User login
It’s board recertification time!
Kernohan’s notch false localizing sign. PPRF. The 7th nerve fascicle wraps around the 6th nerve nucleus. (Or is it the other way around?)

Yes, I’m studying for my 10-year boards.
It’s funny how many of these details you forget over time. I used to be able to rattle off names, syndromes, and pathways at the dreaded Thursday morning differential conference in residency. To not know them would get you a dreaded glare from the chairman. Now ... not as much.
Granted, the names of such things become less important over time. What’s important is the instinctive understanding of them that comes with experience. Remembering the specific name of a neural pathway becomes less relevant compared to recognizing where the problem is when you see that patient, and translating that into appropriate testing and treatment.
But, every 10 years, I have to go back to the books. Relearn the faded details of enzyme pathways, miscellaneous receptor actions, and courses of nerve tracts.
A lot of it is done on my iPad, a gadget I never imagined back in medical school, but it’s still the same routine I knew so well back then: Reading a page, staring blankly off to commit some point to memory, taking a practice test, and reviewing the answers. Occasionally, wandering off to get a can of soda or make tea.
Of course, today I have to work that around my family and job, concerns I didn’t have to split my time with in medical school. I had classmates who were married and had kids, and this always gives me a new respect for how they managed it.
Does knowing these details again make me a better doctor? I have no idea. I understand the idea that we need some way of showing we’re still on top of things after 20 years in the field. I’m not sure the current maintenance of certification practices are the best way to do that, but admittedly I don’t have any better ideas.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Kernohan’s notch false localizing sign. PPRF. The 7th nerve fascicle wraps around the 6th nerve nucleus. (Or is it the other way around?)
Yes, I’m studying for my 10-year boards.
It’s funny how many of these details you forget over time. I used to be able to rattle off names, syndromes, and pathways at the dreaded Thursday morning differential conference in residency. To not know them would get you a dreaded glare from the chairman. Now ... not as much.
Granted, the names of such things become less important over time. What’s important is the instinctive understanding of them that comes with experience. Remembering the specific name of a neural pathway becomes less relevant compared to recognizing where the problem is when you see that patient, and translating that into appropriate testing and treatment.
But, every 10 years, I have to go back to the books. Relearn the faded details of enzyme pathways, miscellaneous receptor actions, and courses of nerve tracts.
A lot of it is done on my iPad, a gadget I never imagined back in medical school, but it’s still the same routine I knew so well back then: Reading a page, staring blankly off to commit some point to memory, taking a practice test, and reviewing the answers. Occasionally, wandering off to get a can of soda or make tea.
Of course, today I have to work that around my family and job, concerns I didn’t have to split my time with in medical school. I had classmates who were married and had kids, and this always gives me a new respect for how they managed it.
Does knowing these details again make me a better doctor? I have no idea. I understand the idea that we need some way of showing we’re still on top of things after 20 years in the field. I’m not sure the current maintenance of certification practices are the best way to do that, but admittedly I don’t have any better ideas.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Kernohan’s notch false localizing sign. PPRF. The 7th nerve fascicle wraps around the 6th nerve nucleus. (Or is it the other way around?)
Yes, I’m studying for my 10-year boards.
It’s funny how many of these details you forget over time. I used to be able to rattle off names, syndromes, and pathways at the dreaded Thursday morning differential conference in residency. To not know them would get you a dreaded glare from the chairman. Now ... not as much.
Granted, the names of such things become less important over time. What’s important is the instinctive understanding of them that comes with experience. Remembering the specific name of a neural pathway becomes less relevant compared to recognizing where the problem is when you see that patient, and translating that into appropriate testing and treatment.
But, every 10 years, I have to go back to the books. Relearn the faded details of enzyme pathways, miscellaneous receptor actions, and courses of nerve tracts.
A lot of it is done on my iPad, a gadget I never imagined back in medical school, but it’s still the same routine I knew so well back then: Reading a page, staring blankly off to commit some point to memory, taking a practice test, and reviewing the answers. Occasionally, wandering off to get a can of soda or make tea.
Of course, today I have to work that around my family and job, concerns I didn’t have to split my time with in medical school. I had classmates who were married and had kids, and this always gives me a new respect for how they managed it.
Does knowing these details again make me a better doctor? I have no idea. I understand the idea that we need some way of showing we’re still on top of things after 20 years in the field. I’m not sure the current maintenance of certification practices are the best way to do that, but admittedly I don’t have any better ideas.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
ID Blog: The story of syphilis, part I
Rise of a global scourge
The Great Pox, the French Disease, Cupid’s Disease – syphilis has had many names throughout history.

Why should we care about the history of syphilis? Surely syphilis has reached the status of a nonentity disease – in-and-out of the doctor’s office with a course of antibiotics and farewell to the problem. And on the surface, that is certainly true. For now. In the developed world. For those with access to reasonable health care.
But that is all the shiny surface of modern medical triumph. Despite successes in prevention throughout the late 20th and early 21st century, syphilis is making comeback. A growing reservoir of syphilis, often untreated, lies hidden by the invisibility of poorer nations and increasingly in the lower economic strata of the developed world. And the danger is increased by the rise of antibiotic-resistant strains of the disease.
Over the last decade, the European Union and several other high-income countries observed an increasing syphilis trend, according to a recent report by the European Centre for Disease Prevention and Control. And in the United States, the Centers for Disease Control and Prevention has expressed concern over “the rising tide of syphilis” and a “devastating surge in congenital syphilis.” Many reasons have been suggested for this resurgence of syphilis, including the prevalence of unprotected sex and the overall increase in multiple sexual partners in the sexually active population. This trend has been ascribed to a reduced fear of acquiring HIV from condomless sex because of the rise of antiretroviral therapies, which make HIV infection no longer a death sentence for those who have access to and can afford the drugs.
Men who have sex with men are the most affected population cited, which may in part be related to the trend in unprotected sex that has accompanied the decreasing fear of HIV. But in some countries, syphilis rates among heterosexual populations are on the increase as well. Even more troubling were the increases in syphilis diagnosed among pregnant women that were reported in high-income settings outside of the European Union, which led to increases in congenital syphilis infections.
According to a 2018 update on the global epidemiology of syphilis, each year an estimated 6 million new cases are diagnosed in people aged 15-49 years, with more than 300,000 fetal and neonatal deaths attributed to the disease. An additional 215,000 infants are at increased risk of early death because of prenatal infection.
For syphilis is indeed a nasty disease. But a remarkable one as well. It presents an almost textbook example of disease evolution and adaptation writ large. It is also a disease with equally remarkable properties – acute, systemic, latent, eruptive, and congenital in its various manifestations. As Sir William Osler, one of the brightest lights of medical education of his time, said in 1897: “I often tell my students that it [syphilis] is the only disease which they require to know thoroughly. Know syphilis in all its manifestations and relations, and all other things clinical will be added unto you.”
Syphilis is caused by the spirochete Treponema pallidum subspecies pallidum and is generally acquired by sexual contact. Congenital syphilis infection occurs by transplacental transmission.
In its modern manifestation, the disease evolves through several stages – primary, secondary, and tertiary. Primary, noncongenital infection is characterized by a lesion. This chancre, as it is called, occurs at the original site of infection, typically between 10 days and 3 months after exposure. The chancre usually appears on the genitals, but given the variety of sexual behaviors, chancres can also occur on the rectum, tongue, pharynx, breast, and so on. The myth of only choosing “a clean partner,” one without visible lesions, is misleading because vaginal and rectal lesions may not be easy to spot yet still remain profoundly infectious.
The secondary stage of an untreated infection occurs 2-3 months after the onset of chancre, and results in multisystem involvement as the spirochetes spread through the bloodstream. Symptoms include skin rash (involving the palms and the soles of the feet) and potentially a variety of other dermatologic manifestations. Fever and swollen lymph nodes may also be present before the disease moves into a latent stage, in which no clinical symptoms are evident. Following this, tertiary syphilis can occur 10-30 years after the initial infection in about 30% of the untreated population, resulting in neurosyphilis, cardiovascular syphilis, or late benign syphilis. Disease progression in tertiary syphilis can lead to dementia, disfigurement, and death.
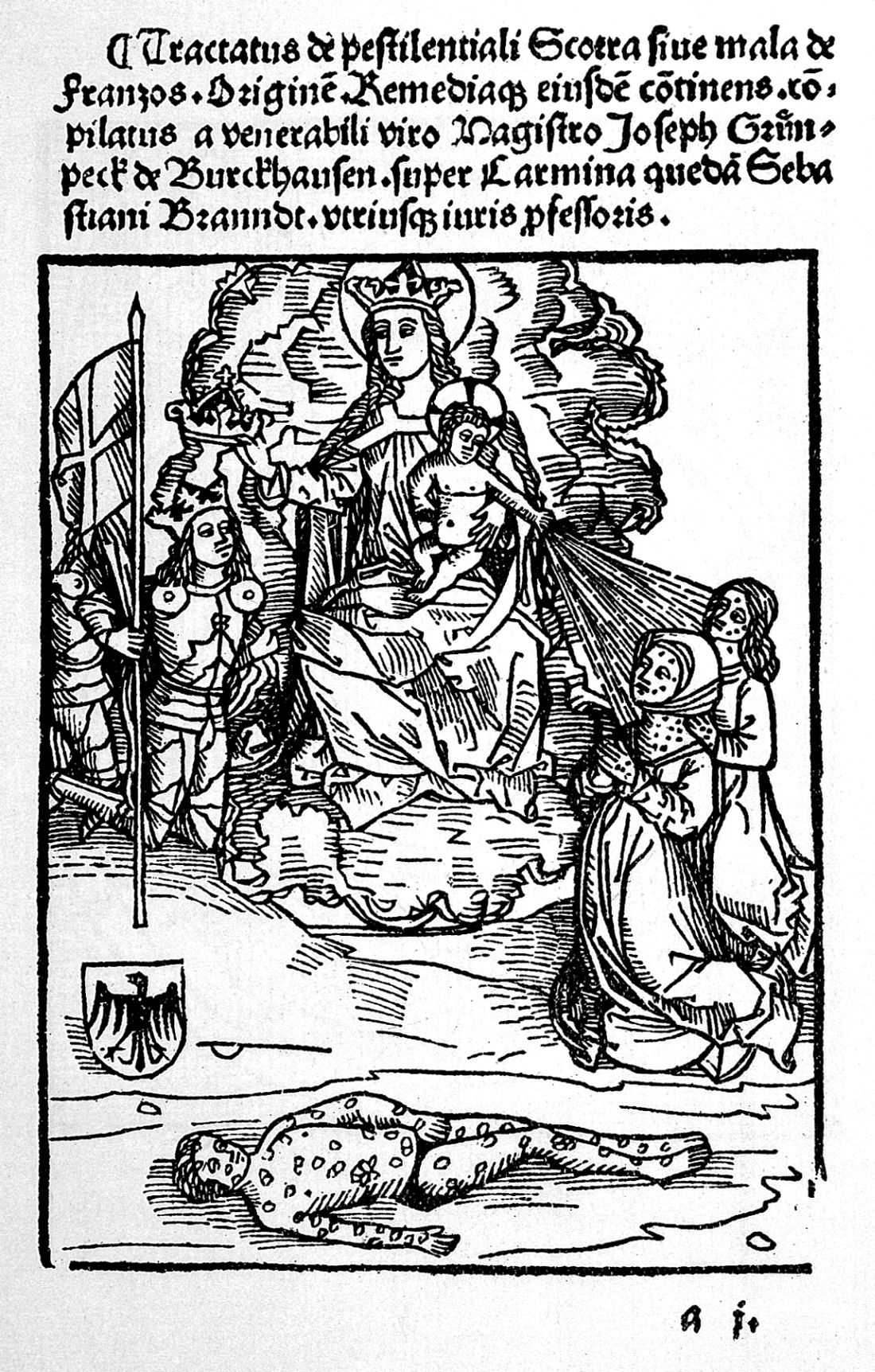
Sounds bad, doesn’t it? But what we’ve just recounted is the relatively benign disease that modern syphilis has become. Syphilis began as a sweeping, lethal epidemic in the late 15th century spreading dread across the world from the Americas to Europe and then to Asia at a speed equal to the fastest sailing ships of the era.
Syphilis first appeared in Naples in its epidemic form in 1495. Recent anthropological and historical consensus has suggested that syphilis, as we know it today, like tobacco, potatoes, and maize is a product of the Americas that was brought to the Old World by the intrepid exploits of one Christopher Columbus in 1493. Just as the Spanish inadvertently brought smallpox to devastate the population of the New World, Christopher Columbus appears to have brought epidemic syphilis to the Old World in an ironic twist of fate.
Ruy Diaz de Isla, one of two Spanish physicians present when Christopher Columbus returned from his first voyage to America, wrote in a manuscript that Pinzon de Palos, the pilot of Columbus, and also other members of the crew already suffered from symptoms of what was likely syphilis on their return from the New World
Although there has been some controversy regarding the origin of the syphilis epidemic, a recent molecular study using a large collection of pathogenic Treponema strains indicated that venereal syphilis arose relatively recently in human history, and that the closest related syphilis-causing strains were found in South America, providing support for the Columbian theory of syphilis’s origin.
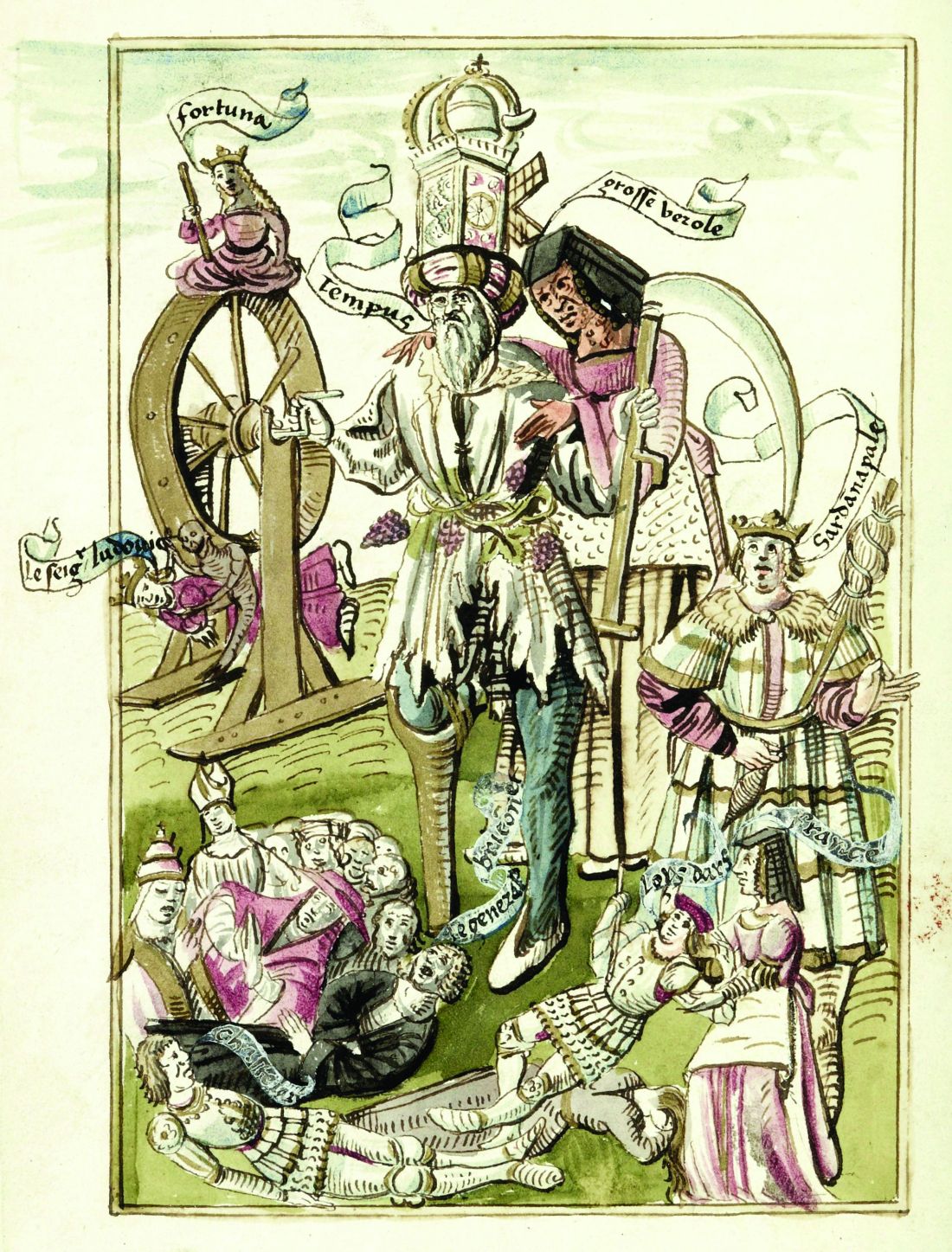
Syphilis flamed across Europe like wildfire, lit by a series of small wars that started shortly after Columbus’s return. Soldiers throughout history have indulged themselves in activities well primed for the spread of venereal disease, and the doughty warriors of the late 15th century were no exception. And throughout the next 500-plus years, syphilis and war rode across the world in tandem, like the white and red horsemen of the Apocalypse.
In its initial launch, syphilis had the help of Charles VIII, the King of France, who had invaded Italy in early 1495 with an army of more than 30,000 mercenaries recruited from across Europe. His forces conquered Naples, which was primarily defended by Spanish mercenaries.
When Charles VIII broke up his army, “mercenaries, infected with a mysterious, serious disease, returned to their native lands or moved elsewhere to wage war, spreading the disease across Europe.” The “Great Pox” initially struck Italy, France, Germany, and Switzerland in 1495; then Holland and Greece in the following year, reaching England and Scotland by 1497; and then Hungary, Poland, and the Scandinavian countries by 1500.
As this period was the Age of Exploration, French, Dutch, and English sailors soon carried syphilis across the rest of an unsuspecting world, with the disease reaching India in 1498 before moving also to Africa and then throughout the rest of Asia in the early 16th century.
And yet, one of the most remarkable parts of the story is the rapid transformation of syphilis from a deadly virulent epidemic to a (comparatively) benign endemic status. Which will be the subject of my next posting.
Mark Lesney is the managing editor of MDedge.com/IDPractioner . He has a PhD in Plant Virology and a PhD in the History of Science, with a focus on the history of biotechnology and medicine. He has served as an adjunct assistant professor at the Georgetown University School of Medicine, Department of Biochemistry and Molecular & Cellular Biology, Washington, DC.
Rise of a global scourge
Rise of a global scourge
The Great Pox, the French Disease, Cupid’s Disease – syphilis has had many names throughout history.
Why should we care about the history of syphilis? Surely syphilis has reached the status of a nonentity disease – in-and-out of the doctor’s office with a course of antibiotics and farewell to the problem. And on the surface, that is certainly true. For now. In the developed world. For those with access to reasonable health care.
But that is all the shiny surface of modern medical triumph. Despite successes in prevention throughout the late 20th and early 21st century, syphilis is making comeback. A growing reservoir of syphilis, often untreated, lies hidden by the invisibility of poorer nations and increasingly in the lower economic strata of the developed world. And the danger is increased by the rise of antibiotic-resistant strains of the disease.
Over the last decade, the European Union and several other high-income countries observed an increasing syphilis trend, according to a recent report by the European Centre for Disease Prevention and Control. And in the United States, the Centers for Disease Control and Prevention has expressed concern over “the rising tide of syphilis” and a “devastating surge in congenital syphilis.” Many reasons have been suggested for this resurgence of syphilis, including the prevalence of unprotected sex and the overall increase in multiple sexual partners in the sexually active population. This trend has been ascribed to a reduced fear of acquiring HIV from condomless sex because of the rise of antiretroviral therapies, which make HIV infection no longer a death sentence for those who have access to and can afford the drugs.
Men who have sex with men are the most affected population cited, which may in part be related to the trend in unprotected sex that has accompanied the decreasing fear of HIV. But in some countries, syphilis rates among heterosexual populations are on the increase as well. Even more troubling were the increases in syphilis diagnosed among pregnant women that were reported in high-income settings outside of the European Union, which led to increases in congenital syphilis infections.
According to a 2018 update on the global epidemiology of syphilis, each year an estimated 6 million new cases are diagnosed in people aged 15-49 years, with more than 300,000 fetal and neonatal deaths attributed to the disease. An additional 215,000 infants are at increased risk of early death because of prenatal infection.
For syphilis is indeed a nasty disease. But a remarkable one as well. It presents an almost textbook example of disease evolution and adaptation writ large. It is also a disease with equally remarkable properties – acute, systemic, latent, eruptive, and congenital in its various manifestations. As Sir William Osler, one of the brightest lights of medical education of his time, said in 1897: “I often tell my students that it [syphilis] is the only disease which they require to know thoroughly. Know syphilis in all its manifestations and relations, and all other things clinical will be added unto you.”
Syphilis is caused by the spirochete Treponema pallidum subspecies pallidum and is generally acquired by sexual contact. Congenital syphilis infection occurs by transplacental transmission.
In its modern manifestation, the disease evolves through several stages – primary, secondary, and tertiary. Primary, noncongenital infection is characterized by a lesion. This chancre, as it is called, occurs at the original site of infection, typically between 10 days and 3 months after exposure. The chancre usually appears on the genitals, but given the variety of sexual behaviors, chancres can also occur on the rectum, tongue, pharynx, breast, and so on. The myth of only choosing “a clean partner,” one without visible lesions, is misleading because vaginal and rectal lesions may not be easy to spot yet still remain profoundly infectious.
The secondary stage of an untreated infection occurs 2-3 months after the onset of chancre, and results in multisystem involvement as the spirochetes spread through the bloodstream. Symptoms include skin rash (involving the palms and the soles of the feet) and potentially a variety of other dermatologic manifestations. Fever and swollen lymph nodes may also be present before the disease moves into a latent stage, in which no clinical symptoms are evident. Following this, tertiary syphilis can occur 10-30 years after the initial infection in about 30% of the untreated population, resulting in neurosyphilis, cardiovascular syphilis, or late benign syphilis. Disease progression in tertiary syphilis can lead to dementia, disfigurement, and death.
Sounds bad, doesn’t it? But what we’ve just recounted is the relatively benign disease that modern syphilis has become. Syphilis began as a sweeping, lethal epidemic in the late 15th century spreading dread across the world from the Americas to Europe and then to Asia at a speed equal to the fastest sailing ships of the era.
Syphilis first appeared in Naples in its epidemic form in 1495. Recent anthropological and historical consensus has suggested that syphilis, as we know it today, like tobacco, potatoes, and maize is a product of the Americas that was brought to the Old World by the intrepid exploits of one Christopher Columbus in 1493. Just as the Spanish inadvertently brought smallpox to devastate the population of the New World, Christopher Columbus appears to have brought epidemic syphilis to the Old World in an ironic twist of fate.
Ruy Diaz de Isla, one of two Spanish physicians present when Christopher Columbus returned from his first voyage to America, wrote in a manuscript that Pinzon de Palos, the pilot of Columbus, and also other members of the crew already suffered from symptoms of what was likely syphilis on their return from the New World
Although there has been some controversy regarding the origin of the syphilis epidemic, a recent molecular study using a large collection of pathogenic Treponema strains indicated that venereal syphilis arose relatively recently in human history, and that the closest related syphilis-causing strains were found in South America, providing support for the Columbian theory of syphilis’s origin.
Syphilis flamed across Europe like wildfire, lit by a series of small wars that started shortly after Columbus’s return. Soldiers throughout history have indulged themselves in activities well primed for the spread of venereal disease, and the doughty warriors of the late 15th century were no exception. And throughout the next 500-plus years, syphilis and war rode across the world in tandem, like the white and red horsemen of the Apocalypse.
In its initial launch, syphilis had the help of Charles VIII, the King of France, who had invaded Italy in early 1495 with an army of more than 30,000 mercenaries recruited from across Europe. His forces conquered Naples, which was primarily defended by Spanish mercenaries.
When Charles VIII broke up his army, “mercenaries, infected with a mysterious, serious disease, returned to their native lands or moved elsewhere to wage war, spreading the disease across Europe.” The “Great Pox” initially struck Italy, France, Germany, and Switzerland in 1495; then Holland and Greece in the following year, reaching England and Scotland by 1497; and then Hungary, Poland, and the Scandinavian countries by 1500.
As this period was the Age of Exploration, French, Dutch, and English sailors soon carried syphilis across the rest of an unsuspecting world, with the disease reaching India in 1498 before moving also to Africa and then throughout the rest of Asia in the early 16th century.
And yet, one of the most remarkable parts of the story is the rapid transformation of syphilis from a deadly virulent epidemic to a (comparatively) benign endemic status. Which will be the subject of my next posting.
Mark Lesney is the managing editor of MDedge.com/IDPractioner . He has a PhD in Plant Virology and a PhD in the History of Science, with a focus on the history of biotechnology and medicine. He has served as an adjunct assistant professor at the Georgetown University School of Medicine, Department of Biochemistry and Molecular & Cellular Biology, Washington, DC.
The Great Pox, the French Disease, Cupid’s Disease – syphilis has had many names throughout history.
Why should we care about the history of syphilis? Surely syphilis has reached the status of a nonentity disease – in-and-out of the doctor’s office with a course of antibiotics and farewell to the problem. And on the surface, that is certainly true. For now. In the developed world. For those with access to reasonable health care.
But that is all the shiny surface of modern medical triumph. Despite successes in prevention throughout the late 20th and early 21st century, syphilis is making comeback. A growing reservoir of syphilis, often untreated, lies hidden by the invisibility of poorer nations and increasingly in the lower economic strata of the developed world. And the danger is increased by the rise of antibiotic-resistant strains of the disease.
Over the last decade, the European Union and several other high-income countries observed an increasing syphilis trend, according to a recent report by the European Centre for Disease Prevention and Control. And in the United States, the Centers for Disease Control and Prevention has expressed concern over “the rising tide of syphilis” and a “devastating surge in congenital syphilis.” Many reasons have been suggested for this resurgence of syphilis, including the prevalence of unprotected sex and the overall increase in multiple sexual partners in the sexually active population. This trend has been ascribed to a reduced fear of acquiring HIV from condomless sex because of the rise of antiretroviral therapies, which make HIV infection no longer a death sentence for those who have access to and can afford the drugs.
Men who have sex with men are the most affected population cited, which may in part be related to the trend in unprotected sex that has accompanied the decreasing fear of HIV. But in some countries, syphilis rates among heterosexual populations are on the increase as well. Even more troubling were the increases in syphilis diagnosed among pregnant women that were reported in high-income settings outside of the European Union, which led to increases in congenital syphilis infections.
According to a 2018 update on the global epidemiology of syphilis, each year an estimated 6 million new cases are diagnosed in people aged 15-49 years, with more than 300,000 fetal and neonatal deaths attributed to the disease. An additional 215,000 infants are at increased risk of early death because of prenatal infection.
For syphilis is indeed a nasty disease. But a remarkable one as well. It presents an almost textbook example of disease evolution and adaptation writ large. It is also a disease with equally remarkable properties – acute, systemic, latent, eruptive, and congenital in its various manifestations. As Sir William Osler, one of the brightest lights of medical education of his time, said in 1897: “I often tell my students that it [syphilis] is the only disease which they require to know thoroughly. Know syphilis in all its manifestations and relations, and all other things clinical will be added unto you.”
Syphilis is caused by the spirochete Treponema pallidum subspecies pallidum and is generally acquired by sexual contact. Congenital syphilis infection occurs by transplacental transmission.
In its modern manifestation, the disease evolves through several stages – primary, secondary, and tertiary. Primary, noncongenital infection is characterized by a lesion. This chancre, as it is called, occurs at the original site of infection, typically between 10 days and 3 months after exposure. The chancre usually appears on the genitals, but given the variety of sexual behaviors, chancres can also occur on the rectum, tongue, pharynx, breast, and so on. The myth of only choosing “a clean partner,” one without visible lesions, is misleading because vaginal and rectal lesions may not be easy to spot yet still remain profoundly infectious.
The secondary stage of an untreated infection occurs 2-3 months after the onset of chancre, and results in multisystem involvement as the spirochetes spread through the bloodstream. Symptoms include skin rash (involving the palms and the soles of the feet) and potentially a variety of other dermatologic manifestations. Fever and swollen lymph nodes may also be present before the disease moves into a latent stage, in which no clinical symptoms are evident. Following this, tertiary syphilis can occur 10-30 years after the initial infection in about 30% of the untreated population, resulting in neurosyphilis, cardiovascular syphilis, or late benign syphilis. Disease progression in tertiary syphilis can lead to dementia, disfigurement, and death.
Sounds bad, doesn’t it? But what we’ve just recounted is the relatively benign disease that modern syphilis has become. Syphilis began as a sweeping, lethal epidemic in the late 15th century spreading dread across the world from the Americas to Europe and then to Asia at a speed equal to the fastest sailing ships of the era.
Syphilis first appeared in Naples in its epidemic form in 1495. Recent anthropological and historical consensus has suggested that syphilis, as we know it today, like tobacco, potatoes, and maize is a product of the Americas that was brought to the Old World by the intrepid exploits of one Christopher Columbus in 1493. Just as the Spanish inadvertently brought smallpox to devastate the population of the New World, Christopher Columbus appears to have brought epidemic syphilis to the Old World in an ironic twist of fate.
Ruy Diaz de Isla, one of two Spanish physicians present when Christopher Columbus returned from his first voyage to America, wrote in a manuscript that Pinzon de Palos, the pilot of Columbus, and also other members of the crew already suffered from symptoms of what was likely syphilis on their return from the New World
Although there has been some controversy regarding the origin of the syphilis epidemic, a recent molecular study using a large collection of pathogenic Treponema strains indicated that venereal syphilis arose relatively recently in human history, and that the closest related syphilis-causing strains were found in South America, providing support for the Columbian theory of syphilis’s origin.
Syphilis flamed across Europe like wildfire, lit by a series of small wars that started shortly after Columbus’s return. Soldiers throughout history have indulged themselves in activities well primed for the spread of venereal disease, and the doughty warriors of the late 15th century were no exception. And throughout the next 500-plus years, syphilis and war rode across the world in tandem, like the white and red horsemen of the Apocalypse.
In its initial launch, syphilis had the help of Charles VIII, the King of France, who had invaded Italy in early 1495 with an army of more than 30,000 mercenaries recruited from across Europe. His forces conquered Naples, which was primarily defended by Spanish mercenaries.
When Charles VIII broke up his army, “mercenaries, infected with a mysterious, serious disease, returned to their native lands or moved elsewhere to wage war, spreading the disease across Europe.” The “Great Pox” initially struck Italy, France, Germany, and Switzerland in 1495; then Holland and Greece in the following year, reaching England and Scotland by 1497; and then Hungary, Poland, and the Scandinavian countries by 1500.
As this period was the Age of Exploration, French, Dutch, and English sailors soon carried syphilis across the rest of an unsuspecting world, with the disease reaching India in 1498 before moving also to Africa and then throughout the rest of Asia in the early 16th century.
And yet, one of the most remarkable parts of the story is the rapid transformation of syphilis from a deadly virulent epidemic to a (comparatively) benign endemic status. Which will be the subject of my next posting.
Mark Lesney is the managing editor of MDedge.com/IDPractioner . He has a PhD in Plant Virology and a PhD in the History of Science, with a focus on the history of biotechnology and medicine. He has served as an adjunct assistant professor at the Georgetown University School of Medicine, Department of Biochemistry and Molecular & Cellular Biology, Washington, DC.
Our EHRs have a drug problem
The “opioid epidemic” has become, perhaps, the most talked-about health crisis of the 21st century. It is a pervasive topic of discussion in the health literature and beyond, written about on the front pages of national newspapers and even mentioned in presidential state-of-the-union addresses.

As practicing physicians, we are all too familiar with the ills of chronic opioid use and have dealt with the implications of the crisis long before the issue attracted the public’s attention. In many ways, we have felt alone in bearing the burdens of caring for patients on chronic controlled substances. Until this point it has been our sacred duty to determine which patients are truly in need of those medications, and which are merely dependent on or – even worse – abusing them.
Health care providers have been largely blamed for the creation of this crisis, but we are not alone. Responsibility must also be shared by the pharmaceutical industry, health insurers, and even the government. Marketing practices, inadequate coverage of pain-relieving procedures and rehabilitation, and poorly-conceived drug policies have created an environment where it has been far too difficult to provide appropriate care for patients with chronic pain. As a result, patients who may have had an alternative to opioids were still started on these medications, and we – their physicians – have been left alone to manage the outcome.
Recently, however, health policy and public awareness have signaled a dramatic shift in the management of long-term pain medication. Significant legislation has been enacted on national, state, and local levels, and parties who are perceived to be responsible for the crisis are being held to task. For example, in August a landmark legal case was decided in an Oklahoma district court. Johnson & Johnson Pharmaceuticals was found guilty of promoting drug addiction through false and misleading marketing and was thus ordered to pay $572 million to the state to fund drug rehabilitation programs. This is likely a harbinger of many more such decisions to come, and the industry as a whole is bracing for the worst.
Physician prescribing practices are also being carefully scrutinized by the DEA, and a significant number of new “checks and balances” have been put in place to address dependence and addiction concerns. Unfortunately, as with all sweeping reform programs, there are good – and not-so-good – aspects to these changes. In many ways, the new tools at our disposal are a powerful way of mitigating drug dependence and diversion while protecting the sanctity of our “prescription pads.” Yet, as with so many other government mandates, we are burdened with the onus of complying with the new mandates for each and every opioid prescription, while our EHRs provide little help. This means more “clicks” for us, which can feel quite burdensome. It doesn’t need to be this way. Below are two straightforward things that can and should occur in order for providers to feel unburdened and to fully embrace the changes.
PDMP integration
One of the major ways of controlling prescription opioid abuse is through effective monitoring. Forty-nine of the 50 U.S. states have developed Prescription Drug Monitoring Programs (PDMPs), with Missouri being the only holdout (due to the politics of individual privacy concerns and conflation with gun control legislation). Most – though not all – of the states with a PDMP also mandate that physicians query a database prior to prescribing controlled substances. While noble and helpful in principle, querying a PDMP can be cumbersome, and the process is rarely integrated into the EHR workflow. Instead, physicians typically need to login to a separate website and manually transpose patient data to search the database. While most states have offered to subsidize PDMP integration with electronic records, EHR vendors have been very slow to develop the capability, leaving most physicians with no choice but to continue the aforementioned workflow. That is, if they comply at all; many well-meaning physicians have told us that they find themselves too harried to use the PDMP consistently. This reduces the value of these databases and places the physicians at significant risk. In some states, failure to query the database can lead to loss of a doctor’s medical license. It is high time that EHR vendors step up and integrate with every state’s prescription drug database.
Electronic prescribing of controlled substances
The other major milestone in prescription opioid management is the electronic prescribing of controlled substances (EPCS). This received national priority when the SUPPORT for Patients and Communities Act was signed into federal law in October of 2018. Included in this act is a requirement that, by January of 2021, all controlled substance prescriptions covered under Medicare Part D be sent electronically. Taking this as inspiration, many states and private companies have adopted more aggressive policies, choosing to implement electronic prescription requirements prior to the 2021 deadline. In Pennsylvania, where we practice, an EPCS requirement goes into effect in October of this year (2019). National pharmacy chains have also taken a more proactive approach. Walmart, for example, has decided that it will require EPCS nationwide in all of its stores beginning in January of 2020.
Essentially physicians have no choice – if they plan to continue to prescribe controlled substances, they will need to begin doing so electronically. Unfortunately, this may not be a straightforward process. While most EHRs offer some sort of EPCS solution, it is typically far from user friendly. Setting up EPCS can be costly and incredibly time consuming, and the procedure of actually submitting controlled prescriptions can be onerous and add many extra clicks. If vendors are serious about assisting in solving the opioid crisis, they need to make streamlining the steps of EPCS a high priority.
A prescription for success
As with so many other topics we’ve written about, we face an ever-increasing burden to provide quality patient care while complying with cumbersome and often unfunded external mandates. In the case of the opioid crisis, we believe we can do better. Our prescription for success? Streamlined workflow, smarter EHRs, and fewer clicks. There is no question that physicians and patients will benefit from effective implementation of the new tools at our disposal, but we need EHR vendors to step up and help carry the load.
Dr. Notte is a family physician and associate chief medical information officer for Abington (Pa.) Jefferson Health. Follow him on Twitter @doctornotte. Dr. Skolnik is professor of family and community medicine at Jefferson Medical College, Philadelphia, and an associate director of the family medicine residency program at Abington (Pa.) Jefferson Health.
The “opioid epidemic” has become, perhaps, the most talked-about health crisis of the 21st century. It is a pervasive topic of discussion in the health literature and beyond, written about on the front pages of national newspapers and even mentioned in presidential state-of-the-union addresses.
As practicing physicians, we are all too familiar with the ills of chronic opioid use and have dealt with the implications of the crisis long before the issue attracted the public’s attention. In many ways, we have felt alone in bearing the burdens of caring for patients on chronic controlled substances. Until this point it has been our sacred duty to determine which patients are truly in need of those medications, and which are merely dependent on or – even worse – abusing them.
Health care providers have been largely blamed for the creation of this crisis, but we are not alone. Responsibility must also be shared by the pharmaceutical industry, health insurers, and even the government. Marketing practices, inadequate coverage of pain-relieving procedures and rehabilitation, and poorly-conceived drug policies have created an environment where it has been far too difficult to provide appropriate care for patients with chronic pain. As a result, patients who may have had an alternative to opioids were still started on these medications, and we – their physicians – have been left alone to manage the outcome.
Recently, however, health policy and public awareness have signaled a dramatic shift in the management of long-term pain medication. Significant legislation has been enacted on national, state, and local levels, and parties who are perceived to be responsible for the crisis are being held to task. For example, in August a landmark legal case was decided in an Oklahoma district court. Johnson & Johnson Pharmaceuticals was found guilty of promoting drug addiction through false and misleading marketing and was thus ordered to pay $572 million to the state to fund drug rehabilitation programs. This is likely a harbinger of many more such decisions to come, and the industry as a whole is bracing for the worst.
Physician prescribing practices are also being carefully scrutinized by the DEA, and a significant number of new “checks and balances” have been put in place to address dependence and addiction concerns. Unfortunately, as with all sweeping reform programs, there are good – and not-so-good – aspects to these changes. In many ways, the new tools at our disposal are a powerful way of mitigating drug dependence and diversion while protecting the sanctity of our “prescription pads.” Yet, as with so many other government mandates, we are burdened with the onus of complying with the new mandates for each and every opioid prescription, while our EHRs provide little help. This means more “clicks” for us, which can feel quite burdensome. It doesn’t need to be this way. Below are two straightforward things that can and should occur in order for providers to feel unburdened and to fully embrace the changes.
PDMP integration
One of the major ways of controlling prescription opioid abuse is through effective monitoring. Forty-nine of the 50 U.S. states have developed Prescription Drug Monitoring Programs (PDMPs), with Missouri being the only holdout (due to the politics of individual privacy concerns and conflation with gun control legislation). Most – though not all – of the states with a PDMP also mandate that physicians query a database prior to prescribing controlled substances. While noble and helpful in principle, querying a PDMP can be cumbersome, and the process is rarely integrated into the EHR workflow. Instead, physicians typically need to login to a separate website and manually transpose patient data to search the database. While most states have offered to subsidize PDMP integration with electronic records, EHR vendors have been very slow to develop the capability, leaving most physicians with no choice but to continue the aforementioned workflow. That is, if they comply at all; many well-meaning physicians have told us that they find themselves too harried to use the PDMP consistently. This reduces the value of these databases and places the physicians at significant risk. In some states, failure to query the database can lead to loss of a doctor’s medical license. It is high time that EHR vendors step up and integrate with every state’s prescription drug database.
Electronic prescribing of controlled substances
The other major milestone in prescription opioid management is the electronic prescribing of controlled substances (EPCS). This received national priority when the SUPPORT for Patients and Communities Act was signed into federal law in October of 2018. Included in this act is a requirement that, by January of 2021, all controlled substance prescriptions covered under Medicare Part D be sent electronically. Taking this as inspiration, many states and private companies have adopted more aggressive policies, choosing to implement electronic prescription requirements prior to the 2021 deadline. In Pennsylvania, where we practice, an EPCS requirement goes into effect in October of this year (2019). National pharmacy chains have also taken a more proactive approach. Walmart, for example, has decided that it will require EPCS nationwide in all of its stores beginning in January of 2020.
Essentially physicians have no choice – if they plan to continue to prescribe controlled substances, they will need to begin doing so electronically. Unfortunately, this may not be a straightforward process. While most EHRs offer some sort of EPCS solution, it is typically far from user friendly. Setting up EPCS can be costly and incredibly time consuming, and the procedure of actually submitting controlled prescriptions can be onerous and add many extra clicks. If vendors are serious about assisting in solving the opioid crisis, they need to make streamlining the steps of EPCS a high priority.
A prescription for success
As with so many other topics we’ve written about, we face an ever-increasing burden to provide quality patient care while complying with cumbersome and often unfunded external mandates. In the case of the opioid crisis, we believe we can do better. Our prescription for success? Streamlined workflow, smarter EHRs, and fewer clicks. There is no question that physicians and patients will benefit from effective implementation of the new tools at our disposal, but we need EHR vendors to step up and help carry the load.
Dr. Notte is a family physician and associate chief medical information officer for Abington (Pa.) Jefferson Health. Follow him on Twitter @doctornotte. Dr. Skolnik is professor of family and community medicine at Jefferson Medical College, Philadelphia, and an associate director of the family medicine residency program at Abington (Pa.) Jefferson Health.
The “opioid epidemic” has become, perhaps, the most talked-about health crisis of the 21st century. It is a pervasive topic of discussion in the health literature and beyond, written about on the front pages of national newspapers and even mentioned in presidential state-of-the-union addresses.
As practicing physicians, we are all too familiar with the ills of chronic opioid use and have dealt with the implications of the crisis long before the issue attracted the public’s attention. In many ways, we have felt alone in bearing the burdens of caring for patients on chronic controlled substances. Until this point it has been our sacred duty to determine which patients are truly in need of those medications, and which are merely dependent on or – even worse – abusing them.
Health care providers have been largely blamed for the creation of this crisis, but we are not alone. Responsibility must also be shared by the pharmaceutical industry, health insurers, and even the government. Marketing practices, inadequate coverage of pain-relieving procedures and rehabilitation, and poorly-conceived drug policies have created an environment where it has been far too difficult to provide appropriate care for patients with chronic pain. As a result, patients who may have had an alternative to opioids were still started on these medications, and we – their physicians – have been left alone to manage the outcome.
Recently, however, health policy and public awareness have signaled a dramatic shift in the management of long-term pain medication. Significant legislation has been enacted on national, state, and local levels, and parties who are perceived to be responsible for the crisis are being held to task. For example, in August a landmark legal case was decided in an Oklahoma district court. Johnson & Johnson Pharmaceuticals was found guilty of promoting drug addiction through false and misleading marketing and was thus ordered to pay $572 million to the state to fund drug rehabilitation programs. This is likely a harbinger of many more such decisions to come, and the industry as a whole is bracing for the worst.
Physician prescribing practices are also being carefully scrutinized by the DEA, and a significant number of new “checks and balances” have been put in place to address dependence and addiction concerns. Unfortunately, as with all sweeping reform programs, there are good – and not-so-good – aspects to these changes. In many ways, the new tools at our disposal are a powerful way of mitigating drug dependence and diversion while protecting the sanctity of our “prescription pads.” Yet, as with so many other government mandates, we are burdened with the onus of complying with the new mandates for each and every opioid prescription, while our EHRs provide little help. This means more “clicks” for us, which can feel quite burdensome. It doesn’t need to be this way. Below are two straightforward things that can and should occur in order for providers to feel unburdened and to fully embrace the changes.
PDMP integration
One of the major ways of controlling prescription opioid abuse is through effective monitoring. Forty-nine of the 50 U.S. states have developed Prescription Drug Monitoring Programs (PDMPs), with Missouri being the only holdout (due to the politics of individual privacy concerns and conflation with gun control legislation). Most – though not all – of the states with a PDMP also mandate that physicians query a database prior to prescribing controlled substances. While noble and helpful in principle, querying a PDMP can be cumbersome, and the process is rarely integrated into the EHR workflow. Instead, physicians typically need to login to a separate website and manually transpose patient data to search the database. While most states have offered to subsidize PDMP integration with electronic records, EHR vendors have been very slow to develop the capability, leaving most physicians with no choice but to continue the aforementioned workflow. That is, if they comply at all; many well-meaning physicians have told us that they find themselves too harried to use the PDMP consistently. This reduces the value of these databases and places the physicians at significant risk. In some states, failure to query the database can lead to loss of a doctor’s medical license. It is high time that EHR vendors step up and integrate with every state’s prescription drug database.
Electronic prescribing of controlled substances
The other major milestone in prescription opioid management is the electronic prescribing of controlled substances (EPCS). This received national priority when the SUPPORT for Patients and Communities Act was signed into federal law in October of 2018. Included in this act is a requirement that, by January of 2021, all controlled substance prescriptions covered under Medicare Part D be sent electronically. Taking this as inspiration, many states and private companies have adopted more aggressive policies, choosing to implement electronic prescription requirements prior to the 2021 deadline. In Pennsylvania, where we practice, an EPCS requirement goes into effect in October of this year (2019). National pharmacy chains have also taken a more proactive approach. Walmart, for example, has decided that it will require EPCS nationwide in all of its stores beginning in January of 2020.
Essentially physicians have no choice – if they plan to continue to prescribe controlled substances, they will need to begin doing so electronically. Unfortunately, this may not be a straightforward process. While most EHRs offer some sort of EPCS solution, it is typically far from user friendly. Setting up EPCS can be costly and incredibly time consuming, and the procedure of actually submitting controlled prescriptions can be onerous and add many extra clicks. If vendors are serious about assisting in solving the opioid crisis, they need to make streamlining the steps of EPCS a high priority.
A prescription for success
As with so many other topics we’ve written about, we face an ever-increasing burden to provide quality patient care while complying with cumbersome and often unfunded external mandates. In the case of the opioid crisis, we believe we can do better. Our prescription for success? Streamlined workflow, smarter EHRs, and fewer clicks. There is no question that physicians and patients will benefit from effective implementation of the new tools at our disposal, but we need EHR vendors to step up and help carry the load.
Dr. Notte is a family physician and associate chief medical information officer for Abington (Pa.) Jefferson Health. Follow him on Twitter @doctornotte. Dr. Skolnik is professor of family and community medicine at Jefferson Medical College, Philadelphia, and an associate director of the family medicine residency program at Abington (Pa.) Jefferson Health.
Curative intent and palliative care – compatible goals?
The first signs are always vague. Katie (not her real name) was 33 years old and loved to spend her weekends hiking. First, it was fatigue when doing elevation. Then fatigue even while walking across flat ground. One day she just sat in bed and noticed her heart racing.

One blood test, and her primary care doctor called her at home with the results. Go to the emergency room, she said. Katie’s red blood cells were dangerously low. She would need a blood transfusion.
Something was wrong, but the list of possibilities remained broad. Someone in the emergency room tossed out the word “leukemia.” Katie froze. She liked the resident who tossed out “internal bleeding” better.
This was the start of the ups and downs; the good news and bad news; the branch points that opened and closed her future.
The hematologist-oncologist came by. You need to be admitted to the hospital, and we need to do a bone marrow biopsy, she told Katie. It could be – and then the word was said again – this time by a specialist, making it all the more real: leukemia.
Katie had a few days to sit with this. The bone marrow biopsy was done. Now, what type of leukemia? She read on her computer. She knew there were lots of kinds, some better than others. Now, she was praying for a “good” cancer.
It was one of the bad ones. But.
We sent off additional molecular and genetics testing from your bone marrow, the doctor explained. This type of leukemia can be divided into three groups: high risk, standard risk, and low risk. All the signs so far point to low risk. This is good news, Katie thought.
Six days later. The final cytogenetics came back. Actually, Katie had a rare mutation that automatically put her in the high risk category. It meant she would definitely need a bone marrow transplant to be cured. Bad.
And so she underwent induction chemotherapy. The nurse posted a big calendar on her wall and filled it with her daily blood counts. The counts are dropping, Katie noted. This is good, right? It means the leukemia is responding to chemo? Yes. Good news.
Four days later. The blast count in her blood crept up. It could be anything. It could be reactive. It doesn’t necessarily mean refractory leukemia. But. It’s bad news.
In the interim, some more testing came back. You have one sister, right? Sharon? Yes, Katie confirmed. Looks like Sharon is a perfect match for a bone marrow transplant. Katie cried. Such good news.
Two weeks later the next bone marrow biopsy was done. This shows how you responded to the chemotherapy, the doctors explained. Will it be in remission? Will it be refractory? It’s in remission. Wow, good news.
But the window to transplant is small. In the few weeks to get there, another test came back. Even though the cancer is technically in remission, you have something called minimal residual disease. Meaning there are small amounts of leukemia left over. We should bridge with more chemo before transplant.
Was this good news? Bad news? Who knew anymore?

It’s well known in the hematology and oncology world that – even with advanced disease and poor prognoses – patients with blood cancers are less likely to see palliative care than patients with solid tumors. At conferences and in academic journals, leaders in the field expound on why this may be. One reason is the inability for most hospice agencies to offer blood transfusions. That’s certainly a big piece.
Then there’s Katie. When Katie was diagnosed, she asked me what stage her cancer was. It’s a question I hear a lot. With leukemia, I explained, we don’t think about staging the same way we do for conditions like breast cancer or prostate cancer. Since it’s in the blood, it’s stage 4 by definition, I said, but that doesn’t mean anything about prognosis. Our model of thinking is fundamentally different.
With a solid stage 4 cancer, there is generally no chance for cure. The goal is stabilization: We want to keep the cancer where it is for as long as possible. A stable CT scan, in which the disease burden is identical to 3 months before, is a success. The difference between good news and bad news is in lifespan. Receiving bad news is the difference between projecting 2 years and 6 months to live.
With a stage 4 blood cancer like Katie’s leukemia, there is generally a chance for cure. The goal is to make the cancer disappear completely and have someone live a normal lifespan. The outcomes are binary. The difference between good news and bad news is not a difference in lifespan, but a difference in probability of cure. Receiving bad news is the difference between an 80% chance of cure and a 20% chance.
Whenever I order chemotherapy, the electronic record prompts me for my intent: Is this palliative or curative intent? I always type curative intent. The intent is curative until we choose to stop pursuing cure.
Grappling with uncertainty is an enormous challenge for anyone after a diagnosis of cancer. Not knowing whether cure is even possible makes it that much more complex. The outcomes are as diverse as can be. The next branch point can literally be the difference between no more cancer and no more options.
Which raises the question, at what point – if any – should we have asked palliative care to see Katie? I wish we would have done it sooner, not because patients like Katie won’t be cured, but to help them sit with the toughest of uncertainties; prepare for it; live in it as best as possible.
As I write this, Katie is undergoing a bone marrow transplant from her sister, the match. In a few weeks she will face her next branch point – whether the transplant worked. It will move her closer or further from a cure.
Dr. Yurkiewicz is a fellow in hematology and oncology at Stanford (Calif.) University. Follow her on Twitter @ilanayurkiewicz and listen to her each week on the Blood & Cancer podcast.
The first signs are always vague. Katie (not her real name) was 33 years old and loved to spend her weekends hiking. First, it was fatigue when doing elevation. Then fatigue even while walking across flat ground. One day she just sat in bed and noticed her heart racing.
One blood test, and her primary care doctor called her at home with the results. Go to the emergency room, she said. Katie’s red blood cells were dangerously low. She would need a blood transfusion.
Something was wrong, but the list of possibilities remained broad. Someone in the emergency room tossed out the word “leukemia.” Katie froze. She liked the resident who tossed out “internal bleeding” better.
This was the start of the ups and downs; the good news and bad news; the branch points that opened and closed her future.
The hematologist-oncologist came by. You need to be admitted to the hospital, and we need to do a bone marrow biopsy, she told Katie. It could be – and then the word was said again – this time by a specialist, making it all the more real: leukemia.
Katie had a few days to sit with this. The bone marrow biopsy was done. Now, what type of leukemia? She read on her computer. She knew there were lots of kinds, some better than others. Now, she was praying for a “good” cancer.
It was one of the bad ones. But.
We sent off additional molecular and genetics testing from your bone marrow, the doctor explained. This type of leukemia can be divided into three groups: high risk, standard risk, and low risk. All the signs so far point to low risk. This is good news, Katie thought.
Six days later. The final cytogenetics came back. Actually, Katie had a rare mutation that automatically put her in the high risk category. It meant she would definitely need a bone marrow transplant to be cured. Bad.
And so she underwent induction chemotherapy. The nurse posted a big calendar on her wall and filled it with her daily blood counts. The counts are dropping, Katie noted. This is good, right? It means the leukemia is responding to chemo? Yes. Good news.
Four days later. The blast count in her blood crept up. It could be anything. It could be reactive. It doesn’t necessarily mean refractory leukemia. But. It’s bad news.
In the interim, some more testing came back. You have one sister, right? Sharon? Yes, Katie confirmed. Looks like Sharon is a perfect match for a bone marrow transplant. Katie cried. Such good news.
Two weeks later the next bone marrow biopsy was done. This shows how you responded to the chemotherapy, the doctors explained. Will it be in remission? Will it be refractory? It’s in remission. Wow, good news.
But the window to transplant is small. In the few weeks to get there, another test came back. Even though the cancer is technically in remission, you have something called minimal residual disease. Meaning there are small amounts of leukemia left over. We should bridge with more chemo before transplant.
Was this good news? Bad news? Who knew anymore?
It’s well known in the hematology and oncology world that – even with advanced disease and poor prognoses – patients with blood cancers are less likely to see palliative care than patients with solid tumors. At conferences and in academic journals, leaders in the field expound on why this may be. One reason is the inability for most hospice agencies to offer blood transfusions. That’s certainly a big piece.
Then there’s Katie. When Katie was diagnosed, she asked me what stage her cancer was. It’s a question I hear a lot. With leukemia, I explained, we don’t think about staging the same way we do for conditions like breast cancer or prostate cancer. Since it’s in the blood, it’s stage 4 by definition, I said, but that doesn’t mean anything about prognosis. Our model of thinking is fundamentally different.
With a solid stage 4 cancer, there is generally no chance for cure. The goal is stabilization: We want to keep the cancer where it is for as long as possible. A stable CT scan, in which the disease burden is identical to 3 months before, is a success. The difference between good news and bad news is in lifespan. Receiving bad news is the difference between projecting 2 years and 6 months to live.
With a stage 4 blood cancer like Katie’s leukemia, there is generally a chance for cure. The goal is to make the cancer disappear completely and have someone live a normal lifespan. The outcomes are binary. The difference between good news and bad news is not a difference in lifespan, but a difference in probability of cure. Receiving bad news is the difference between an 80% chance of cure and a 20% chance.
Whenever I order chemotherapy, the electronic record prompts me for my intent: Is this palliative or curative intent? I always type curative intent. The intent is curative until we choose to stop pursuing cure.
Grappling with uncertainty is an enormous challenge for anyone after a diagnosis of cancer. Not knowing whether cure is even possible makes it that much more complex. The outcomes are as diverse as can be. The next branch point can literally be the difference between no more cancer and no more options.
Which raises the question, at what point – if any – should we have asked palliative care to see Katie? I wish we would have done it sooner, not because patients like Katie won’t be cured, but to help them sit with the toughest of uncertainties; prepare for it; live in it as best as possible.
As I write this, Katie is undergoing a bone marrow transplant from her sister, the match. In a few weeks she will face her next branch point – whether the transplant worked. It will move her closer or further from a cure.
Dr. Yurkiewicz is a fellow in hematology and oncology at Stanford (Calif.) University. Follow her on Twitter @ilanayurkiewicz and listen to her each week on the Blood & Cancer podcast.
The first signs are always vague. Katie (not her real name) was 33 years old and loved to spend her weekends hiking. First, it was fatigue when doing elevation. Then fatigue even while walking across flat ground. One day she just sat in bed and noticed her heart racing.
One blood test, and her primary care doctor called her at home with the results. Go to the emergency room, she said. Katie’s red blood cells were dangerously low. She would need a blood transfusion.
Something was wrong, but the list of possibilities remained broad. Someone in the emergency room tossed out the word “leukemia.” Katie froze. She liked the resident who tossed out “internal bleeding” better.
This was the start of the ups and downs; the good news and bad news; the branch points that opened and closed her future.
The hematologist-oncologist came by. You need to be admitted to the hospital, and we need to do a bone marrow biopsy, she told Katie. It could be – and then the word was said again – this time by a specialist, making it all the more real: leukemia.
Katie had a few days to sit with this. The bone marrow biopsy was done. Now, what type of leukemia? She read on her computer. She knew there were lots of kinds, some better than others. Now, she was praying for a “good” cancer.
It was one of the bad ones. But.
We sent off additional molecular and genetics testing from your bone marrow, the doctor explained. This type of leukemia can be divided into three groups: high risk, standard risk, and low risk. All the signs so far point to low risk. This is good news, Katie thought.
Six days later. The final cytogenetics came back. Actually, Katie had a rare mutation that automatically put her in the high risk category. It meant she would definitely need a bone marrow transplant to be cured. Bad.
And so she underwent induction chemotherapy. The nurse posted a big calendar on her wall and filled it with her daily blood counts. The counts are dropping, Katie noted. This is good, right? It means the leukemia is responding to chemo? Yes. Good news.
Four days later. The blast count in her blood crept up. It could be anything. It could be reactive. It doesn’t necessarily mean refractory leukemia. But. It’s bad news.
In the interim, some more testing came back. You have one sister, right? Sharon? Yes, Katie confirmed. Looks like Sharon is a perfect match for a bone marrow transplant. Katie cried. Such good news.
Two weeks later the next bone marrow biopsy was done. This shows how you responded to the chemotherapy, the doctors explained. Will it be in remission? Will it be refractory? It’s in remission. Wow, good news.
But the window to transplant is small. In the few weeks to get there, another test came back. Even though the cancer is technically in remission, you have something called minimal residual disease. Meaning there are small amounts of leukemia left over. We should bridge with more chemo before transplant.
Was this good news? Bad news? Who knew anymore?
It’s well known in the hematology and oncology world that – even with advanced disease and poor prognoses – patients with blood cancers are less likely to see palliative care than patients with solid tumors. At conferences and in academic journals, leaders in the field expound on why this may be. One reason is the inability for most hospice agencies to offer blood transfusions. That’s certainly a big piece.
Then there’s Katie. When Katie was diagnosed, she asked me what stage her cancer was. It’s a question I hear a lot. With leukemia, I explained, we don’t think about staging the same way we do for conditions like breast cancer or prostate cancer. Since it’s in the blood, it’s stage 4 by definition, I said, but that doesn’t mean anything about prognosis. Our model of thinking is fundamentally different.
With a solid stage 4 cancer, there is generally no chance for cure. The goal is stabilization: We want to keep the cancer where it is for as long as possible. A stable CT scan, in which the disease burden is identical to 3 months before, is a success. The difference between good news and bad news is in lifespan. Receiving bad news is the difference between projecting 2 years and 6 months to live.
With a stage 4 blood cancer like Katie’s leukemia, there is generally a chance for cure. The goal is to make the cancer disappear completely and have someone live a normal lifespan. The outcomes are binary. The difference between good news and bad news is not a difference in lifespan, but a difference in probability of cure. Receiving bad news is the difference between an 80% chance of cure and a 20% chance.
Whenever I order chemotherapy, the electronic record prompts me for my intent: Is this palliative or curative intent? I always type curative intent. The intent is curative until we choose to stop pursuing cure.
Grappling with uncertainty is an enormous challenge for anyone after a diagnosis of cancer. Not knowing whether cure is even possible makes it that much more complex. The outcomes are as diverse as can be. The next branch point can literally be the difference between no more cancer and no more options.
Which raises the question, at what point – if any – should we have asked palliative care to see Katie? I wish we would have done it sooner, not because patients like Katie won’t be cured, but to help them sit with the toughest of uncertainties; prepare for it; live in it as best as possible.
As I write this, Katie is undergoing a bone marrow transplant from her sister, the match. In a few weeks she will face her next branch point – whether the transplant worked. It will move her closer or further from a cure.
Dr. Yurkiewicz is a fellow in hematology and oncology at Stanford (Calif.) University. Follow her on Twitter @ilanayurkiewicz and listen to her each week on the Blood & Cancer podcast.
Reunion
We were catching up during our 35th college reunion at our old fraternity house overlooking Cayuga Lake in Ithaca, N.Y. About 50 of us lived in the Tudor-style house, complete with secret basement room, and there was a ladder that allowed access to the relatively flat, painted aluminum roof. When the weather allowed, we climbed the ladder to sun ourselves on top of the house. We also flung water balloons at unsuspecting pedestrians with a sling shot device made by attaching rubber tubing to a funnel. The “funnelator” was very accurate to about 50 yards away. We were kids, and climbing that ladder meant fun, and we climbed it as often as we could.

Despite what many would have predicted when we graduated, my fraternity brothers became a very successful group of CEOs, vice presidents, doctors, lawyers, chairmen, and consultants. Our house was just off Cornell University’s campus at the top of Ithaca Falls, an idyllic setting on a beautiful June evening for my brothers to sit around, laugh about the old times, and philosophize about life. We recounted our life after college and reveled in each others’ accomplishments.
After climbing the roof ladder for fun, we had each climbed a different kind of ladder to success in our respective fields. We all really enjoyed the climb. I don’t think it is a coincidence that many of my brothers and I are now done climbing our ladders. Many of us are getting out of the rat race.
One of my friends is resigning as chairman of an academic ENT department. I remember his discipline in college, leaving the house after dinner every night to climb the hill where he studied in the quiet of Uris Library, which is attached to the iconic McGraw Tower. His hard work paid off with an acceptance to a prestigious medical school where he continued to excel. The author of more than 200 published manuscripts, with four senior-authored papers already this year, he is at the pinnacle of his academic success. Yet, he resigned.
Similarly, another of my fraternity brothers had recently resigned from his position as Senior Vice President and Chief Medical Officer for a large health care system. He would have been in line for the CEO position had he stayed. He has written well-received books on leadership and financial acumen for physicians. As a result, he is a frequent public speaker on similar topics. Yet, he resigned.
They were not the only ones resigning positions that others covet. I, too, resigned my position as Department Chairman earlier this year. None of us were fired, none of us were asked to leave, and none of us are burned out. So here we were, three accomplished physicians all resigning from powerful posts at the same time for what turns out to be similar reasons. Our priorities changed as our children moved out.
I would like to say that we all had the wisdom to know that our leadership skills were deteriorating and that we all wanted to get out while we are at the top of our game. Had Arthur Brooks written “Your Professional Decline Is Coming (Much) Sooner Than You Think” in The Atlantic (July 2019) before we made our decisions, I may have made that argument, but it would not have been true. All three of us feel like we have accomplished what we sought to achieve when we took our respective roles and now we wanted to leverage that experience into something different, if not better. None of us have settled into new roles yet, and all of us are still trying to define exactly what it is we want to do next, but all of us agree that we are no longer interested in driving ourselves to succeed at the expense of our family, friends, and relationships.
My fraternity brothers and I gushed with pride talking about our children and their success. Our progeny are starting their individual climbs up the ladder of opportunity in whatever field they have chosen. My friends and I, on the other hand, had already climbed a ladder and feel comfortable stopping. Or maybe we just want to start climbing a different ladder.
Dr. Kalaycio is editor in chief of Hematology News. He chairs the department of hematology and medical oncology at Cleveland Clinic Taussig Cancer Institute. Contact him at kalaycm@ccf.org.
We were catching up during our 35th college reunion at our old fraternity house overlooking Cayuga Lake in Ithaca, N.Y. About 50 of us lived in the Tudor-style house, complete with secret basement room, and there was a ladder that allowed access to the relatively flat, painted aluminum roof. When the weather allowed, we climbed the ladder to sun ourselves on top of the house. We also flung water balloons at unsuspecting pedestrians with a sling shot device made by attaching rubber tubing to a funnel. The “funnelator” was very accurate to about 50 yards away. We were kids, and climbing that ladder meant fun, and we climbed it as often as we could.
Despite what many would have predicted when we graduated, my fraternity brothers became a very successful group of CEOs, vice presidents, doctors, lawyers, chairmen, and consultants. Our house was just off Cornell University’s campus at the top of Ithaca Falls, an idyllic setting on a beautiful June evening for my brothers to sit around, laugh about the old times, and philosophize about life. We recounted our life after college and reveled in each others’ accomplishments.
After climbing the roof ladder for fun, we had each climbed a different kind of ladder to success in our respective fields. We all really enjoyed the climb. I don’t think it is a coincidence that many of my brothers and I are now done climbing our ladders. Many of us are getting out of the rat race.
One of my friends is resigning as chairman of an academic ENT department. I remember his discipline in college, leaving the house after dinner every night to climb the hill where he studied in the quiet of Uris Library, which is attached to the iconic McGraw Tower. His hard work paid off with an acceptance to a prestigious medical school where he continued to excel. The author of more than 200 published manuscripts, with four senior-authored papers already this year, he is at the pinnacle of his academic success. Yet, he resigned.
Similarly, another of my fraternity brothers had recently resigned from his position as Senior Vice President and Chief Medical Officer for a large health care system. He would have been in line for the CEO position had he stayed. He has written well-received books on leadership and financial acumen for physicians. As a result, he is a frequent public speaker on similar topics. Yet, he resigned.
They were not the only ones resigning positions that others covet. I, too, resigned my position as Department Chairman earlier this year. None of us were fired, none of us were asked to leave, and none of us are burned out. So here we were, three accomplished physicians all resigning from powerful posts at the same time for what turns out to be similar reasons. Our priorities changed as our children moved out.
I would like to say that we all had the wisdom to know that our leadership skills were deteriorating and that we all wanted to get out while we are at the top of our game. Had Arthur Brooks written “Your Professional Decline Is Coming (Much) Sooner Than You Think” in The Atlantic (July 2019) before we made our decisions, I may have made that argument, but it would not have been true. All three of us feel like we have accomplished what we sought to achieve when we took our respective roles and now we wanted to leverage that experience into something different, if not better. None of us have settled into new roles yet, and all of us are still trying to define exactly what it is we want to do next, but all of us agree that we are no longer interested in driving ourselves to succeed at the expense of our family, friends, and relationships.
My fraternity brothers and I gushed with pride talking about our children and their success. Our progeny are starting their individual climbs up the ladder of opportunity in whatever field they have chosen. My friends and I, on the other hand, had already climbed a ladder and feel comfortable stopping. Or maybe we just want to start climbing a different ladder.
Dr. Kalaycio is editor in chief of Hematology News. He chairs the department of hematology and medical oncology at Cleveland Clinic Taussig Cancer Institute. Contact him at kalaycm@ccf.org.
We were catching up during our 35th college reunion at our old fraternity house overlooking Cayuga Lake in Ithaca, N.Y. About 50 of us lived in the Tudor-style house, complete with secret basement room, and there was a ladder that allowed access to the relatively flat, painted aluminum roof. When the weather allowed, we climbed the ladder to sun ourselves on top of the house. We also flung water balloons at unsuspecting pedestrians with a sling shot device made by attaching rubber tubing to a funnel. The “funnelator” was very accurate to about 50 yards away. We were kids, and climbing that ladder meant fun, and we climbed it as often as we could.
Despite what many would have predicted when we graduated, my fraternity brothers became a very successful group of CEOs, vice presidents, doctors, lawyers, chairmen, and consultants. Our house was just off Cornell University’s campus at the top of Ithaca Falls, an idyllic setting on a beautiful June evening for my brothers to sit around, laugh about the old times, and philosophize about life. We recounted our life after college and reveled in each others’ accomplishments.
After climbing the roof ladder for fun, we had each climbed a different kind of ladder to success in our respective fields. We all really enjoyed the climb. I don’t think it is a coincidence that many of my brothers and I are now done climbing our ladders. Many of us are getting out of the rat race.
One of my friends is resigning as chairman of an academic ENT department. I remember his discipline in college, leaving the house after dinner every night to climb the hill where he studied in the quiet of Uris Library, which is attached to the iconic McGraw Tower. His hard work paid off with an acceptance to a prestigious medical school where he continued to excel. The author of more than 200 published manuscripts, with four senior-authored papers already this year, he is at the pinnacle of his academic success. Yet, he resigned.
Similarly, another of my fraternity brothers had recently resigned from his position as Senior Vice President and Chief Medical Officer for a large health care system. He would have been in line for the CEO position had he stayed. He has written well-received books on leadership and financial acumen for physicians. As a result, he is a frequent public speaker on similar topics. Yet, he resigned.
They were not the only ones resigning positions that others covet. I, too, resigned my position as Department Chairman earlier this year. None of us were fired, none of us were asked to leave, and none of us are burned out. So here we were, three accomplished physicians all resigning from powerful posts at the same time for what turns out to be similar reasons. Our priorities changed as our children moved out.
I would like to say that we all had the wisdom to know that our leadership skills were deteriorating and that we all wanted to get out while we are at the top of our game. Had Arthur Brooks written “Your Professional Decline Is Coming (Much) Sooner Than You Think” in The Atlantic (July 2019) before we made our decisions, I may have made that argument, but it would not have been true. All three of us feel like we have accomplished what we sought to achieve when we took our respective roles and now we wanted to leverage that experience into something different, if not better. None of us have settled into new roles yet, and all of us are still trying to define exactly what it is we want to do next, but all of us agree that we are no longer interested in driving ourselves to succeed at the expense of our family, friends, and relationships.
My fraternity brothers and I gushed with pride talking about our children and their success. Our progeny are starting their individual climbs up the ladder of opportunity in whatever field they have chosen. My friends and I, on the other hand, had already climbed a ladder and feel comfortable stopping. Or maybe we just want to start climbing a different ladder.
Dr. Kalaycio is editor in chief of Hematology News. He chairs the department of hematology and medical oncology at Cleveland Clinic Taussig Cancer Institute. Contact him at kalaycm@ccf.org.
The month of new beginnings is here
This month’s Letter from the Editor is guest authored by Dr. Megan A. Adams, GI & Hepatology News Associate Editor
September is a month of new beginnings, as summer transitions to fall, kids go back to school, and we return to more consistent work routines, refreshed and reinvigorated after some well-deserved time off with family and friends. Among our cover stories this month is a study showing a novel application of deep learning to inform clinical care of patients with pancreatic cysts. We also feature several high-impact studies from AGA’s journals, including a large randomized controlled trial by Dr. Paul Moayyedi and colleagues, demonstrating that PPI therapy may be unnecessary in the majority of patients on oral anticoagulants, despite current guideline recommendations. This study has the potential to substantially change clinical practice, particularly in the context of the current discussion regarding PPI benefits and harms, and our transition to value-based care.
We also highlight a proof-of-concept study demonstrating a potential role for probiotics (specifically Bifidobacteria) in reducing the risk of NSAID-related gastrointestinal bleeding, and another study showing a possible role for clopidogrel in chemoprevention of colorectal cancer. Both articles are accompanied by expert commentaries highlighting their potential effect on clinical practice.

Our September issue also emphasizes the importance of professional advocacy by chronicling the participation of four AGA leaders (Dr. Carr, Dr. Kaufman, Dr. Ketwaroo, and Dr. Mathews) in the 2019 Alliance of Specialty Medicine Fly In, a multisociety effort to lobby legislators on key issues such as reducing prior authorization burdens and minimizing the strict constraints of step-therapy protocols. We also are pleased to acknowledge the future leaders of gastroenterology by recognizing the 17 exceptional fellows who demonstrated their passion for advancing GI clinical care by presenting their institutional quality improvement projects at a special session at DDW® 2019. We hope you find these stories to be thought provoking, inspiring, and directly relevant to your clinical practice – thank you for reading!
Megan A. Adams, MD, JD, MSc
Associate Editor
This month’s Letter from the Editor is guest authored by Dr. Megan A. Adams, GI & Hepatology News Associate Editor
September is a month of new beginnings, as summer transitions to fall, kids go back to school, and we return to more consistent work routines, refreshed and reinvigorated after some well-deserved time off with family and friends. Among our cover stories this month is a study showing a novel application of deep learning to inform clinical care of patients with pancreatic cysts. We also feature several high-impact studies from AGA’s journals, including a large randomized controlled trial by Dr. Paul Moayyedi and colleagues, demonstrating that PPI therapy may be unnecessary in the majority of patients on oral anticoagulants, despite current guideline recommendations. This study has the potential to substantially change clinical practice, particularly in the context of the current discussion regarding PPI benefits and harms, and our transition to value-based care.
We also highlight a proof-of-concept study demonstrating a potential role for probiotics (specifically Bifidobacteria) in reducing the risk of NSAID-related gastrointestinal bleeding, and another study showing a possible role for clopidogrel in chemoprevention of colorectal cancer. Both articles are accompanied by expert commentaries highlighting their potential effect on clinical practice.
Our September issue also emphasizes the importance of professional advocacy by chronicling the participation of four AGA leaders (Dr. Carr, Dr. Kaufman, Dr. Ketwaroo, and Dr. Mathews) in the 2019 Alliance of Specialty Medicine Fly In, a multisociety effort to lobby legislators on key issues such as reducing prior authorization burdens and minimizing the strict constraints of step-therapy protocols. We also are pleased to acknowledge the future leaders of gastroenterology by recognizing the 17 exceptional fellows who demonstrated their passion for advancing GI clinical care by presenting their institutional quality improvement projects at a special session at DDW® 2019. We hope you find these stories to be thought provoking, inspiring, and directly relevant to your clinical practice – thank you for reading!
Megan A. Adams, MD, JD, MSc
Associate Editor
This month’s Letter from the Editor is guest authored by Dr. Megan A. Adams, GI & Hepatology News Associate Editor
September is a month of new beginnings, as summer transitions to fall, kids go back to school, and we return to more consistent work routines, refreshed and reinvigorated after some well-deserved time off with family and friends. Among our cover stories this month is a study showing a novel application of deep learning to inform clinical care of patients with pancreatic cysts. We also feature several high-impact studies from AGA’s journals, including a large randomized controlled trial by Dr. Paul Moayyedi and colleagues, demonstrating that PPI therapy may be unnecessary in the majority of patients on oral anticoagulants, despite current guideline recommendations. This study has the potential to substantially change clinical practice, particularly in the context of the current discussion regarding PPI benefits and harms, and our transition to value-based care.
We also highlight a proof-of-concept study demonstrating a potential role for probiotics (specifically Bifidobacteria) in reducing the risk of NSAID-related gastrointestinal bleeding, and another study showing a possible role for clopidogrel in chemoprevention of colorectal cancer. Both articles are accompanied by expert commentaries highlighting their potential effect on clinical practice.
Our September issue also emphasizes the importance of professional advocacy by chronicling the participation of four AGA leaders (Dr. Carr, Dr. Kaufman, Dr. Ketwaroo, and Dr. Mathews) in the 2019 Alliance of Specialty Medicine Fly In, a multisociety effort to lobby legislators on key issues such as reducing prior authorization burdens and minimizing the strict constraints of step-therapy protocols. We also are pleased to acknowledge the future leaders of gastroenterology by recognizing the 17 exceptional fellows who demonstrated their passion for advancing GI clinical care by presenting their institutional quality improvement projects at a special session at DDW® 2019. We hope you find these stories to be thought provoking, inspiring, and directly relevant to your clinical practice – thank you for reading!
Megan A. Adams, MD, JD, MSc
Associate Editor
Studies reinforce clinical experience and intuition
In this edition of “How I will treat my next patient,” I examine two recently published efforts to enlighten our sensitivity to the seriousness of immune-related adverse events (IrAEs) in patients on immune checkpoint inhibitors (ICIs) and the effect of delays in initiating systemic adjuvant therapy on the long-term outcomes of patients with resected pancreatic cancer.
IrAEs requiring hospitalization
Investigators led by Aanika Balaji of the Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins University, Baltimore, reviewed a 6-month audit of inpatient oncology admissions of solid-tumor patients who had ever received ICIs and ascertained the prevalence of hospitalization for management of IrAEs (J Oncol Pract. 2019 Aug 6. doi: 10.1200/JOP.18.00703). To determine that an IrAE had occurred they required: consensus among two oncologists, clinical improvement with immune-directed therapy, exclusion of alternative diagnoses or pathologic confirmation of an IrAE, or chronic management of an IrAE for more than 6 months.

The bottom line: They found a cumulative incidence of a confirmed IrAEs among hospitalized ICI-treated solid tumor patients of 23%. As expected, the majority (65%) were grade 3-4 in severity. In total, 91% required multidisciplinary management, and 65% improved or resolved. But 87% of patients never received an ICI again.
Patients with preexisting autoimmune disease (25% of patients, although they included hypothyroidism in that group) were not more vulnerable to an IrAE with ICI therapy (odds ratio, 1.0; 95% confidence interval, 0.3-4.0). Not unsurprisingly, the median age was higher for ICI-treated patients who were admitted for IrAEs than for those not admitted (68 years vs. 59 years; OR, 5.4; 95% CI, 1.6-17.8), and more admitted patients had received combination ICIs than single agents (OR, 6.8; 95% CI, 2.0-23.2).
The median time from beginning ICIs to an IrAE-related hospitalization was 64 days, and the median number of ICI doses was one, with a wide range for both days and doses. The authors were quick to comment that this is a small, academic, single-institution survey over a brief period of time and that the generalizability of the results is uncertain.
What this means in practice
This publication changes very little for most practicing oncologists, but it does reinforce that ICI therapy can cause unpredictable, severe IrAEs. Clinical markers for selecting patients at highest risk are imperfect. As with chemotherapy, the patients we worry about the most – older individuals and patients treated with drug combinations – are, in fact, the ones we should be worrying about the most.
In view of the potential severity and impact of IrAEs, research efforts should place equal priority on identifying biomarkers of toxicity, such as tumor mutation burden, and biomarkers of efficacy (JAMA Oncol. 2019 Aug 22. doi: 10.1001/jamaoncol.2019.3221). The potential financial and societal effects, as well as lost opportunity costs in the form of alternative therapies and early referral to hospice, demand no less, particularly in an era of value-based health care reimbursement.
Timing of adjuvant treatment
Sung Jun Ma, MD, department of radiation medicine at Roswell Park Comprehensive Cancer Center, Buffalo, N.Y., and colleagues analyzed data from the more than 7,500 stage I-II resected pancreatic cancer patients in the National Cancer Database, of whom more than 5,400 ultimately received adjuvant therapy (chemotherapy with or without radiation). The patients were treated during 2004-2015. Appropriately, the investigators focused on correlating survival duration with the interval between surgery and initiation of adjuvant therapy. Other endpoints would be hard to accurately measure and verify without detailed clinical information (JAMA Network Open. 2019 Aug 14. doi: 10.1001/jamanetworkopen.2019.9126).
They found that the best overall survival was associated with starting adjuvant treatment 28-59 days after surgery – not earlier (17% higher mortality) and not later (9% higher). Patients who did not start adjuvant treatment until more than 90 days post operatively still had an overall survival benefit (hazard ratio, 0.75; 95% confidence interval, 0.66-0.85; P less than .001), a more impressive hazard ratio than that seen for any particular interval between surgery and adjuvant treatment. Overall survival at 2 years was 47.2% versus 38% for the adjuvant therapy and surgery alone cohorts, respectively, with no overlap in the 95% confidence intervals.
As expected, longer delays to receive adjuvant treatment were associated with longer inpatient surgical stays, advanced age, black race, lower income, and a readmission for a postoperative complication within 30 days.
What this means in practice
This is another study that verifies that the patients we worry about most – older patients, those with a complicated recovery from surgery, and those with fewer supportive resources – are exactly the patients we should worry about most. It changes very little for most practicing oncologists. The analysis validates the importance of adjuvant therapy for patients who are able to receive it – whenever that is.
The data collection in this publication precedes recent improvements in adjuvant chemotherapy for resected pancreatic cancer, such as FOLFIRINOX or gemcitabine plus capecitabine. In an era of improved treatment, delays in initiating therapy may be less important since better treatment overcomes many prognostic variables that are significant for less effective therapy.
In my opinion, this large-data analysis is not really hypothesis-generating or practice-changing, but it does compel us to continue research efforts to improve surgical morbidity, identify better adjuvant and advanced disease regimens, and consider neoadjuvant treatment so that more than 72% of patients can receive all components of the multimodality treatment they need.
Dr. Lyss has been a community-based medical oncologist and clinical researcher for more than 35 years, practicing in St. Louis. His clinical and research interests are in the prevention, diagnosis, and treatment of breast and lung cancers and in expanding access to clinical trials to medically underserved populations.
In this edition of “How I will treat my next patient,” I examine two recently published efforts to enlighten our sensitivity to the seriousness of immune-related adverse events (IrAEs) in patients on immune checkpoint inhibitors (ICIs) and the effect of delays in initiating systemic adjuvant therapy on the long-term outcomes of patients with resected pancreatic cancer.
IrAEs requiring hospitalization
Investigators led by Aanika Balaji of the Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins University, Baltimore, reviewed a 6-month audit of inpatient oncology admissions of solid-tumor patients who had ever received ICIs and ascertained the prevalence of hospitalization for management of IrAEs (J Oncol Pract. 2019 Aug 6. doi: 10.1200/JOP.18.00703). To determine that an IrAE had occurred they required: consensus among two oncologists, clinical improvement with immune-directed therapy, exclusion of alternative diagnoses or pathologic confirmation of an IrAE, or chronic management of an IrAE for more than 6 months.
The bottom line: They found a cumulative incidence of a confirmed IrAEs among hospitalized ICI-treated solid tumor patients of 23%. As expected, the majority (65%) were grade 3-4 in severity. In total, 91% required multidisciplinary management, and 65% improved or resolved. But 87% of patients never received an ICI again.
Patients with preexisting autoimmune disease (25% of patients, although they included hypothyroidism in that group) were not more vulnerable to an IrAE with ICI therapy (odds ratio, 1.0; 95% confidence interval, 0.3-4.0). Not unsurprisingly, the median age was higher for ICI-treated patients who were admitted for IrAEs than for those not admitted (68 years vs. 59 years; OR, 5.4; 95% CI, 1.6-17.8), and more admitted patients had received combination ICIs than single agents (OR, 6.8; 95% CI, 2.0-23.2).
The median time from beginning ICIs to an IrAE-related hospitalization was 64 days, and the median number of ICI doses was one, with a wide range for both days and doses. The authors were quick to comment that this is a small, academic, single-institution survey over a brief period of time and that the generalizability of the results is uncertain.
What this means in practice
This publication changes very little for most practicing oncologists, but it does reinforce that ICI therapy can cause unpredictable, severe IrAEs. Clinical markers for selecting patients at highest risk are imperfect. As with chemotherapy, the patients we worry about the most – older individuals and patients treated with drug combinations – are, in fact, the ones we should be worrying about the most.
In view of the potential severity and impact of IrAEs, research efforts should place equal priority on identifying biomarkers of toxicity, such as tumor mutation burden, and biomarkers of efficacy (JAMA Oncol. 2019 Aug 22. doi: 10.1001/jamaoncol.2019.3221). The potential financial and societal effects, as well as lost opportunity costs in the form of alternative therapies and early referral to hospice, demand no less, particularly in an era of value-based health care reimbursement.
Timing of adjuvant treatment
Sung Jun Ma, MD, department of radiation medicine at Roswell Park Comprehensive Cancer Center, Buffalo, N.Y., and colleagues analyzed data from the more than 7,500 stage I-II resected pancreatic cancer patients in the National Cancer Database, of whom more than 5,400 ultimately received adjuvant therapy (chemotherapy with or without radiation). The patients were treated during 2004-2015. Appropriately, the investigators focused on correlating survival duration with the interval between surgery and initiation of adjuvant therapy. Other endpoints would be hard to accurately measure and verify without detailed clinical information (JAMA Network Open. 2019 Aug 14. doi: 10.1001/jamanetworkopen.2019.9126).
They found that the best overall survival was associated with starting adjuvant treatment 28-59 days after surgery – not earlier (17% higher mortality) and not later (9% higher). Patients who did not start adjuvant treatment until more than 90 days post operatively still had an overall survival benefit (hazard ratio, 0.75; 95% confidence interval, 0.66-0.85; P less than .001), a more impressive hazard ratio than that seen for any particular interval between surgery and adjuvant treatment. Overall survival at 2 years was 47.2% versus 38% for the adjuvant therapy and surgery alone cohorts, respectively, with no overlap in the 95% confidence intervals.
As expected, longer delays to receive adjuvant treatment were associated with longer inpatient surgical stays, advanced age, black race, lower income, and a readmission for a postoperative complication within 30 days.
What this means in practice
This is another study that verifies that the patients we worry about most – older patients, those with a complicated recovery from surgery, and those with fewer supportive resources – are exactly the patients we should worry about most. It changes very little for most practicing oncologists. The analysis validates the importance of adjuvant therapy for patients who are able to receive it – whenever that is.
The data collection in this publication precedes recent improvements in adjuvant chemotherapy for resected pancreatic cancer, such as FOLFIRINOX or gemcitabine plus capecitabine. In an era of improved treatment, delays in initiating therapy may be less important since better treatment overcomes many prognostic variables that are significant for less effective therapy.
In my opinion, this large-data analysis is not really hypothesis-generating or practice-changing, but it does compel us to continue research efforts to improve surgical morbidity, identify better adjuvant and advanced disease regimens, and consider neoadjuvant treatment so that more than 72% of patients can receive all components of the multimodality treatment they need.
Dr. Lyss has been a community-based medical oncologist and clinical researcher for more than 35 years, practicing in St. Louis. His clinical and research interests are in the prevention, diagnosis, and treatment of breast and lung cancers and in expanding access to clinical trials to medically underserved populations.
In this edition of “How I will treat my next patient,” I examine two recently published efforts to enlighten our sensitivity to the seriousness of immune-related adverse events (IrAEs) in patients on immune checkpoint inhibitors (ICIs) and the effect of delays in initiating systemic adjuvant therapy on the long-term outcomes of patients with resected pancreatic cancer.
IrAEs requiring hospitalization
Investigators led by Aanika Balaji of the Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins University, Baltimore, reviewed a 6-month audit of inpatient oncology admissions of solid-tumor patients who had ever received ICIs and ascertained the prevalence of hospitalization for management of IrAEs (J Oncol Pract. 2019 Aug 6. doi: 10.1200/JOP.18.00703). To determine that an IrAE had occurred they required: consensus among two oncologists, clinical improvement with immune-directed therapy, exclusion of alternative diagnoses or pathologic confirmation of an IrAE, or chronic management of an IrAE for more than 6 months.
The bottom line: They found a cumulative incidence of a confirmed IrAEs among hospitalized ICI-treated solid tumor patients of 23%. As expected, the majority (65%) were grade 3-4 in severity. In total, 91% required multidisciplinary management, and 65% improved or resolved. But 87% of patients never received an ICI again.
Patients with preexisting autoimmune disease (25% of patients, although they included hypothyroidism in that group) were not more vulnerable to an IrAE with ICI therapy (odds ratio, 1.0; 95% confidence interval, 0.3-4.0). Not unsurprisingly, the median age was higher for ICI-treated patients who were admitted for IrAEs than for those not admitted (68 years vs. 59 years; OR, 5.4; 95% CI, 1.6-17.8), and more admitted patients had received combination ICIs than single agents (OR, 6.8; 95% CI, 2.0-23.2).
The median time from beginning ICIs to an IrAE-related hospitalization was 64 days, and the median number of ICI doses was one, with a wide range for both days and doses. The authors were quick to comment that this is a small, academic, single-institution survey over a brief period of time and that the generalizability of the results is uncertain.
What this means in practice
This publication changes very little for most practicing oncologists, but it does reinforce that ICI therapy can cause unpredictable, severe IrAEs. Clinical markers for selecting patients at highest risk are imperfect. As with chemotherapy, the patients we worry about the most – older individuals and patients treated with drug combinations – are, in fact, the ones we should be worrying about the most.
In view of the potential severity and impact of IrAEs, research efforts should place equal priority on identifying biomarkers of toxicity, such as tumor mutation burden, and biomarkers of efficacy (JAMA Oncol. 2019 Aug 22. doi: 10.1001/jamaoncol.2019.3221). The potential financial and societal effects, as well as lost opportunity costs in the form of alternative therapies and early referral to hospice, demand no less, particularly in an era of value-based health care reimbursement.
Timing of adjuvant treatment
Sung Jun Ma, MD, department of radiation medicine at Roswell Park Comprehensive Cancer Center, Buffalo, N.Y., and colleagues analyzed data from the more than 7,500 stage I-II resected pancreatic cancer patients in the National Cancer Database, of whom more than 5,400 ultimately received adjuvant therapy (chemotherapy with or without radiation). The patients were treated during 2004-2015. Appropriately, the investigators focused on correlating survival duration with the interval between surgery and initiation of adjuvant therapy. Other endpoints would be hard to accurately measure and verify without detailed clinical information (JAMA Network Open. 2019 Aug 14. doi: 10.1001/jamanetworkopen.2019.9126).
They found that the best overall survival was associated with starting adjuvant treatment 28-59 days after surgery – not earlier (17% higher mortality) and not later (9% higher). Patients who did not start adjuvant treatment until more than 90 days post operatively still had an overall survival benefit (hazard ratio, 0.75; 95% confidence interval, 0.66-0.85; P less than .001), a more impressive hazard ratio than that seen for any particular interval between surgery and adjuvant treatment. Overall survival at 2 years was 47.2% versus 38% for the adjuvant therapy and surgery alone cohorts, respectively, with no overlap in the 95% confidence intervals.
As expected, longer delays to receive adjuvant treatment were associated with longer inpatient surgical stays, advanced age, black race, lower income, and a readmission for a postoperative complication within 30 days.
What this means in practice
This is another study that verifies that the patients we worry about most – older patients, those with a complicated recovery from surgery, and those with fewer supportive resources – are exactly the patients we should worry about most. It changes very little for most practicing oncologists. The analysis validates the importance of adjuvant therapy for patients who are able to receive it – whenever that is.
The data collection in this publication precedes recent improvements in adjuvant chemotherapy for resected pancreatic cancer, such as FOLFIRINOX or gemcitabine plus capecitabine. In an era of improved treatment, delays in initiating therapy may be less important since better treatment overcomes many prognostic variables that are significant for less effective therapy.
In my opinion, this large-data analysis is not really hypothesis-generating or practice-changing, but it does compel us to continue research efforts to improve surgical morbidity, identify better adjuvant and advanced disease regimens, and consider neoadjuvant treatment so that more than 72% of patients can receive all components of the multimodality treatment they need.
Dr. Lyss has been a community-based medical oncologist and clinical researcher for more than 35 years, practicing in St. Louis. His clinical and research interests are in the prevention, diagnosis, and treatment of breast and lung cancers and in expanding access to clinical trials to medically underserved populations.
Time or money?
The authors of a recent study published in the Annals of Internal Medicine estimate that physician burnout is costing this country’s health care system $4.6 billion annually, using a conservative base-case model (Ann Intern Med. 2019;170[11]:784-90). I guess we shouldn’t be surprised at the magnitude of the drain on our economy caused by unhappy physicians. We all know colleagues who are showing signs of burnout. And, you may be feeling yourself that the challenges of work are taking too great a toll on your physical and mental health? Would you be happier if you had more time?

A study reported in Harvard Business Review has looked at recent college graduates to determine if how they prioritize time and money can predict their future happiness (“Are New Graduates Happier Making More Money or Having More Time?” July 25, 2019). The researchers at the Harvard Business School surveyed 1,000 college students in the 2015 and 2016 classes of the University of British Columbia, Vancouver. The students were asked to match themselves with descriptions of fictitious individuals to determine whether in general they prioritized time or money. The researchers then assessed the students’ level of happiness by asking them, “How satisfied are you with life overall?”
At a 2-year follow-up, the researchers found that, even taking into account the students’ level of happiness at the beginning of the study, “those who prioritized time were happier.” The authors also found that time-oriented people don’t necessarily work less or even earn more money, prompting their conclusion there is “strong evidence that valuing time puts people on a trajectory toward job satisfaction and well-being.”
Do the results of this study of Canadian college students provide any answers for our epidemic of physician burnout? One could argue that, if we wanted to minimize burnout, medical schools should include an assessment of each applicant’s level of happiness and how she or he prioritizes time and money using methods similar those used in this study? The problem is that some students are so heavily committed to becoming physicians that they would game the system and provide answers that will project the image that they are happy and prioritize time over money, when in reality they are ticking time bombs of discontent.

The bigger problem with interpreting the results of this study is that the subjects were Canadians who have significantly less educational debt than the medical students in this country. And as the authors observe, “people with objective financial constraints ... are more likely to focus on having more money.” Until we solve the problem of the high cost of medical education the system will continue to select for physicians whose decisions are too heavily influenced by their educational debt.
Finally, it is important to consider that time-oriented individuals don’t always work less, rather they make decisions that make it more likely that they will pursue activities they find enjoyable. For example, accepting a higher-paying job that requires an additional 3 hours of commute each day lays the foundation for a life in which a large portion of one’s day is expended in an activity that few of us find enjoyable. Choosing a long commute is a personal decision. Spending nearly 2 hours each day tethered to an EHR system was not something most physicians anticipated when they were choosing a career.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@mdedge.com.
The authors of a recent study published in the Annals of Internal Medicine estimate that physician burnout is costing this country’s health care system $4.6 billion annually, using a conservative base-case model (Ann Intern Med. 2019;170[11]:784-90). I guess we shouldn’t be surprised at the magnitude of the drain on our economy caused by unhappy physicians. We all know colleagues who are showing signs of burnout. And, you may be feeling yourself that the challenges of work are taking too great a toll on your physical and mental health? Would you be happier if you had more time?
A study reported in Harvard Business Review has looked at recent college graduates to determine if how they prioritize time and money can predict their future happiness (“Are New Graduates Happier Making More Money or Having More Time?” July 25, 2019). The researchers at the Harvard Business School surveyed 1,000 college students in the 2015 and 2016 classes of the University of British Columbia, Vancouver. The students were asked to match themselves with descriptions of fictitious individuals to determine whether in general they prioritized time or money. The researchers then assessed the students’ level of happiness by asking them, “How satisfied are you with life overall?”
At a 2-year follow-up, the researchers found that, even taking into account the students’ level of happiness at the beginning of the study, “those who prioritized time were happier.” The authors also found that time-oriented people don’t necessarily work less or even earn more money, prompting their conclusion there is “strong evidence that valuing time puts people on a trajectory toward job satisfaction and well-being.”
Do the results of this study of Canadian college students provide any answers for our epidemic of physician burnout? One could argue that, if we wanted to minimize burnout, medical schools should include an assessment of each applicant’s level of happiness and how she or he prioritizes time and money using methods similar those used in this study? The problem is that some students are so heavily committed to becoming physicians that they would game the system and provide answers that will project the image that they are happy and prioritize time over money, when in reality they are ticking time bombs of discontent.
The bigger problem with interpreting the results of this study is that the subjects were Canadians who have significantly less educational debt than the medical students in this country. And as the authors observe, “people with objective financial constraints ... are more likely to focus on having more money.” Until we solve the problem of the high cost of medical education the system will continue to select for physicians whose decisions are too heavily influenced by their educational debt.
Finally, it is important to consider that time-oriented individuals don’t always work less, rather they make decisions that make it more likely that they will pursue activities they find enjoyable. For example, accepting a higher-paying job that requires an additional 3 hours of commute each day lays the foundation for a life in which a large portion of one’s day is expended in an activity that few of us find enjoyable. Choosing a long commute is a personal decision. Spending nearly 2 hours each day tethered to an EHR system was not something most physicians anticipated when they were choosing a career.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@mdedge.com.
The authors of a recent study published in the Annals of Internal Medicine estimate that physician burnout is costing this country’s health care system $4.6 billion annually, using a conservative base-case model (Ann Intern Med. 2019;170[11]:784-90). I guess we shouldn’t be surprised at the magnitude of the drain on our economy caused by unhappy physicians. We all know colleagues who are showing signs of burnout. And, you may be feeling yourself that the challenges of work are taking too great a toll on your physical and mental health? Would you be happier if you had more time?
A study reported in Harvard Business Review has looked at recent college graduates to determine if how they prioritize time and money can predict their future happiness (“Are New Graduates Happier Making More Money or Having More Time?” July 25, 2019). The researchers at the Harvard Business School surveyed 1,000 college students in the 2015 and 2016 classes of the University of British Columbia, Vancouver. The students were asked to match themselves with descriptions of fictitious individuals to determine whether in general they prioritized time or money. The researchers then assessed the students’ level of happiness by asking them, “How satisfied are you with life overall?”
At a 2-year follow-up, the researchers found that, even taking into account the students’ level of happiness at the beginning of the study, “those who prioritized time were happier.” The authors also found that time-oriented people don’t necessarily work less or even earn more money, prompting their conclusion there is “strong evidence that valuing time puts people on a trajectory toward job satisfaction and well-being.”
Do the results of this study of Canadian college students provide any answers for our epidemic of physician burnout? One could argue that, if we wanted to minimize burnout, medical schools should include an assessment of each applicant’s level of happiness and how she or he prioritizes time and money using methods similar those used in this study? The problem is that some students are so heavily committed to becoming physicians that they would game the system and provide answers that will project the image that they are happy and prioritize time over money, when in reality they are ticking time bombs of discontent.
The bigger problem with interpreting the results of this study is that the subjects were Canadians who have significantly less educational debt than the medical students in this country. And as the authors observe, “people with objective financial constraints ... are more likely to focus on having more money.” Until we solve the problem of the high cost of medical education the system will continue to select for physicians whose decisions are too heavily influenced by their educational debt.
Finally, it is important to consider that time-oriented individuals don’t always work less, rather they make decisions that make it more likely that they will pursue activities they find enjoyable. For example, accepting a higher-paying job that requires an additional 3 hours of commute each day lays the foundation for a life in which a large portion of one’s day is expended in an activity that few of us find enjoyable. Choosing a long commute is a personal decision. Spending nearly 2 hours each day tethered to an EHR system was not something most physicians anticipated when they were choosing a career.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@mdedge.com.
Customer service in the medical practice – Are you losing additional revenue opportunities?
If you work in health care or manage a medical practice, you are aware of all the radical changes in technology, medicine, social values, and interpersonal relations over the past few years and you probably do not expect the next several years to be less stressful and less uncertain. To ensure your practice and your provider’s success, you may need to adjust how your team interacts with patients – starting with the first area of patient interaction.
Patients who seek care for their health problems are looking for some measure of kindness when they approach the window of your office’s receptionist. Many are already apprehensive about their clinical condition and adding to that problem is their concern about the financial impact of their visit on the family’s budget. The medical group’s unwillingness to rethink how it greets patients as they approach the receptionist sets the stage for the patient to feel mishandled or underappreciated.
This initial patient interaction stage must be evaluated and recognized as an area of improvement. If not handled properly, it will significantly affect how a medical practice or provider is graded as a group in the field of patient experience and managing patient expectations. Every medical office needs to recognize that people hold on to negative experiences and are not likely to change their mind after that negative experience. The best way to avoid negative bias is to prevent it from happening in the first place.
Listed below are the five additional patient experience mistakes that can cost your group, if they are not recognized as being priorities for both your staff and your patients.
Mistake #1 - Educated patients are taking control of their health care.
When health care is treated like any other paid service, an unhappy patient will move along to a new facility or doctor if they have a bad interaction – whether it is with the doctor or the support staff. Educating, training, or adjusting staff to make changes needed is required to ensure that your staff understands the value of patient appreciation and providing the patient with a positive experience.
Mistake #2 - Patients are customers, and just like customers, patients have options.
It should be recognized that patients are customers who are concerned about their future and do not want to be in a medical practice requesting help. They feel vulnerable and out of their routine comfort zone. Reminding your staff that a patient is a customer who has multiple health care choices, but chose to come to your practice, will help your staff understand the value of providing your patient with a positive experience.
Mistake #3 – Dr. Google is becoming the patient’s best friend.
Research indicates that many patients arrive at the doctor’s office already with some information on their condition. Various websites already have provided the patient with free access to learn about their health condition. Popular medical sites such as WebMD.com give the patient the preliminary education they are looking for, so they are already armed with medical information even before they see the doctor or their support staff.
Mistake # 4 - Surveys are carrying more weight.
Outside surveys are becoming even more popular and are carrying additional weight when combined with various social media outlets. All types of surveys and reviews are being used to measure not only the care the patient received, but also the interpersonal relationship between the patient and the doctor, and the patient’s experience with the medical practice’s support staff. Some surveys cover all levels in the practice area, down to the cleanliness of the reception area or the patient’s treatment area, and even the adequacy of the parking lot. These surveys are conditioning patients to recall their entire experience. With a patient experience plan in place, excellent service becomes second nature and will be recognized by those surveyed.
Mistake #5 - Patient-centered care is customer service, too.
It’s not just about the obvious. Excellent patient (customer) service extends beyond a pleasant demeanor. The patient experience does not start or end at the doctor’s office. Perception is built by gathering information from multiple channels, whether it is through review sites, office visits, or surveys. It is necessary to consider the importance of those channels when looking to build patient loyalty.
To avoid the mistakes listed above, the more progressive medical practices are training their staff to anticipate the customer service needs of their patients, much like other major service industries. By rolling out a patient/customer experience training program, they can prevent these mistakes from ever happening and affecting their potential revenue. This training should focus on integrating the following strategies into their daily work habits to provide their patients with exceptional customer service while they are guests in their practice.
1) Patients are the lifeline to building the future of their practice.
Patients are comparing their health care services to other companies that routinely provide high-end services to their clients. Whether groups like it or not, their front-line personnel are compared to five-star hotel receptionists, who are expected to greet their customers both pleasantly and professionally after a long day of traveling and required business functions. Every medical group must understand that patients have options when they select a medical practice and they expect to be treated with respect and transparency, and not just another person to be cared for at the end of a long day. The same level of service needs to be delivered in the doctor’s office no matter what time of day it is because for that patient, the personal problems and subsequent disposition of the medical staff is not their problem. All they want is someone to listen and help them take care of their medical problem. Their long-term loyalty to the group will be solely dependent on how well each personal interaction is handled. Remember that the patient is a person first and not just a customer. We must approach each patient with humanity first, and then customer service.
2) Be courteous and respectful.
Remind your staff to be courteous, always polite and to use good manners. By treating a patient how they expect to be treated, you are showing the patient that you respect them and care for not only their health but also their feelings. The health care worker must understand that the patient is viewing their interactions with staff and providers as being symbolic of the overall group’s brand identity. The group’s leadership needs to select and train their workforce to recognize their importance in how patients view their clinical offerings and their interactions with the patient.
3) Never show indifference to patients.
Losing patients before they complete their treatment regimen is a significant liability issue for any medical practice. In an article written by Strive Labs CEO and Co-Founder, Scott Hebert, DPT, wrote: “Patient churn is too big of a problem to ignore, and it can have a profound impact on your clinic’s bottom line.” In addition to the rather obvious missed revenue opportunity, a churning patient represents a practice liability, because an unsatisfied patient is significantly more likely to leave you a negative review online — or turn the experience with your practice into a cautionary tale for friends and family members. Either way, it’s bad for business — and your reputation.
4) Don’t contradict, argue, or match wits.
It’s tough for a health care worker who is continually being bombarded in a high-pressure environment to agree to disagree. When a person feels they are right or that their perception is the only logical one, they can be very stubborn in their understanding, and they will dig in their heels. It takes a strong person to allow others to have their opinion and not be judgmental about it. Any customer or patient relations training program to be deployed in a medical office must include skill training to teach the staff member how to diffuse an argument or disagreement. This situation can be dispersed by training your staff to consider the source of the conflict, respect the patient’s perception, and then teach the staff member to tell the patient that they never thought of it that way and ease away from the discussion. Their absence will help diffuse the situation.
5) Tell patients you appreciate their business.
How you relate to a patient will speak volumes to them about how much you appreciate their loyalty, all because they chose your practice for their health care. All patient and customer training programs should include discussions on making eye contact, shaking with a firm grasp, and always closing a personal encounter on a sincere and positive note. Health care workers need to understand that they are in the service business and that the patients they care for have options and they can easily walk out of the medical practice and share any negative experience on social media. Educating and reminding your staff on how easily a patient can leave your practice or share their experience with others, needs to be recognized and discussed at all the group’s town hall meetings.
6) Use plain terms and simple explanations.
We all want to appear to be super intelligent by trying to use complex terms to describe a situation because it creates leverage with the other parties engaged in the conversation. While some of this may be necessary when educating patients on their condition, any additional complex terms can easily annoy or even confuse the patient who is only there seeking help. Health care workers need to talk in a manner that keeps the patients engaged and helps them understand the topic at hand. The worker needs to use every day vernacular examples, so the patient quickly understands the reason that brought them to the clinic and what they need to do to get some relief from what ails them. The phrase “plain and simple” means precisely that – explain the topic using basic and simple terms, so the listener understands it. Using this method when discussing a patient’s condition isn’t just for the patient’s benefit because many confused patients ultimately call the office later in the day only to ask additional questions, which uses your staff’s time.
7) Good manners will get you everywhere.
Emily Post wrote, “Manners are a sensitive awareness of the feelings of others. If you have that awareness, you have good manners, no matter what fork you use.” Proper manners are behaving in a way that is both aware of and considerate of the people around us. A person with good manners treats everyone with kindness and respect. It is knowing how to get along without causing offense or harm, no matter how much the current interaction is going south – especially when you are engaged in a tough conversation.
8) Keep seeing health care as a calling.
All health care workers need to know that their vocation of caring for sick and injured patients is a calling and not just a job and all training programs designed to teach customer service need to stress this point. Practicing your vocation means that you will work hard to eliminate all barriers that exist between the patient and the health care worker. Too often we underestimate the power of a simple touch, a smile, a kind word, a listening ear, an honest compliment, or the smallest act of caring – all of which have the potential to turn a life or a bad interaction into a magical moment for both the patient and the health care worker. One that has meaning and a bit of affirmation of the dignity of both individuals interacting to find some common ground.
9) Stay in touch with patients.
The group needs to find ways to keep in contact with their patients, whether it is by giving them tips on how to remain healthy or the need for proactive and preventive medicine. The use of technology and social media, as well as handing out freebies at health fairs, giving patients informational brochures upon discharge, or even cards telling them how to contact the practice in case of emergencies, is quite helpful. Calling your patients is a significant signal that your group values the health and welfare of your patients. A phone call from either the doctor or their assistant goes further than any advertisement when building brand and doctor loyalty.
10) Keep your promises.
Do what you say you are going to do, should be a commonly shared mantra for the medical practice. While changing your mind from time to time when circumstances prevent you from keeping a promise, is just part of being flexible in life, regularly breaking promises to other people isn’t healthy. Here’s how to keep your promises: Pay close attention to your words – every word you communicate (through speaking or writing), as a patient may take your words as a promise. Study your patterns of making promises. Figure out when you tend to make careless promises and study the situations in which you do, so you can understand why you’re promising what you don’t intend to do. Take time and careful consideration before making a promise to someone. Don’t rush yourself into a promise that you won’t be able to keep. Even when you’re in a hurry, you usually don’t have an immediate sense of urgency about promising to do something. Stop yourself before you make a vow, delaying your decision long enough to think it through carefully. The more careful you become about making promises, the easier it will be to keep them.
The last step of deploying a patient/customer service program is handling the change in management that is required to train the staff. Accepting “No, we are not changing any part of the group to meet the needs of our patients better.” is unacceptable. Usually, you will be introducing this program to employees that have been in a group for a while and so to get them to buy into the new ideas will require constant reinforcement. It may take some time to align the focus of the group from the neutral zone to the notion that there are new deliverables that would better serve your patients. The following rules will be helpful when beginning your training program:
Rule #1 – Be consistent. Every policy, procedure, and list of priorities sends a message – make sure it’s the right message.
Rule #2 – Ensure quick successes. Look for ways to get the group’s employees to buy into the program – early on after its deployment.
Rule# 3 – Symbolize the new identity. Make sure the group’s logos and branding support the new identity of the group and the culture change.
Rule #4 – Celebrate all the group’s successes. Make sure the group’s employees recognize the work efforts involved as well as the success the group will enjoy. Stress the fact that the work completed will significantly enhance the care and service levels to the patients, which should feed the ego of the group to do more and more in the future.
And lastly, do not forget how vital the buy-in is of the clinicians of the group. They must be introduced early to the new patient/customer service program and embrace it so that their employees will recognize that these efforts are focused on providing a high quality of care throughout the enterprise. As the French philosopher Albert Schweitzer once stated, “Example is not the main thing in influencing others, it’s the only thing.”
References
1. Peters, T. “The Excellence Dividend: Meeting the Tech Tide with Work that Wows and Jobs that Last.” (New York, Vintage Books, 2018).
2. 10 Strategies to Provide Patients with Superior Customer Service. Becker’s Hospital Review 2010 Dec 20.
3. Shell MA, Buell RW. Why anxious customers prefer human customer service. Harvard Business Review 2019 April 15.
4. Matt Brannon. 13 Ways to improve customer services at your medical practice. Blog post Sept 7, 2018.
5. 5 Reasons Why Customer Service Matters in Healthcare. https://www.pointsgroup.com/5-reasons-why-customer-service-matters-in-healthcare/Feb. 25, 2014
6. Senge P, Kleiner A, Roberts C, et al. “The Dance of Change: A fifth discipline resource.” (New York, Doubleday, 1999).
7. Bridges W. “Managing Transitions: Making the Most of Change.” (Boston, Da Capo Books, 2017)
8. Michelli J. “The New Gold Standard – 5 Leadership Principles for Creating the Legendary Customer Experience Courtesy of the Ritz-Carlton Hotel Company.” (New York, McGraw Hill, 2008).
Mr. Turner is chief executive officer of Indianapolis Gastroenterology and Hepatology.
If you work in health care or manage a medical practice, you are aware of all the radical changes in technology, medicine, social values, and interpersonal relations over the past few years and you probably do not expect the next several years to be less stressful and less uncertain. To ensure your practice and your provider’s success, you may need to adjust how your team interacts with patients – starting with the first area of patient interaction.
Patients who seek care for their health problems are looking for some measure of kindness when they approach the window of your office’s receptionist. Many are already apprehensive about their clinical condition and adding to that problem is their concern about the financial impact of their visit on the family’s budget. The medical group’s unwillingness to rethink how it greets patients as they approach the receptionist sets the stage for the patient to feel mishandled or underappreciated.
This initial patient interaction stage must be evaluated and recognized as an area of improvement. If not handled properly, it will significantly affect how a medical practice or provider is graded as a group in the field of patient experience and managing patient expectations. Every medical office needs to recognize that people hold on to negative experiences and are not likely to change their mind after that negative experience. The best way to avoid negative bias is to prevent it from happening in the first place.
Listed below are the five additional patient experience mistakes that can cost your group, if they are not recognized as being priorities for both your staff and your patients.
Mistake #1 - Educated patients are taking control of their health care.
When health care is treated like any other paid service, an unhappy patient will move along to a new facility or doctor if they have a bad interaction – whether it is with the doctor or the support staff. Educating, training, or adjusting staff to make changes needed is required to ensure that your staff understands the value of patient appreciation and providing the patient with a positive experience.
Mistake #2 - Patients are customers, and just like customers, patients have options.
It should be recognized that patients are customers who are concerned about their future and do not want to be in a medical practice requesting help. They feel vulnerable and out of their routine comfort zone. Reminding your staff that a patient is a customer who has multiple health care choices, but chose to come to your practice, will help your staff understand the value of providing your patient with a positive experience.
Mistake #3 – Dr. Google is becoming the patient’s best friend.
Research indicates that many patients arrive at the doctor’s office already with some information on their condition. Various websites already have provided the patient with free access to learn about their health condition. Popular medical sites such as WebMD.com give the patient the preliminary education they are looking for, so they are already armed with medical information even before they see the doctor or their support staff.
Mistake # 4 - Surveys are carrying more weight.
Outside surveys are becoming even more popular and are carrying additional weight when combined with various social media outlets. All types of surveys and reviews are being used to measure not only the care the patient received, but also the interpersonal relationship between the patient and the doctor, and the patient’s experience with the medical practice’s support staff. Some surveys cover all levels in the practice area, down to the cleanliness of the reception area or the patient’s treatment area, and even the adequacy of the parking lot. These surveys are conditioning patients to recall their entire experience. With a patient experience plan in place, excellent service becomes second nature and will be recognized by those surveyed.
Mistake #5 - Patient-centered care is customer service, too.
It’s not just about the obvious. Excellent patient (customer) service extends beyond a pleasant demeanor. The patient experience does not start or end at the doctor’s office. Perception is built by gathering information from multiple channels, whether it is through review sites, office visits, or surveys. It is necessary to consider the importance of those channels when looking to build patient loyalty.
To avoid the mistakes listed above, the more progressive medical practices are training their staff to anticipate the customer service needs of their patients, much like other major service industries. By rolling out a patient/customer experience training program, they can prevent these mistakes from ever happening and affecting their potential revenue. This training should focus on integrating the following strategies into their daily work habits to provide their patients with exceptional customer service while they are guests in their practice.
1) Patients are the lifeline to building the future of their practice.
Patients are comparing their health care services to other companies that routinely provide high-end services to their clients. Whether groups like it or not, their front-line personnel are compared to five-star hotel receptionists, who are expected to greet their customers both pleasantly and professionally after a long day of traveling and required business functions. Every medical group must understand that patients have options when they select a medical practice and they expect to be treated with respect and transparency, and not just another person to be cared for at the end of a long day. The same level of service needs to be delivered in the doctor’s office no matter what time of day it is because for that patient, the personal problems and subsequent disposition of the medical staff is not their problem. All they want is someone to listen and help them take care of their medical problem. Their long-term loyalty to the group will be solely dependent on how well each personal interaction is handled. Remember that the patient is a person first and not just a customer. We must approach each patient with humanity first, and then customer service.
2) Be courteous and respectful.
Remind your staff to be courteous, always polite and to use good manners. By treating a patient how they expect to be treated, you are showing the patient that you respect them and care for not only their health but also their feelings. The health care worker must understand that the patient is viewing their interactions with staff and providers as being symbolic of the overall group’s brand identity. The group’s leadership needs to select and train their workforce to recognize their importance in how patients view their clinical offerings and their interactions with the patient.
3) Never show indifference to patients.
Losing patients before they complete their treatment regimen is a significant liability issue for any medical practice. In an article written by Strive Labs CEO and Co-Founder, Scott Hebert, DPT, wrote: “Patient churn is too big of a problem to ignore, and it can have a profound impact on your clinic’s bottom line.” In addition to the rather obvious missed revenue opportunity, a churning patient represents a practice liability, because an unsatisfied patient is significantly more likely to leave you a negative review online — or turn the experience with your practice into a cautionary tale for friends and family members. Either way, it’s bad for business — and your reputation.
4) Don’t contradict, argue, or match wits.
It’s tough for a health care worker who is continually being bombarded in a high-pressure environment to agree to disagree. When a person feels they are right or that their perception is the only logical one, they can be very stubborn in their understanding, and they will dig in their heels. It takes a strong person to allow others to have their opinion and not be judgmental about it. Any customer or patient relations training program to be deployed in a medical office must include skill training to teach the staff member how to diffuse an argument or disagreement. This situation can be dispersed by training your staff to consider the source of the conflict, respect the patient’s perception, and then teach the staff member to tell the patient that they never thought of it that way and ease away from the discussion. Their absence will help diffuse the situation.
5) Tell patients you appreciate their business.
How you relate to a patient will speak volumes to them about how much you appreciate their loyalty, all because they chose your practice for their health care. All patient and customer training programs should include discussions on making eye contact, shaking with a firm grasp, and always closing a personal encounter on a sincere and positive note. Health care workers need to understand that they are in the service business and that the patients they care for have options and they can easily walk out of the medical practice and share any negative experience on social media. Educating and reminding your staff on how easily a patient can leave your practice or share their experience with others, needs to be recognized and discussed at all the group’s town hall meetings.
6) Use plain terms and simple explanations.
We all want to appear to be super intelligent by trying to use complex terms to describe a situation because it creates leverage with the other parties engaged in the conversation. While some of this may be necessary when educating patients on their condition, any additional complex terms can easily annoy or even confuse the patient who is only there seeking help. Health care workers need to talk in a manner that keeps the patients engaged and helps them understand the topic at hand. The worker needs to use every day vernacular examples, so the patient quickly understands the reason that brought them to the clinic and what they need to do to get some relief from what ails them. The phrase “plain and simple” means precisely that – explain the topic using basic and simple terms, so the listener understands it. Using this method when discussing a patient’s condition isn’t just for the patient’s benefit because many confused patients ultimately call the office later in the day only to ask additional questions, which uses your staff’s time.
7) Good manners will get you everywhere.
Emily Post wrote, “Manners are a sensitive awareness of the feelings of others. If you have that awareness, you have good manners, no matter what fork you use.” Proper manners are behaving in a way that is both aware of and considerate of the people around us. A person with good manners treats everyone with kindness and respect. It is knowing how to get along without causing offense or harm, no matter how much the current interaction is going south – especially when you are engaged in a tough conversation.
8) Keep seeing health care as a calling.
All health care workers need to know that their vocation of caring for sick and injured patients is a calling and not just a job and all training programs designed to teach customer service need to stress this point. Practicing your vocation means that you will work hard to eliminate all barriers that exist between the patient and the health care worker. Too often we underestimate the power of a simple touch, a smile, a kind word, a listening ear, an honest compliment, or the smallest act of caring – all of which have the potential to turn a life or a bad interaction into a magical moment for both the patient and the health care worker. One that has meaning and a bit of affirmation of the dignity of both individuals interacting to find some common ground.
9) Stay in touch with patients.
The group needs to find ways to keep in contact with their patients, whether it is by giving them tips on how to remain healthy or the need for proactive and preventive medicine. The use of technology and social media, as well as handing out freebies at health fairs, giving patients informational brochures upon discharge, or even cards telling them how to contact the practice in case of emergencies, is quite helpful. Calling your patients is a significant signal that your group values the health and welfare of your patients. A phone call from either the doctor or their assistant goes further than any advertisement when building brand and doctor loyalty.
10) Keep your promises.
Do what you say you are going to do, should be a commonly shared mantra for the medical practice. While changing your mind from time to time when circumstances prevent you from keeping a promise, is just part of being flexible in life, regularly breaking promises to other people isn’t healthy. Here’s how to keep your promises: Pay close attention to your words – every word you communicate (through speaking or writing), as a patient may take your words as a promise. Study your patterns of making promises. Figure out when you tend to make careless promises and study the situations in which you do, so you can understand why you’re promising what you don’t intend to do. Take time and careful consideration before making a promise to someone. Don’t rush yourself into a promise that you won’t be able to keep. Even when you’re in a hurry, you usually don’t have an immediate sense of urgency about promising to do something. Stop yourself before you make a vow, delaying your decision long enough to think it through carefully. The more careful you become about making promises, the easier it will be to keep them.
The last step of deploying a patient/customer service program is handling the change in management that is required to train the staff. Accepting “No, we are not changing any part of the group to meet the needs of our patients better.” is unacceptable. Usually, you will be introducing this program to employees that have been in a group for a while and so to get them to buy into the new ideas will require constant reinforcement. It may take some time to align the focus of the group from the neutral zone to the notion that there are new deliverables that would better serve your patients. The following rules will be helpful when beginning your training program:
Rule #1 – Be consistent. Every policy, procedure, and list of priorities sends a message – make sure it’s the right message.
Rule #2 – Ensure quick successes. Look for ways to get the group’s employees to buy into the program – early on after its deployment.
Rule# 3 – Symbolize the new identity. Make sure the group’s logos and branding support the new identity of the group and the culture change.
Rule #4 – Celebrate all the group’s successes. Make sure the group’s employees recognize the work efforts involved as well as the success the group will enjoy. Stress the fact that the work completed will significantly enhance the care and service levels to the patients, which should feed the ego of the group to do more and more in the future.
And lastly, do not forget how vital the buy-in is of the clinicians of the group. They must be introduced early to the new patient/customer service program and embrace it so that their employees will recognize that these efforts are focused on providing a high quality of care throughout the enterprise. As the French philosopher Albert Schweitzer once stated, “Example is not the main thing in influencing others, it’s the only thing.”
References
1. Peters, T. “The Excellence Dividend: Meeting the Tech Tide with Work that Wows and Jobs that Last.” (New York, Vintage Books, 2018).
2. 10 Strategies to Provide Patients with Superior Customer Service. Becker’s Hospital Review 2010 Dec 20.
3. Shell MA, Buell RW. Why anxious customers prefer human customer service. Harvard Business Review 2019 April 15.
4. Matt Brannon. 13 Ways to improve customer services at your medical practice. Blog post Sept 7, 2018.
5. 5 Reasons Why Customer Service Matters in Healthcare. https://www.pointsgroup.com/5-reasons-why-customer-service-matters-in-healthcare/Feb. 25, 2014
6. Senge P, Kleiner A, Roberts C, et al. “The Dance of Change: A fifth discipline resource.” (New York, Doubleday, 1999).
7. Bridges W. “Managing Transitions: Making the Most of Change.” (Boston, Da Capo Books, 2017)
8. Michelli J. “The New Gold Standard – 5 Leadership Principles for Creating the Legendary Customer Experience Courtesy of the Ritz-Carlton Hotel Company.” (New York, McGraw Hill, 2008).
Mr. Turner is chief executive officer of Indianapolis Gastroenterology and Hepatology.
If you work in health care or manage a medical practice, you are aware of all the radical changes in technology, medicine, social values, and interpersonal relations over the past few years and you probably do not expect the next several years to be less stressful and less uncertain. To ensure your practice and your provider’s success, you may need to adjust how your team interacts with patients – starting with the first area of patient interaction.
Patients who seek care for their health problems are looking for some measure of kindness when they approach the window of your office’s receptionist. Many are already apprehensive about their clinical condition and adding to that problem is their concern about the financial impact of their visit on the family’s budget. The medical group’s unwillingness to rethink how it greets patients as they approach the receptionist sets the stage for the patient to feel mishandled or underappreciated.
This initial patient interaction stage must be evaluated and recognized as an area of improvement. If not handled properly, it will significantly affect how a medical practice or provider is graded as a group in the field of patient experience and managing patient expectations. Every medical office needs to recognize that people hold on to negative experiences and are not likely to change their mind after that negative experience. The best way to avoid negative bias is to prevent it from happening in the first place.
Listed below are the five additional patient experience mistakes that can cost your group, if they are not recognized as being priorities for both your staff and your patients.
Mistake #1 - Educated patients are taking control of their health care.
When health care is treated like any other paid service, an unhappy patient will move along to a new facility or doctor if they have a bad interaction – whether it is with the doctor or the support staff. Educating, training, or adjusting staff to make changes needed is required to ensure that your staff understands the value of patient appreciation and providing the patient with a positive experience.
Mistake #2 - Patients are customers, and just like customers, patients have options.
It should be recognized that patients are customers who are concerned about their future and do not want to be in a medical practice requesting help. They feel vulnerable and out of their routine comfort zone. Reminding your staff that a patient is a customer who has multiple health care choices, but chose to come to your practice, will help your staff understand the value of providing your patient with a positive experience.
Mistake #3 – Dr. Google is becoming the patient’s best friend.
Research indicates that many patients arrive at the doctor’s office already with some information on their condition. Various websites already have provided the patient with free access to learn about their health condition. Popular medical sites such as WebMD.com give the patient the preliminary education they are looking for, so they are already armed with medical information even before they see the doctor or their support staff.
Mistake # 4 - Surveys are carrying more weight.
Outside surveys are becoming even more popular and are carrying additional weight when combined with various social media outlets. All types of surveys and reviews are being used to measure not only the care the patient received, but also the interpersonal relationship between the patient and the doctor, and the patient’s experience with the medical practice’s support staff. Some surveys cover all levels in the practice area, down to the cleanliness of the reception area or the patient’s treatment area, and even the adequacy of the parking lot. These surveys are conditioning patients to recall their entire experience. With a patient experience plan in place, excellent service becomes second nature and will be recognized by those surveyed.
Mistake #5 - Patient-centered care is customer service, too.
It’s not just about the obvious. Excellent patient (customer) service extends beyond a pleasant demeanor. The patient experience does not start or end at the doctor’s office. Perception is built by gathering information from multiple channels, whether it is through review sites, office visits, or surveys. It is necessary to consider the importance of those channels when looking to build patient loyalty.
To avoid the mistakes listed above, the more progressive medical practices are training their staff to anticipate the customer service needs of their patients, much like other major service industries. By rolling out a patient/customer experience training program, they can prevent these mistakes from ever happening and affecting their potential revenue. This training should focus on integrating the following strategies into their daily work habits to provide their patients with exceptional customer service while they are guests in their practice.
1) Patients are the lifeline to building the future of their practice.
Patients are comparing their health care services to other companies that routinely provide high-end services to their clients. Whether groups like it or not, their front-line personnel are compared to five-star hotel receptionists, who are expected to greet their customers both pleasantly and professionally after a long day of traveling and required business functions. Every medical group must understand that patients have options when they select a medical practice and they expect to be treated with respect and transparency, and not just another person to be cared for at the end of a long day. The same level of service needs to be delivered in the doctor’s office no matter what time of day it is because for that patient, the personal problems and subsequent disposition of the medical staff is not their problem. All they want is someone to listen and help them take care of their medical problem. Their long-term loyalty to the group will be solely dependent on how well each personal interaction is handled. Remember that the patient is a person first and not just a customer. We must approach each patient with humanity first, and then customer service.
2) Be courteous and respectful.
Remind your staff to be courteous, always polite and to use good manners. By treating a patient how they expect to be treated, you are showing the patient that you respect them and care for not only their health but also their feelings. The health care worker must understand that the patient is viewing their interactions with staff and providers as being symbolic of the overall group’s brand identity. The group’s leadership needs to select and train their workforce to recognize their importance in how patients view their clinical offerings and their interactions with the patient.
3) Never show indifference to patients.
Losing patients before they complete their treatment regimen is a significant liability issue for any medical practice. In an article written by Strive Labs CEO and Co-Founder, Scott Hebert, DPT, wrote: “Patient churn is too big of a problem to ignore, and it can have a profound impact on your clinic’s bottom line.” In addition to the rather obvious missed revenue opportunity, a churning patient represents a practice liability, because an unsatisfied patient is significantly more likely to leave you a negative review online — or turn the experience with your practice into a cautionary tale for friends and family members. Either way, it’s bad for business — and your reputation.
4) Don’t contradict, argue, or match wits.
It’s tough for a health care worker who is continually being bombarded in a high-pressure environment to agree to disagree. When a person feels they are right or that their perception is the only logical one, they can be very stubborn in their understanding, and they will dig in their heels. It takes a strong person to allow others to have their opinion and not be judgmental about it. Any customer or patient relations training program to be deployed in a medical office must include skill training to teach the staff member how to diffuse an argument or disagreement. This situation can be dispersed by training your staff to consider the source of the conflict, respect the patient’s perception, and then teach the staff member to tell the patient that they never thought of it that way and ease away from the discussion. Their absence will help diffuse the situation.
5) Tell patients you appreciate their business.
How you relate to a patient will speak volumes to them about how much you appreciate their loyalty, all because they chose your practice for their health care. All patient and customer training programs should include discussions on making eye contact, shaking with a firm grasp, and always closing a personal encounter on a sincere and positive note. Health care workers need to understand that they are in the service business and that the patients they care for have options and they can easily walk out of the medical practice and share any negative experience on social media. Educating and reminding your staff on how easily a patient can leave your practice or share their experience with others, needs to be recognized and discussed at all the group’s town hall meetings.
6) Use plain terms and simple explanations.
We all want to appear to be super intelligent by trying to use complex terms to describe a situation because it creates leverage with the other parties engaged in the conversation. While some of this may be necessary when educating patients on their condition, any additional complex terms can easily annoy or even confuse the patient who is only there seeking help. Health care workers need to talk in a manner that keeps the patients engaged and helps them understand the topic at hand. The worker needs to use every day vernacular examples, so the patient quickly understands the reason that brought them to the clinic and what they need to do to get some relief from what ails them. The phrase “plain and simple” means precisely that – explain the topic using basic and simple terms, so the listener understands it. Using this method when discussing a patient’s condition isn’t just for the patient’s benefit because many confused patients ultimately call the office later in the day only to ask additional questions, which uses your staff’s time.
7) Good manners will get you everywhere.
Emily Post wrote, “Manners are a sensitive awareness of the feelings of others. If you have that awareness, you have good manners, no matter what fork you use.” Proper manners are behaving in a way that is both aware of and considerate of the people around us. A person with good manners treats everyone with kindness and respect. It is knowing how to get along without causing offense or harm, no matter how much the current interaction is going south – especially when you are engaged in a tough conversation.
8) Keep seeing health care as a calling.
All health care workers need to know that their vocation of caring for sick and injured patients is a calling and not just a job and all training programs designed to teach customer service need to stress this point. Practicing your vocation means that you will work hard to eliminate all barriers that exist between the patient and the health care worker. Too often we underestimate the power of a simple touch, a smile, a kind word, a listening ear, an honest compliment, or the smallest act of caring – all of which have the potential to turn a life or a bad interaction into a magical moment for both the patient and the health care worker. One that has meaning and a bit of affirmation of the dignity of both individuals interacting to find some common ground.
9) Stay in touch with patients.
The group needs to find ways to keep in contact with their patients, whether it is by giving them tips on how to remain healthy or the need for proactive and preventive medicine. The use of technology and social media, as well as handing out freebies at health fairs, giving patients informational brochures upon discharge, or even cards telling them how to contact the practice in case of emergencies, is quite helpful. Calling your patients is a significant signal that your group values the health and welfare of your patients. A phone call from either the doctor or their assistant goes further than any advertisement when building brand and doctor loyalty.
10) Keep your promises.
Do what you say you are going to do, should be a commonly shared mantra for the medical practice. While changing your mind from time to time when circumstances prevent you from keeping a promise, is just part of being flexible in life, regularly breaking promises to other people isn’t healthy. Here’s how to keep your promises: Pay close attention to your words – every word you communicate (through speaking or writing), as a patient may take your words as a promise. Study your patterns of making promises. Figure out when you tend to make careless promises and study the situations in which you do, so you can understand why you’re promising what you don’t intend to do. Take time and careful consideration before making a promise to someone. Don’t rush yourself into a promise that you won’t be able to keep. Even when you’re in a hurry, you usually don’t have an immediate sense of urgency about promising to do something. Stop yourself before you make a vow, delaying your decision long enough to think it through carefully. The more careful you become about making promises, the easier it will be to keep them.
The last step of deploying a patient/customer service program is handling the change in management that is required to train the staff. Accepting “No, we are not changing any part of the group to meet the needs of our patients better.” is unacceptable. Usually, you will be introducing this program to employees that have been in a group for a while and so to get them to buy into the new ideas will require constant reinforcement. It may take some time to align the focus of the group from the neutral zone to the notion that there are new deliverables that would better serve your patients. The following rules will be helpful when beginning your training program:
Rule #1 – Be consistent. Every policy, procedure, and list of priorities sends a message – make sure it’s the right message.
Rule #2 – Ensure quick successes. Look for ways to get the group’s employees to buy into the program – early on after its deployment.
Rule# 3 – Symbolize the new identity. Make sure the group’s logos and branding support the new identity of the group and the culture change.
Rule #4 – Celebrate all the group’s successes. Make sure the group’s employees recognize the work efforts involved as well as the success the group will enjoy. Stress the fact that the work completed will significantly enhance the care and service levels to the patients, which should feed the ego of the group to do more and more in the future.
And lastly, do not forget how vital the buy-in is of the clinicians of the group. They must be introduced early to the new patient/customer service program and embrace it so that their employees will recognize that these efforts are focused on providing a high quality of care throughout the enterprise. As the French philosopher Albert Schweitzer once stated, “Example is not the main thing in influencing others, it’s the only thing.”
References
1. Peters, T. “The Excellence Dividend: Meeting the Tech Tide with Work that Wows and Jobs that Last.” (New York, Vintage Books, 2018).
2. 10 Strategies to Provide Patients with Superior Customer Service. Becker’s Hospital Review 2010 Dec 20.
3. Shell MA, Buell RW. Why anxious customers prefer human customer service. Harvard Business Review 2019 April 15.
4. Matt Brannon. 13 Ways to improve customer services at your medical practice. Blog post Sept 7, 2018.
5. 5 Reasons Why Customer Service Matters in Healthcare. https://www.pointsgroup.com/5-reasons-why-customer-service-matters-in-healthcare/Feb. 25, 2014
6. Senge P, Kleiner A, Roberts C, et al. “The Dance of Change: A fifth discipline resource.” (New York, Doubleday, 1999).
7. Bridges W. “Managing Transitions: Making the Most of Change.” (Boston, Da Capo Books, 2017)
8. Michelli J. “The New Gold Standard – 5 Leadership Principles for Creating the Legendary Customer Experience Courtesy of the Ritz-Carlton Hotel Company.” (New York, McGraw Hill, 2008).
Mr. Turner is chief executive officer of Indianapolis Gastroenterology and Hepatology.
Ovarian cancer and perineal talc exposure: An epidemiologic dilemma
Many readers may be aware of large payments made by such companies as Johnson & Johnson to compensate women with a history of ovarian cancer who have claimed that perineal application of talc played a causative role in their cancer development. This column serves to review the purported role of perineal talc use in the development of ovarian cancer, and explore some of the pitfalls of observational science.

Talc, a hydrated magnesium silicate, is the softest mineral on earth, and has been sold as a personal hygiene product for many decades. Perineal application of talc to sanitary pads, perineal skin, undergarments, and diapers has been a common practice to decrease friction, moisture build-up, and as a deodorant. Talc is chemically similar, although not identical, to asbestos and is geologically located in close proximity to the known carcinogen. In the 1970s, there were concerns raised regarding the possible contamination of cosmetic-grade talc with asbestos, which led to the development of asbestos-free forms of the substance. Given that a strong causal relationship had been established between asbestos exposure and lung and pleural cancers, there was concern that exposure to perineal talc might increase cancer risk.
In the 1980s, an association between perineal talc exposure and ovarian cancer was observed in a case-control study.1 Since that time, multiple other observational studies, predominately case-control studies, have observed an increased ovarian cancer risk among users of perineal talc including the findings of a meta-analysis which estimated a 24%-39% increased risk for ovarian cancer among users.2 Does this establish a causal relationship? For the purposes of legal cases, these associations are adequate. However, science demands a different standard when determining cause and effect.
It is not unusual to rely on observational studies to establish a causal relationship between exposure and disease when it is unethical to randomize subjects in a clinical trial to exposure of the potential harmful agent. This was the necessary methodology behind establishing that smoking causes lung cancer. Several factors must be present when relying on observational studies to establish plausible causation including an observable biologic mechanism, dose-effect response, temporal relationship, consistent effect observed in multiple study populations, and statistical strength of response. These elements should be present in a consistent and powerful enough way to balance the pitfalls of observational studies, namely biases.
A particularly problematic bias is one of recall bias, which plagues case-control studies. Case-control studies are a popular tool to measure a relationship between an exposure and a rare disease, because they are more feasible than the prospective, observational cohort studies that require very large study populations observed over very long periods of time to capture enough events of interest (in this case, cases of ovarian cancer). In case-control studies, researchers identify a cohort of patients with the outcome of interest (ovarian cancer) and compare this population to a control group of similar demographic features. They then survey directly or indirectly (through medical records) for the exposure of interest (perineal talc use).
Recall bias occurs when subjects who have the disease are more likely to have memory of exposure than do control subjects because of the natural instincts individuals have toward attribution. This is emphasized when there is public commentary, justified or not, about the potential risks of that exposure. Given the significant publicity that these lawsuits have had with companies that produced cosmetic talc, it is plausible that ovarian cancer survivors are more likely to remember and negatively attribute their talc exposure to their cancer than are subjects without cancer. Additionally, their memory of volume and duration of exposure generally is enhanced by the same pressures. The potential for this bias is eliminated in prospective, cohort observational studies such as the Women’s Health Initiative Observational Study which, among 61,576 women, half of whom reported perineal talc exposure, did not measure a difference in the development of ovarian cancers during their 12 years of mean follow-up.3
Given these inherent biases, The biologic mechanism of talc carcinogenesis is largely theoretical. As mentioned earlier, prior to the 1970s, there was some observed contamination of talc with asbestos likely caused by the geologic proximity of these minerals. Asbestos is a known carcinogen, and therefore possibly could be harmful if a contaminant of talc. However, it is not known if this level of contamination was enough to be achieve ovarian carcinogenesis. Most theories of talc carcinogenesis are based on foreign body inflammatory reaction via talc particle ascent through the genital tract. This is proposed to induce an inflammatory release of prostaglandins and cytokines, which could cause a mutagenic effect promoting carcinogenesis. The foreign body inflammatory mechanism is further supported by the observation of a decreased incidence of ovarian cancer after hysterectomy or tubal ligation.4 However, inconsistently, a protective effect of NSAIDs has not been observed in ovarian cancer.5
A recent meta-analysis, which reviewed 27 of the largest, best-quality observational studies, identified a dose-effect response with an increased risk for ovarian cancer with greater than 3,600 lifetime applications, compared with less than 3,600 applications.2 The observed association between perineal talc exposure and increased risk of ovarian cancer appears to be consistent across a number of observational studies, including both case-control studies and prospective cohort studies (although somewhat mitigated in the latter). Additionally, there appears to be consistency in the finding that the risk is present for the epithelial subtypes of serous and endometrioid, but not mucinous or clear cell cancer. However, when considering the magnitude of effect, this remains somewhat small (odds ratio, 1.31; 95% confidence interval, 1.24-1.39) when compared with other better established carcinogenic relationships such as smoking and lung cancer where the hazard ratio is 12.12 (95% CI, 6.94-21.17).2,6
If talc does not cause ovarian cancer, why would this association be observed at all? One explanation could be that talc use is a confounder for the true causative mechanism. A theoretical example of this would be if the genital microbiome (a subject we have reviewed previously in this column) was the true culprit. If a particular microbiome profile promotes both oncogenic change in the ovary while also causing vaginal discharge and odor, it might increase the likelihood that perineal talc use is reported in the history of these cancer patients. This is purely speculative, but it always is important to consider the potential for confounding variables when utilizing observational studies to attribute cause and effect.

Therefore, there is a consistently observed association between perineal talc application and ovarian cancer, however, the relationship does not appear to be strong enough, associated with a proven carcinogenic mechanism, or free from interfering recall bias such to definitively state that perineal talc exposure causes ovarian cancer. Given these findings, it is reasonable to recommend patients avoid the use of perineal talc application until further definitive safety evidence is provided. In the meantime, it should be noted that even though talc-containing products are not commercially labeled as carcinogens, many pharmaceutical and cosmetic companies have replaced the mineral talc with corn starch in their powders.
Dr. Rossi is assistant professor in the division of gynecologic oncology at the University of North Carolina at Chapel Hill. She had no relevant financial disclosures. Email her at obnews@mdedge.com.
References
1. Cancer. 1982 Jul 15;50(2):372-6.
2. Epidemiology. 2018 Jan;29(1):41-9.
3. J Natl Cancer Inst. 2014 Sep 10;106(9). pii: dju208.
4. Am J Epidemiol. 1991 Aug 15;134(4):362-9.
5. Int J Cancer. 2008 Jan 1;122(1):170-6.
6. J Natl Cancer Inst. 2018 Nov 1;110(11):1201-7.
Many readers may be aware of large payments made by such companies as Johnson & Johnson to compensate women with a history of ovarian cancer who have claimed that perineal application of talc played a causative role in their cancer development. This column serves to review the purported role of perineal talc use in the development of ovarian cancer, and explore some of the pitfalls of observational science.
Talc, a hydrated magnesium silicate, is the softest mineral on earth, and has been sold as a personal hygiene product for many decades. Perineal application of talc to sanitary pads, perineal skin, undergarments, and diapers has been a common practice to decrease friction, moisture build-up, and as a deodorant. Talc is chemically similar, although not identical, to asbestos and is geologically located in close proximity to the known carcinogen. In the 1970s, there were concerns raised regarding the possible contamination of cosmetic-grade talc with asbestos, which led to the development of asbestos-free forms of the substance. Given that a strong causal relationship had been established between asbestos exposure and lung and pleural cancers, there was concern that exposure to perineal talc might increase cancer risk.
In the 1980s, an association between perineal talc exposure and ovarian cancer was observed in a case-control study.1 Since that time, multiple other observational studies, predominately case-control studies, have observed an increased ovarian cancer risk among users of perineal talc including the findings of a meta-analysis which estimated a 24%-39% increased risk for ovarian cancer among users.2 Does this establish a causal relationship? For the purposes of legal cases, these associations are adequate. However, science demands a different standard when determining cause and effect.
It is not unusual to rely on observational studies to establish a causal relationship between exposure and disease when it is unethical to randomize subjects in a clinical trial to exposure of the potential harmful agent. This was the necessary methodology behind establishing that smoking causes lung cancer. Several factors must be present when relying on observational studies to establish plausible causation including an observable biologic mechanism, dose-effect response, temporal relationship, consistent effect observed in multiple study populations, and statistical strength of response. These elements should be present in a consistent and powerful enough way to balance the pitfalls of observational studies, namely biases.
A particularly problematic bias is one of recall bias, which plagues case-control studies. Case-control studies are a popular tool to measure a relationship between an exposure and a rare disease, because they are more feasible than the prospective, observational cohort studies that require very large study populations observed over very long periods of time to capture enough events of interest (in this case, cases of ovarian cancer). In case-control studies, researchers identify a cohort of patients with the outcome of interest (ovarian cancer) and compare this population to a control group of similar demographic features. They then survey directly or indirectly (through medical records) for the exposure of interest (perineal talc use).
Recall bias occurs when subjects who have the disease are more likely to have memory of exposure than do control subjects because of the natural instincts individuals have toward attribution. This is emphasized when there is public commentary, justified or not, about the potential risks of that exposure. Given the significant publicity that these lawsuits have had with companies that produced cosmetic talc, it is plausible that ovarian cancer survivors are more likely to remember and negatively attribute their talc exposure to their cancer than are subjects without cancer. Additionally, their memory of volume and duration of exposure generally is enhanced by the same pressures. The potential for this bias is eliminated in prospective, cohort observational studies such as the Women’s Health Initiative Observational Study which, among 61,576 women, half of whom reported perineal talc exposure, did not measure a difference in the development of ovarian cancers during their 12 years of mean follow-up.3
Given these inherent biases, The biologic mechanism of talc carcinogenesis is largely theoretical. As mentioned earlier, prior to the 1970s, there was some observed contamination of talc with asbestos likely caused by the geologic proximity of these minerals. Asbestos is a known carcinogen, and therefore possibly could be harmful if a contaminant of talc. However, it is not known if this level of contamination was enough to be achieve ovarian carcinogenesis. Most theories of talc carcinogenesis are based on foreign body inflammatory reaction via talc particle ascent through the genital tract. This is proposed to induce an inflammatory release of prostaglandins and cytokines, which could cause a mutagenic effect promoting carcinogenesis. The foreign body inflammatory mechanism is further supported by the observation of a decreased incidence of ovarian cancer after hysterectomy or tubal ligation.4 However, inconsistently, a protective effect of NSAIDs has not been observed in ovarian cancer.5
A recent meta-analysis, which reviewed 27 of the largest, best-quality observational studies, identified a dose-effect response with an increased risk for ovarian cancer with greater than 3,600 lifetime applications, compared with less than 3,600 applications.2 The observed association between perineal talc exposure and increased risk of ovarian cancer appears to be consistent across a number of observational studies, including both case-control studies and prospective cohort studies (although somewhat mitigated in the latter). Additionally, there appears to be consistency in the finding that the risk is present for the epithelial subtypes of serous and endometrioid, but not mucinous or clear cell cancer. However, when considering the magnitude of effect, this remains somewhat small (odds ratio, 1.31; 95% confidence interval, 1.24-1.39) when compared with other better established carcinogenic relationships such as smoking and lung cancer where the hazard ratio is 12.12 (95% CI, 6.94-21.17).2,6
If talc does not cause ovarian cancer, why would this association be observed at all? One explanation could be that talc use is a confounder for the true causative mechanism. A theoretical example of this would be if the genital microbiome (a subject we have reviewed previously in this column) was the true culprit. If a particular microbiome profile promotes both oncogenic change in the ovary while also causing vaginal discharge and odor, it might increase the likelihood that perineal talc use is reported in the history of these cancer patients. This is purely speculative, but it always is important to consider the potential for confounding variables when utilizing observational studies to attribute cause and effect.
Therefore, there is a consistently observed association between perineal talc application and ovarian cancer, however, the relationship does not appear to be strong enough, associated with a proven carcinogenic mechanism, or free from interfering recall bias such to definitively state that perineal talc exposure causes ovarian cancer. Given these findings, it is reasonable to recommend patients avoid the use of perineal talc application until further definitive safety evidence is provided. In the meantime, it should be noted that even though talc-containing products are not commercially labeled as carcinogens, many pharmaceutical and cosmetic companies have replaced the mineral talc with corn starch in their powders.
Dr. Rossi is assistant professor in the division of gynecologic oncology at the University of North Carolina at Chapel Hill. She had no relevant financial disclosures. Email her at obnews@mdedge.com.
References
1. Cancer. 1982 Jul 15;50(2):372-6.
2. Epidemiology. 2018 Jan;29(1):41-9.
3. J Natl Cancer Inst. 2014 Sep 10;106(9). pii: dju208.
4. Am J Epidemiol. 1991 Aug 15;134(4):362-9.
5. Int J Cancer. 2008 Jan 1;122(1):170-6.
6. J Natl Cancer Inst. 2018 Nov 1;110(11):1201-7.
Many readers may be aware of large payments made by such companies as Johnson & Johnson to compensate women with a history of ovarian cancer who have claimed that perineal application of talc played a causative role in their cancer development. This column serves to review the purported role of perineal talc use in the development of ovarian cancer, and explore some of the pitfalls of observational science.
Talc, a hydrated magnesium silicate, is the softest mineral on earth, and has been sold as a personal hygiene product for many decades. Perineal application of talc to sanitary pads, perineal skin, undergarments, and diapers has been a common practice to decrease friction, moisture build-up, and as a deodorant. Talc is chemically similar, although not identical, to asbestos and is geologically located in close proximity to the known carcinogen. In the 1970s, there were concerns raised regarding the possible contamination of cosmetic-grade talc with asbestos, which led to the development of asbestos-free forms of the substance. Given that a strong causal relationship had been established between asbestos exposure and lung and pleural cancers, there was concern that exposure to perineal talc might increase cancer risk.
In the 1980s, an association between perineal talc exposure and ovarian cancer was observed in a case-control study.1 Since that time, multiple other observational studies, predominately case-control studies, have observed an increased ovarian cancer risk among users of perineal talc including the findings of a meta-analysis which estimated a 24%-39% increased risk for ovarian cancer among users.2 Does this establish a causal relationship? For the purposes of legal cases, these associations are adequate. However, science demands a different standard when determining cause and effect.
It is not unusual to rely on observational studies to establish a causal relationship between exposure and disease when it is unethical to randomize subjects in a clinical trial to exposure of the potential harmful agent. This was the necessary methodology behind establishing that smoking causes lung cancer. Several factors must be present when relying on observational studies to establish plausible causation including an observable biologic mechanism, dose-effect response, temporal relationship, consistent effect observed in multiple study populations, and statistical strength of response. These elements should be present in a consistent and powerful enough way to balance the pitfalls of observational studies, namely biases.
A particularly problematic bias is one of recall bias, which plagues case-control studies. Case-control studies are a popular tool to measure a relationship between an exposure and a rare disease, because they are more feasible than the prospective, observational cohort studies that require very large study populations observed over very long periods of time to capture enough events of interest (in this case, cases of ovarian cancer). In case-control studies, researchers identify a cohort of patients with the outcome of interest (ovarian cancer) and compare this population to a control group of similar demographic features. They then survey directly or indirectly (through medical records) for the exposure of interest (perineal talc use).
Recall bias occurs when subjects who have the disease are more likely to have memory of exposure than do control subjects because of the natural instincts individuals have toward attribution. This is emphasized when there is public commentary, justified or not, about the potential risks of that exposure. Given the significant publicity that these lawsuits have had with companies that produced cosmetic talc, it is plausible that ovarian cancer survivors are more likely to remember and negatively attribute their talc exposure to their cancer than are subjects without cancer. Additionally, their memory of volume and duration of exposure generally is enhanced by the same pressures. The potential for this bias is eliminated in prospective, cohort observational studies such as the Women’s Health Initiative Observational Study which, among 61,576 women, half of whom reported perineal talc exposure, did not measure a difference in the development of ovarian cancers during their 12 years of mean follow-up.3
Given these inherent biases, The biologic mechanism of talc carcinogenesis is largely theoretical. As mentioned earlier, prior to the 1970s, there was some observed contamination of talc with asbestos likely caused by the geologic proximity of these minerals. Asbestos is a known carcinogen, and therefore possibly could be harmful if a contaminant of talc. However, it is not known if this level of contamination was enough to be achieve ovarian carcinogenesis. Most theories of talc carcinogenesis are based on foreign body inflammatory reaction via talc particle ascent through the genital tract. This is proposed to induce an inflammatory release of prostaglandins and cytokines, which could cause a mutagenic effect promoting carcinogenesis. The foreign body inflammatory mechanism is further supported by the observation of a decreased incidence of ovarian cancer after hysterectomy or tubal ligation.4 However, inconsistently, a protective effect of NSAIDs has not been observed in ovarian cancer.5
A recent meta-analysis, which reviewed 27 of the largest, best-quality observational studies, identified a dose-effect response with an increased risk for ovarian cancer with greater than 3,600 lifetime applications, compared with less than 3,600 applications.2 The observed association between perineal talc exposure and increased risk of ovarian cancer appears to be consistent across a number of observational studies, including both case-control studies and prospective cohort studies (although somewhat mitigated in the latter). Additionally, there appears to be consistency in the finding that the risk is present for the epithelial subtypes of serous and endometrioid, but not mucinous or clear cell cancer. However, when considering the magnitude of effect, this remains somewhat small (odds ratio, 1.31; 95% confidence interval, 1.24-1.39) when compared with other better established carcinogenic relationships such as smoking and lung cancer where the hazard ratio is 12.12 (95% CI, 6.94-21.17).2,6
If talc does not cause ovarian cancer, why would this association be observed at all? One explanation could be that talc use is a confounder for the true causative mechanism. A theoretical example of this would be if the genital microbiome (a subject we have reviewed previously in this column) was the true culprit. If a particular microbiome profile promotes both oncogenic change in the ovary while also causing vaginal discharge and odor, it might increase the likelihood that perineal talc use is reported in the history of these cancer patients. This is purely speculative, but it always is important to consider the potential for confounding variables when utilizing observational studies to attribute cause and effect.
Therefore, there is a consistently observed association between perineal talc application and ovarian cancer, however, the relationship does not appear to be strong enough, associated with a proven carcinogenic mechanism, or free from interfering recall bias such to definitively state that perineal talc exposure causes ovarian cancer. Given these findings, it is reasonable to recommend patients avoid the use of perineal talc application until further definitive safety evidence is provided. In the meantime, it should be noted that even though talc-containing products are not commercially labeled as carcinogens, many pharmaceutical and cosmetic companies have replaced the mineral talc with corn starch in their powders.
Dr. Rossi is assistant professor in the division of gynecologic oncology at the University of North Carolina at Chapel Hill. She had no relevant financial disclosures. Email her at obnews@mdedge.com.
References
1. Cancer. 1982 Jul 15;50(2):372-6.
2. Epidemiology. 2018 Jan;29(1):41-9.
3. J Natl Cancer Inst. 2014 Sep 10;106(9). pii: dju208.
4. Am J Epidemiol. 1991 Aug 15;134(4):362-9.
5. Int J Cancer. 2008 Jan 1;122(1):170-6.
6. J Natl Cancer Inst. 2018 Nov 1;110(11):1201-7.