User login
Expanding the reach of available cancer therapies
In this edition of “How I Will Treat My Next Patient,” I highlight two articles that demonstrate the safety of established treatments – nephrectomy and stereotactic ablative body radiotherapy (SABR) – in patient populations that previously may have been excluded from those treatments at many centers.

Nephrectomy in advanced RCC
Nirmish Singla, MD, and colleagues reported a single-center retrospective cohort study, assessing outcomes of 11 nephrectomies (10 radical, 1 partial) in 10 patients with advanced renal cell carcinoma (RCC) who had received front- or later-line immune checkpoint inhibitor therapy (ICIs). Half had received nivolumab alone; the others received nivolumab plus ipilimumab. Surgery was performed laparoscopically in five cases (Urol Oncol. 2019 Dec;37[12]:924-31).
No patient experienced a major intraoperative complication. Four experienced postoperative complications, the majority of which were addressed with interventional radiology procedures. The median hospital stay was 4 days. One patient died of progressive disease more than 3 months after surgery, and another died of pulmonary embolism and sepsis. Six of the 10 patients did not have any complications or readmissions. There were no immune-related toxicities and no wound-healing issues. ICI therapy was resumed postoperatively in six patients.
At nephrectomy (plus or minus metastatectomy), one patient achieved a response to immunotherapy in the primary tumor, and three of four patients who underwent resection of hepatic, pulmonary, or adrenal metastases had no detectable cancer. All surgical margins were negative.
During a median postoperative follow-up of 180 days, nephrectomy following ICI was safe. Pathologic response in both the primary tumor and metastatic sites was encouraging.
What this means in clinical practice
In medical school, all of us are admonished not to be afraid to unlearn something and to learn something new. Historically, nephrectomy was felt to be helpful in improving overall survival in patients with advanced RCC. Effective targeted therapies and ICIs have caused us to question the role of nephrectomy and its timing, since 20%-40% of patients who have apparently localized RCC at the time of nephrectomy develop recurrences within 3 years. Preoperative therapy could mitigate potentially aggressive tumor biology, treat micrometastatic disease, and help select patients who should not be treated surgically.
In the CARMENA trial of the treatment of advanced RCC patients with the tyrosine kinase inhibitor sunitinib versus nephrectomy followed by sunitinib, most patients could avoid nephrectomy without compromising survival (N Engl J Med. 2018; 379:417-27). Results were updated at the 2019 annual meeting of the American Society of Clinical Oncology. Overall, nephrectomy was not beneficial. However, delayed nephrectomy (after sunitinib) appeared be beneficial for good responders with only one IMDC (International Metastatic RCC Database Consortium) risk factor and only one metastatic site.
The small study by Dr. Singla and colleagues illustrates that nephrectomy is feasible after ICI, plus or minus anti-CTLA4-targeted treatment, and that favorable histologic results can be achieved. With ICI plus or minus anti-CTLA4-targeted treatment, no patient had progressive disease prior to surgery. This experience is germane in view of recently updated results of the CheckMate 214 trial, showing superior overall survival, response rates, and response duration for nivolumab plus ipilimumab, in comparison with sunitinib.
There are still unresolved questions, including whether these favorable outcomes can be achieved in community practice and whether there are genomic or immunohistochemistry expression profiles to select patients who can benefit from this approach. It’s unclear whether there are practical issues that influence outcome, such as type of ICI, number of preoperative treatment cycles, and additional systemic therapies including postoperative treatment. However, the current series rings the starting bell for the study of those questions and a promising era for patients with this deadly disease.
SABR in moderately central NSCLC
SABR to peripheral, small non–small cell lung cancers (NSCLCs) produces high local control rates, with low grade 3-4 toxicity, and is an alternative to resection in patients who are unfit for surgery. In a pragmatic, community-based, prospective cohort experience in Scotland, Robert Rulach, MBChB, and colleagues, treated 50 T1-2N0M0 NSCLC patients with SABR 50-Gy in five fractions (Clin Oncol. 2019 Oct 10. doi: 10.1016/j.clon.2019.09.055). The dose and fractionation schedule was safe and effective in the phase 1/2 RTOG 0813 trial and is concordant with guidelines from the National Comprehensive Cancer Network (NCCN).
All of the tumors were moderately central, as in the RTOG trial. One patient had an additional tumor that was ultracentral. Notably, 84% of patients were deemed medically unfit for surgery.
All patients completed radiotherapy without treatment delays. Two patients died within 90 days of treatment. There were no grade 4 or grade 5 toxicities and the overall rate of grade 3 toxicity was 4%. With a median follow-up of 25.2 months, 34 patients died: 18 from causes unrelated to cancer and 16 from cancer recurrence. The median overall survival was 27 months. The 2-year overall survival rate was 67.6%, commensurate with the rate seen in RTOG 0813.
The researchers concluded that, for frail patients with centrally-located NSCLC treated uniformly in a community practice, SABR with the RTOG 0813 treatment protocol produced acceptable toxicity and overall survival comparable with the published literature.
What this means in clinical practice
The results and conclusions of the study by Dr. Rulach and colleagues are straightforward: SABR can be used for centrally-located NSCLC without producing massive hemoptysis, bronchial stricture, and fistula formation. Since the majority of patients had no histologic diagnosis, T1N0 lesions, and no routine follow-up CT scans beyond 3 months post treatment, conclusions beyond that are unjustified.
In a community-based practice, NCCN guideline–concordant SABR treatment in moderately centrally-located NSCLC was safely delivered. For the burgeoning population of medically inoperable and/or elderly NSCLC patients, this alone is reassuring for clinicians and is helpful information for patients who require and/or desire nonsurgical treatment.
Dr. Lyss has been a community-based medical oncologist and clinical researcher for more than 35 years, practicing in St. Louis. His clinical and research interests are in the prevention, diagnosis, and treatment of breast and lung cancers and in expanding access to clinical trials to medically underserved populations.
In this edition of “How I Will Treat My Next Patient,” I highlight two articles that demonstrate the safety of established treatments – nephrectomy and stereotactic ablative body radiotherapy (SABR) – in patient populations that previously may have been excluded from those treatments at many centers.
Nephrectomy in advanced RCC
Nirmish Singla, MD, and colleagues reported a single-center retrospective cohort study, assessing outcomes of 11 nephrectomies (10 radical, 1 partial) in 10 patients with advanced renal cell carcinoma (RCC) who had received front- or later-line immune checkpoint inhibitor therapy (ICIs). Half had received nivolumab alone; the others received nivolumab plus ipilimumab. Surgery was performed laparoscopically in five cases (Urol Oncol. 2019 Dec;37[12]:924-31).
No patient experienced a major intraoperative complication. Four experienced postoperative complications, the majority of which were addressed with interventional radiology procedures. The median hospital stay was 4 days. One patient died of progressive disease more than 3 months after surgery, and another died of pulmonary embolism and sepsis. Six of the 10 patients did not have any complications or readmissions. There were no immune-related toxicities and no wound-healing issues. ICI therapy was resumed postoperatively in six patients.
At nephrectomy (plus or minus metastatectomy), one patient achieved a response to immunotherapy in the primary tumor, and three of four patients who underwent resection of hepatic, pulmonary, or adrenal metastases had no detectable cancer. All surgical margins were negative.
During a median postoperative follow-up of 180 days, nephrectomy following ICI was safe. Pathologic response in both the primary tumor and metastatic sites was encouraging.
What this means in clinical practice
In medical school, all of us are admonished not to be afraid to unlearn something and to learn something new. Historically, nephrectomy was felt to be helpful in improving overall survival in patients with advanced RCC. Effective targeted therapies and ICIs have caused us to question the role of nephrectomy and its timing, since 20%-40% of patients who have apparently localized RCC at the time of nephrectomy develop recurrences within 3 years. Preoperative therapy could mitigate potentially aggressive tumor biology, treat micrometastatic disease, and help select patients who should not be treated surgically.
In the CARMENA trial of the treatment of advanced RCC patients with the tyrosine kinase inhibitor sunitinib versus nephrectomy followed by sunitinib, most patients could avoid nephrectomy without compromising survival (N Engl J Med. 2018; 379:417-27). Results were updated at the 2019 annual meeting of the American Society of Clinical Oncology. Overall, nephrectomy was not beneficial. However, delayed nephrectomy (after sunitinib) appeared be beneficial for good responders with only one IMDC (International Metastatic RCC Database Consortium) risk factor and only one metastatic site.
The small study by Dr. Singla and colleagues illustrates that nephrectomy is feasible after ICI, plus or minus anti-CTLA4-targeted treatment, and that favorable histologic results can be achieved. With ICI plus or minus anti-CTLA4-targeted treatment, no patient had progressive disease prior to surgery. This experience is germane in view of recently updated results of the CheckMate 214 trial, showing superior overall survival, response rates, and response duration for nivolumab plus ipilimumab, in comparison with sunitinib.
There are still unresolved questions, including whether these favorable outcomes can be achieved in community practice and whether there are genomic or immunohistochemistry expression profiles to select patients who can benefit from this approach. It’s unclear whether there are practical issues that influence outcome, such as type of ICI, number of preoperative treatment cycles, and additional systemic therapies including postoperative treatment. However, the current series rings the starting bell for the study of those questions and a promising era for patients with this deadly disease.
SABR in moderately central NSCLC
SABR to peripheral, small non–small cell lung cancers (NSCLCs) produces high local control rates, with low grade 3-4 toxicity, and is an alternative to resection in patients who are unfit for surgery. In a pragmatic, community-based, prospective cohort experience in Scotland, Robert Rulach, MBChB, and colleagues, treated 50 T1-2N0M0 NSCLC patients with SABR 50-Gy in five fractions (Clin Oncol. 2019 Oct 10. doi: 10.1016/j.clon.2019.09.055). The dose and fractionation schedule was safe and effective in the phase 1/2 RTOG 0813 trial and is concordant with guidelines from the National Comprehensive Cancer Network (NCCN).
All of the tumors were moderately central, as in the RTOG trial. One patient had an additional tumor that was ultracentral. Notably, 84% of patients were deemed medically unfit for surgery.
All patients completed radiotherapy without treatment delays. Two patients died within 90 days of treatment. There were no grade 4 or grade 5 toxicities and the overall rate of grade 3 toxicity was 4%. With a median follow-up of 25.2 months, 34 patients died: 18 from causes unrelated to cancer and 16 from cancer recurrence. The median overall survival was 27 months. The 2-year overall survival rate was 67.6%, commensurate with the rate seen in RTOG 0813.
The researchers concluded that, for frail patients with centrally-located NSCLC treated uniformly in a community practice, SABR with the RTOG 0813 treatment protocol produced acceptable toxicity and overall survival comparable with the published literature.
What this means in clinical practice
The results and conclusions of the study by Dr. Rulach and colleagues are straightforward: SABR can be used for centrally-located NSCLC without producing massive hemoptysis, bronchial stricture, and fistula formation. Since the majority of patients had no histologic diagnosis, T1N0 lesions, and no routine follow-up CT scans beyond 3 months post treatment, conclusions beyond that are unjustified.
In a community-based practice, NCCN guideline–concordant SABR treatment in moderately centrally-located NSCLC was safely delivered. For the burgeoning population of medically inoperable and/or elderly NSCLC patients, this alone is reassuring for clinicians and is helpful information for patients who require and/or desire nonsurgical treatment.
Dr. Lyss has been a community-based medical oncologist and clinical researcher for more than 35 years, practicing in St. Louis. His clinical and research interests are in the prevention, diagnosis, and treatment of breast and lung cancers and in expanding access to clinical trials to medically underserved populations.
In this edition of “How I Will Treat My Next Patient,” I highlight two articles that demonstrate the safety of established treatments – nephrectomy and stereotactic ablative body radiotherapy (SABR) – in patient populations that previously may have been excluded from those treatments at many centers.
Nephrectomy in advanced RCC
Nirmish Singla, MD, and colleagues reported a single-center retrospective cohort study, assessing outcomes of 11 nephrectomies (10 radical, 1 partial) in 10 patients with advanced renal cell carcinoma (RCC) who had received front- or later-line immune checkpoint inhibitor therapy (ICIs). Half had received nivolumab alone; the others received nivolumab plus ipilimumab. Surgery was performed laparoscopically in five cases (Urol Oncol. 2019 Dec;37[12]:924-31).
No patient experienced a major intraoperative complication. Four experienced postoperative complications, the majority of which were addressed with interventional radiology procedures. The median hospital stay was 4 days. One patient died of progressive disease more than 3 months after surgery, and another died of pulmonary embolism and sepsis. Six of the 10 patients did not have any complications or readmissions. There were no immune-related toxicities and no wound-healing issues. ICI therapy was resumed postoperatively in six patients.
At nephrectomy (plus or minus metastatectomy), one patient achieved a response to immunotherapy in the primary tumor, and three of four patients who underwent resection of hepatic, pulmonary, or adrenal metastases had no detectable cancer. All surgical margins were negative.
During a median postoperative follow-up of 180 days, nephrectomy following ICI was safe. Pathologic response in both the primary tumor and metastatic sites was encouraging.
What this means in clinical practice
In medical school, all of us are admonished not to be afraid to unlearn something and to learn something new. Historically, nephrectomy was felt to be helpful in improving overall survival in patients with advanced RCC. Effective targeted therapies and ICIs have caused us to question the role of nephrectomy and its timing, since 20%-40% of patients who have apparently localized RCC at the time of nephrectomy develop recurrences within 3 years. Preoperative therapy could mitigate potentially aggressive tumor biology, treat micrometastatic disease, and help select patients who should not be treated surgically.
In the CARMENA trial of the treatment of advanced RCC patients with the tyrosine kinase inhibitor sunitinib versus nephrectomy followed by sunitinib, most patients could avoid nephrectomy without compromising survival (N Engl J Med. 2018; 379:417-27). Results were updated at the 2019 annual meeting of the American Society of Clinical Oncology. Overall, nephrectomy was not beneficial. However, delayed nephrectomy (after sunitinib) appeared be beneficial for good responders with only one IMDC (International Metastatic RCC Database Consortium) risk factor and only one metastatic site.
The small study by Dr. Singla and colleagues illustrates that nephrectomy is feasible after ICI, plus or minus anti-CTLA4-targeted treatment, and that favorable histologic results can be achieved. With ICI plus or minus anti-CTLA4-targeted treatment, no patient had progressive disease prior to surgery. This experience is germane in view of recently updated results of the CheckMate 214 trial, showing superior overall survival, response rates, and response duration for nivolumab plus ipilimumab, in comparison with sunitinib.
There are still unresolved questions, including whether these favorable outcomes can be achieved in community practice and whether there are genomic or immunohistochemistry expression profiles to select patients who can benefit from this approach. It’s unclear whether there are practical issues that influence outcome, such as type of ICI, number of preoperative treatment cycles, and additional systemic therapies including postoperative treatment. However, the current series rings the starting bell for the study of those questions and a promising era for patients with this deadly disease.
SABR in moderately central NSCLC
SABR to peripheral, small non–small cell lung cancers (NSCLCs) produces high local control rates, with low grade 3-4 toxicity, and is an alternative to resection in patients who are unfit for surgery. In a pragmatic, community-based, prospective cohort experience in Scotland, Robert Rulach, MBChB, and colleagues, treated 50 T1-2N0M0 NSCLC patients with SABR 50-Gy in five fractions (Clin Oncol. 2019 Oct 10. doi: 10.1016/j.clon.2019.09.055). The dose and fractionation schedule was safe and effective in the phase 1/2 RTOG 0813 trial and is concordant with guidelines from the National Comprehensive Cancer Network (NCCN).
All of the tumors were moderately central, as in the RTOG trial. One patient had an additional tumor that was ultracentral. Notably, 84% of patients were deemed medically unfit for surgery.
All patients completed radiotherapy without treatment delays. Two patients died within 90 days of treatment. There were no grade 4 or grade 5 toxicities and the overall rate of grade 3 toxicity was 4%. With a median follow-up of 25.2 months, 34 patients died: 18 from causes unrelated to cancer and 16 from cancer recurrence. The median overall survival was 27 months. The 2-year overall survival rate was 67.6%, commensurate with the rate seen in RTOG 0813.
The researchers concluded that, for frail patients with centrally-located NSCLC treated uniformly in a community practice, SABR with the RTOG 0813 treatment protocol produced acceptable toxicity and overall survival comparable with the published literature.
What this means in clinical practice
The results and conclusions of the study by Dr. Rulach and colleagues are straightforward: SABR can be used for centrally-located NSCLC without producing massive hemoptysis, bronchial stricture, and fistula formation. Since the majority of patients had no histologic diagnosis, T1N0 lesions, and no routine follow-up CT scans beyond 3 months post treatment, conclusions beyond that are unjustified.
In a community-based practice, NCCN guideline–concordant SABR treatment in moderately centrally-located NSCLC was safely delivered. For the burgeoning population of medically inoperable and/or elderly NSCLC patients, this alone is reassuring for clinicians and is helpful information for patients who require and/or desire nonsurgical treatment.
Dr. Lyss has been a community-based medical oncologist and clinical researcher for more than 35 years, practicing in St. Louis. His clinical and research interests are in the prevention, diagnosis, and treatment of breast and lung cancers and in expanding access to clinical trials to medically underserved populations.
Not all lung cancer patients receive treatment
In the United States, just over 15% of patients with lung cancer receive no treatment, according to the American Lung Association.
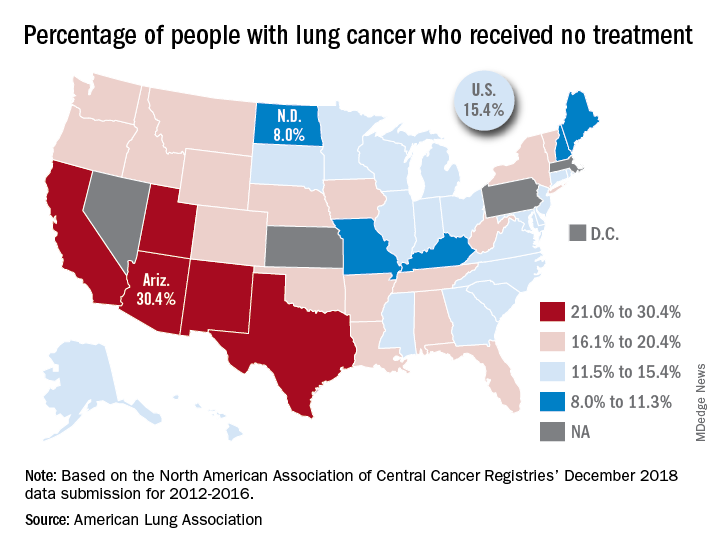
“This can happen for multiple reasons, such as the tumor having spread too far, poor health, or refusal of treatment,” the ALA said in its 2019 State of Lung Cancer report.
On the state level, the disparities were considerable. Arizona had the highest rate of nontreatment at 30.4%, followed by the neighboring states of New Mexico (24.2%) and California (24.0%). The lowest rate in the country, 8.0%, came from North Dakota, with Missouri next at 9.4% and Maine third at 9.6%, based on data from the North American Association of Central Cancer Registries’ December 2018 data submission, which covered the years from 2012 to 2016.
Although some cases of lung cancer may be unavoidable, “no one should go untreated because of lack of provider or patient knowledge, stigma associated with lung cancer, fatalism after diagnosis, or cost of treatment. Dismantling these and other barriers is important to reducing the percent of untreated patients,” the ALA said.
In the United States, just over 15% of patients with lung cancer receive no treatment, according to the American Lung Association.
“This can happen for multiple reasons, such as the tumor having spread too far, poor health, or refusal of treatment,” the ALA said in its 2019 State of Lung Cancer report.
On the state level, the disparities were considerable. Arizona had the highest rate of nontreatment at 30.4%, followed by the neighboring states of New Mexico (24.2%) and California (24.0%). The lowest rate in the country, 8.0%, came from North Dakota, with Missouri next at 9.4% and Maine third at 9.6%, based on data from the North American Association of Central Cancer Registries’ December 2018 data submission, which covered the years from 2012 to 2016.
Although some cases of lung cancer may be unavoidable, “no one should go untreated because of lack of provider or patient knowledge, stigma associated with lung cancer, fatalism after diagnosis, or cost of treatment. Dismantling these and other barriers is important to reducing the percent of untreated patients,” the ALA said.
In the United States, just over 15% of patients with lung cancer receive no treatment, according to the American Lung Association.
“This can happen for multiple reasons, such as the tumor having spread too far, poor health, or refusal of treatment,” the ALA said in its 2019 State of Lung Cancer report.
On the state level, the disparities were considerable. Arizona had the highest rate of nontreatment at 30.4%, followed by the neighboring states of New Mexico (24.2%) and California (24.0%). The lowest rate in the country, 8.0%, came from North Dakota, with Missouri next at 9.4% and Maine third at 9.6%, based on data from the North American Association of Central Cancer Registries’ December 2018 data submission, which covered the years from 2012 to 2016.
Although some cases of lung cancer may be unavoidable, “no one should go untreated because of lack of provider or patient knowledge, stigma associated with lung cancer, fatalism after diagnosis, or cost of treatment. Dismantling these and other barriers is important to reducing the percent of untreated patients,” the ALA said.
Neoantigen vaccine appears safe and active in NSCLC
NATIONAL HARBOR, MD. – Trial results suggest a personalized vaccination approach is feasible and safe, and the vaccine can produce clinical responses in patients with non–small cell lung cancer (NSCLC).

The neoantigen vaccine produced only grade 1 adverse events, yielded responses in patients with epidermal growth factor receptor (EGFR) mutations, and proved particularly effective in patients who were also receiving an EGFR inhibitor.
“EGFR inhibitors seemed to reduce tumor immunosuppression barriers and may enhance antitumor immune responses before and during immunization, suggesting there may be a potential synergy of EGFR with immunotherapies,” Gregory A. Lizee, PhD, of University of Texas MD Anderson Cancer Center, Houston, said at the annual meeting of the Society for Immunotherapy of Cancer.
The research began with an elderly patient who had heavily pretreated NSCLC (Oncoimmunology. 2016;5[12]:e1238539). Dr. Lizee and colleagues used tumor mutational profiling and human leukocyte antigen (HLA) typing to develop a personalized peptide vaccine for the patient. He received the vaccine along with topical imiquimod and had multiple lung tumor nodules regress. However, the patient also had liver metastasis that remained refractory to treatment, and he ultimately died.
To investigate this treatment approach in a larger group, Dr. Lizee and colleagues began a phase 1b trial of patients with advanced NSCLC (ChiCTR-IIR-16009867). As with the prior patient, the researchers designed personalized peptide vaccines for the trial subjects based on mutational profiling of 508 cancer-associated genes and high-resolution HLA typing. The peptides were selected based on nonsynonymous somatic tumor–associated mutations with variant allele frequency greater than 0.04 and the highest predicted neoantigen peptide binding to each patient’s HLA class I and II molecules. The vaccines targeted up to eight independent somatic mutations (mean, 3.75 mutations).
In all, 31 patients provided lung tumor biopsies and peripheral blood for mutational and HLA analyses. The researchers designed 27 personalized neoantigen vaccines, and 24 patients were ultimately vaccinated. This translates to a vaccination rate of 77%, which suggests this treatment approach is feasible, Dr. Lizee said.
Of the 24 vaccinated patients, 18 had adenocarcinoma, and 6 had squamous cell carcinoma. All patients had received multiple prior therapies, including surgery, chemotherapy, radiation, and EGFR inhibitors.
Each patient was vaccinated with a personalized mixture of short and long neoantigen peptides (mean, 9.4 peptides) dissolved in isotonic saline. Patients received at least 12 weekly immunizations and had topical imiquimod applied over the injection site for costimulation through toll-like receptor 7. The 16 patients with EGFR mutations were given the option of continuing on an EGFR inhibitor, and 9 patients elected to do so.
Results
Dr. Lizee said this treatment approach was “very safe,” with only grade 1 treatment-related adverse events. The events were fatigue (n = 2), rash (n = 1), and fever (n = 1).
Seven patients achieved a response after vaccination, and one patient achieved a complete response. All seven responders had EGFR mutations, and four of them were receiving an EGFR inhibitor.
The patients on an EGFR inhibitor had significantly better overall survival than that of EGFR-mutated patients who had stopped taking an EGFR inhibitor – 13.8 months and 7.6 months, respectively (P = .038).
Immune profiling revealed that neoantigen-specific T-cell reactivity was associated with clinical responses. The researchers observed EGFR neoantigen-specific T-cell responses in five responders. In three responders, the strongest response was against a peptide encompassing the L858R driver mutation.
The researchers also found evidence of synergy between EGFR inhibitor therapy and the peptide vaccine. EGFR inhibition caused immunomodulatory pathways in EGFR-mutated cancer cells to favor immune-cell infiltration and HLA-mediated antigen presentation.
“Our mechanistic working model is that, in the circulation, the personalized vaccine increased the T-cell frequency,” Dr. Lizee said. “The EGFR inhibitor increased chemokines and antigen presentation at the tumor site, which then attracted those T cells to migrate to the tumor. Then, recognition of the antigen caused interferon gamma [to increase], which caused, potentially, a feed-forward loop by increasing chemokines and antigen presentation further.”
This research is sponsored by Tianjin Beichen Hospital and funded by Tianjin HengJia Biotechnology Development Co. Ltd. Dr. Lizee disclosed a consulting relationship with Tianjin HengJia Biotechnology Development Co. Ltd.
SOURCE: Lizee G et al. SITC 2019. Abstract O18.
NATIONAL HARBOR, MD. – Trial results suggest a personalized vaccination approach is feasible and safe, and the vaccine can produce clinical responses in patients with non–small cell lung cancer (NSCLC).
The neoantigen vaccine produced only grade 1 adverse events, yielded responses in patients with epidermal growth factor receptor (EGFR) mutations, and proved particularly effective in patients who were also receiving an EGFR inhibitor.
“EGFR inhibitors seemed to reduce tumor immunosuppression barriers and may enhance antitumor immune responses before and during immunization, suggesting there may be a potential synergy of EGFR with immunotherapies,” Gregory A. Lizee, PhD, of University of Texas MD Anderson Cancer Center, Houston, said at the annual meeting of the Society for Immunotherapy of Cancer.
The research began with an elderly patient who had heavily pretreated NSCLC (Oncoimmunology. 2016;5[12]:e1238539). Dr. Lizee and colleagues used tumor mutational profiling and human leukocyte antigen (HLA) typing to develop a personalized peptide vaccine for the patient. He received the vaccine along with topical imiquimod and had multiple lung tumor nodules regress. However, the patient also had liver metastasis that remained refractory to treatment, and he ultimately died.
To investigate this treatment approach in a larger group, Dr. Lizee and colleagues began a phase 1b trial of patients with advanced NSCLC (ChiCTR-IIR-16009867). As with the prior patient, the researchers designed personalized peptide vaccines for the trial subjects based on mutational profiling of 508 cancer-associated genes and high-resolution HLA typing. The peptides were selected based on nonsynonymous somatic tumor–associated mutations with variant allele frequency greater than 0.04 and the highest predicted neoantigen peptide binding to each patient’s HLA class I and II molecules. The vaccines targeted up to eight independent somatic mutations (mean, 3.75 mutations).
In all, 31 patients provided lung tumor biopsies and peripheral blood for mutational and HLA analyses. The researchers designed 27 personalized neoantigen vaccines, and 24 patients were ultimately vaccinated. This translates to a vaccination rate of 77%, which suggests this treatment approach is feasible, Dr. Lizee said.
Of the 24 vaccinated patients, 18 had adenocarcinoma, and 6 had squamous cell carcinoma. All patients had received multiple prior therapies, including surgery, chemotherapy, radiation, and EGFR inhibitors.
Each patient was vaccinated with a personalized mixture of short and long neoantigen peptides (mean, 9.4 peptides) dissolved in isotonic saline. Patients received at least 12 weekly immunizations and had topical imiquimod applied over the injection site for costimulation through toll-like receptor 7. The 16 patients with EGFR mutations were given the option of continuing on an EGFR inhibitor, and 9 patients elected to do so.
Results
Dr. Lizee said this treatment approach was “very safe,” with only grade 1 treatment-related adverse events. The events were fatigue (n = 2), rash (n = 1), and fever (n = 1).
Seven patients achieved a response after vaccination, and one patient achieved a complete response. All seven responders had EGFR mutations, and four of them were receiving an EGFR inhibitor.
The patients on an EGFR inhibitor had significantly better overall survival than that of EGFR-mutated patients who had stopped taking an EGFR inhibitor – 13.8 months and 7.6 months, respectively (P = .038).
Immune profiling revealed that neoantigen-specific T-cell reactivity was associated with clinical responses. The researchers observed EGFR neoantigen-specific T-cell responses in five responders. In three responders, the strongest response was against a peptide encompassing the L858R driver mutation.
The researchers also found evidence of synergy between EGFR inhibitor therapy and the peptide vaccine. EGFR inhibition caused immunomodulatory pathways in EGFR-mutated cancer cells to favor immune-cell infiltration and HLA-mediated antigen presentation.
“Our mechanistic working model is that, in the circulation, the personalized vaccine increased the T-cell frequency,” Dr. Lizee said. “The EGFR inhibitor increased chemokines and antigen presentation at the tumor site, which then attracted those T cells to migrate to the tumor. Then, recognition of the antigen caused interferon gamma [to increase], which caused, potentially, a feed-forward loop by increasing chemokines and antigen presentation further.”
This research is sponsored by Tianjin Beichen Hospital and funded by Tianjin HengJia Biotechnology Development Co. Ltd. Dr. Lizee disclosed a consulting relationship with Tianjin HengJia Biotechnology Development Co. Ltd.
SOURCE: Lizee G et al. SITC 2019. Abstract O18.
NATIONAL HARBOR, MD. – Trial results suggest a personalized vaccination approach is feasible and safe, and the vaccine can produce clinical responses in patients with non–small cell lung cancer (NSCLC).
The neoantigen vaccine produced only grade 1 adverse events, yielded responses in patients with epidermal growth factor receptor (EGFR) mutations, and proved particularly effective in patients who were also receiving an EGFR inhibitor.
“EGFR inhibitors seemed to reduce tumor immunosuppression barriers and may enhance antitumor immune responses before and during immunization, suggesting there may be a potential synergy of EGFR with immunotherapies,” Gregory A. Lizee, PhD, of University of Texas MD Anderson Cancer Center, Houston, said at the annual meeting of the Society for Immunotherapy of Cancer.
The research began with an elderly patient who had heavily pretreated NSCLC (Oncoimmunology. 2016;5[12]:e1238539). Dr. Lizee and colleagues used tumor mutational profiling and human leukocyte antigen (HLA) typing to develop a personalized peptide vaccine for the patient. He received the vaccine along with topical imiquimod and had multiple lung tumor nodules regress. However, the patient also had liver metastasis that remained refractory to treatment, and he ultimately died.
To investigate this treatment approach in a larger group, Dr. Lizee and colleagues began a phase 1b trial of patients with advanced NSCLC (ChiCTR-IIR-16009867). As with the prior patient, the researchers designed personalized peptide vaccines for the trial subjects based on mutational profiling of 508 cancer-associated genes and high-resolution HLA typing. The peptides were selected based on nonsynonymous somatic tumor–associated mutations with variant allele frequency greater than 0.04 and the highest predicted neoantigen peptide binding to each patient’s HLA class I and II molecules. The vaccines targeted up to eight independent somatic mutations (mean, 3.75 mutations).
In all, 31 patients provided lung tumor biopsies and peripheral blood for mutational and HLA analyses. The researchers designed 27 personalized neoantigen vaccines, and 24 patients were ultimately vaccinated. This translates to a vaccination rate of 77%, which suggests this treatment approach is feasible, Dr. Lizee said.
Of the 24 vaccinated patients, 18 had adenocarcinoma, and 6 had squamous cell carcinoma. All patients had received multiple prior therapies, including surgery, chemotherapy, radiation, and EGFR inhibitors.
Each patient was vaccinated with a personalized mixture of short and long neoantigen peptides (mean, 9.4 peptides) dissolved in isotonic saline. Patients received at least 12 weekly immunizations and had topical imiquimod applied over the injection site for costimulation through toll-like receptor 7. The 16 patients with EGFR mutations were given the option of continuing on an EGFR inhibitor, and 9 patients elected to do so.
Results
Dr. Lizee said this treatment approach was “very safe,” with only grade 1 treatment-related adverse events. The events were fatigue (n = 2), rash (n = 1), and fever (n = 1).
Seven patients achieved a response after vaccination, and one patient achieved a complete response. All seven responders had EGFR mutations, and four of them were receiving an EGFR inhibitor.
The patients on an EGFR inhibitor had significantly better overall survival than that of EGFR-mutated patients who had stopped taking an EGFR inhibitor – 13.8 months and 7.6 months, respectively (P = .038).
Immune profiling revealed that neoantigen-specific T-cell reactivity was associated with clinical responses. The researchers observed EGFR neoantigen-specific T-cell responses in five responders. In three responders, the strongest response was against a peptide encompassing the L858R driver mutation.
The researchers also found evidence of synergy between EGFR inhibitor therapy and the peptide vaccine. EGFR inhibition caused immunomodulatory pathways in EGFR-mutated cancer cells to favor immune-cell infiltration and HLA-mediated antigen presentation.
“Our mechanistic working model is that, in the circulation, the personalized vaccine increased the T-cell frequency,” Dr. Lizee said. “The EGFR inhibitor increased chemokines and antigen presentation at the tumor site, which then attracted those T cells to migrate to the tumor. Then, recognition of the antigen caused interferon gamma [to increase], which caused, potentially, a feed-forward loop by increasing chemokines and antigen presentation further.”
This research is sponsored by Tianjin Beichen Hospital and funded by Tianjin HengJia Biotechnology Development Co. Ltd. Dr. Lizee disclosed a consulting relationship with Tianjin HengJia Biotechnology Development Co. Ltd.
SOURCE: Lizee G et al. SITC 2019. Abstract O18.
REPORTING FROM SITC 2019
Lorlatinib induces deep responses in ROS1-positive NSCLC
The tyrosine kinase inhibitor (TKI) lorlatinib showed deep responses and intracranial activity in both TKI-pretreated and TKI-naive patients with advanced ROS1-positive non–small cell lung cancer (NSCLC), according to results from a phase 1-2 trial.
“We investigated the antitumour activity and safety of lorlatinib in advanced, ROS1-positive NSCLC,” wrote Alice T. Shaw, MD, PhD, of Massachusetts General Hospital Cancer Center, Boston, and colleagues. Their report is in The Lancet Oncology.
The single-arm, open-label study included 69 patients with advanced ROS1-positive disease with or without CNS involvement. The effects of lorlatinib were evaluated across 28 institutions in 12 different countries around the globe.
At baseline, the median age of study participants was 54 years (range, 44-61 years), and 57% were positive for brain metastases.
Study participants received 100 mg of oral lorlatinib once daily in repeated 21-day cycles. Drug therapy was continued until death, disease progression, unacceptable toxicity, or withdrawal of consent.
The primary outcome measured was intracranial and overall response. Activity outcomes were evaluated in subjects given a minimum of one dose of lorlatinib.
A total of 58% of patients were previously treated with crizotinib, while 30% of patients were TKI-naive. Among 40 crizotinib-pretreated patients, 14 patients (35%) had an objective response, with a median duration of response and PFS of 13.8 and 8.5 months, respectively.
Among 21 TKI-naive patients, 13 patients (62%) had an objective response, with a median duration of response and PFS of 25.3 and 21 months, respectively.
“Intracranial responses were achieved in seven (64%) of 11 TKI-naive patients and 12 (50%) of 24 previous crizotinib-only patients,” they reported.
With respect to safety, serious lorlatinib-related adverse events were observed in 7% of patients, with no therapy-related deaths reported. The most frequently seen grade 3-4 TEAEs were hypertriglyceridemia (19%) and hypercholesterolemia (14%).
The researchers noted a key limitation of the study was the small sample size; however, due to the rare nature of ROS1 rearrangements in patients with NSCLC, increasing enrollment for future studies could be challenging.
“Because crizotinib-refractory patients have few treatment options, lorlatinib could represent an important next-line targeted agent,” they concluded.
Pfizer funded the study. The authors reported financial affiliations with Ariad, Blueprint Medicines, Chugai Pharmaceutical, Daiichi Sankyo, EMD Serono, Pfizer, KSQ Therapeutics, Servier, TP Therapeutics, and other companies.
SOURCE: Shaw AT et al. Lancet Oncol. 2019 Oct 25. doi: 10.1016/S1470-2045(19)30655-2.
The tyrosine kinase inhibitor (TKI) crizotinib was recently established as an optimal first-line treatment option for patients with ROS1-positive non–small cell lung cancer (NSCLC). Despite strong efficacy seen in clinical trials, disease progression can still occur in patients on crizotinib, often through the development of resistance, which is largely the result of on-target mutations, such as Gly2032Arg.
Early results suggest the novel oral TKI candidate, lorlatinib, a potent inhibitor of the Gly2032Arg mutation, may be a treatment of choice in patients with crizotinib-resistance. Recent phase 1 data showed lorlatinib had antitumor activity in ROS1-positive patients.
Correspondingly, the deep and durable responses reported by Dr. Shaw and colleagues represents a significant milestone for lorlatinib, particularly in the setting of crizotinib resistance, where a paucity of later-line treatment options exist. In comparison to platinum-pemetrexed chemotherapy, lorlatinib is better tolerated and has demonstrated potent intracranial activity, which may prevent or delay CNS progression in the disease.
One question that remains from the current study is whether other ROS1 TKI drug candidates, such as repotrectinib and entrectinib, will show similar results to lorlatinib. Several trials are presently ongoing in an attempt to help answer this, and other remaining questions.
Michaël Duruisseaux, MD, PhD, is affiliated with the Hospices Civils de Lyon (France), Universit é Claude Bernard Lyon. Dr. Duruisseaux reported financial affiliations with Boehringer Ingelheim, Bristol-Myers Squibb, Roche, and Takeda. These comments are adapted from his editorial (Lancet Oncol. 2019 Oct 25. doi: 10.1016/S1470-2045[19]30716-8 ).
The tyrosine kinase inhibitor (TKI) crizotinib was recently established as an optimal first-line treatment option for patients with ROS1-positive non–small cell lung cancer (NSCLC). Despite strong efficacy seen in clinical trials, disease progression can still occur in patients on crizotinib, often through the development of resistance, which is largely the result of on-target mutations, such as Gly2032Arg.
Early results suggest the novel oral TKI candidate, lorlatinib, a potent inhibitor of the Gly2032Arg mutation, may be a treatment of choice in patients with crizotinib-resistance. Recent phase 1 data showed lorlatinib had antitumor activity in ROS1-positive patients.
Correspondingly, the deep and durable responses reported by Dr. Shaw and colleagues represents a significant milestone for lorlatinib, particularly in the setting of crizotinib resistance, where a paucity of later-line treatment options exist. In comparison to platinum-pemetrexed chemotherapy, lorlatinib is better tolerated and has demonstrated potent intracranial activity, which may prevent or delay CNS progression in the disease.
One question that remains from the current study is whether other ROS1 TKI drug candidates, such as repotrectinib and entrectinib, will show similar results to lorlatinib. Several trials are presently ongoing in an attempt to help answer this, and other remaining questions.
Michaël Duruisseaux, MD, PhD, is affiliated with the Hospices Civils de Lyon (France), Universit é Claude Bernard Lyon. Dr. Duruisseaux reported financial affiliations with Boehringer Ingelheim, Bristol-Myers Squibb, Roche, and Takeda. These comments are adapted from his editorial (Lancet Oncol. 2019 Oct 25. doi: 10.1016/S1470-2045[19]30716-8 ).
The tyrosine kinase inhibitor (TKI) crizotinib was recently established as an optimal first-line treatment option for patients with ROS1-positive non–small cell lung cancer (NSCLC). Despite strong efficacy seen in clinical trials, disease progression can still occur in patients on crizotinib, often through the development of resistance, which is largely the result of on-target mutations, such as Gly2032Arg.
Early results suggest the novel oral TKI candidate, lorlatinib, a potent inhibitor of the Gly2032Arg mutation, may be a treatment of choice in patients with crizotinib-resistance. Recent phase 1 data showed lorlatinib had antitumor activity in ROS1-positive patients.
Correspondingly, the deep and durable responses reported by Dr. Shaw and colleagues represents a significant milestone for lorlatinib, particularly in the setting of crizotinib resistance, where a paucity of later-line treatment options exist. In comparison to platinum-pemetrexed chemotherapy, lorlatinib is better tolerated and has demonstrated potent intracranial activity, which may prevent or delay CNS progression in the disease.
One question that remains from the current study is whether other ROS1 TKI drug candidates, such as repotrectinib and entrectinib, will show similar results to lorlatinib. Several trials are presently ongoing in an attempt to help answer this, and other remaining questions.
Michaël Duruisseaux, MD, PhD, is affiliated with the Hospices Civils de Lyon (France), Universit é Claude Bernard Lyon. Dr. Duruisseaux reported financial affiliations with Boehringer Ingelheim, Bristol-Myers Squibb, Roche, and Takeda. These comments are adapted from his editorial (Lancet Oncol. 2019 Oct 25. doi: 10.1016/S1470-2045[19]30716-8 ).
The tyrosine kinase inhibitor (TKI) lorlatinib showed deep responses and intracranial activity in both TKI-pretreated and TKI-naive patients with advanced ROS1-positive non–small cell lung cancer (NSCLC), according to results from a phase 1-2 trial.
“We investigated the antitumour activity and safety of lorlatinib in advanced, ROS1-positive NSCLC,” wrote Alice T. Shaw, MD, PhD, of Massachusetts General Hospital Cancer Center, Boston, and colleagues. Their report is in The Lancet Oncology.
The single-arm, open-label study included 69 patients with advanced ROS1-positive disease with or without CNS involvement. The effects of lorlatinib were evaluated across 28 institutions in 12 different countries around the globe.
At baseline, the median age of study participants was 54 years (range, 44-61 years), and 57% were positive for brain metastases.
Study participants received 100 mg of oral lorlatinib once daily in repeated 21-day cycles. Drug therapy was continued until death, disease progression, unacceptable toxicity, or withdrawal of consent.
The primary outcome measured was intracranial and overall response. Activity outcomes were evaluated in subjects given a minimum of one dose of lorlatinib.
A total of 58% of patients were previously treated with crizotinib, while 30% of patients were TKI-naive. Among 40 crizotinib-pretreated patients, 14 patients (35%) had an objective response, with a median duration of response and PFS of 13.8 and 8.5 months, respectively.
Among 21 TKI-naive patients, 13 patients (62%) had an objective response, with a median duration of response and PFS of 25.3 and 21 months, respectively.
“Intracranial responses were achieved in seven (64%) of 11 TKI-naive patients and 12 (50%) of 24 previous crizotinib-only patients,” they reported.
With respect to safety, serious lorlatinib-related adverse events were observed in 7% of patients, with no therapy-related deaths reported. The most frequently seen grade 3-4 TEAEs were hypertriglyceridemia (19%) and hypercholesterolemia (14%).
The researchers noted a key limitation of the study was the small sample size; however, due to the rare nature of ROS1 rearrangements in patients with NSCLC, increasing enrollment for future studies could be challenging.
“Because crizotinib-refractory patients have few treatment options, lorlatinib could represent an important next-line targeted agent,” they concluded.
Pfizer funded the study. The authors reported financial affiliations with Ariad, Blueprint Medicines, Chugai Pharmaceutical, Daiichi Sankyo, EMD Serono, Pfizer, KSQ Therapeutics, Servier, TP Therapeutics, and other companies.
SOURCE: Shaw AT et al. Lancet Oncol. 2019 Oct 25. doi: 10.1016/S1470-2045(19)30655-2.
The tyrosine kinase inhibitor (TKI) lorlatinib showed deep responses and intracranial activity in both TKI-pretreated and TKI-naive patients with advanced ROS1-positive non–small cell lung cancer (NSCLC), according to results from a phase 1-2 trial.
“We investigated the antitumour activity and safety of lorlatinib in advanced, ROS1-positive NSCLC,” wrote Alice T. Shaw, MD, PhD, of Massachusetts General Hospital Cancer Center, Boston, and colleagues. Their report is in The Lancet Oncology.
The single-arm, open-label study included 69 patients with advanced ROS1-positive disease with or without CNS involvement. The effects of lorlatinib were evaluated across 28 institutions in 12 different countries around the globe.
At baseline, the median age of study participants was 54 years (range, 44-61 years), and 57% were positive for brain metastases.
Study participants received 100 mg of oral lorlatinib once daily in repeated 21-day cycles. Drug therapy was continued until death, disease progression, unacceptable toxicity, or withdrawal of consent.
The primary outcome measured was intracranial and overall response. Activity outcomes were evaluated in subjects given a minimum of one dose of lorlatinib.
A total of 58% of patients were previously treated with crizotinib, while 30% of patients were TKI-naive. Among 40 crizotinib-pretreated patients, 14 patients (35%) had an objective response, with a median duration of response and PFS of 13.8 and 8.5 months, respectively.
Among 21 TKI-naive patients, 13 patients (62%) had an objective response, with a median duration of response and PFS of 25.3 and 21 months, respectively.
“Intracranial responses were achieved in seven (64%) of 11 TKI-naive patients and 12 (50%) of 24 previous crizotinib-only patients,” they reported.
With respect to safety, serious lorlatinib-related adverse events were observed in 7% of patients, with no therapy-related deaths reported. The most frequently seen grade 3-4 TEAEs were hypertriglyceridemia (19%) and hypercholesterolemia (14%).
The researchers noted a key limitation of the study was the small sample size; however, due to the rare nature of ROS1 rearrangements in patients with NSCLC, increasing enrollment for future studies could be challenging.
“Because crizotinib-refractory patients have few treatment options, lorlatinib could represent an important next-line targeted agent,” they concluded.
Pfizer funded the study. The authors reported financial affiliations with Ariad, Blueprint Medicines, Chugai Pharmaceutical, Daiichi Sankyo, EMD Serono, Pfizer, KSQ Therapeutics, Servier, TP Therapeutics, and other companies.
SOURCE: Shaw AT et al. Lancet Oncol. 2019 Oct 25. doi: 10.1016/S1470-2045(19)30655-2.
FROM THE LANCET ONCOLOGY
‘You had me at hello’: ESMO studies confirm survival benefits in NSCLC and breast cancer
In this edition of “How I will treat my next patient,” I highlight two studies that previously reported significant progression-free survival (PFS) improvements and more recently, at the European Society for Medical Oncology Congress, overall survival (OS) benefit. I reflect on the significance of these new reports in the wake of previously reported data and guidelines from the National Comprehensive Cancer Network (NCCN).
Osimertinib in advanced NSCLC
In the double-blind, phase 3 FLAURA trial, 556 patients with EGFR-mutated (EGFRm), advanced non–small cell lung cancer (NSCLC) received osimertinib or a standard tyrosine kinase inhibitor (TKI) as initial treatment. PFS, the primary endpoint, was clinically and statistically better for osimertinib (18.9 months vs. 10.2 months; hazard ratio 0.46; P less than .001), overall and in all major subgroups. There were fewer grade 3-4 adverse events and fewer permanent treatment discontinuations with osimertinib.
At the time of initial publication, OS data were immature, but because of the substantial survival improvements previously noted, osimertinib was approved by the Food and Drug Administration for first-line treatment of EGFRm stage IV NSCLC patients in April 2018 (N Engl J Med. 2018; 378:113-25).
More recently, at ESMO 2019, Suresh Ramalingam, MD, of the department of hematology and medical oncology at Emory University, Atlanta, and colleagues reported the OS results. Crossover to osimertinib was allowed for patients on the standard TKI arm when they had progressive disease and a T790M mutation. Osimertinib produced a median OS of 38.6 months, compared with 31.8 months for standard TKI (HR, 0.799; P = .0462), a 24-month OS rate of 74% vs. 59% (with no overlap in the 95% confidence intervals), and a 36-month OS rate of 54% vs. 44%. These benefits were interpreted to be statistically significant and clinically meaningful.
The 31.8-month median OS for standard TKI was competitive with the highest reported OS for standard therapy, perhaps because crossover to osimertinib was permitted.
What this means in clinical practice
The report by Dr. Ramalingam and colleagues – and the next abstract I will review – remind me of the famous “You had me at Hello” line from “Jerry Maguire.”
For patient education – and perhaps for some national regulatory agencies – it is good that we now have definition of what the average OS is with osimertinib, compared with standard TKI followed by osimertinib. However, very few oncologists in the United States likely use the latter strategy anymore. It was clear when the impressive PFS and toxicity information appeared in 2018 in the New England Journal of Medicine that osimertinib is the best tolerated, most durably effective front-line treatment for EGFRm mNSCLC, regardless of disease extent, sex, nationality, type of EGFRm (L858R amino acid substitution in exon 21 or exon 19 deletion), or presence/absence of central nervous system metastases.
In NCCN guidelines, osimertinib was listed as the preferred TKI, prior to the OS report at ESMO 2019. The challenges going forward will be to identify high-risk patient subsets who might benefit from drug combinations or novel new agents.
MONARCH 2: Abemaciclib plus fulvestrant
In the MONARCH 2, randomized, placebo-controlled, phase 3 trial, abemaciclib plus fulvestrant (abema-F) significantly improved PFS, in comparison with placebo plus fulvestrant (placebo-F; 16.9 months vs. 9.3 months; HR, 0.563) in 669 premenopausal (with concurrent ovarian function suppression) and postmenopausal women with metastatic breast cancer (mBC) who had disease progression on one to two lines of prior hormonal therapy (J Clin Oncol. 2017;35[25]:2875-84).
At ESMO 2019, George W. Sledge Jr., MD, of Stanford (Calif.) Medical Center, and colleagues reported the OS results, a secondary endpoint for the trial (JAMA Oncol. 2019 Sep 29. doi. 10.1001/jamaoncol.2019.4782). At the prespecified interim analysis point, median OS for abema-F was 46.7 months vs. 37.3 months for placebo-F (HR, 0.757; 95% CI 0.505-0.945; P = .0137). Patients with greatest benefit from abema-F were exactly the patients who needed the most help – those with visceral metastases (HR 0.675) and with primary resistance to prior hormonal therapy (HR, 0.686).
At 3 years, at least three times as many patients remained progression free with abema-F, compared with placebo-F, and the abema-F patients experienced prolongation in time to eventual chemotherapy (50.2 months vs. 22.1 months; HR, 0.625).
What this means in clinical practice
Many times I find myself sitting at the annual meeting of the American Society of Clinical Oncology and thinking, “Only a medical oncologist like me would find this result exciting.” Prior to ESMO 2019, MONARCH 2 (and a similar study presented at ESMO 2019, MONALEESA-3, which employed an alternative CDK 4/6 inhibitor, ribociclib, with similar OS results) added to the body of literature that caused NCCN guidelines to list all of the approved CDK 4/6 inhibitors plus endocrine therapy for first- or second-line use in patients with hormone-receptor positive, HER2/neu-negative mBC. NCCN guidelines have the caveat that, among patients with disease progression on CDK 4/6 inhibitors in the first-line setting, there are no data to support continuing the CDK 4/6 inhibitor or switching to an alternative CDK 4/6 inhibitor thereafter.
For that shrinking group of patients and doctors who choose to avoid CDK 4/6 inhibitors for first-line treatment, as we describe risks and benefits of using a CDK 4/6 inhibitor for second- or third-line therapy, we have high-quality OS information from ESMO 2019 to answer the “Is it worth it?” question.
Are the results of MONARCH 2 and MONALEESA-3 practice changing? No. We were already convinced. Should we be excited that we have this new information for discussions with our patients? Absolutely.
Dr. Lyss has been a community-based medical oncologist and clinical researcher for more than 35 years, practicing in St. Louis. His clinical and research interests are in the prevention, diagnosis, and treatment of breast and lung cancers and in expanding access to clinical trials to medically underserved populations.
In this edition of “How I will treat my next patient,” I highlight two studies that previously reported significant progression-free survival (PFS) improvements and more recently, at the European Society for Medical Oncology Congress, overall survival (OS) benefit. I reflect on the significance of these new reports in the wake of previously reported data and guidelines from the National Comprehensive Cancer Network (NCCN).
Osimertinib in advanced NSCLC
In the double-blind, phase 3 FLAURA trial, 556 patients with EGFR-mutated (EGFRm), advanced non–small cell lung cancer (NSCLC) received osimertinib or a standard tyrosine kinase inhibitor (TKI) as initial treatment. PFS, the primary endpoint, was clinically and statistically better for osimertinib (18.9 months vs. 10.2 months; hazard ratio 0.46; P less than .001), overall and in all major subgroups. There were fewer grade 3-4 adverse events and fewer permanent treatment discontinuations with osimertinib.
At the time of initial publication, OS data were immature, but because of the substantial survival improvements previously noted, osimertinib was approved by the Food and Drug Administration for first-line treatment of EGFRm stage IV NSCLC patients in April 2018 (N Engl J Med. 2018; 378:113-25).
More recently, at ESMO 2019, Suresh Ramalingam, MD, of the department of hematology and medical oncology at Emory University, Atlanta, and colleagues reported the OS results. Crossover to osimertinib was allowed for patients on the standard TKI arm when they had progressive disease and a T790M mutation. Osimertinib produced a median OS of 38.6 months, compared with 31.8 months for standard TKI (HR, 0.799; P = .0462), a 24-month OS rate of 74% vs. 59% (with no overlap in the 95% confidence intervals), and a 36-month OS rate of 54% vs. 44%. These benefits were interpreted to be statistically significant and clinically meaningful.
The 31.8-month median OS for standard TKI was competitive with the highest reported OS for standard therapy, perhaps because crossover to osimertinib was permitted.
What this means in clinical practice
The report by Dr. Ramalingam and colleagues – and the next abstract I will review – remind me of the famous “You had me at Hello” line from “Jerry Maguire.”
For patient education – and perhaps for some national regulatory agencies – it is good that we now have definition of what the average OS is with osimertinib, compared with standard TKI followed by osimertinib. However, very few oncologists in the United States likely use the latter strategy anymore. It was clear when the impressive PFS and toxicity information appeared in 2018 in the New England Journal of Medicine that osimertinib is the best tolerated, most durably effective front-line treatment for EGFRm mNSCLC, regardless of disease extent, sex, nationality, type of EGFRm (L858R amino acid substitution in exon 21 or exon 19 deletion), or presence/absence of central nervous system metastases.
In NCCN guidelines, osimertinib was listed as the preferred TKI, prior to the OS report at ESMO 2019. The challenges going forward will be to identify high-risk patient subsets who might benefit from drug combinations or novel new agents.
MONARCH 2: Abemaciclib plus fulvestrant
In the MONARCH 2, randomized, placebo-controlled, phase 3 trial, abemaciclib plus fulvestrant (abema-F) significantly improved PFS, in comparison with placebo plus fulvestrant (placebo-F; 16.9 months vs. 9.3 months; HR, 0.563) in 669 premenopausal (with concurrent ovarian function suppression) and postmenopausal women with metastatic breast cancer (mBC) who had disease progression on one to two lines of prior hormonal therapy (J Clin Oncol. 2017;35[25]:2875-84).
At ESMO 2019, George W. Sledge Jr., MD, of Stanford (Calif.) Medical Center, and colleagues reported the OS results, a secondary endpoint for the trial (JAMA Oncol. 2019 Sep 29. doi. 10.1001/jamaoncol.2019.4782). At the prespecified interim analysis point, median OS for abema-F was 46.7 months vs. 37.3 months for placebo-F (HR, 0.757; 95% CI 0.505-0.945; P = .0137). Patients with greatest benefit from abema-F were exactly the patients who needed the most help – those with visceral metastases (HR 0.675) and with primary resistance to prior hormonal therapy (HR, 0.686).
At 3 years, at least three times as many patients remained progression free with abema-F, compared with placebo-F, and the abema-F patients experienced prolongation in time to eventual chemotherapy (50.2 months vs. 22.1 months; HR, 0.625).
What this means in clinical practice
Many times I find myself sitting at the annual meeting of the American Society of Clinical Oncology and thinking, “Only a medical oncologist like me would find this result exciting.” Prior to ESMO 2019, MONARCH 2 (and a similar study presented at ESMO 2019, MONALEESA-3, which employed an alternative CDK 4/6 inhibitor, ribociclib, with similar OS results) added to the body of literature that caused NCCN guidelines to list all of the approved CDK 4/6 inhibitors plus endocrine therapy for first- or second-line use in patients with hormone-receptor positive, HER2/neu-negative mBC. NCCN guidelines have the caveat that, among patients with disease progression on CDK 4/6 inhibitors in the first-line setting, there are no data to support continuing the CDK 4/6 inhibitor or switching to an alternative CDK 4/6 inhibitor thereafter.
For that shrinking group of patients and doctors who choose to avoid CDK 4/6 inhibitors for first-line treatment, as we describe risks and benefits of using a CDK 4/6 inhibitor for second- or third-line therapy, we have high-quality OS information from ESMO 2019 to answer the “Is it worth it?” question.
Are the results of MONARCH 2 and MONALEESA-3 practice changing? No. We were already convinced. Should we be excited that we have this new information for discussions with our patients? Absolutely.
Dr. Lyss has been a community-based medical oncologist and clinical researcher for more than 35 years, practicing in St. Louis. His clinical and research interests are in the prevention, diagnosis, and treatment of breast and lung cancers and in expanding access to clinical trials to medically underserved populations.
In this edition of “How I will treat my next patient,” I highlight two studies that previously reported significant progression-free survival (PFS) improvements and more recently, at the European Society for Medical Oncology Congress, overall survival (OS) benefit. I reflect on the significance of these new reports in the wake of previously reported data and guidelines from the National Comprehensive Cancer Network (NCCN).
Osimertinib in advanced NSCLC
In the double-blind, phase 3 FLAURA trial, 556 patients with EGFR-mutated (EGFRm), advanced non–small cell lung cancer (NSCLC) received osimertinib or a standard tyrosine kinase inhibitor (TKI) as initial treatment. PFS, the primary endpoint, was clinically and statistically better for osimertinib (18.9 months vs. 10.2 months; hazard ratio 0.46; P less than .001), overall and in all major subgroups. There were fewer grade 3-4 adverse events and fewer permanent treatment discontinuations with osimertinib.
At the time of initial publication, OS data were immature, but because of the substantial survival improvements previously noted, osimertinib was approved by the Food and Drug Administration for first-line treatment of EGFRm stage IV NSCLC patients in April 2018 (N Engl J Med. 2018; 378:113-25).
More recently, at ESMO 2019, Suresh Ramalingam, MD, of the department of hematology and medical oncology at Emory University, Atlanta, and colleagues reported the OS results. Crossover to osimertinib was allowed for patients on the standard TKI arm when they had progressive disease and a T790M mutation. Osimertinib produced a median OS of 38.6 months, compared with 31.8 months for standard TKI (HR, 0.799; P = .0462), a 24-month OS rate of 74% vs. 59% (with no overlap in the 95% confidence intervals), and a 36-month OS rate of 54% vs. 44%. These benefits were interpreted to be statistically significant and clinically meaningful.
The 31.8-month median OS for standard TKI was competitive with the highest reported OS for standard therapy, perhaps because crossover to osimertinib was permitted.
What this means in clinical practice
The report by Dr. Ramalingam and colleagues – and the next abstract I will review – remind me of the famous “You had me at Hello” line from “Jerry Maguire.”
For patient education – and perhaps for some national regulatory agencies – it is good that we now have definition of what the average OS is with osimertinib, compared with standard TKI followed by osimertinib. However, very few oncologists in the United States likely use the latter strategy anymore. It was clear when the impressive PFS and toxicity information appeared in 2018 in the New England Journal of Medicine that osimertinib is the best tolerated, most durably effective front-line treatment for EGFRm mNSCLC, regardless of disease extent, sex, nationality, type of EGFRm (L858R amino acid substitution in exon 21 or exon 19 deletion), or presence/absence of central nervous system metastases.
In NCCN guidelines, osimertinib was listed as the preferred TKI, prior to the OS report at ESMO 2019. The challenges going forward will be to identify high-risk patient subsets who might benefit from drug combinations or novel new agents.
MONARCH 2: Abemaciclib plus fulvestrant
In the MONARCH 2, randomized, placebo-controlled, phase 3 trial, abemaciclib plus fulvestrant (abema-F) significantly improved PFS, in comparison with placebo plus fulvestrant (placebo-F; 16.9 months vs. 9.3 months; HR, 0.563) in 669 premenopausal (with concurrent ovarian function suppression) and postmenopausal women with metastatic breast cancer (mBC) who had disease progression on one to two lines of prior hormonal therapy (J Clin Oncol. 2017;35[25]:2875-84).
At ESMO 2019, George W. Sledge Jr., MD, of Stanford (Calif.) Medical Center, and colleagues reported the OS results, a secondary endpoint for the trial (JAMA Oncol. 2019 Sep 29. doi. 10.1001/jamaoncol.2019.4782). At the prespecified interim analysis point, median OS for abema-F was 46.7 months vs. 37.3 months for placebo-F (HR, 0.757; 95% CI 0.505-0.945; P = .0137). Patients with greatest benefit from abema-F were exactly the patients who needed the most help – those with visceral metastases (HR 0.675) and with primary resistance to prior hormonal therapy (HR, 0.686).
At 3 years, at least three times as many patients remained progression free with abema-F, compared with placebo-F, and the abema-F patients experienced prolongation in time to eventual chemotherapy (50.2 months vs. 22.1 months; HR, 0.625).
What this means in clinical practice
Many times I find myself sitting at the annual meeting of the American Society of Clinical Oncology and thinking, “Only a medical oncologist like me would find this result exciting.” Prior to ESMO 2019, MONARCH 2 (and a similar study presented at ESMO 2019, MONALEESA-3, which employed an alternative CDK 4/6 inhibitor, ribociclib, with similar OS results) added to the body of literature that caused NCCN guidelines to list all of the approved CDK 4/6 inhibitors plus endocrine therapy for first- or second-line use in patients with hormone-receptor positive, HER2/neu-negative mBC. NCCN guidelines have the caveat that, among patients with disease progression on CDK 4/6 inhibitors in the first-line setting, there are no data to support continuing the CDK 4/6 inhibitor or switching to an alternative CDK 4/6 inhibitor thereafter.
For that shrinking group of patients and doctors who choose to avoid CDK 4/6 inhibitors for first-line treatment, as we describe risks and benefits of using a CDK 4/6 inhibitor for second- or third-line therapy, we have high-quality OS information from ESMO 2019 to answer the “Is it worth it?” question.
Are the results of MONARCH 2 and MONALEESA-3 practice changing? No. We were already convinced. Should we be excited that we have this new information for discussions with our patients? Absolutely.
Dr. Lyss has been a community-based medical oncologist and clinical researcher for more than 35 years, practicing in St. Louis. His clinical and research interests are in the prevention, diagnosis, and treatment of breast and lung cancers and in expanding access to clinical trials to medically underserved populations.
Atezolizumab bests chemo in NSCLC patients with high PD-L1 expression
NATIONAL HARBOR, MD – interim results of a phase 3 trial suggest.

When compared with platinum-based chemotherapy, atezolizumab significantly improved OS in patients who had PD-L1 expression of 50% or greater on tumor cells (TC) or 10% or greater on tumor-infiltrating immune cells (IC).
Patients with lower levels of PD-L1 expression had a numerical, but not statistically significant, benefit in OS with atezolizumab.
Giuseppe Giaccone, MD, PhD, of Georgetown University, Washington, presented these results, from the IMpower110 trial, as a late-breaking abstract at the annual meeting of the Society for Immunotherapy of Cancer.
The trial enrolled treatment-naive, PD-L1–selected patients with stage IV NSCLC. Patients with EGFR-positive or ALK-positive NSCLC were excluded.
The overall population consisted of 554 patients with PD-L1 expression of at least 1% on TC or IC (TC1/2/3 or IC1/2/3). There were 328 patients with PD-L1 expression of at least 5% on TC or IC (TC2/3 or IC2/3) and 205 patients with PD-L1 expression of at least 50% on TC or 10% on IC (TC3 or IC3).
All patients were randomized to receive atezolizumab or platinum-based chemotherapy. Atezolizumab was given at 1,200 mg every 3 weeks until disease progression or loss of clinical benefit. In the chemotherapy arm, patients with nonsquamous NSCLC received cisplatin or carboplatin plus pemetrexed, and patients with squamous NSCLC received cisplatin or carboplatin plus gemcitabine. Chemotherapy was given for 4-6 cycles, after which patients received pemetrexed (nonsquamous) or best supportive care (squamous) until progression.
Baseline characteristics were similar between the treatment arms and across the PD-L1 subgroups.
Overall survival
OS was evaluated hierarchically, starting with the TC3 or IC3 population. This group had a significant improvement in OS with atezolizumab. At a median follow-up of 15.7 months, the median OS was 13.1 months with chemotherapy and 20.2 months with atezolizumab (hazard ratio, 0.59; P = .0106).
The TC2/3 or IC2/3 population had a numerical, but not significant, improvement in OS with atezolizumab. At a median follow-up of 15.2 months, the median OS was 14.9 months with chemotherapy and 18.2 months with atezolizumab (HR, 0.72; P = .0416).
“The prespecified alpha boundary was not crossed in this analysis,” Dr. Giaccone said. “Therefore, it cannot be considered statistically significant, although, numerically, there is clearly an advantage with atezolizumab versus chemotherapy.”
There was no significant improvement in OS in the overall population (TC1/2/3 or IC1/2/3). At a median follow-up of 13.4 months, the median OS was 14.1 months in the chemotherapy arm and 17.5 months in the atezolizumab arm (HR, 0.83; P = .1481).
Dr. Giaccone noted that 29.6% of patients in the atezolizumab arm and 49.5% of those in the chemotherapy arm received at least one subsequent cancer therapy. The proportion of patients that received second-line cancer therapies was similar across the PD-L1 subgroups.
Progression-free survival
Progression-free survival (PFS) was significantly better with atezolizumab, regardless of PD-L1 expression.
In the TC3/IC3 population, the median PFS was 5.0 months with chemotherapy and 8.1 months with atezolizumab (HR, 0.63; P = .0070). In the TC2/3 or IC2/3 group, the median PFS was 5.5 months with chemotherapy and 7.2 months with atezolizumab (HR, 0.67; P = .0030). In the overall population, the median PFS was 5.5 months with chemotherapy and 5.7 months with atezolizumab (HR, 0.77; P = .0104).
Safety
“The safety profile of atezolizumab was consistent with prior observations,” Dr. Giaccone said.
The incidence of treatment-related adverse events (AEs) was 90.2% in the atezolizumab arm and 94.7% in the chemotherapy arm. Rates of grade 3/4 related AEs were 12.9% and 44.1%, respectively. There was one grade 5 AE in the chemotherapy arm and none in the atezolizumab arm.
AEs that were more frequent with atezolizumab included increased aspartate aminotransferase, pruritus, and hypothyroidism.
This trial is sponsored by Hoffmann-La Roche, and Dr. Giaccone disclosed grants and nonfinancial support from the company.
SOURCE: Giaccone G et al. SITC 2019, Abstract O81.
NATIONAL HARBOR, MD – interim results of a phase 3 trial suggest.
When compared with platinum-based chemotherapy, atezolizumab significantly improved OS in patients who had PD-L1 expression of 50% or greater on tumor cells (TC) or 10% or greater on tumor-infiltrating immune cells (IC).
Patients with lower levels of PD-L1 expression had a numerical, but not statistically significant, benefit in OS with atezolizumab.
Giuseppe Giaccone, MD, PhD, of Georgetown University, Washington, presented these results, from the IMpower110 trial, as a late-breaking abstract at the annual meeting of the Society for Immunotherapy of Cancer.
The trial enrolled treatment-naive, PD-L1–selected patients with stage IV NSCLC. Patients with EGFR-positive or ALK-positive NSCLC were excluded.
The overall population consisted of 554 patients with PD-L1 expression of at least 1% on TC or IC (TC1/2/3 or IC1/2/3). There were 328 patients with PD-L1 expression of at least 5% on TC or IC (TC2/3 or IC2/3) and 205 patients with PD-L1 expression of at least 50% on TC or 10% on IC (TC3 or IC3).
All patients were randomized to receive atezolizumab or platinum-based chemotherapy. Atezolizumab was given at 1,200 mg every 3 weeks until disease progression or loss of clinical benefit. In the chemotherapy arm, patients with nonsquamous NSCLC received cisplatin or carboplatin plus pemetrexed, and patients with squamous NSCLC received cisplatin or carboplatin plus gemcitabine. Chemotherapy was given for 4-6 cycles, after which patients received pemetrexed (nonsquamous) or best supportive care (squamous) until progression.
Baseline characteristics were similar between the treatment arms and across the PD-L1 subgroups.
Overall survival
OS was evaluated hierarchically, starting with the TC3 or IC3 population. This group had a significant improvement in OS with atezolizumab. At a median follow-up of 15.7 months, the median OS was 13.1 months with chemotherapy and 20.2 months with atezolizumab (hazard ratio, 0.59; P = .0106).
The TC2/3 or IC2/3 population had a numerical, but not significant, improvement in OS with atezolizumab. At a median follow-up of 15.2 months, the median OS was 14.9 months with chemotherapy and 18.2 months with atezolizumab (HR, 0.72; P = .0416).
“The prespecified alpha boundary was not crossed in this analysis,” Dr. Giaccone said. “Therefore, it cannot be considered statistically significant, although, numerically, there is clearly an advantage with atezolizumab versus chemotherapy.”
There was no significant improvement in OS in the overall population (TC1/2/3 or IC1/2/3). At a median follow-up of 13.4 months, the median OS was 14.1 months in the chemotherapy arm and 17.5 months in the atezolizumab arm (HR, 0.83; P = .1481).
Dr. Giaccone noted that 29.6% of patients in the atezolizumab arm and 49.5% of those in the chemotherapy arm received at least one subsequent cancer therapy. The proportion of patients that received second-line cancer therapies was similar across the PD-L1 subgroups.
Progression-free survival
Progression-free survival (PFS) was significantly better with atezolizumab, regardless of PD-L1 expression.
In the TC3/IC3 population, the median PFS was 5.0 months with chemotherapy and 8.1 months with atezolizumab (HR, 0.63; P = .0070). In the TC2/3 or IC2/3 group, the median PFS was 5.5 months with chemotherapy and 7.2 months with atezolizumab (HR, 0.67; P = .0030). In the overall population, the median PFS was 5.5 months with chemotherapy and 5.7 months with atezolizumab (HR, 0.77; P = .0104).
Safety
“The safety profile of atezolizumab was consistent with prior observations,” Dr. Giaccone said.
The incidence of treatment-related adverse events (AEs) was 90.2% in the atezolizumab arm and 94.7% in the chemotherapy arm. Rates of grade 3/4 related AEs were 12.9% and 44.1%, respectively. There was one grade 5 AE in the chemotherapy arm and none in the atezolizumab arm.
AEs that were more frequent with atezolizumab included increased aspartate aminotransferase, pruritus, and hypothyroidism.
This trial is sponsored by Hoffmann-La Roche, and Dr. Giaccone disclosed grants and nonfinancial support from the company.
SOURCE: Giaccone G et al. SITC 2019, Abstract O81.
NATIONAL HARBOR, MD – interim results of a phase 3 trial suggest.
When compared with platinum-based chemotherapy, atezolizumab significantly improved OS in patients who had PD-L1 expression of 50% or greater on tumor cells (TC) or 10% or greater on tumor-infiltrating immune cells (IC).
Patients with lower levels of PD-L1 expression had a numerical, but not statistically significant, benefit in OS with atezolizumab.
Giuseppe Giaccone, MD, PhD, of Georgetown University, Washington, presented these results, from the IMpower110 trial, as a late-breaking abstract at the annual meeting of the Society for Immunotherapy of Cancer.
The trial enrolled treatment-naive, PD-L1–selected patients with stage IV NSCLC. Patients with EGFR-positive or ALK-positive NSCLC were excluded.
The overall population consisted of 554 patients with PD-L1 expression of at least 1% on TC or IC (TC1/2/3 or IC1/2/3). There were 328 patients with PD-L1 expression of at least 5% on TC or IC (TC2/3 or IC2/3) and 205 patients with PD-L1 expression of at least 50% on TC or 10% on IC (TC3 or IC3).
All patients were randomized to receive atezolizumab or platinum-based chemotherapy. Atezolizumab was given at 1,200 mg every 3 weeks until disease progression or loss of clinical benefit. In the chemotherapy arm, patients with nonsquamous NSCLC received cisplatin or carboplatin plus pemetrexed, and patients with squamous NSCLC received cisplatin or carboplatin plus gemcitabine. Chemotherapy was given for 4-6 cycles, after which patients received pemetrexed (nonsquamous) or best supportive care (squamous) until progression.
Baseline characteristics were similar between the treatment arms and across the PD-L1 subgroups.
Overall survival
OS was evaluated hierarchically, starting with the TC3 or IC3 population. This group had a significant improvement in OS with atezolizumab. At a median follow-up of 15.7 months, the median OS was 13.1 months with chemotherapy and 20.2 months with atezolizumab (hazard ratio, 0.59; P = .0106).
The TC2/3 or IC2/3 population had a numerical, but not significant, improvement in OS with atezolizumab. At a median follow-up of 15.2 months, the median OS was 14.9 months with chemotherapy and 18.2 months with atezolizumab (HR, 0.72; P = .0416).
“The prespecified alpha boundary was not crossed in this analysis,” Dr. Giaccone said. “Therefore, it cannot be considered statistically significant, although, numerically, there is clearly an advantage with atezolizumab versus chemotherapy.”
There was no significant improvement in OS in the overall population (TC1/2/3 or IC1/2/3). At a median follow-up of 13.4 months, the median OS was 14.1 months in the chemotherapy arm and 17.5 months in the atezolizumab arm (HR, 0.83; P = .1481).
Dr. Giaccone noted that 29.6% of patients in the atezolizumab arm and 49.5% of those in the chemotherapy arm received at least one subsequent cancer therapy. The proportion of patients that received second-line cancer therapies was similar across the PD-L1 subgroups.
Progression-free survival
Progression-free survival (PFS) was significantly better with atezolizumab, regardless of PD-L1 expression.
In the TC3/IC3 population, the median PFS was 5.0 months with chemotherapy and 8.1 months with atezolizumab (HR, 0.63; P = .0070). In the TC2/3 or IC2/3 group, the median PFS was 5.5 months with chemotherapy and 7.2 months with atezolizumab (HR, 0.67; P = .0030). In the overall population, the median PFS was 5.5 months with chemotherapy and 5.7 months with atezolizumab (HR, 0.77; P = .0104).
Safety
“The safety profile of atezolizumab was consistent with prior observations,” Dr. Giaccone said.
The incidence of treatment-related adverse events (AEs) was 90.2% in the atezolizumab arm and 94.7% in the chemotherapy arm. Rates of grade 3/4 related AEs were 12.9% and 44.1%, respectively. There was one grade 5 AE in the chemotherapy arm and none in the atezolizumab arm.
AEs that were more frequent with atezolizumab included increased aspartate aminotransferase, pruritus, and hypothyroidism.
This trial is sponsored by Hoffmann-La Roche, and Dr. Giaccone disclosed grants and nonfinancial support from the company.
SOURCE: Giaccone G et al. SITC 2019, Abstract O81.
REPORTING FROM SITC 2019
Lung cancer screening, early diagnosis still lower among blacks, Hispanics
SAN FRANCISCO – A review of lung cancer cases in New York suggests that 2011 guidelines issued by the National Comprehensive Cancer Network (NCCN) have made little difference in addressing ethnic and socioeconomic disparities in lung cancer diagnosis. The review showed some progress; however, . The researchers also found a reduced incidence of lung cancer only in whites.
The guidelines call for CT screening for smokers aged 55-74 years that have a 30 pack-year history within the past 15 years and were based on a lung cancer screening trial showing that annual low-dose CT led to a 20% reduction in lung cancer deaths, compared with chest x-ray (N Eng J Med. 2011;365:395-409).
Nonwhites “aren’t always exposed to screening opportunities, and may be taken care of by providers who haven’t necessarily bought into screening or aren’t necessarily aware of it. So the downstream effects of the lack of access to screening hurts them doubly, because they’re diagnosed later and they also have disparities in access to treatment,” said Elizabeth David, MD, in an interview. Dr. David is an associate professor of surgery of University of Southern California, Los Angeles. She comoderated a session at the annual congress of the American College of Surgeons, where the research was presented.
The findings underscore the need to get the word out to primary care providers in all communities that catching lung cancer early can make all the difference to patients. “The more we can do to talk about lung cancer as a treatable disease and a cancer that can become a chronically managed medical problem for patients, rather than a death sentence, which it has the misperception of being, the more we can encourage people to seek treatment when they have a symptom, instead of being afraid and doing nothing,” said Dr. David.
The researchers considered metropolitan New York to be a good test case to examine the impact of the screening guidelines since it is socioeconomically and racially diverse. “New York presents a microcosm of what’s going on nationally in other urban areas,” said Tamar Nobel, MD, from Mount Sinai Hospital, New York, who presented the study.
The researchers analyzed records from the New York State Cancer Registry from the period 2008-201 and compared that with data from 2012-2015 (total, n = 18,284). The incidence of lung cancer declined among whites from the first period to the second, at an average annual percent change of –1.5% (95% confidence interval, –1.0% to –2.0%). A similar result was seen in Hispanics (–1.7%; 95% CI, –0.4% to –2.9%), but not among blacks (–1.2%; not significant). There was an increase among Asians/Pacific Islanders (+1.4%; 95% CI, 0.6% to 2.2%).
There were also inequalities when it came to the odds of a stage I diagnosis. Although the percentages increased in whites (+3.5%; 95% CI, 0.6%-6.4%) and blacks (+6.0%; 95% CI, 2.3%-9.7%), the median percentage was higher among whites (27.6% versus 18.2%; no overlap among 95% CIs; odds ratio, 0.62; 95% CI, 0.56-0.68). Hispanics and Asians/Pacific Islanders experienced no significant changes in their odds of a stage I diagnosis, and both groups remained significantly less likely than whites to be diagnosed with stage I disease (OR, 0.72 and 0.86, respectively, both significant).
No funding was disclosed. Dr. David and Dr. Nobel have no relevant financial disclosures.
SOURCE: Nobel T et al. ACS Clinical Congress 2019. Abstract, doi: 10.1016/j.jamcollsurg.2019.08.607.
SAN FRANCISCO – A review of lung cancer cases in New York suggests that 2011 guidelines issued by the National Comprehensive Cancer Network (NCCN) have made little difference in addressing ethnic and socioeconomic disparities in lung cancer diagnosis. The review showed some progress; however, . The researchers also found a reduced incidence of lung cancer only in whites.
The guidelines call for CT screening for smokers aged 55-74 years that have a 30 pack-year history within the past 15 years and were based on a lung cancer screening trial showing that annual low-dose CT led to a 20% reduction in lung cancer deaths, compared with chest x-ray (N Eng J Med. 2011;365:395-409).
Nonwhites “aren’t always exposed to screening opportunities, and may be taken care of by providers who haven’t necessarily bought into screening or aren’t necessarily aware of it. So the downstream effects of the lack of access to screening hurts them doubly, because they’re diagnosed later and they also have disparities in access to treatment,” said Elizabeth David, MD, in an interview. Dr. David is an associate professor of surgery of University of Southern California, Los Angeles. She comoderated a session at the annual congress of the American College of Surgeons, where the research was presented.
The findings underscore the need to get the word out to primary care providers in all communities that catching lung cancer early can make all the difference to patients. “The more we can do to talk about lung cancer as a treatable disease and a cancer that can become a chronically managed medical problem for patients, rather than a death sentence, which it has the misperception of being, the more we can encourage people to seek treatment when they have a symptom, instead of being afraid and doing nothing,” said Dr. David.
The researchers considered metropolitan New York to be a good test case to examine the impact of the screening guidelines since it is socioeconomically and racially diverse. “New York presents a microcosm of what’s going on nationally in other urban areas,” said Tamar Nobel, MD, from Mount Sinai Hospital, New York, who presented the study.
The researchers analyzed records from the New York State Cancer Registry from the period 2008-201 and compared that with data from 2012-2015 (total, n = 18,284). The incidence of lung cancer declined among whites from the first period to the second, at an average annual percent change of –1.5% (95% confidence interval, –1.0% to –2.0%). A similar result was seen in Hispanics (–1.7%; 95% CI, –0.4% to –2.9%), but not among blacks (–1.2%; not significant). There was an increase among Asians/Pacific Islanders (+1.4%; 95% CI, 0.6% to 2.2%).
There were also inequalities when it came to the odds of a stage I diagnosis. Although the percentages increased in whites (+3.5%; 95% CI, 0.6%-6.4%) and blacks (+6.0%; 95% CI, 2.3%-9.7%), the median percentage was higher among whites (27.6% versus 18.2%; no overlap among 95% CIs; odds ratio, 0.62; 95% CI, 0.56-0.68). Hispanics and Asians/Pacific Islanders experienced no significant changes in their odds of a stage I diagnosis, and both groups remained significantly less likely than whites to be diagnosed with stage I disease (OR, 0.72 and 0.86, respectively, both significant).
No funding was disclosed. Dr. David and Dr. Nobel have no relevant financial disclosures.
SOURCE: Nobel T et al. ACS Clinical Congress 2019. Abstract, doi: 10.1016/j.jamcollsurg.2019.08.607.
SAN FRANCISCO – A review of lung cancer cases in New York suggests that 2011 guidelines issued by the National Comprehensive Cancer Network (NCCN) have made little difference in addressing ethnic and socioeconomic disparities in lung cancer diagnosis. The review showed some progress; however, . The researchers also found a reduced incidence of lung cancer only in whites.
The guidelines call for CT screening for smokers aged 55-74 years that have a 30 pack-year history within the past 15 years and were based on a lung cancer screening trial showing that annual low-dose CT led to a 20% reduction in lung cancer deaths, compared with chest x-ray (N Eng J Med. 2011;365:395-409).
Nonwhites “aren’t always exposed to screening opportunities, and may be taken care of by providers who haven’t necessarily bought into screening or aren’t necessarily aware of it. So the downstream effects of the lack of access to screening hurts them doubly, because they’re diagnosed later and they also have disparities in access to treatment,” said Elizabeth David, MD, in an interview. Dr. David is an associate professor of surgery of University of Southern California, Los Angeles. She comoderated a session at the annual congress of the American College of Surgeons, where the research was presented.
The findings underscore the need to get the word out to primary care providers in all communities that catching lung cancer early can make all the difference to patients. “The more we can do to talk about lung cancer as a treatable disease and a cancer that can become a chronically managed medical problem for patients, rather than a death sentence, which it has the misperception of being, the more we can encourage people to seek treatment when they have a symptom, instead of being afraid and doing nothing,” said Dr. David.
The researchers considered metropolitan New York to be a good test case to examine the impact of the screening guidelines since it is socioeconomically and racially diverse. “New York presents a microcosm of what’s going on nationally in other urban areas,” said Tamar Nobel, MD, from Mount Sinai Hospital, New York, who presented the study.
The researchers analyzed records from the New York State Cancer Registry from the period 2008-201 and compared that with data from 2012-2015 (total, n = 18,284). The incidence of lung cancer declined among whites from the first period to the second, at an average annual percent change of –1.5% (95% confidence interval, –1.0% to –2.0%). A similar result was seen in Hispanics (–1.7%; 95% CI, –0.4% to –2.9%), but not among blacks (–1.2%; not significant). There was an increase among Asians/Pacific Islanders (+1.4%; 95% CI, 0.6% to 2.2%).
There were also inequalities when it came to the odds of a stage I diagnosis. Although the percentages increased in whites (+3.5%; 95% CI, 0.6%-6.4%) and blacks (+6.0%; 95% CI, 2.3%-9.7%), the median percentage was higher among whites (27.6% versus 18.2%; no overlap among 95% CIs; odds ratio, 0.62; 95% CI, 0.56-0.68). Hispanics and Asians/Pacific Islanders experienced no significant changes in their odds of a stage I diagnosis, and both groups remained significantly less likely than whites to be diagnosed with stage I disease (OR, 0.72 and 0.86, respectively, both significant).
No funding was disclosed. Dr. David and Dr. Nobel have no relevant financial disclosures.
SOURCE: Nobel T et al. ACS Clinical Congress 2019. Abstract, doi: 10.1016/j.jamcollsurg.2019.08.607.
REPORTING FROM CLINICAL CONGRESS 2019
Lung cancer on the decline, but still higher among men than women
according to the Centers for Disease Control and Prevention.
![]()
From 2007 to 2016, rates dropped among both sexes in metropolitan and nonmetropolitan areas, according to Mary Elizabeth O’Neil, MPH, and colleagues. Their report is in Morbidity and Mortality Weekly Report (MMWR Morb Mortal Wkly Rep. 2019 Nov 8;68[44];993-8). But lung cancer incidence in 2016 was still 40% higher among men than among women, said Ms. O’Neil, an epidemiologist at the CDC.
Rather than narrowly focusing on the “just stop smoking” message, “a comprehensive approach to lung cancer prevention and control includes such population-based strategies as screening for tobacco dependence, promoting tobacco cessation, implementing comprehensive smoke-free laws, testing all homes for radon and using proven methods to lower high radon levels, and reducing exposure to lung carcinogens such as asbestos.” According to the authors of the report, “increasing the implementation of these strategies, particularly among persons living in nonmetropolitan counties, might help to reduce disparities in the decline of lung cancer incidence.”
The recommendation is based on data extracted from the U.S. Cancer Statistics Database for 2007-2016. The data cover 97% of the population.
In nonmetropolitan counties in 2007, incidence rates among men were 60% higher (99 vs. 61 per 100,000). Although rates decreased in both sexes, they were still elevated compared with women in 2016 (82 vs. 58 per 100,000; 40%).
Over the 10-year period, the rate declined more among men than among women (–2.9% vs. –1.5%) in metropolitan areas. The pattern repeated in nonmetropolitan areas (–2.1% and –0.5%, respectively).
There were different declines in different age groups by region, the authors noted.
Men aged 45-54 years in metropolitan areas experienced the largest decline (–5.2%).
Among women, the largest decline occurred in metropolitan areas among those aged 35-44 years (–5%). In nonmetropolitan areas, women in this age group experienced a 3.6% decline and women aged 65-74 years, a 1.3% decline.
Among persons aged 35-54 years, incidence rates in nonmetropolitan and metropolitan counties did not differ by sex but were higher in nonmetropolitan counties than in metropolitan counties.
There were also overall changes in smoking patterns. According to 2017 data from the National Health Interview Survey data, more adults in metropolitan areas than nonmetropolitan areas smoked (23% versus 13%) but fewer had tried to quit (50% vs. 56%). Successful quitting attempts also were lower (5% vs. 9%).
Although it is a large contributing factor, smoking is not the only risk factor for lung cancer, the authors wrote. About 10%-15% of lung cancer patients have never smoked tobacco. Nonsmoked tobacco products and second-hand exposure to cigarette smoke are risks, as are indoor radon and asbestos exposure.
Clinicians can help improve this scenario by screening at each office visit, the authors said. The recommendation is based on U.S. Preventive Services Task Force guidance.
“Lung cancer screening is recommended for adults at high risk for developing lung cancer because of their age and cigarette smoking history. Screening efforts can identify lung cancer in its early stages and provide an important opportunity to promote tobacco smoking cessation.”
However, lack of insurance among residents of nonmetropolitan areas may hamper access to these services, they said. In those regions, “a higher percentage of residents aged less than 65 years report being uninsured compared with those in metropolitan areas.”
SOURCE: O’Neil ME et al. MMWR Morb Mortal Wkly Rep. 2019 Nov 8: 68(44);993-8.
according to the Centers for Disease Control and Prevention.
![]()
From 2007 to 2016, rates dropped among both sexes in metropolitan and nonmetropolitan areas, according to Mary Elizabeth O’Neil, MPH, and colleagues. Their report is in Morbidity and Mortality Weekly Report (MMWR Morb Mortal Wkly Rep. 2019 Nov 8;68[44];993-8). But lung cancer incidence in 2016 was still 40% higher among men than among women, said Ms. O’Neil, an epidemiologist at the CDC.
Rather than narrowly focusing on the “just stop smoking” message, “a comprehensive approach to lung cancer prevention and control includes such population-based strategies as screening for tobacco dependence, promoting tobacco cessation, implementing comprehensive smoke-free laws, testing all homes for radon and using proven methods to lower high radon levels, and reducing exposure to lung carcinogens such as asbestos.” According to the authors of the report, “increasing the implementation of these strategies, particularly among persons living in nonmetropolitan counties, might help to reduce disparities in the decline of lung cancer incidence.”
The recommendation is based on data extracted from the U.S. Cancer Statistics Database for 2007-2016. The data cover 97% of the population.
In nonmetropolitan counties in 2007, incidence rates among men were 60% higher (99 vs. 61 per 100,000). Although rates decreased in both sexes, they were still elevated compared with women in 2016 (82 vs. 58 per 100,000; 40%).
Over the 10-year period, the rate declined more among men than among women (–2.9% vs. –1.5%) in metropolitan areas. The pattern repeated in nonmetropolitan areas (–2.1% and –0.5%, respectively).
There were different declines in different age groups by region, the authors noted.
Men aged 45-54 years in metropolitan areas experienced the largest decline (–5.2%).
Among women, the largest decline occurred in metropolitan areas among those aged 35-44 years (–5%). In nonmetropolitan areas, women in this age group experienced a 3.6% decline and women aged 65-74 years, a 1.3% decline.
Among persons aged 35-54 years, incidence rates in nonmetropolitan and metropolitan counties did not differ by sex but were higher in nonmetropolitan counties than in metropolitan counties.
There were also overall changes in smoking patterns. According to 2017 data from the National Health Interview Survey data, more adults in metropolitan areas than nonmetropolitan areas smoked (23% versus 13%) but fewer had tried to quit (50% vs. 56%). Successful quitting attempts also were lower (5% vs. 9%).
Although it is a large contributing factor, smoking is not the only risk factor for lung cancer, the authors wrote. About 10%-15% of lung cancer patients have never smoked tobacco. Nonsmoked tobacco products and second-hand exposure to cigarette smoke are risks, as are indoor radon and asbestos exposure.
Clinicians can help improve this scenario by screening at each office visit, the authors said. The recommendation is based on U.S. Preventive Services Task Force guidance.
“Lung cancer screening is recommended for adults at high risk for developing lung cancer because of their age and cigarette smoking history. Screening efforts can identify lung cancer in its early stages and provide an important opportunity to promote tobacco smoking cessation.”
However, lack of insurance among residents of nonmetropolitan areas may hamper access to these services, they said. In those regions, “a higher percentage of residents aged less than 65 years report being uninsured compared with those in metropolitan areas.”
SOURCE: O’Neil ME et al. MMWR Morb Mortal Wkly Rep. 2019 Nov 8: 68(44);993-8.
according to the Centers for Disease Control and Prevention.
![]()
From 2007 to 2016, rates dropped among both sexes in metropolitan and nonmetropolitan areas, according to Mary Elizabeth O’Neil, MPH, and colleagues. Their report is in Morbidity and Mortality Weekly Report (MMWR Morb Mortal Wkly Rep. 2019 Nov 8;68[44];993-8). But lung cancer incidence in 2016 was still 40% higher among men than among women, said Ms. O’Neil, an epidemiologist at the CDC.
Rather than narrowly focusing on the “just stop smoking” message, “a comprehensive approach to lung cancer prevention and control includes such population-based strategies as screening for tobacco dependence, promoting tobacco cessation, implementing comprehensive smoke-free laws, testing all homes for radon and using proven methods to lower high radon levels, and reducing exposure to lung carcinogens such as asbestos.” According to the authors of the report, “increasing the implementation of these strategies, particularly among persons living in nonmetropolitan counties, might help to reduce disparities in the decline of lung cancer incidence.”
The recommendation is based on data extracted from the U.S. Cancer Statistics Database for 2007-2016. The data cover 97% of the population.
In nonmetropolitan counties in 2007, incidence rates among men were 60% higher (99 vs. 61 per 100,000). Although rates decreased in both sexes, they were still elevated compared with women in 2016 (82 vs. 58 per 100,000; 40%).
Over the 10-year period, the rate declined more among men than among women (–2.9% vs. –1.5%) in metropolitan areas. The pattern repeated in nonmetropolitan areas (–2.1% and –0.5%, respectively).
There were different declines in different age groups by region, the authors noted.
Men aged 45-54 years in metropolitan areas experienced the largest decline (–5.2%).
Among women, the largest decline occurred in metropolitan areas among those aged 35-44 years (–5%). In nonmetropolitan areas, women in this age group experienced a 3.6% decline and women aged 65-74 years, a 1.3% decline.
Among persons aged 35-54 years, incidence rates in nonmetropolitan and metropolitan counties did not differ by sex but were higher in nonmetropolitan counties than in metropolitan counties.
There were also overall changes in smoking patterns. According to 2017 data from the National Health Interview Survey data, more adults in metropolitan areas than nonmetropolitan areas smoked (23% versus 13%) but fewer had tried to quit (50% vs. 56%). Successful quitting attempts also were lower (5% vs. 9%).
Although it is a large contributing factor, smoking is not the only risk factor for lung cancer, the authors wrote. About 10%-15% of lung cancer patients have never smoked tobacco. Nonsmoked tobacco products and second-hand exposure to cigarette smoke are risks, as are indoor radon and asbestos exposure.
Clinicians can help improve this scenario by screening at each office visit, the authors said. The recommendation is based on U.S. Preventive Services Task Force guidance.
“Lung cancer screening is recommended for adults at high risk for developing lung cancer because of their age and cigarette smoking history. Screening efforts can identify lung cancer in its early stages and provide an important opportunity to promote tobacco smoking cessation.”
However, lack of insurance among residents of nonmetropolitan areas may hamper access to these services, they said. In those regions, “a higher percentage of residents aged less than 65 years report being uninsured compared with those in metropolitan areas.”
SOURCE: O’Neil ME et al. MMWR Morb Mortal Wkly Rep. 2019 Nov 8: 68(44);993-8.
FROM MMWR
Nivolumab benefit for NSCLC persists at 5-year follow-up
BARCELONA – Nivolumab, compared with docetaxel chemotherapy, led to a fivefold improvement in 5-year overall survival among previously treated patients with non–small cell lung cancer (NSCLC), according to a pooled analysis of data from the phase 3 CheckMate 017 and 057 trials.

The 5-year overall survival (OS) rates from the two randomized registrational trials, which established the programmed death-1 (PD-1) inhibitor nivolumab as the standard salvage therapy for NSCLC, were 13.4% vs. 2.6% (median, 11.1 vs. 8.1 months) with nivolumab and docetaxel, respectively, Scott Gettinger, MD, reported at the World Conference on Lung Cancer.
“These are the first randomized trials to report 5-year outcomes for a PD-1 axis inhibitor in patients with previously treated advanced non–small lung cancer,” said Dr. Gettinger, a professor at the Yale Comprehensive Cancer Center, New Haven, Conn. “This is really unprecedented; we wouldn’t expect many patients to be out 5 years in this scenario.”
Notably, the 5-year OS benefit was seen in both trials, he said, explaining that each compared nivolumab and docetaxel, but CheckMate 017 included patients with only squamous NSCLC, and CheckMate 057 included only non–squamous NSCLC patients.
The trials randomized 272 and 582 patients, respectively, and both demonstrated significantly improved 12-month OS with nivolumab – regardless of programmed death-ligand 1 (PD-L1) expression levels. Common eligibility criteria included stage IIIb/IV disease, good performance status (ECOG performance score of 0-1), and 1 prior platinum-based chemotherapy; CheckMate 057 further allowed prior tyrosine kinase inhibitor treatment for known anaplastic lymphoma kinase (ALK) translocation or epidermal growth factor receptor (EGFR) mutation, and allowed prior maintenance therapy. Doses in both trials were 3 mg/kg of nivolumab every 2 weeks or 75 mg/m2 of intravenous docetaxel every 3 weeks until disease progression or unacceptable toxicity.
The pooled data also showed an improvement in progression-free survival (PFS) at 5 years (8% vs. 0%) with nivolumab vs. docetaxel groups.
“Again, we don’t see this in trials – more commonly we see zero patients without progression, and that’s what we saw with the docetaxel arm,” said Dr. Gettinger, who also is the Disease Aligned Research Team Leader, Thoracic Oncology Program, at the cancer center.
The median duration of responses with nivolumab was 19.9 months vs. 5.6 months with docetaxel, and 32.2% of nivolumab responders were still without progression at 5 years, he noted.
A common question in the clinic relates to the prognosis in patients who do well with PD-1 axis inhibitors, which prompted an additional analysis across the two trials, he said, noting that 60%, 78%, and 88% of patients who had not progressed at 2, 3, or 4 years, respectively, also had not progressed at 5 years, and 80%, 93%, and 100%, of patients in those groups were alive at 5 years. In the docetaxel arm, only 4, 1, and 0 patients had PFS at 2, 3, and 4, years, respectively, and none of those patients survived to 5 years, he said.
No new safety signals were seen with long-term follow-up, he added.
“In fact there was only one grade 3 or higher toxicity that was related to treatment in the nivolumab arm, and this was a grade 3 lipase elevation. There was one patient who discontinued nivolumab after 3 years, and this was for a grade 2 rash and eczema that had waxed and waned since starting nivolumab,” he said.
Also of note, 10% of nivolumab-treated patients who were off treatment at 5 years – for variable periods of time – had not progressed and had not received subsequent therapy.
“So we clearly see benefit in our patients long after they finish a course or stop for some reason,” he said.
CheckMate 017 and 057 were funded by Bristol-Myers Squibb. Dr. Gettinger reported advisory board and/or consulting work for, and/or research funding from Bristol-Myers Squibb, Nektar Therapeutics, Genentech/Roche, Iovance, and Takeda/Ariad.
SOURCE: Gettinger S et al. WCLC 2019, Abstract PR04.03.
BARCELONA – Nivolumab, compared with docetaxel chemotherapy, led to a fivefold improvement in 5-year overall survival among previously treated patients with non–small cell lung cancer (NSCLC), according to a pooled analysis of data from the phase 3 CheckMate 017 and 057 trials.
The 5-year overall survival (OS) rates from the two randomized registrational trials, which established the programmed death-1 (PD-1) inhibitor nivolumab as the standard salvage therapy for NSCLC, were 13.4% vs. 2.6% (median, 11.1 vs. 8.1 months) with nivolumab and docetaxel, respectively, Scott Gettinger, MD, reported at the World Conference on Lung Cancer.
“These are the first randomized trials to report 5-year outcomes for a PD-1 axis inhibitor in patients with previously treated advanced non–small lung cancer,” said Dr. Gettinger, a professor at the Yale Comprehensive Cancer Center, New Haven, Conn. “This is really unprecedented; we wouldn’t expect many patients to be out 5 years in this scenario.”
Notably, the 5-year OS benefit was seen in both trials, he said, explaining that each compared nivolumab and docetaxel, but CheckMate 017 included patients with only squamous NSCLC, and CheckMate 057 included only non–squamous NSCLC patients.
The trials randomized 272 and 582 patients, respectively, and both demonstrated significantly improved 12-month OS with nivolumab – regardless of programmed death-ligand 1 (PD-L1) expression levels. Common eligibility criteria included stage IIIb/IV disease, good performance status (ECOG performance score of 0-1), and 1 prior platinum-based chemotherapy; CheckMate 057 further allowed prior tyrosine kinase inhibitor treatment for known anaplastic lymphoma kinase (ALK) translocation or epidermal growth factor receptor (EGFR) mutation, and allowed prior maintenance therapy. Doses in both trials were 3 mg/kg of nivolumab every 2 weeks or 75 mg/m2 of intravenous docetaxel every 3 weeks until disease progression or unacceptable toxicity.
The pooled data also showed an improvement in progression-free survival (PFS) at 5 years (8% vs. 0%) with nivolumab vs. docetaxel groups.
“Again, we don’t see this in trials – more commonly we see zero patients without progression, and that’s what we saw with the docetaxel arm,” said Dr. Gettinger, who also is the Disease Aligned Research Team Leader, Thoracic Oncology Program, at the cancer center.
The median duration of responses with nivolumab was 19.9 months vs. 5.6 months with docetaxel, and 32.2% of nivolumab responders were still without progression at 5 years, he noted.
A common question in the clinic relates to the prognosis in patients who do well with PD-1 axis inhibitors, which prompted an additional analysis across the two trials, he said, noting that 60%, 78%, and 88% of patients who had not progressed at 2, 3, or 4 years, respectively, also had not progressed at 5 years, and 80%, 93%, and 100%, of patients in those groups were alive at 5 years. In the docetaxel arm, only 4, 1, and 0 patients had PFS at 2, 3, and 4, years, respectively, and none of those patients survived to 5 years, he said.
No new safety signals were seen with long-term follow-up, he added.
“In fact there was only one grade 3 or higher toxicity that was related to treatment in the nivolumab arm, and this was a grade 3 lipase elevation. There was one patient who discontinued nivolumab after 3 years, and this was for a grade 2 rash and eczema that had waxed and waned since starting nivolumab,” he said.
Also of note, 10% of nivolumab-treated patients who were off treatment at 5 years – for variable periods of time – had not progressed and had not received subsequent therapy.
“So we clearly see benefit in our patients long after they finish a course or stop for some reason,” he said.
CheckMate 017 and 057 were funded by Bristol-Myers Squibb. Dr. Gettinger reported advisory board and/or consulting work for, and/or research funding from Bristol-Myers Squibb, Nektar Therapeutics, Genentech/Roche, Iovance, and Takeda/Ariad.
SOURCE: Gettinger S et al. WCLC 2019, Abstract PR04.03.
BARCELONA – Nivolumab, compared with docetaxel chemotherapy, led to a fivefold improvement in 5-year overall survival among previously treated patients with non–small cell lung cancer (NSCLC), according to a pooled analysis of data from the phase 3 CheckMate 017 and 057 trials.
The 5-year overall survival (OS) rates from the two randomized registrational trials, which established the programmed death-1 (PD-1) inhibitor nivolumab as the standard salvage therapy for NSCLC, were 13.4% vs. 2.6% (median, 11.1 vs. 8.1 months) with nivolumab and docetaxel, respectively, Scott Gettinger, MD, reported at the World Conference on Lung Cancer.
“These are the first randomized trials to report 5-year outcomes for a PD-1 axis inhibitor in patients with previously treated advanced non–small lung cancer,” said Dr. Gettinger, a professor at the Yale Comprehensive Cancer Center, New Haven, Conn. “This is really unprecedented; we wouldn’t expect many patients to be out 5 years in this scenario.”
Notably, the 5-year OS benefit was seen in both trials, he said, explaining that each compared nivolumab and docetaxel, but CheckMate 017 included patients with only squamous NSCLC, and CheckMate 057 included only non–squamous NSCLC patients.
The trials randomized 272 and 582 patients, respectively, and both demonstrated significantly improved 12-month OS with nivolumab – regardless of programmed death-ligand 1 (PD-L1) expression levels. Common eligibility criteria included stage IIIb/IV disease, good performance status (ECOG performance score of 0-1), and 1 prior platinum-based chemotherapy; CheckMate 057 further allowed prior tyrosine kinase inhibitor treatment for known anaplastic lymphoma kinase (ALK) translocation or epidermal growth factor receptor (EGFR) mutation, and allowed prior maintenance therapy. Doses in both trials were 3 mg/kg of nivolumab every 2 weeks or 75 mg/m2 of intravenous docetaxel every 3 weeks until disease progression or unacceptable toxicity.
The pooled data also showed an improvement in progression-free survival (PFS) at 5 years (8% vs. 0%) with nivolumab vs. docetaxel groups.
“Again, we don’t see this in trials – more commonly we see zero patients without progression, and that’s what we saw with the docetaxel arm,” said Dr. Gettinger, who also is the Disease Aligned Research Team Leader, Thoracic Oncology Program, at the cancer center.
The median duration of responses with nivolumab was 19.9 months vs. 5.6 months with docetaxel, and 32.2% of nivolumab responders were still without progression at 5 years, he noted.
A common question in the clinic relates to the prognosis in patients who do well with PD-1 axis inhibitors, which prompted an additional analysis across the two trials, he said, noting that 60%, 78%, and 88% of patients who had not progressed at 2, 3, or 4 years, respectively, also had not progressed at 5 years, and 80%, 93%, and 100%, of patients in those groups were alive at 5 years. In the docetaxel arm, only 4, 1, and 0 patients had PFS at 2, 3, and 4, years, respectively, and none of those patients survived to 5 years, he said.
No new safety signals were seen with long-term follow-up, he added.
“In fact there was only one grade 3 or higher toxicity that was related to treatment in the nivolumab arm, and this was a grade 3 lipase elevation. There was one patient who discontinued nivolumab after 3 years, and this was for a grade 2 rash and eczema that had waxed and waned since starting nivolumab,” he said.
Also of note, 10% of nivolumab-treated patients who were off treatment at 5 years – for variable periods of time – had not progressed and had not received subsequent therapy.
“So we clearly see benefit in our patients long after they finish a course or stop for some reason,” he said.
CheckMate 017 and 057 were funded by Bristol-Myers Squibb. Dr. Gettinger reported advisory board and/or consulting work for, and/or research funding from Bristol-Myers Squibb, Nektar Therapeutics, Genentech/Roche, Iovance, and Takeda/Ariad.
SOURCE: Gettinger S et al. WCLC 2019, Abstract PR04.03.
REPORTING FROM WCLC 2019
Robotic bronchoscopy beat standard techniques for targeting lung nodules
NEW ORLEANS –
A prospective study in a cadaver model showed that robotic bronchoscopy targeted nodules more effectively than electromagnetic navigation or an ultrathin bronchoscope with radial endobronchial ultrasound (UTB-rEBUS).
“This is really the first study to randomize, blind, and compare procedural outcomes between existing technologies in advanced bronchoscopy,” said Lonny Yarmus, DO, of Johns Hopkins Medicine in Baltimore.
Dr. Yarmus described this study, PRECISION-1, at the annual meeting of the American Society of Chest Physicians. The study was designed to compare the following:
- UTB-rEBUS (3.0 mm outer diameter and 1.7 mm working channel).
- Electromagnetic navigation bronchoscopy (Superdimension version 7.1).
- Robotic bronchoscopy (3.5 mm outer diameter and 2.0-mm working channel).
With all methods, a 21-gauge needle was used. For each nodule, UTB-rEBUS was done first to eliminate potential localization bias. The subsequent order of electromagnetic navigation and robotic bronchoscopy was determined based on block randomization.
Eight bronchoscopists performed a total of 60 procedures using each of the methods to target 20 nodules implanted in cadavers. The nodules were distributed across all lobes, 80% were in the outer third of the lung, and 50% had a positive bronchus sign on computed tomography (CT). The mean nodule size was 16.5 plus or minus 1.5 mm.
The study’s primary endpoint was the ability to localize and puncture target nodules within a maximum of three attempts per method. This includes center, peripheral, and distal punctures of nodules. Cone-beam CT was used to confirm that needles punctured the target lesions. The bronchoscopists were blinded to cone-beam CT results, and a blinded, independent investigator assessed whether nodule punctures were successful. The primary endpoint was met in 25% of UTB-rEBUS procedures, 45% of electromagnetic navigation procedures, and 80% of robotic bronchoscopy procedures.
The study’s secondary endpoint was localization success, which was defined as navigation to within needle biopsy distance of the nodule. This includes center, peripheral, and distal punctures of nodules, as well as adjacent punctures (touching the nodule but not within it). The secondary endpoint was met in 35% of UTB-rEBUS procedures, 65% of electromagnetic navigation procedures, and 90% of robotic bronchoscopy procedures.
The researchers also assessed successful navigation, which was defined as the provider localizing with software or radial ultrasound and passing the needle to make a biopsy attempt. Navigation was successful in 65% of UTB-rEBUS procedures, 85% of electromagnetic navigation procedures, and 100% of robotic bronchoscopy procedures.
“Utilization of robotic bronchoscopy with shape-sensing technology can significantly increase the ability to localize and puncture lesions when compared with standard existing technologies,” Dr. Yarmus said in closing.
He did note that this research was done in a cadaveric model, so “prospective, randomized, and comparative in vivo studies are needed.”
This study was funded by the Association of Interventional Pulmonary Program Directors. Dr. Yarmus disclosed government and societal funding and relationships with Boston Scientific, Veran, Medtronic, Intuitive, Auris, Erbe, Olympus, BD, Rocket, Ambu, Inspire Medical, and AstraZeneca.
SOURCE: Yarmus L et al. CHEST 2019. Abstract, doi: 10.1016/j.chest.2019.08.311.
NEW ORLEANS –
A prospective study in a cadaver model showed that robotic bronchoscopy targeted nodules more effectively than electromagnetic navigation or an ultrathin bronchoscope with radial endobronchial ultrasound (UTB-rEBUS).
“This is really the first study to randomize, blind, and compare procedural outcomes between existing technologies in advanced bronchoscopy,” said Lonny Yarmus, DO, of Johns Hopkins Medicine in Baltimore.
Dr. Yarmus described this study, PRECISION-1, at the annual meeting of the American Society of Chest Physicians. The study was designed to compare the following:
- UTB-rEBUS (3.0 mm outer diameter and 1.7 mm working channel).
- Electromagnetic navigation bronchoscopy (Superdimension version 7.1).
- Robotic bronchoscopy (3.5 mm outer diameter and 2.0-mm working channel).
With all methods, a 21-gauge needle was used. For each nodule, UTB-rEBUS was done first to eliminate potential localization bias. The subsequent order of electromagnetic navigation and robotic bronchoscopy was determined based on block randomization.
Eight bronchoscopists performed a total of 60 procedures using each of the methods to target 20 nodules implanted in cadavers. The nodules were distributed across all lobes, 80% were in the outer third of the lung, and 50% had a positive bronchus sign on computed tomography (CT). The mean nodule size was 16.5 plus or minus 1.5 mm.
The study’s primary endpoint was the ability to localize and puncture target nodules within a maximum of three attempts per method. This includes center, peripheral, and distal punctures of nodules. Cone-beam CT was used to confirm that needles punctured the target lesions. The bronchoscopists were blinded to cone-beam CT results, and a blinded, independent investigator assessed whether nodule punctures were successful. The primary endpoint was met in 25% of UTB-rEBUS procedures, 45% of electromagnetic navigation procedures, and 80% of robotic bronchoscopy procedures.
The study’s secondary endpoint was localization success, which was defined as navigation to within needle biopsy distance of the nodule. This includes center, peripheral, and distal punctures of nodules, as well as adjacent punctures (touching the nodule but not within it). The secondary endpoint was met in 35% of UTB-rEBUS procedures, 65% of electromagnetic navigation procedures, and 90% of robotic bronchoscopy procedures.
The researchers also assessed successful navigation, which was defined as the provider localizing with software or radial ultrasound and passing the needle to make a biopsy attempt. Navigation was successful in 65% of UTB-rEBUS procedures, 85% of electromagnetic navigation procedures, and 100% of robotic bronchoscopy procedures.
“Utilization of robotic bronchoscopy with shape-sensing technology can significantly increase the ability to localize and puncture lesions when compared with standard existing technologies,” Dr. Yarmus said in closing.
He did note that this research was done in a cadaveric model, so “prospective, randomized, and comparative in vivo studies are needed.”
This study was funded by the Association of Interventional Pulmonary Program Directors. Dr. Yarmus disclosed government and societal funding and relationships with Boston Scientific, Veran, Medtronic, Intuitive, Auris, Erbe, Olympus, BD, Rocket, Ambu, Inspire Medical, and AstraZeneca.
SOURCE: Yarmus L et al. CHEST 2019. Abstract, doi: 10.1016/j.chest.2019.08.311.
NEW ORLEANS –
A prospective study in a cadaver model showed that robotic bronchoscopy targeted nodules more effectively than electromagnetic navigation or an ultrathin bronchoscope with radial endobronchial ultrasound (UTB-rEBUS).
“This is really the first study to randomize, blind, and compare procedural outcomes between existing technologies in advanced bronchoscopy,” said Lonny Yarmus, DO, of Johns Hopkins Medicine in Baltimore.
Dr. Yarmus described this study, PRECISION-1, at the annual meeting of the American Society of Chest Physicians. The study was designed to compare the following:
- UTB-rEBUS (3.0 mm outer diameter and 1.7 mm working channel).
- Electromagnetic navigation bronchoscopy (Superdimension version 7.1).
- Robotic bronchoscopy (3.5 mm outer diameter and 2.0-mm working channel).
With all methods, a 21-gauge needle was used. For each nodule, UTB-rEBUS was done first to eliminate potential localization bias. The subsequent order of electromagnetic navigation and robotic bronchoscopy was determined based on block randomization.
Eight bronchoscopists performed a total of 60 procedures using each of the methods to target 20 nodules implanted in cadavers. The nodules were distributed across all lobes, 80% were in the outer third of the lung, and 50% had a positive bronchus sign on computed tomography (CT). The mean nodule size was 16.5 plus or minus 1.5 mm.
The study’s primary endpoint was the ability to localize and puncture target nodules within a maximum of three attempts per method. This includes center, peripheral, and distal punctures of nodules. Cone-beam CT was used to confirm that needles punctured the target lesions. The bronchoscopists were blinded to cone-beam CT results, and a blinded, independent investigator assessed whether nodule punctures were successful. The primary endpoint was met in 25% of UTB-rEBUS procedures, 45% of electromagnetic navigation procedures, and 80% of robotic bronchoscopy procedures.
The study’s secondary endpoint was localization success, which was defined as navigation to within needle biopsy distance of the nodule. This includes center, peripheral, and distal punctures of nodules, as well as adjacent punctures (touching the nodule but not within it). The secondary endpoint was met in 35% of UTB-rEBUS procedures, 65% of electromagnetic navigation procedures, and 90% of robotic bronchoscopy procedures.
The researchers also assessed successful navigation, which was defined as the provider localizing with software or radial ultrasound and passing the needle to make a biopsy attempt. Navigation was successful in 65% of UTB-rEBUS procedures, 85% of electromagnetic navigation procedures, and 100% of robotic bronchoscopy procedures.
“Utilization of robotic bronchoscopy with shape-sensing technology can significantly increase the ability to localize and puncture lesions when compared with standard existing technologies,” Dr. Yarmus said in closing.
He did note that this research was done in a cadaveric model, so “prospective, randomized, and comparative in vivo studies are needed.”
This study was funded by the Association of Interventional Pulmonary Program Directors. Dr. Yarmus disclosed government and societal funding and relationships with Boston Scientific, Veran, Medtronic, Intuitive, Auris, Erbe, Olympus, BD, Rocket, Ambu, Inspire Medical, and AstraZeneca.
SOURCE: Yarmus L et al. CHEST 2019. Abstract, doi: 10.1016/j.chest.2019.08.311.
REPORTING FROM CHEST 2019