User login
Meaningful Use Gets Mixed Reviews From Users
Many physicians are frustrated and confused by the meaningful use criteria that spell out how they can receive incentive payments from Medicare and Medicaid for their use of electronic health records.
With that uncertainty, physicians are not jumping in with both feet to participate in the incentive program, even if they have purchased EHR systems. The Medical Group Management Association (MGMA), in an April survey of its members, found that 80% of those who had adopted an EHR system intended to participate. But at that time, only 14% said they were able to meet all the criteria.
The American Medical Association held a special session on meaningful use at its House of Delegates meeting in June. When Dr. Michael L. Hodgkins, AMA chief medical information officer, asked how many physicians were confused about what was expected of them, more than half raised their hands.
Physicians in smaller practices are especially challenged, Dr. Hodgkins said, citing data that some 300,000 doctors are in practices of 10 or fewer physicians. Among those, fewer than 15% have implemented an EHR system, and most are not yet capable of meeting the meaningful use criteria.
According to Dr. Hodgkins, there are many obstacles to meeting meaningful use, including selecting from the more than 400 EHR products certified by the federal Office of the National Coordinator (ONC) for Health Information Technology, part of the Health and Human Services department.
Another problem: “Aggressive” timelines set by the government, according to Dr. Steve Waldren, director of the Center for Health Information Technology at the American Academy of Family Physicians (AAFP). He says it takes 6-18 months from purchase to active meaningful use of a system.
It's been a tough road, he said. Physicians who don't have EHRs or who have just gotten on board are struggling to get them operational and to achieve meaningful use. Those who have owned systems for awhile may face upgrades to meet the meaningful use criteria.
Meanwhile, there's the system's financial cost, its training and maintenance issues, and workflow changes once a system is in place.
The Long-Time User
Some physicians aren't in a panic about the impending deadlines. Dr. Michael Mirro of Ft. Wayne (Ind.) Cardiology, a 24-physician group, said his practice has been using health IT since 1996.
“We knew that we had to ultimately modernize our practice,” Dr. Mirro said in an interview. Their current system has improved efficiency and quality, and has “supported a higher level of coding and reimbursement.”
The system has “pretty much complete functionality,” said Dr. Mirro. It provides the EHR, offers e-prescribing and decision-support tools, and can be used for direct quality reporting to the American College of Cardiology's PINNACLE registry.
The system is Web based, which reduces maintenance costs and IT headaches. The practice does not own the servers; it has local computers that interact with the vendor's servers and software. The system is certified by the Certification Commission for Health Information Technology and was updated to ensure that the practice would meet the meaningful use criteria. One helpful tool, according to Dr. Mirro: A meaningful use “meter” that tells the physicians how well they are meeting the goals.
Ft. Wayne Cardiology has already attested to the government that it was a meaningful user and has received the maximum $18,000 per physician incentive for 2011, Dr. Mirro said.
The annual cost is about $2,000 per physician per year. That's low, said Dr. Mirro, because his practice is owned by a hospital. The system is already ahead of the curve, as it already incorporates a patient Web portal (a stage 2 goal).
He said that he is sympathetic to physicians who are just getting started. “Any time you adopt technology at the point of care, it's going to require a change in workflow,” he said. That was definitely the case at Ft. Wayne Cardiology.
Dr. Mirro said that physicians looking to buy or expand their health IT should talk with one of the 60 regional extension centers established by the ONC. These centers have been charged to help rural and primary care physicians especially. They offer vendor recommendations, practice audits, and other advice for free.
A Model for Her Peers
In 2005, Dr. Jennifer Brull figured that she needed to get on board with health IT, even though it might be expensive and difficult for a family physician in a rural Kansas solo practice. A younger physician with whom she was collaborating suggested that having an EHR was the wave of the future, and would likely be a necessity going forward. She also had a practice-sharing arrangement with another physician, who was older. He was not as sure, Dr. Brull said in an interview.
But they moved ahead and spent 3 years selecting, buying, and implementing an EHR system that they could all use, said Dr. Brull, who practices in Plainview. She took out a loan for $50,000 to buy the equipment; her colleagues contributed to the software and other costs.
Because they practice in a rural area, there was no possibility of using a Web-based model; broadband access in her area is still not robust enough, said Dr. Brull. So she has a server onsite at her office, and recently purchased a second server for $3,000. The net cost so far has been about $30,000 per physician, Dr. Brull said.
The first 6 months were a challenge, she said. “Anytime you do something that's a complete paradigm shift, it's hard. It's hard mentally to think about all those changes, hard physically because you're investing more time and effort, and hard emotionally because your staff gets freaked out.”
In addition to allowing the practice to meet meaningful use criteria, the system also has a patient portal. The physicians are preparing to be able to participate in the state's health information exchange.
Dr. Brull said that she disagrees with physicians who say that adopting an EHR interrupts the workflow or comes between the physician and patient.
“I've found it easier to be more collaborative [with my patients],” she said. One example: She recently used an EHR-generated graph to show a patient that she had gained 40 pounds over 3 years. The graph made much more of an impression on the patient than Dr. Brull could have done by reading numbers off a paper chart, she said.
“This whole project has resulted in dramatic quality improvement for my practice,” Dr. Brull added. Another example: She implemented a quality measure on breast cancer screening. Just by having a flag in the EHR, she went from screening 50% of patients to almost 100%. “Having the data at your fingertips makes you aware of where you do a good job and where you don't,” Dr. Brull said.
In April, Dr. Brull collected the full Medicare incentive payment for 2011. Her colleagues weren't ready, but that didn't matter. Physicians can choose to attest to meaningful use on their own time frame, regardless of where their colleagues might be, she said.
Dr. Brull has become an evangelist for the power of the EHR and meaningful use. She was chosen to speak at a CMS press conference announcing the first round of Medicare incentive payments. And she is a member of the regional extension center in Kansas. The ONC also named her a “MUVer” – someone who serves as a local leader and adviser.
The Reluctant Adopter
Dr. Michael Machen is one of the physicians who consulted with Dr. Brull. He practices with four other family physicians in nearby Quinter, Kan. (population, 980). The impetus for taking on an EHR came from his younger partners, Dr. Machen said in an interview. They were also motivated by the meaningful use program, and got started in July 2010.
One junior partner became the EHR champion, doing much of the legwork to find appropriate vendors and systems. The physicians also attended seminars and webinars offered by the Kansas Medical Society and the Kansas chapter of the AAFP. A team from the regional extension center visited their practice too, Dr. Machen said.
They borrowed $75,000 to purchase hardware and software. The biggest cost is the $2,000-$4,000 they spend monthly on IT support – a necessity when there is no one with such expertise in the practice or locally. The IT help comes from more than an hour away. Dr. Machen and his colleagues house the server themselves; broadband is no better in Quinter than it is in Plainview.
Dr. Machen said that the younger physicians have all done well with the system, but he is struggling.
“I'm not technically inclined, and I have very little computer knowledge,” he said. It has also been difficult for his nurse, who is spending more time on data entry and less on interacting with patients, Dr. Machen said, adding that they are both in their late 50s and are more frustrated with the system than are their younger colleagues.
His staff has been happy; there's no more searching for charts, and coding is easier, he said. And he does see the potential for improving quality, especially with the data-collection effort, warnings about drug interactions, and prompts for screening tests.
But for now, “it's horrible with the workflow and the patient flow.” On days of 15-20 patient visits, using the EHR is not as much of an issue. But on days of 30 patient visits, “it's not doable,” he said.
So far, patients haven't been wild about the transition, either. They don't like the physician to be working on a computer during the visit, he said. And “I don't like it much, either,” said Dr. Machen. “When I was in medical school, I was taught that the second you enter the exam room, the patient has your undivided attention.” That's not really possible with an EHR, at least the way he sees it currently, although he also can see possible solutions, such as having a scribe.
{kind=link}
Source Elsevier Global Medical News
Making Sense of Meaningful Use: How, Where, and When
The ONC provides the central leadership for the Medicare and Medicaid EHR incentive programs. The HITECH (Health Information Technology for Economic and Clinical Health) Act directly appropriated $2 billion to the ONC to spend on incentives and administration of the program. The federal regulation governing the incentive program (some 800 pages) was issued in July 2010.
This year – 2011 – is the first year in which physicians can participate; they have until Oct. 1 to attest that they are meaningful users. To be eligible for incentive payments, physicians have to meet the meaningful use criteria for 90 consecutive days.
The criteria are being introduced in stages over the next 4-5 years. Stage 1 outlines what is expected in 2011 and 2012. Stage 2 was expected to be put into place in 2013, but in June, the Health IT Policy Committee of the Centers for Medicare and Medicaid Services voted to delay implementation until 2014, but only for physicians who were already participating.
Physicians who wait until 2012 or later would still be expected to meet stage 2 criteria in 2013.
Physicians who want to participate have to choose between the Medicare or Medicaid incentive program.
Those who take part in the Medicare program are eligible to receive incentive payments of $44,000 over 5 years. However, the payments will be made only through 2016. Physicians who wait until 2012 to start would still earn the $44,000 maximum; those who start later would receive prorated payments.
Physicians who practice in designated Health Professional Shortage Areas (HPSA) may be eligible for an additional 10% in each year's incentive payment.
Importantly, Medicare begins to penalize nonparticipating physicians starting in 2016.
The Medicaid incentives are more generous: A total of $63,750 can be paid out over 6 years. And there's a longer time frame. Eligible professionals can wait until 2016 to start participating and still receive the maximum payout over a 6-year period.
In late May, the CMS announced that $75 million in Medicare incentives had been awarded to physicians and hospitals in the first 2 weeks of the program. Some states began paying out Medicaid incentives in January. By late May, $83 million had been issued.
Meaningful use of EHRs is critical, according to Dr. Farzad Mostashari, the national coordinator, who testified to the House Small Business Committee's Subcommittee on Healthcare and Technology in June.
“If all we do is put an EHR in every provider's office or hospital, we will have failed to realize health IT's full potential,” he said. “Instead, doctors, hospitals, and other providers need to use robust EHR technology in a meaningful and interoperable way to improve care.”
Many physicians are frustrated and confused by the meaningful use criteria that spell out how they can receive incentive payments from Medicare and Medicaid for their use of electronic health records.
With that uncertainty, physicians are not jumping in with both feet to participate in the incentive program, even if they have purchased EHR systems. The Medical Group Management Association (MGMA), in an April survey of its members, found that 80% of those who had adopted an EHR system intended to participate. But at that time, only 14% said they were able to meet all the criteria.
The American Medical Association held a special session on meaningful use at its House of Delegates meeting in June. When Dr. Michael L. Hodgkins, AMA chief medical information officer, asked how many physicians were confused about what was expected of them, more than half raised their hands.
Physicians in smaller practices are especially challenged, Dr. Hodgkins said, citing data that some 300,000 doctors are in practices of 10 or fewer physicians. Among those, fewer than 15% have implemented an EHR system, and most are not yet capable of meeting the meaningful use criteria.
According to Dr. Hodgkins, there are many obstacles to meeting meaningful use, including selecting from the more than 400 EHR products certified by the federal Office of the National Coordinator (ONC) for Health Information Technology, part of the Health and Human Services department.
Another problem: “Aggressive” timelines set by the government, according to Dr. Steve Waldren, director of the Center for Health Information Technology at the American Academy of Family Physicians (AAFP). He says it takes 6-18 months from purchase to active meaningful use of a system.
It's been a tough road, he said. Physicians who don't have EHRs or who have just gotten on board are struggling to get them operational and to achieve meaningful use. Those who have owned systems for awhile may face upgrades to meet the meaningful use criteria.
Meanwhile, there's the system's financial cost, its training and maintenance issues, and workflow changes once a system is in place.
The Long-Time User
Some physicians aren't in a panic about the impending deadlines. Dr. Michael Mirro of Ft. Wayne (Ind.) Cardiology, a 24-physician group, said his practice has been using health IT since 1996.
“We knew that we had to ultimately modernize our practice,” Dr. Mirro said in an interview. Their current system has improved efficiency and quality, and has “supported a higher level of coding and reimbursement.”
The system has “pretty much complete functionality,” said Dr. Mirro. It provides the EHR, offers e-prescribing and decision-support tools, and can be used for direct quality reporting to the American College of Cardiology's PINNACLE registry.
The system is Web based, which reduces maintenance costs and IT headaches. The practice does not own the servers; it has local computers that interact with the vendor's servers and software. The system is certified by the Certification Commission for Health Information Technology and was updated to ensure that the practice would meet the meaningful use criteria. One helpful tool, according to Dr. Mirro: A meaningful use “meter” that tells the physicians how well they are meeting the goals.
Ft. Wayne Cardiology has already attested to the government that it was a meaningful user and has received the maximum $18,000 per physician incentive for 2011, Dr. Mirro said.
The annual cost is about $2,000 per physician per year. That's low, said Dr. Mirro, because his practice is owned by a hospital. The system is already ahead of the curve, as it already incorporates a patient Web portal (a stage 2 goal).
He said that he is sympathetic to physicians who are just getting started. “Any time you adopt technology at the point of care, it's going to require a change in workflow,” he said. That was definitely the case at Ft. Wayne Cardiology.
Dr. Mirro said that physicians looking to buy or expand their health IT should talk with one of the 60 regional extension centers established by the ONC. These centers have been charged to help rural and primary care physicians especially. They offer vendor recommendations, practice audits, and other advice for free.
A Model for Her Peers
In 2005, Dr. Jennifer Brull figured that she needed to get on board with health IT, even though it might be expensive and difficult for a family physician in a rural Kansas solo practice. A younger physician with whom she was collaborating suggested that having an EHR was the wave of the future, and would likely be a necessity going forward. She also had a practice-sharing arrangement with another physician, who was older. He was not as sure, Dr. Brull said in an interview.
But they moved ahead and spent 3 years selecting, buying, and implementing an EHR system that they could all use, said Dr. Brull, who practices in Plainview. She took out a loan for $50,000 to buy the equipment; her colleagues contributed to the software and other costs.
Because they practice in a rural area, there was no possibility of using a Web-based model; broadband access in her area is still not robust enough, said Dr. Brull. So she has a server onsite at her office, and recently purchased a second server for $3,000. The net cost so far has been about $30,000 per physician, Dr. Brull said.
The first 6 months were a challenge, she said. “Anytime you do something that's a complete paradigm shift, it's hard. It's hard mentally to think about all those changes, hard physically because you're investing more time and effort, and hard emotionally because your staff gets freaked out.”
In addition to allowing the practice to meet meaningful use criteria, the system also has a patient portal. The physicians are preparing to be able to participate in the state's health information exchange.
Dr. Brull said that she disagrees with physicians who say that adopting an EHR interrupts the workflow or comes between the physician and patient.
“I've found it easier to be more collaborative [with my patients],” she said. One example: She recently used an EHR-generated graph to show a patient that she had gained 40 pounds over 3 years. The graph made much more of an impression on the patient than Dr. Brull could have done by reading numbers off a paper chart, she said.
“This whole project has resulted in dramatic quality improvement for my practice,” Dr. Brull added. Another example: She implemented a quality measure on breast cancer screening. Just by having a flag in the EHR, she went from screening 50% of patients to almost 100%. “Having the data at your fingertips makes you aware of where you do a good job and where you don't,” Dr. Brull said.
In April, Dr. Brull collected the full Medicare incentive payment for 2011. Her colleagues weren't ready, but that didn't matter. Physicians can choose to attest to meaningful use on their own time frame, regardless of where their colleagues might be, she said.
Dr. Brull has become an evangelist for the power of the EHR and meaningful use. She was chosen to speak at a CMS press conference announcing the first round of Medicare incentive payments. And she is a member of the regional extension center in Kansas. The ONC also named her a “MUVer” – someone who serves as a local leader and adviser.
The Reluctant Adopter
Dr. Michael Machen is one of the physicians who consulted with Dr. Brull. He practices with four other family physicians in nearby Quinter, Kan. (population, 980). The impetus for taking on an EHR came from his younger partners, Dr. Machen said in an interview. They were also motivated by the meaningful use program, and got started in July 2010.
One junior partner became the EHR champion, doing much of the legwork to find appropriate vendors and systems. The physicians also attended seminars and webinars offered by the Kansas Medical Society and the Kansas chapter of the AAFP. A team from the regional extension center visited their practice too, Dr. Machen said.
They borrowed $75,000 to purchase hardware and software. The biggest cost is the $2,000-$4,000 they spend monthly on IT support – a necessity when there is no one with such expertise in the practice or locally. The IT help comes from more than an hour away. Dr. Machen and his colleagues house the server themselves; broadband is no better in Quinter than it is in Plainview.
Dr. Machen said that the younger physicians have all done well with the system, but he is struggling.
“I'm not technically inclined, and I have very little computer knowledge,” he said. It has also been difficult for his nurse, who is spending more time on data entry and less on interacting with patients, Dr. Machen said, adding that they are both in their late 50s and are more frustrated with the system than are their younger colleagues.
His staff has been happy; there's no more searching for charts, and coding is easier, he said. And he does see the potential for improving quality, especially with the data-collection effort, warnings about drug interactions, and prompts for screening tests.
But for now, “it's horrible with the workflow and the patient flow.” On days of 15-20 patient visits, using the EHR is not as much of an issue. But on days of 30 patient visits, “it's not doable,” he said.
So far, patients haven't been wild about the transition, either. They don't like the physician to be working on a computer during the visit, he said. And “I don't like it much, either,” said Dr. Machen. “When I was in medical school, I was taught that the second you enter the exam room, the patient has your undivided attention.” That's not really possible with an EHR, at least the way he sees it currently, although he also can see possible solutions, such as having a scribe.
Source Elsevier Global Medical News
Making Sense of Meaningful Use: How, Where, and When
The ONC provides the central leadership for the Medicare and Medicaid EHR incentive programs. The HITECH (Health Information Technology for Economic and Clinical Health) Act directly appropriated $2 billion to the ONC to spend on incentives and administration of the program. The federal regulation governing the incentive program (some 800 pages) was issued in July 2010.
This year – 2011 – is the first year in which physicians can participate; they have until Oct. 1 to attest that they are meaningful users. To be eligible for incentive payments, physicians have to meet the meaningful use criteria for 90 consecutive days.
The criteria are being introduced in stages over the next 4-5 years. Stage 1 outlines what is expected in 2011 and 2012. Stage 2 was expected to be put into place in 2013, but in June, the Health IT Policy Committee of the Centers for Medicare and Medicaid Services voted to delay implementation until 2014, but only for physicians who were already participating.
Physicians who wait until 2012 or later would still be expected to meet stage 2 criteria in 2013.
Physicians who want to participate have to choose between the Medicare or Medicaid incentive program.
Those who take part in the Medicare program are eligible to receive incentive payments of $44,000 over 5 years. However, the payments will be made only through 2016. Physicians who wait until 2012 to start would still earn the $44,000 maximum; those who start later would receive prorated payments.
Physicians who practice in designated Health Professional Shortage Areas (HPSA) may be eligible for an additional 10% in each year's incentive payment.
Importantly, Medicare begins to penalize nonparticipating physicians starting in 2016.
The Medicaid incentives are more generous: A total of $63,750 can be paid out over 6 years. And there's a longer time frame. Eligible professionals can wait until 2016 to start participating and still receive the maximum payout over a 6-year period.
In late May, the CMS announced that $75 million in Medicare incentives had been awarded to physicians and hospitals in the first 2 weeks of the program. Some states began paying out Medicaid incentives in January. By late May, $83 million had been issued.
Meaningful use of EHRs is critical, according to Dr. Farzad Mostashari, the national coordinator, who testified to the House Small Business Committee's Subcommittee on Healthcare and Technology in June.
“If all we do is put an EHR in every provider's office or hospital, we will have failed to realize health IT's full potential,” he said. “Instead, doctors, hospitals, and other providers need to use robust EHR technology in a meaningful and interoperable way to improve care.”
Many physicians are frustrated and confused by the meaningful use criteria that spell out how they can receive incentive payments from Medicare and Medicaid for their use of electronic health records.
With that uncertainty, physicians are not jumping in with both feet to participate in the incentive program, even if they have purchased EHR systems. The Medical Group Management Association (MGMA), in an April survey of its members, found that 80% of those who had adopted an EHR system intended to participate. But at that time, only 14% said they were able to meet all the criteria.
The American Medical Association held a special session on meaningful use at its House of Delegates meeting in June. When Dr. Michael L. Hodgkins, AMA chief medical information officer, asked how many physicians were confused about what was expected of them, more than half raised their hands.
Physicians in smaller practices are especially challenged, Dr. Hodgkins said, citing data that some 300,000 doctors are in practices of 10 or fewer physicians. Among those, fewer than 15% have implemented an EHR system, and most are not yet capable of meeting the meaningful use criteria.
According to Dr. Hodgkins, there are many obstacles to meeting meaningful use, including selecting from the more than 400 EHR products certified by the federal Office of the National Coordinator (ONC) for Health Information Technology, part of the Health and Human Services department.
Another problem: “Aggressive” timelines set by the government, according to Dr. Steve Waldren, director of the Center for Health Information Technology at the American Academy of Family Physicians (AAFP). He says it takes 6-18 months from purchase to active meaningful use of a system.
It's been a tough road, he said. Physicians who don't have EHRs or who have just gotten on board are struggling to get them operational and to achieve meaningful use. Those who have owned systems for awhile may face upgrades to meet the meaningful use criteria.
Meanwhile, there's the system's financial cost, its training and maintenance issues, and workflow changes once a system is in place.
The Long-Time User
Some physicians aren't in a panic about the impending deadlines. Dr. Michael Mirro of Ft. Wayne (Ind.) Cardiology, a 24-physician group, said his practice has been using health IT since 1996.
“We knew that we had to ultimately modernize our practice,” Dr. Mirro said in an interview. Their current system has improved efficiency and quality, and has “supported a higher level of coding and reimbursement.”
The system has “pretty much complete functionality,” said Dr. Mirro. It provides the EHR, offers e-prescribing and decision-support tools, and can be used for direct quality reporting to the American College of Cardiology's PINNACLE registry.
The system is Web based, which reduces maintenance costs and IT headaches. The practice does not own the servers; it has local computers that interact with the vendor's servers and software. The system is certified by the Certification Commission for Health Information Technology and was updated to ensure that the practice would meet the meaningful use criteria. One helpful tool, according to Dr. Mirro: A meaningful use “meter” that tells the physicians how well they are meeting the goals.
Ft. Wayne Cardiology has already attested to the government that it was a meaningful user and has received the maximum $18,000 per physician incentive for 2011, Dr. Mirro said.
The annual cost is about $2,000 per physician per year. That's low, said Dr. Mirro, because his practice is owned by a hospital. The system is already ahead of the curve, as it already incorporates a patient Web portal (a stage 2 goal).
He said that he is sympathetic to physicians who are just getting started. “Any time you adopt technology at the point of care, it's going to require a change in workflow,” he said. That was definitely the case at Ft. Wayne Cardiology.
Dr. Mirro said that physicians looking to buy or expand their health IT should talk with one of the 60 regional extension centers established by the ONC. These centers have been charged to help rural and primary care physicians especially. They offer vendor recommendations, practice audits, and other advice for free.
A Model for Her Peers
In 2005, Dr. Jennifer Brull figured that she needed to get on board with health IT, even though it might be expensive and difficult for a family physician in a rural Kansas solo practice. A younger physician with whom she was collaborating suggested that having an EHR was the wave of the future, and would likely be a necessity going forward. She also had a practice-sharing arrangement with another physician, who was older. He was not as sure, Dr. Brull said in an interview.
But they moved ahead and spent 3 years selecting, buying, and implementing an EHR system that they could all use, said Dr. Brull, who practices in Plainview. She took out a loan for $50,000 to buy the equipment; her colleagues contributed to the software and other costs.
Because they practice in a rural area, there was no possibility of using a Web-based model; broadband access in her area is still not robust enough, said Dr. Brull. So she has a server onsite at her office, and recently purchased a second server for $3,000. The net cost so far has been about $30,000 per physician, Dr. Brull said.
The first 6 months were a challenge, she said. “Anytime you do something that's a complete paradigm shift, it's hard. It's hard mentally to think about all those changes, hard physically because you're investing more time and effort, and hard emotionally because your staff gets freaked out.”
In addition to allowing the practice to meet meaningful use criteria, the system also has a patient portal. The physicians are preparing to be able to participate in the state's health information exchange.
Dr. Brull said that she disagrees with physicians who say that adopting an EHR interrupts the workflow or comes between the physician and patient.
“I've found it easier to be more collaborative [with my patients],” she said. One example: She recently used an EHR-generated graph to show a patient that she had gained 40 pounds over 3 years. The graph made much more of an impression on the patient than Dr. Brull could have done by reading numbers off a paper chart, she said.
“This whole project has resulted in dramatic quality improvement for my practice,” Dr. Brull added. Another example: She implemented a quality measure on breast cancer screening. Just by having a flag in the EHR, she went from screening 50% of patients to almost 100%. “Having the data at your fingertips makes you aware of where you do a good job and where you don't,” Dr. Brull said.
In April, Dr. Brull collected the full Medicare incentive payment for 2011. Her colleagues weren't ready, but that didn't matter. Physicians can choose to attest to meaningful use on their own time frame, regardless of where their colleagues might be, she said.
Dr. Brull has become an evangelist for the power of the EHR and meaningful use. She was chosen to speak at a CMS press conference announcing the first round of Medicare incentive payments. And she is a member of the regional extension center in Kansas. The ONC also named her a “MUVer” – someone who serves as a local leader and adviser.
The Reluctant Adopter
Dr. Michael Machen is one of the physicians who consulted with Dr. Brull. He practices with four other family physicians in nearby Quinter, Kan. (population, 980). The impetus for taking on an EHR came from his younger partners, Dr. Machen said in an interview. They were also motivated by the meaningful use program, and got started in July 2010.
One junior partner became the EHR champion, doing much of the legwork to find appropriate vendors and systems. The physicians also attended seminars and webinars offered by the Kansas Medical Society and the Kansas chapter of the AAFP. A team from the regional extension center visited their practice too, Dr. Machen said.
They borrowed $75,000 to purchase hardware and software. The biggest cost is the $2,000-$4,000 they spend monthly on IT support – a necessity when there is no one with such expertise in the practice or locally. The IT help comes from more than an hour away. Dr. Machen and his colleagues house the server themselves; broadband is no better in Quinter than it is in Plainview.
Dr. Machen said that the younger physicians have all done well with the system, but he is struggling.
“I'm not technically inclined, and I have very little computer knowledge,” he said. It has also been difficult for his nurse, who is spending more time on data entry and less on interacting with patients, Dr. Machen said, adding that they are both in their late 50s and are more frustrated with the system than are their younger colleagues.
His staff has been happy; there's no more searching for charts, and coding is easier, he said. And he does see the potential for improving quality, especially with the data-collection effort, warnings about drug interactions, and prompts for screening tests.
But for now, “it's horrible with the workflow and the patient flow.” On days of 15-20 patient visits, using the EHR is not as much of an issue. But on days of 30 patient visits, “it's not doable,” he said.
So far, patients haven't been wild about the transition, either. They don't like the physician to be working on a computer during the visit, he said. And “I don't like it much, either,” said Dr. Machen. “When I was in medical school, I was taught that the second you enter the exam room, the patient has your undivided attention.” That's not really possible with an EHR, at least the way he sees it currently, although he also can see possible solutions, such as having a scribe.
Source Elsevier Global Medical News
Making Sense of Meaningful Use: How, Where, and When
The ONC provides the central leadership for the Medicare and Medicaid EHR incentive programs. The HITECH (Health Information Technology for Economic and Clinical Health) Act directly appropriated $2 billion to the ONC to spend on incentives and administration of the program. The federal regulation governing the incentive program (some 800 pages) was issued in July 2010.
This year – 2011 – is the first year in which physicians can participate; they have until Oct. 1 to attest that they are meaningful users. To be eligible for incentive payments, physicians have to meet the meaningful use criteria for 90 consecutive days.
The criteria are being introduced in stages over the next 4-5 years. Stage 1 outlines what is expected in 2011 and 2012. Stage 2 was expected to be put into place in 2013, but in June, the Health IT Policy Committee of the Centers for Medicare and Medicaid Services voted to delay implementation until 2014, but only for physicians who were already participating.
Physicians who wait until 2012 or later would still be expected to meet stage 2 criteria in 2013.
Physicians who want to participate have to choose between the Medicare or Medicaid incentive program.
Those who take part in the Medicare program are eligible to receive incentive payments of $44,000 over 5 years. However, the payments will be made only through 2016. Physicians who wait until 2012 to start would still earn the $44,000 maximum; those who start later would receive prorated payments.
Physicians who practice in designated Health Professional Shortage Areas (HPSA) may be eligible for an additional 10% in each year's incentive payment.
Importantly, Medicare begins to penalize nonparticipating physicians starting in 2016.
The Medicaid incentives are more generous: A total of $63,750 can be paid out over 6 years. And there's a longer time frame. Eligible professionals can wait until 2016 to start participating and still receive the maximum payout over a 6-year period.
In late May, the CMS announced that $75 million in Medicare incentives had been awarded to physicians and hospitals in the first 2 weeks of the program. Some states began paying out Medicaid incentives in January. By late May, $83 million had been issued.
Meaningful use of EHRs is critical, according to Dr. Farzad Mostashari, the national coordinator, who testified to the House Small Business Committee's Subcommittee on Healthcare and Technology in June.
“If all we do is put an EHR in every provider's office or hospital, we will have failed to realize health IT's full potential,” he said. “Instead, doctors, hospitals, and other providers need to use robust EHR technology in a meaningful and interoperable way to improve care.”
Less-Frequent Call Is More Important Than Higher Pay
Physicians are more concerned about the burden of taking call than about how much they get paid for providing coverage at hospital emergency departments, according to a survey.
About 50 medical groups participated, primarily from independently owned, large, multispecialty groups.
When physicians were asked to choose between reduced call burden or payment, 58% of those surveyed said it was more important to reduce call burden was high. AMGA said the survey shows that there is a big gulf between hospitals and physicians on this issue.
According to the AMGA, its members deliver health care to 110 million patients in 49 states.
To access the free report online, go to https://ecommerce.amga.org/iMISPublic/Core/Orders/product.aspx?catid=12&prodid=2022
Physicians are more concerned about the burden of taking call than about how much they get paid for providing coverage at hospital emergency departments, according to a survey.
About 50 medical groups participated, primarily from independently owned, large, multispecialty groups.
When physicians were asked to choose between reduced call burden or payment, 58% of those surveyed said it was more important to reduce call burden was high. AMGA said the survey shows that there is a big gulf between hospitals and physicians on this issue.
According to the AMGA, its members deliver health care to 110 million patients in 49 states.
To access the free report online, go to https://ecommerce.amga.org/iMISPublic/Core/Orders/product.aspx?catid=12&prodid=2022
Physicians are more concerned about the burden of taking call than about how much they get paid for providing coverage at hospital emergency departments, according to a survey.
About 50 medical groups participated, primarily from independently owned, large, multispecialty groups.
When physicians were asked to choose between reduced call burden or payment, 58% of those surveyed said it was more important to reduce call burden was high. AMGA said the survey shows that there is a big gulf between hospitals and physicians on this issue.
According to the AMGA, its members deliver health care to 110 million patients in 49 states.
To access the free report online, go to https://ecommerce.amga.org/iMISPublic/Core/Orders/product.aspx?catid=12&prodid=2022
Recession Kept Health Spending Growth Low in 2010
Major Finding: The nation's health spending rose by 3.9% in 2010 to $2.6 trillion. It is projected to rise by about 6% each year over the next decade, with the exception of an 8% increase in 2014, when the Affordable Care Act is in full effect.
Data Source: An actuarial and econometric analysis of data from the 2011 Medicare Trustees Report, done under a current-law framework.
Disclosures: The authors are all employees of the Centers for Medicare and Medicaid Services.
Despite a huge increase in the number of Americans who will have insurance coverage when the main provisions of the Affordable Care Act take effect in 2014, the nation's overall health spending in that year is projected to rise only 2% above the expected yearly average increase for the rest of the decade, economists from the Centers for Medicare and Medicaid Services said.
The 8% growth in spending expected in 2014 is in line with the average 5.8% annual rise in health spending expected each year from 2010 to 2020 and is relatively small given that, by 2014, an estimated 23 million more Americans will have health insurance coverage under the Affordable Care Act (ACA), said Sean P. Keehan, an economist in the Office of the Actuary at the Centers for Medicare and Medicaid Services (CMS).
Over the next decade, the ACA is projected to add only a tenth of a percentage point to the nation's overall health spending, Mr. Keehan and his colleagues reported in the journal Health Affairs (August [doi:10.1377/hlthaff.2011.0662]).
The ACA is expected to drive a 20% increase in Medicaid costs and a 9% increase in private insurance spending in 2014. The economists said many of the newly insured will be younger and healthier than the existing populations covered by Medicaid and private insurance.
With the new coverage, they are likely to use more physician services (a projected 9% increase in 2014) and pharmaceuticals (a projected 11% increase in 2014), the authors said.
The increases in spending will not be offset by Medicare cuts in the first year, according to the report, an actuarial and econometric analysis of data from the 2011 Medicare Trustees Report, done under a current-law framework.
The projections could be substantially affected by the outcome of the ongoing federal debt ceiling talks and, in a few years, by any potential changes in the Medicare Sustainable Growth Rate (SGR) formula.
In 2012, the SGR calls for an-almost 30% cut in Medicare physician payments. If that happens, Medicare spending would only grow by 1.7%, instead of by 5.9%, according to the study. If the Congress decides to try an alternative, such as tying fee increases to the Medicare Economic Index, Medicare spending would rise by 6.6%.
In 2010, growth in health spending was, for the second year in a row, near a historic low, driven largely by the recession. The $2.6 trillion represented almost 18% of the gross domestic product (GDP). That was about the same share as 2009, as both health spending and the GDP grew relatively slowly, according to the report.
Medicare spending growth slowed because of less spending on private Medicare Advantage plans. Private health insurance spending grew only 2.6% in 2010, as more people lost jobs and coverage. Americans for the second year in a row also spent less out-of-pocket.
Overall, spending on physician and clinical services grew only 2.4% in 2010. The economists said they expect that figure to rebound by 4% in 2011, but to slow again in 2012, largely because of the SGR cut. That year, physician spending may only rise by 0.8%.
With many major provisions of the ACA taking effect in 2014, physician spending is expected to grow by 8.9% that year, a $17.8 billion increase over what would have been expected without health reform, according to the report.
Major Finding: The nation's health spending rose by 3.9% in 2010 to $2.6 trillion. It is projected to rise by about 6% each year over the next decade, with the exception of an 8% increase in 2014, when the Affordable Care Act is in full effect.
Data Source: An actuarial and econometric analysis of data from the 2011 Medicare Trustees Report, done under a current-law framework.
Disclosures: The authors are all employees of the Centers for Medicare and Medicaid Services.
Despite a huge increase in the number of Americans who will have insurance coverage when the main provisions of the Affordable Care Act take effect in 2014, the nation's overall health spending in that year is projected to rise only 2% above the expected yearly average increase for the rest of the decade, economists from the Centers for Medicare and Medicaid Services said.
The 8% growth in spending expected in 2014 is in line with the average 5.8% annual rise in health spending expected each year from 2010 to 2020 and is relatively small given that, by 2014, an estimated 23 million more Americans will have health insurance coverage under the Affordable Care Act (ACA), said Sean P. Keehan, an economist in the Office of the Actuary at the Centers for Medicare and Medicaid Services (CMS).
Over the next decade, the ACA is projected to add only a tenth of a percentage point to the nation's overall health spending, Mr. Keehan and his colleagues reported in the journal Health Affairs (August [doi:10.1377/hlthaff.2011.0662]).
The ACA is expected to drive a 20% increase in Medicaid costs and a 9% increase in private insurance spending in 2014. The economists said many of the newly insured will be younger and healthier than the existing populations covered by Medicaid and private insurance.
With the new coverage, they are likely to use more physician services (a projected 9% increase in 2014) and pharmaceuticals (a projected 11% increase in 2014), the authors said.
The increases in spending will not be offset by Medicare cuts in the first year, according to the report, an actuarial and econometric analysis of data from the 2011 Medicare Trustees Report, done under a current-law framework.
The projections could be substantially affected by the outcome of the ongoing federal debt ceiling talks and, in a few years, by any potential changes in the Medicare Sustainable Growth Rate (SGR) formula.
In 2012, the SGR calls for an-almost 30% cut in Medicare physician payments. If that happens, Medicare spending would only grow by 1.7%, instead of by 5.9%, according to the study. If the Congress decides to try an alternative, such as tying fee increases to the Medicare Economic Index, Medicare spending would rise by 6.6%.
In 2010, growth in health spending was, for the second year in a row, near a historic low, driven largely by the recession. The $2.6 trillion represented almost 18% of the gross domestic product (GDP). That was about the same share as 2009, as both health spending and the GDP grew relatively slowly, according to the report.
Medicare spending growth slowed because of less spending on private Medicare Advantage plans. Private health insurance spending grew only 2.6% in 2010, as more people lost jobs and coverage. Americans for the second year in a row also spent less out-of-pocket.
Overall, spending on physician and clinical services grew only 2.4% in 2010. The economists said they expect that figure to rebound by 4% in 2011, but to slow again in 2012, largely because of the SGR cut. That year, physician spending may only rise by 0.8%.
With many major provisions of the ACA taking effect in 2014, physician spending is expected to grow by 8.9% that year, a $17.8 billion increase over what would have been expected without health reform, according to the report.
Major Finding: The nation's health spending rose by 3.9% in 2010 to $2.6 trillion. It is projected to rise by about 6% each year over the next decade, with the exception of an 8% increase in 2014, when the Affordable Care Act is in full effect.
Data Source: An actuarial and econometric analysis of data from the 2011 Medicare Trustees Report, done under a current-law framework.
Disclosures: The authors are all employees of the Centers for Medicare and Medicaid Services.
Despite a huge increase in the number of Americans who will have insurance coverage when the main provisions of the Affordable Care Act take effect in 2014, the nation's overall health spending in that year is projected to rise only 2% above the expected yearly average increase for the rest of the decade, economists from the Centers for Medicare and Medicaid Services said.
The 8% growth in spending expected in 2014 is in line with the average 5.8% annual rise in health spending expected each year from 2010 to 2020 and is relatively small given that, by 2014, an estimated 23 million more Americans will have health insurance coverage under the Affordable Care Act (ACA), said Sean P. Keehan, an economist in the Office of the Actuary at the Centers for Medicare and Medicaid Services (CMS).
Over the next decade, the ACA is projected to add only a tenth of a percentage point to the nation's overall health spending, Mr. Keehan and his colleagues reported in the journal Health Affairs (August [doi:10.1377/hlthaff.2011.0662]).
The ACA is expected to drive a 20% increase in Medicaid costs and a 9% increase in private insurance spending in 2014. The economists said many of the newly insured will be younger and healthier than the existing populations covered by Medicaid and private insurance.
With the new coverage, they are likely to use more physician services (a projected 9% increase in 2014) and pharmaceuticals (a projected 11% increase in 2014), the authors said.
The increases in spending will not be offset by Medicare cuts in the first year, according to the report, an actuarial and econometric analysis of data from the 2011 Medicare Trustees Report, done under a current-law framework.
The projections could be substantially affected by the outcome of the ongoing federal debt ceiling talks and, in a few years, by any potential changes in the Medicare Sustainable Growth Rate (SGR) formula.
In 2012, the SGR calls for an-almost 30% cut in Medicare physician payments. If that happens, Medicare spending would only grow by 1.7%, instead of by 5.9%, according to the study. If the Congress decides to try an alternative, such as tying fee increases to the Medicare Economic Index, Medicare spending would rise by 6.6%.
In 2010, growth in health spending was, for the second year in a row, near a historic low, driven largely by the recession. The $2.6 trillion represented almost 18% of the gross domestic product (GDP). That was about the same share as 2009, as both health spending and the GDP grew relatively slowly, according to the report.
Medicare spending growth slowed because of less spending on private Medicare Advantage plans. Private health insurance spending grew only 2.6% in 2010, as more people lost jobs and coverage. Americans for the second year in a row also spent less out-of-pocket.
Overall, spending on physician and clinical services grew only 2.4% in 2010. The economists said they expect that figure to rebound by 4% in 2011, but to slow again in 2012, largely because of the SGR cut. That year, physician spending may only rise by 0.8%.
With many major provisions of the ACA taking effect in 2014, physician spending is expected to grow by 8.9% that year, a $17.8 billion increase over what would have been expected without health reform, according to the report.
Meaningful Use: Some Struggle, Others Thrive
Many physicians continue to be frustrated and confused by the meaningful use criteria that spell out how they can receive incentive payments from Medicare and Medicaid for their use of electronic health records.
With that uncertainty, physicians are not jumping in with both feet to participate in the incentive program, even if they have purchased EHR systems. The Medical Group Management Association (MGMA) surveyed its members in April and found that 80% of those who already had adopted an EHR system said that they intended to participate. But at that time, only about 14% said that they were able to meet all of the criteria.
Physicians in smaller practices are especially challenged, Dr. Michael L. Hodgkins, a chief medical information officer at the American Medical Association, said at the AMA's House of Delegates meeting in June. He cited data that some 300,000 doctors are in practices of 10 or fewer physicians. Among those, fewer than 15% have implemented an EHR system, and most are not yet capable of meeting the meaningful use criteria.
According to Dr. Hodgkins, there are many obstacles to meeting meaningful use, including selecting from the more than 400 EHR products certified by the federal Office of the National Coordinator (ONC) for Health Information Technology, part of the Health and Human Services Department.
Another problem: “Aggressive” timelines set by the government, according to Dr. Steve Waldren, director of the Center for Health Information Technology at the American Academy of Family Physicians (AAFP).
Dr. Waldren says it takes generally 6-18 months from purchase to active meaningful use of a system.
It's been a tough road, he said. Physicians who don't have EHRs or who have just gotten on board are struggling to get them operational and to achieve meaningful use. Those who have owned systems for awhile may face upgrades in order to meet the meaningful use criteria.
Meanwhile, there's the system's financial cost, training, and maintenance issues, and workflow changes once a system is in place.
The Long-Time User
Some physicians are not in a panic about the impending deadlines. Dr. Michael Mirro of Ft. Wayne (Ind.) Cardiology, a 24-physician group, said that his practice has been using health IT since 1996.
“We knew that we had to ultimately modernize our practice,” Dr. Mirro said in an interview. Their current system has improved efficiency and quality, and has “supported a higher level of coding and reimbursement.”
The system has “pretty much complete functionality,” said Dr. Mirro. It provides the EHR, offers e-prescribing and decision-support tools, and can be used for direct quality reporting to the American College of Cardiology's PINNACLE registry.
The system is web based, which reduces maintenance costs and IT headaches. The practice does not own the servers; it merely has local computers that interact with the vendor's servers and software. The system is certified by the Certification Commission for Health Information Technology and was updated to ensure that the practice would meet the meaningful use criteria. One helpful tool, according to Dr. Mirro: A meaningful use “meter” that tells the physicians how well they are meeting the goals.
Ft. Wayne Cardiology has already attested to the government that it was a meaningful user and has received the maximum $18,000 per physician incentive for 2011, Dr. Mirro said.
The annual cost is about $2,000 per physician per year. That's low, said Dr. Mirro, because his practice is owned by a hospital. The system is already somewhat ahead of the curve, as it already incorporates a patient web portal (a stage 2 goal).
Dr. Mirro said that physicians who are looking to buy or expand their health IT should talk with one of the 60 regional extension centers established by the ONC. These centers have been charged to help rural physicians and primary care physicians especially, and they offer vendor recommendations, practice audits, and other advice for free.
Dr. Mirro said that he believes most cardiologists will be forced to purchase an EHR sooner rather than later. With the decline in reimbursement (particularly for imaging services), cardiologists are increasingly being employed by hospitals. Those institutions – which themselves are facing a huge penalty if they don't comply with meaningful use by 2017 – will want to have a lot of connectivity with the physician practice.
A Model For Her Peers
In 2005, Dr. Jennifer Brull figured that she needed to get on board with health IT, even though it might be expensive and difficult for a family physician in a rural Kansas solo practice. A younger physician with whom she was collaborating suggested that having an EHR was the wave of the future, and would likely be a necessity going forward. She also had a practice-sharing arrangement with another physician, who was older. He wasn't as sure, said Dr. Brull in an interview.
But they moved ahead and spent 3 years selecting, buying, and implementing an EHR system that they could all use, said Dr. Brull, who practices in Plainview. She took out a loan for $50,000 to buy the equipment; her colleagues contributed to the software and other costs.
Because they practice in a rural area, there was no possibility of using a web-based model, so Dr. Brull has a server onsite at her office, and recently purchased a second server for $3,000. The net cost so far has been about $30,000 per physician, Dr. Brull said.
The first 6 months were a challenge, she said. “Anytime you do something that's a complete paradigm shift, it's hard. It's hard mentally to think about all those changes, hard physically because you're investing more time and effort, and hard emotionally because your staff gets freaked out.”
In addition to allowing the practice to meet meaningful use criteria, the system also has a patient portal. The physicians are preparing to be able to participate in the state's health information exchange.
Dr. Brull said that she disagrees with physicians who say that adopting an EHR interrupts the workflow or comes between the physician and patient.
“This whole project has resulted in dramatic quality improvement for my practice,” Dr. Brull added. Another example: She implemented a quality measure on breast cancer screening. Just by having a flag in the EHR, she went from screening 50% of patients to almost 100%. “Having the data at your fingertips makes you aware of where you do a good job and where you don't,” Dr. Brull said.
{kind=link}
Vitals
Source Elsevier Global Medical News
Meaningful Use: How, Where, When
The ONC provides the central leadership for the Medicare and Medicaid EHR incentive programs. The HITECH (Health Information Technology for Economic and Clinical Health) Act directly appropriated $2 billion to the ONC to spend on incentives and administration of the program.
The federal regulation governing the incentive program (some 800 pages) was issued in July 2010.
This year – 2011 – is the first year in which physicians can participate; they have until Oct. 1 to attest that they are meaningful users. To be eligible for incentive payments, physicians have to meet the meaningful use criteria for 90 consecutive days.
The criteria are being introduced in stages over the next 4-5 years. Stage 1 outlines what is expected in 2011 and 2012.
Stage 2 was expected to be put into place in 2013, but in June, the Health IT Policy Committee of the Centers for Medicare and Medicaid Services voted to delay implementation until 2014, but only for physicians who were already participating.
Physicians who wait until 2012 or later would still be expected to meet stage 2 criteria in 2013.
Physicians who want to participate have to choose between the Medicare or Medicaid incentive program. Those who take part in the Medicare program are eligible to receive incentive payments of $44,000 over 5 years. However, the payments will be made only through 2016.
Physicians who wait until 2012 to start would still earn the $44,000 maximum; those who start later would receive prorated payments.
Physicians who practice in designated Health Professional Shortage Areas may be eligible for an additional 10% in each year's incentive payment.
Importantly, Medicare begins to penalize nonparticipating physicians starting in 2016.
The Medicaid incentives are more generous: A total of $63,750 can be paid out over 6 years. And there's a longer time frame. Eligible professionals can wait until 2016 to start participating and still receive the maximum payout over a 6-year period.
In late May, the CMS announced that $75 million in Medicare incentives had been awarded to physicians and hospitals in the first 2 weeks of the program. Some states began paying out Medicaid incentives in January.
Many physicians continue to be frustrated and confused by the meaningful use criteria that spell out how they can receive incentive payments from Medicare and Medicaid for their use of electronic health records.
With that uncertainty, physicians are not jumping in with both feet to participate in the incentive program, even if they have purchased EHR systems. The Medical Group Management Association (MGMA) surveyed its members in April and found that 80% of those who already had adopted an EHR system said that they intended to participate. But at that time, only about 14% said that they were able to meet all of the criteria.
Physicians in smaller practices are especially challenged, Dr. Michael L. Hodgkins, a chief medical information officer at the American Medical Association, said at the AMA's House of Delegates meeting in June. He cited data that some 300,000 doctors are in practices of 10 or fewer physicians. Among those, fewer than 15% have implemented an EHR system, and most are not yet capable of meeting the meaningful use criteria.
According to Dr. Hodgkins, there are many obstacles to meeting meaningful use, including selecting from the more than 400 EHR products certified by the federal Office of the National Coordinator (ONC) for Health Information Technology, part of the Health and Human Services Department.
Another problem: “Aggressive” timelines set by the government, according to Dr. Steve Waldren, director of the Center for Health Information Technology at the American Academy of Family Physicians (AAFP).
Dr. Waldren says it takes generally 6-18 months from purchase to active meaningful use of a system.
It's been a tough road, he said. Physicians who don't have EHRs or who have just gotten on board are struggling to get them operational and to achieve meaningful use. Those who have owned systems for awhile may face upgrades in order to meet the meaningful use criteria.
Meanwhile, there's the system's financial cost, training, and maintenance issues, and workflow changes once a system is in place.
The Long-Time User
Some physicians are not in a panic about the impending deadlines. Dr. Michael Mirro of Ft. Wayne (Ind.) Cardiology, a 24-physician group, said that his practice has been using health IT since 1996.
“We knew that we had to ultimately modernize our practice,” Dr. Mirro said in an interview. Their current system has improved efficiency and quality, and has “supported a higher level of coding and reimbursement.”
The system has “pretty much complete functionality,” said Dr. Mirro. It provides the EHR, offers e-prescribing and decision-support tools, and can be used for direct quality reporting to the American College of Cardiology's PINNACLE registry.
The system is web based, which reduces maintenance costs and IT headaches. The practice does not own the servers; it merely has local computers that interact with the vendor's servers and software. The system is certified by the Certification Commission for Health Information Technology and was updated to ensure that the practice would meet the meaningful use criteria. One helpful tool, according to Dr. Mirro: A meaningful use “meter” that tells the physicians how well they are meeting the goals.
Ft. Wayne Cardiology has already attested to the government that it was a meaningful user and has received the maximum $18,000 per physician incentive for 2011, Dr. Mirro said.
The annual cost is about $2,000 per physician per year. That's low, said Dr. Mirro, because his practice is owned by a hospital. The system is already somewhat ahead of the curve, as it already incorporates a patient web portal (a stage 2 goal).
Dr. Mirro said that physicians who are looking to buy or expand their health IT should talk with one of the 60 regional extension centers established by the ONC. These centers have been charged to help rural physicians and primary care physicians especially, and they offer vendor recommendations, practice audits, and other advice for free.
Dr. Mirro said that he believes most cardiologists will be forced to purchase an EHR sooner rather than later. With the decline in reimbursement (particularly for imaging services), cardiologists are increasingly being employed by hospitals. Those institutions – which themselves are facing a huge penalty if they don't comply with meaningful use by 2017 – will want to have a lot of connectivity with the physician practice.
A Model For Her Peers
In 2005, Dr. Jennifer Brull figured that she needed to get on board with health IT, even though it might be expensive and difficult for a family physician in a rural Kansas solo practice. A younger physician with whom she was collaborating suggested that having an EHR was the wave of the future, and would likely be a necessity going forward. She also had a practice-sharing arrangement with another physician, who was older. He wasn't as sure, said Dr. Brull in an interview.
But they moved ahead and spent 3 years selecting, buying, and implementing an EHR system that they could all use, said Dr. Brull, who practices in Plainview. She took out a loan for $50,000 to buy the equipment; her colleagues contributed to the software and other costs.
Because they practice in a rural area, there was no possibility of using a web-based model, so Dr. Brull has a server onsite at her office, and recently purchased a second server for $3,000. The net cost so far has been about $30,000 per physician, Dr. Brull said.
The first 6 months were a challenge, she said. “Anytime you do something that's a complete paradigm shift, it's hard. It's hard mentally to think about all those changes, hard physically because you're investing more time and effort, and hard emotionally because your staff gets freaked out.”
In addition to allowing the practice to meet meaningful use criteria, the system also has a patient portal. The physicians are preparing to be able to participate in the state's health information exchange.
Dr. Brull said that she disagrees with physicians who say that adopting an EHR interrupts the workflow or comes between the physician and patient.
“This whole project has resulted in dramatic quality improvement for my practice,” Dr. Brull added. Another example: She implemented a quality measure on breast cancer screening. Just by having a flag in the EHR, she went from screening 50% of patients to almost 100%. “Having the data at your fingertips makes you aware of where you do a good job and where you don't,” Dr. Brull said.
Vitals
Source Elsevier Global Medical News
Meaningful Use: How, Where, When
The ONC provides the central leadership for the Medicare and Medicaid EHR incentive programs. The HITECH (Health Information Technology for Economic and Clinical Health) Act directly appropriated $2 billion to the ONC to spend on incentives and administration of the program.
The federal regulation governing the incentive program (some 800 pages) was issued in July 2010.
This year – 2011 – is the first year in which physicians can participate; they have until Oct. 1 to attest that they are meaningful users. To be eligible for incentive payments, physicians have to meet the meaningful use criteria for 90 consecutive days.
The criteria are being introduced in stages over the next 4-5 years. Stage 1 outlines what is expected in 2011 and 2012.
Stage 2 was expected to be put into place in 2013, but in June, the Health IT Policy Committee of the Centers for Medicare and Medicaid Services voted to delay implementation until 2014, but only for physicians who were already participating.
Physicians who wait until 2012 or later would still be expected to meet stage 2 criteria in 2013.
Physicians who want to participate have to choose between the Medicare or Medicaid incentive program. Those who take part in the Medicare program are eligible to receive incentive payments of $44,000 over 5 years. However, the payments will be made only through 2016.
Physicians who wait until 2012 to start would still earn the $44,000 maximum; those who start later would receive prorated payments.
Physicians who practice in designated Health Professional Shortage Areas may be eligible for an additional 10% in each year's incentive payment.
Importantly, Medicare begins to penalize nonparticipating physicians starting in 2016.
The Medicaid incentives are more generous: A total of $63,750 can be paid out over 6 years. And there's a longer time frame. Eligible professionals can wait until 2016 to start participating and still receive the maximum payout over a 6-year period.
In late May, the CMS announced that $75 million in Medicare incentives had been awarded to physicians and hospitals in the first 2 weeks of the program. Some states began paying out Medicaid incentives in January.
Many physicians continue to be frustrated and confused by the meaningful use criteria that spell out how they can receive incentive payments from Medicare and Medicaid for their use of electronic health records.
With that uncertainty, physicians are not jumping in with both feet to participate in the incentive program, even if they have purchased EHR systems. The Medical Group Management Association (MGMA) surveyed its members in April and found that 80% of those who already had adopted an EHR system said that they intended to participate. But at that time, only about 14% said that they were able to meet all of the criteria.
Physicians in smaller practices are especially challenged, Dr. Michael L. Hodgkins, a chief medical information officer at the American Medical Association, said at the AMA's House of Delegates meeting in June. He cited data that some 300,000 doctors are in practices of 10 or fewer physicians. Among those, fewer than 15% have implemented an EHR system, and most are not yet capable of meeting the meaningful use criteria.
According to Dr. Hodgkins, there are many obstacles to meeting meaningful use, including selecting from the more than 400 EHR products certified by the federal Office of the National Coordinator (ONC) for Health Information Technology, part of the Health and Human Services Department.
Another problem: “Aggressive” timelines set by the government, according to Dr. Steve Waldren, director of the Center for Health Information Technology at the American Academy of Family Physicians (AAFP).
Dr. Waldren says it takes generally 6-18 months from purchase to active meaningful use of a system.
It's been a tough road, he said. Physicians who don't have EHRs or who have just gotten on board are struggling to get them operational and to achieve meaningful use. Those who have owned systems for awhile may face upgrades in order to meet the meaningful use criteria.
Meanwhile, there's the system's financial cost, training, and maintenance issues, and workflow changes once a system is in place.
The Long-Time User
Some physicians are not in a panic about the impending deadlines. Dr. Michael Mirro of Ft. Wayne (Ind.) Cardiology, a 24-physician group, said that his practice has been using health IT since 1996.
“We knew that we had to ultimately modernize our practice,” Dr. Mirro said in an interview. Their current system has improved efficiency and quality, and has “supported a higher level of coding and reimbursement.”
The system has “pretty much complete functionality,” said Dr. Mirro. It provides the EHR, offers e-prescribing and decision-support tools, and can be used for direct quality reporting to the American College of Cardiology's PINNACLE registry.
The system is web based, which reduces maintenance costs and IT headaches. The practice does not own the servers; it merely has local computers that interact with the vendor's servers and software. The system is certified by the Certification Commission for Health Information Technology and was updated to ensure that the practice would meet the meaningful use criteria. One helpful tool, according to Dr. Mirro: A meaningful use “meter” that tells the physicians how well they are meeting the goals.
Ft. Wayne Cardiology has already attested to the government that it was a meaningful user and has received the maximum $18,000 per physician incentive for 2011, Dr. Mirro said.
The annual cost is about $2,000 per physician per year. That's low, said Dr. Mirro, because his practice is owned by a hospital. The system is already somewhat ahead of the curve, as it already incorporates a patient web portal (a stage 2 goal).
Dr. Mirro said that physicians who are looking to buy or expand their health IT should talk with one of the 60 regional extension centers established by the ONC. These centers have been charged to help rural physicians and primary care physicians especially, and they offer vendor recommendations, practice audits, and other advice for free.
Dr. Mirro said that he believes most cardiologists will be forced to purchase an EHR sooner rather than later. With the decline in reimbursement (particularly for imaging services), cardiologists are increasingly being employed by hospitals. Those institutions – which themselves are facing a huge penalty if they don't comply with meaningful use by 2017 – will want to have a lot of connectivity with the physician practice.
A Model For Her Peers
In 2005, Dr. Jennifer Brull figured that she needed to get on board with health IT, even though it might be expensive and difficult for a family physician in a rural Kansas solo practice. A younger physician with whom she was collaborating suggested that having an EHR was the wave of the future, and would likely be a necessity going forward. She also had a practice-sharing arrangement with another physician, who was older. He wasn't as sure, said Dr. Brull in an interview.
But they moved ahead and spent 3 years selecting, buying, and implementing an EHR system that they could all use, said Dr. Brull, who practices in Plainview. She took out a loan for $50,000 to buy the equipment; her colleagues contributed to the software and other costs.
Because they practice in a rural area, there was no possibility of using a web-based model, so Dr. Brull has a server onsite at her office, and recently purchased a second server for $3,000. The net cost so far has been about $30,000 per physician, Dr. Brull said.
The first 6 months were a challenge, she said. “Anytime you do something that's a complete paradigm shift, it's hard. It's hard mentally to think about all those changes, hard physically because you're investing more time and effort, and hard emotionally because your staff gets freaked out.”
In addition to allowing the practice to meet meaningful use criteria, the system also has a patient portal. The physicians are preparing to be able to participate in the state's health information exchange.
Dr. Brull said that she disagrees with physicians who say that adopting an EHR interrupts the workflow or comes between the physician and patient.
“This whole project has resulted in dramatic quality improvement for my practice,” Dr. Brull added. Another example: She implemented a quality measure on breast cancer screening. Just by having a flag in the EHR, she went from screening 50% of patients to almost 100%. “Having the data at your fingertips makes you aware of where you do a good job and where you don't,” Dr. Brull said.
Vitals
Source Elsevier Global Medical News
Meaningful Use: How, Where, When
The ONC provides the central leadership for the Medicare and Medicaid EHR incentive programs. The HITECH (Health Information Technology for Economic and Clinical Health) Act directly appropriated $2 billion to the ONC to spend on incentives and administration of the program.
The federal regulation governing the incentive program (some 800 pages) was issued in July 2010.
This year – 2011 – is the first year in which physicians can participate; they have until Oct. 1 to attest that they are meaningful users. To be eligible for incentive payments, physicians have to meet the meaningful use criteria for 90 consecutive days.
The criteria are being introduced in stages over the next 4-5 years. Stage 1 outlines what is expected in 2011 and 2012.
Stage 2 was expected to be put into place in 2013, but in June, the Health IT Policy Committee of the Centers for Medicare and Medicaid Services voted to delay implementation until 2014, but only for physicians who were already participating.
Physicians who wait until 2012 or later would still be expected to meet stage 2 criteria in 2013.
Physicians who want to participate have to choose between the Medicare or Medicaid incentive program. Those who take part in the Medicare program are eligible to receive incentive payments of $44,000 over 5 years. However, the payments will be made only through 2016.
Physicians who wait until 2012 to start would still earn the $44,000 maximum; those who start later would receive prorated payments.
Physicians who practice in designated Health Professional Shortage Areas may be eligible for an additional 10% in each year's incentive payment.
Importantly, Medicare begins to penalize nonparticipating physicians starting in 2016.
The Medicaid incentives are more generous: A total of $63,750 can be paid out over 6 years. And there's a longer time frame. Eligible professionals can wait until 2016 to start participating and still receive the maximum payout over a 6-year period.
In late May, the CMS announced that $75 million in Medicare incentives had been awarded to physicians and hospitals in the first 2 weeks of the program. Some states began paying out Medicaid incentives in January.
Meaningful Use: Some Physicians Struggle, Others Thrive
Many physicians continue to be frustrated and confused by the meaningful use criteria that spell out how they can receive incentive payments from Medicare and Medicaid for their use of electronic health records.
With that uncertainty, physicians are not jumping in with both feet to participate in the incentive program, even if they have purchased EHR systems. The Medical Group Management Association (MGMA) surveyed its members in April and found that 80% of those who already had adopted an EHR system said that they intended to participate. But at that time, only about 14% said that they were able to meet all of the criteria.
The American Medical Association held a special session on meaningful use at its House of Delegates meeting in June. When the speaker – Dr. Michael L. Hodgkins, an AMA chief medical information officer – asked how many physicians were confused about what was expected of them, more than half raised their hands.
Physicians in smaller practices are especially challenged, Dr. Hodgkins said, citing data that some 300,000 doctors are in practices of 10 or fewer physicians. Among those, fewer than 15% have implemented an EHR system, and most are not yet capable of meeting the meaningful use criteria.
According to Dr. Hodgkins, there are many obstacles to meeting meaningful use, including selecting from the more than 400 EHR products certified by the federal Office of the National Coordinator (ONC) for Health Information Technology, part of the Health and Human Services department.
Another problem: "Aggressive" timelines set by the government, according to Dr. Steve Waldren, director of the Center for Health Information Technology at the American Academy of Family Physicians (AAFP).
Dr. Waldren says it takes generally 6-18 months from purchase to active meaningful use of a system.
It’s been a tough road, he said. Physicians who don’t have EHRs or who have just gotten on board are struggling to get them operational and to achieve meaningful use. Those who have owned systems for awhile may face upgrades in order to meet the meaningful use criteria.
Meanwhile, there’s the system’s financial cost, training, and maintenance issues, and workflow changes once a system is in place.
The Long-Time User
Some physicians aren’t in a panic about the impending deadlines. Dr. Michael Mirro of Ft. Wayne (Ind.) Cardiology, a 24-physician group, said that his practice has been using health IT since 1996.
"We knew that we had to ultimately modernize our practice," Dr. Mirro said in an interview. Their current system has improved efficiency and quality, and has "supported a higher level of coding and reimbursement."
The system has "pretty much complete functionality," said Dr. Mirro. It provides the EHR, offers e-prescribing and decision-support tools, and can be used for direct quality reporting to the American College of Cardiology’s PINNACLE registry.
The system is web based, which reduces maintenance costs and IT headaches. The practice does not own the servers; it merely has local computers that interact with the vendor’s servers and software. The system is certified by the Certification Commission for Health Information Technology and was updated to ensure that the practice would meet the meaningful use criteria. One helpful tool, according to Dr. Mirro: A meaningful use "meter" that tells the physicians how well they are meeting the goals.
Ft. Wayne Cardiology has already attested to the government that it was a meaningful user and has received the maximum $18,000 per physician incentive for 2011, Dr. Mirro said.
The annual cost is about $2,000 per physician per year. That’s low, said Dr. Mirro, because his practice is owned by a hospital. The system is already somewhat ahead of the curve, as it already incorporates a patient web portal (a stage 2 goal).
He said that he is sympathetic to physicians who are just getting started.
"Any time you adopt technology at the point of care, it’s going to require a change in workflow," he said. That was definitely the case at Ft. Wayne Cardiology. For example, because some of the practice’s physicians still don’t know how to type, the system has templates that require point-and-click data entry to avoid errors.
Dr. Mirro said that physicians who are looking to buy or expand their health IT should talk with one of the 60 regional extension centers established by the ONC. These centers have been charged to help rural physicians and primary care physicians especially, and they offer vendor recommendations, practice audits, and other advice for free.
Dr. Mirro said that he believes most cardiologists will be forced to purchase an EHR sooner rather than later. With the decline in reimbursement (particularly for imaging services), cardiologists are increasingly being employed by hospitals. Those institutions – which themselves are facing a huge penalty if they don’t comply with meaningful use by 2017 – will want to have a lot of connectivity with the physician practice.
A Model For Her Peers
In 2005, Dr. Jennifer Brull figured that she needed to get on board with health IT, even though it might be expensive and difficult for a family physician in a rural Kansas solo practice. A younger physician with whom she was collaborating suggested that having an EHR was the wave of the future, and would likely be a necessity going forward. She also had a practice-sharing arrangement with another physician, who was older. He wasn’t as sure, said Dr. Brull in an interview.

But they moved ahead and spent 3 years selecting, buying, and implementing an EHR system that they could all use, said Dr. Brull, who practices in Plainview. She took out a loan for $50,000 to buy the equipment; her colleagues contributed to the software and other costs.
Because they practice in a rural area, there was no possibility of using a web-based model; broadband access in her area is still not robust enough, said Dr. Brull. So she has a server onsite at her office, and recently purchased a second server for $3,000. The net cost so far has been about $30,000 per physician, Dr. Brull said.
The first 6 months were a challenge, she said. "Anytime you do something that’s a complete paradigm shift, it’s hard. It’s hard mentally to think about all those changes, hard physically because you’re investing more time and effort, and hard emotionally because your staff gets freaked out."
In addition to allowing the practice to meet meaningful use criteria, the system also has a patient portal. The physicians are preparing to be able to participate in the state’s health information exchange.
Dr. Brull said that she disagrees with physicians who say that adopting an EHR interrupts the workflow or comes between the physician and patient.
"I’ve found it easier to be more collaborative [with my patients]," she said. One example: She recently used an EHR-generated graph to show a patient that she had gained 40 pounds over 3 years. The graph made much more of an impression on the patient than Dr. Brull could have done by reading numbers off a paper chart, she said.
"This whole project has resulted in dramatic quality improvement for my practice," Dr. Brull added.
Another example: She implemented a quality measure on breast cancer screening. Just by having a flag in the EHR, she went from screening 50% of patients to almost 100%. "Having the data at your fingertips makes you aware of where you do a good job and where you don’t," Dr. Brull said.
In April, Dr. Brull collected the full Medicare incentive payment for 2011. Her colleagues weren’t ready, but that didn’t matter. Physicians can choose to attest to meaningful use on their own time frame, regardless of where their colleagues might be, she said.
Dr. Brull has become an evangelist for the power of the EHR and meaningful use. She was chosen to speak at a CMS press conference announcing the first round of Medicare incentive payments. And she is a member of the regional extension center in Kansas. The ONC also named her a "MUVer" – someone who serves as a local leader and adviser.
The Reluctant Adopter
Dr. Michael Machen is one of the physicians who consulted with Dr. Brull. He practices with four other family physicians in nearby Quinter, Kan. (population, 980). The impetus for taking on an EHR came from his younger partners, Dr. Machen said in an interview. They were also motivated by the meaningful use program, and got started in July 2010.
One junior partner became the EHR champion, doing much of the legwork to find appropriate vendors and systems. The physicians also attended seminars and webinars offered by the Kansas Medical Society and the Kansas chapter of the AAFP. A team from the regional extension center visited their practice too, Dr. Machen said.
They borrowed $75,000 to purchase hardware and software. The biggest cost is the $2,000-$4,000 they spend monthly on IT support – a necessity when there is no one with such expertise in the practice or locally. The IT help comes from more than an hour away. Dr. Machen and his colleagues house the server themselves; broadband is no better in Quinter than it is in Plainview.
Dr. Machen said that the younger physicians have all done well with the system, but he is struggling.
"I’m not technically inclined, and I have very little computer knowledge," he said.
It has also been difficult for his nurse, who is spending more time on data entry and less on interacting with patients, Dr. Machen said, adding that they are both in their late 50s and are more frustrated with the system than are their younger colleagues.
His staff has been happy; there’s no more searching for charts, and coding is easier, he said. And he does see the potential for improving quality, especially with the data-collection effort, warnings about drug interactions, and prompts for screening tests.
But for the time being, "it’s horrible with the workflow and the patient flow." On days of 15-20 patient visits, using the EHR is not as much of an issue. But on days of 30 patient visits, "it’s not doable," he said.
So far, patients haven’t been wild about the transition, either. They don’t like the physician to be working on a computer during the visit, he said. And "I don’t like it much, either," said Dr. Machen. "When I was in medical school, I was taught that the second you enter the exam room, the patient has your undivided attention." That’s not really possible with an EHR, at least the way he sees it currently, although he also can see possible solutions, such as having a scribe.
Dr. Machen also said he has concerns about whether it’s possible to truly secure an EHR, and, whether the systems will truly improve patient outcomes. The jury is still out on that, he said.
But, he added, "I don’t want to be a naysayer." He said that he’s "on the upward slope of the learning curve," and expects to get more comfortable eventually.
In September, he’ll begin his 90-day period of meaningful use, with the aim of receiving an incentive payment by the end of the year.
Medicare and Medicaid Incentives
The ONC provides the central leadership for the Medicare and Medicaid EHR incentive programs. The HITECH (Health Information Technology for Economic and Clinical Health) Act directly appropriated $2 billion to the ONC to spend on incentives and administration of the program. The federal regulation governing the incentive program (some 800 pages) was issued in July 2010.
This year – 2011 – is the first year in which physicians can participate; they have until Oct. 1 to attest that they are meaningful users. To be eligible for incentive payments, physicians have to meet the meaningful use criteria for 90 consecutive days.
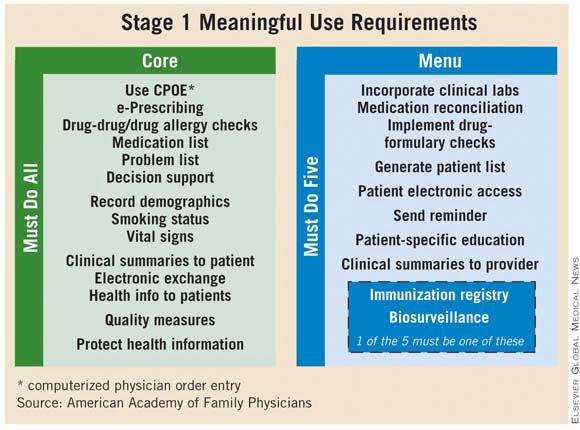
The criteria are being introduced in stages over the next 4-5 years. Stage 1 outlines what is expected in 2011 and 2012. Stage 2 was expected to be put into place in 2013, but in June, the Health IT Policy Committee of the Centers for Medicare and Medicaid Services voted to delay implementation until 2014, but only for physicians who were already participating. Physicians who wait until 2012 or later would still be expected to meet stage 2 criteria in 2013.
Physicians who want to participate have to choose between the Medicare or Medicaid incentive program. Those who take part in the Medicare program are eligible to receive incentive payments of $44,000 over 5 years. However, the payments will be made only through 2016. Physicians who wait until 2012 to start would still earn the $44,000 maximum; those who start later would receive prorated payments.
Physicians who practice in designated Health Professional Shortage Areas (HPSA) may be eligible for an additional 10% in each year’s incentive payment.
Importantly, Medicare begins to penalize nonparticipating physicians starting in 2016.
The Medicaid incentives are more generous: A total of $63,750 can be paid out over 6 years. And there’s a longer time frame. Eligible professionals can wait until 2016 to start participating and still receive the maximum payout over a 6-year period.
In late May, the CMS announced that $75 million in Medicare incentives had been awarded to physicians and hospitals in the first 2 weeks of the program. Some states began paying out Medicaid incentives in January. By late May, $83 million had been issued.
Meaningful use of EHRs is critical, according to Dr. Farzad Mostashari, the National Coordinator, who testified to the House Small Business Committee’s Subcommittee on Healthcare and Technology in June.
"If all we do is put an EHR in every provider’s office or hospital, we will have failed to realize health IT’s full potential," he said. "Instead, doctors, hospitals, and other providers need to use robust EHR technology in a meaningful and interoperable way to improve care."
Many physicians continue to be frustrated and confused by the meaningful use criteria that spell out how they can receive incentive payments from Medicare and Medicaid for their use of electronic health records.
With that uncertainty, physicians are not jumping in with both feet to participate in the incentive program, even if they have purchased EHR systems. The Medical Group Management Association (MGMA) surveyed its members in April and found that 80% of those who already had adopted an EHR system said that they intended to participate. But at that time, only about 14% said that they were able to meet all of the criteria.
The American Medical Association held a special session on meaningful use at its House of Delegates meeting in June. When the speaker – Dr. Michael L. Hodgkins, an AMA chief medical information officer – asked how many physicians were confused about what was expected of them, more than half raised their hands.
Physicians in smaller practices are especially challenged, Dr. Hodgkins said, citing data that some 300,000 doctors are in practices of 10 or fewer physicians. Among those, fewer than 15% have implemented an EHR system, and most are not yet capable of meeting the meaningful use criteria.
According to Dr. Hodgkins, there are many obstacles to meeting meaningful use, including selecting from the more than 400 EHR products certified by the federal Office of the National Coordinator (ONC) for Health Information Technology, part of the Health and Human Services department.
Another problem: "Aggressive" timelines set by the government, according to Dr. Steve Waldren, director of the Center for Health Information Technology at the American Academy of Family Physicians (AAFP).
Dr. Waldren says it takes generally 6-18 months from purchase to active meaningful use of a system.
It’s been a tough road, he said. Physicians who don’t have EHRs or who have just gotten on board are struggling to get them operational and to achieve meaningful use. Those who have owned systems for awhile may face upgrades in order to meet the meaningful use criteria.
Meanwhile, there’s the system’s financial cost, training, and maintenance issues, and workflow changes once a system is in place.
The Long-Time User
Some physicians aren’t in a panic about the impending deadlines. Dr. Michael Mirro of Ft. Wayne (Ind.) Cardiology, a 24-physician group, said that his practice has been using health IT since 1996.
"We knew that we had to ultimately modernize our practice," Dr. Mirro said in an interview. Their current system has improved efficiency and quality, and has "supported a higher level of coding and reimbursement."
The system has "pretty much complete functionality," said Dr. Mirro. It provides the EHR, offers e-prescribing and decision-support tools, and can be used for direct quality reporting to the American College of Cardiology’s PINNACLE registry.
The system is web based, which reduces maintenance costs and IT headaches. The practice does not own the servers; it merely has local computers that interact with the vendor’s servers and software. The system is certified by the Certification Commission for Health Information Technology and was updated to ensure that the practice would meet the meaningful use criteria. One helpful tool, according to Dr. Mirro: A meaningful use "meter" that tells the physicians how well they are meeting the goals.
Ft. Wayne Cardiology has already attested to the government that it was a meaningful user and has received the maximum $18,000 per physician incentive for 2011, Dr. Mirro said.
The annual cost is about $2,000 per physician per year. That’s low, said Dr. Mirro, because his practice is owned by a hospital. The system is already somewhat ahead of the curve, as it already incorporates a patient web portal (a stage 2 goal).
He said that he is sympathetic to physicians who are just getting started.
"Any time you adopt technology at the point of care, it’s going to require a change in workflow," he said. That was definitely the case at Ft. Wayne Cardiology. For example, because some of the practice’s physicians still don’t know how to type, the system has templates that require point-and-click data entry to avoid errors.
Dr. Mirro said that physicians who are looking to buy or expand their health IT should talk with one of the 60 regional extension centers established by the ONC. These centers have been charged to help rural physicians and primary care physicians especially, and they offer vendor recommendations, practice audits, and other advice for free.
Dr. Mirro said that he believes most cardiologists will be forced to purchase an EHR sooner rather than later. With the decline in reimbursement (particularly for imaging services), cardiologists are increasingly being employed by hospitals. Those institutions – which themselves are facing a huge penalty if they don’t comply with meaningful use by 2017 – will want to have a lot of connectivity with the physician practice.
A Model For Her Peers
In 2005, Dr. Jennifer Brull figured that she needed to get on board with health IT, even though it might be expensive and difficult for a family physician in a rural Kansas solo practice. A younger physician with whom she was collaborating suggested that having an EHR was the wave of the future, and would likely be a necessity going forward. She also had a practice-sharing arrangement with another physician, who was older. He wasn’t as sure, said Dr. Brull in an interview.
But they moved ahead and spent 3 years selecting, buying, and implementing an EHR system that they could all use, said Dr. Brull, who practices in Plainview. She took out a loan for $50,000 to buy the equipment; her colleagues contributed to the software and other costs.
Because they practice in a rural area, there was no possibility of using a web-based model; broadband access in her area is still not robust enough, said Dr. Brull. So she has a server onsite at her office, and recently purchased a second server for $3,000. The net cost so far has been about $30,000 per physician, Dr. Brull said.
The first 6 months were a challenge, she said. "Anytime you do something that’s a complete paradigm shift, it’s hard. It’s hard mentally to think about all those changes, hard physically because you’re investing more time and effort, and hard emotionally because your staff gets freaked out."
In addition to allowing the practice to meet meaningful use criteria, the system also has a patient portal. The physicians are preparing to be able to participate in the state’s health information exchange.
Dr. Brull said that she disagrees with physicians who say that adopting an EHR interrupts the workflow or comes between the physician and patient.
"I’ve found it easier to be more collaborative [with my patients]," she said. One example: She recently used an EHR-generated graph to show a patient that she had gained 40 pounds over 3 years. The graph made much more of an impression on the patient than Dr. Brull could have done by reading numbers off a paper chart, she said.
"This whole project has resulted in dramatic quality improvement for my practice," Dr. Brull added.
Another example: She implemented a quality measure on breast cancer screening. Just by having a flag in the EHR, she went from screening 50% of patients to almost 100%. "Having the data at your fingertips makes you aware of where you do a good job and where you don’t," Dr. Brull said.
In April, Dr. Brull collected the full Medicare incentive payment for 2011. Her colleagues weren’t ready, but that didn’t matter. Physicians can choose to attest to meaningful use on their own time frame, regardless of where their colleagues might be, she said.
Dr. Brull has become an evangelist for the power of the EHR and meaningful use. She was chosen to speak at a CMS press conference announcing the first round of Medicare incentive payments. And she is a member of the regional extension center in Kansas. The ONC also named her a "MUVer" – someone who serves as a local leader and adviser.
The Reluctant Adopter
Dr. Michael Machen is one of the physicians who consulted with Dr. Brull. He practices with four other family physicians in nearby Quinter, Kan. (population, 980). The impetus for taking on an EHR came from his younger partners, Dr. Machen said in an interview. They were also motivated by the meaningful use program, and got started in July 2010.
One junior partner became the EHR champion, doing much of the legwork to find appropriate vendors and systems. The physicians also attended seminars and webinars offered by the Kansas Medical Society and the Kansas chapter of the AAFP. A team from the regional extension center visited their practice too, Dr. Machen said.
They borrowed $75,000 to purchase hardware and software. The biggest cost is the $2,000-$4,000 they spend monthly on IT support – a necessity when there is no one with such expertise in the practice or locally. The IT help comes from more than an hour away. Dr. Machen and his colleagues house the server themselves; broadband is no better in Quinter than it is in Plainview.
Dr. Machen said that the younger physicians have all done well with the system, but he is struggling.
"I’m not technically inclined, and I have very little computer knowledge," he said.
It has also been difficult for his nurse, who is spending more time on data entry and less on interacting with patients, Dr. Machen said, adding that they are both in their late 50s and are more frustrated with the system than are their younger colleagues.
His staff has been happy; there’s no more searching for charts, and coding is easier, he said. And he does see the potential for improving quality, especially with the data-collection effort, warnings about drug interactions, and prompts for screening tests.
But for the time being, "it’s horrible with the workflow and the patient flow." On days of 15-20 patient visits, using the EHR is not as much of an issue. But on days of 30 patient visits, "it’s not doable," he said.
So far, patients haven’t been wild about the transition, either. They don’t like the physician to be working on a computer during the visit, he said. And "I don’t like it much, either," said Dr. Machen. "When I was in medical school, I was taught that the second you enter the exam room, the patient has your undivided attention." That’s not really possible with an EHR, at least the way he sees it currently, although he also can see possible solutions, such as having a scribe.
Dr. Machen also said he has concerns about whether it’s possible to truly secure an EHR, and, whether the systems will truly improve patient outcomes. The jury is still out on that, he said.
But, he added, "I don’t want to be a naysayer." He said that he’s "on the upward slope of the learning curve," and expects to get more comfortable eventually.
In September, he’ll begin his 90-day period of meaningful use, with the aim of receiving an incentive payment by the end of the year.
Medicare and Medicaid Incentives
The ONC provides the central leadership for the Medicare and Medicaid EHR incentive programs. The HITECH (Health Information Technology for Economic and Clinical Health) Act directly appropriated $2 billion to the ONC to spend on incentives and administration of the program. The federal regulation governing the incentive program (some 800 pages) was issued in July 2010.
This year – 2011 – is the first year in which physicians can participate; they have until Oct. 1 to attest that they are meaningful users. To be eligible for incentive payments, physicians have to meet the meaningful use criteria for 90 consecutive days.
The criteria are being introduced in stages over the next 4-5 years. Stage 1 outlines what is expected in 2011 and 2012. Stage 2 was expected to be put into place in 2013, but in June, the Health IT Policy Committee of the Centers for Medicare and Medicaid Services voted to delay implementation until 2014, but only for physicians who were already participating. Physicians who wait until 2012 or later would still be expected to meet stage 2 criteria in 2013.
Physicians who want to participate have to choose between the Medicare or Medicaid incentive program. Those who take part in the Medicare program are eligible to receive incentive payments of $44,000 over 5 years. However, the payments will be made only through 2016. Physicians who wait until 2012 to start would still earn the $44,000 maximum; those who start later would receive prorated payments.
Physicians who practice in designated Health Professional Shortage Areas (HPSA) may be eligible for an additional 10% in each year’s incentive payment.
Importantly, Medicare begins to penalize nonparticipating physicians starting in 2016.
The Medicaid incentives are more generous: A total of $63,750 can be paid out over 6 years. And there’s a longer time frame. Eligible professionals can wait until 2016 to start participating and still receive the maximum payout over a 6-year period.
In late May, the CMS announced that $75 million in Medicare incentives had been awarded to physicians and hospitals in the first 2 weeks of the program. Some states began paying out Medicaid incentives in January. By late May, $83 million had been issued.
Meaningful use of EHRs is critical, according to Dr. Farzad Mostashari, the National Coordinator, who testified to the House Small Business Committee’s Subcommittee on Healthcare and Technology in June.
"If all we do is put an EHR in every provider’s office or hospital, we will have failed to realize health IT’s full potential," he said. "Instead, doctors, hospitals, and other providers need to use robust EHR technology in a meaningful and interoperable way to improve care."
Many physicians continue to be frustrated and confused by the meaningful use criteria that spell out how they can receive incentive payments from Medicare and Medicaid for their use of electronic health records.
With that uncertainty, physicians are not jumping in with both feet to participate in the incentive program, even if they have purchased EHR systems. The Medical Group Management Association (MGMA) surveyed its members in April and found that 80% of those who already had adopted an EHR system said that they intended to participate. But at that time, only about 14% said that they were able to meet all of the criteria.
The American Medical Association held a special session on meaningful use at its House of Delegates meeting in June. When the speaker – Dr. Michael L. Hodgkins, an AMA chief medical information officer – asked how many physicians were confused about what was expected of them, more than half raised their hands.
Physicians in smaller practices are especially challenged, Dr. Hodgkins said, citing data that some 300,000 doctors are in practices of 10 or fewer physicians. Among those, fewer than 15% have implemented an EHR system, and most are not yet capable of meeting the meaningful use criteria.
According to Dr. Hodgkins, there are many obstacles to meeting meaningful use, including selecting from the more than 400 EHR products certified by the federal Office of the National Coordinator (ONC) for Health Information Technology, part of the Health and Human Services department.
Another problem: "Aggressive" timelines set by the government, according to Dr. Steve Waldren, director of the Center for Health Information Technology at the American Academy of Family Physicians (AAFP).
Dr. Waldren says it takes generally 6-18 months from purchase to active meaningful use of a system.
It’s been a tough road, he said. Physicians who don’t have EHRs or who have just gotten on board are struggling to get them operational and to achieve meaningful use. Those who have owned systems for awhile may face upgrades in order to meet the meaningful use criteria.
Meanwhile, there’s the system’s financial cost, training, and maintenance issues, and workflow changes once a system is in place.
The Long-Time User
Some physicians aren’t in a panic about the impending deadlines. Dr. Michael Mirro of Ft. Wayne (Ind.) Cardiology, a 24-physician group, said that his practice has been using health IT since 1996.
"We knew that we had to ultimately modernize our practice," Dr. Mirro said in an interview. Their current system has improved efficiency and quality, and has "supported a higher level of coding and reimbursement."
The system has "pretty much complete functionality," said Dr. Mirro. It provides the EHR, offers e-prescribing and decision-support tools, and can be used for direct quality reporting to the American College of Cardiology’s PINNACLE registry.
The system is web based, which reduces maintenance costs and IT headaches. The practice does not own the servers; it merely has local computers that interact with the vendor’s servers and software. The system is certified by the Certification Commission for Health Information Technology and was updated to ensure that the practice would meet the meaningful use criteria. One helpful tool, according to Dr. Mirro: A meaningful use "meter" that tells the physicians how well they are meeting the goals.
Ft. Wayne Cardiology has already attested to the government that it was a meaningful user and has received the maximum $18,000 per physician incentive for 2011, Dr. Mirro said.
The annual cost is about $2,000 per physician per year. That’s low, said Dr. Mirro, because his practice is owned by a hospital. The system is already somewhat ahead of the curve, as it already incorporates a patient web portal (a stage 2 goal).
He said that he is sympathetic to physicians who are just getting started.
"Any time you adopt technology at the point of care, it’s going to require a change in workflow," he said. That was definitely the case at Ft. Wayne Cardiology. For example, because some of the practice’s physicians still don’t know how to type, the system has templates that require point-and-click data entry to avoid errors.
Dr. Mirro said that physicians who are looking to buy or expand their health IT should talk with one of the 60 regional extension centers established by the ONC. These centers have been charged to help rural physicians and primary care physicians especially, and they offer vendor recommendations, practice audits, and other advice for free.
Dr. Mirro said that he believes most cardiologists will be forced to purchase an EHR sooner rather than later. With the decline in reimbursement (particularly for imaging services), cardiologists are increasingly being employed by hospitals. Those institutions – which themselves are facing a huge penalty if they don’t comply with meaningful use by 2017 – will want to have a lot of connectivity with the physician practice.
A Model For Her Peers
In 2005, Dr. Jennifer Brull figured that she needed to get on board with health IT, even though it might be expensive and difficult for a family physician in a rural Kansas solo practice. A younger physician with whom she was collaborating suggested that having an EHR was the wave of the future, and would likely be a necessity going forward. She also had a practice-sharing arrangement with another physician, who was older. He wasn’t as sure, said Dr. Brull in an interview.
But they moved ahead and spent 3 years selecting, buying, and implementing an EHR system that they could all use, said Dr. Brull, who practices in Plainview. She took out a loan for $50,000 to buy the equipment; her colleagues contributed to the software and other costs.
Because they practice in a rural area, there was no possibility of using a web-based model; broadband access in her area is still not robust enough, said Dr. Brull. So she has a server onsite at her office, and recently purchased a second server for $3,000. The net cost so far has been about $30,000 per physician, Dr. Brull said.
The first 6 months were a challenge, she said. "Anytime you do something that’s a complete paradigm shift, it’s hard. It’s hard mentally to think about all those changes, hard physically because you’re investing more time and effort, and hard emotionally because your staff gets freaked out."
In addition to allowing the practice to meet meaningful use criteria, the system also has a patient portal. The physicians are preparing to be able to participate in the state’s health information exchange.
Dr. Brull said that she disagrees with physicians who say that adopting an EHR interrupts the workflow or comes between the physician and patient.
"I’ve found it easier to be more collaborative [with my patients]," she said. One example: She recently used an EHR-generated graph to show a patient that she had gained 40 pounds over 3 years. The graph made much more of an impression on the patient than Dr. Brull could have done by reading numbers off a paper chart, she said.
"This whole project has resulted in dramatic quality improvement for my practice," Dr. Brull added.
Another example: She implemented a quality measure on breast cancer screening. Just by having a flag in the EHR, she went from screening 50% of patients to almost 100%. "Having the data at your fingertips makes you aware of where you do a good job and where you don’t," Dr. Brull said.
In April, Dr. Brull collected the full Medicare incentive payment for 2011. Her colleagues weren’t ready, but that didn’t matter. Physicians can choose to attest to meaningful use on their own time frame, regardless of where their colleagues might be, she said.
Dr. Brull has become an evangelist for the power of the EHR and meaningful use. She was chosen to speak at a CMS press conference announcing the first round of Medicare incentive payments. And she is a member of the regional extension center in Kansas. The ONC also named her a "MUVer" – someone who serves as a local leader and adviser.
The Reluctant Adopter
Dr. Michael Machen is one of the physicians who consulted with Dr. Brull. He practices with four other family physicians in nearby Quinter, Kan. (population, 980). The impetus for taking on an EHR came from his younger partners, Dr. Machen said in an interview. They were also motivated by the meaningful use program, and got started in July 2010.
One junior partner became the EHR champion, doing much of the legwork to find appropriate vendors and systems. The physicians also attended seminars and webinars offered by the Kansas Medical Society and the Kansas chapter of the AAFP. A team from the regional extension center visited their practice too, Dr. Machen said.
They borrowed $75,000 to purchase hardware and software. The biggest cost is the $2,000-$4,000 they spend monthly on IT support – a necessity when there is no one with such expertise in the practice or locally. The IT help comes from more than an hour away. Dr. Machen and his colleagues house the server themselves; broadband is no better in Quinter than it is in Plainview.
Dr. Machen said that the younger physicians have all done well with the system, but he is struggling.
"I’m not technically inclined, and I have very little computer knowledge," he said.
It has also been difficult for his nurse, who is spending more time on data entry and less on interacting with patients, Dr. Machen said, adding that they are both in their late 50s and are more frustrated with the system than are their younger colleagues.
His staff has been happy; there’s no more searching for charts, and coding is easier, he said. And he does see the potential for improving quality, especially with the data-collection effort, warnings about drug interactions, and prompts for screening tests.
But for the time being, "it’s horrible with the workflow and the patient flow." On days of 15-20 patient visits, using the EHR is not as much of an issue. But on days of 30 patient visits, "it’s not doable," he said.
So far, patients haven’t been wild about the transition, either. They don’t like the physician to be working on a computer during the visit, he said. And "I don’t like it much, either," said Dr. Machen. "When I was in medical school, I was taught that the second you enter the exam room, the patient has your undivided attention." That’s not really possible with an EHR, at least the way he sees it currently, although he also can see possible solutions, such as having a scribe.
Dr. Machen also said he has concerns about whether it’s possible to truly secure an EHR, and, whether the systems will truly improve patient outcomes. The jury is still out on that, he said.
But, he added, "I don’t want to be a naysayer." He said that he’s "on the upward slope of the learning curve," and expects to get more comfortable eventually.
In September, he’ll begin his 90-day period of meaningful use, with the aim of receiving an incentive payment by the end of the year.
Medicare and Medicaid Incentives
The ONC provides the central leadership for the Medicare and Medicaid EHR incentive programs. The HITECH (Health Information Technology for Economic and Clinical Health) Act directly appropriated $2 billion to the ONC to spend on incentives and administration of the program. The federal regulation governing the incentive program (some 800 pages) was issued in July 2010.
This year – 2011 – is the first year in which physicians can participate; they have until Oct. 1 to attest that they are meaningful users. To be eligible for incentive payments, physicians have to meet the meaningful use criteria for 90 consecutive days.
The criteria are being introduced in stages over the next 4-5 years. Stage 1 outlines what is expected in 2011 and 2012. Stage 2 was expected to be put into place in 2013, but in June, the Health IT Policy Committee of the Centers for Medicare and Medicaid Services voted to delay implementation until 2014, but only for physicians who were already participating. Physicians who wait until 2012 or later would still be expected to meet stage 2 criteria in 2013.
Physicians who want to participate have to choose between the Medicare or Medicaid incentive program. Those who take part in the Medicare program are eligible to receive incentive payments of $44,000 over 5 years. However, the payments will be made only through 2016. Physicians who wait until 2012 to start would still earn the $44,000 maximum; those who start later would receive prorated payments.
Physicians who practice in designated Health Professional Shortage Areas (HPSA) may be eligible for an additional 10% in each year’s incentive payment.
Importantly, Medicare begins to penalize nonparticipating physicians starting in 2016.
The Medicaid incentives are more generous: A total of $63,750 can be paid out over 6 years. And there’s a longer time frame. Eligible professionals can wait until 2016 to start participating and still receive the maximum payout over a 6-year period.
In late May, the CMS announced that $75 million in Medicare incentives had been awarded to physicians and hospitals in the first 2 weeks of the program. Some states began paying out Medicaid incentives in January. By late May, $83 million had been issued.
Meaningful use of EHRs is critical, according to Dr. Farzad Mostashari, the National Coordinator, who testified to the House Small Business Committee’s Subcommittee on Healthcare and Technology in June.
"If all we do is put an EHR in every provider’s office or hospital, we will have failed to realize health IT’s full potential," he said. "Instead, doctors, hospitals, and other providers need to use robust EHR technology in a meaningful and interoperable way to improve care."
Appeals Court Upholds Individual Mandate For Health Reform
In the first appeals court ruling on the Affordable Care Act, a three-judge panel of the 6th U.S. Circuit Court of Appeals ruled that the individual mandate requirement is constitutional.
The three judges – two Democratic appointees and one Republican appointee – said that requiring individuals to buy health insurance or face a penalty is legitimate and a “valid exercise of Congress's authority under the Commerce Clause.”
“The provision regulates active participation in the health care market, and in any case, the Constitution imposes no categorical bar on regulating inactivity,” the judges concluded in their opinion.
Judge James Graham dissented somewhat from the majority, stating that he was concerned that if Congress was allowed to use its power to levy the mandate, there might not be any limit to that ability in the future.
Challenges to the individual mandate have asserted that Congress does not have the ability to regulate inactivity, that is, the choice to not buy insurance. They also have argued that if Congress can order someone to purchase insurance, it could require Americans to do other things.
The plaintiffs in the 6th Circuit case had appealed a lower court ruling upholding the constitutionality of the individual mandate. Those plaintiffs – the Thomas More Law Center, a public interest law firm in Ann Arbor, Mich., and three individuals – presented oral arguments to the 6th Circuit on June 1, as did the Department of Justice (DOJ), as the defendant.
In a statement issued after the ruling, DOJ spokeswoman Tracy Schmaler said the government welcomed the judges' opinion. “We will continue to vigorously defend the health care reform statute in any litigation challenging it,” she said
Ron Pollack, executive director of the advocacy group Families USA, also praised the ruling. “The court – made up of judges appointed by both Republican and Democratic presidents – recognized that health care makes up a substantial portion of the national economy and that Congress has the power to regulate that market,” he said in a statement.
Opinions from those other appellate courts – the 4th U.S. Circuit in Richmond, Va., and the 11th U.S. Circuit in Atlanta – are expected soon.
In the first appeals court ruling on the Affordable Care Act, a three-judge panel of the 6th U.S. Circuit Court of Appeals ruled that the individual mandate requirement is constitutional.
The three judges – two Democratic appointees and one Republican appointee – said that requiring individuals to buy health insurance or face a penalty is legitimate and a “valid exercise of Congress's authority under the Commerce Clause.”
“The provision regulates active participation in the health care market, and in any case, the Constitution imposes no categorical bar on regulating inactivity,” the judges concluded in their opinion.
Judge James Graham dissented somewhat from the majority, stating that he was concerned that if Congress was allowed to use its power to levy the mandate, there might not be any limit to that ability in the future.
Challenges to the individual mandate have asserted that Congress does not have the ability to regulate inactivity, that is, the choice to not buy insurance. They also have argued that if Congress can order someone to purchase insurance, it could require Americans to do other things.
The plaintiffs in the 6th Circuit case had appealed a lower court ruling upholding the constitutionality of the individual mandate. Those plaintiffs – the Thomas More Law Center, a public interest law firm in Ann Arbor, Mich., and three individuals – presented oral arguments to the 6th Circuit on June 1, as did the Department of Justice (DOJ), as the defendant.
In a statement issued after the ruling, DOJ spokeswoman Tracy Schmaler said the government welcomed the judges' opinion. “We will continue to vigorously defend the health care reform statute in any litigation challenging it,” she said
Ron Pollack, executive director of the advocacy group Families USA, also praised the ruling. “The court – made up of judges appointed by both Republican and Democratic presidents – recognized that health care makes up a substantial portion of the national economy and that Congress has the power to regulate that market,” he said in a statement.
Opinions from those other appellate courts – the 4th U.S. Circuit in Richmond, Va., and the 11th U.S. Circuit in Atlanta – are expected soon.
In the first appeals court ruling on the Affordable Care Act, a three-judge panel of the 6th U.S. Circuit Court of Appeals ruled that the individual mandate requirement is constitutional.
The three judges – two Democratic appointees and one Republican appointee – said that requiring individuals to buy health insurance or face a penalty is legitimate and a “valid exercise of Congress's authority under the Commerce Clause.”
“The provision regulates active participation in the health care market, and in any case, the Constitution imposes no categorical bar on regulating inactivity,” the judges concluded in their opinion.
Judge James Graham dissented somewhat from the majority, stating that he was concerned that if Congress was allowed to use its power to levy the mandate, there might not be any limit to that ability in the future.
Challenges to the individual mandate have asserted that Congress does not have the ability to regulate inactivity, that is, the choice to not buy insurance. They also have argued that if Congress can order someone to purchase insurance, it could require Americans to do other things.
The plaintiffs in the 6th Circuit case had appealed a lower court ruling upholding the constitutionality of the individual mandate. Those plaintiffs – the Thomas More Law Center, a public interest law firm in Ann Arbor, Mich., and three individuals – presented oral arguments to the 6th Circuit on June 1, as did the Department of Justice (DOJ), as the defendant.
In a statement issued after the ruling, DOJ spokeswoman Tracy Schmaler said the government welcomed the judges' opinion. “We will continue to vigorously defend the health care reform statute in any litigation challenging it,” she said
Ron Pollack, executive director of the advocacy group Families USA, also praised the ruling. “The court – made up of judges appointed by both Republican and Democratic presidents – recognized that health care makes up a substantial portion of the national economy and that Congress has the power to regulate that market,” he said in a statement.
Opinions from those other appellate courts – the 4th U.S. Circuit in Richmond, Va., and the 11th U.S. Circuit in Atlanta – are expected soon.
Costs Rise With Spreading Drug Shortages
The persistent shortages of several medications, especially injectable and infusion products, are now affecting virtually every hospital department, according to data released July 12.
The American Hospital Association and the American Society of Health System Pharmacists surveyed their memberships and found that 99.5% of hospitals had experienced one or more drug shortages in the last 6 months. Most hospitals reported delaying treatment or rationing certain products, and almost all said that the shortages have led to increased drug costs. This is not the first time the shortages have been reported to be a major problem. But it appears from the new data that shortages have grown from affecting mostly oncology departments to affecting the majority of clinical care areas at the hospital.
The June 2011 AHA survey included responses from 820 hospitals. Of all respondents, 90%-95% said that within the last 6 months they had experienced shortages of medications for the following clinical uses: surgery/anesthesia, emergency care, cardiovascular, gastrointestinal/nutrition, and pain management. Shortages were also noted in infectious diseases, oncology, neurology, endocrinology, obstetrics/gynecology, allergy, and psychiatry. Three-quarters of hospitals said they rarely or never received advance notice of the shortages.
In a separate study, researchers from the University of Michigan and the ASHP reported that the number of shortages in 2010 (211) was the highest ever recorded in a single year. The researchers surveyed ASHP members about the impact of 30 recent shortages; 353 pharmacists responded.
Pharmacists spent about 9 hrs/wk managing shortages, with an estimated annual labor cost of $216 million. Shortages seemed to hit bigger hospitals harder. When asked if drug shortages created an increased burden, 97% of respondents agreed or strongly agreed; 93% said shortages increased costs, and 55% said shortages compromised care (Am. J. Health-Syst. Pharm. 2011;68:e13-21 [doi:10.2146/ajhp110210]).
The shortage problem is attracting more attention in Congress. In February, Sen. Amy Klobuchar (D-Minn.) introduced the Preserving Access to Life-Saving Medications Act (S. 296), which would give the Food and Drug Administration the authority to require early notification from pharmaceutical companies when a shortage appears to be imminent. At press time, the bill had 11 cosponsors.
Rep. Diana DeGette (D-Col.) and Rep. Tom Rooney (R-Fla.) introduced the bill in the House in mid-July.
{kind=link}
Elsevier Global Medical News
The persistent shortages of several medications, especially injectable and infusion products, are now affecting virtually every hospital department, according to data released July 12.
The American Hospital Association and the American Society of Health System Pharmacists surveyed their memberships and found that 99.5% of hospitals had experienced one or more drug shortages in the last 6 months. Most hospitals reported delaying treatment or rationing certain products, and almost all said that the shortages have led to increased drug costs. This is not the first time the shortages have been reported to be a major problem. But it appears from the new data that shortages have grown from affecting mostly oncology departments to affecting the majority of clinical care areas at the hospital.
The June 2011 AHA survey included responses from 820 hospitals. Of all respondents, 90%-95% said that within the last 6 months they had experienced shortages of medications for the following clinical uses: surgery/anesthesia, emergency care, cardiovascular, gastrointestinal/nutrition, and pain management. Shortages were also noted in infectious diseases, oncology, neurology, endocrinology, obstetrics/gynecology, allergy, and psychiatry. Three-quarters of hospitals said they rarely or never received advance notice of the shortages.
In a separate study, researchers from the University of Michigan and the ASHP reported that the number of shortages in 2010 (211) was the highest ever recorded in a single year. The researchers surveyed ASHP members about the impact of 30 recent shortages; 353 pharmacists responded.
Pharmacists spent about 9 hrs/wk managing shortages, with an estimated annual labor cost of $216 million. Shortages seemed to hit bigger hospitals harder. When asked if drug shortages created an increased burden, 97% of respondents agreed or strongly agreed; 93% said shortages increased costs, and 55% said shortages compromised care (Am. J. Health-Syst. Pharm. 2011;68:e13-21 [doi:10.2146/ajhp110210]).
The shortage problem is attracting more attention in Congress. In February, Sen. Amy Klobuchar (D-Minn.) introduced the Preserving Access to Life-Saving Medications Act (S. 296), which would give the Food and Drug Administration the authority to require early notification from pharmaceutical companies when a shortage appears to be imminent. At press time, the bill had 11 cosponsors.
Rep. Diana DeGette (D-Col.) and Rep. Tom Rooney (R-Fla.) introduced the bill in the House in mid-July.
Elsevier Global Medical News
The persistent shortages of several medications, especially injectable and infusion products, are now affecting virtually every hospital department, according to data released July 12.
The American Hospital Association and the American Society of Health System Pharmacists surveyed their memberships and found that 99.5% of hospitals had experienced one or more drug shortages in the last 6 months. Most hospitals reported delaying treatment or rationing certain products, and almost all said that the shortages have led to increased drug costs. This is not the first time the shortages have been reported to be a major problem. But it appears from the new data that shortages have grown from affecting mostly oncology departments to affecting the majority of clinical care areas at the hospital.
The June 2011 AHA survey included responses from 820 hospitals. Of all respondents, 90%-95% said that within the last 6 months they had experienced shortages of medications for the following clinical uses: surgery/anesthesia, emergency care, cardiovascular, gastrointestinal/nutrition, and pain management. Shortages were also noted in infectious diseases, oncology, neurology, endocrinology, obstetrics/gynecology, allergy, and psychiatry. Three-quarters of hospitals said they rarely or never received advance notice of the shortages.
In a separate study, researchers from the University of Michigan and the ASHP reported that the number of shortages in 2010 (211) was the highest ever recorded in a single year. The researchers surveyed ASHP members about the impact of 30 recent shortages; 353 pharmacists responded.
Pharmacists spent about 9 hrs/wk managing shortages, with an estimated annual labor cost of $216 million. Shortages seemed to hit bigger hospitals harder. When asked if drug shortages created an increased burden, 97% of respondents agreed or strongly agreed; 93% said shortages increased costs, and 55% said shortages compromised care (Am. J. Health-Syst. Pharm. 2011;68:e13-21 [doi:10.2146/ajhp110210]).
The shortage problem is attracting more attention in Congress. In February, Sen. Amy Klobuchar (D-Minn.) introduced the Preserving Access to Life-Saving Medications Act (S. 296), which would give the Food and Drug Administration the authority to require early notification from pharmaceutical companies when a shortage appears to be imminent. At press time, the bill had 11 cosponsors.
Rep. Diana DeGette (D-Col.) and Rep. Tom Rooney (R-Fla.) introduced the bill in the House in mid-July.
Elsevier Global Medical News
CMS Proposes 30% Physician Pay Cut for 2012 : Quality, cost measures may be used to set incentive payments.
As expected, the Centers for Medicare and Medicaid Services proposed that physician fees for 2012 would be reduced by 29.5%. The proposed rule was released in the Federal Register July 1.
The reduction is required by the Sustainable Growth Rate (SGR) formula that was part of the Balanced Budget Act of 1997. But Dr. Donald M. Berwick, CMS administrator, said in a statement that the agency is hoping to find a way to avoid the statutory decrease.
“This payment cut would have serious consequences and we cannot and will not allow it to happen,” Dr. Berwick said. “We need a permanent SGR fix to solve this problem once and for all. That's why the president's budget and his fiscal framework call for averting these cuts and why we are determined to pass and implement a permanent and sustainable fix.”
Dr. Peter W. Carmel, president of the American Medical Association, said that the reductions called for by the SGR formula are a constant threat to physicians' stability. “We are pleased that there is support from the administration and bipartisan members of congress for permanent reform of this broken system, but agreement is not enough,” Dr. Carmel said in a statement.
The AMA has been seeking a review and revision of the Medicare Economic Index (MEI), a measure of cost increases that affect physician practices. Dr. Carmel said that such a review was promised in the 2011 Medicare Physician Fee Schedule final rule, but the newly released proposed rule for 2012 shows it has not yet begun. Revisions in the MEI could significantly reduce the legislative cost of permanent reform of the Medicare physician payment formula,” said Dr. Carmel, noting that cost is an estimated $300 billion over the next 10 years, and is on its way to hit half a trillion dollars in a few years.
The reductions could be deeper for some specialties – especially for radiation oncology and diagnostic imaging – based on the impact of the Physician Practice Information Survey. The changes would reflect the third year of a 4-year transition to new practice expense relative value units.
And more payment changes may be looming. The CMS said in a statement that it is proposing to continue its efforts to identify what it calls “potentially misvalued codes.” As part of those efforts, it will be taking a look at all evaluation and management (E/M) codes to determine if they are undervalued. The agency also proposes to examine the highest non–E/M expenditure codes for each specialty to see if they are overvalued.
The agency said that the reviews will improve payment accuracy, in particular ensuring that primary care services are appropriately reimbursed. It's the first time the agency has looked across all specialties, according to the CMS.
“We believe strong efforts are needed to evaluate Medicare's fee schedule to ensure that it is paying accurately and ensuring that Medicare beneficiaries continue to have access to vital services, such as primary care services,” Jonathan Blum, director of the Center for Medicare, said in a statement.
Diagnostic imaging has been a target for Medicare, and it is again in this proposal. The agency wants to extend the multiple procedure payment reduction (MPPR) policy to the professional component of advanced imaging services, which includes computed tomography (CT) scans, MRI, and ultrasound.
The agency said the reduction would affect about 100 types of services. It is also the first time that the CMS has taken aim at the professional component of these services. That component would be reduced by 50% for subsequent procedures furnished to the same patient, on the same day, in the same session, resulting in an estimated $200 million in savings, according to the CMS.
For the first time, the agency is proposing quality and cost measures to be used in setting incentive payments for physicians who provide higher quality and more efficient care. That lays the groundwork for 2015, when the Affordable Care Act requires the CMS to begin making payment adjustments for certain physicians and physician groups. The requirement goes into effect for all physicians in 2017. The agency is proposing to use 2013 as the initial performance year.
In other issues addressed by the proposed rule, CMS seeks to add smoking cessation to the list of services that can be provided through telehealth. In the future, new services would be examined according to the clinical benefit they provide rather than on whether they are equivalent to a corresponding in-person service.
Finally, the CMS proposed some changes to the Physician Quality Reporting System, the ePrescribing Incentive Program, and the Electronic Health Records Incentive Program. The agency, for instance, is expanding the ways physicians can qualify for incentive payments under the meaningful use criteria.
Comments to the proposed rule can be submitted until Aug. 30 at http://www.regulations.gov
As expected, the Centers for Medicare and Medicaid Services proposed that physician fees for 2012 would be reduced by 29.5%. The proposed rule was released in the Federal Register July 1.
The reduction is required by the Sustainable Growth Rate (SGR) formula that was part of the Balanced Budget Act of 1997. But Dr. Donald M. Berwick, CMS administrator, said in a statement that the agency is hoping to find a way to avoid the statutory decrease.
“This payment cut would have serious consequences and we cannot and will not allow it to happen,” Dr. Berwick said. “We need a permanent SGR fix to solve this problem once and for all. That's why the president's budget and his fiscal framework call for averting these cuts and why we are determined to pass and implement a permanent and sustainable fix.”
Dr. Peter W. Carmel, president of the American Medical Association, said that the reductions called for by the SGR formula are a constant threat to physicians' stability. “We are pleased that there is support from the administration and bipartisan members of congress for permanent reform of this broken system, but agreement is not enough,” Dr. Carmel said in a statement.
The AMA has been seeking a review and revision of the Medicare Economic Index (MEI), a measure of cost increases that affect physician practices. Dr. Carmel said that such a review was promised in the 2011 Medicare Physician Fee Schedule final rule, but the newly released proposed rule for 2012 shows it has not yet begun. Revisions in the MEI could significantly reduce the legislative cost of permanent reform of the Medicare physician payment formula,” said Dr. Carmel, noting that cost is an estimated $300 billion over the next 10 years, and is on its way to hit half a trillion dollars in a few years.
The reductions could be deeper for some specialties – especially for radiation oncology and diagnostic imaging – based on the impact of the Physician Practice Information Survey. The changes would reflect the third year of a 4-year transition to new practice expense relative value units.
And more payment changes may be looming. The CMS said in a statement that it is proposing to continue its efforts to identify what it calls “potentially misvalued codes.” As part of those efforts, it will be taking a look at all evaluation and management (E/M) codes to determine if they are undervalued. The agency also proposes to examine the highest non–E/M expenditure codes for each specialty to see if they are overvalued.
The agency said that the reviews will improve payment accuracy, in particular ensuring that primary care services are appropriately reimbursed. It's the first time the agency has looked across all specialties, according to the CMS.
“We believe strong efforts are needed to evaluate Medicare's fee schedule to ensure that it is paying accurately and ensuring that Medicare beneficiaries continue to have access to vital services, such as primary care services,” Jonathan Blum, director of the Center for Medicare, said in a statement.
Diagnostic imaging has been a target for Medicare, and it is again in this proposal. The agency wants to extend the multiple procedure payment reduction (MPPR) policy to the professional component of advanced imaging services, which includes computed tomography (CT) scans, MRI, and ultrasound.
The agency said the reduction would affect about 100 types of services. It is also the first time that the CMS has taken aim at the professional component of these services. That component would be reduced by 50% for subsequent procedures furnished to the same patient, on the same day, in the same session, resulting in an estimated $200 million in savings, according to the CMS.
For the first time, the agency is proposing quality and cost measures to be used in setting incentive payments for physicians who provide higher quality and more efficient care. That lays the groundwork for 2015, when the Affordable Care Act requires the CMS to begin making payment adjustments for certain physicians and physician groups. The requirement goes into effect for all physicians in 2017. The agency is proposing to use 2013 as the initial performance year.
In other issues addressed by the proposed rule, CMS seeks to add smoking cessation to the list of services that can be provided through telehealth. In the future, new services would be examined according to the clinical benefit they provide rather than on whether they are equivalent to a corresponding in-person service.
Finally, the CMS proposed some changes to the Physician Quality Reporting System, the ePrescribing Incentive Program, and the Electronic Health Records Incentive Program. The agency, for instance, is expanding the ways physicians can qualify for incentive payments under the meaningful use criteria.
Comments to the proposed rule can be submitted until Aug. 30 at http://www.regulations.gov
As expected, the Centers for Medicare and Medicaid Services proposed that physician fees for 2012 would be reduced by 29.5%. The proposed rule was released in the Federal Register July 1.
The reduction is required by the Sustainable Growth Rate (SGR) formula that was part of the Balanced Budget Act of 1997. But Dr. Donald M. Berwick, CMS administrator, said in a statement that the agency is hoping to find a way to avoid the statutory decrease.
“This payment cut would have serious consequences and we cannot and will not allow it to happen,” Dr. Berwick said. “We need a permanent SGR fix to solve this problem once and for all. That's why the president's budget and his fiscal framework call for averting these cuts and why we are determined to pass and implement a permanent and sustainable fix.”
Dr. Peter W. Carmel, president of the American Medical Association, said that the reductions called for by the SGR formula are a constant threat to physicians' stability. “We are pleased that there is support from the administration and bipartisan members of congress for permanent reform of this broken system, but agreement is not enough,” Dr. Carmel said in a statement.
The AMA has been seeking a review and revision of the Medicare Economic Index (MEI), a measure of cost increases that affect physician practices. Dr. Carmel said that such a review was promised in the 2011 Medicare Physician Fee Schedule final rule, but the newly released proposed rule for 2012 shows it has not yet begun. Revisions in the MEI could significantly reduce the legislative cost of permanent reform of the Medicare physician payment formula,” said Dr. Carmel, noting that cost is an estimated $300 billion over the next 10 years, and is on its way to hit half a trillion dollars in a few years.
The reductions could be deeper for some specialties – especially for radiation oncology and diagnostic imaging – based on the impact of the Physician Practice Information Survey. The changes would reflect the third year of a 4-year transition to new practice expense relative value units.
And more payment changes may be looming. The CMS said in a statement that it is proposing to continue its efforts to identify what it calls “potentially misvalued codes.” As part of those efforts, it will be taking a look at all evaluation and management (E/M) codes to determine if they are undervalued. The agency also proposes to examine the highest non–E/M expenditure codes for each specialty to see if they are overvalued.
The agency said that the reviews will improve payment accuracy, in particular ensuring that primary care services are appropriately reimbursed. It's the first time the agency has looked across all specialties, according to the CMS.
“We believe strong efforts are needed to evaluate Medicare's fee schedule to ensure that it is paying accurately and ensuring that Medicare beneficiaries continue to have access to vital services, such as primary care services,” Jonathan Blum, director of the Center for Medicare, said in a statement.
Diagnostic imaging has been a target for Medicare, and it is again in this proposal. The agency wants to extend the multiple procedure payment reduction (MPPR) policy to the professional component of advanced imaging services, which includes computed tomography (CT) scans, MRI, and ultrasound.
The agency said the reduction would affect about 100 types of services. It is also the first time that the CMS has taken aim at the professional component of these services. That component would be reduced by 50% for subsequent procedures furnished to the same patient, on the same day, in the same session, resulting in an estimated $200 million in savings, according to the CMS.
For the first time, the agency is proposing quality and cost measures to be used in setting incentive payments for physicians who provide higher quality and more efficient care. That lays the groundwork for 2015, when the Affordable Care Act requires the CMS to begin making payment adjustments for certain physicians and physician groups. The requirement goes into effect for all physicians in 2017. The agency is proposing to use 2013 as the initial performance year.
In other issues addressed by the proposed rule, CMS seeks to add smoking cessation to the list of services that can be provided through telehealth. In the future, new services would be examined according to the clinical benefit they provide rather than on whether they are equivalent to a corresponding in-person service.
Finally, the CMS proposed some changes to the Physician Quality Reporting System, the ePrescribing Incentive Program, and the Electronic Health Records Incentive Program. The agency, for instance, is expanding the ways physicians can qualify for incentive payments under the meaningful use criteria.
Comments to the proposed rule can be submitted until Aug. 30 at http://www.regulations.gov
Court Upholds Individual Mandate
In the first appeals court ruling on the Affordable Care Act, a three-judge panel of the 6th U.S. Circuit Court of Appeals ruled that the individual mandate requirement is constitutional.
The three judges – two Democratic appointees and one Republican appointee – said that requiring individuals to buy health insurance or face a penalty is legitimate and a “valid exercise of Congress's authority under the Commerce Clause.”
“The provision regulates active participation in the health care market, and in any case, the Constitution imposes no categorical bar on regulating inactivity,” the judges concluded.
Judge James Graham dissented somewhat from the majority, stating that he was concerned that if Congress was allowed to use its power to levy the mandate, there might not be any limit to that ability in the future.
Challenges to the individual mandate have asserted that Congress does not have the ability to regulate inactivity, that is, the choice to not buy insurance. They also have argued that if Congress can order someone to purchase insurance, it could require Americans to do other things.
The plaintiffs in the 6th Circuit case had appealed a lower court ruling upholding the constitutionality of the individual mandate. Those plaintiffs – the Thomas More Law Center, a public interest law firm in Ann Arbor, Mich., and three individuals – presented oral arguments to the appeals court on June 1, as did the Department of Justice (DOJ), as the defendant.
In a statement issued after the ruling, DOJ spokeswoman Tracy Schmaler said that the government welcomed the judges' opinion. “We will continue to vigorously defend the health care reform statute in any litigation challenging it,” said Ms. Schmaler, adding that challenges to other landmark laws such as the Social Security Act and the Civil Rights Act had failed.
Ron Pollack, executive director of the advocacy group Families USA, also praised the ruling. “The court – made up of judges appointed by both Republican and Democratic presidents – recognized that health care makes up a substantial portion of the national economy and that Congress has the power to regulate that market,” he said in a statement. “We expect that other appellate courts, and ultimately the Supreme Court, will reach the same decision.”
Opinions from those other appellate courts – the 4th U.S. Circuit in Richmond, Va., and the 11th U.S. Circuit in Atlanta – are expected soon.
In the first appeals court ruling on the Affordable Care Act, a three-judge panel of the 6th U.S. Circuit Court of Appeals ruled that the individual mandate requirement is constitutional.
The three judges – two Democratic appointees and one Republican appointee – said that requiring individuals to buy health insurance or face a penalty is legitimate and a “valid exercise of Congress's authority under the Commerce Clause.”
“The provision regulates active participation in the health care market, and in any case, the Constitution imposes no categorical bar on regulating inactivity,” the judges concluded.
Judge James Graham dissented somewhat from the majority, stating that he was concerned that if Congress was allowed to use its power to levy the mandate, there might not be any limit to that ability in the future.
Challenges to the individual mandate have asserted that Congress does not have the ability to regulate inactivity, that is, the choice to not buy insurance. They also have argued that if Congress can order someone to purchase insurance, it could require Americans to do other things.
The plaintiffs in the 6th Circuit case had appealed a lower court ruling upholding the constitutionality of the individual mandate. Those plaintiffs – the Thomas More Law Center, a public interest law firm in Ann Arbor, Mich., and three individuals – presented oral arguments to the appeals court on June 1, as did the Department of Justice (DOJ), as the defendant.
In a statement issued after the ruling, DOJ spokeswoman Tracy Schmaler said that the government welcomed the judges' opinion. “We will continue to vigorously defend the health care reform statute in any litigation challenging it,” said Ms. Schmaler, adding that challenges to other landmark laws such as the Social Security Act and the Civil Rights Act had failed.
Ron Pollack, executive director of the advocacy group Families USA, also praised the ruling. “The court – made up of judges appointed by both Republican and Democratic presidents – recognized that health care makes up a substantial portion of the national economy and that Congress has the power to regulate that market,” he said in a statement. “We expect that other appellate courts, and ultimately the Supreme Court, will reach the same decision.”
Opinions from those other appellate courts – the 4th U.S. Circuit in Richmond, Va., and the 11th U.S. Circuit in Atlanta – are expected soon.
In the first appeals court ruling on the Affordable Care Act, a three-judge panel of the 6th U.S. Circuit Court of Appeals ruled that the individual mandate requirement is constitutional.
The three judges – two Democratic appointees and one Republican appointee – said that requiring individuals to buy health insurance or face a penalty is legitimate and a “valid exercise of Congress's authority under the Commerce Clause.”
“The provision regulates active participation in the health care market, and in any case, the Constitution imposes no categorical bar on regulating inactivity,” the judges concluded.
Judge James Graham dissented somewhat from the majority, stating that he was concerned that if Congress was allowed to use its power to levy the mandate, there might not be any limit to that ability in the future.
Challenges to the individual mandate have asserted that Congress does not have the ability to regulate inactivity, that is, the choice to not buy insurance. They also have argued that if Congress can order someone to purchase insurance, it could require Americans to do other things.
The plaintiffs in the 6th Circuit case had appealed a lower court ruling upholding the constitutionality of the individual mandate. Those plaintiffs – the Thomas More Law Center, a public interest law firm in Ann Arbor, Mich., and three individuals – presented oral arguments to the appeals court on June 1, as did the Department of Justice (DOJ), as the defendant.
In a statement issued after the ruling, DOJ spokeswoman Tracy Schmaler said that the government welcomed the judges' opinion. “We will continue to vigorously defend the health care reform statute in any litigation challenging it,” said Ms. Schmaler, adding that challenges to other landmark laws such as the Social Security Act and the Civil Rights Act had failed.
Ron Pollack, executive director of the advocacy group Families USA, also praised the ruling. “The court – made up of judges appointed by both Republican and Democratic presidents – recognized that health care makes up a substantial portion of the national economy and that Congress has the power to regulate that market,” he said in a statement. “We expect that other appellate courts, and ultimately the Supreme Court, will reach the same decision.”
Opinions from those other appellate courts – the 4th U.S. Circuit in Richmond, Va., and the 11th U.S. Circuit in Atlanta – are expected soon.
AMA House Adopts Conflict of Interest Policy
CHICAGO – After 5 years of discussion and attempts at passage, the American Medical Association's House of Delegates adopted a conflict of interest policy to help guide physicians on the ethics of receiving pharmaceutical or device company funding for continuing medical education.
The House was asked to approve a report on financial arrangements prepared by the AMA Council on Ethical and Judicial Affairs (CEJA). But because so many members continued to be divided on what the AMA policy should be, the Reference Committee on Amendments to Constitution and Bylaws recommended that delegates put off any formal action and refer the matter yet again, this time to the AMA Board of Trustees.
When the resolution to refer came to the House floor, the vote was close, with 48% of delegates wanting to put off any action, and 52% voting against referral. Delegates were then asked whether to adopt the CEJA report. The vote was less ambiguous, with 60% voting in favor of adoption.
The report was supported by primary care delegations and many state delegations. Dr. Lori J. Heim, board chair of the American Academy of Family Physicians, said on the House floor that the latest iteration of the report addressed her organization's concerns and should be adopted.
“I hope we can deal with this today rather than refer it back,” said Dr. Heim, a family physician and hospitalist in Laurinburg, N.C. “The CEJA has found a compromise that we can all live with.”
Dr. William Golden, a delegate from the American College of Physicians, and a professor of medicine and public health at the University of Arkansas, Little Rock, said on the House floor that “version 5.0 is ready for distribution,” and urged passage of the policy.
Several delegates said that although most specialty societies have conflict of interest policies, it was important for the AMA to have its own.
But some delegates from surgical societies said that passage of the policy might harm important relationships between surgeons and industry.
The American College of Surgeons spoke against adoption of the policy.
In the report, the CEJA said it recognized that it could have looked more broadly at conflict of interest issues, but decided to focus on pharmaceutical, biotechnology, and medical device company sponsorship of continuing medical education.
“Narrowing our focus to CME allows us to explore the complex considerations at stake in a manageable context and to provide practical ethical guidance on issues that increasingly challenge physicians as professionals,” according to the CEJA report.
The CEJA concluded that “physicians should strive to avoid financial relationships with industry.”
Instead, physicians should “cultivate alternative sources of support” and “design and conduct educational activities so as to reduce costs.”
They also “should insist that content developers and faculty members not have problematic ties with industry, to ensure independent, unbiased, high-quality educational programming that best meets physicians' needs and is accessible and affordable for all practitioners,” according to the report.
The report recognized that “it is not always feasible, or necessarily desirable, for professional education to disengage from industry completely.” In the cases where industry funding could not be avoided, “vigorous efforts must be made to mitigate the potential influence of financial relationships.”
CHICAGO – After 5 years of discussion and attempts at passage, the American Medical Association's House of Delegates adopted a conflict of interest policy to help guide physicians on the ethics of receiving pharmaceutical or device company funding for continuing medical education.
The House was asked to approve a report on financial arrangements prepared by the AMA Council on Ethical and Judicial Affairs (CEJA). But because so many members continued to be divided on what the AMA policy should be, the Reference Committee on Amendments to Constitution and Bylaws recommended that delegates put off any formal action and refer the matter yet again, this time to the AMA Board of Trustees.
When the resolution to refer came to the House floor, the vote was close, with 48% of delegates wanting to put off any action, and 52% voting against referral. Delegates were then asked whether to adopt the CEJA report. The vote was less ambiguous, with 60% voting in favor of adoption.
The report was supported by primary care delegations and many state delegations. Dr. Lori J. Heim, board chair of the American Academy of Family Physicians, said on the House floor that the latest iteration of the report addressed her organization's concerns and should be adopted.
“I hope we can deal with this today rather than refer it back,” said Dr. Heim, a family physician and hospitalist in Laurinburg, N.C. “The CEJA has found a compromise that we can all live with.”
Dr. William Golden, a delegate from the American College of Physicians, and a professor of medicine and public health at the University of Arkansas, Little Rock, said on the House floor that “version 5.0 is ready for distribution,” and urged passage of the policy.
Several delegates said that although most specialty societies have conflict of interest policies, it was important for the AMA to have its own.
But some delegates from surgical societies said that passage of the policy might harm important relationships between surgeons and industry.
The American College of Surgeons spoke against adoption of the policy.
In the report, the CEJA said it recognized that it could have looked more broadly at conflict of interest issues, but decided to focus on pharmaceutical, biotechnology, and medical device company sponsorship of continuing medical education.
“Narrowing our focus to CME allows us to explore the complex considerations at stake in a manageable context and to provide practical ethical guidance on issues that increasingly challenge physicians as professionals,” according to the CEJA report.
The CEJA concluded that “physicians should strive to avoid financial relationships with industry.”
Instead, physicians should “cultivate alternative sources of support” and “design and conduct educational activities so as to reduce costs.”
They also “should insist that content developers and faculty members not have problematic ties with industry, to ensure independent, unbiased, high-quality educational programming that best meets physicians' needs and is accessible and affordable for all practitioners,” according to the report.
The report recognized that “it is not always feasible, or necessarily desirable, for professional education to disengage from industry completely.” In the cases where industry funding could not be avoided, “vigorous efforts must be made to mitigate the potential influence of financial relationships.”
CHICAGO – After 5 years of discussion and attempts at passage, the American Medical Association's House of Delegates adopted a conflict of interest policy to help guide physicians on the ethics of receiving pharmaceutical or device company funding for continuing medical education.
The House was asked to approve a report on financial arrangements prepared by the AMA Council on Ethical and Judicial Affairs (CEJA). But because so many members continued to be divided on what the AMA policy should be, the Reference Committee on Amendments to Constitution and Bylaws recommended that delegates put off any formal action and refer the matter yet again, this time to the AMA Board of Trustees.
When the resolution to refer came to the House floor, the vote was close, with 48% of delegates wanting to put off any action, and 52% voting against referral. Delegates were then asked whether to adopt the CEJA report. The vote was less ambiguous, with 60% voting in favor of adoption.
The report was supported by primary care delegations and many state delegations. Dr. Lori J. Heim, board chair of the American Academy of Family Physicians, said on the House floor that the latest iteration of the report addressed her organization's concerns and should be adopted.
“I hope we can deal with this today rather than refer it back,” said Dr. Heim, a family physician and hospitalist in Laurinburg, N.C. “The CEJA has found a compromise that we can all live with.”
Dr. William Golden, a delegate from the American College of Physicians, and a professor of medicine and public health at the University of Arkansas, Little Rock, said on the House floor that “version 5.0 is ready for distribution,” and urged passage of the policy.
Several delegates said that although most specialty societies have conflict of interest policies, it was important for the AMA to have its own.
But some delegates from surgical societies said that passage of the policy might harm important relationships between surgeons and industry.
The American College of Surgeons spoke against adoption of the policy.
In the report, the CEJA said it recognized that it could have looked more broadly at conflict of interest issues, but decided to focus on pharmaceutical, biotechnology, and medical device company sponsorship of continuing medical education.
“Narrowing our focus to CME allows us to explore the complex considerations at stake in a manageable context and to provide practical ethical guidance on issues that increasingly challenge physicians as professionals,” according to the CEJA report.
The CEJA concluded that “physicians should strive to avoid financial relationships with industry.”
Instead, physicians should “cultivate alternative sources of support” and “design and conduct educational activities so as to reduce costs.”
They also “should insist that content developers and faculty members not have problematic ties with industry, to ensure independent, unbiased, high-quality educational programming that best meets physicians' needs and is accessible and affordable for all practitioners,” according to the report.
The report recognized that “it is not always feasible, or necessarily desirable, for professional education to disengage from industry completely.” In the cases where industry funding could not be avoided, “vigorous efforts must be made to mitigate the potential influence of financial relationships.”