User login
VEXAS Syndrome: Study Highlights Cutaneous Symptoms
Additionally, the most common histologic findings include leukocytoclastic vasculitis, neutrophilic dermatosis, and perivascular dermatitis; different variants in the UBA1 gene are associated with specific skin manifestations.
Those are key findings from a cohort study of 112 patients with VEXAS published online in JAMA Dermatology. The study, conducted by researchers at the National Institutes of Health (NIH) and several other institutions, aimed to define the spectrum of cutaneous manifestations in VEXAS in association with genetic, histologic, and other clinical findings.
First described in 2020, VEXAS syndrome is an adult-onset multisystem disease that can pose a diagnostic challenge to clinicians, the study’s corresponding author, Edward W. Cowen, MD, MHSc, of the dermatology branch at the National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS), said in an interview. The disease is caused by pathogenic variants in the UBA1 gene, located on the X chromosome. Affected individuals exhibit a wide range of manifestations, including cytopenia/myelodysplasia, multiorgan systemic inflammation, and cutaneous involvement.
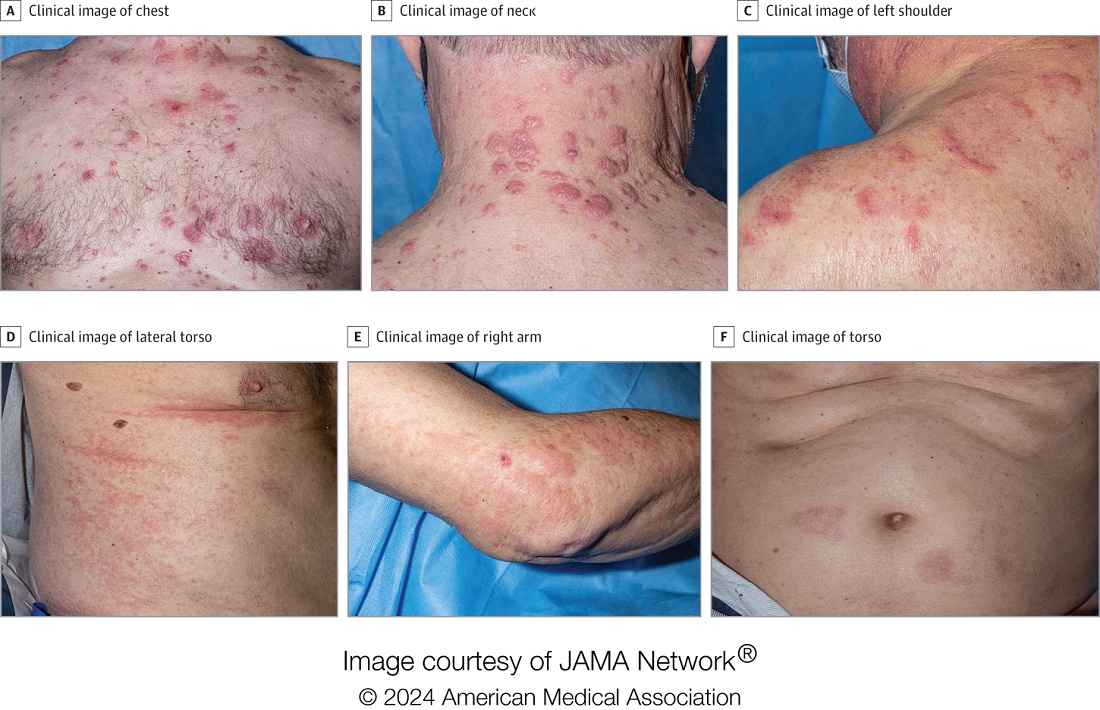
“Patients may present to a variety of disease specialists depending on their symptoms and providers may not immediately consider a genetic etiology in an older individual,” Dr. Cowen said in an interview. “Although skin involvement occurs in more than 80% of patients, it is pleomorphic and may resemble a variety of other conditions such as vasculitis and Sweet syndrome.”
To better understand the cutaneous manifestations of VEXAS syndrome, the researchers evaluated data from 112 patients with VEXAS-defining genetic variants in the UBA1 gene between 2019 and 2023. Of the 112 patients, 73 underwent medical record review only, and 39 were prospectively evaluated at NIH. All but one of the patients were men, 94% were White individuals, and their mean age was 64 years. Skin involvement occurred in 83% of cases and was the most common presenting feature of VEXAS in 61% of cases.
Of the 64 histopathologic reports available from 60 patients, the main skin histopathologic findings were leukocytoclastic vasculitis in 23 patients (36%), neutrophilic dermatosis in 22 patients (34%), and perivascular dermatitis in 19 patients (30%). According to Dr. Cowen, one key histologic finding was a distinct pattern of “histiocytoid” dermal neutrophilic inflammation, which was present in 13 of 15 specimens (86%) that underwent central re-review. “This pattern can occasionally also be seen in patients with Sweet syndrome, unrelated to VEXAS, but was a hallmark feature found in the majority of skin biopsies of patients with VEXAS,” he said.
“Together with another pathologic finding, leukocytoclasia, these features can be useful clues to alert the pathologist to a potential diagnosis of VEXAS. This myeloid predominant pattern of skin inflammation was also most strongly associated with the leucine pathogenic variant of the UBA1 gene.” In contrast, cutaneous vasculitis was most strongly associated with the valine pathogenic variant of UBA1. “This is important because the valine variant has been previously independently linked to decreased survival,” he said.
In findings related to pathogenic genetic variants, the researchers observed that the p.Met41Leu variant was most frequently associated with neutrophilic dermal infiltrates in 14 of 17 patients (82%) with this variant and often resembled histiocytoid Sweet syndrome. In addition, the p.Met41Val variant was associated with vasculitic lesions in 11 of 20 patients (55%) with this variant and with a mixed leukocytic infiltrate in 17 of these 20 patients (85%).
Treatment Outcomes
In the realm of therapies, skin manifestations improved in 67 of 73 patients (92%) treated with oral prednisone, while treatment with the interleukin-1 receptor antagonist anakinra improved cutaneous disease in 9 of the 16 (56%) who received it. However, 12 (75%) of those who received anakinra developed severe injection-site reactions, including ulceration in two patients and abscess formation in one patient.
Dr. Cowen noted that VEXAS is associated with high mortality (22% in this cohort), and a high degree of suspicion is required to diagnose patients with VEXAS before significant end organ damage has occurred. “This diagnosis should be considered in all older male patients who present with neutrophilic dermatosis — particularly histiocytoid Sweet syndrome, vasculitis, or leukocytoclasia without vasculitis. Patients who appear to have isolated skin involvement may have cytopenias and acute phase reactants. Therefore, complete blood count with differential and ESR and CRP should be considered to investigate for macrocytosis, cytopenias, and systemic inflammation.”
He acknowledged certain limitations of the study, including the fact that many patients were first evaluated at the NIH after having disease symptoms for many months or years. “It is possible that patients with VEXAS referred to the NIH, either for genetic testing or in person evaluation, represent a population with more aggressive disease.”
Christine Ko, MD, professor of dermatology and pathology at Yale University, New Haven, Connecticut, who was asked to comment on the study, emphasized the importance of the UBA1 mutation in the diagnosis of this complex syndrome. “Dermatologists should be aware of VEXAS syndrome as the majority of patients present with skin lesions, which can range from urticarial to Sweet syndrome–like to palpable purpura,” Dr. Ko said.
“Chondritis and periorbital edema, sometimes unilateral, are also associated. Histopathologic clues include a predominantly histiocytoid infiltrate,” she noted. In addition, “the prominent myxoid stroma around blood vessels and adnexal structures as a clue to VEXAS syndrome surprised me; I had not read that before.”
The study was supported by the Intramural Research Program of NIAMS. One of the study authors reported personal fees from Alexion, Novartis, and Sobi outside of the submitted work. No other disclosures were reported. Dr. Ko reported having no disclosures.
A version of this article appeared on Medscape.com .
Additionally, the most common histologic findings include leukocytoclastic vasculitis, neutrophilic dermatosis, and perivascular dermatitis; different variants in the UBA1 gene are associated with specific skin manifestations.
Those are key findings from a cohort study of 112 patients with VEXAS published online in JAMA Dermatology. The study, conducted by researchers at the National Institutes of Health (NIH) and several other institutions, aimed to define the spectrum of cutaneous manifestations in VEXAS in association with genetic, histologic, and other clinical findings.
First described in 2020, VEXAS syndrome is an adult-onset multisystem disease that can pose a diagnostic challenge to clinicians, the study’s corresponding author, Edward W. Cowen, MD, MHSc, of the dermatology branch at the National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS), said in an interview. The disease is caused by pathogenic variants in the UBA1 gene, located on the X chromosome. Affected individuals exhibit a wide range of manifestations, including cytopenia/myelodysplasia, multiorgan systemic inflammation, and cutaneous involvement.
“Patients may present to a variety of disease specialists depending on their symptoms and providers may not immediately consider a genetic etiology in an older individual,” Dr. Cowen said in an interview. “Although skin involvement occurs in more than 80% of patients, it is pleomorphic and may resemble a variety of other conditions such as vasculitis and Sweet syndrome.”
To better understand the cutaneous manifestations of VEXAS syndrome, the researchers evaluated data from 112 patients with VEXAS-defining genetic variants in the UBA1 gene between 2019 and 2023. Of the 112 patients, 73 underwent medical record review only, and 39 were prospectively evaluated at NIH. All but one of the patients were men, 94% were White individuals, and their mean age was 64 years. Skin involvement occurred in 83% of cases and was the most common presenting feature of VEXAS in 61% of cases.
Of the 64 histopathologic reports available from 60 patients, the main skin histopathologic findings were leukocytoclastic vasculitis in 23 patients (36%), neutrophilic dermatosis in 22 patients (34%), and perivascular dermatitis in 19 patients (30%). According to Dr. Cowen, one key histologic finding was a distinct pattern of “histiocytoid” dermal neutrophilic inflammation, which was present in 13 of 15 specimens (86%) that underwent central re-review. “This pattern can occasionally also be seen in patients with Sweet syndrome, unrelated to VEXAS, but was a hallmark feature found in the majority of skin biopsies of patients with VEXAS,” he said.
“Together with another pathologic finding, leukocytoclasia, these features can be useful clues to alert the pathologist to a potential diagnosis of VEXAS. This myeloid predominant pattern of skin inflammation was also most strongly associated with the leucine pathogenic variant of the UBA1 gene.” In contrast, cutaneous vasculitis was most strongly associated with the valine pathogenic variant of UBA1. “This is important because the valine variant has been previously independently linked to decreased survival,” he said.
In findings related to pathogenic genetic variants, the researchers observed that the p.Met41Leu variant was most frequently associated with neutrophilic dermal infiltrates in 14 of 17 patients (82%) with this variant and often resembled histiocytoid Sweet syndrome. In addition, the p.Met41Val variant was associated with vasculitic lesions in 11 of 20 patients (55%) with this variant and with a mixed leukocytic infiltrate in 17 of these 20 patients (85%).
Treatment Outcomes
In the realm of therapies, skin manifestations improved in 67 of 73 patients (92%) treated with oral prednisone, while treatment with the interleukin-1 receptor antagonist anakinra improved cutaneous disease in 9 of the 16 (56%) who received it. However, 12 (75%) of those who received anakinra developed severe injection-site reactions, including ulceration in two patients and abscess formation in one patient.
Dr. Cowen noted that VEXAS is associated with high mortality (22% in this cohort), and a high degree of suspicion is required to diagnose patients with VEXAS before significant end organ damage has occurred. “This diagnosis should be considered in all older male patients who present with neutrophilic dermatosis — particularly histiocytoid Sweet syndrome, vasculitis, or leukocytoclasia without vasculitis. Patients who appear to have isolated skin involvement may have cytopenias and acute phase reactants. Therefore, complete blood count with differential and ESR and CRP should be considered to investigate for macrocytosis, cytopenias, and systemic inflammation.”
He acknowledged certain limitations of the study, including the fact that many patients were first evaluated at the NIH after having disease symptoms for many months or years. “It is possible that patients with VEXAS referred to the NIH, either for genetic testing or in person evaluation, represent a population with more aggressive disease.”
Christine Ko, MD, professor of dermatology and pathology at Yale University, New Haven, Connecticut, who was asked to comment on the study, emphasized the importance of the UBA1 mutation in the diagnosis of this complex syndrome. “Dermatologists should be aware of VEXAS syndrome as the majority of patients present with skin lesions, which can range from urticarial to Sweet syndrome–like to palpable purpura,” Dr. Ko said.
“Chondritis and periorbital edema, sometimes unilateral, are also associated. Histopathologic clues include a predominantly histiocytoid infiltrate,” she noted. In addition, “the prominent myxoid stroma around blood vessels and adnexal structures as a clue to VEXAS syndrome surprised me; I had not read that before.”
The study was supported by the Intramural Research Program of NIAMS. One of the study authors reported personal fees from Alexion, Novartis, and Sobi outside of the submitted work. No other disclosures were reported. Dr. Ko reported having no disclosures.
A version of this article appeared on Medscape.com .
Additionally, the most common histologic findings include leukocytoclastic vasculitis, neutrophilic dermatosis, and perivascular dermatitis; different variants in the UBA1 gene are associated with specific skin manifestations.
Those are key findings from a cohort study of 112 patients with VEXAS published online in JAMA Dermatology. The study, conducted by researchers at the National Institutes of Health (NIH) and several other institutions, aimed to define the spectrum of cutaneous manifestations in VEXAS in association with genetic, histologic, and other clinical findings.
First described in 2020, VEXAS syndrome is an adult-onset multisystem disease that can pose a diagnostic challenge to clinicians, the study’s corresponding author, Edward W. Cowen, MD, MHSc, of the dermatology branch at the National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS), said in an interview. The disease is caused by pathogenic variants in the UBA1 gene, located on the X chromosome. Affected individuals exhibit a wide range of manifestations, including cytopenia/myelodysplasia, multiorgan systemic inflammation, and cutaneous involvement.
“Patients may present to a variety of disease specialists depending on their symptoms and providers may not immediately consider a genetic etiology in an older individual,” Dr. Cowen said in an interview. “Although skin involvement occurs in more than 80% of patients, it is pleomorphic and may resemble a variety of other conditions such as vasculitis and Sweet syndrome.”
To better understand the cutaneous manifestations of VEXAS syndrome, the researchers evaluated data from 112 patients with VEXAS-defining genetic variants in the UBA1 gene between 2019 and 2023. Of the 112 patients, 73 underwent medical record review only, and 39 were prospectively evaluated at NIH. All but one of the patients were men, 94% were White individuals, and their mean age was 64 years. Skin involvement occurred in 83% of cases and was the most common presenting feature of VEXAS in 61% of cases.
Of the 64 histopathologic reports available from 60 patients, the main skin histopathologic findings were leukocytoclastic vasculitis in 23 patients (36%), neutrophilic dermatosis in 22 patients (34%), and perivascular dermatitis in 19 patients (30%). According to Dr. Cowen, one key histologic finding was a distinct pattern of “histiocytoid” dermal neutrophilic inflammation, which was present in 13 of 15 specimens (86%) that underwent central re-review. “This pattern can occasionally also be seen in patients with Sweet syndrome, unrelated to VEXAS, but was a hallmark feature found in the majority of skin biopsies of patients with VEXAS,” he said.
“Together with another pathologic finding, leukocytoclasia, these features can be useful clues to alert the pathologist to a potential diagnosis of VEXAS. This myeloid predominant pattern of skin inflammation was also most strongly associated with the leucine pathogenic variant of the UBA1 gene.” In contrast, cutaneous vasculitis was most strongly associated with the valine pathogenic variant of UBA1. “This is important because the valine variant has been previously independently linked to decreased survival,” he said.
In findings related to pathogenic genetic variants, the researchers observed that the p.Met41Leu variant was most frequently associated with neutrophilic dermal infiltrates in 14 of 17 patients (82%) with this variant and often resembled histiocytoid Sweet syndrome. In addition, the p.Met41Val variant was associated with vasculitic lesions in 11 of 20 patients (55%) with this variant and with a mixed leukocytic infiltrate in 17 of these 20 patients (85%).
Treatment Outcomes
In the realm of therapies, skin manifestations improved in 67 of 73 patients (92%) treated with oral prednisone, while treatment with the interleukin-1 receptor antagonist anakinra improved cutaneous disease in 9 of the 16 (56%) who received it. However, 12 (75%) of those who received anakinra developed severe injection-site reactions, including ulceration in two patients and abscess formation in one patient.
Dr. Cowen noted that VEXAS is associated with high mortality (22% in this cohort), and a high degree of suspicion is required to diagnose patients with VEXAS before significant end organ damage has occurred. “This diagnosis should be considered in all older male patients who present with neutrophilic dermatosis — particularly histiocytoid Sweet syndrome, vasculitis, or leukocytoclasia without vasculitis. Patients who appear to have isolated skin involvement may have cytopenias and acute phase reactants. Therefore, complete blood count with differential and ESR and CRP should be considered to investigate for macrocytosis, cytopenias, and systemic inflammation.”
He acknowledged certain limitations of the study, including the fact that many patients were first evaluated at the NIH after having disease symptoms for many months or years. “It is possible that patients with VEXAS referred to the NIH, either for genetic testing or in person evaluation, represent a population with more aggressive disease.”
Christine Ko, MD, professor of dermatology and pathology at Yale University, New Haven, Connecticut, who was asked to comment on the study, emphasized the importance of the UBA1 mutation in the diagnosis of this complex syndrome. “Dermatologists should be aware of VEXAS syndrome as the majority of patients present with skin lesions, which can range from urticarial to Sweet syndrome–like to palpable purpura,” Dr. Ko said.
“Chondritis and periorbital edema, sometimes unilateral, are also associated. Histopathologic clues include a predominantly histiocytoid infiltrate,” she noted. In addition, “the prominent myxoid stroma around blood vessels and adnexal structures as a clue to VEXAS syndrome surprised me; I had not read that before.”
The study was supported by the Intramural Research Program of NIAMS. One of the study authors reported personal fees from Alexion, Novartis, and Sobi outside of the submitted work. No other disclosures were reported. Dr. Ko reported having no disclosures.
A version of this article appeared on Medscape.com .
FROM JAMA DERMATOLOGY
Hidradenitis Suppurativa: Clinical Outcomes for Bimekizumab Positive in Phase 3 Studies
TOPLINE:
, in two phase 3 studies.
METHODOLOGY:
- To assess the efficacy and safety of bimekizumab, an interleukin (IL)-17A and IL-17F antagonist, 320 mg for HS, researchers conducted two 48-week phase 3 trials BE HEARD I (n = 505) and II (n = 509), which enrolled patients with moderate to severe HS and a history of inadequate response to systemic antibiotics.
- Patients were randomly assigned to one of four groups: Bimekizumab every 2 weeks, bimekizumab every 2 weeks for 16 weeks followed by every 4 weeks of dosing, bimekizumab every 4 weeks, or placebo for 16 weeks followed by bimekizumab every 2 weeks.
- The primary outcome was an HS clinical response of at least 50% (HiSCR50) at week 16, defined as at least a 50% reduction in total abscess and inflammatory nodule count.
TAKEAWAY:
- A higher proportion of patients receiving bimekizumab every 2 weeks vs placebo achieved an HiSCR50 response at week 16 in BE HEARD I (48% vs 29%; odds ratio [OR], 2.23; P = .006) and II (52% vs 32%; OR, 2.29; P = .0032) trials.
- Patients receiving bimekizumab every 4 weeks also achieved a higher HiSCR50 response at week 16 vs placebo in the BE HEARD II trial (54% vs 32%; OR, 2.42; P = .0038).
- At week 16, a higher proportion of patients receiving bimekizumab every 2 weeks vs placebo achieved at least a 75% HiSCR (HiSCR75) in both trials, and a higher proportion of those receiving bimekizumab every 4 weeks achieved HiSCR75 in the BE HEARD II trial.
- At week 48, 45%-68% of patients achieved HiSCR50 in both trials.
- Patients who received bimekizumab vs placebo for the initial 16 weeks had greater improvements in patient-reported outcomes, and bimekizumab was well tolerated with a low number of serious or severe treatment-emergent adverse events.
IN PRACTICE:
“Bimekizumab was well tolerated by patients with hidradenitis suppurativa and produced rapid and deep clinically meaningful responses that were maintained up to 48 weeks,” the authors wrote. “These data support the use of bimekizumab as a promising new therapeutic option for patients with moderate to severe hidradenitis suppurativa.”
SOURCE:
Alexa B. Kimball, MD, MPH, from Beth Israel Deaconess Medical Center and Harvard Medical School, Boston, led this study, which was published online in The Lancet.
LIMITATIONS:
The placebo-controlled part of this trial was relatively short at 16 weeks and may affect the interpretation of later efficacy data, there was a lack of an active comparator group, and the efficacy of treatment was evaluated in the presence of rescue treatment with systemic antibiotics.
DISCLOSURES:
The studies were funded by bimekizumab manufacturer UCB Pharma. Seven authors disclosed being current or former employees of UCB Pharma. Other authors reported several ties with many companies, including UCB Pharma.
A version of this article first appeared on Medscape.com.
TOPLINE:
, in two phase 3 studies.
METHODOLOGY:
- To assess the efficacy and safety of bimekizumab, an interleukin (IL)-17A and IL-17F antagonist, 320 mg for HS, researchers conducted two 48-week phase 3 trials BE HEARD I (n = 505) and II (n = 509), which enrolled patients with moderate to severe HS and a history of inadequate response to systemic antibiotics.
- Patients were randomly assigned to one of four groups: Bimekizumab every 2 weeks, bimekizumab every 2 weeks for 16 weeks followed by every 4 weeks of dosing, bimekizumab every 4 weeks, or placebo for 16 weeks followed by bimekizumab every 2 weeks.
- The primary outcome was an HS clinical response of at least 50% (HiSCR50) at week 16, defined as at least a 50% reduction in total abscess and inflammatory nodule count.
TAKEAWAY:
- A higher proportion of patients receiving bimekizumab every 2 weeks vs placebo achieved an HiSCR50 response at week 16 in BE HEARD I (48% vs 29%; odds ratio [OR], 2.23; P = .006) and II (52% vs 32%; OR, 2.29; P = .0032) trials.
- Patients receiving bimekizumab every 4 weeks also achieved a higher HiSCR50 response at week 16 vs placebo in the BE HEARD II trial (54% vs 32%; OR, 2.42; P = .0038).
- At week 16, a higher proportion of patients receiving bimekizumab every 2 weeks vs placebo achieved at least a 75% HiSCR (HiSCR75) in both trials, and a higher proportion of those receiving bimekizumab every 4 weeks achieved HiSCR75 in the BE HEARD II trial.
- At week 48, 45%-68% of patients achieved HiSCR50 in both trials.
- Patients who received bimekizumab vs placebo for the initial 16 weeks had greater improvements in patient-reported outcomes, and bimekizumab was well tolerated with a low number of serious or severe treatment-emergent adverse events.
IN PRACTICE:
“Bimekizumab was well tolerated by patients with hidradenitis suppurativa and produced rapid and deep clinically meaningful responses that were maintained up to 48 weeks,” the authors wrote. “These data support the use of bimekizumab as a promising new therapeutic option for patients with moderate to severe hidradenitis suppurativa.”
SOURCE:
Alexa B. Kimball, MD, MPH, from Beth Israel Deaconess Medical Center and Harvard Medical School, Boston, led this study, which was published online in The Lancet.
LIMITATIONS:
The placebo-controlled part of this trial was relatively short at 16 weeks and may affect the interpretation of later efficacy data, there was a lack of an active comparator group, and the efficacy of treatment was evaluated in the presence of rescue treatment with systemic antibiotics.
DISCLOSURES:
The studies were funded by bimekizumab manufacturer UCB Pharma. Seven authors disclosed being current or former employees of UCB Pharma. Other authors reported several ties with many companies, including UCB Pharma.
A version of this article first appeared on Medscape.com.
TOPLINE:
, in two phase 3 studies.
METHODOLOGY:
- To assess the efficacy and safety of bimekizumab, an interleukin (IL)-17A and IL-17F antagonist, 320 mg for HS, researchers conducted two 48-week phase 3 trials BE HEARD I (n = 505) and II (n = 509), which enrolled patients with moderate to severe HS and a history of inadequate response to systemic antibiotics.
- Patients were randomly assigned to one of four groups: Bimekizumab every 2 weeks, bimekizumab every 2 weeks for 16 weeks followed by every 4 weeks of dosing, bimekizumab every 4 weeks, or placebo for 16 weeks followed by bimekizumab every 2 weeks.
- The primary outcome was an HS clinical response of at least 50% (HiSCR50) at week 16, defined as at least a 50% reduction in total abscess and inflammatory nodule count.
TAKEAWAY:
- A higher proportion of patients receiving bimekizumab every 2 weeks vs placebo achieved an HiSCR50 response at week 16 in BE HEARD I (48% vs 29%; odds ratio [OR], 2.23; P = .006) and II (52% vs 32%; OR, 2.29; P = .0032) trials.
- Patients receiving bimekizumab every 4 weeks also achieved a higher HiSCR50 response at week 16 vs placebo in the BE HEARD II trial (54% vs 32%; OR, 2.42; P = .0038).
- At week 16, a higher proportion of patients receiving bimekizumab every 2 weeks vs placebo achieved at least a 75% HiSCR (HiSCR75) in both trials, and a higher proportion of those receiving bimekizumab every 4 weeks achieved HiSCR75 in the BE HEARD II trial.
- At week 48, 45%-68% of patients achieved HiSCR50 in both trials.
- Patients who received bimekizumab vs placebo for the initial 16 weeks had greater improvements in patient-reported outcomes, and bimekizumab was well tolerated with a low number of serious or severe treatment-emergent adverse events.
IN PRACTICE:
“Bimekizumab was well tolerated by patients with hidradenitis suppurativa and produced rapid and deep clinically meaningful responses that were maintained up to 48 weeks,” the authors wrote. “These data support the use of bimekizumab as a promising new therapeutic option for patients with moderate to severe hidradenitis suppurativa.”
SOURCE:
Alexa B. Kimball, MD, MPH, from Beth Israel Deaconess Medical Center and Harvard Medical School, Boston, led this study, which was published online in The Lancet.
LIMITATIONS:
The placebo-controlled part of this trial was relatively short at 16 weeks and may affect the interpretation of later efficacy data, there was a lack of an active comparator group, and the efficacy of treatment was evaluated in the presence of rescue treatment with systemic antibiotics.
DISCLOSURES:
The studies were funded by bimekizumab manufacturer UCB Pharma. Seven authors disclosed being current or former employees of UCB Pharma. Other authors reported several ties with many companies, including UCB Pharma.
A version of this article first appeared on Medscape.com.
Treatments for Early HS Range From Topical Therapies to Laser Hair Removal
This can be challenging because to date, no Food and Drug Administration–approved treatments exist for early-stage HS and only two biologics exist for moderate to severe disease.
“For someone with occasional nodules and abscesses, we often use antibiotics and topical antiseptics,” Christopher Sayed, MD, a dermatologist at the HS and Follicular Disorders Clinic at the University of North Carolina, Chapel Hill, told this news organization. “We may use these daily for weeks or months or just provide them to use for 1-2 weeks at a time for intermittent flares if a patient doesn’t want to take a pill every day,” he said. “For women, hormonal options like oral contraceptive pills and spironolactone can be a great option” if they don’t mind taking a daily pill.
Topical options that Jennifer L. Hsiao, MD, reaches for in her role as director of the HS clinic at the University of Southern California, Los Angeles, include chlorhexidine wash, topical clindamycin, and topical resorcinol. Systemic medications include oral antibiotics such as doxycycline or clindamycin, while hormonal options include oral contraceptives and/or spironolactone for women and finasteride for men.
Laser hair removal for both men and women can also help treat lesions and abscesses in the groin and axillae, since reducing hair follicles tends to result in fewer follicles that become inflamed and form nodules and abscesses over time, “but it requires multiple visits and not all patients have access to it,” Dr. Sayed said. “Once patients start to develop tunnels or scars or fail to respond to some of these other treatments, I am quick to open the conversation on biologics to help avoid progression and long-term need for surgery.”
Metformin Among Options to Consider
According to Dr. Hsiao, other treatment options to consider trying in patients with mild HS include metformin, “especially in patients who also have prediabetes, PCOS, or obesity;” isotretinoin if the patient has concomitant severe acne; botulinum toxin injections; apremilast or topical roflumilast, and antihyperhidrosis medications such as prescription aluminum chloride topicals, glycopyrronium wipes, and glycopyrrolate.
Recommending lifestyle modifications such as smoking cessation and weight loss for patients diagnosed with early-stage HS is “challenging,” Dr. Sayed said, “because the evidence on different triggers and lifestyle modifications isn’t very strong. There can also be a lot of stigmas around weight and smoking in HS, and it can alienate patients to go straight to these topics in the first visit.”

Many patients also ask what dietary changes they can make to improve their HS. “The most common things patients tend to bring up are dairy avoidance and reducing carbohydrates,” he said. “Supplements like zinc and turmeric are also frequently brought up by patients and some find them helpful. Once rapport is built, I may discuss smoking cessation as potentially helping prevent as much activity over time or weight loss as possibly helping improve response to treatments, but I don’t promise that these things always help since modifying them doesn’t always lead to improvement.”
Dr. Hsiao noted that existing research suggests that following a Mediterranean diet may benefit HS symptoms.
Early Data on Ruxolitinib Cream Promising
At the 2024 annual meeting of the American Academy of Dermatology, researchers reported on the results of a phase 2 study, which found that topical 1.5% ruxolitinib, a Janus kinase (JAK) inhibitor (currently FDA-approved for atopic dermatitis) was effective in reducing abscess and inflammatory nodule count in patients with mild HS. “There is a major need for this kind of option, and the early results are promising,” said Dr. Sayed, who was not involved with the study. “It’s very difficult to get this covered for patients currently since it is off label for HS. We’ve gotten it for a few patients, and one has really liked it, but it’s unclear how consistent the others were with their use, and their level of improvement was not clear to me.”
For mild HS, he added, “the most important area in which we’ve seen growing evidence is around hair removal lasers such as Nd:YAG and alexandrite lasers. Improving access for patients is a major priority in the coming years.”
According to Dr. Hsiao, other approaches being studied for treating mild HS include a topical aryl hydrocarbon receptor agonist known as AT193, and oral medications, such as phosphodiesterase-4 inhibitors. Laser therapies are also being studied, “such as fractional ablative CO2 laser therapy combined with topical triamcinolone,” she said. “However, the majority of ongoing HS trials are for moderate to severe disease, so there is certainly a need for more investigation into mild HS treatment approaches.”
Dr. Sayed disclosed that he is secretary of the HS Foundation and a member of the European HS Foundation. He has served as a consultant for AbbVie, Alumis, AstraZeneca, Incyte, InflaRx, Novartis, Sanofi, Sonoma Biotherapeutics, and UCB; as a speaker for AbbVie, Novartis, and UCB; and as an investigator for Chemocentryx, Incyte, InflaRx, Novartis, and UCB. Dr. Hsiao disclosed that she is a member of the board of directors for the HS Foundation and has served as a consultant for AbbVie, Aclaris, Boehringer Ingelheim, Incyte, Novartis, and UCB; as a speaker for AbbVie, Novartis, Sanofi Regeneron, and UCB; and as an investigator for Amgen, Boehringer Ingelheim, and Incyte.
A version of this article first appeared on Medscape.com.
This can be challenging because to date, no Food and Drug Administration–approved treatments exist for early-stage HS and only two biologics exist for moderate to severe disease.
“For someone with occasional nodules and abscesses, we often use antibiotics and topical antiseptics,” Christopher Sayed, MD, a dermatologist at the HS and Follicular Disorders Clinic at the University of North Carolina, Chapel Hill, told this news organization. “We may use these daily for weeks or months or just provide them to use for 1-2 weeks at a time for intermittent flares if a patient doesn’t want to take a pill every day,” he said. “For women, hormonal options like oral contraceptive pills and spironolactone can be a great option” if they don’t mind taking a daily pill.
Topical options that Jennifer L. Hsiao, MD, reaches for in her role as director of the HS clinic at the University of Southern California, Los Angeles, include chlorhexidine wash, topical clindamycin, and topical resorcinol. Systemic medications include oral antibiotics such as doxycycline or clindamycin, while hormonal options include oral contraceptives and/or spironolactone for women and finasteride for men.
Laser hair removal for both men and women can also help treat lesions and abscesses in the groin and axillae, since reducing hair follicles tends to result in fewer follicles that become inflamed and form nodules and abscesses over time, “but it requires multiple visits and not all patients have access to it,” Dr. Sayed said. “Once patients start to develop tunnels or scars or fail to respond to some of these other treatments, I am quick to open the conversation on biologics to help avoid progression and long-term need for surgery.”
Metformin Among Options to Consider
According to Dr. Hsiao, other treatment options to consider trying in patients with mild HS include metformin, “especially in patients who also have prediabetes, PCOS, or obesity;” isotretinoin if the patient has concomitant severe acne; botulinum toxin injections; apremilast or topical roflumilast, and antihyperhidrosis medications such as prescription aluminum chloride topicals, glycopyrronium wipes, and glycopyrrolate.
Recommending lifestyle modifications such as smoking cessation and weight loss for patients diagnosed with early-stage HS is “challenging,” Dr. Sayed said, “because the evidence on different triggers and lifestyle modifications isn’t very strong. There can also be a lot of stigmas around weight and smoking in HS, and it can alienate patients to go straight to these topics in the first visit.”
Many patients also ask what dietary changes they can make to improve their HS. “The most common things patients tend to bring up are dairy avoidance and reducing carbohydrates,” he said. “Supplements like zinc and turmeric are also frequently brought up by patients and some find them helpful. Once rapport is built, I may discuss smoking cessation as potentially helping prevent as much activity over time or weight loss as possibly helping improve response to treatments, but I don’t promise that these things always help since modifying them doesn’t always lead to improvement.”
Dr. Hsiao noted that existing research suggests that following a Mediterranean diet may benefit HS symptoms.
Early Data on Ruxolitinib Cream Promising
At the 2024 annual meeting of the American Academy of Dermatology, researchers reported on the results of a phase 2 study, which found that topical 1.5% ruxolitinib, a Janus kinase (JAK) inhibitor (currently FDA-approved for atopic dermatitis) was effective in reducing abscess and inflammatory nodule count in patients with mild HS. “There is a major need for this kind of option, and the early results are promising,” said Dr. Sayed, who was not involved with the study. “It’s very difficult to get this covered for patients currently since it is off label for HS. We’ve gotten it for a few patients, and one has really liked it, but it’s unclear how consistent the others were with their use, and their level of improvement was not clear to me.”
For mild HS, he added, “the most important area in which we’ve seen growing evidence is around hair removal lasers such as Nd:YAG and alexandrite lasers. Improving access for patients is a major priority in the coming years.”
According to Dr. Hsiao, other approaches being studied for treating mild HS include a topical aryl hydrocarbon receptor agonist known as AT193, and oral medications, such as phosphodiesterase-4 inhibitors. Laser therapies are also being studied, “such as fractional ablative CO2 laser therapy combined with topical triamcinolone,” she said. “However, the majority of ongoing HS trials are for moderate to severe disease, so there is certainly a need for more investigation into mild HS treatment approaches.”
Dr. Sayed disclosed that he is secretary of the HS Foundation and a member of the European HS Foundation. He has served as a consultant for AbbVie, Alumis, AstraZeneca, Incyte, InflaRx, Novartis, Sanofi, Sonoma Biotherapeutics, and UCB; as a speaker for AbbVie, Novartis, and UCB; and as an investigator for Chemocentryx, Incyte, InflaRx, Novartis, and UCB. Dr. Hsiao disclosed that she is a member of the board of directors for the HS Foundation and has served as a consultant for AbbVie, Aclaris, Boehringer Ingelheim, Incyte, Novartis, and UCB; as a speaker for AbbVie, Novartis, Sanofi Regeneron, and UCB; and as an investigator for Amgen, Boehringer Ingelheim, and Incyte.
A version of this article first appeared on Medscape.com.
This can be challenging because to date, no Food and Drug Administration–approved treatments exist for early-stage HS and only two biologics exist for moderate to severe disease.
“For someone with occasional nodules and abscesses, we often use antibiotics and topical antiseptics,” Christopher Sayed, MD, a dermatologist at the HS and Follicular Disorders Clinic at the University of North Carolina, Chapel Hill, told this news organization. “We may use these daily for weeks or months or just provide them to use for 1-2 weeks at a time for intermittent flares if a patient doesn’t want to take a pill every day,” he said. “For women, hormonal options like oral contraceptive pills and spironolactone can be a great option” if they don’t mind taking a daily pill.
Topical options that Jennifer L. Hsiao, MD, reaches for in her role as director of the HS clinic at the University of Southern California, Los Angeles, include chlorhexidine wash, topical clindamycin, and topical resorcinol. Systemic medications include oral antibiotics such as doxycycline or clindamycin, while hormonal options include oral contraceptives and/or spironolactone for women and finasteride for men.
Laser hair removal for both men and women can also help treat lesions and abscesses in the groin and axillae, since reducing hair follicles tends to result in fewer follicles that become inflamed and form nodules and abscesses over time, “but it requires multiple visits and not all patients have access to it,” Dr. Sayed said. “Once patients start to develop tunnels or scars or fail to respond to some of these other treatments, I am quick to open the conversation on biologics to help avoid progression and long-term need for surgery.”
Metformin Among Options to Consider
According to Dr. Hsiao, other treatment options to consider trying in patients with mild HS include metformin, “especially in patients who also have prediabetes, PCOS, or obesity;” isotretinoin if the patient has concomitant severe acne; botulinum toxin injections; apremilast or topical roflumilast, and antihyperhidrosis medications such as prescription aluminum chloride topicals, glycopyrronium wipes, and glycopyrrolate.
Recommending lifestyle modifications such as smoking cessation and weight loss for patients diagnosed with early-stage HS is “challenging,” Dr. Sayed said, “because the evidence on different triggers and lifestyle modifications isn’t very strong. There can also be a lot of stigmas around weight and smoking in HS, and it can alienate patients to go straight to these topics in the first visit.”
Many patients also ask what dietary changes they can make to improve their HS. “The most common things patients tend to bring up are dairy avoidance and reducing carbohydrates,” he said. “Supplements like zinc and turmeric are also frequently brought up by patients and some find them helpful. Once rapport is built, I may discuss smoking cessation as potentially helping prevent as much activity over time or weight loss as possibly helping improve response to treatments, but I don’t promise that these things always help since modifying them doesn’t always lead to improvement.”
Dr. Hsiao noted that existing research suggests that following a Mediterranean diet may benefit HS symptoms.
Early Data on Ruxolitinib Cream Promising
At the 2024 annual meeting of the American Academy of Dermatology, researchers reported on the results of a phase 2 study, which found that topical 1.5% ruxolitinib, a Janus kinase (JAK) inhibitor (currently FDA-approved for atopic dermatitis) was effective in reducing abscess and inflammatory nodule count in patients with mild HS. “There is a major need for this kind of option, and the early results are promising,” said Dr. Sayed, who was not involved with the study. “It’s very difficult to get this covered for patients currently since it is off label for HS. We’ve gotten it for a few patients, and one has really liked it, but it’s unclear how consistent the others were with their use, and their level of improvement was not clear to me.”
For mild HS, he added, “the most important area in which we’ve seen growing evidence is around hair removal lasers such as Nd:YAG and alexandrite lasers. Improving access for patients is a major priority in the coming years.”
According to Dr. Hsiao, other approaches being studied for treating mild HS include a topical aryl hydrocarbon receptor agonist known as AT193, and oral medications, such as phosphodiesterase-4 inhibitors. Laser therapies are also being studied, “such as fractional ablative CO2 laser therapy combined with topical triamcinolone,” she said. “However, the majority of ongoing HS trials are for moderate to severe disease, so there is certainly a need for more investigation into mild HS treatment approaches.”
Dr. Sayed disclosed that he is secretary of the HS Foundation and a member of the European HS Foundation. He has served as a consultant for AbbVie, Alumis, AstraZeneca, Incyte, InflaRx, Novartis, Sanofi, Sonoma Biotherapeutics, and UCB; as a speaker for AbbVie, Novartis, and UCB; and as an investigator for Chemocentryx, Incyte, InflaRx, Novartis, and UCB. Dr. Hsiao disclosed that she is a member of the board of directors for the HS Foundation and has served as a consultant for AbbVie, Aclaris, Boehringer Ingelheim, Incyte, Novartis, and UCB; as a speaker for AbbVie, Novartis, Sanofi Regeneron, and UCB; and as an investigator for Amgen, Boehringer Ingelheim, and Incyte.
A version of this article first appeared on Medscape.com.
Diagnosing Mild Hidradenitis Suppurativa: Early Stage Can Mimic Other Diseases
, such as an infection, folliculitis, and acne.
According to 2019 guidelines from the United States and Canadian hidradenitis suppurativa foundations, the diagnostic criteria for HS in general are the presence of typical lesions such as abscesses, nodules, and tunnels in classic locations such as underarms, groins, and buttocks that recur over the course of at least 6 months. “There is no need for additional testing or imaging to make the diagnosis,” said Dr. Sayed, co-chair of the 2019 guidelines work group, who sees patients at the HS and Follicular Disorders Clinic at the University of North Carolina, Chapel Hill. “In many ways, the diagnosis should be very simple since the presentation is classic in most cases, though it can be confusing in the first 6 months or so.”

Persistence, Recurrence Major Clues
Prior to being diagnosed with Hurley stage I HS — characterized by recurrent nodules and abscesses with minimal scars, according to the guidelines — most people figure they’ve been getting recurrent Staphylococcus aureus infections or are having trouble with ingrown hairs from shaving, he continued. They may also say they get “boils” without an understanding of what has been causing them.
“Early HS can mimic an intense folliculitis or furuncles that can sometimes be caused by Staphylococcus infections, but the history of persistence or recurrence for months, despite treatment that should cover something like a Staph infection is a major clue,” Dr. Sayed said. “Thanks to improved resources on the internet, more patients, compared to several years ago, come in asking about HS after they’ve done their own research. As public awareness improves, hopefully this trend will grow, and patients will be diagnosed and treated earlier.” Family history is also a strong predictor of HS, since about half of patients have first-degree relatives who have a history of HS, he noted.

Clinicians can use the Hurley staging system to characterize the extent of disease and the Dermatology Life Quality Index to measure the impact of HS on quality of life. “We perform these assessments in our specialty clinic at each visit, but they are not necessary for diagnosis,” Dr. Sayed told this news organization.
The ‘2-2-6 Rule’
When she sees a patient who might have HS, Jennifer L. Hsiao, MD, a dermatologist who directs the HS clinic at the University of Southern California, Los Angeles, follows the “2-2-6 rule,” which involves asking patients if they have had 2 episodes of 2 or more abscesses in 6 months. “If the patient answers yes, there’s a high likelihood that person has HS,” she said.
Hurley stage I HS is defined as nodules and abscesses without sinus tracts (tunnels) or scarring. But in Dr. Hsiao’s opinion, the Hurley staging system “is not the best way to characterize disease activity” because some patients meet criteria for Hurley stage I disease, meaning they do not have any scars or sinus tracts/tunnels, “but they have high disease activity with several inflammatory nodules and large painful abscesses that are limiting their quality of life and ability to function.”

Most cases of early-stage HS can be diagnosed in a single clinic visit, but some patients may present with a limited history of disease. For example, they may report having only had one episode of an axillary abscess or one episode of a few folliculitis-like papules in the groin. “In the absence of other physical exam findings suggestive of HS, such as open or double-headed comedones in flexural regions, I tell the patient that it is too early to call their condition HS, and I recommend that if they have another episode to call the office for an appointment for evaluation,” Dr. Hsiao said in an interview.
“What sets HS apart from an isolated incidence of a Staphylococcus aureus furuncle is the history of recurrence,” she added. To better characterize HS disease severity, she uses the six-point HS Physician Global Assessment score, a scale from 0 to 5, which classifies a patient as having moderate HS if they have five or more inflammatory nodules, or one abscess and one or more inflammatory nodule(s), without the requirement of demonstrating a scar or tunnel on a physical exam.
To help guide management decisions, Dr. Hsiao also considers asking patients with early-stage HS the following questions:
- Do you have a primary care provider (PCP)? PCPs are important care partners for patients with HS doctor to help screen for the comorbidities associated with the condition.
- What seems to make your HS worse? This can help identify potential triggers to avoid.
- What other medical conditions do you have?
- How would you describe the impact HS has on your quality of life?
- For women: Does your HS get worse around your period? “This can help to identify a potential hormonal trigger,” she said. “If the patient answers ‘yes,’ I would strongly consider a combined oral contraceptive pill and/or spironolactone as part of the patient’s treatment regimen.”
‘Window of Opportunity’ to Intervene
According to Dr. Hsiao, there has been a paradigm shift in the approach to HS management that emphasizes a “window of opportunity,” where earlier initiation of appropriate long-term immunomodulator therapy is recommended to try to mitigate disease progression. The development of tunnels and scars is a telltale sign that permanent tissue destruction is occurring, and the patient’s HS is no longer mild.
Ideally, a conversation about adalimumab, a tumor necrosis factor inhibitor, and secukinumab, an interleukin-17A antagonist (the two currently Food and Drug Administration–approved medications for HS, for moderate to severe disease/Hurley stage II/III) will have already been started with patients prior to development of a high tunnel or scar burden, signs of later-stage disease.
“Medications like this have the potential to slow and prevent that progression and reduce the surgical burden patients face over time, which is a major priority,” Dr. Sayed said. He noted that while comfort level with managing HS can vary among clinicians, “I’d encourage dermatologists to stay engaged with these patients because our training in the medical and surgical management of complex diseases like this is unmatched among other specialties,” he said. “Education of colleagues in other specialties should also be a big priority, especially for those in urgent care, emergency medicine, surgery, and ob.gyn. who often encounter these patients and may be less familiar” with HS.
Besides the North American clinical management guidelines for HS, which are expected to be updated in the next 18-24 months, as well as comorbidity screening recommendations for HS published in 2022, another resource Dr. Sayed and Dr. Hsiao recommend is the HS Foundation website, which features a link to Continuing Medical Education video lectures. The foundation also hosts an annual Symposium on HS Advances. This year’s event is scheduled in November in Austin, Texas.
Dr. Sayed disclosed that he is secretary of the HS Foundation and a member of the European HS Foundation. He has served as a consultant for AbbVie, Alumis, AstraZeneca, Incyte, InflaRx, Novartis, Sanofi, Sonoma Biotherapeutics, and UCB; as a speaker for AbbVie, Novartis, and UCB; and as an investigator for Chemocentryx, Incyte, InflaRx, Novartis, and UCB. Dr. Hsiao disclosed that she is a member of the board of directors for the HS Foundation and has served as a consultant for AbbVie, Aclaris, Boehringer Ingelheim, Incyte, Novartis, and UCB; as a speaker for AbbVie, Novartis, Sanofi Regeneron, and UCB; and as an investigator for Amgen, Boehringer Ingelheim, and Incyte.
A version of this article first appeared on Medscape.com.
, such as an infection, folliculitis, and acne.
According to 2019 guidelines from the United States and Canadian hidradenitis suppurativa foundations, the diagnostic criteria for HS in general are the presence of typical lesions such as abscesses, nodules, and tunnels in classic locations such as underarms, groins, and buttocks that recur over the course of at least 6 months. “There is no need for additional testing or imaging to make the diagnosis,” said Dr. Sayed, co-chair of the 2019 guidelines work group, who sees patients at the HS and Follicular Disorders Clinic at the University of North Carolina, Chapel Hill. “In many ways, the diagnosis should be very simple since the presentation is classic in most cases, though it can be confusing in the first 6 months or so.”
Persistence, Recurrence Major Clues
Prior to being diagnosed with Hurley stage I HS — characterized by recurrent nodules and abscesses with minimal scars, according to the guidelines — most people figure they’ve been getting recurrent Staphylococcus aureus infections or are having trouble with ingrown hairs from shaving, he continued. They may also say they get “boils” without an understanding of what has been causing them.
“Early HS can mimic an intense folliculitis or furuncles that can sometimes be caused by Staphylococcus infections, but the history of persistence or recurrence for months, despite treatment that should cover something like a Staph infection is a major clue,” Dr. Sayed said. “Thanks to improved resources on the internet, more patients, compared to several years ago, come in asking about HS after they’ve done their own research. As public awareness improves, hopefully this trend will grow, and patients will be diagnosed and treated earlier.” Family history is also a strong predictor of HS, since about half of patients have first-degree relatives who have a history of HS, he noted.
Clinicians can use the Hurley staging system to characterize the extent of disease and the Dermatology Life Quality Index to measure the impact of HS on quality of life. “We perform these assessments in our specialty clinic at each visit, but they are not necessary for diagnosis,” Dr. Sayed told this news organization.
The ‘2-2-6 Rule’
When she sees a patient who might have HS, Jennifer L. Hsiao, MD, a dermatologist who directs the HS clinic at the University of Southern California, Los Angeles, follows the “2-2-6 rule,” which involves asking patients if they have had 2 episodes of 2 or more abscesses in 6 months. “If the patient answers yes, there’s a high likelihood that person has HS,” she said.
Hurley stage I HS is defined as nodules and abscesses without sinus tracts (tunnels) or scarring. But in Dr. Hsiao’s opinion, the Hurley staging system “is not the best way to characterize disease activity” because some patients meet criteria for Hurley stage I disease, meaning they do not have any scars or sinus tracts/tunnels, “but they have high disease activity with several inflammatory nodules and large painful abscesses that are limiting their quality of life and ability to function.”
Most cases of early-stage HS can be diagnosed in a single clinic visit, but some patients may present with a limited history of disease. For example, they may report having only had one episode of an axillary abscess or one episode of a few folliculitis-like papules in the groin. “In the absence of other physical exam findings suggestive of HS, such as open or double-headed comedones in flexural regions, I tell the patient that it is too early to call their condition HS, and I recommend that if they have another episode to call the office for an appointment for evaluation,” Dr. Hsiao said in an interview.
“What sets HS apart from an isolated incidence of a Staphylococcus aureus furuncle is the history of recurrence,” she added. To better characterize HS disease severity, she uses the six-point HS Physician Global Assessment score, a scale from 0 to 5, which classifies a patient as having moderate HS if they have five or more inflammatory nodules, or one abscess and one or more inflammatory nodule(s), without the requirement of demonstrating a scar or tunnel on a physical exam.
To help guide management decisions, Dr. Hsiao also considers asking patients with early-stage HS the following questions:
- Do you have a primary care provider (PCP)? PCPs are important care partners for patients with HS doctor to help screen for the comorbidities associated with the condition.
- What seems to make your HS worse? This can help identify potential triggers to avoid.
- What other medical conditions do you have?
- How would you describe the impact HS has on your quality of life?
- For women: Does your HS get worse around your period? “This can help to identify a potential hormonal trigger,” she said. “If the patient answers ‘yes,’ I would strongly consider a combined oral contraceptive pill and/or spironolactone as part of the patient’s treatment regimen.”
‘Window of Opportunity’ to Intervene
According to Dr. Hsiao, there has been a paradigm shift in the approach to HS management that emphasizes a “window of opportunity,” where earlier initiation of appropriate long-term immunomodulator therapy is recommended to try to mitigate disease progression. The development of tunnels and scars is a telltale sign that permanent tissue destruction is occurring, and the patient’s HS is no longer mild.
Ideally, a conversation about adalimumab, a tumor necrosis factor inhibitor, and secukinumab, an interleukin-17A antagonist (the two currently Food and Drug Administration–approved medications for HS, for moderate to severe disease/Hurley stage II/III) will have already been started with patients prior to development of a high tunnel or scar burden, signs of later-stage disease.
“Medications like this have the potential to slow and prevent that progression and reduce the surgical burden patients face over time, which is a major priority,” Dr. Sayed said. He noted that while comfort level with managing HS can vary among clinicians, “I’d encourage dermatologists to stay engaged with these patients because our training in the medical and surgical management of complex diseases like this is unmatched among other specialties,” he said. “Education of colleagues in other specialties should also be a big priority, especially for those in urgent care, emergency medicine, surgery, and ob.gyn. who often encounter these patients and may be less familiar” with HS.
Besides the North American clinical management guidelines for HS, which are expected to be updated in the next 18-24 months, as well as comorbidity screening recommendations for HS published in 2022, another resource Dr. Sayed and Dr. Hsiao recommend is the HS Foundation website, which features a link to Continuing Medical Education video lectures. The foundation also hosts an annual Symposium on HS Advances. This year’s event is scheduled in November in Austin, Texas.
Dr. Sayed disclosed that he is secretary of the HS Foundation and a member of the European HS Foundation. He has served as a consultant for AbbVie, Alumis, AstraZeneca, Incyte, InflaRx, Novartis, Sanofi, Sonoma Biotherapeutics, and UCB; as a speaker for AbbVie, Novartis, and UCB; and as an investigator for Chemocentryx, Incyte, InflaRx, Novartis, and UCB. Dr. Hsiao disclosed that she is a member of the board of directors for the HS Foundation and has served as a consultant for AbbVie, Aclaris, Boehringer Ingelheim, Incyte, Novartis, and UCB; as a speaker for AbbVie, Novartis, Sanofi Regeneron, and UCB; and as an investigator for Amgen, Boehringer Ingelheim, and Incyte.
A version of this article first appeared on Medscape.com.
, such as an infection, folliculitis, and acne.
According to 2019 guidelines from the United States and Canadian hidradenitis suppurativa foundations, the diagnostic criteria for HS in general are the presence of typical lesions such as abscesses, nodules, and tunnels in classic locations such as underarms, groins, and buttocks that recur over the course of at least 6 months. “There is no need for additional testing or imaging to make the diagnosis,” said Dr. Sayed, co-chair of the 2019 guidelines work group, who sees patients at the HS and Follicular Disorders Clinic at the University of North Carolina, Chapel Hill. “In many ways, the diagnosis should be very simple since the presentation is classic in most cases, though it can be confusing in the first 6 months or so.”
Persistence, Recurrence Major Clues
Prior to being diagnosed with Hurley stage I HS — characterized by recurrent nodules and abscesses with minimal scars, according to the guidelines — most people figure they’ve been getting recurrent Staphylococcus aureus infections or are having trouble with ingrown hairs from shaving, he continued. They may also say they get “boils” without an understanding of what has been causing them.
“Early HS can mimic an intense folliculitis or furuncles that can sometimes be caused by Staphylococcus infections, but the history of persistence or recurrence for months, despite treatment that should cover something like a Staph infection is a major clue,” Dr. Sayed said. “Thanks to improved resources on the internet, more patients, compared to several years ago, come in asking about HS after they’ve done their own research. As public awareness improves, hopefully this trend will grow, and patients will be diagnosed and treated earlier.” Family history is also a strong predictor of HS, since about half of patients have first-degree relatives who have a history of HS, he noted.
Clinicians can use the Hurley staging system to characterize the extent of disease and the Dermatology Life Quality Index to measure the impact of HS on quality of life. “We perform these assessments in our specialty clinic at each visit, but they are not necessary for diagnosis,” Dr. Sayed told this news organization.
The ‘2-2-6 Rule’
When she sees a patient who might have HS, Jennifer L. Hsiao, MD, a dermatologist who directs the HS clinic at the University of Southern California, Los Angeles, follows the “2-2-6 rule,” which involves asking patients if they have had 2 episodes of 2 or more abscesses in 6 months. “If the patient answers yes, there’s a high likelihood that person has HS,” she said.
Hurley stage I HS is defined as nodules and abscesses without sinus tracts (tunnels) or scarring. But in Dr. Hsiao’s opinion, the Hurley staging system “is not the best way to characterize disease activity” because some patients meet criteria for Hurley stage I disease, meaning they do not have any scars or sinus tracts/tunnels, “but they have high disease activity with several inflammatory nodules and large painful abscesses that are limiting their quality of life and ability to function.”
Most cases of early-stage HS can be diagnosed in a single clinic visit, but some patients may present with a limited history of disease. For example, they may report having only had one episode of an axillary abscess or one episode of a few folliculitis-like papules in the groin. “In the absence of other physical exam findings suggestive of HS, such as open or double-headed comedones in flexural regions, I tell the patient that it is too early to call their condition HS, and I recommend that if they have another episode to call the office for an appointment for evaluation,” Dr. Hsiao said in an interview.
“What sets HS apart from an isolated incidence of a Staphylococcus aureus furuncle is the history of recurrence,” she added. To better characterize HS disease severity, she uses the six-point HS Physician Global Assessment score, a scale from 0 to 5, which classifies a patient as having moderate HS if they have five or more inflammatory nodules, or one abscess and one or more inflammatory nodule(s), without the requirement of demonstrating a scar or tunnel on a physical exam.
To help guide management decisions, Dr. Hsiao also considers asking patients with early-stage HS the following questions:
- Do you have a primary care provider (PCP)? PCPs are important care partners for patients with HS doctor to help screen for the comorbidities associated with the condition.
- What seems to make your HS worse? This can help identify potential triggers to avoid.
- What other medical conditions do you have?
- How would you describe the impact HS has on your quality of life?
- For women: Does your HS get worse around your period? “This can help to identify a potential hormonal trigger,” she said. “If the patient answers ‘yes,’ I would strongly consider a combined oral contraceptive pill and/or spironolactone as part of the patient’s treatment regimen.”
‘Window of Opportunity’ to Intervene
According to Dr. Hsiao, there has been a paradigm shift in the approach to HS management that emphasizes a “window of opportunity,” where earlier initiation of appropriate long-term immunomodulator therapy is recommended to try to mitigate disease progression. The development of tunnels and scars is a telltale sign that permanent tissue destruction is occurring, and the patient’s HS is no longer mild.
Ideally, a conversation about adalimumab, a tumor necrosis factor inhibitor, and secukinumab, an interleukin-17A antagonist (the two currently Food and Drug Administration–approved medications for HS, for moderate to severe disease/Hurley stage II/III) will have already been started with patients prior to development of a high tunnel or scar burden, signs of later-stage disease.
“Medications like this have the potential to slow and prevent that progression and reduce the surgical burden patients face over time, which is a major priority,” Dr. Sayed said. He noted that while comfort level with managing HS can vary among clinicians, “I’d encourage dermatologists to stay engaged with these patients because our training in the medical and surgical management of complex diseases like this is unmatched among other specialties,” he said. “Education of colleagues in other specialties should also be a big priority, especially for those in urgent care, emergency medicine, surgery, and ob.gyn. who often encounter these patients and may be less familiar” with HS.
Besides the North American clinical management guidelines for HS, which are expected to be updated in the next 18-24 months, as well as comorbidity screening recommendations for HS published in 2022, another resource Dr. Sayed and Dr. Hsiao recommend is the HS Foundation website, which features a link to Continuing Medical Education video lectures. The foundation also hosts an annual Symposium on HS Advances. This year’s event is scheduled in November in Austin, Texas.
Dr. Sayed disclosed that he is secretary of the HS Foundation and a member of the European HS Foundation. He has served as a consultant for AbbVie, Alumis, AstraZeneca, Incyte, InflaRx, Novartis, Sanofi, Sonoma Biotherapeutics, and UCB; as a speaker for AbbVie, Novartis, and UCB; and as an investigator for Chemocentryx, Incyte, InflaRx, Novartis, and UCB. Dr. Hsiao disclosed that she is a member of the board of directors for the HS Foundation and has served as a consultant for AbbVie, Aclaris, Boehringer Ingelheim, Incyte, Novartis, and UCB; as a speaker for AbbVie, Novartis, Sanofi Regeneron, and UCB; and as an investigator for Amgen, Boehringer Ingelheim, and Incyte.
A version of this article first appeared on Medscape.com.
Global Analysis Identifies Drugs Associated With SJS-TEN in Children
TOPLINE:
METHODOLOGY:
- SJS and TEN are rare, life-threatening mucocutaneous reactions mainly associated with medications, but large pharmacovigilance studies of drugs associated with SJS-TEN in the pediatric population are still lacking.
- Using the WHO’s pharmacovigilance database (VigiBase) containing individual case safety reports from January 1967 to July 2022, researchers identified 7342 adverse drug reaction reports of SJS-TEN in children (younger than 18 years; median age, 9 years) in all six continents. Median onset was 5 days, and 3.2% were fatal.
- They analyzed drugs reported as suspected treatments, and for each molecule, they performed a case–non-case study to assess a potential pharmacovigilance signal by computing the information component (IC).
- A positive IC value suggested more frequent reporting of a specific drug-adverse reaction pair. A positive IC025, a traditional threshold for statistical signal detection, is suggestive of a potential pharmacovigilance signal.
TAKEAWAY:
- Overall, 165 drugs were associated with a diagnosis of SJS-TEN; antiepileptic and anti-infectious drugs were the most common drug classes represented.
- The five most frequently reported drugs were carbamazepine (11.7%), lamotrigine (10.6%), sulfamethoxazole-trimethoprim (9%), acetaminophen (8.4%), and phenytoin (6.6%). The five drugs with the highest IC025 were lamotrigine, carbamazepine, phenobarbital, phenytoin, and nimesulide.
- All antiepileptics, many antibiotic families, dapsone, antiretroviral drugs, some antifungal drugs, and nonsteroidal anti-inflammatory drugs were identified in reports, with penicillins the most frequently reported antibiotic family and sulfonamides having the strongest pharmacovigilance signal.
- Vaccines were not associated with significant signals.
IN PRACTICE:
The study provides an update on “the spectrum of drugs potentially associated with SJS-TEN in the pediatric population,” the authors concluded, and “underlines the importance of reporting to pharmacovigilance the suspicion of this severe side effect of drugs with the most precise and detailed clinical description possible.”
SOURCE:
The study, led by Pauline Bataille, MD, of the Department of Pediatric Dermatology, Hôpital Necker-Enfants Malades, Paris City University, France, was published online in the Journal of the European Academy of Dermatology and Venereology.
LIMITATIONS:
Limitations include the possibility that some cases could have had an infectious or idiopathic cause not related to a drug and the lack of detailed clinical data in the database.
DISCLOSURES:
This study did not receive any funding. The authors declared no conflict of interest.
A version of this article first appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- SJS and TEN are rare, life-threatening mucocutaneous reactions mainly associated with medications, but large pharmacovigilance studies of drugs associated with SJS-TEN in the pediatric population are still lacking.
- Using the WHO’s pharmacovigilance database (VigiBase) containing individual case safety reports from January 1967 to July 2022, researchers identified 7342 adverse drug reaction reports of SJS-TEN in children (younger than 18 years; median age, 9 years) in all six continents. Median onset was 5 days, and 3.2% were fatal.
- They analyzed drugs reported as suspected treatments, and for each molecule, they performed a case–non-case study to assess a potential pharmacovigilance signal by computing the information component (IC).
- A positive IC value suggested more frequent reporting of a specific drug-adverse reaction pair. A positive IC025, a traditional threshold for statistical signal detection, is suggestive of a potential pharmacovigilance signal.
TAKEAWAY:
- Overall, 165 drugs were associated with a diagnosis of SJS-TEN; antiepileptic and anti-infectious drugs were the most common drug classes represented.
- The five most frequently reported drugs were carbamazepine (11.7%), lamotrigine (10.6%), sulfamethoxazole-trimethoprim (9%), acetaminophen (8.4%), and phenytoin (6.6%). The five drugs with the highest IC025 were lamotrigine, carbamazepine, phenobarbital, phenytoin, and nimesulide.
- All antiepileptics, many antibiotic families, dapsone, antiretroviral drugs, some antifungal drugs, and nonsteroidal anti-inflammatory drugs were identified in reports, with penicillins the most frequently reported antibiotic family and sulfonamides having the strongest pharmacovigilance signal.
- Vaccines were not associated with significant signals.
IN PRACTICE:
The study provides an update on “the spectrum of drugs potentially associated with SJS-TEN in the pediatric population,” the authors concluded, and “underlines the importance of reporting to pharmacovigilance the suspicion of this severe side effect of drugs with the most precise and detailed clinical description possible.”
SOURCE:
The study, led by Pauline Bataille, MD, of the Department of Pediatric Dermatology, Hôpital Necker-Enfants Malades, Paris City University, France, was published online in the Journal of the European Academy of Dermatology and Venereology.
LIMITATIONS:
Limitations include the possibility that some cases could have had an infectious or idiopathic cause not related to a drug and the lack of detailed clinical data in the database.
DISCLOSURES:
This study did not receive any funding. The authors declared no conflict of interest.
A version of this article first appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- SJS and TEN are rare, life-threatening mucocutaneous reactions mainly associated with medications, but large pharmacovigilance studies of drugs associated with SJS-TEN in the pediatric population are still lacking.
- Using the WHO’s pharmacovigilance database (VigiBase) containing individual case safety reports from January 1967 to July 2022, researchers identified 7342 adverse drug reaction reports of SJS-TEN in children (younger than 18 years; median age, 9 years) in all six continents. Median onset was 5 days, and 3.2% were fatal.
- They analyzed drugs reported as suspected treatments, and for each molecule, they performed a case–non-case study to assess a potential pharmacovigilance signal by computing the information component (IC).
- A positive IC value suggested more frequent reporting of a specific drug-adverse reaction pair. A positive IC025, a traditional threshold for statistical signal detection, is suggestive of a potential pharmacovigilance signal.
TAKEAWAY:
- Overall, 165 drugs were associated with a diagnosis of SJS-TEN; antiepileptic and anti-infectious drugs were the most common drug classes represented.
- The five most frequently reported drugs were carbamazepine (11.7%), lamotrigine (10.6%), sulfamethoxazole-trimethoprim (9%), acetaminophen (8.4%), and phenytoin (6.6%). The five drugs with the highest IC025 were lamotrigine, carbamazepine, phenobarbital, phenytoin, and nimesulide.
- All antiepileptics, many antibiotic families, dapsone, antiretroviral drugs, some antifungal drugs, and nonsteroidal anti-inflammatory drugs were identified in reports, with penicillins the most frequently reported antibiotic family and sulfonamides having the strongest pharmacovigilance signal.
- Vaccines were not associated with significant signals.
IN PRACTICE:
The study provides an update on “the spectrum of drugs potentially associated with SJS-TEN in the pediatric population,” the authors concluded, and “underlines the importance of reporting to pharmacovigilance the suspicion of this severe side effect of drugs with the most precise and detailed clinical description possible.”
SOURCE:
The study, led by Pauline Bataille, MD, of the Department of Pediatric Dermatology, Hôpital Necker-Enfants Malades, Paris City University, France, was published online in the Journal of the European Academy of Dermatology and Venereology.
LIMITATIONS:
Limitations include the possibility that some cases could have had an infectious or idiopathic cause not related to a drug and the lack of detailed clinical data in the database.
DISCLOSURES:
This study did not receive any funding. The authors declared no conflict of interest.
A version of this article first appeared on Medscape.com.
Aquagenic Wrinkling Among Skin-Related Signs of Cystic Fibrosis
TOPLINE:
METHODOLOGY:
- Patients with CF, caused by a mutation in the CF Transmembrane Conductance Regulator (CFTR) gene, can develop diverse dermatologic manifestations.
- Researchers reviewed the literature and provided their own clinical experience regarding dermatologic manifestations of CF.
- They also reviewed the cutaneous side effects of CFTR modulators and antibiotics used to treat CF.
TAKEAWAY:
- Aquagenic wrinkling of the palm is common in individuals with CF, affecting up to 80% of patients (and 25% of CF gene carriers), and can be an early manifestation of CF. Treatments include topical medications (such as aluminum chloride, corticosteroids, and salicylic acid), botulinum toxin injections, and recently, CFTR-modulating treatments.
- CF nutrient deficiency dermatitis, often in a diaper distribution, usually appears in infancy and, before newborn screening was available, was sometimes the first sign of CF in some cases. It usually resolves with an adequate diet, pancreatic enzymes, and/or nutritional supplements. Zinc and essential fatty acid deficiencies can lead to acrodermatitis enteropathica–like symptoms and psoriasiform rashes, respectively.
- CF is also associated with vascular disorders, including cutaneous and, rarely, systemic vasculitis. Treatment includes topical and oral steroids and immune-modulating therapies.
- CFTR modulators, now the most common and highly effective treatment for CF, are associated with several skin reactions, which can be managed with treatments that include topical steroids and oral antihistamines. Frequent antibiotic treatment can also trigger skin reactions.
IN PRACTICE:
“Recognition and familiarity with dermatologic clinical manifestations of CF are important for multidisciplinary care” for patients with CF, the authors wrote, adding that “dermatology providers may play a significant role in the diagnosis and management of CF cutaneous comorbidities.”
SOURCE:
Aaron D. Smith, BS, from the University of Virginia (UVA) School of Medicine, Charlottesville, and coauthors were from the departments of dermatology and pulmonology/critical care medicine at UVA. The study was published online in the Journal of the American Academy of Dermatology.
LIMITATIONS:
The authors did not make a comment about the limitations of their review.
DISCLOSURES:
No funding was received for the review. The authors had no disclosures.
A version of this article first appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- Patients with CF, caused by a mutation in the CF Transmembrane Conductance Regulator (CFTR) gene, can develop diverse dermatologic manifestations.
- Researchers reviewed the literature and provided their own clinical experience regarding dermatologic manifestations of CF.
- They also reviewed the cutaneous side effects of CFTR modulators and antibiotics used to treat CF.
TAKEAWAY:
- Aquagenic wrinkling of the palm is common in individuals with CF, affecting up to 80% of patients (and 25% of CF gene carriers), and can be an early manifestation of CF. Treatments include topical medications (such as aluminum chloride, corticosteroids, and salicylic acid), botulinum toxin injections, and recently, CFTR-modulating treatments.
- CF nutrient deficiency dermatitis, often in a diaper distribution, usually appears in infancy and, before newborn screening was available, was sometimes the first sign of CF in some cases. It usually resolves with an adequate diet, pancreatic enzymes, and/or nutritional supplements. Zinc and essential fatty acid deficiencies can lead to acrodermatitis enteropathica–like symptoms and psoriasiform rashes, respectively.
- CF is also associated with vascular disorders, including cutaneous and, rarely, systemic vasculitis. Treatment includes topical and oral steroids and immune-modulating therapies.
- CFTR modulators, now the most common and highly effective treatment for CF, are associated with several skin reactions, which can be managed with treatments that include topical steroids and oral antihistamines. Frequent antibiotic treatment can also trigger skin reactions.
IN PRACTICE:
“Recognition and familiarity with dermatologic clinical manifestations of CF are important for multidisciplinary care” for patients with CF, the authors wrote, adding that “dermatology providers may play a significant role in the diagnosis and management of CF cutaneous comorbidities.”
SOURCE:
Aaron D. Smith, BS, from the University of Virginia (UVA) School of Medicine, Charlottesville, and coauthors were from the departments of dermatology and pulmonology/critical care medicine at UVA. The study was published online in the Journal of the American Academy of Dermatology.
LIMITATIONS:
The authors did not make a comment about the limitations of their review.
DISCLOSURES:
No funding was received for the review. The authors had no disclosures.
A version of this article first appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- Patients with CF, caused by a mutation in the CF Transmembrane Conductance Regulator (CFTR) gene, can develop diverse dermatologic manifestations.
- Researchers reviewed the literature and provided their own clinical experience regarding dermatologic manifestations of CF.
- They also reviewed the cutaneous side effects of CFTR modulators and antibiotics used to treat CF.
TAKEAWAY:
- Aquagenic wrinkling of the palm is common in individuals with CF, affecting up to 80% of patients (and 25% of CF gene carriers), and can be an early manifestation of CF. Treatments include topical medications (such as aluminum chloride, corticosteroids, and salicylic acid), botulinum toxin injections, and recently, CFTR-modulating treatments.
- CF nutrient deficiency dermatitis, often in a diaper distribution, usually appears in infancy and, before newborn screening was available, was sometimes the first sign of CF in some cases. It usually resolves with an adequate diet, pancreatic enzymes, and/or nutritional supplements. Zinc and essential fatty acid deficiencies can lead to acrodermatitis enteropathica–like symptoms and psoriasiform rashes, respectively.
- CF is also associated with vascular disorders, including cutaneous and, rarely, systemic vasculitis. Treatment includes topical and oral steroids and immune-modulating therapies.
- CFTR modulators, now the most common and highly effective treatment for CF, are associated with several skin reactions, which can be managed with treatments that include topical steroids and oral antihistamines. Frequent antibiotic treatment can also trigger skin reactions.
IN PRACTICE:
“Recognition and familiarity with dermatologic clinical manifestations of CF are important for multidisciplinary care” for patients with CF, the authors wrote, adding that “dermatology providers may play a significant role in the diagnosis and management of CF cutaneous comorbidities.”
SOURCE:
Aaron D. Smith, BS, from the University of Virginia (UVA) School of Medicine, Charlottesville, and coauthors were from the departments of dermatology and pulmonology/critical care medicine at UVA. The study was published online in the Journal of the American Academy of Dermatology.
LIMITATIONS:
The authors did not make a comment about the limitations of their review.
DISCLOSURES:
No funding was received for the review. The authors had no disclosures.
A version of this article first appeared on Medscape.com.
Study Evaluates CVD, Mortality Risks In Patients With Prurigo Nodularis
TOPLINE:
, particularly among women and White patients.
METHODOLOGY:
- Studies have shown increased risks for cardiovascular diseases in patients with PN, but limited sample sizes have hindered further subgroup analysis. Given PN’s pronounced sex and ethnicity skew, it is important to examine underrepresented groups to accurately assess their cardiovascular risk.
- In this propensity-score matched analysis, researchers identified 64,801 patients (59.44% women) with PN using electronic health reports from the Global Collaborative Network of TriNetX and matched to individuals without PN.
- Researchers calculated risks for 15 cardiovascular endpoints and all-cause mortality within 10 years of diagnosis. Major adverse cardiovascular events (MACE) included acute cerebral and myocardial infarction (MI), heart failure, ventricular arrhythmia, and sudden cardiac death.
TAKEAWAY:
- Patients with PN showed a higher risk for death (hazard ratio [HR], 1.1243) and MACE (HR, 1.117) (P < .0001 for both).
- PN was also associated with a higher risk for heart failure (HR, 1.062), thrombotic venous disease (HR, 1.26), angina pectoris (HR, 1.096), and peripheral arterial diseases (HR, 1.082) (P < .0001 for all) and for acute MI (HR, 1.11; P = .0015) and valve disorders (HR, 1.08; P = .0018).
- White patients with PN had a significantly increased risk for MACE, death, heart failure, cardiac arrest, vascular diseases, and acute MI, but this was not observed in people of color.
- Women exhibited a higher risk for MACE, heart failure, peripheral artery disease, acute MI, conduction disease, and valve disorders, while men did not have an increased risk for major or acute cardiovascular events. Both men and women had a higher risk for death, chronic ischemic heart disease, and venous disease.
IN PRACTICE:
“Although no novel PN-specific treatment rationale can be derived from the presented data, the potential risk of subsequent cardiovascular disease should be considered in the care of patients with PN, which includes screening and optimal management of other additional cardiovascular risk factors,” the authors wrote.
LIMITATIONS:
Retrospective observational design introduced inherent biases. Misdiagnosis or false coding in electronic health records could affect the data accuracy and ethnicity-specific analyses.
SOURCE:
This work, led by Henning Olbrich, from the Department of Dermatology, University of Lübeck, Germany, was published online in eBioMedicine.
DISCLOSURES:
The study was supported by the University of Lübeck, the Deutsche Forschungsgemeinschaft, and the State of Schleswig-Holstein. One author declared financial ties outside this work, and one author is an employee of TriNetX.
A version of this article appeared on Medscape.com.
TOPLINE:
, particularly among women and White patients.
METHODOLOGY:
- Studies have shown increased risks for cardiovascular diseases in patients with PN, but limited sample sizes have hindered further subgroup analysis. Given PN’s pronounced sex and ethnicity skew, it is important to examine underrepresented groups to accurately assess their cardiovascular risk.
- In this propensity-score matched analysis, researchers identified 64,801 patients (59.44% women) with PN using electronic health reports from the Global Collaborative Network of TriNetX and matched to individuals without PN.
- Researchers calculated risks for 15 cardiovascular endpoints and all-cause mortality within 10 years of diagnosis. Major adverse cardiovascular events (MACE) included acute cerebral and myocardial infarction (MI), heart failure, ventricular arrhythmia, and sudden cardiac death.
TAKEAWAY:
- Patients with PN showed a higher risk for death (hazard ratio [HR], 1.1243) and MACE (HR, 1.117) (P < .0001 for both).
- PN was also associated with a higher risk for heart failure (HR, 1.062), thrombotic venous disease (HR, 1.26), angina pectoris (HR, 1.096), and peripheral arterial diseases (HR, 1.082) (P < .0001 for all) and for acute MI (HR, 1.11; P = .0015) and valve disorders (HR, 1.08; P = .0018).
- White patients with PN had a significantly increased risk for MACE, death, heart failure, cardiac arrest, vascular diseases, and acute MI, but this was not observed in people of color.
- Women exhibited a higher risk for MACE, heart failure, peripheral artery disease, acute MI, conduction disease, and valve disorders, while men did not have an increased risk for major or acute cardiovascular events. Both men and women had a higher risk for death, chronic ischemic heart disease, and venous disease.
IN PRACTICE:
“Although no novel PN-specific treatment rationale can be derived from the presented data, the potential risk of subsequent cardiovascular disease should be considered in the care of patients with PN, which includes screening and optimal management of other additional cardiovascular risk factors,” the authors wrote.
LIMITATIONS:
Retrospective observational design introduced inherent biases. Misdiagnosis or false coding in electronic health records could affect the data accuracy and ethnicity-specific analyses.
SOURCE:
This work, led by Henning Olbrich, from the Department of Dermatology, University of Lübeck, Germany, was published online in eBioMedicine.
DISCLOSURES:
The study was supported by the University of Lübeck, the Deutsche Forschungsgemeinschaft, and the State of Schleswig-Holstein. One author declared financial ties outside this work, and one author is an employee of TriNetX.
A version of this article appeared on Medscape.com.
TOPLINE:
, particularly among women and White patients.
METHODOLOGY:
- Studies have shown increased risks for cardiovascular diseases in patients with PN, but limited sample sizes have hindered further subgroup analysis. Given PN’s pronounced sex and ethnicity skew, it is important to examine underrepresented groups to accurately assess their cardiovascular risk.
- In this propensity-score matched analysis, researchers identified 64,801 patients (59.44% women) with PN using electronic health reports from the Global Collaborative Network of TriNetX and matched to individuals without PN.
- Researchers calculated risks for 15 cardiovascular endpoints and all-cause mortality within 10 years of diagnosis. Major adverse cardiovascular events (MACE) included acute cerebral and myocardial infarction (MI), heart failure, ventricular arrhythmia, and sudden cardiac death.
TAKEAWAY:
- Patients with PN showed a higher risk for death (hazard ratio [HR], 1.1243) and MACE (HR, 1.117) (P < .0001 for both).
- PN was also associated with a higher risk for heart failure (HR, 1.062), thrombotic venous disease (HR, 1.26), angina pectoris (HR, 1.096), and peripheral arterial diseases (HR, 1.082) (P < .0001 for all) and for acute MI (HR, 1.11; P = .0015) and valve disorders (HR, 1.08; P = .0018).
- White patients with PN had a significantly increased risk for MACE, death, heart failure, cardiac arrest, vascular diseases, and acute MI, but this was not observed in people of color.
- Women exhibited a higher risk for MACE, heart failure, peripheral artery disease, acute MI, conduction disease, and valve disorders, while men did not have an increased risk for major or acute cardiovascular events. Both men and women had a higher risk for death, chronic ischemic heart disease, and venous disease.
IN PRACTICE:
“Although no novel PN-specific treatment rationale can be derived from the presented data, the potential risk of subsequent cardiovascular disease should be considered in the care of patients with PN, which includes screening and optimal management of other additional cardiovascular risk factors,” the authors wrote.
LIMITATIONS:
Retrospective observational design introduced inherent biases. Misdiagnosis or false coding in electronic health records could affect the data accuracy and ethnicity-specific analyses.
SOURCE:
This work, led by Henning Olbrich, from the Department of Dermatology, University of Lübeck, Germany, was published online in eBioMedicine.
DISCLOSURES:
The study was supported by the University of Lübeck, the Deutsche Forschungsgemeinschaft, and the State of Schleswig-Holstein. One author declared financial ties outside this work, and one author is an employee of TriNetX.
A version of this article appeared on Medscape.com.
Diabetic Foot Ulcers: Life-Threatening Issue in Need of Help
The photo of the patient’s foot, sent from his campsite, included a cheeky note: “I remember you telling me that getting in trouble doing something was better than getting in trouble doing nothing. This lets me get out there and know that I have feedback.”
The “this” was the patient’s “foot selfie,” an approach that allows patients at a risk for diabetic foot ulcers (DFUs) to snap a picture and send it to their healthcare providers for evaluation.
This particular patient had an extensive history of previous wounds. Some had essentially kept him house-bound in the past, as he was afraid to get another one.
This time, however, he got an all-clear to keep on camping, “and we scheduled him in on the following Tuesday [for follow-up],” said the camper’s physician David G. Armstrong, DPM, MD, PhD, professor of surgery and neurological surgery, USC Keck School of Medicine, Los Angeles.
Dr. Armstrong is one of the researchers evaluating the concept of foot selfies. It’s a welcome advance, he and others said, and has been shown to help heal wounds and reverse pre-ulcer lesions. Research on foot selfies continues, but much more is needed to solve the issue of DFUs, diabetic foot infections (DFIs), and the high rates of reinfection, experts know.
Worldwide, about 18.6 million people have a DFU each year, including 1.6 million in the United States. About 50%-60% of ulcers become infected, with 20% of moderate to severe infections requiring amputation of the limb. The 5-year mortality rate for DFUs is 30%, but it climbs to 70% after amputation. While about 40% of ulcers heal within 12 weeks, 42% recur at the 1-year mark, setting up a vicious and costly cycle. Healthcare costs for patients with diabetes and DFUs are five times as high as costs for patients with diabetes but no DFUs. The per capita cost to treat a DFU in America is $17,500.
While the statistics paint a grim picture, progress is being made on several fronts:
- US Food and Drug Administration (FDA) guidance on the development of drugs for DFUs, under evaluation, is forthcoming.
- New treatments are under study.
- A multidisciplinary team approach is known to improve outcomes.
Anatomy of a DFU
When neuropathy develops in those with diabetes, they no longer have what Dr. Armstrong calls the “gift” of pain perception. “They can wear a hole in their foot like you and I wear a hole in our sock or shoe,” he said. “That hole is called a diabetic foot ulcer.”
A DFU is an open wound on the foot, often occurring when bleeding develops beneath a callus and then the callus wears away. Deeper tissues of the foot are then exposed.
About half of the DFUs get infected, hence the FDA guidance, said Dr. Armstrong, who is also founding president of the American Limb Preservation Society, which aims to eliminate preventable amputations within the next generation. Every 20 seconds, Dr. Armstrong said, someone in the world loses a leg due to diabetes.
FDA Guidance on Drug Development for DFIs
In October, the FDA issued draft guidance for industry to articulate the design of clinical trials for developing antibacterial drugs to treat DFIs without concomitant bone and joint involvement. Comments closed on December 18. Among the points in the guidance, which is nonbinding, are to include DFIs of varying depths and extent in phase 3 trials and ideally to include only those patients who have not had prior antibacterial treatment for the current DFI.
According to an FDA spokesperson, “The agency is working to finalize the guidance. However, a timeline for its release has not yet been established.”
The good news about the upcoming FDA guidance, Dr. Armstrong said, is that the agency has realized the importance of treating the infections. Fully one third of direct costs of care for diabetes are spent on the lower extremities, he said. Keeping patients out of the hospital, uninfected, and “keeping legs on bodies” are all important goals, he said.
Pharmaceutical firms need to understand that “you aren’t dealing with a normal ulcer,” said Andrew J.M. Boulton, MD, professor of medicine at the University of Manchester and physician consultant at the Manchester Royal Infirmary, Manchester, England, and a visiting professor at the University of Miami. For research, “the most important thing is to take account of off-loading the ulcers,” he said. “Most ulcers will heal if put in a boot.”
Dr. Boulton, like Dr. Armstrong, a long-time expert in the field, contended that pharma has not understood this concept and has wasted millions over the last three decades doing studies that were poorly designed and controlled.
Treatments: Current, Under Study
Currently, DFIs are treated with antimicrobial therapy, without or without debridement, along with a clinical assessment for ischemia. If ischemia is found, care progresses to wound care and off-loading devices, such as healing sandals. Clinicians then assess the likelihood of improved outcomes with revascularization based on operative risks and distribution of lower extremity artery disease and proceed depending on the likelihood. If osteomyelitis testing shows it is present, providers proceed to wound debridement, limb-sparing amputation, and prolonged antimicrobials, as needed.
More options are needed, Dr. Armstrong said.
Among the many approaches under study:
- DFUs can be accurately detected by applying artificial intelligence to the “foot selfie” images taken by patients on smartphones, research by Dr. and has found.
- After a phase 3 study of for DFUs originally intending to enroll 300 subjects was discontinued because of slow patient recruitment, an interim analysis was conducted on 44 participants. It showed a positive trend toward wound closure in the group receiving the injected gene therapy, VM202 (ENGENSIS), in their calf muscles. VM202 is a plasmid DNA-encoding human hepatocyte growth factor. While those in both the intervention and placebo groups showed wound-closing effects at month 6, in 23 patients with neuro-ischemic ulcers, the percentage of those reaching complete closure of the DFU was significantly higher in the treated group at months 3, 4, and 5 (P = .0391, .0391, and .0361, respectively). After excluding two outliers, the difference in months 3-6 became more significant (P = .03).
- An closed more DFUs than standard care after 12 weeks — 70% vs 34% (P = .00032). Of the 100 participants randomized, 50 per group, 42% of the treatment group and 56% of the control group experienced adverse events, with eight withdrawn due to serious adverse events (such as osteomyelitis).
- A closed more refractory DFUs over a 16-week study than standard sharp debridement, with 65% of water-treated ulcers healed but just 42% of the standard care group (P = .021, unadjusted).
- Researchers from UC Davis and VA Northern California Healthcare are evaluating timolol, a beta adrenergic receptor blocker already approved for topical administration for glaucoma, as a way to heal chronic DFUs faster. After demonstrating that the medication worked in animal models, researchers then launched a study to use it off-label for DFUs. While data are still being analyzed, researcher Roslyn (Rivkah) Isseroff, MD, of UC Davis and VA, said that data so far demonstrate that the timolol reduced transepidermal water loss in the healed wounds, and that is linked with a decrease in re-ulceration.
The Power of a Team
Multidisciplinary approaches to treatment are effective in reducing amputation, with one review of 33 studies finding the approach worked to decrease amputation in 94% of them. “The American Limb Preservation Society (ALPS) lists 30 programs,” said Dr. Armstrong, the founding president of the organization. “There may be as many as 100.”
Team compositions vary but usually include at least one medical specialty clinician, such as infectious disease, primary care, or endocrinology, and two or more specialty clinicians, such as vascular, podiatric, orthopedic, or plastic surgery. A shoe specialist is needed to prescribe and manage footwear. Other important team members include nutrition experts and behavioral health professionals to deal with associated depression.
Johns Hopkins’ Multidisciplinary Diabetic Foot and Wound Service launched in 2012 and includes vascular surgeons, surgical podiatrists, endocrinologists, wound care nurses, advanced practice staff, board-certified wound care specialists, orthopedic surgeons, infection disease experts, physical therapists, and certified orthotists.
“This interdisciplinary care model has been repeatedly validated by research as superior for limb salvage and wound healing,” said Nestoras Mathioudakis, MD, codirector of the service. “For instance, endocrinologists and diabetes educators are crucial for managing uncontrolled diabetes — a key factor in infection and delayed wound healing. Similarly, vascular surgeons play a vital role in addressing peripheral arterial disease to improve blood flow to the affected area.”
“Diabetic foot ulcers might require prolonged periods of specialized care, including meticulous wound management and off-loading, overseen by surgical podiatrists and wound care experts,” he said. “In cases where infection is present, particularly with multidrug resistant organisms or when standard antibiotics are contraindicated, the insight of an infectious disease specialist is invaluable.”
While the makeup of teams varies from location to location, he said “the hallmark of effective teams is their ability to comprehensively manage glycemic control, foot wounds, vascular disease, and infections.”
The power of teams, Dr. Armstrong said, is very much evident after his weekly “foot selfie rounds” conducted Mondays at 7 AM, with an “all feet on deck” approach. “Not a week goes by when we don’t stop a hospitalization,” he said of the team evaluating the photos, due to detecting issues early, while still in the manageable state.
Teams can trump technology, Dr. Armstrong said. A team of just a primary care doctor and a podiatrist can make a significant reduction in amputations, he said, just by a “Knock your socks off” approach. He reminds primary care doctors that observing the feet of their patients with diabetes can go a long way to reducing DFUs and the hospitalizations and amputations that can result.
Dr. Mathioudakis and Dr. Isseroff reported no disclosures. Dr. Boulton consults for Urgo Medical, Nevro Corporation, and AOT, Inc. Dr. Armstrong reported receiving consulting fees from Podimetrics; Molnlycke; Cardiovascular Systems, Inc.; Endo Pharmaceuticals; and Averitas Pharma (GRT US).
A version of this article first appeared on Medscape.com.
The photo of the patient’s foot, sent from his campsite, included a cheeky note: “I remember you telling me that getting in trouble doing something was better than getting in trouble doing nothing. This lets me get out there and know that I have feedback.”
The “this” was the patient’s “foot selfie,” an approach that allows patients at a risk for diabetic foot ulcers (DFUs) to snap a picture and send it to their healthcare providers for evaluation.
This particular patient had an extensive history of previous wounds. Some had essentially kept him house-bound in the past, as he was afraid to get another one.
This time, however, he got an all-clear to keep on camping, “and we scheduled him in on the following Tuesday [for follow-up],” said the camper’s physician David G. Armstrong, DPM, MD, PhD, professor of surgery and neurological surgery, USC Keck School of Medicine, Los Angeles.
Dr. Armstrong is one of the researchers evaluating the concept of foot selfies. It’s a welcome advance, he and others said, and has been shown to help heal wounds and reverse pre-ulcer lesions. Research on foot selfies continues, but much more is needed to solve the issue of DFUs, diabetic foot infections (DFIs), and the high rates of reinfection, experts know.
Worldwide, about 18.6 million people have a DFU each year, including 1.6 million in the United States. About 50%-60% of ulcers become infected, with 20% of moderate to severe infections requiring amputation of the limb. The 5-year mortality rate for DFUs is 30%, but it climbs to 70% after amputation. While about 40% of ulcers heal within 12 weeks, 42% recur at the 1-year mark, setting up a vicious and costly cycle. Healthcare costs for patients with diabetes and DFUs are five times as high as costs for patients with diabetes but no DFUs. The per capita cost to treat a DFU in America is $17,500.
While the statistics paint a grim picture, progress is being made on several fronts:
- US Food and Drug Administration (FDA) guidance on the development of drugs for DFUs, under evaluation, is forthcoming.
- New treatments are under study.
- A multidisciplinary team approach is known to improve outcomes.
Anatomy of a DFU
When neuropathy develops in those with diabetes, they no longer have what Dr. Armstrong calls the “gift” of pain perception. “They can wear a hole in their foot like you and I wear a hole in our sock or shoe,” he said. “That hole is called a diabetic foot ulcer.”
A DFU is an open wound on the foot, often occurring when bleeding develops beneath a callus and then the callus wears away. Deeper tissues of the foot are then exposed.
About half of the DFUs get infected, hence the FDA guidance, said Dr. Armstrong, who is also founding president of the American Limb Preservation Society, which aims to eliminate preventable amputations within the next generation. Every 20 seconds, Dr. Armstrong said, someone in the world loses a leg due to diabetes.
FDA Guidance on Drug Development for DFIs
In October, the FDA issued draft guidance for industry to articulate the design of clinical trials for developing antibacterial drugs to treat DFIs without concomitant bone and joint involvement. Comments closed on December 18. Among the points in the guidance, which is nonbinding, are to include DFIs of varying depths and extent in phase 3 trials and ideally to include only those patients who have not had prior antibacterial treatment for the current DFI.
According to an FDA spokesperson, “The agency is working to finalize the guidance. However, a timeline for its release has not yet been established.”
The good news about the upcoming FDA guidance, Dr. Armstrong said, is that the agency has realized the importance of treating the infections. Fully one third of direct costs of care for diabetes are spent on the lower extremities, he said. Keeping patients out of the hospital, uninfected, and “keeping legs on bodies” are all important goals, he said.
Pharmaceutical firms need to understand that “you aren’t dealing with a normal ulcer,” said Andrew J.M. Boulton, MD, professor of medicine at the University of Manchester and physician consultant at the Manchester Royal Infirmary, Manchester, England, and a visiting professor at the University of Miami. For research, “the most important thing is to take account of off-loading the ulcers,” he said. “Most ulcers will heal if put in a boot.”
Dr. Boulton, like Dr. Armstrong, a long-time expert in the field, contended that pharma has not understood this concept and has wasted millions over the last three decades doing studies that were poorly designed and controlled.
Treatments: Current, Under Study
Currently, DFIs are treated with antimicrobial therapy, without or without debridement, along with a clinical assessment for ischemia. If ischemia is found, care progresses to wound care and off-loading devices, such as healing sandals. Clinicians then assess the likelihood of improved outcomes with revascularization based on operative risks and distribution of lower extremity artery disease and proceed depending on the likelihood. If osteomyelitis testing shows it is present, providers proceed to wound debridement, limb-sparing amputation, and prolonged antimicrobials, as needed.
More options are needed, Dr. Armstrong said.
Among the many approaches under study:
- DFUs can be accurately detected by applying artificial intelligence to the “foot selfie” images taken by patients on smartphones, research by Dr. and has found.
- After a phase 3 study of for DFUs originally intending to enroll 300 subjects was discontinued because of slow patient recruitment, an interim analysis was conducted on 44 participants. It showed a positive trend toward wound closure in the group receiving the injected gene therapy, VM202 (ENGENSIS), in their calf muscles. VM202 is a plasmid DNA-encoding human hepatocyte growth factor. While those in both the intervention and placebo groups showed wound-closing effects at month 6, in 23 patients with neuro-ischemic ulcers, the percentage of those reaching complete closure of the DFU was significantly higher in the treated group at months 3, 4, and 5 (P = .0391, .0391, and .0361, respectively). After excluding two outliers, the difference in months 3-6 became more significant (P = .03).
- An closed more DFUs than standard care after 12 weeks — 70% vs 34% (P = .00032). Of the 100 participants randomized, 50 per group, 42% of the treatment group and 56% of the control group experienced adverse events, with eight withdrawn due to serious adverse events (such as osteomyelitis).
- A closed more refractory DFUs over a 16-week study than standard sharp debridement, with 65% of water-treated ulcers healed but just 42% of the standard care group (P = .021, unadjusted).
- Researchers from UC Davis and VA Northern California Healthcare are evaluating timolol, a beta adrenergic receptor blocker already approved for topical administration for glaucoma, as a way to heal chronic DFUs faster. After demonstrating that the medication worked in animal models, researchers then launched a study to use it off-label for DFUs. While data are still being analyzed, researcher Roslyn (Rivkah) Isseroff, MD, of UC Davis and VA, said that data so far demonstrate that the timolol reduced transepidermal water loss in the healed wounds, and that is linked with a decrease in re-ulceration.
The Power of a Team
Multidisciplinary approaches to treatment are effective in reducing amputation, with one review of 33 studies finding the approach worked to decrease amputation in 94% of them. “The American Limb Preservation Society (ALPS) lists 30 programs,” said Dr. Armstrong, the founding president of the organization. “There may be as many as 100.”
Team compositions vary but usually include at least one medical specialty clinician, such as infectious disease, primary care, or endocrinology, and two or more specialty clinicians, such as vascular, podiatric, orthopedic, or plastic surgery. A shoe specialist is needed to prescribe and manage footwear. Other important team members include nutrition experts and behavioral health professionals to deal with associated depression.
Johns Hopkins’ Multidisciplinary Diabetic Foot and Wound Service launched in 2012 and includes vascular surgeons, surgical podiatrists, endocrinologists, wound care nurses, advanced practice staff, board-certified wound care specialists, orthopedic surgeons, infection disease experts, physical therapists, and certified orthotists.
“This interdisciplinary care model has been repeatedly validated by research as superior for limb salvage and wound healing,” said Nestoras Mathioudakis, MD, codirector of the service. “For instance, endocrinologists and diabetes educators are crucial for managing uncontrolled diabetes — a key factor in infection and delayed wound healing. Similarly, vascular surgeons play a vital role in addressing peripheral arterial disease to improve blood flow to the affected area.”
“Diabetic foot ulcers might require prolonged periods of specialized care, including meticulous wound management and off-loading, overseen by surgical podiatrists and wound care experts,” he said. “In cases where infection is present, particularly with multidrug resistant organisms or when standard antibiotics are contraindicated, the insight of an infectious disease specialist is invaluable.”
While the makeup of teams varies from location to location, he said “the hallmark of effective teams is their ability to comprehensively manage glycemic control, foot wounds, vascular disease, and infections.”
The power of teams, Dr. Armstrong said, is very much evident after his weekly “foot selfie rounds” conducted Mondays at 7 AM, with an “all feet on deck” approach. “Not a week goes by when we don’t stop a hospitalization,” he said of the team evaluating the photos, due to detecting issues early, while still in the manageable state.
Teams can trump technology, Dr. Armstrong said. A team of just a primary care doctor and a podiatrist can make a significant reduction in amputations, he said, just by a “Knock your socks off” approach. He reminds primary care doctors that observing the feet of their patients with diabetes can go a long way to reducing DFUs and the hospitalizations and amputations that can result.
Dr. Mathioudakis and Dr. Isseroff reported no disclosures. Dr. Boulton consults for Urgo Medical, Nevro Corporation, and AOT, Inc. Dr. Armstrong reported receiving consulting fees from Podimetrics; Molnlycke; Cardiovascular Systems, Inc.; Endo Pharmaceuticals; and Averitas Pharma (GRT US).
A version of this article first appeared on Medscape.com.
The photo of the patient’s foot, sent from his campsite, included a cheeky note: “I remember you telling me that getting in trouble doing something was better than getting in trouble doing nothing. This lets me get out there and know that I have feedback.”
The “this” was the patient’s “foot selfie,” an approach that allows patients at a risk for diabetic foot ulcers (DFUs) to snap a picture and send it to their healthcare providers for evaluation.
This particular patient had an extensive history of previous wounds. Some had essentially kept him house-bound in the past, as he was afraid to get another one.
This time, however, he got an all-clear to keep on camping, “and we scheduled him in on the following Tuesday [for follow-up],” said the camper’s physician David G. Armstrong, DPM, MD, PhD, professor of surgery and neurological surgery, USC Keck School of Medicine, Los Angeles.
Dr. Armstrong is one of the researchers evaluating the concept of foot selfies. It’s a welcome advance, he and others said, and has been shown to help heal wounds and reverse pre-ulcer lesions. Research on foot selfies continues, but much more is needed to solve the issue of DFUs, diabetic foot infections (DFIs), and the high rates of reinfection, experts know.
Worldwide, about 18.6 million people have a DFU each year, including 1.6 million in the United States. About 50%-60% of ulcers become infected, with 20% of moderate to severe infections requiring amputation of the limb. The 5-year mortality rate for DFUs is 30%, but it climbs to 70% after amputation. While about 40% of ulcers heal within 12 weeks, 42% recur at the 1-year mark, setting up a vicious and costly cycle. Healthcare costs for patients with diabetes and DFUs are five times as high as costs for patients with diabetes but no DFUs. The per capita cost to treat a DFU in America is $17,500.
While the statistics paint a grim picture, progress is being made on several fronts:
- US Food and Drug Administration (FDA) guidance on the development of drugs for DFUs, under evaluation, is forthcoming.
- New treatments are under study.
- A multidisciplinary team approach is known to improve outcomes.
Anatomy of a DFU
When neuropathy develops in those with diabetes, they no longer have what Dr. Armstrong calls the “gift” of pain perception. “They can wear a hole in their foot like you and I wear a hole in our sock or shoe,” he said. “That hole is called a diabetic foot ulcer.”
A DFU is an open wound on the foot, often occurring when bleeding develops beneath a callus and then the callus wears away. Deeper tissues of the foot are then exposed.
About half of the DFUs get infected, hence the FDA guidance, said Dr. Armstrong, who is also founding president of the American Limb Preservation Society, which aims to eliminate preventable amputations within the next generation. Every 20 seconds, Dr. Armstrong said, someone in the world loses a leg due to diabetes.
FDA Guidance on Drug Development for DFIs
In October, the FDA issued draft guidance for industry to articulate the design of clinical trials for developing antibacterial drugs to treat DFIs without concomitant bone and joint involvement. Comments closed on December 18. Among the points in the guidance, which is nonbinding, are to include DFIs of varying depths and extent in phase 3 trials and ideally to include only those patients who have not had prior antibacterial treatment for the current DFI.
According to an FDA spokesperson, “The agency is working to finalize the guidance. However, a timeline for its release has not yet been established.”
The good news about the upcoming FDA guidance, Dr. Armstrong said, is that the agency has realized the importance of treating the infections. Fully one third of direct costs of care for diabetes are spent on the lower extremities, he said. Keeping patients out of the hospital, uninfected, and “keeping legs on bodies” are all important goals, he said.
Pharmaceutical firms need to understand that “you aren’t dealing with a normal ulcer,” said Andrew J.M. Boulton, MD, professor of medicine at the University of Manchester and physician consultant at the Manchester Royal Infirmary, Manchester, England, and a visiting professor at the University of Miami. For research, “the most important thing is to take account of off-loading the ulcers,” he said. “Most ulcers will heal if put in a boot.”
Dr. Boulton, like Dr. Armstrong, a long-time expert in the field, contended that pharma has not understood this concept and has wasted millions over the last three decades doing studies that were poorly designed and controlled.
Treatments: Current, Under Study
Currently, DFIs are treated with antimicrobial therapy, without or without debridement, along with a clinical assessment for ischemia. If ischemia is found, care progresses to wound care and off-loading devices, such as healing sandals. Clinicians then assess the likelihood of improved outcomes with revascularization based on operative risks and distribution of lower extremity artery disease and proceed depending on the likelihood. If osteomyelitis testing shows it is present, providers proceed to wound debridement, limb-sparing amputation, and prolonged antimicrobials, as needed.
More options are needed, Dr. Armstrong said.
Among the many approaches under study:
- DFUs can be accurately detected by applying artificial intelligence to the “foot selfie” images taken by patients on smartphones, research by Dr. and has found.
- After a phase 3 study of for DFUs originally intending to enroll 300 subjects was discontinued because of slow patient recruitment, an interim analysis was conducted on 44 participants. It showed a positive trend toward wound closure in the group receiving the injected gene therapy, VM202 (ENGENSIS), in their calf muscles. VM202 is a plasmid DNA-encoding human hepatocyte growth factor. While those in both the intervention and placebo groups showed wound-closing effects at month 6, in 23 patients with neuro-ischemic ulcers, the percentage of those reaching complete closure of the DFU was significantly higher in the treated group at months 3, 4, and 5 (P = .0391, .0391, and .0361, respectively). After excluding two outliers, the difference in months 3-6 became more significant (P = .03).
- An closed more DFUs than standard care after 12 weeks — 70% vs 34% (P = .00032). Of the 100 participants randomized, 50 per group, 42% of the treatment group and 56% of the control group experienced adverse events, with eight withdrawn due to serious adverse events (such as osteomyelitis).
- A closed more refractory DFUs over a 16-week study than standard sharp debridement, with 65% of water-treated ulcers healed but just 42% of the standard care group (P = .021, unadjusted).
- Researchers from UC Davis and VA Northern California Healthcare are evaluating timolol, a beta adrenergic receptor blocker already approved for topical administration for glaucoma, as a way to heal chronic DFUs faster. After demonstrating that the medication worked in animal models, researchers then launched a study to use it off-label for DFUs. While data are still being analyzed, researcher Roslyn (Rivkah) Isseroff, MD, of UC Davis and VA, said that data so far demonstrate that the timolol reduced transepidermal water loss in the healed wounds, and that is linked with a decrease in re-ulceration.
The Power of a Team
Multidisciplinary approaches to treatment are effective in reducing amputation, with one review of 33 studies finding the approach worked to decrease amputation in 94% of them. “The American Limb Preservation Society (ALPS) lists 30 programs,” said Dr. Armstrong, the founding president of the organization. “There may be as many as 100.”
Team compositions vary but usually include at least one medical specialty clinician, such as infectious disease, primary care, or endocrinology, and two or more specialty clinicians, such as vascular, podiatric, orthopedic, or plastic surgery. A shoe specialist is needed to prescribe and manage footwear. Other important team members include nutrition experts and behavioral health professionals to deal with associated depression.
Johns Hopkins’ Multidisciplinary Diabetic Foot and Wound Service launched in 2012 and includes vascular surgeons, surgical podiatrists, endocrinologists, wound care nurses, advanced practice staff, board-certified wound care specialists, orthopedic surgeons, infection disease experts, physical therapists, and certified orthotists.
“This interdisciplinary care model has been repeatedly validated by research as superior for limb salvage and wound healing,” said Nestoras Mathioudakis, MD, codirector of the service. “For instance, endocrinologists and diabetes educators are crucial for managing uncontrolled diabetes — a key factor in infection and delayed wound healing. Similarly, vascular surgeons play a vital role in addressing peripheral arterial disease to improve blood flow to the affected area.”
“Diabetic foot ulcers might require prolonged periods of specialized care, including meticulous wound management and off-loading, overseen by surgical podiatrists and wound care experts,” he said. “In cases where infection is present, particularly with multidrug resistant organisms or when standard antibiotics are contraindicated, the insight of an infectious disease specialist is invaluable.”
While the makeup of teams varies from location to location, he said “the hallmark of effective teams is their ability to comprehensively manage glycemic control, foot wounds, vascular disease, and infections.”
The power of teams, Dr. Armstrong said, is very much evident after his weekly “foot selfie rounds” conducted Mondays at 7 AM, with an “all feet on deck” approach. “Not a week goes by when we don’t stop a hospitalization,” he said of the team evaluating the photos, due to detecting issues early, while still in the manageable state.
Teams can trump technology, Dr. Armstrong said. A team of just a primary care doctor and a podiatrist can make a significant reduction in amputations, he said, just by a “Knock your socks off” approach. He reminds primary care doctors that observing the feet of their patients with diabetes can go a long way to reducing DFUs and the hospitalizations and amputations that can result.
Dr. Mathioudakis and Dr. Isseroff reported no disclosures. Dr. Boulton consults for Urgo Medical, Nevro Corporation, and AOT, Inc. Dr. Armstrong reported receiving consulting fees from Podimetrics; Molnlycke; Cardiovascular Systems, Inc.; Endo Pharmaceuticals; and Averitas Pharma (GRT US).
A version of this article first appeared on Medscape.com.
A 30-Year-Old White Female Presented With a 4-Month History of Scaly, Erythematous Patches and Plaques on Her Trunk and Extremities
Tumor necrosis factor (TNF)-alpha inhibitors are used to treat a variety of autoimmune conditions including psoriasis, psoriatic arthritis, rheumatoid arthritis (RA), spondyloarthritis, and inflammatory bowel disease (IBD). Interestingly, they have also been observed to cause paradoxical psoriasis with an incidence between 0.6%-5.3%, most commonly occurring in patients with underlying Crohn’s disease and rheumatoid arthritis (RA). Infliximab is the most common TNF inhibitor associated with this condition (52.6%-62.6% of cases) followed by etanercept (12%-29%). .
Psoriasis is traditionally divided into two types. Patients with type I psoriasis have a family history, develop symptoms before the age of 40 and are often positive for HLA-Cw6. Type II psoriasis is not related to HLA-Cw6, lacks a family history, and typically manifests after age 40. Psoriatic lesions are well-defined, erythematous plaques with silvery scales most commonly appearing on extensor surfaces and the scalp. Variants include nail psoriasis, pustular psoriasis, inverse psoriasis, and guttate psoriasis.
Although psoriasis is typically a clinical diagnosis, histologic examination may be used to differentiate from other dermatoses if necessary. The lesions of TNF inhibitor-induced psoriasis characteristically display patterns similar to primary psoriasis, including parakeratosis, microabscesses, and rete ridges. Eosinophilic hypersensitivity reactions and features overlapping with eczematous hypersensitivity (psoriasiform dermatitis) may also be present.
The pathogenesis of this condition is not well understood, but theories include a variety of immune processes including interferon overproduction, interleukin and T-cell activation, and the presence of an infectious nidus. Classical psoriasis is related to type 1 interferon release, so theoretically, immunosuppression caused by TNF inhibitor treatment may permit uncontrolled production of interferons, resulting in psoriatic lesions. Another theory is that interleukin (IL)-23, a pro-inflammatory cytokine, promotes activation of T-helper 17 (Th17) cells. Th17 cells are part of the pathogenesis of primary psoriasis and other inflammatory conditions, such as RA and inflammatory bowel disease. Of note, individuals with gastrointestinal inflammatory diseases are already known to be at a greater risk for developing psoriasis. Immunosuppression caused by a TNF inhibitor may leave patients more susceptible to other infections, which may induce psoriatic plaques.

There are multiple approaches to treatment depending on the severity of the disease. If the psoriatic eruption is mild, the medication may be continued. This “treat-through” method is often considered when stopping the current immunotherapy would cause the patient significant issues. Moderate to severe cases of TNF inhibitor-induced psoriasis may warrant switching TNF inhibitor therapy or completely changing the drug class used in the treatment of the underlying autoimmune condition. Additional treatments include topical and oral steroids, UV therapy, methotrexate, cyclosporine, and acitretin.
This case and the photo were submitted by Lucas Shapiro, BS, of Nova Southeastern University College of Osteopathic Medicine, Fort Lauderdale, Florida, and Leon S. Maratchi, MD, Gastro Health, Hollywood, Florida. The column was edited by Donna Bilu Martin, MD.
Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Florida. More diagnostic cases are available at mdedge.com/dermatology. To submit a case for possible publication, send an email to dermnews@mdedge.com.
References
1. Li SJ et al. J Psoriasis Psoriatic Arthritis. 2019 Apr;4(2):70-80. doi: 10.1177/2475530318810851.
2. Lu J and Lu Y. J Transl Autoimmun. 2023 Sep 6:7:100211. doi: 10.1016/j.jtauto.2023.100211.
3. Nair PA and Badri T. Psoriasis. [Updated 2023 Apr 3]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: www.ncbi.nlm.nih.gov/books/NBK448194/
Tumor necrosis factor (TNF)-alpha inhibitors are used to treat a variety of autoimmune conditions including psoriasis, psoriatic arthritis, rheumatoid arthritis (RA), spondyloarthritis, and inflammatory bowel disease (IBD). Interestingly, they have also been observed to cause paradoxical psoriasis with an incidence between 0.6%-5.3%, most commonly occurring in patients with underlying Crohn’s disease and rheumatoid arthritis (RA). Infliximab is the most common TNF inhibitor associated with this condition (52.6%-62.6% of cases) followed by etanercept (12%-29%). .
Psoriasis is traditionally divided into two types. Patients with type I psoriasis have a family history, develop symptoms before the age of 40 and are often positive for HLA-Cw6. Type II psoriasis is not related to HLA-Cw6, lacks a family history, and typically manifests after age 40. Psoriatic lesions are well-defined, erythematous plaques with silvery scales most commonly appearing on extensor surfaces and the scalp. Variants include nail psoriasis, pustular psoriasis, inverse psoriasis, and guttate psoriasis.
Although psoriasis is typically a clinical diagnosis, histologic examination may be used to differentiate from other dermatoses if necessary. The lesions of TNF inhibitor-induced psoriasis characteristically display patterns similar to primary psoriasis, including parakeratosis, microabscesses, and rete ridges. Eosinophilic hypersensitivity reactions and features overlapping with eczematous hypersensitivity (psoriasiform dermatitis) may also be present.
The pathogenesis of this condition is not well understood, but theories include a variety of immune processes including interferon overproduction, interleukin and T-cell activation, and the presence of an infectious nidus. Classical psoriasis is related to type 1 interferon release, so theoretically, immunosuppression caused by TNF inhibitor treatment may permit uncontrolled production of interferons, resulting in psoriatic lesions. Another theory is that interleukin (IL)-23, a pro-inflammatory cytokine, promotes activation of T-helper 17 (Th17) cells. Th17 cells are part of the pathogenesis of primary psoriasis and other inflammatory conditions, such as RA and inflammatory bowel disease. Of note, individuals with gastrointestinal inflammatory diseases are already known to be at a greater risk for developing psoriasis. Immunosuppression caused by a TNF inhibitor may leave patients more susceptible to other infections, which may induce psoriatic plaques.
There are multiple approaches to treatment depending on the severity of the disease. If the psoriatic eruption is mild, the medication may be continued. This “treat-through” method is often considered when stopping the current immunotherapy would cause the patient significant issues. Moderate to severe cases of TNF inhibitor-induced psoriasis may warrant switching TNF inhibitor therapy or completely changing the drug class used in the treatment of the underlying autoimmune condition. Additional treatments include topical and oral steroids, UV therapy, methotrexate, cyclosporine, and acitretin.
This case and the photo were submitted by Lucas Shapiro, BS, of Nova Southeastern University College of Osteopathic Medicine, Fort Lauderdale, Florida, and Leon S. Maratchi, MD, Gastro Health, Hollywood, Florida. The column was edited by Donna Bilu Martin, MD.
Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Florida. More diagnostic cases are available at mdedge.com/dermatology. To submit a case for possible publication, send an email to dermnews@mdedge.com.
References
1. Li SJ et al. J Psoriasis Psoriatic Arthritis. 2019 Apr;4(2):70-80. doi: 10.1177/2475530318810851.
2. Lu J and Lu Y. J Transl Autoimmun. 2023 Sep 6:7:100211. doi: 10.1016/j.jtauto.2023.100211.
3. Nair PA and Badri T. Psoriasis. [Updated 2023 Apr 3]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: www.ncbi.nlm.nih.gov/books/NBK448194/
Tumor necrosis factor (TNF)-alpha inhibitors are used to treat a variety of autoimmune conditions including psoriasis, psoriatic arthritis, rheumatoid arthritis (RA), spondyloarthritis, and inflammatory bowel disease (IBD). Interestingly, they have also been observed to cause paradoxical psoriasis with an incidence between 0.6%-5.3%, most commonly occurring in patients with underlying Crohn’s disease and rheumatoid arthritis (RA). Infliximab is the most common TNF inhibitor associated with this condition (52.6%-62.6% of cases) followed by etanercept (12%-29%). .
Psoriasis is traditionally divided into two types. Patients with type I psoriasis have a family history, develop symptoms before the age of 40 and are often positive for HLA-Cw6. Type II psoriasis is not related to HLA-Cw6, lacks a family history, and typically manifests after age 40. Psoriatic lesions are well-defined, erythematous plaques with silvery scales most commonly appearing on extensor surfaces and the scalp. Variants include nail psoriasis, pustular psoriasis, inverse psoriasis, and guttate psoriasis.
Although psoriasis is typically a clinical diagnosis, histologic examination may be used to differentiate from other dermatoses if necessary. The lesions of TNF inhibitor-induced psoriasis characteristically display patterns similar to primary psoriasis, including parakeratosis, microabscesses, and rete ridges. Eosinophilic hypersensitivity reactions and features overlapping with eczematous hypersensitivity (psoriasiform dermatitis) may also be present.
The pathogenesis of this condition is not well understood, but theories include a variety of immune processes including interferon overproduction, interleukin and T-cell activation, and the presence of an infectious nidus. Classical psoriasis is related to type 1 interferon release, so theoretically, immunosuppression caused by TNF inhibitor treatment may permit uncontrolled production of interferons, resulting in psoriatic lesions. Another theory is that interleukin (IL)-23, a pro-inflammatory cytokine, promotes activation of T-helper 17 (Th17) cells. Th17 cells are part of the pathogenesis of primary psoriasis and other inflammatory conditions, such as RA and inflammatory bowel disease. Of note, individuals with gastrointestinal inflammatory diseases are already known to be at a greater risk for developing psoriasis. Immunosuppression caused by a TNF inhibitor may leave patients more susceptible to other infections, which may induce psoriatic plaques.
There are multiple approaches to treatment depending on the severity of the disease. If the psoriatic eruption is mild, the medication may be continued. This “treat-through” method is often considered when stopping the current immunotherapy would cause the patient significant issues. Moderate to severe cases of TNF inhibitor-induced psoriasis may warrant switching TNF inhibitor therapy or completely changing the drug class used in the treatment of the underlying autoimmune condition. Additional treatments include topical and oral steroids, UV therapy, methotrexate, cyclosporine, and acitretin.
This case and the photo were submitted by Lucas Shapiro, BS, of Nova Southeastern University College of Osteopathic Medicine, Fort Lauderdale, Florida, and Leon S. Maratchi, MD, Gastro Health, Hollywood, Florida. The column was edited by Donna Bilu Martin, MD.
Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Florida. More diagnostic cases are available at mdedge.com/dermatology. To submit a case for possible publication, send an email to dermnews@mdedge.com.
References
1. Li SJ et al. J Psoriasis Psoriatic Arthritis. 2019 Apr;4(2):70-80. doi: 10.1177/2475530318810851.
2. Lu J and Lu Y. J Transl Autoimmun. 2023 Sep 6:7:100211. doi: 10.1016/j.jtauto.2023.100211.
3. Nair PA and Badri T. Psoriasis. [Updated 2023 Apr 3]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: www.ncbi.nlm.nih.gov/books/NBK448194/
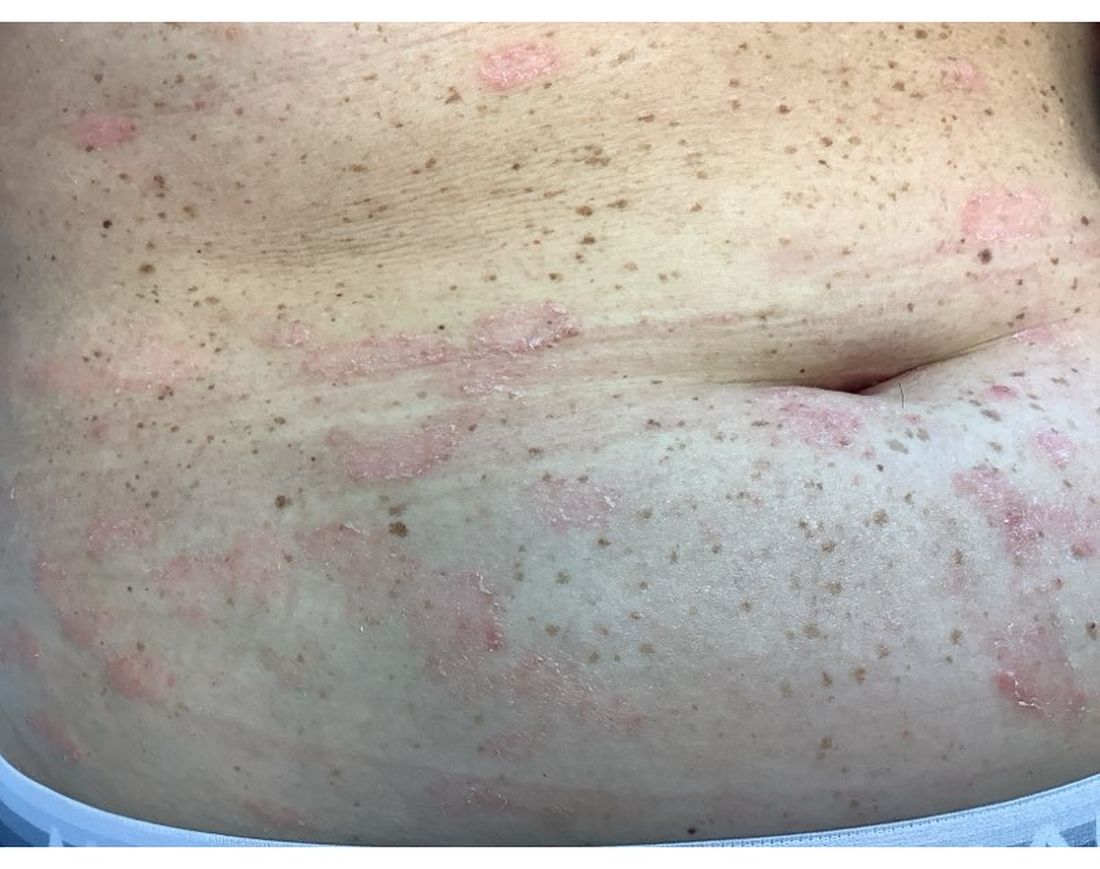
Mild Hidradenitis Suppurativa: Positive Results Reported for Topical Therapy
SAN DIEGO — cream, in a phase 2 trial.
“HS is a chronic, recurring inflammatory skin disease that is associated with painful inflammatory modules and abscesses,” said presenting author Martina J. Porter, MD, a dermatologist at Beth Israel Deaconess Medical Center and Harvard Medical School, both in Boston, Massachusetts. Dr. Porter presented the data during a late-breaking session at the annual meeting of the American Academy of Dermatology.
“Over time, these patients may progress to having tunnels, ulcerations, malodorous discharge, and permanent scarring,” she said. “Currently, there are no approved therapies for milder HS, and the standard treatments that we apply in clinical practice are often inadequate.”
Ruxolitinib is a selective Janus kinase (JAK) 1/JAK2 inhibitor that has demonstrated efficacy in other inflammatory and autoimmune skin diseases. Ruxolitinib cream, 1.5%, is approved for treating mild to moderate atopic dermatitis and nonsegmental vitiligo in patients ages 12 years and older.
The phase 2 double-blind, vehicle-controlled trial evaluated the efficacy and safety of ruxolitinib cream for mild HS. Researchers assigned 69 adults with Hurley stage I or II HS to receive 1.5% ruxolitinib cream or vehicle cream twice daily for 16 weeks. The primary endpoint was the change from baseline in AN count at week 16. To be eligible, patients had to have an AN count between 3 and 10.
“This is much more mild than what we have seen in any systemic therapy trials,” Dr. Porter said. “And, if patients had 3 lesions, they all needed to be in one anatomic area, but if they had 4-10 lesions, they had to have two anatomic areas involved. Also, no patients with active draining tunnels were allowed in the study.”
Of the 69 patients, 34 received ruxolitinib cream and 35 received vehicle. About 51% of patients in the vehicle arm were Black and 34% were White, while about 32% of patients in the ruxolitinib arm were Black and 56% were White.
The mean age of patients overall was 29 years, and about half the patients in both study arms had Hurley stage I disease, while the other half had Hurley stage II disease. Their average AN count ranged between 5.3 and 5.6 — mostly inflammatory nodules and few abscesses. Patients were not allowed to receive any type of intervention or rescue therapy during the study.
Dr. Porter reported that the least square mean change in AN count from baseline to week 16 was -2.42 in the vehicle arm vs -3.61 in the ruxolitinib cream arm (P <.05). The proportion of patients who achieved a 50% decrease in AN count was 79.2% in the ruxolitinib cream arm, compared with 56.5% of patients in the vehicle arm, respectively. More patients in the ruxolitinib cream arm achieved a 75% decrease in AN count (54.2% vs 25%), a 90% decrease in AN count (20.8 vs 12.5%), and a 100% decrease in AN count (20.8% vs 12.5%).
In other findings, 79.2% of patients in the ruxolitinib cream arm achieved a Hidradenitis Suppurativa Clinical Response score from baseline through week 16, compared with 50% of those in the vehicle group. The International Hidradenitis Suppurativa Severity Score System results favored the ruxolitinib cream arm (-4.46 vs -2.66 in the vehicle arm). Skin Pain and Itch numeric rating scale scores were moderate at baseline and improved similarly in both groups during the study.
Ruxolitinib cream was generally well tolerated over 16 weeks. No serious treatment-emergent adverse events were reported. The most common adverse event reported in the ruxolitinib cream group was COVID-19 and nasopharyngitis (two cases each) and one case of an application site reaction.
“Twice-daily 1.5% ruxolitinib cream was effective in patients with milder HS,” Dr. Porter concluded. “Modifications to our traditionally accepted clinical endpoints may be needed in studies of patients with milder HS.”
Jennifer L. Hsiao, MD, a dermatologist who directs the HS clinic at the University of Southern California, Los Angeles, who was asked to comment on the results, characterized the study as exciting for several reasons.
“First, with the global push in recent years to increase HS awareness, I am already seeing more patients earlier in their disease course with milder disease, and there is currently a gap in approved therapies for this patient population,” she told this news organization.
“Second, patients are very interested in topical therapies for HS and are thrilled whenever they learn that topical options are under investigation. This study had small patient numbers, but it was encouraging to see the positive results for ruxolitinib cream and that the treatment appeared well-tolerated.”
The trial was sponsored by the Incyte Corporation. Dr. Porter disclosed that she has received consulting fees from AbbVie, Alumis, Eli Lilly, Incyte, Janssen, Novartis, Pfizer, Prometheus Laboratories, Sanofi, Sonoma Biotherapeutics, Trifecta Clinical, and UCB. Dr. Hsiao disclosed that she is a member of the board of directors for the HS Foundation. She has also served as a consultant for AbbVie, Aclaris, Boehringer Ingelheim, Incyte, Novartis, and UCB; as a speaker for AbbVie, Novartis, and UCB; and as an investigator for Amgen, Boehringer Ingelheim, and Incyte.
A version of this article appeared on Medscape.com .
SAN DIEGO — cream, in a phase 2 trial.
“HS is a chronic, recurring inflammatory skin disease that is associated with painful inflammatory modules and abscesses,” said presenting author Martina J. Porter, MD, a dermatologist at Beth Israel Deaconess Medical Center and Harvard Medical School, both in Boston, Massachusetts. Dr. Porter presented the data during a late-breaking session at the annual meeting of the American Academy of Dermatology.
“Over time, these patients may progress to having tunnels, ulcerations, malodorous discharge, and permanent scarring,” she said. “Currently, there are no approved therapies for milder HS, and the standard treatments that we apply in clinical practice are often inadequate.”
Ruxolitinib is a selective Janus kinase (JAK) 1/JAK2 inhibitor that has demonstrated efficacy in other inflammatory and autoimmune skin diseases. Ruxolitinib cream, 1.5%, is approved for treating mild to moderate atopic dermatitis and nonsegmental vitiligo in patients ages 12 years and older.
The phase 2 double-blind, vehicle-controlled trial evaluated the efficacy and safety of ruxolitinib cream for mild HS. Researchers assigned 69 adults with Hurley stage I or II HS to receive 1.5% ruxolitinib cream or vehicle cream twice daily for 16 weeks. The primary endpoint was the change from baseline in AN count at week 16. To be eligible, patients had to have an AN count between 3 and 10.
“This is much more mild than what we have seen in any systemic therapy trials,” Dr. Porter said. “And, if patients had 3 lesions, they all needed to be in one anatomic area, but if they had 4-10 lesions, they had to have two anatomic areas involved. Also, no patients with active draining tunnels were allowed in the study.”
Of the 69 patients, 34 received ruxolitinib cream and 35 received vehicle. About 51% of patients in the vehicle arm were Black and 34% were White, while about 32% of patients in the ruxolitinib arm were Black and 56% were White.
The mean age of patients overall was 29 years, and about half the patients in both study arms had Hurley stage I disease, while the other half had Hurley stage II disease. Their average AN count ranged between 5.3 and 5.6 — mostly inflammatory nodules and few abscesses. Patients were not allowed to receive any type of intervention or rescue therapy during the study.
Dr. Porter reported that the least square mean change in AN count from baseline to week 16 was -2.42 in the vehicle arm vs -3.61 in the ruxolitinib cream arm (P <.05). The proportion of patients who achieved a 50% decrease in AN count was 79.2% in the ruxolitinib cream arm, compared with 56.5% of patients in the vehicle arm, respectively. More patients in the ruxolitinib cream arm achieved a 75% decrease in AN count (54.2% vs 25%), a 90% decrease in AN count (20.8 vs 12.5%), and a 100% decrease in AN count (20.8% vs 12.5%).
In other findings, 79.2% of patients in the ruxolitinib cream arm achieved a Hidradenitis Suppurativa Clinical Response score from baseline through week 16, compared with 50% of those in the vehicle group. The International Hidradenitis Suppurativa Severity Score System results favored the ruxolitinib cream arm (-4.46 vs -2.66 in the vehicle arm). Skin Pain and Itch numeric rating scale scores were moderate at baseline and improved similarly in both groups during the study.
Ruxolitinib cream was generally well tolerated over 16 weeks. No serious treatment-emergent adverse events were reported. The most common adverse event reported in the ruxolitinib cream group was COVID-19 and nasopharyngitis (two cases each) and one case of an application site reaction.
“Twice-daily 1.5% ruxolitinib cream was effective in patients with milder HS,” Dr. Porter concluded. “Modifications to our traditionally accepted clinical endpoints may be needed in studies of patients with milder HS.”
Jennifer L. Hsiao, MD, a dermatologist who directs the HS clinic at the University of Southern California, Los Angeles, who was asked to comment on the results, characterized the study as exciting for several reasons.
“First, with the global push in recent years to increase HS awareness, I am already seeing more patients earlier in their disease course with milder disease, and there is currently a gap in approved therapies for this patient population,” she told this news organization.
“Second, patients are very interested in topical therapies for HS and are thrilled whenever they learn that topical options are under investigation. This study had small patient numbers, but it was encouraging to see the positive results for ruxolitinib cream and that the treatment appeared well-tolerated.”
The trial was sponsored by the Incyte Corporation. Dr. Porter disclosed that she has received consulting fees from AbbVie, Alumis, Eli Lilly, Incyte, Janssen, Novartis, Pfizer, Prometheus Laboratories, Sanofi, Sonoma Biotherapeutics, Trifecta Clinical, and UCB. Dr. Hsiao disclosed that she is a member of the board of directors for the HS Foundation. She has also served as a consultant for AbbVie, Aclaris, Boehringer Ingelheim, Incyte, Novartis, and UCB; as a speaker for AbbVie, Novartis, and UCB; and as an investigator for Amgen, Boehringer Ingelheim, and Incyte.
A version of this article appeared on Medscape.com .
SAN DIEGO — cream, in a phase 2 trial.
“HS is a chronic, recurring inflammatory skin disease that is associated with painful inflammatory modules and abscesses,” said presenting author Martina J. Porter, MD, a dermatologist at Beth Israel Deaconess Medical Center and Harvard Medical School, both in Boston, Massachusetts. Dr. Porter presented the data during a late-breaking session at the annual meeting of the American Academy of Dermatology.
“Over time, these patients may progress to having tunnels, ulcerations, malodorous discharge, and permanent scarring,” she said. “Currently, there are no approved therapies for milder HS, and the standard treatments that we apply in clinical practice are often inadequate.”
Ruxolitinib is a selective Janus kinase (JAK) 1/JAK2 inhibitor that has demonstrated efficacy in other inflammatory and autoimmune skin diseases. Ruxolitinib cream, 1.5%, is approved for treating mild to moderate atopic dermatitis and nonsegmental vitiligo in patients ages 12 years and older.
The phase 2 double-blind, vehicle-controlled trial evaluated the efficacy and safety of ruxolitinib cream for mild HS. Researchers assigned 69 adults with Hurley stage I or II HS to receive 1.5% ruxolitinib cream or vehicle cream twice daily for 16 weeks. The primary endpoint was the change from baseline in AN count at week 16. To be eligible, patients had to have an AN count between 3 and 10.
“This is much more mild than what we have seen in any systemic therapy trials,” Dr. Porter said. “And, if patients had 3 lesions, they all needed to be in one anatomic area, but if they had 4-10 lesions, they had to have two anatomic areas involved. Also, no patients with active draining tunnels were allowed in the study.”
Of the 69 patients, 34 received ruxolitinib cream and 35 received vehicle. About 51% of patients in the vehicle arm were Black and 34% were White, while about 32% of patients in the ruxolitinib arm were Black and 56% were White.
The mean age of patients overall was 29 years, and about half the patients in both study arms had Hurley stage I disease, while the other half had Hurley stage II disease. Their average AN count ranged between 5.3 and 5.6 — mostly inflammatory nodules and few abscesses. Patients were not allowed to receive any type of intervention or rescue therapy during the study.
Dr. Porter reported that the least square mean change in AN count from baseline to week 16 was -2.42 in the vehicle arm vs -3.61 in the ruxolitinib cream arm (P <.05). The proportion of patients who achieved a 50% decrease in AN count was 79.2% in the ruxolitinib cream arm, compared with 56.5% of patients in the vehicle arm, respectively. More patients in the ruxolitinib cream arm achieved a 75% decrease in AN count (54.2% vs 25%), a 90% decrease in AN count (20.8 vs 12.5%), and a 100% decrease in AN count (20.8% vs 12.5%).
In other findings, 79.2% of patients in the ruxolitinib cream arm achieved a Hidradenitis Suppurativa Clinical Response score from baseline through week 16, compared with 50% of those in the vehicle group. The International Hidradenitis Suppurativa Severity Score System results favored the ruxolitinib cream arm (-4.46 vs -2.66 in the vehicle arm). Skin Pain and Itch numeric rating scale scores were moderate at baseline and improved similarly in both groups during the study.
Ruxolitinib cream was generally well tolerated over 16 weeks. No serious treatment-emergent adverse events were reported. The most common adverse event reported in the ruxolitinib cream group was COVID-19 and nasopharyngitis (two cases each) and one case of an application site reaction.
“Twice-daily 1.5% ruxolitinib cream was effective in patients with milder HS,” Dr. Porter concluded. “Modifications to our traditionally accepted clinical endpoints may be needed in studies of patients with milder HS.”
Jennifer L. Hsiao, MD, a dermatologist who directs the HS clinic at the University of Southern California, Los Angeles, who was asked to comment on the results, characterized the study as exciting for several reasons.
“First, with the global push in recent years to increase HS awareness, I am already seeing more patients earlier in their disease course with milder disease, and there is currently a gap in approved therapies for this patient population,” she told this news organization.
“Second, patients are very interested in topical therapies for HS and are thrilled whenever they learn that topical options are under investigation. This study had small patient numbers, but it was encouraging to see the positive results for ruxolitinib cream and that the treatment appeared well-tolerated.”
The trial was sponsored by the Incyte Corporation. Dr. Porter disclosed that she has received consulting fees from AbbVie, Alumis, Eli Lilly, Incyte, Janssen, Novartis, Pfizer, Prometheus Laboratories, Sanofi, Sonoma Biotherapeutics, Trifecta Clinical, and UCB. Dr. Hsiao disclosed that she is a member of the board of directors for the HS Foundation. She has also served as a consultant for AbbVie, Aclaris, Boehringer Ingelheim, Incyte, Novartis, and UCB; as a speaker for AbbVie, Novartis, and UCB; and as an investigator for Amgen, Boehringer Ingelheim, and Incyte.
A version of this article appeared on Medscape.com .
FROM AAD 2024