User login
Mitchel is a reporter for MDedge based in the Philadelphia area. He started with the company in 1992, when it was International Medical News Group (IMNG), and has since covered a range of medical specialties. Mitchel trained as a virologist at Roswell Park Memorial Institute in Buffalo, and then worked briefly as a researcher at Boston Children's Hospital before pivoting to journalism as a AAAS Mass Media Fellow in 1980. His first reporting job was with Science Digest magazine, and from the mid-1980s to early-1990s he was a reporter with Medical World News. @mitchelzoler
U.K. ahead of U.S. in cancer survivorship planning
BRUSSELS – Cancer survivorship planning in the United Kingdom is ahead of the United States and the rest of Europe with the recent rollout of a model care plan for cancer patients, along with a guide for conversations between cancer-care health care providers and patients at the time they start long-term follow-up surveillance.
A care plan guides patients as they segue from acute cancer treatment to longer-term health maintenance and follow-up. The plan can include a personalized record of treatment received, prognosis, recommended follow-up examinations, symptoms to be alert for, and other critical information when patients transition to life as a cancer survivor.

The U.K.’s National Health System (NHS) first released a hard-copy version of a model care plan for cancer patients along with a guide for conversations with patients at the time they start long-term follow-up surveillance in 2012. Although the hard-copy form is available from the agency’s National Cancer Survivorship Initiative, the NHS continues to test the care plan and simultaneously is finalizing an electronic version planned for release next year, Dr. Jane Maher said at the first EORTC Cancer Survivorship Summit hosted by the European Organisation for Research and Treatment of Cancer.
"The paper version is freely available," while testing continues at 160 U.K. sites," said Dr. Maher, chief medical officer at Macmillan Cancer Support, London, and a clinical leader with the NHS.
"The first evaluation is done. Patients really liked it and found it helpful and it was possible to do, so it’s at the point where it can be spread, but key elements are still in evaluation until 2015," she said in an interview.
"We can now say that we have a tool to shape the conversation" between a cancer patient who has finished the initial phase of treatment and her care provider. "We have a framework for patient education, for treatment, and for review of their cancer care." Patients who have gone through this care-planning conversation "felt more controlled and that their care was more coordinated."
Prevailing attitudes about cancer management pose some of the biggest challenges in developing and implementing cancer plans, Dr. Maher said. "Cancer is seen as an acute illness that is managed acutely by specialists," she noted. Timing the discussions introduces another challenge. "Physicians were prepared to discuss treatment-related consequences at the time of treatment, but patients did not want to hear it then because they were in life-and-death mode," she said.
In contrast, when patients felt ready to get this information, at the end of their treatment, "physicians weren’t prepared to discuss it for fear of frightening patients." But having some type of conversation on long-term prospects is very important, more critical than any of the individual tools, she said.
U.S. efforts still in process
This rollout puts U.K. cancer survivorship planning ahead of the United States and the rest of Europe. The U.S. National Cancer Institute (NCI) "has a research call out to test models for having that conversation with patient-centered goals," said Catherine Alfano, Ph.D., deputy director of survivorship research at the NCI in Bethesda, Md.
"How do you sit with a patient and family members and friends and talk about what just happened and what will happen in the future? Right now we don’t have a best model for this, but I think we owe it to survivors to identify best practices and get it to all of them, and make it patient centered, so it’s not just an oncologist who hands a piece of paper to the cancer patient and says this is what you need to do, because that won’t work. We need a conversation to take place where cancer patients are engaged in setting their survivorship care goals," Dr. Alfano said in an interview.
"We’re talking a lot right now about giving cancer survivors a treatment summary so they know what they received, and equally important a survivorship care plan that talks about what the patient needs to look out for, what providers they’ll see, how often, and how will their care be coordinated. This is implemented in very different ways throughout the U.S. right now. There is a mad rush to do it. What we want is for a conversation to take place so that cancer survivors are engaged in setting goals for their survivorship care," Dr. Alfano said.

Late last year, NCI researchers and their collaborators published results from a recent survey of more than 1,100 U.S. oncologists and more than 1,000 U.S. primary-care physicians about their practice regarding survivor care plans for their cancer patients (J. Natl. Cancer Inst. 2013;105:1579-87). These plans were used by about 20% of the surveyed oncologists and 13% of primary care physicians. Higher numbers reported giving patients treatment summaries at the end of their acute care, usual practice for half of the responding oncologists and about a third of the primary-care physicians.
Survivorship needs grow and diversify
Optimizing care for cancer survivors and better involving them in long-term surveillance and care has become increasingly important as the numbers continue to climb. "The number of cancer survivors is larger than ever, and as U.S. boomers become 65 years and older, there will be a tsunami of more cancer survivors, Dr. Alfano predicted.
"This huge tsunami [of cancer patients] is coming over the next decade, and we are completely unprepared. We have done a poor job of understanding the needs of adult cancer survivors," she warned. "There is a scramble underway now to understand what adult cancer survivors need."
For example, cardiovascular adverse effects from several different cancer treatments often occur many years after treatment. "Usually, these patients are not in surveillance anymore," said Dr. Thomas M. Suter of the Swiss Cardiovascular Centre in Bern, Switzerland. "No one is looking at these patients. They need to be on medical treatment to improve their prognosis," such as treatment with an angiotensin-converting enzyme inhibitor, he said in his talk at the meeting.
Another shortcoming of U.S. cancer survivor care is the fragmented care many patients receive and a glaring lack of coordination.
U.S. cancer survivors "wind up seeing multiple providers for late effects like cardiovascular disease, osteoporosis, and diabetes, which is on top of their surveillance for a recurrence of their primary cancer or appearance of a second primary cancer," said Dr. Alfano. "We have to create a more coordinated form of care that is truly team based to make it easier for patients and relieve the huge burden on them and their families. I hear from cancer survivors and families all the time that it takes hours each week just to coordinate a cancer patient’s care. We need to ease this burden. We have done a poor job understanding the needs of adult cancer survivors."
An especially pressing need is for information on lifestyle change, said Dr. Alfano. "Cancer survivors are looking for things they can do personally to take control back over their morbidity and mortality."
Cancer patients are often highly motivated to take steps to cut their risk of treatment-related adverse outcomes, recurrence, or development of a second primary cancer. In 2012, the American Cancer Society issued nutrition and physical activity guidelines for cancer survivors (CA Cancer J. Clin. 2012;62:30-67), noted Dr. Kevin D. Stein, managing director of the behavioral research center of the ACS in a talk at the meeting.
"We’ve done a poor job of getting lifestyle-change information to cancer survivors. We need to include lifestyle change as part of survivorship plans," said Dr. Alfano.
Despite the shortcomings in survivorship planning in the United States and United Kingdom, it outstrips what currently occurs in most of Europe. "We are far behind the United States," said Dr. Elizabeth Charlotte Moser, professor at the Champalimaud Foundation in Lisbon and chair of the EORTC Survivorship Task Force.
In addition to having Europe follow the United Kingdom and United States in expanding survivor planning, she anticipates a contribution from several European-based cancer-treatment trials for which long-term follow-up data are available. For example, six EORTC-sponsored trials in patients with either early-stage breast cancer or ductal carcinoma in situ together enrolled more than 20,000 patients starting in 1986. EORTC researchers are planning to collect long-term outcome data from as many of these patients as can be tracked down, Dr. Moser said.
Dr. Maher, Dr. Alfano, Dr. Stein, and Dr. Moser said they had no disclosures. Dr. Suter said that he has been a speaker on behalf of Roche, RoboPharma, and Novartis.
On Twitter @mitchelzoler
BRUSSELS – Cancer survivorship planning in the United Kingdom is ahead of the United States and the rest of Europe with the recent rollout of a model care plan for cancer patients, along with a guide for conversations between cancer-care health care providers and patients at the time they start long-term follow-up surveillance.
A care plan guides patients as they segue from acute cancer treatment to longer-term health maintenance and follow-up. The plan can include a personalized record of treatment received, prognosis, recommended follow-up examinations, symptoms to be alert for, and other critical information when patients transition to life as a cancer survivor.
The U.K.’s National Health System (NHS) first released a hard-copy version of a model care plan for cancer patients along with a guide for conversations with patients at the time they start long-term follow-up surveillance in 2012. Although the hard-copy form is available from the agency’s National Cancer Survivorship Initiative, the NHS continues to test the care plan and simultaneously is finalizing an electronic version planned for release next year, Dr. Jane Maher said at the first EORTC Cancer Survivorship Summit hosted by the European Organisation for Research and Treatment of Cancer.
"The paper version is freely available," while testing continues at 160 U.K. sites," said Dr. Maher, chief medical officer at Macmillan Cancer Support, London, and a clinical leader with the NHS.
"The first evaluation is done. Patients really liked it and found it helpful and it was possible to do, so it’s at the point where it can be spread, but key elements are still in evaluation until 2015," she said in an interview.
"We can now say that we have a tool to shape the conversation" between a cancer patient who has finished the initial phase of treatment and her care provider. "We have a framework for patient education, for treatment, and for review of their cancer care." Patients who have gone through this care-planning conversation "felt more controlled and that their care was more coordinated."
Prevailing attitudes about cancer management pose some of the biggest challenges in developing and implementing cancer plans, Dr. Maher said. "Cancer is seen as an acute illness that is managed acutely by specialists," she noted. Timing the discussions introduces another challenge. "Physicians were prepared to discuss treatment-related consequences at the time of treatment, but patients did not want to hear it then because they were in life-and-death mode," she said.
In contrast, when patients felt ready to get this information, at the end of their treatment, "physicians weren’t prepared to discuss it for fear of frightening patients." But having some type of conversation on long-term prospects is very important, more critical than any of the individual tools, she said.
U.S. efforts still in process
This rollout puts U.K. cancer survivorship planning ahead of the United States and the rest of Europe. The U.S. National Cancer Institute (NCI) "has a research call out to test models for having that conversation with patient-centered goals," said Catherine Alfano, Ph.D., deputy director of survivorship research at the NCI in Bethesda, Md.
"How do you sit with a patient and family members and friends and talk about what just happened and what will happen in the future? Right now we don’t have a best model for this, but I think we owe it to survivors to identify best practices and get it to all of them, and make it patient centered, so it’s not just an oncologist who hands a piece of paper to the cancer patient and says this is what you need to do, because that won’t work. We need a conversation to take place where cancer patients are engaged in setting their survivorship care goals," Dr. Alfano said in an interview.
"We’re talking a lot right now about giving cancer survivors a treatment summary so they know what they received, and equally important a survivorship care plan that talks about what the patient needs to look out for, what providers they’ll see, how often, and how will their care be coordinated. This is implemented in very different ways throughout the U.S. right now. There is a mad rush to do it. What we want is for a conversation to take place so that cancer survivors are engaged in setting goals for their survivorship care," Dr. Alfano said.
Late last year, NCI researchers and their collaborators published results from a recent survey of more than 1,100 U.S. oncologists and more than 1,000 U.S. primary-care physicians about their practice regarding survivor care plans for their cancer patients (J. Natl. Cancer Inst. 2013;105:1579-87). These plans were used by about 20% of the surveyed oncologists and 13% of primary care physicians. Higher numbers reported giving patients treatment summaries at the end of their acute care, usual practice for half of the responding oncologists and about a third of the primary-care physicians.
Survivorship needs grow and diversify
Optimizing care for cancer survivors and better involving them in long-term surveillance and care has become increasingly important as the numbers continue to climb. "The number of cancer survivors is larger than ever, and as U.S. boomers become 65 years and older, there will be a tsunami of more cancer survivors, Dr. Alfano predicted.
"This huge tsunami [of cancer patients] is coming over the next decade, and we are completely unprepared. We have done a poor job of understanding the needs of adult cancer survivors," she warned. "There is a scramble underway now to understand what adult cancer survivors need."
For example, cardiovascular adverse effects from several different cancer treatments often occur many years after treatment. "Usually, these patients are not in surveillance anymore," said Dr. Thomas M. Suter of the Swiss Cardiovascular Centre in Bern, Switzerland. "No one is looking at these patients. They need to be on medical treatment to improve their prognosis," such as treatment with an angiotensin-converting enzyme inhibitor, he said in his talk at the meeting.
Another shortcoming of U.S. cancer survivor care is the fragmented care many patients receive and a glaring lack of coordination.
U.S. cancer survivors "wind up seeing multiple providers for late effects like cardiovascular disease, osteoporosis, and diabetes, which is on top of their surveillance for a recurrence of their primary cancer or appearance of a second primary cancer," said Dr. Alfano. "We have to create a more coordinated form of care that is truly team based to make it easier for patients and relieve the huge burden on them and their families. I hear from cancer survivors and families all the time that it takes hours each week just to coordinate a cancer patient’s care. We need to ease this burden. We have done a poor job understanding the needs of adult cancer survivors."
An especially pressing need is for information on lifestyle change, said Dr. Alfano. "Cancer survivors are looking for things they can do personally to take control back over their morbidity and mortality."
Cancer patients are often highly motivated to take steps to cut their risk of treatment-related adverse outcomes, recurrence, or development of a second primary cancer. In 2012, the American Cancer Society issued nutrition and physical activity guidelines for cancer survivors (CA Cancer J. Clin. 2012;62:30-67), noted Dr. Kevin D. Stein, managing director of the behavioral research center of the ACS in a talk at the meeting.
"We’ve done a poor job of getting lifestyle-change information to cancer survivors. We need to include lifestyle change as part of survivorship plans," said Dr. Alfano.
Despite the shortcomings in survivorship planning in the United States and United Kingdom, it outstrips what currently occurs in most of Europe. "We are far behind the United States," said Dr. Elizabeth Charlotte Moser, professor at the Champalimaud Foundation in Lisbon and chair of the EORTC Survivorship Task Force.
In addition to having Europe follow the United Kingdom and United States in expanding survivor planning, she anticipates a contribution from several European-based cancer-treatment trials for which long-term follow-up data are available. For example, six EORTC-sponsored trials in patients with either early-stage breast cancer or ductal carcinoma in situ together enrolled more than 20,000 patients starting in 1986. EORTC researchers are planning to collect long-term outcome data from as many of these patients as can be tracked down, Dr. Moser said.
Dr. Maher, Dr. Alfano, Dr. Stein, and Dr. Moser said they had no disclosures. Dr. Suter said that he has been a speaker on behalf of Roche, RoboPharma, and Novartis.
On Twitter @mitchelzoler
BRUSSELS – Cancer survivorship planning in the United Kingdom is ahead of the United States and the rest of Europe with the recent rollout of a model care plan for cancer patients, along with a guide for conversations between cancer-care health care providers and patients at the time they start long-term follow-up surveillance.
A care plan guides patients as they segue from acute cancer treatment to longer-term health maintenance and follow-up. The plan can include a personalized record of treatment received, prognosis, recommended follow-up examinations, symptoms to be alert for, and other critical information when patients transition to life as a cancer survivor.
The U.K.’s National Health System (NHS) first released a hard-copy version of a model care plan for cancer patients along with a guide for conversations with patients at the time they start long-term follow-up surveillance in 2012. Although the hard-copy form is available from the agency’s National Cancer Survivorship Initiative, the NHS continues to test the care plan and simultaneously is finalizing an electronic version planned for release next year, Dr. Jane Maher said at the first EORTC Cancer Survivorship Summit hosted by the European Organisation for Research and Treatment of Cancer.
"The paper version is freely available," while testing continues at 160 U.K. sites," said Dr. Maher, chief medical officer at Macmillan Cancer Support, London, and a clinical leader with the NHS.
"The first evaluation is done. Patients really liked it and found it helpful and it was possible to do, so it’s at the point where it can be spread, but key elements are still in evaluation until 2015," she said in an interview.
"We can now say that we have a tool to shape the conversation" between a cancer patient who has finished the initial phase of treatment and her care provider. "We have a framework for patient education, for treatment, and for review of their cancer care." Patients who have gone through this care-planning conversation "felt more controlled and that their care was more coordinated."
Prevailing attitudes about cancer management pose some of the biggest challenges in developing and implementing cancer plans, Dr. Maher said. "Cancer is seen as an acute illness that is managed acutely by specialists," she noted. Timing the discussions introduces another challenge. "Physicians were prepared to discuss treatment-related consequences at the time of treatment, but patients did not want to hear it then because they were in life-and-death mode," she said.
In contrast, when patients felt ready to get this information, at the end of their treatment, "physicians weren’t prepared to discuss it for fear of frightening patients." But having some type of conversation on long-term prospects is very important, more critical than any of the individual tools, she said.
U.S. efforts still in process
This rollout puts U.K. cancer survivorship planning ahead of the United States and the rest of Europe. The U.S. National Cancer Institute (NCI) "has a research call out to test models for having that conversation with patient-centered goals," said Catherine Alfano, Ph.D., deputy director of survivorship research at the NCI in Bethesda, Md.
"How do you sit with a patient and family members and friends and talk about what just happened and what will happen in the future? Right now we don’t have a best model for this, but I think we owe it to survivors to identify best practices and get it to all of them, and make it patient centered, so it’s not just an oncologist who hands a piece of paper to the cancer patient and says this is what you need to do, because that won’t work. We need a conversation to take place where cancer patients are engaged in setting their survivorship care goals," Dr. Alfano said in an interview.
"We’re talking a lot right now about giving cancer survivors a treatment summary so they know what they received, and equally important a survivorship care plan that talks about what the patient needs to look out for, what providers they’ll see, how often, and how will their care be coordinated. This is implemented in very different ways throughout the U.S. right now. There is a mad rush to do it. What we want is for a conversation to take place so that cancer survivors are engaged in setting goals for their survivorship care," Dr. Alfano said.
Late last year, NCI researchers and their collaborators published results from a recent survey of more than 1,100 U.S. oncologists and more than 1,000 U.S. primary-care physicians about their practice regarding survivor care plans for their cancer patients (J. Natl. Cancer Inst. 2013;105:1579-87). These plans were used by about 20% of the surveyed oncologists and 13% of primary care physicians. Higher numbers reported giving patients treatment summaries at the end of their acute care, usual practice for half of the responding oncologists and about a third of the primary-care physicians.
Survivorship needs grow and diversify
Optimizing care for cancer survivors and better involving them in long-term surveillance and care has become increasingly important as the numbers continue to climb. "The number of cancer survivors is larger than ever, and as U.S. boomers become 65 years and older, there will be a tsunami of more cancer survivors, Dr. Alfano predicted.
"This huge tsunami [of cancer patients] is coming over the next decade, and we are completely unprepared. We have done a poor job of understanding the needs of adult cancer survivors," she warned. "There is a scramble underway now to understand what adult cancer survivors need."
For example, cardiovascular adverse effects from several different cancer treatments often occur many years after treatment. "Usually, these patients are not in surveillance anymore," said Dr. Thomas M. Suter of the Swiss Cardiovascular Centre in Bern, Switzerland. "No one is looking at these patients. They need to be on medical treatment to improve their prognosis," such as treatment with an angiotensin-converting enzyme inhibitor, he said in his talk at the meeting.
Another shortcoming of U.S. cancer survivor care is the fragmented care many patients receive and a glaring lack of coordination.
U.S. cancer survivors "wind up seeing multiple providers for late effects like cardiovascular disease, osteoporosis, and diabetes, which is on top of their surveillance for a recurrence of their primary cancer or appearance of a second primary cancer," said Dr. Alfano. "We have to create a more coordinated form of care that is truly team based to make it easier for patients and relieve the huge burden on them and their families. I hear from cancer survivors and families all the time that it takes hours each week just to coordinate a cancer patient’s care. We need to ease this burden. We have done a poor job understanding the needs of adult cancer survivors."
An especially pressing need is for information on lifestyle change, said Dr. Alfano. "Cancer survivors are looking for things they can do personally to take control back over their morbidity and mortality."
Cancer patients are often highly motivated to take steps to cut their risk of treatment-related adverse outcomes, recurrence, or development of a second primary cancer. In 2012, the American Cancer Society issued nutrition and physical activity guidelines for cancer survivors (CA Cancer J. Clin. 2012;62:30-67), noted Dr. Kevin D. Stein, managing director of the behavioral research center of the ACS in a talk at the meeting.
"We’ve done a poor job of getting lifestyle-change information to cancer survivors. We need to include lifestyle change as part of survivorship plans," said Dr. Alfano.
Despite the shortcomings in survivorship planning in the United States and United Kingdom, it outstrips what currently occurs in most of Europe. "We are far behind the United States," said Dr. Elizabeth Charlotte Moser, professor at the Champalimaud Foundation in Lisbon and chair of the EORTC Survivorship Task Force.
In addition to having Europe follow the United Kingdom and United States in expanding survivor planning, she anticipates a contribution from several European-based cancer-treatment trials for which long-term follow-up data are available. For example, six EORTC-sponsored trials in patients with either early-stage breast cancer or ductal carcinoma in situ together enrolled more than 20,000 patients starting in 1986. EORTC researchers are planning to collect long-term outcome data from as many of these patients as can be tracked down, Dr. Moser said.
Dr. Maher, Dr. Alfano, Dr. Stein, and Dr. Moser said they had no disclosures. Dr. Suter said that he has been a speaker on behalf of Roche, RoboPharma, and Novartis.
On Twitter @mitchelzoler

Europe’s latest sarcoma guidelines increase emphasis on genetic profiling
MILAN – The 2014 update to the European Society of Medical Oncology’s sarcoma-management guidelines put unprecedented emphasis on genetic assessment and using the data to guide treatment.
"Molecular diagnosis is recommended as standard care" for patients with gastrointestinal stromal tumors (GIST), Dr. Jean-Yves Blay said at Sarcoma and GIST 2014, hosted by the European Society for Medical Oncology (ESMO). Identifying the genetic profile of a newly diagnosed GIST "is predictive and can guide treatment in the adjuvant setting and possibly also in the advanced phase," said Dr. Blay, professor and head of medical oncology at Claude Bernard University in Lyon, France. "Molecular characterization is increasingly an important diagnostic and prognostic tool and also helps select treatment."

The new update also strengthened the advice from past updates to centralize GIST and sarcoma management at reference centers. "What is clear from looking at past guidelines is that since 2008 we have moved toward increasingly stronger recommendations to centralize," although the panel remained unable to settle on a definition of a GIST and sarcoma reference center, Dr. Blay said.
The 2014 revision to ESMO’s guidelines for managing GIST and sarcomas is the fourth biannual revision since these guidelines first appeared in 2008. The new update will soon appear on ESMO’s website. A majority of the guidelines remain based on consensus opinion and not evidence, because the number of randomized controlled trials that have tested various aspects of management remains limited, Dr. Blay said. The lack of trials also leaves many questions unanswered, such as the best treatment for GIST that carry the D842V mutation in their PDGFRA gene or for the "wild-type" GIST that don’t have any of the described GIST mutations. "Everyone agrees we need more studies," he said.
For managing patients with advanced GIST, the new update noted that surgical removal of recurrent lesions has not been proven beneficial to patients, and that the benefit from monitoring trough levels of a tyrosine-kinase inhibitor drug also remains unproven. The new update also acknowledged a possible role for continued imatinib (Gleevec) treatment after relapse, based on results from the RIGHT (Resumption of Imatinib to Control Metastatic or Unresectable GIST After Failure of Imatinib and Sunitinib) trial (Lancet Oncol. 2013;14:1175-82). In addition, the update recognized the potential benefit of trying regorafenib (Stivarga) after patients progress on imatinib or sunitinib (Sutent) treatment, and strongly advised against treating patients with two or more tyrosine-kinase inhibitor drugs simultaneously, as this approach needs further study.
One other change to the GIST guidelines this year was a suggestion to increase the frequency of follow-up examinations during the 1-3 years following the end of adjuvant therapy, also based on consensus opinion and without firm evidence, Dr. Blay said.
The revised soft-tissue sarcoma (STS) guidelines included adoption of the bone and STS classification scheme issued by the World Health Organization last year, and endorsement of genetic analyses when the histologic diagnosis is uncertain or the tumor has an unusual presentation. The revision added stronger language promoting the need to individualize radiotherapy based on factors such as clinical presentation of the sarcoma, patient history, tumor site, and patient’s age. The revision panel could not reach a consensus on a recommended, standard adjuvant regimen.
This inability to recommend adjuvant therapies should be "no surprise because there are no data. We need to look at larger numbers of patients to identify those who would benefit from adjuvant therapy," Dr. Blay said.
For treatment of advanced STSs, the panel added pazopanib (Votrient) as a second-line treatment option, but not for patients with liposarcomas, who were not included in the trial that established pazopanib’s efficacy for metastatic STS (Lancet 2012;379:1879-86). The update also recommended identifying sarcoma subtypes genetically and matching drugs to these types using agents such as sunitinib, crizotinib (Xalkori), and cediranib (Recentin). In addition, the new update highlighted that a role for intensified follow-up of metastatic STS using computed tomography was not supported by the results of a recent randomized, controlled trial.
The 2014 guidelines also include sections for four specific STSs: retroperitoneal, uterine, desmoids, and breast. "The guidelines are expanding to organ-specific locations, something we will probably see more of" in future updates, Dr. Blay said.
Dr. Blay disclosed that he has received honoraria as a consultant to PharmaMar, and that he has received research grants from Roche, GlaxoSmithKline, and Novartis.
On Twitter @mitchelzoler
MILAN – The 2014 update to the European Society of Medical Oncology’s sarcoma-management guidelines put unprecedented emphasis on genetic assessment and using the data to guide treatment.
"Molecular diagnosis is recommended as standard care" for patients with gastrointestinal stromal tumors (GIST), Dr. Jean-Yves Blay said at Sarcoma and GIST 2014, hosted by the European Society for Medical Oncology (ESMO). Identifying the genetic profile of a newly diagnosed GIST "is predictive and can guide treatment in the adjuvant setting and possibly also in the advanced phase," said Dr. Blay, professor and head of medical oncology at Claude Bernard University in Lyon, France. "Molecular characterization is increasingly an important diagnostic and prognostic tool and also helps select treatment."
The new update also strengthened the advice from past updates to centralize GIST and sarcoma management at reference centers. "What is clear from looking at past guidelines is that since 2008 we have moved toward increasingly stronger recommendations to centralize," although the panel remained unable to settle on a definition of a GIST and sarcoma reference center, Dr. Blay said.
The 2014 revision to ESMO’s guidelines for managing GIST and sarcomas is the fourth biannual revision since these guidelines first appeared in 2008. The new update will soon appear on ESMO’s website. A majority of the guidelines remain based on consensus opinion and not evidence, because the number of randomized controlled trials that have tested various aspects of management remains limited, Dr. Blay said. The lack of trials also leaves many questions unanswered, such as the best treatment for GIST that carry the D842V mutation in their PDGFRA gene or for the "wild-type" GIST that don’t have any of the described GIST mutations. "Everyone agrees we need more studies," he said.
For managing patients with advanced GIST, the new update noted that surgical removal of recurrent lesions has not been proven beneficial to patients, and that the benefit from monitoring trough levels of a tyrosine-kinase inhibitor drug also remains unproven. The new update also acknowledged a possible role for continued imatinib (Gleevec) treatment after relapse, based on results from the RIGHT (Resumption of Imatinib to Control Metastatic or Unresectable GIST After Failure of Imatinib and Sunitinib) trial (Lancet Oncol. 2013;14:1175-82). In addition, the update recognized the potential benefit of trying regorafenib (Stivarga) after patients progress on imatinib or sunitinib (Sutent) treatment, and strongly advised against treating patients with two or more tyrosine-kinase inhibitor drugs simultaneously, as this approach needs further study.
One other change to the GIST guidelines this year was a suggestion to increase the frequency of follow-up examinations during the 1-3 years following the end of adjuvant therapy, also based on consensus opinion and without firm evidence, Dr. Blay said.
The revised soft-tissue sarcoma (STS) guidelines included adoption of the bone and STS classification scheme issued by the World Health Organization last year, and endorsement of genetic analyses when the histologic diagnosis is uncertain or the tumor has an unusual presentation. The revision added stronger language promoting the need to individualize radiotherapy based on factors such as clinical presentation of the sarcoma, patient history, tumor site, and patient’s age. The revision panel could not reach a consensus on a recommended, standard adjuvant regimen.
This inability to recommend adjuvant therapies should be "no surprise because there are no data. We need to look at larger numbers of patients to identify those who would benefit from adjuvant therapy," Dr. Blay said.
For treatment of advanced STSs, the panel added pazopanib (Votrient) as a second-line treatment option, but not for patients with liposarcomas, who were not included in the trial that established pazopanib’s efficacy for metastatic STS (Lancet 2012;379:1879-86). The update also recommended identifying sarcoma subtypes genetically and matching drugs to these types using agents such as sunitinib, crizotinib (Xalkori), and cediranib (Recentin). In addition, the new update highlighted that a role for intensified follow-up of metastatic STS using computed tomography was not supported by the results of a recent randomized, controlled trial.
The 2014 guidelines also include sections for four specific STSs: retroperitoneal, uterine, desmoids, and breast. "The guidelines are expanding to organ-specific locations, something we will probably see more of" in future updates, Dr. Blay said.
Dr. Blay disclosed that he has received honoraria as a consultant to PharmaMar, and that he has received research grants from Roche, GlaxoSmithKline, and Novartis.
On Twitter @mitchelzoler
MILAN – The 2014 update to the European Society of Medical Oncology’s sarcoma-management guidelines put unprecedented emphasis on genetic assessment and using the data to guide treatment.
"Molecular diagnosis is recommended as standard care" for patients with gastrointestinal stromal tumors (GIST), Dr. Jean-Yves Blay said at Sarcoma and GIST 2014, hosted by the European Society for Medical Oncology (ESMO). Identifying the genetic profile of a newly diagnosed GIST "is predictive and can guide treatment in the adjuvant setting and possibly also in the advanced phase," said Dr. Blay, professor and head of medical oncology at Claude Bernard University in Lyon, France. "Molecular characterization is increasingly an important diagnostic and prognostic tool and also helps select treatment."
The new update also strengthened the advice from past updates to centralize GIST and sarcoma management at reference centers. "What is clear from looking at past guidelines is that since 2008 we have moved toward increasingly stronger recommendations to centralize," although the panel remained unable to settle on a definition of a GIST and sarcoma reference center, Dr. Blay said.
The 2014 revision to ESMO’s guidelines for managing GIST and sarcomas is the fourth biannual revision since these guidelines first appeared in 2008. The new update will soon appear on ESMO’s website. A majority of the guidelines remain based on consensus opinion and not evidence, because the number of randomized controlled trials that have tested various aspects of management remains limited, Dr. Blay said. The lack of trials also leaves many questions unanswered, such as the best treatment for GIST that carry the D842V mutation in their PDGFRA gene or for the "wild-type" GIST that don’t have any of the described GIST mutations. "Everyone agrees we need more studies," he said.
For managing patients with advanced GIST, the new update noted that surgical removal of recurrent lesions has not been proven beneficial to patients, and that the benefit from monitoring trough levels of a tyrosine-kinase inhibitor drug also remains unproven. The new update also acknowledged a possible role for continued imatinib (Gleevec) treatment after relapse, based on results from the RIGHT (Resumption of Imatinib to Control Metastatic or Unresectable GIST After Failure of Imatinib and Sunitinib) trial (Lancet Oncol. 2013;14:1175-82). In addition, the update recognized the potential benefit of trying regorafenib (Stivarga) after patients progress on imatinib or sunitinib (Sutent) treatment, and strongly advised against treating patients with two or more tyrosine-kinase inhibitor drugs simultaneously, as this approach needs further study.
One other change to the GIST guidelines this year was a suggestion to increase the frequency of follow-up examinations during the 1-3 years following the end of adjuvant therapy, also based on consensus opinion and without firm evidence, Dr. Blay said.
The revised soft-tissue sarcoma (STS) guidelines included adoption of the bone and STS classification scheme issued by the World Health Organization last year, and endorsement of genetic analyses when the histologic diagnosis is uncertain or the tumor has an unusual presentation. The revision added stronger language promoting the need to individualize radiotherapy based on factors such as clinical presentation of the sarcoma, patient history, tumor site, and patient’s age. The revision panel could not reach a consensus on a recommended, standard adjuvant regimen.
This inability to recommend adjuvant therapies should be "no surprise because there are no data. We need to look at larger numbers of patients to identify those who would benefit from adjuvant therapy," Dr. Blay said.
For treatment of advanced STSs, the panel added pazopanib (Votrient) as a second-line treatment option, but not for patients with liposarcomas, who were not included in the trial that established pazopanib’s efficacy for metastatic STS (Lancet 2012;379:1879-86). The update also recommended identifying sarcoma subtypes genetically and matching drugs to these types using agents such as sunitinib, crizotinib (Xalkori), and cediranib (Recentin). In addition, the new update highlighted that a role for intensified follow-up of metastatic STS using computed tomography was not supported by the results of a recent randomized, controlled trial.
The 2014 guidelines also include sections for four specific STSs: retroperitoneal, uterine, desmoids, and breast. "The guidelines are expanding to organ-specific locations, something we will probably see more of" in future updates, Dr. Blay said.
Dr. Blay disclosed that he has received honoraria as a consultant to PharmaMar, and that he has received research grants from Roche, GlaxoSmithKline, and Novartis.
On Twitter @mitchelzoler
EXPERT ANALYSIS FROM SARCOMA AND GIST 2014

Role for GIST genotyping stirs controversy
MILAN – Many U.S. patients with gastrointestinal stromal tumors today start on the wrong adjuvant treatment because their physicians don’t order genetic assessment of the cancer, said two American oncologists.
"Initial treatment for GIST [gastrointestinal stromal tumors] is enhanced by molecular decision making," Dr. Jonathan C. Trent said at Sarcoma and GIST 2014, hosted by the European Society for Medical Oncology.

"I’ve had patients referred to me from academic centers where the patient was treated with imatinib [Gleevec], which didn’t work, sunitinib [Sutent], which didn’t work, and regorafenib [Stivarga], which didn’t work. We did genetic testing, and it was a D842V mutation [in the PDGFRA gene]. This patient should never have been treated with these drugs," because GIST that carry this PDGFRA mutation are resistant to all three of these tyrosine kinase inhibitor [TKI] drugs, said Dr. Trent, professor of medicine and director of the bone and soft tissue program at the University of Miami.
"If you’re thinking of giving adjuvant therapy, you absolutely need molecular profiling because in the primary, resected-disease setting, a full 20% of patients will have a mutation that makes imatinib useless, the D842V mutation," said Dr. George D. Demetri, professor of medicine at Harvard University and director of the Center for Sarcoma and Bone Oncology at Dana Farber Cancer Institute, Boston. The potential consequence of not performing a genetic analysis is "you could overtreat 20% of patients with what is a still moderately expensive drug that will give them side effects for 3 years when they don’t need it. That is bad medicine," Dr. Demetri said in an interview. "I’m flabbergasted that more people are not getting molecular profiling for GIST patients being considered for adjuvant therapy. We have not communicated this well. Genetic testing is easily accessible at reference labs."
Dr. Demetri highlighted that identifying a D842V mutation in the PDGFRA gene of a GIST is good news for patients, because when this mutation appears in a primary tumor it flags a very indolent form of GIST. "The physician can tell patients that they don’t need to take this drug because it won’t do them any good, plus most patients with your mutation don’t have their tumor recur for many years and sometimes never."

In its most recent guidelines for GIST management, the National Comprehensive Cancer Network (NCCN) said: "If tyrosine kinase inhibitors are considered as part of the treatment plan, genetic analysis of the tumor should be considered since the presence of mutations (or absence of mutations) in specific regions of the KIT and PDGFRA tyrosine kinase genes are correlated with response (or lack of a response) to specific tyrosine kinase inhibitors."
Similar language exists in the posted GIST management recommendations of the National Cancer Institute (NCI), which date from 2012: "KIT- and PDGFRA-mutational analysis may be of help in predicting responses to kinase inhibitors for patients with unresectable, metastatic, or recurrent GIST who are undergoing therapy with selective TKIs. However, the data are preliminary and mutational analysis for treatment decisions is not routine. There is currently no evidence that basing treatment decisions on mutational analysis improves OS [overall survival]."
Dr. Trent took issue with these positions and said that the NCCN and NCI need to call genetic assessment of primary GIST necessary, especially for patients considered for adjuvant treatment. But others saw reason for equivocation.
"Since the mutational status of GIST can impact your use of adjuvant therapy or even therapy for metastatic disease, most sarcoma physicians prefer to see it done," noted Dr. Robert G. Maki, professor of medicine and director of the sarcoma program at Mount Sinai Medical Center in New York. "That said, we often do not have clinical trial data to support" this approach to management. For example, no trial results clearly show that GIST that carry a PDGFRA D842V mutation do not respond well to imatinib and have better outcomes when treated with some other drug. "I would like to have these data to discuss the options" with patients, Dr. Maki said in an interview. The relatively well-described patterns of genetic mutation and drug sensitivity seen in GIST make this tumor different from other adult sarcomas, he added.
"We had a patient with the PDGFRA D842V mutation who clearly responded to imatinib," said Dr. Robert S. Benjamin, professor and chairman of sarcoma medical oncology at M.D. Anderson Cancer Center in Houston.

"You use imatinib empirically because it is the most benign drug, especially at the 400-mg/day level," Dr. Benjamin said in an interview. "It’s well tolerated, and it usually works." But Dr. Benjamin acknowledged the added value of learning a tumor’s genetic profile. "It’s analogous to infectious disease," where you might start a patient on an empiric antibiotic but then reconsider once you receive antibiotic-sensitivity results. Genotyping complements the clinical findings made after starting a patient on imatinib, he said.
Based on current data for GIST sensitivity to TKIs, Dr. Trent and Dr. Demetri summarized the current GIST mutation and treatment landscape this way:
• About 60% of GIST have the most common tyrosine kinase mutation, in exon 11 of the KIT gene, and are sensitive to 400 mg/day of imatinib.
• About 7% of GIST have the exon 9 mutation of KIT and are sensitive to a higher dosage of imatinib, ideally 800 mg/day if that is tolerated.
• About 20% of GIST have the D842V mutation in the PDGFRA tyrosine kinase gene, and these patients are candidates for enrollment in a trial, as no regimens are known effective for these tumors.
• About 12% of GIST have a mutation in the SDF gene, which appears to make them resistant to imatinib and sunitinib but which may be sensitive to another TKI, regorafenib.
• The remaining GIST have other, rare mutations.
Dr. Trent said that he had no disclosures. Dr. Demetri said that he has been a consultant to Bayer, Novartis, and other companies. Dr. Maki said that he has been a consultant to Eisai/Morphotek, Bayer, and other companies, and has received research support from Eisai/Morphotek, Tracon, and Bayer. Dr. Benjamin said that he has been a consultant to Johnson & Johnson, Merck, and Pfizer.
On Twitter @mitchelzoler
MILAN – Many U.S. patients with gastrointestinal stromal tumors today start on the wrong adjuvant treatment because their physicians don’t order genetic assessment of the cancer, said two American oncologists.
"Initial treatment for GIST [gastrointestinal stromal tumors] is enhanced by molecular decision making," Dr. Jonathan C. Trent said at Sarcoma and GIST 2014, hosted by the European Society for Medical Oncology.
"I’ve had patients referred to me from academic centers where the patient was treated with imatinib [Gleevec], which didn’t work, sunitinib [Sutent], which didn’t work, and regorafenib [Stivarga], which didn’t work. We did genetic testing, and it was a D842V mutation [in the PDGFRA gene]. This patient should never have been treated with these drugs," because GIST that carry this PDGFRA mutation are resistant to all three of these tyrosine kinase inhibitor [TKI] drugs, said Dr. Trent, professor of medicine and director of the bone and soft tissue program at the University of Miami.
"If you’re thinking of giving adjuvant therapy, you absolutely need molecular profiling because in the primary, resected-disease setting, a full 20% of patients will have a mutation that makes imatinib useless, the D842V mutation," said Dr. George D. Demetri, professor of medicine at Harvard University and director of the Center for Sarcoma and Bone Oncology at Dana Farber Cancer Institute, Boston. The potential consequence of not performing a genetic analysis is "you could overtreat 20% of patients with what is a still moderately expensive drug that will give them side effects for 3 years when they don’t need it. That is bad medicine," Dr. Demetri said in an interview. "I’m flabbergasted that more people are not getting molecular profiling for GIST patients being considered for adjuvant therapy. We have not communicated this well. Genetic testing is easily accessible at reference labs."
Dr. Demetri highlighted that identifying a D842V mutation in the PDGFRA gene of a GIST is good news for patients, because when this mutation appears in a primary tumor it flags a very indolent form of GIST. "The physician can tell patients that they don’t need to take this drug because it won’t do them any good, plus most patients with your mutation don’t have their tumor recur for many years and sometimes never."
In its most recent guidelines for GIST management, the National Comprehensive Cancer Network (NCCN) said: "If tyrosine kinase inhibitors are considered as part of the treatment plan, genetic analysis of the tumor should be considered since the presence of mutations (or absence of mutations) in specific regions of the KIT and PDGFRA tyrosine kinase genes are correlated with response (or lack of a response) to specific tyrosine kinase inhibitors."
Similar language exists in the posted GIST management recommendations of the National Cancer Institute (NCI), which date from 2012: "KIT- and PDGFRA-mutational analysis may be of help in predicting responses to kinase inhibitors for patients with unresectable, metastatic, or recurrent GIST who are undergoing therapy with selective TKIs. However, the data are preliminary and mutational analysis for treatment decisions is not routine. There is currently no evidence that basing treatment decisions on mutational analysis improves OS [overall survival]."
Dr. Trent took issue with these positions and said that the NCCN and NCI need to call genetic assessment of primary GIST necessary, especially for patients considered for adjuvant treatment. But others saw reason for equivocation.
"Since the mutational status of GIST can impact your use of adjuvant therapy or even therapy for metastatic disease, most sarcoma physicians prefer to see it done," noted Dr. Robert G. Maki, professor of medicine and director of the sarcoma program at Mount Sinai Medical Center in New York. "That said, we often do not have clinical trial data to support" this approach to management. For example, no trial results clearly show that GIST that carry a PDGFRA D842V mutation do not respond well to imatinib and have better outcomes when treated with some other drug. "I would like to have these data to discuss the options" with patients, Dr. Maki said in an interview. The relatively well-described patterns of genetic mutation and drug sensitivity seen in GIST make this tumor different from other adult sarcomas, he added.
"We had a patient with the PDGFRA D842V mutation who clearly responded to imatinib," said Dr. Robert S. Benjamin, professor and chairman of sarcoma medical oncology at M.D. Anderson Cancer Center in Houston.
"You use imatinib empirically because it is the most benign drug, especially at the 400-mg/day level," Dr. Benjamin said in an interview. "It’s well tolerated, and it usually works." But Dr. Benjamin acknowledged the added value of learning a tumor’s genetic profile. "It’s analogous to infectious disease," where you might start a patient on an empiric antibiotic but then reconsider once you receive antibiotic-sensitivity results. Genotyping complements the clinical findings made after starting a patient on imatinib, he said.
Based on current data for GIST sensitivity to TKIs, Dr. Trent and Dr. Demetri summarized the current GIST mutation and treatment landscape this way:
• About 60% of GIST have the most common tyrosine kinase mutation, in exon 11 of the KIT gene, and are sensitive to 400 mg/day of imatinib.
• About 7% of GIST have the exon 9 mutation of KIT and are sensitive to a higher dosage of imatinib, ideally 800 mg/day if that is tolerated.
• About 20% of GIST have the D842V mutation in the PDGFRA tyrosine kinase gene, and these patients are candidates for enrollment in a trial, as no regimens are known effective for these tumors.
• About 12% of GIST have a mutation in the SDF gene, which appears to make them resistant to imatinib and sunitinib but which may be sensitive to another TKI, regorafenib.
• The remaining GIST have other, rare mutations.
Dr. Trent said that he had no disclosures. Dr. Demetri said that he has been a consultant to Bayer, Novartis, and other companies. Dr. Maki said that he has been a consultant to Eisai/Morphotek, Bayer, and other companies, and has received research support from Eisai/Morphotek, Tracon, and Bayer. Dr. Benjamin said that he has been a consultant to Johnson & Johnson, Merck, and Pfizer.
On Twitter @mitchelzoler
MILAN – Many U.S. patients with gastrointestinal stromal tumors today start on the wrong adjuvant treatment because their physicians don’t order genetic assessment of the cancer, said two American oncologists.
"Initial treatment for GIST [gastrointestinal stromal tumors] is enhanced by molecular decision making," Dr. Jonathan C. Trent said at Sarcoma and GIST 2014, hosted by the European Society for Medical Oncology.
"I’ve had patients referred to me from academic centers where the patient was treated with imatinib [Gleevec], which didn’t work, sunitinib [Sutent], which didn’t work, and regorafenib [Stivarga], which didn’t work. We did genetic testing, and it was a D842V mutation [in the PDGFRA gene]. This patient should never have been treated with these drugs," because GIST that carry this PDGFRA mutation are resistant to all three of these tyrosine kinase inhibitor [TKI] drugs, said Dr. Trent, professor of medicine and director of the bone and soft tissue program at the University of Miami.
"If you’re thinking of giving adjuvant therapy, you absolutely need molecular profiling because in the primary, resected-disease setting, a full 20% of patients will have a mutation that makes imatinib useless, the D842V mutation," said Dr. George D. Demetri, professor of medicine at Harvard University and director of the Center for Sarcoma and Bone Oncology at Dana Farber Cancer Institute, Boston. The potential consequence of not performing a genetic analysis is "you could overtreat 20% of patients with what is a still moderately expensive drug that will give them side effects for 3 years when they don’t need it. That is bad medicine," Dr. Demetri said in an interview. "I’m flabbergasted that more people are not getting molecular profiling for GIST patients being considered for adjuvant therapy. We have not communicated this well. Genetic testing is easily accessible at reference labs."
Dr. Demetri highlighted that identifying a D842V mutation in the PDGFRA gene of a GIST is good news for patients, because when this mutation appears in a primary tumor it flags a very indolent form of GIST. "The physician can tell patients that they don’t need to take this drug because it won’t do them any good, plus most patients with your mutation don’t have their tumor recur for many years and sometimes never."
In its most recent guidelines for GIST management, the National Comprehensive Cancer Network (NCCN) said: "If tyrosine kinase inhibitors are considered as part of the treatment plan, genetic analysis of the tumor should be considered since the presence of mutations (or absence of mutations) in specific regions of the KIT and PDGFRA tyrosine kinase genes are correlated with response (or lack of a response) to specific tyrosine kinase inhibitors."
Similar language exists in the posted GIST management recommendations of the National Cancer Institute (NCI), which date from 2012: "KIT- and PDGFRA-mutational analysis may be of help in predicting responses to kinase inhibitors for patients with unresectable, metastatic, or recurrent GIST who are undergoing therapy with selective TKIs. However, the data are preliminary and mutational analysis for treatment decisions is not routine. There is currently no evidence that basing treatment decisions on mutational analysis improves OS [overall survival]."
Dr. Trent took issue with these positions and said that the NCCN and NCI need to call genetic assessment of primary GIST necessary, especially for patients considered for adjuvant treatment. But others saw reason for equivocation.
"Since the mutational status of GIST can impact your use of adjuvant therapy or even therapy for metastatic disease, most sarcoma physicians prefer to see it done," noted Dr. Robert G. Maki, professor of medicine and director of the sarcoma program at Mount Sinai Medical Center in New York. "That said, we often do not have clinical trial data to support" this approach to management. For example, no trial results clearly show that GIST that carry a PDGFRA D842V mutation do not respond well to imatinib and have better outcomes when treated with some other drug. "I would like to have these data to discuss the options" with patients, Dr. Maki said in an interview. The relatively well-described patterns of genetic mutation and drug sensitivity seen in GIST make this tumor different from other adult sarcomas, he added.
"We had a patient with the PDGFRA D842V mutation who clearly responded to imatinib," said Dr. Robert S. Benjamin, professor and chairman of sarcoma medical oncology at M.D. Anderson Cancer Center in Houston.
"You use imatinib empirically because it is the most benign drug, especially at the 400-mg/day level," Dr. Benjamin said in an interview. "It’s well tolerated, and it usually works." But Dr. Benjamin acknowledged the added value of learning a tumor’s genetic profile. "It’s analogous to infectious disease," where you might start a patient on an empiric antibiotic but then reconsider once you receive antibiotic-sensitivity results. Genotyping complements the clinical findings made after starting a patient on imatinib, he said.
Based on current data for GIST sensitivity to TKIs, Dr. Trent and Dr. Demetri summarized the current GIST mutation and treatment landscape this way:
• About 60% of GIST have the most common tyrosine kinase mutation, in exon 11 of the KIT gene, and are sensitive to 400 mg/day of imatinib.
• About 7% of GIST have the exon 9 mutation of KIT and are sensitive to a higher dosage of imatinib, ideally 800 mg/day if that is tolerated.
• About 20% of GIST have the D842V mutation in the PDGFRA tyrosine kinase gene, and these patients are candidates for enrollment in a trial, as no regimens are known effective for these tumors.
• About 12% of GIST have a mutation in the SDF gene, which appears to make them resistant to imatinib and sunitinib but which may be sensitive to another TKI, regorafenib.
• The remaining GIST have other, rare mutations.
Dr. Trent said that he had no disclosures. Dr. Demetri said that he has been a consultant to Bayer, Novartis, and other companies. Dr. Maki said that he has been a consultant to Eisai/Morphotek, Bayer, and other companies, and has received research support from Eisai/Morphotek, Tracon, and Bayer. Dr. Benjamin said that he has been a consultant to Johnson & Johnson, Merck, and Pfizer.
On Twitter @mitchelzoler
EXPERT ANALYSIS FROM SARCOMA AND GIST 2014

Liquid biopsies may solve GIST biopsy problem
MILAN – Although genetic analysis has become a key part of gastrointestinal-stromal tumor assessment before treating a primary tumor, its use at the time of recurrence remains problematic because of the heterogeneity of recurrent clones at the time of relapse, according to Dr. George D. Demetri.
"Liquid biopsy" is a new genetic assessment method with the potential to address the heterogeneity by sampling the complete spectrum of a patient’s tumor using free circulating tumor DNA in the patient’s plasma, rather than biopsying specific pieces of the tumor.

"The challenge from multiple, progressing tumors in a patient with GIST who is failing tyrosine-kinase inhibitor treatment is how to get around the limitation of tumor biopsy. How useful are biopsies when each corner of the tumor tells you something different" when a patient has recurrent GIST? said Dr. Demetri at Sarcoma and GIST 2014, hosted by the European Society for Medical Oncology. "Do you think you get a comprehensive look by biopsying the tumor? How many biopsies do you take?" asked Dr. Demetri, professor of medicine at Harvard Medical School and director of the center for sarcoma and bone oncology at Dana Farber Cancer Institute, both in Boston.
Dr. Demetri called for continued research to prove the efficacy and utility of liquid biopsies. "We need to develop liquid biopsies to get around the issue of tumor biopsies," he said.
The approach relies on the concept that tumor cells are constantly dying and releasing their DNA into a patient’s blood, and hence the free DNA circulating reflects the genetic profile, including all mutations and clones the patient’s tumor has at the time; this approach was pioneered by researchers at Johns Hopkins University (Sci. Transl. Med. 2012;4:162ra154).
Last year, researchers in Germany reported good correlations when assessing mutations in free circulating DNA in multiple plasma samples drawn from 38 patients with recurrent GIST and matching the results with the patients’ clinical state (Clin. Cancer Res. 2013;19:4854-67).

Dr. Demetri said his own laboratory recently compared mutational analyses in 32 patients with primary GIST and found that in 29 of 32 cases (91%), the mutational profile seen in the free circulating DNA matched that seen in biopsy specimens from each patient.
Currently, genetic assessment of free circulating DNA relies on looking for known mutations using specific amplification primers for those mutations, but next-generation sequencing could be used instead to search for any type of mutation, Dr. Demetri said.
Genetic analysis of GIST at the time of relapse is important, given today’s treatment options and the need to match the right treatment to the right genetic profile, but the challenge is how to perform this analysis in a meaningful way, commented Dr. Robert S. Benjamin, professor and chairman of sarcoma medical oncology at M.D. Anderson Cancer Center in Houston. "The idea of using free DNA in blood is very exciting," he said in an interview.
Dr. Demetri said he has been a consultant to Bayer, Novartis, Pfizer, Sanofi Oncology, Merck, GlaxoSmithKline, and Ariad. Dr. Benjamin said he has been a consultant to Johnson & Johnson, Merck, and Pfizer.
On Twitter @mitchelzoler
MILAN – Although genetic analysis has become a key part of gastrointestinal-stromal tumor assessment before treating a primary tumor, its use at the time of recurrence remains problematic because of the heterogeneity of recurrent clones at the time of relapse, according to Dr. George D. Demetri.
"Liquid biopsy" is a new genetic assessment method with the potential to address the heterogeneity by sampling the complete spectrum of a patient’s tumor using free circulating tumor DNA in the patient’s plasma, rather than biopsying specific pieces of the tumor.
"The challenge from multiple, progressing tumors in a patient with GIST who is failing tyrosine-kinase inhibitor treatment is how to get around the limitation of tumor biopsy. How useful are biopsies when each corner of the tumor tells you something different" when a patient has recurrent GIST? said Dr. Demetri at Sarcoma and GIST 2014, hosted by the European Society for Medical Oncology. "Do you think you get a comprehensive look by biopsying the tumor? How many biopsies do you take?" asked Dr. Demetri, professor of medicine at Harvard Medical School and director of the center for sarcoma and bone oncology at Dana Farber Cancer Institute, both in Boston.
Dr. Demetri called for continued research to prove the efficacy and utility of liquid biopsies. "We need to develop liquid biopsies to get around the issue of tumor biopsies," he said.
The approach relies on the concept that tumor cells are constantly dying and releasing their DNA into a patient’s blood, and hence the free DNA circulating reflects the genetic profile, including all mutations and clones the patient’s tumor has at the time; this approach was pioneered by researchers at Johns Hopkins University (Sci. Transl. Med. 2012;4:162ra154).
Last year, researchers in Germany reported good correlations when assessing mutations in free circulating DNA in multiple plasma samples drawn from 38 patients with recurrent GIST and matching the results with the patients’ clinical state (Clin. Cancer Res. 2013;19:4854-67).
Dr. Demetri said his own laboratory recently compared mutational analyses in 32 patients with primary GIST and found that in 29 of 32 cases (91%), the mutational profile seen in the free circulating DNA matched that seen in biopsy specimens from each patient.
Currently, genetic assessment of free circulating DNA relies on looking for known mutations using specific amplification primers for those mutations, but next-generation sequencing could be used instead to search for any type of mutation, Dr. Demetri said.
Genetic analysis of GIST at the time of relapse is important, given today’s treatment options and the need to match the right treatment to the right genetic profile, but the challenge is how to perform this analysis in a meaningful way, commented Dr. Robert S. Benjamin, professor and chairman of sarcoma medical oncology at M.D. Anderson Cancer Center in Houston. "The idea of using free DNA in blood is very exciting," he said in an interview.
Dr. Demetri said he has been a consultant to Bayer, Novartis, Pfizer, Sanofi Oncology, Merck, GlaxoSmithKline, and Ariad. Dr. Benjamin said he has been a consultant to Johnson & Johnson, Merck, and Pfizer.
On Twitter @mitchelzoler
MILAN – Although genetic analysis has become a key part of gastrointestinal-stromal tumor assessment before treating a primary tumor, its use at the time of recurrence remains problematic because of the heterogeneity of recurrent clones at the time of relapse, according to Dr. George D. Demetri.
"Liquid biopsy" is a new genetic assessment method with the potential to address the heterogeneity by sampling the complete spectrum of a patient’s tumor using free circulating tumor DNA in the patient’s plasma, rather than biopsying specific pieces of the tumor.
"The challenge from multiple, progressing tumors in a patient with GIST who is failing tyrosine-kinase inhibitor treatment is how to get around the limitation of tumor biopsy. How useful are biopsies when each corner of the tumor tells you something different" when a patient has recurrent GIST? said Dr. Demetri at Sarcoma and GIST 2014, hosted by the European Society for Medical Oncology. "Do you think you get a comprehensive look by biopsying the tumor? How many biopsies do you take?" asked Dr. Demetri, professor of medicine at Harvard Medical School and director of the center for sarcoma and bone oncology at Dana Farber Cancer Institute, both in Boston.
Dr. Demetri called for continued research to prove the efficacy and utility of liquid biopsies. "We need to develop liquid biopsies to get around the issue of tumor biopsies," he said.
The approach relies on the concept that tumor cells are constantly dying and releasing their DNA into a patient’s blood, and hence the free DNA circulating reflects the genetic profile, including all mutations and clones the patient’s tumor has at the time; this approach was pioneered by researchers at Johns Hopkins University (Sci. Transl. Med. 2012;4:162ra154).
Last year, researchers in Germany reported good correlations when assessing mutations in free circulating DNA in multiple plasma samples drawn from 38 patients with recurrent GIST and matching the results with the patients’ clinical state (Clin. Cancer Res. 2013;19:4854-67).
Dr. Demetri said his own laboratory recently compared mutational analyses in 32 patients with primary GIST and found that in 29 of 32 cases (91%), the mutational profile seen in the free circulating DNA matched that seen in biopsy specimens from each patient.
Currently, genetic assessment of free circulating DNA relies on looking for known mutations using specific amplification primers for those mutations, but next-generation sequencing could be used instead to search for any type of mutation, Dr. Demetri said.
Genetic analysis of GIST at the time of relapse is important, given today’s treatment options and the need to match the right treatment to the right genetic profile, but the challenge is how to perform this analysis in a meaningful way, commented Dr. Robert S. Benjamin, professor and chairman of sarcoma medical oncology at M.D. Anderson Cancer Center in Houston. "The idea of using free DNA in blood is very exciting," he said in an interview.
Dr. Demetri said he has been a consultant to Bayer, Novartis, Pfizer, Sanofi Oncology, Merck, GlaxoSmithKline, and Ariad. Dr. Benjamin said he has been a consultant to Johnson & Johnson, Merck, and Pfizer.
On Twitter @mitchelzoler
EXPERT ANALYSIS FROM SARCOMA AND GIST 2014

U.K. ahead of U.S.A. in cancer survivorship planning
BRUSSELS – Cancer survivorship planning in the United Kingdom is ahead of the United States and the rest of Europe with the recent rollout of a model care plan for cancer patients, along with a guide for conversations between cancer-care health care providers and patients at the time they start long-term follow-up surveillance.
A care plan guides patients as they segue from acute cancer treatment to longer-term health maintenance and follow-up. The plan can include a personalized record of treatment received, prognosis, recommended follow-up examinations, symptoms to be alert for, and other critical information when patients transition to life as a cancer survivor.
The U.K.’s National Health System (NHS) first released a hard-copy version of a model care plan for cancer patients along with a guide for conversations with patients at the time they start long-term follow-up surveillance in 2012. Although the hard-copy form is available from the agency’s National Cancer Survivorship Initiative, the NHS continues to test the care plan and simultaneously is finalizing an electronic version planned for release next year, Dr. Jane Maher said at the first EORTC Cancer Survivorship Summit hosted by the European Organisation for Research and Treatment of Cancer.

"The paper version is freely available," while testing continues at 160 U.K. sites," said Dr. Maher, chief medical officer at Macmillan Cancer Support, London, and a clinical leader with the NHS.
"The first evaluation is done. Patients really liked it and found it helpful and it was possible to do, so it’s at the point where it can be spread, but key elements are still in evaluation until 2015," she said in an interview.
"We can now say that we have a tool to shape the conversation" between a cancer patient who has finished the initial phase of treatment and her care provider. "We have a framework for patient education, for treatment, and for review of their cancer care." Patients who have gone through this care-planning conversation "felt more controlled and that their care was more coordinated."

Prevailing attitudes about cancer management pose some of the biggest challenges in developing and implementing cancer plans, Dr. Maher said. "Cancer is seen as an acute illness that is managed acutely by specialists," she noted. Timing the discussions introduces another challenge. "Physicians were prepared to discuss treatment-related consequences at the time of treatment, but patients did not want to hear it then because they were in life-and-death mode," she said.
In contrast, when patients felt ready to get this information, at the end of their treatment, "physicians weren’t prepared to discuss it for fear of frightening patients." But having some type of conversation on long-term prospects is very important, more critical than any of the individual tools, she said.
U.S. efforts still in process
This rollout puts U.K. cancer survivorship planning ahead of the United States and the rest of Europe. The U.S. National Cancer Institute (NCI) "has a research call out to test models for having that conversation with patient-centered goals," said Catherine Alfano, Ph.D., deputy director of survivorship research at the NCI in Bethesda, Md.
"How do you sit with a patient and family members and friends and talk about what just happened and what will happen in the future? Right now we don’t have a best model for this, but I think we owe it to survivors to identify best practices and get it to all of them, and make it patient centered, so it’s not just an oncologist who hands a piece of paper to the cancer patient and says this is what you need to do, because that won’t work. We need a conversation to take place where cancer patients are engaged in setting their survivorship care goals," Dr. Alfano said in an interview.
"We’re talking a lot right now about giving cancer survivors a treatment summary so they know what they received, and equally important a survivorship care plan that talks about what the patient needs to look out for, what providers they’ll see, how often, and how will their care be coordinated. This is implemented in very different ways throughout the U.S. right now. There is a mad rush to do it. What we want is for a conversation to take place so that cancer survivors are engaged in setting goals for their survivorship care," Dr. Alfano said.
Late last year, NCI researchers and their collaborators published results from a recent survey of more than 1,100 U.S. oncologists and more than 1,000 U.S. primary-care physicians about their practice regarding survivor care plans for their cancer patients (J. Natl. Cancer Inst. 2013;105:1579-87). These plans were used by about 20% of the surveyed oncologists and 13% of primary care physicians. Higher numbers reported giving patients treatment summaries at the end of their acute care, usual practice for half of the responding oncologists and about a third of the primary-care physicians.
Survivorship needs grow and diversify
Optimizing care for cancer survivors and better involving them in long-term surveillance and care has become increasingly important as the numbers continue to climb. "The number of cancer survivors is larger than ever, and as U.S. boomers become 65 years and older, there will be a tsunami of more cancer survivors, Dr. Alfano predicted.
"This huge tsunami [of cancer patients] is coming over the next decade, and we are completely unprepared. We have done a poor job of understanding the needs of adult cancer survivors," she warned. "There is a scramble underway now to understand what adult cancer survivors need."
For example, cardiovascular adverse effects from several different cancer treatments often occur many years after treatment. "Usually, these patients are not in surveillance anymore," said Dr. Thomas M. Suter of the Swiss Cardiovascular Center in Bern, Switzerland. "No one is looking at these patients. They need to be on medical treatment to improve their prognosis," such as treatment with an angiotensin-converting enzyme inhibitor, he said in his talk at the meeting.
Another shortcoming of U.S. cancer survivor care is the fragmented care many patients receive and a glaring lack of coordination.
U.S. cancer survivors "wind up seeing multiple providers for late effects like cardiovascular disease, osteoporosis, and diabetes, which is on top of their surveillance for a recurrence of their primary cancer or appearance of a second primary cancer," said Dr. Alfano. "We have to create a more coordinated form of care that is truly team based to make it easier for patients and relieve the huge burden on them and their families. I hear from cancer survivors and families all the time that it takes hours each week just to coordinate a cancer patient’s care. We need to ease this burden. We have done a poor job understanding the needs of adult cancer survivors."
An especially pressing need is for information on lifestyle change, said Dr. Alfano. "Cancer survivors are looking for things they can do personally to take control back over their morbidity and mortality."
Cancer patients are often highly motivated to take steps to cut their risk of treatment-related adverse outcomes, recurrence, or development of a second primary cancer. In 2012, the American Cancer Society issued nutrition and physical activity guidelines for cancer survivors (CA Cancer J. Clin. 2012;62:30-67), noted Dr. Kevin D. Stein, managing director of the behavioral research center of the ACS in a talk at the meeting.
"We’ve done a poor job of getting lifestyle-change information to cancer survivors. We need to include lifestyle change as part of survivorship plans," said Dr. Alfano.
Despite the shortcomings in survivorship planning in the United States and United Kingdom, it outstrips what currently occurs in most of Europe. "We are far behind the United States," said Dr. Elizabeth Charlotte Moser, professor at the Champalimaud Foundation in Lisbon and chair of the EORTC Survivorship Task Force.
In addition to having Europe follow the United Kingdom and United States in expanding survivor planning, she anticipates a contribution from several European-based cancer-treatment trials for which long-term follow-up data are available. For example, six EORTC-sponsored trials in patients with either early-stage breast cancer or ductal carcinoma in situ together enrolled more than 20,000 patients starting in 1986. EORTC researchers are planning to collect long-term outcome data from as many of these patients as can be tracked down, Dr. Moser said.
Dr. Maher, Dr. Alfano, Dr. Stein, and Dr. Moser said they had no disclosures. Dr. Suter said that he has been a speaker on behalf of Roche, RoboPharma, and Novartis.
On Twitter @mitchelzoler
BRUSSELS – Cancer survivorship planning in the United Kingdom is ahead of the United States and the rest of Europe with the recent rollout of a model care plan for cancer patients, along with a guide for conversations between cancer-care health care providers and patients at the time they start long-term follow-up surveillance.
A care plan guides patients as they segue from acute cancer treatment to longer-term health maintenance and follow-up. The plan can include a personalized record of treatment received, prognosis, recommended follow-up examinations, symptoms to be alert for, and other critical information when patients transition to life as a cancer survivor.
The U.K.’s National Health System (NHS) first released a hard-copy version of a model care plan for cancer patients along with a guide for conversations with patients at the time they start long-term follow-up surveillance in 2012. Although the hard-copy form is available from the agency’s National Cancer Survivorship Initiative, the NHS continues to test the care plan and simultaneously is finalizing an electronic version planned for release next year, Dr. Jane Maher said at the first EORTC Cancer Survivorship Summit hosted by the European Organisation for Research and Treatment of Cancer.
"The paper version is freely available," while testing continues at 160 U.K. sites," said Dr. Maher, chief medical officer at Macmillan Cancer Support, London, and a clinical leader with the NHS.
"The first evaluation is done. Patients really liked it and found it helpful and it was possible to do, so it’s at the point where it can be spread, but key elements are still in evaluation until 2015," she said in an interview.
"We can now say that we have a tool to shape the conversation" between a cancer patient who has finished the initial phase of treatment and her care provider. "We have a framework for patient education, for treatment, and for review of their cancer care." Patients who have gone through this care-planning conversation "felt more controlled and that their care was more coordinated."
Prevailing attitudes about cancer management pose some of the biggest challenges in developing and implementing cancer plans, Dr. Maher said. "Cancer is seen as an acute illness that is managed acutely by specialists," she noted. Timing the discussions introduces another challenge. "Physicians were prepared to discuss treatment-related consequences at the time of treatment, but patients did not want to hear it then because they were in life-and-death mode," she said.
In contrast, when patients felt ready to get this information, at the end of their treatment, "physicians weren’t prepared to discuss it for fear of frightening patients." But having some type of conversation on long-term prospects is very important, more critical than any of the individual tools, she said.
U.S. efforts still in process
This rollout puts U.K. cancer survivorship planning ahead of the United States and the rest of Europe. The U.S. National Cancer Institute (NCI) "has a research call out to test models for having that conversation with patient-centered goals," said Catherine Alfano, Ph.D., deputy director of survivorship research at the NCI in Bethesda, Md.
"How do you sit with a patient and family members and friends and talk about what just happened and what will happen in the future? Right now we don’t have a best model for this, but I think we owe it to survivors to identify best practices and get it to all of them, and make it patient centered, so it’s not just an oncologist who hands a piece of paper to the cancer patient and says this is what you need to do, because that won’t work. We need a conversation to take place where cancer patients are engaged in setting their survivorship care goals," Dr. Alfano said in an interview.
"We’re talking a lot right now about giving cancer survivors a treatment summary so they know what they received, and equally important a survivorship care plan that talks about what the patient needs to look out for, what providers they’ll see, how often, and how will their care be coordinated. This is implemented in very different ways throughout the U.S. right now. There is a mad rush to do it. What we want is for a conversation to take place so that cancer survivors are engaged in setting goals for their survivorship care," Dr. Alfano said.
Late last year, NCI researchers and their collaborators published results from a recent survey of more than 1,100 U.S. oncologists and more than 1,000 U.S. primary-care physicians about their practice regarding survivor care plans for their cancer patients (J. Natl. Cancer Inst. 2013;105:1579-87). These plans were used by about 20% of the surveyed oncologists and 13% of primary care physicians. Higher numbers reported giving patients treatment summaries at the end of their acute care, usual practice for half of the responding oncologists and about a third of the primary-care physicians.
Survivorship needs grow and diversify
Optimizing care for cancer survivors and better involving them in long-term surveillance and care has become increasingly important as the numbers continue to climb. "The number of cancer survivors is larger than ever, and as U.S. boomers become 65 years and older, there will be a tsunami of more cancer survivors, Dr. Alfano predicted.
"This huge tsunami [of cancer patients] is coming over the next decade, and we are completely unprepared. We have done a poor job of understanding the needs of adult cancer survivors," she warned. "There is a scramble underway now to understand what adult cancer survivors need."
For example, cardiovascular adverse effects from several different cancer treatments often occur many years after treatment. "Usually, these patients are not in surveillance anymore," said Dr. Thomas M. Suter of the Swiss Cardiovascular Center in Bern, Switzerland. "No one is looking at these patients. They need to be on medical treatment to improve their prognosis," such as treatment with an angiotensin-converting enzyme inhibitor, he said in his talk at the meeting.
Another shortcoming of U.S. cancer survivor care is the fragmented care many patients receive and a glaring lack of coordination.
U.S. cancer survivors "wind up seeing multiple providers for late effects like cardiovascular disease, osteoporosis, and diabetes, which is on top of their surveillance for a recurrence of their primary cancer or appearance of a second primary cancer," said Dr. Alfano. "We have to create a more coordinated form of care that is truly team based to make it easier for patients and relieve the huge burden on them and their families. I hear from cancer survivors and families all the time that it takes hours each week just to coordinate a cancer patient’s care. We need to ease this burden. We have done a poor job understanding the needs of adult cancer survivors."
An especially pressing need is for information on lifestyle change, said Dr. Alfano. "Cancer survivors are looking for things they can do personally to take control back over their morbidity and mortality."
Cancer patients are often highly motivated to take steps to cut their risk of treatment-related adverse outcomes, recurrence, or development of a second primary cancer. In 2012, the American Cancer Society issued nutrition and physical activity guidelines for cancer survivors (CA Cancer J. Clin. 2012;62:30-67), noted Dr. Kevin D. Stein, managing director of the behavioral research center of the ACS in a talk at the meeting.
"We’ve done a poor job of getting lifestyle-change information to cancer survivors. We need to include lifestyle change as part of survivorship plans," said Dr. Alfano.
Despite the shortcomings in survivorship planning in the United States and United Kingdom, it outstrips what currently occurs in most of Europe. "We are far behind the United States," said Dr. Elizabeth Charlotte Moser, professor at the Champalimaud Foundation in Lisbon and chair of the EORTC Survivorship Task Force.
In addition to having Europe follow the United Kingdom and United States in expanding survivor planning, she anticipates a contribution from several European-based cancer-treatment trials for which long-term follow-up data are available. For example, six EORTC-sponsored trials in patients with either early-stage breast cancer or ductal carcinoma in situ together enrolled more than 20,000 patients starting in 1986. EORTC researchers are planning to collect long-term outcome data from as many of these patients as can be tracked down, Dr. Moser said.
Dr. Maher, Dr. Alfano, Dr. Stein, and Dr. Moser said they had no disclosures. Dr. Suter said that he has been a speaker on behalf of Roche, RoboPharma, and Novartis.
On Twitter @mitchelzoler
BRUSSELS – Cancer survivorship planning in the United Kingdom is ahead of the United States and the rest of Europe with the recent rollout of a model care plan for cancer patients, along with a guide for conversations between cancer-care health care providers and patients at the time they start long-term follow-up surveillance.
A care plan guides patients as they segue from acute cancer treatment to longer-term health maintenance and follow-up. The plan can include a personalized record of treatment received, prognosis, recommended follow-up examinations, symptoms to be alert for, and other critical information when patients transition to life as a cancer survivor.
The U.K.’s National Health System (NHS) first released a hard-copy version of a model care plan for cancer patients along with a guide for conversations with patients at the time they start long-term follow-up surveillance in 2012. Although the hard-copy form is available from the agency’s National Cancer Survivorship Initiative, the NHS continues to test the care plan and simultaneously is finalizing an electronic version planned for release next year, Dr. Jane Maher said at the first EORTC Cancer Survivorship Summit hosted by the European Organisation for Research and Treatment of Cancer.
"The paper version is freely available," while testing continues at 160 U.K. sites," said Dr. Maher, chief medical officer at Macmillan Cancer Support, London, and a clinical leader with the NHS.
"The first evaluation is done. Patients really liked it and found it helpful and it was possible to do, so it’s at the point where it can be spread, but key elements are still in evaluation until 2015," she said in an interview.
"We can now say that we have a tool to shape the conversation" between a cancer patient who has finished the initial phase of treatment and her care provider. "We have a framework for patient education, for treatment, and for review of their cancer care." Patients who have gone through this care-planning conversation "felt more controlled and that their care was more coordinated."
Prevailing attitudes about cancer management pose some of the biggest challenges in developing and implementing cancer plans, Dr. Maher said. "Cancer is seen as an acute illness that is managed acutely by specialists," she noted. Timing the discussions introduces another challenge. "Physicians were prepared to discuss treatment-related consequences at the time of treatment, but patients did not want to hear it then because they were in life-and-death mode," she said.
In contrast, when patients felt ready to get this information, at the end of their treatment, "physicians weren’t prepared to discuss it for fear of frightening patients." But having some type of conversation on long-term prospects is very important, more critical than any of the individual tools, she said.
U.S. efforts still in process
This rollout puts U.K. cancer survivorship planning ahead of the United States and the rest of Europe. The U.S. National Cancer Institute (NCI) "has a research call out to test models for having that conversation with patient-centered goals," said Catherine Alfano, Ph.D., deputy director of survivorship research at the NCI in Bethesda, Md.
"How do you sit with a patient and family members and friends and talk about what just happened and what will happen in the future? Right now we don’t have a best model for this, but I think we owe it to survivors to identify best practices and get it to all of them, and make it patient centered, so it’s not just an oncologist who hands a piece of paper to the cancer patient and says this is what you need to do, because that won’t work. We need a conversation to take place where cancer patients are engaged in setting their survivorship care goals," Dr. Alfano said in an interview.
"We’re talking a lot right now about giving cancer survivors a treatment summary so they know what they received, and equally important a survivorship care plan that talks about what the patient needs to look out for, what providers they’ll see, how often, and how will their care be coordinated. This is implemented in very different ways throughout the U.S. right now. There is a mad rush to do it. What we want is for a conversation to take place so that cancer survivors are engaged in setting goals for their survivorship care," Dr. Alfano said.
Late last year, NCI researchers and their collaborators published results from a recent survey of more than 1,100 U.S. oncologists and more than 1,000 U.S. primary-care physicians about their practice regarding survivor care plans for their cancer patients (J. Natl. Cancer Inst. 2013;105:1579-87). These plans were used by about 20% of the surveyed oncologists and 13% of primary care physicians. Higher numbers reported giving patients treatment summaries at the end of their acute care, usual practice for half of the responding oncologists and about a third of the primary-care physicians.
Survivorship needs grow and diversify
Optimizing care for cancer survivors and better involving them in long-term surveillance and care has become increasingly important as the numbers continue to climb. "The number of cancer survivors is larger than ever, and as U.S. boomers become 65 years and older, there will be a tsunami of more cancer survivors, Dr. Alfano predicted.
"This huge tsunami [of cancer patients] is coming over the next decade, and we are completely unprepared. We have done a poor job of understanding the needs of adult cancer survivors," she warned. "There is a scramble underway now to understand what adult cancer survivors need."
For example, cardiovascular adverse effects from several different cancer treatments often occur many years after treatment. "Usually, these patients are not in surveillance anymore," said Dr. Thomas M. Suter of the Swiss Cardiovascular Center in Bern, Switzerland. "No one is looking at these patients. They need to be on medical treatment to improve their prognosis," such as treatment with an angiotensin-converting enzyme inhibitor, he said in his talk at the meeting.
Another shortcoming of U.S. cancer survivor care is the fragmented care many patients receive and a glaring lack of coordination.
U.S. cancer survivors "wind up seeing multiple providers for late effects like cardiovascular disease, osteoporosis, and diabetes, which is on top of their surveillance for a recurrence of their primary cancer or appearance of a second primary cancer," said Dr. Alfano. "We have to create a more coordinated form of care that is truly team based to make it easier for patients and relieve the huge burden on them and their families. I hear from cancer survivors and families all the time that it takes hours each week just to coordinate a cancer patient’s care. We need to ease this burden. We have done a poor job understanding the needs of adult cancer survivors."
An especially pressing need is for information on lifestyle change, said Dr. Alfano. "Cancer survivors are looking for things they can do personally to take control back over their morbidity and mortality."
Cancer patients are often highly motivated to take steps to cut their risk of treatment-related adverse outcomes, recurrence, or development of a second primary cancer. In 2012, the American Cancer Society issued nutrition and physical activity guidelines for cancer survivors (CA Cancer J. Clin. 2012;62:30-67), noted Dr. Kevin D. Stein, managing director of the behavioral research center of the ACS in a talk at the meeting.
"We’ve done a poor job of getting lifestyle-change information to cancer survivors. We need to include lifestyle change as part of survivorship plans," said Dr. Alfano.
Despite the shortcomings in survivorship planning in the United States and United Kingdom, it outstrips what currently occurs in most of Europe. "We are far behind the United States," said Dr. Elizabeth Charlotte Moser, professor at the Champalimaud Foundation in Lisbon and chair of the EORTC Survivorship Task Force.
In addition to having Europe follow the United Kingdom and United States in expanding survivor planning, she anticipates a contribution from several European-based cancer-treatment trials for which long-term follow-up data are available. For example, six EORTC-sponsored trials in patients with either early-stage breast cancer or ductal carcinoma in situ together enrolled more than 20,000 patients starting in 1986. EORTC researchers are planning to collect long-term outcome data from as many of these patients as can be tracked down, Dr. Moser said.
Dr. Maher, Dr. Alfano, Dr. Stein, and Dr. Moser said they had no disclosures. Dr. Suter said that he has been a speaker on behalf of Roche, RoboPharma, and Novartis.
On Twitter @mitchelzoler
AT THE CANCER SURVIVORSHIP SUMMIT

ACC highlights noninvasive cardiovascular imaging issues
Noninvasive cardiovascular imaging in U.S. medical practice today raises two policy challenges, according to a statement released on Feb. 17 by the American College of Cardiology and 13 collaborating medical groups: fostering a volume of imaging that balances patient needs with responsible use of societal resources, and continued improvement in the quality of care based on noninvasive cardiovascular imaging.
"The purpose of this document is to provide a brief exposition of the issues involved [in usage volume of noninvasive cardiovascular imaging] and the possible ways in which the medical care system can balance responsible use of imaging with patient safety concerns while maintaining or even enhancing quality of care," wrote the 20-member panel in a health policy statement (J. Am. Coll. Cardiol. 2014;63:698-721). "Policy makers must take into account the complex interplay between medical care quality (of which proper use of diagnostic testing is an integral part), patient health outcomes, and medical costs," said the statement’s panel, which included representatives from the American Society of Nuclear Cardiology, the American Society of Echocardiography, the Radiological Society of North America, and six other imaging groups.
"The current situation in noninvasive cardiovascular imaging is pretty much unsatisfactory from everyone’s point of view," said Dr. Daniel B. Mark, a cardiologist and professor of medicine at Duke University in Durham, N.C., who chaired the statement-writing committee."However, it is encouraging that we now have much more knowledge and several new informatics tools that can be used to help us apply that knowledge. We have many of the ingredients needed to create a more responsible, cost-conscious approach to imaging that still preserves – at its core – patient-physician decision making," said Dr. Mark in a written statement.
Over the past 20 years, U.S. health care payers implemented three main strategies to control expenditures for diagnostic imaging, the statement said: requiring prior authorization from a radiology benefits manager; requiring prior notification before performing selected, advanced diagnostic imaging methods like MRI and PET; and reduced payments for imaging. The statement characterized all three as "blunt instruments,’ and added these can lead to "limited patient access to necessary services and greater administrative inefficiencies."
One approach that would likely improve imaging-use policy is an "iterative process" that uses high-quality data to guide development of policy interventions with the potential to reduce imaging overuse, underuse, and misuse. Another approach the panel endorsed is integration of appropriate-use software into the process of care. "Development of computerized appropriate-use tools would be efficient and also greatly enhance transparency," the panel said. "Validated patient-specific point-of-care/referral appropriateness tools and other decision-support tools are examples of innovations that could support a higher-quality, more accountable use of cardiovascular imaging."
Recent data show that growth of advanced cardiovascular imaging has substantially slowed since 2006, likely because of a combination of professional society and payer initiatives. "Many clinicians and patients fear that imaging policy decisions will continue to be driven primarily, if not exclusively, by cost considerations without adequate consideration of clinical benefit and value," said the statement.
"The complexity of our current health care system and the competing macro-forces that push it in myriad different directions can make responsible imaging use seem impossibly daunting. What we need is a convergence of will from all key stakeholders to make it happen. This statement is hopefully a step in that direction," Dr. Mark said.
Dr. Mark said that he had no disclosures.
On Twitter @mitchelzoler
Noninvasive cardiovascular imaging in U.S. medical practice today raises two policy challenges, according to a statement released on Feb. 17 by the American College of Cardiology and 13 collaborating medical groups: fostering a volume of imaging that balances patient needs with responsible use of societal resources, and continued improvement in the quality of care based on noninvasive cardiovascular imaging.
"The purpose of this document is to provide a brief exposition of the issues involved [in usage volume of noninvasive cardiovascular imaging] and the possible ways in which the medical care system can balance responsible use of imaging with patient safety concerns while maintaining or even enhancing quality of care," wrote the 20-member panel in a health policy statement (J. Am. Coll. Cardiol. 2014;63:698-721). "Policy makers must take into account the complex interplay between medical care quality (of which proper use of diagnostic testing is an integral part), patient health outcomes, and medical costs," said the statement’s panel, which included representatives from the American Society of Nuclear Cardiology, the American Society of Echocardiography, the Radiological Society of North America, and six other imaging groups.
"The current situation in noninvasive cardiovascular imaging is pretty much unsatisfactory from everyone’s point of view," said Dr. Daniel B. Mark, a cardiologist and professor of medicine at Duke University in Durham, N.C., who chaired the statement-writing committee."However, it is encouraging that we now have much more knowledge and several new informatics tools that can be used to help us apply that knowledge. We have many of the ingredients needed to create a more responsible, cost-conscious approach to imaging that still preserves – at its core – patient-physician decision making," said Dr. Mark in a written statement.
Over the past 20 years, U.S. health care payers implemented three main strategies to control expenditures for diagnostic imaging, the statement said: requiring prior authorization from a radiology benefits manager; requiring prior notification before performing selected, advanced diagnostic imaging methods like MRI and PET; and reduced payments for imaging. The statement characterized all three as "blunt instruments,’ and added these can lead to "limited patient access to necessary services and greater administrative inefficiencies."
One approach that would likely improve imaging-use policy is an "iterative process" that uses high-quality data to guide development of policy interventions with the potential to reduce imaging overuse, underuse, and misuse. Another approach the panel endorsed is integration of appropriate-use software into the process of care. "Development of computerized appropriate-use tools would be efficient and also greatly enhance transparency," the panel said. "Validated patient-specific point-of-care/referral appropriateness tools and other decision-support tools are examples of innovations that could support a higher-quality, more accountable use of cardiovascular imaging."
Recent data show that growth of advanced cardiovascular imaging has substantially slowed since 2006, likely because of a combination of professional society and payer initiatives. "Many clinicians and patients fear that imaging policy decisions will continue to be driven primarily, if not exclusively, by cost considerations without adequate consideration of clinical benefit and value," said the statement.
"The complexity of our current health care system and the competing macro-forces that push it in myriad different directions can make responsible imaging use seem impossibly daunting. What we need is a convergence of will from all key stakeholders to make it happen. This statement is hopefully a step in that direction," Dr. Mark said.
Dr. Mark said that he had no disclosures.
On Twitter @mitchelzoler
Noninvasive cardiovascular imaging in U.S. medical practice today raises two policy challenges, according to a statement released on Feb. 17 by the American College of Cardiology and 13 collaborating medical groups: fostering a volume of imaging that balances patient needs with responsible use of societal resources, and continued improvement in the quality of care based on noninvasive cardiovascular imaging.
"The purpose of this document is to provide a brief exposition of the issues involved [in usage volume of noninvasive cardiovascular imaging] and the possible ways in which the medical care system can balance responsible use of imaging with patient safety concerns while maintaining or even enhancing quality of care," wrote the 20-member panel in a health policy statement (J. Am. Coll. Cardiol. 2014;63:698-721). "Policy makers must take into account the complex interplay between medical care quality (of which proper use of diagnostic testing is an integral part), patient health outcomes, and medical costs," said the statement’s panel, which included representatives from the American Society of Nuclear Cardiology, the American Society of Echocardiography, the Radiological Society of North America, and six other imaging groups.
"The current situation in noninvasive cardiovascular imaging is pretty much unsatisfactory from everyone’s point of view," said Dr. Daniel B. Mark, a cardiologist and professor of medicine at Duke University in Durham, N.C., who chaired the statement-writing committee."However, it is encouraging that we now have much more knowledge and several new informatics tools that can be used to help us apply that knowledge. We have many of the ingredients needed to create a more responsible, cost-conscious approach to imaging that still preserves – at its core – patient-physician decision making," said Dr. Mark in a written statement.
Over the past 20 years, U.S. health care payers implemented three main strategies to control expenditures for diagnostic imaging, the statement said: requiring prior authorization from a radiology benefits manager; requiring prior notification before performing selected, advanced diagnostic imaging methods like MRI and PET; and reduced payments for imaging. The statement characterized all three as "blunt instruments,’ and added these can lead to "limited patient access to necessary services and greater administrative inefficiencies."
One approach that would likely improve imaging-use policy is an "iterative process" that uses high-quality data to guide development of policy interventions with the potential to reduce imaging overuse, underuse, and misuse. Another approach the panel endorsed is integration of appropriate-use software into the process of care. "Development of computerized appropriate-use tools would be efficient and also greatly enhance transparency," the panel said. "Validated patient-specific point-of-care/referral appropriateness tools and other decision-support tools are examples of innovations that could support a higher-quality, more accountable use of cardiovascular imaging."
Recent data show that growth of advanced cardiovascular imaging has substantially slowed since 2006, likely because of a combination of professional society and payer initiatives. "Many clinicians and patients fear that imaging policy decisions will continue to be driven primarily, if not exclusively, by cost considerations without adequate consideration of clinical benefit and value," said the statement.
"The complexity of our current health care system and the competing macro-forces that push it in myriad different directions can make responsible imaging use seem impossibly daunting. What we need is a convergence of will from all key stakeholders to make it happen. This statement is hopefully a step in that direction," Dr. Mark said.
Dr. Mark said that he had no disclosures.
On Twitter @mitchelzoler
FROM THE JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY
Genotyping adds little to optimized warfarin dosing
DALLAS - Genotyping to guide the starting dosage of warfarin treatment showed no added value above tailoring treatment with a panel of clinical features in a randomized, controlled U.S. trial of more than 1,000 patients.
The resounding null result from adding genotype information should spell the end of this practice, said Dr. Stephen E. Kimmel, lead investigator for the study, and professor and director of cardiovascular epidemiology at the University of Pennsylvania in Philadelphia.

"Based on what we've seen, I don't believe there is sufficient evidence to add genetic information on top of the available clinical algorithms," Dr. Kimmel said at the American Heart Association scientific sessions. "I don't think we'll see another genetics trial in warfarin treatment. I think this is it."
Good outcomes in the comparison group largely accounted for the failure of genotyping to significantly improve the percentage of time that patients' international normalized ratios (INRs) were in the target range of 2.0-3.0. The amount of time in the therapeutic INR range (PTTR) averaged 45% in patients in the comparison arm during the first 4 weeks of warfarin treatment.
"When the comparison group does so well, it's more difficult for genotyping to have an effect," said Dr. Elaine M. Hylek, professor of medicine and an anticoagulant specialist at Boston University.
That limitation, coupled with the shifting anticoagulant landscape, knock genotyping out of the picture, she agreed. "It will be difficult funding [another study of genotyping] with all the anticoagulant alternatives that are now out there" for preventing thrombosis in patients with atrial fibrillation or a recent venous thromboembolism.
The Clarification of Optimal Anticoagulant through Genetics (COAG) trial enrolled 1,015 patients initiating warfarin therapy at 18 U.S. centers during September 2009 to April 2013. The study randomized patients to two different ways to calculate their warfarin dosage during the first 5 days of treatment.
Half had their dosage calculated by a formula that took into account seven clinical and demographic factors, including age, race, smoking status, and body surface area. The others had their dosage calculated with the same formula and factors plus added information on the patient's genotype for two genes that affect warfarin activity, CYP2C9 and VKORC1. Patients' average age was 58 years; just over a quarter were African American.

During the first 4 weeks on treatment, the average PTTR was 45% in both arms of the study, the trial's primary endpoint. Adding genotyping information led to a bigger improvement in the PTTR among the non-African American patients compared with those who were African American, but did not produce a significantly increased PTTR in the non-African American subgroup.
Dr. Munir Pirmohamed reported results from a similar study that enrolled 455 patients starting warfarin therapy at any of five centers in the United Kingdom and Sweden.
The EU-Pharmacogenetics of Anticoagulant Therapy (EU-PACT) Warfarin study mainly differed from the COAG study by the background method used to calculate a starting warfarin dosage over the first 3 days of treatment.
In EU-PACT, the warfarin dosage of all patients was adjusted for age but not for other factors. In the intervention arm, the starting dosages were adjusted for the status of the same two genes, CYP2C9 and VKORC1.
During the first 12 weeks after starting warfarin, the cumulative average PTTR was 67% in the patients whose dose was adjusted by genotype and 60% in patients who were not genotyped, a statistically significant difference for this study's primary endpoint, reported Dr. Pirmohamed, professor and head of molecular and clinical pharmacology at the University of Liverpool, England.
Taken together, the findings of the two studies highlight that patients should not start warfarin treatment on a fixed dosage, said Dr. Patrick T. Ellinor, a cardiologist and arrhythmia specialist at Massachusetts General Hospital, Boston, and designated discussant for both reports at the meeting.
The findings support use of a clinical algorithm that takes into account several clinical factors, he added.
Concurrently with the meeting, the reports were published online for COAG (N. Engl. J. Med. 2013 [doi: 10.1056/NEJMoa1310669]) and for EU-PACT (N. Engl. J. Med. 2013 [doi: 10.1056/NEJMoa1311386]).
Warfarin on top despite competition
Warfarin remains the most widely used anticoagulant in the United States. Among patients with atrial fibrillation taking anticoagulation treatment, 72% used warfarin during the third quarter of 2013, data from a large registry show.
The new anticoagulants on the U.S. market - dabigatran (Pradaxa), apixaban (Eliquis), and rivaroxaban (Xarelto) - are gaining ground and widely acknowledged to be better, safer, and easier to manage. But warfarin clings to the market largely because of familiarity and low price, according to several experts.
"There is no doubt that the new anticoagulants look better compared with warfarin, but the clinical fact is that it's what you know versus what you don't know, and warfarin has been used for 60 years," Dr. Kimmel said at the press conference.
"The new drugs perform better than warfarin does; they get patients to where they need to be more quickly, but warfarin has been around a long time. We know its interactions and risks, there is the ability to reverse its effect, and the cost to patients is a real issue. If the new anticoagulants were the same price as warfarin then I think you'd see a lot more patients get a new drug," Dr. Ellinor said in an interview.
Data on current U.S. uptake of the new oral anticoagulants came from the 148,320 unique patients with atrial fibrillation included during June to September of 2013 in the PINNACLE Registry database run by the American College of Cardiology. Among these patients, about 83,000 (56%) were on some anticoagulant treatment, and within this subgroup, 72% were on warfarin, 27% on a new anticoagulant, and the remainder on different treatment, said Dr. John Gordon Harold, ACC president and a cardiologist at Cedars-Sinai Heart Institute in Los Angeles.

"In my own practice the new anticoagulants are being used with increasing frequency, mainly driven by direct-to-consumer advertising," Dr. Harold said in an interview. "We have patients who are completely stable on warfarin. (They) come in because of a consumer ad and they ask if they should switch drugs. When patients are stable I don't encourage them to switch, but we have a shared decision making conversation and go over the pros and cons, the cost, and the outcomes data. A lot of patients prefer to pay the difference" and switch to a new anticoagulant.
Dr. Harold said he also recommends that patients switch off warfarin if they have problems with compliance and variability in their international normalized ratio (INR).
"If you can keep a patient on warfarin in their INR target range 80% or more of the time then I wouldn't change, but most patients on warfarin have a very hard time maintaining an INR of 2-3," said Dr. Mark S. Link, professor and codirector of the cardiac arrhythmia center at Tufts Medical Center, Boston. But he said cost is a major factor keeping many patients on warfarin.
The new anticoagulants "are better than warfarin, but we are often forced by insurers to start with the cheaper drug," Dr. Link said during the news conference.
The COAG and EU-PACT studies did not receive any direct commercial sponsorship. Dr. Kimmel has been a consultant to Pfizer and Janssen. Dr. Hylek has been a consultant or adviser to Bayer, Boehringer Ingelheim, Bristol-Myers Squibb, Daiichi Sankyo, Johnson & Johnson, and Pfizer. Dr. Pirmohamed, Dr. Ellinor, Dr. Harold, and Dr. Link had no relevant disclosures.
On Twitter @mitchelzoler
DALLAS - Genotyping to guide the starting dosage of warfarin treatment showed no added value above tailoring treatment with a panel of clinical features in a randomized, controlled U.S. trial of more than 1,000 patients.
The resounding null result from adding genotype information should spell the end of this practice, said Dr. Stephen E. Kimmel, lead investigator for the study, and professor and director of cardiovascular epidemiology at the University of Pennsylvania in Philadelphia.
"Based on what we've seen, I don't believe there is sufficient evidence to add genetic information on top of the available clinical algorithms," Dr. Kimmel said at the American Heart Association scientific sessions. "I don't think we'll see another genetics trial in warfarin treatment. I think this is it."
Good outcomes in the comparison group largely accounted for the failure of genotyping to significantly improve the percentage of time that patients' international normalized ratios (INRs) were in the target range of 2.0-3.0. The amount of time in the therapeutic INR range (PTTR) averaged 45% in patients in the comparison arm during the first 4 weeks of warfarin treatment.
"When the comparison group does so well, it's more difficult for genotyping to have an effect," said Dr. Elaine M. Hylek, professor of medicine and an anticoagulant specialist at Boston University.
That limitation, coupled with the shifting anticoagulant landscape, knock genotyping out of the picture, she agreed. "It will be difficult funding [another study of genotyping] with all the anticoagulant alternatives that are now out there" for preventing thrombosis in patients with atrial fibrillation or a recent venous thromboembolism.
The Clarification of Optimal Anticoagulant through Genetics (COAG) trial enrolled 1,015 patients initiating warfarin therapy at 18 U.S. centers during September 2009 to April 2013. The study randomized patients to two different ways to calculate their warfarin dosage during the first 5 days of treatment.
Half had their dosage calculated by a formula that took into account seven clinical and demographic factors, including age, race, smoking status, and body surface area. The others had their dosage calculated with the same formula and factors plus added information on the patient's genotype for two genes that affect warfarin activity, CYP2C9 and VKORC1. Patients' average age was 58 years; just over a quarter were African American.
During the first 4 weeks on treatment, the average PTTR was 45% in both arms of the study, the trial's primary endpoint. Adding genotyping information led to a bigger improvement in the PTTR among the non-African American patients compared with those who were African American, but did not produce a significantly increased PTTR in the non-African American subgroup.
Dr. Munir Pirmohamed reported results from a similar study that enrolled 455 patients starting warfarin therapy at any of five centers in the United Kingdom and Sweden.
The EU-Pharmacogenetics of Anticoagulant Therapy (EU-PACT) Warfarin study mainly differed from the COAG study by the background method used to calculate a starting warfarin dosage over the first 3 days of treatment.
In EU-PACT, the warfarin dosage of all patients was adjusted for age but not for other factors. In the intervention arm, the starting dosages were adjusted for the status of the same two genes, CYP2C9 and VKORC1.
During the first 12 weeks after starting warfarin, the cumulative average PTTR was 67% in the patients whose dose was adjusted by genotype and 60% in patients who were not genotyped, a statistically significant difference for this study's primary endpoint, reported Dr. Pirmohamed, professor and head of molecular and clinical pharmacology at the University of Liverpool, England.
Taken together, the findings of the two studies highlight that patients should not start warfarin treatment on a fixed dosage, said Dr. Patrick T. Ellinor, a cardiologist and arrhythmia specialist at Massachusetts General Hospital, Boston, and designated discussant for both reports at the meeting.
The findings support use of a clinical algorithm that takes into account several clinical factors, he added.
Concurrently with the meeting, the reports were published online for COAG (N. Engl. J. Med. 2013 [doi: 10.1056/NEJMoa1310669]) and for EU-PACT (N. Engl. J. Med. 2013 [doi: 10.1056/NEJMoa1311386]).
Warfarin on top despite competition
Warfarin remains the most widely used anticoagulant in the United States. Among patients with atrial fibrillation taking anticoagulation treatment, 72% used warfarin during the third quarter of 2013, data from a large registry show.
The new anticoagulants on the U.S. market - dabigatran (Pradaxa), apixaban (Eliquis), and rivaroxaban (Xarelto) - are gaining ground and widely acknowledged to be better, safer, and easier to manage. But warfarin clings to the market largely because of familiarity and low price, according to several experts.
"There is no doubt that the new anticoagulants look better compared with warfarin, but the clinical fact is that it's what you know versus what you don't know, and warfarin has been used for 60 years," Dr. Kimmel said at the press conference.
"The new drugs perform better than warfarin does; they get patients to where they need to be more quickly, but warfarin has been around a long time. We know its interactions and risks, there is the ability to reverse its effect, and the cost to patients is a real issue. If the new anticoagulants were the same price as warfarin then I think you'd see a lot more patients get a new drug," Dr. Ellinor said in an interview.
Data on current U.S. uptake of the new oral anticoagulants came from the 148,320 unique patients with atrial fibrillation included during June to September of 2013 in the PINNACLE Registry database run by the American College of Cardiology. Among these patients, about 83,000 (56%) were on some anticoagulant treatment, and within this subgroup, 72% were on warfarin, 27% on a new anticoagulant, and the remainder on different treatment, said Dr. John Gordon Harold, ACC president and a cardiologist at Cedars-Sinai Heart Institute in Los Angeles.
"In my own practice the new anticoagulants are being used with increasing frequency, mainly driven by direct-to-consumer advertising," Dr. Harold said in an interview. "We have patients who are completely stable on warfarin. (They) come in because of a consumer ad and they ask if they should switch drugs. When patients are stable I don't encourage them to switch, but we have a shared decision making conversation and go over the pros and cons, the cost, and the outcomes data. A lot of patients prefer to pay the difference" and switch to a new anticoagulant.
Dr. Harold said he also recommends that patients switch off warfarin if they have problems with compliance and variability in their international normalized ratio (INR).
"If you can keep a patient on warfarin in their INR target range 80% or more of the time then I wouldn't change, but most patients on warfarin have a very hard time maintaining an INR of 2-3," said Dr. Mark S. Link, professor and codirector of the cardiac arrhythmia center at Tufts Medical Center, Boston. But he said cost is a major factor keeping many patients on warfarin.
The new anticoagulants "are better than warfarin, but we are often forced by insurers to start with the cheaper drug," Dr. Link said during the news conference.
The COAG and EU-PACT studies did not receive any direct commercial sponsorship. Dr. Kimmel has been a consultant to Pfizer and Janssen. Dr. Hylek has been a consultant or adviser to Bayer, Boehringer Ingelheim, Bristol-Myers Squibb, Daiichi Sankyo, Johnson & Johnson, and Pfizer. Dr. Pirmohamed, Dr. Ellinor, Dr. Harold, and Dr. Link had no relevant disclosures.
On Twitter @mitchelzoler
DALLAS - Genotyping to guide the starting dosage of warfarin treatment showed no added value above tailoring treatment with a panel of clinical features in a randomized, controlled U.S. trial of more than 1,000 patients.
The resounding null result from adding genotype information should spell the end of this practice, said Dr. Stephen E. Kimmel, lead investigator for the study, and professor and director of cardiovascular epidemiology at the University of Pennsylvania in Philadelphia.
"Based on what we've seen, I don't believe there is sufficient evidence to add genetic information on top of the available clinical algorithms," Dr. Kimmel said at the American Heart Association scientific sessions. "I don't think we'll see another genetics trial in warfarin treatment. I think this is it."
Good outcomes in the comparison group largely accounted for the failure of genotyping to significantly improve the percentage of time that patients' international normalized ratios (INRs) were in the target range of 2.0-3.0. The amount of time in the therapeutic INR range (PTTR) averaged 45% in patients in the comparison arm during the first 4 weeks of warfarin treatment.
"When the comparison group does so well, it's more difficult for genotyping to have an effect," said Dr. Elaine M. Hylek, professor of medicine and an anticoagulant specialist at Boston University.
That limitation, coupled with the shifting anticoagulant landscape, knock genotyping out of the picture, she agreed. "It will be difficult funding [another study of genotyping] with all the anticoagulant alternatives that are now out there" for preventing thrombosis in patients with atrial fibrillation or a recent venous thromboembolism.
The Clarification of Optimal Anticoagulant through Genetics (COAG) trial enrolled 1,015 patients initiating warfarin therapy at 18 U.S. centers during September 2009 to April 2013. The study randomized patients to two different ways to calculate their warfarin dosage during the first 5 days of treatment.
Half had their dosage calculated by a formula that took into account seven clinical and demographic factors, including age, race, smoking status, and body surface area. The others had their dosage calculated with the same formula and factors plus added information on the patient's genotype for two genes that affect warfarin activity, CYP2C9 and VKORC1. Patients' average age was 58 years; just over a quarter were African American.
During the first 4 weeks on treatment, the average PTTR was 45% in both arms of the study, the trial's primary endpoint. Adding genotyping information led to a bigger improvement in the PTTR among the non-African American patients compared with those who were African American, but did not produce a significantly increased PTTR in the non-African American subgroup.
Dr. Munir Pirmohamed reported results from a similar study that enrolled 455 patients starting warfarin therapy at any of five centers in the United Kingdom and Sweden.
The EU-Pharmacogenetics of Anticoagulant Therapy (EU-PACT) Warfarin study mainly differed from the COAG study by the background method used to calculate a starting warfarin dosage over the first 3 days of treatment.
In EU-PACT, the warfarin dosage of all patients was adjusted for age but not for other factors. In the intervention arm, the starting dosages were adjusted for the status of the same two genes, CYP2C9 and VKORC1.
During the first 12 weeks after starting warfarin, the cumulative average PTTR was 67% in the patients whose dose was adjusted by genotype and 60% in patients who were not genotyped, a statistically significant difference for this study's primary endpoint, reported Dr. Pirmohamed, professor and head of molecular and clinical pharmacology at the University of Liverpool, England.
Taken together, the findings of the two studies highlight that patients should not start warfarin treatment on a fixed dosage, said Dr. Patrick T. Ellinor, a cardiologist and arrhythmia specialist at Massachusetts General Hospital, Boston, and designated discussant for both reports at the meeting.
The findings support use of a clinical algorithm that takes into account several clinical factors, he added.
Concurrently with the meeting, the reports were published online for COAG (N. Engl. J. Med. 2013 [doi: 10.1056/NEJMoa1310669]) and for EU-PACT (N. Engl. J. Med. 2013 [doi: 10.1056/NEJMoa1311386]).
Warfarin on top despite competition
Warfarin remains the most widely used anticoagulant in the United States. Among patients with atrial fibrillation taking anticoagulation treatment, 72% used warfarin during the third quarter of 2013, data from a large registry show.
The new anticoagulants on the U.S. market - dabigatran (Pradaxa), apixaban (Eliquis), and rivaroxaban (Xarelto) - are gaining ground and widely acknowledged to be better, safer, and easier to manage. But warfarin clings to the market largely because of familiarity and low price, according to several experts.
"There is no doubt that the new anticoagulants look better compared with warfarin, but the clinical fact is that it's what you know versus what you don't know, and warfarin has been used for 60 years," Dr. Kimmel said at the press conference.
"The new drugs perform better than warfarin does; they get patients to where they need to be more quickly, but warfarin has been around a long time. We know its interactions and risks, there is the ability to reverse its effect, and the cost to patients is a real issue. If the new anticoagulants were the same price as warfarin then I think you'd see a lot more patients get a new drug," Dr. Ellinor said in an interview.
Data on current U.S. uptake of the new oral anticoagulants came from the 148,320 unique patients with atrial fibrillation included during June to September of 2013 in the PINNACLE Registry database run by the American College of Cardiology. Among these patients, about 83,000 (56%) were on some anticoagulant treatment, and within this subgroup, 72% were on warfarin, 27% on a new anticoagulant, and the remainder on different treatment, said Dr. John Gordon Harold, ACC president and a cardiologist at Cedars-Sinai Heart Institute in Los Angeles.
"In my own practice the new anticoagulants are being used with increasing frequency, mainly driven by direct-to-consumer advertising," Dr. Harold said in an interview. "We have patients who are completely stable on warfarin. (They) come in because of a consumer ad and they ask if they should switch drugs. When patients are stable I don't encourage them to switch, but we have a shared decision making conversation and go over the pros and cons, the cost, and the outcomes data. A lot of patients prefer to pay the difference" and switch to a new anticoagulant.
Dr. Harold said he also recommends that patients switch off warfarin if they have problems with compliance and variability in their international normalized ratio (INR).
"If you can keep a patient on warfarin in their INR target range 80% or more of the time then I wouldn't change, but most patients on warfarin have a very hard time maintaining an INR of 2-3," said Dr. Mark S. Link, professor and codirector of the cardiac arrhythmia center at Tufts Medical Center, Boston. But he said cost is a major factor keeping many patients on warfarin.
The new anticoagulants "are better than warfarin, but we are often forced by insurers to start with the cheaper drug," Dr. Link said during the news conference.
The COAG and EU-PACT studies did not receive any direct commercial sponsorship. Dr. Kimmel has been a consultant to Pfizer and Janssen. Dr. Hylek has been a consultant or adviser to Bayer, Boehringer Ingelheim, Bristol-Myers Squibb, Daiichi Sankyo, Johnson & Johnson, and Pfizer. Dr. Pirmohamed, Dr. Ellinor, Dr. Harold, and Dr. Link had no relevant disclosures.
On Twitter @mitchelzoler
Major finding: Patients starting warfarin with dosing based on a formula that took into account seven clinical and demographic factors averaged 45% of the time in therapeutic range regardless of whether the starting dosage was adjusted based on genotype results.
Data source: COAG, a randomized trial with 1,015 patients starting warfarin therapy at 18 U.S. centers.
Disclosures: The COAG and EU-PACT studies did not receive any direct commercial sponsorship. Dr. Kimmel has been a consultant to Pfizer and Janssen. Dr. Hylek has been a consultant or adviser to Bayer, Boehringer Ingelheim, Bristol-Myers Squibb, Daiichi Sankyo, Johnson & Johnson, and Pfizer. Dr. Pirmohamed and Dr. Ellinor had no disclosures.

Closing the circle on sentinel lymph node biopsy
Some diagnoses, treatments, or procedures become closely identified with one or two people. Sentinel lymph node biopsy is a cancer-staging technique forever linked to Dr. Donald L. Morton, who in 1978 published his first findings on lymph node drainage and metastasis patterns in patients with malignant melanoma.
Since then, sentinel lymph node biopsy (SLNB) became the standard of care for staging a sizeable subset of patients with newly diagnosed melanoma, based largely on a prespecified interim analysis of data from the first Multicenter Selective Lymphadenectomy Trial (MSLT-I), a study with 2,001 patients launched by Dr. Morton and his associates in 1994 to definitively test the efficacy of SLNB.

On Feb. 13, Dr. Morton and his associates published "the final trial report" from MSLT-I with 10-year follow-up, results that further confirmed the beneficial role of SLNB and brought full closure to a clinical journey that lasted nearly 40 years.
But Dr. Morton did not quite make it to see the article published. He died on Jan. 10 from heart failure, at age 79, at St. John’s Health Center in Santa Monica, Calif.
"Dr. Morton was incredibly pleased to know the paper was to be published. It was very gratifying to him that it was successfully completed and would be out in the New England Journal of Medicine," said Dr. Mark B. Faries, a senior collaborator with Dr. Morton on MSLT-I and director of melanoma research at the John Wayne Cancer Institute in Santa Monica, Calif.
Publication of the final report of the MSLT-I trial "is a capstone on Dr. Morton’s career," said Dr. Charles M. Balch, professor of surgery at the University of Texas Southwestern Medical Center at Dallas, in an interview. In an editorial accompanying the publication, Dr. Balch and a colleague wrote that the final report from the "landmark" MSLT-I trial "caps a 35-year effort to resolve the controversy surrounding the survival benefit of surgical excision of regional lymph nodes as a component of initial treatment of patients with primary melanoma."
Dr. Morton faced strong skepticism when he first presented his findings on the staging role for SLNB at a meeting in 1990 and in the years immediately after. His report describing a method for identifying and assessing sentinel lymph nodes was rejected by several "high-impact journals," recalled Dr. Balch and some of his colleagues in a remembrance that will be published in Annals of Surgical Oncology in March. "Undaunted, he persisted," they wrote, until the report appeared in Archives of Surgery in 1992. Designing, launching, and running MSLT-I came next, with many of the study’s major findings appearing in 2006. By confirming the efficacy of SLNB for staging many melanoma patients, MSLT-I was a "practice-changing trial," wrote Dr. Balch and his associates.
Although the new, 10-year follow-up gives closure to the central thesis of Dr. Morton’s SLNB technique, he didn’t stop there.
"Anyone who knew [Dr. Morton] would know he would never feel he had completed his work until the disease was cured for all," said Dr. Faries. "This is evidenced by the second MSLT trial that is now underway" that Dr. Morton and his associates launched to determine whether patients with positive sentinel lymph nodes benefit from the completion lymph node dissection that now follows as part of standard treatment. MSLT-II has randomized 1,900 patients so far, and the results are expected in a few years.
On Twitter @mitchelzoler
Some diagnoses, treatments, or procedures become closely identified with one or two people. Sentinel lymph node biopsy is a cancer-staging technique forever linked to Dr. Donald L. Morton, who in 1978 published his first findings on lymph node drainage and metastasis patterns in patients with malignant melanoma.
Since then, sentinel lymph node biopsy (SLNB) became the standard of care for staging a sizeable subset of patients with newly diagnosed melanoma, based largely on a prespecified interim analysis of data from the first Multicenter Selective Lymphadenectomy Trial (MSLT-I), a study with 2,001 patients launched by Dr. Morton and his associates in 1994 to definitively test the efficacy of SLNB.
On Feb. 13, Dr. Morton and his associates published "the final trial report" from MSLT-I with 10-year follow-up, results that further confirmed the beneficial role of SLNB and brought full closure to a clinical journey that lasted nearly 40 years.
But Dr. Morton did not quite make it to see the article published. He died on Jan. 10 from heart failure, at age 79, at St. John’s Health Center in Santa Monica, Calif.
"Dr. Morton was incredibly pleased to know the paper was to be published. It was very gratifying to him that it was successfully completed and would be out in the New England Journal of Medicine," said Dr. Mark B. Faries, a senior collaborator with Dr. Morton on MSLT-I and director of melanoma research at the John Wayne Cancer Institute in Santa Monica, Calif.
Publication of the final report of the MSLT-I trial "is a capstone on Dr. Morton’s career," said Dr. Charles M. Balch, professor of surgery at the University of Texas Southwestern Medical Center at Dallas, in an interview. In an editorial accompanying the publication, Dr. Balch and a colleague wrote that the final report from the "landmark" MSLT-I trial "caps a 35-year effort to resolve the controversy surrounding the survival benefit of surgical excision of regional lymph nodes as a component of initial treatment of patients with primary melanoma."
Dr. Morton faced strong skepticism when he first presented his findings on the staging role for SLNB at a meeting in 1990 and in the years immediately after. His report describing a method for identifying and assessing sentinel lymph nodes was rejected by several "high-impact journals," recalled Dr. Balch and some of his colleagues in a remembrance that will be published in Annals of Surgical Oncology in March. "Undaunted, he persisted," they wrote, until the report appeared in Archives of Surgery in 1992. Designing, launching, and running MSLT-I came next, with many of the study’s major findings appearing in 2006. By confirming the efficacy of SLNB for staging many melanoma patients, MSLT-I was a "practice-changing trial," wrote Dr. Balch and his associates.
Although the new, 10-year follow-up gives closure to the central thesis of Dr. Morton’s SLNB technique, he didn’t stop there.
"Anyone who knew [Dr. Morton] would know he would never feel he had completed his work until the disease was cured for all," said Dr. Faries. "This is evidenced by the second MSLT trial that is now underway" that Dr. Morton and his associates launched to determine whether patients with positive sentinel lymph nodes benefit from the completion lymph node dissection that now follows as part of standard treatment. MSLT-II has randomized 1,900 patients so far, and the results are expected in a few years.
On Twitter @mitchelzoler
Some diagnoses, treatments, or procedures become closely identified with one or two people. Sentinel lymph node biopsy is a cancer-staging technique forever linked to Dr. Donald L. Morton, who in 1978 published his first findings on lymph node drainage and metastasis patterns in patients with malignant melanoma.
Since then, sentinel lymph node biopsy (SLNB) became the standard of care for staging a sizeable subset of patients with newly diagnosed melanoma, based largely on a prespecified interim analysis of data from the first Multicenter Selective Lymphadenectomy Trial (MSLT-I), a study with 2,001 patients launched by Dr. Morton and his associates in 1994 to definitively test the efficacy of SLNB.
On Feb. 13, Dr. Morton and his associates published "the final trial report" from MSLT-I with 10-year follow-up, results that further confirmed the beneficial role of SLNB and brought full closure to a clinical journey that lasted nearly 40 years.
But Dr. Morton did not quite make it to see the article published. He died on Jan. 10 from heart failure, at age 79, at St. John’s Health Center in Santa Monica, Calif.
"Dr. Morton was incredibly pleased to know the paper was to be published. It was very gratifying to him that it was successfully completed and would be out in the New England Journal of Medicine," said Dr. Mark B. Faries, a senior collaborator with Dr. Morton on MSLT-I and director of melanoma research at the John Wayne Cancer Institute in Santa Monica, Calif.
Publication of the final report of the MSLT-I trial "is a capstone on Dr. Morton’s career," said Dr. Charles M. Balch, professor of surgery at the University of Texas Southwestern Medical Center at Dallas, in an interview. In an editorial accompanying the publication, Dr. Balch and a colleague wrote that the final report from the "landmark" MSLT-I trial "caps a 35-year effort to resolve the controversy surrounding the survival benefit of surgical excision of regional lymph nodes as a component of initial treatment of patients with primary melanoma."
Dr. Morton faced strong skepticism when he first presented his findings on the staging role for SLNB at a meeting in 1990 and in the years immediately after. His report describing a method for identifying and assessing sentinel lymph nodes was rejected by several "high-impact journals," recalled Dr. Balch and some of his colleagues in a remembrance that will be published in Annals of Surgical Oncology in March. "Undaunted, he persisted," they wrote, until the report appeared in Archives of Surgery in 1992. Designing, launching, and running MSLT-I came next, with many of the study’s major findings appearing in 2006. By confirming the efficacy of SLNB for staging many melanoma patients, MSLT-I was a "practice-changing trial," wrote Dr. Balch and his associates.
Although the new, 10-year follow-up gives closure to the central thesis of Dr. Morton’s SLNB technique, he didn’t stop there.
"Anyone who knew [Dr. Morton] would know he would never feel he had completed his work until the disease was cured for all," said Dr. Faries. "This is evidenced by the second MSLT trial that is now underway" that Dr. Morton and his associates launched to determine whether patients with positive sentinel lymph nodes benefit from the completion lymph node dissection that now follows as part of standard treatment. MSLT-II has randomized 1,900 patients so far, and the results are expected in a few years.
On Twitter @mitchelzoler
Personalization keys vision of improved atrial fib care
Atrial fibrillation is not a single disease, and specialists already have ways to distinguish one type from another and guide management. But new methods are emerging to better distinguish various causes and types of atrial fibrillation, further refine management, and offer new intervention approaches.
This new way of looking at AF has been called personalized management, and while some cardiologists may quibble that a fully personalized approach to managing each AF patient is still likely a decade or more away, there seems to be wide agreement that AF patients are heterogeneous and the more that can be learned about the etiology and character of AF in each patient, the better care will be.
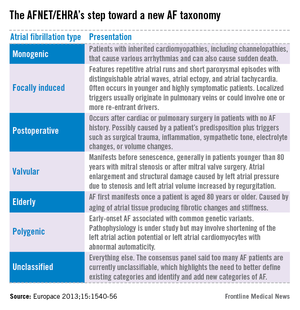
A manifesto on personalized AF management appeared last November from a panel of 72 cardiologists organized by the German AF Competence Network (AFNET) and the European Heart Rhythm Association (EP Europace 2013;15:1540-56).
"Atrial fibrillation is not a disease, it is a syndrome" in which different patients "present with similar ECG patterns and complications, but with completely different causes," said Dr. Paulus Kirchhof, an organizer of the AFNET/EHRA consensus group, during a session on personalized AF at the American Heart Association’s scientific sessions last November. "We are still in the process of trying to understand the individual mechanisms [causing AF], and then we try to translate that into parameters that can be measured. Once we get there, we can probably reclassify AF as a disease with different causes in different people. But we still need more work to better classify AF based on causal mechanisms," said Dr. Kirchhof, professor of cardiovascular medicine at the University of Birmingham, England.
AF classification evolves
More than 2 decades ago, atrial fibrillation was classified as either acute or chronic. Starting about 20 years ago, classification by duration became a little more subdivided, into categories of paroxysmal, persistent, long-term persistent, and permanent. This rough taxonomy, focused on episode duration, guides some facets of management today and has "served a reasonable function, but has done as much as it could. So, we’re searching for a new taxonomy that will help us progress further, a taxonomy based on mechanisms," said Dr. A. John Camm, professor of clinical cardiology at St. George’s, University of London, and another organizer of the AFNET/EHRA group.
"The electrophysiology community and the physician community are starting to get comfortable with the current AF taxonomy of paroxysmal, persistent, and long-standing persistent. But those who spend a lot of time thinking about AF recognize that this scheme is overly simplistic and that other parameters are important," said Dr. Hugh Calkins, professor and director of the cardiac arrhythmia service at Johns Hopkins Medical Center in Baltimore. "I do not believe it is time to make a dramatic shift to a new AF taxonomy now, especially for day-to-day care, but it is likely that over time new parameters will be included when describing AF patients. The proposed new classification scheme may provide a useful framework as this research moves forward," Dr. Calkins said in an interview. Dr. Calkins, president of the U.S.-based Heart Rhythm Society, was one of the 72 coauthors of the AFNET/EHRA consensus statement and one of the few participants not based in Europe.

"Given the complexities of AF, a personalized approach is and will continue to be essential. This is widely accepted and not controversial," said Dr. Peter R. Kowey, chief of cardiovascular diseases at Main Line Health in Wynnewood, Pa. "But each new parameter used to categorize AF will require careful validation before its adoption," he said in an interview. "Subclassification of AF would be helpful, but it will need to be data driven and carefully vetted before it will be accepted," said Dr. Kowey, who was not a member of the AFNET/EHRA group.
"The concept of personalized AF management is not new and not controversial. It is at the core of optimal patient care," Dr. Calkins concurred.
"Our hope is that molecular, genomic, and novel ECG and structural-imaging modalities will guide AF treatment in the future," said Dr. Anne M. Gillis, professor of medicine at the University of Calgary (Alta.), speaking during the AHA session last November. "At present, we start with rate control and move on to rhythm control when dictated by symptoms, with ablation continuing to emerge as the primary option. In the future we think there will be a focus on prevention and a personalized approach, with a greater emphasis on rhythm control that may involve mechanism-directed ablation against foci and rotors."
Dr. Gillis, immediate past president of the Heart Rhythm Society, and some of her colleagues endorsed the concept of a personalized approach to AF management and increasing reliance on new methods to further distinguish various types of AF patients in a commentary last year (Can. J. Cardiol. 2013;29:1141-6).
Preliminary draft of a new AF taxonomy

The consensus statement from the AFNET/EHRA group includes a draft of a new way to classify and think about AF. They divided AF into seven types: monogenic, focally induced, postoperative, valvular, AF in the elderly, polygenic, and unclassified (see table). But the coauthors of the statement cautioned that their proposed classifications were "preliminary," just a "step towards" a new AF taxonomy.
The proposed classification "is useful because it identifies patients with specific causes of AF, but it is preliminary because it is not able to classify many patients. We need better markers for the common mechanisms of AF," said Dr. Kirchhof in an interview. Progress in AF classification and taxonomy and progress in AF management will be "closely intertwined," he said. "We have a relatively decent understanding of several major mechanisms that cause AF, but we need clinically applicable markers that need to be validated. I expect that blood-based markers, and, to some extent, ECG-based markers will become helpful in the near future provided that they are validated."
Factors already accepted as valid tools for discriminating among AF patients include myocardial ischemia, hemodynamic instability, blood cell count, electrolytes, thyroid stimulating hormone level, ECG, and the presence or absence of AF-related symptoms, while decisions about anticoagulation are driven by a patient’s CHA2DS2-VASc score.
According to the consensus statement, factors currently under development and seen as good candidates for additional ways to discriminate among AF patients include:
• More ECG-derived information including evidence of left ventricular hypertrophy, heart failure, QT interval, atrioventricular block, and cardiomyopathy, as well as analysis of the electrical complexity of AF episodes.
• Silent AF episodes detected by prolonged ECG monitoring with a miniaturized device; also using prolonged ECG monitoring to further refine and personalize rhythm-control therapy.
• Brain imaging, particularly magnetic resonance imaging (MRI), to identify silent brain infarctions, white matter hyperintensities, and cerebral microbleeds to further refine anticoagulant treatment.
• Structural heart disease including valve disease, left ventricular hypertrophy, and left ventricular dysfunction detected by MRI or three-dimensional echocardiography.
• Atrial activation time monitored by tissue Doppler to better guide rhythm-control treatment.
• Blood levels of D-dimer, high-sensitive troponin T, and forms of brain natriuretic peptide, biomarkers that might refine stroke-risk assessment and anticoagulation.
• Chronic kidney disease, which might especially affect stroke risk.
• Blood and urine biomarkers of inflammation, cardiac load, cardiac damage, or kidney function that may predict the risk of recurrent AF, including various forms of brain natriuretic peptide, C-reactive protein, and creatinine.
• Genes linked to familial forms of AF, such as genes close to the PITX2 locus on chromosome 4q25 and genes close to the ZFHX3 locus on chromosome 16q22.
What comes next?
Dr. Camm cited two methods in particular as among the closest to becoming the next new ways to assess and discriminate AF patients. One is evaluating atrial remodeling by MRI, which also identifies regions of atrial fibrosis. This is especially promising because several drug classes may stop or perhaps reverse fibrotic changes in atria: angiotensin-converting enzyme inhibitors, angiotensin-receptor blockers, and galectin 3 inhibitor drugs.
Another way to assess AF and personalize management nearing routine use is measuring ECG patterns on the atrial surface with noninvasive sensors placed on a patient’s chest, patterns that may pinpoint conduction lesions or circuits amenable to focused ablation.
It’s also very possible that some new, validated markers of AF will flag some of the earliest pathologic changes that start down the road to AF, markers that could identify potential targets for early intervention, "allowing us to interrupt the AF process before it becomes an end-stage disease and while it can still be more directly managed," Dr. Camm said.
The AFNET/EHRA group plans to reconvene early next year and every 2 years after that to update its assessment of AF personalization, he added.
"Even AF patients treated with the best available treatment today have unacceptably high mortality. Treatments targeting individual mechanisms that cause AF could improve this," Dr. Kirchhof said.
Dr. Kirchhof said he has received consulting fees and honoraria from more than a dozen drug and device companies. Dr. Camm said he has received consulting fees and honoraria from more than 20 drug and device companies. Dr. Gillis said she has received honoraria from Medtronic. Dr. Calkins and Dr. Kowey had no relevant disclosures.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
Atrial fibrillation is not a single disease, and specialists already have ways to distinguish one type from another and guide management. But new methods are emerging to better distinguish various causes and types of atrial fibrillation, further refine management, and offer new intervention approaches.
This new way of looking at AF has been called personalized management, and while some cardiologists may quibble that a fully personalized approach to managing each AF patient is still likely a decade or more away, there seems to be wide agreement that AF patients are heterogeneous and the more that can be learned about the etiology and character of AF in each patient, the better care will be.
A manifesto on personalized AF management appeared last November from a panel of 72 cardiologists organized by the German AF Competence Network (AFNET) and the European Heart Rhythm Association (EP Europace 2013;15:1540-56).
"Atrial fibrillation is not a disease, it is a syndrome" in which different patients "present with similar ECG patterns and complications, but with completely different causes," said Dr. Paulus Kirchhof, an organizer of the AFNET/EHRA consensus group, during a session on personalized AF at the American Heart Association’s scientific sessions last November. "We are still in the process of trying to understand the individual mechanisms [causing AF], and then we try to translate that into parameters that can be measured. Once we get there, we can probably reclassify AF as a disease with different causes in different people. But we still need more work to better classify AF based on causal mechanisms," said Dr. Kirchhof, professor of cardiovascular medicine at the University of Birmingham, England.
AF classification evolves
More than 2 decades ago, atrial fibrillation was classified as either acute or chronic. Starting about 20 years ago, classification by duration became a little more subdivided, into categories of paroxysmal, persistent, long-term persistent, and permanent. This rough taxonomy, focused on episode duration, guides some facets of management today and has "served a reasonable function, but has done as much as it could. So, we’re searching for a new taxonomy that will help us progress further, a taxonomy based on mechanisms," said Dr. A. John Camm, professor of clinical cardiology at St. George’s, University of London, and another organizer of the AFNET/EHRA group.
"The electrophysiology community and the physician community are starting to get comfortable with the current AF taxonomy of paroxysmal, persistent, and long-standing persistent. But those who spend a lot of time thinking about AF recognize that this scheme is overly simplistic and that other parameters are important," said Dr. Hugh Calkins, professor and director of the cardiac arrhythmia service at Johns Hopkins Medical Center in Baltimore. "I do not believe it is time to make a dramatic shift to a new AF taxonomy now, especially for day-to-day care, but it is likely that over time new parameters will be included when describing AF patients. The proposed new classification scheme may provide a useful framework as this research moves forward," Dr. Calkins said in an interview. Dr. Calkins, president of the U.S.-based Heart Rhythm Society, was one of the 72 coauthors of the AFNET/EHRA consensus statement and one of the few participants not based in Europe.
"Given the complexities of AF, a personalized approach is and will continue to be essential. This is widely accepted and not controversial," said Dr. Peter R. Kowey, chief of cardiovascular diseases at Main Line Health in Wynnewood, Pa. "But each new parameter used to categorize AF will require careful validation before its adoption," he said in an interview. "Subclassification of AF would be helpful, but it will need to be data driven and carefully vetted before it will be accepted," said Dr. Kowey, who was not a member of the AFNET/EHRA group.
"The concept of personalized AF management is not new and not controversial. It is at the core of optimal patient care," Dr. Calkins concurred.
"Our hope is that molecular, genomic, and novel ECG and structural-imaging modalities will guide AF treatment in the future," said Dr. Anne M. Gillis, professor of medicine at the University of Calgary (Alta.), speaking during the AHA session last November. "At present, we start with rate control and move on to rhythm control when dictated by symptoms, with ablation continuing to emerge as the primary option. In the future we think there will be a focus on prevention and a personalized approach, with a greater emphasis on rhythm control that may involve mechanism-directed ablation against foci and rotors."
Dr. Gillis, immediate past president of the Heart Rhythm Society, and some of her colleagues endorsed the concept of a personalized approach to AF management and increasing reliance on new methods to further distinguish various types of AF patients in a commentary last year (Can. J. Cardiol. 2013;29:1141-6).
Preliminary draft of a new AF taxonomy
The consensus statement from the AFNET/EHRA group includes a draft of a new way to classify and think about AF. They divided AF into seven types: monogenic, focally induced, postoperative, valvular, AF in the elderly, polygenic, and unclassified (see table). But the coauthors of the statement cautioned that their proposed classifications were "preliminary," just a "step towards" a new AF taxonomy.
The proposed classification "is useful because it identifies patients with specific causes of AF, but it is preliminary because it is not able to classify many patients. We need better markers for the common mechanisms of AF," said Dr. Kirchhof in an interview. Progress in AF classification and taxonomy and progress in AF management will be "closely intertwined," he said. "We have a relatively decent understanding of several major mechanisms that cause AF, but we need clinically applicable markers that need to be validated. I expect that blood-based markers, and, to some extent, ECG-based markers will become helpful in the near future provided that they are validated."
Factors already accepted as valid tools for discriminating among AF patients include myocardial ischemia, hemodynamic instability, blood cell count, electrolytes, thyroid stimulating hormone level, ECG, and the presence or absence of AF-related symptoms, while decisions about anticoagulation are driven by a patient’s CHA2DS2-VASc score.
According to the consensus statement, factors currently under development and seen as good candidates for additional ways to discriminate among AF patients include:
• More ECG-derived information including evidence of left ventricular hypertrophy, heart failure, QT interval, atrioventricular block, and cardiomyopathy, as well as analysis of the electrical complexity of AF episodes.
• Silent AF episodes detected by prolonged ECG monitoring with a miniaturized device; also using prolonged ECG monitoring to further refine and personalize rhythm-control therapy.
• Brain imaging, particularly magnetic resonance imaging (MRI), to identify silent brain infarctions, white matter hyperintensities, and cerebral microbleeds to further refine anticoagulant treatment.
• Structural heart disease including valve disease, left ventricular hypertrophy, and left ventricular dysfunction detected by MRI or three-dimensional echocardiography.
• Atrial activation time monitored by tissue Doppler to better guide rhythm-control treatment.
• Blood levels of D-dimer, high-sensitive troponin T, and forms of brain natriuretic peptide, biomarkers that might refine stroke-risk assessment and anticoagulation.
• Chronic kidney disease, which might especially affect stroke risk.
• Blood and urine biomarkers of inflammation, cardiac load, cardiac damage, or kidney function that may predict the risk of recurrent AF, including various forms of brain natriuretic peptide, C-reactive protein, and creatinine.
• Genes linked to familial forms of AF, such as genes close to the PITX2 locus on chromosome 4q25 and genes close to the ZFHX3 locus on chromosome 16q22.
What comes next?
Dr. Camm cited two methods in particular as among the closest to becoming the next new ways to assess and discriminate AF patients. One is evaluating atrial remodeling by MRI, which also identifies regions of atrial fibrosis. This is especially promising because several drug classes may stop or perhaps reverse fibrotic changes in atria: angiotensin-converting enzyme inhibitors, angiotensin-receptor blockers, and galectin 3 inhibitor drugs.
Another way to assess AF and personalize management nearing routine use is measuring ECG patterns on the atrial surface with noninvasive sensors placed on a patient’s chest, patterns that may pinpoint conduction lesions or circuits amenable to focused ablation.
It’s also very possible that some new, validated markers of AF will flag some of the earliest pathologic changes that start down the road to AF, markers that could identify potential targets for early intervention, "allowing us to interrupt the AF process before it becomes an end-stage disease and while it can still be more directly managed," Dr. Camm said.
The AFNET/EHRA group plans to reconvene early next year and every 2 years after that to update its assessment of AF personalization, he added.
"Even AF patients treated with the best available treatment today have unacceptably high mortality. Treatments targeting individual mechanisms that cause AF could improve this," Dr. Kirchhof said.
Dr. Kirchhof said he has received consulting fees and honoraria from more than a dozen drug and device companies. Dr. Camm said he has received consulting fees and honoraria from more than 20 drug and device companies. Dr. Gillis said she has received honoraria from Medtronic. Dr. Calkins and Dr. Kowey had no relevant disclosures.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
Atrial fibrillation is not a single disease, and specialists already have ways to distinguish one type from another and guide management. But new methods are emerging to better distinguish various causes and types of atrial fibrillation, further refine management, and offer new intervention approaches.
This new way of looking at AF has been called personalized management, and while some cardiologists may quibble that a fully personalized approach to managing each AF patient is still likely a decade or more away, there seems to be wide agreement that AF patients are heterogeneous and the more that can be learned about the etiology and character of AF in each patient, the better care will be.
A manifesto on personalized AF management appeared last November from a panel of 72 cardiologists organized by the German AF Competence Network (AFNET) and the European Heart Rhythm Association (EP Europace 2013;15:1540-56).
"Atrial fibrillation is not a disease, it is a syndrome" in which different patients "present with similar ECG patterns and complications, but with completely different causes," said Dr. Paulus Kirchhof, an organizer of the AFNET/EHRA consensus group, during a session on personalized AF at the American Heart Association’s scientific sessions last November. "We are still in the process of trying to understand the individual mechanisms [causing AF], and then we try to translate that into parameters that can be measured. Once we get there, we can probably reclassify AF as a disease with different causes in different people. But we still need more work to better classify AF based on causal mechanisms," said Dr. Kirchhof, professor of cardiovascular medicine at the University of Birmingham, England.
AF classification evolves
More than 2 decades ago, atrial fibrillation was classified as either acute or chronic. Starting about 20 years ago, classification by duration became a little more subdivided, into categories of paroxysmal, persistent, long-term persistent, and permanent. This rough taxonomy, focused on episode duration, guides some facets of management today and has "served a reasonable function, but has done as much as it could. So, we’re searching for a new taxonomy that will help us progress further, a taxonomy based on mechanisms," said Dr. A. John Camm, professor of clinical cardiology at St. George’s, University of London, and another organizer of the AFNET/EHRA group.
"The electrophysiology community and the physician community are starting to get comfortable with the current AF taxonomy of paroxysmal, persistent, and long-standing persistent. But those who spend a lot of time thinking about AF recognize that this scheme is overly simplistic and that other parameters are important," said Dr. Hugh Calkins, professor and director of the cardiac arrhythmia service at Johns Hopkins Medical Center in Baltimore. "I do not believe it is time to make a dramatic shift to a new AF taxonomy now, especially for day-to-day care, but it is likely that over time new parameters will be included when describing AF patients. The proposed new classification scheme may provide a useful framework as this research moves forward," Dr. Calkins said in an interview. Dr. Calkins, president of the U.S.-based Heart Rhythm Society, was one of the 72 coauthors of the AFNET/EHRA consensus statement and one of the few participants not based in Europe.
"Given the complexities of AF, a personalized approach is and will continue to be essential. This is widely accepted and not controversial," said Dr. Peter R. Kowey, chief of cardiovascular diseases at Main Line Health in Wynnewood, Pa. "But each new parameter used to categorize AF will require careful validation before its adoption," he said in an interview. "Subclassification of AF would be helpful, but it will need to be data driven and carefully vetted before it will be accepted," said Dr. Kowey, who was not a member of the AFNET/EHRA group.
"The concept of personalized AF management is not new and not controversial. It is at the core of optimal patient care," Dr. Calkins concurred.
"Our hope is that molecular, genomic, and novel ECG and structural-imaging modalities will guide AF treatment in the future," said Dr. Anne M. Gillis, professor of medicine at the University of Calgary (Alta.), speaking during the AHA session last November. "At present, we start with rate control and move on to rhythm control when dictated by symptoms, with ablation continuing to emerge as the primary option. In the future we think there will be a focus on prevention and a personalized approach, with a greater emphasis on rhythm control that may involve mechanism-directed ablation against foci and rotors."
Dr. Gillis, immediate past president of the Heart Rhythm Society, and some of her colleagues endorsed the concept of a personalized approach to AF management and increasing reliance on new methods to further distinguish various types of AF patients in a commentary last year (Can. J. Cardiol. 2013;29:1141-6).
Preliminary draft of a new AF taxonomy
The consensus statement from the AFNET/EHRA group includes a draft of a new way to classify and think about AF. They divided AF into seven types: monogenic, focally induced, postoperative, valvular, AF in the elderly, polygenic, and unclassified (see table). But the coauthors of the statement cautioned that their proposed classifications were "preliminary," just a "step towards" a new AF taxonomy.
The proposed classification "is useful because it identifies patients with specific causes of AF, but it is preliminary because it is not able to classify many patients. We need better markers for the common mechanisms of AF," said Dr. Kirchhof in an interview. Progress in AF classification and taxonomy and progress in AF management will be "closely intertwined," he said. "We have a relatively decent understanding of several major mechanisms that cause AF, but we need clinically applicable markers that need to be validated. I expect that blood-based markers, and, to some extent, ECG-based markers will become helpful in the near future provided that they are validated."
Factors already accepted as valid tools for discriminating among AF patients include myocardial ischemia, hemodynamic instability, blood cell count, electrolytes, thyroid stimulating hormone level, ECG, and the presence or absence of AF-related symptoms, while decisions about anticoagulation are driven by a patient’s CHA2DS2-VASc score.
According to the consensus statement, factors currently under development and seen as good candidates for additional ways to discriminate among AF patients include:
• More ECG-derived information including evidence of left ventricular hypertrophy, heart failure, QT interval, atrioventricular block, and cardiomyopathy, as well as analysis of the electrical complexity of AF episodes.
• Silent AF episodes detected by prolonged ECG monitoring with a miniaturized device; also using prolonged ECG monitoring to further refine and personalize rhythm-control therapy.
• Brain imaging, particularly magnetic resonance imaging (MRI), to identify silent brain infarctions, white matter hyperintensities, and cerebral microbleeds to further refine anticoagulant treatment.
• Structural heart disease including valve disease, left ventricular hypertrophy, and left ventricular dysfunction detected by MRI or three-dimensional echocardiography.
• Atrial activation time monitored by tissue Doppler to better guide rhythm-control treatment.
• Blood levels of D-dimer, high-sensitive troponin T, and forms of brain natriuretic peptide, biomarkers that might refine stroke-risk assessment and anticoagulation.
• Chronic kidney disease, which might especially affect stroke risk.
• Blood and urine biomarkers of inflammation, cardiac load, cardiac damage, or kidney function that may predict the risk of recurrent AF, including various forms of brain natriuretic peptide, C-reactive protein, and creatinine.
• Genes linked to familial forms of AF, such as genes close to the PITX2 locus on chromosome 4q25 and genes close to the ZFHX3 locus on chromosome 16q22.
What comes next?
Dr. Camm cited two methods in particular as among the closest to becoming the next new ways to assess and discriminate AF patients. One is evaluating atrial remodeling by MRI, which also identifies regions of atrial fibrosis. This is especially promising because several drug classes may stop or perhaps reverse fibrotic changes in atria: angiotensin-converting enzyme inhibitors, angiotensin-receptor blockers, and galectin 3 inhibitor drugs.
Another way to assess AF and personalize management nearing routine use is measuring ECG patterns on the atrial surface with noninvasive sensors placed on a patient’s chest, patterns that may pinpoint conduction lesions or circuits amenable to focused ablation.
It’s also very possible that some new, validated markers of AF will flag some of the earliest pathologic changes that start down the road to AF, markers that could identify potential targets for early intervention, "allowing us to interrupt the AF process before it becomes an end-stage disease and while it can still be more directly managed," Dr. Camm said.
The AFNET/EHRA group plans to reconvene early next year and every 2 years after that to update its assessment of AF personalization, he added.
"Even AF patients treated with the best available treatment today have unacceptably high mortality. Treatments targeting individual mechanisms that cause AF could improve this," Dr. Kirchhof said.
Dr. Kirchhof said he has received consulting fees and honoraria from more than a dozen drug and device companies. Dr. Camm said he has received consulting fees and honoraria from more than 20 drug and device companies. Dr. Gillis said she has received honoraria from Medtronic. Dr. Calkins and Dr. Kowey had no relevant disclosures.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
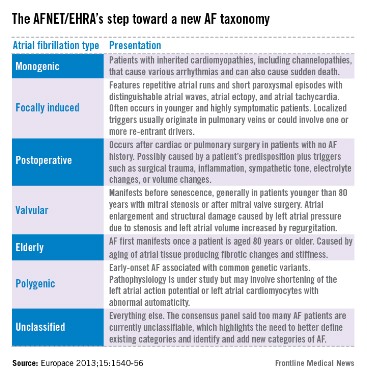
FDA to probe saxagliptin’s heart failure risk
The U.S. Food and Drug Administration will investigate the possible association between treatment with the type 2 diabetes drug saxagliptin and an increased rate of hospitalizations for heart failure using data collected by the drug’s manufacturer during clinical trials. The agency released a "safety announcement" on Feb.11 that it had requested these data from Bristol-Myers Squibb and AstraZeneca, the two companies that together market saxagliptin as Onglyza and Kombiglyze XR.
The agency based its request on results reported last year in the SAVOR (Saxagliptin Assessment of Vascular Outcomes Recorded in Patients With Diabetes Mellitus)–TIMI 53 (Thrombolysis in Myocardial Infarction) trial, a trial with more than 16,000 patients with type 2 diabetes designed to test the cardiovascular safety of saxagliptin (N. Engl. J. Med. 2013;369:1317-26).
Although treatment with the drug produced no excess in the rate of the primary endpoint of all cardiovascular events, compared with a control group, the results showed a statistically significant, 0.7% absolute increase in the rate of hospitalizations for heart failure in the saxagliptin-treated patients, compared with those not on the drug, a 27% relative increase.
While presenting more detailed data on the heart failure hospitalization effect in a poster during the American Heart Association’s Scientific Sessions last November, Dr. Benjamin M. Scirica, lead author for the study, called the effect by saxagliptin on raising heart failure hospitalizations "real."
"Every drug has adverse effects. With these data, the calculation about saxagliptin can be made to a much more certain level. Clinicians need to weigh a patient’s risk factors, which drugs they can or cannot take, and a drug’s overall safety for ischemic events," said Dr. Scirica while presenting his poster last November. "At this point, we have no definitive data to a priori say don’t give saxagliptin to patients with heart failure."
The manufacturers are expected to submit the saxagliptin-trial data to the FDA by March 2014, after which the agency said it will "conduct a thorough analysis and report our findings publically."
The FDA’s statement added this caution to patients and physicians about its action:
"At this time, we consider information from the New England Journal of Medicine study to be preliminary. Our analysis of the saxagliptin clinical trial data is part of a broader evaluation of all type 2 diabetes drug therapies and cardiovascular risk. Patients should not stop taking saxagliptin and should speak with their health care professionals about any questions or concerns. Health care professionals should continue to follow the prescribing recommendations in the drug labels." The FDA also urged health care professionals and patients to report side effects involving saxagliptin products to the FDA MedWatch program.
Dr. Scirica said that he had been a consultant to Bristol-Myers Squibb and to several other drug companies and that he has received research grants from Bristol-Myers Squibb and AstraZeneca and from several other companies.
On Twitter @mitchelzoler
The U.S. Food and Drug Administration will investigate the possible association between treatment with the type 2 diabetes drug saxagliptin and an increased rate of hospitalizations for heart failure using data collected by the drug’s manufacturer during clinical trials. The agency released a "safety announcement" on Feb.11 that it had requested these data from Bristol-Myers Squibb and AstraZeneca, the two companies that together market saxagliptin as Onglyza and Kombiglyze XR.
The agency based its request on results reported last year in the SAVOR (Saxagliptin Assessment of Vascular Outcomes Recorded in Patients With Diabetes Mellitus)–TIMI 53 (Thrombolysis in Myocardial Infarction) trial, a trial with more than 16,000 patients with type 2 diabetes designed to test the cardiovascular safety of saxagliptin (N. Engl. J. Med. 2013;369:1317-26).
Although treatment with the drug produced no excess in the rate of the primary endpoint of all cardiovascular events, compared with a control group, the results showed a statistically significant, 0.7% absolute increase in the rate of hospitalizations for heart failure in the saxagliptin-treated patients, compared with those not on the drug, a 27% relative increase.
While presenting more detailed data on the heart failure hospitalization effect in a poster during the American Heart Association’s Scientific Sessions last November, Dr. Benjamin M. Scirica, lead author for the study, called the effect by saxagliptin on raising heart failure hospitalizations "real."
"Every drug has adverse effects. With these data, the calculation about saxagliptin can be made to a much more certain level. Clinicians need to weigh a patient’s risk factors, which drugs they can or cannot take, and a drug’s overall safety for ischemic events," said Dr. Scirica while presenting his poster last November. "At this point, we have no definitive data to a priori say don’t give saxagliptin to patients with heart failure."
The manufacturers are expected to submit the saxagliptin-trial data to the FDA by March 2014, after which the agency said it will "conduct a thorough analysis and report our findings publically."
The FDA’s statement added this caution to patients and physicians about its action:
"At this time, we consider information from the New England Journal of Medicine study to be preliminary. Our analysis of the saxagliptin clinical trial data is part of a broader evaluation of all type 2 diabetes drug therapies and cardiovascular risk. Patients should not stop taking saxagliptin and should speak with their health care professionals about any questions or concerns. Health care professionals should continue to follow the prescribing recommendations in the drug labels." The FDA also urged health care professionals and patients to report side effects involving saxagliptin products to the FDA MedWatch program.
Dr. Scirica said that he had been a consultant to Bristol-Myers Squibb and to several other drug companies and that he has received research grants from Bristol-Myers Squibb and AstraZeneca and from several other companies.
On Twitter @mitchelzoler
The U.S. Food and Drug Administration will investigate the possible association between treatment with the type 2 diabetes drug saxagliptin and an increased rate of hospitalizations for heart failure using data collected by the drug’s manufacturer during clinical trials. The agency released a "safety announcement" on Feb.11 that it had requested these data from Bristol-Myers Squibb and AstraZeneca, the two companies that together market saxagliptin as Onglyza and Kombiglyze XR.
The agency based its request on results reported last year in the SAVOR (Saxagliptin Assessment of Vascular Outcomes Recorded in Patients With Diabetes Mellitus)–TIMI 53 (Thrombolysis in Myocardial Infarction) trial, a trial with more than 16,000 patients with type 2 diabetes designed to test the cardiovascular safety of saxagliptin (N. Engl. J. Med. 2013;369:1317-26).
Although treatment with the drug produced no excess in the rate of the primary endpoint of all cardiovascular events, compared with a control group, the results showed a statistically significant, 0.7% absolute increase in the rate of hospitalizations for heart failure in the saxagliptin-treated patients, compared with those not on the drug, a 27% relative increase.
While presenting more detailed data on the heart failure hospitalization effect in a poster during the American Heart Association’s Scientific Sessions last November, Dr. Benjamin M. Scirica, lead author for the study, called the effect by saxagliptin on raising heart failure hospitalizations "real."
"Every drug has adverse effects. With these data, the calculation about saxagliptin can be made to a much more certain level. Clinicians need to weigh a patient’s risk factors, which drugs they can or cannot take, and a drug’s overall safety for ischemic events," said Dr. Scirica while presenting his poster last November. "At this point, we have no definitive data to a priori say don’t give saxagliptin to patients with heart failure."
The manufacturers are expected to submit the saxagliptin-trial data to the FDA by March 2014, after which the agency said it will "conduct a thorough analysis and report our findings publically."
The FDA’s statement added this caution to patients and physicians about its action:
"At this time, we consider information from the New England Journal of Medicine study to be preliminary. Our analysis of the saxagliptin clinical trial data is part of a broader evaluation of all type 2 diabetes drug therapies and cardiovascular risk. Patients should not stop taking saxagliptin and should speak with their health care professionals about any questions or concerns. Health care professionals should continue to follow the prescribing recommendations in the drug labels." The FDA also urged health care professionals and patients to report side effects involving saxagliptin products to the FDA MedWatch program.
Dr. Scirica said that he had been a consultant to Bristol-Myers Squibb and to several other drug companies and that he has received research grants from Bristol-Myers Squibb and AstraZeneca and from several other companies.
On Twitter @mitchelzoler