User login
RF, IPL score highest for facial rejuvenation in review
SAN DIEGO – A review of existing research found that newer technologies are safer and more effective at skin rejuvenation than older ones, with two types – intense pulsed laser (IPL) and radiofrequency (RF) – at or near the head of the pack on both fronts.
In addition, 10 types of treatments, including multiple laser technologies, scored higher than facial peels on safety, although the peels beat almost all comers in terms of efficacy, the study’s lead author, Caerwyn Ash, PhD, said in an interview after presenting the results at the annual meeting of the American Society for Laser Medicine and Surgery.

The review is unique because it maps the various treatments on two axes – safety and efficacy – in a chart. Viewers gain an instant perspective on how the individual treatments fare when stacked up against each other. “The study gives credence to the new technologies,” said Dr. Ash, associate professor of medical devices at the University of Wales Trinity Saint David, Swansea. “We’re moving toward safer and more efficacious results.”
He and his colleagues analyzed more than 500 studies published since 1985, which evaluated 15 different types of technology used for facial rejuvenation. They reviewed at least 35 clinical studies per platform. They also reported on the safety and efficacy of facial peels.
The technologies examined included RF, light emitting diode (LED), pulsed dyed laser (PDL), frequency doubled 532-nm potassium-titanyl-phosphate neodymium:YAG laser (which had a low number of clinical studies), 980-nm diode laser, Q-switched Nd:YAG laser, 1320-nm Nd:YAG laser, 1540-nm Erbium:glass laser, 1450-nm diode laser, IPL, long pulsed Nd:YAG laser, plasma, and copper bromide laser.
Another technology reviewed was fractional selective photothermolysis, but studies of this modality were difficult to compare, according to the authors. Also included was the carbon dioxide laser, which the authors described as being hampered by long healing times and discomfort that requires anesthesia.
The review notes that comparisons between studies of the different treatments in the review were limited by such factors as varied beam and tip sizes (even within individual studies), various pulse durations, and different treatment times and intervals.
The researchers mapped the treatments in a single chart on two axes, safety and efficacy.
Three treatments scored the best in terms of efficacy: RF, IPL and chemical peels. However, while RF and IPL scored near the top of all treatments on the safety scale, chemical peels pulled up the rear.
The treatment strategies on the safety scale, ranked from most safe to least safe, were LED, IPL, diode laser, RF, argon laser, PDL and carbon dioxide laser, Nd:YAG, ablative Erbium, plasma, and chemical peel.
Radiofrequency topped the efficacy scale, followed closely by chemical peel and IPL. Following them, from most efficacious to least efficacious, were carbon dioxide laser, ablative Erbium, plasma treatments, and PDL, Nd:YAG and argon laser, diode laser, and LED.
The study was funded by the University of Wales Trinity Saint David. The authors had no disclosures.
SAN DIEGO – A review of existing research found that newer technologies are safer and more effective at skin rejuvenation than older ones, with two types – intense pulsed laser (IPL) and radiofrequency (RF) – at or near the head of the pack on both fronts.
In addition, 10 types of treatments, including multiple laser technologies, scored higher than facial peels on safety, although the peels beat almost all comers in terms of efficacy, the study’s lead author, Caerwyn Ash, PhD, said in an interview after presenting the results at the annual meeting of the American Society for Laser Medicine and Surgery.
The review is unique because it maps the various treatments on two axes – safety and efficacy – in a chart. Viewers gain an instant perspective on how the individual treatments fare when stacked up against each other. “The study gives credence to the new technologies,” said Dr. Ash, associate professor of medical devices at the University of Wales Trinity Saint David, Swansea. “We’re moving toward safer and more efficacious results.”
He and his colleagues analyzed more than 500 studies published since 1985, which evaluated 15 different types of technology used for facial rejuvenation. They reviewed at least 35 clinical studies per platform. They also reported on the safety and efficacy of facial peels.
The technologies examined included RF, light emitting diode (LED), pulsed dyed laser (PDL), frequency doubled 532-nm potassium-titanyl-phosphate neodymium:YAG laser (which had a low number of clinical studies), 980-nm diode laser, Q-switched Nd:YAG laser, 1320-nm Nd:YAG laser, 1540-nm Erbium:glass laser, 1450-nm diode laser, IPL, long pulsed Nd:YAG laser, plasma, and copper bromide laser.
Another technology reviewed was fractional selective photothermolysis, but studies of this modality were difficult to compare, according to the authors. Also included was the carbon dioxide laser, which the authors described as being hampered by long healing times and discomfort that requires anesthesia.
The review notes that comparisons between studies of the different treatments in the review were limited by such factors as varied beam and tip sizes (even within individual studies), various pulse durations, and different treatment times and intervals.
The researchers mapped the treatments in a single chart on two axes, safety and efficacy.
Three treatments scored the best in terms of efficacy: RF, IPL and chemical peels. However, while RF and IPL scored near the top of all treatments on the safety scale, chemical peels pulled up the rear.
The treatment strategies on the safety scale, ranked from most safe to least safe, were LED, IPL, diode laser, RF, argon laser, PDL and carbon dioxide laser, Nd:YAG, ablative Erbium, plasma, and chemical peel.
Radiofrequency topped the efficacy scale, followed closely by chemical peel and IPL. Following them, from most efficacious to least efficacious, were carbon dioxide laser, ablative Erbium, plasma treatments, and PDL, Nd:YAG and argon laser, diode laser, and LED.
The study was funded by the University of Wales Trinity Saint David. The authors had no disclosures.
SAN DIEGO – A review of existing research found that newer technologies are safer and more effective at skin rejuvenation than older ones, with two types – intense pulsed laser (IPL) and radiofrequency (RF) – at or near the head of the pack on both fronts.
In addition, 10 types of treatments, including multiple laser technologies, scored higher than facial peels on safety, although the peels beat almost all comers in terms of efficacy, the study’s lead author, Caerwyn Ash, PhD, said in an interview after presenting the results at the annual meeting of the American Society for Laser Medicine and Surgery.
The review is unique because it maps the various treatments on two axes – safety and efficacy – in a chart. Viewers gain an instant perspective on how the individual treatments fare when stacked up against each other. “The study gives credence to the new technologies,” said Dr. Ash, associate professor of medical devices at the University of Wales Trinity Saint David, Swansea. “We’re moving toward safer and more efficacious results.”
He and his colleagues analyzed more than 500 studies published since 1985, which evaluated 15 different types of technology used for facial rejuvenation. They reviewed at least 35 clinical studies per platform. They also reported on the safety and efficacy of facial peels.
The technologies examined included RF, light emitting diode (LED), pulsed dyed laser (PDL), frequency doubled 532-nm potassium-titanyl-phosphate neodymium:YAG laser (which had a low number of clinical studies), 980-nm diode laser, Q-switched Nd:YAG laser, 1320-nm Nd:YAG laser, 1540-nm Erbium:glass laser, 1450-nm diode laser, IPL, long pulsed Nd:YAG laser, plasma, and copper bromide laser.
Another technology reviewed was fractional selective photothermolysis, but studies of this modality were difficult to compare, according to the authors. Also included was the carbon dioxide laser, which the authors described as being hampered by long healing times and discomfort that requires anesthesia.
The review notes that comparisons between studies of the different treatments in the review were limited by such factors as varied beam and tip sizes (even within individual studies), various pulse durations, and different treatment times and intervals.
The researchers mapped the treatments in a single chart on two axes, safety and efficacy.
Three treatments scored the best in terms of efficacy: RF, IPL and chemical peels. However, while RF and IPL scored near the top of all treatments on the safety scale, chemical peels pulled up the rear.
The treatment strategies on the safety scale, ranked from most safe to least safe, were LED, IPL, diode laser, RF, argon laser, PDL and carbon dioxide laser, Nd:YAG, ablative Erbium, plasma, and chemical peel.
Radiofrequency topped the efficacy scale, followed closely by chemical peel and IPL. Following them, from most efficacious to least efficacious, were carbon dioxide laser, ablative Erbium, plasma treatments, and PDL, Nd:YAG and argon laser, diode laser, and LED.
The study was funded by the University of Wales Trinity Saint David. The authors had no disclosures.
AT LASER 2017
Key clinical point:
Major finding: IPL and RF were among the modalities that were safer and more effective at skin rejuvenation than were older ones.
Data source: An analysis of more than 500 studies published since 1985 evaluating of 15 different types of technology used for facial rejuvenation, reviewing at least 35 clinical studies per platform.
Disclosures: The study was funded by the University of Wales Trinity Saint David. The authors had no disclosures.
Top Acthar prescribers reap hefty payments from drug maker
BOSTON – A new analysis finds that some of the biggest neurologist prescribers of repository corticotropin gel (Acthar) – the extraordinarily expensive multiple sclerosis (MS) relapse drug – reaped extensive payments from its manufacturer, with one taking in $130,307 in a single year.
Together, 51 neurologists accounted for 980 Medicare claims worth more than $39 million in Acthar spending in 2014, almost half of the entire estimated $83 million in Medicare spending on neurologist-prescribed Acthar that year.
“There is a small group of neurologists – less than 1% – who are prescribing Acthar at considerable cost to Medicare and may do this in part because of financial relationships with the company that sells Acthar,” said study lead author Dennis Bourdette, MD, chair and research professor of neurology at Oregon Health and Science University, Portland.

Dr. Bourdette acknowledges that the research doesn’t prove a causal relationship between payments and prescriptions. In response to questions, Acthar manufacturer Mallinckrodt Pharmaceuticals, already under fire for the $34,000-per-vial cost of the drug, questioned the study design and denied wrongdoing in a statement: “Mallinckrodt is committed to following the highest standards for integrity and compliance in all of our business practices, including our collaboration with physicians.”
Acthar, also known as H.P. Acthar, is the poster child for stunningly expensive medication. According to the Federal Trade Commission, the cost of the drug rose from $40 per vial in 2001 to more than $34,000 this year. The New York Times reports that Medicare spending on Acthar topped half a billion in 2015.
Earlier this year, Mallinckrodt ARD (formerly Questcor) and its parent company agreed to pay a $100 million fine to settle charges that it created an illegal monopoly over the drug.
Dr. Bourdette and colleagues released their findings at the annual meeting of the American Academy of Neurology.
In an interview, Dr. Bourdette said the study’s roots lie in his concern about the medication, whose transformation from an inexpensive 1950s-era medication for pulmonary sarcoidosis to high-priced MS treatment has drawn national media attention.
“I believe that Acthar is tremendously overpriced and a waste of health care money,” Dr. Bourdette said. “I wanted to find out how extensive an economic problem it was and how much money Medicare was spending on it since this data was easily accessible.”
According to the study, Medicare spent $1.3 billion from 2011 to 2015 on Acthar, with about 25% of the cost due to prescriptions from neurologists. “When I discovered that a relatively small number of neurologists was prescribing it commonly at a cost of $40-$50 million a year to Medicare, I was interested in determining why they were prescribing this expensive therapy and postulated that it might be related to financial support they were receiving from the manufacturer,” Dr. Bourdette said.
The researchers examined the Medicare Part D Public Use File to determine which neurologists prescribed Acthar frequently in 2014. They identified 51 who prescribed Acthar 10 or more times that year and were frequent prescribers of MS disease-modifying therapy, indicating they treated many people with MS.
The 51 neurologists accounted for a mean of 19 Acthar claims each in 2014 (range, 11-50) totaling a mean annual cost of $770,145 (range, $354,479-$3,623,509). Together, the neurologists accounted for total Medicare spending on Acthar of $39,277,380.
The researchers also chose a control group – 51 neurologists who prescribed glatiramer acetate (Copaxone) more than 10 times in 2014 and also prescribed a similar frequency of all MS disease-modifying therapies as the high-frequency Acthar group.
“Acthar is used episodically to treat MS relapses, and glatiramer acetate is taken chronically to prevent relapses and disability,” Dr. Bourdette said. He added that glatiramer acetate is now available in a generic, but it wasn’t in 2014.
The Acthar and Copaxone groups were nearly identical in terms of gender (about two-thirds men) and years since graduation (a mean of 26), but the Acthar prescribers were more likely to work in small practices (1-10 doctors), file more prescription claims, see more Medicare patients, and practice in the South or West. The demographic information came from CMS Physician Compare.
In terms of overall drug maker payments, neurologists in the Acthar group accepted much more (median, $54,270; range, $623-$369,847) than did the Copaxone group (median, $1,747, range, $0-$256,305, P less than .001). Payment information came from the federal Open Payments database.
As for payments directly from the manufacturers of the two drugs, the Acthar prescribers accepted a median of $5,344 (range, $0-$130,307) from its manufacturer, while the Copaxone prescribers accepted a median of $137 (range, $0-$168,373) from Teva (P = .003).
“The payments are primarily for giving lectures or serving on advisory boards,” Dr. Bourdette said. “These types of payments are commonly made by pharmaceutical companies to physicians who participate in these types of activities.”
In a statement, Mallinckrodt Pharmaceuticals contends that the study inappropriately compares Acthar, often a later-line therapy, to Copaxone, which it says is often a first-line therapy.
Dr. Bourdette responded that the researchers chose a comparison group of top prescribers of Copaxone “as a marker of neurologists who treated a significant number of patients with MS.”
Mallinckrodt also notes that “there may be unmeasured confounding factors in the matching process between the comparator physician groups. These could include differences in the patient characteristics managed by these physicians including disease severity affecting prescribing patterns.”
The researchers agree that there may be differences between the groups, Dr. Bourdette said. However, he added, “the fact remains that the two groups differed in the amount of money they received as open-source payments from pharmaceutical companies. We doubt that the severity of their case mixes should lead to one group receiving more pharmaceutical open-source payments than another.”
Finally, Mallinckrodt says there’s no proof of a causal connection between the payments and the prescriptions; the study authors agree. And, the company says, “this pattern of correlation would be expected in any scenario where a small number of prescribers are the experts in the use of a later-line drug to treat a limited subset of patients.”
Dr. Bourdette rejects this contention. Few of the high Acthar prescribers practice at academic centers, he said, and few are recognized for their MS expertise. “So to suggest that they are experts in the use of Acthar for the treatment of MS when they are not as a group recognized as being experts on the treatment of MS in general is incredible,” he said. “Why a small group of neurologists prescribe Acthar remains a mystery, but it is not because the majority are leaders in the field of MS therapeutics.”
In an interview, Eric G. Campbell, PhD, professor of medicine and director of research at the Mongan Institute Health Policy Center at Harvard Medical School, Boston, said the study findings fit in with previous research that has found that “the more money that people get, the more they use the drug.
“Any reasonable person looking at this data would assume or at least consider very strongly that there is a causal relationship here,” he said.
What should be done? “There are lots of ways to stop this,” Dr. Campbell said. “One could simply impose rules that forbid doctors who accept payments for marketing drugs from billing Medicare or private payers for the care they provide. Large provider organizations could pass rules that forbid this kind of behavior. Finally, the government could vigorously pursue stiff penalties against physicians who accept payments that are really nothing more than incentives to encourage or sustain prescribing practices.”
The study was supported by a National Multiple Sclerosis Society grant. Dr. Bourdette said that he provides consulting to Magellan Healthcare, a company that provides recommendations to insurance companies on the approval of high-cost therapies. Dr. Campbell disclosed that he serves as an expert witness on law cases related to conflicts of interest in medicine.
BOSTON – A new analysis finds that some of the biggest neurologist prescribers of repository corticotropin gel (Acthar) – the extraordinarily expensive multiple sclerosis (MS) relapse drug – reaped extensive payments from its manufacturer, with one taking in $130,307 in a single year.
Together, 51 neurologists accounted for 980 Medicare claims worth more than $39 million in Acthar spending in 2014, almost half of the entire estimated $83 million in Medicare spending on neurologist-prescribed Acthar that year.
“There is a small group of neurologists – less than 1% – who are prescribing Acthar at considerable cost to Medicare and may do this in part because of financial relationships with the company that sells Acthar,” said study lead author Dennis Bourdette, MD, chair and research professor of neurology at Oregon Health and Science University, Portland.
Dr. Bourdette acknowledges that the research doesn’t prove a causal relationship between payments and prescriptions. In response to questions, Acthar manufacturer Mallinckrodt Pharmaceuticals, already under fire for the $34,000-per-vial cost of the drug, questioned the study design and denied wrongdoing in a statement: “Mallinckrodt is committed to following the highest standards for integrity and compliance in all of our business practices, including our collaboration with physicians.”
Acthar, also known as H.P. Acthar, is the poster child for stunningly expensive medication. According to the Federal Trade Commission, the cost of the drug rose from $40 per vial in 2001 to more than $34,000 this year. The New York Times reports that Medicare spending on Acthar topped half a billion in 2015.
Earlier this year, Mallinckrodt ARD (formerly Questcor) and its parent company agreed to pay a $100 million fine to settle charges that it created an illegal monopoly over the drug.
Dr. Bourdette and colleagues released their findings at the annual meeting of the American Academy of Neurology.
In an interview, Dr. Bourdette said the study’s roots lie in his concern about the medication, whose transformation from an inexpensive 1950s-era medication for pulmonary sarcoidosis to high-priced MS treatment has drawn national media attention.
“I believe that Acthar is tremendously overpriced and a waste of health care money,” Dr. Bourdette said. “I wanted to find out how extensive an economic problem it was and how much money Medicare was spending on it since this data was easily accessible.”
According to the study, Medicare spent $1.3 billion from 2011 to 2015 on Acthar, with about 25% of the cost due to prescriptions from neurologists. “When I discovered that a relatively small number of neurologists was prescribing it commonly at a cost of $40-$50 million a year to Medicare, I was interested in determining why they were prescribing this expensive therapy and postulated that it might be related to financial support they were receiving from the manufacturer,” Dr. Bourdette said.
The researchers examined the Medicare Part D Public Use File to determine which neurologists prescribed Acthar frequently in 2014. They identified 51 who prescribed Acthar 10 or more times that year and were frequent prescribers of MS disease-modifying therapy, indicating they treated many people with MS.
The 51 neurologists accounted for a mean of 19 Acthar claims each in 2014 (range, 11-50) totaling a mean annual cost of $770,145 (range, $354,479-$3,623,509). Together, the neurologists accounted for total Medicare spending on Acthar of $39,277,380.
The researchers also chose a control group – 51 neurologists who prescribed glatiramer acetate (Copaxone) more than 10 times in 2014 and also prescribed a similar frequency of all MS disease-modifying therapies as the high-frequency Acthar group.
“Acthar is used episodically to treat MS relapses, and glatiramer acetate is taken chronically to prevent relapses and disability,” Dr. Bourdette said. He added that glatiramer acetate is now available in a generic, but it wasn’t in 2014.
The Acthar and Copaxone groups were nearly identical in terms of gender (about two-thirds men) and years since graduation (a mean of 26), but the Acthar prescribers were more likely to work in small practices (1-10 doctors), file more prescription claims, see more Medicare patients, and practice in the South or West. The demographic information came from CMS Physician Compare.
In terms of overall drug maker payments, neurologists in the Acthar group accepted much more (median, $54,270; range, $623-$369,847) than did the Copaxone group (median, $1,747, range, $0-$256,305, P less than .001). Payment information came from the federal Open Payments database.
As for payments directly from the manufacturers of the two drugs, the Acthar prescribers accepted a median of $5,344 (range, $0-$130,307) from its manufacturer, while the Copaxone prescribers accepted a median of $137 (range, $0-$168,373) from Teva (P = .003).
“The payments are primarily for giving lectures or serving on advisory boards,” Dr. Bourdette said. “These types of payments are commonly made by pharmaceutical companies to physicians who participate in these types of activities.”
In a statement, Mallinckrodt Pharmaceuticals contends that the study inappropriately compares Acthar, often a later-line therapy, to Copaxone, which it says is often a first-line therapy.
Dr. Bourdette responded that the researchers chose a comparison group of top prescribers of Copaxone “as a marker of neurologists who treated a significant number of patients with MS.”
Mallinckrodt also notes that “there may be unmeasured confounding factors in the matching process between the comparator physician groups. These could include differences in the patient characteristics managed by these physicians including disease severity affecting prescribing patterns.”
The researchers agree that there may be differences between the groups, Dr. Bourdette said. However, he added, “the fact remains that the two groups differed in the amount of money they received as open-source payments from pharmaceutical companies. We doubt that the severity of their case mixes should lead to one group receiving more pharmaceutical open-source payments than another.”
Finally, Mallinckrodt says there’s no proof of a causal connection between the payments and the prescriptions; the study authors agree. And, the company says, “this pattern of correlation would be expected in any scenario where a small number of prescribers are the experts in the use of a later-line drug to treat a limited subset of patients.”
Dr. Bourdette rejects this contention. Few of the high Acthar prescribers practice at academic centers, he said, and few are recognized for their MS expertise. “So to suggest that they are experts in the use of Acthar for the treatment of MS when they are not as a group recognized as being experts on the treatment of MS in general is incredible,” he said. “Why a small group of neurologists prescribe Acthar remains a mystery, but it is not because the majority are leaders in the field of MS therapeutics.”
In an interview, Eric G. Campbell, PhD, professor of medicine and director of research at the Mongan Institute Health Policy Center at Harvard Medical School, Boston, said the study findings fit in with previous research that has found that “the more money that people get, the more they use the drug.
“Any reasonable person looking at this data would assume or at least consider very strongly that there is a causal relationship here,” he said.
What should be done? “There are lots of ways to stop this,” Dr. Campbell said. “One could simply impose rules that forbid doctors who accept payments for marketing drugs from billing Medicare or private payers for the care they provide. Large provider organizations could pass rules that forbid this kind of behavior. Finally, the government could vigorously pursue stiff penalties against physicians who accept payments that are really nothing more than incentives to encourage or sustain prescribing practices.”
The study was supported by a National Multiple Sclerosis Society grant. Dr. Bourdette said that he provides consulting to Magellan Healthcare, a company that provides recommendations to insurance companies on the approval of high-cost therapies. Dr. Campbell disclosed that he serves as an expert witness on law cases related to conflicts of interest in medicine.
BOSTON – A new analysis finds that some of the biggest neurologist prescribers of repository corticotropin gel (Acthar) – the extraordinarily expensive multiple sclerosis (MS) relapse drug – reaped extensive payments from its manufacturer, with one taking in $130,307 in a single year.
Together, 51 neurologists accounted for 980 Medicare claims worth more than $39 million in Acthar spending in 2014, almost half of the entire estimated $83 million in Medicare spending on neurologist-prescribed Acthar that year.
“There is a small group of neurologists – less than 1% – who are prescribing Acthar at considerable cost to Medicare and may do this in part because of financial relationships with the company that sells Acthar,” said study lead author Dennis Bourdette, MD, chair and research professor of neurology at Oregon Health and Science University, Portland.
Dr. Bourdette acknowledges that the research doesn’t prove a causal relationship between payments and prescriptions. In response to questions, Acthar manufacturer Mallinckrodt Pharmaceuticals, already under fire for the $34,000-per-vial cost of the drug, questioned the study design and denied wrongdoing in a statement: “Mallinckrodt is committed to following the highest standards for integrity and compliance in all of our business practices, including our collaboration with physicians.”
Acthar, also known as H.P. Acthar, is the poster child for stunningly expensive medication. According to the Federal Trade Commission, the cost of the drug rose from $40 per vial in 2001 to more than $34,000 this year. The New York Times reports that Medicare spending on Acthar topped half a billion in 2015.
Earlier this year, Mallinckrodt ARD (formerly Questcor) and its parent company agreed to pay a $100 million fine to settle charges that it created an illegal monopoly over the drug.
Dr. Bourdette and colleagues released their findings at the annual meeting of the American Academy of Neurology.
In an interview, Dr. Bourdette said the study’s roots lie in his concern about the medication, whose transformation from an inexpensive 1950s-era medication for pulmonary sarcoidosis to high-priced MS treatment has drawn national media attention.
“I believe that Acthar is tremendously overpriced and a waste of health care money,” Dr. Bourdette said. “I wanted to find out how extensive an economic problem it was and how much money Medicare was spending on it since this data was easily accessible.”
According to the study, Medicare spent $1.3 billion from 2011 to 2015 on Acthar, with about 25% of the cost due to prescriptions from neurologists. “When I discovered that a relatively small number of neurologists was prescribing it commonly at a cost of $40-$50 million a year to Medicare, I was interested in determining why they were prescribing this expensive therapy and postulated that it might be related to financial support they were receiving from the manufacturer,” Dr. Bourdette said.
The researchers examined the Medicare Part D Public Use File to determine which neurologists prescribed Acthar frequently in 2014. They identified 51 who prescribed Acthar 10 or more times that year and were frequent prescribers of MS disease-modifying therapy, indicating they treated many people with MS.
The 51 neurologists accounted for a mean of 19 Acthar claims each in 2014 (range, 11-50) totaling a mean annual cost of $770,145 (range, $354,479-$3,623,509). Together, the neurologists accounted for total Medicare spending on Acthar of $39,277,380.
The researchers also chose a control group – 51 neurologists who prescribed glatiramer acetate (Copaxone) more than 10 times in 2014 and also prescribed a similar frequency of all MS disease-modifying therapies as the high-frequency Acthar group.
“Acthar is used episodically to treat MS relapses, and glatiramer acetate is taken chronically to prevent relapses and disability,” Dr. Bourdette said. He added that glatiramer acetate is now available in a generic, but it wasn’t in 2014.
The Acthar and Copaxone groups were nearly identical in terms of gender (about two-thirds men) and years since graduation (a mean of 26), but the Acthar prescribers were more likely to work in small practices (1-10 doctors), file more prescription claims, see more Medicare patients, and practice in the South or West. The demographic information came from CMS Physician Compare.
In terms of overall drug maker payments, neurologists in the Acthar group accepted much more (median, $54,270; range, $623-$369,847) than did the Copaxone group (median, $1,747, range, $0-$256,305, P less than .001). Payment information came from the federal Open Payments database.
As for payments directly from the manufacturers of the two drugs, the Acthar prescribers accepted a median of $5,344 (range, $0-$130,307) from its manufacturer, while the Copaxone prescribers accepted a median of $137 (range, $0-$168,373) from Teva (P = .003).
“The payments are primarily for giving lectures or serving on advisory boards,” Dr. Bourdette said. “These types of payments are commonly made by pharmaceutical companies to physicians who participate in these types of activities.”
In a statement, Mallinckrodt Pharmaceuticals contends that the study inappropriately compares Acthar, often a later-line therapy, to Copaxone, which it says is often a first-line therapy.
Dr. Bourdette responded that the researchers chose a comparison group of top prescribers of Copaxone “as a marker of neurologists who treated a significant number of patients with MS.”
Mallinckrodt also notes that “there may be unmeasured confounding factors in the matching process between the comparator physician groups. These could include differences in the patient characteristics managed by these physicians including disease severity affecting prescribing patterns.”
The researchers agree that there may be differences between the groups, Dr. Bourdette said. However, he added, “the fact remains that the two groups differed in the amount of money they received as open-source payments from pharmaceutical companies. We doubt that the severity of their case mixes should lead to one group receiving more pharmaceutical open-source payments than another.”
Finally, Mallinckrodt says there’s no proof of a causal connection between the payments and the prescriptions; the study authors agree. And, the company says, “this pattern of correlation would be expected in any scenario where a small number of prescribers are the experts in the use of a later-line drug to treat a limited subset of patients.”
Dr. Bourdette rejects this contention. Few of the high Acthar prescribers practice at academic centers, he said, and few are recognized for their MS expertise. “So to suggest that they are experts in the use of Acthar for the treatment of MS when they are not as a group recognized as being experts on the treatment of MS in general is incredible,” he said. “Why a small group of neurologists prescribe Acthar remains a mystery, but it is not because the majority are leaders in the field of MS therapeutics.”
In an interview, Eric G. Campbell, PhD, professor of medicine and director of research at the Mongan Institute Health Policy Center at Harvard Medical School, Boston, said the study findings fit in with previous research that has found that “the more money that people get, the more they use the drug.
“Any reasonable person looking at this data would assume or at least consider very strongly that there is a causal relationship here,” he said.
What should be done? “There are lots of ways to stop this,” Dr. Campbell said. “One could simply impose rules that forbid doctors who accept payments for marketing drugs from billing Medicare or private payers for the care they provide. Large provider organizations could pass rules that forbid this kind of behavior. Finally, the government could vigorously pursue stiff penalties against physicians who accept payments that are really nothing more than incentives to encourage or sustain prescribing practices.”
The study was supported by a National Multiple Sclerosis Society grant. Dr. Bourdette said that he provides consulting to Magellan Healthcare, a company that provides recommendations to insurance companies on the approval of high-cost therapies. Dr. Campbell disclosed that he serves as an expert witness on law cases related to conflicts of interest in medicine.
AT AAN 2017
Key clinical point:
Major finding: The top Acthar prescribers reaped much more in payments from drug makers overall in 2014 than did a control group of top prescribers of another MS drug (median of $54,270 vs. $1,747; P less than .001) and from the manufacturer of each drug (median of $5,344 vs. $137; P = .003).
Data source: Medicare Part D Public Use File, CMS Physician Compare, Open Payments database, 2014.
Disclosures: The work was supported by a National Multiple Sclerosis Society grant. Dr. Bourdette provides consulting to Magellan Healthcare, a company that provides recommendations to insurance companies on the approval of high-cost therapies.
Lasers may be effective for treating xanthelasma
SAN DIEGO – Laser treatments may be effective for xanthelasma palpebrarum lesions, based on a systematic review of existing studies, although the research is limited.
“The number of cases we looked at was relatively small, so you can’t come up with any definite conclusions,” said review coauthor Christopher J. Huerter, MD, head of the division of dermatology at Creighton University, Omaha. “But it’s promising since the lasers we examined all work with some efficacy, with the CO2 and Er:YAG [erbium:YAG] lasers probably having the best results.”
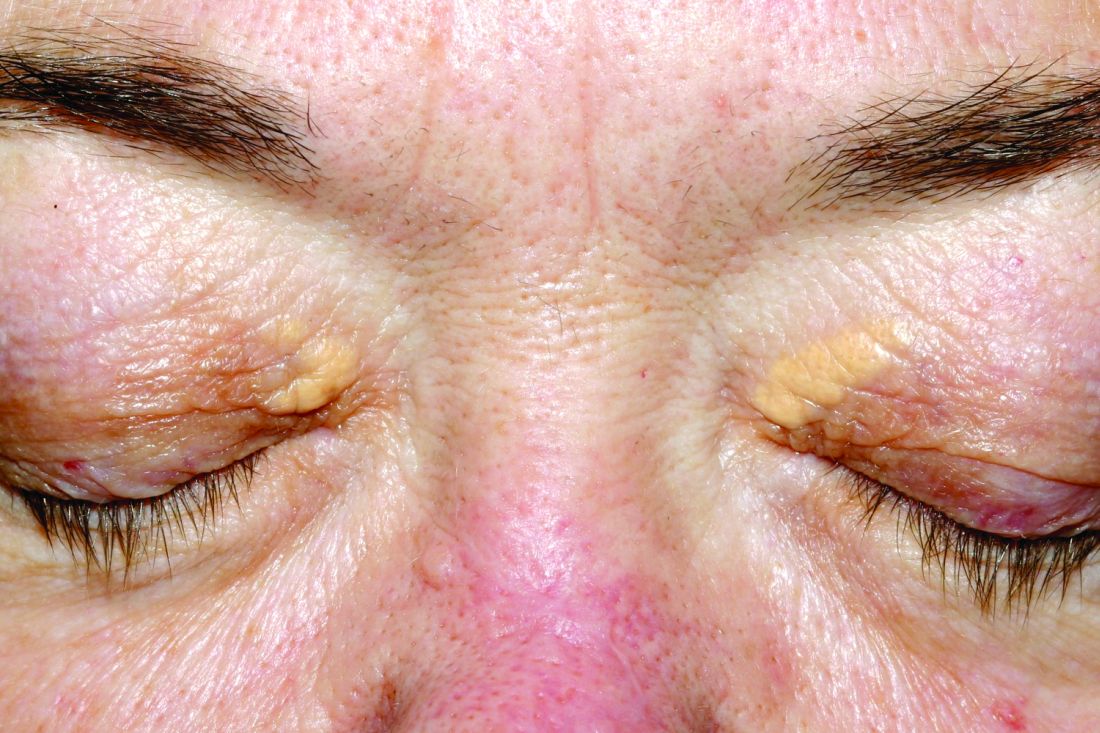
Xanthelasma lesions appear as small yellowish plaques on the eyelids. “About half the people who have it have some blood lipid abnormality,” Dr. Huerter said in an interview. “If a person has it, it’s worthwhile to do a cholesterol screen or a lipid profile.”
Treatment with trichloroacetic acid is one option, although it was more common before lasers began to be used. In addition, “surgical incision can be very effective,” he said, although the review notes that it can create undesirable scarring.
Researchers have studied laser treatment for xanthelasma for at least 30 years. Dr. Huerter and his colleagues examined 21 studies published since 1987, with the following lasers: CO2 laser (three studies), argon laser (one study), Er:YAG laser (four studies), ultrapulse CO2 laser (five studies), 1,450-nm diode laser (one study), pulsed dye laser (PDL, two studies), superpulsed or fractional CO2 laser (one study), and Q-switched neodymium:YAG laser (three studies). An additional study examined both argon and Er:YAG lasers.
The number of treated patients in the studies ranged from 1 to 50, and the number of treated lesions ranged from 1 to 76. (Patients often had more than one lesion.) “It would be nice to have bigger studies and bigger numbers,” Dr. Huerter said at the annual meeting of the American Society for Laser Medicine and Surgery.
Although the studies were limited by small cohorts, short follow-up, and lack of comparison groups, the findings did reveal signs of effectiveness: Clearance rates were 100% in CO2, argon, and PDL cases and about 85% with Er:YAG lasers. Clearance rates were lower with Nd:YAG (about 55%) and 1,450-nm diode (about 48%) lasers.
Edema was reported in all PDL cases and erythema in almost 20% of CO2 cases. Dyspigmentation was most common – at about 30% – in Er:YAG and 1,450-nm diode cases. Visible scars were reported in more than 5% of Er:YAG cases.
The review concluded that “sufficient evidence is available to suggest laser therapies to be a cosmetically excellent treatment option for xanthelasma , particularly applicable in patients who are not good candidates for surgical excision,” he said.
As for advice to dermatologists, Dr. Huerter pointed to the positive results for CO2 and Er:YAG lasers. He said PDL lasers could also be used. As for argon lasers, he noted that it’s not as likely for dermatologists to have them on hand, he said.
In regard to choosing which xanthelasma lesions to treat with laser, he said thicker ones may not be as amenable. “But if you do laser treatment and don’t get the results you want, you can always excise.”
No funding for the study was reported. Dr. Huerter reported no disclosures.
SAN DIEGO – Laser treatments may be effective for xanthelasma palpebrarum lesions, based on a systematic review of existing studies, although the research is limited.
“The number of cases we looked at was relatively small, so you can’t come up with any definite conclusions,” said review coauthor Christopher J. Huerter, MD, head of the division of dermatology at Creighton University, Omaha. “But it’s promising since the lasers we examined all work with some efficacy, with the CO2 and Er:YAG [erbium:YAG] lasers probably having the best results.”
Xanthelasma lesions appear as small yellowish plaques on the eyelids. “About half the people who have it have some blood lipid abnormality,” Dr. Huerter said in an interview. “If a person has it, it’s worthwhile to do a cholesterol screen or a lipid profile.”
Treatment with trichloroacetic acid is one option, although it was more common before lasers began to be used. In addition, “surgical incision can be very effective,” he said, although the review notes that it can create undesirable scarring.
Researchers have studied laser treatment for xanthelasma for at least 30 years. Dr. Huerter and his colleagues examined 21 studies published since 1987, with the following lasers: CO2 laser (three studies), argon laser (one study), Er:YAG laser (four studies), ultrapulse CO2 laser (five studies), 1,450-nm diode laser (one study), pulsed dye laser (PDL, two studies), superpulsed or fractional CO2 laser (one study), and Q-switched neodymium:YAG laser (three studies). An additional study examined both argon and Er:YAG lasers.
The number of treated patients in the studies ranged from 1 to 50, and the number of treated lesions ranged from 1 to 76. (Patients often had more than one lesion.) “It would be nice to have bigger studies and bigger numbers,” Dr. Huerter said at the annual meeting of the American Society for Laser Medicine and Surgery.
Although the studies were limited by small cohorts, short follow-up, and lack of comparison groups, the findings did reveal signs of effectiveness: Clearance rates were 100% in CO2, argon, and PDL cases and about 85% with Er:YAG lasers. Clearance rates were lower with Nd:YAG (about 55%) and 1,450-nm diode (about 48%) lasers.
Edema was reported in all PDL cases and erythema in almost 20% of CO2 cases. Dyspigmentation was most common – at about 30% – in Er:YAG and 1,450-nm diode cases. Visible scars were reported in more than 5% of Er:YAG cases.
The review concluded that “sufficient evidence is available to suggest laser therapies to be a cosmetically excellent treatment option for xanthelasma , particularly applicable in patients who are not good candidates for surgical excision,” he said.
As for advice to dermatologists, Dr. Huerter pointed to the positive results for CO2 and Er:YAG lasers. He said PDL lasers could also be used. As for argon lasers, he noted that it’s not as likely for dermatologists to have them on hand, he said.
In regard to choosing which xanthelasma lesions to treat with laser, he said thicker ones may not be as amenable. “But if you do laser treatment and don’t get the results you want, you can always excise.”
No funding for the study was reported. Dr. Huerter reported no disclosures.
SAN DIEGO – Laser treatments may be effective for xanthelasma palpebrarum lesions, based on a systematic review of existing studies, although the research is limited.
“The number of cases we looked at was relatively small, so you can’t come up with any definite conclusions,” said review coauthor Christopher J. Huerter, MD, head of the division of dermatology at Creighton University, Omaha. “But it’s promising since the lasers we examined all work with some efficacy, with the CO2 and Er:YAG [erbium:YAG] lasers probably having the best results.”
Xanthelasma lesions appear as small yellowish plaques on the eyelids. “About half the people who have it have some blood lipid abnormality,” Dr. Huerter said in an interview. “If a person has it, it’s worthwhile to do a cholesterol screen or a lipid profile.”
Treatment with trichloroacetic acid is one option, although it was more common before lasers began to be used. In addition, “surgical incision can be very effective,” he said, although the review notes that it can create undesirable scarring.
Researchers have studied laser treatment for xanthelasma for at least 30 years. Dr. Huerter and his colleagues examined 21 studies published since 1987, with the following lasers: CO2 laser (three studies), argon laser (one study), Er:YAG laser (four studies), ultrapulse CO2 laser (five studies), 1,450-nm diode laser (one study), pulsed dye laser (PDL, two studies), superpulsed or fractional CO2 laser (one study), and Q-switched neodymium:YAG laser (three studies). An additional study examined both argon and Er:YAG lasers.
The number of treated patients in the studies ranged from 1 to 50, and the number of treated lesions ranged from 1 to 76. (Patients often had more than one lesion.) “It would be nice to have bigger studies and bigger numbers,” Dr. Huerter said at the annual meeting of the American Society for Laser Medicine and Surgery.
Although the studies were limited by small cohorts, short follow-up, and lack of comparison groups, the findings did reveal signs of effectiveness: Clearance rates were 100% in CO2, argon, and PDL cases and about 85% with Er:YAG lasers. Clearance rates were lower with Nd:YAG (about 55%) and 1,450-nm diode (about 48%) lasers.
Edema was reported in all PDL cases and erythema in almost 20% of CO2 cases. Dyspigmentation was most common – at about 30% – in Er:YAG and 1,450-nm diode cases. Visible scars were reported in more than 5% of Er:YAG cases.
The review concluded that “sufficient evidence is available to suggest laser therapies to be a cosmetically excellent treatment option for xanthelasma , particularly applicable in patients who are not good candidates for surgical excision,” he said.
As for advice to dermatologists, Dr. Huerter pointed to the positive results for CO2 and Er:YAG lasers. He said PDL lasers could also be used. As for argon lasers, he noted that it’s not as likely for dermatologists to have them on hand, he said.
In regard to choosing which xanthelasma lesions to treat with laser, he said thicker ones may not be as amenable. “But if you do laser treatment and don’t get the results you want, you can always excise.”
No funding for the study was reported. Dr. Huerter reported no disclosures.
Key clinical point:
Major finding: Clearance rates of about 85%-100% were reported for xanthelasma treatment with CO2, argon, pulsed dye, and Er:YAG laser treatments.
Data source: A systematic review of 21 studies evaluating different laser treatments for xanthelasma.
Disclosures: No funding was reported. Dr. Huerter reported no disclosures.
VIDEO: About 1 in 20 ALS patients in Washington state chose assisted suicide
BOSTON – A new study estimates that 3.4%-6.7% of amyotrophic lateral sclerosis (ALS) patients in Washington state sought to commit physician-assisted suicide over a 5-year period.
The rate is many times higher than that among cancer patients in the state, researchers found. They also discovered that ALS patients were significantly more likely than were other terminally ill people to use the deadly medication after getting prescriptions for it.
The findings appear to reflect the unique hopelessness facing ALS patients. “They’re not afforded as much denial of decline and death as are patients with other terminal illnesses,” said Linda Ganzini, MD, MPH, a professor of psychiatry and medicine at Oregon Health & Science University, Portland, who has studied end of life in ALS patients.
“Many cancer patients, even in the final days of life, receive treatments that they hope will extend their lives,” she said in an interview after reviewing the study findings. “In contrast, treatments for ALS are minimally effective.”
Physician-assisted suicide is legal in California, Colorado, the District of Columbia, Montana, Oregon, Vermont, and Washington.
A team led by Leo H. Wang, MD, PhD, of the University of Washington, Seattle, examined the medical records of 39 ALS patients who sought medication to end their lives at three hospitals in Seattle from March 2009 to Dec. 31, 2014.
Washington’s Death with Dignity (DWD) law, which went into effect in 2009, allows physicians to prescribe lethal medication if the patient has a terminal illness and a prognosis of less than 6 months to live as judged by two physicians.
The researchers reported their findings, a follow-up to a previous study (Neurology. 2016 Nov 15;87[20]:2117-22), at the annual meeting of the American Academy of Neurology.
The median age of the ALS patients at symptom onset was 64 (range, 42-83), and a median of 712 days passed (range, 207-2,407) from the date of diagnosis to date of prescription for lethal medication.
The median time from prescription to death was 22 days, with at least one patient dying immediately (range, 0-386 days). All 39 patients had limb involvement, and 82%-92% had bulbar involvement, dysarthria, dysphagia, and/or dyspnea.
The researchers estimate that 3.4%-6.7% of 1,146 ALS patients in Washington who died over the time period of the study sought a physician-assisted death. The 3.4% figure assumes that the 39 patients at the three hospitals make up all the ALS patients who received medication prescriptions. The 6.7% figure assumes that all patients with neurodegenerative disease who sought DWD in the state over that period had ALS.
“Similarly, 5% (92 of 1,795) of Oregon ALS patient who died sought medication under DWD between 1998 and 2014,” Dr. Wang said. “This is slightly increased compared to the percentage during the first decade, following enactment of the Oregon law (1998-2007), when 2.7% (26 of 962) of ALS patients died using DWD medication.”
Using Washington state data, researchers also estimated that 0.6% of 73,319 cancer patients and 0.2% of 298,178 people in the state who died of all causes sought DWD over the study period.
A total of 30 (77%) ALS patients who received the deadly prescriptions chose to take them, compared with 67% of all-cause patients who took advantage of the DWD law and 60% of cancer patients.
All 30 patients died. The nine who chose to not take the prescribed medication died after a median of 76 days. The patients who did not take the medication were more likely to be married (88% vs. 69%), to be college educated (100% vs. 74%), and to use a motorized wheelchair (78% vs. 31%).
Those who chose to not take the prescribed medication were also less motivated by loss of dignity (63% vs. 93% among those who took the medication) and by being a burden on others (25% vs. 66%). They were more likely to identify themselves as religious (80% vs. 35%).
Multiple factors may explain why ALS patients made different choices regarding the deadly drugs, lead study author Dr. Wang said in an interview. “We thought that the loss of communication may have played a role based on our finding, as most patients who followed through had more substantial trouble speaking,” he said. “For the patients who ultimately did not choose to take the medication, we found more of them had stronger religious beliefs than those who did not.”
As for pain, he reported that it was not a major issue. “Only about 10% of ALS patients were worried about pain, as opposed to 30% of the general Death with Dignity patients,” he said.
Dr. Ganzini noted that some patients who seek the prescribed drugs “want reassurance that, if their quality of life becomes unbearable, they have the option of physician-assisted death. But, they continue to cope and find reasons to live. As such, they ultimately die of their disease without taking the medications. Others lose the ability to ingest the medications, often because of sudden worsening of their disease.”
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
No specific funding was reported. Dr. Ganzini and Dr. Wang had no disclosures.
BOSTON – A new study estimates that 3.4%-6.7% of amyotrophic lateral sclerosis (ALS) patients in Washington state sought to commit physician-assisted suicide over a 5-year period.
The rate is many times higher than that among cancer patients in the state, researchers found. They also discovered that ALS patients were significantly more likely than were other terminally ill people to use the deadly medication after getting prescriptions for it.
The findings appear to reflect the unique hopelessness facing ALS patients. “They’re not afforded as much denial of decline and death as are patients with other terminal illnesses,” said Linda Ganzini, MD, MPH, a professor of psychiatry and medicine at Oregon Health & Science University, Portland, who has studied end of life in ALS patients.
“Many cancer patients, even in the final days of life, receive treatments that they hope will extend their lives,” she said in an interview after reviewing the study findings. “In contrast, treatments for ALS are minimally effective.”
Physician-assisted suicide is legal in California, Colorado, the District of Columbia, Montana, Oregon, Vermont, and Washington.
A team led by Leo H. Wang, MD, PhD, of the University of Washington, Seattle, examined the medical records of 39 ALS patients who sought medication to end their lives at three hospitals in Seattle from March 2009 to Dec. 31, 2014.
Washington’s Death with Dignity (DWD) law, which went into effect in 2009, allows physicians to prescribe lethal medication if the patient has a terminal illness and a prognosis of less than 6 months to live as judged by two physicians.
The researchers reported their findings, a follow-up to a previous study (Neurology. 2016 Nov 15;87[20]:2117-22), at the annual meeting of the American Academy of Neurology.
The median age of the ALS patients at symptom onset was 64 (range, 42-83), and a median of 712 days passed (range, 207-2,407) from the date of diagnosis to date of prescription for lethal medication.
The median time from prescription to death was 22 days, with at least one patient dying immediately (range, 0-386 days). All 39 patients had limb involvement, and 82%-92% had bulbar involvement, dysarthria, dysphagia, and/or dyspnea.
The researchers estimate that 3.4%-6.7% of 1,146 ALS patients in Washington who died over the time period of the study sought a physician-assisted death. The 3.4% figure assumes that the 39 patients at the three hospitals make up all the ALS patients who received medication prescriptions. The 6.7% figure assumes that all patients with neurodegenerative disease who sought DWD in the state over that period had ALS.
“Similarly, 5% (92 of 1,795) of Oregon ALS patient who died sought medication under DWD between 1998 and 2014,” Dr. Wang said. “This is slightly increased compared to the percentage during the first decade, following enactment of the Oregon law (1998-2007), when 2.7% (26 of 962) of ALS patients died using DWD medication.”
Using Washington state data, researchers also estimated that 0.6% of 73,319 cancer patients and 0.2% of 298,178 people in the state who died of all causes sought DWD over the study period.
A total of 30 (77%) ALS patients who received the deadly prescriptions chose to take them, compared with 67% of all-cause patients who took advantage of the DWD law and 60% of cancer patients.
All 30 patients died. The nine who chose to not take the prescribed medication died after a median of 76 days. The patients who did not take the medication were more likely to be married (88% vs. 69%), to be college educated (100% vs. 74%), and to use a motorized wheelchair (78% vs. 31%).
Those who chose to not take the prescribed medication were also less motivated by loss of dignity (63% vs. 93% among those who took the medication) and by being a burden on others (25% vs. 66%). They were more likely to identify themselves as religious (80% vs. 35%).
Multiple factors may explain why ALS patients made different choices regarding the deadly drugs, lead study author Dr. Wang said in an interview. “We thought that the loss of communication may have played a role based on our finding, as most patients who followed through had more substantial trouble speaking,” he said. “For the patients who ultimately did not choose to take the medication, we found more of them had stronger religious beliefs than those who did not.”
As for pain, he reported that it was not a major issue. “Only about 10% of ALS patients were worried about pain, as opposed to 30% of the general Death with Dignity patients,” he said.
Dr. Ganzini noted that some patients who seek the prescribed drugs “want reassurance that, if their quality of life becomes unbearable, they have the option of physician-assisted death. But, they continue to cope and find reasons to live. As such, they ultimately die of their disease without taking the medications. Others lose the ability to ingest the medications, often because of sudden worsening of their disease.”
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
No specific funding was reported. Dr. Ganzini and Dr. Wang had no disclosures.
BOSTON – A new study estimates that 3.4%-6.7% of amyotrophic lateral sclerosis (ALS) patients in Washington state sought to commit physician-assisted suicide over a 5-year period.
The rate is many times higher than that among cancer patients in the state, researchers found. They also discovered that ALS patients were significantly more likely than were other terminally ill people to use the deadly medication after getting prescriptions for it.
The findings appear to reflect the unique hopelessness facing ALS patients. “They’re not afforded as much denial of decline and death as are patients with other terminal illnesses,” said Linda Ganzini, MD, MPH, a professor of psychiatry and medicine at Oregon Health & Science University, Portland, who has studied end of life in ALS patients.
“Many cancer patients, even in the final days of life, receive treatments that they hope will extend their lives,” she said in an interview after reviewing the study findings. “In contrast, treatments for ALS are minimally effective.”
Physician-assisted suicide is legal in California, Colorado, the District of Columbia, Montana, Oregon, Vermont, and Washington.
A team led by Leo H. Wang, MD, PhD, of the University of Washington, Seattle, examined the medical records of 39 ALS patients who sought medication to end their lives at three hospitals in Seattle from March 2009 to Dec. 31, 2014.
Washington’s Death with Dignity (DWD) law, which went into effect in 2009, allows physicians to prescribe lethal medication if the patient has a terminal illness and a prognosis of less than 6 months to live as judged by two physicians.
The researchers reported their findings, a follow-up to a previous study (Neurology. 2016 Nov 15;87[20]:2117-22), at the annual meeting of the American Academy of Neurology.
The median age of the ALS patients at symptom onset was 64 (range, 42-83), and a median of 712 days passed (range, 207-2,407) from the date of diagnosis to date of prescription for lethal medication.
The median time from prescription to death was 22 days, with at least one patient dying immediately (range, 0-386 days). All 39 patients had limb involvement, and 82%-92% had bulbar involvement, dysarthria, dysphagia, and/or dyspnea.
The researchers estimate that 3.4%-6.7% of 1,146 ALS patients in Washington who died over the time period of the study sought a physician-assisted death. The 3.4% figure assumes that the 39 patients at the three hospitals make up all the ALS patients who received medication prescriptions. The 6.7% figure assumes that all patients with neurodegenerative disease who sought DWD in the state over that period had ALS.
“Similarly, 5% (92 of 1,795) of Oregon ALS patient who died sought medication under DWD between 1998 and 2014,” Dr. Wang said. “This is slightly increased compared to the percentage during the first decade, following enactment of the Oregon law (1998-2007), when 2.7% (26 of 962) of ALS patients died using DWD medication.”
Using Washington state data, researchers also estimated that 0.6% of 73,319 cancer patients and 0.2% of 298,178 people in the state who died of all causes sought DWD over the study period.
A total of 30 (77%) ALS patients who received the deadly prescriptions chose to take them, compared with 67% of all-cause patients who took advantage of the DWD law and 60% of cancer patients.
All 30 patients died. The nine who chose to not take the prescribed medication died after a median of 76 days. The patients who did not take the medication were more likely to be married (88% vs. 69%), to be college educated (100% vs. 74%), and to use a motorized wheelchair (78% vs. 31%).
Those who chose to not take the prescribed medication were also less motivated by loss of dignity (63% vs. 93% among those who took the medication) and by being a burden on others (25% vs. 66%). They were more likely to identify themselves as religious (80% vs. 35%).
Multiple factors may explain why ALS patients made different choices regarding the deadly drugs, lead study author Dr. Wang said in an interview. “We thought that the loss of communication may have played a role based on our finding, as most patients who followed through had more substantial trouble speaking,” he said. “For the patients who ultimately did not choose to take the medication, we found more of them had stronger religious beliefs than those who did not.”
As for pain, he reported that it was not a major issue. “Only about 10% of ALS patients were worried about pain, as opposed to 30% of the general Death with Dignity patients,” he said.
Dr. Ganzini noted that some patients who seek the prescribed drugs “want reassurance that, if their quality of life becomes unbearable, they have the option of physician-assisted death. But, they continue to cope and find reasons to live. As such, they ultimately die of their disease without taking the medications. Others lose the ability to ingest the medications, often because of sudden worsening of their disease.”
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
No specific funding was reported. Dr. Ganzini and Dr. Wang had no disclosures.
At AAN 2017
Key clinical point:
Major finding: An estimated 3.4%-6.7% of ALS patients in Washington state sought physician-assisted death, and 77% took the prescribed deadly medication, a higher rate than all-cause (67%) and cancer patients (60%).
Data source: Analysis of 39 ALS patients who sought deadly medication from three Seattle hospitals from March 2009 to Dec. 31, 2014.
Disclosures: No specific funding was reported, and Dr. Wang had no disclosures.

Schizophrenia patients’ mortality is 14.5 years shorter
SAN DIEGO – A new systematic review and meta-analysis, the first of its kind, suggests that most people with schizophrenia – especially men – do not survive past their 60s.
According to findings released at the 2017 International Congress on Schizophrenia Research, schizophrenia patients appear to die a weighted average of 14.5 years earlier than the rest of the population (95% confidence interval, 11.2-17.8).
The weighted average life expectancy for schizophrenia patients was 64.7 years (95% CI, 61.1-71.3) – 59.9 years for men (95% CI, 55.5-64.3) and 67.6 years for women (95% CI, 63.1-72.1).
“There were no indications that this is improving over time,” lead author Carsten Hjorthøj, PhD, senior researcher at the University of Copenhagen, said in an interview.
The researchers launched their paper in order to provide a wider perspective on lives lost in schizophrenia.
Previous studies had used measures like the standardized mortality ratio, which compared schizophrenia patients with a matched group from the general population, Dr. Hjorthøj said. “Saying that people with schizophrenia are, for instance, 2.5 times more likely to die at any given age may be a little difficult to understand. Identifying the actual number of years they die earlier than the rest of the population is easily understood and will probably also make the issue more obvious to policymakers.”
The researchers, whose findings were previously published in Lancet Psychiatry (2017 Apr;4[4]:295-301), examined 11 studies, mostly from Europe (n = 5) and North America (n = 3) with single studies from Africa, Asia, and Australia. (The lowest life expectancies were reported in Asia and Africa.)
One study was published in 1991, and the rest from 2001-2016. Together, the studies tracked 302,691 patients with schizophrenia.
What explains the gap between the life expectancies in men and women? “We did not investigate the reasons for this,” Dr. Hjorthøj said, “but men typically have worse adherence to treatment than women, and men typically also have poorer health-seeking behavior than women even in the general population. Given that schizophrenia is associated with a multitude of adverse somatic outcomes, this could then be aggravated by this difference in health-seeking behavior.”
In addition, he said, “It could also be the case that use of alcohol, tobacco, and illicit substances is even more skewed in schizophrenia than in the general population. Finally, it could also be attributed in part to the fact that men are more likely than women to die from suicide.”
Dr. Hjorthøj said that the findings emphasize the importance of treating physical symptoms in people with schizophrenia.
“I am aware of several cases where physical complaints were not taken seriously because they were raised by people who were known to suffer from delusions,” he said. “But, I do believe that most psychiatrists are aware of this, and the problem is perhaps more that the system in general is underfunded and that somatic and psychiatric hospitals are not good enough at communicating with each other.”
The researchers report no funding and no disclosures.
SAN DIEGO – A new systematic review and meta-analysis, the first of its kind, suggests that most people with schizophrenia – especially men – do not survive past their 60s.
According to findings released at the 2017 International Congress on Schizophrenia Research, schizophrenia patients appear to die a weighted average of 14.5 years earlier than the rest of the population (95% confidence interval, 11.2-17.8).
The weighted average life expectancy for schizophrenia patients was 64.7 years (95% CI, 61.1-71.3) – 59.9 years for men (95% CI, 55.5-64.3) and 67.6 years for women (95% CI, 63.1-72.1).
“There were no indications that this is improving over time,” lead author Carsten Hjorthøj, PhD, senior researcher at the University of Copenhagen, said in an interview.
The researchers launched their paper in order to provide a wider perspective on lives lost in schizophrenia.
Previous studies had used measures like the standardized mortality ratio, which compared schizophrenia patients with a matched group from the general population, Dr. Hjorthøj said. “Saying that people with schizophrenia are, for instance, 2.5 times more likely to die at any given age may be a little difficult to understand. Identifying the actual number of years they die earlier than the rest of the population is easily understood and will probably also make the issue more obvious to policymakers.”
The researchers, whose findings were previously published in Lancet Psychiatry (2017 Apr;4[4]:295-301), examined 11 studies, mostly from Europe (n = 5) and North America (n = 3) with single studies from Africa, Asia, and Australia. (The lowest life expectancies were reported in Asia and Africa.)
One study was published in 1991, and the rest from 2001-2016. Together, the studies tracked 302,691 patients with schizophrenia.
What explains the gap between the life expectancies in men and women? “We did not investigate the reasons for this,” Dr. Hjorthøj said, “but men typically have worse adherence to treatment than women, and men typically also have poorer health-seeking behavior than women even in the general population. Given that schizophrenia is associated with a multitude of adverse somatic outcomes, this could then be aggravated by this difference in health-seeking behavior.”
In addition, he said, “It could also be the case that use of alcohol, tobacco, and illicit substances is even more skewed in schizophrenia than in the general population. Finally, it could also be attributed in part to the fact that men are more likely than women to die from suicide.”
Dr. Hjorthøj said that the findings emphasize the importance of treating physical symptoms in people with schizophrenia.
“I am aware of several cases where physical complaints were not taken seriously because they were raised by people who were known to suffer from delusions,” he said. “But, I do believe that most psychiatrists are aware of this, and the problem is perhaps more that the system in general is underfunded and that somatic and psychiatric hospitals are not good enough at communicating with each other.”
The researchers report no funding and no disclosures.
SAN DIEGO – A new systematic review and meta-analysis, the first of its kind, suggests that most people with schizophrenia – especially men – do not survive past their 60s.
According to findings released at the 2017 International Congress on Schizophrenia Research, schizophrenia patients appear to die a weighted average of 14.5 years earlier than the rest of the population (95% confidence interval, 11.2-17.8).
The weighted average life expectancy for schizophrenia patients was 64.7 years (95% CI, 61.1-71.3) – 59.9 years for men (95% CI, 55.5-64.3) and 67.6 years for women (95% CI, 63.1-72.1).
“There were no indications that this is improving over time,” lead author Carsten Hjorthøj, PhD, senior researcher at the University of Copenhagen, said in an interview.
The researchers launched their paper in order to provide a wider perspective on lives lost in schizophrenia.
Previous studies had used measures like the standardized mortality ratio, which compared schizophrenia patients with a matched group from the general population, Dr. Hjorthøj said. “Saying that people with schizophrenia are, for instance, 2.5 times more likely to die at any given age may be a little difficult to understand. Identifying the actual number of years they die earlier than the rest of the population is easily understood and will probably also make the issue more obvious to policymakers.”
The researchers, whose findings were previously published in Lancet Psychiatry (2017 Apr;4[4]:295-301), examined 11 studies, mostly from Europe (n = 5) and North America (n = 3) with single studies from Africa, Asia, and Australia. (The lowest life expectancies were reported in Asia and Africa.)
One study was published in 1991, and the rest from 2001-2016. Together, the studies tracked 302,691 patients with schizophrenia.
What explains the gap between the life expectancies in men and women? “We did not investigate the reasons for this,” Dr. Hjorthøj said, “but men typically have worse adherence to treatment than women, and men typically also have poorer health-seeking behavior than women even in the general population. Given that schizophrenia is associated with a multitude of adverse somatic outcomes, this could then be aggravated by this difference in health-seeking behavior.”
In addition, he said, “It could also be the case that use of alcohol, tobacco, and illicit substances is even more skewed in schizophrenia than in the general population. Finally, it could also be attributed in part to the fact that men are more likely than women to die from suicide.”
Dr. Hjorthøj said that the findings emphasize the importance of treating physical symptoms in people with schizophrenia.
“I am aware of several cases where physical complaints were not taken seriously because they were raised by people who were known to suffer from delusions,” he said. “But, I do believe that most psychiatrists are aware of this, and the problem is perhaps more that the system in general is underfunded and that somatic and psychiatric hospitals are not good enough at communicating with each other.”
The researchers report no funding and no disclosures.
At the ICSR Biennial Meeting
Key clinical point:
Major finding: Schizophrenia patients die a weighted average of 14.5 years earlier than those in the general population (95% CI, 11.2-17.8), and their weighted average life expectancy is 64.7 years (95% CI, 61-71.3) – 59.9 for men (95% CI, 55.5-64.3) and 67.6 for women (95% CI, 63.1-72.1).
Data source: Review and meta-analysis of 11 studies of 302,691 schizophrenia patients.
Disclosures: No specific funding was reported, and the authors reported no disclosures.
Kids with MS face higher risk of mental disorders
BOSTON – Children with multiple sclerosis (MS) and related conditions are as much as 10 times more likely than the general population to need to be hospitalized for various psychiatric conditions, a study showed.
“The true prevalence of morbidity is almost certainly higher than suggested by our data,” said study lead author Julia Pakpoor, BM BCh, who presented data from her research at the annual meeting of the American Academy of Neurology.
While several studies have examined links between MS and mental illness in adults, there’s been little research into the topic in children. The number of children with the disease is far from tiny, however. According to the National MS Society, an estimated 8,000-10,000 children have the condition in the United States.
The researchers tracked future psychiatric visits by these patients and compared them with a reference cohort of more than 1.1 million children.
The risks of mental conditions in children with MS, compared with the reference cohort, were as follows: psychotic disorders (relative risk [RR] = 10.76; 95% confidence interval [CI], 2.93-27.63; P less than .001), mood disorders (RR = 2.57; 95% CI, 1.03-5.31; P = .022), and intellectual disability (RR = 6.08; 95% CI, 1.25-17.80; P = .004).
The children with other CNS demyelinating diseases also had higher risk levels, compared with the reference cohort: psychotic disorders (RR = 5.77; 95% CI, 2.48-11.41; P less than .001), anxiety, stress-related, and somatoform disorders that cause symptoms like pain (RR = 2.38; 95% CI, 1.39-3.81; P less than .001); intellectual disability (RR = 6.56; 95% CI, 3.66-10.84; P less than .001), and other behavioral disorders (RR = 8.99; 95% CI, 5.13-14.62; P less than .001).
The researchers also reported evidence of a reverse trend. Children with several mental conditions had greater risk than did the reference cohort to go on to develop CNS demyelinating diseases, specifically anxiety, stress-related, and somatoform disorders (RR = 3.15; 95% CI, 1.70-5.39; P less than .001), ADHD (RR = 3.88; 95% CI, 1.75-7.48; P less than .001), autism (RR = 3.80; 95% CI, 2.05-6.50; P less than .001), intellectual disability (RR = 6.33; 95% CI, 2.86-12.21; P less than .001), and other behavioral disorders (RR = 8.30; 95% CI, 5.17-12.75; P less than .001).
“We detected strong associations, and further associations likely exist,” Dr. Pakpoor said.
She acknowledged that the research is limited because it includes information only about patients admitted to a hospital. “There may be many more with psychiatric conditions that are mild,” she said. “We’re probably detecting cases that are more severe.”
In an interview, Flavia M. Nelson, MD, interim chief of the multiple sclerosis division at the University of Texas Health Science Center at Houston, said she often sees psychiatric conditions in her pediatric patients.
Conditions such as depression and anxiety disorders are common, she said, and the pediatric patients often suffer from isolation. “There’s a lot of fear about what this will do to their lives,” she said. Some patients have even refused to go to college because they fear that “they’ll have a disabling attack and everyone will know.”
As for the link between psychiatric illness and MS, Dr. Nelson said the disorders may develop because stress, fear, and anxiety push young people to their limits. “I had one patient who developed tics and rage,” she said. “That was his way of coping with the disease.”
Dr. Nelson suggested doing cognitive testing on young patients and referring them to counseling, especially in light of the fact that teens often put up walls when they don’t know how to express their feelings. Simply asking questions may not be enough to draw them out, she said, so professional counseling can be helpful.
No specific funding was reported. Dr. Pakpoor reported no relevant disclosures. Dr. Nelson has received personal compensation for activities with Bayer, Sanofi-Genzyme, Genentech, Novartis, Teva, and the Consortium of Multiple Sclerosis Centers. She has received research support from the National Institutes of Health, the National MS Society, and Novartis.
BOSTON – Children with multiple sclerosis (MS) and related conditions are as much as 10 times more likely than the general population to need to be hospitalized for various psychiatric conditions, a study showed.
“The true prevalence of morbidity is almost certainly higher than suggested by our data,” said study lead author Julia Pakpoor, BM BCh, who presented data from her research at the annual meeting of the American Academy of Neurology.
While several studies have examined links between MS and mental illness in adults, there’s been little research into the topic in children. The number of children with the disease is far from tiny, however. According to the National MS Society, an estimated 8,000-10,000 children have the condition in the United States.
The researchers tracked future psychiatric visits by these patients and compared them with a reference cohort of more than 1.1 million children.
The risks of mental conditions in children with MS, compared with the reference cohort, were as follows: psychotic disorders (relative risk [RR] = 10.76; 95% confidence interval [CI], 2.93-27.63; P less than .001), mood disorders (RR = 2.57; 95% CI, 1.03-5.31; P = .022), and intellectual disability (RR = 6.08; 95% CI, 1.25-17.80; P = .004).
The children with other CNS demyelinating diseases also had higher risk levels, compared with the reference cohort: psychotic disorders (RR = 5.77; 95% CI, 2.48-11.41; P less than .001), anxiety, stress-related, and somatoform disorders that cause symptoms like pain (RR = 2.38; 95% CI, 1.39-3.81; P less than .001); intellectual disability (RR = 6.56; 95% CI, 3.66-10.84; P less than .001), and other behavioral disorders (RR = 8.99; 95% CI, 5.13-14.62; P less than .001).
The researchers also reported evidence of a reverse trend. Children with several mental conditions had greater risk than did the reference cohort to go on to develop CNS demyelinating diseases, specifically anxiety, stress-related, and somatoform disorders (RR = 3.15; 95% CI, 1.70-5.39; P less than .001), ADHD (RR = 3.88; 95% CI, 1.75-7.48; P less than .001), autism (RR = 3.80; 95% CI, 2.05-6.50; P less than .001), intellectual disability (RR = 6.33; 95% CI, 2.86-12.21; P less than .001), and other behavioral disorders (RR = 8.30; 95% CI, 5.17-12.75; P less than .001).
“We detected strong associations, and further associations likely exist,” Dr. Pakpoor said.
She acknowledged that the research is limited because it includes information only about patients admitted to a hospital. “There may be many more with psychiatric conditions that are mild,” she said. “We’re probably detecting cases that are more severe.”
In an interview, Flavia M. Nelson, MD, interim chief of the multiple sclerosis division at the University of Texas Health Science Center at Houston, said she often sees psychiatric conditions in her pediatric patients.
Conditions such as depression and anxiety disorders are common, she said, and the pediatric patients often suffer from isolation. “There’s a lot of fear about what this will do to their lives,” she said. Some patients have even refused to go to college because they fear that “they’ll have a disabling attack and everyone will know.”
As for the link between psychiatric illness and MS, Dr. Nelson said the disorders may develop because stress, fear, and anxiety push young people to their limits. “I had one patient who developed tics and rage,” she said. “That was his way of coping with the disease.”
Dr. Nelson suggested doing cognitive testing on young patients and referring them to counseling, especially in light of the fact that teens often put up walls when they don’t know how to express their feelings. Simply asking questions may not be enough to draw them out, she said, so professional counseling can be helpful.
No specific funding was reported. Dr. Pakpoor reported no relevant disclosures. Dr. Nelson has received personal compensation for activities with Bayer, Sanofi-Genzyme, Genentech, Novartis, Teva, and the Consortium of Multiple Sclerosis Centers. She has received research support from the National Institutes of Health, the National MS Society, and Novartis.
BOSTON – Children with multiple sclerosis (MS) and related conditions are as much as 10 times more likely than the general population to need to be hospitalized for various psychiatric conditions, a study showed.
“The true prevalence of morbidity is almost certainly higher than suggested by our data,” said study lead author Julia Pakpoor, BM BCh, who presented data from her research at the annual meeting of the American Academy of Neurology.
While several studies have examined links between MS and mental illness in adults, there’s been little research into the topic in children. The number of children with the disease is far from tiny, however. According to the National MS Society, an estimated 8,000-10,000 children have the condition in the United States.
The researchers tracked future psychiatric visits by these patients and compared them with a reference cohort of more than 1.1 million children.
The risks of mental conditions in children with MS, compared with the reference cohort, were as follows: psychotic disorders (relative risk [RR] = 10.76; 95% confidence interval [CI], 2.93-27.63; P less than .001), mood disorders (RR = 2.57; 95% CI, 1.03-5.31; P = .022), and intellectual disability (RR = 6.08; 95% CI, 1.25-17.80; P = .004).
The children with other CNS demyelinating diseases also had higher risk levels, compared with the reference cohort: psychotic disorders (RR = 5.77; 95% CI, 2.48-11.41; P less than .001), anxiety, stress-related, and somatoform disorders that cause symptoms like pain (RR = 2.38; 95% CI, 1.39-3.81; P less than .001); intellectual disability (RR = 6.56; 95% CI, 3.66-10.84; P less than .001), and other behavioral disorders (RR = 8.99; 95% CI, 5.13-14.62; P less than .001).
The researchers also reported evidence of a reverse trend. Children with several mental conditions had greater risk than did the reference cohort to go on to develop CNS demyelinating diseases, specifically anxiety, stress-related, and somatoform disorders (RR = 3.15; 95% CI, 1.70-5.39; P less than .001), ADHD (RR = 3.88; 95% CI, 1.75-7.48; P less than .001), autism (RR = 3.80; 95% CI, 2.05-6.50; P less than .001), intellectual disability (RR = 6.33; 95% CI, 2.86-12.21; P less than .001), and other behavioral disorders (RR = 8.30; 95% CI, 5.17-12.75; P less than .001).
“We detected strong associations, and further associations likely exist,” Dr. Pakpoor said.
She acknowledged that the research is limited because it includes information only about patients admitted to a hospital. “There may be many more with psychiatric conditions that are mild,” she said. “We’re probably detecting cases that are more severe.”
In an interview, Flavia M. Nelson, MD, interim chief of the multiple sclerosis division at the University of Texas Health Science Center at Houston, said she often sees psychiatric conditions in her pediatric patients.
Conditions such as depression and anxiety disorders are common, she said, and the pediatric patients often suffer from isolation. “There’s a lot of fear about what this will do to their lives,” she said. Some patients have even refused to go to college because they fear that “they’ll have a disabling attack and everyone will know.”
As for the link between psychiatric illness and MS, Dr. Nelson said the disorders may develop because stress, fear, and anxiety push young people to their limits. “I had one patient who developed tics and rage,” she said. “That was his way of coping with the disease.”
Dr. Nelson suggested doing cognitive testing on young patients and referring them to counseling, especially in light of the fact that teens often put up walls when they don’t know how to express their feelings. Simply asking questions may not be enough to draw them out, she said, so professional counseling can be helpful.
No specific funding was reported. Dr. Pakpoor reported no relevant disclosures. Dr. Nelson has received personal compensation for activities with Bayer, Sanofi-Genzyme, Genentech, Novartis, Teva, and the Consortium of Multiple Sclerosis Centers. She has received research support from the National Institutes of Health, the National MS Society, and Novartis.
Key clinical point: Children with MS and similar conditions are at higher risk of a long list of psychiatric disorders.
Major finding:
Data source: An analysis of children admitted to hospitals in England from 1999 to 2011 with MS (n = 201) and other CNS demyelinating diseases (n = 1,097) plus a reference cohort of more than 1.1 million.
Disclosures: No specific funding or disclosures were reported.
Study reveals crazy quilt of laser laws across the United States
SAN DIEGO – Laser hair removal isn’t typically in an office cleaner’s job description. So it’s no wonder that Virginia legislators were spooked when they heard from a constituent who was treated by a spa worker who turned out to be a janitor.
Earlier this year, legislators in the Old Dominion passed a bill limiting laser hair removal procedures to a “properly trained” medical doctor, physician assistant, or nurse practitioner – or a “properly trained” person who is supervised by one of these professionals. Therefore, it’s still possible for a “properly trained” person without a degree of any kind to operate a laser in Virginia.
To the north in New Jersey, the rules are much stricter: Only physicians can perform laser procedures. But in New York, it appears that anyone can fire up a laser and go to work on unwanted hair. And in Florida, nonphysicians can perform laser procedures only if they’re physician assistants or nurse practitioners. But they’re only allowed to remove hair with lasers at a clinic that just performs laser hair removal.
Such is the chaotic state of laser law in the United States, a new study finds. The rules, which vary widely from state to state, are often vague and confusing. And, as Virginia’s new law shows, they’re still evolving. (The study is current as of March 2016.)

She and study coauthor Mathew M. Avram, MD, JD, director of the Laser and Cosmetic Center at Massachusetts General, analyzed regulations in the 50 states regarding the operation of lasers. They reported their findings at the annual meeting of the American Society for Laser Medicine and Surgery.
Dr. DiGiorgio said that laser operator laws address three issues:
1. Who can operate a laser?
At other clinics across the country, nonphysician employees — such as nurse practitioners and registered nurses – often operate lasers. Whether they can legally actually do so isn’t always obvious.
New Jersey is the only state that requires laser operators to be physicians. At the other extreme, 11 states, including Massachusetts, Colorado, Florida, Missouri, New York, and Pennsylvania, have “no” limits on who can perform laser procedures. (At Massachusetts General Hospital, physicians perform all laser procedures.)
So does that mean anyone can perform a laser procedure? It’s not clear. “The laws are a lot more vague than they should be,” Dr. DiGiorgio said in an interview.
Eighteen states allow people to perform laser procedures as part of the “practice of medicine,” although legislation can be vague on what that means. Those states include Illinois, Michigan, Minnesota, North Carolina, and Texas.
Another 19 states, including California, Ohio, Washington, Wisconsin, and now Virginia, have specific limits on who can perform laser procedures. In California, for example, physician assistants and registered nurses – but not licensed vocational nurses – are allowed to use lasers to remove hair, spider veins, and tattoos. Unlicensed medical assistants, cosmetologists, electrologists, and estheticians are not allowed to perform the procedures
2. Can someone delegate laser procedures to someone else?
In nine states, including Iowa and New Hampshire, there’s no oversight of delegation or nonphysicians can delegate procedures to someone else.
In another nine states, certain procedures can be delegated with no physician oversight, such as laser hair removal in Alaska and ablative procedures (to advanced practice registered nurses only) in Utah.
3. Is supervision required of nonphysicians?
Physicians don’t need to supervise certain laser procedures in 11 states, including Hawaii, Oregon, and Vermont, where they can be performed by a nonphysician with no supervision or under supervision by a non-physician.
In 17 states, supervision isn’t always required or it’s under the discretion of the supervising physician. These states include California, Michigan, Pennsylvania, and Wisconsin.
In 11 states, including Illinois and Massachusetts, only certain procedures require on-site supervision. Six states, including Connecticut and Maryland, require on-site physician supervision for all laser procedures, but Dr. DiGiorgio said the requirements can be vague about what “on site” actually means.
Idaho requires the physician to be on site or immediately available, and South Carolina allows registered nurses to perform laser hair and leg vein removal if a physician is on site and can respond within 5 minutes.
“We don’t know what the ideal regulation is,” Dr. DiGiorgio said. But she believes laser regulations are crucial to safety, especially as fields such as plastic surgery, ophthalmology, and gynecology embrace cosmetic laser procedures.
Information about state-by-state laser operator laws is available on the American Med Spa Association website.
Dr. DiGiorgio reported no relevant disclosures.
SAN DIEGO – Laser hair removal isn’t typically in an office cleaner’s job description. So it’s no wonder that Virginia legislators were spooked when they heard from a constituent who was treated by a spa worker who turned out to be a janitor.
Earlier this year, legislators in the Old Dominion passed a bill limiting laser hair removal procedures to a “properly trained” medical doctor, physician assistant, or nurse practitioner – or a “properly trained” person who is supervised by one of these professionals. Therefore, it’s still possible for a “properly trained” person without a degree of any kind to operate a laser in Virginia.
To the north in New Jersey, the rules are much stricter: Only physicians can perform laser procedures. But in New York, it appears that anyone can fire up a laser and go to work on unwanted hair. And in Florida, nonphysicians can perform laser procedures only if they’re physician assistants or nurse practitioners. But they’re only allowed to remove hair with lasers at a clinic that just performs laser hair removal.
Such is the chaotic state of laser law in the United States, a new study finds. The rules, which vary widely from state to state, are often vague and confusing. And, as Virginia’s new law shows, they’re still evolving. (The study is current as of March 2016.)
She and study coauthor Mathew M. Avram, MD, JD, director of the Laser and Cosmetic Center at Massachusetts General, analyzed regulations in the 50 states regarding the operation of lasers. They reported their findings at the annual meeting of the American Society for Laser Medicine and Surgery.
Dr. DiGiorgio said that laser operator laws address three issues:
1. Who can operate a laser?
At other clinics across the country, nonphysician employees — such as nurse practitioners and registered nurses – often operate lasers. Whether they can legally actually do so isn’t always obvious.
New Jersey is the only state that requires laser operators to be physicians. At the other extreme, 11 states, including Massachusetts, Colorado, Florida, Missouri, New York, and Pennsylvania, have “no” limits on who can perform laser procedures. (At Massachusetts General Hospital, physicians perform all laser procedures.)
So does that mean anyone can perform a laser procedure? It’s not clear. “The laws are a lot more vague than they should be,” Dr. DiGiorgio said in an interview.
Eighteen states allow people to perform laser procedures as part of the “practice of medicine,” although legislation can be vague on what that means. Those states include Illinois, Michigan, Minnesota, North Carolina, and Texas.
Another 19 states, including California, Ohio, Washington, Wisconsin, and now Virginia, have specific limits on who can perform laser procedures. In California, for example, physician assistants and registered nurses – but not licensed vocational nurses – are allowed to use lasers to remove hair, spider veins, and tattoos. Unlicensed medical assistants, cosmetologists, electrologists, and estheticians are not allowed to perform the procedures
2. Can someone delegate laser procedures to someone else?
In nine states, including Iowa and New Hampshire, there’s no oversight of delegation or nonphysicians can delegate procedures to someone else.
In another nine states, certain procedures can be delegated with no physician oversight, such as laser hair removal in Alaska and ablative procedures (to advanced practice registered nurses only) in Utah.
3. Is supervision required of nonphysicians?
Physicians don’t need to supervise certain laser procedures in 11 states, including Hawaii, Oregon, and Vermont, where they can be performed by a nonphysician with no supervision or under supervision by a non-physician.
In 17 states, supervision isn’t always required or it’s under the discretion of the supervising physician. These states include California, Michigan, Pennsylvania, and Wisconsin.
In 11 states, including Illinois and Massachusetts, only certain procedures require on-site supervision. Six states, including Connecticut and Maryland, require on-site physician supervision for all laser procedures, but Dr. DiGiorgio said the requirements can be vague about what “on site” actually means.
Idaho requires the physician to be on site or immediately available, and South Carolina allows registered nurses to perform laser hair and leg vein removal if a physician is on site and can respond within 5 minutes.
“We don’t know what the ideal regulation is,” Dr. DiGiorgio said. But she believes laser regulations are crucial to safety, especially as fields such as plastic surgery, ophthalmology, and gynecology embrace cosmetic laser procedures.
Information about state-by-state laser operator laws is available on the American Med Spa Association website.
Dr. DiGiorgio reported no relevant disclosures.
SAN DIEGO – Laser hair removal isn’t typically in an office cleaner’s job description. So it’s no wonder that Virginia legislators were spooked when they heard from a constituent who was treated by a spa worker who turned out to be a janitor.
Earlier this year, legislators in the Old Dominion passed a bill limiting laser hair removal procedures to a “properly trained” medical doctor, physician assistant, or nurse practitioner – or a “properly trained” person who is supervised by one of these professionals. Therefore, it’s still possible for a “properly trained” person without a degree of any kind to operate a laser in Virginia.
To the north in New Jersey, the rules are much stricter: Only physicians can perform laser procedures. But in New York, it appears that anyone can fire up a laser and go to work on unwanted hair. And in Florida, nonphysicians can perform laser procedures only if they’re physician assistants or nurse practitioners. But they’re only allowed to remove hair with lasers at a clinic that just performs laser hair removal.
Such is the chaotic state of laser law in the United States, a new study finds. The rules, which vary widely from state to state, are often vague and confusing. And, as Virginia’s new law shows, they’re still evolving. (The study is current as of March 2016.)
She and study coauthor Mathew M. Avram, MD, JD, director of the Laser and Cosmetic Center at Massachusetts General, analyzed regulations in the 50 states regarding the operation of lasers. They reported their findings at the annual meeting of the American Society for Laser Medicine and Surgery.
Dr. DiGiorgio said that laser operator laws address three issues:
1. Who can operate a laser?
At other clinics across the country, nonphysician employees — such as nurse practitioners and registered nurses – often operate lasers. Whether they can legally actually do so isn’t always obvious.
New Jersey is the only state that requires laser operators to be physicians. At the other extreme, 11 states, including Massachusetts, Colorado, Florida, Missouri, New York, and Pennsylvania, have “no” limits on who can perform laser procedures. (At Massachusetts General Hospital, physicians perform all laser procedures.)
So does that mean anyone can perform a laser procedure? It’s not clear. “The laws are a lot more vague than they should be,” Dr. DiGiorgio said in an interview.
Eighteen states allow people to perform laser procedures as part of the “practice of medicine,” although legislation can be vague on what that means. Those states include Illinois, Michigan, Minnesota, North Carolina, and Texas.
Another 19 states, including California, Ohio, Washington, Wisconsin, and now Virginia, have specific limits on who can perform laser procedures. In California, for example, physician assistants and registered nurses – but not licensed vocational nurses – are allowed to use lasers to remove hair, spider veins, and tattoos. Unlicensed medical assistants, cosmetologists, electrologists, and estheticians are not allowed to perform the procedures
2. Can someone delegate laser procedures to someone else?
In nine states, including Iowa and New Hampshire, there’s no oversight of delegation or nonphysicians can delegate procedures to someone else.
In another nine states, certain procedures can be delegated with no physician oversight, such as laser hair removal in Alaska and ablative procedures (to advanced practice registered nurses only) in Utah.
3. Is supervision required of nonphysicians?
Physicians don’t need to supervise certain laser procedures in 11 states, including Hawaii, Oregon, and Vermont, where they can be performed by a nonphysician with no supervision or under supervision by a non-physician.
In 17 states, supervision isn’t always required or it’s under the discretion of the supervising physician. These states include California, Michigan, Pennsylvania, and Wisconsin.
In 11 states, including Illinois and Massachusetts, only certain procedures require on-site supervision. Six states, including Connecticut and Maryland, require on-site physician supervision for all laser procedures, but Dr. DiGiorgio said the requirements can be vague about what “on site” actually means.
Idaho requires the physician to be on site or immediately available, and South Carolina allows registered nurses to perform laser hair and leg vein removal if a physician is on site and can respond within 5 minutes.
“We don’t know what the ideal regulation is,” Dr. DiGiorgio said. But she believes laser regulations are crucial to safety, especially as fields such as plastic surgery, ophthalmology, and gynecology embrace cosmetic laser procedures.
Information about state-by-state laser operator laws is available on the American Med Spa Association website.
Dr. DiGiorgio reported no relevant disclosures.
AT LASER 2017
Key clinical point:
Major finding: The study found wide variations in who can operate lasers, and in regulations regarding the delegation and supervision of laser treatments in the different states.
Data source: Analysis of regulations in the 50 states regarding the operation of lasers.
Disclosures: Dr. DiGiorgio reported no relevant disclosures
Hospital infections top WHO’s list of priority pathogens
The World Health Organization is urging governments to focus antibiotic research efforts on a list of urgent bacterial threats, topped by several increasingly powerful superbugs that cause hospital-based infections and other potentially deadly conditions.
The WHO listed the top 20 bacteria that it believes are most harmful to human health, other than mycobacteria such as Mycobacterium tuberculosis, which causes tuberculosis. The germ was not included in the list because it’s generally accepted to be the most urgent priority for new antibiotic research and development, Marie-Paule Kieny, PhD, a WHO assistant director, said at a press conference.
The priority list is needed because the antibiotic pipeline is “practically dry,” thanks to scientific research challenges and a lack of financial incentives, according to Dr. Kieny. “Antibiotics are generally used for the short term, unlike therapies for chronic diseases, which bring in much higher returns on investment,” she said. The list “is intended to signal to the scientific community and the pharmaceutical industry the areas they should focus on to address urgent public health threats.”
The WHO list begins with Priority 1/“Critical” pathogens that it believes most urgently need to be targeted through antibiotic research and development: Acinetobacter baumannii, carbapenem-resistant; Pseudomonas aeruginosa, carbapenem-resistant; and Enterobacteriaceae (including Klebsiella pneumonia, Escherichia coli, Enterobacter spp., Serratia spp., Proteus spp., Providencia spp., and Morganella spp.), carbapenem-resistant, extended-spectrum beta-lactamase–producing.
“These bacteria are responsible for severe infections and high mortality rates, mostly in hospitalized patients, transplant recipients, those receiving chemotherapy, or patients in intensive care units,” Dr. Kieny said. “While these bacteria are not widespread and do not generally affect healthy individuals, the burden for patients and society is now alarming – and new, effective therapies are imperative.”
Priority 2/”High” pathogens are Enterococcus faecium, vancomycin-resistant; Staphylococcus aureus, methicillin-resistant, vancomycin intermediate and resistant; Helicobacter pylori, clarithromycin-resistant; Campylobacter, fluoroquinolone-resistant; Salmonella spp., fluoroquinolone-resistant; Neisseria gonorrhoeae, third-generation cephalosporin-resistant and fluoroquinolone-resistant.
Pathogens in this category can infect healthy individuals, Dr. Kieny noted. “These infections, although not associated with significant mortality, have a dramatic health and economic impact on communities and, in particular, in low-income countries.”
Priority 3/”Medium” pathogens are Streptococcus pneumoniae, penicillin–non-susceptible; Haemophilus influenzae, ampicillin-resistant; and Shigella spp., fluoroquinolone-resistant.
These pathogens “represent a threat because of increasing resistance but still have some effective antibiotic options available,” Dr. Kieny said.
According to a statement provided by the WHO, the priority list doesn’t include streptococcus A and B or chlamydia, because resistance hasn’t reached the level of a public health threat.
One goal of the list is to focus attention on the development of small-market, gram-negative drugs that combat hospital-based infections, explained Nicola Magrini, MD, a WHO scientist who also spoke at the press conference.
Over the last decade, he said, the pipeline has instead focused more on gram-positive agents – mostly linked to beta-lactamase – that have wider market potential and generate less resistance.
“From a clinical point of view, these multidrug-resistant gram-negative clinical trials are very difficult and expensive to do, more than for gram-positive,” noted Evelina Tacconelli, MD, PhD, a contributor to the WHO report. “Because when we talk about gram-negative, we need to cover multiple pathogens and not just one or two, as in the case of gram-positive.”
Dr. Magrini said he couldn’t provide estimates about how many people worldwide are affected by the listed pathogens. However, he said a full report with numbers will be released by June.
It does appear that patients with severe infection from antibiotic-resistant germs face a mortality rate of up to 60%, while extended-spectrum beta-lactamase–positive E. coli accounts for up to 70% of urinary tract infections in many countries, explained Dr. Tacconelli, head of the division of infectious diseases at the University of Tübingen, Germany.
“Even if we don’t know exactly how many,” she said, “we are talking about millions of people affected.”
The World Health Organization is urging governments to focus antibiotic research efforts on a list of urgent bacterial threats, topped by several increasingly powerful superbugs that cause hospital-based infections and other potentially deadly conditions.
The WHO listed the top 20 bacteria that it believes are most harmful to human health, other than mycobacteria such as Mycobacterium tuberculosis, which causes tuberculosis. The germ was not included in the list because it’s generally accepted to be the most urgent priority for new antibiotic research and development, Marie-Paule Kieny, PhD, a WHO assistant director, said at a press conference.
The priority list is needed because the antibiotic pipeline is “practically dry,” thanks to scientific research challenges and a lack of financial incentives, according to Dr. Kieny. “Antibiotics are generally used for the short term, unlike therapies for chronic diseases, which bring in much higher returns on investment,” she said. The list “is intended to signal to the scientific community and the pharmaceutical industry the areas they should focus on to address urgent public health threats.”
The WHO list begins with Priority 1/“Critical” pathogens that it believes most urgently need to be targeted through antibiotic research and development: Acinetobacter baumannii, carbapenem-resistant; Pseudomonas aeruginosa, carbapenem-resistant; and Enterobacteriaceae (including Klebsiella pneumonia, Escherichia coli, Enterobacter spp., Serratia spp., Proteus spp., Providencia spp., and Morganella spp.), carbapenem-resistant, extended-spectrum beta-lactamase–producing.
“These bacteria are responsible for severe infections and high mortality rates, mostly in hospitalized patients, transplant recipients, those receiving chemotherapy, or patients in intensive care units,” Dr. Kieny said. “While these bacteria are not widespread and do not generally affect healthy individuals, the burden for patients and society is now alarming – and new, effective therapies are imperative.”
Priority 2/”High” pathogens are Enterococcus faecium, vancomycin-resistant; Staphylococcus aureus, methicillin-resistant, vancomycin intermediate and resistant; Helicobacter pylori, clarithromycin-resistant; Campylobacter, fluoroquinolone-resistant; Salmonella spp., fluoroquinolone-resistant; Neisseria gonorrhoeae, third-generation cephalosporin-resistant and fluoroquinolone-resistant.
Pathogens in this category can infect healthy individuals, Dr. Kieny noted. “These infections, although not associated with significant mortality, have a dramatic health and economic impact on communities and, in particular, in low-income countries.”
Priority 3/”Medium” pathogens are Streptococcus pneumoniae, penicillin–non-susceptible; Haemophilus influenzae, ampicillin-resistant; and Shigella spp., fluoroquinolone-resistant.
These pathogens “represent a threat because of increasing resistance but still have some effective antibiotic options available,” Dr. Kieny said.
According to a statement provided by the WHO, the priority list doesn’t include streptococcus A and B or chlamydia, because resistance hasn’t reached the level of a public health threat.
One goal of the list is to focus attention on the development of small-market, gram-negative drugs that combat hospital-based infections, explained Nicola Magrini, MD, a WHO scientist who also spoke at the press conference.
Over the last decade, he said, the pipeline has instead focused more on gram-positive agents – mostly linked to beta-lactamase – that have wider market potential and generate less resistance.
“From a clinical point of view, these multidrug-resistant gram-negative clinical trials are very difficult and expensive to do, more than for gram-positive,” noted Evelina Tacconelli, MD, PhD, a contributor to the WHO report. “Because when we talk about gram-negative, we need to cover multiple pathogens and not just one or two, as in the case of gram-positive.”
Dr. Magrini said he couldn’t provide estimates about how many people worldwide are affected by the listed pathogens. However, he said a full report with numbers will be released by June.
It does appear that patients with severe infection from antibiotic-resistant germs face a mortality rate of up to 60%, while extended-spectrum beta-lactamase–positive E. coli accounts for up to 70% of urinary tract infections in many countries, explained Dr. Tacconelli, head of the division of infectious diseases at the University of Tübingen, Germany.
“Even if we don’t know exactly how many,” she said, “we are talking about millions of people affected.”
The World Health Organization is urging governments to focus antibiotic research efforts on a list of urgent bacterial threats, topped by several increasingly powerful superbugs that cause hospital-based infections and other potentially deadly conditions.
The WHO listed the top 20 bacteria that it believes are most harmful to human health, other than mycobacteria such as Mycobacterium tuberculosis, which causes tuberculosis. The germ was not included in the list because it’s generally accepted to be the most urgent priority for new antibiotic research and development, Marie-Paule Kieny, PhD, a WHO assistant director, said at a press conference.
The priority list is needed because the antibiotic pipeline is “practically dry,” thanks to scientific research challenges and a lack of financial incentives, according to Dr. Kieny. “Antibiotics are generally used for the short term, unlike therapies for chronic diseases, which bring in much higher returns on investment,” she said. The list “is intended to signal to the scientific community and the pharmaceutical industry the areas they should focus on to address urgent public health threats.”
The WHO list begins with Priority 1/“Critical” pathogens that it believes most urgently need to be targeted through antibiotic research and development: Acinetobacter baumannii, carbapenem-resistant; Pseudomonas aeruginosa, carbapenem-resistant; and Enterobacteriaceae (including Klebsiella pneumonia, Escherichia coli, Enterobacter spp., Serratia spp., Proteus spp., Providencia spp., and Morganella spp.), carbapenem-resistant, extended-spectrum beta-lactamase–producing.
“These bacteria are responsible for severe infections and high mortality rates, mostly in hospitalized patients, transplant recipients, those receiving chemotherapy, or patients in intensive care units,” Dr. Kieny said. “While these bacteria are not widespread and do not generally affect healthy individuals, the burden for patients and society is now alarming – and new, effective therapies are imperative.”
Priority 2/”High” pathogens are Enterococcus faecium, vancomycin-resistant; Staphylococcus aureus, methicillin-resistant, vancomycin intermediate and resistant; Helicobacter pylori, clarithromycin-resistant; Campylobacter, fluoroquinolone-resistant; Salmonella spp., fluoroquinolone-resistant; Neisseria gonorrhoeae, third-generation cephalosporin-resistant and fluoroquinolone-resistant.
Pathogens in this category can infect healthy individuals, Dr. Kieny noted. “These infections, although not associated with significant mortality, have a dramatic health and economic impact on communities and, in particular, in low-income countries.”
Priority 3/”Medium” pathogens are Streptococcus pneumoniae, penicillin–non-susceptible; Haemophilus influenzae, ampicillin-resistant; and Shigella spp., fluoroquinolone-resistant.
These pathogens “represent a threat because of increasing resistance but still have some effective antibiotic options available,” Dr. Kieny said.
According to a statement provided by the WHO, the priority list doesn’t include streptococcus A and B or chlamydia, because resistance hasn’t reached the level of a public health threat.
One goal of the list is to focus attention on the development of small-market, gram-negative drugs that combat hospital-based infections, explained Nicola Magrini, MD, a WHO scientist who also spoke at the press conference.
Over the last decade, he said, the pipeline has instead focused more on gram-positive agents – mostly linked to beta-lactamase – that have wider market potential and generate less resistance.
“From a clinical point of view, these multidrug-resistant gram-negative clinical trials are very difficult and expensive to do, more than for gram-positive,” noted Evelina Tacconelli, MD, PhD, a contributor to the WHO report. “Because when we talk about gram-negative, we need to cover multiple pathogens and not just one or two, as in the case of gram-positive.”
Dr. Magrini said he couldn’t provide estimates about how many people worldwide are affected by the listed pathogens. However, he said a full report with numbers will be released by June.
It does appear that patients with severe infection from antibiotic-resistant germs face a mortality rate of up to 60%, while extended-spectrum beta-lactamase–positive E. coli accounts for up to 70% of urinary tract infections in many countries, explained Dr. Tacconelli, head of the division of infectious diseases at the University of Tübingen, Germany.
“Even if we don’t know exactly how many,” she said, “we are talking about millions of people affected.”
VIDEO: Stroke risk in women deserves greater attention
BOSTON – Texas neurologist Louise McCullough, MD, PhD, is determined to help women live longer by urging neurologists to focus on the unique risks and needs involved.
Dr. McCullough, chief of neurology at Memorial Hermann Hospital in Houston, told a plenary audience at the annual meeting of the American Academy of Neurology that both biological and social factors contribute to conditions, such as atrial fibrillation, that are more dangerous in females than in males.
For example, women are less likely than men to be taking blood thinners, she said, possibly because doctors assume they’re frail even when they’ll confirm – if only someone asks – that they haven’t fallen.
At the same time, she said, women with atrial fibrillation are twice as likely as their male counterparts to suffer a stroke. “You need to screen older women for a-fib and have a much lower threshold for treatment.”
Isolation can be another contributing factor to the stroke gender gap, she said. “Women are often living alone – they’ve outlived their spouses; they don’t live near their children; they may not have access to rapid care.”
These factors, she said, may even contribute to the smaller presence of women in clinical trials.
Dr. McCullough discussed these issues and more in a video interview at the meeting.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
BOSTON – Texas neurologist Louise McCullough, MD, PhD, is determined to help women live longer by urging neurologists to focus on the unique risks and needs involved.
Dr. McCullough, chief of neurology at Memorial Hermann Hospital in Houston, told a plenary audience at the annual meeting of the American Academy of Neurology that both biological and social factors contribute to conditions, such as atrial fibrillation, that are more dangerous in females than in males.
For example, women are less likely than men to be taking blood thinners, she said, possibly because doctors assume they’re frail even when they’ll confirm – if only someone asks – that they haven’t fallen.
At the same time, she said, women with atrial fibrillation are twice as likely as their male counterparts to suffer a stroke. “You need to screen older women for a-fib and have a much lower threshold for treatment.”
Isolation can be another contributing factor to the stroke gender gap, she said. “Women are often living alone – they’ve outlived their spouses; they don’t live near their children; they may not have access to rapid care.”
These factors, she said, may even contribute to the smaller presence of women in clinical trials.
Dr. McCullough discussed these issues and more in a video interview at the meeting.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
BOSTON – Texas neurologist Louise McCullough, MD, PhD, is determined to help women live longer by urging neurologists to focus on the unique risks and needs involved.
Dr. McCullough, chief of neurology at Memorial Hermann Hospital in Houston, told a plenary audience at the annual meeting of the American Academy of Neurology that both biological and social factors contribute to conditions, such as atrial fibrillation, that are more dangerous in females than in males.
For example, women are less likely than men to be taking blood thinners, she said, possibly because doctors assume they’re frail even when they’ll confirm – if only someone asks – that they haven’t fallen.
At the same time, she said, women with atrial fibrillation are twice as likely as their male counterparts to suffer a stroke. “You need to screen older women for a-fib and have a much lower threshold for treatment.”
Isolation can be another contributing factor to the stroke gender gap, she said. “Women are often living alone – they’ve outlived their spouses; they don’t live near their children; they may not have access to rapid care.”
These factors, she said, may even contribute to the smaller presence of women in clinical trials.
Dr. McCullough discussed these issues and more in a video interview at the meeting.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
AT AAN 2017

Parkinson’s patients’ quality of life improves after deep brain stimulation
BOSTON– Early results from an industry-funded registry of Parkinson’s disease patients who underwent deep brain stimulation (DBS) reveal that their quality-of-life scores grew by 22% at 6 months.
Patients, their caregivers, and their clinicians all overwhelmingly reported improvement.
The study, which examined two types of technology that are not approved in the United States, aims to fill a gap in DBS research: How do patients fare in normal conditions – “real life” – outside of clinical trials?
While DBS has been widely used for many years, “much of the available information is from controlled trials that usually select the best possible patients – relatively young and in the condition to go through a clinical trial. There’s less information about people who may not be in the best possible shape,” said Michele Tagliati, MD, professor and director of movement disorders at Cedars-Sinai Medical Center in Los Angeles. He did not take part in the study but is familiar with its findings.
The study’s lead author, Günther Deuschl, MD, PhD, of University Hospital Schleswig-Holstein, released preliminary findings at the annual meeting of the American Academy of Neurology.
The researchers have enrolled 203 patients who were treated with Boston Scientific’s Vercise DBS system, which is not approved for use in the United States. The researchers plan to track patients for 3 years.
“This is the first such industry-sponsored registry, which addresses a need in the field to track DBS practice and outcomes across multiple centers,” said Mark Richardson, MD, PhD, associate professor and director of epilepsy and movement disorders surgery at the University of Pittsburgh Medical Center. He did not take part in the study but is familiar with its findings.
The average age of participants is 59 years, which Dr. Deuschl said is a bit younger than many other studies, and 69% are male. Eighty-five serious adverse events were reported in 52 patients; 57 were not linked to the procedure. One patient died of a surgery-related hematoma.
At 6 months, patients reported a 22% improvement (P less than .0001) on the Parkinson’s Disease Questionnaire (PDQ-39), Dr. Deuschl said, and that level was sustained at 1 year.
That level of improvement is significant, Dr. Richardson said in an interview.
“Previous randomized, controlled trials have shown that patients who are candidates for DBS but who continue medical management alone are most likely to have no improvement at all on any quality of life measures,” he said. In addition, “6 months is fairly short, and some patients likely have not reached stable stimulation programming and effectiveness.”
The researchers also reported that more than 90% of patients, their clinicians, and their caregivers reported improvement.
This kind of study is valuable in light of skepticism about DBS, which is used to treat patients who do not respond to medication, Dr. Tagliati noted.
“Despite 15 years of [Food and Drug Administration] approval, there is still some form of resistance out there in referring patients with Parkinson’s at the right time when they can still fully benefit from the procedure,” he said. “Registries have this potential great benefit in terms of awareness and reassuring people.”
As for the high rating of improvement, Dr. Tagliati said it reflects what he sees in the clinic.
“Barring complications, we have very substantial satisfaction in our patients, definitely in the short term after DBS,” he said. “Over the long term, the picture is more difficult to read.”
Dr. Deuschl said researchers would like to add hundreds more patients to the study, and they hope to gain data about the differences between the results from standard and directional-lead DBS systems.
Boston Scientific funded the study, and some of the authors work for the company.
Dr. Richardson reported receiving research grant funding from Medtronic. Dr. Tagliati reported receiving funding from Abbott, Boston Scientific, Medtronic, and all DBS manufacturers, and his clinic is an investigational center for the Vercise DBS system. Dr. Deuschl reported receiving consulting fees from Boston Scientific, grant funding from Medtronic, lecture fees from Almirall and Novartis, and royalties from Thieme Publishers.
BOSTON– Early results from an industry-funded registry of Parkinson’s disease patients who underwent deep brain stimulation (DBS) reveal that their quality-of-life scores grew by 22% at 6 months.
Patients, their caregivers, and their clinicians all overwhelmingly reported improvement.
The study, which examined two types of technology that are not approved in the United States, aims to fill a gap in DBS research: How do patients fare in normal conditions – “real life” – outside of clinical trials?
While DBS has been widely used for many years, “much of the available information is from controlled trials that usually select the best possible patients – relatively young and in the condition to go through a clinical trial. There’s less information about people who may not be in the best possible shape,” said Michele Tagliati, MD, professor and director of movement disorders at Cedars-Sinai Medical Center in Los Angeles. He did not take part in the study but is familiar with its findings.
The study’s lead author, Günther Deuschl, MD, PhD, of University Hospital Schleswig-Holstein, released preliminary findings at the annual meeting of the American Academy of Neurology.
The researchers have enrolled 203 patients who were treated with Boston Scientific’s Vercise DBS system, which is not approved for use in the United States. The researchers plan to track patients for 3 years.
“This is the first such industry-sponsored registry, which addresses a need in the field to track DBS practice and outcomes across multiple centers,” said Mark Richardson, MD, PhD, associate professor and director of epilepsy and movement disorders surgery at the University of Pittsburgh Medical Center. He did not take part in the study but is familiar with its findings.
The average age of participants is 59 years, which Dr. Deuschl said is a bit younger than many other studies, and 69% are male. Eighty-five serious adverse events were reported in 52 patients; 57 were not linked to the procedure. One patient died of a surgery-related hematoma.
At 6 months, patients reported a 22% improvement (P less than .0001) on the Parkinson’s Disease Questionnaire (PDQ-39), Dr. Deuschl said, and that level was sustained at 1 year.
That level of improvement is significant, Dr. Richardson said in an interview.
“Previous randomized, controlled trials have shown that patients who are candidates for DBS but who continue medical management alone are most likely to have no improvement at all on any quality of life measures,” he said. In addition, “6 months is fairly short, and some patients likely have not reached stable stimulation programming and effectiveness.”
The researchers also reported that more than 90% of patients, their clinicians, and their caregivers reported improvement.
This kind of study is valuable in light of skepticism about DBS, which is used to treat patients who do not respond to medication, Dr. Tagliati noted.
“Despite 15 years of [Food and Drug Administration] approval, there is still some form of resistance out there in referring patients with Parkinson’s at the right time when they can still fully benefit from the procedure,” he said. “Registries have this potential great benefit in terms of awareness and reassuring people.”
As for the high rating of improvement, Dr. Tagliati said it reflects what he sees in the clinic.
“Barring complications, we have very substantial satisfaction in our patients, definitely in the short term after DBS,” he said. “Over the long term, the picture is more difficult to read.”
Dr. Deuschl said researchers would like to add hundreds more patients to the study, and they hope to gain data about the differences between the results from standard and directional-lead DBS systems.
Boston Scientific funded the study, and some of the authors work for the company.
Dr. Richardson reported receiving research grant funding from Medtronic. Dr. Tagliati reported receiving funding from Abbott, Boston Scientific, Medtronic, and all DBS manufacturers, and his clinic is an investigational center for the Vercise DBS system. Dr. Deuschl reported receiving consulting fees from Boston Scientific, grant funding from Medtronic, lecture fees from Almirall and Novartis, and royalties from Thieme Publishers.
BOSTON– Early results from an industry-funded registry of Parkinson’s disease patients who underwent deep brain stimulation (DBS) reveal that their quality-of-life scores grew by 22% at 6 months.
Patients, their caregivers, and their clinicians all overwhelmingly reported improvement.
The study, which examined two types of technology that are not approved in the United States, aims to fill a gap in DBS research: How do patients fare in normal conditions – “real life” – outside of clinical trials?
While DBS has been widely used for many years, “much of the available information is from controlled trials that usually select the best possible patients – relatively young and in the condition to go through a clinical trial. There’s less information about people who may not be in the best possible shape,” said Michele Tagliati, MD, professor and director of movement disorders at Cedars-Sinai Medical Center in Los Angeles. He did not take part in the study but is familiar with its findings.
The study’s lead author, Günther Deuschl, MD, PhD, of University Hospital Schleswig-Holstein, released preliminary findings at the annual meeting of the American Academy of Neurology.
The researchers have enrolled 203 patients who were treated with Boston Scientific’s Vercise DBS system, which is not approved for use in the United States. The researchers plan to track patients for 3 years.
“This is the first such industry-sponsored registry, which addresses a need in the field to track DBS practice and outcomes across multiple centers,” said Mark Richardson, MD, PhD, associate professor and director of epilepsy and movement disorders surgery at the University of Pittsburgh Medical Center. He did not take part in the study but is familiar with its findings.
The average age of participants is 59 years, which Dr. Deuschl said is a bit younger than many other studies, and 69% are male. Eighty-five serious adverse events were reported in 52 patients; 57 were not linked to the procedure. One patient died of a surgery-related hematoma.
At 6 months, patients reported a 22% improvement (P less than .0001) on the Parkinson’s Disease Questionnaire (PDQ-39), Dr. Deuschl said, and that level was sustained at 1 year.
That level of improvement is significant, Dr. Richardson said in an interview.
“Previous randomized, controlled trials have shown that patients who are candidates for DBS but who continue medical management alone are most likely to have no improvement at all on any quality of life measures,” he said. In addition, “6 months is fairly short, and some patients likely have not reached stable stimulation programming and effectiveness.”
The researchers also reported that more than 90% of patients, their clinicians, and their caregivers reported improvement.
This kind of study is valuable in light of skepticism about DBS, which is used to treat patients who do not respond to medication, Dr. Tagliati noted.
“Despite 15 years of [Food and Drug Administration] approval, there is still some form of resistance out there in referring patients with Parkinson’s at the right time when they can still fully benefit from the procedure,” he said. “Registries have this potential great benefit in terms of awareness and reassuring people.”
As for the high rating of improvement, Dr. Tagliati said it reflects what he sees in the clinic.
“Barring complications, we have very substantial satisfaction in our patients, definitely in the short term after DBS,” he said. “Over the long term, the picture is more difficult to read.”
Dr. Deuschl said researchers would like to add hundreds more patients to the study, and they hope to gain data about the differences between the results from standard and directional-lead DBS systems.
Boston Scientific funded the study, and some of the authors work for the company.
Dr. Richardson reported receiving research grant funding from Medtronic. Dr. Tagliati reported receiving funding from Abbott, Boston Scientific, Medtronic, and all DBS manufacturers, and his clinic is an investigational center for the Vercise DBS system. Dr. Deuschl reported receiving consulting fees from Boston Scientific, grant funding from Medtronic, lecture fees from Almirall and Novartis, and royalties from Thieme Publishers.