User login
FDA OKs Subcutaneous Atezolizumab Formulation for Multiple Cancer Indications
Approved indications include non–small cell lung cancer (NSCLC), SCLC, hepatocellular carcinoma, melanoma, and alveolar soft part sarcoma. Specific indications are available with the full prescribing information at Drugs@FDA.
This is the first programmed death–ligand 1 inhibitor to gain approval for subcutaneous administration.
“This approval represents a significant option to improve the patient experience,” Ann Fish-Steagall, RN, Senior Vice President of Patient Services at the LUNGevity Foundation stated in a Genentech press release.
Subcutaneous atezolizumab and hyaluronidase-tqjs was evaluated in the open-label, randomized IMscin001 trial of 371 adult patients with locally advanced or metastatic NSCLC who were not previously exposed to cancer immunotherapy and who had disease progression following treatment with platinum-based chemotherapy. Patients were randomized 2:1 to receive subcutaneous or IV administration until disease progression or unacceptable toxicity.
Atezolizumab exposure, the primary outcome measure of the study, met the lower limit of geometric mean ratio above the prespecified threshold of 0.8 (cycle 1C trough, 1.05; area under the curve for days 0-21, 0.87).
No notable differences were observed in overall response rate, progression-free survival, or overall survival between the two formulations, according to the FDA approval notice.
The confirmed overall response rate was 9% in the subcutaneous arm and 8% intravenous arm.
Adverse events of any grade occurring in at least 10% of patients were fatigue, musculoskeletal pain, cough, dyspnea, and decreased appetite.
The recommended dose for subcutaneous injection is one 15 mL injection, which contains 1875 mg of atezolizumab and 30,000 units of hyaluronidase.
Injections should be administered in the thigh over approximately 7 minutes every 3 weeks. By contrast, IV administration generally takes 30-60 minutes.
A version of this article first appeared on Medscape.com.
Approved indications include non–small cell lung cancer (NSCLC), SCLC, hepatocellular carcinoma, melanoma, and alveolar soft part sarcoma. Specific indications are available with the full prescribing information at Drugs@FDA.
This is the first programmed death–ligand 1 inhibitor to gain approval for subcutaneous administration.
“This approval represents a significant option to improve the patient experience,” Ann Fish-Steagall, RN, Senior Vice President of Patient Services at the LUNGevity Foundation stated in a Genentech press release.
Subcutaneous atezolizumab and hyaluronidase-tqjs was evaluated in the open-label, randomized IMscin001 trial of 371 adult patients with locally advanced or metastatic NSCLC who were not previously exposed to cancer immunotherapy and who had disease progression following treatment with platinum-based chemotherapy. Patients were randomized 2:1 to receive subcutaneous or IV administration until disease progression or unacceptable toxicity.
Atezolizumab exposure, the primary outcome measure of the study, met the lower limit of geometric mean ratio above the prespecified threshold of 0.8 (cycle 1C trough, 1.05; area under the curve for days 0-21, 0.87).
No notable differences were observed in overall response rate, progression-free survival, or overall survival between the two formulations, according to the FDA approval notice.
The confirmed overall response rate was 9% in the subcutaneous arm and 8% intravenous arm.
Adverse events of any grade occurring in at least 10% of patients were fatigue, musculoskeletal pain, cough, dyspnea, and decreased appetite.
The recommended dose for subcutaneous injection is one 15 mL injection, which contains 1875 mg of atezolizumab and 30,000 units of hyaluronidase.
Injections should be administered in the thigh over approximately 7 minutes every 3 weeks. By contrast, IV administration generally takes 30-60 minutes.
A version of this article first appeared on Medscape.com.
Approved indications include non–small cell lung cancer (NSCLC), SCLC, hepatocellular carcinoma, melanoma, and alveolar soft part sarcoma. Specific indications are available with the full prescribing information at Drugs@FDA.
This is the first programmed death–ligand 1 inhibitor to gain approval for subcutaneous administration.
“This approval represents a significant option to improve the patient experience,” Ann Fish-Steagall, RN, Senior Vice President of Patient Services at the LUNGevity Foundation stated in a Genentech press release.
Subcutaneous atezolizumab and hyaluronidase-tqjs was evaluated in the open-label, randomized IMscin001 trial of 371 adult patients with locally advanced or metastatic NSCLC who were not previously exposed to cancer immunotherapy and who had disease progression following treatment with platinum-based chemotherapy. Patients were randomized 2:1 to receive subcutaneous or IV administration until disease progression or unacceptable toxicity.
Atezolizumab exposure, the primary outcome measure of the study, met the lower limit of geometric mean ratio above the prespecified threshold of 0.8 (cycle 1C trough, 1.05; area under the curve for days 0-21, 0.87).
No notable differences were observed in overall response rate, progression-free survival, or overall survival between the two formulations, according to the FDA approval notice.
The confirmed overall response rate was 9% in the subcutaneous arm and 8% intravenous arm.
Adverse events of any grade occurring in at least 10% of patients were fatigue, musculoskeletal pain, cough, dyspnea, and decreased appetite.
The recommended dose for subcutaneous injection is one 15 mL injection, which contains 1875 mg of atezolizumab and 30,000 units of hyaluronidase.
Injections should be administered in the thigh over approximately 7 minutes every 3 weeks. By contrast, IV administration generally takes 30-60 minutes.
A version of this article first appeared on Medscape.com.
Osimertinib/Savolitinib Combo Shows Promise in NSCLC
according to results of the phase 2 FLOWERS study.
Compared with EGFR inhibitor osimertinib alone, the combination demonstrated a clinically meaningful improvement in the objective response rate — the study’s primary endpoint — with a positive trend in progression-free survival and a manageable safety profile.
About 30% patients with EGFR-mutated NSCLC fail to respond well to EGFR–tyrosine kinase inhibitors (TKIs), explained Jin-Ji Yang, MD, with Guangdong Lung Cancer Institute, Guangzhou, China, who reported the study results at the annual meeting of the World Conference on Lung Cancer.
Data suggested that de novo MET amplification occurs in up to 5% patients with treatment-naive, EGFR-mutated advanced NSCLC, and MET overexpression occurs in up to 15% these patients.
Coexistence of EGFR mutation and MET amplification/overexpression reduces sensitivity to EGFR-TKI therapy “and is likely the mechanism for mediating primary resistance to first-line EGFR-TKI monotherapy,” Dr. Yang explained in her presentation.
Osimertinib is a third-generation EGFR-TKI recommended as the first-line treatment for EGFR-mutant advanced NSCLC. Savolitinib is a highly selective MET-TKI which has demonstrated antitumor activity in various cancers with MET alterations.
The FLOWERS study is the first to test whether combining the two agents could improve efficacy and overcome MET-driven primary resistance in these patients.
The phase 2 study enrolled 44 treatment-naive patients with de novo MET-aberrant, EGFR-mutant, stage IIIB-IV NSCLC; 23 were randomly allocated to receive oral osimertinib (80 mg once daily) alone and 21 to receive oral osimertinib (80 mg once daily) plus savolitinib (300 mg twice daily).
At a median follow-up of 8.2 months, the objective response rate was 60.9% with osimertinib monotherapy vs 90.5% with combination therapy. The disease control rate was also better with the combination therapy than with monotherapy (95.2% vs 87%).
Median duration of response (not yet mature) was 8.4 months with monotherapy vs 18.6 months with combination therapy.
Preliminary progression-free survival data also showed a trend in favor of combination therapy over monotherapy (a median of 19.3 vs 9.3 months; hazard ratio, 0.59).
Most treatment-related adverse events were grade 1 or 2, and there were no fatal adverse events.
Treatment-related adverse events of grade 3 or higher were more common with combination therapy (57.1% vs 8.7%). The most common events with monotherapy were diarrhea (56.5%), rash (52.2%), and pruritus (43.5%) and with dual therapy were rash (52.4%), thrombocytopenia (52.4%), and peripheral edema (42.9%).
The results showed that the combination therapy has the potential to become a first-line treatment option for patients who do not respond well to EGFR-TKIs alone, Dr. Yang said in a press release.
Discussant for the study Paul Paik, MD, thoracic oncologist at Memorial Sloan Kettering Cancer Center in New York City, said this study “adds to data suggesting high MET expression might be a poor prognostic or predictive marker, the outcomes of which are improved with MET inhibition.”
He cautioned, however, that there appears to be “quality of life, side-effect trade-offs with dual MET plus EGFR TKI upfront.”
Dr. Paik said he looks forward to results from FLOWERS on serial circulating tumor DNA and formal androgen receptor testing, which “might aid in further assessing clonality and characterizing MET as a co-driver in this setting.”
The study was funded by AstraZeneca China. Dr. Yang had no disclosures. Dr. Paik disclosed relationships with EMD Serono, Bicara, Novartis, and Summit.
A version of this article first appeared on Medscape.com.
according to results of the phase 2 FLOWERS study.
Compared with EGFR inhibitor osimertinib alone, the combination demonstrated a clinically meaningful improvement in the objective response rate — the study’s primary endpoint — with a positive trend in progression-free survival and a manageable safety profile.
About 30% patients with EGFR-mutated NSCLC fail to respond well to EGFR–tyrosine kinase inhibitors (TKIs), explained Jin-Ji Yang, MD, with Guangdong Lung Cancer Institute, Guangzhou, China, who reported the study results at the annual meeting of the World Conference on Lung Cancer.
Data suggested that de novo MET amplification occurs in up to 5% patients with treatment-naive, EGFR-mutated advanced NSCLC, and MET overexpression occurs in up to 15% these patients.
Coexistence of EGFR mutation and MET amplification/overexpression reduces sensitivity to EGFR-TKI therapy “and is likely the mechanism for mediating primary resistance to first-line EGFR-TKI monotherapy,” Dr. Yang explained in her presentation.
Osimertinib is a third-generation EGFR-TKI recommended as the first-line treatment for EGFR-mutant advanced NSCLC. Savolitinib is a highly selective MET-TKI which has demonstrated antitumor activity in various cancers with MET alterations.
The FLOWERS study is the first to test whether combining the two agents could improve efficacy and overcome MET-driven primary resistance in these patients.
The phase 2 study enrolled 44 treatment-naive patients with de novo MET-aberrant, EGFR-mutant, stage IIIB-IV NSCLC; 23 were randomly allocated to receive oral osimertinib (80 mg once daily) alone and 21 to receive oral osimertinib (80 mg once daily) plus savolitinib (300 mg twice daily).
At a median follow-up of 8.2 months, the objective response rate was 60.9% with osimertinib monotherapy vs 90.5% with combination therapy. The disease control rate was also better with the combination therapy than with monotherapy (95.2% vs 87%).
Median duration of response (not yet mature) was 8.4 months with monotherapy vs 18.6 months with combination therapy.
Preliminary progression-free survival data also showed a trend in favor of combination therapy over monotherapy (a median of 19.3 vs 9.3 months; hazard ratio, 0.59).
Most treatment-related adverse events were grade 1 or 2, and there were no fatal adverse events.
Treatment-related adverse events of grade 3 or higher were more common with combination therapy (57.1% vs 8.7%). The most common events with monotherapy were diarrhea (56.5%), rash (52.2%), and pruritus (43.5%) and with dual therapy were rash (52.4%), thrombocytopenia (52.4%), and peripheral edema (42.9%).
The results showed that the combination therapy has the potential to become a first-line treatment option for patients who do not respond well to EGFR-TKIs alone, Dr. Yang said in a press release.
Discussant for the study Paul Paik, MD, thoracic oncologist at Memorial Sloan Kettering Cancer Center in New York City, said this study “adds to data suggesting high MET expression might be a poor prognostic or predictive marker, the outcomes of which are improved with MET inhibition.”
He cautioned, however, that there appears to be “quality of life, side-effect trade-offs with dual MET plus EGFR TKI upfront.”
Dr. Paik said he looks forward to results from FLOWERS on serial circulating tumor DNA and formal androgen receptor testing, which “might aid in further assessing clonality and characterizing MET as a co-driver in this setting.”
The study was funded by AstraZeneca China. Dr. Yang had no disclosures. Dr. Paik disclosed relationships with EMD Serono, Bicara, Novartis, and Summit.
A version of this article first appeared on Medscape.com.
according to results of the phase 2 FLOWERS study.
Compared with EGFR inhibitor osimertinib alone, the combination demonstrated a clinically meaningful improvement in the objective response rate — the study’s primary endpoint — with a positive trend in progression-free survival and a manageable safety profile.
About 30% patients with EGFR-mutated NSCLC fail to respond well to EGFR–tyrosine kinase inhibitors (TKIs), explained Jin-Ji Yang, MD, with Guangdong Lung Cancer Institute, Guangzhou, China, who reported the study results at the annual meeting of the World Conference on Lung Cancer.
Data suggested that de novo MET amplification occurs in up to 5% patients with treatment-naive, EGFR-mutated advanced NSCLC, and MET overexpression occurs in up to 15% these patients.
Coexistence of EGFR mutation and MET amplification/overexpression reduces sensitivity to EGFR-TKI therapy “and is likely the mechanism for mediating primary resistance to first-line EGFR-TKI monotherapy,” Dr. Yang explained in her presentation.
Osimertinib is a third-generation EGFR-TKI recommended as the first-line treatment for EGFR-mutant advanced NSCLC. Savolitinib is a highly selective MET-TKI which has demonstrated antitumor activity in various cancers with MET alterations.
The FLOWERS study is the first to test whether combining the two agents could improve efficacy and overcome MET-driven primary resistance in these patients.
The phase 2 study enrolled 44 treatment-naive patients with de novo MET-aberrant, EGFR-mutant, stage IIIB-IV NSCLC; 23 were randomly allocated to receive oral osimertinib (80 mg once daily) alone and 21 to receive oral osimertinib (80 mg once daily) plus savolitinib (300 mg twice daily).
At a median follow-up of 8.2 months, the objective response rate was 60.9% with osimertinib monotherapy vs 90.5% with combination therapy. The disease control rate was also better with the combination therapy than with monotherapy (95.2% vs 87%).
Median duration of response (not yet mature) was 8.4 months with monotherapy vs 18.6 months with combination therapy.
Preliminary progression-free survival data also showed a trend in favor of combination therapy over monotherapy (a median of 19.3 vs 9.3 months; hazard ratio, 0.59).
Most treatment-related adverse events were grade 1 or 2, and there were no fatal adverse events.
Treatment-related adverse events of grade 3 or higher were more common with combination therapy (57.1% vs 8.7%). The most common events with monotherapy were diarrhea (56.5%), rash (52.2%), and pruritus (43.5%) and with dual therapy were rash (52.4%), thrombocytopenia (52.4%), and peripheral edema (42.9%).
The results showed that the combination therapy has the potential to become a first-line treatment option for patients who do not respond well to EGFR-TKIs alone, Dr. Yang said in a press release.
Discussant for the study Paul Paik, MD, thoracic oncologist at Memorial Sloan Kettering Cancer Center in New York City, said this study “adds to data suggesting high MET expression might be a poor prognostic or predictive marker, the outcomes of which are improved with MET inhibition.”
He cautioned, however, that there appears to be “quality of life, side-effect trade-offs with dual MET plus EGFR TKI upfront.”
Dr. Paik said he looks forward to results from FLOWERS on serial circulating tumor DNA and formal androgen receptor testing, which “might aid in further assessing clonality and characterizing MET as a co-driver in this setting.”
The study was funded by AstraZeneca China. Dr. Yang had no disclosures. Dr. Paik disclosed relationships with EMD Serono, Bicara, Novartis, and Summit.
A version of this article first appeared on Medscape.com.
FROM WCLC 2024
Majority of Hospitalized Patients With COPD Misuse Inhalers
Approximately two thirds of hospitalized adults with chronic obstructive pulmonary disease (COPD) received suboptimal treatment with inhalers, mainly resulting from errors, based on data from 96 individuals.
“Numerous studies have highlighted the significant issue of improper inhaler use in outpatient settings, but the extent of this problem within hospital settings remains poorly documented,” said lead author Gaël Grandmaison, MD, of the University of Fribourg in Switzerland, in an interview.
“This gap in knowledge is concerning, especially considering that several factors associated with suboptimal inhaler use, such as improper inhalation techniques, insufficient inspiratory flow, or the use of inhalers that are not suited to the patient’s specific characteristics, are associated with poorer disease control, more frequent exacerbations, and increased costs,” Dr. Grandmaison said.
To better characterize the prevalence of and factors associated with inhaler misuse in hospitalized patients with COPD, the researchers reviewed data from consecutive patients with COPD who were hospitalized in the general internal medicine department of a single institution between August 2022 and April 2023. Patients were assessed for peak inspiratory flow (PIF) and inhaler technique.
The primary outcome was the proportion of misused inhalers, which was defined as any inhaler used with either insufficient PIF and/or a critical error. The mean age of the patients was 71.6 years, 63% were men, and 67% were hospitalized for COPD exacerbations. Patients used 3.0 inhalers on average.
The study included 96 patients and 160 inhalers that were assessed at hospital admission. Overall, 111 were misused. Of those misused, 105 were associated with a critical error in the inhalation technique, and 22 were used with an insufficient PIF. After an episode of misuse, patients received targeted teaching on correct use that was repeated until they performed the technique without errors.
The percentage of inhaler misuse decreased over the course of the teaching sessions. The proportion of inhaler misuse decreased to 20.6%, 9.4%, and 5.6% after one, two, and three sessions, respectively.
“The inhalation technique was classified as ‘non-teachable’ if the patient continued to exhibit critical errors despite receiving three repetitions of the instructions,” the researchers wrote. Factors associated with inhaler misuse included cognitive disorders, fine motor disorders, poor coordination between inhaler activation and aspiration, and the inability to hold one’s breath.
Overall, the proportion of misused inhalers did not vary by age or gender. In an analysis at the patient level, 79 patients used at least one misused inhaler, 78 used at least one inhaler with a critical error, and 21 used inhalers with insufficient PIF.
“This study is particularly timely because reasons for hospitalization, such as COPD exacerbations or confusional states, could exacerbate the problem, leading to a potentially higher prevalence of suboptimal inhaler use compared to outpatient settings,” Dr. Grandmaison said.
The researchers also examined secondary outcomes including the prevalence of inhalers that were not suited to them and the number of patients using at least one misused inhaler.
The study findings confirm that suboptimal inhaler use is a significant problem in the hospital setting and provide new insights into the specific reasons behind this suboptimal usage, Dr. Grandmaison said.
“In the majority of cases, poor inhalation technique is the primary cause, which can generally be corrected through targeted therapeutic education,” she said. However, the study also revealed that 20% of patients are unable to use at least one of their inhalers correctly because of insufficient inspiratory force. Another 10% struggle despite receiving proper instruction, often because of cognitive impairments or difficulty with fine motor skills.
The results underscore the need for a comprehensive approach to inhaler use in hospitalized patients that combines continuous therapeutic education with personalized assessment in order to improve technique and subsequently enhance patient outcomes, she said.
Changing Clinical Practice
“As hospital physicians, these findings have led us to systematically evaluate the inhalers used by COPD patients, regardless of their reason for hospitalization,” Dr. Grandmaison said. Consequently, the hospital has implemented an assessment of inhaler use among patients that includes a review of techniques, an evaluation of the appropriateness of the inhaler prescribed, and an algorithm to help clinicians choose the most appropriate inhaler. Since its inception, the targeted intervention has significantly reduced improper inhaler use at discharge.
Limitations and Next Steps
The findings were limited by several factors including the possible underreporting of misuse caused by inadequate PIF, a lack of consensus on what constitutes a critical error, and the small sample of patients from a single center.
Despite these limitations, the study adds to the understanding of improper inhaler use in the hospital setting, Dr. Grandmaison said. “Our subsequent research demonstrated that a systematic evaluation of inhalers, combined with therapeutic education and an algorithm to select an inhaler suited to the patient’s characteristics, significantly reduces the number of improperly used inhalers at hospital discharge.”
However, several areas require further investigation, said Dr. Grandmaison. The most effective methods and frequency for teaching inhalation techniques must be defined, and more research is needed to understand the factors influencing PIF and its progression over the course of disease. The next steps for the current research are to evaluate the impact of the intervention on long-term symptom control and disease progression.
“Moreover, adapting the strategy developed in our institution for use in outpatient care is a priority, and multicenter studies would be valuable in validating these findings across different hospital settings,” she added.
In-Hospital Inhaler Education Falls Short
“Poor inhaler technique can lead to ineffective inhaler use and suboptimal treatment of COPD,” said Arianne K. Baldomero, MD, a pulmonologist and assistant professor of medicine at the University of Minnesota, Minneapolis, in an interview.
“The results from this study are consistent with prior studies showing a high prevalence of suboptimal inhaler use,” said Dr. Baldomero, who was not involved in the current study.
“The investigators also found that therapeutic education led to a significant reduction in the number of critical errors,” she said.
“What is surprising is that it can take up to three lessons to reduce this critical error down to 3.8%,” Dr. Baldomero said. “In most real-world clinic settings, many patients are not taught how to properly use inhalers, and many patients who receive inhaler technique education only receive instructions once.”
Dr. Baldomero’s takeaway from the study is that teaching patients to properly use their inhalers is critical, but that this education may need to be repeated multiple times. The findings also remind clinicians that some types of inhaler delivery are not suited for patients who cannot generate adequate respiratory flow.
Looking ahead, a larger sample size is needed to better identify which patients need additional teaching, Dr. Baldomero said. Also, the current study is limited by the focus on hospitalized patients. “I am interested in learning about the characteristics of patients in the outpatient settings who would benefit from additional inhaler teaching,” she noted.
The study was supported by a grant from the Hospital of Fribourg in Switzerland. The researchers had no financial conflicts to disclose. Dr. Baldomero had no financial conflicts to disclose.
A version of this article first appeared on Medscape.com.
Approximately two thirds of hospitalized adults with chronic obstructive pulmonary disease (COPD) received suboptimal treatment with inhalers, mainly resulting from errors, based on data from 96 individuals.
“Numerous studies have highlighted the significant issue of improper inhaler use in outpatient settings, but the extent of this problem within hospital settings remains poorly documented,” said lead author Gaël Grandmaison, MD, of the University of Fribourg in Switzerland, in an interview.
“This gap in knowledge is concerning, especially considering that several factors associated with suboptimal inhaler use, such as improper inhalation techniques, insufficient inspiratory flow, or the use of inhalers that are not suited to the patient’s specific characteristics, are associated with poorer disease control, more frequent exacerbations, and increased costs,” Dr. Grandmaison said.
To better characterize the prevalence of and factors associated with inhaler misuse in hospitalized patients with COPD, the researchers reviewed data from consecutive patients with COPD who were hospitalized in the general internal medicine department of a single institution between August 2022 and April 2023. Patients were assessed for peak inspiratory flow (PIF) and inhaler technique.
The primary outcome was the proportion of misused inhalers, which was defined as any inhaler used with either insufficient PIF and/or a critical error. The mean age of the patients was 71.6 years, 63% were men, and 67% were hospitalized for COPD exacerbations. Patients used 3.0 inhalers on average.
The study included 96 patients and 160 inhalers that were assessed at hospital admission. Overall, 111 were misused. Of those misused, 105 were associated with a critical error in the inhalation technique, and 22 were used with an insufficient PIF. After an episode of misuse, patients received targeted teaching on correct use that was repeated until they performed the technique without errors.
The percentage of inhaler misuse decreased over the course of the teaching sessions. The proportion of inhaler misuse decreased to 20.6%, 9.4%, and 5.6% after one, two, and three sessions, respectively.
“The inhalation technique was classified as ‘non-teachable’ if the patient continued to exhibit critical errors despite receiving three repetitions of the instructions,” the researchers wrote. Factors associated with inhaler misuse included cognitive disorders, fine motor disorders, poor coordination between inhaler activation and aspiration, and the inability to hold one’s breath.
Overall, the proportion of misused inhalers did not vary by age or gender. In an analysis at the patient level, 79 patients used at least one misused inhaler, 78 used at least one inhaler with a critical error, and 21 used inhalers with insufficient PIF.
“This study is particularly timely because reasons for hospitalization, such as COPD exacerbations or confusional states, could exacerbate the problem, leading to a potentially higher prevalence of suboptimal inhaler use compared to outpatient settings,” Dr. Grandmaison said.
The researchers also examined secondary outcomes including the prevalence of inhalers that were not suited to them and the number of patients using at least one misused inhaler.
The study findings confirm that suboptimal inhaler use is a significant problem in the hospital setting and provide new insights into the specific reasons behind this suboptimal usage, Dr. Grandmaison said.
“In the majority of cases, poor inhalation technique is the primary cause, which can generally be corrected through targeted therapeutic education,” she said. However, the study also revealed that 20% of patients are unable to use at least one of their inhalers correctly because of insufficient inspiratory force. Another 10% struggle despite receiving proper instruction, often because of cognitive impairments or difficulty with fine motor skills.
The results underscore the need for a comprehensive approach to inhaler use in hospitalized patients that combines continuous therapeutic education with personalized assessment in order to improve technique and subsequently enhance patient outcomes, she said.
Changing Clinical Practice
“As hospital physicians, these findings have led us to systematically evaluate the inhalers used by COPD patients, regardless of their reason for hospitalization,” Dr. Grandmaison said. Consequently, the hospital has implemented an assessment of inhaler use among patients that includes a review of techniques, an evaluation of the appropriateness of the inhaler prescribed, and an algorithm to help clinicians choose the most appropriate inhaler. Since its inception, the targeted intervention has significantly reduced improper inhaler use at discharge.
Limitations and Next Steps
The findings were limited by several factors including the possible underreporting of misuse caused by inadequate PIF, a lack of consensus on what constitutes a critical error, and the small sample of patients from a single center.
Despite these limitations, the study adds to the understanding of improper inhaler use in the hospital setting, Dr. Grandmaison said. “Our subsequent research demonstrated that a systematic evaluation of inhalers, combined with therapeutic education and an algorithm to select an inhaler suited to the patient’s characteristics, significantly reduces the number of improperly used inhalers at hospital discharge.”
However, several areas require further investigation, said Dr. Grandmaison. The most effective methods and frequency for teaching inhalation techniques must be defined, and more research is needed to understand the factors influencing PIF and its progression over the course of disease. The next steps for the current research are to evaluate the impact of the intervention on long-term symptom control and disease progression.
“Moreover, adapting the strategy developed in our institution for use in outpatient care is a priority, and multicenter studies would be valuable in validating these findings across different hospital settings,” she added.
In-Hospital Inhaler Education Falls Short
“Poor inhaler technique can lead to ineffective inhaler use and suboptimal treatment of COPD,” said Arianne K. Baldomero, MD, a pulmonologist and assistant professor of medicine at the University of Minnesota, Minneapolis, in an interview.
“The results from this study are consistent with prior studies showing a high prevalence of suboptimal inhaler use,” said Dr. Baldomero, who was not involved in the current study.
“The investigators also found that therapeutic education led to a significant reduction in the number of critical errors,” she said.
“What is surprising is that it can take up to three lessons to reduce this critical error down to 3.8%,” Dr. Baldomero said. “In most real-world clinic settings, many patients are not taught how to properly use inhalers, and many patients who receive inhaler technique education only receive instructions once.”
Dr. Baldomero’s takeaway from the study is that teaching patients to properly use their inhalers is critical, but that this education may need to be repeated multiple times. The findings also remind clinicians that some types of inhaler delivery are not suited for patients who cannot generate adequate respiratory flow.
Looking ahead, a larger sample size is needed to better identify which patients need additional teaching, Dr. Baldomero said. Also, the current study is limited by the focus on hospitalized patients. “I am interested in learning about the characteristics of patients in the outpatient settings who would benefit from additional inhaler teaching,” she noted.
The study was supported by a grant from the Hospital of Fribourg in Switzerland. The researchers had no financial conflicts to disclose. Dr. Baldomero had no financial conflicts to disclose.
A version of this article first appeared on Medscape.com.
Approximately two thirds of hospitalized adults with chronic obstructive pulmonary disease (COPD) received suboptimal treatment with inhalers, mainly resulting from errors, based on data from 96 individuals.
“Numerous studies have highlighted the significant issue of improper inhaler use in outpatient settings, but the extent of this problem within hospital settings remains poorly documented,” said lead author Gaël Grandmaison, MD, of the University of Fribourg in Switzerland, in an interview.
“This gap in knowledge is concerning, especially considering that several factors associated with suboptimal inhaler use, such as improper inhalation techniques, insufficient inspiratory flow, or the use of inhalers that are not suited to the patient’s specific characteristics, are associated with poorer disease control, more frequent exacerbations, and increased costs,” Dr. Grandmaison said.
To better characterize the prevalence of and factors associated with inhaler misuse in hospitalized patients with COPD, the researchers reviewed data from consecutive patients with COPD who were hospitalized in the general internal medicine department of a single institution between August 2022 and April 2023. Patients were assessed for peak inspiratory flow (PIF) and inhaler technique.
The primary outcome was the proportion of misused inhalers, which was defined as any inhaler used with either insufficient PIF and/or a critical error. The mean age of the patients was 71.6 years, 63% were men, and 67% were hospitalized for COPD exacerbations. Patients used 3.0 inhalers on average.
The study included 96 patients and 160 inhalers that were assessed at hospital admission. Overall, 111 were misused. Of those misused, 105 were associated with a critical error in the inhalation technique, and 22 were used with an insufficient PIF. After an episode of misuse, patients received targeted teaching on correct use that was repeated until they performed the technique without errors.
The percentage of inhaler misuse decreased over the course of the teaching sessions. The proportion of inhaler misuse decreased to 20.6%, 9.4%, and 5.6% after one, two, and three sessions, respectively.
“The inhalation technique was classified as ‘non-teachable’ if the patient continued to exhibit critical errors despite receiving three repetitions of the instructions,” the researchers wrote. Factors associated with inhaler misuse included cognitive disorders, fine motor disorders, poor coordination between inhaler activation and aspiration, and the inability to hold one’s breath.
Overall, the proportion of misused inhalers did not vary by age or gender. In an analysis at the patient level, 79 patients used at least one misused inhaler, 78 used at least one inhaler with a critical error, and 21 used inhalers with insufficient PIF.
“This study is particularly timely because reasons for hospitalization, such as COPD exacerbations or confusional states, could exacerbate the problem, leading to a potentially higher prevalence of suboptimal inhaler use compared to outpatient settings,” Dr. Grandmaison said.
The researchers also examined secondary outcomes including the prevalence of inhalers that were not suited to them and the number of patients using at least one misused inhaler.
The study findings confirm that suboptimal inhaler use is a significant problem in the hospital setting and provide new insights into the specific reasons behind this suboptimal usage, Dr. Grandmaison said.
“In the majority of cases, poor inhalation technique is the primary cause, which can generally be corrected through targeted therapeutic education,” she said. However, the study also revealed that 20% of patients are unable to use at least one of their inhalers correctly because of insufficient inspiratory force. Another 10% struggle despite receiving proper instruction, often because of cognitive impairments or difficulty with fine motor skills.
The results underscore the need for a comprehensive approach to inhaler use in hospitalized patients that combines continuous therapeutic education with personalized assessment in order to improve technique and subsequently enhance patient outcomes, she said.
Changing Clinical Practice
“As hospital physicians, these findings have led us to systematically evaluate the inhalers used by COPD patients, regardless of their reason for hospitalization,” Dr. Grandmaison said. Consequently, the hospital has implemented an assessment of inhaler use among patients that includes a review of techniques, an evaluation of the appropriateness of the inhaler prescribed, and an algorithm to help clinicians choose the most appropriate inhaler. Since its inception, the targeted intervention has significantly reduced improper inhaler use at discharge.
Limitations and Next Steps
The findings were limited by several factors including the possible underreporting of misuse caused by inadequate PIF, a lack of consensus on what constitutes a critical error, and the small sample of patients from a single center.
Despite these limitations, the study adds to the understanding of improper inhaler use in the hospital setting, Dr. Grandmaison said. “Our subsequent research demonstrated that a systematic evaluation of inhalers, combined with therapeutic education and an algorithm to select an inhaler suited to the patient’s characteristics, significantly reduces the number of improperly used inhalers at hospital discharge.”
However, several areas require further investigation, said Dr. Grandmaison. The most effective methods and frequency for teaching inhalation techniques must be defined, and more research is needed to understand the factors influencing PIF and its progression over the course of disease. The next steps for the current research are to evaluate the impact of the intervention on long-term symptom control and disease progression.
“Moreover, adapting the strategy developed in our institution for use in outpatient care is a priority, and multicenter studies would be valuable in validating these findings across different hospital settings,” she added.
In-Hospital Inhaler Education Falls Short
“Poor inhaler technique can lead to ineffective inhaler use and suboptimal treatment of COPD,” said Arianne K. Baldomero, MD, a pulmonologist and assistant professor of medicine at the University of Minnesota, Minneapolis, in an interview.
“The results from this study are consistent with prior studies showing a high prevalence of suboptimal inhaler use,” said Dr. Baldomero, who was not involved in the current study.
“The investigators also found that therapeutic education led to a significant reduction in the number of critical errors,” she said.
“What is surprising is that it can take up to three lessons to reduce this critical error down to 3.8%,” Dr. Baldomero said. “In most real-world clinic settings, many patients are not taught how to properly use inhalers, and many patients who receive inhaler technique education only receive instructions once.”
Dr. Baldomero’s takeaway from the study is that teaching patients to properly use their inhalers is critical, but that this education may need to be repeated multiple times. The findings also remind clinicians that some types of inhaler delivery are not suited for patients who cannot generate adequate respiratory flow.
Looking ahead, a larger sample size is needed to better identify which patients need additional teaching, Dr. Baldomero said. Also, the current study is limited by the focus on hospitalized patients. “I am interested in learning about the characteristics of patients in the outpatient settings who would benefit from additional inhaler teaching,” she noted.
The study was supported by a grant from the Hospital of Fribourg in Switzerland. The researchers had no financial conflicts to disclose. Dr. Baldomero had no financial conflicts to disclose.
A version of this article first appeared on Medscape.com.
FROM CHRONIC OBSTRUCTIVE PULMONARY DISEASES
Genetic Testing and Novel Biomarkers Important in Cystic Fibrosis Diagnosis and Monitoring
VIENNA — Advances in genetic testing and newly discovered biomarkers can help screen newborns and monitor inflammation and pulmonary exacerbations in patients diagnosed with cystic fibrosis.
At the European Respiratory Society (ERS) 2024 International Congress, clinical researchers presented results from the Turkish context.
Cystic fibrosis is the most common genetic disorder among Caucasians. The average prevalence at birth in Europe is 1 in 5000, whereas the overall population averages 1 in 9000. Both rates vary significantly based on geographic area. In the central Anatolia region, one study found that the incidence of cystic fibrosis is 1 in 3400 live births.
Çigdem Korkmaz, a researcher at the Department of Pediatric Pulmonology at the Istanbul University-Cerrahpasa in Istanbul, Turkey, said that diagnosis in Turkey is especially challenging because of the genetic diversity of cystic fibrosis within the population. She said genetic testing might be necessary to catch missed cases by traditional screening methods.
Genetic Testing Picks Up Missed Cases
In 2022, 30 European countries run newborn bloodspot screening for cystic fibrosis, with 26 national programs. Screening protocols vary between countries but generally involve initial screening using an immunoreactive trypsinogen (IRT) blood test. Follow-up testing may include a second IRT test, DNA analysis for common CFTR mutations, and sweat chloride test (SCT).
Turkey introduced newborn screening for cystic fibrosis in 2015. Newborns with an elevated IRT and confirmatory SCT undergo genetic testing. However, in a retrospective study, researchers found that IRT tests turn many false-positive results, and some patients who turn a normal SCT are diagnosed with the disease through genetic testing.
The study included 205 infants referred to a tertiary care center in Istanbul between January 2015 and January 2023 following an elevator IRT result. The researchers analyzed the clinical and sociodemographic data, IRT and SCT values, and genetic analysis results.
“The high false-positive rate of the current screening strategy suggests that the IRT thresholds used in Turkey may be too low,” said Ms. Korkmaz, who presented the study at the ERS Congress. She added that genetic testing might be important, especially in patients with normal SCT results. “Early diagnosis means these patients avoid missing or delaying treatments.”
Biomarkers for Monitoring Cystic Fibrosis Exacerbations
C-reactive protein (CRP) blood testing is typically used in monitoring inflammation and pulmonary exacerbations in patients who have already been diagnosed with cystic fibrosis. CRP is an inflammatory biomarker that increases in patients with cystic fibrosis during pulmonary exacerbations and settles with treatment.
Researchers at Gazi University in Ankara, Turkey, found other biomarkers to identify inflammation and pulmonary exacerbations with great sensitivity and specificity in patients with cystic fibrosis.
Over 3 years, from 2021 to 2024, the researchers analyzed blood samples from 54 children aged 1-18 years during exacerbation and non-exacerbation periods. Besides CRP, they tested CRP/albumin (ALB) ratio, neutrophil-to-lymphocyte ratio (NLR), delivered NLR (dNLR), and systemic immune inflammation (SII).
All biomarkers increased during exacerbation episodes. All showed high specificity and sensitivity:
- CPR/ALB had a specificity of 81% and a sensitivity of 90% at a cutoff of 1.7 mg/dL.
- SII had a specificity of 86% and a sensitivity of 67% at a cutoff of 426 mg/dL.
- NLR had a specificity of 62% and a sensitivity of 79% at a cutoff of 2.2 mg/dL.
- SII had a specificity of 86% and a sensitivity of 67% at a cutoff of 426 mg/dL.
- dNLR had a specificity of 71% and a sensitivity of 66% at a cutoff of 1.15 mg/dL.
- In comparison, CPR had a specificity of 85% and a sensitivity of 84% at a cutoff of 6.2 mg/dL.
Ayse Tana Aslan, a professor at the Department of Pediatric Pulmonology, Faculty of Medicine, at Gazi University in Ankara, Turkey, who presented the results at the ERS Congress, said that these biomarkers can be easily and quickly identified with a blood test while waiting on phlegm culture results, which can take days. “It is important to predict inflammation and exacerbation quickly so that patients can start a course of antibiotics as soon as possible,” she said.
Ms. Korkmaz and Ms. Aslan reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
VIENNA — Advances in genetic testing and newly discovered biomarkers can help screen newborns and monitor inflammation and pulmonary exacerbations in patients diagnosed with cystic fibrosis.
At the European Respiratory Society (ERS) 2024 International Congress, clinical researchers presented results from the Turkish context.
Cystic fibrosis is the most common genetic disorder among Caucasians. The average prevalence at birth in Europe is 1 in 5000, whereas the overall population averages 1 in 9000. Both rates vary significantly based on geographic area. In the central Anatolia region, one study found that the incidence of cystic fibrosis is 1 in 3400 live births.
Çigdem Korkmaz, a researcher at the Department of Pediatric Pulmonology at the Istanbul University-Cerrahpasa in Istanbul, Turkey, said that diagnosis in Turkey is especially challenging because of the genetic diversity of cystic fibrosis within the population. She said genetic testing might be necessary to catch missed cases by traditional screening methods.
Genetic Testing Picks Up Missed Cases
In 2022, 30 European countries run newborn bloodspot screening for cystic fibrosis, with 26 national programs. Screening protocols vary between countries but generally involve initial screening using an immunoreactive trypsinogen (IRT) blood test. Follow-up testing may include a second IRT test, DNA analysis for common CFTR mutations, and sweat chloride test (SCT).
Turkey introduced newborn screening for cystic fibrosis in 2015. Newborns with an elevated IRT and confirmatory SCT undergo genetic testing. However, in a retrospective study, researchers found that IRT tests turn many false-positive results, and some patients who turn a normal SCT are diagnosed with the disease through genetic testing.
The study included 205 infants referred to a tertiary care center in Istanbul between January 2015 and January 2023 following an elevator IRT result. The researchers analyzed the clinical and sociodemographic data, IRT and SCT values, and genetic analysis results.
“The high false-positive rate of the current screening strategy suggests that the IRT thresholds used in Turkey may be too low,” said Ms. Korkmaz, who presented the study at the ERS Congress. She added that genetic testing might be important, especially in patients with normal SCT results. “Early diagnosis means these patients avoid missing or delaying treatments.”
Biomarkers for Monitoring Cystic Fibrosis Exacerbations
C-reactive protein (CRP) blood testing is typically used in monitoring inflammation and pulmonary exacerbations in patients who have already been diagnosed with cystic fibrosis. CRP is an inflammatory biomarker that increases in patients with cystic fibrosis during pulmonary exacerbations and settles with treatment.
Researchers at Gazi University in Ankara, Turkey, found other biomarkers to identify inflammation and pulmonary exacerbations with great sensitivity and specificity in patients with cystic fibrosis.
Over 3 years, from 2021 to 2024, the researchers analyzed blood samples from 54 children aged 1-18 years during exacerbation and non-exacerbation periods. Besides CRP, they tested CRP/albumin (ALB) ratio, neutrophil-to-lymphocyte ratio (NLR), delivered NLR (dNLR), and systemic immune inflammation (SII).
All biomarkers increased during exacerbation episodes. All showed high specificity and sensitivity:
- CPR/ALB had a specificity of 81% and a sensitivity of 90% at a cutoff of 1.7 mg/dL.
- SII had a specificity of 86% and a sensitivity of 67% at a cutoff of 426 mg/dL.
- NLR had a specificity of 62% and a sensitivity of 79% at a cutoff of 2.2 mg/dL.
- SII had a specificity of 86% and a sensitivity of 67% at a cutoff of 426 mg/dL.
- dNLR had a specificity of 71% and a sensitivity of 66% at a cutoff of 1.15 mg/dL.
- In comparison, CPR had a specificity of 85% and a sensitivity of 84% at a cutoff of 6.2 mg/dL.
Ayse Tana Aslan, a professor at the Department of Pediatric Pulmonology, Faculty of Medicine, at Gazi University in Ankara, Turkey, who presented the results at the ERS Congress, said that these biomarkers can be easily and quickly identified with a blood test while waiting on phlegm culture results, which can take days. “It is important to predict inflammation and exacerbation quickly so that patients can start a course of antibiotics as soon as possible,” she said.
Ms. Korkmaz and Ms. Aslan reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
VIENNA — Advances in genetic testing and newly discovered biomarkers can help screen newborns and monitor inflammation and pulmonary exacerbations in patients diagnosed with cystic fibrosis.
At the European Respiratory Society (ERS) 2024 International Congress, clinical researchers presented results from the Turkish context.
Cystic fibrosis is the most common genetic disorder among Caucasians. The average prevalence at birth in Europe is 1 in 5000, whereas the overall population averages 1 in 9000. Both rates vary significantly based on geographic area. In the central Anatolia region, one study found that the incidence of cystic fibrosis is 1 in 3400 live births.
Çigdem Korkmaz, a researcher at the Department of Pediatric Pulmonology at the Istanbul University-Cerrahpasa in Istanbul, Turkey, said that diagnosis in Turkey is especially challenging because of the genetic diversity of cystic fibrosis within the population. She said genetic testing might be necessary to catch missed cases by traditional screening methods.
Genetic Testing Picks Up Missed Cases
In 2022, 30 European countries run newborn bloodspot screening for cystic fibrosis, with 26 national programs. Screening protocols vary between countries but generally involve initial screening using an immunoreactive trypsinogen (IRT) blood test. Follow-up testing may include a second IRT test, DNA analysis for common CFTR mutations, and sweat chloride test (SCT).
Turkey introduced newborn screening for cystic fibrosis in 2015. Newborns with an elevated IRT and confirmatory SCT undergo genetic testing. However, in a retrospective study, researchers found that IRT tests turn many false-positive results, and some patients who turn a normal SCT are diagnosed with the disease through genetic testing.
The study included 205 infants referred to a tertiary care center in Istanbul between January 2015 and January 2023 following an elevator IRT result. The researchers analyzed the clinical and sociodemographic data, IRT and SCT values, and genetic analysis results.
“The high false-positive rate of the current screening strategy suggests that the IRT thresholds used in Turkey may be too low,” said Ms. Korkmaz, who presented the study at the ERS Congress. She added that genetic testing might be important, especially in patients with normal SCT results. “Early diagnosis means these patients avoid missing or delaying treatments.”
Biomarkers for Monitoring Cystic Fibrosis Exacerbations
C-reactive protein (CRP) blood testing is typically used in monitoring inflammation and pulmonary exacerbations in patients who have already been diagnosed with cystic fibrosis. CRP is an inflammatory biomarker that increases in patients with cystic fibrosis during pulmonary exacerbations and settles with treatment.
Researchers at Gazi University in Ankara, Turkey, found other biomarkers to identify inflammation and pulmonary exacerbations with great sensitivity and specificity in patients with cystic fibrosis.
Over 3 years, from 2021 to 2024, the researchers analyzed blood samples from 54 children aged 1-18 years during exacerbation and non-exacerbation periods. Besides CRP, they tested CRP/albumin (ALB) ratio, neutrophil-to-lymphocyte ratio (NLR), delivered NLR (dNLR), and systemic immune inflammation (SII).
All biomarkers increased during exacerbation episodes. All showed high specificity and sensitivity:
- CPR/ALB had a specificity of 81% and a sensitivity of 90% at a cutoff of 1.7 mg/dL.
- SII had a specificity of 86% and a sensitivity of 67% at a cutoff of 426 mg/dL.
- NLR had a specificity of 62% and a sensitivity of 79% at a cutoff of 2.2 mg/dL.
- SII had a specificity of 86% and a sensitivity of 67% at a cutoff of 426 mg/dL.
- dNLR had a specificity of 71% and a sensitivity of 66% at a cutoff of 1.15 mg/dL.
- In comparison, CPR had a specificity of 85% and a sensitivity of 84% at a cutoff of 6.2 mg/dL.
Ayse Tana Aslan, a professor at the Department of Pediatric Pulmonology, Faculty of Medicine, at Gazi University in Ankara, Turkey, who presented the results at the ERS Congress, said that these biomarkers can be easily and quickly identified with a blood test while waiting on phlegm culture results, which can take days. “It is important to predict inflammation and exacerbation quickly so that patients can start a course of antibiotics as soon as possible,” she said.
Ms. Korkmaz and Ms. Aslan reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
Controversy Surrounds Optimal Treatment for High-Risk Pulmonary Embolism
VIENNA — The optimal course of treatment when managing acute, high-risk pulmonary embolism (PE) remains a contentious topic among respiratory specialists.
Systemic thrombolysis, specifically using recombinant tissue plasminogen activator (rtPA), is the current gold standard treatment for high-risk PE. However, the real-world application is less straightforward due to patient complexities.
Here at the European Respiratory Society (ERS) 2024 Congress, respiratory specialists presented contrasting viewpoints and the latest evidence on each side of the issue to provide a comprehensive framework for navigating the complex decision-making process required for effective treatment.
“High-risk PE is a mechanical problem and thus needs a mechanical solution,” said Parth M. Rali, MD, an associate professor in thoracic medicine and surgery at the Lewis Katz School of Medicine at Temple University, Philadelphia.
“The marketing on some of the mechanical techniques is very impressive,” said Olivier Sanchez, MD, a pulmonologist in the Department of Pneumology and Intensive Care at the Georges Pompidou European Hospital in France. “But what is the evidence of such treatment in the setting of pulmonary embolism?”
The Case Against rtPA as the Standard of Care
High-risk PE typically involves hemodynamically unstable patients presenting with conditions such as low blood pressure, cardiac arrest, or the need for mechanical circulatory support. There is a spectrum of severity within high-risk PE, making it a complex condition to manage, especially since many patients have comorbidities like anemia or active cancer, complicating treatment. “It’s a very dynamic and fluid condition, and we can’t take for granted that rtPA is a standard of care,” Dr. Rali said.
Alternative treatments such as catheter-directed therapies, extracorporeal membrane oxygenation (ECMO), and surgical embolectomy are emerging as promising options, especially for patients who do not respond to or cannot receive rtPA. Mechanical treatments offer benefits in reducing clot burden and stabilizing patients, but they come with their own challenges.
ECMO can stabilize patients who are in shock or cardiac arrest, buying time for the clot to resolve or for further interventions like surgery or catheter-based treatments, said Dr. Rali. However, it is an invasive procedure requiring cannulation of large blood vessels, often involving significant resources and expertise.
Catheter-directed thrombolysis is a minimally invasive technique where a catheter is inserted directly into the pulmonary artery to deliver thrombolytic drugs at lower doses. This method allows for more targeted treatment of the clot, reducing the risk for systemic bleeding that comes with higher doses of thrombolytic agents used in systemic therapy, Dr. Rali explained.
Dr. Rali reported results from the FLAME study, which investigated the effectiveness of FlowTriever mechanical thrombectomy compared with conventional therapies for high-risk PE. This prospective, multicenter observational study enrolled 53 patients in the FlowTriever arm and 61 in the context arm, which included patients treated with systemic thrombolysis or anticoagulation. The primary endpoint, a composite of adverse in-hospital outcomes, was reached in 17% of FlowTriever patients, significantly lower than the 32% performance goal and the 63.9% rate in the context arm. In-hospital mortality was dramatically lower in the FlowTriever arm (1.9%) compared to the context arm (29.5%).
When catheter-based treatment fails, surgical pulmonary embolectomy is a last-resort option. “Only a minority of the high-risk PE [patients] would qualify for rtPA without harmful side effects,” Dr. Rali concluded. “So think wise before you pull your trigger.”
rtPA Not a Matter of the Past
In high-risk PE, the therapeutic priority is rapid hemodynamic stabilization and restoration of pulmonary blood flow to prevent cardiovascular collapse. Systemic thrombolysis acts quickly, reducing pulmonary vascular resistance and obstruction within hours, said Dr. Sanchez.
Presenting at the ERS Congress, he reported numerous studies, including 15 randomized controlled trials that demonstrated its effectiveness in high-risk PE. The PEITHO trial, in particular, demonstrated the ability of systemic thrombolysis to reduce all-cause mortality and hemodynamic collapse within 7 days.
However, this benefit comes at the cost of increased bleeding risk, including a 10% rate of major bleeding and a 2% risk for intracranial hemorrhage. “These data come from old studies using invasive diagnostic procedures, and with current diagnostic procedures, the rate of bleeding is probably lower,” Dr. Sanchez said. The risk of bleeding is also related to the type of thrombolytic agent, with tenecteplase being strongly associated with a higher risk of bleeding, while alteplase shows no increase in the risk of major bleeding, he added. New strategies like reduced-dose thrombolysis offer comparable efficacy and improved safety, as demonstrated in ongoing trials like PEITHO-3, which aim to optimize the balance between efficacy and bleeding risk. Dr. Sanchez is the lead investigator of the PEITHO-3 study.
While rtPA might not be optimal for all patients, Dr. Sanchez thinks there is not enough evidence to replace it as a first-line treatment.
Existing studies on catheter-directed therapies often focus on surrogate endpoints, such as right-to-left ventricular ratio changes, rather than clinical outcomes like mortality, he said. Retrospective data suggest that catheter-directed therapies may reduce in-hospital mortality compared with systemic therapies, but they also increase the risk of intracranial bleeding, post-procedure complications, and device-related events.
Sanchez mentioned the same FLAME study described by Dr. Rali, which reported a 23% rate of device-related complications and 11% major bleeding in patients treated with catheter-directed therapies.
“Systemic thrombolysis remains the first treatment of choice,” Dr. Sanchez concluded. “The use of catheter-directed treatment should be discussed as an alternative in case of contraindications.”
The Debate Continues
Numerous ongoing clinical studies, such as the FLARE trial, will address gaps in evidence and refine treatment protocols, potentially reshaping the standard of care in high-risk PE in the near future by providing new data on the efficacy and safety of existing and emerging therapies.
“The coming data will make it clearer what the best option is,” said Thamer Al Khouzaie, MD, a pulmonary medicine consultant at Johns Hopkins Aramco Healthcare in Dhahran, Saudi Arabia. For now, he said, systemic thrombolysis remains the best option for most patients because it is widely available, easily administered with intravenous infusion, and at a limited cost. Catheter-directed treatment and surgical options are only available in specialized centers, require expertise and training, and are also very expensive.
Dr. Rali, Dr. Sanchez, and Dr. Khouzaie report no relevant financial relationships.
A version of this article appeared on Medscape.com.
VIENNA — The optimal course of treatment when managing acute, high-risk pulmonary embolism (PE) remains a contentious topic among respiratory specialists.
Systemic thrombolysis, specifically using recombinant tissue plasminogen activator (rtPA), is the current gold standard treatment for high-risk PE. However, the real-world application is less straightforward due to patient complexities.
Here at the European Respiratory Society (ERS) 2024 Congress, respiratory specialists presented contrasting viewpoints and the latest evidence on each side of the issue to provide a comprehensive framework for navigating the complex decision-making process required for effective treatment.
“High-risk PE is a mechanical problem and thus needs a mechanical solution,” said Parth M. Rali, MD, an associate professor in thoracic medicine and surgery at the Lewis Katz School of Medicine at Temple University, Philadelphia.
“The marketing on some of the mechanical techniques is very impressive,” said Olivier Sanchez, MD, a pulmonologist in the Department of Pneumology and Intensive Care at the Georges Pompidou European Hospital in France. “But what is the evidence of such treatment in the setting of pulmonary embolism?”
The Case Against rtPA as the Standard of Care
High-risk PE typically involves hemodynamically unstable patients presenting with conditions such as low blood pressure, cardiac arrest, or the need for mechanical circulatory support. There is a spectrum of severity within high-risk PE, making it a complex condition to manage, especially since many patients have comorbidities like anemia or active cancer, complicating treatment. “It’s a very dynamic and fluid condition, and we can’t take for granted that rtPA is a standard of care,” Dr. Rali said.
Alternative treatments such as catheter-directed therapies, extracorporeal membrane oxygenation (ECMO), and surgical embolectomy are emerging as promising options, especially for patients who do not respond to or cannot receive rtPA. Mechanical treatments offer benefits in reducing clot burden and stabilizing patients, but they come with their own challenges.
ECMO can stabilize patients who are in shock or cardiac arrest, buying time for the clot to resolve or for further interventions like surgery or catheter-based treatments, said Dr. Rali. However, it is an invasive procedure requiring cannulation of large blood vessels, often involving significant resources and expertise.
Catheter-directed thrombolysis is a minimally invasive technique where a catheter is inserted directly into the pulmonary artery to deliver thrombolytic drugs at lower doses. This method allows for more targeted treatment of the clot, reducing the risk for systemic bleeding that comes with higher doses of thrombolytic agents used in systemic therapy, Dr. Rali explained.
Dr. Rali reported results from the FLAME study, which investigated the effectiveness of FlowTriever mechanical thrombectomy compared with conventional therapies for high-risk PE. This prospective, multicenter observational study enrolled 53 patients in the FlowTriever arm and 61 in the context arm, which included patients treated with systemic thrombolysis or anticoagulation. The primary endpoint, a composite of adverse in-hospital outcomes, was reached in 17% of FlowTriever patients, significantly lower than the 32% performance goal and the 63.9% rate in the context arm. In-hospital mortality was dramatically lower in the FlowTriever arm (1.9%) compared to the context arm (29.5%).
When catheter-based treatment fails, surgical pulmonary embolectomy is a last-resort option. “Only a minority of the high-risk PE [patients] would qualify for rtPA without harmful side effects,” Dr. Rali concluded. “So think wise before you pull your trigger.”
rtPA Not a Matter of the Past
In high-risk PE, the therapeutic priority is rapid hemodynamic stabilization and restoration of pulmonary blood flow to prevent cardiovascular collapse. Systemic thrombolysis acts quickly, reducing pulmonary vascular resistance and obstruction within hours, said Dr. Sanchez.
Presenting at the ERS Congress, he reported numerous studies, including 15 randomized controlled trials that demonstrated its effectiveness in high-risk PE. The PEITHO trial, in particular, demonstrated the ability of systemic thrombolysis to reduce all-cause mortality and hemodynamic collapse within 7 days.
However, this benefit comes at the cost of increased bleeding risk, including a 10% rate of major bleeding and a 2% risk for intracranial hemorrhage. “These data come from old studies using invasive diagnostic procedures, and with current diagnostic procedures, the rate of bleeding is probably lower,” Dr. Sanchez said. The risk of bleeding is also related to the type of thrombolytic agent, with tenecteplase being strongly associated with a higher risk of bleeding, while alteplase shows no increase in the risk of major bleeding, he added. New strategies like reduced-dose thrombolysis offer comparable efficacy and improved safety, as demonstrated in ongoing trials like PEITHO-3, which aim to optimize the balance between efficacy and bleeding risk. Dr. Sanchez is the lead investigator of the PEITHO-3 study.
While rtPA might not be optimal for all patients, Dr. Sanchez thinks there is not enough evidence to replace it as a first-line treatment.
Existing studies on catheter-directed therapies often focus on surrogate endpoints, such as right-to-left ventricular ratio changes, rather than clinical outcomes like mortality, he said. Retrospective data suggest that catheter-directed therapies may reduce in-hospital mortality compared with systemic therapies, but they also increase the risk of intracranial bleeding, post-procedure complications, and device-related events.
Sanchez mentioned the same FLAME study described by Dr. Rali, which reported a 23% rate of device-related complications and 11% major bleeding in patients treated with catheter-directed therapies.
“Systemic thrombolysis remains the first treatment of choice,” Dr. Sanchez concluded. “The use of catheter-directed treatment should be discussed as an alternative in case of contraindications.”
The Debate Continues
Numerous ongoing clinical studies, such as the FLARE trial, will address gaps in evidence and refine treatment protocols, potentially reshaping the standard of care in high-risk PE in the near future by providing new data on the efficacy and safety of existing and emerging therapies.
“The coming data will make it clearer what the best option is,” said Thamer Al Khouzaie, MD, a pulmonary medicine consultant at Johns Hopkins Aramco Healthcare in Dhahran, Saudi Arabia. For now, he said, systemic thrombolysis remains the best option for most patients because it is widely available, easily administered with intravenous infusion, and at a limited cost. Catheter-directed treatment and surgical options are only available in specialized centers, require expertise and training, and are also very expensive.
Dr. Rali, Dr. Sanchez, and Dr. Khouzaie report no relevant financial relationships.
A version of this article appeared on Medscape.com.
VIENNA — The optimal course of treatment when managing acute, high-risk pulmonary embolism (PE) remains a contentious topic among respiratory specialists.
Systemic thrombolysis, specifically using recombinant tissue plasminogen activator (rtPA), is the current gold standard treatment for high-risk PE. However, the real-world application is less straightforward due to patient complexities.
Here at the European Respiratory Society (ERS) 2024 Congress, respiratory specialists presented contrasting viewpoints and the latest evidence on each side of the issue to provide a comprehensive framework for navigating the complex decision-making process required for effective treatment.
“High-risk PE is a mechanical problem and thus needs a mechanical solution,” said Parth M. Rali, MD, an associate professor in thoracic medicine and surgery at the Lewis Katz School of Medicine at Temple University, Philadelphia.
“The marketing on some of the mechanical techniques is very impressive,” said Olivier Sanchez, MD, a pulmonologist in the Department of Pneumology and Intensive Care at the Georges Pompidou European Hospital in France. “But what is the evidence of such treatment in the setting of pulmonary embolism?”
The Case Against rtPA as the Standard of Care
High-risk PE typically involves hemodynamically unstable patients presenting with conditions such as low blood pressure, cardiac arrest, or the need for mechanical circulatory support. There is a spectrum of severity within high-risk PE, making it a complex condition to manage, especially since many patients have comorbidities like anemia or active cancer, complicating treatment. “It’s a very dynamic and fluid condition, and we can’t take for granted that rtPA is a standard of care,” Dr. Rali said.
Alternative treatments such as catheter-directed therapies, extracorporeal membrane oxygenation (ECMO), and surgical embolectomy are emerging as promising options, especially for patients who do not respond to or cannot receive rtPA. Mechanical treatments offer benefits in reducing clot burden and stabilizing patients, but they come with their own challenges.
ECMO can stabilize patients who are in shock or cardiac arrest, buying time for the clot to resolve or for further interventions like surgery or catheter-based treatments, said Dr. Rali. However, it is an invasive procedure requiring cannulation of large blood vessels, often involving significant resources and expertise.
Catheter-directed thrombolysis is a minimally invasive technique where a catheter is inserted directly into the pulmonary artery to deliver thrombolytic drugs at lower doses. This method allows for more targeted treatment of the clot, reducing the risk for systemic bleeding that comes with higher doses of thrombolytic agents used in systemic therapy, Dr. Rali explained.
Dr. Rali reported results from the FLAME study, which investigated the effectiveness of FlowTriever mechanical thrombectomy compared with conventional therapies for high-risk PE. This prospective, multicenter observational study enrolled 53 patients in the FlowTriever arm and 61 in the context arm, which included patients treated with systemic thrombolysis or anticoagulation. The primary endpoint, a composite of adverse in-hospital outcomes, was reached in 17% of FlowTriever patients, significantly lower than the 32% performance goal and the 63.9% rate in the context arm. In-hospital mortality was dramatically lower in the FlowTriever arm (1.9%) compared to the context arm (29.5%).
When catheter-based treatment fails, surgical pulmonary embolectomy is a last-resort option. “Only a minority of the high-risk PE [patients] would qualify for rtPA without harmful side effects,” Dr. Rali concluded. “So think wise before you pull your trigger.”
rtPA Not a Matter of the Past
In high-risk PE, the therapeutic priority is rapid hemodynamic stabilization and restoration of pulmonary blood flow to prevent cardiovascular collapse. Systemic thrombolysis acts quickly, reducing pulmonary vascular resistance and obstruction within hours, said Dr. Sanchez.
Presenting at the ERS Congress, he reported numerous studies, including 15 randomized controlled trials that demonstrated its effectiveness in high-risk PE. The PEITHO trial, in particular, demonstrated the ability of systemic thrombolysis to reduce all-cause mortality and hemodynamic collapse within 7 days.
However, this benefit comes at the cost of increased bleeding risk, including a 10% rate of major bleeding and a 2% risk for intracranial hemorrhage. “These data come from old studies using invasive diagnostic procedures, and with current diagnostic procedures, the rate of bleeding is probably lower,” Dr. Sanchez said. The risk of bleeding is also related to the type of thrombolytic agent, with tenecteplase being strongly associated with a higher risk of bleeding, while alteplase shows no increase in the risk of major bleeding, he added. New strategies like reduced-dose thrombolysis offer comparable efficacy and improved safety, as demonstrated in ongoing trials like PEITHO-3, which aim to optimize the balance between efficacy and bleeding risk. Dr. Sanchez is the lead investigator of the PEITHO-3 study.
While rtPA might not be optimal for all patients, Dr. Sanchez thinks there is not enough evidence to replace it as a first-line treatment.
Existing studies on catheter-directed therapies often focus on surrogate endpoints, such as right-to-left ventricular ratio changes, rather than clinical outcomes like mortality, he said. Retrospective data suggest that catheter-directed therapies may reduce in-hospital mortality compared with systemic therapies, but they also increase the risk of intracranial bleeding, post-procedure complications, and device-related events.
Sanchez mentioned the same FLAME study described by Dr. Rali, which reported a 23% rate of device-related complications and 11% major bleeding in patients treated with catheter-directed therapies.
“Systemic thrombolysis remains the first treatment of choice,” Dr. Sanchez concluded. “The use of catheter-directed treatment should be discussed as an alternative in case of contraindications.”
The Debate Continues
Numerous ongoing clinical studies, such as the FLARE trial, will address gaps in evidence and refine treatment protocols, potentially reshaping the standard of care in high-risk PE in the near future by providing new data on the efficacy and safety of existing and emerging therapies.
“The coming data will make it clearer what the best option is,” said Thamer Al Khouzaie, MD, a pulmonary medicine consultant at Johns Hopkins Aramco Healthcare in Dhahran, Saudi Arabia. For now, he said, systemic thrombolysis remains the best option for most patients because it is widely available, easily administered with intravenous infusion, and at a limited cost. Catheter-directed treatment and surgical options are only available in specialized centers, require expertise and training, and are also very expensive.
Dr. Rali, Dr. Sanchez, and Dr. Khouzaie report no relevant financial relationships.
A version of this article appeared on Medscape.com.
Ivonescimab: Possible New First-Line Standard in PD-L1–Positive Advanced NSCLC?
according to recent findings from the HARMONi-2 trial.
“This is the first randomized, phase 3 study to demonstrate a clinically significant improvement in efficacy with a novel drug compared to pembrolizumab in advanced NSCLC,” said study investigator Caicun Zhou, MD, PhD, with Shanghai Pulmonary Hospital in China,
The results highlight ivonescimab’s potential to become a “new standard of care” in advanced PD-L1–positive advanced NSCLC, said Dr. Zhou, who presented the analysis at the annual International Association for the Study of Lung Cancer (IASLC) World Conference on Lung Cancer in San Diego. Dr. Zhou is president-elect of the IASLC.
Ivonescimab (AK112) is a novel, potentially first-in-class investigational bispecific antibody that targets PD-1 and vascular endothelial growth factor (VEGF) developed by Akeso Biopharma, which funded the HARMONi-2 trial.
Conducted at 55 centers in China, HARMONi-2 enrolled 398 patients with untreated locally advanced or metastatic NSCLC, Eastern Cooperative Oncology Group Performance Status of 0 or 1, PD-L1 positive (with at least 1% of tumor cells expressing PD-L1), and no EGFR mutations or ALK rearrangements.
Patients were randomly allocated (1:1) to receive ivonescimab (20 mg/kg) or pembrolizumab (200 mg) every 3 weeks. The two groups were well balanced, and randomization was stratified by histology (squamous vs nonsquamous), clinical stage (IIIB/IIIC vs IV) and PD-L1 expression (PD-L1 of 1%-49% vs 50% or greater).
Dr. Zhou reported that patients who received ivonescimab were progression free for nearly twice as long as those on pembrolizumab — a median of 11.1 vs 5.8 months, indicating a 49% lower risk for progression or death (stratified hazard ratio [HR], 0.51; P < .0001).
The meaningful improvement in PFS with ivonescimab, compared with pembrolizumab, was “broadly consistent” in all prespecified subgroups, Dr. Zhou noted. That included patients with squamous NSCLC (HR, 0.48) and nonsquamous NSCLC (HR, 0.54), those with PD-L1 expression of 1%-49% (HR, 0.54) and 50% or higher (HR, 0.46), as well as those with liver metastases (HR, 0.47) and brain metastases (HR, 0.55).
The PFS benefit seen with ivonescimab in HARMONi-2 is “striking,” and the results “highlight the potential benefits of combined VEGF and PD-1 blockade together,” said John Heymach, MD, with the University of Texas MD Anderson Cancer Center in Houston, who served as discussant for the study.
Ivonescimab also led to a higher objective response rate (50% vs 38.5%) and disease control rate (89.9% vs 70.5%).
Grade 3 or higher treatment-related adverse events occurred in more patients receiving ivonescimab — 29.4% vs 15.6% on pembrolizumab. The difference largely stemmed from higher rates of proteinuria, hypertension, and lab abnormalities.
The rates of serious treatment-related adverse events were similar between the groups —20.8% in the ivonescimab group and 16.1% in the pembrolizumab group. Rates of grade 3 or higher immune-related adverse events were also similar, occurring in 7% of patients treated with ivonescimab and 8% of those receiving pembrolizumab.
In patients with squamous cell carcinoma, in particular, ivonescimab demonstrated a “very manageable” safety profile, Dr. Zhou noted. In this group, grade 3 or higher treatment-related adverse events occurred in 22.2% of patients (vs 18.7% receiving pembrolizumab).
Ivonescimab was associated with comparable but “numerically better” time to deterioration of global health status, based on the EORTC Core Quality of Life questionnaire, Dr. Zhou said.
Although the “really impressive and clinically meaningful” PFS benefits extended across different subgroups, “we await the overall survival results and additional studies done outside of China to confirm the benefit seen,” Dr. Heymach noted.
He also cautioned that, for patients with low to intermediate PD-L1 expression (1%-49%), pembrolizumab monotherapy “would not be the relevant comparator in the US and the rest of the world, and different study designs are going to be required for those populations.”
Based on the results of HARMONi-2, Akeso’s partner, Summit Therapeutics, plans to initiate HARMONi-7 in early 2025.
HARMONi-7 is currently planned as a multiregional, phase 3 clinical trial that will compare ivonescimab monotherapy to pembrolizumab monotherapy in patients with metastatic NSCLC whose tumors have high PD-L1 expression (50% or more).
Dr. Zhou has received consulting fees from Qilu Pharmaceutical, Hengrui, and TopAlliance Biosciences and honoraria from Eli Lilly China, Boehringer Ingelheim, Roche, Merck Sharp & Dohme, Qilu, Hengrui, Innovent Biologics, Alice, C-Stone, Luye Pharma, TopAlliance Biosciences, Amoy Diagnostics, and AnHeart Therapeutics. Dr. Heymach is a consultant for AbbVie, AnHeart Therapeutics, ArriVent Biopharma, AstraZeneca, BioCurity Pharmaceuticals, BioNTech, Blueprint Medicines, Boehringer Ingelheim, BMS, Eli Lilly, EMD Serono, Genentech, GlaxoSmithKline, Janssen Pharmaceuticals, Mirati Therapeutics, Novartis Pharmaceuticals, Regeneron Pharmaceuticals, Sanofi, Spectrum Pharmaceuticals, and Takeda.
A version of this article first appeared on Medscape.com.
according to recent findings from the HARMONi-2 trial.
“This is the first randomized, phase 3 study to demonstrate a clinically significant improvement in efficacy with a novel drug compared to pembrolizumab in advanced NSCLC,” said study investigator Caicun Zhou, MD, PhD, with Shanghai Pulmonary Hospital in China,
The results highlight ivonescimab’s potential to become a “new standard of care” in advanced PD-L1–positive advanced NSCLC, said Dr. Zhou, who presented the analysis at the annual International Association for the Study of Lung Cancer (IASLC) World Conference on Lung Cancer in San Diego. Dr. Zhou is president-elect of the IASLC.
Ivonescimab (AK112) is a novel, potentially first-in-class investigational bispecific antibody that targets PD-1 and vascular endothelial growth factor (VEGF) developed by Akeso Biopharma, which funded the HARMONi-2 trial.
Conducted at 55 centers in China, HARMONi-2 enrolled 398 patients with untreated locally advanced or metastatic NSCLC, Eastern Cooperative Oncology Group Performance Status of 0 or 1, PD-L1 positive (with at least 1% of tumor cells expressing PD-L1), and no EGFR mutations or ALK rearrangements.
Patients were randomly allocated (1:1) to receive ivonescimab (20 mg/kg) or pembrolizumab (200 mg) every 3 weeks. The two groups were well balanced, and randomization was stratified by histology (squamous vs nonsquamous), clinical stage (IIIB/IIIC vs IV) and PD-L1 expression (PD-L1 of 1%-49% vs 50% or greater).
Dr. Zhou reported that patients who received ivonescimab were progression free for nearly twice as long as those on pembrolizumab — a median of 11.1 vs 5.8 months, indicating a 49% lower risk for progression or death (stratified hazard ratio [HR], 0.51; P < .0001).
The meaningful improvement in PFS with ivonescimab, compared with pembrolizumab, was “broadly consistent” in all prespecified subgroups, Dr. Zhou noted. That included patients with squamous NSCLC (HR, 0.48) and nonsquamous NSCLC (HR, 0.54), those with PD-L1 expression of 1%-49% (HR, 0.54) and 50% or higher (HR, 0.46), as well as those with liver metastases (HR, 0.47) and brain metastases (HR, 0.55).
The PFS benefit seen with ivonescimab in HARMONi-2 is “striking,” and the results “highlight the potential benefits of combined VEGF and PD-1 blockade together,” said John Heymach, MD, with the University of Texas MD Anderson Cancer Center in Houston, who served as discussant for the study.
Ivonescimab also led to a higher objective response rate (50% vs 38.5%) and disease control rate (89.9% vs 70.5%).
Grade 3 or higher treatment-related adverse events occurred in more patients receiving ivonescimab — 29.4% vs 15.6% on pembrolizumab. The difference largely stemmed from higher rates of proteinuria, hypertension, and lab abnormalities.
The rates of serious treatment-related adverse events were similar between the groups —20.8% in the ivonescimab group and 16.1% in the pembrolizumab group. Rates of grade 3 or higher immune-related adverse events were also similar, occurring in 7% of patients treated with ivonescimab and 8% of those receiving pembrolizumab.
In patients with squamous cell carcinoma, in particular, ivonescimab demonstrated a “very manageable” safety profile, Dr. Zhou noted. In this group, grade 3 or higher treatment-related adverse events occurred in 22.2% of patients (vs 18.7% receiving pembrolizumab).
Ivonescimab was associated with comparable but “numerically better” time to deterioration of global health status, based on the EORTC Core Quality of Life questionnaire, Dr. Zhou said.
Although the “really impressive and clinically meaningful” PFS benefits extended across different subgroups, “we await the overall survival results and additional studies done outside of China to confirm the benefit seen,” Dr. Heymach noted.
He also cautioned that, for patients with low to intermediate PD-L1 expression (1%-49%), pembrolizumab monotherapy “would not be the relevant comparator in the US and the rest of the world, and different study designs are going to be required for those populations.”
Based on the results of HARMONi-2, Akeso’s partner, Summit Therapeutics, plans to initiate HARMONi-7 in early 2025.
HARMONi-7 is currently planned as a multiregional, phase 3 clinical trial that will compare ivonescimab monotherapy to pembrolizumab monotherapy in patients with metastatic NSCLC whose tumors have high PD-L1 expression (50% or more).
Dr. Zhou has received consulting fees from Qilu Pharmaceutical, Hengrui, and TopAlliance Biosciences and honoraria from Eli Lilly China, Boehringer Ingelheim, Roche, Merck Sharp & Dohme, Qilu, Hengrui, Innovent Biologics, Alice, C-Stone, Luye Pharma, TopAlliance Biosciences, Amoy Diagnostics, and AnHeart Therapeutics. Dr. Heymach is a consultant for AbbVie, AnHeart Therapeutics, ArriVent Biopharma, AstraZeneca, BioCurity Pharmaceuticals, BioNTech, Blueprint Medicines, Boehringer Ingelheim, BMS, Eli Lilly, EMD Serono, Genentech, GlaxoSmithKline, Janssen Pharmaceuticals, Mirati Therapeutics, Novartis Pharmaceuticals, Regeneron Pharmaceuticals, Sanofi, Spectrum Pharmaceuticals, and Takeda.
A version of this article first appeared on Medscape.com.
according to recent findings from the HARMONi-2 trial.
“This is the first randomized, phase 3 study to demonstrate a clinically significant improvement in efficacy with a novel drug compared to pembrolizumab in advanced NSCLC,” said study investigator Caicun Zhou, MD, PhD, with Shanghai Pulmonary Hospital in China,
The results highlight ivonescimab’s potential to become a “new standard of care” in advanced PD-L1–positive advanced NSCLC, said Dr. Zhou, who presented the analysis at the annual International Association for the Study of Lung Cancer (IASLC) World Conference on Lung Cancer in San Diego. Dr. Zhou is president-elect of the IASLC.
Ivonescimab (AK112) is a novel, potentially first-in-class investigational bispecific antibody that targets PD-1 and vascular endothelial growth factor (VEGF) developed by Akeso Biopharma, which funded the HARMONi-2 trial.
Conducted at 55 centers in China, HARMONi-2 enrolled 398 patients with untreated locally advanced or metastatic NSCLC, Eastern Cooperative Oncology Group Performance Status of 0 or 1, PD-L1 positive (with at least 1% of tumor cells expressing PD-L1), and no EGFR mutations or ALK rearrangements.
Patients were randomly allocated (1:1) to receive ivonescimab (20 mg/kg) or pembrolizumab (200 mg) every 3 weeks. The two groups were well balanced, and randomization was stratified by histology (squamous vs nonsquamous), clinical stage (IIIB/IIIC vs IV) and PD-L1 expression (PD-L1 of 1%-49% vs 50% or greater).
Dr. Zhou reported that patients who received ivonescimab were progression free for nearly twice as long as those on pembrolizumab — a median of 11.1 vs 5.8 months, indicating a 49% lower risk for progression or death (stratified hazard ratio [HR], 0.51; P < .0001).
The meaningful improvement in PFS with ivonescimab, compared with pembrolizumab, was “broadly consistent” in all prespecified subgroups, Dr. Zhou noted. That included patients with squamous NSCLC (HR, 0.48) and nonsquamous NSCLC (HR, 0.54), those with PD-L1 expression of 1%-49% (HR, 0.54) and 50% or higher (HR, 0.46), as well as those with liver metastases (HR, 0.47) and brain metastases (HR, 0.55).
The PFS benefit seen with ivonescimab in HARMONi-2 is “striking,” and the results “highlight the potential benefits of combined VEGF and PD-1 blockade together,” said John Heymach, MD, with the University of Texas MD Anderson Cancer Center in Houston, who served as discussant for the study.
Ivonescimab also led to a higher objective response rate (50% vs 38.5%) and disease control rate (89.9% vs 70.5%).
Grade 3 or higher treatment-related adverse events occurred in more patients receiving ivonescimab — 29.4% vs 15.6% on pembrolizumab. The difference largely stemmed from higher rates of proteinuria, hypertension, and lab abnormalities.
The rates of serious treatment-related adverse events were similar between the groups —20.8% in the ivonescimab group and 16.1% in the pembrolizumab group. Rates of grade 3 or higher immune-related adverse events were also similar, occurring in 7% of patients treated with ivonescimab and 8% of those receiving pembrolizumab.
In patients with squamous cell carcinoma, in particular, ivonescimab demonstrated a “very manageable” safety profile, Dr. Zhou noted. In this group, grade 3 or higher treatment-related adverse events occurred in 22.2% of patients (vs 18.7% receiving pembrolizumab).
Ivonescimab was associated with comparable but “numerically better” time to deterioration of global health status, based on the EORTC Core Quality of Life questionnaire, Dr. Zhou said.
Although the “really impressive and clinically meaningful” PFS benefits extended across different subgroups, “we await the overall survival results and additional studies done outside of China to confirm the benefit seen,” Dr. Heymach noted.
He also cautioned that, for patients with low to intermediate PD-L1 expression (1%-49%), pembrolizumab monotherapy “would not be the relevant comparator in the US and the rest of the world, and different study designs are going to be required for those populations.”
Based on the results of HARMONi-2, Akeso’s partner, Summit Therapeutics, plans to initiate HARMONi-7 in early 2025.
HARMONi-7 is currently planned as a multiregional, phase 3 clinical trial that will compare ivonescimab monotherapy to pembrolizumab monotherapy in patients with metastatic NSCLC whose tumors have high PD-L1 expression (50% or more).
Dr. Zhou has received consulting fees from Qilu Pharmaceutical, Hengrui, and TopAlliance Biosciences and honoraria from Eli Lilly China, Boehringer Ingelheim, Roche, Merck Sharp & Dohme, Qilu, Hengrui, Innovent Biologics, Alice, C-Stone, Luye Pharma, TopAlliance Biosciences, Amoy Diagnostics, and AnHeart Therapeutics. Dr. Heymach is a consultant for AbbVie, AnHeart Therapeutics, ArriVent Biopharma, AstraZeneca, BioCurity Pharmaceuticals, BioNTech, Blueprint Medicines, Boehringer Ingelheim, BMS, Eli Lilly, EMD Serono, Genentech, GlaxoSmithKline, Janssen Pharmaceuticals, Mirati Therapeutics, Novartis Pharmaceuticals, Regeneron Pharmaceuticals, Sanofi, Spectrum Pharmaceuticals, and Takeda.
A version of this article first appeared on Medscape.com.
FROM WCLC 2024
Do Clonal Hematopoiesis and Mosaic Chromosomal Alterations Increase Solid Tumor Risk?
Clonal hematopoiesis of indeterminate potential (CHIP) and mosaic chromosomal alterations (mCAs) are associated with an increased risk for breast cancer, and CHIP is associated with increased mortality in patients with colon cancer, according to the authors of new research.
These findings, drawn from almost 11,000 patients in the Women’s Health Initiative (WHI) study, add further evidence that CHIP and mCA drive solid tumor risk, alongside known associations with hematologic malignancies, reported lead author Pinkal Desai, MD, associate professor of medicine and clinical director of molecular aging at Englander Institute for Precision Medicine, Weill Cornell Medical College, New York City, and colleagues.
How This Study Differs From Others of Breast Cancer Risk Factors
“The independent effect of CHIP and mCA on risk and mortality from solid tumors has not been elucidated due to lack of detailed data on mortality outcomes and risk factors,” the investigators wrote in Cancer, although some previous studies have suggested a link.
In particular, the investigators highlighted a 2022 UK Biobank study, which reported an association between CHIP and lung cancer and a borderline association with breast cancer that did not quite reach statistical significance.
But the UK Biobank study was confined to a UK population, Dr. Desai noted in an interview, and the data were less detailed than those in the present investigation.
“In terms of risk, the part that was lacking in previous studies was a comprehensive assessment of risk factors that increase risk for all these cancers,” Dr. Desai said. “For example, for breast cancer, we had very detailed data on [participants’] Gail risk score, which is known to impact breast cancer risk. We also had mammogram data and colonoscopy data.”
In an accompanying editorial, Koichi Takahashi, MD, PhD , and Nehali Shah, BS, of The University of Texas MD Anderson Cancer Center, Houston, Texas, pointed out the same UK Biobank findings, then noted that CHIP has also been linked with worse overall survival in unselected cancer patients. Still, they wrote, “the impact of CH on cancer risk and mortality remains controversial due to conflicting data and context‐dependent effects,” necessitating studies like this one by Dr. Desai and colleagues.
How Was the Relationship Between CHIP, MCA, and Solid Tumor Risk Assessed?
To explore possible associations between CHIP, mCA, and solid tumors, the investigators analyzed whole genome sequencing data from 10,866 women in the WHI, a multi-study program that began in 1992 and involved 161,808 women in both observational and clinical trial cohorts.
In 2002, the first big data release from the WHI suggested that hormone replacement therapy (HRT) increased breast cancer risk, leading to widespread reduction in HRT use.
More recent reports continue to shape our understanding of these risks, suggesting differences across cancer types. For breast cancer, the WHI data suggested that HRT-associated risk was largely driven by formulations involving progesterone and estrogen, whereas estrogen-only formulations, now more common, are generally considered to present an acceptable risk profile for suitable patients.
The new study accounted for this potential HRT-associated risk, including by adjusting for patients who received HRT, type of HRT received, and duration of HRT received. According to Desai, this approach is commonly used when analyzing data from the WHI, nullifying concerns about the potentially deleterious effects of the hormones used in the study.
“Our question was not ‘does HRT cause cancer?’ ” Dr. Desai said in an interview. “But HRT can be linked to breast cancer risk and has a potential to be a confounder, and hence the above methodology.
“So I can say that the confounding/effect modification that HRT would have contributed to in the relationship between exposure (CH and mCA) and outcome (cancer) is well adjusted for as described above. This is standard in WHI analyses,” she continued.
“Every Women’s Health Initiative analysis that comes out — not just for our study — uses a standard method ... where you account for hormonal therapy,” Dr. Desai added, again noting that many other potential risk factors were considered, enabling a “detailed, robust” analysis.
Dr. Takahashi and Ms. Shah agreed. “A notable strength of this study is its adjustment for many confounding factors,” they wrote. “The cohort’s well‐annotated data on other known cancer risk factors allowed for a robust assessment of CH’s independent risk.”
How Do Findings Compare With Those of the UK Biobank Study?
CHIP was associated with a 30% increased risk for breast cancer (hazard ratio [HR], 1.30; 95% CI, 1.03-1.64; P = .02), strengthening the borderline association reported by the UK Biobank study.
In contrast with the UK Biobank study, CHIP was not associated with lung cancer risk, although this may have been caused by fewer cases of lung cancer and a lack of male patients, Dr. Desai suggested.
“The discrepancy between the studies lies in the risk of lung cancer, although the point estimate in the current study suggested a positive association,” wrote Dr. Takahashi and Ms. Shah.
As in the UK Biobank study, CHIP was not associated with increased risk of developing colorectal cancer.
Mortality analysis, however, which was not conducted in the UK Biobank study, offered a new insight: Patients with existing colorectal cancer and CHIP had a significantly higher mortality risk than those without CHIP. Before stage adjustment, risk for mortality among those with colorectal cancer and CHIP was fourfold higher than those without CHIP (HR, 3.99; 95% CI, 2.41-6.62; P < .001). After stage adjustment, CHIP was still associated with a twofold higher mortality risk (HR, 2.50; 95% CI, 1.32-4.72; P = .004).
The investigators’ first mCA analyses, which employed a cell fraction cutoff greater than 3%, were unfruitful. But raising the cell fraction threshold to 5% in an exploratory analysis showed that autosomal mCA was associated with a 39% increased risk for breast cancer (HR, 1.39; 95% CI, 1.06-1.83; P = .01). No such associations were found between mCA and colorectal or lung cancer, regardless of cell fraction threshold.
The original 3% cell fraction threshold was selected on the basis of previous studies reporting a link between mCA and hematologic malignancies at this cutoff, Dr. Desai said.
She and her colleagues said a higher 5% cutoff might be needed, as they suspected that the link between mCA and solid tumors may not be causal, requiring a higher mutation rate.
Why Do Results Differ Between These Types of Studies?
Dr. Takahashi and Ms. Shah suggested that one possible limitation of the new study, and an obstacle to comparing results with the UK Biobank study and others like it, goes beyond population heterogeneity; incongruent findings could also be explained by differences in whole genome sequencing (WGS) technique.
“Although WGS allows sensitive detection of mCA through broad genomic coverage, it is less effective at detecting CHIP with low variant allele frequency (VAF) due to its relatively shallow depth (30x),” they wrote. “Consequently, the prevalence of mCA (18.8%) was much higher than that of CHIP (8.3%) in this cohort, contrasting with other studies using deeper sequencing.” As a result, the present study may have underestimated CHIP prevalence because of shallow sequencing depth.
“This inconsistency is a common challenge in CH population studies due to the lack of standardized methodologies and the frequent reliance on preexisting data not originally intended for CH detection,” Dr. Takahashi and Ms. Shah said.
Even so, despite the “heavily context-dependent” nature of these reported risks, the body of evidence to date now offers a convincing biological rationale linking CH with cancer development and outcomes, they added.
How Do the CHIP- and mCA-associated Risks Differ Between Solid Tumors and Blood Cancers?
“[These solid tumor risks are] not causal in the way CHIP mutations are causal for blood cancers,” Dr. Desai said. “Here we are talking about solid tumor risk, and it’s kind of scattered. It’s not just breast cancer ... there’s also increased colon cancer mortality. So I feel these mutations are doing something different ... they are sort of an added factor.”
Specific mechanisms remain unclear, Dr. Desai said, although she speculated about possible impacts on the inflammatory state or alterations to the tumor microenvironment.
“These are blood cells, right?” Dr. Desai asked. “They’re everywhere, and they’re changing something inherently in these tumors.”
Future research and therapeutic development
Siddhartha Jaiswal, MD, PhD, assistant professor in the Department of Pathology at Stanford University in California, whose lab focuses on clonal hematopoiesis, said the causality question is central to future research.
“The key question is, are these mutations acting because they alter the function of blood cells in some way to promote cancer risk, or is it reflective of some sort of shared etiology that’s not causal?” Dr. Jaiswal said in an interview.
Available data support both possibilities.
On one side, “reasonable evidence” supports the noncausal view, Dr. Jaiswal noted, because telomere length is one of the most common genetic risk factors for clonal hematopoiesis and also for solid tumors, suggesting a shared genetic factor. On the other hand, CHIP and mCA could be directly protumorigenic via conferred disturbances of immune cell function.
When asked if both causal and noncausal factors could be at play, Dr. Jaiswal said, “yeah, absolutely.”
The presence of a causal association could be promising from a therapeutic standpoint.
“If it turns out that this association is driven by a direct causal effect of the mutations, perhaps related to immune cell function or dysfunction, then targeting that dysfunction could be a therapeutic path to improve outcomes in people, and there’s a lot of interest in this,” Dr. Jaiswal said. He went on to explain how a trial exploring this approach via interleukin-8 inhibition in lung cancer fell short.
Yet earlier intervention may still hold promise, according to experts.
“[This study] provokes the hypothesis that CH‐targeted interventions could potentially reduce cancer risk in the future,” Dr. Takahashi and Ms. Shah said in their editorial.
The WHI program is funded by the National Heart, Lung, and Blood Institute; National Institutes of Health; and the Department of Health & Human Services. The investigators disclosed relationships with Eli Lilly, AbbVie, Celgene, and others. Dr. Jaiswal reported stock equity in a company that has an interest in clonal hematopoiesis.
A version of this article first appeared on Medscape.com.
Clonal hematopoiesis of indeterminate potential (CHIP) and mosaic chromosomal alterations (mCAs) are associated with an increased risk for breast cancer, and CHIP is associated with increased mortality in patients with colon cancer, according to the authors of new research.
These findings, drawn from almost 11,000 patients in the Women’s Health Initiative (WHI) study, add further evidence that CHIP and mCA drive solid tumor risk, alongside known associations with hematologic malignancies, reported lead author Pinkal Desai, MD, associate professor of medicine and clinical director of molecular aging at Englander Institute for Precision Medicine, Weill Cornell Medical College, New York City, and colleagues.
How This Study Differs From Others of Breast Cancer Risk Factors
“The independent effect of CHIP and mCA on risk and mortality from solid tumors has not been elucidated due to lack of detailed data on mortality outcomes and risk factors,” the investigators wrote in Cancer, although some previous studies have suggested a link.
In particular, the investigators highlighted a 2022 UK Biobank study, which reported an association between CHIP and lung cancer and a borderline association with breast cancer that did not quite reach statistical significance.
But the UK Biobank study was confined to a UK population, Dr. Desai noted in an interview, and the data were less detailed than those in the present investigation.
“In terms of risk, the part that was lacking in previous studies was a comprehensive assessment of risk factors that increase risk for all these cancers,” Dr. Desai said. “For example, for breast cancer, we had very detailed data on [participants’] Gail risk score, which is known to impact breast cancer risk. We also had mammogram data and colonoscopy data.”
In an accompanying editorial, Koichi Takahashi, MD, PhD , and Nehali Shah, BS, of The University of Texas MD Anderson Cancer Center, Houston, Texas, pointed out the same UK Biobank findings, then noted that CHIP has also been linked with worse overall survival in unselected cancer patients. Still, they wrote, “the impact of CH on cancer risk and mortality remains controversial due to conflicting data and context‐dependent effects,” necessitating studies like this one by Dr. Desai and colleagues.
How Was the Relationship Between CHIP, MCA, and Solid Tumor Risk Assessed?
To explore possible associations between CHIP, mCA, and solid tumors, the investigators analyzed whole genome sequencing data from 10,866 women in the WHI, a multi-study program that began in 1992 and involved 161,808 women in both observational and clinical trial cohorts.
In 2002, the first big data release from the WHI suggested that hormone replacement therapy (HRT) increased breast cancer risk, leading to widespread reduction in HRT use.
More recent reports continue to shape our understanding of these risks, suggesting differences across cancer types. For breast cancer, the WHI data suggested that HRT-associated risk was largely driven by formulations involving progesterone and estrogen, whereas estrogen-only formulations, now more common, are generally considered to present an acceptable risk profile for suitable patients.
The new study accounted for this potential HRT-associated risk, including by adjusting for patients who received HRT, type of HRT received, and duration of HRT received. According to Desai, this approach is commonly used when analyzing data from the WHI, nullifying concerns about the potentially deleterious effects of the hormones used in the study.
“Our question was not ‘does HRT cause cancer?’ ” Dr. Desai said in an interview. “But HRT can be linked to breast cancer risk and has a potential to be a confounder, and hence the above methodology.
“So I can say that the confounding/effect modification that HRT would have contributed to in the relationship between exposure (CH and mCA) and outcome (cancer) is well adjusted for as described above. This is standard in WHI analyses,” she continued.
“Every Women’s Health Initiative analysis that comes out — not just for our study — uses a standard method ... where you account for hormonal therapy,” Dr. Desai added, again noting that many other potential risk factors were considered, enabling a “detailed, robust” analysis.
Dr. Takahashi and Ms. Shah agreed. “A notable strength of this study is its adjustment for many confounding factors,” they wrote. “The cohort’s well‐annotated data on other known cancer risk factors allowed for a robust assessment of CH’s independent risk.”
How Do Findings Compare With Those of the UK Biobank Study?
CHIP was associated with a 30% increased risk for breast cancer (hazard ratio [HR], 1.30; 95% CI, 1.03-1.64; P = .02), strengthening the borderline association reported by the UK Biobank study.
In contrast with the UK Biobank study, CHIP was not associated with lung cancer risk, although this may have been caused by fewer cases of lung cancer and a lack of male patients, Dr. Desai suggested.
“The discrepancy between the studies lies in the risk of lung cancer, although the point estimate in the current study suggested a positive association,” wrote Dr. Takahashi and Ms. Shah.
As in the UK Biobank study, CHIP was not associated with increased risk of developing colorectal cancer.
Mortality analysis, however, which was not conducted in the UK Biobank study, offered a new insight: Patients with existing colorectal cancer and CHIP had a significantly higher mortality risk than those without CHIP. Before stage adjustment, risk for mortality among those with colorectal cancer and CHIP was fourfold higher than those without CHIP (HR, 3.99; 95% CI, 2.41-6.62; P < .001). After stage adjustment, CHIP was still associated with a twofold higher mortality risk (HR, 2.50; 95% CI, 1.32-4.72; P = .004).
The investigators’ first mCA analyses, which employed a cell fraction cutoff greater than 3%, were unfruitful. But raising the cell fraction threshold to 5% in an exploratory analysis showed that autosomal mCA was associated with a 39% increased risk for breast cancer (HR, 1.39; 95% CI, 1.06-1.83; P = .01). No such associations were found between mCA and colorectal or lung cancer, regardless of cell fraction threshold.
The original 3% cell fraction threshold was selected on the basis of previous studies reporting a link between mCA and hematologic malignancies at this cutoff, Dr. Desai said.
She and her colleagues said a higher 5% cutoff might be needed, as they suspected that the link between mCA and solid tumors may not be causal, requiring a higher mutation rate.
Why Do Results Differ Between These Types of Studies?
Dr. Takahashi and Ms. Shah suggested that one possible limitation of the new study, and an obstacle to comparing results with the UK Biobank study and others like it, goes beyond population heterogeneity; incongruent findings could also be explained by differences in whole genome sequencing (WGS) technique.
“Although WGS allows sensitive detection of mCA through broad genomic coverage, it is less effective at detecting CHIP with low variant allele frequency (VAF) due to its relatively shallow depth (30x),” they wrote. “Consequently, the prevalence of mCA (18.8%) was much higher than that of CHIP (8.3%) in this cohort, contrasting with other studies using deeper sequencing.” As a result, the present study may have underestimated CHIP prevalence because of shallow sequencing depth.
“This inconsistency is a common challenge in CH population studies due to the lack of standardized methodologies and the frequent reliance on preexisting data not originally intended for CH detection,” Dr. Takahashi and Ms. Shah said.
Even so, despite the “heavily context-dependent” nature of these reported risks, the body of evidence to date now offers a convincing biological rationale linking CH with cancer development and outcomes, they added.
How Do the CHIP- and mCA-associated Risks Differ Between Solid Tumors and Blood Cancers?
“[These solid tumor risks are] not causal in the way CHIP mutations are causal for blood cancers,” Dr. Desai said. “Here we are talking about solid tumor risk, and it’s kind of scattered. It’s not just breast cancer ... there’s also increased colon cancer mortality. So I feel these mutations are doing something different ... they are sort of an added factor.”
Specific mechanisms remain unclear, Dr. Desai said, although she speculated about possible impacts on the inflammatory state or alterations to the tumor microenvironment.
“These are blood cells, right?” Dr. Desai asked. “They’re everywhere, and they’re changing something inherently in these tumors.”
Future research and therapeutic development
Siddhartha Jaiswal, MD, PhD, assistant professor in the Department of Pathology at Stanford University in California, whose lab focuses on clonal hematopoiesis, said the causality question is central to future research.
“The key question is, are these mutations acting because they alter the function of blood cells in some way to promote cancer risk, or is it reflective of some sort of shared etiology that’s not causal?” Dr. Jaiswal said in an interview.
Available data support both possibilities.
On one side, “reasonable evidence” supports the noncausal view, Dr. Jaiswal noted, because telomere length is one of the most common genetic risk factors for clonal hematopoiesis and also for solid tumors, suggesting a shared genetic factor. On the other hand, CHIP and mCA could be directly protumorigenic via conferred disturbances of immune cell function.
When asked if both causal and noncausal factors could be at play, Dr. Jaiswal said, “yeah, absolutely.”
The presence of a causal association could be promising from a therapeutic standpoint.
“If it turns out that this association is driven by a direct causal effect of the mutations, perhaps related to immune cell function or dysfunction, then targeting that dysfunction could be a therapeutic path to improve outcomes in people, and there’s a lot of interest in this,” Dr. Jaiswal said. He went on to explain how a trial exploring this approach via interleukin-8 inhibition in lung cancer fell short.
Yet earlier intervention may still hold promise, according to experts.
“[This study] provokes the hypothesis that CH‐targeted interventions could potentially reduce cancer risk in the future,” Dr. Takahashi and Ms. Shah said in their editorial.
The WHI program is funded by the National Heart, Lung, and Blood Institute; National Institutes of Health; and the Department of Health & Human Services. The investigators disclosed relationships with Eli Lilly, AbbVie, Celgene, and others. Dr. Jaiswal reported stock equity in a company that has an interest in clonal hematopoiesis.
A version of this article first appeared on Medscape.com.
Clonal hematopoiesis of indeterminate potential (CHIP) and mosaic chromosomal alterations (mCAs) are associated with an increased risk for breast cancer, and CHIP is associated with increased mortality in patients with colon cancer, according to the authors of new research.
These findings, drawn from almost 11,000 patients in the Women’s Health Initiative (WHI) study, add further evidence that CHIP and mCA drive solid tumor risk, alongside known associations with hematologic malignancies, reported lead author Pinkal Desai, MD, associate professor of medicine and clinical director of molecular aging at Englander Institute for Precision Medicine, Weill Cornell Medical College, New York City, and colleagues.
How This Study Differs From Others of Breast Cancer Risk Factors
“The independent effect of CHIP and mCA on risk and mortality from solid tumors has not been elucidated due to lack of detailed data on mortality outcomes and risk factors,” the investigators wrote in Cancer, although some previous studies have suggested a link.
In particular, the investigators highlighted a 2022 UK Biobank study, which reported an association between CHIP and lung cancer and a borderline association with breast cancer that did not quite reach statistical significance.
But the UK Biobank study was confined to a UK population, Dr. Desai noted in an interview, and the data were less detailed than those in the present investigation.
“In terms of risk, the part that was lacking in previous studies was a comprehensive assessment of risk factors that increase risk for all these cancers,” Dr. Desai said. “For example, for breast cancer, we had very detailed data on [participants’] Gail risk score, which is known to impact breast cancer risk. We also had mammogram data and colonoscopy data.”
In an accompanying editorial, Koichi Takahashi, MD, PhD , and Nehali Shah, BS, of The University of Texas MD Anderson Cancer Center, Houston, Texas, pointed out the same UK Biobank findings, then noted that CHIP has also been linked with worse overall survival in unselected cancer patients. Still, they wrote, “the impact of CH on cancer risk and mortality remains controversial due to conflicting data and context‐dependent effects,” necessitating studies like this one by Dr. Desai and colleagues.
How Was the Relationship Between CHIP, MCA, and Solid Tumor Risk Assessed?
To explore possible associations between CHIP, mCA, and solid tumors, the investigators analyzed whole genome sequencing data from 10,866 women in the WHI, a multi-study program that began in 1992 and involved 161,808 women in both observational and clinical trial cohorts.
In 2002, the first big data release from the WHI suggested that hormone replacement therapy (HRT) increased breast cancer risk, leading to widespread reduction in HRT use.
More recent reports continue to shape our understanding of these risks, suggesting differences across cancer types. For breast cancer, the WHI data suggested that HRT-associated risk was largely driven by formulations involving progesterone and estrogen, whereas estrogen-only formulations, now more common, are generally considered to present an acceptable risk profile for suitable patients.
The new study accounted for this potential HRT-associated risk, including by adjusting for patients who received HRT, type of HRT received, and duration of HRT received. According to Desai, this approach is commonly used when analyzing data from the WHI, nullifying concerns about the potentially deleterious effects of the hormones used in the study.
“Our question was not ‘does HRT cause cancer?’ ” Dr. Desai said in an interview. “But HRT can be linked to breast cancer risk and has a potential to be a confounder, and hence the above methodology.
“So I can say that the confounding/effect modification that HRT would have contributed to in the relationship between exposure (CH and mCA) and outcome (cancer) is well adjusted for as described above. This is standard in WHI analyses,” she continued.
“Every Women’s Health Initiative analysis that comes out — not just for our study — uses a standard method ... where you account for hormonal therapy,” Dr. Desai added, again noting that many other potential risk factors were considered, enabling a “detailed, robust” analysis.
Dr. Takahashi and Ms. Shah agreed. “A notable strength of this study is its adjustment for many confounding factors,” they wrote. “The cohort’s well‐annotated data on other known cancer risk factors allowed for a robust assessment of CH’s independent risk.”
How Do Findings Compare With Those of the UK Biobank Study?
CHIP was associated with a 30% increased risk for breast cancer (hazard ratio [HR], 1.30; 95% CI, 1.03-1.64; P = .02), strengthening the borderline association reported by the UK Biobank study.
In contrast with the UK Biobank study, CHIP was not associated with lung cancer risk, although this may have been caused by fewer cases of lung cancer and a lack of male patients, Dr. Desai suggested.
“The discrepancy between the studies lies in the risk of lung cancer, although the point estimate in the current study suggested a positive association,” wrote Dr. Takahashi and Ms. Shah.
As in the UK Biobank study, CHIP was not associated with increased risk of developing colorectal cancer.
Mortality analysis, however, which was not conducted in the UK Biobank study, offered a new insight: Patients with existing colorectal cancer and CHIP had a significantly higher mortality risk than those without CHIP. Before stage adjustment, risk for mortality among those with colorectal cancer and CHIP was fourfold higher than those without CHIP (HR, 3.99; 95% CI, 2.41-6.62; P < .001). After stage adjustment, CHIP was still associated with a twofold higher mortality risk (HR, 2.50; 95% CI, 1.32-4.72; P = .004).
The investigators’ first mCA analyses, which employed a cell fraction cutoff greater than 3%, were unfruitful. But raising the cell fraction threshold to 5% in an exploratory analysis showed that autosomal mCA was associated with a 39% increased risk for breast cancer (HR, 1.39; 95% CI, 1.06-1.83; P = .01). No such associations were found between mCA and colorectal or lung cancer, regardless of cell fraction threshold.
The original 3% cell fraction threshold was selected on the basis of previous studies reporting a link between mCA and hematologic malignancies at this cutoff, Dr. Desai said.
She and her colleagues said a higher 5% cutoff might be needed, as they suspected that the link between mCA and solid tumors may not be causal, requiring a higher mutation rate.
Why Do Results Differ Between These Types of Studies?
Dr. Takahashi and Ms. Shah suggested that one possible limitation of the new study, and an obstacle to comparing results with the UK Biobank study and others like it, goes beyond population heterogeneity; incongruent findings could also be explained by differences in whole genome sequencing (WGS) technique.
“Although WGS allows sensitive detection of mCA through broad genomic coverage, it is less effective at detecting CHIP with low variant allele frequency (VAF) due to its relatively shallow depth (30x),” they wrote. “Consequently, the prevalence of mCA (18.8%) was much higher than that of CHIP (8.3%) in this cohort, contrasting with other studies using deeper sequencing.” As a result, the present study may have underestimated CHIP prevalence because of shallow sequencing depth.
“This inconsistency is a common challenge in CH population studies due to the lack of standardized methodologies and the frequent reliance on preexisting data not originally intended for CH detection,” Dr. Takahashi and Ms. Shah said.
Even so, despite the “heavily context-dependent” nature of these reported risks, the body of evidence to date now offers a convincing biological rationale linking CH with cancer development and outcomes, they added.
How Do the CHIP- and mCA-associated Risks Differ Between Solid Tumors and Blood Cancers?
“[These solid tumor risks are] not causal in the way CHIP mutations are causal for blood cancers,” Dr. Desai said. “Here we are talking about solid tumor risk, and it’s kind of scattered. It’s not just breast cancer ... there’s also increased colon cancer mortality. So I feel these mutations are doing something different ... they are sort of an added factor.”
Specific mechanisms remain unclear, Dr. Desai said, although she speculated about possible impacts on the inflammatory state or alterations to the tumor microenvironment.
“These are blood cells, right?” Dr. Desai asked. “They’re everywhere, and they’re changing something inherently in these tumors.”
Future research and therapeutic development
Siddhartha Jaiswal, MD, PhD, assistant professor in the Department of Pathology at Stanford University in California, whose lab focuses on clonal hematopoiesis, said the causality question is central to future research.
“The key question is, are these mutations acting because they alter the function of blood cells in some way to promote cancer risk, or is it reflective of some sort of shared etiology that’s not causal?” Dr. Jaiswal said in an interview.
Available data support both possibilities.
On one side, “reasonable evidence” supports the noncausal view, Dr. Jaiswal noted, because telomere length is one of the most common genetic risk factors for clonal hematopoiesis and also for solid tumors, suggesting a shared genetic factor. On the other hand, CHIP and mCA could be directly protumorigenic via conferred disturbances of immune cell function.
When asked if both causal and noncausal factors could be at play, Dr. Jaiswal said, “yeah, absolutely.”
The presence of a causal association could be promising from a therapeutic standpoint.
“If it turns out that this association is driven by a direct causal effect of the mutations, perhaps related to immune cell function or dysfunction, then targeting that dysfunction could be a therapeutic path to improve outcomes in people, and there’s a lot of interest in this,” Dr. Jaiswal said. He went on to explain how a trial exploring this approach via interleukin-8 inhibition in lung cancer fell short.
Yet earlier intervention may still hold promise, according to experts.
“[This study] provokes the hypothesis that CH‐targeted interventions could potentially reduce cancer risk in the future,” Dr. Takahashi and Ms. Shah said in their editorial.
The WHI program is funded by the National Heart, Lung, and Blood Institute; National Institutes of Health; and the Department of Health & Human Services. The investigators disclosed relationships with Eli Lilly, AbbVie, Celgene, and others. Dr. Jaiswal reported stock equity in a company that has an interest in clonal hematopoiesis.
A version of this article first appeared on Medscape.com.
FROM CANCER
RSV Updates: Prophylaxis Approval and Hospitalization for Severe RSV
1. Pfizer announces positive top-line results from phase 3 study of ABRYSVO® in adults aged 18 to 59 at increased risk for RSV disease. Press release. Pfizer; April 9, 2024. Accessed May 22, 2024. https://www.pfizer.com/news/press-release/press-release-detail/pfizer-announces-positive-top-line-results-phase-3-study-1
2. Pfizer announces positive top-line data for full season two efficacy of ABRYSVO® for RSV in older adults. Press release. Pfizer; February 29, 2024. Accessed May 22, 2024. https://www.pfizer.com/news/press-release/press-release-detail/pfizer-announces-positive-top-line-data-full-season-two
3. CDC study shows effectiveness of RSV immunization for infants. Press release. US Centers for Disease Control and Prevention; March 7, 2024. Accessed May 22, 2024. https://www.cdc.gov/media/releases/2024/s0307-rsv-immunization.html
4. Moline HL, Tannis A, Toepfer AP, et al. Early estimate of nirsevimab effectiveness for prevention of respiratory syncytial virus–associated hospitalization among infants entering their first respiratory syncytial virus season — new vaccine surveillance network, October 2023–February 2024. MMWR Morb Mortal Wkly Rep. 2024;73(9):209-214. doi:10.15585/mmwr.mm7309a4
5. Havers FP, Whitaker M, Melgar M, et al; for the RSV-NET Surveillance Team. Characteristics and outcomes among adults aged ≥60 years hospitalized with laboratory-confirmed respiratory syncytial virus ─ RSV-NET, 12 states, July 2022–June 2023. MMWR Morb Mortal Wkly Rep. 2023;72(40):1075-1082. doi:10.15585/mmwr.mm7240a1
6. Walsh EE, Pérez Marc G, Zareba AM, et al; for the RENOIR Clinical Trial Group. Efficacy and safety of a bivalent RSV prefusion F vaccine in older adults. N Engl J Med. 2023;388(16):1465-1477. doi:10.1056/NEJMoa2213836
7. Fleming-Dutra KE, Jones JM, Roper LE, et al. Use of the Pfizer respiratory syncytial virus vaccine during pregnancy for the prevention of respiratory syncytial virus–associated lower respiratory tract disease in infants: recommendations of the Advisory Committee on Immunization Practices — United States, 2023. MMWR Morb Mortal Wkly Rep. 2023;72(41):1115-1122. doi:10.15585/mmwr.mm7241e1
8. Baker J, Aliabadi N, Munjal I, et al. Equivalent immunogenicity across three RSVpreF vaccine lots in healthy adults 18-49 years of age: results of a randomized phase 3 study. Vaccine. 2024;42(13):3172-3179. doi:10.1016/j.vaccine.2024.03.070
9. New data for AREXVY, GSK’s RSV vaccine, show potential to help protect adults aged 50 to 59 at increased risk for RSV disease. Press release. GSK; October 25, 2023. Accessed May 22, 2024. https://us.gsk.com/en-us/media/press-releases/new-data-for-arexvy/
1. Pfizer announces positive top-line results from phase 3 study of ABRYSVO® in adults aged 18 to 59 at increased risk for RSV disease. Press release. Pfizer; April 9, 2024. Accessed May 22, 2024. https://www.pfizer.com/news/press-release/press-release-detail/pfizer-announces-positive-top-line-results-phase-3-study-1
2. Pfizer announces positive top-line data for full season two efficacy of ABRYSVO® for RSV in older adults. Press release. Pfizer; February 29, 2024. Accessed May 22, 2024. https://www.pfizer.com/news/press-release/press-release-detail/pfizer-announces-positive-top-line-data-full-season-two
3. CDC study shows effectiveness of RSV immunization for infants. Press release. US Centers for Disease Control and Prevention; March 7, 2024. Accessed May 22, 2024. https://www.cdc.gov/media/releases/2024/s0307-rsv-immunization.html
4. Moline HL, Tannis A, Toepfer AP, et al. Early estimate of nirsevimab effectiveness for prevention of respiratory syncytial virus–associated hospitalization among infants entering their first respiratory syncytial virus season — new vaccine surveillance network, October 2023–February 2024. MMWR Morb Mortal Wkly Rep. 2024;73(9):209-214. doi:10.15585/mmwr.mm7309a4
5. Havers FP, Whitaker M, Melgar M, et al; for the RSV-NET Surveillance Team. Characteristics and outcomes among adults aged ≥60 years hospitalized with laboratory-confirmed respiratory syncytial virus ─ RSV-NET, 12 states, July 2022–June 2023. MMWR Morb Mortal Wkly Rep. 2023;72(40):1075-1082. doi:10.15585/mmwr.mm7240a1
6. Walsh EE, Pérez Marc G, Zareba AM, et al; for the RENOIR Clinical Trial Group. Efficacy and safety of a bivalent RSV prefusion F vaccine in older adults. N Engl J Med. 2023;388(16):1465-1477. doi:10.1056/NEJMoa2213836
7. Fleming-Dutra KE, Jones JM, Roper LE, et al. Use of the Pfizer respiratory syncytial virus vaccine during pregnancy for the prevention of respiratory syncytial virus–associated lower respiratory tract disease in infants: recommendations of the Advisory Committee on Immunization Practices — United States, 2023. MMWR Morb Mortal Wkly Rep. 2023;72(41):1115-1122. doi:10.15585/mmwr.mm7241e1
8. Baker J, Aliabadi N, Munjal I, et al. Equivalent immunogenicity across three RSVpreF vaccine lots in healthy adults 18-49 years of age: results of a randomized phase 3 study. Vaccine. 2024;42(13):3172-3179. doi:10.1016/j.vaccine.2024.03.070
9. New data for AREXVY, GSK’s RSV vaccine, show potential to help protect adults aged 50 to 59 at increased risk for RSV disease. Press release. GSK; October 25, 2023. Accessed May 22, 2024. https://us.gsk.com/en-us/media/press-releases/new-data-for-arexvy/
1. Pfizer announces positive top-line results from phase 3 study of ABRYSVO® in adults aged 18 to 59 at increased risk for RSV disease. Press release. Pfizer; April 9, 2024. Accessed May 22, 2024. https://www.pfizer.com/news/press-release/press-release-detail/pfizer-announces-positive-top-line-results-phase-3-study-1
2. Pfizer announces positive top-line data for full season two efficacy of ABRYSVO® for RSV in older adults. Press release. Pfizer; February 29, 2024. Accessed May 22, 2024. https://www.pfizer.com/news/press-release/press-release-detail/pfizer-announces-positive-top-line-data-full-season-two
3. CDC study shows effectiveness of RSV immunization for infants. Press release. US Centers for Disease Control and Prevention; March 7, 2024. Accessed May 22, 2024. https://www.cdc.gov/media/releases/2024/s0307-rsv-immunization.html
4. Moline HL, Tannis A, Toepfer AP, et al. Early estimate of nirsevimab effectiveness for prevention of respiratory syncytial virus–associated hospitalization among infants entering their first respiratory syncytial virus season — new vaccine surveillance network, October 2023–February 2024. MMWR Morb Mortal Wkly Rep. 2024;73(9):209-214. doi:10.15585/mmwr.mm7309a4
5. Havers FP, Whitaker M, Melgar M, et al; for the RSV-NET Surveillance Team. Characteristics and outcomes among adults aged ≥60 years hospitalized with laboratory-confirmed respiratory syncytial virus ─ RSV-NET, 12 states, July 2022–June 2023. MMWR Morb Mortal Wkly Rep. 2023;72(40):1075-1082. doi:10.15585/mmwr.mm7240a1
6. Walsh EE, Pérez Marc G, Zareba AM, et al; for the RENOIR Clinical Trial Group. Efficacy and safety of a bivalent RSV prefusion F vaccine in older adults. N Engl J Med. 2023;388(16):1465-1477. doi:10.1056/NEJMoa2213836
7. Fleming-Dutra KE, Jones JM, Roper LE, et al. Use of the Pfizer respiratory syncytial virus vaccine during pregnancy for the prevention of respiratory syncytial virus–associated lower respiratory tract disease in infants: recommendations of the Advisory Committee on Immunization Practices — United States, 2023. MMWR Morb Mortal Wkly Rep. 2023;72(41):1115-1122. doi:10.15585/mmwr.mm7241e1
8. Baker J, Aliabadi N, Munjal I, et al. Equivalent immunogenicity across three RSVpreF vaccine lots in healthy adults 18-49 years of age: results of a randomized phase 3 study. Vaccine. 2024;42(13):3172-3179. doi:10.1016/j.vaccine.2024.03.070
9. New data for AREXVY, GSK’s RSV vaccine, show potential to help protect adults aged 50 to 59 at increased risk for RSV disease. Press release. GSK; October 25, 2023. Accessed May 22, 2024. https://us.gsk.com/en-us/media/press-releases/new-data-for-arexvy/
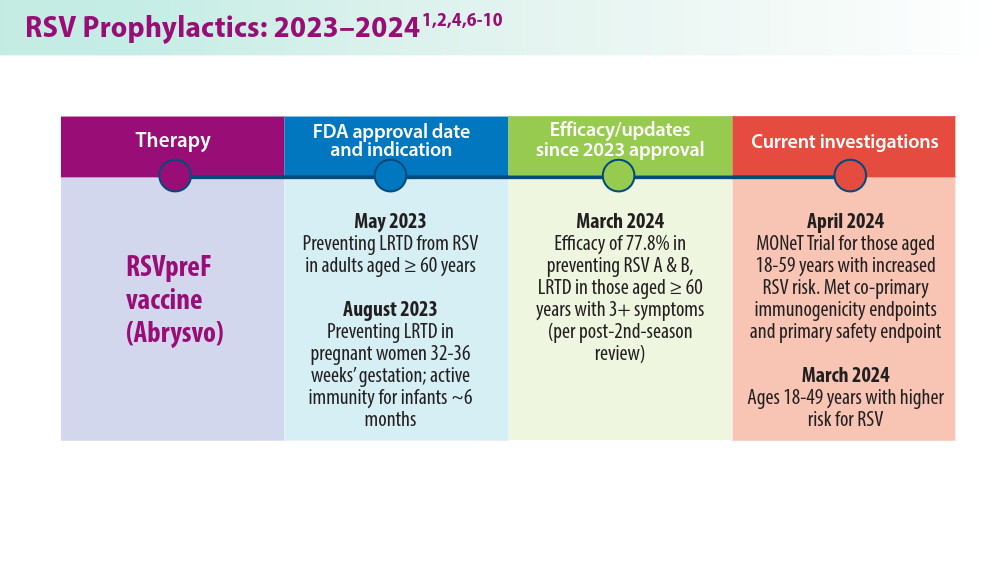
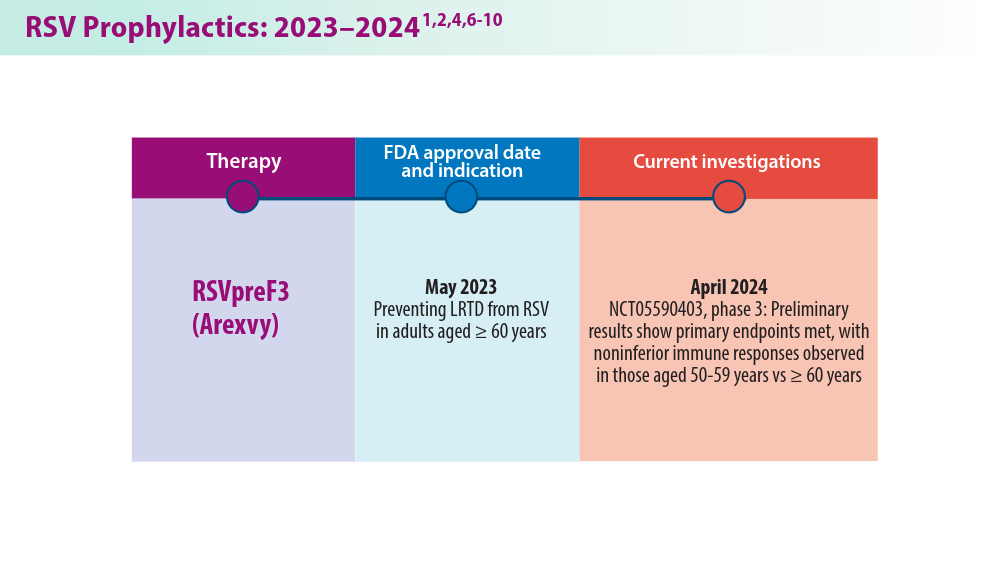
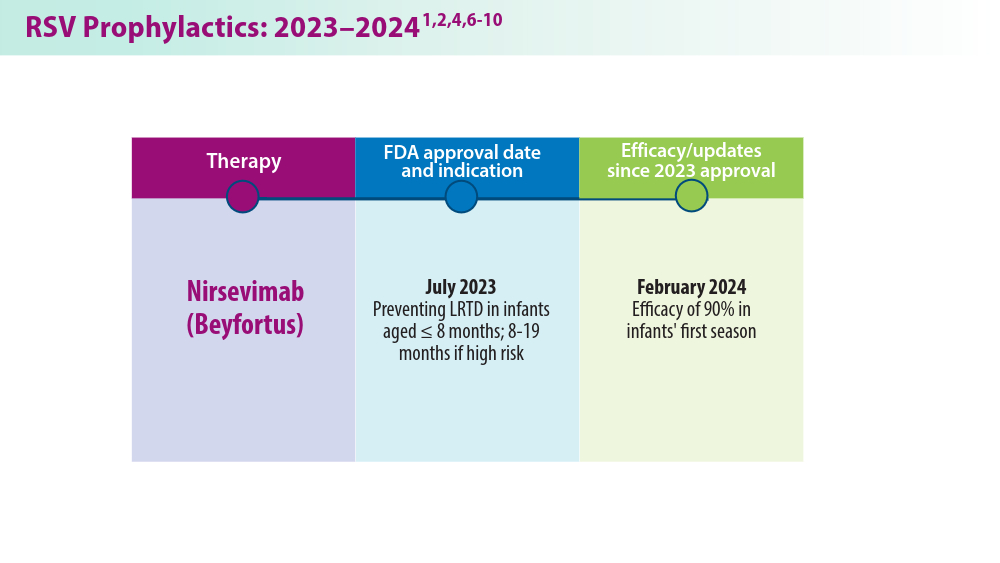
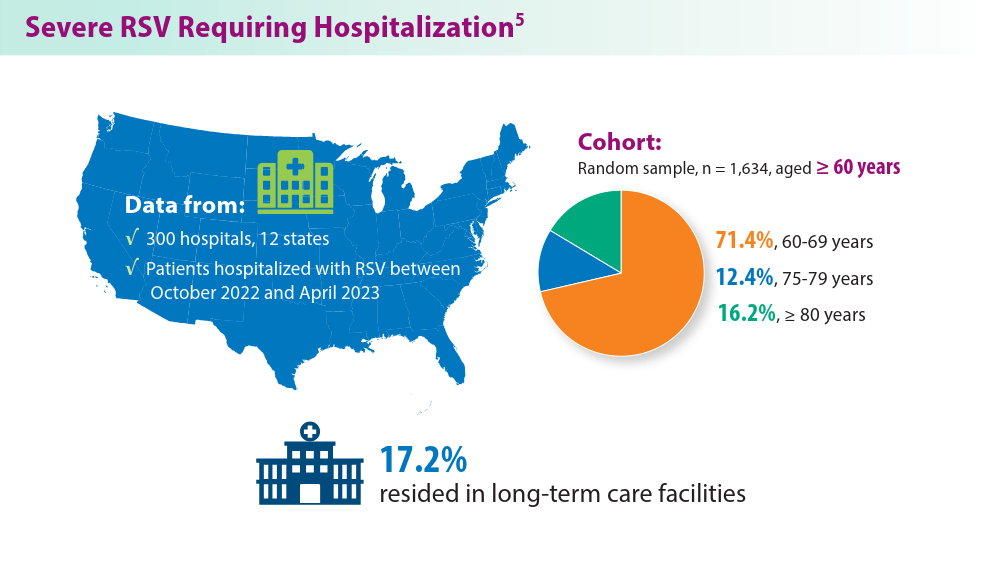
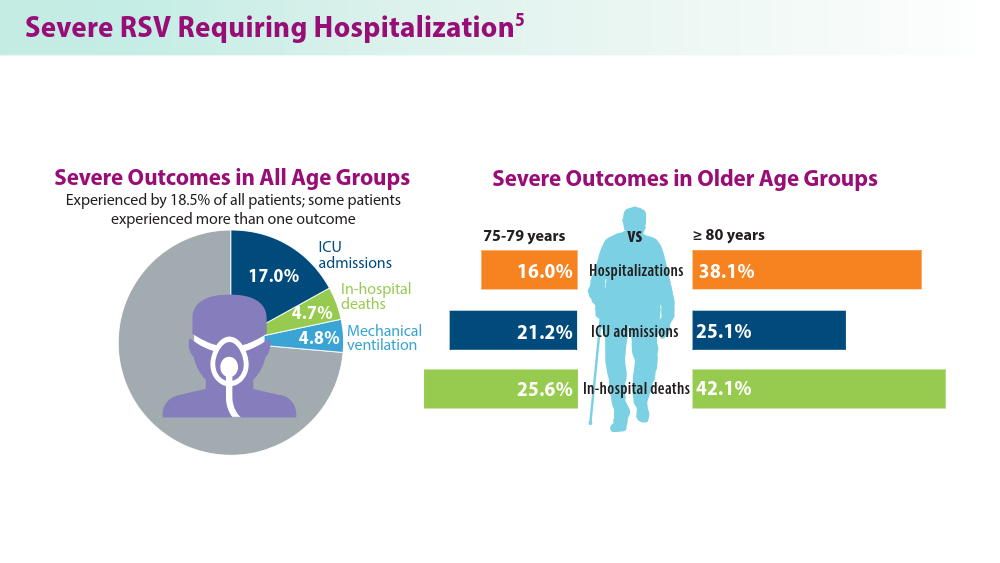
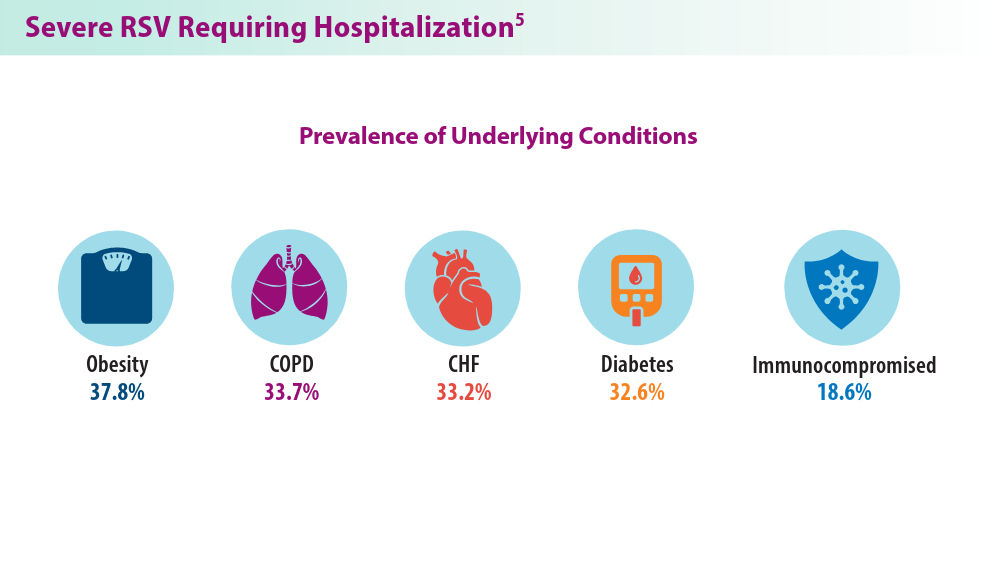
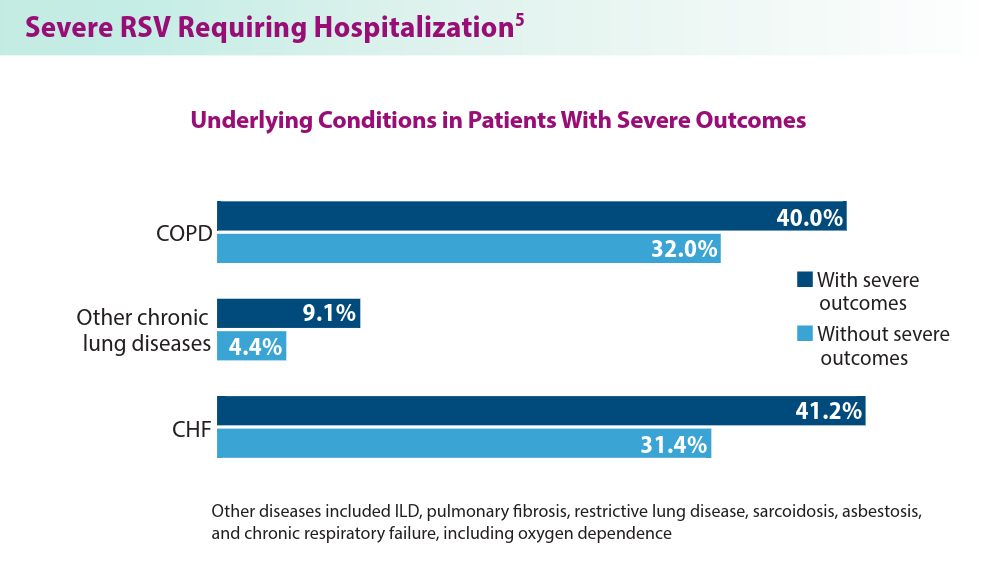
Closing the GAP in Idiopathic Pulmonary Fibrosis
5 things you should know about IPF. American Lung Association. April 12, 2023. Accessed June 21, 2024. https://www.lung.org/blog/idiopathic-pulmonary-fibrosis-things-to-know
Raghu G, Chen SY, Yeh WS, et al. Idiopathic pulmonary fibrosis in US Medicare beneficiaries aged 65 years and older: incidence, prevalence, and survival, 2001-11. Lancet Respir Med. 2014;2(7):566-572. doi:10.1016/S2213-2600(14)70101-8
Morrow T. Improving outcomes and managing costs in idiopathic pulmonary fibrosis. Am J Manag Care. 2019;25(11 suppl):S204-S209. PMID: 31419090
Man RK, Gogikar A, Nanda A, et al. A comparison of the effectiveness of nintedanib and pirfenidone in treating idiopathic pulmonary fibrosis: a systematic review. Cureus. 2024;16(2):e54268. doi:10.7759/cureus.54268
Ley B, Ryerson CJ, Vittinghoff E, et al. A multidimensional index and staging system for idiopathic pulmonary fibrosis. Ann Intern Med. 2012;156(10):684-691. doi:10.7326/0003-4819-156-10-201205150-00004
Raghu G, Remy-Jardin M, Myers JL, et al. Diagnosis of idiopathic pulmonary fibrosis. An official ATS/ERS/JRS/ALAT clinical practice guideline. Am J Respir Crit Care Med. 2018;198(5):e44-e68. doi:10.1164/rccm.201807-1255ST
Collard HR, Ryerson CJ, Corte TJ, et al. Acute exacerbation of idiopathic pulmonary fibrosis. An International Working Group report. Am J Respir Crit Care Med. 2016;194(3):265-275. doi:10.1164/rccm.201604-0801CI
Abuserewa ST, Duff R, Becker G. Treatment of idiopathic pulmonary fibrosis. Cureus. 2021;13(5):e15360. doi:10.7759/cureus.15360
Lee JH, Jang JH, Jang HJ, et al. New prognostic scoring system for mortality in idiopathic pulmonary fibrosis by modifying the gender, age, and physiology model with desaturation during the six-minute walk test. Front Med (Lausanne). 2023;10:1052129. doi:10.3389/fmed.2023.1052129
Chandel A, Pastre J, Valery S, King CS, Nathan SD. Derivation and validation of a simple multidimensional index incorporating exercise capacity parameters for survival prediction in idiopathic pulmonary fibrosis. Thorax. 2023;78(4):368-375. doi:10.1136/thoraxjnl-2021-218440
Chandel A, King CS, Ignacio RV, et al. External validation and longitudinal application of the DO-GAP index to individualise survival prediction in idiopathic pulmonary fibrosis. ERJ Open Res. 2023;9(3):00124-2023. doi:10.1183/23120541.00124-2023
Suzuki Y, Mori K, Aono Y, et al. Combined assessment of the GAP index and body mass index at antifibrotic therapy initiation for prognosis of idiopathic pulmonary fibrosis. Sci Rep. 2021;11(1):18579. doi:10.1038/s41598-021-98161-y
Lacedonia D, De Pace CC, Rea G, et al. Machine learning and BMI improve the prognostic value of GAP index in treated IPF patients. Bioengineering (Basel). 2023;10(2):251. doi:10.3390/bioengineering10020251
Fujii H, Hara Y, Saigusa Y, et al. ILD-GAP combined with the Charlson Comorbidity Index score (ILD-GAPC) as a prognostic prediction model in patients with interstitial lung disease. Can Respir J. 2023;2023:5088207. doi:10.1155/2023/5088207
Ley B, Bradford WZ, Weycker D, Vittinghoff E, du Bois RM, Collard HR. Unified baseline and longitudinal mortality prediction in idiopathic pulmonary fibrosis. Eur Respir J. 2015;45(5):1374-1381. doi:10.1183/09031936.00146314
Kreuter M, Lee JS, Tzouvelekis A, et al. Monocyte count as a prognostic biomarker in patients with idiopathic pulmonary fibrosis. Am J Respir Crit Care Med. 2021;204(1):74-81. doi:10.1164/rccm.202003-0669OC
Kreuter M, Lee JS, Tzouvelekis A, et al. A modified blood cell GAP (cGAP) to prognosticate outcomes in IPF. Poster presented at: European Respiratory Society International Congress; September 4-6, 2022. https://medically.gene.com/global/en/unrestricted/respiratory/ERS-2022/ers-2022-poster-kreuter-a-modified-blood-cell-gap.html
Nishikiori H, Chiba H, Lee SH, et al. A modified GAP model for East-Asian populations with idiopathic pulmonary fibrosis. Respir Investig. 2020;58(5):395-402. doi:10.1016/j.resinv.2020.04.001
5 things you should know about IPF. American Lung Association. April 12, 2023. Accessed June 21, 2024. https://www.lung.org/blog/idiopathic-pulmonary-fibrosis-things-to-know
Raghu G, Chen SY, Yeh WS, et al. Idiopathic pulmonary fibrosis in US Medicare beneficiaries aged 65 years and older: incidence, prevalence, and survival, 2001-11. Lancet Respir Med. 2014;2(7):566-572. doi:10.1016/S2213-2600(14)70101-8
Morrow T. Improving outcomes and managing costs in idiopathic pulmonary fibrosis. Am J Manag Care. 2019;25(11 suppl):S204-S209. PMID: 31419090
Man RK, Gogikar A, Nanda A, et al. A comparison of the effectiveness of nintedanib and pirfenidone in treating idiopathic pulmonary fibrosis: a systematic review. Cureus. 2024;16(2):e54268. doi:10.7759/cureus.54268
Ley B, Ryerson CJ, Vittinghoff E, et al. A multidimensional index and staging system for idiopathic pulmonary fibrosis. Ann Intern Med. 2012;156(10):684-691. doi:10.7326/0003-4819-156-10-201205150-00004
Raghu G, Remy-Jardin M, Myers JL, et al. Diagnosis of idiopathic pulmonary fibrosis. An official ATS/ERS/JRS/ALAT clinical practice guideline. Am J Respir Crit Care Med. 2018;198(5):e44-e68. doi:10.1164/rccm.201807-1255ST
Collard HR, Ryerson CJ, Corte TJ, et al. Acute exacerbation of idiopathic pulmonary fibrosis. An International Working Group report. Am J Respir Crit Care Med. 2016;194(3):265-275. doi:10.1164/rccm.201604-0801CI
Abuserewa ST, Duff R, Becker G. Treatment of idiopathic pulmonary fibrosis. Cureus. 2021;13(5):e15360. doi:10.7759/cureus.15360
Lee JH, Jang JH, Jang HJ, et al. New prognostic scoring system for mortality in idiopathic pulmonary fibrosis by modifying the gender, age, and physiology model with desaturation during the six-minute walk test. Front Med (Lausanne). 2023;10:1052129. doi:10.3389/fmed.2023.1052129
Chandel A, Pastre J, Valery S, King CS, Nathan SD. Derivation and validation of a simple multidimensional index incorporating exercise capacity parameters for survival prediction in idiopathic pulmonary fibrosis. Thorax. 2023;78(4):368-375. doi:10.1136/thoraxjnl-2021-218440
Chandel A, King CS, Ignacio RV, et al. External validation and longitudinal application of the DO-GAP index to individualise survival prediction in idiopathic pulmonary fibrosis. ERJ Open Res. 2023;9(3):00124-2023. doi:10.1183/23120541.00124-2023
Suzuki Y, Mori K, Aono Y, et al. Combined assessment of the GAP index and body mass index at antifibrotic therapy initiation for prognosis of idiopathic pulmonary fibrosis. Sci Rep. 2021;11(1):18579. doi:10.1038/s41598-021-98161-y
Lacedonia D, De Pace CC, Rea G, et al. Machine learning and BMI improve the prognostic value of GAP index in treated IPF patients. Bioengineering (Basel). 2023;10(2):251. doi:10.3390/bioengineering10020251
Fujii H, Hara Y, Saigusa Y, et al. ILD-GAP combined with the Charlson Comorbidity Index score (ILD-GAPC) as a prognostic prediction model in patients with interstitial lung disease. Can Respir J. 2023;2023:5088207. doi:10.1155/2023/5088207
Ley B, Bradford WZ, Weycker D, Vittinghoff E, du Bois RM, Collard HR. Unified baseline and longitudinal mortality prediction in idiopathic pulmonary fibrosis. Eur Respir J. 2015;45(5):1374-1381. doi:10.1183/09031936.00146314
Kreuter M, Lee JS, Tzouvelekis A, et al. Monocyte count as a prognostic biomarker in patients with idiopathic pulmonary fibrosis. Am J Respir Crit Care Med. 2021;204(1):74-81. doi:10.1164/rccm.202003-0669OC
Kreuter M, Lee JS, Tzouvelekis A, et al. A modified blood cell GAP (cGAP) to prognosticate outcomes in IPF. Poster presented at: European Respiratory Society International Congress; September 4-6, 2022. https://medically.gene.com/global/en/unrestricted/respiratory/ERS-2022/ers-2022-poster-kreuter-a-modified-blood-cell-gap.html
Nishikiori H, Chiba H, Lee SH, et al. A modified GAP model for East-Asian populations with idiopathic pulmonary fibrosis. Respir Investig. 2020;58(5):395-402. doi:10.1016/j.resinv.2020.04.001
5 things you should know about IPF. American Lung Association. April 12, 2023. Accessed June 21, 2024. https://www.lung.org/blog/idiopathic-pulmonary-fibrosis-things-to-know
Raghu G, Chen SY, Yeh WS, et al. Idiopathic pulmonary fibrosis in US Medicare beneficiaries aged 65 years and older: incidence, prevalence, and survival, 2001-11. Lancet Respir Med. 2014;2(7):566-572. doi:10.1016/S2213-2600(14)70101-8
Morrow T. Improving outcomes and managing costs in idiopathic pulmonary fibrosis. Am J Manag Care. 2019;25(11 suppl):S204-S209. PMID: 31419090
Man RK, Gogikar A, Nanda A, et al. A comparison of the effectiveness of nintedanib and pirfenidone in treating idiopathic pulmonary fibrosis: a systematic review. Cureus. 2024;16(2):e54268. doi:10.7759/cureus.54268
Ley B, Ryerson CJ, Vittinghoff E, et al. A multidimensional index and staging system for idiopathic pulmonary fibrosis. Ann Intern Med. 2012;156(10):684-691. doi:10.7326/0003-4819-156-10-201205150-00004
Raghu G, Remy-Jardin M, Myers JL, et al. Diagnosis of idiopathic pulmonary fibrosis. An official ATS/ERS/JRS/ALAT clinical practice guideline. Am J Respir Crit Care Med. 2018;198(5):e44-e68. doi:10.1164/rccm.201807-1255ST
Collard HR, Ryerson CJ, Corte TJ, et al. Acute exacerbation of idiopathic pulmonary fibrosis. An International Working Group report. Am J Respir Crit Care Med. 2016;194(3):265-275. doi:10.1164/rccm.201604-0801CI
Abuserewa ST, Duff R, Becker G. Treatment of idiopathic pulmonary fibrosis. Cureus. 2021;13(5):e15360. doi:10.7759/cureus.15360
Lee JH, Jang JH, Jang HJ, et al. New prognostic scoring system for mortality in idiopathic pulmonary fibrosis by modifying the gender, age, and physiology model with desaturation during the six-minute walk test. Front Med (Lausanne). 2023;10:1052129. doi:10.3389/fmed.2023.1052129
Chandel A, Pastre J, Valery S, King CS, Nathan SD. Derivation and validation of a simple multidimensional index incorporating exercise capacity parameters for survival prediction in idiopathic pulmonary fibrosis. Thorax. 2023;78(4):368-375. doi:10.1136/thoraxjnl-2021-218440
Chandel A, King CS, Ignacio RV, et al. External validation and longitudinal application of the DO-GAP index to individualise survival prediction in idiopathic pulmonary fibrosis. ERJ Open Res. 2023;9(3):00124-2023. doi:10.1183/23120541.00124-2023
Suzuki Y, Mori K, Aono Y, et al. Combined assessment of the GAP index and body mass index at antifibrotic therapy initiation for prognosis of idiopathic pulmonary fibrosis. Sci Rep. 2021;11(1):18579. doi:10.1038/s41598-021-98161-y
Lacedonia D, De Pace CC, Rea G, et al. Machine learning and BMI improve the prognostic value of GAP index in treated IPF patients. Bioengineering (Basel). 2023;10(2):251. doi:10.3390/bioengineering10020251
Fujii H, Hara Y, Saigusa Y, et al. ILD-GAP combined with the Charlson Comorbidity Index score (ILD-GAPC) as a prognostic prediction model in patients with interstitial lung disease. Can Respir J. 2023;2023:5088207. doi:10.1155/2023/5088207
Ley B, Bradford WZ, Weycker D, Vittinghoff E, du Bois RM, Collard HR. Unified baseline and longitudinal mortality prediction in idiopathic pulmonary fibrosis. Eur Respir J. 2015;45(5):1374-1381. doi:10.1183/09031936.00146314
Kreuter M, Lee JS, Tzouvelekis A, et al. Monocyte count as a prognostic biomarker in patients with idiopathic pulmonary fibrosis. Am J Respir Crit Care Med. 2021;204(1):74-81. doi:10.1164/rccm.202003-0669OC
Kreuter M, Lee JS, Tzouvelekis A, et al. A modified blood cell GAP (cGAP) to prognosticate outcomes in IPF. Poster presented at: European Respiratory Society International Congress; September 4-6, 2022. https://medically.gene.com/global/en/unrestricted/respiratory/ERS-2022/ers-2022-poster-kreuter-a-modified-blood-cell-gap.html
Nishikiori H, Chiba H, Lee SH, et al. A modified GAP model for East-Asian populations with idiopathic pulmonary fibrosis. Respir Investig. 2020;58(5):395-402. doi:10.1016/j.resinv.2020.04.001
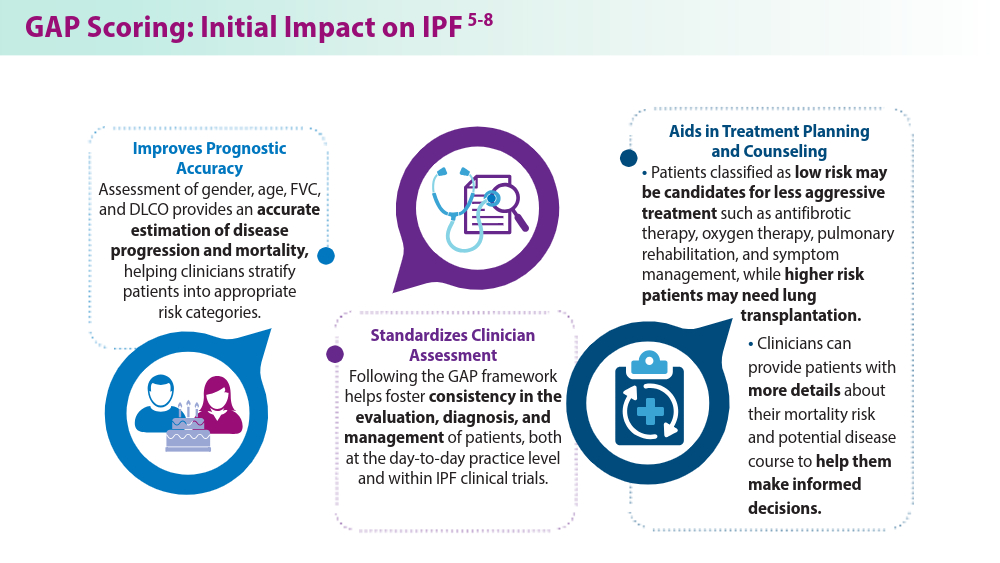
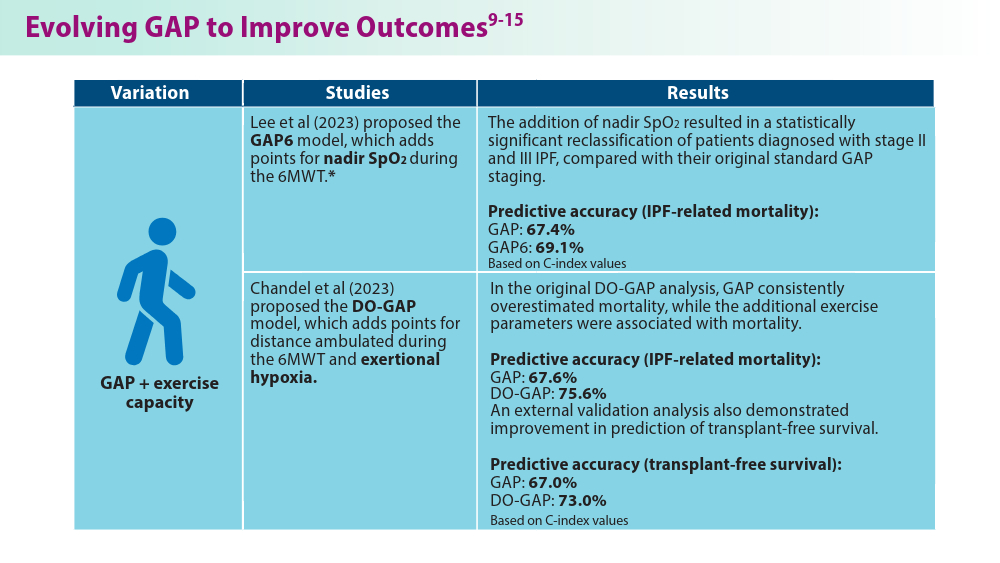
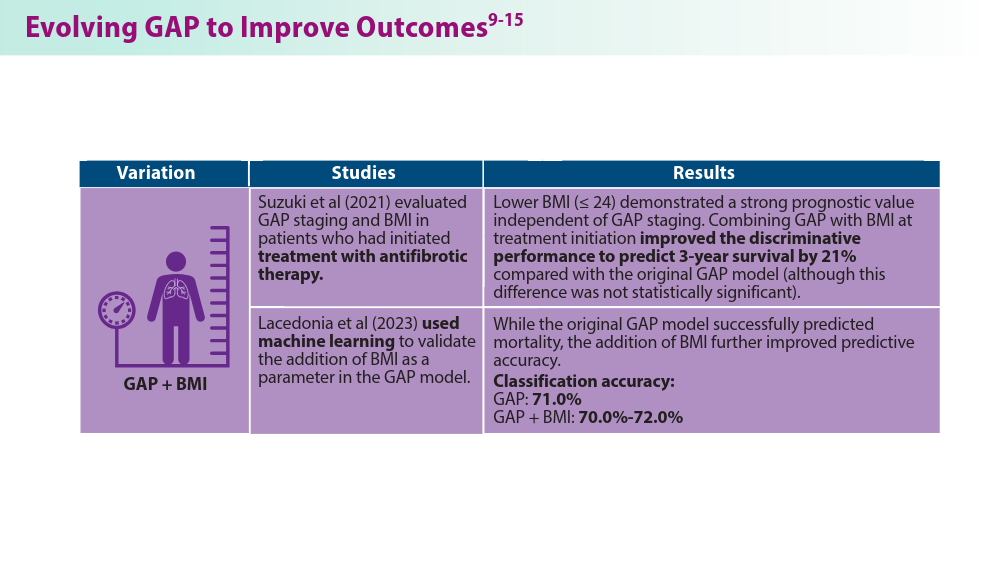
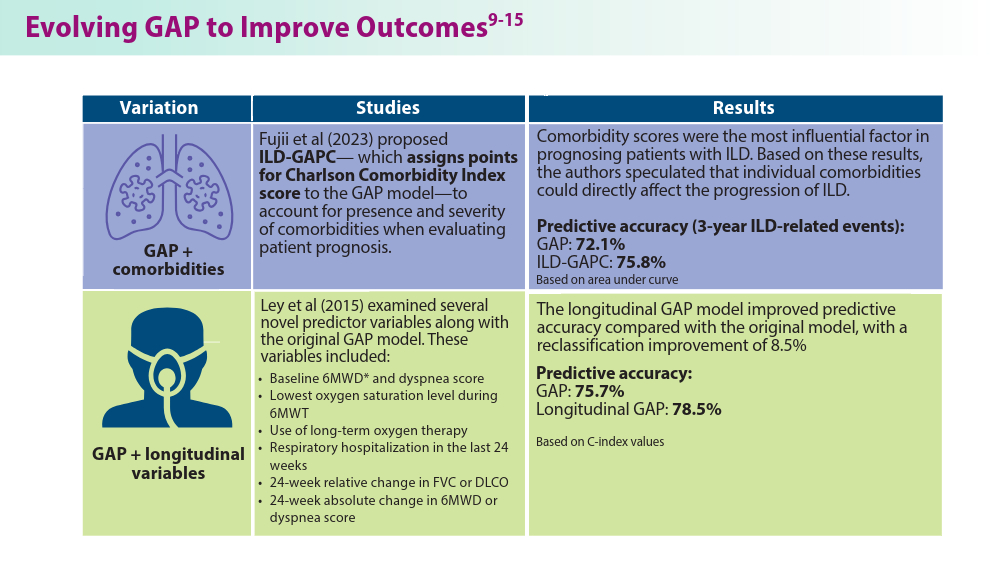
Noninvasive Ventilation in Neuromuscular Disease
- Gong Y, Sankari A. Noninvasive ventilation. StatPearls [Internet]. Treasure Island, FL: StatPearls Publishing; 2024.Updated December 11, 2022. Accessed June 19, 2024. https://www.ncbi.nlm.nih.gov/books/NBK578188/
- Khan A, Frazer-Green L, Amin R, et al. Respiratory management of patients with neuromuscular weakness: an American College of Chest Physicians clinical practice guideline and expert panel report. Chest. 2023;164(2):394-413. doi:10.1016/j.chest.2023.03.011
- Taran S, McCredie VA, Goligher EC. Noninvasive and invasive mechanical ventilation for neurologic disorders. Handb Clin Neurol. 2022;189:361-386. doi:10.1016/B978-0-323-91532-8.00015-X
- Rao F, Garuti G, Vitacca M, et al; for the UILDM Respiratory Group. Management of respiratory complications and rehabilitation in individuals with muscular dystrophies: 1st Consensus Conference report from UILDM - Italian Muscular Dystrophy Association (Milan, January 25-26, 2019). Acta Myol. 2021;40(1):8-42. doi:10.36185/2532-1900-045
- Respiratory assist devices. Centers for Medicare & Medicaid Services. Revised January 1, 2024. Accessed June 19, 2024. https://www.cms.gov/ medicare-coverage-database/view/lcd.aspx?lcdid=33800
- What you need to know about the Philips PAP device recalls. American College of Chest Physicians. February 1, 2024. Accessed June 19, 2024. https://www.chestnet.org/Newsroom/CHEST-News/2021/07/What-YouNeed-to-Know-About-the-Philips-PAP-Device-Recall
- Orr JE, Chen K, Vaida F, et al. Effectiveness of long-term noninvasive ventilation measured by remote monitoring in neuromuscular disease. ERJ Open Res. 2023;9(5):00163-2023. doi:10.1183/23120541.00163-2023
- Kapur VK, Auckley DH, Chowdhuri S, et al. Clinical practice guideline for diagnostic testing for adult obstructive sleep apnea: an American Academy of Sleep Medicine clinical practice guideline. J Clin Sleep Med. 2017;13(3):479-504. doi:10.5664/jcsm.6506
- Phillips Respironics. Trilogy Evo Clinical Manual. 2019
- ResMed. Astral Series Clinical Guide. 2018
- Breas. Vivo 45 LS User Manual. 2023
- Lowenstein Medical. Luisa Life Support Ventilation.
- Ventec Life Systems. VOCSN Clinical and Technical Manual. 2019
- Gong Y, Sankari A. Noninvasive ventilation. StatPearls [Internet]. Treasure Island, FL: StatPearls Publishing; 2024.Updated December 11, 2022. Accessed June 19, 2024. https://www.ncbi.nlm.nih.gov/books/NBK578188/
- Khan A, Frazer-Green L, Amin R, et al. Respiratory management of patients with neuromuscular weakness: an American College of Chest Physicians clinical practice guideline and expert panel report. Chest. 2023;164(2):394-413. doi:10.1016/j.chest.2023.03.011
- Taran S, McCredie VA, Goligher EC. Noninvasive and invasive mechanical ventilation for neurologic disorders. Handb Clin Neurol. 2022;189:361-386. doi:10.1016/B978-0-323-91532-8.00015-X
- Rao F, Garuti G, Vitacca M, et al; for the UILDM Respiratory Group. Management of respiratory complications and rehabilitation in individuals with muscular dystrophies: 1st Consensus Conference report from UILDM - Italian Muscular Dystrophy Association (Milan, January 25-26, 2019). Acta Myol. 2021;40(1):8-42. doi:10.36185/2532-1900-045
- Respiratory assist devices. Centers for Medicare & Medicaid Services. Revised January 1, 2024. Accessed June 19, 2024. https://www.cms.gov/ medicare-coverage-database/view/lcd.aspx?lcdid=33800
- What you need to know about the Philips PAP device recalls. American College of Chest Physicians. February 1, 2024. Accessed June 19, 2024. https://www.chestnet.org/Newsroom/CHEST-News/2021/07/What-YouNeed-to-Know-About-the-Philips-PAP-Device-Recall
- Orr JE, Chen K, Vaida F, et al. Effectiveness of long-term noninvasive ventilation measured by remote monitoring in neuromuscular disease. ERJ Open Res. 2023;9(5):00163-2023. doi:10.1183/23120541.00163-2023
- Kapur VK, Auckley DH, Chowdhuri S, et al. Clinical practice guideline for diagnostic testing for adult obstructive sleep apnea: an American Academy of Sleep Medicine clinical practice guideline. J Clin Sleep Med. 2017;13(3):479-504. doi:10.5664/jcsm.6506
- Phillips Respironics. Trilogy Evo Clinical Manual. 2019
- ResMed. Astral Series Clinical Guide. 2018
- Breas. Vivo 45 LS User Manual. 2023
- Lowenstein Medical. Luisa Life Support Ventilation.
- Ventec Life Systems. VOCSN Clinical and Technical Manual. 2019
- Gong Y, Sankari A. Noninvasive ventilation. StatPearls [Internet]. Treasure Island, FL: StatPearls Publishing; 2024.Updated December 11, 2022. Accessed June 19, 2024. https://www.ncbi.nlm.nih.gov/books/NBK578188/
- Khan A, Frazer-Green L, Amin R, et al. Respiratory management of patients with neuromuscular weakness: an American College of Chest Physicians clinical practice guideline and expert panel report. Chest. 2023;164(2):394-413. doi:10.1016/j.chest.2023.03.011
- Taran S, McCredie VA, Goligher EC. Noninvasive and invasive mechanical ventilation for neurologic disorders. Handb Clin Neurol. 2022;189:361-386. doi:10.1016/B978-0-323-91532-8.00015-X
- Rao F, Garuti G, Vitacca M, et al; for the UILDM Respiratory Group. Management of respiratory complications and rehabilitation in individuals with muscular dystrophies: 1st Consensus Conference report from UILDM - Italian Muscular Dystrophy Association (Milan, January 25-26, 2019). Acta Myol. 2021;40(1):8-42. doi:10.36185/2532-1900-045
- Respiratory assist devices. Centers for Medicare & Medicaid Services. Revised January 1, 2024. Accessed June 19, 2024. https://www.cms.gov/ medicare-coverage-database/view/lcd.aspx?lcdid=33800
- What you need to know about the Philips PAP device recalls. American College of Chest Physicians. February 1, 2024. Accessed June 19, 2024. https://www.chestnet.org/Newsroom/CHEST-News/2021/07/What-YouNeed-to-Know-About-the-Philips-PAP-Device-Recall
- Orr JE, Chen K, Vaida F, et al. Effectiveness of long-term noninvasive ventilation measured by remote monitoring in neuromuscular disease. ERJ Open Res. 2023;9(5):00163-2023. doi:10.1183/23120541.00163-2023
- Kapur VK, Auckley DH, Chowdhuri S, et al. Clinical practice guideline for diagnostic testing for adult obstructive sleep apnea: an American Academy of Sleep Medicine clinical practice guideline. J Clin Sleep Med. 2017;13(3):479-504. doi:10.5664/jcsm.6506
- Phillips Respironics. Trilogy Evo Clinical Manual. 2019
- ResMed. Astral Series Clinical Guide. 2018
- Breas. Vivo 45 LS User Manual. 2023
- Lowenstein Medical. Luisa Life Support Ventilation.
- Ventec Life Systems. VOCSN Clinical and Technical Manual. 2019