User login
Friable Warty Plaque on the Heel
The Diagnosis: Verrucous Hemangioma
Verrucous hemangioma (VH) is a rare vascular anomaly that has not been definitively delineated as a malformation or a tumor, as it has features of both. Verrucous hemangioma presents at birth as a compressible soft mass with a red violaceous hue favoring the legs.1,2 Over time VH will develop a warty, friable, and keratotic surface that can begin to evolve as early as 6 months or as late as 34 years of age.3 Verrucous hemangioma does not involute and tends to grow proportionally with the patient. Thus, VH classically has been considered a vascular malformation.
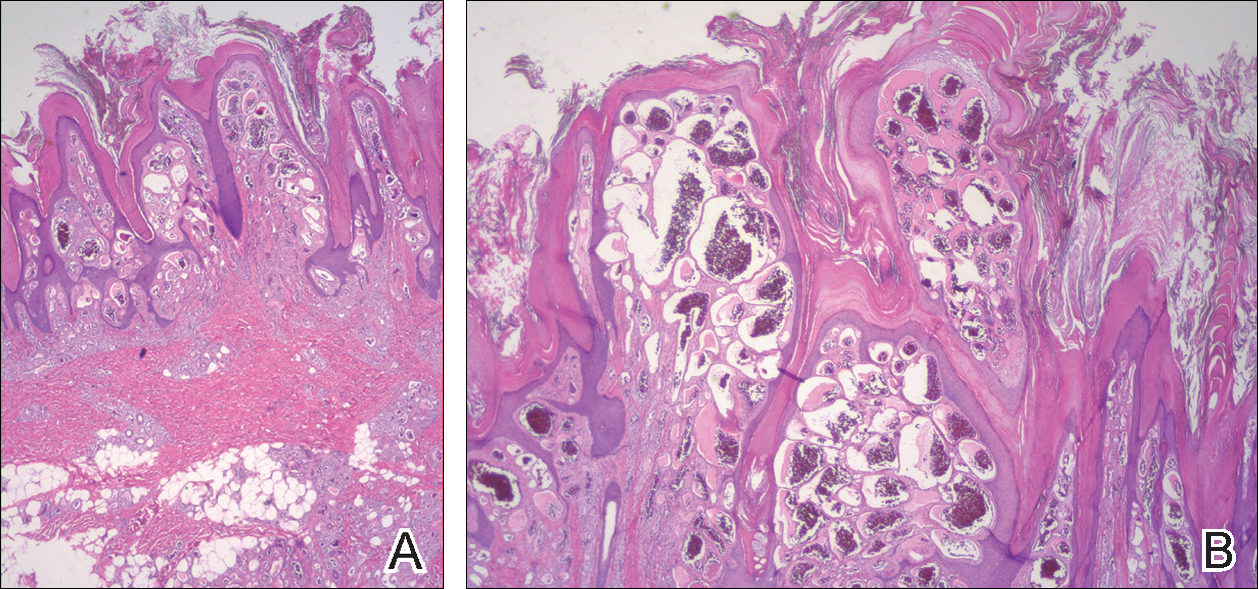
On histopathology VH shows collections of uniform, thin-walled vessels with a multilamellated basement membrane throughout the dermis, similar to an infantile hemangioma (IH). These lesions extend deep into the subcutaneous tissue and often involve the underlying fascia. The papillary dermis has large ectatic vessels, while the epidermis displays verrucous hyperkeratosis, papillomatosis, and irregular acanthosis without viral change (Figure).4,5 The superficial component can resemble an angiokeratoma; however, VH is differentiated by a deeper component that is often larger in size and has a more protracted clinical course.
Similar to IH, immunohistochemical studies have shown that VH expresses Wilms tumor 1 and glucose transporter 1 but is negative for D2-40.4 These findings suggest that VH is a vascular tumor rather than a vascular malformation, as was previously reported.6 Additional research has shown that the immunohistochemical staining profile of VH is nearly identical to IH, which has led to postulation that VH may be of placental mesodermal origin, as has been hypothesized for IH.5
Due to its deep infiltration and tendency for recurrence, VH is most effectively treated with wide local excision.3,6-8 Preoperative planning with magnetic resonance imaging may be indicated. Although laser monotherapy and other local destructive therapies have been largely unsuccessful, postsurgical laser therapy with CO2 lasers as well as dual pulsed dye laser and Nd:YAG laser have shown promise in preventing recurrence.3
- Tennant LB, Mulliken JB, Perez-Atayde AR, et al. Verrucous hemangioma revisited. Pediatr Dermatol. 2006;23:208-215.
- Koc M, Kavala M, Kocatür E, et al. An unusual vascular tumor: verrucous hemangioma. Dermatol Online J. 2009;15:7.
- Yang CH, Ohara K. Successful surgical treatment of verrucous hemangioma: a combined approach. Dermatol Surg. 2002;28:913-919; discussion 920.
- Trindade F, Torrelo A, Requena L, et al. An immunohistochemical study of verrucous hemangiomas. J Cutan Pathol. 2013;40:472-476.
- Laing EL, Brasch HD, Steel R, et al. Verrucous hemangioma expresses primitive markers. J Cutan Pathol. 2013;40:391-396.
- Mankani MH, Dufresne CR. Verrucous malformations: their presentation and management. Ann Plast Surg. 2000;45:31-36.
- Clairwood MQ, Bruckner AL, Dadras SS. Verrucous hemangioma: a report of two cases and review of the literature. J Cutan Pathol. 2011;38:740-746.
- Segura Palacios JM, Boixeda P, Rocha J, et al. Laser treatment for verrucous hemangioma. Laser Med Sci. 2012;27:681-684.
The Diagnosis: Verrucous Hemangioma
Verrucous hemangioma (VH) is a rare vascular anomaly that has not been definitively delineated as a malformation or a tumor, as it has features of both. Verrucous hemangioma presents at birth as a compressible soft mass with a red violaceous hue favoring the legs.1,2 Over time VH will develop a warty, friable, and keratotic surface that can begin to evolve as early as 6 months or as late as 34 years of age.3 Verrucous hemangioma does not involute and tends to grow proportionally with the patient. Thus, VH classically has been considered a vascular malformation.
On histopathology VH shows collections of uniform, thin-walled vessels with a multilamellated basement membrane throughout the dermis, similar to an infantile hemangioma (IH). These lesions extend deep into the subcutaneous tissue and often involve the underlying fascia. The papillary dermis has large ectatic vessels, while the epidermis displays verrucous hyperkeratosis, papillomatosis, and irregular acanthosis without viral change (Figure).4,5 The superficial component can resemble an angiokeratoma; however, VH is differentiated by a deeper component that is often larger in size and has a more protracted clinical course.
Similar to IH, immunohistochemical studies have shown that VH expresses Wilms tumor 1 and glucose transporter 1 but is negative for D2-40.4 These findings suggest that VH is a vascular tumor rather than a vascular malformation, as was previously reported.6 Additional research has shown that the immunohistochemical staining profile of VH is nearly identical to IH, which has led to postulation that VH may be of placental mesodermal origin, as has been hypothesized for IH.5
Due to its deep infiltration and tendency for recurrence, VH is most effectively treated with wide local excision.3,6-8 Preoperative planning with magnetic resonance imaging may be indicated. Although laser monotherapy and other local destructive therapies have been largely unsuccessful, postsurgical laser therapy with CO2 lasers as well as dual pulsed dye laser and Nd:YAG laser have shown promise in preventing recurrence.3
The Diagnosis: Verrucous Hemangioma
Verrucous hemangioma (VH) is a rare vascular anomaly that has not been definitively delineated as a malformation or a tumor, as it has features of both. Verrucous hemangioma presents at birth as a compressible soft mass with a red violaceous hue favoring the legs.1,2 Over time VH will develop a warty, friable, and keratotic surface that can begin to evolve as early as 6 months or as late as 34 years of age.3 Verrucous hemangioma does not involute and tends to grow proportionally with the patient. Thus, VH classically has been considered a vascular malformation.
On histopathology VH shows collections of uniform, thin-walled vessels with a multilamellated basement membrane throughout the dermis, similar to an infantile hemangioma (IH). These lesions extend deep into the subcutaneous tissue and often involve the underlying fascia. The papillary dermis has large ectatic vessels, while the epidermis displays verrucous hyperkeratosis, papillomatosis, and irregular acanthosis without viral change (Figure).4,5 The superficial component can resemble an angiokeratoma; however, VH is differentiated by a deeper component that is often larger in size and has a more protracted clinical course.
Similar to IH, immunohistochemical studies have shown that VH expresses Wilms tumor 1 and glucose transporter 1 but is negative for D2-40.4 These findings suggest that VH is a vascular tumor rather than a vascular malformation, as was previously reported.6 Additional research has shown that the immunohistochemical staining profile of VH is nearly identical to IH, which has led to postulation that VH may be of placental mesodermal origin, as has been hypothesized for IH.5
Due to its deep infiltration and tendency for recurrence, VH is most effectively treated with wide local excision.3,6-8 Preoperative planning with magnetic resonance imaging may be indicated. Although laser monotherapy and other local destructive therapies have been largely unsuccessful, postsurgical laser therapy with CO2 lasers as well as dual pulsed dye laser and Nd:YAG laser have shown promise in preventing recurrence.3
- Tennant LB, Mulliken JB, Perez-Atayde AR, et al. Verrucous hemangioma revisited. Pediatr Dermatol. 2006;23:208-215.
- Koc M, Kavala M, Kocatür E, et al. An unusual vascular tumor: verrucous hemangioma. Dermatol Online J. 2009;15:7.
- Yang CH, Ohara K. Successful surgical treatment of verrucous hemangioma: a combined approach. Dermatol Surg. 2002;28:913-919; discussion 920.
- Trindade F, Torrelo A, Requena L, et al. An immunohistochemical study of verrucous hemangiomas. J Cutan Pathol. 2013;40:472-476.
- Laing EL, Brasch HD, Steel R, et al. Verrucous hemangioma expresses primitive markers. J Cutan Pathol. 2013;40:391-396.
- Mankani MH, Dufresne CR. Verrucous malformations: their presentation and management. Ann Plast Surg. 2000;45:31-36.
- Clairwood MQ, Bruckner AL, Dadras SS. Verrucous hemangioma: a report of two cases and review of the literature. J Cutan Pathol. 2011;38:740-746.
- Segura Palacios JM, Boixeda P, Rocha J, et al. Laser treatment for verrucous hemangioma. Laser Med Sci. 2012;27:681-684.
- Tennant LB, Mulliken JB, Perez-Atayde AR, et al. Verrucous hemangioma revisited. Pediatr Dermatol. 2006;23:208-215.
- Koc M, Kavala M, Kocatür E, et al. An unusual vascular tumor: verrucous hemangioma. Dermatol Online J. 2009;15:7.
- Yang CH, Ohara K. Successful surgical treatment of verrucous hemangioma: a combined approach. Dermatol Surg. 2002;28:913-919; discussion 920.
- Trindade F, Torrelo A, Requena L, et al. An immunohistochemical study of verrucous hemangiomas. J Cutan Pathol. 2013;40:472-476.
- Laing EL, Brasch HD, Steel R, et al. Verrucous hemangioma expresses primitive markers. J Cutan Pathol. 2013;40:391-396.
- Mankani MH, Dufresne CR. Verrucous malformations: their presentation and management. Ann Plast Surg. 2000;45:31-36.
- Clairwood MQ, Bruckner AL, Dadras SS. Verrucous hemangioma: a report of two cases and review of the literature. J Cutan Pathol. 2011;38:740-746.
- Segura Palacios JM, Boixeda P, Rocha J, et al. Laser treatment for verrucous hemangioma. Laser Med Sci. 2012;27:681-684.

A 31-year-old man presented with a large friable and warty plaque on the left heel. He recalled that the lesion had been present since birth as a flat red birthmark that grew proportionally with him. Throughout his adolescence its surface became increasingly rough and bumpy. The patient described receiving laser treatment twice in his early 20s without notable improvement. He wanted the lesion removed because it was easily traumatized, resulting in bleeding, pain, and infection. The patient reported being otherwise healthy.

How to Treat Pediatric MS
VANCOUVER—Pediatric multiple sclerosis (MS) presents unique concerns, making appropriate treatment especially important, according to an overview presented at the 45th Annual Meeting of the Child Neurology Society. Currently, disease-modifying therapies with FDA approval in adult MS have not been approved for the treatment of pediatric MS. In addition, brain growth and cognition are adversely affected in pediatric MS. Furthermore, children with MS tend to become disabled at a younger age, compared with adults.

Diagnosis and Initiation of Therapy
Neurologists should be prepared to engage with children and their families to ensure the most efficacious treatment. “Whenever you are having that conversation or you are considering starting the disease-modifying therapy, you need to balance the need to treat the disease with the idea that you are going to be starting a therapy for a lifetime,” said Dr. Lotze.
Disease-modifying therapies target the inflammatory aspects of pediatric-onset MS and should be initiated in children with a confirmed diagnosis, said Dr. Lotze. Children with clinically isolated syndrome who appear to be at high risk for MS and children with positive oligoclonal bands or elevated IgG index may also need to begin a disease-modifying therapy. Distinguishing between MS, acute disseminated encephalomyelitis (ADEM), and neuromyelitis optica (NMO) poses challenges, especially in children under age 10. Certain interferons can exacerbate NMO and may be harmful in children with ADEM or multiphasic ADEM.
Setting Goals
Neurologists are encouraged to counsel patients about the purpose and side effects of treatment, as well as to establish reasonable expectations for treatment. Additionally, children and families should be aware that another attack may occur during treatment and should be informed about what to do if it does.
No therapy is 100% efficacious in pediatric or adult MS, said Dr. Lotze. Research suggests that 50% of adults have no evidence of disease activity (NEDA) at two years of the disease. After seven years, however, 7% of these adults meet NEDA criteria. As a result, minimal disease progression (defined as less than one attack per year, fewer than three new lesions on a yearly MRI, and no progression in disability) may be a more attainable goal. “We would like to see a drug in a single individual or patient that is effective in achieving NEDA. If that is not possible … you might find that ultimately what you can go for is minimal disease progression,” said Dr. Lotze. He added that there appears to be no clear difference in terms of long-term outcome between children with MS who achieve NEDA and those who achieve minimal disease progression.
First-Line Therapies and Follow-Up Appointments
First-line agents for pediatric MS are the injectable drugs known as platform therapies. The International Pediatric MS Society Group (IPMSSG) recommends that all patients start first-line therapy (ie, interferon β or glatiramer acetate) soon after diagnosis.
Positive results from phase IV observational studies suggest that interferon β and glatiramer acetate are safe and efficacious treatments in pediatric MS. When studied in populations ranging in age from 12 to 17, these therapies decreased relapse rate, stabilized disability, and reduced accrual of new lesions. However, injectable treatments are associated with flu-like symptoms and injection-site reactions. Neurologists should start pediatric patients on interferon β with 25% to 50% of full dosing and titrate to a full adult dosing over four to six weeks. When initiating glatiramer acetate, neurologists should start children with a full adult dosing, 20 mg subcutaneous daily or 40 mg subcutaneous three times per week.
Follow-up appointments should occur every three to six months to assess adherence and determine efficacy of treatment. Neurologists are advised to ask patients whether they are comfortable with taking shots. Patients with needle anxiety, a common problem in pediatric MS, may need assistance from a child psychologist or child life specialist. Asking patients how often the patient or family forgets to take the disease-modifying therapy is also necessary, said Dr. Lotze. In addition, the transition from pediatric to adult care should be addressed in follow-up discussions. Teens must understand that certain disease-modifying therapies are contraindicated for pregnant patients. They also should be aware of how alcohol and other drugs interact with treatment.
Treatment Failure
Research indicates that approximately 30% of patients with pediatric-onset MS will not respond to the first-line therapies, and numerous variables may explain why. Age and disease duration can influence treatment efficacy, as can the number of relapses and the level of disease activity before treatment initiation. Patients who are nonadherent because of side effects and who continue to struggle with needle anxiety may experience treatment failure. The IPMSSG defines treatment failure as adherence to treatment for at least six months with no reduction in relapse rate or in new MRI T2 or contrast-enhancing lesions, or with two or more relapses within a 12-month period.
Second-Line Therapies
Trials of several oral agents are currently under way. The IPMSSG, however, urges neurologists to use extreme caution when considering nonplatform therapies for pediatric patients.
Fingolimod is a second-line drug for pediatric MS that blocks the egress of lymphocytes from the lymph nodes. A small percentage of patients taking this oral agent may develop bradycardia. Monitoring is required for the first six hours of treatment to ensure that the patient has no side effects. Some adverse effects associated with the drug include: first dose bradycardia, macular edema, and herpetic infections.
Dimethyl fumarate is an Nrf2 antioxidant pathway modulator that is associated with adverse effects such as flushing and gastrointestinal upset, said Dr. Lotze. Low-dose aspirin may help with flushing, and a proton pump inhibitor can help to manage the gastrointestinal upset. This treatment requires patients to undergo monitoring for blood count and liver function, as does fingolimod.
Teriflunomide, a pyrimidine synthesis inhibitor, is a Pregnancy Category X drug because it increases the risk of birth defects. Rituximab, an anti-CD20 chimeric monoclonal antibody, is gaining popularity for treating MS. Studies suggest that ocrelizumab may be well tolerated in pediatric MS. Natlizumamb, cladribine, and alemtuzumab are typically used to treat more aggressive forms of MS.
Neurologists rarely prescribe cyclophosphamide or mitoxantrone in pediatric MS. Cyclophosphamide has no formal FDA approval for adult MS or pediatric-onset MS and is associated with increased risks of bladder cancer, secondary leukemia, and infertility. Mitoxantrone is FDA-approved for adults with aggressive relapsing-remitting MS and secondary progressive MS. It is associated with increased cancer risk, however, and is highly cardiotoxic.
“After you have initiated a second-line agent, you need to continue to monitor aspects of disease control, including relapse rate, disability, MRI changes, and other adverse events. If you continue to see breakthrough disease, then you may need to consider … changing to another agent or moving to a more aggressive therapy such as rituximab or natalizumab,” said Dr. Lotze.
—Erica Tricarico
Suggested Reading
Chitnis T, Ghezzi A, Bajer-Korneck B, et al. Pediatric multiple sclerosis: Escalation and emerging treatments. Neurology. 2016;87(9 Suppl 2):S10 3-S109.
Jancic J, Nikolic B, Ivancevic N, et al. Multiple sclerosis in pediatrics: Current concepts and treatment options. Neurol Ther. 2016:5(2):131-1
VANCOUVER—Pediatric multiple sclerosis (MS) presents unique concerns, making appropriate treatment especially important, according to an overview presented at the 45th Annual Meeting of the Child Neurology Society. Currently, disease-modifying therapies with FDA approval in adult MS have not been approved for the treatment of pediatric MS. In addition, brain growth and cognition are adversely affected in pediatric MS. Furthermore, children with MS tend to become disabled at a younger age, compared with adults.
Diagnosis and Initiation of Therapy
Neurologists should be prepared to engage with children and their families to ensure the most efficacious treatment. “Whenever you are having that conversation or you are considering starting the disease-modifying therapy, you need to balance the need to treat the disease with the idea that you are going to be starting a therapy for a lifetime,” said Dr. Lotze.
Disease-modifying therapies target the inflammatory aspects of pediatric-onset MS and should be initiated in children with a confirmed diagnosis, said Dr. Lotze. Children with clinically isolated syndrome who appear to be at high risk for MS and children with positive oligoclonal bands or elevated IgG index may also need to begin a disease-modifying therapy. Distinguishing between MS, acute disseminated encephalomyelitis (ADEM), and neuromyelitis optica (NMO) poses challenges, especially in children under age 10. Certain interferons can exacerbate NMO and may be harmful in children with ADEM or multiphasic ADEM.
Setting Goals
Neurologists are encouraged to counsel patients about the purpose and side effects of treatment, as well as to establish reasonable expectations for treatment. Additionally, children and families should be aware that another attack may occur during treatment and should be informed about what to do if it does.
No therapy is 100% efficacious in pediatric or adult MS, said Dr. Lotze. Research suggests that 50% of adults have no evidence of disease activity (NEDA) at two years of the disease. After seven years, however, 7% of these adults meet NEDA criteria. As a result, minimal disease progression (defined as less than one attack per year, fewer than three new lesions on a yearly MRI, and no progression in disability) may be a more attainable goal. “We would like to see a drug in a single individual or patient that is effective in achieving NEDA. If that is not possible … you might find that ultimately what you can go for is minimal disease progression,” said Dr. Lotze. He added that there appears to be no clear difference in terms of long-term outcome between children with MS who achieve NEDA and those who achieve minimal disease progression.
First-Line Therapies and Follow-Up Appointments
First-line agents for pediatric MS are the injectable drugs known as platform therapies. The International Pediatric MS Society Group (IPMSSG) recommends that all patients start first-line therapy (ie, interferon β or glatiramer acetate) soon after diagnosis.
Positive results from phase IV observational studies suggest that interferon β and glatiramer acetate are safe and efficacious treatments in pediatric MS. When studied in populations ranging in age from 12 to 17, these therapies decreased relapse rate, stabilized disability, and reduced accrual of new lesions. However, injectable treatments are associated with flu-like symptoms and injection-site reactions. Neurologists should start pediatric patients on interferon β with 25% to 50% of full dosing and titrate to a full adult dosing over four to six weeks. When initiating glatiramer acetate, neurologists should start children with a full adult dosing, 20 mg subcutaneous daily or 40 mg subcutaneous three times per week.
Follow-up appointments should occur every three to six months to assess adherence and determine efficacy of treatment. Neurologists are advised to ask patients whether they are comfortable with taking shots. Patients with needle anxiety, a common problem in pediatric MS, may need assistance from a child psychologist or child life specialist. Asking patients how often the patient or family forgets to take the disease-modifying therapy is also necessary, said Dr. Lotze. In addition, the transition from pediatric to adult care should be addressed in follow-up discussions. Teens must understand that certain disease-modifying therapies are contraindicated for pregnant patients. They also should be aware of how alcohol and other drugs interact with treatment.
Treatment Failure
Research indicates that approximately 30% of patients with pediatric-onset MS will not respond to the first-line therapies, and numerous variables may explain why. Age and disease duration can influence treatment efficacy, as can the number of relapses and the level of disease activity before treatment initiation. Patients who are nonadherent because of side effects and who continue to struggle with needle anxiety may experience treatment failure. The IPMSSG defines treatment failure as adherence to treatment for at least six months with no reduction in relapse rate or in new MRI T2 or contrast-enhancing lesions, or with two or more relapses within a 12-month period.
Second-Line Therapies
Trials of several oral agents are currently under way. The IPMSSG, however, urges neurologists to use extreme caution when considering nonplatform therapies for pediatric patients.
Fingolimod is a second-line drug for pediatric MS that blocks the egress of lymphocytes from the lymph nodes. A small percentage of patients taking this oral agent may develop bradycardia. Monitoring is required for the first six hours of treatment to ensure that the patient has no side effects. Some adverse effects associated with the drug include: first dose bradycardia, macular edema, and herpetic infections.
Dimethyl fumarate is an Nrf2 antioxidant pathway modulator that is associated with adverse effects such as flushing and gastrointestinal upset, said Dr. Lotze. Low-dose aspirin may help with flushing, and a proton pump inhibitor can help to manage the gastrointestinal upset. This treatment requires patients to undergo monitoring for blood count and liver function, as does fingolimod.
Teriflunomide, a pyrimidine synthesis inhibitor, is a Pregnancy Category X drug because it increases the risk of birth defects. Rituximab, an anti-CD20 chimeric monoclonal antibody, is gaining popularity for treating MS. Studies suggest that ocrelizumab may be well tolerated in pediatric MS. Natlizumamb, cladribine, and alemtuzumab are typically used to treat more aggressive forms of MS.
Neurologists rarely prescribe cyclophosphamide or mitoxantrone in pediatric MS. Cyclophosphamide has no formal FDA approval for adult MS or pediatric-onset MS and is associated with increased risks of bladder cancer, secondary leukemia, and infertility. Mitoxantrone is FDA-approved for adults with aggressive relapsing-remitting MS and secondary progressive MS. It is associated with increased cancer risk, however, and is highly cardiotoxic.
“After you have initiated a second-line agent, you need to continue to monitor aspects of disease control, including relapse rate, disability, MRI changes, and other adverse events. If you continue to see breakthrough disease, then you may need to consider … changing to another agent or moving to a more aggressive therapy such as rituximab or natalizumab,” said Dr. Lotze.
—Erica Tricarico
Suggested Reading
Chitnis T, Ghezzi A, Bajer-Korneck B, et al. Pediatric multiple sclerosis: Escalation and emerging treatments. Neurology. 2016;87(9 Suppl 2):S10 3-S109.
Jancic J, Nikolic B, Ivancevic N, et al. Multiple sclerosis in pediatrics: Current concepts and treatment options. Neurol Ther. 2016:5(2):131-1
VANCOUVER—Pediatric multiple sclerosis (MS) presents unique concerns, making appropriate treatment especially important, according to an overview presented at the 45th Annual Meeting of the Child Neurology Society. Currently, disease-modifying therapies with FDA approval in adult MS have not been approved for the treatment of pediatric MS. In addition, brain growth and cognition are adversely affected in pediatric MS. Furthermore, children with MS tend to become disabled at a younger age, compared with adults.
Diagnosis and Initiation of Therapy
Neurologists should be prepared to engage with children and their families to ensure the most efficacious treatment. “Whenever you are having that conversation or you are considering starting the disease-modifying therapy, you need to balance the need to treat the disease with the idea that you are going to be starting a therapy for a lifetime,” said Dr. Lotze.
Disease-modifying therapies target the inflammatory aspects of pediatric-onset MS and should be initiated in children with a confirmed diagnosis, said Dr. Lotze. Children with clinically isolated syndrome who appear to be at high risk for MS and children with positive oligoclonal bands or elevated IgG index may also need to begin a disease-modifying therapy. Distinguishing between MS, acute disseminated encephalomyelitis (ADEM), and neuromyelitis optica (NMO) poses challenges, especially in children under age 10. Certain interferons can exacerbate NMO and may be harmful in children with ADEM or multiphasic ADEM.
Setting Goals
Neurologists are encouraged to counsel patients about the purpose and side effects of treatment, as well as to establish reasonable expectations for treatment. Additionally, children and families should be aware that another attack may occur during treatment and should be informed about what to do if it does.
No therapy is 100% efficacious in pediatric or adult MS, said Dr. Lotze. Research suggests that 50% of adults have no evidence of disease activity (NEDA) at two years of the disease. After seven years, however, 7% of these adults meet NEDA criteria. As a result, minimal disease progression (defined as less than one attack per year, fewer than three new lesions on a yearly MRI, and no progression in disability) may be a more attainable goal. “We would like to see a drug in a single individual or patient that is effective in achieving NEDA. If that is not possible … you might find that ultimately what you can go for is minimal disease progression,” said Dr. Lotze. He added that there appears to be no clear difference in terms of long-term outcome between children with MS who achieve NEDA and those who achieve minimal disease progression.
First-Line Therapies and Follow-Up Appointments
First-line agents for pediatric MS are the injectable drugs known as platform therapies. The International Pediatric MS Society Group (IPMSSG) recommends that all patients start first-line therapy (ie, interferon β or glatiramer acetate) soon after diagnosis.
Positive results from phase IV observational studies suggest that interferon β and glatiramer acetate are safe and efficacious treatments in pediatric MS. When studied in populations ranging in age from 12 to 17, these therapies decreased relapse rate, stabilized disability, and reduced accrual of new lesions. However, injectable treatments are associated with flu-like symptoms and injection-site reactions. Neurologists should start pediatric patients on interferon β with 25% to 50% of full dosing and titrate to a full adult dosing over four to six weeks. When initiating glatiramer acetate, neurologists should start children with a full adult dosing, 20 mg subcutaneous daily or 40 mg subcutaneous three times per week.
Follow-up appointments should occur every three to six months to assess adherence and determine efficacy of treatment. Neurologists are advised to ask patients whether they are comfortable with taking shots. Patients with needle anxiety, a common problem in pediatric MS, may need assistance from a child psychologist or child life specialist. Asking patients how often the patient or family forgets to take the disease-modifying therapy is also necessary, said Dr. Lotze. In addition, the transition from pediatric to adult care should be addressed in follow-up discussions. Teens must understand that certain disease-modifying therapies are contraindicated for pregnant patients. They also should be aware of how alcohol and other drugs interact with treatment.
Treatment Failure
Research indicates that approximately 30% of patients with pediatric-onset MS will not respond to the first-line therapies, and numerous variables may explain why. Age and disease duration can influence treatment efficacy, as can the number of relapses and the level of disease activity before treatment initiation. Patients who are nonadherent because of side effects and who continue to struggle with needle anxiety may experience treatment failure. The IPMSSG defines treatment failure as adherence to treatment for at least six months with no reduction in relapse rate or in new MRI T2 or contrast-enhancing lesions, or with two or more relapses within a 12-month period.
Second-Line Therapies
Trials of several oral agents are currently under way. The IPMSSG, however, urges neurologists to use extreme caution when considering nonplatform therapies for pediatric patients.
Fingolimod is a second-line drug for pediatric MS that blocks the egress of lymphocytes from the lymph nodes. A small percentage of patients taking this oral agent may develop bradycardia. Monitoring is required for the first six hours of treatment to ensure that the patient has no side effects. Some adverse effects associated with the drug include: first dose bradycardia, macular edema, and herpetic infections.
Dimethyl fumarate is an Nrf2 antioxidant pathway modulator that is associated with adverse effects such as flushing and gastrointestinal upset, said Dr. Lotze. Low-dose aspirin may help with flushing, and a proton pump inhibitor can help to manage the gastrointestinal upset. This treatment requires patients to undergo monitoring for blood count and liver function, as does fingolimod.
Teriflunomide, a pyrimidine synthesis inhibitor, is a Pregnancy Category X drug because it increases the risk of birth defects. Rituximab, an anti-CD20 chimeric monoclonal antibody, is gaining popularity for treating MS. Studies suggest that ocrelizumab may be well tolerated in pediatric MS. Natlizumamb, cladribine, and alemtuzumab are typically used to treat more aggressive forms of MS.
Neurologists rarely prescribe cyclophosphamide or mitoxantrone in pediatric MS. Cyclophosphamide has no formal FDA approval for adult MS or pediatric-onset MS and is associated with increased risks of bladder cancer, secondary leukemia, and infertility. Mitoxantrone is FDA-approved for adults with aggressive relapsing-remitting MS and secondary progressive MS. It is associated with increased cancer risk, however, and is highly cardiotoxic.
“After you have initiated a second-line agent, you need to continue to monitor aspects of disease control, including relapse rate, disability, MRI changes, and other adverse events. If you continue to see breakthrough disease, then you may need to consider … changing to another agent or moving to a more aggressive therapy such as rituximab or natalizumab,” said Dr. Lotze.
—Erica Tricarico
Suggested Reading
Chitnis T, Ghezzi A, Bajer-Korneck B, et al. Pediatric multiple sclerosis: Escalation and emerging treatments. Neurology. 2016;87(9 Suppl 2):S10 3-S109.
Jancic J, Nikolic B, Ivancevic N, et al. Multiple sclerosis in pediatrics: Current concepts and treatment options. Neurol Ther. 2016:5(2):131-1

Herpes Zoster Following Varicella Vaccination in Children
Varicella-zoster virus (VZV) causes varicella as a primary infection. It is a highly contagious disease characterized by a widespread papulovesicular eruption with fever and malaise.1,2 After the primary infection, the virus remains latent within the sensory dorsal root ganglia and can reactivate as herpes zoster (HZ).1-5 Herpes zoster is characterized by unilateral radicular pain and a vesicular rash in a dermatomal pattern.1,2 It is most common in adults, especially elderly and immunocompromised patients, but rarely occurs in children. Herpes zoster is most often seen in individuals previously infected with VZV, but it also has occurred in individuals without known varicella infection,1-17 possibly because these individuals had a prior subclinical VZV infection.
A live attenuated VZV vaccine was created after isolation of the virus from a child in Japan.2 Since the introduction of the vaccine in 1995 in the United States, the incidence of VZV and HZ has declined.5 Herpes zoster rates after vaccination vary from 14 to 19 per 100,000 individuals.3,5 Breakthrough disease with the wild-type strain does occur in vaccinated children, but vaccine-strain HZ also has been reported.1-5 The risk for HZ caused by reactivated VZV vaccine in healthy children is unknown. We present a case of HZ in an otherwise healthy 19-month-old boy with no known varicella exposure who received the VZV vaccine at 13 months of age.
Case Report
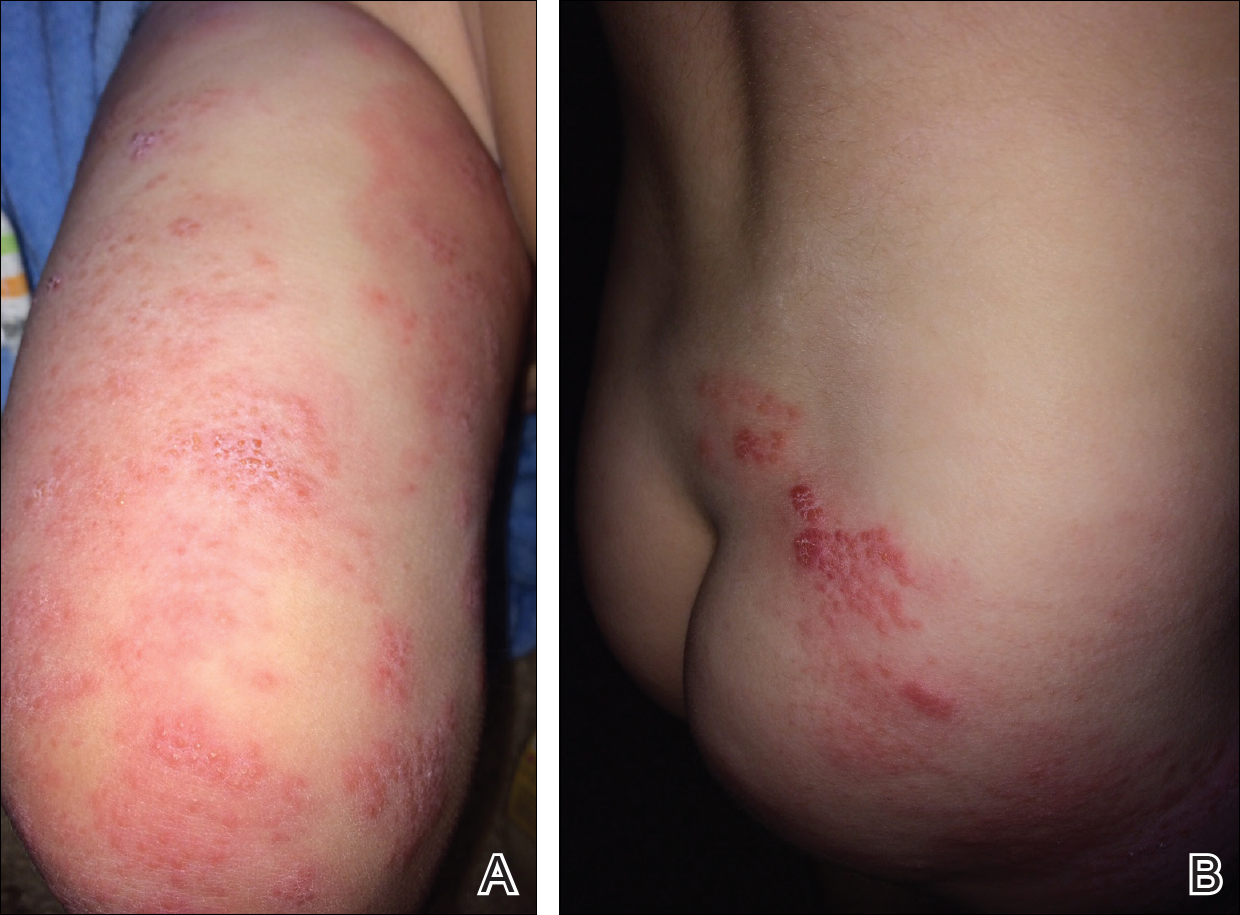
An otherwise healthy 19-month-old boy presented to the dermatology clinic with a rash that began 2 days prior on the right groin and spread to the right leg. The patient’s mother denied that the child had been febrile and noted that the rash did not appear to bother him in any way. The patient was up-to-date on his vaccinations and received the first dose of the varicella series 6 months prior to presentation. He had no personal history of varicella, no exposure to sick contacts with varicella, and no known exposure to the virus. He was otherwise completely healthy with no signs or symptoms of immunocompromise.
Physical examination revealed grouped vesicles on an erythematous base on the right thigh, right sacrum, and lower abdomen that did not cross the midline (Figure). There were no other pertinent physical examination findings. The eruption was most consistent with HZ but concern remained for herpes simplex virus (HSV) or impetigo. A bacterial culture and polymerase chain reaction assay for VZV and HSV from skin swabs was ordered. The patient was prescribed acyclovir 20 mg/kg every 6 hours for 5 days. Laboratory testing revealed a positive result for VZV on polymerase chain reaction and a negative result for HSV. The majority of the patient’s lesions had crusted after 2 days of treatment with acyclovir, and the rash had nearly resolved 1 week after presentation. Subsequent evaluation with a complete blood cell count with differential and basic metabolic profile was normal. Levels of IgG, IgA, and IgM also were normal; IgE was slightly elevated.
Comment
Herpes zoster in children is an uncommon clinical entity. Most children with HZ are immunocompromised, have a history of varicella, or were exposed to varicella during gestation.8 With the introduction of the live VZV vaccine, the incidence of HZ has declined, but reactivation of the live vaccine leading to HZ infection is possible. The vaccine is 90% effective, and breakthrough varicella has been reported in 15% to 20% of vaccinated patients.1-17 The cause of HZ in vaccinated children is unclear due to the potential for either wild-type or vaccine-strain VZV to induce HZ.
Twenty-two cases of HZ in healthy children after vaccination were identified with a PubMed search of articles indexed for MEDLINE using the search terms herpes zoster infection after vaccination and herpes zoster infection AND immunocompetent AND vaccination in separate searches for all English-language studies (Table). The search was limited to immunocompetent children and adolescents who were 18 years or younger with no history of varicella or exposure to varicella during gestation.
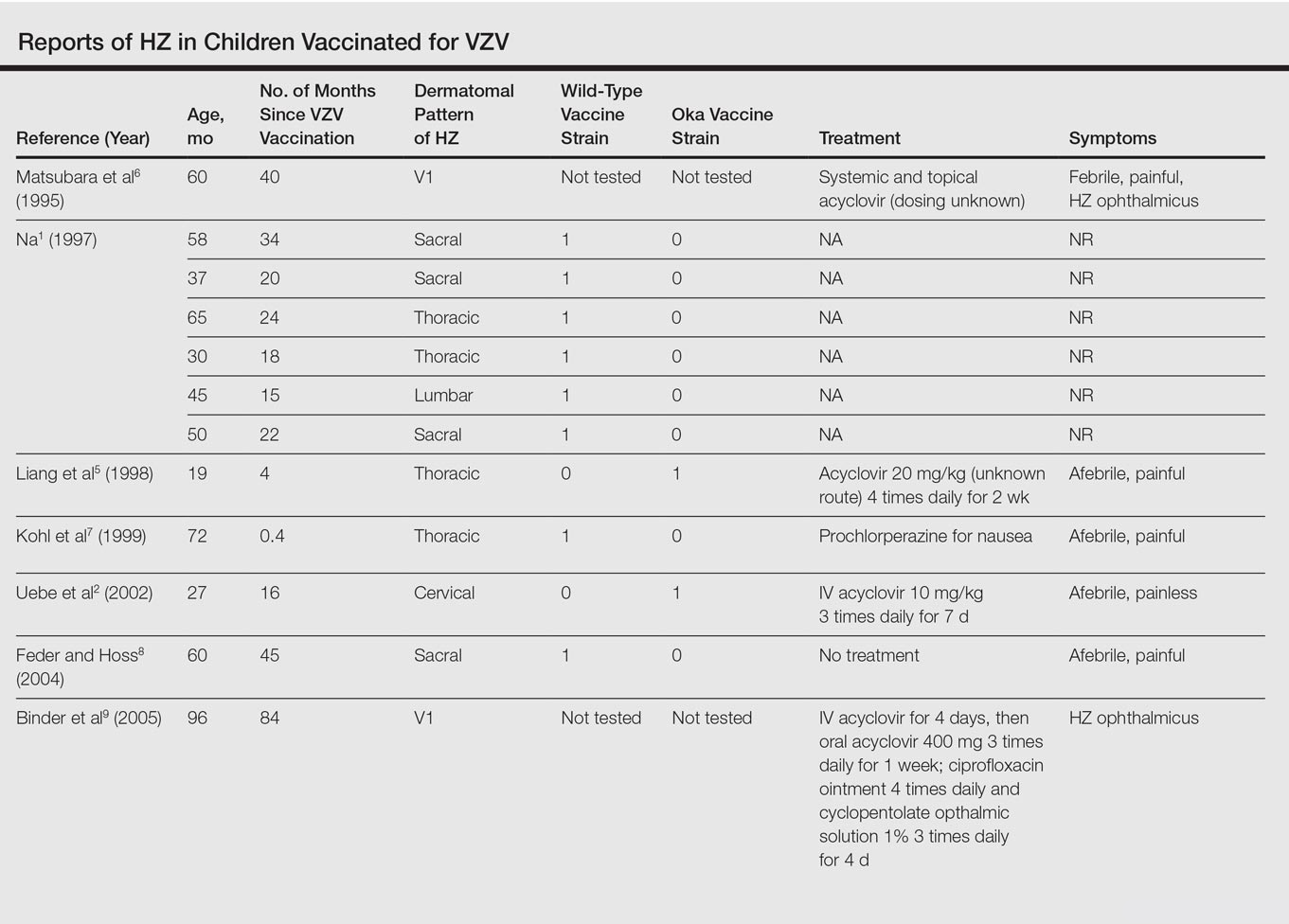

The mean age for HZ infection was 5.3 years. The average time between vaccination and HZ infection was 3.3 years. There was a spread of dermatomal patterns with cases in the first division of the trigeminal nerve, cervical, thoracic, lumbar, and sacral distributions. Of the 22 cases of HZ we reviewed, 16 underwent genotype testing to determine the source of the infection. The Oka vaccine strain virus was identified in 8 (50%) cases, while wild-type virus was found in 8 (50%) cases.1,2,4,5,7,8,10,11,13,14,16 Twelve cases were treated with acyclovir.2,3,5,6,9-12,14-17 The method of delivery, either oral or intravenous, and the length of treatment depended on the severity of the disease. Patients with meningoencephalitis and HZ ophthalmicus received intravenous acyclovir more often and also had a longer course of acyclovir compared to those individuals with involvement limited to the skin.
This review found HZ occurs from reactivation of wild-type or Oka vaccine-strain VZV in immunocompetent children.1-17 It shows that subclinical varicella infection is not the only explanation for HZ in a healthy vaccinated child. It is currently not clear why some healthy children experience HZ from vaccine-strain VZV. When HZ presents in a vaccinated immunocompetent child without a history of varicella infection or exposure, the possibility for vaccine strain–induced HZ should be considered.
- . Herpes zoster in three healthy children immunized with varicella vaccine (Oka/Biken); the causative virus differed from vaccine strain on PCR analysis of the IV variable region (R5) and of a PstI-site region. Br J Dermatol. 1997;137:255-258.
- Uebe B, Sauerbrei A, Burdach S, et al. Herpes zoster by reactivated vaccine varicella zoster virus in a healthy child [published online June 25, 2002]. Eur J Pediatr. 2002;161:442-444.
- Obieta MP, Jacinto SS. Herpes zoster after varicella vaccination in a healthy young child. Int J Dermatol. 2008;47:640-641.
- Ota K, Kim V, Lavi S, et al. Vaccine-strain varicella zoster virus causing recurrent herpes zoster in an immunocompetent 2-year-old. Pediatr Infect Dis J. 2008;27:847-848.
- Liang GL, Heidelberg KA, Jacobson RM, et al. Herpes zoster after varicella vaccination. J Am Acad Dermatol. 1998;38:761-763.
- Matsubara K, Nigami H, Harigaya H, et al. Herpes zoster in a normal child after varicella vaccination. Acta Paediatr Jpn. 1995;37:648-650.
- Kohl S, Rapp J, Larussa P, et al. Natural varicella-zoster virus reactivation shortly after varicella immunization in a child. Pediatr Infect Dis J. 1999;18:1112-1113.
- Feder HM Jr, Hoss DM. Herpes zoster in otherwise healthy children. Pediatr Infect Dis J. 2004;23:451-457; quiz 458-460.
- Binder NR, Holland GN, Hosea S, et al. Herpes zoster ophthalmicus in an otherwise-healthy child. J AAPOS. 2005;9:597-598.
- Levin MJ, DeBiasi RL, Bostik V, et al. Herpes zoster with skin lesions and meningitis caused by 2 different genotypes of the Oka varicella-zoster virus vaccine. J Infect Dis. 2008;198:1444-1447.
- Iyer S, Mittal MK, Hodinka RL. Herpes zoster and meningitis resulting from reactivation of varicella vaccine virus in an immunocompetent child. Ann Emerg Med. 2009;53:792-795.
- Lin P, Yoon MK, Chiu CS. Herpes zoster keratouveitis and inflammatory ocular hypertension 8 years after varicella vaccination. Ocul Immunol Inflamm. 2009;17:33-35.
- Chouliaras G, Spoulou V, Quinlivan M, et al. Vaccine-associated herpes zoster ophthalmicus [correction of opthalmicus] and encephalitis in an immunocompetent child [published online March 1, 2010]. Pediatrics. 2010;125:E969-E972.
- Han JY, Hanson DC, Way SS. Herpes zoster and meningitis due to reactivation of varicella vaccine virus in an immunocompetent child. Pediatr Infect Dis J. 2011;30:266-268.
- Ryu WY, Kim NY, Kwon YH, et al. Herpes zoster ophthalmicus with isolated trochlear nerve palsy in an otherwise healthy 13-year-old girl. J AAPOS. 2014;18:193-195.
- Iwasaki S, Motokura K, Honda Y, et al. Vaccine-strain herpes zoster found in the trigeminal nerve area in a healthy child: a case report [published online November 3, 2016]. J Clin Virol. 2016;85:44-47.
- Peterson N, Goodman S, Peterson M, et al. Herpes zoster in children. Cutis. 2016;98:94-95.
Varicella-zoster virus (VZV) causes varicella as a primary infection. It is a highly contagious disease characterized by a widespread papulovesicular eruption with fever and malaise.1,2 After the primary infection, the virus remains latent within the sensory dorsal root ganglia and can reactivate as herpes zoster (HZ).1-5 Herpes zoster is characterized by unilateral radicular pain and a vesicular rash in a dermatomal pattern.1,2 It is most common in adults, especially elderly and immunocompromised patients, but rarely occurs in children. Herpes zoster is most often seen in individuals previously infected with VZV, but it also has occurred in individuals without known varicella infection,1-17 possibly because these individuals had a prior subclinical VZV infection.
A live attenuated VZV vaccine was created after isolation of the virus from a child in Japan.2 Since the introduction of the vaccine in 1995 in the United States, the incidence of VZV and HZ has declined.5 Herpes zoster rates after vaccination vary from 14 to 19 per 100,000 individuals.3,5 Breakthrough disease with the wild-type strain does occur in vaccinated children, but vaccine-strain HZ also has been reported.1-5 The risk for HZ caused by reactivated VZV vaccine in healthy children is unknown. We present a case of HZ in an otherwise healthy 19-month-old boy with no known varicella exposure who received the VZV vaccine at 13 months of age.
Case Report
An otherwise healthy 19-month-old boy presented to the dermatology clinic with a rash that began 2 days prior on the right groin and spread to the right leg. The patient’s mother denied that the child had been febrile and noted that the rash did not appear to bother him in any way. The patient was up-to-date on his vaccinations and received the first dose of the varicella series 6 months prior to presentation. He had no personal history of varicella, no exposure to sick contacts with varicella, and no known exposure to the virus. He was otherwise completely healthy with no signs or symptoms of immunocompromise.
Physical examination revealed grouped vesicles on an erythematous base on the right thigh, right sacrum, and lower abdomen that did not cross the midline (Figure). There were no other pertinent physical examination findings. The eruption was most consistent with HZ but concern remained for herpes simplex virus (HSV) or impetigo. A bacterial culture and polymerase chain reaction assay for VZV and HSV from skin swabs was ordered. The patient was prescribed acyclovir 20 mg/kg every 6 hours for 5 days. Laboratory testing revealed a positive result for VZV on polymerase chain reaction and a negative result for HSV. The majority of the patient’s lesions had crusted after 2 days of treatment with acyclovir, and the rash had nearly resolved 1 week after presentation. Subsequent evaluation with a complete blood cell count with differential and basic metabolic profile was normal. Levels of IgG, IgA, and IgM also were normal; IgE was slightly elevated.
Comment
Herpes zoster in children is an uncommon clinical entity. Most children with HZ are immunocompromised, have a history of varicella, or were exposed to varicella during gestation.8 With the introduction of the live VZV vaccine, the incidence of HZ has declined, but reactivation of the live vaccine leading to HZ infection is possible. The vaccine is 90% effective, and breakthrough varicella has been reported in 15% to 20% of vaccinated patients.1-17 The cause of HZ in vaccinated children is unclear due to the potential for either wild-type or vaccine-strain VZV to induce HZ.
Twenty-two cases of HZ in healthy children after vaccination were identified with a PubMed search of articles indexed for MEDLINE using the search terms herpes zoster infection after vaccination and herpes zoster infection AND immunocompetent AND vaccination in separate searches for all English-language studies (Table). The search was limited to immunocompetent children and adolescents who were 18 years or younger with no history of varicella or exposure to varicella during gestation.
The mean age for HZ infection was 5.3 years. The average time between vaccination and HZ infection was 3.3 years. There was a spread of dermatomal patterns with cases in the first division of the trigeminal nerve, cervical, thoracic, lumbar, and sacral distributions. Of the 22 cases of HZ we reviewed, 16 underwent genotype testing to determine the source of the infection. The Oka vaccine strain virus was identified in 8 (50%) cases, while wild-type virus was found in 8 (50%) cases.1,2,4,5,7,8,10,11,13,14,16 Twelve cases were treated with acyclovir.2,3,5,6,9-12,14-17 The method of delivery, either oral or intravenous, and the length of treatment depended on the severity of the disease. Patients with meningoencephalitis and HZ ophthalmicus received intravenous acyclovir more often and also had a longer course of acyclovir compared to those individuals with involvement limited to the skin.
This review found HZ occurs from reactivation of wild-type or Oka vaccine-strain VZV in immunocompetent children.1-17 It shows that subclinical varicella infection is not the only explanation for HZ in a healthy vaccinated child. It is currently not clear why some healthy children experience HZ from vaccine-strain VZV. When HZ presents in a vaccinated immunocompetent child without a history of varicella infection or exposure, the possibility for vaccine strain–induced HZ should be considered.
Varicella-zoster virus (VZV) causes varicella as a primary infection. It is a highly contagious disease characterized by a widespread papulovesicular eruption with fever and malaise.1,2 After the primary infection, the virus remains latent within the sensory dorsal root ganglia and can reactivate as herpes zoster (HZ).1-5 Herpes zoster is characterized by unilateral radicular pain and a vesicular rash in a dermatomal pattern.1,2 It is most common in adults, especially elderly and immunocompromised patients, but rarely occurs in children. Herpes zoster is most often seen in individuals previously infected with VZV, but it also has occurred in individuals without known varicella infection,1-17 possibly because these individuals had a prior subclinical VZV infection.
A live attenuated VZV vaccine was created after isolation of the virus from a child in Japan.2 Since the introduction of the vaccine in 1995 in the United States, the incidence of VZV and HZ has declined.5 Herpes zoster rates after vaccination vary from 14 to 19 per 100,000 individuals.3,5 Breakthrough disease with the wild-type strain does occur in vaccinated children, but vaccine-strain HZ also has been reported.1-5 The risk for HZ caused by reactivated VZV vaccine in healthy children is unknown. We present a case of HZ in an otherwise healthy 19-month-old boy with no known varicella exposure who received the VZV vaccine at 13 months of age.
Case Report
An otherwise healthy 19-month-old boy presented to the dermatology clinic with a rash that began 2 days prior on the right groin and spread to the right leg. The patient’s mother denied that the child had been febrile and noted that the rash did not appear to bother him in any way. The patient was up-to-date on his vaccinations and received the first dose of the varicella series 6 months prior to presentation. He had no personal history of varicella, no exposure to sick contacts with varicella, and no known exposure to the virus. He was otherwise completely healthy with no signs or symptoms of immunocompromise.
Physical examination revealed grouped vesicles on an erythematous base on the right thigh, right sacrum, and lower abdomen that did not cross the midline (Figure). There were no other pertinent physical examination findings. The eruption was most consistent with HZ but concern remained for herpes simplex virus (HSV) or impetigo. A bacterial culture and polymerase chain reaction assay for VZV and HSV from skin swabs was ordered. The patient was prescribed acyclovir 20 mg/kg every 6 hours for 5 days. Laboratory testing revealed a positive result for VZV on polymerase chain reaction and a negative result for HSV. The majority of the patient’s lesions had crusted after 2 days of treatment with acyclovir, and the rash had nearly resolved 1 week after presentation. Subsequent evaluation with a complete blood cell count with differential and basic metabolic profile was normal. Levels of IgG, IgA, and IgM also were normal; IgE was slightly elevated.
Comment
Herpes zoster in children is an uncommon clinical entity. Most children with HZ are immunocompromised, have a history of varicella, or were exposed to varicella during gestation.8 With the introduction of the live VZV vaccine, the incidence of HZ has declined, but reactivation of the live vaccine leading to HZ infection is possible. The vaccine is 90% effective, and breakthrough varicella has been reported in 15% to 20% of vaccinated patients.1-17 The cause of HZ in vaccinated children is unclear due to the potential for either wild-type or vaccine-strain VZV to induce HZ.
Twenty-two cases of HZ in healthy children after vaccination were identified with a PubMed search of articles indexed for MEDLINE using the search terms herpes zoster infection after vaccination and herpes zoster infection AND immunocompetent AND vaccination in separate searches for all English-language studies (Table). The search was limited to immunocompetent children and adolescents who were 18 years or younger with no history of varicella or exposure to varicella during gestation.
The mean age for HZ infection was 5.3 years. The average time between vaccination and HZ infection was 3.3 years. There was a spread of dermatomal patterns with cases in the first division of the trigeminal nerve, cervical, thoracic, lumbar, and sacral distributions. Of the 22 cases of HZ we reviewed, 16 underwent genotype testing to determine the source of the infection. The Oka vaccine strain virus was identified in 8 (50%) cases, while wild-type virus was found in 8 (50%) cases.1,2,4,5,7,8,10,11,13,14,16 Twelve cases were treated with acyclovir.2,3,5,6,9-12,14-17 The method of delivery, either oral or intravenous, and the length of treatment depended on the severity of the disease. Patients with meningoencephalitis and HZ ophthalmicus received intravenous acyclovir more often and also had a longer course of acyclovir compared to those individuals with involvement limited to the skin.
This review found HZ occurs from reactivation of wild-type or Oka vaccine-strain VZV in immunocompetent children.1-17 It shows that subclinical varicella infection is not the only explanation for HZ in a healthy vaccinated child. It is currently not clear why some healthy children experience HZ from vaccine-strain VZV. When HZ presents in a vaccinated immunocompetent child without a history of varicella infection or exposure, the possibility for vaccine strain–induced HZ should be considered.
- . Herpes zoster in three healthy children immunized with varicella vaccine (Oka/Biken); the causative virus differed from vaccine strain on PCR analysis of the IV variable region (R5) and of a PstI-site region. Br J Dermatol. 1997;137:255-258.
- Uebe B, Sauerbrei A, Burdach S, et al. Herpes zoster by reactivated vaccine varicella zoster virus in a healthy child [published online June 25, 2002]. Eur J Pediatr. 2002;161:442-444.
- Obieta MP, Jacinto SS. Herpes zoster after varicella vaccination in a healthy young child. Int J Dermatol. 2008;47:640-641.
- Ota K, Kim V, Lavi S, et al. Vaccine-strain varicella zoster virus causing recurrent herpes zoster in an immunocompetent 2-year-old. Pediatr Infect Dis J. 2008;27:847-848.
- Liang GL, Heidelberg KA, Jacobson RM, et al. Herpes zoster after varicella vaccination. J Am Acad Dermatol. 1998;38:761-763.
- Matsubara K, Nigami H, Harigaya H, et al. Herpes zoster in a normal child after varicella vaccination. Acta Paediatr Jpn. 1995;37:648-650.
- Kohl S, Rapp J, Larussa P, et al. Natural varicella-zoster virus reactivation shortly after varicella immunization in a child. Pediatr Infect Dis J. 1999;18:1112-1113.
- Feder HM Jr, Hoss DM. Herpes zoster in otherwise healthy children. Pediatr Infect Dis J. 2004;23:451-457; quiz 458-460.
- Binder NR, Holland GN, Hosea S, et al. Herpes zoster ophthalmicus in an otherwise-healthy child. J AAPOS. 2005;9:597-598.
- Levin MJ, DeBiasi RL, Bostik V, et al. Herpes zoster with skin lesions and meningitis caused by 2 different genotypes of the Oka varicella-zoster virus vaccine. J Infect Dis. 2008;198:1444-1447.
- Iyer S, Mittal MK, Hodinka RL. Herpes zoster and meningitis resulting from reactivation of varicella vaccine virus in an immunocompetent child. Ann Emerg Med. 2009;53:792-795.
- Lin P, Yoon MK, Chiu CS. Herpes zoster keratouveitis and inflammatory ocular hypertension 8 years after varicella vaccination. Ocul Immunol Inflamm. 2009;17:33-35.
- Chouliaras G, Spoulou V, Quinlivan M, et al. Vaccine-associated herpes zoster ophthalmicus [correction of opthalmicus] and encephalitis in an immunocompetent child [published online March 1, 2010]. Pediatrics. 2010;125:E969-E972.
- Han JY, Hanson DC, Way SS. Herpes zoster and meningitis due to reactivation of varicella vaccine virus in an immunocompetent child. Pediatr Infect Dis J. 2011;30:266-268.
- Ryu WY, Kim NY, Kwon YH, et al. Herpes zoster ophthalmicus with isolated trochlear nerve palsy in an otherwise healthy 13-year-old girl. J AAPOS. 2014;18:193-195.
- Iwasaki S, Motokura K, Honda Y, et al. Vaccine-strain herpes zoster found in the trigeminal nerve area in a healthy child: a case report [published online November 3, 2016]. J Clin Virol. 2016;85:44-47.
- Peterson N, Goodman S, Peterson M, et al. Herpes zoster in children. Cutis. 2016;98:94-95.
- . Herpes zoster in three healthy children immunized with varicella vaccine (Oka/Biken); the causative virus differed from vaccine strain on PCR analysis of the IV variable region (R5) and of a PstI-site region. Br J Dermatol. 1997;137:255-258.
- Uebe B, Sauerbrei A, Burdach S, et al. Herpes zoster by reactivated vaccine varicella zoster virus in a healthy child [published online June 25, 2002]. Eur J Pediatr. 2002;161:442-444.
- Obieta MP, Jacinto SS. Herpes zoster after varicella vaccination in a healthy young child. Int J Dermatol. 2008;47:640-641.
- Ota K, Kim V, Lavi S, et al. Vaccine-strain varicella zoster virus causing recurrent herpes zoster in an immunocompetent 2-year-old. Pediatr Infect Dis J. 2008;27:847-848.
- Liang GL, Heidelberg KA, Jacobson RM, et al. Herpes zoster after varicella vaccination. J Am Acad Dermatol. 1998;38:761-763.
- Matsubara K, Nigami H, Harigaya H, et al. Herpes zoster in a normal child after varicella vaccination. Acta Paediatr Jpn. 1995;37:648-650.
- Kohl S, Rapp J, Larussa P, et al. Natural varicella-zoster virus reactivation shortly after varicella immunization in a child. Pediatr Infect Dis J. 1999;18:1112-1113.
- Feder HM Jr, Hoss DM. Herpes zoster in otherwise healthy children. Pediatr Infect Dis J. 2004;23:451-457; quiz 458-460.
- Binder NR, Holland GN, Hosea S, et al. Herpes zoster ophthalmicus in an otherwise-healthy child. J AAPOS. 2005;9:597-598.
- Levin MJ, DeBiasi RL, Bostik V, et al. Herpes zoster with skin lesions and meningitis caused by 2 different genotypes of the Oka varicella-zoster virus vaccine. J Infect Dis. 2008;198:1444-1447.
- Iyer S, Mittal MK, Hodinka RL. Herpes zoster and meningitis resulting from reactivation of varicella vaccine virus in an immunocompetent child. Ann Emerg Med. 2009;53:792-795.
- Lin P, Yoon MK, Chiu CS. Herpes zoster keratouveitis and inflammatory ocular hypertension 8 years after varicella vaccination. Ocul Immunol Inflamm. 2009;17:33-35.
- Chouliaras G, Spoulou V, Quinlivan M, et al. Vaccine-associated herpes zoster ophthalmicus [correction of opthalmicus] and encephalitis in an immunocompetent child [published online March 1, 2010]. Pediatrics. 2010;125:E969-E972.
- Han JY, Hanson DC, Way SS. Herpes zoster and meningitis due to reactivation of varicella vaccine virus in an immunocompetent child. Pediatr Infect Dis J. 2011;30:266-268.
- Ryu WY, Kim NY, Kwon YH, et al. Herpes zoster ophthalmicus with isolated trochlear nerve palsy in an otherwise healthy 13-year-old girl. J AAPOS. 2014;18:193-195.
- Iwasaki S, Motokura K, Honda Y, et al. Vaccine-strain herpes zoster found in the trigeminal nerve area in a healthy child: a case report [published online November 3, 2016]. J Clin Virol. 2016;85:44-47.
- Peterson N, Goodman S, Peterson M, et al. Herpes zoster in children. Cutis. 2016;98:94-95.
Practice Points
- Most children with herpes zoster are immunocompromised, have a history of varicella, or were exposed to varicella in utero.
- Herpes zoster has been reported in immunocompetent children due to either wild-type or vaccine-strain varicella-zoster virus.

Physicians need to take hyperhidrosis in teens seriously
ORLANDO – Not quite a fifth of teens experience excessive, uncontrollable sweating, according to the results of an online survey presented during this year’s annual American Academy of Dermatology.
Because nearly 70% of teens who reported the condition said it interferes with their activities of daily living, late-breaking research presenter, Adelaide A. Hebert, MD, chief of pediatric dermatology at the University of Texas, Houston, said it was time medical schools paid more attention to it.
For the study, Dr. Hebert and her colleagues online-surveyed 1,000 adolescents between 12 and 17 years who meet the accepted diagnostic criteria for primary focal hyperhidrosis. An analysis of the 981 surveys that were complete showed that 17.1% of respondents experienced excessive, uncontrollable sweating and that 68.6% of these reported the sweating was moderate or major, impairing their normal functioning.
The average age of onset for the condition was 11 years, although more than a quarter of respondents said their sweating began at age 10 years. Nearly all those surveyed said they sweat from at least two focal areas, with five areas being the average number of focal areas.
Adolescence is when hyperhidrosis begins for many adults with the condition, yet few if any data exist regarding the condition in this age group, according to Dr. Hebert. “We have to figure out what is going on so maybe we can make a difference later.”
wmcknight@frontlinemedcom.com
On Twitter @whitneymcknight
ORLANDO – Not quite a fifth of teens experience excessive, uncontrollable sweating, according to the results of an online survey presented during this year’s annual American Academy of Dermatology.
Because nearly 70% of teens who reported the condition said it interferes with their activities of daily living, late-breaking research presenter, Adelaide A. Hebert, MD, chief of pediatric dermatology at the University of Texas, Houston, said it was time medical schools paid more attention to it.
For the study, Dr. Hebert and her colleagues online-surveyed 1,000 adolescents between 12 and 17 years who meet the accepted diagnostic criteria for primary focal hyperhidrosis. An analysis of the 981 surveys that were complete showed that 17.1% of respondents experienced excessive, uncontrollable sweating and that 68.6% of these reported the sweating was moderate or major, impairing their normal functioning.
The average age of onset for the condition was 11 years, although more than a quarter of respondents said their sweating began at age 10 years. Nearly all those surveyed said they sweat from at least two focal areas, with five areas being the average number of focal areas.
Adolescence is when hyperhidrosis begins for many adults with the condition, yet few if any data exist regarding the condition in this age group, according to Dr. Hebert. “We have to figure out what is going on so maybe we can make a difference later.”
wmcknight@frontlinemedcom.com
On Twitter @whitneymcknight
ORLANDO – Not quite a fifth of teens experience excessive, uncontrollable sweating, according to the results of an online survey presented during this year’s annual American Academy of Dermatology.
Because nearly 70% of teens who reported the condition said it interferes with their activities of daily living, late-breaking research presenter, Adelaide A. Hebert, MD, chief of pediatric dermatology at the University of Texas, Houston, said it was time medical schools paid more attention to it.
For the study, Dr. Hebert and her colleagues online-surveyed 1,000 adolescents between 12 and 17 years who meet the accepted diagnostic criteria for primary focal hyperhidrosis. An analysis of the 981 surveys that were complete showed that 17.1% of respondents experienced excessive, uncontrollable sweating and that 68.6% of these reported the sweating was moderate or major, impairing their normal functioning.
The average age of onset for the condition was 11 years, although more than a quarter of respondents said their sweating began at age 10 years. Nearly all those surveyed said they sweat from at least two focal areas, with five areas being the average number of focal areas.
Adolescence is when hyperhidrosis begins for many adults with the condition, yet few if any data exist regarding the condition in this age group, according to Dr. Hebert. “We have to figure out what is going on so maybe we can make a difference later.”
wmcknight@frontlinemedcom.com
On Twitter @whitneymcknight
AT AAD 17
Key clinical point:
Major finding: Hyperhidrosis is common in 17% of teens surveyed; 69% of these reported hyperhidrosis interferes with activities of daily living.
Data source: Online survey of 1,000 U.S. teens between 12 and 17 years who reported excessive, uncontrollable sweating.
Disclosures: Dr. Hebert received a grant from GlaxoSmithKline for this study. She is also a board member of the International Hyperhidrosis Society.

VIDEO: Don’t overlook psychosocial concerns of vitiligo patients
ORLANDO – There are ways to assess the psychosocial needs of your patients with vitiligo, even if you don’t believe you have the necessary skills to do a complete mental health work-up, according to Seemal R. Desai, MD.
In an interview recorded at this year’s annual meeting of the American Academy of Dermatology, Dr. Desai, an assistant clinical professor of dermatology at the University of Texas, Dallas, shares his ideas for how to have casual conversations with patients that can help reveal important clues to psychosocial stress patients with this serious medical skin condition might be facing.
“There are subtle clues to look for to know that these patients are uncomfortable with others seeing their skin,” says Dr. Desai.
In the video interview, he also covers taking a multidisciplinary approach to caring for these patients, what treatments are available to those who are suffering psychosocial stress after having failed several interventions, and how patients from many Asian and African counties are especially at risk for ostracization.
“It’s important to let your patients know that you understand this is really affecting them psychosocially, and that you care,” says Dr. Desai.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
wmcknight@frontlinemedcom.com
On Twitter @whitneymcknight
ORLANDO – There are ways to assess the psychosocial needs of your patients with vitiligo, even if you don’t believe you have the necessary skills to do a complete mental health work-up, according to Seemal R. Desai, MD.
In an interview recorded at this year’s annual meeting of the American Academy of Dermatology, Dr. Desai, an assistant clinical professor of dermatology at the University of Texas, Dallas, shares his ideas for how to have casual conversations with patients that can help reveal important clues to psychosocial stress patients with this serious medical skin condition might be facing.
“There are subtle clues to look for to know that these patients are uncomfortable with others seeing their skin,” says Dr. Desai.
In the video interview, he also covers taking a multidisciplinary approach to caring for these patients, what treatments are available to those who are suffering psychosocial stress after having failed several interventions, and how patients from many Asian and African counties are especially at risk for ostracization.
“It’s important to let your patients know that you understand this is really affecting them psychosocially, and that you care,” says Dr. Desai.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
wmcknight@frontlinemedcom.com
On Twitter @whitneymcknight
ORLANDO – There are ways to assess the psychosocial needs of your patients with vitiligo, even if you don’t believe you have the necessary skills to do a complete mental health work-up, according to Seemal R. Desai, MD.
In an interview recorded at this year’s annual meeting of the American Academy of Dermatology, Dr. Desai, an assistant clinical professor of dermatology at the University of Texas, Dallas, shares his ideas for how to have casual conversations with patients that can help reveal important clues to psychosocial stress patients with this serious medical skin condition might be facing.
“There are subtle clues to look for to know that these patients are uncomfortable with others seeing their skin,” says Dr. Desai.
In the video interview, he also covers taking a multidisciplinary approach to caring for these patients, what treatments are available to those who are suffering psychosocial stress after having failed several interventions, and how patients from many Asian and African counties are especially at risk for ostracization.
“It’s important to let your patients know that you understand this is really affecting them psychosocially, and that you care,” says Dr. Desai.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
wmcknight@frontlinemedcom.com
On Twitter @whitneymcknight
EXPERT ANALYSIS FROM AAD 17

Long-term peanut sublingual immunotherapy found safe
ATLANTA – Peanut sublingual immunotherapy induces clinically significant desensitization in the majority of subjects and can induce sustained unresponsiveness in a subset of children treated for 36-60 months, results from a small study suggest.
“Sublingual immunotherapy [SLIT] is an easy-to-administer treatment that appears to be safe, and with extended treatment, may provide a clinically significant amount of protection with the potential for a lasting effect,” one of the study authors, Edwin H. Kim, MD, said in an interview in advance of the annual meeting of the American Academy of Allergy, Asthma, and Immunology.

To find out, the researchers treated 37 patients with 2 mg of peanut SLIT for 36-60 months and then assessed a 5,000-mg peanut oral food challenge to further assess desensitization. Those who passed the challenge discontinued SLIT for 2-4 weeks and were then re-challenged with 5,000 mg of peanut protein to assess for sustained unresponsiveness.
“Existing data suggested that about 50% of patients on oral immunotherapy develop sustained unresponsiveness, which was defined by being able to tolerate the same full amount of peanut 1 month after stopping therapy,” Dr. Kim said. “As the assumption was that SLIT would have a more modest effect, it was unclear if any patients at all on SLIT would develop sustained unresponsiveness.”
Of the 37 subjects who completed the study, 32 (86%) safely ingested more than 300 mg of peanut and 12 (32%) passed the oral food challenge at the end of SLIT therapy. The median amount of peanut tolerated was 1,750 mg (compared with 1,710 mg in the original 12-month paper). The 12 subjects who passed the oral food challenge were re-challenged with 5,000 mg of peanut 2-4 weeks after discontinuing SLIT. Of these, 10 (27%) demonstrated sustained unresponsiveness. Dr. Kim characterized the results as “better than we would have expected.”
He acknowledged certain limitations to the study, including the lack of an entry food challenge to determine a baseline reaction threshold and the lack of a placebo arm for the study’s extended maintenance phase.
Dr. Kim reported having no financial disclosures.
dbrunk@frontlinemedcom.com
ATLANTA – Peanut sublingual immunotherapy induces clinically significant desensitization in the majority of subjects and can induce sustained unresponsiveness in a subset of children treated for 36-60 months, results from a small study suggest.
“Sublingual immunotherapy [SLIT] is an easy-to-administer treatment that appears to be safe, and with extended treatment, may provide a clinically significant amount of protection with the potential for a lasting effect,” one of the study authors, Edwin H. Kim, MD, said in an interview in advance of the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
To find out, the researchers treated 37 patients with 2 mg of peanut SLIT for 36-60 months and then assessed a 5,000-mg peanut oral food challenge to further assess desensitization. Those who passed the challenge discontinued SLIT for 2-4 weeks and were then re-challenged with 5,000 mg of peanut protein to assess for sustained unresponsiveness.
“Existing data suggested that about 50% of patients on oral immunotherapy develop sustained unresponsiveness, which was defined by being able to tolerate the same full amount of peanut 1 month after stopping therapy,” Dr. Kim said. “As the assumption was that SLIT would have a more modest effect, it was unclear if any patients at all on SLIT would develop sustained unresponsiveness.”
Of the 37 subjects who completed the study, 32 (86%) safely ingested more than 300 mg of peanut and 12 (32%) passed the oral food challenge at the end of SLIT therapy. The median amount of peanut tolerated was 1,750 mg (compared with 1,710 mg in the original 12-month paper). The 12 subjects who passed the oral food challenge were re-challenged with 5,000 mg of peanut 2-4 weeks after discontinuing SLIT. Of these, 10 (27%) demonstrated sustained unresponsiveness. Dr. Kim characterized the results as “better than we would have expected.”
He acknowledged certain limitations to the study, including the lack of an entry food challenge to determine a baseline reaction threshold and the lack of a placebo arm for the study’s extended maintenance phase.
Dr. Kim reported having no financial disclosures.
dbrunk@frontlinemedcom.com
ATLANTA – Peanut sublingual immunotherapy induces clinically significant desensitization in the majority of subjects and can induce sustained unresponsiveness in a subset of children treated for 36-60 months, results from a small study suggest.
“Sublingual immunotherapy [SLIT] is an easy-to-administer treatment that appears to be safe, and with extended treatment, may provide a clinically significant amount of protection with the potential for a lasting effect,” one of the study authors, Edwin H. Kim, MD, said in an interview in advance of the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
To find out, the researchers treated 37 patients with 2 mg of peanut SLIT for 36-60 months and then assessed a 5,000-mg peanut oral food challenge to further assess desensitization. Those who passed the challenge discontinued SLIT for 2-4 weeks and were then re-challenged with 5,000 mg of peanut protein to assess for sustained unresponsiveness.
“Existing data suggested that about 50% of patients on oral immunotherapy develop sustained unresponsiveness, which was defined by being able to tolerate the same full amount of peanut 1 month after stopping therapy,” Dr. Kim said. “As the assumption was that SLIT would have a more modest effect, it was unclear if any patients at all on SLIT would develop sustained unresponsiveness.”
Of the 37 subjects who completed the study, 32 (86%) safely ingested more than 300 mg of peanut and 12 (32%) passed the oral food challenge at the end of SLIT therapy. The median amount of peanut tolerated was 1,750 mg (compared with 1,710 mg in the original 12-month paper). The 12 subjects who passed the oral food challenge were re-challenged with 5,000 mg of peanut 2-4 weeks after discontinuing SLIT. Of these, 10 (27%) demonstrated sustained unresponsiveness. Dr. Kim characterized the results as “better than we would have expected.”
He acknowledged certain limitations to the study, including the lack of an entry food challenge to determine a baseline reaction threshold and the lack of a placebo arm for the study’s extended maintenance phase.
Dr. Kim reported having no financial disclosures.
dbrunk@frontlinemedcom.com
AT THE 2017 AAAAI ANNUAL MEETING
Key clinical point:
Major finding: Of the children who completed the study, 86% safely ingested more than 300 mg of peanut and 32% passed the oral food challenge at the end of SLIT therapy.
Data source: A study of 37 patients who were treated with 2 mg of peanut SLIT for 36-60 months.
Disclosures: Dr. Kim reported having no financial disclosures.
Uptick found in severe allergy shot reactions
ATLANTA – Systemic reactions against subcutaneous allergen immunotherapy have trended down overall in recent years, but there has been an uptick in reports of severe grade 4 reactions for reasons that are not yet clear, according to a review of 46.6 million injection office visits from 2008-2015.
The data come from annual surveys of members of the American Academy of Allergy, Asthma, and Immunology and of the American College of Allergy, Asthma, and Immunology, of whom 27%-51% responded each year.

However, on surveys from 2013 to 2015, one grade 4 reaction – hypotension or respiratory failure – was reported for every 160,000 injection visits, up from one per million office visits in previous years. Two-thirds (152/252) of grade 3/4 systemic reactions (SRs) for 2014-2015 occurred in asthmatics. Among the three fatalities directly linked to allergy shots since 2008, all of them occurred in adults; two patients had asthma. The findings highlight the need for good asthma control before shots begin, with a forced expiratory volume of at least 70% in 1 second (J Allergy Clin Immunol. 2017 Feb;139[2]:AB377).
“Asthma remains a major risk factor for severe SRs... [It’s something] allergists need to be vigilant about,” said lead investigator Tolly Epstein, MD, an assistant professor of immunology at the University of Cincinnati.
It’s unclear if there has been a true increase in severe reactions, or simply better reporting of them since the reaction grading system started being used a few years ago. “I was surprised a little bit to see the uptick in severe systemic reactions, but I am not sure if it’s real yet,” Dr. Epstein said. She and her colleagues are collecting more data on the reports of severe reactions.
Dr. Epstein and her colleagues found in previous work that higher maintenance doses may increase the risk of SRs. The right balance between efficacy and safety is still being worked out, she said at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
The surveys started collecting data on infections from allergy shots in 2014, amid concerns about contaminants in compounded medications. The fact that none were reported probably isn’t a surprise to allergists, but it might be news to others who have raised concerns about the possibility, Dr. Epstein said.
Overall safety was good for sublingual allergen immunotherapy, first approved by the Food and Drug Administration in 2014. One of the grade 3 reactions was pharyngeal edema; the other involved throat tightening and lower respiratory symptoms.
One of the asthma patients who died was morbidly obese and under treatment for weed allergies during pollen season, and died from overwhelming laryngeal edema. The patient’s weight made IV access difficult. The other asthma patient had severe disease, and was on the maximum dose of fluticasone/salmeterol. He was on an accelerated buildup for dust mites, pollen, mold, and other allergies, and apparently died of asthma complications triggered by the shots. There were no known risk factors in the third death.
Mortalities are lower than they used to be in the past with allergy shots, Dr. Epstein said.
She said she had no relevant disclosures.
aotto@frontlinemedcom.com
ATLANTA – Systemic reactions against subcutaneous allergen immunotherapy have trended down overall in recent years, but there has been an uptick in reports of severe grade 4 reactions for reasons that are not yet clear, according to a review of 46.6 million injection office visits from 2008-2015.
The data come from annual surveys of members of the American Academy of Allergy, Asthma, and Immunology and of the American College of Allergy, Asthma, and Immunology, of whom 27%-51% responded each year.
However, on surveys from 2013 to 2015, one grade 4 reaction – hypotension or respiratory failure – was reported for every 160,000 injection visits, up from one per million office visits in previous years. Two-thirds (152/252) of grade 3/4 systemic reactions (SRs) for 2014-2015 occurred in asthmatics. Among the three fatalities directly linked to allergy shots since 2008, all of them occurred in adults; two patients had asthma. The findings highlight the need for good asthma control before shots begin, with a forced expiratory volume of at least 70% in 1 second (J Allergy Clin Immunol. 2017 Feb;139[2]:AB377).
“Asthma remains a major risk factor for severe SRs... [It’s something] allergists need to be vigilant about,” said lead investigator Tolly Epstein, MD, an assistant professor of immunology at the University of Cincinnati.
It’s unclear if there has been a true increase in severe reactions, or simply better reporting of them since the reaction grading system started being used a few years ago. “I was surprised a little bit to see the uptick in severe systemic reactions, but I am not sure if it’s real yet,” Dr. Epstein said. She and her colleagues are collecting more data on the reports of severe reactions.
Dr. Epstein and her colleagues found in previous work that higher maintenance doses may increase the risk of SRs. The right balance between efficacy and safety is still being worked out, she said at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
The surveys started collecting data on infections from allergy shots in 2014, amid concerns about contaminants in compounded medications. The fact that none were reported probably isn’t a surprise to allergists, but it might be news to others who have raised concerns about the possibility, Dr. Epstein said.
Overall safety was good for sublingual allergen immunotherapy, first approved by the Food and Drug Administration in 2014. One of the grade 3 reactions was pharyngeal edema; the other involved throat tightening and lower respiratory symptoms.
One of the asthma patients who died was morbidly obese and under treatment for weed allergies during pollen season, and died from overwhelming laryngeal edema. The patient’s weight made IV access difficult. The other asthma patient had severe disease, and was on the maximum dose of fluticasone/salmeterol. He was on an accelerated buildup for dust mites, pollen, mold, and other allergies, and apparently died of asthma complications triggered by the shots. There were no known risk factors in the third death.
Mortalities are lower than they used to be in the past with allergy shots, Dr. Epstein said.
She said she had no relevant disclosures.
aotto@frontlinemedcom.com
ATLANTA – Systemic reactions against subcutaneous allergen immunotherapy have trended down overall in recent years, but there has been an uptick in reports of severe grade 4 reactions for reasons that are not yet clear, according to a review of 46.6 million injection office visits from 2008-2015.
The data come from annual surveys of members of the American Academy of Allergy, Asthma, and Immunology and of the American College of Allergy, Asthma, and Immunology, of whom 27%-51% responded each year.
However, on surveys from 2013 to 2015, one grade 4 reaction – hypotension or respiratory failure – was reported for every 160,000 injection visits, up from one per million office visits in previous years. Two-thirds (152/252) of grade 3/4 systemic reactions (SRs) for 2014-2015 occurred in asthmatics. Among the three fatalities directly linked to allergy shots since 2008, all of them occurred in adults; two patients had asthma. The findings highlight the need for good asthma control before shots begin, with a forced expiratory volume of at least 70% in 1 second (J Allergy Clin Immunol. 2017 Feb;139[2]:AB377).
“Asthma remains a major risk factor for severe SRs... [It’s something] allergists need to be vigilant about,” said lead investigator Tolly Epstein, MD, an assistant professor of immunology at the University of Cincinnati.
It’s unclear if there has been a true increase in severe reactions, or simply better reporting of them since the reaction grading system started being used a few years ago. “I was surprised a little bit to see the uptick in severe systemic reactions, but I am not sure if it’s real yet,” Dr. Epstein said. She and her colleagues are collecting more data on the reports of severe reactions.
Dr. Epstein and her colleagues found in previous work that higher maintenance doses may increase the risk of SRs. The right balance between efficacy and safety is still being worked out, she said at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
The surveys started collecting data on infections from allergy shots in 2014, amid concerns about contaminants in compounded medications. The fact that none were reported probably isn’t a surprise to allergists, but it might be news to others who have raised concerns about the possibility, Dr. Epstein said.
Overall safety was good for sublingual allergen immunotherapy, first approved by the Food and Drug Administration in 2014. One of the grade 3 reactions was pharyngeal edema; the other involved throat tightening and lower respiratory symptoms.
One of the asthma patients who died was morbidly obese and under treatment for weed allergies during pollen season, and died from overwhelming laryngeal edema. The patient’s weight made IV access difficult. The other asthma patient had severe disease, and was on the maximum dose of fluticasone/salmeterol. He was on an accelerated buildup for dust mites, pollen, mold, and other allergies, and apparently died of asthma complications triggered by the shots. There were no known risk factors in the third death.
Mortalities are lower than they used to be in the past with allergy shots, Dr. Epstein said.
She said she had no relevant disclosures.
aotto@frontlinemedcom.com
AT THE 2017 AAAAI ANNUAL MEETING
Key clinical point: for reasons that are not yet clear, according to a review of 46.6 million injection office visits from 2008-2015.
Major finding: On surveys from 2013 to 2015, one grade 4 reaction – hypotension or respiratory failure – was reported for every 160,000 injection visits, up from one per million office visits in previous years. Two-thirds (152/252) of grade 3/4 systemic reactions for 2014-2015 occurred in patients with asthma.
Data source: Allergist surveys from 2008 to 2015.
Disclosures: The lead investigator said she had no relevant disclosures.
Maternal vitamin E isoform levels possible marker for infant wheezing risk
ATLANTA – Increasing maternal postpartum–plasma alpha-tocopherol isoform concentration was associated with a decreased likelihood of wheezing at age 2 years, defined as wheezing in the past 12 months, use of asthma medications in the past 12 months, or diagnosis of asthma, results from a large analysis showed.
“For now, this is an association and not causation,” study author Cosby Stone, MD, MPH, said in an interview in advance of the annual meeting of the American Academy of Allergy, Asthma, and Immunology. “We need a clinical trial to evaluate the effect of giving more alpha-tocopherol to mothers during pregnancy before anyone should jump to giving supplements.”

The median age of children at the time of maternal sample collection was 50 days. 47% were female, and 61% were white. Of the 652 children, 167 (26%) met criteria for wheezing at age 2 years. These children had mothers with significantly lower postpartum concentrations of plasma alpha-tocopherol, compared with those who did not meet criteria for wheezing at 2 years (a mean of 69 micromol/L vs. 75 micromol/L, respectively; P = .02). In multivariable regression analysis, the researchers detected a significant interaction between gamma-tocopherol and alpha-tocopherol, where the highest amounts of maternal gamma-tocopherol modified and mitigated the protective association of maternal alpha-tocopherol with risk of wheezing at 2 years (P = .05).
Dr. Stone cautioned that, what is currently labeled as vitamin E or alpha-tocopherol in foods and supplements, “could be any of eight different isoforms, and alpha-tocopherol may not actually be the dominant isoform being provided. In addition, the oils that we eat are the main sources of tocopherols in our diet, and they vary widely in terms of their tocopherol isoforms. Sunflower and safflower oil, for example, provide predominantly alpha-tocopherol as their isoform of vitamin E, while corn and soy oil provide predominantly gamma-tocopherol.”
For now, he continued, correcting maternal alpha-tocopherol deficiency, currently defined by a serum alpha-tocopherol concentration less than 11.6 micromol/L, is certainly reasonable. Down the road, modification of maternal alpha-tocopherol or gamma-tocopherol concentrations through dietary counseling may provide clinicians with a tool to prevent wheezing or asthma in affected children. “In the future there may be a role for checking tocopherol isoforms in pregnant women and then modifying dietary oil consumption to protect the health of their children,” he said.
He acknowledged certain limitations of the study, including that researchers obtained maternal vitamin E isoform measurements at enrollment, when the infants were, on average, 6 weeks post partum, and not during pregnancy. “However, the literature has shown that postpartum vitamin E levels at this time point are very similar to those during the second trimester of pregnancy,” Dr. Stone said. “The literature has also shown that plasma vitamin E isoform concentrations are tightly tied to diet and body stores and do not change very rapidly (such that a woman would not be likely to go from the highest quartile to the lowest, or vice versa). People’s diets don’t tend to change that much, in general.”
INSPIRE is funded by the National Institutes of Health. Dr. Stone is funded by an NIH training grant through Vanderbilt University. He reported having no relevant financial disclosures.
ATLANTA – Increasing maternal postpartum–plasma alpha-tocopherol isoform concentration was associated with a decreased likelihood of wheezing at age 2 years, defined as wheezing in the past 12 months, use of asthma medications in the past 12 months, or diagnosis of asthma, results from a large analysis showed.
“For now, this is an association and not causation,” study author Cosby Stone, MD, MPH, said in an interview in advance of the annual meeting of the American Academy of Allergy, Asthma, and Immunology. “We need a clinical trial to evaluate the effect of giving more alpha-tocopherol to mothers during pregnancy before anyone should jump to giving supplements.”
The median age of children at the time of maternal sample collection was 50 days. 47% were female, and 61% were white. Of the 652 children, 167 (26%) met criteria for wheezing at age 2 years. These children had mothers with significantly lower postpartum concentrations of plasma alpha-tocopherol, compared with those who did not meet criteria for wheezing at 2 years (a mean of 69 micromol/L vs. 75 micromol/L, respectively; P = .02). In multivariable regression analysis, the researchers detected a significant interaction between gamma-tocopherol and alpha-tocopherol, where the highest amounts of maternal gamma-tocopherol modified and mitigated the protective association of maternal alpha-tocopherol with risk of wheezing at 2 years (P = .05).
Dr. Stone cautioned that, what is currently labeled as vitamin E or alpha-tocopherol in foods and supplements, “could be any of eight different isoforms, and alpha-tocopherol may not actually be the dominant isoform being provided. In addition, the oils that we eat are the main sources of tocopherols in our diet, and they vary widely in terms of their tocopherol isoforms. Sunflower and safflower oil, for example, provide predominantly alpha-tocopherol as their isoform of vitamin E, while corn and soy oil provide predominantly gamma-tocopherol.”
For now, he continued, correcting maternal alpha-tocopherol deficiency, currently defined by a serum alpha-tocopherol concentration less than 11.6 micromol/L, is certainly reasonable. Down the road, modification of maternal alpha-tocopherol or gamma-tocopherol concentrations through dietary counseling may provide clinicians with a tool to prevent wheezing or asthma in affected children. “In the future there may be a role for checking tocopherol isoforms in pregnant women and then modifying dietary oil consumption to protect the health of their children,” he said.
He acknowledged certain limitations of the study, including that researchers obtained maternal vitamin E isoform measurements at enrollment, when the infants were, on average, 6 weeks post partum, and not during pregnancy. “However, the literature has shown that postpartum vitamin E levels at this time point are very similar to those during the second trimester of pregnancy,” Dr. Stone said. “The literature has also shown that plasma vitamin E isoform concentrations are tightly tied to diet and body stores and do not change very rapidly (such that a woman would not be likely to go from the highest quartile to the lowest, or vice versa). People’s diets don’t tend to change that much, in general.”
INSPIRE is funded by the National Institutes of Health. Dr. Stone is funded by an NIH training grant through Vanderbilt University. He reported having no relevant financial disclosures.
ATLANTA – Increasing maternal postpartum–plasma alpha-tocopherol isoform concentration was associated with a decreased likelihood of wheezing at age 2 years, defined as wheezing in the past 12 months, use of asthma medications in the past 12 months, or diagnosis of asthma, results from a large analysis showed.
“For now, this is an association and not causation,” study author Cosby Stone, MD, MPH, said in an interview in advance of the annual meeting of the American Academy of Allergy, Asthma, and Immunology. “We need a clinical trial to evaluate the effect of giving more alpha-tocopherol to mothers during pregnancy before anyone should jump to giving supplements.”
The median age of children at the time of maternal sample collection was 50 days. 47% were female, and 61% were white. Of the 652 children, 167 (26%) met criteria for wheezing at age 2 years. These children had mothers with significantly lower postpartum concentrations of plasma alpha-tocopherol, compared with those who did not meet criteria for wheezing at 2 years (a mean of 69 micromol/L vs. 75 micromol/L, respectively; P = .02). In multivariable regression analysis, the researchers detected a significant interaction between gamma-tocopherol and alpha-tocopherol, where the highest amounts of maternal gamma-tocopherol modified and mitigated the protective association of maternal alpha-tocopherol with risk of wheezing at 2 years (P = .05).
Dr. Stone cautioned that, what is currently labeled as vitamin E or alpha-tocopherol in foods and supplements, “could be any of eight different isoforms, and alpha-tocopherol may not actually be the dominant isoform being provided. In addition, the oils that we eat are the main sources of tocopherols in our diet, and they vary widely in terms of their tocopherol isoforms. Sunflower and safflower oil, for example, provide predominantly alpha-tocopherol as their isoform of vitamin E, while corn and soy oil provide predominantly gamma-tocopherol.”
For now, he continued, correcting maternal alpha-tocopherol deficiency, currently defined by a serum alpha-tocopherol concentration less than 11.6 micromol/L, is certainly reasonable. Down the road, modification of maternal alpha-tocopherol or gamma-tocopherol concentrations through dietary counseling may provide clinicians with a tool to prevent wheezing or asthma in affected children. “In the future there may be a role for checking tocopherol isoforms in pregnant women and then modifying dietary oil consumption to protect the health of their children,” he said.
He acknowledged certain limitations of the study, including that researchers obtained maternal vitamin E isoform measurements at enrollment, when the infants were, on average, 6 weeks post partum, and not during pregnancy. “However, the literature has shown that postpartum vitamin E levels at this time point are very similar to those during the second trimester of pregnancy,” Dr. Stone said. “The literature has also shown that plasma vitamin E isoform concentrations are tightly tied to diet and body stores and do not change very rapidly (such that a woman would not be likely to go from the highest quartile to the lowest, or vice versa). People’s diets don’t tend to change that much, in general.”
INSPIRE is funded by the National Institutes of Health. Dr. Stone is funded by an NIH training grant through Vanderbilt University. He reported having no relevant financial disclosures.
AT THE 2017 AAAAI ANNUAL MEETING
Key clinical point:
Major finding: Increasing maternal postpartum–plasma alpha-tocopherol concentration was associated with a decreased likelihood of wheezing requiring asthma medications at 2 years (P = .02).
Data source: A prospective evaluation of 652 children with maternal postpartum–plasma vitamin E isoforms measured at study enrollment.
Disclosures: INSPIRE is funded by the National Institutes of Health. Dr. Stone is funded by an NIH training grant through Vanderbilt University. He reported having no relevant financial disclosures.
Study advances precision opioid dosing for mucositis

ORLANDO, FL—A pilot study to determine the burden of mucositis in pediatric patients undergoing hematopoietic stem cell transplant (HSCT) showed that more than 50% of patients required a change in their opioids either for toxicity or lack of efficacy.
Investigators also observed that patients’ genotypes were associated with time to optimal pain control, although this needs to be defined more clearly in larger prospective studies.
“Pain from mucositis is a major problem during the early post-transplant period in pediatric patients,” said M. Christa Krupski, DO, of Cincinnati Children’s Hospital Medical Center in Ohio.
The pain frequently requires intravenous (IV) pain medication, but adequate pain management is often delayed by the trial and error of finding the right agent or the right dose, Dr Krupski added.
She and her colleagues tried to find predictors of mucositis that would help optimize pain control and minimize adverse effects of pain medication.
Dr Krupski presented the group’s findings at the 2017 BMT Tandem Meetings as abstract 50*.
Based on the investigators’ previous experience using a pain chip, they hypothesized that host genetic polymorphisms would predict perception of mucositis pain, opioid efficacy, and opioid-induced adverse effects in pediatric patients undergoing HSCT.
The pain chip was comprised of a panel of 46 single-nucleotide polymorphisms (SNPs) in a set of candidate genes known to influence opioid effect.
Study design
In this single-institution, retrospective pilot study, investigators genotyped 100 consecutive HSCT patients using pre-transplant samples.
The team collected demographic and transplant data, information on the utilization of pain medication, and mucositis data according to the standard CTCAE guidelines.
“And it must be noted,” Dr Krupski said, “that many of our patients required total parenteral nutrition during the transplant process, which automatically made them a grade 3 for mucositis.”
The investigators assessed pain using 2 scales, the Face, Legs, Activity, Cry, Consolability (FLACC) Scale, which is an objective measurement, and the more subjective Numeric Rating Scores (NRS).
Demographics
Patients were a median age of 9.9 years (range, 0.5–32.8), 65% were male, 87% were Caucasian, and 13% non-Caucasian.
The main indications for transplant were malignancy (45%), immune deficiency/dysregulation (30%), and bone marrow failure syndrome (19%).
More than two-thirds (68%) of patients had received a myeloablative conditioning regimen.
Results—mucositis
Seventy-six patients experienced mucositis, three-quarters of whom (78%) had received a myeloablative conditioning regimen.
The majority of patients (57%) had severe mucositis, which developed a median of 3 days after transplant (range, -2 to 17).
Regarding treatment, 13 (17%) had medication as needed or no medication, 5 (7%) had scheduled IV opioid, and 58 (76%) had patient-controlled analgesia (PCA).
For analysis purposes, the investigators grouped together the scheduled IV opioid and PCA treatment groups.
Results—opioid efficacy
The opioid efficacy analysis was based on 63 patients.
Time to optimal pain control was a median of 7 days (range, 0–22), and the morphine dose at the time of optimal pain control was a median of 1.5 mg/kg (range, 0.2–15.7).
“You will note, though, the wide inter-patient variability,” Dr Krupski pointed out, “with some of our patients immediately achieving optimal pain control the day the medication was started and others taking over 3 weeks to reach optimal pain control.”
Investigators observed similar inter-patient variability in morphine equivalent use at the time of optimal pain control and total morphine equivalent use.
The total time patients were on PCA was a median of 16 days (range, 1–32), and the median total morphine equivalent use was 0.99 mg/kg/day (range, 0.10–8.07).
“Most interesting, though, was that 18 patients, or nearly one-third of the patients requiring IV opioids, required a change in this opioid due to poor efficacy,” Dr Krupski said.
Results—opioid toxicity
Thirty-two (51%) patients experienced at least 1 adverse effect from their pain medication.
Specific toxicities, based on 32 patients, included pruritus (53%), sedation (16%), and nausea/vomiting (9%). Six patients (19%) had more than one adverse event.
“Similar to what we observed with respect to opioid efficacy,” Dr Krupski said, “another one-third of our patients with mucositis required a change in opioid due to toxicity.”
Results—impact of race
Non-Caucasians patients (n=13) had a significantly higher incidence of mucositis (100%) than Caucasians (n=87, 72%, P=0.03).
Non-Caucasian patients also experienced significantly more pain with mucositis (P=0.03), even though the severity of mucositis did not differ between the 2 groups.
The total equivalent dose of morphine used also did not differ between the groups.
“This raises the question of whether there are factors other than race that may be contributing to this difference,” Dr Krupski said.
Genetic findings
The UGT2B7 gene encodes the main enzyme metabolizer of morphine, and SNPs of this gene (rs7668258 and rs7439366) vary by race.
Non-Caucasian patients had significantly more wild-type SNPs than Caucasian patients (P=0.001). And patients with the wild-type UGT2B7 genotype spent more total days on IV opioids than patients with variant alleles (P=0.03).
On examination of rs4633, a SNP of the COMT gene, which is a key regulator of pain perception, the investigators observed some different findings from what had previously been reported.
There was no difference in mucositis severity between patients with the wild-type and variant allele (P=0.3).
However, patients with the variant allele required more days to optimal pain control than patients with the wild-type allele (P=0.04). This finding confirmed increased pain sensitivity associated with the genotype, irrespective of race.
“[I]f this association holds true in future studies,” Dr Krupski explained, “one may be more aggressive in the initial opioid titration to optimize pain control.”
Despite limitations of sample size, especially with respect to non-Caucasian patients, the pilot study showed association, but not causation, with respect to genetic variants.
“Racial differences affect mucositis pain perception and opioid requirement,” Dr Krupski said. “If genotyping is not feasible, it is important to pay particular attention to this difference while managing patients’ pain from mucositis.”
“We have an opportunity here to improve our care. Therefore, our plan is to validate these findings in additional patients before we use them to achieve our ultimate goal: precision dosing of opioids to individual patients.” ![]()
*Data in the abstract differ slightly from the presentation.
ORLANDO, FL—A pilot study to determine the burden of mucositis in pediatric patients undergoing hematopoietic stem cell transplant (HSCT) showed that more than 50% of patients required a change in their opioids either for toxicity or lack of efficacy.
Investigators also observed that patients’ genotypes were associated with time to optimal pain control, although this needs to be defined more clearly in larger prospective studies.
“Pain from mucositis is a major problem during the early post-transplant period in pediatric patients,” said M. Christa Krupski, DO, of Cincinnati Children’s Hospital Medical Center in Ohio.
The pain frequently requires intravenous (IV) pain medication, but adequate pain management is often delayed by the trial and error of finding the right agent or the right dose, Dr Krupski added.
She and her colleagues tried to find predictors of mucositis that would help optimize pain control and minimize adverse effects of pain medication.
Dr Krupski presented the group’s findings at the 2017 BMT Tandem Meetings as abstract 50*.
Based on the investigators’ previous experience using a pain chip, they hypothesized that host genetic polymorphisms would predict perception of mucositis pain, opioid efficacy, and opioid-induced adverse effects in pediatric patients undergoing HSCT.
The pain chip was comprised of a panel of 46 single-nucleotide polymorphisms (SNPs) in a set of candidate genes known to influence opioid effect.
Study design
In this single-institution, retrospective pilot study, investigators genotyped 100 consecutive HSCT patients using pre-transplant samples.
The team collected demographic and transplant data, information on the utilization of pain medication, and mucositis data according to the standard CTCAE guidelines.
“And it must be noted,” Dr Krupski said, “that many of our patients required total parenteral nutrition during the transplant process, which automatically made them a grade 3 for mucositis.”
The investigators assessed pain using 2 scales, the Face, Legs, Activity, Cry, Consolability (FLACC) Scale, which is an objective measurement, and the more subjective Numeric Rating Scores (NRS).
Demographics
Patients were a median age of 9.9 years (range, 0.5–32.8), 65% were male, 87% were Caucasian, and 13% non-Caucasian.
The main indications for transplant were malignancy (45%), immune deficiency/dysregulation (30%), and bone marrow failure syndrome (19%).
More than two-thirds (68%) of patients had received a myeloablative conditioning regimen.
Results—mucositis
Seventy-six patients experienced mucositis, three-quarters of whom (78%) had received a myeloablative conditioning regimen.
The majority of patients (57%) had severe mucositis, which developed a median of 3 days after transplant (range, -2 to 17).
Regarding treatment, 13 (17%) had medication as needed or no medication, 5 (7%) had scheduled IV opioid, and 58 (76%) had patient-controlled analgesia (PCA).
For analysis purposes, the investigators grouped together the scheduled IV opioid and PCA treatment groups.
Results—opioid efficacy
The opioid efficacy analysis was based on 63 patients.
Time to optimal pain control was a median of 7 days (range, 0–22), and the morphine dose at the time of optimal pain control was a median of 1.5 mg/kg (range, 0.2–15.7).
“You will note, though, the wide inter-patient variability,” Dr Krupski pointed out, “with some of our patients immediately achieving optimal pain control the day the medication was started and others taking over 3 weeks to reach optimal pain control.”
Investigators observed similar inter-patient variability in morphine equivalent use at the time of optimal pain control and total morphine equivalent use.
The total time patients were on PCA was a median of 16 days (range, 1–32), and the median total morphine equivalent use was 0.99 mg/kg/day (range, 0.10–8.07).
“Most interesting, though, was that 18 patients, or nearly one-third of the patients requiring IV opioids, required a change in this opioid due to poor efficacy,” Dr Krupski said.
Results—opioid toxicity
Thirty-two (51%) patients experienced at least 1 adverse effect from their pain medication.
Specific toxicities, based on 32 patients, included pruritus (53%), sedation (16%), and nausea/vomiting (9%). Six patients (19%) had more than one adverse event.
“Similar to what we observed with respect to opioid efficacy,” Dr Krupski said, “another one-third of our patients with mucositis required a change in opioid due to toxicity.”
Results—impact of race
Non-Caucasians patients (n=13) had a significantly higher incidence of mucositis (100%) than Caucasians (n=87, 72%, P=0.03).
Non-Caucasian patients also experienced significantly more pain with mucositis (P=0.03), even though the severity of mucositis did not differ between the 2 groups.
The total equivalent dose of morphine used also did not differ between the groups.
“This raises the question of whether there are factors other than race that may be contributing to this difference,” Dr Krupski said.
Genetic findings
The UGT2B7 gene encodes the main enzyme metabolizer of morphine, and SNPs of this gene (rs7668258 and rs7439366) vary by race.
Non-Caucasian patients had significantly more wild-type SNPs than Caucasian patients (P=0.001). And patients with the wild-type UGT2B7 genotype spent more total days on IV opioids than patients with variant alleles (P=0.03).
On examination of rs4633, a SNP of the COMT gene, which is a key regulator of pain perception, the investigators observed some different findings from what had previously been reported.
There was no difference in mucositis severity between patients with the wild-type and variant allele (P=0.3).
However, patients with the variant allele required more days to optimal pain control than patients with the wild-type allele (P=0.04). This finding confirmed increased pain sensitivity associated with the genotype, irrespective of race.
“[I]f this association holds true in future studies,” Dr Krupski explained, “one may be more aggressive in the initial opioid titration to optimize pain control.”
Despite limitations of sample size, especially with respect to non-Caucasian patients, the pilot study showed association, but not causation, with respect to genetic variants.
“Racial differences affect mucositis pain perception and opioid requirement,” Dr Krupski said. “If genotyping is not feasible, it is important to pay particular attention to this difference while managing patients’ pain from mucositis.”
“We have an opportunity here to improve our care. Therefore, our plan is to validate these findings in additional patients before we use them to achieve our ultimate goal: precision dosing of opioids to individual patients.” ![]()
*Data in the abstract differ slightly from the presentation.
ORLANDO, FL—A pilot study to determine the burden of mucositis in pediatric patients undergoing hematopoietic stem cell transplant (HSCT) showed that more than 50% of patients required a change in their opioids either for toxicity or lack of efficacy.
Investigators also observed that patients’ genotypes were associated with time to optimal pain control, although this needs to be defined more clearly in larger prospective studies.
“Pain from mucositis is a major problem during the early post-transplant period in pediatric patients,” said M. Christa Krupski, DO, of Cincinnati Children’s Hospital Medical Center in Ohio.
The pain frequently requires intravenous (IV) pain medication, but adequate pain management is often delayed by the trial and error of finding the right agent or the right dose, Dr Krupski added.
She and her colleagues tried to find predictors of mucositis that would help optimize pain control and minimize adverse effects of pain medication.
Dr Krupski presented the group’s findings at the 2017 BMT Tandem Meetings as abstract 50*.
Based on the investigators’ previous experience using a pain chip, they hypothesized that host genetic polymorphisms would predict perception of mucositis pain, opioid efficacy, and opioid-induced adverse effects in pediatric patients undergoing HSCT.
The pain chip was comprised of a panel of 46 single-nucleotide polymorphisms (SNPs) in a set of candidate genes known to influence opioid effect.
Study design
In this single-institution, retrospective pilot study, investigators genotyped 100 consecutive HSCT patients using pre-transplant samples.
The team collected demographic and transplant data, information on the utilization of pain medication, and mucositis data according to the standard CTCAE guidelines.
“And it must be noted,” Dr Krupski said, “that many of our patients required total parenteral nutrition during the transplant process, which automatically made them a grade 3 for mucositis.”
The investigators assessed pain using 2 scales, the Face, Legs, Activity, Cry, Consolability (FLACC) Scale, which is an objective measurement, and the more subjective Numeric Rating Scores (NRS).
Demographics
Patients were a median age of 9.9 years (range, 0.5–32.8), 65% were male, 87% were Caucasian, and 13% non-Caucasian.
The main indications for transplant were malignancy (45%), immune deficiency/dysregulation (30%), and bone marrow failure syndrome (19%).
More than two-thirds (68%) of patients had received a myeloablative conditioning regimen.
Results—mucositis
Seventy-six patients experienced mucositis, three-quarters of whom (78%) had received a myeloablative conditioning regimen.
The majority of patients (57%) had severe mucositis, which developed a median of 3 days after transplant (range, -2 to 17).
Regarding treatment, 13 (17%) had medication as needed or no medication, 5 (7%) had scheduled IV opioid, and 58 (76%) had patient-controlled analgesia (PCA).
For analysis purposes, the investigators grouped together the scheduled IV opioid and PCA treatment groups.
Results—opioid efficacy
The opioid efficacy analysis was based on 63 patients.
Time to optimal pain control was a median of 7 days (range, 0–22), and the morphine dose at the time of optimal pain control was a median of 1.5 mg/kg (range, 0.2–15.7).
“You will note, though, the wide inter-patient variability,” Dr Krupski pointed out, “with some of our patients immediately achieving optimal pain control the day the medication was started and others taking over 3 weeks to reach optimal pain control.”
Investigators observed similar inter-patient variability in morphine equivalent use at the time of optimal pain control and total morphine equivalent use.
The total time patients were on PCA was a median of 16 days (range, 1–32), and the median total morphine equivalent use was 0.99 mg/kg/day (range, 0.10–8.07).
“Most interesting, though, was that 18 patients, or nearly one-third of the patients requiring IV opioids, required a change in this opioid due to poor efficacy,” Dr Krupski said.
Results—opioid toxicity
Thirty-two (51%) patients experienced at least 1 adverse effect from their pain medication.
Specific toxicities, based on 32 patients, included pruritus (53%), sedation (16%), and nausea/vomiting (9%). Six patients (19%) had more than one adverse event.
“Similar to what we observed with respect to opioid efficacy,” Dr Krupski said, “another one-third of our patients with mucositis required a change in opioid due to toxicity.”
Results—impact of race
Non-Caucasians patients (n=13) had a significantly higher incidence of mucositis (100%) than Caucasians (n=87, 72%, P=0.03).
Non-Caucasian patients also experienced significantly more pain with mucositis (P=0.03), even though the severity of mucositis did not differ between the 2 groups.
The total equivalent dose of morphine used also did not differ between the groups.
“This raises the question of whether there are factors other than race that may be contributing to this difference,” Dr Krupski said.
Genetic findings
The UGT2B7 gene encodes the main enzyme metabolizer of morphine, and SNPs of this gene (rs7668258 and rs7439366) vary by race.
Non-Caucasian patients had significantly more wild-type SNPs than Caucasian patients (P=0.001). And patients with the wild-type UGT2B7 genotype spent more total days on IV opioids than patients with variant alleles (P=0.03).
On examination of rs4633, a SNP of the COMT gene, which is a key regulator of pain perception, the investigators observed some different findings from what had previously been reported.
There was no difference in mucositis severity between patients with the wild-type and variant allele (P=0.3).
However, patients with the variant allele required more days to optimal pain control than patients with the wild-type allele (P=0.04). This finding confirmed increased pain sensitivity associated with the genotype, irrespective of race.
“[I]f this association holds true in future studies,” Dr Krupski explained, “one may be more aggressive in the initial opioid titration to optimize pain control.”
Despite limitations of sample size, especially with respect to non-Caucasian patients, the pilot study showed association, but not causation, with respect to genetic variants.
“Racial differences affect mucositis pain perception and opioid requirement,” Dr Krupski said. “If genotyping is not feasible, it is important to pay particular attention to this difference while managing patients’ pain from mucositis.”
“We have an opportunity here to improve our care. Therefore, our plan is to validate these findings in additional patients before we use them to achieve our ultimate goal: precision dosing of opioids to individual patients.” ![]()
*Data in the abstract differ slightly from the presentation.
Family-based treatment of anorexia promising
LAS VEGAS – Mounting evidence demonstrates that a family-based approach to treating adolescents with anorexia nervosa usually is more effective than hospitalization.
“In the history of psychiatric literature, families have been blamed a lot for psychiatric problems in their children,” James Lock, MD, PhD, said at the annual psychopharmacology update held by the Nevada Psychiatric Association. “Parents are put off by anorexia nervosa, because it’s a very confusing illness and terrifying for them to have their children radically change their behavior. These are kids who are often high achieving and have generally been easy to manage: self-starters, self-directors. Then, suddenly, over a period of 6-7 months, they go from being very well to being at death’s door.”
Enter family-based treatment (FBT) for anorexia nervosa, an outpatient intervention appropriate for children and adolescents who are medically stable. Developed around 2001, FBT is designed to restore weight and put the patient’s development back on track. It’s a team approach consisting of a primary therapist, a pediatrician, and a child and adolescent psychiatrist. Brief hospitalization sometimes is used to resolve medical concerns. Dr. Lock, professor of psychiatry and behavioral sciences at Stanford (Calif.) University, described FBT as “a highly focused staged treatment that emphasizes behavioral recovery rather than insight and understanding or cognitive change. This approach might indirectly improve family functioning and reduce eating-related cognitive distortions for the adolescent.”
According to Dr. Lock, coauthor with Daniel Le Grange, PhD, of “Treatment Manual for Anorexia Nervosa: A Family-Based Approach” second edition, (New York: Guilford Press, 2015), the current evidence base for FBT is limited, consisting of 879 patients enrolled in 11 studies at 12 different sites in four countries, as well as one meta-analysis. “We have not done the kind of research in anorexia nervosa that we need to do,” he said. “Parents ask me this every time I sit down with them: ‘Why don’t we know more? Why don’t we have more clinical guidance?’ It’s not been a priority despite the seriousness of this problem [and the] lifelong impact it has.”
Interest in FBT emerged in part because of studies demonstrating the limitations of hospitalizing patients with the disorder. One trial from the United Kingdom found that, among 90 children who were randomized to one of two outpatient treatments, to an inpatient arm, or to no treatment, no differences in outcomes were observed among the treatment groups (Br J Psychiatry. 1991;159:325-33). Similar results were found in a trial of 167 children who were randomized to either inpatient psychiatric treatment or two forms of outpatient management (Br J Psychiatry. 2007;191[5]:427-35). “If you think hospitalization will cure kids with anorexia, this study tells you that isn’t true,” Dr. Lock said. “It doesn’t say that it doesn’t benefit some people. What it says is that, on average, it’s not better than outpatient treatment for adolescents with anorexia nervosa. It’s important to build systems of care around that knowledge.”
Dr. Lock has his own opinion as to why inpatient psychiatric treatment alone usually doesn’t help anorexia nervosa patients in the long-term. “Learning in an inpatient setting is not generalizable,” he said. “You cannot learn and apply the learning that you get in the hospital to your real life: in your family and your school and your social processes. You can dress up psychotherapy any way you want to, but ultimately, it’s about learning. Can parents learn to be effective at helping their children with anorexia nervosa recover?”
In general, FBT is delivered in three phases over the course of 6-12 months. Phase I involves helping parents assume control of weight restoration in their child. “It tries to accomplish at home what could have been accomplished at a hospital by a nursing staff who are trained and able to disrupt and manage destructive behaviors that lead to weight loss and reinforce cognitive distortions,” Dr. Lock said. In phase II, parents gradually hand control over eating back to their child, while phase III involves shifting the family back to discussing adolescent issues without anorexia nervosa at the center of their concern. One fundamental assumption of FBT, he continued, is that it takes an agnostic view as to the cause of anorexia.
“We don’t have to address cause in order to have an effective treatment,” said Dr. Lock, also a professor of pediatrics at the university. “We are going to try to help patients and parents feel valued, not blamed. Secondly, we need to engage parents in a consultative way, recognizing their skills around their family, and help them apply that to anorexia nervosa.” The expected outcome should be a healthy weight, based on the child’s age. According to Dr. Lock, 79% of patients who have gained at least 4 pounds after 4 weeks of FBT will have a favorable treatment response, while 71% of those who don’t meet that benchmark are likely to fail treatment. “The therapeutic alliance is important in treatment outcome, but our studies suggest it is not enough,” he said. “You have to engage people in treatment to get them started, but if you don’t help the parents be effective in promoting weight gain, your therapeutic alliance will diminish.”
In a randomized trial that compared FBT with adolescent-focused individual therapy (AFT) for adolescents with anorexia nervosa, Dr. Lock and his associates found that, at both 6- and 12-month follow-up, FBT was significantly superior to AFT in helping patients achieve full remission, which was defined as normal weight for age and a mean global Eating Disorder Examination score within one standard deviation of published means (Arch Gen Psychiatry. 2010;67[10]:1025-32). A separate trial found that, after FBT was implemented at the Royal Children’s Hospital, Melbourne, admissions decreased by 50%, readmissions decreased by 75%, and the overall number of days patients spent in the hospital fell by 51% (J Pediatr Health Care. 2014 Jul-Aug 28[4]:322-30).
During the first FBT meeting with patients and their families, Dr. Lock discusses the hazards of anorexia nervosa, including the increased risk of death by cardiac arrest and suicide. “I instill the fact that we have a crisis on our hands, and we need to block the development of anorexia nervosa,” he said. “We have no evidence-based treatments for anorexia nervosa once it becomes chronic, and that occurs after about 5 years. The onset is about age 14. At age 19, on average, your chances of complete recovery are greatly diminished. Of course, you can still be of help by supporting improvement in the quality of their lives; you may help improve their thinking and you may help them restore weight, but many will live with the ongoing anorexia nervosa. So, our greatest chance to be effective is early intervention and the window of opportunity is 3-4 years.” Emphasizing these realities “stops people,” he said. “It’s meant to bring them into clear awareness of what they’re facing.”
Dr. Lock disclosed that he has received grant or research support from the National Institute of Mental Health. He also is a consultant for the Training Institute for Child and Adolescent Eating Disorders and has received royalties from Guilford Press and Oxford Press.
LAS VEGAS – Mounting evidence demonstrates that a family-based approach to treating adolescents with anorexia nervosa usually is more effective than hospitalization.
“In the history of psychiatric literature, families have been blamed a lot for psychiatric problems in their children,” James Lock, MD, PhD, said at the annual psychopharmacology update held by the Nevada Psychiatric Association. “Parents are put off by anorexia nervosa, because it’s a very confusing illness and terrifying for them to have their children radically change their behavior. These are kids who are often high achieving and have generally been easy to manage: self-starters, self-directors. Then, suddenly, over a period of 6-7 months, they go from being very well to being at death’s door.”
Enter family-based treatment (FBT) for anorexia nervosa, an outpatient intervention appropriate for children and adolescents who are medically stable. Developed around 2001, FBT is designed to restore weight and put the patient’s development back on track. It’s a team approach consisting of a primary therapist, a pediatrician, and a child and adolescent psychiatrist. Brief hospitalization sometimes is used to resolve medical concerns. Dr. Lock, professor of psychiatry and behavioral sciences at Stanford (Calif.) University, described FBT as “a highly focused staged treatment that emphasizes behavioral recovery rather than insight and understanding or cognitive change. This approach might indirectly improve family functioning and reduce eating-related cognitive distortions for the adolescent.”
According to Dr. Lock, coauthor with Daniel Le Grange, PhD, of “Treatment Manual for Anorexia Nervosa: A Family-Based Approach” second edition, (New York: Guilford Press, 2015), the current evidence base for FBT is limited, consisting of 879 patients enrolled in 11 studies at 12 different sites in four countries, as well as one meta-analysis. “We have not done the kind of research in anorexia nervosa that we need to do,” he said. “Parents ask me this every time I sit down with them: ‘Why don’t we know more? Why don’t we have more clinical guidance?’ It’s not been a priority despite the seriousness of this problem [and the] lifelong impact it has.”
Interest in FBT emerged in part because of studies demonstrating the limitations of hospitalizing patients with the disorder. One trial from the United Kingdom found that, among 90 children who were randomized to one of two outpatient treatments, to an inpatient arm, or to no treatment, no differences in outcomes were observed among the treatment groups (Br J Psychiatry. 1991;159:325-33). Similar results were found in a trial of 167 children who were randomized to either inpatient psychiatric treatment or two forms of outpatient management (Br J Psychiatry. 2007;191[5]:427-35). “If you think hospitalization will cure kids with anorexia, this study tells you that isn’t true,” Dr. Lock said. “It doesn’t say that it doesn’t benefit some people. What it says is that, on average, it’s not better than outpatient treatment for adolescents with anorexia nervosa. It’s important to build systems of care around that knowledge.”
Dr. Lock has his own opinion as to why inpatient psychiatric treatment alone usually doesn’t help anorexia nervosa patients in the long-term. “Learning in an inpatient setting is not generalizable,” he said. “You cannot learn and apply the learning that you get in the hospital to your real life: in your family and your school and your social processes. You can dress up psychotherapy any way you want to, but ultimately, it’s about learning. Can parents learn to be effective at helping their children with anorexia nervosa recover?”
In general, FBT is delivered in three phases over the course of 6-12 months. Phase I involves helping parents assume control of weight restoration in their child. “It tries to accomplish at home what could have been accomplished at a hospital by a nursing staff who are trained and able to disrupt and manage destructive behaviors that lead to weight loss and reinforce cognitive distortions,” Dr. Lock said. In phase II, parents gradually hand control over eating back to their child, while phase III involves shifting the family back to discussing adolescent issues without anorexia nervosa at the center of their concern. One fundamental assumption of FBT, he continued, is that it takes an agnostic view as to the cause of anorexia.
“We don’t have to address cause in order to have an effective treatment,” said Dr. Lock, also a professor of pediatrics at the university. “We are going to try to help patients and parents feel valued, not blamed. Secondly, we need to engage parents in a consultative way, recognizing their skills around their family, and help them apply that to anorexia nervosa.” The expected outcome should be a healthy weight, based on the child’s age. According to Dr. Lock, 79% of patients who have gained at least 4 pounds after 4 weeks of FBT will have a favorable treatment response, while 71% of those who don’t meet that benchmark are likely to fail treatment. “The therapeutic alliance is important in treatment outcome, but our studies suggest it is not enough,” he said. “You have to engage people in treatment to get them started, but if you don’t help the parents be effective in promoting weight gain, your therapeutic alliance will diminish.”
In a randomized trial that compared FBT with adolescent-focused individual therapy (AFT) for adolescents with anorexia nervosa, Dr. Lock and his associates found that, at both 6- and 12-month follow-up, FBT was significantly superior to AFT in helping patients achieve full remission, which was defined as normal weight for age and a mean global Eating Disorder Examination score within one standard deviation of published means (Arch Gen Psychiatry. 2010;67[10]:1025-32). A separate trial found that, after FBT was implemented at the Royal Children’s Hospital, Melbourne, admissions decreased by 50%, readmissions decreased by 75%, and the overall number of days patients spent in the hospital fell by 51% (J Pediatr Health Care. 2014 Jul-Aug 28[4]:322-30).
During the first FBT meeting with patients and their families, Dr. Lock discusses the hazards of anorexia nervosa, including the increased risk of death by cardiac arrest and suicide. “I instill the fact that we have a crisis on our hands, and we need to block the development of anorexia nervosa,” he said. “We have no evidence-based treatments for anorexia nervosa once it becomes chronic, and that occurs after about 5 years. The onset is about age 14. At age 19, on average, your chances of complete recovery are greatly diminished. Of course, you can still be of help by supporting improvement in the quality of their lives; you may help improve their thinking and you may help them restore weight, but many will live with the ongoing anorexia nervosa. So, our greatest chance to be effective is early intervention and the window of opportunity is 3-4 years.” Emphasizing these realities “stops people,” he said. “It’s meant to bring them into clear awareness of what they’re facing.”
Dr. Lock disclosed that he has received grant or research support from the National Institute of Mental Health. He also is a consultant for the Training Institute for Child and Adolescent Eating Disorders and has received royalties from Guilford Press and Oxford Press.
LAS VEGAS – Mounting evidence demonstrates that a family-based approach to treating adolescents with anorexia nervosa usually is more effective than hospitalization.
“In the history of psychiatric literature, families have been blamed a lot for psychiatric problems in their children,” James Lock, MD, PhD, said at the annual psychopharmacology update held by the Nevada Psychiatric Association. “Parents are put off by anorexia nervosa, because it’s a very confusing illness and terrifying for them to have their children radically change their behavior. These are kids who are often high achieving and have generally been easy to manage: self-starters, self-directors. Then, suddenly, over a period of 6-7 months, they go from being very well to being at death’s door.”
Enter family-based treatment (FBT) for anorexia nervosa, an outpatient intervention appropriate for children and adolescents who are medically stable. Developed around 2001, FBT is designed to restore weight and put the patient’s development back on track. It’s a team approach consisting of a primary therapist, a pediatrician, and a child and adolescent psychiatrist. Brief hospitalization sometimes is used to resolve medical concerns. Dr. Lock, professor of psychiatry and behavioral sciences at Stanford (Calif.) University, described FBT as “a highly focused staged treatment that emphasizes behavioral recovery rather than insight and understanding or cognitive change. This approach might indirectly improve family functioning and reduce eating-related cognitive distortions for the adolescent.”
According to Dr. Lock, coauthor with Daniel Le Grange, PhD, of “Treatment Manual for Anorexia Nervosa: A Family-Based Approach” second edition, (New York: Guilford Press, 2015), the current evidence base for FBT is limited, consisting of 879 patients enrolled in 11 studies at 12 different sites in four countries, as well as one meta-analysis. “We have not done the kind of research in anorexia nervosa that we need to do,” he said. “Parents ask me this every time I sit down with them: ‘Why don’t we know more? Why don’t we have more clinical guidance?’ It’s not been a priority despite the seriousness of this problem [and the] lifelong impact it has.”
Interest in FBT emerged in part because of studies demonstrating the limitations of hospitalizing patients with the disorder. One trial from the United Kingdom found that, among 90 children who were randomized to one of two outpatient treatments, to an inpatient arm, or to no treatment, no differences in outcomes were observed among the treatment groups (Br J Psychiatry. 1991;159:325-33). Similar results were found in a trial of 167 children who were randomized to either inpatient psychiatric treatment or two forms of outpatient management (Br J Psychiatry. 2007;191[5]:427-35). “If you think hospitalization will cure kids with anorexia, this study tells you that isn’t true,” Dr. Lock said. “It doesn’t say that it doesn’t benefit some people. What it says is that, on average, it’s not better than outpatient treatment for adolescents with anorexia nervosa. It’s important to build systems of care around that knowledge.”
Dr. Lock has his own opinion as to why inpatient psychiatric treatment alone usually doesn’t help anorexia nervosa patients in the long-term. “Learning in an inpatient setting is not generalizable,” he said. “You cannot learn and apply the learning that you get in the hospital to your real life: in your family and your school and your social processes. You can dress up psychotherapy any way you want to, but ultimately, it’s about learning. Can parents learn to be effective at helping their children with anorexia nervosa recover?”
In general, FBT is delivered in three phases over the course of 6-12 months. Phase I involves helping parents assume control of weight restoration in their child. “It tries to accomplish at home what could have been accomplished at a hospital by a nursing staff who are trained and able to disrupt and manage destructive behaviors that lead to weight loss and reinforce cognitive distortions,” Dr. Lock said. In phase II, parents gradually hand control over eating back to their child, while phase III involves shifting the family back to discussing adolescent issues without anorexia nervosa at the center of their concern. One fundamental assumption of FBT, he continued, is that it takes an agnostic view as to the cause of anorexia.
“We don’t have to address cause in order to have an effective treatment,” said Dr. Lock, also a professor of pediatrics at the university. “We are going to try to help patients and parents feel valued, not blamed. Secondly, we need to engage parents in a consultative way, recognizing their skills around their family, and help them apply that to anorexia nervosa.” The expected outcome should be a healthy weight, based on the child’s age. According to Dr. Lock, 79% of patients who have gained at least 4 pounds after 4 weeks of FBT will have a favorable treatment response, while 71% of those who don’t meet that benchmark are likely to fail treatment. “The therapeutic alliance is important in treatment outcome, but our studies suggest it is not enough,” he said. “You have to engage people in treatment to get them started, but if you don’t help the parents be effective in promoting weight gain, your therapeutic alliance will diminish.”
In a randomized trial that compared FBT with adolescent-focused individual therapy (AFT) for adolescents with anorexia nervosa, Dr. Lock and his associates found that, at both 6- and 12-month follow-up, FBT was significantly superior to AFT in helping patients achieve full remission, which was defined as normal weight for age and a mean global Eating Disorder Examination score within one standard deviation of published means (Arch Gen Psychiatry. 2010;67[10]:1025-32). A separate trial found that, after FBT was implemented at the Royal Children’s Hospital, Melbourne, admissions decreased by 50%, readmissions decreased by 75%, and the overall number of days patients spent in the hospital fell by 51% (J Pediatr Health Care. 2014 Jul-Aug 28[4]:322-30).
During the first FBT meeting with patients and their families, Dr. Lock discusses the hazards of anorexia nervosa, including the increased risk of death by cardiac arrest and suicide. “I instill the fact that we have a crisis on our hands, and we need to block the development of anorexia nervosa,” he said. “We have no evidence-based treatments for anorexia nervosa once it becomes chronic, and that occurs after about 5 years. The onset is about age 14. At age 19, on average, your chances of complete recovery are greatly diminished. Of course, you can still be of help by supporting improvement in the quality of their lives; you may help improve their thinking and you may help them restore weight, but many will live with the ongoing anorexia nervosa. So, our greatest chance to be effective is early intervention and the window of opportunity is 3-4 years.” Emphasizing these realities “stops people,” he said. “It’s meant to bring them into clear awareness of what they’re facing.”
Dr. Lock disclosed that he has received grant or research support from the National Institute of Mental Health. He also is a consultant for the Training Institute for Child and Adolescent Eating Disorders and has received royalties from Guilford Press and Oxford Press.