User login
Sharon Worcester is an award-winning medical journalist for MDedge News. She has been with the company since 1996, first as the Southeast Bureau Chief (1996-2009) when the company was known as International Medical News Group, then as a freelance writer (2010-2015) before returning as a reporter in 2015. She previously worked as a daily newspaper reporter covering health and local government. Sharon currently reports primarily on oncology and hematology. She has a BA from Eckerd College and an MA in Mass Communication/Print Journalism from the University of Florida. Connect with her via LinkedIn and follow her on twitter @SW_MedReporter.
Several factors predict postbariatric surgery readmission
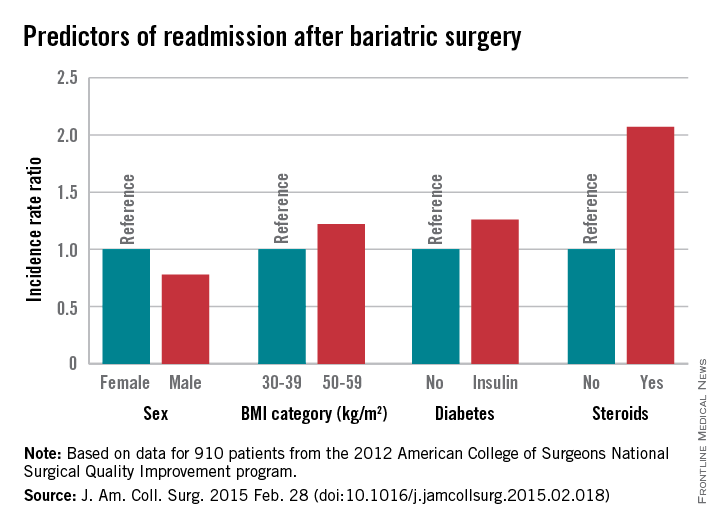
Bariatric surgery is generally safe and readmissions are rare, but prolonged operative time, operation complexity, and major postoperative complications are among several risk factors for readmission identified in a large retrospective cohort.
Of 18,186 patients from the 2012 American College of Surgeons National Surgical Quality Improvement program (ACS NSQIP) database who had bariatric surgery as a primary procedure, 5% were readmitted. Of 815 patients with any major complication, 31% were readmitted. Factors found on multivariate analysis to significantly predict readmission within 30 days were age, sex, body mass index, American Society of Anesthesiology (ASA) risk class, diabetes status, hypertension, and steroid use, Dr. Christa R. Abraham of Albany (N.Y.) Medical College and her colleagues reported online in the Journal of the American College of Surgeons.

Further, all major postoperative complications were significant predictors of readmission, including bleeding requiring transfusion, urinary tract infections, and superficial surgical site infection (SSI). Other significant predictors were deep SSI, organ space SSI, wound disruption, pneumonia, unplanned intubation, mechanical ventilation for more than 48 hours, pulmonary embolism, deep vein thrombosis, and sepsis, the investigators said (J. Am. Coll. Surg. 2015 [doi:10.1016/j.jamcollsurg.2015.02.018]).
Of the patients included in the study, 1,819 had a laparoscopic gastric band, 9,613 had laparoscopic Roux-en-Y gastric bypass, 6,439 had gastroplasties, and 315 had open Roux-en-Y gastric bypass. All had a BMI of at least 30 kg/m2, and had a postsurgery length of stay of 14 days or fewer. Most were ASA risk class 3 or lower, and most were functionally independent.
Complications were more common with laparoscopic and open Roux-en-y gastric bypass (5.5% and 11.8%, respectively) rather than with gastroplasty and sleeve (3.4%) and laparoscopic banding (1.4%).
The findings are of value, because while bariatric surgery is a low-risk procedure, and it is extremely common; in 2013 there were 179,000 such surgeries performed in the United States.
“Bariatric surgery is one of the fastest-growing surgical interest areas, making analysis of patient outcomes and reasons for readmission important,” the investigators explained.
The ability to identify high-risk patients could allow for targeted interventions to prevent readmission, they said.
For example, steroid use, which was identified as a risk factor in the current study, is modifiable.
“In our practice, steroids are discontinued for 6 weeks prior to bariatric surgery and patients who are steroid dependent are unlikely to undergo bariatric surgery,” they said.
Additionally, they “try to minimize readmission for patients with infections by treating with antibiotics following operation and continuing antibiotics at discharge.”
The investigators noted that the ACS NSQIP MORBPROB (estimated probability of morbidity) tool is a good tool for predicting readmission among prospective bariatric patients, although it may not fully capture the effect of preexisting conditions.
“These data led us to change our own practice by risk-stratifying patients with higher ASA and BMI to consider surgical options, and to begin early surveillance soon after discharge,” they said.
The authors reported having no disclosures.
Bariatric surgery is generally safe and readmissions are rare, but prolonged operative time, operation complexity, and major postoperative complications are among several risk factors for readmission identified in a large retrospective cohort.
Of 18,186 patients from the 2012 American College of Surgeons National Surgical Quality Improvement program (ACS NSQIP) database who had bariatric surgery as a primary procedure, 5% were readmitted. Of 815 patients with any major complication, 31% were readmitted. Factors found on multivariate analysis to significantly predict readmission within 30 days were age, sex, body mass index, American Society of Anesthesiology (ASA) risk class, diabetes status, hypertension, and steroid use, Dr. Christa R. Abraham of Albany (N.Y.) Medical College and her colleagues reported online in the Journal of the American College of Surgeons.
Further, all major postoperative complications were significant predictors of readmission, including bleeding requiring transfusion, urinary tract infections, and superficial surgical site infection (SSI). Other significant predictors were deep SSI, organ space SSI, wound disruption, pneumonia, unplanned intubation, mechanical ventilation for more than 48 hours, pulmonary embolism, deep vein thrombosis, and sepsis, the investigators said (J. Am. Coll. Surg. 2015 [doi:10.1016/j.jamcollsurg.2015.02.018]).
Of the patients included in the study, 1,819 had a laparoscopic gastric band, 9,613 had laparoscopic Roux-en-Y gastric bypass, 6,439 had gastroplasties, and 315 had open Roux-en-Y gastric bypass. All had a BMI of at least 30 kg/m2, and had a postsurgery length of stay of 14 days or fewer. Most were ASA risk class 3 or lower, and most were functionally independent.
Complications were more common with laparoscopic and open Roux-en-y gastric bypass (5.5% and 11.8%, respectively) rather than with gastroplasty and sleeve (3.4%) and laparoscopic banding (1.4%).
The findings are of value, because while bariatric surgery is a low-risk procedure, and it is extremely common; in 2013 there were 179,000 such surgeries performed in the United States.
“Bariatric surgery is one of the fastest-growing surgical interest areas, making analysis of patient outcomes and reasons for readmission important,” the investigators explained.
The ability to identify high-risk patients could allow for targeted interventions to prevent readmission, they said.
For example, steroid use, which was identified as a risk factor in the current study, is modifiable.
“In our practice, steroids are discontinued for 6 weeks prior to bariatric surgery and patients who are steroid dependent are unlikely to undergo bariatric surgery,” they said.
Additionally, they “try to minimize readmission for patients with infections by treating with antibiotics following operation and continuing antibiotics at discharge.”
The investigators noted that the ACS NSQIP MORBPROB (estimated probability of morbidity) tool is a good tool for predicting readmission among prospective bariatric patients, although it may not fully capture the effect of preexisting conditions.
“These data led us to change our own practice by risk-stratifying patients with higher ASA and BMI to consider surgical options, and to begin early surveillance soon after discharge,” they said.
The authors reported having no disclosures.
Bariatric surgery is generally safe and readmissions are rare, but prolonged operative time, operation complexity, and major postoperative complications are among several risk factors for readmission identified in a large retrospective cohort.
Of 18,186 patients from the 2012 American College of Surgeons National Surgical Quality Improvement program (ACS NSQIP) database who had bariatric surgery as a primary procedure, 5% were readmitted. Of 815 patients with any major complication, 31% were readmitted. Factors found on multivariate analysis to significantly predict readmission within 30 days were age, sex, body mass index, American Society of Anesthesiology (ASA) risk class, diabetes status, hypertension, and steroid use, Dr. Christa R. Abraham of Albany (N.Y.) Medical College and her colleagues reported online in the Journal of the American College of Surgeons.
Further, all major postoperative complications were significant predictors of readmission, including bleeding requiring transfusion, urinary tract infections, and superficial surgical site infection (SSI). Other significant predictors were deep SSI, organ space SSI, wound disruption, pneumonia, unplanned intubation, mechanical ventilation for more than 48 hours, pulmonary embolism, deep vein thrombosis, and sepsis, the investigators said (J. Am. Coll. Surg. 2015 [doi:10.1016/j.jamcollsurg.2015.02.018]).
Of the patients included in the study, 1,819 had a laparoscopic gastric band, 9,613 had laparoscopic Roux-en-Y gastric bypass, 6,439 had gastroplasties, and 315 had open Roux-en-Y gastric bypass. All had a BMI of at least 30 kg/m2, and had a postsurgery length of stay of 14 days or fewer. Most were ASA risk class 3 or lower, and most were functionally independent.
Complications were more common with laparoscopic and open Roux-en-y gastric bypass (5.5% and 11.8%, respectively) rather than with gastroplasty and sleeve (3.4%) and laparoscopic banding (1.4%).
The findings are of value, because while bariatric surgery is a low-risk procedure, and it is extremely common; in 2013 there were 179,000 such surgeries performed in the United States.
“Bariatric surgery is one of the fastest-growing surgical interest areas, making analysis of patient outcomes and reasons for readmission important,” the investigators explained.
The ability to identify high-risk patients could allow for targeted interventions to prevent readmission, they said.
For example, steroid use, which was identified as a risk factor in the current study, is modifiable.
“In our practice, steroids are discontinued for 6 weeks prior to bariatric surgery and patients who are steroid dependent are unlikely to undergo bariatric surgery,” they said.
Additionally, they “try to minimize readmission for patients with infections by treating with antibiotics following operation and continuing antibiotics at discharge.”
The investigators noted that the ACS NSQIP MORBPROB (estimated probability of morbidity) tool is a good tool for predicting readmission among prospective bariatric patients, although it may not fully capture the effect of preexisting conditions.
“These data led us to change our own practice by risk-stratifying patients with higher ASA and BMI to consider surgical options, and to begin early surveillance soon after discharge,” they said.
The authors reported having no disclosures.
FROM THE JOURNAL OF THE AMERICAN COLLEGE OF SURGEONS
Key clinical point: Knowing risk factors for readmission after bariatric surgery can allow for targeted interventions.
Major finding: Steroid use is among several risk factors for readmission following bariatric surgery (incidence rate ratio, 2.07)
Data source: A retrospective cohort study involving 18,186 patients.
Disclosures: The authors reported having no disclosures.

Household contamination may promote recurrent MRSA skin infections
MIAMI BEACH – Patients with recurrent methicillin-resistant Staphylococcus aureus skin infections should be advised to address their environment, according to Dr. Theodore Rosen.
Toilets, telephones, hairbrushes, and bathroom sink and door handles are particular culprits in harboring MRSA, Dr. Rosen, professor of dermatology at Baylor College of Medicine, Houston, said at the South Beach Symposium.

That was the finding of a recent prospective longitudinal study looking at households in Los Angeles and Chicago with at least one index case of S. aureus skin infection, he said.
Samantha J. Eells of the Los Angeles Biomedical Research Center at Harbor-UCLA Medical Center, Torrance, Calif., and her colleagues enrolled 346 households of adults and children with such infections. Household fomites were surveyed for contamination at baseline and 3 months, and all isolates underwent genetic typing.
Nearly half (49%) of households were contaminated with S. aureus at baseline, and 51% of the 304 that completed follow-up were contaminated at 3 months. Of those with a USA300 MRSA body infection isolate, 58% and 63% had environmental contamination with an indistinguishable MRSA strain at baseline and at 3 months, respectively, the investigators found (Infect. Control. Hosp. Epidemiol. 2014;35:1373-82).
Numerous environmental locations were contaminated up to 3 months after the index case, but among the most common locations with MRSA contamination, with 7%-8% affected among the study households, were toilets, landline phones, index subjects’ hairbrushes, and bathroom sink and door handles. Other areas with contamination detected were children’s toys, television remote controls, kitchen counters, and kitchen sink handles.
“We found that an index subject’s infection isolate frequently persisted for at least 3 months, suggesting that it potentially serves as a reservoir that places all household members at risk for future S. aureus infections. While multiple S. aureus strain types were recovered from some households, the index subject’s infection strain persisted in more than 50% of households after 3 months,” the investigators wrote.
The findings, in the context of the high prevalence of body colonization found in the community-based population, suggests that successful outpatient decolonization may require not only eradication of nasal, skin, and oropharyngeal colonization, but also of environmental contamination, they said.
So not only can patients get MRSA from family members, sex partners, dogs and cats, and raw food sold in grocery stores, as shown in prior studies, they can also get it from the household environment, Dr. Rosen said.
“If you’re doing everything else [to eradicate colonization], you need to make sure someone who is having recurring MRSA outbreaks basically cleans up their environment,” he said.
Dr. Rosen reported having no disclosures.
MIAMI BEACH – Patients with recurrent methicillin-resistant Staphylococcus aureus skin infections should be advised to address their environment, according to Dr. Theodore Rosen.
Toilets, telephones, hairbrushes, and bathroom sink and door handles are particular culprits in harboring MRSA, Dr. Rosen, professor of dermatology at Baylor College of Medicine, Houston, said at the South Beach Symposium.
That was the finding of a recent prospective longitudinal study looking at households in Los Angeles and Chicago with at least one index case of S. aureus skin infection, he said.
Samantha J. Eells of the Los Angeles Biomedical Research Center at Harbor-UCLA Medical Center, Torrance, Calif., and her colleagues enrolled 346 households of adults and children with such infections. Household fomites were surveyed for contamination at baseline and 3 months, and all isolates underwent genetic typing.
Nearly half (49%) of households were contaminated with S. aureus at baseline, and 51% of the 304 that completed follow-up were contaminated at 3 months. Of those with a USA300 MRSA body infection isolate, 58% and 63% had environmental contamination with an indistinguishable MRSA strain at baseline and at 3 months, respectively, the investigators found (Infect. Control. Hosp. Epidemiol. 2014;35:1373-82).
Numerous environmental locations were contaminated up to 3 months after the index case, but among the most common locations with MRSA contamination, with 7%-8% affected among the study households, were toilets, landline phones, index subjects’ hairbrushes, and bathroom sink and door handles. Other areas with contamination detected were children’s toys, television remote controls, kitchen counters, and kitchen sink handles.
“We found that an index subject’s infection isolate frequently persisted for at least 3 months, suggesting that it potentially serves as a reservoir that places all household members at risk for future S. aureus infections. While multiple S. aureus strain types were recovered from some households, the index subject’s infection strain persisted in more than 50% of households after 3 months,” the investigators wrote.
The findings, in the context of the high prevalence of body colonization found in the community-based population, suggests that successful outpatient decolonization may require not only eradication of nasal, skin, and oropharyngeal colonization, but also of environmental contamination, they said.
So not only can patients get MRSA from family members, sex partners, dogs and cats, and raw food sold in grocery stores, as shown in prior studies, they can also get it from the household environment, Dr. Rosen said.
“If you’re doing everything else [to eradicate colonization], you need to make sure someone who is having recurring MRSA outbreaks basically cleans up their environment,” he said.
Dr. Rosen reported having no disclosures.
MIAMI BEACH – Patients with recurrent methicillin-resistant Staphylococcus aureus skin infections should be advised to address their environment, according to Dr. Theodore Rosen.
Toilets, telephones, hairbrushes, and bathroom sink and door handles are particular culprits in harboring MRSA, Dr. Rosen, professor of dermatology at Baylor College of Medicine, Houston, said at the South Beach Symposium.
That was the finding of a recent prospective longitudinal study looking at households in Los Angeles and Chicago with at least one index case of S. aureus skin infection, he said.
Samantha J. Eells of the Los Angeles Biomedical Research Center at Harbor-UCLA Medical Center, Torrance, Calif., and her colleagues enrolled 346 households of adults and children with such infections. Household fomites were surveyed for contamination at baseline and 3 months, and all isolates underwent genetic typing.
Nearly half (49%) of households were contaminated with S. aureus at baseline, and 51% of the 304 that completed follow-up were contaminated at 3 months. Of those with a USA300 MRSA body infection isolate, 58% and 63% had environmental contamination with an indistinguishable MRSA strain at baseline and at 3 months, respectively, the investigators found (Infect. Control. Hosp. Epidemiol. 2014;35:1373-82).
Numerous environmental locations were contaminated up to 3 months after the index case, but among the most common locations with MRSA contamination, with 7%-8% affected among the study households, were toilets, landline phones, index subjects’ hairbrushes, and bathroom sink and door handles. Other areas with contamination detected were children’s toys, television remote controls, kitchen counters, and kitchen sink handles.
“We found that an index subject’s infection isolate frequently persisted for at least 3 months, suggesting that it potentially serves as a reservoir that places all household members at risk for future S. aureus infections. While multiple S. aureus strain types were recovered from some households, the index subject’s infection strain persisted in more than 50% of households after 3 months,” the investigators wrote.
The findings, in the context of the high prevalence of body colonization found in the community-based population, suggests that successful outpatient decolonization may require not only eradication of nasal, skin, and oropharyngeal colonization, but also of environmental contamination, they said.
So not only can patients get MRSA from family members, sex partners, dogs and cats, and raw food sold in grocery stores, as shown in prior studies, they can also get it from the household environment, Dr. Rosen said.
“If you’re doing everything else [to eradicate colonization], you need to make sure someone who is having recurring MRSA outbreaks basically cleans up their environment,” he said.
Dr. Rosen reported having no disclosures.

Newer antifungals shorten tinea pedis treatment duration, promote adherence
MIAMI BEACH – Two new antifungal agents on the market – luliconazole and naftifine – each have something unique to offer when it comes to treating tinea pedis, according to Dr. Boni E. Elewski.
Luliconazole is an azole drug, meaning it is broad spectrum and kills dermatophytes, yeast, and molds. Also, like all azoles, it has some antibacterial activity, she said at the South Beach Symposium.
Naftifine is an allylamine drug, and is mainly an antidermatophyte agent – albeit a “very, very potent antidermatophyte” – with no antibacterial activity, she said.
Both are approved for once-daily use for 2 weeks, and that’s good because the short treatment duration improves adherence to the regimen, especially compared with other drugs that require 4-6 weeks of treatment to eradicate the problem, noted Dr. Elewski, professor of dermatology and director of clinical trials research at the University of Alabama at Birmingham.
Both drugs also stay in the skin and continue working after treatment stops.
Making the choice regarding which drug or class of drugs to use depends on the patient’s symptoms.
“First of all, tinea pedis may not be obvious. People don’t often tell you, ‘This is what I have – it’s tinea pedis,’ ” she said.
Keep in mind that tinea pedis and onychomycosis are related. If you have a patient who you think has onychomycosis, look at the bottom of their foot, she advised.
“If they don’t have tinea pedis, they probably don’t have onychomycosis unless they’ve had tinea pedis recently and got rid of it,” she said.
Also, look for collarettes of scale, which may be very subtle and may look like “tiny little circular pieces of scale on the medial or lateral foot.”
“If you are not sure, just keep looking harder because you might see it,” Dr. Elewski said.
Interdigital tinea pedis will be a little more obvious, with scaling and crusting between the toes, as well as maceration and oozing in many cases.
When the toe web is oozing, you’re likely dealing with intertrigo, she said.
In such cases, an azole cream is the better treatment choice, because azoles will kill Candida, bacteria, and dermatophytes that are there, she said.
“So when I have a moist macerated space, I like an azole. If you have a dry scaly process – with or without the collarettes – you’re probably better with an allylamine, particularly if you use a keratolytic with it, something that has urea or a lactic acid,” she said.
Dr. Elewski is a consultant for Valeant Pharmaceuticals International and a contracted researcher for Anacor Pharmaceuticals.
MIAMI BEACH – Two new antifungal agents on the market – luliconazole and naftifine – each have something unique to offer when it comes to treating tinea pedis, according to Dr. Boni E. Elewski.
Luliconazole is an azole drug, meaning it is broad spectrum and kills dermatophytes, yeast, and molds. Also, like all azoles, it has some antibacterial activity, she said at the South Beach Symposium.
Naftifine is an allylamine drug, and is mainly an antidermatophyte agent – albeit a “very, very potent antidermatophyte” – with no antibacterial activity, she said.
Both are approved for once-daily use for 2 weeks, and that’s good because the short treatment duration improves adherence to the regimen, especially compared with other drugs that require 4-6 weeks of treatment to eradicate the problem, noted Dr. Elewski, professor of dermatology and director of clinical trials research at the University of Alabama at Birmingham.
Both drugs also stay in the skin and continue working after treatment stops.
Making the choice regarding which drug or class of drugs to use depends on the patient’s symptoms.
“First of all, tinea pedis may not be obvious. People don’t often tell you, ‘This is what I have – it’s tinea pedis,’ ” she said.
Keep in mind that tinea pedis and onychomycosis are related. If you have a patient who you think has onychomycosis, look at the bottom of their foot, she advised.
“If they don’t have tinea pedis, they probably don’t have onychomycosis unless they’ve had tinea pedis recently and got rid of it,” she said.
Also, look for collarettes of scale, which may be very subtle and may look like “tiny little circular pieces of scale on the medial or lateral foot.”
“If you are not sure, just keep looking harder because you might see it,” Dr. Elewski said.
Interdigital tinea pedis will be a little more obvious, with scaling and crusting between the toes, as well as maceration and oozing in many cases.
When the toe web is oozing, you’re likely dealing with intertrigo, she said.
In such cases, an azole cream is the better treatment choice, because azoles will kill Candida, bacteria, and dermatophytes that are there, she said.
“So when I have a moist macerated space, I like an azole. If you have a dry scaly process – with or without the collarettes – you’re probably better with an allylamine, particularly if you use a keratolytic with it, something that has urea or a lactic acid,” she said.
Dr. Elewski is a consultant for Valeant Pharmaceuticals International and a contracted researcher for Anacor Pharmaceuticals.
MIAMI BEACH – Two new antifungal agents on the market – luliconazole and naftifine – each have something unique to offer when it comes to treating tinea pedis, according to Dr. Boni E. Elewski.
Luliconazole is an azole drug, meaning it is broad spectrum and kills dermatophytes, yeast, and molds. Also, like all azoles, it has some antibacterial activity, she said at the South Beach Symposium.
Naftifine is an allylamine drug, and is mainly an antidermatophyte agent – albeit a “very, very potent antidermatophyte” – with no antibacterial activity, she said.
Both are approved for once-daily use for 2 weeks, and that’s good because the short treatment duration improves adherence to the regimen, especially compared with other drugs that require 4-6 weeks of treatment to eradicate the problem, noted Dr. Elewski, professor of dermatology and director of clinical trials research at the University of Alabama at Birmingham.
Both drugs also stay in the skin and continue working after treatment stops.
Making the choice regarding which drug or class of drugs to use depends on the patient’s symptoms.
“First of all, tinea pedis may not be obvious. People don’t often tell you, ‘This is what I have – it’s tinea pedis,’ ” she said.
Keep in mind that tinea pedis and onychomycosis are related. If you have a patient who you think has onychomycosis, look at the bottom of their foot, she advised.
“If they don’t have tinea pedis, they probably don’t have onychomycosis unless they’ve had tinea pedis recently and got rid of it,” she said.
Also, look for collarettes of scale, which may be very subtle and may look like “tiny little circular pieces of scale on the medial or lateral foot.”
“If you are not sure, just keep looking harder because you might see it,” Dr. Elewski said.
Interdigital tinea pedis will be a little more obvious, with scaling and crusting between the toes, as well as maceration and oozing in many cases.
When the toe web is oozing, you’re likely dealing with intertrigo, she said.
In such cases, an azole cream is the better treatment choice, because azoles will kill Candida, bacteria, and dermatophytes that are there, she said.
“So when I have a moist macerated space, I like an azole. If you have a dry scaly process – with or without the collarettes – you’re probably better with an allylamine, particularly if you use a keratolytic with it, something that has urea or a lactic acid,” she said.
Dr. Elewski is a consultant for Valeant Pharmaceuticals International and a contracted researcher for Anacor Pharmaceuticals.
AT THE SOUTH BEACH SYMPOSIUM
Behavioral economics may be the key to improving health-related behaviors
The usual approach to improving health-related behaviors involves education and, in some cases, financial incentives; a better approach involves using “behavioral economics” to help patients identify and overcome psychological barriers to behavioral change, according to Dr. David Asch.
During his keynote presentation titled “Using Behavioral Economics to Improve Individual and Population Health” on Thursday morning at the 2015 AGA Technology Summit, Dr. Asch will describe the concept of behavioral economics and discuss ongoing research demonstrating its value in the health care setting.
“In health care, so many of the outcomes that people achieve are highly determined by their own behaviors,” Dr. Asch, an internist at the University of Pennsylvania, Philadelphia , said in an interview.
This is true regarding diet, exercise, and medication adherence, he added, naming just a few examples.
“Human behavior is really the final common pathway toward a lot of the outcomes we care about in health and health care, and until recently there hasn’t been a lot of insight into how to improve people’s health behavior and to advance their own goals,” he said.
One thing that’s known, however, is that being armed with the knowledge that a certain behavior will derail one’s efforts doesn’t necessarily prevent that behavior. A person may know that it’s safer to use a seat belt, but may avoid using one anyway. A dieter may know that piece of chocolate cake is fattening, but will eat it anyway.
That’s why education – though important – is not typically enough on its own to change behaviors, Dr. Asch said, explaining that the premise of the educational approach is that if you tell dieters that chocolate cake is fattening, they won’t eat it, and therefore they won’t get fat.
It’s clear what a weak argument that is, he said.
Similarly, economic incentives – paying patients to take their medication or quit smoking, or, conversely, charging penalties if they don’t – may have some benefit, but these incentives are expensive and off-putting, and their effectiveness is limited, he noted.
Behavioral economics, on the other hand, has much more to do with psychology than with economics, he said, adding that “the basic principle is that all of us are irrational. We do all sorts of things that are irrational, meaning they’re not consistent with our own best interests.”
The key insight of behavioral economics, however, isn’t that people are irrational – it is that they are irrational in highly predictable ways, Dr. Asch said, explaining that people tend to make the same types of mistakes as other people, which allows for the development of solutions with widespread applicability.
“We can harness these same errors that trip us up and use them to create interventions that improve our health,” he said.
At the summit, which is sponsored by the AGA’s Center for GI Innovation and Technology, Dr. Asch will share his recent research showing how health can be improved by “taking advantage of these psychological foibles.”
One study he will discuss is looking at how behavioral economics can promote medication adherence.
“We have a large study in the field right now for patients who have been discharged from the hospital following a heart attack,” he said explaining that such patients are typically discharged on three or four different types of medications, and despite the seriousness of the condition, adherence is only about 40%.
The study uses a multipronged approach that “game-ifies” medication adherence by monitoring pill use via special pill bottles with a computer chip in the cap. A daily lottery is conducted in which patients are randomly selected for monetary prizes if they have been adherent (the data are transmitted through a cell phone signal), resulting in a doubling of compliance rates, he said.
The approach incorporates powerful psychological forces such as regret, which patients will experience if their number is drawn in the lottery and they lose out on the money because of lack of medication adherence, for example. It also enlists the help of a volunteer support person – such as an adult child of the patient – who is notified if a patient misses 2 days of medication in a row. The latter “turns an unwitnessed event into a witnessed event,” providing further impetus for compliance, Dr. Asch said, explaining that no one wants a witness to their failure.
The study is ongoing, and while it remains to be seen whether the behavioral economics approach reduces admissions and proves cost effective, it’s clear that it works to promote adherence, he said.
“And that’s almost certainly a good thing,” he added.
The usual approach to improving health-related behaviors involves education and, in some cases, financial incentives; a better approach involves using “behavioral economics” to help patients identify and overcome psychological barriers to behavioral change, according to Dr. David Asch.
During his keynote presentation titled “Using Behavioral Economics to Improve Individual and Population Health” on Thursday morning at the 2015 AGA Technology Summit, Dr. Asch will describe the concept of behavioral economics and discuss ongoing research demonstrating its value in the health care setting.
“In health care, so many of the outcomes that people achieve are highly determined by their own behaviors,” Dr. Asch, an internist at the University of Pennsylvania, Philadelphia , said in an interview.
This is true regarding diet, exercise, and medication adherence, he added, naming just a few examples.
“Human behavior is really the final common pathway toward a lot of the outcomes we care about in health and health care, and until recently there hasn’t been a lot of insight into how to improve people’s health behavior and to advance their own goals,” he said.
One thing that’s known, however, is that being armed with the knowledge that a certain behavior will derail one’s efforts doesn’t necessarily prevent that behavior. A person may know that it’s safer to use a seat belt, but may avoid using one anyway. A dieter may know that piece of chocolate cake is fattening, but will eat it anyway.
That’s why education – though important – is not typically enough on its own to change behaviors, Dr. Asch said, explaining that the premise of the educational approach is that if you tell dieters that chocolate cake is fattening, they won’t eat it, and therefore they won’t get fat.
It’s clear what a weak argument that is, he said.
Similarly, economic incentives – paying patients to take their medication or quit smoking, or, conversely, charging penalties if they don’t – may have some benefit, but these incentives are expensive and off-putting, and their effectiveness is limited, he noted.
Behavioral economics, on the other hand, has much more to do with psychology than with economics, he said, adding that “the basic principle is that all of us are irrational. We do all sorts of things that are irrational, meaning they’re not consistent with our own best interests.”
The key insight of behavioral economics, however, isn’t that people are irrational – it is that they are irrational in highly predictable ways, Dr. Asch said, explaining that people tend to make the same types of mistakes as other people, which allows for the development of solutions with widespread applicability.
“We can harness these same errors that trip us up and use them to create interventions that improve our health,” he said.
At the summit, which is sponsored by the AGA’s Center for GI Innovation and Technology, Dr. Asch will share his recent research showing how health can be improved by “taking advantage of these psychological foibles.”
One study he will discuss is looking at how behavioral economics can promote medication adherence.
“We have a large study in the field right now for patients who have been discharged from the hospital following a heart attack,” he said explaining that such patients are typically discharged on three or four different types of medications, and despite the seriousness of the condition, adherence is only about 40%.
The study uses a multipronged approach that “game-ifies” medication adherence by monitoring pill use via special pill bottles with a computer chip in the cap. A daily lottery is conducted in which patients are randomly selected for monetary prizes if they have been adherent (the data are transmitted through a cell phone signal), resulting in a doubling of compliance rates, he said.
The approach incorporates powerful psychological forces such as regret, which patients will experience if their number is drawn in the lottery and they lose out on the money because of lack of medication adherence, for example. It also enlists the help of a volunteer support person – such as an adult child of the patient – who is notified if a patient misses 2 days of medication in a row. The latter “turns an unwitnessed event into a witnessed event,” providing further impetus for compliance, Dr. Asch said, explaining that no one wants a witness to their failure.
The study is ongoing, and while it remains to be seen whether the behavioral economics approach reduces admissions and proves cost effective, it’s clear that it works to promote adherence, he said.
“And that’s almost certainly a good thing,” he added.
The usual approach to improving health-related behaviors involves education and, in some cases, financial incentives; a better approach involves using “behavioral economics” to help patients identify and overcome psychological barriers to behavioral change, according to Dr. David Asch.
During his keynote presentation titled “Using Behavioral Economics to Improve Individual and Population Health” on Thursday morning at the 2015 AGA Technology Summit, Dr. Asch will describe the concept of behavioral economics and discuss ongoing research demonstrating its value in the health care setting.
“In health care, so many of the outcomes that people achieve are highly determined by their own behaviors,” Dr. Asch, an internist at the University of Pennsylvania, Philadelphia , said in an interview.
This is true regarding diet, exercise, and medication adherence, he added, naming just a few examples.
“Human behavior is really the final common pathway toward a lot of the outcomes we care about in health and health care, and until recently there hasn’t been a lot of insight into how to improve people’s health behavior and to advance their own goals,” he said.
One thing that’s known, however, is that being armed with the knowledge that a certain behavior will derail one’s efforts doesn’t necessarily prevent that behavior. A person may know that it’s safer to use a seat belt, but may avoid using one anyway. A dieter may know that piece of chocolate cake is fattening, but will eat it anyway.
That’s why education – though important – is not typically enough on its own to change behaviors, Dr. Asch said, explaining that the premise of the educational approach is that if you tell dieters that chocolate cake is fattening, they won’t eat it, and therefore they won’t get fat.
It’s clear what a weak argument that is, he said.
Similarly, economic incentives – paying patients to take their medication or quit smoking, or, conversely, charging penalties if they don’t – may have some benefit, but these incentives are expensive and off-putting, and their effectiveness is limited, he noted.
Behavioral economics, on the other hand, has much more to do with psychology than with economics, he said, adding that “the basic principle is that all of us are irrational. We do all sorts of things that are irrational, meaning they’re not consistent with our own best interests.”
The key insight of behavioral economics, however, isn’t that people are irrational – it is that they are irrational in highly predictable ways, Dr. Asch said, explaining that people tend to make the same types of mistakes as other people, which allows for the development of solutions with widespread applicability.
“We can harness these same errors that trip us up and use them to create interventions that improve our health,” he said.
At the summit, which is sponsored by the AGA’s Center for GI Innovation and Technology, Dr. Asch will share his recent research showing how health can be improved by “taking advantage of these psychological foibles.”
One study he will discuss is looking at how behavioral economics can promote medication adherence.
“We have a large study in the field right now for patients who have been discharged from the hospital following a heart attack,” he said explaining that such patients are typically discharged on three or four different types of medications, and despite the seriousness of the condition, adherence is only about 40%.
The study uses a multipronged approach that “game-ifies” medication adherence by monitoring pill use via special pill bottles with a computer chip in the cap. A daily lottery is conducted in which patients are randomly selected for monetary prizes if they have been adherent (the data are transmitted through a cell phone signal), resulting in a doubling of compliance rates, he said.
The approach incorporates powerful psychological forces such as regret, which patients will experience if their number is drawn in the lottery and they lose out on the money because of lack of medication adherence, for example. It also enlists the help of a volunteer support person – such as an adult child of the patient – who is notified if a patient misses 2 days of medication in a row. The latter “turns an unwitnessed event into a witnessed event,” providing further impetus for compliance, Dr. Asch said, explaining that no one wants a witness to their failure.
The study is ongoing, and while it remains to be seen whether the behavioral economics approach reduces admissions and proves cost effective, it’s clear that it works to promote adherence, he said.
“And that’s almost certainly a good thing,” he added.
ACS NSQIP data: Laparoscopic sleeve gastrectomy is at least as safe as gastric bypass
Laparoscopic sleeve gastrectomy is associated with lower rates of morbidity and similar mortality when compared with laparoscopic Roux-en-Y gastric bypass, according to an analysis of 2010-2011 data from the American College of Surgeons National Surgical Quality Improvement Program database.
Of 24,117 patients included in the analysis, 79.5% underwent laparoscopic Roux-en-Y gastric bypass (LGB), and 20.5% had laparoscopic sleeve gastrectomy (LSG). Of note, the proportion of LSG cases increased from 14.6% in 2010 to 24.8% in 2011, Dr. Monica T. Young of the University of California Irvine Medical Center, Orange, Calif., and her colleagues reported.

Those who underwent LGB had a significantly higher rate of 30-day risk-adjusted morbidity (odds ratio, 1.32). The 30-day mortality rate was 0.15% with bypass and 0.10% for sleeve gastrectomy, the investigators said (J. Am. Coll. Surg. 2015 [doi:
10.1016/j.jamcollsurg.2015.01.059]).
Further, sleeve gastrectomy was associated with shorter operative time (101 vs. 133 minutes) and with lower rates of blood loss requiring transfusion (0.65% vs. 1.5%), deep wound infections (0.06% vs. 0.20%), sepsis (0.34% vs. 0.58%), overall serious morbidity (3.8% vs. 5.8%), and reoperations within 30 days (1.6% vs. 2.5%).
The rate of deep venous thrombosis, however, was significantly higher with sleeve gastrectomy (0.47% vs. 0.21%). Deep vein thrombosis was the only complication found to be higher after LSG, they noted.
Older patients, those with a higher body mass index, and those who smoked or had hypertension were at significantly greater risk of serious morbidity.
Given the increasing popularity and use of sleeve gastrectomy as seen both in this study and nationally – with a reported increase in utilization from 0.9% in 2008 to 36.3% in 2012, it is important to compare outcomes with LSG with those for the preferred Roux-en-Y bypass surgery, the investigators said, noting that few large-scale studies have compared outcomes with the two procedures.
“Over the past decade, laparoscopic sleeve gastrectomy has emerged as a common utilized bariatric procedure. LSG has several advantages over LGB including preservation of endoscopic access to the upper gastrointestinal tract, avoidance of intestinal anastomosis, and prevention of dumping syndrome by pylorus preservation,” they wrote, adding that studies increasingly demonstrate its efficacy for weight loss.
The current findings support those of other recent studies, and a comparison of the data with those from 2007 to 2010 from the ACS NSQIP database showed that while reoperation rates after gastric bypass and sleeve gastrectomy have declined dramatically over time, readmission rates remain elevated.
“Therefore, it appears that further quality improvement initiatives are necessary to reduce the rate of readmissions after bariatric surgery,” the investigators wrote, noting that a national collaborative to reduce 30-day readmissions by 20% (the Metabolic and Bariatric Surgery Accreditation and Quality Improvement Program, or MBSAQIP) is currently enrolling.
Additional randomized controlled trials are also needed to evaluate differences in long-term outcomes between the two procedures, they concluded.
The authors reported having no relevant financial disclosures.
Laparoscopic sleeve gastrectomy is associated with lower rates of morbidity and similar mortality when compared with laparoscopic Roux-en-Y gastric bypass, according to an analysis of 2010-2011 data from the American College of Surgeons National Surgical Quality Improvement Program database.
Of 24,117 patients included in the analysis, 79.5% underwent laparoscopic Roux-en-Y gastric bypass (LGB), and 20.5% had laparoscopic sleeve gastrectomy (LSG). Of note, the proportion of LSG cases increased from 14.6% in 2010 to 24.8% in 2011, Dr. Monica T. Young of the University of California Irvine Medical Center, Orange, Calif., and her colleagues reported.
Those who underwent LGB had a significantly higher rate of 30-day risk-adjusted morbidity (odds ratio, 1.32). The 30-day mortality rate was 0.15% with bypass and 0.10% for sleeve gastrectomy, the investigators said (J. Am. Coll. Surg. 2015 [doi:
10.1016/j.jamcollsurg.2015.01.059]).
Further, sleeve gastrectomy was associated with shorter operative time (101 vs. 133 minutes) and with lower rates of blood loss requiring transfusion (0.65% vs. 1.5%), deep wound infections (0.06% vs. 0.20%), sepsis (0.34% vs. 0.58%), overall serious morbidity (3.8% vs. 5.8%), and reoperations within 30 days (1.6% vs. 2.5%).
The rate of deep venous thrombosis, however, was significantly higher with sleeve gastrectomy (0.47% vs. 0.21%). Deep vein thrombosis was the only complication found to be higher after LSG, they noted.
Older patients, those with a higher body mass index, and those who smoked or had hypertension were at significantly greater risk of serious morbidity.
Given the increasing popularity and use of sleeve gastrectomy as seen both in this study and nationally – with a reported increase in utilization from 0.9% in 2008 to 36.3% in 2012, it is important to compare outcomes with LSG with those for the preferred Roux-en-Y bypass surgery, the investigators said, noting that few large-scale studies have compared outcomes with the two procedures.
“Over the past decade, laparoscopic sleeve gastrectomy has emerged as a common utilized bariatric procedure. LSG has several advantages over LGB including preservation of endoscopic access to the upper gastrointestinal tract, avoidance of intestinal anastomosis, and prevention of dumping syndrome by pylorus preservation,” they wrote, adding that studies increasingly demonstrate its efficacy for weight loss.
The current findings support those of other recent studies, and a comparison of the data with those from 2007 to 2010 from the ACS NSQIP database showed that while reoperation rates after gastric bypass and sleeve gastrectomy have declined dramatically over time, readmission rates remain elevated.
“Therefore, it appears that further quality improvement initiatives are necessary to reduce the rate of readmissions after bariatric surgery,” the investigators wrote, noting that a national collaborative to reduce 30-day readmissions by 20% (the Metabolic and Bariatric Surgery Accreditation and Quality Improvement Program, or MBSAQIP) is currently enrolling.
Additional randomized controlled trials are also needed to evaluate differences in long-term outcomes between the two procedures, they concluded.
The authors reported having no relevant financial disclosures.
Laparoscopic sleeve gastrectomy is associated with lower rates of morbidity and similar mortality when compared with laparoscopic Roux-en-Y gastric bypass, according to an analysis of 2010-2011 data from the American College of Surgeons National Surgical Quality Improvement Program database.
Of 24,117 patients included in the analysis, 79.5% underwent laparoscopic Roux-en-Y gastric bypass (LGB), and 20.5% had laparoscopic sleeve gastrectomy (LSG). Of note, the proportion of LSG cases increased from 14.6% in 2010 to 24.8% in 2011, Dr. Monica T. Young of the University of California Irvine Medical Center, Orange, Calif., and her colleagues reported.
Those who underwent LGB had a significantly higher rate of 30-day risk-adjusted morbidity (odds ratio, 1.32). The 30-day mortality rate was 0.15% with bypass and 0.10% for sleeve gastrectomy, the investigators said (J. Am. Coll. Surg. 2015 [doi:
10.1016/j.jamcollsurg.2015.01.059]).
Further, sleeve gastrectomy was associated with shorter operative time (101 vs. 133 minutes) and with lower rates of blood loss requiring transfusion (0.65% vs. 1.5%), deep wound infections (0.06% vs. 0.20%), sepsis (0.34% vs. 0.58%), overall serious morbidity (3.8% vs. 5.8%), and reoperations within 30 days (1.6% vs. 2.5%).
The rate of deep venous thrombosis, however, was significantly higher with sleeve gastrectomy (0.47% vs. 0.21%). Deep vein thrombosis was the only complication found to be higher after LSG, they noted.
Older patients, those with a higher body mass index, and those who smoked or had hypertension were at significantly greater risk of serious morbidity.
Given the increasing popularity and use of sleeve gastrectomy as seen both in this study and nationally – with a reported increase in utilization from 0.9% in 2008 to 36.3% in 2012, it is important to compare outcomes with LSG with those for the preferred Roux-en-Y bypass surgery, the investigators said, noting that few large-scale studies have compared outcomes with the two procedures.
“Over the past decade, laparoscopic sleeve gastrectomy has emerged as a common utilized bariatric procedure. LSG has several advantages over LGB including preservation of endoscopic access to the upper gastrointestinal tract, avoidance of intestinal anastomosis, and prevention of dumping syndrome by pylorus preservation,” they wrote, adding that studies increasingly demonstrate its efficacy for weight loss.
The current findings support those of other recent studies, and a comparison of the data with those from 2007 to 2010 from the ACS NSQIP database showed that while reoperation rates after gastric bypass and sleeve gastrectomy have declined dramatically over time, readmission rates remain elevated.
“Therefore, it appears that further quality improvement initiatives are necessary to reduce the rate of readmissions after bariatric surgery,” the investigators wrote, noting that a national collaborative to reduce 30-day readmissions by 20% (the Metabolic and Bariatric Surgery Accreditation and Quality Improvement Program, or MBSAQIP) is currently enrolling.
Additional randomized controlled trials are also needed to evaluate differences in long-term outcomes between the two procedures, they concluded.
The authors reported having no relevant financial disclosures.
FROM THE JOURNAL OF THE AMERICAN COLLEGE OF SURGEONS
Key clinical point: Laparoscopic sleeve gastrectomy appears to have numerous advantages over laparoscopic Roux-en-Y gastric bypass.
Major finding: Patients who underwent LGB had a significantly higher rate of 30-day risk-adjusted morbidity (odds ratio, 1.32).
Data source: An analysis of data from the ACS NSQIP database.
Disclosures: The authors reported having no relevant financial disclosures.

CDC: Cancer incidence and survival improve; racial disparities persist
Numerous states have achieved Healthy People 2020 goals for colorectal and cervical cancer incidence, and the proportion of persons with cancer who survive at least 5 years after diagnosis has reached 65%, but racial disparities in survival persist, according to a Centers for Disease Control and Prevention report.
An analysis of data from the U.S. Cancer Statistics for 2011 – the most recent data available – showed that a total of 1,532,066 invasive cancers were reported to cancer registries in the United States that year (annual incidence rate, 451 per 100,000 persons). Invasive cancers were considered all cancers except in situ cancers (excluding situ cancers in the urinary bladder) and basal and squamous cell cancers.
Incidence rates were higher for men than for women (508 vs. 410 per 100,000), and were highest among blacks (458 per 100,000). The 5-year survival rate, calculated for cases diagnosed between 2003 and 2010, was similar among men and women at 65%, but lower among blacks (60%) for every cancer site, S. Jane Henley of the National Center for Chronic Disease Prevention and Health Promotion, CDC, Atlanta and her colleagues reported in the March 13 issue of the Morbidity and Mortality Weekly Report.
Survival was highest among those diagnosed before age 45 years (81%) and decreased with increasing age.
The most common cancer reported was prostate cancer (128 per 100,000 men), followed by female breast cancer (122 per 100,000 women), lung and bronchus cancer (61 per 100,000 persons), and colon and rectum cancer (40 per 100,000 persons). Together these cancers accounted for half of those diagnosed in 2011, and 5-year relative survival in patients diagnosed with these cancers was highest for prostate cancer (97%) and breast cancer (88%), the investigators said (MMWR 2015;63:237-42).
Survival was intermediate for colorectal cancer (63%) and lowest for lung cancer (18%).
The cervical cancer incidence rate was 7.5 per 100,000 the authors noted.
A geographic breakdown shows that incidence ranged from 374 per 100,000 persons in New Mexico to 509 per 100,000 persons in Washington, D.C.
“Healthy People 2020 targets were reached in 37 states for incidence of colorectal cancer and in 28 states for incidence of cervical cancer,” they wrote, noting that this report is the first to include incidence rates in Puerto Rico; those rates were lower for all cancer sites, compared with the states and the District of Columbia (339 per 100,000 persons) – a finding that reflects screening practices and risk factors that may differ from in the states.
The inclusion of survival data is also a first and provides a basis for tracking progress.
“Cancer incidence and survival data can guide the planning and evaluation of cancer prevention and control programs,” the authors said, adding that such data can also assist in long-term planning for cancer diagnostic and treatment services, and help public health officials set priorities for allocating health resources.
Though limited by potential systematic misclassification of race and ethnicity, by the possibility that cancer reporting was delayed thus leading to underestimation of certain cancers, and by the fact that relative survival rates were calculated only for white and black racial groups due to lack of accurate life tables for other racial/ethnic groups, the findings are nonetheless important for helping public health officials to monitor cancer incidence, mortality, and survival and to identify populations that might benefit most from targeted prevention and control efforts, they said.
The findings can also help guide the planning of health care allocation and support services and track progress toward Healthy People 2020 goals, they added.
Dr. Lisa Richardson, the director of the CDC’s Division of Cancer Prevention and Control further stressed the value of monitoring cancer incidence and survival rates in a statement.
“These data are an important reminder that a key to surviving with cancer is making sure everyone has access to care from early diagnosis to treatment. We know, for example, that early detection of colorectal cancer has had the largest impact on long-term survival rates,” she said.
Numerous states have achieved Healthy People 2020 goals for colorectal and cervical cancer incidence, and the proportion of persons with cancer who survive at least 5 years after diagnosis has reached 65%, but racial disparities in survival persist, according to a Centers for Disease Control and Prevention report.
An analysis of data from the U.S. Cancer Statistics for 2011 – the most recent data available – showed that a total of 1,532,066 invasive cancers were reported to cancer registries in the United States that year (annual incidence rate, 451 per 100,000 persons). Invasive cancers were considered all cancers except in situ cancers (excluding situ cancers in the urinary bladder) and basal and squamous cell cancers.
Incidence rates were higher for men than for women (508 vs. 410 per 100,000), and were highest among blacks (458 per 100,000). The 5-year survival rate, calculated for cases diagnosed between 2003 and 2010, was similar among men and women at 65%, but lower among blacks (60%) for every cancer site, S. Jane Henley of the National Center for Chronic Disease Prevention and Health Promotion, CDC, Atlanta and her colleagues reported in the March 13 issue of the Morbidity and Mortality Weekly Report.
Survival was highest among those diagnosed before age 45 years (81%) and decreased with increasing age.
The most common cancer reported was prostate cancer (128 per 100,000 men), followed by female breast cancer (122 per 100,000 women), lung and bronchus cancer (61 per 100,000 persons), and colon and rectum cancer (40 per 100,000 persons). Together these cancers accounted for half of those diagnosed in 2011, and 5-year relative survival in patients diagnosed with these cancers was highest for prostate cancer (97%) and breast cancer (88%), the investigators said (MMWR 2015;63:237-42).
Survival was intermediate for colorectal cancer (63%) and lowest for lung cancer (18%).
The cervical cancer incidence rate was 7.5 per 100,000 the authors noted.
A geographic breakdown shows that incidence ranged from 374 per 100,000 persons in New Mexico to 509 per 100,000 persons in Washington, D.C.
“Healthy People 2020 targets were reached in 37 states for incidence of colorectal cancer and in 28 states for incidence of cervical cancer,” they wrote, noting that this report is the first to include incidence rates in Puerto Rico; those rates were lower for all cancer sites, compared with the states and the District of Columbia (339 per 100,000 persons) – a finding that reflects screening practices and risk factors that may differ from in the states.
The inclusion of survival data is also a first and provides a basis for tracking progress.
“Cancer incidence and survival data can guide the planning and evaluation of cancer prevention and control programs,” the authors said, adding that such data can also assist in long-term planning for cancer diagnostic and treatment services, and help public health officials set priorities for allocating health resources.
Though limited by potential systematic misclassification of race and ethnicity, by the possibility that cancer reporting was delayed thus leading to underestimation of certain cancers, and by the fact that relative survival rates were calculated only for white and black racial groups due to lack of accurate life tables for other racial/ethnic groups, the findings are nonetheless important for helping public health officials to monitor cancer incidence, mortality, and survival and to identify populations that might benefit most from targeted prevention and control efforts, they said.
The findings can also help guide the planning of health care allocation and support services and track progress toward Healthy People 2020 goals, they added.
Dr. Lisa Richardson, the director of the CDC’s Division of Cancer Prevention and Control further stressed the value of monitoring cancer incidence and survival rates in a statement.
“These data are an important reminder that a key to surviving with cancer is making sure everyone has access to care from early diagnosis to treatment. We know, for example, that early detection of colorectal cancer has had the largest impact on long-term survival rates,” she said.
Numerous states have achieved Healthy People 2020 goals for colorectal and cervical cancer incidence, and the proportion of persons with cancer who survive at least 5 years after diagnosis has reached 65%, but racial disparities in survival persist, according to a Centers for Disease Control and Prevention report.
An analysis of data from the U.S. Cancer Statistics for 2011 – the most recent data available – showed that a total of 1,532,066 invasive cancers were reported to cancer registries in the United States that year (annual incidence rate, 451 per 100,000 persons). Invasive cancers were considered all cancers except in situ cancers (excluding situ cancers in the urinary bladder) and basal and squamous cell cancers.
Incidence rates were higher for men than for women (508 vs. 410 per 100,000), and were highest among blacks (458 per 100,000). The 5-year survival rate, calculated for cases diagnosed between 2003 and 2010, was similar among men and women at 65%, but lower among blacks (60%) for every cancer site, S. Jane Henley of the National Center for Chronic Disease Prevention and Health Promotion, CDC, Atlanta and her colleagues reported in the March 13 issue of the Morbidity and Mortality Weekly Report.
Survival was highest among those diagnosed before age 45 years (81%) and decreased with increasing age.
The most common cancer reported was prostate cancer (128 per 100,000 men), followed by female breast cancer (122 per 100,000 women), lung and bronchus cancer (61 per 100,000 persons), and colon and rectum cancer (40 per 100,000 persons). Together these cancers accounted for half of those diagnosed in 2011, and 5-year relative survival in patients diagnosed with these cancers was highest for prostate cancer (97%) and breast cancer (88%), the investigators said (MMWR 2015;63:237-42).
Survival was intermediate for colorectal cancer (63%) and lowest for lung cancer (18%).
The cervical cancer incidence rate was 7.5 per 100,000 the authors noted.
A geographic breakdown shows that incidence ranged from 374 per 100,000 persons in New Mexico to 509 per 100,000 persons in Washington, D.C.
“Healthy People 2020 targets were reached in 37 states for incidence of colorectal cancer and in 28 states for incidence of cervical cancer,” they wrote, noting that this report is the first to include incidence rates in Puerto Rico; those rates were lower for all cancer sites, compared with the states and the District of Columbia (339 per 100,000 persons) – a finding that reflects screening practices and risk factors that may differ from in the states.
The inclusion of survival data is also a first and provides a basis for tracking progress.
“Cancer incidence and survival data can guide the planning and evaluation of cancer prevention and control programs,” the authors said, adding that such data can also assist in long-term planning for cancer diagnostic and treatment services, and help public health officials set priorities for allocating health resources.
Though limited by potential systematic misclassification of race and ethnicity, by the possibility that cancer reporting was delayed thus leading to underestimation of certain cancers, and by the fact that relative survival rates were calculated only for white and black racial groups due to lack of accurate life tables for other racial/ethnic groups, the findings are nonetheless important for helping public health officials to monitor cancer incidence, mortality, and survival and to identify populations that might benefit most from targeted prevention and control efforts, they said.
The findings can also help guide the planning of health care allocation and support services and track progress toward Healthy People 2020 goals, they added.
Dr. Lisa Richardson, the director of the CDC’s Division of Cancer Prevention and Control further stressed the value of monitoring cancer incidence and survival rates in a statement.
“These data are an important reminder that a key to surviving with cancer is making sure everyone has access to care from early diagnosis to treatment. We know, for example, that early detection of colorectal cancer has had the largest impact on long-term survival rates,” she said.
FROM MORBIDITY AND MORTALITY WEEKLY REPORT
Key clinical point: Incidence rates are declining for some cancers, and survival is improving.
Major finding: The 5-year survival rate is 65% among persons with invasive cancer.
Data source: The U.S. Cancer Statistics for 2011.
Disclosures: The study was funded and conducted by the Centers for Disease Control and Prevention.
‘Perfect storm’ of depression, stress raises risk of MI, death
Patients with coronary heart disease who have both depression and stress are at increased risk of myocardial infarction and death, according to findings from a large, prospective, cohort study.
Of 4,487 adults with CHD who were part of the Reasons for Geographic and Racial Differences in Stroke (REGARDS) study, 1,337 experienced MI or death during a median of nearly 6 years of follow-up. Those with both high depressive symptoms and high stress at baseline – about 6% of the study population – were at significantly increased risk of such events (adjusted hazard ratio, 1.48) during the first 2.5 years of follow-up, compared with those with low stress and low depressive symptoms. However, the association was not significant beyond the initial 2.5 years (HR, 0.89), Carmela Alcántara, Ph.D., of Columbia University, New York, and her colleagues reported.
Those with low stress and high depressive symptoms, and those with high stress and low depressive symptoms, were not at increased risk (HR, 0.92 and 0.86, respectively) at any point during follow-up (Circ. Cardiovasc. Qual. Outcomes 2015 March 10 [doi:10.1161/IRCOUTCOMES.114.001180]).
The findings provide initial empirical evidence to support a “psychosocial perfect storm conceptual model” based on the idea that it takes an underlying chronic psychosocial vulnerability such as depression along with a more transient state such as psychological stress to precipitate a clinical event. The confluence of these factors may be particularly destructive in the short term, the investigators concluded, noting that the findings could have implications for the development of preventive treatments that focus on depression and stress during this vulnerable period in CHD patients.
The National Institute of Neurological Disorders and Stroke and the National Heart, Lung, and Blood Institute supported the study. Dr. Alcantara reported having no disclosures, but two other authors received salary support from Amgen for research, and one served as a consultant for DiaDexus.
Patients with coronary heart disease who have both depression and stress are at increased risk of myocardial infarction and death, according to findings from a large, prospective, cohort study.
Of 4,487 adults with CHD who were part of the Reasons for Geographic and Racial Differences in Stroke (REGARDS) study, 1,337 experienced MI or death during a median of nearly 6 years of follow-up. Those with both high depressive symptoms and high stress at baseline – about 6% of the study population – were at significantly increased risk of such events (adjusted hazard ratio, 1.48) during the first 2.5 years of follow-up, compared with those with low stress and low depressive symptoms. However, the association was not significant beyond the initial 2.5 years (HR, 0.89), Carmela Alcántara, Ph.D., of Columbia University, New York, and her colleagues reported.
Those with low stress and high depressive symptoms, and those with high stress and low depressive symptoms, were not at increased risk (HR, 0.92 and 0.86, respectively) at any point during follow-up (Circ. Cardiovasc. Qual. Outcomes 2015 March 10 [doi:10.1161/IRCOUTCOMES.114.001180]).
The findings provide initial empirical evidence to support a “psychosocial perfect storm conceptual model” based on the idea that it takes an underlying chronic psychosocial vulnerability such as depression along with a more transient state such as psychological stress to precipitate a clinical event. The confluence of these factors may be particularly destructive in the short term, the investigators concluded, noting that the findings could have implications for the development of preventive treatments that focus on depression and stress during this vulnerable period in CHD patients.
The National Institute of Neurological Disorders and Stroke and the National Heart, Lung, and Blood Institute supported the study. Dr. Alcantara reported having no disclosures, but two other authors received salary support from Amgen for research, and one served as a consultant for DiaDexus.
Patients with coronary heart disease who have both depression and stress are at increased risk of myocardial infarction and death, according to findings from a large, prospective, cohort study.
Of 4,487 adults with CHD who were part of the Reasons for Geographic and Racial Differences in Stroke (REGARDS) study, 1,337 experienced MI or death during a median of nearly 6 years of follow-up. Those with both high depressive symptoms and high stress at baseline – about 6% of the study population – were at significantly increased risk of such events (adjusted hazard ratio, 1.48) during the first 2.5 years of follow-up, compared with those with low stress and low depressive symptoms. However, the association was not significant beyond the initial 2.5 years (HR, 0.89), Carmela Alcántara, Ph.D., of Columbia University, New York, and her colleagues reported.
Those with low stress and high depressive symptoms, and those with high stress and low depressive symptoms, were not at increased risk (HR, 0.92 and 0.86, respectively) at any point during follow-up (Circ. Cardiovasc. Qual. Outcomes 2015 March 10 [doi:10.1161/IRCOUTCOMES.114.001180]).
The findings provide initial empirical evidence to support a “psychosocial perfect storm conceptual model” based on the idea that it takes an underlying chronic psychosocial vulnerability such as depression along with a more transient state such as psychological stress to precipitate a clinical event. The confluence of these factors may be particularly destructive in the short term, the investigators concluded, noting that the findings could have implications for the development of preventive treatments that focus on depression and stress during this vulnerable period in CHD patients.
The National Institute of Neurological Disorders and Stroke and the National Heart, Lung, and Blood Institute supported the study. Dr. Alcantara reported having no disclosures, but two other authors received salary support from Amgen for research, and one served as a consultant for DiaDexus.
FROM CIRCULATION: CARDIOVASCULAR QUALITY AND OUTCOMES
Key clinical point: Concurrent depression and stress in CHD patients may increase the early risk of MI and death.
Major finding: CHD patients with high depressive symptoms and high stress at baseline had an increased risk of MI and death early during follow-up (adjusted HR, 1.48).
Data source: A prospective cohort study of 4,487 adults.
Disclosures: The National Institute of Neurological Disorders and Stroke and the National Heart, Lung, and Blood Institute supported the study. Dr. Alcantara reported having no disclosures; two other authors received salary support from Amgen for research, and one served as a consultant for DiaDexus.
Novel ‘soft anticholinergic’ shows promise for axillary hyperhidrosis
MIAMI BEACH – A promising new treatment for axillary hyperhidrosis will soon be evaluated in a clinical trial.
The novel molecular compound – a “soft anticholinergic” – was safe and effective as a topical treatment in a recent pilot study, Dr. Brian Berman reported in a session on innovations in clinical therapeutics at the South Beach Symposium.
Currently known as BBI-4000, the product is locally active but quickly metabolized if absorbed, which reduces the risk of treatment-related adverse events, said Dr. Berman of the University of Miami.

No comparable first-line topical prescription treatment exists for axillary hyperhidrosis, he noted.
In the pilot study – the results of which were reported in September by the manufacturer, Brickell Biotech – 18 subjects were randomized to receive once-daily treatment with either a high topical concentration, a low topical concentration, or topical vehicle for 14 days. Of the 12 patients receiving active treatment, 75% achieved at least a 50% sweat reduction, compared with 33% of the 6 patients in the vehicle group.
Further, 67% of those receiving active treatment, compared with 33% in the vehicle group, achieved at least a two-point improvement in their Hyperhidrosis Disease Severity Scale score, indicating substantial improvement, Dr. Berman said.
No treatment-related adverse events were reported, and none of the patients discontinued treatment because of adverse events.
Based on these findings, Brickell Biotech has initiated a randomized, double-blind, vehicle-controlled phase IIb clinical trial with plans to enroll 180 patients with primary axillary hyperhidrosis. The trial will assess the safety and efficacy of three different concentrations of BBI-4000, compared with vehicle.
Dr. Berman is a consultant, researcher, and/or speaker for Beiersdorf, DUSA Pharmaceuticals, Ferndale Pharmaceuticals, Galderma Laboratories, Genentech, Halscion, LEO Pharmaceuticals, Onset Therapeutics, Sensus Healthcare, Tigercat Pharma, and TopMD Skin Care. He also owns stock in TopMD Skin Care.
MIAMI BEACH – A promising new treatment for axillary hyperhidrosis will soon be evaluated in a clinical trial.
The novel molecular compound – a “soft anticholinergic” – was safe and effective as a topical treatment in a recent pilot study, Dr. Brian Berman reported in a session on innovations in clinical therapeutics at the South Beach Symposium.
Currently known as BBI-4000, the product is locally active but quickly metabolized if absorbed, which reduces the risk of treatment-related adverse events, said Dr. Berman of the University of Miami.
No comparable first-line topical prescription treatment exists for axillary hyperhidrosis, he noted.
In the pilot study – the results of which were reported in September by the manufacturer, Brickell Biotech – 18 subjects were randomized to receive once-daily treatment with either a high topical concentration, a low topical concentration, or topical vehicle for 14 days. Of the 12 patients receiving active treatment, 75% achieved at least a 50% sweat reduction, compared with 33% of the 6 patients in the vehicle group.
Further, 67% of those receiving active treatment, compared with 33% in the vehicle group, achieved at least a two-point improvement in their Hyperhidrosis Disease Severity Scale score, indicating substantial improvement, Dr. Berman said.
No treatment-related adverse events were reported, and none of the patients discontinued treatment because of adverse events.
Based on these findings, Brickell Biotech has initiated a randomized, double-blind, vehicle-controlled phase IIb clinical trial with plans to enroll 180 patients with primary axillary hyperhidrosis. The trial will assess the safety and efficacy of three different concentrations of BBI-4000, compared with vehicle.
Dr. Berman is a consultant, researcher, and/or speaker for Beiersdorf, DUSA Pharmaceuticals, Ferndale Pharmaceuticals, Galderma Laboratories, Genentech, Halscion, LEO Pharmaceuticals, Onset Therapeutics, Sensus Healthcare, Tigercat Pharma, and TopMD Skin Care. He also owns stock in TopMD Skin Care.
MIAMI BEACH – A promising new treatment for axillary hyperhidrosis will soon be evaluated in a clinical trial.
The novel molecular compound – a “soft anticholinergic” – was safe and effective as a topical treatment in a recent pilot study, Dr. Brian Berman reported in a session on innovations in clinical therapeutics at the South Beach Symposium.
Currently known as BBI-4000, the product is locally active but quickly metabolized if absorbed, which reduces the risk of treatment-related adverse events, said Dr. Berman of the University of Miami.
No comparable first-line topical prescription treatment exists for axillary hyperhidrosis, he noted.
In the pilot study – the results of which were reported in September by the manufacturer, Brickell Biotech – 18 subjects were randomized to receive once-daily treatment with either a high topical concentration, a low topical concentration, or topical vehicle for 14 days. Of the 12 patients receiving active treatment, 75% achieved at least a 50% sweat reduction, compared with 33% of the 6 patients in the vehicle group.
Further, 67% of those receiving active treatment, compared with 33% in the vehicle group, achieved at least a two-point improvement in their Hyperhidrosis Disease Severity Scale score, indicating substantial improvement, Dr. Berman said.
No treatment-related adverse events were reported, and none of the patients discontinued treatment because of adverse events.
Based on these findings, Brickell Biotech has initiated a randomized, double-blind, vehicle-controlled phase IIb clinical trial with plans to enroll 180 patients with primary axillary hyperhidrosis. The trial will assess the safety and efficacy of three different concentrations of BBI-4000, compared with vehicle.
Dr. Berman is a consultant, researcher, and/or speaker for Beiersdorf, DUSA Pharmaceuticals, Ferndale Pharmaceuticals, Galderma Laboratories, Genentech, Halscion, LEO Pharmaceuticals, Onset Therapeutics, Sensus Healthcare, Tigercat Pharma, and TopMD Skin Care. He also owns stock in TopMD Skin Care.
AT THE SOUTH BEACH SYMPOSIUM

Careful planning, technique, and counseling can minimize pediatric scarring
It’s a myth that children don’t scar like adults, according to Dr. Jon A. Dyer.
In fact, children often scar worse than adults, he said at the Hawaii Dermatology Seminar sponsored by Global Academy for Medical Education/Skin Disease Education Foundation.
Children have more aggressive healing and inflammatory responses, a highly elastic dermis and connective tissues, and a high activity level that increases the risk of stressing the wound, and they may pay less attention to it, he explained.
Additionally, children can be more difficult to treat for scars because they are often more fearful and anxious, they have a short attention span, and they move around – a lot, he said. This leads to greater anxiety on the part of both the dermatologist and the family, which can lead to rapidly completing a procedure, said Dr. Dyer of the University of Missouri, Columbia.
Successful treatment of a wound or lesion – that is, getting the best initial scar possible – requires good planning, proactive application of surgical principles, and careful patient and family counseling and follow-up, he said.
Among Dr. Dyer’s tips for minimizing scarring when treating lesions in children:
• Do the simplest possible procedure.
• Make the scar as small as possible, keeping in mind that pediatric skin is more elastic.
• Remember that fusiform closures in children do not always require a 3:1 ratio. Tips settle, and divots fill in in young children, he said.
• Operate before puberty when the lesion is located in a cosmetically important area.
Also, consider performing a staged excision if possible; this allows a reduction in final scar length, provides tissue expansion, and allows assessment of individual wound healing. Take as much of the lesion as possible the first time, and remember that central excision is preferable to lateral excision, Dr. Dyer said.
The ideal time to wait between stage 1 and 2 is 4-6 weeks. Longer intervals will lead to more spread and more hypertrophy, and will negate the benefits of staging, he said.
Keep in mind that purse-string sutures can be particularly effective for suturing small spaces and for closing dead spaces, he said, adding that use of a purse-string closure for a round defect can reduce the final scar length by at least 50%.
Scar prevention or minimization requires strict adherence to good surgical principles, Dr. Dyer said, explaining that attention must be paid to perfecting the excision through proper use of skin tension lines, clean wound edges, sharp corners with no or minimal boating, undermining, and removing bulk if necessary.
Track marks are more likely on nonfacial skin and can be avoided by using running subcuticular sutures; in some cases of excellent approximation with no tension, the wound surface can be secured with Dermabond, he said.
Dr. Dyer also outlined the best closure choices for specific areas. For the scalp, use running cuticular sutures; for the extremities, trunk, axilla, or groin, use running subcuticular sutures; for the face, feet, or hands, use interrupted sutures; and for a punch biopsy, consider not using any closure, he advised.
If cuticular stitches are used, minimize scarring by pulling them within 5 days on the face, and within 7-10 days on the body. If dehiscence is a concern, pull the cuticulars and follow with either Dermabond or SteriStrips, he said, but strongly consider using running subcuticular sutures.
Once a wound is closed, secure it with Dermabond or with Steri-Strips and Mastisol and provide protective dressing.
“The bulkier and more colorful the dressing, the happier and more compliant the child,” he said.
Minimize postoperative wound tension in high-risk scars or sites and restrict movement and trauma for as long as possible; 6 weeks is ideal, he added, noting that movement restriction is critical for ensuring a good outcome.
To reduce the trauma of suture removal, “cut ’em long and leave ’em long,” and be sure to use proper scissors, he said.
Running subcuticular suture removal doesn’t hurt; enlist parents’ help in convincing the child of this, he suggested.
Finally, be specific when counseling patients about restrictions, discuss possible complications, provide a written summary including contact numbers, address the scar, and give the follow-up appointment time in writing, he said.
If dehiscence occurs – and it’s not uncommon in children – let it heal and restart the process, he said, noting that prevention is best and can be achieved in many cases with aggressive pre- and postop education, restriction of movement, and proper dressing.
Dr. Dyer stressed that good surgical principles for use in children can also be utilized to improve results in adult patients.
Dr. Dyer reported having no disclosures. SDEF and this new organization are owned by the same parent company.
It’s a myth that children don’t scar like adults, according to Dr. Jon A. Dyer.
In fact, children often scar worse than adults, he said at the Hawaii Dermatology Seminar sponsored by Global Academy for Medical Education/Skin Disease Education Foundation.
Children have more aggressive healing and inflammatory responses, a highly elastic dermis and connective tissues, and a high activity level that increases the risk of stressing the wound, and they may pay less attention to it, he explained.
Additionally, children can be more difficult to treat for scars because they are often more fearful and anxious, they have a short attention span, and they move around – a lot, he said. This leads to greater anxiety on the part of both the dermatologist and the family, which can lead to rapidly completing a procedure, said Dr. Dyer of the University of Missouri, Columbia.
Successful treatment of a wound or lesion – that is, getting the best initial scar possible – requires good planning, proactive application of surgical principles, and careful patient and family counseling and follow-up, he said.
Among Dr. Dyer’s tips for minimizing scarring when treating lesions in children:
• Do the simplest possible procedure.
• Make the scar as small as possible, keeping in mind that pediatric skin is more elastic.
• Remember that fusiform closures in children do not always require a 3:1 ratio. Tips settle, and divots fill in in young children, he said.
• Operate before puberty when the lesion is located in a cosmetically important area.
Also, consider performing a staged excision if possible; this allows a reduction in final scar length, provides tissue expansion, and allows assessment of individual wound healing. Take as much of the lesion as possible the first time, and remember that central excision is preferable to lateral excision, Dr. Dyer said.
The ideal time to wait between stage 1 and 2 is 4-6 weeks. Longer intervals will lead to more spread and more hypertrophy, and will negate the benefits of staging, he said.
Keep in mind that purse-string sutures can be particularly effective for suturing small spaces and for closing dead spaces, he said, adding that use of a purse-string closure for a round defect can reduce the final scar length by at least 50%.
Scar prevention or minimization requires strict adherence to good surgical principles, Dr. Dyer said, explaining that attention must be paid to perfecting the excision through proper use of skin tension lines, clean wound edges, sharp corners with no or minimal boating, undermining, and removing bulk if necessary.
Track marks are more likely on nonfacial skin and can be avoided by using running subcuticular sutures; in some cases of excellent approximation with no tension, the wound surface can be secured with Dermabond, he said.
Dr. Dyer also outlined the best closure choices for specific areas. For the scalp, use running cuticular sutures; for the extremities, trunk, axilla, or groin, use running subcuticular sutures; for the face, feet, or hands, use interrupted sutures; and for a punch biopsy, consider not using any closure, he advised.
If cuticular stitches are used, minimize scarring by pulling them within 5 days on the face, and within 7-10 days on the body. If dehiscence is a concern, pull the cuticulars and follow with either Dermabond or SteriStrips, he said, but strongly consider using running subcuticular sutures.
Once a wound is closed, secure it with Dermabond or with Steri-Strips and Mastisol and provide protective dressing.
“The bulkier and more colorful the dressing, the happier and more compliant the child,” he said.
Minimize postoperative wound tension in high-risk scars or sites and restrict movement and trauma for as long as possible; 6 weeks is ideal, he added, noting that movement restriction is critical for ensuring a good outcome.
To reduce the trauma of suture removal, “cut ’em long and leave ’em long,” and be sure to use proper scissors, he said.
Running subcuticular suture removal doesn’t hurt; enlist parents’ help in convincing the child of this, he suggested.
Finally, be specific when counseling patients about restrictions, discuss possible complications, provide a written summary including contact numbers, address the scar, and give the follow-up appointment time in writing, he said.
If dehiscence occurs – and it’s not uncommon in children – let it heal and restart the process, he said, noting that prevention is best and can be achieved in many cases with aggressive pre- and postop education, restriction of movement, and proper dressing.
Dr. Dyer stressed that good surgical principles for use in children can also be utilized to improve results in adult patients.
Dr. Dyer reported having no disclosures. SDEF and this new organization are owned by the same parent company.
It’s a myth that children don’t scar like adults, according to Dr. Jon A. Dyer.
In fact, children often scar worse than adults, he said at the Hawaii Dermatology Seminar sponsored by Global Academy for Medical Education/Skin Disease Education Foundation.
Children have more aggressive healing and inflammatory responses, a highly elastic dermis and connective tissues, and a high activity level that increases the risk of stressing the wound, and they may pay less attention to it, he explained.
Additionally, children can be more difficult to treat for scars because they are often more fearful and anxious, they have a short attention span, and they move around – a lot, he said. This leads to greater anxiety on the part of both the dermatologist and the family, which can lead to rapidly completing a procedure, said Dr. Dyer of the University of Missouri, Columbia.
Successful treatment of a wound or lesion – that is, getting the best initial scar possible – requires good planning, proactive application of surgical principles, and careful patient and family counseling and follow-up, he said.
Among Dr. Dyer’s tips for minimizing scarring when treating lesions in children:
• Do the simplest possible procedure.
• Make the scar as small as possible, keeping in mind that pediatric skin is more elastic.
• Remember that fusiform closures in children do not always require a 3:1 ratio. Tips settle, and divots fill in in young children, he said.
• Operate before puberty when the lesion is located in a cosmetically important area.
Also, consider performing a staged excision if possible; this allows a reduction in final scar length, provides tissue expansion, and allows assessment of individual wound healing. Take as much of the lesion as possible the first time, and remember that central excision is preferable to lateral excision, Dr. Dyer said.
The ideal time to wait between stage 1 and 2 is 4-6 weeks. Longer intervals will lead to more spread and more hypertrophy, and will negate the benefits of staging, he said.
Keep in mind that purse-string sutures can be particularly effective for suturing small spaces and for closing dead spaces, he said, adding that use of a purse-string closure for a round defect can reduce the final scar length by at least 50%.
Scar prevention or minimization requires strict adherence to good surgical principles, Dr. Dyer said, explaining that attention must be paid to perfecting the excision through proper use of skin tension lines, clean wound edges, sharp corners with no or minimal boating, undermining, and removing bulk if necessary.
Track marks are more likely on nonfacial skin and can be avoided by using running subcuticular sutures; in some cases of excellent approximation with no tension, the wound surface can be secured with Dermabond, he said.
Dr. Dyer also outlined the best closure choices for specific areas. For the scalp, use running cuticular sutures; for the extremities, trunk, axilla, or groin, use running subcuticular sutures; for the face, feet, or hands, use interrupted sutures; and for a punch biopsy, consider not using any closure, he advised.
If cuticular stitches are used, minimize scarring by pulling them within 5 days on the face, and within 7-10 days on the body. If dehiscence is a concern, pull the cuticulars and follow with either Dermabond or SteriStrips, he said, but strongly consider using running subcuticular sutures.
Once a wound is closed, secure it with Dermabond or with Steri-Strips and Mastisol and provide protective dressing.
“The bulkier and more colorful the dressing, the happier and more compliant the child,” he said.
Minimize postoperative wound tension in high-risk scars or sites and restrict movement and trauma for as long as possible; 6 weeks is ideal, he added, noting that movement restriction is critical for ensuring a good outcome.
To reduce the trauma of suture removal, “cut ’em long and leave ’em long,” and be sure to use proper scissors, he said.
Running subcuticular suture removal doesn’t hurt; enlist parents’ help in convincing the child of this, he suggested.
Finally, be specific when counseling patients about restrictions, discuss possible complications, provide a written summary including contact numbers, address the scar, and give the follow-up appointment time in writing, he said.
If dehiscence occurs – and it’s not uncommon in children – let it heal and restart the process, he said, noting that prevention is best and can be achieved in many cases with aggressive pre- and postop education, restriction of movement, and proper dressing.
Dr. Dyer stressed that good surgical principles for use in children can also be utilized to improve results in adult patients.
Dr. Dyer reported having no disclosures. SDEF and this new organization are owned by the same parent company.
Hyaluronic acid wrinkle filler also appears useful for midface augmentation
MIAMI BEACH – A large gel particle hyaluronic acid filler with lidocaine (LGP-HAL) was safe and effective for midface augmentation and correction of midface contour deficiencies in a randomized, multicenter, pivotal study.
The product (Perlane, Galderma Laboratories), which is currently approved for moderate to severe facial folds and wrinkles, provided visible, clinically meaningful, aesthetic results for at least 12 months based on assessment by a blinded evaluator, Dr. David E. Bank reported in a poster at the South Beach Symposium.
At 8 weeks after initial treatment, 89% of 150 treated subjects experienced at least a one-point improvement in their combined right and left side Medicis Midface Volume Scale (MMVS) score, compared with 16% of 50 patients who were not treated.
Further, the treated subjects were assessed as having greater midface fullness than the nontreated subjects at every measurement during the first 12 months after treatment, according to Dr. Bank of New York–Presbyterian Hospital/Columbia University Medical Center, New York.
Study participants were men and women aged 18-65 years (mean of 53 years) with MMVS scores of two, three, or four on the validated one- to four-point scale, with one indicating a fairly full midface and four indicating substantial loss of fullness in the midface area. At the initial treatment, the 150 treatment group subjects were injected with a mean volume of 4.21 mL. All but one received subcutaneous injections, and 115 received supraperiosteal injections.
They were evaluated at weeks 2 (when an optional touch-up was allowed) and 4, and months 2, 4, 6, 8, 10, and 12 following the initial treatment.
The treatment group subjects were treated again at 12 months, along with those not treated initially. Another touch-up was allowed at a 2-week assessment, and additional assessments were conducted at weeks 3 and 4.
Treatment was well tolerated. More than 80% of events reported after treatment were mild in severity, and the adverse events that occurred in more than 5% of subjects included implant site hematoma, hemorrhage, pain, swelling, and headache.
One subject had two cases of implant site inflammation that were deemed related by the investigators, and one experienced a serious adverse event (implant site hematoma) deemed related to the procedure as opposed to the device.
No additional risk was seen in those who were treated twice, Dr. Bank noted.
“Facial shape plays an important role in facial attractiveness,” he wrote, adding that full cheeks, in particular, play an important role.
Aging, however, is associated with increased tissue laxity, soft-tissue descent and deflation, and loss of bone, which all contribute to deficiencies in the midface.
Hyaluronic fillers have been used successfully to correct such deficiencies, and the current findings suggest that LGP-HAL also can be used safely to enhance midface aesthetics, he concluded.
This study was funded by Galderma Laboratories.
MIAMI BEACH – A large gel particle hyaluronic acid filler with lidocaine (LGP-HAL) was safe and effective for midface augmentation and correction of midface contour deficiencies in a randomized, multicenter, pivotal study.
The product (Perlane, Galderma Laboratories), which is currently approved for moderate to severe facial folds and wrinkles, provided visible, clinically meaningful, aesthetic results for at least 12 months based on assessment by a blinded evaluator, Dr. David E. Bank reported in a poster at the South Beach Symposium.
At 8 weeks after initial treatment, 89% of 150 treated subjects experienced at least a one-point improvement in their combined right and left side Medicis Midface Volume Scale (MMVS) score, compared with 16% of 50 patients who were not treated.
Further, the treated subjects were assessed as having greater midface fullness than the nontreated subjects at every measurement during the first 12 months after treatment, according to Dr. Bank of New York–Presbyterian Hospital/Columbia University Medical Center, New York.
Study participants were men and women aged 18-65 years (mean of 53 years) with MMVS scores of two, three, or four on the validated one- to four-point scale, with one indicating a fairly full midface and four indicating substantial loss of fullness in the midface area. At the initial treatment, the 150 treatment group subjects were injected with a mean volume of 4.21 mL. All but one received subcutaneous injections, and 115 received supraperiosteal injections.
They were evaluated at weeks 2 (when an optional touch-up was allowed) and 4, and months 2, 4, 6, 8, 10, and 12 following the initial treatment.
The treatment group subjects were treated again at 12 months, along with those not treated initially. Another touch-up was allowed at a 2-week assessment, and additional assessments were conducted at weeks 3 and 4.
Treatment was well tolerated. More than 80% of events reported after treatment were mild in severity, and the adverse events that occurred in more than 5% of subjects included implant site hematoma, hemorrhage, pain, swelling, and headache.
One subject had two cases of implant site inflammation that were deemed related by the investigators, and one experienced a serious adverse event (implant site hematoma) deemed related to the procedure as opposed to the device.
No additional risk was seen in those who were treated twice, Dr. Bank noted.
“Facial shape plays an important role in facial attractiveness,” he wrote, adding that full cheeks, in particular, play an important role.
Aging, however, is associated with increased tissue laxity, soft-tissue descent and deflation, and loss of bone, which all contribute to deficiencies in the midface.
Hyaluronic fillers have been used successfully to correct such deficiencies, and the current findings suggest that LGP-HAL also can be used safely to enhance midface aesthetics, he concluded.
This study was funded by Galderma Laboratories.
MIAMI BEACH – A large gel particle hyaluronic acid filler with lidocaine (LGP-HAL) was safe and effective for midface augmentation and correction of midface contour deficiencies in a randomized, multicenter, pivotal study.
The product (Perlane, Galderma Laboratories), which is currently approved for moderate to severe facial folds and wrinkles, provided visible, clinically meaningful, aesthetic results for at least 12 months based on assessment by a blinded evaluator, Dr. David E. Bank reported in a poster at the South Beach Symposium.
At 8 weeks after initial treatment, 89% of 150 treated subjects experienced at least a one-point improvement in their combined right and left side Medicis Midface Volume Scale (MMVS) score, compared with 16% of 50 patients who were not treated.
Further, the treated subjects were assessed as having greater midface fullness than the nontreated subjects at every measurement during the first 12 months after treatment, according to Dr. Bank of New York–Presbyterian Hospital/Columbia University Medical Center, New York.
Study participants were men and women aged 18-65 years (mean of 53 years) with MMVS scores of two, three, or four on the validated one- to four-point scale, with one indicating a fairly full midface and four indicating substantial loss of fullness in the midface area. At the initial treatment, the 150 treatment group subjects were injected with a mean volume of 4.21 mL. All but one received subcutaneous injections, and 115 received supraperiosteal injections.
They were evaluated at weeks 2 (when an optional touch-up was allowed) and 4, and months 2, 4, 6, 8, 10, and 12 following the initial treatment.
The treatment group subjects were treated again at 12 months, along with those not treated initially. Another touch-up was allowed at a 2-week assessment, and additional assessments were conducted at weeks 3 and 4.
Treatment was well tolerated. More than 80% of events reported after treatment were mild in severity, and the adverse events that occurred in more than 5% of subjects included implant site hematoma, hemorrhage, pain, swelling, and headache.
One subject had two cases of implant site inflammation that were deemed related by the investigators, and one experienced a serious adverse event (implant site hematoma) deemed related to the procedure as opposed to the device.
No additional risk was seen in those who were treated twice, Dr. Bank noted.
“Facial shape plays an important role in facial attractiveness,” he wrote, adding that full cheeks, in particular, play an important role.
Aging, however, is associated with increased tissue laxity, soft-tissue descent and deflation, and loss of bone, which all contribute to deficiencies in the midface.
Hyaluronic fillers have been used successfully to correct such deficiencies, and the current findings suggest that LGP-HAL also can be used safely to enhance midface aesthetics, he concluded.
This study was funded by Galderma Laboratories.
Key clinical point: LGP-HAL (Perlane) is safe and effective for midface augmentation.
Major finding: At 8 weeks, 89% of treated subjects vs. 16% of controls experienced at least a one-point improvement in MMVS score.
Data source: A randomized, multicenter, pivotal study of 200 subjects.
Disclosures This study was funded by Galderma Laboratories.