User login
ACIP votes to scrap LAIV vaccine for 2016-2017 influenza season
The Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices has voted to scrap the use of the live attenuated influenza vaccine for the 2016-2017 flu season.
ACIP’s interim recommendation guidance to the CDC is that “no live attenuated influenza vaccines (LAIV) should be used in any setting,” after reviewing data showing that for three consecutive influenza seasons, LAIV’s vaccine effectiveness (VE) against any flu virus was 3% (95% confidence interval, -49%-37%) in children aged 2-17 years. Meanwhile, injectable inactivated influenza vaccine (IIV) had a VE estimate of 63% (95% CI, 52%-72%) against any flu virus in that age group. Findings were similar across age groups.

CDC epidemiologist Brendan Flannery, Ph.D., painted a damning picture of the intranasal LAIV, presenting preliminary data from the U.S. Flu Vaccine Effectiveness Network for 2015-2016 that showed quadrivalent LAIV offered children “no significant protection against influenza A(H1N1)pdm09.” He also presented 2015-2016 national cohort data from Finland showing that unadjusted vaccine effectiveness (VE) against the H1N1 strain for LAIV in 2-year-olds was 47%, compared with 78% for IIV. Dr. Flannery also cited a series of other U.S. and international studies that did not support the use of LAIV, including unpublished Department of Defense 2015-2016 influenza season data for military families indicating that VE for LAIV against the strain last season was “insignificant” in children aged 2-17 years.
Data from an industry study of the quadrivalent LAIV FluMist (MedImmune) also indicated that in this cohort, for the 2015-2016 influenza season, LAIV underperformed compared with IIV, 46% vs. 65%.
Still more bad news for LAIV came from an English study published online just as the ACIP meeting was getting underway. Those data showed that from October 2015 through May 2016, LAIV in children aged 2-17 years had a VE of 57.6% against influenza A and B.
Debate over whether to pull support for LAIV entirely or to allow the use of it in certain circumstances – such as when a person declined a flu shot – hinged on the projected upheaval pulling LAIV is likely to cause.
Concerns were raised around what would happen in the case of LAIV vaccine orders already placed, over whether pulling LAIV would mean a shortage of other vaccine alternatives, and how communicating contingencies might only confuse the public, but several committee members spoke forcefully in favor of what they said the data compelled them to do.
“The science simply shows that LAIV has not worked for the past 3 years, whereas IIV has,” American Academy of Pediatrics Infectious Disease Committee’s Red Book editor, and AAP liaison to ACIP, Dr. David Kimberlin said before the vote.
Restricting but not prohibiting LAIV also would have allowed for an easier transition back to LAIV if the vaccine were successfully reformulated, ACIP Influenza Work Group Chair Dr. Ruth Karron said while presenting potential policy recommendations.
During the debate over whether to pull or limit support for the inhaled vaccine, Dr. Karron reminded the committee that at the time the Food and Drug Administration approved LAIV, serum antibody responses to both the tri- and quadrivalent vaccine were modest, prompting the FDA to call for effectiveness studies. “So, my question to the FDA now is, ‘What are their plans?’ ”
“We’ve seen the studies, but we’ve not really reviewed all the data,” Dr. Wellington Sun, the FDA’s ACIP liaison responded. “I think we have to acknowledge that LAIV has offered advantages over IIV in the past. At this point, we’re not ready to undertake a program for changing the prescriber’s information. We want to continue to work with MedImmune to find out the root cause of this phenomenon.”
“We’ve increased our research into understanding the biology of the H1N1pdm09 LAIV strains so we can improve their effectiveness in future seasons,” Dr. Chris Ambrose, vice president of U.S. medical affairs for infectious disease at MedImmune’s parent company AstraZeneca, told the committee.
“I think this is a very sad day for the influenza vaccination program,” ACIP chair Dr. Nancy Bennett said before adjourning the meeting. “We all had great hopes. It’s not over. If you’ve seen 1 influenza year, you’ve seen 1 influenza year. We may be back here next year having a very different discussion.”
The CDC is not obligated to adopt ACIP recommendations, but typically does. The committee also accepted a resolution to update the Vaccines for Children program in accordance with the recommendation to deny support for LAIV this flu season.
Thirteen members of the committee voted in favor of the recommendation. Dr. Edward Belongia abstained citing a conflict of interest, and Ms. Cynthia Pelligrini voted no, citing “insufficient time to consider this information.” The ICICLE trial NCT01997450, was sponsored by MedImmune, a subsidiary of AstraZeneca where Dr. Ambrose is vice president of U.S. medical affairs for infectious disease.
On Twitter @whitneymcknight
The Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices has voted to scrap the use of the live attenuated influenza vaccine for the 2016-2017 flu season.
ACIP’s interim recommendation guidance to the CDC is that “no live attenuated influenza vaccines (LAIV) should be used in any setting,” after reviewing data showing that for three consecutive influenza seasons, LAIV’s vaccine effectiveness (VE) against any flu virus was 3% (95% confidence interval, -49%-37%) in children aged 2-17 years. Meanwhile, injectable inactivated influenza vaccine (IIV) had a VE estimate of 63% (95% CI, 52%-72%) against any flu virus in that age group. Findings were similar across age groups.
CDC epidemiologist Brendan Flannery, Ph.D., painted a damning picture of the intranasal LAIV, presenting preliminary data from the U.S. Flu Vaccine Effectiveness Network for 2015-2016 that showed quadrivalent LAIV offered children “no significant protection against influenza A(H1N1)pdm09.” He also presented 2015-2016 national cohort data from Finland showing that unadjusted vaccine effectiveness (VE) against the H1N1 strain for LAIV in 2-year-olds was 47%, compared with 78% for IIV. Dr. Flannery also cited a series of other U.S. and international studies that did not support the use of LAIV, including unpublished Department of Defense 2015-2016 influenza season data for military families indicating that VE for LAIV against the strain last season was “insignificant” in children aged 2-17 years.
Data from an industry study of the quadrivalent LAIV FluMist (MedImmune) also indicated that in this cohort, for the 2015-2016 influenza season, LAIV underperformed compared with IIV, 46% vs. 65%.
Still more bad news for LAIV came from an English study published online just as the ACIP meeting was getting underway. Those data showed that from October 2015 through May 2016, LAIV in children aged 2-17 years had a VE of 57.6% against influenza A and B.
Debate over whether to pull support for LAIV entirely or to allow the use of it in certain circumstances – such as when a person declined a flu shot – hinged on the projected upheaval pulling LAIV is likely to cause.
Concerns were raised around what would happen in the case of LAIV vaccine orders already placed, over whether pulling LAIV would mean a shortage of other vaccine alternatives, and how communicating contingencies might only confuse the public, but several committee members spoke forcefully in favor of what they said the data compelled them to do.
“The science simply shows that LAIV has not worked for the past 3 years, whereas IIV has,” American Academy of Pediatrics Infectious Disease Committee’s Red Book editor, and AAP liaison to ACIP, Dr. David Kimberlin said before the vote.
Restricting but not prohibiting LAIV also would have allowed for an easier transition back to LAIV if the vaccine were successfully reformulated, ACIP Influenza Work Group Chair Dr. Ruth Karron said while presenting potential policy recommendations.
During the debate over whether to pull or limit support for the inhaled vaccine, Dr. Karron reminded the committee that at the time the Food and Drug Administration approved LAIV, serum antibody responses to both the tri- and quadrivalent vaccine were modest, prompting the FDA to call for effectiveness studies. “So, my question to the FDA now is, ‘What are their plans?’ ”
“We’ve seen the studies, but we’ve not really reviewed all the data,” Dr. Wellington Sun, the FDA’s ACIP liaison responded. “I think we have to acknowledge that LAIV has offered advantages over IIV in the past. At this point, we’re not ready to undertake a program for changing the prescriber’s information. We want to continue to work with MedImmune to find out the root cause of this phenomenon.”
“We’ve increased our research into understanding the biology of the H1N1pdm09 LAIV strains so we can improve their effectiveness in future seasons,” Dr. Chris Ambrose, vice president of U.S. medical affairs for infectious disease at MedImmune’s parent company AstraZeneca, told the committee.
“I think this is a very sad day for the influenza vaccination program,” ACIP chair Dr. Nancy Bennett said before adjourning the meeting. “We all had great hopes. It’s not over. If you’ve seen 1 influenza year, you’ve seen 1 influenza year. We may be back here next year having a very different discussion.”
The CDC is not obligated to adopt ACIP recommendations, but typically does. The committee also accepted a resolution to update the Vaccines for Children program in accordance with the recommendation to deny support for LAIV this flu season.
Thirteen members of the committee voted in favor of the recommendation. Dr. Edward Belongia abstained citing a conflict of interest, and Ms. Cynthia Pelligrini voted no, citing “insufficient time to consider this information.” The ICICLE trial NCT01997450, was sponsored by MedImmune, a subsidiary of AstraZeneca where Dr. Ambrose is vice president of U.S. medical affairs for infectious disease.
On Twitter @whitneymcknight
The Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices has voted to scrap the use of the live attenuated influenza vaccine for the 2016-2017 flu season.
ACIP’s interim recommendation guidance to the CDC is that “no live attenuated influenza vaccines (LAIV) should be used in any setting,” after reviewing data showing that for three consecutive influenza seasons, LAIV’s vaccine effectiveness (VE) against any flu virus was 3% (95% confidence interval, -49%-37%) in children aged 2-17 years. Meanwhile, injectable inactivated influenza vaccine (IIV) had a VE estimate of 63% (95% CI, 52%-72%) against any flu virus in that age group. Findings were similar across age groups.
CDC epidemiologist Brendan Flannery, Ph.D., painted a damning picture of the intranasal LAIV, presenting preliminary data from the U.S. Flu Vaccine Effectiveness Network for 2015-2016 that showed quadrivalent LAIV offered children “no significant protection against influenza A(H1N1)pdm09.” He also presented 2015-2016 national cohort data from Finland showing that unadjusted vaccine effectiveness (VE) against the H1N1 strain for LAIV in 2-year-olds was 47%, compared with 78% for IIV. Dr. Flannery also cited a series of other U.S. and international studies that did not support the use of LAIV, including unpublished Department of Defense 2015-2016 influenza season data for military families indicating that VE for LAIV against the strain last season was “insignificant” in children aged 2-17 years.
Data from an industry study of the quadrivalent LAIV FluMist (MedImmune) also indicated that in this cohort, for the 2015-2016 influenza season, LAIV underperformed compared with IIV, 46% vs. 65%.
Still more bad news for LAIV came from an English study published online just as the ACIP meeting was getting underway. Those data showed that from October 2015 through May 2016, LAIV in children aged 2-17 years had a VE of 57.6% against influenza A and B.
Debate over whether to pull support for LAIV entirely or to allow the use of it in certain circumstances – such as when a person declined a flu shot – hinged on the projected upheaval pulling LAIV is likely to cause.
Concerns were raised around what would happen in the case of LAIV vaccine orders already placed, over whether pulling LAIV would mean a shortage of other vaccine alternatives, and how communicating contingencies might only confuse the public, but several committee members spoke forcefully in favor of what they said the data compelled them to do.
“The science simply shows that LAIV has not worked for the past 3 years, whereas IIV has,” American Academy of Pediatrics Infectious Disease Committee’s Red Book editor, and AAP liaison to ACIP, Dr. David Kimberlin said before the vote.
Restricting but not prohibiting LAIV also would have allowed for an easier transition back to LAIV if the vaccine were successfully reformulated, ACIP Influenza Work Group Chair Dr. Ruth Karron said while presenting potential policy recommendations.
During the debate over whether to pull or limit support for the inhaled vaccine, Dr. Karron reminded the committee that at the time the Food and Drug Administration approved LAIV, serum antibody responses to both the tri- and quadrivalent vaccine were modest, prompting the FDA to call for effectiveness studies. “So, my question to the FDA now is, ‘What are their plans?’ ”
“We’ve seen the studies, but we’ve not really reviewed all the data,” Dr. Wellington Sun, the FDA’s ACIP liaison responded. “I think we have to acknowledge that LAIV has offered advantages over IIV in the past. At this point, we’re not ready to undertake a program for changing the prescriber’s information. We want to continue to work with MedImmune to find out the root cause of this phenomenon.”
“We’ve increased our research into understanding the biology of the H1N1pdm09 LAIV strains so we can improve their effectiveness in future seasons,” Dr. Chris Ambrose, vice president of U.S. medical affairs for infectious disease at MedImmune’s parent company AstraZeneca, told the committee.
“I think this is a very sad day for the influenza vaccination program,” ACIP chair Dr. Nancy Bennett said before adjourning the meeting. “We all had great hopes. It’s not over. If you’ve seen 1 influenza year, you’ve seen 1 influenza year. We may be back here next year having a very different discussion.”
The CDC is not obligated to adopt ACIP recommendations, but typically does. The committee also accepted a resolution to update the Vaccines for Children program in accordance with the recommendation to deny support for LAIV this flu season.
Thirteen members of the committee voted in favor of the recommendation. Dr. Edward Belongia abstained citing a conflict of interest, and Ms. Cynthia Pelligrini voted no, citing “insufficient time to consider this information.” The ICICLE trial NCT01997450, was sponsored by MedImmune, a subsidiary of AstraZeneca where Dr. Ambrose is vice president of U.S. medical affairs for infectious disease.
On Twitter @whitneymcknight
FROM AN ACIP MEETING

The Promise of Peanut Allergy Prevention Lies in Draft Guidelines
Updated guidelines from the National Institute of Allergy and Infectious Diseases for the early introduction of peanut-containing foods to children at increased risk for peanut allergies are on the horizon, pending final approval.
“Two studies recently showed that infants at high risk of developing peanut allergy [infants with egg allergy and or severe eczema] were much less likely to have peanut allergy at age 5 years if they were able to incorporate peanut regularly into the diet between 4 and 11 months of age,” said Dr. Scott H. Sicherer, the Elliot and Roslyn Jaffe Professor of Pediatrics, Allergy and Immunology, and chief of the division of allergy and immunology in the department of pediatrics at the Icahn School of Medicine at Mount Sinai, New York.

“However, adding peanut to the diet at this age requires caution because these infants may already be allergic to peanut, and so allergy testing and care in adding peanut to the diet with medical supervision is needed in this high-risk group,” noted Dr. Sicherer, a member of the expert panel that worked on the guidelines.
The draft guidelines include 43 clinical recommendations for the diagnosis and management of food allergies in children, according to the NIAID website. In particular, the draft guidelines recommend introducing peanut-containing foods to infants aged 4-6 months who are at increased risk for peanut allergy because of severe eczema and/or egg allergies, after an evaluation with skin prick testing or peanut-specific IgE testing.
“Peanut allergy is relatively common and often persistent, and so a strategy that could prevent the allergy is very important,” Dr. Sicherer said in an interview. “However, peanut can be a choking hazard as peanuts or peanut butter, and so families should talk to their pediatrician about how and when to incorporate peanut into the diet, and whether allergy testing and referral to an allergist is needed.”
Support for the guidelines comes from several large studies with promising results, notably the LEAP (Learning Early about Peanut Allergy) trial. A recent extension of that study, known as LEAP-On (Persistence of Oral Tolerance to Peanut), showed that regular consumption of peanut-containing foods from infancy to 5 years provided ongoing protection against allergies, even 6 years after peanut consumption was discontinued for a 1-year period in 550 children (N Eng J Med. 2016 Apr 14;374:1435-43).
In the original LEAP study, 640 infants aged 4-11 months with severe eczema, egg allergy, or both were randomized to dietary peanut consumption or avoidance (N Engl J Med. 2015 Feb 26;372[9]:803-13). The prevalence of peanut allergy at 5 years of age was approximately 2% in the peanut-consumption group, compared with 14% in the peanut-avoidance group.
Another significant randomized trial, the EAT study (Enquiring About Tolerance) tested not only peanut, but also the early introduction of cooked egg, cow’s milk, sesame, wheat, and fish to 1,303 infants aged 3 months and older in the general population. The study’s strict protocol made adherence difficult, but researchers found a significant 67% reduction in the prevalence of food allergies at age 3 years among the children who followed the protocol, compared with controls, with relative risk reductions of 100% and 75%, respectively, for peanut and egg allergies (N Engl J Med. 2016 May 5;374:1733-43).
The next steps for research should make early introduction of peanut-containing foods even more effective at allergy prevention, Dr. Sicherer noted.
“We need to learn more about how much peanut should be incorporated into the diet, how long the protein has to be kept in the diet to have the best preventative effect, and whether this strategy applies to other foods,” he said.
Updated guidelines from the National Institute of Allergy and Infectious Diseases for the early introduction of peanut-containing foods to children at increased risk for peanut allergies are on the horizon, pending final approval.
“Two studies recently showed that infants at high risk of developing peanut allergy [infants with egg allergy and or severe eczema] were much less likely to have peanut allergy at age 5 years if they were able to incorporate peanut regularly into the diet between 4 and 11 months of age,” said Dr. Scott H. Sicherer, the Elliot and Roslyn Jaffe Professor of Pediatrics, Allergy and Immunology, and chief of the division of allergy and immunology in the department of pediatrics at the Icahn School of Medicine at Mount Sinai, New York.
“However, adding peanut to the diet at this age requires caution because these infants may already be allergic to peanut, and so allergy testing and care in adding peanut to the diet with medical supervision is needed in this high-risk group,” noted Dr. Sicherer, a member of the expert panel that worked on the guidelines.
The draft guidelines include 43 clinical recommendations for the diagnosis and management of food allergies in children, according to the NIAID website. In particular, the draft guidelines recommend introducing peanut-containing foods to infants aged 4-6 months who are at increased risk for peanut allergy because of severe eczema and/or egg allergies, after an evaluation with skin prick testing or peanut-specific IgE testing.
“Peanut allergy is relatively common and often persistent, and so a strategy that could prevent the allergy is very important,” Dr. Sicherer said in an interview. “However, peanut can be a choking hazard as peanuts or peanut butter, and so families should talk to their pediatrician about how and when to incorporate peanut into the diet, and whether allergy testing and referral to an allergist is needed.”
Support for the guidelines comes from several large studies with promising results, notably the LEAP (Learning Early about Peanut Allergy) trial. A recent extension of that study, known as LEAP-On (Persistence of Oral Tolerance to Peanut), showed that regular consumption of peanut-containing foods from infancy to 5 years provided ongoing protection against allergies, even 6 years after peanut consumption was discontinued for a 1-year period in 550 children (N Eng J Med. 2016 Apr 14;374:1435-43).
In the original LEAP study, 640 infants aged 4-11 months with severe eczema, egg allergy, or both were randomized to dietary peanut consumption or avoidance (N Engl J Med. 2015 Feb 26;372[9]:803-13). The prevalence of peanut allergy at 5 years of age was approximately 2% in the peanut-consumption group, compared with 14% in the peanut-avoidance group.
Another significant randomized trial, the EAT study (Enquiring About Tolerance) tested not only peanut, but also the early introduction of cooked egg, cow’s milk, sesame, wheat, and fish to 1,303 infants aged 3 months and older in the general population. The study’s strict protocol made adherence difficult, but researchers found a significant 67% reduction in the prevalence of food allergies at age 3 years among the children who followed the protocol, compared with controls, with relative risk reductions of 100% and 75%, respectively, for peanut and egg allergies (N Engl J Med. 2016 May 5;374:1733-43).
The next steps for research should make early introduction of peanut-containing foods even more effective at allergy prevention, Dr. Sicherer noted.
“We need to learn more about how much peanut should be incorporated into the diet, how long the protein has to be kept in the diet to have the best preventative effect, and whether this strategy applies to other foods,” he said.
Updated guidelines from the National Institute of Allergy and Infectious Diseases for the early introduction of peanut-containing foods to children at increased risk for peanut allergies are on the horizon, pending final approval.
“Two studies recently showed that infants at high risk of developing peanut allergy [infants with egg allergy and or severe eczema] were much less likely to have peanut allergy at age 5 years if they were able to incorporate peanut regularly into the diet between 4 and 11 months of age,” said Dr. Scott H. Sicherer, the Elliot and Roslyn Jaffe Professor of Pediatrics, Allergy and Immunology, and chief of the division of allergy and immunology in the department of pediatrics at the Icahn School of Medicine at Mount Sinai, New York.
“However, adding peanut to the diet at this age requires caution because these infants may already be allergic to peanut, and so allergy testing and care in adding peanut to the diet with medical supervision is needed in this high-risk group,” noted Dr. Sicherer, a member of the expert panel that worked on the guidelines.
The draft guidelines include 43 clinical recommendations for the diagnosis and management of food allergies in children, according to the NIAID website. In particular, the draft guidelines recommend introducing peanut-containing foods to infants aged 4-6 months who are at increased risk for peanut allergy because of severe eczema and/or egg allergies, after an evaluation with skin prick testing or peanut-specific IgE testing.
“Peanut allergy is relatively common and often persistent, and so a strategy that could prevent the allergy is very important,” Dr. Sicherer said in an interview. “However, peanut can be a choking hazard as peanuts or peanut butter, and so families should talk to their pediatrician about how and when to incorporate peanut into the diet, and whether allergy testing and referral to an allergist is needed.”
Support for the guidelines comes from several large studies with promising results, notably the LEAP (Learning Early about Peanut Allergy) trial. A recent extension of that study, known as LEAP-On (Persistence of Oral Tolerance to Peanut), showed that regular consumption of peanut-containing foods from infancy to 5 years provided ongoing protection against allergies, even 6 years after peanut consumption was discontinued for a 1-year period in 550 children (N Eng J Med. 2016 Apr 14;374:1435-43).
In the original LEAP study, 640 infants aged 4-11 months with severe eczema, egg allergy, or both were randomized to dietary peanut consumption or avoidance (N Engl J Med. 2015 Feb 26;372[9]:803-13). The prevalence of peanut allergy at 5 years of age was approximately 2% in the peanut-consumption group, compared with 14% in the peanut-avoidance group.
Another significant randomized trial, the EAT study (Enquiring About Tolerance) tested not only peanut, but also the early introduction of cooked egg, cow’s milk, sesame, wheat, and fish to 1,303 infants aged 3 months and older in the general population. The study’s strict protocol made adherence difficult, but researchers found a significant 67% reduction in the prevalence of food allergies at age 3 years among the children who followed the protocol, compared with controls, with relative risk reductions of 100% and 75%, respectively, for peanut and egg allergies (N Engl J Med. 2016 May 5;374:1733-43).
The next steps for research should make early introduction of peanut-containing foods even more effective at allergy prevention, Dr. Sicherer noted.
“We need to learn more about how much peanut should be incorporated into the diet, how long the protein has to be kept in the diet to have the best preventative effect, and whether this strategy applies to other foods,” he said.

The promise of peanut allergy prevention lies in draft guidelines
Updated guidelines from the National Institute of Allergy and Infectious Diseases for the early introduction of peanut-containing foods to children at increased risk for peanut allergies are on the horizon, pending final approval.
“Two studies recently showed that infants at high risk of developing peanut allergy [infants with egg allergy and or severe eczema] were much less likely to have peanut allergy at age 5 years if they were able to incorporate peanut regularly into the diet between 4 and 11 months of age,” said Dr. Scott H. Sicherer, the Elliot and Roslyn Jaffe Professor of Pediatrics, Allergy and Immunology, and chief of the division of allergy and immunology in the department of pediatrics at the Icahn School of Medicine at Mount Sinai, New York.

“However, adding peanut to the diet at this age requires caution because these infants may already be allergic to peanut, and so allergy testing and care in adding peanut to the diet with medical supervision is needed in this high-risk group,” noted Dr. Sicherer, a member of the expert panel that worked on the guidelines.
The draft guidelines include 43 clinical recommendations for the diagnosis and management of food allergies in children, according to the NIAID website. In particular, the draft guidelines recommend introducing peanut-containing foods to infants aged 4-6 months who are at increased risk for peanut allergy because of severe eczema and/or egg allergies, after an evaluation with skin prick testing or peanut-specific IgE testing.
“Peanut allergy is relatively common and often persistent, and so a strategy that could prevent the allergy is very important,” Dr. Sicherer said in an interview. “However, peanut can be a choking hazard as peanuts or peanut butter, and so families should talk to their pediatrician about how and when to incorporate peanut into the diet, and whether allergy testing and referral to an allergist is needed.”
Support for the guidelines comes from several large studies with promising results, notably the LEAP (Learning Early about Peanut Allergy) trial. A recent extension of that study, known as LEAP-On (Persistence of Oral Tolerance to Peanut), showed that regular consumption of peanut-containing foods from infancy to 5 years provided ongoing protection against allergies, even 6 years after peanut consumption was discontinued for a 1-year period in 550 children (N Eng J Med. 2016 Apr 14;374:1435-43).
In the original LEAP study, 640 infants aged 4-11 months with severe eczema, egg allergy, or both were randomized to dietary peanut consumption or avoidance (N Engl J Med. 2015 Feb 26;372[9]:803-13). The prevalence of peanut allergy at 5 years of age was approximately 2% in the peanut-consumption group, compared with 14% in the peanut-avoidance group.
Another significant randomized trial, the EAT study (Enquiring About Tolerance) tested not only peanut, but also the early introduction of cooked egg, cow’s milk, sesame, wheat, and fish to 1,303 infants aged 3 months and older in the general population. The study’s strict protocol made adherence difficult, but researchers found a significant 67% reduction in the prevalence of food allergies at age 3 years among the children who followed the protocol, compared with controls, with relative risk reductions of 100% and 75%, respectively, for peanut and egg allergies (N Engl J Med. 2016 May 5;374:1733-43).
The next steps for research should make early introduction of peanut-containing foods even more effective at allergy prevention, Dr. Sicherer noted.
“We need to learn more about how much peanut should be incorporated into the diet, how long the protein has to be kept in the diet to have the best preventative effect, and whether this strategy applies to other foods,” he said.
Updated guidelines from the National Institute of Allergy and Infectious Diseases for the early introduction of peanut-containing foods to children at increased risk for peanut allergies are on the horizon, pending final approval.
“Two studies recently showed that infants at high risk of developing peanut allergy [infants with egg allergy and or severe eczema] were much less likely to have peanut allergy at age 5 years if they were able to incorporate peanut regularly into the diet between 4 and 11 months of age,” said Dr. Scott H. Sicherer, the Elliot and Roslyn Jaffe Professor of Pediatrics, Allergy and Immunology, and chief of the division of allergy and immunology in the department of pediatrics at the Icahn School of Medicine at Mount Sinai, New York.
“However, adding peanut to the diet at this age requires caution because these infants may already be allergic to peanut, and so allergy testing and care in adding peanut to the diet with medical supervision is needed in this high-risk group,” noted Dr. Sicherer, a member of the expert panel that worked on the guidelines.
The draft guidelines include 43 clinical recommendations for the diagnosis and management of food allergies in children, according to the NIAID website. In particular, the draft guidelines recommend introducing peanut-containing foods to infants aged 4-6 months who are at increased risk for peanut allergy because of severe eczema and/or egg allergies, after an evaluation with skin prick testing or peanut-specific IgE testing.
“Peanut allergy is relatively common and often persistent, and so a strategy that could prevent the allergy is very important,” Dr. Sicherer said in an interview. “However, peanut can be a choking hazard as peanuts or peanut butter, and so families should talk to their pediatrician about how and when to incorporate peanut into the diet, and whether allergy testing and referral to an allergist is needed.”
Support for the guidelines comes from several large studies with promising results, notably the LEAP (Learning Early about Peanut Allergy) trial. A recent extension of that study, known as LEAP-On (Persistence of Oral Tolerance to Peanut), showed that regular consumption of peanut-containing foods from infancy to 5 years provided ongoing protection against allergies, even 6 years after peanut consumption was discontinued for a 1-year period in 550 children (N Eng J Med. 2016 Apr 14;374:1435-43).
In the original LEAP study, 640 infants aged 4-11 months with severe eczema, egg allergy, or both were randomized to dietary peanut consumption or avoidance (N Engl J Med. 2015 Feb 26;372[9]:803-13). The prevalence of peanut allergy at 5 years of age was approximately 2% in the peanut-consumption group, compared with 14% in the peanut-avoidance group.
Another significant randomized trial, the EAT study (Enquiring About Tolerance) tested not only peanut, but also the early introduction of cooked egg, cow’s milk, sesame, wheat, and fish to 1,303 infants aged 3 months and older in the general population. The study’s strict protocol made adherence difficult, but researchers found a significant 67% reduction in the prevalence of food allergies at age 3 years among the children who followed the protocol, compared with controls, with relative risk reductions of 100% and 75%, respectively, for peanut and egg allergies (N Engl J Med. 2016 May 5;374:1733-43).
The next steps for research should make early introduction of peanut-containing foods even more effective at allergy prevention, Dr. Sicherer noted.
“We need to learn more about how much peanut should be incorporated into the diet, how long the protein has to be kept in the diet to have the best preventative effect, and whether this strategy applies to other foods,” he said.
Updated guidelines from the National Institute of Allergy and Infectious Diseases for the early introduction of peanut-containing foods to children at increased risk for peanut allergies are on the horizon, pending final approval.
“Two studies recently showed that infants at high risk of developing peanut allergy [infants with egg allergy and or severe eczema] were much less likely to have peanut allergy at age 5 years if they were able to incorporate peanut regularly into the diet between 4 and 11 months of age,” said Dr. Scott H. Sicherer, the Elliot and Roslyn Jaffe Professor of Pediatrics, Allergy and Immunology, and chief of the division of allergy and immunology in the department of pediatrics at the Icahn School of Medicine at Mount Sinai, New York.
“However, adding peanut to the diet at this age requires caution because these infants may already be allergic to peanut, and so allergy testing and care in adding peanut to the diet with medical supervision is needed in this high-risk group,” noted Dr. Sicherer, a member of the expert panel that worked on the guidelines.
The draft guidelines include 43 clinical recommendations for the diagnosis and management of food allergies in children, according to the NIAID website. In particular, the draft guidelines recommend introducing peanut-containing foods to infants aged 4-6 months who are at increased risk for peanut allergy because of severe eczema and/or egg allergies, after an evaluation with skin prick testing or peanut-specific IgE testing.
“Peanut allergy is relatively common and often persistent, and so a strategy that could prevent the allergy is very important,” Dr. Sicherer said in an interview. “However, peanut can be a choking hazard as peanuts or peanut butter, and so families should talk to their pediatrician about how and when to incorporate peanut into the diet, and whether allergy testing and referral to an allergist is needed.”
Support for the guidelines comes from several large studies with promising results, notably the LEAP (Learning Early about Peanut Allergy) trial. A recent extension of that study, known as LEAP-On (Persistence of Oral Tolerance to Peanut), showed that regular consumption of peanut-containing foods from infancy to 5 years provided ongoing protection against allergies, even 6 years after peanut consumption was discontinued for a 1-year period in 550 children (N Eng J Med. 2016 Apr 14;374:1435-43).
In the original LEAP study, 640 infants aged 4-11 months with severe eczema, egg allergy, or both were randomized to dietary peanut consumption or avoidance (N Engl J Med. 2015 Feb 26;372[9]:803-13). The prevalence of peanut allergy at 5 years of age was approximately 2% in the peanut-consumption group, compared with 14% in the peanut-avoidance group.
Another significant randomized trial, the EAT study (Enquiring About Tolerance) tested not only peanut, but also the early introduction of cooked egg, cow’s milk, sesame, wheat, and fish to 1,303 infants aged 3 months and older in the general population. The study’s strict protocol made adherence difficult, but researchers found a significant 67% reduction in the prevalence of food allergies at age 3 years among the children who followed the protocol, compared with controls, with relative risk reductions of 100% and 75%, respectively, for peanut and egg allergies (N Engl J Med. 2016 May 5;374:1733-43).
The next steps for research should make early introduction of peanut-containing foods even more effective at allergy prevention, Dr. Sicherer noted.
“We need to learn more about how much peanut should be incorporated into the diet, how long the protein has to be kept in the diet to have the best preventative effect, and whether this strategy applies to other foods,” he said.

ACIP recommends MenACWY vaccine for HIV-infected persons 2 months and older
The Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices unanimously voted to recommend that all HIV-infected persons aged 2 months and older receive the meningococcal ACWY (MenACWY) vaccine.
Guidance for this recommendation states that persons 2 months and older with HIV who have not been vaccinated previously should receive a two-dose, primary series of MenACWY; and that HIV-infected persons who have been vaccinated previously with one dose of MenACWY should receive a second dose at the earliest opportunity, with an 8-week minimum interval between doses. After that, boosters are to be given at the appropriate intervals.

Committee members voted in favor of immunizing earlier rather than waiting until 11 years of age or older, in part because human complement (hSBA) antibody titers following up to two doses of MenACWY vaccine in HIV-infected children ages 2-10 years is higher than in those ages 11-24 years. Also, the agreed upon recommended policy for earlier immunization is in step with current ACIP recommendations for use of the vaccine in persons with functional/anatomic asplenia or complement component deficiencies.
Despite an overall decline in the risk of meningococcal disease in the United States, there was a 13-fold increased risk in HIV-infected persons aged 25-64 years between 2000 and 2008, according to surveillance data presented to ACIP by Ms. Jessica MacNeil, MPH, an epidemiologist at the National Center for Immunization and Respiratory Diseases at the CDC in Atlanta. A ten-fold increase in risk was recorded in New York City alone in this population between 2000 and 2011.
Although fatality data are mixed, the infections were due primarily to serogroups C, W, and Y, for which the immune response wanes rapidly, according to Ms. MacNeil.
There are no safety or immunogenicity data currently available for the use of serogroup B meningococcal vaccines in HIV-infected persons, she said.
ACIP members also unanimously recommended this vaccine be covered under the Vaccines for Children program.
No information about disclosures was available at press time.
On Twitter @whitneymcknight
The Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices unanimously voted to recommend that all HIV-infected persons aged 2 months and older receive the meningococcal ACWY (MenACWY) vaccine.
Guidance for this recommendation states that persons 2 months and older with HIV who have not been vaccinated previously should receive a two-dose, primary series of MenACWY; and that HIV-infected persons who have been vaccinated previously with one dose of MenACWY should receive a second dose at the earliest opportunity, with an 8-week minimum interval between doses. After that, boosters are to be given at the appropriate intervals.
Committee members voted in favor of immunizing earlier rather than waiting until 11 years of age or older, in part because human complement (hSBA) antibody titers following up to two doses of MenACWY vaccine in HIV-infected children ages 2-10 years is higher than in those ages 11-24 years. Also, the agreed upon recommended policy for earlier immunization is in step with current ACIP recommendations for use of the vaccine in persons with functional/anatomic asplenia or complement component deficiencies.
Despite an overall decline in the risk of meningococcal disease in the United States, there was a 13-fold increased risk in HIV-infected persons aged 25-64 years between 2000 and 2008, according to surveillance data presented to ACIP by Ms. Jessica MacNeil, MPH, an epidemiologist at the National Center for Immunization and Respiratory Diseases at the CDC in Atlanta. A ten-fold increase in risk was recorded in New York City alone in this population between 2000 and 2011.
Although fatality data are mixed, the infections were due primarily to serogroups C, W, and Y, for which the immune response wanes rapidly, according to Ms. MacNeil.
There are no safety or immunogenicity data currently available for the use of serogroup B meningococcal vaccines in HIV-infected persons, she said.
ACIP members also unanimously recommended this vaccine be covered under the Vaccines for Children program.
No information about disclosures was available at press time.
On Twitter @whitneymcknight
The Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices unanimously voted to recommend that all HIV-infected persons aged 2 months and older receive the meningococcal ACWY (MenACWY) vaccine.
Guidance for this recommendation states that persons 2 months and older with HIV who have not been vaccinated previously should receive a two-dose, primary series of MenACWY; and that HIV-infected persons who have been vaccinated previously with one dose of MenACWY should receive a second dose at the earliest opportunity, with an 8-week minimum interval between doses. After that, boosters are to be given at the appropriate intervals.
Committee members voted in favor of immunizing earlier rather than waiting until 11 years of age or older, in part because human complement (hSBA) antibody titers following up to two doses of MenACWY vaccine in HIV-infected children ages 2-10 years is higher than in those ages 11-24 years. Also, the agreed upon recommended policy for earlier immunization is in step with current ACIP recommendations for use of the vaccine in persons with functional/anatomic asplenia or complement component deficiencies.
Despite an overall decline in the risk of meningococcal disease in the United States, there was a 13-fold increased risk in HIV-infected persons aged 25-64 years between 2000 and 2008, according to surveillance data presented to ACIP by Ms. Jessica MacNeil, MPH, an epidemiologist at the National Center for Immunization and Respiratory Diseases at the CDC in Atlanta. A ten-fold increase in risk was recorded in New York City alone in this population between 2000 and 2011.
Although fatality data are mixed, the infections were due primarily to serogroups C, W, and Y, for which the immune response wanes rapidly, according to Ms. MacNeil.
There are no safety or immunogenicity data currently available for the use of serogroup B meningococcal vaccines in HIV-infected persons, she said.
ACIP members also unanimously recommended this vaccine be covered under the Vaccines for Children program.
No information about disclosures was available at press time.
On Twitter @whitneymcknight
FROM AN ACIP MEETING
Autism spectrum disorders in gender-nonconforming youth
Despite the lack of clarity about the exact prevalence in youth, particularly prepubertal youth, it’s clear that an increasing number of children and teenagers are presenting to multidisciplinary clinics for evaluation and management of gender identity issues (Pediatrics. 2012 Mar;129[3]:418-25). Recent literature has indicated that the prevalence of individuals overall identifying as transgender and/or experiencing gender dysphoria is about 0.2%-0.3% of the population (JAMA Pediatr. 2016;170[5]:423-4), while being mindful of the variability in the characteristics of the populations included in certain studies.
Although gender variation, in and of itself, is not a disorder, these youth are a considerably underserved and poorly researched population with specific medical and mental health needs. They are at risk for being victims of abuse and developing a range of mental health struggles, including mood disorders, suicidal thinking, self-harming, and anxiety, possibly because of the stresses they experience socially (family rejection, victimization). In addition to these more discrete psychiatric phenomena, co-occurring autism spectrum disorders (or traits thereof) are increasingly being recognized in transgender youth.
Case summary
Maddie is a 20-year-old college sophomore who presents for an autism diagnostic evaluation after being seen by a mental health colleague for consultation regarding medical treatment associated with female-to-male gender transition. In brief, Maddie reports a longstanding history of feeling “socially overwhelmed.” He is an articulate young adult who shares that he’s frequently uncomfortable in social situations, explaining that he has trouble “reading people,” acknowledging a tendency to become overly focused on the details of others and missing the gestalt of interpersonal interactions. Maddie discloses never having close friendships, and although he identifies as lonely, he doesn’t “understand the appeal of casual social interactions.” Maddie and his mother seek an understanding of such social difficulties, wondering about the possibility of Asperger’s syndrome.

Maddie, whose assigned gender at birth was female, now identifies as male. His mother recalls him to have been a precocious preschooler in terms of language development who had no significant developmental delays and became, per report, increasingly withdrawn in elementary school. Over the years, educators have commented repeatedly on the fact that Maddie has needed to work on his “people skills,” with past providers ascribing such struggles to anxiety and social awkwardness that were thought to inherently accompany gender-variant behaviors and thinking. Maddie socially transitioned from a female to male in grade 11 and began taking prescribed testosterone about 4 years ago.
In the interview, Maddie is a hesitant male-appearing individual whose eye contact and spontaneity are limited. He has a guarded manner, and although he is able to answer questions posed to him, rapport is difficult to establish as he appears interpersonally uncomfortable.
Prior to the visit, Maddie’s mother completed the Social Responsiveness Scales, which revealed elevated scores in the area of Social Communication and Social Motivation. Despite appearing cognitively bright and having an array of academic and creative strengths, Maddie’s troubles forming meaningful relationships are striking. Deficits in social-emotional competence are incommensurate with his suspected cognitive abilities, and although he relates learning social skills from film over the years, he endorses pervasively compromised social-communication aptitudes and enduring functional impairments. “I’m always playing catch-up socially,” he shares, wondering how this will affect him in his nursing career.
Discussion
Maddie and his mother participated in an autism diagnostic evaluation, including the administration of the Autism Diagnostic Interview–Revised (ADI-R) and the Autism Diagnostic Observation Schedule (ADOS). The evaluation revealed a profile of social impairments and inflexible thinking dating back to early childhood that supported a diagnosis of an autism spectrum disorder (ASD). Other diagnoses, including anxiety disorders, a depressive disorder, a social pragmatic communication disorder, and a nonverbal learning disorder, were considered, but ultimately it was concluded that ASD best captured Maddie, who also continued to display features consistent with gender dysphoria.
Over the past 30 years, the relationship between gender-related concerns and ASD has begun to be discussed in the scientific literature, beginning with case reports and more recently with a retrospective chart study that yielded results suggesting that subjects diagnosed with ASD were almost eight times more likely to report gender variance than a nonreferred standardization sample of the Child Behavior Checklist (CBCL) (Transgender Health. 2016 Feb;1[1]:63-8). These results echo those of a prior study showing that 7.8% of individuals presenting for an evaluation in a Dutch gender clinic had an ASD diagnosis (J Autism Dev Disord. 2010 Aug;40[8]:930-6).
With the individual prevalences for ASD and gender dysphoria taken into account, these numbers suggest that the prevalence of ASD in gender-dysphoric youth is about four times higher than that found in the general population (Sex Med Rev. 2016;4:3e14). These data raise questions regarding potential shared etiology and the neurobiology between a disorder of social communication and gender identity–related issues; however, to date, despite several theories attempting to explain the connection (the notion of an “extreme male brain,” role of sex hormones, etc.), the relationship remains puzzling. Some have argued that the rigid thinking that can characterize ASD may lead those individuals who display any gender-variant behaviors to automatically identify as the gender opposite their biologic gender, even though they aren’t necessarily experiencing frank gender dysphoria or a core gender identity that is firmly discordant from their anatomical sex. Thinking about the relationship from another perspective, perhaps those with ASD are less aware of the social constructs of gender and are able to express their gender identity (whether it be crossgender or cisgender) more freely and without the worry of how they may be perceived by others. Undoubtedly, a complex interplay between ASD and gender dysphoria/gender-nonconforming behavior is suspected, and more quality research is needed – research that, at a minimum, is informed by the use of representative sample groups drawn from all developmental periods and well-defined diagnostic constructs.
Clinical pearl
Maddie, a transgender man, received a diagnosis of an autism spectrum disorder as a young adult – a full 16 years after the median age of diagnosis (MMWR Surveill Summ. 2016;65[3]:1-23).
The case illustrates some of the difficulties of attempting to parse out the cause of social impairments in an individual who also may have other phenomena that influence interpersonal functioning (attention-deficit/hyperactivity disorder, anxiety, gender dysphoria, etc.) in a developmental manner. Diagnostic “overshadowing” (mistakenly attributing symptoms to a particular condition and paying little attention to other possibilities) is not uncommon in youth with ASD and co-occurring conditions. Given the overlap between gender-nonconforming youth, individuals with gender dysphoria, and ASD, primary care providers may opt to incorporate mental health professionals familiar with ASD into the assessment and care of these children and adolescents. Getting a complete developmental history and paying attention to the possibility of early red flags for ASD can help to elucidate diagnostic possibilities and inform treatment planning. If a co-occurring diagnosis is confirmed, implementation of evidence-based interventions that are provided through the lens of ASD can help to minimize the risk of developing other co-occurring pathology, build resilience, alleviate social impairment, and foster self-advocacy skills in this very vulnerable population. Regardless of whether gender-variant youth and adolescents have an autistic disorder, mental health providers can have an integral role in assisting these individuals and their families to navigate a complicated system of care, address gender dysphoria, and promote healthy identity development (J Am Acad Child Adolesc Psychiatry. 2016 Jun;55[6]:441-3).
Dr. Dickerson, a child and adolescent psychiatrist, is assistant professor of psychiatry at the University of Vermont, where he is director of the autism diagnostic clinic.
Despite the lack of clarity about the exact prevalence in youth, particularly prepubertal youth, it’s clear that an increasing number of children and teenagers are presenting to multidisciplinary clinics for evaluation and management of gender identity issues (Pediatrics. 2012 Mar;129[3]:418-25). Recent literature has indicated that the prevalence of individuals overall identifying as transgender and/or experiencing gender dysphoria is about 0.2%-0.3% of the population (JAMA Pediatr. 2016;170[5]:423-4), while being mindful of the variability in the characteristics of the populations included in certain studies.
Although gender variation, in and of itself, is not a disorder, these youth are a considerably underserved and poorly researched population with specific medical and mental health needs. They are at risk for being victims of abuse and developing a range of mental health struggles, including mood disorders, suicidal thinking, self-harming, and anxiety, possibly because of the stresses they experience socially (family rejection, victimization). In addition to these more discrete psychiatric phenomena, co-occurring autism spectrum disorders (or traits thereof) are increasingly being recognized in transgender youth.
Case summary
Maddie is a 20-year-old college sophomore who presents for an autism diagnostic evaluation after being seen by a mental health colleague for consultation regarding medical treatment associated with female-to-male gender transition. In brief, Maddie reports a longstanding history of feeling “socially overwhelmed.” He is an articulate young adult who shares that he’s frequently uncomfortable in social situations, explaining that he has trouble “reading people,” acknowledging a tendency to become overly focused on the details of others and missing the gestalt of interpersonal interactions. Maddie discloses never having close friendships, and although he identifies as lonely, he doesn’t “understand the appeal of casual social interactions.” Maddie and his mother seek an understanding of such social difficulties, wondering about the possibility of Asperger’s syndrome.
Maddie, whose assigned gender at birth was female, now identifies as male. His mother recalls him to have been a precocious preschooler in terms of language development who had no significant developmental delays and became, per report, increasingly withdrawn in elementary school. Over the years, educators have commented repeatedly on the fact that Maddie has needed to work on his “people skills,” with past providers ascribing such struggles to anxiety and social awkwardness that were thought to inherently accompany gender-variant behaviors and thinking. Maddie socially transitioned from a female to male in grade 11 and began taking prescribed testosterone about 4 years ago.
In the interview, Maddie is a hesitant male-appearing individual whose eye contact and spontaneity are limited. He has a guarded manner, and although he is able to answer questions posed to him, rapport is difficult to establish as he appears interpersonally uncomfortable.
Prior to the visit, Maddie’s mother completed the Social Responsiveness Scales, which revealed elevated scores in the area of Social Communication and Social Motivation. Despite appearing cognitively bright and having an array of academic and creative strengths, Maddie’s troubles forming meaningful relationships are striking. Deficits in social-emotional competence are incommensurate with his suspected cognitive abilities, and although he relates learning social skills from film over the years, he endorses pervasively compromised social-communication aptitudes and enduring functional impairments. “I’m always playing catch-up socially,” he shares, wondering how this will affect him in his nursing career.
Discussion
Maddie and his mother participated in an autism diagnostic evaluation, including the administration of the Autism Diagnostic Interview–Revised (ADI-R) and the Autism Diagnostic Observation Schedule (ADOS). The evaluation revealed a profile of social impairments and inflexible thinking dating back to early childhood that supported a diagnosis of an autism spectrum disorder (ASD). Other diagnoses, including anxiety disorders, a depressive disorder, a social pragmatic communication disorder, and a nonverbal learning disorder, were considered, but ultimately it was concluded that ASD best captured Maddie, who also continued to display features consistent with gender dysphoria.
Over the past 30 years, the relationship between gender-related concerns and ASD has begun to be discussed in the scientific literature, beginning with case reports and more recently with a retrospective chart study that yielded results suggesting that subjects diagnosed with ASD were almost eight times more likely to report gender variance than a nonreferred standardization sample of the Child Behavior Checklist (CBCL) (Transgender Health. 2016 Feb;1[1]:63-8). These results echo those of a prior study showing that 7.8% of individuals presenting for an evaluation in a Dutch gender clinic had an ASD diagnosis (J Autism Dev Disord. 2010 Aug;40[8]:930-6).
With the individual prevalences for ASD and gender dysphoria taken into account, these numbers suggest that the prevalence of ASD in gender-dysphoric youth is about four times higher than that found in the general population (Sex Med Rev. 2016;4:3e14). These data raise questions regarding potential shared etiology and the neurobiology between a disorder of social communication and gender identity–related issues; however, to date, despite several theories attempting to explain the connection (the notion of an “extreme male brain,” role of sex hormones, etc.), the relationship remains puzzling. Some have argued that the rigid thinking that can characterize ASD may lead those individuals who display any gender-variant behaviors to automatically identify as the gender opposite their biologic gender, even though they aren’t necessarily experiencing frank gender dysphoria or a core gender identity that is firmly discordant from their anatomical sex. Thinking about the relationship from another perspective, perhaps those with ASD are less aware of the social constructs of gender and are able to express their gender identity (whether it be crossgender or cisgender) more freely and without the worry of how they may be perceived by others. Undoubtedly, a complex interplay between ASD and gender dysphoria/gender-nonconforming behavior is suspected, and more quality research is needed – research that, at a minimum, is informed by the use of representative sample groups drawn from all developmental periods and well-defined diagnostic constructs.
Clinical pearl
Maddie, a transgender man, received a diagnosis of an autism spectrum disorder as a young adult – a full 16 years after the median age of diagnosis (MMWR Surveill Summ. 2016;65[3]:1-23).
The case illustrates some of the difficulties of attempting to parse out the cause of social impairments in an individual who also may have other phenomena that influence interpersonal functioning (attention-deficit/hyperactivity disorder, anxiety, gender dysphoria, etc.) in a developmental manner. Diagnostic “overshadowing” (mistakenly attributing symptoms to a particular condition and paying little attention to other possibilities) is not uncommon in youth with ASD and co-occurring conditions. Given the overlap between gender-nonconforming youth, individuals with gender dysphoria, and ASD, primary care providers may opt to incorporate mental health professionals familiar with ASD into the assessment and care of these children and adolescents. Getting a complete developmental history and paying attention to the possibility of early red flags for ASD can help to elucidate diagnostic possibilities and inform treatment planning. If a co-occurring diagnosis is confirmed, implementation of evidence-based interventions that are provided through the lens of ASD can help to minimize the risk of developing other co-occurring pathology, build resilience, alleviate social impairment, and foster self-advocacy skills in this very vulnerable population. Regardless of whether gender-variant youth and adolescents have an autistic disorder, mental health providers can have an integral role in assisting these individuals and their families to navigate a complicated system of care, address gender dysphoria, and promote healthy identity development (J Am Acad Child Adolesc Psychiatry. 2016 Jun;55[6]:441-3).
Dr. Dickerson, a child and adolescent psychiatrist, is assistant professor of psychiatry at the University of Vermont, where he is director of the autism diagnostic clinic.
Despite the lack of clarity about the exact prevalence in youth, particularly prepubertal youth, it’s clear that an increasing number of children and teenagers are presenting to multidisciplinary clinics for evaluation and management of gender identity issues (Pediatrics. 2012 Mar;129[3]:418-25). Recent literature has indicated that the prevalence of individuals overall identifying as transgender and/or experiencing gender dysphoria is about 0.2%-0.3% of the population (JAMA Pediatr. 2016;170[5]:423-4), while being mindful of the variability in the characteristics of the populations included in certain studies.
Although gender variation, in and of itself, is not a disorder, these youth are a considerably underserved and poorly researched population with specific medical and mental health needs. They are at risk for being victims of abuse and developing a range of mental health struggles, including mood disorders, suicidal thinking, self-harming, and anxiety, possibly because of the stresses they experience socially (family rejection, victimization). In addition to these more discrete psychiatric phenomena, co-occurring autism spectrum disorders (or traits thereof) are increasingly being recognized in transgender youth.
Case summary
Maddie is a 20-year-old college sophomore who presents for an autism diagnostic evaluation after being seen by a mental health colleague for consultation regarding medical treatment associated with female-to-male gender transition. In brief, Maddie reports a longstanding history of feeling “socially overwhelmed.” He is an articulate young adult who shares that he’s frequently uncomfortable in social situations, explaining that he has trouble “reading people,” acknowledging a tendency to become overly focused on the details of others and missing the gestalt of interpersonal interactions. Maddie discloses never having close friendships, and although he identifies as lonely, he doesn’t “understand the appeal of casual social interactions.” Maddie and his mother seek an understanding of such social difficulties, wondering about the possibility of Asperger’s syndrome.
Maddie, whose assigned gender at birth was female, now identifies as male. His mother recalls him to have been a precocious preschooler in terms of language development who had no significant developmental delays and became, per report, increasingly withdrawn in elementary school. Over the years, educators have commented repeatedly on the fact that Maddie has needed to work on his “people skills,” with past providers ascribing such struggles to anxiety and social awkwardness that were thought to inherently accompany gender-variant behaviors and thinking. Maddie socially transitioned from a female to male in grade 11 and began taking prescribed testosterone about 4 years ago.
In the interview, Maddie is a hesitant male-appearing individual whose eye contact and spontaneity are limited. He has a guarded manner, and although he is able to answer questions posed to him, rapport is difficult to establish as he appears interpersonally uncomfortable.
Prior to the visit, Maddie’s mother completed the Social Responsiveness Scales, which revealed elevated scores in the area of Social Communication and Social Motivation. Despite appearing cognitively bright and having an array of academic and creative strengths, Maddie’s troubles forming meaningful relationships are striking. Deficits in social-emotional competence are incommensurate with his suspected cognitive abilities, and although he relates learning social skills from film over the years, he endorses pervasively compromised social-communication aptitudes and enduring functional impairments. “I’m always playing catch-up socially,” he shares, wondering how this will affect him in his nursing career.
Discussion
Maddie and his mother participated in an autism diagnostic evaluation, including the administration of the Autism Diagnostic Interview–Revised (ADI-R) and the Autism Diagnostic Observation Schedule (ADOS). The evaluation revealed a profile of social impairments and inflexible thinking dating back to early childhood that supported a diagnosis of an autism spectrum disorder (ASD). Other diagnoses, including anxiety disorders, a depressive disorder, a social pragmatic communication disorder, and a nonverbal learning disorder, were considered, but ultimately it was concluded that ASD best captured Maddie, who also continued to display features consistent with gender dysphoria.
Over the past 30 years, the relationship between gender-related concerns and ASD has begun to be discussed in the scientific literature, beginning with case reports and more recently with a retrospective chart study that yielded results suggesting that subjects diagnosed with ASD were almost eight times more likely to report gender variance than a nonreferred standardization sample of the Child Behavior Checklist (CBCL) (Transgender Health. 2016 Feb;1[1]:63-8). These results echo those of a prior study showing that 7.8% of individuals presenting for an evaluation in a Dutch gender clinic had an ASD diagnosis (J Autism Dev Disord. 2010 Aug;40[8]:930-6).
With the individual prevalences for ASD and gender dysphoria taken into account, these numbers suggest that the prevalence of ASD in gender-dysphoric youth is about four times higher than that found in the general population (Sex Med Rev. 2016;4:3e14). These data raise questions regarding potential shared etiology and the neurobiology between a disorder of social communication and gender identity–related issues; however, to date, despite several theories attempting to explain the connection (the notion of an “extreme male brain,” role of sex hormones, etc.), the relationship remains puzzling. Some have argued that the rigid thinking that can characterize ASD may lead those individuals who display any gender-variant behaviors to automatically identify as the gender opposite their biologic gender, even though they aren’t necessarily experiencing frank gender dysphoria or a core gender identity that is firmly discordant from their anatomical sex. Thinking about the relationship from another perspective, perhaps those with ASD are less aware of the social constructs of gender and are able to express their gender identity (whether it be crossgender or cisgender) more freely and without the worry of how they may be perceived by others. Undoubtedly, a complex interplay between ASD and gender dysphoria/gender-nonconforming behavior is suspected, and more quality research is needed – research that, at a minimum, is informed by the use of representative sample groups drawn from all developmental periods and well-defined diagnostic constructs.
Clinical pearl
Maddie, a transgender man, received a diagnosis of an autism spectrum disorder as a young adult – a full 16 years after the median age of diagnosis (MMWR Surveill Summ. 2016;65[3]:1-23).
The case illustrates some of the difficulties of attempting to parse out the cause of social impairments in an individual who also may have other phenomena that influence interpersonal functioning (attention-deficit/hyperactivity disorder, anxiety, gender dysphoria, etc.) in a developmental manner. Diagnostic “overshadowing” (mistakenly attributing symptoms to a particular condition and paying little attention to other possibilities) is not uncommon in youth with ASD and co-occurring conditions. Given the overlap between gender-nonconforming youth, individuals with gender dysphoria, and ASD, primary care providers may opt to incorporate mental health professionals familiar with ASD into the assessment and care of these children and adolescents. Getting a complete developmental history and paying attention to the possibility of early red flags for ASD can help to elucidate diagnostic possibilities and inform treatment planning. If a co-occurring diagnosis is confirmed, implementation of evidence-based interventions that are provided through the lens of ASD can help to minimize the risk of developing other co-occurring pathology, build resilience, alleviate social impairment, and foster self-advocacy skills in this very vulnerable population. Regardless of whether gender-variant youth and adolescents have an autistic disorder, mental health providers can have an integral role in assisting these individuals and their families to navigate a complicated system of care, address gender dysphoria, and promote healthy identity development (J Am Acad Child Adolesc Psychiatry. 2016 Jun;55[6]:441-3).
Dr. Dickerson, a child and adolescent psychiatrist, is assistant professor of psychiatry at the University of Vermont, where he is director of the autism diagnostic clinic.

Kids and accidents
Summer is upon us, a season of delight for children and teens. School is out, the days are long, warm, and full of activities they get to choose. But we know that summer is also the season of accidents. While adventurous activities can lead to scratches, sprains, and broken bones, many accidents are far more serious. The Centers for Disease Control and Prevention reported that in 2014 (the most recent data available), accidental injuries were the leading cause of death for children from the age of 1 year through young adulthood (age 24 years). Car accidents, drowning, burns, suffocation, poisoning, and being struck while on a bike or other vehicle are the most prominent causes of injury or death in youth.
When something is an “accident,” we understand it to be an unfortunate event that happened by chance, without deliberate cause, and not easily foreseeable or preventable. But many accidents that befall children, while not deliberate, might be more foreseeable and preventable than they first appear. With younger children, parents directly oversee their children, ensuring they wear bike helmets, are placed in appropriate car restraints, cannot play with lighters, are always in sight when learning to swim (with a family pool well fenced and locked), and have no access to guns (and the guns are not loaded and have trigger locks!).

As their children grow older, parents must manage the challenging task of teaching their children to manage risk as they cultivate independence: learning to always put on their bike helmet before riding home from school, avoiding diving into shallow water, and not riding in a car with an impaired driver. Both the direct supervision of younger children and the teaching of older children and teenagers are very demanding of time and energy for parents. Terrible accidents can occur during truly unpredictable moments of distraction, but for too many parents, these moments of distraction are in fact predictable. If parents are strained by financial troubles, a disintegrating marriage, a serious illness in a spouse or elderly parent, or their own mental illness, their ability to be fully present and patient to supervise their children will be predictably impaired. During the summer months, when children may be home all day and looking for adventure, parental stress and distraction result in a high-risk environment that makes serious accidents more likely.
You as a child care provider are wonderful at providing supportive reminders to parents about the basics of child safety and supervision. Every checkup includes questions about whether anyone smokes at home and whether there is a working smoke detector. You ask about bike helmets and booster seats, and whether there are firearms in the home and if so, whether they are properly stored and locked. While there are often no formal questions about the level of family stress at a checkup, it would be simple to add: “Would you say the stress level at home is low, moderate, or high?” Such an open-ended question could lead to discussion of those factors that might be causing stress and give you a quick sense of how equipped the parent (or parents) are to handle it. Without a doubt, physicians’ practices are themselves stressed for time, and asking parents about their own stress may seem like opening Pandora’s box. But by being curious, bringing the important matter of domestic stress into the conversation about a child’s health and well being can by itself be therapeutic. The parents found the time to bring their child to this appointment, despite their stress. By simply bringing their awareness to the impact their stress could have on the safety of their children, you may have made a critical difference.

When parents report a high level of stress, you might follow up with more specific questions about their supports. Who provides them with practical help or a supportive ear? Do they have a strong community of friends, nearby family, or a supportive faith community? Are there practical ways to outsource some of the demands they may be juggling? You should be prepared to offer resources if a parent reports domestic violence. Some pediatric practices will employ social workers who can facilitate connecting stressed families with appropriate resources. But if your practice does not, a little time online can build a database of virtual and community resources that a family can start with.
You are also in a unique position to appreciate that certain children are themselves at higher risk for accidents. Children and adolescents with attention-deficit/hyperactivity disorder may be more distractible and impulsive than their peers. And summer is often a season when families decide to suspend stimulant treatment to promote weight gain or growth. These children and teens are at elevated risk to “leap before they look,” and parents should be reminded of their higher level of risk and need for supervision, at least when having a conversation about whether to suspend stimulant treatment. Children with a history of oppositional behaviors also can prove more challenging to supervise than their peers. Beyond the risk of self-injury or suicide, youth with depressive disorders can have impaired concentration and attention, and may not assess the risk of certain activities very well. These children can be challenging to parent at all times, so their parents likely manage a higher general level of parenting stress, and can benefit from your inquiry and additional resources.
A parent’s task of supervising is different with adolescents than with younger children. It is as much about effective communication and modeling how to assess risk and make judgments as it is about time spent watching the children. But these tasks take time and patience, perhaps even more than the supervision of younger kids. And while a teenager may have good judgment, who her friends are matters as much as her own judgment. Teenagers take more chances when they are with friends, and particularly with thrill-seeking friends. If parents are too distracted or busy to know who their teenager is spending time with, that itself raises the teenager’s chances of risky behaviors and accidental injury.

Of course, when teenagers are experimenting with alcohol or drugs, the risk of serious accidents increases significantly. The Centers for Disease Control and Prevention estimates that approximately half of the nonmedical deaths of 15- to 24-year-olds involve drug or alcohol use. Stressed parents are less likely to be spending time with their teenagers to ask about drugs and alcohol: Who is using them? When and where? What else are they hearing about drugs and alcohol? It also takes time and a calm, clear, and open presence to talk with teenagers about expectations and ground rules around drug or alcohol experimentation (which has been shown to diminish the rate of regular use of drugs or alcohol in teens by as much as half). It takes time for parents to explain to their teenager that they should ALWAYS call home if they are anywhere they do not feel safe, even if it involves drugs or alcohol. It is complex to set rules and expectations while also being clear that their safety always comes first. You can encourage parents to know their teen’s friends, and to have a conversation about the rules around drug and alcohol use and to set a safety plan. Parents who are too stressed to even know where to start will benefit from a longer conversation, and can be referred to some good websites or for a mental health consultation.
Summer should be a time of skill building, adventure, growing independence, and some rest and relaxation. Helping parents to pay attention to their own stress level and access needed supports may be the critical factor in preventing accidents and promoting the health and well being of their children during this wonderful, but risky season.
Dr. Swick is an attending psychiatrist in the division of child psychiatry at Massachusetts General Hospital, Boston, and director of the Parenting at a Challenging Time (PACT) Program at the Vernon Cancer Center at Newton (Mass.) Wellesley Hospital. Dr. Jellinek is professor of psychiatry and of pediatrics at Harvard Medical School, Boston.
Summer is upon us, a season of delight for children and teens. School is out, the days are long, warm, and full of activities they get to choose. But we know that summer is also the season of accidents. While adventurous activities can lead to scratches, sprains, and broken bones, many accidents are far more serious. The Centers for Disease Control and Prevention reported that in 2014 (the most recent data available), accidental injuries were the leading cause of death for children from the age of 1 year through young adulthood (age 24 years). Car accidents, drowning, burns, suffocation, poisoning, and being struck while on a bike or other vehicle are the most prominent causes of injury or death in youth.
When something is an “accident,” we understand it to be an unfortunate event that happened by chance, without deliberate cause, and not easily foreseeable or preventable. But many accidents that befall children, while not deliberate, might be more foreseeable and preventable than they first appear. With younger children, parents directly oversee their children, ensuring they wear bike helmets, are placed in appropriate car restraints, cannot play with lighters, are always in sight when learning to swim (with a family pool well fenced and locked), and have no access to guns (and the guns are not loaded and have trigger locks!).
As their children grow older, parents must manage the challenging task of teaching their children to manage risk as they cultivate independence: learning to always put on their bike helmet before riding home from school, avoiding diving into shallow water, and not riding in a car with an impaired driver. Both the direct supervision of younger children and the teaching of older children and teenagers are very demanding of time and energy for parents. Terrible accidents can occur during truly unpredictable moments of distraction, but for too many parents, these moments of distraction are in fact predictable. If parents are strained by financial troubles, a disintegrating marriage, a serious illness in a spouse or elderly parent, or their own mental illness, their ability to be fully present and patient to supervise their children will be predictably impaired. During the summer months, when children may be home all day and looking for adventure, parental stress and distraction result in a high-risk environment that makes serious accidents more likely.
You as a child care provider are wonderful at providing supportive reminders to parents about the basics of child safety and supervision. Every checkup includes questions about whether anyone smokes at home and whether there is a working smoke detector. You ask about bike helmets and booster seats, and whether there are firearms in the home and if so, whether they are properly stored and locked. While there are often no formal questions about the level of family stress at a checkup, it would be simple to add: “Would you say the stress level at home is low, moderate, or high?” Such an open-ended question could lead to discussion of those factors that might be causing stress and give you a quick sense of how equipped the parent (or parents) are to handle it. Without a doubt, physicians’ practices are themselves stressed for time, and asking parents about their own stress may seem like opening Pandora’s box. But by being curious, bringing the important matter of domestic stress into the conversation about a child’s health and well being can by itself be therapeutic. The parents found the time to bring their child to this appointment, despite their stress. By simply bringing their awareness to the impact their stress could have on the safety of their children, you may have made a critical difference.
When parents report a high level of stress, you might follow up with more specific questions about their supports. Who provides them with practical help or a supportive ear? Do they have a strong community of friends, nearby family, or a supportive faith community? Are there practical ways to outsource some of the demands they may be juggling? You should be prepared to offer resources if a parent reports domestic violence. Some pediatric practices will employ social workers who can facilitate connecting stressed families with appropriate resources. But if your practice does not, a little time online can build a database of virtual and community resources that a family can start with.
You are also in a unique position to appreciate that certain children are themselves at higher risk for accidents. Children and adolescents with attention-deficit/hyperactivity disorder may be more distractible and impulsive than their peers. And summer is often a season when families decide to suspend stimulant treatment to promote weight gain or growth. These children and teens are at elevated risk to “leap before they look,” and parents should be reminded of their higher level of risk and need for supervision, at least when having a conversation about whether to suspend stimulant treatment. Children with a history of oppositional behaviors also can prove more challenging to supervise than their peers. Beyond the risk of self-injury or suicide, youth with depressive disorders can have impaired concentration and attention, and may not assess the risk of certain activities very well. These children can be challenging to parent at all times, so their parents likely manage a higher general level of parenting stress, and can benefit from your inquiry and additional resources.
A parent’s task of supervising is different with adolescents than with younger children. It is as much about effective communication and modeling how to assess risk and make judgments as it is about time spent watching the children. But these tasks take time and patience, perhaps even more than the supervision of younger kids. And while a teenager may have good judgment, who her friends are matters as much as her own judgment. Teenagers take more chances when they are with friends, and particularly with thrill-seeking friends. If parents are too distracted or busy to know who their teenager is spending time with, that itself raises the teenager’s chances of risky behaviors and accidental injury.
Of course, when teenagers are experimenting with alcohol or drugs, the risk of serious accidents increases significantly. The Centers for Disease Control and Prevention estimates that approximately half of the nonmedical deaths of 15- to 24-year-olds involve drug or alcohol use. Stressed parents are less likely to be spending time with their teenagers to ask about drugs and alcohol: Who is using them? When and where? What else are they hearing about drugs and alcohol? It also takes time and a calm, clear, and open presence to talk with teenagers about expectations and ground rules around drug or alcohol experimentation (which has been shown to diminish the rate of regular use of drugs or alcohol in teens by as much as half). It takes time for parents to explain to their teenager that they should ALWAYS call home if they are anywhere they do not feel safe, even if it involves drugs or alcohol. It is complex to set rules and expectations while also being clear that their safety always comes first. You can encourage parents to know their teen’s friends, and to have a conversation about the rules around drug and alcohol use and to set a safety plan. Parents who are too stressed to even know where to start will benefit from a longer conversation, and can be referred to some good websites or for a mental health consultation.
Summer should be a time of skill building, adventure, growing independence, and some rest and relaxation. Helping parents to pay attention to their own stress level and access needed supports may be the critical factor in preventing accidents and promoting the health and well being of their children during this wonderful, but risky season.
Dr. Swick is an attending psychiatrist in the division of child psychiatry at Massachusetts General Hospital, Boston, and director of the Parenting at a Challenging Time (PACT) Program at the Vernon Cancer Center at Newton (Mass.) Wellesley Hospital. Dr. Jellinek is professor of psychiatry and of pediatrics at Harvard Medical School, Boston.
Summer is upon us, a season of delight for children and teens. School is out, the days are long, warm, and full of activities they get to choose. But we know that summer is also the season of accidents. While adventurous activities can lead to scratches, sprains, and broken bones, many accidents are far more serious. The Centers for Disease Control and Prevention reported that in 2014 (the most recent data available), accidental injuries were the leading cause of death for children from the age of 1 year through young adulthood (age 24 years). Car accidents, drowning, burns, suffocation, poisoning, and being struck while on a bike or other vehicle are the most prominent causes of injury or death in youth.
When something is an “accident,” we understand it to be an unfortunate event that happened by chance, without deliberate cause, and not easily foreseeable or preventable. But many accidents that befall children, while not deliberate, might be more foreseeable and preventable than they first appear. With younger children, parents directly oversee their children, ensuring they wear bike helmets, are placed in appropriate car restraints, cannot play with lighters, are always in sight when learning to swim (with a family pool well fenced and locked), and have no access to guns (and the guns are not loaded and have trigger locks!).
As their children grow older, parents must manage the challenging task of teaching their children to manage risk as they cultivate independence: learning to always put on their bike helmet before riding home from school, avoiding diving into shallow water, and not riding in a car with an impaired driver. Both the direct supervision of younger children and the teaching of older children and teenagers are very demanding of time and energy for parents. Terrible accidents can occur during truly unpredictable moments of distraction, but for too many parents, these moments of distraction are in fact predictable. If parents are strained by financial troubles, a disintegrating marriage, a serious illness in a spouse or elderly parent, or their own mental illness, their ability to be fully present and patient to supervise their children will be predictably impaired. During the summer months, when children may be home all day and looking for adventure, parental stress and distraction result in a high-risk environment that makes serious accidents more likely.
You as a child care provider are wonderful at providing supportive reminders to parents about the basics of child safety and supervision. Every checkup includes questions about whether anyone smokes at home and whether there is a working smoke detector. You ask about bike helmets and booster seats, and whether there are firearms in the home and if so, whether they are properly stored and locked. While there are often no formal questions about the level of family stress at a checkup, it would be simple to add: “Would you say the stress level at home is low, moderate, or high?” Such an open-ended question could lead to discussion of those factors that might be causing stress and give you a quick sense of how equipped the parent (or parents) are to handle it. Without a doubt, physicians’ practices are themselves stressed for time, and asking parents about their own stress may seem like opening Pandora’s box. But by being curious, bringing the important matter of domestic stress into the conversation about a child’s health and well being can by itself be therapeutic. The parents found the time to bring their child to this appointment, despite their stress. By simply bringing their awareness to the impact their stress could have on the safety of their children, you may have made a critical difference.
When parents report a high level of stress, you might follow up with more specific questions about their supports. Who provides them with practical help or a supportive ear? Do they have a strong community of friends, nearby family, or a supportive faith community? Are there practical ways to outsource some of the demands they may be juggling? You should be prepared to offer resources if a parent reports domestic violence. Some pediatric practices will employ social workers who can facilitate connecting stressed families with appropriate resources. But if your practice does not, a little time online can build a database of virtual and community resources that a family can start with.
You are also in a unique position to appreciate that certain children are themselves at higher risk for accidents. Children and adolescents with attention-deficit/hyperactivity disorder may be more distractible and impulsive than their peers. And summer is often a season when families decide to suspend stimulant treatment to promote weight gain or growth. These children and teens are at elevated risk to “leap before they look,” and parents should be reminded of their higher level of risk and need for supervision, at least when having a conversation about whether to suspend stimulant treatment. Children with a history of oppositional behaviors also can prove more challenging to supervise than their peers. Beyond the risk of self-injury or suicide, youth with depressive disorders can have impaired concentration and attention, and may not assess the risk of certain activities very well. These children can be challenging to parent at all times, so their parents likely manage a higher general level of parenting stress, and can benefit from your inquiry and additional resources.
A parent’s task of supervising is different with adolescents than with younger children. It is as much about effective communication and modeling how to assess risk and make judgments as it is about time spent watching the children. But these tasks take time and patience, perhaps even more than the supervision of younger kids. And while a teenager may have good judgment, who her friends are matters as much as her own judgment. Teenagers take more chances when they are with friends, and particularly with thrill-seeking friends. If parents are too distracted or busy to know who their teenager is spending time with, that itself raises the teenager’s chances of risky behaviors and accidental injury.
Of course, when teenagers are experimenting with alcohol or drugs, the risk of serious accidents increases significantly. The Centers for Disease Control and Prevention estimates that approximately half of the nonmedical deaths of 15- to 24-year-olds involve drug or alcohol use. Stressed parents are less likely to be spending time with their teenagers to ask about drugs and alcohol: Who is using them? When and where? What else are they hearing about drugs and alcohol? It also takes time and a calm, clear, and open presence to talk with teenagers about expectations and ground rules around drug or alcohol experimentation (which has been shown to diminish the rate of regular use of drugs or alcohol in teens by as much as half). It takes time for parents to explain to their teenager that they should ALWAYS call home if they are anywhere they do not feel safe, even if it involves drugs or alcohol. It is complex to set rules and expectations while also being clear that their safety always comes first. You can encourage parents to know their teen’s friends, and to have a conversation about the rules around drug and alcohol use and to set a safety plan. Parents who are too stressed to even know where to start will benefit from a longer conversation, and can be referred to some good websites or for a mental health consultation.
Summer should be a time of skill building, adventure, growing independence, and some rest and relaxation. Helping parents to pay attention to their own stress level and access needed supports may be the critical factor in preventing accidents and promoting the health and well being of their children during this wonderful, but risky season.
Dr. Swick is an attending psychiatrist in the division of child psychiatry at Massachusetts General Hospital, Boston, and director of the Parenting at a Challenging Time (PACT) Program at the Vernon Cancer Center at Newton (Mass.) Wellesley Hospital. Dr. Jellinek is professor of psychiatry and of pediatrics at Harvard Medical School, Boston.

VIDEO: Depression worsens newly diagnosed juvenile idiopathic arthritis
LONDON – Depression is relatively common among teenagers newly diagnosed with juvenile idiopathic arthritis, and adolescents with both disorders appeared to have a less complete response to their treatment in a study of 102 patients.
Juvenile idiopathic arthritis (JIA) that first manifests when a patient is a teenager comes at a “vulnerable time” that can drive the development and worsening of depression, and depression can potentially exacerbate inflammation and also interfere with treatment compliance, Dr. John Ioannou said at the European Congress of Rheumatology,
Depression and JIA can produce a “vicious cycle in which depression exacerbates the disease and the disease exacerbates depression,” explained Dr. Ioannou, a rheumatologist at University College Hospital in London.
Although no study results have yet identified an effective intervention for depression identified in teenagers with newly diagnosed JIA, the immediate message from these new findings is that clinicians must assess the psychological health of adolescents with JIA both when they are first diagnosed as well as at subsequent visits, and if depression is found it requires some sort of intervention, Dr. Ioannou said in an interview.
He and his associates studied 102 patients from the United Kingdom, who were newly diagnosed with JIA and were 11-16 years old at baseline and enrolled in the Childhood Arthritis Prospective Study (CAPS), a nationwide cohort of patients with childhood-onset arthritis of various types. The average age of the group they studied was just under 13 years old, 57% were girls, 52% had persistent oligoarticular arthritis, 30% had polyarticular arthritis, and 18% had enthesitis-related arthritis. All patients underwent assessment at baseline for depression using the Mood and Feelings Questionnaire and 15 (15%) had a score that flagged them as having “probable” depression.
This depression prevalence is about three- to fourfold higher than for an otherwise healthy group of similarly aged adolescents, Dr. Ioannou said.
At baseline, the subgroup of teens with depression had a significantly higher number of inflamed joints, restricted joints, and also more overall pain and disability as measured on the Childhood Health Assessment Questionnaire.
The 102 teens with JIA underwent follow-up assessment 1-3 years later, after they had received ongoing treatment for their JIA. At follow-up, standard JIA treatment had largely resulted in resolution of joint inflammation and movement restriction among all patients, including those with depression at baseline. However the adolescents who had both JIA and depression at entry continued to have significantly more pain and disability at follow-up than did the nondepressed JIA patients, suggesting a link between depression and refractory pain and disability in JIA patients, the researchers reported.
“We need to ensure that psychological assessments and support are available to all young people diagnosed with JIA, and that this is fully integrated into routine care” for newly diagnosed JIA patients, Dr. Ioannou said. He had no disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @mitchelzoler
Prior study results showed that about a third of adult patients with rheumatoid arthritis are depressed. There seems to be a vulnerability to depression among patients diagnosed with inflammatory arthritis. It makes sense that chronic arthritis can cause depression as it is a painful, debilitating, and long-term disease that is often nonremitting.

|
| Mitchel L. Zoler/Frontline Medical News Susan Barlett, Ph.D. |
Good evidence also suggests that people who are depressed are more vulnerable to develop rheumatoid arthritis or other autoimmune diseases.
The important new findings reported by Dr. Ioannou and his associates underscore the importance of providing psychological support to adolescents newly diagnosed with juvenile idiopathic arthritis. Among its many effects, depression is one of the few robust predictors of nonadherence to medical treatments by patients. Patients who are depressed are less likely to take their medications as prescribed. Depressed patients are also more likely to smoke because tobacco smoking can produce some depression relief. But smoking also contributes to the development and worsening of rheumatoid arthritis and likely other forms of inflammatory arthritis.
Susan Bartlett, Ph.D., is a psychologist and clinical epidemiologist at McGill University, Montreal, who specializes in chronic diseases including arthritis. She had no disclosures. She made these comments during a press conference.
Prior study results showed that about a third of adult patients with rheumatoid arthritis are depressed. There seems to be a vulnerability to depression among patients diagnosed with inflammatory arthritis. It makes sense that chronic arthritis can cause depression as it is a painful, debilitating, and long-term disease that is often nonremitting.
|
|
| Mitchel L. Zoler/Frontline Medical News Susan Barlett, Ph.D. |
Good evidence also suggests that people who are depressed are more vulnerable to develop rheumatoid arthritis or other autoimmune diseases.
The important new findings reported by Dr. Ioannou and his associates underscore the importance of providing psychological support to adolescents newly diagnosed with juvenile idiopathic arthritis. Among its many effects, depression is one of the few robust predictors of nonadherence to medical treatments by patients. Patients who are depressed are less likely to take their medications as prescribed. Depressed patients are also more likely to smoke because tobacco smoking can produce some depression relief. But smoking also contributes to the development and worsening of rheumatoid arthritis and likely other forms of inflammatory arthritis.
Susan Bartlett, Ph.D., is a psychologist and clinical epidemiologist at McGill University, Montreal, who specializes in chronic diseases including arthritis. She had no disclosures. She made these comments during a press conference.
Prior study results showed that about a third of adult patients with rheumatoid arthritis are depressed. There seems to be a vulnerability to depression among patients diagnosed with inflammatory arthritis. It makes sense that chronic arthritis can cause depression as it is a painful, debilitating, and long-term disease that is often nonremitting.
|
|
| Mitchel L. Zoler/Frontline Medical News Susan Barlett, Ph.D. |
Good evidence also suggests that people who are depressed are more vulnerable to develop rheumatoid arthritis or other autoimmune diseases.
The important new findings reported by Dr. Ioannou and his associates underscore the importance of providing psychological support to adolescents newly diagnosed with juvenile idiopathic arthritis. Among its many effects, depression is one of the few robust predictors of nonadherence to medical treatments by patients. Patients who are depressed are less likely to take their medications as prescribed. Depressed patients are also more likely to smoke because tobacco smoking can produce some depression relief. But smoking also contributes to the development and worsening of rheumatoid arthritis and likely other forms of inflammatory arthritis.
Susan Bartlett, Ph.D., is a psychologist and clinical epidemiologist at McGill University, Montreal, who specializes in chronic diseases including arthritis. She had no disclosures. She made these comments during a press conference.
LONDON – Depression is relatively common among teenagers newly diagnosed with juvenile idiopathic arthritis, and adolescents with both disorders appeared to have a less complete response to their treatment in a study of 102 patients.
Juvenile idiopathic arthritis (JIA) that first manifests when a patient is a teenager comes at a “vulnerable time” that can drive the development and worsening of depression, and depression can potentially exacerbate inflammation and also interfere with treatment compliance, Dr. John Ioannou said at the European Congress of Rheumatology,
Depression and JIA can produce a “vicious cycle in which depression exacerbates the disease and the disease exacerbates depression,” explained Dr. Ioannou, a rheumatologist at University College Hospital in London.
Although no study results have yet identified an effective intervention for depression identified in teenagers with newly diagnosed JIA, the immediate message from these new findings is that clinicians must assess the psychological health of adolescents with JIA both when they are first diagnosed as well as at subsequent visits, and if depression is found it requires some sort of intervention, Dr. Ioannou said in an interview.
He and his associates studied 102 patients from the United Kingdom, who were newly diagnosed with JIA and were 11-16 years old at baseline and enrolled in the Childhood Arthritis Prospective Study (CAPS), a nationwide cohort of patients with childhood-onset arthritis of various types. The average age of the group they studied was just under 13 years old, 57% were girls, 52% had persistent oligoarticular arthritis, 30% had polyarticular arthritis, and 18% had enthesitis-related arthritis. All patients underwent assessment at baseline for depression using the Mood and Feelings Questionnaire and 15 (15%) had a score that flagged them as having “probable” depression.
This depression prevalence is about three- to fourfold higher than for an otherwise healthy group of similarly aged adolescents, Dr. Ioannou said.
At baseline, the subgroup of teens with depression had a significantly higher number of inflamed joints, restricted joints, and also more overall pain and disability as measured on the Childhood Health Assessment Questionnaire.
The 102 teens with JIA underwent follow-up assessment 1-3 years later, after they had received ongoing treatment for their JIA. At follow-up, standard JIA treatment had largely resulted in resolution of joint inflammation and movement restriction among all patients, including those with depression at baseline. However the adolescents who had both JIA and depression at entry continued to have significantly more pain and disability at follow-up than did the nondepressed JIA patients, suggesting a link between depression and refractory pain and disability in JIA patients, the researchers reported.
“We need to ensure that psychological assessments and support are available to all young people diagnosed with JIA, and that this is fully integrated into routine care” for newly diagnosed JIA patients, Dr. Ioannou said. He had no disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @mitchelzoler
LONDON – Depression is relatively common among teenagers newly diagnosed with juvenile idiopathic arthritis, and adolescents with both disorders appeared to have a less complete response to their treatment in a study of 102 patients.
Juvenile idiopathic arthritis (JIA) that first manifests when a patient is a teenager comes at a “vulnerable time” that can drive the development and worsening of depression, and depression can potentially exacerbate inflammation and also interfere with treatment compliance, Dr. John Ioannou said at the European Congress of Rheumatology,
Depression and JIA can produce a “vicious cycle in which depression exacerbates the disease and the disease exacerbates depression,” explained Dr. Ioannou, a rheumatologist at University College Hospital in London.
Although no study results have yet identified an effective intervention for depression identified in teenagers with newly diagnosed JIA, the immediate message from these new findings is that clinicians must assess the psychological health of adolescents with JIA both when they are first diagnosed as well as at subsequent visits, and if depression is found it requires some sort of intervention, Dr. Ioannou said in an interview.
He and his associates studied 102 patients from the United Kingdom, who were newly diagnosed with JIA and were 11-16 years old at baseline and enrolled in the Childhood Arthritis Prospective Study (CAPS), a nationwide cohort of patients with childhood-onset arthritis of various types. The average age of the group they studied was just under 13 years old, 57% were girls, 52% had persistent oligoarticular arthritis, 30% had polyarticular arthritis, and 18% had enthesitis-related arthritis. All patients underwent assessment at baseline for depression using the Mood and Feelings Questionnaire and 15 (15%) had a score that flagged them as having “probable” depression.
This depression prevalence is about three- to fourfold higher than for an otherwise healthy group of similarly aged adolescents, Dr. Ioannou said.
At baseline, the subgroup of teens with depression had a significantly higher number of inflamed joints, restricted joints, and also more overall pain and disability as measured on the Childhood Health Assessment Questionnaire.
The 102 teens with JIA underwent follow-up assessment 1-3 years later, after they had received ongoing treatment for their JIA. At follow-up, standard JIA treatment had largely resulted in resolution of joint inflammation and movement restriction among all patients, including those with depression at baseline. However the adolescents who had both JIA and depression at entry continued to have significantly more pain and disability at follow-up than did the nondepressed JIA patients, suggesting a link between depression and refractory pain and disability in JIA patients, the researchers reported.
“We need to ensure that psychological assessments and support are available to all young people diagnosed with JIA, and that this is fully integrated into routine care” for newly diagnosed JIA patients, Dr. Ioannou said. He had no disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @mitchelzoler
AT THE EULAR 2016 CONGRESS
Key clinical point: Pain and disability often persist despite effective antirheumatic treatment in depressed adolescents with juvenile idiopathic arthritis.
Major finding: Disability and pain levels remained significantly elevated among JIA teens with depression, compared with JIA teens without baseline depression.
Data source: The 102 adolescents enrolled in the Childhood Arthritis Prospective Study with juvenile idiopathic arthritis, including 15 patients with depression at baseline.
Disclosures: Dr. Ioannou had no disclosures.

AAP promotes streamlined tools to help screen for pediatric substance use
While the overall American Academy of Pediatrics policy objectives on screening for pediatric substance use have not changed, the academy is highlighting streamlined screening tools in a new clinical report.
The AAP remains focused on pushing for abstinence. That being said, the organization recommends “that pediatricians screen kids for substance use and talk about substance use,” lead author Dr. Sharon Levy said in an interview. “The big picture, bottom line, [is that] nothing has changed. It’s just an opportunity to reemphasize that we think talking about substance use is an important part of pediatric care.”
What has changed are the tools highlighted in the clinical report, published online June 20 (Pediatrics. 2016 Jul. doi: 10.1542/peds.2016-1211).

“We simplified the algorithm quite a bit,” said Dr. Levy, director of the adolescent substance abuse program at Boston Children’s Hospital. “We demonstrated use of more screening tools that are a bit simpler to use, a bit shorter, and lead more directly to intervention. For people who are using the older tools, that’s fine if that’s really been established in their practice and [they] are doing a good job with [those tools].”
However, Dr. Levy noted that many of the established screening tools were not being used, or were being shortened or modified in others ways to render them less effective.
“We recommend … new tools that we call frequency-based screening tools,” she explained. Pediatric patients are given a risk level based on their answer to a question regarding how many times in the past year they’ve used alcohol, marijuana, or tobacco.
Slightly different interventions are recommended based on the child’s risk level, including counseling about substance use and some strategies, especially with kids with heavier use, for conducting the conversation in a way that will make kids more likely to consider behavior change, she sa

The clinical report suggests that when no substance use is disclosed, doctors should offer positive reinforcement about smart decision making. For patients disclosing one or two uses per year with a low likelihood of having a substance use disorder, doctors should be promoting abstaining from use to support a healthy lifestyle, as well as discussions on the negative health effects of substance use. As the response to frequency of use increases and the greater likelihood of substance abuse disorder grows, so does the level of questions, including understanding the types of substances being used, coupled with more counseling on quitting use, and, in severe cases, referring for treatment.
The common theme in all the advice given to patients, though, is the importance of abstinence from substance use.
“The American Academy of Pediatrics recommends abstinence as the best health recommendation for adolescents,” Dr. Levy said. “That sometimes gets lost in the shuffle. That really is something that stands out in the policy, and that substance use is such an important health risk behavior that it should be addressed as part of routine health care for adolescents.”
The authors disclosed no relevant financial conflicts.
While the overall American Academy of Pediatrics policy objectives on screening for pediatric substance use have not changed, the academy is highlighting streamlined screening tools in a new clinical report.
The AAP remains focused on pushing for abstinence. That being said, the organization recommends “that pediatricians screen kids for substance use and talk about substance use,” lead author Dr. Sharon Levy said in an interview. “The big picture, bottom line, [is that] nothing has changed. It’s just an opportunity to reemphasize that we think talking about substance use is an important part of pediatric care.”
What has changed are the tools highlighted in the clinical report, published online June 20 (Pediatrics. 2016 Jul. doi: 10.1542/peds.2016-1211).
“We simplified the algorithm quite a bit,” said Dr. Levy, director of the adolescent substance abuse program at Boston Children’s Hospital. “We demonstrated use of more screening tools that are a bit simpler to use, a bit shorter, and lead more directly to intervention. For people who are using the older tools, that’s fine if that’s really been established in their practice and [they] are doing a good job with [those tools].”
However, Dr. Levy noted that many of the established screening tools were not being used, or were being shortened or modified in others ways to render them less effective.
“We recommend … new tools that we call frequency-based screening tools,” she explained. Pediatric patients are given a risk level based on their answer to a question regarding how many times in the past year they’ve used alcohol, marijuana, or tobacco.
Slightly different interventions are recommended based on the child’s risk level, including counseling about substance use and some strategies, especially with kids with heavier use, for conducting the conversation in a way that will make kids more likely to consider behavior change, she sa
The clinical report suggests that when no substance use is disclosed, doctors should offer positive reinforcement about smart decision making. For patients disclosing one or two uses per year with a low likelihood of having a substance use disorder, doctors should be promoting abstaining from use to support a healthy lifestyle, as well as discussions on the negative health effects of substance use. As the response to frequency of use increases and the greater likelihood of substance abuse disorder grows, so does the level of questions, including understanding the types of substances being used, coupled with more counseling on quitting use, and, in severe cases, referring for treatment.
The common theme in all the advice given to patients, though, is the importance of abstinence from substance use.
“The American Academy of Pediatrics recommends abstinence as the best health recommendation for adolescents,” Dr. Levy said. “That sometimes gets lost in the shuffle. That really is something that stands out in the policy, and that substance use is such an important health risk behavior that it should be addressed as part of routine health care for adolescents.”
The authors disclosed no relevant financial conflicts.
While the overall American Academy of Pediatrics policy objectives on screening for pediatric substance use have not changed, the academy is highlighting streamlined screening tools in a new clinical report.
The AAP remains focused on pushing for abstinence. That being said, the organization recommends “that pediatricians screen kids for substance use and talk about substance use,” lead author Dr. Sharon Levy said in an interview. “The big picture, bottom line, [is that] nothing has changed. It’s just an opportunity to reemphasize that we think talking about substance use is an important part of pediatric care.”
What has changed are the tools highlighted in the clinical report, published online June 20 (Pediatrics. 2016 Jul. doi: 10.1542/peds.2016-1211).
“We simplified the algorithm quite a bit,” said Dr. Levy, director of the adolescent substance abuse program at Boston Children’s Hospital. “We demonstrated use of more screening tools that are a bit simpler to use, a bit shorter, and lead more directly to intervention. For people who are using the older tools, that’s fine if that’s really been established in their practice and [they] are doing a good job with [those tools].”
However, Dr. Levy noted that many of the established screening tools were not being used, or were being shortened or modified in others ways to render them less effective.
“We recommend … new tools that we call frequency-based screening tools,” she explained. Pediatric patients are given a risk level based on their answer to a question regarding how many times in the past year they’ve used alcohol, marijuana, or tobacco.
Slightly different interventions are recommended based on the child’s risk level, including counseling about substance use and some strategies, especially with kids with heavier use, for conducting the conversation in a way that will make kids more likely to consider behavior change, she sa
The clinical report suggests that when no substance use is disclosed, doctors should offer positive reinforcement about smart decision making. For patients disclosing one or two uses per year with a low likelihood of having a substance use disorder, doctors should be promoting abstaining from use to support a healthy lifestyle, as well as discussions on the negative health effects of substance use. As the response to frequency of use increases and the greater likelihood of substance abuse disorder grows, so does the level of questions, including understanding the types of substances being used, coupled with more counseling on quitting use, and, in severe cases, referring for treatment.
The common theme in all the advice given to patients, though, is the importance of abstinence from substance use.
“The American Academy of Pediatrics recommends abstinence as the best health recommendation for adolescents,” Dr. Levy said. “That sometimes gets lost in the shuffle. That really is something that stands out in the policy, and that substance use is such an important health risk behavior that it should be addressed as part of routine health care for adolescents.”
The authors disclosed no relevant financial conflicts.
FROM PEDIATRICS

AAP, NASPAG issue joint guidance on menstruation management in teens with disabilities
For the first time, the American Academy of Pediatrics is offering guidance on managing menstruation and sexuality education in adolescents with disabilities.
Written jointly with the North American Society for Pediatric and Adolescent Gynecology, the clinical report offers guidance on options for menstrual management, sexual education and expression, and protection from sexual abuse. The report gives guidance regarding the care of adolescents with physical and/or intellectual abilities, but not for those with psychiatric illnesses (Pediatrics. 2016 April. doi: 10.1542/peds.2016-0295).
“Taking care of teens with disabilities and figuring out what to do with menstrual management has been all over the map,” Dr. Cora Collette Breuner, chair of the AAP’s committee on adolescence, said in an interview. “So, we tried to clarify it and help clinicians know what to do and when.”

A particular concern for the two groups was the threat of adverse events. “We wanted to cover what’s safe and what’s not in menstruation management, especially around bone health and thromboembolic events,” said Dr. Breuner, a professor of pediatrics and adolescent medicine at the University of Washington, Seattle.
Some of the information will not surprise clinicians, but there are some data that will perhaps come as news, said Dr. Breuner, including the recommendation that long-acting reversible contraception (LARC), such as the levonorgestrel intrauterine device or the progesterone implant rod should be considered first-line management therapies. “We point out that a number of studies show that these are safe.”
The report emphasizes offering anticipatory guidance before menses begins, noting that most teens with disabilities mature at the same rate as teens without disabilities. The report does not recommend premenarchal suppression in these patients, because doing so can interfere with normal bone growth. Such suppression also prevents patients and their families and caregivers from discovering that coping with the onset of menses is perhaps not as difficult as they might fear, the report states.
Although combined oral contraceptives are not contraindicated in teens with mobility issues, to guard against the threat of thromboembolic events in teens who use wheelchairs, the report recommends taking a thorough family history to rule out inherited thrombophilia. Otherwise, the recommendation is to prescribe the lowest-dose estrogen with a first- or second-generation progestin, as these are associated with lower rates of venous thrombotic events.
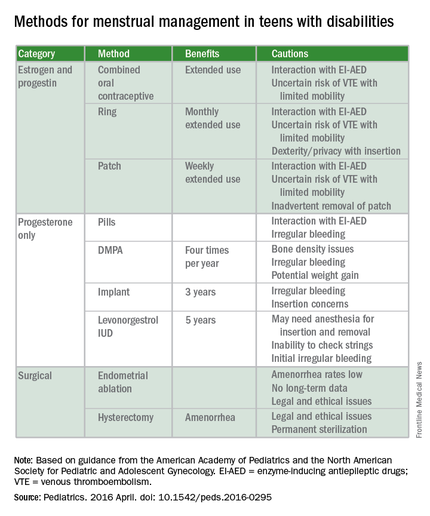
The guidance states that if cycles are creating difficulties in the patient’s life, “as determined by health care providers, patients, and families,” then menstrual management is appropriate. Even though it may take up to 3 years before a menstrual cycle becomes regular, the report cites irregularities caused by certain medications can be reason enough for menstrual management. Specific drugs noted include those affecting the dopaminergic system, valproic acid, and medications that elevate prolactin. Teens with obesity, seizure disorders, and polycystic ovary syndrome also can experience higher rates of irregularity.
The report also warns against the assumption that teens with disabilities are asexual or uninterested in sex. When appropriate, they should be offered the same confidential conversations about sexuality as are recommended for all teenagers by the AAP and the American College of Obstetricians and Gynecologists. “Teenagers with physical disabilities are just as likely to be sexually active as their peers and have a higher incidence of sexual abuse,” the report states. It is typically when a patient is cognitively impaired that consent to confidential services may require “discussion about legal guardianship or medical power of attorney status for families,” according to the report.
The report’s comprehensive review of four main menstrual management techniques – estrogen-containing, progestin-only, nonhormonal methods, and surgical requests and options – begins with the caveat that regardless of the method used, the threat of abuse or sexually transmitted infections remain. When a patient’s family or caregivers request suppression of menarche in a patient, stating fears of abuse or pregnancy, further investigation into the patient’s circumstances is warranted, the report states.
“It’s always worth reminding physicians that in this cohort, endometrial ablation can have legal implications, and it’s not recommended in this age group,” Dr. Breuner said.
On average, 1.5 hormonal methods are tried before achieving management goals, according to the report. Data cited in the study showed that at 42%, oral contraception is the preferred method of menstrual suppression, followed by the patch at 20%. Expectant management was third at 15%, followed by DMPA (depot medroxyprogesterone acetate) at 12%. The least utilized method was the levonorgestrel intrauterine device at 3%. No data were provided for the implantable contraceptive rod.
The clinical report is a companion document to another AAP clinical report, “Sexuality of Children and Adolescents with Developmental Disabilities” (Pediatrics. 2006. doi: 10.1542/peds.2006-1115).
AAP guidance on these matters in teens with psychiatric illnesses is expected to be issued within a few years, Dr. Breuner said.
There was no external funding and the authors have no relevant financial disclosures.
On Twitter @whitneymcknight
Although this guideline focuses on menstrual management and the guidance for you to help teens with disabilities through the pubertal transition, it’s very important to put this topic also into the context of sexuality. I think you have a great opportunity to do this because, often, you already have developed long-term relationships with these teenagers and their families, so the trust is already there. You should be the one to ensure all patients have appropriate sex education and help families with this.

|
Dr. Elisabeth Quint |
For some of these teens who are cognitively impaired, the initial conversations about sex may focus more on safety and abuse prevention. For example, which parts of their body should not be touched by other people. You can help the families really be the educators. Parents can be the ones to teach their kids how to protect themselves by rehearsing the answers to questions like, “What do you do if someone touches you? Who do you tell? Where do you go? What if it happens at school?” As part of the safety aspects, you also can help families assess whether the patient will be able to have a consensual sexual relationship. It’s the teens who have mild cognitive impairment that I worry about most, because often they are friendly and open to people, and can be taken advantage of. You just want to make sure they have the right information at their appropriate level.
Adolescents with physical disabilities are going to be just as interested in sex as any other teens and should be helped with any potential issues that they may have around that issue. They will likely get sex education in schools, but are still often viewed as not interested in sex or sexually active, and they may not get the usual confidential teen questions or appropriate screenings. Menstrual management and sexuality education both are important aspects of reproductive health care for teens with disabilities.
Dr. Elisabeth Quint, lead author of the AAP clinical report “Menstrual Management for Adolescents,” is a clinical professor of obstetrics and gynecology at the University of Michigan, Ann Arbor. She is also a past president of the North American Society for Pediatric and Adolescent Gynecology.
Although this guideline focuses on menstrual management and the guidance for you to help teens with disabilities through the pubertal transition, it’s very important to put this topic also into the context of sexuality. I think you have a great opportunity to do this because, often, you already have developed long-term relationships with these teenagers and their families, so the trust is already there. You should be the one to ensure all patients have appropriate sex education and help families with this.
|
|
Dr. Elisabeth Quint |
For some of these teens who are cognitively impaired, the initial conversations about sex may focus more on safety and abuse prevention. For example, which parts of their body should not be touched by other people. You can help the families really be the educators. Parents can be the ones to teach their kids how to protect themselves by rehearsing the answers to questions like, “What do you do if someone touches you? Who do you tell? Where do you go? What if it happens at school?” As part of the safety aspects, you also can help families assess whether the patient will be able to have a consensual sexual relationship. It’s the teens who have mild cognitive impairment that I worry about most, because often they are friendly and open to people, and can be taken advantage of. You just want to make sure they have the right information at their appropriate level.
Adolescents with physical disabilities are going to be just as interested in sex as any other teens and should be helped with any potential issues that they may have around that issue. They will likely get sex education in schools, but are still often viewed as not interested in sex or sexually active, and they may not get the usual confidential teen questions or appropriate screenings. Menstrual management and sexuality education both are important aspects of reproductive health care for teens with disabilities.
Dr. Elisabeth Quint, lead author of the AAP clinical report “Menstrual Management for Adolescents,” is a clinical professor of obstetrics and gynecology at the University of Michigan, Ann Arbor. She is also a past president of the North American Society for Pediatric and Adolescent Gynecology.
Although this guideline focuses on menstrual management and the guidance for you to help teens with disabilities through the pubertal transition, it’s very important to put this topic also into the context of sexuality. I think you have a great opportunity to do this because, often, you already have developed long-term relationships with these teenagers and their families, so the trust is already there. You should be the one to ensure all patients have appropriate sex education and help families with this.
|
|
Dr. Elisabeth Quint |
For some of these teens who are cognitively impaired, the initial conversations about sex may focus more on safety and abuse prevention. For example, which parts of their body should not be touched by other people. You can help the families really be the educators. Parents can be the ones to teach their kids how to protect themselves by rehearsing the answers to questions like, “What do you do if someone touches you? Who do you tell? Where do you go? What if it happens at school?” As part of the safety aspects, you also can help families assess whether the patient will be able to have a consensual sexual relationship. It’s the teens who have mild cognitive impairment that I worry about most, because often they are friendly and open to people, and can be taken advantage of. You just want to make sure they have the right information at their appropriate level.
Adolescents with physical disabilities are going to be just as interested in sex as any other teens and should be helped with any potential issues that they may have around that issue. They will likely get sex education in schools, but are still often viewed as not interested in sex or sexually active, and they may not get the usual confidential teen questions or appropriate screenings. Menstrual management and sexuality education both are important aspects of reproductive health care for teens with disabilities.
Dr. Elisabeth Quint, lead author of the AAP clinical report “Menstrual Management for Adolescents,” is a clinical professor of obstetrics and gynecology at the University of Michigan, Ann Arbor. She is also a past president of the North American Society for Pediatric and Adolescent Gynecology.
For the first time, the American Academy of Pediatrics is offering guidance on managing menstruation and sexuality education in adolescents with disabilities.
Written jointly with the North American Society for Pediatric and Adolescent Gynecology, the clinical report offers guidance on options for menstrual management, sexual education and expression, and protection from sexual abuse. The report gives guidance regarding the care of adolescents with physical and/or intellectual abilities, but not for those with psychiatric illnesses (Pediatrics. 2016 April. doi: 10.1542/peds.2016-0295).
“Taking care of teens with disabilities and figuring out what to do with menstrual management has been all over the map,” Dr. Cora Collette Breuner, chair of the AAP’s committee on adolescence, said in an interview. “So, we tried to clarify it and help clinicians know what to do and when.”
A particular concern for the two groups was the threat of adverse events. “We wanted to cover what’s safe and what’s not in menstruation management, especially around bone health and thromboembolic events,” said Dr. Breuner, a professor of pediatrics and adolescent medicine at the University of Washington, Seattle.
Some of the information will not surprise clinicians, but there are some data that will perhaps come as news, said Dr. Breuner, including the recommendation that long-acting reversible contraception (LARC), such as the levonorgestrel intrauterine device or the progesterone implant rod should be considered first-line management therapies. “We point out that a number of studies show that these are safe.”
The report emphasizes offering anticipatory guidance before menses begins, noting that most teens with disabilities mature at the same rate as teens without disabilities. The report does not recommend premenarchal suppression in these patients, because doing so can interfere with normal bone growth. Such suppression also prevents patients and their families and caregivers from discovering that coping with the onset of menses is perhaps not as difficult as they might fear, the report states.
Although combined oral contraceptives are not contraindicated in teens with mobility issues, to guard against the threat of thromboembolic events in teens who use wheelchairs, the report recommends taking a thorough family history to rule out inherited thrombophilia. Otherwise, the recommendation is to prescribe the lowest-dose estrogen with a first- or second-generation progestin, as these are associated with lower rates of venous thrombotic events.
The guidance states that if cycles are creating difficulties in the patient’s life, “as determined by health care providers, patients, and families,” then menstrual management is appropriate. Even though it may take up to 3 years before a menstrual cycle becomes regular, the report cites irregularities caused by certain medications can be reason enough for menstrual management. Specific drugs noted include those affecting the dopaminergic system, valproic acid, and medications that elevate prolactin. Teens with obesity, seizure disorders, and polycystic ovary syndrome also can experience higher rates of irregularity.
The report also warns against the assumption that teens with disabilities are asexual or uninterested in sex. When appropriate, they should be offered the same confidential conversations about sexuality as are recommended for all teenagers by the AAP and the American College of Obstetricians and Gynecologists. “Teenagers with physical disabilities are just as likely to be sexually active as their peers and have a higher incidence of sexual abuse,” the report states. It is typically when a patient is cognitively impaired that consent to confidential services may require “discussion about legal guardianship or medical power of attorney status for families,” according to the report.
The report’s comprehensive review of four main menstrual management techniques – estrogen-containing, progestin-only, nonhormonal methods, and surgical requests and options – begins with the caveat that regardless of the method used, the threat of abuse or sexually transmitted infections remain. When a patient’s family or caregivers request suppression of menarche in a patient, stating fears of abuse or pregnancy, further investigation into the patient’s circumstances is warranted, the report states.
“It’s always worth reminding physicians that in this cohort, endometrial ablation can have legal implications, and it’s not recommended in this age group,” Dr. Breuner said.
On average, 1.5 hormonal methods are tried before achieving management goals, according to the report. Data cited in the study showed that at 42%, oral contraception is the preferred method of menstrual suppression, followed by the patch at 20%. Expectant management was third at 15%, followed by DMPA (depot medroxyprogesterone acetate) at 12%. The least utilized method was the levonorgestrel intrauterine device at 3%. No data were provided for the implantable contraceptive rod.
The clinical report is a companion document to another AAP clinical report, “Sexuality of Children and Adolescents with Developmental Disabilities” (Pediatrics. 2006. doi: 10.1542/peds.2006-1115).
AAP guidance on these matters in teens with psychiatric illnesses is expected to be issued within a few years, Dr. Breuner said.
There was no external funding and the authors have no relevant financial disclosures.
On Twitter @whitneymcknight
For the first time, the American Academy of Pediatrics is offering guidance on managing menstruation and sexuality education in adolescents with disabilities.
Written jointly with the North American Society for Pediatric and Adolescent Gynecology, the clinical report offers guidance on options for menstrual management, sexual education and expression, and protection from sexual abuse. The report gives guidance regarding the care of adolescents with physical and/or intellectual abilities, but not for those with psychiatric illnesses (Pediatrics. 2016 April. doi: 10.1542/peds.2016-0295).
“Taking care of teens with disabilities and figuring out what to do with menstrual management has been all over the map,” Dr. Cora Collette Breuner, chair of the AAP’s committee on adolescence, said in an interview. “So, we tried to clarify it and help clinicians know what to do and when.”
A particular concern for the two groups was the threat of adverse events. “We wanted to cover what’s safe and what’s not in menstruation management, especially around bone health and thromboembolic events,” said Dr. Breuner, a professor of pediatrics and adolescent medicine at the University of Washington, Seattle.
Some of the information will not surprise clinicians, but there are some data that will perhaps come as news, said Dr. Breuner, including the recommendation that long-acting reversible contraception (LARC), such as the levonorgestrel intrauterine device or the progesterone implant rod should be considered first-line management therapies. “We point out that a number of studies show that these are safe.”
The report emphasizes offering anticipatory guidance before menses begins, noting that most teens with disabilities mature at the same rate as teens without disabilities. The report does not recommend premenarchal suppression in these patients, because doing so can interfere with normal bone growth. Such suppression also prevents patients and their families and caregivers from discovering that coping with the onset of menses is perhaps not as difficult as they might fear, the report states.
Although combined oral contraceptives are not contraindicated in teens with mobility issues, to guard against the threat of thromboembolic events in teens who use wheelchairs, the report recommends taking a thorough family history to rule out inherited thrombophilia. Otherwise, the recommendation is to prescribe the lowest-dose estrogen with a first- or second-generation progestin, as these are associated with lower rates of venous thrombotic events.
The guidance states that if cycles are creating difficulties in the patient’s life, “as determined by health care providers, patients, and families,” then menstrual management is appropriate. Even though it may take up to 3 years before a menstrual cycle becomes regular, the report cites irregularities caused by certain medications can be reason enough for menstrual management. Specific drugs noted include those affecting the dopaminergic system, valproic acid, and medications that elevate prolactin. Teens with obesity, seizure disorders, and polycystic ovary syndrome also can experience higher rates of irregularity.
The report also warns against the assumption that teens with disabilities are asexual or uninterested in sex. When appropriate, they should be offered the same confidential conversations about sexuality as are recommended for all teenagers by the AAP and the American College of Obstetricians and Gynecologists. “Teenagers with physical disabilities are just as likely to be sexually active as their peers and have a higher incidence of sexual abuse,” the report states. It is typically when a patient is cognitively impaired that consent to confidential services may require “discussion about legal guardianship or medical power of attorney status for families,” according to the report.
The report’s comprehensive review of four main menstrual management techniques – estrogen-containing, progestin-only, nonhormonal methods, and surgical requests and options – begins with the caveat that regardless of the method used, the threat of abuse or sexually transmitted infections remain. When a patient’s family or caregivers request suppression of menarche in a patient, stating fears of abuse or pregnancy, further investigation into the patient’s circumstances is warranted, the report states.
“It’s always worth reminding physicians that in this cohort, endometrial ablation can have legal implications, and it’s not recommended in this age group,” Dr. Breuner said.
On average, 1.5 hormonal methods are tried before achieving management goals, according to the report. Data cited in the study showed that at 42%, oral contraception is the preferred method of menstrual suppression, followed by the patch at 20%. Expectant management was third at 15%, followed by DMPA (depot medroxyprogesterone acetate) at 12%. The least utilized method was the levonorgestrel intrauterine device at 3%. No data were provided for the implantable contraceptive rod.
The clinical report is a companion document to another AAP clinical report, “Sexuality of Children and Adolescents with Developmental Disabilities” (Pediatrics. 2006. doi: 10.1542/peds.2006-1115).
AAP guidance on these matters in teens with psychiatric illnesses is expected to be issued within a few years, Dr. Breuner said.
There was no external funding and the authors have no relevant financial disclosures.
On Twitter @whitneymcknight
FROM PEDIATRICS

Consider Fusobacterium in culture-negative pharyngitis
BOSTON – An underappreciated cause of bacterial pharyngitis had a similar clinical presentation to group A Streptococcus (GAS), although prevalence was low in the population of 300 pediatric patients in a single-site study.
The 10 patients (3.3%) who had positive cultures for Fusobacterium necrophorum were about as likely as those with GAS to have fever, sore throat, exudate, and absence of cough. GAS cultures were positive in 57 (19%) of the patients.

F. necrophorum is a common cause of serious bacterial pharyngitis, especially in adolescents and young adults. The gram-negative species, an obligate anaerobe, is a cause of Lemierre’s syndrome, and “has recently been identified to be an important pathogen of bacterial pharyngitis with higher prevalence than group A Streptococcus (GAS) in adolescents and young adults,” wrote Tam Van, Ph.D., and her colleagues in a poster presented at the annual meeting of the American Society for Microbiology.
To examine the prevalence and disease characteristics of F. necrophorum in the emergency department patient population at Children’s Hospital of Los Angeles, Dr Van, a medical microbiology fellow at the hospital, and her colleagues enrolled 300 patients with pharyngitis aged 1-20 years (mean, 7.8 years).
All patients’ throats were swabbed, and investigators conducted a rapid antigen detection test (RADT) for group A beta-hemolytic Streptococcus and cultured samples for Streptococcus on a blood agar plate, according to usual care; samples also were cultured anaerobically and tested via polymerase chain reaction (PCR) for F. necrophorum.
A total of 67 patients had positive culture or PCR results for both species. Fifteen of the RADT tests were positive, while 57 cultures returned positive for GAS growth. Nine of the 10 positive F. necrophorum PCR tests correlated with positive culture results for that species.
Luckily, said Dr. Van, penicillin is an effective treatment for F. necrophorum, although it’s a gram-negative bacterium, so if a patient is coinfected with F. necrophorum and GAS, or treated for GAS empirically, then standard of care treatment should be effective, she said. However, since the species is associated with serious complications such as Lemierre’s disease, close follow-up and a low threshold for aggressive treatment are warranted if F. necrophorum is suspected or identified.
The relatively low positive culture rate of 3.3% for F. necrophorum in the study population was a bit surprising, Dr. Van said in an interview but was perhaps accounted for by the relatively young age of the Children’s Hospital Los Angeles patients. “Previous reports looked at adolescents and young adults,” wrote Dr. Van and her colleagues, while two-thirds of the patients in their study were under the age of 10 years. “This may contribute to the difference in prevalence.”
“Although rare, recovery of F. necrophorum correlated with true signs and symptoms of bacterial pharyngitis,” wrote Dr. Van and her colleagues. Serious pharyngitis with a negative rapid test and culture for group A Streptococcus should prompt clinical suspicion for F. necrophorum, especially in older adolescents and young adults, said Dr. Tam.
Dr. Tam and her coauthors reported no outside sources of funding and reported no relevant financial disclosures.
On Twitter @karioakes
BOSTON – An underappreciated cause of bacterial pharyngitis had a similar clinical presentation to group A Streptococcus (GAS), although prevalence was low in the population of 300 pediatric patients in a single-site study.
The 10 patients (3.3%) who had positive cultures for Fusobacterium necrophorum were about as likely as those with GAS to have fever, sore throat, exudate, and absence of cough. GAS cultures were positive in 57 (19%) of the patients.
F. necrophorum is a common cause of serious bacterial pharyngitis, especially in adolescents and young adults. The gram-negative species, an obligate anaerobe, is a cause of Lemierre’s syndrome, and “has recently been identified to be an important pathogen of bacterial pharyngitis with higher prevalence than group A Streptococcus (GAS) in adolescents and young adults,” wrote Tam Van, Ph.D., and her colleagues in a poster presented at the annual meeting of the American Society for Microbiology.
To examine the prevalence and disease characteristics of F. necrophorum in the emergency department patient population at Children’s Hospital of Los Angeles, Dr Van, a medical microbiology fellow at the hospital, and her colleagues enrolled 300 patients with pharyngitis aged 1-20 years (mean, 7.8 years).
All patients’ throats were swabbed, and investigators conducted a rapid antigen detection test (RADT) for group A beta-hemolytic Streptococcus and cultured samples for Streptococcus on a blood agar plate, according to usual care; samples also were cultured anaerobically and tested via polymerase chain reaction (PCR) for F. necrophorum.
A total of 67 patients had positive culture or PCR results for both species. Fifteen of the RADT tests were positive, while 57 cultures returned positive for GAS growth. Nine of the 10 positive F. necrophorum PCR tests correlated with positive culture results for that species.
Luckily, said Dr. Van, penicillin is an effective treatment for F. necrophorum, although it’s a gram-negative bacterium, so if a patient is coinfected with F. necrophorum and GAS, or treated for GAS empirically, then standard of care treatment should be effective, she said. However, since the species is associated with serious complications such as Lemierre’s disease, close follow-up and a low threshold for aggressive treatment are warranted if F. necrophorum is suspected or identified.
The relatively low positive culture rate of 3.3% for F. necrophorum in the study population was a bit surprising, Dr. Van said in an interview but was perhaps accounted for by the relatively young age of the Children’s Hospital Los Angeles patients. “Previous reports looked at adolescents and young adults,” wrote Dr. Van and her colleagues, while two-thirds of the patients in their study were under the age of 10 years. “This may contribute to the difference in prevalence.”
“Although rare, recovery of F. necrophorum correlated with true signs and symptoms of bacterial pharyngitis,” wrote Dr. Van and her colleagues. Serious pharyngitis with a negative rapid test and culture for group A Streptococcus should prompt clinical suspicion for F. necrophorum, especially in older adolescents and young adults, said Dr. Tam.
Dr. Tam and her coauthors reported no outside sources of funding and reported no relevant financial disclosures.
On Twitter @karioakes
BOSTON – An underappreciated cause of bacterial pharyngitis had a similar clinical presentation to group A Streptococcus (GAS), although prevalence was low in the population of 300 pediatric patients in a single-site study.
The 10 patients (3.3%) who had positive cultures for Fusobacterium necrophorum were about as likely as those with GAS to have fever, sore throat, exudate, and absence of cough. GAS cultures were positive in 57 (19%) of the patients.
F. necrophorum is a common cause of serious bacterial pharyngitis, especially in adolescents and young adults. The gram-negative species, an obligate anaerobe, is a cause of Lemierre’s syndrome, and “has recently been identified to be an important pathogen of bacterial pharyngitis with higher prevalence than group A Streptococcus (GAS) in adolescents and young adults,” wrote Tam Van, Ph.D., and her colleagues in a poster presented at the annual meeting of the American Society for Microbiology.
To examine the prevalence and disease characteristics of F. necrophorum in the emergency department patient population at Children’s Hospital of Los Angeles, Dr Van, a medical microbiology fellow at the hospital, and her colleagues enrolled 300 patients with pharyngitis aged 1-20 years (mean, 7.8 years).
All patients’ throats were swabbed, and investigators conducted a rapid antigen detection test (RADT) for group A beta-hemolytic Streptococcus and cultured samples for Streptococcus on a blood agar plate, according to usual care; samples also were cultured anaerobically and tested via polymerase chain reaction (PCR) for F. necrophorum.
A total of 67 patients had positive culture or PCR results for both species. Fifteen of the RADT tests were positive, while 57 cultures returned positive for GAS growth. Nine of the 10 positive F. necrophorum PCR tests correlated with positive culture results for that species.
Luckily, said Dr. Van, penicillin is an effective treatment for F. necrophorum, although it’s a gram-negative bacterium, so if a patient is coinfected with F. necrophorum and GAS, or treated for GAS empirically, then standard of care treatment should be effective, she said. However, since the species is associated with serious complications such as Lemierre’s disease, close follow-up and a low threshold for aggressive treatment are warranted if F. necrophorum is suspected or identified.
The relatively low positive culture rate of 3.3% for F. necrophorum in the study population was a bit surprising, Dr. Van said in an interview but was perhaps accounted for by the relatively young age of the Children’s Hospital Los Angeles patients. “Previous reports looked at adolescents and young adults,” wrote Dr. Van and her colleagues, while two-thirds of the patients in their study were under the age of 10 years. “This may contribute to the difference in prevalence.”
“Although rare, recovery of F. necrophorum correlated with true signs and symptoms of bacterial pharyngitis,” wrote Dr. Van and her colleagues. Serious pharyngitis with a negative rapid test and culture for group A Streptococcus should prompt clinical suspicion for F. necrophorum, especially in older adolescents and young adults, said Dr. Tam.
Dr. Tam and her coauthors reported no outside sources of funding and reported no relevant financial disclosures.
On Twitter @karioakes
AT ASM MICROBE 2016
Key clinical point: Fusobacterium necrophorum has a similar presentation to group A Streptococcus (GAS) pharyngitis.
Major finding: Pediatric patients with F. necrophorum pharyngitis were about as likely as those with GAS to have fever, exudates, adenopathy, and no cough.
Data source: 300 pediatric emergency department patients with pharyngitis who received antigen testing, cultures, and PCR to identify both causative agents.
Disclosures: The study investigators reported no disclosures.