User login
Primary Care Takes on Greater Role in HIV/AIDS
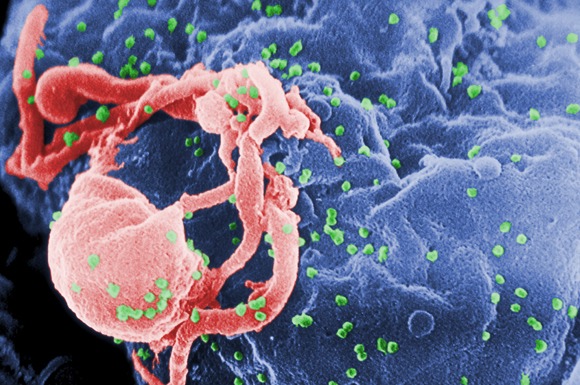
Thirty years after the first U.S. reports of pneumocystis pneumonia, a harbinger of the onslaught of the human immunodeficiency virus (HIV), primary care physicians find themselves again at the front lines of caring for patients with HIV/AIDS.
Like the illness itself, which has gone from a certain death sentence to a chronic disease, primary care practices evolved from first providing simple ministrations to the mostly untreatable to grappling with the specialized care needed for patients with active infectious disease, and the drug toxicities that go with their regimens. Now, HIV/AIDS care has entered a different phase over the past decade or so, in which physicians need both specialized knowledge and basic primary care skills. They must simultaneously address patients’ complications from living longer with the disease, along with their psychosocial issues and age-related comorbidities.
"For the first 15 years, we focused on helping people die," said Dr. Michael Saag, professor of medicine at the University of Alabama at Birmingham (UAB). "For the next 15 years, we’ve focused on helping people live – that’s a remarkable transition."
Dr. Saag said that primary care physicians who care for patients with HIV/AIDS can make an even bigger mark over the next 10-15 years. How? By showing that the care model they’ve been using perfectly demonstrates the power of the medical home.
Primary care physicians can, and should, be at the helm of HIV/AIDS care, agreed Dr. Peter Selwyn, chair of the department of family and social medicine at the Montefiore Medical Center and Albert Einstein College of Medicine, New York.
In HIV/AIDS care, "I’ve seen it start in primary care, then gravitate away, and then gravitate back," Dr. Selwyn said in an interview.
But workforce issues are a problem. Many of the primary care doctors who specialize in HIV/AIDS care now are readying for retirement. Meanwhile, some 50,000 Americans are infected each year, and the number living with the disease continues to rise. That ensures a growing patient population – unless prevention strategies, another challenge, gain more success.
And there are other hurdles, including early diagnosis and ensuring the continuation of funding under the Ryan White CARE Act, the 1990 law that has kept many HIV programs afloat.
Thirty years ago ... and today. According to the Centers for Disease Control and Prevention, the transmission of HIV in the United States has declined by 89% since the 1980s – the peak of the epidemic. With the advent of the first antiretroviral drug, AZT (zidovudine), in 1987, the number of people living with HIV/AIDS began to grow, while the number who died of it declined.
Still, today, there are 56,000 new cases a year, and some 18,000 people die annually, according to the CDC. As it was 30 years ago, men who have sex with men still make up the bulk of those infected (53%) and living with HIV/AIDS (48%). It is also the only group at risk in which new infections continue to increase.
More than a million people are living with HIV, but at least 20% don’t even know they are infected, according to the CDC.
Initially, the epidemic was concentrated in major cities on the two coasts. Now, infections are hitting Southern cities harder, and disproportionately affecting minorities. CDC data show that Miami; Jacksonville; Orlando; New Orleans; Baton Rouge, La.; Baltimore; Washington; Columbia, S.C.; Atlanta; San Juan, P.R.; and Jackson, Miss. have a high incidence of HIV. New York City and San Francisco remain epicenters.
African Americans make up only 14% of the U.S. population, but account for 46% of people living with HIV and 45% of new infections. Latinos make up 16% of the American population, but account for 18% of people living with HIV and 17% of new infections.
Patients also have a much lower socioeconomic status than they did in the past, said Dr. Donna E. Sweet, professor of internal medicine at the University of Kansas, Wichita. In her own practice, 50% of the patients are still men having sex with men, but they are less educated and less affluent, she said in an interview.
"It’s a financially and socioeconomically disenfranchised group of people compared to 20 years ago," she said.
The number of infected women in her practice also has increased. A decade or more ago, less than 10% of her patients were women. Now it’s closer to 26%; most have contracted HIV through unprotected vaginal sex, Dr. Sweet said.
At Southwest Boulevard Family Health Care Services of Greater Kansas City, the epidemic has continued to grow in the largely poor and minority population it serves, said Dr. Sharon Lee, a cofounder and CEO of the nonprofit clinic.
Of the 800-some patients with HIV, about a third are women, said Dr. Lee, professor of medicine in the department of family medicine at the University of Kansas. The women are acquiring the virus through sexual contact. Men having sex with men still make up the largest proportion of patients, and the majority are still white males, but minorities are disproportionately affected, she said in an interview.
Spiraling back around. While many primary care physicians found themselves treating HIV/AIDS patients at the dawn of the epidemic, that changed.
By the early 2000s, many primary care physicians didn’t feel as comfortable caring for HIV/AIDS patients because the field had become so specialized, Dr. Selwyn said.
But in the past 10 years, with HIV becoming a manageable chronic disease in this country, it is "not different in its acuity and time course from other chronic diseases that primary care doctors are used to taking care of," he said.
Dr. Lee said she became known for her specialization and often received referrals from other physicians for HIV care because the drug regimens were so complicated. But now, it makes more sense for HIV/AIDS patients to get care from a family physician or internist, she said. Primary care physicians have specific training to manage chronic diseases like diabetes, hypertension, and hypercholesterolemia, all of which are hitting HIV/AIDS patients hard.
"All of those things are things we are very well trained to care for. In fact, we are better trained than those specialists trained in infectious diseases," Dr. Lee said. The evolutionary path of HIV/AIDS care resembles "a pendulum of sorts, but more like a spiral – it’s spiraling back to primary care but it’s at a different level."
Dr. Sweet said that she’s been speaking around the country to physicians and administrators at community health centers and federally qualified health centers, urging them to funnel their HIV/AIDS patients into primary care. "It’s better to have one primary care physician than a dozen specialists," she tells them.
Building new capacity. Spreading the expertise is gaining urgency because many primary care doctors who focus on HIV/AIDS care are ready to retire. Many of these physicians belong to the HIV Medical Association or the American Academy of HIV Medicine; a majority of those members are within 10-15 years of retirement, said Dr. Selwyn, who has served on the HIVMA board of directors.
Dr. Lee, who currently serves on that board of directors, said that the organization has been seeking ways to increase training of primary care physicians in HIV/AIDS. The University of Kansas Medical Center is hoping to start an HIV medicine residency, she said.
The Albert Einstein College of Medicine has an active teaching program for family practice and internal medicine residents in HIV care and HIV primary care, Dr. Selwyn added.
Physicians and professional societies also are pushing the medical home concept as a viable model for offering lower-cost, high-quality HIV/AIDS care.
The Ryan White CARE Act, named after a teenage boy who died of AIDS in 1990, has become the main support for the AIDS-related medical home, according to Dr. Saag. The program is administered by the Health Resources and Services Administration (HRSA), a division of the Department of Health and Human Services. HRSA awards federal funds that are then used to deliver care and pay for medications. According to HRSA, the Ryan White HIV/AIDS Program is currently funded at $2.1 billion.
Funding via the Ryan White CARE Act led to the creation of multispecialty HIV clinics that deliver care through teams of providers. The clinics offer comprehensive care – from primary care to case management to counseling, social services, substance abuse treatment, palliative care, and pharmacy consultation.
The original model has evolved to helping people live, but "the overall effectiveness is just superb," said Dr. Saag, who says he believes he has data to prove the claim.
He and his colleagues studied the costs and reimbursement of caring for HIV/AIDS patients at the UAB clinic in 2006 (Clin. Infect. Dis. 2006;42:1003-10). Costs ranged from $13,885 per patient per year for those with early infection to $36,532 for those with more advanced disease. Three-quarters of the reimbursement was for medications, regardless of disease stage. Only 2% of the clinic’s actual costs for care was reimbursed. The study concluded that most HIV clinics would not survive without Ryan White CARE Act funds, as they make up a large amount of unreimbursed costs.
In a separate calculation, which has yet to be published, but was part of an editorial supporting the medical home published in the AIDS Reader, Dr. Saag estimated that it costs the UAB clinic about $2,700 per patient per year to offer a medical home.
It is his argument that it would be more efficient – and result in better-quality care – to take a portion of the money going to reimburse medications and instead direct it to primary care and the medical home.
"There’s a lot of money wasted in this field now," said Dr. Saag. "We just need to realign where that money is going."
Thirty years after the first U.S. reports of pneumocystis pneumonia, a harbinger of the onslaught of the human immunodeficiency virus (HIV), primary care physicians find themselves again at the front lines of caring for patients with HIV/AIDS.
Like the illness itself, which has gone from a certain death sentence to a chronic disease, primary care practices evolved from first providing simple ministrations to the mostly untreatable to grappling with the specialized care needed for patients with active infectious disease, and the drug toxicities that go with their regimens. Now, HIV/AIDS care has entered a different phase over the past decade or so, in which physicians need both specialized knowledge and basic primary care skills. They must simultaneously address patients’ complications from living longer with the disease, along with their psychosocial issues and age-related comorbidities.
"For the first 15 years, we focused on helping people die," said Dr. Michael Saag, professor of medicine at the University of Alabama at Birmingham (UAB). "For the next 15 years, we’ve focused on helping people live – that’s a remarkable transition."
Dr. Saag said that primary care physicians who care for patients with HIV/AIDS can make an even bigger mark over the next 10-15 years. How? By showing that the care model they’ve been using perfectly demonstrates the power of the medical home.
Primary care physicians can, and should, be at the helm of HIV/AIDS care, agreed Dr. Peter Selwyn, chair of the department of family and social medicine at the Montefiore Medical Center and Albert Einstein College of Medicine, New York.
In HIV/AIDS care, "I’ve seen it start in primary care, then gravitate away, and then gravitate back," Dr. Selwyn said in an interview.
But workforce issues are a problem. Many of the primary care doctors who specialize in HIV/AIDS care now are readying for retirement. Meanwhile, some 50,000 Americans are infected each year, and the number living with the disease continues to rise. That ensures a growing patient population – unless prevention strategies, another challenge, gain more success.
And there are other hurdles, including early diagnosis and ensuring the continuation of funding under the Ryan White CARE Act, the 1990 law that has kept many HIV programs afloat.
Thirty years ago ... and today. According to the Centers for Disease Control and Prevention, the transmission of HIV in the United States has declined by 89% since the 1980s – the peak of the epidemic. With the advent of the first antiretroviral drug, AZT (zidovudine), in 1987, the number of people living with HIV/AIDS began to grow, while the number who died of it declined.
Still, today, there are 56,000 new cases a year, and some 18,000 people die annually, according to the CDC. As it was 30 years ago, men who have sex with men still make up the bulk of those infected (53%) and living with HIV/AIDS (48%). It is also the only group at risk in which new infections continue to increase.
More than a million people are living with HIV, but at least 20% don’t even know they are infected, according to the CDC.
Initially, the epidemic was concentrated in major cities on the two coasts. Now, infections are hitting Southern cities harder, and disproportionately affecting minorities. CDC data show that Miami; Jacksonville; Orlando; New Orleans; Baton Rouge, La.; Baltimore; Washington; Columbia, S.C.; Atlanta; San Juan, P.R.; and Jackson, Miss. have a high incidence of HIV. New York City and San Francisco remain epicenters.
African Americans make up only 14% of the U.S. population, but account for 46% of people living with HIV and 45% of new infections. Latinos make up 16% of the American population, but account for 18% of people living with HIV and 17% of new infections.
Patients also have a much lower socioeconomic status than they did in the past, said Dr. Donna E. Sweet, professor of internal medicine at the University of Kansas, Wichita. In her own practice, 50% of the patients are still men having sex with men, but they are less educated and less affluent, she said in an interview.
"It’s a financially and socioeconomically disenfranchised group of people compared to 20 years ago," she said.
The number of infected women in her practice also has increased. A decade or more ago, less than 10% of her patients were women. Now it’s closer to 26%; most have contracted HIV through unprotected vaginal sex, Dr. Sweet said.
At Southwest Boulevard Family Health Care Services of Greater Kansas City, the epidemic has continued to grow in the largely poor and minority population it serves, said Dr. Sharon Lee, a cofounder and CEO of the nonprofit clinic.
Of the 800-some patients with HIV, about a third are women, said Dr. Lee, professor of medicine in the department of family medicine at the University of Kansas. The women are acquiring the virus through sexual contact. Men having sex with men still make up the largest proportion of patients, and the majority are still white males, but minorities are disproportionately affected, she said in an interview.
Spiraling back around. While many primary care physicians found themselves treating HIV/AIDS patients at the dawn of the epidemic, that changed.
By the early 2000s, many primary care physicians didn’t feel as comfortable caring for HIV/AIDS patients because the field had become so specialized, Dr. Selwyn said.
But in the past 10 years, with HIV becoming a manageable chronic disease in this country, it is "not different in its acuity and time course from other chronic diseases that primary care doctors are used to taking care of," he said.
Dr. Lee said she became known for her specialization and often received referrals from other physicians for HIV care because the drug regimens were so complicated. But now, it makes more sense for HIV/AIDS patients to get care from a family physician or internist, she said. Primary care physicians have specific training to manage chronic diseases like diabetes, hypertension, and hypercholesterolemia, all of which are hitting HIV/AIDS patients hard.
"All of those things are things we are very well trained to care for. In fact, we are better trained than those specialists trained in infectious diseases," Dr. Lee said. The evolutionary path of HIV/AIDS care resembles "a pendulum of sorts, but more like a spiral – it’s spiraling back to primary care but it’s at a different level."
Dr. Sweet said that she’s been speaking around the country to physicians and administrators at community health centers and federally qualified health centers, urging them to funnel their HIV/AIDS patients into primary care. "It’s better to have one primary care physician than a dozen specialists," she tells them.
Building new capacity. Spreading the expertise is gaining urgency because many primary care doctors who focus on HIV/AIDS care are ready to retire. Many of these physicians belong to the HIV Medical Association or the American Academy of HIV Medicine; a majority of those members are within 10-15 years of retirement, said Dr. Selwyn, who has served on the HIVMA board of directors.
Dr. Lee, who currently serves on that board of directors, said that the organization has been seeking ways to increase training of primary care physicians in HIV/AIDS. The University of Kansas Medical Center is hoping to start an HIV medicine residency, she said.
The Albert Einstein College of Medicine has an active teaching program for family practice and internal medicine residents in HIV care and HIV primary care, Dr. Selwyn added.
Physicians and professional societies also are pushing the medical home concept as a viable model for offering lower-cost, high-quality HIV/AIDS care.
The Ryan White CARE Act, named after a teenage boy who died of AIDS in 1990, has become the main support for the AIDS-related medical home, according to Dr. Saag. The program is administered by the Health Resources and Services Administration (HRSA), a division of the Department of Health and Human Services. HRSA awards federal funds that are then used to deliver care and pay for medications. According to HRSA, the Ryan White HIV/AIDS Program is currently funded at $2.1 billion.
Funding via the Ryan White CARE Act led to the creation of multispecialty HIV clinics that deliver care through teams of providers. The clinics offer comprehensive care – from primary care to case management to counseling, social services, substance abuse treatment, palliative care, and pharmacy consultation.
The original model has evolved to helping people live, but "the overall effectiveness is just superb," said Dr. Saag, who says he believes he has data to prove the claim.
He and his colleagues studied the costs and reimbursement of caring for HIV/AIDS patients at the UAB clinic in 2006 (Clin. Infect. Dis. 2006;42:1003-10). Costs ranged from $13,885 per patient per year for those with early infection to $36,532 for those with more advanced disease. Three-quarters of the reimbursement was for medications, regardless of disease stage. Only 2% of the clinic’s actual costs for care was reimbursed. The study concluded that most HIV clinics would not survive without Ryan White CARE Act funds, as they make up a large amount of unreimbursed costs.
In a separate calculation, which has yet to be published, but was part of an editorial supporting the medical home published in the AIDS Reader, Dr. Saag estimated that it costs the UAB clinic about $2,700 per patient per year to offer a medical home.
It is his argument that it would be more efficient – and result in better-quality care – to take a portion of the money going to reimburse medications and instead direct it to primary care and the medical home.
"There’s a lot of money wasted in this field now," said Dr. Saag. "We just need to realign where that money is going."
Thirty years after the first U.S. reports of pneumocystis pneumonia, a harbinger of the onslaught of the human immunodeficiency virus (HIV), primary care physicians find themselves again at the front lines of caring for patients with HIV/AIDS.
Like the illness itself, which has gone from a certain death sentence to a chronic disease, primary care practices evolved from first providing simple ministrations to the mostly untreatable to grappling with the specialized care needed for patients with active infectious disease, and the drug toxicities that go with their regimens. Now, HIV/AIDS care has entered a different phase over the past decade or so, in which physicians need both specialized knowledge and basic primary care skills. They must simultaneously address patients’ complications from living longer with the disease, along with their psychosocial issues and age-related comorbidities.
"For the first 15 years, we focused on helping people die," said Dr. Michael Saag, professor of medicine at the University of Alabama at Birmingham (UAB). "For the next 15 years, we’ve focused on helping people live – that’s a remarkable transition."
Dr. Saag said that primary care physicians who care for patients with HIV/AIDS can make an even bigger mark over the next 10-15 years. How? By showing that the care model they’ve been using perfectly demonstrates the power of the medical home.
Primary care physicians can, and should, be at the helm of HIV/AIDS care, agreed Dr. Peter Selwyn, chair of the department of family and social medicine at the Montefiore Medical Center and Albert Einstein College of Medicine, New York.
In HIV/AIDS care, "I’ve seen it start in primary care, then gravitate away, and then gravitate back," Dr. Selwyn said in an interview.
But workforce issues are a problem. Many of the primary care doctors who specialize in HIV/AIDS care now are readying for retirement. Meanwhile, some 50,000 Americans are infected each year, and the number living with the disease continues to rise. That ensures a growing patient population – unless prevention strategies, another challenge, gain more success.
And there are other hurdles, including early diagnosis and ensuring the continuation of funding under the Ryan White CARE Act, the 1990 law that has kept many HIV programs afloat.
Thirty years ago ... and today. According to the Centers for Disease Control and Prevention, the transmission of HIV in the United States has declined by 89% since the 1980s – the peak of the epidemic. With the advent of the first antiretroviral drug, AZT (zidovudine), in 1987, the number of people living with HIV/AIDS began to grow, while the number who died of it declined.
Still, today, there are 56,000 new cases a year, and some 18,000 people die annually, according to the CDC. As it was 30 years ago, men who have sex with men still make up the bulk of those infected (53%) and living with HIV/AIDS (48%). It is also the only group at risk in which new infections continue to increase.
More than a million people are living with HIV, but at least 20% don’t even know they are infected, according to the CDC.
Initially, the epidemic was concentrated in major cities on the two coasts. Now, infections are hitting Southern cities harder, and disproportionately affecting minorities. CDC data show that Miami; Jacksonville; Orlando; New Orleans; Baton Rouge, La.; Baltimore; Washington; Columbia, S.C.; Atlanta; San Juan, P.R.; and Jackson, Miss. have a high incidence of HIV. New York City and San Francisco remain epicenters.
African Americans make up only 14% of the U.S. population, but account for 46% of people living with HIV and 45% of new infections. Latinos make up 16% of the American population, but account for 18% of people living with HIV and 17% of new infections.
Patients also have a much lower socioeconomic status than they did in the past, said Dr. Donna E. Sweet, professor of internal medicine at the University of Kansas, Wichita. In her own practice, 50% of the patients are still men having sex with men, but they are less educated and less affluent, she said in an interview.
"It’s a financially and socioeconomically disenfranchised group of people compared to 20 years ago," she said.
The number of infected women in her practice also has increased. A decade or more ago, less than 10% of her patients were women. Now it’s closer to 26%; most have contracted HIV through unprotected vaginal sex, Dr. Sweet said.
At Southwest Boulevard Family Health Care Services of Greater Kansas City, the epidemic has continued to grow in the largely poor and minority population it serves, said Dr. Sharon Lee, a cofounder and CEO of the nonprofit clinic.
Of the 800-some patients with HIV, about a third are women, said Dr. Lee, professor of medicine in the department of family medicine at the University of Kansas. The women are acquiring the virus through sexual contact. Men having sex with men still make up the largest proportion of patients, and the majority are still white males, but minorities are disproportionately affected, she said in an interview.
Spiraling back around. While many primary care physicians found themselves treating HIV/AIDS patients at the dawn of the epidemic, that changed.
By the early 2000s, many primary care physicians didn’t feel as comfortable caring for HIV/AIDS patients because the field had become so specialized, Dr. Selwyn said.
But in the past 10 years, with HIV becoming a manageable chronic disease in this country, it is "not different in its acuity and time course from other chronic diseases that primary care doctors are used to taking care of," he said.
Dr. Lee said she became known for her specialization and often received referrals from other physicians for HIV care because the drug regimens were so complicated. But now, it makes more sense for HIV/AIDS patients to get care from a family physician or internist, she said. Primary care physicians have specific training to manage chronic diseases like diabetes, hypertension, and hypercholesterolemia, all of which are hitting HIV/AIDS patients hard.
"All of those things are things we are very well trained to care for. In fact, we are better trained than those specialists trained in infectious diseases," Dr. Lee said. The evolutionary path of HIV/AIDS care resembles "a pendulum of sorts, but more like a spiral – it’s spiraling back to primary care but it’s at a different level."
Dr. Sweet said that she’s been speaking around the country to physicians and administrators at community health centers and federally qualified health centers, urging them to funnel their HIV/AIDS patients into primary care. "It’s better to have one primary care physician than a dozen specialists," she tells them.
Building new capacity. Spreading the expertise is gaining urgency because many primary care doctors who focus on HIV/AIDS care are ready to retire. Many of these physicians belong to the HIV Medical Association or the American Academy of HIV Medicine; a majority of those members are within 10-15 years of retirement, said Dr. Selwyn, who has served on the HIVMA board of directors.
Dr. Lee, who currently serves on that board of directors, said that the organization has been seeking ways to increase training of primary care physicians in HIV/AIDS. The University of Kansas Medical Center is hoping to start an HIV medicine residency, she said.
The Albert Einstein College of Medicine has an active teaching program for family practice and internal medicine residents in HIV care and HIV primary care, Dr. Selwyn added.
Physicians and professional societies also are pushing the medical home concept as a viable model for offering lower-cost, high-quality HIV/AIDS care.
The Ryan White CARE Act, named after a teenage boy who died of AIDS in 1990, has become the main support for the AIDS-related medical home, according to Dr. Saag. The program is administered by the Health Resources and Services Administration (HRSA), a division of the Department of Health and Human Services. HRSA awards federal funds that are then used to deliver care and pay for medications. According to HRSA, the Ryan White HIV/AIDS Program is currently funded at $2.1 billion.
Funding via the Ryan White CARE Act led to the creation of multispecialty HIV clinics that deliver care through teams of providers. The clinics offer comprehensive care – from primary care to case management to counseling, social services, substance abuse treatment, palliative care, and pharmacy consultation.
The original model has evolved to helping people live, but "the overall effectiveness is just superb," said Dr. Saag, who says he believes he has data to prove the claim.
He and his colleagues studied the costs and reimbursement of caring for HIV/AIDS patients at the UAB clinic in 2006 (Clin. Infect. Dis. 2006;42:1003-10). Costs ranged from $13,885 per patient per year for those with early infection to $36,532 for those with more advanced disease. Three-quarters of the reimbursement was for medications, regardless of disease stage. Only 2% of the clinic’s actual costs for care was reimbursed. The study concluded that most HIV clinics would not survive without Ryan White CARE Act funds, as they make up a large amount of unreimbursed costs.
In a separate calculation, which has yet to be published, but was part of an editorial supporting the medical home published in the AIDS Reader, Dr. Saag estimated that it costs the UAB clinic about $2,700 per patient per year to offer a medical home.
It is his argument that it would be more efficient – and result in better-quality care – to take a portion of the money going to reimburse medications and instead direct it to primary care and the medical home.
"There’s a lot of money wasted in this field now," said Dr. Saag. "We just need to realign where that money is going."
HHS Paid Over $150 Million in EHR Incentives
Physician incentives for the meaningful use of electronic health records total $75 million, the Centers for Medicare and Medicaid Services (CMS) announced.
The payments were made to physicians who signed up for the incentive program in the first 2 weeks of eligibility. Beginning April 18, physicians could go to a secure CMS website and “attest” that they had complied with program requirements for a continuous 90-day reporting period during the first year of participation in the Medicare EHR incentive program. The program was created under the Health Information Technology Economic and Clinical Health Act (HITECH), which was part of the American Recovery and Reinvestment Act of 2009.
Physicians, hospitals, and other eligible providers in seven states have received an additional $83.3 million in incentive payments under Medicaid. Each state is launching a separate program; in January, programs began in Alaska, Iowa, Kentucky, Louisiana, Michigan, Mississippi, North Carolina, Oklahoma, South Carolina, Tennessee, and Texas. In April, Alabama and Missouri began programs, and Indiana and Ohio began programs in May.
CMS officials said that they expect incentive payments to grow, and that more professionals and hospitals will register for the Medicare and Medicaid incentives. As of April 30, 42,600 eligible physicians and hospitals had registered for the two programs.
“I'm looking forward to continued growth and greater adoption,” said CMS Administrator Dr. Donald Berwick in a briefing with reporters.
Under Medicare, eligible providers can receive up to $44,000 over 5 years. Under the Medicaid program, eligible providers can get up to $63,750 over 6 years.
According to Dr. Jennifer Brull, the incentive program not only boosted her practice's financial bottom line, but also improved the quality of care delivered to her patients. The Plainville, Kansas–based family physician said during the briefing that her practice began using health information technology in 2008. Initially, she said, she was skeptical that the meaningful use criteria would actually lead to better patient outcomes.
With meaningful use, the EHR system includes, among other things, alerts on drug interactions, clinical care reminders for patients, and assistance in tracking quality measures.
The physicians at Prairie Star Family Practice began tracking colon cancer screening under the program. Initially, only 43% of patients were getting appropriate screening, said Dr. Brull. But the EHR helped the practice improve to “a much more acceptable 82%. It is not perfect, but it is better,” she said.
Dr. Brull said she'd tell her peers that meaningful use is not about the money, but “about making our care better, knowing what our care is doing, and making patients better in the long run.”
Dr. Farzad Mostashari, National Coordinator for Health Information Technology, said that the meaningful use criteria under the Medicare EHR incentive program is “providing [a] model for a coordinated national transition to health information technology.”
He applauded the providers who had already attested to the fact that they were compliant with meaningful use criteria.
“These are providers who are early adopters of health IT and who are promoting health IT to their peers,” said Dr. Mostashari.
Physician incentives for the meaningful use of electronic health records total $75 million, the Centers for Medicare and Medicaid Services (CMS) announced.
The payments were made to physicians who signed up for the incentive program in the first 2 weeks of eligibility. Beginning April 18, physicians could go to a secure CMS website and “attest” that they had complied with program requirements for a continuous 90-day reporting period during the first year of participation in the Medicare EHR incentive program. The program was created under the Health Information Technology Economic and Clinical Health Act (HITECH), which was part of the American Recovery and Reinvestment Act of 2009.
Physicians, hospitals, and other eligible providers in seven states have received an additional $83.3 million in incentive payments under Medicaid. Each state is launching a separate program; in January, programs began in Alaska, Iowa, Kentucky, Louisiana, Michigan, Mississippi, North Carolina, Oklahoma, South Carolina, Tennessee, and Texas. In April, Alabama and Missouri began programs, and Indiana and Ohio began programs in May.
CMS officials said that they expect incentive payments to grow, and that more professionals and hospitals will register for the Medicare and Medicaid incentives. As of April 30, 42,600 eligible physicians and hospitals had registered for the two programs.
“I'm looking forward to continued growth and greater adoption,” said CMS Administrator Dr. Donald Berwick in a briefing with reporters.
Under Medicare, eligible providers can receive up to $44,000 over 5 years. Under the Medicaid program, eligible providers can get up to $63,750 over 6 years.
According to Dr. Jennifer Brull, the incentive program not only boosted her practice's financial bottom line, but also improved the quality of care delivered to her patients. The Plainville, Kansas–based family physician said during the briefing that her practice began using health information technology in 2008. Initially, she said, she was skeptical that the meaningful use criteria would actually lead to better patient outcomes.
With meaningful use, the EHR system includes, among other things, alerts on drug interactions, clinical care reminders for patients, and assistance in tracking quality measures.
The physicians at Prairie Star Family Practice began tracking colon cancer screening under the program. Initially, only 43% of patients were getting appropriate screening, said Dr. Brull. But the EHR helped the practice improve to “a much more acceptable 82%. It is not perfect, but it is better,” she said.
Dr. Brull said she'd tell her peers that meaningful use is not about the money, but “about making our care better, knowing what our care is doing, and making patients better in the long run.”
Dr. Farzad Mostashari, National Coordinator for Health Information Technology, said that the meaningful use criteria under the Medicare EHR incentive program is “providing [a] model for a coordinated national transition to health information technology.”
He applauded the providers who had already attested to the fact that they were compliant with meaningful use criteria.
“These are providers who are early adopters of health IT and who are promoting health IT to their peers,” said Dr. Mostashari.
Physician incentives for the meaningful use of electronic health records total $75 million, the Centers for Medicare and Medicaid Services (CMS) announced.
The payments were made to physicians who signed up for the incentive program in the first 2 weeks of eligibility. Beginning April 18, physicians could go to a secure CMS website and “attest” that they had complied with program requirements for a continuous 90-day reporting period during the first year of participation in the Medicare EHR incentive program. The program was created under the Health Information Technology Economic and Clinical Health Act (HITECH), which was part of the American Recovery and Reinvestment Act of 2009.
Physicians, hospitals, and other eligible providers in seven states have received an additional $83.3 million in incentive payments under Medicaid. Each state is launching a separate program; in January, programs began in Alaska, Iowa, Kentucky, Louisiana, Michigan, Mississippi, North Carolina, Oklahoma, South Carolina, Tennessee, and Texas. In April, Alabama and Missouri began programs, and Indiana and Ohio began programs in May.
CMS officials said that they expect incentive payments to grow, and that more professionals and hospitals will register for the Medicare and Medicaid incentives. As of April 30, 42,600 eligible physicians and hospitals had registered for the two programs.
“I'm looking forward to continued growth and greater adoption,” said CMS Administrator Dr. Donald Berwick in a briefing with reporters.
Under Medicare, eligible providers can receive up to $44,000 over 5 years. Under the Medicaid program, eligible providers can get up to $63,750 over 6 years.
According to Dr. Jennifer Brull, the incentive program not only boosted her practice's financial bottom line, but also improved the quality of care delivered to her patients. The Plainville, Kansas–based family physician said during the briefing that her practice began using health information technology in 2008. Initially, she said, she was skeptical that the meaningful use criteria would actually lead to better patient outcomes.
With meaningful use, the EHR system includes, among other things, alerts on drug interactions, clinical care reminders for patients, and assistance in tracking quality measures.
The physicians at Prairie Star Family Practice began tracking colon cancer screening under the program. Initially, only 43% of patients were getting appropriate screening, said Dr. Brull. But the EHR helped the practice improve to “a much more acceptable 82%. It is not perfect, but it is better,” she said.
Dr. Brull said she'd tell her peers that meaningful use is not about the money, but “about making our care better, knowing what our care is doing, and making patients better in the long run.”
Dr. Farzad Mostashari, National Coordinator for Health Information Technology, said that the meaningful use criteria under the Medicare EHR incentive program is “providing [a] model for a coordinated national transition to health information technology.”
He applauded the providers who had already attested to the fact that they were compliant with meaningful use criteria.
“These are providers who are early adopters of health IT and who are promoting health IT to their peers,” said Dr. Mostashari.
From the Centers for Medicare and Medicaid Services
Enrollment Lags for Pre-Existing Condition Insurance Plan
A federal program to help people with pre-existing conditions obtain health insurance has lagged in terms of the government's projected enrollment, which may be partly because it has largely gone unnoticed as one of the benefits of the health reform law.
The Pre-Existing Condition Insurance Plan (PCIP) was launched in July 2010 with $5 billion in funding from the Affordable Care Act. The goal is to provide an insurance option to people who may be barred from coverage or who have to pay huge surcharges because of a pre-existing condition such as hypercholesterolemia or cancer. The program will be in force until 2014, when the new insurance exchanges go into effect and insurers are prohibited from denying coverage to adults with pre-existing conditions. (They are already barred from doing so for children.)
Although the Department of Health and Human Services initially estimated that several hundred thousand people might benefit from the PCIP, as of early May only about 18,000 people had enrolled, according to the government's statistics.
In an interview, Richard Popper, director of insurance programs at the federal Center for Consumer Information and Insurance Oversight, would not comment on the number of enrollees. He did say, however, that enrollment had been strongest in states with higher populations, such as Texas, California, Pennsylvania, and Illinois.
A “significant number” of patients with cancer, coronary artery disease, chronic obstructive pulmonary disease, and digestive system problems have accessed the program, said Mr. Popper, whose office is a division within the Centers for Medicare and Medicaid Services. The average person who has enrolled has annual medical costs of $20,000 a year, he said.
To be eligible for the PCIP, an individual must have been without insurance for 6 months before enrollment. Mr. Popper said that because he was not working for DHHS at the time the Affordable Care Act was developed, he can't comment on why this waiting period was made an essential part of the eligibility.
After that, the program varies according to whether it is administered by a state or the federal government, although there are minimum coverage criteria. Twenty-three states and the District of Columbia elected to have their PCIP program be federally run, which is essentially the same as the plan offered by Blue Cross/Blue Shield to federal employees.
Twenty-seven states run their own programs.
Patients can apply at the federal government's website (www.pcip.gov
In all cases, the patient gets coverage immediately. There is no waiting period, and premiums will be the same as for a healthy person in the same age range. There are no surcharges for health conditions.
At a meeting of the Association of Community Cancer Centers in March, Mr. Popper cited figures for the plan in Texas, which has a program operated by the federal government. For standard coverage, individuals can expect to pay $174 to $557 monthly, depending on age, with a $2,000 deductible for medical care and a $500 deductible for medications. Higher benefit plans run $234-$749 for premiums, with $1,000 and $250 deductibles, respectively. There is also a health savings account option, with premiums of $181-$578 and a $2,500 deductible.
The out-of-pocket maximum that patients would pay under all plans is $5,950. There is no lifetime limit and no limit on physician visits or prescription drugs.
DHHS is trying to get the word out about the PCIP. When people apply for disability under the Social Security program, they receive notification about the PCIP. Many insurance companies have also been advising patients who are rejected for coverage that the PCIP is a potential alternative, said Mr. Popper.
A federal program to help people with pre-existing conditions obtain health insurance has lagged in terms of the government's projected enrollment, which may be partly because it has largely gone unnoticed as one of the benefits of the health reform law.
The Pre-Existing Condition Insurance Plan (PCIP) was launched in July 2010 with $5 billion in funding from the Affordable Care Act. The goal is to provide an insurance option to people who may be barred from coverage or who have to pay huge surcharges because of a pre-existing condition such as hypercholesterolemia or cancer. The program will be in force until 2014, when the new insurance exchanges go into effect and insurers are prohibited from denying coverage to adults with pre-existing conditions. (They are already barred from doing so for children.)
Although the Department of Health and Human Services initially estimated that several hundred thousand people might benefit from the PCIP, as of early May only about 18,000 people had enrolled, according to the government's statistics.
In an interview, Richard Popper, director of insurance programs at the federal Center for Consumer Information and Insurance Oversight, would not comment on the number of enrollees. He did say, however, that enrollment had been strongest in states with higher populations, such as Texas, California, Pennsylvania, and Illinois.
A “significant number” of patients with cancer, coronary artery disease, chronic obstructive pulmonary disease, and digestive system problems have accessed the program, said Mr. Popper, whose office is a division within the Centers for Medicare and Medicaid Services. The average person who has enrolled has annual medical costs of $20,000 a year, he said.
To be eligible for the PCIP, an individual must have been without insurance for 6 months before enrollment. Mr. Popper said that because he was not working for DHHS at the time the Affordable Care Act was developed, he can't comment on why this waiting period was made an essential part of the eligibility.
After that, the program varies according to whether it is administered by a state or the federal government, although there are minimum coverage criteria. Twenty-three states and the District of Columbia elected to have their PCIP program be federally run, which is essentially the same as the plan offered by Blue Cross/Blue Shield to federal employees.
Twenty-seven states run their own programs.
Patients can apply at the federal government's website (www.pcip.gov
In all cases, the patient gets coverage immediately. There is no waiting period, and premiums will be the same as for a healthy person in the same age range. There are no surcharges for health conditions.
At a meeting of the Association of Community Cancer Centers in March, Mr. Popper cited figures for the plan in Texas, which has a program operated by the federal government. For standard coverage, individuals can expect to pay $174 to $557 monthly, depending on age, with a $2,000 deductible for medical care and a $500 deductible for medications. Higher benefit plans run $234-$749 for premiums, with $1,000 and $250 deductibles, respectively. There is also a health savings account option, with premiums of $181-$578 and a $2,500 deductible.
The out-of-pocket maximum that patients would pay under all plans is $5,950. There is no lifetime limit and no limit on physician visits or prescription drugs.
DHHS is trying to get the word out about the PCIP. When people apply for disability under the Social Security program, they receive notification about the PCIP. Many insurance companies have also been advising patients who are rejected for coverage that the PCIP is a potential alternative, said Mr. Popper.
A federal program to help people with pre-existing conditions obtain health insurance has lagged in terms of the government's projected enrollment, which may be partly because it has largely gone unnoticed as one of the benefits of the health reform law.
The Pre-Existing Condition Insurance Plan (PCIP) was launched in July 2010 with $5 billion in funding from the Affordable Care Act. The goal is to provide an insurance option to people who may be barred from coverage or who have to pay huge surcharges because of a pre-existing condition such as hypercholesterolemia or cancer. The program will be in force until 2014, when the new insurance exchanges go into effect and insurers are prohibited from denying coverage to adults with pre-existing conditions. (They are already barred from doing so for children.)
Although the Department of Health and Human Services initially estimated that several hundred thousand people might benefit from the PCIP, as of early May only about 18,000 people had enrolled, according to the government's statistics.
In an interview, Richard Popper, director of insurance programs at the federal Center for Consumer Information and Insurance Oversight, would not comment on the number of enrollees. He did say, however, that enrollment had been strongest in states with higher populations, such as Texas, California, Pennsylvania, and Illinois.
A “significant number” of patients with cancer, coronary artery disease, chronic obstructive pulmonary disease, and digestive system problems have accessed the program, said Mr. Popper, whose office is a division within the Centers for Medicare and Medicaid Services. The average person who has enrolled has annual medical costs of $20,000 a year, he said.
To be eligible for the PCIP, an individual must have been without insurance for 6 months before enrollment. Mr. Popper said that because he was not working for DHHS at the time the Affordable Care Act was developed, he can't comment on why this waiting period was made an essential part of the eligibility.
After that, the program varies according to whether it is administered by a state or the federal government, although there are minimum coverage criteria. Twenty-three states and the District of Columbia elected to have their PCIP program be federally run, which is essentially the same as the plan offered by Blue Cross/Blue Shield to federal employees.
Twenty-seven states run their own programs.
Patients can apply at the federal government's website (www.pcip.gov
In all cases, the patient gets coverage immediately. There is no waiting period, and premiums will be the same as for a healthy person in the same age range. There are no surcharges for health conditions.
At a meeting of the Association of Community Cancer Centers in March, Mr. Popper cited figures for the plan in Texas, which has a program operated by the federal government. For standard coverage, individuals can expect to pay $174 to $557 monthly, depending on age, with a $2,000 deductible for medical care and a $500 deductible for medications. Higher benefit plans run $234-$749 for premiums, with $1,000 and $250 deductibles, respectively. There is also a health savings account option, with premiums of $181-$578 and a $2,500 deductible.
The out-of-pocket maximum that patients would pay under all plans is $5,950. There is no lifetime limit and no limit on physician visits or prescription drugs.
DHHS is trying to get the word out about the PCIP. When people apply for disability under the Social Security program, they receive notification about the PCIP. Many insurance companies have also been advising patients who are rejected for coverage that the PCIP is a potential alternative, said Mr. Popper.
E-Prescribing Rules May Be Eased by CMS
The Centers for Medicare and Medicaid Services has proposed modifying the rules for e-prescribing so more physicians could claim exemptions from the criteria and therefore avoid being penalized in 2012.
In a conference call, agency officials said the change was in response to indications from providers and professional societies that many prescribers might not be able to meet the requirements of the current incentive program.
“Today's rule demonstrates that CMS is willing to work cooperatively with the medical professional community to encourage participation in electronic prescribing,” Dr. Patrick Conway, chief medical officer at CMS and director of the agency's Office of Clinical Standards and Quality, said in a statement.
Under the current incentive program, eligible prescribers were due to get a 1% bonus payment for 2011 and 2012 and a 0.5% bonus in 2013. For prescribers who did not meet the criteria, there would be a penalty imposed in 2012. The penalty would escalate in 2013 and 2014.
The final Medicare Physician Fee Schedule for 2011 contains exceptions, along with two hardship exemptions. Practices are exempt if they are in a rural area without high-speed internet access or an area without enough available pharmacies for electronic prescribing.
Under the proposed rule, prescribers who use certified EHRs can now claim this as a “qualified” e-prescribing system. This move was designed to more closely align the e-prescribing program with the program that offers incentives for meaningful use of electronic health records. The proposed rule would also create four additional hardship exemption categories.
Prescribers also would be granted an extension, until Oct. 1, 2011, to apply for the hardship exemption.
The Centers for Medicare and Medicaid Services has proposed modifying the rules for e-prescribing so more physicians could claim exemptions from the criteria and therefore avoid being penalized in 2012.
In a conference call, agency officials said the change was in response to indications from providers and professional societies that many prescribers might not be able to meet the requirements of the current incentive program.
“Today's rule demonstrates that CMS is willing to work cooperatively with the medical professional community to encourage participation in electronic prescribing,” Dr. Patrick Conway, chief medical officer at CMS and director of the agency's Office of Clinical Standards and Quality, said in a statement.
Under the current incentive program, eligible prescribers were due to get a 1% bonus payment for 2011 and 2012 and a 0.5% bonus in 2013. For prescribers who did not meet the criteria, there would be a penalty imposed in 2012. The penalty would escalate in 2013 and 2014.
The final Medicare Physician Fee Schedule for 2011 contains exceptions, along with two hardship exemptions. Practices are exempt if they are in a rural area without high-speed internet access or an area without enough available pharmacies for electronic prescribing.
Under the proposed rule, prescribers who use certified EHRs can now claim this as a “qualified” e-prescribing system. This move was designed to more closely align the e-prescribing program with the program that offers incentives for meaningful use of electronic health records. The proposed rule would also create four additional hardship exemption categories.
Prescribers also would be granted an extension, until Oct. 1, 2011, to apply for the hardship exemption.
The Centers for Medicare and Medicaid Services has proposed modifying the rules for e-prescribing so more physicians could claim exemptions from the criteria and therefore avoid being penalized in 2012.
In a conference call, agency officials said the change was in response to indications from providers and professional societies that many prescribers might not be able to meet the requirements of the current incentive program.
“Today's rule demonstrates that CMS is willing to work cooperatively with the medical professional community to encourage participation in electronic prescribing,” Dr. Patrick Conway, chief medical officer at CMS and director of the agency's Office of Clinical Standards and Quality, said in a statement.
Under the current incentive program, eligible prescribers were due to get a 1% bonus payment for 2011 and 2012 and a 0.5% bonus in 2013. For prescribers who did not meet the criteria, there would be a penalty imposed in 2012. The penalty would escalate in 2013 and 2014.
The final Medicare Physician Fee Schedule for 2011 contains exceptions, along with two hardship exemptions. Practices are exempt if they are in a rural area without high-speed internet access or an area without enough available pharmacies for electronic prescribing.
Under the proposed rule, prescribers who use certified EHRs can now claim this as a “qualified” e-prescribing system. This move was designed to more closely align the e-prescribing program with the program that offers incentives for meaningful use of electronic health records. The proposed rule would also create four additional hardship exemption categories.
Prescribers also would be granted an extension, until Oct. 1, 2011, to apply for the hardship exemption.
Physicians Consider Frequent Call Burdensome
Physicians are more concerned about the burden of taking call than about how much they get paid for providing coverage at hospital emergency departments, according to a survey by the American Medical Group Association and a consulting firm.
About 50 medical groups participated, primarily from independently owned, large, multispecialty groups. Dr. Donald W. Fisher, president and CEO of the AMGA, said that most of the data on physicians' opinions on call coverage have been anecdotal. The AMGA survey, conducted with ECG Management Consultants, quantifies better what's actually happening, he said.
According to the survey, when physicians were asked to choose between reduced call burden or payment, 58% of those surveyed said it was more important to reduce call burden. More than half the respondents said their call burden was high.
The survey also asked physicians for some potential solutions to reducing call burden. Respondents said that the advent of hospitalists – which they regarded as favorable – was a potentially important way to reduce call burden. The majority of respondents said that use of nocturnists would be helpful. And 70% said that offering preferred scheduling on the day after call would be a good way to address call burden.
To access the free report online, go to https://ecommerce.amga.org/iMISPublic/Core/Orders/product.aspx?catid=12&prodid=2022
Physicians are more concerned about the burden of taking call than about how much they get paid for providing coverage at hospital emergency departments, according to a survey by the American Medical Group Association and a consulting firm.
About 50 medical groups participated, primarily from independently owned, large, multispecialty groups. Dr. Donald W. Fisher, president and CEO of the AMGA, said that most of the data on physicians' opinions on call coverage have been anecdotal. The AMGA survey, conducted with ECG Management Consultants, quantifies better what's actually happening, he said.
According to the survey, when physicians were asked to choose between reduced call burden or payment, 58% of those surveyed said it was more important to reduce call burden. More than half the respondents said their call burden was high.
The survey also asked physicians for some potential solutions to reducing call burden. Respondents said that the advent of hospitalists – which they regarded as favorable – was a potentially important way to reduce call burden. The majority of respondents said that use of nocturnists would be helpful. And 70% said that offering preferred scheduling on the day after call would be a good way to address call burden.
To access the free report online, go to https://ecommerce.amga.org/iMISPublic/Core/Orders/product.aspx?catid=12&prodid=2022
Physicians are more concerned about the burden of taking call than about how much they get paid for providing coverage at hospital emergency departments, according to a survey by the American Medical Group Association and a consulting firm.
About 50 medical groups participated, primarily from independently owned, large, multispecialty groups. Dr. Donald W. Fisher, president and CEO of the AMGA, said that most of the data on physicians' opinions on call coverage have been anecdotal. The AMGA survey, conducted with ECG Management Consultants, quantifies better what's actually happening, he said.
According to the survey, when physicians were asked to choose between reduced call burden or payment, 58% of those surveyed said it was more important to reduce call burden. More than half the respondents said their call burden was high.
The survey also asked physicians for some potential solutions to reducing call burden. Respondents said that the advent of hospitalists – which they regarded as favorable – was a potentially important way to reduce call burden. The majority of respondents said that use of nocturnists would be helpful. And 70% said that offering preferred scheduling on the day after call would be a good way to address call burden.
To access the free report online, go to https://ecommerce.amga.org/iMISPublic/Core/Orders/product.aspx?catid=12&prodid=2022
From A Survey by the American Medical Group Association
Incentives Boost Quality Reporting, e-Prescribing
About $234 million in bonuses under the Physician Quality Reporting System and $148 million in incentives for ePrescribing were paid out in 2009, according to the Centers for Medicare and Medicaid Services.
Participation in the now-voluntary PQRS has grown 50% per year since the program started in 2007 and currently includes one in five eligible health care professionals. In 2009, some 210,000 physicians and other eligible health care professionals participated, but just 119,804 clinicians reported data in a manner consistent with the necessary criteria for incentive payouts, the CMS said.
Emergency physicians had the highest rate of satisfactory reporting, the CMS said. In 2009, 31,000 reported on at least one quality measure and 79% received an incentive payment.
“Although participation in our pay-for-reporting programs is optional now, it should be regarded as imperative in terms of medical professionals' shared goal of improving quality of care and patient safety,” CMS Administrator Donald Berwick said in a statement.
The average payment per professional was $1,956 and the average payment per practice was $18,525, according to the CMS. Payments, which were sent in the fall of 2010, were equal to 2% of total estimated charges under Medicare Part B.
Physicians and health professionals could report on 194 measures. The three most frequently reported quality measures were performing electrocardiograms in the emergency department to diagnose chest pain; using electronic health records to organize and manage care; and, working with diabetics to control blood glucose levels.
Some notable improvements since the program's inception included a near doubling of the number of physicians reporting that they had talked with diabetic patients about eye-related complications – from 52% in 2007 to 93% in 2009. Also, beta-blockers were recommended to patients with left ventricular systolic dysfunction by 95% of reporting physicians in 2009, as compared to 64% in 2007.
The PQRS program will remain voluntary until 2015, when the Medicare program will start withholding payments for lack of participation.
The first year of the e-Prescribing program was 2009. That year, 48,354 physicians received an e-Prescribing incentive payment, with an average payment of $3,000 per individual and $14,501 per practice.
The deadline for participation in the e-Prescribing program is much sooner than that for the PQRS program. Physicians will see pay reductions beginning in 2012 if they don't participate in ePrescribing.
About $234 million in bonuses under the Physician Quality Reporting System and $148 million in incentives for ePrescribing were paid out in 2009, according to the Centers for Medicare and Medicaid Services.
Participation in the now-voluntary PQRS has grown 50% per year since the program started in 2007 and currently includes one in five eligible health care professionals. In 2009, some 210,000 physicians and other eligible health care professionals participated, but just 119,804 clinicians reported data in a manner consistent with the necessary criteria for incentive payouts, the CMS said.
Emergency physicians had the highest rate of satisfactory reporting, the CMS said. In 2009, 31,000 reported on at least one quality measure and 79% received an incentive payment.
“Although participation in our pay-for-reporting programs is optional now, it should be regarded as imperative in terms of medical professionals' shared goal of improving quality of care and patient safety,” CMS Administrator Donald Berwick said in a statement.
The average payment per professional was $1,956 and the average payment per practice was $18,525, according to the CMS. Payments, which were sent in the fall of 2010, were equal to 2% of total estimated charges under Medicare Part B.
Physicians and health professionals could report on 194 measures. The three most frequently reported quality measures were performing electrocardiograms in the emergency department to diagnose chest pain; using electronic health records to organize and manage care; and, working with diabetics to control blood glucose levels.
Some notable improvements since the program's inception included a near doubling of the number of physicians reporting that they had talked with diabetic patients about eye-related complications – from 52% in 2007 to 93% in 2009. Also, beta-blockers were recommended to patients with left ventricular systolic dysfunction by 95% of reporting physicians in 2009, as compared to 64% in 2007.
The PQRS program will remain voluntary until 2015, when the Medicare program will start withholding payments for lack of participation.
The first year of the e-Prescribing program was 2009. That year, 48,354 physicians received an e-Prescribing incentive payment, with an average payment of $3,000 per individual and $14,501 per practice.
The deadline for participation in the e-Prescribing program is much sooner than that for the PQRS program. Physicians will see pay reductions beginning in 2012 if they don't participate in ePrescribing.
About $234 million in bonuses under the Physician Quality Reporting System and $148 million in incentives for ePrescribing were paid out in 2009, according to the Centers for Medicare and Medicaid Services.
Participation in the now-voluntary PQRS has grown 50% per year since the program started in 2007 and currently includes one in five eligible health care professionals. In 2009, some 210,000 physicians and other eligible health care professionals participated, but just 119,804 clinicians reported data in a manner consistent with the necessary criteria for incentive payouts, the CMS said.
Emergency physicians had the highest rate of satisfactory reporting, the CMS said. In 2009, 31,000 reported on at least one quality measure and 79% received an incentive payment.
“Although participation in our pay-for-reporting programs is optional now, it should be regarded as imperative in terms of medical professionals' shared goal of improving quality of care and patient safety,” CMS Administrator Donald Berwick said in a statement.
The average payment per professional was $1,956 and the average payment per practice was $18,525, according to the CMS. Payments, which were sent in the fall of 2010, were equal to 2% of total estimated charges under Medicare Part B.
Physicians and health professionals could report on 194 measures. The three most frequently reported quality measures were performing electrocardiograms in the emergency department to diagnose chest pain; using electronic health records to organize and manage care; and, working with diabetics to control blood glucose levels.
Some notable improvements since the program's inception included a near doubling of the number of physicians reporting that they had talked with diabetic patients about eye-related complications – from 52% in 2007 to 93% in 2009. Also, beta-blockers were recommended to patients with left ventricular systolic dysfunction by 95% of reporting physicians in 2009, as compared to 64% in 2007.
The PQRS program will remain voluntary until 2015, when the Medicare program will start withholding payments for lack of participation.
The first year of the e-Prescribing program was 2009. That year, 48,354 physicians received an e-Prescribing incentive payment, with an average payment of $3,000 per individual and $14,501 per practice.
The deadline for participation in the e-Prescribing program is much sooner than that for the PQRS program. Physicians will see pay reductions beginning in 2012 if they don't participate in ePrescribing.
Enrollment Lags for Pre-Existing Condition Insurance Plan
A federal program to help people with pre-existing conditions obtain health insurance has lagged in terms of the government's projected enrollment, which may be partly because it has largely gone unnoticed as one of the benefits of the health reform law.
The Pre-Existing Condition Insurance Plan (PCIP) was launched in July 2010 with $5 billion in funding from the Affordable Care Act. The goal is to provide an insurance option to people who may be barred from coverage or who have to pay huge surcharges because of a pre-existing condition such as hypercholesterolemia or cancer. The program will be in force until 2014, when the new insurance exchanges go into effect and insurers are prohibited from denying coverage to adults with pre-existing conditions.
Although the Department of Health and Human Services initially estimated that several hundred thousand people might benefit from the PCIP, as of early May only about 18,000 people had enrolled, according to the government's statistics.
In an interview, Richard Popper, director of insurance programs at the federal Center for Consumer Information and Insurance Oversight, would not comment on the number of enrollees. But he said that enrollment had been strongest in states with higher populations, such as Texas, California, Pennsylvania, and Illinois.
A “significant number” of patients with cancer, coronary artery disease, chronic obstructive pulmonary disease, and digestive system problems have accessed the program, he said. The average person who has enrolled has annual medical costs of $20,000 a year, he said.
To be eligible for the PCIP, an individual must have been without insurance for 6 months before enrollment. Mr. Popper said that because he was not working for DHHS at the time the Affordable Care Act was developed, he couldn't comment on the waiting period.
After that, the program varies according to whether it is administered by a state or the federal government, although there are minimum coverage criteria. Twenty-three states and the District of Columbia went with a federally run PCIP program, which is essentially the same as Blue Cross/Blue Shield's plan for federal employees. Twenty-seven states run their own programs.
Patients can apply at the federal government's website (www.pcip.gov
In all cases, the patient gets coverage immediately. There is no waiting period, and premiums will be the same as for a healthy person in the same age range.
At a meeting of the Association of Community Cancer Centers in March, Mr. Popper cited figures for the plan in Texas, which has a program that is operated by the federal government. For standard coverage, individuals could expect to pay from $174 to $557 monthly, depending on age, with a $2,000 deductible for medical care and a $500 deductible for medications. Higher benefit plans run $234-$749 for premiums, with $1,000 and $250 deductibles, respectively. There is also a health savings account option, with premiums of $181-$578 and a $2,500 deductible.
The out-of-pocket maximum that patients would pay under all plans is $5,950. There is no lifetime limit and no limit on physician visits or prescription drugs.
Relief in Rhode Island
At least one couple – Don and Renee Eddie of Rhode Island – has been thrilled to have stumbled upon the PCIP. The couple had been trying to stay insured over the last 6 years or so, through a patchwork of plans. They also have a son who is disabled.
Initially, they had family coverage through her teaching job, but after a series of back surgeries left her unable to work in 2004, she lost the coverage along with the job. Mr. Eddie had coverage through his workplace, Electric Boat, and when he retired in 2006, the Eddies elected a family plan through the company. But the premiums were $1,299 a month. “We did that for 18 months, and it was draining us,” said Ms. Eddie in an interview.
They found a discount insurance program; the premiums were cheap at $300 a month, but the coverage was paltry. After being left with a $587 bill for a blood test, the family decided to drop the plan. And then, in April 2010, Mr. Eddie complained of chest pain and was taken to the emergency department. Shortly thereafter he had two stents inserted and spent 4 days in intensive care. The bill came to $92,000.
Ms. Eddie went back to trying to find an affordable insurance plan for Mr. Eddie. A few months later, she read about the PCIP in an article in the Providence Journal.
Ms. Eddie applied, and in October her husband got coverage for $519 a month through Blue Cross of Rhode Island. The state runs its own plan, which has a $1,000 deductible. Mr. Eddie's premiums have risen this year, as he just turned 60, but they are still a relatively affordable $567, said Ms. Eddie.
His prescriptions, which include Plavix, simvastatin, and Crestor, are relatively affordable also, she said. The best part of the plan, according to Ms. Eddie, is the monthly call from a Blue Cross nurse coordinator to offer tips and to monitor his care. “It's the first time we've had anything like that, so that's a very nice component,” said Ms. Eddie.
A federal program to help people with pre-existing conditions obtain health insurance has lagged in terms of the government's projected enrollment, which may be partly because it has largely gone unnoticed as one of the benefits of the health reform law.
The Pre-Existing Condition Insurance Plan (PCIP) was launched in July 2010 with $5 billion in funding from the Affordable Care Act. The goal is to provide an insurance option to people who may be barred from coverage or who have to pay huge surcharges because of a pre-existing condition such as hypercholesterolemia or cancer. The program will be in force until 2014, when the new insurance exchanges go into effect and insurers are prohibited from denying coverage to adults with pre-existing conditions.
Although the Department of Health and Human Services initially estimated that several hundred thousand people might benefit from the PCIP, as of early May only about 18,000 people had enrolled, according to the government's statistics.
In an interview, Richard Popper, director of insurance programs at the federal Center for Consumer Information and Insurance Oversight, would not comment on the number of enrollees. But he said that enrollment had been strongest in states with higher populations, such as Texas, California, Pennsylvania, and Illinois.
A “significant number” of patients with cancer, coronary artery disease, chronic obstructive pulmonary disease, and digestive system problems have accessed the program, he said. The average person who has enrolled has annual medical costs of $20,000 a year, he said.
To be eligible for the PCIP, an individual must have been without insurance for 6 months before enrollment. Mr. Popper said that because he was not working for DHHS at the time the Affordable Care Act was developed, he couldn't comment on the waiting period.
After that, the program varies according to whether it is administered by a state or the federal government, although there are minimum coverage criteria. Twenty-three states and the District of Columbia went with a federally run PCIP program, which is essentially the same as Blue Cross/Blue Shield's plan for federal employees. Twenty-seven states run their own programs.
Patients can apply at the federal government's website (www.pcip.gov
In all cases, the patient gets coverage immediately. There is no waiting period, and premiums will be the same as for a healthy person in the same age range.
At a meeting of the Association of Community Cancer Centers in March, Mr. Popper cited figures for the plan in Texas, which has a program that is operated by the federal government. For standard coverage, individuals could expect to pay from $174 to $557 monthly, depending on age, with a $2,000 deductible for medical care and a $500 deductible for medications. Higher benefit plans run $234-$749 for premiums, with $1,000 and $250 deductibles, respectively. There is also a health savings account option, with premiums of $181-$578 and a $2,500 deductible.
The out-of-pocket maximum that patients would pay under all plans is $5,950. There is no lifetime limit and no limit on physician visits or prescription drugs.
Relief in Rhode Island
At least one couple – Don and Renee Eddie of Rhode Island – has been thrilled to have stumbled upon the PCIP. The couple had been trying to stay insured over the last 6 years or so, through a patchwork of plans. They also have a son who is disabled.
Initially, they had family coverage through her teaching job, but after a series of back surgeries left her unable to work in 2004, she lost the coverage along with the job. Mr. Eddie had coverage through his workplace, Electric Boat, and when he retired in 2006, the Eddies elected a family plan through the company. But the premiums were $1,299 a month. “We did that for 18 months, and it was draining us,” said Ms. Eddie in an interview.
They found a discount insurance program; the premiums were cheap at $300 a month, but the coverage was paltry. After being left with a $587 bill for a blood test, the family decided to drop the plan. And then, in April 2010, Mr. Eddie complained of chest pain and was taken to the emergency department. Shortly thereafter he had two stents inserted and spent 4 days in intensive care. The bill came to $92,000.
Ms. Eddie went back to trying to find an affordable insurance plan for Mr. Eddie. A few months later, she read about the PCIP in an article in the Providence Journal.
Ms. Eddie applied, and in October her husband got coverage for $519 a month through Blue Cross of Rhode Island. The state runs its own plan, which has a $1,000 deductible. Mr. Eddie's premiums have risen this year, as he just turned 60, but they are still a relatively affordable $567, said Ms. Eddie.
His prescriptions, which include Plavix, simvastatin, and Crestor, are relatively affordable also, she said. The best part of the plan, according to Ms. Eddie, is the monthly call from a Blue Cross nurse coordinator to offer tips and to monitor his care. “It's the first time we've had anything like that, so that's a very nice component,” said Ms. Eddie.
A federal program to help people with pre-existing conditions obtain health insurance has lagged in terms of the government's projected enrollment, which may be partly because it has largely gone unnoticed as one of the benefits of the health reform law.
The Pre-Existing Condition Insurance Plan (PCIP) was launched in July 2010 with $5 billion in funding from the Affordable Care Act. The goal is to provide an insurance option to people who may be barred from coverage or who have to pay huge surcharges because of a pre-existing condition such as hypercholesterolemia or cancer. The program will be in force until 2014, when the new insurance exchanges go into effect and insurers are prohibited from denying coverage to adults with pre-existing conditions.
Although the Department of Health and Human Services initially estimated that several hundred thousand people might benefit from the PCIP, as of early May only about 18,000 people had enrolled, according to the government's statistics.
In an interview, Richard Popper, director of insurance programs at the federal Center for Consumer Information and Insurance Oversight, would not comment on the number of enrollees. But he said that enrollment had been strongest in states with higher populations, such as Texas, California, Pennsylvania, and Illinois.
A “significant number” of patients with cancer, coronary artery disease, chronic obstructive pulmonary disease, and digestive system problems have accessed the program, he said. The average person who has enrolled has annual medical costs of $20,000 a year, he said.
To be eligible for the PCIP, an individual must have been without insurance for 6 months before enrollment. Mr. Popper said that because he was not working for DHHS at the time the Affordable Care Act was developed, he couldn't comment on the waiting period.
After that, the program varies according to whether it is administered by a state or the federal government, although there are minimum coverage criteria. Twenty-three states and the District of Columbia went with a federally run PCIP program, which is essentially the same as Blue Cross/Blue Shield's plan for federal employees. Twenty-seven states run their own programs.
Patients can apply at the federal government's website (www.pcip.gov
In all cases, the patient gets coverage immediately. There is no waiting period, and premiums will be the same as for a healthy person in the same age range.
At a meeting of the Association of Community Cancer Centers in March, Mr. Popper cited figures for the plan in Texas, which has a program that is operated by the federal government. For standard coverage, individuals could expect to pay from $174 to $557 monthly, depending on age, with a $2,000 deductible for medical care and a $500 deductible for medications. Higher benefit plans run $234-$749 for premiums, with $1,000 and $250 deductibles, respectively. There is also a health savings account option, with premiums of $181-$578 and a $2,500 deductible.
The out-of-pocket maximum that patients would pay under all plans is $5,950. There is no lifetime limit and no limit on physician visits or prescription drugs.
Relief in Rhode Island
At least one couple – Don and Renee Eddie of Rhode Island – has been thrilled to have stumbled upon the PCIP. The couple had been trying to stay insured over the last 6 years or so, through a patchwork of plans. They also have a son who is disabled.
Initially, they had family coverage through her teaching job, but after a series of back surgeries left her unable to work in 2004, she lost the coverage along with the job. Mr. Eddie had coverage through his workplace, Electric Boat, and when he retired in 2006, the Eddies elected a family plan through the company. But the premiums were $1,299 a month. “We did that for 18 months, and it was draining us,” said Ms. Eddie in an interview.
They found a discount insurance program; the premiums were cheap at $300 a month, but the coverage was paltry. After being left with a $587 bill for a blood test, the family decided to drop the plan. And then, in April 2010, Mr. Eddie complained of chest pain and was taken to the emergency department. Shortly thereafter he had two stents inserted and spent 4 days in intensive care. The bill came to $92,000.
Ms. Eddie went back to trying to find an affordable insurance plan for Mr. Eddie. A few months later, she read about the PCIP in an article in the Providence Journal.
Ms. Eddie applied, and in October her husband got coverage for $519 a month through Blue Cross of Rhode Island. The state runs its own plan, which has a $1,000 deductible. Mr. Eddie's premiums have risen this year, as he just turned 60, but they are still a relatively affordable $567, said Ms. Eddie.
His prescriptions, which include Plavix, simvastatin, and Crestor, are relatively affordable also, she said. The best part of the plan, according to Ms. Eddie, is the monthly call from a Blue Cross nurse coordinator to offer tips and to monitor his care. “It's the first time we've had anything like that, so that's a very nice component,” said Ms. Eddie.
Don't-Do Lists Aim to Improve Care, Cut Costs
Research among primary care physicians has outlined “Top 5” practices to avoid in order to deliver better quality, more cost-effective medical care.
For internists and family physicians, the top item on the not-to-do list: Don't do imaging for low-back pain within the first 6 weeks unless red flags are present. For pediatricians, the top quality-promoting, cost-reducing activity is: Don't prescribe antibiotics for pharyngitis unless the patient tests positive for streptococcus.
Working groups convened by the nonprofit National Physicians Alliance sought to find evidence-based activities that were common in primary care. To be included on the top 5 lists, the activities had to lead to significant health benefits, as well as reduce harms to patients and cut health care costs.
The top 5 practices that should be adopted by internists include:
▸ Don't do imaging for low-back pain within the first 6 weeks unless red flags are present.
▸ Don't obtain blood chemistry panels or urinalyses for screening in asymptomatic, healthy adults.
▸ Don't order annual electrocardiograms (ECG) or any other cardiac screening tests for asymptomatic, low-risk adults.
▸ Use only generic statins when initiating lipid-lowering drug therapy.
▸ Don't use dual-energy x-ray absorptiometry (DEXA) screening for osteoporosis in women under age 65 years or men under 70 years with no risk factors.
The top 5 not-to-do list for family physicians is similar, but not identical, and includes:
▸ Don't do imaging for low-back pain within the first 6 weeks unless red flags are present.
▸ Don't routinely prescribe antibiotics for acute mild to moderate sinusitis unless symptoms last for 7 days or more or symptoms worsen after initial clinical improvement
▸ Don't order annual ECG or any other cardiac screening for asymptomatic, low-risk adults.
▸ Don't perform Pap tests on patients younger than 21 years or in women status post hysterectomy for benign disease.
▸ Don't use DEXA screening for osteoporosis in women under age 65 years or men under 70 years with no risk factors.
For pediatricians, the top 5 quality-improving activities include:
▸ Don't prescribe antibiotics for pharyngitis unless the patient tests positive for streptococcus.
▸ Don't obtain diagnostic images for minor head injuries without loss of consciousness or other risk factors.
▸ Don't refer otitis media with effusion early in its course.
▸ Advise patients not to use cough and cold medications.
▸ Use inhaled corticosteroids to control asthma appropriately.
Consensus lists were drawn up by working group members and tested initially with 83 NPA physicians who rated the activity based on how often they engaged in the activity in their practice, its impact on quality of care and cost, the strength of the evidence supporting the activity, and how easy or hard it was to eliminate from their practice.
Field testing then was expanded through an invitation to all NPA members. There were 172 testers in the second round, all of whom completed the same surveys as the initial testers.
Field testing showed support for the evidence that backed the recommendations, and the ease with which they could be implemented, according to the study's authors in the Good Stewardship Working Group. However, they pointed out, field testing physicians might not be representative of all internists, family physicians, and pediatricians.
The authors pointed out that although the groups worked independently, several activities to avoid appeared on more than one list. “This commonality across specialties reinforced the importance and relevance of addressing overuse of these activities,” the authors said (Arch. Intern. Med. 2011[doi: 10.1001/archinternmed.2011.231]).
The NPA plans to distribute the top 5 lists to all its members who are internists, family physicians, and pediatricians. The organization also plans to create a virtual practice community to help members implement the recommendations. And it says it will create a training video that will teach physicians how to enlist their patients' support for the recommendations; another video will be created specifically to explain to patients the rationale behind the lists.
The NPA plans to seek endorsements from patient advocacy and patient safety groups to “help dispel the misconception that these clinical recommendations represent rationing and support the idea that often less is truly more.”
The project was funded by a grant from the American Board of Internal Medicine Foundation.
Research among primary care physicians has outlined “Top 5” practices to avoid in order to deliver better quality, more cost-effective medical care.
For internists and family physicians, the top item on the not-to-do list: Don't do imaging for low-back pain within the first 6 weeks unless red flags are present. For pediatricians, the top quality-promoting, cost-reducing activity is: Don't prescribe antibiotics for pharyngitis unless the patient tests positive for streptococcus.
Working groups convened by the nonprofit National Physicians Alliance sought to find evidence-based activities that were common in primary care. To be included on the top 5 lists, the activities had to lead to significant health benefits, as well as reduce harms to patients and cut health care costs.
The top 5 practices that should be adopted by internists include:
▸ Don't do imaging for low-back pain within the first 6 weeks unless red flags are present.
▸ Don't obtain blood chemistry panels or urinalyses for screening in asymptomatic, healthy adults.
▸ Don't order annual electrocardiograms (ECG) or any other cardiac screening tests for asymptomatic, low-risk adults.
▸ Use only generic statins when initiating lipid-lowering drug therapy.
▸ Don't use dual-energy x-ray absorptiometry (DEXA) screening for osteoporosis in women under age 65 years or men under 70 years with no risk factors.
The top 5 not-to-do list for family physicians is similar, but not identical, and includes:
▸ Don't do imaging for low-back pain within the first 6 weeks unless red flags are present.
▸ Don't routinely prescribe antibiotics for acute mild to moderate sinusitis unless symptoms last for 7 days or more or symptoms worsen after initial clinical improvement
▸ Don't order annual ECG or any other cardiac screening for asymptomatic, low-risk adults.
▸ Don't perform Pap tests on patients younger than 21 years or in women status post hysterectomy for benign disease.
▸ Don't use DEXA screening for osteoporosis in women under age 65 years or men under 70 years with no risk factors.
For pediatricians, the top 5 quality-improving activities include:
▸ Don't prescribe antibiotics for pharyngitis unless the patient tests positive for streptococcus.
▸ Don't obtain diagnostic images for minor head injuries without loss of consciousness or other risk factors.
▸ Don't refer otitis media with effusion early in its course.
▸ Advise patients not to use cough and cold medications.
▸ Use inhaled corticosteroids to control asthma appropriately.
Consensus lists were drawn up by working group members and tested initially with 83 NPA physicians who rated the activity based on how often they engaged in the activity in their practice, its impact on quality of care and cost, the strength of the evidence supporting the activity, and how easy or hard it was to eliminate from their practice.
Field testing then was expanded through an invitation to all NPA members. There were 172 testers in the second round, all of whom completed the same surveys as the initial testers.
Field testing showed support for the evidence that backed the recommendations, and the ease with which they could be implemented, according to the study's authors in the Good Stewardship Working Group. However, they pointed out, field testing physicians might not be representative of all internists, family physicians, and pediatricians.
The authors pointed out that although the groups worked independently, several activities to avoid appeared on more than one list. “This commonality across specialties reinforced the importance and relevance of addressing overuse of these activities,” the authors said (Arch. Intern. Med. 2011[doi: 10.1001/archinternmed.2011.231]).
The NPA plans to distribute the top 5 lists to all its members who are internists, family physicians, and pediatricians. The organization also plans to create a virtual practice community to help members implement the recommendations. And it says it will create a training video that will teach physicians how to enlist their patients' support for the recommendations; another video will be created specifically to explain to patients the rationale behind the lists.
The NPA plans to seek endorsements from patient advocacy and patient safety groups to “help dispel the misconception that these clinical recommendations represent rationing and support the idea that often less is truly more.”
The project was funded by a grant from the American Board of Internal Medicine Foundation.
Research among primary care physicians has outlined “Top 5” practices to avoid in order to deliver better quality, more cost-effective medical care.
For internists and family physicians, the top item on the not-to-do list: Don't do imaging for low-back pain within the first 6 weeks unless red flags are present. For pediatricians, the top quality-promoting, cost-reducing activity is: Don't prescribe antibiotics for pharyngitis unless the patient tests positive for streptococcus.
Working groups convened by the nonprofit National Physicians Alliance sought to find evidence-based activities that were common in primary care. To be included on the top 5 lists, the activities had to lead to significant health benefits, as well as reduce harms to patients and cut health care costs.
The top 5 practices that should be adopted by internists include:
▸ Don't do imaging for low-back pain within the first 6 weeks unless red flags are present.
▸ Don't obtain blood chemistry panels or urinalyses for screening in asymptomatic, healthy adults.
▸ Don't order annual electrocardiograms (ECG) or any other cardiac screening tests for asymptomatic, low-risk adults.
▸ Use only generic statins when initiating lipid-lowering drug therapy.
▸ Don't use dual-energy x-ray absorptiometry (DEXA) screening for osteoporosis in women under age 65 years or men under 70 years with no risk factors.
The top 5 not-to-do list for family physicians is similar, but not identical, and includes:
▸ Don't do imaging for low-back pain within the first 6 weeks unless red flags are present.
▸ Don't routinely prescribe antibiotics for acute mild to moderate sinusitis unless symptoms last for 7 days or more or symptoms worsen after initial clinical improvement
▸ Don't order annual ECG or any other cardiac screening for asymptomatic, low-risk adults.
▸ Don't perform Pap tests on patients younger than 21 years or in women status post hysterectomy for benign disease.
▸ Don't use DEXA screening for osteoporosis in women under age 65 years or men under 70 years with no risk factors.
For pediatricians, the top 5 quality-improving activities include:
▸ Don't prescribe antibiotics for pharyngitis unless the patient tests positive for streptococcus.
▸ Don't obtain diagnostic images for minor head injuries without loss of consciousness or other risk factors.
▸ Don't refer otitis media with effusion early in its course.
▸ Advise patients not to use cough and cold medications.
▸ Use inhaled corticosteroids to control asthma appropriately.
Consensus lists were drawn up by working group members and tested initially with 83 NPA physicians who rated the activity based on how often they engaged in the activity in their practice, its impact on quality of care and cost, the strength of the evidence supporting the activity, and how easy or hard it was to eliminate from their practice.
Field testing then was expanded through an invitation to all NPA members. There were 172 testers in the second round, all of whom completed the same surveys as the initial testers.
Field testing showed support for the evidence that backed the recommendations, and the ease with which they could be implemented, according to the study's authors in the Good Stewardship Working Group. However, they pointed out, field testing physicians might not be representative of all internists, family physicians, and pediatricians.
The authors pointed out that although the groups worked independently, several activities to avoid appeared on more than one list. “This commonality across specialties reinforced the importance and relevance of addressing overuse of these activities,” the authors said (Arch. Intern. Med. 2011[doi: 10.1001/archinternmed.2011.231]).
The NPA plans to distribute the top 5 lists to all its members who are internists, family physicians, and pediatricians. The organization also plans to create a virtual practice community to help members implement the recommendations. And it says it will create a training video that will teach physicians how to enlist their patients' support for the recommendations; another video will be created specifically to explain to patients the rationale behind the lists.
The NPA plans to seek endorsements from patient advocacy and patient safety groups to “help dispel the misconception that these clinical recommendations represent rationing and support the idea that often less is truly more.”
The project was funded by a grant from the American Board of Internal Medicine Foundation.
CMS Aims to Ease E-Prescribing Rules
The Centers for Medicare and Medicaid Services has proposed modifying e-prescribing rules so more physicians could claim exemptions from the criteria and therefore avoid being penalized in 2012.
In a conference call, agency officials said the change was in response to indications from providers and professional societies that many prescribers might not be able to meet the requirements of the current incentive program.
“Today's rule demonstrates that CMS is willing to work cooperatively with the medical professional community to encourage participation in electronic prescribing,” Dr. Patrick Conway, chief medical officer at CMS and director of the agency's Office of Clinical Standards and Quality, said in a statement.
“These proposed changes will continue to encourage adoption of electronic prescribing while acknowledging circumstances that may keep health professionals from realizing the full potential of these systems right away,” he said.
Under the current incentive program, eligible prescribers were due to get a 1% bonus payment for 2011 and 2012 and a 0.5% bonus in 2013. For prescribers who did not meet the criteria, there would be a penalty imposed in 2012. The penalty would escalate in 2013 and 2014.
The final Medicare Physician Fee Schedule for 2011 contains exceptions, along with two hardship exemptions. Practices are exempt if they are in a rural area without high-speed Internet access or an area without enough available pharmacies for electronic prescribing.
Under the proposed rule, prescribers who use certified EHRs can now claim this as a “qualified” e-prescribing system. The move was designed to more closely align the e-prescribing program with the program that offers incentives for meaningful use of EHRs.
The proposed rule would also create four additional hardship exemption categories. Prescribers would have to show that they have:
▸ Registered to participate in the Medicare or Medicaid EHR incentive program and have adopted certified EHR technology.
▸ An inability to electronically prescribe due to local, state, or federal law (this primarily applies to prescribing of narcotics).
▸ Very limited prescribing activity.
▸ Insufficient opportunities to report the electronic prescribing measure due to limitations on the measure's denominator.
Prescribers also would be granted an extension, until Oct. 1, 2011, to apply for the hardship exemption.
The Centers for Medicare and Medicaid Services has proposed modifying e-prescribing rules so more physicians could claim exemptions from the criteria and therefore avoid being penalized in 2012.
In a conference call, agency officials said the change was in response to indications from providers and professional societies that many prescribers might not be able to meet the requirements of the current incentive program.
“Today's rule demonstrates that CMS is willing to work cooperatively with the medical professional community to encourage participation in electronic prescribing,” Dr. Patrick Conway, chief medical officer at CMS and director of the agency's Office of Clinical Standards and Quality, said in a statement.
“These proposed changes will continue to encourage adoption of electronic prescribing while acknowledging circumstances that may keep health professionals from realizing the full potential of these systems right away,” he said.
Under the current incentive program, eligible prescribers were due to get a 1% bonus payment for 2011 and 2012 and a 0.5% bonus in 2013. For prescribers who did not meet the criteria, there would be a penalty imposed in 2012. The penalty would escalate in 2013 and 2014.
The final Medicare Physician Fee Schedule for 2011 contains exceptions, along with two hardship exemptions. Practices are exempt if they are in a rural area without high-speed Internet access or an area without enough available pharmacies for electronic prescribing.
Under the proposed rule, prescribers who use certified EHRs can now claim this as a “qualified” e-prescribing system. The move was designed to more closely align the e-prescribing program with the program that offers incentives for meaningful use of EHRs.
The proposed rule would also create four additional hardship exemption categories. Prescribers would have to show that they have:
▸ Registered to participate in the Medicare or Medicaid EHR incentive program and have adopted certified EHR technology.
▸ An inability to electronically prescribe due to local, state, or federal law (this primarily applies to prescribing of narcotics).
▸ Very limited prescribing activity.
▸ Insufficient opportunities to report the electronic prescribing measure due to limitations on the measure's denominator.
Prescribers also would be granted an extension, until Oct. 1, 2011, to apply for the hardship exemption.
The Centers for Medicare and Medicaid Services has proposed modifying e-prescribing rules so more physicians could claim exemptions from the criteria and therefore avoid being penalized in 2012.
In a conference call, agency officials said the change was in response to indications from providers and professional societies that many prescribers might not be able to meet the requirements of the current incentive program.
“Today's rule demonstrates that CMS is willing to work cooperatively with the medical professional community to encourage participation in electronic prescribing,” Dr. Patrick Conway, chief medical officer at CMS and director of the agency's Office of Clinical Standards and Quality, said in a statement.
“These proposed changes will continue to encourage adoption of electronic prescribing while acknowledging circumstances that may keep health professionals from realizing the full potential of these systems right away,” he said.
Under the current incentive program, eligible prescribers were due to get a 1% bonus payment for 2011 and 2012 and a 0.5% bonus in 2013. For prescribers who did not meet the criteria, there would be a penalty imposed in 2012. The penalty would escalate in 2013 and 2014.
The final Medicare Physician Fee Schedule for 2011 contains exceptions, along with two hardship exemptions. Practices are exempt if they are in a rural area without high-speed Internet access or an area without enough available pharmacies for electronic prescribing.
Under the proposed rule, prescribers who use certified EHRs can now claim this as a “qualified” e-prescribing system. The move was designed to more closely align the e-prescribing program with the program that offers incentives for meaningful use of EHRs.
The proposed rule would also create four additional hardship exemption categories. Prescribers would have to show that they have:
▸ Registered to participate in the Medicare or Medicaid EHR incentive program and have adopted certified EHR technology.
▸ An inability to electronically prescribe due to local, state, or federal law (this primarily applies to prescribing of narcotics).
▸ Very limited prescribing activity.
▸ Insufficient opportunities to report the electronic prescribing measure due to limitations on the measure's denominator.
Prescribers also would be granted an extension, until Oct. 1, 2011, to apply for the hardship exemption.
Policy & Practice : Want more health reform news? Subscribe to our podcast – search 'Policy & Practice' in the iTunes store
Cardiologists Top E-Prescribers
Cardiologists appear to be adopting electronic prescribing more readily than colleagues in other specialties, according to a report by the Surescripts e-prescribing network. The 49% of cardiologists using e-prescribing is ahead of family practitioners (47%) and internists (45%). Behind them, 38% of gastroenterologists and 36% of pediatricians are e-prescribing. About 36% of all office-based physicians were e-prescribing in 2010, and 1 in 10 prescriptions was delivered electronically in 2010, up from 1 in 18 in 2008. E-prescribing is being driven primarily by federal legislation, including health care reform, according to Surescripts.
Bill Would Protect Device Makers
A tort-reform bill that was passed by the House Energy and Commerce Committee in mid-May would exempt medical device makers from paying punitive damages in product liability suits, according to the Gray Sheet, which reports on the medical-device industry. The committee passed the Help Efficient, Accessible, Low-Cost, Timely Healthcare (HEALTH) Act of 2011 (H.R. 5) by a vote of 30-20, largely along party lines. The bill was introduced in January by Rep. Phil Gingrey (R-Ga.), who is a physician. Although Republicans and physicians' organizations have generally favored the bill, Democrats have objected to the exemptions for medical device and pharmaceutical manufacturers. The bill would place a $250,000 cap on noneconomic damages in malpractice cases and would require that most medical liability suits be filed within 3 years of an injury.
Heart Admissions Declined
Hospital admissions for top cardiovascular conditions declined among Medicare beneficiaries from 1998 to 2008, researchers at New York University and Yale University found. While overall Medicare admissions climbed from 11 million to 13 million during the decade, hospitalizations for heart failure, ischemic heart disease, and acute myocardial infarction went down 7%, 24%, and 13%, respectively. In contrast, admissions for cardiac arrhythmia increased 28%. The study was presented as a poster at an American Heart Association meeting in Washington.
Some Pacemakers Okay With MRI
Medicare has proposed ending its blanket ban on MRI in patients with implantable pacemakers. Device maker Medtronic had asked the agency to alter the policy after the company in February won Food and Drug Administration approval of a pacemaker that was designed for use with MRI. In a “Proposed Decision Memo,” the Centers for Medicare and Medicaid services said that “the evidence is adequate to conclude that magnetic resonance imaging (MRI) improves health outcomes for Medicare beneficiaries with implanted permanent pacemakers (PMs) when the PMs are used according to the FDA-approved labeling for use in an MRI environment.”
Heart Failure Certification Begins
The Joint Commission and the American Heart Association announced that their advanced certification program in heart failure will start next month. The program will focus on “safe, successful transitions of care” from inpatient to outpatient settings, according to an AHA statement. Programs seeking certification must have a hospital-based or outpatient heart failure clinic, a collaborative relationship with a cardiology practice, and proof of adherence to the AHA–American College of Cardiology guidelines on diagnosis and management of heart failure. “By achieving advanced certification in heart failure, programs will have demonstrated their commitment to consistently delivering reliable, effective and high quality care to their heart failure patients,” said Dr. Gregg C. Fonarow, who led the AHA's guidelines committee.
CME-Funding Dilemma Persists
Although physicians and other medical professionals say they're concerned that commercial funding of continuing medical education may bias the information provided, most are not willing to pay more to offset or eliminate such funding, a study in Archives of Internal Medicine shows. Researchers surveyed 770 physicians, nurses, nurse practitioners, and physician assistants at CME sessions and found that the vast majority (88%) said that commercial support of CME introduces bias. They also said that the greater the financial support, the greater the bias. However, only 15% would eliminate commercial support from CME activities and only 42% said they were willing to pay more in an effort to cut industry financial involvement. Most CME participants also significantly underestimated the amount of commercial funding for their courses, the authors wrote, adding that “the dilemma remains of how to provide quality CME either with [alternative funding] or at reduced cost.”
Uninsured Can't Afford Hospitals
Few families that lack health insurance hold the financial assets that would be necessary to pay potential hospital bills, according to a report from the DHHS. Each year, nearly 2 million uninsured Americans are hospitalized, and 58% of the resulting bills total more than $10,000 each. On average, uninsured families can afford to pay only about 12% of potential hospital stays in full, and even families of four making up to $89,400 per year – four times the federal poverty level – would be unable to pay for most hospitalizations, HHS found. About 50 million Americans are uninsured, and their median family financial assets are about $20, the report said.
State Smoke-Free Laws Jump
More than half the states now prohibit smoking in indoor work areas, restaurants, and bars, an increase from zero states in 2000, according to the Centers for Disease Control and Prevention. However, regional disparities persist, especially in the South, where no state has adopted a law that prohibits smoking in all three venues, the CDC said. It's still possible for the United States to reach the Healthy People 2000 target of smoke-free indoor work sites in all 50 states by 2020, the report said. “Tremendous progress has been made during the past decade to protect workers and patrons from the hazardous effects of secondhand smoke,” the American Cancer Society Cancer Action Network said in a statement, but the organization called for more states to act quickly.
Cardiologists Top E-Prescribers
Cardiologists appear to be adopting electronic prescribing more readily than colleagues in other specialties, according to a report by the Surescripts e-prescribing network. The 49% of cardiologists using e-prescribing is ahead of family practitioners (47%) and internists (45%). Behind them, 38% of gastroenterologists and 36% of pediatricians are e-prescribing. About 36% of all office-based physicians were e-prescribing in 2010, and 1 in 10 prescriptions was delivered electronically in 2010, up from 1 in 18 in 2008. E-prescribing is being driven primarily by federal legislation, including health care reform, according to Surescripts.
Bill Would Protect Device Makers
A tort-reform bill that was passed by the House Energy and Commerce Committee in mid-May would exempt medical device makers from paying punitive damages in product liability suits, according to the Gray Sheet, which reports on the medical-device industry. The committee passed the Help Efficient, Accessible, Low-Cost, Timely Healthcare (HEALTH) Act of 2011 (H.R. 5) by a vote of 30-20, largely along party lines. The bill was introduced in January by Rep. Phil Gingrey (R-Ga.), who is a physician. Although Republicans and physicians' organizations have generally favored the bill, Democrats have objected to the exemptions for medical device and pharmaceutical manufacturers. The bill would place a $250,000 cap on noneconomic damages in malpractice cases and would require that most medical liability suits be filed within 3 years of an injury.
Heart Admissions Declined
Hospital admissions for top cardiovascular conditions declined among Medicare beneficiaries from 1998 to 2008, researchers at New York University and Yale University found. While overall Medicare admissions climbed from 11 million to 13 million during the decade, hospitalizations for heart failure, ischemic heart disease, and acute myocardial infarction went down 7%, 24%, and 13%, respectively. In contrast, admissions for cardiac arrhythmia increased 28%. The study was presented as a poster at an American Heart Association meeting in Washington.
Some Pacemakers Okay With MRI
Medicare has proposed ending its blanket ban on MRI in patients with implantable pacemakers. Device maker Medtronic had asked the agency to alter the policy after the company in February won Food and Drug Administration approval of a pacemaker that was designed for use with MRI. In a “Proposed Decision Memo,” the Centers for Medicare and Medicaid services said that “the evidence is adequate to conclude that magnetic resonance imaging (MRI) improves health outcomes for Medicare beneficiaries with implanted permanent pacemakers (PMs) when the PMs are used according to the FDA-approved labeling for use in an MRI environment.”
Heart Failure Certification Begins
The Joint Commission and the American Heart Association announced that their advanced certification program in heart failure will start next month. The program will focus on “safe, successful transitions of care” from inpatient to outpatient settings, according to an AHA statement. Programs seeking certification must have a hospital-based or outpatient heart failure clinic, a collaborative relationship with a cardiology practice, and proof of adherence to the AHA–American College of Cardiology guidelines on diagnosis and management of heart failure. “By achieving advanced certification in heart failure, programs will have demonstrated their commitment to consistently delivering reliable, effective and high quality care to their heart failure patients,” said Dr. Gregg C. Fonarow, who led the AHA's guidelines committee.
CME-Funding Dilemma Persists
Although physicians and other medical professionals say they're concerned that commercial funding of continuing medical education may bias the information provided, most are not willing to pay more to offset or eliminate such funding, a study in Archives of Internal Medicine shows. Researchers surveyed 770 physicians, nurses, nurse practitioners, and physician assistants at CME sessions and found that the vast majority (88%) said that commercial support of CME introduces bias. They also said that the greater the financial support, the greater the bias. However, only 15% would eliminate commercial support from CME activities and only 42% said they were willing to pay more in an effort to cut industry financial involvement. Most CME participants also significantly underestimated the amount of commercial funding for their courses, the authors wrote, adding that “the dilemma remains of how to provide quality CME either with [alternative funding] or at reduced cost.”
Uninsured Can't Afford Hospitals
Few families that lack health insurance hold the financial assets that would be necessary to pay potential hospital bills, according to a report from the DHHS. Each year, nearly 2 million uninsured Americans are hospitalized, and 58% of the resulting bills total more than $10,000 each. On average, uninsured families can afford to pay only about 12% of potential hospital stays in full, and even families of four making up to $89,400 per year – four times the federal poverty level – would be unable to pay for most hospitalizations, HHS found. About 50 million Americans are uninsured, and their median family financial assets are about $20, the report said.
State Smoke-Free Laws Jump
More than half the states now prohibit smoking in indoor work areas, restaurants, and bars, an increase from zero states in 2000, according to the Centers for Disease Control and Prevention. However, regional disparities persist, especially in the South, where no state has adopted a law that prohibits smoking in all three venues, the CDC said. It's still possible for the United States to reach the Healthy People 2000 target of smoke-free indoor work sites in all 50 states by 2020, the report said. “Tremendous progress has been made during the past decade to protect workers and patrons from the hazardous effects of secondhand smoke,” the American Cancer Society Cancer Action Network said in a statement, but the organization called for more states to act quickly.
Cardiologists Top E-Prescribers
Cardiologists appear to be adopting electronic prescribing more readily than colleagues in other specialties, according to a report by the Surescripts e-prescribing network. The 49% of cardiologists using e-prescribing is ahead of family practitioners (47%) and internists (45%). Behind them, 38% of gastroenterologists and 36% of pediatricians are e-prescribing. About 36% of all office-based physicians were e-prescribing in 2010, and 1 in 10 prescriptions was delivered electronically in 2010, up from 1 in 18 in 2008. E-prescribing is being driven primarily by federal legislation, including health care reform, according to Surescripts.
Bill Would Protect Device Makers
A tort-reform bill that was passed by the House Energy and Commerce Committee in mid-May would exempt medical device makers from paying punitive damages in product liability suits, according to the Gray Sheet, which reports on the medical-device industry. The committee passed the Help Efficient, Accessible, Low-Cost, Timely Healthcare (HEALTH) Act of 2011 (H.R. 5) by a vote of 30-20, largely along party lines. The bill was introduced in January by Rep. Phil Gingrey (R-Ga.), who is a physician. Although Republicans and physicians' organizations have generally favored the bill, Democrats have objected to the exemptions for medical device and pharmaceutical manufacturers. The bill would place a $250,000 cap on noneconomic damages in malpractice cases and would require that most medical liability suits be filed within 3 years of an injury.
Heart Admissions Declined
Hospital admissions for top cardiovascular conditions declined among Medicare beneficiaries from 1998 to 2008, researchers at New York University and Yale University found. While overall Medicare admissions climbed from 11 million to 13 million during the decade, hospitalizations for heart failure, ischemic heart disease, and acute myocardial infarction went down 7%, 24%, and 13%, respectively. In contrast, admissions for cardiac arrhythmia increased 28%. The study was presented as a poster at an American Heart Association meeting in Washington.
Some Pacemakers Okay With MRI
Medicare has proposed ending its blanket ban on MRI in patients with implantable pacemakers. Device maker Medtronic had asked the agency to alter the policy after the company in February won Food and Drug Administration approval of a pacemaker that was designed for use with MRI. In a “Proposed Decision Memo,” the Centers for Medicare and Medicaid services said that “the evidence is adequate to conclude that magnetic resonance imaging (MRI) improves health outcomes for Medicare beneficiaries with implanted permanent pacemakers (PMs) when the PMs are used according to the FDA-approved labeling for use in an MRI environment.”
Heart Failure Certification Begins
The Joint Commission and the American Heart Association announced that their advanced certification program in heart failure will start next month. The program will focus on “safe, successful transitions of care” from inpatient to outpatient settings, according to an AHA statement. Programs seeking certification must have a hospital-based or outpatient heart failure clinic, a collaborative relationship with a cardiology practice, and proof of adherence to the AHA–American College of Cardiology guidelines on diagnosis and management of heart failure. “By achieving advanced certification in heart failure, programs will have demonstrated their commitment to consistently delivering reliable, effective and high quality care to their heart failure patients,” said Dr. Gregg C. Fonarow, who led the AHA's guidelines committee.
CME-Funding Dilemma Persists
Although physicians and other medical professionals say they're concerned that commercial funding of continuing medical education may bias the information provided, most are not willing to pay more to offset or eliminate such funding, a study in Archives of Internal Medicine shows. Researchers surveyed 770 physicians, nurses, nurse practitioners, and physician assistants at CME sessions and found that the vast majority (88%) said that commercial support of CME introduces bias. They also said that the greater the financial support, the greater the bias. However, only 15% would eliminate commercial support from CME activities and only 42% said they were willing to pay more in an effort to cut industry financial involvement. Most CME participants also significantly underestimated the amount of commercial funding for their courses, the authors wrote, adding that “the dilemma remains of how to provide quality CME either with [alternative funding] or at reduced cost.”
Uninsured Can't Afford Hospitals
Few families that lack health insurance hold the financial assets that would be necessary to pay potential hospital bills, according to a report from the DHHS. Each year, nearly 2 million uninsured Americans are hospitalized, and 58% of the resulting bills total more than $10,000 each. On average, uninsured families can afford to pay only about 12% of potential hospital stays in full, and even families of four making up to $89,400 per year – four times the federal poverty level – would be unable to pay for most hospitalizations, HHS found. About 50 million Americans are uninsured, and their median family financial assets are about $20, the report said.
State Smoke-Free Laws Jump
More than half the states now prohibit smoking in indoor work areas, restaurants, and bars, an increase from zero states in 2000, according to the Centers for Disease Control and Prevention. However, regional disparities persist, especially in the South, where no state has adopted a law that prohibits smoking in all three venues, the CDC said. It's still possible for the United States to reach the Healthy People 2000 target of smoke-free indoor work sites in all 50 states by 2020, the report said. “Tremendous progress has been made during the past decade to protect workers and patrons from the hazardous effects of secondhand smoke,” the American Cancer Society Cancer Action Network said in a statement, but the organization called for more states to act quickly.