User login
Postvaccination anaphylaxis still possible with certain vaccines
New findings confirm that although it is rare, postvaccination anaphylaxis can still occur with certain vaccines.
Dr. Michael M. McNeil of the Centers for Disease Control and Prevention, Atlanta, and his associates identified 17,606,500 vaccination visits from Jan. 1, 2009, through Dec. 31, 2011, at which 25,173,965 vaccine doses were administered. The researchers identified 76 cases of chart-confirmed anaphylaxis; 33 anaphylaxis cases were associated with vaccination, and 43 were attributed to other causes.

Inactivated trivalent influenza vaccine (TIV) was the major contributor to vaccine-triggered anaphylaxis cases in the population, although the rate (1.35 cases per 1 million vaccine doses of TIV given alone) was similar to the rate for all vaccines. The postvaccination anaphylaxis case rate not involving TIV was 1.32 per million vaccine doses.
The study factored in race, age, gender, symptoms, and history of the patients. There were no deaths, and only 1 patient (3%) was hospitalized. A total of 28 of the 33 vaccine-triggered anaphylaxis cases involved patients with a history of atopy.
“Although anaphylaxis after immunization is rare, its immediate onset (usually within minutes) and life-threatening nature require that all personnel and facilities providing vaccinations have procedures in place for anaphylaxis management,” the investigators noted. “Additional provider education concerning current recommendations for treatment and follow-up appears to be warranted.”
Find the full story in the Journal of Allergy and Clinical Immunology (2016 Mar;137[3]:868-78).
New findings confirm that although it is rare, postvaccination anaphylaxis can still occur with certain vaccines.
Dr. Michael M. McNeil of the Centers for Disease Control and Prevention, Atlanta, and his associates identified 17,606,500 vaccination visits from Jan. 1, 2009, through Dec. 31, 2011, at which 25,173,965 vaccine doses were administered. The researchers identified 76 cases of chart-confirmed anaphylaxis; 33 anaphylaxis cases were associated with vaccination, and 43 were attributed to other causes.
Inactivated trivalent influenza vaccine (TIV) was the major contributor to vaccine-triggered anaphylaxis cases in the population, although the rate (1.35 cases per 1 million vaccine doses of TIV given alone) was similar to the rate for all vaccines. The postvaccination anaphylaxis case rate not involving TIV was 1.32 per million vaccine doses.
The study factored in race, age, gender, symptoms, and history of the patients. There were no deaths, and only 1 patient (3%) was hospitalized. A total of 28 of the 33 vaccine-triggered anaphylaxis cases involved patients with a history of atopy.
“Although anaphylaxis after immunization is rare, its immediate onset (usually within minutes) and life-threatening nature require that all personnel and facilities providing vaccinations have procedures in place for anaphylaxis management,” the investigators noted. “Additional provider education concerning current recommendations for treatment and follow-up appears to be warranted.”
Find the full story in the Journal of Allergy and Clinical Immunology (2016 Mar;137[3]:868-78).
New findings confirm that although it is rare, postvaccination anaphylaxis can still occur with certain vaccines.
Dr. Michael M. McNeil of the Centers for Disease Control and Prevention, Atlanta, and his associates identified 17,606,500 vaccination visits from Jan. 1, 2009, through Dec. 31, 2011, at which 25,173,965 vaccine doses were administered. The researchers identified 76 cases of chart-confirmed anaphylaxis; 33 anaphylaxis cases were associated with vaccination, and 43 were attributed to other causes.
Inactivated trivalent influenza vaccine (TIV) was the major contributor to vaccine-triggered anaphylaxis cases in the population, although the rate (1.35 cases per 1 million vaccine doses of TIV given alone) was similar to the rate for all vaccines. The postvaccination anaphylaxis case rate not involving TIV was 1.32 per million vaccine doses.
The study factored in race, age, gender, symptoms, and history of the patients. There were no deaths, and only 1 patient (3%) was hospitalized. A total of 28 of the 33 vaccine-triggered anaphylaxis cases involved patients with a history of atopy.
“Although anaphylaxis after immunization is rare, its immediate onset (usually within minutes) and life-threatening nature require that all personnel and facilities providing vaccinations have procedures in place for anaphylaxis management,” the investigators noted. “Additional provider education concerning current recommendations for treatment and follow-up appears to be warranted.”
Find the full story in the Journal of Allergy and Clinical Immunology (2016 Mar;137[3]:868-78).
FROM THE JOURNAL OF ALLERGY AND CLINICAL IMMUNOLOGY

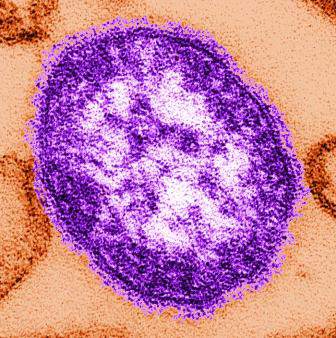
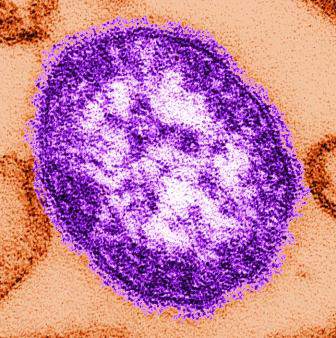
Measles outbreak underscores vulnerability of infants
An outbreak of measles in infants who were too young for routine immunization with the MMR vaccine occurred in an Illinois day care center, highlighting the vulnerability of infants younger than 1 year to measles infection.
“With the continued threat of measles importations from endemic countries and the recent resurgence of cases in the United States, it is critical to institute measures to protect this susceptible population,” researchers led by Dr. Whitney J. Clegg wrote online (J Pediatric Infect Dis Soc. 2016 March 24. doi: 10.1093/jpids/piw011). “Although infection among infants cannot be prevented through routine vaccination and herd immunity does not provide 100% protection, other strategies are effective in protecting this population from measles during future outbreaks. These include maintaining a high index of suspicion for measles in unvaccinated individuals presenting with a febrile rash illness and ensuring that those caring for infants have documented evidence of immunity.”
Dr. Clegg, an applied epidemiology fellow with the Illinois Department of Public Health, and his associates reported on an outbreak of 15 confirmed measles cases that occurred during January and February of 2015 in Cook County, Ill. Of the 15 cases, 12 (80%) occurred in infants aged 3-11 months who attended the same child care center. One of the cases, a 7-month-old male infant, was hospitalized for near-daily fevers and respiratory symptoms. Clinicians suspected Kawasaki disease, but that was ruled out 26 days after initial rash onset through positive measles-specific IgM serology. The child attended the day care only once during the time he was infectious, but delayed recognition of measles “led to continued transmission within the child care center,” the researchers wrote. “High vaccination rates in the community, especially among child care attendees aged [1 year and older] and among staff caring for the infants, likely led to containment of the outbreak primarily among individuals too young to receive their first dose of MMR vaccine.”
Among the 11 other infant cases, 5 visited outpatient clinics during their infectious period, exposing 33 infants. The three remaining confirmed measles cases were adult females who ranged in age from their late 20s to early 40s. One was the mother of a child care center attendee with confirmed measles.
“No direct connection could be made between the other two adults and the child care center attendees other than geographic proximity,” Dr. Clegg and his associates said. “The three adults reported unknown vaccination histories and denied personal or religious objections to immunizations; all had children that were up to date with their vaccinations. All cases resided in or attended child care in the same city within Cook County. No cases in this outbreak reported a travel history or contact with ill individuals who recently traveled.”
In all, 91 contacts of the 15 measles cases were monitored, and 20 received postexposure prophylaxis. The researchers noted that an important part of the outbreak investigation was identifying health care workers and child care center staff who worked closely with susceptible children and ensuring documentation of measles immunity. “Three health care workers with no vaccination records available were identified at the exposed pediatric clinics,” they noted. “Obtaining documentation of vaccinations, time taken away from regular clinic activities, and preventable work exclusions during an outbreak can be costly for health care facilities. These costs, as well as measles infection and transmission, could be avoided by ensuring all health care workers have the necessary documentation readily available at their facility.”
The report was supported in part by an appointment to the Applied Epidemiology Fellowship Program administered by the Council of State and Territorial Epidemiologists and funded by the Centers for Disease Control and Prevention. Dr. Clegg and his associates reported no relevant financial conflicts.
An outbreak of measles in infants who were too young for routine immunization with the MMR vaccine occurred in an Illinois day care center, highlighting the vulnerability of infants younger than 1 year to measles infection.
“With the continued threat of measles importations from endemic countries and the recent resurgence of cases in the United States, it is critical to institute measures to protect this susceptible population,” researchers led by Dr. Whitney J. Clegg wrote online (J Pediatric Infect Dis Soc. 2016 March 24. doi: 10.1093/jpids/piw011). “Although infection among infants cannot be prevented through routine vaccination and herd immunity does not provide 100% protection, other strategies are effective in protecting this population from measles during future outbreaks. These include maintaining a high index of suspicion for measles in unvaccinated individuals presenting with a febrile rash illness and ensuring that those caring for infants have documented evidence of immunity.”
Dr. Clegg, an applied epidemiology fellow with the Illinois Department of Public Health, and his associates reported on an outbreak of 15 confirmed measles cases that occurred during January and February of 2015 in Cook County, Ill. Of the 15 cases, 12 (80%) occurred in infants aged 3-11 months who attended the same child care center. One of the cases, a 7-month-old male infant, was hospitalized for near-daily fevers and respiratory symptoms. Clinicians suspected Kawasaki disease, but that was ruled out 26 days after initial rash onset through positive measles-specific IgM serology. The child attended the day care only once during the time he was infectious, but delayed recognition of measles “led to continued transmission within the child care center,” the researchers wrote. “High vaccination rates in the community, especially among child care attendees aged [1 year and older] and among staff caring for the infants, likely led to containment of the outbreak primarily among individuals too young to receive their first dose of MMR vaccine.”
Among the 11 other infant cases, 5 visited outpatient clinics during their infectious period, exposing 33 infants. The three remaining confirmed measles cases were adult females who ranged in age from their late 20s to early 40s. One was the mother of a child care center attendee with confirmed measles.
“No direct connection could be made between the other two adults and the child care center attendees other than geographic proximity,” Dr. Clegg and his associates said. “The three adults reported unknown vaccination histories and denied personal or religious objections to immunizations; all had children that were up to date with their vaccinations. All cases resided in or attended child care in the same city within Cook County. No cases in this outbreak reported a travel history or contact with ill individuals who recently traveled.”
In all, 91 contacts of the 15 measles cases were monitored, and 20 received postexposure prophylaxis. The researchers noted that an important part of the outbreak investigation was identifying health care workers and child care center staff who worked closely with susceptible children and ensuring documentation of measles immunity. “Three health care workers with no vaccination records available were identified at the exposed pediatric clinics,” they noted. “Obtaining documentation of vaccinations, time taken away from regular clinic activities, and preventable work exclusions during an outbreak can be costly for health care facilities. These costs, as well as measles infection and transmission, could be avoided by ensuring all health care workers have the necessary documentation readily available at their facility.”
The report was supported in part by an appointment to the Applied Epidemiology Fellowship Program administered by the Council of State and Territorial Epidemiologists and funded by the Centers for Disease Control and Prevention. Dr. Clegg and his associates reported no relevant financial conflicts.
An outbreak of measles in infants who were too young for routine immunization with the MMR vaccine occurred in an Illinois day care center, highlighting the vulnerability of infants younger than 1 year to measles infection.
“With the continued threat of measles importations from endemic countries and the recent resurgence of cases in the United States, it is critical to institute measures to protect this susceptible population,” researchers led by Dr. Whitney J. Clegg wrote online (J Pediatric Infect Dis Soc. 2016 March 24. doi: 10.1093/jpids/piw011). “Although infection among infants cannot be prevented through routine vaccination and herd immunity does not provide 100% protection, other strategies are effective in protecting this population from measles during future outbreaks. These include maintaining a high index of suspicion for measles in unvaccinated individuals presenting with a febrile rash illness and ensuring that those caring for infants have documented evidence of immunity.”
Dr. Clegg, an applied epidemiology fellow with the Illinois Department of Public Health, and his associates reported on an outbreak of 15 confirmed measles cases that occurred during January and February of 2015 in Cook County, Ill. Of the 15 cases, 12 (80%) occurred in infants aged 3-11 months who attended the same child care center. One of the cases, a 7-month-old male infant, was hospitalized for near-daily fevers and respiratory symptoms. Clinicians suspected Kawasaki disease, but that was ruled out 26 days after initial rash onset through positive measles-specific IgM serology. The child attended the day care only once during the time he was infectious, but delayed recognition of measles “led to continued transmission within the child care center,” the researchers wrote. “High vaccination rates in the community, especially among child care attendees aged [1 year and older] and among staff caring for the infants, likely led to containment of the outbreak primarily among individuals too young to receive their first dose of MMR vaccine.”
Among the 11 other infant cases, 5 visited outpatient clinics during their infectious period, exposing 33 infants. The three remaining confirmed measles cases were adult females who ranged in age from their late 20s to early 40s. One was the mother of a child care center attendee with confirmed measles.
“No direct connection could be made between the other two adults and the child care center attendees other than geographic proximity,” Dr. Clegg and his associates said. “The three adults reported unknown vaccination histories and denied personal or religious objections to immunizations; all had children that were up to date with their vaccinations. All cases resided in or attended child care in the same city within Cook County. No cases in this outbreak reported a travel history or contact with ill individuals who recently traveled.”
In all, 91 contacts of the 15 measles cases were monitored, and 20 received postexposure prophylaxis. The researchers noted that an important part of the outbreak investigation was identifying health care workers and child care center staff who worked closely with susceptible children and ensuring documentation of measles immunity. “Three health care workers with no vaccination records available were identified at the exposed pediatric clinics,” they noted. “Obtaining documentation of vaccinations, time taken away from regular clinic activities, and preventable work exclusions during an outbreak can be costly for health care facilities. These costs, as well as measles infection and transmission, could be avoided by ensuring all health care workers have the necessary documentation readily available at their facility.”
The report was supported in part by an appointment to the Applied Epidemiology Fellowship Program administered by the Council of State and Territorial Epidemiologists and funded by the Centers for Disease Control and Prevention. Dr. Clegg and his associates reported no relevant financial conflicts.
FROM THE JOURNAL OF THE PEDIATRIC INFECTIOUS DISEASES SOCIETY
Key clinical point: Clinicians should implement measures to protect infants younger than 1 year from measles infection.
Major finding: Of the 15 measles cases, 12 (80%) occurred in infants aged 3-11 months who attended the same child care center.
Data source: The report of a measles outbreak in Cook County, Ill., and the control measures public health officials took to interrupt transmission.
Disclosures: The report was supported in part by an appointment to the Applied Epidemiology Fellowship Program administered by the Council of State and Territorial Epidemiologists and funded by the Centers for Disease Control and Prevention. Dr. Clegg and his associates reported no relevant financial disclosures.
EC approves drug for pediatric ITP

Photo by Logan Tuttle
The European Commission (EC) has approved eltrombopag (Revolade), a once-daily oral thrombopoietin receptor agonist, to treat pediatric patients (age 1 and older) with chronic immune thrombocytopenia (ITP) that is refractory to other therapies.
This approval includes the use of tablets and a new oral suspension formulation of eltrombopag, which is designed for younger children who may not be able to swallow tablets.
The approval applies to all 28 member states of the European Union plus Iceland, Norway, and Liechtenstein.
Eltrombopag was previously approved by the EC for use in adults with refractory chronic ITP. The drug is also approved in the EC to treat adults with severe aplastic anemia and adults with chronic hepatitis C virus infection who have thrombocytopenia.
Eltrombopag is made by Novartis. For more details on the drug, see the full Summary of Product Characteristics, available on the European Medicines Agency’s website.
The EC’s latest approval of eltrombopag was based on data from 2 double-blind, placebo-controlled trials—the phase 2 PETIT trial and the phase 3 PETIT2 trial.
PETIT trials: Efficacy
The PETIT trial included 67 ITP patients stratified by age cohort (12-17 years, 6-11 years, and 1-5 years). They were randomized (2:1) to receive eltrombopag or placebo for 7 weeks. The eltrombopag dose was titrated to a target platelet count of 50-200 x 109/L.
The primary efficacy endpoint was the proportion of subjects achieving platelet counts of 50 x 109/L or higher at least once between days 8 and 43 of the randomized period of the study.
Significantly more patients in the eltrombopag arm met this endpoint—62.2%—compared to 31.8% in the placebo arm (P=0.011).
The PETIT2 trial enrolled 92 patients with chronic ITP who were randomized (2:1) to receive eltrombopag or placebo for 13 weeks. The eltrombopag dose was titrated to a target platelet count of 50-200 x 109/L.
The primary efficacy endpoint was the proportion of subjects who achieved platelet counts of 50 x 109/L or higher for at least 6 out of 8 weeks, between weeks 5 and 12 of the randomized period.
Significantly more patients in the eltrombopag arm met this endpoint—41.3%—compared to 3.4% of patients in the placebo arm (P<0.001).
PETIT trials: Safety
For both trials, there were 107 eltrombopag-treated patients evaluable for safety.
The most common adverse events that occurred more frequently in the eltrombopag arms than the placebo arms were upper respiratory tract infection, nasopharyngitis, cough, diarrhea, pyrexia, rhinitis, abdominal pain, oropharyngeal pain, toothache, increased ALT/AST, rash, and rhinorrhea.
Serious adverse events were reported in 8% of patients during the randomized part of both trials, although no serious adverse event occurred in more than 1 patient.
An ALT elevation of at least 3 times the upper limit of normal occurred in 5% of eltrombopag-treated patients. Of those patients, 2% had ALT increases of at least 5 times the upper limit of normal.
There were no deaths or thromboembolic events during either study. ![]()
Photo by Logan Tuttle
The European Commission (EC) has approved eltrombopag (Revolade), a once-daily oral thrombopoietin receptor agonist, to treat pediatric patients (age 1 and older) with chronic immune thrombocytopenia (ITP) that is refractory to other therapies.
This approval includes the use of tablets and a new oral suspension formulation of eltrombopag, which is designed for younger children who may not be able to swallow tablets.
The approval applies to all 28 member states of the European Union plus Iceland, Norway, and Liechtenstein.
Eltrombopag was previously approved by the EC for use in adults with refractory chronic ITP. The drug is also approved in the EC to treat adults with severe aplastic anemia and adults with chronic hepatitis C virus infection who have thrombocytopenia.
Eltrombopag is made by Novartis. For more details on the drug, see the full Summary of Product Characteristics, available on the European Medicines Agency’s website.
The EC’s latest approval of eltrombopag was based on data from 2 double-blind, placebo-controlled trials—the phase 2 PETIT trial and the phase 3 PETIT2 trial.
PETIT trials: Efficacy
The PETIT trial included 67 ITP patients stratified by age cohort (12-17 years, 6-11 years, and 1-5 years). They were randomized (2:1) to receive eltrombopag or placebo for 7 weeks. The eltrombopag dose was titrated to a target platelet count of 50-200 x 109/L.
The primary efficacy endpoint was the proportion of subjects achieving platelet counts of 50 x 109/L or higher at least once between days 8 and 43 of the randomized period of the study.
Significantly more patients in the eltrombopag arm met this endpoint—62.2%—compared to 31.8% in the placebo arm (P=0.011).
The PETIT2 trial enrolled 92 patients with chronic ITP who were randomized (2:1) to receive eltrombopag or placebo for 13 weeks. The eltrombopag dose was titrated to a target platelet count of 50-200 x 109/L.
The primary efficacy endpoint was the proportion of subjects who achieved platelet counts of 50 x 109/L or higher for at least 6 out of 8 weeks, between weeks 5 and 12 of the randomized period.
Significantly more patients in the eltrombopag arm met this endpoint—41.3%—compared to 3.4% of patients in the placebo arm (P<0.001).
PETIT trials: Safety
For both trials, there were 107 eltrombopag-treated patients evaluable for safety.
The most common adverse events that occurred more frequently in the eltrombopag arms than the placebo arms were upper respiratory tract infection, nasopharyngitis, cough, diarrhea, pyrexia, rhinitis, abdominal pain, oropharyngeal pain, toothache, increased ALT/AST, rash, and rhinorrhea.
Serious adverse events were reported in 8% of patients during the randomized part of both trials, although no serious adverse event occurred in more than 1 patient.
An ALT elevation of at least 3 times the upper limit of normal occurred in 5% of eltrombopag-treated patients. Of those patients, 2% had ALT increases of at least 5 times the upper limit of normal.
There were no deaths or thromboembolic events during either study. ![]()
Photo by Logan Tuttle
The European Commission (EC) has approved eltrombopag (Revolade), a once-daily oral thrombopoietin receptor agonist, to treat pediatric patients (age 1 and older) with chronic immune thrombocytopenia (ITP) that is refractory to other therapies.
This approval includes the use of tablets and a new oral suspension formulation of eltrombopag, which is designed for younger children who may not be able to swallow tablets.
The approval applies to all 28 member states of the European Union plus Iceland, Norway, and Liechtenstein.
Eltrombopag was previously approved by the EC for use in adults with refractory chronic ITP. The drug is also approved in the EC to treat adults with severe aplastic anemia and adults with chronic hepatitis C virus infection who have thrombocytopenia.
Eltrombopag is made by Novartis. For more details on the drug, see the full Summary of Product Characteristics, available on the European Medicines Agency’s website.
The EC’s latest approval of eltrombopag was based on data from 2 double-blind, placebo-controlled trials—the phase 2 PETIT trial and the phase 3 PETIT2 trial.
PETIT trials: Efficacy
The PETIT trial included 67 ITP patients stratified by age cohort (12-17 years, 6-11 years, and 1-5 years). They were randomized (2:1) to receive eltrombopag or placebo for 7 weeks. The eltrombopag dose was titrated to a target platelet count of 50-200 x 109/L.
The primary efficacy endpoint was the proportion of subjects achieving platelet counts of 50 x 109/L or higher at least once between days 8 and 43 of the randomized period of the study.
Significantly more patients in the eltrombopag arm met this endpoint—62.2%—compared to 31.8% in the placebo arm (P=0.011).
The PETIT2 trial enrolled 92 patients with chronic ITP who were randomized (2:1) to receive eltrombopag or placebo for 13 weeks. The eltrombopag dose was titrated to a target platelet count of 50-200 x 109/L.
The primary efficacy endpoint was the proportion of subjects who achieved platelet counts of 50 x 109/L or higher for at least 6 out of 8 weeks, between weeks 5 and 12 of the randomized period.
Significantly more patients in the eltrombopag arm met this endpoint—41.3%—compared to 3.4% of patients in the placebo arm (P<0.001).
PETIT trials: Safety
For both trials, there were 107 eltrombopag-treated patients evaluable for safety.
The most common adverse events that occurred more frequently in the eltrombopag arms than the placebo arms were upper respiratory tract infection, nasopharyngitis, cough, diarrhea, pyrexia, rhinitis, abdominal pain, oropharyngeal pain, toothache, increased ALT/AST, rash, and rhinorrhea.
Serious adverse events were reported in 8% of patients during the randomized part of both trials, although no serious adverse event occurred in more than 1 patient.
An ALT elevation of at least 3 times the upper limit of normal occurred in 5% of eltrombopag-treated patients. Of those patients, 2% had ALT increases of at least 5 times the upper limit of normal.
There were no deaths or thromboembolic events during either study. ![]()
Scare tactics
Okay, let’s try this one more time. We agree that vaccine rates are declining and that the outbreak of measles believed to have spread from an index case at Disneyland is an example of the risk this country faces from those declining rates. In the last few years, there has been at least one study that found that providing vaccine-hesitant families with factual provaccine information failed to change parental attitudes. In fact, the educational effort backfired in some cases, and hesitant parents found other arguments to support their flawed positions. An equally discouraging study presented in the last year suggests that parents have already decided whether they will vaccinate even before they enter into childbearing, long before pediatricians have an opportunity to present their case.
In the face of this dismal landscape of antiscience, some pediatricians have decided to discharge vaccine-refusing families from their practices. Although this approach may create a thin shell of protection against some malpractice suits, and provide their youngest patients a shred of protection from waiting-room acquired infection, it has no effect on the larger problem facing this country.

A study from the University of Illinois published in the Proceedings of the National Academy of Sciences entitled, “Countering anti-vaccine attitudes” (PNAS 2015 Aug 18;112[33]:10321-4) suggests that we may have been too timid in choosing our strategies to combat the antivaccine epidemic. From a group of more than 800 individuals across a broad economic base, a smaller group of 315 was culled using several strategies to ensure that the participants were paying attention. They were then divided into three subgroups whose pretest vaccine attitudes did not differ.
One group was presented with materials that included photographs of ill children with rashes and a testimonial from the mother whose child had had measles. A second group was presented with articles exposing the myth of a relationship between autism and the measles-mumps-rubella vaccine. This group was labeled the “autism correction” group. The control group was presented with several scientific articles unrelated to vaccines.
The researchers found that while the control group and the autism correction group showed no change in their attitudes to vaccines, those individuals presented with graphic evidence of the risk of disease did demonstrate a significant change in attitude. So, the message would seem to be that scaring parents might work.
I’m not sure why pediatricians have been so hesitant to employ scare tactics in the past. While you and I may be more easily convinced by science-based evidence than the average parent, we also have seen children with vaccine-preventable diseases or at least seen pictures and heard their horrible histories. I suspect that our provaccine attitudes are colored more by the horrors that we have seen and heard than by our lip service to the sanctity of science.
We may have been too worried about being labeled as fear mongers if we showed graphic pictures of sick and dying children and promoted tear-jerking testimonials from parents. If we were a business whose bottom line depended on selling vaccines, our marketing and advertising folks would have sent us on the fear-generating pathway long ago.
It is time to ask ourselves if the situation is so dire that it is time to stop pussyfooting around with soft educational messages and begin trying to scare the vaccine deniers into protecting their children – and everyone else’s.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics including “How to Say No to Your Toddler.”
Okay, let’s try this one more time. We agree that vaccine rates are declining and that the outbreak of measles believed to have spread from an index case at Disneyland is an example of the risk this country faces from those declining rates. In the last few years, there has been at least one study that found that providing vaccine-hesitant families with factual provaccine information failed to change parental attitudes. In fact, the educational effort backfired in some cases, and hesitant parents found other arguments to support their flawed positions. An equally discouraging study presented in the last year suggests that parents have already decided whether they will vaccinate even before they enter into childbearing, long before pediatricians have an opportunity to present their case.
In the face of this dismal landscape of antiscience, some pediatricians have decided to discharge vaccine-refusing families from their practices. Although this approach may create a thin shell of protection against some malpractice suits, and provide their youngest patients a shred of protection from waiting-room acquired infection, it has no effect on the larger problem facing this country.
A study from the University of Illinois published in the Proceedings of the National Academy of Sciences entitled, “Countering anti-vaccine attitudes” (PNAS 2015 Aug 18;112[33]:10321-4) suggests that we may have been too timid in choosing our strategies to combat the antivaccine epidemic. From a group of more than 800 individuals across a broad economic base, a smaller group of 315 was culled using several strategies to ensure that the participants were paying attention. They were then divided into three subgroups whose pretest vaccine attitudes did not differ.
One group was presented with materials that included photographs of ill children with rashes and a testimonial from the mother whose child had had measles. A second group was presented with articles exposing the myth of a relationship between autism and the measles-mumps-rubella vaccine. This group was labeled the “autism correction” group. The control group was presented with several scientific articles unrelated to vaccines.
The researchers found that while the control group and the autism correction group showed no change in their attitudes to vaccines, those individuals presented with graphic evidence of the risk of disease did demonstrate a significant change in attitude. So, the message would seem to be that scaring parents might work.
I’m not sure why pediatricians have been so hesitant to employ scare tactics in the past. While you and I may be more easily convinced by science-based evidence than the average parent, we also have seen children with vaccine-preventable diseases or at least seen pictures and heard their horrible histories. I suspect that our provaccine attitudes are colored more by the horrors that we have seen and heard than by our lip service to the sanctity of science.
We may have been too worried about being labeled as fear mongers if we showed graphic pictures of sick and dying children and promoted tear-jerking testimonials from parents. If we were a business whose bottom line depended on selling vaccines, our marketing and advertising folks would have sent us on the fear-generating pathway long ago.
It is time to ask ourselves if the situation is so dire that it is time to stop pussyfooting around with soft educational messages and begin trying to scare the vaccine deniers into protecting their children – and everyone else’s.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics including “How to Say No to Your Toddler.”
Okay, let’s try this one more time. We agree that vaccine rates are declining and that the outbreak of measles believed to have spread from an index case at Disneyland is an example of the risk this country faces from those declining rates. In the last few years, there has been at least one study that found that providing vaccine-hesitant families with factual provaccine information failed to change parental attitudes. In fact, the educational effort backfired in some cases, and hesitant parents found other arguments to support their flawed positions. An equally discouraging study presented in the last year suggests that parents have already decided whether they will vaccinate even before they enter into childbearing, long before pediatricians have an opportunity to present their case.
In the face of this dismal landscape of antiscience, some pediatricians have decided to discharge vaccine-refusing families from their practices. Although this approach may create a thin shell of protection against some malpractice suits, and provide their youngest patients a shred of protection from waiting-room acquired infection, it has no effect on the larger problem facing this country.
A study from the University of Illinois published in the Proceedings of the National Academy of Sciences entitled, “Countering anti-vaccine attitudes” (PNAS 2015 Aug 18;112[33]:10321-4) suggests that we may have been too timid in choosing our strategies to combat the antivaccine epidemic. From a group of more than 800 individuals across a broad economic base, a smaller group of 315 was culled using several strategies to ensure that the participants were paying attention. They were then divided into three subgroups whose pretest vaccine attitudes did not differ.
One group was presented with materials that included photographs of ill children with rashes and a testimonial from the mother whose child had had measles. A second group was presented with articles exposing the myth of a relationship between autism and the measles-mumps-rubella vaccine. This group was labeled the “autism correction” group. The control group was presented with several scientific articles unrelated to vaccines.
The researchers found that while the control group and the autism correction group showed no change in their attitudes to vaccines, those individuals presented with graphic evidence of the risk of disease did demonstrate a significant change in attitude. So, the message would seem to be that scaring parents might work.
I’m not sure why pediatricians have been so hesitant to employ scare tactics in the past. While you and I may be more easily convinced by science-based evidence than the average parent, we also have seen children with vaccine-preventable diseases or at least seen pictures and heard their horrible histories. I suspect that our provaccine attitudes are colored more by the horrors that we have seen and heard than by our lip service to the sanctity of science.
We may have been too worried about being labeled as fear mongers if we showed graphic pictures of sick and dying children and promoted tear-jerking testimonials from parents. If we were a business whose bottom line depended on selling vaccines, our marketing and advertising folks would have sent us on the fear-generating pathway long ago.
It is time to ask ourselves if the situation is so dire that it is time to stop pussyfooting around with soft educational messages and begin trying to scare the vaccine deniers into protecting their children – and everyone else’s.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics including “How to Say No to Your Toddler.”

Intracranial calcification, hypomyelination seen with Zika virus congenital microcephaly
A CT imaging study in 23 infants with Zika virus–linked congenital microcephaly has revealed severe brain anomalies, in particular intracranial calcifications mainly in the frontal and parietal lobes that were mostly punctate, often with a bandlike distribution.
Head CT images were taken between 3 days and 5 months after birth (mean age, 36 days) revealing ventriculomegaly in all infants, which was severe in more than half, according to a letter published online April 6 in the New England Journal of Medicine.

Researchers also observed global hypogyration in the cerebral cortex in all the infants (severe in 78%) and cerebellar hypoplasia in 74%, as well as an abnormally low density of white matter in all cases (N Engl J Med. 2016 April 6. doi: 10.1056/NEJMc1603617).
“The global presence of cortical hypogyration and white-matter hypomyelination or dysmyelination in all the infants, and cerebellar hypoplasia in the majority of them, suggest that ZIKV [Zika virus] is associated with a disruption in brain development rather than a destruction of brain,” wrote Dr. Adriano N. Hazin of the Instituto di Medicina Integral Professor Fernando Figueira, Recife, Brazil, and coauthors who reported the findings for the Microcephaly Epidemic Research Group.
Two authors declared grants from the Conselho Nacional de Desenvolvimento Científico e Tecnológico. No other conflicts of interest were declared.
A CT imaging study in 23 infants with Zika virus–linked congenital microcephaly has revealed severe brain anomalies, in particular intracranial calcifications mainly in the frontal and parietal lobes that were mostly punctate, often with a bandlike distribution.
Head CT images were taken between 3 days and 5 months after birth (mean age, 36 days) revealing ventriculomegaly in all infants, which was severe in more than half, according to a letter published online April 6 in the New England Journal of Medicine.
Researchers also observed global hypogyration in the cerebral cortex in all the infants (severe in 78%) and cerebellar hypoplasia in 74%, as well as an abnormally low density of white matter in all cases (N Engl J Med. 2016 April 6. doi: 10.1056/NEJMc1603617).
“The global presence of cortical hypogyration and white-matter hypomyelination or dysmyelination in all the infants, and cerebellar hypoplasia in the majority of them, suggest that ZIKV [Zika virus] is associated with a disruption in brain development rather than a destruction of brain,” wrote Dr. Adriano N. Hazin of the Instituto di Medicina Integral Professor Fernando Figueira, Recife, Brazil, and coauthors who reported the findings for the Microcephaly Epidemic Research Group.
Two authors declared grants from the Conselho Nacional de Desenvolvimento Científico e Tecnológico. No other conflicts of interest were declared.
A CT imaging study in 23 infants with Zika virus–linked congenital microcephaly has revealed severe brain anomalies, in particular intracranial calcifications mainly in the frontal and parietal lobes that were mostly punctate, often with a bandlike distribution.
Head CT images were taken between 3 days and 5 months after birth (mean age, 36 days) revealing ventriculomegaly in all infants, which was severe in more than half, according to a letter published online April 6 in the New England Journal of Medicine.
Researchers also observed global hypogyration in the cerebral cortex in all the infants (severe in 78%) and cerebellar hypoplasia in 74%, as well as an abnormally low density of white matter in all cases (N Engl J Med. 2016 April 6. doi: 10.1056/NEJMc1603617).
“The global presence of cortical hypogyration and white-matter hypomyelination or dysmyelination in all the infants, and cerebellar hypoplasia in the majority of them, suggest that ZIKV [Zika virus] is associated with a disruption in brain development rather than a destruction of brain,” wrote Dr. Adriano N. Hazin of the Instituto di Medicina Integral Professor Fernando Figueira, Recife, Brazil, and coauthors who reported the findings for the Microcephaly Epidemic Research Group.
Two authors declared grants from the Conselho Nacional de Desenvolvimento Científico e Tecnológico. No other conflicts of interest were declared.
FROM NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point: Zika virus–linked congenital microcephaly is characterized by severe brain anomalies including intracranial calcifications, ventriculomegaly, and hypomyelination.
Major finding: Hypomyelination and ventriculomegaly were present in all infants with Zika virus–associated congenital microcephaly.
Data source: A CT imaging study in 23 infants with Zika virus–associated congenital microcephaly.
Disclosures: Two authors declared grants from the Conselho Nacional de Desenvolvimento Científico e Tecnológico. No other conflicts of interest were declared.

Acute otitis media rates have dropped, but tied to upper respiratory infections
Close to half of all infants have an episode of acute otitis media by age 1 year, but incidence appears to have dropped in the pneumococcal conjugate vaccine era, a recent study found.
“We clearly showed that frequent viral infections, bacterial colonization, and lack of breastfeeding are major acute otitis media (AOM) risk factors,” reported Dr. Tasnee Chonmaitree and her associates at the University of Texas Medical Branch in Galveston (Pediatrics 2016 March 28 doi: 10.1542/peds.2015-3555). “It is likely that medical interventions in the past few decades, such as the use of pneumococcal and influenza virus vaccines, higher breastfeeding rates and decreased smoking, helped reduce AOM incidence.”

Between October 2008 and March 2014, researchers began tracking 367 infants from birth until they experienced their first case of AOM (and then on to age 6 months) or until they reached age 12 months; 85% completed the study. Preterm infants and those with anatomic defects or major medical problems were not included. The researchers collected nasopharyngeal specimens once during each of the first 6 months, once in the child’s 9th month, and during any viral upper respiratory infections to conduct bacterial cultures and viral polymerase chain reactions for 13 respiratory viruses.
During the course of the study, 305 children experienced a total of 887 upper respiratory infections, and 143 children experienced a total of 180 AOM episodes. Upper respiratory infections occurred at a rate of 3.2 episodes per child per year, and lower respiratory infections occurred at a rate of 0.24 episodes per child per year. Clinical sinusitis complications followed 4.6% of the upper respiratory infections, and lower respiratory infections followed 7.6%.
The rate of AOM was 0.67 episodes per child per year. Although only 6% of the infants had experienced AOM by age 3 months, that rose to nearly a quarter (23%) of the children at age 6 months and nearly half (46%) at age 12 months. Still, it remained below the rates of 18% by 3 months and 30%-39% by 6 months that had been reported in the late 1980s and 1990s.
Children who had AOM experienced 4.7 upper respiratory infections per year, compared with 2.3 episodes per year in children without AOM (P less than .002). They also had significantly greater pathogenic bacterial colonization overall and for Haemophilus influenzae and Moraxella catarrhalis, in their monthly nasopharyngeal specimens, although Streptococcus pneumoniae rates were not significantly greater.
“Interestingly, we found that not only viruses increased upper respiratory infection risk; M. catarrhalis and S. pneumoniae also increased upper respiratory infection risk,” the authors wrote “On the other hand, we found better protection for S. pneumoniae (infants born after 2010) associated with decreased upper respiratory infection risk.”
Upper respiratory infections were 74% more likely among children attending day care, and 7% more likely among children with at least one sibling at home. These infections were 37% less likely in children exclusively breastfed at least 6 months, 16% less likely in children born after February 2010, and 4% less likely for each month of any breastfeeding.
Similarly, AOM episodes were 60% less likely in children exclusively breastfed at least 3 months, and 15% less likely for each month children were breastfed.
The research was funded by the National Institutes of Health. The authors reported no disclosures.
Otitis media, or middle ear infection, is one of the most common reasons for office visits to pediatricians, and for outpatient surgery. Indeed, operations to insert ear tubes are the most frequently performed surgical procedures in children in the United States, at more than 500,000 per year. Extensive use of broad-spectrum oral antibiotics in children selects for difficult-to-treat resistant strains of bacteria and alters the normal microbiome of children. Strategies to reduce otitis media in children hold substantial promise in improving child health and reducing the cost of medical care.
Against this backdrop, the data reported in the study by Chonmaitree et al. in the current issue of Pediatrics provide reassurance that we are, indeed, making progress in the fight against otitis media. This study shows that a number of simple interventions can decrease a child’s risk of otitis. Compared with studies of similar design in the late 1980s and early 1990s, the incidence of otitis media was appreciably lower in the current study – compatible with an impact of licensure and implementation of the conjugate pneumococcal vaccine in the 1990s. This study also confirms the risk conferred by cigarette smoke exposure on the incidence of otitis media in children. Finally, and perhaps most importantly, exclusivity of breastfeeding for the first 6 months of life, and total duration of breastfeeding, also had a substantial impact on otitis media. Thus, simple interventions such as ensuring compliance with routine immunization, avoiding cigarette smoke exposure, and encouraging breastfeeding can go a long way in reducing the risk of otitis media.
The study also points out important interactions between viruses that cause infections of the upper respiratory track and pathogenic bacteria that can lead to otitis media. Although we don’t think of otitis media as a viral infection, this study confirms that viruses in fact play a critical role in development of otitis, and antiviral vaccines, such as influenza vaccine, can decrease not only the risk of developing the flu, but also the risk of otitis media and its attendant complications. Future studies of antiviral vaccines will likely further contribute to the progress made in reducing otitis media that this interesting study nicely documents.
These comments were made by Mark R. Schleiss, M.D., professor and division director of pediatric infectious diseases and immunology and the American Legion Endowed Professor of Pediatrics at the University of Minnesota, Minneapolis. Dr. Schleiss had no disclosures.
Otitis media, or middle ear infection, is one of the most common reasons for office visits to pediatricians, and for outpatient surgery. Indeed, operations to insert ear tubes are the most frequently performed surgical procedures in children in the United States, at more than 500,000 per year. Extensive use of broad-spectrum oral antibiotics in children selects for difficult-to-treat resistant strains of bacteria and alters the normal microbiome of children. Strategies to reduce otitis media in children hold substantial promise in improving child health and reducing the cost of medical care.
Against this backdrop, the data reported in the study by Chonmaitree et al. in the current issue of Pediatrics provide reassurance that we are, indeed, making progress in the fight against otitis media. This study shows that a number of simple interventions can decrease a child’s risk of otitis. Compared with studies of similar design in the late 1980s and early 1990s, the incidence of otitis media was appreciably lower in the current study – compatible with an impact of licensure and implementation of the conjugate pneumococcal vaccine in the 1990s. This study also confirms the risk conferred by cigarette smoke exposure on the incidence of otitis media in children. Finally, and perhaps most importantly, exclusivity of breastfeeding for the first 6 months of life, and total duration of breastfeeding, also had a substantial impact on otitis media. Thus, simple interventions such as ensuring compliance with routine immunization, avoiding cigarette smoke exposure, and encouraging breastfeeding can go a long way in reducing the risk of otitis media.
The study also points out important interactions between viruses that cause infections of the upper respiratory track and pathogenic bacteria that can lead to otitis media. Although we don’t think of otitis media as a viral infection, this study confirms that viruses in fact play a critical role in development of otitis, and antiviral vaccines, such as influenza vaccine, can decrease not only the risk of developing the flu, but also the risk of otitis media and its attendant complications. Future studies of antiviral vaccines will likely further contribute to the progress made in reducing otitis media that this interesting study nicely documents.
These comments were made by Mark R. Schleiss, M.D., professor and division director of pediatric infectious diseases and immunology and the American Legion Endowed Professor of Pediatrics at the University of Minnesota, Minneapolis. Dr. Schleiss had no disclosures.
Otitis media, or middle ear infection, is one of the most common reasons for office visits to pediatricians, and for outpatient surgery. Indeed, operations to insert ear tubes are the most frequently performed surgical procedures in children in the United States, at more than 500,000 per year. Extensive use of broad-spectrum oral antibiotics in children selects for difficult-to-treat resistant strains of bacteria and alters the normal microbiome of children. Strategies to reduce otitis media in children hold substantial promise in improving child health and reducing the cost of medical care.
Against this backdrop, the data reported in the study by Chonmaitree et al. in the current issue of Pediatrics provide reassurance that we are, indeed, making progress in the fight against otitis media. This study shows that a number of simple interventions can decrease a child’s risk of otitis. Compared with studies of similar design in the late 1980s and early 1990s, the incidence of otitis media was appreciably lower in the current study – compatible with an impact of licensure and implementation of the conjugate pneumococcal vaccine in the 1990s. This study also confirms the risk conferred by cigarette smoke exposure on the incidence of otitis media in children. Finally, and perhaps most importantly, exclusivity of breastfeeding for the first 6 months of life, and total duration of breastfeeding, also had a substantial impact on otitis media. Thus, simple interventions such as ensuring compliance with routine immunization, avoiding cigarette smoke exposure, and encouraging breastfeeding can go a long way in reducing the risk of otitis media.
The study also points out important interactions between viruses that cause infections of the upper respiratory track and pathogenic bacteria that can lead to otitis media. Although we don’t think of otitis media as a viral infection, this study confirms that viruses in fact play a critical role in development of otitis, and antiviral vaccines, such as influenza vaccine, can decrease not only the risk of developing the flu, but also the risk of otitis media and its attendant complications. Future studies of antiviral vaccines will likely further contribute to the progress made in reducing otitis media that this interesting study nicely documents.
These comments were made by Mark R. Schleiss, M.D., professor and division director of pediatric infectious diseases and immunology and the American Legion Endowed Professor of Pediatrics at the University of Minnesota, Minneapolis. Dr. Schleiss had no disclosures.
Close to half of all infants have an episode of acute otitis media by age 1 year, but incidence appears to have dropped in the pneumococcal conjugate vaccine era, a recent study found.
“We clearly showed that frequent viral infections, bacterial colonization, and lack of breastfeeding are major acute otitis media (AOM) risk factors,” reported Dr. Tasnee Chonmaitree and her associates at the University of Texas Medical Branch in Galveston (Pediatrics 2016 March 28 doi: 10.1542/peds.2015-3555). “It is likely that medical interventions in the past few decades, such as the use of pneumococcal and influenza virus vaccines, higher breastfeeding rates and decreased smoking, helped reduce AOM incidence.”
Between October 2008 and March 2014, researchers began tracking 367 infants from birth until they experienced their first case of AOM (and then on to age 6 months) or until they reached age 12 months; 85% completed the study. Preterm infants and those with anatomic defects or major medical problems were not included. The researchers collected nasopharyngeal specimens once during each of the first 6 months, once in the child’s 9th month, and during any viral upper respiratory infections to conduct bacterial cultures and viral polymerase chain reactions for 13 respiratory viruses.
During the course of the study, 305 children experienced a total of 887 upper respiratory infections, and 143 children experienced a total of 180 AOM episodes. Upper respiratory infections occurred at a rate of 3.2 episodes per child per year, and lower respiratory infections occurred at a rate of 0.24 episodes per child per year. Clinical sinusitis complications followed 4.6% of the upper respiratory infections, and lower respiratory infections followed 7.6%.
The rate of AOM was 0.67 episodes per child per year. Although only 6% of the infants had experienced AOM by age 3 months, that rose to nearly a quarter (23%) of the children at age 6 months and nearly half (46%) at age 12 months. Still, it remained below the rates of 18% by 3 months and 30%-39% by 6 months that had been reported in the late 1980s and 1990s.
Children who had AOM experienced 4.7 upper respiratory infections per year, compared with 2.3 episodes per year in children without AOM (P less than .002). They also had significantly greater pathogenic bacterial colonization overall and for Haemophilus influenzae and Moraxella catarrhalis, in their monthly nasopharyngeal specimens, although Streptococcus pneumoniae rates were not significantly greater.
“Interestingly, we found that not only viruses increased upper respiratory infection risk; M. catarrhalis and S. pneumoniae also increased upper respiratory infection risk,” the authors wrote “On the other hand, we found better protection for S. pneumoniae (infants born after 2010) associated with decreased upper respiratory infection risk.”
Upper respiratory infections were 74% more likely among children attending day care, and 7% more likely among children with at least one sibling at home. These infections were 37% less likely in children exclusively breastfed at least 6 months, 16% less likely in children born after February 2010, and 4% less likely for each month of any breastfeeding.
Similarly, AOM episodes were 60% less likely in children exclusively breastfed at least 3 months, and 15% less likely for each month children were breastfed.
The research was funded by the National Institutes of Health. The authors reported no disclosures.
Close to half of all infants have an episode of acute otitis media by age 1 year, but incidence appears to have dropped in the pneumococcal conjugate vaccine era, a recent study found.
“We clearly showed that frequent viral infections, bacterial colonization, and lack of breastfeeding are major acute otitis media (AOM) risk factors,” reported Dr. Tasnee Chonmaitree and her associates at the University of Texas Medical Branch in Galveston (Pediatrics 2016 March 28 doi: 10.1542/peds.2015-3555). “It is likely that medical interventions in the past few decades, such as the use of pneumococcal and influenza virus vaccines, higher breastfeeding rates and decreased smoking, helped reduce AOM incidence.”
Between October 2008 and March 2014, researchers began tracking 367 infants from birth until they experienced their first case of AOM (and then on to age 6 months) or until they reached age 12 months; 85% completed the study. Preterm infants and those with anatomic defects or major medical problems were not included. The researchers collected nasopharyngeal specimens once during each of the first 6 months, once in the child’s 9th month, and during any viral upper respiratory infections to conduct bacterial cultures and viral polymerase chain reactions for 13 respiratory viruses.
During the course of the study, 305 children experienced a total of 887 upper respiratory infections, and 143 children experienced a total of 180 AOM episodes. Upper respiratory infections occurred at a rate of 3.2 episodes per child per year, and lower respiratory infections occurred at a rate of 0.24 episodes per child per year. Clinical sinusitis complications followed 4.6% of the upper respiratory infections, and lower respiratory infections followed 7.6%.
The rate of AOM was 0.67 episodes per child per year. Although only 6% of the infants had experienced AOM by age 3 months, that rose to nearly a quarter (23%) of the children at age 6 months and nearly half (46%) at age 12 months. Still, it remained below the rates of 18% by 3 months and 30%-39% by 6 months that had been reported in the late 1980s and 1990s.
Children who had AOM experienced 4.7 upper respiratory infections per year, compared with 2.3 episodes per year in children without AOM (P less than .002). They also had significantly greater pathogenic bacterial colonization overall and for Haemophilus influenzae and Moraxella catarrhalis, in their monthly nasopharyngeal specimens, although Streptococcus pneumoniae rates were not significantly greater.
“Interestingly, we found that not only viruses increased upper respiratory infection risk; M. catarrhalis and S. pneumoniae also increased upper respiratory infection risk,” the authors wrote “On the other hand, we found better protection for S. pneumoniae (infants born after 2010) associated with decreased upper respiratory infection risk.”
Upper respiratory infections were 74% more likely among children attending day care, and 7% more likely among children with at least one sibling at home. These infections were 37% less likely in children exclusively breastfed at least 6 months, 16% less likely in children born after February 2010, and 4% less likely for each month of any breastfeeding.
Similarly, AOM episodes were 60% less likely in children exclusively breastfed at least 3 months, and 15% less likely for each month children were breastfed.
The research was funded by the National Institutes of Health. The authors reported no disclosures.
FROM PEDIATRICS
Key clinical point: Acute otitis media rates have declined, but are associated with upper respiratory infections.
Major finding: 46% of children had AOM by age 1 year; rates of upper respiratory infections were 4.7 per year in children with AOM and 2.3 per year in children without it.
Data source: The findings are based on a longitudinal cohort study of 305 children between October 2008 and March 2014, and their incidence of upper and lower respiratory infections and acute otitis media.
Disclosures: The research was funded by the National Institutes of Health. The authors reported no disclosures.

UK Report Shows Prevalence of Antibiotic Resistance in Pediatric Urinary Tract Infection
NEW YORK (Reuters Health) - The prevalence of antibiotic resistance in pediatric urinary tract infection (UTI) has reached such high levels in many countries that existing empiric therapies may no longer be effective, researchers from UK report."
Prevalence of resistance to commonly prescribed antibiotics in primary care in children with urinary tract infections caused by E. coli is high, and there was remarkable variability in E. coli resistance among countries in the study, particularly in countries outside the OECD (Organization for Economic Cooperation and Development), where one possible explanation is the availability of antibiotics over the counter," Ashley Bryce from the University of Bristol in the U.K. and Dr. Céire E. Costelloe from Imperial College London told Reuters Health in a joint email.
"This could render some antibiotics ineffective as first-line treatments for urinary tract infection," they said.
E. coli is responsible for more than 80% of all UTIs and is also the most common cause of bacteremia and foodborne infections and one cause of meningitis in neonates.
Bryce, Dr. Costelloe, and colleagues investigated the prevalence of resistance in community-acquired E. coli UTI to the most commonly prescribed antibiotics given to children in primary care in their systematic review of 58 published reports.
For all antibiotics tested, the prevalence of antibiotic resistance was higher in non-OECD countries than in OECD countries, the team reports in an article online March 15 in The BMJ.
The prevalence of resistance was highest for ampicillin, ranging from 41% in Switzerland to 100% in Ghana and Nigeria.
Resistance to co-trimoxazole and trimethoprim was 30% in OECD countries and 67% in Saudi Arabia, the only non-OECD country for which rates were available.
Pooled prevalences of resistance to ciprofloxacin and ceftazidime were around 2% in OECD countries but over 26% in non-OECD countries.
For all time periods analyzed, the odds of resistance were greater in children exposed to antibiotics than in those who were unexposed.
"The Infectious Diseases Society of America (IDSA) in collaboration with the European Society for Microbiology and Infectious Diseases (ESCMID) recommend that an antibiotic should be selected for first line empirical treatment of urinary tract infection only if the local prevalence of resistance is less than 20%," the researchers note.
"According to these guidelines, our review suggests ampicillin, co-trimoxazole, and trimethoprim are no longer suitable first line treatment options for urinary tract infection in many OECD countries and that as a result many guidelines, such as those published by the National Institute for Health and Care Excellence (NICE), might need updating," they write. "In non-OECD countries, resistance to all first line antibiotics specified for urinary tract infections was in excess of 20%, suggesting that choices of first line treatment might need to be re-evaluated in less well developed countries."
"We are not able to advise clinicians on which antibiotic is best to prescribe as this often depends on the individual case," Bryce and Dr. Costelloe said. "Clinicians should, however, adhere to local or national guidelines wherever possible, which is why it is of great importance that such guidelines are kept up to date and reflect current resistance rates."
"Clinicians may also wish to consider the antibiotic history of the child when they present to primary care with symptoms of an infection, especially in light of the suggestion of our results that previous treatment with an antibiotic is associated with resistance to that same antibiotic, and that this association may be present up to 6 months post treatment," they added.
Dr. Grant Russell from Monash University in Melbourne, Australia, wrote an editorial accompanying the report. He told Reuters Health by email, "I found the extent of the resistance (and the fact that it covered all of the regularly used empiric antibiotics) both concerning and surprising. The fact that choices are diminishing is disturbing, and the fact that the situation is dire in the developing world is deeply troubling."
"We need to do what we can do to prevent bacterial infections, and when treating them to consider that effective antibiotics are a finite resource," he said. "We all have a responsibility in attempting to conserve that resource."
"No new classes of antibiotics have been developed in the last 30 years - this and the dire situation in both the developed and the developing world suggests that the 'global problem' of antibiotic resistance is going to become more and more of an issue in years and decades to come," Dr. Russell concluded.
NEW YORK (Reuters Health) - The prevalence of antibiotic resistance in pediatric urinary tract infection (UTI) has reached such high levels in many countries that existing empiric therapies may no longer be effective, researchers from UK report."
Prevalence of resistance to commonly prescribed antibiotics in primary care in children with urinary tract infections caused by E. coli is high, and there was remarkable variability in E. coli resistance among countries in the study, particularly in countries outside the OECD (Organization for Economic Cooperation and Development), where one possible explanation is the availability of antibiotics over the counter," Ashley Bryce from the University of Bristol in the U.K. and Dr. Céire E. Costelloe from Imperial College London told Reuters Health in a joint email.
"This could render some antibiotics ineffective as first-line treatments for urinary tract infection," they said.
E. coli is responsible for more than 80% of all UTIs and is also the most common cause of bacteremia and foodborne infections and one cause of meningitis in neonates.
Bryce, Dr. Costelloe, and colleagues investigated the prevalence of resistance in community-acquired E. coli UTI to the most commonly prescribed antibiotics given to children in primary care in their systematic review of 58 published reports.
For all antibiotics tested, the prevalence of antibiotic resistance was higher in non-OECD countries than in OECD countries, the team reports in an article online March 15 in The BMJ.
The prevalence of resistance was highest for ampicillin, ranging from 41% in Switzerland to 100% in Ghana and Nigeria.
Resistance to co-trimoxazole and trimethoprim was 30% in OECD countries and 67% in Saudi Arabia, the only non-OECD country for which rates were available.
Pooled prevalences of resistance to ciprofloxacin and ceftazidime were around 2% in OECD countries but over 26% in non-OECD countries.
For all time periods analyzed, the odds of resistance were greater in children exposed to antibiotics than in those who were unexposed.
"The Infectious Diseases Society of America (IDSA) in collaboration with the European Society for Microbiology and Infectious Diseases (ESCMID) recommend that an antibiotic should be selected for first line empirical treatment of urinary tract infection only if the local prevalence of resistance is less than 20%," the researchers note.
"According to these guidelines, our review suggests ampicillin, co-trimoxazole, and trimethoprim are no longer suitable first line treatment options for urinary tract infection in many OECD countries and that as a result many guidelines, such as those published by the National Institute for Health and Care Excellence (NICE), might need updating," they write. "In non-OECD countries, resistance to all first line antibiotics specified for urinary tract infections was in excess of 20%, suggesting that choices of first line treatment might need to be re-evaluated in less well developed countries."
"We are not able to advise clinicians on which antibiotic is best to prescribe as this often depends on the individual case," Bryce and Dr. Costelloe said. "Clinicians should, however, adhere to local or national guidelines wherever possible, which is why it is of great importance that such guidelines are kept up to date and reflect current resistance rates."
"Clinicians may also wish to consider the antibiotic history of the child when they present to primary care with symptoms of an infection, especially in light of the suggestion of our results that previous treatment with an antibiotic is associated with resistance to that same antibiotic, and that this association may be present up to 6 months post treatment," they added.
Dr. Grant Russell from Monash University in Melbourne, Australia, wrote an editorial accompanying the report. He told Reuters Health by email, "I found the extent of the resistance (and the fact that it covered all of the regularly used empiric antibiotics) both concerning and surprising. The fact that choices are diminishing is disturbing, and the fact that the situation is dire in the developing world is deeply troubling."
"We need to do what we can do to prevent bacterial infections, and when treating them to consider that effective antibiotics are a finite resource," he said. "We all have a responsibility in attempting to conserve that resource."
"No new classes of antibiotics have been developed in the last 30 years - this and the dire situation in both the developed and the developing world suggests that the 'global problem' of antibiotic resistance is going to become more and more of an issue in years and decades to come," Dr. Russell concluded.
NEW YORK (Reuters Health) - The prevalence of antibiotic resistance in pediatric urinary tract infection (UTI) has reached such high levels in many countries that existing empiric therapies may no longer be effective, researchers from UK report."
Prevalence of resistance to commonly prescribed antibiotics in primary care in children with urinary tract infections caused by E. coli is high, and there was remarkable variability in E. coli resistance among countries in the study, particularly in countries outside the OECD (Organization for Economic Cooperation and Development), where one possible explanation is the availability of antibiotics over the counter," Ashley Bryce from the University of Bristol in the U.K. and Dr. Céire E. Costelloe from Imperial College London told Reuters Health in a joint email.
"This could render some antibiotics ineffective as first-line treatments for urinary tract infection," they said.
E. coli is responsible for more than 80% of all UTIs and is also the most common cause of bacteremia and foodborne infections and one cause of meningitis in neonates.
Bryce, Dr. Costelloe, and colleagues investigated the prevalence of resistance in community-acquired E. coli UTI to the most commonly prescribed antibiotics given to children in primary care in their systematic review of 58 published reports.
For all antibiotics tested, the prevalence of antibiotic resistance was higher in non-OECD countries than in OECD countries, the team reports in an article online March 15 in The BMJ.
The prevalence of resistance was highest for ampicillin, ranging from 41% in Switzerland to 100% in Ghana and Nigeria.
Resistance to co-trimoxazole and trimethoprim was 30% in OECD countries and 67% in Saudi Arabia, the only non-OECD country for which rates were available.
Pooled prevalences of resistance to ciprofloxacin and ceftazidime were around 2% in OECD countries but over 26% in non-OECD countries.
For all time periods analyzed, the odds of resistance were greater in children exposed to antibiotics than in those who were unexposed.
"The Infectious Diseases Society of America (IDSA) in collaboration with the European Society for Microbiology and Infectious Diseases (ESCMID) recommend that an antibiotic should be selected for first line empirical treatment of urinary tract infection only if the local prevalence of resistance is less than 20%," the researchers note.
"According to these guidelines, our review suggests ampicillin, co-trimoxazole, and trimethoprim are no longer suitable first line treatment options for urinary tract infection in many OECD countries and that as a result many guidelines, such as those published by the National Institute for Health and Care Excellence (NICE), might need updating," they write. "In non-OECD countries, resistance to all first line antibiotics specified for urinary tract infections was in excess of 20%, suggesting that choices of first line treatment might need to be re-evaluated in less well developed countries."
"We are not able to advise clinicians on which antibiotic is best to prescribe as this often depends on the individual case," Bryce and Dr. Costelloe said. "Clinicians should, however, adhere to local or national guidelines wherever possible, which is why it is of great importance that such guidelines are kept up to date and reflect current resistance rates."
"Clinicians may also wish to consider the antibiotic history of the child when they present to primary care with symptoms of an infection, especially in light of the suggestion of our results that previous treatment with an antibiotic is associated with resistance to that same antibiotic, and that this association may be present up to 6 months post treatment," they added.
Dr. Grant Russell from Monash University in Melbourne, Australia, wrote an editorial accompanying the report. He told Reuters Health by email, "I found the extent of the resistance (and the fact that it covered all of the regularly used empiric antibiotics) both concerning and surprising. The fact that choices are diminishing is disturbing, and the fact that the situation is dire in the developing world is deeply troubling."
"We need to do what we can do to prevent bacterial infections, and when treating them to consider that effective antibiotics are a finite resource," he said. "We all have a responsibility in attempting to conserve that resource."
"No new classes of antibiotics have been developed in the last 30 years - this and the dire situation in both the developed and the developing world suggests that the 'global problem' of antibiotic resistance is going to become more and more of an issue in years and decades to come," Dr. Russell concluded.
Dome-Shaped Papule With a Bloody Crust
The Diagnosis: Congenital Folliculosebaceous Cystic Hamartoma
Folliculosebaceous cystic hamartoma (FSCH) is a rare skin condition that is either congenital or acquired. It presents as a slow-growing and flesh-colored papulonodular lesion1 that mainly occurs on the head and neck. Involvement of the nipples, perineum, back, forearms, genital areas, and subcutaneous tissue also has been reported but usually indicates a larger lesion.1,2
Histologically, FSCH is considered a hamartoma composed of both ectodermal and mesodermal elements.1 Folliculosebaceous cystic hamartoma is a more complex lesion composed of infundibulocystic structures connected to maloriented folliculosebaceous units surrounded by whorls of highly vascularized fibrous stroma and adipocytes. Clefts between fibroepithelial units and surrounding stroma usually are present.1
Epithelial components contribute to the adnexal and folliculosebaceous cystic proliferations, and mesenchymal elements include vascular tissue, adipose tissue, and fibroblast-rich stroma.1,2 Acquired lesions arising in adults have been described,1-5 but the congenital presentation of FSCH in infancy is rare.
Histopathologically, some variations of FSCH are mainly composed of epithelial components while others are composed of nonepithelial components. Nonepithelial components include neural proliferation, muscle components, vascular proliferation, and mucin deposition.1-4 In some cases, FSCH may coexist with other diseases, such as nevus lipomatosus cutaneous superficialis and neurofibromatosis type I.4,5
In our case, histopathology showed several dermal infundibulocystic structures that were lined by stratified squamous epithelium and contained horny material (Figure 1). Numerous immature sebaceous lobules and rudimentary hair follicles emanated from some of the cyst walls. Mesenchymal changes around the fibroepithelial units included fibrillary bundles of collagen, clusters of adipocytes, and an increased number of small venules (Figure 2). In addition, the stroma adjacent to the malformed perifollicle contained some amount of mucin. Prominent clefts formed between fibroepithelial units and the surrounding altered stroma.
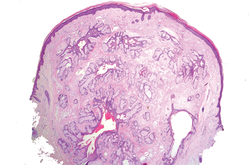
| 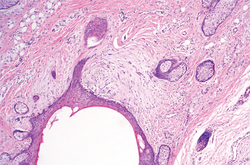
| |
|
The differential diagnosis mainly includes sebaceous trichofolliculoma, molluscum contagiosum, dermoid cysts, pilomatrixoma, Spitz nevus, and nevus lipomatosus superficialis. The differential diagnosis between FSCH and sebaceous trichofolliculoma is challenging. Both lesions show an infundibular cyst and surrounding sebaceous nodules. According to Plewig,6 trichofolliculoma has a wide spectrum ranging from low to high differentiation represented by trichofolliculoma, sebaceous trichofolliculoma, and FSCH, respectively. It is not difficult to distinguish FSCH from other diseases according to its peculiar histopathologic features.
The clinicopathologic features of our case were similar to those of reported FSCH cases, except for the following unique characteristics: congenital lesion, lack of terminal hair, and no sebaceous material extrusion. These features of hair and sebaceous material may be correlated with the patient’s age and hormonal level.1 Androgen may play a key role in sebaceous gland development at puberty, which leads to sebaceous gland hyperplasia and hypertrophy. Therefore, slight pressure from the lesions can make ivory-white sebaceous material discharge. Hence, the dermatologist and pediatrician must be poised and sensitive while making an initial diagnosis of FSCH.
1. Kimura T, Miyazawa H, Aoyagi T, et al. Folliculosebaceous cystic hamartoma: a distinctive malformation of the skin. Am J Dermatopathol. 1991;13:213-220.
2. Moriki M, Ito T, Hirakawa S, et al. Folliculosebaceous cystic hamartoma presenting as a subcutaneous nodule on the thigh. J Dermatol. 2013;40:483-484.
3. Aloi F, Tomasini C, Pippione M. Folliculosebaceous cystic hamartoma with perifollicular mucinosis. Am J Dermatopathol. 1996;18:58-62.
4. Brasanac D, Boricic I. Giant nevus lipomatosus superficialis with multiple folliculosebaceous cystic hamartomas and dermoid cysts. J Eur Acad Dermatol Venereol. 2005;19:84-86.
5. Noh S, Kwon JE, Lee KG, et al. Folliculosebaceous cystic hamartoma in a patient with neurofibromatosis type I. Ann Dermatol. 2011;23(suppl 2):S185-S187.
6. Plewig G. In discussion of: Leserbrief zu Zheng LQ, Han XC, Huang Y, Li HW. Several acneiform papules and nodules on the neck. diagnosis: folliculosebaceous cystic hamartoma. J Dtsch Dermatol Ges. 2014;12:824-825.
The Diagnosis: Congenital Folliculosebaceous Cystic Hamartoma
Folliculosebaceous cystic hamartoma (FSCH) is a rare skin condition that is either congenital or acquired. It presents as a slow-growing and flesh-colored papulonodular lesion1 that mainly occurs on the head and neck. Involvement of the nipples, perineum, back, forearms, genital areas, and subcutaneous tissue also has been reported but usually indicates a larger lesion.1,2
Histologically, FSCH is considered a hamartoma composed of both ectodermal and mesodermal elements.1 Folliculosebaceous cystic hamartoma is a more complex lesion composed of infundibulocystic structures connected to maloriented folliculosebaceous units surrounded by whorls of highly vascularized fibrous stroma and adipocytes. Clefts between fibroepithelial units and surrounding stroma usually are present.1
Epithelial components contribute to the adnexal and folliculosebaceous cystic proliferations, and mesenchymal elements include vascular tissue, adipose tissue, and fibroblast-rich stroma.1,2 Acquired lesions arising in adults have been described,1-5 but the congenital presentation of FSCH in infancy is rare.
Histopathologically, some variations of FSCH are mainly composed of epithelial components while others are composed of nonepithelial components. Nonepithelial components include neural proliferation, muscle components, vascular proliferation, and mucin deposition.1-4 In some cases, FSCH may coexist with other diseases, such as nevus lipomatosus cutaneous superficialis and neurofibromatosis type I.4,5
In our case, histopathology showed several dermal infundibulocystic structures that were lined by stratified squamous epithelium and contained horny material (Figure 1). Numerous immature sebaceous lobules and rudimentary hair follicles emanated from some of the cyst walls. Mesenchymal changes around the fibroepithelial units included fibrillary bundles of collagen, clusters of adipocytes, and an increased number of small venules (Figure 2). In addition, the stroma adjacent to the malformed perifollicle contained some amount of mucin. Prominent clefts formed between fibroepithelial units and the surrounding altered stroma.
|
|
| |
|
The differential diagnosis mainly includes sebaceous trichofolliculoma, molluscum contagiosum, dermoid cysts, pilomatrixoma, Spitz nevus, and nevus lipomatosus superficialis. The differential diagnosis between FSCH and sebaceous trichofolliculoma is challenging. Both lesions show an infundibular cyst and surrounding sebaceous nodules. According to Plewig,6 trichofolliculoma has a wide spectrum ranging from low to high differentiation represented by trichofolliculoma, sebaceous trichofolliculoma, and FSCH, respectively. It is not difficult to distinguish FSCH from other diseases according to its peculiar histopathologic features.
The clinicopathologic features of our case were similar to those of reported FSCH cases, except for the following unique characteristics: congenital lesion, lack of terminal hair, and no sebaceous material extrusion. These features of hair and sebaceous material may be correlated with the patient’s age and hormonal level.1 Androgen may play a key role in sebaceous gland development at puberty, which leads to sebaceous gland hyperplasia and hypertrophy. Therefore, slight pressure from the lesions can make ivory-white sebaceous material discharge. Hence, the dermatologist and pediatrician must be poised and sensitive while making an initial diagnosis of FSCH.
The Diagnosis: Congenital Folliculosebaceous Cystic Hamartoma
Folliculosebaceous cystic hamartoma (FSCH) is a rare skin condition that is either congenital or acquired. It presents as a slow-growing and flesh-colored papulonodular lesion1 that mainly occurs on the head and neck. Involvement of the nipples, perineum, back, forearms, genital areas, and subcutaneous tissue also has been reported but usually indicates a larger lesion.1,2
Histologically, FSCH is considered a hamartoma composed of both ectodermal and mesodermal elements.1 Folliculosebaceous cystic hamartoma is a more complex lesion composed of infundibulocystic structures connected to maloriented folliculosebaceous units surrounded by whorls of highly vascularized fibrous stroma and adipocytes. Clefts between fibroepithelial units and surrounding stroma usually are present.1
Epithelial components contribute to the adnexal and folliculosebaceous cystic proliferations, and mesenchymal elements include vascular tissue, adipose tissue, and fibroblast-rich stroma.1,2 Acquired lesions arising in adults have been described,1-5 but the congenital presentation of FSCH in infancy is rare.
Histopathologically, some variations of FSCH are mainly composed of epithelial components while others are composed of nonepithelial components. Nonepithelial components include neural proliferation, muscle components, vascular proliferation, and mucin deposition.1-4 In some cases, FSCH may coexist with other diseases, such as nevus lipomatosus cutaneous superficialis and neurofibromatosis type I.4,5
In our case, histopathology showed several dermal infundibulocystic structures that were lined by stratified squamous epithelium and contained horny material (Figure 1). Numerous immature sebaceous lobules and rudimentary hair follicles emanated from some of the cyst walls. Mesenchymal changes around the fibroepithelial units included fibrillary bundles of collagen, clusters of adipocytes, and an increased number of small venules (Figure 2). In addition, the stroma adjacent to the malformed perifollicle contained some amount of mucin. Prominent clefts formed between fibroepithelial units and the surrounding altered stroma.
|
|
| |
|
The differential diagnosis mainly includes sebaceous trichofolliculoma, molluscum contagiosum, dermoid cysts, pilomatrixoma, Spitz nevus, and nevus lipomatosus superficialis. The differential diagnosis between FSCH and sebaceous trichofolliculoma is challenging. Both lesions show an infundibular cyst and surrounding sebaceous nodules. According to Plewig,6 trichofolliculoma has a wide spectrum ranging from low to high differentiation represented by trichofolliculoma, sebaceous trichofolliculoma, and FSCH, respectively. It is not difficult to distinguish FSCH from other diseases according to its peculiar histopathologic features.
The clinicopathologic features of our case were similar to those of reported FSCH cases, except for the following unique characteristics: congenital lesion, lack of terminal hair, and no sebaceous material extrusion. These features of hair and sebaceous material may be correlated with the patient’s age and hormonal level.1 Androgen may play a key role in sebaceous gland development at puberty, which leads to sebaceous gland hyperplasia and hypertrophy. Therefore, slight pressure from the lesions can make ivory-white sebaceous material discharge. Hence, the dermatologist and pediatrician must be poised and sensitive while making an initial diagnosis of FSCH.
1. Kimura T, Miyazawa H, Aoyagi T, et al. Folliculosebaceous cystic hamartoma: a distinctive malformation of the skin. Am J Dermatopathol. 1991;13:213-220.
2. Moriki M, Ito T, Hirakawa S, et al. Folliculosebaceous cystic hamartoma presenting as a subcutaneous nodule on the thigh. J Dermatol. 2013;40:483-484.
3. Aloi F, Tomasini C, Pippione M. Folliculosebaceous cystic hamartoma with perifollicular mucinosis. Am J Dermatopathol. 1996;18:58-62.
4. Brasanac D, Boricic I. Giant nevus lipomatosus superficialis with multiple folliculosebaceous cystic hamartomas and dermoid cysts. J Eur Acad Dermatol Venereol. 2005;19:84-86.
5. Noh S, Kwon JE, Lee KG, et al. Folliculosebaceous cystic hamartoma in a patient with neurofibromatosis type I. Ann Dermatol. 2011;23(suppl 2):S185-S187.
6. Plewig G. In discussion of: Leserbrief zu Zheng LQ, Han XC, Huang Y, Li HW. Several acneiform papules and nodules on the neck. diagnosis: folliculosebaceous cystic hamartoma. J Dtsch Dermatol Ges. 2014;12:824-825.
1. Kimura T, Miyazawa H, Aoyagi T, et al. Folliculosebaceous cystic hamartoma: a distinctive malformation of the skin. Am J Dermatopathol. 1991;13:213-220.
2. Moriki M, Ito T, Hirakawa S, et al. Folliculosebaceous cystic hamartoma presenting as a subcutaneous nodule on the thigh. J Dermatol. 2013;40:483-484.
3. Aloi F, Tomasini C, Pippione M. Folliculosebaceous cystic hamartoma with perifollicular mucinosis. Am J Dermatopathol. 1996;18:58-62.
4. Brasanac D, Boricic I. Giant nevus lipomatosus superficialis with multiple folliculosebaceous cystic hamartomas and dermoid cysts. J Eur Acad Dermatol Venereol. 2005;19:84-86.
5. Noh S, Kwon JE, Lee KG, et al. Folliculosebaceous cystic hamartoma in a patient with neurofibromatosis type I. Ann Dermatol. 2011;23(suppl 2):S185-S187.
6. Plewig G. In discussion of: Leserbrief zu Zheng LQ, Han XC, Huang Y, Li HW. Several acneiform papules and nodules on the neck. diagnosis: folliculosebaceous cystic hamartoma. J Dtsch Dermatol Ges. 2014;12:824-825.

A 3-year-old girl was referred to our clinic for a lesion on the face that had been present since birth and had enlarged slowly with slight itching. Physical examination revealed a 1.0×1.0-cm, sessile, flesh-colored, sharply demarcated, and dome-shaped papule with a bloody crust. It was firm and slightly painful to palpation. Dilated hair follicle–like orifices and thick central terminal hair were not found. Sebaceous material was not discharged. There was no notable family history or evidence of systemic disease. The lesion was surgically removed for cosmetic reasons and further histopathologic examination was performed.

Recently identified eczema comorbidities include anemia, obesity
WAIKOLOA, HAWAII – The list of nonatopic comorbid conditions associated with atopic dermatitis is rapidly expanding.
Just in the past year, published studies have linked pediatric atopic dermatitis to increased risks of obesity, high blood pressure, headaches, anemia, and speech disorders. Meanwhile, adult atopic dermatitis was reported to be associated with increased rates of fracture and cardiovascular disease. And in the dermatologic arena, a link between atopic dermatitis, vitiligo, and alopecia areata was identified, Dr. Lawrence F. Eichenfield noted at the Hawaii Dermatology Seminar provided by the Global Academy for Medical Education/Skin Disease Education Foundation.

Actually, these reported associations published in 2015-2016 might best be termed “emerging comorbidities,” as they are first reports and thus need confirmation, said Dr. Eichenfield, professor of dermatology and pediatrics at the University of California, San Diego, and chief of pediatric and adolescent dermatology at Rady Children’s Hospital San Diego.
Much of this work on emerging comorbidities has been done by dermatologist Dr. Jonathan I. Silverberg of Northwestern University, Chicago, and various coinvestigators. They have been prolific.
For example, in a multivariate logistic regression analysis of 207,007 children and adolescents included in the cross-sectional 1997-2013 U.S. National Health Interview Survey, Dr. Silverberg and coinvestigators found that eczema was independently associated with a 1.83-fold increased odds of anemia. They bolstered this observation with an analysis of more than 30,000 children and adolescents in the 1992-2012 National Health and Nutrition Examination Survey (NHANES) in which they found that current eczema was associated with a 1.93-fold increased odds of anemia, particularly microcytic anemia. The underlying mechanism is unknown; however, the investigators noted that chronic inflammation and systemic immunosuppressant drugs have been shown to be associated with anemia (JAMA Pediatr. 2016;170[1]:29-34).
Dr. Silverberg also found in a multivariate logistic regression analysis of data on more than 400,000 pediatric participants in the National Survey of Children’s Health and the National Health Interview Survey that mild and severe eczema were independently associated with 1.79-fold and 2.72-fold, respectively, increased odds of headaches (J Allergy Clin Immunol. 2016 Feb;137[2]:492-9).
Using these same two data sources, with multivariate analysis adjusted for potential confounders, the investigators found that eczema was associated with a 1.81-fold increased risk of speech disorder (J Pediatr. 2016 Jan;168:185-92).
In a case-control study involving 132 children and adolescents with current moderate to severe atopic dermatitis and 143 healthy controls, Dr. Silverberg and coinvestigators found in a logistic regression analysis that atopic dermatitis was independently associated with a doubled risk of having a systolic blood pressure in the 90th percentile or higher – as well as 3.92-fold increased odds of central obesity, as defined by a waist circumference in the 85th percentile or higher (JAMA Dermatol. 2015 Feb;151[2]:144-52).
In a systematic review and meta-analysis of 16 published vitiligo studies and 17 published studies of alopecia areata, Dr. Silverberg and medical student Girish C. Mohan found that patients with vitiligo or alopecia areata were respectively 7.8 and 2.6 times more likely to have atopic dermatitis than controls without those disorders (JAMA Dermatol. 2015 May;151[5]:522-8).
In a logistic regression analysis of data on 34,500 adults with a history of eczema within the prior year who participated in the 2012 National Health Interview Survey, Drs. Nitin Garg and Dr. Silverberg concluded that the results suggested that adult atopic dermatitis is a previously unrecognized risk factor for fracture and other bone or joint injuries causing limitation. Adults with atopic dermatitis were at a 1.67-fold increased risk for such injuries in an analysis controlling for sociodemographics, other forms of atopic disease, and psychiatric and behavioral disorders (JAMA Dermatol. 2015 Jan;151[1]:33-41).
In another large cross-sectional study, Dr. Silverberg found that adults with atopic dermatitis had significantly higher odds of a history of acute MI, coronary artery disease, heart failure, and stroke (Allergy. 2015 Oct;70[10]:1300-8).
Dr. Eichenfield said that while he would like to see these hot-off-the-presses 2015-2016 findings on nonatopic comorbidities backed up by confirmatory studies in other populations, the evidence is stronger for an association between pediatric atopic dermatitis and several mental health disorders. The initial reports came mainly from Europe, but were then supported by a large study by Dr. Eric L. Simpson and coinvestigators at Oregon Health and Science University, Portland.
In their analysis of data on nearly 93,000 noninstitutionalized children and adolescents included in the 2007 National Survey of Children’s Health, the investigators found after controlling for potential confounders that atopic dermatitis was associated with a 1.87-fold increased risk of having attention-deficit/hyperactivity disorder, a 3-fold increased risk of diagnosed autism, an adjusted 1.81-fold increase in depression, and 1.87-fold increased odds of conduct disorder. The Oregon group found a clear dose-dependent relationship between the reported severity of the skin disease and the likelihood of those mental health disorders (J Allergy Clin Immunol. 2013 Feb;131[2]:428-33).
The hope is that emerging strategies to prevent atopic dermatitis or aggressively treat it early on will reduce the risk of many of these comorbid conditions, Dr. Eichenfield said.
SDEF and this news organization are owned by the same parent company.
WAIKOLOA, HAWAII – The list of nonatopic comorbid conditions associated with atopic dermatitis is rapidly expanding.
Just in the past year, published studies have linked pediatric atopic dermatitis to increased risks of obesity, high blood pressure, headaches, anemia, and speech disorders. Meanwhile, adult atopic dermatitis was reported to be associated with increased rates of fracture and cardiovascular disease. And in the dermatologic arena, a link between atopic dermatitis, vitiligo, and alopecia areata was identified, Dr. Lawrence F. Eichenfield noted at the Hawaii Dermatology Seminar provided by the Global Academy for Medical Education/Skin Disease Education Foundation.
Actually, these reported associations published in 2015-2016 might best be termed “emerging comorbidities,” as they are first reports and thus need confirmation, said Dr. Eichenfield, professor of dermatology and pediatrics at the University of California, San Diego, and chief of pediatric and adolescent dermatology at Rady Children’s Hospital San Diego.
Much of this work on emerging comorbidities has been done by dermatologist Dr. Jonathan I. Silverberg of Northwestern University, Chicago, and various coinvestigators. They have been prolific.
For example, in a multivariate logistic regression analysis of 207,007 children and adolescents included in the cross-sectional 1997-2013 U.S. National Health Interview Survey, Dr. Silverberg and coinvestigators found that eczema was independently associated with a 1.83-fold increased odds of anemia. They bolstered this observation with an analysis of more than 30,000 children and adolescents in the 1992-2012 National Health and Nutrition Examination Survey (NHANES) in which they found that current eczema was associated with a 1.93-fold increased odds of anemia, particularly microcytic anemia. The underlying mechanism is unknown; however, the investigators noted that chronic inflammation and systemic immunosuppressant drugs have been shown to be associated with anemia (JAMA Pediatr. 2016;170[1]:29-34).
Dr. Silverberg also found in a multivariate logistic regression analysis of data on more than 400,000 pediatric participants in the National Survey of Children’s Health and the National Health Interview Survey that mild and severe eczema were independently associated with 1.79-fold and 2.72-fold, respectively, increased odds of headaches (J Allergy Clin Immunol. 2016 Feb;137[2]:492-9).
Using these same two data sources, with multivariate analysis adjusted for potential confounders, the investigators found that eczema was associated with a 1.81-fold increased risk of speech disorder (J Pediatr. 2016 Jan;168:185-92).
In a case-control study involving 132 children and adolescents with current moderate to severe atopic dermatitis and 143 healthy controls, Dr. Silverberg and coinvestigators found in a logistic regression analysis that atopic dermatitis was independently associated with a doubled risk of having a systolic blood pressure in the 90th percentile or higher – as well as 3.92-fold increased odds of central obesity, as defined by a waist circumference in the 85th percentile or higher (JAMA Dermatol. 2015 Feb;151[2]:144-52).
In a systematic review and meta-analysis of 16 published vitiligo studies and 17 published studies of alopecia areata, Dr. Silverberg and medical student Girish C. Mohan found that patients with vitiligo or alopecia areata were respectively 7.8 and 2.6 times more likely to have atopic dermatitis than controls without those disorders (JAMA Dermatol. 2015 May;151[5]:522-8).
In a logistic regression analysis of data on 34,500 adults with a history of eczema within the prior year who participated in the 2012 National Health Interview Survey, Drs. Nitin Garg and Dr. Silverberg concluded that the results suggested that adult atopic dermatitis is a previously unrecognized risk factor for fracture and other bone or joint injuries causing limitation. Adults with atopic dermatitis were at a 1.67-fold increased risk for such injuries in an analysis controlling for sociodemographics, other forms of atopic disease, and psychiatric and behavioral disorders (JAMA Dermatol. 2015 Jan;151[1]:33-41).
In another large cross-sectional study, Dr. Silverberg found that adults with atopic dermatitis had significantly higher odds of a history of acute MI, coronary artery disease, heart failure, and stroke (Allergy. 2015 Oct;70[10]:1300-8).
Dr. Eichenfield said that while he would like to see these hot-off-the-presses 2015-2016 findings on nonatopic comorbidities backed up by confirmatory studies in other populations, the evidence is stronger for an association between pediatric atopic dermatitis and several mental health disorders. The initial reports came mainly from Europe, but were then supported by a large study by Dr. Eric L. Simpson and coinvestigators at Oregon Health and Science University, Portland.
In their analysis of data on nearly 93,000 noninstitutionalized children and adolescents included in the 2007 National Survey of Children’s Health, the investigators found after controlling for potential confounders that atopic dermatitis was associated with a 1.87-fold increased risk of having attention-deficit/hyperactivity disorder, a 3-fold increased risk of diagnosed autism, an adjusted 1.81-fold increase in depression, and 1.87-fold increased odds of conduct disorder. The Oregon group found a clear dose-dependent relationship between the reported severity of the skin disease and the likelihood of those mental health disorders (J Allergy Clin Immunol. 2013 Feb;131[2]:428-33).
The hope is that emerging strategies to prevent atopic dermatitis or aggressively treat it early on will reduce the risk of many of these comorbid conditions, Dr. Eichenfield said.
SDEF and this news organization are owned by the same parent company.
WAIKOLOA, HAWAII – The list of nonatopic comorbid conditions associated with atopic dermatitis is rapidly expanding.
Just in the past year, published studies have linked pediatric atopic dermatitis to increased risks of obesity, high blood pressure, headaches, anemia, and speech disorders. Meanwhile, adult atopic dermatitis was reported to be associated with increased rates of fracture and cardiovascular disease. And in the dermatologic arena, a link between atopic dermatitis, vitiligo, and alopecia areata was identified, Dr. Lawrence F. Eichenfield noted at the Hawaii Dermatology Seminar provided by the Global Academy for Medical Education/Skin Disease Education Foundation.
Actually, these reported associations published in 2015-2016 might best be termed “emerging comorbidities,” as they are first reports and thus need confirmation, said Dr. Eichenfield, professor of dermatology and pediatrics at the University of California, San Diego, and chief of pediatric and adolescent dermatology at Rady Children’s Hospital San Diego.
Much of this work on emerging comorbidities has been done by dermatologist Dr. Jonathan I. Silverberg of Northwestern University, Chicago, and various coinvestigators. They have been prolific.
For example, in a multivariate logistic regression analysis of 207,007 children and adolescents included in the cross-sectional 1997-2013 U.S. National Health Interview Survey, Dr. Silverberg and coinvestigators found that eczema was independently associated with a 1.83-fold increased odds of anemia. They bolstered this observation with an analysis of more than 30,000 children and adolescents in the 1992-2012 National Health and Nutrition Examination Survey (NHANES) in which they found that current eczema was associated with a 1.93-fold increased odds of anemia, particularly microcytic anemia. The underlying mechanism is unknown; however, the investigators noted that chronic inflammation and systemic immunosuppressant drugs have been shown to be associated with anemia (JAMA Pediatr. 2016;170[1]:29-34).
Dr. Silverberg also found in a multivariate logistic regression analysis of data on more than 400,000 pediatric participants in the National Survey of Children’s Health and the National Health Interview Survey that mild and severe eczema were independently associated with 1.79-fold and 2.72-fold, respectively, increased odds of headaches (J Allergy Clin Immunol. 2016 Feb;137[2]:492-9).
Using these same two data sources, with multivariate analysis adjusted for potential confounders, the investigators found that eczema was associated with a 1.81-fold increased risk of speech disorder (J Pediatr. 2016 Jan;168:185-92).
In a case-control study involving 132 children and adolescents with current moderate to severe atopic dermatitis and 143 healthy controls, Dr. Silverberg and coinvestigators found in a logistic regression analysis that atopic dermatitis was independently associated with a doubled risk of having a systolic blood pressure in the 90th percentile or higher – as well as 3.92-fold increased odds of central obesity, as defined by a waist circumference in the 85th percentile or higher (JAMA Dermatol. 2015 Feb;151[2]:144-52).
In a systematic review and meta-analysis of 16 published vitiligo studies and 17 published studies of alopecia areata, Dr. Silverberg and medical student Girish C. Mohan found that patients with vitiligo or alopecia areata were respectively 7.8 and 2.6 times more likely to have atopic dermatitis than controls without those disorders (JAMA Dermatol. 2015 May;151[5]:522-8).
In a logistic regression analysis of data on 34,500 adults with a history of eczema within the prior year who participated in the 2012 National Health Interview Survey, Drs. Nitin Garg and Dr. Silverberg concluded that the results suggested that adult atopic dermatitis is a previously unrecognized risk factor for fracture and other bone or joint injuries causing limitation. Adults with atopic dermatitis were at a 1.67-fold increased risk for such injuries in an analysis controlling for sociodemographics, other forms of atopic disease, and psychiatric and behavioral disorders (JAMA Dermatol. 2015 Jan;151[1]:33-41).
In another large cross-sectional study, Dr. Silverberg found that adults with atopic dermatitis had significantly higher odds of a history of acute MI, coronary artery disease, heart failure, and stroke (Allergy. 2015 Oct;70[10]:1300-8).
Dr. Eichenfield said that while he would like to see these hot-off-the-presses 2015-2016 findings on nonatopic comorbidities backed up by confirmatory studies in other populations, the evidence is stronger for an association between pediatric atopic dermatitis and several mental health disorders. The initial reports came mainly from Europe, but were then supported by a large study by Dr. Eric L. Simpson and coinvestigators at Oregon Health and Science University, Portland.
In their analysis of data on nearly 93,000 noninstitutionalized children and adolescents included in the 2007 National Survey of Children’s Health, the investigators found after controlling for potential confounders that atopic dermatitis was associated with a 1.87-fold increased risk of having attention-deficit/hyperactivity disorder, a 3-fold increased risk of diagnosed autism, an adjusted 1.81-fold increase in depression, and 1.87-fold increased odds of conduct disorder. The Oregon group found a clear dose-dependent relationship between the reported severity of the skin disease and the likelihood of those mental health disorders (J Allergy Clin Immunol. 2013 Feb;131[2]:428-33).
The hope is that emerging strategies to prevent atopic dermatitis or aggressively treat it early on will reduce the risk of many of these comorbid conditions, Dr. Eichenfield said.
SDEF and this news organization are owned by the same parent company.
EXPERT ANALYSIS FROM THE SDEF HAWAII DERMATOLOGY SEMINAR

Haplo-HSCT approach appears safe, effective for nonmalignant disorders

Image courtesy of NIAID
VALENCIA, SPAIN—Interim results of a phase 1/2 trial suggest the adjunct T-cell therapy BPX-501 can safely accelerate immune recovery after haploidentical hematopoietic stem cell transplant (haplo-HSCT) in pediatric patients with nonmalignant disorders.
Twenty-four such patients received BPX-501 after haplo-HSCT on this trial.
At a median follow-up of 7 months, all 24 were still alive and disease-free.
In addition, the incidence of graft-versus-host disease (GVHD) was considered “very low.”
Pietro Merli, MD, of Bambino Gesù Children’s Hospital in Rome, Italy, presented these results during the Presidential Symposium of the 42nd Annual Meeting of the European Society for Blood and Marrow Transplantation (EBMT) as abstract O007.*
The trial, known as BP-004, was sponsored by Bellicum Pharmaceuticals, the company developing BPX-501.
About BPX-501
BPX-501 consists of genetically modified donor T cells incorporating the CaspaCIDe safety switch, which is designed to eliminate cells in the event of toxicity.
The goal is to allow physicians to more safely perform haplo-HSCTs by giving patients BPX-501 to speed immune reconstitution and provide control over viral infections. But the technology is designed to provide a safety net to eliminate BPX-501 alloreactive T cells if severe GVHD occurs.
The CaspaCIDe switch consists of the CID-binding domain coupled to the signaling domain of caspase-9, an enzyme that is part of the apoptotic pathway. The idea is that, if a patient develops severe GVHD, he can receive an infusion with the small molecule rimiducid. And this will trigger activation of the domain of caspase-9, which leads to selective apoptosis of the CaspaCIDe-containing cells.
About BP-004
In late 2014, Bellicum initiated BP-004, a phase 1/2 trial in children with leukemias, lymphomas, or orphan inherited blood disorders. The trial is being conducted in European and US pediatric transplant centers and is set to enroll up to 90 patients.
At the EBMT meeting, investigators reported results in 41 patients treated on this trial.
Dr Merli presented data on the 24 patients with nonmalignant disorders, including Fanconi anemia (n=5), beta-thalassemia major (n=5), severe combined immunodeficiency (n=5), Wiskott-Aldrich syndrome (n=4), Diamond-Blackfan anemia (n=1), hemophagocytic lymphohistiocytosis (n=1), immune deficiency due to mutation of XIAP gene (n=1), osteopetrosis (n=1), and sickle cell disease (n=1).
All of these patients received a T-cell-depleted haplo-HSCT without post-transplant GVHD prophylaxis.
The patients received BPX-501 within 14 ± 4 days after haplo-HSCT. The phase 1 portion of the trial consisted of a classical 3+3 design, with 3 cohorts receiving escalating doses of BPX-501 cells—2.5 x 105, 5 x 105, and 1 x 106 cells/kg.
In the phase 2 portion, patients received 1 X 106 BPX-501 cells/kg. Rimiducid was only to be used in the event of uncontrollable GVHD.
Results
The median time to platelet recovery was 10 days (range, 7-16), and the median time to neutrophil recovery was 15 days (range, 10-33).
At a median follow-up of 220 days (range, 61-486), there were no reports of transplant-related mortality.
All 24 patients were still alive and disease-free. And none of the patients developed post-transplant lymphoproliferative disorder.
The cumulative incidence of skin-only acute GVHD was 16.6% (n=4), and the cumulative incidence of mild chronic GVHD was 5% (n=1).
This trial also included 17 patients with acute leukemias. Results in these patients were presented at the EBMT meeting as abstract WP16. ![]()
*Information in the abstract differs from that presented at the meeting.
Image courtesy of NIAID
VALENCIA, SPAIN—Interim results of a phase 1/2 trial suggest the adjunct T-cell therapy BPX-501 can safely accelerate immune recovery after haploidentical hematopoietic stem cell transplant (haplo-HSCT) in pediatric patients with nonmalignant disorders.
Twenty-four such patients received BPX-501 after haplo-HSCT on this trial.
At a median follow-up of 7 months, all 24 were still alive and disease-free.
In addition, the incidence of graft-versus-host disease (GVHD) was considered “very low.”
Pietro Merli, MD, of Bambino Gesù Children’s Hospital in Rome, Italy, presented these results during the Presidential Symposium of the 42nd Annual Meeting of the European Society for Blood and Marrow Transplantation (EBMT) as abstract O007.*
The trial, known as BP-004, was sponsored by Bellicum Pharmaceuticals, the company developing BPX-501.
About BPX-501
BPX-501 consists of genetically modified donor T cells incorporating the CaspaCIDe safety switch, which is designed to eliminate cells in the event of toxicity.
The goal is to allow physicians to more safely perform haplo-HSCTs by giving patients BPX-501 to speed immune reconstitution and provide control over viral infections. But the technology is designed to provide a safety net to eliminate BPX-501 alloreactive T cells if severe GVHD occurs.
The CaspaCIDe switch consists of the CID-binding domain coupled to the signaling domain of caspase-9, an enzyme that is part of the apoptotic pathway. The idea is that, if a patient develops severe GVHD, he can receive an infusion with the small molecule rimiducid. And this will trigger activation of the domain of caspase-9, which leads to selective apoptosis of the CaspaCIDe-containing cells.
About BP-004
In late 2014, Bellicum initiated BP-004, a phase 1/2 trial in children with leukemias, lymphomas, or orphan inherited blood disorders. The trial is being conducted in European and US pediatric transplant centers and is set to enroll up to 90 patients.
At the EBMT meeting, investigators reported results in 41 patients treated on this trial.
Dr Merli presented data on the 24 patients with nonmalignant disorders, including Fanconi anemia (n=5), beta-thalassemia major (n=5), severe combined immunodeficiency (n=5), Wiskott-Aldrich syndrome (n=4), Diamond-Blackfan anemia (n=1), hemophagocytic lymphohistiocytosis (n=1), immune deficiency due to mutation of XIAP gene (n=1), osteopetrosis (n=1), and sickle cell disease (n=1).
All of these patients received a T-cell-depleted haplo-HSCT without post-transplant GVHD prophylaxis.
The patients received BPX-501 within 14 ± 4 days after haplo-HSCT. The phase 1 portion of the trial consisted of a classical 3+3 design, with 3 cohorts receiving escalating doses of BPX-501 cells—2.5 x 105, 5 x 105, and 1 x 106 cells/kg.
In the phase 2 portion, patients received 1 X 106 BPX-501 cells/kg. Rimiducid was only to be used in the event of uncontrollable GVHD.
Results
The median time to platelet recovery was 10 days (range, 7-16), and the median time to neutrophil recovery was 15 days (range, 10-33).
At a median follow-up of 220 days (range, 61-486), there were no reports of transplant-related mortality.
All 24 patients were still alive and disease-free. And none of the patients developed post-transplant lymphoproliferative disorder.
The cumulative incidence of skin-only acute GVHD was 16.6% (n=4), and the cumulative incidence of mild chronic GVHD was 5% (n=1).
This trial also included 17 patients with acute leukemias. Results in these patients were presented at the EBMT meeting as abstract WP16. ![]()
*Information in the abstract differs from that presented at the meeting.
Image courtesy of NIAID
VALENCIA, SPAIN—Interim results of a phase 1/2 trial suggest the adjunct T-cell therapy BPX-501 can safely accelerate immune recovery after haploidentical hematopoietic stem cell transplant (haplo-HSCT) in pediatric patients with nonmalignant disorders.
Twenty-four such patients received BPX-501 after haplo-HSCT on this trial.
At a median follow-up of 7 months, all 24 were still alive and disease-free.
In addition, the incidence of graft-versus-host disease (GVHD) was considered “very low.”
Pietro Merli, MD, of Bambino Gesù Children’s Hospital in Rome, Italy, presented these results during the Presidential Symposium of the 42nd Annual Meeting of the European Society for Blood and Marrow Transplantation (EBMT) as abstract O007.*
The trial, known as BP-004, was sponsored by Bellicum Pharmaceuticals, the company developing BPX-501.
About BPX-501
BPX-501 consists of genetically modified donor T cells incorporating the CaspaCIDe safety switch, which is designed to eliminate cells in the event of toxicity.
The goal is to allow physicians to more safely perform haplo-HSCTs by giving patients BPX-501 to speed immune reconstitution and provide control over viral infections. But the technology is designed to provide a safety net to eliminate BPX-501 alloreactive T cells if severe GVHD occurs.
The CaspaCIDe switch consists of the CID-binding domain coupled to the signaling domain of caspase-9, an enzyme that is part of the apoptotic pathway. The idea is that, if a patient develops severe GVHD, he can receive an infusion with the small molecule rimiducid. And this will trigger activation of the domain of caspase-9, which leads to selective apoptosis of the CaspaCIDe-containing cells.
About BP-004
In late 2014, Bellicum initiated BP-004, a phase 1/2 trial in children with leukemias, lymphomas, or orphan inherited blood disorders. The trial is being conducted in European and US pediatric transplant centers and is set to enroll up to 90 patients.
At the EBMT meeting, investigators reported results in 41 patients treated on this trial.
Dr Merli presented data on the 24 patients with nonmalignant disorders, including Fanconi anemia (n=5), beta-thalassemia major (n=5), severe combined immunodeficiency (n=5), Wiskott-Aldrich syndrome (n=4), Diamond-Blackfan anemia (n=1), hemophagocytic lymphohistiocytosis (n=1), immune deficiency due to mutation of XIAP gene (n=1), osteopetrosis (n=1), and sickle cell disease (n=1).
All of these patients received a T-cell-depleted haplo-HSCT without post-transplant GVHD prophylaxis.
The patients received BPX-501 within 14 ± 4 days after haplo-HSCT. The phase 1 portion of the trial consisted of a classical 3+3 design, with 3 cohorts receiving escalating doses of BPX-501 cells—2.5 x 105, 5 x 105, and 1 x 106 cells/kg.
In the phase 2 portion, patients received 1 X 106 BPX-501 cells/kg. Rimiducid was only to be used in the event of uncontrollable GVHD.
Results
The median time to platelet recovery was 10 days (range, 7-16), and the median time to neutrophil recovery was 15 days (range, 10-33).
At a median follow-up of 220 days (range, 61-486), there were no reports of transplant-related mortality.
All 24 patients were still alive and disease-free. And none of the patients developed post-transplant lymphoproliferative disorder.
The cumulative incidence of skin-only acute GVHD was 16.6% (n=4), and the cumulative incidence of mild chronic GVHD was 5% (n=1).
This trial also included 17 patients with acute leukemias. Results in these patients were presented at the EBMT meeting as abstract WP16. ![]()
*Information in the abstract differs from that presented at the meeting.