User login
Anti-CCP antibodies associated with increased mortality in RA
Postmenopausal women with rheumatoid arthritis were almost three times more likely to die over a 10-year period than were those who did not have the disease in a subanalysis of participants in the Women’s Health Initiative study.
Using stored serum from Women’s Health Initiative (WHI) subjects, investigators found that the increased risk was mostly attributable to women with anti-cyclic citrullinated peptide (anti-CCP) antibodies – a marker used to identify those in the sample who probably had true rheumatoid arthritis (RA). This finding stayed significant even when the analysis controlled for the use of disease-modifying antirheumatic drugs (DMARDs), and also in several models that controlled for health and lifestyle risk factors, Dr. Lewis H. Kuller and his colleagues reported in Arthritis & Rheumatism.
"The increased risk of death for anti-CCP positive women was not explained by age, rheumatoid factor positivity, ANA [antinuclear antibody] positivity, or DMARD use," wrote Dr. Kuller of the University of Pittsburgh and his coauthors (Arthritis Rheum. 2014 Dec. 23 [doi:10.1002/art.38268]).

"Traditional risk factors (e.g., smoking, diabetes), kidney disease, joint pain, health status or [white blood cell] count also did not statistically explain the increased risk for anti-CCP-positivity, despite their independent associations with higher mortality," they said.
The study focused on 9,988 women from the WHI, all of whom self-reported having RA at baseline or at follow-up visits. To further refine the sample, the investigators defined probable RA as the presence of anti-CCP antibodies, with or without the use of DMARDs (8% of the sample), or the absence of anti-CCP antibodies reported with DMARD use (7%). Thus, a total of 1,029 women were considered to have probable RA. The remainder of the sample probably had osteoarthritis, the authors suggested.
The mortality analysis further considered the timing of RA onset by whether it was reported at baseline or during follow-up.
During the 10-year study period, 13% of the group died, including 14% of those with RA at baseline and follow-up, 16% of those with RA only at baseline, and 10% of those who reported it only at follow-up. The median times to death were 8 years for those with baseline RA, 7 years for those with baseline and follow-up RA, and 6 years for those with RA at follow-up.
Women with anti-CCP antibodies had the highest age-adjusted death rate (19 per 1,000 person-years), followed by those who did not have anti-CCP antibodies but were taking DMARDs (18 per 1,000 person-years) and those who probably did not have RA (no antibodies and no DMARDS; 10 per 1,000 person-years).
ANA positivity occurred in 16% of the women, but two-thirds of them were negative for anti-CCP and rheumatoid factor and "therefore probably did not have clinical RA." Age-adjusted death rates were lower for ANA-positive women than for anti-CCP–positive and rheumatoid factor–positive women and were not higher for anti-CPP–positive women with or without rheumatoid factor, or for anti-CPP–negative women with rheumatoid factor. This suggested to the investigators that "anti-CCP positivity rather than rheumatoid factor positivity was the correlate of increased death rates."
Mortality was similar for those using DMARDs and those not using them, and for the use of methotrexate, compared with other DMARDs.
There were no between-group differences in causes of death, which were most frequently cardiovascular disease and cancers. Smoking, diabetes, less physical activity, poor overall health, and a history of coronary heart disease all increased the death rate among those with anti-CCP antibodies. About a quarter of those with the antibodies reported poor health status, with a death rate four times higher than those who probably didn’t have RA and who also said they had excellent health.
Joint pain in the 4 weeks before the baseline interview was another indicator of mortality. Among all antibody-positive women, those who reported severe pain were twice as likely to die during the follow-up as were those who reported no pain or mild pain. Additionally, among all women with severe joint pain, the death rates were significantly higher for those with the antibodies (35.5 per 1,000 person-years) than for those who reported RA but were antibody negative (17.2 per 1,000 person-years), those who reported arthritis but not RA (12.1 per 1,000 person-years), and those who reported no arthritis (11.4 per 1,000 person-years).
In a multivariate, age-adjusted model, anti-CCP–positive women using DMARDs were almost three times more likely to die (hazard ratio [HR], 2.8) than were women without RA. The risk was also significantly elevated in anti-CCP–positive women who weren’t taking DMARDs (HR, 2.2) and for those who were anti-CCP–negative but who used DMARDs (HR, 1.8).
The study was funded by the National Heart, Lung, and Blood Institute. No financial disclosures were listed.
Postmenopausal women with rheumatoid arthritis were almost three times more likely to die over a 10-year period than were those who did not have the disease in a subanalysis of participants in the Women’s Health Initiative study.
Using stored serum from Women’s Health Initiative (WHI) subjects, investigators found that the increased risk was mostly attributable to women with anti-cyclic citrullinated peptide (anti-CCP) antibodies – a marker used to identify those in the sample who probably had true rheumatoid arthritis (RA). This finding stayed significant even when the analysis controlled for the use of disease-modifying antirheumatic drugs (DMARDs), and also in several models that controlled for health and lifestyle risk factors, Dr. Lewis H. Kuller and his colleagues reported in Arthritis & Rheumatism.
"The increased risk of death for anti-CCP positive women was not explained by age, rheumatoid factor positivity, ANA [antinuclear antibody] positivity, or DMARD use," wrote Dr. Kuller of the University of Pittsburgh and his coauthors (Arthritis Rheum. 2014 Dec. 23 [doi:10.1002/art.38268]).
"Traditional risk factors (e.g., smoking, diabetes), kidney disease, joint pain, health status or [white blood cell] count also did not statistically explain the increased risk for anti-CCP-positivity, despite their independent associations with higher mortality," they said.
The study focused on 9,988 women from the WHI, all of whom self-reported having RA at baseline or at follow-up visits. To further refine the sample, the investigators defined probable RA as the presence of anti-CCP antibodies, with or without the use of DMARDs (8% of the sample), or the absence of anti-CCP antibodies reported with DMARD use (7%). Thus, a total of 1,029 women were considered to have probable RA. The remainder of the sample probably had osteoarthritis, the authors suggested.
The mortality analysis further considered the timing of RA onset by whether it was reported at baseline or during follow-up.
During the 10-year study period, 13% of the group died, including 14% of those with RA at baseline and follow-up, 16% of those with RA only at baseline, and 10% of those who reported it only at follow-up. The median times to death were 8 years for those with baseline RA, 7 years for those with baseline and follow-up RA, and 6 years for those with RA at follow-up.
Women with anti-CCP antibodies had the highest age-adjusted death rate (19 per 1,000 person-years), followed by those who did not have anti-CCP antibodies but were taking DMARDs (18 per 1,000 person-years) and those who probably did not have RA (no antibodies and no DMARDS; 10 per 1,000 person-years).
ANA positivity occurred in 16% of the women, but two-thirds of them were negative for anti-CCP and rheumatoid factor and "therefore probably did not have clinical RA." Age-adjusted death rates were lower for ANA-positive women than for anti-CCP–positive and rheumatoid factor–positive women and were not higher for anti-CPP–positive women with or without rheumatoid factor, or for anti-CPP–negative women with rheumatoid factor. This suggested to the investigators that "anti-CCP positivity rather than rheumatoid factor positivity was the correlate of increased death rates."
Mortality was similar for those using DMARDs and those not using them, and for the use of methotrexate, compared with other DMARDs.
There were no between-group differences in causes of death, which were most frequently cardiovascular disease and cancers. Smoking, diabetes, less physical activity, poor overall health, and a history of coronary heart disease all increased the death rate among those with anti-CCP antibodies. About a quarter of those with the antibodies reported poor health status, with a death rate four times higher than those who probably didn’t have RA and who also said they had excellent health.
Joint pain in the 4 weeks before the baseline interview was another indicator of mortality. Among all antibody-positive women, those who reported severe pain were twice as likely to die during the follow-up as were those who reported no pain or mild pain. Additionally, among all women with severe joint pain, the death rates were significantly higher for those with the antibodies (35.5 per 1,000 person-years) than for those who reported RA but were antibody negative (17.2 per 1,000 person-years), those who reported arthritis but not RA (12.1 per 1,000 person-years), and those who reported no arthritis (11.4 per 1,000 person-years).
In a multivariate, age-adjusted model, anti-CCP–positive women using DMARDs were almost three times more likely to die (hazard ratio [HR], 2.8) than were women without RA. The risk was also significantly elevated in anti-CCP–positive women who weren’t taking DMARDs (HR, 2.2) and for those who were anti-CCP–negative but who used DMARDs (HR, 1.8).
The study was funded by the National Heart, Lung, and Blood Institute. No financial disclosures were listed.
Postmenopausal women with rheumatoid arthritis were almost three times more likely to die over a 10-year period than were those who did not have the disease in a subanalysis of participants in the Women’s Health Initiative study.
Using stored serum from Women’s Health Initiative (WHI) subjects, investigators found that the increased risk was mostly attributable to women with anti-cyclic citrullinated peptide (anti-CCP) antibodies – a marker used to identify those in the sample who probably had true rheumatoid arthritis (RA). This finding stayed significant even when the analysis controlled for the use of disease-modifying antirheumatic drugs (DMARDs), and also in several models that controlled for health and lifestyle risk factors, Dr. Lewis H. Kuller and his colleagues reported in Arthritis & Rheumatism.
"The increased risk of death for anti-CCP positive women was not explained by age, rheumatoid factor positivity, ANA [antinuclear antibody] positivity, or DMARD use," wrote Dr. Kuller of the University of Pittsburgh and his coauthors (Arthritis Rheum. 2014 Dec. 23 [doi:10.1002/art.38268]).
"Traditional risk factors (e.g., smoking, diabetes), kidney disease, joint pain, health status or [white blood cell] count also did not statistically explain the increased risk for anti-CCP-positivity, despite their independent associations with higher mortality," they said.
The study focused on 9,988 women from the WHI, all of whom self-reported having RA at baseline or at follow-up visits. To further refine the sample, the investigators defined probable RA as the presence of anti-CCP antibodies, with or without the use of DMARDs (8% of the sample), or the absence of anti-CCP antibodies reported with DMARD use (7%). Thus, a total of 1,029 women were considered to have probable RA. The remainder of the sample probably had osteoarthritis, the authors suggested.
The mortality analysis further considered the timing of RA onset by whether it was reported at baseline or during follow-up.
During the 10-year study period, 13% of the group died, including 14% of those with RA at baseline and follow-up, 16% of those with RA only at baseline, and 10% of those who reported it only at follow-up. The median times to death were 8 years for those with baseline RA, 7 years for those with baseline and follow-up RA, and 6 years for those with RA at follow-up.
Women with anti-CCP antibodies had the highest age-adjusted death rate (19 per 1,000 person-years), followed by those who did not have anti-CCP antibodies but were taking DMARDs (18 per 1,000 person-years) and those who probably did not have RA (no antibodies and no DMARDS; 10 per 1,000 person-years).
ANA positivity occurred in 16% of the women, but two-thirds of them were negative for anti-CCP and rheumatoid factor and "therefore probably did not have clinical RA." Age-adjusted death rates were lower for ANA-positive women than for anti-CCP–positive and rheumatoid factor–positive women and were not higher for anti-CPP–positive women with or without rheumatoid factor, or for anti-CPP–negative women with rheumatoid factor. This suggested to the investigators that "anti-CCP positivity rather than rheumatoid factor positivity was the correlate of increased death rates."
Mortality was similar for those using DMARDs and those not using them, and for the use of methotrexate, compared with other DMARDs.
There were no between-group differences in causes of death, which were most frequently cardiovascular disease and cancers. Smoking, diabetes, less physical activity, poor overall health, and a history of coronary heart disease all increased the death rate among those with anti-CCP antibodies. About a quarter of those with the antibodies reported poor health status, with a death rate four times higher than those who probably didn’t have RA and who also said they had excellent health.
Joint pain in the 4 weeks before the baseline interview was another indicator of mortality. Among all antibody-positive women, those who reported severe pain were twice as likely to die during the follow-up as were those who reported no pain or mild pain. Additionally, among all women with severe joint pain, the death rates were significantly higher for those with the antibodies (35.5 per 1,000 person-years) than for those who reported RA but were antibody negative (17.2 per 1,000 person-years), those who reported arthritis but not RA (12.1 per 1,000 person-years), and those who reported no arthritis (11.4 per 1,000 person-years).
In a multivariate, age-adjusted model, anti-CCP–positive women using DMARDs were almost three times more likely to die (hazard ratio [HR], 2.8) than were women without RA. The risk was also significantly elevated in anti-CCP–positive women who weren’t taking DMARDs (HR, 2.2) and for those who were anti-CCP–negative but who used DMARDs (HR, 1.8).
The study was funded by the National Heart, Lung, and Blood Institute. No financial disclosures were listed.
FROM ARTHRITIS & RHEUMATISM
Major finding: Anti-CCP–positive women using DMARDs were almost three times more likely to die (hazard ratio, 2.8) than were women without RA in a multivariate, age-adjusted model.
Data source: The study involved 9,988 women who had been in the Women’s Health Initiative and reported RA at baseline or at follow-up visits.
Disclosures: The study was sponsored by the National Heart, Lung, and Blood Institutes. No financial disclosures were listed.

Newly recognized autoantibody found in blood sera years before RA diagnosis
Anti-carbamylated protein antibodies, a recently identified autoantibody system against carbamylated proteins, can be detected years before symptoms develop in rheumatoid arthritis, according to a retrospective study.
The finding suggests "another source of antibodies which can potentially contribute to RA pathogenesis. ... The moment of first appearance of anti-CarP [anti-carbamylated protein] antibodies is comparable with ACPA [anti-citrullinated protein antibodies] and earlier than IgM-RF [IgM-rheumatoid factor]," both now included in American College of Rheumatology/European League Against Rheumatism RA criteria, said senior author Dr. Leendert A. Trouw and lead author Jing Shi, Ph.D., of the department of rheumatology at Leiden (the Netherlands) University Medical Center and their colleagues.

Identifying people who could benefit most from early RA intervention "is a challenge, but the presence of autoantibodies could be a useful marker," the investigators said (Ann. Rheum. Dis. 2013 Dec. 13 [doi:10.1136/annrheumdis-2013-204154]).
Anti-CarP antibodies presented in both ACPA-positive and ACPA-negative patients; they "appear by and large [to be] two different autoantibody systems," the investigators said.
The authors tested years of blood samples from 79 donors in the Sanquin Blood Bank – the Dutch national blood bank – who were eventually diagnosed with RA, for the presence of anti-carbamylated-fetal calf serum (anti-Ca-FCS), anti-carbamylated-fibrinogen (anti-Ca-Fib), anticyclic citrullinated-peptide 2 (anti-CCP2) antibodies, and IgM-RF, all by enzyme-linked immunosorbent assay. Levels were considered elevated if they were two standard deviations above the mean of 141 age and sex-matched controls who did not develop RA. The subjects were white, with a median of five sequential sera obtained from blood samples 1-6 years apart. The future-RA group included 48 women; the mean age at diagnosis was 51 years.
Six years before diagnosis, more than half of the future-RA patients harbored one autoantibody, and at least 30% had all three autoantibody families within 4 years of diagnosis. Median levels of autoantibodies started to increase around 5-7 years before the diagnosis.
"IgM-RF, anti-Ca-FCS, anti-Ca-Fib and anti-CCP2 antibodies were [first] detectable [at] 10, 14, 14, and 14 years before diagnosis, respectively. These are the time points when the first samples of these donors were collected. The median of time points when anti-CCP2, anti-Ca-FCS, anti-Ca-Fib antibodies and IgM-RF were detectable were 6, 5, 7, and 2 years before the diagnosis," the investigators found.
Anti-Ca-FCS antibodies were present in 27% and anti-Ca-Fib antibodies in 38% of patients at their last blood draw, which came at a mean of 1.4 years before diagnosis.
Although "anti-CCP antibodies or IgM-RF can be found in both patients and their healthy first-degree relatives, the combination of both anti-CCP and RF is predominantly found in the RA patients. This supports the notion that ACPA and anti-CarP antibodies may initiate the primary target recognition but that amplification of IgM-RF is important for progression towards clinical RA, for example, by enhancing complement activation," they wrote.
The study was funded by the Dutch Arthritis Foundation, the Netherlands Organisation for Scientific Research, Masterswitch project FP7, the Innovative Medicines Initiative Joint Undertaking funded project BeTheCure (through a Pfizer contract), and the Netherlands Proteomics Center and the Center for Medical Systems Biology (as part of the Netherlands Genomics Initiative). Dr. Trouw is supported by a Janssen Biologics fellowship.
Anti-carbamylated protein antibodies, a recently identified autoantibody system against carbamylated proteins, can be detected years before symptoms develop in rheumatoid arthritis, according to a retrospective study.
The finding suggests "another source of antibodies which can potentially contribute to RA pathogenesis. ... The moment of first appearance of anti-CarP [anti-carbamylated protein] antibodies is comparable with ACPA [anti-citrullinated protein antibodies] and earlier than IgM-RF [IgM-rheumatoid factor]," both now included in American College of Rheumatology/European League Against Rheumatism RA criteria, said senior author Dr. Leendert A. Trouw and lead author Jing Shi, Ph.D., of the department of rheumatology at Leiden (the Netherlands) University Medical Center and their colleagues.
Identifying people who could benefit most from early RA intervention "is a challenge, but the presence of autoantibodies could be a useful marker," the investigators said (Ann. Rheum. Dis. 2013 Dec. 13 [doi:10.1136/annrheumdis-2013-204154]).
Anti-CarP antibodies presented in both ACPA-positive and ACPA-negative patients; they "appear by and large [to be] two different autoantibody systems," the investigators said.
The authors tested years of blood samples from 79 donors in the Sanquin Blood Bank – the Dutch national blood bank – who were eventually diagnosed with RA, for the presence of anti-carbamylated-fetal calf serum (anti-Ca-FCS), anti-carbamylated-fibrinogen (anti-Ca-Fib), anticyclic citrullinated-peptide 2 (anti-CCP2) antibodies, and IgM-RF, all by enzyme-linked immunosorbent assay. Levels were considered elevated if they were two standard deviations above the mean of 141 age and sex-matched controls who did not develop RA. The subjects were white, with a median of five sequential sera obtained from blood samples 1-6 years apart. The future-RA group included 48 women; the mean age at diagnosis was 51 years.
Six years before diagnosis, more than half of the future-RA patients harbored one autoantibody, and at least 30% had all three autoantibody families within 4 years of diagnosis. Median levels of autoantibodies started to increase around 5-7 years before the diagnosis.
"IgM-RF, anti-Ca-FCS, anti-Ca-Fib and anti-CCP2 antibodies were [first] detectable [at] 10, 14, 14, and 14 years before diagnosis, respectively. These are the time points when the first samples of these donors were collected. The median of time points when anti-CCP2, anti-Ca-FCS, anti-Ca-Fib antibodies and IgM-RF were detectable were 6, 5, 7, and 2 years before the diagnosis," the investigators found.
Anti-Ca-FCS antibodies were present in 27% and anti-Ca-Fib antibodies in 38% of patients at their last blood draw, which came at a mean of 1.4 years before diagnosis.
Although "anti-CCP antibodies or IgM-RF can be found in both patients and their healthy first-degree relatives, the combination of both anti-CCP and RF is predominantly found in the RA patients. This supports the notion that ACPA and anti-CarP antibodies may initiate the primary target recognition but that amplification of IgM-RF is important for progression towards clinical RA, for example, by enhancing complement activation," they wrote.
The study was funded by the Dutch Arthritis Foundation, the Netherlands Organisation for Scientific Research, Masterswitch project FP7, the Innovative Medicines Initiative Joint Undertaking funded project BeTheCure (through a Pfizer contract), and the Netherlands Proteomics Center and the Center for Medical Systems Biology (as part of the Netherlands Genomics Initiative). Dr. Trouw is supported by a Janssen Biologics fellowship.
Anti-carbamylated protein antibodies, a recently identified autoantibody system against carbamylated proteins, can be detected years before symptoms develop in rheumatoid arthritis, according to a retrospective study.
The finding suggests "another source of antibodies which can potentially contribute to RA pathogenesis. ... The moment of first appearance of anti-CarP [anti-carbamylated protein] antibodies is comparable with ACPA [anti-citrullinated protein antibodies] and earlier than IgM-RF [IgM-rheumatoid factor]," both now included in American College of Rheumatology/European League Against Rheumatism RA criteria, said senior author Dr. Leendert A. Trouw and lead author Jing Shi, Ph.D., of the department of rheumatology at Leiden (the Netherlands) University Medical Center and their colleagues.
Identifying people who could benefit most from early RA intervention "is a challenge, but the presence of autoantibodies could be a useful marker," the investigators said (Ann. Rheum. Dis. 2013 Dec. 13 [doi:10.1136/annrheumdis-2013-204154]).
Anti-CarP antibodies presented in both ACPA-positive and ACPA-negative patients; they "appear by and large [to be] two different autoantibody systems," the investigators said.
The authors tested years of blood samples from 79 donors in the Sanquin Blood Bank – the Dutch national blood bank – who were eventually diagnosed with RA, for the presence of anti-carbamylated-fetal calf serum (anti-Ca-FCS), anti-carbamylated-fibrinogen (anti-Ca-Fib), anticyclic citrullinated-peptide 2 (anti-CCP2) antibodies, and IgM-RF, all by enzyme-linked immunosorbent assay. Levels were considered elevated if they were two standard deviations above the mean of 141 age and sex-matched controls who did not develop RA. The subjects were white, with a median of five sequential sera obtained from blood samples 1-6 years apart. The future-RA group included 48 women; the mean age at diagnosis was 51 years.
Six years before diagnosis, more than half of the future-RA patients harbored one autoantibody, and at least 30% had all three autoantibody families within 4 years of diagnosis. Median levels of autoantibodies started to increase around 5-7 years before the diagnosis.
"IgM-RF, anti-Ca-FCS, anti-Ca-Fib and anti-CCP2 antibodies were [first] detectable [at] 10, 14, 14, and 14 years before diagnosis, respectively. These are the time points when the first samples of these donors were collected. The median of time points when anti-CCP2, anti-Ca-FCS, anti-Ca-Fib antibodies and IgM-RF were detectable were 6, 5, 7, and 2 years before the diagnosis," the investigators found.
Anti-Ca-FCS antibodies were present in 27% and anti-Ca-Fib antibodies in 38% of patients at their last blood draw, which came at a mean of 1.4 years before diagnosis.
Although "anti-CCP antibodies or IgM-RF can be found in both patients and their healthy first-degree relatives, the combination of both anti-CCP and RF is predominantly found in the RA patients. This supports the notion that ACPA and anti-CarP antibodies may initiate the primary target recognition but that amplification of IgM-RF is important for progression towards clinical RA, for example, by enhancing complement activation," they wrote.
The study was funded by the Dutch Arthritis Foundation, the Netherlands Organisation for Scientific Research, Masterswitch project FP7, the Innovative Medicines Initiative Joint Undertaking funded project BeTheCure (through a Pfizer contract), and the Netherlands Proteomics Center and the Center for Medical Systems Biology (as part of the Netherlands Genomics Initiative). Dr. Trouw is supported by a Janssen Biologics fellowship.
FROM ANNALS OF THE RHEUMATIC DISEASES
Major finding: Anti-carbamylated protein antibodies are present in about a third of patients a mean of 1.4 years before rheumatoid arthritis diagnosis.
Data Source: Retrospective study of blood samples from 79 patients before they were diagnosed with RA.
Disclosures: The study was funded by the Dutch Arthritis Foundation, the Netherlands Organisation for Scientific Research, Masterswitch project FP7, the Innovative Medicines Initiative Joint Undertaking funded project BeTheCure (through a Pfizer contract), and the Netherlands Proteomics Center and the Center for Medical Systems Biology (as part of the Netherlands Genomics Initiative). Dr. Trouw is supported by a Janssen Biologics fellowship.

Best cost savings seen with RA treatment aimed at fastest remission
A treat-to-target strategy for treating early rheumatoid arthritis yielded better patient outcomes and long-term cost savings than did usual care for patients in the multicenter Dutch Rheumatoid Arthritis Monitoring registry.
"Treat-to-target" refers to a treatment regime whose goal is to reach and maintain remission in patients as quickly as possible using regular monitoring of disease activity and a fixed protocol for adjusting medication.
"After 2 years of treatment, treat-to-target is cost-effective as it comes with higher costs but also with substantially higher effectiveness," reported Marloes Vermeer, a PhD student at the University of Twente in Enschede, the Netherlands, and her colleagues in (BMC Musculoskelet. Disord. 2013 Dec. 13 [doi:10.1186/1471-2474-14-350]). "Our study suggests that treating to the target of remission is the preferred strategy over usual care in early rheumatoid arthritis," they wrote.
The researchers used the incremental cost-effectiveness ratio (ICER) and the incremental cost-utility ratio (ICUR) to analyze costs after determining the participants’ volume of care and the cost for each volume of consumption, based on the Dutch Guideline for Cost Analyses and the Dutch Board of Health Insurances. The ICER, found in this study to be 3,591 euros (about US $4,900), represents the costs per one more patient in remission while the ICUR, found to be 19,410 euros (US $26,530) in this study, represents the costs per quality-adjusted life-year (QALY) gained. For both the second and third years of follow-up, the treat-to-target strategy was dominant.
The researchers followed two cohorts of rheumatoid arthritis patients from initial diagnosis through at least 2 years of follow-up at 11 centers participating in the Dutch Rheumatoid Arthritis Monitoring registry (DREAM). Both the target-to-treat and usual care groups had been diagnosed according to American College of Rheumatology 1987 classification criteria with symptoms for less than a year and no past treatment with disease-modifying antirheumatic drugs (DMARDs). Comparable age, sex, rheumatoid factor positivity, number of tender joints, and erythrocyte sedimentation rate characteristics existed among both groups.
The treat-to-target cohort, initially composed of 261 patients diagnosed between January 2006 and February 2009, involved initial treatment with methotrexate monotherapy and then sulfasalazine, which was replaced with antitumor necrosis factor (TNF) agents if disease activity continued. Remission was defined as a Disease Activity Score in 28 joints (DAS28) of less than 2.6, after which medication was not changed until remission had been sustained for at least 6 months. After 6 months of remission, medication use was gradually discontinued. After clinic visits every 1-3 months for the first year, patients were assessed every 3 months in the second and third years.
In the usual care group, initially composed of 213 patients diagnosed between January 2000 and February 2009, DAS28 was assessed every 3 months by rheumatology nurses but not usually provided to the treating rheumatologist. Medication regimes were determined without a set protocol by the rheumatologist, most frequently involving "step-up or sequential monotherapy with conventional DMARDs and/or biologic, notably anti-TNF."
Among the patients in the treat-to-target cohort, 64.4% of 261 patients were in remission after 2 years, and 59.8% of 127 patients were in remission after 3 years (P less than .001). Among the patients in the usual care cohort, 34.7% of 213 patients were in remission after 2 years, and 35% of 180 patients were in remission after 3 years (P less than .001). The median QALYs in both the second and third years were higher for the treat-to-target cohort, rising from 1.45 in the second year (compared with 1.39 in the usual care group, P = .04) to 2.19 in the third year (compared with 2.04 in the usual care group, P = .05).
Direct costs per patient after 2 years were initially greater in the treat-to-target group, at 4,791 per patient, than in the usual care group, costing 3,727 euros per patient, a difference driven primarily by hospitalization and anti-TNF therapy costs. The treat-to-target group included 21.5% of patients receiving anti-TNF therapy over the first 2 years, with a mean time of 58 weeks until the first anti-TNF agent was started. Meanwhile, 15% of the usual care group received anti-TNF therapy over the first 2 years, with a mean time of 80 weeks until the first anti-TNF agent was started.
By the third year of follow-up, however, the 6,872 euro costs per patient in the usual care group exceeded the 6,410 euro costs per patient in the treat-to-target group, a difference driven primarily by hospitalization costs. The treat-to-target strategy was determined to be dominant in both the second and third years of follow-up.
Ms. Vermeer and her colleagues wrote that they expected cost savings with the treat-to-target regime to continue increasing over the long term, with better, earlier disease control also allowing for work participation and productivity within society and overall improved quality of life for patients. "Our expectation is that the extra effort and time spent in the first years of the disease ultimately result in a reduction of the number of consultations later in the disease course and the possibility of tapering and discontinuing medication in case of sustained remission, thereby diminishing costs," they wrote.
An unrestricted grant from Abbott in the Netherlands funded the study. The authors reported no disclosures.
A treat-to-target strategy for treating early rheumatoid arthritis yielded better patient outcomes and long-term cost savings than did usual care for patients in the multicenter Dutch Rheumatoid Arthritis Monitoring registry.
"Treat-to-target" refers to a treatment regime whose goal is to reach and maintain remission in patients as quickly as possible using regular monitoring of disease activity and a fixed protocol for adjusting medication.
"After 2 years of treatment, treat-to-target is cost-effective as it comes with higher costs but also with substantially higher effectiveness," reported Marloes Vermeer, a PhD student at the University of Twente in Enschede, the Netherlands, and her colleagues in (BMC Musculoskelet. Disord. 2013 Dec. 13 [doi:10.1186/1471-2474-14-350]). "Our study suggests that treating to the target of remission is the preferred strategy over usual care in early rheumatoid arthritis," they wrote.
The researchers used the incremental cost-effectiveness ratio (ICER) and the incremental cost-utility ratio (ICUR) to analyze costs after determining the participants’ volume of care and the cost for each volume of consumption, based on the Dutch Guideline for Cost Analyses and the Dutch Board of Health Insurances. The ICER, found in this study to be 3,591 euros (about US $4,900), represents the costs per one more patient in remission while the ICUR, found to be 19,410 euros (US $26,530) in this study, represents the costs per quality-adjusted life-year (QALY) gained. For both the second and third years of follow-up, the treat-to-target strategy was dominant.
The researchers followed two cohorts of rheumatoid arthritis patients from initial diagnosis through at least 2 years of follow-up at 11 centers participating in the Dutch Rheumatoid Arthritis Monitoring registry (DREAM). Both the target-to-treat and usual care groups had been diagnosed according to American College of Rheumatology 1987 classification criteria with symptoms for less than a year and no past treatment with disease-modifying antirheumatic drugs (DMARDs). Comparable age, sex, rheumatoid factor positivity, number of tender joints, and erythrocyte sedimentation rate characteristics existed among both groups.
The treat-to-target cohort, initially composed of 261 patients diagnosed between January 2006 and February 2009, involved initial treatment with methotrexate monotherapy and then sulfasalazine, which was replaced with antitumor necrosis factor (TNF) agents if disease activity continued. Remission was defined as a Disease Activity Score in 28 joints (DAS28) of less than 2.6, after which medication was not changed until remission had been sustained for at least 6 months. After 6 months of remission, medication use was gradually discontinued. After clinic visits every 1-3 months for the first year, patients were assessed every 3 months in the second and third years.
In the usual care group, initially composed of 213 patients diagnosed between January 2000 and February 2009, DAS28 was assessed every 3 months by rheumatology nurses but not usually provided to the treating rheumatologist. Medication regimes were determined without a set protocol by the rheumatologist, most frequently involving "step-up or sequential monotherapy with conventional DMARDs and/or biologic, notably anti-TNF."
Among the patients in the treat-to-target cohort, 64.4% of 261 patients were in remission after 2 years, and 59.8% of 127 patients were in remission after 3 years (P less than .001). Among the patients in the usual care cohort, 34.7% of 213 patients were in remission after 2 years, and 35% of 180 patients were in remission after 3 years (P less than .001). The median QALYs in both the second and third years were higher for the treat-to-target cohort, rising from 1.45 in the second year (compared with 1.39 in the usual care group, P = .04) to 2.19 in the third year (compared with 2.04 in the usual care group, P = .05).
Direct costs per patient after 2 years were initially greater in the treat-to-target group, at 4,791 per patient, than in the usual care group, costing 3,727 euros per patient, a difference driven primarily by hospitalization and anti-TNF therapy costs. The treat-to-target group included 21.5% of patients receiving anti-TNF therapy over the first 2 years, with a mean time of 58 weeks until the first anti-TNF agent was started. Meanwhile, 15% of the usual care group received anti-TNF therapy over the first 2 years, with a mean time of 80 weeks until the first anti-TNF agent was started.
By the third year of follow-up, however, the 6,872 euro costs per patient in the usual care group exceeded the 6,410 euro costs per patient in the treat-to-target group, a difference driven primarily by hospitalization costs. The treat-to-target strategy was determined to be dominant in both the second and third years of follow-up.
Ms. Vermeer and her colleagues wrote that they expected cost savings with the treat-to-target regime to continue increasing over the long term, with better, earlier disease control also allowing for work participation and productivity within society and overall improved quality of life for patients. "Our expectation is that the extra effort and time spent in the first years of the disease ultimately result in a reduction of the number of consultations later in the disease course and the possibility of tapering and discontinuing medication in case of sustained remission, thereby diminishing costs," they wrote.
An unrestricted grant from Abbott in the Netherlands funded the study. The authors reported no disclosures.
A treat-to-target strategy for treating early rheumatoid arthritis yielded better patient outcomes and long-term cost savings than did usual care for patients in the multicenter Dutch Rheumatoid Arthritis Monitoring registry.
"Treat-to-target" refers to a treatment regime whose goal is to reach and maintain remission in patients as quickly as possible using regular monitoring of disease activity and a fixed protocol for adjusting medication.
"After 2 years of treatment, treat-to-target is cost-effective as it comes with higher costs but also with substantially higher effectiveness," reported Marloes Vermeer, a PhD student at the University of Twente in Enschede, the Netherlands, and her colleagues in (BMC Musculoskelet. Disord. 2013 Dec. 13 [doi:10.1186/1471-2474-14-350]). "Our study suggests that treating to the target of remission is the preferred strategy over usual care in early rheumatoid arthritis," they wrote.
The researchers used the incremental cost-effectiveness ratio (ICER) and the incremental cost-utility ratio (ICUR) to analyze costs after determining the participants’ volume of care and the cost for each volume of consumption, based on the Dutch Guideline for Cost Analyses and the Dutch Board of Health Insurances. The ICER, found in this study to be 3,591 euros (about US $4,900), represents the costs per one more patient in remission while the ICUR, found to be 19,410 euros (US $26,530) in this study, represents the costs per quality-adjusted life-year (QALY) gained. For both the second and third years of follow-up, the treat-to-target strategy was dominant.
The researchers followed two cohorts of rheumatoid arthritis patients from initial diagnosis through at least 2 years of follow-up at 11 centers participating in the Dutch Rheumatoid Arthritis Monitoring registry (DREAM). Both the target-to-treat and usual care groups had been diagnosed according to American College of Rheumatology 1987 classification criteria with symptoms for less than a year and no past treatment with disease-modifying antirheumatic drugs (DMARDs). Comparable age, sex, rheumatoid factor positivity, number of tender joints, and erythrocyte sedimentation rate characteristics existed among both groups.
The treat-to-target cohort, initially composed of 261 patients diagnosed between January 2006 and February 2009, involved initial treatment with methotrexate monotherapy and then sulfasalazine, which was replaced with antitumor necrosis factor (TNF) agents if disease activity continued. Remission was defined as a Disease Activity Score in 28 joints (DAS28) of less than 2.6, after which medication was not changed until remission had been sustained for at least 6 months. After 6 months of remission, medication use was gradually discontinued. After clinic visits every 1-3 months for the first year, patients were assessed every 3 months in the second and third years.
In the usual care group, initially composed of 213 patients diagnosed between January 2000 and February 2009, DAS28 was assessed every 3 months by rheumatology nurses but not usually provided to the treating rheumatologist. Medication regimes were determined without a set protocol by the rheumatologist, most frequently involving "step-up or sequential monotherapy with conventional DMARDs and/or biologic, notably anti-TNF."
Among the patients in the treat-to-target cohort, 64.4% of 261 patients were in remission after 2 years, and 59.8% of 127 patients were in remission after 3 years (P less than .001). Among the patients in the usual care cohort, 34.7% of 213 patients were in remission after 2 years, and 35% of 180 patients were in remission after 3 years (P less than .001). The median QALYs in both the second and third years were higher for the treat-to-target cohort, rising from 1.45 in the second year (compared with 1.39 in the usual care group, P = .04) to 2.19 in the third year (compared with 2.04 in the usual care group, P = .05).
Direct costs per patient after 2 years were initially greater in the treat-to-target group, at 4,791 per patient, than in the usual care group, costing 3,727 euros per patient, a difference driven primarily by hospitalization and anti-TNF therapy costs. The treat-to-target group included 21.5% of patients receiving anti-TNF therapy over the first 2 years, with a mean time of 58 weeks until the first anti-TNF agent was started. Meanwhile, 15% of the usual care group received anti-TNF therapy over the first 2 years, with a mean time of 80 weeks until the first anti-TNF agent was started.
By the third year of follow-up, however, the 6,872 euro costs per patient in the usual care group exceeded the 6,410 euro costs per patient in the treat-to-target group, a difference driven primarily by hospitalization costs. The treat-to-target strategy was determined to be dominant in both the second and third years of follow-up.
Ms. Vermeer and her colleagues wrote that they expected cost savings with the treat-to-target regime to continue increasing over the long term, with better, earlier disease control also allowing for work participation and productivity within society and overall improved quality of life for patients. "Our expectation is that the extra effort and time spent in the first years of the disease ultimately result in a reduction of the number of consultations later in the disease course and the possibility of tapering and discontinuing medication in case of sustained remission, thereby diminishing costs," they wrote.
An unrestricted grant from Abbott in the Netherlands funded the study. The authors reported no disclosures.
FROM BMC MUSCULOSKELETAL DISORDERS
Major Finding: A treat-to-target regime for early rheumatoid arthritis costs 4,791 euros per patient after 2 years and 6,410 euros per patient after 3 years with remission rates of 64.4% and 59.8%, respectively, compared with a usual care regime’s cost of 3,727 euros after 2 years and 6,872 euros after 3 years with remission rates of 34.7% and 35%, respectively (P less than .001).
Data Source: The findings are based on 2011 cost prices determined in a prospective comparison of two cohorts of 474 total rheumatoid arthritis patients, diagnosed between 2000 and 2009 and treated at 1 of 11 centers participating in the Dutch Rheumatoid Arthritis Monitoring registry.
Disclosures: An unrestricted grant from Abbott in the Netherlands funded the study. The authors reported no disclosures.
Ultrasound-guided synovial tissue biopsies appear safe, reliable in early arthritis
A minimally invasive, ultrasound-guided biopsy technique safely harvested synovial tissue samples for immunohistochemical analysis and RNA extraction from both large and small joints of patients with inflammatory arthritis of less than 1 year duration in a small, single-center study.
Dr. Stephen Kelly of Mile End Hospital at Barts Health NHS Trust in London and his colleagues collected a median of 14 samples per procedure in 57 patients with a mean age of 50 years who were a part of the Pathobiology of Early Arthritis Cohort, a multicenter consortium that recruits patients in the early stages of arthritis. Clinical diagnoses in the patients included rheumatoid arthritis (40); psoriatic arthritis (6); undifferentiated arthritis (10); and monoarthritis (1). The investigators took tissue from the knee, elbow, and wrist, as well as metacarpal phalangeal and proximal interphalangeal joints (Ann. Rheum. Dis. 2013 Dec. 13 [doi:10.1136/annrheumdis-2013-204603]).
Synovial tissue biopsies are performed to collect RNA, identify tissue damage, and monitor early stages of rheumatoid arthritis and other joint disorders. The procedure is usually done using a blind needle examination – the simplest of biopsy options – or with arthroscopy, which the authors argue is a more complicated procedure and can target only larger joints (which is not a problem with the ultrasound-guided procedure). Although arthroscopy is still the ‘gold standard’ for joint tissue collection, the ability to conduct minimally invasive synovial tissue sampling would benefit research and drug development, as well as potentially assisting diagnosis, classification, and monitoring of treatment.
The investigators recorded no major complications and only mild pain or discomfort in 93 procedures in the patients, including 36 who participated in a follow-up procedure. In addition, 86 of the biopsies (93%) yielded high-quality tissue samples, on par with other ultrasound extraction methods like renal biopsies in which suitable tissue for analysis is obtained in 83%-97% of reported cases.
At a follow-up visit 3-7 days after the procedure, the patients did not have infection, hemarthrosis, deep venous thrombosis, thrombophlebitis, or flare of the underlying disease. A total of 18 patients reported mild arthralgia after the procedure, but this resolved within 24 hours with simple analgesia. Although 36 of the 57 patients initially agreed to a follow-up procedure at 6 months, an additional 18 patients also agreed after the database for this study’s analysis had been closed. These results lend additional validation to the good safety and tolerability findings from an initial proof of concept study in nine patients with established rheumatoid arthritis (Arthritis Res. Ther. 2007;9:R101).
The study was supported by a grant from the Medical Research Council, and Dr. Kelly reported receiving a Clinical Research Fellowship from Arthritis Research UK.
A minimally invasive, ultrasound-guided biopsy technique safely harvested synovial tissue samples for immunohistochemical analysis and RNA extraction from both large and small joints of patients with inflammatory arthritis of less than 1 year duration in a small, single-center study.
Dr. Stephen Kelly of Mile End Hospital at Barts Health NHS Trust in London and his colleagues collected a median of 14 samples per procedure in 57 patients with a mean age of 50 years who were a part of the Pathobiology of Early Arthritis Cohort, a multicenter consortium that recruits patients in the early stages of arthritis. Clinical diagnoses in the patients included rheumatoid arthritis (40); psoriatic arthritis (6); undifferentiated arthritis (10); and monoarthritis (1). The investigators took tissue from the knee, elbow, and wrist, as well as metacarpal phalangeal and proximal interphalangeal joints (Ann. Rheum. Dis. 2013 Dec. 13 [doi:10.1136/annrheumdis-2013-204603]).
Synovial tissue biopsies are performed to collect RNA, identify tissue damage, and monitor early stages of rheumatoid arthritis and other joint disorders. The procedure is usually done using a blind needle examination – the simplest of biopsy options – or with arthroscopy, which the authors argue is a more complicated procedure and can target only larger joints (which is not a problem with the ultrasound-guided procedure). Although arthroscopy is still the ‘gold standard’ for joint tissue collection, the ability to conduct minimally invasive synovial tissue sampling would benefit research and drug development, as well as potentially assisting diagnosis, classification, and monitoring of treatment.
The investigators recorded no major complications and only mild pain or discomfort in 93 procedures in the patients, including 36 who participated in a follow-up procedure. In addition, 86 of the biopsies (93%) yielded high-quality tissue samples, on par with other ultrasound extraction methods like renal biopsies in which suitable tissue for analysis is obtained in 83%-97% of reported cases.
At a follow-up visit 3-7 days after the procedure, the patients did not have infection, hemarthrosis, deep venous thrombosis, thrombophlebitis, or flare of the underlying disease. A total of 18 patients reported mild arthralgia after the procedure, but this resolved within 24 hours with simple analgesia. Although 36 of the 57 patients initially agreed to a follow-up procedure at 6 months, an additional 18 patients also agreed after the database for this study’s analysis had been closed. These results lend additional validation to the good safety and tolerability findings from an initial proof of concept study in nine patients with established rheumatoid arthritis (Arthritis Res. Ther. 2007;9:R101).
The study was supported by a grant from the Medical Research Council, and Dr. Kelly reported receiving a Clinical Research Fellowship from Arthritis Research UK.
A minimally invasive, ultrasound-guided biopsy technique safely harvested synovial tissue samples for immunohistochemical analysis and RNA extraction from both large and small joints of patients with inflammatory arthritis of less than 1 year duration in a small, single-center study.
Dr. Stephen Kelly of Mile End Hospital at Barts Health NHS Trust in London and his colleagues collected a median of 14 samples per procedure in 57 patients with a mean age of 50 years who were a part of the Pathobiology of Early Arthritis Cohort, a multicenter consortium that recruits patients in the early stages of arthritis. Clinical diagnoses in the patients included rheumatoid arthritis (40); psoriatic arthritis (6); undifferentiated arthritis (10); and monoarthritis (1). The investigators took tissue from the knee, elbow, and wrist, as well as metacarpal phalangeal and proximal interphalangeal joints (Ann. Rheum. Dis. 2013 Dec. 13 [doi:10.1136/annrheumdis-2013-204603]).
Synovial tissue biopsies are performed to collect RNA, identify tissue damage, and monitor early stages of rheumatoid arthritis and other joint disorders. The procedure is usually done using a blind needle examination – the simplest of biopsy options – or with arthroscopy, which the authors argue is a more complicated procedure and can target only larger joints (which is not a problem with the ultrasound-guided procedure). Although arthroscopy is still the ‘gold standard’ for joint tissue collection, the ability to conduct minimally invasive synovial tissue sampling would benefit research and drug development, as well as potentially assisting diagnosis, classification, and monitoring of treatment.
The investigators recorded no major complications and only mild pain or discomfort in 93 procedures in the patients, including 36 who participated in a follow-up procedure. In addition, 86 of the biopsies (93%) yielded high-quality tissue samples, on par with other ultrasound extraction methods like renal biopsies in which suitable tissue for analysis is obtained in 83%-97% of reported cases.
At a follow-up visit 3-7 days after the procedure, the patients did not have infection, hemarthrosis, deep venous thrombosis, thrombophlebitis, or flare of the underlying disease. A total of 18 patients reported mild arthralgia after the procedure, but this resolved within 24 hours with simple analgesia. Although 36 of the 57 patients initially agreed to a follow-up procedure at 6 months, an additional 18 patients also agreed after the database for this study’s analysis had been closed. These results lend additional validation to the good safety and tolerability findings from an initial proof of concept study in nine patients with established rheumatoid arthritis (Arthritis Res. Ther. 2007;9:R101).
The study was supported by a grant from the Medical Research Council, and Dr. Kelly reported receiving a Clinical Research Fellowship from Arthritis Research UK.
FROM ANNALS OF THE RHEUMATIC DISEASES
Major finding: A total of 93% of ultrasound-guided tissue biopsies resulted in high-quality tissue samples, and a median of 14 biopsy samples were obtained from each procedure without significant complications following the procedure.
Data source: A single-center study of 57 patients with early arthritis in the Pathobiology of Early Arthritis Cohort.
Disclosures: The study was supported by a grant from the Medical Research Council, and Dr. Kelly reported receiving a Clinical Research Fellowship from Arthritis Research UK.
RA patients’ mood, anxiety, and physical disability improved over past 20 years
Psychological distress and physical disability have decreased in patients with rheumatoid arthritis over the past 2 decades, at least partly because of reduced disease activity with earlier and more intensive treatment and shifting recommendations for physical activity, according to an analysis of 1,151 Dutch patients who were monitored at diagnosis and after 3-5 years of treatment during 1990-2011.
Although prior studies have found this trend for improvement for shorter time periods, they had few cross-sectional cohorts and did not examine recent years, said Cécile L. Overman and colleagues at Utrecht (the Netherlands) University and Utrecht University Medical Center.
The investigators assembled the study cohort from a median of 47 patients older than 16 years with a duration of rheumatoid arthritis of less than 1 year who presented each year during 1990-2001 to rheumatology departments across the Netherlands. The patients originally had consented to participate in one of several prospective trials comparing the effectiveness of different drug treatment strategies, including strategies that were conventional at the time.
The rate of depressed mood among patients at the time of diagnosis declined from 43% in 1990-1994 to 32% in 2004-2008, and the corresponding rate at follow-up declined from 25% to 14%. For anxiety, the rate at the time of diagnosis shifted from 34% to 21% and at follow-up changed from 23% to 12%. Physical disability rates at diagnosis decreased from 64% to 60% and at follow-up from 53% to 31% (Arthritis Care Res. 2013 Dec. 3 [doi:10.1002/acr.22211]).
Across the 21 years of the study, there were small, but statistically significant decreases in depressed mood and physical disability and a moderate decline in anxiety. During treatment, these changes were not significant for depressed mood but were significant, yet small for anxiety and moderate to large for physical disability. After time trends were accounted for, measurements associated with decreased disease activity at the time of diagnosis and at follow-up declined over the course of the study, and partly mediated declines in depressed mood, anxiety, and physical disability. Changes in patient composition over time, such as earlier diagnosis over the years as reflected by a decreasing age at the time of diagnosis, increases in education level, and increases in socioeconomic status and life expectancy, were not consistently associated with depressed mood or anxiety or physical disability at diagnosis or follow-up.
"Across the decades, especially the trend of progressively decreasing physical disability after the first years of treatment was noteworthy, and this favorable trend remained significant after having taken account of the reduction of disease activity and change in the composition of patient influx," wrote Ms. Overman, a PhD candidate in the department of clinical and health psychology at the university, and her associates.
The investigators noted that it is impossible to know whether the changes in patient composition played a causal role in affecting psychological distress and physical disability or "only reflect a historic change occurring simultaneously, affecting the improvements statistically but not in real life."
They also suggested that improvements in psychological distress and physical disability might be related not only to pharmacologic reduction of disease activity but also targeted nonpharmacologic therapies such as exercise therapy and cognitive-behavioral therapy as well as "the changed education by rheumatologists and health professionals enhancing physical activity and encouraging patients to live a valued life."
Biologic agents’ inhibition of proinflammatory cytokines and their potential effects on behavior also could have contributed to a reduction in psychological distress and physical disability "not fully explained by reduced disease activity," according to the investigators.
The study was funded by a grant from the Faculty of Social and Behavioral Sciences of Utrecht University and by unrestricted grants from the Dutch Arthritis Foundation. The authors reported no relevant financial conflicts.
Psychological distress and physical disability have decreased in patients with rheumatoid arthritis over the past 2 decades, at least partly because of reduced disease activity with earlier and more intensive treatment and shifting recommendations for physical activity, according to an analysis of 1,151 Dutch patients who were monitored at diagnosis and after 3-5 years of treatment during 1990-2011.
Although prior studies have found this trend for improvement for shorter time periods, they had few cross-sectional cohorts and did not examine recent years, said Cécile L. Overman and colleagues at Utrecht (the Netherlands) University and Utrecht University Medical Center.
The investigators assembled the study cohort from a median of 47 patients older than 16 years with a duration of rheumatoid arthritis of less than 1 year who presented each year during 1990-2001 to rheumatology departments across the Netherlands. The patients originally had consented to participate in one of several prospective trials comparing the effectiveness of different drug treatment strategies, including strategies that were conventional at the time.
The rate of depressed mood among patients at the time of diagnosis declined from 43% in 1990-1994 to 32% in 2004-2008, and the corresponding rate at follow-up declined from 25% to 14%. For anxiety, the rate at the time of diagnosis shifted from 34% to 21% and at follow-up changed from 23% to 12%. Physical disability rates at diagnosis decreased from 64% to 60% and at follow-up from 53% to 31% (Arthritis Care Res. 2013 Dec. 3 [doi:10.1002/acr.22211]).
Across the 21 years of the study, there were small, but statistically significant decreases in depressed mood and physical disability and a moderate decline in anxiety. During treatment, these changes were not significant for depressed mood but were significant, yet small for anxiety and moderate to large for physical disability. After time trends were accounted for, measurements associated with decreased disease activity at the time of diagnosis and at follow-up declined over the course of the study, and partly mediated declines in depressed mood, anxiety, and physical disability. Changes in patient composition over time, such as earlier diagnosis over the years as reflected by a decreasing age at the time of diagnosis, increases in education level, and increases in socioeconomic status and life expectancy, were not consistently associated with depressed mood or anxiety or physical disability at diagnosis or follow-up.
"Across the decades, especially the trend of progressively decreasing physical disability after the first years of treatment was noteworthy, and this favorable trend remained significant after having taken account of the reduction of disease activity and change in the composition of patient influx," wrote Ms. Overman, a PhD candidate in the department of clinical and health psychology at the university, and her associates.
The investigators noted that it is impossible to know whether the changes in patient composition played a causal role in affecting psychological distress and physical disability or "only reflect a historic change occurring simultaneously, affecting the improvements statistically but not in real life."
They also suggested that improvements in psychological distress and physical disability might be related not only to pharmacologic reduction of disease activity but also targeted nonpharmacologic therapies such as exercise therapy and cognitive-behavioral therapy as well as "the changed education by rheumatologists and health professionals enhancing physical activity and encouraging patients to live a valued life."
Biologic agents’ inhibition of proinflammatory cytokines and their potential effects on behavior also could have contributed to a reduction in psychological distress and physical disability "not fully explained by reduced disease activity," according to the investigators.
The study was funded by a grant from the Faculty of Social and Behavioral Sciences of Utrecht University and by unrestricted grants from the Dutch Arthritis Foundation. The authors reported no relevant financial conflicts.
Psychological distress and physical disability have decreased in patients with rheumatoid arthritis over the past 2 decades, at least partly because of reduced disease activity with earlier and more intensive treatment and shifting recommendations for physical activity, according to an analysis of 1,151 Dutch patients who were monitored at diagnosis and after 3-5 years of treatment during 1990-2011.
Although prior studies have found this trend for improvement for shorter time periods, they had few cross-sectional cohorts and did not examine recent years, said Cécile L. Overman and colleagues at Utrecht (the Netherlands) University and Utrecht University Medical Center.
The investigators assembled the study cohort from a median of 47 patients older than 16 years with a duration of rheumatoid arthritis of less than 1 year who presented each year during 1990-2001 to rheumatology departments across the Netherlands. The patients originally had consented to participate in one of several prospective trials comparing the effectiveness of different drug treatment strategies, including strategies that were conventional at the time.
The rate of depressed mood among patients at the time of diagnosis declined from 43% in 1990-1994 to 32% in 2004-2008, and the corresponding rate at follow-up declined from 25% to 14%. For anxiety, the rate at the time of diagnosis shifted from 34% to 21% and at follow-up changed from 23% to 12%. Physical disability rates at diagnosis decreased from 64% to 60% and at follow-up from 53% to 31% (Arthritis Care Res. 2013 Dec. 3 [doi:10.1002/acr.22211]).
Across the 21 years of the study, there were small, but statistically significant decreases in depressed mood and physical disability and a moderate decline in anxiety. During treatment, these changes were not significant for depressed mood but were significant, yet small for anxiety and moderate to large for physical disability. After time trends were accounted for, measurements associated with decreased disease activity at the time of diagnosis and at follow-up declined over the course of the study, and partly mediated declines in depressed mood, anxiety, and physical disability. Changes in patient composition over time, such as earlier diagnosis over the years as reflected by a decreasing age at the time of diagnosis, increases in education level, and increases in socioeconomic status and life expectancy, were not consistently associated with depressed mood or anxiety or physical disability at diagnosis or follow-up.
"Across the decades, especially the trend of progressively decreasing physical disability after the first years of treatment was noteworthy, and this favorable trend remained significant after having taken account of the reduction of disease activity and change in the composition of patient influx," wrote Ms. Overman, a PhD candidate in the department of clinical and health psychology at the university, and her associates.
The investigators noted that it is impossible to know whether the changes in patient composition played a causal role in affecting psychological distress and physical disability or "only reflect a historic change occurring simultaneously, affecting the improvements statistically but not in real life."
They also suggested that improvements in psychological distress and physical disability might be related not only to pharmacologic reduction of disease activity but also targeted nonpharmacologic therapies such as exercise therapy and cognitive-behavioral therapy as well as "the changed education by rheumatologists and health professionals enhancing physical activity and encouraging patients to live a valued life."
Biologic agents’ inhibition of proinflammatory cytokines and their potential effects on behavior also could have contributed to a reduction in psychological distress and physical disability "not fully explained by reduced disease activity," according to the investigators.
The study was funded by a grant from the Faculty of Social and Behavioral Sciences of Utrecht University and by unrestricted grants from the Dutch Arthritis Foundation. The authors reported no relevant financial conflicts.
FROM ARTHRITIS CARE & RESEARCH
Major finding: Physical disability rates at diagnosis decreased from 64% to 60% in 1990-1994 and at follow-up from 53% to 31% in 2004-2008.
Data source: A cross-sectional study of 1,151 patients in the Utrecht Rheumatoid Arthritis Cohort from 1990 to 2011.
Disclosures: The study was funded by a grant from the Faculty of Social and Behavioral Sciences of Utrecht University and by unrestricted grants from the Dutch Arthritis Foundation. The authors reported no relevant financial conflicts.
Investigational interleukin-6 receptor inhibitor for RA shows efficacy, safety
Sarilumab, an investigational fully human monoclonal antibody against interleukin-6 receptor alpha, proved to have good safety and efficacy for methotrexate-nonresponsive rheumatoid arthritis patients with doses given every 2 weeks in a multicenter, phase II dose-ranging study.
The dosing regimens that appeared to have the best balance between efficacy and safety – 150 mg every 2 weeks and 200 mg every 2 weeks – gave American College of Rheumatology 20 (ACR 20) response rates of 67% and 65%, and as with other biologic drugs, had nonserious infections as the most common adverse events, reported Dr. Tom Huizinga of Leiden (the Netherlands) University Medical Center and his associates.

Sarilumab at those doses also was associated with neutropenia and increases in liver function tests and serum lipids, which are similar to laboratory changes observed with tocilizumab (Actemra), a humanized monoclonal antibody directed against interleukin-6 (IL-6) receptor alpha. Tocilizumab has been approved in the United States for the treatment of adults with moderately to severely active rheumatoid arthritis (RA) who have had an inadequate response to one or more disease-modifying antirheumatic drugs.
IL-6 activity is a target for the treatment of rheumatoid arthritis because of the cytokine’s role in driving inflammation and its elevation in the serum and synovial fluid of patients with RA.
Patients in the trial, dubbed SARIL-RA-MOBILITY Part A, had active RA for at least 3 months despite methotrexate treatment for a minimum of 12 weeks on a stable dose (10-25 mg/wk) for at least 6 weeks prior to the screening visit. Participants’ mean age was 52 years (range, 18-75 years), and 79% were women. They continued on methotrexate after being randomized to one of five subcutaneous sarilumab dosing arms or placebo for 12 weeks of treatment plus 6 weeks of posttreatment follow-up.
Of the five active treatment arms in the double-blind, placebo-controlled trial of 306 patients – 100 mg every 2 weeks, 150 mg every 2 weeks, 200 mg every 2 weeks, 100 mg every week, and 150 mg every week – only 100 mg every 2 weeks was ineffective, with an ACR 20 response seen in 49% of patients, compared with 46% of patients who received placebo. The ACR 20 responses in the other sarilumab regimens ranged from 62% at 100 mg every week to 72% at 150 mg every week (Ann. Rheum. Dis. 2013 Dec. 2 [doi: 10.1136/annrheumdis-2013-204405]).
Secondary endpoints in the trial also showed that the lowest dose of sarilumab was ineffective in comparison with placebo, according to ACR 50 and ACR 70 responses, changes from baseline in individual disease activity measures (swollen joint count, tender joint count, physician and patient global assessment of disease activity, patient’s pain score, C-reactive protein levels, and Health Assessment Questionnaire score), as well as Disease Activity Score in 28 joints (DAS28-CRP).
For most of those measures, the doses of 150 mg every 2 weeks and 200 mg every 2 weeks gave results similar to those of two higher doses in terms of statistically significant improvement compared with placebo. In some cases, the responses seen with sarilumab at 200 mg every 2 weeks were numerically similar to or greater than those observed with the highest dose.
"These data, taken together with the more convenient dosing interval, support [biweekly] dosing as optimal for sarilumab when dosed at 150 mg and 200 mg," the investigators wrote.
The investigators were unsure why the placebo arm had such a high ACR 20 response rate (46%), but they noted that investigators in the CHARISMA trial involving tocilizumab suggested that "extending the time period during which patients received stable methotrexate prior to trial entry may reduce the high placebo rate."
Of the 24 patient discontinuations that were due to treatment-emergent adverse events, 22 were a result of neutropenia (as mandated by protocol) and 2 were due to infection (1 Escherichia coli urinary tract infection and 1 herpes zoster infection). Infection rates with sarilumab did not appear to be associated with neutropenia.
All of the efficacious dosing arms increased alanine aminotransferase levels during the dosing period, rising to three to five times the upper limit of normal in seven patients and from 5 to 10 times the upper limit of normal in four patients, most of which resolved on treatment or at the end of the study. Similar rates of increase in aspartate transferase levels were seen with sarilumab treatment.
Increases in the mean total cholesterol level at week 12 ranged from 9% to 21% in the four efficacious treatment arms, compared with 5% in the placebo group.
The trial was funded by Sanofi and Regeneron Pharmaceuticals, which are developing sarilumab. Three investigators reported financial ties to Sanofi and/or Regeneron and other manufacturers of drugs for RA, and the rest are employees and/or shareholders of Sanofi or Regeneron or were during the conduct of the study.
Sarilumab, an investigational fully human monoclonal antibody against interleukin-6 receptor alpha, proved to have good safety and efficacy for methotrexate-nonresponsive rheumatoid arthritis patients with doses given every 2 weeks in a multicenter, phase II dose-ranging study.
The dosing regimens that appeared to have the best balance between efficacy and safety – 150 mg every 2 weeks and 200 mg every 2 weeks – gave American College of Rheumatology 20 (ACR 20) response rates of 67% and 65%, and as with other biologic drugs, had nonserious infections as the most common adverse events, reported Dr. Tom Huizinga of Leiden (the Netherlands) University Medical Center and his associates.
Sarilumab at those doses also was associated with neutropenia and increases in liver function tests and serum lipids, which are similar to laboratory changes observed with tocilizumab (Actemra), a humanized monoclonal antibody directed against interleukin-6 (IL-6) receptor alpha. Tocilizumab has been approved in the United States for the treatment of adults with moderately to severely active rheumatoid arthritis (RA) who have had an inadequate response to one or more disease-modifying antirheumatic drugs.
IL-6 activity is a target for the treatment of rheumatoid arthritis because of the cytokine’s role in driving inflammation and its elevation in the serum and synovial fluid of patients with RA.
Patients in the trial, dubbed SARIL-RA-MOBILITY Part A, had active RA for at least 3 months despite methotrexate treatment for a minimum of 12 weeks on a stable dose (10-25 mg/wk) for at least 6 weeks prior to the screening visit. Participants’ mean age was 52 years (range, 18-75 years), and 79% were women. They continued on methotrexate after being randomized to one of five subcutaneous sarilumab dosing arms or placebo for 12 weeks of treatment plus 6 weeks of posttreatment follow-up.
Of the five active treatment arms in the double-blind, placebo-controlled trial of 306 patients – 100 mg every 2 weeks, 150 mg every 2 weeks, 200 mg every 2 weeks, 100 mg every week, and 150 mg every week – only 100 mg every 2 weeks was ineffective, with an ACR 20 response seen in 49% of patients, compared with 46% of patients who received placebo. The ACR 20 responses in the other sarilumab regimens ranged from 62% at 100 mg every week to 72% at 150 mg every week (Ann. Rheum. Dis. 2013 Dec. 2 [doi: 10.1136/annrheumdis-2013-204405]).
Secondary endpoints in the trial also showed that the lowest dose of sarilumab was ineffective in comparison with placebo, according to ACR 50 and ACR 70 responses, changes from baseline in individual disease activity measures (swollen joint count, tender joint count, physician and patient global assessment of disease activity, patient’s pain score, C-reactive protein levels, and Health Assessment Questionnaire score), as well as Disease Activity Score in 28 joints (DAS28-CRP).
For most of those measures, the doses of 150 mg every 2 weeks and 200 mg every 2 weeks gave results similar to those of two higher doses in terms of statistically significant improvement compared with placebo. In some cases, the responses seen with sarilumab at 200 mg every 2 weeks were numerically similar to or greater than those observed with the highest dose.
"These data, taken together with the more convenient dosing interval, support [biweekly] dosing as optimal for sarilumab when dosed at 150 mg and 200 mg," the investigators wrote.
The investigators were unsure why the placebo arm had such a high ACR 20 response rate (46%), but they noted that investigators in the CHARISMA trial involving tocilizumab suggested that "extending the time period during which patients received stable methotrexate prior to trial entry may reduce the high placebo rate."
Of the 24 patient discontinuations that were due to treatment-emergent adverse events, 22 were a result of neutropenia (as mandated by protocol) and 2 were due to infection (1 Escherichia coli urinary tract infection and 1 herpes zoster infection). Infection rates with sarilumab did not appear to be associated with neutropenia.
All of the efficacious dosing arms increased alanine aminotransferase levels during the dosing period, rising to three to five times the upper limit of normal in seven patients and from 5 to 10 times the upper limit of normal in four patients, most of which resolved on treatment or at the end of the study. Similar rates of increase in aspartate transferase levels were seen with sarilumab treatment.
Increases in the mean total cholesterol level at week 12 ranged from 9% to 21% in the four efficacious treatment arms, compared with 5% in the placebo group.
The trial was funded by Sanofi and Regeneron Pharmaceuticals, which are developing sarilumab. Three investigators reported financial ties to Sanofi and/or Regeneron and other manufacturers of drugs for RA, and the rest are employees and/or shareholders of Sanofi or Regeneron or were during the conduct of the study.
Sarilumab, an investigational fully human monoclonal antibody against interleukin-6 receptor alpha, proved to have good safety and efficacy for methotrexate-nonresponsive rheumatoid arthritis patients with doses given every 2 weeks in a multicenter, phase II dose-ranging study.
The dosing regimens that appeared to have the best balance between efficacy and safety – 150 mg every 2 weeks and 200 mg every 2 weeks – gave American College of Rheumatology 20 (ACR 20) response rates of 67% and 65%, and as with other biologic drugs, had nonserious infections as the most common adverse events, reported Dr. Tom Huizinga of Leiden (the Netherlands) University Medical Center and his associates.
Sarilumab at those doses also was associated with neutropenia and increases in liver function tests and serum lipids, which are similar to laboratory changes observed with tocilizumab (Actemra), a humanized monoclonal antibody directed against interleukin-6 (IL-6) receptor alpha. Tocilizumab has been approved in the United States for the treatment of adults with moderately to severely active rheumatoid arthritis (RA) who have had an inadequate response to one or more disease-modifying antirheumatic drugs.
IL-6 activity is a target for the treatment of rheumatoid arthritis because of the cytokine’s role in driving inflammation and its elevation in the serum and synovial fluid of patients with RA.
Patients in the trial, dubbed SARIL-RA-MOBILITY Part A, had active RA for at least 3 months despite methotrexate treatment for a minimum of 12 weeks on a stable dose (10-25 mg/wk) for at least 6 weeks prior to the screening visit. Participants’ mean age was 52 years (range, 18-75 years), and 79% were women. They continued on methotrexate after being randomized to one of five subcutaneous sarilumab dosing arms or placebo for 12 weeks of treatment plus 6 weeks of posttreatment follow-up.
Of the five active treatment arms in the double-blind, placebo-controlled trial of 306 patients – 100 mg every 2 weeks, 150 mg every 2 weeks, 200 mg every 2 weeks, 100 mg every week, and 150 mg every week – only 100 mg every 2 weeks was ineffective, with an ACR 20 response seen in 49% of patients, compared with 46% of patients who received placebo. The ACR 20 responses in the other sarilumab regimens ranged from 62% at 100 mg every week to 72% at 150 mg every week (Ann. Rheum. Dis. 2013 Dec. 2 [doi: 10.1136/annrheumdis-2013-204405]).
Secondary endpoints in the trial also showed that the lowest dose of sarilumab was ineffective in comparison with placebo, according to ACR 50 and ACR 70 responses, changes from baseline in individual disease activity measures (swollen joint count, tender joint count, physician and patient global assessment of disease activity, patient’s pain score, C-reactive protein levels, and Health Assessment Questionnaire score), as well as Disease Activity Score in 28 joints (DAS28-CRP).
For most of those measures, the doses of 150 mg every 2 weeks and 200 mg every 2 weeks gave results similar to those of two higher doses in terms of statistically significant improvement compared with placebo. In some cases, the responses seen with sarilumab at 200 mg every 2 weeks were numerically similar to or greater than those observed with the highest dose.
"These data, taken together with the more convenient dosing interval, support [biweekly] dosing as optimal for sarilumab when dosed at 150 mg and 200 mg," the investigators wrote.
The investigators were unsure why the placebo arm had such a high ACR 20 response rate (46%), but they noted that investigators in the CHARISMA trial involving tocilizumab suggested that "extending the time period during which patients received stable methotrexate prior to trial entry may reduce the high placebo rate."
Of the 24 patient discontinuations that were due to treatment-emergent adverse events, 22 were a result of neutropenia (as mandated by protocol) and 2 were due to infection (1 Escherichia coli urinary tract infection and 1 herpes zoster infection). Infection rates with sarilumab did not appear to be associated with neutropenia.
All of the efficacious dosing arms increased alanine aminotransferase levels during the dosing period, rising to three to five times the upper limit of normal in seven patients and from 5 to 10 times the upper limit of normal in four patients, most of which resolved on treatment or at the end of the study. Similar rates of increase in aspartate transferase levels were seen with sarilumab treatment.
Increases in the mean total cholesterol level at week 12 ranged from 9% to 21% in the four efficacious treatment arms, compared with 5% in the placebo group.
The trial was funded by Sanofi and Regeneron Pharmaceuticals, which are developing sarilumab. Three investigators reported financial ties to Sanofi and/or Regeneron and other manufacturers of drugs for RA, and the rest are employees and/or shareholders of Sanofi or Regeneron or were during the conduct of the study.
FROM ANNALS OF THE RHEUMATIC DISEASES
Major finding: Sarilumab doses of 150 mg every 2 weeks and 200 mg every 2 weeks gave ACR 20 response rates of 67% and 65%, compared with 46% for placebo.
Data source: A phase II, randomized, double-blind, placebo-controlled, multicenter dose-ranging study of 306 patients with active RA for at least 3 months despite methotrexate treatment for a minimum of 12 weeks on a stable dose.
Disclosures: The trial was funded by Sanofi and Regeneron Pharmaceuticals, which are developing sarilumab. Three investigators reported financial ties to Sanofi and/or Regeneron and other manufacturers of drugs for RA, and the rest are employees and/or shareholders of Sanofi or Regeneron or were during the conduct of the study.

Abatacept, anti-TNFs prove comparable after prior anti-TNFs
Outcomes in patients with rheumatoid arthritis and prior exposure to an anti–tumor necrosis factor drug who switched to a new anti-TNF drug were similar to those in patients with prior anti-TNF exposure who initiated abatacept in a comparative effectiveness trial.
The mean changes in Clinical Disease Activity Index (CDAI) scores; modified American College of Rheumatology (mACR) 20, 50, and 70 responses; modified Health Assessment Questionnaire (mHAQ) scores; and remission rates on the CDAI all were similar at 6 and 12 months after treatment initiation in propensity score-matched groups of patients from the large observational cohort study who either switched anti-TNF drugs or initiated abatacept after exposure to an anti-TNF drug, Dr. Leslie R. Harrold of the University of Massachusetts Medical School, Worcester, and her colleagues reported.
For example, at 6 months in 746 anti-TNF users and 431 abatacept users and at 12 months in 493 anti-TNF users and 311 abatacept users, the mean differences in CDAI scores were 0.46 and –1.64, respectively, after adjustment for number of prior anti-TNF medications, baseline disease activity, rheumatoid arthritis disease severity, and concomitant medications. Also, mACR20 responses at 6 months were 28.2% vs. 31.7%.
At 12 months, 35%-37% of patients in the groups achieved mACR20, 20%-22% achieved mACR50, and 10%-12% achieved mACR70. A meaningful change in mHAQ score was achieved by 30%-33% of patients at 6 months and 29%-30% at 12 months. CDAI remission rates were 9%-10% at 6 months and 12%-14% at 12 months, the investigators said (Ann. Rheum. Dis. 2013 Dec. 2 [doi:10.1136/annrheumdis-2013-203936]).
Patients were Consortium of Rheumatology Researchers of North American (CORRONA) registry participants with exposure to one or more anti-TNF agents but no prior use of non-anti-TNF biologics, according to data from Feb. 1, 2000, to Aug. 1, 2011, the investigators said.
The findings of the current analysis, which is among the first to examine comparative effectiveness of abatacept and anti-TNF agents in those with prior anti-TNF agent exposures, suggest that "just changing the mechanism of action may not be enough to improve disease activity," Dr. Harrold and her associates wrote.
"When discussing next therapeutic interventions in those not responding or unable to take their current anti-TNF agents, these results can potentially contribute to the discussion as patients weigh other factors such as potential adverse events associated with the different agents, out-of pocket costs, and medication route of administration," they said.
Additional comparative effectiveness studies are needed to evaluate the potential benefits of switching to a different non-TNF biologic versus anti-TNF intra-class switching in patients who have an inadequate response to an anti-TNF, they concluded.
CORRONA has received support from Abbott, Amgen, Astra-Zeneca, Genentech, Janssen (Centocor), Eli Lilly, and Pfizer through contracted subscriptions to the database. The investigators reported ties with CORRONA, AbbVie, Amgen, Bristol-Myers Squibb, Genentech, Lilly, Pfizer, UCB, Roche, Janssen, Crescendo, UpToDate, Novartis, the National Institutes of Health, the Agency for Healthcare Research and Quality, the Arthritis Foundation, and/or the Arthritis National Research Foundation.
Outcomes in patients with rheumatoid arthritis and prior exposure to an anti–tumor necrosis factor drug who switched to a new anti-TNF drug were similar to those in patients with prior anti-TNF exposure who initiated abatacept in a comparative effectiveness trial.
The mean changes in Clinical Disease Activity Index (CDAI) scores; modified American College of Rheumatology (mACR) 20, 50, and 70 responses; modified Health Assessment Questionnaire (mHAQ) scores; and remission rates on the CDAI all were similar at 6 and 12 months after treatment initiation in propensity score-matched groups of patients from the large observational cohort study who either switched anti-TNF drugs or initiated abatacept after exposure to an anti-TNF drug, Dr. Leslie R. Harrold of the University of Massachusetts Medical School, Worcester, and her colleagues reported.
For example, at 6 months in 746 anti-TNF users and 431 abatacept users and at 12 months in 493 anti-TNF users and 311 abatacept users, the mean differences in CDAI scores were 0.46 and –1.64, respectively, after adjustment for number of prior anti-TNF medications, baseline disease activity, rheumatoid arthritis disease severity, and concomitant medications. Also, mACR20 responses at 6 months were 28.2% vs. 31.7%.
At 12 months, 35%-37% of patients in the groups achieved mACR20, 20%-22% achieved mACR50, and 10%-12% achieved mACR70. A meaningful change in mHAQ score was achieved by 30%-33% of patients at 6 months and 29%-30% at 12 months. CDAI remission rates were 9%-10% at 6 months and 12%-14% at 12 months, the investigators said (Ann. Rheum. Dis. 2013 Dec. 2 [doi:10.1136/annrheumdis-2013-203936]).
Patients were Consortium of Rheumatology Researchers of North American (CORRONA) registry participants with exposure to one or more anti-TNF agents but no prior use of non-anti-TNF biologics, according to data from Feb. 1, 2000, to Aug. 1, 2011, the investigators said.
The findings of the current analysis, which is among the first to examine comparative effectiveness of abatacept and anti-TNF agents in those with prior anti-TNF agent exposures, suggest that "just changing the mechanism of action may not be enough to improve disease activity," Dr. Harrold and her associates wrote.
"When discussing next therapeutic interventions in those not responding or unable to take their current anti-TNF agents, these results can potentially contribute to the discussion as patients weigh other factors such as potential adverse events associated with the different agents, out-of pocket costs, and medication route of administration," they said.
Additional comparative effectiveness studies are needed to evaluate the potential benefits of switching to a different non-TNF biologic versus anti-TNF intra-class switching in patients who have an inadequate response to an anti-TNF, they concluded.
CORRONA has received support from Abbott, Amgen, Astra-Zeneca, Genentech, Janssen (Centocor), Eli Lilly, and Pfizer through contracted subscriptions to the database. The investigators reported ties with CORRONA, AbbVie, Amgen, Bristol-Myers Squibb, Genentech, Lilly, Pfizer, UCB, Roche, Janssen, Crescendo, UpToDate, Novartis, the National Institutes of Health, the Agency for Healthcare Research and Quality, the Arthritis Foundation, and/or the Arthritis National Research Foundation.
Outcomes in patients with rheumatoid arthritis and prior exposure to an anti–tumor necrosis factor drug who switched to a new anti-TNF drug were similar to those in patients with prior anti-TNF exposure who initiated abatacept in a comparative effectiveness trial.
The mean changes in Clinical Disease Activity Index (CDAI) scores; modified American College of Rheumatology (mACR) 20, 50, and 70 responses; modified Health Assessment Questionnaire (mHAQ) scores; and remission rates on the CDAI all were similar at 6 and 12 months after treatment initiation in propensity score-matched groups of patients from the large observational cohort study who either switched anti-TNF drugs or initiated abatacept after exposure to an anti-TNF drug, Dr. Leslie R. Harrold of the University of Massachusetts Medical School, Worcester, and her colleagues reported.
For example, at 6 months in 746 anti-TNF users and 431 abatacept users and at 12 months in 493 anti-TNF users and 311 abatacept users, the mean differences in CDAI scores were 0.46 and –1.64, respectively, after adjustment for number of prior anti-TNF medications, baseline disease activity, rheumatoid arthritis disease severity, and concomitant medications. Also, mACR20 responses at 6 months were 28.2% vs. 31.7%.
At 12 months, 35%-37% of patients in the groups achieved mACR20, 20%-22% achieved mACR50, and 10%-12% achieved mACR70. A meaningful change in mHAQ score was achieved by 30%-33% of patients at 6 months and 29%-30% at 12 months. CDAI remission rates were 9%-10% at 6 months and 12%-14% at 12 months, the investigators said (Ann. Rheum. Dis. 2013 Dec. 2 [doi:10.1136/annrheumdis-2013-203936]).
Patients were Consortium of Rheumatology Researchers of North American (CORRONA) registry participants with exposure to one or more anti-TNF agents but no prior use of non-anti-TNF biologics, according to data from Feb. 1, 2000, to Aug. 1, 2011, the investigators said.
The findings of the current analysis, which is among the first to examine comparative effectiveness of abatacept and anti-TNF agents in those with prior anti-TNF agent exposures, suggest that "just changing the mechanism of action may not be enough to improve disease activity," Dr. Harrold and her associates wrote.
"When discussing next therapeutic interventions in those not responding or unable to take their current anti-TNF agents, these results can potentially contribute to the discussion as patients weigh other factors such as potential adverse events associated with the different agents, out-of pocket costs, and medication route of administration," they said.
Additional comparative effectiveness studies are needed to evaluate the potential benefits of switching to a different non-TNF biologic versus anti-TNF intra-class switching in patients who have an inadequate response to an anti-TNF, they concluded.
CORRONA has received support from Abbott, Amgen, Astra-Zeneca, Genentech, Janssen (Centocor), Eli Lilly, and Pfizer through contracted subscriptions to the database. The investigators reported ties with CORRONA, AbbVie, Amgen, Bristol-Myers Squibb, Genentech, Lilly, Pfizer, UCB, Roche, Janssen, Crescendo, UpToDate, Novartis, the National Institutes of Health, the Agency for Healthcare Research and Quality, the Arthritis Foundation, and/or the Arthritis National Research Foundation.
FROM ANNALS OF THE RHEUMATIC DISEASES
Major finding: At 6 and 12 months, the adjusted mean differences in CDAI for anti-TNF vs. abatacept users were 0.46 and –1.64, respectively.
Data source: A comparative effectiveness study in CORRONA Registry participants.
Disclosures: CORRONA has received support from Abbott, Amgen, Astra-Zeneca, Genentech, Janssen (Centocor), Eli Lilly, and Pfizer through contracted subscriptions to the database. The investigators reported ties with CORRONA, AbbVie, Amgen, Bristol-Myers Squibb, Genentech, Lilly, Pfizer, UCB, Roche, Janssen, Crescendo, UpToDate, Novartis, the National Institutes of Health, the Agency for Healthcare Research and Quality, the Arthritis Foundation, and/or the Arthritis National Research Foundation.
In memoriam: Dr. Kenneth R. Wilske (1935-2013)
Dr. Kenneth R. Wilske, an editorial adviser to Rheumatology News since 2003, died unexpectedly Sept. 17 of a pulmonary embolism while playing golf. He was 78.
Dr. Wilske was a leader in rheumatology in the Pacific Northwest and was a driving force in what he called the "step-down bridge" approach to treating rheumatoid arthritis. He also made important contributions to medicine’s understanding of giant cell arteritis and polymyalgia rheumatica.
Until his retirement in 2004, Dr. Wilske served as the section head of the division of rheumatology at the Virginia Mason Clinic in Seattle, which acknowledged his legacy by creating the Wilske Center for Translational Research. He also was a clinical professor of rheumatology at the University of Washington, Seattle, where he had trained as one of the first fellows in the division of rheumatology in 1962-1964 under Dr. John Decker.

Dr. Wilske remained an important member of the clinical faculty at the university in retirement. "We saw him regularly. He would come not only to rheumatology programs, but he was also a faithful attendee of medical grand rounds at the university. He saw patients with our fellows and attended our clinical conferences, and he was an insightful, very positive force in our program," said Dr. Peter A. Simkin, emeritus professor of medicine in the division of rheumatology at the university.
Dr. Wilske played a key role in building the Benaroya Research Institute (BRI) at Virginia Mason Clinic and served on many of its advisory boards and committees. Until his death, Dr. Wilske continued to work on the board of the BRI, which recognized his legacy after his retirement by establishing the Kenneth R. Wilske Lecture Series in Science and Medicine.
He served terms as president of the Northwest Society for Clinical Research and the Northwest Rheumatism Society and as a member of the Food and Drug Administration Arthritis Advisory Committee.
In 2000, the American College of Rheumatology honored him as a Master of Rheumatology and in the following year gave him its Distinguished Rheumatologist Award.
Dr. Wilske’s step-down bridge approach to the treatment of rheumatoid arthritis "was really a paradigm shift at the time," noted Dr. Jeffrey Carlin, who succeeded him as the section head of the division of rheumatology at Virginia Mason. In their original editorial on the subject, Dr. Wilske and his Virginia Mason colleague, Dr. Louis Andrew Healey, wrote that the step-down bridge concept involves taking advantage of different medication’s abilities and mechanisms of action in suppressing inflammation by "employing a combination of drugs to control inflammation in the critical early stages of RA," so that medications can be "sequentially withdrawn in contrast to the traditional pyramid, in which they have been sequentially added," without any greater problem of toxicity (J. Rheumatol. 1989;16:565-7).
"This concept has now become accepted and a standard approach to the therapy of rheumatoid arthritis and is becoming a paradigm and strategy for therapy for other rheumatic diseases and chronic inflammatory disorders," said Dr. Keith B. Elkon, head of the division of rheumatology at the University of Washington.
Dr. Wilske published 75 articles and abstracts. He was best known for his clinical research in polymyalgia rheumatica and giant cell arteritis, much of which was conducted with Dr. Healey. The two researchers "literally wrote the book on giant cell arteritis and made a lot of important contributions when it was really just first finding its way into the rheumatology panoply of conditions that we deal with," Dr. Simkin said.
Many of Dr. Wilske’s colleagues held in high regard not only his clinical acumen but also his interpersonal abilities. "He had a remarkably well-organized mindset, so that if you wanted a list of complications of any drug or the manifestations of any disease, it was always right on the tip of his tongue – just an excellent clinician," Dr. Simkin said.
"He was the kind of guy who could see a ridiculous number of people in the course of a day but somehow everybody felt as though they got his full attention. And yet he could still find time to have lunch and interact with his colleagues. I don’t know how he did it," Dr. Carlin said.
Dr. Wilske is survived by his wife, three daughters, and three granddaughters.
Dr. Kenneth R. Wilske, an editorial adviser to Rheumatology News since 2003, died unexpectedly Sept. 17 of a pulmonary embolism while playing golf. He was 78.
Dr. Wilske was a leader in rheumatology in the Pacific Northwest and was a driving force in what he called the "step-down bridge" approach to treating rheumatoid arthritis. He also made important contributions to medicine’s understanding of giant cell arteritis and polymyalgia rheumatica.
Until his retirement in 2004, Dr. Wilske served as the section head of the division of rheumatology at the Virginia Mason Clinic in Seattle, which acknowledged his legacy by creating the Wilske Center for Translational Research. He also was a clinical professor of rheumatology at the University of Washington, Seattle, where he had trained as one of the first fellows in the division of rheumatology in 1962-1964 under Dr. John Decker.
Dr. Wilske remained an important member of the clinical faculty at the university in retirement. "We saw him regularly. He would come not only to rheumatology programs, but he was also a faithful attendee of medical grand rounds at the university. He saw patients with our fellows and attended our clinical conferences, and he was an insightful, very positive force in our program," said Dr. Peter A. Simkin, emeritus professor of medicine in the division of rheumatology at the university.
Dr. Wilske played a key role in building the Benaroya Research Institute (BRI) at Virginia Mason Clinic and served on many of its advisory boards and committees. Until his death, Dr. Wilske continued to work on the board of the BRI, which recognized his legacy after his retirement by establishing the Kenneth R. Wilske Lecture Series in Science and Medicine.
He served terms as president of the Northwest Society for Clinical Research and the Northwest Rheumatism Society and as a member of the Food and Drug Administration Arthritis Advisory Committee.
In 2000, the American College of Rheumatology honored him as a Master of Rheumatology and in the following year gave him its Distinguished Rheumatologist Award.
Dr. Wilske’s step-down bridge approach to the treatment of rheumatoid arthritis "was really a paradigm shift at the time," noted Dr. Jeffrey Carlin, who succeeded him as the section head of the division of rheumatology at Virginia Mason. In their original editorial on the subject, Dr. Wilske and his Virginia Mason colleague, Dr. Louis Andrew Healey, wrote that the step-down bridge concept involves taking advantage of different medication’s abilities and mechanisms of action in suppressing inflammation by "employing a combination of drugs to control inflammation in the critical early stages of RA," so that medications can be "sequentially withdrawn in contrast to the traditional pyramid, in which they have been sequentially added," without any greater problem of toxicity (J. Rheumatol. 1989;16:565-7).
"This concept has now become accepted and a standard approach to the therapy of rheumatoid arthritis and is becoming a paradigm and strategy for therapy for other rheumatic diseases and chronic inflammatory disorders," said Dr. Keith B. Elkon, head of the division of rheumatology at the University of Washington.
Dr. Wilske published 75 articles and abstracts. He was best known for his clinical research in polymyalgia rheumatica and giant cell arteritis, much of which was conducted with Dr. Healey. The two researchers "literally wrote the book on giant cell arteritis and made a lot of important contributions when it was really just first finding its way into the rheumatology panoply of conditions that we deal with," Dr. Simkin said.
Many of Dr. Wilske’s colleagues held in high regard not only his clinical acumen but also his interpersonal abilities. "He had a remarkably well-organized mindset, so that if you wanted a list of complications of any drug or the manifestations of any disease, it was always right on the tip of his tongue – just an excellent clinician," Dr. Simkin said.
"He was the kind of guy who could see a ridiculous number of people in the course of a day but somehow everybody felt as though they got his full attention. And yet he could still find time to have lunch and interact with his colleagues. I don’t know how he did it," Dr. Carlin said.
Dr. Wilske is survived by his wife, three daughters, and three granddaughters.
Dr. Kenneth R. Wilske, an editorial adviser to Rheumatology News since 2003, died unexpectedly Sept. 17 of a pulmonary embolism while playing golf. He was 78.
Dr. Wilske was a leader in rheumatology in the Pacific Northwest and was a driving force in what he called the "step-down bridge" approach to treating rheumatoid arthritis. He also made important contributions to medicine’s understanding of giant cell arteritis and polymyalgia rheumatica.
Until his retirement in 2004, Dr. Wilske served as the section head of the division of rheumatology at the Virginia Mason Clinic in Seattle, which acknowledged his legacy by creating the Wilske Center for Translational Research. He also was a clinical professor of rheumatology at the University of Washington, Seattle, where he had trained as one of the first fellows in the division of rheumatology in 1962-1964 under Dr. John Decker.
Dr. Wilske remained an important member of the clinical faculty at the university in retirement. "We saw him regularly. He would come not only to rheumatology programs, but he was also a faithful attendee of medical grand rounds at the university. He saw patients with our fellows and attended our clinical conferences, and he was an insightful, very positive force in our program," said Dr. Peter A. Simkin, emeritus professor of medicine in the division of rheumatology at the university.
Dr. Wilske played a key role in building the Benaroya Research Institute (BRI) at Virginia Mason Clinic and served on many of its advisory boards and committees. Until his death, Dr. Wilske continued to work on the board of the BRI, which recognized his legacy after his retirement by establishing the Kenneth R. Wilske Lecture Series in Science and Medicine.
He served terms as president of the Northwest Society for Clinical Research and the Northwest Rheumatism Society and as a member of the Food and Drug Administration Arthritis Advisory Committee.
In 2000, the American College of Rheumatology honored him as a Master of Rheumatology and in the following year gave him its Distinguished Rheumatologist Award.
Dr. Wilske’s step-down bridge approach to the treatment of rheumatoid arthritis "was really a paradigm shift at the time," noted Dr. Jeffrey Carlin, who succeeded him as the section head of the division of rheumatology at Virginia Mason. In their original editorial on the subject, Dr. Wilske and his Virginia Mason colleague, Dr. Louis Andrew Healey, wrote that the step-down bridge concept involves taking advantage of different medication’s abilities and mechanisms of action in suppressing inflammation by "employing a combination of drugs to control inflammation in the critical early stages of RA," so that medications can be "sequentially withdrawn in contrast to the traditional pyramid, in which they have been sequentially added," without any greater problem of toxicity (J. Rheumatol. 1989;16:565-7).
"This concept has now become accepted and a standard approach to the therapy of rheumatoid arthritis and is becoming a paradigm and strategy for therapy for other rheumatic diseases and chronic inflammatory disorders," said Dr. Keith B. Elkon, head of the division of rheumatology at the University of Washington.
Dr. Wilske published 75 articles and abstracts. He was best known for his clinical research in polymyalgia rheumatica and giant cell arteritis, much of which was conducted with Dr. Healey. The two researchers "literally wrote the book on giant cell arteritis and made a lot of important contributions when it was really just first finding its way into the rheumatology panoply of conditions that we deal with," Dr. Simkin said.
Many of Dr. Wilske’s colleagues held in high regard not only his clinical acumen but also his interpersonal abilities. "He had a remarkably well-organized mindset, so that if you wanted a list of complications of any drug or the manifestations of any disease, it was always right on the tip of his tongue – just an excellent clinician," Dr. Simkin said.
"He was the kind of guy who could see a ridiculous number of people in the course of a day but somehow everybody felt as though they got his full attention. And yet he could still find time to have lunch and interact with his colleagues. I don’t know how he did it," Dr. Carlin said.
Dr. Wilske is survived by his wife, three daughters, and three granddaughters.

Successful anti-TNF therapy may cancel excess coronary risk in RA
SAN DIEGO – Rheumatoid arthritis patients with a good response to tumor necrosis factor inhibitor therapy when assessed roughly 5 months into treatment had an acute coronary syndrome risk during the next 2 years that was no different than that of the matched general population in a large, Swedish national registry study.
"We could see that the risk of acute coronary syndrome in the TNF inhibitor–exposed population was doubled in the first year compared to the general population. But all this increased risk was carried by patients with a moderate or nonresponse to therapy. We saw no difference in risk between the general population and patients with a good response to treatment. My belief is that this benefit is not due to the TNF inhibitor as such, but rather it’s the control of inflammation that is crucial," Dr. Lotta Ljung said at the annual meeting of the American College of Rheumatology.

‘Good response’ was defined in this study via the EULAR response criteria: that is, a greater than 1.2-point improvement in the widely used Disease Activity Score 28 (DAS28) over baseline to a score of 3.2 or less at the 5-month evaluation.
Dr. Ljung, a senior consultant in rheumatology at Umea (Sweden) University Hospital, presented two analyses drawn from the Swedish Biologics Register, a national registry that captures 90% of all Swedes on biologic therapy for rheumatoid arthritis (RA). The study population included 7,704 RA patients with no history of ischemic heart disease when they started on their first TNF inhibitor during 2001-2010. They were matched by age, gender, and location to 23,112 RA patients who never took a biologic agent and to a second matched control group comprised of 38,520 individuals in the general population.
The crude incidence rate of acute coronary syndrome (ACS) in patients actively on TNF inhibitor therapy throughout follow-up was 5.7 events per 1,000 person-years, compared with 8.6 per 1,000 in biologic-naive RA patients and 3.3 per 1,000 in the matched general population.
In a fully adjusted Cox multivariate regression analysis factoring in socioeconomic variables, RA duration, joint surgery, and baseline atherosclerotic disease and other comorbid conditions, patients on anti-TNF therapy had a highly significant 27% reduction in ACS risk, compared with biologic-naive RA patients.
Nonetheless, patients on TNF inhibitor therapy remained at an adjusted 1.5-fold increased risk of ACS, compared with general population controls. However, this was significantly lower than the 2.3-fold elevated risk in biologic-naive RA patients.
In a separate analysis, the investigators took a closer look at the Swedish Biologics Register subgroup of the 4,931 RA patients on anti-TNF therapy for whom EULAR response data 5 months into treatment were available. Thirty-eight percent of these patients had a EULAR good response, 37% had a moderate response, and 25% had no response.
During 2 years of follow-up starting at the time of the EULAR response evaluation, the crude incidence rate of ACS among all TNF inhibitor–exposed RA patients, with close to 8,600 person-years of follow-up, was 6.9 cases per 1,000 person-years, compared with 3.4 per 1,000 among the matched general population controls. In an adjusted multivariate regression analysis, the ACS risk was 1.94-fold greater in moderate responders to anti-TNF therapy than in the general population and 2.53-fold greater in the nonresponders, but not significantly different between good responders and controls.
In addition, patients with an erythrocyte sedimentation rate (ESR) below 20 mm/hour at the time of their EULAR response evaluation had a subsequent 66% lower 1-year risk of ACS than did those with a higher ESR. And patients with a DAS28 remission at the 5-month evaluation – that is, a DAS28 below 2.6 – had a 79% lower ACS risk than did those with a DAS28 of 2.6 or above.
"This is dramatic," Dr. Ljung said in an interview. "I think it’s the first time we see a population in our RA cohorts that doesn’t have any proven cardiovascular risk increase compared with the general population. But it raises additional questions, of course, such as who are these patients who receive the good response: Is it due to factors related to their disease or background that gives them the opportunity to have the good response? We adjusted for a number of factors, but still ..."
She added that these studies contain two key take-home messages for rheumatologists: "I think the first thing for us to do is to treat our patients’ inflammation perfectly using traditional and biologic DMARDs. And the second thing is to be more aware of the traditional risk factors and start modifying those more aggressively for our patients."
The Swedish Biologics Register is funded by the Swedish Rheumatology Association, with support from half a dozen pharmaceutical companies. Dr. Ljung disclosed ties with AbbVie and Bristol-Myers Squibb.
SAN DIEGO – Rheumatoid arthritis patients with a good response to tumor necrosis factor inhibitor therapy when assessed roughly 5 months into treatment had an acute coronary syndrome risk during the next 2 years that was no different than that of the matched general population in a large, Swedish national registry study.
"We could see that the risk of acute coronary syndrome in the TNF inhibitor–exposed population was doubled in the first year compared to the general population. But all this increased risk was carried by patients with a moderate or nonresponse to therapy. We saw no difference in risk between the general population and patients with a good response to treatment. My belief is that this benefit is not due to the TNF inhibitor as such, but rather it’s the control of inflammation that is crucial," Dr. Lotta Ljung said at the annual meeting of the American College of Rheumatology.
‘Good response’ was defined in this study via the EULAR response criteria: that is, a greater than 1.2-point improvement in the widely used Disease Activity Score 28 (DAS28) over baseline to a score of 3.2 or less at the 5-month evaluation.
Dr. Ljung, a senior consultant in rheumatology at Umea (Sweden) University Hospital, presented two analyses drawn from the Swedish Biologics Register, a national registry that captures 90% of all Swedes on biologic therapy for rheumatoid arthritis (RA). The study population included 7,704 RA patients with no history of ischemic heart disease when they started on their first TNF inhibitor during 2001-2010. They were matched by age, gender, and location to 23,112 RA patients who never took a biologic agent and to a second matched control group comprised of 38,520 individuals in the general population.
The crude incidence rate of acute coronary syndrome (ACS) in patients actively on TNF inhibitor therapy throughout follow-up was 5.7 events per 1,000 person-years, compared with 8.6 per 1,000 in biologic-naive RA patients and 3.3 per 1,000 in the matched general population.
In a fully adjusted Cox multivariate regression analysis factoring in socioeconomic variables, RA duration, joint surgery, and baseline atherosclerotic disease and other comorbid conditions, patients on anti-TNF therapy had a highly significant 27% reduction in ACS risk, compared with biologic-naive RA patients.
Nonetheless, patients on TNF inhibitor therapy remained at an adjusted 1.5-fold increased risk of ACS, compared with general population controls. However, this was significantly lower than the 2.3-fold elevated risk in biologic-naive RA patients.
In a separate analysis, the investigators took a closer look at the Swedish Biologics Register subgroup of the 4,931 RA patients on anti-TNF therapy for whom EULAR response data 5 months into treatment were available. Thirty-eight percent of these patients had a EULAR good response, 37% had a moderate response, and 25% had no response.
During 2 years of follow-up starting at the time of the EULAR response evaluation, the crude incidence rate of ACS among all TNF inhibitor–exposed RA patients, with close to 8,600 person-years of follow-up, was 6.9 cases per 1,000 person-years, compared with 3.4 per 1,000 among the matched general population controls. In an adjusted multivariate regression analysis, the ACS risk was 1.94-fold greater in moderate responders to anti-TNF therapy than in the general population and 2.53-fold greater in the nonresponders, but not significantly different between good responders and controls.
In addition, patients with an erythrocyte sedimentation rate (ESR) below 20 mm/hour at the time of their EULAR response evaluation had a subsequent 66% lower 1-year risk of ACS than did those with a higher ESR. And patients with a DAS28 remission at the 5-month evaluation – that is, a DAS28 below 2.6 – had a 79% lower ACS risk than did those with a DAS28 of 2.6 or above.
"This is dramatic," Dr. Ljung said in an interview. "I think it’s the first time we see a population in our RA cohorts that doesn’t have any proven cardiovascular risk increase compared with the general population. But it raises additional questions, of course, such as who are these patients who receive the good response: Is it due to factors related to their disease or background that gives them the opportunity to have the good response? We adjusted for a number of factors, but still ..."
She added that these studies contain two key take-home messages for rheumatologists: "I think the first thing for us to do is to treat our patients’ inflammation perfectly using traditional and biologic DMARDs. And the second thing is to be more aware of the traditional risk factors and start modifying those more aggressively for our patients."
The Swedish Biologics Register is funded by the Swedish Rheumatology Association, with support from half a dozen pharmaceutical companies. Dr. Ljung disclosed ties with AbbVie and Bristol-Myers Squibb.
SAN DIEGO – Rheumatoid arthritis patients with a good response to tumor necrosis factor inhibitor therapy when assessed roughly 5 months into treatment had an acute coronary syndrome risk during the next 2 years that was no different than that of the matched general population in a large, Swedish national registry study.
"We could see that the risk of acute coronary syndrome in the TNF inhibitor–exposed population was doubled in the first year compared to the general population. But all this increased risk was carried by patients with a moderate or nonresponse to therapy. We saw no difference in risk between the general population and patients with a good response to treatment. My belief is that this benefit is not due to the TNF inhibitor as such, but rather it’s the control of inflammation that is crucial," Dr. Lotta Ljung said at the annual meeting of the American College of Rheumatology.
‘Good response’ was defined in this study via the EULAR response criteria: that is, a greater than 1.2-point improvement in the widely used Disease Activity Score 28 (DAS28) over baseline to a score of 3.2 or less at the 5-month evaluation.
Dr. Ljung, a senior consultant in rheumatology at Umea (Sweden) University Hospital, presented two analyses drawn from the Swedish Biologics Register, a national registry that captures 90% of all Swedes on biologic therapy for rheumatoid arthritis (RA). The study population included 7,704 RA patients with no history of ischemic heart disease when they started on their first TNF inhibitor during 2001-2010. They were matched by age, gender, and location to 23,112 RA patients who never took a biologic agent and to a second matched control group comprised of 38,520 individuals in the general population.
The crude incidence rate of acute coronary syndrome (ACS) in patients actively on TNF inhibitor therapy throughout follow-up was 5.7 events per 1,000 person-years, compared with 8.6 per 1,000 in biologic-naive RA patients and 3.3 per 1,000 in the matched general population.
In a fully adjusted Cox multivariate regression analysis factoring in socioeconomic variables, RA duration, joint surgery, and baseline atherosclerotic disease and other comorbid conditions, patients on anti-TNF therapy had a highly significant 27% reduction in ACS risk, compared with biologic-naive RA patients.
Nonetheless, patients on TNF inhibitor therapy remained at an adjusted 1.5-fold increased risk of ACS, compared with general population controls. However, this was significantly lower than the 2.3-fold elevated risk in biologic-naive RA patients.
In a separate analysis, the investigators took a closer look at the Swedish Biologics Register subgroup of the 4,931 RA patients on anti-TNF therapy for whom EULAR response data 5 months into treatment were available. Thirty-eight percent of these patients had a EULAR good response, 37% had a moderate response, and 25% had no response.
During 2 years of follow-up starting at the time of the EULAR response evaluation, the crude incidence rate of ACS among all TNF inhibitor–exposed RA patients, with close to 8,600 person-years of follow-up, was 6.9 cases per 1,000 person-years, compared with 3.4 per 1,000 among the matched general population controls. In an adjusted multivariate regression analysis, the ACS risk was 1.94-fold greater in moderate responders to anti-TNF therapy than in the general population and 2.53-fold greater in the nonresponders, but not significantly different between good responders and controls.
In addition, patients with an erythrocyte sedimentation rate (ESR) below 20 mm/hour at the time of their EULAR response evaluation had a subsequent 66% lower 1-year risk of ACS than did those with a higher ESR. And patients with a DAS28 remission at the 5-month evaluation – that is, a DAS28 below 2.6 – had a 79% lower ACS risk than did those with a DAS28 of 2.6 or above.
"This is dramatic," Dr. Ljung said in an interview. "I think it’s the first time we see a population in our RA cohorts that doesn’t have any proven cardiovascular risk increase compared with the general population. But it raises additional questions, of course, such as who are these patients who receive the good response: Is it due to factors related to their disease or background that gives them the opportunity to have the good response? We adjusted for a number of factors, but still ..."
She added that these studies contain two key take-home messages for rheumatologists: "I think the first thing for us to do is to treat our patients’ inflammation perfectly using traditional and biologic DMARDs. And the second thing is to be more aware of the traditional risk factors and start modifying those more aggressively for our patients."
The Swedish Biologics Register is funded by the Swedish Rheumatology Association, with support from half a dozen pharmaceutical companies. Dr. Ljung disclosed ties with AbbVie and Bristol-Myers Squibb.
AT THE ACR ANNUAL MEETING
Major finding: The acute coronary syndrome risk was 1.94-fold greater in rheumatoid arthritis patients with a moderate response to anti-TNF therapy than in the general population and 2.53-fold greater in those with no response, but not significantly different between controls and good responders (defined by the degree of improvement in the Disease Activity Score 28 when evaluated 5 months into treatment).
Data source: An observational study of 7,704 rheumatoid arthritis patients in the nationwide Swedish Biologics Register who started on a first tumor necrosis factor inhibitor during 2001-2010, together with 23,112 matched biologic-naive rheumatoid arthritis patients and 38,520 matched controls drawn from the general population.
Disclosures: The Swedish Biologics Register is funded by the Swedish Rheumatology Association, with support from half a dozen pharmaceutical companies. The presenter disclosed ties to AbbVie and Bristol-Myers Squibb.

Minimally important differences defined for CDAI for rheumatoid arthritis
SAN DIEGO – The utility of the Clinical Disease Activity Index as a simple, practical tool to quantify rheumatoid arthritis activity in everyday practice has gotten a big boost as a result of formal determination of the absolute change in the index that constitutes a minimally important difference.
"Our hope and expectation is that these MIDs [minimally important differences] for absolute change in CDAI [Clinical Disease Activity Index] can be used to determine whether patients are improving, and to help manage the patients that we see in clinic in terms of what treatments might need to be altered," Dr. Jeffrey R. Curtis explained at the annual meeting of the American College of Rheumatology.
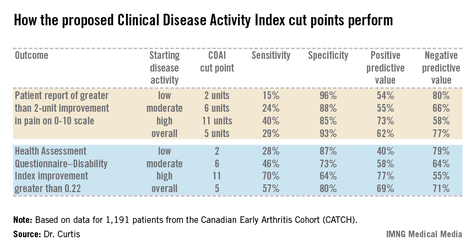
The Disease Activity Score 28 (DAS28) has a widely accepted MID of 1.2 units, making it highly useful in defining a patient’s magnitude of clinical improvement in clinical trial settings. For example, exceeding this MID early after going on tumor necrosis factor inhibitor therapy has been shown to predict high likelihood of low disease activity at 1 year (J. Rheumatol. 2012;39:1326-33). But the DAS28 is impractical except when a real-time measurement of acute phase reactants is available, which is often not the case in everyday practice. The CDAI could be a better option for clinicians who are willing to do a joint count. Until now, however, the MID for the CDAI in real-world settings has not been defined, noted Dr. Curtis of the University of Alabama, Birmingham.
He and his coinvestigators have rectified this situation. They accomplished this by analyzing data from the Canadian Early Arthritis Cohort (CATCH), a large observational cohort of patients with early rheumatoid arthritis. After exclusion of the 8% of CATCH participants with comorbid fibromyalgia, that left 1,191 patients with rheumatologist-diagnosed rheumatoid arthritis, a mean 5.8-month duration of symptoms at enrollment, and a baseline CDAI of 28.5.
The investigators compared changes in DAS28 and CDAI during a total of more than 3,200 pairs of rheumatology patient visits spaced at 3-month intervals during the first 12 months after enrollment.

Overall, the best discriminator between a DAS28 MID indicative of significant clinical improvement as opposed to no improvement or worsening was a CDAI cut point of 5 units. That is, an absolute reduction of more than 5 units on the CDAI correlated well with a DAS28 improvement of at least 1.2 units. Indeed, the area under the receiver operator curve using a CDAI cut point of 5 units was 0.87. But there’s more to the story than that, according to Dr. Curtis.
"If at all possible, it’s preferable to use more specific CDAI MID cut points conditional on where patients are starting in terms of disease activity. Patients need less of a change in order to say that they feel better if they’re already starting out doing pretty well, with low disease activity, than if they’re starting with high disease activity," the rheumatologist said.
The generally accepted CDAI threshold for low disease activity is a score below 10. Moderate disease activity is a score of 10-22, while high disease activity is a CDAI in excess of 22. Dr. Curtis and his coworkers determined that the MID for patients with low disease activity is an absolute difference greater than 2 units. For patients with moderately active disease, it’s greater than 6 units. And for those with high disease activity, an absolute reduction of greater than 11 units defines the MID.
The investigators also tested the utility of their CDAI cut points in comparison to changes in outcomes other than the DAS28, including patient self-reported pain and Health Assessment Questionnaire-Disability Index scores (see chart).
Dr. Curtis reported receiving grants from and serving as a consultant to Amgen and Pfizer, which sponsor the CATCH study. He also receives funding from other companies as well as the National Institutes of Health.
SAN DIEGO – The utility of the Clinical Disease Activity Index as a simple, practical tool to quantify rheumatoid arthritis activity in everyday practice has gotten a big boost as a result of formal determination of the absolute change in the index that constitutes a minimally important difference.
"Our hope and expectation is that these MIDs [minimally important differences] for absolute change in CDAI [Clinical Disease Activity Index] can be used to determine whether patients are improving, and to help manage the patients that we see in clinic in terms of what treatments might need to be altered," Dr. Jeffrey R. Curtis explained at the annual meeting of the American College of Rheumatology.
The Disease Activity Score 28 (DAS28) has a widely accepted MID of 1.2 units, making it highly useful in defining a patient’s magnitude of clinical improvement in clinical trial settings. For example, exceeding this MID early after going on tumor necrosis factor inhibitor therapy has been shown to predict high likelihood of low disease activity at 1 year (J. Rheumatol. 2012;39:1326-33). But the DAS28 is impractical except when a real-time measurement of acute phase reactants is available, which is often not the case in everyday practice. The CDAI could be a better option for clinicians who are willing to do a joint count. Until now, however, the MID for the CDAI in real-world settings has not been defined, noted Dr. Curtis of the University of Alabama, Birmingham.
He and his coinvestigators have rectified this situation. They accomplished this by analyzing data from the Canadian Early Arthritis Cohort (CATCH), a large observational cohort of patients with early rheumatoid arthritis. After exclusion of the 8% of CATCH participants with comorbid fibromyalgia, that left 1,191 patients with rheumatologist-diagnosed rheumatoid arthritis, a mean 5.8-month duration of symptoms at enrollment, and a baseline CDAI of 28.5.
The investigators compared changes in DAS28 and CDAI during a total of more than 3,200 pairs of rheumatology patient visits spaced at 3-month intervals during the first 12 months after enrollment.
Overall, the best discriminator between a DAS28 MID indicative of significant clinical improvement as opposed to no improvement or worsening was a CDAI cut point of 5 units. That is, an absolute reduction of more than 5 units on the CDAI correlated well with a DAS28 improvement of at least 1.2 units. Indeed, the area under the receiver operator curve using a CDAI cut point of 5 units was 0.87. But there’s more to the story than that, according to Dr. Curtis.
"If at all possible, it’s preferable to use more specific CDAI MID cut points conditional on where patients are starting in terms of disease activity. Patients need less of a change in order to say that they feel better if they’re already starting out doing pretty well, with low disease activity, than if they’re starting with high disease activity," the rheumatologist said.
The generally accepted CDAI threshold for low disease activity is a score below 10. Moderate disease activity is a score of 10-22, while high disease activity is a CDAI in excess of 22. Dr. Curtis and his coworkers determined that the MID for patients with low disease activity is an absolute difference greater than 2 units. For patients with moderately active disease, it’s greater than 6 units. And for those with high disease activity, an absolute reduction of greater than 11 units defines the MID.
The investigators also tested the utility of their CDAI cut points in comparison to changes in outcomes other than the DAS28, including patient self-reported pain and Health Assessment Questionnaire-Disability Index scores (see chart).
Dr. Curtis reported receiving grants from and serving as a consultant to Amgen and Pfizer, which sponsor the CATCH study. He also receives funding from other companies as well as the National Institutes of Health.
SAN DIEGO – The utility of the Clinical Disease Activity Index as a simple, practical tool to quantify rheumatoid arthritis activity in everyday practice has gotten a big boost as a result of formal determination of the absolute change in the index that constitutes a minimally important difference.
"Our hope and expectation is that these MIDs [minimally important differences] for absolute change in CDAI [Clinical Disease Activity Index] can be used to determine whether patients are improving, and to help manage the patients that we see in clinic in terms of what treatments might need to be altered," Dr. Jeffrey R. Curtis explained at the annual meeting of the American College of Rheumatology.
The Disease Activity Score 28 (DAS28) has a widely accepted MID of 1.2 units, making it highly useful in defining a patient’s magnitude of clinical improvement in clinical trial settings. For example, exceeding this MID early after going on tumor necrosis factor inhibitor therapy has been shown to predict high likelihood of low disease activity at 1 year (J. Rheumatol. 2012;39:1326-33). But the DAS28 is impractical except when a real-time measurement of acute phase reactants is available, which is often not the case in everyday practice. The CDAI could be a better option for clinicians who are willing to do a joint count. Until now, however, the MID for the CDAI in real-world settings has not been defined, noted Dr. Curtis of the University of Alabama, Birmingham.
He and his coinvestigators have rectified this situation. They accomplished this by analyzing data from the Canadian Early Arthritis Cohort (CATCH), a large observational cohort of patients with early rheumatoid arthritis. After exclusion of the 8% of CATCH participants with comorbid fibromyalgia, that left 1,191 patients with rheumatologist-diagnosed rheumatoid arthritis, a mean 5.8-month duration of symptoms at enrollment, and a baseline CDAI of 28.5.
The investigators compared changes in DAS28 and CDAI during a total of more than 3,200 pairs of rheumatology patient visits spaced at 3-month intervals during the first 12 months after enrollment.
Overall, the best discriminator between a DAS28 MID indicative of significant clinical improvement as opposed to no improvement or worsening was a CDAI cut point of 5 units. That is, an absolute reduction of more than 5 units on the CDAI correlated well with a DAS28 improvement of at least 1.2 units. Indeed, the area under the receiver operator curve using a CDAI cut point of 5 units was 0.87. But there’s more to the story than that, according to Dr. Curtis.
"If at all possible, it’s preferable to use more specific CDAI MID cut points conditional on where patients are starting in terms of disease activity. Patients need less of a change in order to say that they feel better if they’re already starting out doing pretty well, with low disease activity, than if they’re starting with high disease activity," the rheumatologist said.
The generally accepted CDAI threshold for low disease activity is a score below 10. Moderate disease activity is a score of 10-22, while high disease activity is a CDAI in excess of 22. Dr. Curtis and his coworkers determined that the MID for patients with low disease activity is an absolute difference greater than 2 units. For patients with moderately active disease, it’s greater than 6 units. And for those with high disease activity, an absolute reduction of greater than 11 units defines the MID.
The investigators also tested the utility of their CDAI cut points in comparison to changes in outcomes other than the DAS28, including patient self-reported pain and Health Assessment Questionnaire-Disability Index scores (see chart).
Dr. Curtis reported receiving grants from and serving as a consultant to Amgen and Pfizer, which sponsor the CATCH study. He also receives funding from other companies as well as the National Institutes of Health.
AT THE ACR ANNUAL MEETING
Major finding: The minimally important difference on the Clinical Disease Activity Index that defines clinically meaningful improvement in rheumatoid arthritis patients is an absolute reduction greater than 5 units.
Data source: This determination was made by correlating changes in the CDAI and the Disease Activity Score 28 in 1,191 patients with early rheumatoid arthritis in the CATCH cohort.
Disclosures: Dr. Curtis reported receiving grants from and serving as a consultant to Amgen and Pfizer, which sponsor the CATCH study. He also receives funding from other companies as well as the National Institutes of Health.