User login
‘Decapitated’ boy saved by surgery team
This transcript has been edited for clarity.
F. Perry Wilson, MD, MSCE: I am joined today by Dr. Ohad Einav. He’s a staff surgeon in orthopedics at Hadassah Medical Center in Jerusalem. He’s with me to talk about an absolutely incredible surgical case, something that is terrifying to most non–orthopedic surgeons and I imagine is fairly scary for spine surgeons like him as well. But what we don’t have is information about how this works from a medical perspective. So, first of all, Dr. Einav, thank you for taking time to speak with me today.
Ohad Einav, MD: Thank you for having me.
Dr. Wilson: Can you tell us about Suleiman Hassan and what happened to him before he came into your care?
Dr. Einav: Hassan is a 12-year-old child who was riding his bicycle on the West Bank, about 40 minutes from here. Unfortunately, he was involved in a motor vehicle accident and he suffered injuries to his abdomen and cervical spine. He was transported to our service by helicopter from the scene of the accident.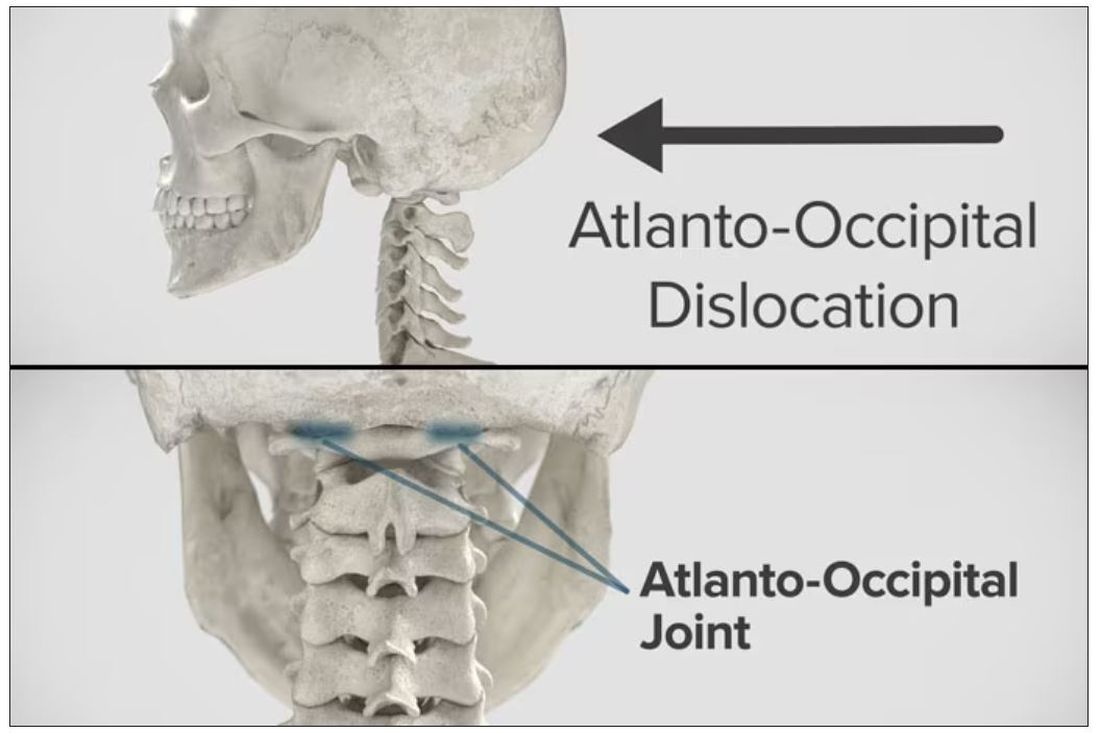
Dr. Wilson: “Injury to the cervical spine” might be something of an understatement. He had what’s called atlanto-occipital dislocation, colloquially often referred to as internal decapitation. Can you tell us what that means? It sounds terrifying.
Dr. Einav: It’s an injury to the ligaments between the occiput and the upper cervical spine, with or without bony fracture. The atlanto-occipital joint is formed by the superior articular facet of the atlas and the occipital condyle, stabilized by an articular capsule between the head and neck, and is supported by various ligaments around it that stabilize the joint and allow joint movements, including flexion, extension, and some rotation in the lower levels.
Dr. Wilson: This joint has several degrees of freedom, which means it needs a lot of support. With this type of injury, where essentially you have severing of the ligaments, is it usually survivable? How dangerous is this?
Dr. Einav: The mortality rate is 50%-60%, depending on the primary impact, the injury, transportation later on, and then the surgery and surgical management.
Dr. Wilson: Tell us a bit about this patient’s status when he came to your medical center. I assume he was in bad shape.
Dr. Einav: Hassan arrived at our medical center with a Glasgow Coma Scale score of 15. He was fully conscious. He was hemodynamically stable except for a bad laceration on his abdomen. He had a Philadelphia collar around his neck. He was transported by chopper because the paramedics suspected that he had a cervical spine injury and decided to bring him to a Level 1 trauma center.
He was monitored and we treated him according to the ATLS [advanced trauma life support] protocol. He didn’t have any gross sensory deficits, but he was a little confused about the whole situation and the accident. Therefore, we could do a general examination but we couldn’t rely on that regarding any sensory deficit that he may or may not have. We decided as a team that it would be better to slow down and control the situation. We decided not to operate on him immediately. We basically stabilized him and made sure that he didn’t have any traumatic internal organ damage. Later on we took him to the OR and performed surgery.
Dr. Wilson: It’s amazing that he had intact motor function, considering the extent of his injury. The spinal cord was spared somewhat during the injury. There must have been a moment when you realized that this kid, who was conscious and could move all four extremities, had a very severe neck injury. Was that due to a CT scan or physical exam? And what was your feeling when you saw that he had atlanto-occipital dislocation?
Dr. Einav: As a surgeon, you have a gut feeling in regard to the general examination of the patient. But I never rely on gut feelings. On the CT, I understood exactly what he had, what we needed to do, and the time frame.
Dr. Wilson: You’ve done these types of surgeries before, right? Obviously, no one has done a lot of them because this isn’t very common. But you knew what to do. Did you have a plan? Where does your experience come into play in a situation like this?
Dr. Einav: I graduated from the spine program of Toronto University, where I did a fellowship in trauma of the spine and complex spine surgery. I had very good teachers, and during my fellowship I treated a few cases in older patients that were similar but not the same. Therefore, I knew exactly what needed to be done.
Dr. Wilson: For those of us who aren’t surgeons, take us into the OR with you. This is obviously an incredibly delicate procedure. You are high up in the spinal cord at the base of the brain. The slightest mistake could have devastating consequences. What are the key elements of this procedure? What can go wrong here? What is the number-one thing you have to look out for when you’re trying to fix an internal decapitation?
Dr. Einav: The key element in surgeries of the cervical spine – trauma and complex spine surgery – is planning. I never go to the OR without knowing what I’m going to do. I have a few plans – plan A, plan B, plan C – in case something fails. So, I definitely know what the next step will be. I always think about the surgery a few hours before, if I have time to prepare.
The second thing that is very important is teamwork. The team needs to be coordinated. Everybody needs to know what their job is. With these types of injuries, it’s not the time for rookies. If you are new, please stand back and let the more experienced people do that job. I’m talking about surgeons, nurses, anesthesiologists – everyone.
Another important thing in planning is choosing the right hardware. For example, in this case we had a problem because most of the hardware is designed for adults, and we had to improvise because there isn’t a lot of hardware on the market for the pediatric population. The adult plates and screws are too big, so we had to improvise.
Dr. Wilson: Tell us more about that. How do you improvise spinal hardware for a 12-year-old?
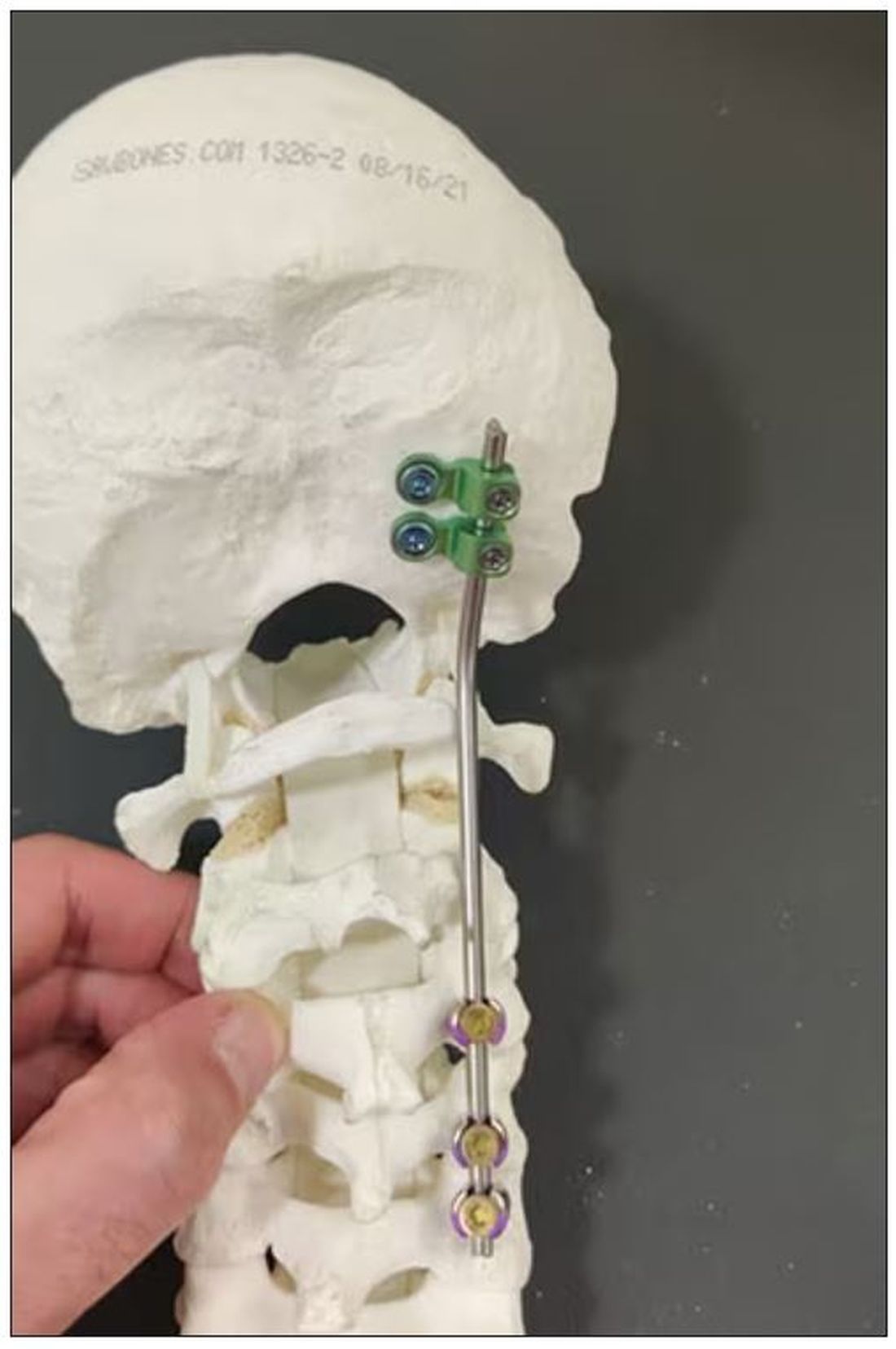
Dr. Einav: In this case, I chose to use hardware from one of the companies that works with us.
You can see in this model the area of the injury, and the area that we worked on. To perform the surgery, I had to use some plates and rods from a different company. This company’s (NuVasive) hardware has a small attachment to the skull, which was helpful for affixing the skull to the cervical spine, instead of using a big plate that would sit at the base of the skull and would not be very good for him. Most of the hardware is made for adults and not for kids.
Dr. Wilson: Will that hardware preserve the motor function of his neck? Will he be able to turn his head and extend and flex it?
Dr. Einav: The injury leads to instability and destruction of both articulations between the head and neck. Therefore, those articulations won’t be able to function the same way in the future. There is a decrease of something like 50% of the flexion and extension of Hassan’s cervical spine. Therefore, I decided that in this case there would be no chance of saving Hassan’s motor function unless we performed a fusion between the head and the neck, and therefore I decided that this would be the best procedure with the best survival rate. So, in the future, he will have some diminished flexion, extension, and rotation of his head.
Dr. Wilson: How long did his surgery take?
Dr. Einav: To be honest, I don’t remember. But I can tell you that it took us time. It was very challenging to coordinate with everyone. The most problematic part of the surgery to perform is what we call “flip-over.”
The anesthesiologist intubated the patient when he was supine, and later on, we flipped him prone to operate on the spine. This maneuver can actually lead to injury by itself, and injury at this level is fatal. So, we took our time and got Hassan into the OR. The anesthesiologist did a great job with the GlideScope – inserting the endotracheal tube. Later on, we neuromonitored him. Basically, we connected Hassan’s peripheral nerves to a computer and monitored his motor function. Gently we flipped him over, and after that we saw a little change in his motor function, so we had to modify his position so we could preserve his motor function. We then started the procedure, which took a few hours. I don’t know exactly how many.
Dr. Wilson: That just speaks to how delicate this is for everything from the intubation, where typically you’re manipulating the head, to the repositioning. Clearly this requires a lot of teamwork.
What happened after the operation? How is he doing?
Dr. Einav: After the operation, Hassan had a great recovery. He’s doing well. He doesn’t have any motor or sensory deficits. He’s able to ambulate without any aid. He had no signs of infection, which can happen after a car accident, neither from his abdominal wound nor from the occipital cervical surgery. He feels well. We saw him in the clinic. We removed his collar. We monitored him at the clinic. He looked amazing.
Dr. Wilson: That’s incredible. Are there long-term risks for him that you need to be looking out for?
Dr. Einav: Yes, and that’s the reason that we are monitoring him post surgery. While he was in the hospital, we monitored his motor and sensory functions, as well as his wound healing. Later on, in the clinic, for a few weeks after surgery we monitored for any failure of the hardware and bone graft. We check for healing of the bone graft and bone substitutes we put in to heal those bones.
Dr. Wilson: He will grow, right? He’s only 12, so he still has some years of growth in him. Is he going to need more surgery or any kind of hardware upgrade?
Dr. Einav: I hope not. In my surgeries, I never rely on the hardware for long durations. If I decide to do, for example, fusion, I rely on the hardware for a certain amount of time. And then I plan that the biology will do the work. If I plan for fusion, I put bone grafts in the preferred area for a fusion. Then if the hardware fails, I wouldn’t need to take out the hardware, and there would be no change in the condition of the patient.
Dr. Wilson: What an incredible story. It’s clear that you and your team kept your cool despite a very high-acuity situation with a ton of risk. What a tremendous outcome that this boy is not only alive but fully functional. So, congratulations to you and your team. That was very strong work.
Dr. Einav: Thank you very much. I would like to thank our team. We have to remember that the surgeon is not standing alone in the war. Hassan’s story is a success story of a very big group of people from various backgrounds and religions. They work day and night to help people and save lives. To the paramedics, the physiologists, the traumatologists, the pediatricians, the nurses, the physiotherapists, and obviously the surgeons, a big thank you. His story is our success story.
Dr. Wilson: It’s inspiring to see so many people come together to do what we all are here for, which is to fight against suffering, disease, and death. Thank you for keeping up that fight. And thank you for joining me here.
Dr. Einav: Thank you very much.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
F. Perry Wilson, MD, MSCE: I am joined today by Dr. Ohad Einav. He’s a staff surgeon in orthopedics at Hadassah Medical Center in Jerusalem. He’s with me to talk about an absolutely incredible surgical case, something that is terrifying to most non–orthopedic surgeons and I imagine is fairly scary for spine surgeons like him as well. But what we don’t have is information about how this works from a medical perspective. So, first of all, Dr. Einav, thank you for taking time to speak with me today.
Ohad Einav, MD: Thank you for having me.
Dr. Wilson: Can you tell us about Suleiman Hassan and what happened to him before he came into your care?
Dr. Einav: Hassan is a 12-year-old child who was riding his bicycle on the West Bank, about 40 minutes from here. Unfortunately, he was involved in a motor vehicle accident and he suffered injuries to his abdomen and cervical spine. He was transported to our service by helicopter from the scene of the accident.
Dr. Wilson: “Injury to the cervical spine” might be something of an understatement. He had what’s called atlanto-occipital dislocation, colloquially often referred to as internal decapitation. Can you tell us what that means? It sounds terrifying.
Dr. Einav: It’s an injury to the ligaments between the occiput and the upper cervical spine, with or without bony fracture. The atlanto-occipital joint is formed by the superior articular facet of the atlas and the occipital condyle, stabilized by an articular capsule between the head and neck, and is supported by various ligaments around it that stabilize the joint and allow joint movements, including flexion, extension, and some rotation in the lower levels.
Dr. Wilson: This joint has several degrees of freedom, which means it needs a lot of support. With this type of injury, where essentially you have severing of the ligaments, is it usually survivable? How dangerous is this?
Dr. Einav: The mortality rate is 50%-60%, depending on the primary impact, the injury, transportation later on, and then the surgery and surgical management.
Dr. Wilson: Tell us a bit about this patient’s status when he came to your medical center. I assume he was in bad shape.
Dr. Einav: Hassan arrived at our medical center with a Glasgow Coma Scale score of 15. He was fully conscious. He was hemodynamically stable except for a bad laceration on his abdomen. He had a Philadelphia collar around his neck. He was transported by chopper because the paramedics suspected that he had a cervical spine injury and decided to bring him to a Level 1 trauma center.
He was monitored and we treated him according to the ATLS [advanced trauma life support] protocol. He didn’t have any gross sensory deficits, but he was a little confused about the whole situation and the accident. Therefore, we could do a general examination but we couldn’t rely on that regarding any sensory deficit that he may or may not have. We decided as a team that it would be better to slow down and control the situation. We decided not to operate on him immediately. We basically stabilized him and made sure that he didn’t have any traumatic internal organ damage. Later on we took him to the OR and performed surgery.
Dr. Wilson: It’s amazing that he had intact motor function, considering the extent of his injury. The spinal cord was spared somewhat during the injury. There must have been a moment when you realized that this kid, who was conscious and could move all four extremities, had a very severe neck injury. Was that due to a CT scan or physical exam? And what was your feeling when you saw that he had atlanto-occipital dislocation?
Dr. Einav: As a surgeon, you have a gut feeling in regard to the general examination of the patient. But I never rely on gut feelings. On the CT, I understood exactly what he had, what we needed to do, and the time frame.
Dr. Wilson: You’ve done these types of surgeries before, right? Obviously, no one has done a lot of them because this isn’t very common. But you knew what to do. Did you have a plan? Where does your experience come into play in a situation like this?
Dr. Einav: I graduated from the spine program of Toronto University, where I did a fellowship in trauma of the spine and complex spine surgery. I had very good teachers, and during my fellowship I treated a few cases in older patients that were similar but not the same. Therefore, I knew exactly what needed to be done.
Dr. Wilson: For those of us who aren’t surgeons, take us into the OR with you. This is obviously an incredibly delicate procedure. You are high up in the spinal cord at the base of the brain. The slightest mistake could have devastating consequences. What are the key elements of this procedure? What can go wrong here? What is the number-one thing you have to look out for when you’re trying to fix an internal decapitation?
Dr. Einav: The key element in surgeries of the cervical spine – trauma and complex spine surgery – is planning. I never go to the OR without knowing what I’m going to do. I have a few plans – plan A, plan B, plan C – in case something fails. So, I definitely know what the next step will be. I always think about the surgery a few hours before, if I have time to prepare.
The second thing that is very important is teamwork. The team needs to be coordinated. Everybody needs to know what their job is. With these types of injuries, it’s not the time for rookies. If you are new, please stand back and let the more experienced people do that job. I’m talking about surgeons, nurses, anesthesiologists – everyone.
Another important thing in planning is choosing the right hardware. For example, in this case we had a problem because most of the hardware is designed for adults, and we had to improvise because there isn’t a lot of hardware on the market for the pediatric population. The adult plates and screws are too big, so we had to improvise.
Dr. Wilson: Tell us more about that. How do you improvise spinal hardware for a 12-year-old?
Dr. Einav: In this case, I chose to use hardware from one of the companies that works with us.
You can see in this model the area of the injury, and the area that we worked on. To perform the surgery, I had to use some plates and rods from a different company. This company’s (NuVasive) hardware has a small attachment to the skull, which was helpful for affixing the skull to the cervical spine, instead of using a big plate that would sit at the base of the skull and would not be very good for him. Most of the hardware is made for adults and not for kids.
Dr. Wilson: Will that hardware preserve the motor function of his neck? Will he be able to turn his head and extend and flex it?
Dr. Einav: The injury leads to instability and destruction of both articulations between the head and neck. Therefore, those articulations won’t be able to function the same way in the future. There is a decrease of something like 50% of the flexion and extension of Hassan’s cervical spine. Therefore, I decided that in this case there would be no chance of saving Hassan’s motor function unless we performed a fusion between the head and the neck, and therefore I decided that this would be the best procedure with the best survival rate. So, in the future, he will have some diminished flexion, extension, and rotation of his head.
Dr. Wilson: How long did his surgery take?
Dr. Einav: To be honest, I don’t remember. But I can tell you that it took us time. It was very challenging to coordinate with everyone. The most problematic part of the surgery to perform is what we call “flip-over.”
The anesthesiologist intubated the patient when he was supine, and later on, we flipped him prone to operate on the spine. This maneuver can actually lead to injury by itself, and injury at this level is fatal. So, we took our time and got Hassan into the OR. The anesthesiologist did a great job with the GlideScope – inserting the endotracheal tube. Later on, we neuromonitored him. Basically, we connected Hassan’s peripheral nerves to a computer and monitored his motor function. Gently we flipped him over, and after that we saw a little change in his motor function, so we had to modify his position so we could preserve his motor function. We then started the procedure, which took a few hours. I don’t know exactly how many.
Dr. Wilson: That just speaks to how delicate this is for everything from the intubation, where typically you’re manipulating the head, to the repositioning. Clearly this requires a lot of teamwork.
What happened after the operation? How is he doing?
Dr. Einav: After the operation, Hassan had a great recovery. He’s doing well. He doesn’t have any motor or sensory deficits. He’s able to ambulate without any aid. He had no signs of infection, which can happen after a car accident, neither from his abdominal wound nor from the occipital cervical surgery. He feels well. We saw him in the clinic. We removed his collar. We monitored him at the clinic. He looked amazing.
Dr. Wilson: That’s incredible. Are there long-term risks for him that you need to be looking out for?
Dr. Einav: Yes, and that’s the reason that we are monitoring him post surgery. While he was in the hospital, we monitored his motor and sensory functions, as well as his wound healing. Later on, in the clinic, for a few weeks after surgery we monitored for any failure of the hardware and bone graft. We check for healing of the bone graft and bone substitutes we put in to heal those bones.
Dr. Wilson: He will grow, right? He’s only 12, so he still has some years of growth in him. Is he going to need more surgery or any kind of hardware upgrade?
Dr. Einav: I hope not. In my surgeries, I never rely on the hardware for long durations. If I decide to do, for example, fusion, I rely on the hardware for a certain amount of time. And then I plan that the biology will do the work. If I plan for fusion, I put bone grafts in the preferred area for a fusion. Then if the hardware fails, I wouldn’t need to take out the hardware, and there would be no change in the condition of the patient.
Dr. Wilson: What an incredible story. It’s clear that you and your team kept your cool despite a very high-acuity situation with a ton of risk. What a tremendous outcome that this boy is not only alive but fully functional. So, congratulations to you and your team. That was very strong work.
Dr. Einav: Thank you very much. I would like to thank our team. We have to remember that the surgeon is not standing alone in the war. Hassan’s story is a success story of a very big group of people from various backgrounds and religions. They work day and night to help people and save lives. To the paramedics, the physiologists, the traumatologists, the pediatricians, the nurses, the physiotherapists, and obviously the surgeons, a big thank you. His story is our success story.
Dr. Wilson: It’s inspiring to see so many people come together to do what we all are here for, which is to fight against suffering, disease, and death. Thank you for keeping up that fight. And thank you for joining me here.
Dr. Einav: Thank you very much.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
F. Perry Wilson, MD, MSCE: I am joined today by Dr. Ohad Einav. He’s a staff surgeon in orthopedics at Hadassah Medical Center in Jerusalem. He’s with me to talk about an absolutely incredible surgical case, something that is terrifying to most non–orthopedic surgeons and I imagine is fairly scary for spine surgeons like him as well. But what we don’t have is information about how this works from a medical perspective. So, first of all, Dr. Einav, thank you for taking time to speak with me today.
Ohad Einav, MD: Thank you for having me.
Dr. Wilson: Can you tell us about Suleiman Hassan and what happened to him before he came into your care?
Dr. Einav: Hassan is a 12-year-old child who was riding his bicycle on the West Bank, about 40 minutes from here. Unfortunately, he was involved in a motor vehicle accident and he suffered injuries to his abdomen and cervical spine. He was transported to our service by helicopter from the scene of the accident.
Dr. Wilson: “Injury to the cervical spine” might be something of an understatement. He had what’s called atlanto-occipital dislocation, colloquially often referred to as internal decapitation. Can you tell us what that means? It sounds terrifying.
Dr. Einav: It’s an injury to the ligaments between the occiput and the upper cervical spine, with or without bony fracture. The atlanto-occipital joint is formed by the superior articular facet of the atlas and the occipital condyle, stabilized by an articular capsule between the head and neck, and is supported by various ligaments around it that stabilize the joint and allow joint movements, including flexion, extension, and some rotation in the lower levels.
Dr. Wilson: This joint has several degrees of freedom, which means it needs a lot of support. With this type of injury, where essentially you have severing of the ligaments, is it usually survivable? How dangerous is this?
Dr. Einav: The mortality rate is 50%-60%, depending on the primary impact, the injury, transportation later on, and then the surgery and surgical management.
Dr. Wilson: Tell us a bit about this patient’s status when he came to your medical center. I assume he was in bad shape.
Dr. Einav: Hassan arrived at our medical center with a Glasgow Coma Scale score of 15. He was fully conscious. He was hemodynamically stable except for a bad laceration on his abdomen. He had a Philadelphia collar around his neck. He was transported by chopper because the paramedics suspected that he had a cervical spine injury and decided to bring him to a Level 1 trauma center.
He was monitored and we treated him according to the ATLS [advanced trauma life support] protocol. He didn’t have any gross sensory deficits, but he was a little confused about the whole situation and the accident. Therefore, we could do a general examination but we couldn’t rely on that regarding any sensory deficit that he may or may not have. We decided as a team that it would be better to slow down and control the situation. We decided not to operate on him immediately. We basically stabilized him and made sure that he didn’t have any traumatic internal organ damage. Later on we took him to the OR and performed surgery.
Dr. Wilson: It’s amazing that he had intact motor function, considering the extent of his injury. The spinal cord was spared somewhat during the injury. There must have been a moment when you realized that this kid, who was conscious and could move all four extremities, had a very severe neck injury. Was that due to a CT scan or physical exam? And what was your feeling when you saw that he had atlanto-occipital dislocation?
Dr. Einav: As a surgeon, you have a gut feeling in regard to the general examination of the patient. But I never rely on gut feelings. On the CT, I understood exactly what he had, what we needed to do, and the time frame.
Dr. Wilson: You’ve done these types of surgeries before, right? Obviously, no one has done a lot of them because this isn’t very common. But you knew what to do. Did you have a plan? Where does your experience come into play in a situation like this?
Dr. Einav: I graduated from the spine program of Toronto University, where I did a fellowship in trauma of the spine and complex spine surgery. I had very good teachers, and during my fellowship I treated a few cases in older patients that were similar but not the same. Therefore, I knew exactly what needed to be done.
Dr. Wilson: For those of us who aren’t surgeons, take us into the OR with you. This is obviously an incredibly delicate procedure. You are high up in the spinal cord at the base of the brain. The slightest mistake could have devastating consequences. What are the key elements of this procedure? What can go wrong here? What is the number-one thing you have to look out for when you’re trying to fix an internal decapitation?
Dr. Einav: The key element in surgeries of the cervical spine – trauma and complex spine surgery – is planning. I never go to the OR without knowing what I’m going to do. I have a few plans – plan A, plan B, plan C – in case something fails. So, I definitely know what the next step will be. I always think about the surgery a few hours before, if I have time to prepare.
The second thing that is very important is teamwork. The team needs to be coordinated. Everybody needs to know what their job is. With these types of injuries, it’s not the time for rookies. If you are new, please stand back and let the more experienced people do that job. I’m talking about surgeons, nurses, anesthesiologists – everyone.
Another important thing in planning is choosing the right hardware. For example, in this case we had a problem because most of the hardware is designed for adults, and we had to improvise because there isn’t a lot of hardware on the market for the pediatric population. The adult plates and screws are too big, so we had to improvise.
Dr. Wilson: Tell us more about that. How do you improvise spinal hardware for a 12-year-old?
Dr. Einav: In this case, I chose to use hardware from one of the companies that works with us.
You can see in this model the area of the injury, and the area that we worked on. To perform the surgery, I had to use some plates and rods from a different company. This company’s (NuVasive) hardware has a small attachment to the skull, which was helpful for affixing the skull to the cervical spine, instead of using a big plate that would sit at the base of the skull and would not be very good for him. Most of the hardware is made for adults and not for kids.
Dr. Wilson: Will that hardware preserve the motor function of his neck? Will he be able to turn his head and extend and flex it?
Dr. Einav: The injury leads to instability and destruction of both articulations between the head and neck. Therefore, those articulations won’t be able to function the same way in the future. There is a decrease of something like 50% of the flexion and extension of Hassan’s cervical spine. Therefore, I decided that in this case there would be no chance of saving Hassan’s motor function unless we performed a fusion between the head and the neck, and therefore I decided that this would be the best procedure with the best survival rate. So, in the future, he will have some diminished flexion, extension, and rotation of his head.
Dr. Wilson: How long did his surgery take?
Dr. Einav: To be honest, I don’t remember. But I can tell you that it took us time. It was very challenging to coordinate with everyone. The most problematic part of the surgery to perform is what we call “flip-over.”
The anesthesiologist intubated the patient when he was supine, and later on, we flipped him prone to operate on the spine. This maneuver can actually lead to injury by itself, and injury at this level is fatal. So, we took our time and got Hassan into the OR. The anesthesiologist did a great job with the GlideScope – inserting the endotracheal tube. Later on, we neuromonitored him. Basically, we connected Hassan’s peripheral nerves to a computer and monitored his motor function. Gently we flipped him over, and after that we saw a little change in his motor function, so we had to modify his position so we could preserve his motor function. We then started the procedure, which took a few hours. I don’t know exactly how many.
Dr. Wilson: That just speaks to how delicate this is for everything from the intubation, where typically you’re manipulating the head, to the repositioning. Clearly this requires a lot of teamwork.
What happened after the operation? How is he doing?
Dr. Einav: After the operation, Hassan had a great recovery. He’s doing well. He doesn’t have any motor or sensory deficits. He’s able to ambulate without any aid. He had no signs of infection, which can happen after a car accident, neither from his abdominal wound nor from the occipital cervical surgery. He feels well. We saw him in the clinic. We removed his collar. We monitored him at the clinic. He looked amazing.
Dr. Wilson: That’s incredible. Are there long-term risks for him that you need to be looking out for?
Dr. Einav: Yes, and that’s the reason that we are monitoring him post surgery. While he was in the hospital, we monitored his motor and sensory functions, as well as his wound healing. Later on, in the clinic, for a few weeks after surgery we monitored for any failure of the hardware and bone graft. We check for healing of the bone graft and bone substitutes we put in to heal those bones.
Dr. Wilson: He will grow, right? He’s only 12, so he still has some years of growth in him. Is he going to need more surgery or any kind of hardware upgrade?
Dr. Einav: I hope not. In my surgeries, I never rely on the hardware for long durations. If I decide to do, for example, fusion, I rely on the hardware for a certain amount of time. And then I plan that the biology will do the work. If I plan for fusion, I put bone grafts in the preferred area for a fusion. Then if the hardware fails, I wouldn’t need to take out the hardware, and there would be no change in the condition of the patient.
Dr. Wilson: What an incredible story. It’s clear that you and your team kept your cool despite a very high-acuity situation with a ton of risk. What a tremendous outcome that this boy is not only alive but fully functional. So, congratulations to you and your team. That was very strong work.
Dr. Einav: Thank you very much. I would like to thank our team. We have to remember that the surgeon is not standing alone in the war. Hassan’s story is a success story of a very big group of people from various backgrounds and religions. They work day and night to help people and save lives. To the paramedics, the physiologists, the traumatologists, the pediatricians, the nurses, the physiotherapists, and obviously the surgeons, a big thank you. His story is our success story.
Dr. Wilson: It’s inspiring to see so many people come together to do what we all are here for, which is to fight against suffering, disease, and death. Thank you for keeping up that fight. And thank you for joining me here.
Dr. Einav: Thank you very much.
A version of this article first appeared on Medscape.com.
Five ways to avert a malpractice lawsuit with better EHR techniques
Although most physicians have gotten used to working with EHRs, despite their irritations, the use of EHRs has contributed to a growing number of malpractice lawsuits. Defense attorneys say that
According to a study in the Journal of Patient Safety, more than 30% of all EHR-related malpractice cases are associated with medication errors; 28% with diagnosis; and 31% with a complication of treatment, such as entering wrong information, entering information in the wrong place, and overlooking EHR flags and warnings for interactions or contraindications.
The study gave these examples of EHR-related errors that led to patient harm and ultimately to malpractice lawsuits:
- A discharge order omitted a patient’s medication that prevented strokes; the patient had a stroke days later.
- An electronic order for morphine failed to state the upper dose limit; the patient died.
- A physician meant to click on “discontinue” for an anticoagulant but mistakenly clicked on “continue” for home use.
Catching potential issues such as drug interactions or critical medical history that should inform treatment is more important than ever. “We know from safety engineering principles that just relying on vigilance is not a long-term safety strategy,” says Aaron Zach Hettinger, MD, chief research information officer at MedStar Health Research Institute, Washington, D.C. “So, it’s critical that we design these safe systems and leverage the data that’s in them.”
Here are five smart EHR practices to help protect your patients’ health and your own liability.
1. Double-check dropdown boxes
When it comes to user error, it’s easy to click the wrong choice from a drop-down menu. Better to take the time to explain your answer in a box, even if it takes a few more minutes. Or if you are choosing from a menu, proofread any information it auto-fills in the chart.
Dr. Hettinger says you can strike a balance between these templated approaches to diagnosis and long-term care by working with third-party systems and your organization or vendor IT department to help with follow-up questions to keep populated data in check.
“Make sure you have a back-end system that can help monitor that structured data,” says Dr. Hettinger. Structured data are the patient’s demographic information, like name, address, age, height, weight, vital signs, and data elements like diagnosis, medications, and lab results. “Wherever you can leverage the underlying tools that are part of the electronic health record to make sure that we’re constantly checking the right results, that helps reduce the workload so that clinicians can focus on taking care of the patients and doing the right thing and not be as focused on entering data into the system.”
2. Supplement EHR notes with direct communication
The failure to diagnose cancer because one physician doesn’t know what another physician saw in an imaging report is one of the most common claims in the cases he tries, says Aaron Boeder, a plaintiff’s medical negligence lawyer in Chicago.
Physicians often assume that if they put a note in the electronic chart, others will look for it, but Mr. Boeder says it’s far more prudent to communicate directly.
“Let’s say a radiologist interprets a scan and sees what might be cancer,” he says. “If the ordering doctor is an orthopedist who’s ordered a CT scan for DVT, there’s going to be a report for that scan. It’s going to get auto-populated back into that physician’s note,” says Mr. Boeder.
The physician may or may not look at it, but it will be in their note, and they’re supposed to follow up on it because they ordered the scan. “But they may not follow up on it, and they may not get a call from the radiologist,” he says.
“Next thing you know, 2 or 3 years later, that patient is diagnosed with very advanced cancer.”
3. Tailor auto-fill information to your common practices
Suppose, as a physician, you find that you need to change a default setting time and time again. Dr. Hettinger says it’s worth your time to take an extra couple of minutes to work with your vendor or your health system to try and make changes to auto-population settings that align with your practices.
“Let’s say a default dose of 20 milligrams of a medication is what automatically pops up, but in reality, your practice is to use a smaller dose because it’s safer, even though they’re all within the acceptable realm of what you would order,” he says. “Rather than have the default to the higher dose, see if you can change the default to a lower dose. And that way, you don’t have to catch yourself every time.”
If your auto-fills are amounts that constantly need changing, an interruption could easily knock you off course before you make that correction.
“If there are ways to have the system defaults be safer or more in line with your clinical practice, and especially across a group, then you’re designing a safer system and not relying on vigilance or memory prone to interruptions,” says Dr. Hettinger.
4. Curb the copy and paste
It’s tempting to copy a note from a previous patient visit and make only minimal changes as needed, but you risk including outdated information if you do. Even if you’re repeating questions asked by the intake nurse, it is safer to not to rely on that information, says Beth Kanik, a defense medical malpractice attorney in Atlanta.
“If it later goes into litigation, the argument then becomes that it looks like you didn’t do your job,” says Ms. Kanik. “Instead, try to ask questions in a way that would elicit responses that may be a little different than what the nurse got, so that it’s clear you asked the questions and didn’t just simply rely upon someone else’s information.”
5. Separate typing from listening
While EHR may be an excellent tool for data collection and safety checking, it’s not a stand-in for doctor-patient interaction. As technology practices push medicine toward more and more efficiency, Mr. Boeder says it’s most often listening over all else that makes the difference in the quality of care. And good listening requires full attention.
“A real concern for physicians is the number of visits they’re expected to accomplish in a set amount of time,” says Mr. Boeder. “Often this translates into a doctor talking to a patient while typing notes or while reading a note from the last time the patient was in.”
Taking the time to pause after entering data and briefly reviewing your understanding of what your patient has told you can be invaluable and may save you – and your patient – problems later.
“In so many cases, it comes down to people not being heard,” says Mr. Boeder. “So listen to what your patients are saying.”
A version of this article first appeared on Medscape.com.
Although most physicians have gotten used to working with EHRs, despite their irritations, the use of EHRs has contributed to a growing number of malpractice lawsuits. Defense attorneys say that
According to a study in the Journal of Patient Safety, more than 30% of all EHR-related malpractice cases are associated with medication errors; 28% with diagnosis; and 31% with a complication of treatment, such as entering wrong information, entering information in the wrong place, and overlooking EHR flags and warnings for interactions or contraindications.
The study gave these examples of EHR-related errors that led to patient harm and ultimately to malpractice lawsuits:
- A discharge order omitted a patient’s medication that prevented strokes; the patient had a stroke days later.
- An electronic order for morphine failed to state the upper dose limit; the patient died.
- A physician meant to click on “discontinue” for an anticoagulant but mistakenly clicked on “continue” for home use.
Catching potential issues such as drug interactions or critical medical history that should inform treatment is more important than ever. “We know from safety engineering principles that just relying on vigilance is not a long-term safety strategy,” says Aaron Zach Hettinger, MD, chief research information officer at MedStar Health Research Institute, Washington, D.C. “So, it’s critical that we design these safe systems and leverage the data that’s in them.”
Here are five smart EHR practices to help protect your patients’ health and your own liability.
1. Double-check dropdown boxes
When it comes to user error, it’s easy to click the wrong choice from a drop-down menu. Better to take the time to explain your answer in a box, even if it takes a few more minutes. Or if you are choosing from a menu, proofread any information it auto-fills in the chart.
Dr. Hettinger says you can strike a balance between these templated approaches to diagnosis and long-term care by working with third-party systems and your organization or vendor IT department to help with follow-up questions to keep populated data in check.
“Make sure you have a back-end system that can help monitor that structured data,” says Dr. Hettinger. Structured data are the patient’s demographic information, like name, address, age, height, weight, vital signs, and data elements like diagnosis, medications, and lab results. “Wherever you can leverage the underlying tools that are part of the electronic health record to make sure that we’re constantly checking the right results, that helps reduce the workload so that clinicians can focus on taking care of the patients and doing the right thing and not be as focused on entering data into the system.”
2. Supplement EHR notes with direct communication
The failure to diagnose cancer because one physician doesn’t know what another physician saw in an imaging report is one of the most common claims in the cases he tries, says Aaron Boeder, a plaintiff’s medical negligence lawyer in Chicago.
Physicians often assume that if they put a note in the electronic chart, others will look for it, but Mr. Boeder says it’s far more prudent to communicate directly.
“Let’s say a radiologist interprets a scan and sees what might be cancer,” he says. “If the ordering doctor is an orthopedist who’s ordered a CT scan for DVT, there’s going to be a report for that scan. It’s going to get auto-populated back into that physician’s note,” says Mr. Boeder.
The physician may or may not look at it, but it will be in their note, and they’re supposed to follow up on it because they ordered the scan. “But they may not follow up on it, and they may not get a call from the radiologist,” he says.
“Next thing you know, 2 or 3 years later, that patient is diagnosed with very advanced cancer.”
3. Tailor auto-fill information to your common practices
Suppose, as a physician, you find that you need to change a default setting time and time again. Dr. Hettinger says it’s worth your time to take an extra couple of minutes to work with your vendor or your health system to try and make changes to auto-population settings that align with your practices.
“Let’s say a default dose of 20 milligrams of a medication is what automatically pops up, but in reality, your practice is to use a smaller dose because it’s safer, even though they’re all within the acceptable realm of what you would order,” he says. “Rather than have the default to the higher dose, see if you can change the default to a lower dose. And that way, you don’t have to catch yourself every time.”
If your auto-fills are amounts that constantly need changing, an interruption could easily knock you off course before you make that correction.
“If there are ways to have the system defaults be safer or more in line with your clinical practice, and especially across a group, then you’re designing a safer system and not relying on vigilance or memory prone to interruptions,” says Dr. Hettinger.
4. Curb the copy and paste
It’s tempting to copy a note from a previous patient visit and make only minimal changes as needed, but you risk including outdated information if you do. Even if you’re repeating questions asked by the intake nurse, it is safer to not to rely on that information, says Beth Kanik, a defense medical malpractice attorney in Atlanta.
“If it later goes into litigation, the argument then becomes that it looks like you didn’t do your job,” says Ms. Kanik. “Instead, try to ask questions in a way that would elicit responses that may be a little different than what the nurse got, so that it’s clear you asked the questions and didn’t just simply rely upon someone else’s information.”
5. Separate typing from listening
While EHR may be an excellent tool for data collection and safety checking, it’s not a stand-in for doctor-patient interaction. As technology practices push medicine toward more and more efficiency, Mr. Boeder says it’s most often listening over all else that makes the difference in the quality of care. And good listening requires full attention.
“A real concern for physicians is the number of visits they’re expected to accomplish in a set amount of time,” says Mr. Boeder. “Often this translates into a doctor talking to a patient while typing notes or while reading a note from the last time the patient was in.”
Taking the time to pause after entering data and briefly reviewing your understanding of what your patient has told you can be invaluable and may save you – and your patient – problems later.
“In so many cases, it comes down to people not being heard,” says Mr. Boeder. “So listen to what your patients are saying.”
A version of this article first appeared on Medscape.com.
Although most physicians have gotten used to working with EHRs, despite their irritations, the use of EHRs has contributed to a growing number of malpractice lawsuits. Defense attorneys say that
According to a study in the Journal of Patient Safety, more than 30% of all EHR-related malpractice cases are associated with medication errors; 28% with diagnosis; and 31% with a complication of treatment, such as entering wrong information, entering information in the wrong place, and overlooking EHR flags and warnings for interactions or contraindications.
The study gave these examples of EHR-related errors that led to patient harm and ultimately to malpractice lawsuits:
- A discharge order omitted a patient’s medication that prevented strokes; the patient had a stroke days later.
- An electronic order for morphine failed to state the upper dose limit; the patient died.
- A physician meant to click on “discontinue” for an anticoagulant but mistakenly clicked on “continue” for home use.
Catching potential issues such as drug interactions or critical medical history that should inform treatment is more important than ever. “We know from safety engineering principles that just relying on vigilance is not a long-term safety strategy,” says Aaron Zach Hettinger, MD, chief research information officer at MedStar Health Research Institute, Washington, D.C. “So, it’s critical that we design these safe systems and leverage the data that’s in them.”
Here are five smart EHR practices to help protect your patients’ health and your own liability.
1. Double-check dropdown boxes
When it comes to user error, it’s easy to click the wrong choice from a drop-down menu. Better to take the time to explain your answer in a box, even if it takes a few more minutes. Or if you are choosing from a menu, proofread any information it auto-fills in the chart.
Dr. Hettinger says you can strike a balance between these templated approaches to diagnosis and long-term care by working with third-party systems and your organization or vendor IT department to help with follow-up questions to keep populated data in check.
“Make sure you have a back-end system that can help monitor that structured data,” says Dr. Hettinger. Structured data are the patient’s demographic information, like name, address, age, height, weight, vital signs, and data elements like diagnosis, medications, and lab results. “Wherever you can leverage the underlying tools that are part of the electronic health record to make sure that we’re constantly checking the right results, that helps reduce the workload so that clinicians can focus on taking care of the patients and doing the right thing and not be as focused on entering data into the system.”
2. Supplement EHR notes with direct communication
The failure to diagnose cancer because one physician doesn’t know what another physician saw in an imaging report is one of the most common claims in the cases he tries, says Aaron Boeder, a plaintiff’s medical negligence lawyer in Chicago.
Physicians often assume that if they put a note in the electronic chart, others will look for it, but Mr. Boeder says it’s far more prudent to communicate directly.
“Let’s say a radiologist interprets a scan and sees what might be cancer,” he says. “If the ordering doctor is an orthopedist who’s ordered a CT scan for DVT, there’s going to be a report for that scan. It’s going to get auto-populated back into that physician’s note,” says Mr. Boeder.
The physician may or may not look at it, but it will be in their note, and they’re supposed to follow up on it because they ordered the scan. “But they may not follow up on it, and they may not get a call from the radiologist,” he says.
“Next thing you know, 2 or 3 years later, that patient is diagnosed with very advanced cancer.”
3. Tailor auto-fill information to your common practices
Suppose, as a physician, you find that you need to change a default setting time and time again. Dr. Hettinger says it’s worth your time to take an extra couple of minutes to work with your vendor or your health system to try and make changes to auto-population settings that align with your practices.
“Let’s say a default dose of 20 milligrams of a medication is what automatically pops up, but in reality, your practice is to use a smaller dose because it’s safer, even though they’re all within the acceptable realm of what you would order,” he says. “Rather than have the default to the higher dose, see if you can change the default to a lower dose. And that way, you don’t have to catch yourself every time.”
If your auto-fills are amounts that constantly need changing, an interruption could easily knock you off course before you make that correction.
“If there are ways to have the system defaults be safer or more in line with your clinical practice, and especially across a group, then you’re designing a safer system and not relying on vigilance or memory prone to interruptions,” says Dr. Hettinger.
4. Curb the copy and paste
It’s tempting to copy a note from a previous patient visit and make only minimal changes as needed, but you risk including outdated information if you do. Even if you’re repeating questions asked by the intake nurse, it is safer to not to rely on that information, says Beth Kanik, a defense medical malpractice attorney in Atlanta.
“If it later goes into litigation, the argument then becomes that it looks like you didn’t do your job,” says Ms. Kanik. “Instead, try to ask questions in a way that would elicit responses that may be a little different than what the nurse got, so that it’s clear you asked the questions and didn’t just simply rely upon someone else’s information.”
5. Separate typing from listening
While EHR may be an excellent tool for data collection and safety checking, it’s not a stand-in for doctor-patient interaction. As technology practices push medicine toward more and more efficiency, Mr. Boeder says it’s most often listening over all else that makes the difference in the quality of care. And good listening requires full attention.
“A real concern for physicians is the number of visits they’re expected to accomplish in a set amount of time,” says Mr. Boeder. “Often this translates into a doctor talking to a patient while typing notes or while reading a note from the last time the patient was in.”
Taking the time to pause after entering data and briefly reviewing your understanding of what your patient has told you can be invaluable and may save you – and your patient – problems later.
“In so many cases, it comes down to people not being heard,” says Mr. Boeder. “So listen to what your patients are saying.”
A version of this article first appeared on Medscape.com.
Could a malpractice insurer drop you when you need it most?
You’ve practiced medicine for years without issues, but now you are facing a medical malpractice case. No worries – you’ve had professional liability insurance all this time, so surely there’s nothing to be concerned about. Undoubtedly, your medical malpractice insurer will cover the costs of defending you. Or will they? One case casts questions on just this issue.
Professional liability insurance
According to the American Medical Association, almost one in three physicians (31%) have had a medical malpractice lawsuit filed against them at some point in their careers. These numbers only increase the longer a physician practices; almost half of doctors 55 and over have been sued, compared with less than 10% of physicians under 40.
And while the majority of cases are dropped or dismissed, and the small minority of cases that do go to trial are mostly won by the defense, the cost of defending these cases can be extremely high. Physicians have medical malpractice insurance to defray these costs.
Malpractice insurance generally covers the costs of attorney fees, court costs, arbitration, compensatory damages, and settlements related to patient injury or death. Insurance sometimes, but not always, pays for the costs of malpractice lawsuits arising out of Health Insurance Portability and Accountability Act (HIPAA) violations.
But it is what the policies don’t pay for that should be of most interest to practitioners.
Exclusions to medical malpractice insurance
All professional liability insurance policies contain exclusions, and it is essential that you know what they are. While the exclusions may vary by policy, most malpractice insurance policies exclude claims stemming from:
- Reckless or intentional acts.
- Illegal/criminal activities, including theft.
- Misrepresentation, including dishonesty, fraudulent activity, falsification, and misrepresentation on forms.
- Practicing under the influence of alcohol or drugs.
- Altering patient or hospital records.
- Sexual misconduct.
- Cyber security issues, which typically require a separate cyber liability policy to protect against cyber attacks and data breaches affecting patient medical records.
It’s essential to know what your specific policy’s exclusions are, or you may be surprised to find that your malpractice liability insurance doesn’t cover you when you expected that it would. Such was the situation in a recently decided case.
Also essential is knowing what type of coverage your policy provides – claims-made or occurrence-based. Occurrence policies offer lifetime coverage for incidents that occurred during the policy period, no matter when the claim is made. Claims-made policies cover only incidents that occur and are reported within the policy’s time period (unless a “tail” policy is purchased to extend the reporting period).
The case
Dr. P was a neurologist specializing in pain management. He had a professional liability insurance policy with an insurance company. In 2012, Dr. P’s insurance agent saw a television news story about the physician being accused by the state medical board for overprescribing opioids, resulting in the deaths of 17 patients. The next day, the agent obtained copies of documents from the state medical board, including a summary suspension order and a notice of contemplated action.
The notice of contemplated action specified that Dr. P had deviated from the standard of care through injudicious prescribing, leading to approximately 17 patient deaths due to drug toxicity. Because the agent realized that lawsuits could be filed against Dr. P for the deaths, she sent the insurance company the paperwork from the medical board so the insurer would be aware of the potential claims.
However, when the insurer received the information, it did not investigate or seek more information as it was required to do. The insurer failed to get medical records, or specific patient names, and none of the 17 deaths were recorded in the insurance company’s claims system (a failure to follow company procedure). Instead, the insurance company decided to cancel Dr. P’s policy effective the following month.
The company sent Dr. P a cancellation letter advising him that his policy was being terminated due to “license suspension, nature of allegations, and practice profile,” and offered him a tail policy to purchase.
The insurance company did not advise Dr. P that he should ensure all potential claims were reported, including the 17 deaths, before his policy expired. The company also did not advise him that he had a claims-made policy and what that meant regarding future lawsuits that might be filed after his policy period expired.
A year later, Dr. P was sued in two wrongful death lawsuits by the families of two of the 17 opioid-related deaths. When he was served with the papers, he promptly notified the insurance company. The insurance company issued a denial letter, incorrectly asserting that the 17 drug-toxicity deaths that they were aware of did not qualify as claims under Dr. P’s policy.
After his insurance company failed to represent him, Dr. P divorced his wife of 35 years and filed for bankruptcy. The only creditors with claims were the two families who had sued him. The bankruptcy trustee filed a lawsuit against the insurance company on behalf of Dr. P for the insurer’s failure to defend and indemnify Dr. P against the wrongful death lawsuits. In 2017, the bankruptcy trustee settled the two wrongful death cases by paying the families a certain amount of cash and assigning the insurance bad faith lawsuit to them.
Court and jury decide
In 2020, the case against the insurance company ended up in court. By 2022, the court had decided some of the issues and left some for the jury to determine.
The court found that the insurance company had breached its obligation to defend and indemnify Dr. P, committed unfair insurance claims practices, and committed bad faith in failing to defend the physician. The court limited the compensation to the amount of cash that had been paid to settle the two cases, and any fees and costs that Dr. P had incurred defending himself.
However, this still left the jury to decide whether the insurance company had committed bad faith in failing to indemnify (secure a person against legal liability for his/her actions) Dr. P, whether it had violated the state’s Unfair Insurance Practices Act, and whether punitive damages should be levied against the insurer.
The jury trial ended in a stunning $52 million verdict against the insurance company after less than 2 hours of deliberation. The jury found that the insurance company had acted in bad faith and willfully violated the Unfair Insurances Practices Act.
While the jury ultimately decided against the insurance company and sent it a strong message with a large verdict, Dr. P’s career was still over. He had stopped practicing medicine, was bankrupt, and his personal life was in shambles. The litigation had taken about a decade. Sometimes a win isn’t a victory.
Protecting yourself
The best way to protect yourself from a situation in which your insurer will not defend you is to really know and understand your insurance policy. Is it occurrence-based or claims-made insurance? What exactly does it cover? How are claims supposed to be made? Your professional liability insurance can be extremely important if you get sued, so it is equally important to choose it carefully and to really understand what is being covered.
Other ways to protect yourself:
- Know your agent. Your agent is key to explaining your policy as well as helping in the event that you need to make a claim. Dr. P’s agent saw a news story about him on television, which is why she submitted the information to the insurance company. Dr. P would have been far better off calling the agent directly when he was being investigated by the state medical board to explain the situation and seek advice.
- Be aware of exclusions to your policy. Many – such as criminal acts, reckless or intentional acts, or practicing under the influence – were mentioned earlier in this article. Some may be unexpected, so it is extremely important that you understand the specific exclusions to your particular policy.
- Be aware of your state law, and how changes might affect you. For example, in states that have outlawed or criminalized abortion, an insurance company would probably not have to represent a policy holder who was sued for malpractice involving an abortion. On the other hand, be aware that not treating a patient who needs life-saving care because you are afraid of running afoul of the law can also get you in trouble if the patient is harmed by not being treated. (For example, the Centers for Medicare & Medicaid Services is currently investigating two hospitals that failed to provide necessary stabilizing abortion care to a patient with an emergency medication condition resulting from a miscarriage.)
- Know how your policy defines ‘intentional’ acts (which are typically excluded from coverage). This is important. In some jurisdictions, the insured clinician has to merely intend to commit the acts in order for the claim to be excluded. In other jurisdictions, the insured doctor has to intend to cause the resulting damage. This can result in a very different outcome.
- The best thing doctors can do is to really understand what the policy covers and be prepared to make some noise if the company is not covering something that it should. Don’t be afraid to ask questions if you think your insurer is doing something wrong, and if the answers don’t satisfy you, consult an attorney.
The future
In the fall of 2022, at least partially in response to the Dobbs v. Jackson Women’s Health Organization decision regarding abortion, one professional liability company (Physician’s Insurance) launched criminal defense reimbursement coverage for physicians and hospitals to pay for defense costs incurred in responding to criminal allegations arising directly from patient care.
The add-on Criminal Defense Reimbursement Endorsement was made available in Washington State in January 2023, and will be offered in other states pending regulatory approval. It reimburses defense costs up to $250,000 when criminal actions have arisen from direct patient care.
In a press release announcing the new coverage, Physician’s Insurance CEO Bill Cotter explained the company’s reasoning in providing it: “The already challenging environment for physicians and hospitals has been made even more difficult as they now navigate the legal ramifications of increased criminal medical negligence claims as seen in the case of the Nashville nurse at the Vanderbilt University Medical Center, the potential for criminal state claims arising out of the U.S. Supreme Court decision in Dobbs v. Jackson Women’s Health Organization, and the subsequent state criminalization of healthcare practices that have long been the professionally accepted standard of care.”
Expect to see more insurance companies offering new coverage options for physicians in the future as they recognize that physicians may be facing more than just medical malpractice lawsuits arising out of patient care.
A version of this article first appeared on Medscape.com.
You’ve practiced medicine for years without issues, but now you are facing a medical malpractice case. No worries – you’ve had professional liability insurance all this time, so surely there’s nothing to be concerned about. Undoubtedly, your medical malpractice insurer will cover the costs of defending you. Or will they? One case casts questions on just this issue.
Professional liability insurance
According to the American Medical Association, almost one in three physicians (31%) have had a medical malpractice lawsuit filed against them at some point in their careers. These numbers only increase the longer a physician practices; almost half of doctors 55 and over have been sued, compared with less than 10% of physicians under 40.
And while the majority of cases are dropped or dismissed, and the small minority of cases that do go to trial are mostly won by the defense, the cost of defending these cases can be extremely high. Physicians have medical malpractice insurance to defray these costs.
Malpractice insurance generally covers the costs of attorney fees, court costs, arbitration, compensatory damages, and settlements related to patient injury or death. Insurance sometimes, but not always, pays for the costs of malpractice lawsuits arising out of Health Insurance Portability and Accountability Act (HIPAA) violations.
But it is what the policies don’t pay for that should be of most interest to practitioners.
Exclusions to medical malpractice insurance
All professional liability insurance policies contain exclusions, and it is essential that you know what they are. While the exclusions may vary by policy, most malpractice insurance policies exclude claims stemming from:
- Reckless or intentional acts.
- Illegal/criminal activities, including theft.
- Misrepresentation, including dishonesty, fraudulent activity, falsification, and misrepresentation on forms.
- Practicing under the influence of alcohol or drugs.
- Altering patient or hospital records.
- Sexual misconduct.
- Cyber security issues, which typically require a separate cyber liability policy to protect against cyber attacks and data breaches affecting patient medical records.
It’s essential to know what your specific policy’s exclusions are, or you may be surprised to find that your malpractice liability insurance doesn’t cover you when you expected that it would. Such was the situation in a recently decided case.
Also essential is knowing what type of coverage your policy provides – claims-made or occurrence-based. Occurrence policies offer lifetime coverage for incidents that occurred during the policy period, no matter when the claim is made. Claims-made policies cover only incidents that occur and are reported within the policy’s time period (unless a “tail” policy is purchased to extend the reporting period).
The case
Dr. P was a neurologist specializing in pain management. He had a professional liability insurance policy with an insurance company. In 2012, Dr. P’s insurance agent saw a television news story about the physician being accused by the state medical board for overprescribing opioids, resulting in the deaths of 17 patients. The next day, the agent obtained copies of documents from the state medical board, including a summary suspension order and a notice of contemplated action.
The notice of contemplated action specified that Dr. P had deviated from the standard of care through injudicious prescribing, leading to approximately 17 patient deaths due to drug toxicity. Because the agent realized that lawsuits could be filed against Dr. P for the deaths, she sent the insurance company the paperwork from the medical board so the insurer would be aware of the potential claims.
However, when the insurer received the information, it did not investigate or seek more information as it was required to do. The insurer failed to get medical records, or specific patient names, and none of the 17 deaths were recorded in the insurance company’s claims system (a failure to follow company procedure). Instead, the insurance company decided to cancel Dr. P’s policy effective the following month.
The company sent Dr. P a cancellation letter advising him that his policy was being terminated due to “license suspension, nature of allegations, and practice profile,” and offered him a tail policy to purchase.
The insurance company did not advise Dr. P that he should ensure all potential claims were reported, including the 17 deaths, before his policy expired. The company also did not advise him that he had a claims-made policy and what that meant regarding future lawsuits that might be filed after his policy period expired.
A year later, Dr. P was sued in two wrongful death lawsuits by the families of two of the 17 opioid-related deaths. When he was served with the papers, he promptly notified the insurance company. The insurance company issued a denial letter, incorrectly asserting that the 17 drug-toxicity deaths that they were aware of did not qualify as claims under Dr. P’s policy.
After his insurance company failed to represent him, Dr. P divorced his wife of 35 years and filed for bankruptcy. The only creditors with claims were the two families who had sued him. The bankruptcy trustee filed a lawsuit against the insurance company on behalf of Dr. P for the insurer’s failure to defend and indemnify Dr. P against the wrongful death lawsuits. In 2017, the bankruptcy trustee settled the two wrongful death cases by paying the families a certain amount of cash and assigning the insurance bad faith lawsuit to them.
Court and jury decide
In 2020, the case against the insurance company ended up in court. By 2022, the court had decided some of the issues and left some for the jury to determine.
The court found that the insurance company had breached its obligation to defend and indemnify Dr. P, committed unfair insurance claims practices, and committed bad faith in failing to defend the physician. The court limited the compensation to the amount of cash that had been paid to settle the two cases, and any fees and costs that Dr. P had incurred defending himself.
However, this still left the jury to decide whether the insurance company had committed bad faith in failing to indemnify (secure a person against legal liability for his/her actions) Dr. P, whether it had violated the state’s Unfair Insurance Practices Act, and whether punitive damages should be levied against the insurer.
The jury trial ended in a stunning $52 million verdict against the insurance company after less than 2 hours of deliberation. The jury found that the insurance company had acted in bad faith and willfully violated the Unfair Insurances Practices Act.
While the jury ultimately decided against the insurance company and sent it a strong message with a large verdict, Dr. P’s career was still over. He had stopped practicing medicine, was bankrupt, and his personal life was in shambles. The litigation had taken about a decade. Sometimes a win isn’t a victory.
Protecting yourself
The best way to protect yourself from a situation in which your insurer will not defend you is to really know and understand your insurance policy. Is it occurrence-based or claims-made insurance? What exactly does it cover? How are claims supposed to be made? Your professional liability insurance can be extremely important if you get sued, so it is equally important to choose it carefully and to really understand what is being covered.
Other ways to protect yourself:
- Know your agent. Your agent is key to explaining your policy as well as helping in the event that you need to make a claim. Dr. P’s agent saw a news story about him on television, which is why she submitted the information to the insurance company. Dr. P would have been far better off calling the agent directly when he was being investigated by the state medical board to explain the situation and seek advice.
- Be aware of exclusions to your policy. Many – such as criminal acts, reckless or intentional acts, or practicing under the influence – were mentioned earlier in this article. Some may be unexpected, so it is extremely important that you understand the specific exclusions to your particular policy.
- Be aware of your state law, and how changes might affect you. For example, in states that have outlawed or criminalized abortion, an insurance company would probably not have to represent a policy holder who was sued for malpractice involving an abortion. On the other hand, be aware that not treating a patient who needs life-saving care because you are afraid of running afoul of the law can also get you in trouble if the patient is harmed by not being treated. (For example, the Centers for Medicare & Medicaid Services is currently investigating two hospitals that failed to provide necessary stabilizing abortion care to a patient with an emergency medication condition resulting from a miscarriage.)
- Know how your policy defines ‘intentional’ acts (which are typically excluded from coverage). This is important. In some jurisdictions, the insured clinician has to merely intend to commit the acts in order for the claim to be excluded. In other jurisdictions, the insured doctor has to intend to cause the resulting damage. This can result in a very different outcome.
- The best thing doctors can do is to really understand what the policy covers and be prepared to make some noise if the company is not covering something that it should. Don’t be afraid to ask questions if you think your insurer is doing something wrong, and if the answers don’t satisfy you, consult an attorney.
The future
In the fall of 2022, at least partially in response to the Dobbs v. Jackson Women’s Health Organization decision regarding abortion, one professional liability company (Physician’s Insurance) launched criminal defense reimbursement coverage for physicians and hospitals to pay for defense costs incurred in responding to criminal allegations arising directly from patient care.
The add-on Criminal Defense Reimbursement Endorsement was made available in Washington State in January 2023, and will be offered in other states pending regulatory approval. It reimburses defense costs up to $250,000 when criminal actions have arisen from direct patient care.
In a press release announcing the new coverage, Physician’s Insurance CEO Bill Cotter explained the company’s reasoning in providing it: “The already challenging environment for physicians and hospitals has been made even more difficult as they now navigate the legal ramifications of increased criminal medical negligence claims as seen in the case of the Nashville nurse at the Vanderbilt University Medical Center, the potential for criminal state claims arising out of the U.S. Supreme Court decision in Dobbs v. Jackson Women’s Health Organization, and the subsequent state criminalization of healthcare practices that have long been the professionally accepted standard of care.”
Expect to see more insurance companies offering new coverage options for physicians in the future as they recognize that physicians may be facing more than just medical malpractice lawsuits arising out of patient care.
A version of this article first appeared on Medscape.com.
You’ve practiced medicine for years without issues, but now you are facing a medical malpractice case. No worries – you’ve had professional liability insurance all this time, so surely there’s nothing to be concerned about. Undoubtedly, your medical malpractice insurer will cover the costs of defending you. Or will they? One case casts questions on just this issue.
Professional liability insurance
According to the American Medical Association, almost one in three physicians (31%) have had a medical malpractice lawsuit filed against them at some point in their careers. These numbers only increase the longer a physician practices; almost half of doctors 55 and over have been sued, compared with less than 10% of physicians under 40.
And while the majority of cases are dropped or dismissed, and the small minority of cases that do go to trial are mostly won by the defense, the cost of defending these cases can be extremely high. Physicians have medical malpractice insurance to defray these costs.
Malpractice insurance generally covers the costs of attorney fees, court costs, arbitration, compensatory damages, and settlements related to patient injury or death. Insurance sometimes, but not always, pays for the costs of malpractice lawsuits arising out of Health Insurance Portability and Accountability Act (HIPAA) violations.
But it is what the policies don’t pay for that should be of most interest to practitioners.
Exclusions to medical malpractice insurance
All professional liability insurance policies contain exclusions, and it is essential that you know what they are. While the exclusions may vary by policy, most malpractice insurance policies exclude claims stemming from:
- Reckless or intentional acts.
- Illegal/criminal activities, including theft.
- Misrepresentation, including dishonesty, fraudulent activity, falsification, and misrepresentation on forms.
- Practicing under the influence of alcohol or drugs.
- Altering patient or hospital records.
- Sexual misconduct.
- Cyber security issues, which typically require a separate cyber liability policy to protect against cyber attacks and data breaches affecting patient medical records.
It’s essential to know what your specific policy’s exclusions are, or you may be surprised to find that your malpractice liability insurance doesn’t cover you when you expected that it would. Such was the situation in a recently decided case.
Also essential is knowing what type of coverage your policy provides – claims-made or occurrence-based. Occurrence policies offer lifetime coverage for incidents that occurred during the policy period, no matter when the claim is made. Claims-made policies cover only incidents that occur and are reported within the policy’s time period (unless a “tail” policy is purchased to extend the reporting period).
The case
Dr. P was a neurologist specializing in pain management. He had a professional liability insurance policy with an insurance company. In 2012, Dr. P’s insurance agent saw a television news story about the physician being accused by the state medical board for overprescribing opioids, resulting in the deaths of 17 patients. The next day, the agent obtained copies of documents from the state medical board, including a summary suspension order and a notice of contemplated action.
The notice of contemplated action specified that Dr. P had deviated from the standard of care through injudicious prescribing, leading to approximately 17 patient deaths due to drug toxicity. Because the agent realized that lawsuits could be filed against Dr. P for the deaths, she sent the insurance company the paperwork from the medical board so the insurer would be aware of the potential claims.
However, when the insurer received the information, it did not investigate or seek more information as it was required to do. The insurer failed to get medical records, or specific patient names, and none of the 17 deaths were recorded in the insurance company’s claims system (a failure to follow company procedure). Instead, the insurance company decided to cancel Dr. P’s policy effective the following month.
The company sent Dr. P a cancellation letter advising him that his policy was being terminated due to “license suspension, nature of allegations, and practice profile,” and offered him a tail policy to purchase.
The insurance company did not advise Dr. P that he should ensure all potential claims were reported, including the 17 deaths, before his policy expired. The company also did not advise him that he had a claims-made policy and what that meant regarding future lawsuits that might be filed after his policy period expired.
A year later, Dr. P was sued in two wrongful death lawsuits by the families of two of the 17 opioid-related deaths. When he was served with the papers, he promptly notified the insurance company. The insurance company issued a denial letter, incorrectly asserting that the 17 drug-toxicity deaths that they were aware of did not qualify as claims under Dr. P’s policy.
After his insurance company failed to represent him, Dr. P divorced his wife of 35 years and filed for bankruptcy. The only creditors with claims were the two families who had sued him. The bankruptcy trustee filed a lawsuit against the insurance company on behalf of Dr. P for the insurer’s failure to defend and indemnify Dr. P against the wrongful death lawsuits. In 2017, the bankruptcy trustee settled the two wrongful death cases by paying the families a certain amount of cash and assigning the insurance bad faith lawsuit to them.
Court and jury decide
In 2020, the case against the insurance company ended up in court. By 2022, the court had decided some of the issues and left some for the jury to determine.
The court found that the insurance company had breached its obligation to defend and indemnify Dr. P, committed unfair insurance claims practices, and committed bad faith in failing to defend the physician. The court limited the compensation to the amount of cash that had been paid to settle the two cases, and any fees and costs that Dr. P had incurred defending himself.
However, this still left the jury to decide whether the insurance company had committed bad faith in failing to indemnify (secure a person against legal liability for his/her actions) Dr. P, whether it had violated the state’s Unfair Insurance Practices Act, and whether punitive damages should be levied against the insurer.
The jury trial ended in a stunning $52 million verdict against the insurance company after less than 2 hours of deliberation. The jury found that the insurance company had acted in bad faith and willfully violated the Unfair Insurances Practices Act.
While the jury ultimately decided against the insurance company and sent it a strong message with a large verdict, Dr. P’s career was still over. He had stopped practicing medicine, was bankrupt, and his personal life was in shambles. The litigation had taken about a decade. Sometimes a win isn’t a victory.
Protecting yourself
The best way to protect yourself from a situation in which your insurer will not defend you is to really know and understand your insurance policy. Is it occurrence-based or claims-made insurance? What exactly does it cover? How are claims supposed to be made? Your professional liability insurance can be extremely important if you get sued, so it is equally important to choose it carefully and to really understand what is being covered.
Other ways to protect yourself:
- Know your agent. Your agent is key to explaining your policy as well as helping in the event that you need to make a claim. Dr. P’s agent saw a news story about him on television, which is why she submitted the information to the insurance company. Dr. P would have been far better off calling the agent directly when he was being investigated by the state medical board to explain the situation and seek advice.
- Be aware of exclusions to your policy. Many – such as criminal acts, reckless or intentional acts, or practicing under the influence – were mentioned earlier in this article. Some may be unexpected, so it is extremely important that you understand the specific exclusions to your particular policy.
- Be aware of your state law, and how changes might affect you. For example, in states that have outlawed or criminalized abortion, an insurance company would probably not have to represent a policy holder who was sued for malpractice involving an abortion. On the other hand, be aware that not treating a patient who needs life-saving care because you are afraid of running afoul of the law can also get you in trouble if the patient is harmed by not being treated. (For example, the Centers for Medicare & Medicaid Services is currently investigating two hospitals that failed to provide necessary stabilizing abortion care to a patient with an emergency medication condition resulting from a miscarriage.)
- Know how your policy defines ‘intentional’ acts (which are typically excluded from coverage). This is important. In some jurisdictions, the insured clinician has to merely intend to commit the acts in order for the claim to be excluded. In other jurisdictions, the insured doctor has to intend to cause the resulting damage. This can result in a very different outcome.
- The best thing doctors can do is to really understand what the policy covers and be prepared to make some noise if the company is not covering something that it should. Don’t be afraid to ask questions if you think your insurer is doing something wrong, and if the answers don’t satisfy you, consult an attorney.
The future
In the fall of 2022, at least partially in response to the Dobbs v. Jackson Women’s Health Organization decision regarding abortion, one professional liability company (Physician’s Insurance) launched criminal defense reimbursement coverage for physicians and hospitals to pay for defense costs incurred in responding to criminal allegations arising directly from patient care.
The add-on Criminal Defense Reimbursement Endorsement was made available in Washington State in January 2023, and will be offered in other states pending regulatory approval. It reimburses defense costs up to $250,000 when criminal actions have arisen from direct patient care.
In a press release announcing the new coverage, Physician’s Insurance CEO Bill Cotter explained the company’s reasoning in providing it: “The already challenging environment for physicians and hospitals has been made even more difficult as they now navigate the legal ramifications of increased criminal medical negligence claims as seen in the case of the Nashville nurse at the Vanderbilt University Medical Center, the potential for criminal state claims arising out of the U.S. Supreme Court decision in Dobbs v. Jackson Women’s Health Organization, and the subsequent state criminalization of healthcare practices that have long been the professionally accepted standard of care.”
Expect to see more insurance companies offering new coverage options for physicians in the future as they recognize that physicians may be facing more than just medical malpractice lawsuits arising out of patient care.
A version of this article first appeared on Medscape.com.
Docs using AI? Some love it, most remain wary
When OpenAI released ChatGPT-3 publicly last November, some doctors decided to try out the free AI tool that learns language and writes human-like text. Some physicians found the chatbot made mistakes and stopped using it, while others were happy with the results and plan to use it more often.
“We’ve played around with it. It was very early on in AI and we noticed it gave us incorrect information with regards to clinical guidance,” said Monalisa Tailor, MD, an internal medicine physician at Norton Health Care in Louisville, Ky. “We decided not to pursue it further,” she said.
Orthopedic spine surgeon Daniel Choi, MD, who owns a small medical/surgical practice in Long Island, New York, tested the chatbot’s performance with a few administrative tasks, including writing a job listing for an administrator and prior authorization letters.
He was enthusiastic. “A well-polished job posting that would usually take me 2-3 hours to write was done in 5 minutes,” Dr. Choi said. “I was blown away by the writing – it was much better than anything I could write.”
The chatbot can also automate administrative tasks in doctors’ practices from appointment scheduling and billing to clinical documentation, saving doctors time and money, experts say.
Most physicians are proceeding cautiously. About 10% of more than 500 medical group leaders, responding to a March poll by the Medical Group Management Association, said their practices regularly use AI tools.
More than half of the respondents not using AI said they first want more evidence that the technology works as intended.
“None of them work as advertised,” said one respondent.
MGMA practice management consultant Dawn Plested acknowledges that many of the physician practices she’s worked with are still wary. “I have yet to encounter a practice that is using any AI tool, even something as low-risk as appointment scheduling,” she said.
Physician groups may be concerned about the costs and logistics of integrating ChatGPT with their electronic health record systems (EHRs) and how that would work, said Ms. Plested.
Doctors may also be skeptical of AI based on their experience with EHRs, she said.
“They were promoted as a panacea to many problems; they were supposed to automate business practice, reduce staff and clinician’s work, and improve billing/coding/documentation. Unfortunately, they have become a major source of frustration for doctors,” said Ms. Plested.
Drawing the line at patient care
Patients are worried about their doctors relying on AI for their care, according to a Pew Research Center poll released in February. About 60% of U.S. adults say they would feel uncomfortable if their own health care professional relied on artificial intelligence to do things like diagnose disease and recommend treatments; about 40% say they would feel comfortable with this.
“We have not yet gone into using ChatGPT for clinical purposes and will be very cautious with these types of applications due to concerns about inaccuracies,” Dr. Choi said.
Practice leaders reported in the MGMA poll that the most common uses of AI were nonclinical, such as:
- Patient communications, including call center answering service to help triage calls, to sort/distribute incoming fax messages, and outreach such as appointment reminders and marketing materials.
- Capturing clinical documentation, often with natural language processing or speech recognition platforms to help virtually scribe.
- Improving billing operations and predictive analytics.
Some doctors told The New York Times that ChatGPT helped them communicate with patients in a more compassionate way.
They used chatbots “to find words to break bad news and express concerns about a patient’s suffering, or to just more clearly explain medical recommendations,” the story noted.
Is regulation needed?
Some legal scholars and medical groups say that AI should be regulated to protect patients and doctors from risks, including medical errors, that could harm patients.
“It’s very important to evaluate the accuracy, safety, and privacy of language learning models (LLMs) before integrating them into the medical system. The same should be true of any new medical tool,” said Mason Marks, MD, JD, a health law professor at the Florida State University College of Law in Tallahassee.
In mid-June, the American Medical Association approved two resolutions calling for greater government oversight of AI. The AMA will develop proposed state and federal regulations and work with the federal government and other organizations to protect patients from false or misleading AI-generated medical advice.
Dr. Marks pointed to existing federal rules that apply to AI. “The Federal Trade Commission already has regulation that can potentially be used to combat unfair or deceptive trade practices associated with chatbots,” he said.
In addition, “the U.S. Food and Drug Administration can also regulate these tools, but it needs to update how it approaches risk when it comes to AI. The FDA has an outdated view of risk as physical harm, for instance, from traditional medical devices. That view of risk needs to be updated and expanded to encompass the unique harms of AI,” Dr. Marks said.
There should also be more transparency about how LLM software is used in medicine, he said. “That could be a norm implemented by the LLM developers and it could also be enforced by federal agencies. For instance, the FDA could require developers to be more transparent regarding training data and methods, and the FTC could require greater transparency regarding how consumer data might be used and opportunities to opt out of certain uses,” said Dr. Marks.
What should doctors do?
Dr. Marks advised doctors to be cautious when using ChatGPT and other LLMs, especially for medical advice. “The same would apply to any new medical tool, but we know that the current generation of LLMs [is] particularly prone to making things up, which could lead to medical errors if relied on in clinical settings,” he said.
There is also potential for breaches of patient confidentiality if doctors input clinical information. ChatGPT and OpenAI-enabled tools may not be compliant with the Health Insurance Portability and Accountability Act, which set national standards to protect individuals’ medical records and individually identifiable health information.
“The best approach is to use chatbots cautiously and with skepticism. Don’t input patient information, confirm the accuracy of information produced, and don’t use them as replacements for professional judgment,” Dr. Marks recommended.
Ms. Plested suggested that doctors who want to experiment with AI start with a low-risk tool such as appointment reminders that could save staff time and money. “I never recommend they start with something as high-stakes as coding/billing,” she said.
A version of this article appeared on Medscape.com.
When OpenAI released ChatGPT-3 publicly last November, some doctors decided to try out the free AI tool that learns language and writes human-like text. Some physicians found the chatbot made mistakes and stopped using it, while others were happy with the results and plan to use it more often.
“We’ve played around with it. It was very early on in AI and we noticed it gave us incorrect information with regards to clinical guidance,” said Monalisa Tailor, MD, an internal medicine physician at Norton Health Care in Louisville, Ky. “We decided not to pursue it further,” she said.
Orthopedic spine surgeon Daniel Choi, MD, who owns a small medical/surgical practice in Long Island, New York, tested the chatbot’s performance with a few administrative tasks, including writing a job listing for an administrator and prior authorization letters.
He was enthusiastic. “A well-polished job posting that would usually take me 2-3 hours to write was done in 5 minutes,” Dr. Choi said. “I was blown away by the writing – it was much better than anything I could write.”
The chatbot can also automate administrative tasks in doctors’ practices from appointment scheduling and billing to clinical documentation, saving doctors time and money, experts say.
Most physicians are proceeding cautiously. About 10% of more than 500 medical group leaders, responding to a March poll by the Medical Group Management Association, said their practices regularly use AI tools.
More than half of the respondents not using AI said they first want more evidence that the technology works as intended.
“None of them work as advertised,” said one respondent.
MGMA practice management consultant Dawn Plested acknowledges that many of the physician practices she’s worked with are still wary. “I have yet to encounter a practice that is using any AI tool, even something as low-risk as appointment scheduling,” she said.
Physician groups may be concerned about the costs and logistics of integrating ChatGPT with their electronic health record systems (EHRs) and how that would work, said Ms. Plested.
Doctors may also be skeptical of AI based on their experience with EHRs, she said.
“They were promoted as a panacea to many problems; they were supposed to automate business practice, reduce staff and clinician’s work, and improve billing/coding/documentation. Unfortunately, they have become a major source of frustration for doctors,” said Ms. Plested.
Drawing the line at patient care
Patients are worried about their doctors relying on AI for their care, according to a Pew Research Center poll released in February. About 60% of U.S. adults say they would feel uncomfortable if their own health care professional relied on artificial intelligence to do things like diagnose disease and recommend treatments; about 40% say they would feel comfortable with this.
“We have not yet gone into using ChatGPT for clinical purposes and will be very cautious with these types of applications due to concerns about inaccuracies,” Dr. Choi said.
Practice leaders reported in the MGMA poll that the most common uses of AI were nonclinical, such as:
- Patient communications, including call center answering service to help triage calls, to sort/distribute incoming fax messages, and outreach such as appointment reminders and marketing materials.
- Capturing clinical documentation, often with natural language processing or speech recognition platforms to help virtually scribe.
- Improving billing operations and predictive analytics.
Some doctors told The New York Times that ChatGPT helped them communicate with patients in a more compassionate way.
They used chatbots “to find words to break bad news and express concerns about a patient’s suffering, or to just more clearly explain medical recommendations,” the story noted.
Is regulation needed?
Some legal scholars and medical groups say that AI should be regulated to protect patients and doctors from risks, including medical errors, that could harm patients.
“It’s very important to evaluate the accuracy, safety, and privacy of language learning models (LLMs) before integrating them into the medical system. The same should be true of any new medical tool,” said Mason Marks, MD, JD, a health law professor at the Florida State University College of Law in Tallahassee.
In mid-June, the American Medical Association approved two resolutions calling for greater government oversight of AI. The AMA will develop proposed state and federal regulations and work with the federal government and other organizations to protect patients from false or misleading AI-generated medical advice.
Dr. Marks pointed to existing federal rules that apply to AI. “The Federal Trade Commission already has regulation that can potentially be used to combat unfair or deceptive trade practices associated with chatbots,” he said.
In addition, “the U.S. Food and Drug Administration can also regulate these tools, but it needs to update how it approaches risk when it comes to AI. The FDA has an outdated view of risk as physical harm, for instance, from traditional medical devices. That view of risk needs to be updated and expanded to encompass the unique harms of AI,” Dr. Marks said.
There should also be more transparency about how LLM software is used in medicine, he said. “That could be a norm implemented by the LLM developers and it could also be enforced by federal agencies. For instance, the FDA could require developers to be more transparent regarding training data and methods, and the FTC could require greater transparency regarding how consumer data might be used and opportunities to opt out of certain uses,” said Dr. Marks.
What should doctors do?
Dr. Marks advised doctors to be cautious when using ChatGPT and other LLMs, especially for medical advice. “The same would apply to any new medical tool, but we know that the current generation of LLMs [is] particularly prone to making things up, which could lead to medical errors if relied on in clinical settings,” he said.
There is also potential for breaches of patient confidentiality if doctors input clinical information. ChatGPT and OpenAI-enabled tools may not be compliant with the Health Insurance Portability and Accountability Act, which set national standards to protect individuals’ medical records and individually identifiable health information.
“The best approach is to use chatbots cautiously and with skepticism. Don’t input patient information, confirm the accuracy of information produced, and don’t use them as replacements for professional judgment,” Dr. Marks recommended.
Ms. Plested suggested that doctors who want to experiment with AI start with a low-risk tool such as appointment reminders that could save staff time and money. “I never recommend they start with something as high-stakes as coding/billing,” she said.
A version of this article appeared on Medscape.com.
When OpenAI released ChatGPT-3 publicly last November, some doctors decided to try out the free AI tool that learns language and writes human-like text. Some physicians found the chatbot made mistakes and stopped using it, while others were happy with the results and plan to use it more often.
“We’ve played around with it. It was very early on in AI and we noticed it gave us incorrect information with regards to clinical guidance,” said Monalisa Tailor, MD, an internal medicine physician at Norton Health Care in Louisville, Ky. “We decided not to pursue it further,” she said.
Orthopedic spine surgeon Daniel Choi, MD, who owns a small medical/surgical practice in Long Island, New York, tested the chatbot’s performance with a few administrative tasks, including writing a job listing for an administrator and prior authorization letters.
He was enthusiastic. “A well-polished job posting that would usually take me 2-3 hours to write was done in 5 minutes,” Dr. Choi said. “I was blown away by the writing – it was much better than anything I could write.”
The chatbot can also automate administrative tasks in doctors’ practices from appointment scheduling and billing to clinical documentation, saving doctors time and money, experts say.
Most physicians are proceeding cautiously. About 10% of more than 500 medical group leaders, responding to a March poll by the Medical Group Management Association, said their practices regularly use AI tools.
More than half of the respondents not using AI said they first want more evidence that the technology works as intended.
“None of them work as advertised,” said one respondent.
MGMA practice management consultant Dawn Plested acknowledges that many of the physician practices she’s worked with are still wary. “I have yet to encounter a practice that is using any AI tool, even something as low-risk as appointment scheduling,” she said.
Physician groups may be concerned about the costs and logistics of integrating ChatGPT with their electronic health record systems (EHRs) and how that would work, said Ms. Plested.
Doctors may also be skeptical of AI based on their experience with EHRs, she said.
“They were promoted as a panacea to many problems; they were supposed to automate business practice, reduce staff and clinician’s work, and improve billing/coding/documentation. Unfortunately, they have become a major source of frustration for doctors,” said Ms. Plested.
Drawing the line at patient care
Patients are worried about their doctors relying on AI for their care, according to a Pew Research Center poll released in February. About 60% of U.S. adults say they would feel uncomfortable if their own health care professional relied on artificial intelligence to do things like diagnose disease and recommend treatments; about 40% say they would feel comfortable with this.
“We have not yet gone into using ChatGPT for clinical purposes and will be very cautious with these types of applications due to concerns about inaccuracies,” Dr. Choi said.
Practice leaders reported in the MGMA poll that the most common uses of AI were nonclinical, such as:
- Patient communications, including call center answering service to help triage calls, to sort/distribute incoming fax messages, and outreach such as appointment reminders and marketing materials.
- Capturing clinical documentation, often with natural language processing or speech recognition platforms to help virtually scribe.
- Improving billing operations and predictive analytics.
Some doctors told The New York Times that ChatGPT helped them communicate with patients in a more compassionate way.
They used chatbots “to find words to break bad news and express concerns about a patient’s suffering, or to just more clearly explain medical recommendations,” the story noted.
Is regulation needed?
Some legal scholars and medical groups say that AI should be regulated to protect patients and doctors from risks, including medical errors, that could harm patients.
“It’s very important to evaluate the accuracy, safety, and privacy of language learning models (LLMs) before integrating them into the medical system. The same should be true of any new medical tool,” said Mason Marks, MD, JD, a health law professor at the Florida State University College of Law in Tallahassee.
In mid-June, the American Medical Association approved two resolutions calling for greater government oversight of AI. The AMA will develop proposed state and federal regulations and work with the federal government and other organizations to protect patients from false or misleading AI-generated medical advice.
Dr. Marks pointed to existing federal rules that apply to AI. “The Federal Trade Commission already has regulation that can potentially be used to combat unfair or deceptive trade practices associated with chatbots,” he said.
In addition, “the U.S. Food and Drug Administration can also regulate these tools, but it needs to update how it approaches risk when it comes to AI. The FDA has an outdated view of risk as physical harm, for instance, from traditional medical devices. That view of risk needs to be updated and expanded to encompass the unique harms of AI,” Dr. Marks said.
There should also be more transparency about how LLM software is used in medicine, he said. “That could be a norm implemented by the LLM developers and it could also be enforced by federal agencies. For instance, the FDA could require developers to be more transparent regarding training data and methods, and the FTC could require greater transparency regarding how consumer data might be used and opportunities to opt out of certain uses,” said Dr. Marks.
What should doctors do?
Dr. Marks advised doctors to be cautious when using ChatGPT and other LLMs, especially for medical advice. “The same would apply to any new medical tool, but we know that the current generation of LLMs [is] particularly prone to making things up, which could lead to medical errors if relied on in clinical settings,” he said.
There is also potential for breaches of patient confidentiality if doctors input clinical information. ChatGPT and OpenAI-enabled tools may not be compliant with the Health Insurance Portability and Accountability Act, which set national standards to protect individuals’ medical records and individually identifiable health information.
“The best approach is to use chatbots cautiously and with skepticism. Don’t input patient information, confirm the accuracy of information produced, and don’t use them as replacements for professional judgment,” Dr. Marks recommended.
Ms. Plested suggested that doctors who want to experiment with AI start with a low-risk tool such as appointment reminders that could save staff time and money. “I never recommend they start with something as high-stakes as coding/billing,” she said.
A version of this article appeared on Medscape.com.
Pig kidneys show ‘life-sustaining’ function in human
– marking another important step toward opening up a new supply of much-needed organs for those with end-stage kidney disease.
A team of researchers in Alabama removed a brain-dead person’s kidneys and transplanted two kidneys that had been taken from a genetically modified pig. The researchers monitored the patient’s response to the organs and tracked the kidneys’ function over a 7-day period. The findings were published in JAMA Surgery.
During the first 24 hours after transplantation, the pig kidneys made more than 37 liters of urine. “It was really a remarkable thing to see,” lead investigator Jayme Locke, MD, professor of surgery and the Arnold G. Diethelm Endowed Chair in Transplantation Surgery, University of Alabama at Birmingham, said in a press release.
The recipient was given standard maintenance immunosuppression - tacrolimus, mycophenolate mofetil, and prednisone. The target tacrolimus level (8-10 ng/dL) was reached by postoperative day 2 and was maintained through study completion.
At the end of the study, the serum creatinine level was 0.9 mg/dL, and creatinine clearance was 200 mL/min. Creatinine levels are an indicator of kidney function and demonstrate the organ’s ability to filter waste from blood, according to Roger Lord, PhD, senior lecturer (medical sciences) in the School of Behavioural and Health Sciences, Australian Catholic University, who was not involved in the research.
This is the first time that it has been demonstrated that a standard immunosuppression regimen may be sufficient to support xenotransplantation with pig kidneys and in which creatinine clearance was achieved.
The finding comes less than 2 years after the same team published results from a similar experiment. In that transplant, the investigators didn’t observe significant creatinine excretion into the urine.
In the team’s previous attempts, kidney function was delayed because the brain-dead recipients had deteriorated physiologically. This time, the subject was stable, and the team was able to observe urine production within 4 minutes of restoration of blood flow to the transplanted pig organs.
“This new work firmly establishes that the xenografts not only make urine but provide life-sustaining kidney function by clearing serum creatinine,” Locke said in an interview. “This is the first time in history this has been shown.”
The investigators are hoping animal-sourced organs could become an alternative for human transplantations, potentially solving the serious shortage of human organs available for patients on transplant waiting lists.
Organ transplantation can treat patients with advanced kidney disease and kidney failure, but there are not enough human organs available to meet the need. More than 92,000 people in the United States are waiting for a kidney, according to the American Kidney Fund.
Organ rejection is a risk with xenotransplants – animal-to-human organ transplants. Investigators in this study used kidneys from pigs with 10 gene modifications. The modifications were intended to decrease the likelihood of the organs being rejected by a human host.
The kidneys were still viable at the end of the 7-day period. In addition, there was no microscopic blood clot formation, another indicator of normal kidney function, according to Dr. Lord, who provided comments to the UK Science Media Centre.
The long-term outcomes of animal-to-human organ transplantation remain unclear. Dr. Lord describes the operation as a “first step” to demonstrate that genetically modified, transplanted pig kidneys can function normally so as to remove creatinine over a 7-day period.
Dr. Locke and colleagues said: “Future research in living human recipients is necessary to determine long-term xenograft kidney function and whether xenografts could serve as a bridge or destination therapy for end-stage kidney disease.
“Because our study represents a single case, generalizability of the findings is limited. This study showcases xenotransplant as a viable potential solution to an organ shortage crisis responsible for thousands of preventable deaths annually,” they concluded.
A version of this article first appeared on Medscape.com .
– marking another important step toward opening up a new supply of much-needed organs for those with end-stage kidney disease.
A team of researchers in Alabama removed a brain-dead person’s kidneys and transplanted two kidneys that had been taken from a genetically modified pig. The researchers monitored the patient’s response to the organs and tracked the kidneys’ function over a 7-day period. The findings were published in JAMA Surgery.
During the first 24 hours after transplantation, the pig kidneys made more than 37 liters of urine. “It was really a remarkable thing to see,” lead investigator Jayme Locke, MD, professor of surgery and the Arnold G. Diethelm Endowed Chair in Transplantation Surgery, University of Alabama at Birmingham, said in a press release.
The recipient was given standard maintenance immunosuppression - tacrolimus, mycophenolate mofetil, and prednisone. The target tacrolimus level (8-10 ng/dL) was reached by postoperative day 2 and was maintained through study completion.
At the end of the study, the serum creatinine level was 0.9 mg/dL, and creatinine clearance was 200 mL/min. Creatinine levels are an indicator of kidney function and demonstrate the organ’s ability to filter waste from blood, according to Roger Lord, PhD, senior lecturer (medical sciences) in the School of Behavioural and Health Sciences, Australian Catholic University, who was not involved in the research.
This is the first time that it has been demonstrated that a standard immunosuppression regimen may be sufficient to support xenotransplantation with pig kidneys and in which creatinine clearance was achieved.
The finding comes less than 2 years after the same team published results from a similar experiment. In that transplant, the investigators didn’t observe significant creatinine excretion into the urine.
In the team’s previous attempts, kidney function was delayed because the brain-dead recipients had deteriorated physiologically. This time, the subject was stable, and the team was able to observe urine production within 4 minutes of restoration of blood flow to the transplanted pig organs.
“This new work firmly establishes that the xenografts not only make urine but provide life-sustaining kidney function by clearing serum creatinine,” Locke said in an interview. “This is the first time in history this has been shown.”
The investigators are hoping animal-sourced organs could become an alternative for human transplantations, potentially solving the serious shortage of human organs available for patients on transplant waiting lists.
Organ transplantation can treat patients with advanced kidney disease and kidney failure, but there are not enough human organs available to meet the need. More than 92,000 people in the United States are waiting for a kidney, according to the American Kidney Fund.
Organ rejection is a risk with xenotransplants – animal-to-human organ transplants. Investigators in this study used kidneys from pigs with 10 gene modifications. The modifications were intended to decrease the likelihood of the organs being rejected by a human host.
The kidneys were still viable at the end of the 7-day period. In addition, there was no microscopic blood clot formation, another indicator of normal kidney function, according to Dr. Lord, who provided comments to the UK Science Media Centre.
The long-term outcomes of animal-to-human organ transplantation remain unclear. Dr. Lord describes the operation as a “first step” to demonstrate that genetically modified, transplanted pig kidneys can function normally so as to remove creatinine over a 7-day period.
Dr. Locke and colleagues said: “Future research in living human recipients is necessary to determine long-term xenograft kidney function and whether xenografts could serve as a bridge or destination therapy for end-stage kidney disease.
“Because our study represents a single case, generalizability of the findings is limited. This study showcases xenotransplant as a viable potential solution to an organ shortage crisis responsible for thousands of preventable deaths annually,” they concluded.
A version of this article first appeared on Medscape.com .
– marking another important step toward opening up a new supply of much-needed organs for those with end-stage kidney disease.
A team of researchers in Alabama removed a brain-dead person’s kidneys and transplanted two kidneys that had been taken from a genetically modified pig. The researchers monitored the patient’s response to the organs and tracked the kidneys’ function over a 7-day period. The findings were published in JAMA Surgery.
During the first 24 hours after transplantation, the pig kidneys made more than 37 liters of urine. “It was really a remarkable thing to see,” lead investigator Jayme Locke, MD, professor of surgery and the Arnold G. Diethelm Endowed Chair in Transplantation Surgery, University of Alabama at Birmingham, said in a press release.
The recipient was given standard maintenance immunosuppression - tacrolimus, mycophenolate mofetil, and prednisone. The target tacrolimus level (8-10 ng/dL) was reached by postoperative day 2 and was maintained through study completion.
At the end of the study, the serum creatinine level was 0.9 mg/dL, and creatinine clearance was 200 mL/min. Creatinine levels are an indicator of kidney function and demonstrate the organ’s ability to filter waste from blood, according to Roger Lord, PhD, senior lecturer (medical sciences) in the School of Behavioural and Health Sciences, Australian Catholic University, who was not involved in the research.
This is the first time that it has been demonstrated that a standard immunosuppression regimen may be sufficient to support xenotransplantation with pig kidneys and in which creatinine clearance was achieved.
The finding comes less than 2 years after the same team published results from a similar experiment. In that transplant, the investigators didn’t observe significant creatinine excretion into the urine.
In the team’s previous attempts, kidney function was delayed because the brain-dead recipients had deteriorated physiologically. This time, the subject was stable, and the team was able to observe urine production within 4 minutes of restoration of blood flow to the transplanted pig organs.
“This new work firmly establishes that the xenografts not only make urine but provide life-sustaining kidney function by clearing serum creatinine,” Locke said in an interview. “This is the first time in history this has been shown.”
The investigators are hoping animal-sourced organs could become an alternative for human transplantations, potentially solving the serious shortage of human organs available for patients on transplant waiting lists.
Organ transplantation can treat patients with advanced kidney disease and kidney failure, but there are not enough human organs available to meet the need. More than 92,000 people in the United States are waiting for a kidney, according to the American Kidney Fund.
Organ rejection is a risk with xenotransplants – animal-to-human organ transplants. Investigators in this study used kidneys from pigs with 10 gene modifications. The modifications were intended to decrease the likelihood of the organs being rejected by a human host.
The kidneys were still viable at the end of the 7-day period. In addition, there was no microscopic blood clot formation, another indicator of normal kidney function, according to Dr. Lord, who provided comments to the UK Science Media Centre.
The long-term outcomes of animal-to-human organ transplantation remain unclear. Dr. Lord describes the operation as a “first step” to demonstrate that genetically modified, transplanted pig kidneys can function normally so as to remove creatinine over a 7-day period.
Dr. Locke and colleagues said: “Future research in living human recipients is necessary to determine long-term xenograft kidney function and whether xenografts could serve as a bridge or destination therapy for end-stage kidney disease.
“Because our study represents a single case, generalizability of the findings is limited. This study showcases xenotransplant as a viable potential solution to an organ shortage crisis responsible for thousands of preventable deaths annually,” they concluded.
A version of this article first appeared on Medscape.com .
FROM JAMA SURGERY
Better than dialysis? Artificial kidney could be the future
Nearly 90,000 patients in the United States are waiting for a lifesaving kidney transplant, yet only about 25,000 kidney transplants were performed last year. Thousands die each year while they wait. Others are not suitable transplant candidates.
Half a million people are on dialysis, the only transplant alternative for those with kidney failure. This greatly impacts their work, relationships, and quality of life.
Researchers from The Kidney Project hope to solve this public health crisis with a futuristic approach: an implantable bioartificial kidney. That hope is slowly approaching reality. Early prototypes have been tested successfully in preclinical research and clinical trials could lie ahead.
This news organization spoke with two researchers who came up with the idea: nephrologist William Dr. Fissell, MD, of Vanderbilt University in Nashville, Tenn., and Shuvo Dr. Roy, PhD, a biomedical engineer at the University of California, San Francisco. This interview has been edited for length and clarity.
Question: Could you summarize the clinical problem with chronic kidney disease?
Dr. Fissell: Dialysis treatment, although lifesaving, is incomplete. Healthy kidneys do a variety of things that dialysis cannot provide. Transplant is absolutely the best remedy, but donor organs are vanishingly scarce.
Do you envision your implantable, bioartificial kidney as a bridge to transplantation? Or can it be even more, like a bionic organ, as good as a natural organ and thus better than a transplant?
Dr. Roy: We see it initially as a bridge to transplantation or as a better option than dialysis for those who will never get a transplant. We’re not trying to create the “Six Million Dollar Man.” The goal is to keep patients off dialysis – to deliver some, but probably not all, of the benefits of a kidney transplant in a mass-produced device that anybody can receive.
Dr. Fissell: The technology is aimed at people in stage 5 renal disease, the final stage, when kidneys are failing, and dialysis is the only option to maintain life. We want to make dialysis a thing of the past, put dialysis machines in museums like the iron lung, which was so vital to keeping people alive several decades ago but is mostly obsolete today.
How did you two come up with this idea? How did you get started working together?
Dr. Roy: I had just begun my career as a research biomedical engineer when I met Dr. William Fissell, who was then contemplating a career in nephrology. He opened my eyes to the problems faced by patients affected by kidney failure. Through our discussions, we quickly realized that while we could improve dialysis machines, patients needed and deserved something better – a treatment that improves their health while also allowing them to keep a job, travel readily, and consume food and drink without restrictions. Basically, something that works more like a kidney transplant.
How does the artificial kidney differ from dialysis?
Dr. Fissell: Dialysis is an intermittent stop-and-start treatment. The artificial kidney is continuous, around-the-clock treatment. There are a couple of advantages to that. The first is that you can maintain your body’s fluid balance. In dialysis, you get rid of 2-3 days’ worth of fluid in a couple of hours, and that’s very stressful to the heart and maybe to the brain as well. Second advantage is that patients will be able to eat a normal diet. Some waste products that are byproducts of our nutritional intake are slow to leave the body. So in dialysis, we restrict the diet severely and add medicines to soak up extra phosphorus. With a continuous treatment, you can balance excretion and intake.
The other aspect is that dialysis requires an immense amount of disposables. Hundreds of liters of water per patient per treatment, hundreds of thousands of dialysis cartridges and IV bags every year. The artificial kidney doesn’t need a water supply, disposable sorbent, or cartridges.
How does the artificial kidney work?
Dr. Fissell: Just like a healthy kidney. We have a unit that filters the blood so that red blood cells, white blood cells, platelets, antibodies, albumin – all the good stuff that your body worked hard to synthesize – stays in the blood, but a watery soup of toxins and waste is separated out. In a second unit, called the bioreactor, kidney cells concentrate those wastes and toxins into urine.
Dr. Roy: We used a technology called silicon micro-machining to invent an entirely new membrane that mimics a healthy kidney’s filters. It filters the blood just using the patient’s heart as a pump. No electric motors, no batteries, no wires. This lets us have something that’s completely implanted.
We also developed a cell culture of kidney cells that function in an artificial kidney. Normally, cells in a dish don’t fully adopt the features of a cell in the body. We looked at the literature around 3-D printing of organs. We learned that, in addition to fluid flow, stiff scaffolds, like cell culture dishes, trigger specific signals that keep the cells from functioning. We overcame that by looking at the physical microenvironment of the cells – not the hormones and proteins, but instead the fundamentals of the laboratory environment. For example, most organs are soft, yet plastic lab dishes are hard. By using tools that replicated the softness and fluid flow of a healthy kidney, remarkably, these cells functioned better than on a plastic dish.
Would patients need immunosuppressive or anticoagulation medication?
Dr. Fissell: They wouldn’t need either. The structure and chemistry of the device prevents blood from clotting. And the membranes in the device are a physical barrier between the host immune system and the donor cells, so the body won’t reject the device.
What is the state of the technology now?
Dr. Fissell: We have shown the function of the filters and the function of the cells, both separately and together, in preclinical in vivo testing. What we now need to do is construct clinical-grade devices and complete sterility and biocompatibility testing to initiate a human trial. That’s going to take between $12 million and $15 million in device manufacturing.
So it’s more a matter of money than time until the first clinical trials?
Dr. Roy: Yes, exactly. We don’t like to say that a clinical trial will start by such-and-such year. From the very start of the project, we have been resource limited.
A version of this article first appeared on Medscape.com.
Nearly 90,000 patients in the United States are waiting for a lifesaving kidney transplant, yet only about 25,000 kidney transplants were performed last year. Thousands die each year while they wait. Others are not suitable transplant candidates.
Half a million people are on dialysis, the only transplant alternative for those with kidney failure. This greatly impacts their work, relationships, and quality of life.
Researchers from The Kidney Project hope to solve this public health crisis with a futuristic approach: an implantable bioartificial kidney. That hope is slowly approaching reality. Early prototypes have been tested successfully in preclinical research and clinical trials could lie ahead.
This news organization spoke with two researchers who came up with the idea: nephrologist William Dr. Fissell, MD, of Vanderbilt University in Nashville, Tenn., and Shuvo Dr. Roy, PhD, a biomedical engineer at the University of California, San Francisco. This interview has been edited for length and clarity.
Question: Could you summarize the clinical problem with chronic kidney disease?
Dr. Fissell: Dialysis treatment, although lifesaving, is incomplete. Healthy kidneys do a variety of things that dialysis cannot provide. Transplant is absolutely the best remedy, but donor organs are vanishingly scarce.
Do you envision your implantable, bioartificial kidney as a bridge to transplantation? Or can it be even more, like a bionic organ, as good as a natural organ and thus better than a transplant?
Dr. Roy: We see it initially as a bridge to transplantation or as a better option than dialysis for those who will never get a transplant. We’re not trying to create the “Six Million Dollar Man.” The goal is to keep patients off dialysis – to deliver some, but probably not all, of the benefits of a kidney transplant in a mass-produced device that anybody can receive.
Dr. Fissell: The technology is aimed at people in stage 5 renal disease, the final stage, when kidneys are failing, and dialysis is the only option to maintain life. We want to make dialysis a thing of the past, put dialysis machines in museums like the iron lung, which was so vital to keeping people alive several decades ago but is mostly obsolete today.
How did you two come up with this idea? How did you get started working together?
Dr. Roy: I had just begun my career as a research biomedical engineer when I met Dr. William Fissell, who was then contemplating a career in nephrology. He opened my eyes to the problems faced by patients affected by kidney failure. Through our discussions, we quickly realized that while we could improve dialysis machines, patients needed and deserved something better – a treatment that improves their health while also allowing them to keep a job, travel readily, and consume food and drink without restrictions. Basically, something that works more like a kidney transplant.
How does the artificial kidney differ from dialysis?
Dr. Fissell: Dialysis is an intermittent stop-and-start treatment. The artificial kidney is continuous, around-the-clock treatment. There are a couple of advantages to that. The first is that you can maintain your body’s fluid balance. In dialysis, you get rid of 2-3 days’ worth of fluid in a couple of hours, and that’s very stressful to the heart and maybe to the brain as well. Second advantage is that patients will be able to eat a normal diet. Some waste products that are byproducts of our nutritional intake are slow to leave the body. So in dialysis, we restrict the diet severely and add medicines to soak up extra phosphorus. With a continuous treatment, you can balance excretion and intake.
The other aspect is that dialysis requires an immense amount of disposables. Hundreds of liters of water per patient per treatment, hundreds of thousands of dialysis cartridges and IV bags every year. The artificial kidney doesn’t need a water supply, disposable sorbent, or cartridges.
How does the artificial kidney work?
Dr. Fissell: Just like a healthy kidney. We have a unit that filters the blood so that red blood cells, white blood cells, platelets, antibodies, albumin – all the good stuff that your body worked hard to synthesize – stays in the blood, but a watery soup of toxins and waste is separated out. In a second unit, called the bioreactor, kidney cells concentrate those wastes and toxins into urine.
Dr. Roy: We used a technology called silicon micro-machining to invent an entirely new membrane that mimics a healthy kidney’s filters. It filters the blood just using the patient’s heart as a pump. No electric motors, no batteries, no wires. This lets us have something that’s completely implanted.
We also developed a cell culture of kidney cells that function in an artificial kidney. Normally, cells in a dish don’t fully adopt the features of a cell in the body. We looked at the literature around 3-D printing of organs. We learned that, in addition to fluid flow, stiff scaffolds, like cell culture dishes, trigger specific signals that keep the cells from functioning. We overcame that by looking at the physical microenvironment of the cells – not the hormones and proteins, but instead the fundamentals of the laboratory environment. For example, most organs are soft, yet plastic lab dishes are hard. By using tools that replicated the softness and fluid flow of a healthy kidney, remarkably, these cells functioned better than on a plastic dish.
Would patients need immunosuppressive or anticoagulation medication?
Dr. Fissell: They wouldn’t need either. The structure and chemistry of the device prevents blood from clotting. And the membranes in the device are a physical barrier between the host immune system and the donor cells, so the body won’t reject the device.
What is the state of the technology now?
Dr. Fissell: We have shown the function of the filters and the function of the cells, both separately and together, in preclinical in vivo testing. What we now need to do is construct clinical-grade devices and complete sterility and biocompatibility testing to initiate a human trial. That’s going to take between $12 million and $15 million in device manufacturing.
So it’s more a matter of money than time until the first clinical trials?
Dr. Roy: Yes, exactly. We don’t like to say that a clinical trial will start by such-and-such year. From the very start of the project, we have been resource limited.
A version of this article first appeared on Medscape.com.
Nearly 90,000 patients in the United States are waiting for a lifesaving kidney transplant, yet only about 25,000 kidney transplants were performed last year. Thousands die each year while they wait. Others are not suitable transplant candidates.
Half a million people are on dialysis, the only transplant alternative for those with kidney failure. This greatly impacts their work, relationships, and quality of life.
Researchers from The Kidney Project hope to solve this public health crisis with a futuristic approach: an implantable bioartificial kidney. That hope is slowly approaching reality. Early prototypes have been tested successfully in preclinical research and clinical trials could lie ahead.
This news organization spoke with two researchers who came up with the idea: nephrologist William Dr. Fissell, MD, of Vanderbilt University in Nashville, Tenn., and Shuvo Dr. Roy, PhD, a biomedical engineer at the University of California, San Francisco. This interview has been edited for length and clarity.
Question: Could you summarize the clinical problem with chronic kidney disease?
Dr. Fissell: Dialysis treatment, although lifesaving, is incomplete. Healthy kidneys do a variety of things that dialysis cannot provide. Transplant is absolutely the best remedy, but donor organs are vanishingly scarce.
Do you envision your implantable, bioartificial kidney as a bridge to transplantation? Or can it be even more, like a bionic organ, as good as a natural organ and thus better than a transplant?
Dr. Roy: We see it initially as a bridge to transplantation or as a better option than dialysis for those who will never get a transplant. We’re not trying to create the “Six Million Dollar Man.” The goal is to keep patients off dialysis – to deliver some, but probably not all, of the benefits of a kidney transplant in a mass-produced device that anybody can receive.
Dr. Fissell: The technology is aimed at people in stage 5 renal disease, the final stage, when kidneys are failing, and dialysis is the only option to maintain life. We want to make dialysis a thing of the past, put dialysis machines in museums like the iron lung, which was so vital to keeping people alive several decades ago but is mostly obsolete today.
How did you two come up with this idea? How did you get started working together?
Dr. Roy: I had just begun my career as a research biomedical engineer when I met Dr. William Fissell, who was then contemplating a career in nephrology. He opened my eyes to the problems faced by patients affected by kidney failure. Through our discussions, we quickly realized that while we could improve dialysis machines, patients needed and deserved something better – a treatment that improves their health while also allowing them to keep a job, travel readily, and consume food and drink without restrictions. Basically, something that works more like a kidney transplant.
How does the artificial kidney differ from dialysis?
Dr. Fissell: Dialysis is an intermittent stop-and-start treatment. The artificial kidney is continuous, around-the-clock treatment. There are a couple of advantages to that. The first is that you can maintain your body’s fluid balance. In dialysis, you get rid of 2-3 days’ worth of fluid in a couple of hours, and that’s very stressful to the heart and maybe to the brain as well. Second advantage is that patients will be able to eat a normal diet. Some waste products that are byproducts of our nutritional intake are slow to leave the body. So in dialysis, we restrict the diet severely and add medicines to soak up extra phosphorus. With a continuous treatment, you can balance excretion and intake.
The other aspect is that dialysis requires an immense amount of disposables. Hundreds of liters of water per patient per treatment, hundreds of thousands of dialysis cartridges and IV bags every year. The artificial kidney doesn’t need a water supply, disposable sorbent, or cartridges.
How does the artificial kidney work?
Dr. Fissell: Just like a healthy kidney. We have a unit that filters the blood so that red blood cells, white blood cells, platelets, antibodies, albumin – all the good stuff that your body worked hard to synthesize – stays in the blood, but a watery soup of toxins and waste is separated out. In a second unit, called the bioreactor, kidney cells concentrate those wastes and toxins into urine.
Dr. Roy: We used a technology called silicon micro-machining to invent an entirely new membrane that mimics a healthy kidney’s filters. It filters the blood just using the patient’s heart as a pump. No electric motors, no batteries, no wires. This lets us have something that’s completely implanted.
We also developed a cell culture of kidney cells that function in an artificial kidney. Normally, cells in a dish don’t fully adopt the features of a cell in the body. We looked at the literature around 3-D printing of organs. We learned that, in addition to fluid flow, stiff scaffolds, like cell culture dishes, trigger specific signals that keep the cells from functioning. We overcame that by looking at the physical microenvironment of the cells – not the hormones and proteins, but instead the fundamentals of the laboratory environment. For example, most organs are soft, yet plastic lab dishes are hard. By using tools that replicated the softness and fluid flow of a healthy kidney, remarkably, these cells functioned better than on a plastic dish.
Would patients need immunosuppressive or anticoagulation medication?
Dr. Fissell: They wouldn’t need either. The structure and chemistry of the device prevents blood from clotting. And the membranes in the device are a physical barrier between the host immune system and the donor cells, so the body won’t reject the device.
What is the state of the technology now?
Dr. Fissell: We have shown the function of the filters and the function of the cells, both separately and together, in preclinical in vivo testing. What we now need to do is construct clinical-grade devices and complete sterility and biocompatibility testing to initiate a human trial. That’s going to take between $12 million and $15 million in device manufacturing.
So it’s more a matter of money than time until the first clinical trials?
Dr. Roy: Yes, exactly. We don’t like to say that a clinical trial will start by such-and-such year. From the very start of the project, we have been resource limited.
A version of this article first appeared on Medscape.com.
New studies inform best practices for pelvic organ prolapse
“Approximately one in five women will undergo surgery for prolapse and/or urinary incontinence by the age of 80, which is more likely than the risk of developing breast cancer,” said David D. Rahn, MD, corresponding author of the study on perioperative vaginal estrogen, in an interview.

“About 13% of women will specifically undergo surgery to repair pelvic organ prolapse,” said Dr. Rahn, of the department of obstetrics and gynecology, University of Texas Southwestern Medical Center, Dallas. Reoperation for recurrent prolapse is not uncommon.
In their study, Dr. Rahn and colleagues examined whether the addition of perioperative vaginal estrogen cream in postmenopausal women with prolapse planning surgical correction could both strengthen the repair and lessen the likelihood of recurrence. The researchers randomized 206 postmenopausal women who were seeking surgical repair for bothersome anterior and apical vaginal prolapse to 1 gram of conjugated estrogen cream or a placebo for nightly vaginal insertion for 2 weeks, then twice weekly for at least 5 weeks of preoperative use. The treatment continued twice weekly for 12 months following surgery.
The primary outcome was the time to a failed prolapse repair by 12 months after surgery. Failure was defined by at least one of three criteria, “anatomical/objective prolapse of anterior or posterior walls beyond the hymen or the apex descending more than one-third of the vaginal length, subjective vaginal bulge symptoms, or repeated prolapse treatment,” the researchers wrote. The mean age of the patients was 65 years, and 90% and 92% of patients in the treatment and placebo groups, respectively, were White; 10% and 5%, respectively, were Black. Other baseline characteristics were similar between the groups.
After 12 months, the surgical failure incidence was not significantly different between the vaginal estrogen and placebo groups (19% vs. 9%, respectively; adjusted hazard ratio, 1.97).
Overall, anatomic recurrence was the most common outcome associated with surgical failure.
However, vaginal atrophy scores for most bothersome symptom was significantly better at 12 months in the vaginal estrogen group, compared with the placebo group, in a subset of 109 patients who reported vaginal atrophy that was at least “moderately bothersome,” the researchers said.
The findings were limited by several factors including the use of a nonvalidated instrument to assess secondary outcomes, the potentially short time period to the primary outcome, and the inclusion of the apex descending below one third total vaginal length as a criterion for surgical failure (which could be considered conservative), the researchers noted.
Unexpected results
“This work followed logically from a pilot study that similarly randomized postmenopausal women with prolapse planning surgical repair to vaginal estrogen cream versus placebo,” Dr. Rahn said. “In that smaller study, full thickness vaginal wall biopsies were collected at the time of surgery. Those participants who received the estrogen had a thicker vaginal epithelium, thicker underlying muscularis, and appeared to have a more robust concentration of strong connective tissue (i.e., type I collagen) with less of the proteases that break down connective tissue.”
This suggested that preoperative estrogen might optimize the vaginal tissue at the time of the repair. Dr. Rahn said. However, “despite evidence that the application of vaginal estrogen cream decreased the symptoms and signs of atrophic vaginal tissues, this did not lessen the likelihood of pelvic organ prolapse recurrence 12 months after surgical repair.”
The current study “would argue against routine prescription of vaginal estrogen to optimize vaginal tissue for prolapse repair, a practice that is recommended by some experts and commonly prescribed anecdotally,” said Dr. Rahn. “However, in those patients with prolapse and bothersome atrophy-related complaints such as vaginal dryness and pain with intercourse, vaginal estrogen may still be appropriate,” and vaginal estrogen also could be useful for postoperatively for patients prone to recurrent urinary tract infections.
Additional research from the study is underway, said Dr. Rahn. “All participants have now been followed to 3 years after surgery, and those clinical results are now being analyzed. In addition, full-thickness vaginal wall biopsies were collected at the time of all 186 surgeries; these are being analyzed and may yield important information regarding how biomarkers for connective tissue health could point to increased (or decreased) risk for prolapse recurrence.”
Manchester technique surpasses sacrospinous hysteropexy
In the second JAMA study, sacrospinous hysteropexy for uterine-sparing surgical management of uterine prolapse was less effective than the older Manchester procedure, based on data from nearly 400 individuals.
“Until now, the optimal uterus-sparing procedure for the treatment of uterine descent remained uncertain,” lead author Rosa Enklaar, MD, of Radboud (the Netherlands) University Medical Center, said in an interview.

“Globally, there has been a lack of scientific evidence comparing the efficacy of these two techniques, and this study aims to bridge that gap,” she said.
In their study, Dr. Enklaar and colleagues randomized 215 women to sacrospinous hysteropexy and 215 to the Manchester procedure. The mean age of the participants was 61.7 years.
The Manchester procedure involves “extraperitoneal plication of the uterosacral ligaments at the posterior side of the uterus and amputation of the cervix,” and “the cardinal ligaments are plicated on the anterior side of the cervix, “ the researchers wrote.
The primary outcome was a composite outcome of surgical success at 2 years after surgery, defined as the absence of three elements: absence of vaginal prolapse beyond the hymen, absence of bothersome bulge symptoms, and absence of retreatment of current prolapse.
Overall, 87.3% of patients in the Manchester group and 77.0% in the sacrospinous hysteropexy group met the primary outcome. At the end of the 2-year follow-up period, perioperative and patient-reported outcomes were not significantly different between the groups.
Dr. Enklaar said she was surprised by the findings. “At the start of this study, we hypothesized that there would be no difference between the two techniques,” as both have been used for a long period of time.
However, “based on the composite outcome of success at 2-year follow-up after the primary uterus-sparing surgery for uterine descent in patients with pelvic organ prolapse, these findings indicate that the sacrospinous hysteropexy is inferior to the Manchester procedure,” she said.
The study findings were limited by several factors including the lack of blinding and the applicability of the results only to women without uterine prolapse past the hymen, as well as the exclusion of patients with higher-stage prolapse, the researchers said. However, the results suggest that sacrospinous hysteropexy is inferior to the Manchester technique for uterine-sparing pelvic organ prolapse surgery.
As for additional research, few studies of prolapse surgery with long-term follow-up data are available, Dr. Enklaar said. “It is important that this current study will be continued to see the results after a longer follow-up period. Personalized health care is increasingly important, and we need to provide adequate information when counselling patients. With studies such as this one, we hope to improve the choices regarding surgical treatment of uterine descent.”
Studies challenge current prolapse protocols
The study by Dr. Rahn and colleagues contradicts the common clinical practice of preoperative vaginal estrogen to reduce recurrence of prolapse, wrote Charles W. Nager, MD, of the University of California San Diego Health, La Jolla, in an accompanying editorial that addressed both studies.
The results suggest that use of perioperative intravaginal estrogen had no impact on outcomes, “despite the surgeon assessment of less atrophy and better vaginal apex tissue in the estrogen group,” he noted. Although vaginal estrogen has other benefits in terms of patient symptoms and effects on the vaginal epithelium, “surgeons should not prescribe vaginal estrogen with the expectation that it will improve surgical success.”
The study by Dr. Enklaar and colleagues reflects the growing interest in uterine-conserving procedures, Dr. Nager wrote. The modified Manchester procedure conforms to professional society guidelines, and the composite outcome conforms to current standards for the treatment of pelvic organ prolapse.
Although suspension of the vaginal apex was quite successful, the researchers interpreted their noninferiority findings with caution, said Dr. Nager. However, they suggested that the modified Manchester procedure as performed in their study “has a role in modern prolapse surgical repair for women with uterine descent that does not protrude beyond the hymen.”
The vaginal estrogen study was supported by the National Institute on Aging, a Bridge Award from the American Board of Obstetrics & Gynecology and the American Association of Obstetricians and Gynecologists Foundation. Dr. Rahn disclosed grants from the National Institute on Aging, the American Board of Obstetrics & Gynecology, and the AAOGF bridge award, as well as nonfinancial support from National Center for Advancing Translational Sciences and Pfizer during the study. The uterine prolapse study was supported by the Netherlands Organisation for Health Research and Development. The researchers had no financial conflicts to disclose. Dr. Nager had no financial conflicts to disclose.
“Approximately one in five women will undergo surgery for prolapse and/or urinary incontinence by the age of 80, which is more likely than the risk of developing breast cancer,” said David D. Rahn, MD, corresponding author of the study on perioperative vaginal estrogen, in an interview.
“About 13% of women will specifically undergo surgery to repair pelvic organ prolapse,” said Dr. Rahn, of the department of obstetrics and gynecology, University of Texas Southwestern Medical Center, Dallas. Reoperation for recurrent prolapse is not uncommon.
In their study, Dr. Rahn and colleagues examined whether the addition of perioperative vaginal estrogen cream in postmenopausal women with prolapse planning surgical correction could both strengthen the repair and lessen the likelihood of recurrence. The researchers randomized 206 postmenopausal women who were seeking surgical repair for bothersome anterior and apical vaginal prolapse to 1 gram of conjugated estrogen cream or a placebo for nightly vaginal insertion for 2 weeks, then twice weekly for at least 5 weeks of preoperative use. The treatment continued twice weekly for 12 months following surgery.
The primary outcome was the time to a failed prolapse repair by 12 months after surgery. Failure was defined by at least one of three criteria, “anatomical/objective prolapse of anterior or posterior walls beyond the hymen or the apex descending more than one-third of the vaginal length, subjective vaginal bulge symptoms, or repeated prolapse treatment,” the researchers wrote. The mean age of the patients was 65 years, and 90% and 92% of patients in the treatment and placebo groups, respectively, were White; 10% and 5%, respectively, were Black. Other baseline characteristics were similar between the groups.
After 12 months, the surgical failure incidence was not significantly different between the vaginal estrogen and placebo groups (19% vs. 9%, respectively; adjusted hazard ratio, 1.97).
Overall, anatomic recurrence was the most common outcome associated with surgical failure.
However, vaginal atrophy scores for most bothersome symptom was significantly better at 12 months in the vaginal estrogen group, compared with the placebo group, in a subset of 109 patients who reported vaginal atrophy that was at least “moderately bothersome,” the researchers said.
The findings were limited by several factors including the use of a nonvalidated instrument to assess secondary outcomes, the potentially short time period to the primary outcome, and the inclusion of the apex descending below one third total vaginal length as a criterion for surgical failure (which could be considered conservative), the researchers noted.
Unexpected results
“This work followed logically from a pilot study that similarly randomized postmenopausal women with prolapse planning surgical repair to vaginal estrogen cream versus placebo,” Dr. Rahn said. “In that smaller study, full thickness vaginal wall biopsies were collected at the time of surgery. Those participants who received the estrogen had a thicker vaginal epithelium, thicker underlying muscularis, and appeared to have a more robust concentration of strong connective tissue (i.e., type I collagen) with less of the proteases that break down connective tissue.”
This suggested that preoperative estrogen might optimize the vaginal tissue at the time of the repair. Dr. Rahn said. However, “despite evidence that the application of vaginal estrogen cream decreased the symptoms and signs of atrophic vaginal tissues, this did not lessen the likelihood of pelvic organ prolapse recurrence 12 months after surgical repair.”
The current study “would argue against routine prescription of vaginal estrogen to optimize vaginal tissue for prolapse repair, a practice that is recommended by some experts and commonly prescribed anecdotally,” said Dr. Rahn. “However, in those patients with prolapse and bothersome atrophy-related complaints such as vaginal dryness and pain with intercourse, vaginal estrogen may still be appropriate,” and vaginal estrogen also could be useful for postoperatively for patients prone to recurrent urinary tract infections.
Additional research from the study is underway, said Dr. Rahn. “All participants have now been followed to 3 years after surgery, and those clinical results are now being analyzed. In addition, full-thickness vaginal wall biopsies were collected at the time of all 186 surgeries; these are being analyzed and may yield important information regarding how biomarkers for connective tissue health could point to increased (or decreased) risk for prolapse recurrence.”
Manchester technique surpasses sacrospinous hysteropexy
In the second JAMA study, sacrospinous hysteropexy for uterine-sparing surgical management of uterine prolapse was less effective than the older Manchester procedure, based on data from nearly 400 individuals.
“Until now, the optimal uterus-sparing procedure for the treatment of uterine descent remained uncertain,” lead author Rosa Enklaar, MD, of Radboud (the Netherlands) University Medical Center, said in an interview.
“Globally, there has been a lack of scientific evidence comparing the efficacy of these two techniques, and this study aims to bridge that gap,” she said.
In their study, Dr. Enklaar and colleagues randomized 215 women to sacrospinous hysteropexy and 215 to the Manchester procedure. The mean age of the participants was 61.7 years.
The Manchester procedure involves “extraperitoneal plication of the uterosacral ligaments at the posterior side of the uterus and amputation of the cervix,” and “the cardinal ligaments are plicated on the anterior side of the cervix, “ the researchers wrote.
The primary outcome was a composite outcome of surgical success at 2 years after surgery, defined as the absence of three elements: absence of vaginal prolapse beyond the hymen, absence of bothersome bulge symptoms, and absence of retreatment of current prolapse.
Overall, 87.3% of patients in the Manchester group and 77.0% in the sacrospinous hysteropexy group met the primary outcome. At the end of the 2-year follow-up period, perioperative and patient-reported outcomes were not significantly different between the groups.
Dr. Enklaar said she was surprised by the findings. “At the start of this study, we hypothesized that there would be no difference between the two techniques,” as both have been used for a long period of time.
However, “based on the composite outcome of success at 2-year follow-up after the primary uterus-sparing surgery for uterine descent in patients with pelvic organ prolapse, these findings indicate that the sacrospinous hysteropexy is inferior to the Manchester procedure,” she said.
The study findings were limited by several factors including the lack of blinding and the applicability of the results only to women without uterine prolapse past the hymen, as well as the exclusion of patients with higher-stage prolapse, the researchers said. However, the results suggest that sacrospinous hysteropexy is inferior to the Manchester technique for uterine-sparing pelvic organ prolapse surgery.
As for additional research, few studies of prolapse surgery with long-term follow-up data are available, Dr. Enklaar said. “It is important that this current study will be continued to see the results after a longer follow-up period. Personalized health care is increasingly important, and we need to provide adequate information when counselling patients. With studies such as this one, we hope to improve the choices regarding surgical treatment of uterine descent.”
Studies challenge current prolapse protocols
The study by Dr. Rahn and colleagues contradicts the common clinical practice of preoperative vaginal estrogen to reduce recurrence of prolapse, wrote Charles W. Nager, MD, of the University of California San Diego Health, La Jolla, in an accompanying editorial that addressed both studies.
The results suggest that use of perioperative intravaginal estrogen had no impact on outcomes, “despite the surgeon assessment of less atrophy and better vaginal apex tissue in the estrogen group,” he noted. Although vaginal estrogen has other benefits in terms of patient symptoms and effects on the vaginal epithelium, “surgeons should not prescribe vaginal estrogen with the expectation that it will improve surgical success.”
The study by Dr. Enklaar and colleagues reflects the growing interest in uterine-conserving procedures, Dr. Nager wrote. The modified Manchester procedure conforms to professional society guidelines, and the composite outcome conforms to current standards for the treatment of pelvic organ prolapse.
Although suspension of the vaginal apex was quite successful, the researchers interpreted their noninferiority findings with caution, said Dr. Nager. However, they suggested that the modified Manchester procedure as performed in their study “has a role in modern prolapse surgical repair for women with uterine descent that does not protrude beyond the hymen.”
The vaginal estrogen study was supported by the National Institute on Aging, a Bridge Award from the American Board of Obstetrics & Gynecology and the American Association of Obstetricians and Gynecologists Foundation. Dr. Rahn disclosed grants from the National Institute on Aging, the American Board of Obstetrics & Gynecology, and the AAOGF bridge award, as well as nonfinancial support from National Center for Advancing Translational Sciences and Pfizer during the study. The uterine prolapse study was supported by the Netherlands Organisation for Health Research and Development. The researchers had no financial conflicts to disclose. Dr. Nager had no financial conflicts to disclose.
“Approximately one in five women will undergo surgery for prolapse and/or urinary incontinence by the age of 80, which is more likely than the risk of developing breast cancer,” said David D. Rahn, MD, corresponding author of the study on perioperative vaginal estrogen, in an interview.
“About 13% of women will specifically undergo surgery to repair pelvic organ prolapse,” said Dr. Rahn, of the department of obstetrics and gynecology, University of Texas Southwestern Medical Center, Dallas. Reoperation for recurrent prolapse is not uncommon.
In their study, Dr. Rahn and colleagues examined whether the addition of perioperative vaginal estrogen cream in postmenopausal women with prolapse planning surgical correction could both strengthen the repair and lessen the likelihood of recurrence. The researchers randomized 206 postmenopausal women who were seeking surgical repair for bothersome anterior and apical vaginal prolapse to 1 gram of conjugated estrogen cream or a placebo for nightly vaginal insertion for 2 weeks, then twice weekly for at least 5 weeks of preoperative use. The treatment continued twice weekly for 12 months following surgery.
The primary outcome was the time to a failed prolapse repair by 12 months after surgery. Failure was defined by at least one of three criteria, “anatomical/objective prolapse of anterior or posterior walls beyond the hymen or the apex descending more than one-third of the vaginal length, subjective vaginal bulge symptoms, or repeated prolapse treatment,” the researchers wrote. The mean age of the patients was 65 years, and 90% and 92% of patients in the treatment and placebo groups, respectively, were White; 10% and 5%, respectively, were Black. Other baseline characteristics were similar between the groups.
After 12 months, the surgical failure incidence was not significantly different between the vaginal estrogen and placebo groups (19% vs. 9%, respectively; adjusted hazard ratio, 1.97).
Overall, anatomic recurrence was the most common outcome associated with surgical failure.
However, vaginal atrophy scores for most bothersome symptom was significantly better at 12 months in the vaginal estrogen group, compared with the placebo group, in a subset of 109 patients who reported vaginal atrophy that was at least “moderately bothersome,” the researchers said.
The findings were limited by several factors including the use of a nonvalidated instrument to assess secondary outcomes, the potentially short time period to the primary outcome, and the inclusion of the apex descending below one third total vaginal length as a criterion for surgical failure (which could be considered conservative), the researchers noted.
Unexpected results
“This work followed logically from a pilot study that similarly randomized postmenopausal women with prolapse planning surgical repair to vaginal estrogen cream versus placebo,” Dr. Rahn said. “In that smaller study, full thickness vaginal wall biopsies were collected at the time of surgery. Those participants who received the estrogen had a thicker vaginal epithelium, thicker underlying muscularis, and appeared to have a more robust concentration of strong connective tissue (i.e., type I collagen) with less of the proteases that break down connective tissue.”
This suggested that preoperative estrogen might optimize the vaginal tissue at the time of the repair. Dr. Rahn said. However, “despite evidence that the application of vaginal estrogen cream decreased the symptoms and signs of atrophic vaginal tissues, this did not lessen the likelihood of pelvic organ prolapse recurrence 12 months after surgical repair.”
The current study “would argue against routine prescription of vaginal estrogen to optimize vaginal tissue for prolapse repair, a practice that is recommended by some experts and commonly prescribed anecdotally,” said Dr. Rahn. “However, in those patients with prolapse and bothersome atrophy-related complaints such as vaginal dryness and pain with intercourse, vaginal estrogen may still be appropriate,” and vaginal estrogen also could be useful for postoperatively for patients prone to recurrent urinary tract infections.
Additional research from the study is underway, said Dr. Rahn. “All participants have now been followed to 3 years after surgery, and those clinical results are now being analyzed. In addition, full-thickness vaginal wall biopsies were collected at the time of all 186 surgeries; these are being analyzed and may yield important information regarding how biomarkers for connective tissue health could point to increased (or decreased) risk for prolapse recurrence.”
Manchester technique surpasses sacrospinous hysteropexy
In the second JAMA study, sacrospinous hysteropexy for uterine-sparing surgical management of uterine prolapse was less effective than the older Manchester procedure, based on data from nearly 400 individuals.
“Until now, the optimal uterus-sparing procedure for the treatment of uterine descent remained uncertain,” lead author Rosa Enklaar, MD, of Radboud (the Netherlands) University Medical Center, said in an interview.
“Globally, there has been a lack of scientific evidence comparing the efficacy of these two techniques, and this study aims to bridge that gap,” she said.
In their study, Dr. Enklaar and colleagues randomized 215 women to sacrospinous hysteropexy and 215 to the Manchester procedure. The mean age of the participants was 61.7 years.
The Manchester procedure involves “extraperitoneal plication of the uterosacral ligaments at the posterior side of the uterus and amputation of the cervix,” and “the cardinal ligaments are plicated on the anterior side of the cervix, “ the researchers wrote.
The primary outcome was a composite outcome of surgical success at 2 years after surgery, defined as the absence of three elements: absence of vaginal prolapse beyond the hymen, absence of bothersome bulge symptoms, and absence of retreatment of current prolapse.
Overall, 87.3% of patients in the Manchester group and 77.0% in the sacrospinous hysteropexy group met the primary outcome. At the end of the 2-year follow-up period, perioperative and patient-reported outcomes were not significantly different between the groups.
Dr. Enklaar said she was surprised by the findings. “At the start of this study, we hypothesized that there would be no difference between the two techniques,” as both have been used for a long period of time.
However, “based on the composite outcome of success at 2-year follow-up after the primary uterus-sparing surgery for uterine descent in patients with pelvic organ prolapse, these findings indicate that the sacrospinous hysteropexy is inferior to the Manchester procedure,” she said.
The study findings were limited by several factors including the lack of blinding and the applicability of the results only to women without uterine prolapse past the hymen, as well as the exclusion of patients with higher-stage prolapse, the researchers said. However, the results suggest that sacrospinous hysteropexy is inferior to the Manchester technique for uterine-sparing pelvic organ prolapse surgery.
As for additional research, few studies of prolapse surgery with long-term follow-up data are available, Dr. Enklaar said. “It is important that this current study will be continued to see the results after a longer follow-up period. Personalized health care is increasingly important, and we need to provide adequate information when counselling patients. With studies such as this one, we hope to improve the choices regarding surgical treatment of uterine descent.”
Studies challenge current prolapse protocols
The study by Dr. Rahn and colleagues contradicts the common clinical practice of preoperative vaginal estrogen to reduce recurrence of prolapse, wrote Charles W. Nager, MD, of the University of California San Diego Health, La Jolla, in an accompanying editorial that addressed both studies.
The results suggest that use of perioperative intravaginal estrogen had no impact on outcomes, “despite the surgeon assessment of less atrophy and better vaginal apex tissue in the estrogen group,” he noted. Although vaginal estrogen has other benefits in terms of patient symptoms and effects on the vaginal epithelium, “surgeons should not prescribe vaginal estrogen with the expectation that it will improve surgical success.”
The study by Dr. Enklaar and colleagues reflects the growing interest in uterine-conserving procedures, Dr. Nager wrote. The modified Manchester procedure conforms to professional society guidelines, and the composite outcome conforms to current standards for the treatment of pelvic organ prolapse.
Although suspension of the vaginal apex was quite successful, the researchers interpreted their noninferiority findings with caution, said Dr. Nager. However, they suggested that the modified Manchester procedure as performed in their study “has a role in modern prolapse surgical repair for women with uterine descent that does not protrude beyond the hymen.”
The vaginal estrogen study was supported by the National Institute on Aging, a Bridge Award from the American Board of Obstetrics & Gynecology and the American Association of Obstetricians and Gynecologists Foundation. Dr. Rahn disclosed grants from the National Institute on Aging, the American Board of Obstetrics & Gynecology, and the AAOGF bridge award, as well as nonfinancial support from National Center for Advancing Translational Sciences and Pfizer during the study. The uterine prolapse study was supported by the Netherlands Organisation for Health Research and Development. The researchers had no financial conflicts to disclose. Dr. Nager had no financial conflicts to disclose.
FROM JAMA
A1c not linked to postop complications in kids with diabetes
TOPLINE:
- Delaying elective surgeries until A1c is consistently normalized may not be warranted, particularly because this is challenging to accomplish rapidly.
METHODOLOGY:
- A retrospective analysis was done of data from surgery and endocrinology medical records of 438 children aged 1-18 years with type 1 (72%) or type 2 diabetes (28%) undergoing elective noncardiac surgery at Texas Children’s Hospital, January 2011 to June 2021.
- Overall, 28% had an A1c less than 7.0%, 42% had A1c 7%-9%, and 30% had A1c greater than 9%.
- The primary outcome was defined as a new-onset postoperative systemic infection, wound complication, or ketosis.
TAKEAWAY:
- The incidence of any postoperative systemic infections was 0.91% (n = 4); postoperative wound disruption, 3.33% (n = 19); and postoperative ketosis, 3.89% (n = 17).
- A1c levels were not associated with any postoperative systemic infections, wound complications, or ketosis.
- No other preoperative factors, including diabetes type, body mass index, or procedure type, were association with these complications.
IN PRACTICE:
“Current recommendations suggest consulting with the diabetes team before surgery and if glycemic status is suboptimal to consider delaying surgery and, if surgery cannot be delayed, considering admission to the hospital before surgery for acute optimization of glycemia, However, there is no guidance on the level of elevated A1c that should prompt consideration of delaying surgery. This issue is of crucial importance because necessary elective surgery or diagnostic procedures may be delayed unnecessarily or for longer than needed in children with elevated A1c because of the difficulty of improving A1c levels rapidly.”
STUDY DETAILS:
The study was led by Grace Kim, MD, of the division of diabetes and endocrinology, Texas Children’s Hospital, Houston. It was published online August 1, 2023, in Diabetes Care.
LIMITATIONS:
- The postoperative complication rate was low.
- Only elective procedures were included.
DISCLOSURES:
The authors have no disclosures.
A version of this article first appeared on Medscape.com.
TOPLINE:
- Delaying elective surgeries until A1c is consistently normalized may not be warranted, particularly because this is challenging to accomplish rapidly.
METHODOLOGY:
- A retrospective analysis was done of data from surgery and endocrinology medical records of 438 children aged 1-18 years with type 1 (72%) or type 2 diabetes (28%) undergoing elective noncardiac surgery at Texas Children’s Hospital, January 2011 to June 2021.
- Overall, 28% had an A1c less than 7.0%, 42% had A1c 7%-9%, and 30% had A1c greater than 9%.
- The primary outcome was defined as a new-onset postoperative systemic infection, wound complication, or ketosis.
TAKEAWAY:
- The incidence of any postoperative systemic infections was 0.91% (n = 4); postoperative wound disruption, 3.33% (n = 19); and postoperative ketosis, 3.89% (n = 17).
- A1c levels were not associated with any postoperative systemic infections, wound complications, or ketosis.
- No other preoperative factors, including diabetes type, body mass index, or procedure type, were association with these complications.
IN PRACTICE:
“Current recommendations suggest consulting with the diabetes team before surgery and if glycemic status is suboptimal to consider delaying surgery and, if surgery cannot be delayed, considering admission to the hospital before surgery for acute optimization of glycemia, However, there is no guidance on the level of elevated A1c that should prompt consideration of delaying surgery. This issue is of crucial importance because necessary elective surgery or diagnostic procedures may be delayed unnecessarily or for longer than needed in children with elevated A1c because of the difficulty of improving A1c levels rapidly.”
STUDY DETAILS:
The study was led by Grace Kim, MD, of the division of diabetes and endocrinology, Texas Children’s Hospital, Houston. It was published online August 1, 2023, in Diabetes Care.
LIMITATIONS:
- The postoperative complication rate was low.
- Only elective procedures were included.
DISCLOSURES:
The authors have no disclosures.
A version of this article first appeared on Medscape.com.
TOPLINE:
- Delaying elective surgeries until A1c is consistently normalized may not be warranted, particularly because this is challenging to accomplish rapidly.
METHODOLOGY:
- A retrospective analysis was done of data from surgery and endocrinology medical records of 438 children aged 1-18 years with type 1 (72%) or type 2 diabetes (28%) undergoing elective noncardiac surgery at Texas Children’s Hospital, January 2011 to June 2021.
- Overall, 28% had an A1c less than 7.0%, 42% had A1c 7%-9%, and 30% had A1c greater than 9%.
- The primary outcome was defined as a new-onset postoperative systemic infection, wound complication, or ketosis.
TAKEAWAY:
- The incidence of any postoperative systemic infections was 0.91% (n = 4); postoperative wound disruption, 3.33% (n = 19); and postoperative ketosis, 3.89% (n = 17).
- A1c levels were not associated with any postoperative systemic infections, wound complications, or ketosis.
- No other preoperative factors, including diabetes type, body mass index, or procedure type, were association with these complications.
IN PRACTICE:
“Current recommendations suggest consulting with the diabetes team before surgery and if glycemic status is suboptimal to consider delaying surgery and, if surgery cannot be delayed, considering admission to the hospital before surgery for acute optimization of glycemia, However, there is no guidance on the level of elevated A1c that should prompt consideration of delaying surgery. This issue is of crucial importance because necessary elective surgery or diagnostic procedures may be delayed unnecessarily or for longer than needed in children with elevated A1c because of the difficulty of improving A1c levels rapidly.”
STUDY DETAILS:
The study was led by Grace Kim, MD, of the division of diabetes and endocrinology, Texas Children’s Hospital, Houston. It was published online August 1, 2023, in Diabetes Care.
LIMITATIONS:
- The postoperative complication rate was low.
- Only elective procedures were included.
DISCLOSURES:
The authors have no disclosures.
A version of this article first appeared on Medscape.com.
FROM DIABETES CARE
Dural-puncture epidural drives faster conversion to cesarean anesthesia
DPE, while not new, has become more popular as an option for initiating labor analgesia, but data comparing DPE with standard epidural in conversion to surgical anesthesia for cesarean deliveries are limited, Nadir Sharawi, MD, of the University of Arkansas for Medical Sciences, Little Rock, and colleagues wrote.

DPE involves no injection of intrathecal drugs, and the potential advantages include easier translocation of epidural medications into the intrathecal space for improved analgesia, but the effects of DPE on the onset and reliability of surgical anesthesia remain unknown, they said.
In a study published in JAMA Network Open, the researchers randomized 70 women scheduled for cesarean delivery of singleton pregnancies to DPE and 70 to a standard epidural. The participants were aged 18 years and older, with a mean age of the 30.1 years; the study was conducted between April 2019 and October 2022 at a single center.
The primary outcome was the time to the loss of sharp sensation at T6, defined as “the start of epidural extension anesthesia (time zero on the stopwatch) to when the patient could no longer feel sharp sensation at T6 (assessed bilaterally at the midclavicular line),” the researchers wrote.
The onset time to surgical anesthesia was faster in the DPE group, compared with the standard group, with a median of 422 seconds versus 655 seconds.
A key secondary outcome was a composite measure of the quality of epidural anesthesia that included failure to achieve a T10 bilateral block preoperatively in the delivery room, failure to achieve a surgical block at T6 within 15 minutes of chloroprocaine administration, requirement for intraoperative analgesia, repeat neuraxial procedure, and conversion to general anesthesia. The composite rates of lower quality anesthesia were significantly less in the DPE group, compared with the standard group (15.7% vs. 36.3%; P = .007).
Additional secondary outcomes included maternal satisfaction and pain score during surgery, adverse events, opioid use in the first 24 hours, maternal vasopressor requirements, epidural block assessments, and neonatal outcomes. No significant differences in these outcomes were noted between the groups, and no instances of local anesthetic systemic toxicity or neurological complications were reported.
The findings were limited by several factors including the study population of women scheduled for cesarean delivery and not in labor, and the inability to detect less frequent complications such as post–dural-puncture headache and accidental dural puncture, the researchers noted.
In addition, the results may vary with the use of other combinations of local anesthetics and opioids. “Chloroprocaine was chosen in this study because of its ease of administration without the need for opioids and other additives along with the low risk of systemic toxic effects, which favors rapid administration for emergent cesarean delivery,” they wrote.
However, the results show an association between DPE within an hour of epidural extension for elective cesarean delivery and a faster onset of anesthesia, improved block quality, and a more favorable ratio of risks versus benefits, compared with the use of standard epidural, the researchers concluded.
No need for general anesthesia?
“There is controversy over whether the dural puncture epidural technique improves labor analgesia when compared to a standard epidural,” Dr. Shawari said in an interview. “However, there are limited data on whether the dural puncture epidural technique decreases the onset time to surgical anesthesia when compared to a standard epidural for cesarean delivery. This is important as a pre-existing epidural is commonly used to convert labor analgesia to surgical anesthesia in the setting of urgent cesarean delivery. A faster onset of epidural anesthesia could potentially avoid the need for general anesthesia in an emergency.”
The researchers were not surprised by the findings given their experience with performing dural puncture epidurals for labor analgesia, Dr. Shawari said. In those cases, DPE provided a faster onset when converting cesarean anesthesia, compared with a standard epidural.
The takeaway from the current study is that DPE also provided “a faster onset and improved quality of anesthesia when compared to standard epidural for elective cesarean delivery,” Dr. Shawari said. However, additional research is needed to confirm the findings for intrapartum cesarean delivery.
Progress in improving pain control
“Adequate pain control during cesarean delivery is incredibly important,” Catherine Albright, MD, a maternal-fetal medicine specialist at the University of Washington, Seattle, said in an interview. “Inadequate pain control leads to the need to provide additional intravenous medications or the need to be put under general anesthesia, which changes the birth experience and is more dangerous for the birthing person and the neonate.

“In my clinical experience, there are many times when patients do not have adequate pain control during a cesarean delivery,” said Dr. Albright, who was not involved in the current study. “I am pleased to see that there is research underway about how to best manage pain on labor and delivery, especially in the setting of conversion from labor anesthesia to cesarean anesthesia.”
The findings may have implications for clinical practice, said Dr. Albright. If the dural puncture epidural can improve cesarean anesthesia following an epidural during labor, rather than anesthesia provided for an elective cesarean), “then I believe it would reduce the number of patients who require additional pain medication, have a poor cesarean experience, and/or need to be put under general anesthesia.”
However, “as noted by the authors, additional research is needed to further determine possible risks and side effects from this technique, and also to ensure that it also works in the setting of labor, rather than for an elective cesarean,” Dr. Albright added.
The study received no outside funding. The researchers had no financial conflicts to disclose. Dr. Albright had no financial conflicts to disclose.
DPE, while not new, has become more popular as an option for initiating labor analgesia, but data comparing DPE with standard epidural in conversion to surgical anesthesia for cesarean deliveries are limited, Nadir Sharawi, MD, of the University of Arkansas for Medical Sciences, Little Rock, and colleagues wrote.
DPE involves no injection of intrathecal drugs, and the potential advantages include easier translocation of epidural medications into the intrathecal space for improved analgesia, but the effects of DPE on the onset and reliability of surgical anesthesia remain unknown, they said.
In a study published in JAMA Network Open, the researchers randomized 70 women scheduled for cesarean delivery of singleton pregnancies to DPE and 70 to a standard epidural. The participants were aged 18 years and older, with a mean age of the 30.1 years; the study was conducted between April 2019 and October 2022 at a single center.
The primary outcome was the time to the loss of sharp sensation at T6, defined as “the start of epidural extension anesthesia (time zero on the stopwatch) to when the patient could no longer feel sharp sensation at T6 (assessed bilaterally at the midclavicular line),” the researchers wrote.
The onset time to surgical anesthesia was faster in the DPE group, compared with the standard group, with a median of 422 seconds versus 655 seconds.
A key secondary outcome was a composite measure of the quality of epidural anesthesia that included failure to achieve a T10 bilateral block preoperatively in the delivery room, failure to achieve a surgical block at T6 within 15 minutes of chloroprocaine administration, requirement for intraoperative analgesia, repeat neuraxial procedure, and conversion to general anesthesia. The composite rates of lower quality anesthesia were significantly less in the DPE group, compared with the standard group (15.7% vs. 36.3%; P = .007).
Additional secondary outcomes included maternal satisfaction and pain score during surgery, adverse events, opioid use in the first 24 hours, maternal vasopressor requirements, epidural block assessments, and neonatal outcomes. No significant differences in these outcomes were noted between the groups, and no instances of local anesthetic systemic toxicity or neurological complications were reported.
The findings were limited by several factors including the study population of women scheduled for cesarean delivery and not in labor, and the inability to detect less frequent complications such as post–dural-puncture headache and accidental dural puncture, the researchers noted.
In addition, the results may vary with the use of other combinations of local anesthetics and opioids. “Chloroprocaine was chosen in this study because of its ease of administration without the need for opioids and other additives along with the low risk of systemic toxic effects, which favors rapid administration for emergent cesarean delivery,” they wrote.
However, the results show an association between DPE within an hour of epidural extension for elective cesarean delivery and a faster onset of anesthesia, improved block quality, and a more favorable ratio of risks versus benefits, compared with the use of standard epidural, the researchers concluded.
No need for general anesthesia?
“There is controversy over whether the dural puncture epidural technique improves labor analgesia when compared to a standard epidural,” Dr. Shawari said in an interview. “However, there are limited data on whether the dural puncture epidural technique decreases the onset time to surgical anesthesia when compared to a standard epidural for cesarean delivery. This is important as a pre-existing epidural is commonly used to convert labor analgesia to surgical anesthesia in the setting of urgent cesarean delivery. A faster onset of epidural anesthesia could potentially avoid the need for general anesthesia in an emergency.”
The researchers were not surprised by the findings given their experience with performing dural puncture epidurals for labor analgesia, Dr. Shawari said. In those cases, DPE provided a faster onset when converting cesarean anesthesia, compared with a standard epidural.
The takeaway from the current study is that DPE also provided “a faster onset and improved quality of anesthesia when compared to standard epidural for elective cesarean delivery,” Dr. Shawari said. However, additional research is needed to confirm the findings for intrapartum cesarean delivery.
Progress in improving pain control
“Adequate pain control during cesarean delivery is incredibly important,” Catherine Albright, MD, a maternal-fetal medicine specialist at the University of Washington, Seattle, said in an interview. “Inadequate pain control leads to the need to provide additional intravenous medications or the need to be put under general anesthesia, which changes the birth experience and is more dangerous for the birthing person and the neonate.
“In my clinical experience, there are many times when patients do not have adequate pain control during a cesarean delivery,” said Dr. Albright, who was not involved in the current study. “I am pleased to see that there is research underway about how to best manage pain on labor and delivery, especially in the setting of conversion from labor anesthesia to cesarean anesthesia.”
The findings may have implications for clinical practice, said Dr. Albright. If the dural puncture epidural can improve cesarean anesthesia following an epidural during labor, rather than anesthesia provided for an elective cesarean), “then I believe it would reduce the number of patients who require additional pain medication, have a poor cesarean experience, and/or need to be put under general anesthesia.”
However, “as noted by the authors, additional research is needed to further determine possible risks and side effects from this technique, and also to ensure that it also works in the setting of labor, rather than for an elective cesarean,” Dr. Albright added.
The study received no outside funding. The researchers had no financial conflicts to disclose. Dr. Albright had no financial conflicts to disclose.
DPE, while not new, has become more popular as an option for initiating labor analgesia, but data comparing DPE with standard epidural in conversion to surgical anesthesia for cesarean deliveries are limited, Nadir Sharawi, MD, of the University of Arkansas for Medical Sciences, Little Rock, and colleagues wrote.
DPE involves no injection of intrathecal drugs, and the potential advantages include easier translocation of epidural medications into the intrathecal space for improved analgesia, but the effects of DPE on the onset and reliability of surgical anesthesia remain unknown, they said.
In a study published in JAMA Network Open, the researchers randomized 70 women scheduled for cesarean delivery of singleton pregnancies to DPE and 70 to a standard epidural. The participants were aged 18 years and older, with a mean age of the 30.1 years; the study was conducted between April 2019 and October 2022 at a single center.
The primary outcome was the time to the loss of sharp sensation at T6, defined as “the start of epidural extension anesthesia (time zero on the stopwatch) to when the patient could no longer feel sharp sensation at T6 (assessed bilaterally at the midclavicular line),” the researchers wrote.
The onset time to surgical anesthesia was faster in the DPE group, compared with the standard group, with a median of 422 seconds versus 655 seconds.
A key secondary outcome was a composite measure of the quality of epidural anesthesia that included failure to achieve a T10 bilateral block preoperatively in the delivery room, failure to achieve a surgical block at T6 within 15 minutes of chloroprocaine administration, requirement for intraoperative analgesia, repeat neuraxial procedure, and conversion to general anesthesia. The composite rates of lower quality anesthesia were significantly less in the DPE group, compared with the standard group (15.7% vs. 36.3%; P = .007).
Additional secondary outcomes included maternal satisfaction and pain score during surgery, adverse events, opioid use in the first 24 hours, maternal vasopressor requirements, epidural block assessments, and neonatal outcomes. No significant differences in these outcomes were noted between the groups, and no instances of local anesthetic systemic toxicity or neurological complications were reported.
The findings were limited by several factors including the study population of women scheduled for cesarean delivery and not in labor, and the inability to detect less frequent complications such as post–dural-puncture headache and accidental dural puncture, the researchers noted.
In addition, the results may vary with the use of other combinations of local anesthetics and opioids. “Chloroprocaine was chosen in this study because of its ease of administration without the need for opioids and other additives along with the low risk of systemic toxic effects, which favors rapid administration for emergent cesarean delivery,” they wrote.
However, the results show an association between DPE within an hour of epidural extension for elective cesarean delivery and a faster onset of anesthesia, improved block quality, and a more favorable ratio of risks versus benefits, compared with the use of standard epidural, the researchers concluded.
No need for general anesthesia?
“There is controversy over whether the dural puncture epidural technique improves labor analgesia when compared to a standard epidural,” Dr. Shawari said in an interview. “However, there are limited data on whether the dural puncture epidural technique decreases the onset time to surgical anesthesia when compared to a standard epidural for cesarean delivery. This is important as a pre-existing epidural is commonly used to convert labor analgesia to surgical anesthesia in the setting of urgent cesarean delivery. A faster onset of epidural anesthesia could potentially avoid the need for general anesthesia in an emergency.”
The researchers were not surprised by the findings given their experience with performing dural puncture epidurals for labor analgesia, Dr. Shawari said. In those cases, DPE provided a faster onset when converting cesarean anesthesia, compared with a standard epidural.
The takeaway from the current study is that DPE also provided “a faster onset and improved quality of anesthesia when compared to standard epidural for elective cesarean delivery,” Dr. Shawari said. However, additional research is needed to confirm the findings for intrapartum cesarean delivery.
Progress in improving pain control
“Adequate pain control during cesarean delivery is incredibly important,” Catherine Albright, MD, a maternal-fetal medicine specialist at the University of Washington, Seattle, said in an interview. “Inadequate pain control leads to the need to provide additional intravenous medications or the need to be put under general anesthesia, which changes the birth experience and is more dangerous for the birthing person and the neonate.
“In my clinical experience, there are many times when patients do not have adequate pain control during a cesarean delivery,” said Dr. Albright, who was not involved in the current study. “I am pleased to see that there is research underway about how to best manage pain on labor and delivery, especially in the setting of conversion from labor anesthesia to cesarean anesthesia.”
The findings may have implications for clinical practice, said Dr. Albright. If the dural puncture epidural can improve cesarean anesthesia following an epidural during labor, rather than anesthesia provided for an elective cesarean), “then I believe it would reduce the number of patients who require additional pain medication, have a poor cesarean experience, and/or need to be put under general anesthesia.”
However, “as noted by the authors, additional research is needed to further determine possible risks and side effects from this technique, and also to ensure that it also works in the setting of labor, rather than for an elective cesarean,” Dr. Albright added.
The study received no outside funding. The researchers had no financial conflicts to disclose. Dr. Albright had no financial conflicts to disclose.
FROM JAMA NETWORK OPEN
Fatalities from breast cancer have ‘improved substantially’
Women diagnosed with early-stage breast cancer are more likely to become long-term survivors of the disease now than they were 20 years ago, a new study found.
Researchers at the University of Oxford (England) conducted an observational study that examined case fatality rates for women with breast cancer and found that the prognosis for women has “improved substantially” over the past few decades. For women diagnosed with early invasive breast cancer during the 1990s, the risk of death within 5 years of diagnosis was just over 14% on average. For women diagnosed during the 2010s, it was nearly 5% on average.
“The take-home message in our study is that it’s good news for women who are diagnosed with early breast cancer today because most of them can expect to become long-term cancer survivors, and so I think our results are reassuring,” said lead study author Carolyn Taylor, DPhil, a clinical oncologist from the Nuffield Department Of Population Health, University of Oxford.
The study was published online in the BMJ.
Although breast cancer survival has improved, recent estimates don’t incorporate detailed data on age, tumor size, tumor grade, and nodal and receptor status. In the current population-based study, researchers explored improvement in survival from early-stage breast cancer. They used nine patient and tumor characteristics as factors in their analysis.
The study is based on data from the National Cancer Registration for 512,447 women in England who were diagnosed with early-stage invasive breast cancer between 1993 and 2015. Women were broken into four groups: those diagnosed during 1993-1999, 2000-2004, 2005-2009, and 2010-2015.
The study focused on women who initially underwent either breast-conserving surgery or mastectomy as their first treatment. Data included age, tumor size, tumor grade, number of positive nodes, and estrogen receptor (ER) status. For women who were diagnosed from 2010 to 2015, HER2 status was included. Data regarding recurrence, receipt of neoadjuvant therapy, and patients who were diagnosed with more than one cancer were not included.
The major finding: Among women diagnosed with early-stage invasive breast cancer, the risk of dying decreased almost threefold between 1993 and 2015. The 5-year cumulative case fatality risk was 14.4% for women diagnosed in the 1990s (1993-1999) versus 4.9% for women diagnosed about 2 decades later (2010-2015).
Dr. Taylor and colleagues found that the case fatality rate was highest during the 5 years after diagnosis; within those years, the rates typically increased during the first 2 years, peaked during the third, and declined thereafter.
The 5-year risk of death, however, varied widely among women in the population. For most (62.8%) who were diagnosed between 2010 and 2015, the case fatality risk was 3% or less; however, for a small subset of women (4.6%), the risk reached 20% or higher.
Patients with ER-negative tumors tended to have worse prognoses in the first decade following their diagnosis. Overall, higher tumor size and grade, more positive nodes, and older age tended to be associated with worse prognoses.
Overall, the annual case fatality rates decreased over time in nearly every patient group.
While Dr. Taylor said these findings are encouraging, she added that the investigators did not analyze why survival rates have improved over 2 decades.
“We didn’t explain how much of the improvement was due to advances treatments, improved screening rates, etc,” Dr. Taylor said. Another limitation is that data on recurrence were not available.
Kathy Miller, MD, who specializes in breast cancer at the Melvin and Bren Simon Cancer Center at Indiana University, Indianapolis, said the 5-year mark for survival is great news for some patients with breast cancer but that the time frame doesn’t apply to all.
While the risk of case fatality from breast cancer may be higher during the first 5 years after diagnosis, Dr. Miller said that is not the case for women with ER-positive breast cancer. In the study, the researchers highlighted this trend for ER status: before the 10-year mark, survival rates for women with ER-positive disease were better, but after the 10-year mark, those with ER-negative tumors seemed to fare slightly better.
“Many patients have heard this very arbitrary 5-year mark, and for patients with ER-positive disease, that 5-year mark has no meaning, because their risk in any given year is very low and it stays at that very low consistent level for at least 15 years, probably longer,” Dr. Miller said in an interview. “I think a better way to think about this for ER-positive patients is that every day that goes by without a problem makes it a tiny bit less likely that you will ever have a problem.”
The authors took a similar view for the overall population, concluding that, “although deaths from breast cancer will continue to occur beyond this [5-year mark], the risk during each subsequent 5-year period is likely to be lower than during the first 5 years.”
The research was funded by Cancer Research UK, the National Institute for Health Research Oxford Biomedical Research Centre, the U.K. Medical Research Council, and the University of Oxford. Some study authors received support for several of these institutions, but they reported no financial relationships with organizations that might have had an interest in the submitted work during the previous 3 years.
A version of this article first appeared on Medscape.com.
Women diagnosed with early-stage breast cancer are more likely to become long-term survivors of the disease now than they were 20 years ago, a new study found.
Researchers at the University of Oxford (England) conducted an observational study that examined case fatality rates for women with breast cancer and found that the prognosis for women has “improved substantially” over the past few decades. For women diagnosed with early invasive breast cancer during the 1990s, the risk of death within 5 years of diagnosis was just over 14% on average. For women diagnosed during the 2010s, it was nearly 5% on average.
“The take-home message in our study is that it’s good news for women who are diagnosed with early breast cancer today because most of them can expect to become long-term cancer survivors, and so I think our results are reassuring,” said lead study author Carolyn Taylor, DPhil, a clinical oncologist from the Nuffield Department Of Population Health, University of Oxford.
The study was published online in the BMJ.
Although breast cancer survival has improved, recent estimates don’t incorporate detailed data on age, tumor size, tumor grade, and nodal and receptor status. In the current population-based study, researchers explored improvement in survival from early-stage breast cancer. They used nine patient and tumor characteristics as factors in their analysis.
The study is based on data from the National Cancer Registration for 512,447 women in England who were diagnosed with early-stage invasive breast cancer between 1993 and 2015. Women were broken into four groups: those diagnosed during 1993-1999, 2000-2004, 2005-2009, and 2010-2015.
The study focused on women who initially underwent either breast-conserving surgery or mastectomy as their first treatment. Data included age, tumor size, tumor grade, number of positive nodes, and estrogen receptor (ER) status. For women who were diagnosed from 2010 to 2015, HER2 status was included. Data regarding recurrence, receipt of neoadjuvant therapy, and patients who were diagnosed with more than one cancer were not included.
The major finding: Among women diagnosed with early-stage invasive breast cancer, the risk of dying decreased almost threefold between 1993 and 2015. The 5-year cumulative case fatality risk was 14.4% for women diagnosed in the 1990s (1993-1999) versus 4.9% for women diagnosed about 2 decades later (2010-2015).
Dr. Taylor and colleagues found that the case fatality rate was highest during the 5 years after diagnosis; within those years, the rates typically increased during the first 2 years, peaked during the third, and declined thereafter.
The 5-year risk of death, however, varied widely among women in the population. For most (62.8%) who were diagnosed between 2010 and 2015, the case fatality risk was 3% or less; however, for a small subset of women (4.6%), the risk reached 20% or higher.
Patients with ER-negative tumors tended to have worse prognoses in the first decade following their diagnosis. Overall, higher tumor size and grade, more positive nodes, and older age tended to be associated with worse prognoses.
Overall, the annual case fatality rates decreased over time in nearly every patient group.
While Dr. Taylor said these findings are encouraging, she added that the investigators did not analyze why survival rates have improved over 2 decades.
“We didn’t explain how much of the improvement was due to advances treatments, improved screening rates, etc,” Dr. Taylor said. Another limitation is that data on recurrence were not available.
Kathy Miller, MD, who specializes in breast cancer at the Melvin and Bren Simon Cancer Center at Indiana University, Indianapolis, said the 5-year mark for survival is great news for some patients with breast cancer but that the time frame doesn’t apply to all.
While the risk of case fatality from breast cancer may be higher during the first 5 years after diagnosis, Dr. Miller said that is not the case for women with ER-positive breast cancer. In the study, the researchers highlighted this trend for ER status: before the 10-year mark, survival rates for women with ER-positive disease were better, but after the 10-year mark, those with ER-negative tumors seemed to fare slightly better.
“Many patients have heard this very arbitrary 5-year mark, and for patients with ER-positive disease, that 5-year mark has no meaning, because their risk in any given year is very low and it stays at that very low consistent level for at least 15 years, probably longer,” Dr. Miller said in an interview. “I think a better way to think about this for ER-positive patients is that every day that goes by without a problem makes it a tiny bit less likely that you will ever have a problem.”
The authors took a similar view for the overall population, concluding that, “although deaths from breast cancer will continue to occur beyond this [5-year mark], the risk during each subsequent 5-year period is likely to be lower than during the first 5 years.”
The research was funded by Cancer Research UK, the National Institute for Health Research Oxford Biomedical Research Centre, the U.K. Medical Research Council, and the University of Oxford. Some study authors received support for several of these institutions, but they reported no financial relationships with organizations that might have had an interest in the submitted work during the previous 3 years.
A version of this article first appeared on Medscape.com.
Women diagnosed with early-stage breast cancer are more likely to become long-term survivors of the disease now than they were 20 years ago, a new study found.
Researchers at the University of Oxford (England) conducted an observational study that examined case fatality rates for women with breast cancer and found that the prognosis for women has “improved substantially” over the past few decades. For women diagnosed with early invasive breast cancer during the 1990s, the risk of death within 5 years of diagnosis was just over 14% on average. For women diagnosed during the 2010s, it was nearly 5% on average.
“The take-home message in our study is that it’s good news for women who are diagnosed with early breast cancer today because most of them can expect to become long-term cancer survivors, and so I think our results are reassuring,” said lead study author Carolyn Taylor, DPhil, a clinical oncologist from the Nuffield Department Of Population Health, University of Oxford.
The study was published online in the BMJ.
Although breast cancer survival has improved, recent estimates don’t incorporate detailed data on age, tumor size, tumor grade, and nodal and receptor status. In the current population-based study, researchers explored improvement in survival from early-stage breast cancer. They used nine patient and tumor characteristics as factors in their analysis.
The study is based on data from the National Cancer Registration for 512,447 women in England who were diagnosed with early-stage invasive breast cancer between 1993 and 2015. Women were broken into four groups: those diagnosed during 1993-1999, 2000-2004, 2005-2009, and 2010-2015.
The study focused on women who initially underwent either breast-conserving surgery or mastectomy as their first treatment. Data included age, tumor size, tumor grade, number of positive nodes, and estrogen receptor (ER) status. For women who were diagnosed from 2010 to 2015, HER2 status was included. Data regarding recurrence, receipt of neoadjuvant therapy, and patients who were diagnosed with more than one cancer were not included.
The major finding: Among women diagnosed with early-stage invasive breast cancer, the risk of dying decreased almost threefold between 1993 and 2015. The 5-year cumulative case fatality risk was 14.4% for women diagnosed in the 1990s (1993-1999) versus 4.9% for women diagnosed about 2 decades later (2010-2015).
Dr. Taylor and colleagues found that the case fatality rate was highest during the 5 years after diagnosis; within those years, the rates typically increased during the first 2 years, peaked during the third, and declined thereafter.
The 5-year risk of death, however, varied widely among women in the population. For most (62.8%) who were diagnosed between 2010 and 2015, the case fatality risk was 3% or less; however, for a small subset of women (4.6%), the risk reached 20% or higher.
Patients with ER-negative tumors tended to have worse prognoses in the first decade following their diagnosis. Overall, higher tumor size and grade, more positive nodes, and older age tended to be associated with worse prognoses.
Overall, the annual case fatality rates decreased over time in nearly every patient group.
While Dr. Taylor said these findings are encouraging, she added that the investigators did not analyze why survival rates have improved over 2 decades.
“We didn’t explain how much of the improvement was due to advances treatments, improved screening rates, etc,” Dr. Taylor said. Another limitation is that data on recurrence were not available.
Kathy Miller, MD, who specializes in breast cancer at the Melvin and Bren Simon Cancer Center at Indiana University, Indianapolis, said the 5-year mark for survival is great news for some patients with breast cancer but that the time frame doesn’t apply to all.
While the risk of case fatality from breast cancer may be higher during the first 5 years after diagnosis, Dr. Miller said that is not the case for women with ER-positive breast cancer. In the study, the researchers highlighted this trend for ER status: before the 10-year mark, survival rates for women with ER-positive disease were better, but after the 10-year mark, those with ER-negative tumors seemed to fare slightly better.
“Many patients have heard this very arbitrary 5-year mark, and for patients with ER-positive disease, that 5-year mark has no meaning, because their risk in any given year is very low and it stays at that very low consistent level for at least 15 years, probably longer,” Dr. Miller said in an interview. “I think a better way to think about this for ER-positive patients is that every day that goes by without a problem makes it a tiny bit less likely that you will ever have a problem.”
The authors took a similar view for the overall population, concluding that, “although deaths from breast cancer will continue to occur beyond this [5-year mark], the risk during each subsequent 5-year period is likely to be lower than during the first 5 years.”
The research was funded by Cancer Research UK, the National Institute for Health Research Oxford Biomedical Research Centre, the U.K. Medical Research Council, and the University of Oxford. Some study authors received support for several of these institutions, but they reported no financial relationships with organizations that might have had an interest in the submitted work during the previous 3 years.
A version of this article first appeared on Medscape.com.
FROM THE BMJ