User login
Sharon Worcester is an award-winning medical journalist for MDedge News. She has been with the company since 1996, first as the Southeast Bureau Chief (1996-2009) when the company was known as International Medical News Group, then as a freelance writer (2010-2015) before returning as a reporter in 2015. She previously worked as a daily newspaper reporter covering health and local government. Sharon currently reports primarily on oncology and hematology. She has a BA from Eckerd College and an MA in Mass Communication/Print Journalism from the University of Florida. Connect with her via LinkedIn and follow her on twitter @SW_MedReporter.
Radiation to Pancreas Linked with Diabetes in Childhood Cancer Survivors
Radiation therapy to the pancreas during childhood confers an increased risk of diabetes during adulthood, according to findings from a retrospective cohort study involving more than 2,500 survivors of childhood cancer.
Specifically, a dose-response relationship was seen between radiation to the tail of the pancreas – where the islets of Langerhans are concentrated – and subsequent diabetes development, reported Florent de Vathaire, Ph.D., of the Center for Epidemiology and Public Health of INSERM at Gustave Roussy Institute in Villejuif, France, and colleagues.

The findings are published online in the Aug. 23 issue of The Lancet Oncology.
Of 2,520 survivors of childhood cancer who returned a survey for the study, 1,632 received radiotherapy during childhood, and 65 had verifiable diabetes, which the authors said was likely type II in most cases. The cumulative incidence of diabetes at age 45 years was significantly greater in those who received radiation therapy (6.6% vs. 2.3%), and those who received radiotherapy to the tail of the pancreas at a dose of 10 Gy or more during childhood were significantly more likely to develop diabetes than were those who did not receive radiotherapy (cumulative incidence of 16.3%).
This relationship persisted even after adjustment for body-mass index (relative risk of 12.6 at a mean radiation dose of 24.2 Gy), the investigators said.
The risk, which was similar in men and women, increased strongly in a dose-dependent fashion up to 20-29 Gy, reaching a plateau at higher doses, they noted (Lancet Oncology 2012 Aug. 23 [doi:10/1016/S1470-2045(12)70323-6]).
No association was found between radiotherapy to other parts of the pancreas and subsequent diabetes development.
Of note, diabetes was diagnosed in 3% of 739 patients who were younger than age 2 years at diagnosis, and the increase per Gy was higher in these patients, compared with older patients. Also, diabetes incidence strongly varied based on the type of childhood cancer, with a cumulative incidence of diabetes at age 45 of 14.7% in survivors of nephroblastoma, compared with 3.1% in survivors of other cancers.
Although these variations by cancer type were explained by differences in age at radiotherapy and by radiation dose to the pancreas tail, patients with nephroblastoma comprised the majority of patients who received high radiation doses to the tail of the pancreas, which raises uncertainty about the attribution of cause, the investigators noted.
No evidence of a significant role for chemotherapy in the calculation of diabetes risk or for chemotherapy overall acting as a modifier of the dose-response for radiation was found in this study, they said.
For the study, the investigators surveyed survivors of childhood cancer – including solid cancer or lymphoma, but excluding leukemia – who were treated in eight centers in France and the United Kingdom before 1986 and followed for a mean of 30 years. Radiation doses to the tail, body, and head of the pancreas were estimated using mathematical modeling, details from the patients’ records, and information about equipment, treatment techniques, and guideline used at the time of treatment.
Though limited by factors such as the high proportion of survivors not included in the analysis and inherent difficulties with estimating radiation dose, the findings of the specificity of the radiation dose to the tail of the pancreas is "plausibly explained by the fact that the islet of Langerhans concentration is higher in the tail than in the body and head of the pancreas," they noted.
"Our investigation emphasizes the importance of long-term follow-up of childhood cancer survivors; almost no diabetes mellitus was seen in our cohort, or those of others, before 20 years of follow-up," they said, noting that the findings also underscore the need for contouring the pancreas when planning radiation therapy to achieve the lowest possible radiation dose to the organ.
This study was funded by Ligue National Contre le Cancer, Institut de Recherche en Santé Publique, Programme Hospitalier de Recherche Clinique, Institut National du Cancer, Agence Française de Sécurité Sanitaire et des Produits de Santé and Fondation Pfizer pour la santé de l’enfant et de l’adolescent. The authors reported having no conflicts of interest.
The findings of Dr. de Vathaire and colleagues substantially extend the current understanding of the late effect of cancer therapy on diabetes development, and have important clinical implications, Dr. Kevin C. Oeffinger and Dr. Charles A. Sklar wrote in an accompanying editorial.
The investigators demonstrate a dose-response relationship between radiation to the tail of the pancreas and subsequent development of diabetes, and since radiation remains an integral part of therapy for many children with Wilms’ tumor or neuroblastoma, concerns about diabetes – a major risk factor for all-cause cardiovascular mortality – are valid in these patients (Lancet Oncology 2012 Aug. 23 [doi:10/1016/S1470-2045(12)70340-6]).
"Additionally, visceral adiposity and insulin resistance are important in tumorigenesis," they said, noting that further study is needed to elucidate the mechanisms underlying diabetes after abdominal radiation.
"Understanding these mechanisms will, hopefully, result in the development of targeted interventions that will lead to a reduction in risk in this population."
Dr. Oeffinger and Dr. Sklar are with Memorial Sloan-Kettering Cancer Center, New York. They reported receiving research grants from the National Institutes of Health, but had no conflicts of interest to report.
The findings of Dr. de Vathaire and colleagues substantially extend the current understanding of the late effect of cancer therapy on diabetes development, and have important clinical implications, Dr. Kevin C. Oeffinger and Dr. Charles A. Sklar wrote in an accompanying editorial.
The investigators demonstrate a dose-response relationship between radiation to the tail of the pancreas and subsequent development of diabetes, and since radiation remains an integral part of therapy for many children with Wilms’ tumor or neuroblastoma, concerns about diabetes – a major risk factor for all-cause cardiovascular mortality – are valid in these patients (Lancet Oncology 2012 Aug. 23 [doi:10/1016/S1470-2045(12)70340-6]).
"Additionally, visceral adiposity and insulin resistance are important in tumorigenesis," they said, noting that further study is needed to elucidate the mechanisms underlying diabetes after abdominal radiation.
"Understanding these mechanisms will, hopefully, result in the development of targeted interventions that will lead to a reduction in risk in this population."
Dr. Oeffinger and Dr. Sklar are with Memorial Sloan-Kettering Cancer Center, New York. They reported receiving research grants from the National Institutes of Health, but had no conflicts of interest to report.
The findings of Dr. de Vathaire and colleagues substantially extend the current understanding of the late effect of cancer therapy on diabetes development, and have important clinical implications, Dr. Kevin C. Oeffinger and Dr. Charles A. Sklar wrote in an accompanying editorial.
The investigators demonstrate a dose-response relationship between radiation to the tail of the pancreas and subsequent development of diabetes, and since radiation remains an integral part of therapy for many children with Wilms’ tumor or neuroblastoma, concerns about diabetes – a major risk factor for all-cause cardiovascular mortality – are valid in these patients (Lancet Oncology 2012 Aug. 23 [doi:10/1016/S1470-2045(12)70340-6]).
"Additionally, visceral adiposity and insulin resistance are important in tumorigenesis," they said, noting that further study is needed to elucidate the mechanisms underlying diabetes after abdominal radiation.
"Understanding these mechanisms will, hopefully, result in the development of targeted interventions that will lead to a reduction in risk in this population."
Dr. Oeffinger and Dr. Sklar are with Memorial Sloan-Kettering Cancer Center, New York. They reported receiving research grants from the National Institutes of Health, but had no conflicts of interest to report.
Radiation therapy to the pancreas during childhood confers an increased risk of diabetes during adulthood, according to findings from a retrospective cohort study involving more than 2,500 survivors of childhood cancer.
Specifically, a dose-response relationship was seen between radiation to the tail of the pancreas – where the islets of Langerhans are concentrated – and subsequent diabetes development, reported Florent de Vathaire, Ph.D., of the Center for Epidemiology and Public Health of INSERM at Gustave Roussy Institute in Villejuif, France, and colleagues.
The findings are published online in the Aug. 23 issue of The Lancet Oncology.
Of 2,520 survivors of childhood cancer who returned a survey for the study, 1,632 received radiotherapy during childhood, and 65 had verifiable diabetes, which the authors said was likely type II in most cases. The cumulative incidence of diabetes at age 45 years was significantly greater in those who received radiation therapy (6.6% vs. 2.3%), and those who received radiotherapy to the tail of the pancreas at a dose of 10 Gy or more during childhood were significantly more likely to develop diabetes than were those who did not receive radiotherapy (cumulative incidence of 16.3%).
This relationship persisted even after adjustment for body-mass index (relative risk of 12.6 at a mean radiation dose of 24.2 Gy), the investigators said.
The risk, which was similar in men and women, increased strongly in a dose-dependent fashion up to 20-29 Gy, reaching a plateau at higher doses, they noted (Lancet Oncology 2012 Aug. 23 [doi:10/1016/S1470-2045(12)70323-6]).
No association was found between radiotherapy to other parts of the pancreas and subsequent diabetes development.
Of note, diabetes was diagnosed in 3% of 739 patients who were younger than age 2 years at diagnosis, and the increase per Gy was higher in these patients, compared with older patients. Also, diabetes incidence strongly varied based on the type of childhood cancer, with a cumulative incidence of diabetes at age 45 of 14.7% in survivors of nephroblastoma, compared with 3.1% in survivors of other cancers.
Although these variations by cancer type were explained by differences in age at radiotherapy and by radiation dose to the pancreas tail, patients with nephroblastoma comprised the majority of patients who received high radiation doses to the tail of the pancreas, which raises uncertainty about the attribution of cause, the investigators noted.
No evidence of a significant role for chemotherapy in the calculation of diabetes risk or for chemotherapy overall acting as a modifier of the dose-response for radiation was found in this study, they said.
For the study, the investigators surveyed survivors of childhood cancer – including solid cancer or lymphoma, but excluding leukemia – who were treated in eight centers in France and the United Kingdom before 1986 and followed for a mean of 30 years. Radiation doses to the tail, body, and head of the pancreas were estimated using mathematical modeling, details from the patients’ records, and information about equipment, treatment techniques, and guideline used at the time of treatment.
Though limited by factors such as the high proportion of survivors not included in the analysis and inherent difficulties with estimating radiation dose, the findings of the specificity of the radiation dose to the tail of the pancreas is "plausibly explained by the fact that the islet of Langerhans concentration is higher in the tail than in the body and head of the pancreas," they noted.
"Our investigation emphasizes the importance of long-term follow-up of childhood cancer survivors; almost no diabetes mellitus was seen in our cohort, or those of others, before 20 years of follow-up," they said, noting that the findings also underscore the need for contouring the pancreas when planning radiation therapy to achieve the lowest possible radiation dose to the organ.
This study was funded by Ligue National Contre le Cancer, Institut de Recherche en Santé Publique, Programme Hospitalier de Recherche Clinique, Institut National du Cancer, Agence Française de Sécurité Sanitaire et des Produits de Santé and Fondation Pfizer pour la santé de l’enfant et de l’adolescent. The authors reported having no conflicts of interest.
Radiation therapy to the pancreas during childhood confers an increased risk of diabetes during adulthood, according to findings from a retrospective cohort study involving more than 2,500 survivors of childhood cancer.
Specifically, a dose-response relationship was seen between radiation to the tail of the pancreas – where the islets of Langerhans are concentrated – and subsequent diabetes development, reported Florent de Vathaire, Ph.D., of the Center for Epidemiology and Public Health of INSERM at Gustave Roussy Institute in Villejuif, France, and colleagues.
The findings are published online in the Aug. 23 issue of The Lancet Oncology.
Of 2,520 survivors of childhood cancer who returned a survey for the study, 1,632 received radiotherapy during childhood, and 65 had verifiable diabetes, which the authors said was likely type II in most cases. The cumulative incidence of diabetes at age 45 years was significantly greater in those who received radiation therapy (6.6% vs. 2.3%), and those who received radiotherapy to the tail of the pancreas at a dose of 10 Gy or more during childhood were significantly more likely to develop diabetes than were those who did not receive radiotherapy (cumulative incidence of 16.3%).
This relationship persisted even after adjustment for body-mass index (relative risk of 12.6 at a mean radiation dose of 24.2 Gy), the investigators said.
The risk, which was similar in men and women, increased strongly in a dose-dependent fashion up to 20-29 Gy, reaching a plateau at higher doses, they noted (Lancet Oncology 2012 Aug. 23 [doi:10/1016/S1470-2045(12)70323-6]).
No association was found between radiotherapy to other parts of the pancreas and subsequent diabetes development.
Of note, diabetes was diagnosed in 3% of 739 patients who were younger than age 2 years at diagnosis, and the increase per Gy was higher in these patients, compared with older patients. Also, diabetes incidence strongly varied based on the type of childhood cancer, with a cumulative incidence of diabetes at age 45 of 14.7% in survivors of nephroblastoma, compared with 3.1% in survivors of other cancers.
Although these variations by cancer type were explained by differences in age at radiotherapy and by radiation dose to the pancreas tail, patients with nephroblastoma comprised the majority of patients who received high radiation doses to the tail of the pancreas, which raises uncertainty about the attribution of cause, the investigators noted.
No evidence of a significant role for chemotherapy in the calculation of diabetes risk or for chemotherapy overall acting as a modifier of the dose-response for radiation was found in this study, they said.
For the study, the investigators surveyed survivors of childhood cancer – including solid cancer or lymphoma, but excluding leukemia – who were treated in eight centers in France and the United Kingdom before 1986 and followed for a mean of 30 years. Radiation doses to the tail, body, and head of the pancreas were estimated using mathematical modeling, details from the patients’ records, and information about equipment, treatment techniques, and guideline used at the time of treatment.
Though limited by factors such as the high proportion of survivors not included in the analysis and inherent difficulties with estimating radiation dose, the findings of the specificity of the radiation dose to the tail of the pancreas is "plausibly explained by the fact that the islet of Langerhans concentration is higher in the tail than in the body and head of the pancreas," they noted.
"Our investigation emphasizes the importance of long-term follow-up of childhood cancer survivors; almost no diabetes mellitus was seen in our cohort, or those of others, before 20 years of follow-up," they said, noting that the findings also underscore the need for contouring the pancreas when planning radiation therapy to achieve the lowest possible radiation dose to the organ.
This study was funded by Ligue National Contre le Cancer, Institut de Recherche en Santé Publique, Programme Hospitalier de Recherche Clinique, Institut National du Cancer, Agence Française de Sécurité Sanitaire et des Produits de Santé and Fondation Pfizer pour la santé de l’enfant et de l’adolescent. The authors reported having no conflicts of interest.
FROM THE LANCET ONCOLOGY
Major Finding: Cancer survivors who received radiotherapy to the tail of the pancreas at a dose of 10 Gy or more during childhood were significantly more likely to develop diabetes than were those who did not receive radiotherapy (cumulative incidence of 16%).
Data Source: Childhood cancer survivors from France and the United Kingdom returned 2,520 questionnaires in this retrospective cohort study.
Disclosures: This study was funded by Ligue National Contre le Cancer, Institut de Recherche en Santé Publique, Programme Hospitalier de Recherche Clinique, Institut National du Cancer, Agence Française de Sécurité Sanitaire et des Produits de Santé and Fondation Pfizer pour la santé de l’enfant et de l’adolescent. The authors reported having no conflicts of interest.

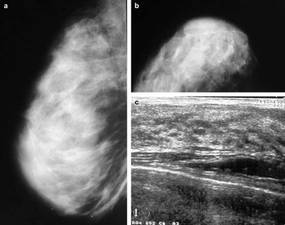
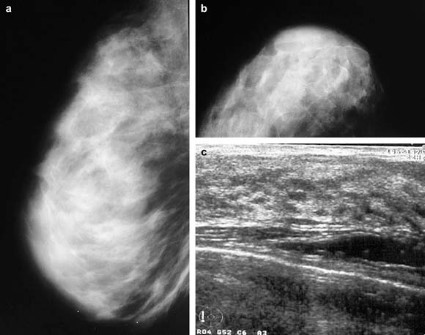
Dense Breasts Don't Increase Risk of Breast Cancer Death
High mammographic breast density is associated with increased risk of developing breast cancer, but not with increased risk of death among those diagnosed with breast cancer, according to an analysis of data from the U.S. Breast Cancer Surveillance Consortium.
Low breast density is associated with an increased risk of breast cancer death, however, in women who are obese or who have large or high-grade tumors, Gretchen L. Gierach, Ph.D., of the National Cancer Institute and her colleagues reported.
Specifically, the elevated risk was apparent for obese women (body mass index 30 kg/m2 or greater) with "almost entirely fatty breasts." This association was not apparent in overweight or lean women.
"One explanation for the increased risks associated with low density among some subgroups is that breasts with a higher percentage of fat may contribute to a tumor microenvironment that facilitates cancer growth and progression," the investigators suggested.
The findings were published Aug. 20 online in the Journal of the National Cancer Institute.
Prior studies have demonstrated that elevated mammographic breast density is among the strongest risk factors for nonfamilial breast cancer. High breast density is also associated with breast cancer risk factors including nulliparity, a positive family history of breast cancer, and menopausal hormone therapy use, but studies have consistently demonstrated that "compared with low density, high density confers relative risks of four- to fivefold for breast cancer, independent of these and other factors," the investigators said.
The association between breast density and death among those diagnosed with breast cancer has remained unclear, however. To assess this relationship, they analyzed data from the U.S. Breast Cancer Surveillance Consortium (BCSC) – a National Cancer Institute–sponsored population-based registry of breast imaging facilities.
"The BCSC offers several advantages for studying these associations relative to other studies, including the prospective follow-up of a large number of breast cancer patients with detailed information regarding potential confounding factors, including BMI, as well as on screening history, tumor characteristics, and treatment," the investigators noted.
The analysis was restricted to women aged 30 years and older at the time of diagnosis with primary incident invasive breast carcinoma. Breast cancer pathology and vital status data were obtained through the Surveillance, Epidemiology, and End Results (SEER) program and by linkage to state cancer registries and/or pathology databases. Breast density data were collected according to the American College of Radiology’s Breast Imaging Reporting and Data System, or BI-RADS, which rates density in categories from 1 (almost entirely fat) to 4 (extremely dense).
The study population comprised 9,232 women diagnosed with primary invasive breast cancer between 1996 and 2005 and followed for a mean of 6.6 years (60,759 person-years) as part of the consortium. Of these 1,795 died, including 889 who died from their breast cancer.
After adjustment for site, age at diagnosis, year of diagnosis, American Joint Committee on Cancer stage, BMI, mode of detection, treatment, and income, no significant association was found between BI-RADS 4 density and death from breast cancer (hazard ratio, 0.92) or death from all causes (HR, 0.83), compared with BI-RADS 2 (scattered fibroglandular densities).
Women with BI-RADS 1 density had an elevated risk for breast cancer death (HR, 1.36), and that risk was further increased among those with tumors of at least 2.0 cm (HR, 1.55), and those with high-grade tumors (HR, 1.45), the investigators reported (J. Natl. Cancer Inst. 2012 Aug. 20 [doi: 10.1093/jnci/djs327]).
BMI was found to modify the relationship between breast density and risk of breast cancer death (P for interaction = .007). The investigators reported a hazard ratio of 2.02 in obese women with "almost entirely fatty" breasts, and noted that it remained apparent even if morbidly obese women with BMI greater than 40 were excluded.
Although the study is limited by "moderate interobserver reliability" with respect to BI-RADS density assessment, and by the fact that that detailed, cumulative information on treatment, comorbidities, and changes in weight after diagnosis was limited, the findings raise additional questions about possible interactions between breast density, other patient characteristics, and subsequent treatment, the investigators said.
"It is reassuring that elevated breast density, a prevalent and strong breast cancer risk factor, was not associated with risk of breast cancer death or death from any cause in this large, prospective study," they said.
"However, we identified subsets of women with breast cancer for whom low density was associated with adverse prognoses, highlighting the possibility of integrating breast density with epidemiological data and other measurements to understand mechanisms of breast carcinogenesis and to identify women who are likely to develop aggressive cancers, which might be preventable or detectable through specific interventions," they said.
The findings underscore the need for improved understanding of the biological characteristics of, and the relationships between breast tissue components responsible for inter-individual variations in breast density, they added.
This study was supported by the Intramural Research Program of the National Institutes of Health, the National Cancer Institute (NCI), and the NCI-funded BCSC.
High mammographic breast density is associated with increased risk of developing breast cancer, but not with increased risk of death among those diagnosed with breast cancer, according to an analysis of data from the U.S. Breast Cancer Surveillance Consortium.
Low breast density is associated with an increased risk of breast cancer death, however, in women who are obese or who have large or high-grade tumors, Gretchen L. Gierach, Ph.D., of the National Cancer Institute and her colleagues reported.
Specifically, the elevated risk was apparent for obese women (body mass index 30 kg/m2 or greater) with "almost entirely fatty breasts." This association was not apparent in overweight or lean women.
"One explanation for the increased risks associated with low density among some subgroups is that breasts with a higher percentage of fat may contribute to a tumor microenvironment that facilitates cancer growth and progression," the investigators suggested.
The findings were published Aug. 20 online in the Journal of the National Cancer Institute.
Prior studies have demonstrated that elevated mammographic breast density is among the strongest risk factors for nonfamilial breast cancer. High breast density is also associated with breast cancer risk factors including nulliparity, a positive family history of breast cancer, and menopausal hormone therapy use, but studies have consistently demonstrated that "compared with low density, high density confers relative risks of four- to fivefold for breast cancer, independent of these and other factors," the investigators said.
The association between breast density and death among those diagnosed with breast cancer has remained unclear, however. To assess this relationship, they analyzed data from the U.S. Breast Cancer Surveillance Consortium (BCSC) – a National Cancer Institute–sponsored population-based registry of breast imaging facilities.
"The BCSC offers several advantages for studying these associations relative to other studies, including the prospective follow-up of a large number of breast cancer patients with detailed information regarding potential confounding factors, including BMI, as well as on screening history, tumor characteristics, and treatment," the investigators noted.
The analysis was restricted to women aged 30 years and older at the time of diagnosis with primary incident invasive breast carcinoma. Breast cancer pathology and vital status data were obtained through the Surveillance, Epidemiology, and End Results (SEER) program and by linkage to state cancer registries and/or pathology databases. Breast density data were collected according to the American College of Radiology’s Breast Imaging Reporting and Data System, or BI-RADS, which rates density in categories from 1 (almost entirely fat) to 4 (extremely dense).
The study population comprised 9,232 women diagnosed with primary invasive breast cancer between 1996 and 2005 and followed for a mean of 6.6 years (60,759 person-years) as part of the consortium. Of these 1,795 died, including 889 who died from their breast cancer.
After adjustment for site, age at diagnosis, year of diagnosis, American Joint Committee on Cancer stage, BMI, mode of detection, treatment, and income, no significant association was found between BI-RADS 4 density and death from breast cancer (hazard ratio, 0.92) or death from all causes (HR, 0.83), compared with BI-RADS 2 (scattered fibroglandular densities).
Women with BI-RADS 1 density had an elevated risk for breast cancer death (HR, 1.36), and that risk was further increased among those with tumors of at least 2.0 cm (HR, 1.55), and those with high-grade tumors (HR, 1.45), the investigators reported (J. Natl. Cancer Inst. 2012 Aug. 20 [doi: 10.1093/jnci/djs327]).
BMI was found to modify the relationship between breast density and risk of breast cancer death (P for interaction = .007). The investigators reported a hazard ratio of 2.02 in obese women with "almost entirely fatty" breasts, and noted that it remained apparent even if morbidly obese women with BMI greater than 40 were excluded.
Although the study is limited by "moderate interobserver reliability" with respect to BI-RADS density assessment, and by the fact that that detailed, cumulative information on treatment, comorbidities, and changes in weight after diagnosis was limited, the findings raise additional questions about possible interactions between breast density, other patient characteristics, and subsequent treatment, the investigators said.
"It is reassuring that elevated breast density, a prevalent and strong breast cancer risk factor, was not associated with risk of breast cancer death or death from any cause in this large, prospective study," they said.
"However, we identified subsets of women with breast cancer for whom low density was associated with adverse prognoses, highlighting the possibility of integrating breast density with epidemiological data and other measurements to understand mechanisms of breast carcinogenesis and to identify women who are likely to develop aggressive cancers, which might be preventable or detectable through specific interventions," they said.
The findings underscore the need for improved understanding of the biological characteristics of, and the relationships between breast tissue components responsible for inter-individual variations in breast density, they added.
This study was supported by the Intramural Research Program of the National Institutes of Health, the National Cancer Institute (NCI), and the NCI-funded BCSC.
High mammographic breast density is associated with increased risk of developing breast cancer, but not with increased risk of death among those diagnosed with breast cancer, according to an analysis of data from the U.S. Breast Cancer Surveillance Consortium.
Low breast density is associated with an increased risk of breast cancer death, however, in women who are obese or who have large or high-grade tumors, Gretchen L. Gierach, Ph.D., of the National Cancer Institute and her colleagues reported.
Specifically, the elevated risk was apparent for obese women (body mass index 30 kg/m2 or greater) with "almost entirely fatty breasts." This association was not apparent in overweight or lean women.
"One explanation for the increased risks associated with low density among some subgroups is that breasts with a higher percentage of fat may contribute to a tumor microenvironment that facilitates cancer growth and progression," the investigators suggested.
The findings were published Aug. 20 online in the Journal of the National Cancer Institute.
Prior studies have demonstrated that elevated mammographic breast density is among the strongest risk factors for nonfamilial breast cancer. High breast density is also associated with breast cancer risk factors including nulliparity, a positive family history of breast cancer, and menopausal hormone therapy use, but studies have consistently demonstrated that "compared with low density, high density confers relative risks of four- to fivefold for breast cancer, independent of these and other factors," the investigators said.
The association between breast density and death among those diagnosed with breast cancer has remained unclear, however. To assess this relationship, they analyzed data from the U.S. Breast Cancer Surveillance Consortium (BCSC) – a National Cancer Institute–sponsored population-based registry of breast imaging facilities.
"The BCSC offers several advantages for studying these associations relative to other studies, including the prospective follow-up of a large number of breast cancer patients with detailed information regarding potential confounding factors, including BMI, as well as on screening history, tumor characteristics, and treatment," the investigators noted.
The analysis was restricted to women aged 30 years and older at the time of diagnosis with primary incident invasive breast carcinoma. Breast cancer pathology and vital status data were obtained through the Surveillance, Epidemiology, and End Results (SEER) program and by linkage to state cancer registries and/or pathology databases. Breast density data were collected according to the American College of Radiology’s Breast Imaging Reporting and Data System, or BI-RADS, which rates density in categories from 1 (almost entirely fat) to 4 (extremely dense).
The study population comprised 9,232 women diagnosed with primary invasive breast cancer between 1996 and 2005 and followed for a mean of 6.6 years (60,759 person-years) as part of the consortium. Of these 1,795 died, including 889 who died from their breast cancer.
After adjustment for site, age at diagnosis, year of diagnosis, American Joint Committee on Cancer stage, BMI, mode of detection, treatment, and income, no significant association was found between BI-RADS 4 density and death from breast cancer (hazard ratio, 0.92) or death from all causes (HR, 0.83), compared with BI-RADS 2 (scattered fibroglandular densities).
Women with BI-RADS 1 density had an elevated risk for breast cancer death (HR, 1.36), and that risk was further increased among those with tumors of at least 2.0 cm (HR, 1.55), and those with high-grade tumors (HR, 1.45), the investigators reported (J. Natl. Cancer Inst. 2012 Aug. 20 [doi: 10.1093/jnci/djs327]).
BMI was found to modify the relationship between breast density and risk of breast cancer death (P for interaction = .007). The investigators reported a hazard ratio of 2.02 in obese women with "almost entirely fatty" breasts, and noted that it remained apparent even if morbidly obese women with BMI greater than 40 were excluded.
Although the study is limited by "moderate interobserver reliability" with respect to BI-RADS density assessment, and by the fact that that detailed, cumulative information on treatment, comorbidities, and changes in weight after diagnosis was limited, the findings raise additional questions about possible interactions between breast density, other patient characteristics, and subsequent treatment, the investigators said.
"It is reassuring that elevated breast density, a prevalent and strong breast cancer risk factor, was not associated with risk of breast cancer death or death from any cause in this large, prospective study," they said.
"However, we identified subsets of women with breast cancer for whom low density was associated with adverse prognoses, highlighting the possibility of integrating breast density with epidemiological data and other measurements to understand mechanisms of breast carcinogenesis and to identify women who are likely to develop aggressive cancers, which might be preventable or detectable through specific interventions," they said.
The findings underscore the need for improved understanding of the biological characteristics of, and the relationships between breast tissue components responsible for inter-individual variations in breast density, they added.
This study was supported by the Intramural Research Program of the National Institutes of Health, the National Cancer Institute (NCI), and the NCI-funded BCSC.
FROM THE JOURNAL OF THE NATIONAL CANCER INSTITUTE
Enzalutamide Prolongs Prostate Cancer Survival After Chemotherapy Fails
Enzalutamide – formerly known as MDV3100 – prolonged overall survival by a median of 4.8 months and reduced the risk of death by 37%, according to newly published data from the phase III, placebo-controlled AFFIRM study of men with metastatic, castration-resistant prostate cancer.
An experimental oral agent inhibiting signaling by the androgen receptor, enzalutamide is under priority review by the Food and Drug Administration with an action date of Nov. 22, 2012, trial sponsors Medivation and Astellas Pharma have announced.

The randomized, double-blind AFFIRM trial underpins their New Drug Application in men with castration-resistant prostate cancer previously treated with docetaxel (Taxotere)-based chemotherapy. Based on the findings, an independent data and safety monitoring committee halted the trial, and those receiving placebo were offered treatment with enzalutamide.
At the time of a planned interim analysis, median overall survival was 18.4 months among 800 men randomized to receive a daily 160-mg oral dose of enzalutamide. It was 13.6 months in 399 men who received a placebo, Dr. Howard I. Scher of Memorial Sloan-Kettering Cancer Center, New York, and his colleagues reported "online first" Aug. 15 in the New England Journal of Medicine.
The drug was also superior to placebo with respect to all secondary end points, including prostate-specific antigen (PSA) response rate (54% vs. 2%), soft-tissue response rate (29% vs. 4%), FACT-P quality of life response (43% vs. 18%), time to PSA progression (8.3 vs. 3.0 months; hazard ratio, 0.25), radiographic progression-free survival (8.3 vs. 2.9 months; HR, 0.40), and time to first skeletal-related event (16.7 vs. 13.3 months; HR, 0.69). The results were consistent across all subgroups, and were maintained after adjustment for stratification factors and baseline prognostic factors.
They confirm that the androgen receptor and androgen-receptor signaling have a central role in the progression of prostate cancer "throughout the spectrum of disease," the investigators said (N. Engl. J. Med. 2012 [doi: 10.1056/NEJMoa1207506]).
Participants in AFFIRM (A Study Evaluating the Efficacy and Safety of the Investigational Drug MDV3100) were men with progressive prostate cancer that had been treated with one or two chemotherapy regimens, at least one of which included docetaxel. The subjects, who were enrolled at 156 sites in 15 countries between September 2009 and November 2010, had a histologically or cytologically confirmed diagnosis of prostate cancer and testosterone levels of less than 50 ng/dL.
Despite longer observation with enzalutamide, adverse event rates were generally similar between the treatment and control groups; of note, those in the enzalutamide group experienced a lower incidence of adverse events of grade 3 or above (45.3% vs. 53.1%).
"The median time to any initial adverse event of grade 3 or higher was 8.4 months longer in the enzalutamide group than in the placebo groups (12.6 vs. 4.2 months) owing to improved long-term control of disease-related symptoms without an increase in drug reactions of grade 3 or higher," the investigators said.
More patients in the treatment group, however, experienced fatigue, diarrhea, hot flashes, musculoskeletal pain, and headache. In addition, seizures occurred in five (0.6%) patients in the treatment group, whereas no seizures were reported in those receiving placebo. Predisposing factors were present in several patients experiencing seizures, including brain metastases in two patients, inadvertent IV administration of lidocaine in one patient, and brain atrophy in one patient.
The findings of this study substantiate preclinical work showing that androgen-receptor signaling contributes to disease progression despite castrate levels of testosterone and despite prior treatment with conventional antiandrogen therapy, the investigators said. This – coupled with other recent findings – establishes that these tumors are not refractory to hormones as previously thought, even after chemotherapy has been administered, they added.
"This novel agent is anticipated to join the therapeutic armamentarium of anticancer drugs with diverse mechanisms of action that confer a survival benefit in men with castration-resistant prostate cancer. These results validate androgen-receptor signaling as a key therapeutic target throughout the clinical spectrum of prostate cancer, including in men who have received previous chemotherapy," they concluded, noting that clinical trials of the drug in earlier-stage prostate cancer are ongoing.
Earlier studies of enzalutamide have been announced in patients with metastatic chemotherapy-naive prostate cancer.
This study was supported by Medivation, the maker of enzalutamide, and Astellas Pharma Global Development. Dr. Scher reported relationships with Aragon Pharmaceuticals, Centocor Ortho Biotech, and other companies. He holds stock or stock options in Johnson & Johnson. Other study authors also made disclosures; details are available with the full text of the article at NEJM.org.
Dr. Scher presented results from the AFFIRM trial at the American Society of Clinical Oncology’s Genitourinary Cancers Symposium in February 2012.
Click here to see a 2009 video of Dr. Scher discussing the rationale behind MDV3100 efficacy in advanced prostate cancer.
Enzalutamide – formerly known as MDV3100 – prolonged overall survival by a median of 4.8 months and reduced the risk of death by 37%, according to newly published data from the phase III, placebo-controlled AFFIRM study of men with metastatic, castration-resistant prostate cancer.
An experimental oral agent inhibiting signaling by the androgen receptor, enzalutamide is under priority review by the Food and Drug Administration with an action date of Nov. 22, 2012, trial sponsors Medivation and Astellas Pharma have announced.
The randomized, double-blind AFFIRM trial underpins their New Drug Application in men with castration-resistant prostate cancer previously treated with docetaxel (Taxotere)-based chemotherapy. Based on the findings, an independent data and safety monitoring committee halted the trial, and those receiving placebo were offered treatment with enzalutamide.
At the time of a planned interim analysis, median overall survival was 18.4 months among 800 men randomized to receive a daily 160-mg oral dose of enzalutamide. It was 13.6 months in 399 men who received a placebo, Dr. Howard I. Scher of Memorial Sloan-Kettering Cancer Center, New York, and his colleagues reported "online first" Aug. 15 in the New England Journal of Medicine.
The drug was also superior to placebo with respect to all secondary end points, including prostate-specific antigen (PSA) response rate (54% vs. 2%), soft-tissue response rate (29% vs. 4%), FACT-P quality of life response (43% vs. 18%), time to PSA progression (8.3 vs. 3.0 months; hazard ratio, 0.25), radiographic progression-free survival (8.3 vs. 2.9 months; HR, 0.40), and time to first skeletal-related event (16.7 vs. 13.3 months; HR, 0.69). The results were consistent across all subgroups, and were maintained after adjustment for stratification factors and baseline prognostic factors.
They confirm that the androgen receptor and androgen-receptor signaling have a central role in the progression of prostate cancer "throughout the spectrum of disease," the investigators said (N. Engl. J. Med. 2012 [doi: 10.1056/NEJMoa1207506]).
Participants in AFFIRM (A Study Evaluating the Efficacy and Safety of the Investigational Drug MDV3100) were men with progressive prostate cancer that had been treated with one or two chemotherapy regimens, at least one of which included docetaxel. The subjects, who were enrolled at 156 sites in 15 countries between September 2009 and November 2010, had a histologically or cytologically confirmed diagnosis of prostate cancer and testosterone levels of less than 50 ng/dL.
Despite longer observation with enzalutamide, adverse event rates were generally similar between the treatment and control groups; of note, those in the enzalutamide group experienced a lower incidence of adverse events of grade 3 or above (45.3% vs. 53.1%).
"The median time to any initial adverse event of grade 3 or higher was 8.4 months longer in the enzalutamide group than in the placebo groups (12.6 vs. 4.2 months) owing to improved long-term control of disease-related symptoms without an increase in drug reactions of grade 3 or higher," the investigators said.
More patients in the treatment group, however, experienced fatigue, diarrhea, hot flashes, musculoskeletal pain, and headache. In addition, seizures occurred in five (0.6%) patients in the treatment group, whereas no seizures were reported in those receiving placebo. Predisposing factors were present in several patients experiencing seizures, including brain metastases in two patients, inadvertent IV administration of lidocaine in one patient, and brain atrophy in one patient.
The findings of this study substantiate preclinical work showing that androgen-receptor signaling contributes to disease progression despite castrate levels of testosterone and despite prior treatment with conventional antiandrogen therapy, the investigators said. This – coupled with other recent findings – establishes that these tumors are not refractory to hormones as previously thought, even after chemotherapy has been administered, they added.
"This novel agent is anticipated to join the therapeutic armamentarium of anticancer drugs with diverse mechanisms of action that confer a survival benefit in men with castration-resistant prostate cancer. These results validate androgen-receptor signaling as a key therapeutic target throughout the clinical spectrum of prostate cancer, including in men who have received previous chemotherapy," they concluded, noting that clinical trials of the drug in earlier-stage prostate cancer are ongoing.
Earlier studies of enzalutamide have been announced in patients with metastatic chemotherapy-naive prostate cancer.
This study was supported by Medivation, the maker of enzalutamide, and Astellas Pharma Global Development. Dr. Scher reported relationships with Aragon Pharmaceuticals, Centocor Ortho Biotech, and other companies. He holds stock or stock options in Johnson & Johnson. Other study authors also made disclosures; details are available with the full text of the article at NEJM.org.
Dr. Scher presented results from the AFFIRM trial at the American Society of Clinical Oncology’s Genitourinary Cancers Symposium in February 2012.
Click here to see a 2009 video of Dr. Scher discussing the rationale behind MDV3100 efficacy in advanced prostate cancer.
Enzalutamide – formerly known as MDV3100 – prolonged overall survival by a median of 4.8 months and reduced the risk of death by 37%, according to newly published data from the phase III, placebo-controlled AFFIRM study of men with metastatic, castration-resistant prostate cancer.
An experimental oral agent inhibiting signaling by the androgen receptor, enzalutamide is under priority review by the Food and Drug Administration with an action date of Nov. 22, 2012, trial sponsors Medivation and Astellas Pharma have announced.
The randomized, double-blind AFFIRM trial underpins their New Drug Application in men with castration-resistant prostate cancer previously treated with docetaxel (Taxotere)-based chemotherapy. Based on the findings, an independent data and safety monitoring committee halted the trial, and those receiving placebo were offered treatment with enzalutamide.
At the time of a planned interim analysis, median overall survival was 18.4 months among 800 men randomized to receive a daily 160-mg oral dose of enzalutamide. It was 13.6 months in 399 men who received a placebo, Dr. Howard I. Scher of Memorial Sloan-Kettering Cancer Center, New York, and his colleagues reported "online first" Aug. 15 in the New England Journal of Medicine.
The drug was also superior to placebo with respect to all secondary end points, including prostate-specific antigen (PSA) response rate (54% vs. 2%), soft-tissue response rate (29% vs. 4%), FACT-P quality of life response (43% vs. 18%), time to PSA progression (8.3 vs. 3.0 months; hazard ratio, 0.25), radiographic progression-free survival (8.3 vs. 2.9 months; HR, 0.40), and time to first skeletal-related event (16.7 vs. 13.3 months; HR, 0.69). The results were consistent across all subgroups, and were maintained after adjustment for stratification factors and baseline prognostic factors.
They confirm that the androgen receptor and androgen-receptor signaling have a central role in the progression of prostate cancer "throughout the spectrum of disease," the investigators said (N. Engl. J. Med. 2012 [doi: 10.1056/NEJMoa1207506]).
Participants in AFFIRM (A Study Evaluating the Efficacy and Safety of the Investigational Drug MDV3100) were men with progressive prostate cancer that had been treated with one or two chemotherapy regimens, at least one of which included docetaxel. The subjects, who were enrolled at 156 sites in 15 countries between September 2009 and November 2010, had a histologically or cytologically confirmed diagnosis of prostate cancer and testosterone levels of less than 50 ng/dL.
Despite longer observation with enzalutamide, adverse event rates were generally similar between the treatment and control groups; of note, those in the enzalutamide group experienced a lower incidence of adverse events of grade 3 or above (45.3% vs. 53.1%).
"The median time to any initial adverse event of grade 3 or higher was 8.4 months longer in the enzalutamide group than in the placebo groups (12.6 vs. 4.2 months) owing to improved long-term control of disease-related symptoms without an increase in drug reactions of grade 3 or higher," the investigators said.
More patients in the treatment group, however, experienced fatigue, diarrhea, hot flashes, musculoskeletal pain, and headache. In addition, seizures occurred in five (0.6%) patients in the treatment group, whereas no seizures were reported in those receiving placebo. Predisposing factors were present in several patients experiencing seizures, including brain metastases in two patients, inadvertent IV administration of lidocaine in one patient, and brain atrophy in one patient.
The findings of this study substantiate preclinical work showing that androgen-receptor signaling contributes to disease progression despite castrate levels of testosterone and despite prior treatment with conventional antiandrogen therapy, the investigators said. This – coupled with other recent findings – establishes that these tumors are not refractory to hormones as previously thought, even after chemotherapy has been administered, they added.
"This novel agent is anticipated to join the therapeutic armamentarium of anticancer drugs with diverse mechanisms of action that confer a survival benefit in men with castration-resistant prostate cancer. These results validate androgen-receptor signaling as a key therapeutic target throughout the clinical spectrum of prostate cancer, including in men who have received previous chemotherapy," they concluded, noting that clinical trials of the drug in earlier-stage prostate cancer are ongoing.
Earlier studies of enzalutamide have been announced in patients with metastatic chemotherapy-naive prostate cancer.
This study was supported by Medivation, the maker of enzalutamide, and Astellas Pharma Global Development. Dr. Scher reported relationships with Aragon Pharmaceuticals, Centocor Ortho Biotech, and other companies. He holds stock or stock options in Johnson & Johnson. Other study authors also made disclosures; details are available with the full text of the article at NEJM.org.
Dr. Scher presented results from the AFFIRM trial at the American Society of Clinical Oncology’s Genitourinary Cancers Symposium in February 2012.
Click here to see a 2009 video of Dr. Scher discussing the rationale behind MDV3100 efficacy in advanced prostate cancer.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE

Troponin T-Based Algorithm Rules AMI In or Out
A simple algorithm using baseline values and absolute changes in high-sensitivity cardiac troponin T allows for rapid rule-in and rule-out of acute myocardial infarction in most patients who present with chest pain, according to findings from a prospective, multicenter study.
The algorithm, which was developed in a randomly selected derivation cohort of 436 patients and validated in an additional 436 subjects from the APACE (Advantageous Predictors of Acute Coronary Syndrome Evaluation) study, safely ruled out and accurately ruled in acute myocardial infarction within 1 hour in 77% of patients with chest pain, Dr. Tobias Reichlin of University Hospital Basel (Switzerland) and his colleagues reported online Aug. 13 in Archives of Internal Medicine.
In the validation cohort, the algorithm had 100% sensitivity and negative predictive value for ruling out acute myocardial infarction, and 97% specificity and 84% positive predictive value for ruling in AMI, the investigators said (Arch. Intern. Med. 2012 Aug. 13 [doi: 10.1001/archinternmed.2012.3698]).
Use of the algorithm "may obviate the need for prolonged monitoring and serial blood sampling in 3 of 4 patients with chest pain," they noted.
APACE participants presented during April 2006-June 2009 with acute chest pain symptoms suggestive of AMI, and were tested at baseline and after 1 hour for serum levels of high-sensitivity cardiac troponin T (hs-cTnT), a highly specific biomarker of myocardial necrosis.
Baseline levels of hs-cTnT were significantly higher in patients with AMI, compared with patients having other final diagnoses, and the prevalence of AMI in those presenting with acute chest pain differed significantly based on quantitative levels of hs-cTnT.
"In patients with hs-cTnT levels lower than 14 ng/L (99th percentile of healthy individuals) at presentation, the incidence of AMI was 3.2%, and there was a rise to 21% in patients with levels between 14 and 49 ng/L, 65% in patients with levels between 50 and 99 ng/L, 88% in patients with levels between 100 and 199 ng/L, and 93% in patients with levels of 200 ng/L or higher," the investigators said.
The optimal rule-out threshold was determined to be a baseline hs-cTnT level lower than 12 ng/L, and an absolute change of less than 3 ng/L in the first hour; the optimal rule-in threshold for AMI was either a baseline hs-cTnT of 52 ng/L or higher at presentation, or an absolute change of 5 ng/L or higher in the first hour.
The cumulative 30-day survival rates among 259 patients in whom AMI was ruled out, 76 in whom AMI was ruled in, and 101 who did not meet criteria for rule-in or rule-out (those considered to be in an "observational zone") were 99.8%, 95.3%, and 98.6%, respectively.
The low 30-day mortality of 0.2% in patients ruled out for AMI "underscores the suitability of these patients for early discharge," the investigators wrote.
"Our findings extend and corroborate recent results regarding hs-cTnT assays and are of great clinical importance," they said, explaining that they provide some clarification about how to use the assays for decision making in daily clinical practice. Because the proportion of patients with AMI continuously increases with increasing hs-cTnT values, it is important to interpret levels as quantitative rather than qualitative, avoiding the terms positive and negative with respect to the levels.
Given the potential limitations of the study – including the fact that it was conducted in emergency department patients with symptoms suggestive of AMI (the pretest probability setting where the algorithm should be used), and the fact that the proportion of patients with MI (17%) was high compared with other chest pain studies – the algorithm requires confirmation and external validation in a second multicenter study in a lower-risk cohort, the investigators said.
This study was supported by research grants from the Swiss National Science Foundation, the Swiss Heart Foundation, Abbott, Roche, Siemens, and the department of internal medicine at University Hospital Basel. The hs-cTnT assay was donated by Roche. Dr. Reichlin and coauthor Dr. Christian Mueller each disclosed receiving speaker honoraria from Abbott, Biosite, and other companies. In addition, Dr. Reichlin disclosed receiving grant support from the Professor Max Cloetta Foundation, and Dr. Mueller reported receiving research support from the Novartis Foundation, the Krokus Foundation, Abbott, AstraZeneca, and other companies.
The algorithmic approach to ruling in and ruling out AMI in patients presenting with chest pain as presented by Dr. Reichlin and his colleagues provides an important step forward in the application of high-sensitivity cardiac troponin as a tool for the triage of emergency department patients with possible MI, and could – with continued development – substantially improve the evaluation of such patients, Dr. L. Kristin Newby wrote in an accompanying editorial.
"However, much work remains to develop the evidence to bring hsTn testing and the algorithms they have developed to use in clinical practice," she wrote (Arch. Intern. Med. 2012 Aug. 13 [doi: 10/1001/archinternmed.2012.1808]).
Most importantly, the algorithm requires validation in prospective studies that assess implications for clinical outcomes in addition to the sensitivity and negative predictive value, and specificity and positive predictive value, she noted.
Such studies will help confirm that the thresholds used in the current study are satisfactory across age groups, and help determine whether factors such as sex and time from symptom onset should also be considered.
"Finally, although touted as ‘simple’ by the authors, the need for multi-component algorithms that are different for rule-in and rule-out and that vary by age group or other parameters will challenge application by busy clinicians unlikely to remember or accurately process the proposed algorithm. As such, it will be imperative that hsTn algorithms, if validated, are built into clinical decision support layered onto electronic health records so that testing results are provided electronically to physicians along with the algorithmic interpretation to allow systematic application in triage and treatment," she wrote.
Dr. Newby is with the division of cardiology at the Duke Clinical Research Institute in Durham, N.C. She reported receiving personal income from consulting or other service, and/or support from research grants or contracts from Amgen, AstraZeneca, and other companies, as well as the National Heart, Lung, and Blood Institute.
The algorithmic approach to ruling in and ruling out AMI in patients presenting with chest pain as presented by Dr. Reichlin and his colleagues provides an important step forward in the application of high-sensitivity cardiac troponin as a tool for the triage of emergency department patients with possible MI, and could – with continued development – substantially improve the evaluation of such patients, Dr. L. Kristin Newby wrote in an accompanying editorial.
"However, much work remains to develop the evidence to bring hsTn testing and the algorithms they have developed to use in clinical practice," she wrote (Arch. Intern. Med. 2012 Aug. 13 [doi: 10/1001/archinternmed.2012.1808]).
Most importantly, the algorithm requires validation in prospective studies that assess implications for clinical outcomes in addition to the sensitivity and negative predictive value, and specificity and positive predictive value, she noted.
Such studies will help confirm that the thresholds used in the current study are satisfactory across age groups, and help determine whether factors such as sex and time from symptom onset should also be considered.
"Finally, although touted as ‘simple’ by the authors, the need for multi-component algorithms that are different for rule-in and rule-out and that vary by age group or other parameters will challenge application by busy clinicians unlikely to remember or accurately process the proposed algorithm. As such, it will be imperative that hsTn algorithms, if validated, are built into clinical decision support layered onto electronic health records so that testing results are provided electronically to physicians along with the algorithmic interpretation to allow systematic application in triage and treatment," she wrote.
Dr. Newby is with the division of cardiology at the Duke Clinical Research Institute in Durham, N.C. She reported receiving personal income from consulting or other service, and/or support from research grants or contracts from Amgen, AstraZeneca, and other companies, as well as the National Heart, Lung, and Blood Institute.
The algorithmic approach to ruling in and ruling out AMI in patients presenting with chest pain as presented by Dr. Reichlin and his colleagues provides an important step forward in the application of high-sensitivity cardiac troponin as a tool for the triage of emergency department patients with possible MI, and could – with continued development – substantially improve the evaluation of such patients, Dr. L. Kristin Newby wrote in an accompanying editorial.
"However, much work remains to develop the evidence to bring hsTn testing and the algorithms they have developed to use in clinical practice," she wrote (Arch. Intern. Med. 2012 Aug. 13 [doi: 10/1001/archinternmed.2012.1808]).
Most importantly, the algorithm requires validation in prospective studies that assess implications for clinical outcomes in addition to the sensitivity and negative predictive value, and specificity and positive predictive value, she noted.
Such studies will help confirm that the thresholds used in the current study are satisfactory across age groups, and help determine whether factors such as sex and time from symptom onset should also be considered.
"Finally, although touted as ‘simple’ by the authors, the need for multi-component algorithms that are different for rule-in and rule-out and that vary by age group or other parameters will challenge application by busy clinicians unlikely to remember or accurately process the proposed algorithm. As such, it will be imperative that hsTn algorithms, if validated, are built into clinical decision support layered onto electronic health records so that testing results are provided electronically to physicians along with the algorithmic interpretation to allow systematic application in triage and treatment," she wrote.
Dr. Newby is with the division of cardiology at the Duke Clinical Research Institute in Durham, N.C. She reported receiving personal income from consulting or other service, and/or support from research grants or contracts from Amgen, AstraZeneca, and other companies, as well as the National Heart, Lung, and Blood Institute.
A simple algorithm using baseline values and absolute changes in high-sensitivity cardiac troponin T allows for rapid rule-in and rule-out of acute myocardial infarction in most patients who present with chest pain, according to findings from a prospective, multicenter study.
The algorithm, which was developed in a randomly selected derivation cohort of 436 patients and validated in an additional 436 subjects from the APACE (Advantageous Predictors of Acute Coronary Syndrome Evaluation) study, safely ruled out and accurately ruled in acute myocardial infarction within 1 hour in 77% of patients with chest pain, Dr. Tobias Reichlin of University Hospital Basel (Switzerland) and his colleagues reported online Aug. 13 in Archives of Internal Medicine.
In the validation cohort, the algorithm had 100% sensitivity and negative predictive value for ruling out acute myocardial infarction, and 97% specificity and 84% positive predictive value for ruling in AMI, the investigators said (Arch. Intern. Med. 2012 Aug. 13 [doi: 10.1001/archinternmed.2012.3698]).
Use of the algorithm "may obviate the need for prolonged monitoring and serial blood sampling in 3 of 4 patients with chest pain," they noted.
APACE participants presented during April 2006-June 2009 with acute chest pain symptoms suggestive of AMI, and were tested at baseline and after 1 hour for serum levels of high-sensitivity cardiac troponin T (hs-cTnT), a highly specific biomarker of myocardial necrosis.
Baseline levels of hs-cTnT were significantly higher in patients with AMI, compared with patients having other final diagnoses, and the prevalence of AMI in those presenting with acute chest pain differed significantly based on quantitative levels of hs-cTnT.
"In patients with hs-cTnT levels lower than 14 ng/L (99th percentile of healthy individuals) at presentation, the incidence of AMI was 3.2%, and there was a rise to 21% in patients with levels between 14 and 49 ng/L, 65% in patients with levels between 50 and 99 ng/L, 88% in patients with levels between 100 and 199 ng/L, and 93% in patients with levels of 200 ng/L or higher," the investigators said.
The optimal rule-out threshold was determined to be a baseline hs-cTnT level lower than 12 ng/L, and an absolute change of less than 3 ng/L in the first hour; the optimal rule-in threshold for AMI was either a baseline hs-cTnT of 52 ng/L or higher at presentation, or an absolute change of 5 ng/L or higher in the first hour.
The cumulative 30-day survival rates among 259 patients in whom AMI was ruled out, 76 in whom AMI was ruled in, and 101 who did not meet criteria for rule-in or rule-out (those considered to be in an "observational zone") were 99.8%, 95.3%, and 98.6%, respectively.
The low 30-day mortality of 0.2% in patients ruled out for AMI "underscores the suitability of these patients for early discharge," the investigators wrote.
"Our findings extend and corroborate recent results regarding hs-cTnT assays and are of great clinical importance," they said, explaining that they provide some clarification about how to use the assays for decision making in daily clinical practice. Because the proportion of patients with AMI continuously increases with increasing hs-cTnT values, it is important to interpret levels as quantitative rather than qualitative, avoiding the terms positive and negative with respect to the levels.
Given the potential limitations of the study – including the fact that it was conducted in emergency department patients with symptoms suggestive of AMI (the pretest probability setting where the algorithm should be used), and the fact that the proportion of patients with MI (17%) was high compared with other chest pain studies – the algorithm requires confirmation and external validation in a second multicenter study in a lower-risk cohort, the investigators said.
This study was supported by research grants from the Swiss National Science Foundation, the Swiss Heart Foundation, Abbott, Roche, Siemens, and the department of internal medicine at University Hospital Basel. The hs-cTnT assay was donated by Roche. Dr. Reichlin and coauthor Dr. Christian Mueller each disclosed receiving speaker honoraria from Abbott, Biosite, and other companies. In addition, Dr. Reichlin disclosed receiving grant support from the Professor Max Cloetta Foundation, and Dr. Mueller reported receiving research support from the Novartis Foundation, the Krokus Foundation, Abbott, AstraZeneca, and other companies.
A simple algorithm using baseline values and absolute changes in high-sensitivity cardiac troponin T allows for rapid rule-in and rule-out of acute myocardial infarction in most patients who present with chest pain, according to findings from a prospective, multicenter study.
The algorithm, which was developed in a randomly selected derivation cohort of 436 patients and validated in an additional 436 subjects from the APACE (Advantageous Predictors of Acute Coronary Syndrome Evaluation) study, safely ruled out and accurately ruled in acute myocardial infarction within 1 hour in 77% of patients with chest pain, Dr. Tobias Reichlin of University Hospital Basel (Switzerland) and his colleagues reported online Aug. 13 in Archives of Internal Medicine.
In the validation cohort, the algorithm had 100% sensitivity and negative predictive value for ruling out acute myocardial infarction, and 97% specificity and 84% positive predictive value for ruling in AMI, the investigators said (Arch. Intern. Med. 2012 Aug. 13 [doi: 10.1001/archinternmed.2012.3698]).
Use of the algorithm "may obviate the need for prolonged monitoring and serial blood sampling in 3 of 4 patients with chest pain," they noted.
APACE participants presented during April 2006-June 2009 with acute chest pain symptoms suggestive of AMI, and were tested at baseline and after 1 hour for serum levels of high-sensitivity cardiac troponin T (hs-cTnT), a highly specific biomarker of myocardial necrosis.
Baseline levels of hs-cTnT were significantly higher in patients with AMI, compared with patients having other final diagnoses, and the prevalence of AMI in those presenting with acute chest pain differed significantly based on quantitative levels of hs-cTnT.
"In patients with hs-cTnT levels lower than 14 ng/L (99th percentile of healthy individuals) at presentation, the incidence of AMI was 3.2%, and there was a rise to 21% in patients with levels between 14 and 49 ng/L, 65% in patients with levels between 50 and 99 ng/L, 88% in patients with levels between 100 and 199 ng/L, and 93% in patients with levels of 200 ng/L or higher," the investigators said.
The optimal rule-out threshold was determined to be a baseline hs-cTnT level lower than 12 ng/L, and an absolute change of less than 3 ng/L in the first hour; the optimal rule-in threshold for AMI was either a baseline hs-cTnT of 52 ng/L or higher at presentation, or an absolute change of 5 ng/L or higher in the first hour.
The cumulative 30-day survival rates among 259 patients in whom AMI was ruled out, 76 in whom AMI was ruled in, and 101 who did not meet criteria for rule-in or rule-out (those considered to be in an "observational zone") were 99.8%, 95.3%, and 98.6%, respectively.
The low 30-day mortality of 0.2% in patients ruled out for AMI "underscores the suitability of these patients for early discharge," the investigators wrote.
"Our findings extend and corroborate recent results regarding hs-cTnT assays and are of great clinical importance," they said, explaining that they provide some clarification about how to use the assays for decision making in daily clinical practice. Because the proportion of patients with AMI continuously increases with increasing hs-cTnT values, it is important to interpret levels as quantitative rather than qualitative, avoiding the terms positive and negative with respect to the levels.
Given the potential limitations of the study – including the fact that it was conducted in emergency department patients with symptoms suggestive of AMI (the pretest probability setting where the algorithm should be used), and the fact that the proportion of patients with MI (17%) was high compared with other chest pain studies – the algorithm requires confirmation and external validation in a second multicenter study in a lower-risk cohort, the investigators said.
This study was supported by research grants from the Swiss National Science Foundation, the Swiss Heart Foundation, Abbott, Roche, Siemens, and the department of internal medicine at University Hospital Basel. The hs-cTnT assay was donated by Roche. Dr. Reichlin and coauthor Dr. Christian Mueller each disclosed receiving speaker honoraria from Abbott, Biosite, and other companies. In addition, Dr. Reichlin disclosed receiving grant support from the Professor Max Cloetta Foundation, and Dr. Mueller reported receiving research support from the Novartis Foundation, the Krokus Foundation, Abbott, AstraZeneca, and other companies.
FROM ARCHIVES OF INTERNAL MEDICINE
Major Finding: In the validation cohort, a high-sensitivity cardiac troponin T algorithm had 100% sensitivity and negative predictive value for ruling out AMI, and 97% specificity and 84% positive predictive value for ruling in AMI.
Data Source: Data are from the prospective, multicenter APACE study.
Disclosures: This study was supported by research grants from the Swiss National Science Foundation, the Swiss Heart Foundation, Abbott, Roche, Siemens, and the department of internal medicine at University Hospital Basel. The hs-cTnT assay was donated by Roche. Dr. Reichlin and coauthor Dr. Christian Mueller each disclosed receiving speaker honoraria from Abbott, Biosite, and other companies. In addition, Dr. Reichlin disclosed receiving grant support from the Professor Max Cloetta Foundation, and Dr. Mueller reported receiving research support from the Novartis Foundation, the Krokus Foundation, Abbott, AstraZeneca, and other companies.
EMS Prenotification of Hospitals Lags for Incoming Stroke Patients
When emergency medical services personnel alert hospitals of incoming stroke patients, evaluation and treatment are improved, but prenotification occurs in only about two-thirds of cases, according to findings from two new American Heart Association/American Stroke Association (AHA/ASA) studies.
Both of the Get With The Guidelines–Stroke program studies involved the same group of nearly 372,000 patients with acute ischemic stroke, who were transported by emergency medical services to one of 1,585 participating hospitals between April 2003 and April 2011. One of the studies showed that compared with no notification, prenotification of an incoming stroke patient was associated with significantly more rapid evaluation and treatment, and with a significantly greater likelihood of treatment with tissue plasminogen activator (TPA) within 3 hours, Cheryl B. Lin of the Duke–National University of Singapore Graduate Medical School, Singapore, and her colleagues reported online in Circulation: Cardiovascular Quality and Outcomes.
For example, among patients who arrived at the hospital within 3 hours of symptom onset, median door-to-imaging time was 26 minutes, compared with 31 minutes for those without prenotification. Door-to-imaging time was within 25 minutes for 48.8% and 40.5% of those with and without prenotification, respectively. Also, symptom onset–to-door times were lower with prenotification (113 vs. 150 minutes) (Circ. Cardiovasc. Qual. Outcomes 2012 July 10 [doi: 10.1161/circoutcomes.112.965210]).
Prenotification also significantly improved door-to-needle time and symptom onset–to-needle time, and more eligible patients who arrived at the hospital within 2 hours were treated with TPA within 3 hours (71.8% vs. 62.2%).
The problem is that prenotification occurred in only 67% of cases, the authors said.
"Our analysis supports the role [of EMS prenotification] as a potentially important but underused means to improving rapid triage, evaluation, and treatment of patients with acute ischemic stroke," they wrote, noting that although prenotification is recommended in guidelines from both the AHA/ ASA and the National Association of Emergency Medical Services Physicians, it appears many hospitals "still find difficulty in meeting these performance goals."
In the related study published online in the Journal of the American Heart Association, Ms. Lin and her colleagues found that prenotification varied widely by hospital and region, with rates of prenotification ranging from 0% to 100%.
In Washington, D.C., for example, the prenotification rate was 19.7%, compared with 93.4% in Montana, the investigators said (J. Am. Heart Assoc. 2012 July 10 [doi: 10.1161/jaha.112.002345]).
Patient factors associated with increased likelihood of prenotification were younger age, white race, past history of atrial fibrillation, no medical history of previous stroke or transient ischemic attack, diabetes mellitus, and peripheral vascular disease.
"In particular, black patients had decreased odds [of EMS prenotification] when compared to their white counterparts, with adjusted odds ratio of 0.94," the investigators noted.
Hospital factors associated with reduced likelihood of prenotification were academic affiliation, location in the northeastern United States, and lower annual volume of TPA administration.
Rates of prenotification did increase modestly and significantly over time, from 58% to 67% between 2003 and 2011, with a high of 71.1% in 2008, followed by a decline to about 65% in 2009 and 2010, and an increase to 67.3% in 2011, but targeted improvements in rates of EMS prenotification are needed, they said.
"These findings demonstrate gaps in the quality of stroke care provided and support the need for initiatives targeted to improve [EMS prenotification rates] on a national level," they concluded, explaining that a systems approach is needed involving increasing symptom recognition and rapid activation of EMS, adequate training of EMS staff in proper use of stroke-screening instruments and the need for hospital prenotification, and implementation of systems of care in receiving hospitals.
A stroke system-of-care process measure reporting the use of EMS prenotification should be considered, they said.
The Get With the Guidelines (GWTG)–Stroke program is provided by the AHA/ASA and is supported in part by a charitable contribution from the Bristol-Myers Squibb/Sanofi Pharmaceuticals Partnership and the AHA Pharmaceutical Roundtable. Past support has been provided by Boehringer Ingelheim and Merck. Ms. Lin reported having no relevant conflicts of interest. Several coauthors have worked with GWTG committees, and some have received research grant support from pharmaceutical companies. Some researchers are employees of the University of California, which holds a patent on retriever devices for stroke.
When emergency medical services personnel alert hospitals of incoming stroke patients, evaluation and treatment are improved, but prenotification occurs in only about two-thirds of cases, according to findings from two new American Heart Association/American Stroke Association (AHA/ASA) studies.
Both of the Get With The Guidelines–Stroke program studies involved the same group of nearly 372,000 patients with acute ischemic stroke, who were transported by emergency medical services to one of 1,585 participating hospitals between April 2003 and April 2011. One of the studies showed that compared with no notification, prenotification of an incoming stroke patient was associated with significantly more rapid evaluation and treatment, and with a significantly greater likelihood of treatment with tissue plasminogen activator (TPA) within 3 hours, Cheryl B. Lin of the Duke–National University of Singapore Graduate Medical School, Singapore, and her colleagues reported online in Circulation: Cardiovascular Quality and Outcomes.
For example, among patients who arrived at the hospital within 3 hours of symptom onset, median door-to-imaging time was 26 minutes, compared with 31 minutes for those without prenotification. Door-to-imaging time was within 25 minutes for 48.8% and 40.5% of those with and without prenotification, respectively. Also, symptom onset–to-door times were lower with prenotification (113 vs. 150 minutes) (Circ. Cardiovasc. Qual. Outcomes 2012 July 10 [doi: 10.1161/circoutcomes.112.965210]).
Prenotification also significantly improved door-to-needle time and symptom onset–to-needle time, and more eligible patients who arrived at the hospital within 2 hours were treated with TPA within 3 hours (71.8% vs. 62.2%).
The problem is that prenotification occurred in only 67% of cases, the authors said.
"Our analysis supports the role [of EMS prenotification] as a potentially important but underused means to improving rapid triage, evaluation, and treatment of patients with acute ischemic stroke," they wrote, noting that although prenotification is recommended in guidelines from both the AHA/ ASA and the National Association of Emergency Medical Services Physicians, it appears many hospitals "still find difficulty in meeting these performance goals."
In the related study published online in the Journal of the American Heart Association, Ms. Lin and her colleagues found that prenotification varied widely by hospital and region, with rates of prenotification ranging from 0% to 100%.
In Washington, D.C., for example, the prenotification rate was 19.7%, compared with 93.4% in Montana, the investigators said (J. Am. Heart Assoc. 2012 July 10 [doi: 10.1161/jaha.112.002345]).
Patient factors associated with increased likelihood of prenotification were younger age, white race, past history of atrial fibrillation, no medical history of previous stroke or transient ischemic attack, diabetes mellitus, and peripheral vascular disease.
"In particular, black patients had decreased odds [of EMS prenotification] when compared to their white counterparts, with adjusted odds ratio of 0.94," the investigators noted.
Hospital factors associated with reduced likelihood of prenotification were academic affiliation, location in the northeastern United States, and lower annual volume of TPA administration.
Rates of prenotification did increase modestly and significantly over time, from 58% to 67% between 2003 and 2011, with a high of 71.1% in 2008, followed by a decline to about 65% in 2009 and 2010, and an increase to 67.3% in 2011, but targeted improvements in rates of EMS prenotification are needed, they said.
"These findings demonstrate gaps in the quality of stroke care provided and support the need for initiatives targeted to improve [EMS prenotification rates] on a national level," they concluded, explaining that a systems approach is needed involving increasing symptom recognition and rapid activation of EMS, adequate training of EMS staff in proper use of stroke-screening instruments and the need for hospital prenotification, and implementation of systems of care in receiving hospitals.
A stroke system-of-care process measure reporting the use of EMS prenotification should be considered, they said.
The Get With the Guidelines (GWTG)–Stroke program is provided by the AHA/ASA and is supported in part by a charitable contribution from the Bristol-Myers Squibb/Sanofi Pharmaceuticals Partnership and the AHA Pharmaceutical Roundtable. Past support has been provided by Boehringer Ingelheim and Merck. Ms. Lin reported having no relevant conflicts of interest. Several coauthors have worked with GWTG committees, and some have received research grant support from pharmaceutical companies. Some researchers are employees of the University of California, which holds a patent on retriever devices for stroke.
When emergency medical services personnel alert hospitals of incoming stroke patients, evaluation and treatment are improved, but prenotification occurs in only about two-thirds of cases, according to findings from two new American Heart Association/American Stroke Association (AHA/ASA) studies.
Both of the Get With The Guidelines–Stroke program studies involved the same group of nearly 372,000 patients with acute ischemic stroke, who were transported by emergency medical services to one of 1,585 participating hospitals between April 2003 and April 2011. One of the studies showed that compared with no notification, prenotification of an incoming stroke patient was associated with significantly more rapid evaluation and treatment, and with a significantly greater likelihood of treatment with tissue plasminogen activator (TPA) within 3 hours, Cheryl B. Lin of the Duke–National University of Singapore Graduate Medical School, Singapore, and her colleagues reported online in Circulation: Cardiovascular Quality and Outcomes.
For example, among patients who arrived at the hospital within 3 hours of symptom onset, median door-to-imaging time was 26 minutes, compared with 31 minutes for those without prenotification. Door-to-imaging time was within 25 minutes for 48.8% and 40.5% of those with and without prenotification, respectively. Also, symptom onset–to-door times were lower with prenotification (113 vs. 150 minutes) (Circ. Cardiovasc. Qual. Outcomes 2012 July 10 [doi: 10.1161/circoutcomes.112.965210]).
Prenotification also significantly improved door-to-needle time and symptom onset–to-needle time, and more eligible patients who arrived at the hospital within 2 hours were treated with TPA within 3 hours (71.8% vs. 62.2%).
The problem is that prenotification occurred in only 67% of cases, the authors said.
"Our analysis supports the role [of EMS prenotification] as a potentially important but underused means to improving rapid triage, evaluation, and treatment of patients with acute ischemic stroke," they wrote, noting that although prenotification is recommended in guidelines from both the AHA/ ASA and the National Association of Emergency Medical Services Physicians, it appears many hospitals "still find difficulty in meeting these performance goals."
In the related study published online in the Journal of the American Heart Association, Ms. Lin and her colleagues found that prenotification varied widely by hospital and region, with rates of prenotification ranging from 0% to 100%.
In Washington, D.C., for example, the prenotification rate was 19.7%, compared with 93.4% in Montana, the investigators said (J. Am. Heart Assoc. 2012 July 10 [doi: 10.1161/jaha.112.002345]).
Patient factors associated with increased likelihood of prenotification were younger age, white race, past history of atrial fibrillation, no medical history of previous stroke or transient ischemic attack, diabetes mellitus, and peripheral vascular disease.
"In particular, black patients had decreased odds [of EMS prenotification] when compared to their white counterparts, with adjusted odds ratio of 0.94," the investigators noted.
Hospital factors associated with reduced likelihood of prenotification were academic affiliation, location in the northeastern United States, and lower annual volume of TPA administration.
Rates of prenotification did increase modestly and significantly over time, from 58% to 67% between 2003 and 2011, with a high of 71.1% in 2008, followed by a decline to about 65% in 2009 and 2010, and an increase to 67.3% in 2011, but targeted improvements in rates of EMS prenotification are needed, they said.
"These findings demonstrate gaps in the quality of stroke care provided and support the need for initiatives targeted to improve [EMS prenotification rates] on a national level," they concluded, explaining that a systems approach is needed involving increasing symptom recognition and rapid activation of EMS, adequate training of EMS staff in proper use of stroke-screening instruments and the need for hospital prenotification, and implementation of systems of care in receiving hospitals.
A stroke system-of-care process measure reporting the use of EMS prenotification should be considered, they said.
The Get With the Guidelines (GWTG)–Stroke program is provided by the AHA/ASA and is supported in part by a charitable contribution from the Bristol-Myers Squibb/Sanofi Pharmaceuticals Partnership and the AHA Pharmaceutical Roundtable. Past support has been provided by Boehringer Ingelheim and Merck. Ms. Lin reported having no relevant conflicts of interest. Several coauthors have worked with GWTG committees, and some have received research grant support from pharmaceutical companies. Some researchers are employees of the University of California, which holds a patent on retriever devices for stroke.
FROM CIRCULATION: CARDIOVASCULAR QUALITY AND OUTCOMES, AND THE JOURNAL OF THE AMERICAN HEART ASSOCIATION
Biopsy Must Guide Lupus Nephritis Management
The management of adult and pediatric lupus nephritis should be guided by renal biopsy, with a goal of achieving complete renal response, according to updated recommendations from the European League Against Rheumatism and the European Renal Association–European Dialysis and Transplant Association.
The update, including 28 final statements on lupus nephritis (LN) management derived using an evidence-based approach and expert consensus, is the first since 2008, when EULAR recommendations on the management of systemic lupus erythematosus (SLE) were issued.
"Since then, several controlled trials have been published upon which updated recommendations can be based," Dr. George K. Bertsias of the University of Crete, Iraklion, Greece, and his colleagues reported. The study was published online July 31 in Annals of the Rheumatic Diseases.
The new recommendations call for renal biopsy in patients with any sign of kidney involvement, particularly those with reproducible proteinuria of 0.5 g/24 h or greater, and especially if glomerular hematuria and/or cellular casts are present (Ann. Rheum. Dis. 2012 July 31 [doi:10.1136/annrheumdis-2012-201940]).
"Because of the potentially aggressive nature of [lupus nephritis], the thresholds for performing a renal biopsy should be low," the investigators said, noting that biopsy can also be considered in cases of persisting isolated glomerular hematuria, isolated leucocyturia (after other causes such as infection or drugs are excluded), and the rare occurrence of unexplained renal insufficiency with normal urinary findings.
Biopsy should be performed within a month of disease onset – ideally before institution of immunosuppressive therapy. But treatment with high-dose glucocorticoids should not be delayed if biopsy cannot be readily performed, the investigators said.
The aim of immunosuppressive treatment should be complete response, defined as a urine protein:creatinine ratio of less than 50 mg/mmol, which is roughly equivalent to proteinuria of less than 0.5 g/24 h.
"Ultimate goals of treatment are long-term preservation of renal function, prevention of flares, avoidance of treatment-related harms, and improved quality of life and survival," the investigators said, adding that treatment choices must be based on a decision reached jointly by patient and physician.
Immunosuppressive therapy is generally not warranted in classes I and VI LN, unless there is extra-renal lupus activity.
In adults, the recommended initial treatment for most cases of class III-IV disease is mycophenolate mofetil (target dose of 3 g/day for 6 months) or an equivalent dose of enteric-coated mycophenolic acid sodium, or low-dose intravenous cyclophosphamide at a total dose of 3 g over 3 months in combination with oral glucocorticoids (0.5 mg/kg per day). To increase efficacy, treatment should be combined initially with three consecutive pulses of intravenous methylprednisolone at 500-750 mg, followed by oral prednisone at 0.5 mg/kg per day for 4 weeks, with this dosage reduced to 10 mg/day or less by 4-6 months.
In pure class V disease with nephrotic-range proteinuria, the recommended treatment is mycophenolate mofetil at a target dose of 3 g/day for 6 months in combination with oral prednisone at a dose of 0.5 mg/kg per day.
In children whose LN tends to be more severe with increased damage accrual, management and monitoring recommendations are similar to those for adults. Management should include "a coordinated transition program to adult specialists" to optimize long-term outcomes.
The joint European League Against Rheumatism and the European Renal Association–European Dialysis and Transplant Association recommendations also address:
• Adjunctive treatments. For example, angiotensin-converting enzyme inhibitors or angiotensin receptor blockers are recommended for patients with proteinuria or hypertension, and hydroxychloroquine is recommended to improve outcomes by reducing renal flares and limiting accrual of renal and cardiovascular damage.
• Monitoring and prognosis of lupus nephritis. Visits are recommended every 2-4 weeks for the first 2-4 months after diagnosis, and repeat biopsies in certain patients, such as those experiencing relapse, are also recommended.
• Management of end-stage renal disease in LN. The recommendations state that all types of renal replacement can be used in patients with lupus, and transplantation can be performed when lupus activity has been absent or at a low level for 3-6 months.
• Antiphospholipid syndrome–associated nephropathy. Hydroxychloroquine and/or antiplatelet/ anticoagulant treatment should be considered.
• LN in pregnancy. Hydroxychloroquine can be used, as can low-dose prednisone, azathioprine and/or calcineurin inhibitors when needed. Acetylsalicylic acid should be considered to reduce risk of preeclampsia.
The recommendations are important, given that about half of all patients with SLE will develop LN, thereby increasing their risk of renal failure, cardiovascular disease, and death.
"The realization that in the case of patients with LN internists/rheumatologists and nephrologists are involved, prompted us to develop recommendations for LN under the joint auspices of the EULAR and the [ERA-EDTA], with experts from both disciplines," they explained, noting that "the panel was enriched with renal pathologists and pediatricians with expertise on LN."
The American College of Rheumatology similarly released updated recommendations on LN in May.
Support for the development of the EULAR/ERA-EDTA recommendations was provided via grants from the EULAR Standing Committee on Clinical Affairs and the ERA-EDTA. The authors reported having no competing interests.
The management of adult and pediatric lupus nephritis should be guided by renal biopsy, with a goal of achieving complete renal response, according to updated recommendations from the European League Against Rheumatism and the European Renal Association–European Dialysis and Transplant Association.
The update, including 28 final statements on lupus nephritis (LN) management derived using an evidence-based approach and expert consensus, is the first since 2008, when EULAR recommendations on the management of systemic lupus erythematosus (SLE) were issued.
"Since then, several controlled trials have been published upon which updated recommendations can be based," Dr. George K. Bertsias of the University of Crete, Iraklion, Greece, and his colleagues reported. The study was published online July 31 in Annals of the Rheumatic Diseases.
The new recommendations call for renal biopsy in patients with any sign of kidney involvement, particularly those with reproducible proteinuria of 0.5 g/24 h or greater, and especially if glomerular hematuria and/or cellular casts are present (Ann. Rheum. Dis. 2012 July 31 [doi:10.1136/annrheumdis-2012-201940]).
"Because of the potentially aggressive nature of [lupus nephritis], the thresholds for performing a renal biopsy should be low," the investigators said, noting that biopsy can also be considered in cases of persisting isolated glomerular hematuria, isolated leucocyturia (after other causes such as infection or drugs are excluded), and the rare occurrence of unexplained renal insufficiency with normal urinary findings.
Biopsy should be performed within a month of disease onset – ideally before institution of immunosuppressive therapy. But treatment with high-dose glucocorticoids should not be delayed if biopsy cannot be readily performed, the investigators said.
The aim of immunosuppressive treatment should be complete response, defined as a urine protein:creatinine ratio of less than 50 mg/mmol, which is roughly equivalent to proteinuria of less than 0.5 g/24 h.
"Ultimate goals of treatment are long-term preservation of renal function, prevention of flares, avoidance of treatment-related harms, and improved quality of life and survival," the investigators said, adding that treatment choices must be based on a decision reached jointly by patient and physician.
Immunosuppressive therapy is generally not warranted in classes I and VI LN, unless there is extra-renal lupus activity.
In adults, the recommended initial treatment for most cases of class III-IV disease is mycophenolate mofetil (target dose of 3 g/day for 6 months) or an equivalent dose of enteric-coated mycophenolic acid sodium, or low-dose intravenous cyclophosphamide at a total dose of 3 g over 3 months in combination with oral glucocorticoids (0.5 mg/kg per day). To increase efficacy, treatment should be combined initially with three consecutive pulses of intravenous methylprednisolone at 500-750 mg, followed by oral prednisone at 0.5 mg/kg per day for 4 weeks, with this dosage reduced to 10 mg/day or less by 4-6 months.
In pure class V disease with nephrotic-range proteinuria, the recommended treatment is mycophenolate mofetil at a target dose of 3 g/day for 6 months in combination with oral prednisone at a dose of 0.5 mg/kg per day.
In children whose LN tends to be more severe with increased damage accrual, management and monitoring recommendations are similar to those for adults. Management should include "a coordinated transition program to adult specialists" to optimize long-term outcomes.
The joint European League Against Rheumatism and the European Renal Association–European Dialysis and Transplant Association recommendations also address:
• Adjunctive treatments. For example, angiotensin-converting enzyme inhibitors or angiotensin receptor blockers are recommended for patients with proteinuria or hypertension, and hydroxychloroquine is recommended to improve outcomes by reducing renal flares and limiting accrual of renal and cardiovascular damage.
• Monitoring and prognosis of lupus nephritis. Visits are recommended every 2-4 weeks for the first 2-4 months after diagnosis, and repeat biopsies in certain patients, such as those experiencing relapse, are also recommended.
• Management of end-stage renal disease in LN. The recommendations state that all types of renal replacement can be used in patients with lupus, and transplantation can be performed when lupus activity has been absent or at a low level for 3-6 months.
• Antiphospholipid syndrome–associated nephropathy. Hydroxychloroquine and/or antiplatelet/ anticoagulant treatment should be considered.
• LN in pregnancy. Hydroxychloroquine can be used, as can low-dose prednisone, azathioprine and/or calcineurin inhibitors when needed. Acetylsalicylic acid should be considered to reduce risk of preeclampsia.
The recommendations are important, given that about half of all patients with SLE will develop LN, thereby increasing their risk of renal failure, cardiovascular disease, and death.
"The realization that in the case of patients with LN internists/rheumatologists and nephrologists are involved, prompted us to develop recommendations for LN under the joint auspices of the EULAR and the [ERA-EDTA], with experts from both disciplines," they explained, noting that "the panel was enriched with renal pathologists and pediatricians with expertise on LN."
The American College of Rheumatology similarly released updated recommendations on LN in May.
Support for the development of the EULAR/ERA-EDTA recommendations was provided via grants from the EULAR Standing Committee on Clinical Affairs and the ERA-EDTA. The authors reported having no competing interests.
The management of adult and pediatric lupus nephritis should be guided by renal biopsy, with a goal of achieving complete renal response, according to updated recommendations from the European League Against Rheumatism and the European Renal Association–European Dialysis and Transplant Association.
The update, including 28 final statements on lupus nephritis (LN) management derived using an evidence-based approach and expert consensus, is the first since 2008, when EULAR recommendations on the management of systemic lupus erythematosus (SLE) were issued.
"Since then, several controlled trials have been published upon which updated recommendations can be based," Dr. George K. Bertsias of the University of Crete, Iraklion, Greece, and his colleagues reported. The study was published online July 31 in Annals of the Rheumatic Diseases.
The new recommendations call for renal biopsy in patients with any sign of kidney involvement, particularly those with reproducible proteinuria of 0.5 g/24 h or greater, and especially if glomerular hematuria and/or cellular casts are present (Ann. Rheum. Dis. 2012 July 31 [doi:10.1136/annrheumdis-2012-201940]).
"Because of the potentially aggressive nature of [lupus nephritis], the thresholds for performing a renal biopsy should be low," the investigators said, noting that biopsy can also be considered in cases of persisting isolated glomerular hematuria, isolated leucocyturia (after other causes such as infection or drugs are excluded), and the rare occurrence of unexplained renal insufficiency with normal urinary findings.
Biopsy should be performed within a month of disease onset – ideally before institution of immunosuppressive therapy. But treatment with high-dose glucocorticoids should not be delayed if biopsy cannot be readily performed, the investigators said.
The aim of immunosuppressive treatment should be complete response, defined as a urine protein:creatinine ratio of less than 50 mg/mmol, which is roughly equivalent to proteinuria of less than 0.5 g/24 h.
"Ultimate goals of treatment are long-term preservation of renal function, prevention of flares, avoidance of treatment-related harms, and improved quality of life and survival," the investigators said, adding that treatment choices must be based on a decision reached jointly by patient and physician.
Immunosuppressive therapy is generally not warranted in classes I and VI LN, unless there is extra-renal lupus activity.
In adults, the recommended initial treatment for most cases of class III-IV disease is mycophenolate mofetil (target dose of 3 g/day for 6 months) or an equivalent dose of enteric-coated mycophenolic acid sodium, or low-dose intravenous cyclophosphamide at a total dose of 3 g over 3 months in combination with oral glucocorticoids (0.5 mg/kg per day). To increase efficacy, treatment should be combined initially with three consecutive pulses of intravenous methylprednisolone at 500-750 mg, followed by oral prednisone at 0.5 mg/kg per day for 4 weeks, with this dosage reduced to 10 mg/day or less by 4-6 months.
In pure class V disease with nephrotic-range proteinuria, the recommended treatment is mycophenolate mofetil at a target dose of 3 g/day for 6 months in combination with oral prednisone at a dose of 0.5 mg/kg per day.
In children whose LN tends to be more severe with increased damage accrual, management and monitoring recommendations are similar to those for adults. Management should include "a coordinated transition program to adult specialists" to optimize long-term outcomes.
The joint European League Against Rheumatism and the European Renal Association–European Dialysis and Transplant Association recommendations also address:
• Adjunctive treatments. For example, angiotensin-converting enzyme inhibitors or angiotensin receptor blockers are recommended for patients with proteinuria or hypertension, and hydroxychloroquine is recommended to improve outcomes by reducing renal flares and limiting accrual of renal and cardiovascular damage.
• Monitoring and prognosis of lupus nephritis. Visits are recommended every 2-4 weeks for the first 2-4 months after diagnosis, and repeat biopsies in certain patients, such as those experiencing relapse, are also recommended.
• Management of end-stage renal disease in LN. The recommendations state that all types of renal replacement can be used in patients with lupus, and transplantation can be performed when lupus activity has been absent or at a low level for 3-6 months.
• Antiphospholipid syndrome–associated nephropathy. Hydroxychloroquine and/or antiplatelet/ anticoagulant treatment should be considered.
• LN in pregnancy. Hydroxychloroquine can be used, as can low-dose prednisone, azathioprine and/or calcineurin inhibitors when needed. Acetylsalicylic acid should be considered to reduce risk of preeclampsia.
The recommendations are important, given that about half of all patients with SLE will develop LN, thereby increasing their risk of renal failure, cardiovascular disease, and death.
"The realization that in the case of patients with LN internists/rheumatologists and nephrologists are involved, prompted us to develop recommendations for LN under the joint auspices of the EULAR and the [ERA-EDTA], with experts from both disciplines," they explained, noting that "the panel was enriched with renal pathologists and pediatricians with expertise on LN."
The American College of Rheumatology similarly released updated recommendations on LN in May.
Support for the development of the EULAR/ERA-EDTA recommendations was provided via grants from the EULAR Standing Committee on Clinical Affairs and the ERA-EDTA. The authors reported having no competing interests.
FROM ANNALS OF THE RHEUMATIC DISEASES
Spray-On Cells Promote Venous Ulcer Healing
A spray formulation of allogeneic neonatal keratinocytes and fibroblasts significantly improved wound healing in a multicenter, randomized, placebo-controlled phase II study of more than 200 patients with venous leg ulcers.
The mean reduction in wound area was significantly greater among 177 patients who received 12 weeks of active treatment with the novel cell therapy, known as HP802-247, than among 50 patients who were treated with application vehicle of a modified fibrin spray alone. HP802-247 consists of cryopreserved, allogenic, growth-arrested fibroblasts and keratinocytes derived from neonatal foreskin. The largest improvement (16% on average over placebo) was seen in 44 patients assigned to treatment with 5.0x106 cells per mL every 14 days, Dr. Robert S. Kirsner of the University of Miami and his colleagues reported. The study was published online in the Aug. 3 issue of The Lancet.
Reduction in wound area was between 8% and 12% over that seen with placebo in 45 patients treated with 5.0x106 cells per mL every 7 days, 44 patients treated with 5.0x106 cells per mL every 14 days, and 43 patients treated with 0.5x106 cells per mL every 7 days, the investigators said (Lancet 2012 Aug. 3 [doi:10.1016/S0140-6736(12)60644-8]).
The study investigators included vascular surgeons, dermatologists, and podiatrists at universities and in private practice. All patients were treated with standard compression bandaging as well as the study treatment.
"Wound area began to decrease rapidly after initiation of treatment. After one application of the 0.5x106/mL every 14 days dose, the mean reduction in wound area was 40%, compared with 23% for the vehicle group. This effect persisted with the maximum difference in mean reduction between the group assigned [0.5x106 cells per mL] every 14 days and the vehicle group occurring at week 7 of treatment (87% vs. 65%)," they wrote.
At week 12 of treatment, the mean wound area in the group treated with 0.5x106 cells per mL every 14 days was reduced by 91%, compared with 80% with vehicle, and for the other treatment groups, the mean wound area was reduced by between 84% and 87%.
"Overall, patients treated with cells had higher proportions of healed wounds than did those assigned vehicle alone, but only the group assigned [0.5x106 cells per mL] every 14 days differed significantly compared with control," they noted.
Adverse events were similar across all groups, and most were nonserious, mild to moderate events that resolved. Only new skin ulcers and cellulitis occurred at a frequency of greater than 5%. Immunotoxicity testing showed that there was no treatment-induced alloantibody formation or induction of autoimmunity.
Included in this study were adult outpatients enrolled from 28 centers in the United States and Canada between 2009 and 2011. All had venous reflux confirmed by duplex Doppler ultrasonography, and up to three venous leg ulcers. Those assigned to the placebo group received vehicle alone applied every 7 days for the 12 weeks of the trial.
The findings may have important implications for the treatment of venous leg ulcers, which affect an estimated 1.65% to 1.74% of adults aged 65 years and older. Standard treatment with infection control, primary dressings, and high-strength compressions heal between 30% and 75% of such ulcers, compared with the 84%-91% healing seen with HP802-247 in this study, with the remainder becoming "chronic, with unresolved inflammatory processes within the extracellular matrix of the wound bed and dysfunction of wound fibroblasts and keratinocytes," the investigators noted.
"The results are sufficiently promising that larger randomized trials comparing HP802-247 to standard treatment for venous leg ulcers are now warranted," they concluded.
The researchers reported that their study was limited by the wound upper end boundary of 12 cm3, which represents 80% of all venous leg ulcers, but a smaller proportion of chronic venous ulcers.
The research trial is registered with ClinicalTrials.gov as NCT00852995.
Dr. Kirsner received consulting fees for his assistance with protocol design and data interpretation. Two of his coauthors also received such consulting fees, and other authors on the study disclosed that they are employed by Healthpoint, and/or hold adjunct academic appointments at the University of North Texas Health Sciences Center in Fort Worth, Tex.
The findings of this "well-done clinical trial" highlight the potential of cell-based therapies not only for venous leg ulcer treatment, but for the treatment of other chronic wounds as well, Dr. Matthias Augustin and Dr. Wolfgang Vanscheidt wrote in an accompanying editorial.
The authors have "clearly shown that a specific cell therapy for venous leg ulcers can lead to a significantly higher healing rate than for vehicle alone in hard-to-treat wounds for which compression treatment has been applied unsuccessfully," they noted, adding that "the benefits identified by Kirsner and colleagues could well be applicable in other chronic wounds such as ischemic and diabetic foot ulcers."
Dr. Augustin and Dr. Vanscheidt stressed the importance of gaining insight into the mechanism of action to further understand the best potential uses of these types of therapies, and called on the scientific community and industry to investigate the effects of tissue and cell therapy products in patients with mixed arterial-venous leg ulcers in whom revascularization is not possible (Lancet 2012 Aug. 3 [doi:10.1016/S0140-6736(12)61255-0]).
"In this indication, bioengineered tissue and cell therapy products are presumably among the very few methods that could achieve sustained healing. Because of aging of the population in most societies, this fatal combination of venous insufficiency and arterial occlusive disease will become an ever-growing problem. We believe that biotherapy of such ulcers will be a challenge but will also offer hope to wound researchers in the coming decades," they said.
Dr. Augustin and Dr. Vanscheidt are with the Institute for Health Services Research in Dermatology and Nursing and Comprehensive Wound Center, University Medical Center Hamburg (Germany), and Freiburg, Germany, respectively. They reported having no conflicts of interest.
The findings of this "well-done clinical trial" highlight the potential of cell-based therapies not only for venous leg ulcer treatment, but for the treatment of other chronic wounds as well, Dr. Matthias Augustin and Dr. Wolfgang Vanscheidt wrote in an accompanying editorial.
The authors have "clearly shown that a specific cell therapy for venous leg ulcers can lead to a significantly higher healing rate than for vehicle alone in hard-to-treat wounds for which compression treatment has been applied unsuccessfully," they noted, adding that "the benefits identified by Kirsner and colleagues could well be applicable in other chronic wounds such as ischemic and diabetic foot ulcers."
Dr. Augustin and Dr. Vanscheidt stressed the importance of gaining insight into the mechanism of action to further understand the best potential uses of these types of therapies, and called on the scientific community and industry to investigate the effects of tissue and cell therapy products in patients with mixed arterial-venous leg ulcers in whom revascularization is not possible (Lancet 2012 Aug. 3 [doi:10.1016/S0140-6736(12)61255-0]).
"In this indication, bioengineered tissue and cell therapy products are presumably among the very few methods that could achieve sustained healing. Because of aging of the population in most societies, this fatal combination of venous insufficiency and arterial occlusive disease will become an ever-growing problem. We believe that biotherapy of such ulcers will be a challenge but will also offer hope to wound researchers in the coming decades," they said.
Dr. Augustin and Dr. Vanscheidt are with the Institute for Health Services Research in Dermatology and Nursing and Comprehensive Wound Center, University Medical Center Hamburg (Germany), and Freiburg, Germany, respectively. They reported having no conflicts of interest.
The findings of this "well-done clinical trial" highlight the potential of cell-based therapies not only for venous leg ulcer treatment, but for the treatment of other chronic wounds as well, Dr. Matthias Augustin and Dr. Wolfgang Vanscheidt wrote in an accompanying editorial.
The authors have "clearly shown that a specific cell therapy for venous leg ulcers can lead to a significantly higher healing rate than for vehicle alone in hard-to-treat wounds for which compression treatment has been applied unsuccessfully," they noted, adding that "the benefits identified by Kirsner and colleagues could well be applicable in other chronic wounds such as ischemic and diabetic foot ulcers."
Dr. Augustin and Dr. Vanscheidt stressed the importance of gaining insight into the mechanism of action to further understand the best potential uses of these types of therapies, and called on the scientific community and industry to investigate the effects of tissue and cell therapy products in patients with mixed arterial-venous leg ulcers in whom revascularization is not possible (Lancet 2012 Aug. 3 [doi:10.1016/S0140-6736(12)61255-0]).
"In this indication, bioengineered tissue and cell therapy products are presumably among the very few methods that could achieve sustained healing. Because of aging of the population in most societies, this fatal combination of venous insufficiency and arterial occlusive disease will become an ever-growing problem. We believe that biotherapy of such ulcers will be a challenge but will also offer hope to wound researchers in the coming decades," they said.
Dr. Augustin and Dr. Vanscheidt are with the Institute for Health Services Research in Dermatology and Nursing and Comprehensive Wound Center, University Medical Center Hamburg (Germany), and Freiburg, Germany, respectively. They reported having no conflicts of interest.
A spray formulation of allogeneic neonatal keratinocytes and fibroblasts significantly improved wound healing in a multicenter, randomized, placebo-controlled phase II study of more than 200 patients with venous leg ulcers.
The mean reduction in wound area was significantly greater among 177 patients who received 12 weeks of active treatment with the novel cell therapy, known as HP802-247, than among 50 patients who were treated with application vehicle of a modified fibrin spray alone. HP802-247 consists of cryopreserved, allogenic, growth-arrested fibroblasts and keratinocytes derived from neonatal foreskin. The largest improvement (16% on average over placebo) was seen in 44 patients assigned to treatment with 5.0x106 cells per mL every 14 days, Dr. Robert S. Kirsner of the University of Miami and his colleagues reported. The study was published online in the Aug. 3 issue of The Lancet.
Reduction in wound area was between 8% and 12% over that seen with placebo in 45 patients treated with 5.0x106 cells per mL every 7 days, 44 patients treated with 5.0x106 cells per mL every 14 days, and 43 patients treated with 0.5x106 cells per mL every 7 days, the investigators said (Lancet 2012 Aug. 3 [doi:10.1016/S0140-6736(12)60644-8]).
The study investigators included vascular surgeons, dermatologists, and podiatrists at universities and in private practice. All patients were treated with standard compression bandaging as well as the study treatment.
"Wound area began to decrease rapidly after initiation of treatment. After one application of the 0.5x106/mL every 14 days dose, the mean reduction in wound area was 40%, compared with 23% for the vehicle group. This effect persisted with the maximum difference in mean reduction between the group assigned [0.5x106 cells per mL] every 14 days and the vehicle group occurring at week 7 of treatment (87% vs. 65%)," they wrote.
At week 12 of treatment, the mean wound area in the group treated with 0.5x106 cells per mL every 14 days was reduced by 91%, compared with 80% with vehicle, and for the other treatment groups, the mean wound area was reduced by between 84% and 87%.
"Overall, patients treated with cells had higher proportions of healed wounds than did those assigned vehicle alone, but only the group assigned [0.5x106 cells per mL] every 14 days differed significantly compared with control," they noted.
Adverse events were similar across all groups, and most were nonserious, mild to moderate events that resolved. Only new skin ulcers and cellulitis occurred at a frequency of greater than 5%. Immunotoxicity testing showed that there was no treatment-induced alloantibody formation or induction of autoimmunity.
Included in this study were adult outpatients enrolled from 28 centers in the United States and Canada between 2009 and 2011. All had venous reflux confirmed by duplex Doppler ultrasonography, and up to three venous leg ulcers. Those assigned to the placebo group received vehicle alone applied every 7 days for the 12 weeks of the trial.
The findings may have important implications for the treatment of venous leg ulcers, which affect an estimated 1.65% to 1.74% of adults aged 65 years and older. Standard treatment with infection control, primary dressings, and high-strength compressions heal between 30% and 75% of such ulcers, compared with the 84%-91% healing seen with HP802-247 in this study, with the remainder becoming "chronic, with unresolved inflammatory processes within the extracellular matrix of the wound bed and dysfunction of wound fibroblasts and keratinocytes," the investigators noted.
"The results are sufficiently promising that larger randomized trials comparing HP802-247 to standard treatment for venous leg ulcers are now warranted," they concluded.
The researchers reported that their study was limited by the wound upper end boundary of 12 cm3, which represents 80% of all venous leg ulcers, but a smaller proportion of chronic venous ulcers.
The research trial is registered with ClinicalTrials.gov as NCT00852995.
Dr. Kirsner received consulting fees for his assistance with protocol design and data interpretation. Two of his coauthors also received such consulting fees, and other authors on the study disclosed that they are employed by Healthpoint, and/or hold adjunct academic appointments at the University of North Texas Health Sciences Center in Fort Worth, Tex.
A spray formulation of allogeneic neonatal keratinocytes and fibroblasts significantly improved wound healing in a multicenter, randomized, placebo-controlled phase II study of more than 200 patients with venous leg ulcers.
The mean reduction in wound area was significantly greater among 177 patients who received 12 weeks of active treatment with the novel cell therapy, known as HP802-247, than among 50 patients who were treated with application vehicle of a modified fibrin spray alone. HP802-247 consists of cryopreserved, allogenic, growth-arrested fibroblasts and keratinocytes derived from neonatal foreskin. The largest improvement (16% on average over placebo) was seen in 44 patients assigned to treatment with 5.0x106 cells per mL every 14 days, Dr. Robert S. Kirsner of the University of Miami and his colleagues reported. The study was published online in the Aug. 3 issue of The Lancet.
Reduction in wound area was between 8% and 12% over that seen with placebo in 45 patients treated with 5.0x106 cells per mL every 7 days, 44 patients treated with 5.0x106 cells per mL every 14 days, and 43 patients treated with 0.5x106 cells per mL every 7 days, the investigators said (Lancet 2012 Aug. 3 [doi:10.1016/S0140-6736(12)60644-8]).
The study investigators included vascular surgeons, dermatologists, and podiatrists at universities and in private practice. All patients were treated with standard compression bandaging as well as the study treatment.
"Wound area began to decrease rapidly after initiation of treatment. After one application of the 0.5x106/mL every 14 days dose, the mean reduction in wound area was 40%, compared with 23% for the vehicle group. This effect persisted with the maximum difference in mean reduction between the group assigned [0.5x106 cells per mL] every 14 days and the vehicle group occurring at week 7 of treatment (87% vs. 65%)," they wrote.
At week 12 of treatment, the mean wound area in the group treated with 0.5x106 cells per mL every 14 days was reduced by 91%, compared with 80% with vehicle, and for the other treatment groups, the mean wound area was reduced by between 84% and 87%.
"Overall, patients treated with cells had higher proportions of healed wounds than did those assigned vehicle alone, but only the group assigned [0.5x106 cells per mL] every 14 days differed significantly compared with control," they noted.
Adverse events were similar across all groups, and most were nonserious, mild to moderate events that resolved. Only new skin ulcers and cellulitis occurred at a frequency of greater than 5%. Immunotoxicity testing showed that there was no treatment-induced alloantibody formation or induction of autoimmunity.
Included in this study were adult outpatients enrolled from 28 centers in the United States and Canada between 2009 and 2011. All had venous reflux confirmed by duplex Doppler ultrasonography, and up to three venous leg ulcers. Those assigned to the placebo group received vehicle alone applied every 7 days for the 12 weeks of the trial.
The findings may have important implications for the treatment of venous leg ulcers, which affect an estimated 1.65% to 1.74% of adults aged 65 years and older. Standard treatment with infection control, primary dressings, and high-strength compressions heal between 30% and 75% of such ulcers, compared with the 84%-91% healing seen with HP802-247 in this study, with the remainder becoming "chronic, with unresolved inflammatory processes within the extracellular matrix of the wound bed and dysfunction of wound fibroblasts and keratinocytes," the investigators noted.
"The results are sufficiently promising that larger randomized trials comparing HP802-247 to standard treatment for venous leg ulcers are now warranted," they concluded.
The researchers reported that their study was limited by the wound upper end boundary of 12 cm3, which represents 80% of all venous leg ulcers, but a smaller proportion of chronic venous ulcers.
The research trial is registered with ClinicalTrials.gov as NCT00852995.
Dr. Kirsner received consulting fees for his assistance with protocol design and data interpretation. Two of his coauthors also received such consulting fees, and other authors on the study disclosed that they are employed by Healthpoint, and/or hold adjunct academic appointments at the University of North Texas Health Sciences Center in Fort Worth, Tex.
FROM THE LANCET
Major Finding: At week 12 of treatment, the mean wound area in the group treated with 0.5x106 cells per mL every 14 days was reduced by 91%, compared with 80% with vehicle, and for the other treatment groups the mean wound area was reduced by between 84% and 87%.
Data Source: This was a randomized, placebo-controlled phase II trial.
Disclosures: Dr. Kirsner received consulting fees for his assistance with protocol design and data interpretation. Two of his coauthors also received such consulting fees, and other authors on the study disclosed that they are employed by Healthpoint, and/or hold adjunct academic appointments at the University of North Texas Health Sciences Center in Fort Worth, Tex. The authors of the editorial reported having no disclosures.
Tobacco, Drug Use High Early in Course of Schizophrenia
Illicit drug use is common among heavy cigarette smokers in the general population, but among outpatients with schizophrenia who are heavy smokers, it is most common in the first decade of illness, according to findings from a study of 70 patients and 97 controls.
The findings have important implications for the management of schizophrenia patients who are in the early stages of their disease, Kristen M. Mackowick of the National Institute on Drug Abuse and her colleagues reported in the August issue of Schizophrenia Research.
The prevalence of cigarette smoking among those with schizophrenia is 58%-90%, compared with about 20% in the general population, a particular problem given that those with mental illness or substance use disorders are more susceptible to smoking-related illnesses because they smoke more cigarettes per day and have more difficulty quitting.

"A significant cause for concern in the schizophrenia population, in addition to increased morbidity and mortality rates, is that cigarette smoking and use of other drugs often covary," the investigators said, noting that one study showed that the odds of someone with a substance abuse diagnosis also having a diagnosis of schizophrenia was 4.6 times higher than for the rest of the population. Other studies show that the combination of psychiatric disorders with a substance use disorder greatly increases the likelihood that an individual will need psychological health services, be more aggressive, and be less compliant with medication.
In the current study, lifetime drug use was similar among the participants with schizophrenia and controls, except that more of those with schizophrenia reported ever using hallucinogens (49% vs. 25%) and inhalants (21% vs. 5%).
Notably, fewer than 3% of schizophrenia participants "reported current use of any drug other than alcohol (17% current use), whereas considerably higher percentages of controls reported current use of some drug (alcohol 69%, heroin 12%, cocaine 25%, marijuana 45%). However, more schizophrenia participants than controls reported past, but not current, use of some substances (alcohol 71% vs. 29%, cocaine 51% vs. 34%, marijuana, 84% vs. 49%) with most having not used for more than a year," the investigators found (Schizophrenia Research 2012;139:194-200).
After controlling for age, they also found that most current substance use occurred between at age 20-30 years in both patients and controls, with discrepancies becoming greater with increasing age. The rates of current use declined for schizophrenia patients, but not for controls, they noted.
The findings suggest that the co-occurrence of schizophrenia, tobacco dependence, and drug use remains a serious health concern, as well as a barrier to improving health and quality of life in those with schizophrenia, they said, noting that the finding that schizophrenia participants reported more past substance use than controls is a concern, because "early-onset drug use may increase an already vulnerable individual’s chance of developing psychosis."
Research has shown, for example, that individuals who possess the Val allele on the COMT gene and who had early-onset cannabis use were at an increased risk of developing psychotic symptoms, they noted.
The finding with respect to inhalant use also is of concern, as it has been shown to have the potential to produce persistent psychotic symptoms in those at risk for psychosis, they added.
Participants in this study were adults aged 18-65 years who smoked at least five cigarettes daily, and who had a breath carbon monoxide (CO) level of at least 8 parts per million. Patients were outpatients with a DSM-IV diagnosis of schizophrenia or schizoaffective disorder; controls had no major Axis I psychotic disorder as determined by the SCID-I (Structured Clinical Interview for DSM-IV Axis I Disorders).
The study consisted of one 2- to 3-hour session involving screening (the CO measurement and SCID), smoking of one cigarette to standardize the time since last tobacco exposure, and completion of a semistructured interview and research questionnaires.
The findings – particularly the substantial history of past substance use among schizophrenia participants aged 20-30 years – underscore the need for enhanced efforts to treat tobacco dependence in those with schizophrenia, both for the obvious health benefits and to help protect against initiation of drug use, the investigators said.
"Clinicians should also be vigilant when treating schizophrenia patients who are in the early stages of their illness, as prodromal and first-episode patients may be more vulnerable to drug use, as we observed more past drug use than current use in our schizophrenia participants," they concluded.
This study was supported by the Intramural Research Program of the National Institutes of Health, the National Institute on Drug Abuse, and by a NIDA Residential Research Support Services contract. Ms. Mackowick had no disclosures to report. Coauthor Robert P. McMahon reported serving as a consultant to Amgen. Coauthor Deanna L. Kelly reported receiving grant support from Janssen Pharmaceuticals and Bristol-Myers Squibb.
Illicit drug use is common among heavy cigarette smokers in the general population, but among outpatients with schizophrenia who are heavy smokers, it is most common in the first decade of illness, according to findings from a study of 70 patients and 97 controls.
The findings have important implications for the management of schizophrenia patients who are in the early stages of their disease, Kristen M. Mackowick of the National Institute on Drug Abuse and her colleagues reported in the August issue of Schizophrenia Research.
The prevalence of cigarette smoking among those with schizophrenia is 58%-90%, compared with about 20% in the general population, a particular problem given that those with mental illness or substance use disorders are more susceptible to smoking-related illnesses because they smoke more cigarettes per day and have more difficulty quitting.
"A significant cause for concern in the schizophrenia population, in addition to increased morbidity and mortality rates, is that cigarette smoking and use of other drugs often covary," the investigators said, noting that one study showed that the odds of someone with a substance abuse diagnosis also having a diagnosis of schizophrenia was 4.6 times higher than for the rest of the population. Other studies show that the combination of psychiatric disorders with a substance use disorder greatly increases the likelihood that an individual will need psychological health services, be more aggressive, and be less compliant with medication.
In the current study, lifetime drug use was similar among the participants with schizophrenia and controls, except that more of those with schizophrenia reported ever using hallucinogens (49% vs. 25%) and inhalants (21% vs. 5%).
Notably, fewer than 3% of schizophrenia participants "reported current use of any drug other than alcohol (17% current use), whereas considerably higher percentages of controls reported current use of some drug (alcohol 69%, heroin 12%, cocaine 25%, marijuana 45%). However, more schizophrenia participants than controls reported past, but not current, use of some substances (alcohol 71% vs. 29%, cocaine 51% vs. 34%, marijuana, 84% vs. 49%) with most having not used for more than a year," the investigators found (Schizophrenia Research 2012;139:194-200).
After controlling for age, they also found that most current substance use occurred between at age 20-30 years in both patients and controls, with discrepancies becoming greater with increasing age. The rates of current use declined for schizophrenia patients, but not for controls, they noted.
The findings suggest that the co-occurrence of schizophrenia, tobacco dependence, and drug use remains a serious health concern, as well as a barrier to improving health and quality of life in those with schizophrenia, they said, noting that the finding that schizophrenia participants reported more past substance use than controls is a concern, because "early-onset drug use may increase an already vulnerable individual’s chance of developing psychosis."
Research has shown, for example, that individuals who possess the Val allele on the COMT gene and who had early-onset cannabis use were at an increased risk of developing psychotic symptoms, they noted.
The finding with respect to inhalant use also is of concern, as it has been shown to have the potential to produce persistent psychotic symptoms in those at risk for psychosis, they added.
Participants in this study were adults aged 18-65 years who smoked at least five cigarettes daily, and who had a breath carbon monoxide (CO) level of at least 8 parts per million. Patients were outpatients with a DSM-IV diagnosis of schizophrenia or schizoaffective disorder; controls had no major Axis I psychotic disorder as determined by the SCID-I (Structured Clinical Interview for DSM-IV Axis I Disorders).
The study consisted of one 2- to 3-hour session involving screening (the CO measurement and SCID), smoking of one cigarette to standardize the time since last tobacco exposure, and completion of a semistructured interview and research questionnaires.
The findings – particularly the substantial history of past substance use among schizophrenia participants aged 20-30 years – underscore the need for enhanced efforts to treat tobacco dependence in those with schizophrenia, both for the obvious health benefits and to help protect against initiation of drug use, the investigators said.
"Clinicians should also be vigilant when treating schizophrenia patients who are in the early stages of their illness, as prodromal and first-episode patients may be more vulnerable to drug use, as we observed more past drug use than current use in our schizophrenia participants," they concluded.
This study was supported by the Intramural Research Program of the National Institutes of Health, the National Institute on Drug Abuse, and by a NIDA Residential Research Support Services contract. Ms. Mackowick had no disclosures to report. Coauthor Robert P. McMahon reported serving as a consultant to Amgen. Coauthor Deanna L. Kelly reported receiving grant support from Janssen Pharmaceuticals and Bristol-Myers Squibb.
Illicit drug use is common among heavy cigarette smokers in the general population, but among outpatients with schizophrenia who are heavy smokers, it is most common in the first decade of illness, according to findings from a study of 70 patients and 97 controls.
The findings have important implications for the management of schizophrenia patients who are in the early stages of their disease, Kristen M. Mackowick of the National Institute on Drug Abuse and her colleagues reported in the August issue of Schizophrenia Research.
The prevalence of cigarette smoking among those with schizophrenia is 58%-90%, compared with about 20% in the general population, a particular problem given that those with mental illness or substance use disorders are more susceptible to smoking-related illnesses because they smoke more cigarettes per day and have more difficulty quitting.
"A significant cause for concern in the schizophrenia population, in addition to increased morbidity and mortality rates, is that cigarette smoking and use of other drugs often covary," the investigators said, noting that one study showed that the odds of someone with a substance abuse diagnosis also having a diagnosis of schizophrenia was 4.6 times higher than for the rest of the population. Other studies show that the combination of psychiatric disorders with a substance use disorder greatly increases the likelihood that an individual will need psychological health services, be more aggressive, and be less compliant with medication.
In the current study, lifetime drug use was similar among the participants with schizophrenia and controls, except that more of those with schizophrenia reported ever using hallucinogens (49% vs. 25%) and inhalants (21% vs. 5%).
Notably, fewer than 3% of schizophrenia participants "reported current use of any drug other than alcohol (17% current use), whereas considerably higher percentages of controls reported current use of some drug (alcohol 69%, heroin 12%, cocaine 25%, marijuana 45%). However, more schizophrenia participants than controls reported past, but not current, use of some substances (alcohol 71% vs. 29%, cocaine 51% vs. 34%, marijuana, 84% vs. 49%) with most having not used for more than a year," the investigators found (Schizophrenia Research 2012;139:194-200).
After controlling for age, they also found that most current substance use occurred between at age 20-30 years in both patients and controls, with discrepancies becoming greater with increasing age. The rates of current use declined for schizophrenia patients, but not for controls, they noted.
The findings suggest that the co-occurrence of schizophrenia, tobacco dependence, and drug use remains a serious health concern, as well as a barrier to improving health and quality of life in those with schizophrenia, they said, noting that the finding that schizophrenia participants reported more past substance use than controls is a concern, because "early-onset drug use may increase an already vulnerable individual’s chance of developing psychosis."
Research has shown, for example, that individuals who possess the Val allele on the COMT gene and who had early-onset cannabis use were at an increased risk of developing psychotic symptoms, they noted.
The finding with respect to inhalant use also is of concern, as it has been shown to have the potential to produce persistent psychotic symptoms in those at risk for psychosis, they added.
Participants in this study were adults aged 18-65 years who smoked at least five cigarettes daily, and who had a breath carbon monoxide (CO) level of at least 8 parts per million. Patients were outpatients with a DSM-IV diagnosis of schizophrenia or schizoaffective disorder; controls had no major Axis I psychotic disorder as determined by the SCID-I (Structured Clinical Interview for DSM-IV Axis I Disorders).
The study consisted of one 2- to 3-hour session involving screening (the CO measurement and SCID), smoking of one cigarette to standardize the time since last tobacco exposure, and completion of a semistructured interview and research questionnaires.
The findings – particularly the substantial history of past substance use among schizophrenia participants aged 20-30 years – underscore the need for enhanced efforts to treat tobacco dependence in those with schizophrenia, both for the obvious health benefits and to help protect against initiation of drug use, the investigators said.
"Clinicians should also be vigilant when treating schizophrenia patients who are in the early stages of their illness, as prodromal and first-episode patients may be more vulnerable to drug use, as we observed more past drug use than current use in our schizophrenia participants," they concluded.
This study was supported by the Intramural Research Program of the National Institutes of Health, the National Institute on Drug Abuse, and by a NIDA Residential Research Support Services contract. Ms. Mackowick had no disclosures to report. Coauthor Robert P. McMahon reported serving as a consultant to Amgen. Coauthor Deanna L. Kelly reported receiving grant support from Janssen Pharmaceuticals and Bristol-Myers Squibb.
FROM SCHIZOPHRENIA RESEARCH
Major Finding: More schizophrenia participants than controls reported past – but not current – use of some substances (alcohol, 71% vs. 29%; cocaine, 51% vs. 34%; marijuana, 84% vs. 49%), with most having not used for more than a year. After controlling for age, the investigators found that most current substance use occurred at age 20-30 years in both patients and controls, with discrepancies becoming greater with increasing age.
Data Source: This was a study of illicit drug use among heavy smokers with and without schizophrenia.
Disclosures: This study was supported by the Intramural Research Program of the National Institutes of Health, the National Institute on Drug Abuse, and by a NIDA Residential Research Support Services contract. Ms. Mackowick had no disclosures to report. Coauthor Robert P. McMahon reported serving as a consultant to Amgen. Coauthor Deanna L. Kelly reported receiving grant support from Janssen Pharmaceuticals and Bristol-Myers Squibb.

Egg-White Powder Immunotherapy Desensitizes Children With Egg Allergy
Oral immunotherapy using egg-white powder represents a highly promising therapeutic intervention for children with egg allergy, according to findings from a randomized, placebo-controlled trial reported online in the July 19 issue of the New England Journal of Medicine.
After 10 months of immunotherapy, none of the 15 children with egg allergy who received placebo as part of the double-blind study passed an oral food challenge of 5 g of egg-white powder, whereas 22 (55%) of 40 children who received oral immunotherapy passed the oral food challenge and were considered to be desensitized. At 22 months, 30 (75%) of the 40 children who received oral immunotherapy passed an oral food challenge with 10 g of egg-white powder, Dr. A. Wesley Burks, chair of the department of pediatrics at the University of North Carolina and chief physician of N.C. Children’s Hospital, his colleagues reported on behalf of the Consortium of Food Allergy Research.

Of the 30 children who passed the oral food challenge at 22 months, 29 were rechallenged at 24 months with 10 g of egg-white powder, followed 1 hour later with one whole cooked egg (after having discontinued immunotherapy and egg consumption for 4-6 weeks); 11 (28%) passed the challenge and were considered to have "sustained unresponsiveness," the investigators reported (N. Engl. J. Med. 2012 July 19 [doi:10.1056/NEJMoa1200435]).
These 11 children then were instructed to add egg to their diet ad libitum. No adverse events were reported at the 30- and 36-month follow-ups.
Study participants were children aged 5-18 years (median, 7 years) with a convincing clinical history of egg allergy and a serum egg-specific IgE antibody level of more than 5 kU/L for those aged 6 years and older, and 12 kU/L or more for those aged 5 years. Those with a history of severe anaphylaxis after egg consumption were excluded.
The protocol for oral immunotherapy consisted of an initial-day dose escalation, a build-up phase, and a maintenance phase involving ingestion of up to 2 g of egg-white powder (equivalent of about one-third of an egg) daily.
Factors that were found to be associated with sustained unresponsiveness at 24 months were higher egg-specific IgG4 antibody levels at 10 months, smaller wheal diameter on skin-prick allergy testing at 22 months, and a decrease in wheal size from baseline to 22 months, the investigators noted.
Oral immunotherapy in this study was generally well tolerated, with adverse events occurring most frequently in association with oral-immunotherapy dosing. Most of the events were mild (grade 1), with only 1% being graded as moderate (grade 2). No severe adverse events occurred. Most events were oral or pharyngeal, and were associated with 25% of the 11,860 doses of oral immunotherapy, and with 3.9% of the 4,018 doses of placebo. The rate of symptoms decreased to 8.3% of 15,815 doses in the oral immunotherapy group after 10 months.
The findings could have important implications, given that the cumulative prevalence of egg allergy is approximately 2.6% by 2.5 years of age, and that egg avoidance (which is difficult and can adversely affect quality of life) is the only available treatment for egg allergy, investigators said.
However, for oral immunotherapy to be recommended as a standard of care, it is important to better define risks, compared with allergen avoidance; to determine the dosing regimens with the most favorable outcomes; to identify the patients most likely to benefit; and to develop postdesensitization strategies, the investigators concluded.
This study was supported by the National Institute of Allergy and Infectious Diseases and the National Institutes of Health–National Center for Research Resources Clinical Translational Science Awards and Clinical Research Centers. Dr. A. Wesley Burks has been a consultant for companies including Dannon Co. Probiotic, McNeil Nutritionals, Merck, the Food Allergy & Anaphylaxis Network, and Novartis, and has grants or grants pending from the Food Allergy Initiative, the NIH, the National Peanut Board, and others. Some of his associates were consultants for companies including DBV Technologies, Allertein Therapeutics, and Sunovion, or received grants from various companies; other associates had no relevant financial disclosures.
CLARIFICATION 7/20/2012: The institutional affiliation of Dr. Burks has been updated to reflect his current position.
Oral immunotherapy using egg-white powder represents a highly promising therapeutic intervention for children with egg allergy, according to findings from a randomized, placebo-controlled trial reported online in the July 19 issue of the New England Journal of Medicine.
After 10 months of immunotherapy, none of the 15 children with egg allergy who received placebo as part of the double-blind study passed an oral food challenge of 5 g of egg-white powder, whereas 22 (55%) of 40 children who received oral immunotherapy passed the oral food challenge and were considered to be desensitized. At 22 months, 30 (75%) of the 40 children who received oral immunotherapy passed an oral food challenge with 10 g of egg-white powder, Dr. A. Wesley Burks, chair of the department of pediatrics at the University of North Carolina and chief physician of N.C. Children’s Hospital, his colleagues reported on behalf of the Consortium of Food Allergy Research.
Of the 30 children who passed the oral food challenge at 22 months, 29 were rechallenged at 24 months with 10 g of egg-white powder, followed 1 hour later with one whole cooked egg (after having discontinued immunotherapy and egg consumption for 4-6 weeks); 11 (28%) passed the challenge and were considered to have "sustained unresponsiveness," the investigators reported (N. Engl. J. Med. 2012 July 19 [doi:10.1056/NEJMoa1200435]).
These 11 children then were instructed to add egg to their diet ad libitum. No adverse events were reported at the 30- and 36-month follow-ups.
Study participants were children aged 5-18 years (median, 7 years) with a convincing clinical history of egg allergy and a serum egg-specific IgE antibody level of more than 5 kU/L for those aged 6 years and older, and 12 kU/L or more for those aged 5 years. Those with a history of severe anaphylaxis after egg consumption were excluded.
The protocol for oral immunotherapy consisted of an initial-day dose escalation, a build-up phase, and a maintenance phase involving ingestion of up to 2 g of egg-white powder (equivalent of about one-third of an egg) daily.
Factors that were found to be associated with sustained unresponsiveness at 24 months were higher egg-specific IgG4 antibody levels at 10 months, smaller wheal diameter on skin-prick allergy testing at 22 months, and a decrease in wheal size from baseline to 22 months, the investigators noted.
Oral immunotherapy in this study was generally well tolerated, with adverse events occurring most frequently in association with oral-immunotherapy dosing. Most of the events were mild (grade 1), with only 1% being graded as moderate (grade 2). No severe adverse events occurred. Most events were oral or pharyngeal, and were associated with 25% of the 11,860 doses of oral immunotherapy, and with 3.9% of the 4,018 doses of placebo. The rate of symptoms decreased to 8.3% of 15,815 doses in the oral immunotherapy group after 10 months.
The findings could have important implications, given that the cumulative prevalence of egg allergy is approximately 2.6% by 2.5 years of age, and that egg avoidance (which is difficult and can adversely affect quality of life) is the only available treatment for egg allergy, investigators said.
However, for oral immunotherapy to be recommended as a standard of care, it is important to better define risks, compared with allergen avoidance; to determine the dosing regimens with the most favorable outcomes; to identify the patients most likely to benefit; and to develop postdesensitization strategies, the investigators concluded.
This study was supported by the National Institute of Allergy and Infectious Diseases and the National Institutes of Health–National Center for Research Resources Clinical Translational Science Awards and Clinical Research Centers. Dr. A. Wesley Burks has been a consultant for companies including Dannon Co. Probiotic, McNeil Nutritionals, Merck, the Food Allergy & Anaphylaxis Network, and Novartis, and has grants or grants pending from the Food Allergy Initiative, the NIH, the National Peanut Board, and others. Some of his associates were consultants for companies including DBV Technologies, Allertein Therapeutics, and Sunovion, or received grants from various companies; other associates had no relevant financial disclosures.
CLARIFICATION 7/20/2012: The institutional affiliation of Dr. Burks has been updated to reflect his current position.
Oral immunotherapy using egg-white powder represents a highly promising therapeutic intervention for children with egg allergy, according to findings from a randomized, placebo-controlled trial reported online in the July 19 issue of the New England Journal of Medicine.
After 10 months of immunotherapy, none of the 15 children with egg allergy who received placebo as part of the double-blind study passed an oral food challenge of 5 g of egg-white powder, whereas 22 (55%) of 40 children who received oral immunotherapy passed the oral food challenge and were considered to be desensitized. At 22 months, 30 (75%) of the 40 children who received oral immunotherapy passed an oral food challenge with 10 g of egg-white powder, Dr. A. Wesley Burks, chair of the department of pediatrics at the University of North Carolina and chief physician of N.C. Children’s Hospital, his colleagues reported on behalf of the Consortium of Food Allergy Research.
Of the 30 children who passed the oral food challenge at 22 months, 29 were rechallenged at 24 months with 10 g of egg-white powder, followed 1 hour later with one whole cooked egg (after having discontinued immunotherapy and egg consumption for 4-6 weeks); 11 (28%) passed the challenge and were considered to have "sustained unresponsiveness," the investigators reported (N. Engl. J. Med. 2012 July 19 [doi:10.1056/NEJMoa1200435]).
These 11 children then were instructed to add egg to their diet ad libitum. No adverse events were reported at the 30- and 36-month follow-ups.
Study participants were children aged 5-18 years (median, 7 years) with a convincing clinical history of egg allergy and a serum egg-specific IgE antibody level of more than 5 kU/L for those aged 6 years and older, and 12 kU/L or more for those aged 5 years. Those with a history of severe anaphylaxis after egg consumption were excluded.
The protocol for oral immunotherapy consisted of an initial-day dose escalation, a build-up phase, and a maintenance phase involving ingestion of up to 2 g of egg-white powder (equivalent of about one-third of an egg) daily.
Factors that were found to be associated with sustained unresponsiveness at 24 months were higher egg-specific IgG4 antibody levels at 10 months, smaller wheal diameter on skin-prick allergy testing at 22 months, and a decrease in wheal size from baseline to 22 months, the investigators noted.
Oral immunotherapy in this study was generally well tolerated, with adverse events occurring most frequently in association with oral-immunotherapy dosing. Most of the events were mild (grade 1), with only 1% being graded as moderate (grade 2). No severe adverse events occurred. Most events were oral or pharyngeal, and were associated with 25% of the 11,860 doses of oral immunotherapy, and with 3.9% of the 4,018 doses of placebo. The rate of symptoms decreased to 8.3% of 15,815 doses in the oral immunotherapy group after 10 months.
The findings could have important implications, given that the cumulative prevalence of egg allergy is approximately 2.6% by 2.5 years of age, and that egg avoidance (which is difficult and can adversely affect quality of life) is the only available treatment for egg allergy, investigators said.
However, for oral immunotherapy to be recommended as a standard of care, it is important to better define risks, compared with allergen avoidance; to determine the dosing regimens with the most favorable outcomes; to identify the patients most likely to benefit; and to develop postdesensitization strategies, the investigators concluded.
This study was supported by the National Institute of Allergy and Infectious Diseases and the National Institutes of Health–National Center for Research Resources Clinical Translational Science Awards and Clinical Research Centers. Dr. A. Wesley Burks has been a consultant for companies including Dannon Co. Probiotic, McNeil Nutritionals, Merck, the Food Allergy & Anaphylaxis Network, and Novartis, and has grants or grants pending from the Food Allergy Initiative, the NIH, the National Peanut Board, and others. Some of his associates were consultants for companies including DBV Technologies, Allertein Therapeutics, and Sunovion, or received grants from various companies; other associates had no relevant financial disclosures.
CLARIFICATION 7/20/2012: The institutional affiliation of Dr. Burks has been updated to reflect his current position.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Major Finding: At 22 months, 30 (75%) of 40 children who received oral immunotherapy passed an oral food challenge with 10 g of egg-white powder and were considered desensitized. After discontinuing immunotherapy and egg consumption for 4-6 weeks, 29 of these children were rechallenged at 24 months with 10 g of egg-white powder, followed 1 hour later with one whole cooked egg; 11 (28%) of them passed and were considered to have "sustained unresponsiveness."
Data Source: This was a double-blind, randomized, placebo-controlled study.
Disclosures: This study was supported by the National Institute of Allergy and Infectious Diseases and the National Institutes of Health–National Center for Research Resources Clinical Translational Science Awards and Clinical Research Centers. Dr. A. Wesley Burks has been a consultant for companies including Dannon Co. Probiotic, McNeil Nutritionals, Merck, the Food Allergy & Anaphylaxis Network, and Novartis, and has grants or grants pending from the Food Allergy Initiative, the NIH, the National Peanut Board, and others. Some of his associates were consultants for companies including DBV Technologies, Allertein Therapeutics, and Sunovion, or received grants from various companies; other associates had no relevant financial disclosures.

Genotypes in ANCA-Associated Vasculitis May Guide Therapy
Genes play a key role in the pathogenesis of antineutrophil cytoplasmic antibody-associated vasculitis, and genetic distinctions exist between two of the condition’s main clinical syndromes: granulomatosis with polyangiitis and microscopic polyangiitis, judging from data from a genomewide association study.
The findings also support the concept that proteinase 3 ANCA-associated vasculitis and myeloperoxidase ANCA-associated vasculitis are distinct autoimmune syndromes. If true, those findings could have both immunopathogenic and therapeutic implications, according to Paul A. Lyons, Ph.D., of the Cambridge (England) Institute for Medical Research, and his colleagues in their online report in the July 19 issue of the New England Journal of Medicine.
"There is debate as to whether the clinical syndromes of granulomatosis with polyangiitis and microscopic polyangiitis represent distinct diseases or are part of a single disease spectrum," the investigators wrote. The concept of a single disease spectrum has resulted in similar treatment strategies being used in trials regardless of which of these two clinical syndromes are present, and also in the suggestion that genetic studies should consider the two syndromes together, they explained.
"Clear evidence that these clinical syndromes are etiologically distinct might provide a rationale for devising syndrome-specific therapeutic strategies," the investigators noted (N. Engl. J. Med. 2012 July 19 [doi: 10.1056/NEJMoa1108735]).
To identify genetic risk factors and evaluate whether a common or distinct genetic background exists for granulomatosis with polyangiitis and microscopic polyangiitis, they performed genotyping in a discovery cohort of 1,233 patients with ANCA-associated vasculitis from the United Kingdom and 5,884 controls, as well as in a replication cohort of 1,454 Northern European case patients and 1,666 controls.
Combined analysis of the discovery and replication cohorts demonstrated that four single nucleotide polymorphisms (SNPs) exceeded the significance threshold for genomewide association, including three from the major histocompatibility complex (MHC). The most significant of these three was within the gene encoding HLA-DPB1. The fourth was in the SERPINA1 locus at 14q32.
Another SNP in PRTN3, which was added to the replication analysis on the bases of a priori hypotheses, was also found to be significantly associated with disease.
"Together, these data provide evidence of a genetic base of ANCA-associated vasculitis that extends beyond the MHC," the investigators said.
Additional analysis of the discovery cohort after subdivision on the basis of whether patients were diagnosed with granulomatosis with polyangiitis or with microscopic polyangiitis showed that all three MHC-associated SNPs differed between the two groups, with "essentially all of the association" found in those with granulomatosis with polyangiitis.
"This was also true of SERPINA1 – while it did not show a significant difference when granulomatosis with polyangiitis and microscopic polyangiitis were compared directly, perhaps owing to small numbers of patients and thus reduced power, it was associated with granulomatosis with polyangiitis, but not microscopic polyangiitis, when each subtype was compared with controls," they added.
There also was a suggestion of an association between PRTN3 and granulomatosis with polyangiitis rather than with microscopic polyangiitis, and also between some less significant SNPs and granulomatosis with polyangiitis, they said.
"Overall, there was evidence that granulomatosis with polyangiitis had genetic associations distinct from microscopic polyangiitis at both the MHC and SERPIN loci," they said.
Additional subgroup analysis based on proteinase 3 and myeloperoxidase ANCA specificity showed significant differences at the MHC, SERPINA1, and PRTN3 loci, all of which included a genetic association with proteinase 3 ANCA but not with myeloperoxidase ANCA. Further analysis demonstrated associations of HLA-DP and the related SNPs SERPINA1 and PRTN3 in patients with proteinase 3 ANCA associated with granulomatosis with polyangiitis but not myeloperoxidase ANCA. The findings were the same in the microscopic polyangiitis group, showing an association of proteinase 3 ANCA and the HLA-DP SNP and SERPINA1. The converse was true for the HLA-DQ SNP, which was associated with myeloperoxidase ANCA rather than proteinase 3 ANCA in patients with microscopic polyangiitis.
The clear association of genetic background with autoantibody specificity suggests that it might contribute to the clinical classifications of granulomatosis with polyangiitis and microscopic polyangiitis, the investigators said.
"The genetic difference between proteinase 3 ANCA and myeloperoxidase ANCA polyangiitis could have immunopathogenic and therapeutic implications, ... and will require future genetic studies powered to detect associations with these conditions rather than with ANCA-associated vasculitis as a whole," they said.
The investigators concluded that this study "provides clear evidence of a genetic contribution to disease susceptibility, which differs between granulomatosis with polyangiitis and microscopic polyangiitis."
Further, "associations with HLA, SERPINA1, and PRTN3 are primarily aligned with ANCA specificity rather than with the clinically defined syndromes granulomatosis with polyangiitis and microscopic polyangiitis, making it logical to consider including ANCA specificity in the diagnostic criteria for ANCA-associated vasculitis," they argued.
Dr. Lyons and his associates disclosed that they had no relevant financial disclosures relevant to this research other than its funding. This study was supported by the British Heart Foundation; the Wellcome Trust; the National Institute of Health Research Biomedical Research Centres of Cambridge, Imperial College, and Manchester; the Medical Research Council and Kidney Research UK; the West Anglia Comprehensive Local Research Network; the Norfolk and Suffolk Comprehensive Local Research network; the German Research Foundation; and the European Union FP7 Infectious Triggers of Chronic Autoimmunity Consortium. Author disclosure forms for both the study authors and editorial author are available with the full text of the article at NEMJ.org.
Direct clinical implications of this study in terms of disease classification or diagnosis are premature, given that the data indicate that carriers of certain SNPs have only a slightly or moderately increased probability of having a subtype of a rare disease for which the general likelihood is already very low. But despite these limitations, the findings represent a major step forward, Dr. Maria C. Cid wrote in an accompanying editorial.
The findings also pose interesting questions for future studies, she said.
"Patients with the Churg-Strauss syndrome, ANCA-negative patients, and patients of different ethnic groups are interesting populations to be explored," she said (N. Engl. J. Med. 2012 July 19 [doi: 10.1056/NEJMe1203592]).
Fine mapping of selected regions, along with the search for rare SNPs, SNPs influencing severity, and non-SNP variants might also provide interesting information, she added, noting that the collaborative network supporting the study "provides a strong basis for more comprehensive studies with new-generation technologies."
Dr. Cid is with the University of Barcelona and Institut d’Investigacions Biomediques August Pi i Sunyer. She reported having financial relationships with Bristol-Myers-Squibb, Centocor, and Roche.
Direct clinical implications of this study in terms of disease classification or diagnosis are premature, given that the data indicate that carriers of certain SNPs have only a slightly or moderately increased probability of having a subtype of a rare disease for which the general likelihood is already very low. But despite these limitations, the findings represent a major step forward, Dr. Maria C. Cid wrote in an accompanying editorial.
The findings also pose interesting questions for future studies, she said.
"Patients with the Churg-Strauss syndrome, ANCA-negative patients, and patients of different ethnic groups are interesting populations to be explored," she said (N. Engl. J. Med. 2012 July 19 [doi: 10.1056/NEJMe1203592]).
Fine mapping of selected regions, along with the search for rare SNPs, SNPs influencing severity, and non-SNP variants might also provide interesting information, she added, noting that the collaborative network supporting the study "provides a strong basis for more comprehensive studies with new-generation technologies."
Dr. Cid is with the University of Barcelona and Institut d’Investigacions Biomediques August Pi i Sunyer. She reported having financial relationships with Bristol-Myers-Squibb, Centocor, and Roche.
Direct clinical implications of this study in terms of disease classification or diagnosis are premature, given that the data indicate that carriers of certain SNPs have only a slightly or moderately increased probability of having a subtype of a rare disease for which the general likelihood is already very low. But despite these limitations, the findings represent a major step forward, Dr. Maria C. Cid wrote in an accompanying editorial.
The findings also pose interesting questions for future studies, she said.
"Patients with the Churg-Strauss syndrome, ANCA-negative patients, and patients of different ethnic groups are interesting populations to be explored," she said (N. Engl. J. Med. 2012 July 19 [doi: 10.1056/NEJMe1203592]).
Fine mapping of selected regions, along with the search for rare SNPs, SNPs influencing severity, and non-SNP variants might also provide interesting information, she added, noting that the collaborative network supporting the study "provides a strong basis for more comprehensive studies with new-generation technologies."
Dr. Cid is with the University of Barcelona and Institut d’Investigacions Biomediques August Pi i Sunyer. She reported having financial relationships with Bristol-Myers-Squibb, Centocor, and Roche.
Genes play a key role in the pathogenesis of antineutrophil cytoplasmic antibody-associated vasculitis, and genetic distinctions exist between two of the condition’s main clinical syndromes: granulomatosis with polyangiitis and microscopic polyangiitis, judging from data from a genomewide association study.
The findings also support the concept that proteinase 3 ANCA-associated vasculitis and myeloperoxidase ANCA-associated vasculitis are distinct autoimmune syndromes. If true, those findings could have both immunopathogenic and therapeutic implications, according to Paul A. Lyons, Ph.D., of the Cambridge (England) Institute for Medical Research, and his colleagues in their online report in the July 19 issue of the New England Journal of Medicine.
"There is debate as to whether the clinical syndromes of granulomatosis with polyangiitis and microscopic polyangiitis represent distinct diseases or are part of a single disease spectrum," the investigators wrote. The concept of a single disease spectrum has resulted in similar treatment strategies being used in trials regardless of which of these two clinical syndromes are present, and also in the suggestion that genetic studies should consider the two syndromes together, they explained.
"Clear evidence that these clinical syndromes are etiologically distinct might provide a rationale for devising syndrome-specific therapeutic strategies," the investigators noted (N. Engl. J. Med. 2012 July 19 [doi: 10.1056/NEJMoa1108735]).
To identify genetic risk factors and evaluate whether a common or distinct genetic background exists for granulomatosis with polyangiitis and microscopic polyangiitis, they performed genotyping in a discovery cohort of 1,233 patients with ANCA-associated vasculitis from the United Kingdom and 5,884 controls, as well as in a replication cohort of 1,454 Northern European case patients and 1,666 controls.
Combined analysis of the discovery and replication cohorts demonstrated that four single nucleotide polymorphisms (SNPs) exceeded the significance threshold for genomewide association, including three from the major histocompatibility complex (MHC). The most significant of these three was within the gene encoding HLA-DPB1. The fourth was in the SERPINA1 locus at 14q32.
Another SNP in PRTN3, which was added to the replication analysis on the bases of a priori hypotheses, was also found to be significantly associated with disease.
"Together, these data provide evidence of a genetic base of ANCA-associated vasculitis that extends beyond the MHC," the investigators said.
Additional analysis of the discovery cohort after subdivision on the basis of whether patients were diagnosed with granulomatosis with polyangiitis or with microscopic polyangiitis showed that all three MHC-associated SNPs differed between the two groups, with "essentially all of the association" found in those with granulomatosis with polyangiitis.
"This was also true of SERPINA1 – while it did not show a significant difference when granulomatosis with polyangiitis and microscopic polyangiitis were compared directly, perhaps owing to small numbers of patients and thus reduced power, it was associated with granulomatosis with polyangiitis, but not microscopic polyangiitis, when each subtype was compared with controls," they added.
There also was a suggestion of an association between PRTN3 and granulomatosis with polyangiitis rather than with microscopic polyangiitis, and also between some less significant SNPs and granulomatosis with polyangiitis, they said.
"Overall, there was evidence that granulomatosis with polyangiitis had genetic associations distinct from microscopic polyangiitis at both the MHC and SERPIN loci," they said.
Additional subgroup analysis based on proteinase 3 and myeloperoxidase ANCA specificity showed significant differences at the MHC, SERPINA1, and PRTN3 loci, all of which included a genetic association with proteinase 3 ANCA but not with myeloperoxidase ANCA. Further analysis demonstrated associations of HLA-DP and the related SNPs SERPINA1 and PRTN3 in patients with proteinase 3 ANCA associated with granulomatosis with polyangiitis but not myeloperoxidase ANCA. The findings were the same in the microscopic polyangiitis group, showing an association of proteinase 3 ANCA and the HLA-DP SNP and SERPINA1. The converse was true for the HLA-DQ SNP, which was associated with myeloperoxidase ANCA rather than proteinase 3 ANCA in patients with microscopic polyangiitis.
The clear association of genetic background with autoantibody specificity suggests that it might contribute to the clinical classifications of granulomatosis with polyangiitis and microscopic polyangiitis, the investigators said.
"The genetic difference between proteinase 3 ANCA and myeloperoxidase ANCA polyangiitis could have immunopathogenic and therapeutic implications, ... and will require future genetic studies powered to detect associations with these conditions rather than with ANCA-associated vasculitis as a whole," they said.
The investigators concluded that this study "provides clear evidence of a genetic contribution to disease susceptibility, which differs between granulomatosis with polyangiitis and microscopic polyangiitis."
Further, "associations with HLA, SERPINA1, and PRTN3 are primarily aligned with ANCA specificity rather than with the clinically defined syndromes granulomatosis with polyangiitis and microscopic polyangiitis, making it logical to consider including ANCA specificity in the diagnostic criteria for ANCA-associated vasculitis," they argued.
Dr. Lyons and his associates disclosed that they had no relevant financial disclosures relevant to this research other than its funding. This study was supported by the British Heart Foundation; the Wellcome Trust; the National Institute of Health Research Biomedical Research Centres of Cambridge, Imperial College, and Manchester; the Medical Research Council and Kidney Research UK; the West Anglia Comprehensive Local Research Network; the Norfolk and Suffolk Comprehensive Local Research network; the German Research Foundation; and the European Union FP7 Infectious Triggers of Chronic Autoimmunity Consortium. Author disclosure forms for both the study authors and editorial author are available with the full text of the article at NEMJ.org.
Genes play a key role in the pathogenesis of antineutrophil cytoplasmic antibody-associated vasculitis, and genetic distinctions exist between two of the condition’s main clinical syndromes: granulomatosis with polyangiitis and microscopic polyangiitis, judging from data from a genomewide association study.
The findings also support the concept that proteinase 3 ANCA-associated vasculitis and myeloperoxidase ANCA-associated vasculitis are distinct autoimmune syndromes. If true, those findings could have both immunopathogenic and therapeutic implications, according to Paul A. Lyons, Ph.D., of the Cambridge (England) Institute for Medical Research, and his colleagues in their online report in the July 19 issue of the New England Journal of Medicine.
"There is debate as to whether the clinical syndromes of granulomatosis with polyangiitis and microscopic polyangiitis represent distinct diseases or are part of a single disease spectrum," the investigators wrote. The concept of a single disease spectrum has resulted in similar treatment strategies being used in trials regardless of which of these two clinical syndromes are present, and also in the suggestion that genetic studies should consider the two syndromes together, they explained.
"Clear evidence that these clinical syndromes are etiologically distinct might provide a rationale for devising syndrome-specific therapeutic strategies," the investigators noted (N. Engl. J. Med. 2012 July 19 [doi: 10.1056/NEJMoa1108735]).
To identify genetic risk factors and evaluate whether a common or distinct genetic background exists for granulomatosis with polyangiitis and microscopic polyangiitis, they performed genotyping in a discovery cohort of 1,233 patients with ANCA-associated vasculitis from the United Kingdom and 5,884 controls, as well as in a replication cohort of 1,454 Northern European case patients and 1,666 controls.
Combined analysis of the discovery and replication cohorts demonstrated that four single nucleotide polymorphisms (SNPs) exceeded the significance threshold for genomewide association, including three from the major histocompatibility complex (MHC). The most significant of these three was within the gene encoding HLA-DPB1. The fourth was in the SERPINA1 locus at 14q32.
Another SNP in PRTN3, which was added to the replication analysis on the bases of a priori hypotheses, was also found to be significantly associated with disease.
"Together, these data provide evidence of a genetic base of ANCA-associated vasculitis that extends beyond the MHC," the investigators said.
Additional analysis of the discovery cohort after subdivision on the basis of whether patients were diagnosed with granulomatosis with polyangiitis or with microscopic polyangiitis showed that all three MHC-associated SNPs differed between the two groups, with "essentially all of the association" found in those with granulomatosis with polyangiitis.
"This was also true of SERPINA1 – while it did not show a significant difference when granulomatosis with polyangiitis and microscopic polyangiitis were compared directly, perhaps owing to small numbers of patients and thus reduced power, it was associated with granulomatosis with polyangiitis, but not microscopic polyangiitis, when each subtype was compared with controls," they added.
There also was a suggestion of an association between PRTN3 and granulomatosis with polyangiitis rather than with microscopic polyangiitis, and also between some less significant SNPs and granulomatosis with polyangiitis, they said.
"Overall, there was evidence that granulomatosis with polyangiitis had genetic associations distinct from microscopic polyangiitis at both the MHC and SERPIN loci," they said.
Additional subgroup analysis based on proteinase 3 and myeloperoxidase ANCA specificity showed significant differences at the MHC, SERPINA1, and PRTN3 loci, all of which included a genetic association with proteinase 3 ANCA but not with myeloperoxidase ANCA. Further analysis demonstrated associations of HLA-DP and the related SNPs SERPINA1 and PRTN3 in patients with proteinase 3 ANCA associated with granulomatosis with polyangiitis but not myeloperoxidase ANCA. The findings were the same in the microscopic polyangiitis group, showing an association of proteinase 3 ANCA and the HLA-DP SNP and SERPINA1. The converse was true for the HLA-DQ SNP, which was associated with myeloperoxidase ANCA rather than proteinase 3 ANCA in patients with microscopic polyangiitis.
The clear association of genetic background with autoantibody specificity suggests that it might contribute to the clinical classifications of granulomatosis with polyangiitis and microscopic polyangiitis, the investigators said.
"The genetic difference between proteinase 3 ANCA and myeloperoxidase ANCA polyangiitis could have immunopathogenic and therapeutic implications, ... and will require future genetic studies powered to detect associations with these conditions rather than with ANCA-associated vasculitis as a whole," they said.
The investigators concluded that this study "provides clear evidence of a genetic contribution to disease susceptibility, which differs between granulomatosis with polyangiitis and microscopic polyangiitis."
Further, "associations with HLA, SERPINA1, and PRTN3 are primarily aligned with ANCA specificity rather than with the clinically defined syndromes granulomatosis with polyangiitis and microscopic polyangiitis, making it logical to consider including ANCA specificity in the diagnostic criteria for ANCA-associated vasculitis," they argued.
Dr. Lyons and his associates disclosed that they had no relevant financial disclosures relevant to this research other than its funding. This study was supported by the British Heart Foundation; the Wellcome Trust; the National Institute of Health Research Biomedical Research Centres of Cambridge, Imperial College, and Manchester; the Medical Research Council and Kidney Research UK; the West Anglia Comprehensive Local Research Network; the Norfolk and Suffolk Comprehensive Local Research network; the German Research Foundation; and the European Union FP7 Infectious Triggers of Chronic Autoimmunity Consortium. Author disclosure forms for both the study authors and editorial author are available with the full text of the article at NEMJ.org.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE