User login
Body Fat and Cardiovascular Risk: Location, Location, Location!
DALLAS – It’s not obesity per se that affects cardiovascular risk, it’s where that excess body fat is stored, according to the results of a novel adipose tissue–imaging study.
Excess visceral adipose tissue is independently associated with increased risk of developing cardiovascular disease. In contrast, increased lower body subcutaneous adipose tissue – that is, fat around the hips and a big butt – actually seems to protect against cardiovascular disease, Dr. Ian J. Neeland reported at the American Heart Association scientific sessions.
He presented an analysis of 972 obese participants in the Dallas Heart Study with a mean age of 44 years at enrollment and no baseline cardiovascular disease. All underwent dual-energy x-ray absorptiometry and MRI assessment of their body fat distribution, focusing on the visceral, abdominal subcutaneous, and lower body subcutaneous adipose tissue depots. Participants were then followed prospectively for a median 8.1 years, during which 91 cardiovascular events occurred in 68 subjects.
The impetus for the adipose tissue imaging study was the researchers’ recognition that obesity is a heterogeneous disorder.
"Currently, we know that obesity is associated with incident cardiovascular disease at a general population level. However, body mass index alone is really an inadequate marker of risk among the obese. Many individuals with even high BMIs do not develop cardiovascular disease. Marked abdominal obesity is a stronger predictor of cardiovascular disease but still lacks the necessary specificity. So there’s really a clinical need for tools to differentiate obese individuals who will develop cardiovascular disease from those who will be free of cardiovascular disease for their lifetime," explained Dr. Neeland, a fellow in cardiovascular medicine at the University of Texas Southwestern Medical Center, Dallas.
In a multivariate analysis adjusted for age, sex, race, and the conventional cardiovascular risk factors, each 1–standard deviation increase in visceral adipose tissue was independently associated with a 24% increase in the risk of developing cardiovascular disease during follow-up. Dividing the study population into quartiles on the basis of their extent of visceral adipose tissue, the cumulative incidence of cardiovascular disease rose in stepwise fashion, with subjects in the lowest quartile having the least cardiovascular events and those in the top quartile having the most.
Having more lower body subcutaneous fat had the opposite effect. For every 1–standard deviation increase in the amount of fat at that location, the cardiovascular event risk dropped by 27%.
Participants’ amount of abdominal subcutaneous fat didn’t affect their cardiovascular event risk one way or another. Nor did BMI, waist circumference, waist-hip ratio, or the amount of liver fat on MRI show any significant association with cardiovascular disease risk.
"These results really underscore the biologic importance of body fat distribution with regard to cardiovascular disease risk in obesity and suggest a possible prognostic role for imaging-based assessment of body fat distribution in high-risk obese patients," according to Dr. Neeland.
One intriguing clinical implication of this study is that preventing accumulation of visceral adipose tissue may have benefit in terms of cardiovascular disease prevention even in the absence of meaningful weight loss. It’s possible that new drugs could be developed that lower cardiovascular risk in obese patients by changing their body fat distribution profile rather than lopping off pounds.
In the Dallas study, increased visceral abdominal tissue was consistently associated with a higher risk of cardiovascular disease across subgroups based upon age, race, sex, and BMI.
"Interestingly, those with increased visceral abdominal fat who were less than 40 years of age had greater risk for cardiovascular disease than [did] those over 40. This could suggest that visceral abdominal tissue has a greater impact on the young, in whom other cardiovascular risk factors have not yet accumulated over time," Dr. Neeland observed.
The cardiovascular event endpoint in the study was a composite of cardiovascular death, acute MI, stroke, heart failure, atrial fibrillation, or event-driven coronary or peripheral artery revascularization.
The Dallas Heart Study is funded by the Donald W. Reynolds Foundation. Dr. Neeland reported having no financial conflicts.
DALLAS – It’s not obesity per se that affects cardiovascular risk, it’s where that excess body fat is stored, according to the results of a novel adipose tissue–imaging study.
Excess visceral adipose tissue is independently associated with increased risk of developing cardiovascular disease. In contrast, increased lower body subcutaneous adipose tissue – that is, fat around the hips and a big butt – actually seems to protect against cardiovascular disease, Dr. Ian J. Neeland reported at the American Heart Association scientific sessions.
He presented an analysis of 972 obese participants in the Dallas Heart Study with a mean age of 44 years at enrollment and no baseline cardiovascular disease. All underwent dual-energy x-ray absorptiometry and MRI assessment of their body fat distribution, focusing on the visceral, abdominal subcutaneous, and lower body subcutaneous adipose tissue depots. Participants were then followed prospectively for a median 8.1 years, during which 91 cardiovascular events occurred in 68 subjects.
The impetus for the adipose tissue imaging study was the researchers’ recognition that obesity is a heterogeneous disorder.
"Currently, we know that obesity is associated with incident cardiovascular disease at a general population level. However, body mass index alone is really an inadequate marker of risk among the obese. Many individuals with even high BMIs do not develop cardiovascular disease. Marked abdominal obesity is a stronger predictor of cardiovascular disease but still lacks the necessary specificity. So there’s really a clinical need for tools to differentiate obese individuals who will develop cardiovascular disease from those who will be free of cardiovascular disease for their lifetime," explained Dr. Neeland, a fellow in cardiovascular medicine at the University of Texas Southwestern Medical Center, Dallas.
In a multivariate analysis adjusted for age, sex, race, and the conventional cardiovascular risk factors, each 1–standard deviation increase in visceral adipose tissue was independently associated with a 24% increase in the risk of developing cardiovascular disease during follow-up. Dividing the study population into quartiles on the basis of their extent of visceral adipose tissue, the cumulative incidence of cardiovascular disease rose in stepwise fashion, with subjects in the lowest quartile having the least cardiovascular events and those in the top quartile having the most.
Having more lower body subcutaneous fat had the opposite effect. For every 1–standard deviation increase in the amount of fat at that location, the cardiovascular event risk dropped by 27%.
Participants’ amount of abdominal subcutaneous fat didn’t affect their cardiovascular event risk one way or another. Nor did BMI, waist circumference, waist-hip ratio, or the amount of liver fat on MRI show any significant association with cardiovascular disease risk.
"These results really underscore the biologic importance of body fat distribution with regard to cardiovascular disease risk in obesity and suggest a possible prognostic role for imaging-based assessment of body fat distribution in high-risk obese patients," according to Dr. Neeland.
One intriguing clinical implication of this study is that preventing accumulation of visceral adipose tissue may have benefit in terms of cardiovascular disease prevention even in the absence of meaningful weight loss. It’s possible that new drugs could be developed that lower cardiovascular risk in obese patients by changing their body fat distribution profile rather than lopping off pounds.
In the Dallas study, increased visceral abdominal tissue was consistently associated with a higher risk of cardiovascular disease across subgroups based upon age, race, sex, and BMI.
"Interestingly, those with increased visceral abdominal fat who were less than 40 years of age had greater risk for cardiovascular disease than [did] those over 40. This could suggest that visceral abdominal tissue has a greater impact on the young, in whom other cardiovascular risk factors have not yet accumulated over time," Dr. Neeland observed.
The cardiovascular event endpoint in the study was a composite of cardiovascular death, acute MI, stroke, heart failure, atrial fibrillation, or event-driven coronary or peripheral artery revascularization.
The Dallas Heart Study is funded by the Donald W. Reynolds Foundation. Dr. Neeland reported having no financial conflicts.
DALLAS – It’s not obesity per se that affects cardiovascular risk, it’s where that excess body fat is stored, according to the results of a novel adipose tissue–imaging study.
Excess visceral adipose tissue is independently associated with increased risk of developing cardiovascular disease. In contrast, increased lower body subcutaneous adipose tissue – that is, fat around the hips and a big butt – actually seems to protect against cardiovascular disease, Dr. Ian J. Neeland reported at the American Heart Association scientific sessions.
He presented an analysis of 972 obese participants in the Dallas Heart Study with a mean age of 44 years at enrollment and no baseline cardiovascular disease. All underwent dual-energy x-ray absorptiometry and MRI assessment of their body fat distribution, focusing on the visceral, abdominal subcutaneous, and lower body subcutaneous adipose tissue depots. Participants were then followed prospectively for a median 8.1 years, during which 91 cardiovascular events occurred in 68 subjects.
The impetus for the adipose tissue imaging study was the researchers’ recognition that obesity is a heterogeneous disorder.
"Currently, we know that obesity is associated with incident cardiovascular disease at a general population level. However, body mass index alone is really an inadequate marker of risk among the obese. Many individuals with even high BMIs do not develop cardiovascular disease. Marked abdominal obesity is a stronger predictor of cardiovascular disease but still lacks the necessary specificity. So there’s really a clinical need for tools to differentiate obese individuals who will develop cardiovascular disease from those who will be free of cardiovascular disease for their lifetime," explained Dr. Neeland, a fellow in cardiovascular medicine at the University of Texas Southwestern Medical Center, Dallas.
In a multivariate analysis adjusted for age, sex, race, and the conventional cardiovascular risk factors, each 1–standard deviation increase in visceral adipose tissue was independently associated with a 24% increase in the risk of developing cardiovascular disease during follow-up. Dividing the study population into quartiles on the basis of their extent of visceral adipose tissue, the cumulative incidence of cardiovascular disease rose in stepwise fashion, with subjects in the lowest quartile having the least cardiovascular events and those in the top quartile having the most.
Having more lower body subcutaneous fat had the opposite effect. For every 1–standard deviation increase in the amount of fat at that location, the cardiovascular event risk dropped by 27%.
Participants’ amount of abdominal subcutaneous fat didn’t affect their cardiovascular event risk one way or another. Nor did BMI, waist circumference, waist-hip ratio, or the amount of liver fat on MRI show any significant association with cardiovascular disease risk.
"These results really underscore the biologic importance of body fat distribution with regard to cardiovascular disease risk in obesity and suggest a possible prognostic role for imaging-based assessment of body fat distribution in high-risk obese patients," according to Dr. Neeland.
One intriguing clinical implication of this study is that preventing accumulation of visceral adipose tissue may have benefit in terms of cardiovascular disease prevention even in the absence of meaningful weight loss. It’s possible that new drugs could be developed that lower cardiovascular risk in obese patients by changing their body fat distribution profile rather than lopping off pounds.
In the Dallas study, increased visceral abdominal tissue was consistently associated with a higher risk of cardiovascular disease across subgroups based upon age, race, sex, and BMI.
"Interestingly, those with increased visceral abdominal fat who were less than 40 years of age had greater risk for cardiovascular disease than [did] those over 40. This could suggest that visceral abdominal tissue has a greater impact on the young, in whom other cardiovascular risk factors have not yet accumulated over time," Dr. Neeland observed.
The cardiovascular event endpoint in the study was a composite of cardiovascular death, acute MI, stroke, heart failure, atrial fibrillation, or event-driven coronary or peripheral artery revascularization.
The Dallas Heart Study is funded by the Donald W. Reynolds Foundation. Dr. Neeland reported having no financial conflicts.
AT THE AHA SCIENTIFIC SESSIONS

Antiphospholipid, thrombosis histories differently affect pregnancy antithrombotic needs
SNOWMASS, COLO. – Whether a woman with antiphospholipid antibodies meets diagnostic criteria for antiphospholipid syndrome makes a huge difference in her risk of pregnancy failure.
Having antiphospholipid antibodies alone confers only a modest increase in the risks of thrombosis and/or pregnancy mishap, Dr. Megan E.B. Clowse said at the Winter Rheumatology Symposium, sponsored by the American College of Rheumatology.
"You don’t have to jump all over these patients and get them worked up into a tizzy that they’re going to have blood clots or major pregnancy problems if they’ve never had them before," said Dr. Clowse, director of the Duke University Autoimmunity in Pregnancy registry in Durham, N.C.
The published experience indicates that women with antiphospholipid antibodies (aPL) but not antiphospholipid syndrome (APS) have roughly a 15% rate of pregnancy loss in their first pregnancy, not much different than the 11% rate in the general population. In contrast, women with untreated APS have up to a 90% pregnancy loss rate. With aspirin at 81 mg/day, this rate drops to 50%, and with dual therapy of low-dose aspirin plus either low-molecular-weight (LMW) or unfractionated heparin, the risk falls further to 25%, still twice that of the general population.

Thus, the distinction between aPL and APS is key. In addition to its implications for pregnancy outcome, it also guides the duration of anticoagulation following thrombosis. Anticoagulation needs to continue indefinitely in patients with APS because of their high risk of another clotting event. Indeed, patients with APS, if left untreated after a thrombotic event, have a 25% chance of another event within the next year, the rheumatologist noted.
"The diagnosis of APS is actually straightforward, but in patients referred to our lupus clinic from outside I see the term being used pretty fast and loose, and I think it’s somewhat inappropriate to do so. There are many patients with antiphospholipid antibodies who don’t have APS," she continued.
The current diagnostic criteria for APS – the so-called Sydney criteria (J. Thromb. Haemost. 2006;4:295-306) – require both laboratory and clinical findings. The laboratory criteria require a finding of lupus anticoagulant, medium- or high-titer IgG or IgM anticardiolipin antibodies, and/or medium- or high-titer anti-beta2-glycoprotein-1 antibody. The test results need to be positive on two occasions 12 weeks apart, although treatment for presumptive APS can start after tentative diagnosis based upon the first positive test.
To meet the vascular criteria for APS, a patient simply has to have had an arterial, venous, or small vessel thrombosis in any tissue or organ. The pregnancy criteria are more elaborate. To qualify, a woman must have had spontaneous abortions at less than 10 weeks’ gestation in at least three or more consecutive pregnancies, or a second- or third-trimester pregnancy loss of a normal fetus, or premature birth of a morphologically normal fetus before week 34 due to preeclampsia or placental insufficiency.
In women with full-blown APS, antibody titers matter quite a bit in terms of pregnancy outcome. In a study of 51 women with APS who were treated with LMW heparin and aspirin throughout 55 pregnancies, the 20 women with antibody titers greater than four times the upper limit of normal had a 35% rate of delivering an appropriately grown baby after 32 weeks’ gestation. The 35 antibody-positive women with titers less than four times the upper limit of normal had a 77% rate of normal delivery (Acta Obstet. Gynecol. Scand. 2011;90:1428-33).
In women with aPL only, the risk of pregnancy loss may be so low that aspirin isn’t protective. In an intriguing Italian study of 139 pregnancies in 114 women with aPL but not APS, the pregnancy loss rate in 104 pregnancies treated throughout with low-dose aspirin was 7.7%, while in 35 untreated pregnancies the rate was 2.9% (J. Rheumatol. 2013;40:425-9).
"The conclusion here is you can go ahead and use aspirin, but we don’t know that it’s doing a whole lot. Maybe we’re really just treating ourselves," Dr. Clowse mused.
Evidence from the PROMISSE trial, the largest-ever U.S. study of pregnancy loss in lupus patients, points to lupus anticoagulant as the main driver of pregnancy morbidity in patients with aPL. Thirty-nine percent of lupus anticoagulant–positive patients had adverse pregnancy outcomes, compared with just 3% of those without lupus anticoagulant. Unfortunately, treatment with heparin, aspirin, prednisone, or hydroxychloroquine didn’t mitigate the risk (Arthritis Rheum. 2012;64:2311-8).
While pregnancy loss is the biggest concern among most women with APS, it’s important to watch for maternal complications, including early severe preeclampsia, HELLP (hemolysis, elevated liver enzymes, and low platelet count) syndrome, and thrombotic events.
"It’s worth talking to the woman before pregnancy and explaining that, unfortunately, pregnancy loss is not necessarily the worst thing that can happen. Her health can also be at risk," Dr. Clowse observed.
In her own practice, everybody with APS goes on aspirin at 81 mg/day throughout pregnancy, even if there has been no prior pregnancy loss. With a history of three or more consecutive pregnancy losses, the treatment is low-dose LMW heparin plus low-dose aspirin. In women with a history of pregnancy loss that doesn’t reach that level, there is no good evidence to provide guidance as to whether to use low-dose LMW heparin plus aspirin or aspirin alone; however, she tends to be more aggressive in women with lupus anticoagulant or very high titers of the other aPLs. Women with a history of thrombosis, whether arterial or venous, are encouraged to remain on full-dose LMW heparin plus low-dose aspirin throughout pregnancy.
Dr. Clowse reported serving as a consultant to UCB.
SNOWMASS, COLO. – Whether a woman with antiphospholipid antibodies meets diagnostic criteria for antiphospholipid syndrome makes a huge difference in her risk of pregnancy failure.
Having antiphospholipid antibodies alone confers only a modest increase in the risks of thrombosis and/or pregnancy mishap, Dr. Megan E.B. Clowse said at the Winter Rheumatology Symposium, sponsored by the American College of Rheumatology.
"You don’t have to jump all over these patients and get them worked up into a tizzy that they’re going to have blood clots or major pregnancy problems if they’ve never had them before," said Dr. Clowse, director of the Duke University Autoimmunity in Pregnancy registry in Durham, N.C.
The published experience indicates that women with antiphospholipid antibodies (aPL) but not antiphospholipid syndrome (APS) have roughly a 15% rate of pregnancy loss in their first pregnancy, not much different than the 11% rate in the general population. In contrast, women with untreated APS have up to a 90% pregnancy loss rate. With aspirin at 81 mg/day, this rate drops to 50%, and with dual therapy of low-dose aspirin plus either low-molecular-weight (LMW) or unfractionated heparin, the risk falls further to 25%, still twice that of the general population.
Thus, the distinction between aPL and APS is key. In addition to its implications for pregnancy outcome, it also guides the duration of anticoagulation following thrombosis. Anticoagulation needs to continue indefinitely in patients with APS because of their high risk of another clotting event. Indeed, patients with APS, if left untreated after a thrombotic event, have a 25% chance of another event within the next year, the rheumatologist noted.
"The diagnosis of APS is actually straightforward, but in patients referred to our lupus clinic from outside I see the term being used pretty fast and loose, and I think it’s somewhat inappropriate to do so. There are many patients with antiphospholipid antibodies who don’t have APS," she continued.
The current diagnostic criteria for APS – the so-called Sydney criteria (J. Thromb. Haemost. 2006;4:295-306) – require both laboratory and clinical findings. The laboratory criteria require a finding of lupus anticoagulant, medium- or high-titer IgG or IgM anticardiolipin antibodies, and/or medium- or high-titer anti-beta2-glycoprotein-1 antibody. The test results need to be positive on two occasions 12 weeks apart, although treatment for presumptive APS can start after tentative diagnosis based upon the first positive test.
To meet the vascular criteria for APS, a patient simply has to have had an arterial, venous, or small vessel thrombosis in any tissue or organ. The pregnancy criteria are more elaborate. To qualify, a woman must have had spontaneous abortions at less than 10 weeks’ gestation in at least three or more consecutive pregnancies, or a second- or third-trimester pregnancy loss of a normal fetus, or premature birth of a morphologically normal fetus before week 34 due to preeclampsia or placental insufficiency.
In women with full-blown APS, antibody titers matter quite a bit in terms of pregnancy outcome. In a study of 51 women with APS who were treated with LMW heparin and aspirin throughout 55 pregnancies, the 20 women with antibody titers greater than four times the upper limit of normal had a 35% rate of delivering an appropriately grown baby after 32 weeks’ gestation. The 35 antibody-positive women with titers less than four times the upper limit of normal had a 77% rate of normal delivery (Acta Obstet. Gynecol. Scand. 2011;90:1428-33).
In women with aPL only, the risk of pregnancy loss may be so low that aspirin isn’t protective. In an intriguing Italian study of 139 pregnancies in 114 women with aPL but not APS, the pregnancy loss rate in 104 pregnancies treated throughout with low-dose aspirin was 7.7%, while in 35 untreated pregnancies the rate was 2.9% (J. Rheumatol. 2013;40:425-9).
"The conclusion here is you can go ahead and use aspirin, but we don’t know that it’s doing a whole lot. Maybe we’re really just treating ourselves," Dr. Clowse mused.
Evidence from the PROMISSE trial, the largest-ever U.S. study of pregnancy loss in lupus patients, points to lupus anticoagulant as the main driver of pregnancy morbidity in patients with aPL. Thirty-nine percent of lupus anticoagulant–positive patients had adverse pregnancy outcomes, compared with just 3% of those without lupus anticoagulant. Unfortunately, treatment with heparin, aspirin, prednisone, or hydroxychloroquine didn’t mitigate the risk (Arthritis Rheum. 2012;64:2311-8).
While pregnancy loss is the biggest concern among most women with APS, it’s important to watch for maternal complications, including early severe preeclampsia, HELLP (hemolysis, elevated liver enzymes, and low platelet count) syndrome, and thrombotic events.
"It’s worth talking to the woman before pregnancy and explaining that, unfortunately, pregnancy loss is not necessarily the worst thing that can happen. Her health can also be at risk," Dr. Clowse observed.
In her own practice, everybody with APS goes on aspirin at 81 mg/day throughout pregnancy, even if there has been no prior pregnancy loss. With a history of three or more consecutive pregnancy losses, the treatment is low-dose LMW heparin plus low-dose aspirin. In women with a history of pregnancy loss that doesn’t reach that level, there is no good evidence to provide guidance as to whether to use low-dose LMW heparin plus aspirin or aspirin alone; however, she tends to be more aggressive in women with lupus anticoagulant or very high titers of the other aPLs. Women with a history of thrombosis, whether arterial or venous, are encouraged to remain on full-dose LMW heparin plus low-dose aspirin throughout pregnancy.
Dr. Clowse reported serving as a consultant to UCB.
SNOWMASS, COLO. – Whether a woman with antiphospholipid antibodies meets diagnostic criteria for antiphospholipid syndrome makes a huge difference in her risk of pregnancy failure.
Having antiphospholipid antibodies alone confers only a modest increase in the risks of thrombosis and/or pregnancy mishap, Dr. Megan E.B. Clowse said at the Winter Rheumatology Symposium, sponsored by the American College of Rheumatology.
"You don’t have to jump all over these patients and get them worked up into a tizzy that they’re going to have blood clots or major pregnancy problems if they’ve never had them before," said Dr. Clowse, director of the Duke University Autoimmunity in Pregnancy registry in Durham, N.C.
The published experience indicates that women with antiphospholipid antibodies (aPL) but not antiphospholipid syndrome (APS) have roughly a 15% rate of pregnancy loss in their first pregnancy, not much different than the 11% rate in the general population. In contrast, women with untreated APS have up to a 90% pregnancy loss rate. With aspirin at 81 mg/day, this rate drops to 50%, and with dual therapy of low-dose aspirin plus either low-molecular-weight (LMW) or unfractionated heparin, the risk falls further to 25%, still twice that of the general population.
Thus, the distinction between aPL and APS is key. In addition to its implications for pregnancy outcome, it also guides the duration of anticoagulation following thrombosis. Anticoagulation needs to continue indefinitely in patients with APS because of their high risk of another clotting event. Indeed, patients with APS, if left untreated after a thrombotic event, have a 25% chance of another event within the next year, the rheumatologist noted.
"The diagnosis of APS is actually straightforward, but in patients referred to our lupus clinic from outside I see the term being used pretty fast and loose, and I think it’s somewhat inappropriate to do so. There are many patients with antiphospholipid antibodies who don’t have APS," she continued.
The current diagnostic criteria for APS – the so-called Sydney criteria (J. Thromb. Haemost. 2006;4:295-306) – require both laboratory and clinical findings. The laboratory criteria require a finding of lupus anticoagulant, medium- or high-titer IgG or IgM anticardiolipin antibodies, and/or medium- or high-titer anti-beta2-glycoprotein-1 antibody. The test results need to be positive on two occasions 12 weeks apart, although treatment for presumptive APS can start after tentative diagnosis based upon the first positive test.
To meet the vascular criteria for APS, a patient simply has to have had an arterial, venous, or small vessel thrombosis in any tissue or organ. The pregnancy criteria are more elaborate. To qualify, a woman must have had spontaneous abortions at less than 10 weeks’ gestation in at least three or more consecutive pregnancies, or a second- or third-trimester pregnancy loss of a normal fetus, or premature birth of a morphologically normal fetus before week 34 due to preeclampsia or placental insufficiency.
In women with full-blown APS, antibody titers matter quite a bit in terms of pregnancy outcome. In a study of 51 women with APS who were treated with LMW heparin and aspirin throughout 55 pregnancies, the 20 women with antibody titers greater than four times the upper limit of normal had a 35% rate of delivering an appropriately grown baby after 32 weeks’ gestation. The 35 antibody-positive women with titers less than four times the upper limit of normal had a 77% rate of normal delivery (Acta Obstet. Gynecol. Scand. 2011;90:1428-33).
In women with aPL only, the risk of pregnancy loss may be so low that aspirin isn’t protective. In an intriguing Italian study of 139 pregnancies in 114 women with aPL but not APS, the pregnancy loss rate in 104 pregnancies treated throughout with low-dose aspirin was 7.7%, while in 35 untreated pregnancies the rate was 2.9% (J. Rheumatol. 2013;40:425-9).
"The conclusion here is you can go ahead and use aspirin, but we don’t know that it’s doing a whole lot. Maybe we’re really just treating ourselves," Dr. Clowse mused.
Evidence from the PROMISSE trial, the largest-ever U.S. study of pregnancy loss in lupus patients, points to lupus anticoagulant as the main driver of pregnancy morbidity in patients with aPL. Thirty-nine percent of lupus anticoagulant–positive patients had adverse pregnancy outcomes, compared with just 3% of those without lupus anticoagulant. Unfortunately, treatment with heparin, aspirin, prednisone, or hydroxychloroquine didn’t mitigate the risk (Arthritis Rheum. 2012;64:2311-8).
While pregnancy loss is the biggest concern among most women with APS, it’s important to watch for maternal complications, including early severe preeclampsia, HELLP (hemolysis, elevated liver enzymes, and low platelet count) syndrome, and thrombotic events.
"It’s worth talking to the woman before pregnancy and explaining that, unfortunately, pregnancy loss is not necessarily the worst thing that can happen. Her health can also be at risk," Dr. Clowse observed.
In her own practice, everybody with APS goes on aspirin at 81 mg/day throughout pregnancy, even if there has been no prior pregnancy loss. With a history of three or more consecutive pregnancy losses, the treatment is low-dose LMW heparin plus low-dose aspirin. In women with a history of pregnancy loss that doesn’t reach that level, there is no good evidence to provide guidance as to whether to use low-dose LMW heparin plus aspirin or aspirin alone; however, she tends to be more aggressive in women with lupus anticoagulant or very high titers of the other aPLs. Women with a history of thrombosis, whether arterial or venous, are encouraged to remain on full-dose LMW heparin plus low-dose aspirin throughout pregnancy.
Dr. Clowse reported serving as a consultant to UCB.
EXPERT ANALYSIS FROM THE WINTER RHEUMATOLOGY SYMPOSIUM

Gut-joint connection promising in psoriatic arthritis
SNOWMASS, COLO. – Mounting circumstantial evidence points to perturbation of bacterial communities in the gut and skin as important environmental triggers for psoriasis and psoriatic arthritis.
A distinctive pattern of alterations in the skin microbiota, termed bacterial "cutaneotypes," has recently been documented in lesional and uninvolved skin of psoriasis patients. Similarly, psoriatic arthritis patients show decreased diversity of their intestinal bacterial community in a pattern similar to patients with inflammatory bowel disease, Dr. Jose U. Scher said at the Winter Rheumatology Symposium sponsored by the American College of Rheumatology.

The current working hypothesis of disease pathogenesis is that, in individuals genetically predisposed to psoriasis or psoriatic arthritis, this microbial dysbiosis at the cutaneous and gut levels provides an environmental trigger for overt expression of clinical disease.
"This dysbiosis is potentially relevant as a diagnostic and/or therapeutic target in psoriasis and psoriatic arthritis. For example, it may eventually become possible to assess the gut microbiota to predict which psoriasis patients will later develop psoriatic arthritis. And reconstituting the gut flora may turn out to have therapeutic benefit. But much more work is needed," explained Dr. Scher, director of the Microbiome Center for Rheumatology and Autoimmunity at New York University.
About 25%-30% of psoriasis patients develop inflammatory psoriatic arthritis, most often roughly 7 years after onset of their skin disease. Genetics clearly plays a role, as shown in a classic Danish twin registry study with more than 21,000 subjects. Fifty-five percent of the siblings of monozygotic twins with psoriatic arthritis had skin psoriasis, but only 10% of the siblings had psoriatic arthritis, as did 3.8% of siblings of dizygotic twins with psoriatic arthritis. The lesser concordance rate seen for psoriatic arthritis hinted at the importance of environmental factors in disease genesis (Ann. Rheum. Dis. 2008;67:1417-21).
Subclinical gut inflammation is common in psoriatic arthritis. In one early study, histologic evidence of mild or moderate gut mucosal inflammation was detected in 45% of a group of psoriatic arthritis patients, compared with 15% of patients with rheumatoid arthritis and 0% of controls (Scand. J. Rheumatol. 1997;26:92-8).
Also, psoriasis patients are at a roughly 3.5-fold increased risk of developing Crohn’s disease. Among patients with established psoriatic arthritis, this risk climbs to 6.5-fold greater than in nonpsoriatic controls (Ann. Rheum. Dis. 2013;72:1200-5).
In a soon-to-be-published study, Dr. Scher and his coworkers have taken the field a step further, employing high-throughput gene sequencing to analyze the gut bacterial communities of psoriatic arthritis patients and controls. These were all new-onset psoriatic arthritis patients who had never been exposed to systemic corticosteroids, biologic agents, or conventional disease-modifying antirheumatic drugs.
Compared with the stool samples of healthy controls, several major bacterial species were underrepresented or absent in the gut microbiota of psoriatic arthritis patients. These included Akkermansia, the most common mucolytic bacterium in healthy subjects. Intriguingly, Akkermansia counts are decreased 15-fold in Crohn’s disease and 92-fold in ulcerative colitis, according to the rheumatologist.
Other bacterial species markedly less abundant in the psoriatic arthritis patients’ gut flora were Ruminoccocus, Alistipes, and Roseburia. Like Akkermansia, these are mucin-degrading bacteria that promote a healthy gut environment, and they, too, are reduced in inflammatory bowel disease, Dr. Scher said.
He theorized that these disruptions of the bacterial ecosystem might arise from a course of antibiotics, a change in diet, or other insults. The result is activation of dendritic cells to produce interleukin-23, which triggers a proinflammatory cascade including tumor necrosis factor-alpha, interleukin-22, and antimicrobial peptides.
As shown by other investigators (Mucosal Immunol. 2013;6:666-77), these proinflammatory cytokines inhibit RANK ligand, which is the critical factor for differentiation of microfold cells in the gut. These microfold cells, or M cells, are specialized epithelial cells that transport antigens across the gut epithelium and play an important role in maintenance of an efficient immune response. It’s plausible that, when these M cells are defective, the resultant loss of tolerance and chronic inflammatory state can result in psoriatic arthritis, he explained.
Dr. Scher’s colleagues at New York University have used high-throughput gene sequencing to analyze the cutaneous microbiota of lesional and nonlesional skin in psoriasis patients, as well as skin samples from the same sites in healthy controls. The impetus for this study was a hypothesis that psoriasis might represent an inappropriate cutaneous immune response directed against offending bacteria in the skin microbiota.
Sure enough, the bacterial community present in psoriatic lesions displayed a markedly decreased diversity, compared with controls. This decreased diversity also was present, albeit to a lesser extent, in the psoriasis patients’ nonlesional skin. Both the lesional and nonlesional skin of psoriasis patients contained an increased abundance of Corynebacterium, Staphylococcus, and Streptococcus, compared with controls.
In addition, the skin microbiota could be classified into one of two characteristic patterns, which the investigators termed "cutaneotypes." Cutaneotype 1, which predominated in the skin of normal controls, contained an abundance of Proteobacteria. In contrast, cutaneotype 2, which was 3.5-fold more prevalent in psoriatic lesions than in controls, was enriched in Firmicutes and Actinobacteria. The psoriatic patients’ nonlesional skin contained a balance of cutaneotypes 1 and 2 (Microbiome 2013 Dec. 23 [doi:10.1186/2049-2618-1-31]).
Dr. Scher said that the next step in his own research is to learn whether the gut microbiota of psoriasis patients differs from that of psoriatic arthritis patients.
"That’s to me the most important piece of data. I think there’s a lot of work to do, and we’re doing it now, in prospective fashion. We’re following patients with psoriasis, and for those who later convert to psoriatic arthritis we’ll want to know if there’s alteration of their bacterial immunity, both in the gut and the skin," he explained.
Dr. Scher reported having no financial conflicts.
SNOWMASS, COLO. – Mounting circumstantial evidence points to perturbation of bacterial communities in the gut and skin as important environmental triggers for psoriasis and psoriatic arthritis.
A distinctive pattern of alterations in the skin microbiota, termed bacterial "cutaneotypes," has recently been documented in lesional and uninvolved skin of psoriasis patients. Similarly, psoriatic arthritis patients show decreased diversity of their intestinal bacterial community in a pattern similar to patients with inflammatory bowel disease, Dr. Jose U. Scher said at the Winter Rheumatology Symposium sponsored by the American College of Rheumatology.
The current working hypothesis of disease pathogenesis is that, in individuals genetically predisposed to psoriasis or psoriatic arthritis, this microbial dysbiosis at the cutaneous and gut levels provides an environmental trigger for overt expression of clinical disease.
"This dysbiosis is potentially relevant as a diagnostic and/or therapeutic target in psoriasis and psoriatic arthritis. For example, it may eventually become possible to assess the gut microbiota to predict which psoriasis patients will later develop psoriatic arthritis. And reconstituting the gut flora may turn out to have therapeutic benefit. But much more work is needed," explained Dr. Scher, director of the Microbiome Center for Rheumatology and Autoimmunity at New York University.
About 25%-30% of psoriasis patients develop inflammatory psoriatic arthritis, most often roughly 7 years after onset of their skin disease. Genetics clearly plays a role, as shown in a classic Danish twin registry study with more than 21,000 subjects. Fifty-five percent of the siblings of monozygotic twins with psoriatic arthritis had skin psoriasis, but only 10% of the siblings had psoriatic arthritis, as did 3.8% of siblings of dizygotic twins with psoriatic arthritis. The lesser concordance rate seen for psoriatic arthritis hinted at the importance of environmental factors in disease genesis (Ann. Rheum. Dis. 2008;67:1417-21).
Subclinical gut inflammation is common in psoriatic arthritis. In one early study, histologic evidence of mild or moderate gut mucosal inflammation was detected in 45% of a group of psoriatic arthritis patients, compared with 15% of patients with rheumatoid arthritis and 0% of controls (Scand. J. Rheumatol. 1997;26:92-8).
Also, psoriasis patients are at a roughly 3.5-fold increased risk of developing Crohn’s disease. Among patients with established psoriatic arthritis, this risk climbs to 6.5-fold greater than in nonpsoriatic controls (Ann. Rheum. Dis. 2013;72:1200-5).
In a soon-to-be-published study, Dr. Scher and his coworkers have taken the field a step further, employing high-throughput gene sequencing to analyze the gut bacterial communities of psoriatic arthritis patients and controls. These were all new-onset psoriatic arthritis patients who had never been exposed to systemic corticosteroids, biologic agents, or conventional disease-modifying antirheumatic drugs.
Compared with the stool samples of healthy controls, several major bacterial species were underrepresented or absent in the gut microbiota of psoriatic arthritis patients. These included Akkermansia, the most common mucolytic bacterium in healthy subjects. Intriguingly, Akkermansia counts are decreased 15-fold in Crohn’s disease and 92-fold in ulcerative colitis, according to the rheumatologist.
Other bacterial species markedly less abundant in the psoriatic arthritis patients’ gut flora were Ruminoccocus, Alistipes, and Roseburia. Like Akkermansia, these are mucin-degrading bacteria that promote a healthy gut environment, and they, too, are reduced in inflammatory bowel disease, Dr. Scher said.
He theorized that these disruptions of the bacterial ecosystem might arise from a course of antibiotics, a change in diet, or other insults. The result is activation of dendritic cells to produce interleukin-23, which triggers a proinflammatory cascade including tumor necrosis factor-alpha, interleukin-22, and antimicrobial peptides.
As shown by other investigators (Mucosal Immunol. 2013;6:666-77), these proinflammatory cytokines inhibit RANK ligand, which is the critical factor for differentiation of microfold cells in the gut. These microfold cells, or M cells, are specialized epithelial cells that transport antigens across the gut epithelium and play an important role in maintenance of an efficient immune response. It’s plausible that, when these M cells are defective, the resultant loss of tolerance and chronic inflammatory state can result in psoriatic arthritis, he explained.
Dr. Scher’s colleagues at New York University have used high-throughput gene sequencing to analyze the cutaneous microbiota of lesional and nonlesional skin in psoriasis patients, as well as skin samples from the same sites in healthy controls. The impetus for this study was a hypothesis that psoriasis might represent an inappropriate cutaneous immune response directed against offending bacteria in the skin microbiota.
Sure enough, the bacterial community present in psoriatic lesions displayed a markedly decreased diversity, compared with controls. This decreased diversity also was present, albeit to a lesser extent, in the psoriasis patients’ nonlesional skin. Both the lesional and nonlesional skin of psoriasis patients contained an increased abundance of Corynebacterium, Staphylococcus, and Streptococcus, compared with controls.
In addition, the skin microbiota could be classified into one of two characteristic patterns, which the investigators termed "cutaneotypes." Cutaneotype 1, which predominated in the skin of normal controls, contained an abundance of Proteobacteria. In contrast, cutaneotype 2, which was 3.5-fold more prevalent in psoriatic lesions than in controls, was enriched in Firmicutes and Actinobacteria. The psoriatic patients’ nonlesional skin contained a balance of cutaneotypes 1 and 2 (Microbiome 2013 Dec. 23 [doi:10.1186/2049-2618-1-31]).
Dr. Scher said that the next step in his own research is to learn whether the gut microbiota of psoriasis patients differs from that of psoriatic arthritis patients.
"That’s to me the most important piece of data. I think there’s a lot of work to do, and we’re doing it now, in prospective fashion. We’re following patients with psoriasis, and for those who later convert to psoriatic arthritis we’ll want to know if there’s alteration of their bacterial immunity, both in the gut and the skin," he explained.
Dr. Scher reported having no financial conflicts.
SNOWMASS, COLO. – Mounting circumstantial evidence points to perturbation of bacterial communities in the gut and skin as important environmental triggers for psoriasis and psoriatic arthritis.
A distinctive pattern of alterations in the skin microbiota, termed bacterial "cutaneotypes," has recently been documented in lesional and uninvolved skin of psoriasis patients. Similarly, psoriatic arthritis patients show decreased diversity of their intestinal bacterial community in a pattern similar to patients with inflammatory bowel disease, Dr. Jose U. Scher said at the Winter Rheumatology Symposium sponsored by the American College of Rheumatology.
The current working hypothesis of disease pathogenesis is that, in individuals genetically predisposed to psoriasis or psoriatic arthritis, this microbial dysbiosis at the cutaneous and gut levels provides an environmental trigger for overt expression of clinical disease.
"This dysbiosis is potentially relevant as a diagnostic and/or therapeutic target in psoriasis and psoriatic arthritis. For example, it may eventually become possible to assess the gut microbiota to predict which psoriasis patients will later develop psoriatic arthritis. And reconstituting the gut flora may turn out to have therapeutic benefit. But much more work is needed," explained Dr. Scher, director of the Microbiome Center for Rheumatology and Autoimmunity at New York University.
About 25%-30% of psoriasis patients develop inflammatory psoriatic arthritis, most often roughly 7 years after onset of their skin disease. Genetics clearly plays a role, as shown in a classic Danish twin registry study with more than 21,000 subjects. Fifty-five percent of the siblings of monozygotic twins with psoriatic arthritis had skin psoriasis, but only 10% of the siblings had psoriatic arthritis, as did 3.8% of siblings of dizygotic twins with psoriatic arthritis. The lesser concordance rate seen for psoriatic arthritis hinted at the importance of environmental factors in disease genesis (Ann. Rheum. Dis. 2008;67:1417-21).
Subclinical gut inflammation is common in psoriatic arthritis. In one early study, histologic evidence of mild or moderate gut mucosal inflammation was detected in 45% of a group of psoriatic arthritis patients, compared with 15% of patients with rheumatoid arthritis and 0% of controls (Scand. J. Rheumatol. 1997;26:92-8).
Also, psoriasis patients are at a roughly 3.5-fold increased risk of developing Crohn’s disease. Among patients with established psoriatic arthritis, this risk climbs to 6.5-fold greater than in nonpsoriatic controls (Ann. Rheum. Dis. 2013;72:1200-5).
In a soon-to-be-published study, Dr. Scher and his coworkers have taken the field a step further, employing high-throughput gene sequencing to analyze the gut bacterial communities of psoriatic arthritis patients and controls. These were all new-onset psoriatic arthritis patients who had never been exposed to systemic corticosteroids, biologic agents, or conventional disease-modifying antirheumatic drugs.
Compared with the stool samples of healthy controls, several major bacterial species were underrepresented or absent in the gut microbiota of psoriatic arthritis patients. These included Akkermansia, the most common mucolytic bacterium in healthy subjects. Intriguingly, Akkermansia counts are decreased 15-fold in Crohn’s disease and 92-fold in ulcerative colitis, according to the rheumatologist.
Other bacterial species markedly less abundant in the psoriatic arthritis patients’ gut flora were Ruminoccocus, Alistipes, and Roseburia. Like Akkermansia, these are mucin-degrading bacteria that promote a healthy gut environment, and they, too, are reduced in inflammatory bowel disease, Dr. Scher said.
He theorized that these disruptions of the bacterial ecosystem might arise from a course of antibiotics, a change in diet, or other insults. The result is activation of dendritic cells to produce interleukin-23, which triggers a proinflammatory cascade including tumor necrosis factor-alpha, interleukin-22, and antimicrobial peptides.
As shown by other investigators (Mucosal Immunol. 2013;6:666-77), these proinflammatory cytokines inhibit RANK ligand, which is the critical factor for differentiation of microfold cells in the gut. These microfold cells, or M cells, are specialized epithelial cells that transport antigens across the gut epithelium and play an important role in maintenance of an efficient immune response. It’s plausible that, when these M cells are defective, the resultant loss of tolerance and chronic inflammatory state can result in psoriatic arthritis, he explained.
Dr. Scher’s colleagues at New York University have used high-throughput gene sequencing to analyze the cutaneous microbiota of lesional and nonlesional skin in psoriasis patients, as well as skin samples from the same sites in healthy controls. The impetus for this study was a hypothesis that psoriasis might represent an inappropriate cutaneous immune response directed against offending bacteria in the skin microbiota.
Sure enough, the bacterial community present in psoriatic lesions displayed a markedly decreased diversity, compared with controls. This decreased diversity also was present, albeit to a lesser extent, in the psoriasis patients’ nonlesional skin. Both the lesional and nonlesional skin of psoriasis patients contained an increased abundance of Corynebacterium, Staphylococcus, and Streptococcus, compared with controls.
In addition, the skin microbiota could be classified into one of two characteristic patterns, which the investigators termed "cutaneotypes." Cutaneotype 1, which predominated in the skin of normal controls, contained an abundance of Proteobacteria. In contrast, cutaneotype 2, which was 3.5-fold more prevalent in psoriatic lesions than in controls, was enriched in Firmicutes and Actinobacteria. The psoriatic patients’ nonlesional skin contained a balance of cutaneotypes 1 and 2 (Microbiome 2013 Dec. 23 [doi:10.1186/2049-2618-1-31]).
Dr. Scher said that the next step in his own research is to learn whether the gut microbiota of psoriasis patients differs from that of psoriatic arthritis patients.
"That’s to me the most important piece of data. I think there’s a lot of work to do, and we’re doing it now, in prospective fashion. We’re following patients with psoriasis, and for those who later convert to psoriatic arthritis we’ll want to know if there’s alteration of their bacterial immunity, both in the gut and the skin," he explained.
Dr. Scher reported having no financial conflicts.
EXPERT ANALYSIS FROM THE WINTER RHEUMATOLOGY SYMPOSIUM

Latest heart failure guidelines break new ground
SNOWMASS, COLO. – The latest heart failure guidelines from the American College of Cardiology/American Heart Association place a new emphasis on aldosterone antagonists as a central aspect of the management of symptomatic or previously symptomatic heart failure with reduced ejection fraction – while underscoring important caveats to their use.
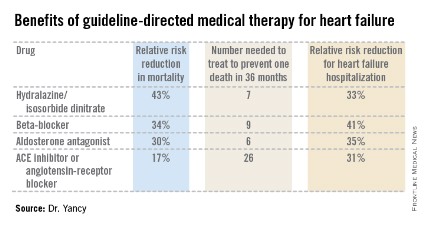
Aldosterone antagonist therapy earns the strongest possible designation in the guidelines: a Class I/Level of Evidence A recommendation. This is based on data from multiple randomized trials showing that, used appropriately, these agents result in a 30% relative risk reduction in mortality and a 35% reduction in the relative risk of heart failure hospitalization, with a number needed to treat for 36 months of just six patients to prevent one additional death. Those figures place the aldosterone antagonists on a par with the other Class I/A heart failure medications – beta-blockers, ACE inhibitors or angiotensin receptor blockers, and hydralazine/isosorbide dinitrate in African Americans – in terms of benefits (see chart).

"These data are quite striking," Dr. Clyde W. Yancy observed in presenting highlights of the 2013 ACC/AHA guidelines at the Annual Cardiovascular Conference at Snowmass.
"For many years, we’ve functioned in a space where we thought there’s not that much we can do for heart failure, and I would now argue stridently against that. You can see the incredibly low numbers needed to treat here. Only a handful of patients need to be exposed to these therapies to derive a significant benefit on mortality. These are data we should incorporate in our clinical practice without exclusion," declared Dr. Yancy, who chaired the heart failure guideline-writing committee.
The important caveat regarding the aldosterone antagonists is that they should be used only in patients with an estimated glomerular filtration rate greater than 30 mL/min per 1.73 m2 and a serum potassium level below 5.0 mEq/dL. Otherwise that Class I/A recommendation plummets to III/B, meaning the treatment is inappropriate and potentially harmful, continued Dr. Yancy, professor of medicine and of medical social sciences and chief of cardiology at Northwestern University, Chicago.
The guidelines emphasize the imperative to implement what has come to be termed guideline-directed medical therapy, known by the acronym GDMT. The panel found persuasive an analysis showing that heart failure patients with reduced ejection fraction who were on two of seven evidence-based, guideline-directed management interventions had an adjusted 38% reduction in 2-year mortality risk compared with those on none or one, while those on three interventions had a 62% decrease in the odds of mortality and patients on four or more had mortality reductions of about 70% (J. Am. Heart Assoc. 2012;1:16-26).
The seven interventions are beta-blockers, ACE inhibitors or ARBs, aldosterone antagonists, anticoagulation for atrial fibrillation, cardiac resynchronization therapy, implantable cardioverter-defibrillators, and heart failure education for eligible patients.
The guidelines advise strongly against the combined use of an ACE inhibitor and ARB. It’s an either/or treatment strategy. Studies indicate there is no additive benefit with the combination, only an increased risk of side effects.
An important innovation in the guidelines is the new prominence afforded to heart failure with preserved ejection fraction, known as HFpEF (pronounced heff-peff).

"What’s most different in the new heart failure guidelines is that we have uploaded HFpEF to the front page," said Dr. Yancy. "We want you to appreciate how important it is. We recognize that there’s no evidence-based intervention that changes its natural history; rather, the focus is on identification and treatment of the comorbidities. It’s important to emphasize that this is a novel way of thinking about heart failure for a very important iteration of that disease."
Among the other highlights of the guidelines is a clarification of the current role for biomarker-guided heart failure therapy. B-type natriuretic peptide (BNP) or N-terminal pro-BNP measurements are deemed useful in making the diagnosis of heart failure as well as in establishing prognosis. Serial measurements can be used to titrate GDMT to optimal doses. But there are as yet no data to show that using the biomarkers to titrate GDMT to higher doses improves mortality.
The 2013 ACC/AHA Guideline for the Management of Heart Failure was developed in collaboration with the American Academy of Family Physicians, the American College of Chest Physicians, the Heart Rhythm Society, and the International Society for Heart and Lung Transplantation (J. Am. Coll. Cardiol. 2013;62:e147-e239).
Dr. Yancy reported having no financial conflicts.
SNOWMASS, COLO. – The latest heart failure guidelines from the American College of Cardiology/American Heart Association place a new emphasis on aldosterone antagonists as a central aspect of the management of symptomatic or previously symptomatic heart failure with reduced ejection fraction – while underscoring important caveats to their use.
Aldosterone antagonist therapy earns the strongest possible designation in the guidelines: a Class I/Level of Evidence A recommendation. This is based on data from multiple randomized trials showing that, used appropriately, these agents result in a 30% relative risk reduction in mortality and a 35% reduction in the relative risk of heart failure hospitalization, with a number needed to treat for 36 months of just six patients to prevent one additional death. Those figures place the aldosterone antagonists on a par with the other Class I/A heart failure medications – beta-blockers, ACE inhibitors or angiotensin receptor blockers, and hydralazine/isosorbide dinitrate in African Americans – in terms of benefits (see chart).
"These data are quite striking," Dr. Clyde W. Yancy observed in presenting highlights of the 2013 ACC/AHA guidelines at the Annual Cardiovascular Conference at Snowmass.
"For many years, we’ve functioned in a space where we thought there’s not that much we can do for heart failure, and I would now argue stridently against that. You can see the incredibly low numbers needed to treat here. Only a handful of patients need to be exposed to these therapies to derive a significant benefit on mortality. These are data we should incorporate in our clinical practice without exclusion," declared Dr. Yancy, who chaired the heart failure guideline-writing committee.
The important caveat regarding the aldosterone antagonists is that they should be used only in patients with an estimated glomerular filtration rate greater than 30 mL/min per 1.73 m2 and a serum potassium level below 5.0 mEq/dL. Otherwise that Class I/A recommendation plummets to III/B, meaning the treatment is inappropriate and potentially harmful, continued Dr. Yancy, professor of medicine and of medical social sciences and chief of cardiology at Northwestern University, Chicago.
The guidelines emphasize the imperative to implement what has come to be termed guideline-directed medical therapy, known by the acronym GDMT. The panel found persuasive an analysis showing that heart failure patients with reduced ejection fraction who were on two of seven evidence-based, guideline-directed management interventions had an adjusted 38% reduction in 2-year mortality risk compared with those on none or one, while those on three interventions had a 62% decrease in the odds of mortality and patients on four or more had mortality reductions of about 70% (J. Am. Heart Assoc. 2012;1:16-26).
The seven interventions are beta-blockers, ACE inhibitors or ARBs, aldosterone antagonists, anticoagulation for atrial fibrillation, cardiac resynchronization therapy, implantable cardioverter-defibrillators, and heart failure education for eligible patients.
The guidelines advise strongly against the combined use of an ACE inhibitor and ARB. It’s an either/or treatment strategy. Studies indicate there is no additive benefit with the combination, only an increased risk of side effects.
An important innovation in the guidelines is the new prominence afforded to heart failure with preserved ejection fraction, known as HFpEF (pronounced heff-peff).
"What’s most different in the new heart failure guidelines is that we have uploaded HFpEF to the front page," said Dr. Yancy. "We want you to appreciate how important it is. We recognize that there’s no evidence-based intervention that changes its natural history; rather, the focus is on identification and treatment of the comorbidities. It’s important to emphasize that this is a novel way of thinking about heart failure for a very important iteration of that disease."
Among the other highlights of the guidelines is a clarification of the current role for biomarker-guided heart failure therapy. B-type natriuretic peptide (BNP) or N-terminal pro-BNP measurements are deemed useful in making the diagnosis of heart failure as well as in establishing prognosis. Serial measurements can be used to titrate GDMT to optimal doses. But there are as yet no data to show that using the biomarkers to titrate GDMT to higher doses improves mortality.
The 2013 ACC/AHA Guideline for the Management of Heart Failure was developed in collaboration with the American Academy of Family Physicians, the American College of Chest Physicians, the Heart Rhythm Society, and the International Society for Heart and Lung Transplantation (J. Am. Coll. Cardiol. 2013;62:e147-e239).
Dr. Yancy reported having no financial conflicts.
SNOWMASS, COLO. – The latest heart failure guidelines from the American College of Cardiology/American Heart Association place a new emphasis on aldosterone antagonists as a central aspect of the management of symptomatic or previously symptomatic heart failure with reduced ejection fraction – while underscoring important caveats to their use.
Aldosterone antagonist therapy earns the strongest possible designation in the guidelines: a Class I/Level of Evidence A recommendation. This is based on data from multiple randomized trials showing that, used appropriately, these agents result in a 30% relative risk reduction in mortality and a 35% reduction in the relative risk of heart failure hospitalization, with a number needed to treat for 36 months of just six patients to prevent one additional death. Those figures place the aldosterone antagonists on a par with the other Class I/A heart failure medications – beta-blockers, ACE inhibitors or angiotensin receptor blockers, and hydralazine/isosorbide dinitrate in African Americans – in terms of benefits (see chart).
"These data are quite striking," Dr. Clyde W. Yancy observed in presenting highlights of the 2013 ACC/AHA guidelines at the Annual Cardiovascular Conference at Snowmass.
"For many years, we’ve functioned in a space where we thought there’s not that much we can do for heart failure, and I would now argue stridently against that. You can see the incredibly low numbers needed to treat here. Only a handful of patients need to be exposed to these therapies to derive a significant benefit on mortality. These are data we should incorporate in our clinical practice without exclusion," declared Dr. Yancy, who chaired the heart failure guideline-writing committee.
The important caveat regarding the aldosterone antagonists is that they should be used only in patients with an estimated glomerular filtration rate greater than 30 mL/min per 1.73 m2 and a serum potassium level below 5.0 mEq/dL. Otherwise that Class I/A recommendation plummets to III/B, meaning the treatment is inappropriate and potentially harmful, continued Dr. Yancy, professor of medicine and of medical social sciences and chief of cardiology at Northwestern University, Chicago.
The guidelines emphasize the imperative to implement what has come to be termed guideline-directed medical therapy, known by the acronym GDMT. The panel found persuasive an analysis showing that heart failure patients with reduced ejection fraction who were on two of seven evidence-based, guideline-directed management interventions had an adjusted 38% reduction in 2-year mortality risk compared with those on none or one, while those on three interventions had a 62% decrease in the odds of mortality and patients on four or more had mortality reductions of about 70% (J. Am. Heart Assoc. 2012;1:16-26).
The seven interventions are beta-blockers, ACE inhibitors or ARBs, aldosterone antagonists, anticoagulation for atrial fibrillation, cardiac resynchronization therapy, implantable cardioverter-defibrillators, and heart failure education for eligible patients.
The guidelines advise strongly against the combined use of an ACE inhibitor and ARB. It’s an either/or treatment strategy. Studies indicate there is no additive benefit with the combination, only an increased risk of side effects.
An important innovation in the guidelines is the new prominence afforded to heart failure with preserved ejection fraction, known as HFpEF (pronounced heff-peff).
"What’s most different in the new heart failure guidelines is that we have uploaded HFpEF to the front page," said Dr. Yancy. "We want you to appreciate how important it is. We recognize that there’s no evidence-based intervention that changes its natural history; rather, the focus is on identification and treatment of the comorbidities. It’s important to emphasize that this is a novel way of thinking about heart failure for a very important iteration of that disease."
Among the other highlights of the guidelines is a clarification of the current role for biomarker-guided heart failure therapy. B-type natriuretic peptide (BNP) or N-terminal pro-BNP measurements are deemed useful in making the diagnosis of heart failure as well as in establishing prognosis. Serial measurements can be used to titrate GDMT to optimal doses. But there are as yet no data to show that using the biomarkers to titrate GDMT to higher doses improves mortality.
The 2013 ACC/AHA Guideline for the Management of Heart Failure was developed in collaboration with the American Academy of Family Physicians, the American College of Chest Physicians, the Heart Rhythm Society, and the International Society for Heart and Lung Transplantation (J. Am. Coll. Cardiol. 2013;62:e147-e239).
Dr. Yancy reported having no financial conflicts.
EXPERT ANALYSIS FROM THE CARDIOVASCULAR CONFERENCE AT SNOWMASS
Photodynamic therapy: ‘Often not worth the trouble’
WAIKOLOA, HAWAII – Just because a dermatologist has photodynamic therapy equipment in the office doesn’t mean it should be applied to every skin condition that comes through the door, Dr. Jerome M. Garden cautioned at the Hawaii Dermatology Seminar sponsored by the Global Academy for Medical Education/Skin Disease Education Foundation.
"Used selectively, I think PDT can be truly worthwhile in some of our patients. But we run into problems when we decide it’s a cure-all for everything. Just because it’s available does not always make it the best choice around," said Dr. Garden, who is director of the Physicians Laser and Dermatology Institute as well as a professor of clinical dermatology and biomedical engineering at Northwestern University in Chicago.
Looking through the literature, it’s quickly apparent that PDT has been used to treat a bewildering array of dermatologic disorders, in most cases with less than stellar results.

"In my practice, I’m using PDT to treat just two things: actinic keratoses and actinic cheilitis, which is a close cousin. Why am I not using it to treat more disease processes? Because it has to be worth it. PDT is not simple to do. It takes a lot of your time and it costs you money. Insurance doesn’t necessarily help you with this. Either the patient’s insurance will reimburse you at an incredibly low rate, where it’s basically costing you money to do it, or you go outside of the insurance – and PDT is an expensive procedure," he noted.
The substantial time expenditure involved in PDT stems from the need to use microdermabrasion or another method of skin preparation to help the topical photosensitizing agent penetrate better. This is followed by an incubation time of 1-3 hours as the photosensitizer finds its target, and then light therapy to create the reactive oxygen species, which kills the targeted cells. The duration of light therapy is source dependent; blue light, for example, must be applied for 15-20 minutes.
PDT has other shortcomings in addition to the cost and time involved. It can be painful and entails several days of down time because of scaling and crusting. Plus, multiple treatment sessions are usually required, the dermatologist continued.
The 2012 American Society for Dermatologic Surgery member survey found that dermatologic surgeons performed roughly 205,000 PDT procedures during the year. The bulk was for actinic keratoses, acne, and rosacea.
"I didn’t even know until I saw this list that anybody treats rosacea with PDT," noted Dr. Garden. "A lot of people out there who are doing PDT use it for many more things than I do. But I’m just telling you what I do."
"I’ve tried it for acne. It helps, but depending on the light source, it can be a painful procedure. There’s a lot of desquamation afterward, and you have to go through it a few times. So you have to have a highly motivated patient – and even then, it doesn’t work all the time," he said.
Dr. Garden cited a Danish split-face study of pulsed-dye laser-assisted PDT vs. pulsed-dye laser therapy alone. Twelve weeks after completing three treatment sessions, the PDT side showed an 80% reduction in inflammatory acne lesions, compared with a 67% drop with pulsed-dye laser, and a 53% decrease in noninflammatory lesions compared to a 42% reduction with laser alone (J. Am. Acad. Dermatol. 2008; 58:387-94).
"Even without the topical photosensitizer, patients did pretty well," he commented.
As for PDT in cutaneous malignancies, Dr. Garden highlighted a recent literature review by dermatologists at the University of South Florida, Tampa, which concluded that the therapy is equivalent or superior to cryosurgery for actinic keratoses. The investigators also deemed PDT suitable for Bowen’s disease lesions provided they are large, widespread, or on difficult to treat areas, as well as for squamous cell carcinomas, but only when surgery is contraindicated. PDT may also provide better cosmetic outcomes than surgery or cryosurgery for superficial basal cell carcinomas (Dermatol. Surg. 2013;39:1733-44).
Dr. Garden called PDT his current first-line treatment for actinic cheilitis.
"I used to use the CO2 laser exclusively. It works very well, much better than PDT. But when I’d strip off the top layer of skin with the CO2 laser, patients would end up with an open wound that took a long time to heal. That’s hard for the patient to tolerate. And occasionally we’d see fibrosis of the lip. You don’t see that with PDT, although with PDT you usually need to do two or three treatments, and the area is red and swollen for 2-4 days. I like PDT. It’s my go-to therapy. When it fails, I turn on the CO2 laser," he said.
In treating actinic keratoses, he reserves PDT for patients with numerous lesions over a large field.
"It does work, but it’s a lot of effort. So if you’re just going after a handful of [actinic keratoses] do you need PDT? Probably not," Dr. Garden said.
Ending on an encouraging note, the dermatologist pointed to the ongoing substantial research commitment to PDT as very promising. Finding more specific photosensitizers is a priority. And ablative fractional laser-assisted delivery of the standard photosensitizer methyl aminolevulinic acid appears to be "an exciting development," in Dr. Garden’s view, although to date the work is limited to animal studies.
Dr. Garden reported having financial relationships with Alma, Candela & Syneron, and Palomar/Cynosure.
The SDEF and this news organization are owned by the same parent company.
WAIKOLOA, HAWAII – Just because a dermatologist has photodynamic therapy equipment in the office doesn’t mean it should be applied to every skin condition that comes through the door, Dr. Jerome M. Garden cautioned at the Hawaii Dermatology Seminar sponsored by the Global Academy for Medical Education/Skin Disease Education Foundation.
"Used selectively, I think PDT can be truly worthwhile in some of our patients. But we run into problems when we decide it’s a cure-all for everything. Just because it’s available does not always make it the best choice around," said Dr. Garden, who is director of the Physicians Laser and Dermatology Institute as well as a professor of clinical dermatology and biomedical engineering at Northwestern University in Chicago.
Looking through the literature, it’s quickly apparent that PDT has been used to treat a bewildering array of dermatologic disorders, in most cases with less than stellar results.
"In my practice, I’m using PDT to treat just two things: actinic keratoses and actinic cheilitis, which is a close cousin. Why am I not using it to treat more disease processes? Because it has to be worth it. PDT is not simple to do. It takes a lot of your time and it costs you money. Insurance doesn’t necessarily help you with this. Either the patient’s insurance will reimburse you at an incredibly low rate, where it’s basically costing you money to do it, or you go outside of the insurance – and PDT is an expensive procedure," he noted.
The substantial time expenditure involved in PDT stems from the need to use microdermabrasion or another method of skin preparation to help the topical photosensitizing agent penetrate better. This is followed by an incubation time of 1-3 hours as the photosensitizer finds its target, and then light therapy to create the reactive oxygen species, which kills the targeted cells. The duration of light therapy is source dependent; blue light, for example, must be applied for 15-20 minutes.
PDT has other shortcomings in addition to the cost and time involved. It can be painful and entails several days of down time because of scaling and crusting. Plus, multiple treatment sessions are usually required, the dermatologist continued.
The 2012 American Society for Dermatologic Surgery member survey found that dermatologic surgeons performed roughly 205,000 PDT procedures during the year. The bulk was for actinic keratoses, acne, and rosacea.
"I didn’t even know until I saw this list that anybody treats rosacea with PDT," noted Dr. Garden. "A lot of people out there who are doing PDT use it for many more things than I do. But I’m just telling you what I do."
"I’ve tried it for acne. It helps, but depending on the light source, it can be a painful procedure. There’s a lot of desquamation afterward, and you have to go through it a few times. So you have to have a highly motivated patient – and even then, it doesn’t work all the time," he said.
Dr. Garden cited a Danish split-face study of pulsed-dye laser-assisted PDT vs. pulsed-dye laser therapy alone. Twelve weeks after completing three treatment sessions, the PDT side showed an 80% reduction in inflammatory acne lesions, compared with a 67% drop with pulsed-dye laser, and a 53% decrease in noninflammatory lesions compared to a 42% reduction with laser alone (J. Am. Acad. Dermatol. 2008; 58:387-94).
"Even without the topical photosensitizer, patients did pretty well," he commented.
As for PDT in cutaneous malignancies, Dr. Garden highlighted a recent literature review by dermatologists at the University of South Florida, Tampa, which concluded that the therapy is equivalent or superior to cryosurgery for actinic keratoses. The investigators also deemed PDT suitable for Bowen’s disease lesions provided they are large, widespread, or on difficult to treat areas, as well as for squamous cell carcinomas, but only when surgery is contraindicated. PDT may also provide better cosmetic outcomes than surgery or cryosurgery for superficial basal cell carcinomas (Dermatol. Surg. 2013;39:1733-44).
Dr. Garden called PDT his current first-line treatment for actinic cheilitis.
"I used to use the CO2 laser exclusively. It works very well, much better than PDT. But when I’d strip off the top layer of skin with the CO2 laser, patients would end up with an open wound that took a long time to heal. That’s hard for the patient to tolerate. And occasionally we’d see fibrosis of the lip. You don’t see that with PDT, although with PDT you usually need to do two or three treatments, and the area is red and swollen for 2-4 days. I like PDT. It’s my go-to therapy. When it fails, I turn on the CO2 laser," he said.
In treating actinic keratoses, he reserves PDT for patients with numerous lesions over a large field.
"It does work, but it’s a lot of effort. So if you’re just going after a handful of [actinic keratoses] do you need PDT? Probably not," Dr. Garden said.
Ending on an encouraging note, the dermatologist pointed to the ongoing substantial research commitment to PDT as very promising. Finding more specific photosensitizers is a priority. And ablative fractional laser-assisted delivery of the standard photosensitizer methyl aminolevulinic acid appears to be "an exciting development," in Dr. Garden’s view, although to date the work is limited to animal studies.
Dr. Garden reported having financial relationships with Alma, Candela & Syneron, and Palomar/Cynosure.
The SDEF and this news organization are owned by the same parent company.
WAIKOLOA, HAWAII – Just because a dermatologist has photodynamic therapy equipment in the office doesn’t mean it should be applied to every skin condition that comes through the door, Dr. Jerome M. Garden cautioned at the Hawaii Dermatology Seminar sponsored by the Global Academy for Medical Education/Skin Disease Education Foundation.
"Used selectively, I think PDT can be truly worthwhile in some of our patients. But we run into problems when we decide it’s a cure-all for everything. Just because it’s available does not always make it the best choice around," said Dr. Garden, who is director of the Physicians Laser and Dermatology Institute as well as a professor of clinical dermatology and biomedical engineering at Northwestern University in Chicago.
Looking through the literature, it’s quickly apparent that PDT has been used to treat a bewildering array of dermatologic disorders, in most cases with less than stellar results.
"In my practice, I’m using PDT to treat just two things: actinic keratoses and actinic cheilitis, which is a close cousin. Why am I not using it to treat more disease processes? Because it has to be worth it. PDT is not simple to do. It takes a lot of your time and it costs you money. Insurance doesn’t necessarily help you with this. Either the patient’s insurance will reimburse you at an incredibly low rate, where it’s basically costing you money to do it, or you go outside of the insurance – and PDT is an expensive procedure," he noted.
The substantial time expenditure involved in PDT stems from the need to use microdermabrasion or another method of skin preparation to help the topical photosensitizing agent penetrate better. This is followed by an incubation time of 1-3 hours as the photosensitizer finds its target, and then light therapy to create the reactive oxygen species, which kills the targeted cells. The duration of light therapy is source dependent; blue light, for example, must be applied for 15-20 minutes.
PDT has other shortcomings in addition to the cost and time involved. It can be painful and entails several days of down time because of scaling and crusting. Plus, multiple treatment sessions are usually required, the dermatologist continued.
The 2012 American Society for Dermatologic Surgery member survey found that dermatologic surgeons performed roughly 205,000 PDT procedures during the year. The bulk was for actinic keratoses, acne, and rosacea.
"I didn’t even know until I saw this list that anybody treats rosacea with PDT," noted Dr. Garden. "A lot of people out there who are doing PDT use it for many more things than I do. But I’m just telling you what I do."
"I’ve tried it for acne. It helps, but depending on the light source, it can be a painful procedure. There’s a lot of desquamation afterward, and you have to go through it a few times. So you have to have a highly motivated patient – and even then, it doesn’t work all the time," he said.
Dr. Garden cited a Danish split-face study of pulsed-dye laser-assisted PDT vs. pulsed-dye laser therapy alone. Twelve weeks after completing three treatment sessions, the PDT side showed an 80% reduction in inflammatory acne lesions, compared with a 67% drop with pulsed-dye laser, and a 53% decrease in noninflammatory lesions compared to a 42% reduction with laser alone (J. Am. Acad. Dermatol. 2008; 58:387-94).
"Even without the topical photosensitizer, patients did pretty well," he commented.
As for PDT in cutaneous malignancies, Dr. Garden highlighted a recent literature review by dermatologists at the University of South Florida, Tampa, which concluded that the therapy is equivalent or superior to cryosurgery for actinic keratoses. The investigators also deemed PDT suitable for Bowen’s disease lesions provided they are large, widespread, or on difficult to treat areas, as well as for squamous cell carcinomas, but only when surgery is contraindicated. PDT may also provide better cosmetic outcomes than surgery or cryosurgery for superficial basal cell carcinomas (Dermatol. Surg. 2013;39:1733-44).
Dr. Garden called PDT his current first-line treatment for actinic cheilitis.
"I used to use the CO2 laser exclusively. It works very well, much better than PDT. But when I’d strip off the top layer of skin with the CO2 laser, patients would end up with an open wound that took a long time to heal. That’s hard for the patient to tolerate. And occasionally we’d see fibrosis of the lip. You don’t see that with PDT, although with PDT you usually need to do two or three treatments, and the area is red and swollen for 2-4 days. I like PDT. It’s my go-to therapy. When it fails, I turn on the CO2 laser," he said.
In treating actinic keratoses, he reserves PDT for patients with numerous lesions over a large field.
"It does work, but it’s a lot of effort. So if you’re just going after a handful of [actinic keratoses] do you need PDT? Probably not," Dr. Garden said.
Ending on an encouraging note, the dermatologist pointed to the ongoing substantial research commitment to PDT as very promising. Finding more specific photosensitizers is a priority. And ablative fractional laser-assisted delivery of the standard photosensitizer methyl aminolevulinic acid appears to be "an exciting development," in Dr. Garden’s view, although to date the work is limited to animal studies.
Dr. Garden reported having financial relationships with Alma, Candela & Syneron, and Palomar/Cynosure.
The SDEF and this news organization are owned by the same parent company.
EXPERT ANALYSIS FROM SDEF HAWAII DERMATOLOGY SEMINAR

Don’t overlook venerable benzoyl peroxide for acne
WAIKOLOA, HAWAII – Benzoyl peroxide has stood the test of time amid a diverse field of acne therapies, according to Dr. Linda Stein Gold. She spoke with us in a video interview about why benzoyl peroxide "should still play a central role in the treatment of acne."
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
WAIKOLOA, HAWAII – Benzoyl peroxide has stood the test of time amid a diverse field of acne therapies, according to Dr. Linda Stein Gold. She spoke with us in a video interview about why benzoyl peroxide "should still play a central role in the treatment of acne."
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
WAIKOLOA, HAWAII – Benzoyl peroxide has stood the test of time amid a diverse field of acne therapies, according to Dr. Linda Stein Gold. She spoke with us in a video interview about why benzoyl peroxide "should still play a central role in the treatment of acne."
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
EXPERT ANALYSIS FROM SDEF HAWAII DERMATOLOGY SYMPOSIUM
Novel topical rosacea drug sails through phase III
WAIKOLOA, HAWAII – Ivermectin 1% cream for the treatment of papulopustular rosacea convincingly hit all of its primary efficacy and safety endpoints in two pivotal phase III clinical trials.
The studies included 1,371 subjects randomized in a double-blind fashion 2:1 to 3 months of once-daily topical invermectin 1% or vehicle. These were patients with significant papulopustular rosacea (PPR): In one trial, 75% of patients were rated at baseline as having moderate disease and 25% severe, while in the other study the percentages were 80% and 20%, respectively, Dr. Hilary E. Baldwin reported at the SDEF Hawaii Dermatology Seminar sponsored by the Global Academy for Medical Education/Skin Disease Education Foundation.
The two prespecified coprimary endpoints were treatment success as defined by an Investigator Global Assessment rating of clear or almost clear at 12 weeks, along with reduction in inflammatory lesions from baseline through 12 weeks.

Roughly 40% of topical ivermectin–treated patients met the clear or almost-clear treatment success standard, a rate two- to fourfold greater than in controls in the two trials. The difference between the active treatment group and controls became statistically significant as early as week 4.
In addition, the inflammatory lesion count dropped by an average of more than 20 lesions at 12 weeks in the topical ivermectin–treated patients, an effect more than one-third larger than documented in controls. Here again, the benefit was significant by week 4, according to Dr. Baldwin, a dermatologist at SUNY Downstate Medical Center, Brooklyn.
The incidence of treatment-related dermatologic adverse events was 2.5% in patients on topical ivermectin, compared with 6.3% in controls.
Moreover, in a related single-blind, 9-month safety study involving 910 patients on ivermectin 1% cream once daily and 481 on topical azelaic acid 15% twice daily, the rate of treatment-related dermatologic adverse events was 1.3% in the ivermectin arm, compared with 5.3% with azelaic acid.
Stepping back from these compelling clinical trial data, Dr. Baldwin observed that the exact mechanism of benefit for topical invermectin in PPR has yet to be determined. The medication is certainly acaricidal and is known to kill the demodex mites that reside in the pilosebaceous units of patients with PPR. But it’s tough to think of demodex mites as causative in rosacea because they are also present in the pilosebaceous units of individuals without rosacea.
The latest thinking regarding the pathogenesis of rosacea is that this common chronic inflammatory skin disease is not caused by demodex mites, Propionibacterium acnes, or any other pathogen, she explained. In the current concept, cathelicidin proteins that are present in the epidermis as part of the vanguard of the innate immune system play a key role. When these proteins detect a foreign invader on the skin – bacterial, viral, or fungal – they release toxic enzymes, including cathelicidin LL-37, which kill the offending organism. High levels of LL-37 are proinflammatory, angiogenic, and activate the acquired immune system, effects that would explain the chronic skin redness and telangiectasias of rosacea. The trouble is, demodex is not a foreign invader.
"The innate immune system is not supposed to be triggered by demodex or P. acnes. They’re supposed to be in the follicle. They live there," Dr. Baldwin said.
Why the innate immune system of patients with PPR is apparently alerted by demodex, part of the normal fauna, requires further study, she added.
She anticipates that the full results of the recently completed pivotal phase III trials, sponsored by Galderma, will be published later this year.
SDEF and this news organization are owned by the same parent company.
Dr. Baldwin is on the advisory boards and/or speakers bureaus of Galderma and 10 other pharmaceutical and cosmetics companies.
WAIKOLOA, HAWAII – Ivermectin 1% cream for the treatment of papulopustular rosacea convincingly hit all of its primary efficacy and safety endpoints in two pivotal phase III clinical trials.
The studies included 1,371 subjects randomized in a double-blind fashion 2:1 to 3 months of once-daily topical invermectin 1% or vehicle. These were patients with significant papulopustular rosacea (PPR): In one trial, 75% of patients were rated at baseline as having moderate disease and 25% severe, while in the other study the percentages were 80% and 20%, respectively, Dr. Hilary E. Baldwin reported at the SDEF Hawaii Dermatology Seminar sponsored by the Global Academy for Medical Education/Skin Disease Education Foundation.
The two prespecified coprimary endpoints were treatment success as defined by an Investigator Global Assessment rating of clear or almost clear at 12 weeks, along with reduction in inflammatory lesions from baseline through 12 weeks.
Roughly 40% of topical ivermectin–treated patients met the clear or almost-clear treatment success standard, a rate two- to fourfold greater than in controls in the two trials. The difference between the active treatment group and controls became statistically significant as early as week 4.
In addition, the inflammatory lesion count dropped by an average of more than 20 lesions at 12 weeks in the topical ivermectin–treated patients, an effect more than one-third larger than documented in controls. Here again, the benefit was significant by week 4, according to Dr. Baldwin, a dermatologist at SUNY Downstate Medical Center, Brooklyn.
The incidence of treatment-related dermatologic adverse events was 2.5% in patients on topical ivermectin, compared with 6.3% in controls.
Moreover, in a related single-blind, 9-month safety study involving 910 patients on ivermectin 1% cream once daily and 481 on topical azelaic acid 15% twice daily, the rate of treatment-related dermatologic adverse events was 1.3% in the ivermectin arm, compared with 5.3% with azelaic acid.
Stepping back from these compelling clinical trial data, Dr. Baldwin observed that the exact mechanism of benefit for topical invermectin in PPR has yet to be determined. The medication is certainly acaricidal and is known to kill the demodex mites that reside in the pilosebaceous units of patients with PPR. But it’s tough to think of demodex mites as causative in rosacea because they are also present in the pilosebaceous units of individuals without rosacea.
The latest thinking regarding the pathogenesis of rosacea is that this common chronic inflammatory skin disease is not caused by demodex mites, Propionibacterium acnes, or any other pathogen, she explained. In the current concept, cathelicidin proteins that are present in the epidermis as part of the vanguard of the innate immune system play a key role. When these proteins detect a foreign invader on the skin – bacterial, viral, or fungal – they release toxic enzymes, including cathelicidin LL-37, which kill the offending organism. High levels of LL-37 are proinflammatory, angiogenic, and activate the acquired immune system, effects that would explain the chronic skin redness and telangiectasias of rosacea. The trouble is, demodex is not a foreign invader.
"The innate immune system is not supposed to be triggered by demodex or P. acnes. They’re supposed to be in the follicle. They live there," Dr. Baldwin said.
Why the innate immune system of patients with PPR is apparently alerted by demodex, part of the normal fauna, requires further study, she added.
She anticipates that the full results of the recently completed pivotal phase III trials, sponsored by Galderma, will be published later this year.
SDEF and this news organization are owned by the same parent company.
Dr. Baldwin is on the advisory boards and/or speakers bureaus of Galderma and 10 other pharmaceutical and cosmetics companies.
WAIKOLOA, HAWAII – Ivermectin 1% cream for the treatment of papulopustular rosacea convincingly hit all of its primary efficacy and safety endpoints in two pivotal phase III clinical trials.
The studies included 1,371 subjects randomized in a double-blind fashion 2:1 to 3 months of once-daily topical invermectin 1% or vehicle. These were patients with significant papulopustular rosacea (PPR): In one trial, 75% of patients were rated at baseline as having moderate disease and 25% severe, while in the other study the percentages were 80% and 20%, respectively, Dr. Hilary E. Baldwin reported at the SDEF Hawaii Dermatology Seminar sponsored by the Global Academy for Medical Education/Skin Disease Education Foundation.
The two prespecified coprimary endpoints were treatment success as defined by an Investigator Global Assessment rating of clear or almost clear at 12 weeks, along with reduction in inflammatory lesions from baseline through 12 weeks.
Roughly 40% of topical ivermectin–treated patients met the clear or almost-clear treatment success standard, a rate two- to fourfold greater than in controls in the two trials. The difference between the active treatment group and controls became statistically significant as early as week 4.
In addition, the inflammatory lesion count dropped by an average of more than 20 lesions at 12 weeks in the topical ivermectin–treated patients, an effect more than one-third larger than documented in controls. Here again, the benefit was significant by week 4, according to Dr. Baldwin, a dermatologist at SUNY Downstate Medical Center, Brooklyn.
The incidence of treatment-related dermatologic adverse events was 2.5% in patients on topical ivermectin, compared with 6.3% in controls.
Moreover, in a related single-blind, 9-month safety study involving 910 patients on ivermectin 1% cream once daily and 481 on topical azelaic acid 15% twice daily, the rate of treatment-related dermatologic adverse events was 1.3% in the ivermectin arm, compared with 5.3% with azelaic acid.
Stepping back from these compelling clinical trial data, Dr. Baldwin observed that the exact mechanism of benefit for topical invermectin in PPR has yet to be determined. The medication is certainly acaricidal and is known to kill the demodex mites that reside in the pilosebaceous units of patients with PPR. But it’s tough to think of demodex mites as causative in rosacea because they are also present in the pilosebaceous units of individuals without rosacea.
The latest thinking regarding the pathogenesis of rosacea is that this common chronic inflammatory skin disease is not caused by demodex mites, Propionibacterium acnes, or any other pathogen, she explained. In the current concept, cathelicidin proteins that are present in the epidermis as part of the vanguard of the innate immune system play a key role. When these proteins detect a foreign invader on the skin – bacterial, viral, or fungal – they release toxic enzymes, including cathelicidin LL-37, which kill the offending organism. High levels of LL-37 are proinflammatory, angiogenic, and activate the acquired immune system, effects that would explain the chronic skin redness and telangiectasias of rosacea. The trouble is, demodex is not a foreign invader.
"The innate immune system is not supposed to be triggered by demodex or P. acnes. They’re supposed to be in the follicle. They live there," Dr. Baldwin said.
Why the innate immune system of patients with PPR is apparently alerted by demodex, part of the normal fauna, requires further study, she added.
She anticipates that the full results of the recently completed pivotal phase III trials, sponsored by Galderma, will be published later this year.
SDEF and this news organization are owned by the same parent company.
Dr. Baldwin is on the advisory boards and/or speakers bureaus of Galderma and 10 other pharmaceutical and cosmetics companies.
EXPERT ANALYSIS FROM SDEF HAWAII DERMATOLOGY SEMINAR

Beta-blockers lose luster for hypertension therapy
SNOWMASS, COLO. – Beta-blockers have lost their decades-long status as first-line therapy for hypertension.
"Generally, I think there is a consensus that beta-blockers are a poor choice for uncomplicated hypertension," Dr. Clive Rosendorff observed at the Annual Cardiovascular Conference at Snowmass.

Abundant evidence indicates that beta-blockers provide less protection against stroke, MI, and overall mortality than other classes of antihypertensive agents. They offer less renal protection than ramipril and achieve less regression of left ventricular hypertrophy than other antihypertensive drugs.
Moreover, as was shown in the Conduit Artery Function Evaluation (CAFE) study, beta-blockers have what has been termed "pseudo-antihypertensive efficacy": that is, they fail to reduce central aortic blood pressure to the same extent they lower systolic blood pressure, which may explain why they are less cardioprotective than other antihypertensive drugs. They also are associated with an increase in insulin resistance, reduced exercise tolerance, weight gain, and a high rate of withdrawal because of side effects, said Dr. Rosendorff, professor of medicine at Mount Sinai School of Medicine, New York.
Dr. Rosdendorff chaired the joint American College of Cardiology/American Heart Association/American Society for Hypertension committee that wrote the soon-to-be-released revised scientific statement on the treatment of hypertension in the prevention and management of ischemic heart disease. He also chaired the 2007 AHA scientific statement on the subject (Circulation 2007;115:2761-88).
One of the most persuasive pieces of evidence of the shortcomings of beta-blockers as first-line agents for uncomplicated hypertension to appear since the release of the 2007 AHA scientific statement was a meta-analysis of six meta-analyses. The six meta-analyses incorporated a total of 26 randomized trials of beta-blockers versus placebo. The conclusion: beta-blockers were no better than placebo in preventing MI or mortality, although they did result in a 16%-22% relative reduction in stroke risk (J. Am. Coll. Cardiol. 2007;50:563-72).
This meta-meta-analysis also included three meta-analyses of comparative trials of beta-blockers versus diuretics and three meta-analyses of beta-blockers compared with other drugs. Beta-blockers turned out to be significantly worse than the other antihypertensive agents in terms of the three endpoints of MI, stroke, and mortality.
A caveat: these clinical trials and meta-analyses were nearly all restricted to atenolol and short-acting metoprolol.
"We don’t have any comparable data for newer beta-blockers. Carvedilol has never been looked at from the point of view of outcomes in hypertension. Bisoprolol likewise, and nabivolol, too. It’s possible that the paradigm might be changed quite considerably when we have data to support the use of these newer beta-blockers in the treatment of hypertension," the cardiologist said.
Dr. Rosendorff noted that he wasn’t at liberty to discuss the recommendations of the forthcoming ACC/AHA/ASH scientific statement in advance of its release. He stressed that his comments on the drawbacks of beta-blockers for uncomplicated hypertension represented his own views and not necessarily the panel’s.
Of note, however, is that the recently published report of the Eighth Joint National Committee (JNC 8) doesn’t list beta-blockers among the four classes of antihypertensive medications recommended for the initial treatment of hypertension (JAMA 2014;311:507-20).
Dr. Rosendorff reported having no financial conflicts of interest.
SNOWMASS, COLO. – Beta-blockers have lost their decades-long status as first-line therapy for hypertension.
"Generally, I think there is a consensus that beta-blockers are a poor choice for uncomplicated hypertension," Dr. Clive Rosendorff observed at the Annual Cardiovascular Conference at Snowmass.
Abundant evidence indicates that beta-blockers provide less protection against stroke, MI, and overall mortality than other classes of antihypertensive agents. They offer less renal protection than ramipril and achieve less regression of left ventricular hypertrophy than other antihypertensive drugs.
Moreover, as was shown in the Conduit Artery Function Evaluation (CAFE) study, beta-blockers have what has been termed "pseudo-antihypertensive efficacy": that is, they fail to reduce central aortic blood pressure to the same extent they lower systolic blood pressure, which may explain why they are less cardioprotective than other antihypertensive drugs. They also are associated with an increase in insulin resistance, reduced exercise tolerance, weight gain, and a high rate of withdrawal because of side effects, said Dr. Rosendorff, professor of medicine at Mount Sinai School of Medicine, New York.
Dr. Rosdendorff chaired the joint American College of Cardiology/American Heart Association/American Society for Hypertension committee that wrote the soon-to-be-released revised scientific statement on the treatment of hypertension in the prevention and management of ischemic heart disease. He also chaired the 2007 AHA scientific statement on the subject (Circulation 2007;115:2761-88).
One of the most persuasive pieces of evidence of the shortcomings of beta-blockers as first-line agents for uncomplicated hypertension to appear since the release of the 2007 AHA scientific statement was a meta-analysis of six meta-analyses. The six meta-analyses incorporated a total of 26 randomized trials of beta-blockers versus placebo. The conclusion: beta-blockers were no better than placebo in preventing MI or mortality, although they did result in a 16%-22% relative reduction in stroke risk (J. Am. Coll. Cardiol. 2007;50:563-72).
This meta-meta-analysis also included three meta-analyses of comparative trials of beta-blockers versus diuretics and three meta-analyses of beta-blockers compared with other drugs. Beta-blockers turned out to be significantly worse than the other antihypertensive agents in terms of the three endpoints of MI, stroke, and mortality.
A caveat: these clinical trials and meta-analyses were nearly all restricted to atenolol and short-acting metoprolol.
"We don’t have any comparable data for newer beta-blockers. Carvedilol has never been looked at from the point of view of outcomes in hypertension. Bisoprolol likewise, and nabivolol, too. It’s possible that the paradigm might be changed quite considerably when we have data to support the use of these newer beta-blockers in the treatment of hypertension," the cardiologist said.
Dr. Rosendorff noted that he wasn’t at liberty to discuss the recommendations of the forthcoming ACC/AHA/ASH scientific statement in advance of its release. He stressed that his comments on the drawbacks of beta-blockers for uncomplicated hypertension represented his own views and not necessarily the panel’s.
Of note, however, is that the recently published report of the Eighth Joint National Committee (JNC 8) doesn’t list beta-blockers among the four classes of antihypertensive medications recommended for the initial treatment of hypertension (JAMA 2014;311:507-20).
Dr. Rosendorff reported having no financial conflicts of interest.
SNOWMASS, COLO. – Beta-blockers have lost their decades-long status as first-line therapy for hypertension.
"Generally, I think there is a consensus that beta-blockers are a poor choice for uncomplicated hypertension," Dr. Clive Rosendorff observed at the Annual Cardiovascular Conference at Snowmass.
Abundant evidence indicates that beta-blockers provide less protection against stroke, MI, and overall mortality than other classes of antihypertensive agents. They offer less renal protection than ramipril and achieve less regression of left ventricular hypertrophy than other antihypertensive drugs.
Moreover, as was shown in the Conduit Artery Function Evaluation (CAFE) study, beta-blockers have what has been termed "pseudo-antihypertensive efficacy": that is, they fail to reduce central aortic blood pressure to the same extent they lower systolic blood pressure, which may explain why they are less cardioprotective than other antihypertensive drugs. They also are associated with an increase in insulin resistance, reduced exercise tolerance, weight gain, and a high rate of withdrawal because of side effects, said Dr. Rosendorff, professor of medicine at Mount Sinai School of Medicine, New York.
Dr. Rosdendorff chaired the joint American College of Cardiology/American Heart Association/American Society for Hypertension committee that wrote the soon-to-be-released revised scientific statement on the treatment of hypertension in the prevention and management of ischemic heart disease. He also chaired the 2007 AHA scientific statement on the subject (Circulation 2007;115:2761-88).
One of the most persuasive pieces of evidence of the shortcomings of beta-blockers as first-line agents for uncomplicated hypertension to appear since the release of the 2007 AHA scientific statement was a meta-analysis of six meta-analyses. The six meta-analyses incorporated a total of 26 randomized trials of beta-blockers versus placebo. The conclusion: beta-blockers were no better than placebo in preventing MI or mortality, although they did result in a 16%-22% relative reduction in stroke risk (J. Am. Coll. Cardiol. 2007;50:563-72).
This meta-meta-analysis also included three meta-analyses of comparative trials of beta-blockers versus diuretics and three meta-analyses of beta-blockers compared with other drugs. Beta-blockers turned out to be significantly worse than the other antihypertensive agents in terms of the three endpoints of MI, stroke, and mortality.
A caveat: these clinical trials and meta-analyses were nearly all restricted to atenolol and short-acting metoprolol.
"We don’t have any comparable data for newer beta-blockers. Carvedilol has never been looked at from the point of view of outcomes in hypertension. Bisoprolol likewise, and nabivolol, too. It’s possible that the paradigm might be changed quite considerably when we have data to support the use of these newer beta-blockers in the treatment of hypertension," the cardiologist said.
Dr. Rosendorff noted that he wasn’t at liberty to discuss the recommendations of the forthcoming ACC/AHA/ASH scientific statement in advance of its release. He stressed that his comments on the drawbacks of beta-blockers for uncomplicated hypertension represented his own views and not necessarily the panel’s.
Of note, however, is that the recently published report of the Eighth Joint National Committee (JNC 8) doesn’t list beta-blockers among the four classes of antihypertensive medications recommended for the initial treatment of hypertension (JAMA 2014;311:507-20).
Dr. Rosendorff reported having no financial conflicts of interest.
EXPERT ANALYSIS FROM THE CARDIOVASCULAR CONFERENCE AT SNOWMASS
Latest studies fine-tune ACC/AHA dietary guidelines
SNOWMASS, COLO. – Recent large studies validate and fine-tune the 2013 American Heart Association/American College of Cardiology guidelines on diet and lifestyle management to reduce cardiovascular risk.
The guidelines recommend a dietary pattern that emphasizes fruits and vegetables, whole grains, legumes, fish, poultry, nuts and vegetable oils for fat, and restricted consumption of saturated and trans fats, sugar, sodium, and red meat. It’s a dietary pattern evocative of the Mediterranean or DASH-type diet (J. Am. Coll. Cardiol. 2014 Jan. 28 [doi:10.1016/j.jacc.2013.11.003]).

"There’s nothing particularly controversial here. I support all these recommendations," Dr. Robert A. Vogel commented at the Annual Cardiovascular Conference at Snowmass.
A fair number of important studies bearing on the topic of diet and longevity have appeared since the AHA/ACC guidelines were developed. Dr. Vogel shared highlights of these randomized and cohort studies, some of which were published in journals most physicians don’t read regularly.
• Fruits and veggies: Conventional dietary guidance has emphasized the importance of eating a wide range of fruits and vegetables.
"You’ve been told to eat vegetables and fruits of every different color. Variety is the cornerstone of dietary advice, right? Wrong!" said Dr. Vogel, a cardiologist at the University of Colorado, Denver.
He cited a prospective study of the independent roles of quantity and variety in vegetable and fruit consumption in association with incident coronary heart disease in 71,141 women and 42,135 men participating in the Nurses’ Health Study and the Health Professionals Follow-Up Study. During follow-up there were 2,582 documented cases of CHD in women and 3,607 in men. In a multivariate analysis, subjects in the highest quintile of daily fruit and vegetable consumption had a 17% lower risk of CHD. The absolute quantity of fruit and vegetable intake, but not the variety, was associated with a significantly lower risk of CHD. (Am. J. Clin. Nutr. 2013;98:1514-23).
• Nuts: In a separate analysis of more than 3 million person-years of prospective follow-up data from the Nurses’ Health Study and the Health Professionals Follow-Up Study, increasing consumption of nuts was associated with a stepwise reduction in all-cause mortality. People who consumed nuts less than once a week had a statistically significant 7% reduction in the risk of total mortality, compared with those who didn’t eat nuts. Subjects who ate nuts once per week had an 11% reduction in risk; those who ate nuts 2-4 times per week had a 13% reduction; nut eaters 5 or 6 times per week had a 15% reduction in risk; and subjects who ate nuts 7 or more times per week had a 20% reduction in the risk of total mortality. Also, significant inverse relationships were seen between nut intake and specific common causes of death, including cancer, heart disease, and pulmonary disease.
Investigators reanalyzed the data separately for consumption of tree nuts and peanuts, which are actually legumes. The mortality risk reduction was the same for both (N. Engl. J. Med. 2013;369:2001-11).
"Peanuts are not nuts, but they work like nuts," Dr. Vogel observed.
• Meat: An analysis of 448,568 participants in the EPIC (European Prospective Investigation into Cancer and Nutrition) trial, 26,344 of whom have died, showed what investigators termed "a moderate positive association" between processed meat consumption and mortality, especially deaths from cardiovascular disease and cancer. In a multivariate analysis, daily consumption of red meat at an average of 160 g or more – that’s 5.6 oz. – was independently associated with 14% higher all-cause mortality than in individuals who consumed an average of 10-19.9/day.
The association was more striking for processed meat, such as salami: Subjects who ate an average of 5.6 oz/day had 44% greater all-cause mortality. The investigators estimated that if all study participants limited their processed meat consumption to less than 20 g/day, 3.3% of deaths could be prevented (BMC Med. 2013;11:63 [doi:10.1186/1741-7015-11-63]).

The EPIC findings call to mind an earlier study by investigators at Loma Linda (Calif.) University, who reviewed six prospective cohort studies and concluded that very low meat consumption – less than once weekly – was associated with increased longevity, but that how long subjects had been on such a diet was a key factor. Individuals who had at least a 20-year history of very low meat intake lived an average of 3.6 years longer than those who had adopted the dietary practice more recently (Am. J. Clin. Nutr. 2003;78:526S-532S).
"When you make the changes to adopt a healthier lifestyle substantially matters in terms of longevity. It’s great to change your diet after your first non-ST-elevation MI, but in fact you want to do it before," Dr. Vogel observed.
• Which components of the Mediterranean diet are most beneficial? Greek investigators involved in the EPIC study addressed this question in 23,349 subjects followed for a mean of 8.5 years, during which 1,075 deaths occurred. Greater adherence to the Mediterranean diet was associated with larger reductions in total mortality. By analyzing Mediterranean diet adherence scores, the investigators determined that 16% of the mortality benefit was attributable to high vegetable consumption, 11% to high fruit and nut intake, 10% to legume consumption, 24% was from moderate alcohol consumption, 17% to low intake of meats, and just 11% to fats and oils having a high monounsaturated-to-saturated lipid ratio (BMJ 2009;338:b2337).
"We think that the Mediterranean diet is olive oil, but probably olive oil is good because you put it on a salad; and fruits and vegetables are the best part of a diet," the cardiologist said.
• How to maximize longevity: "If I had one recommendation based upon all the data I’ve reviewed," Dr. Vogel said, "it would be to become a pesco-vegetarian. They in fact are the longest-living Americans. That’s a vegetarian diet with the addition of fish."
Seventh-Day Adventists as a group have the longest life expectancy among all Americans. And analysis of 73,308 Seventh-day Adventists participating in the Adventist Health Study 2 showed that during a mean follow-up of 5.8 years, the adjusted risk of all-cause mortality was 12% lower among all vegetarians than in non-vegetarians, and 19% lower in the subgroup composed of pesco-vegetarians (JAMA Intern. Med. 2013;173:1230-8).
Dr. Vogel serves as a consultant to the Pritikin Longevity Center.
SNOWMASS, COLO. – Recent large studies validate and fine-tune the 2013 American Heart Association/American College of Cardiology guidelines on diet and lifestyle management to reduce cardiovascular risk.
The guidelines recommend a dietary pattern that emphasizes fruits and vegetables, whole grains, legumes, fish, poultry, nuts and vegetable oils for fat, and restricted consumption of saturated and trans fats, sugar, sodium, and red meat. It’s a dietary pattern evocative of the Mediterranean or DASH-type diet (J. Am. Coll. Cardiol. 2014 Jan. 28 [doi:10.1016/j.jacc.2013.11.003]).
"There’s nothing particularly controversial here. I support all these recommendations," Dr. Robert A. Vogel commented at the Annual Cardiovascular Conference at Snowmass.
A fair number of important studies bearing on the topic of diet and longevity have appeared since the AHA/ACC guidelines were developed. Dr. Vogel shared highlights of these randomized and cohort studies, some of which were published in journals most physicians don’t read regularly.
• Fruits and veggies: Conventional dietary guidance has emphasized the importance of eating a wide range of fruits and vegetables.
"You’ve been told to eat vegetables and fruits of every different color. Variety is the cornerstone of dietary advice, right? Wrong!" said Dr. Vogel, a cardiologist at the University of Colorado, Denver.
He cited a prospective study of the independent roles of quantity and variety in vegetable and fruit consumption in association with incident coronary heart disease in 71,141 women and 42,135 men participating in the Nurses’ Health Study and the Health Professionals Follow-Up Study. During follow-up there were 2,582 documented cases of CHD in women and 3,607 in men. In a multivariate analysis, subjects in the highest quintile of daily fruit and vegetable consumption had a 17% lower risk of CHD. The absolute quantity of fruit and vegetable intake, but not the variety, was associated with a significantly lower risk of CHD. (Am. J. Clin. Nutr. 2013;98:1514-23).
• Nuts: In a separate analysis of more than 3 million person-years of prospective follow-up data from the Nurses’ Health Study and the Health Professionals Follow-Up Study, increasing consumption of nuts was associated with a stepwise reduction in all-cause mortality. People who consumed nuts less than once a week had a statistically significant 7% reduction in the risk of total mortality, compared with those who didn’t eat nuts. Subjects who ate nuts once per week had an 11% reduction in risk; those who ate nuts 2-4 times per week had a 13% reduction; nut eaters 5 or 6 times per week had a 15% reduction in risk; and subjects who ate nuts 7 or more times per week had a 20% reduction in the risk of total mortality. Also, significant inverse relationships were seen between nut intake and specific common causes of death, including cancer, heart disease, and pulmonary disease.
Investigators reanalyzed the data separately for consumption of tree nuts and peanuts, which are actually legumes. The mortality risk reduction was the same for both (N. Engl. J. Med. 2013;369:2001-11).
"Peanuts are not nuts, but they work like nuts," Dr. Vogel observed.
• Meat: An analysis of 448,568 participants in the EPIC (European Prospective Investigation into Cancer and Nutrition) trial, 26,344 of whom have died, showed what investigators termed "a moderate positive association" between processed meat consumption and mortality, especially deaths from cardiovascular disease and cancer. In a multivariate analysis, daily consumption of red meat at an average of 160 g or more – that’s 5.6 oz. – was independently associated with 14% higher all-cause mortality than in individuals who consumed an average of 10-19.9/day.
The association was more striking for processed meat, such as salami: Subjects who ate an average of 5.6 oz/day had 44% greater all-cause mortality. The investigators estimated that if all study participants limited their processed meat consumption to less than 20 g/day, 3.3% of deaths could be prevented (BMC Med. 2013;11:63 [doi:10.1186/1741-7015-11-63]).
The EPIC findings call to mind an earlier study by investigators at Loma Linda (Calif.) University, who reviewed six prospective cohort studies and concluded that very low meat consumption – less than once weekly – was associated with increased longevity, but that how long subjects had been on such a diet was a key factor. Individuals who had at least a 20-year history of very low meat intake lived an average of 3.6 years longer than those who had adopted the dietary practice more recently (Am. J. Clin. Nutr. 2003;78:526S-532S).
"When you make the changes to adopt a healthier lifestyle substantially matters in terms of longevity. It’s great to change your diet after your first non-ST-elevation MI, but in fact you want to do it before," Dr. Vogel observed.
• Which components of the Mediterranean diet are most beneficial? Greek investigators involved in the EPIC study addressed this question in 23,349 subjects followed for a mean of 8.5 years, during which 1,075 deaths occurred. Greater adherence to the Mediterranean diet was associated with larger reductions in total mortality. By analyzing Mediterranean diet adherence scores, the investigators determined that 16% of the mortality benefit was attributable to high vegetable consumption, 11% to high fruit and nut intake, 10% to legume consumption, 24% was from moderate alcohol consumption, 17% to low intake of meats, and just 11% to fats and oils having a high monounsaturated-to-saturated lipid ratio (BMJ 2009;338:b2337).
"We think that the Mediterranean diet is olive oil, but probably olive oil is good because you put it on a salad; and fruits and vegetables are the best part of a diet," the cardiologist said.
• How to maximize longevity: "If I had one recommendation based upon all the data I’ve reviewed," Dr. Vogel said, "it would be to become a pesco-vegetarian. They in fact are the longest-living Americans. That’s a vegetarian diet with the addition of fish."
Seventh-Day Adventists as a group have the longest life expectancy among all Americans. And analysis of 73,308 Seventh-day Adventists participating in the Adventist Health Study 2 showed that during a mean follow-up of 5.8 years, the adjusted risk of all-cause mortality was 12% lower among all vegetarians than in non-vegetarians, and 19% lower in the subgroup composed of pesco-vegetarians (JAMA Intern. Med. 2013;173:1230-8).
Dr. Vogel serves as a consultant to the Pritikin Longevity Center.
SNOWMASS, COLO. – Recent large studies validate and fine-tune the 2013 American Heart Association/American College of Cardiology guidelines on diet and lifestyle management to reduce cardiovascular risk.
The guidelines recommend a dietary pattern that emphasizes fruits and vegetables, whole grains, legumes, fish, poultry, nuts and vegetable oils for fat, and restricted consumption of saturated and trans fats, sugar, sodium, and red meat. It’s a dietary pattern evocative of the Mediterranean or DASH-type diet (J. Am. Coll. Cardiol. 2014 Jan. 28 [doi:10.1016/j.jacc.2013.11.003]).
"There’s nothing particularly controversial here. I support all these recommendations," Dr. Robert A. Vogel commented at the Annual Cardiovascular Conference at Snowmass.
A fair number of important studies bearing on the topic of diet and longevity have appeared since the AHA/ACC guidelines were developed. Dr. Vogel shared highlights of these randomized and cohort studies, some of which were published in journals most physicians don’t read regularly.
• Fruits and veggies: Conventional dietary guidance has emphasized the importance of eating a wide range of fruits and vegetables.
"You’ve been told to eat vegetables and fruits of every different color. Variety is the cornerstone of dietary advice, right? Wrong!" said Dr. Vogel, a cardiologist at the University of Colorado, Denver.
He cited a prospective study of the independent roles of quantity and variety in vegetable and fruit consumption in association with incident coronary heart disease in 71,141 women and 42,135 men participating in the Nurses’ Health Study and the Health Professionals Follow-Up Study. During follow-up there were 2,582 documented cases of CHD in women and 3,607 in men. In a multivariate analysis, subjects in the highest quintile of daily fruit and vegetable consumption had a 17% lower risk of CHD. The absolute quantity of fruit and vegetable intake, but not the variety, was associated with a significantly lower risk of CHD. (Am. J. Clin. Nutr. 2013;98:1514-23).
• Nuts: In a separate analysis of more than 3 million person-years of prospective follow-up data from the Nurses’ Health Study and the Health Professionals Follow-Up Study, increasing consumption of nuts was associated with a stepwise reduction in all-cause mortality. People who consumed nuts less than once a week had a statistically significant 7% reduction in the risk of total mortality, compared with those who didn’t eat nuts. Subjects who ate nuts once per week had an 11% reduction in risk; those who ate nuts 2-4 times per week had a 13% reduction; nut eaters 5 or 6 times per week had a 15% reduction in risk; and subjects who ate nuts 7 or more times per week had a 20% reduction in the risk of total mortality. Also, significant inverse relationships were seen between nut intake and specific common causes of death, including cancer, heart disease, and pulmonary disease.
Investigators reanalyzed the data separately for consumption of tree nuts and peanuts, which are actually legumes. The mortality risk reduction was the same for both (N. Engl. J. Med. 2013;369:2001-11).
"Peanuts are not nuts, but they work like nuts," Dr. Vogel observed.
• Meat: An analysis of 448,568 participants in the EPIC (European Prospective Investigation into Cancer and Nutrition) trial, 26,344 of whom have died, showed what investigators termed "a moderate positive association" between processed meat consumption and mortality, especially deaths from cardiovascular disease and cancer. In a multivariate analysis, daily consumption of red meat at an average of 160 g or more – that’s 5.6 oz. – was independently associated with 14% higher all-cause mortality than in individuals who consumed an average of 10-19.9/day.
The association was more striking for processed meat, such as salami: Subjects who ate an average of 5.6 oz/day had 44% greater all-cause mortality. The investigators estimated that if all study participants limited their processed meat consumption to less than 20 g/day, 3.3% of deaths could be prevented (BMC Med. 2013;11:63 [doi:10.1186/1741-7015-11-63]).
The EPIC findings call to mind an earlier study by investigators at Loma Linda (Calif.) University, who reviewed six prospective cohort studies and concluded that very low meat consumption – less than once weekly – was associated with increased longevity, but that how long subjects had been on such a diet was a key factor. Individuals who had at least a 20-year history of very low meat intake lived an average of 3.6 years longer than those who had adopted the dietary practice more recently (Am. J. Clin. Nutr. 2003;78:526S-532S).
"When you make the changes to adopt a healthier lifestyle substantially matters in terms of longevity. It’s great to change your diet after your first non-ST-elevation MI, but in fact you want to do it before," Dr. Vogel observed.
• Which components of the Mediterranean diet are most beneficial? Greek investigators involved in the EPIC study addressed this question in 23,349 subjects followed for a mean of 8.5 years, during which 1,075 deaths occurred. Greater adherence to the Mediterranean diet was associated with larger reductions in total mortality. By analyzing Mediterranean diet adherence scores, the investigators determined that 16% of the mortality benefit was attributable to high vegetable consumption, 11% to high fruit and nut intake, 10% to legume consumption, 24% was from moderate alcohol consumption, 17% to low intake of meats, and just 11% to fats and oils having a high monounsaturated-to-saturated lipid ratio (BMJ 2009;338:b2337).
"We think that the Mediterranean diet is olive oil, but probably olive oil is good because you put it on a salad; and fruits and vegetables are the best part of a diet," the cardiologist said.
• How to maximize longevity: "If I had one recommendation based upon all the data I’ve reviewed," Dr. Vogel said, "it would be to become a pesco-vegetarian. They in fact are the longest-living Americans. That’s a vegetarian diet with the addition of fish."
Seventh-Day Adventists as a group have the longest life expectancy among all Americans. And analysis of 73,308 Seventh-day Adventists participating in the Adventist Health Study 2 showed that during a mean follow-up of 5.8 years, the adjusted risk of all-cause mortality was 12% lower among all vegetarians than in non-vegetarians, and 19% lower in the subgroup composed of pesco-vegetarians (JAMA Intern. Med. 2013;173:1230-8).
Dr. Vogel serves as a consultant to the Pritikin Longevity Center.
EXPERT ANALYSIS FROM THE CARDIOVASCULAR CONFERENCE AT SNOWMASS

Myocardial fibrosis assessment fine-tunes ICD selection
SNOWMASS, COLO. – Detection of myocardial midwall fibrosis via cardiovascular magnetic resonance in patients with nonischemic dilated cardiomyopathy provides prognostic information independent of left ventricular ejection fraction.
"Low LVEF and fibrosis uniquely identify the need for an ICD [implantable cardioverter-defibrillator]. This is new information that helps refine our understanding of whom it is that’s uniquely at risk. We’ve always had these troublesome questions in patients with nonischemic heart failure," Dr. Clyde W. Yancy observed at the Annual Cardiovascular Conference at Snowmass.
He highlighted what he called "very provocative data" in a recent study led by Dr. Sanjay K. Prasad of Royal Brompton Hospital in London. The investigators evaluated 472 consecutive patients with nonischemic dilated cardiomyopathy using late gadolinium cardiovascular magnetic resonance (CMR). Thirty percent of them were found to have midwall fibrosis. Their all-cause mortality rate during a median 5.3 years of prospective follow-up was 26.8%, compared with 10.6% in the 330 patients without fibrosis. An arrhythmic composite event comprising sudden cardiac death (SCD), aborted SCD, or sustained ventricular tachycardia occurred in 29.6% of the group with fibrosis vs. 7% of patients without fibrosis.

In a multivariate analysis adjusted for LVEF and other prognostic factors, the presence of midwall fibrosis was independently associated with a 2.43-fold increased risk of all-cause mortality, a 3.2-fold greater risk of cardiovascular mortality or heart transplantation, a 4.6-fold increase in SCD or aborted SCD, and a 1.6-fold increased likelihood of a composite of heart failure hospitalization, mortality from heart failure, or cardiac transplantation (JAMA 2013;309:896-908).
Dr. Yancy, who chaired the writing committee for the 2013 ACC/AHA Guideline for the Management of Heart Failure, noted that the guidelines grant a strong Class I/Level of Evidence B recommendation for implantation of an ICD for primary prevention in nonischemic dilated cardiomyopathy patients who are in New York Heart Association functional class II or III and have an LVEF of 35% or less. But there is a pressing need for refined implantation criteria. Basing the ICD decision on only these criteria results in a low rate of appropriate shocks, a high frequency of inappropriate shocks, and exclusion from device therapy of a group of patients with a high relative risk of SCD.
The British study provides reason for optimism in this regard. Using a greater than 15% estimated SCD risk based upon LVEF plus midwall fibrosis as a proposed indication for ICD implantation, the investigators found that an additional 12 patients in their cohort would receive an ICD and 43 others would now avoid ICD implantation, noted Dr. Yancy, professor of medicine and of medical social sciences and chief of cardiology at Northwestern University, Chicago.
He reported having no financial conflicts.
SNOWMASS, COLO. – Detection of myocardial midwall fibrosis via cardiovascular magnetic resonance in patients with nonischemic dilated cardiomyopathy provides prognostic information independent of left ventricular ejection fraction.
"Low LVEF and fibrosis uniquely identify the need for an ICD [implantable cardioverter-defibrillator]. This is new information that helps refine our understanding of whom it is that’s uniquely at risk. We’ve always had these troublesome questions in patients with nonischemic heart failure," Dr. Clyde W. Yancy observed at the Annual Cardiovascular Conference at Snowmass.
He highlighted what he called "very provocative data" in a recent study led by Dr. Sanjay K. Prasad of Royal Brompton Hospital in London. The investigators evaluated 472 consecutive patients with nonischemic dilated cardiomyopathy using late gadolinium cardiovascular magnetic resonance (CMR). Thirty percent of them were found to have midwall fibrosis. Their all-cause mortality rate during a median 5.3 years of prospective follow-up was 26.8%, compared with 10.6% in the 330 patients without fibrosis. An arrhythmic composite event comprising sudden cardiac death (SCD), aborted SCD, or sustained ventricular tachycardia occurred in 29.6% of the group with fibrosis vs. 7% of patients without fibrosis.
In a multivariate analysis adjusted for LVEF and other prognostic factors, the presence of midwall fibrosis was independently associated with a 2.43-fold increased risk of all-cause mortality, a 3.2-fold greater risk of cardiovascular mortality or heart transplantation, a 4.6-fold increase in SCD or aborted SCD, and a 1.6-fold increased likelihood of a composite of heart failure hospitalization, mortality from heart failure, or cardiac transplantation (JAMA 2013;309:896-908).
Dr. Yancy, who chaired the writing committee for the 2013 ACC/AHA Guideline for the Management of Heart Failure, noted that the guidelines grant a strong Class I/Level of Evidence B recommendation for implantation of an ICD for primary prevention in nonischemic dilated cardiomyopathy patients who are in New York Heart Association functional class II or III and have an LVEF of 35% or less. But there is a pressing need for refined implantation criteria. Basing the ICD decision on only these criteria results in a low rate of appropriate shocks, a high frequency of inappropriate shocks, and exclusion from device therapy of a group of patients with a high relative risk of SCD.
The British study provides reason for optimism in this regard. Using a greater than 15% estimated SCD risk based upon LVEF plus midwall fibrosis as a proposed indication for ICD implantation, the investigators found that an additional 12 patients in their cohort would receive an ICD and 43 others would now avoid ICD implantation, noted Dr. Yancy, professor of medicine and of medical social sciences and chief of cardiology at Northwestern University, Chicago.
He reported having no financial conflicts.
SNOWMASS, COLO. – Detection of myocardial midwall fibrosis via cardiovascular magnetic resonance in patients with nonischemic dilated cardiomyopathy provides prognostic information independent of left ventricular ejection fraction.
"Low LVEF and fibrosis uniquely identify the need for an ICD [implantable cardioverter-defibrillator]. This is new information that helps refine our understanding of whom it is that’s uniquely at risk. We’ve always had these troublesome questions in patients with nonischemic heart failure," Dr. Clyde W. Yancy observed at the Annual Cardiovascular Conference at Snowmass.
He highlighted what he called "very provocative data" in a recent study led by Dr. Sanjay K. Prasad of Royal Brompton Hospital in London. The investigators evaluated 472 consecutive patients with nonischemic dilated cardiomyopathy using late gadolinium cardiovascular magnetic resonance (CMR). Thirty percent of them were found to have midwall fibrosis. Their all-cause mortality rate during a median 5.3 years of prospective follow-up was 26.8%, compared with 10.6% in the 330 patients without fibrosis. An arrhythmic composite event comprising sudden cardiac death (SCD), aborted SCD, or sustained ventricular tachycardia occurred in 29.6% of the group with fibrosis vs. 7% of patients without fibrosis.
In a multivariate analysis adjusted for LVEF and other prognostic factors, the presence of midwall fibrosis was independently associated with a 2.43-fold increased risk of all-cause mortality, a 3.2-fold greater risk of cardiovascular mortality or heart transplantation, a 4.6-fold increase in SCD or aborted SCD, and a 1.6-fold increased likelihood of a composite of heart failure hospitalization, mortality from heart failure, or cardiac transplantation (JAMA 2013;309:896-908).
Dr. Yancy, who chaired the writing committee for the 2013 ACC/AHA Guideline for the Management of Heart Failure, noted that the guidelines grant a strong Class I/Level of Evidence B recommendation for implantation of an ICD for primary prevention in nonischemic dilated cardiomyopathy patients who are in New York Heart Association functional class II or III and have an LVEF of 35% or less. But there is a pressing need for refined implantation criteria. Basing the ICD decision on only these criteria results in a low rate of appropriate shocks, a high frequency of inappropriate shocks, and exclusion from device therapy of a group of patients with a high relative risk of SCD.
The British study provides reason for optimism in this regard. Using a greater than 15% estimated SCD risk based upon LVEF plus midwall fibrosis as a proposed indication for ICD implantation, the investigators found that an additional 12 patients in their cohort would receive an ICD and 43 others would now avoid ICD implantation, noted Dr. Yancy, professor of medicine and of medical social sciences and chief of cardiology at Northwestern University, Chicago.
He reported having no financial conflicts.
EXPERT ANALYSIS FROM THE CARDIOVASCULAR CONFERENCE AT SNOWMASS