User login
Same-day discharge after PCI gets a boost
PARIS – Same-day discharge after uncomplicated transradial-access percutaneous coronary intervention (PCI) in patients with stable coronary artery disease is both feasible and safe, according to the findings of a multicenter prospective Spanish registry study.
Under the Spanish investigators’ protocol for same-day discharge, roughly three-quarters of patients successfully completed the 4- to 12-hour post-PCI surveillance period and were expeditiously sent home without spending a night in the hospital, Juan Gabriel Cordoba Soriano, MD, reported at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.

The other 26% of patients were admitted, most often because they showed clinical instability during the surveillance period, less frequently due to a suboptimal angiographic result, explained Dr. Cordoba Soriano of the University of Albacete, Spain.
The rationale for same-day discharge post PCI – provided it has first been shown to be safe, as was the case using the Spanish criteria – is that it reduces costs by avoiding an expensive hospital bed. Also, most patients prefer to sleep in their own bed and avoid a hospital stay, he continued.
Eligibility for same-day discharge in the Spanish study was restricted to patients with stable coronary artery disease undergoing elective transradial PCI with no complications during the procedure and with clinical stability during the subsequent 4- to 12-hour observation period. Patients undergoing complex PCIs – for example, treatment of left main lesions, complex bifurcation lesions, or chronic total occlusions – were ineligible.
Why restrict eligibility to patients undergoing transradial PCI? Multiple studies convincingly show it is safer than femoral access. And outside of the United States, it is by far the more popular access route. In a show of hands, virtually all of Dr. Cordoba Soriano’s audience indicated they perform more than 70% of their PCIs via transradial access. And patients with stable CAD are less likely to experience stent thrombosis or acute occlusion of the treated artery or side branches, he continued.
Of 989 patients who presented to the three participating Spanish medical centers for elective PCI, 257 were immediately excluded from the registry because they underwent elective femoral access. That left 732 patients, 74% of whom got same-day discharge.
The same-day discharge and hospital admission groups were closely similar in terms of baseline characteristics with two exceptions: The prevalence of peripheral arterial disease in the same-day discharge group was less than half of the 10% figure in the hospitalized group, and kidney function was better in patients who ultimately received same-day discharge as evidenced by a serum creatinine of 0.9 mg/dL, half that of the hospitalized patients.
Procedural characteristics were mostly similar for the two groups as well. Although the same-day discharge group had a 26-minute shorter median procedure time, were less likely to undergo multivessel PCI, and had fewer stents implanted per patient, in a multivariate regression analysis the only independent predictors of admission post PCI were the presence of peripheral arterial disease, with an associated 2.2-fold increased risk; multivessel PCI, with a 1.8-fold risk; ad hoc as opposed to a scheduled PCI, with a 4.0-fold increased risk; and a history of prior transradial catheterization, which cut the risk of hospitalization in half.
Turning to the safety of same-day discharge, the cardiologist deemed the rate of major complications in the first 24 hours to be acceptable at 0.18% for a single case of significant bleeding. Minor complications were confined to a 1.8% incidence of hematomas greater than 5 cm in size.
The major complication rate from 24 hours to 30 days post PCI was 0.54% (two deaths, one stroke), with a 2.2% incidence of minor complications.
Dr. Cordoba Soriano noted that investigators at the Quebec Heart and Lung Institute have published a meta-analysis of 13 studies of same-day discharge after PCI totaling more than 111,000 patients (JACC Cardiovasc Interv. 2013 Feb;6[2]:99-112). The investigators concluded that a definitive randomized trial would require more than 17,000 subjects, and in the absence of such evidence same-day discharge after uncomplicated PCI “seems a reasonable approach in selected patients.”
Stanford University investigators have published a separate meta-analysis of same-day discharge after PCI in nearly 13,000 patients in 30 observational and 7 randomized controlled trials. They concluded that it appears to be as safe as overnight observation (J Am Coll Cardiol. 2013 Jul 23;62[4]:275-85).
Nevertheless, the Society for Cardiovascular Angiography and Interventions has yet to update its 2009 expert consensus document stating that the standard of care is an overnight stay following PCI (Catheter Cardiovasc Interv. 2009 Jun 1;73[7]:847-58), Dr. Cordoba Soriano observed.
He reported having no financial conflicts regarding the registry study, which was conducted with university research funds.
PARIS – Same-day discharge after uncomplicated transradial-access percutaneous coronary intervention (PCI) in patients with stable coronary artery disease is both feasible and safe, according to the findings of a multicenter prospective Spanish registry study.
Under the Spanish investigators’ protocol for same-day discharge, roughly three-quarters of patients successfully completed the 4- to 12-hour post-PCI surveillance period and were expeditiously sent home without spending a night in the hospital, Juan Gabriel Cordoba Soriano, MD, reported at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
The other 26% of patients were admitted, most often because they showed clinical instability during the surveillance period, less frequently due to a suboptimal angiographic result, explained Dr. Cordoba Soriano of the University of Albacete, Spain.
The rationale for same-day discharge post PCI – provided it has first been shown to be safe, as was the case using the Spanish criteria – is that it reduces costs by avoiding an expensive hospital bed. Also, most patients prefer to sleep in their own bed and avoid a hospital stay, he continued.
Eligibility for same-day discharge in the Spanish study was restricted to patients with stable coronary artery disease undergoing elective transradial PCI with no complications during the procedure and with clinical stability during the subsequent 4- to 12-hour observation period. Patients undergoing complex PCIs – for example, treatment of left main lesions, complex bifurcation lesions, or chronic total occlusions – were ineligible.
Why restrict eligibility to patients undergoing transradial PCI? Multiple studies convincingly show it is safer than femoral access. And outside of the United States, it is by far the more popular access route. In a show of hands, virtually all of Dr. Cordoba Soriano’s audience indicated they perform more than 70% of their PCIs via transradial access. And patients with stable CAD are less likely to experience stent thrombosis or acute occlusion of the treated artery or side branches, he continued.
Of 989 patients who presented to the three participating Spanish medical centers for elective PCI, 257 were immediately excluded from the registry because they underwent elective femoral access. That left 732 patients, 74% of whom got same-day discharge.
The same-day discharge and hospital admission groups were closely similar in terms of baseline characteristics with two exceptions: The prevalence of peripheral arterial disease in the same-day discharge group was less than half of the 10% figure in the hospitalized group, and kidney function was better in patients who ultimately received same-day discharge as evidenced by a serum creatinine of 0.9 mg/dL, half that of the hospitalized patients.
Procedural characteristics were mostly similar for the two groups as well. Although the same-day discharge group had a 26-minute shorter median procedure time, were less likely to undergo multivessel PCI, and had fewer stents implanted per patient, in a multivariate regression analysis the only independent predictors of admission post PCI were the presence of peripheral arterial disease, with an associated 2.2-fold increased risk; multivessel PCI, with a 1.8-fold risk; ad hoc as opposed to a scheduled PCI, with a 4.0-fold increased risk; and a history of prior transradial catheterization, which cut the risk of hospitalization in half.
Turning to the safety of same-day discharge, the cardiologist deemed the rate of major complications in the first 24 hours to be acceptable at 0.18% for a single case of significant bleeding. Minor complications were confined to a 1.8% incidence of hematomas greater than 5 cm in size.
The major complication rate from 24 hours to 30 days post PCI was 0.54% (two deaths, one stroke), with a 2.2% incidence of minor complications.
Dr. Cordoba Soriano noted that investigators at the Quebec Heart and Lung Institute have published a meta-analysis of 13 studies of same-day discharge after PCI totaling more than 111,000 patients (JACC Cardiovasc Interv. 2013 Feb;6[2]:99-112). The investigators concluded that a definitive randomized trial would require more than 17,000 subjects, and in the absence of such evidence same-day discharge after uncomplicated PCI “seems a reasonable approach in selected patients.”
Stanford University investigators have published a separate meta-analysis of same-day discharge after PCI in nearly 13,000 patients in 30 observational and 7 randomized controlled trials. They concluded that it appears to be as safe as overnight observation (J Am Coll Cardiol. 2013 Jul 23;62[4]:275-85).
Nevertheless, the Society for Cardiovascular Angiography and Interventions has yet to update its 2009 expert consensus document stating that the standard of care is an overnight stay following PCI (Catheter Cardiovasc Interv. 2009 Jun 1;73[7]:847-58), Dr. Cordoba Soriano observed.
He reported having no financial conflicts regarding the registry study, which was conducted with university research funds.
PARIS – Same-day discharge after uncomplicated transradial-access percutaneous coronary intervention (PCI) in patients with stable coronary artery disease is both feasible and safe, according to the findings of a multicenter prospective Spanish registry study.
Under the Spanish investigators’ protocol for same-day discharge, roughly three-quarters of patients successfully completed the 4- to 12-hour post-PCI surveillance period and were expeditiously sent home without spending a night in the hospital, Juan Gabriel Cordoba Soriano, MD, reported at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
The other 26% of patients were admitted, most often because they showed clinical instability during the surveillance period, less frequently due to a suboptimal angiographic result, explained Dr. Cordoba Soriano of the University of Albacete, Spain.
The rationale for same-day discharge post PCI – provided it has first been shown to be safe, as was the case using the Spanish criteria – is that it reduces costs by avoiding an expensive hospital bed. Also, most patients prefer to sleep in their own bed and avoid a hospital stay, he continued.
Eligibility for same-day discharge in the Spanish study was restricted to patients with stable coronary artery disease undergoing elective transradial PCI with no complications during the procedure and with clinical stability during the subsequent 4- to 12-hour observation period. Patients undergoing complex PCIs – for example, treatment of left main lesions, complex bifurcation lesions, or chronic total occlusions – were ineligible.
Why restrict eligibility to patients undergoing transradial PCI? Multiple studies convincingly show it is safer than femoral access. And outside of the United States, it is by far the more popular access route. In a show of hands, virtually all of Dr. Cordoba Soriano’s audience indicated they perform more than 70% of their PCIs via transradial access. And patients with stable CAD are less likely to experience stent thrombosis or acute occlusion of the treated artery or side branches, he continued.
Of 989 patients who presented to the three participating Spanish medical centers for elective PCI, 257 were immediately excluded from the registry because they underwent elective femoral access. That left 732 patients, 74% of whom got same-day discharge.
The same-day discharge and hospital admission groups were closely similar in terms of baseline characteristics with two exceptions: The prevalence of peripheral arterial disease in the same-day discharge group was less than half of the 10% figure in the hospitalized group, and kidney function was better in patients who ultimately received same-day discharge as evidenced by a serum creatinine of 0.9 mg/dL, half that of the hospitalized patients.
Procedural characteristics were mostly similar for the two groups as well. Although the same-day discharge group had a 26-minute shorter median procedure time, were less likely to undergo multivessel PCI, and had fewer stents implanted per patient, in a multivariate regression analysis the only independent predictors of admission post PCI were the presence of peripheral arterial disease, with an associated 2.2-fold increased risk; multivessel PCI, with a 1.8-fold risk; ad hoc as opposed to a scheduled PCI, with a 4.0-fold increased risk; and a history of prior transradial catheterization, which cut the risk of hospitalization in half.
Turning to the safety of same-day discharge, the cardiologist deemed the rate of major complications in the first 24 hours to be acceptable at 0.18% for a single case of significant bleeding. Minor complications were confined to a 1.8% incidence of hematomas greater than 5 cm in size.
The major complication rate from 24 hours to 30 days post PCI was 0.54% (two deaths, one stroke), with a 2.2% incidence of minor complications.
Dr. Cordoba Soriano noted that investigators at the Quebec Heart and Lung Institute have published a meta-analysis of 13 studies of same-day discharge after PCI totaling more than 111,000 patients (JACC Cardiovasc Interv. 2013 Feb;6[2]:99-112). The investigators concluded that a definitive randomized trial would require more than 17,000 subjects, and in the absence of such evidence same-day discharge after uncomplicated PCI “seems a reasonable approach in selected patients.”
Stanford University investigators have published a separate meta-analysis of same-day discharge after PCI in nearly 13,000 patients in 30 observational and 7 randomized controlled trials. They concluded that it appears to be as safe as overnight observation (J Am Coll Cardiol. 2013 Jul 23;62[4]:275-85).
Nevertheless, the Society for Cardiovascular Angiography and Interventions has yet to update its 2009 expert consensus document stating that the standard of care is an overnight stay following PCI (Catheter Cardiovasc Interv. 2009 Jun 1;73[7]:847-58), Dr. Cordoba Soriano observed.
He reported having no financial conflicts regarding the registry study, which was conducted with university research funds.
AT EUROPCR 2016
Key clinical point: Same-day discharge following uncomplicated elective transradial PCI is feasible and safe.
Major finding: The rates of major and minor complications in the 24 hours following PCI with same-day discharge were 0.18% and 1.8%, respectively.
Data source: A prospective observational registry study including 989 PCI patients at three Spanish university hospitals.
Disclosures: The presenter reported having no financial conflicts regarding the registry study, which was conducted with university research funds.

Using transcatheter aortic valves for severe mitral annular calcification
PARIS – Transcatheter mitral valve replacement using a repurposed transcatheter aortic valve in patients with severe symptomatic native mitral valve disease and severe mitral annular calcification is feasible and may be an option in carefully selected patients who aren’t candidates for surgery, Mayra Guerrero, MD, said at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
However, at this early point in development, the procedure is associated with an exceptionally steep learning curve, said Dr. Guerrero, director of cardiac structural interventions at the NorthShore University Health System in Evanston, Ill.

She presented the procedural and 30-day outcomes for the first 104 patients entered into a global registry encompassing 47 centers in 11 countries. Nearly 90% of patients received an Edwards SAPIEN XT or SAPIEN 3 valve. The EuroPCR results update an earlier report on the first 64 patients in the registry (JACC Cardiovasc Interv. 2016 Jul 11;9[13]:1361-71).
The results, she said, are reminiscent of the early days in transcatheter aortic valve replacement, which were marked by an initial very high early mortality rate that fell dramatically as technology and techniques improved.
“We know that there are important things we need to improve. Left ventricular outflow tract obstruction is the Achilles heel of this procedure; we need to work on its prevention and management. We need better annulus sizing methods. We need to find the best delivery method and improve our patient selection in order to avoid taking on patients who are too sick. Still, even during this early experience, the technical success rate has improved, and 30-day mortality continues to drop,” Dr. Guerrero said.
Indeed, the 30-day all-cause mortality rate of 25% in the first 104 patients doesn’t tell the whole story. The rate was 37.5% in the first third of patients, fell to 21.9% in the second tertile, and then to 15% in the most recent tertile.
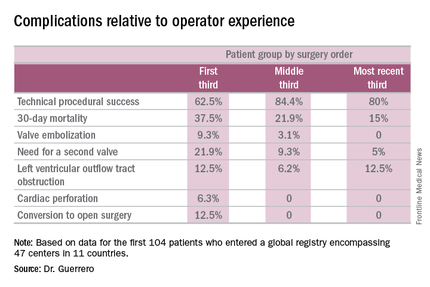
Similarly, the technical success rate of the procedure according to Mitral Valve Academic Research Consortium criteria improved from 62.5% in the first tertile of patients to 84.4% and 80% in the second and third, respectively, she continued.
The rates of almost all complications went down with greater operator experience, too. The notable exception was left ventricular outflow tract obstruction (LVOTO). It occurred in 12.5% of patients in the first tertile and remained unchanged in the third.
It’s noteworthy that the majority of deaths were noncardiac in nature. Patients with mitral annular calcification are a high-risk group even before they develop valvular dysfunction. They are typically older and have multiple comorbidities. Participants in the global registry had a mean Society of Thoracic Surgeons score of 14.4; 38% had diabetes, 45% had chronic obstructive pulmonary disease, 35% had heart failure, 34% had previously undergone coronary artery bypass surgery, and roughly half of patients had a prior aortic valve replacement.
Causes of noncardiac mortality within 30 days included multiorgan failure in 8.6% of subjects, pneumonia in 2.9%, infection in 1.9%, and one fatal thoracentesis-related bleeding complication.
Cardiovascular deaths included two cases due to left ventricular perforation, two fatal strokes, an MI due to air emboli, a lethal complete atrioventricular block, and three deaths owing to LVOTO.
Alcohol ablation met with some success as a bailout treatment in cases of LVOTO with hemodynamic compromise after transmitral valve replacement in the global registry. All six treated patients had significant improvement initially, although the LVOTO recurred the next day in one instance. Four of the six patients were discharged from the hospital. One patient died because of atrioventricular block, and another from multiorgan failure 3 weeks after alcohol ablation of the LVOTO.
Dr. Guerrero has been a leader in this new field. She reported the first percutaneous implantation of a balloon expandable transcatheter valve in a native mitral valve without a surgical incision (Catheter Cardiovasc Interv. 2014 Jun 1;83[7]:E287-91), and more recently, together with coworkers developed a percutaneous alcohol ablation technique for acute reduction of LVOTO due to transcatheter mitral valve replacement (Catheter Cardiovasc Interv. 2016 Jul 5. doi:10.1002/ccd.26649).
She is now the principal investigator in the ongoing Mitral Implantation of Transcatheter Valves (MITRAL) trial, a physician-sponsored, 90-patient pilot study underway at six U.S. sites. MITRAL is recruiting three patient populations for transcatheter mitral valve replacement: patients like those in the global registry, with native mitral valve disease and severe mitral annular calcification; those with a symptomatic failing surgical ring with severe mitral regurgitation or stenosis; and patients with a symptomatic failing surgical bioprosthesis with severe mitral regurgitation or stenosis.

Discussant Nicolo Piazza, MD, of McGill University, Montreal, said transcatheter mitral valve replacement in mitral valve disease with severe mitral annular calcification in patients unsuitable for surgery “definitely represents an unmet clinical need in our practice today.” But he urged caution in interpreting the global registry data.
“This is a real world registry study with inherent selection bias and physician reporting bias,” the cardiologist said.
“We are leveraging a therapy from the aortic field into the mitral field. Of course, we do not have dedicated devices yet to treat these patients. The main finding of this study is that the procedure is actually feasible,” Dr. Piazza said.
Still, it’s sobering that at least 1 in 10 treated patients experiences LVOTO, 1 in 10 requires a second valve, and technical success is achieved in 3 out of 4 patients, he added.
Dr. Piazza predicted that multislice CT scans will be “extremely important” in refining patient selection criteria for the procedure, and echocardiography will be helpful in understanding the optimal procedural techniques and viewing angles. Work also needs to be done on developing optimal anticoagulation protocols in order to avoid valve thrombosis.
Dr. Guerrero reported serving as a consultant to Edwards Lifesciences. Dr. Piazza is a consultant to Medtronic and MicroPort.
PARIS – Transcatheter mitral valve replacement using a repurposed transcatheter aortic valve in patients with severe symptomatic native mitral valve disease and severe mitral annular calcification is feasible and may be an option in carefully selected patients who aren’t candidates for surgery, Mayra Guerrero, MD, said at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
However, at this early point in development, the procedure is associated with an exceptionally steep learning curve, said Dr. Guerrero, director of cardiac structural interventions at the NorthShore University Health System in Evanston, Ill.
She presented the procedural and 30-day outcomes for the first 104 patients entered into a global registry encompassing 47 centers in 11 countries. Nearly 90% of patients received an Edwards SAPIEN XT or SAPIEN 3 valve. The EuroPCR results update an earlier report on the first 64 patients in the registry (JACC Cardiovasc Interv. 2016 Jul 11;9[13]:1361-71).
The results, she said, are reminiscent of the early days in transcatheter aortic valve replacement, which were marked by an initial very high early mortality rate that fell dramatically as technology and techniques improved.
“We know that there are important things we need to improve. Left ventricular outflow tract obstruction is the Achilles heel of this procedure; we need to work on its prevention and management. We need better annulus sizing methods. We need to find the best delivery method and improve our patient selection in order to avoid taking on patients who are too sick. Still, even during this early experience, the technical success rate has improved, and 30-day mortality continues to drop,” Dr. Guerrero said.
Indeed, the 30-day all-cause mortality rate of 25% in the first 104 patients doesn’t tell the whole story. The rate was 37.5% in the first third of patients, fell to 21.9% in the second tertile, and then to 15% in the most recent tertile.
Similarly, the technical success rate of the procedure according to Mitral Valve Academic Research Consortium criteria improved from 62.5% in the first tertile of patients to 84.4% and 80% in the second and third, respectively, she continued.
The rates of almost all complications went down with greater operator experience, too. The notable exception was left ventricular outflow tract obstruction (LVOTO). It occurred in 12.5% of patients in the first tertile and remained unchanged in the third.
It’s noteworthy that the majority of deaths were noncardiac in nature. Patients with mitral annular calcification are a high-risk group even before they develop valvular dysfunction. They are typically older and have multiple comorbidities. Participants in the global registry had a mean Society of Thoracic Surgeons score of 14.4; 38% had diabetes, 45% had chronic obstructive pulmonary disease, 35% had heart failure, 34% had previously undergone coronary artery bypass surgery, and roughly half of patients had a prior aortic valve replacement.
Causes of noncardiac mortality within 30 days included multiorgan failure in 8.6% of subjects, pneumonia in 2.9%, infection in 1.9%, and one fatal thoracentesis-related bleeding complication.
Cardiovascular deaths included two cases due to left ventricular perforation, two fatal strokes, an MI due to air emboli, a lethal complete atrioventricular block, and three deaths owing to LVOTO.
Alcohol ablation met with some success as a bailout treatment in cases of LVOTO with hemodynamic compromise after transmitral valve replacement in the global registry. All six treated patients had significant improvement initially, although the LVOTO recurred the next day in one instance. Four of the six patients were discharged from the hospital. One patient died because of atrioventricular block, and another from multiorgan failure 3 weeks after alcohol ablation of the LVOTO.
Dr. Guerrero has been a leader in this new field. She reported the first percutaneous implantation of a balloon expandable transcatheter valve in a native mitral valve without a surgical incision (Catheter Cardiovasc Interv. 2014 Jun 1;83[7]:E287-91), and more recently, together with coworkers developed a percutaneous alcohol ablation technique for acute reduction of LVOTO due to transcatheter mitral valve replacement (Catheter Cardiovasc Interv. 2016 Jul 5. doi:10.1002/ccd.26649).
She is now the principal investigator in the ongoing Mitral Implantation of Transcatheter Valves (MITRAL) trial, a physician-sponsored, 90-patient pilot study underway at six U.S. sites. MITRAL is recruiting three patient populations for transcatheter mitral valve replacement: patients like those in the global registry, with native mitral valve disease and severe mitral annular calcification; those with a symptomatic failing surgical ring with severe mitral regurgitation or stenosis; and patients with a symptomatic failing surgical bioprosthesis with severe mitral regurgitation or stenosis.
Discussant Nicolo Piazza, MD, of McGill University, Montreal, said transcatheter mitral valve replacement in mitral valve disease with severe mitral annular calcification in patients unsuitable for surgery “definitely represents an unmet clinical need in our practice today.” But he urged caution in interpreting the global registry data.
“This is a real world registry study with inherent selection bias and physician reporting bias,” the cardiologist said.
“We are leveraging a therapy from the aortic field into the mitral field. Of course, we do not have dedicated devices yet to treat these patients. The main finding of this study is that the procedure is actually feasible,” Dr. Piazza said.
Still, it’s sobering that at least 1 in 10 treated patients experiences LVOTO, 1 in 10 requires a second valve, and technical success is achieved in 3 out of 4 patients, he added.
Dr. Piazza predicted that multislice CT scans will be “extremely important” in refining patient selection criteria for the procedure, and echocardiography will be helpful in understanding the optimal procedural techniques and viewing angles. Work also needs to be done on developing optimal anticoagulation protocols in order to avoid valve thrombosis.
Dr. Guerrero reported serving as a consultant to Edwards Lifesciences. Dr. Piazza is a consultant to Medtronic and MicroPort.
PARIS – Transcatheter mitral valve replacement using a repurposed transcatheter aortic valve in patients with severe symptomatic native mitral valve disease and severe mitral annular calcification is feasible and may be an option in carefully selected patients who aren’t candidates for surgery, Mayra Guerrero, MD, said at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
However, at this early point in development, the procedure is associated with an exceptionally steep learning curve, said Dr. Guerrero, director of cardiac structural interventions at the NorthShore University Health System in Evanston, Ill.
She presented the procedural and 30-day outcomes for the first 104 patients entered into a global registry encompassing 47 centers in 11 countries. Nearly 90% of patients received an Edwards SAPIEN XT or SAPIEN 3 valve. The EuroPCR results update an earlier report on the first 64 patients in the registry (JACC Cardiovasc Interv. 2016 Jul 11;9[13]:1361-71).
The results, she said, are reminiscent of the early days in transcatheter aortic valve replacement, which were marked by an initial very high early mortality rate that fell dramatically as technology and techniques improved.
“We know that there are important things we need to improve. Left ventricular outflow tract obstruction is the Achilles heel of this procedure; we need to work on its prevention and management. We need better annulus sizing methods. We need to find the best delivery method and improve our patient selection in order to avoid taking on patients who are too sick. Still, even during this early experience, the technical success rate has improved, and 30-day mortality continues to drop,” Dr. Guerrero said.
Indeed, the 30-day all-cause mortality rate of 25% in the first 104 patients doesn’t tell the whole story. The rate was 37.5% in the first third of patients, fell to 21.9% in the second tertile, and then to 15% in the most recent tertile.
Similarly, the technical success rate of the procedure according to Mitral Valve Academic Research Consortium criteria improved from 62.5% in the first tertile of patients to 84.4% and 80% in the second and third, respectively, she continued.
The rates of almost all complications went down with greater operator experience, too. The notable exception was left ventricular outflow tract obstruction (LVOTO). It occurred in 12.5% of patients in the first tertile and remained unchanged in the third.
It’s noteworthy that the majority of deaths were noncardiac in nature. Patients with mitral annular calcification are a high-risk group even before they develop valvular dysfunction. They are typically older and have multiple comorbidities. Participants in the global registry had a mean Society of Thoracic Surgeons score of 14.4; 38% had diabetes, 45% had chronic obstructive pulmonary disease, 35% had heart failure, 34% had previously undergone coronary artery bypass surgery, and roughly half of patients had a prior aortic valve replacement.
Causes of noncardiac mortality within 30 days included multiorgan failure in 8.6% of subjects, pneumonia in 2.9%, infection in 1.9%, and one fatal thoracentesis-related bleeding complication.
Cardiovascular deaths included two cases due to left ventricular perforation, two fatal strokes, an MI due to air emboli, a lethal complete atrioventricular block, and three deaths owing to LVOTO.
Alcohol ablation met with some success as a bailout treatment in cases of LVOTO with hemodynamic compromise after transmitral valve replacement in the global registry. All six treated patients had significant improvement initially, although the LVOTO recurred the next day in one instance. Four of the six patients were discharged from the hospital. One patient died because of atrioventricular block, and another from multiorgan failure 3 weeks after alcohol ablation of the LVOTO.
Dr. Guerrero has been a leader in this new field. She reported the first percutaneous implantation of a balloon expandable transcatheter valve in a native mitral valve without a surgical incision (Catheter Cardiovasc Interv. 2014 Jun 1;83[7]:E287-91), and more recently, together with coworkers developed a percutaneous alcohol ablation technique for acute reduction of LVOTO due to transcatheter mitral valve replacement (Catheter Cardiovasc Interv. 2016 Jul 5. doi:10.1002/ccd.26649).
She is now the principal investigator in the ongoing Mitral Implantation of Transcatheter Valves (MITRAL) trial, a physician-sponsored, 90-patient pilot study underway at six U.S. sites. MITRAL is recruiting three patient populations for transcatheter mitral valve replacement: patients like those in the global registry, with native mitral valve disease and severe mitral annular calcification; those with a symptomatic failing surgical ring with severe mitral regurgitation or stenosis; and patients with a symptomatic failing surgical bioprosthesis with severe mitral regurgitation or stenosis.
Discussant Nicolo Piazza, MD, of McGill University, Montreal, said transcatheter mitral valve replacement in mitral valve disease with severe mitral annular calcification in patients unsuitable for surgery “definitely represents an unmet clinical need in our practice today.” But he urged caution in interpreting the global registry data.
“This is a real world registry study with inherent selection bias and physician reporting bias,” the cardiologist said.
“We are leveraging a therapy from the aortic field into the mitral field. Of course, we do not have dedicated devices yet to treat these patients. The main finding of this study is that the procedure is actually feasible,” Dr. Piazza said.
Still, it’s sobering that at least 1 in 10 treated patients experiences LVOTO, 1 in 10 requires a second valve, and technical success is achieved in 3 out of 4 patients, he added.
Dr. Piazza predicted that multislice CT scans will be “extremely important” in refining patient selection criteria for the procedure, and echocardiography will be helpful in understanding the optimal procedural techniques and viewing angles. Work also needs to be done on developing optimal anticoagulation protocols in order to avoid valve thrombosis.
Dr. Guerrero reported serving as a consultant to Edwards Lifesciences. Dr. Piazza is a consultant to Medtronic and MicroPort.
AT EUROPCR 2016
Key clinical point: A report from a global registry of transcatheter aortic valve implantation in the mitral position shows the procedure is feasible.
Major finding: Thirty-day mortality fell from 37.5% in the first third of treated patients to 15% in the most recent tertile.
Data source: A real world registry that includes 104 patients at 47 centers in 11 countries to date.
Disclosures: The study presenter reported serving as a consultant to Edwards Lifesciences.

Extended-release naltrexone helps alcohol-dependent HIV-positive prisoners transition to community
DURBAN, SOUTH AFRICA – Extended-release naltrexone provides clinically meaningful benefits in HIV-infected prisoners with alcohol use disorder and multiple comorbid conditions as they transition back into the community, according to the findings of a double-blind randomized clinical trial.
“I think it’s important to know that a very effective medication, which has not previously been given to this population, was accepted by this group. It may be a feasible conduit to care as they transition to the community, even among those with severe psychosocial disparities like homelessness and mental illness,” Sandra A. Springer, MD, said in presenting the study findings at the 21st International AIDS Conference.
Extended-release naltrexone (Vivitrol) is a mu-opioid receptor antagonist approved for the treatment of alcohol use disorder, where it has been shown to decrease consumption. But prior to her study, the once-monthly injectable drug hadn’t been studied in alcohol-dependent prisoners living with HIV who are transitioning from jail or prison into the community, noted Dr. Springer, an infectious disease specialist at Yale University in New Haven, Conn.
This is a large, important, and seriously neglected patient population, she observed. The United States has the highest incarceration rate in the world. The prevalence of HIV infection is at least three times greater in U.S. criminal justice settings than in the general population. Alcohol use disorders are eightfold more common. Release from prison or jail in affected individuals often is complicated by relapse to alcohol use, which in turn is associated with poor HIV treatment outcomes.
Dr. Springer reported on 100 HIV-positive adult prisoners with alcohol use disorder diagnosed by DSM-IV criteria who were randomized double-blind two-to-one to 6 monthly 380-mg intramuscular injections of extended-release naltrexone or placebo, with the first dose given 3-7 days prior to release. Participants were required to have no baseline clinical evidence of cirrhosis or very high liver enzyme levels.
Half of participants had chronic hepatitis C. Eighty-seven percent of subjects scored 20 or higher on the Alcohol Use Disorders Identification test, indicating alcohol dependence. On the Mini International Neuropsychiatric Interview, 15% of participants met criteria for major depressive disorder, 16% for bipolar disorder, 59% for cocaine use disorder, 16% for narcotic use disorder, and 16% for cannabis use disorder. Most of the subjects were homeless or had an unstable housing situation.
Alcohol outcomes were assessed monthly during the 6-month trial. Not surprisingly, the better the treatment adherence, the better the outcomes. During the 90 days before incarceration, patients self-reported that 70% of those days were heavy drinking days, defined in men as having five or more drinks per day and in women as four or more. Their average consumption on those heavy drinking days was 28 drinks per day. In contrast, patients who accepted four or more extended-release naltrexone injections during 180 days of follow-up after release from custody drank heavily on just 7.6% of days, with an average of 8.6 drinks per day on those heavy drinking days. Subjects who received four or more placebo injections drank heavily on 11.6% of days, consuming an average of 12 drinks per heavy drinking day.
The time to first heavy drinking day was longer in patients who accepted 4-6 monthly injections of extended-release naltrexone than in those with 4-6 placebo injections. However, the difference achieved statistical significance only in the younger subgroup of participants aged 21-29 years. In that subgroup, the average time to the first heavy drinking day was 24.1 days, compared with 9.5 days with placebo.
On a composite alcohol consumption index comprised of time to first heavy drinking day after release, mean number of drinks per drinking day, change from before to after incarceration in average number of drinks per drinking day, alcohol craving score, and total number of drinking days, subjects who received four or more extended-release naltrexone injections had a significantly more favorable result, with a mean score of 3.15, compared with 2.93 in patients who took four or more placebo injections.
Moreover, consistent use of extended-release naltrexone was associated with significantly lower HIV viral load counts, compared with placebo-treated controls.
Treatment with extended-release naltrexone was safe. No serious side effects occurred, even in patients with comorbid hepatitis C who were on antiretroviral therapy. The most common side effects were the same as in seen in studies of the drug in other populations: mild to moderate nausea, headache, decreased appetite, fatigue, and dizziness.
Elsewhere at AIDS 2016, Chris Beyrer, MD, president of the International AIDS Society, included prisoners on his list of the populations most vulnerable to HIV because of discriminatory laws and policies in many parts of the world. Others on the list were transgender people, sex workers, men who have sex with men, and injection drug users.
“We’ll never be able to end AIDS without addressing the needs of these most vulnerable individuals and communities, and yet we know in 2016 far too many are being left behind,” said Dr. Beyrer, professor of epidemiology at Johns Hopkins University, Baltimore.
Transgender individuals, for example, are 49 times more likely to have HIV infection than other adults. Injection drug users and men who have sex with men are each 24-fold more likely to become HIV infected than the general population. Sex workers are 10 times more likely to acquire HIV infection than others in their reproductive years. And prisoners have a fivefold greater prevalence of HIV.
“In 2014 these vulnerable groups accounted for more than one-third of all new HIV infections. That’s an extraordinary proportion of HIV,” he observed. “This truly is the undone work of the HIV response. If there’s any silver lining in this cloud, it’s this: We’re talking about a relatively small number of people who are at high risk of infection relative to the world’s population. And that means that turning this around doesn’t require massive new commitments to very large populations. What it does require is an honest acknowledgment of where the epidemic is hitting hardest and directing resources to that need.”
Unfortunately, screening and treatment programs are rarely tailored to reach these highly vulnerable groups effectively, he added.
Dr. Beyrer was a contributor to a special issue of the Lancet devoted to HIV infection among prisoners published with the AIDS 2016 conference.
Dr. Springer’s study was funded by the National Institute on Alcohol Abuse and Alcoholism, and the National Institute on Drug Abuse. She reported having no financial conflicts of interest.
DURBAN, SOUTH AFRICA – Extended-release naltrexone provides clinically meaningful benefits in HIV-infected prisoners with alcohol use disorder and multiple comorbid conditions as they transition back into the community, according to the findings of a double-blind randomized clinical trial.
“I think it’s important to know that a very effective medication, which has not previously been given to this population, was accepted by this group. It may be a feasible conduit to care as they transition to the community, even among those with severe psychosocial disparities like homelessness and mental illness,” Sandra A. Springer, MD, said in presenting the study findings at the 21st International AIDS Conference.
Extended-release naltrexone (Vivitrol) is a mu-opioid receptor antagonist approved for the treatment of alcohol use disorder, where it has been shown to decrease consumption. But prior to her study, the once-monthly injectable drug hadn’t been studied in alcohol-dependent prisoners living with HIV who are transitioning from jail or prison into the community, noted Dr. Springer, an infectious disease specialist at Yale University in New Haven, Conn.
This is a large, important, and seriously neglected patient population, she observed. The United States has the highest incarceration rate in the world. The prevalence of HIV infection is at least three times greater in U.S. criminal justice settings than in the general population. Alcohol use disorders are eightfold more common. Release from prison or jail in affected individuals often is complicated by relapse to alcohol use, which in turn is associated with poor HIV treatment outcomes.
Dr. Springer reported on 100 HIV-positive adult prisoners with alcohol use disorder diagnosed by DSM-IV criteria who were randomized double-blind two-to-one to 6 monthly 380-mg intramuscular injections of extended-release naltrexone or placebo, with the first dose given 3-7 days prior to release. Participants were required to have no baseline clinical evidence of cirrhosis or very high liver enzyme levels.
Half of participants had chronic hepatitis C. Eighty-seven percent of subjects scored 20 or higher on the Alcohol Use Disorders Identification test, indicating alcohol dependence. On the Mini International Neuropsychiatric Interview, 15% of participants met criteria for major depressive disorder, 16% for bipolar disorder, 59% for cocaine use disorder, 16% for narcotic use disorder, and 16% for cannabis use disorder. Most of the subjects were homeless or had an unstable housing situation.
Alcohol outcomes were assessed monthly during the 6-month trial. Not surprisingly, the better the treatment adherence, the better the outcomes. During the 90 days before incarceration, patients self-reported that 70% of those days were heavy drinking days, defined in men as having five or more drinks per day and in women as four or more. Their average consumption on those heavy drinking days was 28 drinks per day. In contrast, patients who accepted four or more extended-release naltrexone injections during 180 days of follow-up after release from custody drank heavily on just 7.6% of days, with an average of 8.6 drinks per day on those heavy drinking days. Subjects who received four or more placebo injections drank heavily on 11.6% of days, consuming an average of 12 drinks per heavy drinking day.
The time to first heavy drinking day was longer in patients who accepted 4-6 monthly injections of extended-release naltrexone than in those with 4-6 placebo injections. However, the difference achieved statistical significance only in the younger subgroup of participants aged 21-29 years. In that subgroup, the average time to the first heavy drinking day was 24.1 days, compared with 9.5 days with placebo.
On a composite alcohol consumption index comprised of time to first heavy drinking day after release, mean number of drinks per drinking day, change from before to after incarceration in average number of drinks per drinking day, alcohol craving score, and total number of drinking days, subjects who received four or more extended-release naltrexone injections had a significantly more favorable result, with a mean score of 3.15, compared with 2.93 in patients who took four or more placebo injections.
Moreover, consistent use of extended-release naltrexone was associated with significantly lower HIV viral load counts, compared with placebo-treated controls.
Treatment with extended-release naltrexone was safe. No serious side effects occurred, even in patients with comorbid hepatitis C who were on antiretroviral therapy. The most common side effects were the same as in seen in studies of the drug in other populations: mild to moderate nausea, headache, decreased appetite, fatigue, and dizziness.
Elsewhere at AIDS 2016, Chris Beyrer, MD, president of the International AIDS Society, included prisoners on his list of the populations most vulnerable to HIV because of discriminatory laws and policies in many parts of the world. Others on the list were transgender people, sex workers, men who have sex with men, and injection drug users.
“We’ll never be able to end AIDS without addressing the needs of these most vulnerable individuals and communities, and yet we know in 2016 far too many are being left behind,” said Dr. Beyrer, professor of epidemiology at Johns Hopkins University, Baltimore.
Transgender individuals, for example, are 49 times more likely to have HIV infection than other adults. Injection drug users and men who have sex with men are each 24-fold more likely to become HIV infected than the general population. Sex workers are 10 times more likely to acquire HIV infection than others in their reproductive years. And prisoners have a fivefold greater prevalence of HIV.
“In 2014 these vulnerable groups accounted for more than one-third of all new HIV infections. That’s an extraordinary proportion of HIV,” he observed. “This truly is the undone work of the HIV response. If there’s any silver lining in this cloud, it’s this: We’re talking about a relatively small number of people who are at high risk of infection relative to the world’s population. And that means that turning this around doesn’t require massive new commitments to very large populations. What it does require is an honest acknowledgment of where the epidemic is hitting hardest and directing resources to that need.”
Unfortunately, screening and treatment programs are rarely tailored to reach these highly vulnerable groups effectively, he added.
Dr. Beyrer was a contributor to a special issue of the Lancet devoted to HIV infection among prisoners published with the AIDS 2016 conference.
Dr. Springer’s study was funded by the National Institute on Alcohol Abuse and Alcoholism, and the National Institute on Drug Abuse. She reported having no financial conflicts of interest.
DURBAN, SOUTH AFRICA – Extended-release naltrexone provides clinically meaningful benefits in HIV-infected prisoners with alcohol use disorder and multiple comorbid conditions as they transition back into the community, according to the findings of a double-blind randomized clinical trial.
“I think it’s important to know that a very effective medication, which has not previously been given to this population, was accepted by this group. It may be a feasible conduit to care as they transition to the community, even among those with severe psychosocial disparities like homelessness and mental illness,” Sandra A. Springer, MD, said in presenting the study findings at the 21st International AIDS Conference.
Extended-release naltrexone (Vivitrol) is a mu-opioid receptor antagonist approved for the treatment of alcohol use disorder, where it has been shown to decrease consumption. But prior to her study, the once-monthly injectable drug hadn’t been studied in alcohol-dependent prisoners living with HIV who are transitioning from jail or prison into the community, noted Dr. Springer, an infectious disease specialist at Yale University in New Haven, Conn.
This is a large, important, and seriously neglected patient population, she observed. The United States has the highest incarceration rate in the world. The prevalence of HIV infection is at least three times greater in U.S. criminal justice settings than in the general population. Alcohol use disorders are eightfold more common. Release from prison or jail in affected individuals often is complicated by relapse to alcohol use, which in turn is associated with poor HIV treatment outcomes.
Dr. Springer reported on 100 HIV-positive adult prisoners with alcohol use disorder diagnosed by DSM-IV criteria who were randomized double-blind two-to-one to 6 monthly 380-mg intramuscular injections of extended-release naltrexone or placebo, with the first dose given 3-7 days prior to release. Participants were required to have no baseline clinical evidence of cirrhosis or very high liver enzyme levels.
Half of participants had chronic hepatitis C. Eighty-seven percent of subjects scored 20 or higher on the Alcohol Use Disorders Identification test, indicating alcohol dependence. On the Mini International Neuropsychiatric Interview, 15% of participants met criteria for major depressive disorder, 16% for bipolar disorder, 59% for cocaine use disorder, 16% for narcotic use disorder, and 16% for cannabis use disorder. Most of the subjects were homeless or had an unstable housing situation.
Alcohol outcomes were assessed monthly during the 6-month trial. Not surprisingly, the better the treatment adherence, the better the outcomes. During the 90 days before incarceration, patients self-reported that 70% of those days were heavy drinking days, defined in men as having five or more drinks per day and in women as four or more. Their average consumption on those heavy drinking days was 28 drinks per day. In contrast, patients who accepted four or more extended-release naltrexone injections during 180 days of follow-up after release from custody drank heavily on just 7.6% of days, with an average of 8.6 drinks per day on those heavy drinking days. Subjects who received four or more placebo injections drank heavily on 11.6% of days, consuming an average of 12 drinks per heavy drinking day.
The time to first heavy drinking day was longer in patients who accepted 4-6 monthly injections of extended-release naltrexone than in those with 4-6 placebo injections. However, the difference achieved statistical significance only in the younger subgroup of participants aged 21-29 years. In that subgroup, the average time to the first heavy drinking day was 24.1 days, compared with 9.5 days with placebo.
On a composite alcohol consumption index comprised of time to first heavy drinking day after release, mean number of drinks per drinking day, change from before to after incarceration in average number of drinks per drinking day, alcohol craving score, and total number of drinking days, subjects who received four or more extended-release naltrexone injections had a significantly more favorable result, with a mean score of 3.15, compared with 2.93 in patients who took four or more placebo injections.
Moreover, consistent use of extended-release naltrexone was associated with significantly lower HIV viral load counts, compared with placebo-treated controls.
Treatment with extended-release naltrexone was safe. No serious side effects occurred, even in patients with comorbid hepatitis C who were on antiretroviral therapy. The most common side effects were the same as in seen in studies of the drug in other populations: mild to moderate nausea, headache, decreased appetite, fatigue, and dizziness.
Elsewhere at AIDS 2016, Chris Beyrer, MD, president of the International AIDS Society, included prisoners on his list of the populations most vulnerable to HIV because of discriminatory laws and policies in many parts of the world. Others on the list were transgender people, sex workers, men who have sex with men, and injection drug users.
“We’ll never be able to end AIDS without addressing the needs of these most vulnerable individuals and communities, and yet we know in 2016 far too many are being left behind,” said Dr. Beyrer, professor of epidemiology at Johns Hopkins University, Baltimore.
Transgender individuals, for example, are 49 times more likely to have HIV infection than other adults. Injection drug users and men who have sex with men are each 24-fold more likely to become HIV infected than the general population. Sex workers are 10 times more likely to acquire HIV infection than others in their reproductive years. And prisoners have a fivefold greater prevalence of HIV.
“In 2014 these vulnerable groups accounted for more than one-third of all new HIV infections. That’s an extraordinary proportion of HIV,” he observed. “This truly is the undone work of the HIV response. If there’s any silver lining in this cloud, it’s this: We’re talking about a relatively small number of people who are at high risk of infection relative to the world’s population. And that means that turning this around doesn’t require massive new commitments to very large populations. What it does require is an honest acknowledgment of where the epidemic is hitting hardest and directing resources to that need.”
Unfortunately, screening and treatment programs are rarely tailored to reach these highly vulnerable groups effectively, he added.
Dr. Beyrer was a contributor to a special issue of the Lancet devoted to HIV infection among prisoners published with the AIDS 2016 conference.
Dr. Springer’s study was funded by the National Institute on Alcohol Abuse and Alcoholism, and the National Institute on Drug Abuse. She reported having no financial conflicts of interest.
AT AIDS 2016
Key clinical point: Extended-release naltrexone helps HIV-infected prisoners with alcohol use disorder in transitioning to the community.
Major finding: The mean time to the first heavy drinking day among 21- to 29-year-old HIV-infected prisoners with an alcohol use disorder was 24.1 days following release from prison or jail in those on extended-release naltrexone versus 9.5 days with placebo.
Data source: This randomized, double-blind clinical trial included 100 HIV-positive prisoners with alcohol use disorder who were released into the community. Two-thirds received six monthly injections of extended-release naltrexone, the rest placebo.
Disclosures: The study was funded by the National Institute on Alcohol Abuse and Alcoholism and the National Institute on Drug Abuse. The presenter reported having no financial conflicts of interest.
Psychiatric disorders often impair antiretroviral adherence in perinatally HIV-infected teens
DURBAN, SOUTH AFRICA – Adolescents who were perinatally infected with HIV have a high prevalence of selected psychiatric disorders that impede their adherence to antiretroviral therapy, Claude Ann Mellins, PhD, reported at the 21st International AIDS Conference.
Those psychiatric diagnoses were predictive of viremia over the ensuing 2-3 years in a new analysis from the ongoing Child and Adolescent Self-Awareness and Health (CASAH) study, according to Dr. Mellins, professor of medical psychology at Columbia University, New York, and codirector of CASAH.

The clinical implications of the CASAH findings are clear, she added. “Assessing and treating specific categories of psychiatric and substance abuse problems may enhance efforts to improve adherence and prevent poor health outcomes in these adolescents and young adults, who are especially vulnerable due to their very challenging circumstances,” Dr. Mellins said.
CASAH is a longitudinal study of perinatally HIV-infected and perinatally HIV-exposed but uninfected New York City youth. They were enrolled during 2003-2008, when they were 9-16 years old. They and their caregivers undergo detailed psychosocial interviews every 12-18 months. The goal is to identify risk factors as well as protective factors influencing their behavioral health outcomes, the clinical psychologist explained.
She reported on 179 perinatally infected adolescents who were at least 13 years old at the first of their three interviews conducted over a 2.7-year period. Of note, 53% of them met Diagnostic Interview Schedule for Children (DISC-IV) criteria for one or more psychiatric diagnoses at all three time points. The pattern of psychopathology was somewhat different from that previously described in adults with HIV, who have been studied much more extensively than perinatally infected teens.
“Much of the literature on adults has focused on depression and mood disorders as predictors of poor health outcomes. Our data suggest that among youth, disruptive behavioral disorders – things like [attention-deficit/hyperactivity disorder], conduct disorder, or oppositional defiant disorder – may be just as important, if not more so. Substance abuse was also a critical factor,” Dr. Mellins said.
In a cross-sectional multivariate logistic regression analysis, a behavior disorder diagnosed at the first interview was associated with a 2.57-fold increased likelihood of contemporaneous viremia as evidenced by a plasma HIV RNA viral load greater than 1,000 copies/mL, and with a threefold increased likelihood of self-reported missed doses of antiretroviral medications during the previous week.
Anxiety disorder was the most common psychiatric diagnosis at the initial interview, followed by disruptive behavior disorder and substance use disorder. A diagnosis of any psychiatric disorder at the time of the first interview was associated with a significantly increased risk of viremia across the next 2.7 years. Forty-seven percent of subjects had viremia at 2.7 years of follow-up, reflective of chronic suboptimal medication adherence.
She noted that the pattern of psychiatric disorders in perinatally infected patients shifts between adolescence and young adulthood.
“By the time perinatally infected adolescents become young adults, I will say that anxiety and mood disorders become much more prevalent. But the number of psychiatric problems actually goes down by young adulthood,” according to Dr. Mellins.
Indeed, in another CASAH analysis she presented at AIDS 2016, this one involving 136 perinatally infected young adults and 86 perinatally exposed but uninfected controls, the vast majority living in impoverished communities, there was no difference between the two groups in rates of psychiatric or substance use disorders, although the 27% prevalence of substance use disorders is higher than that found in the age-matched general population.
Eighty-four percent of the perinatally infected 18- to 28-year-olds had graduated from high school, 94% were in a stable housing situation, 59% were currently working or in school, 54% were paying rent, and 95% reported ever being in a romantic relationship. Rates were similar in the perinatally exposed but uninfected group with the exception that these individuals were less likely to be paying rent.
“In spite of substantive risks, there is a relatively large portion of both groups with positive behavioral health outcomes, achieving normative young adult transition milestones. We need to understand why. Identification of protective factors conferring resilience can inform evidence-based prevention efforts, which are critical given the staggering numbers of children and young adolescents worldwide affected by HIV who will be transitioning to adulthood,” she said.
Dr. Mellins said the CASAH findings constitute a persuasive argument in favor of integrating mental health as a component of HIV care.
“Young people don’t always go to mental health appointments that are separate from medical care, so integrating mental health as a component of HIV care might be one of the most effective ways to identify and treat mental health problems in infected youth while simultaneously improving medication adherence and health outcomes,” Dr. Mellins said.
The ongoing CASAH study is funded by the National Institute of Mental Health. Dr. Mellins reported having no relevant financial conflicts.
DURBAN, SOUTH AFRICA – Adolescents who were perinatally infected with HIV have a high prevalence of selected psychiatric disorders that impede their adherence to antiretroviral therapy, Claude Ann Mellins, PhD, reported at the 21st International AIDS Conference.
Those psychiatric diagnoses were predictive of viremia over the ensuing 2-3 years in a new analysis from the ongoing Child and Adolescent Self-Awareness and Health (CASAH) study, according to Dr. Mellins, professor of medical psychology at Columbia University, New York, and codirector of CASAH.
The clinical implications of the CASAH findings are clear, she added. “Assessing and treating specific categories of psychiatric and substance abuse problems may enhance efforts to improve adherence and prevent poor health outcomes in these adolescents and young adults, who are especially vulnerable due to their very challenging circumstances,” Dr. Mellins said.
CASAH is a longitudinal study of perinatally HIV-infected and perinatally HIV-exposed but uninfected New York City youth. They were enrolled during 2003-2008, when they were 9-16 years old. They and their caregivers undergo detailed psychosocial interviews every 12-18 months. The goal is to identify risk factors as well as protective factors influencing their behavioral health outcomes, the clinical psychologist explained.
She reported on 179 perinatally infected adolescents who were at least 13 years old at the first of their three interviews conducted over a 2.7-year period. Of note, 53% of them met Diagnostic Interview Schedule for Children (DISC-IV) criteria for one or more psychiatric diagnoses at all three time points. The pattern of psychopathology was somewhat different from that previously described in adults with HIV, who have been studied much more extensively than perinatally infected teens.
“Much of the literature on adults has focused on depression and mood disorders as predictors of poor health outcomes. Our data suggest that among youth, disruptive behavioral disorders – things like [attention-deficit/hyperactivity disorder], conduct disorder, or oppositional defiant disorder – may be just as important, if not more so. Substance abuse was also a critical factor,” Dr. Mellins said.
In a cross-sectional multivariate logistic regression analysis, a behavior disorder diagnosed at the first interview was associated with a 2.57-fold increased likelihood of contemporaneous viremia as evidenced by a plasma HIV RNA viral load greater than 1,000 copies/mL, and with a threefold increased likelihood of self-reported missed doses of antiretroviral medications during the previous week.
Anxiety disorder was the most common psychiatric diagnosis at the initial interview, followed by disruptive behavior disorder and substance use disorder. A diagnosis of any psychiatric disorder at the time of the first interview was associated with a significantly increased risk of viremia across the next 2.7 years. Forty-seven percent of subjects had viremia at 2.7 years of follow-up, reflective of chronic suboptimal medication adherence.
She noted that the pattern of psychiatric disorders in perinatally infected patients shifts between adolescence and young adulthood.
“By the time perinatally infected adolescents become young adults, I will say that anxiety and mood disorders become much more prevalent. But the number of psychiatric problems actually goes down by young adulthood,” according to Dr. Mellins.
Indeed, in another CASAH analysis she presented at AIDS 2016, this one involving 136 perinatally infected young adults and 86 perinatally exposed but uninfected controls, the vast majority living in impoverished communities, there was no difference between the two groups in rates of psychiatric or substance use disorders, although the 27% prevalence of substance use disorders is higher than that found in the age-matched general population.
Eighty-four percent of the perinatally infected 18- to 28-year-olds had graduated from high school, 94% were in a stable housing situation, 59% were currently working or in school, 54% were paying rent, and 95% reported ever being in a romantic relationship. Rates were similar in the perinatally exposed but uninfected group with the exception that these individuals were less likely to be paying rent.
“In spite of substantive risks, there is a relatively large portion of both groups with positive behavioral health outcomes, achieving normative young adult transition milestones. We need to understand why. Identification of protective factors conferring resilience can inform evidence-based prevention efforts, which are critical given the staggering numbers of children and young adolescents worldwide affected by HIV who will be transitioning to adulthood,” she said.
Dr. Mellins said the CASAH findings constitute a persuasive argument in favor of integrating mental health as a component of HIV care.
“Young people don’t always go to mental health appointments that are separate from medical care, so integrating mental health as a component of HIV care might be one of the most effective ways to identify and treat mental health problems in infected youth while simultaneously improving medication adherence and health outcomes,” Dr. Mellins said.
The ongoing CASAH study is funded by the National Institute of Mental Health. Dr. Mellins reported having no relevant financial conflicts.
DURBAN, SOUTH AFRICA – Adolescents who were perinatally infected with HIV have a high prevalence of selected psychiatric disorders that impede their adherence to antiretroviral therapy, Claude Ann Mellins, PhD, reported at the 21st International AIDS Conference.
Those psychiatric diagnoses were predictive of viremia over the ensuing 2-3 years in a new analysis from the ongoing Child and Adolescent Self-Awareness and Health (CASAH) study, according to Dr. Mellins, professor of medical psychology at Columbia University, New York, and codirector of CASAH.
The clinical implications of the CASAH findings are clear, she added. “Assessing and treating specific categories of psychiatric and substance abuse problems may enhance efforts to improve adherence and prevent poor health outcomes in these adolescents and young adults, who are especially vulnerable due to their very challenging circumstances,” Dr. Mellins said.
CASAH is a longitudinal study of perinatally HIV-infected and perinatally HIV-exposed but uninfected New York City youth. They were enrolled during 2003-2008, when they were 9-16 years old. They and their caregivers undergo detailed psychosocial interviews every 12-18 months. The goal is to identify risk factors as well as protective factors influencing their behavioral health outcomes, the clinical psychologist explained.
She reported on 179 perinatally infected adolescents who were at least 13 years old at the first of their three interviews conducted over a 2.7-year period. Of note, 53% of them met Diagnostic Interview Schedule for Children (DISC-IV) criteria for one or more psychiatric diagnoses at all three time points. The pattern of psychopathology was somewhat different from that previously described in adults with HIV, who have been studied much more extensively than perinatally infected teens.
“Much of the literature on adults has focused on depression and mood disorders as predictors of poor health outcomes. Our data suggest that among youth, disruptive behavioral disorders – things like [attention-deficit/hyperactivity disorder], conduct disorder, or oppositional defiant disorder – may be just as important, if not more so. Substance abuse was also a critical factor,” Dr. Mellins said.
In a cross-sectional multivariate logistic regression analysis, a behavior disorder diagnosed at the first interview was associated with a 2.57-fold increased likelihood of contemporaneous viremia as evidenced by a plasma HIV RNA viral load greater than 1,000 copies/mL, and with a threefold increased likelihood of self-reported missed doses of antiretroviral medications during the previous week.
Anxiety disorder was the most common psychiatric diagnosis at the initial interview, followed by disruptive behavior disorder and substance use disorder. A diagnosis of any psychiatric disorder at the time of the first interview was associated with a significantly increased risk of viremia across the next 2.7 years. Forty-seven percent of subjects had viremia at 2.7 years of follow-up, reflective of chronic suboptimal medication adherence.
She noted that the pattern of psychiatric disorders in perinatally infected patients shifts between adolescence and young adulthood.
“By the time perinatally infected adolescents become young adults, I will say that anxiety and mood disorders become much more prevalent. But the number of psychiatric problems actually goes down by young adulthood,” according to Dr. Mellins.
Indeed, in another CASAH analysis she presented at AIDS 2016, this one involving 136 perinatally infected young adults and 86 perinatally exposed but uninfected controls, the vast majority living in impoverished communities, there was no difference between the two groups in rates of psychiatric or substance use disorders, although the 27% prevalence of substance use disorders is higher than that found in the age-matched general population.
Eighty-four percent of the perinatally infected 18- to 28-year-olds had graduated from high school, 94% were in a stable housing situation, 59% were currently working or in school, 54% were paying rent, and 95% reported ever being in a romantic relationship. Rates were similar in the perinatally exposed but uninfected group with the exception that these individuals were less likely to be paying rent.
“In spite of substantive risks, there is a relatively large portion of both groups with positive behavioral health outcomes, achieving normative young adult transition milestones. We need to understand why. Identification of protective factors conferring resilience can inform evidence-based prevention efforts, which are critical given the staggering numbers of children and young adolescents worldwide affected by HIV who will be transitioning to adulthood,” she said.
Dr. Mellins said the CASAH findings constitute a persuasive argument in favor of integrating mental health as a component of HIV care.
“Young people don’t always go to mental health appointments that are separate from medical care, so integrating mental health as a component of HIV care might be one of the most effective ways to identify and treat mental health problems in infected youth while simultaneously improving medication adherence and health outcomes,” Dr. Mellins said.
The ongoing CASAH study is funded by the National Institute of Mental Health. Dr. Mellins reported having no relevant financial conflicts.
AT AIDS 2016
Key clinical point: Look for and treat psychiatric disorders in perinatally HIV-infected adolescents as a means of optimizing their antiretroviral medication adherence.
Major finding: A majority of perinatally HIV-infected adolescents meet the criteria for at least one psychiatric diagnosis, and they are at significantly increased risk for poor medication adherence and viremia during the next 2-3 years.
Data source: The longitudinal CASAH study involving prospective follow-up of several hundred perinatally HIV-infected and perinatally exposed but uninfected subjects through adolescence and young adulthood.
Disclosures: The ongoing CASAH study is funded by the National Institute of Mental Health. Dr. Mellins reported having no relevant financial conflicts.

Who benefits most from immediate HIV therapy?
DURBAN, SOUTH AFRICA – Immediate initiation of antiretroviral therapy in asymptomatic treatment-naive HIV-infected adults with a CD4+ cell count greater than 500/mL brings considerably more bang for the buck in selected patient subgroups, according to a secondary analysis from the landmark START trial.
Four subgroups in START stood out as having larger absolute risk reductions and lower numbers-needed-to-treat with a strategy of immediate treatment: patients above age 50, those with a baseline Framingham Risk Score in excess of 10%, individuals whose plasma HIV RNA level exceeds 50,000 copies/mL, and patients with a CD4:CD8 ratio below 0.5, Dr. Jean-Michel Molina reported at the 21st International AIDS Conference.
“These patients might be prioritized for immediate access to ART,” observed Dr. Molina, professor of infectious diseases at the University of Paris-Diderot and head of the infectious diseases department at Saint-Louis Hospital, also in Paris.
The START (Strategic Timing of AntiRetroviral Treatment) study was a major clinical trial conducted in 35 countries. Investigators randomized 4,685 treatment-naive HIV-infected men and women with CD4+ cell counts in the normal range to immediate antiretroviral therapy or to deferral of treatment until their CD4+ cell count dropped to 350 cells/mL. After 3 years of prospective follow-up, the immediate-treatment strategy was associated with a 47% reduction in risk for the primary endpoint, a composite of AIDS, major cardiovascular or other non-AIDS events, and death. The number needed to treat immediately for 1 year in order to prevent one major event was 128 (N Engl J Med. 2015;373:795-807).
The START findings prompted a revision in World Health Organization guidelines, which now recommend universal antiretroviral treatment (ART) in patients with HIV infection regardless of their CD4+ cell count.
But some patients are reluctant to go on lifetime ART, particularly since they still feel normal while in the initial phases of HIV infection. In such cases, these new subgroup data may tip the balance in decision-making. Moreover, the new START findings should help physicians and policy makers in prioritizing access to immediate ART in settings where it isn’t universally available, according to Dr. Molina.
In the prespecified subgroup analysis, patients aged 50 and up at enrollment had a 2.9% incidence of the primary composite endpoint at 3 years if randomized to immediate ART and an 11.7% rate if they were assigned to deferred ART. The number of 50-plus-year-olds needed to treat (NNT) immediately for 1 year in order to prevent one additional case of AIDS, a major non-AIDS event, or death was just 45, compared to NNTs of 151 and 206 in patients aged 30-49 and younger than 30, respectively. Patients aged 50 and older accounted for nearly 12% of the overall study population.
For the roughly 28% of START participants whose baseline CD4:CD8 ratio was less than 0.5, the NNT for immediate rather than deferred therapy was 60, substantially more favorable than the NNTs of 214 in patients with a baseline ratio of 0.5-0.8 and 248 in patients with a CD4:CD8 ratio greater than 0.8. The incidence of the primary endpoint at 3 years of follow-up in patients with a CD4:CD8 ratio of less than 0.5 was 0.5% in the immediate ART group and 6.3% with deferred therapy.
Similarly, patients with a baseline 10-year Framingham Risk Score (FRS) of 10% or higher had an NNT of 69, compared with NNTs of 111 in subjects with an FRS of 1%-9.9% and 276 in those with an FRS of less than 1%. Patients with an FRS of 10% or more had a 2.4% incidence of the primary endpoint at 3 years if assigned to immediate ART and a 10.1% rate with deferred therapy. Patients with an FRS of 10% or more comprised only 9.6% of the study population, Dr. Molina continued.
Patients with a heavy baseline viral load as evidenced by a plasma HIV RNA level of at least 50,000 copies/mL accounted for roughly 22% of the total study sample. Their 3-year rate of the primary outcome was 2.1% with immediate ART and 6.9% with deferred treatment. The NNT was 67, compared to an NNT of 122 in patients with 3,000-49,999 copies/mL and 992 in the one-quarter of START participants with a baseline plasma HIV RNA level of less than 3,000 copies/mL.
Variables that weren’t related to the magnitude of absolute risk reduction and NNT in the START subgroup analysis were race, gender, geographic region, baseline CD4 cell count, and whether an individual resided in a high- or lower-income country.
Several audience members rose to assert that the CD4:CD8 ratio and viral load might very well be redundant predictors measuring the same thing, since they are typically tightly correlated. Dr. Molina replied that the START investigators are planning to conduct a multivariate analysis of the data in the near future, which should provide a definitive answer.
Another audience member expressed surprise at what struck him as a low cardiovascular event rate in the START study, given that HIV infection is known to be associated with accelerated atherosclerosis. Dr. Molina said the explanation for the low number of cardiovascular events lies in the fact that cardiovascular risk is so heavily age-dependent, and START participants were relatively young, with a median age of 36 years.
The START trial was carried out by the International Network for Strategic Initiatives in Global HIV Trials (INSIGHT) with funding provided mainly by the National Institutes of Health. Dr. Molina reported having no financial conflicts of interest.
DURBAN, SOUTH AFRICA – Immediate initiation of antiretroviral therapy in asymptomatic treatment-naive HIV-infected adults with a CD4+ cell count greater than 500/mL brings considerably more bang for the buck in selected patient subgroups, according to a secondary analysis from the landmark START trial.
Four subgroups in START stood out as having larger absolute risk reductions and lower numbers-needed-to-treat with a strategy of immediate treatment: patients above age 50, those with a baseline Framingham Risk Score in excess of 10%, individuals whose plasma HIV RNA level exceeds 50,000 copies/mL, and patients with a CD4:CD8 ratio below 0.5, Dr. Jean-Michel Molina reported at the 21st International AIDS Conference.
“These patients might be prioritized for immediate access to ART,” observed Dr. Molina, professor of infectious diseases at the University of Paris-Diderot and head of the infectious diseases department at Saint-Louis Hospital, also in Paris.
The START (Strategic Timing of AntiRetroviral Treatment) study was a major clinical trial conducted in 35 countries. Investigators randomized 4,685 treatment-naive HIV-infected men and women with CD4+ cell counts in the normal range to immediate antiretroviral therapy or to deferral of treatment until their CD4+ cell count dropped to 350 cells/mL. After 3 years of prospective follow-up, the immediate-treatment strategy was associated with a 47% reduction in risk for the primary endpoint, a composite of AIDS, major cardiovascular or other non-AIDS events, and death. The number needed to treat immediately for 1 year in order to prevent one major event was 128 (N Engl J Med. 2015;373:795-807).
The START findings prompted a revision in World Health Organization guidelines, which now recommend universal antiretroviral treatment (ART) in patients with HIV infection regardless of their CD4+ cell count.
But some patients are reluctant to go on lifetime ART, particularly since they still feel normal while in the initial phases of HIV infection. In such cases, these new subgroup data may tip the balance in decision-making. Moreover, the new START findings should help physicians and policy makers in prioritizing access to immediate ART in settings where it isn’t universally available, according to Dr. Molina.
In the prespecified subgroup analysis, patients aged 50 and up at enrollment had a 2.9% incidence of the primary composite endpoint at 3 years if randomized to immediate ART and an 11.7% rate if they were assigned to deferred ART. The number of 50-plus-year-olds needed to treat (NNT) immediately for 1 year in order to prevent one additional case of AIDS, a major non-AIDS event, or death was just 45, compared to NNTs of 151 and 206 in patients aged 30-49 and younger than 30, respectively. Patients aged 50 and older accounted for nearly 12% of the overall study population.
For the roughly 28% of START participants whose baseline CD4:CD8 ratio was less than 0.5, the NNT for immediate rather than deferred therapy was 60, substantially more favorable than the NNTs of 214 in patients with a baseline ratio of 0.5-0.8 and 248 in patients with a CD4:CD8 ratio greater than 0.8. The incidence of the primary endpoint at 3 years of follow-up in patients with a CD4:CD8 ratio of less than 0.5 was 0.5% in the immediate ART group and 6.3% with deferred therapy.
Similarly, patients with a baseline 10-year Framingham Risk Score (FRS) of 10% or higher had an NNT of 69, compared with NNTs of 111 in subjects with an FRS of 1%-9.9% and 276 in those with an FRS of less than 1%. Patients with an FRS of 10% or more had a 2.4% incidence of the primary endpoint at 3 years if assigned to immediate ART and a 10.1% rate with deferred therapy. Patients with an FRS of 10% or more comprised only 9.6% of the study population, Dr. Molina continued.
Patients with a heavy baseline viral load as evidenced by a plasma HIV RNA level of at least 50,000 copies/mL accounted for roughly 22% of the total study sample. Their 3-year rate of the primary outcome was 2.1% with immediate ART and 6.9% with deferred treatment. The NNT was 67, compared to an NNT of 122 in patients with 3,000-49,999 copies/mL and 992 in the one-quarter of START participants with a baseline plasma HIV RNA level of less than 3,000 copies/mL.
Variables that weren’t related to the magnitude of absolute risk reduction and NNT in the START subgroup analysis were race, gender, geographic region, baseline CD4 cell count, and whether an individual resided in a high- or lower-income country.
Several audience members rose to assert that the CD4:CD8 ratio and viral load might very well be redundant predictors measuring the same thing, since they are typically tightly correlated. Dr. Molina replied that the START investigators are planning to conduct a multivariate analysis of the data in the near future, which should provide a definitive answer.
Another audience member expressed surprise at what struck him as a low cardiovascular event rate in the START study, given that HIV infection is known to be associated with accelerated atherosclerosis. Dr. Molina said the explanation for the low number of cardiovascular events lies in the fact that cardiovascular risk is so heavily age-dependent, and START participants were relatively young, with a median age of 36 years.
The START trial was carried out by the International Network for Strategic Initiatives in Global HIV Trials (INSIGHT) with funding provided mainly by the National Institutes of Health. Dr. Molina reported having no financial conflicts of interest.
DURBAN, SOUTH AFRICA – Immediate initiation of antiretroviral therapy in asymptomatic treatment-naive HIV-infected adults with a CD4+ cell count greater than 500/mL brings considerably more bang for the buck in selected patient subgroups, according to a secondary analysis from the landmark START trial.
Four subgroups in START stood out as having larger absolute risk reductions and lower numbers-needed-to-treat with a strategy of immediate treatment: patients above age 50, those with a baseline Framingham Risk Score in excess of 10%, individuals whose plasma HIV RNA level exceeds 50,000 copies/mL, and patients with a CD4:CD8 ratio below 0.5, Dr. Jean-Michel Molina reported at the 21st International AIDS Conference.
“These patients might be prioritized for immediate access to ART,” observed Dr. Molina, professor of infectious diseases at the University of Paris-Diderot and head of the infectious diseases department at Saint-Louis Hospital, also in Paris.
The START (Strategic Timing of AntiRetroviral Treatment) study was a major clinical trial conducted in 35 countries. Investigators randomized 4,685 treatment-naive HIV-infected men and women with CD4+ cell counts in the normal range to immediate antiretroviral therapy or to deferral of treatment until their CD4+ cell count dropped to 350 cells/mL. After 3 years of prospective follow-up, the immediate-treatment strategy was associated with a 47% reduction in risk for the primary endpoint, a composite of AIDS, major cardiovascular or other non-AIDS events, and death. The number needed to treat immediately for 1 year in order to prevent one major event was 128 (N Engl J Med. 2015;373:795-807).
The START findings prompted a revision in World Health Organization guidelines, which now recommend universal antiretroviral treatment (ART) in patients with HIV infection regardless of their CD4+ cell count.
But some patients are reluctant to go on lifetime ART, particularly since they still feel normal while in the initial phases of HIV infection. In such cases, these new subgroup data may tip the balance in decision-making. Moreover, the new START findings should help physicians and policy makers in prioritizing access to immediate ART in settings where it isn’t universally available, according to Dr. Molina.
In the prespecified subgroup analysis, patients aged 50 and up at enrollment had a 2.9% incidence of the primary composite endpoint at 3 years if randomized to immediate ART and an 11.7% rate if they were assigned to deferred ART. The number of 50-plus-year-olds needed to treat (NNT) immediately for 1 year in order to prevent one additional case of AIDS, a major non-AIDS event, or death was just 45, compared to NNTs of 151 and 206 in patients aged 30-49 and younger than 30, respectively. Patients aged 50 and older accounted for nearly 12% of the overall study population.
For the roughly 28% of START participants whose baseline CD4:CD8 ratio was less than 0.5, the NNT for immediate rather than deferred therapy was 60, substantially more favorable than the NNTs of 214 in patients with a baseline ratio of 0.5-0.8 and 248 in patients with a CD4:CD8 ratio greater than 0.8. The incidence of the primary endpoint at 3 years of follow-up in patients with a CD4:CD8 ratio of less than 0.5 was 0.5% in the immediate ART group and 6.3% with deferred therapy.
Similarly, patients with a baseline 10-year Framingham Risk Score (FRS) of 10% or higher had an NNT of 69, compared with NNTs of 111 in subjects with an FRS of 1%-9.9% and 276 in those with an FRS of less than 1%. Patients with an FRS of 10% or more had a 2.4% incidence of the primary endpoint at 3 years if assigned to immediate ART and a 10.1% rate with deferred therapy. Patients with an FRS of 10% or more comprised only 9.6% of the study population, Dr. Molina continued.
Patients with a heavy baseline viral load as evidenced by a plasma HIV RNA level of at least 50,000 copies/mL accounted for roughly 22% of the total study sample. Their 3-year rate of the primary outcome was 2.1% with immediate ART and 6.9% with deferred treatment. The NNT was 67, compared to an NNT of 122 in patients with 3,000-49,999 copies/mL and 992 in the one-quarter of START participants with a baseline plasma HIV RNA level of less than 3,000 copies/mL.
Variables that weren’t related to the magnitude of absolute risk reduction and NNT in the START subgroup analysis were race, gender, geographic region, baseline CD4 cell count, and whether an individual resided in a high- or lower-income country.
Several audience members rose to assert that the CD4:CD8 ratio and viral load might very well be redundant predictors measuring the same thing, since they are typically tightly correlated. Dr. Molina replied that the START investigators are planning to conduct a multivariate analysis of the data in the near future, which should provide a definitive answer.
Another audience member expressed surprise at what struck him as a low cardiovascular event rate in the START study, given that HIV infection is known to be associated with accelerated atherosclerosis. Dr. Molina said the explanation for the low number of cardiovascular events lies in the fact that cardiovascular risk is so heavily age-dependent, and START participants were relatively young, with a median age of 36 years.
The START trial was carried out by the International Network for Strategic Initiatives in Global HIV Trials (INSIGHT) with funding provided mainly by the National Institutes of Health. Dr. Molina reported having no financial conflicts of interest.
AT AIDS 2016
Key clinical point: Four specific subgroups of asymptomatic HIV-infected adults who obtain the most clinical benefit from immediate rather than deferred antiretroviral therapy have been identified.
Major finding: The number of asymptomatic HIV-infected adults needed to treat immediately with antiretroviral therapy for 1 year instead of deferring treatment in order to avoid one case of AIDS or serious non-AIDS illness is 45 in patients aged 50 and older, compared with NNTs of 151 in 30- to 49-year-olds and 206 in patients younger than age 30.
Data source: This was a prespecified subgroup analysis of the landmark START trial, in which 4,685 treatment-naive asymptomatic HIV-infected adults with more than 500 CD4+ cells/mL were randomized to immediate or deferred antiretroviral therapy.
Disclosures: The START trial was funded chiefly by the National Institutes of Health. The presenter reported having no financial conflicts of interest.
Gay and Bisexual Male High Schoolers Have High Injected Drug Use
DURBAN, SOUTH AFRICA – The first-ever nationally representative survey on sexual identity and behaviors in U.S. male high school students has exposed a high prevalence of illicit injected drug use among those who have sex with males or with both males and females.
About 10% of high school boys who identify as gay or bisexual reported having ever used a needle to inject any illegal drug into their bodies, compared with 1.5% of high school boys who identify as heterosexual.
“This is a cause for great concern because of the efficiency with which injected drug use transmits not only HIV but hepatitis and other diseases,” Laura Kann, PhD, said in reporting the results of the 2015 National Youth Risk Behavior Survey (YRBS) at the 21st International AIDS Conference.
Dr. Kann of the Centers for Disease Control and Prevention’s division of adolescent and school health directs the YRBS, an annual, multiple-choice, anonymous voluntary survey that addresses six areas of risk: behaviors that contribute to unintentional injuries and violence, tobacco use, alcohol and other drug use, sexual behaviors, inadequate physical activity, and unhealthy diet behaviors.

The 2015 survey was the first ever to include questions regarding sexual identity and behaviors.
“Twenty-two percent of all new HIV diagnoses in the U.S. occur in 13- to 24-year-olds. Most occur in males who have sex with males. This makes young males an important focus for HIV prevention efforts,” Dr. Kann said.
Yet until the 2015 YRBS, no reliable estimates existed regarding the number of gay or bisexual male high school students. “Reducing HIV infection among young sexual minority males is key to reducing HIV infection in the U.S.,” she said. “It’s hard to respond appropriately to a population that has not been counted.”
The 15,624 male students in public and private school grades 9-12 who participated in the YRBS were demographically representative of the nation’s roughly 8 million male high schoolers.
About 2% of male students identified themselves as gay, another 2.4% declared themselves bisexual, 93.1% said they were heterosexual, and 2.6% were unsure. With regard to sexual behaviors, 53.3% of respondents indicated they had sexual contact with females only, 1.3% with males only, and 1.9% with both males and females; 43.6% reported they hadn’t ever had sexual contact. Respondents could interpret “sexual contact” as they wished, ranging from kissing and hugging to intercourse.
Large differences in illicit drug use behaviors were found between the sexual minorities – that is, males who had sexual contact with males or with females as well as males – and those with only heterosexual contacts.
“We need to conduct new research on injected drug use among young males who have sex with males and determine what can be done to minimize, if not eliminate, this very high-risk behavior that is occurring at alarming rates,” Dr. Kann said.
The sexual minority students were also more likely to have engaged in various forms of noninjected illicit drug use known to boost the risk of HIV infection indirectly by increasing the likelihood of having unsafe sex. The sexual minority males had significantly higher rates of having ever used cocaine in any form, of having ever used amphetamines, and of having taken prescription drugs without a physician’s prescription. For instance, 14.8% of sexual minority males reported ever using amphetamines, compared with 2.5% of heterosexual males surveyed.
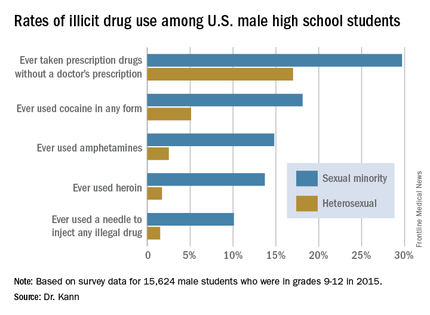
She noted that the YRBS results provided no evidence that the disparity in HIV diagnoses between young males who have sex with males and young males who have sex with females are caused by differences in the prevalence of HIV-related sexual behaviors. There were no statistically significant differences between heterosexual and sexual minority students in rates of ever having had sexual intercourse, having had intercourse with four or more persons, having sexual activity currently, or having used a condom at last intercourse.
Dr. Kann called for more research in the neglected area of social issues affecting young sexual minority males that likely increase their sense of marginalization and may promote behaviors placing them at increased risk for HIV acquisition.
“Many young males who have sex with males suffer from social isolation, stress from self-concealment and from coming out, discrimination, and even hatred, which may occur at home, at school, and in communities among both their peers and the adults responsible for their care and protection,” she said. “These factors may lead to harmful coping behaviors, such as drug use, that can further increase risk for HIV infection. It’s hard to imagine how even the best intervention technology will be able to eliminate the disparities in HIV diagnosis unless these social issues are addressed first and foremost.”
One clinician from New York rose from the audience to chastise the CDC for taking decades to incorporate questions about sexual minority youth into the YRBS.
“It’s important for the rest of the world to know how long it took the U.S. to collect this data. It’s not right. For those of you in the rest of the world who struggle to get information about your youth, don’t think that America is way ahead of you because it took us a long time,” she said.
Dr. Kann noted that such data have been collected for some time by some state and city public health agencies. As local officials began clamoring for a more comprehensive national picture, “it reached a tipping point” at the CDC.
Dr. Kann reported having no relevant financial conflicts.
DURBAN, SOUTH AFRICA – The first-ever nationally representative survey on sexual identity and behaviors in U.S. male high school students has exposed a high prevalence of illicit injected drug use among those who have sex with males or with both males and females.
About 10% of high school boys who identify as gay or bisexual reported having ever used a needle to inject any illegal drug into their bodies, compared with 1.5% of high school boys who identify as heterosexual.
“This is a cause for great concern because of the efficiency with which injected drug use transmits not only HIV but hepatitis and other diseases,” Laura Kann, PhD, said in reporting the results of the 2015 National Youth Risk Behavior Survey (YRBS) at the 21st International AIDS Conference.
Dr. Kann of the Centers for Disease Control and Prevention’s division of adolescent and school health directs the YRBS, an annual, multiple-choice, anonymous voluntary survey that addresses six areas of risk: behaviors that contribute to unintentional injuries and violence, tobacco use, alcohol and other drug use, sexual behaviors, inadequate physical activity, and unhealthy diet behaviors.
The 2015 survey was the first ever to include questions regarding sexual identity and behaviors.
“Twenty-two percent of all new HIV diagnoses in the U.S. occur in 13- to 24-year-olds. Most occur in males who have sex with males. This makes young males an important focus for HIV prevention efforts,” Dr. Kann said.
Yet until the 2015 YRBS, no reliable estimates existed regarding the number of gay or bisexual male high school students. “Reducing HIV infection among young sexual minority males is key to reducing HIV infection in the U.S.,” she said. “It’s hard to respond appropriately to a population that has not been counted.”
The 15,624 male students in public and private school grades 9-12 who participated in the YRBS were demographically representative of the nation’s roughly 8 million male high schoolers.
About 2% of male students identified themselves as gay, another 2.4% declared themselves bisexual, 93.1% said they were heterosexual, and 2.6% were unsure. With regard to sexual behaviors, 53.3% of respondents indicated they had sexual contact with females only, 1.3% with males only, and 1.9% with both males and females; 43.6% reported they hadn’t ever had sexual contact. Respondents could interpret “sexual contact” as they wished, ranging from kissing and hugging to intercourse.
Large differences in illicit drug use behaviors were found between the sexual minorities – that is, males who had sexual contact with males or with females as well as males – and those with only heterosexual contacts.
“We need to conduct new research on injected drug use among young males who have sex with males and determine what can be done to minimize, if not eliminate, this very high-risk behavior that is occurring at alarming rates,” Dr. Kann said.
The sexual minority students were also more likely to have engaged in various forms of noninjected illicit drug use known to boost the risk of HIV infection indirectly by increasing the likelihood of having unsafe sex. The sexual minority males had significantly higher rates of having ever used cocaine in any form, of having ever used amphetamines, and of having taken prescription drugs without a physician’s prescription. For instance, 14.8% of sexual minority males reported ever using amphetamines, compared with 2.5% of heterosexual males surveyed.
She noted that the YRBS results provided no evidence that the disparity in HIV diagnoses between young males who have sex with males and young males who have sex with females are caused by differences in the prevalence of HIV-related sexual behaviors. There were no statistically significant differences between heterosexual and sexual minority students in rates of ever having had sexual intercourse, having had intercourse with four or more persons, having sexual activity currently, or having used a condom at last intercourse.
Dr. Kann called for more research in the neglected area of social issues affecting young sexual minority males that likely increase their sense of marginalization and may promote behaviors placing them at increased risk for HIV acquisition.
“Many young males who have sex with males suffer from social isolation, stress from self-concealment and from coming out, discrimination, and even hatred, which may occur at home, at school, and in communities among both their peers and the adults responsible for their care and protection,” she said. “These factors may lead to harmful coping behaviors, such as drug use, that can further increase risk for HIV infection. It’s hard to imagine how even the best intervention technology will be able to eliminate the disparities in HIV diagnosis unless these social issues are addressed first and foremost.”
One clinician from New York rose from the audience to chastise the CDC for taking decades to incorporate questions about sexual minority youth into the YRBS.
“It’s important for the rest of the world to know how long it took the U.S. to collect this data. It’s not right. For those of you in the rest of the world who struggle to get information about your youth, don’t think that America is way ahead of you because it took us a long time,” she said.
Dr. Kann noted that such data have been collected for some time by some state and city public health agencies. As local officials began clamoring for a more comprehensive national picture, “it reached a tipping point” at the CDC.
Dr. Kann reported having no relevant financial conflicts.
DURBAN, SOUTH AFRICA – The first-ever nationally representative survey on sexual identity and behaviors in U.S. male high school students has exposed a high prevalence of illicit injected drug use among those who have sex with males or with both males and females.
About 10% of high school boys who identify as gay or bisexual reported having ever used a needle to inject any illegal drug into their bodies, compared with 1.5% of high school boys who identify as heterosexual.
“This is a cause for great concern because of the efficiency with which injected drug use transmits not only HIV but hepatitis and other diseases,” Laura Kann, PhD, said in reporting the results of the 2015 National Youth Risk Behavior Survey (YRBS) at the 21st International AIDS Conference.
Dr. Kann of the Centers for Disease Control and Prevention’s division of adolescent and school health directs the YRBS, an annual, multiple-choice, anonymous voluntary survey that addresses six areas of risk: behaviors that contribute to unintentional injuries and violence, tobacco use, alcohol and other drug use, sexual behaviors, inadequate physical activity, and unhealthy diet behaviors.
The 2015 survey was the first ever to include questions regarding sexual identity and behaviors.
“Twenty-two percent of all new HIV diagnoses in the U.S. occur in 13- to 24-year-olds. Most occur in males who have sex with males. This makes young males an important focus for HIV prevention efforts,” Dr. Kann said.
Yet until the 2015 YRBS, no reliable estimates existed regarding the number of gay or bisexual male high school students. “Reducing HIV infection among young sexual minority males is key to reducing HIV infection in the U.S.,” she said. “It’s hard to respond appropriately to a population that has not been counted.”
The 15,624 male students in public and private school grades 9-12 who participated in the YRBS were demographically representative of the nation’s roughly 8 million male high schoolers.
About 2% of male students identified themselves as gay, another 2.4% declared themselves bisexual, 93.1% said they were heterosexual, and 2.6% were unsure. With regard to sexual behaviors, 53.3% of respondents indicated they had sexual contact with females only, 1.3% with males only, and 1.9% with both males and females; 43.6% reported they hadn’t ever had sexual contact. Respondents could interpret “sexual contact” as they wished, ranging from kissing and hugging to intercourse.
Large differences in illicit drug use behaviors were found between the sexual minorities – that is, males who had sexual contact with males or with females as well as males – and those with only heterosexual contacts.
“We need to conduct new research on injected drug use among young males who have sex with males and determine what can be done to minimize, if not eliminate, this very high-risk behavior that is occurring at alarming rates,” Dr. Kann said.
The sexual minority students were also more likely to have engaged in various forms of noninjected illicit drug use known to boost the risk of HIV infection indirectly by increasing the likelihood of having unsafe sex. The sexual minority males had significantly higher rates of having ever used cocaine in any form, of having ever used amphetamines, and of having taken prescription drugs without a physician’s prescription. For instance, 14.8% of sexual minority males reported ever using amphetamines, compared with 2.5% of heterosexual males surveyed.
She noted that the YRBS results provided no evidence that the disparity in HIV diagnoses between young males who have sex with males and young males who have sex with females are caused by differences in the prevalence of HIV-related sexual behaviors. There were no statistically significant differences between heterosexual and sexual minority students in rates of ever having had sexual intercourse, having had intercourse with four or more persons, having sexual activity currently, or having used a condom at last intercourse.
Dr. Kann called for more research in the neglected area of social issues affecting young sexual minority males that likely increase their sense of marginalization and may promote behaviors placing them at increased risk for HIV acquisition.
“Many young males who have sex with males suffer from social isolation, stress from self-concealment and from coming out, discrimination, and even hatred, which may occur at home, at school, and in communities among both their peers and the adults responsible for their care and protection,” she said. “These factors may lead to harmful coping behaviors, such as drug use, that can further increase risk for HIV infection. It’s hard to imagine how even the best intervention technology will be able to eliminate the disparities in HIV diagnosis unless these social issues are addressed first and foremost.”
One clinician from New York rose from the audience to chastise the CDC for taking decades to incorporate questions about sexual minority youth into the YRBS.
“It’s important for the rest of the world to know how long it took the U.S. to collect this data. It’s not right. For those of you in the rest of the world who struggle to get information about your youth, don’t think that America is way ahead of you because it took us a long time,” she said.
Dr. Kann noted that such data have been collected for some time by some state and city public health agencies. As local officials began clamoring for a more comprehensive national picture, “it reached a tipping point” at the CDC.
Dr. Kann reported having no relevant financial conflicts.
AT AIDS 2016

Gay and bisexual male high schoolers have high injected drug use
DURBAN, SOUTH AFRICA – The first-ever nationally representative survey on sexual identity and behaviors in U.S. male high school students has exposed a high prevalence of illicit injected drug use among those who have sex with males or with both males and females.
About 10% of high school boys who identify as gay or bisexual reported having ever used a needle to inject any illegal drug into their bodies, compared with 1.5% of high school boys who identify as heterosexual.
“This is a cause for great concern because of the efficiency with which injected drug use transmits not only HIV but hepatitis and other diseases,” Laura Kann, PhD, said in reporting the results of the 2015 National Youth Risk Behavior Survey (YRBS) at the 21st International AIDS Conference.
Dr. Kann of the Centers for Disease Control and Prevention’s division of adolescent and school health directs the YRBS, an annual, multiple-choice, anonymous voluntary survey that addresses six areas of risk: behaviors that contribute to unintentional injuries and violence, tobacco use, alcohol and other drug use, sexual behaviors, inadequate physical activity, and unhealthy diet behaviors.

The 2015 survey was the first ever to include questions regarding sexual identity and behaviors.
“Twenty-two percent of all new HIV diagnoses in the U.S. occur in 13- to 24-year-olds. Most occur in males who have sex with males. This makes young males an important focus for HIV prevention efforts,” Dr. Kann said.
Yet until the 2015 YRBS, no reliable estimates existed regarding the number of gay or bisexual male high school students. “Reducing HIV infection among young sexual minority males is key to reducing HIV infection in the U.S.,” she said. “It’s hard to respond appropriately to a population that has not been counted.”
The 15,624 male students in public and private school grades 9-12 who participated in the YRBS were demographically representative of the nation’s roughly 8 million male high schoolers.
About 2% of male students identified themselves as gay, another 2.4% declared themselves bisexual, 93.1% said they were heterosexual, and 2.6% were unsure. With regard to sexual behaviors, 53.3% of respondents indicated they had sexual contact with females only, 1.3% with males only, and 1.9% with both males and females; 43.6% reported they hadn’t ever had sexual contact. Respondents could interpret “sexual contact” as they wished, ranging from kissing and hugging to intercourse.
Large differences in illicit drug use behaviors were found between the sexual minorities – that is, males who had sexual contact with males or with females as well as males – and those with only heterosexual contacts.
“We need to conduct new research on injected drug use among young males who have sex with males and determine what can be done to minimize, if not eliminate, this very high-risk behavior that is occurring at alarming rates,” Dr. Kann said.
The sexual minority students were also more likely to have engaged in various forms of noninjected illicit drug use known to boost the risk of HIV infection indirectly by increasing the likelihood of having unsafe sex. The sexual minority males had significantly higher rates of having ever used cocaine in any form, of having ever used amphetamines, and of having taken prescription drugs without a physician’s prescription. For instance, 14.8% of sexual minority males reported ever using amphetamines, compared with 2.5% of heterosexual males surveyed.
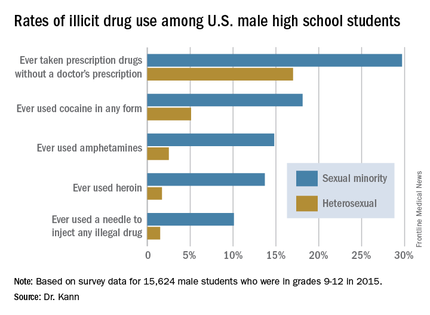
She noted that the YRBS results provided no evidence that the disparity in HIV diagnoses between young males who have sex with males and young males who have sex with females are caused by differences in the prevalence of HIV-related sexual behaviors. There were no statistically significant differences between heterosexual and sexual minority students in rates of ever having had sexual intercourse, having had intercourse with four or more persons, having sexual activity currently, or having used a condom at last intercourse.
Dr. Kann called for more research in the neglected area of social issues affecting young sexual minority males that likely increase their sense of marginalization and may promote behaviors placing them at increased risk for HIV acquisition.
“Many young males who have sex with males suffer from social isolation, stress from self-concealment and from coming out, discrimination, and even hatred, which may occur at home, at school, and in communities among both their peers and the adults responsible for their care and protection,” she said. “These factors may lead to harmful coping behaviors, such as drug use, that can further increase risk for HIV infection. It’s hard to imagine how even the best intervention technology will be able to eliminate the disparities in HIV diagnosis unless these social issues are addressed first and foremost.”
One clinician from New York rose from the audience to chastise the CDC for taking decades to incorporate questions about sexual minority youth into the YRBS.
“It’s important for the rest of the world to know how long it took the U.S. to collect this data. It’s not right. For those of you in the rest of the world who struggle to get information about your youth, don’t think that America is way ahead of you because it took us a long time,” she said.
Dr. Kann noted that such data have been collected for some time by some state and city public health agencies. As local officials began clamoring for a more comprehensive national picture, “it reached a tipping point” at the CDC.
Dr. Kann reported having no relevant financial conflicts.
DURBAN, SOUTH AFRICA – The first-ever nationally representative survey on sexual identity and behaviors in U.S. male high school students has exposed a high prevalence of illicit injected drug use among those who have sex with males or with both males and females.
About 10% of high school boys who identify as gay or bisexual reported having ever used a needle to inject any illegal drug into their bodies, compared with 1.5% of high school boys who identify as heterosexual.
“This is a cause for great concern because of the efficiency with which injected drug use transmits not only HIV but hepatitis and other diseases,” Laura Kann, PhD, said in reporting the results of the 2015 National Youth Risk Behavior Survey (YRBS) at the 21st International AIDS Conference.
Dr. Kann of the Centers for Disease Control and Prevention’s division of adolescent and school health directs the YRBS, an annual, multiple-choice, anonymous voluntary survey that addresses six areas of risk: behaviors that contribute to unintentional injuries and violence, tobacco use, alcohol and other drug use, sexual behaviors, inadequate physical activity, and unhealthy diet behaviors.
The 2015 survey was the first ever to include questions regarding sexual identity and behaviors.
“Twenty-two percent of all new HIV diagnoses in the U.S. occur in 13- to 24-year-olds. Most occur in males who have sex with males. This makes young males an important focus for HIV prevention efforts,” Dr. Kann said.
Yet until the 2015 YRBS, no reliable estimates existed regarding the number of gay or bisexual male high school students. “Reducing HIV infection among young sexual minority males is key to reducing HIV infection in the U.S.,” she said. “It’s hard to respond appropriately to a population that has not been counted.”
The 15,624 male students in public and private school grades 9-12 who participated in the YRBS were demographically representative of the nation’s roughly 8 million male high schoolers.
About 2% of male students identified themselves as gay, another 2.4% declared themselves bisexual, 93.1% said they were heterosexual, and 2.6% were unsure. With regard to sexual behaviors, 53.3% of respondents indicated they had sexual contact with females only, 1.3% with males only, and 1.9% with both males and females; 43.6% reported they hadn’t ever had sexual contact. Respondents could interpret “sexual contact” as they wished, ranging from kissing and hugging to intercourse.
Large differences in illicit drug use behaviors were found between the sexual minorities – that is, males who had sexual contact with males or with females as well as males – and those with only heterosexual contacts.
“We need to conduct new research on injected drug use among young males who have sex with males and determine what can be done to minimize, if not eliminate, this very high-risk behavior that is occurring at alarming rates,” Dr. Kann said.
The sexual minority students were also more likely to have engaged in various forms of noninjected illicit drug use known to boost the risk of HIV infection indirectly by increasing the likelihood of having unsafe sex. The sexual minority males had significantly higher rates of having ever used cocaine in any form, of having ever used amphetamines, and of having taken prescription drugs without a physician’s prescription. For instance, 14.8% of sexual minority males reported ever using amphetamines, compared with 2.5% of heterosexual males surveyed.
She noted that the YRBS results provided no evidence that the disparity in HIV diagnoses between young males who have sex with males and young males who have sex with females are caused by differences in the prevalence of HIV-related sexual behaviors. There were no statistically significant differences between heterosexual and sexual minority students in rates of ever having had sexual intercourse, having had intercourse with four or more persons, having sexual activity currently, or having used a condom at last intercourse.
Dr. Kann called for more research in the neglected area of social issues affecting young sexual minority males that likely increase their sense of marginalization and may promote behaviors placing them at increased risk for HIV acquisition.
“Many young males who have sex with males suffer from social isolation, stress from self-concealment and from coming out, discrimination, and even hatred, which may occur at home, at school, and in communities among both their peers and the adults responsible for their care and protection,” she said. “These factors may lead to harmful coping behaviors, such as drug use, that can further increase risk for HIV infection. It’s hard to imagine how even the best intervention technology will be able to eliminate the disparities in HIV diagnosis unless these social issues are addressed first and foremost.”
One clinician from New York rose from the audience to chastise the CDC for taking decades to incorporate questions about sexual minority youth into the YRBS.
“It’s important for the rest of the world to know how long it took the U.S. to collect this data. It’s not right. For those of you in the rest of the world who struggle to get information about your youth, don’t think that America is way ahead of you because it took us a long time,” she said.
Dr. Kann noted that such data have been collected for some time by some state and city public health agencies. As local officials began clamoring for a more comprehensive national picture, “it reached a tipping point” at the CDC.
Dr. Kann reported having no relevant financial conflicts.
DURBAN, SOUTH AFRICA – The first-ever nationally representative survey on sexual identity and behaviors in U.S. male high school students has exposed a high prevalence of illicit injected drug use among those who have sex with males or with both males and females.
About 10% of high school boys who identify as gay or bisexual reported having ever used a needle to inject any illegal drug into their bodies, compared with 1.5% of high school boys who identify as heterosexual.
“This is a cause for great concern because of the efficiency with which injected drug use transmits not only HIV but hepatitis and other diseases,” Laura Kann, PhD, said in reporting the results of the 2015 National Youth Risk Behavior Survey (YRBS) at the 21st International AIDS Conference.
Dr. Kann of the Centers for Disease Control and Prevention’s division of adolescent and school health directs the YRBS, an annual, multiple-choice, anonymous voluntary survey that addresses six areas of risk: behaviors that contribute to unintentional injuries and violence, tobacco use, alcohol and other drug use, sexual behaviors, inadequate physical activity, and unhealthy diet behaviors.
The 2015 survey was the first ever to include questions regarding sexual identity and behaviors.
“Twenty-two percent of all new HIV diagnoses in the U.S. occur in 13- to 24-year-olds. Most occur in males who have sex with males. This makes young males an important focus for HIV prevention efforts,” Dr. Kann said.
Yet until the 2015 YRBS, no reliable estimates existed regarding the number of gay or bisexual male high school students. “Reducing HIV infection among young sexual minority males is key to reducing HIV infection in the U.S.,” she said. “It’s hard to respond appropriately to a population that has not been counted.”
The 15,624 male students in public and private school grades 9-12 who participated in the YRBS were demographically representative of the nation’s roughly 8 million male high schoolers.
About 2% of male students identified themselves as gay, another 2.4% declared themselves bisexual, 93.1% said they were heterosexual, and 2.6% were unsure. With regard to sexual behaviors, 53.3% of respondents indicated they had sexual contact with females only, 1.3% with males only, and 1.9% with both males and females; 43.6% reported they hadn’t ever had sexual contact. Respondents could interpret “sexual contact” as they wished, ranging from kissing and hugging to intercourse.
Large differences in illicit drug use behaviors were found between the sexual minorities – that is, males who had sexual contact with males or with females as well as males – and those with only heterosexual contacts.
“We need to conduct new research on injected drug use among young males who have sex with males and determine what can be done to minimize, if not eliminate, this very high-risk behavior that is occurring at alarming rates,” Dr. Kann said.
The sexual minority students were also more likely to have engaged in various forms of noninjected illicit drug use known to boost the risk of HIV infection indirectly by increasing the likelihood of having unsafe sex. The sexual minority males had significantly higher rates of having ever used cocaine in any form, of having ever used amphetamines, and of having taken prescription drugs without a physician’s prescription. For instance, 14.8% of sexual minority males reported ever using amphetamines, compared with 2.5% of heterosexual males surveyed.
She noted that the YRBS results provided no evidence that the disparity in HIV diagnoses between young males who have sex with males and young males who have sex with females are caused by differences in the prevalence of HIV-related sexual behaviors. There were no statistically significant differences between heterosexual and sexual minority students in rates of ever having had sexual intercourse, having had intercourse with four or more persons, having sexual activity currently, or having used a condom at last intercourse.
Dr. Kann called for more research in the neglected area of social issues affecting young sexual minority males that likely increase their sense of marginalization and may promote behaviors placing them at increased risk for HIV acquisition.
“Many young males who have sex with males suffer from social isolation, stress from self-concealment and from coming out, discrimination, and even hatred, which may occur at home, at school, and in communities among both their peers and the adults responsible for their care and protection,” she said. “These factors may lead to harmful coping behaviors, such as drug use, that can further increase risk for HIV infection. It’s hard to imagine how even the best intervention technology will be able to eliminate the disparities in HIV diagnosis unless these social issues are addressed first and foremost.”
One clinician from New York rose from the audience to chastise the CDC for taking decades to incorporate questions about sexual minority youth into the YRBS.
“It’s important for the rest of the world to know how long it took the U.S. to collect this data. It’s not right. For those of you in the rest of the world who struggle to get information about your youth, don’t think that America is way ahead of you because it took us a long time,” she said.
Dr. Kann noted that such data have been collected for some time by some state and city public health agencies. As local officials began clamoring for a more comprehensive national picture, “it reached a tipping point” at the CDC.
Dr. Kann reported having no relevant financial conflicts.
AT AIDS 2016
Key clinical point: Male U.S. students in grades 9-12 who identify themselves as sexual minorities have markedly higher rates of illicit drug use than their heterosexual peers.
Major finding: A total of 4.4% of U.S. male high school students identify themselves as gay or bisexual, and they are about sevenfold more likely than heterosexual students to have ever injected illegal drugs.
Data source: A national population-based survey of 15,624 male students in grades 9-12.
Disclosures: The presenter is an employee of the Centers for Disease Control and Prevention, which sponsored the annual Youth Risk Behavior Survey.

Dapivirine vaginal ring sharply reduces HIV infection risk
DURBAN, SOUTH AFRICA – Women who consistently used a monthly vaginal ring containing the antiretroviral drug dapivirine reduced their risk of acquiring HIV infection by 75%-91% in exploratory analyses of the phase III ASPIRE study, Elizabeth R. Brown, ScD, reported at the 21st International AIDS Conference.
ASPIRE (A Study to Prevent Infection with a Ring for Extended use), also known as the Microbicide Trials Network-020 trial, was a multicenter, randomized, double-blind, placebo-controlled, phase III trial of a silicone vaginal ring containing 25 mg of the non-nucleoside reverse transcriptase inhibitor dapivirine. ASPIRE involved 2,629 HIV-uninfected women aged 18-45 years from four Southern African countries with extremely high HIV infection rates: South Africa, Uganda, Malawi, and Zimbabwe. They were prospectively followed monthly for 12-33 months.

As reported at a conference earlier in 2016, seroconversion occurred in 71 women assigned to the dapivirine ring and 97 on a placebo ring during 4,280 person-years of follow-up. The resultant 27% relative risk reduction in an intent-to-treat analysis, while statistically significant, was less than hoped for by investigators.
However, the device only works if it’s used consistently, so the investigators decided to conduct exploratory analyses using an objective measure of adherence: the amount of dapivirine remaining in a ring after a month’s use. This was possible because the rings had been stored for analysis in a central laboratory.
The vaginal ring is self-inserted, then meant to be kept in place continuously for a month before being self-removed and replaced with a fresh ring. Dapivirine is released continuously while the ring is in place, so the less residual dapivirine contained in a used ring, the greater the adherence during that month, explained Dr. Brown, a biostatistician at the University of Washington, Seattle.
A dose-response effect was observed. In the most encouraging of the exploratory time-dependent use analyses, the rate of HIV acquisition was 4.7 cases per 100 person-years with placebo, 4.9/100 person-years in women defined as nonadherent based upon a residual dapivirine level of 23.5 mg or more, 3.1 with low use, 1.9 with moderate use, and 0.4 cases/100 person-years with consistent use as directed, meaning a patient left the device in place continuously for a month as reflected in a residual dapivirine rate below 22 mg.
This translates into a 91% reduction in risk, compared with placebo, in the most consistent users, a 58% relative risk reduction with moderate use, and a 29% reduction with low use, she continued.
The new results were hailed as a major advance in preventing HIV infection.
“We’re meeting here at AIDS 2016 in Durban, capital of the KwaZulu-Natal province of South Africa, which is one of the hardest-hit areas of the world for HIV. Over the course of their lifetime, women in Southern Africa have more than a 50% chance of HIV infection. So a new prevention tool that women can use on their own discretely to protect themselves against HIV would be a game changer,” Jared Baeten, MD, PhD, said in an interview.

“I see this as having an important potential role in the [United States] as well for women who face an increased risk of HIV. It’s extremely valuable for them to have a method of protection that they can control and feel good about and safely use for an extended period of time,” added Dr. Baeten, professor and vice chair of global health, as well as professor of allergy and infectious diseases at the University of Washington, Seattle.
The challenges involved in consistent use of the dapivirine ring are less formidable than are those posed by consistent use of a daily oral medication for preexposure prevention, he noted.
Dr. Baeten was a leader of ASPIRE and is codirector of the HOPE (HIV Open-label Prevention Extension) study, which is now underway. The expectation is that adherence to the dapivirine vaginal ring will be better in HOPE than in ASPIRE because participants can now be counseled that the ring works, it’s safe, and there is no chance of getting a placebo device, he said.
“There is an urgent unmet need to expand long-acting HIV prevention options for women and girls,” Zeda Rosenberg, ScD, founder and chief executive officer of the nonprofit International Partnership for Microbicides (IPM) in Silver Spring, Md., which is the sponsor and developer of the ring.

Toward that end, in the next several months the ASPIRE data will be combined with those from the IPM-sponsored Ring Study, another completed large phase III trial of the dapivirine ring conducted in Africa. The goals will be to try to identify potentially modifiable sociodemographic and behavioral correlates of adherence and to further strengthen the safety and efficacy findings. The plan is to submit the full data package to the Food and Drug Administration and regulat ory agencies in other countries in the spring of 2017.
“Hopefully, the product will receive marketing approval in 2018,” Dr. Rosenberg said.
In addition to sponsoring HOPE, IPM is also sponsoring the ongoing open-label DREAM (Dapivirine Ring Extended Access and Monitoring) study. IPM is also partnering with the Microbicides Trial Network to conduct a separate study of the vaginal ring in adolescents and young women in Africa.
A dapivirine vaginal ring that’s active for 3 months rather than 1 month will begin safety studies later in 2016. The potential advantages of this product are reduced annual cost and fewer clinic visits. Also, a 3-month version of the ring with an added contraceptive has been developed and will begin safety studies in the United States in fall 2016. The possibility that suboptimal adherence can be overcome by a ring containing a higher dose of dapivirine will also be explored, according to Dr. Rosenberg.
Dr. Brown, Dr. Baeten, and Dr. Rosenberg reported having no financial conflicts of interest.
DURBAN, SOUTH AFRICA – Women who consistently used a monthly vaginal ring containing the antiretroviral drug dapivirine reduced their risk of acquiring HIV infection by 75%-91% in exploratory analyses of the phase III ASPIRE study, Elizabeth R. Brown, ScD, reported at the 21st International AIDS Conference.
ASPIRE (A Study to Prevent Infection with a Ring for Extended use), also known as the Microbicide Trials Network-020 trial, was a multicenter, randomized, double-blind, placebo-controlled, phase III trial of a silicone vaginal ring containing 25 mg of the non-nucleoside reverse transcriptase inhibitor dapivirine. ASPIRE involved 2,629 HIV-uninfected women aged 18-45 years from four Southern African countries with extremely high HIV infection rates: South Africa, Uganda, Malawi, and Zimbabwe. They were prospectively followed monthly for 12-33 months.
As reported at a conference earlier in 2016, seroconversion occurred in 71 women assigned to the dapivirine ring and 97 on a placebo ring during 4,280 person-years of follow-up. The resultant 27% relative risk reduction in an intent-to-treat analysis, while statistically significant, was less than hoped for by investigators.
However, the device only works if it’s used consistently, so the investigators decided to conduct exploratory analyses using an objective measure of adherence: the amount of dapivirine remaining in a ring after a month’s use. This was possible because the rings had been stored for analysis in a central laboratory.
The vaginal ring is self-inserted, then meant to be kept in place continuously for a month before being self-removed and replaced with a fresh ring. Dapivirine is released continuously while the ring is in place, so the less residual dapivirine contained in a used ring, the greater the adherence during that month, explained Dr. Brown, a biostatistician at the University of Washington, Seattle.
A dose-response effect was observed. In the most encouraging of the exploratory time-dependent use analyses, the rate of HIV acquisition was 4.7 cases per 100 person-years with placebo, 4.9/100 person-years in women defined as nonadherent based upon a residual dapivirine level of 23.5 mg or more, 3.1 with low use, 1.9 with moderate use, and 0.4 cases/100 person-years with consistent use as directed, meaning a patient left the device in place continuously for a month as reflected in a residual dapivirine rate below 22 mg.
This translates into a 91% reduction in risk, compared with placebo, in the most consistent users, a 58% relative risk reduction with moderate use, and a 29% reduction with low use, she continued.
The new results were hailed as a major advance in preventing HIV infection.
“We’re meeting here at AIDS 2016 in Durban, capital of the KwaZulu-Natal province of South Africa, which is one of the hardest-hit areas of the world for HIV. Over the course of their lifetime, women in Southern Africa have more than a 50% chance of HIV infection. So a new prevention tool that women can use on their own discretely to protect themselves against HIV would be a game changer,” Jared Baeten, MD, PhD, said in an interview.
“I see this as having an important potential role in the [United States] as well for women who face an increased risk of HIV. It’s extremely valuable for them to have a method of protection that they can control and feel good about and safely use for an extended period of time,” added Dr. Baeten, professor and vice chair of global health, as well as professor of allergy and infectious diseases at the University of Washington, Seattle.
The challenges involved in consistent use of the dapivirine ring are less formidable than are those posed by consistent use of a daily oral medication for preexposure prevention, he noted.
Dr. Baeten was a leader of ASPIRE and is codirector of the HOPE (HIV Open-label Prevention Extension) study, which is now underway. The expectation is that adherence to the dapivirine vaginal ring will be better in HOPE than in ASPIRE because participants can now be counseled that the ring works, it’s safe, and there is no chance of getting a placebo device, he said.
“There is an urgent unmet need to expand long-acting HIV prevention options for women and girls,” Zeda Rosenberg, ScD, founder and chief executive officer of the nonprofit International Partnership for Microbicides (IPM) in Silver Spring, Md., which is the sponsor and developer of the ring.
Toward that end, in the next several months the ASPIRE data will be combined with those from the IPM-sponsored Ring Study, another completed large phase III trial of the dapivirine ring conducted in Africa. The goals will be to try to identify potentially modifiable sociodemographic and behavioral correlates of adherence and to further strengthen the safety and efficacy findings. The plan is to submit the full data package to the Food and Drug Administration and regulat ory agencies in other countries in the spring of 2017.
“Hopefully, the product will receive marketing approval in 2018,” Dr. Rosenberg said.
In addition to sponsoring HOPE, IPM is also sponsoring the ongoing open-label DREAM (Dapivirine Ring Extended Access and Monitoring) study. IPM is also partnering with the Microbicides Trial Network to conduct a separate study of the vaginal ring in adolescents and young women in Africa.
A dapivirine vaginal ring that’s active for 3 months rather than 1 month will begin safety studies later in 2016. The potential advantages of this product are reduced annual cost and fewer clinic visits. Also, a 3-month version of the ring with an added contraceptive has been developed and will begin safety studies in the United States in fall 2016. The possibility that suboptimal adherence can be overcome by a ring containing a higher dose of dapivirine will also be explored, according to Dr. Rosenberg.
Dr. Brown, Dr. Baeten, and Dr. Rosenberg reported having no financial conflicts of interest.
DURBAN, SOUTH AFRICA – Women who consistently used a monthly vaginal ring containing the antiretroviral drug dapivirine reduced their risk of acquiring HIV infection by 75%-91% in exploratory analyses of the phase III ASPIRE study, Elizabeth R. Brown, ScD, reported at the 21st International AIDS Conference.
ASPIRE (A Study to Prevent Infection with a Ring for Extended use), also known as the Microbicide Trials Network-020 trial, was a multicenter, randomized, double-blind, placebo-controlled, phase III trial of a silicone vaginal ring containing 25 mg of the non-nucleoside reverse transcriptase inhibitor dapivirine. ASPIRE involved 2,629 HIV-uninfected women aged 18-45 years from four Southern African countries with extremely high HIV infection rates: South Africa, Uganda, Malawi, and Zimbabwe. They were prospectively followed monthly for 12-33 months.
As reported at a conference earlier in 2016, seroconversion occurred in 71 women assigned to the dapivirine ring and 97 on a placebo ring during 4,280 person-years of follow-up. The resultant 27% relative risk reduction in an intent-to-treat analysis, while statistically significant, was less than hoped for by investigators.
However, the device only works if it’s used consistently, so the investigators decided to conduct exploratory analyses using an objective measure of adherence: the amount of dapivirine remaining in a ring after a month’s use. This was possible because the rings had been stored for analysis in a central laboratory.
The vaginal ring is self-inserted, then meant to be kept in place continuously for a month before being self-removed and replaced with a fresh ring. Dapivirine is released continuously while the ring is in place, so the less residual dapivirine contained in a used ring, the greater the adherence during that month, explained Dr. Brown, a biostatistician at the University of Washington, Seattle.
A dose-response effect was observed. In the most encouraging of the exploratory time-dependent use analyses, the rate of HIV acquisition was 4.7 cases per 100 person-years with placebo, 4.9/100 person-years in women defined as nonadherent based upon a residual dapivirine level of 23.5 mg or more, 3.1 with low use, 1.9 with moderate use, and 0.4 cases/100 person-years with consistent use as directed, meaning a patient left the device in place continuously for a month as reflected in a residual dapivirine rate below 22 mg.
This translates into a 91% reduction in risk, compared with placebo, in the most consistent users, a 58% relative risk reduction with moderate use, and a 29% reduction with low use, she continued.
The new results were hailed as a major advance in preventing HIV infection.
“We’re meeting here at AIDS 2016 in Durban, capital of the KwaZulu-Natal province of South Africa, which is one of the hardest-hit areas of the world for HIV. Over the course of their lifetime, women in Southern Africa have more than a 50% chance of HIV infection. So a new prevention tool that women can use on their own discretely to protect themselves against HIV would be a game changer,” Jared Baeten, MD, PhD, said in an interview.
“I see this as having an important potential role in the [United States] as well for women who face an increased risk of HIV. It’s extremely valuable for them to have a method of protection that they can control and feel good about and safely use for an extended period of time,” added Dr. Baeten, professor and vice chair of global health, as well as professor of allergy and infectious diseases at the University of Washington, Seattle.
The challenges involved in consistent use of the dapivirine ring are less formidable than are those posed by consistent use of a daily oral medication for preexposure prevention, he noted.
Dr. Baeten was a leader of ASPIRE and is codirector of the HOPE (HIV Open-label Prevention Extension) study, which is now underway. The expectation is that adherence to the dapivirine vaginal ring will be better in HOPE than in ASPIRE because participants can now be counseled that the ring works, it’s safe, and there is no chance of getting a placebo device, he said.
“There is an urgent unmet need to expand long-acting HIV prevention options for women and girls,” Zeda Rosenberg, ScD, founder and chief executive officer of the nonprofit International Partnership for Microbicides (IPM) in Silver Spring, Md., which is the sponsor and developer of the ring.
Toward that end, in the next several months the ASPIRE data will be combined with those from the IPM-sponsored Ring Study, another completed large phase III trial of the dapivirine ring conducted in Africa. The goals will be to try to identify potentially modifiable sociodemographic and behavioral correlates of adherence and to further strengthen the safety and efficacy findings. The plan is to submit the full data package to the Food and Drug Administration and regulat ory agencies in other countries in the spring of 2017.
“Hopefully, the product will receive marketing approval in 2018,” Dr. Rosenberg said.
In addition to sponsoring HOPE, IPM is also sponsoring the ongoing open-label DREAM (Dapivirine Ring Extended Access and Monitoring) study. IPM is also partnering with the Microbicides Trial Network to conduct a separate study of the vaginal ring in adolescents and young women in Africa.
A dapivirine vaginal ring that’s active for 3 months rather than 1 month will begin safety studies later in 2016. The potential advantages of this product are reduced annual cost and fewer clinic visits. Also, a 3-month version of the ring with an added contraceptive has been developed and will begin safety studies in the United States in fall 2016. The possibility that suboptimal adherence can be overcome by a ring containing a higher dose of dapivirine will also be explored, according to Dr. Rosenberg.
Dr. Brown, Dr. Baeten, and Dr. Rosenberg reported having no financial conflicts of interest.
AT AIDS 2016
Key clinical point: Consistent use of monthly vaginal ring containing dapivirine resulted in significant risk reductions in HIV acquisition, compared with placebo.
Major finding: Women at increased risk for HIV infection who used a dapivirine-impregnated silicone vaginal ring as directed – leaving it in place for a full month and then exchanging it for a new one – had 75%-91% relative risk reductions in HIV acquisition.
Data source: Exploratory analyses of data from ASPIRE, a randomized, placebo-controlled, phase III multicenter clinical trial in which 2,629 women in four Southern African countries were followed monthly for 12-33 months.
Disclosures: The ASPIRE study was supported by the National Institutes of Health–funded Microbicide Trials Network. The presenter reported having no financial conflicts of interest.

Flumazenil effective in refractory hypersomnolence
DENVER – Transdermal or sublingual flumazenil is well worth considering for treatment of carefully selected patients with hypersomnolence refractory to conventional wake-promoting medications, Lynn Marie Trotti, MD, said at the annual meeting of the Associated Professional Sleep Societies.
Her retrospective chart review of 153 consecutive patients treated with flumazenil (Romazicon) showed that 63% derived symptomatic benefit, and 39% of patients remained on the drug at the end of the review period, which averaged 6.8 months, reported Dr. Trotti, a neurologist and sleep scientist at Emory University in Atlanta.

Make no mistake: This is off-label therapy. Flumazenil’s approved indication is as intravenous therapy for benzodiazepine sedation. Given orally, the drug is almost entirely eliminated on first-pass metabolism, so she and her coinvestigators had flumazenil compounded at a pharmacy in two formulations: a 6-mg sublingual lozenge and a transcutaneous lotion in a dispenser providing 3 mg of flumazenil per click of the device.
This novel therapy is supported by a plausible mechanistic rationale. Dr. Trotti and colleagues have previously shown that most patients with central hypersomnolence have abnormal potentiation of GABA-A receptors in their cerebrospinal fluid (CSF).
“Functionally speaking, it’s as though they’re producing an endogenous benzodiazepinelike substance,” she explained.
The investigators showed further that the macrolide antibiotic clarithromycin, a negative allosteric modulator of GABA-A receptors, reduced sleepiness in patients with central hypersomnolence syndromes in a randomized, double-blind, crossover trial (Ann Neurol. 2015 Sep;78[3]:454-65).
“It’s not great to use an antibiotic to treat people who don’t have a bacterial infection, so it would be really lovely if we had a GABA antagonist or negative allosteric modulator of GABA-A receptors that was not clarithromycin. And that’s where flumazenil comes into the picture,” according to Dr. Trotti.
As a requirement for receiving flumazenil at the Emory sleep disorders center, patients had to have been refractory to all conventional therapies. Indeed, they had been refractory to an average of 4.6 medications for excessive sleepiness. Also, their hypersomnolence had to have a serious impact on their daily life, for example a job at risk because of inability to drive to and from work safely. Initially, it was further required as a condition for treatment that patients had to show abnormal CSF potentiation of GABA-A receptors; however, the investigators quit requiring a CSF sample after roughly the first 100 candidates proved positive.
Dosing of the sublingual flumazenil lozenges began at one 6-mg lozenge four times daily, titrating up by adding an extra lozenge every 4-5 days until reaching a maximum of 12 per day. The lotion is rubbed on the inside of the forearm at a dose of 3 mg on each arm up to four times per day.
Among the 40 treatment responders who completed the Epworth Sleepiness Scale at baseline and after an average of 6.8 months on flumazenil, the average score improved from 15 to 10.3.
Fifty-seven patients obtained no benefit from flumazenil, 10 stopped the drug because of side effects, 3 quit because they preferred clarithromycin, 8 stopped owing to the cost, and the rest dropped the drug for an assortment of reasons, including planned pregnancy.
The most common treatment-emergent adverse events included dizziness in 13% of subjects, anxiety in 7%, and other mood disturbances in 6%.
Two serious adverse events occurred. One patient with a history of atrial fibrillation experienced a transient ischemic attack. And a patient with systemic lupus erythematous developed asymptomatic CNS lupus vasculopathy. It’s not possible to say whether these events were treatment related because the experience with chronic flumazenil therapy is so limited. After all, the drug is given for its approved indication for no longer than a few days, Dr. Trotti observed.
“This is all clinical data. Obviously I’m not suggesting that everybody should start prescribing flumazenil. That being said, we really need better treatment options,” she said.
The long-term treatment continuation rate with modafinil for hypersomnolence is about 50%, anywhere from 29% to 66% for amphetamines, 38% for clarithromycin, and 37% for pitolisant.
“If you look globally at how likely people with idiopathic hypersomnolence or narcolepsy are to get a satisfactory response to conventional therapies, probably 15%-20% do not get satisfactorily treated with what we currently have available. Prospective controlled studies of flumazenil for treatment of hypersomnolence are certainly needed, but in the absence of those data there’s at least a rationale for people who are severely affected and have nowhere else to turn to consider flumazenil,” Dr. Trotti concluded.
She reported having no financial conflicts regarding her study, supported by the National Institutes of Health.
DENVER – Transdermal or sublingual flumazenil is well worth considering for treatment of carefully selected patients with hypersomnolence refractory to conventional wake-promoting medications, Lynn Marie Trotti, MD, said at the annual meeting of the Associated Professional Sleep Societies.
Her retrospective chart review of 153 consecutive patients treated with flumazenil (Romazicon) showed that 63% derived symptomatic benefit, and 39% of patients remained on the drug at the end of the review period, which averaged 6.8 months, reported Dr. Trotti, a neurologist and sleep scientist at Emory University in Atlanta.
Make no mistake: This is off-label therapy. Flumazenil’s approved indication is as intravenous therapy for benzodiazepine sedation. Given orally, the drug is almost entirely eliminated on first-pass metabolism, so she and her coinvestigators had flumazenil compounded at a pharmacy in two formulations: a 6-mg sublingual lozenge and a transcutaneous lotion in a dispenser providing 3 mg of flumazenil per click of the device.
This novel therapy is supported by a plausible mechanistic rationale. Dr. Trotti and colleagues have previously shown that most patients with central hypersomnolence have abnormal potentiation of GABA-A receptors in their cerebrospinal fluid (CSF).
“Functionally speaking, it’s as though they’re producing an endogenous benzodiazepinelike substance,” she explained.
The investigators showed further that the macrolide antibiotic clarithromycin, a negative allosteric modulator of GABA-A receptors, reduced sleepiness in patients with central hypersomnolence syndromes in a randomized, double-blind, crossover trial (Ann Neurol. 2015 Sep;78[3]:454-65).
“It’s not great to use an antibiotic to treat people who don’t have a bacterial infection, so it would be really lovely if we had a GABA antagonist or negative allosteric modulator of GABA-A receptors that was not clarithromycin. And that’s where flumazenil comes into the picture,” according to Dr. Trotti.
As a requirement for receiving flumazenil at the Emory sleep disorders center, patients had to have been refractory to all conventional therapies. Indeed, they had been refractory to an average of 4.6 medications for excessive sleepiness. Also, their hypersomnolence had to have a serious impact on their daily life, for example a job at risk because of inability to drive to and from work safely. Initially, it was further required as a condition for treatment that patients had to show abnormal CSF potentiation of GABA-A receptors; however, the investigators quit requiring a CSF sample after roughly the first 100 candidates proved positive.
Dosing of the sublingual flumazenil lozenges began at one 6-mg lozenge four times daily, titrating up by adding an extra lozenge every 4-5 days until reaching a maximum of 12 per day. The lotion is rubbed on the inside of the forearm at a dose of 3 mg on each arm up to four times per day.
Among the 40 treatment responders who completed the Epworth Sleepiness Scale at baseline and after an average of 6.8 months on flumazenil, the average score improved from 15 to 10.3.
Fifty-seven patients obtained no benefit from flumazenil, 10 stopped the drug because of side effects, 3 quit because they preferred clarithromycin, 8 stopped owing to the cost, and the rest dropped the drug for an assortment of reasons, including planned pregnancy.
The most common treatment-emergent adverse events included dizziness in 13% of subjects, anxiety in 7%, and other mood disturbances in 6%.
Two serious adverse events occurred. One patient with a history of atrial fibrillation experienced a transient ischemic attack. And a patient with systemic lupus erythematous developed asymptomatic CNS lupus vasculopathy. It’s not possible to say whether these events were treatment related because the experience with chronic flumazenil therapy is so limited. After all, the drug is given for its approved indication for no longer than a few days, Dr. Trotti observed.
“This is all clinical data. Obviously I’m not suggesting that everybody should start prescribing flumazenil. That being said, we really need better treatment options,” she said.
The long-term treatment continuation rate with modafinil for hypersomnolence is about 50%, anywhere from 29% to 66% for amphetamines, 38% for clarithromycin, and 37% for pitolisant.
“If you look globally at how likely people with idiopathic hypersomnolence or narcolepsy are to get a satisfactory response to conventional therapies, probably 15%-20% do not get satisfactorily treated with what we currently have available. Prospective controlled studies of flumazenil for treatment of hypersomnolence are certainly needed, but in the absence of those data there’s at least a rationale for people who are severely affected and have nowhere else to turn to consider flumazenil,” Dr. Trotti concluded.
She reported having no financial conflicts regarding her study, supported by the National Institutes of Health.
DENVER – Transdermal or sublingual flumazenil is well worth considering for treatment of carefully selected patients with hypersomnolence refractory to conventional wake-promoting medications, Lynn Marie Trotti, MD, said at the annual meeting of the Associated Professional Sleep Societies.
Her retrospective chart review of 153 consecutive patients treated with flumazenil (Romazicon) showed that 63% derived symptomatic benefit, and 39% of patients remained on the drug at the end of the review period, which averaged 6.8 months, reported Dr. Trotti, a neurologist and sleep scientist at Emory University in Atlanta.
Make no mistake: This is off-label therapy. Flumazenil’s approved indication is as intravenous therapy for benzodiazepine sedation. Given orally, the drug is almost entirely eliminated on first-pass metabolism, so she and her coinvestigators had flumazenil compounded at a pharmacy in two formulations: a 6-mg sublingual lozenge and a transcutaneous lotion in a dispenser providing 3 mg of flumazenil per click of the device.
This novel therapy is supported by a plausible mechanistic rationale. Dr. Trotti and colleagues have previously shown that most patients with central hypersomnolence have abnormal potentiation of GABA-A receptors in their cerebrospinal fluid (CSF).
“Functionally speaking, it’s as though they’re producing an endogenous benzodiazepinelike substance,” she explained.
The investigators showed further that the macrolide antibiotic clarithromycin, a negative allosteric modulator of GABA-A receptors, reduced sleepiness in patients with central hypersomnolence syndromes in a randomized, double-blind, crossover trial (Ann Neurol. 2015 Sep;78[3]:454-65).
“It’s not great to use an antibiotic to treat people who don’t have a bacterial infection, so it would be really lovely if we had a GABA antagonist or negative allosteric modulator of GABA-A receptors that was not clarithromycin. And that’s where flumazenil comes into the picture,” according to Dr. Trotti.
As a requirement for receiving flumazenil at the Emory sleep disorders center, patients had to have been refractory to all conventional therapies. Indeed, they had been refractory to an average of 4.6 medications for excessive sleepiness. Also, their hypersomnolence had to have a serious impact on their daily life, for example a job at risk because of inability to drive to and from work safely. Initially, it was further required as a condition for treatment that patients had to show abnormal CSF potentiation of GABA-A receptors; however, the investigators quit requiring a CSF sample after roughly the first 100 candidates proved positive.
Dosing of the sublingual flumazenil lozenges began at one 6-mg lozenge four times daily, titrating up by adding an extra lozenge every 4-5 days until reaching a maximum of 12 per day. The lotion is rubbed on the inside of the forearm at a dose of 3 mg on each arm up to four times per day.
Among the 40 treatment responders who completed the Epworth Sleepiness Scale at baseline and after an average of 6.8 months on flumazenil, the average score improved from 15 to 10.3.
Fifty-seven patients obtained no benefit from flumazenil, 10 stopped the drug because of side effects, 3 quit because they preferred clarithromycin, 8 stopped owing to the cost, and the rest dropped the drug for an assortment of reasons, including planned pregnancy.
The most common treatment-emergent adverse events included dizziness in 13% of subjects, anxiety in 7%, and other mood disturbances in 6%.
Two serious adverse events occurred. One patient with a history of atrial fibrillation experienced a transient ischemic attack. And a patient with systemic lupus erythematous developed asymptomatic CNS lupus vasculopathy. It’s not possible to say whether these events were treatment related because the experience with chronic flumazenil therapy is so limited. After all, the drug is given for its approved indication for no longer than a few days, Dr. Trotti observed.
“This is all clinical data. Obviously I’m not suggesting that everybody should start prescribing flumazenil. That being said, we really need better treatment options,” she said.
The long-term treatment continuation rate with modafinil for hypersomnolence is about 50%, anywhere from 29% to 66% for amphetamines, 38% for clarithromycin, and 37% for pitolisant.
“If you look globally at how likely people with idiopathic hypersomnolence or narcolepsy are to get a satisfactory response to conventional therapies, probably 15%-20% do not get satisfactorily treated with what we currently have available. Prospective controlled studies of flumazenil for treatment of hypersomnolence are certainly needed, but in the absence of those data there’s at least a rationale for people who are severely affected and have nowhere else to turn to consider flumazenil,” Dr. Trotti concluded.
She reported having no financial conflicts regarding her study, supported by the National Institutes of Health.
AT SLEEP 2016
Key clinical point: Flumazenil offers a new option for refractory hypersomnolence.
Major finding: Sixty-three percent of patients with highly refractory hypersomnolence derived symptomatic benefit from flumazenil, and 39% of treated patients remained on the drug at a mean 6.8 months of follow-up.
Data source: This was a retrospective chart review of 153 consecutive patients with severe hypersomnolence refractory to all standard therapies who were treated with sublingual or topical flumazenil.
Disclosures: The presenter reported having no financial conflicts regarding her study, supported by the National Institutes of Health.

GERD and Sleep Disorders Often Go Hand in Glove
DENVER – Gastroesophageal reflux disease is fertile soil for medical and psychiatric comorbid conditions, with sleep disorders leading the way, Maurice M. Ohayon, MD, reported at the annual meeting of the Associated Professional Sleep Societies.
He presented a very large, longitudinal, population-based study of gastroesophageal reflux disease (GERD) and its fellow travelers. The study entailed telephone interviews with 12,218 nationally representative subjects in 8 states at time 1, and reinterviews with 10,830 of them 3 years later. The interviews were guided by Sleep-EVAL, a validated computerized diagnostic interview system.

At time 1, 10.6% of subjects reported that they were told by a physician they have GERD and/or they were taking a medication for it. At time 2 (3 years later), the prevalence had increased to 12.4%, according to Dr. Ohayon, professor of psychiatry and behavioral sciences, chief of the division of public mental health and population sciences, and director of the sleep epidemiology research center at Stanford (Calif.) University.
Chronic GERD – that is, GERD at both time points – was present in 3.9% of subjects; 6% of subjects were remitters, meaning that they had GERD at time 1 but not at time 2. Another 8.5% of the total sample had incident GERD, meaning they had GERD at time 2 but not time 1.
The prevalence of GERD rose stepwise with increasing age, from the low single digits in 18- to 34-year-olds to a peak in the 55- to 64-year-old age group, where the prevalence was 13.5% at time 1 and 17% at time 2.
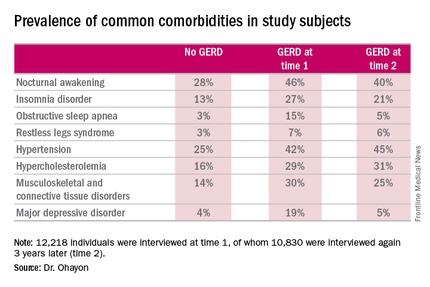
GERD was significantly more common in women. At time 2, the prevalence was 10% in men and 14.4% in women.
Nocturnal awakening was the sleep disorder symptom most commonly associated with GERD. It was a complaint in 28% of subjects who never had GERD, 46% of those with GERD at time 1, and 40% of those with GERD at time 2.
Insomnia, obstructive sleep apnea, and restless legs syndrome were also significantly more common among subjects with GERD. So were musculoskeletal and connective tissue diseases, hypertension, hypercholesterolemia, and major depressive disorder.
The study was supported by the John Arrillaga Foundation and Takeda Pharmaceuticals. Dr. Ohayon reported no financial conflicts of interest.
DENVER – Gastroesophageal reflux disease is fertile soil for medical and psychiatric comorbid conditions, with sleep disorders leading the way, Maurice M. Ohayon, MD, reported at the annual meeting of the Associated Professional Sleep Societies.
He presented a very large, longitudinal, population-based study of gastroesophageal reflux disease (GERD) and its fellow travelers. The study entailed telephone interviews with 12,218 nationally representative subjects in 8 states at time 1, and reinterviews with 10,830 of them 3 years later. The interviews were guided by Sleep-EVAL, a validated computerized diagnostic interview system.
At time 1, 10.6% of subjects reported that they were told by a physician they have GERD and/or they were taking a medication for it. At time 2 (3 years later), the prevalence had increased to 12.4%, according to Dr. Ohayon, professor of psychiatry and behavioral sciences, chief of the division of public mental health and population sciences, and director of the sleep epidemiology research center at Stanford (Calif.) University.
Chronic GERD – that is, GERD at both time points – was present in 3.9% of subjects; 6% of subjects were remitters, meaning that they had GERD at time 1 but not at time 2. Another 8.5% of the total sample had incident GERD, meaning they had GERD at time 2 but not time 1.
The prevalence of GERD rose stepwise with increasing age, from the low single digits in 18- to 34-year-olds to a peak in the 55- to 64-year-old age group, where the prevalence was 13.5% at time 1 and 17% at time 2.
GERD was significantly more common in women. At time 2, the prevalence was 10% in men and 14.4% in women.
Nocturnal awakening was the sleep disorder symptom most commonly associated with GERD. It was a complaint in 28% of subjects who never had GERD, 46% of those with GERD at time 1, and 40% of those with GERD at time 2.
Insomnia, obstructive sleep apnea, and restless legs syndrome were also significantly more common among subjects with GERD. So were musculoskeletal and connective tissue diseases, hypertension, hypercholesterolemia, and major depressive disorder.
The study was supported by the John Arrillaga Foundation and Takeda Pharmaceuticals. Dr. Ohayon reported no financial conflicts of interest.
DENVER – Gastroesophageal reflux disease is fertile soil for medical and psychiatric comorbid conditions, with sleep disorders leading the way, Maurice M. Ohayon, MD, reported at the annual meeting of the Associated Professional Sleep Societies.
He presented a very large, longitudinal, population-based study of gastroesophageal reflux disease (GERD) and its fellow travelers. The study entailed telephone interviews with 12,218 nationally representative subjects in 8 states at time 1, and reinterviews with 10,830 of them 3 years later. The interviews were guided by Sleep-EVAL, a validated computerized diagnostic interview system.
At time 1, 10.6% of subjects reported that they were told by a physician they have GERD and/or they were taking a medication for it. At time 2 (3 years later), the prevalence had increased to 12.4%, according to Dr. Ohayon, professor of psychiatry and behavioral sciences, chief of the division of public mental health and population sciences, and director of the sleep epidemiology research center at Stanford (Calif.) University.
Chronic GERD – that is, GERD at both time points – was present in 3.9% of subjects; 6% of subjects were remitters, meaning that they had GERD at time 1 but not at time 2. Another 8.5% of the total sample had incident GERD, meaning they had GERD at time 2 but not time 1.
The prevalence of GERD rose stepwise with increasing age, from the low single digits in 18- to 34-year-olds to a peak in the 55- to 64-year-old age group, where the prevalence was 13.5% at time 1 and 17% at time 2.
GERD was significantly more common in women. At time 2, the prevalence was 10% in men and 14.4% in women.
Nocturnal awakening was the sleep disorder symptom most commonly associated with GERD. It was a complaint in 28% of subjects who never had GERD, 46% of those with GERD at time 1, and 40% of those with GERD at time 2.
Insomnia, obstructive sleep apnea, and restless legs syndrome were also significantly more common among subjects with GERD. So were musculoskeletal and connective tissue diseases, hypertension, hypercholesterolemia, and major depressive disorder.
The study was supported by the John Arrillaga Foundation and Takeda Pharmaceuticals. Dr. Ohayon reported no financial conflicts of interest.
AT SLEEP 2016
