User login
Parental online sharing involves balancing risks, benefits
SAN FRANCISCO – More than two-thirds of parents worry about their children’s privacy online and/or that photos of their children might be reshared on the wider Web, according to a survey conducted by C.S. Mott Children’s Hospital.
Those fears are not baseless, and they need to be considered more often by parents themselves in posting about their children online, presenters agreed at a symposium on the media at the annual meeting of the American Academy of Pediatrics.
“The first children of social media are just now entering adulthood, entering the job market,” said Stacey Steinberg, JD, a legal skills professor at the University of Florida Levin College of Law, Gainesville. She is also with the law school’s center on children and families.
She and Bahareh Keith, DO, a pediatrician at the University of Florida, discussed the challenges and risks of “sharenting” – parents’ sharing information and photos of their children online – and pediatricians’ role in advising parents and looking out for children’s best interests.
“The dearth of discussion on this topic leaves even the most well-intentioned parents without enough information to thoroughly analyze this,” Ms. Steinberg said. “We’re not sitting here saying we know what the answers are. But we’re saying this is an important issue that affects families, and these children require a voice in this discussion.”
The way social media and blogging have changed the landscape for children coming of age today means that they often have a digital footprint shaped by their parents long before they create their own first account. This reality means it’s necessary to consider how to balance children’s right to privacy with parents’ right to free speech and expression.
The 2015 C.S. Mott survey asked 569 parents of children aged 4 years and younger about how they use social media as parents, and reported that more than half of mothers (56%) and a third of fathers (34%) discuss parenting and child health topics on Facebook, Twitter, blogs, online forums, and other online platforms.
The risks of this sharenting can range from embarrassment of the child to significantly more sinister repercussions. Just over half of the parents (52%) in the Mott survey reported that they are concerned their child might feel embarrassed when they grow older and discover what their parents shared online. But that embarrassment also can lead to bullying or determent of psychosocial development, Ms. Steinberg and Dr. Keith explained.
More serious, if less common, risks include the possibility that data brokers could access and use information about the children or that online child pornographers could repurpose the photos inappropriately. One worst case scenario of the former is digital kidnapping, a disturbing practice in which a stranger uses baby photos and information that is not their own to pass off the child as their own or to invite others to “invent” identities for the child. The Children’s Online Privacy Protection Rule of the Federal Trade Commission addresses only online use by those under age 13 years, not others’ use of those images.
Regarding the latter, Ms. Steinberg and Dr. Keith showed an example of a bare-bottomed baby standing in front of a bathtub that had been reshared hundreds of times, but other images that have been shared on child pornography sites depict children in everyday situations such as playing on a playground, running at the beach, or doing gymnastics.
“These are images that many of us would think are innocent, but pornographers would categorize these into folders,” Dr. Keith said. “It’s not even naked or half-naked pictures.”
A study conducted by an e-safety commission in Australia, for example, found that half of the thousands of photos shared on a sample of child pornography sites had originated from parental sharing.
But Ms. Steinberg and Dr. Keith pointed out that benefits of parents’ online sharing exist as well, as the Mott survey found. In that survey, 72% of parents who discuss parenting and/or their children on social media reported that doing so helps them feel less alone. Similarly, 70% said they learn what not to do through those experiences, 67% said they receive advice from more experienced parents, and 62% said they consequently worry less. Common topics they discussed included sleep, nutrition, discipline, day care, and behavior management.
Other benefits, Ms. Steinberg pointed out, are that families geographically spread apart can stay connected, and communities can grow stronger with shared communal experiences of parents meeting others online.
“For some parents, it gives them an opportunity for advocacy work and raises awareness for important social issues,” Ms. Steinberg said, although she added, “If you’re going to share your children’s behavioral problems, consider sharing anonymously.”
Neither Ms. Steinberg and Dr. Keith said they had simple solutions to these challenges. Rather, they recommended using the public health model of raising awareness and encouraging open dialogue among pediatricians, parents, and their children to look for ways to balance competing interests.
“Social media offers many positive benefits, and we don’t want to silence the many voices of parents who take part in online sharing,” Ms. Steinberg explained. But she and Ms. Keith said it’s also worth considering children’s potential interest in controlling what their digital footprint is as they become adults.
For example, one study they cited found that, among 249 pairs of parents and their children, three times more children than parents wanted the parents to have and follow rules regarding what they could share on social media about their children.
Although guidance for parents on monitoring children’s social media use is a part of the AAP policy statement on media, only one recommendation obliquely addresses how parents should or shouldn’t use social media by advising them to model appropriate use for their children.
“It’s just like any medical decision: What is the benefit, and what is the risk, and does the benefit outweigh the risk?” said Wendy Sue Swanson, MD, executive director of digital health at Seattle Children’s Hospital. She recommended that parents ask their child for permission before posting a story or photo if their kids are aged 6 or older.
Ms. Steinberg and Dr. Keith recommended that pediatricians broach this subject with parents to help them think about risks they simply might not have considered before.
“When we looked at what sorts of best practices could be encouraged or doctors could talk to parents about – the tangible harms, such as whether data brokers or people interested in child pornography could access the information – we didn’t want to create any unnecessary panic,” Ms. Steinberg said. “But we did find some concerns that were troublesome, and we thought that parents or at least physicians [should] be aware of those potential risks.”
Ms. Steinberg and Dr. Keith reported that they had no relevant financial disclosures.
SAN FRANCISCO – More than two-thirds of parents worry about their children’s privacy online and/or that photos of their children might be reshared on the wider Web, according to a survey conducted by C.S. Mott Children’s Hospital.
Those fears are not baseless, and they need to be considered more often by parents themselves in posting about their children online, presenters agreed at a symposium on the media at the annual meeting of the American Academy of Pediatrics.
“The first children of social media are just now entering adulthood, entering the job market,” said Stacey Steinberg, JD, a legal skills professor at the University of Florida Levin College of Law, Gainesville. She is also with the law school’s center on children and families.
She and Bahareh Keith, DO, a pediatrician at the University of Florida, discussed the challenges and risks of “sharenting” – parents’ sharing information and photos of their children online – and pediatricians’ role in advising parents and looking out for children’s best interests.
“The dearth of discussion on this topic leaves even the most well-intentioned parents without enough information to thoroughly analyze this,” Ms. Steinberg said. “We’re not sitting here saying we know what the answers are. But we’re saying this is an important issue that affects families, and these children require a voice in this discussion.”
The way social media and blogging have changed the landscape for children coming of age today means that they often have a digital footprint shaped by their parents long before they create their own first account. This reality means it’s necessary to consider how to balance children’s right to privacy with parents’ right to free speech and expression.
The 2015 C.S. Mott survey asked 569 parents of children aged 4 years and younger about how they use social media as parents, and reported that more than half of mothers (56%) and a third of fathers (34%) discuss parenting and child health topics on Facebook, Twitter, blogs, online forums, and other online platforms.
The risks of this sharenting can range from embarrassment of the child to significantly more sinister repercussions. Just over half of the parents (52%) in the Mott survey reported that they are concerned their child might feel embarrassed when they grow older and discover what their parents shared online. But that embarrassment also can lead to bullying or determent of psychosocial development, Ms. Steinberg and Dr. Keith explained.
More serious, if less common, risks include the possibility that data brokers could access and use information about the children or that online child pornographers could repurpose the photos inappropriately. One worst case scenario of the former is digital kidnapping, a disturbing practice in which a stranger uses baby photos and information that is not their own to pass off the child as their own or to invite others to “invent” identities for the child. The Children’s Online Privacy Protection Rule of the Federal Trade Commission addresses only online use by those under age 13 years, not others’ use of those images.
Regarding the latter, Ms. Steinberg and Dr. Keith showed an example of a bare-bottomed baby standing in front of a bathtub that had been reshared hundreds of times, but other images that have been shared on child pornography sites depict children in everyday situations such as playing on a playground, running at the beach, or doing gymnastics.
“These are images that many of us would think are innocent, but pornographers would categorize these into folders,” Dr. Keith said. “It’s not even naked or half-naked pictures.”
A study conducted by an e-safety commission in Australia, for example, found that half of the thousands of photos shared on a sample of child pornography sites had originated from parental sharing.
But Ms. Steinberg and Dr. Keith pointed out that benefits of parents’ online sharing exist as well, as the Mott survey found. In that survey, 72% of parents who discuss parenting and/or their children on social media reported that doing so helps them feel less alone. Similarly, 70% said they learn what not to do through those experiences, 67% said they receive advice from more experienced parents, and 62% said they consequently worry less. Common topics they discussed included sleep, nutrition, discipline, day care, and behavior management.
Other benefits, Ms. Steinberg pointed out, are that families geographically spread apart can stay connected, and communities can grow stronger with shared communal experiences of parents meeting others online.
“For some parents, it gives them an opportunity for advocacy work and raises awareness for important social issues,” Ms. Steinberg said, although she added, “If you’re going to share your children’s behavioral problems, consider sharing anonymously.”
Neither Ms. Steinberg and Dr. Keith said they had simple solutions to these challenges. Rather, they recommended using the public health model of raising awareness and encouraging open dialogue among pediatricians, parents, and their children to look for ways to balance competing interests.
“Social media offers many positive benefits, and we don’t want to silence the many voices of parents who take part in online sharing,” Ms. Steinberg explained. But she and Ms. Keith said it’s also worth considering children’s potential interest in controlling what their digital footprint is as they become adults.
For example, one study they cited found that, among 249 pairs of parents and their children, three times more children than parents wanted the parents to have and follow rules regarding what they could share on social media about their children.
Although guidance for parents on monitoring children’s social media use is a part of the AAP policy statement on media, only one recommendation obliquely addresses how parents should or shouldn’t use social media by advising them to model appropriate use for their children.
“It’s just like any medical decision: What is the benefit, and what is the risk, and does the benefit outweigh the risk?” said Wendy Sue Swanson, MD, executive director of digital health at Seattle Children’s Hospital. She recommended that parents ask their child for permission before posting a story or photo if their kids are aged 6 or older.
Ms. Steinberg and Dr. Keith recommended that pediatricians broach this subject with parents to help them think about risks they simply might not have considered before.
“When we looked at what sorts of best practices could be encouraged or doctors could talk to parents about – the tangible harms, such as whether data brokers or people interested in child pornography could access the information – we didn’t want to create any unnecessary panic,” Ms. Steinberg said. “But we did find some concerns that were troublesome, and we thought that parents or at least physicians [should] be aware of those potential risks.”
Ms. Steinberg and Dr. Keith reported that they had no relevant financial disclosures.
SAN FRANCISCO – More than two-thirds of parents worry about their children’s privacy online and/or that photos of their children might be reshared on the wider Web, according to a survey conducted by C.S. Mott Children’s Hospital.
Those fears are not baseless, and they need to be considered more often by parents themselves in posting about their children online, presenters agreed at a symposium on the media at the annual meeting of the American Academy of Pediatrics.
“The first children of social media are just now entering adulthood, entering the job market,” said Stacey Steinberg, JD, a legal skills professor at the University of Florida Levin College of Law, Gainesville. She is also with the law school’s center on children and families.
She and Bahareh Keith, DO, a pediatrician at the University of Florida, discussed the challenges and risks of “sharenting” – parents’ sharing information and photos of their children online – and pediatricians’ role in advising parents and looking out for children’s best interests.
“The dearth of discussion on this topic leaves even the most well-intentioned parents without enough information to thoroughly analyze this,” Ms. Steinberg said. “We’re not sitting here saying we know what the answers are. But we’re saying this is an important issue that affects families, and these children require a voice in this discussion.”
The way social media and blogging have changed the landscape for children coming of age today means that they often have a digital footprint shaped by their parents long before they create their own first account. This reality means it’s necessary to consider how to balance children’s right to privacy with parents’ right to free speech and expression.
The 2015 C.S. Mott survey asked 569 parents of children aged 4 years and younger about how they use social media as parents, and reported that more than half of mothers (56%) and a third of fathers (34%) discuss parenting and child health topics on Facebook, Twitter, blogs, online forums, and other online platforms.
The risks of this sharenting can range from embarrassment of the child to significantly more sinister repercussions. Just over half of the parents (52%) in the Mott survey reported that they are concerned their child might feel embarrassed when they grow older and discover what their parents shared online. But that embarrassment also can lead to bullying or determent of psychosocial development, Ms. Steinberg and Dr. Keith explained.
More serious, if less common, risks include the possibility that data brokers could access and use information about the children or that online child pornographers could repurpose the photos inappropriately. One worst case scenario of the former is digital kidnapping, a disturbing practice in which a stranger uses baby photos and information that is not their own to pass off the child as their own or to invite others to “invent” identities for the child. The Children’s Online Privacy Protection Rule of the Federal Trade Commission addresses only online use by those under age 13 years, not others’ use of those images.
Regarding the latter, Ms. Steinberg and Dr. Keith showed an example of a bare-bottomed baby standing in front of a bathtub that had been reshared hundreds of times, but other images that have been shared on child pornography sites depict children in everyday situations such as playing on a playground, running at the beach, or doing gymnastics.
“These are images that many of us would think are innocent, but pornographers would categorize these into folders,” Dr. Keith said. “It’s not even naked or half-naked pictures.”
A study conducted by an e-safety commission in Australia, for example, found that half of the thousands of photos shared on a sample of child pornography sites had originated from parental sharing.
But Ms. Steinberg and Dr. Keith pointed out that benefits of parents’ online sharing exist as well, as the Mott survey found. In that survey, 72% of parents who discuss parenting and/or their children on social media reported that doing so helps them feel less alone. Similarly, 70% said they learn what not to do through those experiences, 67% said they receive advice from more experienced parents, and 62% said they consequently worry less. Common topics they discussed included sleep, nutrition, discipline, day care, and behavior management.
Other benefits, Ms. Steinberg pointed out, are that families geographically spread apart can stay connected, and communities can grow stronger with shared communal experiences of parents meeting others online.
“For some parents, it gives them an opportunity for advocacy work and raises awareness for important social issues,” Ms. Steinberg said, although she added, “If you’re going to share your children’s behavioral problems, consider sharing anonymously.”
Neither Ms. Steinberg and Dr. Keith said they had simple solutions to these challenges. Rather, they recommended using the public health model of raising awareness and encouraging open dialogue among pediatricians, parents, and their children to look for ways to balance competing interests.
“Social media offers many positive benefits, and we don’t want to silence the many voices of parents who take part in online sharing,” Ms. Steinberg explained. But she and Ms. Keith said it’s also worth considering children’s potential interest in controlling what their digital footprint is as they become adults.
For example, one study they cited found that, among 249 pairs of parents and their children, three times more children than parents wanted the parents to have and follow rules regarding what they could share on social media about their children.
Although guidance for parents on monitoring children’s social media use is a part of the AAP policy statement on media, only one recommendation obliquely addresses how parents should or shouldn’t use social media by advising them to model appropriate use for their children.
“It’s just like any medical decision: What is the benefit, and what is the risk, and does the benefit outweigh the risk?” said Wendy Sue Swanson, MD, executive director of digital health at Seattle Children’s Hospital. She recommended that parents ask their child for permission before posting a story or photo if their kids are aged 6 or older.
Ms. Steinberg and Dr. Keith recommended that pediatricians broach this subject with parents to help them think about risks they simply might not have considered before.
“When we looked at what sorts of best practices could be encouraged or doctors could talk to parents about – the tangible harms, such as whether data brokers or people interested in child pornography could access the information – we didn’t want to create any unnecessary panic,” Ms. Steinberg said. “But we did find some concerns that were troublesome, and we thought that parents or at least physicians [should] be aware of those potential risks.”
Ms. Steinberg and Dr. Keith reported that they had no relevant financial disclosures.
AT AAP 2016
Does breastfeeding affect the risk of childhood obesity?
EVIDENCE SUMMARY
A systematic review and meta-analysis of prospective cohort studies evaluating infant risk factors for childhood obesity found that breastfeeding was associated with a lower risk of obesity.1 The authors identified 10 trials (primarily from the United States and Europe) with more than 76,000 infants that compared the effect of some breastfeeding in the first year to no breastfeeding. Follow-up ranged from 2 to 14 years (median 6 years).
Having ever breastfed decreased the odds of future overweight (BMI >85th percentile) or obesity (BMI >95th percentile) by 15% (adjusted odds ratio [AOR]=0.85; 95% confidence interval [CI], 0.74-0.99).
Subsequent studies suggest increased risk with formula feeding
Three large, prospective, longitudinal cohort studies have been published since the meta-analysis. One, which followed 43,367 term infants in Japan, found that formula feeding before 6 months was associated with increased risk of obesity compared with continuous breastfeeding for 6 months.2 Researchers evaluated weight at 7 years and adjusted for child and maternal factors associated with weight gain (AOR for obesity, formula-fed infants=1.8; 95% CI, 1.3-2.6).
A similar prospective longitudinal cohort study of 2868 infants in Australia analyzed maternal breastfeeding diaries and followed children’s weight to age 20 years.3 Introducing a milk other than breast milk before 6 months of age was linked to increased risk of obesity at age 20 (odds ratio [OR]=1.5; 95% CI, 1.1-1.9).
Finally, in a prospective cohort of 568 children in India, 17% of children who breastfed for fewer than 6 months were above the 90th percentile for weight at age 5 years, compared with 10% of children who were breastfed for at least 18 months.4 The result didn’t reach statistical significance, however (P=.08).
Interventions that increase breastfeeding don’t seem to have an impact
An RCT of an intervention to promote breastfeeding didn’t find any effect on subsequent obesity rates. Researchers in Belarus randomized 17,046 mother-infant pairs to breastfeeding promotion, modeled on the UNICEF Baby-Friendly Hospital Initiative, or usual care. The intervention increased the prevalence of exclusive breastfeeding (at 3 months, 43% vs 6%; at 6 months, 7% vs 0.6%; P values not given).
When researchers evaluated 13,879 children at 11 or 12 years by intention-to-treat analysis, however, they found no difference in mean BMI between the children whose mothers received the intervention and those whose mothers didn’t (BMI difference=0.16; 95% CI, -0.02 to 0.35).5
Introduction of solid foods: Later is better
A systematic review investigated the association between the timing of introducing complementary (solid) foods and childhood obesity in 23 primarily cross-sectional and cohort studies (17 from the United States, Canada, and Europe) with more than 33,000 patients. Follow-up ranged from 4 to 19 years.
Eight of the 21 studies that used BMI as an outcome found that early introduction of complementary foods was associated with a higher childhood BMI. In the largest study (a cohort of 17,561 infants), introducing complementary foods before 3 months was associated with higher risk of obesity at age 5 years than introducing them thereafter (OR=1.3; 95% CI, 1.1-1.6).6 Introduction of solids after 4 months was not associated with childhood obesity.
A systematic review of 10 primarily cross-sectional and cohort studies with more than 3000 infants evaluated associations between the types of complementary foods given and the development of childhood obesity.7 Six of the 10 studies were from Europe and none were from the United States. Follow-up ages ranged from 4 to 11 years.
Outcomes were heterogeneous, and no meta-analysis could be performed. The authors cited 3 studies (total 1174 infants) that found various positive associations between total caloric intake during complementary feeding and childhood obesity. No consistent evidence pointed to increased risk from specific foods or food groups.
Scheduled feeding is linked to rapid infant weight gain
A cohort study evaluated the baseline data of an Australian RCT (on an intervention to promote proper nutrition) in 612 infants, mean age 4.3 months.8 Researchers looked at the relationship between feeding on demand vs scheduled feeding (assessed by parental report) and weight gain in infancy. “Rapid weight gain” was defined as >0.67 change in weight-for-age Z-score between birth and enrollment.
Scheduled feeding was associated with rapid weight gain at a higher rate than feeding on demand (OR=2.3; 95% CI, 1.1-4.6). This study didn’t use childhood obesity as an outcome.
1. Weng SF, Redsell SA, Swift JA, et al. Systematic review and meta-analyses of risk factors for childhood overweight identifiable during infancy. Arch Dis Child. 2012;97:1019-1026.
2. Yamakawa M, Yorifuji T, Inoue S, et al. Breastfeeding and obesity among schoolchildren: a national longitudinal survey in Japan. JAMA Pediatr. 2013;167:919-925.
3. Oddy WH, Mari TA, Huang RC, et al. Early infant feeding and adiposity risk: from infancy to adulthood. Ann Nutr Metab. 2014;64:262-270.
4. Caleyachetty A, Krishnaveni GV, Veena SR, et al. Breast-feeding duration, age of starting solids, and high BMI risk and adiposity in Indian children. Matern Child Nutr. 2013;9:199-216.
5. Martin RM, Patel, R, Kramer MS, et al. Effects of promoting longer-term and exclusive breastfeeding on adiposity and insulin-like growth factor-I at age 11.5 years: a randomized trial. JAMA. 2013;309:1005-1013.
6. Pearce J, Taylor MA, Langley-Evans SC. Timing of the introduction of complementary feeding and risk of childhood obesity: a systematic review. Int J Obes (Lond). 2013;37:1295-1306.
7. Pearce J, Langley-Evans. The types of food introduced during complementary feeding and risk of childhood obesity: a systematic review. Int J Obes (Lond). 2013;37:477-485.
8. Mihrshahi S, Battistutta D, Magarey A, et al. Determinants of rapid weight gain during infancy: baseline results from the NOURISH randomised controlled trial. BMC Pediatr. 2011;11:99.
EVIDENCE SUMMARY
A systematic review and meta-analysis of prospective cohort studies evaluating infant risk factors for childhood obesity found that breastfeeding was associated with a lower risk of obesity.1 The authors identified 10 trials (primarily from the United States and Europe) with more than 76,000 infants that compared the effect of some breastfeeding in the first year to no breastfeeding. Follow-up ranged from 2 to 14 years (median 6 years).
Having ever breastfed decreased the odds of future overweight (BMI >85th percentile) or obesity (BMI >95th percentile) by 15% (adjusted odds ratio [AOR]=0.85; 95% confidence interval [CI], 0.74-0.99).
Subsequent studies suggest increased risk with formula feeding
Three large, prospective, longitudinal cohort studies have been published since the meta-analysis. One, which followed 43,367 term infants in Japan, found that formula feeding before 6 months was associated with increased risk of obesity compared with continuous breastfeeding for 6 months.2 Researchers evaluated weight at 7 years and adjusted for child and maternal factors associated with weight gain (AOR for obesity, formula-fed infants=1.8; 95% CI, 1.3-2.6).
A similar prospective longitudinal cohort study of 2868 infants in Australia analyzed maternal breastfeeding diaries and followed children’s weight to age 20 years.3 Introducing a milk other than breast milk before 6 months of age was linked to increased risk of obesity at age 20 (odds ratio [OR]=1.5; 95% CI, 1.1-1.9).
Finally, in a prospective cohort of 568 children in India, 17% of children who breastfed for fewer than 6 months were above the 90th percentile for weight at age 5 years, compared with 10% of children who were breastfed for at least 18 months.4 The result didn’t reach statistical significance, however (P=.08).
Interventions that increase breastfeeding don’t seem to have an impact
An RCT of an intervention to promote breastfeeding didn’t find any effect on subsequent obesity rates. Researchers in Belarus randomized 17,046 mother-infant pairs to breastfeeding promotion, modeled on the UNICEF Baby-Friendly Hospital Initiative, or usual care. The intervention increased the prevalence of exclusive breastfeeding (at 3 months, 43% vs 6%; at 6 months, 7% vs 0.6%; P values not given).
When researchers evaluated 13,879 children at 11 or 12 years by intention-to-treat analysis, however, they found no difference in mean BMI between the children whose mothers received the intervention and those whose mothers didn’t (BMI difference=0.16; 95% CI, -0.02 to 0.35).5
Introduction of solid foods: Later is better
A systematic review investigated the association between the timing of introducing complementary (solid) foods and childhood obesity in 23 primarily cross-sectional and cohort studies (17 from the United States, Canada, and Europe) with more than 33,000 patients. Follow-up ranged from 4 to 19 years.
Eight of the 21 studies that used BMI as an outcome found that early introduction of complementary foods was associated with a higher childhood BMI. In the largest study (a cohort of 17,561 infants), introducing complementary foods before 3 months was associated with higher risk of obesity at age 5 years than introducing them thereafter (OR=1.3; 95% CI, 1.1-1.6).6 Introduction of solids after 4 months was not associated with childhood obesity.
A systematic review of 10 primarily cross-sectional and cohort studies with more than 3000 infants evaluated associations between the types of complementary foods given and the development of childhood obesity.7 Six of the 10 studies were from Europe and none were from the United States. Follow-up ages ranged from 4 to 11 years.
Outcomes were heterogeneous, and no meta-analysis could be performed. The authors cited 3 studies (total 1174 infants) that found various positive associations between total caloric intake during complementary feeding and childhood obesity. No consistent evidence pointed to increased risk from specific foods or food groups.
Scheduled feeding is linked to rapid infant weight gain
A cohort study evaluated the baseline data of an Australian RCT (on an intervention to promote proper nutrition) in 612 infants, mean age 4.3 months.8 Researchers looked at the relationship between feeding on demand vs scheduled feeding (assessed by parental report) and weight gain in infancy. “Rapid weight gain” was defined as >0.67 change in weight-for-age Z-score between birth and enrollment.
Scheduled feeding was associated with rapid weight gain at a higher rate than feeding on demand (OR=2.3; 95% CI, 1.1-4.6). This study didn’t use childhood obesity as an outcome.
EVIDENCE SUMMARY
A systematic review and meta-analysis of prospective cohort studies evaluating infant risk factors for childhood obesity found that breastfeeding was associated with a lower risk of obesity.1 The authors identified 10 trials (primarily from the United States and Europe) with more than 76,000 infants that compared the effect of some breastfeeding in the first year to no breastfeeding. Follow-up ranged from 2 to 14 years (median 6 years).
Having ever breastfed decreased the odds of future overweight (BMI >85th percentile) or obesity (BMI >95th percentile) by 15% (adjusted odds ratio [AOR]=0.85; 95% confidence interval [CI], 0.74-0.99).
Subsequent studies suggest increased risk with formula feeding
Three large, prospective, longitudinal cohort studies have been published since the meta-analysis. One, which followed 43,367 term infants in Japan, found that formula feeding before 6 months was associated with increased risk of obesity compared with continuous breastfeeding for 6 months.2 Researchers evaluated weight at 7 years and adjusted for child and maternal factors associated with weight gain (AOR for obesity, formula-fed infants=1.8; 95% CI, 1.3-2.6).
A similar prospective longitudinal cohort study of 2868 infants in Australia analyzed maternal breastfeeding diaries and followed children’s weight to age 20 years.3 Introducing a milk other than breast milk before 6 months of age was linked to increased risk of obesity at age 20 (odds ratio [OR]=1.5; 95% CI, 1.1-1.9).
Finally, in a prospective cohort of 568 children in India, 17% of children who breastfed for fewer than 6 months were above the 90th percentile for weight at age 5 years, compared with 10% of children who were breastfed for at least 18 months.4 The result didn’t reach statistical significance, however (P=.08).
Interventions that increase breastfeeding don’t seem to have an impact
An RCT of an intervention to promote breastfeeding didn’t find any effect on subsequent obesity rates. Researchers in Belarus randomized 17,046 mother-infant pairs to breastfeeding promotion, modeled on the UNICEF Baby-Friendly Hospital Initiative, or usual care. The intervention increased the prevalence of exclusive breastfeeding (at 3 months, 43% vs 6%; at 6 months, 7% vs 0.6%; P values not given).
When researchers evaluated 13,879 children at 11 or 12 years by intention-to-treat analysis, however, they found no difference in mean BMI between the children whose mothers received the intervention and those whose mothers didn’t (BMI difference=0.16; 95% CI, -0.02 to 0.35).5
Introduction of solid foods: Later is better
A systematic review investigated the association between the timing of introducing complementary (solid) foods and childhood obesity in 23 primarily cross-sectional and cohort studies (17 from the United States, Canada, and Europe) with more than 33,000 patients. Follow-up ranged from 4 to 19 years.
Eight of the 21 studies that used BMI as an outcome found that early introduction of complementary foods was associated with a higher childhood BMI. In the largest study (a cohort of 17,561 infants), introducing complementary foods before 3 months was associated with higher risk of obesity at age 5 years than introducing them thereafter (OR=1.3; 95% CI, 1.1-1.6).6 Introduction of solids after 4 months was not associated with childhood obesity.
A systematic review of 10 primarily cross-sectional and cohort studies with more than 3000 infants evaluated associations between the types of complementary foods given and the development of childhood obesity.7 Six of the 10 studies were from Europe and none were from the United States. Follow-up ages ranged from 4 to 11 years.
Outcomes were heterogeneous, and no meta-analysis could be performed. The authors cited 3 studies (total 1174 infants) that found various positive associations between total caloric intake during complementary feeding and childhood obesity. No consistent evidence pointed to increased risk from specific foods or food groups.
Scheduled feeding is linked to rapid infant weight gain
A cohort study evaluated the baseline data of an Australian RCT (on an intervention to promote proper nutrition) in 612 infants, mean age 4.3 months.8 Researchers looked at the relationship between feeding on demand vs scheduled feeding (assessed by parental report) and weight gain in infancy. “Rapid weight gain” was defined as >0.67 change in weight-for-age Z-score between birth and enrollment.
Scheduled feeding was associated with rapid weight gain at a higher rate than feeding on demand (OR=2.3; 95% CI, 1.1-4.6). This study didn’t use childhood obesity as an outcome.
1. Weng SF, Redsell SA, Swift JA, et al. Systematic review and meta-analyses of risk factors for childhood overweight identifiable during infancy. Arch Dis Child. 2012;97:1019-1026.
2. Yamakawa M, Yorifuji T, Inoue S, et al. Breastfeeding and obesity among schoolchildren: a national longitudinal survey in Japan. JAMA Pediatr. 2013;167:919-925.
3. Oddy WH, Mari TA, Huang RC, et al. Early infant feeding and adiposity risk: from infancy to adulthood. Ann Nutr Metab. 2014;64:262-270.
4. Caleyachetty A, Krishnaveni GV, Veena SR, et al. Breast-feeding duration, age of starting solids, and high BMI risk and adiposity in Indian children. Matern Child Nutr. 2013;9:199-216.
5. Martin RM, Patel, R, Kramer MS, et al. Effects of promoting longer-term and exclusive breastfeeding on adiposity and insulin-like growth factor-I at age 11.5 years: a randomized trial. JAMA. 2013;309:1005-1013.
6. Pearce J, Taylor MA, Langley-Evans SC. Timing of the introduction of complementary feeding and risk of childhood obesity: a systematic review. Int J Obes (Lond). 2013;37:1295-1306.
7. Pearce J, Langley-Evans. The types of food introduced during complementary feeding and risk of childhood obesity: a systematic review. Int J Obes (Lond). 2013;37:477-485.
8. Mihrshahi S, Battistutta D, Magarey A, et al. Determinants of rapid weight gain during infancy: baseline results from the NOURISH randomised controlled trial. BMC Pediatr. 2011;11:99.
1. Weng SF, Redsell SA, Swift JA, et al. Systematic review and meta-analyses of risk factors for childhood overweight identifiable during infancy. Arch Dis Child. 2012;97:1019-1026.
2. Yamakawa M, Yorifuji T, Inoue S, et al. Breastfeeding and obesity among schoolchildren: a national longitudinal survey in Japan. JAMA Pediatr. 2013;167:919-925.
3. Oddy WH, Mari TA, Huang RC, et al. Early infant feeding and adiposity risk: from infancy to adulthood. Ann Nutr Metab. 2014;64:262-270.
4. Caleyachetty A, Krishnaveni GV, Veena SR, et al. Breast-feeding duration, age of starting solids, and high BMI risk and adiposity in Indian children. Matern Child Nutr. 2013;9:199-216.
5. Martin RM, Patel, R, Kramer MS, et al. Effects of promoting longer-term and exclusive breastfeeding on adiposity and insulin-like growth factor-I at age 11.5 years: a randomized trial. JAMA. 2013;309:1005-1013.
6. Pearce J, Taylor MA, Langley-Evans SC. Timing of the introduction of complementary feeding and risk of childhood obesity: a systematic review. Int J Obes (Lond). 2013;37:1295-1306.
7. Pearce J, Langley-Evans. The types of food introduced during complementary feeding and risk of childhood obesity: a systematic review. Int J Obes (Lond). 2013;37:477-485.
8. Mihrshahi S, Battistutta D, Magarey A, et al. Determinants of rapid weight gain during infancy: baseline results from the NOURISH randomised controlled trial. BMC Pediatr. 2011;11:99.
Evidence-based answers from the Family Physicians Inquiries Network
EVIDENCE-BASED ANSWER:
Yes. Ever having breastfed during the first year of life is associated with a 15% lower risk of overweight or obesity over the next 2 to 14 years compared with never having breastfed. Breastfeeding exclusively for 6 months is associated with a 30% to 50% reduction in risk (strength of recommendation [SOR]: B, meta-analysis of cohort studies and subsequent cohort studies). However, interventions that increase breastfeeding rates during the first 3 to 6 months of life don’t appear to alter body mass index (BMI) at 11 to 12 years of age (SOR: B, randomized clinical trial [RCT]).
Introducing complementary (solid) foods before 3 months is associated with a 30% greater risk of childhood obesity than later introduction; starting solid foods after 4 months isn’t linked to increased obesity. High caloric density of complementary feedings may be associated with greater childhood obesity (SOR: C, systematic reviews of heterogeneous cohort studies).
Scheduled feeding doubles the risk of rapid infant weight gain compared with on-demand feeding, although it’s unclear whether a direct relationship exists between rapid infant weight gain and childhood obesity (SOR: B, cohort study).

A more palatable alternative to oral rehydration therapy for kids
ILLUSTRATIVE CASE
A 3-year-old boy is brought by his mother to the office for vomiting and diarrhea that started in the middle of the night. On examination he is slightly dehydrated, but does not have an acute abdomen or other source of infection. He is drinking out of a sippy cup. What fluids should you recommend?
Acute gastroenteritis is a common cause of vomiting and/or diarrhea in children, leading to 1.5 million outpatient visits and 200,000 hospital admissions annually in the United States.2 Children with gastroenteritis are at risk for dehydration, and the recommended treatment for anything less than severe dehydration is oral rehydration therapy (ORT) and early resumption of feeding upon rehydration.2
In 2002, the World Health Organization recommended an ORT with an osmolarity of 245 mOsm/L.3 However, cultural preferences, cost,4 taste,5 availability, and caregiver and professional preference for intravenous hydration6-8 have all been barriers to the use of recommended ORT.2 In fact, a study of ORT preferences in 66 children ages 5 to 10 years found that fewer than half of the children would voluntarily drink the ORT again.5 This study evaluated the use of diluted apple juice as a more palatable alternative to ORT in children with vomiting and/or diarrhea.
STUDY SUMMARY
In kids older than 2, apple juice will do
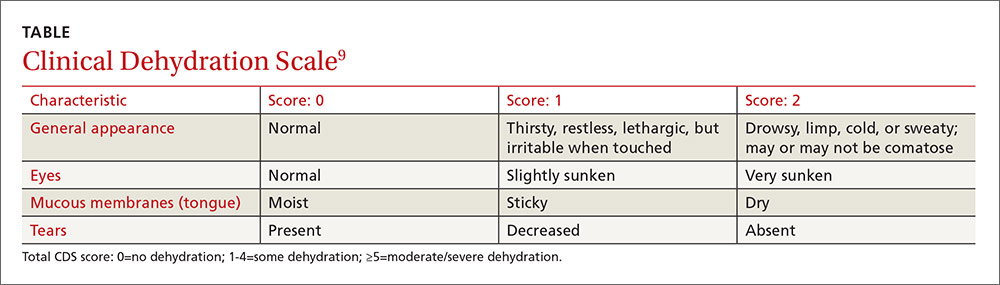
This study was a single-center, single-blind, non-inferiority randomized controlled trial conducted in the emergency department (ED) of a tertiary care pediatric hospital in Canada. The researchers compared the use of half-strength apple juice to a standard ORT for rehydration in simple gastroenteritis.1 Participants were 6 months to 5 years of age, weighed more than 8 kg (17.7 lbs), and had vomiting and/or diarrhea for less than 96 hours (with ≥3 episodes over the last 24 hours). They also had a Clinical Dehydration Scale (CDS) Score9 <5 and a capillary refill of <2 seconds (TABLE). Of the total, 68% of the children had a CDS score of 0, 25.5% scored 1 to 2; and 6.4% scored 3 to 4. Children with chronic gastrointestinal disease or other significant comorbidities that could affect the clinical state (eg, diabetes mellitus) and potential acute abdominal pathology were excluded.
Children were randomized to receive half-strength apple juice (AJ) (intervention group, n=323) or apple-flavored sucralose-sweetened Pediatric Electrolyte (Pharmascience) (control group, n=324), a common electrolyte maintenance solution (EMS). Immediately on triage, each child received 2 L of their assigned solution, to be used while in the ED and then at home. The children received 5 mL of fluid every 2 to 5 minutes. If a child vomited after starting the fluid, he or she was given oral ondansetron.
At discharge, caregivers were encouraged to replace 2 mL/kg of fluid for a vomiting episode and 10 mL/kg of fluid for a diarrhea episode. At home, children in the AJ group could also drink any other preferred fluid, including sports beverages. The EMS group was instructed to drink only the solution provided or a comparable ORT. Caregivers were contacted daily by phone until the child had no symptoms for 24 hours. They were also asked to keep a daily log of vomiting and diarrhea frequency and any subsequent health care visits. At least one follow-up contact occurred with 99.5% of the children.
The primary outcome was treatment failure defined as a composite measure of any of the following occurring within 7 days of the ED visit: hospitalization, intravenous rehydration, further health care visits for diarrhea/vomiting in any setting, protracted symptoms (ie, ≥3 episodes of vomiting or diarrhea within a 24-hour period occurring >7 days after enrollment), 3% or greater weight loss, or CDS score ≥5 at follow-up.
Treatment failure occurred in 16.7% of the AJ group compared to 25% of the EMS group (difference, -8.3%; 97.5% confidence interval [CI], -∞ to -2; number needed to treat [NNT]=12), consistent with non-inferior effectiveness. The benefit was seen primarily in children ≥24 months of age. In children <24 months, the treatment failure for AJ was 23.9% compared to 24.1% in the EMS group (P=not significant). In older children (≥24 months to 5 years), the treatment failure with AJ was 9.8% compared to 25.9% in the EMS group (difference, -16.2%; 95% CI, -24.2% to -8%; NNT=6.2). Intravenous rehydration in the ED or within 7 days of the initial visit was needed in 2.5% of the AJ group and in 9% of the EMS group (difference, -6.5%; 99% CI, -11.6% to -1.8%; NNT=15.4). There were no differences in hospitalization rate or in diarrhea or vomiting frequency between the 2 groups.
WHAT’S NEW
Kids drink more of what they like
This study, in a developed country, found rehydration with diluted apple juice worked just as well as ORT. In children ≥24 months of age, there were fewer treatment failures.
CAVEATS
Infants may not benefit,and ondansetron played a role
In this study, children were only mildly dehydrated. Also, the study did not include infants younger than 6 months of age, and the greatest benefit was in children ≥24 months of age.
Also noteworthy was the role that oral ondansetron played. Most (67.4%) of the children received an oral dose of ondansetron (0.1 mg/kg). Although expensive, if one dose prevents a hospitalization, it is cost-effective. Previous studies of oral ondansetron show it reduces vomiting (NNT=5); lowers the rate of intravenous hydration in the ED (NNT=5); and reduces the hospitalization rate from the ED (NNT=17).10
Lastly, there are a variety of fluid replacement guidelines. In this study, fluid replacement was 2 mL/kg for a vomiting episode and 10 mL/kg for a diarrhea episode.
CHALLENGES TO IMPLEMENTATION
Given the ease of swapping diluted apple juice for oral rehydration therapy, we see no barriers to implementation.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
1. Freedman SB, Willan AR, Boutis K, et al. Effect of dilute apple juice and preferred fluids vs electrolyte maintenance solution on treatment failure among children with mild gastroenteritis: a randomized clinical trial. JAMA. 2016;315:1966-1974.
2. King CK, Glass R, Bresee JS, et al. Managing acute gastroenteritis among children: oral rehydration, maintenance, and nutritional therapy. MMWR Recomm Rep. 2003;52:1-16.
3. Essential medicines and health products information portal. A World Health Organization resource. WHO Drug Information. 2002;16(2). Available at: http://apps.who.int/medicinedocs/en/d/Js4950e/2.4.html. Accessed October 20, 2016.
4. Cohen MB, Hardin J. Medicaid coverage of oral rehydration solutions. N Engl J Med. 1993;329:211.
5. Freedman SB, Cho D, Boutis K, et al. Assessing the palatability of oral rehydration solutions in school-aged children: a randomized crossover trial. Arch Pediatr Adolesc Med. 2010;164:696-702.
6. Reis EC, Goepp JG, Katz S, et al. Barriers to use of oral rehydration therapy. Pediatrics. 1994;93:708-711.
7. Karpas A, Finkelstein M, Reid S. Parental preference for rehydration method for children in the emergency department. Pediatr Emerg Care. 2009;25:301-306.
8. Ozuah PO, Avner JR, Stein RE. Oral rehydration, emergency physicians, and practice parameters: a national survey. Pediatrics. 2002;109:259-261.
9. Goldman RD, Friedman JN, Parkin PC. Validation of the clinical dehydration scale for children with acute gastroenteritis. Pediatrics. 2008;122:545-549.
10. Fedorowicz Z, Jagannath VA, Carter B. Antiemetics for reducing vomiting related to acute gastroenteritis in children and adolescents. Cochrane Database Syst Rev. 2011;CD005506.
ILLUSTRATIVE CASE
A 3-year-old boy is brought by his mother to the office for vomiting and diarrhea that started in the middle of the night. On examination he is slightly dehydrated, but does not have an acute abdomen or other source of infection. He is drinking out of a sippy cup. What fluids should you recommend?
Acute gastroenteritis is a common cause of vomiting and/or diarrhea in children, leading to 1.5 million outpatient visits and 200,000 hospital admissions annually in the United States.2 Children with gastroenteritis are at risk for dehydration, and the recommended treatment for anything less than severe dehydration is oral rehydration therapy (ORT) and early resumption of feeding upon rehydration.2
In 2002, the World Health Organization recommended an ORT with an osmolarity of 245 mOsm/L.3 However, cultural preferences, cost,4 taste,5 availability, and caregiver and professional preference for intravenous hydration6-8 have all been barriers to the use of recommended ORT.2 In fact, a study of ORT preferences in 66 children ages 5 to 10 years found that fewer than half of the children would voluntarily drink the ORT again.5 This study evaluated the use of diluted apple juice as a more palatable alternative to ORT in children with vomiting and/or diarrhea.
STUDY SUMMARY
In kids older than 2, apple juice will do
This study was a single-center, single-blind, non-inferiority randomized controlled trial conducted in the emergency department (ED) of a tertiary care pediatric hospital in Canada. The researchers compared the use of half-strength apple juice to a standard ORT for rehydration in simple gastroenteritis.1 Participants were 6 months to 5 years of age, weighed more than 8 kg (17.7 lbs), and had vomiting and/or diarrhea for less than 96 hours (with ≥3 episodes over the last 24 hours). They also had a Clinical Dehydration Scale (CDS) Score9 <5 and a capillary refill of <2 seconds (TABLE). Of the total, 68% of the children had a CDS score of 0, 25.5% scored 1 to 2; and 6.4% scored 3 to 4. Children with chronic gastrointestinal disease or other significant comorbidities that could affect the clinical state (eg, diabetes mellitus) and potential acute abdominal pathology were excluded.
Children were randomized to receive half-strength apple juice (AJ) (intervention group, n=323) or apple-flavored sucralose-sweetened Pediatric Electrolyte (Pharmascience) (control group, n=324), a common electrolyte maintenance solution (EMS). Immediately on triage, each child received 2 L of their assigned solution, to be used while in the ED and then at home. The children received 5 mL of fluid every 2 to 5 minutes. If a child vomited after starting the fluid, he or she was given oral ondansetron.
At discharge, caregivers were encouraged to replace 2 mL/kg of fluid for a vomiting episode and 10 mL/kg of fluid for a diarrhea episode. At home, children in the AJ group could also drink any other preferred fluid, including sports beverages. The EMS group was instructed to drink only the solution provided or a comparable ORT. Caregivers were contacted daily by phone until the child had no symptoms for 24 hours. They were also asked to keep a daily log of vomiting and diarrhea frequency and any subsequent health care visits. At least one follow-up contact occurred with 99.5% of the children.
The primary outcome was treatment failure defined as a composite measure of any of the following occurring within 7 days of the ED visit: hospitalization, intravenous rehydration, further health care visits for diarrhea/vomiting in any setting, protracted symptoms (ie, ≥3 episodes of vomiting or diarrhea within a 24-hour period occurring >7 days after enrollment), 3% or greater weight loss, or CDS score ≥5 at follow-up.
Treatment failure occurred in 16.7% of the AJ group compared to 25% of the EMS group (difference, -8.3%; 97.5% confidence interval [CI], -∞ to -2; number needed to treat [NNT]=12), consistent with non-inferior effectiveness. The benefit was seen primarily in children ≥24 months of age. In children <24 months, the treatment failure for AJ was 23.9% compared to 24.1% in the EMS group (P=not significant). In older children (≥24 months to 5 years), the treatment failure with AJ was 9.8% compared to 25.9% in the EMS group (difference, -16.2%; 95% CI, -24.2% to -8%; NNT=6.2). Intravenous rehydration in the ED or within 7 days of the initial visit was needed in 2.5% of the AJ group and in 9% of the EMS group (difference, -6.5%; 99% CI, -11.6% to -1.8%; NNT=15.4). There were no differences in hospitalization rate or in diarrhea or vomiting frequency between the 2 groups.
WHAT’S NEW
Kids drink more of what they like
This study, in a developed country, found rehydration with diluted apple juice worked just as well as ORT. In children ≥24 months of age, there were fewer treatment failures.
CAVEATS
Infants may not benefit,and ondansetron played a role
In this study, children were only mildly dehydrated. Also, the study did not include infants younger than 6 months of age, and the greatest benefit was in children ≥24 months of age.
Also noteworthy was the role that oral ondansetron played. Most (67.4%) of the children received an oral dose of ondansetron (0.1 mg/kg). Although expensive, if one dose prevents a hospitalization, it is cost-effective. Previous studies of oral ondansetron show it reduces vomiting (NNT=5); lowers the rate of intravenous hydration in the ED (NNT=5); and reduces the hospitalization rate from the ED (NNT=17).10
Lastly, there are a variety of fluid replacement guidelines. In this study, fluid replacement was 2 mL/kg for a vomiting episode and 10 mL/kg for a diarrhea episode.
CHALLENGES TO IMPLEMENTATION
Given the ease of swapping diluted apple juice for oral rehydration therapy, we see no barriers to implementation.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
ILLUSTRATIVE CASE
A 3-year-old boy is brought by his mother to the office for vomiting and diarrhea that started in the middle of the night. On examination he is slightly dehydrated, but does not have an acute abdomen or other source of infection. He is drinking out of a sippy cup. What fluids should you recommend?
Acute gastroenteritis is a common cause of vomiting and/or diarrhea in children, leading to 1.5 million outpatient visits and 200,000 hospital admissions annually in the United States.2 Children with gastroenteritis are at risk for dehydration, and the recommended treatment for anything less than severe dehydration is oral rehydration therapy (ORT) and early resumption of feeding upon rehydration.2
In 2002, the World Health Organization recommended an ORT with an osmolarity of 245 mOsm/L.3 However, cultural preferences, cost,4 taste,5 availability, and caregiver and professional preference for intravenous hydration6-8 have all been barriers to the use of recommended ORT.2 In fact, a study of ORT preferences in 66 children ages 5 to 10 years found that fewer than half of the children would voluntarily drink the ORT again.5 This study evaluated the use of diluted apple juice as a more palatable alternative to ORT in children with vomiting and/or diarrhea.
STUDY SUMMARY
In kids older than 2, apple juice will do
This study was a single-center, single-blind, non-inferiority randomized controlled trial conducted in the emergency department (ED) of a tertiary care pediatric hospital in Canada. The researchers compared the use of half-strength apple juice to a standard ORT for rehydration in simple gastroenteritis.1 Participants were 6 months to 5 years of age, weighed more than 8 kg (17.7 lbs), and had vomiting and/or diarrhea for less than 96 hours (with ≥3 episodes over the last 24 hours). They also had a Clinical Dehydration Scale (CDS) Score9 <5 and a capillary refill of <2 seconds (TABLE). Of the total, 68% of the children had a CDS score of 0, 25.5% scored 1 to 2; and 6.4% scored 3 to 4. Children with chronic gastrointestinal disease or other significant comorbidities that could affect the clinical state (eg, diabetes mellitus) and potential acute abdominal pathology were excluded.
Children were randomized to receive half-strength apple juice (AJ) (intervention group, n=323) or apple-flavored sucralose-sweetened Pediatric Electrolyte (Pharmascience) (control group, n=324), a common electrolyte maintenance solution (EMS). Immediately on triage, each child received 2 L of their assigned solution, to be used while in the ED and then at home. The children received 5 mL of fluid every 2 to 5 minutes. If a child vomited after starting the fluid, he or she was given oral ondansetron.
At discharge, caregivers were encouraged to replace 2 mL/kg of fluid for a vomiting episode and 10 mL/kg of fluid for a diarrhea episode. At home, children in the AJ group could also drink any other preferred fluid, including sports beverages. The EMS group was instructed to drink only the solution provided or a comparable ORT. Caregivers were contacted daily by phone until the child had no symptoms for 24 hours. They were also asked to keep a daily log of vomiting and diarrhea frequency and any subsequent health care visits. At least one follow-up contact occurred with 99.5% of the children.
The primary outcome was treatment failure defined as a composite measure of any of the following occurring within 7 days of the ED visit: hospitalization, intravenous rehydration, further health care visits for diarrhea/vomiting in any setting, protracted symptoms (ie, ≥3 episodes of vomiting or diarrhea within a 24-hour period occurring >7 days after enrollment), 3% or greater weight loss, or CDS score ≥5 at follow-up.
Treatment failure occurred in 16.7% of the AJ group compared to 25% of the EMS group (difference, -8.3%; 97.5% confidence interval [CI], -∞ to -2; number needed to treat [NNT]=12), consistent with non-inferior effectiveness. The benefit was seen primarily in children ≥24 months of age. In children <24 months, the treatment failure for AJ was 23.9% compared to 24.1% in the EMS group (P=not significant). In older children (≥24 months to 5 years), the treatment failure with AJ was 9.8% compared to 25.9% in the EMS group (difference, -16.2%; 95% CI, -24.2% to -8%; NNT=6.2). Intravenous rehydration in the ED or within 7 days of the initial visit was needed in 2.5% of the AJ group and in 9% of the EMS group (difference, -6.5%; 99% CI, -11.6% to -1.8%; NNT=15.4). There were no differences in hospitalization rate or in diarrhea or vomiting frequency between the 2 groups.
WHAT’S NEW
Kids drink more of what they like
This study, in a developed country, found rehydration with diluted apple juice worked just as well as ORT. In children ≥24 months of age, there were fewer treatment failures.
CAVEATS
Infants may not benefit,and ondansetron played a role
In this study, children were only mildly dehydrated. Also, the study did not include infants younger than 6 months of age, and the greatest benefit was in children ≥24 months of age.
Also noteworthy was the role that oral ondansetron played. Most (67.4%) of the children received an oral dose of ondansetron (0.1 mg/kg). Although expensive, if one dose prevents a hospitalization, it is cost-effective. Previous studies of oral ondansetron show it reduces vomiting (NNT=5); lowers the rate of intravenous hydration in the ED (NNT=5); and reduces the hospitalization rate from the ED (NNT=17).10
Lastly, there are a variety of fluid replacement guidelines. In this study, fluid replacement was 2 mL/kg for a vomiting episode and 10 mL/kg for a diarrhea episode.
CHALLENGES TO IMPLEMENTATION
Given the ease of swapping diluted apple juice for oral rehydration therapy, we see no barriers to implementation.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
1. Freedman SB, Willan AR, Boutis K, et al. Effect of dilute apple juice and preferred fluids vs electrolyte maintenance solution on treatment failure among children with mild gastroenteritis: a randomized clinical trial. JAMA. 2016;315:1966-1974.
2. King CK, Glass R, Bresee JS, et al. Managing acute gastroenteritis among children: oral rehydration, maintenance, and nutritional therapy. MMWR Recomm Rep. 2003;52:1-16.
3. Essential medicines and health products information portal. A World Health Organization resource. WHO Drug Information. 2002;16(2). Available at: http://apps.who.int/medicinedocs/en/d/Js4950e/2.4.html. Accessed October 20, 2016.
4. Cohen MB, Hardin J. Medicaid coverage of oral rehydration solutions. N Engl J Med. 1993;329:211.
5. Freedman SB, Cho D, Boutis K, et al. Assessing the palatability of oral rehydration solutions in school-aged children: a randomized crossover trial. Arch Pediatr Adolesc Med. 2010;164:696-702.
6. Reis EC, Goepp JG, Katz S, et al. Barriers to use of oral rehydration therapy. Pediatrics. 1994;93:708-711.
7. Karpas A, Finkelstein M, Reid S. Parental preference for rehydration method for children in the emergency department. Pediatr Emerg Care. 2009;25:301-306.
8. Ozuah PO, Avner JR, Stein RE. Oral rehydration, emergency physicians, and practice parameters: a national survey. Pediatrics. 2002;109:259-261.
9. Goldman RD, Friedman JN, Parkin PC. Validation of the clinical dehydration scale for children with acute gastroenteritis. Pediatrics. 2008;122:545-549.
10. Fedorowicz Z, Jagannath VA, Carter B. Antiemetics for reducing vomiting related to acute gastroenteritis in children and adolescents. Cochrane Database Syst Rev. 2011;CD005506.
1. Freedman SB, Willan AR, Boutis K, et al. Effect of dilute apple juice and preferred fluids vs electrolyte maintenance solution on treatment failure among children with mild gastroenteritis: a randomized clinical trial. JAMA. 2016;315:1966-1974.
2. King CK, Glass R, Bresee JS, et al. Managing acute gastroenteritis among children: oral rehydration, maintenance, and nutritional therapy. MMWR Recomm Rep. 2003;52:1-16.
3. Essential medicines and health products information portal. A World Health Organization resource. WHO Drug Information. 2002;16(2). Available at: http://apps.who.int/medicinedocs/en/d/Js4950e/2.4.html. Accessed October 20, 2016.
4. Cohen MB, Hardin J. Medicaid coverage of oral rehydration solutions. N Engl J Med. 1993;329:211.
5. Freedman SB, Cho D, Boutis K, et al. Assessing the palatability of oral rehydration solutions in school-aged children: a randomized crossover trial. Arch Pediatr Adolesc Med. 2010;164:696-702.
6. Reis EC, Goepp JG, Katz S, et al. Barriers to use of oral rehydration therapy. Pediatrics. 1994;93:708-711.
7. Karpas A, Finkelstein M, Reid S. Parental preference for rehydration method for children in the emergency department. Pediatr Emerg Care. 2009;25:301-306.
8. Ozuah PO, Avner JR, Stein RE. Oral rehydration, emergency physicians, and practice parameters: a national survey. Pediatrics. 2002;109:259-261.
9. Goldman RD, Friedman JN, Parkin PC. Validation of the clinical dehydration scale for children with acute gastroenteritis. Pediatrics. 2008;122:545-549.
10. Fedorowicz Z, Jagannath VA, Carter B. Antiemetics for reducing vomiting related to acute gastroenteritis in children and adolescents. Cochrane Database Syst Rev. 2011;CD005506.
Copyright © 2016. The Family Physicians Inquiries Network. All rights reserved.
PRACTICE CHANGER
Recommend that parents give half-strength apple juice to children ≥24 months of age who are minimally dehydrated following a case of simple viral gastroenteritis. The juice reduces the need for further interventions better than oral hydration therapy.
Freedman SB, Willan AR, Boutis K, et al. Effect of dilute apple juice and preferred fluids vs electrolyte maintenance solution on treatment failure among children with mild gastroenteritis: a randomized clinical trial. JAMA. 2016;315:1966-1974.1
STRENGTH OF RECOMMENDATION
B: Based on a single, good quality randomized controlled trial.

Pediatric update: 2 vaccine changes and the latest word on media time

Managing stress in children, parents can reduce obesity risk
SAN FRANCISCO – Obesity is a multifactorial problem, influenced by factors ranging from genetics to lifestyle to the environment. Yet stress can play an outsize role in obesity as well, Elizabeth Prout Parks, MD, said at the annual meeting of the American Academy of Pediatrics.
Although the calorie-in/calorie-out model of energy balance has driven much of the thought about obesity, it’s not that simple, suggested Dr. Parks, the medical director of the Healthy Weight Adolescent Bariatrics Program at the Children’s Hospital of Philadelphia. Physical activity accounts for an estimated 15%-30% of energy expenditure, and thermogenesis accounts for an estimated 10%. But the energy expenditure required for basal metabolism can range from 60% to 75%, a sufficiently wide range for significant variation across different individuals.
The psychosocial effects can lead to anxiety, depression, disordered eating behaviors such as emotional eating, a sedentary lifestyle, poor sleep, and low maintenance with self-care activities. Further, poor sleep on its own is additionally associated with childhood obesity. The combination of these physiologic and psychosocial effects can increase the risk of metabolic syndrome, type 2 diabetes, and cardiovascular disease or events. While acute stress and chronic stress follow similar pathways in the brain, it’s chronic stress that carries the greater risk of behavioral and physical conditions.
Measuring and understanding child and parental stress
Several clinical assessments can measure stress in children, including the Daily Hassles Scale, which looks at everyday interactions in the environment and factors such as children’s school, family, neighborhood, peers, and lack of resources. The Multidimensional Life Events Rating Questionnaire and Adolescent Stress Questionnaire both are more appropriate for middle school and older adolescents.
In children, the primary biologic indicators of stress are cortisol levels, heart rate, and blood pressure, but it is perceived stress that has been most clearly linked to emotional eating and other disordered eating behaviors, Dr. Parks said. One 2008 study found perceived stress to be associated with emotional eating among middle school students both with and without obesity. A high level of perceived stress in adolescents was associated with a greater waist circumference and body mass index in a 2009 study.
The findings are somewhat more mixed, however, when it comes to parental stress and child weight. A 2012 study identified a link between parents’ perception of their stress and increased fast food consumption in their children, and a 2008 study identified a link between parenting stress and both overweight and underweight children. Yet a different study in 2008 found no association between child obesity and parenting stress. Research in 2011 found a relationship between children’s consumption of fruits and vegetables and their family’s overall functioning, as well as parental psychological stress and child behavior. Within a family, stress can come from financial strain (such as poverty or changes in employment or insurance), the family’s structure, and changes in physical or mental health of one or more family members.
Addressing the effects of stress on diet
Clinicians can help families manage the ways stress can lead to obesity by helping them with ideas for increasing fruit and vegetable intake, and planning ahead for on-the-go eating. For example, to ensure children get in their recommended five servings of fruit and vegetables each day, parents can serve fruit with breakfast every day and offer vegetables and/or fruit as a snack. Including side salads and a frozen vegetable with dinner will add two more servings, and children can munch on chopped veggies while parents prepare dinner. Offering fruit as a dessert provides another opportunity to bump up kids’ fruit and veggie intake, Dr. Parks said.
To manage the risk of unhealthy eating when out and about, Dr. Parks recommends planning ahead by packing a snack such as yogurt, fruit and vegetables, a sandwich or wrap, and water.
She described the “apple test” for determining whether someone is eating because of boredom or stress or because of actual hunger.“The next time you are thinking about a mini meal or second helpings at a meal, ask yourself, ‘Would I eat an apple instead?’ ” Dr. Parks said. “If the answer is no, then you probably are not really hungry and just need to get away from food.”
Other things people can consider when about to eat something are whether they are actually hungry and whether a distraction such as the television is contributing to distracted eating. “People may eat when they’re happy, sad, or bored,” Dr. Parks said, noting that outside messages such as commercials, advertisements, and passing restaurants may make someone feel like eating even if they don’t need sustenance at that moment. “Consider whether you really are hungry before you eat,” she said.
Avoiding emotional eating and using mindfulness
Additionally, parents and children can avoid emotional eating by skipping the food when they feel angry, tired, nervous, bored, or sad, instead choosing activities such as journaling, taking a walk, listening to music, reading a book, or taking deep breaths while thinking pleasant thoughts. It’s only time to eat if you physically feel hungry, your stomach is rumbling, you are not craving some specific sweet or salty food, or it’s a meal or snack time (or at least 2.5-4 hours since the last time you ate).
Dr. Parks also reviewed ways that mindfulness may help reduce the risk of obesity by reducing stress, enhancing a person’s ability to regulate their everyday behaviors, and teaching individuals to accept discomfort. Another stress reduction strategy is repeated use of “4-7-8 breathing,” which begins with exhalation while the mouth is closed. Then, inhale through the nose for 4 seconds, hold the breath for 7 seconds and slowly exhale out the mouth for 8 seconds.
Reducing the risk of obesity from stress comes from learning to manage stress. Clinicians can play a role in helping both parents and children learn strategies to manage and cope with stress in the short term while developing resilience over the longer term and reducing the likelihood of poor eating and emotional eating.
Dr. Parks reported no disclosures.
SAN FRANCISCO – Obesity is a multifactorial problem, influenced by factors ranging from genetics to lifestyle to the environment. Yet stress can play an outsize role in obesity as well, Elizabeth Prout Parks, MD, said at the annual meeting of the American Academy of Pediatrics.
Although the calorie-in/calorie-out model of energy balance has driven much of the thought about obesity, it’s not that simple, suggested Dr. Parks, the medical director of the Healthy Weight Adolescent Bariatrics Program at the Children’s Hospital of Philadelphia. Physical activity accounts for an estimated 15%-30% of energy expenditure, and thermogenesis accounts for an estimated 10%. But the energy expenditure required for basal metabolism can range from 60% to 75%, a sufficiently wide range for significant variation across different individuals.
The psychosocial effects can lead to anxiety, depression, disordered eating behaviors such as emotional eating, a sedentary lifestyle, poor sleep, and low maintenance with self-care activities. Further, poor sleep on its own is additionally associated with childhood obesity. The combination of these physiologic and psychosocial effects can increase the risk of metabolic syndrome, type 2 diabetes, and cardiovascular disease or events. While acute stress and chronic stress follow similar pathways in the brain, it’s chronic stress that carries the greater risk of behavioral and physical conditions.
Measuring and understanding child and parental stress
Several clinical assessments can measure stress in children, including the Daily Hassles Scale, which looks at everyday interactions in the environment and factors such as children’s school, family, neighborhood, peers, and lack of resources. The Multidimensional Life Events Rating Questionnaire and Adolescent Stress Questionnaire both are more appropriate for middle school and older adolescents.
In children, the primary biologic indicators of stress are cortisol levels, heart rate, and blood pressure, but it is perceived stress that has been most clearly linked to emotional eating and other disordered eating behaviors, Dr. Parks said. One 2008 study found perceived stress to be associated with emotional eating among middle school students both with and without obesity. A high level of perceived stress in adolescents was associated with a greater waist circumference and body mass index in a 2009 study.
The findings are somewhat more mixed, however, when it comes to parental stress and child weight. A 2012 study identified a link between parents’ perception of their stress and increased fast food consumption in their children, and a 2008 study identified a link between parenting stress and both overweight and underweight children. Yet a different study in 2008 found no association between child obesity and parenting stress. Research in 2011 found a relationship between children’s consumption of fruits and vegetables and their family’s overall functioning, as well as parental psychological stress and child behavior. Within a family, stress can come from financial strain (such as poverty or changes in employment or insurance), the family’s structure, and changes in physical or mental health of one or more family members.
Addressing the effects of stress on diet
Clinicians can help families manage the ways stress can lead to obesity by helping them with ideas for increasing fruit and vegetable intake, and planning ahead for on-the-go eating. For example, to ensure children get in their recommended five servings of fruit and vegetables each day, parents can serve fruit with breakfast every day and offer vegetables and/or fruit as a snack. Including side salads and a frozen vegetable with dinner will add two more servings, and children can munch on chopped veggies while parents prepare dinner. Offering fruit as a dessert provides another opportunity to bump up kids’ fruit and veggie intake, Dr. Parks said.
To manage the risk of unhealthy eating when out and about, Dr. Parks recommends planning ahead by packing a snack such as yogurt, fruit and vegetables, a sandwich or wrap, and water.
She described the “apple test” for determining whether someone is eating because of boredom or stress or because of actual hunger.“The next time you are thinking about a mini meal or second helpings at a meal, ask yourself, ‘Would I eat an apple instead?’ ” Dr. Parks said. “If the answer is no, then you probably are not really hungry and just need to get away from food.”
Other things people can consider when about to eat something are whether they are actually hungry and whether a distraction such as the television is contributing to distracted eating. “People may eat when they’re happy, sad, or bored,” Dr. Parks said, noting that outside messages such as commercials, advertisements, and passing restaurants may make someone feel like eating even if they don’t need sustenance at that moment. “Consider whether you really are hungry before you eat,” she said.
Avoiding emotional eating and using mindfulness
Additionally, parents and children can avoid emotional eating by skipping the food when they feel angry, tired, nervous, bored, or sad, instead choosing activities such as journaling, taking a walk, listening to music, reading a book, or taking deep breaths while thinking pleasant thoughts. It’s only time to eat if you physically feel hungry, your stomach is rumbling, you are not craving some specific sweet or salty food, or it’s a meal or snack time (or at least 2.5-4 hours since the last time you ate).
Dr. Parks also reviewed ways that mindfulness may help reduce the risk of obesity by reducing stress, enhancing a person’s ability to regulate their everyday behaviors, and teaching individuals to accept discomfort. Another stress reduction strategy is repeated use of “4-7-8 breathing,” which begins with exhalation while the mouth is closed. Then, inhale through the nose for 4 seconds, hold the breath for 7 seconds and slowly exhale out the mouth for 8 seconds.
Reducing the risk of obesity from stress comes from learning to manage stress. Clinicians can play a role in helping both parents and children learn strategies to manage and cope with stress in the short term while developing resilience over the longer term and reducing the likelihood of poor eating and emotional eating.
Dr. Parks reported no disclosures.
SAN FRANCISCO – Obesity is a multifactorial problem, influenced by factors ranging from genetics to lifestyle to the environment. Yet stress can play an outsize role in obesity as well, Elizabeth Prout Parks, MD, said at the annual meeting of the American Academy of Pediatrics.
Although the calorie-in/calorie-out model of energy balance has driven much of the thought about obesity, it’s not that simple, suggested Dr. Parks, the medical director of the Healthy Weight Adolescent Bariatrics Program at the Children’s Hospital of Philadelphia. Physical activity accounts for an estimated 15%-30% of energy expenditure, and thermogenesis accounts for an estimated 10%. But the energy expenditure required for basal metabolism can range from 60% to 75%, a sufficiently wide range for significant variation across different individuals.
The psychosocial effects can lead to anxiety, depression, disordered eating behaviors such as emotional eating, a sedentary lifestyle, poor sleep, and low maintenance with self-care activities. Further, poor sleep on its own is additionally associated with childhood obesity. The combination of these physiologic and psychosocial effects can increase the risk of metabolic syndrome, type 2 diabetes, and cardiovascular disease or events. While acute stress and chronic stress follow similar pathways in the brain, it’s chronic stress that carries the greater risk of behavioral and physical conditions.
Measuring and understanding child and parental stress
Several clinical assessments can measure stress in children, including the Daily Hassles Scale, which looks at everyday interactions in the environment and factors such as children’s school, family, neighborhood, peers, and lack of resources. The Multidimensional Life Events Rating Questionnaire and Adolescent Stress Questionnaire both are more appropriate for middle school and older adolescents.
In children, the primary biologic indicators of stress are cortisol levels, heart rate, and blood pressure, but it is perceived stress that has been most clearly linked to emotional eating and other disordered eating behaviors, Dr. Parks said. One 2008 study found perceived stress to be associated with emotional eating among middle school students both with and without obesity. A high level of perceived stress in adolescents was associated with a greater waist circumference and body mass index in a 2009 study.
The findings are somewhat more mixed, however, when it comes to parental stress and child weight. A 2012 study identified a link between parents’ perception of their stress and increased fast food consumption in their children, and a 2008 study identified a link between parenting stress and both overweight and underweight children. Yet a different study in 2008 found no association between child obesity and parenting stress. Research in 2011 found a relationship between children’s consumption of fruits and vegetables and their family’s overall functioning, as well as parental psychological stress and child behavior. Within a family, stress can come from financial strain (such as poverty or changes in employment or insurance), the family’s structure, and changes in physical or mental health of one or more family members.
Addressing the effects of stress on diet
Clinicians can help families manage the ways stress can lead to obesity by helping them with ideas for increasing fruit and vegetable intake, and planning ahead for on-the-go eating. For example, to ensure children get in their recommended five servings of fruit and vegetables each day, parents can serve fruit with breakfast every day and offer vegetables and/or fruit as a snack. Including side salads and a frozen vegetable with dinner will add two more servings, and children can munch on chopped veggies while parents prepare dinner. Offering fruit as a dessert provides another opportunity to bump up kids’ fruit and veggie intake, Dr. Parks said.
To manage the risk of unhealthy eating when out and about, Dr. Parks recommends planning ahead by packing a snack such as yogurt, fruit and vegetables, a sandwich or wrap, and water.
She described the “apple test” for determining whether someone is eating because of boredom or stress or because of actual hunger.“The next time you are thinking about a mini meal or second helpings at a meal, ask yourself, ‘Would I eat an apple instead?’ ” Dr. Parks said. “If the answer is no, then you probably are not really hungry and just need to get away from food.”
Other things people can consider when about to eat something are whether they are actually hungry and whether a distraction such as the television is contributing to distracted eating. “People may eat when they’re happy, sad, or bored,” Dr. Parks said, noting that outside messages such as commercials, advertisements, and passing restaurants may make someone feel like eating even if they don’t need sustenance at that moment. “Consider whether you really are hungry before you eat,” she said.
Avoiding emotional eating and using mindfulness
Additionally, parents and children can avoid emotional eating by skipping the food when they feel angry, tired, nervous, bored, or sad, instead choosing activities such as journaling, taking a walk, listening to music, reading a book, or taking deep breaths while thinking pleasant thoughts. It’s only time to eat if you physically feel hungry, your stomach is rumbling, you are not craving some specific sweet or salty food, or it’s a meal or snack time (or at least 2.5-4 hours since the last time you ate).
Dr. Parks also reviewed ways that mindfulness may help reduce the risk of obesity by reducing stress, enhancing a person’s ability to regulate their everyday behaviors, and teaching individuals to accept discomfort. Another stress reduction strategy is repeated use of “4-7-8 breathing,” which begins with exhalation while the mouth is closed. Then, inhale through the nose for 4 seconds, hold the breath for 7 seconds and slowly exhale out the mouth for 8 seconds.
Reducing the risk of obesity from stress comes from learning to manage stress. Clinicians can play a role in helping both parents and children learn strategies to manage and cope with stress in the short term while developing resilience over the longer term and reducing the likelihood of poor eating and emotional eating.
Dr. Parks reported no disclosures.
Early paternal emotional involvement tied to children’s preadolescent behavior
Children whose fathers have a positive emotional response to parenting and provide a sense of security early on are less likely to exhibit behavioral problems at age 9, a cohort study of more than 13,000 children shows. However, the researchers found no association between behavioral problems and paternal involvement with child care and household tasks.
The researchers used data from the Avon Longitudinal Study of Parents and Children, a birth cohort study of children in southwest England that is also known as Children of the 90s. In this study, the children’s fathers completed questionnaires at 8 weeks (37 questions) and 8 months (21 questions) after the birth. They were asked to rate their level of agreement with 58 statements related to several issues, including direct care, household tasks, attitudes about parenting, and relationships with the child. The mothers were interviewed at child age 9 (N = 6,898) and 11 (N = 6,328) to determine the presence or absence of behavioral problems, which were measured via the total difficulties score of the Strengths and Difficulties Questionnaire.
Previous studies have tended toward the assumption that paternal involvement with the child is unidimensional, which might explain why other studies have not found a clear association with behavioral problems. This study is the first to look at paternal involvement as multidimensional, reported Charles Opondo, PhD, of the University of Oxford (England), and his colleagues (BMJ Open. 2016;6:e012034. doi: 10.1136/bmjopen-2016-012034).
The questions for fathers related to emotional response to the childhood, how often fathers participated in domestic and child care activity, and feelings of security about their paternal role.
Children of fathers who scored high on questions about emotional response were less likely to have behavioral problems at age 9 (odds ratio, 0.86; 95% confidence interval, 0.79-0.94; P = .001), as were children of fathers who scored high on their sense of security (OR, 0.87; 95% CI, 0.79-0.96; P = .006). The same patterns were true at age 11.
The impact of paternal involvement on mothers could be an important factor. “There is evidence that fathers’ involvement can also alleviate the impact of factors such as maternal depression, which are known to increase children’s risk of behavioral problems,” the researchers wrote.
Meanwhile, Dr. Opondo and his colleagues found no significant relationship between behavioral problems, and time spent in domestic and child care activity at either age.
“The findings of this research study suggest that it is psychological and emotional aspects of paternal involvement in a child’s infancy that are most powerful in influencing later child behavior and not the amount of time that fathers are engaged in child care or domestic tasks in the household,” Dr. Opondo and his colleagues said.
The researchers cited several limitations. The study was observational, for example, and could be subject to unobserved confounders. In addition, the study relied on self-reporting, which can produce bias.
The Policy Research Program in the Department of Health, England, funded the study. The authors reported having no financial disclosures.
Children whose fathers have a positive emotional response to parenting and provide a sense of security early on are less likely to exhibit behavioral problems at age 9, a cohort study of more than 13,000 children shows. However, the researchers found no association between behavioral problems and paternal involvement with child care and household tasks.
The researchers used data from the Avon Longitudinal Study of Parents and Children, a birth cohort study of children in southwest England that is also known as Children of the 90s. In this study, the children’s fathers completed questionnaires at 8 weeks (37 questions) and 8 months (21 questions) after the birth. They were asked to rate their level of agreement with 58 statements related to several issues, including direct care, household tasks, attitudes about parenting, and relationships with the child. The mothers were interviewed at child age 9 (N = 6,898) and 11 (N = 6,328) to determine the presence or absence of behavioral problems, which were measured via the total difficulties score of the Strengths and Difficulties Questionnaire.
Previous studies have tended toward the assumption that paternal involvement with the child is unidimensional, which might explain why other studies have not found a clear association with behavioral problems. This study is the first to look at paternal involvement as multidimensional, reported Charles Opondo, PhD, of the University of Oxford (England), and his colleagues (BMJ Open. 2016;6:e012034. doi: 10.1136/bmjopen-2016-012034).
The questions for fathers related to emotional response to the childhood, how often fathers participated in domestic and child care activity, and feelings of security about their paternal role.
Children of fathers who scored high on questions about emotional response were less likely to have behavioral problems at age 9 (odds ratio, 0.86; 95% confidence interval, 0.79-0.94; P = .001), as were children of fathers who scored high on their sense of security (OR, 0.87; 95% CI, 0.79-0.96; P = .006). The same patterns were true at age 11.
The impact of paternal involvement on mothers could be an important factor. “There is evidence that fathers’ involvement can also alleviate the impact of factors such as maternal depression, which are known to increase children’s risk of behavioral problems,” the researchers wrote.
Meanwhile, Dr. Opondo and his colleagues found no significant relationship between behavioral problems, and time spent in domestic and child care activity at either age.
“The findings of this research study suggest that it is psychological and emotional aspects of paternal involvement in a child’s infancy that are most powerful in influencing later child behavior and not the amount of time that fathers are engaged in child care or domestic tasks in the household,” Dr. Opondo and his colleagues said.
The researchers cited several limitations. The study was observational, for example, and could be subject to unobserved confounders. In addition, the study relied on self-reporting, which can produce bias.
The Policy Research Program in the Department of Health, England, funded the study. The authors reported having no financial disclosures.
Children whose fathers have a positive emotional response to parenting and provide a sense of security early on are less likely to exhibit behavioral problems at age 9, a cohort study of more than 13,000 children shows. However, the researchers found no association between behavioral problems and paternal involvement with child care and household tasks.
The researchers used data from the Avon Longitudinal Study of Parents and Children, a birth cohort study of children in southwest England that is also known as Children of the 90s. In this study, the children’s fathers completed questionnaires at 8 weeks (37 questions) and 8 months (21 questions) after the birth. They were asked to rate their level of agreement with 58 statements related to several issues, including direct care, household tasks, attitudes about parenting, and relationships with the child. The mothers were interviewed at child age 9 (N = 6,898) and 11 (N = 6,328) to determine the presence or absence of behavioral problems, which were measured via the total difficulties score of the Strengths and Difficulties Questionnaire.
Previous studies have tended toward the assumption that paternal involvement with the child is unidimensional, which might explain why other studies have not found a clear association with behavioral problems. This study is the first to look at paternal involvement as multidimensional, reported Charles Opondo, PhD, of the University of Oxford (England), and his colleagues (BMJ Open. 2016;6:e012034. doi: 10.1136/bmjopen-2016-012034).
The questions for fathers related to emotional response to the childhood, how often fathers participated in domestic and child care activity, and feelings of security about their paternal role.
Children of fathers who scored high on questions about emotional response were less likely to have behavioral problems at age 9 (odds ratio, 0.86; 95% confidence interval, 0.79-0.94; P = .001), as were children of fathers who scored high on their sense of security (OR, 0.87; 95% CI, 0.79-0.96; P = .006). The same patterns were true at age 11.
The impact of paternal involvement on mothers could be an important factor. “There is evidence that fathers’ involvement can also alleviate the impact of factors such as maternal depression, which are known to increase children’s risk of behavioral problems,” the researchers wrote.
Meanwhile, Dr. Opondo and his colleagues found no significant relationship between behavioral problems, and time spent in domestic and child care activity at either age.
“The findings of this research study suggest that it is psychological and emotional aspects of paternal involvement in a child’s infancy that are most powerful in influencing later child behavior and not the amount of time that fathers are engaged in child care or domestic tasks in the household,” Dr. Opondo and his colleagues said.
The researchers cited several limitations. The study was observational, for example, and could be subject to unobserved confounders. In addition, the study relied on self-reporting, which can produce bias.
The Policy Research Program in the Department of Health, England, funded the study. The authors reported having no financial disclosures.
Key clinical point:
Major finding: The children of fathers who reported strong emotional attachment and security as a parent had a lower risk of behavioral problems.
Data source: Cohort study of 14,440 children in southwest England.
Disclosures: The Policy Research Program in the Department of Health, England, funded the study. The authors reported having no financial disclosures.
The art of persuasion
With the advent of the Internet, many parents and teen patients come in armed with information and sometimes even a diagnosis. Much of our time is spent dispelling falsehoods that were posted on the Internet or clarifying information that was misinterpreted. Although generally more information is a good thing, too much false information can result in limiting health care.
Vaccine administration has suffered significantly because of this. With a simple Google search, you can find articles that do everything just short of proving that vaccines are harmful, and tear-jerking stories about children who were harmed by the administration of vaccines. Many sites – Vaxtruth.org, healthwyze.org, naturalnews.com – all present convincing data that would scare any concerned parent to not vaccinate their child. So how do medical professionals regain the trust of their parents and/or patients?

The strategies put forth by the Centers for Disease Control and Prevention for talking to parents about vaccines begin with listening.1 Many parents come with fears that are unfounded and unrealistic that can simply be discussed and resolved. Others present with information from the Internet that discourages vaccines or life experiences such as another family member who was thought to be harmed by vaccines; this discussion is more complex.
It is imperative to become familiar with the most popular information sources on the Internet so that you can speak directly to the validity of the source. As well, countering with a more reliable source will substantiate your position. Healthychildren.org2 is an excellent reference for the AAP recommendations and further references. Vaccinesafety.edu is an independent source that reviews vaccine safety and current research.

Being proactive also builds trust. Provide families with the list of ingredients (vaccinesafety.edu), what their role is in keeping vaccines safe (tell them to go to cdc.gov and search under “vaccines for parents”), and help them understand how vaccines work. Parents then see that you are well informed and are passionate about the health of their children. The AAP provides physicians with a tool kit for the HPV vaccine, and the CDC has an HPV tipsheet entitled “Addressing Parents’ Top Questions about HPV Vaccine” that gives suggestions for what you can say or that can save you time if you provide it while the family waits to be seen.
Probably the most important strategy is believing in what you’re doing. No matter what you’re promoting, if you truly believe in it, then you will encourage others to believe in it as well. This requires educating yourself on current research and recommendations, as well as what is being reported in the news so you can be armed with factual data when parents have questions.
Today, health care is a partnership, and we must embrace our role as educators to empower patients to make good choices for themselves as well as their families.
References
1. http://www.cdc.gov/vaccines/hcp/conversations/conv-materials.html
2. https://www.healthychildren.org/English/safety-prevention/immunizations/Pages/Vaccine-Safety-The-Facts.aspx
3. http://www.immunize.org
Dr. Pearce is a pediatrician in Frankfort, Ill. Email her at pdnews@frontlinemedcom.com.
With the advent of the Internet, many parents and teen patients come in armed with information and sometimes even a diagnosis. Much of our time is spent dispelling falsehoods that were posted on the Internet or clarifying information that was misinterpreted. Although generally more information is a good thing, too much false information can result in limiting health care.
Vaccine administration has suffered significantly because of this. With a simple Google search, you can find articles that do everything just short of proving that vaccines are harmful, and tear-jerking stories about children who were harmed by the administration of vaccines. Many sites – Vaxtruth.org, healthwyze.org, naturalnews.com – all present convincing data that would scare any concerned parent to not vaccinate their child. So how do medical professionals regain the trust of their parents and/or patients?
The strategies put forth by the Centers for Disease Control and Prevention for talking to parents about vaccines begin with listening.1 Many parents come with fears that are unfounded and unrealistic that can simply be discussed and resolved. Others present with information from the Internet that discourages vaccines or life experiences such as another family member who was thought to be harmed by vaccines; this discussion is more complex.
It is imperative to become familiar with the most popular information sources on the Internet so that you can speak directly to the validity of the source. As well, countering with a more reliable source will substantiate your position. Healthychildren.org2 is an excellent reference for the AAP recommendations and further references. Vaccinesafety.edu is an independent source that reviews vaccine safety and current research.
Being proactive also builds trust. Provide families with the list of ingredients (vaccinesafety.edu), what their role is in keeping vaccines safe (tell them to go to cdc.gov and search under “vaccines for parents”), and help them understand how vaccines work. Parents then see that you are well informed and are passionate about the health of their children. The AAP provides physicians with a tool kit for the HPV vaccine, and the CDC has an HPV tipsheet entitled “Addressing Parents’ Top Questions about HPV Vaccine” that gives suggestions for what you can say or that can save you time if you provide it while the family waits to be seen.
Probably the most important strategy is believing in what you’re doing. No matter what you’re promoting, if you truly believe in it, then you will encourage others to believe in it as well. This requires educating yourself on current research and recommendations, as well as what is being reported in the news so you can be armed with factual data when parents have questions.
Today, health care is a partnership, and we must embrace our role as educators to empower patients to make good choices for themselves as well as their families.
References
1. http://www.cdc.gov/vaccines/hcp/conversations/conv-materials.html
2. https://www.healthychildren.org/English/safety-prevention/immunizations/Pages/Vaccine-Safety-The-Facts.aspx
3. http://www.immunize.org
Dr. Pearce is a pediatrician in Frankfort, Ill. Email her at pdnews@frontlinemedcom.com.
With the advent of the Internet, many parents and teen patients come in armed with information and sometimes even a diagnosis. Much of our time is spent dispelling falsehoods that were posted on the Internet or clarifying information that was misinterpreted. Although generally more information is a good thing, too much false information can result in limiting health care.
Vaccine administration has suffered significantly because of this. With a simple Google search, you can find articles that do everything just short of proving that vaccines are harmful, and tear-jerking stories about children who were harmed by the administration of vaccines. Many sites – Vaxtruth.org, healthwyze.org, naturalnews.com – all present convincing data that would scare any concerned parent to not vaccinate their child. So how do medical professionals regain the trust of their parents and/or patients?
The strategies put forth by the Centers for Disease Control and Prevention for talking to parents about vaccines begin with listening.1 Many parents come with fears that are unfounded and unrealistic that can simply be discussed and resolved. Others present with information from the Internet that discourages vaccines or life experiences such as another family member who was thought to be harmed by vaccines; this discussion is more complex.
It is imperative to become familiar with the most popular information sources on the Internet so that you can speak directly to the validity of the source. As well, countering with a more reliable source will substantiate your position. Healthychildren.org2 is an excellent reference for the AAP recommendations and further references. Vaccinesafety.edu is an independent source that reviews vaccine safety and current research.
Being proactive also builds trust. Provide families with the list of ingredients (vaccinesafety.edu), what their role is in keeping vaccines safe (tell them to go to cdc.gov and search under “vaccines for parents”), and help them understand how vaccines work. Parents then see that you are well informed and are passionate about the health of their children. The AAP provides physicians with a tool kit for the HPV vaccine, and the CDC has an HPV tipsheet entitled “Addressing Parents’ Top Questions about HPV Vaccine” that gives suggestions for what you can say or that can save you time if you provide it while the family waits to be seen.
Probably the most important strategy is believing in what you’re doing. No matter what you’re promoting, if you truly believe in it, then you will encourage others to believe in it as well. This requires educating yourself on current research and recommendations, as well as what is being reported in the news so you can be armed with factual data when parents have questions.
Today, health care is a partnership, and we must embrace our role as educators to empower patients to make good choices for themselves as well as their families.
References
1. http://www.cdc.gov/vaccines/hcp/conversations/conv-materials.html
2. https://www.healthychildren.org/English/safety-prevention/immunizations/Pages/Vaccine-Safety-The-Facts.aspx
3. http://www.immunize.org
Dr. Pearce is a pediatrician in Frankfort, Ill. Email her at pdnews@frontlinemedcom.com.
Texas reports local Zika transmission
On Nov. 28, public health officials there reported a case of Zika virus in a Brownsville woman who hadn’t traveled to Mexico or any other area with active Zika transmission. Brownsville sits on the border of Mexico at the state’s southern tip, and is home to Aedes species mosquitoes known to carry the virus. The area had recently been sprayed for mosquitoes.
Zika’s telltale genetic thumbprint was found in the woman’s urine, but her blood was negative, so the virus could no longer be spread from her by mosquito. She was not pregnant. There are no other suspected cases of local transmission, according to Texas officials.
“We knew it was only a matter of time before we saw a Zika case spread by a mosquito in Texas,” John Hellerstedt, MD, commissioner of the Texas Department of State Health Services, said in a statement. “We still don’t believe the virus will become widespread in Texas, but there could be more cases, so people need to protect themselves from mosquito bites, especially in parts of the state that stay relatively warm in the fall and winter.”
The state public health officials recommend testing all pregnant women who have traveled – or who have sexual partners who have traveled – to areas with active Zika transmission. In addition to Mexico, the list includes Southeast Asia, Central and South America, the Caribbean, Cape Verde, and Pacific islands including Tonga, Samoa, and Papua New Guinea.
Texas officials also recommend antibody testing of pregnant women in southern Texas if they have two or more symptoms – fever, itchy rash, joint pain, and eye redness – and anyone statewide with at least three symptoms.
As of Nov. 23, a total of 4,444 Zika cases have been reported to the Centers for Disease Control and Prevention in U.S. states and the District of Columbia. Just 182 of those cases were the result of local spread by mosquitoes in Florida. Puerto Rico has reported nearly 32,000 locally-transmitted cases.
The 257 previously confirmed cases in Texas were all associated with travel. Most were in the Houston and Dallas–Fort Worth areas.
Local and state health officials are working with the CDC to pinpoint how and where the Brownsville infection occurred. Mosquitoes are being trapped, and workers are going door to door to educate people about Zika and request urine samples to screen for infection.
On Nov. 28, public health officials there reported a case of Zika virus in a Brownsville woman who hadn’t traveled to Mexico or any other area with active Zika transmission. Brownsville sits on the border of Mexico at the state’s southern tip, and is home to Aedes species mosquitoes known to carry the virus. The area had recently been sprayed for mosquitoes.
Zika’s telltale genetic thumbprint was found in the woman’s urine, but her blood was negative, so the virus could no longer be spread from her by mosquito. She was not pregnant. There are no other suspected cases of local transmission, according to Texas officials.
“We knew it was only a matter of time before we saw a Zika case spread by a mosquito in Texas,” John Hellerstedt, MD, commissioner of the Texas Department of State Health Services, said in a statement. “We still don’t believe the virus will become widespread in Texas, but there could be more cases, so people need to protect themselves from mosquito bites, especially in parts of the state that stay relatively warm in the fall and winter.”
The state public health officials recommend testing all pregnant women who have traveled – or who have sexual partners who have traveled – to areas with active Zika transmission. In addition to Mexico, the list includes Southeast Asia, Central and South America, the Caribbean, Cape Verde, and Pacific islands including Tonga, Samoa, and Papua New Guinea.
Texas officials also recommend antibody testing of pregnant women in southern Texas if they have two or more symptoms – fever, itchy rash, joint pain, and eye redness – and anyone statewide with at least three symptoms.
As of Nov. 23, a total of 4,444 Zika cases have been reported to the Centers for Disease Control and Prevention in U.S. states and the District of Columbia. Just 182 of those cases were the result of local spread by mosquitoes in Florida. Puerto Rico has reported nearly 32,000 locally-transmitted cases.
The 257 previously confirmed cases in Texas were all associated with travel. Most were in the Houston and Dallas–Fort Worth areas.
Local and state health officials are working with the CDC to pinpoint how and where the Brownsville infection occurred. Mosquitoes are being trapped, and workers are going door to door to educate people about Zika and request urine samples to screen for infection.
On Nov. 28, public health officials there reported a case of Zika virus in a Brownsville woman who hadn’t traveled to Mexico or any other area with active Zika transmission. Brownsville sits on the border of Mexico at the state’s southern tip, and is home to Aedes species mosquitoes known to carry the virus. The area had recently been sprayed for mosquitoes.
Zika’s telltale genetic thumbprint was found in the woman’s urine, but her blood was negative, so the virus could no longer be spread from her by mosquito. She was not pregnant. There are no other suspected cases of local transmission, according to Texas officials.
“We knew it was only a matter of time before we saw a Zika case spread by a mosquito in Texas,” John Hellerstedt, MD, commissioner of the Texas Department of State Health Services, said in a statement. “We still don’t believe the virus will become widespread in Texas, but there could be more cases, so people need to protect themselves from mosquito bites, especially in parts of the state that stay relatively warm in the fall and winter.”
The state public health officials recommend testing all pregnant women who have traveled – or who have sexual partners who have traveled – to areas with active Zika transmission. In addition to Mexico, the list includes Southeast Asia, Central and South America, the Caribbean, Cape Verde, and Pacific islands including Tonga, Samoa, and Papua New Guinea.
Texas officials also recommend antibody testing of pregnant women in southern Texas if they have two or more symptoms – fever, itchy rash, joint pain, and eye redness – and anyone statewide with at least three symptoms.
As of Nov. 23, a total of 4,444 Zika cases have been reported to the Centers for Disease Control and Prevention in U.S. states and the District of Columbia. Just 182 of those cases were the result of local spread by mosquitoes in Florida. Puerto Rico has reported nearly 32,000 locally-transmitted cases.
The 257 previously confirmed cases in Texas were all associated with travel. Most were in the Houston and Dallas–Fort Worth areas.
Local and state health officials are working with the CDC to pinpoint how and where the Brownsville infection occurred. Mosquitoes are being trapped, and workers are going door to door to educate people about Zika and request urine samples to screen for infection.
Recognizing, addressing giftedness can be challenging
SAN FRANCISCO – Gifted children are far too commonly misunderstood, mislabeled, and misdiagnosed, leading to a mismatch between their needs and others’ perceptions of their needs, Dan Peters, PhD, a licensed psychologist and executive director of the Summit Center in the greater San Francisco and Los Angeles areas, explained at the annual meeting of the American Academy of Pediatrics.
Too often, one or more of these children’s health, developmental, social-emotional or learning needs are overlooked, or they receive an inappropriate mental health, developmental and/or learning disorder diagnosis. In fact, many of the risk factors for giftedness resemble those of other conditions: underachievement, difficulties with peers, social isolation, power struggles, perfectionism, anxiety, and depression.
Further, those who are culturally or linguistically diverse may not be recognized if a non-English first language obscures their performance ability or their socioeconomic status or lack of resources and enrichment opportunities leads them to be overlooked. It’s therefore important that practitioners understand what giftedness actually is and the characteristics gifted children might exhibit.
Understanding giftedness
A simple definition of giftedness is demonstrating a performance or the capacity for performance that significantly exceeds age or grade-level expectations, according to one school district’s gifted and talented education program.
A more involved description provided by the Columbus Group in 1991 defines giftedness as an “asynchronous development in which advanced cognitive abilities and heightened intensity combine to create inner experiences and awareness that are qualitatively different from the norm.” This asynchrony increases with higher intellectual capacity, they wrote. “The uniqueness of the gifted renders them vulnerable and requires modifications in parenting, teaching, and counseling in order for them to develop optimally.”
The level of a child’s giftedness makes a difference in their needs as well; these levels include advanced learners (IQ of 120-129), moderately gifted (130-144), highly gifted (145-159), exceptionally gifted (160-179), and profoundly gifted (180 and greater). Different spheres of giftedness can include intellectual ability, creative or productive thinking, leadership ability, and visual or performing arts. Consider the list of common characteristics of gifted children that Dr. Peters provided:
- Rapid learners.
- Strong memory.
- Large vocabulary.
- Advanced comprehension of nuances.
- Largely self-taught.
- Unusual emotional depth.
- Abstract/complex/logical/insightful thinking.
- Idealism and a sense of justice.
- Intense feelings and reactions.
- Highly sensitive.
- Long attention span and persistence.
- Preoccupied with own thoughts.
- Impatient with self and others’ inabilities and slowness.
- Asks probing questions (able to go beyond what is taught).
- Wide range of interests.
- Highly developed curiosity.
- Interest in experimenting and doing things differently.
- Divergent thinking.
- Keen and unusual sense of humor.
Dr. Peters cited Kazimierz Dabrowski, MD, PhD, a Polish psychiatrist of the mid-20th century, as explaining the sensitivity and intensity experienced by many gifted individuals in terms of overexcitabilities – a “greater capacity to be stimulated by and respond to external and internal stimuli.”
“Overexcitability permeates a gifted person’s existence and gives energy to their intelligence, talents, and personality,” Dr. Peters explained of Dabrowski’s ideas. This enhancement manifests in psychomotor terms as a strong drive, a lot of energy or movement, or extended bouts of activity. Intellectually, gifted children have an “insatiable curiosity, and voracious appetite and capacity for intellectual effort and stimulation,” Dr. Peters said. They may have heightened sensual experience in seeing, smelling, tasting, touching, or hearing, and they have an active imaginary and fantasy life. They also exhibit a capacity for great emotional depth and empathy – they deeply feel their own and others’ emotions.
How giftedness can be misdiagnosed
It is the combination of these very characteristics that can lead gifted children to receive an inappropriate mental or developmental diagnosis instead of being recognized as gifted.
“By current estimates, at any given time, approximately 11%-20% of children in the United States have a behavioral or emotional disorder as defined in the DSM-5,” Dr. Peters cited. Further, one study found that diagnoses of attention-deficit/hyperactivity disorder have increased 66% between 2000 and 2010, with 90% of those children taking psychostimulant medications – yet a study in the Journal of Health Economics estimated that one in five children diagnosed with ADHD are probably misdiagnosed and are receiving those medications.
Other incorrect diagnoses besides ADHD that gifted youth may commonly receive include anger diagnoses, ideational or anxiety disorders, developmental and personality disorders, mood disorders, and learning disorders.
Twice exceptionalism (2e)
Even more challenging are twice exceptional children, or 2e, those who are both gifted and have a learning or emotional disability or challenge. Common dual diagnoses in gifted children include anxiety disorders, depression (or existential depression), sleep disorders (such as nightmares, night terrors, or sleep walking), allergies, asthma, ADHD, oppositional-defiant disorder, obsessive-compulsive personality disorder, autism spectrum disorder, nonverbal learning disability, social/pragmatic communication disorder, and learning disorders such as dyslexia, dyscalculia, central auditory processing disorder, or sensory-motor integration disorder.
“It’s very complex. What happens is, a lot of people think you’re either gifted or not,” Dr. Peters said. “In the classroom, sometimes the advanced ability overshadows the weakness and so we get a lot of readers with an IQ of 130-150 and reading at the 50% percentile, and everyone says they’re fine, but they’re dyslexic.”
Other times, the weakness overshadows the strength, and sometimes they’re right in the middle where neither their giftedness nor their disability is recognized or addressed, Peters said. 2e children are very difficult to diagnose but also at higher risk for difficulties if one or both (or more) of their diagnoses are missed.
Maximizing gifted children’s developmental potential
Pediatricians have an opportunity to support gifted children by recognizing and accepting them for who they are, while also acknowledging that they want to feel “normal,” and therefore need extra reassurance and support from adults. Pediatricians should seek information about giftedness and 2e children from state and national gifted organizations, and, in the office, frame conversations with families and children’s differential diagnoses in terms of a child’s giftedness. If a pediatrician is themself gifted, they may be “a supportive and kindred spirit” to the child, Dr. Peters said.
In daily life, as well, gifted children need to be accepted for who they are, provided opportunities to be with their intellectual and academic peers, and provided challenges in their areas of strength, interests, or passions. Parents and teachers should follow their lead in learning: Keep up the pace for those who want to learn fast, and go deeper for those who want slower, more in-depth learning. Adults also need to understand their intensities and sensitivities and lead with their strengths in discussions.
Dr. Peters reported no disclosures.
SAN FRANCISCO – Gifted children are far too commonly misunderstood, mislabeled, and misdiagnosed, leading to a mismatch between their needs and others’ perceptions of their needs, Dan Peters, PhD, a licensed psychologist and executive director of the Summit Center in the greater San Francisco and Los Angeles areas, explained at the annual meeting of the American Academy of Pediatrics.
Too often, one or more of these children’s health, developmental, social-emotional or learning needs are overlooked, or they receive an inappropriate mental health, developmental and/or learning disorder diagnosis. In fact, many of the risk factors for giftedness resemble those of other conditions: underachievement, difficulties with peers, social isolation, power struggles, perfectionism, anxiety, and depression.
Further, those who are culturally or linguistically diverse may not be recognized if a non-English first language obscures their performance ability or their socioeconomic status or lack of resources and enrichment opportunities leads them to be overlooked. It’s therefore important that practitioners understand what giftedness actually is and the characteristics gifted children might exhibit.
Understanding giftedness
A simple definition of giftedness is demonstrating a performance or the capacity for performance that significantly exceeds age or grade-level expectations, according to one school district’s gifted and talented education program.
A more involved description provided by the Columbus Group in 1991 defines giftedness as an “asynchronous development in which advanced cognitive abilities and heightened intensity combine to create inner experiences and awareness that are qualitatively different from the norm.” This asynchrony increases with higher intellectual capacity, they wrote. “The uniqueness of the gifted renders them vulnerable and requires modifications in parenting, teaching, and counseling in order for them to develop optimally.”
The level of a child’s giftedness makes a difference in their needs as well; these levels include advanced learners (IQ of 120-129), moderately gifted (130-144), highly gifted (145-159), exceptionally gifted (160-179), and profoundly gifted (180 and greater). Different spheres of giftedness can include intellectual ability, creative or productive thinking, leadership ability, and visual or performing arts. Consider the list of common characteristics of gifted children that Dr. Peters provided:
- Rapid learners.
- Strong memory.
- Large vocabulary.
- Advanced comprehension of nuances.
- Largely self-taught.
- Unusual emotional depth.
- Abstract/complex/logical/insightful thinking.
- Idealism and a sense of justice.
- Intense feelings and reactions.
- Highly sensitive.
- Long attention span and persistence.
- Preoccupied with own thoughts.
- Impatient with self and others’ inabilities and slowness.
- Asks probing questions (able to go beyond what is taught).
- Wide range of interests.
- Highly developed curiosity.
- Interest in experimenting and doing things differently.
- Divergent thinking.
- Keen and unusual sense of humor.
Dr. Peters cited Kazimierz Dabrowski, MD, PhD, a Polish psychiatrist of the mid-20th century, as explaining the sensitivity and intensity experienced by many gifted individuals in terms of overexcitabilities – a “greater capacity to be stimulated by and respond to external and internal stimuli.”
“Overexcitability permeates a gifted person’s existence and gives energy to their intelligence, talents, and personality,” Dr. Peters explained of Dabrowski’s ideas. This enhancement manifests in psychomotor terms as a strong drive, a lot of energy or movement, or extended bouts of activity. Intellectually, gifted children have an “insatiable curiosity, and voracious appetite and capacity for intellectual effort and stimulation,” Dr. Peters said. They may have heightened sensual experience in seeing, smelling, tasting, touching, or hearing, and they have an active imaginary and fantasy life. They also exhibit a capacity for great emotional depth and empathy – they deeply feel their own and others’ emotions.
How giftedness can be misdiagnosed
It is the combination of these very characteristics that can lead gifted children to receive an inappropriate mental or developmental diagnosis instead of being recognized as gifted.
“By current estimates, at any given time, approximately 11%-20% of children in the United States have a behavioral or emotional disorder as defined in the DSM-5,” Dr. Peters cited. Further, one study found that diagnoses of attention-deficit/hyperactivity disorder have increased 66% between 2000 and 2010, with 90% of those children taking psychostimulant medications – yet a study in the Journal of Health Economics estimated that one in five children diagnosed with ADHD are probably misdiagnosed and are receiving those medications.
Other incorrect diagnoses besides ADHD that gifted youth may commonly receive include anger diagnoses, ideational or anxiety disorders, developmental and personality disorders, mood disorders, and learning disorders.
Twice exceptionalism (2e)
Even more challenging are twice exceptional children, or 2e, those who are both gifted and have a learning or emotional disability or challenge. Common dual diagnoses in gifted children include anxiety disorders, depression (or existential depression), sleep disorders (such as nightmares, night terrors, or sleep walking), allergies, asthma, ADHD, oppositional-defiant disorder, obsessive-compulsive personality disorder, autism spectrum disorder, nonverbal learning disability, social/pragmatic communication disorder, and learning disorders such as dyslexia, dyscalculia, central auditory processing disorder, or sensory-motor integration disorder.
“It’s very complex. What happens is, a lot of people think you’re either gifted or not,” Dr. Peters said. “In the classroom, sometimes the advanced ability overshadows the weakness and so we get a lot of readers with an IQ of 130-150 and reading at the 50% percentile, and everyone says they’re fine, but they’re dyslexic.”
Other times, the weakness overshadows the strength, and sometimes they’re right in the middle where neither their giftedness nor their disability is recognized or addressed, Peters said. 2e children are very difficult to diagnose but also at higher risk for difficulties if one or both (or more) of their diagnoses are missed.
Maximizing gifted children’s developmental potential
Pediatricians have an opportunity to support gifted children by recognizing and accepting them for who they are, while also acknowledging that they want to feel “normal,” and therefore need extra reassurance and support from adults. Pediatricians should seek information about giftedness and 2e children from state and national gifted organizations, and, in the office, frame conversations with families and children’s differential diagnoses in terms of a child’s giftedness. If a pediatrician is themself gifted, they may be “a supportive and kindred spirit” to the child, Dr. Peters said.
In daily life, as well, gifted children need to be accepted for who they are, provided opportunities to be with their intellectual and academic peers, and provided challenges in their areas of strength, interests, or passions. Parents and teachers should follow their lead in learning: Keep up the pace for those who want to learn fast, and go deeper for those who want slower, more in-depth learning. Adults also need to understand their intensities and sensitivities and lead with their strengths in discussions.
Dr. Peters reported no disclosures.
SAN FRANCISCO – Gifted children are far too commonly misunderstood, mislabeled, and misdiagnosed, leading to a mismatch between their needs and others’ perceptions of their needs, Dan Peters, PhD, a licensed psychologist and executive director of the Summit Center in the greater San Francisco and Los Angeles areas, explained at the annual meeting of the American Academy of Pediatrics.
Too often, one or more of these children’s health, developmental, social-emotional or learning needs are overlooked, or they receive an inappropriate mental health, developmental and/or learning disorder diagnosis. In fact, many of the risk factors for giftedness resemble those of other conditions: underachievement, difficulties with peers, social isolation, power struggles, perfectionism, anxiety, and depression.
Further, those who are culturally or linguistically diverse may not be recognized if a non-English first language obscures their performance ability or their socioeconomic status or lack of resources and enrichment opportunities leads them to be overlooked. It’s therefore important that practitioners understand what giftedness actually is and the characteristics gifted children might exhibit.
Understanding giftedness
A simple definition of giftedness is demonstrating a performance or the capacity for performance that significantly exceeds age or grade-level expectations, according to one school district’s gifted and talented education program.
A more involved description provided by the Columbus Group in 1991 defines giftedness as an “asynchronous development in which advanced cognitive abilities and heightened intensity combine to create inner experiences and awareness that are qualitatively different from the norm.” This asynchrony increases with higher intellectual capacity, they wrote. “The uniqueness of the gifted renders them vulnerable and requires modifications in parenting, teaching, and counseling in order for them to develop optimally.”
The level of a child’s giftedness makes a difference in their needs as well; these levels include advanced learners (IQ of 120-129), moderately gifted (130-144), highly gifted (145-159), exceptionally gifted (160-179), and profoundly gifted (180 and greater). Different spheres of giftedness can include intellectual ability, creative or productive thinking, leadership ability, and visual or performing arts. Consider the list of common characteristics of gifted children that Dr. Peters provided:
- Rapid learners.
- Strong memory.
- Large vocabulary.
- Advanced comprehension of nuances.
- Largely self-taught.
- Unusual emotional depth.
- Abstract/complex/logical/insightful thinking.
- Idealism and a sense of justice.
- Intense feelings and reactions.
- Highly sensitive.
- Long attention span and persistence.
- Preoccupied with own thoughts.
- Impatient with self and others’ inabilities and slowness.
- Asks probing questions (able to go beyond what is taught).
- Wide range of interests.
- Highly developed curiosity.
- Interest in experimenting and doing things differently.
- Divergent thinking.
- Keen and unusual sense of humor.
Dr. Peters cited Kazimierz Dabrowski, MD, PhD, a Polish psychiatrist of the mid-20th century, as explaining the sensitivity and intensity experienced by many gifted individuals in terms of overexcitabilities – a “greater capacity to be stimulated by and respond to external and internal stimuli.”
“Overexcitability permeates a gifted person’s existence and gives energy to their intelligence, talents, and personality,” Dr. Peters explained of Dabrowski’s ideas. This enhancement manifests in psychomotor terms as a strong drive, a lot of energy or movement, or extended bouts of activity. Intellectually, gifted children have an “insatiable curiosity, and voracious appetite and capacity for intellectual effort and stimulation,” Dr. Peters said. They may have heightened sensual experience in seeing, smelling, tasting, touching, or hearing, and they have an active imaginary and fantasy life. They also exhibit a capacity for great emotional depth and empathy – they deeply feel their own and others’ emotions.
How giftedness can be misdiagnosed
It is the combination of these very characteristics that can lead gifted children to receive an inappropriate mental or developmental diagnosis instead of being recognized as gifted.
“By current estimates, at any given time, approximately 11%-20% of children in the United States have a behavioral or emotional disorder as defined in the DSM-5,” Dr. Peters cited. Further, one study found that diagnoses of attention-deficit/hyperactivity disorder have increased 66% between 2000 and 2010, with 90% of those children taking psychostimulant medications – yet a study in the Journal of Health Economics estimated that one in five children diagnosed with ADHD are probably misdiagnosed and are receiving those medications.
Other incorrect diagnoses besides ADHD that gifted youth may commonly receive include anger diagnoses, ideational or anxiety disorders, developmental and personality disorders, mood disorders, and learning disorders.
Twice exceptionalism (2e)
Even more challenging are twice exceptional children, or 2e, those who are both gifted and have a learning or emotional disability or challenge. Common dual diagnoses in gifted children include anxiety disorders, depression (or existential depression), sleep disorders (such as nightmares, night terrors, or sleep walking), allergies, asthma, ADHD, oppositional-defiant disorder, obsessive-compulsive personality disorder, autism spectrum disorder, nonverbal learning disability, social/pragmatic communication disorder, and learning disorders such as dyslexia, dyscalculia, central auditory processing disorder, or sensory-motor integration disorder.
“It’s very complex. What happens is, a lot of people think you’re either gifted or not,” Dr. Peters said. “In the classroom, sometimes the advanced ability overshadows the weakness and so we get a lot of readers with an IQ of 130-150 and reading at the 50% percentile, and everyone says they’re fine, but they’re dyslexic.”
Other times, the weakness overshadows the strength, and sometimes they’re right in the middle where neither their giftedness nor their disability is recognized or addressed, Peters said. 2e children are very difficult to diagnose but also at higher risk for difficulties if one or both (or more) of their diagnoses are missed.
Maximizing gifted children’s developmental potential
Pediatricians have an opportunity to support gifted children by recognizing and accepting them for who they are, while also acknowledging that they want to feel “normal,” and therefore need extra reassurance and support from adults. Pediatricians should seek information about giftedness and 2e children from state and national gifted organizations, and, in the office, frame conversations with families and children’s differential diagnoses in terms of a child’s giftedness. If a pediatrician is themself gifted, they may be “a supportive and kindred spirit” to the child, Dr. Peters said.
In daily life, as well, gifted children need to be accepted for who they are, provided opportunities to be with their intellectual and academic peers, and provided challenges in their areas of strength, interests, or passions. Parents and teachers should follow their lead in learning: Keep up the pace for those who want to learn fast, and go deeper for those who want slower, more in-depth learning. Adults also need to understand their intensities and sensitivities and lead with their strengths in discussions.
Dr. Peters reported no disclosures.
EXPERT ANALYSIS FROM AAP 16
Adding metronomic chemo provides no benefit to MAP for osteosarcoma
Adding low-dose metronomic chemotherapy (oral cyclophosphamide and methotrexate) to standard methotrexate, adriamycin, and platinum (MAP) maintenance treatment did not extend event-free survival in adolescents and young adults with high-grade, resectable osteosarcoma of the extremities, according to investigators.
“In pediatric tumors such as localized osteosarcomas, in situ tumor angiogenesis and levels of circulating angiogenic factors correlate with metastatic disease and a poor prognosis,” noted Andreza A. Senerchia, MD, of the Institute of Pediatric Oncology/Support Group for Adolescents and Children With Cancer, Federal University of Sao Paulo (Brazil), and her associates.
Since metronomic chemotherapy can prevent tumor angiogenesis and is a readily available, low-cost treatment with low toxicity, it could serve as a useful add-on to established MAP maintenance therapy in this patient population, they speculated.
The investigators assessed this approach in a prospective clinical trial involving 296 patients aged younger than 30 (mean age, 14 years; range, 0-29 years) who were treated at 27 medical centers in Brazil, Argentina, and Uruguay. All the study participants had high-grade but nonmetastatic operable osteosarcomas of the extremities, and all underwent preoperative chemotherapy followed by surgical resection, with limb salvage whenever possible.
A total of 139 patients were then randomly assigned to receive MAP plus metronomic chemotherapy (intervention group) and 157 to receive MAP alone (control group). However, 35% of the intervention group never started metronomic chemotherapy for a variety of reasons, and another 10% stopped the treatment very early.
At 5 years, cumulative event-free survival was 61% with MAP plus metronomic chemotherapy and 64% with MAP alone, a nonsignificant difference. When the analysis was restricted to only the patients in the intervention group who actually received metronomic chemotherapy, there still was no evidence that the add-on treatment made any difference in event-free survival. Similarly, mean overall survival was not significantly different between the two study groups, at 76% and 73%, respectively, Dr. Senerchia and her associates wrote (Cancer 2016 Nov 7. doi: 10.1002/cncr.30411).
There were 27 deaths (19%) in the intervention group, 81% of which were due to disease progression and 11% of which were due to treatment-related toxicity. Similarly, there were 24 deaths (15%) in the control group, of which 83% were due to disease progression and 17% to treatment-related toxicity.
These findings “do not support the routine use of cyclophosphamide and methotrexate as metronomic agents after standard chemotherapy for nonmetastatic osteosarcoma. However, our results should not preclude further investigation into the potential of maintenance for patients with osteosarcoma ... The combination tested here may not be optimal. In addition, adding a targeted-like effect through drug repositioning could allow more potent treatment with the addition of, for instance, valproic acid or beta-blockers,” the investigators said.
Adding low-dose metronomic chemotherapy (oral cyclophosphamide and methotrexate) to standard methotrexate, adriamycin, and platinum (MAP) maintenance treatment did not extend event-free survival in adolescents and young adults with high-grade, resectable osteosarcoma of the extremities, according to investigators.
“In pediatric tumors such as localized osteosarcomas, in situ tumor angiogenesis and levels of circulating angiogenic factors correlate with metastatic disease and a poor prognosis,” noted Andreza A. Senerchia, MD, of the Institute of Pediatric Oncology/Support Group for Adolescents and Children With Cancer, Federal University of Sao Paulo (Brazil), and her associates.
Since metronomic chemotherapy can prevent tumor angiogenesis and is a readily available, low-cost treatment with low toxicity, it could serve as a useful add-on to established MAP maintenance therapy in this patient population, they speculated.
The investigators assessed this approach in a prospective clinical trial involving 296 patients aged younger than 30 (mean age, 14 years; range, 0-29 years) who were treated at 27 medical centers in Brazil, Argentina, and Uruguay. All the study participants had high-grade but nonmetastatic operable osteosarcomas of the extremities, and all underwent preoperative chemotherapy followed by surgical resection, with limb salvage whenever possible.
A total of 139 patients were then randomly assigned to receive MAP plus metronomic chemotherapy (intervention group) and 157 to receive MAP alone (control group). However, 35% of the intervention group never started metronomic chemotherapy for a variety of reasons, and another 10% stopped the treatment very early.
At 5 years, cumulative event-free survival was 61% with MAP plus metronomic chemotherapy and 64% with MAP alone, a nonsignificant difference. When the analysis was restricted to only the patients in the intervention group who actually received metronomic chemotherapy, there still was no evidence that the add-on treatment made any difference in event-free survival. Similarly, mean overall survival was not significantly different between the two study groups, at 76% and 73%, respectively, Dr. Senerchia and her associates wrote (Cancer 2016 Nov 7. doi: 10.1002/cncr.30411).
There were 27 deaths (19%) in the intervention group, 81% of which were due to disease progression and 11% of which were due to treatment-related toxicity. Similarly, there were 24 deaths (15%) in the control group, of which 83% were due to disease progression and 17% to treatment-related toxicity.
These findings “do not support the routine use of cyclophosphamide and methotrexate as metronomic agents after standard chemotherapy for nonmetastatic osteosarcoma. However, our results should not preclude further investigation into the potential of maintenance for patients with osteosarcoma ... The combination tested here may not be optimal. In addition, adding a targeted-like effect through drug repositioning could allow more potent treatment with the addition of, for instance, valproic acid or beta-blockers,” the investigators said.
Adding low-dose metronomic chemotherapy (oral cyclophosphamide and methotrexate) to standard methotrexate, adriamycin, and platinum (MAP) maintenance treatment did not extend event-free survival in adolescents and young adults with high-grade, resectable osteosarcoma of the extremities, according to investigators.
“In pediatric tumors such as localized osteosarcomas, in situ tumor angiogenesis and levels of circulating angiogenic factors correlate with metastatic disease and a poor prognosis,” noted Andreza A. Senerchia, MD, of the Institute of Pediatric Oncology/Support Group for Adolescents and Children With Cancer, Federal University of Sao Paulo (Brazil), and her associates.
Since metronomic chemotherapy can prevent tumor angiogenesis and is a readily available, low-cost treatment with low toxicity, it could serve as a useful add-on to established MAP maintenance therapy in this patient population, they speculated.
The investigators assessed this approach in a prospective clinical trial involving 296 patients aged younger than 30 (mean age, 14 years; range, 0-29 years) who were treated at 27 medical centers in Brazil, Argentina, and Uruguay. All the study participants had high-grade but nonmetastatic operable osteosarcomas of the extremities, and all underwent preoperative chemotherapy followed by surgical resection, with limb salvage whenever possible.
A total of 139 patients were then randomly assigned to receive MAP plus metronomic chemotherapy (intervention group) and 157 to receive MAP alone (control group). However, 35% of the intervention group never started metronomic chemotherapy for a variety of reasons, and another 10% stopped the treatment very early.
At 5 years, cumulative event-free survival was 61% with MAP plus metronomic chemotherapy and 64% with MAP alone, a nonsignificant difference. When the analysis was restricted to only the patients in the intervention group who actually received metronomic chemotherapy, there still was no evidence that the add-on treatment made any difference in event-free survival. Similarly, mean overall survival was not significantly different between the two study groups, at 76% and 73%, respectively, Dr. Senerchia and her associates wrote (Cancer 2016 Nov 7. doi: 10.1002/cncr.30411).
There were 27 deaths (19%) in the intervention group, 81% of which were due to disease progression and 11% of which were due to treatment-related toxicity. Similarly, there were 24 deaths (15%) in the control group, of which 83% were due to disease progression and 17% to treatment-related toxicity.
These findings “do not support the routine use of cyclophosphamide and methotrexate as metronomic agents after standard chemotherapy for nonmetastatic osteosarcoma. However, our results should not preclude further investigation into the potential of maintenance for patients with osteosarcoma ... The combination tested here may not be optimal. In addition, adding a targeted-like effect through drug repositioning could allow more potent treatment with the addition of, for instance, valproic acid or beta-blockers,” the investigators said.
FROM CANCER
Key clinical point: Adding low-dose metronomic chemotherapy to MAP as maintenance treatment did not extend event-free survival in adolescents and young adults with high-grade, resectable osteosarcoma of the extremities.
Major finding: At 5 years, cumulative event-free survival was 61% with MAP plus metronomic chemotherapy and 64% with MAP alone, a nonsignificant difference.
Data source: A prospective randomized clinical trial involving 296 patients in South America followed for 5 years.
Disclosures: The authors did not provide information on the funding of this study and did not report any conflict-of-interest disclosures.