User login
FDA panel supports injectable midface filler
GAITHERSBURG, MD. – A Food and Drug Administration advisory panel unanimously recommended approval of an injectable filler specifically for use in the midface.
At a May 2 meeting, the members of the FDA’s General and Plastic Surgery Devices Panel supported approval of Allergan’s Juvéderm Voluma XC (Voluma) for the correction of age-related volume loss in the midface. The FDA usually follows the recommendations of its advisory panels, which are not binding.
The meeting was held for the panel to discuss, make recommendations, and vote on information related to the premarket approval application for Voluma. Voluma is a biodegradable dermal filler that combines low- and high-molecular-weight hyaluronic acid (20 mg/mL) and 0.3% lidocaine in phosphate-buffered saline.
This new formulation distinguishes Voluma from other injectable products, noted Joseph Nielsen, Ph.D., a biologist with the FDA’s Center for Drug Evaluation and Research.
Voluma’s combination of high- and low-molecular-weight hyaluronic acid creates a thicker product with a jamlike consistency that is designed for deeper injections, said Dr. Rui Avelar, chief medical officer for Allergan. Voluma is indicated specifically for deep injections (subcutaneous and/or supraperiosteal) to correct age-related volume loss in the midface. No products are currently approved in the United States for this indication, although Voluma is approved in 65 countries, including Canada and Australia.
The approval was based on data from a randomized clinical trial. The study population included adults aged 35-65 years (mean age, 55 years). Approximately 80% of the patients were women, more than half were white, and 44% were Fitzpatrick skin types IV, V, and VI. A total of 235 patients were randomized to immediate treatment with Voluma, and 47 served as nontreatment controls to receive injections 6 months later; 208 treatment patients and 36 nontreatment controls had complete data for evaluation at 6 months.
Primary effectiveness was based on the blinded live evaluation of two investigators using the Mid-Face Volume Deficit Scale (MFVDS), a 0-5 point scale approved and validated for the study. Significant response was defined as at least a 1-point change in the MFVDS. In addition, three-dimensional imaging was used to assess changes in volume. Imaging data were not collected from nonresponders.
At 6 months, 86% of the treatment patients and 35% of the untreated controls met the response criteria. In addition, the evaluators rated 82% of treatment patients and 22% of controls as "improved" or "much improved," compared with pretreatment photos using the Global Aesthetic Improvement Scale, and 93% of treated patients rated themselves as improved or much improved, compared with pretreatment photos.
The average initial treatment was 5.2 mL, and 82% of treated patients received an optional touch-up injection of an average of 2 mL 30 days after the first treatment. The injection techniques were consistent with the methods used for other currently available fillers.
Individuals were excluded from the study if they had permanent or semipermanent facial aesthetic procedures, temporary facial aesthetic procedures within the washout period, midface volume loss unrelated to age, or very thin skin in the midface.
Greater baseline volume deficit was a stronger predictor than age of the volume of filler injected, although both factors were associated with a greater volume injected, said Todd Gross, Ph.D., a biostatistician for Allergan.
However, age, volume of product injected, and tunneling technique were associated with an increased risk of adverse events, said Dr. Janette Alexander, an FDA medical officer.
A total of 33% of the participants reported treatment-related adverse events. Five patients had late-onset adverse events; three of these were deemed severe and device related. The three severe treatment-related events involved lumps at the injection sites, all of which were treated with hyaluronidase, Dr. Alexander said.
The other two serious events included a death caused by stroke 1 year after treatment, and an ischemic optic neuropathy that the FDA could not definitely deem device related.
Approximately 78% of subjects reported an injection site response, but the majority of these resolved within 30 days. Injection site responses included firmness, lumps or bumps, tenderness, swelling, pain, bruising, redness, and discoloration. Approximately 20% of treated patients reported firmness or lumps/bumps persisting longer than 30 days.
The safety profile appears similar to that of other hyaluronic acid fillers except for the duration of firmness and lumps/bumps, and the occurrence of late adverse events, Dr. Alexander said.
No increase in risk of adverse events was observed in darker skin types, said Alvin Van Orden, of the FDA’s division of biostatistics.
The panel agreed that the postapproval study of 12 months’ follow-up proposed by Allergan is adequate, but extra attention should be paid to the subset of patients with darker skin, who might respond differently to the treatment, said panel chair Dr. Joseph LoCicero III, of the State University of New York, Brooklyn.
The panelists’ comments in support of their votes included acknowledgment of the safety profile and the reversibility of the product if needed, and the benefits of having an FDA-approved product for volume enhancement.
During their discussion, the panel members also agreed that setting upper limits on filler volume, age, and relative skin thickness should be left to clinical judgment, and not contraindicated.
Members of FDA advisory panels have been cleared of potential conflicts of interest related to the products under discussion prior to the meeting.
GAITHERSBURG, MD. – A Food and Drug Administration advisory panel unanimously recommended approval of an injectable filler specifically for use in the midface.
At a May 2 meeting, the members of the FDA’s General and Plastic Surgery Devices Panel supported approval of Allergan’s Juvéderm Voluma XC (Voluma) for the correction of age-related volume loss in the midface. The FDA usually follows the recommendations of its advisory panels, which are not binding.
The meeting was held for the panel to discuss, make recommendations, and vote on information related to the premarket approval application for Voluma. Voluma is a biodegradable dermal filler that combines low- and high-molecular-weight hyaluronic acid (20 mg/mL) and 0.3% lidocaine in phosphate-buffered saline.
This new formulation distinguishes Voluma from other injectable products, noted Joseph Nielsen, Ph.D., a biologist with the FDA’s Center for Drug Evaluation and Research.
Voluma’s combination of high- and low-molecular-weight hyaluronic acid creates a thicker product with a jamlike consistency that is designed for deeper injections, said Dr. Rui Avelar, chief medical officer for Allergan. Voluma is indicated specifically for deep injections (subcutaneous and/or supraperiosteal) to correct age-related volume loss in the midface. No products are currently approved in the United States for this indication, although Voluma is approved in 65 countries, including Canada and Australia.
The approval was based on data from a randomized clinical trial. The study population included adults aged 35-65 years (mean age, 55 years). Approximately 80% of the patients were women, more than half were white, and 44% were Fitzpatrick skin types IV, V, and VI. A total of 235 patients were randomized to immediate treatment with Voluma, and 47 served as nontreatment controls to receive injections 6 months later; 208 treatment patients and 36 nontreatment controls had complete data for evaluation at 6 months.
Primary effectiveness was based on the blinded live evaluation of two investigators using the Mid-Face Volume Deficit Scale (MFVDS), a 0-5 point scale approved and validated for the study. Significant response was defined as at least a 1-point change in the MFVDS. In addition, three-dimensional imaging was used to assess changes in volume. Imaging data were not collected from nonresponders.
At 6 months, 86% of the treatment patients and 35% of the untreated controls met the response criteria. In addition, the evaluators rated 82% of treatment patients and 22% of controls as "improved" or "much improved," compared with pretreatment photos using the Global Aesthetic Improvement Scale, and 93% of treated patients rated themselves as improved or much improved, compared with pretreatment photos.
The average initial treatment was 5.2 mL, and 82% of treated patients received an optional touch-up injection of an average of 2 mL 30 days after the first treatment. The injection techniques were consistent with the methods used for other currently available fillers.
Individuals were excluded from the study if they had permanent or semipermanent facial aesthetic procedures, temporary facial aesthetic procedures within the washout period, midface volume loss unrelated to age, or very thin skin in the midface.
Greater baseline volume deficit was a stronger predictor than age of the volume of filler injected, although both factors were associated with a greater volume injected, said Todd Gross, Ph.D., a biostatistician for Allergan.
However, age, volume of product injected, and tunneling technique were associated with an increased risk of adverse events, said Dr. Janette Alexander, an FDA medical officer.
A total of 33% of the participants reported treatment-related adverse events. Five patients had late-onset adverse events; three of these were deemed severe and device related. The three severe treatment-related events involved lumps at the injection sites, all of which were treated with hyaluronidase, Dr. Alexander said.
The other two serious events included a death caused by stroke 1 year after treatment, and an ischemic optic neuropathy that the FDA could not definitely deem device related.
Approximately 78% of subjects reported an injection site response, but the majority of these resolved within 30 days. Injection site responses included firmness, lumps or bumps, tenderness, swelling, pain, bruising, redness, and discoloration. Approximately 20% of treated patients reported firmness or lumps/bumps persisting longer than 30 days.
The safety profile appears similar to that of other hyaluronic acid fillers except for the duration of firmness and lumps/bumps, and the occurrence of late adverse events, Dr. Alexander said.
No increase in risk of adverse events was observed in darker skin types, said Alvin Van Orden, of the FDA’s division of biostatistics.
The panel agreed that the postapproval study of 12 months’ follow-up proposed by Allergan is adequate, but extra attention should be paid to the subset of patients with darker skin, who might respond differently to the treatment, said panel chair Dr. Joseph LoCicero III, of the State University of New York, Brooklyn.
The panelists’ comments in support of their votes included acknowledgment of the safety profile and the reversibility of the product if needed, and the benefits of having an FDA-approved product for volume enhancement.
During their discussion, the panel members also agreed that setting upper limits on filler volume, age, and relative skin thickness should be left to clinical judgment, and not contraindicated.
Members of FDA advisory panels have been cleared of potential conflicts of interest related to the products under discussion prior to the meeting.
GAITHERSBURG, MD. – A Food and Drug Administration advisory panel unanimously recommended approval of an injectable filler specifically for use in the midface.
At a May 2 meeting, the members of the FDA’s General and Plastic Surgery Devices Panel supported approval of Allergan’s Juvéderm Voluma XC (Voluma) for the correction of age-related volume loss in the midface. The FDA usually follows the recommendations of its advisory panels, which are not binding.
The meeting was held for the panel to discuss, make recommendations, and vote on information related to the premarket approval application for Voluma. Voluma is a biodegradable dermal filler that combines low- and high-molecular-weight hyaluronic acid (20 mg/mL) and 0.3% lidocaine in phosphate-buffered saline.
This new formulation distinguishes Voluma from other injectable products, noted Joseph Nielsen, Ph.D., a biologist with the FDA’s Center for Drug Evaluation and Research.
Voluma’s combination of high- and low-molecular-weight hyaluronic acid creates a thicker product with a jamlike consistency that is designed for deeper injections, said Dr. Rui Avelar, chief medical officer for Allergan. Voluma is indicated specifically for deep injections (subcutaneous and/or supraperiosteal) to correct age-related volume loss in the midface. No products are currently approved in the United States for this indication, although Voluma is approved in 65 countries, including Canada and Australia.
The approval was based on data from a randomized clinical trial. The study population included adults aged 35-65 years (mean age, 55 years). Approximately 80% of the patients were women, more than half were white, and 44% were Fitzpatrick skin types IV, V, and VI. A total of 235 patients were randomized to immediate treatment with Voluma, and 47 served as nontreatment controls to receive injections 6 months later; 208 treatment patients and 36 nontreatment controls had complete data for evaluation at 6 months.
Primary effectiveness was based on the blinded live evaluation of two investigators using the Mid-Face Volume Deficit Scale (MFVDS), a 0-5 point scale approved and validated for the study. Significant response was defined as at least a 1-point change in the MFVDS. In addition, three-dimensional imaging was used to assess changes in volume. Imaging data were not collected from nonresponders.
At 6 months, 86% of the treatment patients and 35% of the untreated controls met the response criteria. In addition, the evaluators rated 82% of treatment patients and 22% of controls as "improved" or "much improved," compared with pretreatment photos using the Global Aesthetic Improvement Scale, and 93% of treated patients rated themselves as improved or much improved, compared with pretreatment photos.
The average initial treatment was 5.2 mL, and 82% of treated patients received an optional touch-up injection of an average of 2 mL 30 days after the first treatment. The injection techniques were consistent with the methods used for other currently available fillers.
Individuals were excluded from the study if they had permanent or semipermanent facial aesthetic procedures, temporary facial aesthetic procedures within the washout period, midface volume loss unrelated to age, or very thin skin in the midface.
Greater baseline volume deficit was a stronger predictor than age of the volume of filler injected, although both factors were associated with a greater volume injected, said Todd Gross, Ph.D., a biostatistician for Allergan.
However, age, volume of product injected, and tunneling technique were associated with an increased risk of adverse events, said Dr. Janette Alexander, an FDA medical officer.
A total of 33% of the participants reported treatment-related adverse events. Five patients had late-onset adverse events; three of these were deemed severe and device related. The three severe treatment-related events involved lumps at the injection sites, all of which were treated with hyaluronidase, Dr. Alexander said.
The other two serious events included a death caused by stroke 1 year after treatment, and an ischemic optic neuropathy that the FDA could not definitely deem device related.
Approximately 78% of subjects reported an injection site response, but the majority of these resolved within 30 days. Injection site responses included firmness, lumps or bumps, tenderness, swelling, pain, bruising, redness, and discoloration. Approximately 20% of treated patients reported firmness or lumps/bumps persisting longer than 30 days.
The safety profile appears similar to that of other hyaluronic acid fillers except for the duration of firmness and lumps/bumps, and the occurrence of late adverse events, Dr. Alexander said.
No increase in risk of adverse events was observed in darker skin types, said Alvin Van Orden, of the FDA’s division of biostatistics.
The panel agreed that the postapproval study of 12 months’ follow-up proposed by Allergan is adequate, but extra attention should be paid to the subset of patients with darker skin, who might respond differently to the treatment, said panel chair Dr. Joseph LoCicero III, of the State University of New York, Brooklyn.
The panelists’ comments in support of their votes included acknowledgment of the safety profile and the reversibility of the product if needed, and the benefits of having an FDA-approved product for volume enhancement.
During their discussion, the panel members also agreed that setting upper limits on filler volume, age, and relative skin thickness should be left to clinical judgment, and not contraindicated.
Members of FDA advisory panels have been cleared of potential conflicts of interest related to the products under discussion prior to the meeting.
AT AN FDA ADVISORY COMMITTEE MEETING
Don't miss these emerging hair diseases
WASHINGTON – Potentially puzzling hair diseases might be one of three emerging types of alopecia: psoriatic, frontal fibrosing, and permanent chemotherapy induced, according to Dr. Leonard Sperling.
"You have a good chance of seeing these in the coming year," he said.
Psoriatic alopecia claims features of both cicatricial and noncicatricial alopecia, said Dr. Sperling of the Uniformed Services University of the Health Sciences, Bethesda, Md. "It is a histological mimic of alopecia areata," he noted.
However, sebaceous gland atrophy is evident on histology and is a dependable diagnostic feature. "That’s what sets this disease apart," Dr. Sperling said.
A clinical differential diagnosis of psoriatic alopecia may include tinea capitis, chronic cutaneous systemic lupus erythematosus, seborrheic dermatitis, syphilitic alopecia, and psoriasis plus alopecia areata, he said.
Psoriatic alopecia is not new; a case was reported in 1972 (Br. J. Dermatol. 1972;87:73-7).
Clinical studies of treatment outcomes are limited, but one review of data from 47 cases of psoriatic alopecia showed that most patients had complete hair regrowth, although five patients developed residual scarring, Dr. Sperling noted (Dermatology 1992;185:82-7).
"The prognosis for hair regrowth seems to be favorable, but we have more to learn about this condition," he said.
Another emerging hair disease, psoriatic alopecialike reaction to tumor necrosis factor–inhibitor therapy is becoming increasingly common, Dr. Sperling said.
"If you haven’t seen this yet, I predict that you will, as the biologics are more utilized," he said. All the TNF-alpha inhibitors have been associated with this.
It is psoriasis from hell.
"The follicular findings resemble those seen in alopecia areata, in that there is a lot of hair miniaturization" and inflammation, Dr. Sperling said. Numerous different plasma cells and eosinophils are evident on histology, which would be unusual in alopecia areata, he noted. Atrophy of the sebaceous glands also is evident. Recognizing the role of the underlying drug is important to make the diagnosis, he added.
The reason for the atrophy of the sebaceous glands in these cases, as in patients with psoriatic alopecia, remains unknown, Dr. Sperling said.
Frontal fibrosing alopecia is becoming more common, "It’s like an epidemic," said Dr. Sperling. It is becoming more common, especially in the black community, although it was historically described in postmenopausal white women, he said. Frontal fibrosing alopecia can be mistaken for traction alopecia in black women in particular, he noted. However, it can be distinguished from traction alopecia by the loss of eyebrow hair, which might be a clue to consider a biopsy. "The histology is what you would expect in lichen planopilaris," he noted.
Fibrosing alopecia in a pattern distribution is another condition that might be mistaken for lichen planopilaris, Dr. Sperling said. The pattern of hair loss resembles common balding, "but there is inflammation in the zone of thinning," he said. If a biopsy also shows lichenoid changes and obliteration of follicles, consider a diagnosis of fibrosing alopecia in a pattern distribution. "A lot of the inflammation is concentrated around miniaturized hair follicles," he said, but terminal hair follicles are involved as well.
Permanent chemotherapy-induced alopecia occurs in some chemotherapy patients.
"A sizable number of chemotherapy patients develop some type of permanent hair loss after treatment," Dr. Sperling said. Data from biopsies have shown areas of permanent hair loss, but also telogenlike structures, with a curious, amoeboid shape, he said. However, similar structures have been identified in patients with linear morphea, suggesting that these features are not uniquely characteristic of postchemotherapy permanent alopecia, he said.
Instead, they seem to be some sort of end-stage marker for a follicle that isn’t going to grow back, he said.
Dr. Sperling said he had no relevant financial conflicts.
On Twitter @hsplete
WASHINGTON – Potentially puzzling hair diseases might be one of three emerging types of alopecia: psoriatic, frontal fibrosing, and permanent chemotherapy induced, according to Dr. Leonard Sperling.
"You have a good chance of seeing these in the coming year," he said.
Psoriatic alopecia claims features of both cicatricial and noncicatricial alopecia, said Dr. Sperling of the Uniformed Services University of the Health Sciences, Bethesda, Md. "It is a histological mimic of alopecia areata," he noted.
However, sebaceous gland atrophy is evident on histology and is a dependable diagnostic feature. "That’s what sets this disease apart," Dr. Sperling said.
A clinical differential diagnosis of psoriatic alopecia may include tinea capitis, chronic cutaneous systemic lupus erythematosus, seborrheic dermatitis, syphilitic alopecia, and psoriasis plus alopecia areata, he said.
Psoriatic alopecia is not new; a case was reported in 1972 (Br. J. Dermatol. 1972;87:73-7).
Clinical studies of treatment outcomes are limited, but one review of data from 47 cases of psoriatic alopecia showed that most patients had complete hair regrowth, although five patients developed residual scarring, Dr. Sperling noted (Dermatology 1992;185:82-7).
"The prognosis for hair regrowth seems to be favorable, but we have more to learn about this condition," he said.
Another emerging hair disease, psoriatic alopecialike reaction to tumor necrosis factor–inhibitor therapy is becoming increasingly common, Dr. Sperling said.
"If you haven’t seen this yet, I predict that you will, as the biologics are more utilized," he said. All the TNF-alpha inhibitors have been associated with this.
It is psoriasis from hell.
"The follicular findings resemble those seen in alopecia areata, in that there is a lot of hair miniaturization" and inflammation, Dr. Sperling said. Numerous different plasma cells and eosinophils are evident on histology, which would be unusual in alopecia areata, he noted. Atrophy of the sebaceous glands also is evident. Recognizing the role of the underlying drug is important to make the diagnosis, he added.
The reason for the atrophy of the sebaceous glands in these cases, as in patients with psoriatic alopecia, remains unknown, Dr. Sperling said.
Frontal fibrosing alopecia is becoming more common, "It’s like an epidemic," said Dr. Sperling. It is becoming more common, especially in the black community, although it was historically described in postmenopausal white women, he said. Frontal fibrosing alopecia can be mistaken for traction alopecia in black women in particular, he noted. However, it can be distinguished from traction alopecia by the loss of eyebrow hair, which might be a clue to consider a biopsy. "The histology is what you would expect in lichen planopilaris," he noted.
Fibrosing alopecia in a pattern distribution is another condition that might be mistaken for lichen planopilaris, Dr. Sperling said. The pattern of hair loss resembles common balding, "but there is inflammation in the zone of thinning," he said. If a biopsy also shows lichenoid changes and obliteration of follicles, consider a diagnosis of fibrosing alopecia in a pattern distribution. "A lot of the inflammation is concentrated around miniaturized hair follicles," he said, but terminal hair follicles are involved as well.
Permanent chemotherapy-induced alopecia occurs in some chemotherapy patients.
"A sizable number of chemotherapy patients develop some type of permanent hair loss after treatment," Dr. Sperling said. Data from biopsies have shown areas of permanent hair loss, but also telogenlike structures, with a curious, amoeboid shape, he said. However, similar structures have been identified in patients with linear morphea, suggesting that these features are not uniquely characteristic of postchemotherapy permanent alopecia, he said.
Instead, they seem to be some sort of end-stage marker for a follicle that isn’t going to grow back, he said.
Dr. Sperling said he had no relevant financial conflicts.
On Twitter @hsplete
WASHINGTON – Potentially puzzling hair diseases might be one of three emerging types of alopecia: psoriatic, frontal fibrosing, and permanent chemotherapy induced, according to Dr. Leonard Sperling.
"You have a good chance of seeing these in the coming year," he said.
Psoriatic alopecia claims features of both cicatricial and noncicatricial alopecia, said Dr. Sperling of the Uniformed Services University of the Health Sciences, Bethesda, Md. "It is a histological mimic of alopecia areata," he noted.
However, sebaceous gland atrophy is evident on histology and is a dependable diagnostic feature. "That’s what sets this disease apart," Dr. Sperling said.
A clinical differential diagnosis of psoriatic alopecia may include tinea capitis, chronic cutaneous systemic lupus erythematosus, seborrheic dermatitis, syphilitic alopecia, and psoriasis plus alopecia areata, he said.
Psoriatic alopecia is not new; a case was reported in 1972 (Br. J. Dermatol. 1972;87:73-7).
Clinical studies of treatment outcomes are limited, but one review of data from 47 cases of psoriatic alopecia showed that most patients had complete hair regrowth, although five patients developed residual scarring, Dr. Sperling noted (Dermatology 1992;185:82-7).
"The prognosis for hair regrowth seems to be favorable, but we have more to learn about this condition," he said.
Another emerging hair disease, psoriatic alopecialike reaction to tumor necrosis factor–inhibitor therapy is becoming increasingly common, Dr. Sperling said.
"If you haven’t seen this yet, I predict that you will, as the biologics are more utilized," he said. All the TNF-alpha inhibitors have been associated with this.
It is psoriasis from hell.
"The follicular findings resemble those seen in alopecia areata, in that there is a lot of hair miniaturization" and inflammation, Dr. Sperling said. Numerous different plasma cells and eosinophils are evident on histology, which would be unusual in alopecia areata, he noted. Atrophy of the sebaceous glands also is evident. Recognizing the role of the underlying drug is important to make the diagnosis, he added.
The reason for the atrophy of the sebaceous glands in these cases, as in patients with psoriatic alopecia, remains unknown, Dr. Sperling said.
Frontal fibrosing alopecia is becoming more common, "It’s like an epidemic," said Dr. Sperling. It is becoming more common, especially in the black community, although it was historically described in postmenopausal white women, he said. Frontal fibrosing alopecia can be mistaken for traction alopecia in black women in particular, he noted. However, it can be distinguished from traction alopecia by the loss of eyebrow hair, which might be a clue to consider a biopsy. "The histology is what you would expect in lichen planopilaris," he noted.
Fibrosing alopecia in a pattern distribution is another condition that might be mistaken for lichen planopilaris, Dr. Sperling said. The pattern of hair loss resembles common balding, "but there is inflammation in the zone of thinning," he said. If a biopsy also shows lichenoid changes and obliteration of follicles, consider a diagnosis of fibrosing alopecia in a pattern distribution. "A lot of the inflammation is concentrated around miniaturized hair follicles," he said, but terminal hair follicles are involved as well.
Permanent chemotherapy-induced alopecia occurs in some chemotherapy patients.
"A sizable number of chemotherapy patients develop some type of permanent hair loss after treatment," Dr. Sperling said. Data from biopsies have shown areas of permanent hair loss, but also telogenlike structures, with a curious, amoeboid shape, he said. However, similar structures have been identified in patients with linear morphea, suggesting that these features are not uniquely characteristic of postchemotherapy permanent alopecia, he said.
Instead, they seem to be some sort of end-stage marker for a follicle that isn’t going to grow back, he said.
Dr. Sperling said he had no relevant financial conflicts.
On Twitter @hsplete
EXPERT ANALYSIS FROM THE ATLANTIC DERMATOLOGICAL CONFERENCE
Hold your hoarseness: Tips for tackling challenging cases
WASHINGTON – If your patient complains of hoarseness, how do you handle it? Although the causes of hoarseness are often obvious, many patients with hoarseness have vocal folds that appear normal, which can create a diagnostic challenge, said Dr. Seth M. Cohen of Duke University Medical Center in Durham, N.C., and Dr. J. Pieter Noordzij of Boston Medical Center.
Some of the most common causes of hoarseness in patients with normal-looking vocal folds are muscle tension/functional dysphonia, spasmodic dysphonia, vocal fold tremor, Parkinson’s disease, presbylaryngis (vocal fold atrophy), and amyotrophic lateral sclerosis. Dr. Cohen and Dr. Noordzij reviewed these conditions and shared cases at the annual meeting of the American Academy of Otolaryngology – Head and Neck Surgery Foundation.
The Work-Up
When evaluating a patient’s hoarseness, start with a history and physical exam. The history should include the duration of hoarseness, how it started, family history of hoarseness, and the patient’s vocal demands that could contribute to overuse of the voice, Dr. Cohen said. Fluid intake (or lack of) can play a role, as can certain medical conditions such as gastroesophageal reflux disease (GERD) and allergies involving postnasal drip, he said.
The complete evaluation of a hoarse patient should include a full head and neck exam and a full cranial nerve exam, as well as an assessment of general appearance, facial expression, and endolaryngeal findings, Dr. Cohen said.
In addition, clinicians can use a perceptual voice analysis to try to characterize the general voice quality in terms of roughness (raspy), breathiness, strain (voice breaking), pitch (may be lower than normal), articulation, and speed, Dr. Cohen said. Techniques to evaluate patients include asking them to whisper, sing, make sustained vowel sounds (aaah, eee, ooo), and count from 60 to 69 and from 80 to 89.
Although some patients with hoarseness may benefit from surgical procedures, voice therapy is usually the first choice for treatment, he noted.
"Listen to the patient, listen to what they tell you, and listen to what they sound like," Dr. Cohen said.
Muscle Tension/Functional Dysphonia
Patients with muscle tension and functional dysphonia have excessive tension or poor coordination of the muscles in and near the voice box. The hoarseness in these patients often occurs after a cold and may be worse at the end of the day, said Dr. Noordzij.
On physical exam, this patient’s voice may be raspy and lower in pitch than normal. Someone who puts heavy demands on their voice might be susceptible to this condition, Dr. Noordzij said. They perceive their voice as strained and lower pitched, and they feel that are talking at the end of a breath. An endolaryngeal exam may show a gap between the vocal folds and squeezing of the larynx above the vocal folds (called a supraglottic constriction).
Spasmodic Dysphonia
Spasmodic dysphonia (SD) most often occurs in adulthood and can be triggered by a major life stress, Dr. Noordzij said. SD is a neurologic problem, not a functional one, he noted. SD is a movement disorder that involves involuntary, repetitive contractions of the laryngeal muscles. SD may be one of two types: adductor (a spasm that pushes the vocal folds together) or abductor (a spasm that causes the vocal cords to pull apart). Adductor spasmodic dysphonia is the most common form. Vocal characteristics include a strained or strangled voice that breaks on voiced syllables. However, voice breaks do not occur when the patient whispers, sings, or speaks in a falsetto, Dr. Noordzij said.
Vocal Fold Tremor
Vocal tremor is a central nervous system disorder that can be associated with other tremor conditions such as Parkinson’s disease, cerebellar ataxia, and spasmodic dysphonia, Dr. Cohen said.
"The hallmark of the condition is a rhythmic alteration in both the pitch and the loudness," he said. Vocal tremor may be exacerbated by stress or fatigue, and there may be a family history of tremor, he added.
On physical exam, patients with vocal tremor also may have tremor of the hands, head, jaw, voice, pharynx, tongue, or palate. Oscillations of pitch and amplitude are most noticeable during sustained vowels.
Parkinson’s Disease
Patients with Parkinson’s disease can present with voice complaints before they have a Parkinson’s diagnosis, although they also may exhibit Parkinson’s symptoms including hand tremor, rigidity, drooling, or a shuffling gait, Dr. Cohen said.
Hoarseness in these patients is characterized by breathy, flat voice, in a monotone, with breaths at inappropriate times. Patients also may have decreased blinking and a lack of facial expression.
Parkinson’s patients may have a history of not realizing the low volume of their voices, and they may take breaths at inappropriate times, Dr. Cohen noted. An endolaryngeal exam may show evidence of vocal fold bowing and a pooling of secretions, he said.
Presbylaryngis
Presbylaryngis, also known as vocal fold atrophy, is caused by age-related changes in the vocal folds, including ossification of laryngeal cartilage, decreased muscle bulk, decreased mucus production, and thickening or thinning of the epithelium.
"This is one of the hardest problems to treat surgically," Dr. Cohen said. Therefore, voice therapy is the first line treatment, he said.
In general, the pitch of men’s voices rises in cases of presbylaryngis, while the pitch of women’s voices decreases, Dr. Cohen noted. Patients perceive their voices as breathy and weak, with vocal fatigue and decreased ability to project their voices.
Amyotrophic Lateral Sclerosis
Approximately 25% of patients with amyotrophic lateral sclerosis (ALS) present with speech and swallowing problems. ALS is a progressive degeneration of the upper and lower motor neurons. Speech in these patients is typically slow, weak, and hypernasal, said Dr. Cohen. ALS patients may have dysarthria (disturbance of articulation) as well as dysphonia, and involuntary twitches of the tongue, he added.
Neither Dr. Cohen nor Dr. Noordzij had any financial conflicts to disclose.
WASHINGTON – If your patient complains of hoarseness, how do you handle it? Although the causes of hoarseness are often obvious, many patients with hoarseness have vocal folds that appear normal, which can create a diagnostic challenge, said Dr. Seth M. Cohen of Duke University Medical Center in Durham, N.C., and Dr. J. Pieter Noordzij of Boston Medical Center.
Some of the most common causes of hoarseness in patients with normal-looking vocal folds are muscle tension/functional dysphonia, spasmodic dysphonia, vocal fold tremor, Parkinson’s disease, presbylaryngis (vocal fold atrophy), and amyotrophic lateral sclerosis. Dr. Cohen and Dr. Noordzij reviewed these conditions and shared cases at the annual meeting of the American Academy of Otolaryngology – Head and Neck Surgery Foundation.
The Work-Up
When evaluating a patient’s hoarseness, start with a history and physical exam. The history should include the duration of hoarseness, how it started, family history of hoarseness, and the patient’s vocal demands that could contribute to overuse of the voice, Dr. Cohen said. Fluid intake (or lack of) can play a role, as can certain medical conditions such as gastroesophageal reflux disease (GERD) and allergies involving postnasal drip, he said.
The complete evaluation of a hoarse patient should include a full head and neck exam and a full cranial nerve exam, as well as an assessment of general appearance, facial expression, and endolaryngeal findings, Dr. Cohen said.
In addition, clinicians can use a perceptual voice analysis to try to characterize the general voice quality in terms of roughness (raspy), breathiness, strain (voice breaking), pitch (may be lower than normal), articulation, and speed, Dr. Cohen said. Techniques to evaluate patients include asking them to whisper, sing, make sustained vowel sounds (aaah, eee, ooo), and count from 60 to 69 and from 80 to 89.
Although some patients with hoarseness may benefit from surgical procedures, voice therapy is usually the first choice for treatment, he noted.
"Listen to the patient, listen to what they tell you, and listen to what they sound like," Dr. Cohen said.
Muscle Tension/Functional Dysphonia
Patients with muscle tension and functional dysphonia have excessive tension or poor coordination of the muscles in and near the voice box. The hoarseness in these patients often occurs after a cold and may be worse at the end of the day, said Dr. Noordzij.
On physical exam, this patient’s voice may be raspy and lower in pitch than normal. Someone who puts heavy demands on their voice might be susceptible to this condition, Dr. Noordzij said. They perceive their voice as strained and lower pitched, and they feel that are talking at the end of a breath. An endolaryngeal exam may show a gap between the vocal folds and squeezing of the larynx above the vocal folds (called a supraglottic constriction).
Spasmodic Dysphonia
Spasmodic dysphonia (SD) most often occurs in adulthood and can be triggered by a major life stress, Dr. Noordzij said. SD is a neurologic problem, not a functional one, he noted. SD is a movement disorder that involves involuntary, repetitive contractions of the laryngeal muscles. SD may be one of two types: adductor (a spasm that pushes the vocal folds together) or abductor (a spasm that causes the vocal cords to pull apart). Adductor spasmodic dysphonia is the most common form. Vocal characteristics include a strained or strangled voice that breaks on voiced syllables. However, voice breaks do not occur when the patient whispers, sings, or speaks in a falsetto, Dr. Noordzij said.
Vocal Fold Tremor
Vocal tremor is a central nervous system disorder that can be associated with other tremor conditions such as Parkinson’s disease, cerebellar ataxia, and spasmodic dysphonia, Dr. Cohen said.
"The hallmark of the condition is a rhythmic alteration in both the pitch and the loudness," he said. Vocal tremor may be exacerbated by stress or fatigue, and there may be a family history of tremor, he added.
On physical exam, patients with vocal tremor also may have tremor of the hands, head, jaw, voice, pharynx, tongue, or palate. Oscillations of pitch and amplitude are most noticeable during sustained vowels.
Parkinson’s Disease
Patients with Parkinson’s disease can present with voice complaints before they have a Parkinson’s diagnosis, although they also may exhibit Parkinson’s symptoms including hand tremor, rigidity, drooling, or a shuffling gait, Dr. Cohen said.
Hoarseness in these patients is characterized by breathy, flat voice, in a monotone, with breaths at inappropriate times. Patients also may have decreased blinking and a lack of facial expression.
Parkinson’s patients may have a history of not realizing the low volume of their voices, and they may take breaths at inappropriate times, Dr. Cohen noted. An endolaryngeal exam may show evidence of vocal fold bowing and a pooling of secretions, he said.
Presbylaryngis
Presbylaryngis, also known as vocal fold atrophy, is caused by age-related changes in the vocal folds, including ossification of laryngeal cartilage, decreased muscle bulk, decreased mucus production, and thickening or thinning of the epithelium.
"This is one of the hardest problems to treat surgically," Dr. Cohen said. Therefore, voice therapy is the first line treatment, he said.
In general, the pitch of men’s voices rises in cases of presbylaryngis, while the pitch of women’s voices decreases, Dr. Cohen noted. Patients perceive their voices as breathy and weak, with vocal fatigue and decreased ability to project their voices.
Amyotrophic Lateral Sclerosis
Approximately 25% of patients with amyotrophic lateral sclerosis (ALS) present with speech and swallowing problems. ALS is a progressive degeneration of the upper and lower motor neurons. Speech in these patients is typically slow, weak, and hypernasal, said Dr. Cohen. ALS patients may have dysarthria (disturbance of articulation) as well as dysphonia, and involuntary twitches of the tongue, he added.
Neither Dr. Cohen nor Dr. Noordzij had any financial conflicts to disclose.
WASHINGTON – If your patient complains of hoarseness, how do you handle it? Although the causes of hoarseness are often obvious, many patients with hoarseness have vocal folds that appear normal, which can create a diagnostic challenge, said Dr. Seth M. Cohen of Duke University Medical Center in Durham, N.C., and Dr. J. Pieter Noordzij of Boston Medical Center.
Some of the most common causes of hoarseness in patients with normal-looking vocal folds are muscle tension/functional dysphonia, spasmodic dysphonia, vocal fold tremor, Parkinson’s disease, presbylaryngis (vocal fold atrophy), and amyotrophic lateral sclerosis. Dr. Cohen and Dr. Noordzij reviewed these conditions and shared cases at the annual meeting of the American Academy of Otolaryngology – Head and Neck Surgery Foundation.
The Work-Up
When evaluating a patient’s hoarseness, start with a history and physical exam. The history should include the duration of hoarseness, how it started, family history of hoarseness, and the patient’s vocal demands that could contribute to overuse of the voice, Dr. Cohen said. Fluid intake (or lack of) can play a role, as can certain medical conditions such as gastroesophageal reflux disease (GERD) and allergies involving postnasal drip, he said.
The complete evaluation of a hoarse patient should include a full head and neck exam and a full cranial nerve exam, as well as an assessment of general appearance, facial expression, and endolaryngeal findings, Dr. Cohen said.
In addition, clinicians can use a perceptual voice analysis to try to characterize the general voice quality in terms of roughness (raspy), breathiness, strain (voice breaking), pitch (may be lower than normal), articulation, and speed, Dr. Cohen said. Techniques to evaluate patients include asking them to whisper, sing, make sustained vowel sounds (aaah, eee, ooo), and count from 60 to 69 and from 80 to 89.
Although some patients with hoarseness may benefit from surgical procedures, voice therapy is usually the first choice for treatment, he noted.
"Listen to the patient, listen to what they tell you, and listen to what they sound like," Dr. Cohen said.
Muscle Tension/Functional Dysphonia
Patients with muscle tension and functional dysphonia have excessive tension or poor coordination of the muscles in and near the voice box. The hoarseness in these patients often occurs after a cold and may be worse at the end of the day, said Dr. Noordzij.
On physical exam, this patient’s voice may be raspy and lower in pitch than normal. Someone who puts heavy demands on their voice might be susceptible to this condition, Dr. Noordzij said. They perceive their voice as strained and lower pitched, and they feel that are talking at the end of a breath. An endolaryngeal exam may show a gap between the vocal folds and squeezing of the larynx above the vocal folds (called a supraglottic constriction).
Spasmodic Dysphonia
Spasmodic dysphonia (SD) most often occurs in adulthood and can be triggered by a major life stress, Dr. Noordzij said. SD is a neurologic problem, not a functional one, he noted. SD is a movement disorder that involves involuntary, repetitive contractions of the laryngeal muscles. SD may be one of two types: adductor (a spasm that pushes the vocal folds together) or abductor (a spasm that causes the vocal cords to pull apart). Adductor spasmodic dysphonia is the most common form. Vocal characteristics include a strained or strangled voice that breaks on voiced syllables. However, voice breaks do not occur when the patient whispers, sings, or speaks in a falsetto, Dr. Noordzij said.
Vocal Fold Tremor
Vocal tremor is a central nervous system disorder that can be associated with other tremor conditions such as Parkinson’s disease, cerebellar ataxia, and spasmodic dysphonia, Dr. Cohen said.
"The hallmark of the condition is a rhythmic alteration in both the pitch and the loudness," he said. Vocal tremor may be exacerbated by stress or fatigue, and there may be a family history of tremor, he added.
On physical exam, patients with vocal tremor also may have tremor of the hands, head, jaw, voice, pharynx, tongue, or palate. Oscillations of pitch and amplitude are most noticeable during sustained vowels.
Parkinson’s Disease
Patients with Parkinson’s disease can present with voice complaints before they have a Parkinson’s diagnosis, although they also may exhibit Parkinson’s symptoms including hand tremor, rigidity, drooling, or a shuffling gait, Dr. Cohen said.
Hoarseness in these patients is characterized by breathy, flat voice, in a monotone, with breaths at inappropriate times. Patients also may have decreased blinking and a lack of facial expression.
Parkinson’s patients may have a history of not realizing the low volume of their voices, and they may take breaths at inappropriate times, Dr. Cohen noted. An endolaryngeal exam may show evidence of vocal fold bowing and a pooling of secretions, he said.
Presbylaryngis
Presbylaryngis, also known as vocal fold atrophy, is caused by age-related changes in the vocal folds, including ossification of laryngeal cartilage, decreased muscle bulk, decreased mucus production, and thickening or thinning of the epithelium.
"This is one of the hardest problems to treat surgically," Dr. Cohen said. Therefore, voice therapy is the first line treatment, he said.
In general, the pitch of men’s voices rises in cases of presbylaryngis, while the pitch of women’s voices decreases, Dr. Cohen noted. Patients perceive their voices as breathy and weak, with vocal fatigue and decreased ability to project their voices.
Amyotrophic Lateral Sclerosis
Approximately 25% of patients with amyotrophic lateral sclerosis (ALS) present with speech and swallowing problems. ALS is a progressive degeneration of the upper and lower motor neurons. Speech in these patients is typically slow, weak, and hypernasal, said Dr. Cohen. ALS patients may have dysarthria (disturbance of articulation) as well as dysphonia, and involuntary twitches of the tongue, he added.
Neither Dr. Cohen nor Dr. Noordzij had any financial conflicts to disclose.
AT THE ANNUAL MEETING OF THE AMERICAN ACADEMY OF OTOLARYNGOLOGY HEAD AND NECK SURGERY FOUNDATION
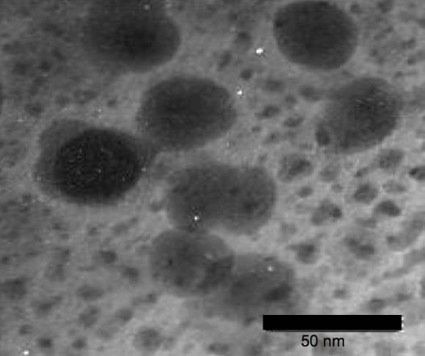
Nanoparticles take aim at acne
Nanotechnology stands to make a big difference in the way acne is treated.
A 0.1% concentration of benzoyl peroxide encapsulated in chitosan-alginate nanoparticles showed more antimicrobial activity against acne bacteria than typical benzoyl peroxide or the nanoparticles alone in a recently published in vitro study (J. Invest. Dermatol. 2012 Nov. 29 [doi:10.1038/jid.2012.399]).
Chitosan-alginate has both antimicrobial and anti-inflammatory impact on Propionibacterium acnes, wrote Dr. Adam Friedman of Albert Einstein College of Medicine, New York, and his colleagues. The nanoparticle structure preserves the antimicrobial and immunological properties of chitosan while alginate lends stability.
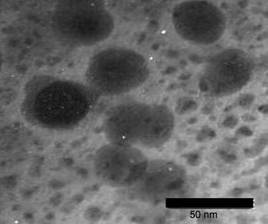
Benzoyl peroxide is, of course, already a first-line therapy for acne, but encapsulating benzoyl peroxide in the nanoparticles stands to reduce the irritating side effects common with topical benzoyl peroxide use, the researchers noted. Less irritation could greatly improve patient compliance.
In the study, scanning electron microscopy and transmission electron microscopy showed "severe disruption, destruction, and ‘peeling’ of the cell wall," the researchers wrote. "These images suggest that the cell damage is due to an osmotic disturbance" created by the encapsulated benzoyl peroxide.
Nanoparticle encapsulation "provides previously undescribed therapeutic opportunities, including delivery of multidrug regimens to combat resistant microbes and inflammatory disease states," the researchers said.
Nanotechnology stands to make a big difference in the way acne is treated.
A 0.1% concentration of benzoyl peroxide encapsulated in chitosan-alginate nanoparticles showed more antimicrobial activity against acne bacteria than typical benzoyl peroxide or the nanoparticles alone in a recently published in vitro study (J. Invest. Dermatol. 2012 Nov. 29 [doi:10.1038/jid.2012.399]).
Chitosan-alginate has both antimicrobial and anti-inflammatory impact on Propionibacterium acnes, wrote Dr. Adam Friedman of Albert Einstein College of Medicine, New York, and his colleagues. The nanoparticle structure preserves the antimicrobial and immunological properties of chitosan while alginate lends stability.
Benzoyl peroxide is, of course, already a first-line therapy for acne, but encapsulating benzoyl peroxide in the nanoparticles stands to reduce the irritating side effects common with topical benzoyl peroxide use, the researchers noted. Less irritation could greatly improve patient compliance.
In the study, scanning electron microscopy and transmission electron microscopy showed "severe disruption, destruction, and ‘peeling’ of the cell wall," the researchers wrote. "These images suggest that the cell damage is due to an osmotic disturbance" created by the encapsulated benzoyl peroxide.
Nanoparticle encapsulation "provides previously undescribed therapeutic opportunities, including delivery of multidrug regimens to combat resistant microbes and inflammatory disease states," the researchers said.
Nanotechnology stands to make a big difference in the way acne is treated.
A 0.1% concentration of benzoyl peroxide encapsulated in chitosan-alginate nanoparticles showed more antimicrobial activity against acne bacteria than typical benzoyl peroxide or the nanoparticles alone in a recently published in vitro study (J. Invest. Dermatol. 2012 Nov. 29 [doi:10.1038/jid.2012.399]).
Chitosan-alginate has both antimicrobial and anti-inflammatory impact on Propionibacterium acnes, wrote Dr. Adam Friedman of Albert Einstein College of Medicine, New York, and his colleagues. The nanoparticle structure preserves the antimicrobial and immunological properties of chitosan while alginate lends stability.
Benzoyl peroxide is, of course, already a first-line therapy for acne, but encapsulating benzoyl peroxide in the nanoparticles stands to reduce the irritating side effects common with topical benzoyl peroxide use, the researchers noted. Less irritation could greatly improve patient compliance.
In the study, scanning electron microscopy and transmission electron microscopy showed "severe disruption, destruction, and ‘peeling’ of the cell wall," the researchers wrote. "These images suggest that the cell damage is due to an osmotic disturbance" created by the encapsulated benzoyl peroxide.
Nanoparticle encapsulation "provides previously undescribed therapeutic opportunities, including delivery of multidrug regimens to combat resistant microbes and inflammatory disease states," the researchers said.
TORS: Postop bleeding risk rises with antithrombotic use
The risk of postoperative hemorrhage after transoral robotic-assisted surgery was significantly higher in patients taking antithrombotic medication than in those not taking it, based on data from 147 consecutive patients.
"Even with this small sample size, we were able to identify that increased risk was associated with antithrombotic medication use," said Dr. Scott Asher of the University of Alabama at Birmingham.
Transoral robotic-assisted surgery (TORS) is gaining in popularity among head and neck surgeons, but the potential for postop bleeding in patients taking antithrombotic medication remains a problem, Dr. Asher said at the annual meeting of the American Academy of Otolaryngology – Head and Neck Surgery Foundation.
To assess the postop bleeding complications in TORS patients, Dr. Asher and his colleagues reviewed data from patients seen at a single tertiary academic medical center between March 2007 and September 2011.
Overall, 11 patients (8%) experienced some postop hemorrhage, but 8 of these hemorrhages (72%) occurred in patients taking antithrombotics, Dr. Asher said. Nine patients who hemorrhaged returned to the operating room for further examination and bleeding control, he noted. All postop hemorrhage events were controlled with standard techniques.
The incidence of postop hemorrhage was significantly higher among patients on antithrombotics (17%) compared with those not on antithrombotics (3%). However, no significant difference in the incidence of bleeding occurred between patients undergoing primary surgery and those undergoing salvage surgery (7% vs. 10%). Bleeding occurred an average of 11 days after surgery.
The bleeding events occurred past the time points when most patients would resume their antithrombotic medications, Dr. Asher noted.
"Our recommendation is that patients taking these meds should receive additional preop counseling when considering a TORS procedure," he said.
"A second recommendation is to collaborate preoperatively with the physicians who are prescribing," as well as the anesthesia team, to closely analyze the indications for use of antithrombotics, Dr. Asher added. "If you can safely discontinue them, you can potentially improve your TORS outcomes," he said.
Additional long-term safety and outcomes data are needed for TORS procedures, said Dr. Asher. "We are constantly reflecting on our own experience," he said. "We would encourage other institutions to collect and publish their complications-related data to continue to improve TORS outcomes."
Dr. Asher said he had no relevant financial conflicts.
The risk of postoperative hemorrhage after transoral robotic-assisted surgery was significantly higher in patients taking antithrombotic medication than in those not taking it, based on data from 147 consecutive patients.
"Even with this small sample size, we were able to identify that increased risk was associated with antithrombotic medication use," said Dr. Scott Asher of the University of Alabama at Birmingham.
Transoral robotic-assisted surgery (TORS) is gaining in popularity among head and neck surgeons, but the potential for postop bleeding in patients taking antithrombotic medication remains a problem, Dr. Asher said at the annual meeting of the American Academy of Otolaryngology – Head and Neck Surgery Foundation.
To assess the postop bleeding complications in TORS patients, Dr. Asher and his colleagues reviewed data from patients seen at a single tertiary academic medical center between March 2007 and September 2011.
Overall, 11 patients (8%) experienced some postop hemorrhage, but 8 of these hemorrhages (72%) occurred in patients taking antithrombotics, Dr. Asher said. Nine patients who hemorrhaged returned to the operating room for further examination and bleeding control, he noted. All postop hemorrhage events were controlled with standard techniques.
The incidence of postop hemorrhage was significantly higher among patients on antithrombotics (17%) compared with those not on antithrombotics (3%). However, no significant difference in the incidence of bleeding occurred between patients undergoing primary surgery and those undergoing salvage surgery (7% vs. 10%). Bleeding occurred an average of 11 days after surgery.
The bleeding events occurred past the time points when most patients would resume their antithrombotic medications, Dr. Asher noted.
"Our recommendation is that patients taking these meds should receive additional preop counseling when considering a TORS procedure," he said.
"A second recommendation is to collaborate preoperatively with the physicians who are prescribing," as well as the anesthesia team, to closely analyze the indications for use of antithrombotics, Dr. Asher added. "If you can safely discontinue them, you can potentially improve your TORS outcomes," he said.
Additional long-term safety and outcomes data are needed for TORS procedures, said Dr. Asher. "We are constantly reflecting on our own experience," he said. "We would encourage other institutions to collect and publish their complications-related data to continue to improve TORS outcomes."
Dr. Asher said he had no relevant financial conflicts.
The risk of postoperative hemorrhage after transoral robotic-assisted surgery was significantly higher in patients taking antithrombotic medication than in those not taking it, based on data from 147 consecutive patients.
"Even with this small sample size, we were able to identify that increased risk was associated with antithrombotic medication use," said Dr. Scott Asher of the University of Alabama at Birmingham.
Transoral robotic-assisted surgery (TORS) is gaining in popularity among head and neck surgeons, but the potential for postop bleeding in patients taking antithrombotic medication remains a problem, Dr. Asher said at the annual meeting of the American Academy of Otolaryngology – Head and Neck Surgery Foundation.
To assess the postop bleeding complications in TORS patients, Dr. Asher and his colleagues reviewed data from patients seen at a single tertiary academic medical center between March 2007 and September 2011.
Overall, 11 patients (8%) experienced some postop hemorrhage, but 8 of these hemorrhages (72%) occurred in patients taking antithrombotics, Dr. Asher said. Nine patients who hemorrhaged returned to the operating room for further examination and bleeding control, he noted. All postop hemorrhage events were controlled with standard techniques.
The incidence of postop hemorrhage was significantly higher among patients on antithrombotics (17%) compared with those not on antithrombotics (3%). However, no significant difference in the incidence of bleeding occurred between patients undergoing primary surgery and those undergoing salvage surgery (7% vs. 10%). Bleeding occurred an average of 11 days after surgery.
The bleeding events occurred past the time points when most patients would resume their antithrombotic medications, Dr. Asher noted.
"Our recommendation is that patients taking these meds should receive additional preop counseling when considering a TORS procedure," he said.
"A second recommendation is to collaborate preoperatively with the physicians who are prescribing," as well as the anesthesia team, to closely analyze the indications for use of antithrombotics, Dr. Asher added. "If you can safely discontinue them, you can potentially improve your TORS outcomes," he said.
Additional long-term safety and outcomes data are needed for TORS procedures, said Dr. Asher. "We are constantly reflecting on our own experience," he said. "We would encourage other institutions to collect and publish their complications-related data to continue to improve TORS outcomes."
Dr. Asher said he had no relevant financial conflicts.
AT THE ANNUAL MEETING OF THE AMERICAN ACADEMY OF OTOLARYNGOLOGY; HEAD AND NECK SURGERY FOUNDATION
Major Finding: Approximately three-quarters of patients (8 of 11) who underwent TORS and experienced some postop bleeding were on an antithrombotic medication.
Data Source: A review of 147 consecutive patients at a single surgery center.
Disclosures: Dr. Asher said he had no relevant financial conflicts.
COPD varies by state, peaks above 9%
The prevalence of chronic obstructive pulmonary disease is 6% nationwide, but varies from less than 4% in Washington and Minnesota to more than 9% in Alabama and Kentucky, according to data from the Centers for Disease Control and Prevention. The findings were published in the CDC’s Morbidity and Mortality Weekly Report.
A total of 13,306 adults who reported having chronic obstructive pulmonary disease (COPD) in the national survey also responded to the COPD module. Of these, 76% reported undergoing a diagnostic breathing test, 64% reported that COPD symptoms (specifically shortness of breath) had an adverse effect on their quality of life, and 51% reported taking at least one COPD medication (MMWR 2012;61:938-43).
In age-adjusted comparisons, women were more likely to report COPD compared with men (7% vs. 5%, respectively). COPD prevalence decreased from an average of 10% among individuals making less than $25,000 per year to 3% in those making more than $75,000 per year, and the prevalence was lower among employed individuals, homemakers, and students compared with those who were unemployed, retired, or otherwise unable to work. The prevalence of COPD was highest in current smokers (13%) compared with former smokers (7%) and never smokers (3%).
Data were taken from the 2011 Behavioral Risk Factor Surveillance System (BRFSS) survey. Additional COPD data were collected in an optional COPD module about COPD diagnosis and quality of life. This module was part of the BRFSS in 21 states, the District of Columbia, and Puerto Rico.
The 2011 BRFSS was conducted via telephone, either landline or mobile. The survey population included adults aged 18 years and older throughout the United States.
The findings were limited by several factors including the absence of data on individuals in institutions or nursing homes and by the use of self-reports for COPD diagnosis, the researchers said. However, the report is the first to analyze data on COPD prevalence in all 50 states, the District of Columbia, and Puerto Rico, they noted. State-level health officials should focus surveillance efforts, educational campaigns, and interventions on areas of highest COPD prevalence, they added.
The study was supported by the CDC and the National Heart, Lung, and Blood Institute of the National Institutes of Health.
The prevalence of chronic obstructive pulmonary disease is 6% nationwide, but varies from less than 4% in Washington and Minnesota to more than 9% in Alabama and Kentucky, according to data from the Centers for Disease Control and Prevention. The findings were published in the CDC’s Morbidity and Mortality Weekly Report.
A total of 13,306 adults who reported having chronic obstructive pulmonary disease (COPD) in the national survey also responded to the COPD module. Of these, 76% reported undergoing a diagnostic breathing test, 64% reported that COPD symptoms (specifically shortness of breath) had an adverse effect on their quality of life, and 51% reported taking at least one COPD medication (MMWR 2012;61:938-43).
In age-adjusted comparisons, women were more likely to report COPD compared with men (7% vs. 5%, respectively). COPD prevalence decreased from an average of 10% among individuals making less than $25,000 per year to 3% in those making more than $75,000 per year, and the prevalence was lower among employed individuals, homemakers, and students compared with those who were unemployed, retired, or otherwise unable to work. The prevalence of COPD was highest in current smokers (13%) compared with former smokers (7%) and never smokers (3%).
Data were taken from the 2011 Behavioral Risk Factor Surveillance System (BRFSS) survey. Additional COPD data were collected in an optional COPD module about COPD diagnosis and quality of life. This module was part of the BRFSS in 21 states, the District of Columbia, and Puerto Rico.
The 2011 BRFSS was conducted via telephone, either landline or mobile. The survey population included adults aged 18 years and older throughout the United States.
The findings were limited by several factors including the absence of data on individuals in institutions or nursing homes and by the use of self-reports for COPD diagnosis, the researchers said. However, the report is the first to analyze data on COPD prevalence in all 50 states, the District of Columbia, and Puerto Rico, they noted. State-level health officials should focus surveillance efforts, educational campaigns, and interventions on areas of highest COPD prevalence, they added.
The study was supported by the CDC and the National Heart, Lung, and Blood Institute of the National Institutes of Health.
The prevalence of chronic obstructive pulmonary disease is 6% nationwide, but varies from less than 4% in Washington and Minnesota to more than 9% in Alabama and Kentucky, according to data from the Centers for Disease Control and Prevention. The findings were published in the CDC’s Morbidity and Mortality Weekly Report.
A total of 13,306 adults who reported having chronic obstructive pulmonary disease (COPD) in the national survey also responded to the COPD module. Of these, 76% reported undergoing a diagnostic breathing test, 64% reported that COPD symptoms (specifically shortness of breath) had an adverse effect on their quality of life, and 51% reported taking at least one COPD medication (MMWR 2012;61:938-43).
In age-adjusted comparisons, women were more likely to report COPD compared with men (7% vs. 5%, respectively). COPD prevalence decreased from an average of 10% among individuals making less than $25,000 per year to 3% in those making more than $75,000 per year, and the prevalence was lower among employed individuals, homemakers, and students compared with those who were unemployed, retired, or otherwise unable to work. The prevalence of COPD was highest in current smokers (13%) compared with former smokers (7%) and never smokers (3%).
Data were taken from the 2011 Behavioral Risk Factor Surveillance System (BRFSS) survey. Additional COPD data were collected in an optional COPD module about COPD diagnosis and quality of life. This module was part of the BRFSS in 21 states, the District of Columbia, and Puerto Rico.
The 2011 BRFSS was conducted via telephone, either landline or mobile. The survey population included adults aged 18 years and older throughout the United States.
The findings were limited by several factors including the absence of data on individuals in institutions or nursing homes and by the use of self-reports for COPD diagnosis, the researchers said. However, the report is the first to analyze data on COPD prevalence in all 50 states, the District of Columbia, and Puerto Rico, they noted. State-level health officials should focus surveillance efforts, educational campaigns, and interventions on areas of highest COPD prevalence, they added.
The study was supported by the CDC and the National Heart, Lung, and Blood Institute of the National Institutes of Health.
Major Finding: The overall prevalence of chronic obstructive pulmonary disease in the United States is approximately 6%.
Data Source: The data come from the 2011 Behavioral Risk Factor Surveillance System (BRFSS) survey.
Disclosures: The study was supported by the CDC and the National Heart, Lung, and Blood Institute of the National Institutes of Health.
Seropositivity predicts progressive joint damage in established RA
WASHINGTON – Seropositivity for either rheumatoid factor or anti-cyclic citrullinated peptide was significantly associated with progressive joint damage in adults with established rheumatoid arthritis, based on a single-center, observational cohort study of 390 patients.
Most rheumatoid arthritis (RA) patients in clinical practice have established disease, but the predictors and proportion of disease progression in these patients has not been well studied, Dr. Siri Lillegraven of Diakonhjemmet Hospital in Oslo said at the annual meeting of the American College of Rheumatology.
Dr. Lillegraven and her colleagues reviewed data from BRASS (the Brigham and Women’s Hospital Rheumatoid Arthritis Sequential Study). Joint damage was assessed using baseline and 2-year radiographic data for patients with disease duration of at least 5 years. The average age of the patients was 60 years, 84% were women, and 44% received biologic treatment in the form of disease-modifying antirheumatic drugs (DMARDs). The median disease duration was 17 years. Disease progression was defined as a change in Sharp/van der Heijde score of 1 or more units per year.
Overall, 44% of the patients showed disease progression after 2 years. A total of 68% of the patients were positive for both rheumatoid factor (RF) and anticyclic citrullinated peptide (anti-CCP), 16% were positive for either RF or anti-CCP, and 16% were negative for both.
Seropositivity was the only significant independent predictor of disease progression after controlling for factors including age, gender, body-mass index, smoking status, treatment, DMARD use, disease duration, and presence of subcutaneous nodules, Dr. Lillegraven said.
Patients who were seropositive for either RF or anti-CCP were five times more likely than were seronegative patients to have disease progression (odds ratio 5.0), while seropositivity for both was associated with four times greater odds for disease progression (odds ratio 4.1).
"Although the odds ratios for progressive joint damage were similar if patients were positive for one or both of RF and anti-CCP, patients who were positive for both RF and anti-CCP tended to experience more joint damage," Dr. Lillegraven said. Rapid progression of joint damage (defined as a change in van der Heijde-Sharp score of 5 or more units per year) was noted in 16% patients who were seropositive for both RF and anti-CCP, compared with 9% of those who were positive for either RF or anti-CCP, although this difference was not statistically significant.
The results were limited by the use of data from a single center and by the challenge of fully adjusting for treatment in patients with established RA, Dr. Lillegraven noted. However, the findings suggest that seropositivity could be used to inform treatment decisions for these patients, she said.
Dr. Lillegraven had no financial conflicts to disclose. Several of the study coauthors disclosed relationships with multiple pharmaceutical companies, including Amgen, Abbott, Merck, and MedImmune.
WASHINGTON – Seropositivity for either rheumatoid factor or anti-cyclic citrullinated peptide was significantly associated with progressive joint damage in adults with established rheumatoid arthritis, based on a single-center, observational cohort study of 390 patients.
Most rheumatoid arthritis (RA) patients in clinical practice have established disease, but the predictors and proportion of disease progression in these patients has not been well studied, Dr. Siri Lillegraven of Diakonhjemmet Hospital in Oslo said at the annual meeting of the American College of Rheumatology.
Dr. Lillegraven and her colleagues reviewed data from BRASS (the Brigham and Women’s Hospital Rheumatoid Arthritis Sequential Study). Joint damage was assessed using baseline and 2-year radiographic data for patients with disease duration of at least 5 years. The average age of the patients was 60 years, 84% were women, and 44% received biologic treatment in the form of disease-modifying antirheumatic drugs (DMARDs). The median disease duration was 17 years. Disease progression was defined as a change in Sharp/van der Heijde score of 1 or more units per year.
Overall, 44% of the patients showed disease progression after 2 years. A total of 68% of the patients were positive for both rheumatoid factor (RF) and anticyclic citrullinated peptide (anti-CCP), 16% were positive for either RF or anti-CCP, and 16% were negative for both.
Seropositivity was the only significant independent predictor of disease progression after controlling for factors including age, gender, body-mass index, smoking status, treatment, DMARD use, disease duration, and presence of subcutaneous nodules, Dr. Lillegraven said.
Patients who were seropositive for either RF or anti-CCP were five times more likely than were seronegative patients to have disease progression (odds ratio 5.0), while seropositivity for both was associated with four times greater odds for disease progression (odds ratio 4.1).
"Although the odds ratios for progressive joint damage were similar if patients were positive for one or both of RF and anti-CCP, patients who were positive for both RF and anti-CCP tended to experience more joint damage," Dr. Lillegraven said. Rapid progression of joint damage (defined as a change in van der Heijde-Sharp score of 5 or more units per year) was noted in 16% patients who were seropositive for both RF and anti-CCP, compared with 9% of those who were positive for either RF or anti-CCP, although this difference was not statistically significant.
The results were limited by the use of data from a single center and by the challenge of fully adjusting for treatment in patients with established RA, Dr. Lillegraven noted. However, the findings suggest that seropositivity could be used to inform treatment decisions for these patients, she said.
Dr. Lillegraven had no financial conflicts to disclose. Several of the study coauthors disclosed relationships with multiple pharmaceutical companies, including Amgen, Abbott, Merck, and MedImmune.
WASHINGTON – Seropositivity for either rheumatoid factor or anti-cyclic citrullinated peptide was significantly associated with progressive joint damage in adults with established rheumatoid arthritis, based on a single-center, observational cohort study of 390 patients.
Most rheumatoid arthritis (RA) patients in clinical practice have established disease, but the predictors and proportion of disease progression in these patients has not been well studied, Dr. Siri Lillegraven of Diakonhjemmet Hospital in Oslo said at the annual meeting of the American College of Rheumatology.
Dr. Lillegraven and her colleagues reviewed data from BRASS (the Brigham and Women’s Hospital Rheumatoid Arthritis Sequential Study). Joint damage was assessed using baseline and 2-year radiographic data for patients with disease duration of at least 5 years. The average age of the patients was 60 years, 84% were women, and 44% received biologic treatment in the form of disease-modifying antirheumatic drugs (DMARDs). The median disease duration was 17 years. Disease progression was defined as a change in Sharp/van der Heijde score of 1 or more units per year.
Overall, 44% of the patients showed disease progression after 2 years. A total of 68% of the patients were positive for both rheumatoid factor (RF) and anticyclic citrullinated peptide (anti-CCP), 16% were positive for either RF or anti-CCP, and 16% were negative for both.
Seropositivity was the only significant independent predictor of disease progression after controlling for factors including age, gender, body-mass index, smoking status, treatment, DMARD use, disease duration, and presence of subcutaneous nodules, Dr. Lillegraven said.
Patients who were seropositive for either RF or anti-CCP were five times more likely than were seronegative patients to have disease progression (odds ratio 5.0), while seropositivity for both was associated with four times greater odds for disease progression (odds ratio 4.1).
"Although the odds ratios for progressive joint damage were similar if patients were positive for one or both of RF and anti-CCP, patients who were positive for both RF and anti-CCP tended to experience more joint damage," Dr. Lillegraven said. Rapid progression of joint damage (defined as a change in van der Heijde-Sharp score of 5 or more units per year) was noted in 16% patients who were seropositive for both RF and anti-CCP, compared with 9% of those who were positive for either RF or anti-CCP, although this difference was not statistically significant.
The results were limited by the use of data from a single center and by the challenge of fully adjusting for treatment in patients with established RA, Dr. Lillegraven noted. However, the findings suggest that seropositivity could be used to inform treatment decisions for these patients, she said.
Dr. Lillegraven had no financial conflicts to disclose. Several of the study coauthors disclosed relationships with multiple pharmaceutical companies, including Amgen, Abbott, Merck, and MedImmune.
AT THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF RHEUMATOLOGY
Major Finding: Patients with established rheumatoid arthritis and seropositivity for either RF or anti-CCP were five times more likely to have disease progression after 2 years than were seronegative patients.
Data Source: The Brigham and Women’s Hospital Rheumatoid Arthritis Sequential Study (BRASS), a single-center, observational cohort study of 390 patients.
Disclosures: Dr. Lillegraven had no financial conflicts to disclose. Several of the study coauthors disclosed relationships with multiple pharmaceutical companies including Amgen, Abbott, Merck, and MedImmune.
SurgiSIS myringoplasty shortens operative time
WASHINGTON – SurgiSIS, a material derived from porcine small intestinal mucosa, can be safely and effectively used for myringoplasty in children, based on data from a prospective, blinded study of 404 patients.
Patients’ tissue is not always available for tympanic membrane repair, and harvesting the graft may increase intraoperative time, said Dr. Riccardo D’Eredita of Vincenza (Italy) Civil Hospital. SurgiSIS (SIS) "promotes early vessel growth, provides scaffolding for remodeling tissues, and is inexpensive and ready to use." He presented the findings at the annual meeting of the American Academy of Otolaryngology – Head and Neck Surgery Foundation.
The material has been used widely in children, and data from previous studies show that SurgiSIS is gradually replaced by host cells, said Dr. D’Eredita. After 30 days, host cells invade SurgiSIS. After 1 year, SurgiSIS is no longer evident, and has been replaced by the patients’ collagen.
In this study, 404 children underwent tympanic membrane repair in 432 ears; 217 were randomized to myringoplasty with SurgiSIS and 215 were randomized to repair using the patients’ own temporalis fascia.
Overall, the group without SurgiSIS had a 97% rate of stable closures and the group with SurgiSIS had a 95% rate. Surgical time was approximately 15 minutes less for SurgiSIS-treated patients, Dr. D’Eredita said.
The researchers assessed the healing of the tympanic membranes over a 10-year period and found comparable reduction of inflammation in the two groups. There were no adverse reactions in the SIS group.
Dr. D’Eredita had no financial conflicts to disclose.
WASHINGTON – SurgiSIS, a material derived from porcine small intestinal mucosa, can be safely and effectively used for myringoplasty in children, based on data from a prospective, blinded study of 404 patients.
Patients’ tissue is not always available for tympanic membrane repair, and harvesting the graft may increase intraoperative time, said Dr. Riccardo D’Eredita of Vincenza (Italy) Civil Hospital. SurgiSIS (SIS) "promotes early vessel growth, provides scaffolding for remodeling tissues, and is inexpensive and ready to use." He presented the findings at the annual meeting of the American Academy of Otolaryngology – Head and Neck Surgery Foundation.
The material has been used widely in children, and data from previous studies show that SurgiSIS is gradually replaced by host cells, said Dr. D’Eredita. After 30 days, host cells invade SurgiSIS. After 1 year, SurgiSIS is no longer evident, and has been replaced by the patients’ collagen.
In this study, 404 children underwent tympanic membrane repair in 432 ears; 217 were randomized to myringoplasty with SurgiSIS and 215 were randomized to repair using the patients’ own temporalis fascia.
Overall, the group without SurgiSIS had a 97% rate of stable closures and the group with SurgiSIS had a 95% rate. Surgical time was approximately 15 minutes less for SurgiSIS-treated patients, Dr. D’Eredita said.
The researchers assessed the healing of the tympanic membranes over a 10-year period and found comparable reduction of inflammation in the two groups. There were no adverse reactions in the SIS group.
Dr. D’Eredita had no financial conflicts to disclose.
WASHINGTON – SurgiSIS, a material derived from porcine small intestinal mucosa, can be safely and effectively used for myringoplasty in children, based on data from a prospective, blinded study of 404 patients.
Patients’ tissue is not always available for tympanic membrane repair, and harvesting the graft may increase intraoperative time, said Dr. Riccardo D’Eredita of Vincenza (Italy) Civil Hospital. SurgiSIS (SIS) "promotes early vessel growth, provides scaffolding for remodeling tissues, and is inexpensive and ready to use." He presented the findings at the annual meeting of the American Academy of Otolaryngology – Head and Neck Surgery Foundation.
The material has been used widely in children, and data from previous studies show that SurgiSIS is gradually replaced by host cells, said Dr. D’Eredita. After 30 days, host cells invade SurgiSIS. After 1 year, SurgiSIS is no longer evident, and has been replaced by the patients’ collagen.
In this study, 404 children underwent tympanic membrane repair in 432 ears; 217 were randomized to myringoplasty with SurgiSIS and 215 were randomized to repair using the patients’ own temporalis fascia.
Overall, the group without SurgiSIS had a 97% rate of stable closures and the group with SurgiSIS had a 95% rate. Surgical time was approximately 15 minutes less for SurgiSIS-treated patients, Dr. D’Eredita said.
The researchers assessed the healing of the tympanic membranes over a 10-year period and found comparable reduction of inflammation in the two groups. There were no adverse reactions in the SIS group.
Dr. D’Eredita had no financial conflicts to disclose.
AT THE ANNUAL MEETING OF THE AMERICAN ACADEMY OF OTOLARYNGOLOGY - HEAD AND NECK SURGERY FOUNDATION
Major Finding: The number of stable surgical closures was similar in children who had tympanic membrane repair with porcine small intestinal mucosa (212) compared with use of their own tissue (204).
Data Source: The data comprise 432 ears in 404 children.
Disclosures: Dr. D’Eredita had no financial conflicts to disclose.
Facial Nerve Dysfunction Seen in 25% of Pediatric Parotidectomy Patients
WASHINGTON – Facial nerve dysfunction affected 23% of 43 children who had parotidectomies in a single-center study presented at the annual meeting of the American Academy of Otolaryngology–Head and Neck Surgery Foundation.
The findings suggest that facial nerve dysfunction after parotidectomy is common enough in children to merit preoperative counseling, said Dr. James A. Owusu of the University of Minnesota, Minneapolis.
Facial nerve dysfunction rates reported in the literature range from 9% to 60% in adults after parotidectomy, but the condition has not been well studied in children.
Dr. Owusu and his colleagues reviewed the charts of 43 patients younger than age 18 years who underwent parotidectomies at a single tertiary care center between 1999 and 2011. Patients who only had parotid biopsies and those without follow-up data were excluded from the study. The average age of the patients was 4 years, and 58% were girls.
Postoperatively, 33 children (77%) had normal nerve function and 10 (23%) had abnormal nerve function. One patient experienced immediate facial nerve paralysis and nine experienced immediate facial nerve paresis. The marginal mandibular branch was affected in seven patients, the frontal branch in one patient, the buccal branch in one, and both marginal mandibular and frontal branches in one.
The most common diagnosis that led to a parotidectomy was atypical mycobacterium infection (37%), followed by branchial cleft abnormality (19%) and lymphangioma (16%). Nearly all (41) of the children underwent superficial parotidectomy; 2 underwent total parotidectomy.
"Age, gender, and pathologic diagnosis were not predictive of postoperative nerve dysfunction," Dr. Owusu said.
In patients with paresis, full nerve recovery occurred within 1 month for 2 patients, within 2 months for 1 patient, within 6 months for 3 patients, and within 10 months for 2 patients. Final nerve status was not available for 1 patient.
The study was limited by its small size and focus on a single center, Dr. Owusu said.
Dr. Owusu had no financial conflicts to disclose.
WASHINGTON – Facial nerve dysfunction affected 23% of 43 children who had parotidectomies in a single-center study presented at the annual meeting of the American Academy of Otolaryngology–Head and Neck Surgery Foundation.
The findings suggest that facial nerve dysfunction after parotidectomy is common enough in children to merit preoperative counseling, said Dr. James A. Owusu of the University of Minnesota, Minneapolis.
Facial nerve dysfunction rates reported in the literature range from 9% to 60% in adults after parotidectomy, but the condition has not been well studied in children.
Dr. Owusu and his colleagues reviewed the charts of 43 patients younger than age 18 years who underwent parotidectomies at a single tertiary care center between 1999 and 2011. Patients who only had parotid biopsies and those without follow-up data were excluded from the study. The average age of the patients was 4 years, and 58% were girls.
Postoperatively, 33 children (77%) had normal nerve function and 10 (23%) had abnormal nerve function. One patient experienced immediate facial nerve paralysis and nine experienced immediate facial nerve paresis. The marginal mandibular branch was affected in seven patients, the frontal branch in one patient, the buccal branch in one, and both marginal mandibular and frontal branches in one.
The most common diagnosis that led to a parotidectomy was atypical mycobacterium infection (37%), followed by branchial cleft abnormality (19%) and lymphangioma (16%). Nearly all (41) of the children underwent superficial parotidectomy; 2 underwent total parotidectomy.
"Age, gender, and pathologic diagnosis were not predictive of postoperative nerve dysfunction," Dr. Owusu said.
In patients with paresis, full nerve recovery occurred within 1 month for 2 patients, within 2 months for 1 patient, within 6 months for 3 patients, and within 10 months for 2 patients. Final nerve status was not available for 1 patient.
The study was limited by its small size and focus on a single center, Dr. Owusu said.
Dr. Owusu had no financial conflicts to disclose.
WASHINGTON – Facial nerve dysfunction affected 23% of 43 children who had parotidectomies in a single-center study presented at the annual meeting of the American Academy of Otolaryngology–Head and Neck Surgery Foundation.
The findings suggest that facial nerve dysfunction after parotidectomy is common enough in children to merit preoperative counseling, said Dr. James A. Owusu of the University of Minnesota, Minneapolis.
Facial nerve dysfunction rates reported in the literature range from 9% to 60% in adults after parotidectomy, but the condition has not been well studied in children.
Dr. Owusu and his colleagues reviewed the charts of 43 patients younger than age 18 years who underwent parotidectomies at a single tertiary care center between 1999 and 2011. Patients who only had parotid biopsies and those without follow-up data were excluded from the study. The average age of the patients was 4 years, and 58% were girls.
Postoperatively, 33 children (77%) had normal nerve function and 10 (23%) had abnormal nerve function. One patient experienced immediate facial nerve paralysis and nine experienced immediate facial nerve paresis. The marginal mandibular branch was affected in seven patients, the frontal branch in one patient, the buccal branch in one, and both marginal mandibular and frontal branches in one.
The most common diagnosis that led to a parotidectomy was atypical mycobacterium infection (37%), followed by branchial cleft abnormality (19%) and lymphangioma (16%). Nearly all (41) of the children underwent superficial parotidectomy; 2 underwent total parotidectomy.
"Age, gender, and pathologic diagnosis were not predictive of postoperative nerve dysfunction," Dr. Owusu said.
In patients with paresis, full nerve recovery occurred within 1 month for 2 patients, within 2 months for 1 patient, within 6 months for 3 patients, and within 10 months for 2 patients. Final nerve status was not available for 1 patient.
The study was limited by its small size and focus on a single center, Dr. Owusu said.
Dr. Owusu had no financial conflicts to disclose.
AT THE ANNUAL MEETING OF THE AMERICAN ACADEMY OF OTOLARYNGOLOGY - HEAD AND NECK SURGERY FOUNDATION
Major Finding: After parotidectomies, 23% of children experienced facial nerve dysfunction, but most were fully recovered within 6 months.
Data Source: Investigators reviewed the charts of 43 children who underwent parotidectomies at a single center between 1999 and 2011.
Disclosures: Dr. Owusu had no financial conflicts to disclose.
Antibodies May Link to Lung Disease in RA
WASHINGTON – Specific anticitrullinated peptide antibody levels were significantly higher in rheumatoid arthritis patients with interstitial lung disease than in those without lung disease, based on data from 177 patients.
Complications and death are common in rheumatoid arthritis (RA) patients with interstitial lung disease (ILD), and the findings "may implicate the lung as a site in which protein citrullination initiates epitope spreading and propagation of RA," said Dr. Jon T. Giles of Columbia University in New York.

To determine the association of anticitrullinated peptide antibodies (ACPA) with ILD, Dr. Giles and his colleagues reviewed data from multidetector computed tomography images and concurrent serum samples for 177 RA patients. The mean age of the patients was 59 years, 60% were women, and 11% were smokers.
A total of 57 patients (32%) showed some evidence of ILD on imaging, and 32 (18%) had ILD scores of 3 U or higher, Dr. Giles said at the meeting. Overall, levels of anticyclic citrullinated peptide (anti-CCP) and 17 specific ACPAs ranged from 46% to 273% higher in patients with ILD than in those without ILD. Patients with ILD were more likely to be male, to smoke, and to have a history of prednisone and leflunomide use as well as rheumatoid factor and anti-CCP seropositivity compared with patients without ILD, said Dr. Giles.
Anti-CCP seropositivity was significantly more common among patients with any ILD vs. those without ILD (89% vs. 69%), and the seropositivity was even more common (94%) in patients with ILD scores of 3 U or higher.
Higher levels of seven or more ACPAs were significantly more common in patients with reticulation, honeycombing, or traction bronchiectasis than in those with no ILD (40% vs. 18%).
In addition, higher levels of seven or more ACPAs were significantly more common in patients with evidence of restriction on a pulmonary function test and/or decreased results on a diffusing capacity of the lungs for carbon monoxide test compared with those without ILD (39% vs. 20%). The differences were significant after adjustment for age, sex, smoking status, disease activity score (using DAS28), and current prednisone and leflunomide use.
Levels of antibodies targeting noncitrullinated proteins were not significantly higher in patients with ILD, which "suggests a specificity for ACPA in the association," Dr. Giles said.
"Another mechanistic possibility is that ACPA[s] targeting citrullinated synovial antigens are generated and mediate remote pathogenic effects upon circulating to the lungs, where their cognate citrullinated proteins may also be present," he said.
The findings were limited in part by the use of multidetector computed tomography, which differs in slice thickness from high-resolution CT, Dr. Giles noted. But the strengths of the research include the multiple measures of pulmonary disease, he said.
Dr. Giles said he had no financial conflicts to disclose. The study was supported in part by the National Institute of Arthritis and Musculoskeletal and Skin Diseases and the American College of Rheumatology’s Within Our Reach Campaign.
WASHINGTON – Specific anticitrullinated peptide antibody levels were significantly higher in rheumatoid arthritis patients with interstitial lung disease than in those without lung disease, based on data from 177 patients.
Complications and death are common in rheumatoid arthritis (RA) patients with interstitial lung disease (ILD), and the findings "may implicate the lung as a site in which protein citrullination initiates epitope spreading and propagation of RA," said Dr. Jon T. Giles of Columbia University in New York.
To determine the association of anticitrullinated peptide antibodies (ACPA) with ILD, Dr. Giles and his colleagues reviewed data from multidetector computed tomography images and concurrent serum samples for 177 RA patients. The mean age of the patients was 59 years, 60% were women, and 11% were smokers.
A total of 57 patients (32%) showed some evidence of ILD on imaging, and 32 (18%) had ILD scores of 3 U or higher, Dr. Giles said at the meeting. Overall, levels of anticyclic citrullinated peptide (anti-CCP) and 17 specific ACPAs ranged from 46% to 273% higher in patients with ILD than in those without ILD. Patients with ILD were more likely to be male, to smoke, and to have a history of prednisone and leflunomide use as well as rheumatoid factor and anti-CCP seropositivity compared with patients without ILD, said Dr. Giles.
Anti-CCP seropositivity was significantly more common among patients with any ILD vs. those without ILD (89% vs. 69%), and the seropositivity was even more common (94%) in patients with ILD scores of 3 U or higher.
Higher levels of seven or more ACPAs were significantly more common in patients with reticulation, honeycombing, or traction bronchiectasis than in those with no ILD (40% vs. 18%).
In addition, higher levels of seven or more ACPAs were significantly more common in patients with evidence of restriction on a pulmonary function test and/or decreased results on a diffusing capacity of the lungs for carbon monoxide test compared with those without ILD (39% vs. 20%). The differences were significant after adjustment for age, sex, smoking status, disease activity score (using DAS28), and current prednisone and leflunomide use.
Levels of antibodies targeting noncitrullinated proteins were not significantly higher in patients with ILD, which "suggests a specificity for ACPA in the association," Dr. Giles said.
"Another mechanistic possibility is that ACPA[s] targeting citrullinated synovial antigens are generated and mediate remote pathogenic effects upon circulating to the lungs, where their cognate citrullinated proteins may also be present," he said.
The findings were limited in part by the use of multidetector computed tomography, which differs in slice thickness from high-resolution CT, Dr. Giles noted. But the strengths of the research include the multiple measures of pulmonary disease, he said.
Dr. Giles said he had no financial conflicts to disclose. The study was supported in part by the National Institute of Arthritis and Musculoskeletal and Skin Diseases and the American College of Rheumatology’s Within Our Reach Campaign.
WASHINGTON – Specific anticitrullinated peptide antibody levels were significantly higher in rheumatoid arthritis patients with interstitial lung disease than in those without lung disease, based on data from 177 patients.
Complications and death are common in rheumatoid arthritis (RA) patients with interstitial lung disease (ILD), and the findings "may implicate the lung as a site in which protein citrullination initiates epitope spreading and propagation of RA," said Dr. Jon T. Giles of Columbia University in New York.
To determine the association of anticitrullinated peptide antibodies (ACPA) with ILD, Dr. Giles and his colleagues reviewed data from multidetector computed tomography images and concurrent serum samples for 177 RA patients. The mean age of the patients was 59 years, 60% were women, and 11% were smokers.
A total of 57 patients (32%) showed some evidence of ILD on imaging, and 32 (18%) had ILD scores of 3 U or higher, Dr. Giles said at the meeting. Overall, levels of anticyclic citrullinated peptide (anti-CCP) and 17 specific ACPAs ranged from 46% to 273% higher in patients with ILD than in those without ILD. Patients with ILD were more likely to be male, to smoke, and to have a history of prednisone and leflunomide use as well as rheumatoid factor and anti-CCP seropositivity compared with patients without ILD, said Dr. Giles.
Anti-CCP seropositivity was significantly more common among patients with any ILD vs. those without ILD (89% vs. 69%), and the seropositivity was even more common (94%) in patients with ILD scores of 3 U or higher.
Higher levels of seven or more ACPAs were significantly more common in patients with reticulation, honeycombing, or traction bronchiectasis than in those with no ILD (40% vs. 18%).
In addition, higher levels of seven or more ACPAs were significantly more common in patients with evidence of restriction on a pulmonary function test and/or decreased results on a diffusing capacity of the lungs for carbon monoxide test compared with those without ILD (39% vs. 20%). The differences were significant after adjustment for age, sex, smoking status, disease activity score (using DAS28), and current prednisone and leflunomide use.
Levels of antibodies targeting noncitrullinated proteins were not significantly higher in patients with ILD, which "suggests a specificity for ACPA in the association," Dr. Giles said.
"Another mechanistic possibility is that ACPA[s] targeting citrullinated synovial antigens are generated and mediate remote pathogenic effects upon circulating to the lungs, where their cognate citrullinated proteins may also be present," he said.
The findings were limited in part by the use of multidetector computed tomography, which differs in slice thickness from high-resolution CT, Dr. Giles noted. But the strengths of the research include the multiple measures of pulmonary disease, he said.
Dr. Giles said he had no financial conflicts to disclose. The study was supported in part by the National Institute of Arthritis and Musculoskeletal and Skin Diseases and the American College of Rheumatology’s Within Our Reach Campaign.
AT THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF RHEUMATOLOGY
Major Finding: Levels of anticyclic citrullinated peptide and 17 specific anticitrullinated peptide antibodies ranged from 46% to 273% higher in rheumatoid arthritis patients with interstitial lung disease than in those without.
Data Source: The data come from chest imaging and serum samples from 177 adults with RA.
Disclosures: Dr. Giles said he had no relevant financial conflicts to disclose. The study was supported in part by the National Institute of Arthritis and Musculoskeletal and Skin Diseases and the American College of Rheumatology’s Within Our Reach Campaign.
