User login
POLICY CORNER: An inside look at the most pressing policy issues
On Feb. 16, the Agency for Healthcare Research and Quality (AHRQ) listed SHM as a patient safety organization (PSO). A PSO serves as an independent, external, expert organization that can collect, analyze, and aggregate information in order to develop insights into the underlying causes of patient-safety events. PSOs are designed to help clinicians, hospitals, and healthcare organizations improve patient safety and the quality of healthcare delivery.
PSO status allows SHM’s current quality-improvement (QI) activities to be conducted in a secure environment that is protected from legal discovery. AHRQ currently lists 78 PSOs, including the Society for Vascular Surgery PSO, the Emergency Medicine Patient Safety Foundation, and the Biomedical Research and Education Foundation. A full list is available at www.pso.ahrq.gov/listing/psolist.htm.
To achieve PSO status, SHM worked closely with AHRQ to meet specific guidelines and requirements. One of the requirements is that the mission and primary activity of a PSO must be to conduct activities that are designed to improve patient safety and the quality of healthcare delivery.
To comply, SHM formed a separate component within the Quality Initiatives Department strictly to pursue patient safety and quality activities.
The SHM PSO will be unique. While PSOs are required to collect patient-safety data and provide some form of feedback to contracted sites, few have their own QI initiatives, and even fewer are established by a national physician’s professional society.
These differences will help the SHM PSO stand out from the crowd and will present opportunities within the healthcare reform framework. The Affordable Care Act (ACA) requires significant QI among the nation’s hospitals.
Specifically pertaining to PSOs, Section 399KK, a rarely mentioned section of the ACA, requires the Health and Human Services to establish a program for hospitals with high readmission rates to improve their rates through the use of PSOs. The details of this program remain unclear, but based upon the little bit of information currently available, there could be positive overlap between SHM’s Project BOOST (Better Outcomes for Older Adults through Safe Transitions) and the provision.
AHRQ’s recognition of the SHM PSO exemplifies SHM’s commitment to improving the quality of healthcare delivery. It also provides additional value to sites that implement SHM’s QI initiatives and will hopefully open new doors to SHM’s members. TH
On Feb. 16, the Agency for Healthcare Research and Quality (AHRQ) listed SHM as a patient safety organization (PSO). A PSO serves as an independent, external, expert organization that can collect, analyze, and aggregate information in order to develop insights into the underlying causes of patient-safety events. PSOs are designed to help clinicians, hospitals, and healthcare organizations improve patient safety and the quality of healthcare delivery.
PSO status allows SHM’s current quality-improvement (QI) activities to be conducted in a secure environment that is protected from legal discovery. AHRQ currently lists 78 PSOs, including the Society for Vascular Surgery PSO, the Emergency Medicine Patient Safety Foundation, and the Biomedical Research and Education Foundation. A full list is available at www.pso.ahrq.gov/listing/psolist.htm.
To achieve PSO status, SHM worked closely with AHRQ to meet specific guidelines and requirements. One of the requirements is that the mission and primary activity of a PSO must be to conduct activities that are designed to improve patient safety and the quality of healthcare delivery.
To comply, SHM formed a separate component within the Quality Initiatives Department strictly to pursue patient safety and quality activities.
The SHM PSO will be unique. While PSOs are required to collect patient-safety data and provide some form of feedback to contracted sites, few have their own QI initiatives, and even fewer are established by a national physician’s professional society.
These differences will help the SHM PSO stand out from the crowd and will present opportunities within the healthcare reform framework. The Affordable Care Act (ACA) requires significant QI among the nation’s hospitals.
Specifically pertaining to PSOs, Section 399KK, a rarely mentioned section of the ACA, requires the Health and Human Services to establish a program for hospitals with high readmission rates to improve their rates through the use of PSOs. The details of this program remain unclear, but based upon the little bit of information currently available, there could be positive overlap between SHM’s Project BOOST (Better Outcomes for Older Adults through Safe Transitions) and the provision.
AHRQ’s recognition of the SHM PSO exemplifies SHM’s commitment to improving the quality of healthcare delivery. It also provides additional value to sites that implement SHM’s QI initiatives and will hopefully open new doors to SHM’s members. TH
On Feb. 16, the Agency for Healthcare Research and Quality (AHRQ) listed SHM as a patient safety organization (PSO). A PSO serves as an independent, external, expert organization that can collect, analyze, and aggregate information in order to develop insights into the underlying causes of patient-safety events. PSOs are designed to help clinicians, hospitals, and healthcare organizations improve patient safety and the quality of healthcare delivery.
PSO status allows SHM’s current quality-improvement (QI) activities to be conducted in a secure environment that is protected from legal discovery. AHRQ currently lists 78 PSOs, including the Society for Vascular Surgery PSO, the Emergency Medicine Patient Safety Foundation, and the Biomedical Research and Education Foundation. A full list is available at www.pso.ahrq.gov/listing/psolist.htm.
To achieve PSO status, SHM worked closely with AHRQ to meet specific guidelines and requirements. One of the requirements is that the mission and primary activity of a PSO must be to conduct activities that are designed to improve patient safety and the quality of healthcare delivery.
To comply, SHM formed a separate component within the Quality Initiatives Department strictly to pursue patient safety and quality activities.
The SHM PSO will be unique. While PSOs are required to collect patient-safety data and provide some form of feedback to contracted sites, few have their own QI initiatives, and even fewer are established by a national physician’s professional society.
These differences will help the SHM PSO stand out from the crowd and will present opportunities within the healthcare reform framework. The Affordable Care Act (ACA) requires significant QI among the nation’s hospitals.
Specifically pertaining to PSOs, Section 399KK, a rarely mentioned section of the ACA, requires the Health and Human Services to establish a program for hospitals with high readmission rates to improve their rates through the use of PSOs. The details of this program remain unclear, but based upon the little bit of information currently available, there could be positive overlap between SHM’s Project BOOST (Better Outcomes for Older Adults through Safe Transitions) and the provision.
AHRQ’s recognition of the SHM PSO exemplifies SHM’s commitment to improving the quality of healthcare delivery. It also provides additional value to sites that implement SHM’s QI initiatives and will hopefully open new doors to SHM’s members. TH
Minivan, Major Lesson

I recently visited my parents in my ancestral home of Wisconsin. As parents of a certain age, they inexplicably are genetically predisposed to owning a minivan. Another quirk of their DNA is that they must own a new minivan. No sooner has the last wisp of new-car smell osmosed from the burled walnut interior than they are trading up to the newest, tricked-out minivan. Perhaps more puzzling is the manner of pride they display in their minivan.
Now, my dad, as if not readily apparent, is not cool. And to see him folded into the driver’s seat, his furry-ear-to-furry-ear grin signaling a self-satisfaction customarily reserved for his grandchildren, painstakingly recounting glory-day stories and 4:30 p.m. dinner buffets, further solidifies his place in the Annals of Uncool.
When I’m home, they tend to employ my chauffeur services (most likely in retribution for my peri-pubescent years), and on the first day back home, I stopped their newest ride near the back door of the house, foot idling on the brake while this exchange occurred: “That’s a fascinating story about how much more challenging the world was when you were my age, Dad. You are a true American hero. Would you like to get out here or in the garage?”
“Here,” he replied.
“OK, then get out,” I countered.
“I can’t,” he responded knowingly.
“Why not?” I queried, the patience seeping from my voice.
“Because the door’s not open,” he answered, seemingly mocking me.
“Then open it,” I replied, silently recounting the evidence for his institutionalization.
“I can’t,” he responded.
“Why not?” I replied again, this time calculating the likelihood that I was adopted.
“Because it’s locked,” came his retort.
“Then unlock it,” I answered, reconfirming my decision to move away for college.
“I can’t,” he replied, ostensibly encouraging parenticide.
“Why not?” I queried, strongly contemplating parenticide.
“Because you haven’t put the car in park,” he responded triumphantly.
A System So Safe
As a safety feature, the minivan needed to be in park before you could open the door to exit. I’ve never heard of anyone actually falling out of a moving car, but recollecting high school, I can fathom the right mix, type, and number of teenagers where possibility would meet inevitability. But, apparently, enough people are falling out of moving vehicles that car engineers have built a system that is so safe, this can’t happen. So no matter how hard someone tries, it just isn’t possible to fall out of a moving car (believe me, toward the end of a week of my father’s car stories, my mind had worked every possible angle).
Likewise, newer vehicles employ occupant-sensitive sensors that detect the weight, size, and position of the passenger to determine if the airbag should deploy. Rather than depending on the driver to turn the passenger-side airbag on or off, the car does it for you: heavy enough to trigger the sensor, and the airbag will deploy; too light, and the car assumes you are a child and doesn’t deploy. It’s a system that is so safe because it doesn’t depend on the operator to get it right.
Ditto motion sensors that detect objects behind the car while reversing (avoiding accidental back-overs), antilock brakes (to maintain control during panicked braking), traction control (improves stability during acceleration), electronic stability control (foils spinouts), tire-pressure-monitoring systems (avoids blowouts), daytime running lights (ensures others see you), rollover airbags (they stay inflated to keep you in the car), lane-departure warning (alerts you if you stray from your lane), and doors that automatically lock after the car starts (again, falling out of cars).
For all the negative press of late, car manufacturers understand safety.
A System Not So Safe
Contrast this to healthcare, in which 10% of patients will suffer a serious, preventable, adverse event during their hospital stay.1 Read that sentence again. That’s 10%; that’s preventable; that’s a number that has largely remained unchanged in the past decade. If 1 in 10 drivers suffered a serious adverse preventable auto accident, Congress would do nothing but hold automotive safety hearings.
In medicine, we still largely employ unsafe systems in which even the best doctors can, and do, hurt patients. Sure, we have made strides in this arena (oxygen tubing that only works if hooked up properly, smart pumps that avert IV dosing errors, CO2 monitors to detect proper endotracheal tube placement), but remarkably, in this era of patient safety, we still utilize systems that largely depend on the heroism of the individual.
As physicians, we are famously autonomous and value our professional independence, even to the degree that it might harm patients. We generally eschew standardization, believing that each patient is inherently different. In fact, the thrill of the improvisational theater that follows every patient’s chief compliant is one of the great satisfiers in medicine. We love that feeling that comes from sleuthing each case, deftly enacting a plan of action to shepherd the patient to health.
To suggest following protocols, guidelines, and checklists is derisively dismissed as “cookbook medicine.” To work in teams in which certain tasks are delegated to others is seen as weakness—we don’t need a system that utilizes a pharmacist; rather, we should know the doses of all medicines, their interactions, and the effect of renal and liver impairment on their clearance. To suggest otherwise is an insult to our Oslerian roots. To examine our errors, our system breakdowns, our patient harms is anathema to our practice, an admission of failure.
The result is that most of us continue to toil in systems that have become exponentially unsafe as healthcare has become more complex. Today, we still have a system that will more or less allow us to kill a patient by doing nothing more than forgetting the letter “g.” I can go to my hospital today and intend to write “4 grams of magnesium sulfate (MgSO4)” and inadvertently forget the “g” in “Mg.” This could result in an order for a lethal dose of morphine sulfate (MSO4). It’s that easy to hurt a patient. Now, you might say that would never happen, because the pharmacy would catch it. And this is likely. But is it guaranteed? Can you 100% ensure it wouldn’t happen? Consider that nearly 20% of medication doses administered in a hospital are done so incorrectly.2 Nearly 1 in 5. This is the type of system we are employing to stop this lethal overdose. Is this system, which depends on another human to prevent an error, foolproof, or just a snare waiting to prove you the fool?
This represents our opportunity. As hospitalists, the hospital is our tapestry, our system of care, our responsibility. Few others are as well-positioned to ensure that the systems that envelop our patients are highly functional, reliable, and safe. This will take work—work that will feel burdensome, underappreciated, undercompensated. And, fully recognizing that none of us went into medicine to become systems engineers, this will be hard.
However, if not us, who? Who will ensure that our fathers, our mothers, our children will be as safe in the hospital as they are on the drive to the hospital? TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
References
- Global health leaders join the World Health Organization to announce accelerated efforts to improve patient safety. World Health Organization website. Available at: www.who.int/mediacentre/news/releases/2004/pr74/en/. Accessed Feb. 14, 2011.
- Barker KN, Flynn EA, Pepper GA, Bates DW, Mikeal RL. Medication errors observed in 36 health care facilities. Arch Intern Med. 2002;162(16):1897-1903.
I recently visited my parents in my ancestral home of Wisconsin. As parents of a certain age, they inexplicably are genetically predisposed to owning a minivan. Another quirk of their DNA is that they must own a new minivan. No sooner has the last wisp of new-car smell osmosed from the burled walnut interior than they are trading up to the newest, tricked-out minivan. Perhaps more puzzling is the manner of pride they display in their minivan.
Now, my dad, as if not readily apparent, is not cool. And to see him folded into the driver’s seat, his furry-ear-to-furry-ear grin signaling a self-satisfaction customarily reserved for his grandchildren, painstakingly recounting glory-day stories and 4:30 p.m. dinner buffets, further solidifies his place in the Annals of Uncool.
When I’m home, they tend to employ my chauffeur services (most likely in retribution for my peri-pubescent years), and on the first day back home, I stopped their newest ride near the back door of the house, foot idling on the brake while this exchange occurred: “That’s a fascinating story about how much more challenging the world was when you were my age, Dad. You are a true American hero. Would you like to get out here or in the garage?”
“Here,” he replied.
“OK, then get out,” I countered.
“I can’t,” he responded knowingly.
“Why not?” I queried, the patience seeping from my voice.
“Because the door’s not open,” he answered, seemingly mocking me.
“Then open it,” I replied, silently recounting the evidence for his institutionalization.
“I can’t,” he responded.
“Why not?” I replied again, this time calculating the likelihood that I was adopted.
“Because it’s locked,” came his retort.
“Then unlock it,” I answered, reconfirming my decision to move away for college.
“I can’t,” he replied, ostensibly encouraging parenticide.
“Why not?” I queried, strongly contemplating parenticide.
“Because you haven’t put the car in park,” he responded triumphantly.
A System So Safe
As a safety feature, the minivan needed to be in park before you could open the door to exit. I’ve never heard of anyone actually falling out of a moving car, but recollecting high school, I can fathom the right mix, type, and number of teenagers where possibility would meet inevitability. But, apparently, enough people are falling out of moving vehicles that car engineers have built a system that is so safe, this can’t happen. So no matter how hard someone tries, it just isn’t possible to fall out of a moving car (believe me, toward the end of a week of my father’s car stories, my mind had worked every possible angle).
Likewise, newer vehicles employ occupant-sensitive sensors that detect the weight, size, and position of the passenger to determine if the airbag should deploy. Rather than depending on the driver to turn the passenger-side airbag on or off, the car does it for you: heavy enough to trigger the sensor, and the airbag will deploy; too light, and the car assumes you are a child and doesn’t deploy. It’s a system that is so safe because it doesn’t depend on the operator to get it right.
Ditto motion sensors that detect objects behind the car while reversing (avoiding accidental back-overs), antilock brakes (to maintain control during panicked braking), traction control (improves stability during acceleration), electronic stability control (foils spinouts), tire-pressure-monitoring systems (avoids blowouts), daytime running lights (ensures others see you), rollover airbags (they stay inflated to keep you in the car), lane-departure warning (alerts you if you stray from your lane), and doors that automatically lock after the car starts (again, falling out of cars).
For all the negative press of late, car manufacturers understand safety.
A System Not So Safe
Contrast this to healthcare, in which 10% of patients will suffer a serious, preventable, adverse event during their hospital stay.1 Read that sentence again. That’s 10%; that’s preventable; that’s a number that has largely remained unchanged in the past decade. If 1 in 10 drivers suffered a serious adverse preventable auto accident, Congress would do nothing but hold automotive safety hearings.
In medicine, we still largely employ unsafe systems in which even the best doctors can, and do, hurt patients. Sure, we have made strides in this arena (oxygen tubing that only works if hooked up properly, smart pumps that avert IV dosing errors, CO2 monitors to detect proper endotracheal tube placement), but remarkably, in this era of patient safety, we still utilize systems that largely depend on the heroism of the individual.
As physicians, we are famously autonomous and value our professional independence, even to the degree that it might harm patients. We generally eschew standardization, believing that each patient is inherently different. In fact, the thrill of the improvisational theater that follows every patient’s chief compliant is one of the great satisfiers in medicine. We love that feeling that comes from sleuthing each case, deftly enacting a plan of action to shepherd the patient to health.
To suggest following protocols, guidelines, and checklists is derisively dismissed as “cookbook medicine.” To work in teams in which certain tasks are delegated to others is seen as weakness—we don’t need a system that utilizes a pharmacist; rather, we should know the doses of all medicines, their interactions, and the effect of renal and liver impairment on their clearance. To suggest otherwise is an insult to our Oslerian roots. To examine our errors, our system breakdowns, our patient harms is anathema to our practice, an admission of failure.
The result is that most of us continue to toil in systems that have become exponentially unsafe as healthcare has become more complex. Today, we still have a system that will more or less allow us to kill a patient by doing nothing more than forgetting the letter “g.” I can go to my hospital today and intend to write “4 grams of magnesium sulfate (MgSO4)” and inadvertently forget the “g” in “Mg.” This could result in an order for a lethal dose of morphine sulfate (MSO4). It’s that easy to hurt a patient. Now, you might say that would never happen, because the pharmacy would catch it. And this is likely. But is it guaranteed? Can you 100% ensure it wouldn’t happen? Consider that nearly 20% of medication doses administered in a hospital are done so incorrectly.2 Nearly 1 in 5. This is the type of system we are employing to stop this lethal overdose. Is this system, which depends on another human to prevent an error, foolproof, or just a snare waiting to prove you the fool?
This represents our opportunity. As hospitalists, the hospital is our tapestry, our system of care, our responsibility. Few others are as well-positioned to ensure that the systems that envelop our patients are highly functional, reliable, and safe. This will take work—work that will feel burdensome, underappreciated, undercompensated. And, fully recognizing that none of us went into medicine to become systems engineers, this will be hard.
However, if not us, who? Who will ensure that our fathers, our mothers, our children will be as safe in the hospital as they are on the drive to the hospital? TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
References
- Global health leaders join the World Health Organization to announce accelerated efforts to improve patient safety. World Health Organization website. Available at: www.who.int/mediacentre/news/releases/2004/pr74/en/. Accessed Feb. 14, 2011.
- Barker KN, Flynn EA, Pepper GA, Bates DW, Mikeal RL. Medication errors observed in 36 health care facilities. Arch Intern Med. 2002;162(16):1897-1903.
I recently visited my parents in my ancestral home of Wisconsin. As parents of a certain age, they inexplicably are genetically predisposed to owning a minivan. Another quirk of their DNA is that they must own a new minivan. No sooner has the last wisp of new-car smell osmosed from the burled walnut interior than they are trading up to the newest, tricked-out minivan. Perhaps more puzzling is the manner of pride they display in their minivan.
Now, my dad, as if not readily apparent, is not cool. And to see him folded into the driver’s seat, his furry-ear-to-furry-ear grin signaling a self-satisfaction customarily reserved for his grandchildren, painstakingly recounting glory-day stories and 4:30 p.m. dinner buffets, further solidifies his place in the Annals of Uncool.
When I’m home, they tend to employ my chauffeur services (most likely in retribution for my peri-pubescent years), and on the first day back home, I stopped their newest ride near the back door of the house, foot idling on the brake while this exchange occurred: “That’s a fascinating story about how much more challenging the world was when you were my age, Dad. You are a true American hero. Would you like to get out here or in the garage?”
“Here,” he replied.
“OK, then get out,” I countered.
“I can’t,” he responded knowingly.
“Why not?” I queried, the patience seeping from my voice.
“Because the door’s not open,” he answered, seemingly mocking me.
“Then open it,” I replied, silently recounting the evidence for his institutionalization.
“I can’t,” he responded.
“Why not?” I replied again, this time calculating the likelihood that I was adopted.
“Because it’s locked,” came his retort.
“Then unlock it,” I answered, reconfirming my decision to move away for college.
“I can’t,” he replied, ostensibly encouraging parenticide.
“Why not?” I queried, strongly contemplating parenticide.
“Because you haven’t put the car in park,” he responded triumphantly.
A System So Safe
As a safety feature, the minivan needed to be in park before you could open the door to exit. I’ve never heard of anyone actually falling out of a moving car, but recollecting high school, I can fathom the right mix, type, and number of teenagers where possibility would meet inevitability. But, apparently, enough people are falling out of moving vehicles that car engineers have built a system that is so safe, this can’t happen. So no matter how hard someone tries, it just isn’t possible to fall out of a moving car (believe me, toward the end of a week of my father’s car stories, my mind had worked every possible angle).
Likewise, newer vehicles employ occupant-sensitive sensors that detect the weight, size, and position of the passenger to determine if the airbag should deploy. Rather than depending on the driver to turn the passenger-side airbag on or off, the car does it for you: heavy enough to trigger the sensor, and the airbag will deploy; too light, and the car assumes you are a child and doesn’t deploy. It’s a system that is so safe because it doesn’t depend on the operator to get it right.
Ditto motion sensors that detect objects behind the car while reversing (avoiding accidental back-overs), antilock brakes (to maintain control during panicked braking), traction control (improves stability during acceleration), electronic stability control (foils spinouts), tire-pressure-monitoring systems (avoids blowouts), daytime running lights (ensures others see you), rollover airbags (they stay inflated to keep you in the car), lane-departure warning (alerts you if you stray from your lane), and doors that automatically lock after the car starts (again, falling out of cars).
For all the negative press of late, car manufacturers understand safety.
A System Not So Safe
Contrast this to healthcare, in which 10% of patients will suffer a serious, preventable, adverse event during their hospital stay.1 Read that sentence again. That’s 10%; that’s preventable; that’s a number that has largely remained unchanged in the past decade. If 1 in 10 drivers suffered a serious adverse preventable auto accident, Congress would do nothing but hold automotive safety hearings.
In medicine, we still largely employ unsafe systems in which even the best doctors can, and do, hurt patients. Sure, we have made strides in this arena (oxygen tubing that only works if hooked up properly, smart pumps that avert IV dosing errors, CO2 monitors to detect proper endotracheal tube placement), but remarkably, in this era of patient safety, we still utilize systems that largely depend on the heroism of the individual.
As physicians, we are famously autonomous and value our professional independence, even to the degree that it might harm patients. We generally eschew standardization, believing that each patient is inherently different. In fact, the thrill of the improvisational theater that follows every patient’s chief compliant is one of the great satisfiers in medicine. We love that feeling that comes from sleuthing each case, deftly enacting a plan of action to shepherd the patient to health.
To suggest following protocols, guidelines, and checklists is derisively dismissed as “cookbook medicine.” To work in teams in which certain tasks are delegated to others is seen as weakness—we don’t need a system that utilizes a pharmacist; rather, we should know the doses of all medicines, their interactions, and the effect of renal and liver impairment on their clearance. To suggest otherwise is an insult to our Oslerian roots. To examine our errors, our system breakdowns, our patient harms is anathema to our practice, an admission of failure.
The result is that most of us continue to toil in systems that have become exponentially unsafe as healthcare has become more complex. Today, we still have a system that will more or less allow us to kill a patient by doing nothing more than forgetting the letter “g.” I can go to my hospital today and intend to write “4 grams of magnesium sulfate (MgSO4)” and inadvertently forget the “g” in “Mg.” This could result in an order for a lethal dose of morphine sulfate (MSO4). It’s that easy to hurt a patient. Now, you might say that would never happen, because the pharmacy would catch it. And this is likely. But is it guaranteed? Can you 100% ensure it wouldn’t happen? Consider that nearly 20% of medication doses administered in a hospital are done so incorrectly.2 Nearly 1 in 5. This is the type of system we are employing to stop this lethal overdose. Is this system, which depends on another human to prevent an error, foolproof, or just a snare waiting to prove you the fool?
This represents our opportunity. As hospitalists, the hospital is our tapestry, our system of care, our responsibility. Few others are as well-positioned to ensure that the systems that envelop our patients are highly functional, reliable, and safe. This will take work—work that will feel burdensome, underappreciated, undercompensated. And, fully recognizing that none of us went into medicine to become systems engineers, this will be hard.
However, if not us, who? Who will ensure that our fathers, our mothers, our children will be as safe in the hospital as they are on the drive to the hospital? TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
References
- Global health leaders join the World Health Organization to announce accelerated efforts to improve patient safety. World Health Organization website. Available at: www.who.int/mediacentre/news/releases/2004/pr74/en/. Accessed Feb. 14, 2011.
- Barker KN, Flynn EA, Pepper GA, Bates DW, Mikeal RL. Medication errors observed in 36 health care facilities. Arch Intern Med. 2002;162(16):1897-1903.
All Aboard
Ten years ago, Stephen Jencks, MD, MPH, was hospitalized after taking a nasty spill and rupturing a kidney, breaking two ribs, and fracturing two transverse processes. The independent healthcare safety and quality consultant based in Baltimore still laughs ruefully at what happened next.
Dr. Jencks was stabilized and given OxyContin to treat his considerable pain, and then he was discharged—without his wife or another caregiver present, with a prescription for nothing more than Tylenol, and without any instructions on what to do if his condition worsened. Twelve hours after returning home, his pain re-emerged with such a vengeance that he experienced severe muscle spasms.
Dr. Jencks suspects his doctor was so focused on his ruptured kidney that pain management and follow-up fell by the wayside. “I am not an unassertive individual, so why didn’t I say something?” he asks. “The simple answer is that, at least for me, if I’m taking OxyContin, there are no problems. People tend not to be at the very top of their game when they’re on opioids and traumatized.”
He made it through the night at home and received better pain medication in the morning, but his experience, he says, “beautifully illustrates” the chronic problem of less-than-graceful transfers of care that can lead to unnecessary hospital readmissions. If it nearly happened to him, it can happen to anyone.
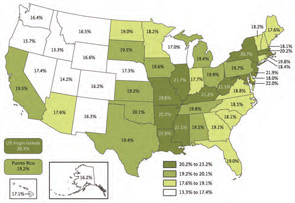
And, based on his research, it often does. In an influential 2009 New England Journal of Medicine study coauthored with Mark Williams, MD, FACP, FHM, professor and chief of the division of hospital medicine at Northwestern University’s Feinberg School of Medicine in Chicago, and principal investigator of SHM’s Project BOOST, and Eric Coleman, MD, MPH, FACP, associate professor of medicine and director of the care transitions program at the University of Colorado Denver, Dr. Jencks helped uncover some startling statistics: During a 15-month period from 2003 to 2004, nearly 20% of the roughly 12 million Medicare beneficiaries discharged from hospitals were readmitted within 30 days (see “State-by-State Breakdown of 30-Day Rehospitalizations of Medicare Beneficiaries,” p. 7).1 Of those patients discharged to the community and then rehospitalized, half had not seen their own primary-care physician (PCP) in the interim. In all, the authors estimated Medicare’s financial toll from unplanned rehospitalizations at $17.4 billion for 2004 alone.

Surprisingly, Dr. Jencks’ study and a 2007 Medicare Payment Advisory Commission report to Congress provided the first estimates of the overall burden of rehospitalization in nearly a quarter-century. Since then, however, the topic has been a mainstay in conversations about the kinds of interventions that could yield major improvements in healthcare.
“The thing that has propelled this to the front is the recognition that we really can do better,” Dr. Jencks says. “What had tended to be seen as just an evitable consequence of people being sick is now increasingly seen as often being the consequence of not having done as good a job as we should have.”
Beyond the potential for poor patient outcomes and wasted money, healthcare experts say excessive readmissions have the potential to undermine the reputations of hospitalists just as they are moving to center stage in national quality-improvement (QI) efforts.
“I see, basically every day, patients that come back to the hospital because the discharge process is broken,” says Eric Howell, MD, SFHM, director of the hospitalist division at Johns Hopkins Bayview Medical Center in Baltimore. Dr. Howell says communication difficulties between the hospital and a nursing home have plagued one “revolving door” case involving a patient with a stomach ulcer that requires surgical resection. Hospital surgeons have repeatedly arranged to see her as an outpatient and schedule the surgery, but before the surgery can take place, the patient vomits up blood and is rehospitalized.
Another contributing factor, Dr. Howell argues, is the lack of incentives for both hospitals and hospitalists to work hard at preventing the next readmission. Although Dr. Jencks’ study suggests readmissions might not always be profitable, Dr. Howell and others say the sizeable contribution of rehospitalizations to overall admission numbers and the single-digit profit margins of most hospitals offer little motivation to change the status quo. “I think there are good people who want to fix it,” says Dr. Howell, an SHM board member and Project BOOST mentor. But changing the reimbursement system so that hospitalists can better focus on reducing readmissions, he adds, “will really go a long way.”
A New Landscape
Change is in the air. As part of the federal Affordable Care Act of 2010, the Centers for Medicare & Medicaid Services (CMS) is expanding a pilot project on bundling payments to doctors and hospitals around episodes of care. Starting Jan. 1, 2013, the bundling pilot will define “episodes” as all medical services administered three days before a hospital admission until 30 days after discharge. A rehospitalization within that timeframe would net reduced reimbursements.
CMS also has begun accepting applications for what’s known as the Community-Based Care Transitions Program, with $500 million over five years authorized by the healthcare reform act to fund collaborative, readmission-reducing efforts between hospitals and community-based organizations. Linda Magno, CMS director of the Medicare Demonstrations Program Group (www.cms.gov/CMSLeadership/19_Office_ORDI.asp), says program participants will form a learning network so the agency can quickly deliver information about who’s doing well and what approaches are working better than others. The participating organizations, she says, can then help teach best practices to other hospitals around the country.
CMS has adopted public reporting requirements as another tactic. The “Hospital Compare” website (www.hospitalcompare.hhs.gov/) set up by CMS, for example, uses discharge data to publish rehospitalization rates for heart failure, acute myocardial infarction, and pneumonia. More published rates will be added soon. More importantly, Medicare will begin penalizing poorly performing institutions in October 2012 by withholding a percentage of their payments, starting at 1% and rising to 3% within three years, as part of the value-based purchasing initiative.
For hospitals, the looming deadline has prompted widespread concern about the potential financial impact. With a growing number of models and projects springing up around the country, however, hospitalists and other healthcare providers are finding encouraging signs that even relatively simple interventions might help profoundly change the trajectory of care transitions.
Rachel George, MD, MBA, FHM, regional medical director and vice president of operations for West Cogent Healthcare Inc., says Cogent has found success with one tactic—ensuring that all patients are called after being discharged. The call helps to verify that prescribed medications have been picked up and that other care-related questions have been answered. Even before discharge, Dr. George says, Cogent also tries to ensure that a follow-up appointment with every patient’s PCP is on the calendar.
Debbie White, project coordinator for the Little Rock, Ark.-based National Transitions of Care Coalition (NTOCC), says it helps to frame the entire process as a transition plan rather than a discharge. White says patients—and often their family caregivers—are the one constant in every transition. “Some older Americans, including the baby boomers, came from a culture where you don’t question your physician or even an RN,” White says. “So they’ve had a hard time speaking up and learning to ask for a list of their medications, or who’s going to make their next follow-up appointment.” Among its tools, NTOCC offers resources to teach patients how to take more responsibility for their own care (see “Patient Interaction,” p. 5).

On the other side of the equation, the most downloaded tool on the coalition’s website is an evaluation and implementation plan that helps healthcare professionals find the gaps in care transitions. Other tools, including case scenarios and checklists, help healthcare providers consider specific steps, and a compendium of evidence offers a look at successful models and projects.
Dr. Bradley M. Sherman, MD, FHM, chairman of the department of medicine at Glen Cove Hospital/North Shore-LIJ University Health System in New York, led one such project, sponsored by the Greater New York Hospital Association. Dr. Sherman targeted heart failure, the condition with the highest readmission rate for both Glen Cove Hospital and the North Shore/LIJ system. By placing special emphasis on medication compliance, dietary adherence, and physician follow-up, Dr. Sherman says, the hospital cut its readmission rates by more than half, to well below the national average.
Another effort led by Johns Hopkins’ Dr. Howell, known as Safe and Successful Transition of Elderly Patients (Safe STEP), used a collaborative staff approach in general medicine wards overseen by hospitalists to reduce 30-day readmission rates from 22% to 14%. The encouraging results, first reported at SHM’s annual meeting in 2008, provided the impetus for a project called Better Outcomes for Older Adults through Safe Transitions, or Project BOOST (www.hospitalmedicine.org/BOOST).
Developed by SHM, BOOST features a yearlong mentoring program to help sites implement the QI project. It began at six hospitals and has since spread to 62 active mentor sites. Enrollment may swell to between 100 and 120 sites by the end of 2011, according to project director Tina Budnitz, MPH. Data from the first phase revealed a 21% reduction in 30-day readmission rates at the six pilot sites, to 11.2% from 14.2%. Follow-up data from the larger cohort are expected this spring.
Eric Siegal, MD, SFHM, an SHM board member, past chair of SHM’s Public Policy Committee, and a clinical assistant professor of medicine at the University of Wisconsin School of Medicine and Public Health, says BOOST has benefited from being solidly in place at the right time, gaining momentum and garnering significant national attention as the focus on better care transitions has intensified.

“If BOOST demonstrates substantial and reproducible decreases in rehospitalizations, improvements in quality, and presumed projected cost reductions, I think that it’s going to go off like a bomb,” he says, “in a good way.”
Lakshmi Halasyamani, MD, SFHM, vice president for medical affairs for the Saint Joseph Mercy Health System in Michigan and an SHM board member, says BOOST encourages hospitalists to think about ways in which a discharge might fail. “And then we need to actively mitigate those risks,” she says.
National Collaborations
CMS has tapped a network of technical assistance and QI contractors in all 50 states, known as quality-improvement organizations (QIOs), for its own project addressing rehospitalizations. In 2008, these QIOs began working with communities in 14 states to implement what’s known as the Care Transitions Program.
The program has helped community leaders highlight three root causes of high readmission rates: patients’ lack of knowledge and understanding about their chronic conditions, lack of communication among providers, and the healthcare system’s lack of known standards.
The 14 communities, 70 hospitals, and 1.25 million Medicare beneficiaries being followed to date suggest that 30-day readmission rates can be significantly decreased, says Paul McGann, MD, CMS deputy chief medical officer. Preliminary data based on the number of readmissions per 1,000 Medicare beneficiaries, he says, show that participating communities have improved by an average of 4.7% over the first two years of the project, with the top performer improving 14% (for more information, visit www.cfmc.org/caretransitions).
Dr. Halasyamani says no single program has necessarily found the “secret sauce” to improve readmission rates across the board. “And we definitely haven’t figured out how to implement that in as cost-effective a way as possible,” she says.
But optimism is clearly building. With the initial focus on coaching low-performing institutions to improve their rates, Medicare could tap programs that demonstrate early promise as the main go-to teaching aids.
More importantly, hospitals around the country are finding what it takes to help their own patients.
“The question isn’t, ‘Is our number better than St. Elsewhere’s down the street?’ ” Dr. Jencks concludes. “The real question is, ‘Are there things we could reasonably have done for this patient and could do for the next patient that will keep this from happening to them?’ ” TH
Bryn Nelson is a freelance medical writer based in Seattle.
Reference
- Jencks SJ, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med. 2009;360(14):1418-1428.
Ten years ago, Stephen Jencks, MD, MPH, was hospitalized after taking a nasty spill and rupturing a kidney, breaking two ribs, and fracturing two transverse processes. The independent healthcare safety and quality consultant based in Baltimore still laughs ruefully at what happened next.
Dr. Jencks was stabilized and given OxyContin to treat his considerable pain, and then he was discharged—without his wife or another caregiver present, with a prescription for nothing more than Tylenol, and without any instructions on what to do if his condition worsened. Twelve hours after returning home, his pain re-emerged with such a vengeance that he experienced severe muscle spasms.
Dr. Jencks suspects his doctor was so focused on his ruptured kidney that pain management and follow-up fell by the wayside. “I am not an unassertive individual, so why didn’t I say something?” he asks. “The simple answer is that, at least for me, if I’m taking OxyContin, there are no problems. People tend not to be at the very top of their game when they’re on opioids and traumatized.”
He made it through the night at home and received better pain medication in the morning, but his experience, he says, “beautifully illustrates” the chronic problem of less-than-graceful transfers of care that can lead to unnecessary hospital readmissions. If it nearly happened to him, it can happen to anyone.
And, based on his research, it often does. In an influential 2009 New England Journal of Medicine study coauthored with Mark Williams, MD, FACP, FHM, professor and chief of the division of hospital medicine at Northwestern University’s Feinberg School of Medicine in Chicago, and principal investigator of SHM’s Project BOOST, and Eric Coleman, MD, MPH, FACP, associate professor of medicine and director of the care transitions program at the University of Colorado Denver, Dr. Jencks helped uncover some startling statistics: During a 15-month period from 2003 to 2004, nearly 20% of the roughly 12 million Medicare beneficiaries discharged from hospitals were readmitted within 30 days (see “State-by-State Breakdown of 30-Day Rehospitalizations of Medicare Beneficiaries,” p. 7).1 Of those patients discharged to the community and then rehospitalized, half had not seen their own primary-care physician (PCP) in the interim. In all, the authors estimated Medicare’s financial toll from unplanned rehospitalizations at $17.4 billion for 2004 alone.
Surprisingly, Dr. Jencks’ study and a 2007 Medicare Payment Advisory Commission report to Congress provided the first estimates of the overall burden of rehospitalization in nearly a quarter-century. Since then, however, the topic has been a mainstay in conversations about the kinds of interventions that could yield major improvements in healthcare.
“The thing that has propelled this to the front is the recognition that we really can do better,” Dr. Jencks says. “What had tended to be seen as just an evitable consequence of people being sick is now increasingly seen as often being the consequence of not having done as good a job as we should have.”
Beyond the potential for poor patient outcomes and wasted money, healthcare experts say excessive readmissions have the potential to undermine the reputations of hospitalists just as they are moving to center stage in national quality-improvement (QI) efforts.
“I see, basically every day, patients that come back to the hospital because the discharge process is broken,” says Eric Howell, MD, SFHM, director of the hospitalist division at Johns Hopkins Bayview Medical Center in Baltimore. Dr. Howell says communication difficulties between the hospital and a nursing home have plagued one “revolving door” case involving a patient with a stomach ulcer that requires surgical resection. Hospital surgeons have repeatedly arranged to see her as an outpatient and schedule the surgery, but before the surgery can take place, the patient vomits up blood and is rehospitalized.
Another contributing factor, Dr. Howell argues, is the lack of incentives for both hospitals and hospitalists to work hard at preventing the next readmission. Although Dr. Jencks’ study suggests readmissions might not always be profitable, Dr. Howell and others say the sizeable contribution of rehospitalizations to overall admission numbers and the single-digit profit margins of most hospitals offer little motivation to change the status quo. “I think there are good people who want to fix it,” says Dr. Howell, an SHM board member and Project BOOST mentor. But changing the reimbursement system so that hospitalists can better focus on reducing readmissions, he adds, “will really go a long way.”
A New Landscape
Change is in the air. As part of the federal Affordable Care Act of 2010, the Centers for Medicare & Medicaid Services (CMS) is expanding a pilot project on bundling payments to doctors and hospitals around episodes of care. Starting Jan. 1, 2013, the bundling pilot will define “episodes” as all medical services administered three days before a hospital admission until 30 days after discharge. A rehospitalization within that timeframe would net reduced reimbursements.
CMS also has begun accepting applications for what’s known as the Community-Based Care Transitions Program, with $500 million over five years authorized by the healthcare reform act to fund collaborative, readmission-reducing efforts between hospitals and community-based organizations. Linda Magno, CMS director of the Medicare Demonstrations Program Group (www.cms.gov/CMSLeadership/19_Office_ORDI.asp), says program participants will form a learning network so the agency can quickly deliver information about who’s doing well and what approaches are working better than others. The participating organizations, she says, can then help teach best practices to other hospitals around the country.
CMS has adopted public reporting requirements as another tactic. The “Hospital Compare” website (www.hospitalcompare.hhs.gov/) set up by CMS, for example, uses discharge data to publish rehospitalization rates for heart failure, acute myocardial infarction, and pneumonia. More published rates will be added soon. More importantly, Medicare will begin penalizing poorly performing institutions in October 2012 by withholding a percentage of their payments, starting at 1% and rising to 3% within three years, as part of the value-based purchasing initiative.
For hospitals, the looming deadline has prompted widespread concern about the potential financial impact. With a growing number of models and projects springing up around the country, however, hospitalists and other healthcare providers are finding encouraging signs that even relatively simple interventions might help profoundly change the trajectory of care transitions.
Rachel George, MD, MBA, FHM, regional medical director and vice president of operations for West Cogent Healthcare Inc., says Cogent has found success with one tactic—ensuring that all patients are called after being discharged. The call helps to verify that prescribed medications have been picked up and that other care-related questions have been answered. Even before discharge, Dr. George says, Cogent also tries to ensure that a follow-up appointment with every patient’s PCP is on the calendar.
Debbie White, project coordinator for the Little Rock, Ark.-based National Transitions of Care Coalition (NTOCC), says it helps to frame the entire process as a transition plan rather than a discharge. White says patients—and often their family caregivers—are the one constant in every transition. “Some older Americans, including the baby boomers, came from a culture where you don’t question your physician or even an RN,” White says. “So they’ve had a hard time speaking up and learning to ask for a list of their medications, or who’s going to make their next follow-up appointment.” Among its tools, NTOCC offers resources to teach patients how to take more responsibility for their own care (see “Patient Interaction,” p. 5).
On the other side of the equation, the most downloaded tool on the coalition’s website is an evaluation and implementation plan that helps healthcare professionals find the gaps in care transitions. Other tools, including case scenarios and checklists, help healthcare providers consider specific steps, and a compendium of evidence offers a look at successful models and projects.
Dr. Bradley M. Sherman, MD, FHM, chairman of the department of medicine at Glen Cove Hospital/North Shore-LIJ University Health System in New York, led one such project, sponsored by the Greater New York Hospital Association. Dr. Sherman targeted heart failure, the condition with the highest readmission rate for both Glen Cove Hospital and the North Shore/LIJ system. By placing special emphasis on medication compliance, dietary adherence, and physician follow-up, Dr. Sherman says, the hospital cut its readmission rates by more than half, to well below the national average.
Another effort led by Johns Hopkins’ Dr. Howell, known as Safe and Successful Transition of Elderly Patients (Safe STEP), used a collaborative staff approach in general medicine wards overseen by hospitalists to reduce 30-day readmission rates from 22% to 14%. The encouraging results, first reported at SHM’s annual meeting in 2008, provided the impetus for a project called Better Outcomes for Older Adults through Safe Transitions, or Project BOOST (www.hospitalmedicine.org/BOOST).
Developed by SHM, BOOST features a yearlong mentoring program to help sites implement the QI project. It began at six hospitals and has since spread to 62 active mentor sites. Enrollment may swell to between 100 and 120 sites by the end of 2011, according to project director Tina Budnitz, MPH. Data from the first phase revealed a 21% reduction in 30-day readmission rates at the six pilot sites, to 11.2% from 14.2%. Follow-up data from the larger cohort are expected this spring.
Eric Siegal, MD, SFHM, an SHM board member, past chair of SHM’s Public Policy Committee, and a clinical assistant professor of medicine at the University of Wisconsin School of Medicine and Public Health, says BOOST has benefited from being solidly in place at the right time, gaining momentum and garnering significant national attention as the focus on better care transitions has intensified.
“If BOOST demonstrates substantial and reproducible decreases in rehospitalizations, improvements in quality, and presumed projected cost reductions, I think that it’s going to go off like a bomb,” he says, “in a good way.”
Lakshmi Halasyamani, MD, SFHM, vice president for medical affairs for the Saint Joseph Mercy Health System in Michigan and an SHM board member, says BOOST encourages hospitalists to think about ways in which a discharge might fail. “And then we need to actively mitigate those risks,” she says.
National Collaborations
CMS has tapped a network of technical assistance and QI contractors in all 50 states, known as quality-improvement organizations (QIOs), for its own project addressing rehospitalizations. In 2008, these QIOs began working with communities in 14 states to implement what’s known as the Care Transitions Program.
The program has helped community leaders highlight three root causes of high readmission rates: patients’ lack of knowledge and understanding about their chronic conditions, lack of communication among providers, and the healthcare system’s lack of known standards.
The 14 communities, 70 hospitals, and 1.25 million Medicare beneficiaries being followed to date suggest that 30-day readmission rates can be significantly decreased, says Paul McGann, MD, CMS deputy chief medical officer. Preliminary data based on the number of readmissions per 1,000 Medicare beneficiaries, he says, show that participating communities have improved by an average of 4.7% over the first two years of the project, with the top performer improving 14% (for more information, visit www.cfmc.org/caretransitions).
Dr. Halasyamani says no single program has necessarily found the “secret sauce” to improve readmission rates across the board. “And we definitely haven’t figured out how to implement that in as cost-effective a way as possible,” she says.
But optimism is clearly building. With the initial focus on coaching low-performing institutions to improve their rates, Medicare could tap programs that demonstrate early promise as the main go-to teaching aids.
More importantly, hospitals around the country are finding what it takes to help their own patients.
“The question isn’t, ‘Is our number better than St. Elsewhere’s down the street?’ ” Dr. Jencks concludes. “The real question is, ‘Are there things we could reasonably have done for this patient and could do for the next patient that will keep this from happening to them?’ ” TH
Bryn Nelson is a freelance medical writer based in Seattle.
Reference
- Jencks SJ, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med. 2009;360(14):1418-1428.
Ten years ago, Stephen Jencks, MD, MPH, was hospitalized after taking a nasty spill and rupturing a kidney, breaking two ribs, and fracturing two transverse processes. The independent healthcare safety and quality consultant based in Baltimore still laughs ruefully at what happened next.
Dr. Jencks was stabilized and given OxyContin to treat his considerable pain, and then he was discharged—without his wife or another caregiver present, with a prescription for nothing more than Tylenol, and without any instructions on what to do if his condition worsened. Twelve hours after returning home, his pain re-emerged with such a vengeance that he experienced severe muscle spasms.
Dr. Jencks suspects his doctor was so focused on his ruptured kidney that pain management and follow-up fell by the wayside. “I am not an unassertive individual, so why didn’t I say something?” he asks. “The simple answer is that, at least for me, if I’m taking OxyContin, there are no problems. People tend not to be at the very top of their game when they’re on opioids and traumatized.”
He made it through the night at home and received better pain medication in the morning, but his experience, he says, “beautifully illustrates” the chronic problem of less-than-graceful transfers of care that can lead to unnecessary hospital readmissions. If it nearly happened to him, it can happen to anyone.
And, based on his research, it often does. In an influential 2009 New England Journal of Medicine study coauthored with Mark Williams, MD, FACP, FHM, professor and chief of the division of hospital medicine at Northwestern University’s Feinberg School of Medicine in Chicago, and principal investigator of SHM’s Project BOOST, and Eric Coleman, MD, MPH, FACP, associate professor of medicine and director of the care transitions program at the University of Colorado Denver, Dr. Jencks helped uncover some startling statistics: During a 15-month period from 2003 to 2004, nearly 20% of the roughly 12 million Medicare beneficiaries discharged from hospitals were readmitted within 30 days (see “State-by-State Breakdown of 30-Day Rehospitalizations of Medicare Beneficiaries,” p. 7).1 Of those patients discharged to the community and then rehospitalized, half had not seen their own primary-care physician (PCP) in the interim. In all, the authors estimated Medicare’s financial toll from unplanned rehospitalizations at $17.4 billion for 2004 alone.
Surprisingly, Dr. Jencks’ study and a 2007 Medicare Payment Advisory Commission report to Congress provided the first estimates of the overall burden of rehospitalization in nearly a quarter-century. Since then, however, the topic has been a mainstay in conversations about the kinds of interventions that could yield major improvements in healthcare.
“The thing that has propelled this to the front is the recognition that we really can do better,” Dr. Jencks says. “What had tended to be seen as just an evitable consequence of people being sick is now increasingly seen as often being the consequence of not having done as good a job as we should have.”
Beyond the potential for poor patient outcomes and wasted money, healthcare experts say excessive readmissions have the potential to undermine the reputations of hospitalists just as they are moving to center stage in national quality-improvement (QI) efforts.
“I see, basically every day, patients that come back to the hospital because the discharge process is broken,” says Eric Howell, MD, SFHM, director of the hospitalist division at Johns Hopkins Bayview Medical Center in Baltimore. Dr. Howell says communication difficulties between the hospital and a nursing home have plagued one “revolving door” case involving a patient with a stomach ulcer that requires surgical resection. Hospital surgeons have repeatedly arranged to see her as an outpatient and schedule the surgery, but before the surgery can take place, the patient vomits up blood and is rehospitalized.
Another contributing factor, Dr. Howell argues, is the lack of incentives for both hospitals and hospitalists to work hard at preventing the next readmission. Although Dr. Jencks’ study suggests readmissions might not always be profitable, Dr. Howell and others say the sizeable contribution of rehospitalizations to overall admission numbers and the single-digit profit margins of most hospitals offer little motivation to change the status quo. “I think there are good people who want to fix it,” says Dr. Howell, an SHM board member and Project BOOST mentor. But changing the reimbursement system so that hospitalists can better focus on reducing readmissions, he adds, “will really go a long way.”
A New Landscape
Change is in the air. As part of the federal Affordable Care Act of 2010, the Centers for Medicare & Medicaid Services (CMS) is expanding a pilot project on bundling payments to doctors and hospitals around episodes of care. Starting Jan. 1, 2013, the bundling pilot will define “episodes” as all medical services administered three days before a hospital admission until 30 days after discharge. A rehospitalization within that timeframe would net reduced reimbursements.
CMS also has begun accepting applications for what’s known as the Community-Based Care Transitions Program, with $500 million over five years authorized by the healthcare reform act to fund collaborative, readmission-reducing efforts between hospitals and community-based organizations. Linda Magno, CMS director of the Medicare Demonstrations Program Group (www.cms.gov/CMSLeadership/19_Office_ORDI.asp), says program participants will form a learning network so the agency can quickly deliver information about who’s doing well and what approaches are working better than others. The participating organizations, she says, can then help teach best practices to other hospitals around the country.
CMS has adopted public reporting requirements as another tactic. The “Hospital Compare” website (www.hospitalcompare.hhs.gov/) set up by CMS, for example, uses discharge data to publish rehospitalization rates for heart failure, acute myocardial infarction, and pneumonia. More published rates will be added soon. More importantly, Medicare will begin penalizing poorly performing institutions in October 2012 by withholding a percentage of their payments, starting at 1% and rising to 3% within three years, as part of the value-based purchasing initiative.
For hospitals, the looming deadline has prompted widespread concern about the potential financial impact. With a growing number of models and projects springing up around the country, however, hospitalists and other healthcare providers are finding encouraging signs that even relatively simple interventions might help profoundly change the trajectory of care transitions.
Rachel George, MD, MBA, FHM, regional medical director and vice president of operations for West Cogent Healthcare Inc., says Cogent has found success with one tactic—ensuring that all patients are called after being discharged. The call helps to verify that prescribed medications have been picked up and that other care-related questions have been answered. Even before discharge, Dr. George says, Cogent also tries to ensure that a follow-up appointment with every patient’s PCP is on the calendar.
Debbie White, project coordinator for the Little Rock, Ark.-based National Transitions of Care Coalition (NTOCC), says it helps to frame the entire process as a transition plan rather than a discharge. White says patients—and often their family caregivers—are the one constant in every transition. “Some older Americans, including the baby boomers, came from a culture where you don’t question your physician or even an RN,” White says. “So they’ve had a hard time speaking up and learning to ask for a list of their medications, or who’s going to make their next follow-up appointment.” Among its tools, NTOCC offers resources to teach patients how to take more responsibility for their own care (see “Patient Interaction,” p. 5).
On the other side of the equation, the most downloaded tool on the coalition’s website is an evaluation and implementation plan that helps healthcare professionals find the gaps in care transitions. Other tools, including case scenarios and checklists, help healthcare providers consider specific steps, and a compendium of evidence offers a look at successful models and projects.
Dr. Bradley M. Sherman, MD, FHM, chairman of the department of medicine at Glen Cove Hospital/North Shore-LIJ University Health System in New York, led one such project, sponsored by the Greater New York Hospital Association. Dr. Sherman targeted heart failure, the condition with the highest readmission rate for both Glen Cove Hospital and the North Shore/LIJ system. By placing special emphasis on medication compliance, dietary adherence, and physician follow-up, Dr. Sherman says, the hospital cut its readmission rates by more than half, to well below the national average.
Another effort led by Johns Hopkins’ Dr. Howell, known as Safe and Successful Transition of Elderly Patients (Safe STEP), used a collaborative staff approach in general medicine wards overseen by hospitalists to reduce 30-day readmission rates from 22% to 14%. The encouraging results, first reported at SHM’s annual meeting in 2008, provided the impetus for a project called Better Outcomes for Older Adults through Safe Transitions, or Project BOOST (www.hospitalmedicine.org/BOOST).
Developed by SHM, BOOST features a yearlong mentoring program to help sites implement the QI project. It began at six hospitals and has since spread to 62 active mentor sites. Enrollment may swell to between 100 and 120 sites by the end of 2011, according to project director Tina Budnitz, MPH. Data from the first phase revealed a 21% reduction in 30-day readmission rates at the six pilot sites, to 11.2% from 14.2%. Follow-up data from the larger cohort are expected this spring.
Eric Siegal, MD, SFHM, an SHM board member, past chair of SHM’s Public Policy Committee, and a clinical assistant professor of medicine at the University of Wisconsin School of Medicine and Public Health, says BOOST has benefited from being solidly in place at the right time, gaining momentum and garnering significant national attention as the focus on better care transitions has intensified.
“If BOOST demonstrates substantial and reproducible decreases in rehospitalizations, improvements in quality, and presumed projected cost reductions, I think that it’s going to go off like a bomb,” he says, “in a good way.”
Lakshmi Halasyamani, MD, SFHM, vice president for medical affairs for the Saint Joseph Mercy Health System in Michigan and an SHM board member, says BOOST encourages hospitalists to think about ways in which a discharge might fail. “And then we need to actively mitigate those risks,” she says.
National Collaborations
CMS has tapped a network of technical assistance and QI contractors in all 50 states, known as quality-improvement organizations (QIOs), for its own project addressing rehospitalizations. In 2008, these QIOs began working with communities in 14 states to implement what’s known as the Care Transitions Program.
The program has helped community leaders highlight three root causes of high readmission rates: patients’ lack of knowledge and understanding about their chronic conditions, lack of communication among providers, and the healthcare system’s lack of known standards.
The 14 communities, 70 hospitals, and 1.25 million Medicare beneficiaries being followed to date suggest that 30-day readmission rates can be significantly decreased, says Paul McGann, MD, CMS deputy chief medical officer. Preliminary data based on the number of readmissions per 1,000 Medicare beneficiaries, he says, show that participating communities have improved by an average of 4.7% over the first two years of the project, with the top performer improving 14% (for more information, visit www.cfmc.org/caretransitions).
Dr. Halasyamani says no single program has necessarily found the “secret sauce” to improve readmission rates across the board. “And we definitely haven’t figured out how to implement that in as cost-effective a way as possible,” she says.
But optimism is clearly building. With the initial focus on coaching low-performing institutions to improve their rates, Medicare could tap programs that demonstrate early promise as the main go-to teaching aids.
More importantly, hospitals around the country are finding what it takes to help their own patients.
“The question isn’t, ‘Is our number better than St. Elsewhere’s down the street?’ ” Dr. Jencks concludes. “The real question is, ‘Are there things we could reasonably have done for this patient and could do for the next patient that will keep this from happening to them?’ ” TH
Bryn Nelson is a freelance medical writer based in Seattle.
Reference
- Jencks SJ, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med. 2009;360(14):1418-1428.
Gettin’ Dirty

Several months ago, my toilet broke. You should also know that I’m not particularly handy. So when I first realized that the toilet bowl seemed to fill constantly, I got a little stressed out.
How much was it going cost to call in a plumber on the weekend?
What kind of a water bill was I going to have?
Was this a serious problem?
I took a quick peek in the tank, but that just made me more confused. I was paralyzed by a lack of know-how.
Normally, I would have just Googled a local plumber. But that day, I decided to do something different. Maybe it was because it was the fantasy football offseason. Maybe it was because my wife had started to ask my father-in-law to change light bulbs around the house. Or, maybe, I wanted to learn to actually fix the problem. A few hours later, after an Internet lesson in toilet physiology, a $4.12 trip to Home Depot, and a wet pair of hands, I had replaced my first toilet flapper.
This wasn’t the rebuilding of a car engine, but it was a clear DIY step toward self-improvement. Easily the most memorable moment here was my sense of accomplishment.
I felt empowered.
One Part Science, One Part Art
It’s taken me a while to realize this, but I’ve begun to take advantage of improvement opportunities at work as well. No, I haven’t been moonlighting as a plumber for my hospital. I’ve just been fortunate to be part of a trifecta of rewarding quality-improvement (QI) projects over the past year. Before I’d gotten my hands dirty with these, my understanding of QI was fairly naive. I’d heard about Plan-Do-Study-Act many times. I had listened to a talk at a national conference. And I had kept up with the general medical literature on the subject.
But none of those activities had truly prepared me for experience of actually doing the work on my own.
By taking on a project, an ambitious attempt to reduce continuous pulse oximetry use, I experienced a crash course in both the science and the art of process improvement. I was forced to overcome my “I don’t know how” inertia. And with expert guidance in the form of a clinical safety and effectiveness class, I learned the importance of run charts (science) and a well-crafted multidisciplinary team (art) in changing established but inefficient behavior.
Our rates of continuous pulse oximetry usage dropped by 50%, and cost savings were $12,000 per year on one unit. These results made my prior attempts at change—years of complaining about ingrained nursing culture—look infantile. (OK, maybe it was ineffective, but who hasn’t complained about the overuse of continuous monitoring?)
I haven’t met a pediatric hospitalist who wouldn’t understand the symbolic importance of this success. But I know of many hospitalists who have not yet participated in meaningful QI project. Imagine calling a plumber who grasped the flush and fill mechanism of a toilet but had never touched real porcelain. Here’s an even better analogy: What if doctors could get licensed without having touched real patients?
If pediatric hospitalists are to transform the care delivery of hospitalized children, and quality learning only comes through hands-on training, then we need some more hands in the pot.
Discharge Improvement
On the heels of my first project, I was fortunate enough to augment my education through another effort—this time with a cohort of fellow pediatric hospitalists. This was a national collaborative to improve discharge handoffs, and I will admit that, at the outset, I was as puzzled as the first time I pulled the lid off the tank of the toilet. There were just too many permutations on PCP communication at the participating institutions, and some felt our aim of timely discharge handoffs was unattainable.
What carried me through, however, was the collective and infectious DIY—no, QIY (Quality Improve-it-Yourself) attitude of the group. We were all learning, and regular participation in the collaborative essentially guaranteed improvement. We achieved our aim of 90% communication with PCPs within two days of discharge. The secret was simple: The more you do, the more you learn.
Pediatric hospitalists can transform care delivery through a focus on safe and quality care, but the tools to accomplish this must come through post-residency, on-the-job learning. This QI know-how must efficiently spread among our ranks through practical and project-based educational efforts. It’s “see one, do one, teach one,” but we’re not talking about lumbar punctures anymore.
This is a journey in which we all take on the responsibility of rolling up our sleeves and simply learn by doing. And here is where the third leg of my as-yet-unfinished QI course unfolds.
Through my involvement with the Value in Inpatient Pediatrics (VIP) Network, I’ve gained a newfound vision for what the future might hold. VIP has evolved from a benchmarking project focused on bronchiolitis to an improvement network that will incorporate projects similar to the discharge handoff collaborative above.
In the process, a model for how to rapidly spread QI learning has emerged. The capacity lies in the network’s rapidly growing connectivity. The power comes from the individuals: motivated, card-carrying pediatric hospitalists from a wide array of sites. Collaborative learning harbors the potential to exponentially increase the pace at which we improve.
The future of our quality care is bright. I see an open network of improvement doers and learners. I see collaboration on quality and safety initiatives in all manner of hospitals and communities. I see that this will all be built upon a foundation of hard work and a QIY attitude.
You, too, will play a role.
Just don’t be afraid to get your hands a little dirty. TH
Dr. Shen is medical director of hospital medicine at Dell Children’s Medical Center in Austin, Texas. He is pediatric editor of The Hospitalist.
Several months ago, my toilet broke. You should also know that I’m not particularly handy. So when I first realized that the toilet bowl seemed to fill constantly, I got a little stressed out.
How much was it going cost to call in a plumber on the weekend?
What kind of a water bill was I going to have?
Was this a serious problem?
I took a quick peek in the tank, but that just made me more confused. I was paralyzed by a lack of know-how.
Normally, I would have just Googled a local plumber. But that day, I decided to do something different. Maybe it was because it was the fantasy football offseason. Maybe it was because my wife had started to ask my father-in-law to change light bulbs around the house. Or, maybe, I wanted to learn to actually fix the problem. A few hours later, after an Internet lesson in toilet physiology, a $4.12 trip to Home Depot, and a wet pair of hands, I had replaced my first toilet flapper.
This wasn’t the rebuilding of a car engine, but it was a clear DIY step toward self-improvement. Easily the most memorable moment here was my sense of accomplishment.
I felt empowered.
One Part Science, One Part Art
It’s taken me a while to realize this, but I’ve begun to take advantage of improvement opportunities at work as well. No, I haven’t been moonlighting as a plumber for my hospital. I’ve just been fortunate to be part of a trifecta of rewarding quality-improvement (QI) projects over the past year. Before I’d gotten my hands dirty with these, my understanding of QI was fairly naive. I’d heard about Plan-Do-Study-Act many times. I had listened to a talk at a national conference. And I had kept up with the general medical literature on the subject.
But none of those activities had truly prepared me for experience of actually doing the work on my own.
By taking on a project, an ambitious attempt to reduce continuous pulse oximetry use, I experienced a crash course in both the science and the art of process improvement. I was forced to overcome my “I don’t know how” inertia. And with expert guidance in the form of a clinical safety and effectiveness class, I learned the importance of run charts (science) and a well-crafted multidisciplinary team (art) in changing established but inefficient behavior.
Our rates of continuous pulse oximetry usage dropped by 50%, and cost savings were $12,000 per year on one unit. These results made my prior attempts at change—years of complaining about ingrained nursing culture—look infantile. (OK, maybe it was ineffective, but who hasn’t complained about the overuse of continuous monitoring?)
I haven’t met a pediatric hospitalist who wouldn’t understand the symbolic importance of this success. But I know of many hospitalists who have not yet participated in meaningful QI project. Imagine calling a plumber who grasped the flush and fill mechanism of a toilet but had never touched real porcelain. Here’s an even better analogy: What if doctors could get licensed without having touched real patients?
If pediatric hospitalists are to transform the care delivery of hospitalized children, and quality learning only comes through hands-on training, then we need some more hands in the pot.
Discharge Improvement
On the heels of my first project, I was fortunate enough to augment my education through another effort—this time with a cohort of fellow pediatric hospitalists. This was a national collaborative to improve discharge handoffs, and I will admit that, at the outset, I was as puzzled as the first time I pulled the lid off the tank of the toilet. There were just too many permutations on PCP communication at the participating institutions, and some felt our aim of timely discharge handoffs was unattainable.
What carried me through, however, was the collective and infectious DIY—no, QIY (Quality Improve-it-Yourself) attitude of the group. We were all learning, and regular participation in the collaborative essentially guaranteed improvement. We achieved our aim of 90% communication with PCPs within two days of discharge. The secret was simple: The more you do, the more you learn.
Pediatric hospitalists can transform care delivery through a focus on safe and quality care, but the tools to accomplish this must come through post-residency, on-the-job learning. This QI know-how must efficiently spread among our ranks through practical and project-based educational efforts. It’s “see one, do one, teach one,” but we’re not talking about lumbar punctures anymore.
This is a journey in which we all take on the responsibility of rolling up our sleeves and simply learn by doing. And here is where the third leg of my as-yet-unfinished QI course unfolds.
Through my involvement with the Value in Inpatient Pediatrics (VIP) Network, I’ve gained a newfound vision for what the future might hold. VIP has evolved from a benchmarking project focused on bronchiolitis to an improvement network that will incorporate projects similar to the discharge handoff collaborative above.
In the process, a model for how to rapidly spread QI learning has emerged. The capacity lies in the network’s rapidly growing connectivity. The power comes from the individuals: motivated, card-carrying pediatric hospitalists from a wide array of sites. Collaborative learning harbors the potential to exponentially increase the pace at which we improve.
The future of our quality care is bright. I see an open network of improvement doers and learners. I see collaboration on quality and safety initiatives in all manner of hospitals and communities. I see that this will all be built upon a foundation of hard work and a QIY attitude.
You, too, will play a role.
Just don’t be afraid to get your hands a little dirty. TH
Dr. Shen is medical director of hospital medicine at Dell Children’s Medical Center in Austin, Texas. He is pediatric editor of The Hospitalist.
Several months ago, my toilet broke. You should also know that I’m not particularly handy. So when I first realized that the toilet bowl seemed to fill constantly, I got a little stressed out.
How much was it going cost to call in a plumber on the weekend?
What kind of a water bill was I going to have?
Was this a serious problem?
I took a quick peek in the tank, but that just made me more confused. I was paralyzed by a lack of know-how.
Normally, I would have just Googled a local plumber. But that day, I decided to do something different. Maybe it was because it was the fantasy football offseason. Maybe it was because my wife had started to ask my father-in-law to change light bulbs around the house. Or, maybe, I wanted to learn to actually fix the problem. A few hours later, after an Internet lesson in toilet physiology, a $4.12 trip to Home Depot, and a wet pair of hands, I had replaced my first toilet flapper.
This wasn’t the rebuilding of a car engine, but it was a clear DIY step toward self-improvement. Easily the most memorable moment here was my sense of accomplishment.
I felt empowered.
One Part Science, One Part Art
It’s taken me a while to realize this, but I’ve begun to take advantage of improvement opportunities at work as well. No, I haven’t been moonlighting as a plumber for my hospital. I’ve just been fortunate to be part of a trifecta of rewarding quality-improvement (QI) projects over the past year. Before I’d gotten my hands dirty with these, my understanding of QI was fairly naive. I’d heard about Plan-Do-Study-Act many times. I had listened to a talk at a national conference. And I had kept up with the general medical literature on the subject.
But none of those activities had truly prepared me for experience of actually doing the work on my own.
By taking on a project, an ambitious attempt to reduce continuous pulse oximetry use, I experienced a crash course in both the science and the art of process improvement. I was forced to overcome my “I don’t know how” inertia. And with expert guidance in the form of a clinical safety and effectiveness class, I learned the importance of run charts (science) and a well-crafted multidisciplinary team (art) in changing established but inefficient behavior.
Our rates of continuous pulse oximetry usage dropped by 50%, and cost savings were $12,000 per year on one unit. These results made my prior attempts at change—years of complaining about ingrained nursing culture—look infantile. (OK, maybe it was ineffective, but who hasn’t complained about the overuse of continuous monitoring?)
I haven’t met a pediatric hospitalist who wouldn’t understand the symbolic importance of this success. But I know of many hospitalists who have not yet participated in meaningful QI project. Imagine calling a plumber who grasped the flush and fill mechanism of a toilet but had never touched real porcelain. Here’s an even better analogy: What if doctors could get licensed without having touched real patients?
If pediatric hospitalists are to transform the care delivery of hospitalized children, and quality learning only comes through hands-on training, then we need some more hands in the pot.
Discharge Improvement
On the heels of my first project, I was fortunate enough to augment my education through another effort—this time with a cohort of fellow pediatric hospitalists. This was a national collaborative to improve discharge handoffs, and I will admit that, at the outset, I was as puzzled as the first time I pulled the lid off the tank of the toilet. There were just too many permutations on PCP communication at the participating institutions, and some felt our aim of timely discharge handoffs was unattainable.
What carried me through, however, was the collective and infectious DIY—no, QIY (Quality Improve-it-Yourself) attitude of the group. We were all learning, and regular participation in the collaborative essentially guaranteed improvement. We achieved our aim of 90% communication with PCPs within two days of discharge. The secret was simple: The more you do, the more you learn.
Pediatric hospitalists can transform care delivery through a focus on safe and quality care, but the tools to accomplish this must come through post-residency, on-the-job learning. This QI know-how must efficiently spread among our ranks through practical and project-based educational efforts. It’s “see one, do one, teach one,” but we’re not talking about lumbar punctures anymore.
This is a journey in which we all take on the responsibility of rolling up our sleeves and simply learn by doing. And here is where the third leg of my as-yet-unfinished QI course unfolds.
Through my involvement with the Value in Inpatient Pediatrics (VIP) Network, I’ve gained a newfound vision for what the future might hold. VIP has evolved from a benchmarking project focused on bronchiolitis to an improvement network that will incorporate projects similar to the discharge handoff collaborative above.
In the process, a model for how to rapidly spread QI learning has emerged. The capacity lies in the network’s rapidly growing connectivity. The power comes from the individuals: motivated, card-carrying pediatric hospitalists from a wide array of sites. Collaborative learning harbors the potential to exponentially increase the pace at which we improve.
The future of our quality care is bright. I see an open network of improvement doers and learners. I see collaboration on quality and safety initiatives in all manner of hospitals and communities. I see that this will all be built upon a foundation of hard work and a QIY attitude.
You, too, will play a role.
Just don’t be afraid to get your hands a little dirty. TH
Dr. Shen is medical director of hospital medicine at Dell Children’s Medical Center in Austin, Texas. He is pediatric editor of The Hospitalist.
Designed to Harm

If every system is perfectly designed to get the results it gets …
And if 15 million patients are harmed every year from medical care …
And if as many as 98,000 people die every year due to medical errors in hospitals …
Then what does that say about the system we have designed?
A System Designed to Competently Hurt Many
By now you’ve no doubt heard, read, and possibly even uttered the above facts and figures yourself. I think we all have our opinions about the veracity of these numbers, but I don’t think any of us would argue with the sentiment. The U.S. healthcare system comprises the most competent, compassionate, well-meaning, and caring professionals on this planet—who harm, maim, and kill countless people every year.
What a discomforting paradox.
Equity: The Overlooked Quality Domain
Many years back, the Institute of Medicine (IOM) published a list of six “domains” of healthcare quality. You’ve no doubt stumbled across the IOM’s Safe … Timely … Effective … Efficient … Equitable … Patient-Centered mnemonic recipe—STEEEP—for high-quality care.1 In fact, it’s hard to read a journal, attend a medical presentation, or open a local newspaper without finding reference to these domains. It’s all the rage to talk about wrong-site surgery (safe), access to care (timely), comparative-effectiveness research (effective), lean concepts (efficient), and individualized medicine (patient-centered). However, the sixth domain often seems to get the Jan Brady treatment—minimized, marginalized, and oft-forgotten.
The IOM defines equitable care as that which “does not vary in quality because of personal characteristics such as gender, ethnicity, geographic location, and socioeconomic status.”1 To be sure, there is some hum at the national level about issues of equity, especially around healthcare coverage for all. And this is important. However, what appears lost in the rant surrounding the inherent inequities in our tiered health insurance system is that we have blantant inequalities baked into the everyday machinery of our hospitals. And they affect all, regardless of skin color, gender, or insurance status.
Think for a moment about your hospital. Are the type, level, and access to care equal at all times? Does the level of care change when the streetlights come on? How about on weekends and holidays? Do your operating rooms run on Saturdays and Sundays? Can patients get chemotherapy on the weekends? Does your hospital alter its nursing staff ratios after hours? Can you get an ultrasound at midnight? How about a urology or neurosurgery consult at 2 a.m.? How about getting interventional radiology to place an IVC filter on a holiday?
Now scratch a bit closer to home. Does your hospitalist group downstaff on weekends and holidays, even though the volumes probably warrant more coverage? Are your night providers part of your group, or are they moonlighters? Do your after-hours providers cross-cover and admit a reasonable number of patients, or are they frequently overwhelmed? Do they cover patients or admit for services that they don’t typically care for during the day (e.g. ICU, neurosurgical, subspecialty cardiology or oncology patients)? For the intensely ill patients admitted to U.S. hospitals today, should the type and availability of care differ when it’s delivered at 3 p.m. or 3 a.m., Sunday or Monday?
Disregarding the macro-inequities in our societal approach to healthcare, can we even ensure equitable care within our own hospital walls 24 hours a day, seven days a week?
The Answer: An Unfortunate “No”
For the record, I hate working nights, abhor working weekends, and resent working holidays. But the thing I’d hate even more than working nights, weekends, and holidays would be being a patient admitted during a night, weekend, or holiday. To understand why, I have to look no further than my hospital parking lot. During bankers’ hours, I can barely find a parking spot on the top floor of our multilevel parking structure.
Fast-forward to Saturday, and I have my pick of empty football fields’ worth of spots on all floors. Ditto Sundays, nights, and holidays.
Why is it that nationally, a collectively near-trillion-dollar hospital enterprise finds it acceptable to effectively shutter itself for a quarter to a third of the week? Especially when doing so seems to counter their primary mission of providing safe, timely, effective, efficient, equitable, and patient-centered care.
The Weekend Effect
There are, of course, economic and operational reasons to downshift during off hours—some hospitals don’t have the elective procedures to run operating rooms seven days a week, and very few patients want to have their elective colonoscopy at 11 p.m. or their chemotherapy during Thanksgiving dinner. However, in most cases, the reasons for doing so center on hospital staff and physician satisfaction. Most us of just don’t like working off hours. As a result, studies have shown significantly less access to such high-level care as coronary angiography and percutaneous coronary intervention on weekends.2,3
And the effects of this “weekend effect” can be devastating.
A recent paper in the New England Journal of Medicine reported that for every 1,000 patients admitted with a myocardial infarction on a weekend, nine more would die than a comparable group admitted during the week.4 Their offense? Having the misfortune to get ill on a Saturday morning. The authors concluded that this higher mortality was secondary to a lower rate of invasive cardiac procedures, presumably because they were less available. And the weekend effect isn’t just limited to coronary care. Poorer outcomes, including higher mortality rates, have been reported for weekend admissions to the neonatal ICU and adult ICU, as well as admission for epiglottitis, ruptured abdominal aortic aneurysms, and pulmonary embolism.5,6,7
So let’s connect the dots: A system designed with inequal access to lifesaving therapies and appropriate staffing results in worse outcomes, more harm, more deaths.
To be clear, 98,000 people don’t die every year because of my disdain for working nights and weekends. This is a much deeper problem that hinges on many unsatisfactory systems working unsatisfactorily in tandem (e.g. see the other five IOM domains of quality care). Furthermore, I don’t mean to suggest that hospitalists necessarily have a lot of say in cardiac catheterization schedules. Yet we do control our own systems of care—how many patients we admit and cover during a shift, how strongly we advocate for timely testing and consultation, how we staff weekends and cover patients at night.
And, more and more, we are in a position to enhance the care delivery systems of the hospital and its providers that surround us. With that comes a responsibility to ensure that these systems are highly functioning and equitable, regardless of the time of day, day of the week.
If we are going to fundamentally enhance the quality of care, then we have to design safer systems of care. It will take time and resources to alter many of our bruised systems of care, but we can begin by at least ensuring equity in how we deliver care at our own institutions. That is, unless we are comfortable with a system perfectly designed to harm. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
References
- Institute of Medicine (IOM). Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, D.C.: National Academy Press; 2001.
- Bell CM, Redelmeier DA. Waiting for urgent procedures on the weekend among emergently hospitalized patients. Am J Med. 2004:117(3):175-181.
- Magid DJ, Wang Y, Herrin J, et al. Relationship between time of day, day of week, timeliness of reperfusion, and in-hospital mortality for patients with acute ST-segment elevation myocardial infarction. JAMA. 2005;294(7):803-812.
- Kostis WJ, Demissie K, Marcella SW, Shao YH, Wilson AC, Moreyra AE. Weekend versus weekday admission and mortality from myocardial infarction. N Eng J Med. 2007;356 (11):1099-1109.
- Hendry RA. The weekend—a dangerous time to be born? Br J Obstet Gynaecol. 1981;88(12):1200-1203.
- Barnett MJ, Kaboli PJ, Sirio CA, Rosenthal GE. Day of the week of intensive care admission and patient outcomes: a multisite regional evaluation. Med Care. 2002;40(6):530-539.
- Bell CM, Redelmeier DA. Mortality among patients admitted to hospitals on weekends as compared with weekdays. N Eng J Med. 2001;345(9):663-668.
If every system is perfectly designed to get the results it gets …
And if 15 million patients are harmed every year from medical care …
And if as many as 98,000 people die every year due to medical errors in hospitals …
Then what does that say about the system we have designed?
A System Designed to Competently Hurt Many
By now you’ve no doubt heard, read, and possibly even uttered the above facts and figures yourself. I think we all have our opinions about the veracity of these numbers, but I don’t think any of us would argue with the sentiment. The U.S. healthcare system comprises the most competent, compassionate, well-meaning, and caring professionals on this planet—who harm, maim, and kill countless people every year.
What a discomforting paradox.
Equity: The Overlooked Quality Domain
Many years back, the Institute of Medicine (IOM) published a list of six “domains” of healthcare quality. You’ve no doubt stumbled across the IOM’s Safe … Timely … Effective … Efficient … Equitable … Patient-Centered mnemonic recipe—STEEEP—for high-quality care.1 In fact, it’s hard to read a journal, attend a medical presentation, or open a local newspaper without finding reference to these domains. It’s all the rage to talk about wrong-site surgery (safe), access to care (timely), comparative-effectiveness research (effective), lean concepts (efficient), and individualized medicine (patient-centered). However, the sixth domain often seems to get the Jan Brady treatment—minimized, marginalized, and oft-forgotten.
The IOM defines equitable care as that which “does not vary in quality because of personal characteristics such as gender, ethnicity, geographic location, and socioeconomic status.”1 To be sure, there is some hum at the national level about issues of equity, especially around healthcare coverage for all. And this is important. However, what appears lost in the rant surrounding the inherent inequities in our tiered health insurance system is that we have blantant inequalities baked into the everyday machinery of our hospitals. And they affect all, regardless of skin color, gender, or insurance status.
Think for a moment about your hospital. Are the type, level, and access to care equal at all times? Does the level of care change when the streetlights come on? How about on weekends and holidays? Do your operating rooms run on Saturdays and Sundays? Can patients get chemotherapy on the weekends? Does your hospital alter its nursing staff ratios after hours? Can you get an ultrasound at midnight? How about a urology or neurosurgery consult at 2 a.m.? How about getting interventional radiology to place an IVC filter on a holiday?
Now scratch a bit closer to home. Does your hospitalist group downstaff on weekends and holidays, even though the volumes probably warrant more coverage? Are your night providers part of your group, or are they moonlighters? Do your after-hours providers cross-cover and admit a reasonable number of patients, or are they frequently overwhelmed? Do they cover patients or admit for services that they don’t typically care for during the day (e.g. ICU, neurosurgical, subspecialty cardiology or oncology patients)? For the intensely ill patients admitted to U.S. hospitals today, should the type and availability of care differ when it’s delivered at 3 p.m. or 3 a.m., Sunday or Monday?
Disregarding the macro-inequities in our societal approach to healthcare, can we even ensure equitable care within our own hospital walls 24 hours a day, seven days a week?
The Answer: An Unfortunate “No”
For the record, I hate working nights, abhor working weekends, and resent working holidays. But the thing I’d hate even more than working nights, weekends, and holidays would be being a patient admitted during a night, weekend, or holiday. To understand why, I have to look no further than my hospital parking lot. During bankers’ hours, I can barely find a parking spot on the top floor of our multilevel parking structure.
Fast-forward to Saturday, and I have my pick of empty football fields’ worth of spots on all floors. Ditto Sundays, nights, and holidays.
Why is it that nationally, a collectively near-trillion-dollar hospital enterprise finds it acceptable to effectively shutter itself for a quarter to a third of the week? Especially when doing so seems to counter their primary mission of providing safe, timely, effective, efficient, equitable, and patient-centered care.
The Weekend Effect
There are, of course, economic and operational reasons to downshift during off hours—some hospitals don’t have the elective procedures to run operating rooms seven days a week, and very few patients want to have their elective colonoscopy at 11 p.m. or their chemotherapy during Thanksgiving dinner. However, in most cases, the reasons for doing so center on hospital staff and physician satisfaction. Most us of just don’t like working off hours. As a result, studies have shown significantly less access to such high-level care as coronary angiography and percutaneous coronary intervention on weekends.2,3
And the effects of this “weekend effect” can be devastating.
A recent paper in the New England Journal of Medicine reported that for every 1,000 patients admitted with a myocardial infarction on a weekend, nine more would die than a comparable group admitted during the week.4 Their offense? Having the misfortune to get ill on a Saturday morning. The authors concluded that this higher mortality was secondary to a lower rate of invasive cardiac procedures, presumably because they were less available. And the weekend effect isn’t just limited to coronary care. Poorer outcomes, including higher mortality rates, have been reported for weekend admissions to the neonatal ICU and adult ICU, as well as admission for epiglottitis, ruptured abdominal aortic aneurysms, and pulmonary embolism.5,6,7
So let’s connect the dots: A system designed with inequal access to lifesaving therapies and appropriate staffing results in worse outcomes, more harm, more deaths.
To be clear, 98,000 people don’t die every year because of my disdain for working nights and weekends. This is a much deeper problem that hinges on many unsatisfactory systems working unsatisfactorily in tandem (e.g. see the other five IOM domains of quality care). Furthermore, I don’t mean to suggest that hospitalists necessarily have a lot of say in cardiac catheterization schedules. Yet we do control our own systems of care—how many patients we admit and cover during a shift, how strongly we advocate for timely testing and consultation, how we staff weekends and cover patients at night.
And, more and more, we are in a position to enhance the care delivery systems of the hospital and its providers that surround us. With that comes a responsibility to ensure that these systems are highly functioning and equitable, regardless of the time of day, day of the week.
If we are going to fundamentally enhance the quality of care, then we have to design safer systems of care. It will take time and resources to alter many of our bruised systems of care, but we can begin by at least ensuring equity in how we deliver care at our own institutions. That is, unless we are comfortable with a system perfectly designed to harm. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
References
- Institute of Medicine (IOM). Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, D.C.: National Academy Press; 2001.
- Bell CM, Redelmeier DA. Waiting for urgent procedures on the weekend among emergently hospitalized patients. Am J Med. 2004:117(3):175-181.
- Magid DJ, Wang Y, Herrin J, et al. Relationship between time of day, day of week, timeliness of reperfusion, and in-hospital mortality for patients with acute ST-segment elevation myocardial infarction. JAMA. 2005;294(7):803-812.
- Kostis WJ, Demissie K, Marcella SW, Shao YH, Wilson AC, Moreyra AE. Weekend versus weekday admission and mortality from myocardial infarction. N Eng J Med. 2007;356 (11):1099-1109.
- Hendry RA. The weekend—a dangerous time to be born? Br J Obstet Gynaecol. 1981;88(12):1200-1203.
- Barnett MJ, Kaboli PJ, Sirio CA, Rosenthal GE. Day of the week of intensive care admission and patient outcomes: a multisite regional evaluation. Med Care. 2002;40(6):530-539.
- Bell CM, Redelmeier DA. Mortality among patients admitted to hospitals on weekends as compared with weekdays. N Eng J Med. 2001;345(9):663-668.
If every system is perfectly designed to get the results it gets …
And if 15 million patients are harmed every year from medical care …
And if as many as 98,000 people die every year due to medical errors in hospitals …
Then what does that say about the system we have designed?
A System Designed to Competently Hurt Many
By now you’ve no doubt heard, read, and possibly even uttered the above facts and figures yourself. I think we all have our opinions about the veracity of these numbers, but I don’t think any of us would argue with the sentiment. The U.S. healthcare system comprises the most competent, compassionate, well-meaning, and caring professionals on this planet—who harm, maim, and kill countless people every year.
What a discomforting paradox.
Equity: The Overlooked Quality Domain
Many years back, the Institute of Medicine (IOM) published a list of six “domains” of healthcare quality. You’ve no doubt stumbled across the IOM’s Safe … Timely … Effective … Efficient … Equitable … Patient-Centered mnemonic recipe—STEEEP—for high-quality care.1 In fact, it’s hard to read a journal, attend a medical presentation, or open a local newspaper without finding reference to these domains. It’s all the rage to talk about wrong-site surgery (safe), access to care (timely), comparative-effectiveness research (effective), lean concepts (efficient), and individualized medicine (patient-centered). However, the sixth domain often seems to get the Jan Brady treatment—minimized, marginalized, and oft-forgotten.
The IOM defines equitable care as that which “does not vary in quality because of personal characteristics such as gender, ethnicity, geographic location, and socioeconomic status.”1 To be sure, there is some hum at the national level about issues of equity, especially around healthcare coverage for all. And this is important. However, what appears lost in the rant surrounding the inherent inequities in our tiered health insurance system is that we have blantant inequalities baked into the everyday machinery of our hospitals. And they affect all, regardless of skin color, gender, or insurance status.
Think for a moment about your hospital. Are the type, level, and access to care equal at all times? Does the level of care change when the streetlights come on? How about on weekends and holidays? Do your operating rooms run on Saturdays and Sundays? Can patients get chemotherapy on the weekends? Does your hospital alter its nursing staff ratios after hours? Can you get an ultrasound at midnight? How about a urology or neurosurgery consult at 2 a.m.? How about getting interventional radiology to place an IVC filter on a holiday?
Now scratch a bit closer to home. Does your hospitalist group downstaff on weekends and holidays, even though the volumes probably warrant more coverage? Are your night providers part of your group, or are they moonlighters? Do your after-hours providers cross-cover and admit a reasonable number of patients, or are they frequently overwhelmed? Do they cover patients or admit for services that they don’t typically care for during the day (e.g. ICU, neurosurgical, subspecialty cardiology or oncology patients)? For the intensely ill patients admitted to U.S. hospitals today, should the type and availability of care differ when it’s delivered at 3 p.m. or 3 a.m., Sunday or Monday?
Disregarding the macro-inequities in our societal approach to healthcare, can we even ensure equitable care within our own hospital walls 24 hours a day, seven days a week?
The Answer: An Unfortunate “No”
For the record, I hate working nights, abhor working weekends, and resent working holidays. But the thing I’d hate even more than working nights, weekends, and holidays would be being a patient admitted during a night, weekend, or holiday. To understand why, I have to look no further than my hospital parking lot. During bankers’ hours, I can barely find a parking spot on the top floor of our multilevel parking structure.
Fast-forward to Saturday, and I have my pick of empty football fields’ worth of spots on all floors. Ditto Sundays, nights, and holidays.
Why is it that nationally, a collectively near-trillion-dollar hospital enterprise finds it acceptable to effectively shutter itself for a quarter to a third of the week? Especially when doing so seems to counter their primary mission of providing safe, timely, effective, efficient, equitable, and patient-centered care.
The Weekend Effect
There are, of course, economic and operational reasons to downshift during off hours—some hospitals don’t have the elective procedures to run operating rooms seven days a week, and very few patients want to have their elective colonoscopy at 11 p.m. or their chemotherapy during Thanksgiving dinner. However, in most cases, the reasons for doing so center on hospital staff and physician satisfaction. Most us of just don’t like working off hours. As a result, studies have shown significantly less access to such high-level care as coronary angiography and percutaneous coronary intervention on weekends.2,3
And the effects of this “weekend effect” can be devastating.
A recent paper in the New England Journal of Medicine reported that for every 1,000 patients admitted with a myocardial infarction on a weekend, nine more would die than a comparable group admitted during the week.4 Their offense? Having the misfortune to get ill on a Saturday morning. The authors concluded that this higher mortality was secondary to a lower rate of invasive cardiac procedures, presumably because they were less available. And the weekend effect isn’t just limited to coronary care. Poorer outcomes, including higher mortality rates, have been reported for weekend admissions to the neonatal ICU and adult ICU, as well as admission for epiglottitis, ruptured abdominal aortic aneurysms, and pulmonary embolism.5,6,7
So let’s connect the dots: A system designed with inequal access to lifesaving therapies and appropriate staffing results in worse outcomes, more harm, more deaths.
To be clear, 98,000 people don’t die every year because of my disdain for working nights and weekends. This is a much deeper problem that hinges on many unsatisfactory systems working unsatisfactorily in tandem (e.g. see the other five IOM domains of quality care). Furthermore, I don’t mean to suggest that hospitalists necessarily have a lot of say in cardiac catheterization schedules. Yet we do control our own systems of care—how many patients we admit and cover during a shift, how strongly we advocate for timely testing and consultation, how we staff weekends and cover patients at night.
And, more and more, we are in a position to enhance the care delivery systems of the hospital and its providers that surround us. With that comes a responsibility to ensure that these systems are highly functioning and equitable, regardless of the time of day, day of the week.
If we are going to fundamentally enhance the quality of care, then we have to design safer systems of care. It will take time and resources to alter many of our bruised systems of care, but we can begin by at least ensuring equity in how we deliver care at our own institutions. That is, unless we are comfortable with a system perfectly designed to harm. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
References
- Institute of Medicine (IOM). Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, D.C.: National Academy Press; 2001.
- Bell CM, Redelmeier DA. Waiting for urgent procedures on the weekend among emergently hospitalized patients. Am J Med. 2004:117(3):175-181.
- Magid DJ, Wang Y, Herrin J, et al. Relationship between time of day, day of week, timeliness of reperfusion, and in-hospital mortality for patients with acute ST-segment elevation myocardial infarction. JAMA. 2005;294(7):803-812.
- Kostis WJ, Demissie K, Marcella SW, Shao YH, Wilson AC, Moreyra AE. Weekend versus weekday admission and mortality from myocardial infarction. N Eng J Med. 2007;356 (11):1099-1109.
- Hendry RA. The weekend—a dangerous time to be born? Br J Obstet Gynaecol. 1981;88(12):1200-1203.
- Barnett MJ, Kaboli PJ, Sirio CA, Rosenthal GE. Day of the week of intensive care admission and patient outcomes: a multisite regional evaluation. Med Care. 2002;40(6):530-539.
- Bell CM, Redelmeier DA. Mortality among patients admitted to hospitals on weekends as compared with weekdays. N Eng J Med. 2001;345(9):663-668.
Market Watch
New Drugs, Devices, Indications, and Approvals
- Alglucosidase alfa (Lumizyme) has been approved by the FDA for the treatment of patients older than 8 with late (noninfantile) onset Pompe disease (GAA deficiency) who do not have evidence of cardiac hypertrophy.1
- Dutasteride and tamsulosin (Jalyn) has been approved by the FDA in a fixed-dose combination product for treating symptomatic benign prostatic hypertrophy.2
- Gatifloxacin ophthalmic solution 0.5% (Zymaxid) has been approved by the FDA to treat bacterial conjunctivitis caused by susceptible bacterial strains.3 It has the highest concentration of gatifloxacin ophthalmic on the U.S. market.
- Memantine hydrochloride (Namenda XR) has been approved by the FDA as an extended-release product to treat moderate to severe dementia of the Alzheimer's type.4 It is available as a 28 mg, once-daily dosage form. The immediate-release product is dosed twice daily.
- Mesenchymal stem cells for intravenous infusion (MSCs, Prochymal) formulated into Prochymal has been granted orphan drug status to treat Type 1 diabetes mellitus (T1DM).5 This agent is in Phase 2 clinical trials in a collaboration with the Juvenile Diabetes Research Foundation as a treatment for patients with newly diagnosed T1DM.
- Mometasone furoate/formoterol fumarate (Dulera) has been approved by the FDA as a combination treatment for asthmatics aged 12 and older.6
- Naproxen/esomeprazole (Vimovo) has been approved by the FDA as a fixed combination for patients with arthritis who are at risk for developing gastric ulcers.7
- Pioglitazone/metformin (ACTOplus met XR) has been approved by the FDA in an extended-release fixed combination for treating Type 2 diabetes mellitus (T2DM) as an adjunct to diet and exercise.8
- Ranibizumab (Lucentis) has received a new indication from the FDA for treating retinal vein occlusion.9 The original approval of ranibizumab was for wet age-related macular degeneration.
- Tramadol HCl, orally disintegrating tablets (Rybix ODT), have been approved by the FDA for treating moderate to moderately severe pain in patients 16 years of age and older.10
Pipeline
- Dronedarone (Multaq) is being investigated as to whether it can reduce major cardiovascular events in patients being treated with the agent for atrial fibrillation.11 Study endpoints will include a reduction in a major cardiovascular event such as stroke or myocardial infarction, or a reduction in cardiovascular hospitalization or death.
- The combination product ibuprofen and famotidine (to be known as Duexa) has been filed as a new drug application (NDA) for reducing the risk of developing upper gastrointestinal (GI) ulcers in patients with pain and arthritis.12 Two Phase 3 trials showed about a 50% reduction in GI ulcers in combination treatment compared with ibuprofen alone.
- Rifaximin (Xifaxan) has been submitted to the FDA at its higher dose (550 mg) for treatment of nonconstipation irritable bowel syndrome (Non-C-IBS) and IBS-related bloating.13 Rifaximin already has approval from the FDA for hepatic encephalopathy and diarrhea.
- TC-5214 has begun Phase 3 clinical trials.14 It is a nicotinic channel blocker for the adjunctive treatment of major depressive disorder in adults who have had an inadequate response to selective serotonin reuptake inhibitors (SSRIs) or serotonin/norepinephrine reuptake inhibitors (SNRIs). A Phase 2 study evaluating TC-5214 as a second-line (“switch”) monotherapy is planned for this year.
- An NDA for vilazodone has been filed for treating major depressive disorder.15 It is a dual-acting potent and selective serotonin reuptake inhibitor and a 5-HT1A receptor partial agonist.
Safety, Warnings, and Label Changes
- Tramadol and tramadol/acetaminophen have undergone a label change related to strengthened warnings of the risk of suicide for patients who are addiction-prone, taking tranquilizers, drinking alcohol, or taking other central-nervous-system-active drugs.16 Addictive effects might occur when tramadol is combined with alcohol, other opioids, or illicit drugs that have central-nervous-system-depressive effects. Serious potential consequences of overdosage are CNS and/or respiratory depression, and death.
- Earlier this year, the FDA once again updated the warning related to severe liver injury related to the use of propylthiouracil (PTU).17 This time, PTU has garnered a boxed warning, which includes reports of severe hepatotoxicity and acute liver failure in both adults and children. Some of these reactions were fatal. Use of PTU should be reserved for patients who do not tolerate other treatments for hyperthyroidism, such as methimazole, radioactive iodine, or are not surgery candidates. PTU might be preferred over methimazole just before and/or during the first trimester of pregnancy due to the occurrence of birth defects with methimazole during this timeframe. A medication guide has been developed and is to be given to patients when they fill PTU prescriptions. The guide alerts patients to the signs and symptoms of hepatotoxicity. TH
Michele B. Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City and a clinical pharmacist at New York Downtown Hospital.
References
- Genzyme receives FDA approval for lumizyme for Pompe disease. Business Wire website. Available at: www.businesswire.com/portal/site/home/email/alert/?ndmViewId=news_view&newsLang=en&newsId=20100525006514. Accessed June 30, 2010.
- Dennis M. FDA approves GlaxoSmithKline’s combination BPH drug Jalyn. FirstWord website. Available at: http://www.firstwordplus.com/Fws.do?articleid=B5F703CADB0347DF970A7B7542D99982&logRowId=369156. Accessed June 30, 2010.
- Allergan receives FDA approval for Zymaxid ophthalmic solution. Medical News Today website. Available at: http://www.medicalnewstoday.com/articles/189397.php. Accessed June 29, 2010.
- Forest and Merz announce FDA approval of Namenda XR for the treatment of moderate to severe dementia of the Alzheimer’s type. Forest Laboratories website. Available at: http://www.frx.com/news/PressRelease.aspx?ID=1440385. Accessed June 30, 2010.
- Osiris Therapeutics receives FDA orphan drug designation for stem cell treatment for Type 1 diabetes. Osiris Therapeutics website. Available at: http://osiris.com/pdf/2010-05-04%20T1D%20Orphan%20Drug%20Designation.pdf. Accessed June 30, 2010.
- FDA approves Merck’s new lung drug Dulera. The Economic Times website. Available at: http://economictimes.indiatimes.com/articleshow/6087079.cms. Accessed June 30, 2010.
- Dane L. FDA approves AstraZeneca, Pozen’s Vimovo. FirstWord website. Available at: http://www.firstwordplus.com/Fws.do?articleid=0C2915EE4D2D47D287D41D90DFE4240D. Accessed June 30, 2010.
- ACTOplus met XR available for diabetes. Monthly Prescribing Reference website. Available at: http://www.empr.com/actoplus-met-xr-available-for-diabetes/article/172985/. Accessed June 30, 2010.
- Dennis M. Roche’s Lucentis garners expanded FDA approval for macular oedema. FirstWord website. Available at: http://www.firstwordplus.com/Fws.do?articleid=5146664F5A4C48108209D15EA744A614&logRowId=370643. Accessed June 30, 2010.
- Rybix ODT launched for moderate to moderately severe pain. Monthly Prescribing Reference website. Available at: http://www.empr.com/rybix-odt-launched-for-moderate-to-moderately-severe-pain/article/172743/. Accessed June 30, 3010.
- Dennis M. Sanofi-Aventis begins late-stage study of Multaq in patients with permanent AF. FirstWord website. Available at: http://www.firstwordplus.com/Fws.do?articleid=E43104A2DB604649A812E69C58F89304&logRowId=364228. Accessed July 7, 2010.
- FDA accepts NDA for Duexa for ulcer risk reduction in arthritis patients. Monthly Prescribing Reference website. Available at: http://www.empr.com/fda-accepts-nda-for-duexa-for-ulcer-risk-reduction-in-arthritis-patients/article/171054/. Accessed July 7, 2010.
- Salix Pharmaceuticals announces NDA submission for Xifaxan550 for treatment of non-constipation irritable bowel syndrome. Salix Pharmaceuticals website. Available at: http://salix.com/news/stories/20100608.aspx. Accessed June 9, 2010.
- AstraZeneca and Targacept initiate Phase 3 clinical development of TC-5214 as an adjunct treatment for major depressive disorder. Targacept website. Available at: http://www.targacept.com/wt/page/pr_1277240993. Accessed June 29, 2010.
- Clinical Data, Inc. announces FDA acceptance of new drug application for Vilazodone for the treatment of major depressive disorder. Clinical Data Inc. website. Available at: http://clda.com/uploads/CLDA%20NDA%20acceptance%20FINAL.pdf. Accessed July 7, 2010.
- Ultram (tramadol hydrochloride), Ultracet (tramadol hydrochloride/acetaminophen): Label change. U.S. Food and Drug Administration website. Available at: http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm213264.htm. Accessed July 8, 2010.
- FDA Drug Safety Communication: New boxed warning on severe liver injury with propylthiouracil. U.S. Food and Drug Administration website. Available at: http://www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/ucm209023.htm. Accessed July 8, 2010.
New Drugs, Devices, Indications, and Approvals
- Alglucosidase alfa (Lumizyme) has been approved by the FDA for the treatment of patients older than 8 with late (noninfantile) onset Pompe disease (GAA deficiency) who do not have evidence of cardiac hypertrophy.1
- Dutasteride and tamsulosin (Jalyn) has been approved by the FDA in a fixed-dose combination product for treating symptomatic benign prostatic hypertrophy.2
- Gatifloxacin ophthalmic solution 0.5% (Zymaxid) has been approved by the FDA to treat bacterial conjunctivitis caused by susceptible bacterial strains.3 It has the highest concentration of gatifloxacin ophthalmic on the U.S. market.
- Memantine hydrochloride (Namenda XR) has been approved by the FDA as an extended-release product to treat moderate to severe dementia of the Alzheimer's type.4 It is available as a 28 mg, once-daily dosage form. The immediate-release product is dosed twice daily.
- Mesenchymal stem cells for intravenous infusion (MSCs, Prochymal) formulated into Prochymal has been granted orphan drug status to treat Type 1 diabetes mellitus (T1DM).5 This agent is in Phase 2 clinical trials in a collaboration with the Juvenile Diabetes Research Foundation as a treatment for patients with newly diagnosed T1DM.
- Mometasone furoate/formoterol fumarate (Dulera) has been approved by the FDA as a combination treatment for asthmatics aged 12 and older.6
- Naproxen/esomeprazole (Vimovo) has been approved by the FDA as a fixed combination for patients with arthritis who are at risk for developing gastric ulcers.7
- Pioglitazone/metformin (ACTOplus met XR) has been approved by the FDA in an extended-release fixed combination for treating Type 2 diabetes mellitus (T2DM) as an adjunct to diet and exercise.8
- Ranibizumab (Lucentis) has received a new indication from the FDA for treating retinal vein occlusion.9 The original approval of ranibizumab was for wet age-related macular degeneration.
- Tramadol HCl, orally disintegrating tablets (Rybix ODT), have been approved by the FDA for treating moderate to moderately severe pain in patients 16 years of age and older.10
Pipeline
- Dronedarone (Multaq) is being investigated as to whether it can reduce major cardiovascular events in patients being treated with the agent for atrial fibrillation.11 Study endpoints will include a reduction in a major cardiovascular event such as stroke or myocardial infarction, or a reduction in cardiovascular hospitalization or death.
- The combination product ibuprofen and famotidine (to be known as Duexa) has been filed as a new drug application (NDA) for reducing the risk of developing upper gastrointestinal (GI) ulcers in patients with pain and arthritis.12 Two Phase 3 trials showed about a 50% reduction in GI ulcers in combination treatment compared with ibuprofen alone.
- Rifaximin (Xifaxan) has been submitted to the FDA at its higher dose (550 mg) for treatment of nonconstipation irritable bowel syndrome (Non-C-IBS) and IBS-related bloating.13 Rifaximin already has approval from the FDA for hepatic encephalopathy and diarrhea.
- TC-5214 has begun Phase 3 clinical trials.14 It is a nicotinic channel blocker for the adjunctive treatment of major depressive disorder in adults who have had an inadequate response to selective serotonin reuptake inhibitors (SSRIs) or serotonin/norepinephrine reuptake inhibitors (SNRIs). A Phase 2 study evaluating TC-5214 as a second-line (“switch”) monotherapy is planned for this year.
- An NDA for vilazodone has been filed for treating major depressive disorder.15 It is a dual-acting potent and selective serotonin reuptake inhibitor and a 5-HT1A receptor partial agonist.
Safety, Warnings, and Label Changes
- Tramadol and tramadol/acetaminophen have undergone a label change related to strengthened warnings of the risk of suicide for patients who are addiction-prone, taking tranquilizers, drinking alcohol, or taking other central-nervous-system-active drugs.16 Addictive effects might occur when tramadol is combined with alcohol, other opioids, or illicit drugs that have central-nervous-system-depressive effects. Serious potential consequences of overdosage are CNS and/or respiratory depression, and death.
- Earlier this year, the FDA once again updated the warning related to severe liver injury related to the use of propylthiouracil (PTU).17 This time, PTU has garnered a boxed warning, which includes reports of severe hepatotoxicity and acute liver failure in both adults and children. Some of these reactions were fatal. Use of PTU should be reserved for patients who do not tolerate other treatments for hyperthyroidism, such as methimazole, radioactive iodine, or are not surgery candidates. PTU might be preferred over methimazole just before and/or during the first trimester of pregnancy due to the occurrence of birth defects with methimazole during this timeframe. A medication guide has been developed and is to be given to patients when they fill PTU prescriptions. The guide alerts patients to the signs and symptoms of hepatotoxicity. TH
Michele B. Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City and a clinical pharmacist at New York Downtown Hospital.
References
- Genzyme receives FDA approval for lumizyme for Pompe disease. Business Wire website. Available at: www.businesswire.com/portal/site/home/email/alert/?ndmViewId=news_view&newsLang=en&newsId=20100525006514. Accessed June 30, 2010.
- Dennis M. FDA approves GlaxoSmithKline’s combination BPH drug Jalyn. FirstWord website. Available at: http://www.firstwordplus.com/Fws.do?articleid=B5F703CADB0347DF970A7B7542D99982&logRowId=369156. Accessed June 30, 2010.
- Allergan receives FDA approval for Zymaxid ophthalmic solution. Medical News Today website. Available at: http://www.medicalnewstoday.com/articles/189397.php. Accessed June 29, 2010.
- Forest and Merz announce FDA approval of Namenda XR for the treatment of moderate to severe dementia of the Alzheimer’s type. Forest Laboratories website. Available at: http://www.frx.com/news/PressRelease.aspx?ID=1440385. Accessed June 30, 2010.
- Osiris Therapeutics receives FDA orphan drug designation for stem cell treatment for Type 1 diabetes. Osiris Therapeutics website. Available at: http://osiris.com/pdf/2010-05-04%20T1D%20Orphan%20Drug%20Designation.pdf. Accessed June 30, 2010.
- FDA approves Merck’s new lung drug Dulera. The Economic Times website. Available at: http://economictimes.indiatimes.com/articleshow/6087079.cms. Accessed June 30, 2010.
- Dane L. FDA approves AstraZeneca, Pozen’s Vimovo. FirstWord website. Available at: http://www.firstwordplus.com/Fws.do?articleid=0C2915EE4D2D47D287D41D90DFE4240D. Accessed June 30, 2010.
- ACTOplus met XR available for diabetes. Monthly Prescribing Reference website. Available at: http://www.empr.com/actoplus-met-xr-available-for-diabetes/article/172985/. Accessed June 30, 2010.
- Dennis M. Roche’s Lucentis garners expanded FDA approval for macular oedema. FirstWord website. Available at: http://www.firstwordplus.com/Fws.do?articleid=5146664F5A4C48108209D15EA744A614&logRowId=370643. Accessed June 30, 2010.
- Rybix ODT launched for moderate to moderately severe pain. Monthly Prescribing Reference website. Available at: http://www.empr.com/rybix-odt-launched-for-moderate-to-moderately-severe-pain/article/172743/. Accessed June 30, 3010.
- Dennis M. Sanofi-Aventis begins late-stage study of Multaq in patients with permanent AF. FirstWord website. Available at: http://www.firstwordplus.com/Fws.do?articleid=E43104A2DB604649A812E69C58F89304&logRowId=364228. Accessed July 7, 2010.
- FDA accepts NDA for Duexa for ulcer risk reduction in arthritis patients. Monthly Prescribing Reference website. Available at: http://www.empr.com/fda-accepts-nda-for-duexa-for-ulcer-risk-reduction-in-arthritis-patients/article/171054/. Accessed July 7, 2010.
- Salix Pharmaceuticals announces NDA submission for Xifaxan550 for treatment of non-constipation irritable bowel syndrome. Salix Pharmaceuticals website. Available at: http://salix.com/news/stories/20100608.aspx. Accessed June 9, 2010.
- AstraZeneca and Targacept initiate Phase 3 clinical development of TC-5214 as an adjunct treatment for major depressive disorder. Targacept website. Available at: http://www.targacept.com/wt/page/pr_1277240993. Accessed June 29, 2010.
- Clinical Data, Inc. announces FDA acceptance of new drug application for Vilazodone for the treatment of major depressive disorder. Clinical Data Inc. website. Available at: http://clda.com/uploads/CLDA%20NDA%20acceptance%20FINAL.pdf. Accessed July 7, 2010.
- Ultram (tramadol hydrochloride), Ultracet (tramadol hydrochloride/acetaminophen): Label change. U.S. Food and Drug Administration website. Available at: http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm213264.htm. Accessed July 8, 2010.
- FDA Drug Safety Communication: New boxed warning on severe liver injury with propylthiouracil. U.S. Food and Drug Administration website. Available at: http://www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/ucm209023.htm. Accessed July 8, 2010.
New Drugs, Devices, Indications, and Approvals
- Alglucosidase alfa (Lumizyme) has been approved by the FDA for the treatment of patients older than 8 with late (noninfantile) onset Pompe disease (GAA deficiency) who do not have evidence of cardiac hypertrophy.1
- Dutasteride and tamsulosin (Jalyn) has been approved by the FDA in a fixed-dose combination product for treating symptomatic benign prostatic hypertrophy.2
- Gatifloxacin ophthalmic solution 0.5% (Zymaxid) has been approved by the FDA to treat bacterial conjunctivitis caused by susceptible bacterial strains.3 It has the highest concentration of gatifloxacin ophthalmic on the U.S. market.
- Memantine hydrochloride (Namenda XR) has been approved by the FDA as an extended-release product to treat moderate to severe dementia of the Alzheimer's type.4 It is available as a 28 mg, once-daily dosage form. The immediate-release product is dosed twice daily.
- Mesenchymal stem cells for intravenous infusion (MSCs, Prochymal) formulated into Prochymal has been granted orphan drug status to treat Type 1 diabetes mellitus (T1DM).5 This agent is in Phase 2 clinical trials in a collaboration with the Juvenile Diabetes Research Foundation as a treatment for patients with newly diagnosed T1DM.
- Mometasone furoate/formoterol fumarate (Dulera) has been approved by the FDA as a combination treatment for asthmatics aged 12 and older.6
- Naproxen/esomeprazole (Vimovo) has been approved by the FDA as a fixed combination for patients with arthritis who are at risk for developing gastric ulcers.7
- Pioglitazone/metformin (ACTOplus met XR) has been approved by the FDA in an extended-release fixed combination for treating Type 2 diabetes mellitus (T2DM) as an adjunct to diet and exercise.8
- Ranibizumab (Lucentis) has received a new indication from the FDA for treating retinal vein occlusion.9 The original approval of ranibizumab was for wet age-related macular degeneration.
- Tramadol HCl, orally disintegrating tablets (Rybix ODT), have been approved by the FDA for treating moderate to moderately severe pain in patients 16 years of age and older.10
Pipeline
- Dronedarone (Multaq) is being investigated as to whether it can reduce major cardiovascular events in patients being treated with the agent for atrial fibrillation.11 Study endpoints will include a reduction in a major cardiovascular event such as stroke or myocardial infarction, or a reduction in cardiovascular hospitalization or death.
- The combination product ibuprofen and famotidine (to be known as Duexa) has been filed as a new drug application (NDA) for reducing the risk of developing upper gastrointestinal (GI) ulcers in patients with pain and arthritis.12 Two Phase 3 trials showed about a 50% reduction in GI ulcers in combination treatment compared with ibuprofen alone.
- Rifaximin (Xifaxan) has been submitted to the FDA at its higher dose (550 mg) for treatment of nonconstipation irritable bowel syndrome (Non-C-IBS) and IBS-related bloating.13 Rifaximin already has approval from the FDA for hepatic encephalopathy and diarrhea.
- TC-5214 has begun Phase 3 clinical trials.14 It is a nicotinic channel blocker for the adjunctive treatment of major depressive disorder in adults who have had an inadequate response to selective serotonin reuptake inhibitors (SSRIs) or serotonin/norepinephrine reuptake inhibitors (SNRIs). A Phase 2 study evaluating TC-5214 as a second-line (“switch”) monotherapy is planned for this year.
- An NDA for vilazodone has been filed for treating major depressive disorder.15 It is a dual-acting potent and selective serotonin reuptake inhibitor and a 5-HT1A receptor partial agonist.
Safety, Warnings, and Label Changes
- Tramadol and tramadol/acetaminophen have undergone a label change related to strengthened warnings of the risk of suicide for patients who are addiction-prone, taking tranquilizers, drinking alcohol, or taking other central-nervous-system-active drugs.16 Addictive effects might occur when tramadol is combined with alcohol, other opioids, or illicit drugs that have central-nervous-system-depressive effects. Serious potential consequences of overdosage are CNS and/or respiratory depression, and death.
- Earlier this year, the FDA once again updated the warning related to severe liver injury related to the use of propylthiouracil (PTU).17 This time, PTU has garnered a boxed warning, which includes reports of severe hepatotoxicity and acute liver failure in both adults and children. Some of these reactions were fatal. Use of PTU should be reserved for patients who do not tolerate other treatments for hyperthyroidism, such as methimazole, radioactive iodine, or are not surgery candidates. PTU might be preferred over methimazole just before and/or during the first trimester of pregnancy due to the occurrence of birth defects with methimazole during this timeframe. A medication guide has been developed and is to be given to patients when they fill PTU prescriptions. The guide alerts patients to the signs and symptoms of hepatotoxicity. TH
Michele B. Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City and a clinical pharmacist at New York Downtown Hospital.
References
- Genzyme receives FDA approval for lumizyme for Pompe disease. Business Wire website. Available at: www.businesswire.com/portal/site/home/email/alert/?ndmViewId=news_view&newsLang=en&newsId=20100525006514. Accessed June 30, 2010.
- Dennis M. FDA approves GlaxoSmithKline’s combination BPH drug Jalyn. FirstWord website. Available at: http://www.firstwordplus.com/Fws.do?articleid=B5F703CADB0347DF970A7B7542D99982&logRowId=369156. Accessed June 30, 2010.
- Allergan receives FDA approval for Zymaxid ophthalmic solution. Medical News Today website. Available at: http://www.medicalnewstoday.com/articles/189397.php. Accessed June 29, 2010.
- Forest and Merz announce FDA approval of Namenda XR for the treatment of moderate to severe dementia of the Alzheimer’s type. Forest Laboratories website. Available at: http://www.frx.com/news/PressRelease.aspx?ID=1440385. Accessed June 30, 2010.
- Osiris Therapeutics receives FDA orphan drug designation for stem cell treatment for Type 1 diabetes. Osiris Therapeutics website. Available at: http://osiris.com/pdf/2010-05-04%20T1D%20Orphan%20Drug%20Designation.pdf. Accessed June 30, 2010.
- FDA approves Merck’s new lung drug Dulera. The Economic Times website. Available at: http://economictimes.indiatimes.com/articleshow/6087079.cms. Accessed June 30, 2010.
- Dane L. FDA approves AstraZeneca, Pozen’s Vimovo. FirstWord website. Available at: http://www.firstwordplus.com/Fws.do?articleid=0C2915EE4D2D47D287D41D90DFE4240D. Accessed June 30, 2010.
- ACTOplus met XR available for diabetes. Monthly Prescribing Reference website. Available at: http://www.empr.com/actoplus-met-xr-available-for-diabetes/article/172985/. Accessed June 30, 2010.
- Dennis M. Roche’s Lucentis garners expanded FDA approval for macular oedema. FirstWord website. Available at: http://www.firstwordplus.com/Fws.do?articleid=5146664F5A4C48108209D15EA744A614&logRowId=370643. Accessed June 30, 2010.
- Rybix ODT launched for moderate to moderately severe pain. Monthly Prescribing Reference website. Available at: http://www.empr.com/rybix-odt-launched-for-moderate-to-moderately-severe-pain/article/172743/. Accessed June 30, 3010.
- Dennis M. Sanofi-Aventis begins late-stage study of Multaq in patients with permanent AF. FirstWord website. Available at: http://www.firstwordplus.com/Fws.do?articleid=E43104A2DB604649A812E69C58F89304&logRowId=364228. Accessed July 7, 2010.
- FDA accepts NDA for Duexa for ulcer risk reduction in arthritis patients. Monthly Prescribing Reference website. Available at: http://www.empr.com/fda-accepts-nda-for-duexa-for-ulcer-risk-reduction-in-arthritis-patients/article/171054/. Accessed July 7, 2010.
- Salix Pharmaceuticals announces NDA submission for Xifaxan550 for treatment of non-constipation irritable bowel syndrome. Salix Pharmaceuticals website. Available at: http://salix.com/news/stories/20100608.aspx. Accessed June 9, 2010.
- AstraZeneca and Targacept initiate Phase 3 clinical development of TC-5214 as an adjunct treatment for major depressive disorder. Targacept website. Available at: http://www.targacept.com/wt/page/pr_1277240993. Accessed June 29, 2010.
- Clinical Data, Inc. announces FDA acceptance of new drug application for Vilazodone for the treatment of major depressive disorder. Clinical Data Inc. website. Available at: http://clda.com/uploads/CLDA%20NDA%20acceptance%20FINAL.pdf. Accessed July 7, 2010.
- Ultram (tramadol hydrochloride), Ultracet (tramadol hydrochloride/acetaminophen): Label change. U.S. Food and Drug Administration website. Available at: http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm213264.htm. Accessed July 8, 2010.
- FDA Drug Safety Communication: New boxed warning on severe liver injury with propylthiouracil. U.S. Food and Drug Administration website. Available at: http://www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/ucm209023.htm. Accessed July 8, 2010.
Innovators Descend on Annual Pediatric HM Conference
More than 400 people attended the Pediatric Hospital Medicine annual conference July 22-25 in Minneapolis. The annual meeting is the premier networking and educational event for pediatric hospitalists and is sponsored by the American Academy of Pediatrics (AAP), SHM, and the Academic Pediatric Association (APA).
Innovation and improvement were popular topics throughout the conference. Keynote speaker George Buckley, CEO of manufacturing and technology conglomerate 3M, spoke about inspiring innovation, and a large percentage of the sessions and posters had quality-improvement (QI) themes. Experts from Cincinnati Children’s Hospital, led by Steve Muething, MD, assistant vice president of patient safety, and Shannon Phillips, MD, MPH, Cleveland Clinic’s patient safety officer, guided several popular sessions on QI.
A major innovation announced at the conference was the planned launch of a journal of pediatric hospital medicine, which will be sponsored by the AAP. (Update 09.14.2010--The journal has yet to officially announce an editor).
Research presentations have continued to increase in this young field, and the meeting was full of poster and platform presentations in the areas of clinical research, QI, educational research, and health services research. Vineeta Mittal, MD, of the University of Texas Southwestern and Children’s Medical Center in Dallas presented research on family-centered rounds, which was recently published in Pediatrics and picked up by the National Association of Children’s Hospitals (NACHRI) for dissemination.1 Patrick Brady, MD, of Cincinnati Children’s Hospital presented his research on short- versus long-course IV therapy for pediatric urinary tract infections, also published in Pediatrics.2
Other buzzed-about sessions included Vanderbilt University pediatric hospitalist Dr. Paul Hain’s ambitious attempt to create a PHM performance dashboard, and a case of “situational” epilepsy presented by Dr. Lisa Zaoutis of CHOP.
As in years past, the hottest ticket was for the luncheon presentation of the “Top Articles in Pediatric Hospital Medicine,” paneled this year by Drs. John Pope, Kris Rehm, and Brian Alverson. Raj Srivastava, MD, of Primary Children’s Medical Center in Salt Lake City and chairperson of the Pediatric Research in Inpatient Settings network, announced that the network had been awarded major grant funding.
Dan Rauch, MD, chair of the AAP’s Section on Hospital Medicine, dropped the biggest bombshell of all: He announced that the American Board of Pediatrics will support the development of pediatric HM as a full-fledged subspecialty in the near future. TH
Dr. Ralston is associate professor of pediatrics and chief of the division of inpatient pediatrics at the University of Texas Health Science Center in San Antonio, and medical director of inpatient services at Christus Santa Rosa Children’s Hospital.
References
- Mittal VS, Sigrest T, Ottolini MC, et al. Family-centered rounds on pediatric wards: a PRIS network survey of U.S. and Canadian hospitalists. Pediatrics. 2010;126(1):37-43.
- Brady PW, Conway PH, Goudie A. Length of intravenous antibiotic therapy and treatment failure in infants with urinary track infections. Pediatrics. 2010;126(2):196-203.
More than 400 people attended the Pediatric Hospital Medicine annual conference July 22-25 in Minneapolis. The annual meeting is the premier networking and educational event for pediatric hospitalists and is sponsored by the American Academy of Pediatrics (AAP), SHM, and the Academic Pediatric Association (APA).
Innovation and improvement were popular topics throughout the conference. Keynote speaker George Buckley, CEO of manufacturing and technology conglomerate 3M, spoke about inspiring innovation, and a large percentage of the sessions and posters had quality-improvement (QI) themes. Experts from Cincinnati Children’s Hospital, led by Steve Muething, MD, assistant vice president of patient safety, and Shannon Phillips, MD, MPH, Cleveland Clinic’s patient safety officer, guided several popular sessions on QI.
A major innovation announced at the conference was the planned launch of a journal of pediatric hospital medicine, which will be sponsored by the AAP. (Update 09.14.2010--The journal has yet to officially announce an editor).
Research presentations have continued to increase in this young field, and the meeting was full of poster and platform presentations in the areas of clinical research, QI, educational research, and health services research. Vineeta Mittal, MD, of the University of Texas Southwestern and Children’s Medical Center in Dallas presented research on family-centered rounds, which was recently published in Pediatrics and picked up by the National Association of Children’s Hospitals (NACHRI) for dissemination.1 Patrick Brady, MD, of Cincinnati Children’s Hospital presented his research on short- versus long-course IV therapy for pediatric urinary tract infections, also published in Pediatrics.2
Other buzzed-about sessions included Vanderbilt University pediatric hospitalist Dr. Paul Hain’s ambitious attempt to create a PHM performance dashboard, and a case of “situational” epilepsy presented by Dr. Lisa Zaoutis of CHOP.
As in years past, the hottest ticket was for the luncheon presentation of the “Top Articles in Pediatric Hospital Medicine,” paneled this year by Drs. John Pope, Kris Rehm, and Brian Alverson. Raj Srivastava, MD, of Primary Children’s Medical Center in Salt Lake City and chairperson of the Pediatric Research in Inpatient Settings network, announced that the network had been awarded major grant funding.
Dan Rauch, MD, chair of the AAP’s Section on Hospital Medicine, dropped the biggest bombshell of all: He announced that the American Board of Pediatrics will support the development of pediatric HM as a full-fledged subspecialty in the near future. TH
Dr. Ralston is associate professor of pediatrics and chief of the division of inpatient pediatrics at the University of Texas Health Science Center in San Antonio, and medical director of inpatient services at Christus Santa Rosa Children’s Hospital.
References
- Mittal VS, Sigrest T, Ottolini MC, et al. Family-centered rounds on pediatric wards: a PRIS network survey of U.S. and Canadian hospitalists. Pediatrics. 2010;126(1):37-43.
- Brady PW, Conway PH, Goudie A. Length of intravenous antibiotic therapy and treatment failure in infants with urinary track infections. Pediatrics. 2010;126(2):196-203.
More than 400 people attended the Pediatric Hospital Medicine annual conference July 22-25 in Minneapolis. The annual meeting is the premier networking and educational event for pediatric hospitalists and is sponsored by the American Academy of Pediatrics (AAP), SHM, and the Academic Pediatric Association (APA).
Innovation and improvement were popular topics throughout the conference. Keynote speaker George Buckley, CEO of manufacturing and technology conglomerate 3M, spoke about inspiring innovation, and a large percentage of the sessions and posters had quality-improvement (QI) themes. Experts from Cincinnati Children’s Hospital, led by Steve Muething, MD, assistant vice president of patient safety, and Shannon Phillips, MD, MPH, Cleveland Clinic’s patient safety officer, guided several popular sessions on QI.
A major innovation announced at the conference was the planned launch of a journal of pediatric hospital medicine, which will be sponsored by the AAP. (Update 09.14.2010--The journal has yet to officially announce an editor).
Research presentations have continued to increase in this young field, and the meeting was full of poster and platform presentations in the areas of clinical research, QI, educational research, and health services research. Vineeta Mittal, MD, of the University of Texas Southwestern and Children’s Medical Center in Dallas presented research on family-centered rounds, which was recently published in Pediatrics and picked up by the National Association of Children’s Hospitals (NACHRI) for dissemination.1 Patrick Brady, MD, of Cincinnati Children’s Hospital presented his research on short- versus long-course IV therapy for pediatric urinary tract infections, also published in Pediatrics.2
Other buzzed-about sessions included Vanderbilt University pediatric hospitalist Dr. Paul Hain’s ambitious attempt to create a PHM performance dashboard, and a case of “situational” epilepsy presented by Dr. Lisa Zaoutis of CHOP.
As in years past, the hottest ticket was for the luncheon presentation of the “Top Articles in Pediatric Hospital Medicine,” paneled this year by Drs. John Pope, Kris Rehm, and Brian Alverson. Raj Srivastava, MD, of Primary Children’s Medical Center in Salt Lake City and chairperson of the Pediatric Research in Inpatient Settings network, announced that the network had been awarded major grant funding.
Dan Rauch, MD, chair of the AAP’s Section on Hospital Medicine, dropped the biggest bombshell of all: He announced that the American Board of Pediatrics will support the development of pediatric HM as a full-fledged subspecialty in the near future. TH
Dr. Ralston is associate professor of pediatrics and chief of the division of inpatient pediatrics at the University of Texas Health Science Center in San Antonio, and medical director of inpatient services at Christus Santa Rosa Children’s Hospital.
References
- Mittal VS, Sigrest T, Ottolini MC, et al. Family-centered rounds on pediatric wards: a PRIS network survey of U.S. and Canadian hospitalists. Pediatrics. 2010;126(1):37-43.
- Brady PW, Conway PH, Goudie A. Length of intravenous antibiotic therapy and treatment failure in infants with urinary track infections. Pediatrics. 2010;126(2):196-203.
Hospitalist/Intensivist Model Lowers Costs, Maintains Quality of Care
As the field of HM continues to mature, branch out, and is called upon to lead in the care of a larger cross-section of hospitalized patients, it is only natural that this includes the critically ill patient. Hospitalists already care for—and are the attending of record for—this patient population in most U.S. hospitals. It is my position that a technically proficient hospitalist service, which is facility-exclusive and offers 24/7 coverage, is able to offer the same quality of care as an intensivist group. An important feature of this model is the inclusion and “buy in” from community pulmonologists in order to provide backup and consultative assistance when warranted.
Our program at Westside Regional Medical Center in Plantation, Fla., has made great strides as we continue to integrate this model in the hospital. We are actively tracking ICU length of stay and throughput, incidence of ventilator-associated pneumonia (VAP), central-line infection rates, and ICU mortality.
I believe that a clinically competent and aggressive HM service is able to drive down costs and generate revenue by establishing clinically beneficial quality-improvement (QI) protocols; drive down ICU length of stay; provide effective and timely procedural services; and incur a lower cost burden (i.e., hospitalists cost less than intensivists). And I believe all of these benefits are available without sacrificing quality or patient care.
Leadership from medical staff and administration is imperative to establish the appropriate vision and drive toward hospitalist/intensivist implementation. Finding the right supporting physicians who bring excitement and energy is equally as important. Establishing expectations for skill sets, as well as the opportunity and mechanism by which these skill sets might be acquired and refined, is a must. The following technical skills should be required of hospitalist/intensivists:
- Ultrasound-guided central line insertion;
- PICC line insertion;
- Endotracheal intubation;
- Advanced airway management;
- Thoracostomy tube insertion;
- Arterial-line insertion;
- Transvenous pacing wire insertion;
- Lumbar puncture;
- Thoracentesis; and
- Paracentesis.
An important starting point is the identification of skill sets for each hospitalist. Once this information is ascertained, the next step is to understand what the credentialing requirements for the individual procedures are. This usually consists of a certain number of “logged” cases, which must be put forward for review by the medical staff leadership. Most physicians completing residency are required to keep a procedural log where cases are documented. Any deficiencies within the log can be supplemented by establishing a practice log where proctored cases are documented until the recommended number of cases are completed and put forward for credentialing.
Obtaining buy-in from the medical staff is important. They can serve as allies in many areas, specifically as proctors in the credentialing process. The key to successful interface is in awakening them to the beneficial impact a service such as this can have on patients and on the lifestyle of providers.
As an example, before our group started the hybrid model at Westside, the nursing staff would call anesthesia to evaluate patients for endotracheal intubation. This system took anesthesia away from its OR cases, causing delays and frustration. After a conversation, the anesthesia director realized the benefits that would come with assisting the hospitalists in becoming more proficient with intubations. This same scenario has been true in our experience with ED physicians, cardiothoracic surgeons (chest tubes), and so on.
Other resources for hospitalists include the National Procedure Institute, which offers CME credit and certification toward “Hospitalist Procedures.” Additionally, difficult airway or advanced airway courses provide certification.
Hospitalists have long been called on to provide emergency services for unstable patients via rapid response or codes. In many facilities hospitalists serve as the lead physicians in the management of critically ill patients. Our hospitalist model serves as a great launching pad for the development and evolution of this new breed of physician.
There exists no clinical evidence to assert inferiority between the care provided by an in-house, 24/7 hospitalist group with assistance from pulmonary medicine versus an intensivist group. It is my belief that if the appropriate infrastructure, fostered skill sets, pulmonologist partnership, and QI protocols are implemented, there will be no measurable difference in scope of care or outcomes.
The inpatient management of critically ill and unstable patients continues to be a significant and important subgroup of hospital patient populations. As patients continue to live longer with debilitating chronic diseases, the fallout from decompensation can be devastating. Many facilities have hospitalists leading the charge in the care of these patients. It is undeniable that the next evolution in HM will require a more proactive inpatient physician, with both the clinical and technical acumen to manage all patients across the hospital spectrum.
Ulises A. Perez, MD,
medical director, hospitalist division,
Westside Regional Medical Center, Plantation, Fla.,
Kendall Regional Medical Center, Miami
As the field of HM continues to mature, branch out, and is called upon to lead in the care of a larger cross-section of hospitalized patients, it is only natural that this includes the critically ill patient. Hospitalists already care for—and are the attending of record for—this patient population in most U.S. hospitals. It is my position that a technically proficient hospitalist service, which is facility-exclusive and offers 24/7 coverage, is able to offer the same quality of care as an intensivist group. An important feature of this model is the inclusion and “buy in” from community pulmonologists in order to provide backup and consultative assistance when warranted.
Our program at Westside Regional Medical Center in Plantation, Fla., has made great strides as we continue to integrate this model in the hospital. We are actively tracking ICU length of stay and throughput, incidence of ventilator-associated pneumonia (VAP), central-line infection rates, and ICU mortality.
I believe that a clinically competent and aggressive HM service is able to drive down costs and generate revenue by establishing clinically beneficial quality-improvement (QI) protocols; drive down ICU length of stay; provide effective and timely procedural services; and incur a lower cost burden (i.e., hospitalists cost less than intensivists). And I believe all of these benefits are available without sacrificing quality or patient care.
Leadership from medical staff and administration is imperative to establish the appropriate vision and drive toward hospitalist/intensivist implementation. Finding the right supporting physicians who bring excitement and energy is equally as important. Establishing expectations for skill sets, as well as the opportunity and mechanism by which these skill sets might be acquired and refined, is a must. The following technical skills should be required of hospitalist/intensivists:
- Ultrasound-guided central line insertion;
- PICC line insertion;
- Endotracheal intubation;
- Advanced airway management;
- Thoracostomy tube insertion;
- Arterial-line insertion;
- Transvenous pacing wire insertion;
- Lumbar puncture;
- Thoracentesis; and
- Paracentesis.
An important starting point is the identification of skill sets for each hospitalist. Once this information is ascertained, the next step is to understand what the credentialing requirements for the individual procedures are. This usually consists of a certain number of “logged” cases, which must be put forward for review by the medical staff leadership. Most physicians completing residency are required to keep a procedural log where cases are documented. Any deficiencies within the log can be supplemented by establishing a practice log where proctored cases are documented until the recommended number of cases are completed and put forward for credentialing.
Obtaining buy-in from the medical staff is important. They can serve as allies in many areas, specifically as proctors in the credentialing process. The key to successful interface is in awakening them to the beneficial impact a service such as this can have on patients and on the lifestyle of providers.
As an example, before our group started the hybrid model at Westside, the nursing staff would call anesthesia to evaluate patients for endotracheal intubation. This system took anesthesia away from its OR cases, causing delays and frustration. After a conversation, the anesthesia director realized the benefits that would come with assisting the hospitalists in becoming more proficient with intubations. This same scenario has been true in our experience with ED physicians, cardiothoracic surgeons (chest tubes), and so on.
Other resources for hospitalists include the National Procedure Institute, which offers CME credit and certification toward “Hospitalist Procedures.” Additionally, difficult airway or advanced airway courses provide certification.
Hospitalists have long been called on to provide emergency services for unstable patients via rapid response or codes. In many facilities hospitalists serve as the lead physicians in the management of critically ill patients. Our hospitalist model serves as a great launching pad for the development and evolution of this new breed of physician.
There exists no clinical evidence to assert inferiority between the care provided by an in-house, 24/7 hospitalist group with assistance from pulmonary medicine versus an intensivist group. It is my belief that if the appropriate infrastructure, fostered skill sets, pulmonologist partnership, and QI protocols are implemented, there will be no measurable difference in scope of care or outcomes.
The inpatient management of critically ill and unstable patients continues to be a significant and important subgroup of hospital patient populations. As patients continue to live longer with debilitating chronic diseases, the fallout from decompensation can be devastating. Many facilities have hospitalists leading the charge in the care of these patients. It is undeniable that the next evolution in HM will require a more proactive inpatient physician, with both the clinical and technical acumen to manage all patients across the hospital spectrum.
Ulises A. Perez, MD,
medical director, hospitalist division,
Westside Regional Medical Center, Plantation, Fla.,
Kendall Regional Medical Center, Miami
As the field of HM continues to mature, branch out, and is called upon to lead in the care of a larger cross-section of hospitalized patients, it is only natural that this includes the critically ill patient. Hospitalists already care for—and are the attending of record for—this patient population in most U.S. hospitals. It is my position that a technically proficient hospitalist service, which is facility-exclusive and offers 24/7 coverage, is able to offer the same quality of care as an intensivist group. An important feature of this model is the inclusion and “buy in” from community pulmonologists in order to provide backup and consultative assistance when warranted.
Our program at Westside Regional Medical Center in Plantation, Fla., has made great strides as we continue to integrate this model in the hospital. We are actively tracking ICU length of stay and throughput, incidence of ventilator-associated pneumonia (VAP), central-line infection rates, and ICU mortality.
I believe that a clinically competent and aggressive HM service is able to drive down costs and generate revenue by establishing clinically beneficial quality-improvement (QI) protocols; drive down ICU length of stay; provide effective and timely procedural services; and incur a lower cost burden (i.e., hospitalists cost less than intensivists). And I believe all of these benefits are available without sacrificing quality or patient care.
Leadership from medical staff and administration is imperative to establish the appropriate vision and drive toward hospitalist/intensivist implementation. Finding the right supporting physicians who bring excitement and energy is equally as important. Establishing expectations for skill sets, as well as the opportunity and mechanism by which these skill sets might be acquired and refined, is a must. The following technical skills should be required of hospitalist/intensivists:
- Ultrasound-guided central line insertion;
- PICC line insertion;
- Endotracheal intubation;
- Advanced airway management;
- Thoracostomy tube insertion;
- Arterial-line insertion;
- Transvenous pacing wire insertion;
- Lumbar puncture;
- Thoracentesis; and
- Paracentesis.
An important starting point is the identification of skill sets for each hospitalist. Once this information is ascertained, the next step is to understand what the credentialing requirements for the individual procedures are. This usually consists of a certain number of “logged” cases, which must be put forward for review by the medical staff leadership. Most physicians completing residency are required to keep a procedural log where cases are documented. Any deficiencies within the log can be supplemented by establishing a practice log where proctored cases are documented until the recommended number of cases are completed and put forward for credentialing.
Obtaining buy-in from the medical staff is important. They can serve as allies in many areas, specifically as proctors in the credentialing process. The key to successful interface is in awakening them to the beneficial impact a service such as this can have on patients and on the lifestyle of providers.
As an example, before our group started the hybrid model at Westside, the nursing staff would call anesthesia to evaluate patients for endotracheal intubation. This system took anesthesia away from its OR cases, causing delays and frustration. After a conversation, the anesthesia director realized the benefits that would come with assisting the hospitalists in becoming more proficient with intubations. This same scenario has been true in our experience with ED physicians, cardiothoracic surgeons (chest tubes), and so on.
Other resources for hospitalists include the National Procedure Institute, which offers CME credit and certification toward “Hospitalist Procedures.” Additionally, difficult airway or advanced airway courses provide certification.
Hospitalists have long been called on to provide emergency services for unstable patients via rapid response or codes. In many facilities hospitalists serve as the lead physicians in the management of critically ill patients. Our hospitalist model serves as a great launching pad for the development and evolution of this new breed of physician.
There exists no clinical evidence to assert inferiority between the care provided by an in-house, 24/7 hospitalist group with assistance from pulmonary medicine versus an intensivist group. It is my belief that if the appropriate infrastructure, fostered skill sets, pulmonologist partnership, and QI protocols are implemented, there will be no measurable difference in scope of care or outcomes.
The inpatient management of critically ill and unstable patients continues to be a significant and important subgroup of hospital patient populations. As patients continue to live longer with debilitating chronic diseases, the fallout from decompensation can be devastating. Many facilities have hospitalists leading the charge in the care of these patients. It is undeniable that the next evolution in HM will require a more proactive inpatient physician, with both the clinical and technical acumen to manage all patients across the hospital spectrum.
Ulises A. Perez, MD,
medical director, hospitalist division,
Westside Regional Medical Center, Plantation, Fla.,
Kendall Regional Medical Center, Miami
Productivity Capacity

The mark of any great society is balance—balance between the production realized today and the preservation of “production capacity” to ensure the same or greater production in the future. HM is not exempt from this fundamental tenet. What we do now in the way of advancing quality, efficiency, and patient safety will matter little if our contributions are not sustained by the generation that follows us.
It is tempting to think that the issue of how we train residents is germane only to universities, but the reality is that it affects us all. There are 126 “university” medical school programs, but there are 384 residency programs, most of which are within community-based hospitals. The result is that most hospitalists encounter resident physicians in some capacity, and all hospitalists will encounter the results of residency training when they welcome a new recruit to their ranks.
The education and socialization of our residents will define the character of the hospitalists of the future. But the “residency” in which most of us trained does not exist anymore: The duty-hours changes and additional training requirements have dramatically changed the landscape of residency training in the past 10 years, and another series of sea changes is underway. As with all things HM, we again have a choice: Be reactive, wait for the dust to clear, and then lament the results, or be proactive and see this change for what it is—an opportunity to improve healthcare quality now, and in the future.
The ACGME
HM felt the impact of the first wave of duty-hours restrictions beginning in 2003, as many training programs opted to employ hospitalists to provide the coverage that could no longer be maintained by residents working under tighter admission caps and duty-hour restrictions. In doing so, hospitalists have provided a valuable service in preserving the integrity of training environments and fidelity to the Accreditation Council for Graduate Medical Education (ACGME) regulations (more than 85% of training programs have hospitalists working in their systems). But the model of hospitalists working solely as “resident-extenders” is not sustainable.
First, hospitalists who work solely on nonteaching services are at great risk of burning out, especially if the distribution of patients has been manipulated such that the more interesting patients are funneled away from the hospitalist’s service to the teaching service. Second, there is a risk in perception: In models in which the hospitalist is solely the “overflow cap coverage” or the night-float physician (i.e., the resident-extender), residents come to see hospitalists as the “PGY-4, 5, 6 …” physicians—that is, the physician who becomes a resident for life. The result is a serious pipeline issue for us, as the most talented resident physicians are unlikely to forego subspecialty training for a career in HM if hospitalists are perceived as perpetual residents.
The solution is simple: The hospitalist’s role in training environments has to be more than merely solving admission cap or duty-hour issues. It is fine for hospitalists to operate nonteaching services, but the hospitalist also has to be a part of the fulfillment that comes with overseeing teaching services. Further, residents have to see the hospitalist career for what it actually is: Academic or not, HM is much more than merely clinical service. HM is about the value-added services of system interventions to improve quality and patient safety; it is about developing a career as a systems architect. Getting the best and brightest residents to choose HM as a career is contingent upon residents seeing hospitalists in the training environment who are happy and fulfilled in the execution of this career goal.
The hospitalist’s plight was helped substantially on June 23, when ACGME released for comment the revised Common Program Requirements (www.acgme.org). The duty-hours changes are unlikely to substantially alter hospitalists’ lives; the only significant change was a limitation on intern shift durations to fewer than 16 hours in a row (upper-level residents still operate under the 24+6 hour rule, with increased flexibility to stay longer by volition). But the interesting part of the new requirements is an augmented focus on teaching residents transitions-of-care skills, improving direct supervision of residents, and constructing educational systems that minimize handoffs.
There is no specialty that is as suited as HM for fulfilling these unique (and, as of yet, unmet) requirements. Transitions, quality, being present on the hospital wards … this is what we do. And requiring instruction in transitions and quality is an unprecedented leverage point for HM to advance the quality of future physicians. How great it would be to attend HM20 and realize that the attendees had already learned the “Quality 101” lessons (i.e., those we are currently teaching at our annual meeting) as part of their residency? Freed from the need to do basic quality sessions, the content of the annual meeting could escalate to even higher-level principles that would result in substantial and sustainable quality improvement (QI).
MedPAC and GME Funding
Simultaneous with the ACGME changes are changes at the Medicare Payment Advisory Committee (MedPAC), the advisory organization responsible for recommending changes in the distribution of Centers for Medicare and Medicaid Services (CMS) funds to support graduate medical education. CMS is the primary funding agent for residency training. Each hospital receives direct medical expenditures to cover a resident’s salary and benefits. Each hospital has a pre-set per-resident allotment, or PRA. This number varies by hospital, but the average is $100,000 per resident. CMS reimburses the hospital a percentage of this number based upon the percentage of hospital days occupied by Medicare patients (e.g., 35% Medicare days=$35,000 per resident).
The hospital also receives indirect medical expenditures, or IME. IME is not a distinct payment to the hospital, but rather an “inflator” of the clinical-care payments the hospital receives from CMS. IME is paid to the hospital under the presumption that a typical training facility incurs greater cost due to higher patient severity, a higher indigent care percentage, and has higher resource utilization due to residents’ excessive testing, etc. The final presumption is that support is needed for the educational infrastructure (i.e., supervision and teaching).
IME is not inconsequential to a hospital; depending upon the payor mix, a 200-bed hospital might have from $4 million to $8 million in annual IME payments. CMS’ total IME payments to hospitals is more than $6 billion a year. Each hospital’s IME revenue can be found at www.graham-center.org/online/graham/home/tools-resources/data-tables/dt001-gme-2007.html.
The game-changing event occurred in April, when MedPAC announced its intent to reassess the mechanisms of IME funding, with a vision of IME funding eventually being linked to a hospital’s training programs’ ability to demonstrate substantial improvement in quality and patient safety. And here is the leverage point that is a unique opportunity for hospitalists in the training environment. For many hospitalists, especially if employed directly by the hospital, there is little financial incentive to engaging on a teaching service. The ACGME caps limit the service size, and this in turn limits the possible RVUs. Up until now, asking the hospital to compensate for teaching time (i.e., EVUs) was a pipe dream. But the linking of IME funding to quality outcomes (and quality instruction to residents) could change all of that.
If you put the two together: ACGME calling for instruction in quality and transitions, plus MedPAC calling for payments linked to resident outcomes in quality and patient safety, you have one inescapable conclusion—the residency of the future will hinge upon having supervisors with the necessary expertise to ensure that residents participate in, and understand the principles of, patient safety and quality as a part of the residency curriculum. And the people who can ensure that goal are likely to be in a position to warrant compensation for doing so.
Who is better to do this than the hospitalist?
SHM’s Proactive Strategy
This is the opportune time for HM to advance its stature as a profession and to ensure its future via a pipeline of residents adequately training in quality and patient safety. But it is not enough to merely wish for this to happen. There are real barriers that have kept hospitalists from being more intimately involved in physician training, the first of which is age.
HM is a young specialty (the average hospitalist is 37; the average HM leader is 41), and its youth makes it hard to compete with older subspecialists/generalists who have more experience in education. But deficits in experience can be compensated by additional training.
The Academic Hospitalist Academy (AHA)—cosponsored by SHM, the Society of General Internal Medicine (SGIM), and the Association of Chiefs and Leaders of General Internal Medicine (ACLGIM)—is the key to the strategy of catching up quickly. The academy will convene this month outside of Atlanta, and it is very important that each training facility think about sending one of its hospitalists to receive the advanced training in education necessary to compensate for not having years of experience in medical education. Academy details are available at http://academichospitalist.org.
SHM’s initiatives on this front do not stop with the academy. Over the past three months, Kevin O’Leary, MD, and his Quality Improvement Education Committee have been furiously building a “Quality and Patient Safety” curriculum, with a target audience of new hospitalists and resident physicians. The vision is to create a Web-based, interactive curriculum that teaches resident physicians the basics of quality and patient safety, design projects with their colleagues (under the supervision of their hospitalist mentor), and track their data to see real-time results.
Unlike other curricula on the market, the SHM Quality Curriculum for residents will be dynamic, requiring participating institutions commit to SHM’s modus operandi of mentored implementation by sponsoring a hospitalist to receive the training necessary to put the curriculum in motion. To this end, SHM has collaborated with the Alliance for Internal Medicine (AIM) in co-sponsoring the Quality Academy, with a focus on how to teach quality and patient safety. Jen Meyers, MD, FHM, and Jeff Glasheen, MD, SFHM, will be leading the team responsible for the development of this Quality Training Course, which should emerge in the fall of 2011.
As this project proceeds, Paul Grant, MD, chair of the Early Career Hospitalist Committee, and Cheryl O’Malley, MD, chair of the Pipeline Committee, will provide counsel. Both of these groups will continue efforts to improve the process by which residents transition from residency to HM practice, and supporting young physicians with distance mentoring.
The SHM vision of our production capacity is simple: Bring in the best and brightest hospitalists who are interested in teaching quality and patient safety, train them in the fundamentals of medical education, provide them with an “off the net” curriculum for how to teach quality, then return them to their respective training environments to coach residents on the principles of quality.
Training programs that invest in this vision will reap the rewards of fidelity to the new ACGME requirements. Hospitals that support such a vision will receive assurances, should MedPAC’s recommendation come to fruition, that DME and IME funding is secure. Hospitalists investing in this vision will find a fulfilling career in quality education.
And all of us will find assurances that, for as good as things are right now for HM, the future will be even better. TH
Dr. Wiese is president of SHM.
The mark of any great society is balance—balance between the production realized today and the preservation of “production capacity” to ensure the same or greater production in the future. HM is not exempt from this fundamental tenet. What we do now in the way of advancing quality, efficiency, and patient safety will matter little if our contributions are not sustained by the generation that follows us.
It is tempting to think that the issue of how we train residents is germane only to universities, but the reality is that it affects us all. There are 126 “university” medical school programs, but there are 384 residency programs, most of which are within community-based hospitals. The result is that most hospitalists encounter resident physicians in some capacity, and all hospitalists will encounter the results of residency training when they welcome a new recruit to their ranks.
The education and socialization of our residents will define the character of the hospitalists of the future. But the “residency” in which most of us trained does not exist anymore: The duty-hours changes and additional training requirements have dramatically changed the landscape of residency training in the past 10 years, and another series of sea changes is underway. As with all things HM, we again have a choice: Be reactive, wait for the dust to clear, and then lament the results, or be proactive and see this change for what it is—an opportunity to improve healthcare quality now, and in the future.
The ACGME
HM felt the impact of the first wave of duty-hours restrictions beginning in 2003, as many training programs opted to employ hospitalists to provide the coverage that could no longer be maintained by residents working under tighter admission caps and duty-hour restrictions. In doing so, hospitalists have provided a valuable service in preserving the integrity of training environments and fidelity to the Accreditation Council for Graduate Medical Education (ACGME) regulations (more than 85% of training programs have hospitalists working in their systems). But the model of hospitalists working solely as “resident-extenders” is not sustainable.
First, hospitalists who work solely on nonteaching services are at great risk of burning out, especially if the distribution of patients has been manipulated such that the more interesting patients are funneled away from the hospitalist’s service to the teaching service. Second, there is a risk in perception: In models in which the hospitalist is solely the “overflow cap coverage” or the night-float physician (i.e., the resident-extender), residents come to see hospitalists as the “PGY-4, 5, 6 …” physicians—that is, the physician who becomes a resident for life. The result is a serious pipeline issue for us, as the most talented resident physicians are unlikely to forego subspecialty training for a career in HM if hospitalists are perceived as perpetual residents.
The solution is simple: The hospitalist’s role in training environments has to be more than merely solving admission cap or duty-hour issues. It is fine for hospitalists to operate nonteaching services, but the hospitalist also has to be a part of the fulfillment that comes with overseeing teaching services. Further, residents have to see the hospitalist career for what it actually is: Academic or not, HM is much more than merely clinical service. HM is about the value-added services of system interventions to improve quality and patient safety; it is about developing a career as a systems architect. Getting the best and brightest residents to choose HM as a career is contingent upon residents seeing hospitalists in the training environment who are happy and fulfilled in the execution of this career goal.
The hospitalist’s plight was helped substantially on June 23, when ACGME released for comment the revised Common Program Requirements (www.acgme.org). The duty-hours changes are unlikely to substantially alter hospitalists’ lives; the only significant change was a limitation on intern shift durations to fewer than 16 hours in a row (upper-level residents still operate under the 24+6 hour rule, with increased flexibility to stay longer by volition). But the interesting part of the new requirements is an augmented focus on teaching residents transitions-of-care skills, improving direct supervision of residents, and constructing educational systems that minimize handoffs.
There is no specialty that is as suited as HM for fulfilling these unique (and, as of yet, unmet) requirements. Transitions, quality, being present on the hospital wards … this is what we do. And requiring instruction in transitions and quality is an unprecedented leverage point for HM to advance the quality of future physicians. How great it would be to attend HM20 and realize that the attendees had already learned the “Quality 101” lessons (i.e., those we are currently teaching at our annual meeting) as part of their residency? Freed from the need to do basic quality sessions, the content of the annual meeting could escalate to even higher-level principles that would result in substantial and sustainable quality improvement (QI).
MedPAC and GME Funding
Simultaneous with the ACGME changes are changes at the Medicare Payment Advisory Committee (MedPAC), the advisory organization responsible for recommending changes in the distribution of Centers for Medicare and Medicaid Services (CMS) funds to support graduate medical education. CMS is the primary funding agent for residency training. Each hospital receives direct medical expenditures to cover a resident’s salary and benefits. Each hospital has a pre-set per-resident allotment, or PRA. This number varies by hospital, but the average is $100,000 per resident. CMS reimburses the hospital a percentage of this number based upon the percentage of hospital days occupied by Medicare patients (e.g., 35% Medicare days=$35,000 per resident).
The hospital also receives indirect medical expenditures, or IME. IME is not a distinct payment to the hospital, but rather an “inflator” of the clinical-care payments the hospital receives from CMS. IME is paid to the hospital under the presumption that a typical training facility incurs greater cost due to higher patient severity, a higher indigent care percentage, and has higher resource utilization due to residents’ excessive testing, etc. The final presumption is that support is needed for the educational infrastructure (i.e., supervision and teaching).
IME is not inconsequential to a hospital; depending upon the payor mix, a 200-bed hospital might have from $4 million to $8 million in annual IME payments. CMS’ total IME payments to hospitals is more than $6 billion a year. Each hospital’s IME revenue can be found at www.graham-center.org/online/graham/home/tools-resources/data-tables/dt001-gme-2007.html.
The game-changing event occurred in April, when MedPAC announced its intent to reassess the mechanisms of IME funding, with a vision of IME funding eventually being linked to a hospital’s training programs’ ability to demonstrate substantial improvement in quality and patient safety. And here is the leverage point that is a unique opportunity for hospitalists in the training environment. For many hospitalists, especially if employed directly by the hospital, there is little financial incentive to engaging on a teaching service. The ACGME caps limit the service size, and this in turn limits the possible RVUs. Up until now, asking the hospital to compensate for teaching time (i.e., EVUs) was a pipe dream. But the linking of IME funding to quality outcomes (and quality instruction to residents) could change all of that.
If you put the two together: ACGME calling for instruction in quality and transitions, plus MedPAC calling for payments linked to resident outcomes in quality and patient safety, you have one inescapable conclusion—the residency of the future will hinge upon having supervisors with the necessary expertise to ensure that residents participate in, and understand the principles of, patient safety and quality as a part of the residency curriculum. And the people who can ensure that goal are likely to be in a position to warrant compensation for doing so.
Who is better to do this than the hospitalist?
SHM’s Proactive Strategy
This is the opportune time for HM to advance its stature as a profession and to ensure its future via a pipeline of residents adequately training in quality and patient safety. But it is not enough to merely wish for this to happen. There are real barriers that have kept hospitalists from being more intimately involved in physician training, the first of which is age.
HM is a young specialty (the average hospitalist is 37; the average HM leader is 41), and its youth makes it hard to compete with older subspecialists/generalists who have more experience in education. But deficits in experience can be compensated by additional training.
The Academic Hospitalist Academy (AHA)—cosponsored by SHM, the Society of General Internal Medicine (SGIM), and the Association of Chiefs and Leaders of General Internal Medicine (ACLGIM)—is the key to the strategy of catching up quickly. The academy will convene this month outside of Atlanta, and it is very important that each training facility think about sending one of its hospitalists to receive the advanced training in education necessary to compensate for not having years of experience in medical education. Academy details are available at http://academichospitalist.org.
SHM’s initiatives on this front do not stop with the academy. Over the past three months, Kevin O’Leary, MD, and his Quality Improvement Education Committee have been furiously building a “Quality and Patient Safety” curriculum, with a target audience of new hospitalists and resident physicians. The vision is to create a Web-based, interactive curriculum that teaches resident physicians the basics of quality and patient safety, design projects with their colleagues (under the supervision of their hospitalist mentor), and track their data to see real-time results.
Unlike other curricula on the market, the SHM Quality Curriculum for residents will be dynamic, requiring participating institutions commit to SHM’s modus operandi of mentored implementation by sponsoring a hospitalist to receive the training necessary to put the curriculum in motion. To this end, SHM has collaborated with the Alliance for Internal Medicine (AIM) in co-sponsoring the Quality Academy, with a focus on how to teach quality and patient safety. Jen Meyers, MD, FHM, and Jeff Glasheen, MD, SFHM, will be leading the team responsible for the development of this Quality Training Course, which should emerge in the fall of 2011.
As this project proceeds, Paul Grant, MD, chair of the Early Career Hospitalist Committee, and Cheryl O’Malley, MD, chair of the Pipeline Committee, will provide counsel. Both of these groups will continue efforts to improve the process by which residents transition from residency to HM practice, and supporting young physicians with distance mentoring.
The SHM vision of our production capacity is simple: Bring in the best and brightest hospitalists who are interested in teaching quality and patient safety, train them in the fundamentals of medical education, provide them with an “off the net” curriculum for how to teach quality, then return them to their respective training environments to coach residents on the principles of quality.
Training programs that invest in this vision will reap the rewards of fidelity to the new ACGME requirements. Hospitals that support such a vision will receive assurances, should MedPAC’s recommendation come to fruition, that DME and IME funding is secure. Hospitalists investing in this vision will find a fulfilling career in quality education.
And all of us will find assurances that, for as good as things are right now for HM, the future will be even better. TH
Dr. Wiese is president of SHM.
The mark of any great society is balance—balance between the production realized today and the preservation of “production capacity” to ensure the same or greater production in the future. HM is not exempt from this fundamental tenet. What we do now in the way of advancing quality, efficiency, and patient safety will matter little if our contributions are not sustained by the generation that follows us.
It is tempting to think that the issue of how we train residents is germane only to universities, but the reality is that it affects us all. There are 126 “university” medical school programs, but there are 384 residency programs, most of which are within community-based hospitals. The result is that most hospitalists encounter resident physicians in some capacity, and all hospitalists will encounter the results of residency training when they welcome a new recruit to their ranks.
The education and socialization of our residents will define the character of the hospitalists of the future. But the “residency” in which most of us trained does not exist anymore: The duty-hours changes and additional training requirements have dramatically changed the landscape of residency training in the past 10 years, and another series of sea changes is underway. As with all things HM, we again have a choice: Be reactive, wait for the dust to clear, and then lament the results, or be proactive and see this change for what it is—an opportunity to improve healthcare quality now, and in the future.
The ACGME
HM felt the impact of the first wave of duty-hours restrictions beginning in 2003, as many training programs opted to employ hospitalists to provide the coverage that could no longer be maintained by residents working under tighter admission caps and duty-hour restrictions. In doing so, hospitalists have provided a valuable service in preserving the integrity of training environments and fidelity to the Accreditation Council for Graduate Medical Education (ACGME) regulations (more than 85% of training programs have hospitalists working in their systems). But the model of hospitalists working solely as “resident-extenders” is not sustainable.
First, hospitalists who work solely on nonteaching services are at great risk of burning out, especially if the distribution of patients has been manipulated such that the more interesting patients are funneled away from the hospitalist’s service to the teaching service. Second, there is a risk in perception: In models in which the hospitalist is solely the “overflow cap coverage” or the night-float physician (i.e., the resident-extender), residents come to see hospitalists as the “PGY-4, 5, 6 …” physicians—that is, the physician who becomes a resident for life. The result is a serious pipeline issue for us, as the most talented resident physicians are unlikely to forego subspecialty training for a career in HM if hospitalists are perceived as perpetual residents.
The solution is simple: The hospitalist’s role in training environments has to be more than merely solving admission cap or duty-hour issues. It is fine for hospitalists to operate nonteaching services, but the hospitalist also has to be a part of the fulfillment that comes with overseeing teaching services. Further, residents have to see the hospitalist career for what it actually is: Academic or not, HM is much more than merely clinical service. HM is about the value-added services of system interventions to improve quality and patient safety; it is about developing a career as a systems architect. Getting the best and brightest residents to choose HM as a career is contingent upon residents seeing hospitalists in the training environment who are happy and fulfilled in the execution of this career goal.
The hospitalist’s plight was helped substantially on June 23, when ACGME released for comment the revised Common Program Requirements (www.acgme.org). The duty-hours changes are unlikely to substantially alter hospitalists’ lives; the only significant change was a limitation on intern shift durations to fewer than 16 hours in a row (upper-level residents still operate under the 24+6 hour rule, with increased flexibility to stay longer by volition). But the interesting part of the new requirements is an augmented focus on teaching residents transitions-of-care skills, improving direct supervision of residents, and constructing educational systems that minimize handoffs.
There is no specialty that is as suited as HM for fulfilling these unique (and, as of yet, unmet) requirements. Transitions, quality, being present on the hospital wards … this is what we do. And requiring instruction in transitions and quality is an unprecedented leverage point for HM to advance the quality of future physicians. How great it would be to attend HM20 and realize that the attendees had already learned the “Quality 101” lessons (i.e., those we are currently teaching at our annual meeting) as part of their residency? Freed from the need to do basic quality sessions, the content of the annual meeting could escalate to even higher-level principles that would result in substantial and sustainable quality improvement (QI).
MedPAC and GME Funding
Simultaneous with the ACGME changes are changes at the Medicare Payment Advisory Committee (MedPAC), the advisory organization responsible for recommending changes in the distribution of Centers for Medicare and Medicaid Services (CMS) funds to support graduate medical education. CMS is the primary funding agent for residency training. Each hospital receives direct medical expenditures to cover a resident’s salary and benefits. Each hospital has a pre-set per-resident allotment, or PRA. This number varies by hospital, but the average is $100,000 per resident. CMS reimburses the hospital a percentage of this number based upon the percentage of hospital days occupied by Medicare patients (e.g., 35% Medicare days=$35,000 per resident).
The hospital also receives indirect medical expenditures, or IME. IME is not a distinct payment to the hospital, but rather an “inflator” of the clinical-care payments the hospital receives from CMS. IME is paid to the hospital under the presumption that a typical training facility incurs greater cost due to higher patient severity, a higher indigent care percentage, and has higher resource utilization due to residents’ excessive testing, etc. The final presumption is that support is needed for the educational infrastructure (i.e., supervision and teaching).
IME is not inconsequential to a hospital; depending upon the payor mix, a 200-bed hospital might have from $4 million to $8 million in annual IME payments. CMS’ total IME payments to hospitals is more than $6 billion a year. Each hospital’s IME revenue can be found at www.graham-center.org/online/graham/home/tools-resources/data-tables/dt001-gme-2007.html.
The game-changing event occurred in April, when MedPAC announced its intent to reassess the mechanisms of IME funding, with a vision of IME funding eventually being linked to a hospital’s training programs’ ability to demonstrate substantial improvement in quality and patient safety. And here is the leverage point that is a unique opportunity for hospitalists in the training environment. For many hospitalists, especially if employed directly by the hospital, there is little financial incentive to engaging on a teaching service. The ACGME caps limit the service size, and this in turn limits the possible RVUs. Up until now, asking the hospital to compensate for teaching time (i.e., EVUs) was a pipe dream. But the linking of IME funding to quality outcomes (and quality instruction to residents) could change all of that.
If you put the two together: ACGME calling for instruction in quality and transitions, plus MedPAC calling for payments linked to resident outcomes in quality and patient safety, you have one inescapable conclusion—the residency of the future will hinge upon having supervisors with the necessary expertise to ensure that residents participate in, and understand the principles of, patient safety and quality as a part of the residency curriculum. And the people who can ensure that goal are likely to be in a position to warrant compensation for doing so.
Who is better to do this than the hospitalist?
SHM’s Proactive Strategy
This is the opportune time for HM to advance its stature as a profession and to ensure its future via a pipeline of residents adequately training in quality and patient safety. But it is not enough to merely wish for this to happen. There are real barriers that have kept hospitalists from being more intimately involved in physician training, the first of which is age.
HM is a young specialty (the average hospitalist is 37; the average HM leader is 41), and its youth makes it hard to compete with older subspecialists/generalists who have more experience in education. But deficits in experience can be compensated by additional training.
The Academic Hospitalist Academy (AHA)—cosponsored by SHM, the Society of General Internal Medicine (SGIM), and the Association of Chiefs and Leaders of General Internal Medicine (ACLGIM)—is the key to the strategy of catching up quickly. The academy will convene this month outside of Atlanta, and it is very important that each training facility think about sending one of its hospitalists to receive the advanced training in education necessary to compensate for not having years of experience in medical education. Academy details are available at http://academichospitalist.org.
SHM’s initiatives on this front do not stop with the academy. Over the past three months, Kevin O’Leary, MD, and his Quality Improvement Education Committee have been furiously building a “Quality and Patient Safety” curriculum, with a target audience of new hospitalists and resident physicians. The vision is to create a Web-based, interactive curriculum that teaches resident physicians the basics of quality and patient safety, design projects with their colleagues (under the supervision of their hospitalist mentor), and track their data to see real-time results.
Unlike other curricula on the market, the SHM Quality Curriculum for residents will be dynamic, requiring participating institutions commit to SHM’s modus operandi of mentored implementation by sponsoring a hospitalist to receive the training necessary to put the curriculum in motion. To this end, SHM has collaborated with the Alliance for Internal Medicine (AIM) in co-sponsoring the Quality Academy, with a focus on how to teach quality and patient safety. Jen Meyers, MD, FHM, and Jeff Glasheen, MD, SFHM, will be leading the team responsible for the development of this Quality Training Course, which should emerge in the fall of 2011.
As this project proceeds, Paul Grant, MD, chair of the Early Career Hospitalist Committee, and Cheryl O’Malley, MD, chair of the Pipeline Committee, will provide counsel. Both of these groups will continue efforts to improve the process by which residents transition from residency to HM practice, and supporting young physicians with distance mentoring.
The SHM vision of our production capacity is simple: Bring in the best and brightest hospitalists who are interested in teaching quality and patient safety, train them in the fundamentals of medical education, provide them with an “off the net” curriculum for how to teach quality, then return them to their respective training environments to coach residents on the principles of quality.
Training programs that invest in this vision will reap the rewards of fidelity to the new ACGME requirements. Hospitals that support such a vision will receive assurances, should MedPAC’s recommendation come to fruition, that DME and IME funding is secure. Hospitalists investing in this vision will find a fulfilling career in quality education.
And all of us will find assurances that, for as good as things are right now for HM, the future will be even better. TH
Dr. Wiese is president of SHM.
Change You Should Believe In
Christina Payne, MD, is a third-year resident at Emory University Hospital in Atlanta who will begin her first hospitalist job, with Emory in September. In spite of her dearth of practical experience, she already has experience researching one of the most vexing problems confronting HM: how to improve transitions of care.
Dr. Payne has been studying the benefits of a structured electronic tool that generates a standardized sign-out list of a hospital team’s full census at the time of shift change, compared with the usual, highly variable sign-out practices of medical residents. At a poster presentation at Internal Medicine 2010 in April in Toronto, Dr. Payne and colleagues reported that residents using the tool were twice as confident at performing handoffs, had lower rates of perceived near-miss events, and were happier.1
“Hospitalists everywhere are starting to realize the importance of trying to reduce opportunities for human error that occur during care transitions,” Dr. Payne says. “The biggest thing I learned from this research is the importance of standardizing the handoff process [with information communicated consistently].
“It is essential to keep communication lines open,” Dr. Payne adds. “No tool can replace the importance of communication between doctors and the need to sit down and talk. The ideal signout happens in a quiet room where the two of you can talk about active patients and achieve rapport. But, realistically, how often does that happen?”
Standardization is one of a handful of strategies hospitalists, researchers, and policymakers are using to tackle transitions—both in-hospital handoffs and post-discharge transitions—with outpatient care. Some hospitalists are using practice simulations and training strategies; others have implemented medication reconciliation checks at every discharge, checklists and other communication strategies, team-based quality-improvement (QI) initiatives, and new technologies to enhance and streamline communication. Some interventions follow the patient from the hospital to the community physician with a phone call, follow-up clinic, or other contact; others aim to empower the patient to be a better self-advocate. But for hospitalists, the challenge is to communicate the right amount of transfer information to the right receiver at the right time.
No matter the technique, the goal is the same: Improve the handoff and discharge process in a way that promotes efficiency and patient safety. And hospitalists are at the forefront of the changing landscape of care transitions.
Under the Microscope
Care transitions of all kinds are under the magnifying glass of national healthcare reform, with growing recognition of the need to make care safer and reduce the preventable, costly hospital readmissions caused by incomplete handoffs. Care transitions for hospitalists include internal handoffs, both at daily shift changes and at service changes when an outgoing provider is leaving after a period of consecutive daily shifts. These typically involve a sign-out process and face-to-face encounter, with some kind of written backup. One teaching institution reported that such handoffs take place 4,000 times per day in the hospital, or 1.6 million times per year.2

—Arpana Vidyarthi, MD, University of California at San Francisco
Geographical transitions can be from one floor or department to another, or out the hospital door to another facility or home. Transitions typically involve a discharge process and a written discharge summary. Care transitions also include hospital admissions, which put the hospitalist in the role of handoff receiver rather than initiator, plus a variety of other transitions involving nurses, physician extenders, and other practitioners.
Each transition is a major decision point in the course of a patient’s hospitalization; each transition also presents a time of heightened vulnerability (e.g., potential communication breakdowns, medication errors, patient anxiety or confusion, etc.). In fact, according to a Transitions of Care Consensus Policy Statement published in 2009 by SHM and five other medical societies, handoffs are ubiquitous in HM, with significant patient safety and quality deficiencies in handoffs existing in the current system.3
Poor communication at the time of handoff has been implicated in near-misses and adverse events in a variety of healthcare contexts, including 70% of hospital sentinel events studied by The Joint Commission, which named standardized handoffs (with an opportunity for interactive communication) as a National Patient Safety Goal in 2006.4 The federal government is studying care transitions, supporting demonstration projects for Medicare enrollees, and including readmission rates in national hospital report card data.

“Transitions of care and handoffs are a huge focus right now because of the increased fragmentation of care in the United States. Hospitalists are in charge of a greater percentage of hospitalized patients, which means more coordination of care is needed,” says Vineet Arora, MD, MA, FHM, assistant professor of medicine and associate director of the internal-medicine residency at the University of Chicago, and chair of the SHM task force on handoffs.
Inadequate communication and poor care transitions can undermine hospitalists’ best care-planning efforts, erode patients’ and families’ confidence and satisfaction with hospital care, and leave primary-care physicians (PCPs) feeling unsatisfied with the relationship. As many as 1 in 5 Medicare beneficiary hospitalizations result in a readmission within 30 days, and while not all of these are preventable, far too many are.5 Another prospective cohort study found that 1 in 5 patients discharged from the hospital to the home experienced an adverse event within three weeks of discharge.6 Complex comorbidities, advanced age, unknown PCP, and limited healthcare literacy present hospitalists with extremely difficult transitions.
Patient safety and cost control are the linchpins to national efforts to improve transitions of care. Dr. Arora recently coauthored an original research paper, which will be published in the Journal of Hospital Medicine in September, showing older hospitalized patients are twice as likely to report problems after discharge if their PCPs were not aware they were hospitalized.
“With escalating healthcare costs, people are looking at ways to save money and reduce redundant care,” Dr. Arora explains, pointing out, as an example, repeated tests resulting from inadequate communication between healthcare providers.
The System Must Change
“All of the effort we put into saving someone’s life—the years of experience, training, medical school, and residency—all of it comes to bear on that hospitalized patient. And it can all be unraveled at the time of discharge if it’s not handled properly,” says Arpana Vidyarthi, MD, a hospitalist and director of quality at the University of California at San Francisco.
Dr. Vidyarthi views in-hospital and discharge transitions as integrally related. “The analysis is similar, even if different techniques may be needed,” she says, adding that, fundamentally, it involves having a system that allows people—or forces them—to do the “right thing.”
That’s why achieving effective care transitions will require more than just a standardized tool or process, Dr. Vidyarthi says. “This is about understanding the ways people communicate and finding ways to train them to communicate better,” she says. “The problem we have is not a lack of information, but how to communicate what, to whom, and when.”
What’s really needed, Dr. Vidyarthi says, is a hospital’s commitment to more effective transitions and its hospitalists’ leadership in driving a comprehensive, multidisciplinary, team- and evidence-based QI process. The new process should be a QI-based solution to a hospital’s care-transitions issues. “Before you can standardize your process, you need to understand it,” she says. “This is a complex problem, and it needs a multifaceted solution. But this lies squarely within the hospitalist arena. We’re part of everything that happens in the hospital.

—Anuj Dalal, MD, Brigham and Women’s Hospital, Boston
Hospital administrators are looking to HM to solve transition and readmission problems now, says Tina Budnitz, MPH, BOOST Project Director (Better Outcomes for Older Adults through Safe Transitions). She expects the scrutiny from the C-suite, legislators, and watchdog groups to increase as the spotlight continues to shine on the healthcare system.
“Any hospitalist can act as a leader in their institution,” Budnitz says. “Be a change agent, pull a group together, and start asking questions: Do we have safe care-transitions practices and processes in place? Just by asking the right question, you can be a catalyst for the system.”
Budnitz also emphasizes the importance of teamwork in the hospital setting. “How can I help my teammates? What am I communicating to the nurses on rounds?” she says. “Can you initiate dialogue with your outpatient medical groups: ‘These faxes we’re sending you—is that information getting to you in ways and times that are helpful? And, by the way, when your patient is admitted, this information would really help me.’ ”

Innovative Strategies
One of the most important initiatives responding to concerns about care transitions is Project BOOST (www.hos pitalmedicine.org/BOOST), a comprehensive toolkit for improving a hospital’s transitions of care. The project aims to build a national consensus for best practices in transitions; collaborate with representatives from the Agency for Healthcare Research and Quality (AHRQ), the Centers for Medicare and Medicaid Services (CMS), and the Joint Commission; and develop a national resource library, Budnitz says.
“Project BOOST not only puts forth best practices for admitting patients, planning for discharge, and then doing the discharge, it also helps show facilities how to change their systems, with resources and tools for analyzing and re-engineering the system,” she says. “Sites get one-to-one assistance from a mentor.”
Six hospitals signed on to the pilot program in 2008; 24 more joined last year. In January, SHM announced a collaborative with the University of Michigan and Blue Cross Blue Shield of Michigan for 15 Michigan hospitals to receive training and mentorship starting in May. And last month, SHM and the California HealthCare Foundation announced a Project BOOST initiative for 20 of the health system’s hospitals (see “California Dreamin’”, p. 6). Other free resources offered on the BOOST Web portal include clinical, data collection, and project management tools. SHM also has a DVD that explains how to use the “teachback” method to improve communication with patients.
Jennifer Myers, MD, FHM, assistant professor of clinical medicine and patient-safety officer at the Hospital of the University of Pennsylvania in Philadelphia, is a Project BOOST participant who spearheaded a process change to improve the quality of her facility’s discharge summary, along with accompanying resident education.7 The discharge summary recently was integrated with the hospital’s electronic health record (EHR) system.
“We’ve gone from dictating the discharge summary to an electronic version completed by the hospitalist, with prompts for key components of the summary, which allows us to create summaries more efficiently—ideally on the day of discharge, but usually within 48 hours,” Dr. Myers says. “We previously researched whether teaching made a difference in the quality of discharges; we found that it did. So we look forward to standardizing our teaching approach around this important topic for all residents.”
Another care-transitions innovation receiving a lot of attention from the government and the private sector is Project RED (Re-Engineered Discharge), led by Brian Jack, MD, vice chair of the department of family medicine at Boston Medical Center. The Project RED research group develops and tests strategies to improve the hospital discharge process to promote patient safety and reduce rehospitalization rates.
“We used re-engineering tools borrowed from other fields, brought together experts from all over the hospital, divided up the whole discharge process, and identified key principles,” Dr. Jack explains. The resulting discharge strategy is reflected in an 11-item checklist of discrete, mutually reinforcing components, which have been shown to reduce rehospitalization rates by 32% while raising patient satisfaction.8 It includes comprehensive discharge and after-hospital plans, a nurse discharge advocate, and a medication reconciliation phone call to the patient. A virtual “patient advocate,” a computerized avatar named Louise, is now being tested. If successful, it will allow patients to interact with a touch-screen teacher of the after-care plan who has time to work at the patient’s pace.
Technology and Transitions

Informatics can be a key player in facilitating care transitions, says Anuj Dalal, MD, a hospitalist and instructor in medicine at Brigham and Women’s Hospital in Boston. He is using one of his hospital’s technological strengths—a well-established, firewall-protected e-mail system—to help improve the discharge process.
“We decided to try to improve awareness of test results pending at the time of discharge,” Dr. Dalal explains. “We created an intervention that automatically triggers an e-mail with the finalized test results to the responsible providers. The intervention creates a loop of communication between the inpatient attending and the PCP. What we hope to show in our research over the next year or two is whether the intervention actually increases awareness of test results by providers.”
One thing to remember is that “all kinds of things can go wrong with care transitions,” no matter the size of the institution, the experience of the staff, or technological limitations, says Vineet Chopra, MD, FACP, a hospitalist at the University of Michigan Health System in Ann Arbor. “The problems of transitions vary from place to place, day to day, time of day, shift changes; and let’s not forget physician extenders and the other members of the healthcare team,” he says. “The more complicated the team, the more complicated the information needing to be handed off becomes.”
Who Else Is Looking at Transitions of Care?

SHM convened the Handoffs Task Force in 2006. The team systematically reviewed the literature and published recommendations in the September 2009 Journal of Hospital Medicine.9 The recommendations are aimed at both community and academic hospitals, as well as hospitalists and other healthcare providers. A new collaborative designed to supplement Project BOOST for hospitalist group handoffs and help put the guidelines into practice is in the works, says Dr. Arora, the task force’s chair.
SHM and five medical groups, including the American College of Physicians, issued a Transitions of Care Consensus Statement, published in the July 2009 issue of the Journal of Hospital Medicine.5 Guiding principles relate to education, measurement, accountability, timely interchange of information, inclusion of patient and family, respect for the medical home, and the need for national standards.
The Joint Commission’s Center for Transforming Health Care, established in 2009 to solve healthcare’s most critical safety and quality problems, has made handoff communications its second major target, and is now working with 10 healthcare systems. Standardized handoff processes and communications were the subject of the Joint Commission’s 2006 National Patient Safety Goal, while the Comprehensive Accreditation Manual for Hospitals also specifies that before a hospital discharges or transfers a patient, it should inform and educate the patient about his or her follow-up care and services.
“We now have a safety goal under review dealing with medication reconciliation, and there are relevant standards related to culturally sensitive communication and low-literacy-level communication,” says Deborah Zadzam, PhD, RN, FAAN, director of international quality and performance measures for Joint Commission Resources. “The essential message the Joint Commission has for hospitalists is to communicate clearly, effectively and thoroughly; don’t assume you are understood or that you understand.”—LB
Before he joined the group at the university, Dr. Chopra worked at a community hospital, St. Joseph’s Mercy Hospital in Hot Springs, Ark. “It’s hard to come up with a one-size-fits-all solution when there are so many variables,” he says. At the community hospital, “we mandated that the hospitalist call the PCP at the time of discharge. At the academic medical center, we share an EHR with the PCPs and can reach them electronically. We are required to have the discharge summary in the computer before the patient leaves the hospital, and we mandate that hospitalists are reachable by e-mail or phone when they are off.
“I’m not a believer in throwing more technology at problems and just adding more layers of information tools,” Dr. Chopra adds. “Hospitalists who used to carry stethoscopes now also have a clipboard, phone, pager, PDA, and nine different signouts in their pockets. What we want to do is make their life easier. Here, we are looking at technology as a means to do that.”
Dr. Chopra and hospitalist colleague Prasanth Gosineni, MD, have been working with an Ann Arbor tech company called Synaptin to develop a lightweight, mobile client application designed to work on smartphones. Still in pilot testing, it would allow for task-oriented and priority-based messaging in real time and the systematic transfer of important information for the next hospitalist shift.
“You need to be able to share information in a systematic way, but that’s only half of the answer. The other half is the ability to ask specific questions,” Dr. Chopra says. “Technology doesn’t take away from the face-to-face encounter that needs to happen. Nothing will replace face time, but part of the solution is to provide data efficiently and in a way that is easily accessible.”
Dr. Chopra admits that EHR presents both positives and negatives to improved transitions and patient care, “depending on how well it works and what smart features it offers,” he says, “but also recognizing that EHR and other technologies have also taken us farther away from face-to-face exchanges. Some would say that’s part of the problem.”
Handoffs, discharges, and other transitions are ubiquitous in HM—and fraught with the potential for costly and harmful errors. The ideal of an interactive, face-to-face handoff simply is not available for many care transitions. However, hospitalists are challenged to find solutions that will work in their hospitals, with their teams, and their types of patients. Patients and policymakers expect nothing less. TH
Larry Beresford is a freelance writer based in Oakland, Calif.
References
- Payne C, Stein J, Dressler D. Implementation of a structured electronic tool to improve patient handoffs and resident satisfaction. Poster abstract: Internal Medicine 2010, April 21-24, 2010, Toronto.
- Vidyarthi AR. Triple Handoff. AHRQ WebM&M website. Available at: webmm.ahrq.gov/case.aspx? caseID=134. Published May 2006. Accessed May 29, 2010.
- Snow V, Beck D, Budnitz T, et al. Transitions of Care Consensus Policy Statement: American College of Physicians, Society of General Internal Medicine, Society of Hospital Medicine, American Geriatrics Society, American College of Emergency Physicians, and Society for Academic Emergency Medicine. J Hosp Med. 2009;4(6):364-370.
- 2006 National Patient Safety Goals. The Joint Commission website. Available at: www.jointcommission.org/PatientSafety/NationalPatientSafetyGoals/06_npsgs.htm. Accessed June 8, 2010.
- Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med. 2009; 2:360:1418-1428.
- Forster AJ, Murff HJ, Peterson JF, Gandhi TK, Bates DW. The incidence and severity of adverse events affecting patients after discharge from the hospital. Ann Intern Med. 2003;138(3):161-167.
- Myers JS, Jaipaul CK, Kogan JR, Krekun S, Bellini LM, Shea JA. Are discharge summaries teachable? The effects of a discharge summary curriculum on the quality of discharge summaries in an internal medicine residency program. Acad Med. 2006; 81(10):S5-S8.
- Jack BW, Chetty VK, Anthony D, et al. A reengineered hospital discharge program to decrease rehospitalization: a randomized trial. Ann Intern Med. 2009;150(3):178-187.
- Arora VM, Manjarrez E, Dressler DD, Basaviah P, Halasyamani L, Kripalani S. Hospitalist handoffs: a systematic review and task force recommendations. J Hosp Med. 2009;4(7): 433-440.
- Halasyamani L, Kripalani S, Coleman E, et al. Transition of care for hospitalized elderly patients—development of a discharge checklist for hospitalists. J Hosp Med. 2006;1(6):354-360.
- Schnipper JL, Kirwin JL, Cotugno MC, et al. Role of pharmacist counseling in preventing adverse drug events after hospitalization. Arch Int Med. 2006;166(5):565-571.
- Dudas V, Bookwalter T, Kerr KM, Pantilat SZ. The impact of follow-up telephone calls to patients after hospitalization. Am J Med. 2001;111(9B): 26S-30S.
Care Transition Tips for Hospitalists and Groups

One recognized key to effective internal handoffs is the face-to-face verbal update, with opportunities to ask questions, priority given to sicker patients, and a written backup filling in the blanks with information that might become important as the patient’s condition changes. But if that is not practical for your HM group, what tools and processes will come closest to the ideal?
A key to effective discharge from the hospital is connection with the PCP, although face-to-face encounters with PCPs are highly unlikely. Hospitalists say there are levels of connection with PCPs, from the urgent (“I need to talk to someone right now”) to the routine (“It’s OK if they get this information tomorrow”). Many often wonder if there should be two levels of discharge communication with PCPs: an immediate message relaying crucial information and a formal discharge summary coming later.
For HM groups, the following is a list of suggestions from transitions-of-care researchers:
- Keep accurate and up-to-date contact information, including preferred communication medium, on referring physicians; survey them on their satisfaction with the discharge communications they receive from hospitalists.
- Partner with hospital administrators and with patient-safety and quality officers to address handoff issues.
- Partner with IT staff to help bridge the divide between clinicians and information technology.
- Track such outcomes as rehospitalization rates.
- Offer formal training on handoffs, discharges, and effective communication to physicians and other providers.
- Standardize the signout process, with computerized tools when appropriate, and create automated systems for following up on tests and lab results that come back after discharge.
- Structure shifts and their overlaps to help facilitate signouts.
- Consider implementing a discharge checklist.10
- Develop a strategy for medication reconciliation, with someone assigned to the process, be that a hospitalist, pharmacist or nurse.11
- Advocate for a post-discharge call-back policy by assigned staff at defined intervals, either for every patient discharged or for those targeted as higher-risk.12
- Consider creating a post-discharge clinic and/or a phone number that discharged patients can call to clarify post-discharge questions and concerns.
For individual hospitalists:
- Understand the transition process, where it fails, and why.
- Be open to changing the way you do things. Be accountable for transitions, and a role model for others.
- Focus on the present—today’s baseline, current to-do items, and what to expect next in the patient’s care.
- Track patients and their future discharge needs from the day of admission. What’s the likely date for going home? What does the patient need to learn in the meantime? Help nurses focus on achieving those needs and, if possible, schedule the initial outpatient clinic appointment before the patient leaves the hospital.
- Take time to talk your patients, listen to their concerns and confirm their understanding of what lies ahead.
For hospitalists on the receiving end of transition messages:
- Actively listen—stay focused, limit interruptions, take notes.
- Ask questions to ensure your understanding and read back what you understand to be the communication.
- Have a system for keeping track of to-do items requiring follow-up.—LB
Christina Payne, MD, is a third-year resident at Emory University Hospital in Atlanta who will begin her first hospitalist job, with Emory in September. In spite of her dearth of practical experience, she already has experience researching one of the most vexing problems confronting HM: how to improve transitions of care.
Dr. Payne has been studying the benefits of a structured electronic tool that generates a standardized sign-out list of a hospital team’s full census at the time of shift change, compared with the usual, highly variable sign-out practices of medical residents. At a poster presentation at Internal Medicine 2010 in April in Toronto, Dr. Payne and colleagues reported that residents using the tool were twice as confident at performing handoffs, had lower rates of perceived near-miss events, and were happier.1
“Hospitalists everywhere are starting to realize the importance of trying to reduce opportunities for human error that occur during care transitions,” Dr. Payne says. “The biggest thing I learned from this research is the importance of standardizing the handoff process [with information communicated consistently].
“It is essential to keep communication lines open,” Dr. Payne adds. “No tool can replace the importance of communication between doctors and the need to sit down and talk. The ideal signout happens in a quiet room where the two of you can talk about active patients and achieve rapport. But, realistically, how often does that happen?”
Standardization is one of a handful of strategies hospitalists, researchers, and policymakers are using to tackle transitions—both in-hospital handoffs and post-discharge transitions—with outpatient care. Some hospitalists are using practice simulations and training strategies; others have implemented medication reconciliation checks at every discharge, checklists and other communication strategies, team-based quality-improvement (QI) initiatives, and new technologies to enhance and streamline communication. Some interventions follow the patient from the hospital to the community physician with a phone call, follow-up clinic, or other contact; others aim to empower the patient to be a better self-advocate. But for hospitalists, the challenge is to communicate the right amount of transfer information to the right receiver at the right time.
No matter the technique, the goal is the same: Improve the handoff and discharge process in a way that promotes efficiency and patient safety. And hospitalists are at the forefront of the changing landscape of care transitions.
Under the Microscope
Care transitions of all kinds are under the magnifying glass of national healthcare reform, with growing recognition of the need to make care safer and reduce the preventable, costly hospital readmissions caused by incomplete handoffs. Care transitions for hospitalists include internal handoffs, both at daily shift changes and at service changes when an outgoing provider is leaving after a period of consecutive daily shifts. These typically involve a sign-out process and face-to-face encounter, with some kind of written backup. One teaching institution reported that such handoffs take place 4,000 times per day in the hospital, or 1.6 million times per year.2
—Arpana Vidyarthi, MD, University of California at San Francisco
Geographical transitions can be from one floor or department to another, or out the hospital door to another facility or home. Transitions typically involve a discharge process and a written discharge summary. Care transitions also include hospital admissions, which put the hospitalist in the role of handoff receiver rather than initiator, plus a variety of other transitions involving nurses, physician extenders, and other practitioners.
Each transition is a major decision point in the course of a patient’s hospitalization; each transition also presents a time of heightened vulnerability (e.g., potential communication breakdowns, medication errors, patient anxiety or confusion, etc.). In fact, according to a Transitions of Care Consensus Policy Statement published in 2009 by SHM and five other medical societies, handoffs are ubiquitous in HM, with significant patient safety and quality deficiencies in handoffs existing in the current system.3
Poor communication at the time of handoff has been implicated in near-misses and adverse events in a variety of healthcare contexts, including 70% of hospital sentinel events studied by The Joint Commission, which named standardized handoffs (with an opportunity for interactive communication) as a National Patient Safety Goal in 2006.4 The federal government is studying care transitions, supporting demonstration projects for Medicare enrollees, and including readmission rates in national hospital report card data.
“Transitions of care and handoffs are a huge focus right now because of the increased fragmentation of care in the United States. Hospitalists are in charge of a greater percentage of hospitalized patients, which means more coordination of care is needed,” says Vineet Arora, MD, MA, FHM, assistant professor of medicine and associate director of the internal-medicine residency at the University of Chicago, and chair of the SHM task force on handoffs.
Inadequate communication and poor care transitions can undermine hospitalists’ best care-planning efforts, erode patients’ and families’ confidence and satisfaction with hospital care, and leave primary-care physicians (PCPs) feeling unsatisfied with the relationship. As many as 1 in 5 Medicare beneficiary hospitalizations result in a readmission within 30 days, and while not all of these are preventable, far too many are.5 Another prospective cohort study found that 1 in 5 patients discharged from the hospital to the home experienced an adverse event within three weeks of discharge.6 Complex comorbidities, advanced age, unknown PCP, and limited healthcare literacy present hospitalists with extremely difficult transitions.
Patient safety and cost control are the linchpins to national efforts to improve transitions of care. Dr. Arora recently coauthored an original research paper, which will be published in the Journal of Hospital Medicine in September, showing older hospitalized patients are twice as likely to report problems after discharge if their PCPs were not aware they were hospitalized.
“With escalating healthcare costs, people are looking at ways to save money and reduce redundant care,” Dr. Arora explains, pointing out, as an example, repeated tests resulting from inadequate communication between healthcare providers.
The System Must Change
“All of the effort we put into saving someone’s life—the years of experience, training, medical school, and residency—all of it comes to bear on that hospitalized patient. And it can all be unraveled at the time of discharge if it’s not handled properly,” says Arpana Vidyarthi, MD, a hospitalist and director of quality at the University of California at San Francisco.
Dr. Vidyarthi views in-hospital and discharge transitions as integrally related. “The analysis is similar, even if different techniques may be needed,” she says, adding that, fundamentally, it involves having a system that allows people—or forces them—to do the “right thing.”
That’s why achieving effective care transitions will require more than just a standardized tool or process, Dr. Vidyarthi says. “This is about understanding the ways people communicate and finding ways to train them to communicate better,” she says. “The problem we have is not a lack of information, but how to communicate what, to whom, and when.”
What’s really needed, Dr. Vidyarthi says, is a hospital’s commitment to more effective transitions and its hospitalists’ leadership in driving a comprehensive, multidisciplinary, team- and evidence-based QI process. The new process should be a QI-based solution to a hospital’s care-transitions issues. “Before you can standardize your process, you need to understand it,” she says. “This is a complex problem, and it needs a multifaceted solution. But this lies squarely within the hospitalist arena. We’re part of everything that happens in the hospital.
—Anuj Dalal, MD, Brigham and Women’s Hospital, Boston
Hospital administrators are looking to HM to solve transition and readmission problems now, says Tina Budnitz, MPH, BOOST Project Director (Better Outcomes for Older Adults through Safe Transitions). She expects the scrutiny from the C-suite, legislators, and watchdog groups to increase as the spotlight continues to shine on the healthcare system.
“Any hospitalist can act as a leader in their institution,” Budnitz says. “Be a change agent, pull a group together, and start asking questions: Do we have safe care-transitions practices and processes in place? Just by asking the right question, you can be a catalyst for the system.”
Budnitz also emphasizes the importance of teamwork in the hospital setting. “How can I help my teammates? What am I communicating to the nurses on rounds?” she says. “Can you initiate dialogue with your outpatient medical groups: ‘These faxes we’re sending you—is that information getting to you in ways and times that are helpful? And, by the way, when your patient is admitted, this information would really help me.’ ”
Innovative Strategies
One of the most important initiatives responding to concerns about care transitions is Project BOOST (www.hos pitalmedicine.org/BOOST), a comprehensive toolkit for improving a hospital’s transitions of care. The project aims to build a national consensus for best practices in transitions; collaborate with representatives from the Agency for Healthcare Research and Quality (AHRQ), the Centers for Medicare and Medicaid Services (CMS), and the Joint Commission; and develop a national resource library, Budnitz says.
“Project BOOST not only puts forth best practices for admitting patients, planning for discharge, and then doing the discharge, it also helps show facilities how to change their systems, with resources and tools for analyzing and re-engineering the system,” she says. “Sites get one-to-one assistance from a mentor.”
Six hospitals signed on to the pilot program in 2008; 24 more joined last year. In January, SHM announced a collaborative with the University of Michigan and Blue Cross Blue Shield of Michigan for 15 Michigan hospitals to receive training and mentorship starting in May. And last month, SHM and the California HealthCare Foundation announced a Project BOOST initiative for 20 of the health system’s hospitals (see “California Dreamin’”, p. 6). Other free resources offered on the BOOST Web portal include clinical, data collection, and project management tools. SHM also has a DVD that explains how to use the “teachback” method to improve communication with patients.
Jennifer Myers, MD, FHM, assistant professor of clinical medicine and patient-safety officer at the Hospital of the University of Pennsylvania in Philadelphia, is a Project BOOST participant who spearheaded a process change to improve the quality of her facility’s discharge summary, along with accompanying resident education.7 The discharge summary recently was integrated with the hospital’s electronic health record (EHR) system.
“We’ve gone from dictating the discharge summary to an electronic version completed by the hospitalist, with prompts for key components of the summary, which allows us to create summaries more efficiently—ideally on the day of discharge, but usually within 48 hours,” Dr. Myers says. “We previously researched whether teaching made a difference in the quality of discharges; we found that it did. So we look forward to standardizing our teaching approach around this important topic for all residents.”
Another care-transitions innovation receiving a lot of attention from the government and the private sector is Project RED (Re-Engineered Discharge), led by Brian Jack, MD, vice chair of the department of family medicine at Boston Medical Center. The Project RED research group develops and tests strategies to improve the hospital discharge process to promote patient safety and reduce rehospitalization rates.
“We used re-engineering tools borrowed from other fields, brought together experts from all over the hospital, divided up the whole discharge process, and identified key principles,” Dr. Jack explains. The resulting discharge strategy is reflected in an 11-item checklist of discrete, mutually reinforcing components, which have been shown to reduce rehospitalization rates by 32% while raising patient satisfaction.8 It includes comprehensive discharge and after-hospital plans, a nurse discharge advocate, and a medication reconciliation phone call to the patient. A virtual “patient advocate,” a computerized avatar named Louise, is now being tested. If successful, it will allow patients to interact with a touch-screen teacher of the after-care plan who has time to work at the patient’s pace.
Technology and Transitions
Informatics can be a key player in facilitating care transitions, says Anuj Dalal, MD, a hospitalist and instructor in medicine at Brigham and Women’s Hospital in Boston. He is using one of his hospital’s technological strengths—a well-established, firewall-protected e-mail system—to help improve the discharge process.
“We decided to try to improve awareness of test results pending at the time of discharge,” Dr. Dalal explains. “We created an intervention that automatically triggers an e-mail with the finalized test results to the responsible providers. The intervention creates a loop of communication between the inpatient attending and the PCP. What we hope to show in our research over the next year or two is whether the intervention actually increases awareness of test results by providers.”
One thing to remember is that “all kinds of things can go wrong with care transitions,” no matter the size of the institution, the experience of the staff, or technological limitations, says Vineet Chopra, MD, FACP, a hospitalist at the University of Michigan Health System in Ann Arbor. “The problems of transitions vary from place to place, day to day, time of day, shift changes; and let’s not forget physician extenders and the other members of the healthcare team,” he says. “The more complicated the team, the more complicated the information needing to be handed off becomes.”
Who Else Is Looking at Transitions of Care?
SHM convened the Handoffs Task Force in 2006. The team systematically reviewed the literature and published recommendations in the September 2009 Journal of Hospital Medicine.9 The recommendations are aimed at both community and academic hospitals, as well as hospitalists and other healthcare providers. A new collaborative designed to supplement Project BOOST for hospitalist group handoffs and help put the guidelines into practice is in the works, says Dr. Arora, the task force’s chair.
SHM and five medical groups, including the American College of Physicians, issued a Transitions of Care Consensus Statement, published in the July 2009 issue of the Journal of Hospital Medicine.5 Guiding principles relate to education, measurement, accountability, timely interchange of information, inclusion of patient and family, respect for the medical home, and the need for national standards.
The Joint Commission’s Center for Transforming Health Care, established in 2009 to solve healthcare’s most critical safety and quality problems, has made handoff communications its second major target, and is now working with 10 healthcare systems. Standardized handoff processes and communications were the subject of the Joint Commission’s 2006 National Patient Safety Goal, while the Comprehensive Accreditation Manual for Hospitals also specifies that before a hospital discharges or transfers a patient, it should inform and educate the patient about his or her follow-up care and services.
“We now have a safety goal under review dealing with medication reconciliation, and there are relevant standards related to culturally sensitive communication and low-literacy-level communication,” says Deborah Zadzam, PhD, RN, FAAN, director of international quality and performance measures for Joint Commission Resources. “The essential message the Joint Commission has for hospitalists is to communicate clearly, effectively and thoroughly; don’t assume you are understood or that you understand.”—LB
Before he joined the group at the university, Dr. Chopra worked at a community hospital, St. Joseph’s Mercy Hospital in Hot Springs, Ark. “It’s hard to come up with a one-size-fits-all solution when there are so many variables,” he says. At the community hospital, “we mandated that the hospitalist call the PCP at the time of discharge. At the academic medical center, we share an EHR with the PCPs and can reach them electronically. We are required to have the discharge summary in the computer before the patient leaves the hospital, and we mandate that hospitalists are reachable by e-mail or phone when they are off.
“I’m not a believer in throwing more technology at problems and just adding more layers of information tools,” Dr. Chopra adds. “Hospitalists who used to carry stethoscopes now also have a clipboard, phone, pager, PDA, and nine different signouts in their pockets. What we want to do is make their life easier. Here, we are looking at technology as a means to do that.”
Dr. Chopra and hospitalist colleague Prasanth Gosineni, MD, have been working with an Ann Arbor tech company called Synaptin to develop a lightweight, mobile client application designed to work on smartphones. Still in pilot testing, it would allow for task-oriented and priority-based messaging in real time and the systematic transfer of important information for the next hospitalist shift.
“You need to be able to share information in a systematic way, but that’s only half of the answer. The other half is the ability to ask specific questions,” Dr. Chopra says. “Technology doesn’t take away from the face-to-face encounter that needs to happen. Nothing will replace face time, but part of the solution is to provide data efficiently and in a way that is easily accessible.”
Dr. Chopra admits that EHR presents both positives and negatives to improved transitions and patient care, “depending on how well it works and what smart features it offers,” he says, “but also recognizing that EHR and other technologies have also taken us farther away from face-to-face exchanges. Some would say that’s part of the problem.”
Handoffs, discharges, and other transitions are ubiquitous in HM—and fraught with the potential for costly and harmful errors. The ideal of an interactive, face-to-face handoff simply is not available for many care transitions. However, hospitalists are challenged to find solutions that will work in their hospitals, with their teams, and their types of patients. Patients and policymakers expect nothing less. TH
Larry Beresford is a freelance writer based in Oakland, Calif.
References
- Payne C, Stein J, Dressler D. Implementation of a structured electronic tool to improve patient handoffs and resident satisfaction. Poster abstract: Internal Medicine 2010, April 21-24, 2010, Toronto.
- Vidyarthi AR. Triple Handoff. AHRQ WebM&M website. Available at: webmm.ahrq.gov/case.aspx? caseID=134. Published May 2006. Accessed May 29, 2010.
- Snow V, Beck D, Budnitz T, et al. Transitions of Care Consensus Policy Statement: American College of Physicians, Society of General Internal Medicine, Society of Hospital Medicine, American Geriatrics Society, American College of Emergency Physicians, and Society for Academic Emergency Medicine. J Hosp Med. 2009;4(6):364-370.
- 2006 National Patient Safety Goals. The Joint Commission website. Available at: www.jointcommission.org/PatientSafety/NationalPatientSafetyGoals/06_npsgs.htm. Accessed June 8, 2010.
- Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med. 2009; 2:360:1418-1428.
- Forster AJ, Murff HJ, Peterson JF, Gandhi TK, Bates DW. The incidence and severity of adverse events affecting patients after discharge from the hospital. Ann Intern Med. 2003;138(3):161-167.
- Myers JS, Jaipaul CK, Kogan JR, Krekun S, Bellini LM, Shea JA. Are discharge summaries teachable? The effects of a discharge summary curriculum on the quality of discharge summaries in an internal medicine residency program. Acad Med. 2006; 81(10):S5-S8.
- Jack BW, Chetty VK, Anthony D, et al. A reengineered hospital discharge program to decrease rehospitalization: a randomized trial. Ann Intern Med. 2009;150(3):178-187.
- Arora VM, Manjarrez E, Dressler DD, Basaviah P, Halasyamani L, Kripalani S. Hospitalist handoffs: a systematic review and task force recommendations. J Hosp Med. 2009;4(7): 433-440.
- Halasyamani L, Kripalani S, Coleman E, et al. Transition of care for hospitalized elderly patients—development of a discharge checklist for hospitalists. J Hosp Med. 2006;1(6):354-360.
- Schnipper JL, Kirwin JL, Cotugno MC, et al. Role of pharmacist counseling in preventing adverse drug events after hospitalization. Arch Int Med. 2006;166(5):565-571.
- Dudas V, Bookwalter T, Kerr KM, Pantilat SZ. The impact of follow-up telephone calls to patients after hospitalization. Am J Med. 2001;111(9B): 26S-30S.
Care Transition Tips for Hospitalists and Groups
One recognized key to effective internal handoffs is the face-to-face verbal update, with opportunities to ask questions, priority given to sicker patients, and a written backup filling in the blanks with information that might become important as the patient’s condition changes. But if that is not practical for your HM group, what tools and processes will come closest to the ideal?
A key to effective discharge from the hospital is connection with the PCP, although face-to-face encounters with PCPs are highly unlikely. Hospitalists say there are levels of connection with PCPs, from the urgent (“I need to talk to someone right now”) to the routine (“It’s OK if they get this information tomorrow”). Many often wonder if there should be two levels of discharge communication with PCPs: an immediate message relaying crucial information and a formal discharge summary coming later.
For HM groups, the following is a list of suggestions from transitions-of-care researchers:
- Keep accurate and up-to-date contact information, including preferred communication medium, on referring physicians; survey them on their satisfaction with the discharge communications they receive from hospitalists.
- Partner with hospital administrators and with patient-safety and quality officers to address handoff issues.
- Partner with IT staff to help bridge the divide between clinicians and information technology.
- Track such outcomes as rehospitalization rates.
- Offer formal training on handoffs, discharges, and effective communication to physicians and other providers.
- Standardize the signout process, with computerized tools when appropriate, and create automated systems for following up on tests and lab results that come back after discharge.
- Structure shifts and their overlaps to help facilitate signouts.
- Consider implementing a discharge checklist.10
- Develop a strategy for medication reconciliation, with someone assigned to the process, be that a hospitalist, pharmacist or nurse.11
- Advocate for a post-discharge call-back policy by assigned staff at defined intervals, either for every patient discharged or for those targeted as higher-risk.12
- Consider creating a post-discharge clinic and/or a phone number that discharged patients can call to clarify post-discharge questions and concerns.
For individual hospitalists:
- Understand the transition process, where it fails, and why.
- Be open to changing the way you do things. Be accountable for transitions, and a role model for others.
- Focus on the present—today’s baseline, current to-do items, and what to expect next in the patient’s care.
- Track patients and their future discharge needs from the day of admission. What’s the likely date for going home? What does the patient need to learn in the meantime? Help nurses focus on achieving those needs and, if possible, schedule the initial outpatient clinic appointment before the patient leaves the hospital.
- Take time to talk your patients, listen to their concerns and confirm their understanding of what lies ahead.
For hospitalists on the receiving end of transition messages:
- Actively listen—stay focused, limit interruptions, take notes.
- Ask questions to ensure your understanding and read back what you understand to be the communication.
- Have a system for keeping track of to-do items requiring follow-up.—LB
Christina Payne, MD, is a third-year resident at Emory University Hospital in Atlanta who will begin her first hospitalist job, with Emory in September. In spite of her dearth of practical experience, she already has experience researching one of the most vexing problems confronting HM: how to improve transitions of care.
Dr. Payne has been studying the benefits of a structured electronic tool that generates a standardized sign-out list of a hospital team’s full census at the time of shift change, compared with the usual, highly variable sign-out practices of medical residents. At a poster presentation at Internal Medicine 2010 in April in Toronto, Dr. Payne and colleagues reported that residents using the tool were twice as confident at performing handoffs, had lower rates of perceived near-miss events, and were happier.1
“Hospitalists everywhere are starting to realize the importance of trying to reduce opportunities for human error that occur during care transitions,” Dr. Payne says. “The biggest thing I learned from this research is the importance of standardizing the handoff process [with information communicated consistently].
“It is essential to keep communication lines open,” Dr. Payne adds. “No tool can replace the importance of communication between doctors and the need to sit down and talk. The ideal signout happens in a quiet room where the two of you can talk about active patients and achieve rapport. But, realistically, how often does that happen?”
Standardization is one of a handful of strategies hospitalists, researchers, and policymakers are using to tackle transitions—both in-hospital handoffs and post-discharge transitions—with outpatient care. Some hospitalists are using practice simulations and training strategies; others have implemented medication reconciliation checks at every discharge, checklists and other communication strategies, team-based quality-improvement (QI) initiatives, and new technologies to enhance and streamline communication. Some interventions follow the patient from the hospital to the community physician with a phone call, follow-up clinic, or other contact; others aim to empower the patient to be a better self-advocate. But for hospitalists, the challenge is to communicate the right amount of transfer information to the right receiver at the right time.
No matter the technique, the goal is the same: Improve the handoff and discharge process in a way that promotes efficiency and patient safety. And hospitalists are at the forefront of the changing landscape of care transitions.
Under the Microscope
Care transitions of all kinds are under the magnifying glass of national healthcare reform, with growing recognition of the need to make care safer and reduce the preventable, costly hospital readmissions caused by incomplete handoffs. Care transitions for hospitalists include internal handoffs, both at daily shift changes and at service changes when an outgoing provider is leaving after a period of consecutive daily shifts. These typically involve a sign-out process and face-to-face encounter, with some kind of written backup. One teaching institution reported that such handoffs take place 4,000 times per day in the hospital, or 1.6 million times per year.2
—Arpana Vidyarthi, MD, University of California at San Francisco
Geographical transitions can be from one floor or department to another, or out the hospital door to another facility or home. Transitions typically involve a discharge process and a written discharge summary. Care transitions also include hospital admissions, which put the hospitalist in the role of handoff receiver rather than initiator, plus a variety of other transitions involving nurses, physician extenders, and other practitioners.
Each transition is a major decision point in the course of a patient’s hospitalization; each transition also presents a time of heightened vulnerability (e.g., potential communication breakdowns, medication errors, patient anxiety or confusion, etc.). In fact, according to a Transitions of Care Consensus Policy Statement published in 2009 by SHM and five other medical societies, handoffs are ubiquitous in HM, with significant patient safety and quality deficiencies in handoffs existing in the current system.3
Poor communication at the time of handoff has been implicated in near-misses and adverse events in a variety of healthcare contexts, including 70% of hospital sentinel events studied by The Joint Commission, which named standardized handoffs (with an opportunity for interactive communication) as a National Patient Safety Goal in 2006.4 The federal government is studying care transitions, supporting demonstration projects for Medicare enrollees, and including readmission rates in national hospital report card data.
“Transitions of care and handoffs are a huge focus right now because of the increased fragmentation of care in the United States. Hospitalists are in charge of a greater percentage of hospitalized patients, which means more coordination of care is needed,” says Vineet Arora, MD, MA, FHM, assistant professor of medicine and associate director of the internal-medicine residency at the University of Chicago, and chair of the SHM task force on handoffs.
Inadequate communication and poor care transitions can undermine hospitalists’ best care-planning efforts, erode patients’ and families’ confidence and satisfaction with hospital care, and leave primary-care physicians (PCPs) feeling unsatisfied with the relationship. As many as 1 in 5 Medicare beneficiary hospitalizations result in a readmission within 30 days, and while not all of these are preventable, far too many are.5 Another prospective cohort study found that 1 in 5 patients discharged from the hospital to the home experienced an adverse event within three weeks of discharge.6 Complex comorbidities, advanced age, unknown PCP, and limited healthcare literacy present hospitalists with extremely difficult transitions.
Patient safety and cost control are the linchpins to national efforts to improve transitions of care. Dr. Arora recently coauthored an original research paper, which will be published in the Journal of Hospital Medicine in September, showing older hospitalized patients are twice as likely to report problems after discharge if their PCPs were not aware they were hospitalized.
“With escalating healthcare costs, people are looking at ways to save money and reduce redundant care,” Dr. Arora explains, pointing out, as an example, repeated tests resulting from inadequate communication between healthcare providers.
The System Must Change
“All of the effort we put into saving someone’s life—the years of experience, training, medical school, and residency—all of it comes to bear on that hospitalized patient. And it can all be unraveled at the time of discharge if it’s not handled properly,” says Arpana Vidyarthi, MD, a hospitalist and director of quality at the University of California at San Francisco.
Dr. Vidyarthi views in-hospital and discharge transitions as integrally related. “The analysis is similar, even if different techniques may be needed,” she says, adding that, fundamentally, it involves having a system that allows people—or forces them—to do the “right thing.”
That’s why achieving effective care transitions will require more than just a standardized tool or process, Dr. Vidyarthi says. “This is about understanding the ways people communicate and finding ways to train them to communicate better,” she says. “The problem we have is not a lack of information, but how to communicate what, to whom, and when.”
What’s really needed, Dr. Vidyarthi says, is a hospital’s commitment to more effective transitions and its hospitalists’ leadership in driving a comprehensive, multidisciplinary, team- and evidence-based QI process. The new process should be a QI-based solution to a hospital’s care-transitions issues. “Before you can standardize your process, you need to understand it,” she says. “This is a complex problem, and it needs a multifaceted solution. But this lies squarely within the hospitalist arena. We’re part of everything that happens in the hospital.
—Anuj Dalal, MD, Brigham and Women’s Hospital, Boston
Hospital administrators are looking to HM to solve transition and readmission problems now, says Tina Budnitz, MPH, BOOST Project Director (Better Outcomes for Older Adults through Safe Transitions). She expects the scrutiny from the C-suite, legislators, and watchdog groups to increase as the spotlight continues to shine on the healthcare system.
“Any hospitalist can act as a leader in their institution,” Budnitz says. “Be a change agent, pull a group together, and start asking questions: Do we have safe care-transitions practices and processes in place? Just by asking the right question, you can be a catalyst for the system.”
Budnitz also emphasizes the importance of teamwork in the hospital setting. “How can I help my teammates? What am I communicating to the nurses on rounds?” she says. “Can you initiate dialogue with your outpatient medical groups: ‘These faxes we’re sending you—is that information getting to you in ways and times that are helpful? And, by the way, when your patient is admitted, this information would really help me.’ ”
Innovative Strategies
One of the most important initiatives responding to concerns about care transitions is Project BOOST (www.hos pitalmedicine.org/BOOST), a comprehensive toolkit for improving a hospital’s transitions of care. The project aims to build a national consensus for best practices in transitions; collaborate with representatives from the Agency for Healthcare Research and Quality (AHRQ), the Centers for Medicare and Medicaid Services (CMS), and the Joint Commission; and develop a national resource library, Budnitz says.
“Project BOOST not only puts forth best practices for admitting patients, planning for discharge, and then doing the discharge, it also helps show facilities how to change their systems, with resources and tools for analyzing and re-engineering the system,” she says. “Sites get one-to-one assistance from a mentor.”
Six hospitals signed on to the pilot program in 2008; 24 more joined last year. In January, SHM announced a collaborative with the University of Michigan and Blue Cross Blue Shield of Michigan for 15 Michigan hospitals to receive training and mentorship starting in May. And last month, SHM and the California HealthCare Foundation announced a Project BOOST initiative for 20 of the health system’s hospitals (see “California Dreamin’”, p. 6). Other free resources offered on the BOOST Web portal include clinical, data collection, and project management tools. SHM also has a DVD that explains how to use the “teachback” method to improve communication with patients.
Jennifer Myers, MD, FHM, assistant professor of clinical medicine and patient-safety officer at the Hospital of the University of Pennsylvania in Philadelphia, is a Project BOOST participant who spearheaded a process change to improve the quality of her facility’s discharge summary, along with accompanying resident education.7 The discharge summary recently was integrated with the hospital’s electronic health record (EHR) system.
“We’ve gone from dictating the discharge summary to an electronic version completed by the hospitalist, with prompts for key components of the summary, which allows us to create summaries more efficiently—ideally on the day of discharge, but usually within 48 hours,” Dr. Myers says. “We previously researched whether teaching made a difference in the quality of discharges; we found that it did. So we look forward to standardizing our teaching approach around this important topic for all residents.”
Another care-transitions innovation receiving a lot of attention from the government and the private sector is Project RED (Re-Engineered Discharge), led by Brian Jack, MD, vice chair of the department of family medicine at Boston Medical Center. The Project RED research group develops and tests strategies to improve the hospital discharge process to promote patient safety and reduce rehospitalization rates.
“We used re-engineering tools borrowed from other fields, brought together experts from all over the hospital, divided up the whole discharge process, and identified key principles,” Dr. Jack explains. The resulting discharge strategy is reflected in an 11-item checklist of discrete, mutually reinforcing components, which have been shown to reduce rehospitalization rates by 32% while raising patient satisfaction.8 It includes comprehensive discharge and after-hospital plans, a nurse discharge advocate, and a medication reconciliation phone call to the patient. A virtual “patient advocate,” a computerized avatar named Louise, is now being tested. If successful, it will allow patients to interact with a touch-screen teacher of the after-care plan who has time to work at the patient’s pace.
Technology and Transitions
Informatics can be a key player in facilitating care transitions, says Anuj Dalal, MD, a hospitalist and instructor in medicine at Brigham and Women’s Hospital in Boston. He is using one of his hospital’s technological strengths—a well-established, firewall-protected e-mail system—to help improve the discharge process.
“We decided to try to improve awareness of test results pending at the time of discharge,” Dr. Dalal explains. “We created an intervention that automatically triggers an e-mail with the finalized test results to the responsible providers. The intervention creates a loop of communication between the inpatient attending and the PCP. What we hope to show in our research over the next year or two is whether the intervention actually increases awareness of test results by providers.”
One thing to remember is that “all kinds of things can go wrong with care transitions,” no matter the size of the institution, the experience of the staff, or technological limitations, says Vineet Chopra, MD, FACP, a hospitalist at the University of Michigan Health System in Ann Arbor. “The problems of transitions vary from place to place, day to day, time of day, shift changes; and let’s not forget physician extenders and the other members of the healthcare team,” he says. “The more complicated the team, the more complicated the information needing to be handed off becomes.”
Who Else Is Looking at Transitions of Care?
SHM convened the Handoffs Task Force in 2006. The team systematically reviewed the literature and published recommendations in the September 2009 Journal of Hospital Medicine.9 The recommendations are aimed at both community and academic hospitals, as well as hospitalists and other healthcare providers. A new collaborative designed to supplement Project BOOST for hospitalist group handoffs and help put the guidelines into practice is in the works, says Dr. Arora, the task force’s chair.
SHM and five medical groups, including the American College of Physicians, issued a Transitions of Care Consensus Statement, published in the July 2009 issue of the Journal of Hospital Medicine.5 Guiding principles relate to education, measurement, accountability, timely interchange of information, inclusion of patient and family, respect for the medical home, and the need for national standards.
The Joint Commission’s Center for Transforming Health Care, established in 2009 to solve healthcare’s most critical safety and quality problems, has made handoff communications its second major target, and is now working with 10 healthcare systems. Standardized handoff processes and communications were the subject of the Joint Commission’s 2006 National Patient Safety Goal, while the Comprehensive Accreditation Manual for Hospitals also specifies that before a hospital discharges or transfers a patient, it should inform and educate the patient about his or her follow-up care and services.
“We now have a safety goal under review dealing with medication reconciliation, and there are relevant standards related to culturally sensitive communication and low-literacy-level communication,” says Deborah Zadzam, PhD, RN, FAAN, director of international quality and performance measures for Joint Commission Resources. “The essential message the Joint Commission has for hospitalists is to communicate clearly, effectively and thoroughly; don’t assume you are understood or that you understand.”—LB
Before he joined the group at the university, Dr. Chopra worked at a community hospital, St. Joseph’s Mercy Hospital in Hot Springs, Ark. “It’s hard to come up with a one-size-fits-all solution when there are so many variables,” he says. At the community hospital, “we mandated that the hospitalist call the PCP at the time of discharge. At the academic medical center, we share an EHR with the PCPs and can reach them electronically. We are required to have the discharge summary in the computer before the patient leaves the hospital, and we mandate that hospitalists are reachable by e-mail or phone when they are off.
“I’m not a believer in throwing more technology at problems and just adding more layers of information tools,” Dr. Chopra adds. “Hospitalists who used to carry stethoscopes now also have a clipboard, phone, pager, PDA, and nine different signouts in their pockets. What we want to do is make their life easier. Here, we are looking at technology as a means to do that.”
Dr. Chopra and hospitalist colleague Prasanth Gosineni, MD, have been working with an Ann Arbor tech company called Synaptin to develop a lightweight, mobile client application designed to work on smartphones. Still in pilot testing, it would allow for task-oriented and priority-based messaging in real time and the systematic transfer of important information for the next hospitalist shift.
“You need to be able to share information in a systematic way, but that’s only half of the answer. The other half is the ability to ask specific questions,” Dr. Chopra says. “Technology doesn’t take away from the face-to-face encounter that needs to happen. Nothing will replace face time, but part of the solution is to provide data efficiently and in a way that is easily accessible.”
Dr. Chopra admits that EHR presents both positives and negatives to improved transitions and patient care, “depending on how well it works and what smart features it offers,” he says, “but also recognizing that EHR and other technologies have also taken us farther away from face-to-face exchanges. Some would say that’s part of the problem.”
Handoffs, discharges, and other transitions are ubiquitous in HM—and fraught with the potential for costly and harmful errors. The ideal of an interactive, face-to-face handoff simply is not available for many care transitions. However, hospitalists are challenged to find solutions that will work in their hospitals, with their teams, and their types of patients. Patients and policymakers expect nothing less. TH
Larry Beresford is a freelance writer based in Oakland, Calif.
References
- Payne C, Stein J, Dressler D. Implementation of a structured electronic tool to improve patient handoffs and resident satisfaction. Poster abstract: Internal Medicine 2010, April 21-24, 2010, Toronto.
- Vidyarthi AR. Triple Handoff. AHRQ WebM&M website. Available at: webmm.ahrq.gov/case.aspx? caseID=134. Published May 2006. Accessed May 29, 2010.
- Snow V, Beck D, Budnitz T, et al. Transitions of Care Consensus Policy Statement: American College of Physicians, Society of General Internal Medicine, Society of Hospital Medicine, American Geriatrics Society, American College of Emergency Physicians, and Society for Academic Emergency Medicine. J Hosp Med. 2009;4(6):364-370.
- 2006 National Patient Safety Goals. The Joint Commission website. Available at: www.jointcommission.org/PatientSafety/NationalPatientSafetyGoals/06_npsgs.htm. Accessed June 8, 2010.
- Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med. 2009; 2:360:1418-1428.
- Forster AJ, Murff HJ, Peterson JF, Gandhi TK, Bates DW. The incidence and severity of adverse events affecting patients after discharge from the hospital. Ann Intern Med. 2003;138(3):161-167.
- Myers JS, Jaipaul CK, Kogan JR, Krekun S, Bellini LM, Shea JA. Are discharge summaries teachable? The effects of a discharge summary curriculum on the quality of discharge summaries in an internal medicine residency program. Acad Med. 2006; 81(10):S5-S8.
- Jack BW, Chetty VK, Anthony D, et al. A reengineered hospital discharge program to decrease rehospitalization: a randomized trial. Ann Intern Med. 2009;150(3):178-187.
- Arora VM, Manjarrez E, Dressler DD, Basaviah P, Halasyamani L, Kripalani S. Hospitalist handoffs: a systematic review and task force recommendations. J Hosp Med. 2009;4(7): 433-440.
- Halasyamani L, Kripalani S, Coleman E, et al. Transition of care for hospitalized elderly patients—development of a discharge checklist for hospitalists. J Hosp Med. 2006;1(6):354-360.
- Schnipper JL, Kirwin JL, Cotugno MC, et al. Role of pharmacist counseling in preventing adverse drug events after hospitalization. Arch Int Med. 2006;166(5):565-571.
- Dudas V, Bookwalter T, Kerr KM, Pantilat SZ. The impact of follow-up telephone calls to patients after hospitalization. Am J Med. 2001;111(9B): 26S-30S.
Care Transition Tips for Hospitalists and Groups
One recognized key to effective internal handoffs is the face-to-face verbal update, with opportunities to ask questions, priority given to sicker patients, and a written backup filling in the blanks with information that might become important as the patient’s condition changes. But if that is not practical for your HM group, what tools and processes will come closest to the ideal?
A key to effective discharge from the hospital is connection with the PCP, although face-to-face encounters with PCPs are highly unlikely. Hospitalists say there are levels of connection with PCPs, from the urgent (“I need to talk to someone right now”) to the routine (“It’s OK if they get this information tomorrow”). Many often wonder if there should be two levels of discharge communication with PCPs: an immediate message relaying crucial information and a formal discharge summary coming later.
For HM groups, the following is a list of suggestions from transitions-of-care researchers:
- Keep accurate and up-to-date contact information, including preferred communication medium, on referring physicians; survey them on their satisfaction with the discharge communications they receive from hospitalists.
- Partner with hospital administrators and with patient-safety and quality officers to address handoff issues.
- Partner with IT staff to help bridge the divide between clinicians and information technology.
- Track such outcomes as rehospitalization rates.
- Offer formal training on handoffs, discharges, and effective communication to physicians and other providers.
- Standardize the signout process, with computerized tools when appropriate, and create automated systems for following up on tests and lab results that come back after discharge.
- Structure shifts and their overlaps to help facilitate signouts.
- Consider implementing a discharge checklist.10
- Develop a strategy for medication reconciliation, with someone assigned to the process, be that a hospitalist, pharmacist or nurse.11
- Advocate for a post-discharge call-back policy by assigned staff at defined intervals, either for every patient discharged or for those targeted as higher-risk.12
- Consider creating a post-discharge clinic and/or a phone number that discharged patients can call to clarify post-discharge questions and concerns.
For individual hospitalists:
- Understand the transition process, where it fails, and why.
- Be open to changing the way you do things. Be accountable for transitions, and a role model for others.
- Focus on the present—today’s baseline, current to-do items, and what to expect next in the patient’s care.
- Track patients and their future discharge needs from the day of admission. What’s the likely date for going home? What does the patient need to learn in the meantime? Help nurses focus on achieving those needs and, if possible, schedule the initial outpatient clinic appointment before the patient leaves the hospital.
- Take time to talk your patients, listen to their concerns and confirm their understanding of what lies ahead.
For hospitalists on the receiving end of transition messages:
- Actively listen—stay focused, limit interruptions, take notes.
- Ask questions to ensure your understanding and read back what you understand to be the communication.
- Have a system for keeping track of to-do items requiring follow-up.—LB