User login
AACR Launches Immunology Journal
The American Association for Cancer Research has announced the launch of Cancer Immunology Research, a peer-reviewed journal for original articles on advances in cancer immunology.
The new journal is receiving manuscripts for consideration for publication through its website, according to a press release. The journal is scheduled to launch online at the 2013 AACR annual meeting, and in print with monthly issues starting in June 2013.

The journal will highlight research from all areas of cancer immunology. Potential topics include: tumor-promoting inflammation, cancer antigens, vaccines, antibodies, cellular therapy, cytokines, endogenous antitumor immunity, immune regulation, immune suppression, immunomodulatory effects of cancer treatment, emerging technologies, and clinical investigations.
Plans for regular features include Masters of Immunology – primers on immunology topics from leaders in the field – and Cancer Immunology at the Crossroads – perspectives on the relationship between immunology and other areas of cancer research and allied disciplines.
Dr. Glenn Dranoff, professor of medicine at Dana-Farber Cancer Institute and Harvard Medical School, Boston, is slated to serve as the founding editor-in-chief of Cancer Immunology Research. Dr. Dranoff also leads the Dana-Farber/Harvard Cancer Center Program in Cancer Immunology.
The American Association for Cancer Research has announced the launch of Cancer Immunology Research, a peer-reviewed journal for original articles on advances in cancer immunology.
The new journal is receiving manuscripts for consideration for publication through its website, according to a press release. The journal is scheduled to launch online at the 2013 AACR annual meeting, and in print with monthly issues starting in June 2013.
The journal will highlight research from all areas of cancer immunology. Potential topics include: tumor-promoting inflammation, cancer antigens, vaccines, antibodies, cellular therapy, cytokines, endogenous antitumor immunity, immune regulation, immune suppression, immunomodulatory effects of cancer treatment, emerging technologies, and clinical investigations.
Plans for regular features include Masters of Immunology – primers on immunology topics from leaders in the field – and Cancer Immunology at the Crossroads – perspectives on the relationship between immunology and other areas of cancer research and allied disciplines.
Dr. Glenn Dranoff, professor of medicine at Dana-Farber Cancer Institute and Harvard Medical School, Boston, is slated to serve as the founding editor-in-chief of Cancer Immunology Research. Dr. Dranoff also leads the Dana-Farber/Harvard Cancer Center Program in Cancer Immunology.
The American Association for Cancer Research has announced the launch of Cancer Immunology Research, a peer-reviewed journal for original articles on advances in cancer immunology.
The new journal is receiving manuscripts for consideration for publication through its website, according to a press release. The journal is scheduled to launch online at the 2013 AACR annual meeting, and in print with monthly issues starting in June 2013.
The journal will highlight research from all areas of cancer immunology. Potential topics include: tumor-promoting inflammation, cancer antigens, vaccines, antibodies, cellular therapy, cytokines, endogenous antitumor immunity, immune regulation, immune suppression, immunomodulatory effects of cancer treatment, emerging technologies, and clinical investigations.
Plans for regular features include Masters of Immunology – primers on immunology topics from leaders in the field – and Cancer Immunology at the Crossroads – perspectives on the relationship between immunology and other areas of cancer research and allied disciplines.
Dr. Glenn Dranoff, professor of medicine at Dana-Farber Cancer Institute and Harvard Medical School, Boston, is slated to serve as the founding editor-in-chief of Cancer Immunology Research. Dr. Dranoff also leads the Dana-Farber/Harvard Cancer Center Program in Cancer Immunology.

Teduglutide Trims Parenteral Support in Short Bowel Syndrome
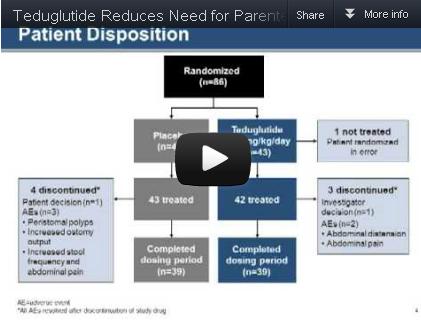
Teduglutide significantly reduced the need for parenteral support in patients with short bowel syndrome and intestinal failure, based on data from 85 adults in a randomized, controlled multicenter trial. The findings were published in the December issue of Gastroenterology.
Patients with short bowel syndrome and intestinal failure (SBS-IF) have inadequate intestinal absorption and require parenteral support (PS) to maintain fluids, electrolytes, trace elements, vitamins, and nutrient balances, said Dr. Palle Bekker Jeppesen of Rigshospitalet in Copenhagen and colleagues.
Source: American Gastroenterological Association
Data from previous open-label studies suggest an association between teduglutide and clinically meaningful reductions in wet weight and energy, which may reduce the need for PS in these patients, the investigators noted.
The researchers randomized 86 adults with SBS-IF to either 0.05 mg/kg per day of teduglutide or a placebo. One patient was randomized in error; complete data were available for 42 teduglutide patients and 43 placebo patients.
Significantly more patients in the teduglutide group responded to treatment, compared with the placebo group (63% vs. 30%). This response was defined as sustaining a 20%-100% reduction from baseline in weekly PS volume during weeks 20-24. "Small bowel length did not appear to be a predictor of response," the researchers noted.
The high placebo response may be explained by examining the fluid composite effect, a measure of the combined effects of teduglutide on PS volume reduction as well as the ability to reduce oral fluid intake and increase urine output volume, the researchers noted.
"In the current study, where protocol modifications encouraged earlier and more aggressive PS reductions, significantly larger PS reductions were also achieved in patients receiving placebo, but subsequently these patients had to increase their oral fluid intake significantly to maintain urine production and hydration constant," they said.
After 24 weeks, overall PS volume was reduced by 32% from baseline in teduglutide patients, compared with 21% in placebo patients. Although no patients in either group were completely weaned from parenteral support at 24 weeks, the difference in PS volume reduction was significantly greater in the teduglutide group.
The average weekly PS volume in teduglutide patients decreased significantly from 12.5 L/wk at baseline to 8.1 L/wk at week 24. The placebo patients also had a significant decrease in average weekly PS volume, from 13.4 L/wk at baseline to 11.1 L/wk at week 24.
Treatment-ending adverse events were similar between the two groups; 5% of teduglutide patients and 7% of placebo patients discontinued treatment because of such events during the study period. The most frequently reported treatment-emergent adverse events included abdominal pain, abdominal distension, nausea, and gastrointestinal stoma complications.
Although the study did not specifically assess quality of life measures, significantly more teduglutide patients had at least 1 day off PS, compared with placebo patients, which could help to "liberate considerable time for unhindered daytime activities or undisturbed sleep," the researchers said.
The study did not address the possible benefit of teduglutide therapy earlier in the course of SBS, or the duration of effect after patients discontinued teduglutide, the researchers added.
However, the findings indicate that teduglutide was safe and well tolerated, and "could positively add to the limited treatment armamentarium" for patients with SBS-IF.
Dr. Jeppesen and several coauthors have served on the advisory board of and as consultants to NPS Pharmaceuticals, the company that funded the study. One author is an employee of NPS Pharmaceuticals.
Patients with short bowel syndrome whose absorption is insufficient to maintain nutritional or fluid autonomy have intestinal failure. These patients, particularly those with proximal jejunostomies, who may actually secrete more fluid than they ingest, are among the most complex and challenging to manage of patients with any gastrointestinal disease. Patients with short bowel syndrome and intestinal failure are dependent on parenteral nutrition and/or fluid support (PS) to maintain life. This therapy has substantial implications for employment, activities, sleep, and finances. Numerous, often life-threatening, complications develop.

|
|
A myriad of growth factors may be involved in the process of postresection intestinal adaptation, including glucagonlike peptide-2 (GLP-2), wherein intestinal epithelial growth is promoted. Teduglutide is a long-acting analog of native GLP-2 and is somewhat more resistant to enzymatic degradation in the enterocyte than is the native enzyme. Dr. Jeppesen and colleagues reported a sustained 20%-100% decrease in PS volume requirements during weeks 20-24 of treatment in 63% of patients who received teduglutide, compared with 30% of placebo-treated patients. The mean drop in weekly PS volume from baseline to week 24 totaled 4.4 L in patients who received teduglutide, which equates to a decrease of 1-2 nights of infusion weekly, a very profound improvement for individual patients. The PS weaning protocol used was similar to that used in most centers experienced in the care of these patients.
As would be expected in the SBS-IF patient population, there were many adverse events, although these were equally distributed across teduglutide and placebo groups. Stomal changes, primarily related to enlargement, were evident in a significant minority of patients in the teduglutide group, as would be expected given the hyperplastic effect of the medication on intestinal epithelial tissue.Concern has been raised about GLP-2’s potential to stimulate the development of colonic adenomas in rodent models. Although the risk for malignancy is hypothetical in humans, colonoscopy should be considered at baseline for those patients with residual colons and perhaps as frequently as annually while the patients are on therapy until more long-term safety data are available.
Is teduglutide a "game changer"? The only patients who will be able to discontinue PS completely will be those who are on the borderline between nutritional autonomy and PS dependence. It is important to realize that teduglutide should be used to augment, not replace conventional management. What happens when teduglutide is stopped? Preliminary evidence suggests the effects on adaptation may be persistent, although earlier study noted that histologic changes trended toward baseline within 4 weeks of discontinuation. Perhaps longer treatment or maintenance will be required. The real future is an artificially grown and harvested intestine; even intestinal transplantation represents a bridge at best.
Dr. Alan L. Buchman is a former professor of medicine and surgery at the Feinberg School of Medicine at Northwestern University, Chicago. Within the past 12 months he has consulted for Takeda Pharmaceuticals and NPS Pharmaceuticals.
Patients with short bowel syndrome whose absorption is insufficient to maintain nutritional or fluid autonomy have intestinal failure. These patients, particularly those with proximal jejunostomies, who may actually secrete more fluid than they ingest, are among the most complex and challenging to manage of patients with any gastrointestinal disease. Patients with short bowel syndrome and intestinal failure are dependent on parenteral nutrition and/or fluid support (PS) to maintain life. This therapy has substantial implications for employment, activities, sleep, and finances. Numerous, often life-threatening, complications develop.
|
|
|
A myriad of growth factors may be involved in the process of postresection intestinal adaptation, including glucagonlike peptide-2 (GLP-2), wherein intestinal epithelial growth is promoted. Teduglutide is a long-acting analog of native GLP-2 and is somewhat more resistant to enzymatic degradation in the enterocyte than is the native enzyme. Dr. Jeppesen and colleagues reported a sustained 20%-100% decrease in PS volume requirements during weeks 20-24 of treatment in 63% of patients who received teduglutide, compared with 30% of placebo-treated patients. The mean drop in weekly PS volume from baseline to week 24 totaled 4.4 L in patients who received teduglutide, which equates to a decrease of 1-2 nights of infusion weekly, a very profound improvement for individual patients. The PS weaning protocol used was similar to that used in most centers experienced in the care of these patients.
As would be expected in the SBS-IF patient population, there were many adverse events, although these were equally distributed across teduglutide and placebo groups. Stomal changes, primarily related to enlargement, were evident in a significant minority of patients in the teduglutide group, as would be expected given the hyperplastic effect of the medication on intestinal epithelial tissue.Concern has been raised about GLP-2’s potential to stimulate the development of colonic adenomas in rodent models. Although the risk for malignancy is hypothetical in humans, colonoscopy should be considered at baseline for those patients with residual colons and perhaps as frequently as annually while the patients are on therapy until more long-term safety data are available.
Is teduglutide a "game changer"? The only patients who will be able to discontinue PS completely will be those who are on the borderline between nutritional autonomy and PS dependence. It is important to realize that teduglutide should be used to augment, not replace conventional management. What happens when teduglutide is stopped? Preliminary evidence suggests the effects on adaptation may be persistent, although earlier study noted that histologic changes trended toward baseline within 4 weeks of discontinuation. Perhaps longer treatment or maintenance will be required. The real future is an artificially grown and harvested intestine; even intestinal transplantation represents a bridge at best.
Dr. Alan L. Buchman is a former professor of medicine and surgery at the Feinberg School of Medicine at Northwestern University, Chicago. Within the past 12 months he has consulted for Takeda Pharmaceuticals and NPS Pharmaceuticals.
Patients with short bowel syndrome whose absorption is insufficient to maintain nutritional or fluid autonomy have intestinal failure. These patients, particularly those with proximal jejunostomies, who may actually secrete more fluid than they ingest, are among the most complex and challenging to manage of patients with any gastrointestinal disease. Patients with short bowel syndrome and intestinal failure are dependent on parenteral nutrition and/or fluid support (PS) to maintain life. This therapy has substantial implications for employment, activities, sleep, and finances. Numerous, often life-threatening, complications develop.
|
|
|
A myriad of growth factors may be involved in the process of postresection intestinal adaptation, including glucagonlike peptide-2 (GLP-2), wherein intestinal epithelial growth is promoted. Teduglutide is a long-acting analog of native GLP-2 and is somewhat more resistant to enzymatic degradation in the enterocyte than is the native enzyme. Dr. Jeppesen and colleagues reported a sustained 20%-100% decrease in PS volume requirements during weeks 20-24 of treatment in 63% of patients who received teduglutide, compared with 30% of placebo-treated patients. The mean drop in weekly PS volume from baseline to week 24 totaled 4.4 L in patients who received teduglutide, which equates to a decrease of 1-2 nights of infusion weekly, a very profound improvement for individual patients. The PS weaning protocol used was similar to that used in most centers experienced in the care of these patients.
As would be expected in the SBS-IF patient population, there were many adverse events, although these were equally distributed across teduglutide and placebo groups. Stomal changes, primarily related to enlargement, were evident in a significant minority of patients in the teduglutide group, as would be expected given the hyperplastic effect of the medication on intestinal epithelial tissue.Concern has been raised about GLP-2’s potential to stimulate the development of colonic adenomas in rodent models. Although the risk for malignancy is hypothetical in humans, colonoscopy should be considered at baseline for those patients with residual colons and perhaps as frequently as annually while the patients are on therapy until more long-term safety data are available.
Is teduglutide a "game changer"? The only patients who will be able to discontinue PS completely will be those who are on the borderline between nutritional autonomy and PS dependence. It is important to realize that teduglutide should be used to augment, not replace conventional management. What happens when teduglutide is stopped? Preliminary evidence suggests the effects on adaptation may be persistent, although earlier study noted that histologic changes trended toward baseline within 4 weeks of discontinuation. Perhaps longer treatment or maintenance will be required. The real future is an artificially grown and harvested intestine; even intestinal transplantation represents a bridge at best.
Dr. Alan L. Buchman is a former professor of medicine and surgery at the Feinberg School of Medicine at Northwestern University, Chicago. Within the past 12 months he has consulted for Takeda Pharmaceuticals and NPS Pharmaceuticals.
Teduglutide significantly reduced the need for parenteral support in patients with short bowel syndrome and intestinal failure, based on data from 85 adults in a randomized, controlled multicenter trial. The findings were published in the December issue of Gastroenterology.
Patients with short bowel syndrome and intestinal failure (SBS-IF) have inadequate intestinal absorption and require parenteral support (PS) to maintain fluids, electrolytes, trace elements, vitamins, and nutrient balances, said Dr. Palle Bekker Jeppesen of Rigshospitalet in Copenhagen and colleagues.
Source: American Gastroenterological Association
Data from previous open-label studies suggest an association between teduglutide and clinically meaningful reductions in wet weight and energy, which may reduce the need for PS in these patients, the investigators noted.
The researchers randomized 86 adults with SBS-IF to either 0.05 mg/kg per day of teduglutide or a placebo. One patient was randomized in error; complete data were available for 42 teduglutide patients and 43 placebo patients.
Significantly more patients in the teduglutide group responded to treatment, compared with the placebo group (63% vs. 30%). This response was defined as sustaining a 20%-100% reduction from baseline in weekly PS volume during weeks 20-24. "Small bowel length did not appear to be a predictor of response," the researchers noted.
The high placebo response may be explained by examining the fluid composite effect, a measure of the combined effects of teduglutide on PS volume reduction as well as the ability to reduce oral fluid intake and increase urine output volume, the researchers noted.
"In the current study, where protocol modifications encouraged earlier and more aggressive PS reductions, significantly larger PS reductions were also achieved in patients receiving placebo, but subsequently these patients had to increase their oral fluid intake significantly to maintain urine production and hydration constant," they said.
After 24 weeks, overall PS volume was reduced by 32% from baseline in teduglutide patients, compared with 21% in placebo patients. Although no patients in either group were completely weaned from parenteral support at 24 weeks, the difference in PS volume reduction was significantly greater in the teduglutide group.
The average weekly PS volume in teduglutide patients decreased significantly from 12.5 L/wk at baseline to 8.1 L/wk at week 24. The placebo patients also had a significant decrease in average weekly PS volume, from 13.4 L/wk at baseline to 11.1 L/wk at week 24.
Treatment-ending adverse events were similar between the two groups; 5% of teduglutide patients and 7% of placebo patients discontinued treatment because of such events during the study period. The most frequently reported treatment-emergent adverse events included abdominal pain, abdominal distension, nausea, and gastrointestinal stoma complications.
Although the study did not specifically assess quality of life measures, significantly more teduglutide patients had at least 1 day off PS, compared with placebo patients, which could help to "liberate considerable time for unhindered daytime activities or undisturbed sleep," the researchers said.
The study did not address the possible benefit of teduglutide therapy earlier in the course of SBS, or the duration of effect after patients discontinued teduglutide, the researchers added.
However, the findings indicate that teduglutide was safe and well tolerated, and "could positively add to the limited treatment armamentarium" for patients with SBS-IF.
Dr. Jeppesen and several coauthors have served on the advisory board of and as consultants to NPS Pharmaceuticals, the company that funded the study. One author is an employee of NPS Pharmaceuticals.
Teduglutide significantly reduced the need for parenteral support in patients with short bowel syndrome and intestinal failure, based on data from 85 adults in a randomized, controlled multicenter trial. The findings were published in the December issue of Gastroenterology.
Patients with short bowel syndrome and intestinal failure (SBS-IF) have inadequate intestinal absorption and require parenteral support (PS) to maintain fluids, electrolytes, trace elements, vitamins, and nutrient balances, said Dr. Palle Bekker Jeppesen of Rigshospitalet in Copenhagen and colleagues.
Source: American Gastroenterological Association
Data from previous open-label studies suggest an association between teduglutide and clinically meaningful reductions in wet weight and energy, which may reduce the need for PS in these patients, the investigators noted.
The researchers randomized 86 adults with SBS-IF to either 0.05 mg/kg per day of teduglutide or a placebo. One patient was randomized in error; complete data were available for 42 teduglutide patients and 43 placebo patients.
Significantly more patients in the teduglutide group responded to treatment, compared with the placebo group (63% vs. 30%). This response was defined as sustaining a 20%-100% reduction from baseline in weekly PS volume during weeks 20-24. "Small bowel length did not appear to be a predictor of response," the researchers noted.
The high placebo response may be explained by examining the fluid composite effect, a measure of the combined effects of teduglutide on PS volume reduction as well as the ability to reduce oral fluid intake and increase urine output volume, the researchers noted.
"In the current study, where protocol modifications encouraged earlier and more aggressive PS reductions, significantly larger PS reductions were also achieved in patients receiving placebo, but subsequently these patients had to increase their oral fluid intake significantly to maintain urine production and hydration constant," they said.
After 24 weeks, overall PS volume was reduced by 32% from baseline in teduglutide patients, compared with 21% in placebo patients. Although no patients in either group were completely weaned from parenteral support at 24 weeks, the difference in PS volume reduction was significantly greater in the teduglutide group.
The average weekly PS volume in teduglutide patients decreased significantly from 12.5 L/wk at baseline to 8.1 L/wk at week 24. The placebo patients also had a significant decrease in average weekly PS volume, from 13.4 L/wk at baseline to 11.1 L/wk at week 24.
Treatment-ending adverse events were similar between the two groups; 5% of teduglutide patients and 7% of placebo patients discontinued treatment because of such events during the study period. The most frequently reported treatment-emergent adverse events included abdominal pain, abdominal distension, nausea, and gastrointestinal stoma complications.
Although the study did not specifically assess quality of life measures, significantly more teduglutide patients had at least 1 day off PS, compared with placebo patients, which could help to "liberate considerable time for unhindered daytime activities or undisturbed sleep," the researchers said.
The study did not address the possible benefit of teduglutide therapy earlier in the course of SBS, or the duration of effect after patients discontinued teduglutide, the researchers added.
However, the findings indicate that teduglutide was safe and well tolerated, and "could positively add to the limited treatment armamentarium" for patients with SBS-IF.
Dr. Jeppesen and several coauthors have served on the advisory board of and as consultants to NPS Pharmaceuticals, the company that funded the study. One author is an employee of NPS Pharmaceuticals.
FROM GASTROENTEROLOGY
Major Finding: Significantly more patients who received 0.05 mg/kg per day of teduglutide had a sustained response to treatment during weeks 20-24, compared with the placebo group (63% vs. 30%).
Data Source: The data come from a randomized, controlled multicenter trial of 85 adults with short bowel syndrome and intestinal failure.
Disclosures: Dr. Jeppesen and several coauthors have served on the advisory board of and as consultants to NPS Pharmaceuticals, the company that funded the study. One author is an employee of NPS Pharmaceuticals.
Recurrent Acute Pancreatitis No Better After Dual Sphincterotomy
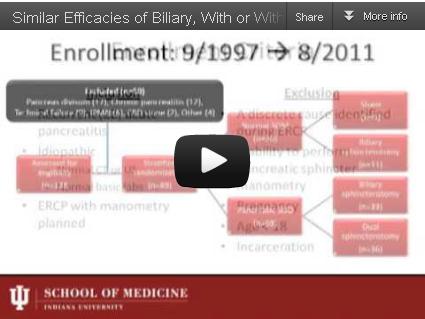
Performance of either biliary endoscopic sphincterotomy alone or dual biliary and pancreatic sphincterotomy similarly prevented approximately half of idiopathic recurrent acute pancreatitis cases in a trial in which 89 patients were randomized to treatments based on the presence or absence of sphincter of Oddi dysfunction.
The study is "the largest randomized clinical trial studying ERCP [endoscopic retrograde cholangiopancreatography] with SOM [sphincter of Oddi manometry] in this population" with long-term follow-up data, Dr. Gregory A. Coté of Indiana University in Indianapolis and his colleagues reported in the December issue of Gastroenterology (2012 [doi: 10.1053/j.gastro.2012.09.006]).
Source: American Gastroenterological Institute
Finding therapeutic equivalence between biliary endoscopic sphincterotomy (BES) and dual endoscopic sphincterotomy (DES) in preventing at least one episode of acute pancreatitis during follow-up is important, because the addition of pancreatic sphincterotomy to ERCP carries the risk of post-ERCP pancreatitis, bleeding, perforation, and sphincter restenosis, according to Dr. Coté and his associates.
To assess the therapeutic value of two types of sphincterotomy and the prognostic value of pancreatic SOD for patients with idiopathic recurrent acute pancreatitis (RAP), the researchers randomized 69 adults with SOD to BES or DES. The other 20 patients who did not have SOD were randomized to BES or a sham therapy. SOD was defined as basal pressure of 40 mm Hg or greater, "sustained for at least 30 seconds across two transducers," the researchers noted.
The patients were aged 18 years and older, and those with chronic pancreatitis or an identified cause of RAP were excluded from the study.
Of the 69 patients with SOD, RAP occurred in 49% of patients who underwent BES and 47% who underwent DES. There was no significant difference in rates of RAP between non-SOD patients who had BES and those who had a sham procedure (27% vs. 11%, respectively).
The risk of RAP was approximately four times higher in patients with SOD than in those without SOD, they added.
"Most RAP events occurred within 30 months of randomization in all subgroups," the researchers said.
Overall, chronic pancreatitis developed in 17% of all patients over a median of 78 months, and there was no difference in the probability of developing chronic pancreatitis in patients with and without SOD.
The study was limited by several factors, including its small sample size for the non-SOD population and the impact of environmental and genetic risk factors on idiopathic RAP, the researchers noted.
The small sample of patients with normal SOM meant that the researchers could draw no conclusions about the benefit of BES in these patients, but the results "represent preliminary data for estimating the sample size of a future definitive trial of ERCP with empiric biliary sphincterotomy," they noted.
In addition, the findings suggest that SOD "may be a secondary marker of more significant inflammation related to previous acute pancreatitis," and that pancreatic sphincterotomy "cannot be recommended as a curative treatment of unexplained RAP alone," they wrote.
None of the study authors had any financial conflicts to disclose.
Performance of either biliary endoscopic sphincterotomy alone or dual biliary and pancreatic sphincterotomy similarly prevented approximately half of idiopathic recurrent acute pancreatitis cases in a trial in which 89 patients were randomized to treatments based on the presence or absence of sphincter of Oddi dysfunction.
The study is "the largest randomized clinical trial studying ERCP [endoscopic retrograde cholangiopancreatography] with SOM [sphincter of Oddi manometry] in this population" with long-term follow-up data, Dr. Gregory A. Coté of Indiana University in Indianapolis and his colleagues reported in the December issue of Gastroenterology (2012 [doi: 10.1053/j.gastro.2012.09.006]).
Source: American Gastroenterological Institute
Finding therapeutic equivalence between biliary endoscopic sphincterotomy (BES) and dual endoscopic sphincterotomy (DES) in preventing at least one episode of acute pancreatitis during follow-up is important, because the addition of pancreatic sphincterotomy to ERCP carries the risk of post-ERCP pancreatitis, bleeding, perforation, and sphincter restenosis, according to Dr. Coté and his associates.
To assess the therapeutic value of two types of sphincterotomy and the prognostic value of pancreatic SOD for patients with idiopathic recurrent acute pancreatitis (RAP), the researchers randomized 69 adults with SOD to BES or DES. The other 20 patients who did not have SOD were randomized to BES or a sham therapy. SOD was defined as basal pressure of 40 mm Hg or greater, "sustained for at least 30 seconds across two transducers," the researchers noted.
The patients were aged 18 years and older, and those with chronic pancreatitis or an identified cause of RAP were excluded from the study.
Of the 69 patients with SOD, RAP occurred in 49% of patients who underwent BES and 47% who underwent DES. There was no significant difference in rates of RAP between non-SOD patients who had BES and those who had a sham procedure (27% vs. 11%, respectively).
The risk of RAP was approximately four times higher in patients with SOD than in those without SOD, they added.
"Most RAP events occurred within 30 months of randomization in all subgroups," the researchers said.
Overall, chronic pancreatitis developed in 17% of all patients over a median of 78 months, and there was no difference in the probability of developing chronic pancreatitis in patients with and without SOD.
The study was limited by several factors, including its small sample size for the non-SOD population and the impact of environmental and genetic risk factors on idiopathic RAP, the researchers noted.
The small sample of patients with normal SOM meant that the researchers could draw no conclusions about the benefit of BES in these patients, but the results "represent preliminary data for estimating the sample size of a future definitive trial of ERCP with empiric biliary sphincterotomy," they noted.
In addition, the findings suggest that SOD "may be a secondary marker of more significant inflammation related to previous acute pancreatitis," and that pancreatic sphincterotomy "cannot be recommended as a curative treatment of unexplained RAP alone," they wrote.
None of the study authors had any financial conflicts to disclose.
Performance of either biliary endoscopic sphincterotomy alone or dual biliary and pancreatic sphincterotomy similarly prevented approximately half of idiopathic recurrent acute pancreatitis cases in a trial in which 89 patients were randomized to treatments based on the presence or absence of sphincter of Oddi dysfunction.
The study is "the largest randomized clinical trial studying ERCP [endoscopic retrograde cholangiopancreatography] with SOM [sphincter of Oddi manometry] in this population" with long-term follow-up data, Dr. Gregory A. Coté of Indiana University in Indianapolis and his colleagues reported in the December issue of Gastroenterology (2012 [doi: 10.1053/j.gastro.2012.09.006]).
Source: American Gastroenterological Institute
Finding therapeutic equivalence between biliary endoscopic sphincterotomy (BES) and dual endoscopic sphincterotomy (DES) in preventing at least one episode of acute pancreatitis during follow-up is important, because the addition of pancreatic sphincterotomy to ERCP carries the risk of post-ERCP pancreatitis, bleeding, perforation, and sphincter restenosis, according to Dr. Coté and his associates.
To assess the therapeutic value of two types of sphincterotomy and the prognostic value of pancreatic SOD for patients with idiopathic recurrent acute pancreatitis (RAP), the researchers randomized 69 adults with SOD to BES or DES. The other 20 patients who did not have SOD were randomized to BES or a sham therapy. SOD was defined as basal pressure of 40 mm Hg or greater, "sustained for at least 30 seconds across two transducers," the researchers noted.
The patients were aged 18 years and older, and those with chronic pancreatitis or an identified cause of RAP were excluded from the study.
Of the 69 patients with SOD, RAP occurred in 49% of patients who underwent BES and 47% who underwent DES. There was no significant difference in rates of RAP between non-SOD patients who had BES and those who had a sham procedure (27% vs. 11%, respectively).
The risk of RAP was approximately four times higher in patients with SOD than in those without SOD, they added.
"Most RAP events occurred within 30 months of randomization in all subgroups," the researchers said.
Overall, chronic pancreatitis developed in 17% of all patients over a median of 78 months, and there was no difference in the probability of developing chronic pancreatitis in patients with and without SOD.
The study was limited by several factors, including its small sample size for the non-SOD population and the impact of environmental and genetic risk factors on idiopathic RAP, the researchers noted.
The small sample of patients with normal SOM meant that the researchers could draw no conclusions about the benefit of BES in these patients, but the results "represent preliminary data for estimating the sample size of a future definitive trial of ERCP with empiric biliary sphincterotomy," they noted.
In addition, the findings suggest that SOD "may be a secondary marker of more significant inflammation related to previous acute pancreatitis," and that pancreatic sphincterotomy "cannot be recommended as a curative treatment of unexplained RAP alone," they wrote.
None of the study authors had any financial conflicts to disclose.
FROM GASTROENTEROLOGY
Major Finding: Of 69 patients with sphincter of Oddi dysfunction, recurrent acute pancreatitis occurred in 49% of patients who underwent biliary endoscopic sphincterectomy and 47% who had dual biliary and pancreatic endoscopic sphincterectomy.
Data Source: The data come from a randomized trial of 89 adults with idiopathic recurrent acute pancreatitis.
Disclosures: None of the study authors had any financial conflicts to disclose.
COPD Varies By State, Peaks Above 9%
The prevalence of chronic obstructive pulmonary disease is 6% nationwide, but varies from less than 4% in Washington and Minnesota to more than 9% in Alabama and Kentucky, according to data from the Centers for Disease Control and Prevention. The findings were published in the CDC’s Morbidity and Mortality Weekly Report on Nov. 23.
A total of 13,306 adults who reported having chronic obstructive pulmonary disease (COPD) in the national survey also responded to the COPD module. Of these, 76% reported undergoing a diagnostic breathing test, 64% reported that COPD symptoms (specifically shortness of breath) had an adverse effect on their quality of life, and 51% reported taking at least one COPD medication (MMWR 2012; 61:938-43).
In age-adjusted comparisons, women were more likely to report COPD compared with men (7% vs. 5%, respectively). COPD prevalence decreased from an average of 10% among individuals making less than $25,000 per year to 3% in those making more than $75,000 per year, and the prevalence was lower among employed individuals, homemakers, and students compared with those who were unemployed, retired, or otherwise unable to work. The prevalence of COPD was highest in current smokers (13%) compared with former smokers (7%) and never smokers (3%).
Data were taken from the 2011 Behavioral Risk Factor Surveillance System (BRFSS) survey. Additional COPD data were collected in an optional COPD module about COPD diagnosis and quality of life. This module was part of the BRFSS in 21 states, the District of Columbia, and Puerto Rico.
The 2011 BRFSS was conducted via telephone, either landline or mobile. The survey population included adults aged 18 years and older throughout the United States.
The findings were limited by several factors including the absence of data on individuals in institutions or nursing homes and by the use of self-reports for COPD diagnosis, the researchers said. However, the report is the first to analyze data on COPD prevalence in all 50 states, the District of Columbia, and Puerto Rico, they noted. State-level health officials should focus surveillance efforts, educational campaigns, and interventions on areas of highest COPD prevalence, they added.
The study was supported by the CDC and the National Heart, Lung, and Blood Institute of the National Institutes of Health.
The prevalence of chronic obstructive pulmonary disease is 6% nationwide, but varies from less than 4% in Washington and Minnesota to more than 9% in Alabama and Kentucky, according to data from the Centers for Disease Control and Prevention. The findings were published in the CDC’s Morbidity and Mortality Weekly Report on Nov. 23.
A total of 13,306 adults who reported having chronic obstructive pulmonary disease (COPD) in the national survey also responded to the COPD module. Of these, 76% reported undergoing a diagnostic breathing test, 64% reported that COPD symptoms (specifically shortness of breath) had an adverse effect on their quality of life, and 51% reported taking at least one COPD medication (MMWR 2012; 61:938-43).
In age-adjusted comparisons, women were more likely to report COPD compared with men (7% vs. 5%, respectively). COPD prevalence decreased from an average of 10% among individuals making less than $25,000 per year to 3% in those making more than $75,000 per year, and the prevalence was lower among employed individuals, homemakers, and students compared with those who were unemployed, retired, or otherwise unable to work. The prevalence of COPD was highest in current smokers (13%) compared with former smokers (7%) and never smokers (3%).
Data were taken from the 2011 Behavioral Risk Factor Surveillance System (BRFSS) survey. Additional COPD data were collected in an optional COPD module about COPD diagnosis and quality of life. This module was part of the BRFSS in 21 states, the District of Columbia, and Puerto Rico.
The 2011 BRFSS was conducted via telephone, either landline or mobile. The survey population included adults aged 18 years and older throughout the United States.
The findings were limited by several factors including the absence of data on individuals in institutions or nursing homes and by the use of self-reports for COPD diagnosis, the researchers said. However, the report is the first to analyze data on COPD prevalence in all 50 states, the District of Columbia, and Puerto Rico, they noted. State-level health officials should focus surveillance efforts, educational campaigns, and interventions on areas of highest COPD prevalence, they added.
The study was supported by the CDC and the National Heart, Lung, and Blood Institute of the National Institutes of Health.
The prevalence of chronic obstructive pulmonary disease is 6% nationwide, but varies from less than 4% in Washington and Minnesota to more than 9% in Alabama and Kentucky, according to data from the Centers for Disease Control and Prevention. The findings were published in the CDC’s Morbidity and Mortality Weekly Report on Nov. 23.
A total of 13,306 adults who reported having chronic obstructive pulmonary disease (COPD) in the national survey also responded to the COPD module. Of these, 76% reported undergoing a diagnostic breathing test, 64% reported that COPD symptoms (specifically shortness of breath) had an adverse effect on their quality of life, and 51% reported taking at least one COPD medication (MMWR 2012; 61:938-43).
In age-adjusted comparisons, women were more likely to report COPD compared with men (7% vs. 5%, respectively). COPD prevalence decreased from an average of 10% among individuals making less than $25,000 per year to 3% in those making more than $75,000 per year, and the prevalence was lower among employed individuals, homemakers, and students compared with those who were unemployed, retired, or otherwise unable to work. The prevalence of COPD was highest in current smokers (13%) compared with former smokers (7%) and never smokers (3%).
Data were taken from the 2011 Behavioral Risk Factor Surveillance System (BRFSS) survey. Additional COPD data were collected in an optional COPD module about COPD diagnosis and quality of life. This module was part of the BRFSS in 21 states, the District of Columbia, and Puerto Rico.
The 2011 BRFSS was conducted via telephone, either landline or mobile. The survey population included adults aged 18 years and older throughout the United States.
The findings were limited by several factors including the absence of data on individuals in institutions or nursing homes and by the use of self-reports for COPD diagnosis, the researchers said. However, the report is the first to analyze data on COPD prevalence in all 50 states, the District of Columbia, and Puerto Rico, they noted. State-level health officials should focus surveillance efforts, educational campaigns, and interventions on areas of highest COPD prevalence, they added.
The study was supported by the CDC and the National Heart, Lung, and Blood Institute of the National Institutes of Health.
FROM THE CENTERS FOR DISEASE CONTROL AND PREVENTION'S MORBIDITY AND MORTALITY WEEKLY REPORT
Major Finding: The overall prevalence of chronic obstructive pulmonary disease in the United States is approximately 6%.
Data Source: The data come from the 2011 Behavioral Risk Factor Surveillance System (BRFSS) survey.
Disclosures: The study was supported by the CDC and the National Heart, Lung, and Blood Institute of the National Institutes of Health.
Ranbaxy Recalls Atorvastatin
Ranbaxy Inc. voluntarily recalled 41 lots of Atorvastatin calcium tablets in 10-mg, 20-mg, and 40-mg doses because of potential contamination with ground glass, the company and the Food and Drug Administration announced Nov. 28.
The small size of the particles (less than 1 mm) makes safety concerns unlikely, according to the statement from MedWatch, the FDA Safety Information and Adverse Event Reporting Program.
"However, the possibility of adverse experiences arising primarily due to physical irritation cannot be ruled out," according to the statement.
The recall does not affect the 80-mg dosage of Atorvastatin calcium tablets, according to the Ranbaxy company press release, which lists the specific lots included in the recall.
Ranbaxy initiated the recall on Nov. 9. Distributors have ceased distribution of the affected lots and are in the process of returning these products to Ranbaxy, according to the statement. The affected tablet is white in color, with the imprint RX12 on 10-mg tablets, RX828 on 20-mg tablets, and RX829 on 40-mg tablets.
Atorvastatin is prescribed not only for lowering blood cholesterol, but also for the prevention of cardiovascular disease in patients at high risk for cardiovascular conditions, and for the prevention of cardiovascular events in patients with heart disease.
Adverse reactions or quality problems with the affected atorvastatin lots may be reported to the FDA online, by mail (use Form FDA 3500), or by fax (1-800-FDA-0178).
Ranbaxy Inc. voluntarily recalled 41 lots of Atorvastatin calcium tablets in 10-mg, 20-mg, and 40-mg doses because of potential contamination with ground glass, the company and the Food and Drug Administration announced Nov. 28.
The small size of the particles (less than 1 mm) makes safety concerns unlikely, according to the statement from MedWatch, the FDA Safety Information and Adverse Event Reporting Program.
"However, the possibility of adverse experiences arising primarily due to physical irritation cannot be ruled out," according to the statement.
The recall does not affect the 80-mg dosage of Atorvastatin calcium tablets, according to the Ranbaxy company press release, which lists the specific lots included in the recall.
Ranbaxy initiated the recall on Nov. 9. Distributors have ceased distribution of the affected lots and are in the process of returning these products to Ranbaxy, according to the statement. The affected tablet is white in color, with the imprint RX12 on 10-mg tablets, RX828 on 20-mg tablets, and RX829 on 40-mg tablets.
Atorvastatin is prescribed not only for lowering blood cholesterol, but also for the prevention of cardiovascular disease in patients at high risk for cardiovascular conditions, and for the prevention of cardiovascular events in patients with heart disease.
Adverse reactions or quality problems with the affected atorvastatin lots may be reported to the FDA online, by mail (use Form FDA 3500), or by fax (1-800-FDA-0178).
Ranbaxy Inc. voluntarily recalled 41 lots of Atorvastatin calcium tablets in 10-mg, 20-mg, and 40-mg doses because of potential contamination with ground glass, the company and the Food and Drug Administration announced Nov. 28.
The small size of the particles (less than 1 mm) makes safety concerns unlikely, according to the statement from MedWatch, the FDA Safety Information and Adverse Event Reporting Program.
"However, the possibility of adverse experiences arising primarily due to physical irritation cannot be ruled out," according to the statement.
The recall does not affect the 80-mg dosage of Atorvastatin calcium tablets, according to the Ranbaxy company press release, which lists the specific lots included in the recall.
Ranbaxy initiated the recall on Nov. 9. Distributors have ceased distribution of the affected lots and are in the process of returning these products to Ranbaxy, according to the statement. The affected tablet is white in color, with the imprint RX12 on 10-mg tablets, RX828 on 20-mg tablets, and RX829 on 40-mg tablets.
Atorvastatin is prescribed not only for lowering blood cholesterol, but also for the prevention of cardiovascular disease in patients at high risk for cardiovascular conditions, and for the prevention of cardiovascular events in patients with heart disease.
Adverse reactions or quality problems with the affected atorvastatin lots may be reported to the FDA online, by mail (use Form FDA 3500), or by fax (1-800-FDA-0178).
Youth Account for Quarter of New HIV Infections
Approximately 1 in 4 new HIV infections in the United States in 2010 occurred in youth aged 13-24 years, according to data from the Centers for Disease Control and Prevention.
Nearly two-thirds (60%) of infected youth are unaware of their condition, according to a study published online Nov. 27 in Morbidity and Mortality Weekly Report.
"The bottom line is that every month, 1,000 youth are becoming infected with HIV," CDC director Dr. Thomas Frieden said in a telebriefing. "The cost of care of a single patient is approximately $400,000 over their lifetime," he said. "That means every month we are accruing about 400 million dollars of health care costs from preventable infections in youth."

"Reducing HIV among young people is a top priority for CDC," said Dr. Frieden. "This is about the health of a new generation, and protecting them from an entirely preventable disease."
In 2010, youth aged 13-24 years accounted for 12,200 new cases of HIV, which was 26% of the total estimated 45,700 new HIV infections. Of these 12,200, approximately 8,000 (72%) occurred in young men who have sex with men (MSM). Approximately 57% of the new cases among young MSM occurred in black youth, compared with 20% among both white and Hispanic youth, he noted.
An estimated 7,000 (57%) newly infected youths were black, 2,390 (20%) were Hispanic, and 2,380 (20%) were white. The report did not account for the ethnicity of the remaining 3% of the cohort. The majority of the newly infected youth were male (83%).
Although the CDC currently recommends routine HIV testing in medical settings, only 13% of high school students, 22% of sexually active high school students, and 35% of young adults aged 18-34 years have been tested, according to the report (MMWR 2012;61:1-6).
The researchers also reviewed data on risky behaviors among high school students in 12 states and 9 large urban school districts. Overall, young MSM were significantly less likely than their heterosexual peers to have used a condom during their most recent sexual encounters (44% vs. 70%), significantly more likely to have had four or more sexual partners (39% vs. 27%), and significantly less likely to report learning about HIV or AIDS in school (75% vs. 86%).
"We know there are many young people who are not routinely seeing health care providers," Dr. Frieden said. However, health care providers have a role to play in preventing the spread of HIV.
"The key for clinicians is to make it [HIV testing] routine," said Dr. Frieden. "Just as we screen adults for high cholesterol, we screen people for HIV infection. If someone refuses testing, that is their right," he said, but clinicians can have a policy of "this is what we do."
CDC researchers used data from the National HIV Surveillance System to estimate the incidence of new HIV infections in 2010. Data from the 2010 National Health Interview Survey and the Youth Risk Behavior Surveillance System were used to assess risk factors and testing rates.
The study was supported by the Centers for Disease Control and Prevention.
Approximately 1 in 4 new HIV infections in the United States in 2010 occurred in youth aged 13-24 years, according to data from the Centers for Disease Control and Prevention.
Nearly two-thirds (60%) of infected youth are unaware of their condition, according to a study published online Nov. 27 in Morbidity and Mortality Weekly Report.
"The bottom line is that every month, 1,000 youth are becoming infected with HIV," CDC director Dr. Thomas Frieden said in a telebriefing. "The cost of care of a single patient is approximately $400,000 over their lifetime," he said. "That means every month we are accruing about 400 million dollars of health care costs from preventable infections in youth."
"Reducing HIV among young people is a top priority for CDC," said Dr. Frieden. "This is about the health of a new generation, and protecting them from an entirely preventable disease."
In 2010, youth aged 13-24 years accounted for 12,200 new cases of HIV, which was 26% of the total estimated 45,700 new HIV infections. Of these 12,200, approximately 8,000 (72%) occurred in young men who have sex with men (MSM). Approximately 57% of the new cases among young MSM occurred in black youth, compared with 20% among both white and Hispanic youth, he noted.
An estimated 7,000 (57%) newly infected youths were black, 2,390 (20%) were Hispanic, and 2,380 (20%) were white. The report did not account for the ethnicity of the remaining 3% of the cohort. The majority of the newly infected youth were male (83%).
Although the CDC currently recommends routine HIV testing in medical settings, only 13% of high school students, 22% of sexually active high school students, and 35% of young adults aged 18-34 years have been tested, according to the report (MMWR 2012;61:1-6).
The researchers also reviewed data on risky behaviors among high school students in 12 states and 9 large urban school districts. Overall, young MSM were significantly less likely than their heterosexual peers to have used a condom during their most recent sexual encounters (44% vs. 70%), significantly more likely to have had four or more sexual partners (39% vs. 27%), and significantly less likely to report learning about HIV or AIDS in school (75% vs. 86%).
"We know there are many young people who are not routinely seeing health care providers," Dr. Frieden said. However, health care providers have a role to play in preventing the spread of HIV.
"The key for clinicians is to make it [HIV testing] routine," said Dr. Frieden. "Just as we screen adults for high cholesterol, we screen people for HIV infection. If someone refuses testing, that is their right," he said, but clinicians can have a policy of "this is what we do."
CDC researchers used data from the National HIV Surveillance System to estimate the incidence of new HIV infections in 2010. Data from the 2010 National Health Interview Survey and the Youth Risk Behavior Surveillance System were used to assess risk factors and testing rates.
The study was supported by the Centers for Disease Control and Prevention.
Approximately 1 in 4 new HIV infections in the United States in 2010 occurred in youth aged 13-24 years, according to data from the Centers for Disease Control and Prevention.
Nearly two-thirds (60%) of infected youth are unaware of their condition, according to a study published online Nov. 27 in Morbidity and Mortality Weekly Report.
"The bottom line is that every month, 1,000 youth are becoming infected with HIV," CDC director Dr. Thomas Frieden said in a telebriefing. "The cost of care of a single patient is approximately $400,000 over their lifetime," he said. "That means every month we are accruing about 400 million dollars of health care costs from preventable infections in youth."
"Reducing HIV among young people is a top priority for CDC," said Dr. Frieden. "This is about the health of a new generation, and protecting them from an entirely preventable disease."
In 2010, youth aged 13-24 years accounted for 12,200 new cases of HIV, which was 26% of the total estimated 45,700 new HIV infections. Of these 12,200, approximately 8,000 (72%) occurred in young men who have sex with men (MSM). Approximately 57% of the new cases among young MSM occurred in black youth, compared with 20% among both white and Hispanic youth, he noted.
An estimated 7,000 (57%) newly infected youths were black, 2,390 (20%) were Hispanic, and 2,380 (20%) were white. The report did not account for the ethnicity of the remaining 3% of the cohort. The majority of the newly infected youth were male (83%).
Although the CDC currently recommends routine HIV testing in medical settings, only 13% of high school students, 22% of sexually active high school students, and 35% of young adults aged 18-34 years have been tested, according to the report (MMWR 2012;61:1-6).
The researchers also reviewed data on risky behaviors among high school students in 12 states and 9 large urban school districts. Overall, young MSM were significantly less likely than their heterosexual peers to have used a condom during their most recent sexual encounters (44% vs. 70%), significantly more likely to have had four or more sexual partners (39% vs. 27%), and significantly less likely to report learning about HIV or AIDS in school (75% vs. 86%).
"We know there are many young people who are not routinely seeing health care providers," Dr. Frieden said. However, health care providers have a role to play in preventing the spread of HIV.
"The key for clinicians is to make it [HIV testing] routine," said Dr. Frieden. "Just as we screen adults for high cholesterol, we screen people for HIV infection. If someone refuses testing, that is their right," he said, but clinicians can have a policy of "this is what we do."
CDC researchers used data from the National HIV Surveillance System to estimate the incidence of new HIV infections in 2010. Data from the 2010 National Health Interview Survey and the Youth Risk Behavior Surveillance System were used to assess risk factors and testing rates.
The study was supported by the Centers for Disease Control and Prevention.
FROM MORBIDITY AND MORTALITY WEEKLY REPORT
Major Finding: An estimated 12,200 new cases of HIV were reported in youth aged 13-24 years in 2010, which was 26% of the total estimated 45,700 new HIV infections. Approximately 72% of cases occurred in young men who have sex with men.
Data Source: The data were taken from the National HIV Surveillance System to estimate the incidence of new HIV infections in 2010, and from the 2010 National Health Interview Survey and the Youth Risk Behavior Surveillance System to assess risk factors and testing rates.
Disclosures: The study was supported by the Centers for Disease Control and Prevention.

Half of Early RA Patients Achieve Sustained Remission
WASHINGTON – Younger age, lower baseline pain, and shorter time to remission were significant predictors of sustained remission for early rheumatoid arthritis patients, based on data from more than 1,000 patients older than 16 years.
The prevalence of and predictive factors for sustained remission in early rheumatoid arthritis (RA) is not well understood, "particularly in the context of new stringent definitions," said Dr. Vivian P. Bykerk, who is on the staff of the Inflammatory Arthritis Center of the Hospital for Special Surgery in New York.

Dr. Bykerk and her colleagues reviewed data from the Canadian Early Arthritis Cohort (CATCH) study. Their selected study population included 1,244 adults with probable or confirmed RA. The average age of the patients was 54 years, 83% were white, and 73% were women. The researchers presented the data at the annual American College of Rheumatology meeting.
Remission was defined using the Simple Disease Activity Index (SDAI) and the ACR/EULAR clinical practice and clinical trial definitions. The remission definition using SDAI was a score of 3.3 or less. The ACR/EULAR clinical practice remission definition included a tender joint count, swollen joint count, and patient global assessment scores of 1 or less; the clinical trial definition added a CRP level of 1 mg/dL or less to the clinical practice definition.
Overall, 40% of the patients achieved SDAI remission, 42% achieved ACR/EULAR clinical practice remission, and 35% achieved ACR/EULAR clinical trial remission. The median time to remission based on the three definitions was 10 months, 8 months, and 9 months, respectively.
Of the patients who achieved SDAI, ACR/EULAR clinical practice, and ACR/EULAR clinical trial remission, 56%, 59%, and 54%, respectively, achieved sustained remission (defined as remission lasting at least 12 months).
The average duration of symptoms was 6 months. Patients were either treatment naïve or in the early stages of treatment. In the first 3 months, 44% of the patients received combination therapy, 32% received methotrexate monotherapy, 30% received oral corticosteroids, and 2% received biologics.
The average SDAI score at baseline was 29, and the baseline number of tender and swollen joints was approximately 8. Patients were evaluated every 3 months for the first year, followed by evaluations every 6 months.
After researchers adjusted for confounding variables, they determined that younger age, lower baseline pain score, and shorter time to remission were significantly associated with sustained remission. The effect of shorter time to remission on sustained remission supports striving for early remission in early RA patients, Dr. Bykerk noted.
Variables that were not associated with sustained remission included smoking status, symptom duration, tender or swollen joint counts, morning stiffness, and initial treatment with oral corticosteroids or biologics.
Methotrexate monotherapy was associated with lower sustained remission, and the data could not prove an association between combination disease-modifying antirheumatic drugs (DMARD) therapy and sustained remission, said Dr. Bykerk.
In addition, laboratory values for erythrocyte sedimentation rate, C-reactive protein, rheumatoid factor, and anticitrullinated protein antibodies (ACPA) were not associated with sustained remission, she said.
The study findings were limited by several factors including a lack of data on medication changes and the limited follow-up times of 3- and 6-month intervals, Dr. Bykerk said. But the results are strengthened by the use of a real-world observational cohort and suggest that more work is needed to determine the best patient-specific treatment strategies, she said.
Dr. Bykerk disclosed financial relationships with multiple companies including Abbott, Amgen, Pfizer, and Roche.
WASHINGTON – Younger age, lower baseline pain, and shorter time to remission were significant predictors of sustained remission for early rheumatoid arthritis patients, based on data from more than 1,000 patients older than 16 years.
The prevalence of and predictive factors for sustained remission in early rheumatoid arthritis (RA) is not well understood, "particularly in the context of new stringent definitions," said Dr. Vivian P. Bykerk, who is on the staff of the Inflammatory Arthritis Center of the Hospital for Special Surgery in New York.
Dr. Bykerk and her colleagues reviewed data from the Canadian Early Arthritis Cohort (CATCH) study. Their selected study population included 1,244 adults with probable or confirmed RA. The average age of the patients was 54 years, 83% were white, and 73% were women. The researchers presented the data at the annual American College of Rheumatology meeting.
Remission was defined using the Simple Disease Activity Index (SDAI) and the ACR/EULAR clinical practice and clinical trial definitions. The remission definition using SDAI was a score of 3.3 or less. The ACR/EULAR clinical practice remission definition included a tender joint count, swollen joint count, and patient global assessment scores of 1 or less; the clinical trial definition added a CRP level of 1 mg/dL or less to the clinical practice definition.
Overall, 40% of the patients achieved SDAI remission, 42% achieved ACR/EULAR clinical practice remission, and 35% achieved ACR/EULAR clinical trial remission. The median time to remission based on the three definitions was 10 months, 8 months, and 9 months, respectively.
Of the patients who achieved SDAI, ACR/EULAR clinical practice, and ACR/EULAR clinical trial remission, 56%, 59%, and 54%, respectively, achieved sustained remission (defined as remission lasting at least 12 months).
The average duration of symptoms was 6 months. Patients were either treatment naïve or in the early stages of treatment. In the first 3 months, 44% of the patients received combination therapy, 32% received methotrexate monotherapy, 30% received oral corticosteroids, and 2% received biologics.
The average SDAI score at baseline was 29, and the baseline number of tender and swollen joints was approximately 8. Patients were evaluated every 3 months for the first year, followed by evaluations every 6 months.
After researchers adjusted for confounding variables, they determined that younger age, lower baseline pain score, and shorter time to remission were significantly associated with sustained remission. The effect of shorter time to remission on sustained remission supports striving for early remission in early RA patients, Dr. Bykerk noted.
Variables that were not associated with sustained remission included smoking status, symptom duration, tender or swollen joint counts, morning stiffness, and initial treatment with oral corticosteroids or biologics.
Methotrexate monotherapy was associated with lower sustained remission, and the data could not prove an association between combination disease-modifying antirheumatic drugs (DMARD) therapy and sustained remission, said Dr. Bykerk.
In addition, laboratory values for erythrocyte sedimentation rate, C-reactive protein, rheumatoid factor, and anticitrullinated protein antibodies (ACPA) were not associated with sustained remission, she said.
The study findings were limited by several factors including a lack of data on medication changes and the limited follow-up times of 3- and 6-month intervals, Dr. Bykerk said. But the results are strengthened by the use of a real-world observational cohort and suggest that more work is needed to determine the best patient-specific treatment strategies, she said.
Dr. Bykerk disclosed financial relationships with multiple companies including Abbott, Amgen, Pfizer, and Roche.
WASHINGTON – Younger age, lower baseline pain, and shorter time to remission were significant predictors of sustained remission for early rheumatoid arthritis patients, based on data from more than 1,000 patients older than 16 years.
The prevalence of and predictive factors for sustained remission in early rheumatoid arthritis (RA) is not well understood, "particularly in the context of new stringent definitions," said Dr. Vivian P. Bykerk, who is on the staff of the Inflammatory Arthritis Center of the Hospital for Special Surgery in New York.
Dr. Bykerk and her colleagues reviewed data from the Canadian Early Arthritis Cohort (CATCH) study. Their selected study population included 1,244 adults with probable or confirmed RA. The average age of the patients was 54 years, 83% were white, and 73% were women. The researchers presented the data at the annual American College of Rheumatology meeting.
Remission was defined using the Simple Disease Activity Index (SDAI) and the ACR/EULAR clinical practice and clinical trial definitions. The remission definition using SDAI was a score of 3.3 or less. The ACR/EULAR clinical practice remission definition included a tender joint count, swollen joint count, and patient global assessment scores of 1 or less; the clinical trial definition added a CRP level of 1 mg/dL or less to the clinical practice definition.
Overall, 40% of the patients achieved SDAI remission, 42% achieved ACR/EULAR clinical practice remission, and 35% achieved ACR/EULAR clinical trial remission. The median time to remission based on the three definitions was 10 months, 8 months, and 9 months, respectively.
Of the patients who achieved SDAI, ACR/EULAR clinical practice, and ACR/EULAR clinical trial remission, 56%, 59%, and 54%, respectively, achieved sustained remission (defined as remission lasting at least 12 months).
The average duration of symptoms was 6 months. Patients were either treatment naïve or in the early stages of treatment. In the first 3 months, 44% of the patients received combination therapy, 32% received methotrexate monotherapy, 30% received oral corticosteroids, and 2% received biologics.
The average SDAI score at baseline was 29, and the baseline number of tender and swollen joints was approximately 8. Patients were evaluated every 3 months for the first year, followed by evaluations every 6 months.
After researchers adjusted for confounding variables, they determined that younger age, lower baseline pain score, and shorter time to remission were significantly associated with sustained remission. The effect of shorter time to remission on sustained remission supports striving for early remission in early RA patients, Dr. Bykerk noted.
Variables that were not associated with sustained remission included smoking status, symptom duration, tender or swollen joint counts, morning stiffness, and initial treatment with oral corticosteroids or biologics.
Methotrexate monotherapy was associated with lower sustained remission, and the data could not prove an association between combination disease-modifying antirheumatic drugs (DMARD) therapy and sustained remission, said Dr. Bykerk.
In addition, laboratory values for erythrocyte sedimentation rate, C-reactive protein, rheumatoid factor, and anticitrullinated protein antibodies (ACPA) were not associated with sustained remission, she said.
The study findings were limited by several factors including a lack of data on medication changes and the limited follow-up times of 3- and 6-month intervals, Dr. Bykerk said. But the results are strengthened by the use of a real-world observational cohort and suggest that more work is needed to determine the best patient-specific treatment strategies, she said.
Dr. Bykerk disclosed financial relationships with multiple companies including Abbott, Amgen, Pfizer, and Roche.
AT THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF RHEUMATOLOGY
Major Finding: A total of 56%, 59%, and 54% of adults with early RA achieved sustained remission based on SDAI remission criteria, ACR/EULAR clinical practice remission criteria, and ACR/EULAR clinical trial remission criteria, respectively.
Data Source: The data come from 1,244 adults in the Canadian Early Arthritis Cohort (CATCH) study.
Disclosures: Dr. Bykerk disclosed financial relationships with multiple companies including Abbott, Amgen, Pfizer, and Roche.

Many Postop Problems After Discharge
CHICAGO – Approximately one-third of surgical complications were diagnosed after patients left the hospital, based on data from nearly 60,000 procedures performed at 112 hospitals.
Reporting postoperative complications, including surgical site infections, has become a mandatory quality reporting initiative for hospitals, and the Affordable Care Act requires reporting of readmissions, said Dr. Melanie Morris of the University of Alabama at Birmingham.
"Some postoperative complications may lead to readmissions, but this may not tell the whole story," she noted at the annual clinical congress of the American College of Surgeons.
To determine the timing of postoperative complications and the nature of readmissions, Dr. Morris and her colleagues reviewed Veterans Affairs data from the noncardiac Surgical Care Improvement Project (SCIP) cohort from 2005 to 2009 for 59,464 surgical procedures in which there was at least one complication.
Surgical cases were classified by specialty into gastrointestinal, gynecologic, orthopedic, and vascular. Complications were grouped into organ-based systems. For example, urinary complications included renal failure, renal insufficiency, and urinary tract infections; respiratory complications included failure to wean, pneumonia, and reintubation; and surgical site infections (SSIs) included both deep and superficial wounds.
The overall complication rate was approximately 15%, and 32% of complications were diagnosed after hospital discharge, Dr. Morris said. More than half (56%) of all SSIs were diagnosed after discharge, she added.
A statistically significant difference appeared in postdischarge complications by surgical specialty. The SSI rate was 5.4%, followed by respiratory complications (5.0%), urinary tract infection (4.9%), cardiac complications (3.2%), and venous thromboembolism (1.2%).
"Our GI surgical patients had the highest overall complication rate," Dr. Morris noted. Among GI patients, colectomy patients had the highest SSI rate (11%), and 23% of the GI complications were diagnosed after hospital discharge.
In addition, 78% of SSIs in orthopedic patients were diagnosed after discharge, as were 39% of SSIs in GI patients, 77% of SSIs in vascular surgery patients, and 95% of SSIs in gynecologic patients, said Dr. Morris.
There were no significant differences in length of hospital stay based on complications, Dr. Morris said.
The overall readmission rate was 11.9%, and 70% of these patients had no identifiable postoperative complication. Of those who did have an identifiable postop complication, 72% were diagnosed before discharge from the hospital.
The probability of being readmitted to the hospital over time was highest in patients with a postdischarge diagnosis of a complication. The overall length of stay was 5 days, and the average length of stay for patients with any complication was 9 days.
Patient-specific factors associated with an increased risk of readmission included a history of heart failure, renal failure, diabetes, weight loss, and smoking. Procedure-specific factors associated with an increased risk of readmission included a longer operating time, a more contaminated wound, and a higher ASA (American Society of Anesthesiologists) class.
Length of stay was slightly protective for readmission, and the presence of any complication was associated with a high risk of readmission.
"It’s very important that patients are accurately educated on the signs and symptoms of complications so they know to seek timely care after discharge," said Dr. Morris.
"Postoperative complications must be measured beyond hospital discharge to capture the whole story.
"Systematic collection of postoperative complications must include postdischarge data as well as readmissions to accurately measure quality," she said.
Dr. Morris said she had no relevant financial disclosures.
Hospital acquired complications are well defined. Once discharged, the incidence of surgical complications in the perioperative time period is a matter of definition, and of who looks and how hard. It has been established that prolonged prevention of DVT is indicated in high risk surgical groups undergoing orthopedic procedures. This has been shown to be safe and effective however more work is needed. The exact duration of prophylaxis remains to be determined.
| Dr. Lohr |
The Caprini risk assessment tool was recently validated in patients undergoing plastic and reconstructive procedures. In this study, 50% of high-risk patients developed DVT late in the postoperative period (15-60 days postoperatively). In higher-risk patients, there was no evidence that DVT risk is limited to the immediate postoperative period. The transition from inpatient to outpatient care is a key event in the coordination of the continuity of care, but specific transition guidelines are currently limited. Work is needed to define appropriate guidelines for post discharge patient management. Specific "at risk" populations may need more prolonged post discharge interventions to decrease the risk of DVT, surgical site infections, UTI’s, and respiratory and cardiac complications which may develop after their procedures and hospitalizations. This is an area where further guidelines need to be developed for specific at risk populations and therapies. Improving patient outcomes and quality does not stop at the hospital door.
Dr. Joann M. Lohr is associate program director, Good Samaritan Hospital Vascular Surgery Program She is also an associate medical editor for Vascular Specialist.
Hospital acquired complications are well defined. Once discharged, the incidence of surgical complications in the perioperative time period is a matter of definition, and of who looks and how hard. It has been established that prolonged prevention of DVT is indicated in high risk surgical groups undergoing orthopedic procedures. This has been shown to be safe and effective however more work is needed. The exact duration of prophylaxis remains to be determined.
| Dr. Lohr |
The Caprini risk assessment tool was recently validated in patients undergoing plastic and reconstructive procedures. In this study, 50% of high-risk patients developed DVT late in the postoperative period (15-60 days postoperatively). In higher-risk patients, there was no evidence that DVT risk is limited to the immediate postoperative period. The transition from inpatient to outpatient care is a key event in the coordination of the continuity of care, but specific transition guidelines are currently limited. Work is needed to define appropriate guidelines for post discharge patient management. Specific "at risk" populations may need more prolonged post discharge interventions to decrease the risk of DVT, surgical site infections, UTI’s, and respiratory and cardiac complications which may develop after their procedures and hospitalizations. This is an area where further guidelines need to be developed for specific at risk populations and therapies. Improving patient outcomes and quality does not stop at the hospital door.
Dr. Joann M. Lohr is associate program director, Good Samaritan Hospital Vascular Surgery Program She is also an associate medical editor for Vascular Specialist.
Hospital acquired complications are well defined. Once discharged, the incidence of surgical complications in the perioperative time period is a matter of definition, and of who looks and how hard. It has been established that prolonged prevention of DVT is indicated in high risk surgical groups undergoing orthopedic procedures. This has been shown to be safe and effective however more work is needed. The exact duration of prophylaxis remains to be determined.
| Dr. Lohr |
The Caprini risk assessment tool was recently validated in patients undergoing plastic and reconstructive procedures. In this study, 50% of high-risk patients developed DVT late in the postoperative period (15-60 days postoperatively). In higher-risk patients, there was no evidence that DVT risk is limited to the immediate postoperative period. The transition from inpatient to outpatient care is a key event in the coordination of the continuity of care, but specific transition guidelines are currently limited. Work is needed to define appropriate guidelines for post discharge patient management. Specific "at risk" populations may need more prolonged post discharge interventions to decrease the risk of DVT, surgical site infections, UTI’s, and respiratory and cardiac complications which may develop after their procedures and hospitalizations. This is an area where further guidelines need to be developed for specific at risk populations and therapies. Improving patient outcomes and quality does not stop at the hospital door.
Dr. Joann M. Lohr is associate program director, Good Samaritan Hospital Vascular Surgery Program She is also an associate medical editor for Vascular Specialist.
CHICAGO – Approximately one-third of surgical complications were diagnosed after patients left the hospital, based on data from nearly 60,000 procedures performed at 112 hospitals.
Reporting postoperative complications, including surgical site infections, has become a mandatory quality reporting initiative for hospitals, and the Affordable Care Act requires reporting of readmissions, said Dr. Melanie Morris of the University of Alabama at Birmingham.
"Some postoperative complications may lead to readmissions, but this may not tell the whole story," she noted at the annual clinical congress of the American College of Surgeons.
To determine the timing of postoperative complications and the nature of readmissions, Dr. Morris and her colleagues reviewed Veterans Affairs data from the noncardiac Surgical Care Improvement Project (SCIP) cohort from 2005 to 2009 for 59,464 surgical procedures in which there was at least one complication.
Surgical cases were classified by specialty into gastrointestinal, gynecologic, orthopedic, and vascular. Complications were grouped into organ-based systems. For example, urinary complications included renal failure, renal insufficiency, and urinary tract infections; respiratory complications included failure to wean, pneumonia, and reintubation; and surgical site infections (SSIs) included both deep and superficial wounds.
The overall complication rate was approximately 15%, and 32% of complications were diagnosed after hospital discharge, Dr. Morris said. More than half (56%) of all SSIs were diagnosed after discharge, she added.
A statistically significant difference appeared in postdischarge complications by surgical specialty. The SSI rate was 5.4%, followed by respiratory complications (5.0%), urinary tract infection (4.9%), cardiac complications (3.2%), and venous thromboembolism (1.2%).
"Our GI surgical patients had the highest overall complication rate," Dr. Morris noted. Among GI patients, colectomy patients had the highest SSI rate (11%), and 23% of the GI complications were diagnosed after hospital discharge.
In addition, 78% of SSIs in orthopedic patients were diagnosed after discharge, as were 39% of SSIs in GI patients, 77% of SSIs in vascular surgery patients, and 95% of SSIs in gynecologic patients, said Dr. Morris.
There were no significant differences in length of hospital stay based on complications, Dr. Morris said.
The overall readmission rate was 11.9%, and 70% of these patients had no identifiable postoperative complication. Of those who did have an identifiable postop complication, 72% were diagnosed before discharge from the hospital.
The probability of being readmitted to the hospital over time was highest in patients with a postdischarge diagnosis of a complication. The overall length of stay was 5 days, and the average length of stay for patients with any complication was 9 days.
Patient-specific factors associated with an increased risk of readmission included a history of heart failure, renal failure, diabetes, weight loss, and smoking. Procedure-specific factors associated with an increased risk of readmission included a longer operating time, a more contaminated wound, and a higher ASA (American Society of Anesthesiologists) class.
Length of stay was slightly protective for readmission, and the presence of any complication was associated with a high risk of readmission.
"It’s very important that patients are accurately educated on the signs and symptoms of complications so they know to seek timely care after discharge," said Dr. Morris.
"Postoperative complications must be measured beyond hospital discharge to capture the whole story.
"Systematic collection of postoperative complications must include postdischarge data as well as readmissions to accurately measure quality," she said.
Dr. Morris said she had no relevant financial disclosures.
CHICAGO – Approximately one-third of surgical complications were diagnosed after patients left the hospital, based on data from nearly 60,000 procedures performed at 112 hospitals.
Reporting postoperative complications, including surgical site infections, has become a mandatory quality reporting initiative for hospitals, and the Affordable Care Act requires reporting of readmissions, said Dr. Melanie Morris of the University of Alabama at Birmingham.
"Some postoperative complications may lead to readmissions, but this may not tell the whole story," she noted at the annual clinical congress of the American College of Surgeons.
To determine the timing of postoperative complications and the nature of readmissions, Dr. Morris and her colleagues reviewed Veterans Affairs data from the noncardiac Surgical Care Improvement Project (SCIP) cohort from 2005 to 2009 for 59,464 surgical procedures in which there was at least one complication.
Surgical cases were classified by specialty into gastrointestinal, gynecologic, orthopedic, and vascular. Complications were grouped into organ-based systems. For example, urinary complications included renal failure, renal insufficiency, and urinary tract infections; respiratory complications included failure to wean, pneumonia, and reintubation; and surgical site infections (SSIs) included both deep and superficial wounds.
The overall complication rate was approximately 15%, and 32% of complications were diagnosed after hospital discharge, Dr. Morris said. More than half (56%) of all SSIs were diagnosed after discharge, she added.
A statistically significant difference appeared in postdischarge complications by surgical specialty. The SSI rate was 5.4%, followed by respiratory complications (5.0%), urinary tract infection (4.9%), cardiac complications (3.2%), and venous thromboembolism (1.2%).
"Our GI surgical patients had the highest overall complication rate," Dr. Morris noted. Among GI patients, colectomy patients had the highest SSI rate (11%), and 23% of the GI complications were diagnosed after hospital discharge.
In addition, 78% of SSIs in orthopedic patients were diagnosed after discharge, as were 39% of SSIs in GI patients, 77% of SSIs in vascular surgery patients, and 95% of SSIs in gynecologic patients, said Dr. Morris.
There were no significant differences in length of hospital stay based on complications, Dr. Morris said.
The overall readmission rate was 11.9%, and 70% of these patients had no identifiable postoperative complication. Of those who did have an identifiable postop complication, 72% were diagnosed before discharge from the hospital.
The probability of being readmitted to the hospital over time was highest in patients with a postdischarge diagnosis of a complication. The overall length of stay was 5 days, and the average length of stay for patients with any complication was 9 days.
Patient-specific factors associated with an increased risk of readmission included a history of heart failure, renal failure, diabetes, weight loss, and smoking. Procedure-specific factors associated with an increased risk of readmission included a longer operating time, a more contaminated wound, and a higher ASA (American Society of Anesthesiologists) class.
Length of stay was slightly protective for readmission, and the presence of any complication was associated with a high risk of readmission.
"It’s very important that patients are accurately educated on the signs and symptoms of complications so they know to seek timely care after discharge," said Dr. Morris.
"Postoperative complications must be measured beyond hospital discharge to capture the whole story.
"Systematic collection of postoperative complications must include postdischarge data as well as readmissions to accurately measure quality," she said.
Dr. Morris said she had no relevant financial disclosures.
Major Finding: Approximately 32% of surgical complications, including 56% of surgical site infections, were diagnosed after patients were discharged from the hospital.
Data Source: The data come from a review of 59,464 surgical procedures performed at 112 VA hospitals.
Disclosures: Dr. Morris said she had no relevant financial disclosures.

Does an Active Childhood Build Strong Knees?
WASHINGTON – Active children may have stronger knees as adults, based on data from a long-term follow-up study of approximately 300 children. The findings were presented at the annual meeting of the American College of Rheumatology.
Although physical activity is recommended for children to improve joint health and function, the correlation between childhood exercise and adult bone structure has not been well studied, said Dr. Graeme Jones, who is professor of rheumatology and epidemiology and head of the musculoskeletal unit at the Menzies Research Institute as well as head of the department of rheumatology at Royal Hobart Hospital, both in Hobart, Australia.

Data from previous studies have shown that children who engaged in vigorous activity in childhood had greater cartilage deposition in their knees compared with less active children, said Dr. Jones.
"The idea would be that if you develop more cartilage in childhood and it lasts until adult life, you can prevent the development of osteoarthritis," he said.
In 1985, data were collected on 8,500 Australian children in the population-based Childhood Determinants of Adult Health study. In that study, researchers measured the children’s fitness based on measures of hand strength, leg strength, run times, sit-ups, and physical work capacity at 170 beats per minute (PWC170).
To measure the long-term impact of exercise on knee structure, Dr. Jones and his colleagues reviewed data from 298 study participants at ages 31-41 years. Approximately half of the participants were female.
The researchers assessed tibial bone area (the size of the knee joint) and the amount of cartilage using T1-weighted fat-suppressed magnetic resonance imaging.
All measures of childhood physical activity levels were significantly associated with increased tibial bone area. These associations included 0.48 cm2 per 100 mW (a measure of work) for PWC170, 1.49 cm2 per 100 g of hand muscle strength, 0.29 cm2 per 100 g of leg muscle strength, and 0.28 cm2 per 10 sit-ups.
In addition, childhood PWC170 was significantly associated with an increased medial tibial cartilage volume in adulthood (0.1 mm3 per 100 mW). This association was approximately 33% weaker, though still significant, after adjusting for tibial bone area, Dr. Jones said. Hand muscle strength and sit-ups were significantly associated with increased medial tibial cartilage volume before adjusting for bone area, but the association became nonsignificant after adjusting for bone area.
"What this suggests to us is that the response to physical activity in childhood is to increase the size of the bone to adjust for this and to spread the load out, and the cartilage will then expand to cover the bone area or the area of contact," said Dr. Jones.
These associations were independent of fitness performance measures and medial tibial cartilage volume in adulthood, he added.
The findings suggest that childhood exposure to physical activity has a long-term protective effect on knee joint health. Therefore, "we need to get children as active as we can," he said.
The study was funded by the National Health and Medical Research Council of Australia. Dr. Jones had no financial conflicts to disclose.
WASHINGTON – Active children may have stronger knees as adults, based on data from a long-term follow-up study of approximately 300 children. The findings were presented at the annual meeting of the American College of Rheumatology.
Although physical activity is recommended for children to improve joint health and function, the correlation between childhood exercise and adult bone structure has not been well studied, said Dr. Graeme Jones, who is professor of rheumatology and epidemiology and head of the musculoskeletal unit at the Menzies Research Institute as well as head of the department of rheumatology at Royal Hobart Hospital, both in Hobart, Australia.
Data from previous studies have shown that children who engaged in vigorous activity in childhood had greater cartilage deposition in their knees compared with less active children, said Dr. Jones.
"The idea would be that if you develop more cartilage in childhood and it lasts until adult life, you can prevent the development of osteoarthritis," he said.
In 1985, data were collected on 8,500 Australian children in the population-based Childhood Determinants of Adult Health study. In that study, researchers measured the children’s fitness based on measures of hand strength, leg strength, run times, sit-ups, and physical work capacity at 170 beats per minute (PWC170).
To measure the long-term impact of exercise on knee structure, Dr. Jones and his colleagues reviewed data from 298 study participants at ages 31-41 years. Approximately half of the participants were female.
The researchers assessed tibial bone area (the size of the knee joint) and the amount of cartilage using T1-weighted fat-suppressed magnetic resonance imaging.
All measures of childhood physical activity levels were significantly associated with increased tibial bone area. These associations included 0.48 cm2 per 100 mW (a measure of work) for PWC170, 1.49 cm2 per 100 g of hand muscle strength, 0.29 cm2 per 100 g of leg muscle strength, and 0.28 cm2 per 10 sit-ups.
In addition, childhood PWC170 was significantly associated with an increased medial tibial cartilage volume in adulthood (0.1 mm3 per 100 mW). This association was approximately 33% weaker, though still significant, after adjusting for tibial bone area, Dr. Jones said. Hand muscle strength and sit-ups were significantly associated with increased medial tibial cartilage volume before adjusting for bone area, but the association became nonsignificant after adjusting for bone area.
"What this suggests to us is that the response to physical activity in childhood is to increase the size of the bone to adjust for this and to spread the load out, and the cartilage will then expand to cover the bone area or the area of contact," said Dr. Jones.
These associations were independent of fitness performance measures and medial tibial cartilage volume in adulthood, he added.
The findings suggest that childhood exposure to physical activity has a long-term protective effect on knee joint health. Therefore, "we need to get children as active as we can," he said.
The study was funded by the National Health and Medical Research Council of Australia. Dr. Jones had no financial conflicts to disclose.
WASHINGTON – Active children may have stronger knees as adults, based on data from a long-term follow-up study of approximately 300 children. The findings were presented at the annual meeting of the American College of Rheumatology.
Although physical activity is recommended for children to improve joint health and function, the correlation between childhood exercise and adult bone structure has not been well studied, said Dr. Graeme Jones, who is professor of rheumatology and epidemiology and head of the musculoskeletal unit at the Menzies Research Institute as well as head of the department of rheumatology at Royal Hobart Hospital, both in Hobart, Australia.
Data from previous studies have shown that children who engaged in vigorous activity in childhood had greater cartilage deposition in their knees compared with less active children, said Dr. Jones.
"The idea would be that if you develop more cartilage in childhood and it lasts until adult life, you can prevent the development of osteoarthritis," he said.
In 1985, data were collected on 8,500 Australian children in the population-based Childhood Determinants of Adult Health study. In that study, researchers measured the children’s fitness based on measures of hand strength, leg strength, run times, sit-ups, and physical work capacity at 170 beats per minute (PWC170).
To measure the long-term impact of exercise on knee structure, Dr. Jones and his colleagues reviewed data from 298 study participants at ages 31-41 years. Approximately half of the participants were female.
The researchers assessed tibial bone area (the size of the knee joint) and the amount of cartilage using T1-weighted fat-suppressed magnetic resonance imaging.
All measures of childhood physical activity levels were significantly associated with increased tibial bone area. These associations included 0.48 cm2 per 100 mW (a measure of work) for PWC170, 1.49 cm2 per 100 g of hand muscle strength, 0.29 cm2 per 100 g of leg muscle strength, and 0.28 cm2 per 10 sit-ups.
In addition, childhood PWC170 was significantly associated with an increased medial tibial cartilage volume in adulthood (0.1 mm3 per 100 mW). This association was approximately 33% weaker, though still significant, after adjusting for tibial bone area, Dr. Jones said. Hand muscle strength and sit-ups were significantly associated with increased medial tibial cartilage volume before adjusting for bone area, but the association became nonsignificant after adjusting for bone area.
"What this suggests to us is that the response to physical activity in childhood is to increase the size of the bone to adjust for this and to spread the load out, and the cartilage will then expand to cover the bone area or the area of contact," said Dr. Jones.
These associations were independent of fitness performance measures and medial tibial cartilage volume in adulthood, he added.
The findings suggest that childhood exposure to physical activity has a long-term protective effect on knee joint health. Therefore, "we need to get children as active as we can," he said.
The study was funded by the National Health and Medical Research Council of Australia. Dr. Jones had no financial conflicts to disclose.
AT THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF RHEUMATOLOGY
Major Finding: Childhood physical activity was significantly associated with increased tibial bone area in early adulthood, including an improvement of 0.29 cm2 per 100 g as a measure of leg muscle strength.
Data Source: The data come from 298 participants in the Childhood Determinants of Adult Health study.
Disclosures: The study was funded by the National Health and Medical Research Council of Australia. Dr. Jones had no financial conflicts to disclose.

Depressed RA patients more likely to die, especially men
WASHINGTON – Men with rheumatoid arthritis who have depression or depressive symptoms were significantly more likely to die compared with RA patients who were not depressed, according to data from a longitudinal cohort study of 530 patients. The findings were presented at the annual meeting of the American College of Rheumatology.
The deleterious effect of depression on early mortality also was seen in women with RA, but to a lesser extent.
"Depression is often underdiagnosed in RA," but the risk of mortality associated with depression in RA has not been well studied, said Patricia Katz, Ph.D., of the University of California, San Francisco.
Dr. Katz and colleagues conducted annual telephone surveys of 530 adults with RA over a 7-year period, with an average of 5 years’ follow-up. The average age of the patients was 60 years, 84% were women, the average disease duration was 19 years, and 46% reported at least one cardiovascular risk factor. Depression was defined as a score of 5 or higher on the 15-item Geriatric Depression Scale (GDS).
"Even though depression is very common in RA, it is not normal."
A total of 63 patients (12%) died during the study period. The risk of death in depressed men and women with RA was approximately three times that of RA patients who were not depressed (hazard ratio 3.5), according to the results of a bivariate analysis.
"People who were depressed at their last interview were more likely to die," Dr. Katz said. In a multivariate analysis, depression remained a significant predictor of mortality.
In particular, men with RA who met criteria for depression had the highest risk of mortality.
"Overall, men were two and half times more likely to die than women," Dr. Katz said, but men with depression had a risk that was six times higher than women with no depression (who served as a reference group), she added. Women with depression had a risk of death of two and half times that of women with no depression.
In addition, a change in depressive symptoms that did not meet the criteria for depression (defined as a worsening of GDS scores by at least 2 points) was associated with an approximately twofold increased risk of death in depressed women compared to women with no depression. Men with an increase in depressive symptom scores had an increase in risk five times that of women with no depression.
"Both depression and an increase in depressive symptoms are significant risk factors for all-cause mortality in RA," Dr. Katz noted.
"I think it is important to recognize that depression is a treatable condition," said Dr. Katz. "Even though depression is very common in RA, it is not normal. It needs to be treated, and to be treated it needs to be recognized," she said.
"This is the clinical challenge; there needs to be some sort of regular monitoring to recognize these changes early, so intervention can happen at an appropriate time," she added.
The study was funded in part by the National Institute for Arthritis, Musculoskeletal, and Skin Diseases of the National Institutes of Health. Dr. Katz had no financial conflicts to disclose.
WASHINGTON – Men with rheumatoid arthritis who have depression or depressive symptoms were significantly more likely to die compared with RA patients who were not depressed, according to data from a longitudinal cohort study of 530 patients. The findings were presented at the annual meeting of the American College of Rheumatology.
The deleterious effect of depression on early mortality also was seen in women with RA, but to a lesser extent.
"Depression is often underdiagnosed in RA," but the risk of mortality associated with depression in RA has not been well studied, said Patricia Katz, Ph.D., of the University of California, San Francisco.
Dr. Katz and colleagues conducted annual telephone surveys of 530 adults with RA over a 7-year period, with an average of 5 years’ follow-up. The average age of the patients was 60 years, 84% were women, the average disease duration was 19 years, and 46% reported at least one cardiovascular risk factor. Depression was defined as a score of 5 or higher on the 15-item Geriatric Depression Scale (GDS).
"Even though depression is very common in RA, it is not normal."
A total of 63 patients (12%) died during the study period. The risk of death in depressed men and women with RA was approximately three times that of RA patients who were not depressed (hazard ratio 3.5), according to the results of a bivariate analysis.
"People who were depressed at their last interview were more likely to die," Dr. Katz said. In a multivariate analysis, depression remained a significant predictor of mortality.
In particular, men with RA who met criteria for depression had the highest risk of mortality.
"Overall, men were two and half times more likely to die than women," Dr. Katz said, but men with depression had a risk that was six times higher than women with no depression (who served as a reference group), she added. Women with depression had a risk of death of two and half times that of women with no depression.
In addition, a change in depressive symptoms that did not meet the criteria for depression (defined as a worsening of GDS scores by at least 2 points) was associated with an approximately twofold increased risk of death in depressed women compared to women with no depression. Men with an increase in depressive symptom scores had an increase in risk five times that of women with no depression.
"Both depression and an increase in depressive symptoms are significant risk factors for all-cause mortality in RA," Dr. Katz noted.
"I think it is important to recognize that depression is a treatable condition," said Dr. Katz. "Even though depression is very common in RA, it is not normal. It needs to be treated, and to be treated it needs to be recognized," she said.
"This is the clinical challenge; there needs to be some sort of regular monitoring to recognize these changes early, so intervention can happen at an appropriate time," she added.
The study was funded in part by the National Institute for Arthritis, Musculoskeletal, and Skin Diseases of the National Institutes of Health. Dr. Katz had no financial conflicts to disclose.
WASHINGTON – Men with rheumatoid arthritis who have depression or depressive symptoms were significantly more likely to die compared with RA patients who were not depressed, according to data from a longitudinal cohort study of 530 patients. The findings were presented at the annual meeting of the American College of Rheumatology.
The deleterious effect of depression on early mortality also was seen in women with RA, but to a lesser extent.
"Depression is often underdiagnosed in RA," but the risk of mortality associated with depression in RA has not been well studied, said Patricia Katz, Ph.D., of the University of California, San Francisco.
Dr. Katz and colleagues conducted annual telephone surveys of 530 adults with RA over a 7-year period, with an average of 5 years’ follow-up. The average age of the patients was 60 years, 84% were women, the average disease duration was 19 years, and 46% reported at least one cardiovascular risk factor. Depression was defined as a score of 5 or higher on the 15-item Geriatric Depression Scale (GDS).
"Even though depression is very common in RA, it is not normal."
A total of 63 patients (12%) died during the study period. The risk of death in depressed men and women with RA was approximately three times that of RA patients who were not depressed (hazard ratio 3.5), according to the results of a bivariate analysis.
"People who were depressed at their last interview were more likely to die," Dr. Katz said. In a multivariate analysis, depression remained a significant predictor of mortality.
In particular, men with RA who met criteria for depression had the highest risk of mortality.
"Overall, men were two and half times more likely to die than women," Dr. Katz said, but men with depression had a risk that was six times higher than women with no depression (who served as a reference group), she added. Women with depression had a risk of death of two and half times that of women with no depression.
In addition, a change in depressive symptoms that did not meet the criteria for depression (defined as a worsening of GDS scores by at least 2 points) was associated with an approximately twofold increased risk of death in depressed women compared to women with no depression. Men with an increase in depressive symptom scores had an increase in risk five times that of women with no depression.
"Both depression and an increase in depressive symptoms are significant risk factors for all-cause mortality in RA," Dr. Katz noted.
"I think it is important to recognize that depression is a treatable condition," said Dr. Katz. "Even though depression is very common in RA, it is not normal. It needs to be treated, and to be treated it needs to be recognized," she said.
"This is the clinical challenge; there needs to be some sort of regular monitoring to recognize these changes early, so intervention can happen at an appropriate time," she added.
The study was funded in part by the National Institute for Arthritis, Musculoskeletal, and Skin Diseases of the National Institutes of Health. Dr. Katz had no financial conflicts to disclose.
AT THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF RHEUMATOLOGY
Major Finding: Depression was associated with an approximately threefold increase in mortality among rheumatoid arthritis patients.
Data Source: The data come from a longitudinal cohort study of 530 adults in California.
Disclosures: The study was funded in part by the National Institute for Arthritis, Musculoskeletal, and Skin Diseases of the National Institutes of Health. Dr. Katz had no financial conflicts to disclose.