User login
Poststroke depression often poorly managed
HONOLULU – Poststroke depression is a common condition that is underdiagnosed and inadequately treated, according to Dr. Linda S. Williams, a neurologist at Indiana University and the Roudebush VA Medical Center, both in Indianapolis.
But it doesn’t have to be this way. "There are many, many treatments, and they’re easy to give. It’s something that should be within the grasp of every provider to do," she said at the International Stroke Conference, sponsored by the American Heart Association.

Yet many of her fellow neurologists don’t see it this way. Dr. Williams said she faults her specialty for playing a major role in the generally poor management of poststroke depression (PSD).
"I’ve always wanted to write an editorial called, ‘What’s the ‘P’ in ABPN?’ because neurologists are boarded by the American Board of Psychiatry and Neurology, but many neurologists – even though we get some training in psychiatry – don’t want to initiate treatment for depression. We somehow think it’s not our job. That might be fine if you have great communication with the patient’s primary care doctor in an integrated health care system and you can be sure that doctor is going to see that the patient gets started on antidepressant therapy, but I think reality would suggest that’s not very often the case," she said.
"So I strongly feel that whoever detects the depression first should get the patient started on treatment and should make sure the patient is seen again in 6 weeks to see if there has been improvement in symptoms and to figure out who’ll get called if the patient has medication side effects and needs to switch," the neurologist continued.
An estimated 25%-30% of the 700,000 new stroke survivors each year will develop PSD, although it’s unclear how many cases are new onset after the neurovascular event, as opposed to undiagnosed depression present beforehand. Depression is, after all, an independent risk factor for both stroke and ischemic heart disease. In any case, PSD is associated with increased morbidity and mortality and greater health care utilization.
The keys to improved outcomes in PSD are to set up a systematic screening program for all patients beginning about 1 month after a stroke, start treatment promptly once the diagnosis is made, and then monitor symptomatic progress and adjust the antidepressant medication as needed, she said.
Lots of screening tools for depression are available. Dr. Williams said she favors the Patient Health Questionnaire-9 (PHQ-9) because it’s quick – just nine simple questions, it was developed specifically with primary care physicians in mind, and it’s one of the few screening tools that allows a busy nonpsychiatrist to reliably diagnose major depression based upon the results.
She conducted a study in which 316 stroke survivors were assessed for depression using both the PHQ-9 and the gold standard, time-consuming Structured Clinical Interview for DSM-IV Disorders (SCID). One hundred forty-five patients met SCID criteria for major depression. A PHQ-9 score of 10 or more out of a possible 27 had 91% sensitivity and 89% specificity for major depression. A PHQ-2 of 3 or more, in which only the first two of the nine questions are asked, had 83% sensitivity and 84% specificity for the diagnosis.
"Even in stroke patients, I feel pretty confident in using this scale and knowing it’s going to give me an accurate diagnosis," the neurologist said.
That being said, Dr. Williams acknowledged that the diagnosis of PSD is somewhat trickier than for other forms of depression because a stroke may have lingering physical or cognitive effects that can mimic the symptoms of the mood disorder. Conversely, stroke-induced severe right hemisphere damage or aphasia can mask depressive symptoms.
Epidemiologic studies suggest only about half of patients with PSD are diagnosed. It’s easy for busy physicians to forget to screen. That’s why a systematic screening plan is important, she said. An automated electronic reminder system to screen for PSD 1-6 months after a stroke is an effective way to boost detection and treatment rates. Dr. Williams and her coinvestigators developed such a system for primary care physicians and neurologists for inclusion in patients’ electronic medical record within the VA medical system. When the investigators put the automated reminder system to the test in a controlled trial, it boosted screening rates 1-6 months after a stroke by 6.2-fold and treatment rates in screen-positive patients by 2.45-fold, compared with usual care (J. Gen. Intern. Med. 2011;26:852-7).
PSD responds to the same therapies that are effective in nonstroke major depression. The recent literature suggests the proportion of patients with PSD who are on antidepressant therapy has been rising in the past few years; however, the majority of treated patients stop taking their medication after the first several weeks or stay on the initial dose without ever having it titrated upward. It’s crucial to check in with the patient after about 6 weeks of therapy to learn if symptoms are improving; if not, it’s time to switch to an antidepressant from another class, Dr. Williams said.
"I do think that ongoing monitoring of treatment and adjustment of medications is really fundamental to patients having good outcomes," she said.
A hot topic in the stroke literature in recent years has been whether it makes sense to simply initiate prophylactic antidepressant therapy in all poststroke patients as a means of preventing a full-blown depressive episode. "My answer is, ‘Not yet,’ " she said, noting that the randomized trials to date looking at this approach have been small and have yielded conflicting results.
Dr. Williams reported having no relevant financial conflicts.
HONOLULU – Poststroke depression is a common condition that is underdiagnosed and inadequately treated, according to Dr. Linda S. Williams, a neurologist at Indiana University and the Roudebush VA Medical Center, both in Indianapolis.
But it doesn’t have to be this way. "There are many, many treatments, and they’re easy to give. It’s something that should be within the grasp of every provider to do," she said at the International Stroke Conference, sponsored by the American Heart Association.
Yet many of her fellow neurologists don’t see it this way. Dr. Williams said she faults her specialty for playing a major role in the generally poor management of poststroke depression (PSD).
"I’ve always wanted to write an editorial called, ‘What’s the ‘P’ in ABPN?’ because neurologists are boarded by the American Board of Psychiatry and Neurology, but many neurologists – even though we get some training in psychiatry – don’t want to initiate treatment for depression. We somehow think it’s not our job. That might be fine if you have great communication with the patient’s primary care doctor in an integrated health care system and you can be sure that doctor is going to see that the patient gets started on antidepressant therapy, but I think reality would suggest that’s not very often the case," she said.
"So I strongly feel that whoever detects the depression first should get the patient started on treatment and should make sure the patient is seen again in 6 weeks to see if there has been improvement in symptoms and to figure out who’ll get called if the patient has medication side effects and needs to switch," the neurologist continued.
An estimated 25%-30% of the 700,000 new stroke survivors each year will develop PSD, although it’s unclear how many cases are new onset after the neurovascular event, as opposed to undiagnosed depression present beforehand. Depression is, after all, an independent risk factor for both stroke and ischemic heart disease. In any case, PSD is associated with increased morbidity and mortality and greater health care utilization.
The keys to improved outcomes in PSD are to set up a systematic screening program for all patients beginning about 1 month after a stroke, start treatment promptly once the diagnosis is made, and then monitor symptomatic progress and adjust the antidepressant medication as needed, she said.
Lots of screening tools for depression are available. Dr. Williams said she favors the Patient Health Questionnaire-9 (PHQ-9) because it’s quick – just nine simple questions, it was developed specifically with primary care physicians in mind, and it’s one of the few screening tools that allows a busy nonpsychiatrist to reliably diagnose major depression based upon the results.
She conducted a study in which 316 stroke survivors were assessed for depression using both the PHQ-9 and the gold standard, time-consuming Structured Clinical Interview for DSM-IV Disorders (SCID). One hundred forty-five patients met SCID criteria for major depression. A PHQ-9 score of 10 or more out of a possible 27 had 91% sensitivity and 89% specificity for major depression. A PHQ-2 of 3 or more, in which only the first two of the nine questions are asked, had 83% sensitivity and 84% specificity for the diagnosis.
"Even in stroke patients, I feel pretty confident in using this scale and knowing it’s going to give me an accurate diagnosis," the neurologist said.
That being said, Dr. Williams acknowledged that the diagnosis of PSD is somewhat trickier than for other forms of depression because a stroke may have lingering physical or cognitive effects that can mimic the symptoms of the mood disorder. Conversely, stroke-induced severe right hemisphere damage or aphasia can mask depressive symptoms.
Epidemiologic studies suggest only about half of patients with PSD are diagnosed. It’s easy for busy physicians to forget to screen. That’s why a systematic screening plan is important, she said. An automated electronic reminder system to screen for PSD 1-6 months after a stroke is an effective way to boost detection and treatment rates. Dr. Williams and her coinvestigators developed such a system for primary care physicians and neurologists for inclusion in patients’ electronic medical record within the VA medical system. When the investigators put the automated reminder system to the test in a controlled trial, it boosted screening rates 1-6 months after a stroke by 6.2-fold and treatment rates in screen-positive patients by 2.45-fold, compared with usual care (J. Gen. Intern. Med. 2011;26:852-7).
PSD responds to the same therapies that are effective in nonstroke major depression. The recent literature suggests the proportion of patients with PSD who are on antidepressant therapy has been rising in the past few years; however, the majority of treated patients stop taking their medication after the first several weeks or stay on the initial dose without ever having it titrated upward. It’s crucial to check in with the patient after about 6 weeks of therapy to learn if symptoms are improving; if not, it’s time to switch to an antidepressant from another class, Dr. Williams said.
"I do think that ongoing monitoring of treatment and adjustment of medications is really fundamental to patients having good outcomes," she said.
A hot topic in the stroke literature in recent years has been whether it makes sense to simply initiate prophylactic antidepressant therapy in all poststroke patients as a means of preventing a full-blown depressive episode. "My answer is, ‘Not yet,’ " she said, noting that the randomized trials to date looking at this approach have been small and have yielded conflicting results.
Dr. Williams reported having no relevant financial conflicts.
HONOLULU – Poststroke depression is a common condition that is underdiagnosed and inadequately treated, according to Dr. Linda S. Williams, a neurologist at Indiana University and the Roudebush VA Medical Center, both in Indianapolis.
But it doesn’t have to be this way. "There are many, many treatments, and they’re easy to give. It’s something that should be within the grasp of every provider to do," she said at the International Stroke Conference, sponsored by the American Heart Association.
Yet many of her fellow neurologists don’t see it this way. Dr. Williams said she faults her specialty for playing a major role in the generally poor management of poststroke depression (PSD).
"I’ve always wanted to write an editorial called, ‘What’s the ‘P’ in ABPN?’ because neurologists are boarded by the American Board of Psychiatry and Neurology, but many neurologists – even though we get some training in psychiatry – don’t want to initiate treatment for depression. We somehow think it’s not our job. That might be fine if you have great communication with the patient’s primary care doctor in an integrated health care system and you can be sure that doctor is going to see that the patient gets started on antidepressant therapy, but I think reality would suggest that’s not very often the case," she said.
"So I strongly feel that whoever detects the depression first should get the patient started on treatment and should make sure the patient is seen again in 6 weeks to see if there has been improvement in symptoms and to figure out who’ll get called if the patient has medication side effects and needs to switch," the neurologist continued.
An estimated 25%-30% of the 700,000 new stroke survivors each year will develop PSD, although it’s unclear how many cases are new onset after the neurovascular event, as opposed to undiagnosed depression present beforehand. Depression is, after all, an independent risk factor for both stroke and ischemic heart disease. In any case, PSD is associated with increased morbidity and mortality and greater health care utilization.
The keys to improved outcomes in PSD are to set up a systematic screening program for all patients beginning about 1 month after a stroke, start treatment promptly once the diagnosis is made, and then monitor symptomatic progress and adjust the antidepressant medication as needed, she said.
Lots of screening tools for depression are available. Dr. Williams said she favors the Patient Health Questionnaire-9 (PHQ-9) because it’s quick – just nine simple questions, it was developed specifically with primary care physicians in mind, and it’s one of the few screening tools that allows a busy nonpsychiatrist to reliably diagnose major depression based upon the results.
She conducted a study in which 316 stroke survivors were assessed for depression using both the PHQ-9 and the gold standard, time-consuming Structured Clinical Interview for DSM-IV Disorders (SCID). One hundred forty-five patients met SCID criteria for major depression. A PHQ-9 score of 10 or more out of a possible 27 had 91% sensitivity and 89% specificity for major depression. A PHQ-2 of 3 or more, in which only the first two of the nine questions are asked, had 83% sensitivity and 84% specificity for the diagnosis.
"Even in stroke patients, I feel pretty confident in using this scale and knowing it’s going to give me an accurate diagnosis," the neurologist said.
That being said, Dr. Williams acknowledged that the diagnosis of PSD is somewhat trickier than for other forms of depression because a stroke may have lingering physical or cognitive effects that can mimic the symptoms of the mood disorder. Conversely, stroke-induced severe right hemisphere damage or aphasia can mask depressive symptoms.
Epidemiologic studies suggest only about half of patients with PSD are diagnosed. It’s easy for busy physicians to forget to screen. That’s why a systematic screening plan is important, she said. An automated electronic reminder system to screen for PSD 1-6 months after a stroke is an effective way to boost detection and treatment rates. Dr. Williams and her coinvestigators developed such a system for primary care physicians and neurologists for inclusion in patients’ electronic medical record within the VA medical system. When the investigators put the automated reminder system to the test in a controlled trial, it boosted screening rates 1-6 months after a stroke by 6.2-fold and treatment rates in screen-positive patients by 2.45-fold, compared with usual care (J. Gen. Intern. Med. 2011;26:852-7).
PSD responds to the same therapies that are effective in nonstroke major depression. The recent literature suggests the proportion of patients with PSD who are on antidepressant therapy has been rising in the past few years; however, the majority of treated patients stop taking their medication after the first several weeks or stay on the initial dose without ever having it titrated upward. It’s crucial to check in with the patient after about 6 weeks of therapy to learn if symptoms are improving; if not, it’s time to switch to an antidepressant from another class, Dr. Williams said.
"I do think that ongoing monitoring of treatment and adjustment of medications is really fundamental to patients having good outcomes," she said.
A hot topic in the stroke literature in recent years has been whether it makes sense to simply initiate prophylactic antidepressant therapy in all poststroke patients as a means of preventing a full-blown depressive episode. "My answer is, ‘Not yet,’ " she said, noting that the randomized trials to date looking at this approach have been small and have yielded conflicting results.
Dr. Williams reported having no relevant financial conflicts.
EXPERT ANALYSIS FROM THE INTERNATIONAL STROKE CONFERENCE

Skin capillary density drop reliably predicts preeclampsia
SAN FRANCISCO – A reduction in skin capillary density during pregnancy constitutes a novel independent and reliable noninvasive predictor of preeclampsia, according to Dr. Tarek Antonios of the University of London.
"Capillary density rarefaction is the most sensitive and specific predictor of preeclampsia to date. Combining capillary density rarefaction and the uterine artery Doppler pulsatility index increases the sensitivity of prediction to 86% and the specificity to 80%, figures that are by far more significant than any other published evidence about the clinical prediction of preeclampsia," he declared at the annual meeting of the American College of Cardiology.
Measurement of skin capillary density changes in pregnancy is inexpensive once the essential equipment – an intravital video microscope suitable for capillaroscopy – has been acquired, he added.
Cardiovascular risk factors known to predispose to preeclampsia include essential hypertension, diabetes, and obesity. Dr. Antonios and coworkers have surmised that the mechanism by which these disorders boost the risk of preeclampsia involves microcirculatory abnormalities and impaired tissue perfusion.
The investigators have developed a reproducible method of measuring skin capillary density on the dorsum of the hand. Further, they have demonstrated that reduced capillary density – which they term "structural capillary rarefaction" – beginning at about 20 weeks of gestation is a harbinger of subsequent onset of preeclampsia.
Dr. Antonios reported on 322 consecutive white women with singleton pregnancies, of whom 13 had a history of preeclampsia, 11 had a history of untreated stage 1 essential hypertension, and the rest were normotensive. They underwent five structured capillaroscopy assessments at 11-16 weeks’ of gestation, 20-24 weeks, 27-32 weeks, 34-38 weeks, and finally at 5-15 weeks post partum. The capillary density measurements were done in a temperature-controlled laboratory with a standardized technique.
Among the 305 women who completed the study, 16 (5%) developed preeclampsia. Four of the 16 (25%) had a history of preeclampsia, compared with just 3% of the 289 (1%) subjects with a normal pregnancy.
The women who became preeclamptic were also set apart by their mean 6.1 capillary/mm2 reduction in density between the weeks 20-24 measurement and the weeks 11-16 baseline. In contrast, the women with normal pregnancies averaged a 1.0 capillary/mm2 decrease during that time frame. Capillary rarefaction further increased over time in women who later developed preeclampsia: their mean reduction in density at the weeks 27-32 measurement was 11.4/mm2, compared with the weeks 11-16 baseline, while the controls averaged a 2.1 capillary/mm2 decrease.
In a multivariate regression analysis, the single strongest predictor of preeclampsia was a history of previous preeclampsia or essential hypertension, which was associated with a 35-fold increase in risk. Each 1 capillary/mm2 reduction in density at 20-24 weeks was associated with a 3% increase in risk, while at 27-32 weeks every 1 capillary/mm2 reduction in density conferred a 26% increase in the risk of preeclampsia.
Significant structural capillary rarefaction at weeks 27-32 had a 77% sensitivity and 77% specificity for subsequent preeclampsia. Combining an increased uterine artery Doppler pulsatility index with a finding of significant capillary density reduction at weeks 27-32 boosted the sensitivity to 86% and the specificity to 80%.
Given that only 16 participants in this study developed preeclampsia, the next step in this research is to conduct a large clinical trial to validate capillaroscopy as a clinical risk prediction tool with an eye toward its eventual integration into routine clinical practice, according to Dr. Antonios.
This study was funded by the British Heart Foundation. Dr. Antonios reported having no financial conflicts.
SAN FRANCISCO – A reduction in skin capillary density during pregnancy constitutes a novel independent and reliable noninvasive predictor of preeclampsia, according to Dr. Tarek Antonios of the University of London.
"Capillary density rarefaction is the most sensitive and specific predictor of preeclampsia to date. Combining capillary density rarefaction and the uterine artery Doppler pulsatility index increases the sensitivity of prediction to 86% and the specificity to 80%, figures that are by far more significant than any other published evidence about the clinical prediction of preeclampsia," he declared at the annual meeting of the American College of Cardiology.
Measurement of skin capillary density changes in pregnancy is inexpensive once the essential equipment – an intravital video microscope suitable for capillaroscopy – has been acquired, he added.
Cardiovascular risk factors known to predispose to preeclampsia include essential hypertension, diabetes, and obesity. Dr. Antonios and coworkers have surmised that the mechanism by which these disorders boost the risk of preeclampsia involves microcirculatory abnormalities and impaired tissue perfusion.
The investigators have developed a reproducible method of measuring skin capillary density on the dorsum of the hand. Further, they have demonstrated that reduced capillary density – which they term "structural capillary rarefaction" – beginning at about 20 weeks of gestation is a harbinger of subsequent onset of preeclampsia.
Dr. Antonios reported on 322 consecutive white women with singleton pregnancies, of whom 13 had a history of preeclampsia, 11 had a history of untreated stage 1 essential hypertension, and the rest were normotensive. They underwent five structured capillaroscopy assessments at 11-16 weeks’ of gestation, 20-24 weeks, 27-32 weeks, 34-38 weeks, and finally at 5-15 weeks post partum. The capillary density measurements were done in a temperature-controlled laboratory with a standardized technique.
Among the 305 women who completed the study, 16 (5%) developed preeclampsia. Four of the 16 (25%) had a history of preeclampsia, compared with just 3% of the 289 (1%) subjects with a normal pregnancy.
The women who became preeclamptic were also set apart by their mean 6.1 capillary/mm2 reduction in density between the weeks 20-24 measurement and the weeks 11-16 baseline. In contrast, the women with normal pregnancies averaged a 1.0 capillary/mm2 decrease during that time frame. Capillary rarefaction further increased over time in women who later developed preeclampsia: their mean reduction in density at the weeks 27-32 measurement was 11.4/mm2, compared with the weeks 11-16 baseline, while the controls averaged a 2.1 capillary/mm2 decrease.
In a multivariate regression analysis, the single strongest predictor of preeclampsia was a history of previous preeclampsia or essential hypertension, which was associated with a 35-fold increase in risk. Each 1 capillary/mm2 reduction in density at 20-24 weeks was associated with a 3% increase in risk, while at 27-32 weeks every 1 capillary/mm2 reduction in density conferred a 26% increase in the risk of preeclampsia.
Significant structural capillary rarefaction at weeks 27-32 had a 77% sensitivity and 77% specificity for subsequent preeclampsia. Combining an increased uterine artery Doppler pulsatility index with a finding of significant capillary density reduction at weeks 27-32 boosted the sensitivity to 86% and the specificity to 80%.
Given that only 16 participants in this study developed preeclampsia, the next step in this research is to conduct a large clinical trial to validate capillaroscopy as a clinical risk prediction tool with an eye toward its eventual integration into routine clinical practice, according to Dr. Antonios.
This study was funded by the British Heart Foundation. Dr. Antonios reported having no financial conflicts.
SAN FRANCISCO – A reduction in skin capillary density during pregnancy constitutes a novel independent and reliable noninvasive predictor of preeclampsia, according to Dr. Tarek Antonios of the University of London.
"Capillary density rarefaction is the most sensitive and specific predictor of preeclampsia to date. Combining capillary density rarefaction and the uterine artery Doppler pulsatility index increases the sensitivity of prediction to 86% and the specificity to 80%, figures that are by far more significant than any other published evidence about the clinical prediction of preeclampsia," he declared at the annual meeting of the American College of Cardiology.
Measurement of skin capillary density changes in pregnancy is inexpensive once the essential equipment – an intravital video microscope suitable for capillaroscopy – has been acquired, he added.
Cardiovascular risk factors known to predispose to preeclampsia include essential hypertension, diabetes, and obesity. Dr. Antonios and coworkers have surmised that the mechanism by which these disorders boost the risk of preeclampsia involves microcirculatory abnormalities and impaired tissue perfusion.
The investigators have developed a reproducible method of measuring skin capillary density on the dorsum of the hand. Further, they have demonstrated that reduced capillary density – which they term "structural capillary rarefaction" – beginning at about 20 weeks of gestation is a harbinger of subsequent onset of preeclampsia.
Dr. Antonios reported on 322 consecutive white women with singleton pregnancies, of whom 13 had a history of preeclampsia, 11 had a history of untreated stage 1 essential hypertension, and the rest were normotensive. They underwent five structured capillaroscopy assessments at 11-16 weeks’ of gestation, 20-24 weeks, 27-32 weeks, 34-38 weeks, and finally at 5-15 weeks post partum. The capillary density measurements were done in a temperature-controlled laboratory with a standardized technique.
Among the 305 women who completed the study, 16 (5%) developed preeclampsia. Four of the 16 (25%) had a history of preeclampsia, compared with just 3% of the 289 (1%) subjects with a normal pregnancy.
The women who became preeclamptic were also set apart by their mean 6.1 capillary/mm2 reduction in density between the weeks 20-24 measurement and the weeks 11-16 baseline. In contrast, the women with normal pregnancies averaged a 1.0 capillary/mm2 decrease during that time frame. Capillary rarefaction further increased over time in women who later developed preeclampsia: their mean reduction in density at the weeks 27-32 measurement was 11.4/mm2, compared with the weeks 11-16 baseline, while the controls averaged a 2.1 capillary/mm2 decrease.
In a multivariate regression analysis, the single strongest predictor of preeclampsia was a history of previous preeclampsia or essential hypertension, which was associated with a 35-fold increase in risk. Each 1 capillary/mm2 reduction in density at 20-24 weeks was associated with a 3% increase in risk, while at 27-32 weeks every 1 capillary/mm2 reduction in density conferred a 26% increase in the risk of preeclampsia.
Significant structural capillary rarefaction at weeks 27-32 had a 77% sensitivity and 77% specificity for subsequent preeclampsia. Combining an increased uterine artery Doppler pulsatility index with a finding of significant capillary density reduction at weeks 27-32 boosted the sensitivity to 86% and the specificity to 80%.
Given that only 16 participants in this study developed preeclampsia, the next step in this research is to conduct a large clinical trial to validate capillaroscopy as a clinical risk prediction tool with an eye toward its eventual integration into routine clinical practice, according to Dr. Antonios.
This study was funded by the British Heart Foundation. Dr. Antonios reported having no financial conflicts.
AT ACC 13
Major finding: A marked reduction in capillary density in the skin on the dorsum of the hand between gestational weeks 11-16 and 27-32 was associated with 77% sensitivity and 77% specificity for subsequent preeclampsia.
Data source: This was a prospective study involving 322 consecutive white women with singleton pregnancies who underwent structured measurement of skin capillary density on four designated occasions during pregnancy and once post partum.
Disclosures: The study was funded by the British Heart Foundation. Dr. Antonios reported having no financial conflicts.
Consider treatment urgency when prescribing for psoriasis
WAILEA, HAWAII – While psoriasis experts typically emphasize the disease’s chronic nature and the importance of effective long-term therapy, in reality the first big question when a patient presents to the office should be, ‘What’s the urgency of treatment?’ according to Dr. Kenneth B. Gordon, professor of dermatology at Northwestern University, Chicago.
Two patients can have equally extensive disease yet dissimilar treatment urgencies – and different treatments of choice as a result, he said at the Hawaii Dermatology Seminar, sponsored by the Global Academy for Medical Education/Skin Disease Education Foundation.
The list of preferred medications for patients with high treatment urgency is short: "When you need to get people better fast, infliximab and cyclosporine are the go-to drugs," the dermatologist stressed.
Insurance companies will often insist that a patient try methotrexate before resorting to a far costlier biologic agent. That’s unreasonable when the treatment urgency is high.
"Methotrexate doesn’t have a high enough level of predictability or efficacy of response. Additionally, it takes a long time to act. When someone is acutely ill, you don’t want to have to wait 16 weeks to figure out what’s the highest level of efficacy you’re going to get. You want to know that answer in 10 weeks, like you do with infliximab. Infliximab is a wonderful short-term therapy for patients who have urgent disease. And with cyclosporine you see effects in 4-8 weeks," Dr. Gordon continued.
He noted that in the open-label RESTORE 1 trial, in which 868 psoriasis patients were randomized to infliximab or methotrexate, the PASI-75 response rate at week 6 in the infliximab group was already close to 60%. By week 10, the PASI-75 rate was 75% in the infliximab group and 27% in the methotrexate group (Br. J. Dermatol. 2011;165:1109-17).
The main safety concern with cyclosporine is renal toxicity, which doesn’t emerge as a real problem until after about a year on the drug, Dr. Gordon said. The safety concerns associated with short-term use (6-8 weeks) to treat an acute exacerbation of psoriasis before transitioning to a different medication are modest, and limited to relatively uncommon increases in blood pressure.
Factors that might raise a patient’s treatment urgency level range from sleep deprivation because of psoriasis pain and itching to workplace hassles because of extensive sick leave, to an important public appearance scheduled within 6-8 weeks.
Session moderator Dr. Craig L. Leonardi remarked that getting payer approval for infliximab often takes a month.
"Unless you’re university based, it’s unlikely you’re going to get infliximab fast, so cyclosporine becomes a real mainstay of treatment when it’s hot and bothersome psoriasis," he said. "And it’s the treatment of choice for psoriasis during pregnancy, absolutely. It’s category C, but there’s a lot of experience with it in the transplant population," noted Dr. Leonardi of St. Louis University.
Dr. Gordon also described a clinical scenario completely different from high treatment urgency – the patient with extensive, yet stable disease. In such a case, the priority is to select a drug the patient can tolerate for a year or more, with good long-term safety and little loss of efficacy over time.
The therapeutic responses to infliximab and adalimumab tend to fade over time, but the majority of patients still do well after 1-3 years of continuous therapy, said Dr. Gordon. His analysis of the phase III REVEAL trial extension showed that 83% of patients with at least a PASI-75 response through the first 33 weeks of adalimumab therapy continued to have a PASI-75 or better response through 100 weeks, and 76% of the original responders were still in that category after 160 weeks of therapy (J. Am. Acad. Dermatol. 2012;66:241-51).
The data on the long-term safety of antitumor necrosis factor agents are extensive and largely reassuring, Dr. Gordon noted.
"I make the argument that there is more known about anti-TNF therapy in terms of safety than any other medicines ever," Dr. Gordon said. Much of the data come courtesy of Europe, where most patients are able to get on anti-TNF therapy only if a physician enrolls them in a registry, he added.
The primary safety risk posed by biologic therapy is serious infections, in Dr. Gordon’s opinion. The collective registry experience in rheumatoid arthritis patients suggests that risk is about 20% greater than in patients on methotrexate, and this risk appears to be stable over time. But it’s probably a mistake to extrapolate from the rheumatologic experience to psoriasis, Dr. Gordon said. He and his colleagues have shown that rheumatoid arthritis patients on biologic therapy tend to be older and more likely to be on concomitant systemic corticosteroids and other immunosuppressive drugs than are psoriasis patients (Ann. Rheum. Dis. 2009;68:1863-9). More data on the risks of biologic therapies in psoriasis patients are anticipated from PSOLAR and other large ongoing patient registries, he said.
A key issue in long-term therapy is the desire of many psoriasis patients to see how they will fare without medication, and the issue has been studied extensively in clinical trials. Dr. Gordon tells patients who would like to discontinue therapy until they relapse, and that there is a one in three chance that they won’t improve upon retreatment. These patients would then need to try another medication. Today there are other medications, and there will likely be more in the coming years, he said.
"But there is a group of patients – and I think we all have them – who are just burning through these medications and don’t respond as well as they did before. So I think we have to be careful and try to convince patients they might be better off staying on their medicine," he said.
SDEF and this news organization are owned by the same parent company.
Dr. Gordon reported receiving research support and/or serving as a consultant to several pharmaceutical companies including Abbott, Amgen, Lilly, and Pfizer.
WAILEA, HAWAII – While psoriasis experts typically emphasize the disease’s chronic nature and the importance of effective long-term therapy, in reality the first big question when a patient presents to the office should be, ‘What’s the urgency of treatment?’ according to Dr. Kenneth B. Gordon, professor of dermatology at Northwestern University, Chicago.
Two patients can have equally extensive disease yet dissimilar treatment urgencies – and different treatments of choice as a result, he said at the Hawaii Dermatology Seminar, sponsored by the Global Academy for Medical Education/Skin Disease Education Foundation.
The list of preferred medications for patients with high treatment urgency is short: "When you need to get people better fast, infliximab and cyclosporine are the go-to drugs," the dermatologist stressed.
Insurance companies will often insist that a patient try methotrexate before resorting to a far costlier biologic agent. That’s unreasonable when the treatment urgency is high.
"Methotrexate doesn’t have a high enough level of predictability or efficacy of response. Additionally, it takes a long time to act. When someone is acutely ill, you don’t want to have to wait 16 weeks to figure out what’s the highest level of efficacy you’re going to get. You want to know that answer in 10 weeks, like you do with infliximab. Infliximab is a wonderful short-term therapy for patients who have urgent disease. And with cyclosporine you see effects in 4-8 weeks," Dr. Gordon continued.
He noted that in the open-label RESTORE 1 trial, in which 868 psoriasis patients were randomized to infliximab or methotrexate, the PASI-75 response rate at week 6 in the infliximab group was already close to 60%. By week 10, the PASI-75 rate was 75% in the infliximab group and 27% in the methotrexate group (Br. J. Dermatol. 2011;165:1109-17).
The main safety concern with cyclosporine is renal toxicity, which doesn’t emerge as a real problem until after about a year on the drug, Dr. Gordon said. The safety concerns associated with short-term use (6-8 weeks) to treat an acute exacerbation of psoriasis before transitioning to a different medication are modest, and limited to relatively uncommon increases in blood pressure.
Factors that might raise a patient’s treatment urgency level range from sleep deprivation because of psoriasis pain and itching to workplace hassles because of extensive sick leave, to an important public appearance scheduled within 6-8 weeks.
Session moderator Dr. Craig L. Leonardi remarked that getting payer approval for infliximab often takes a month.
"Unless you’re university based, it’s unlikely you’re going to get infliximab fast, so cyclosporine becomes a real mainstay of treatment when it’s hot and bothersome psoriasis," he said. "And it’s the treatment of choice for psoriasis during pregnancy, absolutely. It’s category C, but there’s a lot of experience with it in the transplant population," noted Dr. Leonardi of St. Louis University.
Dr. Gordon also described a clinical scenario completely different from high treatment urgency – the patient with extensive, yet stable disease. In such a case, the priority is to select a drug the patient can tolerate for a year or more, with good long-term safety and little loss of efficacy over time.
The therapeutic responses to infliximab and adalimumab tend to fade over time, but the majority of patients still do well after 1-3 years of continuous therapy, said Dr. Gordon. His analysis of the phase III REVEAL trial extension showed that 83% of patients with at least a PASI-75 response through the first 33 weeks of adalimumab therapy continued to have a PASI-75 or better response through 100 weeks, and 76% of the original responders were still in that category after 160 weeks of therapy (J. Am. Acad. Dermatol. 2012;66:241-51).
The data on the long-term safety of antitumor necrosis factor agents are extensive and largely reassuring, Dr. Gordon noted.
"I make the argument that there is more known about anti-TNF therapy in terms of safety than any other medicines ever," Dr. Gordon said. Much of the data come courtesy of Europe, where most patients are able to get on anti-TNF therapy only if a physician enrolls them in a registry, he added.
The primary safety risk posed by biologic therapy is serious infections, in Dr. Gordon’s opinion. The collective registry experience in rheumatoid arthritis patients suggests that risk is about 20% greater than in patients on methotrexate, and this risk appears to be stable over time. But it’s probably a mistake to extrapolate from the rheumatologic experience to psoriasis, Dr. Gordon said. He and his colleagues have shown that rheumatoid arthritis patients on biologic therapy tend to be older and more likely to be on concomitant systemic corticosteroids and other immunosuppressive drugs than are psoriasis patients (Ann. Rheum. Dis. 2009;68:1863-9). More data on the risks of biologic therapies in psoriasis patients are anticipated from PSOLAR and other large ongoing patient registries, he said.
A key issue in long-term therapy is the desire of many psoriasis patients to see how they will fare without medication, and the issue has been studied extensively in clinical trials. Dr. Gordon tells patients who would like to discontinue therapy until they relapse, and that there is a one in three chance that they won’t improve upon retreatment. These patients would then need to try another medication. Today there are other medications, and there will likely be more in the coming years, he said.
"But there is a group of patients – and I think we all have them – who are just burning through these medications and don’t respond as well as they did before. So I think we have to be careful and try to convince patients they might be better off staying on their medicine," he said.
SDEF and this news organization are owned by the same parent company.
Dr. Gordon reported receiving research support and/or serving as a consultant to several pharmaceutical companies including Abbott, Amgen, Lilly, and Pfizer.
WAILEA, HAWAII – While psoriasis experts typically emphasize the disease’s chronic nature and the importance of effective long-term therapy, in reality the first big question when a patient presents to the office should be, ‘What’s the urgency of treatment?’ according to Dr. Kenneth B. Gordon, professor of dermatology at Northwestern University, Chicago.
Two patients can have equally extensive disease yet dissimilar treatment urgencies – and different treatments of choice as a result, he said at the Hawaii Dermatology Seminar, sponsored by the Global Academy for Medical Education/Skin Disease Education Foundation.
The list of preferred medications for patients with high treatment urgency is short: "When you need to get people better fast, infliximab and cyclosporine are the go-to drugs," the dermatologist stressed.
Insurance companies will often insist that a patient try methotrexate before resorting to a far costlier biologic agent. That’s unreasonable when the treatment urgency is high.
"Methotrexate doesn’t have a high enough level of predictability or efficacy of response. Additionally, it takes a long time to act. When someone is acutely ill, you don’t want to have to wait 16 weeks to figure out what’s the highest level of efficacy you’re going to get. You want to know that answer in 10 weeks, like you do with infliximab. Infliximab is a wonderful short-term therapy for patients who have urgent disease. And with cyclosporine you see effects in 4-8 weeks," Dr. Gordon continued.
He noted that in the open-label RESTORE 1 trial, in which 868 psoriasis patients were randomized to infliximab or methotrexate, the PASI-75 response rate at week 6 in the infliximab group was already close to 60%. By week 10, the PASI-75 rate was 75% in the infliximab group and 27% in the methotrexate group (Br. J. Dermatol. 2011;165:1109-17).
The main safety concern with cyclosporine is renal toxicity, which doesn’t emerge as a real problem until after about a year on the drug, Dr. Gordon said. The safety concerns associated with short-term use (6-8 weeks) to treat an acute exacerbation of psoriasis before transitioning to a different medication are modest, and limited to relatively uncommon increases in blood pressure.
Factors that might raise a patient’s treatment urgency level range from sleep deprivation because of psoriasis pain and itching to workplace hassles because of extensive sick leave, to an important public appearance scheduled within 6-8 weeks.
Session moderator Dr. Craig L. Leonardi remarked that getting payer approval for infliximab often takes a month.
"Unless you’re university based, it’s unlikely you’re going to get infliximab fast, so cyclosporine becomes a real mainstay of treatment when it’s hot and bothersome psoriasis," he said. "And it’s the treatment of choice for psoriasis during pregnancy, absolutely. It’s category C, but there’s a lot of experience with it in the transplant population," noted Dr. Leonardi of St. Louis University.
Dr. Gordon also described a clinical scenario completely different from high treatment urgency – the patient with extensive, yet stable disease. In such a case, the priority is to select a drug the patient can tolerate for a year or more, with good long-term safety and little loss of efficacy over time.
The therapeutic responses to infliximab and adalimumab tend to fade over time, but the majority of patients still do well after 1-3 years of continuous therapy, said Dr. Gordon. His analysis of the phase III REVEAL trial extension showed that 83% of patients with at least a PASI-75 response through the first 33 weeks of adalimumab therapy continued to have a PASI-75 or better response through 100 weeks, and 76% of the original responders were still in that category after 160 weeks of therapy (J. Am. Acad. Dermatol. 2012;66:241-51).
The data on the long-term safety of antitumor necrosis factor agents are extensive and largely reassuring, Dr. Gordon noted.
"I make the argument that there is more known about anti-TNF therapy in terms of safety than any other medicines ever," Dr. Gordon said. Much of the data come courtesy of Europe, where most patients are able to get on anti-TNF therapy only if a physician enrolls them in a registry, he added.
The primary safety risk posed by biologic therapy is serious infections, in Dr. Gordon’s opinion. The collective registry experience in rheumatoid arthritis patients suggests that risk is about 20% greater than in patients on methotrexate, and this risk appears to be stable over time. But it’s probably a mistake to extrapolate from the rheumatologic experience to psoriasis, Dr. Gordon said. He and his colleagues have shown that rheumatoid arthritis patients on biologic therapy tend to be older and more likely to be on concomitant systemic corticosteroids and other immunosuppressive drugs than are psoriasis patients (Ann. Rheum. Dis. 2009;68:1863-9). More data on the risks of biologic therapies in psoriasis patients are anticipated from PSOLAR and other large ongoing patient registries, he said.
A key issue in long-term therapy is the desire of many psoriasis patients to see how they will fare without medication, and the issue has been studied extensively in clinical trials. Dr. Gordon tells patients who would like to discontinue therapy until they relapse, and that there is a one in three chance that they won’t improve upon retreatment. These patients would then need to try another medication. Today there are other medications, and there will likely be more in the coming years, he said.
"But there is a group of patients – and I think we all have them – who are just burning through these medications and don’t respond as well as they did before. So I think we have to be careful and try to convince patients they might be better off staying on their medicine," he said.
SDEF and this news organization are owned by the same parent company.
Dr. Gordon reported receiving research support and/or serving as a consultant to several pharmaceutical companies including Abbott, Amgen, Lilly, and Pfizer.
EXPERT ANALYSIS FROM SDEF HAWAII DERMATOLOGY SEMINAR
Progress, obstacles cited in building STEMI networks
SNOWMASS, COLO. – Competition among hospitals and between cardiology groups constitutes the greatest barrier to well-functioning regional networks for ST-elevation myocardial infarction therapy, according to Dr. Bernard J. Gersh.
"We’ve got the resources in this country, but we are competitive. That’s the name of the game. So this is a real challenge," said Dr. Gersh, professor of medicine at the Mayo Clinic, Rochester, Minn.

The 2013 ACC/American Heart Association STEMI (ST-elevation myocardial infarction) guidelines list as a class I recommendation that "each community should develop a STEMI system of care."
But a one-size-fits-all approach won’t work. Creating an efficient network to deliver reperfusion therapy to as many STEMI patients as quickly as possible in Los Angeles, where there is seemingly a percutaneous coronary intervention (PCI) center every few blocks, poses a very different set of challenges than in, say, Wyoming, with two cardiac catheterization laboratories to serve nearly a 100,000-quare-mile area, he said.
He recalled a recent conversation with a colleague from a midsize Eastern city with four PCI hospitals. All four run three call schedules per 24 hours so an interventional cardiologist is always available. But collectively the hospitals handle an average of only five or six STEMIs per week.
"Can you really justify that? Furthermore, if you look at all the epidemiology coming out of the U.S. and the Western World, STEMI is in decline. Only about 30% of MIs now are STEMIs, and it’s going to be less and less," Dr. Gersh continued.
Dr. Gersh noted that the American Heart Association Mission: Lifeline program, which was created to increase timely access to PCI for STEMI patients, recently published the first-ever national survey of regional STEMI systems. The purpose was to identify best practices, financing strategies, and barriers to system implementation. Responses were obtained from 381 STEMI networks with 899 PCI hospitals.
The single most commonly cited barrier to network implementation and optimal functioning was hospital competition, identified as a significant problem in 37% of the systems. Next came emergency medical services (EMS) transport and finances, cited by 26% of respondents. The third most common barrier was competition between cardiology groups, which was an issue in 21% of networks.
The predominant funding sources for STEMI systems were PCI hospitals and cardiology practices.
Based on his favorable personal experience with the Mayo Clinic STEMI network, which uses three helicopters, an airplane, and ground ambulances to serve 28 hospitals as far as 150 miles away, Dr. Gersh said it’s clear from the national survey results that most STEMI systems around the country are doing a lot of the important things right.
For example, 92% of systems activate the cath lab with a single phone call, 97% of PCI hospitals accept a STEMI patient 24/7 regardless of bed availability, and 84% of programs operate a data registry with continuous audit.
Two-thirds of STEMI systems have the capability to transmit ECGs from at least some of their ambulances (Circ. Cardiovasc. Qual. Outcomes 2012;5:423-8).
In 87% of the networks nationwide, an emergency department physician can activate the cath lab without cardiology consultation. However, the Mayo Clinic network takes a different approach: Transferred patients bypass the emergency department and are taken straight to the coronary care unit or cath lab.
In an editorial accompanying the report, Dr. Timothy D. Henry, who in 2002 helped organize the nation’s first regional STEMI system at the Minneapolis Heart Institute, said: "Public policy changes to provide financial incentives for more rational use of resources to support regional STEMI systems rather than building more catheterization laboratories would ... be helpful" (Circulation 2012;126:166-8).
Dr. Gersh reported that he serves as a consultant to a number of device and pharmaceutical companies.
SNOWMASS, COLO. – Competition among hospitals and between cardiology groups constitutes the greatest barrier to well-functioning regional networks for ST-elevation myocardial infarction therapy, according to Dr. Bernard J. Gersh.
"We’ve got the resources in this country, but we are competitive. That’s the name of the game. So this is a real challenge," said Dr. Gersh, professor of medicine at the Mayo Clinic, Rochester, Minn.
The 2013 ACC/American Heart Association STEMI (ST-elevation myocardial infarction) guidelines list as a class I recommendation that "each community should develop a STEMI system of care."
But a one-size-fits-all approach won’t work. Creating an efficient network to deliver reperfusion therapy to as many STEMI patients as quickly as possible in Los Angeles, where there is seemingly a percutaneous coronary intervention (PCI) center every few blocks, poses a very different set of challenges than in, say, Wyoming, with two cardiac catheterization laboratories to serve nearly a 100,000-quare-mile area, he said.
He recalled a recent conversation with a colleague from a midsize Eastern city with four PCI hospitals. All four run three call schedules per 24 hours so an interventional cardiologist is always available. But collectively the hospitals handle an average of only five or six STEMIs per week.
"Can you really justify that? Furthermore, if you look at all the epidemiology coming out of the U.S. and the Western World, STEMI is in decline. Only about 30% of MIs now are STEMIs, and it’s going to be less and less," Dr. Gersh continued.
Dr. Gersh noted that the American Heart Association Mission: Lifeline program, which was created to increase timely access to PCI for STEMI patients, recently published the first-ever national survey of regional STEMI systems. The purpose was to identify best practices, financing strategies, and barriers to system implementation. Responses were obtained from 381 STEMI networks with 899 PCI hospitals.
The single most commonly cited barrier to network implementation and optimal functioning was hospital competition, identified as a significant problem in 37% of the systems. Next came emergency medical services (EMS) transport and finances, cited by 26% of respondents. The third most common barrier was competition between cardiology groups, which was an issue in 21% of networks.
The predominant funding sources for STEMI systems were PCI hospitals and cardiology practices.
Based on his favorable personal experience with the Mayo Clinic STEMI network, which uses three helicopters, an airplane, and ground ambulances to serve 28 hospitals as far as 150 miles away, Dr. Gersh said it’s clear from the national survey results that most STEMI systems around the country are doing a lot of the important things right.
For example, 92% of systems activate the cath lab with a single phone call, 97% of PCI hospitals accept a STEMI patient 24/7 regardless of bed availability, and 84% of programs operate a data registry with continuous audit.
Two-thirds of STEMI systems have the capability to transmit ECGs from at least some of their ambulances (Circ. Cardiovasc. Qual. Outcomes 2012;5:423-8).
In 87% of the networks nationwide, an emergency department physician can activate the cath lab without cardiology consultation. However, the Mayo Clinic network takes a different approach: Transferred patients bypass the emergency department and are taken straight to the coronary care unit or cath lab.
In an editorial accompanying the report, Dr. Timothy D. Henry, who in 2002 helped organize the nation’s first regional STEMI system at the Minneapolis Heart Institute, said: "Public policy changes to provide financial incentives for more rational use of resources to support regional STEMI systems rather than building more catheterization laboratories would ... be helpful" (Circulation 2012;126:166-8).
Dr. Gersh reported that he serves as a consultant to a number of device and pharmaceutical companies.
SNOWMASS, COLO. – Competition among hospitals and between cardiology groups constitutes the greatest barrier to well-functioning regional networks for ST-elevation myocardial infarction therapy, according to Dr. Bernard J. Gersh.
"We’ve got the resources in this country, but we are competitive. That’s the name of the game. So this is a real challenge," said Dr. Gersh, professor of medicine at the Mayo Clinic, Rochester, Minn.
The 2013 ACC/American Heart Association STEMI (ST-elevation myocardial infarction) guidelines list as a class I recommendation that "each community should develop a STEMI system of care."
But a one-size-fits-all approach won’t work. Creating an efficient network to deliver reperfusion therapy to as many STEMI patients as quickly as possible in Los Angeles, where there is seemingly a percutaneous coronary intervention (PCI) center every few blocks, poses a very different set of challenges than in, say, Wyoming, with two cardiac catheterization laboratories to serve nearly a 100,000-quare-mile area, he said.
He recalled a recent conversation with a colleague from a midsize Eastern city with four PCI hospitals. All four run three call schedules per 24 hours so an interventional cardiologist is always available. But collectively the hospitals handle an average of only five or six STEMIs per week.
"Can you really justify that? Furthermore, if you look at all the epidemiology coming out of the U.S. and the Western World, STEMI is in decline. Only about 30% of MIs now are STEMIs, and it’s going to be less and less," Dr. Gersh continued.
Dr. Gersh noted that the American Heart Association Mission: Lifeline program, which was created to increase timely access to PCI for STEMI patients, recently published the first-ever national survey of regional STEMI systems. The purpose was to identify best practices, financing strategies, and barriers to system implementation. Responses were obtained from 381 STEMI networks with 899 PCI hospitals.
The single most commonly cited barrier to network implementation and optimal functioning was hospital competition, identified as a significant problem in 37% of the systems. Next came emergency medical services (EMS) transport and finances, cited by 26% of respondents. The third most common barrier was competition between cardiology groups, which was an issue in 21% of networks.
The predominant funding sources for STEMI systems were PCI hospitals and cardiology practices.
Based on his favorable personal experience with the Mayo Clinic STEMI network, which uses three helicopters, an airplane, and ground ambulances to serve 28 hospitals as far as 150 miles away, Dr. Gersh said it’s clear from the national survey results that most STEMI systems around the country are doing a lot of the important things right.
For example, 92% of systems activate the cath lab with a single phone call, 97% of PCI hospitals accept a STEMI patient 24/7 regardless of bed availability, and 84% of programs operate a data registry with continuous audit.
Two-thirds of STEMI systems have the capability to transmit ECGs from at least some of their ambulances (Circ. Cardiovasc. Qual. Outcomes 2012;5:423-8).
In 87% of the networks nationwide, an emergency department physician can activate the cath lab without cardiology consultation. However, the Mayo Clinic network takes a different approach: Transferred patients bypass the emergency department and are taken straight to the coronary care unit or cath lab.
In an editorial accompanying the report, Dr. Timothy D. Henry, who in 2002 helped organize the nation’s first regional STEMI system at the Minneapolis Heart Institute, said: "Public policy changes to provide financial incentives for more rational use of resources to support regional STEMI systems rather than building more catheterization laboratories would ... be helpful" (Circulation 2012;126:166-8).
Dr. Gersh reported that he serves as a consultant to a number of device and pharmaceutical companies.

Screen all psoriasis patients for hepatitis before immunosuppressive therapy
MAUI, HAWAII – Routine screening for hepatitis B and C has become a must prior to initiation of chronic immunosuppressive therapy for psoriasis, Dr. Craig L. Leonardi said.
"Universal screening for hepatitis B and hepatitis C infection is not optional in 2013," he stressed at the Hawaii Dermatology Seminar sponsored by Global Academy for Medical Education/Skin Disease Education Foundation.
That said, professional society guidelines are at odds and in flux on this issue. The American Association for the Study of Liver Diseases, the European Association for the Study of the Liver, and the Centers for Disease Control and Prevention all recommend routine screening for hepatitis B surface antigen and hepatitis B core antibody prior to initiation of immunosuppressive therapy. The CDC also recommends universal pretreatment testing for antibody to hepatitis B surface antibody.
In contrast, the American College of Rheumatology recommends HBV screening only in high-risk patients and those treated with specific drugs (Arthritis Rheum. 2008;59:762-84).
For now, the American Academy of Dermatology guidelines take a middle-of-the-road position, which Dr. Leonardi said he finds unconvincing. The current guidelines recommend hepatitis B screening in the appropriate setting (J. Am. Acad. Dermatol. 2008;58:826-50).

"Well, the appropriate setting is when you’re going to use immunosuppressive agents," he asserted. "So I think we all need to start ordering these tests and be on the lookout for the problem. Prophylactic antiviral therapy may be more than the average dermatologist wants to take on. Nonetheless, you want to do the testing and then refer affected patients to an experienced hepatology center."
Chronic immunosuppressive therapy for psoriasis encompasses all the biologics agents – the tumor necrosis factor inhibitors as well as the interleukin 12/23 inhibitor ustekinumab, said Dr. Leonardi of the dermatology department at St. Louis University.
It seems likely that the next iteration of the AAD psoriasis guidelines will firmly recommend universal pretreatment screening for hepatitis. That hand was tipped in a recent review article coauthored by Dr. Alan Menter, chair of the AAD psoriasis guidelines committee.
Dr. Menter and his coauthors endorsed universal screening for hepatitis B surface antigen and HBV core antigen prior to initiating anti-TNF therapy in psoriasis patients. And while the American College of Rheumatology guidelines say anti-TNF therapy is contraindicated in patients with chronic hepatitis B, Dr. Menter and his colleagues took issue. They argued that these important biologic therapies can be used safely for psoriasis, citing evidence that the risk of reactivation of hepatitis B can be greatly minimized or eliminated altogether by preemptive antiviral therapy (J. Am. Acad. Dermatol. 2012;67:1349-61).
They advocated preferential consideration of etanercept over the other TNF-inhibitors in light of evidence suggesting it renders HBV reactivation less likely. They further recommended monthly testing of serum transaminase levels for the first 6 months of therapy in patients with chronic HBV, quarterly testing thereafter, and referral to a hepatologist if liver enzyme levels climb above three times baseline.
A major impetus behind the increased attention being given to screening for hepatitis in patients prior to long-term immunosuppressive therapy was an influential paper published last year by investigators at the CDC, the American Association for the Study of Liver Diseases, and other institutions. The authors underscored the risk of HBV reactivation during such therapy, calling it a neglected danger that is poorly recognized in some professional medical groups’ treatment guidelines (Ann. Intern. Med. 2012;156:743-5).
The risk of HBV reactivation is substantial with anti-TNF therapy in patients who express surface antigen – in the 40% range in one review – but less than 5% in those who are core antibody–positive only.
The risk of hepatitis B reactivation during immunosuppressive therapy has gotten most of the recent attention because of the vast scope of HBV worldwide, with close to 400 million people being chronically infected. In his own busy, universally screened psoriasis practice, however, Dr. Leonardi said that uncovering chronic hepatitis C comes up far more commonly.
The medical board at the National Psoriasis Foundation has cautioned that standard interferon-alpha therapy for HCV seriously exacerbates psoriasis. The group recommends considering the full range of therapeutic options in treating psoriasis in HCV-positive patients. Topical therapies are called the best option for those with limited skin disease. Second-line therapies include UVB phototherapy, acitretin, etanercept, PUVA, and possibly the other TNF-antagonists, with cyclosporine and azathioprine held in reserve as the third line (J. Am. Acad. Dermatol. 2009;61:1044-55).
The recommendation is to monitor quantitative hepatitis C viral counts and liver enzymes during psoriasis therapy and refer to a hepatologist early should levels spike.
As yet, there are very few data on the impact of ustekinumab in patients who are HBV or HCV positive, and no meaningful conclusions as to risk are possible yet, Dr. Leonardi said.
He reported that he serves as a consultant to and recipient of research grants from all the major pharmaceutical companies having an interest in biologic therapies for psoriasis. SDEF and this news organization are owned by the same parent company.
MAUI, HAWAII – Routine screening for hepatitis B and C has become a must prior to initiation of chronic immunosuppressive therapy for psoriasis, Dr. Craig L. Leonardi said.
"Universal screening for hepatitis B and hepatitis C infection is not optional in 2013," he stressed at the Hawaii Dermatology Seminar sponsored by Global Academy for Medical Education/Skin Disease Education Foundation.
That said, professional society guidelines are at odds and in flux on this issue. The American Association for the Study of Liver Diseases, the European Association for the Study of the Liver, and the Centers for Disease Control and Prevention all recommend routine screening for hepatitis B surface antigen and hepatitis B core antibody prior to initiation of immunosuppressive therapy. The CDC also recommends universal pretreatment testing for antibody to hepatitis B surface antibody.
In contrast, the American College of Rheumatology recommends HBV screening only in high-risk patients and those treated with specific drugs (Arthritis Rheum. 2008;59:762-84).
For now, the American Academy of Dermatology guidelines take a middle-of-the-road position, which Dr. Leonardi said he finds unconvincing. The current guidelines recommend hepatitis B screening in the appropriate setting (J. Am. Acad. Dermatol. 2008;58:826-50).
"Well, the appropriate setting is when you’re going to use immunosuppressive agents," he asserted. "So I think we all need to start ordering these tests and be on the lookout for the problem. Prophylactic antiviral therapy may be more than the average dermatologist wants to take on. Nonetheless, you want to do the testing and then refer affected patients to an experienced hepatology center."
Chronic immunosuppressive therapy for psoriasis encompasses all the biologics agents – the tumor necrosis factor inhibitors as well as the interleukin 12/23 inhibitor ustekinumab, said Dr. Leonardi of the dermatology department at St. Louis University.
It seems likely that the next iteration of the AAD psoriasis guidelines will firmly recommend universal pretreatment screening for hepatitis. That hand was tipped in a recent review article coauthored by Dr. Alan Menter, chair of the AAD psoriasis guidelines committee.
Dr. Menter and his coauthors endorsed universal screening for hepatitis B surface antigen and HBV core antigen prior to initiating anti-TNF therapy in psoriasis patients. And while the American College of Rheumatology guidelines say anti-TNF therapy is contraindicated in patients with chronic hepatitis B, Dr. Menter and his colleagues took issue. They argued that these important biologic therapies can be used safely for psoriasis, citing evidence that the risk of reactivation of hepatitis B can be greatly minimized or eliminated altogether by preemptive antiviral therapy (J. Am. Acad. Dermatol. 2012;67:1349-61).
They advocated preferential consideration of etanercept over the other TNF-inhibitors in light of evidence suggesting it renders HBV reactivation less likely. They further recommended monthly testing of serum transaminase levels for the first 6 months of therapy in patients with chronic HBV, quarterly testing thereafter, and referral to a hepatologist if liver enzyme levels climb above three times baseline.
A major impetus behind the increased attention being given to screening for hepatitis in patients prior to long-term immunosuppressive therapy was an influential paper published last year by investigators at the CDC, the American Association for the Study of Liver Diseases, and other institutions. The authors underscored the risk of HBV reactivation during such therapy, calling it a neglected danger that is poorly recognized in some professional medical groups’ treatment guidelines (Ann. Intern. Med. 2012;156:743-5).
The risk of HBV reactivation is substantial with anti-TNF therapy in patients who express surface antigen – in the 40% range in one review – but less than 5% in those who are core antibody–positive only.
The risk of hepatitis B reactivation during immunosuppressive therapy has gotten most of the recent attention because of the vast scope of HBV worldwide, with close to 400 million people being chronically infected. In his own busy, universally screened psoriasis practice, however, Dr. Leonardi said that uncovering chronic hepatitis C comes up far more commonly.
The medical board at the National Psoriasis Foundation has cautioned that standard interferon-alpha therapy for HCV seriously exacerbates psoriasis. The group recommends considering the full range of therapeutic options in treating psoriasis in HCV-positive patients. Topical therapies are called the best option for those with limited skin disease. Second-line therapies include UVB phototherapy, acitretin, etanercept, PUVA, and possibly the other TNF-antagonists, with cyclosporine and azathioprine held in reserve as the third line (J. Am. Acad. Dermatol. 2009;61:1044-55).
The recommendation is to monitor quantitative hepatitis C viral counts and liver enzymes during psoriasis therapy and refer to a hepatologist early should levels spike.
As yet, there are very few data on the impact of ustekinumab in patients who are HBV or HCV positive, and no meaningful conclusions as to risk are possible yet, Dr. Leonardi said.
He reported that he serves as a consultant to and recipient of research grants from all the major pharmaceutical companies having an interest in biologic therapies for psoriasis. SDEF and this news organization are owned by the same parent company.
MAUI, HAWAII – Routine screening for hepatitis B and C has become a must prior to initiation of chronic immunosuppressive therapy for psoriasis, Dr. Craig L. Leonardi said.
"Universal screening for hepatitis B and hepatitis C infection is not optional in 2013," he stressed at the Hawaii Dermatology Seminar sponsored by Global Academy for Medical Education/Skin Disease Education Foundation.
That said, professional society guidelines are at odds and in flux on this issue. The American Association for the Study of Liver Diseases, the European Association for the Study of the Liver, and the Centers for Disease Control and Prevention all recommend routine screening for hepatitis B surface antigen and hepatitis B core antibody prior to initiation of immunosuppressive therapy. The CDC also recommends universal pretreatment testing for antibody to hepatitis B surface antibody.
In contrast, the American College of Rheumatology recommends HBV screening only in high-risk patients and those treated with specific drugs (Arthritis Rheum. 2008;59:762-84).
For now, the American Academy of Dermatology guidelines take a middle-of-the-road position, which Dr. Leonardi said he finds unconvincing. The current guidelines recommend hepatitis B screening in the appropriate setting (J. Am. Acad. Dermatol. 2008;58:826-50).
"Well, the appropriate setting is when you’re going to use immunosuppressive agents," he asserted. "So I think we all need to start ordering these tests and be on the lookout for the problem. Prophylactic antiviral therapy may be more than the average dermatologist wants to take on. Nonetheless, you want to do the testing and then refer affected patients to an experienced hepatology center."
Chronic immunosuppressive therapy for psoriasis encompasses all the biologics agents – the tumor necrosis factor inhibitors as well as the interleukin 12/23 inhibitor ustekinumab, said Dr. Leonardi of the dermatology department at St. Louis University.
It seems likely that the next iteration of the AAD psoriasis guidelines will firmly recommend universal pretreatment screening for hepatitis. That hand was tipped in a recent review article coauthored by Dr. Alan Menter, chair of the AAD psoriasis guidelines committee.
Dr. Menter and his coauthors endorsed universal screening for hepatitis B surface antigen and HBV core antigen prior to initiating anti-TNF therapy in psoriasis patients. And while the American College of Rheumatology guidelines say anti-TNF therapy is contraindicated in patients with chronic hepatitis B, Dr. Menter and his colleagues took issue. They argued that these important biologic therapies can be used safely for psoriasis, citing evidence that the risk of reactivation of hepatitis B can be greatly minimized or eliminated altogether by preemptive antiviral therapy (J. Am. Acad. Dermatol. 2012;67:1349-61).
They advocated preferential consideration of etanercept over the other TNF-inhibitors in light of evidence suggesting it renders HBV reactivation less likely. They further recommended monthly testing of serum transaminase levels for the first 6 months of therapy in patients with chronic HBV, quarterly testing thereafter, and referral to a hepatologist if liver enzyme levels climb above three times baseline.
A major impetus behind the increased attention being given to screening for hepatitis in patients prior to long-term immunosuppressive therapy was an influential paper published last year by investigators at the CDC, the American Association for the Study of Liver Diseases, and other institutions. The authors underscored the risk of HBV reactivation during such therapy, calling it a neglected danger that is poorly recognized in some professional medical groups’ treatment guidelines (Ann. Intern. Med. 2012;156:743-5).
The risk of HBV reactivation is substantial with anti-TNF therapy in patients who express surface antigen – in the 40% range in one review – but less than 5% in those who are core antibody–positive only.
The risk of hepatitis B reactivation during immunosuppressive therapy has gotten most of the recent attention because of the vast scope of HBV worldwide, with close to 400 million people being chronically infected. In his own busy, universally screened psoriasis practice, however, Dr. Leonardi said that uncovering chronic hepatitis C comes up far more commonly.
The medical board at the National Psoriasis Foundation has cautioned that standard interferon-alpha therapy for HCV seriously exacerbates psoriasis. The group recommends considering the full range of therapeutic options in treating psoriasis in HCV-positive patients. Topical therapies are called the best option for those with limited skin disease. Second-line therapies include UVB phototherapy, acitretin, etanercept, PUVA, and possibly the other TNF-antagonists, with cyclosporine and azathioprine held in reserve as the third line (J. Am. Acad. Dermatol. 2009;61:1044-55).
The recommendation is to monitor quantitative hepatitis C viral counts and liver enzymes during psoriasis therapy and refer to a hepatologist early should levels spike.
As yet, there are very few data on the impact of ustekinumab in patients who are HBV or HCV positive, and no meaningful conclusions as to risk are possible yet, Dr. Leonardi said.
He reported that he serves as a consultant to and recipient of research grants from all the major pharmaceutical companies having an interest in biologic therapies for psoriasis. SDEF and this news organization are owned by the same parent company.
EXPERT OPINION FROM SDEF HAWAII DERMATOLOGY SEMINAR

Seizure risk substantial after pediatric intracerebral hemorrhage
HONOLULU – In the first 2 years following pediatric intracerebral hemorrhage, one-third of patients will experience a single remote symptomatic seizure and 13% will develop epilepsy, according to a large prospective study.
Twenty-eight percent of study participants who underwent continuous EEG monitoring were found to have subclinical EEG-only seizures. Additional follow-up will determine whether these subclinical seizures constitute a risk factor for later epilepsy, Dr. Lauren A. Beslow said at the International Stroke Conference sponsored by the American Heart Association.
She presented a three-center prospective cohort study involving 20 neonates and 53 other patients up to 18 years of age who experienced an intracerebral hemorrhage (ICH).
While 73 subjects may not sound like a lot, this is in fact an exceptionally large cohort, as pediatric ICH is an understudied topic. The incidence of stroke in U.S. children is 6.4 cases per 100,000 per year, a rate approaching that of pediatric brain tumors. And while intracerebral hemorrhage accounts for only about 15% of adult strokes, it is the cause of half of all strokes in children, according to Dr. Beslow, a pediatric neurologist at Yale University, New Haven, Conn.
Acute symptomatic seizures – that is, seizures occurring at presentation of ICH or up to 7 days afterward – were documented in 12 of 20 neonates (60%) and 23 of 53 older subjects (43%). The median age of non-neonates with acute symptomatic seizures was 2.2 years, compared with 10.8 years for subjects without such seizures.
Nine of 32 (28%) subjects placed on continuous EEG monitoring experienced EEG-only seizures. These subclinical seizures were treated medically in the same way that’s standard for symptomatic seizures.
Seizures occurring more than 7 days post ICH are deemed "remote." Eighteen percent of study participants experienced a remote symptomatic seizure during the first year of follow-up. At 2 years, 24 subjects (33%) had a remote symptomatic seizure.
Epilepsy, defined as two or more unprovoked remote symptomatic seizures, was diagnosed in 4% of patients during the first year. The cumulative rate through 2 years of follow-up was 13%.
This study contains several important new observations for clinical practice, Dr. Beslow said. One involves the high rate of EEG-only seizures. Previously, the decision to place a child on continuous EEG monitoring following ICH was often based upon physician intuition, and monitoring was more likely in those who presented with seizures at the time of their stroke.
"We hope our findings will encourage clinicians to consider more routine use of continuous EEG monitoring in children with ICH," she said.
The conventional wisdom has been that children who don’t have seizures at the time of their ICH are at reduced likelihood of developing seizures or epilepsy later on; these data suggest otherwise. Also, the parents of a young child with ICH are always deeply distraught and desperate to know what will happen to their child in the future. Now there are concrete risk figures for use in counseling, Dr. Beslow added.
Nearly a dozen prespecified potential risk factors for remote symptomatic seizures and epilepsy were scrutinized in the study. Only one proved statistically significant: elevated intracranial pressure requiring urgent intervention. The investigators anticipate that epilepsy rates will increase at planned 5- and 10-year follow-up. In addition, the researchers plan to recruit additional patients with pediatric ICH in order to strengthen the validity of their findings.
This ongoing study is funded by the National Institutes of Health. Dr. Beslow reported having no relevant financial interests.
HONOLULU – In the first 2 years following pediatric intracerebral hemorrhage, one-third of patients will experience a single remote symptomatic seizure and 13% will develop epilepsy, according to a large prospective study.
Twenty-eight percent of study participants who underwent continuous EEG monitoring were found to have subclinical EEG-only seizures. Additional follow-up will determine whether these subclinical seizures constitute a risk factor for later epilepsy, Dr. Lauren A. Beslow said at the International Stroke Conference sponsored by the American Heart Association.
She presented a three-center prospective cohort study involving 20 neonates and 53 other patients up to 18 years of age who experienced an intracerebral hemorrhage (ICH).
While 73 subjects may not sound like a lot, this is in fact an exceptionally large cohort, as pediatric ICH is an understudied topic. The incidence of stroke in U.S. children is 6.4 cases per 100,000 per year, a rate approaching that of pediatric brain tumors. And while intracerebral hemorrhage accounts for only about 15% of adult strokes, it is the cause of half of all strokes in children, according to Dr. Beslow, a pediatric neurologist at Yale University, New Haven, Conn.
Acute symptomatic seizures – that is, seizures occurring at presentation of ICH or up to 7 days afterward – were documented in 12 of 20 neonates (60%) and 23 of 53 older subjects (43%). The median age of non-neonates with acute symptomatic seizures was 2.2 years, compared with 10.8 years for subjects without such seizures.
Nine of 32 (28%) subjects placed on continuous EEG monitoring experienced EEG-only seizures. These subclinical seizures were treated medically in the same way that’s standard for symptomatic seizures.
Seizures occurring more than 7 days post ICH are deemed "remote." Eighteen percent of study participants experienced a remote symptomatic seizure during the first year of follow-up. At 2 years, 24 subjects (33%) had a remote symptomatic seizure.
Epilepsy, defined as two or more unprovoked remote symptomatic seizures, was diagnosed in 4% of patients during the first year. The cumulative rate through 2 years of follow-up was 13%.
This study contains several important new observations for clinical practice, Dr. Beslow said. One involves the high rate of EEG-only seizures. Previously, the decision to place a child on continuous EEG monitoring following ICH was often based upon physician intuition, and monitoring was more likely in those who presented with seizures at the time of their stroke.
"We hope our findings will encourage clinicians to consider more routine use of continuous EEG monitoring in children with ICH," she said.
The conventional wisdom has been that children who don’t have seizures at the time of their ICH are at reduced likelihood of developing seizures or epilepsy later on; these data suggest otherwise. Also, the parents of a young child with ICH are always deeply distraught and desperate to know what will happen to their child in the future. Now there are concrete risk figures for use in counseling, Dr. Beslow added.
Nearly a dozen prespecified potential risk factors for remote symptomatic seizures and epilepsy were scrutinized in the study. Only one proved statistically significant: elevated intracranial pressure requiring urgent intervention. The investigators anticipate that epilepsy rates will increase at planned 5- and 10-year follow-up. In addition, the researchers plan to recruit additional patients with pediatric ICH in order to strengthen the validity of their findings.
This ongoing study is funded by the National Institutes of Health. Dr. Beslow reported having no relevant financial interests.
HONOLULU – In the first 2 years following pediatric intracerebral hemorrhage, one-third of patients will experience a single remote symptomatic seizure and 13% will develop epilepsy, according to a large prospective study.
Twenty-eight percent of study participants who underwent continuous EEG monitoring were found to have subclinical EEG-only seizures. Additional follow-up will determine whether these subclinical seizures constitute a risk factor for later epilepsy, Dr. Lauren A. Beslow said at the International Stroke Conference sponsored by the American Heart Association.
She presented a three-center prospective cohort study involving 20 neonates and 53 other patients up to 18 years of age who experienced an intracerebral hemorrhage (ICH).
While 73 subjects may not sound like a lot, this is in fact an exceptionally large cohort, as pediatric ICH is an understudied topic. The incidence of stroke in U.S. children is 6.4 cases per 100,000 per year, a rate approaching that of pediatric brain tumors. And while intracerebral hemorrhage accounts for only about 15% of adult strokes, it is the cause of half of all strokes in children, according to Dr. Beslow, a pediatric neurologist at Yale University, New Haven, Conn.
Acute symptomatic seizures – that is, seizures occurring at presentation of ICH or up to 7 days afterward – were documented in 12 of 20 neonates (60%) and 23 of 53 older subjects (43%). The median age of non-neonates with acute symptomatic seizures was 2.2 years, compared with 10.8 years for subjects without such seizures.
Nine of 32 (28%) subjects placed on continuous EEG monitoring experienced EEG-only seizures. These subclinical seizures were treated medically in the same way that’s standard for symptomatic seizures.
Seizures occurring more than 7 days post ICH are deemed "remote." Eighteen percent of study participants experienced a remote symptomatic seizure during the first year of follow-up. At 2 years, 24 subjects (33%) had a remote symptomatic seizure.
Epilepsy, defined as two or more unprovoked remote symptomatic seizures, was diagnosed in 4% of patients during the first year. The cumulative rate through 2 years of follow-up was 13%.
This study contains several important new observations for clinical practice, Dr. Beslow said. One involves the high rate of EEG-only seizures. Previously, the decision to place a child on continuous EEG monitoring following ICH was often based upon physician intuition, and monitoring was more likely in those who presented with seizures at the time of their stroke.
"We hope our findings will encourage clinicians to consider more routine use of continuous EEG monitoring in children with ICH," she said.
The conventional wisdom has been that children who don’t have seizures at the time of their ICH are at reduced likelihood of developing seizures or epilepsy later on; these data suggest otherwise. Also, the parents of a young child with ICH are always deeply distraught and desperate to know what will happen to their child in the future. Now there are concrete risk figures for use in counseling, Dr. Beslow added.
Nearly a dozen prespecified potential risk factors for remote symptomatic seizures and epilepsy were scrutinized in the study. Only one proved statistically significant: elevated intracranial pressure requiring urgent intervention. The investigators anticipate that epilepsy rates will increase at planned 5- and 10-year follow-up. In addition, the researchers plan to recruit additional patients with pediatric ICH in order to strengthen the validity of their findings.
This ongoing study is funded by the National Institutes of Health. Dr. Beslow reported having no relevant financial interests.
AT THE INTERNATIONAL STROKE CONFERENCE
Major finding: Twenty-four of 73 (33%) children and adolescents who had a spontaneous intracerebral hemorrhage experienced a remote symptomatic seizure within the next 2 years.
Data source: This prospective cohort study includes 20 subjects who experienced an intracerebral hemorrhage as neonates and 53 who were older children or adolescents at the time of their stroke.
Disclosures: This ongoing study is funded by the National Institutes of Health. Dr. Beslow reported having no relevant financial interests.
CORE320: CT angiography bests SPECT for CAD diagnosis
SAN FRANCISCO – Coronary CT angiography outperformed myocardial perfusion single-photon emission CT for the diagnosis of obstructive coronary artery disease in a prospective multicenter head-to-head comparative study.
The CORE320 (Coronary Artery Evaluation Using 320-Row Multidetector Computed Tomography Angiography and Myocardial Perfusion) study included 381 patients with suspected or known coronary artery disease (CAD) who were scheduled for invasive quantitative coronary angiography. But first they all underwent coronary CT angiography (CTA) and single-photon emission CT (SPECT), with images analyzed in blinded independent core laboratories. The time interval between the two imaging studies was a mean of 9.4 days. Invasive coronary angiography served as the diagnostic reference standard in the 16-center, 8-country study, Dr. Marcelo F. Di Carli explained at the annual meeting of the American College of Cardiology.
The primary study endpoint was test accuracy as defined by the area under the receiver operating characteristic curve for identifying the 59% of subjects with at least a 50% stenosis by invasive coronary angiography. The rate was significantly better for CTA than SPECT: 89% vs. 69%.
CTA’s superior performance was driven by its greater sensitivity in detecting stenoses of 50% or more: 91% vs. 62% for SPECT. The two imaging modalities displayed similar specificity: 74% for CTA and 67% for SPECT.
CTA had a positive predictive value of 83% and a negative predictive value of 85%, compared with 73% and 55%, respectively, for SPECT, according to Dr. Di Carli of Brigham and Women’s Hospital, Boston.
The same pattern of results was seen with regard to diagnostic accuracy in detecting patients with at least a 70% stenosis, a prespecified secondary endpoint. CTA had 94% sensitivity, 60% specificity, a positive predictive value of 66%, and a negative predictive value of 92%. SPECT showed 72% sensitivity, 67% specificity, a 64% positive predictive value, and a 73% negative predictive value.
The average radiation dose was markedly lower with CTA: 3.54 mSv compared with 10.48 mSv for SPECT.
The study was funded by Toshiba. Dr. Di Carli reported having no relevant financial conflicts.
SAN FRANCISCO – Coronary CT angiography outperformed myocardial perfusion single-photon emission CT for the diagnosis of obstructive coronary artery disease in a prospective multicenter head-to-head comparative study.
The CORE320 (Coronary Artery Evaluation Using 320-Row Multidetector Computed Tomography Angiography and Myocardial Perfusion) study included 381 patients with suspected or known coronary artery disease (CAD) who were scheduled for invasive quantitative coronary angiography. But first they all underwent coronary CT angiography (CTA) and single-photon emission CT (SPECT), with images analyzed in blinded independent core laboratories. The time interval between the two imaging studies was a mean of 9.4 days. Invasive coronary angiography served as the diagnostic reference standard in the 16-center, 8-country study, Dr. Marcelo F. Di Carli explained at the annual meeting of the American College of Cardiology.
The primary study endpoint was test accuracy as defined by the area under the receiver operating characteristic curve for identifying the 59% of subjects with at least a 50% stenosis by invasive coronary angiography. The rate was significantly better for CTA than SPECT: 89% vs. 69%.
CTA’s superior performance was driven by its greater sensitivity in detecting stenoses of 50% or more: 91% vs. 62% for SPECT. The two imaging modalities displayed similar specificity: 74% for CTA and 67% for SPECT.
CTA had a positive predictive value of 83% and a negative predictive value of 85%, compared with 73% and 55%, respectively, for SPECT, according to Dr. Di Carli of Brigham and Women’s Hospital, Boston.
The same pattern of results was seen with regard to diagnostic accuracy in detecting patients with at least a 70% stenosis, a prespecified secondary endpoint. CTA had 94% sensitivity, 60% specificity, a positive predictive value of 66%, and a negative predictive value of 92%. SPECT showed 72% sensitivity, 67% specificity, a 64% positive predictive value, and a 73% negative predictive value.
The average radiation dose was markedly lower with CTA: 3.54 mSv compared with 10.48 mSv for SPECT.
The study was funded by Toshiba. Dr. Di Carli reported having no relevant financial conflicts.
SAN FRANCISCO – Coronary CT angiography outperformed myocardial perfusion single-photon emission CT for the diagnosis of obstructive coronary artery disease in a prospective multicenter head-to-head comparative study.
The CORE320 (Coronary Artery Evaluation Using 320-Row Multidetector Computed Tomography Angiography and Myocardial Perfusion) study included 381 patients with suspected or known coronary artery disease (CAD) who were scheduled for invasive quantitative coronary angiography. But first they all underwent coronary CT angiography (CTA) and single-photon emission CT (SPECT), with images analyzed in blinded independent core laboratories. The time interval between the two imaging studies was a mean of 9.4 days. Invasive coronary angiography served as the diagnostic reference standard in the 16-center, 8-country study, Dr. Marcelo F. Di Carli explained at the annual meeting of the American College of Cardiology.
The primary study endpoint was test accuracy as defined by the area under the receiver operating characteristic curve for identifying the 59% of subjects with at least a 50% stenosis by invasive coronary angiography. The rate was significantly better for CTA than SPECT: 89% vs. 69%.
CTA’s superior performance was driven by its greater sensitivity in detecting stenoses of 50% or more: 91% vs. 62% for SPECT. The two imaging modalities displayed similar specificity: 74% for CTA and 67% for SPECT.
CTA had a positive predictive value of 83% and a negative predictive value of 85%, compared with 73% and 55%, respectively, for SPECT, according to Dr. Di Carli of Brigham and Women’s Hospital, Boston.
The same pattern of results was seen with regard to diagnostic accuracy in detecting patients with at least a 70% stenosis, a prespecified secondary endpoint. CTA had 94% sensitivity, 60% specificity, a positive predictive value of 66%, and a negative predictive value of 92%. SPECT showed 72% sensitivity, 67% specificity, a 64% positive predictive value, and a 73% negative predictive value.
The average radiation dose was markedly lower with CTA: 3.54 mSv compared with 10.48 mSv for SPECT.
The study was funded by Toshiba. Dr. Di Carli reported having no relevant financial conflicts.
AT ACC 13
Major Finding: Coronary CT angiography had a 91% sensitivity and a 74% specificity for the detection of at least 50% stenosis in 381 patients with known or suspected CAD, superior to the 62% sensitivity and 67% specificity for myocardial perfusion single-photon emission CT in the same patients.
Data Source: CORE320, an ongoing prospective 16-center study comparing the diagnostic accuracy of two widely utilized noninvasive imaging methods in detecting obstructive CAD, with invasive quantitative coronary angiography serving as the reference standard.
Disclosures: The study is funded by Toshiba. The presenter reported having no relevant financial conflicts.
STREAM trial endorses fibrinolysis-first in selected STEMIs
SAN FRANCISCO – Selected patients with ST-elevation myocardial infarction fare just as well with a treatment strategy of early fibrinolysis followed by transfer to a PCI center for timely coronary angiography as they do with primary PCI, according to the landmark STREAM trial.
The large patient population for whom this so-called "pharmacoinvasive" or fibrinolysis-first strategy is applicable comprises those STEMI patients whose symptoms are less than 3 hours old at first medical contact and who cannot undergo primary percutaneous coronary intervention (PCI) within the following hour, Dr. Frans Van de Werf explained in presenting the results of the STREAM (Strategic Reperfusion Early After Myocardial infarction) trial at the annual meeting of the American College of Cardiology.

Guidelines are clear that primary PCI is the preferred reperfusion method in STEMI patients with recent onset of symptoms, but only when the intervention can be performed promptly by an experienced team. That’s a huge caveat. The fact is that primary PCI doesn’t get done within guideline-recommended times for most patients who present to a non–PCI-capable hospital. Large registries consistently show this to be the case because of lengthy transfer times and other logistic issues, noted Dr. Van de Werf, professor of cardiology at the Catholic University of Leuven (Belgium).
"This study is not a challenge to primary PCI, it’s a study in a population who can’t get primary PCI in a short period of time," he stressed.
STREAM was an international, prospective, randomized trial involving 1,892 STEMI patients who presented to a non-PCI center within 3 hours of symptom onset and were unable to undergo primary PCI within the next hour. They were randomized to direct transfer for primary PCI or to fibrinolytic therapy with tenecteplase along with clopidogrel and enoxaparin, followed by transfer to a PCI-capable center.
If an ECG obtained 90 minutes after bolus tenecteplase showed at least 50% ST resolution, patients underwent coronary angiography 6-24 hours later – after the increased procedural bleeding risk associated with fibrinolytic therapy had worn off – with PCI or coronary artery bypass graft (CABG) surgery if indicated. However, if the ECG did not show reperfusion, emergency angiography was performed with an eye toward PCI.
The median time to the start of reperfusion therapy was 100 minutes from symptom onset in the pharmacoinvasive group, compared with 178 minutes in patients assigned to primary PCI.
The primary study endpoint was the 30-day cumulative rate of death, shock, congestive heart failure, or reinfarction. It occurred in 12.4% of the fibrinolysis-first group and 14.3% of those who underwent primary PCI, a nonsignificant difference (P = .21).
The ECG showed that fibrinolysis failed, requiring emergency angiography, in 36% of patients, with rescue PCI performed an average of 2.2 hours after randomization. The other 64% of patients in the pharmacoinvasive group underwent nonurgent catheterization at a median of 17 hours.
"The study results provide the opportunity for a measured approach to invasive coronary interventions, circumventing an urgent procedure in about two-thirds of fibrinolytic-treated STEMI patients," Dr. Van de Werf observed. "Drug therapy before transfer is at least as effective as PCI, and an urgent catheterization was avoided in two-thirds of patients. This gives physicians time to consider other options, such as CABG and medical therapy."
Indeed, CABG was significantly more frequent in the pharmacoinvasive strategy group than with primary PCI, by a margin of 4.7% to 2.1%. As CABG is probably a better revascularization procedure, this is a good thing, the cardiologist continued.
Intracranial hemorrhage occurred significantly more frequently in the fibrinolysis group than with primary PCI, by a margin of 1.0% to 0.2%. However, after one-fifth of STREAM participants had been enrolled, investigators realized that those aged 75 years or older had an excess risk of intracranial hemorrhage with full-dose bolus tenectaplase. Thereafter, the tenectaplase dose was reduced by 50% in elderly patients. It’s worth noting that in the more than 1,500 patients enrolled after the dosing adjustment, the intracranial hemorrhage rate was similar in both study arms and the fibrinolysis-first group’s lower rate of the study’s primary composite endpoint nearly reached statistical significance, Dr. Van de Werf said.

Probably as a result of earlier recanalization in the fibrinolysis group, their rate of heart failure was 6.1%, compared with 7.6% with primary PCI. Cardiogenic shock was also less common in the fibrinolysis group, by a margin of 4.4% to 5.9%.
"These are important observations. They were not statistically significant differences, but nonetheless I think we might see an effect on long-term mortality. So we are collecting long-term mortality data," he continued.
Discussant Dr. Freek Verheugt called STREAM "an important step forward" and applauded the investigators for pursuing "a courageous trial to do in this era of primary PCI."
"This was the first trial to show that early fibrinolysis followed by mandatory timely angiography is as effective as primary PCI in patients who are more than 1 hour away from a PCI hospital. The strength of this study is two-thirds of patients don’t need urgent intervention when they have the lytic before. I think that’s very important because we know that off-hours primary PCI procedures have a worse outcome than daytime procedures. And you have more patients getting deferred intervention and CABG with the lytic strategy. It’s good for the patients, good for their relatives, and good for the interventional cardiologists and the cath lab personnel," said Dr. Verheugt, professor of cardiology at Nijmegen (the Netherlands) University.
"I don’t think STREAM will change the guidelines because it is within the guidelines, but I think it will change practice in certain parts of the world with long drive times to PCI hospitals," he predicted.
Dr. C. Michael Gibson noted that out of more than a dozen prespecified patient subgroups analyzed in STREAM, the outcomes for the two treatment strategies differed significantly in only one: patients with an inferior infarct location. They accounted for roughly half of study participants, and their primary endpoint rate was 7.3% with fibrinolysis compared with 12.3% with primary PCI. It seems counterintuitive that they would do significantly better with the pharmacoinvasive strategy, observed Dr. Gibson, professor of medicine at Harvard University, Boston.
Dr. Van de Werf replied that while the explanation for this finding is unclear, there is some evidence from earlier studies that fibrinolysis is more effective in reperfusing an occluded right rather than left coronary artery.
ACC conference cochair Dr. Neal Kleiman of Methodist Hospital, Houston, declared STREAM "a fantastic study on a very important issue. I think you’ve provided a beacon of light in the fog here."
Simultaneous with his presentation of the STREAM data in San Francisco, the study results were published online (N. Engl. J. Med. 2013 March 10 [doi: 10.1056/NEJMoa1301092]).
STREAM was funded by Boehringer Ingelheim. Dr. Van de Werf is a consultant to the company.
SAN FRANCISCO – Selected patients with ST-elevation myocardial infarction fare just as well with a treatment strategy of early fibrinolysis followed by transfer to a PCI center for timely coronary angiography as they do with primary PCI, according to the landmark STREAM trial.
The large patient population for whom this so-called "pharmacoinvasive" or fibrinolysis-first strategy is applicable comprises those STEMI patients whose symptoms are less than 3 hours old at first medical contact and who cannot undergo primary percutaneous coronary intervention (PCI) within the following hour, Dr. Frans Van de Werf explained in presenting the results of the STREAM (Strategic Reperfusion Early After Myocardial infarction) trial at the annual meeting of the American College of Cardiology.
Guidelines are clear that primary PCI is the preferred reperfusion method in STEMI patients with recent onset of symptoms, but only when the intervention can be performed promptly by an experienced team. That’s a huge caveat. The fact is that primary PCI doesn’t get done within guideline-recommended times for most patients who present to a non–PCI-capable hospital. Large registries consistently show this to be the case because of lengthy transfer times and other logistic issues, noted Dr. Van de Werf, professor of cardiology at the Catholic University of Leuven (Belgium).
"This study is not a challenge to primary PCI, it’s a study in a population who can’t get primary PCI in a short period of time," he stressed.
STREAM was an international, prospective, randomized trial involving 1,892 STEMI patients who presented to a non-PCI center within 3 hours of symptom onset and were unable to undergo primary PCI within the next hour. They were randomized to direct transfer for primary PCI or to fibrinolytic therapy with tenecteplase along with clopidogrel and enoxaparin, followed by transfer to a PCI-capable center.
If an ECG obtained 90 minutes after bolus tenecteplase showed at least 50% ST resolution, patients underwent coronary angiography 6-24 hours later – after the increased procedural bleeding risk associated with fibrinolytic therapy had worn off – with PCI or coronary artery bypass graft (CABG) surgery if indicated. However, if the ECG did not show reperfusion, emergency angiography was performed with an eye toward PCI.
The median time to the start of reperfusion therapy was 100 minutes from symptom onset in the pharmacoinvasive group, compared with 178 minutes in patients assigned to primary PCI.
The primary study endpoint was the 30-day cumulative rate of death, shock, congestive heart failure, or reinfarction. It occurred in 12.4% of the fibrinolysis-first group and 14.3% of those who underwent primary PCI, a nonsignificant difference (P = .21).
The ECG showed that fibrinolysis failed, requiring emergency angiography, in 36% of patients, with rescue PCI performed an average of 2.2 hours after randomization. The other 64% of patients in the pharmacoinvasive group underwent nonurgent catheterization at a median of 17 hours.
"The study results provide the opportunity for a measured approach to invasive coronary interventions, circumventing an urgent procedure in about two-thirds of fibrinolytic-treated STEMI patients," Dr. Van de Werf observed. "Drug therapy before transfer is at least as effective as PCI, and an urgent catheterization was avoided in two-thirds of patients. This gives physicians time to consider other options, such as CABG and medical therapy."
Indeed, CABG was significantly more frequent in the pharmacoinvasive strategy group than with primary PCI, by a margin of 4.7% to 2.1%. As CABG is probably a better revascularization procedure, this is a good thing, the cardiologist continued.
Intracranial hemorrhage occurred significantly more frequently in the fibrinolysis group than with primary PCI, by a margin of 1.0% to 0.2%. However, after one-fifth of STREAM participants had been enrolled, investigators realized that those aged 75 years or older had an excess risk of intracranial hemorrhage with full-dose bolus tenectaplase. Thereafter, the tenectaplase dose was reduced by 50% in elderly patients. It’s worth noting that in the more than 1,500 patients enrolled after the dosing adjustment, the intracranial hemorrhage rate was similar in both study arms and the fibrinolysis-first group’s lower rate of the study’s primary composite endpoint nearly reached statistical significance, Dr. Van de Werf said.
Probably as a result of earlier recanalization in the fibrinolysis group, their rate of heart failure was 6.1%, compared with 7.6% with primary PCI. Cardiogenic shock was also less common in the fibrinolysis group, by a margin of 4.4% to 5.9%.
"These are important observations. They were not statistically significant differences, but nonetheless I think we might see an effect on long-term mortality. So we are collecting long-term mortality data," he continued.
Discussant Dr. Freek Verheugt called STREAM "an important step forward" and applauded the investigators for pursuing "a courageous trial to do in this era of primary PCI."
"This was the first trial to show that early fibrinolysis followed by mandatory timely angiography is as effective as primary PCI in patients who are more than 1 hour away from a PCI hospital. The strength of this study is two-thirds of patients don’t need urgent intervention when they have the lytic before. I think that’s very important because we know that off-hours primary PCI procedures have a worse outcome than daytime procedures. And you have more patients getting deferred intervention and CABG with the lytic strategy. It’s good for the patients, good for their relatives, and good for the interventional cardiologists and the cath lab personnel," said Dr. Verheugt, professor of cardiology at Nijmegen (the Netherlands) University.
"I don’t think STREAM will change the guidelines because it is within the guidelines, but I think it will change practice in certain parts of the world with long drive times to PCI hospitals," he predicted.
Dr. C. Michael Gibson noted that out of more than a dozen prespecified patient subgroups analyzed in STREAM, the outcomes for the two treatment strategies differed significantly in only one: patients with an inferior infarct location. They accounted for roughly half of study participants, and their primary endpoint rate was 7.3% with fibrinolysis compared with 12.3% with primary PCI. It seems counterintuitive that they would do significantly better with the pharmacoinvasive strategy, observed Dr. Gibson, professor of medicine at Harvard University, Boston.
Dr. Van de Werf replied that while the explanation for this finding is unclear, there is some evidence from earlier studies that fibrinolysis is more effective in reperfusing an occluded right rather than left coronary artery.
ACC conference cochair Dr. Neal Kleiman of Methodist Hospital, Houston, declared STREAM "a fantastic study on a very important issue. I think you’ve provided a beacon of light in the fog here."
Simultaneous with his presentation of the STREAM data in San Francisco, the study results were published online (N. Engl. J. Med. 2013 March 10 [doi: 10.1056/NEJMoa1301092]).
STREAM was funded by Boehringer Ingelheim. Dr. Van de Werf is a consultant to the company.
SAN FRANCISCO – Selected patients with ST-elevation myocardial infarction fare just as well with a treatment strategy of early fibrinolysis followed by transfer to a PCI center for timely coronary angiography as they do with primary PCI, according to the landmark STREAM trial.
The large patient population for whom this so-called "pharmacoinvasive" or fibrinolysis-first strategy is applicable comprises those STEMI patients whose symptoms are less than 3 hours old at first medical contact and who cannot undergo primary percutaneous coronary intervention (PCI) within the following hour, Dr. Frans Van de Werf explained in presenting the results of the STREAM (Strategic Reperfusion Early After Myocardial infarction) trial at the annual meeting of the American College of Cardiology.
Guidelines are clear that primary PCI is the preferred reperfusion method in STEMI patients with recent onset of symptoms, but only when the intervention can be performed promptly by an experienced team. That’s a huge caveat. The fact is that primary PCI doesn’t get done within guideline-recommended times for most patients who present to a non–PCI-capable hospital. Large registries consistently show this to be the case because of lengthy transfer times and other logistic issues, noted Dr. Van de Werf, professor of cardiology at the Catholic University of Leuven (Belgium).
"This study is not a challenge to primary PCI, it’s a study in a population who can’t get primary PCI in a short period of time," he stressed.
STREAM was an international, prospective, randomized trial involving 1,892 STEMI patients who presented to a non-PCI center within 3 hours of symptom onset and were unable to undergo primary PCI within the next hour. They were randomized to direct transfer for primary PCI or to fibrinolytic therapy with tenecteplase along with clopidogrel and enoxaparin, followed by transfer to a PCI-capable center.
If an ECG obtained 90 minutes after bolus tenecteplase showed at least 50% ST resolution, patients underwent coronary angiography 6-24 hours later – after the increased procedural bleeding risk associated with fibrinolytic therapy had worn off – with PCI or coronary artery bypass graft (CABG) surgery if indicated. However, if the ECG did not show reperfusion, emergency angiography was performed with an eye toward PCI.
The median time to the start of reperfusion therapy was 100 minutes from symptom onset in the pharmacoinvasive group, compared with 178 minutes in patients assigned to primary PCI.
The primary study endpoint was the 30-day cumulative rate of death, shock, congestive heart failure, or reinfarction. It occurred in 12.4% of the fibrinolysis-first group and 14.3% of those who underwent primary PCI, a nonsignificant difference (P = .21).
The ECG showed that fibrinolysis failed, requiring emergency angiography, in 36% of patients, with rescue PCI performed an average of 2.2 hours after randomization. The other 64% of patients in the pharmacoinvasive group underwent nonurgent catheterization at a median of 17 hours.
"The study results provide the opportunity for a measured approach to invasive coronary interventions, circumventing an urgent procedure in about two-thirds of fibrinolytic-treated STEMI patients," Dr. Van de Werf observed. "Drug therapy before transfer is at least as effective as PCI, and an urgent catheterization was avoided in two-thirds of patients. This gives physicians time to consider other options, such as CABG and medical therapy."
Indeed, CABG was significantly more frequent in the pharmacoinvasive strategy group than with primary PCI, by a margin of 4.7% to 2.1%. As CABG is probably a better revascularization procedure, this is a good thing, the cardiologist continued.
Intracranial hemorrhage occurred significantly more frequently in the fibrinolysis group than with primary PCI, by a margin of 1.0% to 0.2%. However, after one-fifth of STREAM participants had been enrolled, investigators realized that those aged 75 years or older had an excess risk of intracranial hemorrhage with full-dose bolus tenectaplase. Thereafter, the tenectaplase dose was reduced by 50% in elderly patients. It’s worth noting that in the more than 1,500 patients enrolled after the dosing adjustment, the intracranial hemorrhage rate was similar in both study arms and the fibrinolysis-first group’s lower rate of the study’s primary composite endpoint nearly reached statistical significance, Dr. Van de Werf said.
Probably as a result of earlier recanalization in the fibrinolysis group, their rate of heart failure was 6.1%, compared with 7.6% with primary PCI. Cardiogenic shock was also less common in the fibrinolysis group, by a margin of 4.4% to 5.9%.
"These are important observations. They were not statistically significant differences, but nonetheless I think we might see an effect on long-term mortality. So we are collecting long-term mortality data," he continued.
Discussant Dr. Freek Verheugt called STREAM "an important step forward" and applauded the investigators for pursuing "a courageous trial to do in this era of primary PCI."
"This was the first trial to show that early fibrinolysis followed by mandatory timely angiography is as effective as primary PCI in patients who are more than 1 hour away from a PCI hospital. The strength of this study is two-thirds of patients don’t need urgent intervention when they have the lytic before. I think that’s very important because we know that off-hours primary PCI procedures have a worse outcome than daytime procedures. And you have more patients getting deferred intervention and CABG with the lytic strategy. It’s good for the patients, good for their relatives, and good for the interventional cardiologists and the cath lab personnel," said Dr. Verheugt, professor of cardiology at Nijmegen (the Netherlands) University.
"I don’t think STREAM will change the guidelines because it is within the guidelines, but I think it will change practice in certain parts of the world with long drive times to PCI hospitals," he predicted.
Dr. C. Michael Gibson noted that out of more than a dozen prespecified patient subgroups analyzed in STREAM, the outcomes for the two treatment strategies differed significantly in only one: patients with an inferior infarct location. They accounted for roughly half of study participants, and their primary endpoint rate was 7.3% with fibrinolysis compared with 12.3% with primary PCI. It seems counterintuitive that they would do significantly better with the pharmacoinvasive strategy, observed Dr. Gibson, professor of medicine at Harvard University, Boston.
Dr. Van de Werf replied that while the explanation for this finding is unclear, there is some evidence from earlier studies that fibrinolysis is more effective in reperfusing an occluded right rather than left coronary artery.
ACC conference cochair Dr. Neal Kleiman of Methodist Hospital, Houston, declared STREAM "a fantastic study on a very important issue. I think you’ve provided a beacon of light in the fog here."
Simultaneous with his presentation of the STREAM data in San Francisco, the study results were published online (N. Engl. J. Med. 2013 March 10 [doi: 10.1056/NEJMoa1301092]).
STREAM was funded by Boehringer Ingelheim. Dr. Van de Werf is a consultant to the company.
AT ACC 13
Major finding: The 30-day composite rate of death, shock, congestive heart failure, or reinfarction in STEMI patients was 12.4% in those randomized to a fibrinolysis-first pharmacoinvasive strategy versus 14.3% with primary PCI.
Data source: STREAM, a randomized prospective study in 1,892 patients whose first medical contact was less than 3 hours since symptom onset and who were unable to undergo primary PCI within the next hour.
Disclosures: STREAM was funded by Boehringer Ingelheim. Dr. Van de Werf is a consultant to the company.

Consider topical therapy for kids' nail fungus
MAUI, HAWAII – Conventional wisdom holds that systemic therapy is necessary for effective treatment of onychomycosis. Not so in children, according to Dr. Sheila F. Friedlander.
"You can have different treatment plans depending on the severity of disease. If you have a child with minimal involvement – not involving the nail matrix – I would consider topical therapy rather than systemic," Dr. Friedlander said at the Hawaii Dermatology Seminar sponsored by Global Academy for Medical Education/Skin Disease Education Foundation.

Dr. Friedlander and her coinvestigators conducted a prospective trial of 40 children and teens aged 2-16 years with nonmatrix onychomycosis. The patients were randomized 3 to 1 to receive topical ciclopirox nail lacquer or a vehicle control. The lacquer was applied daily, with weekly removal and nail trimming, for the duration of the 32-week trial.
At 32 weeks, the mycologic cure and effective treatment rates were 77% and 71%, respectively, in the ciclopirox group compared with 22% for both mycologic cure and effective treatment rates in controls.
"Those treatment success rates in excess of 70% were exciting to us. Those are data you never see in adults," said Dr. Friedlander, professor of clinical medicine and pediatrics at the University of California, San Diego, and president of the Society for Pediatric Dermatology. "If you were to do this study of ciclopirox in adults, the numbers would be in the teens or twenties," she said.
Ninety-two percent of patients with mycologic cure at 32 weeks remained clear after 1 year, and the only adverse effect noted was transient discoloration of the nails.
Topical therapy is so much more effective in children and teens because they have thinner, faster-growing nails than adults, Dr. Friedlander explained.
The families of the patients loved this treatment, she added. More than 90% said they would definitely or probably undergo the treatment again.
Eighty-two percent of study participants had one or more family members with onychomycosis, which raises the question of whether the participants’ fungal diseases were caused by environmental exposure or genetic susceptibility, Dr. Friedlander said.
Systemic antifungal therapy is clearly more effective than is topical therapy, Dr. Friedlander noted. But her preferred oral therapy, terbinafine, requires 3 months of daily use to cure a pediatric toenail infection. Also, the Food and Drug Administration recommends that patients get liver function tests when using this drug, which makes terbinafine a tough sell to parents.
"Families are loath to put their children on prolonged systemic therapy. And they do not want their children poked for lab studies," she observed.
Dr. Friedlander reported having no financial conflicts. SDEF and this news organization are owned by the same parent company.
MAUI, HAWAII – Conventional wisdom holds that systemic therapy is necessary for effective treatment of onychomycosis. Not so in children, according to Dr. Sheila F. Friedlander.
"You can have different treatment plans depending on the severity of disease. If you have a child with minimal involvement – not involving the nail matrix – I would consider topical therapy rather than systemic," Dr. Friedlander said at the Hawaii Dermatology Seminar sponsored by Global Academy for Medical Education/Skin Disease Education Foundation.
Dr. Friedlander and her coinvestigators conducted a prospective trial of 40 children and teens aged 2-16 years with nonmatrix onychomycosis. The patients were randomized 3 to 1 to receive topical ciclopirox nail lacquer or a vehicle control. The lacquer was applied daily, with weekly removal and nail trimming, for the duration of the 32-week trial.
At 32 weeks, the mycologic cure and effective treatment rates were 77% and 71%, respectively, in the ciclopirox group compared with 22% for both mycologic cure and effective treatment rates in controls.
"Those treatment success rates in excess of 70% were exciting to us. Those are data you never see in adults," said Dr. Friedlander, professor of clinical medicine and pediatrics at the University of California, San Diego, and president of the Society for Pediatric Dermatology. "If you were to do this study of ciclopirox in adults, the numbers would be in the teens or twenties," she said.
Ninety-two percent of patients with mycologic cure at 32 weeks remained clear after 1 year, and the only adverse effect noted was transient discoloration of the nails.
Topical therapy is so much more effective in children and teens because they have thinner, faster-growing nails than adults, Dr. Friedlander explained.
The families of the patients loved this treatment, she added. More than 90% said they would definitely or probably undergo the treatment again.
Eighty-two percent of study participants had one or more family members with onychomycosis, which raises the question of whether the participants’ fungal diseases were caused by environmental exposure or genetic susceptibility, Dr. Friedlander said.
Systemic antifungal therapy is clearly more effective than is topical therapy, Dr. Friedlander noted. But her preferred oral therapy, terbinafine, requires 3 months of daily use to cure a pediatric toenail infection. Also, the Food and Drug Administration recommends that patients get liver function tests when using this drug, which makes terbinafine a tough sell to parents.
"Families are loath to put their children on prolonged systemic therapy. And they do not want their children poked for lab studies," she observed.
Dr. Friedlander reported having no financial conflicts. SDEF and this news organization are owned by the same parent company.
MAUI, HAWAII – Conventional wisdom holds that systemic therapy is necessary for effective treatment of onychomycosis. Not so in children, according to Dr. Sheila F. Friedlander.
"You can have different treatment plans depending on the severity of disease. If you have a child with minimal involvement – not involving the nail matrix – I would consider topical therapy rather than systemic," Dr. Friedlander said at the Hawaii Dermatology Seminar sponsored by Global Academy for Medical Education/Skin Disease Education Foundation.
Dr. Friedlander and her coinvestigators conducted a prospective trial of 40 children and teens aged 2-16 years with nonmatrix onychomycosis. The patients were randomized 3 to 1 to receive topical ciclopirox nail lacquer or a vehicle control. The lacquer was applied daily, with weekly removal and nail trimming, for the duration of the 32-week trial.
At 32 weeks, the mycologic cure and effective treatment rates were 77% and 71%, respectively, in the ciclopirox group compared with 22% for both mycologic cure and effective treatment rates in controls.
"Those treatment success rates in excess of 70% were exciting to us. Those are data you never see in adults," said Dr. Friedlander, professor of clinical medicine and pediatrics at the University of California, San Diego, and president of the Society for Pediatric Dermatology. "If you were to do this study of ciclopirox in adults, the numbers would be in the teens or twenties," she said.
Ninety-two percent of patients with mycologic cure at 32 weeks remained clear after 1 year, and the only adverse effect noted was transient discoloration of the nails.
Topical therapy is so much more effective in children and teens because they have thinner, faster-growing nails than adults, Dr. Friedlander explained.
The families of the patients loved this treatment, she added. More than 90% said they would definitely or probably undergo the treatment again.
Eighty-two percent of study participants had one or more family members with onychomycosis, which raises the question of whether the participants’ fungal diseases were caused by environmental exposure or genetic susceptibility, Dr. Friedlander said.
Systemic antifungal therapy is clearly more effective than is topical therapy, Dr. Friedlander noted. But her preferred oral therapy, terbinafine, requires 3 months of daily use to cure a pediatric toenail infection. Also, the Food and Drug Administration recommends that patients get liver function tests when using this drug, which makes terbinafine a tough sell to parents.
"Families are loath to put their children on prolonged systemic therapy. And they do not want their children poked for lab studies," she observed.
Dr. Friedlander reported having no financial conflicts. SDEF and this news organization are owned by the same parent company.
EXPERT ANALYSIS FROM SDEF HAWAII DERMATOLOGY SEMINAR

HPS2-THRIVE drives another nail in niacin's coffin
SAN FRANCISCO – The largest-ever randomized trial of niacin for cardiovascular protection has not only failed to show clinical benefit, it spotlighted a hitherto underrecognized and disturbingly high range of serious harms in users of the HDL-raising drug.
The HPS2-THRIVE (Heart Protection Study 2–Treatment of HDL to Reduce the Incidence of Vascular Events) trial found a rate of serious adverse events warranting hospitalization of 30 cases per 1,000 treated patients. Although many of these adverse events were already known to be associated with niacin therapy, two types of serious adverse events not previously recognized as niacin related were also identified: infections and bleeding, Dr. Jane Armitage reported at the annual meeting of the American College of Cardiology.
"The role of extended-release niacin for the treatment and prevention of cardiovascular disease needs to be reconsidered in light of these findings," said Dr. Armitage, professor of clinical trials and epidemiology at the University of Oxford (England).

That’s exactly what is now happening, as the European Medicine Agency has announced it is reviewing niacin’s status and considering its possible withdrawal from the marketplace.
The HPS2-THRIVE study involved 25,673 high-cardiovascular-risk patients in six countries, all of whom were placed on simvastatin 40 mg/day, with ezetimibe added if necessary in order to achieve a target total cholesterol level below 135 mg/dL. On that regimen, their mean LDL was an impressively favorable 63 mg/dL, with an HDL of 44 mg/dL and triglycerides of 125 mg/dL. This was a high-risk population. Roughly 80% of participants had a history of coronary artery disease, one-third had a history of cerebrovascular disease, and one-third had diabetes at baseline. After the investigators established during a run-in period that all participants could tolerate full-dose niacin, they were randomized to 2 g/day of extended-release niacin plus 40 mg of laropiprant to mitigate flushing or to placebo.
The active treatment arm had an average further 10-mg/dL reduction in LDL, a 6-mg/dL rise in HDL, and a 33-mg/dL drop in triglycerides. Extrapolating from earlier studies, Dr. Armitage and his coworkers anticipated that these lipid improvements would lead to an estimated 10%-15% reduction in the primary study endpoint, a composite of cardiac death, MI, stroke, or revascularization. But that’s not what transpired.
Indeed, during a median follow-up of 3.9 years, the primary endpoint occurred in 14.5% of patients on niacin/laropiprant and 15% on placebo, a nonsignificant difference.
Diabetic complications among the more than 8,200 patients with diabetes at baseline occurred at an absolute 3.7% greater rate and 55% increased relative rate in the niacin group, compared with controls. Most of these diabetic complications led to multiday hospitalizations. Leading the way were major hyperglycemic episodes, which were 3.1-fold more common in the active treatment arm.

Among the other serious events that occurred at a significantly higher rate in the niacin group were serious infections in a variety of different organ systems, with a 22% increased rate; serious bleeding into the brain or gut, with a 38% increase; new-onset diabetes, with a 27% increase; myopathy and other serious musculoskeletal problems, with a 26% rise; and serious rash and other skin issues, which increased by 67%.
On the basis of prior studies, the most plausible culprit in the increased rates of serious adverse events is niacin rather than laropiprant, according to Dr. Armitage.
Discussant Donna Arnett, Ph.D., called HPS2-THRIVE "an exceptionally well-conducted study that definitively tells us the story of this drug combination in the setting of very well-controlled LDL."
"The results call into question the concept that increasing a low HDL in the context of a low LDL is really an important clinical problem," added Dr. Arnett, president of the American Heart Association and professor and chair of the department of epidemiology at the University of Alabama at Birmingham.

But panelist Dr. Christie M. Ballantyne indicated he has a big issue with the study: "If your LDL is 60, how important is your HDL, anyway? If I saw a patient who came to me with an LDL of 63, an HDL of 44, and triglycerides of 125, like the subjects in this trial, I would never even think of adding niacin because I know the drug has some risk and there is in my mind very little likelihood of seeing any benefit. But the majority of people in the U.S. who get niacin have LDLs greater than 70. I have high-risk patients who can only get their LDL down to 110 mg/dL with maximum statin therapy, and they can lower it by a further 30-40 mg/dL with niacin. What do I tell those patients now?
"Niacin has always been known as a drug that’s not easy to use, one with lots of side effects. It’s never been a first- or second-line therapy. It’s always been the drug where, when you can’t get there any other way, then you use it," observed Dr. Ballantyne, professor of medicine and chief of cardiology at Baylor College of Medicine, Houston.
Dr. Spencer B. King III called HPS2-THRIVE "another nail in the coffin for niacin," coming after the negative results of the National Institutes of Health–sponsored AIM-HIGH (Niacin Plus Statin to Prevent Vascular Events) study.
"I think the practice-changing part of this study is that many of us have been piling on a lot of niacin in people with low HDL. What you’ve shown is going to change attitudes among many physicians," predicted Dr. King, president of the Saint Joseph’s Heart and Vascular Institute, Atlanta.

When he asked Dr. Armitage whether any room remains now for individualized niacin therapy in selected patients, she replied that the investigators couldn’t identify any patient subgroup in whom the benefit outweighed the greater risk.
Dr. Rory Collins, chair of the HPS2-THRIVE trial, chimed in, adding: "Is niacin dead? I think in the light of these findings, it’s not healthy. The default position should change. It should be, Is there a good reason for using this therapy in any particular patient when there are additional ways, besides statins, of lowering LDL cholesterol, and where we don’t as yet have evidence that raising HDL cholesterol produces benefit?"
The HPS2-THRIVE trial was funded by Merck. Dr. Armitage, Dr. Collins, Dr. Arnett, and Dr. King reported having no relevant financial conflicts. Dr. Ballantyne serves as a consultant to numerous pharmaceutical companies, including Merck.
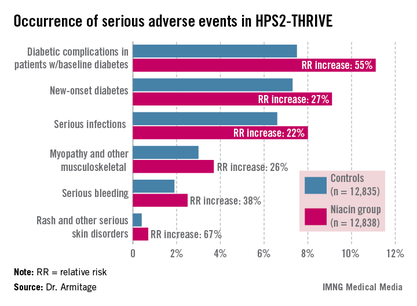
SAN FRANCISCO – The largest-ever randomized trial of niacin for cardiovascular protection has not only failed to show clinical benefit, it spotlighted a hitherto underrecognized and disturbingly high range of serious harms in users of the HDL-raising drug.
The HPS2-THRIVE (Heart Protection Study 2–Treatment of HDL to Reduce the Incidence of Vascular Events) trial found a rate of serious adverse events warranting hospitalization of 30 cases per 1,000 treated patients. Although many of these adverse events were already known to be associated with niacin therapy, two types of serious adverse events not previously recognized as niacin related were also identified: infections and bleeding, Dr. Jane Armitage reported at the annual meeting of the American College of Cardiology.
"The role of extended-release niacin for the treatment and prevention of cardiovascular disease needs to be reconsidered in light of these findings," said Dr. Armitage, professor of clinical trials and epidemiology at the University of Oxford (England).
That’s exactly what is now happening, as the European Medicine Agency has announced it is reviewing niacin’s status and considering its possible withdrawal from the marketplace.
The HPS2-THRIVE study involved 25,673 high-cardiovascular-risk patients in six countries, all of whom were placed on simvastatin 40 mg/day, with ezetimibe added if necessary in order to achieve a target total cholesterol level below 135 mg/dL. On that regimen, their mean LDL was an impressively favorable 63 mg/dL, with an HDL of 44 mg/dL and triglycerides of 125 mg/dL. This was a high-risk population. Roughly 80% of participants had a history of coronary artery disease, one-third had a history of cerebrovascular disease, and one-third had diabetes at baseline. After the investigators established during a run-in period that all participants could tolerate full-dose niacin, they were randomized to 2 g/day of extended-release niacin plus 40 mg of laropiprant to mitigate flushing or to placebo.
The active treatment arm had an average further 10-mg/dL reduction in LDL, a 6-mg/dL rise in HDL, and a 33-mg/dL drop in triglycerides. Extrapolating from earlier studies, Dr. Armitage and his coworkers anticipated that these lipid improvements would lead to an estimated 10%-15% reduction in the primary study endpoint, a composite of cardiac death, MI, stroke, or revascularization. But that’s not what transpired.
Indeed, during a median follow-up of 3.9 years, the primary endpoint occurred in 14.5% of patients on niacin/laropiprant and 15% on placebo, a nonsignificant difference.
Diabetic complications among the more than 8,200 patients with diabetes at baseline occurred at an absolute 3.7% greater rate and 55% increased relative rate in the niacin group, compared with controls. Most of these diabetic complications led to multiday hospitalizations. Leading the way were major hyperglycemic episodes, which were 3.1-fold more common in the active treatment arm.
Among the other serious events that occurred at a significantly higher rate in the niacin group were serious infections in a variety of different organ systems, with a 22% increased rate; serious bleeding into the brain or gut, with a 38% increase; new-onset diabetes, with a 27% increase; myopathy and other serious musculoskeletal problems, with a 26% rise; and serious rash and other skin issues, which increased by 67%.
On the basis of prior studies, the most plausible culprit in the increased rates of serious adverse events is niacin rather than laropiprant, according to Dr. Armitage.
Discussant Donna Arnett, Ph.D., called HPS2-THRIVE "an exceptionally well-conducted study that definitively tells us the story of this drug combination in the setting of very well-controlled LDL."
"The results call into question the concept that increasing a low HDL in the context of a low LDL is really an important clinical problem," added Dr. Arnett, president of the American Heart Association and professor and chair of the department of epidemiology at the University of Alabama at Birmingham.
But panelist Dr. Christie M. Ballantyne indicated he has a big issue with the study: "If your LDL is 60, how important is your HDL, anyway? If I saw a patient who came to me with an LDL of 63, an HDL of 44, and triglycerides of 125, like the subjects in this trial, I would never even think of adding niacin because I know the drug has some risk and there is in my mind very little likelihood of seeing any benefit. But the majority of people in the U.S. who get niacin have LDLs greater than 70. I have high-risk patients who can only get their LDL down to 110 mg/dL with maximum statin therapy, and they can lower it by a further 30-40 mg/dL with niacin. What do I tell those patients now?
"Niacin has always been known as a drug that’s not easy to use, one with lots of side effects. It’s never been a first- or second-line therapy. It’s always been the drug where, when you can’t get there any other way, then you use it," observed Dr. Ballantyne, professor of medicine and chief of cardiology at Baylor College of Medicine, Houston.
Dr. Spencer B. King III called HPS2-THRIVE "another nail in the coffin for niacin," coming after the negative results of the National Institutes of Health–sponsored AIM-HIGH (Niacin Plus Statin to Prevent Vascular Events) study.
"I think the practice-changing part of this study is that many of us have been piling on a lot of niacin in people with low HDL. What you’ve shown is going to change attitudes among many physicians," predicted Dr. King, president of the Saint Joseph’s Heart and Vascular Institute, Atlanta.
When he asked Dr. Armitage whether any room remains now for individualized niacin therapy in selected patients, she replied that the investigators couldn’t identify any patient subgroup in whom the benefit outweighed the greater risk.
Dr. Rory Collins, chair of the HPS2-THRIVE trial, chimed in, adding: "Is niacin dead? I think in the light of these findings, it’s not healthy. The default position should change. It should be, Is there a good reason for using this therapy in any particular patient when there are additional ways, besides statins, of lowering LDL cholesterol, and where we don’t as yet have evidence that raising HDL cholesterol produces benefit?"
The HPS2-THRIVE trial was funded by Merck. Dr. Armitage, Dr. Collins, Dr. Arnett, and Dr. King reported having no relevant financial conflicts. Dr. Ballantyne serves as a consultant to numerous pharmaceutical companies, including Merck.
SAN FRANCISCO – The largest-ever randomized trial of niacin for cardiovascular protection has not only failed to show clinical benefit, it spotlighted a hitherto underrecognized and disturbingly high range of serious harms in users of the HDL-raising drug.
The HPS2-THRIVE (Heart Protection Study 2–Treatment of HDL to Reduce the Incidence of Vascular Events) trial found a rate of serious adverse events warranting hospitalization of 30 cases per 1,000 treated patients. Although many of these adverse events were already known to be associated with niacin therapy, two types of serious adverse events not previously recognized as niacin related were also identified: infections and bleeding, Dr. Jane Armitage reported at the annual meeting of the American College of Cardiology.
"The role of extended-release niacin for the treatment and prevention of cardiovascular disease needs to be reconsidered in light of these findings," said Dr. Armitage, professor of clinical trials and epidemiology at the University of Oxford (England).
That’s exactly what is now happening, as the European Medicine Agency has announced it is reviewing niacin’s status and considering its possible withdrawal from the marketplace.
The HPS2-THRIVE study involved 25,673 high-cardiovascular-risk patients in six countries, all of whom were placed on simvastatin 40 mg/day, with ezetimibe added if necessary in order to achieve a target total cholesterol level below 135 mg/dL. On that regimen, their mean LDL was an impressively favorable 63 mg/dL, with an HDL of 44 mg/dL and triglycerides of 125 mg/dL. This was a high-risk population. Roughly 80% of participants had a history of coronary artery disease, one-third had a history of cerebrovascular disease, and one-third had diabetes at baseline. After the investigators established during a run-in period that all participants could tolerate full-dose niacin, they were randomized to 2 g/day of extended-release niacin plus 40 mg of laropiprant to mitigate flushing or to placebo.
The active treatment arm had an average further 10-mg/dL reduction in LDL, a 6-mg/dL rise in HDL, and a 33-mg/dL drop in triglycerides. Extrapolating from earlier studies, Dr. Armitage and his coworkers anticipated that these lipid improvements would lead to an estimated 10%-15% reduction in the primary study endpoint, a composite of cardiac death, MI, stroke, or revascularization. But that’s not what transpired.
Indeed, during a median follow-up of 3.9 years, the primary endpoint occurred in 14.5% of patients on niacin/laropiprant and 15% on placebo, a nonsignificant difference.
Diabetic complications among the more than 8,200 patients with diabetes at baseline occurred at an absolute 3.7% greater rate and 55% increased relative rate in the niacin group, compared with controls. Most of these diabetic complications led to multiday hospitalizations. Leading the way were major hyperglycemic episodes, which were 3.1-fold more common in the active treatment arm.
Among the other serious events that occurred at a significantly higher rate in the niacin group were serious infections in a variety of different organ systems, with a 22% increased rate; serious bleeding into the brain or gut, with a 38% increase; new-onset diabetes, with a 27% increase; myopathy and other serious musculoskeletal problems, with a 26% rise; and serious rash and other skin issues, which increased by 67%.
On the basis of prior studies, the most plausible culprit in the increased rates of serious adverse events is niacin rather than laropiprant, according to Dr. Armitage.
Discussant Donna Arnett, Ph.D., called HPS2-THRIVE "an exceptionally well-conducted study that definitively tells us the story of this drug combination in the setting of very well-controlled LDL."
"The results call into question the concept that increasing a low HDL in the context of a low LDL is really an important clinical problem," added Dr. Arnett, president of the American Heart Association and professor and chair of the department of epidemiology at the University of Alabama at Birmingham.
But panelist Dr. Christie M. Ballantyne indicated he has a big issue with the study: "If your LDL is 60, how important is your HDL, anyway? If I saw a patient who came to me with an LDL of 63, an HDL of 44, and triglycerides of 125, like the subjects in this trial, I would never even think of adding niacin because I know the drug has some risk and there is in my mind very little likelihood of seeing any benefit. But the majority of people in the U.S. who get niacin have LDLs greater than 70. I have high-risk patients who can only get their LDL down to 110 mg/dL with maximum statin therapy, and they can lower it by a further 30-40 mg/dL with niacin. What do I tell those patients now?
"Niacin has always been known as a drug that’s not easy to use, one with lots of side effects. It’s never been a first- or second-line therapy. It’s always been the drug where, when you can’t get there any other way, then you use it," observed Dr. Ballantyne, professor of medicine and chief of cardiology at Baylor College of Medicine, Houston.
Dr. Spencer B. King III called HPS2-THRIVE "another nail in the coffin for niacin," coming after the negative results of the National Institutes of Health–sponsored AIM-HIGH (Niacin Plus Statin to Prevent Vascular Events) study.
"I think the practice-changing part of this study is that many of us have been piling on a lot of niacin in people with low HDL. What you’ve shown is going to change attitudes among many physicians," predicted Dr. King, president of the Saint Joseph’s Heart and Vascular Institute, Atlanta.
When he asked Dr. Armitage whether any room remains now for individualized niacin therapy in selected patients, she replied that the investigators couldn’t identify any patient subgroup in whom the benefit outweighed the greater risk.
Dr. Rory Collins, chair of the HPS2-THRIVE trial, chimed in, adding: "Is niacin dead? I think in the light of these findings, it’s not healthy. The default position should change. It should be, Is there a good reason for using this therapy in any particular patient when there are additional ways, besides statins, of lowering LDL cholesterol, and where we don’t as yet have evidence that raising HDL cholesterol produces benefit?"
The HPS2-THRIVE trial was funded by Merck. Dr. Armitage, Dr. Collins, Dr. Arnett, and Dr. King reported having no relevant financial conflicts. Dr. Ballantyne serves as a consultant to numerous pharmaceutical companies, including Merck.
AT ACC 13
Major Finding: During an average 3.9-year prospective follow-up, the rate of the combined endpoint of coronary death, nonfatal MI, stroke, or revascularization occurred in 14.5% of patients on 2 g of extended-release niacin plus 40 mg of laropiprant per day and 15% of placebo-treated controls, a nonsignificant difference. Serious adverse events warranting hospitalization occurred in the niacin group at a rate of 30/1,000 treated patients.
Data Source: HPS2-THRIVE, which randomized 25,673 high-cardiovascular-risk patients with low baseline LDL levels on simvastatin with or without ezetimibe to niacin/laropiprant or placebo.
Disclosures: The study was sponsored by Merck. The presenter reported having no relevant financial conflicts.