User login
Cannabis users struggle to quit cigarettes
a large national survey has found.

“Over the past decade, there has been an increase in the use of cannabis among cigarette smokers and prevalence of cigarettes and cannabis co-use, suggesting that the negative consequences of cigarette–cannabis co-use may also become more prevalent over time,” wrote Andrea H. Weinberger, PhD, of Yeshiva University, New York, and colleagues. They noted that the prevalence of cigarette smoking is nearly three times higher among persons who use cannabis and have cannabis use disorders relative to those who do not.
The 2019 National Survey of Drug Use and Health estimated that 15.9% of Americans aged 12 years or older used cannabis in the past year. This number has been rising throughout the 2000s.
In that same report, cannabis use disorder (or marijuana use disorder) was defined as when an individual experiences clinically significant impairment caused by the recurrent use of marijuana, including health problems, persistent or increasing use, and failure to meet major responsibilities at work, school, or home. The report stated that approximately 1.6% of Americans aged 12 or older in 2018 had marijuana use disorder.
In the study published in Tobacco Control, the researchers used the National Survey on Drug Use and Health data to analyze cigarette smoking quit ratios among U.S. adults with and without cannabis use and cannabis use disorders. “Quit ratio was calculated as the proportion of former smokers among lifetime smokers and is considered a measure of total cessation in a population,” the researchers said.
In 2016, the quit ratios for adults with a history of cannabis use or cannabis use disorders were 23% and 15%, respectively, compared with 51% and 48%, respectively, in those with no cannabis use or cannabis use disorders.
Overall, quit ratios did not change significantly from 2002 to 2016 for individuals with cannabis use disorders after controlling for multiple demographic factors and other substance use disorders. However, during the same time period, quit ratios showed a nonlinear increase in cannabis users, nonusers, and individuals without cannabis use disorders.
The study findings were limited by several factors including the inability to generalize results to youth or individuals living outside the United States, the use of DSM-IV criteria to identify cannabis use disorder, the use of self-reports, and the inability to examine the timing of cannabis use as related to attempts to quit smoking, the researchers noted. However, the results highlight the need to consider offering smoking cessation treatment to individuals being treated for cannabis use disorders, and to include cannabis users in smoking cessation programs, the researchers noted.
“Based on our results, both public health and clinical efforts to improve cigarette quit outcomes may benefit from including those with any cannabis use,” they said. More research is needed to determine whether trends in the quit ratio change over time for cannabis users or those with cannabis use disorder, they added.
The study was funded by the National Institute on Drug Abuse. The researchers had no financial conflicts to disclose.
SOURCE: Weinberger AH et al. Tob Control. 2020;29(1):74-80. doi: 10.1136/tobaccocontrol-2018-054590.
a large national survey has found.
“Over the past decade, there has been an increase in the use of cannabis among cigarette smokers and prevalence of cigarettes and cannabis co-use, suggesting that the negative consequences of cigarette–cannabis co-use may also become more prevalent over time,” wrote Andrea H. Weinberger, PhD, of Yeshiva University, New York, and colleagues. They noted that the prevalence of cigarette smoking is nearly three times higher among persons who use cannabis and have cannabis use disorders relative to those who do not.
The 2019 National Survey of Drug Use and Health estimated that 15.9% of Americans aged 12 years or older used cannabis in the past year. This number has been rising throughout the 2000s.
In that same report, cannabis use disorder (or marijuana use disorder) was defined as when an individual experiences clinically significant impairment caused by the recurrent use of marijuana, including health problems, persistent or increasing use, and failure to meet major responsibilities at work, school, or home. The report stated that approximately 1.6% of Americans aged 12 or older in 2018 had marijuana use disorder.
In the study published in Tobacco Control, the researchers used the National Survey on Drug Use and Health data to analyze cigarette smoking quit ratios among U.S. adults with and without cannabis use and cannabis use disorders. “Quit ratio was calculated as the proportion of former smokers among lifetime smokers and is considered a measure of total cessation in a population,” the researchers said.
In 2016, the quit ratios for adults with a history of cannabis use or cannabis use disorders were 23% and 15%, respectively, compared with 51% and 48%, respectively, in those with no cannabis use or cannabis use disorders.
Overall, quit ratios did not change significantly from 2002 to 2016 for individuals with cannabis use disorders after controlling for multiple demographic factors and other substance use disorders. However, during the same time period, quit ratios showed a nonlinear increase in cannabis users, nonusers, and individuals without cannabis use disorders.
The study findings were limited by several factors including the inability to generalize results to youth or individuals living outside the United States, the use of DSM-IV criteria to identify cannabis use disorder, the use of self-reports, and the inability to examine the timing of cannabis use as related to attempts to quit smoking, the researchers noted. However, the results highlight the need to consider offering smoking cessation treatment to individuals being treated for cannabis use disorders, and to include cannabis users in smoking cessation programs, the researchers noted.
“Based on our results, both public health and clinical efforts to improve cigarette quit outcomes may benefit from including those with any cannabis use,” they said. More research is needed to determine whether trends in the quit ratio change over time for cannabis users or those with cannabis use disorder, they added.
The study was funded by the National Institute on Drug Abuse. The researchers had no financial conflicts to disclose.
SOURCE: Weinberger AH et al. Tob Control. 2020;29(1):74-80. doi: 10.1136/tobaccocontrol-2018-054590.
a large national survey has found.
“Over the past decade, there has been an increase in the use of cannabis among cigarette smokers and prevalence of cigarettes and cannabis co-use, suggesting that the negative consequences of cigarette–cannabis co-use may also become more prevalent over time,” wrote Andrea H. Weinberger, PhD, of Yeshiva University, New York, and colleagues. They noted that the prevalence of cigarette smoking is nearly three times higher among persons who use cannabis and have cannabis use disorders relative to those who do not.
The 2019 National Survey of Drug Use and Health estimated that 15.9% of Americans aged 12 years or older used cannabis in the past year. This number has been rising throughout the 2000s.
In that same report, cannabis use disorder (or marijuana use disorder) was defined as when an individual experiences clinically significant impairment caused by the recurrent use of marijuana, including health problems, persistent or increasing use, and failure to meet major responsibilities at work, school, or home. The report stated that approximately 1.6% of Americans aged 12 or older in 2018 had marijuana use disorder.
In the study published in Tobacco Control, the researchers used the National Survey on Drug Use and Health data to analyze cigarette smoking quit ratios among U.S. adults with and without cannabis use and cannabis use disorders. “Quit ratio was calculated as the proportion of former smokers among lifetime smokers and is considered a measure of total cessation in a population,” the researchers said.
In 2016, the quit ratios for adults with a history of cannabis use or cannabis use disorders were 23% and 15%, respectively, compared with 51% and 48%, respectively, in those with no cannabis use or cannabis use disorders.
Overall, quit ratios did not change significantly from 2002 to 2016 for individuals with cannabis use disorders after controlling for multiple demographic factors and other substance use disorders. However, during the same time period, quit ratios showed a nonlinear increase in cannabis users, nonusers, and individuals without cannabis use disorders.
The study findings were limited by several factors including the inability to generalize results to youth or individuals living outside the United States, the use of DSM-IV criteria to identify cannabis use disorder, the use of self-reports, and the inability to examine the timing of cannabis use as related to attempts to quit smoking, the researchers noted. However, the results highlight the need to consider offering smoking cessation treatment to individuals being treated for cannabis use disorders, and to include cannabis users in smoking cessation programs, the researchers noted.
“Based on our results, both public health and clinical efforts to improve cigarette quit outcomes may benefit from including those with any cannabis use,” they said. More research is needed to determine whether trends in the quit ratio change over time for cannabis users or those with cannabis use disorder, they added.
The study was funded by the National Institute on Drug Abuse. The researchers had no financial conflicts to disclose.
SOURCE: Weinberger AH et al. Tob Control. 2020;29(1):74-80. doi: 10.1136/tobaccocontrol-2018-054590.
FROM TOBACCO CONTROL
‘Simple’ model predicts severe neutropenia risk in lung cancer patients
A new and simple model for predicting risk of severe neutropenia in advanced lung cancer could ease the evaluation process and help inform patient management decisions, according to investigators.
The model, based on 10 pretreatment variables, appears to overcome limitations of a comprehensive risk prediction model that is not specific to lung cancer, according to Xiaowen Cao of Duke University, Durham, N.C., and coinvestigators.
“We believe that this model, once validated, will help oncologists accurately identify those patients with lung cancer who are at a high risk of developing severe neutropenia, based on simple, readily available information,” the researchers said in a report on their work, which appears in the journal Lung Cancer.
Oncologists could then make “proactive” decisions about monitoring of high-risk patients, modifying the dose of chemotherapy, and using prophylactic growth factors, the authors added.
Accurate, lung cancer–specific prediction models would be useful to estimate risk of neutropenia, which the investigators acknowledged as a serious chemotherapy-induced toxicity linked to life-threatening infections, dose delays, and reductions that can compromise treatment efficacy, and reduced health-related quality of life.
There are other, previously developed models to predict chemotherapy-induced neutropenia, but those have significant limitations, including development based on small patient sample sizes, according to the researchers.
A comprehensive risk model for neutropenic complications has been developed by Gary H. Lyman, MD, and colleagues, based on a large, prospective cohort including nearly 3,800 patients. That model performs well and had a 90% sensitivity and 96% predictive value; however, it’s not lung cancer specific, and hasn’t been externally validated, according to Ms. Cao and coauthors.
Accordingly, they set out to develop a new risk prediction model based on a lung cancer data set encompassing 11,352 patients from 67 phase 2 or 3 cooperative group studies conducted between 1991 and 2010.
The Lyman model in this data set had an area under the curve (AUC) of 0.8772 in patients with small cell lung cancer (SCLC), but an AUC of just 0.6787 in non–small cell lung cancer (NSCLC), suggesting “much better predictive performance in the SCLC,” the researchers noted.
They used stepwise logistic regression and lasso regression to develop a new model, which was derived based on about two-thirds of the patients, randomly selected, while the validation was conducted using the remaining third.
Variables included in the final model included age, gender, weight, BMI, insurance status, disease stage, number of metastatic sites, chemotherapy agents used, number of chemotherapy agents, planned growth factor use, duration of planned therapy, pleural effusion, presence of symptoms, and performance status.
That model had a good AUC, according to investigators, in both the training set and the testing set (0.8348 and 0.8234, respectively).
“It is worth noticing that our final model compensated for the deficiency of Lyman’s risk model in NSCLC patients,” the researchers noted in a discussion of their results.
The study was supported in part by grants from the National Institutes of Health, the National Center for Advancing Translational Sciences, and the Health and Medical Research Fund of Hong Kong. One study coauthor reported a conflict of interest outside the submitted work related to Genentech.
SOURCE: Cao X et al. Lung Cancer 2020 Jan 5. doi: 10.1016/j.lungcan.2020.01.004.
A new and simple model for predicting risk of severe neutropenia in advanced lung cancer could ease the evaluation process and help inform patient management decisions, according to investigators.
The model, based on 10 pretreatment variables, appears to overcome limitations of a comprehensive risk prediction model that is not specific to lung cancer, according to Xiaowen Cao of Duke University, Durham, N.C., and coinvestigators.
“We believe that this model, once validated, will help oncologists accurately identify those patients with lung cancer who are at a high risk of developing severe neutropenia, based on simple, readily available information,” the researchers said in a report on their work, which appears in the journal Lung Cancer.
Oncologists could then make “proactive” decisions about monitoring of high-risk patients, modifying the dose of chemotherapy, and using prophylactic growth factors, the authors added.
Accurate, lung cancer–specific prediction models would be useful to estimate risk of neutropenia, which the investigators acknowledged as a serious chemotherapy-induced toxicity linked to life-threatening infections, dose delays, and reductions that can compromise treatment efficacy, and reduced health-related quality of life.
There are other, previously developed models to predict chemotherapy-induced neutropenia, but those have significant limitations, including development based on small patient sample sizes, according to the researchers.
A comprehensive risk model for neutropenic complications has been developed by Gary H. Lyman, MD, and colleagues, based on a large, prospective cohort including nearly 3,800 patients. That model performs well and had a 90% sensitivity and 96% predictive value; however, it’s not lung cancer specific, and hasn’t been externally validated, according to Ms. Cao and coauthors.
Accordingly, they set out to develop a new risk prediction model based on a lung cancer data set encompassing 11,352 patients from 67 phase 2 or 3 cooperative group studies conducted between 1991 and 2010.
The Lyman model in this data set had an area under the curve (AUC) of 0.8772 in patients with small cell lung cancer (SCLC), but an AUC of just 0.6787 in non–small cell lung cancer (NSCLC), suggesting “much better predictive performance in the SCLC,” the researchers noted.
They used stepwise logistic regression and lasso regression to develop a new model, which was derived based on about two-thirds of the patients, randomly selected, while the validation was conducted using the remaining third.
Variables included in the final model included age, gender, weight, BMI, insurance status, disease stage, number of metastatic sites, chemotherapy agents used, number of chemotherapy agents, planned growth factor use, duration of planned therapy, pleural effusion, presence of symptoms, and performance status.
That model had a good AUC, according to investigators, in both the training set and the testing set (0.8348 and 0.8234, respectively).
“It is worth noticing that our final model compensated for the deficiency of Lyman’s risk model in NSCLC patients,” the researchers noted in a discussion of their results.
The study was supported in part by grants from the National Institutes of Health, the National Center for Advancing Translational Sciences, and the Health and Medical Research Fund of Hong Kong. One study coauthor reported a conflict of interest outside the submitted work related to Genentech.
SOURCE: Cao X et al. Lung Cancer 2020 Jan 5. doi: 10.1016/j.lungcan.2020.01.004.
A new and simple model for predicting risk of severe neutropenia in advanced lung cancer could ease the evaluation process and help inform patient management decisions, according to investigators.
The model, based on 10 pretreatment variables, appears to overcome limitations of a comprehensive risk prediction model that is not specific to lung cancer, according to Xiaowen Cao of Duke University, Durham, N.C., and coinvestigators.
“We believe that this model, once validated, will help oncologists accurately identify those patients with lung cancer who are at a high risk of developing severe neutropenia, based on simple, readily available information,” the researchers said in a report on their work, which appears in the journal Lung Cancer.
Oncologists could then make “proactive” decisions about monitoring of high-risk patients, modifying the dose of chemotherapy, and using prophylactic growth factors, the authors added.
Accurate, lung cancer–specific prediction models would be useful to estimate risk of neutropenia, which the investigators acknowledged as a serious chemotherapy-induced toxicity linked to life-threatening infections, dose delays, and reductions that can compromise treatment efficacy, and reduced health-related quality of life.
There are other, previously developed models to predict chemotherapy-induced neutropenia, but those have significant limitations, including development based on small patient sample sizes, according to the researchers.
A comprehensive risk model for neutropenic complications has been developed by Gary H. Lyman, MD, and colleagues, based on a large, prospective cohort including nearly 3,800 patients. That model performs well and had a 90% sensitivity and 96% predictive value; however, it’s not lung cancer specific, and hasn’t been externally validated, according to Ms. Cao and coauthors.
Accordingly, they set out to develop a new risk prediction model based on a lung cancer data set encompassing 11,352 patients from 67 phase 2 or 3 cooperative group studies conducted between 1991 and 2010.
The Lyman model in this data set had an area under the curve (AUC) of 0.8772 in patients with small cell lung cancer (SCLC), but an AUC of just 0.6787 in non–small cell lung cancer (NSCLC), suggesting “much better predictive performance in the SCLC,” the researchers noted.
They used stepwise logistic regression and lasso regression to develop a new model, which was derived based on about two-thirds of the patients, randomly selected, while the validation was conducted using the remaining third.
Variables included in the final model included age, gender, weight, BMI, insurance status, disease stage, number of metastatic sites, chemotherapy agents used, number of chemotherapy agents, planned growth factor use, duration of planned therapy, pleural effusion, presence of symptoms, and performance status.
That model had a good AUC, according to investigators, in both the training set and the testing set (0.8348 and 0.8234, respectively).
“It is worth noticing that our final model compensated for the deficiency of Lyman’s risk model in NSCLC patients,” the researchers noted in a discussion of their results.
The study was supported in part by grants from the National Institutes of Health, the National Center for Advancing Translational Sciences, and the Health and Medical Research Fund of Hong Kong. One study coauthor reported a conflict of interest outside the submitted work related to Genentech.
SOURCE: Cao X et al. Lung Cancer 2020 Jan 5. doi: 10.1016/j.lungcan.2020.01.004.
FROM LUNG CANCER
Sharp declines for lung cancer, melanoma deaths fuel record drop in cancer mortality
, the American Cancer Society says.
Lung cancer death rates, which were falling by 3% in men and 2% in women annually in 2008 through 2013, dropped by 5% in men and nearly 4% per year in women annually from 2013 to 2017, according to the society’s 2020 statistical report.
Those accelerating reductions in death rates helped fuel the biggest-ever single year decline in overall cancer mortality, of 2.2%, from 2016 to 2017, their report shows.
According to the investigators, the decline in melanoma death rates escalated to 6.9% per year among 20- to 49-year-olds over 2013-2017, compared with a decline of just 2.9% per year during 2006-2010. Likewise, the melanoma death rate decline was 7.2% annually for the more recent time period, compared with just 1.3% annually in the earlier time period. The finding was even more remarkable for those 65 years of age and older, according to investigators, since the declines in melanoma death rates reached 6.2% annually, compared with a 0.9% annual increase in the years before immunotherapy.
Smoking cessation has been the main driver of progress in cutting lung cancer death rates, according to the report, while in melanoma, death rates have dropped after the introduction of immune checkpoint inhibitors and targeted therapies.
By contrast, reductions in death rates have slowed for colorectal cancers and female breast cancers, and have stabilized for prostate cancer, Ms. Siegel and coauthors stated, adding that racial and geographic disparities persist in preventable cancers, including those of the lung and cervix.
“Increased investment in both the equitable application of existing cancer control interventions and basic and clinical research to further advance treatment options would undoubtedly accelerate progress against cancer,” said the investigators. The report appears in CA: A Cancer Journal for Clinicians.
While the decline in lung cancer death rates is good news, the disease remains a major killer, responsible for more deaths than breast, colorectal, and ovarian cancer combined, said Jacques P. Fontaine, MD, a thoracic surgeon at Moffitt Cancer Center in Tampa, Fla.
“Five-year survival rates are still around the 18%-20% range, which is much lower than breast and prostate cancer,” Dr. Fontaine said in an interview. “Nonetheless, we’ve made a little dent in that, and we’re improving.”
Two other factors that have helped spur that improvement, according to Dr. Fontaine, are the reduced incidence of squamous cell carcinomas, which are linked to smoking, and the increased use of lung cancer screening with low-dose computed tomography.
Squamous cell carcinomas tend to be a central rather than peripheral, which makes the tumors harder to resect: “Surgery is sometimes not an option, and even to this day in 2020, the single most effective treatment for lung cancer remains surgical resection,” said Dr. Fontaine.
Likewise, centrally located tumors may preclude giving high-dose radiation and may result in more “collateral damage” to healthy tissue, he added.
Landmark studies show that low-dose CT scans reduce lung cancer deaths by 20% or more; however, screening can have false-positive results that lead to unnecessary biopsies and other harms, suggesting that the procedures should be done in centers of excellence that provide high-quality, responsible screening for early lung cancer, Dr. Fontaine said.
While the drop in melanoma death rates is encouraging and, not surprising in light of new cutting-edge therapies, an ongoing unmet treatment need still exists, according to Vishal Anil Patel, MD, director of cutaneous oncology at the George Washington Cancer Center in Washington.
“We still have a lot to learn, and a way to go, because we’ve really just made the first breakthrough,” Dr. Patel said in an interview.

Mortality data for melanoma can be challenging to interpret, according to Dr. Patel, given that more widespread screening may increase the number of documented melanoma cases with a lower risk of mortality.
Nevertheless, it’s not surprising that advanced melanoma death rates have declined precipitously, said Dr. Patel, since the diseases carries a high tumor mutational burden, which may explain the improved efficacy of immune checkpoint inhibitors.
“Without a doubt, the reason that people are living longer and doing better with this disease is because of these cutting-edge treatments that provide patients options that previously had no options at all, or a tailored option personalized to their tumor and focusing on what the patient really needs,” Dr. Patel said.
That said, response rates remain lower from other cancers, sparking interest in combining current immunotherapies with costimulatory molecules that may further improve survival rates, according to Dr. Patel.
In 2020, 606,000 cancer deaths are projected, according to the American Cancer Society statistical report. Of those deaths, nearly 136,000 are attributable to cancers of the lung and bronchus, while melanoma of the skin accounts for nearly 7,000 deaths.
The report notes that variation in cancer incidence reflects geographical differences in medical detection practices and the prevalence of risk factors, such as smoking, obesity, and other health behaviors. “For example, lung cancer incidence and mortality rates in Kentucky, where smoking prevalence was historically highest, are 3 to 4 times higher than those in Utah, where it was lowest. Even in 2018, 1 in 4 residents of Kentucky, Arkansas, and West Virginia were current smokers compared with 1 in 10 in Utah and California,” the investigators wrote.
Cancer mortality rates have fallen 29% since 1991, translating into 2.9 million fewer cancer deaths, the report says.
Dr. Siegel and coauthors are employed by the American Cancer Society, which receives grants from private and corporate foundations, and their salaries are solely funded through the American Cancer Society, according to the report.
SOURCE: Siegel RL et al. CA Cancer J Clin. 2020;70(1):7-30. doi: 10.3322/caac.21590.
, the American Cancer Society says.
Lung cancer death rates, which were falling by 3% in men and 2% in women annually in 2008 through 2013, dropped by 5% in men and nearly 4% per year in women annually from 2013 to 2017, according to the society’s 2020 statistical report.
Those accelerating reductions in death rates helped fuel the biggest-ever single year decline in overall cancer mortality, of 2.2%, from 2016 to 2017, their report shows.
According to the investigators, the decline in melanoma death rates escalated to 6.9% per year among 20- to 49-year-olds over 2013-2017, compared with a decline of just 2.9% per year during 2006-2010. Likewise, the melanoma death rate decline was 7.2% annually for the more recent time period, compared with just 1.3% annually in the earlier time period. The finding was even more remarkable for those 65 years of age and older, according to investigators, since the declines in melanoma death rates reached 6.2% annually, compared with a 0.9% annual increase in the years before immunotherapy.
Smoking cessation has been the main driver of progress in cutting lung cancer death rates, according to the report, while in melanoma, death rates have dropped after the introduction of immune checkpoint inhibitors and targeted therapies.
By contrast, reductions in death rates have slowed for colorectal cancers and female breast cancers, and have stabilized for prostate cancer, Ms. Siegel and coauthors stated, adding that racial and geographic disparities persist in preventable cancers, including those of the lung and cervix.
“Increased investment in both the equitable application of existing cancer control interventions and basic and clinical research to further advance treatment options would undoubtedly accelerate progress against cancer,” said the investigators. The report appears in CA: A Cancer Journal for Clinicians.
While the decline in lung cancer death rates is good news, the disease remains a major killer, responsible for more deaths than breast, colorectal, and ovarian cancer combined, said Jacques P. Fontaine, MD, a thoracic surgeon at Moffitt Cancer Center in Tampa, Fla.
“Five-year survival rates are still around the 18%-20% range, which is much lower than breast and prostate cancer,” Dr. Fontaine said in an interview. “Nonetheless, we’ve made a little dent in that, and we’re improving.”
Two other factors that have helped spur that improvement, according to Dr. Fontaine, are the reduced incidence of squamous cell carcinomas, which are linked to smoking, and the increased use of lung cancer screening with low-dose computed tomography.
Squamous cell carcinomas tend to be a central rather than peripheral, which makes the tumors harder to resect: “Surgery is sometimes not an option, and even to this day in 2020, the single most effective treatment for lung cancer remains surgical resection,” said Dr. Fontaine.
Likewise, centrally located tumors may preclude giving high-dose radiation and may result in more “collateral damage” to healthy tissue, he added.
Landmark studies show that low-dose CT scans reduce lung cancer deaths by 20% or more; however, screening can have false-positive results that lead to unnecessary biopsies and other harms, suggesting that the procedures should be done in centers of excellence that provide high-quality, responsible screening for early lung cancer, Dr. Fontaine said.
While the drop in melanoma death rates is encouraging and, not surprising in light of new cutting-edge therapies, an ongoing unmet treatment need still exists, according to Vishal Anil Patel, MD, director of cutaneous oncology at the George Washington Cancer Center in Washington.
“We still have a lot to learn, and a way to go, because we’ve really just made the first breakthrough,” Dr. Patel said in an interview.
Mortality data for melanoma can be challenging to interpret, according to Dr. Patel, given that more widespread screening may increase the number of documented melanoma cases with a lower risk of mortality.
Nevertheless, it’s not surprising that advanced melanoma death rates have declined precipitously, said Dr. Patel, since the diseases carries a high tumor mutational burden, which may explain the improved efficacy of immune checkpoint inhibitors.
“Without a doubt, the reason that people are living longer and doing better with this disease is because of these cutting-edge treatments that provide patients options that previously had no options at all, or a tailored option personalized to their tumor and focusing on what the patient really needs,” Dr. Patel said.
That said, response rates remain lower from other cancers, sparking interest in combining current immunotherapies with costimulatory molecules that may further improve survival rates, according to Dr. Patel.
In 2020, 606,000 cancer deaths are projected, according to the American Cancer Society statistical report. Of those deaths, nearly 136,000 are attributable to cancers of the lung and bronchus, while melanoma of the skin accounts for nearly 7,000 deaths.
The report notes that variation in cancer incidence reflects geographical differences in medical detection practices and the prevalence of risk factors, such as smoking, obesity, and other health behaviors. “For example, lung cancer incidence and mortality rates in Kentucky, where smoking prevalence was historically highest, are 3 to 4 times higher than those in Utah, where it was lowest. Even in 2018, 1 in 4 residents of Kentucky, Arkansas, and West Virginia were current smokers compared with 1 in 10 in Utah and California,” the investigators wrote.
Cancer mortality rates have fallen 29% since 1991, translating into 2.9 million fewer cancer deaths, the report says.
Dr. Siegel and coauthors are employed by the American Cancer Society, which receives grants from private and corporate foundations, and their salaries are solely funded through the American Cancer Society, according to the report.
SOURCE: Siegel RL et al. CA Cancer J Clin. 2020;70(1):7-30. doi: 10.3322/caac.21590.
, the American Cancer Society says.
Lung cancer death rates, which were falling by 3% in men and 2% in women annually in 2008 through 2013, dropped by 5% in men and nearly 4% per year in women annually from 2013 to 2017, according to the society’s 2020 statistical report.
Those accelerating reductions in death rates helped fuel the biggest-ever single year decline in overall cancer mortality, of 2.2%, from 2016 to 2017, their report shows.
According to the investigators, the decline in melanoma death rates escalated to 6.9% per year among 20- to 49-year-olds over 2013-2017, compared with a decline of just 2.9% per year during 2006-2010. Likewise, the melanoma death rate decline was 7.2% annually for the more recent time period, compared with just 1.3% annually in the earlier time period. The finding was even more remarkable for those 65 years of age and older, according to investigators, since the declines in melanoma death rates reached 6.2% annually, compared with a 0.9% annual increase in the years before immunotherapy.
Smoking cessation has been the main driver of progress in cutting lung cancer death rates, according to the report, while in melanoma, death rates have dropped after the introduction of immune checkpoint inhibitors and targeted therapies.
By contrast, reductions in death rates have slowed for colorectal cancers and female breast cancers, and have stabilized for prostate cancer, Ms. Siegel and coauthors stated, adding that racial and geographic disparities persist in preventable cancers, including those of the lung and cervix.
“Increased investment in both the equitable application of existing cancer control interventions and basic and clinical research to further advance treatment options would undoubtedly accelerate progress against cancer,” said the investigators. The report appears in CA: A Cancer Journal for Clinicians.
While the decline in lung cancer death rates is good news, the disease remains a major killer, responsible for more deaths than breast, colorectal, and ovarian cancer combined, said Jacques P. Fontaine, MD, a thoracic surgeon at Moffitt Cancer Center in Tampa, Fla.
“Five-year survival rates are still around the 18%-20% range, which is much lower than breast and prostate cancer,” Dr. Fontaine said in an interview. “Nonetheless, we’ve made a little dent in that, and we’re improving.”
Two other factors that have helped spur that improvement, according to Dr. Fontaine, are the reduced incidence of squamous cell carcinomas, which are linked to smoking, and the increased use of lung cancer screening with low-dose computed tomography.
Squamous cell carcinomas tend to be a central rather than peripheral, which makes the tumors harder to resect: “Surgery is sometimes not an option, and even to this day in 2020, the single most effective treatment for lung cancer remains surgical resection,” said Dr. Fontaine.
Likewise, centrally located tumors may preclude giving high-dose radiation and may result in more “collateral damage” to healthy tissue, he added.
Landmark studies show that low-dose CT scans reduce lung cancer deaths by 20% or more; however, screening can have false-positive results that lead to unnecessary biopsies and other harms, suggesting that the procedures should be done in centers of excellence that provide high-quality, responsible screening for early lung cancer, Dr. Fontaine said.
While the drop in melanoma death rates is encouraging and, not surprising in light of new cutting-edge therapies, an ongoing unmet treatment need still exists, according to Vishal Anil Patel, MD, director of cutaneous oncology at the George Washington Cancer Center in Washington.
“We still have a lot to learn, and a way to go, because we’ve really just made the first breakthrough,” Dr. Patel said in an interview.
Mortality data for melanoma can be challenging to interpret, according to Dr. Patel, given that more widespread screening may increase the number of documented melanoma cases with a lower risk of mortality.
Nevertheless, it’s not surprising that advanced melanoma death rates have declined precipitously, said Dr. Patel, since the diseases carries a high tumor mutational burden, which may explain the improved efficacy of immune checkpoint inhibitors.
“Without a doubt, the reason that people are living longer and doing better with this disease is because of these cutting-edge treatments that provide patients options that previously had no options at all, or a tailored option personalized to their tumor and focusing on what the patient really needs,” Dr. Patel said.
That said, response rates remain lower from other cancers, sparking interest in combining current immunotherapies with costimulatory molecules that may further improve survival rates, according to Dr. Patel.
In 2020, 606,000 cancer deaths are projected, according to the American Cancer Society statistical report. Of those deaths, nearly 136,000 are attributable to cancers of the lung and bronchus, while melanoma of the skin accounts for nearly 7,000 deaths.
The report notes that variation in cancer incidence reflects geographical differences in medical detection practices and the prevalence of risk factors, such as smoking, obesity, and other health behaviors. “For example, lung cancer incidence and mortality rates in Kentucky, where smoking prevalence was historically highest, are 3 to 4 times higher than those in Utah, where it was lowest. Even in 2018, 1 in 4 residents of Kentucky, Arkansas, and West Virginia were current smokers compared with 1 in 10 in Utah and California,” the investigators wrote.
Cancer mortality rates have fallen 29% since 1991, translating into 2.9 million fewer cancer deaths, the report says.
Dr. Siegel and coauthors are employed by the American Cancer Society, which receives grants from private and corporate foundations, and their salaries are solely funded through the American Cancer Society, according to the report.
SOURCE: Siegel RL et al. CA Cancer J Clin. 2020;70(1):7-30. doi: 10.3322/caac.21590.
FROM CA: A CANCER JOURNAL FOR CLINICIANS
New toxicity subscale measures QOL in cancer patients on checkpoint inhibitors
developed based on direct patient involvement, picks up on cutaneous and other side effects that would be missed using traditional quality of life questionnaires, investigators say.
The 25-item list represents the first-ever health-related quality of life (HRQOL) toxicity subscale developed for patients receiving checkpoint inhibitors, according to the investigators, led by Aaron R. Hansen, MBBS, of the division of medical oncology and hematology in the department of medicine at the University of Toronto.
The toxicity subscale is combined with the Functional Assessment of Cancer Therapy–General (FACT-G), which measures physical, emotional, family and social, and functional domains, to form the Functional Assessment of Cancer Therapy–Immune Checkpoint Modulator (FACT-ICM), Dr. Hansen stated in a recent report that describes initial development and early validation efforts.
The FACT-ICM could become an important tool for measuring HRQOL in patients receiving checkpoint inhibitors, depending on results of further investigations including more patients, the authors wrote in that report.
“Currently, we would recommend that our toxicity subscale be validated first before use in clinical care, or in trials with QOL as a primary or secondary endpoint,” wrote Dr. Hansen and colleagues in the report, which appears in Cancer.
The toxicity subscale asks patients to rate items such as “I am bothered by dry skin,” “I feel pain, soreness or aches in some of my muscles,” and “My fatigue keeps me from doing the things I want do” on a scale of 0 (not at all) to 4 (very much).
Development of the toxicity subscale was based on focus groups and interviews with 37 patients with a variety of cancer types who were being treated with a PD-1, PD-L1, and CTLA-4 immune checkpoint inhibitors. Sixteen physicians were surveyed to evaluate the patient input, while 11 of them also participated in follow-up interviews.
“At every step in this process, the patients were central,” the investigators wrote in their report.
According to the investigators, that approach is in line with guidance from the Food and Drug Administration, which has said that meaningful patient input should be used in the upfront development of patient-reported outcome (PRO) measures, rather than obtaining patient endorsement after the fact.
By contrast, an electronic PRO immune-oncology module recently developed, based on 19 immune-related adverse events from drug labels and clinical trial reports, had “no evaluation” of effects on HRQOL, according to Dr. Hansen and coauthors, who added that the tool “did not adhere” to the FDA call for meaningful patient input.
Some previous studies of quality of life in immune checkpoint inhibitor–treated patients have used tumor-specific PROs and the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire–Core 30 Items (EORTC-QLQ-C30).
The new, immune checkpoint inhibitor–specific toxicity subscale has “broader coverage” of side effects that reportedly affect HRQOL in patients treated with these agents, including taste disturbance, cough, and fever or chills, according to the investigators.
Moreover, the EORTC-QLQ-C30 and the EORTC head and neck cancer–specific-35 module (EORTC QLQ-H&N35), do not include items related to cutaneous adverse events such as itch, rash, and dry skin that have been seen in some checkpoint inhibitor clinical trials, they noted.
“This represents a clear limitation of such preexisting PRO instruments, which should be addressed with our immune checkpoint moduator–specific tool,” they wrote.
The study was supported by a grant from the University of Toronto. Authors of the study provided disclosures related to Merck, Bristol-Myers Squibb, Karyopharm, Boston Biomedical, Novartis, Genentech, Hoffmann La Roche, GlaxoSmithKline, and others.
SOURCE: Hansen AR et al. Cancer. 2020 Jan 8. doi: 10.1002/cncr.32692.
developed based on direct patient involvement, picks up on cutaneous and other side effects that would be missed using traditional quality of life questionnaires, investigators say.
The 25-item list represents the first-ever health-related quality of life (HRQOL) toxicity subscale developed for patients receiving checkpoint inhibitors, according to the investigators, led by Aaron R. Hansen, MBBS, of the division of medical oncology and hematology in the department of medicine at the University of Toronto.
The toxicity subscale is combined with the Functional Assessment of Cancer Therapy–General (FACT-G), which measures physical, emotional, family and social, and functional domains, to form the Functional Assessment of Cancer Therapy–Immune Checkpoint Modulator (FACT-ICM), Dr. Hansen stated in a recent report that describes initial development and early validation efforts.
The FACT-ICM could become an important tool for measuring HRQOL in patients receiving checkpoint inhibitors, depending on results of further investigations including more patients, the authors wrote in that report.
“Currently, we would recommend that our toxicity subscale be validated first before use in clinical care, or in trials with QOL as a primary or secondary endpoint,” wrote Dr. Hansen and colleagues in the report, which appears in Cancer.
The toxicity subscale asks patients to rate items such as “I am bothered by dry skin,” “I feel pain, soreness or aches in some of my muscles,” and “My fatigue keeps me from doing the things I want do” on a scale of 0 (not at all) to 4 (very much).
Development of the toxicity subscale was based on focus groups and interviews with 37 patients with a variety of cancer types who were being treated with a PD-1, PD-L1, and CTLA-4 immune checkpoint inhibitors. Sixteen physicians were surveyed to evaluate the patient input, while 11 of them also participated in follow-up interviews.
“At every step in this process, the patients were central,” the investigators wrote in their report.
According to the investigators, that approach is in line with guidance from the Food and Drug Administration, which has said that meaningful patient input should be used in the upfront development of patient-reported outcome (PRO) measures, rather than obtaining patient endorsement after the fact.
By contrast, an electronic PRO immune-oncology module recently developed, based on 19 immune-related adverse events from drug labels and clinical trial reports, had “no evaluation” of effects on HRQOL, according to Dr. Hansen and coauthors, who added that the tool “did not adhere” to the FDA call for meaningful patient input.
Some previous studies of quality of life in immune checkpoint inhibitor–treated patients have used tumor-specific PROs and the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire–Core 30 Items (EORTC-QLQ-C30).
The new, immune checkpoint inhibitor–specific toxicity subscale has “broader coverage” of side effects that reportedly affect HRQOL in patients treated with these agents, including taste disturbance, cough, and fever or chills, according to the investigators.
Moreover, the EORTC-QLQ-C30 and the EORTC head and neck cancer–specific-35 module (EORTC QLQ-H&N35), do not include items related to cutaneous adverse events such as itch, rash, and dry skin that have been seen in some checkpoint inhibitor clinical trials, they noted.
“This represents a clear limitation of such preexisting PRO instruments, which should be addressed with our immune checkpoint moduator–specific tool,” they wrote.
The study was supported by a grant from the University of Toronto. Authors of the study provided disclosures related to Merck, Bristol-Myers Squibb, Karyopharm, Boston Biomedical, Novartis, Genentech, Hoffmann La Roche, GlaxoSmithKline, and others.
SOURCE: Hansen AR et al. Cancer. 2020 Jan 8. doi: 10.1002/cncr.32692.
developed based on direct patient involvement, picks up on cutaneous and other side effects that would be missed using traditional quality of life questionnaires, investigators say.
The 25-item list represents the first-ever health-related quality of life (HRQOL) toxicity subscale developed for patients receiving checkpoint inhibitors, according to the investigators, led by Aaron R. Hansen, MBBS, of the division of medical oncology and hematology in the department of medicine at the University of Toronto.
The toxicity subscale is combined with the Functional Assessment of Cancer Therapy–General (FACT-G), which measures physical, emotional, family and social, and functional domains, to form the Functional Assessment of Cancer Therapy–Immune Checkpoint Modulator (FACT-ICM), Dr. Hansen stated in a recent report that describes initial development and early validation efforts.
The FACT-ICM could become an important tool for measuring HRQOL in patients receiving checkpoint inhibitors, depending on results of further investigations including more patients, the authors wrote in that report.
“Currently, we would recommend that our toxicity subscale be validated first before use in clinical care, or in trials with QOL as a primary or secondary endpoint,” wrote Dr. Hansen and colleagues in the report, which appears in Cancer.
The toxicity subscale asks patients to rate items such as “I am bothered by dry skin,” “I feel pain, soreness or aches in some of my muscles,” and “My fatigue keeps me from doing the things I want do” on a scale of 0 (not at all) to 4 (very much).
Development of the toxicity subscale was based on focus groups and interviews with 37 patients with a variety of cancer types who were being treated with a PD-1, PD-L1, and CTLA-4 immune checkpoint inhibitors. Sixteen physicians were surveyed to evaluate the patient input, while 11 of them also participated in follow-up interviews.
“At every step in this process, the patients were central,” the investigators wrote in their report.
According to the investigators, that approach is in line with guidance from the Food and Drug Administration, which has said that meaningful patient input should be used in the upfront development of patient-reported outcome (PRO) measures, rather than obtaining patient endorsement after the fact.
By contrast, an electronic PRO immune-oncology module recently developed, based on 19 immune-related adverse events from drug labels and clinical trial reports, had “no evaluation” of effects on HRQOL, according to Dr. Hansen and coauthors, who added that the tool “did not adhere” to the FDA call for meaningful patient input.
Some previous studies of quality of life in immune checkpoint inhibitor–treated patients have used tumor-specific PROs and the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire–Core 30 Items (EORTC-QLQ-C30).
The new, immune checkpoint inhibitor–specific toxicity subscale has “broader coverage” of side effects that reportedly affect HRQOL in patients treated with these agents, including taste disturbance, cough, and fever or chills, according to the investigators.
Moreover, the EORTC-QLQ-C30 and the EORTC head and neck cancer–specific-35 module (EORTC QLQ-H&N35), do not include items related to cutaneous adverse events such as itch, rash, and dry skin that have been seen in some checkpoint inhibitor clinical trials, they noted.
“This represents a clear limitation of such preexisting PRO instruments, which should be addressed with our immune checkpoint moduator–specific tool,” they wrote.
The study was supported by a grant from the University of Toronto. Authors of the study provided disclosures related to Merck, Bristol-Myers Squibb, Karyopharm, Boston Biomedical, Novartis, Genentech, Hoffmann La Roche, GlaxoSmithKline, and others.
SOURCE: Hansen AR et al. Cancer. 2020 Jan 8. doi: 10.1002/cncr.32692.
FROM CANCER
Standard-dose RT with concurrent chemo found superior for unresectable NSCLC
More is not better when it comes to radiation therapy administered with concurrent chemotherapy for unresectable stage III non–small cell lung cancer (NSCLC), suggests a long-term update of the RTOG 0617 trial.
Initial results of the phase 3 randomized controlled trial, at a median follow-up of 1.9 years, showed that median overall survival was about 8 months longer with the 60-Gy standard dose of radiation compared with a 74-Gy high dose, each given along with paclitaxel and carboplatin (Lancet Oncol. 2015;16:187-99).
The update, now at a median follow-up of 5.1 years and reported in the Journal of Clinical Oncology, recapitulates that finding, again showing a roughly 8-month longer overall survival with the standard dose of radiation. Results continue to show no benefit of adding the anti-EGFR antibody cetuximab (Erbitux) to treatment.
“The 5-year overall survival estimate for the standard-dose radiation arm of RTOG 0617, regardless of cetuximab delivery, was 32.1%. This is among the highest overall survival results of any phase III trial for patients with stage III NSCLC,” noted the investigators, led by Jeffrey D. Bradley, MD, department of radiation oncology, Emory University, Atlanta.
“These results argue strongly that the current standard-of-care radiation dose should be 60 Gy given in 2-Gy daily fractions to a target volume directed at tumor plus margin on the basis of CT and PET/CT, excluding elective nodal irradiation.”
The RTOG 0617 trial was conducted among 496 patients with unresectable stage III NSCLC in the United States and Canada. They were randomized to receive standard-dose or high-dose radiation in addition to concurrent chemotherapy, and randomized again to receive cetuximab or not.
Median overall survival as of the update was 28.7 months with standard-dose radiation therapy, compared with 20.3 months with high-dose radiation therapy (P = .0072), Dr. Bradley and coinvestigators reported. This survival benefit stood up in multivariate analysis (hazard ratio, 1.30; P = .0315).
The standard dose of radiation also yielded better 5-year overall survival (32.1% vs. 23%; P = .007) and 5-year progression-free survival (18.3% vs. 13%; P = .055). Further analyses suggested that these differences were not due to differential radiation therapy compliance.
The high-dose radiation group had more grade 5 adverse events (nine vs. three events), as well as higher rates of treatment-related grade 3 or worse dysphagia (12.1% vs. 3.2%; P = .0005) and esophagitis (17.4% vs. 5.0%; P less than .0001). Pulmonary toxicity was statistically indistinguishable between groups.
Since the RTOG 0617 results were first reported, the standard of care for unresectable stage III NSCLC has changed, as the PACIFIC trial showed an overall survival advantage of adding the immune checkpoint inhibitor durvalumab (Imfinzi) as maintenance therapy after concurrent chemoradiotherapy (N Engl J Med. 2018;379:2342-50).
However, the 2-year overall survival rate with chemoradiation using the standard radiation dose in the former trial (59.6%) is fairly close to that seen with chemoradiation plus maintenance durvalumab in the latter trial (66.3%), the investigators noted.
Dr. Bradley disclosed having a consulting or advisory role with AstraZeneca. The trial was supported by the National Cancer Institute and Eli Lilly.
SOURCE: Bradley JD et al. J Clin Oncol. 2019 Dec 16. doi: 10.1200/JCO.19.01162.
More is not better when it comes to radiation therapy administered with concurrent chemotherapy for unresectable stage III non–small cell lung cancer (NSCLC), suggests a long-term update of the RTOG 0617 trial.
Initial results of the phase 3 randomized controlled trial, at a median follow-up of 1.9 years, showed that median overall survival was about 8 months longer with the 60-Gy standard dose of radiation compared with a 74-Gy high dose, each given along with paclitaxel and carboplatin (Lancet Oncol. 2015;16:187-99).
The update, now at a median follow-up of 5.1 years and reported in the Journal of Clinical Oncology, recapitulates that finding, again showing a roughly 8-month longer overall survival with the standard dose of radiation. Results continue to show no benefit of adding the anti-EGFR antibody cetuximab (Erbitux) to treatment.
“The 5-year overall survival estimate for the standard-dose radiation arm of RTOG 0617, regardless of cetuximab delivery, was 32.1%. This is among the highest overall survival results of any phase III trial for patients with stage III NSCLC,” noted the investigators, led by Jeffrey D. Bradley, MD, department of radiation oncology, Emory University, Atlanta.
“These results argue strongly that the current standard-of-care radiation dose should be 60 Gy given in 2-Gy daily fractions to a target volume directed at tumor plus margin on the basis of CT and PET/CT, excluding elective nodal irradiation.”
The RTOG 0617 trial was conducted among 496 patients with unresectable stage III NSCLC in the United States and Canada. They were randomized to receive standard-dose or high-dose radiation in addition to concurrent chemotherapy, and randomized again to receive cetuximab or not.
Median overall survival as of the update was 28.7 months with standard-dose radiation therapy, compared with 20.3 months with high-dose radiation therapy (P = .0072), Dr. Bradley and coinvestigators reported. This survival benefit stood up in multivariate analysis (hazard ratio, 1.30; P = .0315).
The standard dose of radiation also yielded better 5-year overall survival (32.1% vs. 23%; P = .007) and 5-year progression-free survival (18.3% vs. 13%; P = .055). Further analyses suggested that these differences were not due to differential radiation therapy compliance.
The high-dose radiation group had more grade 5 adverse events (nine vs. three events), as well as higher rates of treatment-related grade 3 or worse dysphagia (12.1% vs. 3.2%; P = .0005) and esophagitis (17.4% vs. 5.0%; P less than .0001). Pulmonary toxicity was statistically indistinguishable between groups.
Since the RTOG 0617 results were first reported, the standard of care for unresectable stage III NSCLC has changed, as the PACIFIC trial showed an overall survival advantage of adding the immune checkpoint inhibitor durvalumab (Imfinzi) as maintenance therapy after concurrent chemoradiotherapy (N Engl J Med. 2018;379:2342-50).
However, the 2-year overall survival rate with chemoradiation using the standard radiation dose in the former trial (59.6%) is fairly close to that seen with chemoradiation plus maintenance durvalumab in the latter trial (66.3%), the investigators noted.
Dr. Bradley disclosed having a consulting or advisory role with AstraZeneca. The trial was supported by the National Cancer Institute and Eli Lilly.
SOURCE: Bradley JD et al. J Clin Oncol. 2019 Dec 16. doi: 10.1200/JCO.19.01162.
More is not better when it comes to radiation therapy administered with concurrent chemotherapy for unresectable stage III non–small cell lung cancer (NSCLC), suggests a long-term update of the RTOG 0617 trial.
Initial results of the phase 3 randomized controlled trial, at a median follow-up of 1.9 years, showed that median overall survival was about 8 months longer with the 60-Gy standard dose of radiation compared with a 74-Gy high dose, each given along with paclitaxel and carboplatin (Lancet Oncol. 2015;16:187-99).
The update, now at a median follow-up of 5.1 years and reported in the Journal of Clinical Oncology, recapitulates that finding, again showing a roughly 8-month longer overall survival with the standard dose of radiation. Results continue to show no benefit of adding the anti-EGFR antibody cetuximab (Erbitux) to treatment.
“The 5-year overall survival estimate for the standard-dose radiation arm of RTOG 0617, regardless of cetuximab delivery, was 32.1%. This is among the highest overall survival results of any phase III trial for patients with stage III NSCLC,” noted the investigators, led by Jeffrey D. Bradley, MD, department of radiation oncology, Emory University, Atlanta.
“These results argue strongly that the current standard-of-care radiation dose should be 60 Gy given in 2-Gy daily fractions to a target volume directed at tumor plus margin on the basis of CT and PET/CT, excluding elective nodal irradiation.”
The RTOG 0617 trial was conducted among 496 patients with unresectable stage III NSCLC in the United States and Canada. They were randomized to receive standard-dose or high-dose radiation in addition to concurrent chemotherapy, and randomized again to receive cetuximab or not.
Median overall survival as of the update was 28.7 months with standard-dose radiation therapy, compared with 20.3 months with high-dose radiation therapy (P = .0072), Dr. Bradley and coinvestigators reported. This survival benefit stood up in multivariate analysis (hazard ratio, 1.30; P = .0315).
The standard dose of radiation also yielded better 5-year overall survival (32.1% vs. 23%; P = .007) and 5-year progression-free survival (18.3% vs. 13%; P = .055). Further analyses suggested that these differences were not due to differential radiation therapy compliance.
The high-dose radiation group had more grade 5 adverse events (nine vs. three events), as well as higher rates of treatment-related grade 3 or worse dysphagia (12.1% vs. 3.2%; P = .0005) and esophagitis (17.4% vs. 5.0%; P less than .0001). Pulmonary toxicity was statistically indistinguishable between groups.
Since the RTOG 0617 results were first reported, the standard of care for unresectable stage III NSCLC has changed, as the PACIFIC trial showed an overall survival advantage of adding the immune checkpoint inhibitor durvalumab (Imfinzi) as maintenance therapy after concurrent chemoradiotherapy (N Engl J Med. 2018;379:2342-50).
However, the 2-year overall survival rate with chemoradiation using the standard radiation dose in the former trial (59.6%) is fairly close to that seen with chemoradiation plus maintenance durvalumab in the latter trial (66.3%), the investigators noted.
Dr. Bradley disclosed having a consulting or advisory role with AstraZeneca. The trial was supported by the National Cancer Institute and Eli Lilly.
SOURCE: Bradley JD et al. J Clin Oncol. 2019 Dec 16. doi: 10.1200/JCO.19.01162.
FROM THE JOURNAL OF CLINICAL ONCOLOGY
Benefits and drawbacks found for risk-based lung cancer screening tools
Risk-based lung cancer screening tools can prevent significantly more lung cancer deaths than the current United States Preventive Services Task Force recommendations, but life-year gains were negligible or reduced and patients would experience greater overdiagnosis, according to new research.
“Current guidelines propose screening eligibility using age and smoking-related criteria, through combinations of accumulated pack-years and years since smoking cessation,” Kevin ten Haaf, PhD, of the department of public health at Erasmus Medical Center in Rotterdam, the Netherlands, and associates wrote in the Journal of the National Cancer Institute. “The USPSTF recommends annual screening between the ages of 55 and 80 years for current and former smokers (quit less than 15 years) who smoked 30 or more pack-years.”
Individual risk assessment utilizing established lung cancer risk–prediction models may have some superiority over pack-years in identifying those most likely to benefit from screening, they wrote, because the models incorporate smoking history in greater detail and consider risk factors such as chronic obstructive pulmonary disease.
Three risk-assessment models were used for the study, in addition to the USPSTF guidelines: the Bach, PLCOm2012, and Lung Cancer Death Risk Assessment Tool (LCDRAT). The study population was a simulated 1950 U.S. cohort from the Smoking History Generator aged between 55 years and 80 years; each simulated smoking history consists of whether and when the person initiates and ceases smoking, average number of cigarettes smoked per day by age, and the age of death from non–lung cancer causes.
The number of lung cancer deaths averted was significantly higher in the risk-based models, compared with the USPSTF recommendations (Bach, 693 per 100,000 population; PLCOm2012, 698 per 100,000 population; LCDRAT, 696 per 100,000 population; USPSTF, 613 per 100,000 population).
However, life-years gained was only modestly higher in the models, compared with the guideline (Bach, 8,660 per 100,000 life-years; PLCOm2012, 8,862 per 100,000 life-years; LCDRAT, 8,631 per 100,000 life-years; USPSTF, 8,590 per 100,000 life-years). In addition, life-years gained for every lung cancer death prevented was greater in the guideline (14.0 years) than in the risk-based models (12.1-12.4 years).
Overdiagnosis was also more common using risk-based tools (Bach, 149 per 100,000; PLCOm2012, 147 per 100,000; LCDRAT, 150 per 100,000; USPSTF, 115 per 100,000). This was mainly because of eligibility for risk-based screening tools increasing with age, the investigators noted.
According to a sensitivity analysis, risk-based models would retain the life-years gained by the USPSTF model if individuals with limited life expectancies (less than 5 years) were excluded. This would also reduce overdiagnosis by 65.3%.
“Future studies should investigate the cost-effectiveness of risk-based screening and the potential for reducing overdiagnosis in high-risk individuals,” the investigators concluded.
One coauthor developed the PLCOm2012 model, but the model is available free to noncommercial users, and the investigator has received no money from its usage. No other conflicts of interest were reported.
SOURCE: ten Haaf K et al. J Natl Cancer Inst. 2019 Nov 29. doi: 10.1093/jnci/djz164.
Risk-based lung cancer screening tools can prevent significantly more lung cancer deaths than the current United States Preventive Services Task Force recommendations, but life-year gains were negligible or reduced and patients would experience greater overdiagnosis, according to new research.
“Current guidelines propose screening eligibility using age and smoking-related criteria, through combinations of accumulated pack-years and years since smoking cessation,” Kevin ten Haaf, PhD, of the department of public health at Erasmus Medical Center in Rotterdam, the Netherlands, and associates wrote in the Journal of the National Cancer Institute. “The USPSTF recommends annual screening between the ages of 55 and 80 years for current and former smokers (quit less than 15 years) who smoked 30 or more pack-years.”
Individual risk assessment utilizing established lung cancer risk–prediction models may have some superiority over pack-years in identifying those most likely to benefit from screening, they wrote, because the models incorporate smoking history in greater detail and consider risk factors such as chronic obstructive pulmonary disease.
Three risk-assessment models were used for the study, in addition to the USPSTF guidelines: the Bach, PLCOm2012, and Lung Cancer Death Risk Assessment Tool (LCDRAT). The study population was a simulated 1950 U.S. cohort from the Smoking History Generator aged between 55 years and 80 years; each simulated smoking history consists of whether and when the person initiates and ceases smoking, average number of cigarettes smoked per day by age, and the age of death from non–lung cancer causes.
The number of lung cancer deaths averted was significantly higher in the risk-based models, compared with the USPSTF recommendations (Bach, 693 per 100,000 population; PLCOm2012, 698 per 100,000 population; LCDRAT, 696 per 100,000 population; USPSTF, 613 per 100,000 population).
However, life-years gained was only modestly higher in the models, compared with the guideline (Bach, 8,660 per 100,000 life-years; PLCOm2012, 8,862 per 100,000 life-years; LCDRAT, 8,631 per 100,000 life-years; USPSTF, 8,590 per 100,000 life-years). In addition, life-years gained for every lung cancer death prevented was greater in the guideline (14.0 years) than in the risk-based models (12.1-12.4 years).
Overdiagnosis was also more common using risk-based tools (Bach, 149 per 100,000; PLCOm2012, 147 per 100,000; LCDRAT, 150 per 100,000; USPSTF, 115 per 100,000). This was mainly because of eligibility for risk-based screening tools increasing with age, the investigators noted.
According to a sensitivity analysis, risk-based models would retain the life-years gained by the USPSTF model if individuals with limited life expectancies (less than 5 years) were excluded. This would also reduce overdiagnosis by 65.3%.
“Future studies should investigate the cost-effectiveness of risk-based screening and the potential for reducing overdiagnosis in high-risk individuals,” the investigators concluded.
One coauthor developed the PLCOm2012 model, but the model is available free to noncommercial users, and the investigator has received no money from its usage. No other conflicts of interest were reported.
SOURCE: ten Haaf K et al. J Natl Cancer Inst. 2019 Nov 29. doi: 10.1093/jnci/djz164.
Risk-based lung cancer screening tools can prevent significantly more lung cancer deaths than the current United States Preventive Services Task Force recommendations, but life-year gains were negligible or reduced and patients would experience greater overdiagnosis, according to new research.
“Current guidelines propose screening eligibility using age and smoking-related criteria, through combinations of accumulated pack-years and years since smoking cessation,” Kevin ten Haaf, PhD, of the department of public health at Erasmus Medical Center in Rotterdam, the Netherlands, and associates wrote in the Journal of the National Cancer Institute. “The USPSTF recommends annual screening between the ages of 55 and 80 years for current and former smokers (quit less than 15 years) who smoked 30 or more pack-years.”
Individual risk assessment utilizing established lung cancer risk–prediction models may have some superiority over pack-years in identifying those most likely to benefit from screening, they wrote, because the models incorporate smoking history in greater detail and consider risk factors such as chronic obstructive pulmonary disease.
Three risk-assessment models were used for the study, in addition to the USPSTF guidelines: the Bach, PLCOm2012, and Lung Cancer Death Risk Assessment Tool (LCDRAT). The study population was a simulated 1950 U.S. cohort from the Smoking History Generator aged between 55 years and 80 years; each simulated smoking history consists of whether and when the person initiates and ceases smoking, average number of cigarettes smoked per day by age, and the age of death from non–lung cancer causes.
The number of lung cancer deaths averted was significantly higher in the risk-based models, compared with the USPSTF recommendations (Bach, 693 per 100,000 population; PLCOm2012, 698 per 100,000 population; LCDRAT, 696 per 100,000 population; USPSTF, 613 per 100,000 population).
However, life-years gained was only modestly higher in the models, compared with the guideline (Bach, 8,660 per 100,000 life-years; PLCOm2012, 8,862 per 100,000 life-years; LCDRAT, 8,631 per 100,000 life-years; USPSTF, 8,590 per 100,000 life-years). In addition, life-years gained for every lung cancer death prevented was greater in the guideline (14.0 years) than in the risk-based models (12.1-12.4 years).
Overdiagnosis was also more common using risk-based tools (Bach, 149 per 100,000; PLCOm2012, 147 per 100,000; LCDRAT, 150 per 100,000; USPSTF, 115 per 100,000). This was mainly because of eligibility for risk-based screening tools increasing with age, the investigators noted.
According to a sensitivity analysis, risk-based models would retain the life-years gained by the USPSTF model if individuals with limited life expectancies (less than 5 years) were excluded. This would also reduce overdiagnosis by 65.3%.
“Future studies should investigate the cost-effectiveness of risk-based screening and the potential for reducing overdiagnosis in high-risk individuals,” the investigators concluded.
One coauthor developed the PLCOm2012 model, but the model is available free to noncommercial users, and the investigator has received no money from its usage. No other conflicts of interest were reported.
SOURCE: ten Haaf K et al. J Natl Cancer Inst. 2019 Nov 29. doi: 10.1093/jnci/djz164.
FROM THE JOURNAL OF THE NATIONAL CANCER INSTITUTE
Patient-reported outcomes support first-line pembrolizumab for NSCLC
Patient-reported outcomes support pembrolizumab plus chemotherapy for first-line treatment of metastatic non–small cell lung cancer (NSCLC), based on results from the KEYNOTE-407 trial.
At week 18, patients given pembrolizumab more often reported clinically meaningful health-related quality of life improvements than those in the placebo group, according to lead author Julien Mazieres, MD, PhD, of Paul Sabatier University in Toulouse, France, and colleagues.
Writing in the Journal of Clinical Oncology, the investigators explained that these findings build upon previously published results from KEYNOTE-407, which showed that adding pembrolizumab to chemotherapy in the first line could extend both progression-free and overall survival among patients with NSCLC. The benefits to quality of life associated with pembrolizumab align with similar findings from the KEYNOTE-024 and KEYNOTE-189 trials, they added.
The present analysis involved 559 patients with treatment-naive metastatic NSCLC. Patients were randomized to receive 4 cycles of placebo or pembrolizumab once every 3 weeks with carboplatin-based chemotherapy, followed by pembrolizumab or placebo for an additional 31 cycles. Health-related quality of life was assessed by two measures: the European Organisation for the Research and Treatment of Cancer Quality of Life Questionnaire–Core 30 (QLQ-C30) and QLQ–Lung Cancer Module 13 (QLQ-LC13).
Of the 559 patients enrolled, 554 completed at least one QLQ-C30 assessment and 553 completed at least one QLQ-LC13 assessment. These quality of life scores were compared temporally within treatment groups, from baseline to week 9 and week 18, and between groups. The investigators also analyzed median time to deterioration in chest pain, cough, and dyspnea.
Results showed that patients in the pembrolizumab group had statistically significant improvements in patient-reported outcomes over time and more frequently reported improvements than patients in the placebo group. Specifically, in the pembrolizumab group, least-squares mean score improved from baseline to week 9 (1.8) and week 18 (4.3); in comparison, least-squares mean score deteriorated in the placebo group from baseline to week 9 (–1.8) and week 18 (–0.57). Compared with placebo, treatment with pembrolizumab was associated with a least-squares mean change of 3.6 at week 9 (nominal P = .0337) and 4.9 at week 18 (nominal P = .0060). Stated differently, at week 18, compared with placebo, more patients in the pembrolizumab group reported clinically meaningful improvements in health-related quality of life (36.2% vs. 27.7%), and relatively fewer reported deterioration (22.8% vs. 31.3%). Median time to deterioration in symptoms was not reached in either treatment arm.
“These health-related quality of life findings, along with the improved efficacy (including overall survival benefit) of pembrolizumab plus carboplatin and paclitaxel/nab-paclitaxel, support its use as a first-line treatment of metastatic squamous NSCLC, regardless of programmed death–ligand 1 expression,” the investigators concluded.
The study was funded by Merck. The investigators reported additional relationships with Novartis, Genentech, Pfizer, and others.
SOURCE: Mazieres J et al. J Clin Oncol. 2019 Nov 21. doi: 10.1200/JCO.19.01348.
Patient-reported outcomes support pembrolizumab plus chemotherapy for first-line treatment of metastatic non–small cell lung cancer (NSCLC), based on results from the KEYNOTE-407 trial.
At week 18, patients given pembrolizumab more often reported clinically meaningful health-related quality of life improvements than those in the placebo group, according to lead author Julien Mazieres, MD, PhD, of Paul Sabatier University in Toulouse, France, and colleagues.
Writing in the Journal of Clinical Oncology, the investigators explained that these findings build upon previously published results from KEYNOTE-407, which showed that adding pembrolizumab to chemotherapy in the first line could extend both progression-free and overall survival among patients with NSCLC. The benefits to quality of life associated with pembrolizumab align with similar findings from the KEYNOTE-024 and KEYNOTE-189 trials, they added.
The present analysis involved 559 patients with treatment-naive metastatic NSCLC. Patients were randomized to receive 4 cycles of placebo or pembrolizumab once every 3 weeks with carboplatin-based chemotherapy, followed by pembrolizumab or placebo for an additional 31 cycles. Health-related quality of life was assessed by two measures: the European Organisation for the Research and Treatment of Cancer Quality of Life Questionnaire–Core 30 (QLQ-C30) and QLQ–Lung Cancer Module 13 (QLQ-LC13).
Of the 559 patients enrolled, 554 completed at least one QLQ-C30 assessment and 553 completed at least one QLQ-LC13 assessment. These quality of life scores were compared temporally within treatment groups, from baseline to week 9 and week 18, and between groups. The investigators also analyzed median time to deterioration in chest pain, cough, and dyspnea.
Results showed that patients in the pembrolizumab group had statistically significant improvements in patient-reported outcomes over time and more frequently reported improvements than patients in the placebo group. Specifically, in the pembrolizumab group, least-squares mean score improved from baseline to week 9 (1.8) and week 18 (4.3); in comparison, least-squares mean score deteriorated in the placebo group from baseline to week 9 (–1.8) and week 18 (–0.57). Compared with placebo, treatment with pembrolizumab was associated with a least-squares mean change of 3.6 at week 9 (nominal P = .0337) and 4.9 at week 18 (nominal P = .0060). Stated differently, at week 18, compared with placebo, more patients in the pembrolizumab group reported clinically meaningful improvements in health-related quality of life (36.2% vs. 27.7%), and relatively fewer reported deterioration (22.8% vs. 31.3%). Median time to deterioration in symptoms was not reached in either treatment arm.
“These health-related quality of life findings, along with the improved efficacy (including overall survival benefit) of pembrolizumab plus carboplatin and paclitaxel/nab-paclitaxel, support its use as a first-line treatment of metastatic squamous NSCLC, regardless of programmed death–ligand 1 expression,” the investigators concluded.
The study was funded by Merck. The investigators reported additional relationships with Novartis, Genentech, Pfizer, and others.
SOURCE: Mazieres J et al. J Clin Oncol. 2019 Nov 21. doi: 10.1200/JCO.19.01348.
Patient-reported outcomes support pembrolizumab plus chemotherapy for first-line treatment of metastatic non–small cell lung cancer (NSCLC), based on results from the KEYNOTE-407 trial.
At week 18, patients given pembrolizumab more often reported clinically meaningful health-related quality of life improvements than those in the placebo group, according to lead author Julien Mazieres, MD, PhD, of Paul Sabatier University in Toulouse, France, and colleagues.
Writing in the Journal of Clinical Oncology, the investigators explained that these findings build upon previously published results from KEYNOTE-407, which showed that adding pembrolizumab to chemotherapy in the first line could extend both progression-free and overall survival among patients with NSCLC. The benefits to quality of life associated with pembrolizumab align with similar findings from the KEYNOTE-024 and KEYNOTE-189 trials, they added.
The present analysis involved 559 patients with treatment-naive metastatic NSCLC. Patients were randomized to receive 4 cycles of placebo or pembrolizumab once every 3 weeks with carboplatin-based chemotherapy, followed by pembrolizumab or placebo for an additional 31 cycles. Health-related quality of life was assessed by two measures: the European Organisation for the Research and Treatment of Cancer Quality of Life Questionnaire–Core 30 (QLQ-C30) and QLQ–Lung Cancer Module 13 (QLQ-LC13).
Of the 559 patients enrolled, 554 completed at least one QLQ-C30 assessment and 553 completed at least one QLQ-LC13 assessment. These quality of life scores were compared temporally within treatment groups, from baseline to week 9 and week 18, and between groups. The investigators also analyzed median time to deterioration in chest pain, cough, and dyspnea.
Results showed that patients in the pembrolizumab group had statistically significant improvements in patient-reported outcomes over time and more frequently reported improvements than patients in the placebo group. Specifically, in the pembrolizumab group, least-squares mean score improved from baseline to week 9 (1.8) and week 18 (4.3); in comparison, least-squares mean score deteriorated in the placebo group from baseline to week 9 (–1.8) and week 18 (–0.57). Compared with placebo, treatment with pembrolizumab was associated with a least-squares mean change of 3.6 at week 9 (nominal P = .0337) and 4.9 at week 18 (nominal P = .0060). Stated differently, at week 18, compared with placebo, more patients in the pembrolizumab group reported clinically meaningful improvements in health-related quality of life (36.2% vs. 27.7%), and relatively fewer reported deterioration (22.8% vs. 31.3%). Median time to deterioration in symptoms was not reached in either treatment arm.
“These health-related quality of life findings, along with the improved efficacy (including overall survival benefit) of pembrolizumab plus carboplatin and paclitaxel/nab-paclitaxel, support its use as a first-line treatment of metastatic squamous NSCLC, regardless of programmed death–ligand 1 expression,” the investigators concluded.
The study was funded by Merck. The investigators reported additional relationships with Novartis, Genentech, Pfizer, and others.
SOURCE: Mazieres J et al. J Clin Oncol. 2019 Nov 21. doi: 10.1200/JCO.19.01348.
FROM THE JOURNAL OF CLINICAL ONCOLOGY
FDA approves atezolizumab combo as first line for advanced NSCLC
chemotherapy for first-line treatment of adults with metastatic, nonsquamous non–small cell lung cancer (NSCLC) with no EGFR or ALK genomic tumor aberrations.

Atezolizumab has been previously approved in combination with bevacizumab, paclitaxel, and carboplatin for the first-line treatment of adults with metastatic NSCLC with no EGFR or ALK genomic tumor aberrations. The monoclonal antibody is also approved to treat adults with metastatic NSCLC who have disease progression during or following chemotherapy, and for those with extensive-stage SCLC.
The current approval was based on a demonstrated improvement in overall survival in the phase 3 IMpower130 trial (NCT02367781). Median overall survival for advanced NSCLC patients who received atezolizumab in combination with chemotherapy was 18.6 months, compared with 13.9 months for patients who received chemotherapy alone (hazard ratio, 0.80; 95% confidence interval, 0.64-0.99; P = .0384) in the intention-to-treat wild-type population of 681 patients.
Grade 3-4 treatment-related adverse events were reported in 73.2% of people receiving atezolizumab plus chemotherapy, compared with 60.3% of people receiving chemotherapy alone, according to the company press release.
chemotherapy for first-line treatment of adults with metastatic, nonsquamous non–small cell lung cancer (NSCLC) with no EGFR or ALK genomic tumor aberrations.
Atezolizumab has been previously approved in combination with bevacizumab, paclitaxel, and carboplatin for the first-line treatment of adults with metastatic NSCLC with no EGFR or ALK genomic tumor aberrations. The monoclonal antibody is also approved to treat adults with metastatic NSCLC who have disease progression during or following chemotherapy, and for those with extensive-stage SCLC.
The current approval was based on a demonstrated improvement in overall survival in the phase 3 IMpower130 trial (NCT02367781). Median overall survival for advanced NSCLC patients who received atezolizumab in combination with chemotherapy was 18.6 months, compared with 13.9 months for patients who received chemotherapy alone (hazard ratio, 0.80; 95% confidence interval, 0.64-0.99; P = .0384) in the intention-to-treat wild-type population of 681 patients.
Grade 3-4 treatment-related adverse events were reported in 73.2% of people receiving atezolizumab plus chemotherapy, compared with 60.3% of people receiving chemotherapy alone, according to the company press release.
chemotherapy for first-line treatment of adults with metastatic, nonsquamous non–small cell lung cancer (NSCLC) with no EGFR or ALK genomic tumor aberrations.
Atezolizumab has been previously approved in combination with bevacizumab, paclitaxel, and carboplatin for the first-line treatment of adults with metastatic NSCLC with no EGFR or ALK genomic tumor aberrations. The monoclonal antibody is also approved to treat adults with metastatic NSCLC who have disease progression during or following chemotherapy, and for those with extensive-stage SCLC.
The current approval was based on a demonstrated improvement in overall survival in the phase 3 IMpower130 trial (NCT02367781). Median overall survival for advanced NSCLC patients who received atezolizumab in combination with chemotherapy was 18.6 months, compared with 13.9 months for patients who received chemotherapy alone (hazard ratio, 0.80; 95% confidence interval, 0.64-0.99; P = .0384) in the intention-to-treat wild-type population of 681 patients.
Grade 3-4 treatment-related adverse events were reported in 73.2% of people receiving atezolizumab plus chemotherapy, compared with 60.3% of people receiving chemotherapy alone, according to the company press release.
Single-fraction radiation just misses mark for spinal compression relief
Single-fraction radiation could not be shown to be noninferior to multi-fraction radiation at improving walking function in patients with spinal compression from metastatic cancer, but the small differences seen in a noninferiority trial may not matter to patients, investigators suggest.
Among 686 patients with spinal compression from metastatic cancer randomly assigned in a clinical trial to receive either 8 Gy of radiation in a single fraction or 20 Gy delivered in 5 fractions over 5 consecutive days, 69.3% of patients in the single-fraction arm had good ambulatory status at 8 weeks, compared with 72.7% of patients in the multi-fraction arm (P for noninferiority = .06), reported Peter J Hoskin, BSc, MBBS, MD, of Mount Vernon Cancer Centre in Northwood, England, and colleagues.
The trial did not meet the endpoint of noninferiority of single-fraction radiation for improving ambulation at 8 weeks because the lower limit of the 95% confidence interval (CI) was –11.5%, overlapping the noninferiority margin of –11%.
“However, for all other time points, the CI limits were within the noninferiority margin, and the observed risk differences between single-fraction and multi-fraction radiotherapy groups in ambulatory status were small and unlikely to be of clinical importance,” the investigators wrote in JAMA.
The authors note that although radiotherapy is widely used as a palliative measure for patients with spinal canal compression caused my metastatic disease, there is no agreement on the optimum schedule, with some guidelines recommending higher doses in multiple fractions, and others recommending a single 8 Gy does for patients with painful spinal sites.
To see whether single-fraction radiation could be noninferior to multi-fraction, the investigators enrolled patients in 42 sites in the United Kingdom and 5 in Australia into the SCORAD trial, and randomly assigned them to either single-fraction (345 patients) or multi-fraction (341 patients) radiation. The median age of those enrolled was 70 years, and 44% had prostate cancer, 19% had lung cancer, and 12% had breast cancer.
As noted, the primary endpoint of noninferiority of single-fraction radiation at improving ambulatory status at week 8 was not met. Ambulatory status was based on a 4-point scale and was classified as either grade 1: ambulatory without the use of aids and grade 5 of 5 of muscle power, or grade 2: ambulatory with aids or grade 4 of 5 of muscle power.
An analysis of secondary endpoints showed that the difference in ambulatory status grade 1 or 2 in the single- vs. multi-fraction group at week 1 was −0.4% (P value for noninferiority = .004), at week 4 it was −0.7% (P value for noninferiority = .01), and at week 12 it was 4.1% (P value for noninferiority = .002).
Overall survival rates at 12 weeks were 50% in the single-fraction group vs. 55% in the multi-fraction group; this difference was not statistically significant.
Of 11 other secondary endpoints analyzed, including ambulatory and safety endpoints, the between-group differences were not statistically significant or did not meet noninferiority criteria, the authors noted.
They concluded that although the trial did not meet the primary endpoint, ”the extent to which the lower bound of the CI overlapped with the noninferiority margin should be taken into account when interpreting the clinical importance of these findings.”
Cancer Research UK and Cancer Council Queensland funded the trial. Dr. Hoskin reported being supported by the National Institute for Health Research Manchester Biomedical Research Centre.
SOURCE: Hoskin PJ et al. JAMA 2019 Dec 3. doi: 10.1001/jama.2019.17913.
Single-fraction radiation could not be shown to be noninferior to multi-fraction radiation at improving walking function in patients with spinal compression from metastatic cancer, but the small differences seen in a noninferiority trial may not matter to patients, investigators suggest.
Among 686 patients with spinal compression from metastatic cancer randomly assigned in a clinical trial to receive either 8 Gy of radiation in a single fraction or 20 Gy delivered in 5 fractions over 5 consecutive days, 69.3% of patients in the single-fraction arm had good ambulatory status at 8 weeks, compared with 72.7% of patients in the multi-fraction arm (P for noninferiority = .06), reported Peter J Hoskin, BSc, MBBS, MD, of Mount Vernon Cancer Centre in Northwood, England, and colleagues.
The trial did not meet the endpoint of noninferiority of single-fraction radiation for improving ambulation at 8 weeks because the lower limit of the 95% confidence interval (CI) was –11.5%, overlapping the noninferiority margin of –11%.
“However, for all other time points, the CI limits were within the noninferiority margin, and the observed risk differences between single-fraction and multi-fraction radiotherapy groups in ambulatory status were small and unlikely to be of clinical importance,” the investigators wrote in JAMA.
The authors note that although radiotherapy is widely used as a palliative measure for patients with spinal canal compression caused my metastatic disease, there is no agreement on the optimum schedule, with some guidelines recommending higher doses in multiple fractions, and others recommending a single 8 Gy does for patients with painful spinal sites.
To see whether single-fraction radiation could be noninferior to multi-fraction, the investigators enrolled patients in 42 sites in the United Kingdom and 5 in Australia into the SCORAD trial, and randomly assigned them to either single-fraction (345 patients) or multi-fraction (341 patients) radiation. The median age of those enrolled was 70 years, and 44% had prostate cancer, 19% had lung cancer, and 12% had breast cancer.
As noted, the primary endpoint of noninferiority of single-fraction radiation at improving ambulatory status at week 8 was not met. Ambulatory status was based on a 4-point scale and was classified as either grade 1: ambulatory without the use of aids and grade 5 of 5 of muscle power, or grade 2: ambulatory with aids or grade 4 of 5 of muscle power.
An analysis of secondary endpoints showed that the difference in ambulatory status grade 1 or 2 in the single- vs. multi-fraction group at week 1 was −0.4% (P value for noninferiority = .004), at week 4 it was −0.7% (P value for noninferiority = .01), and at week 12 it was 4.1% (P value for noninferiority = .002).
Overall survival rates at 12 weeks were 50% in the single-fraction group vs. 55% in the multi-fraction group; this difference was not statistically significant.
Of 11 other secondary endpoints analyzed, including ambulatory and safety endpoints, the between-group differences were not statistically significant or did not meet noninferiority criteria, the authors noted.
They concluded that although the trial did not meet the primary endpoint, ”the extent to which the lower bound of the CI overlapped with the noninferiority margin should be taken into account when interpreting the clinical importance of these findings.”
Cancer Research UK and Cancer Council Queensland funded the trial. Dr. Hoskin reported being supported by the National Institute for Health Research Manchester Biomedical Research Centre.
SOURCE: Hoskin PJ et al. JAMA 2019 Dec 3. doi: 10.1001/jama.2019.17913.
Single-fraction radiation could not be shown to be noninferior to multi-fraction radiation at improving walking function in patients with spinal compression from metastatic cancer, but the small differences seen in a noninferiority trial may not matter to patients, investigators suggest.
Among 686 patients with spinal compression from metastatic cancer randomly assigned in a clinical trial to receive either 8 Gy of radiation in a single fraction or 20 Gy delivered in 5 fractions over 5 consecutive days, 69.3% of patients in the single-fraction arm had good ambulatory status at 8 weeks, compared with 72.7% of patients in the multi-fraction arm (P for noninferiority = .06), reported Peter J Hoskin, BSc, MBBS, MD, of Mount Vernon Cancer Centre in Northwood, England, and colleagues.
The trial did not meet the endpoint of noninferiority of single-fraction radiation for improving ambulation at 8 weeks because the lower limit of the 95% confidence interval (CI) was –11.5%, overlapping the noninferiority margin of –11%.
“However, for all other time points, the CI limits were within the noninferiority margin, and the observed risk differences between single-fraction and multi-fraction radiotherapy groups in ambulatory status were small and unlikely to be of clinical importance,” the investigators wrote in JAMA.
The authors note that although radiotherapy is widely used as a palliative measure for patients with spinal canal compression caused my metastatic disease, there is no agreement on the optimum schedule, with some guidelines recommending higher doses in multiple fractions, and others recommending a single 8 Gy does for patients with painful spinal sites.
To see whether single-fraction radiation could be noninferior to multi-fraction, the investigators enrolled patients in 42 sites in the United Kingdom and 5 in Australia into the SCORAD trial, and randomly assigned them to either single-fraction (345 patients) or multi-fraction (341 patients) radiation. The median age of those enrolled was 70 years, and 44% had prostate cancer, 19% had lung cancer, and 12% had breast cancer.
As noted, the primary endpoint of noninferiority of single-fraction radiation at improving ambulatory status at week 8 was not met. Ambulatory status was based on a 4-point scale and was classified as either grade 1: ambulatory without the use of aids and grade 5 of 5 of muscle power, or grade 2: ambulatory with aids or grade 4 of 5 of muscle power.
An analysis of secondary endpoints showed that the difference in ambulatory status grade 1 or 2 in the single- vs. multi-fraction group at week 1 was −0.4% (P value for noninferiority = .004), at week 4 it was −0.7% (P value for noninferiority = .01), and at week 12 it was 4.1% (P value for noninferiority = .002).
Overall survival rates at 12 weeks were 50% in the single-fraction group vs. 55% in the multi-fraction group; this difference was not statistically significant.
Of 11 other secondary endpoints analyzed, including ambulatory and safety endpoints, the between-group differences were not statistically significant or did not meet noninferiority criteria, the authors noted.
They concluded that although the trial did not meet the primary endpoint, ”the extent to which the lower bound of the CI overlapped with the noninferiority margin should be taken into account when interpreting the clinical importance of these findings.”
Cancer Research UK and Cancer Council Queensland funded the trial. Dr. Hoskin reported being supported by the National Institute for Health Research Manchester Biomedical Research Centre.
SOURCE: Hoskin PJ et al. JAMA 2019 Dec 3. doi: 10.1001/jama.2019.17913.
FROM JAMA
Large state disparities seen for lung cancer screening
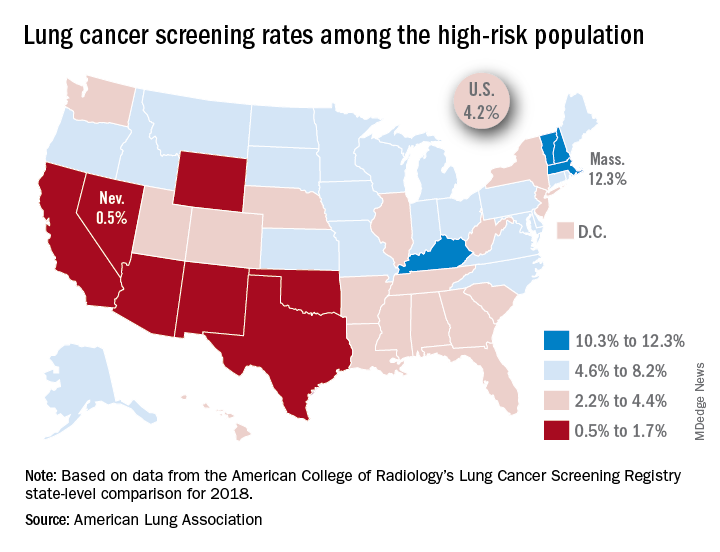
That disparity might suggest that Massachusetts has an exceptionally high rate, but it’s only 12.3%. And that means Nevada’s rate is very low, which it is: Only 0.5% of those at high risk are getting screened with annual low-dose CT scans, the ALA said in its 2019 State of Lung Cancer report.
“[The low rate of screening] may be because of a lack of access or low awareness and knowledge among patients and providers. As rates vary tremendously between states, it is clear that more can be done to increase screening rates,” the ALA stated.
Nationally, the screening rate is 4.2% among those at high risk for lung cancer, but “if everyone currently eligible were screened, close to 48,000 lives could be saved,” the ALA noted in its report.
Six states other than Nevada are below the 2% mark: Arizona, California, New Mexico, Oklahoma, Texas, and Wyoming. Besides Massachusetts, the three other states above 10% are Kentucky, New Hampshire, and Vermont, according to data from the American College of Radiology’s Lung Cancer Screening Registry state-level comparison for 2018.
For individuals at high risk for lung cancer – those aged 55-80 years who have at least a 30 pack-year history and either still smoke or have quit within 15 years – “screening with annual low-dose CT scans can reduce the lung cancer death rate by up to 20% by detecting tumors at early stages when the cancer is more likely to be curable,” the ALA wrote.
That disparity might suggest that Massachusetts has an exceptionally high rate, but it’s only 12.3%. And that means Nevada’s rate is very low, which it is: Only 0.5% of those at high risk are getting screened with annual low-dose CT scans, the ALA said in its 2019 State of Lung Cancer report.
“[The low rate of screening] may be because of a lack of access or low awareness and knowledge among patients and providers. As rates vary tremendously between states, it is clear that more can be done to increase screening rates,” the ALA stated.
Nationally, the screening rate is 4.2% among those at high risk for lung cancer, but “if everyone currently eligible were screened, close to 48,000 lives could be saved,” the ALA noted in its report.
Six states other than Nevada are below the 2% mark: Arizona, California, New Mexico, Oklahoma, Texas, and Wyoming. Besides Massachusetts, the three other states above 10% are Kentucky, New Hampshire, and Vermont, according to data from the American College of Radiology’s Lung Cancer Screening Registry state-level comparison for 2018.
For individuals at high risk for lung cancer – those aged 55-80 years who have at least a 30 pack-year history and either still smoke or have quit within 15 years – “screening with annual low-dose CT scans can reduce the lung cancer death rate by up to 20% by detecting tumors at early stages when the cancer is more likely to be curable,” the ALA wrote.
That disparity might suggest that Massachusetts has an exceptionally high rate, but it’s only 12.3%. And that means Nevada’s rate is very low, which it is: Only 0.5% of those at high risk are getting screened with annual low-dose CT scans, the ALA said in its 2019 State of Lung Cancer report.
“[The low rate of screening] may be because of a lack of access or low awareness and knowledge among patients and providers. As rates vary tremendously between states, it is clear that more can be done to increase screening rates,” the ALA stated.
Nationally, the screening rate is 4.2% among those at high risk for lung cancer, but “if everyone currently eligible were screened, close to 48,000 lives could be saved,” the ALA noted in its report.
Six states other than Nevada are below the 2% mark: Arizona, California, New Mexico, Oklahoma, Texas, and Wyoming. Besides Massachusetts, the three other states above 10% are Kentucky, New Hampshire, and Vermont, according to data from the American College of Radiology’s Lung Cancer Screening Registry state-level comparison for 2018.
For individuals at high risk for lung cancer – those aged 55-80 years who have at least a 30 pack-year history and either still smoke or have quit within 15 years – “screening with annual low-dose CT scans can reduce the lung cancer death rate by up to 20% by detecting tumors at early stages when the cancer is more likely to be curable,” the ALA wrote.