User login
Protein discovery points the way to sepsis treatment

Credit: Eric Smith
A protein that helps the innate immune system target bacteria and viruses can fight sepsis by interacting with histones, according to research
published in Science Signaling.
The pattern recognition protein pentraxin 3 (PTX3) is known to activate the body’s immune system in response to sepsis conditions.
But researchers thought the protein might have an additional role in sepsis pathogenesis, in the form of host protection against extracellular histones.
They knew that, during sepsis, histones escape from dead cells and kill nearby healthy cells, causing inflammation.
And the team’s experiments showed that PTX3 forms strong bonds with histones and disrupts their cellular toxicity, specifically by bundling the histones into aggregates that no longer kill healthy cells.
“We observed extraordinarily rapid and tight interaction with histone, which we recognized as coaggregation after a variety of experiments,” said study author Takao Hamakubo, MD, PhD, of the University of Tokyo in Japan.
The researchers also found that mice pretreated with PTX3 and infused with histones showed reduced inflammation.
So the team decided to investigate the effects of PTX3 in 2 mouse models of sepsis. In both models, the protein substantially reduced mortality.
PTX3 worked even when administered hours after a sepsis-inducing procedure called cecal ligation and puncture, in which fecal material is released into the abdomen to generate a strong immune response.
The researchers said these results suggest the host-protective effects of PTX3 in sepsis are a result of its coaggregation with histones rather than its ability to mediate pattern recognition. And this effect provides a potential basis for treating sepsis by protecting cells from the toxic effects of extracellular histones.
“To our knowledge, this is the first report of coaggregation between different proteins that is protective to the host,” Dr Hamakubo said. “We expect our findings lead to a novel understanding of protein interaction and that they will benefit people who are suffering from severe illness.” ![]()
Credit: Eric Smith
A protein that helps the innate immune system target bacteria and viruses can fight sepsis by interacting with histones, according to research
published in Science Signaling.
The pattern recognition protein pentraxin 3 (PTX3) is known to activate the body’s immune system in response to sepsis conditions.
But researchers thought the protein might have an additional role in sepsis pathogenesis, in the form of host protection against extracellular histones.
They knew that, during sepsis, histones escape from dead cells and kill nearby healthy cells, causing inflammation.
And the team’s experiments showed that PTX3 forms strong bonds with histones and disrupts their cellular toxicity, specifically by bundling the histones into aggregates that no longer kill healthy cells.
“We observed extraordinarily rapid and tight interaction with histone, which we recognized as coaggregation after a variety of experiments,” said study author Takao Hamakubo, MD, PhD, of the University of Tokyo in Japan.
The researchers also found that mice pretreated with PTX3 and infused with histones showed reduced inflammation.
So the team decided to investigate the effects of PTX3 in 2 mouse models of sepsis. In both models, the protein substantially reduced mortality.
PTX3 worked even when administered hours after a sepsis-inducing procedure called cecal ligation and puncture, in which fecal material is released into the abdomen to generate a strong immune response.
The researchers said these results suggest the host-protective effects of PTX3 in sepsis are a result of its coaggregation with histones rather than its ability to mediate pattern recognition. And this effect provides a potential basis for treating sepsis by protecting cells from the toxic effects of extracellular histones.
“To our knowledge, this is the first report of coaggregation between different proteins that is protective to the host,” Dr Hamakubo said. “We expect our findings lead to a novel understanding of protein interaction and that they will benefit people who are suffering from severe illness.” ![]()
Credit: Eric Smith
A protein that helps the innate immune system target bacteria and viruses can fight sepsis by interacting with histones, according to research
published in Science Signaling.
The pattern recognition protein pentraxin 3 (PTX3) is known to activate the body’s immune system in response to sepsis conditions.
But researchers thought the protein might have an additional role in sepsis pathogenesis, in the form of host protection against extracellular histones.
They knew that, during sepsis, histones escape from dead cells and kill nearby healthy cells, causing inflammation.
And the team’s experiments showed that PTX3 forms strong bonds with histones and disrupts their cellular toxicity, specifically by bundling the histones into aggregates that no longer kill healthy cells.
“We observed extraordinarily rapid and tight interaction with histone, which we recognized as coaggregation after a variety of experiments,” said study author Takao Hamakubo, MD, PhD, of the University of Tokyo in Japan.
The researchers also found that mice pretreated with PTX3 and infused with histones showed reduced inflammation.
So the team decided to investigate the effects of PTX3 in 2 mouse models of sepsis. In both models, the protein substantially reduced mortality.
PTX3 worked even when administered hours after a sepsis-inducing procedure called cecal ligation and puncture, in which fecal material is released into the abdomen to generate a strong immune response.
The researchers said these results suggest the host-protective effects of PTX3 in sepsis are a result of its coaggregation with histones rather than its ability to mediate pattern recognition. And this effect provides a potential basis for treating sepsis by protecting cells from the toxic effects of extracellular histones.
“To our knowledge, this is the first report of coaggregation between different proteins that is protective to the host,” Dr Hamakubo said. “We expect our findings lead to a novel understanding of protein interaction and that they will benefit people who are suffering from severe illness.” ![]()
New assay could prove useful in HSCT
![]()
Credit: Chad McNeeley
Researchers say they’ve developed an assay that allows for ultrasensitive DNA detection.
This haplotype-based assay could be used to detect relapse in patients who have undergone hematopoietic stem cell transplant (HSCT).
In fact, the researchers believe it would enable relapse detection earlier than existing microsatellite-based assays.
The new assay could also be used to detect microchimerism in solid organ transplants, in forensics, and for patient identification.
James Eshleman, MD, PhD, of the Johns Hopkins University School of Medicine in Baltimore, Maryland, and his colleagues described this assay in The Journal of Molecular Diagnostics.
The team noted that most bone marrow engraftment testing currently uses microsatellites or short tandem repeats that are resolved by capillary electrophoresis.
“Repeat testing will only detect DNA that makes up at least 1% of a DNA sample, so it’s not great for situations in which results depend on small amounts of material within a larger sample,” Dr Eshleman said.
In these situations, evaluating single-nucleotide polymorphisms (SNPs) might seem like a better choice, but this method has a high error rate. Dr Eshleman and his colleagues found they could circumvent this problem by analyzing blocks of closely spaced SNPs, or haplotypes.
To test their method, the researchers chose the HLA-A locus. They aligned common HLA-A alleles and identified a region containing 18 closely spaced SNPs. The team then tested a series of primers surrounding this region and selected the best pair on the basis of amplification efficiency and specificity.
They found it easy to differentiate some combinations of HLA-A alleles but not others. For instance, they discovered that 11 SNPs differentiate allele A*01 from A*02. But A*02 and HLA-A* 68:01:01:01 have a single SNP difference.
To test the possible cross talk between molecules that vary by 11 SNPs, the researchers sequenced 2 samples—one homozygous for A*01 and another homozygous for A*02—and analyzed each for the other allele. They found that, when there are enough discriminating SNPs between 2 individuals’ alleles, the haplotype assay is highly specific.
To evaluate the assay’s accuracy and limit of detection, the researchers generated various dilutions of 2 cell lines with known HLA-A genotypes. They made dilutions with cell mixes varying from 1 in 1 million (0.0001%) to 1 in 100 (1%), using 10 million cells for each dilution.
The team isolated DNA and performed PCR using 600 ng of DNA. And they sequenced each sample at least twice.
The assay proved highly precise at the 0.1% cell mix but less precise at the 0.01% cell mix.
“[Nevertheless,] we could detect cells when they made up just 0.01% of the mixture, which is a big improvement over the current method, which can only detect DNA that makes up 1% to 5% of a sample,” Dr Eshleman said.
The researchers also used their assay to test samples from 18 HSCT patients whose donor-patient HLA genotypes varied by at least 4 SNPs. All but 1 sample tested positive for some level of patient DNA, and the positives ranged from 0.001% to 1.47% patient DNA.
Finally, the team analyzed the human genome using the 1000 Genomes database and identified many additional loci that could be used with their assay. ![]()
![]()
Credit: Chad McNeeley
Researchers say they’ve developed an assay that allows for ultrasensitive DNA detection.
This haplotype-based assay could be used to detect relapse in patients who have undergone hematopoietic stem cell transplant (HSCT).
In fact, the researchers believe it would enable relapse detection earlier than existing microsatellite-based assays.
The new assay could also be used to detect microchimerism in solid organ transplants, in forensics, and for patient identification.
James Eshleman, MD, PhD, of the Johns Hopkins University School of Medicine in Baltimore, Maryland, and his colleagues described this assay in The Journal of Molecular Diagnostics.
The team noted that most bone marrow engraftment testing currently uses microsatellites or short tandem repeats that are resolved by capillary electrophoresis.
“Repeat testing will only detect DNA that makes up at least 1% of a DNA sample, so it’s not great for situations in which results depend on small amounts of material within a larger sample,” Dr Eshleman said.
In these situations, evaluating single-nucleotide polymorphisms (SNPs) might seem like a better choice, but this method has a high error rate. Dr Eshleman and his colleagues found they could circumvent this problem by analyzing blocks of closely spaced SNPs, or haplotypes.
To test their method, the researchers chose the HLA-A locus. They aligned common HLA-A alleles and identified a region containing 18 closely spaced SNPs. The team then tested a series of primers surrounding this region and selected the best pair on the basis of amplification efficiency and specificity.
They found it easy to differentiate some combinations of HLA-A alleles but not others. For instance, they discovered that 11 SNPs differentiate allele A*01 from A*02. But A*02 and HLA-A* 68:01:01:01 have a single SNP difference.
To test the possible cross talk between molecules that vary by 11 SNPs, the researchers sequenced 2 samples—one homozygous for A*01 and another homozygous for A*02—and analyzed each for the other allele. They found that, when there are enough discriminating SNPs between 2 individuals’ alleles, the haplotype assay is highly specific.
To evaluate the assay’s accuracy and limit of detection, the researchers generated various dilutions of 2 cell lines with known HLA-A genotypes. They made dilutions with cell mixes varying from 1 in 1 million (0.0001%) to 1 in 100 (1%), using 10 million cells for each dilution.
The team isolated DNA and performed PCR using 600 ng of DNA. And they sequenced each sample at least twice.
The assay proved highly precise at the 0.1% cell mix but less precise at the 0.01% cell mix.
“[Nevertheless,] we could detect cells when they made up just 0.01% of the mixture, which is a big improvement over the current method, which can only detect DNA that makes up 1% to 5% of a sample,” Dr Eshleman said.
The researchers also used their assay to test samples from 18 HSCT patients whose donor-patient HLA genotypes varied by at least 4 SNPs. All but 1 sample tested positive for some level of patient DNA, and the positives ranged from 0.001% to 1.47% patient DNA.
Finally, the team analyzed the human genome using the 1000 Genomes database and identified many additional loci that could be used with their assay. ![]()
![]()
Credit: Chad McNeeley
Researchers say they’ve developed an assay that allows for ultrasensitive DNA detection.
This haplotype-based assay could be used to detect relapse in patients who have undergone hematopoietic stem cell transplant (HSCT).
In fact, the researchers believe it would enable relapse detection earlier than existing microsatellite-based assays.
The new assay could also be used to detect microchimerism in solid organ transplants, in forensics, and for patient identification.
James Eshleman, MD, PhD, of the Johns Hopkins University School of Medicine in Baltimore, Maryland, and his colleagues described this assay in The Journal of Molecular Diagnostics.
The team noted that most bone marrow engraftment testing currently uses microsatellites or short tandem repeats that are resolved by capillary electrophoresis.
“Repeat testing will only detect DNA that makes up at least 1% of a DNA sample, so it’s not great for situations in which results depend on small amounts of material within a larger sample,” Dr Eshleman said.
In these situations, evaluating single-nucleotide polymorphisms (SNPs) might seem like a better choice, but this method has a high error rate. Dr Eshleman and his colleagues found they could circumvent this problem by analyzing blocks of closely spaced SNPs, or haplotypes.
To test their method, the researchers chose the HLA-A locus. They aligned common HLA-A alleles and identified a region containing 18 closely spaced SNPs. The team then tested a series of primers surrounding this region and selected the best pair on the basis of amplification efficiency and specificity.
They found it easy to differentiate some combinations of HLA-A alleles but not others. For instance, they discovered that 11 SNPs differentiate allele A*01 from A*02. But A*02 and HLA-A* 68:01:01:01 have a single SNP difference.
To test the possible cross talk between molecules that vary by 11 SNPs, the researchers sequenced 2 samples—one homozygous for A*01 and another homozygous for A*02—and analyzed each for the other allele. They found that, when there are enough discriminating SNPs between 2 individuals’ alleles, the haplotype assay is highly specific.
To evaluate the assay’s accuracy and limit of detection, the researchers generated various dilutions of 2 cell lines with known HLA-A genotypes. They made dilutions with cell mixes varying from 1 in 1 million (0.0001%) to 1 in 100 (1%), using 10 million cells for each dilution.
The team isolated DNA and performed PCR using 600 ng of DNA. And they sequenced each sample at least twice.
The assay proved highly precise at the 0.1% cell mix but less precise at the 0.01% cell mix.
“[Nevertheless,] we could detect cells when they made up just 0.01% of the mixture, which is a big improvement over the current method, which can only detect DNA that makes up 1% to 5% of a sample,” Dr Eshleman said.
The researchers also used their assay to test samples from 18 HSCT patients whose donor-patient HLA genotypes varied by at least 4 SNPs. All but 1 sample tested positive for some level of patient DNA, and the positives ranged from 0.001% to 1.47% patient DNA.
Finally, the team analyzed the human genome using the 1000 Genomes database and identified many additional loci that could be used with their assay. ![]()
Hemostats may decrease costs, use of resources

Credit: Piotr Bodzek
HOUSTON—A family of hemostatic products can decrease the need for blood transfusions, reduce hospital stays, and cut the cost of care for certain surgical patients, a retrospective study suggests.
Researchers compared the SURGICEL family of topical, absorbable hemostats—which are based on oxidized regenerated cellulose—to other adjunctive hemostats—flowables, gelatin, and thrombin—in patients undergoing a range of surgical procedures.
The team presented their findings in a poster at the Society for the Advancement of Blood Management Annual Meeting. The study was sponsored by Ethicon, makers of the SURGICEL products.
The goal of this research was to compare the healthcare resource utilization, costs, and outcomes associated with SURGICEL products—SURGICEL® ORIGINAL, SURGICEL® NU-KNIT®, SURGICEL® FIBRILLAR™, and SURGICEL® SNOW™—to those associated with other adjunctive hemostats.
The researchers analyzed data from adult patients (18 years and older) from the Premier Research Database who were discharged from the hospital between January 1, 2011, and December 31, 2012.
Patients had undergone cholecystectomy (n=3045), cardiovascular surgery (n=11,359), hysterectomy (n=4674), or carotid endarterectomy (5445).
The researchers found that fewer units of hemostat were used per discharge among patients who received SURGICEL products than among those who received other hemostats, regardless of the type of surgery.
Hemostat use was 18% lower for cholecystectomy patients (P<0.0001), 28% lower for cardiovascular patients (P<0.0001), 16% lower for hysterectomy patients (P<0.05), and 41% for carotid endarterectomy patients (P<0.0001).
SURGICEL products were also associated with a reduction in blood transfusions for some patients. Transfusions were reduced by 5% among hysterectomy patients (not significant), 18% in cholecystectomy patients (P<0.05), and 32% for carotid endarterectomy patients (P<0.0001).
The mean length of hospital stay and the mean length of stay in the intensive care unit (ICU) were both lower for certain patients who received SURGICEL products.
Hospital stays were 12% lower in cholecystectomy patients (P<0.05) and 8% lower in carotid endarterectomy patients (P<0.0001). And ICU stays were 3% lower in cholecystectomy patients (not significant) and 8% lower in carotid endarterectomy patients (P<0.05).
ICU costs were not significantly lower for patients who received SURGICEL products. However, the costs of hemostats and all-cause costs were lower with SURGICEL products than with other hemostats.
The cost of hemostats was 59% lower for in cholecystectomy patients (P<0.0001), 33% lower in cardiovascular patients (P<0.0001), 57% lower in hysterectomy patients (P<0.0001), and 49% lower in carotid endarterectomy patients (P<0.0001).
The all-cause costs per discharge were 1% lower for hysterectomy patients (P<0.05), 6% lower for carotid endarterectomy patients (P<0.0001), and 14% lower for cholecystectomy patients (P<0.0001).
Cost savings ranged from $71 to $155 per procedure.
“This study adds to the growing body of evidence that suggests the SURGICEL family of topical, absorbable hemostats has the potential to reduce burdens associated with bleeding and bleeding-related complications, which translates into cost and resource-use savings for healthcare providers,” said study investigator Jerome Riebman, MD, director of medical affairs at Ethicon.
Dr Riebman and his colleagues did note that this study was subject to limitations. For example, not all of the factors influencing the physicians’ choice of treatment were available in the dataset.
Furthermore, it’s not clear whether the hospitals studied are representative of all US hospitals. And coding errors or omitted procedure/product codes could have led to patient misclassification and potential bias in the results. ![]()
Credit: Piotr Bodzek
HOUSTON—A family of hemostatic products can decrease the need for blood transfusions, reduce hospital stays, and cut the cost of care for certain surgical patients, a retrospective study suggests.
Researchers compared the SURGICEL family of topical, absorbable hemostats—which are based on oxidized regenerated cellulose—to other adjunctive hemostats—flowables, gelatin, and thrombin—in patients undergoing a range of surgical procedures.
The team presented their findings in a poster at the Society for the Advancement of Blood Management Annual Meeting. The study was sponsored by Ethicon, makers of the SURGICEL products.
The goal of this research was to compare the healthcare resource utilization, costs, and outcomes associated with SURGICEL products—SURGICEL® ORIGINAL, SURGICEL® NU-KNIT®, SURGICEL® FIBRILLAR™, and SURGICEL® SNOW™—to those associated with other adjunctive hemostats.
The researchers analyzed data from adult patients (18 years and older) from the Premier Research Database who were discharged from the hospital between January 1, 2011, and December 31, 2012.
Patients had undergone cholecystectomy (n=3045), cardiovascular surgery (n=11,359), hysterectomy (n=4674), or carotid endarterectomy (5445).
The researchers found that fewer units of hemostat were used per discharge among patients who received SURGICEL products than among those who received other hemostats, regardless of the type of surgery.
Hemostat use was 18% lower for cholecystectomy patients (P<0.0001), 28% lower for cardiovascular patients (P<0.0001), 16% lower for hysterectomy patients (P<0.05), and 41% for carotid endarterectomy patients (P<0.0001).
SURGICEL products were also associated with a reduction in blood transfusions for some patients. Transfusions were reduced by 5% among hysterectomy patients (not significant), 18% in cholecystectomy patients (P<0.05), and 32% for carotid endarterectomy patients (P<0.0001).
The mean length of hospital stay and the mean length of stay in the intensive care unit (ICU) were both lower for certain patients who received SURGICEL products.
Hospital stays were 12% lower in cholecystectomy patients (P<0.05) and 8% lower in carotid endarterectomy patients (P<0.0001). And ICU stays were 3% lower in cholecystectomy patients (not significant) and 8% lower in carotid endarterectomy patients (P<0.05).
ICU costs were not significantly lower for patients who received SURGICEL products. However, the costs of hemostats and all-cause costs were lower with SURGICEL products than with other hemostats.
The cost of hemostats was 59% lower for in cholecystectomy patients (P<0.0001), 33% lower in cardiovascular patients (P<0.0001), 57% lower in hysterectomy patients (P<0.0001), and 49% lower in carotid endarterectomy patients (P<0.0001).
The all-cause costs per discharge were 1% lower for hysterectomy patients (P<0.05), 6% lower for carotid endarterectomy patients (P<0.0001), and 14% lower for cholecystectomy patients (P<0.0001).
Cost savings ranged from $71 to $155 per procedure.
“This study adds to the growing body of evidence that suggests the SURGICEL family of topical, absorbable hemostats has the potential to reduce burdens associated with bleeding and bleeding-related complications, which translates into cost and resource-use savings for healthcare providers,” said study investigator Jerome Riebman, MD, director of medical affairs at Ethicon.
Dr Riebman and his colleagues did note that this study was subject to limitations. For example, not all of the factors influencing the physicians’ choice of treatment were available in the dataset.
Furthermore, it’s not clear whether the hospitals studied are representative of all US hospitals. And coding errors or omitted procedure/product codes could have led to patient misclassification and potential bias in the results. ![]()
Credit: Piotr Bodzek
HOUSTON—A family of hemostatic products can decrease the need for blood transfusions, reduce hospital stays, and cut the cost of care for certain surgical patients, a retrospective study suggests.
Researchers compared the SURGICEL family of topical, absorbable hemostats—which are based on oxidized regenerated cellulose—to other adjunctive hemostats—flowables, gelatin, and thrombin—in patients undergoing a range of surgical procedures.
The team presented their findings in a poster at the Society for the Advancement of Blood Management Annual Meeting. The study was sponsored by Ethicon, makers of the SURGICEL products.
The goal of this research was to compare the healthcare resource utilization, costs, and outcomes associated with SURGICEL products—SURGICEL® ORIGINAL, SURGICEL® NU-KNIT®, SURGICEL® FIBRILLAR™, and SURGICEL® SNOW™—to those associated with other adjunctive hemostats.
The researchers analyzed data from adult patients (18 years and older) from the Premier Research Database who were discharged from the hospital between January 1, 2011, and December 31, 2012.
Patients had undergone cholecystectomy (n=3045), cardiovascular surgery (n=11,359), hysterectomy (n=4674), or carotid endarterectomy (5445).
The researchers found that fewer units of hemostat were used per discharge among patients who received SURGICEL products than among those who received other hemostats, regardless of the type of surgery.
Hemostat use was 18% lower for cholecystectomy patients (P<0.0001), 28% lower for cardiovascular patients (P<0.0001), 16% lower for hysterectomy patients (P<0.05), and 41% for carotid endarterectomy patients (P<0.0001).
SURGICEL products were also associated with a reduction in blood transfusions for some patients. Transfusions were reduced by 5% among hysterectomy patients (not significant), 18% in cholecystectomy patients (P<0.05), and 32% for carotid endarterectomy patients (P<0.0001).
The mean length of hospital stay and the mean length of stay in the intensive care unit (ICU) were both lower for certain patients who received SURGICEL products.
Hospital stays were 12% lower in cholecystectomy patients (P<0.05) and 8% lower in carotid endarterectomy patients (P<0.0001). And ICU stays were 3% lower in cholecystectomy patients (not significant) and 8% lower in carotid endarterectomy patients (P<0.05).
ICU costs were not significantly lower for patients who received SURGICEL products. However, the costs of hemostats and all-cause costs were lower with SURGICEL products than with other hemostats.
The cost of hemostats was 59% lower for in cholecystectomy patients (P<0.0001), 33% lower in cardiovascular patients (P<0.0001), 57% lower in hysterectomy patients (P<0.0001), and 49% lower in carotid endarterectomy patients (P<0.0001).
The all-cause costs per discharge were 1% lower for hysterectomy patients (P<0.05), 6% lower for carotid endarterectomy patients (P<0.0001), and 14% lower for cholecystectomy patients (P<0.0001).
Cost savings ranged from $71 to $155 per procedure.
“This study adds to the growing body of evidence that suggests the SURGICEL family of topical, absorbable hemostats has the potential to reduce burdens associated with bleeding and bleeding-related complications, which translates into cost and resource-use savings for healthcare providers,” said study investigator Jerome Riebman, MD, director of medical affairs at Ethicon.
Dr Riebman and his colleagues did note that this study was subject to limitations. For example, not all of the factors influencing the physicians’ choice of treatment were available in the dataset.
Furthermore, it’s not clear whether the hospitals studied are representative of all US hospitals. And coding errors or omitted procedure/product codes could have led to patient misclassification and potential bias in the results. ![]()
Drug shows activity in models of pediatric ALL

Credit: Aaron Logan
A compound that has demonstrated efficacy in older adults with acute myeloid leukemia (AML) may be a viable option for childhood acute lymphoblastic
leukemia (ALL) as well.
The drug, CPX-351, is a fixed-ratio combination of cytarabine and daunorubicin inside a lipid vesicle.
It previously showed promise in a phase 2 trial of AML patients ages 60 to 75 years. Now, preclinical results suggest CPX-351 can work against aggressive
pediatric ALL too.
The research appears in Pediatric Blood & Cancer. It was supported by the National Cancer Institute.
“Cytarabine and anthracyclines such as daunorubicin are commonly used to treat ALL in pediatric patients, and while these drug are very effective in front-line, multidrug, combination chemotherapy regimens, there remains room for improvement, especially in pediatric patients who relapse within 36 months of diagnosis,” said study author Richard Lock, PhD, of Children’s Cancer Institute in Sydney, Australia.
“We are very encouraged by these preclinical results, indicating that the proprietary CPX-351 formulation of cytarabine and daunorubicin may be an important tool to maximize efficacy outcomes in relapsed ALL, and we believe these data substantiate the need for additional, clinical study in pediatric patients.”
Dr Lock and his colleagues studied CPX-351 in mice inoculated with leukemia cells from 5 children who had died from ALL. Three of the children, 2 with B-precursor ALL and 1 with T-cell ALL, had relapsed disease at the time of biopsy.
The researchers inoculated up to 18 mice for each of the 5 leukemia types and then randomized the mice to treatment or control.
The maximum-tolerated dose of CPX-351 was 5 units/kg (corresponding to 5 mg/kg cytarabine and 2.2 mg/kg daunorubicin). This dose provided clinically relevant plasma drug exposure and correlated to the pharmacokinetic properties observed in patients with AML.
The researchers found that all 5 models of ALL were “highly responsive” to CPX-351. In the 4 models of B-precursor ALL, the median group response was a complete response. In the mice inoculated with T-cell ALL, the median group response was a partial response.
Among treated mice, event-free survival ranged from 32.8 days to 41.9 days. And among controls, event-free survival ranged from 2.4 days to 10.8 days.
Dr Lock and his colleagues believe these results suggest CPX-351 may be a promising treatment for ALL and support its testing in pediatric leukemia patients.
CPX-351 is currently under investigation in a phase 3 trial in older patients with high-risk (secondary) AML. ![]()
Credit: Aaron Logan
A compound that has demonstrated efficacy in older adults with acute myeloid leukemia (AML) may be a viable option for childhood acute lymphoblastic
leukemia (ALL) as well.
The drug, CPX-351, is a fixed-ratio combination of cytarabine and daunorubicin inside a lipid vesicle.
It previously showed promise in a phase 2 trial of AML patients ages 60 to 75 years. Now, preclinical results suggest CPX-351 can work against aggressive
pediatric ALL too.
The research appears in Pediatric Blood & Cancer. It was supported by the National Cancer Institute.
“Cytarabine and anthracyclines such as daunorubicin are commonly used to treat ALL in pediatric patients, and while these drug are very effective in front-line, multidrug, combination chemotherapy regimens, there remains room for improvement, especially in pediatric patients who relapse within 36 months of diagnosis,” said study author Richard Lock, PhD, of Children’s Cancer Institute in Sydney, Australia.
“We are very encouraged by these preclinical results, indicating that the proprietary CPX-351 formulation of cytarabine and daunorubicin may be an important tool to maximize efficacy outcomes in relapsed ALL, and we believe these data substantiate the need for additional, clinical study in pediatric patients.”
Dr Lock and his colleagues studied CPX-351 in mice inoculated with leukemia cells from 5 children who had died from ALL. Three of the children, 2 with B-precursor ALL and 1 with T-cell ALL, had relapsed disease at the time of biopsy.
The researchers inoculated up to 18 mice for each of the 5 leukemia types and then randomized the mice to treatment or control.
The maximum-tolerated dose of CPX-351 was 5 units/kg (corresponding to 5 mg/kg cytarabine and 2.2 mg/kg daunorubicin). This dose provided clinically relevant plasma drug exposure and correlated to the pharmacokinetic properties observed in patients with AML.
The researchers found that all 5 models of ALL were “highly responsive” to CPX-351. In the 4 models of B-precursor ALL, the median group response was a complete response. In the mice inoculated with T-cell ALL, the median group response was a partial response.
Among treated mice, event-free survival ranged from 32.8 days to 41.9 days. And among controls, event-free survival ranged from 2.4 days to 10.8 days.
Dr Lock and his colleagues believe these results suggest CPX-351 may be a promising treatment for ALL and support its testing in pediatric leukemia patients.
CPX-351 is currently under investigation in a phase 3 trial in older patients with high-risk (secondary) AML. ![]()
Credit: Aaron Logan
A compound that has demonstrated efficacy in older adults with acute myeloid leukemia (AML) may be a viable option for childhood acute lymphoblastic
leukemia (ALL) as well.
The drug, CPX-351, is a fixed-ratio combination of cytarabine and daunorubicin inside a lipid vesicle.
It previously showed promise in a phase 2 trial of AML patients ages 60 to 75 years. Now, preclinical results suggest CPX-351 can work against aggressive
pediatric ALL too.
The research appears in Pediatric Blood & Cancer. It was supported by the National Cancer Institute.
“Cytarabine and anthracyclines such as daunorubicin are commonly used to treat ALL in pediatric patients, and while these drug are very effective in front-line, multidrug, combination chemotherapy regimens, there remains room for improvement, especially in pediatric patients who relapse within 36 months of diagnosis,” said study author Richard Lock, PhD, of Children’s Cancer Institute in Sydney, Australia.
“We are very encouraged by these preclinical results, indicating that the proprietary CPX-351 formulation of cytarabine and daunorubicin may be an important tool to maximize efficacy outcomes in relapsed ALL, and we believe these data substantiate the need for additional, clinical study in pediatric patients.”
Dr Lock and his colleagues studied CPX-351 in mice inoculated with leukemia cells from 5 children who had died from ALL. Three of the children, 2 with B-precursor ALL and 1 with T-cell ALL, had relapsed disease at the time of biopsy.
The researchers inoculated up to 18 mice for each of the 5 leukemia types and then randomized the mice to treatment or control.
The maximum-tolerated dose of CPX-351 was 5 units/kg (corresponding to 5 mg/kg cytarabine and 2.2 mg/kg daunorubicin). This dose provided clinically relevant plasma drug exposure and correlated to the pharmacokinetic properties observed in patients with AML.
The researchers found that all 5 models of ALL were “highly responsive” to CPX-351. In the 4 models of B-precursor ALL, the median group response was a complete response. In the mice inoculated with T-cell ALL, the median group response was a partial response.
Among treated mice, event-free survival ranged from 32.8 days to 41.9 days. And among controls, event-free survival ranged from 2.4 days to 10.8 days.
Dr Lock and his colleagues believe these results suggest CPX-351 may be a promising treatment for ALL and support its testing in pediatric leukemia patients.
CPX-351 is currently under investigation in a phase 3 trial in older patients with high-risk (secondary) AML. ![]()
RT use on decline in early HL despite survival benefit

Credit: Rhoda Baer
SAN FRANCISCO—Results of a large study suggest that consolidation radiation therapy (RT) can improve survival in patients with stage I and II Hodgkin lymphoma (HL), but the use of RT in these patients may be on the decline.
In this study of more than 40,000 patients, the 10-year survival rate was 84% among those who received RT and 76% among those who did not.
Despite this benefit, the use of RT declined during the period studied, from 56% in 1998 to 41% in 2011.
These data were presented at the American Society for Radiation Oncology’s 56th Annual Meeting (abstract 1042).
“Multiple prospective, randomized trials have shown a significant improvement in disease control with the addition of RT,” said lead study author Rahul R. Parikh, MD, of the Mount Sinai Health System in New York.
“However, previous trials were limited by low patient numbers and limited follow-up and, thus, were unable to demonstrate an overall survival benefit. This is the largest dataset in this patient population to demonstrate a survival benefit with the addition of RT.”
Dr Parikh and his colleagues studied 41,502 patients who were diagnosed with stage I and II HL from 1998 to 2011. They were included in the National Cancer Data Base, which consists of cases from 1500 sites and represents more than 75% of all cancers diagnosed in the US.
The average patient age was 37 years (range, 18 to 90). The median follow-up was 7.5 years. Ninety-six percent of patients (n=39,842) received multi-agent chemotherapy, and 49% (n=20,441) received a median RT dose of 30.6 Gy.
The 10-year overall survival of the entire group was 80.8%. Patients receiving RT had significantly better overall survival than those who did not (84.4% vs 76.4%; P<0.00001).
When adjusting for age, stage, comorbidity, transplant, chemotherapy use, and socioeconomic status, RT use was still associated with significantly improved overall survival (hazard ratio=0.51; P<0.00001).
The study also showed that omitting RT was related to higher rates of salvage transplant procedures, a surrogate for persistent/relapsed disease (P=0.04).
Nevertheless, RT use decreased at the study sites from 56% to 41% between 1998 and 2011.
In 88.4% of patients who did not receive RT, the physician-reported reason was that RT was not part of the planned initial treatment strategy.
The research also indicated that RT use was more likely among younger patients (40 years or younger), those in a higher socioeconomic status, those who had access to health insurance, and those who received treatment at comprehensive cancer centers (all P<0.0001).
“[W]e have highlighted ongoing disparities in Hodgkin’s disease treatment, and it is important that we recognize these findings as potential barriers to care,” Dr Parikh said.
“Given the survival benefit demonstrated in this study, radiotherapy should be included in the combined modality approach of multi-agent chemotherapy followed by consolidation RT in order to maintain high overall survival rates for this curable disease.” ![]()
Credit: Rhoda Baer
SAN FRANCISCO—Results of a large study suggest that consolidation radiation therapy (RT) can improve survival in patients with stage I and II Hodgkin lymphoma (HL), but the use of RT in these patients may be on the decline.
In this study of more than 40,000 patients, the 10-year survival rate was 84% among those who received RT and 76% among those who did not.
Despite this benefit, the use of RT declined during the period studied, from 56% in 1998 to 41% in 2011.
These data were presented at the American Society for Radiation Oncology’s 56th Annual Meeting (abstract 1042).
“Multiple prospective, randomized trials have shown a significant improvement in disease control with the addition of RT,” said lead study author Rahul R. Parikh, MD, of the Mount Sinai Health System in New York.
“However, previous trials were limited by low patient numbers and limited follow-up and, thus, were unable to demonstrate an overall survival benefit. This is the largest dataset in this patient population to demonstrate a survival benefit with the addition of RT.”
Dr Parikh and his colleagues studied 41,502 patients who were diagnosed with stage I and II HL from 1998 to 2011. They were included in the National Cancer Data Base, which consists of cases from 1500 sites and represents more than 75% of all cancers diagnosed in the US.
The average patient age was 37 years (range, 18 to 90). The median follow-up was 7.5 years. Ninety-six percent of patients (n=39,842) received multi-agent chemotherapy, and 49% (n=20,441) received a median RT dose of 30.6 Gy.
The 10-year overall survival of the entire group was 80.8%. Patients receiving RT had significantly better overall survival than those who did not (84.4% vs 76.4%; P<0.00001).
When adjusting for age, stage, comorbidity, transplant, chemotherapy use, and socioeconomic status, RT use was still associated with significantly improved overall survival (hazard ratio=0.51; P<0.00001).
The study also showed that omitting RT was related to higher rates of salvage transplant procedures, a surrogate for persistent/relapsed disease (P=0.04).
Nevertheless, RT use decreased at the study sites from 56% to 41% between 1998 and 2011.
In 88.4% of patients who did not receive RT, the physician-reported reason was that RT was not part of the planned initial treatment strategy.
The research also indicated that RT use was more likely among younger patients (40 years or younger), those in a higher socioeconomic status, those who had access to health insurance, and those who received treatment at comprehensive cancer centers (all P<0.0001).
“[W]e have highlighted ongoing disparities in Hodgkin’s disease treatment, and it is important that we recognize these findings as potential barriers to care,” Dr Parikh said.
“Given the survival benefit demonstrated in this study, radiotherapy should be included in the combined modality approach of multi-agent chemotherapy followed by consolidation RT in order to maintain high overall survival rates for this curable disease.” ![]()
Credit: Rhoda Baer
SAN FRANCISCO—Results of a large study suggest that consolidation radiation therapy (RT) can improve survival in patients with stage I and II Hodgkin lymphoma (HL), but the use of RT in these patients may be on the decline.
In this study of more than 40,000 patients, the 10-year survival rate was 84% among those who received RT and 76% among those who did not.
Despite this benefit, the use of RT declined during the period studied, from 56% in 1998 to 41% in 2011.
These data were presented at the American Society for Radiation Oncology’s 56th Annual Meeting (abstract 1042).
“Multiple prospective, randomized trials have shown a significant improvement in disease control with the addition of RT,” said lead study author Rahul R. Parikh, MD, of the Mount Sinai Health System in New York.
“However, previous trials were limited by low patient numbers and limited follow-up and, thus, were unable to demonstrate an overall survival benefit. This is the largest dataset in this patient population to demonstrate a survival benefit with the addition of RT.”
Dr Parikh and his colleagues studied 41,502 patients who were diagnosed with stage I and II HL from 1998 to 2011. They were included in the National Cancer Data Base, which consists of cases from 1500 sites and represents more than 75% of all cancers diagnosed in the US.
The average patient age was 37 years (range, 18 to 90). The median follow-up was 7.5 years. Ninety-six percent of patients (n=39,842) received multi-agent chemotherapy, and 49% (n=20,441) received a median RT dose of 30.6 Gy.
The 10-year overall survival of the entire group was 80.8%. Patients receiving RT had significantly better overall survival than those who did not (84.4% vs 76.4%; P<0.00001).
When adjusting for age, stage, comorbidity, transplant, chemotherapy use, and socioeconomic status, RT use was still associated with significantly improved overall survival (hazard ratio=0.51; P<0.00001).
The study also showed that omitting RT was related to higher rates of salvage transplant procedures, a surrogate for persistent/relapsed disease (P=0.04).
Nevertheless, RT use decreased at the study sites from 56% to 41% between 1998 and 2011.
In 88.4% of patients who did not receive RT, the physician-reported reason was that RT was not part of the planned initial treatment strategy.
The research also indicated that RT use was more likely among younger patients (40 years or younger), those in a higher socioeconomic status, those who had access to health insurance, and those who received treatment at comprehensive cancer centers (all P<0.0001).
“[W]e have highlighted ongoing disparities in Hodgkin’s disease treatment, and it is important that we recognize these findings as potential barriers to care,” Dr Parikh said.
“Given the survival benefit demonstrated in this study, radiotherapy should be included in the combined modality approach of multi-agent chemotherapy followed by consolidation RT in order to maintain high overall survival rates for this curable disease.” ![]()
AB blood type linked to cognitive impairment

Credit: Graham Colm
Individuals with type AB blood may be more likely than those with other blood types to develop memory loss in later years, according to a study published in Neurology.
Investigators found that people with AB blood were 82% more likely to develop cognitive impairment, which can lead to dementia.
Previous studies have shown that individuals with type O blood have a lower risk of heart disease and stroke, factors that can increase the risk of memory loss and dementia.
The new research was part of a larger study—the REasons for Geographic And Racial Differences in Stroke (REGARDS) Study—of more than 30,000 subjects who were followed for an average of 3.4 years.
“Our study looks at blood type and risk of cognitive impairment, but several studies have shown that factors such as high blood pressure, high cholesterol, and diabetes increase the risk of cognitive impairment and dementia,” said Mary Cushman, MD, of the University of Vermont College of Medicine in Burlington.
“Blood type is also related to other vascular conditions like stroke, so the findings highlight the connections between vascular issues and brain health. More research is needed to confirm these results.”
Dr Cushman and her colleagues had set out to assess the relationship between ABO group, factor VIII (FVIII), and incident cognitive impairment in a large, prospective cohort of black and white adults in the US.
The team used cognitive domain tests to assess cognitive impairment. They identified 495 subjects who had no cognitive impairment at baseline but became impaired during follow-up. The investigators then compared these cases with 587 control subjects.
It turned out that subjects with AB blood made up 6% of the group that developed cognitive impairment, which is higher than the 4% of AB individuals found in the general population.
Multivariate analysis—adjusted for age, race, region, and sex—suggested that subjects with AB blood and those with higher FVIII had an increased risk of cognitive impairment. The odds ratios were 1.82 and 1.24, respectively.
Subjects with AB blood had a higher average level of FVIII than subjects with other blood types. The mean level of FVIII was 142 IU/dL among AB subjects and 104 IU/dL among subjects with type O blood.
However, the investigators also found that FVIII mediated only 18% of the association between AB blood type and cognitive impairment. ![]()
Credit: Graham Colm
Individuals with type AB blood may be more likely than those with other blood types to develop memory loss in later years, according to a study published in Neurology.
Investigators found that people with AB blood were 82% more likely to develop cognitive impairment, which can lead to dementia.
Previous studies have shown that individuals with type O blood have a lower risk of heart disease and stroke, factors that can increase the risk of memory loss and dementia.
The new research was part of a larger study—the REasons for Geographic And Racial Differences in Stroke (REGARDS) Study—of more than 30,000 subjects who were followed for an average of 3.4 years.
“Our study looks at blood type and risk of cognitive impairment, but several studies have shown that factors such as high blood pressure, high cholesterol, and diabetes increase the risk of cognitive impairment and dementia,” said Mary Cushman, MD, of the University of Vermont College of Medicine in Burlington.
“Blood type is also related to other vascular conditions like stroke, so the findings highlight the connections between vascular issues and brain health. More research is needed to confirm these results.”
Dr Cushman and her colleagues had set out to assess the relationship between ABO group, factor VIII (FVIII), and incident cognitive impairment in a large, prospective cohort of black and white adults in the US.
The team used cognitive domain tests to assess cognitive impairment. They identified 495 subjects who had no cognitive impairment at baseline but became impaired during follow-up. The investigators then compared these cases with 587 control subjects.
It turned out that subjects with AB blood made up 6% of the group that developed cognitive impairment, which is higher than the 4% of AB individuals found in the general population.
Multivariate analysis—adjusted for age, race, region, and sex—suggested that subjects with AB blood and those with higher FVIII had an increased risk of cognitive impairment. The odds ratios were 1.82 and 1.24, respectively.
Subjects with AB blood had a higher average level of FVIII than subjects with other blood types. The mean level of FVIII was 142 IU/dL among AB subjects and 104 IU/dL among subjects with type O blood.
However, the investigators also found that FVIII mediated only 18% of the association between AB blood type and cognitive impairment. ![]()
Credit: Graham Colm
Individuals with type AB blood may be more likely than those with other blood types to develop memory loss in later years, according to a study published in Neurology.
Investigators found that people with AB blood were 82% more likely to develop cognitive impairment, which can lead to dementia.
Previous studies have shown that individuals with type O blood have a lower risk of heart disease and stroke, factors that can increase the risk of memory loss and dementia.
The new research was part of a larger study—the REasons for Geographic And Racial Differences in Stroke (REGARDS) Study—of more than 30,000 subjects who were followed for an average of 3.4 years.
“Our study looks at blood type and risk of cognitive impairment, but several studies have shown that factors such as high blood pressure, high cholesterol, and diabetes increase the risk of cognitive impairment and dementia,” said Mary Cushman, MD, of the University of Vermont College of Medicine in Burlington.
“Blood type is also related to other vascular conditions like stroke, so the findings highlight the connections between vascular issues and brain health. More research is needed to confirm these results.”
Dr Cushman and her colleagues had set out to assess the relationship between ABO group, factor VIII (FVIII), and incident cognitive impairment in a large, prospective cohort of black and white adults in the US.
The team used cognitive domain tests to assess cognitive impairment. They identified 495 subjects who had no cognitive impairment at baseline but became impaired during follow-up. The investigators then compared these cases with 587 control subjects.
It turned out that subjects with AB blood made up 6% of the group that developed cognitive impairment, which is higher than the 4% of AB individuals found in the general population.
Multivariate analysis—adjusted for age, race, region, and sex—suggested that subjects with AB blood and those with higher FVIII had an increased risk of cognitive impairment. The odds ratios were 1.82 and 1.24, respectively.
Subjects with AB blood had a higher average level of FVIII than subjects with other blood types. The mean level of FVIII was 142 IU/dL among AB subjects and 104 IU/dL among subjects with type O blood.
However, the investigators also found that FVIII mediated only 18% of the association between AB blood type and cognitive impairment. ![]()
Spleen-like device could solve problems in treating sepsis
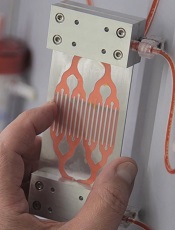
Credit: Wyss Institute
A device inspired by the human spleen could change the way we treat sepsis, researchers say.
This “biospleen” was able to cleanse human blood in lab tests and increase survival in animals with infected blood.
Experiments showed that, in a matter of hours, the biospleen can filter live and dead pathogens from the blood, as well as dangerous toxins released from the pathogens.
The researchers detailed these experiments in Nature Medicine.
“Sepsis is a major medical threat, which is increasing because of antibiotic resistance,” said study author Donald Ingber, MD, PhD, of the Wyss Institute for Biologically Inspired Engineering in Boston, Massachusetts.
“We’re excited by the biospleen because it potentially provides a way to treat patients quickly without having to wait days to identify the source of infection, and it works equally well with antibiotic-resistant organisms. We hope to move this toward human testing [by] advancing to large animal studies as quickly as possible.”
The biospleen is a microfluidic device that works outside the body like a dialysis machine and removes living and dead microbes of all varieties, as well as toxins.
It consists of 2 adjacent, hollow channels that are connected to each other by a series of slits. One channel contains flowing blood, and the other has a saline solution that collects and removes the pathogens that travel through the slits.
Key to the success of the device are nanometer-sized magnetic beads coated with a genetically engineered version of the protein mannose binding lectin (MBL).
In its innate state, MBL has a branch-like “head” and a stick-like “tail.” The head binds to specific sugars on the surfaces of all sorts of bacteria, fungi, viruses, protozoa, and toxins, and the tail cues the immune system to destroy them.
However, other immune system proteins sometimes bind to the MBL tail and activate clotting and organ damage. So Dr Ingber and his colleagues used genetic engineering tools to lop off the tail and graft on a similar one from an antibody protein that does not cause these problems.
The team then attached the hybrid proteins to magnetic beads measuring 128 nanometers in diameter. These novel beads could be added to infected blood to bind to the pathogens and toxins without having to first identify the type of infectious agent.
The biospleen has a magnet that pulls the pathogen-coated magnetic beads through the channels to cleanse the blood flowing through the device, which can then be returned to the patient.
The researchers first tested the biospleen using human blood spiked with pathogens. They were able to filter blood faster than ever before, and the magnets efficiently pulled the beads—coated with pathogens—out of the blood.
More than 90% of key sepsis pathogens were bound and removed when the blood flowed through a single device at a rate of about 0.5 L to 1 L per hour. Many devices can be linked together to obtain levels required for human blood cleansing at dialysis-like rates.
Next, the researchers tested the device using rats infected with E coli, S aureus, and toxins—mimicking many of the bloodstream infections human sepsis patients experience. After 5 hours of filtering, about 90% of the bacteria and toxins were removed from the rats’ bloodstreams.
“We didn’t have to kill the pathogens,” said Michael Super, PhD, also of the Wyss Institute. “We just captured and removed them.”
What’s more, 90% of the treated animals survived, compared to 14% of the controls. And the modified MBL prevented the activation of complement factors and coagulation. ![]()
Credit: Wyss Institute
A device inspired by the human spleen could change the way we treat sepsis, researchers say.
This “biospleen” was able to cleanse human blood in lab tests and increase survival in animals with infected blood.
Experiments showed that, in a matter of hours, the biospleen can filter live and dead pathogens from the blood, as well as dangerous toxins released from the pathogens.
The researchers detailed these experiments in Nature Medicine.
“Sepsis is a major medical threat, which is increasing because of antibiotic resistance,” said study author Donald Ingber, MD, PhD, of the Wyss Institute for Biologically Inspired Engineering in Boston, Massachusetts.
“We’re excited by the biospleen because it potentially provides a way to treat patients quickly without having to wait days to identify the source of infection, and it works equally well with antibiotic-resistant organisms. We hope to move this toward human testing [by] advancing to large animal studies as quickly as possible.”
The biospleen is a microfluidic device that works outside the body like a dialysis machine and removes living and dead microbes of all varieties, as well as toxins.
It consists of 2 adjacent, hollow channels that are connected to each other by a series of slits. One channel contains flowing blood, and the other has a saline solution that collects and removes the pathogens that travel through the slits.
Key to the success of the device are nanometer-sized magnetic beads coated with a genetically engineered version of the protein mannose binding lectin (MBL).
In its innate state, MBL has a branch-like “head” and a stick-like “tail.” The head binds to specific sugars on the surfaces of all sorts of bacteria, fungi, viruses, protozoa, and toxins, and the tail cues the immune system to destroy them.
However, other immune system proteins sometimes bind to the MBL tail and activate clotting and organ damage. So Dr Ingber and his colleagues used genetic engineering tools to lop off the tail and graft on a similar one from an antibody protein that does not cause these problems.
The team then attached the hybrid proteins to magnetic beads measuring 128 nanometers in diameter. These novel beads could be added to infected blood to bind to the pathogens and toxins without having to first identify the type of infectious agent.
The biospleen has a magnet that pulls the pathogen-coated magnetic beads through the channels to cleanse the blood flowing through the device, which can then be returned to the patient.
The researchers first tested the biospleen using human blood spiked with pathogens. They were able to filter blood faster than ever before, and the magnets efficiently pulled the beads—coated with pathogens—out of the blood.
More than 90% of key sepsis pathogens were bound and removed when the blood flowed through a single device at a rate of about 0.5 L to 1 L per hour. Many devices can be linked together to obtain levels required for human blood cleansing at dialysis-like rates.
Next, the researchers tested the device using rats infected with E coli, S aureus, and toxins—mimicking many of the bloodstream infections human sepsis patients experience. After 5 hours of filtering, about 90% of the bacteria and toxins were removed from the rats’ bloodstreams.
“We didn’t have to kill the pathogens,” said Michael Super, PhD, also of the Wyss Institute. “We just captured and removed them.”
What’s more, 90% of the treated animals survived, compared to 14% of the controls. And the modified MBL prevented the activation of complement factors and coagulation. ![]()
Credit: Wyss Institute
A device inspired by the human spleen could change the way we treat sepsis, researchers say.
This “biospleen” was able to cleanse human blood in lab tests and increase survival in animals with infected blood.
Experiments showed that, in a matter of hours, the biospleen can filter live and dead pathogens from the blood, as well as dangerous toxins released from the pathogens.
The researchers detailed these experiments in Nature Medicine.
“Sepsis is a major medical threat, which is increasing because of antibiotic resistance,” said study author Donald Ingber, MD, PhD, of the Wyss Institute for Biologically Inspired Engineering in Boston, Massachusetts.
“We’re excited by the biospleen because it potentially provides a way to treat patients quickly without having to wait days to identify the source of infection, and it works equally well with antibiotic-resistant organisms. We hope to move this toward human testing [by] advancing to large animal studies as quickly as possible.”
The biospleen is a microfluidic device that works outside the body like a dialysis machine and removes living and dead microbes of all varieties, as well as toxins.
It consists of 2 adjacent, hollow channels that are connected to each other by a series of slits. One channel contains flowing blood, and the other has a saline solution that collects and removes the pathogens that travel through the slits.
Key to the success of the device are nanometer-sized magnetic beads coated with a genetically engineered version of the protein mannose binding lectin (MBL).
In its innate state, MBL has a branch-like “head” and a stick-like “tail.” The head binds to specific sugars on the surfaces of all sorts of bacteria, fungi, viruses, protozoa, and toxins, and the tail cues the immune system to destroy them.
However, other immune system proteins sometimes bind to the MBL tail and activate clotting and organ damage. So Dr Ingber and his colleagues used genetic engineering tools to lop off the tail and graft on a similar one from an antibody protein that does not cause these problems.
The team then attached the hybrid proteins to magnetic beads measuring 128 nanometers in diameter. These novel beads could be added to infected blood to bind to the pathogens and toxins without having to first identify the type of infectious agent.
The biospleen has a magnet that pulls the pathogen-coated magnetic beads through the channels to cleanse the blood flowing through the device, which can then be returned to the patient.
The researchers first tested the biospleen using human blood spiked with pathogens. They were able to filter blood faster than ever before, and the magnets efficiently pulled the beads—coated with pathogens—out of the blood.
More than 90% of key sepsis pathogens were bound and removed when the blood flowed through a single device at a rate of about 0.5 L to 1 L per hour. Many devices can be linked together to obtain levels required for human blood cleansing at dialysis-like rates.
Next, the researchers tested the device using rats infected with E coli, S aureus, and toxins—mimicking many of the bloodstream infections human sepsis patients experience. After 5 hours of filtering, about 90% of the bacteria and toxins were removed from the rats’ bloodstreams.
“We didn’t have to kill the pathogens,” said Michael Super, PhD, also of the Wyss Institute. “We just captured and removed them.”
What’s more, 90% of the treated animals survived, compared to 14% of the controls. And the modified MBL prevented the activation of complement factors and coagulation.
FDA approves new treatment for PI

Credit: Baxter
The US Food and Drug Administration (FDA) has approved a subcutaneous immune globulin product for use in adults with primary immunodeficiency (PI).
The product, HyQvia, is an immune globulin with a recombinant human hyaluronidase. It requires a single infusion every 3 to 4 weeks and 1 injection site per infusion to deliver a full therapeutic dose of immune globulin.
Current therapies require weekly or bi-weekly treatment with multiple infusion sites per treatment.
Baxter International Inc. expects to launch HyQvia in the US in the coming weeks. The product has been FDA-approved with a black-box warning detailing the risk of thrombosis associated with immune globulin products.
The immune globulin component of HyQvia is a 10% solution prepared from large pools of human plasma consisting of at least 98% IgG. The recombinant human hyaluronidase increases the dispersion and absorption of the immune globulin.
In a phase 3 trial, HyQvia compared well with intravenous human immune globulin 10% (IVIG).
Researchers compared the treatments at different time periods in a cohort of PI patients with a median age of 35 (range, 4-78 years). All 87 patients studied received IVIG, and 83 of the patients received at least 1 dose of HyQvia.
Patients received HyQvia for a median of 366 days and IVIG for a median of 91 days. The median ratio (HyQvia:IVIG) for the IgG dosage administered was 1.088 (range, 0.986–1.382).
Trough IgG concentrations, the incidence of infection, and rates of adverse events were generally similar during the HyQvia treatment period and the IVIG treatment period.
For patients aged 12 years and older, the median IgG Ctrough values with HyQvia were approximately the same as with IVIG. The median trough ratio (HyQvia:IVIG) was 0.985.
For patients younger than 12 (n=11), the median IgG Ctrough values were 10.0 and 9.6 g/L after HyQvia and IVIG, respectively, with a median trough ratio of 1.038.
The overall infection rates were 2.97 per patient-year with HyQvia and 4.51 per patient-year with IVIG.
During the HyQvia treatment period, the rate of acute serious bacterial infection (SBI) was 0.025 per patient-year. The rate of acute SBIs occurring during IVIG treatment was not reported.
In patients age 18 and older (n=59), the rate of acute SBIs was 0.00 per patient-year, and the overall infection rate was 3.20 per patient-year.
For this same patient group, the local adverse reaction rate was 0.286 per infusion.
The rate of systemic adverse events temporally related to an infusion was 0.20 per infusion with HyQvia and 0.33 per infusion with IVIG. There were no serious adverse events reported in these patients with either treatment.
HyQvia was approved in Europe in 2013 for adults with PI syndromes and myeloma or chronic lymphocytic leukemia with severe secondary hypogammaglobulinemia and recurrent infections.
For more details on HyQvia, see the prescribing information.
Credit: Baxter
The US Food and Drug Administration (FDA) has approved a subcutaneous immune globulin product for use in adults with primary immunodeficiency (PI).
The product, HyQvia, is an immune globulin with a recombinant human hyaluronidase. It requires a single infusion every 3 to 4 weeks and 1 injection site per infusion to deliver a full therapeutic dose of immune globulin.
Current therapies require weekly or bi-weekly treatment with multiple infusion sites per treatment.
Baxter International Inc. expects to launch HyQvia in the US in the coming weeks. The product has been FDA-approved with a black-box warning detailing the risk of thrombosis associated with immune globulin products.
The immune globulin component of HyQvia is a 10% solution prepared from large pools of human plasma consisting of at least 98% IgG. The recombinant human hyaluronidase increases the dispersion and absorption of the immune globulin.
In a phase 3 trial, HyQvia compared well with intravenous human immune globulin 10% (IVIG).
Researchers compared the treatments at different time periods in a cohort of PI patients with a median age of 35 (range, 4-78 years). All 87 patients studied received IVIG, and 83 of the patients received at least 1 dose of HyQvia.
Patients received HyQvia for a median of 366 days and IVIG for a median of 91 days. The median ratio (HyQvia:IVIG) for the IgG dosage administered was 1.088 (range, 0.986–1.382).
Trough IgG concentrations, the incidence of infection, and rates of adverse events were generally similar during the HyQvia treatment period and the IVIG treatment period.
For patients aged 12 years and older, the median IgG Ctrough values with HyQvia were approximately the same as with IVIG. The median trough ratio (HyQvia:IVIG) was 0.985.
For patients younger than 12 (n=11), the median IgG Ctrough values were 10.0 and 9.6 g/L after HyQvia and IVIG, respectively, with a median trough ratio of 1.038.
The overall infection rates were 2.97 per patient-year with HyQvia and 4.51 per patient-year with IVIG.
During the HyQvia treatment period, the rate of acute serious bacterial infection (SBI) was 0.025 per patient-year. The rate of acute SBIs occurring during IVIG treatment was not reported.
In patients age 18 and older (n=59), the rate of acute SBIs was 0.00 per patient-year, and the overall infection rate was 3.20 per patient-year.
For this same patient group, the local adverse reaction rate was 0.286 per infusion.
The rate of systemic adverse events temporally related to an infusion was 0.20 per infusion with HyQvia and 0.33 per infusion with IVIG. There were no serious adverse events reported in these patients with either treatment.
HyQvia was approved in Europe in 2013 for adults with PI syndromes and myeloma or chronic lymphocytic leukemia with severe secondary hypogammaglobulinemia and recurrent infections.
For more details on HyQvia, see the prescribing information.
Credit: Baxter
The US Food and Drug Administration (FDA) has approved a subcutaneous immune globulin product for use in adults with primary immunodeficiency (PI).
The product, HyQvia, is an immune globulin with a recombinant human hyaluronidase. It requires a single infusion every 3 to 4 weeks and 1 injection site per infusion to deliver a full therapeutic dose of immune globulin.
Current therapies require weekly or bi-weekly treatment with multiple infusion sites per treatment.
Baxter International Inc. expects to launch HyQvia in the US in the coming weeks. The product has been FDA-approved with a black-box warning detailing the risk of thrombosis associated with immune globulin products.
The immune globulin component of HyQvia is a 10% solution prepared from large pools of human plasma consisting of at least 98% IgG. The recombinant human hyaluronidase increases the dispersion and absorption of the immune globulin.
In a phase 3 trial, HyQvia compared well with intravenous human immune globulin 10% (IVIG).
Researchers compared the treatments at different time periods in a cohort of PI patients with a median age of 35 (range, 4-78 years). All 87 patients studied received IVIG, and 83 of the patients received at least 1 dose of HyQvia.
Patients received HyQvia for a median of 366 days and IVIG for a median of 91 days. The median ratio (HyQvia:IVIG) for the IgG dosage administered was 1.088 (range, 0.986–1.382).
Trough IgG concentrations, the incidence of infection, and rates of adverse events were generally similar during the HyQvia treatment period and the IVIG treatment period.
For patients aged 12 years and older, the median IgG Ctrough values with HyQvia were approximately the same as with IVIG. The median trough ratio (HyQvia:IVIG) was 0.985.
For patients younger than 12 (n=11), the median IgG Ctrough values were 10.0 and 9.6 g/L after HyQvia and IVIG, respectively, with a median trough ratio of 1.038.
The overall infection rates were 2.97 per patient-year with HyQvia and 4.51 per patient-year with IVIG.
During the HyQvia treatment period, the rate of acute serious bacterial infection (SBI) was 0.025 per patient-year. The rate of acute SBIs occurring during IVIG treatment was not reported.
In patients age 18 and older (n=59), the rate of acute SBIs was 0.00 per patient-year, and the overall infection rate was 3.20 per patient-year.
For this same patient group, the local adverse reaction rate was 0.286 per infusion.
The rate of systemic adverse events temporally related to an infusion was 0.20 per infusion with HyQvia and 0.33 per infusion with IVIG. There were no serious adverse events reported in these patients with either treatment.
HyQvia was approved in Europe in 2013 for adults with PI syndromes and myeloma or chronic lymphocytic leukemia with severe secondary hypogammaglobulinemia and recurrent infections.
For more details on HyQvia, see the prescribing information.
Test allows for rapid diagnosis of anemia

Credit: Gary Meek
A simple device could provide more rapid diagnosis of anemia and allow for inexpensive at-home monitoring, according to a paper published in The Journal of Clinical Investigation.
The disposable device analyzes a single droplet of blood using a chemical reagent that produces visible color changes corresponding to different levels of anemia.
The test produces results in about 60 seconds, and a smartphone application can correlate the visual results to specific hemoglobin levels.
“Our goal is to get this device into patients’ hands so they can diagnose and monitor anemia themselves,” said Wilbur Lam, MD, PhD, of the Georgia Institute of Technology and Emory University in Atlanta.
“Patients could use this device in a way that’s very similar to how diabetics use glucose-monitoring devices, but this will be even simpler because this is a visual-based test that doesn’t require an additional electrical device to analyze the results.”
The device was developed through a collaboration between Emory University, Children’s Healthcare of Atlanta, and Georgia Tech. It grew out of a 2011 undergraduate senior design project in the Wallace H. Coulter Department of Biomedical Engineering at Georgia Tech and Emory University.
Using a 2-piece prototype device, the test works this way: A patient sticks a finger with a lance to produce a droplet of blood. The device’s cap, a small vial, is touched to the droplet, drawing in a precise amount of blood using capillary action.
The cap containing the blood sample is then placed onto the body of the clear plastic test kit, which contains the chemical reagent. After the cap is closed, the device is briefly shaken to mix the blood and reagent.
“When the capillary is filled, we have a very precise volume of blood, about 5 microliters, which is less than a droplet—much less than what is required by other anemia tests,” explained Erika Tyburski, the paper’s first author and leader of the team that developed the device.
Hemoglobin then serves as a catalyst for a reduction-oxidation reaction that takes place in the device. After about 45 seconds, the reaction is complete, and the user sees a color ranging from green-blue to red, indicating the degree of anemia.
A label on the device helps with interpretation of the color, or patients could use a smartphone app that automatically correlates the color to a specific hemoglobin level.
To evaluate sensitivity and specificity of the device, Tyburski studied blood taken from 238 pediatric and adult patients. Each blood sample was tested 4 times using the device, and the results were compared to reports provided by conventional hematology analyzers.
The results of the 1-minute test were consistent with those of the conventional analyses. The smartphone app produced the best results for measuring severe anemia.
“The test doesn’t require a skilled technician or a draw of venous blood, and you see the results immediately,” Dr Lam said. “We think this is an empowering system, both for the general public and for our patients.”
Tyburski and Dr Lam have teamed up with 2 other partners to launch a startup company called Sanguina to commercialize the test, which will be known as AnemoCheck™.
The test will require approval from the US Food and Drug Administration, but the researchers believe the device could be on pharmacy shelves sometime in 2016.
The team also plans to study how the test may be applied to sickle cell anemia and other diseases.
Credit: Gary Meek
A simple device could provide more rapid diagnosis of anemia and allow for inexpensive at-home monitoring, according to a paper published in The Journal of Clinical Investigation.
The disposable device analyzes a single droplet of blood using a chemical reagent that produces visible color changes corresponding to different levels of anemia.
The test produces results in about 60 seconds, and a smartphone application can correlate the visual results to specific hemoglobin levels.
“Our goal is to get this device into patients’ hands so they can diagnose and monitor anemia themselves,” said Wilbur Lam, MD, PhD, of the Georgia Institute of Technology and Emory University in Atlanta.
“Patients could use this device in a way that’s very similar to how diabetics use glucose-monitoring devices, but this will be even simpler because this is a visual-based test that doesn’t require an additional electrical device to analyze the results.”
The device was developed through a collaboration between Emory University, Children’s Healthcare of Atlanta, and Georgia Tech. It grew out of a 2011 undergraduate senior design project in the Wallace H. Coulter Department of Biomedical Engineering at Georgia Tech and Emory University.
Using a 2-piece prototype device, the test works this way: A patient sticks a finger with a lance to produce a droplet of blood. The device’s cap, a small vial, is touched to the droplet, drawing in a precise amount of blood using capillary action.
The cap containing the blood sample is then placed onto the body of the clear plastic test kit, which contains the chemical reagent. After the cap is closed, the device is briefly shaken to mix the blood and reagent.
“When the capillary is filled, we have a very precise volume of blood, about 5 microliters, which is less than a droplet—much less than what is required by other anemia tests,” explained Erika Tyburski, the paper’s first author and leader of the team that developed the device.
Hemoglobin then serves as a catalyst for a reduction-oxidation reaction that takes place in the device. After about 45 seconds, the reaction is complete, and the user sees a color ranging from green-blue to red, indicating the degree of anemia.
A label on the device helps with interpretation of the color, or patients could use a smartphone app that automatically correlates the color to a specific hemoglobin level.
To evaluate sensitivity and specificity of the device, Tyburski studied blood taken from 238 pediatric and adult patients. Each blood sample was tested 4 times using the device, and the results were compared to reports provided by conventional hematology analyzers.
The results of the 1-minute test were consistent with those of the conventional analyses. The smartphone app produced the best results for measuring severe anemia.
“The test doesn’t require a skilled technician or a draw of venous blood, and you see the results immediately,” Dr Lam said. “We think this is an empowering system, both for the general public and for our patients.”
Tyburski and Dr Lam have teamed up with 2 other partners to launch a startup company called Sanguina to commercialize the test, which will be known as AnemoCheck™.
The test will require approval from the US Food and Drug Administration, but the researchers believe the device could be on pharmacy shelves sometime in 2016.
The team also plans to study how the test may be applied to sickle cell anemia and other diseases.
Credit: Gary Meek
A simple device could provide more rapid diagnosis of anemia and allow for inexpensive at-home monitoring, according to a paper published in The Journal of Clinical Investigation.
The disposable device analyzes a single droplet of blood using a chemical reagent that produces visible color changes corresponding to different levels of anemia.
The test produces results in about 60 seconds, and a smartphone application can correlate the visual results to specific hemoglobin levels.
“Our goal is to get this device into patients’ hands so they can diagnose and monitor anemia themselves,” said Wilbur Lam, MD, PhD, of the Georgia Institute of Technology and Emory University in Atlanta.
“Patients could use this device in a way that’s very similar to how diabetics use glucose-monitoring devices, but this will be even simpler because this is a visual-based test that doesn’t require an additional electrical device to analyze the results.”
The device was developed through a collaboration between Emory University, Children’s Healthcare of Atlanta, and Georgia Tech. It grew out of a 2011 undergraduate senior design project in the Wallace H. Coulter Department of Biomedical Engineering at Georgia Tech and Emory University.
Using a 2-piece prototype device, the test works this way: A patient sticks a finger with a lance to produce a droplet of blood. The device’s cap, a small vial, is touched to the droplet, drawing in a precise amount of blood using capillary action.
The cap containing the blood sample is then placed onto the body of the clear plastic test kit, which contains the chemical reagent. After the cap is closed, the device is briefly shaken to mix the blood and reagent.
“When the capillary is filled, we have a very precise volume of blood, about 5 microliters, which is less than a droplet—much less than what is required by other anemia tests,” explained Erika Tyburski, the paper’s first author and leader of the team that developed the device.
Hemoglobin then serves as a catalyst for a reduction-oxidation reaction that takes place in the device. After about 45 seconds, the reaction is complete, and the user sees a color ranging from green-blue to red, indicating the degree of anemia.
A label on the device helps with interpretation of the color, or patients could use a smartphone app that automatically correlates the color to a specific hemoglobin level.
To evaluate sensitivity and specificity of the device, Tyburski studied blood taken from 238 pediatric and adult patients. Each blood sample was tested 4 times using the device, and the results were compared to reports provided by conventional hematology analyzers.
The results of the 1-minute test were consistent with those of the conventional analyses. The smartphone app produced the best results for measuring severe anemia.
“The test doesn’t require a skilled technician or a draw of venous blood, and you see the results immediately,” Dr Lam said. “We think this is an empowering system, both for the general public and for our patients.”
Tyburski and Dr Lam have teamed up with 2 other partners to launch a startup company called Sanguina to commercialize the test, which will be known as AnemoCheck™.
The test will require approval from the US Food and Drug Administration, but the researchers believe the device could be on pharmacy shelves sometime in 2016.
The team also plans to study how the test may be applied to sickle cell anemia and other diseases.
Heparin lot recalled due to particulate

Hospira Inc. has initiated a US-wide recall of 1 lot of heparin sodium, following a customer report of particulate in a single unit.
The recall affects lot 41-046-JT of 1000 USP Heparin Units/500 mL (2 USP Heparin Units/mL), in 0.9% Sodium Chloride Injection, 500 mL (NDC 0409-7620-03; expiration date November 1, 2015).
The foreign particle found in a unit from this lot was a human hair sealed between the tube and the film at the round seal of the unused administrative port on the non-print side of the container.
To date, Hospira has not received reports of any adverse events associated with this issue. The root cause has not been determined and is under investigation.
Heparin sodium injection is indicated as an anticoagulant to maintain catheter patency. In the event that a particulate breaks and pieces are able to pass through the intravenous catheter, injected particulate material may result in local inflammation, phlebitis, and/or low-level allergic response.
Capillaries may become occluded. Patients with a pre-existing condition of trauma or another medical condition that adversely affects the microvascular blood supply are at an increased risk.
The lot of heparin affected by this recall was distributed nationwide between June 2014 and August 2014 to wholesalers/distributors, hospitals, and pharmacies.
Anyone with existing inventory should stop use and distribution and quarantine the product immediately. Customers should also inform potential users of this product about the recall.
Hospira will be notifying its direct distributors/customers via a recall letter and will arrange for the impacted product to be returned to Stericycle. For additional assistance, call Stericycle at 1-855-201-4337 between the hours of 8 am and 5pm ET, Monday through Friday.
For clinical inquiries, contact Hospira. To report adverse events or product complaints, call 1-800-441-4100 (8 am to 5 pm CT, Monday through Friday) or email ProductComplaintsPP@hospira.com.
For medical inquiries, call 1-800-615-0187 (available 24 hours a day, 7 days per week) or email medcom@hospira.com.
Adverse reactions or quality problems associated with this product can be reported to the US Food and Drug Administration’s MedWatch Adverse Event Reporting Program.
Hospira Inc. has initiated a US-wide recall of 1 lot of heparin sodium, following a customer report of particulate in a single unit.
The recall affects lot 41-046-JT of 1000 USP Heparin Units/500 mL (2 USP Heparin Units/mL), in 0.9% Sodium Chloride Injection, 500 mL (NDC 0409-7620-03; expiration date November 1, 2015).
The foreign particle found in a unit from this lot was a human hair sealed between the tube and the film at the round seal of the unused administrative port on the non-print side of the container.
To date, Hospira has not received reports of any adverse events associated with this issue. The root cause has not been determined and is under investigation.
Heparin sodium injection is indicated as an anticoagulant to maintain catheter patency. In the event that a particulate breaks and pieces are able to pass through the intravenous catheter, injected particulate material may result in local inflammation, phlebitis, and/or low-level allergic response.
Capillaries may become occluded. Patients with a pre-existing condition of trauma or another medical condition that adversely affects the microvascular blood supply are at an increased risk.
The lot of heparin affected by this recall was distributed nationwide between June 2014 and August 2014 to wholesalers/distributors, hospitals, and pharmacies.
Anyone with existing inventory should stop use and distribution and quarantine the product immediately. Customers should also inform potential users of this product about the recall.
Hospira will be notifying its direct distributors/customers via a recall letter and will arrange for the impacted product to be returned to Stericycle. For additional assistance, call Stericycle at 1-855-201-4337 between the hours of 8 am and 5pm ET, Monday through Friday.
For clinical inquiries, contact Hospira. To report adverse events or product complaints, call 1-800-441-4100 (8 am to 5 pm CT, Monday through Friday) or email ProductComplaintsPP@hospira.com.
For medical inquiries, call 1-800-615-0187 (available 24 hours a day, 7 days per week) or email medcom@hospira.com.
Adverse reactions or quality problems associated with this product can be reported to the US Food and Drug Administration’s MedWatch Adverse Event Reporting Program.
Hospira Inc. has initiated a US-wide recall of 1 lot of heparin sodium, following a customer report of particulate in a single unit.
The recall affects lot 41-046-JT of 1000 USP Heparin Units/500 mL (2 USP Heparin Units/mL), in 0.9% Sodium Chloride Injection, 500 mL (NDC 0409-7620-03; expiration date November 1, 2015).
The foreign particle found in a unit from this lot was a human hair sealed between the tube and the film at the round seal of the unused administrative port on the non-print side of the container.
To date, Hospira has not received reports of any adverse events associated with this issue. The root cause has not been determined and is under investigation.
Heparin sodium injection is indicated as an anticoagulant to maintain catheter patency. In the event that a particulate breaks and pieces are able to pass through the intravenous catheter, injected particulate material may result in local inflammation, phlebitis, and/or low-level allergic response.
Capillaries may become occluded. Patients with a pre-existing condition of trauma or another medical condition that adversely affects the microvascular blood supply are at an increased risk.
The lot of heparin affected by this recall was distributed nationwide between June 2014 and August 2014 to wholesalers/distributors, hospitals, and pharmacies.
Anyone with existing inventory should stop use and distribution and quarantine the product immediately. Customers should also inform potential users of this product about the recall.
Hospira will be notifying its direct distributors/customers via a recall letter and will arrange for the impacted product to be returned to Stericycle. For additional assistance, call Stericycle at 1-855-201-4337 between the hours of 8 am and 5pm ET, Monday through Friday.
For clinical inquiries, contact Hospira. To report adverse events or product complaints, call 1-800-441-4100 (8 am to 5 pm CT, Monday through Friday) or email ProductComplaintsPP@hospira.com.
For medical inquiries, call 1-800-615-0187 (available 24 hours a day, 7 days per week) or email medcom@hospira.com.
Adverse reactions or quality problems associated with this product can be reported to the US Food and Drug Administration’s MedWatch Adverse Event Reporting Program.