User login
New models predict post-op pain in TKA
two-thirds of the time. Major risk factors include pre-operative pain, sensory testing results, anxiety and anticipated pain.
“The results of this study provide some basis for the identification of patients at risk of PPP after TKA and highlight several modifiable factors that may be targeted by clinicians in an attempt to reduce the risk of developing PPP,” write the authors of the study, which appeared in the British Journal of Anaesthesia.
The authors, led by David Rice, PhD, of Auckland University of Technology, note that moderate to severe levels of PPP affect an estimated 10%-34% of patients at least 3 months after TKA surgery. “PPP adversely affects quality of life, is the most important predictor of patient dissatisfaction after TKA, and is a common reason for undergoing revision surgery.”
The researchers, who launched the study to gain insight into the risk factors that can predict PPP, recruited 300 New Zealand volunteers (average age = 69, 48% female, 92% white, average body mass index [BMI] = 31 kg/m2) to be surveyed before and after TKA surgery. They monitored pain and tracked a long list of possible risk factors including psychological traits (such as anxiety, pain catastrophizing and depression), physical traits (such as gender, BMI), and surgical traits (such as total surgery time).
At 6 months, 21% of 291 patients reported moderate to severe pain, and the percentage fell to 16% in 288 patients at 12 months.
The researchers developed two models that successfully predicted moderate-to-severe PPP.
The 6-month model relied on higher levels of preoperative pain intensity, temporal summation (a statistic that’s based on quantitative sensory testing), trait anxiety (a measure of individual anxiety level), and expected pain. It correctly predicted moderate to severe PPP 66% of the time (area under the curve [AUC] = 0.70, sensitivity = 0.72, specificity = 0.64).
The 12-month model relied on higher levels of all the risk factors except for temporal summation and correctly predicted moderate-to-severe PPP 66% of the time (AUC = 0.66, sensitivity = 0.61, specificity = 0.67).
The researchers noted that other research has linked trait anxiety and expected pain to PPP. In regard to anxiety, “cognitive behavioral interventions in the perioperative period aimed at reducing the threat value of surgery and of postoperative pain, improving patients’ coping strategies, and enhancing self-efficacy might help to reduce the risk of PPP after TKA,” the researchers write. “Furthermore, there is some evidence that anxiolytic medications can diminish perioperative anxiety and reduce APOP [acute postoperative pain] although its effects on PPP are unclear.”
Moving forward, the authors write, “strategies to minimize intraoperative nerve injury, reduce preoperative pain intensity, and address preoperative psychological factors such as expected pain and anxiety may lead to improved outcomes after TKA and should be explored.”
The Australia New Zealand College of Anesthetists and Auckland University of Technology funded the study. The study authors report no relevant disclosures.
SOURCE: Rice D et al. Br J Anaesth 2018;804-12. doi: https://doi.org/10.1016/j.bja.2018.05.070.
two-thirds of the time. Major risk factors include pre-operative pain, sensory testing results, anxiety and anticipated pain.
“The results of this study provide some basis for the identification of patients at risk of PPP after TKA and highlight several modifiable factors that may be targeted by clinicians in an attempt to reduce the risk of developing PPP,” write the authors of the study, which appeared in the British Journal of Anaesthesia.
The authors, led by David Rice, PhD, of Auckland University of Technology, note that moderate to severe levels of PPP affect an estimated 10%-34% of patients at least 3 months after TKA surgery. “PPP adversely affects quality of life, is the most important predictor of patient dissatisfaction after TKA, and is a common reason for undergoing revision surgery.”
The researchers, who launched the study to gain insight into the risk factors that can predict PPP, recruited 300 New Zealand volunteers (average age = 69, 48% female, 92% white, average body mass index [BMI] = 31 kg/m2) to be surveyed before and after TKA surgery. They monitored pain and tracked a long list of possible risk factors including psychological traits (such as anxiety, pain catastrophizing and depression), physical traits (such as gender, BMI), and surgical traits (such as total surgery time).
At 6 months, 21% of 291 patients reported moderate to severe pain, and the percentage fell to 16% in 288 patients at 12 months.
The researchers developed two models that successfully predicted moderate-to-severe PPP.
The 6-month model relied on higher levels of preoperative pain intensity, temporal summation (a statistic that’s based on quantitative sensory testing), trait anxiety (a measure of individual anxiety level), and expected pain. It correctly predicted moderate to severe PPP 66% of the time (area under the curve [AUC] = 0.70, sensitivity = 0.72, specificity = 0.64).
The 12-month model relied on higher levels of all the risk factors except for temporal summation and correctly predicted moderate-to-severe PPP 66% of the time (AUC = 0.66, sensitivity = 0.61, specificity = 0.67).
The researchers noted that other research has linked trait anxiety and expected pain to PPP. In regard to anxiety, “cognitive behavioral interventions in the perioperative period aimed at reducing the threat value of surgery and of postoperative pain, improving patients’ coping strategies, and enhancing self-efficacy might help to reduce the risk of PPP after TKA,” the researchers write. “Furthermore, there is some evidence that anxiolytic medications can diminish perioperative anxiety and reduce APOP [acute postoperative pain] although its effects on PPP are unclear.”
Moving forward, the authors write, “strategies to minimize intraoperative nerve injury, reduce preoperative pain intensity, and address preoperative psychological factors such as expected pain and anxiety may lead to improved outcomes after TKA and should be explored.”
The Australia New Zealand College of Anesthetists and Auckland University of Technology funded the study. The study authors report no relevant disclosures.
SOURCE: Rice D et al. Br J Anaesth 2018;804-12. doi: https://doi.org/10.1016/j.bja.2018.05.070.
two-thirds of the time. Major risk factors include pre-operative pain, sensory testing results, anxiety and anticipated pain.
“The results of this study provide some basis for the identification of patients at risk of PPP after TKA and highlight several modifiable factors that may be targeted by clinicians in an attempt to reduce the risk of developing PPP,” write the authors of the study, which appeared in the British Journal of Anaesthesia.
The authors, led by David Rice, PhD, of Auckland University of Technology, note that moderate to severe levels of PPP affect an estimated 10%-34% of patients at least 3 months after TKA surgery. “PPP adversely affects quality of life, is the most important predictor of patient dissatisfaction after TKA, and is a common reason for undergoing revision surgery.”
The researchers, who launched the study to gain insight into the risk factors that can predict PPP, recruited 300 New Zealand volunteers (average age = 69, 48% female, 92% white, average body mass index [BMI] = 31 kg/m2) to be surveyed before and after TKA surgery. They monitored pain and tracked a long list of possible risk factors including psychological traits (such as anxiety, pain catastrophizing and depression), physical traits (such as gender, BMI), and surgical traits (such as total surgery time).
At 6 months, 21% of 291 patients reported moderate to severe pain, and the percentage fell to 16% in 288 patients at 12 months.
The researchers developed two models that successfully predicted moderate-to-severe PPP.
The 6-month model relied on higher levels of preoperative pain intensity, temporal summation (a statistic that’s based on quantitative sensory testing), trait anxiety (a measure of individual anxiety level), and expected pain. It correctly predicted moderate to severe PPP 66% of the time (area under the curve [AUC] = 0.70, sensitivity = 0.72, specificity = 0.64).
The 12-month model relied on higher levels of all the risk factors except for temporal summation and correctly predicted moderate-to-severe PPP 66% of the time (AUC = 0.66, sensitivity = 0.61, specificity = 0.67).
The researchers noted that other research has linked trait anxiety and expected pain to PPP. In regard to anxiety, “cognitive behavioral interventions in the perioperative period aimed at reducing the threat value of surgery and of postoperative pain, improving patients’ coping strategies, and enhancing self-efficacy might help to reduce the risk of PPP after TKA,” the researchers write. “Furthermore, there is some evidence that anxiolytic medications can diminish perioperative anxiety and reduce APOP [acute postoperative pain] although its effects on PPP are unclear.”
Moving forward, the authors write, “strategies to minimize intraoperative nerve injury, reduce preoperative pain intensity, and address preoperative psychological factors such as expected pain and anxiety may lead to improved outcomes after TKA and should be explored.”
The Australia New Zealand College of Anesthetists and Auckland University of Technology funded the study. The study authors report no relevant disclosures.
SOURCE: Rice D et al. Br J Anaesth 2018;804-12. doi: https://doi.org/10.1016/j.bja.2018.05.070.
FROM BRITISH JOURNAL OF ANESTHESIA
What’s the proper place of benzodiazepines in psychiatry?
Tread carefully, but do not eliminate them as an option, two experts advise.
SAN DIEGO – Not long before his presentation at Psych Congress 2019, psychiatrist Rakesh Jain, MD, MPH, chatted with a fellow attendee, a nurse practitioner from Tyler, Tex. As Dr. Jain recalled later, his fellow Texan told him that “it’s not unusual to see patients on three benzodiazepines.”
The nurse practitioner “talks to them about how they need to do things differently, and they forget,” Dr. Jain said. “He’s very worried about them.”
Dr. Jain is familiar with the feeling. Like many mental health professionals, he worries about the role of benzodiazepines, which seem to be both widely used and misused. Figuring out their proper place in psychiatry “may require us to raise our game,” said Dr. Jain, of Texas Tech University in Midland.
What to do? Dr. Jain and a colleague offered the same answer – tread carefully, but do not eliminate them as an option – in two separate sessions at the annual Psych Congress.
As Dr. Jain noted, benzodiazepines are popular, and for good reason. “There are many patients, perhaps hundreds of thousands, who are using benzodiazepines chronically, and they’re doing it right. There’s not a CVS in America where benzodiazepines aren’t well stocked. They’re very inexpensive, and the most costly benzodiazepine is still cheaper than Motrin.”
On the other hand, he said, the medications are linked to addiction and physical dependence. “Thirty percent of those who die of opioid overdoses may not have died if they didn’t have benzodiazepines [in their systems].”
In another presentation, psychiatrist Murray B. Stein, MD, MPH, of the University of California at San Diego and VA San Diego Healthcare System, offered these tips about prescribing benzodiazepines for patients with anxiety.
Be very cautious about prescribing as needed
“It’s rarely indicated to prescribe benzodiazepine [as needed] when you’re treating people with anxiety,” he said. “The main reason is patients don’t know when they need it. They take their pills either when they’re so anxious that they’ve already been freaking out for a long time, or they take it when they’re first starting to feel at least a bit anxious. That leads to taking it to prevent being anxious.”
Allow an as-needed approach in certain situations
However, he said, advise patients to try the medication beforehand so they understand its effects. “I’ve had one occasion where I thought we had a dose worked out well. Somebody had to do a work presentation, and he took the medicine and got up in front of the group. He wasn’t anxious at all. But he couldn’t remember a single thing.”
Don’t use them as patients start SSRIs
Patients can get anxious as they start SSRIs, especially for panic disorders, Dr. Stein said. So it might seem reasonable, as some psychiatrists believe, to add benzodiazepines on a short-term basis.
But Dr. Stein said he is not a fan of this approach. As he noted, benzodiazepines are hard to stop. He prefers to help patients understand possible side effects of SSRIs instead, and he emphasized the importance of being available to help patients get through them.
Dr. Jain and Dr. Stein each reported multiple relationships with industry.
Tread carefully, but do not eliminate them as an option, two experts advise.
Tread carefully, but do not eliminate them as an option, two experts advise.
SAN DIEGO – Not long before his presentation at Psych Congress 2019, psychiatrist Rakesh Jain, MD, MPH, chatted with a fellow attendee, a nurse practitioner from Tyler, Tex. As Dr. Jain recalled later, his fellow Texan told him that “it’s not unusual to see patients on three benzodiazepines.”
The nurse practitioner “talks to them about how they need to do things differently, and they forget,” Dr. Jain said. “He’s very worried about them.”
Dr. Jain is familiar with the feeling. Like many mental health professionals, he worries about the role of benzodiazepines, which seem to be both widely used and misused. Figuring out their proper place in psychiatry “may require us to raise our game,” said Dr. Jain, of Texas Tech University in Midland.
What to do? Dr. Jain and a colleague offered the same answer – tread carefully, but do not eliminate them as an option – in two separate sessions at the annual Psych Congress.
As Dr. Jain noted, benzodiazepines are popular, and for good reason. “There are many patients, perhaps hundreds of thousands, who are using benzodiazepines chronically, and they’re doing it right. There’s not a CVS in America where benzodiazepines aren’t well stocked. They’re very inexpensive, and the most costly benzodiazepine is still cheaper than Motrin.”
On the other hand, he said, the medications are linked to addiction and physical dependence. “Thirty percent of those who die of opioid overdoses may not have died if they didn’t have benzodiazepines [in their systems].”
In another presentation, psychiatrist Murray B. Stein, MD, MPH, of the University of California at San Diego and VA San Diego Healthcare System, offered these tips about prescribing benzodiazepines for patients with anxiety.
Be very cautious about prescribing as needed
“It’s rarely indicated to prescribe benzodiazepine [as needed] when you’re treating people with anxiety,” he said. “The main reason is patients don’t know when they need it. They take their pills either when they’re so anxious that they’ve already been freaking out for a long time, or they take it when they’re first starting to feel at least a bit anxious. That leads to taking it to prevent being anxious.”
Allow an as-needed approach in certain situations
However, he said, advise patients to try the medication beforehand so they understand its effects. “I’ve had one occasion where I thought we had a dose worked out well. Somebody had to do a work presentation, and he took the medicine and got up in front of the group. He wasn’t anxious at all. But he couldn’t remember a single thing.”
Don’t use them as patients start SSRIs
Patients can get anxious as they start SSRIs, especially for panic disorders, Dr. Stein said. So it might seem reasonable, as some psychiatrists believe, to add benzodiazepines on a short-term basis.
But Dr. Stein said he is not a fan of this approach. As he noted, benzodiazepines are hard to stop. He prefers to help patients understand possible side effects of SSRIs instead, and he emphasized the importance of being available to help patients get through them.
Dr. Jain and Dr. Stein each reported multiple relationships with industry.
SAN DIEGO – Not long before his presentation at Psych Congress 2019, psychiatrist Rakesh Jain, MD, MPH, chatted with a fellow attendee, a nurse practitioner from Tyler, Tex. As Dr. Jain recalled later, his fellow Texan told him that “it’s not unusual to see patients on three benzodiazepines.”
The nurse practitioner “talks to them about how they need to do things differently, and they forget,” Dr. Jain said. “He’s very worried about them.”
Dr. Jain is familiar with the feeling. Like many mental health professionals, he worries about the role of benzodiazepines, which seem to be both widely used and misused. Figuring out their proper place in psychiatry “may require us to raise our game,” said Dr. Jain, of Texas Tech University in Midland.
What to do? Dr. Jain and a colleague offered the same answer – tread carefully, but do not eliminate them as an option – in two separate sessions at the annual Psych Congress.
As Dr. Jain noted, benzodiazepines are popular, and for good reason. “There are many patients, perhaps hundreds of thousands, who are using benzodiazepines chronically, and they’re doing it right. There’s not a CVS in America where benzodiazepines aren’t well stocked. They’re very inexpensive, and the most costly benzodiazepine is still cheaper than Motrin.”
On the other hand, he said, the medications are linked to addiction and physical dependence. “Thirty percent of those who die of opioid overdoses may not have died if they didn’t have benzodiazepines [in their systems].”
In another presentation, psychiatrist Murray B. Stein, MD, MPH, of the University of California at San Diego and VA San Diego Healthcare System, offered these tips about prescribing benzodiazepines for patients with anxiety.
Be very cautious about prescribing as needed
“It’s rarely indicated to prescribe benzodiazepine [as needed] when you’re treating people with anxiety,” he said. “The main reason is patients don’t know when they need it. They take their pills either when they’re so anxious that they’ve already been freaking out for a long time, or they take it when they’re first starting to feel at least a bit anxious. That leads to taking it to prevent being anxious.”
Allow an as-needed approach in certain situations
However, he said, advise patients to try the medication beforehand so they understand its effects. “I’ve had one occasion where I thought we had a dose worked out well. Somebody had to do a work presentation, and he took the medicine and got up in front of the group. He wasn’t anxious at all. But he couldn’t remember a single thing.”
Don’t use them as patients start SSRIs
Patients can get anxious as they start SSRIs, especially for panic disorders, Dr. Stein said. So it might seem reasonable, as some psychiatrists believe, to add benzodiazepines on a short-term basis.
But Dr. Stein said he is not a fan of this approach. As he noted, benzodiazepines are hard to stop. He prefers to help patients understand possible side effects of SSRIs instead, and he emphasized the importance of being available to help patients get through them.
Dr. Jain and Dr. Stein each reported multiple relationships with industry.
REPORTING FROM PSYCH CONGRESS 2019
Acoustic pulse boosts laser tattoo removal
In tattoo removal, the impact of laser treatments in single office visits is limited because of the laser’s effects on the skin. Now, a new study suggests that a
“As a result,” the authors of the study wrote, “a lower total number of office visits will likely be required for complete tattoo removal leading to improved convenience and efficiency as well as increased satisfaction for both patients and clinicians.” The study, led by cosmetic surgeon Michael S. Kaminer, MD, of SkinCare Physicians in Chestnut Hill, Mass., appeared in Lasers in Surgery and Medicine.
In the study, he and his coauthors pointed out that tattoos are most frequently removed with short-pulse high-fluence lasers, such as a 1064-nm Nd:YAG Q‐switched (QS) laser. However, “the QS laser has a limited ability to affect the tattoo ink pigment particles in each treatment session due to shielding of the pigment particles caused by both the agglomeration of the pigment particles and laser‐induced epidermal and dermal vacuoles known as ‘whitening.’ ” Therefore, “use of the QS laser often requires 10 or more single‐pass office sessions to achieve acceptable fading results.”
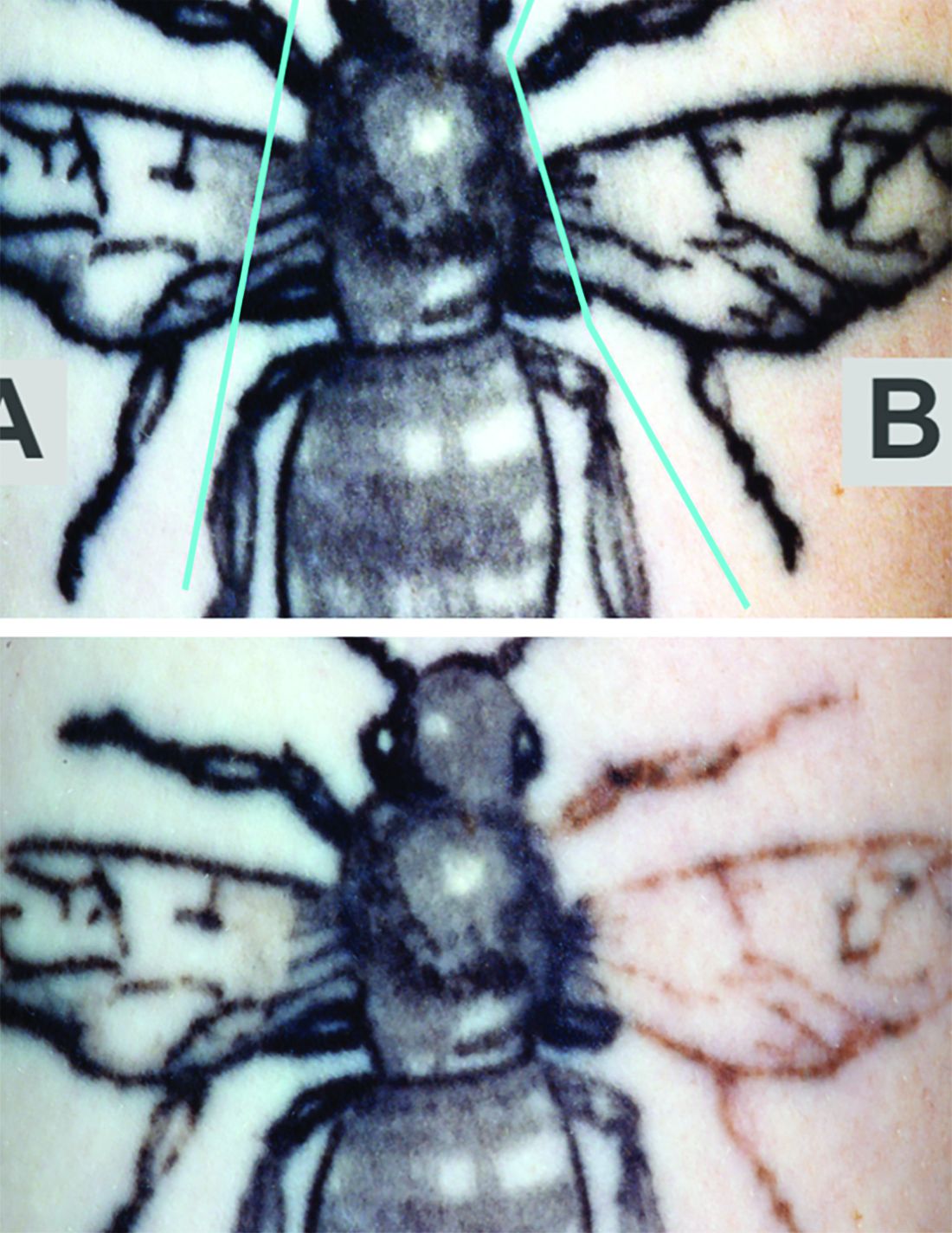
The study evaluated whether the use of a rapid acoustic pulse (RAP) device could reduce the whitening effect by clearing vacuoles and make it possible to increase the number of potential laser passes. In the single-center, prospective trial, they treated 32 black-ink tattoos in 21 patients, dividing the tattoos into zones and treating them differently: One zone received at least three consecutive laser passes alternating with a minute of treatment with the RAP device, one received single-pass laser treatment, and one received no treatment.
Reviewers assessed the tattoos for fading at 12 weeks. Average percent fading was higher in the laser/RAP group, compared with the laser-only group (44% and 25%, respectively, P less than .01). The percentages of tattoos with more than 50% fading (38% vs. 9%, P less than .01) and more than 75% fading (22% vs. 3%, P less than .05) were also higher in the laser/RAP group, compared with the laser-only group.
“Further clinical studies will be performed to investigate the broader applicability of the RAP device as an accessory device to reduce the number of laser tattoo removal sessions for other tattoo ink colors in a broader range of skin types,” the researchers commented, noting that the study included patients with Fitzpatrick skin types I-III.
The study was funded by Soliton, which provided the equipment. One of the six authors is an employee of the company The other authors reported no relevant disclosures.
SOURCE: Kaminer MS et al. Lasers Surg Med. 2019 Sep 19. doi: 10.1002/lsm.23163.
In tattoo removal, the impact of laser treatments in single office visits is limited because of the laser’s effects on the skin. Now, a new study suggests that a
“As a result,” the authors of the study wrote, “a lower total number of office visits will likely be required for complete tattoo removal leading to improved convenience and efficiency as well as increased satisfaction for both patients and clinicians.” The study, led by cosmetic surgeon Michael S. Kaminer, MD, of SkinCare Physicians in Chestnut Hill, Mass., appeared in Lasers in Surgery and Medicine.
In the study, he and his coauthors pointed out that tattoos are most frequently removed with short-pulse high-fluence lasers, such as a 1064-nm Nd:YAG Q‐switched (QS) laser. However, “the QS laser has a limited ability to affect the tattoo ink pigment particles in each treatment session due to shielding of the pigment particles caused by both the agglomeration of the pigment particles and laser‐induced epidermal and dermal vacuoles known as ‘whitening.’ ” Therefore, “use of the QS laser often requires 10 or more single‐pass office sessions to achieve acceptable fading results.”
The study evaluated whether the use of a rapid acoustic pulse (RAP) device could reduce the whitening effect by clearing vacuoles and make it possible to increase the number of potential laser passes. In the single-center, prospective trial, they treated 32 black-ink tattoos in 21 patients, dividing the tattoos into zones and treating them differently: One zone received at least three consecutive laser passes alternating with a minute of treatment with the RAP device, one received single-pass laser treatment, and one received no treatment.
Reviewers assessed the tattoos for fading at 12 weeks. Average percent fading was higher in the laser/RAP group, compared with the laser-only group (44% and 25%, respectively, P less than .01). The percentages of tattoos with more than 50% fading (38% vs. 9%, P less than .01) and more than 75% fading (22% vs. 3%, P less than .05) were also higher in the laser/RAP group, compared with the laser-only group.
“Further clinical studies will be performed to investigate the broader applicability of the RAP device as an accessory device to reduce the number of laser tattoo removal sessions for other tattoo ink colors in a broader range of skin types,” the researchers commented, noting that the study included patients with Fitzpatrick skin types I-III.
The study was funded by Soliton, which provided the equipment. One of the six authors is an employee of the company The other authors reported no relevant disclosures.
SOURCE: Kaminer MS et al. Lasers Surg Med. 2019 Sep 19. doi: 10.1002/lsm.23163.
In tattoo removal, the impact of laser treatments in single office visits is limited because of the laser’s effects on the skin. Now, a new study suggests that a
“As a result,” the authors of the study wrote, “a lower total number of office visits will likely be required for complete tattoo removal leading to improved convenience and efficiency as well as increased satisfaction for both patients and clinicians.” The study, led by cosmetic surgeon Michael S. Kaminer, MD, of SkinCare Physicians in Chestnut Hill, Mass., appeared in Lasers in Surgery and Medicine.
In the study, he and his coauthors pointed out that tattoos are most frequently removed with short-pulse high-fluence lasers, such as a 1064-nm Nd:YAG Q‐switched (QS) laser. However, “the QS laser has a limited ability to affect the tattoo ink pigment particles in each treatment session due to shielding of the pigment particles caused by both the agglomeration of the pigment particles and laser‐induced epidermal and dermal vacuoles known as ‘whitening.’ ” Therefore, “use of the QS laser often requires 10 or more single‐pass office sessions to achieve acceptable fading results.”
The study evaluated whether the use of a rapid acoustic pulse (RAP) device could reduce the whitening effect by clearing vacuoles and make it possible to increase the number of potential laser passes. In the single-center, prospective trial, they treated 32 black-ink tattoos in 21 patients, dividing the tattoos into zones and treating them differently: One zone received at least three consecutive laser passes alternating with a minute of treatment with the RAP device, one received single-pass laser treatment, and one received no treatment.
Reviewers assessed the tattoos for fading at 12 weeks. Average percent fading was higher in the laser/RAP group, compared with the laser-only group (44% and 25%, respectively, P less than .01). The percentages of tattoos with more than 50% fading (38% vs. 9%, P less than .01) and more than 75% fading (22% vs. 3%, P less than .05) were also higher in the laser/RAP group, compared with the laser-only group.
“Further clinical studies will be performed to investigate the broader applicability of the RAP device as an accessory device to reduce the number of laser tattoo removal sessions for other tattoo ink colors in a broader range of skin types,” the researchers commented, noting that the study included patients with Fitzpatrick skin types I-III.
The study was funded by Soliton, which provided the equipment. One of the six authors is an employee of the company The other authors reported no relevant disclosures.
SOURCE: Kaminer MS et al. Lasers Surg Med. 2019 Sep 19. doi: 10.1002/lsm.23163.
FROM LASERS IN SURGERY AND MEDICINE
Treating comorbid ADHD-SUD presents challenges
Consider medications that might improve both conditions
SAN DIEGO – Research suggests that as many as 23% of patients with substance use disorder (SUD) also have ADHD, adding an extra layer of complexity to a difficult-to-treat condition. What to do?
“Treating the ADHD can be useful in reducing the severity of symptoms without worsening the substance use disorder. It shouldn’t be avoided,” said psychiatrist Larissa J. Mooney, MD, of the University of California, Los Angeles, and the Veterans Affairs Greater Los Angeles Healthcare System, in a presentation at the annual Psych Congress.
When ADHD is on board, “it’s a more complicated and challenging clinical course,” Dr. Mooney said. The duo of disorders is linked to higher rates of polysubstance abuse and other psychiatric conditions, such as anxiety, bipolar disorder, posttraumatic stress, and antisocial/borderline conditions (Eur Addict Res. 2018;24[1]:43-51).
“These individuals typically have more difficulty with [drug] abstinence, more health consequences, and reduced quality of life, and social and professional consequences,” she said. “Some studies have suggested that they may not respond to lower doses of medication for attention-deficit/hyperactivity disorder and may require doses in the higher range.”
Research has hinted that several drugs that might prove helpful in these patients by improving both conditions, Dr. Mooney said. These include up to 180 mg/day of methylphenidate (Ritalin), 60- and 80-mg doses of mixed amphetamine salts/extended release, atomoxetine (Strattera), and bupropion.
In regard to bupropion, she said, “I find it to be a good choice in my substance use disorder patients for their depression and concentration problems. I have a greater number of individuals at 450 milligrams per day and the XL formulation.”
“We need more research to show if this is helpful,” she said. “It’s a reasonable choice in terms of weighing pros and cons, because it’s not [a controlled substance].”
Still, some of those medications are stimulants, Dr. Mooney said, and their use in patients with SUD is controversial. There are concerns about misuse and diversion.
“We want to have some flexibility,” she said, but it’s important to think about risks and priorities. In certain cases, ADHD may be a secondary concern.
“Some patients have a severe substance use disorder that keeps landing them in the emergency room or causing them to be hospitalized,” she said. “I’m more worried about that than the impairment function from ADHD.”
If you do consider stimulants, she said, longer-acting formulations can be less risky because there’s less potential for diversion. “Also, think about their treatment plan: Is their functioning improving? Are they or showing up for appointments? These are factors that will say: ‘Oh, I’m on the right path with this medication.’ ”
Behavioral treatment also can be helpful in these patients, she said, although “some may not be willing or motivated to put in the time that it takes to do the behavioral work.”
Dr. Mooney disclosed an advisory board relationship with Alkermes and grant/research support from the National Institute on Drug Abuse.
Consider medications that might improve both conditions
Consider medications that might improve both conditions
SAN DIEGO – Research suggests that as many as 23% of patients with substance use disorder (SUD) also have ADHD, adding an extra layer of complexity to a difficult-to-treat condition. What to do?
“Treating the ADHD can be useful in reducing the severity of symptoms without worsening the substance use disorder. It shouldn’t be avoided,” said psychiatrist Larissa J. Mooney, MD, of the University of California, Los Angeles, and the Veterans Affairs Greater Los Angeles Healthcare System, in a presentation at the annual Psych Congress.
When ADHD is on board, “it’s a more complicated and challenging clinical course,” Dr. Mooney said. The duo of disorders is linked to higher rates of polysubstance abuse and other psychiatric conditions, such as anxiety, bipolar disorder, posttraumatic stress, and antisocial/borderline conditions (Eur Addict Res. 2018;24[1]:43-51).
“These individuals typically have more difficulty with [drug] abstinence, more health consequences, and reduced quality of life, and social and professional consequences,” she said. “Some studies have suggested that they may not respond to lower doses of medication for attention-deficit/hyperactivity disorder and may require doses in the higher range.”
Research has hinted that several drugs that might prove helpful in these patients by improving both conditions, Dr. Mooney said. These include up to 180 mg/day of methylphenidate (Ritalin), 60- and 80-mg doses of mixed amphetamine salts/extended release, atomoxetine (Strattera), and bupropion.
In regard to bupropion, she said, “I find it to be a good choice in my substance use disorder patients for their depression and concentration problems. I have a greater number of individuals at 450 milligrams per day and the XL formulation.”
“We need more research to show if this is helpful,” she said. “It’s a reasonable choice in terms of weighing pros and cons, because it’s not [a controlled substance].”
Still, some of those medications are stimulants, Dr. Mooney said, and their use in patients with SUD is controversial. There are concerns about misuse and diversion.
“We want to have some flexibility,” she said, but it’s important to think about risks and priorities. In certain cases, ADHD may be a secondary concern.
“Some patients have a severe substance use disorder that keeps landing them in the emergency room or causing them to be hospitalized,” she said. “I’m more worried about that than the impairment function from ADHD.”
If you do consider stimulants, she said, longer-acting formulations can be less risky because there’s less potential for diversion. “Also, think about their treatment plan: Is their functioning improving? Are they or showing up for appointments? These are factors that will say: ‘Oh, I’m on the right path with this medication.’ ”
Behavioral treatment also can be helpful in these patients, she said, although “some may not be willing or motivated to put in the time that it takes to do the behavioral work.”
Dr. Mooney disclosed an advisory board relationship with Alkermes and grant/research support from the National Institute on Drug Abuse.
SAN DIEGO – Research suggests that as many as 23% of patients with substance use disorder (SUD) also have ADHD, adding an extra layer of complexity to a difficult-to-treat condition. What to do?
“Treating the ADHD can be useful in reducing the severity of symptoms without worsening the substance use disorder. It shouldn’t be avoided,” said psychiatrist Larissa J. Mooney, MD, of the University of California, Los Angeles, and the Veterans Affairs Greater Los Angeles Healthcare System, in a presentation at the annual Psych Congress.
When ADHD is on board, “it’s a more complicated and challenging clinical course,” Dr. Mooney said. The duo of disorders is linked to higher rates of polysubstance abuse and other psychiatric conditions, such as anxiety, bipolar disorder, posttraumatic stress, and antisocial/borderline conditions (Eur Addict Res. 2018;24[1]:43-51).
“These individuals typically have more difficulty with [drug] abstinence, more health consequences, and reduced quality of life, and social and professional consequences,” she said. “Some studies have suggested that they may not respond to lower doses of medication for attention-deficit/hyperactivity disorder and may require doses in the higher range.”
Research has hinted that several drugs that might prove helpful in these patients by improving both conditions, Dr. Mooney said. These include up to 180 mg/day of methylphenidate (Ritalin), 60- and 80-mg doses of mixed amphetamine salts/extended release, atomoxetine (Strattera), and bupropion.
In regard to bupropion, she said, “I find it to be a good choice in my substance use disorder patients for their depression and concentration problems. I have a greater number of individuals at 450 milligrams per day and the XL formulation.”
“We need more research to show if this is helpful,” she said. “It’s a reasonable choice in terms of weighing pros and cons, because it’s not [a controlled substance].”
Still, some of those medications are stimulants, Dr. Mooney said, and their use in patients with SUD is controversial. There are concerns about misuse and diversion.
“We want to have some flexibility,” she said, but it’s important to think about risks and priorities. In certain cases, ADHD may be a secondary concern.
“Some patients have a severe substance use disorder that keeps landing them in the emergency room or causing them to be hospitalized,” she said. “I’m more worried about that than the impairment function from ADHD.”
If you do consider stimulants, she said, longer-acting formulations can be less risky because there’s less potential for diversion. “Also, think about their treatment plan: Is their functioning improving? Are they or showing up for appointments? These are factors that will say: ‘Oh, I’m on the right path with this medication.’ ”
Behavioral treatment also can be helpful in these patients, she said, although “some may not be willing or motivated to put in the time that it takes to do the behavioral work.”
Dr. Mooney disclosed an advisory board relationship with Alkermes and grant/research support from the National Institute on Drug Abuse.
EXPERT ANALYSIS FROM PSYCH CONGRESS 2019
Low P values shouldn’t always impress you
SAN DIEGO – Even if a P value hints at statistical significance by dipping under .05, it might not tell you anything worthwhile. Effect sizes are hugely important – as long as accompanying P values measure up. And pharmaceutical companies often keep revealing numbers under wraps unless you know what – and whom – to ask.
Those lessons come courtesy of Leslie Citrome, MD, MPH, who spoke to colleagues about study numbers at Psych Congress 2019.
Dr. Citrome, clinical professor of psychiatry and behavioral sciences at New York Medical College, Valhalla, offered several tips about interpreting medical statistics as you make clinical decisions.
Don’t get hung up on the P value.
The P value helps you understand how likely it is that a difference in a study is statistically significant. In medical research, P values under .05 are considered especially desirable. They suggest that an outcome – drug A performed better than drug B, for example – didn’t happen purely by chance.
Here’s the hitch: The P value might not matter at all. “Clinicians often assume that if the P value is less than.05, the result must be important. But even a P value of less than .05 is meaningless outside of the context of how big the treatment effect is,” Dr. Citrome said. “If a clinical trial result shows us a small effect size, then who cares?”
Understand what effect sizes tell you.
Effect size measurements evaluate clinical impact and include number needed to treat (NNT) and number needed to harm (NNH). NNT refers to the number of patients needed to treat with an intervention in order to get a positive effect in one additional patient; NNH is the reverse and examines negative effects that can range from the minor (mild dry mouth) to the devastating (death).
What’s a good size for an NNT? “I respect any NNT versus placebo of less than 10,” Dr. Citrome said. “It’s something I’ll probably consider in day-to-day practice.” Double-digit and triple-digit NNTs “are usually irrelevant unless we’re dealing with very specific outcomes that have long-term consequences.”
As for the opposite side of the picture – NNH – values higher than 10 are ideal.
He cautioned that NNT and NNH, like P values, cannot stand alone. In fact, they work together. In order to have value, NNT or NNH must be statistically significant, and P values provide this crucial insight.
Consider Dr. Citrome’s blood pressure.
As Dr. Citrome noted, research suggests that, among patients with diastolic BP from 90 to 109 mm Hg, 1 additional person will avoid death, stroke, or heart attack for every 141 people who take an antihypertensive medication, compared to those who do not, over a 5-year period. That’s a lot of people taking medication for a long time, with potential side effects, for a fairly small effect size. However, the outcomes are dire, so it is still worth it.
Then there’s Dr. Citrome himself, who has had diastolic BP in the range of 115 to 129 mm Hg. The NNT is 3. For every 3 people who take an antihypertensive vs. not over a 5-year period, 1 additional person will avoid a potentially catastrophic cardiovascular event.
“Guess who’s pretty adherent to taking his antihypertensive medication?” he asked. “I am.”
Ask for effect sizes if you don’t see them.
It’s not unusual for pharmaceutical representatives to avoid providing information about medication effect sizes. “The sales representatives as well as speakers at [Food and Drug Administration]–regulated promotional speaking events can only speak to basically what’s on the label. NNT and NNH are not currently found on product labels. But they are very relevant, and we need to know this information.”
What to do? “There is a workaround here,” he said. “Ask the sales rep to talk to a medical science liaison, who is free to come to your office and talk about all the data that they have.”
Dr. Citrome reported multiple disclosures, including various relationships with pharmaceutical companies.
SAN DIEGO – Even if a P value hints at statistical significance by dipping under .05, it might not tell you anything worthwhile. Effect sizes are hugely important – as long as accompanying P values measure up. And pharmaceutical companies often keep revealing numbers under wraps unless you know what – and whom – to ask.
Those lessons come courtesy of Leslie Citrome, MD, MPH, who spoke to colleagues about study numbers at Psych Congress 2019.
Dr. Citrome, clinical professor of psychiatry and behavioral sciences at New York Medical College, Valhalla, offered several tips about interpreting medical statistics as you make clinical decisions.
Don’t get hung up on the P value.
The P value helps you understand how likely it is that a difference in a study is statistically significant. In medical research, P values under .05 are considered especially desirable. They suggest that an outcome – drug A performed better than drug B, for example – didn’t happen purely by chance.
Here’s the hitch: The P value might not matter at all. “Clinicians often assume that if the P value is less than.05, the result must be important. But even a P value of less than .05 is meaningless outside of the context of how big the treatment effect is,” Dr. Citrome said. “If a clinical trial result shows us a small effect size, then who cares?”
Understand what effect sizes tell you.
Effect size measurements evaluate clinical impact and include number needed to treat (NNT) and number needed to harm (NNH). NNT refers to the number of patients needed to treat with an intervention in order to get a positive effect in one additional patient; NNH is the reverse and examines negative effects that can range from the minor (mild dry mouth) to the devastating (death).
What’s a good size for an NNT? “I respect any NNT versus placebo of less than 10,” Dr. Citrome said. “It’s something I’ll probably consider in day-to-day practice.” Double-digit and triple-digit NNTs “are usually irrelevant unless we’re dealing with very specific outcomes that have long-term consequences.”
As for the opposite side of the picture – NNH – values higher than 10 are ideal.
He cautioned that NNT and NNH, like P values, cannot stand alone. In fact, they work together. In order to have value, NNT or NNH must be statistically significant, and P values provide this crucial insight.
Consider Dr. Citrome’s blood pressure.
As Dr. Citrome noted, research suggests that, among patients with diastolic BP from 90 to 109 mm Hg, 1 additional person will avoid death, stroke, or heart attack for every 141 people who take an antihypertensive medication, compared to those who do not, over a 5-year period. That’s a lot of people taking medication for a long time, with potential side effects, for a fairly small effect size. However, the outcomes are dire, so it is still worth it.
Then there’s Dr. Citrome himself, who has had diastolic BP in the range of 115 to 129 mm Hg. The NNT is 3. For every 3 people who take an antihypertensive vs. not over a 5-year period, 1 additional person will avoid a potentially catastrophic cardiovascular event.
“Guess who’s pretty adherent to taking his antihypertensive medication?” he asked. “I am.”
Ask for effect sizes if you don’t see them.
It’s not unusual for pharmaceutical representatives to avoid providing information about medication effect sizes. “The sales representatives as well as speakers at [Food and Drug Administration]–regulated promotional speaking events can only speak to basically what’s on the label. NNT and NNH are not currently found on product labels. But they are very relevant, and we need to know this information.”
What to do? “There is a workaround here,” he said. “Ask the sales rep to talk to a medical science liaison, who is free to come to your office and talk about all the data that they have.”
Dr. Citrome reported multiple disclosures, including various relationships with pharmaceutical companies.
SAN DIEGO – Even if a P value hints at statistical significance by dipping under .05, it might not tell you anything worthwhile. Effect sizes are hugely important – as long as accompanying P values measure up. And pharmaceutical companies often keep revealing numbers under wraps unless you know what – and whom – to ask.
Those lessons come courtesy of Leslie Citrome, MD, MPH, who spoke to colleagues about study numbers at Psych Congress 2019.
Dr. Citrome, clinical professor of psychiatry and behavioral sciences at New York Medical College, Valhalla, offered several tips about interpreting medical statistics as you make clinical decisions.
Don’t get hung up on the P value.
The P value helps you understand how likely it is that a difference in a study is statistically significant. In medical research, P values under .05 are considered especially desirable. They suggest that an outcome – drug A performed better than drug B, for example – didn’t happen purely by chance.
Here’s the hitch: The P value might not matter at all. “Clinicians often assume that if the P value is less than.05, the result must be important. But even a P value of less than .05 is meaningless outside of the context of how big the treatment effect is,” Dr. Citrome said. “If a clinical trial result shows us a small effect size, then who cares?”
Understand what effect sizes tell you.
Effect size measurements evaluate clinical impact and include number needed to treat (NNT) and number needed to harm (NNH). NNT refers to the number of patients needed to treat with an intervention in order to get a positive effect in one additional patient; NNH is the reverse and examines negative effects that can range from the minor (mild dry mouth) to the devastating (death).
What’s a good size for an NNT? “I respect any NNT versus placebo of less than 10,” Dr. Citrome said. “It’s something I’ll probably consider in day-to-day practice.” Double-digit and triple-digit NNTs “are usually irrelevant unless we’re dealing with very specific outcomes that have long-term consequences.”
As for the opposite side of the picture – NNH – values higher than 10 are ideal.
He cautioned that NNT and NNH, like P values, cannot stand alone. In fact, they work together. In order to have value, NNT or NNH must be statistically significant, and P values provide this crucial insight.
Consider Dr. Citrome’s blood pressure.
As Dr. Citrome noted, research suggests that, among patients with diastolic BP from 90 to 109 mm Hg, 1 additional person will avoid death, stroke, or heart attack for every 141 people who take an antihypertensive medication, compared to those who do not, over a 5-year period. That’s a lot of people taking medication for a long time, with potential side effects, for a fairly small effect size. However, the outcomes are dire, so it is still worth it.
Then there’s Dr. Citrome himself, who has had diastolic BP in the range of 115 to 129 mm Hg. The NNT is 3. For every 3 people who take an antihypertensive vs. not over a 5-year period, 1 additional person will avoid a potentially catastrophic cardiovascular event.
“Guess who’s pretty adherent to taking his antihypertensive medication?” he asked. “I am.”
Ask for effect sizes if you don’t see them.
It’s not unusual for pharmaceutical representatives to avoid providing information about medication effect sizes. “The sales representatives as well as speakers at [Food and Drug Administration]–regulated promotional speaking events can only speak to basically what’s on the label. NNT and NNH are not currently found on product labels. But they are very relevant, and we need to know this information.”
What to do? “There is a workaround here,” he said. “Ask the sales rep to talk to a medical science liaison, who is free to come to your office and talk about all the data that they have.”
Dr. Citrome reported multiple disclosures, including various relationships with pharmaceutical companies.
REPORTING FROM PSYCH CONGRESS 2019
State medical boards under fire in physician suicides
SAN DIEGO – Physician suicide is “a public health crisis because of the sheer volume of people who are dying,” and many medical authorities are contributing to stigma through “invasive” questionnaires, a prevention advocate said at the annual Psych Congress.

“Physicians fear sharing their mental health struggles with the state medical health board,” said Pamela Wible, MD, a family physician who practices in Eugene, Ore., at the meeting. They “pretend, deny, and lie,” she said, and sometimes they seek care and medication hours away in order to avoid detection.
including the “very worst,” which is that of Alaska.
Dr. Wible, who speaks of suffering from suicidal feelings herself as physician in 2004, is a leading advocate for suicide prevention in the medical profession.
She told colleagues at the Psych Congress that anesthesiologists face the highest risk of suicide, followed by surgeons, ob.gyns., and psychiatrists.
“They end their lives not because they want to die but because they want to stop the pain and they can’t find any other way,” she said. “They have a great work ethic until the end: They’re smiling, doing complex surgeries, and cracking jokes to the surgical team, then they shoot themselves in the closet.”
Colleagues are often shocked, she said: “ ‘Wait a minute. He was just joking with me yesterday. What do you mean he hung himself in his office?’ ‘She just had a newborn baby and she was so happy!’ If you see the smile, you don’t see the pain.”
In 2018, she wrote a Washington Post commentary titled “What I’ve learned from my tally of 757 doctor suicides” that was based on her registry of physician suicides. In the United States, she wrote, 1 million patients lose a physician to suicide each year. Factors contributing to suicides include patient deaths, malpractice suits, “academic distress,” and overwork. “Doctors who need help don’t seek it because they fear mental health care won’t remain confidential,” she wrote. “So they drive out of town, pay cash, and use fake names to hide from state medical boards, hospitals, and insurance plans out of fear that they will lose state licensure, hospital privileges, and health plan participation.”
Dr. Wible oversaw a 2019 research project that analyzed state medical board applications. The goal was to grade the state boards by how intrusively their application questions grill applicants about their mental health history. “Physicians fear sharing their mental health struggles with the state medical health board and with each other,” she said. Some lie, and others – “the really honest physicians” – are so dedicated to telling the truth that “they’ll withhold getting care because they want to correctly check the ‘no’ box.”
Seven states – Alabama, Alaska, Delaware, Florida, Mississippi, Rhode Island, and Washington –received “F” grades for “highly invasive mental health questions unlinked to current impairment that contain confusing, punitive, or adversarial language.”
Alaska, Dr. Wible said, asks multiple 25 yes-or-no questions about mental health. One question lists 14 conditions, almost all related to mental health – including depression, “any organic mental disorder,” and “any condition requiring chronic medical or behavioral treatment” – and asks, “Have you ever been diagnosed with, treated for, or do you currently have” any of them. This is “the most invasive mental health question we found on any application,” Dr. Wible wrote on her website.
States also hurt applicants by asking peers of applicants about their mental health, she said. “I’m not against getting peer references, but can we stop getting into everyone’s business with their psych history? What we really want to know is: ‘Are you are safe with patients today?’ ”
Dr. Wible also criticizes state medical boards for asking about mental health impairment over the last 5 years: They don’t get higher than a “C.”
The 13 states with “A” grades either don’t ask about mental health or simply ask about general impairment: Connecticut, Hawaii, Indiana, Kentucky, New Jersey, Maine, Maryland, Massachusetts, Michigan, Nevada, New York, Pennsylvania, and Wyoming.
Massachusetts, for example, asks, “Do you have a medical or physical condition that currently impairs your ability to practice medicine?”
“That is a question anyone can understand,” Dr. Wible said. “I think that’s good wording.”
Going forward, she said, “we’ve got to remove these mental health questions. If we could do this, our profession would be so much better, and we’d lose so many fewer people.”
And, she added, “what we really need to do is share our stories. It’s therapeutic for you and your colleagues, it creates collegial trust and bonding, and it destigmatizes physician mental health.”
Dr. Wible reported no relevant disclosures.
SAN DIEGO – Physician suicide is “a public health crisis because of the sheer volume of people who are dying,” and many medical authorities are contributing to stigma through “invasive” questionnaires, a prevention advocate said at the annual Psych Congress.
“Physicians fear sharing their mental health struggles with the state medical health board,” said Pamela Wible, MD, a family physician who practices in Eugene, Ore., at the meeting. They “pretend, deny, and lie,” she said, and sometimes they seek care and medication hours away in order to avoid detection.
including the “very worst,” which is that of Alaska.
Dr. Wible, who speaks of suffering from suicidal feelings herself as physician in 2004, is a leading advocate for suicide prevention in the medical profession.
She told colleagues at the Psych Congress that anesthesiologists face the highest risk of suicide, followed by surgeons, ob.gyns., and psychiatrists.
“They end their lives not because they want to die but because they want to stop the pain and they can’t find any other way,” she said. “They have a great work ethic until the end: They’re smiling, doing complex surgeries, and cracking jokes to the surgical team, then they shoot themselves in the closet.”
Colleagues are often shocked, she said: “ ‘Wait a minute. He was just joking with me yesterday. What do you mean he hung himself in his office?’ ‘She just had a newborn baby and she was so happy!’ If you see the smile, you don’t see the pain.”
In 2018, she wrote a Washington Post commentary titled “What I’ve learned from my tally of 757 doctor suicides” that was based on her registry of physician suicides. In the United States, she wrote, 1 million patients lose a physician to suicide each year. Factors contributing to suicides include patient deaths, malpractice suits, “academic distress,” and overwork. “Doctors who need help don’t seek it because they fear mental health care won’t remain confidential,” she wrote. “So they drive out of town, pay cash, and use fake names to hide from state medical boards, hospitals, and insurance plans out of fear that they will lose state licensure, hospital privileges, and health plan participation.”
Dr. Wible oversaw a 2019 research project that analyzed state medical board applications. The goal was to grade the state boards by how intrusively their application questions grill applicants about their mental health history. “Physicians fear sharing their mental health struggles with the state medical health board and with each other,” she said. Some lie, and others – “the really honest physicians” – are so dedicated to telling the truth that “they’ll withhold getting care because they want to correctly check the ‘no’ box.”
Seven states – Alabama, Alaska, Delaware, Florida, Mississippi, Rhode Island, and Washington –received “F” grades for “highly invasive mental health questions unlinked to current impairment that contain confusing, punitive, or adversarial language.”
Alaska, Dr. Wible said, asks multiple 25 yes-or-no questions about mental health. One question lists 14 conditions, almost all related to mental health – including depression, “any organic mental disorder,” and “any condition requiring chronic medical or behavioral treatment” – and asks, “Have you ever been diagnosed with, treated for, or do you currently have” any of them. This is “the most invasive mental health question we found on any application,” Dr. Wible wrote on her website.
States also hurt applicants by asking peers of applicants about their mental health, she said. “I’m not against getting peer references, but can we stop getting into everyone’s business with their psych history? What we really want to know is: ‘Are you are safe with patients today?’ ”
Dr. Wible also criticizes state medical boards for asking about mental health impairment over the last 5 years: They don’t get higher than a “C.”
The 13 states with “A” grades either don’t ask about mental health or simply ask about general impairment: Connecticut, Hawaii, Indiana, Kentucky, New Jersey, Maine, Maryland, Massachusetts, Michigan, Nevada, New York, Pennsylvania, and Wyoming.
Massachusetts, for example, asks, “Do you have a medical or physical condition that currently impairs your ability to practice medicine?”
“That is a question anyone can understand,” Dr. Wible said. “I think that’s good wording.”
Going forward, she said, “we’ve got to remove these mental health questions. If we could do this, our profession would be so much better, and we’d lose so many fewer people.”
And, she added, “what we really need to do is share our stories. It’s therapeutic for you and your colleagues, it creates collegial trust and bonding, and it destigmatizes physician mental health.”
Dr. Wible reported no relevant disclosures.
SAN DIEGO – Physician suicide is “a public health crisis because of the sheer volume of people who are dying,” and many medical authorities are contributing to stigma through “invasive” questionnaires, a prevention advocate said at the annual Psych Congress.
“Physicians fear sharing their mental health struggles with the state medical health board,” said Pamela Wible, MD, a family physician who practices in Eugene, Ore., at the meeting. They “pretend, deny, and lie,” she said, and sometimes they seek care and medication hours away in order to avoid detection.
including the “very worst,” which is that of Alaska.
Dr. Wible, who speaks of suffering from suicidal feelings herself as physician in 2004, is a leading advocate for suicide prevention in the medical profession.
She told colleagues at the Psych Congress that anesthesiologists face the highest risk of suicide, followed by surgeons, ob.gyns., and psychiatrists.
“They end their lives not because they want to die but because they want to stop the pain and they can’t find any other way,” she said. “They have a great work ethic until the end: They’re smiling, doing complex surgeries, and cracking jokes to the surgical team, then they shoot themselves in the closet.”
Colleagues are often shocked, she said: “ ‘Wait a minute. He was just joking with me yesterday. What do you mean he hung himself in his office?’ ‘She just had a newborn baby and she was so happy!’ If you see the smile, you don’t see the pain.”
In 2018, she wrote a Washington Post commentary titled “What I’ve learned from my tally of 757 doctor suicides” that was based on her registry of physician suicides. In the United States, she wrote, 1 million patients lose a physician to suicide each year. Factors contributing to suicides include patient deaths, malpractice suits, “academic distress,” and overwork. “Doctors who need help don’t seek it because they fear mental health care won’t remain confidential,” she wrote. “So they drive out of town, pay cash, and use fake names to hide from state medical boards, hospitals, and insurance plans out of fear that they will lose state licensure, hospital privileges, and health plan participation.”
Dr. Wible oversaw a 2019 research project that analyzed state medical board applications. The goal was to grade the state boards by how intrusively their application questions grill applicants about their mental health history. “Physicians fear sharing their mental health struggles with the state medical health board and with each other,” she said. Some lie, and others – “the really honest physicians” – are so dedicated to telling the truth that “they’ll withhold getting care because they want to correctly check the ‘no’ box.”
Seven states – Alabama, Alaska, Delaware, Florida, Mississippi, Rhode Island, and Washington –received “F” grades for “highly invasive mental health questions unlinked to current impairment that contain confusing, punitive, or adversarial language.”
Alaska, Dr. Wible said, asks multiple 25 yes-or-no questions about mental health. One question lists 14 conditions, almost all related to mental health – including depression, “any organic mental disorder,” and “any condition requiring chronic medical or behavioral treatment” – and asks, “Have you ever been diagnosed with, treated for, or do you currently have” any of them. This is “the most invasive mental health question we found on any application,” Dr. Wible wrote on her website.
States also hurt applicants by asking peers of applicants about their mental health, she said. “I’m not against getting peer references, but can we stop getting into everyone’s business with their psych history? What we really want to know is: ‘Are you are safe with patients today?’ ”
Dr. Wible also criticizes state medical boards for asking about mental health impairment over the last 5 years: They don’t get higher than a “C.”
The 13 states with “A” grades either don’t ask about mental health or simply ask about general impairment: Connecticut, Hawaii, Indiana, Kentucky, New Jersey, Maine, Maryland, Massachusetts, Michigan, Nevada, New York, Pennsylvania, and Wyoming.
Massachusetts, for example, asks, “Do you have a medical or physical condition that currently impairs your ability to practice medicine?”
“That is a question anyone can understand,” Dr. Wible said. “I think that’s good wording.”
Going forward, she said, “we’ve got to remove these mental health questions. If we could do this, our profession would be so much better, and we’d lose so many fewer people.”
And, she added, “what we really need to do is share our stories. It’s therapeutic for you and your colleagues, it creates collegial trust and bonding, and it destigmatizes physician mental health.”
Dr. Wible reported no relevant disclosures.
EXPERT ANALYSIS FROM PSYCH CONGRESS 2019
Agitation in psychosis: Still no ‘magic bullet’
SAN DIEGO – The Food and Drug Administration has not approved a drug to treat agitation in dementia, and the absence of medication candidates is only part of the picture. As a geriatric psychiatrist explained to colleagues, the FDA has not taken the step of recognizing that the condition exists. But there are still options to treat this dangerous disorder – although none is ideal.
Research into efficacy of potential treatments for agitation is limited, variable, and “have high placebo effects,” said Marc E. Agronin, MD, of the MIND Institute and Miami Jewish Health, at the annual Psych Congress. “There is no one single magic bullet, especially since there are so many manifestations of agitation, and there are side effects of medication. This is a tough area to focus on.”
What can clinicians do? Dr. Agronin recommended starting with the steps in the DICE algorithm.
- Describe: Learn about the aspects of agitation by talking to caregivers and understanding the circumstances when symptoms develop.
- Investigate: Identify contributing factors, such as those related to illness, medication, and the environment.
- Create: Come up with a team strategy to address the contributing factors. Delirium is especially dangerous since it can lead to injury and subacute cognitive decline. And keep in mind, Dr. Agorin said, that it may be risky to do nothing or undertreat.
- Evaluate: Track the results of the strategy while realizing that there’s “not always a quick fix.” Research suggests that therapeutic approaches such as music, aromatherapy, exercise, group activities, hand massage, and thermal baths can be helpful, Dr. Agronin said.
As for medications, he advised starting with lower doses, perhaps 50%, because older people are less tolerant of medication. And beware of oversedation, dizziness, and lowered blood pressure, which can lead to falls. A hip fracture can “spiral down to someone’s demise very quickly,” he said.
Here’s a closer look at Dr. Agronin’s comments regarding specific medications.
- Antipsychotics: “Every antipsychotic has been used for agitation,” he said, “and they probably have the best efficacy,” compared with other drugs. But the risk of side effects is moderate to high, and atypical antipsychotics have a black-box warning about their use in dementia-related psychosis in elderly patients. Also, discontinuation of antipsychotics can trigger worsening symptoms in some patients. There has been tremendous controversy in recent years over the use of antipsychotics in older patients, but other drugs might be less effective than antipsychotics while still having similar side effect profiles, he said. And clinicians might be too cautious about doses even when they do use these drugs.
- Benzodiazepines: They can work quickly but come with a risk of sedation. Trazodone is an “excellent” alternative to reduce agitation in the short-term, he said.
- Antidepressants: These drugs can address underlying depression. Study results have been mixed.
- Mood stabilizers: Study results are mixed. “Unfortunately, in many situations [clinicians] get scared away from antipsychotics and use mood stabilizers, but there is less data for them in terms of efficacy, and there are a lot of side effects that have to be monitored,” he said.
Dr. Agronin is the author of “How We Age” (Da Capo Lifelong Books, 2012) and “The End of Old Age” (Da Capo Lifelong Books, 2018). He has no relevant disclosures.
SAN DIEGO – The Food and Drug Administration has not approved a drug to treat agitation in dementia, and the absence of medication candidates is only part of the picture. As a geriatric psychiatrist explained to colleagues, the FDA has not taken the step of recognizing that the condition exists. But there are still options to treat this dangerous disorder – although none is ideal.
Research into efficacy of potential treatments for agitation is limited, variable, and “have high placebo effects,” said Marc E. Agronin, MD, of the MIND Institute and Miami Jewish Health, at the annual Psych Congress. “There is no one single magic bullet, especially since there are so many manifestations of agitation, and there are side effects of medication. This is a tough area to focus on.”
What can clinicians do? Dr. Agronin recommended starting with the steps in the DICE algorithm.
- Describe: Learn about the aspects of agitation by talking to caregivers and understanding the circumstances when symptoms develop.
- Investigate: Identify contributing factors, such as those related to illness, medication, and the environment.
- Create: Come up with a team strategy to address the contributing factors. Delirium is especially dangerous since it can lead to injury and subacute cognitive decline. And keep in mind, Dr. Agorin said, that it may be risky to do nothing or undertreat.
- Evaluate: Track the results of the strategy while realizing that there’s “not always a quick fix.” Research suggests that therapeutic approaches such as music, aromatherapy, exercise, group activities, hand massage, and thermal baths can be helpful, Dr. Agronin said.
As for medications, he advised starting with lower doses, perhaps 50%, because older people are less tolerant of medication. And beware of oversedation, dizziness, and lowered blood pressure, which can lead to falls. A hip fracture can “spiral down to someone’s demise very quickly,” he said.
Here’s a closer look at Dr. Agronin’s comments regarding specific medications.
- Antipsychotics: “Every antipsychotic has been used for agitation,” he said, “and they probably have the best efficacy,” compared with other drugs. But the risk of side effects is moderate to high, and atypical antipsychotics have a black-box warning about their use in dementia-related psychosis in elderly patients. Also, discontinuation of antipsychotics can trigger worsening symptoms in some patients. There has been tremendous controversy in recent years over the use of antipsychotics in older patients, but other drugs might be less effective than antipsychotics while still having similar side effect profiles, he said. And clinicians might be too cautious about doses even when they do use these drugs.
- Benzodiazepines: They can work quickly but come with a risk of sedation. Trazodone is an “excellent” alternative to reduce agitation in the short-term, he said.
- Antidepressants: These drugs can address underlying depression. Study results have been mixed.
- Mood stabilizers: Study results are mixed. “Unfortunately, in many situations [clinicians] get scared away from antipsychotics and use mood stabilizers, but there is less data for them in terms of efficacy, and there are a lot of side effects that have to be monitored,” he said.
Dr. Agronin is the author of “How We Age” (Da Capo Lifelong Books, 2012) and “The End of Old Age” (Da Capo Lifelong Books, 2018). He has no relevant disclosures.
SAN DIEGO – The Food and Drug Administration has not approved a drug to treat agitation in dementia, and the absence of medication candidates is only part of the picture. As a geriatric psychiatrist explained to colleagues, the FDA has not taken the step of recognizing that the condition exists. But there are still options to treat this dangerous disorder – although none is ideal.
Research into efficacy of potential treatments for agitation is limited, variable, and “have high placebo effects,” said Marc E. Agronin, MD, of the MIND Institute and Miami Jewish Health, at the annual Psych Congress. “There is no one single magic bullet, especially since there are so many manifestations of agitation, and there are side effects of medication. This is a tough area to focus on.”
What can clinicians do? Dr. Agronin recommended starting with the steps in the DICE algorithm.
- Describe: Learn about the aspects of agitation by talking to caregivers and understanding the circumstances when symptoms develop.
- Investigate: Identify contributing factors, such as those related to illness, medication, and the environment.
- Create: Come up with a team strategy to address the contributing factors. Delirium is especially dangerous since it can lead to injury and subacute cognitive decline. And keep in mind, Dr. Agorin said, that it may be risky to do nothing or undertreat.
- Evaluate: Track the results of the strategy while realizing that there’s “not always a quick fix.” Research suggests that therapeutic approaches such as music, aromatherapy, exercise, group activities, hand massage, and thermal baths can be helpful, Dr. Agronin said.
As for medications, he advised starting with lower doses, perhaps 50%, because older people are less tolerant of medication. And beware of oversedation, dizziness, and lowered blood pressure, which can lead to falls. A hip fracture can “spiral down to someone’s demise very quickly,” he said.
Here’s a closer look at Dr. Agronin’s comments regarding specific medications.
- Antipsychotics: “Every antipsychotic has been used for agitation,” he said, “and they probably have the best efficacy,” compared with other drugs. But the risk of side effects is moderate to high, and atypical antipsychotics have a black-box warning about their use in dementia-related psychosis in elderly patients. Also, discontinuation of antipsychotics can trigger worsening symptoms in some patients. There has been tremendous controversy in recent years over the use of antipsychotics in older patients, but other drugs might be less effective than antipsychotics while still having similar side effect profiles, he said. And clinicians might be too cautious about doses even when they do use these drugs.
- Benzodiazepines: They can work quickly but come with a risk of sedation. Trazodone is an “excellent” alternative to reduce agitation in the short-term, he said.
- Antidepressants: These drugs can address underlying depression. Study results have been mixed.
- Mood stabilizers: Study results are mixed. “Unfortunately, in many situations [clinicians] get scared away from antipsychotics and use mood stabilizers, but there is less data for them in terms of efficacy, and there are a lot of side effects that have to be monitored,” he said.
Dr. Agronin is the author of “How We Age” (Da Capo Lifelong Books, 2012) and “The End of Old Age” (Da Capo Lifelong Books, 2018). He has no relevant disclosures.
REPORTING FROM PSYCH CONGRESS 2019
In methamphetamine use disorder, consider off-label drugs
SAN DIEGO – Its toll is obscured by the opioid crisis, but methamphetamine use is on the rise in the United States. There are no approved treatments for methamphetamine use, but a psychiatrist told colleagues that several off-label medications might prove helpful.
However, the evidence supporting the use of these medications for patients taking methamphetamine is not robust, “and none are even close to [Food and Drug Administration] approval,” said Larissa J. Mooney, MD, of the University of California, Los Angeles, and the VA Greater Los Angeles Healthcare System. “But if I use something that’s approved for depression or might be helpful for anxiety symptoms, maybe it would also help reduce their likelihood of relapse in conjunction with an evidence-based behavioral program or treatment with a therapist.”
Dr. Mooney, who spoke at the annual Psych Congress, highlighted a federal report estimating that 0.4% of people aged 18-25 in 2017 used the drug within the past month, compared with 0.3% of those aged 26 and higher.
There were about 758,000 current adult users of methamphetamine in 2017, the report found.
Meanwhile, (Drug Alcohol Depend. 2018 Dec 1;193:14-20). And, Dr. Mooney said, deaths from stimulants are rising, even independent of opioid deaths.
Stimulant users typically have other psychiatric conditions, such as depression, anxiety, and concentration problems, Dr. Mooney said. In those cases, she said, treating those conditions might help with the substance use, too.
For methamphetamine use disorder, she highlighted some medications that might be helpful, although, again, she cautioned that evidence is not strong:
- Bupropion (Wellbutrin). Research suggests that this drug is more effective in patients with less severe methamphetamine use disorder, Dr. Mooney said. “It’s a more stimulating antidepressant, and can be helpful with concentration and attention.”
- Mirtazapine (Remeron). “I keep it in my list of options for some [who are] really anxious and not sleeping well,” she said. “It might be beneficial.”
- Naltrexone (ReVia, Depade, Vivitrol). “There are some early signs of efficacy,” she said, and a randomized, controlled trial is in progress.
- Methylphenidate (Ritalin, Concerta) and topiramate (Topamax). There’s “low-strength” evidence that the drugs can be helpful and lower use of methamphetamine, she said. However, methylphenidate is a stimulant. There’s controversy over the use of stimulants to treat patients with substance use disorders, Dr. Mooney said, and she tends to be conservative about their use in this population.
Why not use them to treat methamphetamine users in the same way that opioids such as methadone are used to treat opioid use addiction? “We don’t have an equivalent stimulant that works in the same way,” she said. “They don’t stay in the system for 24 hours. If you take a prescription stimulant, by the end of the day it wears off. It won’t stay in the same way as agonist treatments for opioid disorder.”
Even so, she said, “it makes sense that stimulants might be helpful.”
Dr. Mooney disclosed an advisory board relationship with Alkermes and grant/research support from the National Institute on Drug Abuse.
SAN DIEGO – Its toll is obscured by the opioid crisis, but methamphetamine use is on the rise in the United States. There are no approved treatments for methamphetamine use, but a psychiatrist told colleagues that several off-label medications might prove helpful.
However, the evidence supporting the use of these medications for patients taking methamphetamine is not robust, “and none are even close to [Food and Drug Administration] approval,” said Larissa J. Mooney, MD, of the University of California, Los Angeles, and the VA Greater Los Angeles Healthcare System. “But if I use something that’s approved for depression or might be helpful for anxiety symptoms, maybe it would also help reduce their likelihood of relapse in conjunction with an evidence-based behavioral program or treatment with a therapist.”
Dr. Mooney, who spoke at the annual Psych Congress, highlighted a federal report estimating that 0.4% of people aged 18-25 in 2017 used the drug within the past month, compared with 0.3% of those aged 26 and higher.
There were about 758,000 current adult users of methamphetamine in 2017, the report found.
Meanwhile, (Drug Alcohol Depend. 2018 Dec 1;193:14-20). And, Dr. Mooney said, deaths from stimulants are rising, even independent of opioid deaths.
Stimulant users typically have other psychiatric conditions, such as depression, anxiety, and concentration problems, Dr. Mooney said. In those cases, she said, treating those conditions might help with the substance use, too.
For methamphetamine use disorder, she highlighted some medications that might be helpful, although, again, she cautioned that evidence is not strong:
- Bupropion (Wellbutrin). Research suggests that this drug is more effective in patients with less severe methamphetamine use disorder, Dr. Mooney said. “It’s a more stimulating antidepressant, and can be helpful with concentration and attention.”
- Mirtazapine (Remeron). “I keep it in my list of options for some [who are] really anxious and not sleeping well,” she said. “It might be beneficial.”
- Naltrexone (ReVia, Depade, Vivitrol). “There are some early signs of efficacy,” she said, and a randomized, controlled trial is in progress.
- Methylphenidate (Ritalin, Concerta) and topiramate (Topamax). There’s “low-strength” evidence that the drugs can be helpful and lower use of methamphetamine, she said. However, methylphenidate is a stimulant. There’s controversy over the use of stimulants to treat patients with substance use disorders, Dr. Mooney said, and she tends to be conservative about their use in this population.
Why not use them to treat methamphetamine users in the same way that opioids such as methadone are used to treat opioid use addiction? “We don’t have an equivalent stimulant that works in the same way,” she said. “They don’t stay in the system for 24 hours. If you take a prescription stimulant, by the end of the day it wears off. It won’t stay in the same way as agonist treatments for opioid disorder.”
Even so, she said, “it makes sense that stimulants might be helpful.”
Dr. Mooney disclosed an advisory board relationship with Alkermes and grant/research support from the National Institute on Drug Abuse.
SAN DIEGO – Its toll is obscured by the opioid crisis, but methamphetamine use is on the rise in the United States. There are no approved treatments for methamphetamine use, but a psychiatrist told colleagues that several off-label medications might prove helpful.
However, the evidence supporting the use of these medications for patients taking methamphetamine is not robust, “and none are even close to [Food and Drug Administration] approval,” said Larissa J. Mooney, MD, of the University of California, Los Angeles, and the VA Greater Los Angeles Healthcare System. “But if I use something that’s approved for depression or might be helpful for anxiety symptoms, maybe it would also help reduce their likelihood of relapse in conjunction with an evidence-based behavioral program or treatment with a therapist.”
Dr. Mooney, who spoke at the annual Psych Congress, highlighted a federal report estimating that 0.4% of people aged 18-25 in 2017 used the drug within the past month, compared with 0.3% of those aged 26 and higher.
There were about 758,000 current adult users of methamphetamine in 2017, the report found.
Meanwhile, (Drug Alcohol Depend. 2018 Dec 1;193:14-20). And, Dr. Mooney said, deaths from stimulants are rising, even independent of opioid deaths.
Stimulant users typically have other psychiatric conditions, such as depression, anxiety, and concentration problems, Dr. Mooney said. In those cases, she said, treating those conditions might help with the substance use, too.
For methamphetamine use disorder, she highlighted some medications that might be helpful, although, again, she cautioned that evidence is not strong:
- Bupropion (Wellbutrin). Research suggests that this drug is more effective in patients with less severe methamphetamine use disorder, Dr. Mooney said. “It’s a more stimulating antidepressant, and can be helpful with concentration and attention.”
- Mirtazapine (Remeron). “I keep it in my list of options for some [who are] really anxious and not sleeping well,” she said. “It might be beneficial.”
- Naltrexone (ReVia, Depade, Vivitrol). “There are some early signs of efficacy,” she said, and a randomized, controlled trial is in progress.
- Methylphenidate (Ritalin, Concerta) and topiramate (Topamax). There’s “low-strength” evidence that the drugs can be helpful and lower use of methamphetamine, she said. However, methylphenidate is a stimulant. There’s controversy over the use of stimulants to treat patients with substance use disorders, Dr. Mooney said, and she tends to be conservative about their use in this population.
Why not use them to treat methamphetamine users in the same way that opioids such as methadone are used to treat opioid use addiction? “We don’t have an equivalent stimulant that works in the same way,” she said. “They don’t stay in the system for 24 hours. If you take a prescription stimulant, by the end of the day it wears off. It won’t stay in the same way as agonist treatments for opioid disorder.”
Even so, she said, “it makes sense that stimulants might be helpful.”
Dr. Mooney disclosed an advisory board relationship with Alkermes and grant/research support from the National Institute on Drug Abuse.
REPORTING FROM PSYCH CONGRESS 2019
Suicide attempts up in black U.S. teens
New research presents a complex picture of self-reported suicidal behavior in U.S. teenagers over the last few decades. Rates of suicidal ideation and plans dipped overall from 1991 to 2017, but the rate of suicide attempts grew slightly in black adolescents.
White young people “have historically had higher rates of suicide attempts...compared with their black counterparts; however, this study provides some evidence to the contrary,” wrote the authors of the report, which appears in the November issue of Pediatrics.
The investigators, led by Michael A. Lindsey, PhD, executive director of the McSilver Institute for Poverty Policy and Research at New York University, New York, note that suicide is the second leading cause of death in the United States in those aged 12-17. (Accidents rank first.) According to recent research, black children younger than 12 are at higher risk for death by suicide, compared with whites.
For the new study, researchers analyzed data from the Youth Risk Behavior Survey, which is conducted every 2 years among high school students in all 50 states and the District of Columbia. They examined data from 198,540 teens (mean age=16, 51% male; 49% female).
During the study period, the weighted overall prevalences rates of suicidal ideation, planning, attempt, and injury due to attempt were 19%, 15%, 8%, and 3%, respectively. “Our findings reveal that over that span of time, almost 1 in 5 adolescents are thinking about suicide... and > 1 in 10 has a suicide plan,” the researchers wrote.
Rates of suicidal ideation and planning fell overall, and among females, the rate of suicide attempts fell significantly (odds ratio [OR]=0.98). But self-reported suicide attempts grew significantly among black teens (OR=1.02), and injuries due to suicide attempts grew among black males (OR=1.04).
The findings are “troubling because attempts are the most prominent risk factor associated with suicide death,” the study authors wrote. “Findings regarding the rising rates of suicide attempts in black youth may be related to the documented disparities in mental health treatment and common social etiologic factors disproportionately experienced by black youth.”
In an accompanying commentary, psychiatrist Benjamin N. Shain, MD, PhD, of the University of Chicago, noted a seemingly “counterintuitive” fact: Black teens still have lower rates of suicide than whites teens “despite the greater, long-standing difficulties encountered by black adolescents, including disparities in mental health treatment and disproportionately higher stressors, racial discrimination, and childhood abuse and neglect, as well as other adverse experiences, such as poverty.”
It’s not clear why the reported suicide rate is lower in black adolescents than their white counterparts, Dr. Shain wrote, but misclassification and “undercount as a result of violence with suicidal intent, for example, ‘suicide by cop’” may play a role. Additionally, protective factors may have kept suicide rates down. “External attributional orientation (eg, blaming others or ‘the system’ for difficulties) among blacks may have buffered this group from internalizing blame related to psychological stressors,” he wrote.
Among black adolescents, the growing rate of suicidal behavior is concerning and may be due to a weakening of the hypothesized protective mechanism. Perhaps, Dr. Shain wrote, they now are blaming themselves more for difficulties encountered, “thus leading to an increase in suicide risk factors, particularly depression.” He stressed that, regardless of the reasons for the increase in suicide and suicide attempts, prevention and intervention efforts remain critical.
No study funding is reported, and authors report no relevant disclosures. Dr. Shain reports no relevant disclosures.
SOURCE: Lindsey MA et al, Pediatrics. 2019;144(5): e20191187, DOI:10.1542/peds.2019-1187.
New research presents a complex picture of self-reported suicidal behavior in U.S. teenagers over the last few decades. Rates of suicidal ideation and plans dipped overall from 1991 to 2017, but the rate of suicide attempts grew slightly in black adolescents.
White young people “have historically had higher rates of suicide attempts...compared with their black counterparts; however, this study provides some evidence to the contrary,” wrote the authors of the report, which appears in the November issue of Pediatrics.
The investigators, led by Michael A. Lindsey, PhD, executive director of the McSilver Institute for Poverty Policy and Research at New York University, New York, note that suicide is the second leading cause of death in the United States in those aged 12-17. (Accidents rank first.) According to recent research, black children younger than 12 are at higher risk for death by suicide, compared with whites.
For the new study, researchers analyzed data from the Youth Risk Behavior Survey, which is conducted every 2 years among high school students in all 50 states and the District of Columbia. They examined data from 198,540 teens (mean age=16, 51% male; 49% female).
During the study period, the weighted overall prevalences rates of suicidal ideation, planning, attempt, and injury due to attempt were 19%, 15%, 8%, and 3%, respectively. “Our findings reveal that over that span of time, almost 1 in 5 adolescents are thinking about suicide... and > 1 in 10 has a suicide plan,” the researchers wrote.
Rates of suicidal ideation and planning fell overall, and among females, the rate of suicide attempts fell significantly (odds ratio [OR]=0.98). But self-reported suicide attempts grew significantly among black teens (OR=1.02), and injuries due to suicide attempts grew among black males (OR=1.04).
The findings are “troubling because attempts are the most prominent risk factor associated with suicide death,” the study authors wrote. “Findings regarding the rising rates of suicide attempts in black youth may be related to the documented disparities in mental health treatment and common social etiologic factors disproportionately experienced by black youth.”
In an accompanying commentary, psychiatrist Benjamin N. Shain, MD, PhD, of the University of Chicago, noted a seemingly “counterintuitive” fact: Black teens still have lower rates of suicide than whites teens “despite the greater, long-standing difficulties encountered by black adolescents, including disparities in mental health treatment and disproportionately higher stressors, racial discrimination, and childhood abuse and neglect, as well as other adverse experiences, such as poverty.”
It’s not clear why the reported suicide rate is lower in black adolescents than their white counterparts, Dr. Shain wrote, but misclassification and “undercount as a result of violence with suicidal intent, for example, ‘suicide by cop’” may play a role. Additionally, protective factors may have kept suicide rates down. “External attributional orientation (eg, blaming others or ‘the system’ for difficulties) among blacks may have buffered this group from internalizing blame related to psychological stressors,” he wrote.
Among black adolescents, the growing rate of suicidal behavior is concerning and may be due to a weakening of the hypothesized protective mechanism. Perhaps, Dr. Shain wrote, they now are blaming themselves more for difficulties encountered, “thus leading to an increase in suicide risk factors, particularly depression.” He stressed that, regardless of the reasons for the increase in suicide and suicide attempts, prevention and intervention efforts remain critical.
No study funding is reported, and authors report no relevant disclosures. Dr. Shain reports no relevant disclosures.
SOURCE: Lindsey MA et al, Pediatrics. 2019;144(5): e20191187, DOI:10.1542/peds.2019-1187.
New research presents a complex picture of self-reported suicidal behavior in U.S. teenagers over the last few decades. Rates of suicidal ideation and plans dipped overall from 1991 to 2017, but the rate of suicide attempts grew slightly in black adolescents.
White young people “have historically had higher rates of suicide attempts...compared with their black counterparts; however, this study provides some evidence to the contrary,” wrote the authors of the report, which appears in the November issue of Pediatrics.
The investigators, led by Michael A. Lindsey, PhD, executive director of the McSilver Institute for Poverty Policy and Research at New York University, New York, note that suicide is the second leading cause of death in the United States in those aged 12-17. (Accidents rank first.) According to recent research, black children younger than 12 are at higher risk for death by suicide, compared with whites.
For the new study, researchers analyzed data from the Youth Risk Behavior Survey, which is conducted every 2 years among high school students in all 50 states and the District of Columbia. They examined data from 198,540 teens (mean age=16, 51% male; 49% female).
During the study period, the weighted overall prevalences rates of suicidal ideation, planning, attempt, and injury due to attempt were 19%, 15%, 8%, and 3%, respectively. “Our findings reveal that over that span of time, almost 1 in 5 adolescents are thinking about suicide... and > 1 in 10 has a suicide plan,” the researchers wrote.
Rates of suicidal ideation and planning fell overall, and among females, the rate of suicide attempts fell significantly (odds ratio [OR]=0.98). But self-reported suicide attempts grew significantly among black teens (OR=1.02), and injuries due to suicide attempts grew among black males (OR=1.04).
The findings are “troubling because attempts are the most prominent risk factor associated with suicide death,” the study authors wrote. “Findings regarding the rising rates of suicide attempts in black youth may be related to the documented disparities in mental health treatment and common social etiologic factors disproportionately experienced by black youth.”
In an accompanying commentary, psychiatrist Benjamin N. Shain, MD, PhD, of the University of Chicago, noted a seemingly “counterintuitive” fact: Black teens still have lower rates of suicide than whites teens “despite the greater, long-standing difficulties encountered by black adolescents, including disparities in mental health treatment and disproportionately higher stressors, racial discrimination, and childhood abuse and neglect, as well as other adverse experiences, such as poverty.”
It’s not clear why the reported suicide rate is lower in black adolescents than their white counterparts, Dr. Shain wrote, but misclassification and “undercount as a result of violence with suicidal intent, for example, ‘suicide by cop’” may play a role. Additionally, protective factors may have kept suicide rates down. “External attributional orientation (eg, blaming others or ‘the system’ for difficulties) among blacks may have buffered this group from internalizing blame related to psychological stressors,” he wrote.
Among black adolescents, the growing rate of suicidal behavior is concerning and may be due to a weakening of the hypothesized protective mechanism. Perhaps, Dr. Shain wrote, they now are blaming themselves more for difficulties encountered, “thus leading to an increase in suicide risk factors, particularly depression.” He stressed that, regardless of the reasons for the increase in suicide and suicide attempts, prevention and intervention efforts remain critical.
No study funding is reported, and authors report no relevant disclosures. Dr. Shain reports no relevant disclosures.
SOURCE: Lindsey MA et al, Pediatrics. 2019;144(5): e20191187, DOI:10.1542/peds.2019-1187.
FROM PEDIATRICS
Key clinical point: Overall self-reported suicidal behavior is down in U.S. teens, but attempts are up in black adolescents.
Major finding: Self-reported suicide attempts grew significantly among black teens (OR=1.02).
Study details: Retrospective analysis of 1991-2017 surveys of 198,540 U.S. teens (mean age=16, 51% male; 49% female).
Disclosures: No study funding is reported, and the study authors report no relevant disclosures.
Source: Lindsey MA et al, Pediatrics. 2019;144(5): e20191187,https://doi.org/10.1542/peds.2019-1187.
Smoking Out the Truth About Pot and Cancer
MINNEAPOLIS -- Medical professionals within the US Department of Veterans Affairs (VA) can’t prescribe cannabis or certify patients to be able to get it. VA pharmacists can’t dispense it. Still, “we’re asked about it plenty,” a hospice and palliative care specialist told colleagues, at the annual meeting of the Association of VA Hematology/Oncology (AVAHO).
That brings up a big question, said Michael Stellini, MD, MS, FACP, FAAHPM, of Wayne State University, Karmanos Cancer Center, and the John D. Dingell VA Medical Center, in Detroit Michigan: “Should sick people be smoking pot?”
Even the question itself isn’t a simple one to answer since smoking isn’t the only way to consume cannabis for medical purposes. And figuring out the best advice is difficult. As Dr. Stellini said, there’s plenty of uncertainty about crucial cannabis topics like safety and benefits.
Dr. Stellini offered a number of facts and tips about cannabis in medicine.
Understand ‘qualifying conditions’ in your state
In states with legal medical marijuana, he said, physicians do not prescribe marijuana. However, they may certify that patients are eligible to get the drug for medical purposes if they meet certain qualifications.
A typical list of qualifying conditions includes diseases such as cancer, glaucoma, HIV/AIDS and Crohn’s disease. Qualifying conditions also tend to include treatments for severe diseases that produce wasting syndrome, severe and chronic pain, severe nausea, seizures and severe and persistent muscle spasm.
In Michigan, where Dr. Stellini practices, a panel in 2018 approved a long list of added qualifying conditions such as chronic pain, obsessive compulsive disorder and arthritis. But the panel rejected other conditions such as anxiety, asthma, panic attacks and schizophrenia.
Vaporizers are an alternative to joints, but...
Vaporizers are commonly used as an alternative to smoking marijuana joints, Dr. Stellini said, and they don’t significantly release tars or much if any carbon monoxide. While research is limited, he said, use of vaporizers hasn’t been linked to more lung cancer or chronic obstructive pulmonary disease.
“Vaping” is another option, but it’s been linked to dozens of deaths and hundreds of cases of illness in recent weeks. Many patients have reported using products that contain THC, a component of marijuana.
Other delivery methods exist
Marijuana can be ingested in liquid and solid food. “But edibles can have a slow onset of action compared to vaporizing or smoking,” Dr. Stellini said. “You might over-indulge. When users get to their steady state, they might have some adverse effects [AEs].”
Marijuana still has risks
Cannabis use has a long list of well-known AEs linked to the THC component. The most common are drowsiness, fatigue, dizziness, dry mouth, anxiety, cognitive effects, cough, and nausea, Dr. Stellini said. More serious AEs such as psychosis have been reported.
And, of course, users of cannabis with THC get high if they use enough.
A 2017 National Academies of Sciences, Engineering and Medicine report linked cannabis use to a higher risk of motor vehicle accidents. Still, Dr. Stellini said, “it’s relatively safe with respect to mortality, especially compared to opioids.”1
Risk of use in cancer may be low
Research suggest that patients with cancer use cannabis as much as other people and perhaps even more, Dr. Stellini said. But are they facing any extra risks? In general, he said, it doesn’t appear that way.
Cannabis seems to be safe when used with chemotherapy, he said, and drug-drug interactions in cancer appear to be rare. Some studies have suggested that cannabinoids—a component of marijuana—may be an effective treatment for chemotherapy-induced peripheral neuropathy.
However, he said, 1 study has raised a red flag about a possible interaction with cancer immunotherapy. Researchers found evidence that patients who used cannabis had lower tumor response rates to nivolomab for advanced melanoma, non-small cell lung cancer, and renal clear cell carcinoma. However, survival wasn’t affected.2
Meanwhile, he said, there’s no strong evidence that cannabis is a useful treatment for cancer, he said, although it’s worth investigating.
Cannabidiol is the hot new product
Cannabidiol, also known as CBD, has become hugely popular, Dr. Stellini said. It is derived from hemp and doesn’t cause a “buzz” like cannabis.
Due to lack of regulation, he said, buyers should beware. And, he said, CBD has multiple EAs. Standard doses can cause drowsiness, fatigue, dizziness, dry mouth, hypotension and lightheadedness.
Dr. Stellini reports no relevant disclosures.
1. National Academies of Sciences, Engineering, and Medicine. The Health Effects of Cannabis and Cannabinoids: The Current State of Evidence and Recommendations for Research. Washington, DC: The National Academies Press; 2017.
2. Taha T, Meiri D, Talhamy S, Wollner M, Peer A, Bar-Sela G. Cannabis impacts tumor response rate to nivolumab in patients with advanced malignancies. Oncologist. 2019;24(4):549-554.
MINNEAPOLIS -- Medical professionals within the US Department of Veterans Affairs (VA) can’t prescribe cannabis or certify patients to be able to get it. VA pharmacists can’t dispense it. Still, “we’re asked about it plenty,” a hospice and palliative care specialist told colleagues, at the annual meeting of the Association of VA Hematology/Oncology (AVAHO).
That brings up a big question, said Michael Stellini, MD, MS, FACP, FAAHPM, of Wayne State University, Karmanos Cancer Center, and the John D. Dingell VA Medical Center, in Detroit Michigan: “Should sick people be smoking pot?”
Even the question itself isn’t a simple one to answer since smoking isn’t the only way to consume cannabis for medical purposes. And figuring out the best advice is difficult. As Dr. Stellini said, there’s plenty of uncertainty about crucial cannabis topics like safety and benefits.
Dr. Stellini offered a number of facts and tips about cannabis in medicine.
Understand ‘qualifying conditions’ in your state
In states with legal medical marijuana, he said, physicians do not prescribe marijuana. However, they may certify that patients are eligible to get the drug for medical purposes if they meet certain qualifications.
A typical list of qualifying conditions includes diseases such as cancer, glaucoma, HIV/AIDS and Crohn’s disease. Qualifying conditions also tend to include treatments for severe diseases that produce wasting syndrome, severe and chronic pain, severe nausea, seizures and severe and persistent muscle spasm.
In Michigan, where Dr. Stellini practices, a panel in 2018 approved a long list of added qualifying conditions such as chronic pain, obsessive compulsive disorder and arthritis. But the panel rejected other conditions such as anxiety, asthma, panic attacks and schizophrenia.
Vaporizers are an alternative to joints, but...
Vaporizers are commonly used as an alternative to smoking marijuana joints, Dr. Stellini said, and they don’t significantly release tars or much if any carbon monoxide. While research is limited, he said, use of vaporizers hasn’t been linked to more lung cancer or chronic obstructive pulmonary disease.
“Vaping” is another option, but it’s been linked to dozens of deaths and hundreds of cases of illness in recent weeks. Many patients have reported using products that contain THC, a component of marijuana.
Other delivery methods exist
Marijuana can be ingested in liquid and solid food. “But edibles can have a slow onset of action compared to vaporizing or smoking,” Dr. Stellini said. “You might over-indulge. When users get to their steady state, they might have some adverse effects [AEs].”
Marijuana still has risks
Cannabis use has a long list of well-known AEs linked to the THC component. The most common are drowsiness, fatigue, dizziness, dry mouth, anxiety, cognitive effects, cough, and nausea, Dr. Stellini said. More serious AEs such as psychosis have been reported.
And, of course, users of cannabis with THC get high if they use enough.
A 2017 National Academies of Sciences, Engineering and Medicine report linked cannabis use to a higher risk of motor vehicle accidents. Still, Dr. Stellini said, “it’s relatively safe with respect to mortality, especially compared to opioids.”1
Risk of use in cancer may be low
Research suggest that patients with cancer use cannabis as much as other people and perhaps even more, Dr. Stellini said. But are they facing any extra risks? In general, he said, it doesn’t appear that way.
Cannabis seems to be safe when used with chemotherapy, he said, and drug-drug interactions in cancer appear to be rare. Some studies have suggested that cannabinoids—a component of marijuana—may be an effective treatment for chemotherapy-induced peripheral neuropathy.
However, he said, 1 study has raised a red flag about a possible interaction with cancer immunotherapy. Researchers found evidence that patients who used cannabis had lower tumor response rates to nivolomab for advanced melanoma, non-small cell lung cancer, and renal clear cell carcinoma. However, survival wasn’t affected.2
Meanwhile, he said, there’s no strong evidence that cannabis is a useful treatment for cancer, he said, although it’s worth investigating.
Cannabidiol is the hot new product
Cannabidiol, also known as CBD, has become hugely popular, Dr. Stellini said. It is derived from hemp and doesn’t cause a “buzz” like cannabis.
Due to lack of regulation, he said, buyers should beware. And, he said, CBD has multiple EAs. Standard doses can cause drowsiness, fatigue, dizziness, dry mouth, hypotension and lightheadedness.
Dr. Stellini reports no relevant disclosures.
MINNEAPOLIS -- Medical professionals within the US Department of Veterans Affairs (VA) can’t prescribe cannabis or certify patients to be able to get it. VA pharmacists can’t dispense it. Still, “we’re asked about it plenty,” a hospice and palliative care specialist told colleagues, at the annual meeting of the Association of VA Hematology/Oncology (AVAHO).
That brings up a big question, said Michael Stellini, MD, MS, FACP, FAAHPM, of Wayne State University, Karmanos Cancer Center, and the John D. Dingell VA Medical Center, in Detroit Michigan: “Should sick people be smoking pot?”
Even the question itself isn’t a simple one to answer since smoking isn’t the only way to consume cannabis for medical purposes. And figuring out the best advice is difficult. As Dr. Stellini said, there’s plenty of uncertainty about crucial cannabis topics like safety and benefits.
Dr. Stellini offered a number of facts and tips about cannabis in medicine.
Understand ‘qualifying conditions’ in your state
In states with legal medical marijuana, he said, physicians do not prescribe marijuana. However, they may certify that patients are eligible to get the drug for medical purposes if they meet certain qualifications.
A typical list of qualifying conditions includes diseases such as cancer, glaucoma, HIV/AIDS and Crohn’s disease. Qualifying conditions also tend to include treatments for severe diseases that produce wasting syndrome, severe and chronic pain, severe nausea, seizures and severe and persistent muscle spasm.
In Michigan, where Dr. Stellini practices, a panel in 2018 approved a long list of added qualifying conditions such as chronic pain, obsessive compulsive disorder and arthritis. But the panel rejected other conditions such as anxiety, asthma, panic attacks and schizophrenia.
Vaporizers are an alternative to joints, but...
Vaporizers are commonly used as an alternative to smoking marijuana joints, Dr. Stellini said, and they don’t significantly release tars or much if any carbon monoxide. While research is limited, he said, use of vaporizers hasn’t been linked to more lung cancer or chronic obstructive pulmonary disease.
“Vaping” is another option, but it’s been linked to dozens of deaths and hundreds of cases of illness in recent weeks. Many patients have reported using products that contain THC, a component of marijuana.
Other delivery methods exist
Marijuana can be ingested in liquid and solid food. “But edibles can have a slow onset of action compared to vaporizing or smoking,” Dr. Stellini said. “You might over-indulge. When users get to their steady state, they might have some adverse effects [AEs].”
Marijuana still has risks
Cannabis use has a long list of well-known AEs linked to the THC component. The most common are drowsiness, fatigue, dizziness, dry mouth, anxiety, cognitive effects, cough, and nausea, Dr. Stellini said. More serious AEs such as psychosis have been reported.
And, of course, users of cannabis with THC get high if they use enough.
A 2017 National Academies of Sciences, Engineering and Medicine report linked cannabis use to a higher risk of motor vehicle accidents. Still, Dr. Stellini said, “it’s relatively safe with respect to mortality, especially compared to opioids.”1
Risk of use in cancer may be low
Research suggest that patients with cancer use cannabis as much as other people and perhaps even more, Dr. Stellini said. But are they facing any extra risks? In general, he said, it doesn’t appear that way.
Cannabis seems to be safe when used with chemotherapy, he said, and drug-drug interactions in cancer appear to be rare. Some studies have suggested that cannabinoids—a component of marijuana—may be an effective treatment for chemotherapy-induced peripheral neuropathy.
However, he said, 1 study has raised a red flag about a possible interaction with cancer immunotherapy. Researchers found evidence that patients who used cannabis had lower tumor response rates to nivolomab for advanced melanoma, non-small cell lung cancer, and renal clear cell carcinoma. However, survival wasn’t affected.2
Meanwhile, he said, there’s no strong evidence that cannabis is a useful treatment for cancer, he said, although it’s worth investigating.
Cannabidiol is the hot new product
Cannabidiol, also known as CBD, has become hugely popular, Dr. Stellini said. It is derived from hemp and doesn’t cause a “buzz” like cannabis.
Due to lack of regulation, he said, buyers should beware. And, he said, CBD has multiple EAs. Standard doses can cause drowsiness, fatigue, dizziness, dry mouth, hypotension and lightheadedness.
Dr. Stellini reports no relevant disclosures.
1. National Academies of Sciences, Engineering, and Medicine. The Health Effects of Cannabis and Cannabinoids: The Current State of Evidence and Recommendations for Research. Washington, DC: The National Academies Press; 2017.
2. Taha T, Meiri D, Talhamy S, Wollner M, Peer A, Bar-Sela G. Cannabis impacts tumor response rate to nivolumab in patients with advanced malignancies. Oncologist. 2019;24(4):549-554.
1. National Academies of Sciences, Engineering, and Medicine. The Health Effects of Cannabis and Cannabinoids: The Current State of Evidence and Recommendations for Research. Washington, DC: The National Academies Press; 2017.
2. Taha T, Meiri D, Talhamy S, Wollner M, Peer A, Bar-Sela G. Cannabis impacts tumor response rate to nivolumab in patients with advanced malignancies. Oncologist. 2019;24(4):549-554.