User login
Warfarin is best for anticoagulation in prosthetic heart valve pregnancies
SNOWMASS, COLO. – How would you manage anticoagulation in a newly pregnant 23-year-old with a mechanical heart valve who has been on warfarin at 3 mg/day?
A) Weight-adjusted low-molecular-weight heparin during the first trimester, then warfarin in the second and third until switching to unfractionated heparin for delivery.
B) Low-molecular-weight heparin throughout pregnancy.
C) Warfarin throughout pregnancy.
D) Unfractionated heparin in the first trimester, warfarin in the second and third until returning to unfractionated heparin peridelivery.
The correct answer, according to both the ACC/AHA guidelines (Circulation. 2014 Jun 10;129[23]:e521-643) and European Society of Cardiology guidelines (Eur Heart J. 2011 Dec;32[24]:3147-97), is C in women who are on 5 mg/day of warfarin or less.

“Oral anticoagulants throughout pregnancy are much better for the mother, and this is where the guidelines have moved,” Dr. Carole A. Warnes said at the Annual Cardiovascular Conference at Snowmass.
Both sets of guidelines give a class I recommendation to warfarin during the second and third trimesters, because the risk of warfarin embryopathy is confined to weeks 6-12. During the first trimester, warfarin at 5 mg/day or less gets a class IIa rating – making it preferable to unfractionated or low-molecular-weight heparin – because heparin is a far less effective anticoagulant. Plus, multiple small studies indicate the risk of embryopathy is low – roughly 1%-2% – when the mother is on warfarin at 5 mg/day or less.
In a woman on more than 5 mg/day of warfarin, the risk of warfarin embryopathy is about 6%, so the guidelines recommend replacing the drug with heparin during weeks 6-12.
“It’s not a walk in the park,” said Dr. Warnes, director of the Snowmass conference and professor of medicine at the Mayo Clinic in Rochester, Minn.
The major concern in using heparin for anticoagulation in pregnancy is valve thrombosis. It doubles the risk.
“Pregnancy is the most prothrombotic state there is,” she said. “It’s not like managing a patient through a hip replacement or prostate surgery. Women with a mechanical prosthetic valve should be managed by a heart valve team with expertise in treatment during pregnancy.”
The alternatives to warfarin are adjusted-dose unfractionated heparin, which must be given in a continuous intravenous infusion with meticulous monitoring of activated partial thromboplastin time, or twice-daily low-molecular-weight heparin with dose adjustment by weight and maintenance of a target anti–Factor Xa level of 1.0-1.2 IU/mL.
“If you use low-molecular-weight heparin, you’re going to be seeing that patient every week to monitor anti–Factor Xa 4-6 hours post injection. You’ll find it’s not that easy to stay in the sweet spot, with excellent anticoagulation without an increased risk of maternal thromboembolism, or at the other extreme, fetal bleeding. What might look initially as a relatively easy strategy with a lot of appeal turns out to entail considerable risk,” Dr. Warnes said.
This was underscored in a cautionary report by highly experienced University of Toronto investigators. In their series of 23 pregnancies in 17 women with mechanical heart valves on low-molecular-weight heparin throughout pregnancy with careful monitoring, there was one maternal thromboembolic event resulting in maternal and fetal death despite a documented therapeutic anti–Factor Xa level (Am J Cardiol. 2009 Nov 1;104[9]:1259-63).
Although warfarin is clearly the better anticoagulant for the mother, the fetus pays the price. This was highlighted in a recent report from the ESC Registry of Pregnancy and Cardiac Disease (ROPAC) that compared pregnancy outcomes in 212 patients with a mechanical heart valve, 134 with a tissue valve, and 2,620 women without a prosthetic heart valve. Use of warfarin or another vitamin K antagonist in the first trimester was associated with a higher rate of miscarriage than heparin – 28.6% vs. 9.2% – as well as a 7.1% incidence of late fetal death, compared with just 0.7% with heparin.
On the other hand, the mechanical valve thrombosis rate was 4.7%, with half of those serious events occurring during the first trimester in patients after they’d been switched to heparin (Circulation. 2015 Jul 14;132[2]:132-42).
Hemorrhagic events occurred in 23.1% of mothers with a mechanical heart valve, 5.1% of those with a bioprosthetic valve, and 4.9% of patients without a prosthetic valve. A point worth incorporating into prepregnancy patient counseling, Dr. Warnes noted, is that only 58% of ROPAC participants with a mechanical heart valve had an uncomplicated pregnancy with a live birth, in contrast to 79% of those with a tissue valve and 78% of controls.
Because warfarin crosses the placenta, and it takes about a week for the fetus to eliminate the drug following maternal discontinuation, the guidelines recommend stopping warfarin at about week 36 and changing to a continuous infusion of dose-adjusted unfractionated heparin peridelivery. The heparin should be stopped for as short a time as possible before delivery and resumed 6-12 hours post delivery in order to protect against valve thrombosis.
Of course, opting for a bioprosthetic rather than a mechanical heart valve avoids all these difficult anticoagulation-related issues. But it poses a different serious problem: The younger the patient at the time of tissue valve implantation, the greater the risk of rapid calcification and structural valve deterioration. Indeed, among patients who are age 16-39 when they receive a bioprosthetic valve, the rate of structural valve deterioration is 50% at 10 years and 90% at 15 years.
“There is no ideal valve prosthesis. If you elect a tissue prosthesis, you have to discuss the risk of reoperation in that young woman,” Dr. Warnes advised.
Recent data from the Society of Thoracic Surgeons database indicate the mortality associated with redo elective aortic valve replacement in a 35-year-old woman with no comorbidities averages 1.63%, with a 2% mortality rate for redo mitral valve replacement.
Dr. Warnes reported having no financial conflicts regarding her presentation.
SNOWMASS, COLO. – How would you manage anticoagulation in a newly pregnant 23-year-old with a mechanical heart valve who has been on warfarin at 3 mg/day?
A) Weight-adjusted low-molecular-weight heparin during the first trimester, then warfarin in the second and third until switching to unfractionated heparin for delivery.
B) Low-molecular-weight heparin throughout pregnancy.
C) Warfarin throughout pregnancy.
D) Unfractionated heparin in the first trimester, warfarin in the second and third until returning to unfractionated heparin peridelivery.
The correct answer, according to both the ACC/AHA guidelines (Circulation. 2014 Jun 10;129[23]:e521-643) and European Society of Cardiology guidelines (Eur Heart J. 2011 Dec;32[24]:3147-97), is C in women who are on 5 mg/day of warfarin or less.
“Oral anticoagulants throughout pregnancy are much better for the mother, and this is where the guidelines have moved,” Dr. Carole A. Warnes said at the Annual Cardiovascular Conference at Snowmass.
Both sets of guidelines give a class I recommendation to warfarin during the second and third trimesters, because the risk of warfarin embryopathy is confined to weeks 6-12. During the first trimester, warfarin at 5 mg/day or less gets a class IIa rating – making it preferable to unfractionated or low-molecular-weight heparin – because heparin is a far less effective anticoagulant. Plus, multiple small studies indicate the risk of embryopathy is low – roughly 1%-2% – when the mother is on warfarin at 5 mg/day or less.
In a woman on more than 5 mg/day of warfarin, the risk of warfarin embryopathy is about 6%, so the guidelines recommend replacing the drug with heparin during weeks 6-12.
“It’s not a walk in the park,” said Dr. Warnes, director of the Snowmass conference and professor of medicine at the Mayo Clinic in Rochester, Minn.
The major concern in using heparin for anticoagulation in pregnancy is valve thrombosis. It doubles the risk.
“Pregnancy is the most prothrombotic state there is,” she said. “It’s not like managing a patient through a hip replacement or prostate surgery. Women with a mechanical prosthetic valve should be managed by a heart valve team with expertise in treatment during pregnancy.”
The alternatives to warfarin are adjusted-dose unfractionated heparin, which must be given in a continuous intravenous infusion with meticulous monitoring of activated partial thromboplastin time, or twice-daily low-molecular-weight heparin with dose adjustment by weight and maintenance of a target anti–Factor Xa level of 1.0-1.2 IU/mL.
“If you use low-molecular-weight heparin, you’re going to be seeing that patient every week to monitor anti–Factor Xa 4-6 hours post injection. You’ll find it’s not that easy to stay in the sweet spot, with excellent anticoagulation without an increased risk of maternal thromboembolism, or at the other extreme, fetal bleeding. What might look initially as a relatively easy strategy with a lot of appeal turns out to entail considerable risk,” Dr. Warnes said.
This was underscored in a cautionary report by highly experienced University of Toronto investigators. In their series of 23 pregnancies in 17 women with mechanical heart valves on low-molecular-weight heparin throughout pregnancy with careful monitoring, there was one maternal thromboembolic event resulting in maternal and fetal death despite a documented therapeutic anti–Factor Xa level (Am J Cardiol. 2009 Nov 1;104[9]:1259-63).
Although warfarin is clearly the better anticoagulant for the mother, the fetus pays the price. This was highlighted in a recent report from the ESC Registry of Pregnancy and Cardiac Disease (ROPAC) that compared pregnancy outcomes in 212 patients with a mechanical heart valve, 134 with a tissue valve, and 2,620 women without a prosthetic heart valve. Use of warfarin or another vitamin K antagonist in the first trimester was associated with a higher rate of miscarriage than heparin – 28.6% vs. 9.2% – as well as a 7.1% incidence of late fetal death, compared with just 0.7% with heparin.
On the other hand, the mechanical valve thrombosis rate was 4.7%, with half of those serious events occurring during the first trimester in patients after they’d been switched to heparin (Circulation. 2015 Jul 14;132[2]:132-42).
Hemorrhagic events occurred in 23.1% of mothers with a mechanical heart valve, 5.1% of those with a bioprosthetic valve, and 4.9% of patients without a prosthetic valve. A point worth incorporating into prepregnancy patient counseling, Dr. Warnes noted, is that only 58% of ROPAC participants with a mechanical heart valve had an uncomplicated pregnancy with a live birth, in contrast to 79% of those with a tissue valve and 78% of controls.
Because warfarin crosses the placenta, and it takes about a week for the fetus to eliminate the drug following maternal discontinuation, the guidelines recommend stopping warfarin at about week 36 and changing to a continuous infusion of dose-adjusted unfractionated heparin peridelivery. The heparin should be stopped for as short a time as possible before delivery and resumed 6-12 hours post delivery in order to protect against valve thrombosis.
Of course, opting for a bioprosthetic rather than a mechanical heart valve avoids all these difficult anticoagulation-related issues. But it poses a different serious problem: The younger the patient at the time of tissue valve implantation, the greater the risk of rapid calcification and structural valve deterioration. Indeed, among patients who are age 16-39 when they receive a bioprosthetic valve, the rate of structural valve deterioration is 50% at 10 years and 90% at 15 years.
“There is no ideal valve prosthesis. If you elect a tissue prosthesis, you have to discuss the risk of reoperation in that young woman,” Dr. Warnes advised.
Recent data from the Society of Thoracic Surgeons database indicate the mortality associated with redo elective aortic valve replacement in a 35-year-old woman with no comorbidities averages 1.63%, with a 2% mortality rate for redo mitral valve replacement.
Dr. Warnes reported having no financial conflicts regarding her presentation.
SNOWMASS, COLO. – How would you manage anticoagulation in a newly pregnant 23-year-old with a mechanical heart valve who has been on warfarin at 3 mg/day?
A) Weight-adjusted low-molecular-weight heparin during the first trimester, then warfarin in the second and third until switching to unfractionated heparin for delivery.
B) Low-molecular-weight heparin throughout pregnancy.
C) Warfarin throughout pregnancy.
D) Unfractionated heparin in the first trimester, warfarin in the second and third until returning to unfractionated heparin peridelivery.
The correct answer, according to both the ACC/AHA guidelines (Circulation. 2014 Jun 10;129[23]:e521-643) and European Society of Cardiology guidelines (Eur Heart J. 2011 Dec;32[24]:3147-97), is C in women who are on 5 mg/day of warfarin or less.
“Oral anticoagulants throughout pregnancy are much better for the mother, and this is where the guidelines have moved,” Dr. Carole A. Warnes said at the Annual Cardiovascular Conference at Snowmass.
Both sets of guidelines give a class I recommendation to warfarin during the second and third trimesters, because the risk of warfarin embryopathy is confined to weeks 6-12. During the first trimester, warfarin at 5 mg/day or less gets a class IIa rating – making it preferable to unfractionated or low-molecular-weight heparin – because heparin is a far less effective anticoagulant. Plus, multiple small studies indicate the risk of embryopathy is low – roughly 1%-2% – when the mother is on warfarin at 5 mg/day or less.
In a woman on more than 5 mg/day of warfarin, the risk of warfarin embryopathy is about 6%, so the guidelines recommend replacing the drug with heparin during weeks 6-12.
“It’s not a walk in the park,” said Dr. Warnes, director of the Snowmass conference and professor of medicine at the Mayo Clinic in Rochester, Minn.
The major concern in using heparin for anticoagulation in pregnancy is valve thrombosis. It doubles the risk.
“Pregnancy is the most prothrombotic state there is,” she said. “It’s not like managing a patient through a hip replacement or prostate surgery. Women with a mechanical prosthetic valve should be managed by a heart valve team with expertise in treatment during pregnancy.”
The alternatives to warfarin are adjusted-dose unfractionated heparin, which must be given in a continuous intravenous infusion with meticulous monitoring of activated partial thromboplastin time, or twice-daily low-molecular-weight heparin with dose adjustment by weight and maintenance of a target anti–Factor Xa level of 1.0-1.2 IU/mL.
“If you use low-molecular-weight heparin, you’re going to be seeing that patient every week to monitor anti–Factor Xa 4-6 hours post injection. You’ll find it’s not that easy to stay in the sweet spot, with excellent anticoagulation without an increased risk of maternal thromboembolism, or at the other extreme, fetal bleeding. What might look initially as a relatively easy strategy with a lot of appeal turns out to entail considerable risk,” Dr. Warnes said.
This was underscored in a cautionary report by highly experienced University of Toronto investigators. In their series of 23 pregnancies in 17 women with mechanical heart valves on low-molecular-weight heparin throughout pregnancy with careful monitoring, there was one maternal thromboembolic event resulting in maternal and fetal death despite a documented therapeutic anti–Factor Xa level (Am J Cardiol. 2009 Nov 1;104[9]:1259-63).
Although warfarin is clearly the better anticoagulant for the mother, the fetus pays the price. This was highlighted in a recent report from the ESC Registry of Pregnancy and Cardiac Disease (ROPAC) that compared pregnancy outcomes in 212 patients with a mechanical heart valve, 134 with a tissue valve, and 2,620 women without a prosthetic heart valve. Use of warfarin or another vitamin K antagonist in the first trimester was associated with a higher rate of miscarriage than heparin – 28.6% vs. 9.2% – as well as a 7.1% incidence of late fetal death, compared with just 0.7% with heparin.
On the other hand, the mechanical valve thrombosis rate was 4.7%, with half of those serious events occurring during the first trimester in patients after they’d been switched to heparin (Circulation. 2015 Jul 14;132[2]:132-42).
Hemorrhagic events occurred in 23.1% of mothers with a mechanical heart valve, 5.1% of those with a bioprosthetic valve, and 4.9% of patients without a prosthetic valve. A point worth incorporating into prepregnancy patient counseling, Dr. Warnes noted, is that only 58% of ROPAC participants with a mechanical heart valve had an uncomplicated pregnancy with a live birth, in contrast to 79% of those with a tissue valve and 78% of controls.
Because warfarin crosses the placenta, and it takes about a week for the fetus to eliminate the drug following maternal discontinuation, the guidelines recommend stopping warfarin at about week 36 and changing to a continuous infusion of dose-adjusted unfractionated heparin peridelivery. The heparin should be stopped for as short a time as possible before delivery and resumed 6-12 hours post delivery in order to protect against valve thrombosis.
Of course, opting for a bioprosthetic rather than a mechanical heart valve avoids all these difficult anticoagulation-related issues. But it poses a different serious problem: The younger the patient at the time of tissue valve implantation, the greater the risk of rapid calcification and structural valve deterioration. Indeed, among patients who are age 16-39 when they receive a bioprosthetic valve, the rate of structural valve deterioration is 50% at 10 years and 90% at 15 years.
“There is no ideal valve prosthesis. If you elect a tissue prosthesis, you have to discuss the risk of reoperation in that young woman,” Dr. Warnes advised.
Recent data from the Society of Thoracic Surgeons database indicate the mortality associated with redo elective aortic valve replacement in a 35-year-old woman with no comorbidities averages 1.63%, with a 2% mortality rate for redo mitral valve replacement.
Dr. Warnes reported having no financial conflicts regarding her presentation.
EXPERT ANALYSIS FROM THE CARDIOVASCULAR CONFERENCE AT SNOWMASS

Acupressure improves persistent fatigue in breast cancer survivors
SAN ANTONIO – Self-administered acupressure focused on enhancing relaxation significantly reduced persistent fatigue symptoms in breast cancer survivors, according to a randomized clinical trial presented at the San Antonio Breast Cancer Symposium.
“Self-administered relaxation acupressure offers an inexpensive, easy-to-learn method to manage fatigue and co-occurring poor sleep quality and overall quality of life in breast cancer survivors with persistent fatigue,” said Suzanna M. Zick, N.D., MPH, of the department of family medicine, and the complementary and alternative medicine research center at the University of Michigan, Ann Arbor.

She conducted the study because persistent fatigue is arguably the most common and debilitating symptom experienced by breast cancer survivors, affecting 30% of women for up to 10 years after they’ve completed their breast cancer therapy. Yet treatment options remain limited, she said.
Acupressure is a form of traditional Chinese medicine in which pressure is applied to a few specific acupoints on the body using the fingers, thumbs, or a device. Two forms were evaluated in the three-arm, single-blind clinical trial: relaxation acupressure, traditionally used to improve sleep, and stimulation acupressure, which targets pressure points that boost energy.
Dr. Zick presented a 10-week study in which 288 breast cancer survivors who had completed cancer therapy other than hormone treatment at least 12 months before and who still experienced persistent fatigue as defined by a score of 4 or more on the validated Brief Fatigue Inventory. Participants were randomized single-blind to usual care as directed by their physician or to 6 weeks of relaxation or stimulation acupressure, which they administered on their own after receiving instruction. After 6 weeks, women were instructed to stop the acupressure. They were reassessed at week 10 to determine whether acupressure had a sustained carryover effect.
At 6 weeks, 66% of the relaxation acupressure group and 61% of the stimulation acupressure cohort had achieved a normal Brief Fatigue Inventory score of less than 4, as did only 31% of the usual-care controls. Both acupressure groups showed maintenance of benefit at week 10, after 4 weeks of no acupressure, indicating the self-treatment isn’t something patients need to do continuously in order to derive the desired effect.
While both forms of acupressure were similarly effective at reducing complaints of fatigue, there was an important difference between the two. Only relaxation acupressure resulted in significant improvement in sleep quality as measured on the Pittsburgh Sleep Quality Index. Moreover, relaxation acupressure but not stimulation acupressure resulted in quality-of-life improvements on the somatic, fitness, and social support subscales of the Long-Term Quality of Life scale. However, neither form of acupressure had a significant on the spiritual subscale, the quality-of-life instrument’s fourth subscale.
“We really have to conclude that even though both forms of acupressure reduce fatigue to a similar extent, relaxation acupressure is the one we should think about as being more effective,” Dr. Zick said.
One might have predicted, incorrectly as it turns out, that breast cancer survivors complaining of persistent fatigue would find stimulation acupressure to be more beneficial than relaxation acupressure. Dr. Zick suspects the two techniques might reduce chronic fatigue via different mechanisms. She and her coinvestigators have conducted brain imaging studies that show patients with persistent cancer-related fatigue have three neurochemical markers: elevated brain levels of insular glutamate, which causes excitation, as well as high brain levels of creatine phosphokinase and proinflammatory cytokines. In their next round of imaging studies, the investigators plan to see whether the two forms of acupressure have differing effects on this markers.
Session moderator Dr. Norah Lynn Henry liked the concept of self-administered acupressure.
“The great thing about this is you don’t have to make appointments with an acupuncturist. You can do it at home. But is acupressure ready for prime time in clinical practice?” asked Dr. Henry, a medical oncologist at the University of Michigan.
“My answer is yes,” Dr. Zick replied, “because it’s got pretty much zero side effects, it’s inexpensive, and it’s easy to learn. If it doesn’t work for a person then they can just stop, but if it works, great.”
As the next step in this research, Dr. Zick and her coinvestigators hope to develop a smartphone app to deliver instruction in self-administered relaxation acupressure in a readily accessible way.
Her clinical trial was funded by the National Cancer Institute. She reported having no financial conflicts.
SAN ANTONIO – Self-administered acupressure focused on enhancing relaxation significantly reduced persistent fatigue symptoms in breast cancer survivors, according to a randomized clinical trial presented at the San Antonio Breast Cancer Symposium.
“Self-administered relaxation acupressure offers an inexpensive, easy-to-learn method to manage fatigue and co-occurring poor sleep quality and overall quality of life in breast cancer survivors with persistent fatigue,” said Suzanna M. Zick, N.D., MPH, of the department of family medicine, and the complementary and alternative medicine research center at the University of Michigan, Ann Arbor.
She conducted the study because persistent fatigue is arguably the most common and debilitating symptom experienced by breast cancer survivors, affecting 30% of women for up to 10 years after they’ve completed their breast cancer therapy. Yet treatment options remain limited, she said.
Acupressure is a form of traditional Chinese medicine in which pressure is applied to a few specific acupoints on the body using the fingers, thumbs, or a device. Two forms were evaluated in the three-arm, single-blind clinical trial: relaxation acupressure, traditionally used to improve sleep, and stimulation acupressure, which targets pressure points that boost energy.
Dr. Zick presented a 10-week study in which 288 breast cancer survivors who had completed cancer therapy other than hormone treatment at least 12 months before and who still experienced persistent fatigue as defined by a score of 4 or more on the validated Brief Fatigue Inventory. Participants were randomized single-blind to usual care as directed by their physician or to 6 weeks of relaxation or stimulation acupressure, which they administered on their own after receiving instruction. After 6 weeks, women were instructed to stop the acupressure. They were reassessed at week 10 to determine whether acupressure had a sustained carryover effect.
At 6 weeks, 66% of the relaxation acupressure group and 61% of the stimulation acupressure cohort had achieved a normal Brief Fatigue Inventory score of less than 4, as did only 31% of the usual-care controls. Both acupressure groups showed maintenance of benefit at week 10, after 4 weeks of no acupressure, indicating the self-treatment isn’t something patients need to do continuously in order to derive the desired effect.
While both forms of acupressure were similarly effective at reducing complaints of fatigue, there was an important difference between the two. Only relaxation acupressure resulted in significant improvement in sleep quality as measured on the Pittsburgh Sleep Quality Index. Moreover, relaxation acupressure but not stimulation acupressure resulted in quality-of-life improvements on the somatic, fitness, and social support subscales of the Long-Term Quality of Life scale. However, neither form of acupressure had a significant on the spiritual subscale, the quality-of-life instrument’s fourth subscale.
“We really have to conclude that even though both forms of acupressure reduce fatigue to a similar extent, relaxation acupressure is the one we should think about as being more effective,” Dr. Zick said.
One might have predicted, incorrectly as it turns out, that breast cancer survivors complaining of persistent fatigue would find stimulation acupressure to be more beneficial than relaxation acupressure. Dr. Zick suspects the two techniques might reduce chronic fatigue via different mechanisms. She and her coinvestigators have conducted brain imaging studies that show patients with persistent cancer-related fatigue have three neurochemical markers: elevated brain levels of insular glutamate, which causes excitation, as well as high brain levels of creatine phosphokinase and proinflammatory cytokines. In their next round of imaging studies, the investigators plan to see whether the two forms of acupressure have differing effects on this markers.
Session moderator Dr. Norah Lynn Henry liked the concept of self-administered acupressure.
“The great thing about this is you don’t have to make appointments with an acupuncturist. You can do it at home. But is acupressure ready for prime time in clinical practice?” asked Dr. Henry, a medical oncologist at the University of Michigan.
“My answer is yes,” Dr. Zick replied, “because it’s got pretty much zero side effects, it’s inexpensive, and it’s easy to learn. If it doesn’t work for a person then they can just stop, but if it works, great.”
As the next step in this research, Dr. Zick and her coinvestigators hope to develop a smartphone app to deliver instruction in self-administered relaxation acupressure in a readily accessible way.
Her clinical trial was funded by the National Cancer Institute. She reported having no financial conflicts.
SAN ANTONIO – Self-administered acupressure focused on enhancing relaxation significantly reduced persistent fatigue symptoms in breast cancer survivors, according to a randomized clinical trial presented at the San Antonio Breast Cancer Symposium.
“Self-administered relaxation acupressure offers an inexpensive, easy-to-learn method to manage fatigue and co-occurring poor sleep quality and overall quality of life in breast cancer survivors with persistent fatigue,” said Suzanna M. Zick, N.D., MPH, of the department of family medicine, and the complementary and alternative medicine research center at the University of Michigan, Ann Arbor.
She conducted the study because persistent fatigue is arguably the most common and debilitating symptom experienced by breast cancer survivors, affecting 30% of women for up to 10 years after they’ve completed their breast cancer therapy. Yet treatment options remain limited, she said.
Acupressure is a form of traditional Chinese medicine in which pressure is applied to a few specific acupoints on the body using the fingers, thumbs, or a device. Two forms were evaluated in the three-arm, single-blind clinical trial: relaxation acupressure, traditionally used to improve sleep, and stimulation acupressure, which targets pressure points that boost energy.
Dr. Zick presented a 10-week study in which 288 breast cancer survivors who had completed cancer therapy other than hormone treatment at least 12 months before and who still experienced persistent fatigue as defined by a score of 4 or more on the validated Brief Fatigue Inventory. Participants were randomized single-blind to usual care as directed by their physician or to 6 weeks of relaxation or stimulation acupressure, which they administered on their own after receiving instruction. After 6 weeks, women were instructed to stop the acupressure. They were reassessed at week 10 to determine whether acupressure had a sustained carryover effect.
At 6 weeks, 66% of the relaxation acupressure group and 61% of the stimulation acupressure cohort had achieved a normal Brief Fatigue Inventory score of less than 4, as did only 31% of the usual-care controls. Both acupressure groups showed maintenance of benefit at week 10, after 4 weeks of no acupressure, indicating the self-treatment isn’t something patients need to do continuously in order to derive the desired effect.
While both forms of acupressure were similarly effective at reducing complaints of fatigue, there was an important difference between the two. Only relaxation acupressure resulted in significant improvement in sleep quality as measured on the Pittsburgh Sleep Quality Index. Moreover, relaxation acupressure but not stimulation acupressure resulted in quality-of-life improvements on the somatic, fitness, and social support subscales of the Long-Term Quality of Life scale. However, neither form of acupressure had a significant on the spiritual subscale, the quality-of-life instrument’s fourth subscale.
“We really have to conclude that even though both forms of acupressure reduce fatigue to a similar extent, relaxation acupressure is the one we should think about as being more effective,” Dr. Zick said.
One might have predicted, incorrectly as it turns out, that breast cancer survivors complaining of persistent fatigue would find stimulation acupressure to be more beneficial than relaxation acupressure. Dr. Zick suspects the two techniques might reduce chronic fatigue via different mechanisms. She and her coinvestigators have conducted brain imaging studies that show patients with persistent cancer-related fatigue have three neurochemical markers: elevated brain levels of insular glutamate, which causes excitation, as well as high brain levels of creatine phosphokinase and proinflammatory cytokines. In their next round of imaging studies, the investigators plan to see whether the two forms of acupressure have differing effects on this markers.
Session moderator Dr. Norah Lynn Henry liked the concept of self-administered acupressure.
“The great thing about this is you don’t have to make appointments with an acupuncturist. You can do it at home. But is acupressure ready for prime time in clinical practice?” asked Dr. Henry, a medical oncologist at the University of Michigan.
“My answer is yes,” Dr. Zick replied, “because it’s got pretty much zero side effects, it’s inexpensive, and it’s easy to learn. If it doesn’t work for a person then they can just stop, but if it works, great.”
As the next step in this research, Dr. Zick and her coinvestigators hope to develop a smartphone app to deliver instruction in self-administered relaxation acupressure in a readily accessible way.
Her clinical trial was funded by the National Cancer Institute. She reported having no financial conflicts.
AT SABCS 2015
Key clinical point: Acupressure is an easily learned, effective method for self-treatment of persistent fatigue in breast cancer survivors.
Major finding: Two-thirds of breast cancer survivors with persistent fatigue experienced significant improvement in response to 6 weeks of self-administered relaxation acupressure, compared with 31% of usual-care controls.
Data source: This was a 10-week, single-blind study involving 288 breast cancer survivors with persistent fatigue who were randomized to relaxation acupressure, stimulation acupressure, or usual care.
Disclosures: The study was sponsored by the National Cancer Institute. Dr. Zick reported having no financial conflicts.

Hypertrophic cardiomyopathy: Who should get an ICD?
SNOWMASS, COLO. – Since the 2011 release of the current American College of Cardiology/American Heart Association guidelines on hypertrophic cardiomyopathy, several new evidence-based tools have emerged as being helpful in decision making regarding which patients should receive an implantable cardioverter-defibrillator (ICD) for primary prevention of sudden cardiac death, Dr. Rick A. Nishimura said at the annual Cardiovascular Conference at Snowmass.
These three tools – gadolinium-enhanced cardiovascular magnetic resonance imaging, a novel European risk score calculator, and a new appreciation of the importance of age-related risk – are most useful in the many cases of hypertrophic cardiomyopathy (HCM) where the cardiologist is on the fence regarding ICD placement because the patient doesn’t clearly meet the conventional major criteria for an ICD, according to Dr. Nishimura, professor of medicine at the Mayo Clinic in Rochester, Minn.
Dr. Nishimura, a member of the writing panel for the current guidelines (Circulation. 2011 Dec 13;124[24]:2761-96), predicted these tools will be incorporated into the next iteration of the HCM guidelines.
Notably absent from Dr. Nishimura’s list of useful tools was genetic testing for assessment of SCD risk in a patient with HCM.
“You should not spend $6,000 to do a genetic study to try to predict who’s at risk for sudden death. It turns out that most mutations are neither inherently benign nor malignant. High-risk mutations come from high-risk families, so you can do just as well by taking a family history,” according to the cardiologist.
Dr. Nishimura explained that the clinical dilemma in trying to evaluate SCD risk in a patient who presents with HCM is that the overall risk is quite low – probably 1% or less per year in the total HCM population – yet HCM is the number-one cause of SCD in younger patients. And it can occur unpredictably years or decades after diagnosis of HCM.
While ICDs are of proven effectiveness in preventing SCD in patients with HCM, reliance solely upon the conventional risk predictors to identify those who should get a device is clearly inadequate. Those criteria have a positive predictive accuracy of less than 15%; in other words, roughly 85% of HCM patients who get an ICD never receive an appropriate, life-saving shock, Dr. Nishimura said.
“We have a lot of work left to do in order to better identify these patients. In our own data from the Mayo Clinic, 20%-25% of patients have inappropriate ICD shocks despite efforts to program the device to prevent such shocks. That’s especially common in younger, active patients with HCM, and when it occurs patients find it absolutely devastating,” according to the cardiologist.
As stated in the current guidelines, the established SCD risk factors that provide a strong indication for an ICD in a patient with HCM are prior documented cardiac arrest, ventricular fibrillation, or hemodynamically significant ventricular tachycardia. Additionally, risk factors which, in Dr. Nishimura’s view, probably warrant insertion of an ICD and, at the very least should trigger a physician-patient discussion about the risks and benefits of preventive device therapy, include a family history of HCM-related sudden death in a first-degree relative, massive left ventricular (LV) hypertrophy as defined by a maximum wall thickness of at least 30 mm, and recent unexplained syncope inconsistent with neurocardiogenic origin.
Less potent risk predictors where savvy clinical judgment becomes imperative include nonsustained ventricular tachycardia on 24-hour Holter monitoring, a hypotensive blood pressure response to exercise, and an increased LV wall thickness in a younger patient that doesn’t rise to the 30-mm standard. These are situations where gadolinium-enhanced MRI, consideration of patient age, and the European risk scoring system can help in the decision-making process, he said.
Gadolinium-enhanced MRI: Contrast-enhanced cardiovascular MRI with late gadolinium enhancement has emerged as a reliable marker of the myocyte disarray and interstitial fibrosis which serves as a substrate for ventricular arrhythmias. In a recent study of 1,293 HCM patients followed for a median of 3.3 years, the incidence of SCD events increased progressively with the extent of late gadolinium enhancement. Extensive late gadolinium enhancement, defined as involving at least 15% of LV mass, was associated with a doubled risk of SCD events in patients otherwise considered at low risk (Circulation. 2014 Aug 5;130[6]:484-95).
“This is probably going to become one of the key markers that can help you when you’re on the fence as to whether or not to put in an ICD. We’re getting MRIs with gadolinium now in all of our HCM patients. What matters is not gadolinium enhancement at the insertion of the left ventricle into the septum – a lot of people have that – but diffuse gadolinium enhancement throughout the septum,” Dr. Nishimura said.
Because SCD risk increases linearly with greater maximal LV wall thickness, gadolinium-enhanced MRI is particularly helpful in assessing risk in a younger patient with a maximal LV wall thickness of, say, 26 mm, he added.
Age: A study by led by Dr. Barry J. Maron, the cochair of the 2011 guideline committee and director of the HCM center at the Minneapolis Heart Institute, provides a new understanding that prophylactic ICD implantation is not warranted in patients with HCM who present at age 60 or older. In their study of 428 consecutive patients presenting with HCM at age 60 or above, the investigators found during 5.8 years of follow-up that the incidence of arrhythmic sudden death events was just 0.2% per year (Circulation. 2013 Feb 5;127[5]:585-93).
“They’ve shown that if you look at patients age 60 or above who have HCM, the risk of sudden cardiac death is almost nonexistent. That’s incredibly important to remember. Sudden death is something that’s going to happen in the younger population, under age 30,” Dr. Nishimura emphasized.
European SCD risk prediction tool: This tool was hailed as a major advance in the current European Society of Cardiology guidelines on HCM (Eur Heart J. 2014;35:2733-2779). The tool was incorporated into the guidelines. It is also available as a smartphone app.
The risk prediction tool (Eur Heart J. 2014 Aug 7;35[30]:2010-20) is a complex equation that incorporates seven predictive factors: age, maximal LV wall thickness, left atrial diameter, LV outflow tract gradient, family history of SCD, nonsustained VT, and unexplained syncope. After input on these seven factors, the equation spits out an individual’s estimated 5-year SCD risk. Based on the study of 3,675 consecutive HCM patients with a median 5.7 years of follow-up that was used to develop the risk equation, the current ESC guidelines state that an ICD is not warranted in HCM patients with a 5-year risk below 4%, device implantation should be considered in those whose risk is 4%-6%, and an ICD should be even more strongly considered in patients with a 5-year risk in excess of 6%.
“A lot of people across the pond are using this risk score. But there are some problems with it,” according to Dr. Nishimura.
In his view, it “doesn’t make much sense” to include left ventricular outflow tract gradient or left atrial diameter in the risk equation. Nor is unexplained syncope carefully defined. Also, the equation would be improved by incorporation of late gadolinium enhancement on MRI, left ventricular dysfunction, and presence or absence of apical aneurysm as predictive variables. But on the plus side, the European equation treats maximal LV wall thickness as a continuous variable, which is more appropriate than the single 30-mm cutoff used in the ACC/AHA guidelines.
The biggest limitation of the European prognostic score, however, is that it hasn’t yet been validated in an independent patient cohort, Dr. Nishimura said. He noted that when Dr. Maron and coworkers recently applied the European SCD risk equation retrospectively to 1,629 consecutive U.S. patients with HCM, the investigators concluded that the risk equation proved unreliable for prediction of future SCD events. Fifty-nine percent of patients who got an appropriate ICD shock or experienced SCD were misclassified as low risk and hence would not have received an ICD under the European guidelines (Am J Cardiol. 2015 Sep 1;116[5]:757-64).
Nonetheless, because of the limited predictive accuracy of today’s standard methods of assessing SCD risk, Dr. Nishimura considers application of the European risk score to be “reasonable” in HCM patients who don’t have any of the strong indications for an ICD.
“If it comes up with an estimated 5-year risk greater than 6%, I think it’s very reasonable to consider implantation of an ICD,” he said.
Dr. Nishimura observed that in addition to assessing SCD risk, cardiologists have two other separate essential tasks when a patient presents with HCM. One is to screen and counsel the first-degree relatives. The other is to determine whether a left ventricular outflow tract obstruction is present in a symptomatic patient and, if so, to improve symptoms by treating the associated hemodynamic abnormalities medically and if need be by septal ablation or septal myectomy.
He reported having no financial conflicts of interest regarding his presentation.
SNOWMASS, COLO. – Since the 2011 release of the current American College of Cardiology/American Heart Association guidelines on hypertrophic cardiomyopathy, several new evidence-based tools have emerged as being helpful in decision making regarding which patients should receive an implantable cardioverter-defibrillator (ICD) for primary prevention of sudden cardiac death, Dr. Rick A. Nishimura said at the annual Cardiovascular Conference at Snowmass.
These three tools – gadolinium-enhanced cardiovascular magnetic resonance imaging, a novel European risk score calculator, and a new appreciation of the importance of age-related risk – are most useful in the many cases of hypertrophic cardiomyopathy (HCM) where the cardiologist is on the fence regarding ICD placement because the patient doesn’t clearly meet the conventional major criteria for an ICD, according to Dr. Nishimura, professor of medicine at the Mayo Clinic in Rochester, Minn.
Dr. Nishimura, a member of the writing panel for the current guidelines (Circulation. 2011 Dec 13;124[24]:2761-96), predicted these tools will be incorporated into the next iteration of the HCM guidelines.
Notably absent from Dr. Nishimura’s list of useful tools was genetic testing for assessment of SCD risk in a patient with HCM.
“You should not spend $6,000 to do a genetic study to try to predict who’s at risk for sudden death. It turns out that most mutations are neither inherently benign nor malignant. High-risk mutations come from high-risk families, so you can do just as well by taking a family history,” according to the cardiologist.
Dr. Nishimura explained that the clinical dilemma in trying to evaluate SCD risk in a patient who presents with HCM is that the overall risk is quite low – probably 1% or less per year in the total HCM population – yet HCM is the number-one cause of SCD in younger patients. And it can occur unpredictably years or decades after diagnosis of HCM.
While ICDs are of proven effectiveness in preventing SCD in patients with HCM, reliance solely upon the conventional risk predictors to identify those who should get a device is clearly inadequate. Those criteria have a positive predictive accuracy of less than 15%; in other words, roughly 85% of HCM patients who get an ICD never receive an appropriate, life-saving shock, Dr. Nishimura said.
“We have a lot of work left to do in order to better identify these patients. In our own data from the Mayo Clinic, 20%-25% of patients have inappropriate ICD shocks despite efforts to program the device to prevent such shocks. That’s especially common in younger, active patients with HCM, and when it occurs patients find it absolutely devastating,” according to the cardiologist.
As stated in the current guidelines, the established SCD risk factors that provide a strong indication for an ICD in a patient with HCM are prior documented cardiac arrest, ventricular fibrillation, or hemodynamically significant ventricular tachycardia. Additionally, risk factors which, in Dr. Nishimura’s view, probably warrant insertion of an ICD and, at the very least should trigger a physician-patient discussion about the risks and benefits of preventive device therapy, include a family history of HCM-related sudden death in a first-degree relative, massive left ventricular (LV) hypertrophy as defined by a maximum wall thickness of at least 30 mm, and recent unexplained syncope inconsistent with neurocardiogenic origin.
Less potent risk predictors where savvy clinical judgment becomes imperative include nonsustained ventricular tachycardia on 24-hour Holter monitoring, a hypotensive blood pressure response to exercise, and an increased LV wall thickness in a younger patient that doesn’t rise to the 30-mm standard. These are situations where gadolinium-enhanced MRI, consideration of patient age, and the European risk scoring system can help in the decision-making process, he said.
Gadolinium-enhanced MRI: Contrast-enhanced cardiovascular MRI with late gadolinium enhancement has emerged as a reliable marker of the myocyte disarray and interstitial fibrosis which serves as a substrate for ventricular arrhythmias. In a recent study of 1,293 HCM patients followed for a median of 3.3 years, the incidence of SCD events increased progressively with the extent of late gadolinium enhancement. Extensive late gadolinium enhancement, defined as involving at least 15% of LV mass, was associated with a doubled risk of SCD events in patients otherwise considered at low risk (Circulation. 2014 Aug 5;130[6]:484-95).
“This is probably going to become one of the key markers that can help you when you’re on the fence as to whether or not to put in an ICD. We’re getting MRIs with gadolinium now in all of our HCM patients. What matters is not gadolinium enhancement at the insertion of the left ventricle into the septum – a lot of people have that – but diffuse gadolinium enhancement throughout the septum,” Dr. Nishimura said.
Because SCD risk increases linearly with greater maximal LV wall thickness, gadolinium-enhanced MRI is particularly helpful in assessing risk in a younger patient with a maximal LV wall thickness of, say, 26 mm, he added.
Age: A study by led by Dr. Barry J. Maron, the cochair of the 2011 guideline committee and director of the HCM center at the Minneapolis Heart Institute, provides a new understanding that prophylactic ICD implantation is not warranted in patients with HCM who present at age 60 or older. In their study of 428 consecutive patients presenting with HCM at age 60 or above, the investigators found during 5.8 years of follow-up that the incidence of arrhythmic sudden death events was just 0.2% per year (Circulation. 2013 Feb 5;127[5]:585-93).
“They’ve shown that if you look at patients age 60 or above who have HCM, the risk of sudden cardiac death is almost nonexistent. That’s incredibly important to remember. Sudden death is something that’s going to happen in the younger population, under age 30,” Dr. Nishimura emphasized.
European SCD risk prediction tool: This tool was hailed as a major advance in the current European Society of Cardiology guidelines on HCM (Eur Heart J. 2014;35:2733-2779). The tool was incorporated into the guidelines. It is also available as a smartphone app.
The risk prediction tool (Eur Heart J. 2014 Aug 7;35[30]:2010-20) is a complex equation that incorporates seven predictive factors: age, maximal LV wall thickness, left atrial diameter, LV outflow tract gradient, family history of SCD, nonsustained VT, and unexplained syncope. After input on these seven factors, the equation spits out an individual’s estimated 5-year SCD risk. Based on the study of 3,675 consecutive HCM patients with a median 5.7 years of follow-up that was used to develop the risk equation, the current ESC guidelines state that an ICD is not warranted in HCM patients with a 5-year risk below 4%, device implantation should be considered in those whose risk is 4%-6%, and an ICD should be even more strongly considered in patients with a 5-year risk in excess of 6%.
“A lot of people across the pond are using this risk score. But there are some problems with it,” according to Dr. Nishimura.
In his view, it “doesn’t make much sense” to include left ventricular outflow tract gradient or left atrial diameter in the risk equation. Nor is unexplained syncope carefully defined. Also, the equation would be improved by incorporation of late gadolinium enhancement on MRI, left ventricular dysfunction, and presence or absence of apical aneurysm as predictive variables. But on the plus side, the European equation treats maximal LV wall thickness as a continuous variable, which is more appropriate than the single 30-mm cutoff used in the ACC/AHA guidelines.
The biggest limitation of the European prognostic score, however, is that it hasn’t yet been validated in an independent patient cohort, Dr. Nishimura said. He noted that when Dr. Maron and coworkers recently applied the European SCD risk equation retrospectively to 1,629 consecutive U.S. patients with HCM, the investigators concluded that the risk equation proved unreliable for prediction of future SCD events. Fifty-nine percent of patients who got an appropriate ICD shock or experienced SCD were misclassified as low risk and hence would not have received an ICD under the European guidelines (Am J Cardiol. 2015 Sep 1;116[5]:757-64).
Nonetheless, because of the limited predictive accuracy of today’s standard methods of assessing SCD risk, Dr. Nishimura considers application of the European risk score to be “reasonable” in HCM patients who don’t have any of the strong indications for an ICD.
“If it comes up with an estimated 5-year risk greater than 6%, I think it’s very reasonable to consider implantation of an ICD,” he said.
Dr. Nishimura observed that in addition to assessing SCD risk, cardiologists have two other separate essential tasks when a patient presents with HCM. One is to screen and counsel the first-degree relatives. The other is to determine whether a left ventricular outflow tract obstruction is present in a symptomatic patient and, if so, to improve symptoms by treating the associated hemodynamic abnormalities medically and if need be by septal ablation or septal myectomy.
He reported having no financial conflicts of interest regarding his presentation.
SNOWMASS, COLO. – Since the 2011 release of the current American College of Cardiology/American Heart Association guidelines on hypertrophic cardiomyopathy, several new evidence-based tools have emerged as being helpful in decision making regarding which patients should receive an implantable cardioverter-defibrillator (ICD) for primary prevention of sudden cardiac death, Dr. Rick A. Nishimura said at the annual Cardiovascular Conference at Snowmass.
These three tools – gadolinium-enhanced cardiovascular magnetic resonance imaging, a novel European risk score calculator, and a new appreciation of the importance of age-related risk – are most useful in the many cases of hypertrophic cardiomyopathy (HCM) where the cardiologist is on the fence regarding ICD placement because the patient doesn’t clearly meet the conventional major criteria for an ICD, according to Dr. Nishimura, professor of medicine at the Mayo Clinic in Rochester, Minn.
Dr. Nishimura, a member of the writing panel for the current guidelines (Circulation. 2011 Dec 13;124[24]:2761-96), predicted these tools will be incorporated into the next iteration of the HCM guidelines.
Notably absent from Dr. Nishimura’s list of useful tools was genetic testing for assessment of SCD risk in a patient with HCM.
“You should not spend $6,000 to do a genetic study to try to predict who’s at risk for sudden death. It turns out that most mutations are neither inherently benign nor malignant. High-risk mutations come from high-risk families, so you can do just as well by taking a family history,” according to the cardiologist.
Dr. Nishimura explained that the clinical dilemma in trying to evaluate SCD risk in a patient who presents with HCM is that the overall risk is quite low – probably 1% or less per year in the total HCM population – yet HCM is the number-one cause of SCD in younger patients. And it can occur unpredictably years or decades after diagnosis of HCM.
While ICDs are of proven effectiveness in preventing SCD in patients with HCM, reliance solely upon the conventional risk predictors to identify those who should get a device is clearly inadequate. Those criteria have a positive predictive accuracy of less than 15%; in other words, roughly 85% of HCM patients who get an ICD never receive an appropriate, life-saving shock, Dr. Nishimura said.
“We have a lot of work left to do in order to better identify these patients. In our own data from the Mayo Clinic, 20%-25% of patients have inappropriate ICD shocks despite efforts to program the device to prevent such shocks. That’s especially common in younger, active patients with HCM, and when it occurs patients find it absolutely devastating,” according to the cardiologist.
As stated in the current guidelines, the established SCD risk factors that provide a strong indication for an ICD in a patient with HCM are prior documented cardiac arrest, ventricular fibrillation, or hemodynamically significant ventricular tachycardia. Additionally, risk factors which, in Dr. Nishimura’s view, probably warrant insertion of an ICD and, at the very least should trigger a physician-patient discussion about the risks and benefits of preventive device therapy, include a family history of HCM-related sudden death in a first-degree relative, massive left ventricular (LV) hypertrophy as defined by a maximum wall thickness of at least 30 mm, and recent unexplained syncope inconsistent with neurocardiogenic origin.
Less potent risk predictors where savvy clinical judgment becomes imperative include nonsustained ventricular tachycardia on 24-hour Holter monitoring, a hypotensive blood pressure response to exercise, and an increased LV wall thickness in a younger patient that doesn’t rise to the 30-mm standard. These are situations where gadolinium-enhanced MRI, consideration of patient age, and the European risk scoring system can help in the decision-making process, he said.
Gadolinium-enhanced MRI: Contrast-enhanced cardiovascular MRI with late gadolinium enhancement has emerged as a reliable marker of the myocyte disarray and interstitial fibrosis which serves as a substrate for ventricular arrhythmias. In a recent study of 1,293 HCM patients followed for a median of 3.3 years, the incidence of SCD events increased progressively with the extent of late gadolinium enhancement. Extensive late gadolinium enhancement, defined as involving at least 15% of LV mass, was associated with a doubled risk of SCD events in patients otherwise considered at low risk (Circulation. 2014 Aug 5;130[6]:484-95).
“This is probably going to become one of the key markers that can help you when you’re on the fence as to whether or not to put in an ICD. We’re getting MRIs with gadolinium now in all of our HCM patients. What matters is not gadolinium enhancement at the insertion of the left ventricle into the septum – a lot of people have that – but diffuse gadolinium enhancement throughout the septum,” Dr. Nishimura said.
Because SCD risk increases linearly with greater maximal LV wall thickness, gadolinium-enhanced MRI is particularly helpful in assessing risk in a younger patient with a maximal LV wall thickness of, say, 26 mm, he added.
Age: A study by led by Dr. Barry J. Maron, the cochair of the 2011 guideline committee and director of the HCM center at the Minneapolis Heart Institute, provides a new understanding that prophylactic ICD implantation is not warranted in patients with HCM who present at age 60 or older. In their study of 428 consecutive patients presenting with HCM at age 60 or above, the investigators found during 5.8 years of follow-up that the incidence of arrhythmic sudden death events was just 0.2% per year (Circulation. 2013 Feb 5;127[5]:585-93).
“They’ve shown that if you look at patients age 60 or above who have HCM, the risk of sudden cardiac death is almost nonexistent. That’s incredibly important to remember. Sudden death is something that’s going to happen in the younger population, under age 30,” Dr. Nishimura emphasized.
European SCD risk prediction tool: This tool was hailed as a major advance in the current European Society of Cardiology guidelines on HCM (Eur Heart J. 2014;35:2733-2779). The tool was incorporated into the guidelines. It is also available as a smartphone app.
The risk prediction tool (Eur Heart J. 2014 Aug 7;35[30]:2010-20) is a complex equation that incorporates seven predictive factors: age, maximal LV wall thickness, left atrial diameter, LV outflow tract gradient, family history of SCD, nonsustained VT, and unexplained syncope. After input on these seven factors, the equation spits out an individual’s estimated 5-year SCD risk. Based on the study of 3,675 consecutive HCM patients with a median 5.7 years of follow-up that was used to develop the risk equation, the current ESC guidelines state that an ICD is not warranted in HCM patients with a 5-year risk below 4%, device implantation should be considered in those whose risk is 4%-6%, and an ICD should be even more strongly considered in patients with a 5-year risk in excess of 6%.
“A lot of people across the pond are using this risk score. But there are some problems with it,” according to Dr. Nishimura.
In his view, it “doesn’t make much sense” to include left ventricular outflow tract gradient or left atrial diameter in the risk equation. Nor is unexplained syncope carefully defined. Also, the equation would be improved by incorporation of late gadolinium enhancement on MRI, left ventricular dysfunction, and presence or absence of apical aneurysm as predictive variables. But on the plus side, the European equation treats maximal LV wall thickness as a continuous variable, which is more appropriate than the single 30-mm cutoff used in the ACC/AHA guidelines.
The biggest limitation of the European prognostic score, however, is that it hasn’t yet been validated in an independent patient cohort, Dr. Nishimura said. He noted that when Dr. Maron and coworkers recently applied the European SCD risk equation retrospectively to 1,629 consecutive U.S. patients with HCM, the investigators concluded that the risk equation proved unreliable for prediction of future SCD events. Fifty-nine percent of patients who got an appropriate ICD shock or experienced SCD were misclassified as low risk and hence would not have received an ICD under the European guidelines (Am J Cardiol. 2015 Sep 1;116[5]:757-64).
Nonetheless, because of the limited predictive accuracy of today’s standard methods of assessing SCD risk, Dr. Nishimura considers application of the European risk score to be “reasonable” in HCM patients who don’t have any of the strong indications for an ICD.
“If it comes up with an estimated 5-year risk greater than 6%, I think it’s very reasonable to consider implantation of an ICD,” he said.
Dr. Nishimura observed that in addition to assessing SCD risk, cardiologists have two other separate essential tasks when a patient presents with HCM. One is to screen and counsel the first-degree relatives. The other is to determine whether a left ventricular outflow tract obstruction is present in a symptomatic patient and, if so, to improve symptoms by treating the associated hemodynamic abnormalities medically and if need be by septal ablation or septal myectomy.
He reported having no financial conflicts of interest regarding his presentation.
EXPERT ANALYSIS FROM THE CARDIOVASCULAR CONFERENCE AT SNOWMASS
Experts say abandon aspirin for stroke prevention in atrial fib
SNOWMASS, COLO. – It’s time to eliminate the practice of prescribing aspirin for stroke prevention in patients with atrial fibrillation and a CHA2DS2-VASc score of 1, two eminent cardiologists agreed at the Annual Cardiovascular Conference at Snowmass.
“The European guidelines have done away with aspirin for stroke prevention in atrial fibrillation. It barely made it into our current U.S. guidelines. I don’t think aspirin should be in there and I don’t think it will be there in the next guidelines. The role of aspirin will fall away,” predicted Dr. Bernard J. Gersh, professor of medicine at the Mayo Clinic in Rochester, Minn.

“It’s not that aspirin is less effective than the oral anticoagulants, it’s that there’s no role for it. There are no good data to support aspirin in the prevention of stroke in atrial fibrillation,” he declared.
Dr. N.A. Mark Estes III agreed the aspirin evidence is seriously flawed.
“The use of aspirin has probably been misguided, based upon a single trial which showed a profound effect and was probably just an anomaly,” according to Dr. Estes, a past president of the Heart Rhythm Society who is professor of medicine and director of the New England Cardiac Arrhythmia Center at Tufts University, Boston.

The sole positive clinical trial of aspirin versus placebo, the 25-year-old Stroke Prevention in Atrial Fibrillation (SPAF) study (Circulation. 1991 Aug;84[2]:527-39), found an unrealistically high stroke protection benefit for aspirin, a result made implausible by multiple other randomized trials showing no benefit, the cardiologists agreed.
“In our current guidelines for atrial fibrillation (Circulation. 2014 Dec 2;130[23]:2071-104), aspirin can be considered as a Class IIb level of evidence C recommendation in patients with a CHA2DS2-VASc of 1. But I would just take it off of your clinical armamentarium because the best available data indicates that it doesn’t prevent strokes. I’m certainly not using it in my patients. Increasingly in my patients with a CHA2DS2-VASc of 1, I’m discussing the risks and benefits of a NOAC [novel oral anticoagulant],” Dr. Estes said.
Dr. Gersh was also critical of another common practice in stroke prevention in atrial fibrillation: concomitant use of aspirin with an oral anticoagulant.
“We use too much aspirin in patients on oral anticoagulation. Aspirin is perhaps the major cause of bleeding in patients on an oral anticoagulant. Other than in people with a drug-eluting stent, there’s no role at all for aspirin in stroke prevention,” he asserted.
He was coauthor of an analysis of 7,347 participants in the Outcomes Registry for Better Informed Treatment of Atrial Fibrillation (ORBIT-AF) who were on an oral anticoagulant. Fully 35% of them were also on aspirin. In a multivariate analysis, concomitant aspirin and oral anticoagulation was independently associated with a 53% increased risk of major bleeding and a 52% increase in hospitalization for bleeding, compared with atrial fibrillation patients on an oral anticoagulant alone (Circulation. 2013 Aug 13;128[7]:721-8).
Moreover, the widespread use of dual therapy in this real-world registry didn’t appear to be rational. Thirty-nine percent of those on aspirin plus an oral anticoagulant had no history of atherosclerotic disease, the presence of which would be an indication for considering aspirin. And 17% of dual therapy patients had an elevated Anticoagulation and Risk Factors in Atrial Fibrillation (ATRIA) risk score of 5 or more, making dual therapy particularly risky.
This clinically important interaction between aspirin and oral anticoagulation was recently underscored in an analysis of rivaroxaban-treated patients in the ROCKET AF trial, Dr. Gersh observed. Long-term use of aspirin at entry into this pivotal randomized trial of rivaroxaban (Xarelto) versus warfarin in patients with atrial fibrillation proved to be an independent predictor of a 47% increase in the risk of gastrointestinal bleeding, compared with patients on rivaroxaban alone (J Am Coll Cardiol. 2015 Dec 1;66[21]:2271-81).
He added that there is no evidence that combining aspirin and oral anticoagulation enhances stroke prevention beyond the marked benefit achieved with oral anticoagulation alone.
Dr. Gersh reported serving on the leadership of the ORBIT-AF Registry, which was sponsored by Janssen Pharmaceuticals. Dr. Estes reported having no financial conflicts relevant to this discussion.
SNOWMASS, COLO. – It’s time to eliminate the practice of prescribing aspirin for stroke prevention in patients with atrial fibrillation and a CHA2DS2-VASc score of 1, two eminent cardiologists agreed at the Annual Cardiovascular Conference at Snowmass.
“The European guidelines have done away with aspirin for stroke prevention in atrial fibrillation. It barely made it into our current U.S. guidelines. I don’t think aspirin should be in there and I don’t think it will be there in the next guidelines. The role of aspirin will fall away,” predicted Dr. Bernard J. Gersh, professor of medicine at the Mayo Clinic in Rochester, Minn.
“It’s not that aspirin is less effective than the oral anticoagulants, it’s that there’s no role for it. There are no good data to support aspirin in the prevention of stroke in atrial fibrillation,” he declared.
Dr. N.A. Mark Estes III agreed the aspirin evidence is seriously flawed.
“The use of aspirin has probably been misguided, based upon a single trial which showed a profound effect and was probably just an anomaly,” according to Dr. Estes, a past president of the Heart Rhythm Society who is professor of medicine and director of the New England Cardiac Arrhythmia Center at Tufts University, Boston.
The sole positive clinical trial of aspirin versus placebo, the 25-year-old Stroke Prevention in Atrial Fibrillation (SPAF) study (Circulation. 1991 Aug;84[2]:527-39), found an unrealistically high stroke protection benefit for aspirin, a result made implausible by multiple other randomized trials showing no benefit, the cardiologists agreed.
“In our current guidelines for atrial fibrillation (Circulation. 2014 Dec 2;130[23]:2071-104), aspirin can be considered as a Class IIb level of evidence C recommendation in patients with a CHA2DS2-VASc of 1. But I would just take it off of your clinical armamentarium because the best available data indicates that it doesn’t prevent strokes. I’m certainly not using it in my patients. Increasingly in my patients with a CHA2DS2-VASc of 1, I’m discussing the risks and benefits of a NOAC [novel oral anticoagulant],” Dr. Estes said.
Dr. Gersh was also critical of another common practice in stroke prevention in atrial fibrillation: concomitant use of aspirin with an oral anticoagulant.
“We use too much aspirin in patients on oral anticoagulation. Aspirin is perhaps the major cause of bleeding in patients on an oral anticoagulant. Other than in people with a drug-eluting stent, there’s no role at all for aspirin in stroke prevention,” he asserted.
He was coauthor of an analysis of 7,347 participants in the Outcomes Registry for Better Informed Treatment of Atrial Fibrillation (ORBIT-AF) who were on an oral anticoagulant. Fully 35% of them were also on aspirin. In a multivariate analysis, concomitant aspirin and oral anticoagulation was independently associated with a 53% increased risk of major bleeding and a 52% increase in hospitalization for bleeding, compared with atrial fibrillation patients on an oral anticoagulant alone (Circulation. 2013 Aug 13;128[7]:721-8).
Moreover, the widespread use of dual therapy in this real-world registry didn’t appear to be rational. Thirty-nine percent of those on aspirin plus an oral anticoagulant had no history of atherosclerotic disease, the presence of which would be an indication for considering aspirin. And 17% of dual therapy patients had an elevated Anticoagulation and Risk Factors in Atrial Fibrillation (ATRIA) risk score of 5 or more, making dual therapy particularly risky.
This clinically important interaction between aspirin and oral anticoagulation was recently underscored in an analysis of rivaroxaban-treated patients in the ROCKET AF trial, Dr. Gersh observed. Long-term use of aspirin at entry into this pivotal randomized trial of rivaroxaban (Xarelto) versus warfarin in patients with atrial fibrillation proved to be an independent predictor of a 47% increase in the risk of gastrointestinal bleeding, compared with patients on rivaroxaban alone (J Am Coll Cardiol. 2015 Dec 1;66[21]:2271-81).
He added that there is no evidence that combining aspirin and oral anticoagulation enhances stroke prevention beyond the marked benefit achieved with oral anticoagulation alone.
Dr. Gersh reported serving on the leadership of the ORBIT-AF Registry, which was sponsored by Janssen Pharmaceuticals. Dr. Estes reported having no financial conflicts relevant to this discussion.
SNOWMASS, COLO. – It’s time to eliminate the practice of prescribing aspirin for stroke prevention in patients with atrial fibrillation and a CHA2DS2-VASc score of 1, two eminent cardiologists agreed at the Annual Cardiovascular Conference at Snowmass.
“The European guidelines have done away with aspirin for stroke prevention in atrial fibrillation. It barely made it into our current U.S. guidelines. I don’t think aspirin should be in there and I don’t think it will be there in the next guidelines. The role of aspirin will fall away,” predicted Dr. Bernard J. Gersh, professor of medicine at the Mayo Clinic in Rochester, Minn.
“It’s not that aspirin is less effective than the oral anticoagulants, it’s that there’s no role for it. There are no good data to support aspirin in the prevention of stroke in atrial fibrillation,” he declared.
Dr. N.A. Mark Estes III agreed the aspirin evidence is seriously flawed.
“The use of aspirin has probably been misguided, based upon a single trial which showed a profound effect and was probably just an anomaly,” according to Dr. Estes, a past president of the Heart Rhythm Society who is professor of medicine and director of the New England Cardiac Arrhythmia Center at Tufts University, Boston.
The sole positive clinical trial of aspirin versus placebo, the 25-year-old Stroke Prevention in Atrial Fibrillation (SPAF) study (Circulation. 1991 Aug;84[2]:527-39), found an unrealistically high stroke protection benefit for aspirin, a result made implausible by multiple other randomized trials showing no benefit, the cardiologists agreed.
“In our current guidelines for atrial fibrillation (Circulation. 2014 Dec 2;130[23]:2071-104), aspirin can be considered as a Class IIb level of evidence C recommendation in patients with a CHA2DS2-VASc of 1. But I would just take it off of your clinical armamentarium because the best available data indicates that it doesn’t prevent strokes. I’m certainly not using it in my patients. Increasingly in my patients with a CHA2DS2-VASc of 1, I’m discussing the risks and benefits of a NOAC [novel oral anticoagulant],” Dr. Estes said.
Dr. Gersh was also critical of another common practice in stroke prevention in atrial fibrillation: concomitant use of aspirin with an oral anticoagulant.
“We use too much aspirin in patients on oral anticoagulation. Aspirin is perhaps the major cause of bleeding in patients on an oral anticoagulant. Other than in people with a drug-eluting stent, there’s no role at all for aspirin in stroke prevention,” he asserted.
He was coauthor of an analysis of 7,347 participants in the Outcomes Registry for Better Informed Treatment of Atrial Fibrillation (ORBIT-AF) who were on an oral anticoagulant. Fully 35% of them were also on aspirin. In a multivariate analysis, concomitant aspirin and oral anticoagulation was independently associated with a 53% increased risk of major bleeding and a 52% increase in hospitalization for bleeding, compared with atrial fibrillation patients on an oral anticoagulant alone (Circulation. 2013 Aug 13;128[7]:721-8).
Moreover, the widespread use of dual therapy in this real-world registry didn’t appear to be rational. Thirty-nine percent of those on aspirin plus an oral anticoagulant had no history of atherosclerotic disease, the presence of which would be an indication for considering aspirin. And 17% of dual therapy patients had an elevated Anticoagulation and Risk Factors in Atrial Fibrillation (ATRIA) risk score of 5 or more, making dual therapy particularly risky.
This clinically important interaction between aspirin and oral anticoagulation was recently underscored in an analysis of rivaroxaban-treated patients in the ROCKET AF trial, Dr. Gersh observed. Long-term use of aspirin at entry into this pivotal randomized trial of rivaroxaban (Xarelto) versus warfarin in patients with atrial fibrillation proved to be an independent predictor of a 47% increase in the risk of gastrointestinal bleeding, compared with patients on rivaroxaban alone (J Am Coll Cardiol. 2015 Dec 1;66[21]:2271-81).
He added that there is no evidence that combining aspirin and oral anticoagulation enhances stroke prevention beyond the marked benefit achieved with oral anticoagulation alone.
Dr. Gersh reported serving on the leadership of the ORBIT-AF Registry, which was sponsored by Janssen Pharmaceuticals. Dr. Estes reported having no financial conflicts relevant to this discussion.
EXPERT ANALYSIS FROM THE CARDIOVASCULAR CONFERENCE AT SNOWMASS

A call for definitive trial of statins in breast cancer
SAN ANTONIO – A definitive phase III randomized controlled trial of statin therapy during adjuvant endocrine therapy for breast cancer is warranted in light of recent encouraging evidence pointing to a protective effect against disease recurrence, Melissa L. Bondy, Ph.D., said at the San Antonio Breast Cancer Symposium.
“The next phase of research in this area is to learn whether we can improve survival in breast cancer patients by having them take cholesterol-lowering medication. We really need to have a phase III trial in the adjuvant setting that includes these cholesterol-lowering drugs,” said Dr. Bondy, professor of cancer prevention and population sciences at Baylor Medical College, Houston.
Her call for a formal, randomized trial came while serving as discussant for two positive reports of an apparent beneficial effect of statins on breast cancer recurrence-free survival: one from the BIG 1-98 trial of adjuvant endocrine therapy for early-stage breast cancer, the other a meta-analysis of 12 published studies totaling 72,774 breast cancer patients.

Dr. Bondy found particularly compelling the Breast International Group (BIG) 1-98 study results presented by Dr. Signe Borgquist, an oncologist at Lund (Sweden) University. This secondary analysis of the impact of cholesterol-lowering medication included 7,963 postmenopausal women with early-stage, estrogen receptor–positive invasive breast cancer who were randomized to 5 years of tamoxifen, the aromatase inhibitor letrozole (Femara), or the two drugs in sequence. Serum total cholesterol levels and the use of cholesterol-lowering medications – a decision left up to individual physicians and patients – were assessed at baseline and again every 6 months for 5.5 years.
With a median 8 years of prospective follow-up, during which 1,432 patients experienced breast cancer recurrence, the disease-free survival rate was 18% higher in the 637 patients already on cholesterol-lowering medication – mainly statins – at enrollment, compared with those who were not. The distant recurrence-free interval was 19% better as well, with both analyses adjusted for their form of endocrine therapy, tumor size and grade, nodal status, local therapy, peritumoral vascular invasion, and other potential confounders.
Another 697 BIG 1-98 participants initiated cholesterol-lowering medication during their adjuvant endocrine therapy. In multivariate adjusted analyses, their disease-free survival rate was 21% greater and distant recurrence-free interval was 26% better than in participants not on a statin or other cholesterol-lowering medication during the trial.
As a possible mechanism by which statins might exert anticancer effects, Dr. Borgquist proposed that lowering cholesterol levels may deprive tumor cells of the ability to satisfy their increased demand for cholesterol uptake. This is a result of attenuated signaling through the estrogen receptor by the cholesterol metabolite 27-hydroxycholesterol, levels of which correlate with systemic total cholesterol.
Dr. Bondy offered another possible explanation for the reduced risk of breast cancer recurrence seen in women on cholesterol-lowering medication in BIG 1-98: “Many groups have shown that LDL affects the immune system by binding and inactivating all kinds of microorganisms and their toxic products. In other words, statins appear to affect the microbiome.”
She commented that, although the use of statins was nonrandomized in BIG 1-98, she was favorably impressed by the 8-year follow-up and careful monitoring of total cholesterol levels at 6-month intervals throughout the 5 years of adjuvant endocrine therapy.
Dr. Bondy noted that other studies – again, nonrandomized – suggest statins also interrupt the growth of colorectal cancer and other malignancies.

Dr. Sashidhar Manthravadi presented a meta-analysis of the 12 published studies that have reported data on the association of statins with recurrence-free and/or overall survival in breast cancer patients. Statin use was associated with a significant 34% improvement in recurrence-free survival.
Moreover, this benefit was confined to breast cancer patients on the lipophilic statins atorvastatin and simvastatin; the use of hydrophilic statins was not associated with a significant improvement in recurrence-free survival, according to Dr. Manthravadi, an internal medicine resident at the University of Missouri, Kansas City.
The use of statins also was associated with a 27% improvement in breast cancer–specific survival and a 33% improvement in overall survival, compared with statin nonusers; however, neither of these results achieved statistical significance, he added.
Dr. Bondy cautioned against making too much of the apparent distinction between lipophilic and hydrophilic statin in terms of protection against breast cancer recurrence, given the inherent limitations of a meta-analysis.
“There’s always a lot of missing information, as well as a failure to adjust for comorbidities. And follow-up times in these 12 studies ranged from 2.5 to 11.5 years,” she noted.
The ongoing BIG 1-98 trial is sponsored by the International Breast Cancer Study Group. Dr. Borgquist, Dr. Bondy, and Dr. Manthravadi reported having no financial conflicts of interest.
SAN ANTONIO – A definitive phase III randomized controlled trial of statin therapy during adjuvant endocrine therapy for breast cancer is warranted in light of recent encouraging evidence pointing to a protective effect against disease recurrence, Melissa L. Bondy, Ph.D., said at the San Antonio Breast Cancer Symposium.
“The next phase of research in this area is to learn whether we can improve survival in breast cancer patients by having them take cholesterol-lowering medication. We really need to have a phase III trial in the adjuvant setting that includes these cholesterol-lowering drugs,” said Dr. Bondy, professor of cancer prevention and population sciences at Baylor Medical College, Houston.
Her call for a formal, randomized trial came while serving as discussant for two positive reports of an apparent beneficial effect of statins on breast cancer recurrence-free survival: one from the BIG 1-98 trial of adjuvant endocrine therapy for early-stage breast cancer, the other a meta-analysis of 12 published studies totaling 72,774 breast cancer patients.
Dr. Bondy found particularly compelling the Breast International Group (BIG) 1-98 study results presented by Dr. Signe Borgquist, an oncologist at Lund (Sweden) University. This secondary analysis of the impact of cholesterol-lowering medication included 7,963 postmenopausal women with early-stage, estrogen receptor–positive invasive breast cancer who were randomized to 5 years of tamoxifen, the aromatase inhibitor letrozole (Femara), or the two drugs in sequence. Serum total cholesterol levels and the use of cholesterol-lowering medications – a decision left up to individual physicians and patients – were assessed at baseline and again every 6 months for 5.5 years.
With a median 8 years of prospective follow-up, during which 1,432 patients experienced breast cancer recurrence, the disease-free survival rate was 18% higher in the 637 patients already on cholesterol-lowering medication – mainly statins – at enrollment, compared with those who were not. The distant recurrence-free interval was 19% better as well, with both analyses adjusted for their form of endocrine therapy, tumor size and grade, nodal status, local therapy, peritumoral vascular invasion, and other potential confounders.
Another 697 BIG 1-98 participants initiated cholesterol-lowering medication during their adjuvant endocrine therapy. In multivariate adjusted analyses, their disease-free survival rate was 21% greater and distant recurrence-free interval was 26% better than in participants not on a statin or other cholesterol-lowering medication during the trial.
As a possible mechanism by which statins might exert anticancer effects, Dr. Borgquist proposed that lowering cholesterol levels may deprive tumor cells of the ability to satisfy their increased demand for cholesterol uptake. This is a result of attenuated signaling through the estrogen receptor by the cholesterol metabolite 27-hydroxycholesterol, levels of which correlate with systemic total cholesterol.
Dr. Bondy offered another possible explanation for the reduced risk of breast cancer recurrence seen in women on cholesterol-lowering medication in BIG 1-98: “Many groups have shown that LDL affects the immune system by binding and inactivating all kinds of microorganisms and their toxic products. In other words, statins appear to affect the microbiome.”
She commented that, although the use of statins was nonrandomized in BIG 1-98, she was favorably impressed by the 8-year follow-up and careful monitoring of total cholesterol levels at 6-month intervals throughout the 5 years of adjuvant endocrine therapy.
Dr. Bondy noted that other studies – again, nonrandomized – suggest statins also interrupt the growth of colorectal cancer and other malignancies.
Dr. Sashidhar Manthravadi presented a meta-analysis of the 12 published studies that have reported data on the association of statins with recurrence-free and/or overall survival in breast cancer patients. Statin use was associated with a significant 34% improvement in recurrence-free survival.
Moreover, this benefit was confined to breast cancer patients on the lipophilic statins atorvastatin and simvastatin; the use of hydrophilic statins was not associated with a significant improvement in recurrence-free survival, according to Dr. Manthravadi, an internal medicine resident at the University of Missouri, Kansas City.
The use of statins also was associated with a 27% improvement in breast cancer–specific survival and a 33% improvement in overall survival, compared with statin nonusers; however, neither of these results achieved statistical significance, he added.
Dr. Bondy cautioned against making too much of the apparent distinction between lipophilic and hydrophilic statin in terms of protection against breast cancer recurrence, given the inherent limitations of a meta-analysis.
“There’s always a lot of missing information, as well as a failure to adjust for comorbidities. And follow-up times in these 12 studies ranged from 2.5 to 11.5 years,” she noted.
The ongoing BIG 1-98 trial is sponsored by the International Breast Cancer Study Group. Dr. Borgquist, Dr. Bondy, and Dr. Manthravadi reported having no financial conflicts of interest.
SAN ANTONIO – A definitive phase III randomized controlled trial of statin therapy during adjuvant endocrine therapy for breast cancer is warranted in light of recent encouraging evidence pointing to a protective effect against disease recurrence, Melissa L. Bondy, Ph.D., said at the San Antonio Breast Cancer Symposium.
“The next phase of research in this area is to learn whether we can improve survival in breast cancer patients by having them take cholesterol-lowering medication. We really need to have a phase III trial in the adjuvant setting that includes these cholesterol-lowering drugs,” said Dr. Bondy, professor of cancer prevention and population sciences at Baylor Medical College, Houston.
Her call for a formal, randomized trial came while serving as discussant for two positive reports of an apparent beneficial effect of statins on breast cancer recurrence-free survival: one from the BIG 1-98 trial of adjuvant endocrine therapy for early-stage breast cancer, the other a meta-analysis of 12 published studies totaling 72,774 breast cancer patients.
Dr. Bondy found particularly compelling the Breast International Group (BIG) 1-98 study results presented by Dr. Signe Borgquist, an oncologist at Lund (Sweden) University. This secondary analysis of the impact of cholesterol-lowering medication included 7,963 postmenopausal women with early-stage, estrogen receptor–positive invasive breast cancer who were randomized to 5 years of tamoxifen, the aromatase inhibitor letrozole (Femara), or the two drugs in sequence. Serum total cholesterol levels and the use of cholesterol-lowering medications – a decision left up to individual physicians and patients – were assessed at baseline and again every 6 months for 5.5 years.
With a median 8 years of prospective follow-up, during which 1,432 patients experienced breast cancer recurrence, the disease-free survival rate was 18% higher in the 637 patients already on cholesterol-lowering medication – mainly statins – at enrollment, compared with those who were not. The distant recurrence-free interval was 19% better as well, with both analyses adjusted for their form of endocrine therapy, tumor size and grade, nodal status, local therapy, peritumoral vascular invasion, and other potential confounders.
Another 697 BIG 1-98 participants initiated cholesterol-lowering medication during their adjuvant endocrine therapy. In multivariate adjusted analyses, their disease-free survival rate was 21% greater and distant recurrence-free interval was 26% better than in participants not on a statin or other cholesterol-lowering medication during the trial.
As a possible mechanism by which statins might exert anticancer effects, Dr. Borgquist proposed that lowering cholesterol levels may deprive tumor cells of the ability to satisfy their increased demand for cholesterol uptake. This is a result of attenuated signaling through the estrogen receptor by the cholesterol metabolite 27-hydroxycholesterol, levels of which correlate with systemic total cholesterol.
Dr. Bondy offered another possible explanation for the reduced risk of breast cancer recurrence seen in women on cholesterol-lowering medication in BIG 1-98: “Many groups have shown that LDL affects the immune system by binding and inactivating all kinds of microorganisms and their toxic products. In other words, statins appear to affect the microbiome.”
She commented that, although the use of statins was nonrandomized in BIG 1-98, she was favorably impressed by the 8-year follow-up and careful monitoring of total cholesterol levels at 6-month intervals throughout the 5 years of adjuvant endocrine therapy.
Dr. Bondy noted that other studies – again, nonrandomized – suggest statins also interrupt the growth of colorectal cancer and other malignancies.
Dr. Sashidhar Manthravadi presented a meta-analysis of the 12 published studies that have reported data on the association of statins with recurrence-free and/or overall survival in breast cancer patients. Statin use was associated with a significant 34% improvement in recurrence-free survival.
Moreover, this benefit was confined to breast cancer patients on the lipophilic statins atorvastatin and simvastatin; the use of hydrophilic statins was not associated with a significant improvement in recurrence-free survival, according to Dr. Manthravadi, an internal medicine resident at the University of Missouri, Kansas City.
The use of statins also was associated with a 27% improvement in breast cancer–specific survival and a 33% improvement in overall survival, compared with statin nonusers; however, neither of these results achieved statistical significance, he added.
Dr. Bondy cautioned against making too much of the apparent distinction between lipophilic and hydrophilic statin in terms of protection against breast cancer recurrence, given the inherent limitations of a meta-analysis.
“There’s always a lot of missing information, as well as a failure to adjust for comorbidities. And follow-up times in these 12 studies ranged from 2.5 to 11.5 years,” she noted.
The ongoing BIG 1-98 trial is sponsored by the International Breast Cancer Study Group. Dr. Borgquist, Dr. Bondy, and Dr. Manthravadi reported having no financial conflicts of interest.
EXPERT ANALYSIS FROM SABCS 2015

New-onset AF During Hospitalization Is More Lethal in Women
ORLANDO – Women are at lower risk than men for new-onset atrial fibrillation during hospitalization, but when it does occur it’s associated with significantly greater in-hospital mortality, according to a massive retrospective study presented at the American Heart Association scientific sessions.
Dr. Philip W. Chui analyzed 38,403,360 cases of new-onset atrial fibrillation during hospitalization (NOAF) in 2001-2011. The source was the National Inpatient Sample database. Fully 85% of all cases occurred in patients admitted for noncardiac surgery, which also was the cause of admission with the lowest incidence of NOAF. Among the patients hospitalized for sepsis, women were 27% less likely than men to develop new-onset atrial fibrillation, but when they did they were 13% more likely to die in-hospital.
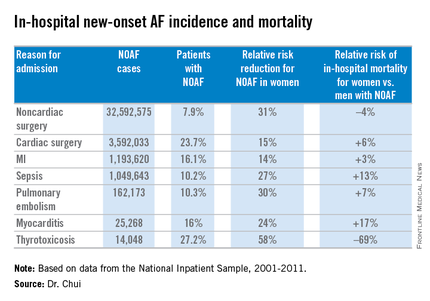
In a multivariate logistic regression analysis extensively adjusted for numerous comorbid conditions and demographic factors, female gender was associated with a significantly reduced risk of NOAF across the board for all major admitting conditions known to be triggers for NOAF. The magnitude of this relative risk reduction favoring women ranged from as low as 14% for patients with an admitting diagnosis of acute MI to 58% with admission for thyrotoxicosis, reported Dr. Chui, an internal medicine resident at the University of California, Irvine.
The most provocative study finding was the significantly higher in-hospital mortality for women, compared with men with NOAF for all but two of the seven major reasons for admission studied: noncardiac surgery and thyrotoxicosis. Dr. Chui asserted that this appears to be a quality of care issue.
“The overwhelming majority of new-onset AF in-hospital occurs in postsurgical patients, who may be under the care of providers with less experience in managing AF,” he said. “Our results suggest clinicians need to be aware of the subtleties in presentation and management of female new-onset AF patients compared to their male counterparts.”
Dr. Chui reported having no financial conflicts regarding his study, which was financially supported by the university’s department of internal medicine.
ORLANDO – Women are at lower risk than men for new-onset atrial fibrillation during hospitalization, but when it does occur it’s associated with significantly greater in-hospital mortality, according to a massive retrospective study presented at the American Heart Association scientific sessions.
Dr. Philip W. Chui analyzed 38,403,360 cases of new-onset atrial fibrillation during hospitalization (NOAF) in 2001-2011. The source was the National Inpatient Sample database. Fully 85% of all cases occurred in patients admitted for noncardiac surgery, which also was the cause of admission with the lowest incidence of NOAF. Among the patients hospitalized for sepsis, women were 27% less likely than men to develop new-onset atrial fibrillation, but when they did they were 13% more likely to die in-hospital.
In a multivariate logistic regression analysis extensively adjusted for numerous comorbid conditions and demographic factors, female gender was associated with a significantly reduced risk of NOAF across the board for all major admitting conditions known to be triggers for NOAF. The magnitude of this relative risk reduction favoring women ranged from as low as 14% for patients with an admitting diagnosis of acute MI to 58% with admission for thyrotoxicosis, reported Dr. Chui, an internal medicine resident at the University of California, Irvine.
The most provocative study finding was the significantly higher in-hospital mortality for women, compared with men with NOAF for all but two of the seven major reasons for admission studied: noncardiac surgery and thyrotoxicosis. Dr. Chui asserted that this appears to be a quality of care issue.
“The overwhelming majority of new-onset AF in-hospital occurs in postsurgical patients, who may be under the care of providers with less experience in managing AF,” he said. “Our results suggest clinicians need to be aware of the subtleties in presentation and management of female new-onset AF patients compared to their male counterparts.”
Dr. Chui reported having no financial conflicts regarding his study, which was financially supported by the university’s department of internal medicine.
ORLANDO – Women are at lower risk than men for new-onset atrial fibrillation during hospitalization, but when it does occur it’s associated with significantly greater in-hospital mortality, according to a massive retrospective study presented at the American Heart Association scientific sessions.
Dr. Philip W. Chui analyzed 38,403,360 cases of new-onset atrial fibrillation during hospitalization (NOAF) in 2001-2011. The source was the National Inpatient Sample database. Fully 85% of all cases occurred in patients admitted for noncardiac surgery, which also was the cause of admission with the lowest incidence of NOAF. Among the patients hospitalized for sepsis, women were 27% less likely than men to develop new-onset atrial fibrillation, but when they did they were 13% more likely to die in-hospital.
In a multivariate logistic regression analysis extensively adjusted for numerous comorbid conditions and demographic factors, female gender was associated with a significantly reduced risk of NOAF across the board for all major admitting conditions known to be triggers for NOAF. The magnitude of this relative risk reduction favoring women ranged from as low as 14% for patients with an admitting diagnosis of acute MI to 58% with admission for thyrotoxicosis, reported Dr. Chui, an internal medicine resident at the University of California, Irvine.
The most provocative study finding was the significantly higher in-hospital mortality for women, compared with men with NOAF for all but two of the seven major reasons for admission studied: noncardiac surgery and thyrotoxicosis. Dr. Chui asserted that this appears to be a quality of care issue.
“The overwhelming majority of new-onset AF in-hospital occurs in postsurgical patients, who may be under the care of providers with less experience in managing AF,” he said. “Our results suggest clinicians need to be aware of the subtleties in presentation and management of female new-onset AF patients compared to their male counterparts.”
Dr. Chui reported having no financial conflicts regarding his study, which was financially supported by the university’s department of internal medicine.
AT THE AHA SCIENTIFIC SESSIONS
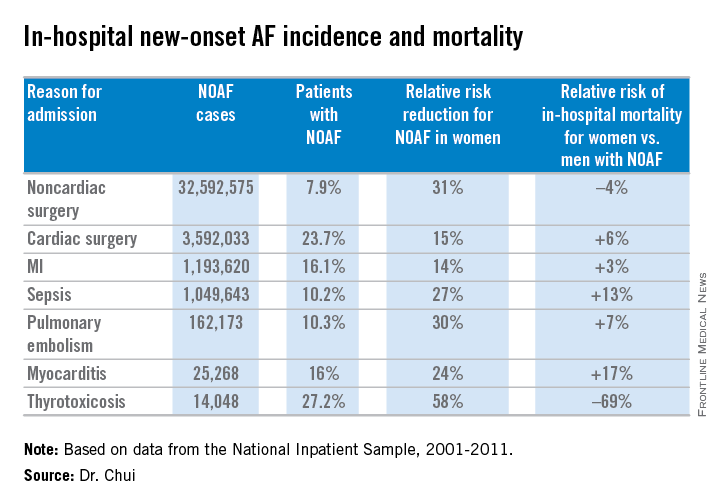
New-onset AF during hospitalization is more lethal in women
ORLANDO – Women are at lower risk than men for new-onset atrial fibrillation during hospitalization, but when it does occur it’s associated with significantly greater in-hospital mortality, according to a massive retrospective study presented at the American Heart Association scientific sessions.
Dr. Philip W. Chui analyzed 38,403,360 cases of new-onset atrial fibrillation during hospitalization (NOAF) in 2001-2011. The source was the National Inpatient Sample database. Fully 85% of all cases occurred in patients admitted for noncardiac surgery, which also was the cause of admission with the lowest incidence of NOAF. Among the patients hospitalized for sepsis, women were 27% less likely than men to develop new-onset atrial fibrillation, but when they did they were 13% more likely to die in-hospital.
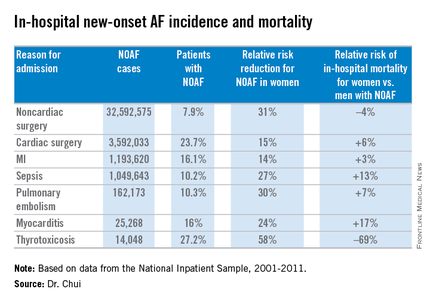
In a multivariate logistic regression analysis extensively adjusted for numerous comorbid conditions and demographic factors, female gender was associated with a significantly reduced risk of NOAF across the board for all major admitting conditions known to be triggers for NOAF. The magnitude of this relative risk reduction favoring women ranged from as low as 14% for patients with an admitting diagnosis of acute MI to 58% with admission for thyrotoxicosis, reported Dr. Chui, an internal medicine resident at the University of California, Irvine.
The most provocative study finding was the significantly higher in-hospital mortality for women, compared with men with NOAF for all but two of the seven major reasons for admission studied: noncardiac surgery and thyrotoxicosis. Dr. Chui asserted that this appears to be a quality of care issue.
“The overwhelming majority of new-onset AF in-hospital occurs in postsurgical patients, who may be under the care of providers with less experience in managing AF,” he said. “Our results suggest clinicians need to be aware of the subtleties in presentation and management of female new-onset AF patients compared to their male counterparts.”
Dr. Chui reported having no financial conflicts regarding his study, which was financially supported by the university’s department of internal medicine.
ORLANDO – Women are at lower risk than men for new-onset atrial fibrillation during hospitalization, but when it does occur it’s associated with significantly greater in-hospital mortality, according to a massive retrospective study presented at the American Heart Association scientific sessions.
Dr. Philip W. Chui analyzed 38,403,360 cases of new-onset atrial fibrillation during hospitalization (NOAF) in 2001-2011. The source was the National Inpatient Sample database. Fully 85% of all cases occurred in patients admitted for noncardiac surgery, which also was the cause of admission with the lowest incidence of NOAF. Among the patients hospitalized for sepsis, women were 27% less likely than men to develop new-onset atrial fibrillation, but when they did they were 13% more likely to die in-hospital.
In a multivariate logistic regression analysis extensively adjusted for numerous comorbid conditions and demographic factors, female gender was associated with a significantly reduced risk of NOAF across the board for all major admitting conditions known to be triggers for NOAF. The magnitude of this relative risk reduction favoring women ranged from as low as 14% for patients with an admitting diagnosis of acute MI to 58% with admission for thyrotoxicosis, reported Dr. Chui, an internal medicine resident at the University of California, Irvine.
The most provocative study finding was the significantly higher in-hospital mortality for women, compared with men with NOAF for all but two of the seven major reasons for admission studied: noncardiac surgery and thyrotoxicosis. Dr. Chui asserted that this appears to be a quality of care issue.
“The overwhelming majority of new-onset AF in-hospital occurs in postsurgical patients, who may be under the care of providers with less experience in managing AF,” he said. “Our results suggest clinicians need to be aware of the subtleties in presentation and management of female new-onset AF patients compared to their male counterparts.”
Dr. Chui reported having no financial conflicts regarding his study, which was financially supported by the university’s department of internal medicine.
ORLANDO – Women are at lower risk than men for new-onset atrial fibrillation during hospitalization, but when it does occur it’s associated with significantly greater in-hospital mortality, according to a massive retrospective study presented at the American Heart Association scientific sessions.
Dr. Philip W. Chui analyzed 38,403,360 cases of new-onset atrial fibrillation during hospitalization (NOAF) in 2001-2011. The source was the National Inpatient Sample database. Fully 85% of all cases occurred in patients admitted for noncardiac surgery, which also was the cause of admission with the lowest incidence of NOAF. Among the patients hospitalized for sepsis, women were 27% less likely than men to develop new-onset atrial fibrillation, but when they did they were 13% more likely to die in-hospital.
In a multivariate logistic regression analysis extensively adjusted for numerous comorbid conditions and demographic factors, female gender was associated with a significantly reduced risk of NOAF across the board for all major admitting conditions known to be triggers for NOAF. The magnitude of this relative risk reduction favoring women ranged from as low as 14% for patients with an admitting diagnosis of acute MI to 58% with admission for thyrotoxicosis, reported Dr. Chui, an internal medicine resident at the University of California, Irvine.
The most provocative study finding was the significantly higher in-hospital mortality for women, compared with men with NOAF for all but two of the seven major reasons for admission studied: noncardiac surgery and thyrotoxicosis. Dr. Chui asserted that this appears to be a quality of care issue.
“The overwhelming majority of new-onset AF in-hospital occurs in postsurgical patients, who may be under the care of providers with less experience in managing AF,” he said. “Our results suggest clinicians need to be aware of the subtleties in presentation and management of female new-onset AF patients compared to their male counterparts.”
Dr. Chui reported having no financial conflicts regarding his study, which was financially supported by the university’s department of internal medicine.
AT THE AHA SCIENTIFIC SESSIONS
Key clinical point: New-onset atrial fibrillation has a higher associated in-hospital mortality in women than in men, suggesting a potential quality of care issue.
Major finding: Among more than 1 million patients hospitalized for sepsis, women were 27% less likely than men to develop new-onset atrial fibrillation, but when they did they were 13% more likely to die in-hospital.
Data source: This was a retrospective study of gender differences in more than 38 million cases of new-onset atrial fibrillation during hospitalization.
Disclosures: The presenter reported having no financial conflicts regarding his study, which was financially supported by the University of California, Irvine, department of internal medicine.
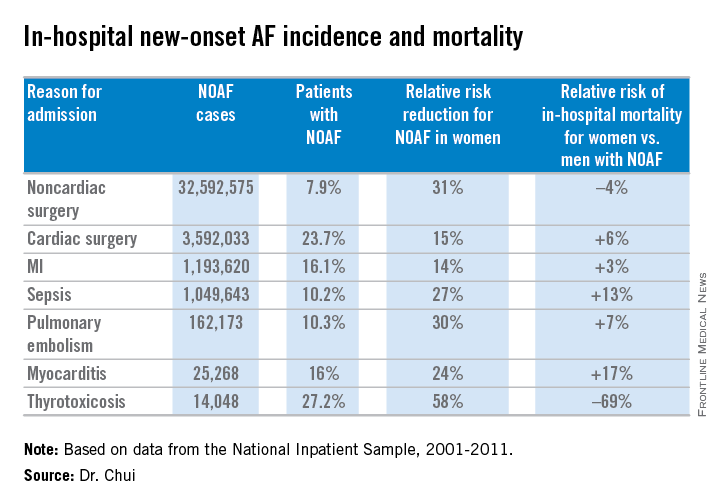
SABCS: Longer overnight fasting may reduce breast cancer recurrence risk
SAN ANTONIO – Breast cancer survivors who typically didn’t eat for at least 13 hours overnight had a 36% reduction in the risk of breast cancer recurrence compared to those with a shorter duration of overnight fasting in a secondary analysis of the Women’s Healthy Eating and Living Study presented at the San Antonio Breast Cancer Symposium.

“Prolonging the length of the nighttime fasting interval may be a simple nonpharmacologic strategy for reducing the risk of breast cancer recurrence as well as other chronic conditions with etiologic ties to breast cancer, like type 2 diabetes,” concluded to Catherine R. Marinac, a doctoral candidate in public health at the University of California, San Diego.
“A lot of dietary recommendations for cancer prevention really focus on what to eat in order to prevent or recover from breast cancer. For a lot of people that can be a really complicated recommendation, like ‘count your carbs, count your fat, don’t eat this/don’t eat that.’ We think timing of food intake in order to prolong the length of the nightly fasting interval can be a simple strategy most women can understand and adopt and that may reduce their risk of breast cancer,” she added.
The new results from the Women’s Healthy Eating and Living (WHEL) study are encouragingly consistent with the findings of earlier rodent studies demonstrating that intermittent fasting regimens aligned with the sleep cycle bring better glycemic control and protection against carcinogenesis, Ms. Marinac noted.
She presented an analysis of 2,413 nondiabetic breast cancer survivors who participated in the multicenter WHEL study and for whom multiple detailed 24-hour dietary recall records were obtained at baseline and 4 years of followup.
“The diets were very well characterized. We analyzed roughly 30,000 time-stamped dietary recalls,” she said in an interview.
During 7.3 years of follow-up, 390 women experienced recurrent breast cancer. Those in the top tertile for duration of overnight fasting, at 13 hours or longer, were 36% less likely to have a recurrence, according to a Cox proportionate hazard analysis and a multivariate linear regression analysis controlling for patient demographics; calorie consumption and other dietary variables; breast cancer stage, grade, and treatment; body mass index; comorbid conditions; and sleep duration.
During 11.4 years of follow-up, 329 subjects died of their breast cancer. All-cause mortality occurred in 420. Women with an overnight fasting duration of 13 hours or greater were 21% less likely to experience breast cancer mortality and 22% less likely to die of any cause. Neither trend achieved statistical significance.
Looking for potential mechanisms to explain the observed relationship between overnight fasting duration and breast cancer recurrence, Ms. Marinac and coinvestigators considered as evaluable possibilities systemic inflammation, glucoregulation, adiposity, and sleep duration.
C-reactive protein levels and body mass index proved to be unrelated to recurrence risk. However, glucoregulation and sleep duration were. Women with an overnight fasting length of at least 13 hours had a significantly lower glycated hemoglobin level and slept longer than those with a shorter overnight fast. The lower HbA1c seen in women who fasted for longer at night mimics an intriguing finding from the classic mouse studies that showed fasting is related to better glycemic control, she observed.
The WHEL study is sponsored by the National Cancer Institute, the University of California at San Diego, and a Ruth L. Kirschstein National Research Service Award. Ms. Marinac reported having no financial conflicts of interest.
SAN ANTONIO – Breast cancer survivors who typically didn’t eat for at least 13 hours overnight had a 36% reduction in the risk of breast cancer recurrence compared to those with a shorter duration of overnight fasting in a secondary analysis of the Women’s Healthy Eating and Living Study presented at the San Antonio Breast Cancer Symposium.
“Prolonging the length of the nighttime fasting interval may be a simple nonpharmacologic strategy for reducing the risk of breast cancer recurrence as well as other chronic conditions with etiologic ties to breast cancer, like type 2 diabetes,” concluded to Catherine R. Marinac, a doctoral candidate in public health at the University of California, San Diego.
“A lot of dietary recommendations for cancer prevention really focus on what to eat in order to prevent or recover from breast cancer. For a lot of people that can be a really complicated recommendation, like ‘count your carbs, count your fat, don’t eat this/don’t eat that.’ We think timing of food intake in order to prolong the length of the nightly fasting interval can be a simple strategy most women can understand and adopt and that may reduce their risk of breast cancer,” she added.
The new results from the Women’s Healthy Eating and Living (WHEL) study are encouragingly consistent with the findings of earlier rodent studies demonstrating that intermittent fasting regimens aligned with the sleep cycle bring better glycemic control and protection against carcinogenesis, Ms. Marinac noted.
She presented an analysis of 2,413 nondiabetic breast cancer survivors who participated in the multicenter WHEL study and for whom multiple detailed 24-hour dietary recall records were obtained at baseline and 4 years of followup.
“The diets were very well characterized. We analyzed roughly 30,000 time-stamped dietary recalls,” she said in an interview.
During 7.3 years of follow-up, 390 women experienced recurrent breast cancer. Those in the top tertile for duration of overnight fasting, at 13 hours or longer, were 36% less likely to have a recurrence, according to a Cox proportionate hazard analysis and a multivariate linear regression analysis controlling for patient demographics; calorie consumption and other dietary variables; breast cancer stage, grade, and treatment; body mass index; comorbid conditions; and sleep duration.
During 11.4 years of follow-up, 329 subjects died of their breast cancer. All-cause mortality occurred in 420. Women with an overnight fasting duration of 13 hours or greater were 21% less likely to experience breast cancer mortality and 22% less likely to die of any cause. Neither trend achieved statistical significance.
Looking for potential mechanisms to explain the observed relationship between overnight fasting duration and breast cancer recurrence, Ms. Marinac and coinvestigators considered as evaluable possibilities systemic inflammation, glucoregulation, adiposity, and sleep duration.
C-reactive protein levels and body mass index proved to be unrelated to recurrence risk. However, glucoregulation and sleep duration were. Women with an overnight fasting length of at least 13 hours had a significantly lower glycated hemoglobin level and slept longer than those with a shorter overnight fast. The lower HbA1c seen in women who fasted for longer at night mimics an intriguing finding from the classic mouse studies that showed fasting is related to better glycemic control, she observed.
The WHEL study is sponsored by the National Cancer Institute, the University of California at San Diego, and a Ruth L. Kirschstein National Research Service Award. Ms. Marinac reported having no financial conflicts of interest.
SAN ANTONIO – Breast cancer survivors who typically didn’t eat for at least 13 hours overnight had a 36% reduction in the risk of breast cancer recurrence compared to those with a shorter duration of overnight fasting in a secondary analysis of the Women’s Healthy Eating and Living Study presented at the San Antonio Breast Cancer Symposium.
“Prolonging the length of the nighttime fasting interval may be a simple nonpharmacologic strategy for reducing the risk of breast cancer recurrence as well as other chronic conditions with etiologic ties to breast cancer, like type 2 diabetes,” concluded to Catherine R. Marinac, a doctoral candidate in public health at the University of California, San Diego.
“A lot of dietary recommendations for cancer prevention really focus on what to eat in order to prevent or recover from breast cancer. For a lot of people that can be a really complicated recommendation, like ‘count your carbs, count your fat, don’t eat this/don’t eat that.’ We think timing of food intake in order to prolong the length of the nightly fasting interval can be a simple strategy most women can understand and adopt and that may reduce their risk of breast cancer,” she added.
The new results from the Women’s Healthy Eating and Living (WHEL) study are encouragingly consistent with the findings of earlier rodent studies demonstrating that intermittent fasting regimens aligned with the sleep cycle bring better glycemic control and protection against carcinogenesis, Ms. Marinac noted.
She presented an analysis of 2,413 nondiabetic breast cancer survivors who participated in the multicenter WHEL study and for whom multiple detailed 24-hour dietary recall records were obtained at baseline and 4 years of followup.
“The diets were very well characterized. We analyzed roughly 30,000 time-stamped dietary recalls,” she said in an interview.
During 7.3 years of follow-up, 390 women experienced recurrent breast cancer. Those in the top tertile for duration of overnight fasting, at 13 hours or longer, were 36% less likely to have a recurrence, according to a Cox proportionate hazard analysis and a multivariate linear regression analysis controlling for patient demographics; calorie consumption and other dietary variables; breast cancer stage, grade, and treatment; body mass index; comorbid conditions; and sleep duration.
During 11.4 years of follow-up, 329 subjects died of their breast cancer. All-cause mortality occurred in 420. Women with an overnight fasting duration of 13 hours or greater were 21% less likely to experience breast cancer mortality and 22% less likely to die of any cause. Neither trend achieved statistical significance.
Looking for potential mechanisms to explain the observed relationship between overnight fasting duration and breast cancer recurrence, Ms. Marinac and coinvestigators considered as evaluable possibilities systemic inflammation, glucoregulation, adiposity, and sleep duration.
C-reactive protein levels and body mass index proved to be unrelated to recurrence risk. However, glucoregulation and sleep duration were. Women with an overnight fasting length of at least 13 hours had a significantly lower glycated hemoglobin level and slept longer than those with a shorter overnight fast. The lower HbA1c seen in women who fasted for longer at night mimics an intriguing finding from the classic mouse studies that showed fasting is related to better glycemic control, she observed.
The WHEL study is sponsored by the National Cancer Institute, the University of California at San Diego, and a Ruth L. Kirschstein National Research Service Award. Ms. Marinac reported having no financial conflicts of interest.
AT SABCS 2015
Key clinical point: Lengthening the overnight fasting interval to at least 13 hours may be a novel, easily adoptable strategy to reduce breast cancer risk.
Major finding: Breast cancer survivors who typically went without eating for at least 13 hours overnight were 36% less likely to experience recurrent breast cancer than those with a shorter overnight fast.
Data source: This was a secondary analysis of a long-term prospective dietary study in 2,413 nondiabetic breast cancer survivors.
Disclosures: The WHEL study is sponsored by the National Cancer Institute, the University of California at San Diego, and a Ruth L. Kirschstein National Research Service Award. The presenter reported having no financial conflicts of interest.

AHA: Bariatric surgery slashes heart failure exacerbations
ORLANDO – Bariatric surgery in obese patients with heart failure was associated with a marked decrease in the subsequent rate of ED visits and hospitalizations for heart failure in a large, real-world, case-control study presented at the American Heart Association scientific sessions.
“This decline in the rate of heart failure morbidity was rapid in onset and sustained for at least 2 years after bariatric surgery,” according to Dr. Yuichi J. Shimada of Massachusetts General Hospital, Boston.
In a separate study, however, he found that bariatric surgery for obesity in patients with atrial fibrillation didn’t produce a reduction in ED visits and hospitalizations for the arrhythmia.
The heart failure study was a case-control study of 1,664 consecutive obese patients with heart failure who underwent a single bariatric surgical procedure in California, Florida, or Nebraska. Their median age was 49 years. Women accounted for 70% of the participants. Drawing upon federal Healthcare Cost and Utility Project databases on ED visits and hospital admissions in those three states, Dr. Shimada and coinvestigators compared the group’s rates of ED visits and hospitalizations for heart failure for 2 years before and 2 years after bariatric surgery. Thus, the subjects served as their own controls.
During the reference period, which lasted from months 13-24 presurgery, the group’s combined rate of ED visits and hospital admission for heart failure exacerbation was 14.4%. The rate wasn’t significantly different during the 12 months immediately prior to surgery, at 13.3%.
The rate dropped to 8.7% during the first 12 months after bariatric surgery and remained rock solid at 8.7% during months 13-24 postsurgery. In a logistic regression analysis, this translated to a 44% reduction in the risk of ED visits or hospital admission for heart failure during the first 2 years following bariatric surgery.
These findings are consistent with previous work by other investigators showing a link between obesity and heart failure exacerbations. The new data advance the field by providing the best evidence to date of the effectiveness of substantial weight loss on heart failure morbidity, Dr. Shimada observed.
Nonbariatric surgeries such as hysterectomy or cholecysectomy in the study population had no effect on the rate of heart failure exacerbations.
Dr. Shimada’s atrial fibrillation study was structured in the same way. It included 1,056 patients with atrial fibrillation who underwent bariatric surgery for obesity in the same three states. The rate of ED visits or hospitalization for heart failure was 12.1% in months 13-24 prior to bariatric surgery, 12.6% in presurgical months 1-12, 14.2% in the first 12 months post-bariatric surgery, and 13.4% during postsurgical months 13-24. These rates weren’t statistically different.
Dr. Shimada reported having no financial conflicts of interest regarding the two studies.
ORLANDO – Bariatric surgery in obese patients with heart failure was associated with a marked decrease in the subsequent rate of ED visits and hospitalizations for heart failure in a large, real-world, case-control study presented at the American Heart Association scientific sessions.
“This decline in the rate of heart failure morbidity was rapid in onset and sustained for at least 2 years after bariatric surgery,” according to Dr. Yuichi J. Shimada of Massachusetts General Hospital, Boston.
In a separate study, however, he found that bariatric surgery for obesity in patients with atrial fibrillation didn’t produce a reduction in ED visits and hospitalizations for the arrhythmia.
The heart failure study was a case-control study of 1,664 consecutive obese patients with heart failure who underwent a single bariatric surgical procedure in California, Florida, or Nebraska. Their median age was 49 years. Women accounted for 70% of the participants. Drawing upon federal Healthcare Cost and Utility Project databases on ED visits and hospital admissions in those three states, Dr. Shimada and coinvestigators compared the group’s rates of ED visits and hospitalizations for heart failure for 2 years before and 2 years after bariatric surgery. Thus, the subjects served as their own controls.
During the reference period, which lasted from months 13-24 presurgery, the group’s combined rate of ED visits and hospital admission for heart failure exacerbation was 14.4%. The rate wasn’t significantly different during the 12 months immediately prior to surgery, at 13.3%.
The rate dropped to 8.7% during the first 12 months after bariatric surgery and remained rock solid at 8.7% during months 13-24 postsurgery. In a logistic regression analysis, this translated to a 44% reduction in the risk of ED visits or hospital admission for heart failure during the first 2 years following bariatric surgery.
These findings are consistent with previous work by other investigators showing a link between obesity and heart failure exacerbations. The new data advance the field by providing the best evidence to date of the effectiveness of substantial weight loss on heart failure morbidity, Dr. Shimada observed.
Nonbariatric surgeries such as hysterectomy or cholecysectomy in the study population had no effect on the rate of heart failure exacerbations.
Dr. Shimada’s atrial fibrillation study was structured in the same way. It included 1,056 patients with atrial fibrillation who underwent bariatric surgery for obesity in the same three states. The rate of ED visits or hospitalization for heart failure was 12.1% in months 13-24 prior to bariatric surgery, 12.6% in presurgical months 1-12, 14.2% in the first 12 months post-bariatric surgery, and 13.4% during postsurgical months 13-24. These rates weren’t statistically different.
Dr. Shimada reported having no financial conflicts of interest regarding the two studies.
ORLANDO – Bariatric surgery in obese patients with heart failure was associated with a marked decrease in the subsequent rate of ED visits and hospitalizations for heart failure in a large, real-world, case-control study presented at the American Heart Association scientific sessions.
“This decline in the rate of heart failure morbidity was rapid in onset and sustained for at least 2 years after bariatric surgery,” according to Dr. Yuichi J. Shimada of Massachusetts General Hospital, Boston.
In a separate study, however, he found that bariatric surgery for obesity in patients with atrial fibrillation didn’t produce a reduction in ED visits and hospitalizations for the arrhythmia.
The heart failure study was a case-control study of 1,664 consecutive obese patients with heart failure who underwent a single bariatric surgical procedure in California, Florida, or Nebraska. Their median age was 49 years. Women accounted for 70% of the participants. Drawing upon federal Healthcare Cost and Utility Project databases on ED visits and hospital admissions in those three states, Dr. Shimada and coinvestigators compared the group’s rates of ED visits and hospitalizations for heart failure for 2 years before and 2 years after bariatric surgery. Thus, the subjects served as their own controls.
During the reference period, which lasted from months 13-24 presurgery, the group’s combined rate of ED visits and hospital admission for heart failure exacerbation was 14.4%. The rate wasn’t significantly different during the 12 months immediately prior to surgery, at 13.3%.
The rate dropped to 8.7% during the first 12 months after bariatric surgery and remained rock solid at 8.7% during months 13-24 postsurgery. In a logistic regression analysis, this translated to a 44% reduction in the risk of ED visits or hospital admission for heart failure during the first 2 years following bariatric surgery.
These findings are consistent with previous work by other investigators showing a link between obesity and heart failure exacerbations. The new data advance the field by providing the best evidence to date of the effectiveness of substantial weight loss on heart failure morbidity, Dr. Shimada observed.
Nonbariatric surgeries such as hysterectomy or cholecysectomy in the study population had no effect on the rate of heart failure exacerbations.
Dr. Shimada’s atrial fibrillation study was structured in the same way. It included 1,056 patients with atrial fibrillation who underwent bariatric surgery for obesity in the same three states. The rate of ED visits or hospitalization for heart failure was 12.1% in months 13-24 prior to bariatric surgery, 12.6% in presurgical months 1-12, 14.2% in the first 12 months post-bariatric surgery, and 13.4% during postsurgical months 13-24. These rates weren’t statistically different.
Dr. Shimada reported having no financial conflicts of interest regarding the two studies.
AT THE AHA SCIENTIFIC SESSIONS
Key clinical point: Bariatric surgery in obese patients with heart failure results in a dramatic reduction in ED visits and hospital admission for heart failure.
Major finding: The combined rate of ED visits and hospital admissions for heart failure dropped by 44% during the 2 years after a large group of patients with heart failure underwent bariatric surgery for obesity.
Data source: This case-control study compared the rates of ED visits and hospital admissions for worsening heart failure in 1,664 patients with heart failure during the 2 years before and 2 years after they underwent bariatric surgery for obesity.
Disclosures: The presenter reported having no financial conflicts of interest regarding the study, which utilized publicly available patient data.
AHA: Poor Real-world Adherence to NOACs
ORLANDO – Adherence to the novel oral anticoagulants (NOACs) is surprisingly poor in clinical practice, Xiaoxi Yao, Ph.D., reported at the American Heart Association scientific sessions.
Her retrospective study of nearly 65,000 patients with atrial fibrillation who initiated therapy with apixaban, dabigatran, rivaroxaban, or warfarin showed that during a median 1.1 years of follow-up fewer than half of all patients were treatment adherent, with adherence defined as possession of sufficient medication to cover at least 80% of days.

Adherence rates, while uniformly suboptimal, nevertheless varied considerably: lowest at 38.5% for dabigatran, followed by 40.2% for warfarin, 50.5% for rivaroxaban, and 61.9% for apixaban.
This poor adherence to NOACs in real-world clinical practice is surprising in light of the drugs’ greater convenience, with fewer drug interactions than warfarin and no need for laboratory monitoring, observed Dr. Yao of the Mayo Clinic in Rochester, Minn.
It’s possible, although speculative, that the NOACs’ greater convenience paradoxically contributes to the low adherence rates, since unlike warfarin, NOACs don’t require regular interactions with the health care system for INR monitoring. And then there is the hefty cost of the novel agents, she added.
The study population consisted of 3,900 patients with atrial fibrillation who initiated oral anticoagulation with apixaban (Eliquis), 10,235 who started on dabigatran (Pradaxa), 12,366 on rivaroxaban (Xarelto), and 38,190 on warfarin. The analysis utilized claims data from a large U.S. commercial insurance database.
Adherence rates were better among patients with greater stroke risk as reflected by their CHA2DS2-VASc scores. For example, at the high end of the adherence spectrum, the adherence rate for apixaban was 50% in patients with a CHA2DS2-VASc score of 0-1, rising to 62% with a score of 2-3 and 64% with a score of 4 or more. The corresponding adherence rates for dabigatran were 25% in patients with a CHA2DS2-VASc of 0-1, 40% among those with a score of 2-3, and 42% in patients with a score of 4 or higher.
Dr. Yao and coinvestigators were interested in whether lower adherence to oral anticoagulation was associated with worse outcomes. This proved to be the case with regard to stroke rate for patients with a CHA2DS2-VASc score of 2 or more, where a clear dose-response relationship was evident between the event rate and cumulative time off oral anticoagulation during follow-up.
Among patients with a CHA2DS2-VASc of 2 or 3, the stroke rate was nearly twice as high among those off oral anticoagulation for a total of 3-6 months and three times greater if off therapy for more than 6 months than in those with a total time off of less than 1 week. The stroke rate was even higher in patients with a CHA2DS2-VASc of 4 or more who had suboptimal adherence.
An unexpected finding, she continued, was that among patients with a CHA2DS2-VASc score of 2 or more there was no significant relationship between cumulative time off oral anticoagulation and the risk of major bleeding unless they were off treatment for a total of 6 months or more; only then was the major bleeding risk lower than in patients whose total time off therapy was less than a week. Also, one would expect that when patients are off oral anticoagulation they should be at significantly lower risk of intracranial hemorrhage than when on-therapy, but this proved not to be the case.
For patients at substantial stroke risk as indicated by a CHA2DS2-VASc score of at least 2, this finding about off-treatment bleeding risk actually constitutes a good argument for sticking to their medication, in Dr. Yao’s view.
“Physicians and patients often fear bleeding, especially intracranial hemorrhage, but we found that for patients at higher risk for stroke there is little difference in intracranial hemorrhage risk whether you’re on or off of oral anticoagulation. So higher-risk patients should definitely adhere to their medication because of the stroke prevention benefit. However, in low-risk patients with a CHA2DS2-VASc of 0-1, the benefits of oral anticoagulation may not always outweigh the harm,” she said.
Dr. Yao reported having no financial conflicts of interest regarding her study.
ORLANDO – Adherence to the novel oral anticoagulants (NOACs) is surprisingly poor in clinical practice, Xiaoxi Yao, Ph.D., reported at the American Heart Association scientific sessions.
Her retrospective study of nearly 65,000 patients with atrial fibrillation who initiated therapy with apixaban, dabigatran, rivaroxaban, or warfarin showed that during a median 1.1 years of follow-up fewer than half of all patients were treatment adherent, with adherence defined as possession of sufficient medication to cover at least 80% of days.
Adherence rates, while uniformly suboptimal, nevertheless varied considerably: lowest at 38.5% for dabigatran, followed by 40.2% for warfarin, 50.5% for rivaroxaban, and 61.9% for apixaban.
This poor adherence to NOACs in real-world clinical practice is surprising in light of the drugs’ greater convenience, with fewer drug interactions than warfarin and no need for laboratory monitoring, observed Dr. Yao of the Mayo Clinic in Rochester, Minn.
It’s possible, although speculative, that the NOACs’ greater convenience paradoxically contributes to the low adherence rates, since unlike warfarin, NOACs don’t require regular interactions with the health care system for INR monitoring. And then there is the hefty cost of the novel agents, she added.
The study population consisted of 3,900 patients with atrial fibrillation who initiated oral anticoagulation with apixaban (Eliquis), 10,235 who started on dabigatran (Pradaxa), 12,366 on rivaroxaban (Xarelto), and 38,190 on warfarin. The analysis utilized claims data from a large U.S. commercial insurance database.
Adherence rates were better among patients with greater stroke risk as reflected by their CHA2DS2-VASc scores. For example, at the high end of the adherence spectrum, the adherence rate for apixaban was 50% in patients with a CHA2DS2-VASc score of 0-1, rising to 62% with a score of 2-3 and 64% with a score of 4 or more. The corresponding adherence rates for dabigatran were 25% in patients with a CHA2DS2-VASc of 0-1, 40% among those with a score of 2-3, and 42% in patients with a score of 4 or higher.
Dr. Yao and coinvestigators were interested in whether lower adherence to oral anticoagulation was associated with worse outcomes. This proved to be the case with regard to stroke rate for patients with a CHA2DS2-VASc score of 2 or more, where a clear dose-response relationship was evident between the event rate and cumulative time off oral anticoagulation during follow-up.
Among patients with a CHA2DS2-VASc of 2 or 3, the stroke rate was nearly twice as high among those off oral anticoagulation for a total of 3-6 months and three times greater if off therapy for more than 6 months than in those with a total time off of less than 1 week. The stroke rate was even higher in patients with a CHA2DS2-VASc of 4 or more who had suboptimal adherence.
An unexpected finding, she continued, was that among patients with a CHA2DS2-VASc score of 2 or more there was no significant relationship between cumulative time off oral anticoagulation and the risk of major bleeding unless they were off treatment for a total of 6 months or more; only then was the major bleeding risk lower than in patients whose total time off therapy was less than a week. Also, one would expect that when patients are off oral anticoagulation they should be at significantly lower risk of intracranial hemorrhage than when on-therapy, but this proved not to be the case.
For patients at substantial stroke risk as indicated by a CHA2DS2-VASc score of at least 2, this finding about off-treatment bleeding risk actually constitutes a good argument for sticking to their medication, in Dr. Yao’s view.
“Physicians and patients often fear bleeding, especially intracranial hemorrhage, but we found that for patients at higher risk for stroke there is little difference in intracranial hemorrhage risk whether you’re on or off of oral anticoagulation. So higher-risk patients should definitely adhere to their medication because of the stroke prevention benefit. However, in low-risk patients with a CHA2DS2-VASc of 0-1, the benefits of oral anticoagulation may not always outweigh the harm,” she said.
Dr. Yao reported having no financial conflicts of interest regarding her study.
ORLANDO – Adherence to the novel oral anticoagulants (NOACs) is surprisingly poor in clinical practice, Xiaoxi Yao, Ph.D., reported at the American Heart Association scientific sessions.
Her retrospective study of nearly 65,000 patients with atrial fibrillation who initiated therapy with apixaban, dabigatran, rivaroxaban, or warfarin showed that during a median 1.1 years of follow-up fewer than half of all patients were treatment adherent, with adherence defined as possession of sufficient medication to cover at least 80% of days.
Adherence rates, while uniformly suboptimal, nevertheless varied considerably: lowest at 38.5% for dabigatran, followed by 40.2% for warfarin, 50.5% for rivaroxaban, and 61.9% for apixaban.
This poor adherence to NOACs in real-world clinical practice is surprising in light of the drugs’ greater convenience, with fewer drug interactions than warfarin and no need for laboratory monitoring, observed Dr. Yao of the Mayo Clinic in Rochester, Minn.
It’s possible, although speculative, that the NOACs’ greater convenience paradoxically contributes to the low adherence rates, since unlike warfarin, NOACs don’t require regular interactions with the health care system for INR monitoring. And then there is the hefty cost of the novel agents, she added.
The study population consisted of 3,900 patients with atrial fibrillation who initiated oral anticoagulation with apixaban (Eliquis), 10,235 who started on dabigatran (Pradaxa), 12,366 on rivaroxaban (Xarelto), and 38,190 on warfarin. The analysis utilized claims data from a large U.S. commercial insurance database.
Adherence rates were better among patients with greater stroke risk as reflected by their CHA2DS2-VASc scores. For example, at the high end of the adherence spectrum, the adherence rate for apixaban was 50% in patients with a CHA2DS2-VASc score of 0-1, rising to 62% with a score of 2-3 and 64% with a score of 4 or more. The corresponding adherence rates for dabigatran were 25% in patients with a CHA2DS2-VASc of 0-1, 40% among those with a score of 2-3, and 42% in patients with a score of 4 or higher.
Dr. Yao and coinvestigators were interested in whether lower adherence to oral anticoagulation was associated with worse outcomes. This proved to be the case with regard to stroke rate for patients with a CHA2DS2-VASc score of 2 or more, where a clear dose-response relationship was evident between the event rate and cumulative time off oral anticoagulation during follow-up.
Among patients with a CHA2DS2-VASc of 2 or 3, the stroke rate was nearly twice as high among those off oral anticoagulation for a total of 3-6 months and three times greater if off therapy for more than 6 months than in those with a total time off of less than 1 week. The stroke rate was even higher in patients with a CHA2DS2-VASc of 4 or more who had suboptimal adherence.
An unexpected finding, she continued, was that among patients with a CHA2DS2-VASc score of 2 or more there was no significant relationship between cumulative time off oral anticoagulation and the risk of major bleeding unless they were off treatment for a total of 6 months or more; only then was the major bleeding risk lower than in patients whose total time off therapy was less than a week. Also, one would expect that when patients are off oral anticoagulation they should be at significantly lower risk of intracranial hemorrhage than when on-therapy, but this proved not to be the case.
For patients at substantial stroke risk as indicated by a CHA2DS2-VASc score of at least 2, this finding about off-treatment bleeding risk actually constitutes a good argument for sticking to their medication, in Dr. Yao’s view.
“Physicians and patients often fear bleeding, especially intracranial hemorrhage, but we found that for patients at higher risk for stroke there is little difference in intracranial hemorrhage risk whether you’re on or off of oral anticoagulation. So higher-risk patients should definitely adhere to their medication because of the stroke prevention benefit. However, in low-risk patients with a CHA2DS2-VASc of 0-1, the benefits of oral anticoagulation may not always outweigh the harm,” she said.
Dr. Yao reported having no financial conflicts of interest regarding her study.
AT THE AHA SCIENTIFIC SESSIONS
