User login
Sharon Worcester is an award-winning medical journalist for MDedge News. She has been with the company since 1996, first as the Southeast Bureau Chief (1996-2009) when the company was known as International Medical News Group, then as a freelance writer (2010-2015) before returning as a reporter in 2015. She previously worked as a daily newspaper reporter covering health and local government. Sharon currently reports primarily on oncology and hematology. She has a BA from Eckerd College and an MA in Mass Communication/Print Journalism from the University of Florida. Connect with her via LinkedIn and follow her on twitter @SW_MedReporter.
High-flow nasal cannulas support children outside the ICU
LAKE BUENA VISTA, FLA. – The use of high-flow nasal cannulas for respiratory support in young children with acute bronchiolitis is safe outside the intensive care unit setting, according to a retrospective cohort study.
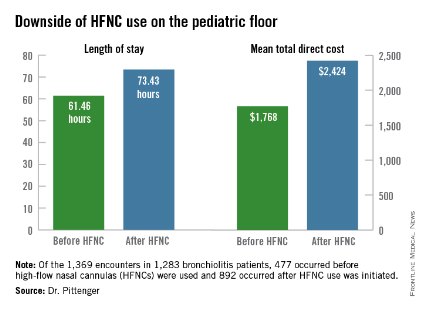
However, initiating the use of high-flow nasal cannulas (HFNCs) on the pediatric floor increases length of stay and direct cost, Dr. Jaime Pittenger of the University of Kentucky, Lexington, reported in a poster at the Pediatric Hospital Medicine 2014 meeting.
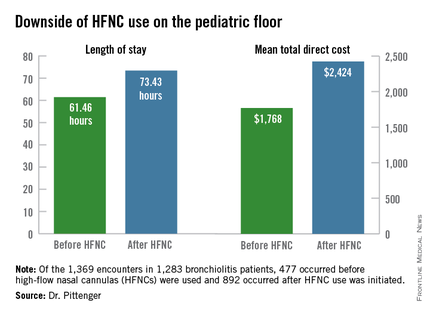
Of 1,369 encounters in 1,283 non-ICU bronchiolitis patients under age 2 who were seen between October 2008 and May 2013, 477 occurred before HFNC use on the floor was initiated in 2010, and 892 occurred after such use was initiated. Of these, 139 involved receipt of HFNCs outside the ICU, Dr. Pittenger reported at the meeting, which was sponsored by the Society of Hospital Medicine, the American Academy of Pediatrics, the AAP Section on Hospital Medicine, and the Academic Pediatric Association.
Of those who received HFNCs outside the ICU, 66% who would have previously gone to the ICU remained on the floor, she noted.
Furthermore, a reduction was seen in noninvasive and invasive ventilation in the ICU after HFNC use outside the ICU was initiated, although this did not reach significance (P = .19).
Use of HFNCs on the floor was associated with a relatively low frequency of complications, but mean length of stay was 61.46 hours before HFNC was used outside the ICU, compared with 73.43 hours. Mean total direct cost was $1,768 before HFNC was used outside the ICU, vs. $2,424 after it began to be used outside the ICU after non-ICU HFNC initiation.
HFNC use outside the ICU for respiratory support in pediatric patients with bronchiolitis has increased in recent years, but there has been little evidence to support the safety and effectiveness of this paradigm shift. Though limited by lack of standardization, patient and treatment selection biases, and a small cohort size for ascertaining the frequency of complications, these findings suggest that the practice is feasible.
However, future studies should evaluate the cost-effectiveness of using HFNC on the floor, Dr. Pittenger concluded, noting that standardization of initiation, escalation, and de-escalation of HFNC are also needed.
Dr. Pittenger reported having no disclosures.
LAKE BUENA VISTA, FLA. – The use of high-flow nasal cannulas for respiratory support in young children with acute bronchiolitis is safe outside the intensive care unit setting, according to a retrospective cohort study.
However, initiating the use of high-flow nasal cannulas (HFNCs) on the pediatric floor increases length of stay and direct cost, Dr. Jaime Pittenger of the University of Kentucky, Lexington, reported in a poster at the Pediatric Hospital Medicine 2014 meeting.
Of 1,369 encounters in 1,283 non-ICU bronchiolitis patients under age 2 who were seen between October 2008 and May 2013, 477 occurred before HFNC use on the floor was initiated in 2010, and 892 occurred after such use was initiated. Of these, 139 involved receipt of HFNCs outside the ICU, Dr. Pittenger reported at the meeting, which was sponsored by the Society of Hospital Medicine, the American Academy of Pediatrics, the AAP Section on Hospital Medicine, and the Academic Pediatric Association.
Of those who received HFNCs outside the ICU, 66% who would have previously gone to the ICU remained on the floor, she noted.
Furthermore, a reduction was seen in noninvasive and invasive ventilation in the ICU after HFNC use outside the ICU was initiated, although this did not reach significance (P = .19).
Use of HFNCs on the floor was associated with a relatively low frequency of complications, but mean length of stay was 61.46 hours before HFNC was used outside the ICU, compared with 73.43 hours. Mean total direct cost was $1,768 before HFNC was used outside the ICU, vs. $2,424 after it began to be used outside the ICU after non-ICU HFNC initiation.
HFNC use outside the ICU for respiratory support in pediatric patients with bronchiolitis has increased in recent years, but there has been little evidence to support the safety and effectiveness of this paradigm shift. Though limited by lack of standardization, patient and treatment selection biases, and a small cohort size for ascertaining the frequency of complications, these findings suggest that the practice is feasible.
However, future studies should evaluate the cost-effectiveness of using HFNC on the floor, Dr. Pittenger concluded, noting that standardization of initiation, escalation, and de-escalation of HFNC are also needed.
Dr. Pittenger reported having no disclosures.
LAKE BUENA VISTA, FLA. – The use of high-flow nasal cannulas for respiratory support in young children with acute bronchiolitis is safe outside the intensive care unit setting, according to a retrospective cohort study.
However, initiating the use of high-flow nasal cannulas (HFNCs) on the pediatric floor increases length of stay and direct cost, Dr. Jaime Pittenger of the University of Kentucky, Lexington, reported in a poster at the Pediatric Hospital Medicine 2014 meeting.
Of 1,369 encounters in 1,283 non-ICU bronchiolitis patients under age 2 who were seen between October 2008 and May 2013, 477 occurred before HFNC use on the floor was initiated in 2010, and 892 occurred after such use was initiated. Of these, 139 involved receipt of HFNCs outside the ICU, Dr. Pittenger reported at the meeting, which was sponsored by the Society of Hospital Medicine, the American Academy of Pediatrics, the AAP Section on Hospital Medicine, and the Academic Pediatric Association.
Of those who received HFNCs outside the ICU, 66% who would have previously gone to the ICU remained on the floor, she noted.
Furthermore, a reduction was seen in noninvasive and invasive ventilation in the ICU after HFNC use outside the ICU was initiated, although this did not reach significance (P = .19).
Use of HFNCs on the floor was associated with a relatively low frequency of complications, but mean length of stay was 61.46 hours before HFNC was used outside the ICU, compared with 73.43 hours. Mean total direct cost was $1,768 before HFNC was used outside the ICU, vs. $2,424 after it began to be used outside the ICU after non-ICU HFNC initiation.
HFNC use outside the ICU for respiratory support in pediatric patients with bronchiolitis has increased in recent years, but there has been little evidence to support the safety and effectiveness of this paradigm shift. Though limited by lack of standardization, patient and treatment selection biases, and a small cohort size for ascertaining the frequency of complications, these findings suggest that the practice is feasible.
However, future studies should evaluate the cost-effectiveness of using HFNC on the floor, Dr. Pittenger concluded, noting that standardization of initiation, escalation, and de-escalation of HFNC are also needed.
Dr. Pittenger reported having no disclosures.
AT PEDIATRIC HOSPITAL MEDICINE 2014
Key clinical point: HFNC use outside the ICU is feasible for respiratory support in young children with bronchiolitis.
Major finding: A total of 66% of HFNC patients who would have been sent to the ICU remained on the pediatric floor.
Data source: A retrospective cohort study of 1,369 encounters in 1,283 non-ICU bronchiolitis patients under age 2.
Disclosures: Dr. Pittenger reported having no disclosures.
RCT: 3% hypertonic saline fails to improve bronchiolitis outcomes
LAKE BUENA VISTA, FLA. – The median length of stay and rate of readmission did not differ between infants with bronchiolitis who were treated with nebulized 3% hypertonic saline and those treated with normal saline in the first U.S. prospective, double-blind, randomized controlled trial comparing the two treatments.*
The median length of stay was 2.0 days in 93 infants younger than age 12 months who were admitted to an urban tertiary care children’s hospital with a diagnosis of bronchiolitis and who were randomized to receive the hypertonic saline treatments without concomitant bronchodilators, and 2.0 days in 97 such infants who received normal saline without bronchodilators, Dr. Alyssa Silver reported at the Pediatric Hospital Medicine 2014 meeting.
The mean length of stay also did not differ significantly between the groups, nor did the rate of readmission and rate of adverse event, Dr. Silver, a pediatric hospitalist and director of pediatric inpatient physician assistant services at the Children’s Hospital at Montefiore, Bronx, N.Y., reported at the meeting, which was sponsored by the Society of Hospital Medicine, the American Academy of Pediatrics, the AAP Section on Hospital Medicine, and the Academic Pediatric Association.
Infants offered enrollment were those admitted with bronchiolitis to an urban tertiary care children’s hospital in a population with a high endemic prevalence of asthma. Those with status asthmaticus, certain chronic diseases, and prior exposure to hypertonic saline were among those excluded.
The infants included in the study were enrolled within 12 hours of admission between 2011 and 2014, received 4 mL of hypertonic or normal saline every 4 hours via standard hospital wall nebulizer until discharge and were assessed daily by study personnel who made follow-up calls at 1 week and 1 month after discharge to document readmissions.
To address the theoretical concern of bronchospasm with hypertonic saline, patients were evaluated using the Respiratory Distress Assessment Instrument prior to first study treatment and at 30 minutes after the treatment as a safety measure and were withdrawn if the measure increased by four or more points, Dr. Silver said.
The treatment and control groups were similar with respect to demographic factors.
Subgroup analyses showed no differences in length of stay between infants in the treatment and control groups who were respiratory syncytial virus positive, had a history of wheezing, or had a history of prematurity, Dr. Silver noted.
Enrollment in the study was halted at the time of an interim analysis because of the demonstrated lack of difference in length of stay between the groups.
Bronchiolitis is the leading cause of hospitalization for children under 12 months of age – at a cost of about $500 million each year. The national average length of stay for infants with bronchiolitis is 3.3 days.
"Despite the high incidence of bronchiolitis, there is a lack of a unified inpatient treatment plan beyond supportive care of oxygen and intravenous hydration. Many different approaches have been used, but none have proven useful," Dr. Silver said, adding that interest in the use of nebulized hypertonic saline has been on the rise.
Based on literature from its use in patients with cystic fibrosis, the proposed mechanism of action is hydration of the airway surface liquid, which decreases airway wall edema and improves ciliary function, thereby assisting with the clearance of secretions, she explained.
A Cochrane review suggested benefit, but there are a number of concerns about generalizing the findings. For example, all of the included studies were performed outside of the United States, included varying dosing regimens, and excluded patients with a history of wheeze, and most allowed the use of adjunctive bronchodilators and were performed in areas with a much longer length of stay than occurs in the United States.
More recent studies in the United States questioned the utility of hypertonic saline, but also allowed the use of bronchodilators and excluded patients with a history of wheezing.
The findings of the current study suggest that although 3% hypertonic saline is safe in infants with bronchiolitis – including those with a history of wheeze, and even in a population with high endemic prevalence of asthma – there is no utility for the routine use of 3% hypertonic saline vs. normal saline without adjunctive bronchodilators in this population, she said.
However, the study is limited by the single-center design, and lack of complete coverage for recruiting of admitted patients (the study was unfunded and relied on voluntary study personnel), although more than 75% of patients admitted for bronchiolitis were offered enrollment.
Future studies might benefit by enrolling patients earlier than within 12 hours of admission with a minimum severity score to enter, assessing similar outcomes using higher concentrations of nebulized sodium chloride, studying on demand vs. scheduled saline treatments for bronchiolitis, and/or by comparing either intervention to supportive care alone, Dr. Silver said.
Dr. Silver reported having no disclosures.
*An earlier version of this article misstated the city name in the dateline.
LAKE BUENA VISTA, FLA. – The median length of stay and rate of readmission did not differ between infants with bronchiolitis who were treated with nebulized 3% hypertonic saline and those treated with normal saline in the first U.S. prospective, double-blind, randomized controlled trial comparing the two treatments.*
The median length of stay was 2.0 days in 93 infants younger than age 12 months who were admitted to an urban tertiary care children’s hospital with a diagnosis of bronchiolitis and who were randomized to receive the hypertonic saline treatments without concomitant bronchodilators, and 2.0 days in 97 such infants who received normal saline without bronchodilators, Dr. Alyssa Silver reported at the Pediatric Hospital Medicine 2014 meeting.
The mean length of stay also did not differ significantly between the groups, nor did the rate of readmission and rate of adverse event, Dr. Silver, a pediatric hospitalist and director of pediatric inpatient physician assistant services at the Children’s Hospital at Montefiore, Bronx, N.Y., reported at the meeting, which was sponsored by the Society of Hospital Medicine, the American Academy of Pediatrics, the AAP Section on Hospital Medicine, and the Academic Pediatric Association.
Infants offered enrollment were those admitted with bronchiolitis to an urban tertiary care children’s hospital in a population with a high endemic prevalence of asthma. Those with status asthmaticus, certain chronic diseases, and prior exposure to hypertonic saline were among those excluded.
The infants included in the study were enrolled within 12 hours of admission between 2011 and 2014, received 4 mL of hypertonic or normal saline every 4 hours via standard hospital wall nebulizer until discharge and were assessed daily by study personnel who made follow-up calls at 1 week and 1 month after discharge to document readmissions.
To address the theoretical concern of bronchospasm with hypertonic saline, patients were evaluated using the Respiratory Distress Assessment Instrument prior to first study treatment and at 30 minutes after the treatment as a safety measure and were withdrawn if the measure increased by four or more points, Dr. Silver said.
The treatment and control groups were similar with respect to demographic factors.
Subgroup analyses showed no differences in length of stay between infants in the treatment and control groups who were respiratory syncytial virus positive, had a history of wheezing, or had a history of prematurity, Dr. Silver noted.
Enrollment in the study was halted at the time of an interim analysis because of the demonstrated lack of difference in length of stay between the groups.
Bronchiolitis is the leading cause of hospitalization for children under 12 months of age – at a cost of about $500 million each year. The national average length of stay for infants with bronchiolitis is 3.3 days.
"Despite the high incidence of bronchiolitis, there is a lack of a unified inpatient treatment plan beyond supportive care of oxygen and intravenous hydration. Many different approaches have been used, but none have proven useful," Dr. Silver said, adding that interest in the use of nebulized hypertonic saline has been on the rise.
Based on literature from its use in patients with cystic fibrosis, the proposed mechanism of action is hydration of the airway surface liquid, which decreases airway wall edema and improves ciliary function, thereby assisting with the clearance of secretions, she explained.
A Cochrane review suggested benefit, but there are a number of concerns about generalizing the findings. For example, all of the included studies were performed outside of the United States, included varying dosing regimens, and excluded patients with a history of wheeze, and most allowed the use of adjunctive bronchodilators and were performed in areas with a much longer length of stay than occurs in the United States.
More recent studies in the United States questioned the utility of hypertonic saline, but also allowed the use of bronchodilators and excluded patients with a history of wheezing.
The findings of the current study suggest that although 3% hypertonic saline is safe in infants with bronchiolitis – including those with a history of wheeze, and even in a population with high endemic prevalence of asthma – there is no utility for the routine use of 3% hypertonic saline vs. normal saline without adjunctive bronchodilators in this population, she said.
However, the study is limited by the single-center design, and lack of complete coverage for recruiting of admitted patients (the study was unfunded and relied on voluntary study personnel), although more than 75% of patients admitted for bronchiolitis were offered enrollment.
Future studies might benefit by enrolling patients earlier than within 12 hours of admission with a minimum severity score to enter, assessing similar outcomes using higher concentrations of nebulized sodium chloride, studying on demand vs. scheduled saline treatments for bronchiolitis, and/or by comparing either intervention to supportive care alone, Dr. Silver said.
Dr. Silver reported having no disclosures.
*An earlier version of this article misstated the city name in the dateline.
LAKE BUENA VISTA, FLA. – The median length of stay and rate of readmission did not differ between infants with bronchiolitis who were treated with nebulized 3% hypertonic saline and those treated with normal saline in the first U.S. prospective, double-blind, randomized controlled trial comparing the two treatments.*
The median length of stay was 2.0 days in 93 infants younger than age 12 months who were admitted to an urban tertiary care children’s hospital with a diagnosis of bronchiolitis and who were randomized to receive the hypertonic saline treatments without concomitant bronchodilators, and 2.0 days in 97 such infants who received normal saline without bronchodilators, Dr. Alyssa Silver reported at the Pediatric Hospital Medicine 2014 meeting.
The mean length of stay also did not differ significantly between the groups, nor did the rate of readmission and rate of adverse event, Dr. Silver, a pediatric hospitalist and director of pediatric inpatient physician assistant services at the Children’s Hospital at Montefiore, Bronx, N.Y., reported at the meeting, which was sponsored by the Society of Hospital Medicine, the American Academy of Pediatrics, the AAP Section on Hospital Medicine, and the Academic Pediatric Association.
Infants offered enrollment were those admitted with bronchiolitis to an urban tertiary care children’s hospital in a population with a high endemic prevalence of asthma. Those with status asthmaticus, certain chronic diseases, and prior exposure to hypertonic saline were among those excluded.
The infants included in the study were enrolled within 12 hours of admission between 2011 and 2014, received 4 mL of hypertonic or normal saline every 4 hours via standard hospital wall nebulizer until discharge and were assessed daily by study personnel who made follow-up calls at 1 week and 1 month after discharge to document readmissions.
To address the theoretical concern of bronchospasm with hypertonic saline, patients were evaluated using the Respiratory Distress Assessment Instrument prior to first study treatment and at 30 minutes after the treatment as a safety measure and were withdrawn if the measure increased by four or more points, Dr. Silver said.
The treatment and control groups were similar with respect to demographic factors.
Subgroup analyses showed no differences in length of stay between infants in the treatment and control groups who were respiratory syncytial virus positive, had a history of wheezing, or had a history of prematurity, Dr. Silver noted.
Enrollment in the study was halted at the time of an interim analysis because of the demonstrated lack of difference in length of stay between the groups.
Bronchiolitis is the leading cause of hospitalization for children under 12 months of age – at a cost of about $500 million each year. The national average length of stay for infants with bronchiolitis is 3.3 days.
"Despite the high incidence of bronchiolitis, there is a lack of a unified inpatient treatment plan beyond supportive care of oxygen and intravenous hydration. Many different approaches have been used, but none have proven useful," Dr. Silver said, adding that interest in the use of nebulized hypertonic saline has been on the rise.
Based on literature from its use in patients with cystic fibrosis, the proposed mechanism of action is hydration of the airway surface liquid, which decreases airway wall edema and improves ciliary function, thereby assisting with the clearance of secretions, she explained.
A Cochrane review suggested benefit, but there are a number of concerns about generalizing the findings. For example, all of the included studies were performed outside of the United States, included varying dosing regimens, and excluded patients with a history of wheeze, and most allowed the use of adjunctive bronchodilators and were performed in areas with a much longer length of stay than occurs in the United States.
More recent studies in the United States questioned the utility of hypertonic saline, but also allowed the use of bronchodilators and excluded patients with a history of wheezing.
The findings of the current study suggest that although 3% hypertonic saline is safe in infants with bronchiolitis – including those with a history of wheeze, and even in a population with high endemic prevalence of asthma – there is no utility for the routine use of 3% hypertonic saline vs. normal saline without adjunctive bronchodilators in this population, she said.
However, the study is limited by the single-center design, and lack of complete coverage for recruiting of admitted patients (the study was unfunded and relied on voluntary study personnel), although more than 75% of patients admitted for bronchiolitis were offered enrollment.
Future studies might benefit by enrolling patients earlier than within 12 hours of admission with a minimum severity score to enter, assessing similar outcomes using higher concentrations of nebulized sodium chloride, studying on demand vs. scheduled saline treatments for bronchiolitis, and/or by comparing either intervention to supportive care alone, Dr. Silver said.
Dr. Silver reported having no disclosures.
*An earlier version of this article misstated the city name in the dateline.
AT PEDIATRIC HOSPITAL MEDICINE 2014
Key clinical point: There is no reason for routine use of 3% hypertonic saline vs. normal saline without adjunctive bronchodilators in infants.
Major finding: Length of stay was approximately 2.0 days in both the treatment and control groups.
Data source: A prospective, double-blind, randomized, controlled study of 190 bronchiolitic infants younger than 12 months.
Disclosures: Dr. Silver reported no disclosures.
Low extragenital STD screening rates result in missed infections
ATLANTA – Extragenital chlamydia and gonorrhea infections are common among men who have sex with men, but screening for extragenital infection is far less common than urethral testing, according to a study of clinic patients.
The lack of extragenital testing likely resulted in a substantial number of missed infections in the clinic population, Roberta Scheinmann of Public Health Solutions, New York, reported at a conference on STD prevention sponsored by the Centers for Disease Control and Prevention.
The prevalence of urethral testing among 300 HIV-positive men evaluated at a federally qualified health center in 2011 was 71%, compared with 47% for rectal testing and 40% for pharyngeal testing. Just over a third of the men were tested at all three sites.
Overall, 9% of patients tested positive for chlamydia at any anatomic site, and 9% tested positive for gonorrhea at any anatomic site. Among those who had a rectal test, 14% and 9% were positive for chlamydia and gonorrhea, respectively, Ms. Scheinmann said.
Of the chlamydia cases, about half were rectal. Of the gonorrhea cases 35% were rectal and 23% were pharyngeal.
Based on these findings and the testing rates in this study, an estimated 143 extragenital gonorrhea infections were missed in the clinic population during the study year, and an estimated 223 extragenital chlamydia infections were missed, Ms. Scheinmann said.
Patients were selected randomly from among about 3,000 HIV-positive men who have sex with men who were seen at least once at the center during 2011, and demographic data and data regarding anatomic sites of testing in the year prior to the visit were abstracted from medical records. The patients had a median age of 39 years, more than half were aged 40 or older, 40% were on Medicaid, and about a third were part of the AIDS Drug Assistance Programs.
The median number of medical visits during the study period was six, so the patients "were quite connected to care," she said.
The rates of coinfection among HIV-positive men who have sex with men is high, and the findings of this study are consistent with those from prior studies showing low rates of extragenital testing and high rates of missed infection in this population. In one study, HIV-positive men were rectally screened only 2%-9% of the time, and in another, half of all chlamydia cases and about two-thirds of gonorrhea cases were missed, Ms. Scheinmann said.
Further evaluation to identify potential barriers to screening and missed opportunities for screening is currently underway, as is an effort to improve screening rates, she said.
Ms. Scheinmann reported having no relevant financial disclosures.
ATLANTA – Extragenital chlamydia and gonorrhea infections are common among men who have sex with men, but screening for extragenital infection is far less common than urethral testing, according to a study of clinic patients.
The lack of extragenital testing likely resulted in a substantial number of missed infections in the clinic population, Roberta Scheinmann of Public Health Solutions, New York, reported at a conference on STD prevention sponsored by the Centers for Disease Control and Prevention.
The prevalence of urethral testing among 300 HIV-positive men evaluated at a federally qualified health center in 2011 was 71%, compared with 47% for rectal testing and 40% for pharyngeal testing. Just over a third of the men were tested at all three sites.
Overall, 9% of patients tested positive for chlamydia at any anatomic site, and 9% tested positive for gonorrhea at any anatomic site. Among those who had a rectal test, 14% and 9% were positive for chlamydia and gonorrhea, respectively, Ms. Scheinmann said.
Of the chlamydia cases, about half were rectal. Of the gonorrhea cases 35% were rectal and 23% were pharyngeal.
Based on these findings and the testing rates in this study, an estimated 143 extragenital gonorrhea infections were missed in the clinic population during the study year, and an estimated 223 extragenital chlamydia infections were missed, Ms. Scheinmann said.
Patients were selected randomly from among about 3,000 HIV-positive men who have sex with men who were seen at least once at the center during 2011, and demographic data and data regarding anatomic sites of testing in the year prior to the visit were abstracted from medical records. The patients had a median age of 39 years, more than half were aged 40 or older, 40% were on Medicaid, and about a third were part of the AIDS Drug Assistance Programs.
The median number of medical visits during the study period was six, so the patients "were quite connected to care," she said.
The rates of coinfection among HIV-positive men who have sex with men is high, and the findings of this study are consistent with those from prior studies showing low rates of extragenital testing and high rates of missed infection in this population. In one study, HIV-positive men were rectally screened only 2%-9% of the time, and in another, half of all chlamydia cases and about two-thirds of gonorrhea cases were missed, Ms. Scheinmann said.
Further evaluation to identify potential barriers to screening and missed opportunities for screening is currently underway, as is an effort to improve screening rates, she said.
Ms. Scheinmann reported having no relevant financial disclosures.
ATLANTA – Extragenital chlamydia and gonorrhea infections are common among men who have sex with men, but screening for extragenital infection is far less common than urethral testing, according to a study of clinic patients.
The lack of extragenital testing likely resulted in a substantial number of missed infections in the clinic population, Roberta Scheinmann of Public Health Solutions, New York, reported at a conference on STD prevention sponsored by the Centers for Disease Control and Prevention.
The prevalence of urethral testing among 300 HIV-positive men evaluated at a federally qualified health center in 2011 was 71%, compared with 47% for rectal testing and 40% for pharyngeal testing. Just over a third of the men were tested at all three sites.
Overall, 9% of patients tested positive for chlamydia at any anatomic site, and 9% tested positive for gonorrhea at any anatomic site. Among those who had a rectal test, 14% and 9% were positive for chlamydia and gonorrhea, respectively, Ms. Scheinmann said.
Of the chlamydia cases, about half were rectal. Of the gonorrhea cases 35% were rectal and 23% were pharyngeal.
Based on these findings and the testing rates in this study, an estimated 143 extragenital gonorrhea infections were missed in the clinic population during the study year, and an estimated 223 extragenital chlamydia infections were missed, Ms. Scheinmann said.
Patients were selected randomly from among about 3,000 HIV-positive men who have sex with men who were seen at least once at the center during 2011, and demographic data and data regarding anatomic sites of testing in the year prior to the visit were abstracted from medical records. The patients had a median age of 39 years, more than half were aged 40 or older, 40% were on Medicaid, and about a third were part of the AIDS Drug Assistance Programs.
The median number of medical visits during the study period was six, so the patients "were quite connected to care," she said.
The rates of coinfection among HIV-positive men who have sex with men is high, and the findings of this study are consistent with those from prior studies showing low rates of extragenital testing and high rates of missed infection in this population. In one study, HIV-positive men were rectally screened only 2%-9% of the time, and in another, half of all chlamydia cases and about two-thirds of gonorrhea cases were missed, Ms. Scheinmann said.
Further evaluation to identify potential barriers to screening and missed opportunities for screening is currently underway, as is an effort to improve screening rates, she said.
Ms. Scheinmann reported having no relevant financial disclosures.
AT THE 2014 STD PREVENTION CONFERENCE
Key clinical point: If physicians don’t look for extragenital STDs in men, they won’t find them.
Major finding: Failure to screen resulted in an estimated 143 and 223 cases of extragenital gonorrhea and chlamydia infection, respectively, being missed.
Data source: An evaluation and review of records for 300 HIV clinic patients.
Disclosures: Ms. Scheinmann reported having no disclosures.
Birth Registry Data Demonstrate Familial Cerebral Palsy Risk
Cerebral palsy appears to have a genetic component, with increased risk extending to third-degree relatives (first cousins), according to findings from a population-based cohort study.
These data "offer additional evidence that the underlying causes of cerebral palsy extend beyond the clinical management of delivery. However, the similar risks of cerebral palsy of co-twins of affected like-sex and unlike-sex twin pairs suggest that genetic influences are only part of a wide range of causes," the researchers concluded, noting that future studies should consider the possibility of genetic causes and genetic susceptibility to environmental causes.
Of over 2 million Norwegians born between 1967 and 2002 and included in the Medical Birth Registry of Norway, 3,649 were diagnosed with cerebral palsy, Dr. Mette C. Tollånes of the University of Bergen and her colleagues reported online July 15 in the British Journal of Medicine.
Individuals who had a twin with cerebral palsy had a 15.6-fold increase in the risk of cerebral palsy. Subsequent full or half siblings of a child with cerebral palsy had a 9.2-fold and 3.0-fold increase in the risk of cerebral palsy, respectively, and parents with cerebral palsy had a 6.5-fold increase in the risk of having an affected child, the investigators found (BMJ 2014 July 15 [doi:10.1136/bmj.g4294]).
Although the risk was lower than for first- and second-degree relatives, even those who had a first cousin with cerebral palsy were at a 1.5-fold increased risk of cerebral palsy, they said.
There was no evidence of a difference in the rate of transmission by affected mothers or fathers, and the risks seen in siblings and cousins were independent of the sex of the index case, Dr. Tollånes and her associates noted.
Prior studies have shown that, in addition to a number of risk factors in pregnancy and during the perinatal period – such as preterm delivery, multiple fetuses, birth asphyxia, and perinatal stroke – there also is a possible heritable component. In fact, a number of candidate genes and single nucleotide polymorphisms have been investigated to explain familial clustering of cerebral palsy, and some studies have extended the investigation to interactions with clinical factors and other genes.
Positive findings, however, have been difficult to replicate, the investigators said.
"We used data from a large population based cohort to ... shed light on patterns of inheritance," they wrote.
Although limited by a number of factors, including lack of information on cerebral palsy subtypes, an inability to identify cases with postneonatal causes, and a possible underestimation of recurrence risk because of the exclusion of those who didn’t survive past 3 years, the findings "suggest that cerebral palsy includes a genetic component, with a stronger recurrence among relatives with closer genetic relationship," Dr. Tollånes and her associates said.
This study was supported by grants from the University of Bergen; the Western Norway Regional Health Authority; and the Intramural Research Program of the National Institute of Environmental Health Sciences, National Institutes of Health. The authors reported having no disclosures other than support from these funding sources.
Cerebral palsy appears to have a genetic component, with increased risk extending to third-degree relatives (first cousins), according to findings from a population-based cohort study.
These data "offer additional evidence that the underlying causes of cerebral palsy extend beyond the clinical management of delivery. However, the similar risks of cerebral palsy of co-twins of affected like-sex and unlike-sex twin pairs suggest that genetic influences are only part of a wide range of causes," the researchers concluded, noting that future studies should consider the possibility of genetic causes and genetic susceptibility to environmental causes.
Of over 2 million Norwegians born between 1967 and 2002 and included in the Medical Birth Registry of Norway, 3,649 were diagnosed with cerebral palsy, Dr. Mette C. Tollånes of the University of Bergen and her colleagues reported online July 15 in the British Journal of Medicine.
Individuals who had a twin with cerebral palsy had a 15.6-fold increase in the risk of cerebral palsy. Subsequent full or half siblings of a child with cerebral palsy had a 9.2-fold and 3.0-fold increase in the risk of cerebral palsy, respectively, and parents with cerebral palsy had a 6.5-fold increase in the risk of having an affected child, the investigators found (BMJ 2014 July 15 [doi:10.1136/bmj.g4294]).
Although the risk was lower than for first- and second-degree relatives, even those who had a first cousin with cerebral palsy were at a 1.5-fold increased risk of cerebral palsy, they said.
There was no evidence of a difference in the rate of transmission by affected mothers or fathers, and the risks seen in siblings and cousins were independent of the sex of the index case, Dr. Tollånes and her associates noted.
Prior studies have shown that, in addition to a number of risk factors in pregnancy and during the perinatal period – such as preterm delivery, multiple fetuses, birth asphyxia, and perinatal stroke – there also is a possible heritable component. In fact, a number of candidate genes and single nucleotide polymorphisms have been investigated to explain familial clustering of cerebral palsy, and some studies have extended the investigation to interactions with clinical factors and other genes.
Positive findings, however, have been difficult to replicate, the investigators said.
"We used data from a large population based cohort to ... shed light on patterns of inheritance," they wrote.
Although limited by a number of factors, including lack of information on cerebral palsy subtypes, an inability to identify cases with postneonatal causes, and a possible underestimation of recurrence risk because of the exclusion of those who didn’t survive past 3 years, the findings "suggest that cerebral palsy includes a genetic component, with a stronger recurrence among relatives with closer genetic relationship," Dr. Tollånes and her associates said.
This study was supported by grants from the University of Bergen; the Western Norway Regional Health Authority; and the Intramural Research Program of the National Institute of Environmental Health Sciences, National Institutes of Health. The authors reported having no disclosures other than support from these funding sources.
Cerebral palsy appears to have a genetic component, with increased risk extending to third-degree relatives (first cousins), according to findings from a population-based cohort study.
These data "offer additional evidence that the underlying causes of cerebral palsy extend beyond the clinical management of delivery. However, the similar risks of cerebral palsy of co-twins of affected like-sex and unlike-sex twin pairs suggest that genetic influences are only part of a wide range of causes," the researchers concluded, noting that future studies should consider the possibility of genetic causes and genetic susceptibility to environmental causes.
Of over 2 million Norwegians born between 1967 and 2002 and included in the Medical Birth Registry of Norway, 3,649 were diagnosed with cerebral palsy, Dr. Mette C. Tollånes of the University of Bergen and her colleagues reported online July 15 in the British Journal of Medicine.
Individuals who had a twin with cerebral palsy had a 15.6-fold increase in the risk of cerebral palsy. Subsequent full or half siblings of a child with cerebral palsy had a 9.2-fold and 3.0-fold increase in the risk of cerebral palsy, respectively, and parents with cerebral palsy had a 6.5-fold increase in the risk of having an affected child, the investigators found (BMJ 2014 July 15 [doi:10.1136/bmj.g4294]).
Although the risk was lower than for first- and second-degree relatives, even those who had a first cousin with cerebral palsy were at a 1.5-fold increased risk of cerebral palsy, they said.
There was no evidence of a difference in the rate of transmission by affected mothers or fathers, and the risks seen in siblings and cousins were independent of the sex of the index case, Dr. Tollånes and her associates noted.
Prior studies have shown that, in addition to a number of risk factors in pregnancy and during the perinatal period – such as preterm delivery, multiple fetuses, birth asphyxia, and perinatal stroke – there also is a possible heritable component. In fact, a number of candidate genes and single nucleotide polymorphisms have been investigated to explain familial clustering of cerebral palsy, and some studies have extended the investigation to interactions with clinical factors and other genes.
Positive findings, however, have been difficult to replicate, the investigators said.
"We used data from a large population based cohort to ... shed light on patterns of inheritance," they wrote.
Although limited by a number of factors, including lack of information on cerebral palsy subtypes, an inability to identify cases with postneonatal causes, and a possible underestimation of recurrence risk because of the exclusion of those who didn’t survive past 3 years, the findings "suggest that cerebral palsy includes a genetic component, with a stronger recurrence among relatives with closer genetic relationship," Dr. Tollånes and her associates said.
This study was supported by grants from the University of Bergen; the Western Norway Regional Health Authority; and the Intramural Research Program of the National Institute of Environmental Health Sciences, National Institutes of Health. The authors reported having no disclosures other than support from these funding sources.
FROM BMJ
New ACOG opinions address gynecologic concerns in young cancer patients
Cancer treatments in children and adolescents can adversely affect reproductive health and future pregnancy outcomes, so gynecologists should be aware of these effects and be involved in patient care, according to a new committee opinion from the American College of Obstetricians and Gynecologists.
The opinion, entitled "Gynecologic Concerns in Children and Adolescents with Cancer," is one of two released July 22 regarding the preservation of reproductive health among young cancer patients. The other opinion specifically addresses prevention and management of heavy menstrual bleeding that can result from cancer and cancer treatments.
Both opinions were developed by the ACOG Committee on Adolescent Health Care and are published in the August 2014 issue of Obstetrics & Gynecology.
Advancements in radiation therapy, chemotherapy, surgery, and multimodal treatment have dramatically improved childhood cancer survival; 5-year survival rates have reached nearly 80%, but the treatments – and the cancer itself – can have immediate or delayed adverse effect on reproductive health, the authors wrote in the first opinion (Obstet. Gynecol. 2014;124:403-8).
Gynecologists should be aware of the potential effects that can occur both during and after each type of therapy, they said.
For example, primary ovarian insufficiency can occur following pelvic radiation therapy and can lead to future adverse pregnancy outcomes. Chemotherapy also can affect ovarian function, and the risk of toxicity is directly proportional to the age and pubertal status of the patient at the time of exposure, with older patients having higher risk.
Surgery, such as resection of the vagina, uterus, ovaries, or fallopian tubes, can lead to adhesions and infertility, and can also lead to pelvic pain, sexual dysfunction, and fistula formation, they said.
Cancer treatments also can lead to precocious or delayed puberty.
Gynecologists should be prepared to manage gynecologic concerns in young patients and survivors, as they may be consulted regarding pubertal concerns, heavy menstrual bleeding and anemia, sexuality, contraception, ovarian function, and breast and cervical cancer screening, the authors noted.
The committee opinion provides information and guidance on managing each of these circumstances. With respect to fertility preservation, the opinion states that anti-Müllerian hormone level is the optimal screening tool for assessing ovarian reserve in survivors and stresses that potential options for fertility preservation should be discussed prior to treatment in those at risk for infertility. Options may include oophoropexy to move the gonads away from the radiation field in those to be treated with pelvic irradiation, and ovarian stimulation and cryopreservation of either oocytes or embryos.
"The science of fertility preservation is a rapidly evolving field; therefore, a referral to a reproductive endocrinologist is recommended to explore the full range of available options," the authors said, adding that for young women who have completed sexual development, gonadotropin-releasing hormone agonists have been used to induce ovarian quiescence in an effort to preserve ovarian function and fertility. Results of this approach have been mixed, and the evidence is not currently strong enough to recommend this therapy, although randomized trials are underway, they said.
In the second opinion, "Options for Prevention and Management of Heavy Menstrual Bleeding in Adolescent Patients Undergoing Cancer Treatment", the authors note that even normal menstrual blood loss can pose a threat to adolescents who are already anemic because of hematologic malignancies or cancer treatment (Obstet. Gynecol. 2014;124:397-402).
"Disruption of the hypothalamic-pituitary-gonadal axis during cancer treatment also may cause anovulatory uterine bleeding," they wrote, adding that gynecologists may, therefore, be consulted regarding strategies for suppressing menstruation prior to treatment or during an episode of severe heavy bleeding to stop the bleeding emergency.
Therapy in both situations should be tailored to the patient and her desires for contraception and fertility.
"Because of the complex nature of cancer care, collaboration with the adolescent’s oncologist is highly recommended," according to the opinion, which outlines options for prophylactic menstrual suppression (combined hormonal contraceptives, progestin-only therapy, and gonadotropin-releasing hormone agonists) and emergent treatment of acute uterine bleeding (hormonal therapy, antifibrinolytics, and surgical options for patients who fail medical therapy).
Surgical options may include dilation and curettage, uterine packing, tamponade with a Foley balloon, or uterine artery embolization, but "evidence for these treatments in adolescents is lacking, and their consideration is based on extrapolation from the literature on adult patients. Also, uterine artery embolization is not suitable as a first-line therapy given its effect on fertility, but may be considered as an alternative to hysterectomy in an acutely ill patient," the authors said.
A treatment algorithm for patients without contraindications to estrogen therapy is included in the opinion, with surgical options listed as a last resort.
"Addressing menstrual issues of adolescent patients undergoing cancer treatment is an important part of long-term management and will require collaborative involvement of obstetrician-gynecologists in the care of such patients," the authors concluded.
These two committee opinions provide important guidance for gynecologists, who will likely be called upon to care for survivors of adolescent and childhood cancer.
"As ob.gyns. and advocates for women’s reproductive health, it is our important role to help patients and families understand the effects of their treatment on fertility and optimize the potential for childbearing if that young woman so chooses after treatment is complete," Dr. Julie L. Strickland, chair of the Committee on Adolescent Health Care, said in a press statement.
"As gynecologists, we must be prepared with the most up-to-date information to help manage and treat the gynecological issues and be willing to work in collaboration with other specialties, such as oncologists and reproductive endocrinologists, to ensure the best options for our patients," she added.
Dr. Strickland reported having no disclosures.
Cancer in young female patients is rare, and the literature to guide the management of gynecologic issues related to treatment is limited. Thus, these two new ACOG committee opinions provide a useful resource for gynecologists who encounter young cancer patients and cancer survivors in their practice or who are consulted on the management of a bleeding emergency in a young cancer patient, Dr. Frances Ginsburg said in an interview.
Importantly, the opinions stress the need for collaboration and involvement of gynecologic care early in the course of treatment or prior to treatment initiation, she said.
"My feeling about a young woman or child who is facing this kind of situation is that the younger they are the more likely that everybody is focusing on a million other things. ... A lot of times I will get a call after the fact about a patient who had chemotherapy at 18 and at 20 is not getting her period. It’s a little late at that point," she said.
However, the committee opinion on gynecologic concerns is not forceful enough in its statement on the use of gonadotropin-releasing agonists to induce ovarian quiescence in an effort to preserve ovarian function and fertility after cytotoxic treatment in those who have reached sexual development, she said, explaining that the opinion states that results have been mixed, that a meta-analysis showed only a slight increase in ovarian function, and that evidence is currently not strong enough to recommend their use for this purpose.
In fact, compelling randomized trial data showing a benefit with these agents were presented at a recent conference.
"The results were really very dramatic. I think the results were dramatic enough that probably all women undergoing chemotherapy who desire future fertility ought to be offered it as one of their options," she said.
Dr. Ginsburg is director of reproductive endocrinology and infertility in the department of obstetrics and gynecology at Stamford (Conn.) Hospital and assistant professor of clinical obstetrics and gynecology at Columbia University, New York. She had no relevant financial disclosures and is not a member of the ACOG committee.
Cancer in young female patients is rare, and the literature to guide the management of gynecologic issues related to treatment is limited. Thus, these two new ACOG committee opinions provide a useful resource for gynecologists who encounter young cancer patients and cancer survivors in their practice or who are consulted on the management of a bleeding emergency in a young cancer patient, Dr. Frances Ginsburg said in an interview.
Importantly, the opinions stress the need for collaboration and involvement of gynecologic care early in the course of treatment or prior to treatment initiation, she said.
"My feeling about a young woman or child who is facing this kind of situation is that the younger they are the more likely that everybody is focusing on a million other things. ... A lot of times I will get a call after the fact about a patient who had chemotherapy at 18 and at 20 is not getting her period. It’s a little late at that point," she said.
However, the committee opinion on gynecologic concerns is not forceful enough in its statement on the use of gonadotropin-releasing agonists to induce ovarian quiescence in an effort to preserve ovarian function and fertility after cytotoxic treatment in those who have reached sexual development, she said, explaining that the opinion states that results have been mixed, that a meta-analysis showed only a slight increase in ovarian function, and that evidence is currently not strong enough to recommend their use for this purpose.
In fact, compelling randomized trial data showing a benefit with these agents were presented at a recent conference.
"The results were really very dramatic. I think the results were dramatic enough that probably all women undergoing chemotherapy who desire future fertility ought to be offered it as one of their options," she said.
Dr. Ginsburg is director of reproductive endocrinology and infertility in the department of obstetrics and gynecology at Stamford (Conn.) Hospital and assistant professor of clinical obstetrics and gynecology at Columbia University, New York. She had no relevant financial disclosures and is not a member of the ACOG committee.
Cancer in young female patients is rare, and the literature to guide the management of gynecologic issues related to treatment is limited. Thus, these two new ACOG committee opinions provide a useful resource for gynecologists who encounter young cancer patients and cancer survivors in their practice or who are consulted on the management of a bleeding emergency in a young cancer patient, Dr. Frances Ginsburg said in an interview.
Importantly, the opinions stress the need for collaboration and involvement of gynecologic care early in the course of treatment or prior to treatment initiation, she said.
"My feeling about a young woman or child who is facing this kind of situation is that the younger they are the more likely that everybody is focusing on a million other things. ... A lot of times I will get a call after the fact about a patient who had chemotherapy at 18 and at 20 is not getting her period. It’s a little late at that point," she said.
However, the committee opinion on gynecologic concerns is not forceful enough in its statement on the use of gonadotropin-releasing agonists to induce ovarian quiescence in an effort to preserve ovarian function and fertility after cytotoxic treatment in those who have reached sexual development, she said, explaining that the opinion states that results have been mixed, that a meta-analysis showed only a slight increase in ovarian function, and that evidence is currently not strong enough to recommend their use for this purpose.
In fact, compelling randomized trial data showing a benefit with these agents were presented at a recent conference.
"The results were really very dramatic. I think the results were dramatic enough that probably all women undergoing chemotherapy who desire future fertility ought to be offered it as one of their options," she said.
Dr. Ginsburg is director of reproductive endocrinology and infertility in the department of obstetrics and gynecology at Stamford (Conn.) Hospital and assistant professor of clinical obstetrics and gynecology at Columbia University, New York. She had no relevant financial disclosures and is not a member of the ACOG committee.
Cancer treatments in children and adolescents can adversely affect reproductive health and future pregnancy outcomes, so gynecologists should be aware of these effects and be involved in patient care, according to a new committee opinion from the American College of Obstetricians and Gynecologists.
The opinion, entitled "Gynecologic Concerns in Children and Adolescents with Cancer," is one of two released July 22 regarding the preservation of reproductive health among young cancer patients. The other opinion specifically addresses prevention and management of heavy menstrual bleeding that can result from cancer and cancer treatments.
Both opinions were developed by the ACOG Committee on Adolescent Health Care and are published in the August 2014 issue of Obstetrics & Gynecology.
Advancements in radiation therapy, chemotherapy, surgery, and multimodal treatment have dramatically improved childhood cancer survival; 5-year survival rates have reached nearly 80%, but the treatments – and the cancer itself – can have immediate or delayed adverse effect on reproductive health, the authors wrote in the first opinion (Obstet. Gynecol. 2014;124:403-8).
Gynecologists should be aware of the potential effects that can occur both during and after each type of therapy, they said.
For example, primary ovarian insufficiency can occur following pelvic radiation therapy and can lead to future adverse pregnancy outcomes. Chemotherapy also can affect ovarian function, and the risk of toxicity is directly proportional to the age and pubertal status of the patient at the time of exposure, with older patients having higher risk.
Surgery, such as resection of the vagina, uterus, ovaries, or fallopian tubes, can lead to adhesions and infertility, and can also lead to pelvic pain, sexual dysfunction, and fistula formation, they said.
Cancer treatments also can lead to precocious or delayed puberty.
Gynecologists should be prepared to manage gynecologic concerns in young patients and survivors, as they may be consulted regarding pubertal concerns, heavy menstrual bleeding and anemia, sexuality, contraception, ovarian function, and breast and cervical cancer screening, the authors noted.
The committee opinion provides information and guidance on managing each of these circumstances. With respect to fertility preservation, the opinion states that anti-Müllerian hormone level is the optimal screening tool for assessing ovarian reserve in survivors and stresses that potential options for fertility preservation should be discussed prior to treatment in those at risk for infertility. Options may include oophoropexy to move the gonads away from the radiation field in those to be treated with pelvic irradiation, and ovarian stimulation and cryopreservation of either oocytes or embryos.
"The science of fertility preservation is a rapidly evolving field; therefore, a referral to a reproductive endocrinologist is recommended to explore the full range of available options," the authors said, adding that for young women who have completed sexual development, gonadotropin-releasing hormone agonists have been used to induce ovarian quiescence in an effort to preserve ovarian function and fertility. Results of this approach have been mixed, and the evidence is not currently strong enough to recommend this therapy, although randomized trials are underway, they said.
In the second opinion, "Options for Prevention and Management of Heavy Menstrual Bleeding in Adolescent Patients Undergoing Cancer Treatment", the authors note that even normal menstrual blood loss can pose a threat to adolescents who are already anemic because of hematologic malignancies or cancer treatment (Obstet. Gynecol. 2014;124:397-402).
"Disruption of the hypothalamic-pituitary-gonadal axis during cancer treatment also may cause anovulatory uterine bleeding," they wrote, adding that gynecologists may, therefore, be consulted regarding strategies for suppressing menstruation prior to treatment or during an episode of severe heavy bleeding to stop the bleeding emergency.
Therapy in both situations should be tailored to the patient and her desires for contraception and fertility.
"Because of the complex nature of cancer care, collaboration with the adolescent’s oncologist is highly recommended," according to the opinion, which outlines options for prophylactic menstrual suppression (combined hormonal contraceptives, progestin-only therapy, and gonadotropin-releasing hormone agonists) and emergent treatment of acute uterine bleeding (hormonal therapy, antifibrinolytics, and surgical options for patients who fail medical therapy).
Surgical options may include dilation and curettage, uterine packing, tamponade with a Foley balloon, or uterine artery embolization, but "evidence for these treatments in adolescents is lacking, and their consideration is based on extrapolation from the literature on adult patients. Also, uterine artery embolization is not suitable as a first-line therapy given its effect on fertility, but may be considered as an alternative to hysterectomy in an acutely ill patient," the authors said.
A treatment algorithm for patients without contraindications to estrogen therapy is included in the opinion, with surgical options listed as a last resort.
"Addressing menstrual issues of adolescent patients undergoing cancer treatment is an important part of long-term management and will require collaborative involvement of obstetrician-gynecologists in the care of such patients," the authors concluded.
These two committee opinions provide important guidance for gynecologists, who will likely be called upon to care for survivors of adolescent and childhood cancer.
"As ob.gyns. and advocates for women’s reproductive health, it is our important role to help patients and families understand the effects of their treatment on fertility and optimize the potential for childbearing if that young woman so chooses after treatment is complete," Dr. Julie L. Strickland, chair of the Committee on Adolescent Health Care, said in a press statement.
"As gynecologists, we must be prepared with the most up-to-date information to help manage and treat the gynecological issues and be willing to work in collaboration with other specialties, such as oncologists and reproductive endocrinologists, to ensure the best options for our patients," she added.
Dr. Strickland reported having no disclosures.
Cancer treatments in children and adolescents can adversely affect reproductive health and future pregnancy outcomes, so gynecologists should be aware of these effects and be involved in patient care, according to a new committee opinion from the American College of Obstetricians and Gynecologists.
The opinion, entitled "Gynecologic Concerns in Children and Adolescents with Cancer," is one of two released July 22 regarding the preservation of reproductive health among young cancer patients. The other opinion specifically addresses prevention and management of heavy menstrual bleeding that can result from cancer and cancer treatments.
Both opinions were developed by the ACOG Committee on Adolescent Health Care and are published in the August 2014 issue of Obstetrics & Gynecology.
Advancements in radiation therapy, chemotherapy, surgery, and multimodal treatment have dramatically improved childhood cancer survival; 5-year survival rates have reached nearly 80%, but the treatments – and the cancer itself – can have immediate or delayed adverse effect on reproductive health, the authors wrote in the first opinion (Obstet. Gynecol. 2014;124:403-8).
Gynecologists should be aware of the potential effects that can occur both during and after each type of therapy, they said.
For example, primary ovarian insufficiency can occur following pelvic radiation therapy and can lead to future adverse pregnancy outcomes. Chemotherapy also can affect ovarian function, and the risk of toxicity is directly proportional to the age and pubertal status of the patient at the time of exposure, with older patients having higher risk.
Surgery, such as resection of the vagina, uterus, ovaries, or fallopian tubes, can lead to adhesions and infertility, and can also lead to pelvic pain, sexual dysfunction, and fistula formation, they said.
Cancer treatments also can lead to precocious or delayed puberty.
Gynecologists should be prepared to manage gynecologic concerns in young patients and survivors, as they may be consulted regarding pubertal concerns, heavy menstrual bleeding and anemia, sexuality, contraception, ovarian function, and breast and cervical cancer screening, the authors noted.
The committee opinion provides information and guidance on managing each of these circumstances. With respect to fertility preservation, the opinion states that anti-Müllerian hormone level is the optimal screening tool for assessing ovarian reserve in survivors and stresses that potential options for fertility preservation should be discussed prior to treatment in those at risk for infertility. Options may include oophoropexy to move the gonads away from the radiation field in those to be treated with pelvic irradiation, and ovarian stimulation and cryopreservation of either oocytes or embryos.
"The science of fertility preservation is a rapidly evolving field; therefore, a referral to a reproductive endocrinologist is recommended to explore the full range of available options," the authors said, adding that for young women who have completed sexual development, gonadotropin-releasing hormone agonists have been used to induce ovarian quiescence in an effort to preserve ovarian function and fertility. Results of this approach have been mixed, and the evidence is not currently strong enough to recommend this therapy, although randomized trials are underway, they said.
In the second opinion, "Options for Prevention and Management of Heavy Menstrual Bleeding in Adolescent Patients Undergoing Cancer Treatment", the authors note that even normal menstrual blood loss can pose a threat to adolescents who are already anemic because of hematologic malignancies or cancer treatment (Obstet. Gynecol. 2014;124:397-402).
"Disruption of the hypothalamic-pituitary-gonadal axis during cancer treatment also may cause anovulatory uterine bleeding," they wrote, adding that gynecologists may, therefore, be consulted regarding strategies for suppressing menstruation prior to treatment or during an episode of severe heavy bleeding to stop the bleeding emergency.
Therapy in both situations should be tailored to the patient and her desires for contraception and fertility.
"Because of the complex nature of cancer care, collaboration with the adolescent’s oncologist is highly recommended," according to the opinion, which outlines options for prophylactic menstrual suppression (combined hormonal contraceptives, progestin-only therapy, and gonadotropin-releasing hormone agonists) and emergent treatment of acute uterine bleeding (hormonal therapy, antifibrinolytics, and surgical options for patients who fail medical therapy).
Surgical options may include dilation and curettage, uterine packing, tamponade with a Foley balloon, or uterine artery embolization, but "evidence for these treatments in adolescents is lacking, and their consideration is based on extrapolation from the literature on adult patients. Also, uterine artery embolization is not suitable as a first-line therapy given its effect on fertility, but may be considered as an alternative to hysterectomy in an acutely ill patient," the authors said.
A treatment algorithm for patients without contraindications to estrogen therapy is included in the opinion, with surgical options listed as a last resort.
"Addressing menstrual issues of adolescent patients undergoing cancer treatment is an important part of long-term management and will require collaborative involvement of obstetrician-gynecologists in the care of such patients," the authors concluded.
These two committee opinions provide important guidance for gynecologists, who will likely be called upon to care for survivors of adolescent and childhood cancer.
"As ob.gyns. and advocates for women’s reproductive health, it is our important role to help patients and families understand the effects of their treatment on fertility and optimize the potential for childbearing if that young woman so chooses after treatment is complete," Dr. Julie L. Strickland, chair of the Committee on Adolescent Health Care, said in a press statement.
"As gynecologists, we must be prepared with the most up-to-date information to help manage and treat the gynecological issues and be willing to work in collaboration with other specialties, such as oncologists and reproductive endocrinologists, to ensure the best options for our patients," she added.
Dr. Strickland reported having no disclosures.
FROM OBSTETRICS & GYNECOLOGY
Natalizumab discontinuation ups MS reactivation risk
The risk of disease reactivation rises in adults with multiple sclerosis who discontinue natalizumab treatment after 24 doses, according to findings from the prospective, multicenter, observational TY-STOP Study.
In an intent-to-treat analysis, disease activity was significantly lower among 43 patients who continued natalizumab treatment, compared with 81 who had interrupted treatment (odds ratios, 0.33 for clinical activity and 0.35 for radiologic activity). In an as-treated analysis, clinical disease activity was more than three times higher in 16 patients who switched treatments (OR, 3.28), and more than four times higher in natalizumab quitters (OR, 4.40), compared with 35 patients who continued on natalizumab. Dr. Marinella Clerico of the University of Turin, San Luigi Gonzaga University Hospital, Orbassano, Italy, and her colleagues reported the findings online June 30 in JAMA Neurology.
One patient who discontinued treatment developed progressive multifocal leukoencephalopathy (PML) during the observation period, but recovered completely (JAMA Neurol. 2014 [doi:10.1001/jamaneurol.2014.1200]).
Continuing natalizumab seems to be the most efficacious therapeutic strategy in those who have already received 24 doses and who must – according to a "meticulous risk management plan" implemented by the European Medicines Agency in the wake of increased incidence of PML among natalizumab users – renew consent to continue treatment after 24 doses. However, given the risk of PML, the decision to continue treatment should take into account the risk of disease reactivation associated with discontinuation as well as the risk of PML with continuation, and treatment should be continued, along with meticulous monitoring for PML, in all patients in whom risk is not considered too high, they concluded.
Dr. Clerico reported receiving travel grants from Merck Serono and Biogen Idec. Other authors also made financial disclosures, the details of which are available with the full text of the article at jamaneurology.com.
The findings by Dr. Clerico and her colleagues confirm that natalizumab effectively suppresses disease activity, and that disease activity may return upon treatment withdrawal, but the authors, like others before them, failed to identify a safe exit strategy that minimizes the return of disease activity and lowers the risk of PML, according to Dr. Olaf Stüve and Gary R. Cutter, Ph.D.
"To make a rational decision [about continuing natalizumab] on the recommendation by the authors, the following important information is unavailable to patients and their neurologists: Are the reduction in disease activity and therapeutic benefits gained during natalizumab therapy maintained in the long term and, most important, after treatment cessation?" they wrote in an editorial. (JAMA Neurol. 2014 [doi:10.1001/jamaneurol.2014.1201]).
Natalizumab has had positive effects on many patients, and these effects are relevant even if they are time limited and reversed upon treatment withdrawal, but long-term data are needed to characterize potential long-term benefits and to "calculate discounts to these benefits if there is an accelerated decline after treatment cessation," they said, concluding that answers are needed regarding whom and how long to treat, how to most effectively initiate sequential therapies, and whether disease reactivation after natalizumab withdrawal is a risk factor for increased long-term disability.
Dr. Stüve is with the Veterans Affairs North Texas Health Care System and the University of Texas Southwestern Medical Center, Dallas, and with Klinikum Rechts der Isar, Technische Universität München, Munich. He also is associate editor for JAMA Neurology. Dr. Cutter is a professor of biostatistics with the University of Alabama at Birmingham. Dr. Stüve reported serving on editorial boards for Multiple Sclerosis Journal, Clinical and Experimental Immunology, and Therapeutic Advances in Neurological Disorders, and participating in data and safety monitoring committees for Pfizer and Sanofi-Aventis. He received grant support from Teva. Dr. Cutter is president of Pythagoras Inc., a private consulting firm and has received numerous National Institutes of Health and Department of Defense grants. Additional disclosures details are available with the editorial at jamaneurology.com.
The findings by Dr. Clerico and her colleagues confirm that natalizumab effectively suppresses disease activity, and that disease activity may return upon treatment withdrawal, but the authors, like others before them, failed to identify a safe exit strategy that minimizes the return of disease activity and lowers the risk of PML, according to Dr. Olaf Stüve and Gary R. Cutter, Ph.D.
"To make a rational decision [about continuing natalizumab] on the recommendation by the authors, the following important information is unavailable to patients and their neurologists: Are the reduction in disease activity and therapeutic benefits gained during natalizumab therapy maintained in the long term and, most important, after treatment cessation?" they wrote in an editorial. (JAMA Neurol. 2014 [doi:10.1001/jamaneurol.2014.1201]).
Natalizumab has had positive effects on many patients, and these effects are relevant even if they are time limited and reversed upon treatment withdrawal, but long-term data are needed to characterize potential long-term benefits and to "calculate discounts to these benefits if there is an accelerated decline after treatment cessation," they said, concluding that answers are needed regarding whom and how long to treat, how to most effectively initiate sequential therapies, and whether disease reactivation after natalizumab withdrawal is a risk factor for increased long-term disability.
Dr. Stüve is with the Veterans Affairs North Texas Health Care System and the University of Texas Southwestern Medical Center, Dallas, and with Klinikum Rechts der Isar, Technische Universität München, Munich. He also is associate editor for JAMA Neurology. Dr. Cutter is a professor of biostatistics with the University of Alabama at Birmingham. Dr. Stüve reported serving on editorial boards for Multiple Sclerosis Journal, Clinical and Experimental Immunology, and Therapeutic Advances in Neurological Disorders, and participating in data and safety monitoring committees for Pfizer and Sanofi-Aventis. He received grant support from Teva. Dr. Cutter is president of Pythagoras Inc., a private consulting firm and has received numerous National Institutes of Health and Department of Defense grants. Additional disclosures details are available with the editorial at jamaneurology.com.
The findings by Dr. Clerico and her colleagues confirm that natalizumab effectively suppresses disease activity, and that disease activity may return upon treatment withdrawal, but the authors, like others before them, failed to identify a safe exit strategy that minimizes the return of disease activity and lowers the risk of PML, according to Dr. Olaf Stüve and Gary R. Cutter, Ph.D.
"To make a rational decision [about continuing natalizumab] on the recommendation by the authors, the following important information is unavailable to patients and their neurologists: Are the reduction in disease activity and therapeutic benefits gained during natalizumab therapy maintained in the long term and, most important, after treatment cessation?" they wrote in an editorial. (JAMA Neurol. 2014 [doi:10.1001/jamaneurol.2014.1201]).
Natalizumab has had positive effects on many patients, and these effects are relevant even if they are time limited and reversed upon treatment withdrawal, but long-term data are needed to characterize potential long-term benefits and to "calculate discounts to these benefits if there is an accelerated decline after treatment cessation," they said, concluding that answers are needed regarding whom and how long to treat, how to most effectively initiate sequential therapies, and whether disease reactivation after natalizumab withdrawal is a risk factor for increased long-term disability.
Dr. Stüve is with the Veterans Affairs North Texas Health Care System and the University of Texas Southwestern Medical Center, Dallas, and with Klinikum Rechts der Isar, Technische Universität München, Munich. He also is associate editor for JAMA Neurology. Dr. Cutter is a professor of biostatistics with the University of Alabama at Birmingham. Dr. Stüve reported serving on editorial boards for Multiple Sclerosis Journal, Clinical and Experimental Immunology, and Therapeutic Advances in Neurological Disorders, and participating in data and safety monitoring committees for Pfizer and Sanofi-Aventis. He received grant support from Teva. Dr. Cutter is president of Pythagoras Inc., a private consulting firm and has received numerous National Institutes of Health and Department of Defense grants. Additional disclosures details are available with the editorial at jamaneurology.com.
The risk of disease reactivation rises in adults with multiple sclerosis who discontinue natalizumab treatment after 24 doses, according to findings from the prospective, multicenter, observational TY-STOP Study.
In an intent-to-treat analysis, disease activity was significantly lower among 43 patients who continued natalizumab treatment, compared with 81 who had interrupted treatment (odds ratios, 0.33 for clinical activity and 0.35 for radiologic activity). In an as-treated analysis, clinical disease activity was more than three times higher in 16 patients who switched treatments (OR, 3.28), and more than four times higher in natalizumab quitters (OR, 4.40), compared with 35 patients who continued on natalizumab. Dr. Marinella Clerico of the University of Turin, San Luigi Gonzaga University Hospital, Orbassano, Italy, and her colleagues reported the findings online June 30 in JAMA Neurology.
One patient who discontinued treatment developed progressive multifocal leukoencephalopathy (PML) during the observation period, but recovered completely (JAMA Neurol. 2014 [doi:10.1001/jamaneurol.2014.1200]).
Continuing natalizumab seems to be the most efficacious therapeutic strategy in those who have already received 24 doses and who must – according to a "meticulous risk management plan" implemented by the European Medicines Agency in the wake of increased incidence of PML among natalizumab users – renew consent to continue treatment after 24 doses. However, given the risk of PML, the decision to continue treatment should take into account the risk of disease reactivation associated with discontinuation as well as the risk of PML with continuation, and treatment should be continued, along with meticulous monitoring for PML, in all patients in whom risk is not considered too high, they concluded.
Dr. Clerico reported receiving travel grants from Merck Serono and Biogen Idec. Other authors also made financial disclosures, the details of which are available with the full text of the article at jamaneurology.com.
The risk of disease reactivation rises in adults with multiple sclerosis who discontinue natalizumab treatment after 24 doses, according to findings from the prospective, multicenter, observational TY-STOP Study.
In an intent-to-treat analysis, disease activity was significantly lower among 43 patients who continued natalizumab treatment, compared with 81 who had interrupted treatment (odds ratios, 0.33 for clinical activity and 0.35 for radiologic activity). In an as-treated analysis, clinical disease activity was more than three times higher in 16 patients who switched treatments (OR, 3.28), and more than four times higher in natalizumab quitters (OR, 4.40), compared with 35 patients who continued on natalizumab. Dr. Marinella Clerico of the University of Turin, San Luigi Gonzaga University Hospital, Orbassano, Italy, and her colleagues reported the findings online June 30 in JAMA Neurology.
One patient who discontinued treatment developed progressive multifocal leukoencephalopathy (PML) during the observation period, but recovered completely (JAMA Neurol. 2014 [doi:10.1001/jamaneurol.2014.1200]).
Continuing natalizumab seems to be the most efficacious therapeutic strategy in those who have already received 24 doses and who must – according to a "meticulous risk management plan" implemented by the European Medicines Agency in the wake of increased incidence of PML among natalizumab users – renew consent to continue treatment after 24 doses. However, given the risk of PML, the decision to continue treatment should take into account the risk of disease reactivation associated with discontinuation as well as the risk of PML with continuation, and treatment should be continued, along with meticulous monitoring for PML, in all patients in whom risk is not considered too high, they concluded.
Dr. Clerico reported receiving travel grants from Merck Serono and Biogen Idec. Other authors also made financial disclosures, the details of which are available with the full text of the article at jamaneurology.com.
FROM JAMA NEUROLOGY
Key clinical point: Discontinuing natalizumab in patients who respond should only be considered if the risk of multifocal leukoencephalopathy is high enough to outweigh the benefits of the drug.
Major finding: Clinical disease activity was higher in patients who switched treatment (OR, 3.28), and who quit natalizumab (OR, 4.40), compared with those who continued natalizumab.
Data source: A prospective observational study involving 124 patients.
Disclosures: Dr. Clerico reported receiving travel grants from Merck Serono and Biogen Idec. Other authors also made financial disclosures, the details of which are available with the full text of the article at jamaneurology.com.
Findings support endovascular-first approach for ruptured VAAs
BOSTON – Endovascular interventions for ruptured visceral artery aneurysms are associated with reduced morbidity and mortality, compared with open interventions, according to findings from a retrospective chart review.
Both endovascular and open repairs are safe and durable for intact visceral artery aneurysms, Dr. Ankur J. Shukla reported at a meeting hosted by the Society for Vascular Surgery.
Of 261 patients who presented with visceral artery aneurysms (VAAs), 174 underwent repair: 74 who presented with ruptured VAA and 100 who presented with intact VAA. The majority – 73% of ruptured VAA and 62% of intact VAA – were repaired with an endovascular approach.
Among those with ruptured VAA, 30-day mortality was 7.4% following endovascular repair, compared with 28.6% following open repair, a significant difference, said Dr. Shukla of the University of Pittsburgh Medical Center.
Survival at 3 years of ruptured VAA was about 70% vs. 46.4% in the endovascular and open repair groups, respectively, he said.
About 65% of patients with ruptured VAA presented with pain, and about 30% presented in hemodynamic shock. The most commonly identified etiology was "inflammatory/pancreatitis inflammatory," and 80% of the aneurysms were pseudoaneurysmal in nature.
A large proportion of the aneurysms were in the splenic and arterial beds, but 26% were located in the pancreaticoduodenal arcade, and those had a mean size of 12.7 mm. Most (95%) were pseudoaneurysms.
The outcomes with ruptured VAA were quite good, Dr. Shukla said, noting that the technical success rate was 98.7%.
Although the 30-day reintervention rate with endovascular repair was higher, the difference between the groups was not statistically significant, and there was a trend toward a lower rate of major complications with endovascular repair.
Factors found to be predictors of mortality risk were older age and steroid use, while endovascular repair was found to be protective.
As for the patients with intact VAA, most presented without symptoms, and the most common etiology was atherosclerosis.
"When we looked at the distribution, this was very consistent with what has been reported in the literature, with the splenic and arterial beds really making up the lion’s share of this group. Notable is the fact that 6.7% of our patients had intact aneurysms in the pancreaticoduodenal arcade," he said.
Outcomes in those with intact aneurysms were good. A slightly higher 30-day reintervention rate in those who underwent endovascular repair did not reach statistical significance, and both the endovascular and open repair groups had low rates of major complications.
Survival at 3 years for intact aneurysms did not differ in the endovascular and open repair groups. This was partly due to a 0% 30-day mortality, and – despite the fact that the overall mortality in those with intact aneurysms was 10% – there was zero overall aneurysm-related mortality, he said.
Patients in the study were treated at a single institution between 2003 and 2013. Most were in their mid to late 50s, and there were more men and more individuals on immunosuppressive therapy in the ruptured VAA group. However, comorbidities were similar in the ruptured and intact VAA groups.
Visceral artery aneurysms occur only rarely, affecting 0.1% to 2% of the general population, but because of the increasing use of noninvasive imaging, more of these aneurysms are being detected incidentally.
When they are not found incidentally, they often go undetected and present when they rupture, Dr. Shukla said.
"Because of the increasing utilization and improvement of endovascular technology, we now have a lot of options to fix these aneurysms. But the outcomes are not well defined. Even less well defined is the outcome of ruptured visceral artery aneurysms," he said, noting that most studies have a small sample size or look only at endovascular or open repairs.
Overall, the current study showed that there is "an acute and sharp drop-off in survival with open repair," related, most likely, to operative mortality, he said.
"Based on the findings, we recommend aggressive treatment of pseudoaneurysms and true aneurysms in the pancreaticoduodenal arcade, and advocate for an endovascular-first approach to treating ruptured visceral artery aneurysms, acknowledging that success in this is really predicated on good planning based on advanced imaging and endovascular set-up," he concluded.
Dr. Shukla reported having no disclosures.
BOSTON – Endovascular interventions for ruptured visceral artery aneurysms are associated with reduced morbidity and mortality, compared with open interventions, according to findings from a retrospective chart review.
Both endovascular and open repairs are safe and durable for intact visceral artery aneurysms, Dr. Ankur J. Shukla reported at a meeting hosted by the Society for Vascular Surgery.
Of 261 patients who presented with visceral artery aneurysms (VAAs), 174 underwent repair: 74 who presented with ruptured VAA and 100 who presented with intact VAA. The majority – 73% of ruptured VAA and 62% of intact VAA – were repaired with an endovascular approach.
Among those with ruptured VAA, 30-day mortality was 7.4% following endovascular repair, compared with 28.6% following open repair, a significant difference, said Dr. Shukla of the University of Pittsburgh Medical Center.
Survival at 3 years of ruptured VAA was about 70% vs. 46.4% in the endovascular and open repair groups, respectively, he said.
About 65% of patients with ruptured VAA presented with pain, and about 30% presented in hemodynamic shock. The most commonly identified etiology was "inflammatory/pancreatitis inflammatory," and 80% of the aneurysms were pseudoaneurysmal in nature.
A large proportion of the aneurysms were in the splenic and arterial beds, but 26% were located in the pancreaticoduodenal arcade, and those had a mean size of 12.7 mm. Most (95%) were pseudoaneurysms.
The outcomes with ruptured VAA were quite good, Dr. Shukla said, noting that the technical success rate was 98.7%.
Although the 30-day reintervention rate with endovascular repair was higher, the difference between the groups was not statistically significant, and there was a trend toward a lower rate of major complications with endovascular repair.
Factors found to be predictors of mortality risk were older age and steroid use, while endovascular repair was found to be protective.
As for the patients with intact VAA, most presented without symptoms, and the most common etiology was atherosclerosis.
"When we looked at the distribution, this was very consistent with what has been reported in the literature, with the splenic and arterial beds really making up the lion’s share of this group. Notable is the fact that 6.7% of our patients had intact aneurysms in the pancreaticoduodenal arcade," he said.
Outcomes in those with intact aneurysms were good. A slightly higher 30-day reintervention rate in those who underwent endovascular repair did not reach statistical significance, and both the endovascular and open repair groups had low rates of major complications.
Survival at 3 years for intact aneurysms did not differ in the endovascular and open repair groups. This was partly due to a 0% 30-day mortality, and – despite the fact that the overall mortality in those with intact aneurysms was 10% – there was zero overall aneurysm-related mortality, he said.
Patients in the study were treated at a single institution between 2003 and 2013. Most were in their mid to late 50s, and there were more men and more individuals on immunosuppressive therapy in the ruptured VAA group. However, comorbidities were similar in the ruptured and intact VAA groups.
Visceral artery aneurysms occur only rarely, affecting 0.1% to 2% of the general population, but because of the increasing use of noninvasive imaging, more of these aneurysms are being detected incidentally.
When they are not found incidentally, they often go undetected and present when they rupture, Dr. Shukla said.
"Because of the increasing utilization and improvement of endovascular technology, we now have a lot of options to fix these aneurysms. But the outcomes are not well defined. Even less well defined is the outcome of ruptured visceral artery aneurysms," he said, noting that most studies have a small sample size or look only at endovascular or open repairs.
Overall, the current study showed that there is "an acute and sharp drop-off in survival with open repair," related, most likely, to operative mortality, he said.
"Based on the findings, we recommend aggressive treatment of pseudoaneurysms and true aneurysms in the pancreaticoduodenal arcade, and advocate for an endovascular-first approach to treating ruptured visceral artery aneurysms, acknowledging that success in this is really predicated on good planning based on advanced imaging and endovascular set-up," he concluded.
Dr. Shukla reported having no disclosures.
BOSTON – Endovascular interventions for ruptured visceral artery aneurysms are associated with reduced morbidity and mortality, compared with open interventions, according to findings from a retrospective chart review.
Both endovascular and open repairs are safe and durable for intact visceral artery aneurysms, Dr. Ankur J. Shukla reported at a meeting hosted by the Society for Vascular Surgery.
Of 261 patients who presented with visceral artery aneurysms (VAAs), 174 underwent repair: 74 who presented with ruptured VAA and 100 who presented with intact VAA. The majority – 73% of ruptured VAA and 62% of intact VAA – were repaired with an endovascular approach.
Among those with ruptured VAA, 30-day mortality was 7.4% following endovascular repair, compared with 28.6% following open repair, a significant difference, said Dr. Shukla of the University of Pittsburgh Medical Center.
Survival at 3 years of ruptured VAA was about 70% vs. 46.4% in the endovascular and open repair groups, respectively, he said.
About 65% of patients with ruptured VAA presented with pain, and about 30% presented in hemodynamic shock. The most commonly identified etiology was "inflammatory/pancreatitis inflammatory," and 80% of the aneurysms were pseudoaneurysmal in nature.
A large proportion of the aneurysms were in the splenic and arterial beds, but 26% were located in the pancreaticoduodenal arcade, and those had a mean size of 12.7 mm. Most (95%) were pseudoaneurysms.
The outcomes with ruptured VAA were quite good, Dr. Shukla said, noting that the technical success rate was 98.7%.
Although the 30-day reintervention rate with endovascular repair was higher, the difference between the groups was not statistically significant, and there was a trend toward a lower rate of major complications with endovascular repair.
Factors found to be predictors of mortality risk were older age and steroid use, while endovascular repair was found to be protective.
As for the patients with intact VAA, most presented without symptoms, and the most common etiology was atherosclerosis.
"When we looked at the distribution, this was very consistent with what has been reported in the literature, with the splenic and arterial beds really making up the lion’s share of this group. Notable is the fact that 6.7% of our patients had intact aneurysms in the pancreaticoduodenal arcade," he said.
Outcomes in those with intact aneurysms were good. A slightly higher 30-day reintervention rate in those who underwent endovascular repair did not reach statistical significance, and both the endovascular and open repair groups had low rates of major complications.
Survival at 3 years for intact aneurysms did not differ in the endovascular and open repair groups. This was partly due to a 0% 30-day mortality, and – despite the fact that the overall mortality in those with intact aneurysms was 10% – there was zero overall aneurysm-related mortality, he said.
Patients in the study were treated at a single institution between 2003 and 2013. Most were in their mid to late 50s, and there were more men and more individuals on immunosuppressive therapy in the ruptured VAA group. However, comorbidities were similar in the ruptured and intact VAA groups.
Visceral artery aneurysms occur only rarely, affecting 0.1% to 2% of the general population, but because of the increasing use of noninvasive imaging, more of these aneurysms are being detected incidentally.
When they are not found incidentally, they often go undetected and present when they rupture, Dr. Shukla said.
"Because of the increasing utilization and improvement of endovascular technology, we now have a lot of options to fix these aneurysms. But the outcomes are not well defined. Even less well defined is the outcome of ruptured visceral artery aneurysms," he said, noting that most studies have a small sample size or look only at endovascular or open repairs.
Overall, the current study showed that there is "an acute and sharp drop-off in survival with open repair," related, most likely, to operative mortality, he said.
"Based on the findings, we recommend aggressive treatment of pseudoaneurysms and true aneurysms in the pancreaticoduodenal arcade, and advocate for an endovascular-first approach to treating ruptured visceral artery aneurysms, acknowledging that success in this is really predicated on good planning based on advanced imaging and endovascular set-up," he concluded.
Dr. Shukla reported having no disclosures.
AT THE 2014 VASCULAR ANNUAL MEETING
Key clinical point: The researchers recommend aggressive treatment of visceral artery pseudoaneurysms and true aneurysms, with an endovascular-first approach to treating ruptured aneurysms.
Major finding: Thirty-day mortality was 7.4% vs. 26% with endovascular vs. open repair of ruptured VAAs.
Data source: A retrospective chart review involving 174 cases.
Disclosures: Dr. Shukla reported having no disclosures.
A teen-focused STD prevention program reduced gonorrhea incidence
ATLANTA – A communitywide condom distribution program is proving successful for expanding access to and awareness of free condoms, and for reducing the incidence of sexually transmitted diseases among teens in Philadelphia.
The program, which includes the Philadelphia Freedom Condom program and Take Control Philly, is a comprehensive, youth-targeted STD prevention initiative launched in April 2011 by the Philadelphia Department of Public Health (PDPH). A 2013 assessment, including interviews with 301 black/African American and/or Hispanic/Latino individuals aged 13-24 years showed that knowledge of at least one aspect of the campaign had almost doubled since 2011, when baseline data were collected from 300 individuals in that age group (97% vs. 52%), Matthew Prior of the PDPH reported in a poster at a conference on STD prevention sponsored by the Centers for Disease Control and Prevention.

Furthermore, 82% of respondents in 2013 vs. 18% in 2011 reported having seen information about the Freedom Condom program, 9% in 2013 vs. 1% in 2011 said they had received a free condom from a commercial business, and 70% in 2013 vs. 58% in 2011 knew where to get free condoms.
Although there was no significant change in reported condom use at last sexual encounter between 2011 and 2013, the overall number of gonorrhea cases declined significantly from approximately 1,600 cases in the first quarter of 2011 to approximately 1,400 cases in the first quarter of 2104; the greatest decline was among adolescents, who accounted for about 8% of cases in the first quarter of 2011 vs. about 5% in the first quarter of 2014, Mr. Prior found.
This followed a 38% increase in the number of gonorrhea cases among adolescents from 2009 to 2010, he noted.
The Freedom Condom program aimed to improve access to condoms, in part through a free condom mailing program, and Take Control Philly aimed to prevent STDs among adolescents through a sexual health awareness campaign and by addressing sexual risk-taking behaviors among a target population. Baseline data showed that 61% of adolescents surveyed had ever had sexual intercourse, 15% had sexual intercourse before the age of 13 years, 40.4% did not use a condom during their last sexual intercourse, and 27.2% had sexual intercourse with four or more persons during their lifetime.
"Multiple strategies were used to promote the Take Control Philly website and the Freedom Condom [program], including social media advertisement, traditional media advertisement, expanded condom distribution, community event outreach, and promotion in Philadelphia public high schools," Mr. Prior wrote.
Between April 2011 and 2014, more than 8.2 million condoms were distributed through the program. The success in promoting the program is due in part to the Philadelphia health commissioner and other city health leaders, whose support was pivotal to the planning and launch of the initiative, he noted.
Also, promotion of the program website through traditional media avenues and Facebook advertising was effective for increasing website traffic and condom mailing requests, he said.
"Communitywide condom distribution expansion is a promising approach for addressing STDs in youth," he concluded, adding that using multiple strategies for increasing program awareness is necessary for reaching youth.
Mr. Prior reported having no relevant financial disclosures.
ATLANTA – A communitywide condom distribution program is proving successful for expanding access to and awareness of free condoms, and for reducing the incidence of sexually transmitted diseases among teens in Philadelphia.
The program, which includes the Philadelphia Freedom Condom program and Take Control Philly, is a comprehensive, youth-targeted STD prevention initiative launched in April 2011 by the Philadelphia Department of Public Health (PDPH). A 2013 assessment, including interviews with 301 black/African American and/or Hispanic/Latino individuals aged 13-24 years showed that knowledge of at least one aspect of the campaign had almost doubled since 2011, when baseline data were collected from 300 individuals in that age group (97% vs. 52%), Matthew Prior of the PDPH reported in a poster at a conference on STD prevention sponsored by the Centers for Disease Control and Prevention.
Furthermore, 82% of respondents in 2013 vs. 18% in 2011 reported having seen information about the Freedom Condom program, 9% in 2013 vs. 1% in 2011 said they had received a free condom from a commercial business, and 70% in 2013 vs. 58% in 2011 knew where to get free condoms.
Although there was no significant change in reported condom use at last sexual encounter between 2011 and 2013, the overall number of gonorrhea cases declined significantly from approximately 1,600 cases in the first quarter of 2011 to approximately 1,400 cases in the first quarter of 2104; the greatest decline was among adolescents, who accounted for about 8% of cases in the first quarter of 2011 vs. about 5% in the first quarter of 2014, Mr. Prior found.
This followed a 38% increase in the number of gonorrhea cases among adolescents from 2009 to 2010, he noted.
The Freedom Condom program aimed to improve access to condoms, in part through a free condom mailing program, and Take Control Philly aimed to prevent STDs among adolescents through a sexual health awareness campaign and by addressing sexual risk-taking behaviors among a target population. Baseline data showed that 61% of adolescents surveyed had ever had sexual intercourse, 15% had sexual intercourse before the age of 13 years, 40.4% did not use a condom during their last sexual intercourse, and 27.2% had sexual intercourse with four or more persons during their lifetime.
"Multiple strategies were used to promote the Take Control Philly website and the Freedom Condom [program], including social media advertisement, traditional media advertisement, expanded condom distribution, community event outreach, and promotion in Philadelphia public high schools," Mr. Prior wrote.
Between April 2011 and 2014, more than 8.2 million condoms were distributed through the program. The success in promoting the program is due in part to the Philadelphia health commissioner and other city health leaders, whose support was pivotal to the planning and launch of the initiative, he noted.
Also, promotion of the program website through traditional media avenues and Facebook advertising was effective for increasing website traffic and condom mailing requests, he said.
"Communitywide condom distribution expansion is a promising approach for addressing STDs in youth," he concluded, adding that using multiple strategies for increasing program awareness is necessary for reaching youth.
Mr. Prior reported having no relevant financial disclosures.
ATLANTA – A communitywide condom distribution program is proving successful for expanding access to and awareness of free condoms, and for reducing the incidence of sexually transmitted diseases among teens in Philadelphia.
The program, which includes the Philadelphia Freedom Condom program and Take Control Philly, is a comprehensive, youth-targeted STD prevention initiative launched in April 2011 by the Philadelphia Department of Public Health (PDPH). A 2013 assessment, including interviews with 301 black/African American and/or Hispanic/Latino individuals aged 13-24 years showed that knowledge of at least one aspect of the campaign had almost doubled since 2011, when baseline data were collected from 300 individuals in that age group (97% vs. 52%), Matthew Prior of the PDPH reported in a poster at a conference on STD prevention sponsored by the Centers for Disease Control and Prevention.
Furthermore, 82% of respondents in 2013 vs. 18% in 2011 reported having seen information about the Freedom Condom program, 9% in 2013 vs. 1% in 2011 said they had received a free condom from a commercial business, and 70% in 2013 vs. 58% in 2011 knew where to get free condoms.
Although there was no significant change in reported condom use at last sexual encounter between 2011 and 2013, the overall number of gonorrhea cases declined significantly from approximately 1,600 cases in the first quarter of 2011 to approximately 1,400 cases in the first quarter of 2104; the greatest decline was among adolescents, who accounted for about 8% of cases in the first quarter of 2011 vs. about 5% in the first quarter of 2014, Mr. Prior found.
This followed a 38% increase in the number of gonorrhea cases among adolescents from 2009 to 2010, he noted.
The Freedom Condom program aimed to improve access to condoms, in part through a free condom mailing program, and Take Control Philly aimed to prevent STDs among adolescents through a sexual health awareness campaign and by addressing sexual risk-taking behaviors among a target population. Baseline data showed that 61% of adolescents surveyed had ever had sexual intercourse, 15% had sexual intercourse before the age of 13 years, 40.4% did not use a condom during their last sexual intercourse, and 27.2% had sexual intercourse with four or more persons during their lifetime.
"Multiple strategies were used to promote the Take Control Philly website and the Freedom Condom [program], including social media advertisement, traditional media advertisement, expanded condom distribution, community event outreach, and promotion in Philadelphia public high schools," Mr. Prior wrote.
Between April 2011 and 2014, more than 8.2 million condoms were distributed through the program. The success in promoting the program is due in part to the Philadelphia health commissioner and other city health leaders, whose support was pivotal to the planning and launch of the initiative, he noted.
Also, promotion of the program website through traditional media avenues and Facebook advertising was effective for increasing website traffic and condom mailing requests, he said.
"Communitywide condom distribution expansion is a promising approach for addressing STDs in youth," he concluded, adding that using multiple strategies for increasing program awareness is necessary for reaching youth.
Mr. Prior reported having no relevant financial disclosures.
AT THE 2014 STD PREVENTION CONFERENCE
Key clinical point: Making condoms available to youths may reduce gonorrhea incidence.
Major finding: Adolescents accounted for about 8% of cases in the first quarter of 2011 vs. about 5% in the first quarter of 2014.
Data source: A follow-up survey of 301 subjects.
Disclosures: Mr. Prior reported having no disclosures.
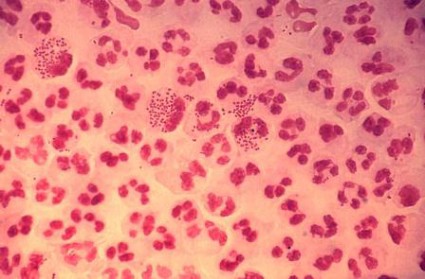
Meds fall short for type B dissection
BOSTON – Medical therapy for acute uncomplicated type B aortic dissections was effective in the short term, but was associated with low 6-year intervention-free survival in a review of 298 cases.
Furthermore, patients who received medical therapy without operative intervention had increased mortality at 6 years, compared with those who received intervention, Dr. Christopher A. Durham reported at the Vascular Annual Meeting.
During a mean follow-up of nearly 4.3 years, medical therapy failed in almost 60% of the patients; 114 died after an average of 2.7 years, and 87 required aortic intervention.
Aneurysmal degeneration was the indication for intervention in 65% of patients requiring intervention, and six of these patients experienced a ruptured aneurysm. "Only six of these patients underwent stent placement, with the remainder receiving open aortic replacement," said Dr. Durham of Massachusetts General Hospital, Boston.
The average time to operation in this subset of patients was 2.3 years. Visceral malperfusion was the indication for intervention in 18 patients (21%), and most underwent an endovascular intervention including either stenting or endovascular fenestration. A less common indication for intervention was retrograde type A dissection development in two patients. These patients underwent open replacement.
The average time to intervention in the subset of patients whose indication was not aneurysmal degeneration was 24 days. Early treatment failure – within 15 days of presentation – occurred in 37 patients (12%) and included 12 deaths and 25 interventions.
"In this group of patients who ultimately required an intervention within the acute period, aneurysmal degeneration was the indication in 25% of patients, all of whom were treated with an open approach," Dr. Durham said. Visceral malperfusion was the indication in half of the early interventions.
The 30-day mortality rate among patients with early intervention after initial medical therapy was 12%.
Freedom from intervention was 74% at 6 years, with most interventions occurring within the first 12 months. Intervention-free survival was 55% at 3 years and 41% at 6 years. Only end-stage renal disease was found to be predictive of failure, and age over 70 years was protective against failure (hazard ratio, 0.97), Dr. Durham said, adding that no variables associated with progression to intervention were identified.
Notably, although survival was similar during the first 3 years in those who remained on medical management and those who required intervention (73% and 78%, respectively), survival at 6 years was 58% and 76% in the groups, respectively.
"These data join emerging data demonstrating a survival benefit in patients undergoing intervention when compared to those who are treated with medical therapy alone," he said.
Study subjects were all patients who were initially managed medically for acute uncomplicated type B aortic dissection between March 1999 and March 2011 in a health care system. The patients had a mean age of 66 years at presentation, about 62% were men, and most were white. Nearly 75% had hypertension, and most of those were on therapy. About 5% had end-stage renal disease.
Failure of medical therapy was defined as any death or aortic-related intervention. Early failure was defined as failure within 15 days of presentation.
"Aortic dissection is the most common catastrophic event affecting the aorta, with an incidence exceeding that of ruptured abdominal aortic aneurysm.
"The majority of patients with type B aortic dissections, where the entry tear originates distal to the left subclavian artery, are treated with medical therapy," he said. In fact, medical management aimed at lowering the systolic blood pressure and pulse remains the standard of care, and a number of studies have demonstrated a favorable 1-year survival – ranging from 70% to 90% – with medical therapy alone in this population.
"However, at what cost?" Dr. Durham asked.
"The principal late complication of aortic dissection is aneurysmal degeneration of the outer wall of the false lumen, which has been reported to occur in up to 40% of medically treated patients," he said, adding that, because of a paucity of contemporary data regarding the natural history of medically treated patients, it has been unclear whether the natural history has been altered with current medical therapy.
The current findings suggest that operative intervention is associated with a survival benefit.
As Food and Drug Administration "approval has just been granted for thoracic stent grafts to be used in aortic dissection, it is clear that endovascular coverage of proximal aortic entry tears will become more common in the acute phase. As such, further study is needed to determine which patients presenting with type B dissections will benefit from early intervention," he said.
Dr. Durham reported having no disclosures.
Editor’s Note: The treatment of type B dissection is a controversial subject and this controversy will be addressed in an upcoming Point/Counterpoint article in Vascular Specialist.
BOSTON – Medical therapy for acute uncomplicated type B aortic dissections was effective in the short term, but was associated with low 6-year intervention-free survival in a review of 298 cases.
Furthermore, patients who received medical therapy without operative intervention had increased mortality at 6 years, compared with those who received intervention, Dr. Christopher A. Durham reported at the Vascular Annual Meeting.
During a mean follow-up of nearly 4.3 years, medical therapy failed in almost 60% of the patients; 114 died after an average of 2.7 years, and 87 required aortic intervention.
Aneurysmal degeneration was the indication for intervention in 65% of patients requiring intervention, and six of these patients experienced a ruptured aneurysm. "Only six of these patients underwent stent placement, with the remainder receiving open aortic replacement," said Dr. Durham of Massachusetts General Hospital, Boston.
The average time to operation in this subset of patients was 2.3 years. Visceral malperfusion was the indication for intervention in 18 patients (21%), and most underwent an endovascular intervention including either stenting or endovascular fenestration. A less common indication for intervention was retrograde type A dissection development in two patients. These patients underwent open replacement.
The average time to intervention in the subset of patients whose indication was not aneurysmal degeneration was 24 days. Early treatment failure – within 15 days of presentation – occurred in 37 patients (12%) and included 12 deaths and 25 interventions.
"In this group of patients who ultimately required an intervention within the acute period, aneurysmal degeneration was the indication in 25% of patients, all of whom were treated with an open approach," Dr. Durham said. Visceral malperfusion was the indication in half of the early interventions.
The 30-day mortality rate among patients with early intervention after initial medical therapy was 12%.
Freedom from intervention was 74% at 6 years, with most interventions occurring within the first 12 months. Intervention-free survival was 55% at 3 years and 41% at 6 years. Only end-stage renal disease was found to be predictive of failure, and age over 70 years was protective against failure (hazard ratio, 0.97), Dr. Durham said, adding that no variables associated with progression to intervention were identified.
Notably, although survival was similar during the first 3 years in those who remained on medical management and those who required intervention (73% and 78%, respectively), survival at 6 years was 58% and 76% in the groups, respectively.
"These data join emerging data demonstrating a survival benefit in patients undergoing intervention when compared to those who are treated with medical therapy alone," he said.
Study subjects were all patients who were initially managed medically for acute uncomplicated type B aortic dissection between March 1999 and March 2011 in a health care system. The patients had a mean age of 66 years at presentation, about 62% were men, and most were white. Nearly 75% had hypertension, and most of those were on therapy. About 5% had end-stage renal disease.
Failure of medical therapy was defined as any death or aortic-related intervention. Early failure was defined as failure within 15 days of presentation.
"Aortic dissection is the most common catastrophic event affecting the aorta, with an incidence exceeding that of ruptured abdominal aortic aneurysm.
"The majority of patients with type B aortic dissections, where the entry tear originates distal to the left subclavian artery, are treated with medical therapy," he said. In fact, medical management aimed at lowering the systolic blood pressure and pulse remains the standard of care, and a number of studies have demonstrated a favorable 1-year survival – ranging from 70% to 90% – with medical therapy alone in this population.
"However, at what cost?" Dr. Durham asked.
"The principal late complication of aortic dissection is aneurysmal degeneration of the outer wall of the false lumen, which has been reported to occur in up to 40% of medically treated patients," he said, adding that, because of a paucity of contemporary data regarding the natural history of medically treated patients, it has been unclear whether the natural history has been altered with current medical therapy.
The current findings suggest that operative intervention is associated with a survival benefit.
As Food and Drug Administration "approval has just been granted for thoracic stent grafts to be used in aortic dissection, it is clear that endovascular coverage of proximal aortic entry tears will become more common in the acute phase. As such, further study is needed to determine which patients presenting with type B dissections will benefit from early intervention," he said.
Dr. Durham reported having no disclosures.
Editor’s Note: The treatment of type B dissection is a controversial subject and this controversy will be addressed in an upcoming Point/Counterpoint article in Vascular Specialist.
BOSTON – Medical therapy for acute uncomplicated type B aortic dissections was effective in the short term, but was associated with low 6-year intervention-free survival in a review of 298 cases.
Furthermore, patients who received medical therapy without operative intervention had increased mortality at 6 years, compared with those who received intervention, Dr. Christopher A. Durham reported at the Vascular Annual Meeting.
During a mean follow-up of nearly 4.3 years, medical therapy failed in almost 60% of the patients; 114 died after an average of 2.7 years, and 87 required aortic intervention.
Aneurysmal degeneration was the indication for intervention in 65% of patients requiring intervention, and six of these patients experienced a ruptured aneurysm. "Only six of these patients underwent stent placement, with the remainder receiving open aortic replacement," said Dr. Durham of Massachusetts General Hospital, Boston.
The average time to operation in this subset of patients was 2.3 years. Visceral malperfusion was the indication for intervention in 18 patients (21%), and most underwent an endovascular intervention including either stenting or endovascular fenestration. A less common indication for intervention was retrograde type A dissection development in two patients. These patients underwent open replacement.
The average time to intervention in the subset of patients whose indication was not aneurysmal degeneration was 24 days. Early treatment failure – within 15 days of presentation – occurred in 37 patients (12%) and included 12 deaths and 25 interventions.
"In this group of patients who ultimately required an intervention within the acute period, aneurysmal degeneration was the indication in 25% of patients, all of whom were treated with an open approach," Dr. Durham said. Visceral malperfusion was the indication in half of the early interventions.
The 30-day mortality rate among patients with early intervention after initial medical therapy was 12%.
Freedom from intervention was 74% at 6 years, with most interventions occurring within the first 12 months. Intervention-free survival was 55% at 3 years and 41% at 6 years. Only end-stage renal disease was found to be predictive of failure, and age over 70 years was protective against failure (hazard ratio, 0.97), Dr. Durham said, adding that no variables associated with progression to intervention were identified.
Notably, although survival was similar during the first 3 years in those who remained on medical management and those who required intervention (73% and 78%, respectively), survival at 6 years was 58% and 76% in the groups, respectively.
"These data join emerging data demonstrating a survival benefit in patients undergoing intervention when compared to those who are treated with medical therapy alone," he said.
Study subjects were all patients who were initially managed medically for acute uncomplicated type B aortic dissection between March 1999 and March 2011 in a health care system. The patients had a mean age of 66 years at presentation, about 62% were men, and most were white. Nearly 75% had hypertension, and most of those were on therapy. About 5% had end-stage renal disease.
Failure of medical therapy was defined as any death or aortic-related intervention. Early failure was defined as failure within 15 days of presentation.
"Aortic dissection is the most common catastrophic event affecting the aorta, with an incidence exceeding that of ruptured abdominal aortic aneurysm.
"The majority of patients with type B aortic dissections, where the entry tear originates distal to the left subclavian artery, are treated with medical therapy," he said. In fact, medical management aimed at lowering the systolic blood pressure and pulse remains the standard of care, and a number of studies have demonstrated a favorable 1-year survival – ranging from 70% to 90% – with medical therapy alone in this population.
"However, at what cost?" Dr. Durham asked.
"The principal late complication of aortic dissection is aneurysmal degeneration of the outer wall of the false lumen, which has been reported to occur in up to 40% of medically treated patients," he said, adding that, because of a paucity of contemporary data regarding the natural history of medically treated patients, it has been unclear whether the natural history has been altered with current medical therapy.
The current findings suggest that operative intervention is associated with a survival benefit.
As Food and Drug Administration "approval has just been granted for thoracic stent grafts to be used in aortic dissection, it is clear that endovascular coverage of proximal aortic entry tears will become more common in the acute phase. As such, further study is needed to determine which patients presenting with type B dissections will benefit from early intervention," he said.
Dr. Durham reported having no disclosures.
Editor’s Note: The treatment of type B dissection is a controversial subject and this controversy will be addressed in an upcoming Point/Counterpoint article in Vascular Specialist.
Major finding: Medical therapy failed in nearly 60% of patients during 4.3 years of follow-up.
Data source: A series of 298 cases.
Disclosures: Dr. Durham reported having no disclosures.
Birth registry data demonstrate familial cerebral palsy risk
Cerebral palsy appears to have a genetic component, with increased risk extending to third-degree relatives (first cousins), according to findings from a population-based cohort study.
These data "offer additional evidence that the underlying causes of cerebral palsy extend beyond the clinical management of delivery. However, the similar risks of cerebral palsy of co-twins of affected like-sex and unlike-sex twin pairs suggest that genetic influences are only part of a wide range of causes," the researchers concluded, noting that future studies should consider the possibility of genetic causes and genetic susceptibility to environmental causes.
Of over 2 million Norwegians born between 1967 and 2002 and included in the Medical Birth Registry of Norway, 3,649 were diagnosed with cerebral palsy, Dr. Mette C. Tollånes of the University of Bergen and her colleagues reported online July 15 in the British Journal of Medicine.
Individuals who had a twin with cerebral palsy had a 15.6-fold increase in the risk of cerebral palsy. Subsequent full or half siblings of a child with cerebral palsy had a 9.2-fold and 3.0-fold increase in the risk of cerebral palsy, respectively, and parents with cerebral palsy had a 6.5-fold increase in the risk of having an affected child, the investigators found (BMJ 2014 July 15 [doi:10.1136/bmj.g4294]).
Although the risk was lower than for first- and second-degree relatives, even those who had a first cousin with cerebral palsy were at a 1.5-fold increased risk of cerebral palsy, they said.
There was no evidence of a difference in the rate of transmission by affected mothers or fathers, and the risks seen in siblings and cousins were independent of the sex of the index case, Dr. Tollånes and her associates noted.
Prior studies have shown that, in addition to a number of risk factors in pregnancy and during the perinatal period – such as preterm delivery, multiple fetuses, birth asphyxia, and perinatal stroke – there also is a possible heritable component. In fact, a number of candidate genes and single nucleotide polymorphisms have been investigated to explain familial clustering of cerebral palsy, and some studies have extended the investigation to interactions with clinical factors and other genes.
Positive findings, however, have been difficult to replicate, the investigators said.
"We used data from a large population based cohort to ... shed light on patterns of inheritance," they wrote.
Although limited by a number of factors, including lack of information on cerebral palsy subtypes, an inability to identify cases with postneonatal causes, and a possible underestimation of recurrence risk because of the exclusion of those who didn’t survive past 3 years, the findings "suggest that cerebral palsy includes a genetic component, with a stronger recurrence among relatives with closer genetic relationship," Dr. Tollånes and her associates said.
This study was supported by grants from the University of Bergen; the Western Norway Regional Health Authority; and the Intramural Research Program of the National Institute of Environmental Health Sciences, National Institutes of Health. The authors reported having no disclosures other than support from these funding sources.
Cerebral palsy appears to have a genetic component, with increased risk extending to third-degree relatives (first cousins), according to findings from a population-based cohort study.
These data "offer additional evidence that the underlying causes of cerebral palsy extend beyond the clinical management of delivery. However, the similar risks of cerebral palsy of co-twins of affected like-sex and unlike-sex twin pairs suggest that genetic influences are only part of a wide range of causes," the researchers concluded, noting that future studies should consider the possibility of genetic causes and genetic susceptibility to environmental causes.
Of over 2 million Norwegians born between 1967 and 2002 and included in the Medical Birth Registry of Norway, 3,649 were diagnosed with cerebral palsy, Dr. Mette C. Tollånes of the University of Bergen and her colleagues reported online July 15 in the British Journal of Medicine.
Individuals who had a twin with cerebral palsy had a 15.6-fold increase in the risk of cerebral palsy. Subsequent full or half siblings of a child with cerebral palsy had a 9.2-fold and 3.0-fold increase in the risk of cerebral palsy, respectively, and parents with cerebral palsy had a 6.5-fold increase in the risk of having an affected child, the investigators found (BMJ 2014 July 15 [doi:10.1136/bmj.g4294]).
Although the risk was lower than for first- and second-degree relatives, even those who had a first cousin with cerebral palsy were at a 1.5-fold increased risk of cerebral palsy, they said.
There was no evidence of a difference in the rate of transmission by affected mothers or fathers, and the risks seen in siblings and cousins were independent of the sex of the index case, Dr. Tollånes and her associates noted.
Prior studies have shown that, in addition to a number of risk factors in pregnancy and during the perinatal period – such as preterm delivery, multiple fetuses, birth asphyxia, and perinatal stroke – there also is a possible heritable component. In fact, a number of candidate genes and single nucleotide polymorphisms have been investigated to explain familial clustering of cerebral palsy, and some studies have extended the investigation to interactions with clinical factors and other genes.
Positive findings, however, have been difficult to replicate, the investigators said.
"We used data from a large population based cohort to ... shed light on patterns of inheritance," they wrote.
Although limited by a number of factors, including lack of information on cerebral palsy subtypes, an inability to identify cases with postneonatal causes, and a possible underestimation of recurrence risk because of the exclusion of those who didn’t survive past 3 years, the findings "suggest that cerebral palsy includes a genetic component, with a stronger recurrence among relatives with closer genetic relationship," Dr. Tollånes and her associates said.
This study was supported by grants from the University of Bergen; the Western Norway Regional Health Authority; and the Intramural Research Program of the National Institute of Environmental Health Sciences, National Institutes of Health. The authors reported having no disclosures other than support from these funding sources.
Cerebral palsy appears to have a genetic component, with increased risk extending to third-degree relatives (first cousins), according to findings from a population-based cohort study.
These data "offer additional evidence that the underlying causes of cerebral palsy extend beyond the clinical management of delivery. However, the similar risks of cerebral palsy of co-twins of affected like-sex and unlike-sex twin pairs suggest that genetic influences are only part of a wide range of causes," the researchers concluded, noting that future studies should consider the possibility of genetic causes and genetic susceptibility to environmental causes.
Of over 2 million Norwegians born between 1967 and 2002 and included in the Medical Birth Registry of Norway, 3,649 were diagnosed with cerebral palsy, Dr. Mette C. Tollånes of the University of Bergen and her colleagues reported online July 15 in the British Journal of Medicine.
Individuals who had a twin with cerebral palsy had a 15.6-fold increase in the risk of cerebral palsy. Subsequent full or half siblings of a child with cerebral palsy had a 9.2-fold and 3.0-fold increase in the risk of cerebral palsy, respectively, and parents with cerebral palsy had a 6.5-fold increase in the risk of having an affected child, the investigators found (BMJ 2014 July 15 [doi:10.1136/bmj.g4294]).
Although the risk was lower than for first- and second-degree relatives, even those who had a first cousin with cerebral palsy were at a 1.5-fold increased risk of cerebral palsy, they said.
There was no evidence of a difference in the rate of transmission by affected mothers or fathers, and the risks seen in siblings and cousins were independent of the sex of the index case, Dr. Tollånes and her associates noted.
Prior studies have shown that, in addition to a number of risk factors in pregnancy and during the perinatal period – such as preterm delivery, multiple fetuses, birth asphyxia, and perinatal stroke – there also is a possible heritable component. In fact, a number of candidate genes and single nucleotide polymorphisms have been investigated to explain familial clustering of cerebral palsy, and some studies have extended the investigation to interactions with clinical factors and other genes.
Positive findings, however, have been difficult to replicate, the investigators said.
"We used data from a large population based cohort to ... shed light on patterns of inheritance," they wrote.
Although limited by a number of factors, including lack of information on cerebral palsy subtypes, an inability to identify cases with postneonatal causes, and a possible underestimation of recurrence risk because of the exclusion of those who didn’t survive past 3 years, the findings "suggest that cerebral palsy includes a genetic component, with a stronger recurrence among relatives with closer genetic relationship," Dr. Tollånes and her associates said.
This study was supported by grants from the University of Bergen; the Western Norway Regional Health Authority; and the Intramural Research Program of the National Institute of Environmental Health Sciences, National Institutes of Health. The authors reported having no disclosures other than support from these funding sources.
FROM BMJ
Key clinical finding: It appears that cerebral palsy runs in families.
Major finding: The risk of cerebral palsy was increased 15.6-fold among twins, 6.5- to 9-fold among first-degree relatives, up to 3-fold among second-degree relatives, and 1.5-fold among third-degree relatives.
Data source: A population-based cohort study involving 2,036,741 Norwegians.
Disclosures: This study was supported by grants from the University of Bergen; the Western Norway Regional Health Authority; and the Intramural Research Program of the National Institute of Environmental Health Sciences, National Institutes of Health. The authors reported having no disclosures other than support from these funding sources.