User login
BIMA’s benefits extend to high-risk CABG patients
COLORADO SPRINGS – The survival advantage of bilateral internal over left internal mammary artery grafts persists even among multivessel CABG patients perceived to be at high surgical risk, Nishant Saran, MD, reported at the annual meeting of the Western Thoracic Surgical Association.
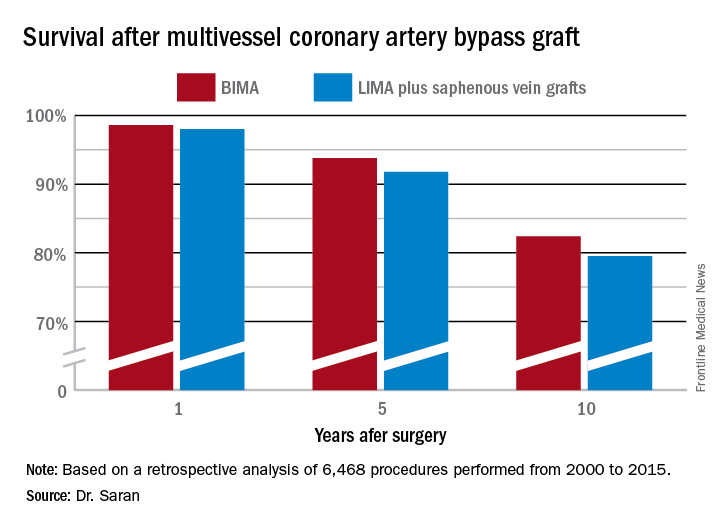
Many surgeons hesitate to perform bilateral internal mammary artery (BIMA) grafting in high-risk patients on the presumption that BIMA might not benefit them. It’s a concern that appears to be without merit, however, based on a retrospective analysis of the 6,468 multivessel CABG procedures performed at the Mayo Clinic during 2000-2015, said Dr. Saran of the Mayo Clinic in Rochester, Minn.

The BIMA patients were as a whole significantly younger, primarily men, and less likely to have diabetes or to be obese than the LIMA patients. Also, LIMA patients were fourfold more likely to have baseline heart failure, twice as likely to have a history of stroke, and had a twofold greater prevalence of chronic lung disease.
“The unmatched comparison shows the clear treatment selection bias we have: BIMA goes to the healthier patients,” Dr. Saran observed.
But is that bias justified? To find out, he and his coinvestigators performed extensive propensity score matching using several dozen baseline variables in order to identify 1,011 closely matched patient pairs. In this propensity score-matched analysis, 5- and 10-year survival rates were significantly better in the BIMA group. The gap between the two survival curves widened after about 7 years and continued to expand steadily through year 10. Incision time averaged 298 minutes in the BIMA group and 254 minutes in the propensity-matched LIMA group.
Discussant Eric J. Lehr, MD, a cardiac surgeon at Swedish Medical Center in Seattle, noted that the impressive survival benefit for BIMA in the retrospective Mayo Clinic study came at what he termed “a modest cost”: a doubled incidence of sternal site infections, from 1.4% in the LIMA group to 3% with BIMA. Importantly, though, there was no significant difference in the more serious deep sternal wound infections.
He agreed with Dr. Saran that BIMA is seriously underutilized, noting that only one cardiothoracic surgery program in the state of Washington uses BIMA more than 10% of the time in multivessel CABG.
Dr. Lehr then posed a provocative question: “Should BIMA grafting be considered a quality metric in coronary revascularization surgery, despite the small increase in sternal site infections, even though sternal wound infections have been declared a ‘never’ event and are tied to reimbursement?”
“I think BIMA should be a gold standard,” Dr. Saran replied. “The first thing that a cardiac surgeon should always think of when a patient is going to have CABG is ‘BIMA first,’ and only then look into reasons for not doing it. But I guess in current real-world practice, things are different.”
Howard K. Song, MD, commented, “I think a study like this doesn’t necessarily show that every surgeon should be using BIMA liberally, it shows that surgeons in your practice who do that have excellent outcomes.”
Dr. Song, professor of surgery and chief of the division of cardiothoracic surgery at Oregon Health and Science University, Portland, added that he believes extensive use of BIMA is actually a surrogate marker for a highly skilled subspecialist who would be expected to have very good outcomes as a matter of course.
“That may be one way of looking at it; however, I do think that even very skilled surgeons still have an inherent resistance to doing BIMA,” Dr. Saran responded.
“In the current era, the surgeon is pressured to achieve improved short-term outcomes and improved OR turnover times. An extra half hour for BIMA tends to push the surgeon away,” he added.
Dr. Saran reported having no financial conflicts of interest.
COLORADO SPRINGS – The survival advantage of bilateral internal over left internal mammary artery grafts persists even among multivessel CABG patients perceived to be at high surgical risk, Nishant Saran, MD, reported at the annual meeting of the Western Thoracic Surgical Association.
Many surgeons hesitate to perform bilateral internal mammary artery (BIMA) grafting in high-risk patients on the presumption that BIMA might not benefit them. It’s a concern that appears to be without merit, however, based on a retrospective analysis of the 6,468 multivessel CABG procedures performed at the Mayo Clinic during 2000-2015, said Dr. Saran of the Mayo Clinic in Rochester, Minn.
The BIMA patients were as a whole significantly younger, primarily men, and less likely to have diabetes or to be obese than the LIMA patients. Also, LIMA patients were fourfold more likely to have baseline heart failure, twice as likely to have a history of stroke, and had a twofold greater prevalence of chronic lung disease.
“The unmatched comparison shows the clear treatment selection bias we have: BIMA goes to the healthier patients,” Dr. Saran observed.
But is that bias justified? To find out, he and his coinvestigators performed extensive propensity score matching using several dozen baseline variables in order to identify 1,011 closely matched patient pairs. In this propensity score-matched analysis, 5- and 10-year survival rates were significantly better in the BIMA group. The gap between the two survival curves widened after about 7 years and continued to expand steadily through year 10. Incision time averaged 298 minutes in the BIMA group and 254 minutes in the propensity-matched LIMA group.
Discussant Eric J. Lehr, MD, a cardiac surgeon at Swedish Medical Center in Seattle, noted that the impressive survival benefit for BIMA in the retrospective Mayo Clinic study came at what he termed “a modest cost”: a doubled incidence of sternal site infections, from 1.4% in the LIMA group to 3% with BIMA. Importantly, though, there was no significant difference in the more serious deep sternal wound infections.
He agreed with Dr. Saran that BIMA is seriously underutilized, noting that only one cardiothoracic surgery program in the state of Washington uses BIMA more than 10% of the time in multivessel CABG.
Dr. Lehr then posed a provocative question: “Should BIMA grafting be considered a quality metric in coronary revascularization surgery, despite the small increase in sternal site infections, even though sternal wound infections have been declared a ‘never’ event and are tied to reimbursement?”
“I think BIMA should be a gold standard,” Dr. Saran replied. “The first thing that a cardiac surgeon should always think of when a patient is going to have CABG is ‘BIMA first,’ and only then look into reasons for not doing it. But I guess in current real-world practice, things are different.”
Howard K. Song, MD, commented, “I think a study like this doesn’t necessarily show that every surgeon should be using BIMA liberally, it shows that surgeons in your practice who do that have excellent outcomes.”
Dr. Song, professor of surgery and chief of the division of cardiothoracic surgery at Oregon Health and Science University, Portland, added that he believes extensive use of BIMA is actually a surrogate marker for a highly skilled subspecialist who would be expected to have very good outcomes as a matter of course.
“That may be one way of looking at it; however, I do think that even very skilled surgeons still have an inherent resistance to doing BIMA,” Dr. Saran responded.
“In the current era, the surgeon is pressured to achieve improved short-term outcomes and improved OR turnover times. An extra half hour for BIMA tends to push the surgeon away,” he added.
Dr. Saran reported having no financial conflicts of interest.
COLORADO SPRINGS – The survival advantage of bilateral internal over left internal mammary artery grafts persists even among multivessel CABG patients perceived to be at high surgical risk, Nishant Saran, MD, reported at the annual meeting of the Western Thoracic Surgical Association.
Many surgeons hesitate to perform bilateral internal mammary artery (BIMA) grafting in high-risk patients on the presumption that BIMA might not benefit them. It’s a concern that appears to be without merit, however, based on a retrospective analysis of the 6,468 multivessel CABG procedures performed at the Mayo Clinic during 2000-2015, said Dr. Saran of the Mayo Clinic in Rochester, Minn.
The BIMA patients were as a whole significantly younger, primarily men, and less likely to have diabetes or to be obese than the LIMA patients. Also, LIMA patients were fourfold more likely to have baseline heart failure, twice as likely to have a history of stroke, and had a twofold greater prevalence of chronic lung disease.
“The unmatched comparison shows the clear treatment selection bias we have: BIMA goes to the healthier patients,” Dr. Saran observed.
But is that bias justified? To find out, he and his coinvestigators performed extensive propensity score matching using several dozen baseline variables in order to identify 1,011 closely matched patient pairs. In this propensity score-matched analysis, 5- and 10-year survival rates were significantly better in the BIMA group. The gap between the two survival curves widened after about 7 years and continued to expand steadily through year 10. Incision time averaged 298 minutes in the BIMA group and 254 minutes in the propensity-matched LIMA group.
Discussant Eric J. Lehr, MD, a cardiac surgeon at Swedish Medical Center in Seattle, noted that the impressive survival benefit for BIMA in the retrospective Mayo Clinic study came at what he termed “a modest cost”: a doubled incidence of sternal site infections, from 1.4% in the LIMA group to 3% with BIMA. Importantly, though, there was no significant difference in the more serious deep sternal wound infections.
He agreed with Dr. Saran that BIMA is seriously underutilized, noting that only one cardiothoracic surgery program in the state of Washington uses BIMA more than 10% of the time in multivessel CABG.
Dr. Lehr then posed a provocative question: “Should BIMA grafting be considered a quality metric in coronary revascularization surgery, despite the small increase in sternal site infections, even though sternal wound infections have been declared a ‘never’ event and are tied to reimbursement?”
“I think BIMA should be a gold standard,” Dr. Saran replied. “The first thing that a cardiac surgeon should always think of when a patient is going to have CABG is ‘BIMA first,’ and only then look into reasons for not doing it. But I guess in current real-world practice, things are different.”
Howard K. Song, MD, commented, “I think a study like this doesn’t necessarily show that every surgeon should be using BIMA liberally, it shows that surgeons in your practice who do that have excellent outcomes.”
Dr. Song, professor of surgery and chief of the division of cardiothoracic surgery at Oregon Health and Science University, Portland, added that he believes extensive use of BIMA is actually a surrogate marker for a highly skilled subspecialist who would be expected to have very good outcomes as a matter of course.
“That may be one way of looking at it; however, I do think that even very skilled surgeons still have an inherent resistance to doing BIMA,” Dr. Saran responded.
“In the current era, the surgeon is pressured to achieve improved short-term outcomes and improved OR turnover times. An extra half hour for BIMA tends to push the surgeon away,” he added.
Dr. Saran reported having no financial conflicts of interest.
AT THE WTSA ANNUAL MEETING
Key clinical point:
Major finding: Ten-year survival following multivessel CABG using bilateral internal mammary artery grafting was 82.4%, significantly better than the 79.5% rate with left internal mammary artery grafting plus saphenous vein grafts.
Data source: This retrospective observational single-center included 6,468 patients who underwent multivessel CABG during 2000-2015.
Disclosures: Dr. Saran reported having no financial conflicts of interest.
Domperidone appears safe galactagogue for mothers and infants
Denver – Prescribing domperidone to support breastfeeding effectively reduced the use of infant formula without significant adverse effects in mothers and infants in a large retrospective study, Mitko Madjunkov, MD, reported at the annual meeting of the Teratology Society.
His study included 985 mothers who began taking domperidone to initiate and support breastfeeding after a visit to the International Breastfeeding Centre in Toronto. Collectively, the women had 1,005 infants.
The study was undertaken because few data exist on the dosing and safety of domperidone during lactation. Additionally, the Food and Drug Administration issued a warning in 2004 regarding the use of domperidone as a galactagogue in response to reports of cardiac arrhythmias and sudden deaths when the drug was prescribed as an antiemetic, explained Dr. Madjunkov of the Hospital for Sick Children in Toronto.
The FDA has not approved domperidone for any indication in the United States, though it is available in Canada and other countries.
Domperidone was used by the Toronto women for a median of 20 days. The maximum daily dose was 107 mg. The infants were an average of 38 days old at the time of the visit when domperidone was prescribed and 72 days of age at their last follow-up visit related to the study.
The drug was effective as a galactagogue: 63% of women were using infant formula before going on domperidone; after using the drug, 41% were still using formula, for an absolute 22% reduction. The drug was similarly effective in promoting breastfeeding in infants with or without tongue-tie/lip-tie defects.
In total, 18% of mothers reported minor side effects. Headaches were the most common, reported by 9.2% of domperidone users. Dose reduction was employed in just 0.6% of women in the study; 0.4% of participants discontinued treatment. Rapid heart rate and other minor cardiac side effects were reported by 0.7% of women, uniformly in conjunction with trigger factors such as anxiety or caffeine use, but none of these women discontinued treatment. No treatment-associated adverse effects occurred in the infants.
Dr. Madjunkov reported having no financial conflicts related to his study.
Denver – Prescribing domperidone to support breastfeeding effectively reduced the use of infant formula without significant adverse effects in mothers and infants in a large retrospective study, Mitko Madjunkov, MD, reported at the annual meeting of the Teratology Society.
His study included 985 mothers who began taking domperidone to initiate and support breastfeeding after a visit to the International Breastfeeding Centre in Toronto. Collectively, the women had 1,005 infants.
The study was undertaken because few data exist on the dosing and safety of domperidone during lactation. Additionally, the Food and Drug Administration issued a warning in 2004 regarding the use of domperidone as a galactagogue in response to reports of cardiac arrhythmias and sudden deaths when the drug was prescribed as an antiemetic, explained Dr. Madjunkov of the Hospital for Sick Children in Toronto.
The FDA has not approved domperidone for any indication in the United States, though it is available in Canada and other countries.
Domperidone was used by the Toronto women for a median of 20 days. The maximum daily dose was 107 mg. The infants were an average of 38 days old at the time of the visit when domperidone was prescribed and 72 days of age at their last follow-up visit related to the study.
The drug was effective as a galactagogue: 63% of women were using infant formula before going on domperidone; after using the drug, 41% were still using formula, for an absolute 22% reduction. The drug was similarly effective in promoting breastfeeding in infants with or without tongue-tie/lip-tie defects.
In total, 18% of mothers reported minor side effects. Headaches were the most common, reported by 9.2% of domperidone users. Dose reduction was employed in just 0.6% of women in the study; 0.4% of participants discontinued treatment. Rapid heart rate and other minor cardiac side effects were reported by 0.7% of women, uniformly in conjunction with trigger factors such as anxiety or caffeine use, but none of these women discontinued treatment. No treatment-associated adverse effects occurred in the infants.
Dr. Madjunkov reported having no financial conflicts related to his study.
Denver – Prescribing domperidone to support breastfeeding effectively reduced the use of infant formula without significant adverse effects in mothers and infants in a large retrospective study, Mitko Madjunkov, MD, reported at the annual meeting of the Teratology Society.
His study included 985 mothers who began taking domperidone to initiate and support breastfeeding after a visit to the International Breastfeeding Centre in Toronto. Collectively, the women had 1,005 infants.
The study was undertaken because few data exist on the dosing and safety of domperidone during lactation. Additionally, the Food and Drug Administration issued a warning in 2004 regarding the use of domperidone as a galactagogue in response to reports of cardiac arrhythmias and sudden deaths when the drug was prescribed as an antiemetic, explained Dr. Madjunkov of the Hospital for Sick Children in Toronto.
The FDA has not approved domperidone for any indication in the United States, though it is available in Canada and other countries.
Domperidone was used by the Toronto women for a median of 20 days. The maximum daily dose was 107 mg. The infants were an average of 38 days old at the time of the visit when domperidone was prescribed and 72 days of age at their last follow-up visit related to the study.
The drug was effective as a galactagogue: 63% of women were using infant formula before going on domperidone; after using the drug, 41% were still using formula, for an absolute 22% reduction. The drug was similarly effective in promoting breastfeeding in infants with or without tongue-tie/lip-tie defects.
In total, 18% of mothers reported minor side effects. Headaches were the most common, reported by 9.2% of domperidone users. Dose reduction was employed in just 0.6% of women in the study; 0.4% of participants discontinued treatment. Rapid heart rate and other minor cardiac side effects were reported by 0.7% of women, uniformly in conjunction with trigger factors such as anxiety or caffeine use, but none of these women discontinued treatment. No treatment-associated adverse effects occurred in the infants.
Dr. Madjunkov reported having no financial conflicts related to his study.
EXPERT ANALYSIS FROM TERATOLOGY SOCIETY 2017
Key clinical point:
Major finding: The use of the domperidone reduced the proportion of women using infant formula by an absolute 22%.
Data source: A retrospective study of 985 women who were prescribed domperidone as a galactagogue at the International Breastfeeding Centre in Toronto.
Disclosures: Dr. Madjunkov reported having no financial conflicts of interest related to the study.
Minimally invasive esophagectomy may mean less major morbidity
COLORADO SPRINGS – Minimally invasive esophagectomy was associated with a significantly lower rate of postoperative major morbidity as well as a mean 1-day briefer length of stay than open esophagectomy in a propensity-matched analysis of the real-world American College of Surgeons-National Quality Improvement Program database, Mark F. Berry, MD, reported at the annual meeting of the Western Thoracic Surgical Association.
However, both of the study’s discussants questioned whether the reported modest absolute reduction in major morbidity was really attributable to the minimally invasive approach or could instead have resulted from one of several potential confounders that couldn’t be fully adjusted for, given inherent limitations of the ACS-NSQIP database.
“There was a statistically significant difference in morbidity,” replied Dr. Berry of Stanford (Calif.) University. “It was a 4% absolute difference, which I think is probably clinically meaningful, but certainly it’s not really, really dramatic.”

“What I think we found is that it’s safe to do a minimally invasive esophagectomy and safe for people to introduce it into their practice. But it’s not necessarily something that’s a game changer, unlike what’s been seen with minimally invasive approaches for some other things,” said Dr. Berry, who added that he didn’t wish to overstate the importance of the observed difference in morbidity.
Studies from high-volume centers show that minimally-invasive esophagectomy (MIE) reduces length of stay, postoperative major morbidity, and features equivalent or even slightly lower mortality than traditional open esophagectomy, the generalizability of these findings beyond such centers is questionable. That’s why Dr. Berry and his coinvestigators turned to the ACS-NSQIP database, which includes all esophagectomies performed for esophageal cancer at roughly 700 U.S. hospitals, not just those done by board-certified thoracic surgeons.
He presented a retrospective cohort study of 3,901 esophagectomy patients during 2005-2013 who met study criteria, 16.4% of whom had MIE. The use of this approach increased steadily from 6.5% of all esophagectomies in 2005 to 22.3% in 2013. A propensity-matched analysis designed to neutralize potentially confounding differences included 638 MIE and 1,914 open esophagectomy patients.
The primary outcome was the 30-day rate of composite major morbidity in the realms of various wound, respiratory, renal, and cardiovascular complications. The rate was 36.1% in the MIE group and 40.5% with open esophagectomy in the propensity-matched analysis, an absolute risk reduction of 4.4% and a relative risk reduction of 17%. Although rates were consistently slightly lower in each of the categories of major morbidity, those individual differences didn’t achieve statistical significance. The difference in major morbidity became significant only when major morbidity was considered as a whole.
Mean length of stay was 9 days with MIE and 10 days with open surgery.
There was no significant difference between the two study groups in 30-day rates of readmission, reoperation, or mortality.
Discussant Donald E. Low said “esophagectomy is being analysed regarding its place in all sorts of presentations, stages, and situations, so the aspect of making sure that we’re delivering the services as efficiently as possible is going to become more important, not less important.”
That being said, he noted that there is no specific CPT code for MIE. That raises the possibility of an uncertain amount of procedural misclassification in the ACS-NSQIP database.
Also, the only significant difference in major morbidity between the two study groups was in the subcategory of intra- or postoperative bleeding requiring transfusion, which occurred in 10.8% of the MIE and 16.7% of the open esophagectomy groups, observed Dr. Low, director of the Esophageal Center of Excellence at Virginia Mason Medical Center, Seattle.
“Some of us believe that blood utilization and transfusion requirement is really a quality measure and not a complication,” the surgeon said. And if that outcome is excluded from consideration, then there is no significant difference in major morbidity.
Discussant Douglas E. Wood, MD, professor and chair of the department of surgery at the University of Washington, Seattle, took the opportunity to share a self-described “pet peeve” about analyses of national surgical databases: these databases typically don’t contain key details necessary to correct for provider and hospital characteristics.
“The small differences that you demonstrate could easily have been completely driven by providers who choose to do minimally invasive esophagectomy and are in higher-volume, more specialized centers,” he said. “I’m not convinced of your conclusion that MIE produces less morbidity based on a 4% difference and no analysis of provider characteristics.”
COLORADO SPRINGS – Minimally invasive esophagectomy was associated with a significantly lower rate of postoperative major morbidity as well as a mean 1-day briefer length of stay than open esophagectomy in a propensity-matched analysis of the real-world American College of Surgeons-National Quality Improvement Program database, Mark F. Berry, MD, reported at the annual meeting of the Western Thoracic Surgical Association.
However, both of the study’s discussants questioned whether the reported modest absolute reduction in major morbidity was really attributable to the minimally invasive approach or could instead have resulted from one of several potential confounders that couldn’t be fully adjusted for, given inherent limitations of the ACS-NSQIP database.
“There was a statistically significant difference in morbidity,” replied Dr. Berry of Stanford (Calif.) University. “It was a 4% absolute difference, which I think is probably clinically meaningful, but certainly it’s not really, really dramatic.”
“What I think we found is that it’s safe to do a minimally invasive esophagectomy and safe for people to introduce it into their practice. But it’s not necessarily something that’s a game changer, unlike what’s been seen with minimally invasive approaches for some other things,” said Dr. Berry, who added that he didn’t wish to overstate the importance of the observed difference in morbidity.
Studies from high-volume centers show that minimally-invasive esophagectomy (MIE) reduces length of stay, postoperative major morbidity, and features equivalent or even slightly lower mortality than traditional open esophagectomy, the generalizability of these findings beyond such centers is questionable. That’s why Dr. Berry and his coinvestigators turned to the ACS-NSQIP database, which includes all esophagectomies performed for esophageal cancer at roughly 700 U.S. hospitals, not just those done by board-certified thoracic surgeons.
He presented a retrospective cohort study of 3,901 esophagectomy patients during 2005-2013 who met study criteria, 16.4% of whom had MIE. The use of this approach increased steadily from 6.5% of all esophagectomies in 2005 to 22.3% in 2013. A propensity-matched analysis designed to neutralize potentially confounding differences included 638 MIE and 1,914 open esophagectomy patients.
The primary outcome was the 30-day rate of composite major morbidity in the realms of various wound, respiratory, renal, and cardiovascular complications. The rate was 36.1% in the MIE group and 40.5% with open esophagectomy in the propensity-matched analysis, an absolute risk reduction of 4.4% and a relative risk reduction of 17%. Although rates were consistently slightly lower in each of the categories of major morbidity, those individual differences didn’t achieve statistical significance. The difference in major morbidity became significant only when major morbidity was considered as a whole.
Mean length of stay was 9 days with MIE and 10 days with open surgery.
There was no significant difference between the two study groups in 30-day rates of readmission, reoperation, or mortality.
Discussant Donald E. Low said “esophagectomy is being analysed regarding its place in all sorts of presentations, stages, and situations, so the aspect of making sure that we’re delivering the services as efficiently as possible is going to become more important, not less important.”
That being said, he noted that there is no specific CPT code for MIE. That raises the possibility of an uncertain amount of procedural misclassification in the ACS-NSQIP database.
Also, the only significant difference in major morbidity between the two study groups was in the subcategory of intra- or postoperative bleeding requiring transfusion, which occurred in 10.8% of the MIE and 16.7% of the open esophagectomy groups, observed Dr. Low, director of the Esophageal Center of Excellence at Virginia Mason Medical Center, Seattle.
“Some of us believe that blood utilization and transfusion requirement is really a quality measure and not a complication,” the surgeon said. And if that outcome is excluded from consideration, then there is no significant difference in major morbidity.
Discussant Douglas E. Wood, MD, professor and chair of the department of surgery at the University of Washington, Seattle, took the opportunity to share a self-described “pet peeve” about analyses of national surgical databases: these databases typically don’t contain key details necessary to correct for provider and hospital characteristics.
“The small differences that you demonstrate could easily have been completely driven by providers who choose to do minimally invasive esophagectomy and are in higher-volume, more specialized centers,” he said. “I’m not convinced of your conclusion that MIE produces less morbidity based on a 4% difference and no analysis of provider characteristics.”
COLORADO SPRINGS – Minimally invasive esophagectomy was associated with a significantly lower rate of postoperative major morbidity as well as a mean 1-day briefer length of stay than open esophagectomy in a propensity-matched analysis of the real-world American College of Surgeons-National Quality Improvement Program database, Mark F. Berry, MD, reported at the annual meeting of the Western Thoracic Surgical Association.
However, both of the study’s discussants questioned whether the reported modest absolute reduction in major morbidity was really attributable to the minimally invasive approach or could instead have resulted from one of several potential confounders that couldn’t be fully adjusted for, given inherent limitations of the ACS-NSQIP database.
“There was a statistically significant difference in morbidity,” replied Dr. Berry of Stanford (Calif.) University. “It was a 4% absolute difference, which I think is probably clinically meaningful, but certainly it’s not really, really dramatic.”
“What I think we found is that it’s safe to do a minimally invasive esophagectomy and safe for people to introduce it into their practice. But it’s not necessarily something that’s a game changer, unlike what’s been seen with minimally invasive approaches for some other things,” said Dr. Berry, who added that he didn’t wish to overstate the importance of the observed difference in morbidity.
Studies from high-volume centers show that minimally-invasive esophagectomy (MIE) reduces length of stay, postoperative major morbidity, and features equivalent or even slightly lower mortality than traditional open esophagectomy, the generalizability of these findings beyond such centers is questionable. That’s why Dr. Berry and his coinvestigators turned to the ACS-NSQIP database, which includes all esophagectomies performed for esophageal cancer at roughly 700 U.S. hospitals, not just those done by board-certified thoracic surgeons.
He presented a retrospective cohort study of 3,901 esophagectomy patients during 2005-2013 who met study criteria, 16.4% of whom had MIE. The use of this approach increased steadily from 6.5% of all esophagectomies in 2005 to 22.3% in 2013. A propensity-matched analysis designed to neutralize potentially confounding differences included 638 MIE and 1,914 open esophagectomy patients.
The primary outcome was the 30-day rate of composite major morbidity in the realms of various wound, respiratory, renal, and cardiovascular complications. The rate was 36.1% in the MIE group and 40.5% with open esophagectomy in the propensity-matched analysis, an absolute risk reduction of 4.4% and a relative risk reduction of 17%. Although rates were consistently slightly lower in each of the categories of major morbidity, those individual differences didn’t achieve statistical significance. The difference in major morbidity became significant only when major morbidity was considered as a whole.
Mean length of stay was 9 days with MIE and 10 days with open surgery.
There was no significant difference between the two study groups in 30-day rates of readmission, reoperation, or mortality.
Discussant Donald E. Low said “esophagectomy is being analysed regarding its place in all sorts of presentations, stages, and situations, so the aspect of making sure that we’re delivering the services as efficiently as possible is going to become more important, not less important.”
That being said, he noted that there is no specific CPT code for MIE. That raises the possibility of an uncertain amount of procedural misclassification in the ACS-NSQIP database.
Also, the only significant difference in major morbidity between the two study groups was in the subcategory of intra- or postoperative bleeding requiring transfusion, which occurred in 10.8% of the MIE and 16.7% of the open esophagectomy groups, observed Dr. Low, director of the Esophageal Center of Excellence at Virginia Mason Medical Center, Seattle.
“Some of us believe that blood utilization and transfusion requirement is really a quality measure and not a complication,” the surgeon said. And if that outcome is excluded from consideration, then there is no significant difference in major morbidity.
Discussant Douglas E. Wood, MD, professor and chair of the department of surgery at the University of Washington, Seattle, took the opportunity to share a self-described “pet peeve” about analyses of national surgical databases: these databases typically don’t contain key details necessary to correct for provider and hospital characteristics.
“The small differences that you demonstrate could easily have been completely driven by providers who choose to do minimally invasive esophagectomy and are in higher-volume, more specialized centers,” he said. “I’m not convinced of your conclusion that MIE produces less morbidity based on a 4% difference and no analysis of provider characteristics.”
AT WTSA 2017
Key clinical point:
Major finding: The 30-day rate of major morbidity was 36.1% in patients who underwent minimally invasive esophagectomy, significantly lower than the 40.5% rate with open esophagectomy in a propensity-matched analysis.
Data source: This retrospective cohort study included 3,901 patients who underwent esophagectomy for esophageal cancer as recorded in the American College of Surgeons-National Quality Improvement Program database for 2005-2013.
Disclosures: The study presenter reported having no financial conflicts of interest.
For interstitial cystitis, restrictive diet pays off
ESTES PARK, CO. – When patients with interstitial cystitis (IC) learn that first-line therapy is a rigorous diet designed to eliminate common bladder irritants, they tend to react in one of two ways, according to Julie A. Chacko, MD, a urologist in private practice in Santa Barbara, Calif.
Some “are just so grateful that they’re not crazy, which is what they’ve been told after 15 negative urine cultures. (Others) “look at the diet and think I’m sentencing them to death,” she said.
The sole medication approved by the Food and Drug Administration for IC is pentosan polysulfate sodium (Elmiron), and it should be reserved for the minority of patients who don’t experience significant improvement after giving the diet a reasonable shot, Dr. Chako advised. “When Elmiron works it’s great, but it’s not usually my go-to agent because it’s very expensive, you have to take it for 3-6 months to know for sure if it’s efficacious, and it has to be taken on an empty stomach. It’s a difficult medication.”

She advises patients to work with the diet. “Over time, they’re going to be able to find what I call their island – a point where they know very well their limitations and become quite comfortable with them,” she said at a conference on internal medicine sponsored by the University of Colorado.
A poorly understood yet common disorder, IC has a prevalence estimated at 0.5%-4% in women, less in men. Although typically diagnosed in the fourth decade or later, IC occurs at all ages. In some studies, the delay from first appearance of symptoms to arrival at a diagnosis is up to 8 years.
Interstitial cystitis is increasingly being called bladder pain syndrome in the literature, said Dr. Chako, who added, “I personally don’t love bladder pain syndrome as a description for this process. This syndrome has variable symptoms, and patients can have no pain at all.”
The mechanisms that result in IC are a mystery. The leading theory is that a bladder permeability problem allows urinary irritants to reach the interstitium. Nearly 80% of patients with IC can, with coaxing, identify dietary triggers for their symptoms, thereby basically establishing the diagnosis.
Other proposed mechanisms include an infectious agent that’s yet to be identified, allergic reaction, and neuromodulatory dysfunction. Common triggers other than foods include menses, copulation, emotional distress, and bladder trauma, including transvaginal ultrasound.
Conditions commonly associated with IC include fibromyalgia, irritable bowel syndrome, chronic fatigue, vulvodynia, migraines, depression, and anxiety.
The most common symptoms of IC are urinary urgency and frequency. Many affected patients have dysuria. Some have pain, which is typically suprapubic. However, pain can be present anywhere in a band circumscribing the whole central section of the torso, including the lower back, lower abdomen, urethra, vagina, and vulva. Patients describe a range of pain – burning, aching, stabbing, itching, buzzing, or a feeling of pressure.
“Most women who come in with IC are married to the idea that they’re having recurrent UTIs. They’re going to get antibiotics any way they can for their UTIs: over the phone, at urgent care. You need to get them to buy into the idea that even though UTIs are common, maybe not all of their flares are infections. They ask, ‘Then why do I feel better when I’m on antibiotics for recurrent UTI even though the cultures are negative?’ I say, ‘You feel less stress and anxiety because you think you’re on effective treatment,” Dr. Chacko said.
The diagnosis of IC is one of exclusions. Diagnoses to rule out before arriving at IC include recurrent UTI; overactive bladder, which should present with pure urge frequency and respond to medications for that condition; kidney stone disease present at the end of the ureter where it enters the bladder; gastrointestinal pathology; bladder cancer; and ovarian or uterine pathology.
Referral to a urologist for cystoscopy and cytology is appropriate in patients with microscopic hematuria, a significant smoking history predisposing to bladder cancer, or severe pain with severe frequency, which raises the possibility of Hunner’s ulcers, considered pathognomic for IC, respond “beautifully” to fulguration, she said.
Otherwise, IC can readily be managed by interested primary care physicians. The IC diet initially calls for 2 weeks of strict avoidance of all high-risk foods, most of which are acidic foods. These include fruits and fruit juices, especially citrus and cranberry juices; tomatoes and tomato products, including ketchup; yogurt; chocolate; coffee and tea, including decaf; vinegar; spicy foods; and carbonated beverages, water included.
These foods can later be added back one at a time to the diet while watching for IC flares, which typically occur within hours to several days of re-introducing the food. The return to coffee consumption, if that’s something important to the patient, should be with low-acid coffee. If that triggers an IC flare, try decaf. In time, many patients find they can consume some trigger foods in modest amounts.
“I tell patients it will take 12-18 months to get a good handle on their IC,” Dr. Chacko noted.
The use of OTC alkalizing agents such as Prelief may diffuse dietary triggers. A teaspoon of baking soda in water is also effective.
Second-line treatments include oral hydroxyzine 10-20 mg at bedtime; amitriptyline 10-20 mg at bedtime, mainly for patients with predominant pain symptoms; cimeditine; and pentosan polysulfate at 100 mg TID.
For IC patients with pelvic muscle tightness on pelvic examination, referral to a physical therapist adept at pelvic floor trigger point release can work wonders, she added.
One second-line option is bladder instillations of dimethyl sulfoxide weekly for 6 weeks, cutting back to once monthly maintenance therapy if the more intensive regimen is effective. Instillation of “heparin with lidocaine is a rescue solution. If it’s going to work, it kicks in within a few hours and usually lasts for 24-72 hours. It gets patients through a weekend, a wedding, or a funeral. A response can help make the IC diagnosis, too,” Dr. Chacko said.
She reported having no financial conflicts of interest regarding her presentation.
bjancin@frontlinemedcom.com
ESTES PARK, CO. – When patients with interstitial cystitis (IC) learn that first-line therapy is a rigorous diet designed to eliminate common bladder irritants, they tend to react in one of two ways, according to Julie A. Chacko, MD, a urologist in private practice in Santa Barbara, Calif.
Some “are just so grateful that they’re not crazy, which is what they’ve been told after 15 negative urine cultures. (Others) “look at the diet and think I’m sentencing them to death,” she said.
The sole medication approved by the Food and Drug Administration for IC is pentosan polysulfate sodium (Elmiron), and it should be reserved for the minority of patients who don’t experience significant improvement after giving the diet a reasonable shot, Dr. Chako advised. “When Elmiron works it’s great, but it’s not usually my go-to agent because it’s very expensive, you have to take it for 3-6 months to know for sure if it’s efficacious, and it has to be taken on an empty stomach. It’s a difficult medication.”
She advises patients to work with the diet. “Over time, they’re going to be able to find what I call their island – a point where they know very well their limitations and become quite comfortable with them,” she said at a conference on internal medicine sponsored by the University of Colorado.
A poorly understood yet common disorder, IC has a prevalence estimated at 0.5%-4% in women, less in men. Although typically diagnosed in the fourth decade or later, IC occurs at all ages. In some studies, the delay from first appearance of symptoms to arrival at a diagnosis is up to 8 years.
Interstitial cystitis is increasingly being called bladder pain syndrome in the literature, said Dr. Chako, who added, “I personally don’t love bladder pain syndrome as a description for this process. This syndrome has variable symptoms, and patients can have no pain at all.”
The mechanisms that result in IC are a mystery. The leading theory is that a bladder permeability problem allows urinary irritants to reach the interstitium. Nearly 80% of patients with IC can, with coaxing, identify dietary triggers for their symptoms, thereby basically establishing the diagnosis.
Other proposed mechanisms include an infectious agent that’s yet to be identified, allergic reaction, and neuromodulatory dysfunction. Common triggers other than foods include menses, copulation, emotional distress, and bladder trauma, including transvaginal ultrasound.
Conditions commonly associated with IC include fibromyalgia, irritable bowel syndrome, chronic fatigue, vulvodynia, migraines, depression, and anxiety.
The most common symptoms of IC are urinary urgency and frequency. Many affected patients have dysuria. Some have pain, which is typically suprapubic. However, pain can be present anywhere in a band circumscribing the whole central section of the torso, including the lower back, lower abdomen, urethra, vagina, and vulva. Patients describe a range of pain – burning, aching, stabbing, itching, buzzing, or a feeling of pressure.
“Most women who come in with IC are married to the idea that they’re having recurrent UTIs. They’re going to get antibiotics any way they can for their UTIs: over the phone, at urgent care. You need to get them to buy into the idea that even though UTIs are common, maybe not all of their flares are infections. They ask, ‘Then why do I feel better when I’m on antibiotics for recurrent UTI even though the cultures are negative?’ I say, ‘You feel less stress and anxiety because you think you’re on effective treatment,” Dr. Chacko said.
The diagnosis of IC is one of exclusions. Diagnoses to rule out before arriving at IC include recurrent UTI; overactive bladder, which should present with pure urge frequency and respond to medications for that condition; kidney stone disease present at the end of the ureter where it enters the bladder; gastrointestinal pathology; bladder cancer; and ovarian or uterine pathology.
Referral to a urologist for cystoscopy and cytology is appropriate in patients with microscopic hematuria, a significant smoking history predisposing to bladder cancer, or severe pain with severe frequency, which raises the possibility of Hunner’s ulcers, considered pathognomic for IC, respond “beautifully” to fulguration, she said.
Otherwise, IC can readily be managed by interested primary care physicians. The IC diet initially calls for 2 weeks of strict avoidance of all high-risk foods, most of which are acidic foods. These include fruits and fruit juices, especially citrus and cranberry juices; tomatoes and tomato products, including ketchup; yogurt; chocolate; coffee and tea, including decaf; vinegar; spicy foods; and carbonated beverages, water included.
These foods can later be added back one at a time to the diet while watching for IC flares, which typically occur within hours to several days of re-introducing the food. The return to coffee consumption, if that’s something important to the patient, should be with low-acid coffee. If that triggers an IC flare, try decaf. In time, many patients find they can consume some trigger foods in modest amounts.
“I tell patients it will take 12-18 months to get a good handle on their IC,” Dr. Chacko noted.
The use of OTC alkalizing agents such as Prelief may diffuse dietary triggers. A teaspoon of baking soda in water is also effective.
Second-line treatments include oral hydroxyzine 10-20 mg at bedtime; amitriptyline 10-20 mg at bedtime, mainly for patients with predominant pain symptoms; cimeditine; and pentosan polysulfate at 100 mg TID.
For IC patients with pelvic muscle tightness on pelvic examination, referral to a physical therapist adept at pelvic floor trigger point release can work wonders, she added.
One second-line option is bladder instillations of dimethyl sulfoxide weekly for 6 weeks, cutting back to once monthly maintenance therapy if the more intensive regimen is effective. Instillation of “heparin with lidocaine is a rescue solution. If it’s going to work, it kicks in within a few hours and usually lasts for 24-72 hours. It gets patients through a weekend, a wedding, or a funeral. A response can help make the IC diagnosis, too,” Dr. Chacko said.
She reported having no financial conflicts of interest regarding her presentation.
bjancin@frontlinemedcom.com
ESTES PARK, CO. – When patients with interstitial cystitis (IC) learn that first-line therapy is a rigorous diet designed to eliminate common bladder irritants, they tend to react in one of two ways, according to Julie A. Chacko, MD, a urologist in private practice in Santa Barbara, Calif.
Some “are just so grateful that they’re not crazy, which is what they’ve been told after 15 negative urine cultures. (Others) “look at the diet and think I’m sentencing them to death,” she said.
The sole medication approved by the Food and Drug Administration for IC is pentosan polysulfate sodium (Elmiron), and it should be reserved for the minority of patients who don’t experience significant improvement after giving the diet a reasonable shot, Dr. Chako advised. “When Elmiron works it’s great, but it’s not usually my go-to agent because it’s very expensive, you have to take it for 3-6 months to know for sure if it’s efficacious, and it has to be taken on an empty stomach. It’s a difficult medication.”
She advises patients to work with the diet. “Over time, they’re going to be able to find what I call their island – a point where they know very well their limitations and become quite comfortable with them,” she said at a conference on internal medicine sponsored by the University of Colorado.
A poorly understood yet common disorder, IC has a prevalence estimated at 0.5%-4% in women, less in men. Although typically diagnosed in the fourth decade or later, IC occurs at all ages. In some studies, the delay from first appearance of symptoms to arrival at a diagnosis is up to 8 years.
Interstitial cystitis is increasingly being called bladder pain syndrome in the literature, said Dr. Chako, who added, “I personally don’t love bladder pain syndrome as a description for this process. This syndrome has variable symptoms, and patients can have no pain at all.”
The mechanisms that result in IC are a mystery. The leading theory is that a bladder permeability problem allows urinary irritants to reach the interstitium. Nearly 80% of patients with IC can, with coaxing, identify dietary triggers for their symptoms, thereby basically establishing the diagnosis.
Other proposed mechanisms include an infectious agent that’s yet to be identified, allergic reaction, and neuromodulatory dysfunction. Common triggers other than foods include menses, copulation, emotional distress, and bladder trauma, including transvaginal ultrasound.
Conditions commonly associated with IC include fibromyalgia, irritable bowel syndrome, chronic fatigue, vulvodynia, migraines, depression, and anxiety.
The most common symptoms of IC are urinary urgency and frequency. Many affected patients have dysuria. Some have pain, which is typically suprapubic. However, pain can be present anywhere in a band circumscribing the whole central section of the torso, including the lower back, lower abdomen, urethra, vagina, and vulva. Patients describe a range of pain – burning, aching, stabbing, itching, buzzing, or a feeling of pressure.
“Most women who come in with IC are married to the idea that they’re having recurrent UTIs. They’re going to get antibiotics any way they can for their UTIs: over the phone, at urgent care. You need to get them to buy into the idea that even though UTIs are common, maybe not all of their flares are infections. They ask, ‘Then why do I feel better when I’m on antibiotics for recurrent UTI even though the cultures are negative?’ I say, ‘You feel less stress and anxiety because you think you’re on effective treatment,” Dr. Chacko said.
The diagnosis of IC is one of exclusions. Diagnoses to rule out before arriving at IC include recurrent UTI; overactive bladder, which should present with pure urge frequency and respond to medications for that condition; kidney stone disease present at the end of the ureter where it enters the bladder; gastrointestinal pathology; bladder cancer; and ovarian or uterine pathology.
Referral to a urologist for cystoscopy and cytology is appropriate in patients with microscopic hematuria, a significant smoking history predisposing to bladder cancer, or severe pain with severe frequency, which raises the possibility of Hunner’s ulcers, considered pathognomic for IC, respond “beautifully” to fulguration, she said.
Otherwise, IC can readily be managed by interested primary care physicians. The IC diet initially calls for 2 weeks of strict avoidance of all high-risk foods, most of which are acidic foods. These include fruits and fruit juices, especially citrus and cranberry juices; tomatoes and tomato products, including ketchup; yogurt; chocolate; coffee and tea, including decaf; vinegar; spicy foods; and carbonated beverages, water included.
These foods can later be added back one at a time to the diet while watching for IC flares, which typically occur within hours to several days of re-introducing the food. The return to coffee consumption, if that’s something important to the patient, should be with low-acid coffee. If that triggers an IC flare, try decaf. In time, many patients find they can consume some trigger foods in modest amounts.
“I tell patients it will take 12-18 months to get a good handle on their IC,” Dr. Chacko noted.
The use of OTC alkalizing agents such as Prelief may diffuse dietary triggers. A teaspoon of baking soda in water is also effective.
Second-line treatments include oral hydroxyzine 10-20 mg at bedtime; amitriptyline 10-20 mg at bedtime, mainly for patients with predominant pain symptoms; cimeditine; and pentosan polysulfate at 100 mg TID.
For IC patients with pelvic muscle tightness on pelvic examination, referral to a physical therapist adept at pelvic floor trigger point release can work wonders, she added.
One second-line option is bladder instillations of dimethyl sulfoxide weekly for 6 weeks, cutting back to once monthly maintenance therapy if the more intensive regimen is effective. Instillation of “heparin with lidocaine is a rescue solution. If it’s going to work, it kicks in within a few hours and usually lasts for 24-72 hours. It gets patients through a weekend, a wedding, or a funeral. A response can help make the IC diagnosis, too,” Dr. Chacko said.
She reported having no financial conflicts of interest regarding her presentation.
bjancin@frontlinemedcom.com
EXPERT ANALYSIS FROM THE ANNUAL INTERNAL MEDICINE PROGRAM

Opioid use disorder: Simplifying diagnosis and treatment in primary care
ESTES PARK, COLO. – Have a low threshold for diagnosing opioid use disorder in chronic pain patients, Joshua Blum, MD, advised at a conference on internal medicine sponsored by the University of Colorado.
Be alert to so-called ‘chemical copers’ as they skate through your practice, he said. “Maybe they call in here and there for an early refill; maybe they go to the ER and get a few pills here and there. But they never really surface to the level where we recognize them as an opioid use disorder patient.
“Some of them cross that line where they go from use and maybe intermittent misuse to meeting the criteria for opioid use disorder. I think we underdiagnose this in our chronic pain patients. I spend a lot of time trying to convince patients who tell me I just need to take their pain seriously that, yes, you’re in pain, and you have a pain diagnosis, but you also have an opioid use disorder. Medicalizing it makes things a lot easier for them; it helps take away the blame,” said Dr. Blum, program coordinator for the HIV primary care clinic at Denver Health.

Chemical copers, a well-established term in addiction medicine, are not the glaringly obvious substance abusers or addicts. “They’re the ones in your practice who are on four or five different psychoactive drugs. They’ve never met a psychoactive drug they didn’t like. When they hurt their back, they’re on Flexoril [cyclobenzaprine]; they’re on an antidepressant, a neuropathic pain agent; they’re on a sedative or sleeping agent or trazadone. If you took the five pills they’re on, you’d be knocked out for 2 days. And they always go to the maximum dose,” he said.
As newly described in the the Diagnostic and Statistical Manual of Mental Disorders, DSM-5, the diagnosis of opioid use disorder (OUD) requires that any 2 of the following 11 criteria be met:
- Taking more opioids than intended.
- Unsuccessful efforts to control opioid use.
- Spending a great deal of time in activities aimed at obtaining, using, or recovering from the effects of opioids.
- Craving opioids.
- Failure to fulfill major work, school, or home obligations because of opioid use.
- Worsening interpersonal problems related to opioid use.
- Giving up or reducing involvement in important social, recreational, or occupational activities because of opioid use.
- Recurrent use in situations where it’s physically hazardous, such as driving under the influence.
- Continued use despite physical or psychological problems stemming from opioid use.
- And finally, two special criteria applicable only if the opioid wasn’t prescribed and therefore isn’t being used under medical supervision: tolerance for opioids and withdrawal symptoms when they aren’t taken.
“Even if you can’t remember all these criteria, all you basically have to remember is ‘control.’ Many of these criteria describe situations where the patient is losing control of the drug. When they’re not controlling their drug use, the drug use is controlling them – and that’s addiction. All you need is for a patient to tell you ‘I tried to cut back on these drugs and I couldn’t,’ and that they’re experiencing some health consequences related to use yet still want to stay on the drugs, and, boom, they meet criteria for at least mild opioid use disorder,” he explained.
The standard treatment for OUD is opioid replacement therapy using methadone or buprenorphine (Subutex).
This approach is evidence-based therapy, Dr. Blum said, citing a recent meta-analysis of studies totaling nearly 123,000 opioid-dependent patients treated long-term with methadone and 16,000 treated with buprenorphine. The risk of all-cause mortality dropped by two-thirds when patients went on methadone, from 36.1% while out of treatment to 11.3% while on treatment. Similarly, all-cause mortality was 4.3% in patients on buprenorphine, compared with 9.5% in those out of treatment (BMJ. 2017 Apr 26;357:j1550. doi: 10.1136/bmj.j1550).
Access to methadone for treatment of OUD is available only through authorized methadone clinics, typically found only in big cities. But buprenorphine is a very useful alternative to methodone, Dr. Blum said.
“Buprenorphine is a schedule III drug that’s safe to prescribe in an office-based setting. It’s a partial mu opioid agonist with a ceiling effect, so people using buprenorphine can’t die from taking excessive amounts of it. You can even write refills on the prescription. And in head-to-head studies, it looks about as effective as moderate-dose methodone at 60 mg/day,” he said.
Opioid replacement therapy reduces euphoria and extinguishes craving. When methadone or buprenorphine is on board, saturating the opioid receptors, patients can use prescription or illicit opioids, but they won’t get high.
“People can really get their brains back online again,” Dr. Blum said.
Opioid maintenance therapy is consistent with the principles of harm reduction, a philosophy Dr. Blum said he embraces. Harm reduction can be summarized as “a set of practical strategies that reduce negative consequences of drug use, incorporating a spectrum of strategies from safer use, to managed use, to abstinence,” according to the Harm Reduction Coalition.
“Primary care doctors are very used to meeting patients where they are. We don’t require perfectionism from our patients. We don’t withhold insulin from diabetic patients because they’re not exercising, for example. In the case of drug use, there is complete abstinence on one end and really severe misuse on the other, and there’s a whole lot of life that happens in the middle. We’re addressing that part in the middle,” Dr. Blum said.
Dr. Blum reported having no financial conflicts of interest regarding his presentation.
ESTES PARK, COLO. – Have a low threshold for diagnosing opioid use disorder in chronic pain patients, Joshua Blum, MD, advised at a conference on internal medicine sponsored by the University of Colorado.
Be alert to so-called ‘chemical copers’ as they skate through your practice, he said. “Maybe they call in here and there for an early refill; maybe they go to the ER and get a few pills here and there. But they never really surface to the level where we recognize them as an opioid use disorder patient.
“Some of them cross that line where they go from use and maybe intermittent misuse to meeting the criteria for opioid use disorder. I think we underdiagnose this in our chronic pain patients. I spend a lot of time trying to convince patients who tell me I just need to take their pain seriously that, yes, you’re in pain, and you have a pain diagnosis, but you also have an opioid use disorder. Medicalizing it makes things a lot easier for them; it helps take away the blame,” said Dr. Blum, program coordinator for the HIV primary care clinic at Denver Health.
Chemical copers, a well-established term in addiction medicine, are not the glaringly obvious substance abusers or addicts. “They’re the ones in your practice who are on four or five different psychoactive drugs. They’ve never met a psychoactive drug they didn’t like. When they hurt their back, they’re on Flexoril [cyclobenzaprine]; they’re on an antidepressant, a neuropathic pain agent; they’re on a sedative or sleeping agent or trazadone. If you took the five pills they’re on, you’d be knocked out for 2 days. And they always go to the maximum dose,” he said.
As newly described in the the Diagnostic and Statistical Manual of Mental Disorders, DSM-5, the diagnosis of opioid use disorder (OUD) requires that any 2 of the following 11 criteria be met:
- Taking more opioids than intended.
- Unsuccessful efforts to control opioid use.
- Spending a great deal of time in activities aimed at obtaining, using, or recovering from the effects of opioids.
- Craving opioids.
- Failure to fulfill major work, school, or home obligations because of opioid use.
- Worsening interpersonal problems related to opioid use.
- Giving up or reducing involvement in important social, recreational, or occupational activities because of opioid use.
- Recurrent use in situations where it’s physically hazardous, such as driving under the influence.
- Continued use despite physical or psychological problems stemming from opioid use.
- And finally, two special criteria applicable only if the opioid wasn’t prescribed and therefore isn’t being used under medical supervision: tolerance for opioids and withdrawal symptoms when they aren’t taken.
“Even if you can’t remember all these criteria, all you basically have to remember is ‘control.’ Many of these criteria describe situations where the patient is losing control of the drug. When they’re not controlling their drug use, the drug use is controlling them – and that’s addiction. All you need is for a patient to tell you ‘I tried to cut back on these drugs and I couldn’t,’ and that they’re experiencing some health consequences related to use yet still want to stay on the drugs, and, boom, they meet criteria for at least mild opioid use disorder,” he explained.
The standard treatment for OUD is opioid replacement therapy using methadone or buprenorphine (Subutex).
This approach is evidence-based therapy, Dr. Blum said, citing a recent meta-analysis of studies totaling nearly 123,000 opioid-dependent patients treated long-term with methadone and 16,000 treated with buprenorphine. The risk of all-cause mortality dropped by two-thirds when patients went on methadone, from 36.1% while out of treatment to 11.3% while on treatment. Similarly, all-cause mortality was 4.3% in patients on buprenorphine, compared with 9.5% in those out of treatment (BMJ. 2017 Apr 26;357:j1550. doi: 10.1136/bmj.j1550).
Access to methadone for treatment of OUD is available only through authorized methadone clinics, typically found only in big cities. But buprenorphine is a very useful alternative to methodone, Dr. Blum said.
“Buprenorphine is a schedule III drug that’s safe to prescribe in an office-based setting. It’s a partial mu opioid agonist with a ceiling effect, so people using buprenorphine can’t die from taking excessive amounts of it. You can even write refills on the prescription. And in head-to-head studies, it looks about as effective as moderate-dose methodone at 60 mg/day,” he said.
Opioid replacement therapy reduces euphoria and extinguishes craving. When methadone or buprenorphine is on board, saturating the opioid receptors, patients can use prescription or illicit opioids, but they won’t get high.
“People can really get their brains back online again,” Dr. Blum said.
Opioid maintenance therapy is consistent with the principles of harm reduction, a philosophy Dr. Blum said he embraces. Harm reduction can be summarized as “a set of practical strategies that reduce negative consequences of drug use, incorporating a spectrum of strategies from safer use, to managed use, to abstinence,” according to the Harm Reduction Coalition.
“Primary care doctors are very used to meeting patients where they are. We don’t require perfectionism from our patients. We don’t withhold insulin from diabetic patients because they’re not exercising, for example. In the case of drug use, there is complete abstinence on one end and really severe misuse on the other, and there’s a whole lot of life that happens in the middle. We’re addressing that part in the middle,” Dr. Blum said.
Dr. Blum reported having no financial conflicts of interest regarding his presentation.
ESTES PARK, COLO. – Have a low threshold for diagnosing opioid use disorder in chronic pain patients, Joshua Blum, MD, advised at a conference on internal medicine sponsored by the University of Colorado.
Be alert to so-called ‘chemical copers’ as they skate through your practice, he said. “Maybe they call in here and there for an early refill; maybe they go to the ER and get a few pills here and there. But they never really surface to the level where we recognize them as an opioid use disorder patient.
“Some of them cross that line where they go from use and maybe intermittent misuse to meeting the criteria for opioid use disorder. I think we underdiagnose this in our chronic pain patients. I spend a lot of time trying to convince patients who tell me I just need to take their pain seriously that, yes, you’re in pain, and you have a pain diagnosis, but you also have an opioid use disorder. Medicalizing it makes things a lot easier for them; it helps take away the blame,” said Dr. Blum, program coordinator for the HIV primary care clinic at Denver Health.
Chemical copers, a well-established term in addiction medicine, are not the glaringly obvious substance abusers or addicts. “They’re the ones in your practice who are on four or five different psychoactive drugs. They’ve never met a psychoactive drug they didn’t like. When they hurt their back, they’re on Flexoril [cyclobenzaprine]; they’re on an antidepressant, a neuropathic pain agent; they’re on a sedative or sleeping agent or trazadone. If you took the five pills they’re on, you’d be knocked out for 2 days. And they always go to the maximum dose,” he said.
As newly described in the the Diagnostic and Statistical Manual of Mental Disorders, DSM-5, the diagnosis of opioid use disorder (OUD) requires that any 2 of the following 11 criteria be met:
- Taking more opioids than intended.
- Unsuccessful efforts to control opioid use.
- Spending a great deal of time in activities aimed at obtaining, using, or recovering from the effects of opioids.
- Craving opioids.
- Failure to fulfill major work, school, or home obligations because of opioid use.
- Worsening interpersonal problems related to opioid use.
- Giving up or reducing involvement in important social, recreational, or occupational activities because of opioid use.
- Recurrent use in situations where it’s physically hazardous, such as driving under the influence.
- Continued use despite physical or psychological problems stemming from opioid use.
- And finally, two special criteria applicable only if the opioid wasn’t prescribed and therefore isn’t being used under medical supervision: tolerance for opioids and withdrawal symptoms when they aren’t taken.
“Even if you can’t remember all these criteria, all you basically have to remember is ‘control.’ Many of these criteria describe situations where the patient is losing control of the drug. When they’re not controlling their drug use, the drug use is controlling them – and that’s addiction. All you need is for a patient to tell you ‘I tried to cut back on these drugs and I couldn’t,’ and that they’re experiencing some health consequences related to use yet still want to stay on the drugs, and, boom, they meet criteria for at least mild opioid use disorder,” he explained.
The standard treatment for OUD is opioid replacement therapy using methadone or buprenorphine (Subutex).
This approach is evidence-based therapy, Dr. Blum said, citing a recent meta-analysis of studies totaling nearly 123,000 opioid-dependent patients treated long-term with methadone and 16,000 treated with buprenorphine. The risk of all-cause mortality dropped by two-thirds when patients went on methadone, from 36.1% while out of treatment to 11.3% while on treatment. Similarly, all-cause mortality was 4.3% in patients on buprenorphine, compared with 9.5% in those out of treatment (BMJ. 2017 Apr 26;357:j1550. doi: 10.1136/bmj.j1550).
Access to methadone for treatment of OUD is available only through authorized methadone clinics, typically found only in big cities. But buprenorphine is a very useful alternative to methodone, Dr. Blum said.
“Buprenorphine is a schedule III drug that’s safe to prescribe in an office-based setting. It’s a partial mu opioid agonist with a ceiling effect, so people using buprenorphine can’t die from taking excessive amounts of it. You can even write refills on the prescription. And in head-to-head studies, it looks about as effective as moderate-dose methodone at 60 mg/day,” he said.
Opioid replacement therapy reduces euphoria and extinguishes craving. When methadone or buprenorphine is on board, saturating the opioid receptors, patients can use prescription or illicit opioids, but they won’t get high.
“People can really get their brains back online again,” Dr. Blum said.
Opioid maintenance therapy is consistent with the principles of harm reduction, a philosophy Dr. Blum said he embraces. Harm reduction can be summarized as “a set of practical strategies that reduce negative consequences of drug use, incorporating a spectrum of strategies from safer use, to managed use, to abstinence,” according to the Harm Reduction Coalition.
“Primary care doctors are very used to meeting patients where they are. We don’t require perfectionism from our patients. We don’t withhold insulin from diabetic patients because they’re not exercising, for example. In the case of drug use, there is complete abstinence on one end and really severe misuse on the other, and there’s a whole lot of life that happens in the middle. We’re addressing that part in the middle,” Dr. Blum said.
Dr. Blum reported having no financial conflicts of interest regarding his presentation.
EXPERT ANALYSIS AT THE ANNUAL INTERNAL MEDICINE PROGRAM
Ivabradine cut mortality in HFrEF patients not on beta-blocker
BARCELONA – The time is right for a placebo-controlled, randomized trial of ivabradine in patients with heart failure with reduced ejection fraction who are unwilling or unable to take a beta-blocker as recommended in the guidelines, John G.F. Cleland, MD, asserted at the annual congress of the European Society of Cardiology.
He cited as the rationale for such a study a new post-hoc analysis of data from the SHIFT trial showing that ivabradine (Corlanor) significantly reduced both cardiovascular and all-cause mortality, as well as hospitalizations for heart failure, in the subset of study participants who weren’t on beta-blocker therapy.

“I think there would be ethical equipoise,” he added. “If patients are unwilling or unable to take a beta-blocker, or their cardiologist feels it’s not in their best interest, then I certainly think a placebo-controlled trial would not only be appropriate, but there’s also an onus on the cardiology community to do such a trial.”
Ivabradine slows heart rate by a unique mechanism that doesn’t involve blockade of adrenergic receptors. In the SHIFT trial (Lancet. 2010 Sep 11;376[9744]:875-85), more than 6,500 patients with heart failure with reduced ejection fraction (HFrEF) in sinus rhythm and with a heart rate greater than 70 bpm were randomized to ivabradine or placebo on top of guideline-directed medical therapy for heart failure. During a median 23 months of follow-up, heart failure hospitalizations were significantly reduced by 26% in the ivabradine group, although cardiovascular deaths were not significantly affected.
As a result of the SHIFT findings, the drug was approved with an indication for use only in combination with a beta-blocker in patients with HFrEF whose on-treatment heart rate exceeds 70 bpm. Ivabradine is not currently recommended as an alternative to beta-blocker therapy. However, in real-world clinical practice a large number of heart failure patients are not managed with a beta-blocker, the cardiologist noted.
His post-hoc analysis focused on the 685 SHIFT participants who were not on a beta-blocker at randomization. During follow-up, there were 93 deaths among patients who were on placebo and only 71 in those randomized to ivabradine, for a statistically significant 30% reduction in all-cause mortality. Cardiovascular mortality was reduced to a similar extent. These hazard ratios remained similar after adjusting for differences in heart rate and other clinical characteristics.
“Beta-blockers are a highly effective therapy for heart failure with reduced ejection fraction, but the mechanism of benefit remains uncertain. It might simply be due to heart rate reduction. And I would point out that we have no evidence of a dose response for beta-blockers: It may well be that you get most of the effect of a beta-blocker with the lowest dose. Titrating to the full dose of a beta-blocker might only be helpful in that it lowers your heart rate. I would argue that 6.25 mg/day of carvedilol plus ivabradine might be as good as 50 mg twice daily of carvedilol but with much higher patient acceptability. We don’t know,” said Dr. Cleland.
“This is an interesting, hypothesis-generating analysis, and we need confirmation now that ivabradine reduces mortality in heart failure patients who are unwilling or unable to take a beta-blocker,” he concluded.
The SHIFT trial was sponsored by Servier. Dr. Cleland reported serving as a consultant to and receiving research funding from that company and others.
BARCELONA – The time is right for a placebo-controlled, randomized trial of ivabradine in patients with heart failure with reduced ejection fraction who are unwilling or unable to take a beta-blocker as recommended in the guidelines, John G.F. Cleland, MD, asserted at the annual congress of the European Society of Cardiology.
He cited as the rationale for such a study a new post-hoc analysis of data from the SHIFT trial showing that ivabradine (Corlanor) significantly reduced both cardiovascular and all-cause mortality, as well as hospitalizations for heart failure, in the subset of study participants who weren’t on beta-blocker therapy.
“I think there would be ethical equipoise,” he added. “If patients are unwilling or unable to take a beta-blocker, or their cardiologist feels it’s not in their best interest, then I certainly think a placebo-controlled trial would not only be appropriate, but there’s also an onus on the cardiology community to do such a trial.”
Ivabradine slows heart rate by a unique mechanism that doesn’t involve blockade of adrenergic receptors. In the SHIFT trial (Lancet. 2010 Sep 11;376[9744]:875-85), more than 6,500 patients with heart failure with reduced ejection fraction (HFrEF) in sinus rhythm and with a heart rate greater than 70 bpm were randomized to ivabradine or placebo on top of guideline-directed medical therapy for heart failure. During a median 23 months of follow-up, heart failure hospitalizations were significantly reduced by 26% in the ivabradine group, although cardiovascular deaths were not significantly affected.
As a result of the SHIFT findings, the drug was approved with an indication for use only in combination with a beta-blocker in patients with HFrEF whose on-treatment heart rate exceeds 70 bpm. Ivabradine is not currently recommended as an alternative to beta-blocker therapy. However, in real-world clinical practice a large number of heart failure patients are not managed with a beta-blocker, the cardiologist noted.
His post-hoc analysis focused on the 685 SHIFT participants who were not on a beta-blocker at randomization. During follow-up, there were 93 deaths among patients who were on placebo and only 71 in those randomized to ivabradine, for a statistically significant 30% reduction in all-cause mortality. Cardiovascular mortality was reduced to a similar extent. These hazard ratios remained similar after adjusting for differences in heart rate and other clinical characteristics.
“Beta-blockers are a highly effective therapy for heart failure with reduced ejection fraction, but the mechanism of benefit remains uncertain. It might simply be due to heart rate reduction. And I would point out that we have no evidence of a dose response for beta-blockers: It may well be that you get most of the effect of a beta-blocker with the lowest dose. Titrating to the full dose of a beta-blocker might only be helpful in that it lowers your heart rate. I would argue that 6.25 mg/day of carvedilol plus ivabradine might be as good as 50 mg twice daily of carvedilol but with much higher patient acceptability. We don’t know,” said Dr. Cleland.
“This is an interesting, hypothesis-generating analysis, and we need confirmation now that ivabradine reduces mortality in heart failure patients who are unwilling or unable to take a beta-blocker,” he concluded.
The SHIFT trial was sponsored by Servier. Dr. Cleland reported serving as a consultant to and receiving research funding from that company and others.
BARCELONA – The time is right for a placebo-controlled, randomized trial of ivabradine in patients with heart failure with reduced ejection fraction who are unwilling or unable to take a beta-blocker as recommended in the guidelines, John G.F. Cleland, MD, asserted at the annual congress of the European Society of Cardiology.
He cited as the rationale for such a study a new post-hoc analysis of data from the SHIFT trial showing that ivabradine (Corlanor) significantly reduced both cardiovascular and all-cause mortality, as well as hospitalizations for heart failure, in the subset of study participants who weren’t on beta-blocker therapy.
“I think there would be ethical equipoise,” he added. “If patients are unwilling or unable to take a beta-blocker, or their cardiologist feels it’s not in their best interest, then I certainly think a placebo-controlled trial would not only be appropriate, but there’s also an onus on the cardiology community to do such a trial.”
Ivabradine slows heart rate by a unique mechanism that doesn’t involve blockade of adrenergic receptors. In the SHIFT trial (Lancet. 2010 Sep 11;376[9744]:875-85), more than 6,500 patients with heart failure with reduced ejection fraction (HFrEF) in sinus rhythm and with a heart rate greater than 70 bpm were randomized to ivabradine or placebo on top of guideline-directed medical therapy for heart failure. During a median 23 months of follow-up, heart failure hospitalizations were significantly reduced by 26% in the ivabradine group, although cardiovascular deaths were not significantly affected.
As a result of the SHIFT findings, the drug was approved with an indication for use only in combination with a beta-blocker in patients with HFrEF whose on-treatment heart rate exceeds 70 bpm. Ivabradine is not currently recommended as an alternative to beta-blocker therapy. However, in real-world clinical practice a large number of heart failure patients are not managed with a beta-blocker, the cardiologist noted.
His post-hoc analysis focused on the 685 SHIFT participants who were not on a beta-blocker at randomization. During follow-up, there were 93 deaths among patients who were on placebo and only 71 in those randomized to ivabradine, for a statistically significant 30% reduction in all-cause mortality. Cardiovascular mortality was reduced to a similar extent. These hazard ratios remained similar after adjusting for differences in heart rate and other clinical characteristics.
“Beta-blockers are a highly effective therapy for heart failure with reduced ejection fraction, but the mechanism of benefit remains uncertain. It might simply be due to heart rate reduction. And I would point out that we have no evidence of a dose response for beta-blockers: It may well be that you get most of the effect of a beta-blocker with the lowest dose. Titrating to the full dose of a beta-blocker might only be helpful in that it lowers your heart rate. I would argue that 6.25 mg/day of carvedilol plus ivabradine might be as good as 50 mg twice daily of carvedilol but with much higher patient acceptability. We don’t know,” said Dr. Cleland.
“This is an interesting, hypothesis-generating analysis, and we need confirmation now that ivabradine reduces mortality in heart failure patients who are unwilling or unable to take a beta-blocker,” he concluded.
The SHIFT trial was sponsored by Servier. Dr. Cleland reported serving as a consultant to and receiving research funding from that company and others.
AT THE ESC CONGRESS 2017
Key clinical point:
Major finding: All-cause mortality was reduced by 30%, compared with placebo, in ivabradine-treated patients with heart failure with reduced ejection fraction who were not on a beta-blocker.
Data source: A post-hoc analysis of the 685 patients in a much larger randomized, placebo-controlled clinical trial of ivabradine in patients with heart failure with reduced ejection fraction.
Disclosures: The SHIFT trial was funded by Servier. The presenter reported serving as a consultant to and recipient of research grants from that and other companies.
Preventive upstream therapy prevents progression of atrial fib
BARCELONA – Aggressive treatment of known risk factors for atrial fibrillation resulted in improved 1-year maintenance of sinus rhythm in patients with recent-onset atrial fibrillation and heart failure in the randomized multicenter RACE 3 trial, Isabelle C. van Gelder, MD, reported at the annual congress of the European Society of Cardiology.
“We now screen for AF, making it possible to catch patients early. That’s what we’ve learned from this trial: if we start treating patients after their first episode of AF and aggressively reduce risk factors for AF, it may help the sinus rhythm. I think that’s an important message: do not wait too long, start treatment early,” said Dr. van Gelder, professor of cardiology at the University of Groningen, the Netherlands.
She calls the interventional strategy tested in RACE 3 “risk factor-driven upstream therapy.” The four-pronged strategy consisted of statin therapy, a mineralcorticoid receptor antagonist, an ACE inhibitor and/or an angiotensin receptor blocker, and a 9- to 11-week supervised cardiac rehabilitation program emphasizing lifestyle modification through physical training and dietary changes supported by professional counseling to promote adherence.
“These are interventions designed to improve the atrial substrate,” Dr. van Gelder explained.
RACE 3 (Routine versus Aggressive Upstream Rhythm Control for Prevention of Early Atrial Fibrillation in Heart Failure 3) was a multicenter, randomized, nonblinded clinical trial including 245 patients with, on average, a 3-month history of AF, a 2-month history of persistent AF, and a 2-month history of mild to moderate heart failure, either with preserved or reduced ejection fraction. All participants received guideline-directed rhythm control and heart failure therapies. In addition, half of participants were randomized to the upstream intervention. Three weeks after enrollment, all patients underwent electrical cardioversion.
The primary outcome was maintenance of sinus rhythm at 1 year as determined by 7-day Holter monitoring analyzed in blinded fashion at a central laboratory. The rate was 75% in the upstream intervention group, significantly better than the 63% in controls. This represented a 76% greater likelihood of sinus rhythm at 1 year in the upstream intervention group. They also showed significant reductions in systolic and diastolic blood pressure, N-terminal pro-brain natriuretic peptide, and LDL cholesterol, compared with controls. However, at 1 year, the two groups didn’t differ significantly in body mass index or left atrial volume. The lack of impact on left atrial volume was disappointing, Dr. van Gelder said.
“The remodeling process starts long before the first episode of AF, although we don’t know exactly when. Although we intended to intervene early in the remodeling process, I think we weren’t that early,” according to the cardiologist.
Discussant Josep Brugada, MD, applauded the Dutch investigators for opening the door to evidence-based preventive upstream therapy for AF, which he declared is vital given the worsening AF epidemic.

“In recent years enormous efforts have been put into treating symptoms of AF, but clearly we have failed to control the epidemic of AF in our societies, probably because we’ve been aiming only at treating symptoms, not treating the causes,” observed Dr. Brugada of the University of Barcelona.
He added, however, that the RACE 3 intervention didn’t go far enough.
“It’s a bit of a disappointment that there is no change in BMI seen after 1 year. Zero. That probably means the rehabilitation program wasn’t strong enough. Yet, the study results are positive, so if we used physical training in a stronger way to get a reduction in body weight and BMI, probably the outcome would be even greater,” he said.
To be maximally effective, an upstream intervention for AF should also address two other important risk factors for the arrhythmia: heavy alcohol drinking and obstructive sleep apnea, the electrophysiologist added.
The RACE 3 trial was supported by the Netherlands Heart Foundation and the Netherlands Heart Institute. Dr. van Gelder reported having no relevant financial interests.
Dr. van Gelder discussed the RACE 3 trial and results in a video interview.
BARCELONA – Aggressive treatment of known risk factors for atrial fibrillation resulted in improved 1-year maintenance of sinus rhythm in patients with recent-onset atrial fibrillation and heart failure in the randomized multicenter RACE 3 trial, Isabelle C. van Gelder, MD, reported at the annual congress of the European Society of Cardiology.
“We now screen for AF, making it possible to catch patients early. That’s what we’ve learned from this trial: if we start treating patients after their first episode of AF and aggressively reduce risk factors for AF, it may help the sinus rhythm. I think that’s an important message: do not wait too long, start treatment early,” said Dr. van Gelder, professor of cardiology at the University of Groningen, the Netherlands.
She calls the interventional strategy tested in RACE 3 “risk factor-driven upstream therapy.” The four-pronged strategy consisted of statin therapy, a mineralcorticoid receptor antagonist, an ACE inhibitor and/or an angiotensin receptor blocker, and a 9- to 11-week supervised cardiac rehabilitation program emphasizing lifestyle modification through physical training and dietary changes supported by professional counseling to promote adherence.
“These are interventions designed to improve the atrial substrate,” Dr. van Gelder explained.
RACE 3 (Routine versus Aggressive Upstream Rhythm Control for Prevention of Early Atrial Fibrillation in Heart Failure 3) was a multicenter, randomized, nonblinded clinical trial including 245 patients with, on average, a 3-month history of AF, a 2-month history of persistent AF, and a 2-month history of mild to moderate heart failure, either with preserved or reduced ejection fraction. All participants received guideline-directed rhythm control and heart failure therapies. In addition, half of participants were randomized to the upstream intervention. Three weeks after enrollment, all patients underwent electrical cardioversion.
The primary outcome was maintenance of sinus rhythm at 1 year as determined by 7-day Holter monitoring analyzed in blinded fashion at a central laboratory. The rate was 75% in the upstream intervention group, significantly better than the 63% in controls. This represented a 76% greater likelihood of sinus rhythm at 1 year in the upstream intervention group. They also showed significant reductions in systolic and diastolic blood pressure, N-terminal pro-brain natriuretic peptide, and LDL cholesterol, compared with controls. However, at 1 year, the two groups didn’t differ significantly in body mass index or left atrial volume. The lack of impact on left atrial volume was disappointing, Dr. van Gelder said.
“The remodeling process starts long before the first episode of AF, although we don’t know exactly when. Although we intended to intervene early in the remodeling process, I think we weren’t that early,” according to the cardiologist.
Discussant Josep Brugada, MD, applauded the Dutch investigators for opening the door to evidence-based preventive upstream therapy for AF, which he declared is vital given the worsening AF epidemic.
“In recent years enormous efforts have been put into treating symptoms of AF, but clearly we have failed to control the epidemic of AF in our societies, probably because we’ve been aiming only at treating symptoms, not treating the causes,” observed Dr. Brugada of the University of Barcelona.
He added, however, that the RACE 3 intervention didn’t go far enough.
“It’s a bit of a disappointment that there is no change in BMI seen after 1 year. Zero. That probably means the rehabilitation program wasn’t strong enough. Yet, the study results are positive, so if we used physical training in a stronger way to get a reduction in body weight and BMI, probably the outcome would be even greater,” he said.
To be maximally effective, an upstream intervention for AF should also address two other important risk factors for the arrhythmia: heavy alcohol drinking and obstructive sleep apnea, the electrophysiologist added.
The RACE 3 trial was supported by the Netherlands Heart Foundation and the Netherlands Heart Institute. Dr. van Gelder reported having no relevant financial interests.
Dr. van Gelder discussed the RACE 3 trial and results in a video interview.
BARCELONA – Aggressive treatment of known risk factors for atrial fibrillation resulted in improved 1-year maintenance of sinus rhythm in patients with recent-onset atrial fibrillation and heart failure in the randomized multicenter RACE 3 trial, Isabelle C. van Gelder, MD, reported at the annual congress of the European Society of Cardiology.
“We now screen for AF, making it possible to catch patients early. That’s what we’ve learned from this trial: if we start treating patients after their first episode of AF and aggressively reduce risk factors for AF, it may help the sinus rhythm. I think that’s an important message: do not wait too long, start treatment early,” said Dr. van Gelder, professor of cardiology at the University of Groningen, the Netherlands.
She calls the interventional strategy tested in RACE 3 “risk factor-driven upstream therapy.” The four-pronged strategy consisted of statin therapy, a mineralcorticoid receptor antagonist, an ACE inhibitor and/or an angiotensin receptor blocker, and a 9- to 11-week supervised cardiac rehabilitation program emphasizing lifestyle modification through physical training and dietary changes supported by professional counseling to promote adherence.
“These are interventions designed to improve the atrial substrate,” Dr. van Gelder explained.
RACE 3 (Routine versus Aggressive Upstream Rhythm Control for Prevention of Early Atrial Fibrillation in Heart Failure 3) was a multicenter, randomized, nonblinded clinical trial including 245 patients with, on average, a 3-month history of AF, a 2-month history of persistent AF, and a 2-month history of mild to moderate heart failure, either with preserved or reduced ejection fraction. All participants received guideline-directed rhythm control and heart failure therapies. In addition, half of participants were randomized to the upstream intervention. Three weeks after enrollment, all patients underwent electrical cardioversion.
The primary outcome was maintenance of sinus rhythm at 1 year as determined by 7-day Holter monitoring analyzed in blinded fashion at a central laboratory. The rate was 75% in the upstream intervention group, significantly better than the 63% in controls. This represented a 76% greater likelihood of sinus rhythm at 1 year in the upstream intervention group. They also showed significant reductions in systolic and diastolic blood pressure, N-terminal pro-brain natriuretic peptide, and LDL cholesterol, compared with controls. However, at 1 year, the two groups didn’t differ significantly in body mass index or left atrial volume. The lack of impact on left atrial volume was disappointing, Dr. van Gelder said.
“The remodeling process starts long before the first episode of AF, although we don’t know exactly when. Although we intended to intervene early in the remodeling process, I think we weren’t that early,” according to the cardiologist.
Discussant Josep Brugada, MD, applauded the Dutch investigators for opening the door to evidence-based preventive upstream therapy for AF, which he declared is vital given the worsening AF epidemic.
“In recent years enormous efforts have been put into treating symptoms of AF, but clearly we have failed to control the epidemic of AF in our societies, probably because we’ve been aiming only at treating symptoms, not treating the causes,” observed Dr. Brugada of the University of Barcelona.
He added, however, that the RACE 3 intervention didn’t go far enough.
“It’s a bit of a disappointment that there is no change in BMI seen after 1 year. Zero. That probably means the rehabilitation program wasn’t strong enough. Yet, the study results are positive, so if we used physical training in a stronger way to get a reduction in body weight and BMI, probably the outcome would be even greater,” he said.
To be maximally effective, an upstream intervention for AF should also address two other important risk factors for the arrhythmia: heavy alcohol drinking and obstructive sleep apnea, the electrophysiologist added.
The RACE 3 trial was supported by the Netherlands Heart Foundation and the Netherlands Heart Institute. Dr. van Gelder reported having no relevant financial interests.
Dr. van Gelder discussed the RACE 3 trial and results in a video interview.
AT THE ESC CONGRESS 2017
Key clinical point:
Major finding: At 1 year, 75% of patients with baseline persistent atrial fibrillation who received a four-pronged program of upstream risk factor modification were in sinus rhythm, compared with 63% of controls.
Data source: RACE 3 was a multicenter, randomized, nonblinded clinical trial including 245 patients with a recent history of persistent atrial fibrillation and heart failure.
Disclosures: The RACE 3 trial was supported by the Netherlands Heart Foundation and the Netherlands Heart Institute. The presenter reported having no relevant financial interests.
Developing vaccines against enterovirus-A71 called a priority
MADRID – Is there a need for an enterovirus-A71 vaccine?
This is a new question for North American and European physicians, but not so new in Asia.
“China says yes, with more than 15 million cases of hand, foot, and mouth disease resulting in 3,500 deaths since surveillance started in 2009,” Heli Harvala, MD, said at the annual meeting of the European Society for Paediatric Infectious Diseases.
Seroconversion rates 28 days after the second dose of these vaccines, both directed specifically against viral subgenotype C-4, are 92%-100%. Vaccine efficacy is 91%-97%, according to Dr. Harvala, a consultant medical virologist at University College London.
It remains a mystery why major outbreaks of severe EV-A71 disease have mostly occurred in Asia, with the notable exception of a Spanish outbreak of EV-A71 encephalitis in 2016. The possibility of much wider spread is concerning.
The Chinese monovalent EV-A71 vaccines, however, are seen as a stopgap. For one thing, recent evidence suggests that it’s probably not the specific EV-A71 C-4 viral subgenotype that accounts for all severe disease.
“I think we have to aim for a multivalent vaccine,” Dr. Harvala said.
Now in clinical trials, investigational bivalent vaccines are directed against other EV-A71 subgenotypes in addition to C-4, and also against another enterovirus, coxsackievirus serotype A16, the most common cause of classic hand, foot, and mouth disease in the United States. But that’s probably not enough, according to Dr. Harvala. She noted that coxsackievirus A6, which was first identified more than 50 years ago, abruptly became the main cause of mild hand, foot, and mouth disease in China in 2013 and again in 2015. Moreover, its role in severe cases is growing, and there have been important outbreaks in the United States in recent years. These severe cases come in three main presentations, resembling either erythema multiforme, chicken pox, or eczema herpeticum.
Dr. Harvala added that a next-generation vaccine probably also should offer protection against enterovirus-D68. In 2014, there were 1,153 laboratory-confirmed EV-D68 infections and 14 deaths in the United States and Canada. This infection poses a diagnostic challenge: while the virus is readily detectable on throat swabs, it’s only rarely present in stool or cerebrospinal fluid samples.
“It’s important to keep in mind that this infection is still underdiagnosed. We are not really looking for it,” she said.
No specific treatment for enterovirus infections is available. Three capsid-binding antiviral agents now are in clinical trials: pleconaril, vapendavir, and pocapavir. In addition, translational studies have demonstrated that the SSRI fluoxetine inhibits enterovirus replication, but there have been no clinical trials as yet.
Although development of antivirals effective against enterovirus is an active area of research, Dr. Harvala thinks drug resistance will be an issue, underscoring the importance of vaccine development.
She reported having no financial conflicts of interest regarding her presentation.
MADRID – Is there a need for an enterovirus-A71 vaccine?
This is a new question for North American and European physicians, but not so new in Asia.
“China says yes, with more than 15 million cases of hand, foot, and mouth disease resulting in 3,500 deaths since surveillance started in 2009,” Heli Harvala, MD, said at the annual meeting of the European Society for Paediatric Infectious Diseases.
Seroconversion rates 28 days after the second dose of these vaccines, both directed specifically against viral subgenotype C-4, are 92%-100%. Vaccine efficacy is 91%-97%, according to Dr. Harvala, a consultant medical virologist at University College London.
It remains a mystery why major outbreaks of severe EV-A71 disease have mostly occurred in Asia, with the notable exception of a Spanish outbreak of EV-A71 encephalitis in 2016. The possibility of much wider spread is concerning.
The Chinese monovalent EV-A71 vaccines, however, are seen as a stopgap. For one thing, recent evidence suggests that it’s probably not the specific EV-A71 C-4 viral subgenotype that accounts for all severe disease.
“I think we have to aim for a multivalent vaccine,” Dr. Harvala said.
Now in clinical trials, investigational bivalent vaccines are directed against other EV-A71 subgenotypes in addition to C-4, and also against another enterovirus, coxsackievirus serotype A16, the most common cause of classic hand, foot, and mouth disease in the United States. But that’s probably not enough, according to Dr. Harvala. She noted that coxsackievirus A6, which was first identified more than 50 years ago, abruptly became the main cause of mild hand, foot, and mouth disease in China in 2013 and again in 2015. Moreover, its role in severe cases is growing, and there have been important outbreaks in the United States in recent years. These severe cases come in three main presentations, resembling either erythema multiforme, chicken pox, or eczema herpeticum.
Dr. Harvala added that a next-generation vaccine probably also should offer protection against enterovirus-D68. In 2014, there were 1,153 laboratory-confirmed EV-D68 infections and 14 deaths in the United States and Canada. This infection poses a diagnostic challenge: while the virus is readily detectable on throat swabs, it’s only rarely present in stool or cerebrospinal fluid samples.
“It’s important to keep in mind that this infection is still underdiagnosed. We are not really looking for it,” she said.
No specific treatment for enterovirus infections is available. Three capsid-binding antiviral agents now are in clinical trials: pleconaril, vapendavir, and pocapavir. In addition, translational studies have demonstrated that the SSRI fluoxetine inhibits enterovirus replication, but there have been no clinical trials as yet.
Although development of antivirals effective against enterovirus is an active area of research, Dr. Harvala thinks drug resistance will be an issue, underscoring the importance of vaccine development.
She reported having no financial conflicts of interest regarding her presentation.
MADRID – Is there a need for an enterovirus-A71 vaccine?
This is a new question for North American and European physicians, but not so new in Asia.
“China says yes, with more than 15 million cases of hand, foot, and mouth disease resulting in 3,500 deaths since surveillance started in 2009,” Heli Harvala, MD, said at the annual meeting of the European Society for Paediatric Infectious Diseases.
Seroconversion rates 28 days after the second dose of these vaccines, both directed specifically against viral subgenotype C-4, are 92%-100%. Vaccine efficacy is 91%-97%, according to Dr. Harvala, a consultant medical virologist at University College London.
It remains a mystery why major outbreaks of severe EV-A71 disease have mostly occurred in Asia, with the notable exception of a Spanish outbreak of EV-A71 encephalitis in 2016. The possibility of much wider spread is concerning.
The Chinese monovalent EV-A71 vaccines, however, are seen as a stopgap. For one thing, recent evidence suggests that it’s probably not the specific EV-A71 C-4 viral subgenotype that accounts for all severe disease.
“I think we have to aim for a multivalent vaccine,” Dr. Harvala said.
Now in clinical trials, investigational bivalent vaccines are directed against other EV-A71 subgenotypes in addition to C-4, and also against another enterovirus, coxsackievirus serotype A16, the most common cause of classic hand, foot, and mouth disease in the United States. But that’s probably not enough, according to Dr. Harvala. She noted that coxsackievirus A6, which was first identified more than 50 years ago, abruptly became the main cause of mild hand, foot, and mouth disease in China in 2013 and again in 2015. Moreover, its role in severe cases is growing, and there have been important outbreaks in the United States in recent years. These severe cases come in three main presentations, resembling either erythema multiforme, chicken pox, or eczema herpeticum.
Dr. Harvala added that a next-generation vaccine probably also should offer protection against enterovirus-D68. In 2014, there were 1,153 laboratory-confirmed EV-D68 infections and 14 deaths in the United States and Canada. This infection poses a diagnostic challenge: while the virus is readily detectable on throat swabs, it’s only rarely present in stool or cerebrospinal fluid samples.
“It’s important to keep in mind that this infection is still underdiagnosed. We are not really looking for it,” she said.
No specific treatment for enterovirus infections is available. Three capsid-binding antiviral agents now are in clinical trials: pleconaril, vapendavir, and pocapavir. In addition, translational studies have demonstrated that the SSRI fluoxetine inhibits enterovirus replication, but there have been no clinical trials as yet.
Although development of antivirals effective against enterovirus is an active area of research, Dr. Harvala thinks drug resistance will be an issue, underscoring the importance of vaccine development.
She reported having no financial conflicts of interest regarding her presentation.
EXPERT ANALYSIS FROM ESPID 2017
VIDEO: Clopidogrel bests ticagrelor in PCI for ACS in real-world study
BARCELONA – Patients who underwent percutaneous coronary intervention for acute coronary syndrome using newer-generation drug-eluting stents backed by ticagrelor-based dual-antiplatelet therapy had significantly higher net adverse event rates at 1 year than did those with clopidogrel-based DAPT in the CHANGE DAPT study, Clemens von Birgelen, MD, reported at the annual congress of the European Society of Cardiology.
Based upon the CHANGE DAPT findings and those from other recent studies, it would be appropriate to revise ESC and American College of Cardiology/American Heart Association guidelines, which now give the newer, more potent platelet inhibitors ticagrelor (Brilinta) or prasugrel (Effient) preferential status as the P2Y12 inhibitor of choice over clopidogrel, added Dr. von Birgelen, professor of cardiology at the University of Twente in Enschede, the Netherlands, and codirector of the department of cardiology at Thoraxcentrum Twente.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
“With the newer drug-eluting stents we see lower ischemic event rates, so the DAPT side effects due to bleeding become more important at this time. It could be that patients with ACS who are undergoing PCI may no longer need the most potent DAPT. Perhaps less potent DAPT with clopidogrel may be sufficient when using these more modern devices,” Dr. von Birgelen said in an interview.
CHANGE DAPT was a prospective, observational registry study that compared 1-year clinical outcomes in 2,062 consecutive ACS patients treated by PCI at Thoraxcentrum Twente, a high-volume PCI center. Half of the patients were treated before the primary DAPT regimen in the region changed from clopidogrel-based to ticagrelor-based DAPT on May 1, 2014, while the other half underwent PCI after the switch. This unique registry study design avoids selection bias, whereby cardiologists might preferentially use clopidogrel – the less potent P2Y12 inhibitor – in frailer patients.
The primary endpoint was the 1-year composite of all-cause mortality, any MI, stroke, or major bleeding. The rate was 7.8% in the ticagrelor period and significantly lower at 5.1% in the clopidogrel period. This difference was driven by the significantly lower major bleeding rate in the clopidogrel group: 1.2% versus 2.7% with ticagrelor-based DAPT.
The increased risk of bleeding associated with ticagrelor wasn’t offset by any advantage in term of ischemic events; indeed, the rate of such events was actually numerically lower with clopidogrel-based DAPT, albeit not statistically significantly so. Definite or probable stent thrombosis occurred in 0.6% of the clopidogrel group and 0.8% of the ticagrelor group, while the composite of cardiac death, MI, or stroke occurred in 3.7% of patients on clopidogrel-based DAPT compared with 4.7% on ticagrelor.
The two patient groups were closely similar at baseline in most respects, although the ticagrelor group was, on average, 1 year older, reflecting the more recent increased willingness of interventional cardiologists to utilize PCI in patients of advanced age. In terms of procedural differences, the ticagrelor group was more likely to undergo a transradial rather than transfemoral approach, less likely to receive a glycoprotein IIb/IIIa inhibitor, and more likely to get a proton pump inhibitor.
“All three of those factors should have reduced the bleeding risk during that second period,” Dr. von Birgelen observed.
In a propensity score–adjusted analysis taking account of the few between-group differences, ticagrelor-based DAPT was associated with a 1.75-fold increased risk of the primary endpoint and a 2.75-fold increased risk of major bleeding.
He noted that the CHANGE DAPT results are consistent with those of TOPIC, a 646-patient, single-center randomized trial conducted in Marseille. In TOPIC, after 1 month on ticagrelor- or prasugrel-backed DAPT, half of patients were switched to vastly less expensive clopidogrel for the remaining 11 months of DAPT. The result in the switched group was a marked decrease in bleeding with no increased risk of ischemic events.
“I see our study as a piece in a mosaic of studies and real-world registries with a similar message that have recently been reported,” the cardiologist said. “I hope the ESC looks carefully at these data.”
Session cochair Laura Mauri, MD, said that while it’s important to look at real-world observational data such as CHANGE DAPT to see if the results of randomized trials are generalizable, she’s not surprised by the evidence of increased risk of bleeding with a more potent agent such as ticagrelor.
“Why there’s a lack of benefit demonstrated, I think, is the bigger question,” said Dr. Mauri, professor of medicine at Harvard Medical School, Boston. “It could be related to changes in procedures over time, with procedures being conducted in a more complex manner, or some other residual confounding. I think whenever we see an observational study that changes the nature of the benefit that we see, it needs to be investigated more deeply. I don’t think it’s time to dismiss the results of very large randomized trials that show a meaningful benefit for the potent agents in the setting of ACS.”
CHANGE DAPT was an investigator-initiated study conducted without external funding. Dr. von Birgelen reported having no financial conflicts of interest.
BARCELONA – Patients who underwent percutaneous coronary intervention for acute coronary syndrome using newer-generation drug-eluting stents backed by ticagrelor-based dual-antiplatelet therapy had significantly higher net adverse event rates at 1 year than did those with clopidogrel-based DAPT in the CHANGE DAPT study, Clemens von Birgelen, MD, reported at the annual congress of the European Society of Cardiology.
Based upon the CHANGE DAPT findings and those from other recent studies, it would be appropriate to revise ESC and American College of Cardiology/American Heart Association guidelines, which now give the newer, more potent platelet inhibitors ticagrelor (Brilinta) or prasugrel (Effient) preferential status as the P2Y12 inhibitor of choice over clopidogrel, added Dr. von Birgelen, professor of cardiology at the University of Twente in Enschede, the Netherlands, and codirector of the department of cardiology at Thoraxcentrum Twente.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
“With the newer drug-eluting stents we see lower ischemic event rates, so the DAPT side effects due to bleeding become more important at this time. It could be that patients with ACS who are undergoing PCI may no longer need the most potent DAPT. Perhaps less potent DAPT with clopidogrel may be sufficient when using these more modern devices,” Dr. von Birgelen said in an interview.
CHANGE DAPT was a prospective, observational registry study that compared 1-year clinical outcomes in 2,062 consecutive ACS patients treated by PCI at Thoraxcentrum Twente, a high-volume PCI center. Half of the patients were treated before the primary DAPT regimen in the region changed from clopidogrel-based to ticagrelor-based DAPT on May 1, 2014, while the other half underwent PCI after the switch. This unique registry study design avoids selection bias, whereby cardiologists might preferentially use clopidogrel – the less potent P2Y12 inhibitor – in frailer patients.
The primary endpoint was the 1-year composite of all-cause mortality, any MI, stroke, or major bleeding. The rate was 7.8% in the ticagrelor period and significantly lower at 5.1% in the clopidogrel period. This difference was driven by the significantly lower major bleeding rate in the clopidogrel group: 1.2% versus 2.7% with ticagrelor-based DAPT.
The increased risk of bleeding associated with ticagrelor wasn’t offset by any advantage in term of ischemic events; indeed, the rate of such events was actually numerically lower with clopidogrel-based DAPT, albeit not statistically significantly so. Definite or probable stent thrombosis occurred in 0.6% of the clopidogrel group and 0.8% of the ticagrelor group, while the composite of cardiac death, MI, or stroke occurred in 3.7% of patients on clopidogrel-based DAPT compared with 4.7% on ticagrelor.
The two patient groups were closely similar at baseline in most respects, although the ticagrelor group was, on average, 1 year older, reflecting the more recent increased willingness of interventional cardiologists to utilize PCI in patients of advanced age. In terms of procedural differences, the ticagrelor group was more likely to undergo a transradial rather than transfemoral approach, less likely to receive a glycoprotein IIb/IIIa inhibitor, and more likely to get a proton pump inhibitor.
“All three of those factors should have reduced the bleeding risk during that second period,” Dr. von Birgelen observed.
In a propensity score–adjusted analysis taking account of the few between-group differences, ticagrelor-based DAPT was associated with a 1.75-fold increased risk of the primary endpoint and a 2.75-fold increased risk of major bleeding.
He noted that the CHANGE DAPT results are consistent with those of TOPIC, a 646-patient, single-center randomized trial conducted in Marseille. In TOPIC, after 1 month on ticagrelor- or prasugrel-backed DAPT, half of patients were switched to vastly less expensive clopidogrel for the remaining 11 months of DAPT. The result in the switched group was a marked decrease in bleeding with no increased risk of ischemic events.
“I see our study as a piece in a mosaic of studies and real-world registries with a similar message that have recently been reported,” the cardiologist said. “I hope the ESC looks carefully at these data.”
Session cochair Laura Mauri, MD, said that while it’s important to look at real-world observational data such as CHANGE DAPT to see if the results of randomized trials are generalizable, she’s not surprised by the evidence of increased risk of bleeding with a more potent agent such as ticagrelor.
“Why there’s a lack of benefit demonstrated, I think, is the bigger question,” said Dr. Mauri, professor of medicine at Harvard Medical School, Boston. “It could be related to changes in procedures over time, with procedures being conducted in a more complex manner, or some other residual confounding. I think whenever we see an observational study that changes the nature of the benefit that we see, it needs to be investigated more deeply. I don’t think it’s time to dismiss the results of very large randomized trials that show a meaningful benefit for the potent agents in the setting of ACS.”
CHANGE DAPT was an investigator-initiated study conducted without external funding. Dr. von Birgelen reported having no financial conflicts of interest.
BARCELONA – Patients who underwent percutaneous coronary intervention for acute coronary syndrome using newer-generation drug-eluting stents backed by ticagrelor-based dual-antiplatelet therapy had significantly higher net adverse event rates at 1 year than did those with clopidogrel-based DAPT in the CHANGE DAPT study, Clemens von Birgelen, MD, reported at the annual congress of the European Society of Cardiology.
Based upon the CHANGE DAPT findings and those from other recent studies, it would be appropriate to revise ESC and American College of Cardiology/American Heart Association guidelines, which now give the newer, more potent platelet inhibitors ticagrelor (Brilinta) or prasugrel (Effient) preferential status as the P2Y12 inhibitor of choice over clopidogrel, added Dr. von Birgelen, professor of cardiology at the University of Twente in Enschede, the Netherlands, and codirector of the department of cardiology at Thoraxcentrum Twente.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
“With the newer drug-eluting stents we see lower ischemic event rates, so the DAPT side effects due to bleeding become more important at this time. It could be that patients with ACS who are undergoing PCI may no longer need the most potent DAPT. Perhaps less potent DAPT with clopidogrel may be sufficient when using these more modern devices,” Dr. von Birgelen said in an interview.
CHANGE DAPT was a prospective, observational registry study that compared 1-year clinical outcomes in 2,062 consecutive ACS patients treated by PCI at Thoraxcentrum Twente, a high-volume PCI center. Half of the patients were treated before the primary DAPT regimen in the region changed from clopidogrel-based to ticagrelor-based DAPT on May 1, 2014, while the other half underwent PCI after the switch. This unique registry study design avoids selection bias, whereby cardiologists might preferentially use clopidogrel – the less potent P2Y12 inhibitor – in frailer patients.
The primary endpoint was the 1-year composite of all-cause mortality, any MI, stroke, or major bleeding. The rate was 7.8% in the ticagrelor period and significantly lower at 5.1% in the clopidogrel period. This difference was driven by the significantly lower major bleeding rate in the clopidogrel group: 1.2% versus 2.7% with ticagrelor-based DAPT.
The increased risk of bleeding associated with ticagrelor wasn’t offset by any advantage in term of ischemic events; indeed, the rate of such events was actually numerically lower with clopidogrel-based DAPT, albeit not statistically significantly so. Definite or probable stent thrombosis occurred in 0.6% of the clopidogrel group and 0.8% of the ticagrelor group, while the composite of cardiac death, MI, or stroke occurred in 3.7% of patients on clopidogrel-based DAPT compared with 4.7% on ticagrelor.
The two patient groups were closely similar at baseline in most respects, although the ticagrelor group was, on average, 1 year older, reflecting the more recent increased willingness of interventional cardiologists to utilize PCI in patients of advanced age. In terms of procedural differences, the ticagrelor group was more likely to undergo a transradial rather than transfemoral approach, less likely to receive a glycoprotein IIb/IIIa inhibitor, and more likely to get a proton pump inhibitor.
“All three of those factors should have reduced the bleeding risk during that second period,” Dr. von Birgelen observed.
In a propensity score–adjusted analysis taking account of the few between-group differences, ticagrelor-based DAPT was associated with a 1.75-fold increased risk of the primary endpoint and a 2.75-fold increased risk of major bleeding.
He noted that the CHANGE DAPT results are consistent with those of TOPIC, a 646-patient, single-center randomized trial conducted in Marseille. In TOPIC, after 1 month on ticagrelor- or prasugrel-backed DAPT, half of patients were switched to vastly less expensive clopidogrel for the remaining 11 months of DAPT. The result in the switched group was a marked decrease in bleeding with no increased risk of ischemic events.
“I see our study as a piece in a mosaic of studies and real-world registries with a similar message that have recently been reported,” the cardiologist said. “I hope the ESC looks carefully at these data.”
Session cochair Laura Mauri, MD, said that while it’s important to look at real-world observational data such as CHANGE DAPT to see if the results of randomized trials are generalizable, she’s not surprised by the evidence of increased risk of bleeding with a more potent agent such as ticagrelor.
“Why there’s a lack of benefit demonstrated, I think, is the bigger question,” said Dr. Mauri, professor of medicine at Harvard Medical School, Boston. “It could be related to changes in procedures over time, with procedures being conducted in a more complex manner, or some other residual confounding. I think whenever we see an observational study that changes the nature of the benefit that we see, it needs to be investigated more deeply. I don’t think it’s time to dismiss the results of very large randomized trials that show a meaningful benefit for the potent agents in the setting of ACS.”
CHANGE DAPT was an investigator-initiated study conducted without external funding. Dr. von Birgelen reported having no financial conflicts of interest.
AT THE ESC CONGRESS 2017
Key clinical point:
Major finding: The 1-year composite endpoint of all-cause mortality, MI, stroke, or major bleeding occurred in 5.1% of ACS patients who underwent PCI using newer-generation drug-eluting stents followed by clopidogrel-based DAPT, compared with 7.8% who received ticagrelor-based DAPT.
Data source: This unique design for a prospective observational registry study compared 1-year outcomes in 2,062 consecutive ACS patients who underwent PCI at a single high-volume center, half before a regional switch from clopidogrel- to ticagrelor-based DAPT and half afterward.
Disclosures: CHANGE DAPT was an investigator-initiated study conducted without external funding. The presenter reported having no financial conflicts of interest.

Dr. Clyde Yancy: CANTOS wows, opens new therapeutic avenues
BARCELONA – For Clyde Yancy, MD, presentation of the bombshell CANTOS trial results at the annual congress of the European Congress of Cardiology made for “a really good day.”
Those results showed that inhibiting the interleukin-1 beta innate immunity pathway with canakinumab reduced recurrent cardiovascular events and lung cancer. But further, they introduced a new way of identifying and treating patients for secondary prevention.
“Here is an alternative way to get to cardiovascular events; here is bringing inflammation right to the front page of what we do as cardiologists to prevent events; here is a brand-new agent that is a monoclonal antibody against interleukin that may be modifying this risk, and … a remarkable advantage that really needs to be replicated,” said Dr. Yancy, chief of medicine-cardiology at Northwestern University in Chicago, in a video interview.
“This is a really good day” because we’ve got new things to think about, new ways to approach our patients, and [we may soon be] entering the realm where we’ll want personalized therapy based on the unique phenotype a patient represents, and think about the pathways to disease through these brand new schemes” that are helping us understand the burden of disease, he declared.
BARCELONA – For Clyde Yancy, MD, presentation of the bombshell CANTOS trial results at the annual congress of the European Congress of Cardiology made for “a really good day.”
Those results showed that inhibiting the interleukin-1 beta innate immunity pathway with canakinumab reduced recurrent cardiovascular events and lung cancer. But further, they introduced a new way of identifying and treating patients for secondary prevention.
“Here is an alternative way to get to cardiovascular events; here is bringing inflammation right to the front page of what we do as cardiologists to prevent events; here is a brand-new agent that is a monoclonal antibody against interleukin that may be modifying this risk, and … a remarkable advantage that really needs to be replicated,” said Dr. Yancy, chief of medicine-cardiology at Northwestern University in Chicago, in a video interview.
“This is a really good day” because we’ve got new things to think about, new ways to approach our patients, and [we may soon be] entering the realm where we’ll want personalized therapy based on the unique phenotype a patient represents, and think about the pathways to disease through these brand new schemes” that are helping us understand the burden of disease, he declared.
BARCELONA – For Clyde Yancy, MD, presentation of the bombshell CANTOS trial results at the annual congress of the European Congress of Cardiology made for “a really good day.”
Those results showed that inhibiting the interleukin-1 beta innate immunity pathway with canakinumab reduced recurrent cardiovascular events and lung cancer. But further, they introduced a new way of identifying and treating patients for secondary prevention.
“Here is an alternative way to get to cardiovascular events; here is bringing inflammation right to the front page of what we do as cardiologists to prevent events; here is a brand-new agent that is a monoclonal antibody against interleukin that may be modifying this risk, and … a remarkable advantage that really needs to be replicated,” said Dr. Yancy, chief of medicine-cardiology at Northwestern University in Chicago, in a video interview.
“This is a really good day” because we’ve got new things to think about, new ways to approach our patients, and [we may soon be] entering the realm where we’ll want personalized therapy based on the unique phenotype a patient represents, and think about the pathways to disease through these brand new schemes” that are helping us understand the burden of disease, he declared.
AT THE ESC CONGRESS 2017
