User login
Monitoring, early intervention key to CAR T safety
GLASGOW – Constant patient monitoring and early intervention with tocilizumab and steroids are essential to the safe delivery of chimeric antigen receptor (CAR) T-cell therapy in patients with non-Hodgkin lymphoma (NHL), according to a leading expert.

As a clinical researcher at MD Anderson Cancer Center in Houston, Loretta Nastoupil, MD has played an active role in the evolution of CAR T-cell therapy, from early trials to ongoing development of treatment protocols. During a presentation at the annual meeting of the British Society for Haematology, Dr. Nastoupil discussed leading topics in CAR T-cell therapy, with an emphasis on safe delivery.
“[Toxicity] is something we don’t talk about as much as we should, partly because this therapy works and it’s really exciting,” Dr. Nastoupil said. “But the toxicity is not something that I minimize, and it’s very challenging. It’s led us to restructure our inpatient services. It’s led to a lot of sleepless nights. These patients can do very, very well, or they can do very, very poorly in terms of toxicity and I think the most important strategy is recognition and early intervention.”
Monitoring
Early recognition depends on close monitoring, Dr. Nastoupil said, which is carried out by highly trained nursing staff who follow therapy-specific decision algorithms.
“We have nurses that are on the front line,” Dr. Nastoupil said. “They’re the most important group. We have staff that round on [patients] daily, but the nurses are there 24 hours a day. We have a flow sheet where they grade cytokine release syndrome and neurotoxicity every 8 hours, or if there is an acute change in symptoms or toxicity, they’ll do it in real time.”
Dr. Nastoupil said that if these toxicities are detected, intervention is occurring sooner than it did with some of the first patients to receive CAR-T cell therapy.
“Initially there was a lot of fear surrounding anything that would abort the CAR-T cell therapy,” Dr. Nastoupil said. “There was concern that if you were trying to mitigate some of the toxicity you might have a negative impact on efficacy ... [W]ith the first iteration of studies, generally we were waiting until grade 3 or higher cytokine release syndrome before initiating either tocilizumab and/or steroids. As the studies evolved, it started to move into grade 2 toxicity that we started using therapy, mostly because we started to see that those patients were still responding.”
At MD Anderson, these earlier interventions have decreased severity of adverse events.
“It’s rare nowadays to have grade 3 or 4 cytokine release syndrome because we are generally introducing abortive therapy at grade 2,” Dr. Nastoupil said, citing increased use of steroids and tocilizumab.
Currently, no consensus exists for managing these events, partly because clinicians are still learning about best management practices.
“There will be a consensus on management,” Dr. Nastoupil said. “I think that’s needed. The problem is, it will probably evolve as we get more experience with managing these patients. I think there’s been a little hesitation to put something out on paper knowing that a year from now that might change.”
Grading toxicity
In contrast, Dr. Nastoupil said that a consensus has been reached for grading acute toxicity. Of note, fever is now considered an essential element of cytokine release syndrome.
“The first thing we see [with cytokine release syndrome] is fever, generally speaking,” Dr. Nastoupil said. “That will prompt a workup for infection because these patients are going to be neutropenic. And we initiate broad spectrum antimicrobials.”
She said that some patients treated with CAR T-cell therapy have had disseminated fungal infections, so clinicians need to be on the lookout for septic shock.
To assess neurotoxicity, the team at MD Anderson uses an objective scoring system, called “CARTOX.” This helps maintain consistency when facing broadly different neurological presentations.
“There’s such a wide ranging spectrum of patients that are undergoing neurotoxicity you can’t expect someone, even myself, to be consistent when you are trying to tease out how serious it is,” Dr. Nastoupil said.
With CARTOX, nurses can easily score patients and call clinicians with results. Still, this doesn’t eliminate difficulties inherent to managing neurotoxicity, particularly when it is severe.
“I’d say one of the areas that is still very challenging is when [patients with neurotoxicity] are no longer responding,” Dr. Nastoupil said. “You have to be very mindful of seizure activity. We’ve had a couple of patients with status [epilepticus]. You don’t see seizure activity physically, but when you do an EEG, you pick it up.”
Dr. Nastoupil added that most centers are now giving patients prophylactic levetiracetam (Keppra) to lower seizure risk.
Choosing therapy
When selecting between the two therapies currently approved by the Food and Drug Administration – tisagenlecleucel (Kymriah) and axicabtagene ciloleucel (Yescarta) – based on safety, Dr. Nastoupil said that rates of cytokine release syndrome appear similar, but neurotoxicity rates may differ.
“Cytokine release syndrome in my opinion is probably more similar than different in terms of grade 3 or higher because tocilizumab and steroids work quite well in aborting those toxicities,” Dr. Nastoupil said. “But neurotoxicity still sticks out in my mind as the most striking difference, where with axicabtagene you see more grade 3 or higher neurotoxicity, though very, very few deaths as a result of this. But it’s very challenging in terms of management.”
According to Dr. Nastoupil, comparisons between CAR T-cell therapies have been complicated by differences in clinical trial methodologies. However, she offered a general conclusion regarding efficacy.
“[W]hat I’ll tell you, at the end of the day, is [that existing CAR T-cell therapies] all seem to sort of settle out around 30%-40% in terms of durable responses,” Dr. Nastoupil said.
Dr. Nastoupil concluded her presentation with an overview and look to the future.
“I do think [CAR T-cell therapy] is transformative, particularly for our chemo refractory patients,” she said. “There is nothing else like it. The problem right now is that it is only durable in 40% of patients. So can we be better at selecting out patients that are more likely to respond? Does introducing this in earlier lines of therapy increase that fraction of patients that are potentially cured?”
Considering these questions, she said: “We need more patients. We need more data. We need longer follow-up to understand the nuances of this therapy.”
Dr. Nastoupil previously reported financial relationships with Celgene, Genentech, Gilead, Merck, Novartis, Spectrum, and TG Therapeutics.
GLASGOW – Constant patient monitoring and early intervention with tocilizumab and steroids are essential to the safe delivery of chimeric antigen receptor (CAR) T-cell therapy in patients with non-Hodgkin lymphoma (NHL), according to a leading expert.
As a clinical researcher at MD Anderson Cancer Center in Houston, Loretta Nastoupil, MD has played an active role in the evolution of CAR T-cell therapy, from early trials to ongoing development of treatment protocols. During a presentation at the annual meeting of the British Society for Haematology, Dr. Nastoupil discussed leading topics in CAR T-cell therapy, with an emphasis on safe delivery.
“[Toxicity] is something we don’t talk about as much as we should, partly because this therapy works and it’s really exciting,” Dr. Nastoupil said. “But the toxicity is not something that I minimize, and it’s very challenging. It’s led us to restructure our inpatient services. It’s led to a lot of sleepless nights. These patients can do very, very well, or they can do very, very poorly in terms of toxicity and I think the most important strategy is recognition and early intervention.”
Monitoring
Early recognition depends on close monitoring, Dr. Nastoupil said, which is carried out by highly trained nursing staff who follow therapy-specific decision algorithms.
“We have nurses that are on the front line,” Dr. Nastoupil said. “They’re the most important group. We have staff that round on [patients] daily, but the nurses are there 24 hours a day. We have a flow sheet where they grade cytokine release syndrome and neurotoxicity every 8 hours, or if there is an acute change in symptoms or toxicity, they’ll do it in real time.”
Dr. Nastoupil said that if these toxicities are detected, intervention is occurring sooner than it did with some of the first patients to receive CAR-T cell therapy.
“Initially there was a lot of fear surrounding anything that would abort the CAR-T cell therapy,” Dr. Nastoupil said. “There was concern that if you were trying to mitigate some of the toxicity you might have a negative impact on efficacy ... [W]ith the first iteration of studies, generally we were waiting until grade 3 or higher cytokine release syndrome before initiating either tocilizumab and/or steroids. As the studies evolved, it started to move into grade 2 toxicity that we started using therapy, mostly because we started to see that those patients were still responding.”
At MD Anderson, these earlier interventions have decreased severity of adverse events.
“It’s rare nowadays to have grade 3 or 4 cytokine release syndrome because we are generally introducing abortive therapy at grade 2,” Dr. Nastoupil said, citing increased use of steroids and tocilizumab.
Currently, no consensus exists for managing these events, partly because clinicians are still learning about best management practices.
“There will be a consensus on management,” Dr. Nastoupil said. “I think that’s needed. The problem is, it will probably evolve as we get more experience with managing these patients. I think there’s been a little hesitation to put something out on paper knowing that a year from now that might change.”
Grading toxicity
In contrast, Dr. Nastoupil said that a consensus has been reached for grading acute toxicity. Of note, fever is now considered an essential element of cytokine release syndrome.
“The first thing we see [with cytokine release syndrome] is fever, generally speaking,” Dr. Nastoupil said. “That will prompt a workup for infection because these patients are going to be neutropenic. And we initiate broad spectrum antimicrobials.”
She said that some patients treated with CAR T-cell therapy have had disseminated fungal infections, so clinicians need to be on the lookout for septic shock.
To assess neurotoxicity, the team at MD Anderson uses an objective scoring system, called “CARTOX.” This helps maintain consistency when facing broadly different neurological presentations.
“There’s such a wide ranging spectrum of patients that are undergoing neurotoxicity you can’t expect someone, even myself, to be consistent when you are trying to tease out how serious it is,” Dr. Nastoupil said.
With CARTOX, nurses can easily score patients and call clinicians with results. Still, this doesn’t eliminate difficulties inherent to managing neurotoxicity, particularly when it is severe.
“I’d say one of the areas that is still very challenging is when [patients with neurotoxicity] are no longer responding,” Dr. Nastoupil said. “You have to be very mindful of seizure activity. We’ve had a couple of patients with status [epilepticus]. You don’t see seizure activity physically, but when you do an EEG, you pick it up.”
Dr. Nastoupil added that most centers are now giving patients prophylactic levetiracetam (Keppra) to lower seizure risk.
Choosing therapy
When selecting between the two therapies currently approved by the Food and Drug Administration – tisagenlecleucel (Kymriah) and axicabtagene ciloleucel (Yescarta) – based on safety, Dr. Nastoupil said that rates of cytokine release syndrome appear similar, but neurotoxicity rates may differ.
“Cytokine release syndrome in my opinion is probably more similar than different in terms of grade 3 or higher because tocilizumab and steroids work quite well in aborting those toxicities,” Dr. Nastoupil said. “But neurotoxicity still sticks out in my mind as the most striking difference, where with axicabtagene you see more grade 3 or higher neurotoxicity, though very, very few deaths as a result of this. But it’s very challenging in terms of management.”
According to Dr. Nastoupil, comparisons between CAR T-cell therapies have been complicated by differences in clinical trial methodologies. However, she offered a general conclusion regarding efficacy.
“[W]hat I’ll tell you, at the end of the day, is [that existing CAR T-cell therapies] all seem to sort of settle out around 30%-40% in terms of durable responses,” Dr. Nastoupil said.
Dr. Nastoupil concluded her presentation with an overview and look to the future.
“I do think [CAR T-cell therapy] is transformative, particularly for our chemo refractory patients,” she said. “There is nothing else like it. The problem right now is that it is only durable in 40% of patients. So can we be better at selecting out patients that are more likely to respond? Does introducing this in earlier lines of therapy increase that fraction of patients that are potentially cured?”
Considering these questions, she said: “We need more patients. We need more data. We need longer follow-up to understand the nuances of this therapy.”
Dr. Nastoupil previously reported financial relationships with Celgene, Genentech, Gilead, Merck, Novartis, Spectrum, and TG Therapeutics.
GLASGOW – Constant patient monitoring and early intervention with tocilizumab and steroids are essential to the safe delivery of chimeric antigen receptor (CAR) T-cell therapy in patients with non-Hodgkin lymphoma (NHL), according to a leading expert.
As a clinical researcher at MD Anderson Cancer Center in Houston, Loretta Nastoupil, MD has played an active role in the evolution of CAR T-cell therapy, from early trials to ongoing development of treatment protocols. During a presentation at the annual meeting of the British Society for Haematology, Dr. Nastoupil discussed leading topics in CAR T-cell therapy, with an emphasis on safe delivery.
“[Toxicity] is something we don’t talk about as much as we should, partly because this therapy works and it’s really exciting,” Dr. Nastoupil said. “But the toxicity is not something that I minimize, and it’s very challenging. It’s led us to restructure our inpatient services. It’s led to a lot of sleepless nights. These patients can do very, very well, or they can do very, very poorly in terms of toxicity and I think the most important strategy is recognition and early intervention.”
Monitoring
Early recognition depends on close monitoring, Dr. Nastoupil said, which is carried out by highly trained nursing staff who follow therapy-specific decision algorithms.
“We have nurses that are on the front line,” Dr. Nastoupil said. “They’re the most important group. We have staff that round on [patients] daily, but the nurses are there 24 hours a day. We have a flow sheet where they grade cytokine release syndrome and neurotoxicity every 8 hours, or if there is an acute change in symptoms or toxicity, they’ll do it in real time.”
Dr. Nastoupil said that if these toxicities are detected, intervention is occurring sooner than it did with some of the first patients to receive CAR-T cell therapy.
“Initially there was a lot of fear surrounding anything that would abort the CAR-T cell therapy,” Dr. Nastoupil said. “There was concern that if you were trying to mitigate some of the toxicity you might have a negative impact on efficacy ... [W]ith the first iteration of studies, generally we were waiting until grade 3 or higher cytokine release syndrome before initiating either tocilizumab and/or steroids. As the studies evolved, it started to move into grade 2 toxicity that we started using therapy, mostly because we started to see that those patients were still responding.”
At MD Anderson, these earlier interventions have decreased severity of adverse events.
“It’s rare nowadays to have grade 3 or 4 cytokine release syndrome because we are generally introducing abortive therapy at grade 2,” Dr. Nastoupil said, citing increased use of steroids and tocilizumab.
Currently, no consensus exists for managing these events, partly because clinicians are still learning about best management practices.
“There will be a consensus on management,” Dr. Nastoupil said. “I think that’s needed. The problem is, it will probably evolve as we get more experience with managing these patients. I think there’s been a little hesitation to put something out on paper knowing that a year from now that might change.”
Grading toxicity
In contrast, Dr. Nastoupil said that a consensus has been reached for grading acute toxicity. Of note, fever is now considered an essential element of cytokine release syndrome.
“The first thing we see [with cytokine release syndrome] is fever, generally speaking,” Dr. Nastoupil said. “That will prompt a workup for infection because these patients are going to be neutropenic. And we initiate broad spectrum antimicrobials.”
She said that some patients treated with CAR T-cell therapy have had disseminated fungal infections, so clinicians need to be on the lookout for septic shock.
To assess neurotoxicity, the team at MD Anderson uses an objective scoring system, called “CARTOX.” This helps maintain consistency when facing broadly different neurological presentations.
“There’s such a wide ranging spectrum of patients that are undergoing neurotoxicity you can’t expect someone, even myself, to be consistent when you are trying to tease out how serious it is,” Dr. Nastoupil said.
With CARTOX, nurses can easily score patients and call clinicians with results. Still, this doesn’t eliminate difficulties inherent to managing neurotoxicity, particularly when it is severe.
“I’d say one of the areas that is still very challenging is when [patients with neurotoxicity] are no longer responding,” Dr. Nastoupil said. “You have to be very mindful of seizure activity. We’ve had a couple of patients with status [epilepticus]. You don’t see seizure activity physically, but when you do an EEG, you pick it up.”
Dr. Nastoupil added that most centers are now giving patients prophylactic levetiracetam (Keppra) to lower seizure risk.
Choosing therapy
When selecting between the two therapies currently approved by the Food and Drug Administration – tisagenlecleucel (Kymriah) and axicabtagene ciloleucel (Yescarta) – based on safety, Dr. Nastoupil said that rates of cytokine release syndrome appear similar, but neurotoxicity rates may differ.
“Cytokine release syndrome in my opinion is probably more similar than different in terms of grade 3 or higher because tocilizumab and steroids work quite well in aborting those toxicities,” Dr. Nastoupil said. “But neurotoxicity still sticks out in my mind as the most striking difference, where with axicabtagene you see more grade 3 or higher neurotoxicity, though very, very few deaths as a result of this. But it’s very challenging in terms of management.”
According to Dr. Nastoupil, comparisons between CAR T-cell therapies have been complicated by differences in clinical trial methodologies. However, she offered a general conclusion regarding efficacy.
“[W]hat I’ll tell you, at the end of the day, is [that existing CAR T-cell therapies] all seem to sort of settle out around 30%-40% in terms of durable responses,” Dr. Nastoupil said.
Dr. Nastoupil concluded her presentation with an overview and look to the future.
“I do think [CAR T-cell therapy] is transformative, particularly for our chemo refractory patients,” she said. “There is nothing else like it. The problem right now is that it is only durable in 40% of patients. So can we be better at selecting out patients that are more likely to respond? Does introducing this in earlier lines of therapy increase that fraction of patients that are potentially cured?”
Considering these questions, she said: “We need more patients. We need more data. We need longer follow-up to understand the nuances of this therapy.”
Dr. Nastoupil previously reported financial relationships with Celgene, Genentech, Gilead, Merck, Novartis, Spectrum, and TG Therapeutics.
EXPERT ANALYSIS FROM BSH 2019
Complementary medicine use common among patients on TKIs
GLASGOW – Many patients receiving tyrosine kinase inhibitors (TKIs) are taking complementary therapies or eating foods that interfere with TKI metabolism, based on results of a British survey of patients with chronic myeloid leukemia.

About one out of three patients with chronic myeloid leukemia (CML) reported taking complementary medicines, according to lead author David Sparksman, MD, of Norfolk and Norwich (England) University Hospital, and his colleagues.
Only a minority of patients were aware of the potential for dietary interactions with TKIs. However, even knowing the potential risk, about a quarter of patients still didn’t exclude these foods from their diets.
“These worrying results are unlikely to be confined to patients with CML,” the investigators wrote in an abstract presented at the annual meeting of the British Society for Haematology. “TKIs are used in the treatment of many other haematological malignancies.”
Because TKIs are metabolized by cytochrome P450 enzymes, inhibition of these enzymes by complementary therapies and foods may alter metabolism, and therefore, safety and efficacy of TKIs, according to the investigators.
“Use of complementary medicines and belief in their effectiveness is common,” the investigators wrote. “In a recent YouGov poll, 51% of those asked believed herbal medicine to be an effective treatment for illness.”
To investigate the prevalence of these beliefs and practices in a subset of cancer patients, the investigators identified 78 patients with CML undergoing follow-up at Norfolk and Norwich University Hospital. The median age of patients was 60 years. Eleven patients were excluded because they were not receiving a TKI and 6 patients declined to participate, leaving 61 patients in the final survey group.
Of these respondents, 41% had considered taking a complementary therapy and 34% were actively doing so. Further questioning revealed that about half of the patients taking a complementary medicine (52%) were taking a drug with known potential to interact with their TKI. Of these 11 patients, 5 were taking a complementary drug that would reduce serum concentrations of their TKI, potentially making it less effective. Conversely, six patients were taking a complementary drug that would increase serum concentrations, potentially increasing the risk of TKI side effects.
About 39% of respondents were aware of possible dietary interactions with TKIs, such as grapefruit. “Surprisingly,” the investigators said, 25% of patients with this knowledge still included such foods in their diet.
Dietary questioning revealed that among the patients who were unaware of food interactions, 67% were consuming foods that interact with TKIs.
Considering these results, the investigators offered some advice on patient communication and management.
“The use of complementary medicine should be discussed with all patients when starting TKIs and written information given to patients should highlight the potential dangers posed by substances which many patients currently regard as harmless,” thy wrote. “Since most patients will remain on treatment for many years, re-discussion about food and drug interactions should take place periodically to remind them of the potential risks.”
The investigators reported having no conflicts of interest.
GLASGOW – Many patients receiving tyrosine kinase inhibitors (TKIs) are taking complementary therapies or eating foods that interfere with TKI metabolism, based on results of a British survey of patients with chronic myeloid leukemia.
About one out of three patients with chronic myeloid leukemia (CML) reported taking complementary medicines, according to lead author David Sparksman, MD, of Norfolk and Norwich (England) University Hospital, and his colleagues.
Only a minority of patients were aware of the potential for dietary interactions with TKIs. However, even knowing the potential risk, about a quarter of patients still didn’t exclude these foods from their diets.
“These worrying results are unlikely to be confined to patients with CML,” the investigators wrote in an abstract presented at the annual meeting of the British Society for Haematology. “TKIs are used in the treatment of many other haematological malignancies.”
Because TKIs are metabolized by cytochrome P450 enzymes, inhibition of these enzymes by complementary therapies and foods may alter metabolism, and therefore, safety and efficacy of TKIs, according to the investigators.
“Use of complementary medicines and belief in their effectiveness is common,” the investigators wrote. “In a recent YouGov poll, 51% of those asked believed herbal medicine to be an effective treatment for illness.”
To investigate the prevalence of these beliefs and practices in a subset of cancer patients, the investigators identified 78 patients with CML undergoing follow-up at Norfolk and Norwich University Hospital. The median age of patients was 60 years. Eleven patients were excluded because they were not receiving a TKI and 6 patients declined to participate, leaving 61 patients in the final survey group.
Of these respondents, 41% had considered taking a complementary therapy and 34% were actively doing so. Further questioning revealed that about half of the patients taking a complementary medicine (52%) were taking a drug with known potential to interact with their TKI. Of these 11 patients, 5 were taking a complementary drug that would reduce serum concentrations of their TKI, potentially making it less effective. Conversely, six patients were taking a complementary drug that would increase serum concentrations, potentially increasing the risk of TKI side effects.
About 39% of respondents were aware of possible dietary interactions with TKIs, such as grapefruit. “Surprisingly,” the investigators said, 25% of patients with this knowledge still included such foods in their diet.
Dietary questioning revealed that among the patients who were unaware of food interactions, 67% were consuming foods that interact with TKIs.
Considering these results, the investigators offered some advice on patient communication and management.
“The use of complementary medicine should be discussed with all patients when starting TKIs and written information given to patients should highlight the potential dangers posed by substances which many patients currently regard as harmless,” thy wrote. “Since most patients will remain on treatment for many years, re-discussion about food and drug interactions should take place periodically to remind them of the potential risks.”
The investigators reported having no conflicts of interest.
GLASGOW – Many patients receiving tyrosine kinase inhibitors (TKIs) are taking complementary therapies or eating foods that interfere with TKI metabolism, based on results of a British survey of patients with chronic myeloid leukemia.
About one out of three patients with chronic myeloid leukemia (CML) reported taking complementary medicines, according to lead author David Sparksman, MD, of Norfolk and Norwich (England) University Hospital, and his colleagues.
Only a minority of patients were aware of the potential for dietary interactions with TKIs. However, even knowing the potential risk, about a quarter of patients still didn’t exclude these foods from their diets.
“These worrying results are unlikely to be confined to patients with CML,” the investigators wrote in an abstract presented at the annual meeting of the British Society for Haematology. “TKIs are used in the treatment of many other haematological malignancies.”
Because TKIs are metabolized by cytochrome P450 enzymes, inhibition of these enzymes by complementary therapies and foods may alter metabolism, and therefore, safety and efficacy of TKIs, according to the investigators.
“Use of complementary medicines and belief in their effectiveness is common,” the investigators wrote. “In a recent YouGov poll, 51% of those asked believed herbal medicine to be an effective treatment for illness.”
To investigate the prevalence of these beliefs and practices in a subset of cancer patients, the investigators identified 78 patients with CML undergoing follow-up at Norfolk and Norwich University Hospital. The median age of patients was 60 years. Eleven patients were excluded because they were not receiving a TKI and 6 patients declined to participate, leaving 61 patients in the final survey group.
Of these respondents, 41% had considered taking a complementary therapy and 34% were actively doing so. Further questioning revealed that about half of the patients taking a complementary medicine (52%) were taking a drug with known potential to interact with their TKI. Of these 11 patients, 5 were taking a complementary drug that would reduce serum concentrations of their TKI, potentially making it less effective. Conversely, six patients were taking a complementary drug that would increase serum concentrations, potentially increasing the risk of TKI side effects.
About 39% of respondents were aware of possible dietary interactions with TKIs, such as grapefruit. “Surprisingly,” the investigators said, 25% of patients with this knowledge still included such foods in their diet.
Dietary questioning revealed that among the patients who were unaware of food interactions, 67% were consuming foods that interact with TKIs.
Considering these results, the investigators offered some advice on patient communication and management.
“The use of complementary medicine should be discussed with all patients when starting TKIs and written information given to patients should highlight the potential dangers posed by substances which many patients currently regard as harmless,” thy wrote. “Since most patients will remain on treatment for many years, re-discussion about food and drug interactions should take place periodically to remind them of the potential risks.”
The investigators reported having no conflicts of interest.
REPORTING FROM BSH 2019
Gene therapy restored immunity in newly diagnosed SCID-X1
For infants with newly diagnosed X-linked severe combined immunodeficiency (SCID-X1), lentiviral gene therapy and targeted busulfan conditioning successfully induced multilineage engraftment of transduced cells, researchers reported.

By 3-4 months after infusion, seven of eight patients had normal numbers of CD3+, CD4+, and naive CD4+ T cells; normal counts of natural killer (NK) cells; and vector marking of T cells, B cells, NK cells, myeloid cells, and bone marrow progenitors, Ewelina Mamcarz, MD, of St. Jude Children’s Research Hospital in Memphis, and her associates reported in the New England Journal of Medicine.
The eighth infant at first lacked a sufficient T-cell response but responded to a boost of gene-corrected cells without busulfan conditioning.
By 6-12 months after infusion, IgM levels also had normalized in seven of the eight infants and showed polyclonal patterns without clonal dominance, according to the investigators. Among four infants who were able to stop intravenous immunoglobulin therapy, three responded to vaccinations with tetanus, diphtheria, pertussis, polio, and pneumococcal polysaccharide. Such restoration of humoral immunity “has not been achieved in previously reported trials of gene therapy for infants with newly diagnosed SCID-X1,” wrote the investigators of this dual-center, phase 1/2 study.
X-linked severe combined immunodeficiency – “bubble boy disease” – is characterized by a lack of T cells, NK cells, and B cells, and is caused by mutations in IL2RG. Some 80% of affected infants have no matched sibling donor for hematopoietic stem cell transplantation, and transplantation from other donors can produce an inadequate response and graft-versus-host disease. Prior attempts at gene therapy with gamma-retroviral vectors had led to vector-induced leukemia or had failed to induce humoral immunity or normal NK cell production.
“Our new lentiviral vector gene therapy combined with nonmyeloablative busulfan conditioning has been successful in restoring immunity in five patients 7-23 years of age in whom a previous allogeneic hematopoietic stem cell transplantation for SCID-X1 had failed,” the investigators wrote. “We hypothesized that the combination of this lentiviral vector and low-exposure busulfan administered by means of pharmacokinetic dose targeting would be safe and effective as the primary treatment in infants with newly diagnosed SCID-X1.”
Their protocol included one to two daily intravenous doses of busulfan, targeting a cumulative area under the curve of 22 mg per hr/L. They calculated the first dose by weight and age using a population-based pharmacokinetic model and adjusted the second dose based on first-dose pharmacokinetics.
After a median of 16.4 months, all infants continued to grow normally and cleared previous infections, and there were no unanticipated side effects from bone marrow harvest, busulfan conditioning, or cell infusion.
“It is hoped that durable, complete adaptive immunity will be achieved in the majority of the patients over time,” the researchers wrote.
They continue to follow the patients to assess therapeutic safety, immune durability, and persistence of the transferred gene in hematopoietic and immune cells.
Study funders included the American Lebanese Syrian Associated Charities, the National Institutes of Health, the California Institute of Regenerative Medicine, and the Assisi Foundation of Memphis. St. Jude Children’s Research Hospital has licensed the gene therapy and partnered with Mustang Bio to develop and commercialize it. Dr. Mamcarz reported receiving grant support from the study funders.
SOURCE: Mamcarz E et al. N Engl J Med. 2019; 380:1525-34.
For infants with newly diagnosed X-linked severe combined immunodeficiency (SCID-X1), lentiviral gene therapy and targeted busulfan conditioning successfully induced multilineage engraftment of transduced cells, researchers reported.
By 3-4 months after infusion, seven of eight patients had normal numbers of CD3+, CD4+, and naive CD4+ T cells; normal counts of natural killer (NK) cells; and vector marking of T cells, B cells, NK cells, myeloid cells, and bone marrow progenitors, Ewelina Mamcarz, MD, of St. Jude Children’s Research Hospital in Memphis, and her associates reported in the New England Journal of Medicine.
The eighth infant at first lacked a sufficient T-cell response but responded to a boost of gene-corrected cells without busulfan conditioning.
By 6-12 months after infusion, IgM levels also had normalized in seven of the eight infants and showed polyclonal patterns without clonal dominance, according to the investigators. Among four infants who were able to stop intravenous immunoglobulin therapy, three responded to vaccinations with tetanus, diphtheria, pertussis, polio, and pneumococcal polysaccharide. Such restoration of humoral immunity “has not been achieved in previously reported trials of gene therapy for infants with newly diagnosed SCID-X1,” wrote the investigators of this dual-center, phase 1/2 study.
X-linked severe combined immunodeficiency – “bubble boy disease” – is characterized by a lack of T cells, NK cells, and B cells, and is caused by mutations in IL2RG. Some 80% of affected infants have no matched sibling donor for hematopoietic stem cell transplantation, and transplantation from other donors can produce an inadequate response and graft-versus-host disease. Prior attempts at gene therapy with gamma-retroviral vectors had led to vector-induced leukemia or had failed to induce humoral immunity or normal NK cell production.
“Our new lentiviral vector gene therapy combined with nonmyeloablative busulfan conditioning has been successful in restoring immunity in five patients 7-23 years of age in whom a previous allogeneic hematopoietic stem cell transplantation for SCID-X1 had failed,” the investigators wrote. “We hypothesized that the combination of this lentiviral vector and low-exposure busulfan administered by means of pharmacokinetic dose targeting would be safe and effective as the primary treatment in infants with newly diagnosed SCID-X1.”
Their protocol included one to two daily intravenous doses of busulfan, targeting a cumulative area under the curve of 22 mg per hr/L. They calculated the first dose by weight and age using a population-based pharmacokinetic model and adjusted the second dose based on first-dose pharmacokinetics.
After a median of 16.4 months, all infants continued to grow normally and cleared previous infections, and there were no unanticipated side effects from bone marrow harvest, busulfan conditioning, or cell infusion.
“It is hoped that durable, complete adaptive immunity will be achieved in the majority of the patients over time,” the researchers wrote.
They continue to follow the patients to assess therapeutic safety, immune durability, and persistence of the transferred gene in hematopoietic and immune cells.
Study funders included the American Lebanese Syrian Associated Charities, the National Institutes of Health, the California Institute of Regenerative Medicine, and the Assisi Foundation of Memphis. St. Jude Children’s Research Hospital has licensed the gene therapy and partnered with Mustang Bio to develop and commercialize it. Dr. Mamcarz reported receiving grant support from the study funders.
SOURCE: Mamcarz E et al. N Engl J Med. 2019; 380:1525-34.
For infants with newly diagnosed X-linked severe combined immunodeficiency (SCID-X1), lentiviral gene therapy and targeted busulfan conditioning successfully induced multilineage engraftment of transduced cells, researchers reported.
By 3-4 months after infusion, seven of eight patients had normal numbers of CD3+, CD4+, and naive CD4+ T cells; normal counts of natural killer (NK) cells; and vector marking of T cells, B cells, NK cells, myeloid cells, and bone marrow progenitors, Ewelina Mamcarz, MD, of St. Jude Children’s Research Hospital in Memphis, and her associates reported in the New England Journal of Medicine.
The eighth infant at first lacked a sufficient T-cell response but responded to a boost of gene-corrected cells without busulfan conditioning.
By 6-12 months after infusion, IgM levels also had normalized in seven of the eight infants and showed polyclonal patterns without clonal dominance, according to the investigators. Among four infants who were able to stop intravenous immunoglobulin therapy, three responded to vaccinations with tetanus, diphtheria, pertussis, polio, and pneumococcal polysaccharide. Such restoration of humoral immunity “has not been achieved in previously reported trials of gene therapy for infants with newly diagnosed SCID-X1,” wrote the investigators of this dual-center, phase 1/2 study.
X-linked severe combined immunodeficiency – “bubble boy disease” – is characterized by a lack of T cells, NK cells, and B cells, and is caused by mutations in IL2RG. Some 80% of affected infants have no matched sibling donor for hematopoietic stem cell transplantation, and transplantation from other donors can produce an inadequate response and graft-versus-host disease. Prior attempts at gene therapy with gamma-retroviral vectors had led to vector-induced leukemia or had failed to induce humoral immunity or normal NK cell production.
“Our new lentiviral vector gene therapy combined with nonmyeloablative busulfan conditioning has been successful in restoring immunity in five patients 7-23 years of age in whom a previous allogeneic hematopoietic stem cell transplantation for SCID-X1 had failed,” the investigators wrote. “We hypothesized that the combination of this lentiviral vector and low-exposure busulfan administered by means of pharmacokinetic dose targeting would be safe and effective as the primary treatment in infants with newly diagnosed SCID-X1.”
Their protocol included one to two daily intravenous doses of busulfan, targeting a cumulative area under the curve of 22 mg per hr/L. They calculated the first dose by weight and age using a population-based pharmacokinetic model and adjusted the second dose based on first-dose pharmacokinetics.
After a median of 16.4 months, all infants continued to grow normally and cleared previous infections, and there were no unanticipated side effects from bone marrow harvest, busulfan conditioning, or cell infusion.
“It is hoped that durable, complete adaptive immunity will be achieved in the majority of the patients over time,” the researchers wrote.
They continue to follow the patients to assess therapeutic safety, immune durability, and persistence of the transferred gene in hematopoietic and immune cells.
Study funders included the American Lebanese Syrian Associated Charities, the National Institutes of Health, the California Institute of Regenerative Medicine, and the Assisi Foundation of Memphis. St. Jude Children’s Research Hospital has licensed the gene therapy and partnered with Mustang Bio to develop and commercialize it. Dr. Mamcarz reported receiving grant support from the study funders.
SOURCE: Mamcarz E et al. N Engl J Med. 2019; 380:1525-34.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Extended half-life clotting factors cut infusions, hike prices
More than a fifth of patients with hemophilia may now be using extended half-life (EHL) clotting factors, although the economic impact of these new treatments remains unclear.
Use of EHL factor VIII (FVIII) and IX (FIX) products surged from 10% of patients to 22% over an 18-month period ending in late 2017, Dr. Stacy E. Croteau and her colleagues reported in Haemophilia.
The increase appears to be mostly driven by prescribed prophylaxis rather than on-demand use of the products, wrote Dr. Croteau of Boston Children’s Hospital, and her coauthors. EHL dosages were similar to standard half-life (SHL) dosages and extended the time between infusions. But in the end, the higher cost of the EHL products actually drove up the price of prophylaxis, with a year of EHL FIX topping $1 million.
“Careful assessment of factor consumption and patient outcomes is needed to ensure general cost neutrality of this expensive therapy,” the researchers wrote. “Unless demonstrably offset by reduction in bleed doses, the net effect could be further increases in annual cost of care for this patient population.”
The study examined the use of SHL and EHL clotting factors in 7,893 adults and children with hemophilia A or B, who were being followed in the American Thrombosis and Hemostasis Network (ATHN) database. The authors sought to characterize changes in usage patterns for SHL and EHL factors, and to identify demographic and economic influences on them.
During the study, the number of patients using EHL products for both on-demand and prophylactic factor replacement increased. EHL FVIII use rose from 9% to 21%, and EHL FIX from 14% to 21%, especially among those with hemophilia B.
There were 6,437 patients with full data at both initial and final sampling. Among these, there was a 9.6% increase in the use of an EHL clotting factor by the end of the study (P less than .001). Patients with hemophilia A were less likely than hemophilia B patients to use an EHL product for prophylaxis.
While the EHL products did reduce the number of prophylactic infusions, they also cost much more, the investigators found.
The standard dose of SHL FVIII is 40 IU/g infused three times a week. The projected cost of 156 annual infusions is $690,144. EHL FVII, dosed at 50 IU/kg, cuts infusions to twice a week. The annual projected cost of the 104 infusions is $753,480.
The standard dose of SHL FIX is 67 IU/kg, infused twice a week. The annual projected cost of 104 infusions is $697,497. EHL FIX, dosed at 75 IU/Kg, halves the number of infusions. But the price for those 52 treatments exceeds $1 million ($1,015,560). Despite the cost, however, just 43 patients switched from an EHL product to a SHL factor product during the study period.
Insurance type appeared to have little influence on the choice of SHL or EHL clotting factors. Across payer types, a similar proportion of patients started using them, and 71% were covered by private insurance or Medicaid.
The study was funded HTRS/ATHN Dataset Research Engagement and a DREAM Award from the Hemostasis and Thrombosis Research Society. Dr. Croteau reported consulting for Bayer, Bioverativ, Biomarin, CSL-Behring, and other companies.
SOURCE: Croteau SE et al. Haemophilia. 2019 Apr 17. doi: 10.1111/hae.13758.
More than a fifth of patients with hemophilia may now be using extended half-life (EHL) clotting factors, although the economic impact of these new treatments remains unclear.
Use of EHL factor VIII (FVIII) and IX (FIX) products surged from 10% of patients to 22% over an 18-month period ending in late 2017, Dr. Stacy E. Croteau and her colleagues reported in Haemophilia.
The increase appears to be mostly driven by prescribed prophylaxis rather than on-demand use of the products, wrote Dr. Croteau of Boston Children’s Hospital, and her coauthors. EHL dosages were similar to standard half-life (SHL) dosages and extended the time between infusions. But in the end, the higher cost of the EHL products actually drove up the price of prophylaxis, with a year of EHL FIX topping $1 million.
“Careful assessment of factor consumption and patient outcomes is needed to ensure general cost neutrality of this expensive therapy,” the researchers wrote. “Unless demonstrably offset by reduction in bleed doses, the net effect could be further increases in annual cost of care for this patient population.”
The study examined the use of SHL and EHL clotting factors in 7,893 adults and children with hemophilia A or B, who were being followed in the American Thrombosis and Hemostasis Network (ATHN) database. The authors sought to characterize changes in usage patterns for SHL and EHL factors, and to identify demographic and economic influences on them.
During the study, the number of patients using EHL products for both on-demand and prophylactic factor replacement increased. EHL FVIII use rose from 9% to 21%, and EHL FIX from 14% to 21%, especially among those with hemophilia B.
There were 6,437 patients with full data at both initial and final sampling. Among these, there was a 9.6% increase in the use of an EHL clotting factor by the end of the study (P less than .001). Patients with hemophilia A were less likely than hemophilia B patients to use an EHL product for prophylaxis.
While the EHL products did reduce the number of prophylactic infusions, they also cost much more, the investigators found.
The standard dose of SHL FVIII is 40 IU/g infused three times a week. The projected cost of 156 annual infusions is $690,144. EHL FVII, dosed at 50 IU/kg, cuts infusions to twice a week. The annual projected cost of the 104 infusions is $753,480.
The standard dose of SHL FIX is 67 IU/kg, infused twice a week. The annual projected cost of 104 infusions is $697,497. EHL FIX, dosed at 75 IU/Kg, halves the number of infusions. But the price for those 52 treatments exceeds $1 million ($1,015,560). Despite the cost, however, just 43 patients switched from an EHL product to a SHL factor product during the study period.
Insurance type appeared to have little influence on the choice of SHL or EHL clotting factors. Across payer types, a similar proportion of patients started using them, and 71% were covered by private insurance or Medicaid.
The study was funded HTRS/ATHN Dataset Research Engagement and a DREAM Award from the Hemostasis and Thrombosis Research Society. Dr. Croteau reported consulting for Bayer, Bioverativ, Biomarin, CSL-Behring, and other companies.
SOURCE: Croteau SE et al. Haemophilia. 2019 Apr 17. doi: 10.1111/hae.13758.
More than a fifth of patients with hemophilia may now be using extended half-life (EHL) clotting factors, although the economic impact of these new treatments remains unclear.
Use of EHL factor VIII (FVIII) and IX (FIX) products surged from 10% of patients to 22% over an 18-month period ending in late 2017, Dr. Stacy E. Croteau and her colleagues reported in Haemophilia.
The increase appears to be mostly driven by prescribed prophylaxis rather than on-demand use of the products, wrote Dr. Croteau of Boston Children’s Hospital, and her coauthors. EHL dosages were similar to standard half-life (SHL) dosages and extended the time between infusions. But in the end, the higher cost of the EHL products actually drove up the price of prophylaxis, with a year of EHL FIX topping $1 million.
“Careful assessment of factor consumption and patient outcomes is needed to ensure general cost neutrality of this expensive therapy,” the researchers wrote. “Unless demonstrably offset by reduction in bleed doses, the net effect could be further increases in annual cost of care for this patient population.”
The study examined the use of SHL and EHL clotting factors in 7,893 adults and children with hemophilia A or B, who were being followed in the American Thrombosis and Hemostasis Network (ATHN) database. The authors sought to characterize changes in usage patterns for SHL and EHL factors, and to identify demographic and economic influences on them.
During the study, the number of patients using EHL products for both on-demand and prophylactic factor replacement increased. EHL FVIII use rose from 9% to 21%, and EHL FIX from 14% to 21%, especially among those with hemophilia B.
There were 6,437 patients with full data at both initial and final sampling. Among these, there was a 9.6% increase in the use of an EHL clotting factor by the end of the study (P less than .001). Patients with hemophilia A were less likely than hemophilia B patients to use an EHL product for prophylaxis.
While the EHL products did reduce the number of prophylactic infusions, they also cost much more, the investigators found.
The standard dose of SHL FVIII is 40 IU/g infused three times a week. The projected cost of 156 annual infusions is $690,144. EHL FVII, dosed at 50 IU/kg, cuts infusions to twice a week. The annual projected cost of the 104 infusions is $753,480.
The standard dose of SHL FIX is 67 IU/kg, infused twice a week. The annual projected cost of 104 infusions is $697,497. EHL FIX, dosed at 75 IU/Kg, halves the number of infusions. But the price for those 52 treatments exceeds $1 million ($1,015,560). Despite the cost, however, just 43 patients switched from an EHL product to a SHL factor product during the study period.
Insurance type appeared to have little influence on the choice of SHL or EHL clotting factors. Across payer types, a similar proportion of patients started using them, and 71% were covered by private insurance or Medicaid.
The study was funded HTRS/ATHN Dataset Research Engagement and a DREAM Award from the Hemostasis and Thrombosis Research Society. Dr. Croteau reported consulting for Bayer, Bioverativ, Biomarin, CSL-Behring, and other companies.
SOURCE: Croteau SE et al. Haemophilia. 2019 Apr 17. doi: 10.1111/hae.13758.
FROM HAEMOPHILIA
HAVEN 4: Monthly emicizumab shows value
For many patients with hemophilia A, with or without inhibitors, a monthly emicizumab injection is enough to ensure a high level of bleed control, based on results from the ongoing HAVEN 4 trial.
Most patients reported three or fewer treated bleeds, while slightly more than half had no treated bleeds at all, according to lead author Steven W. Pipe, MD, of the University of Michigan, Ann Arbor, and his colleagues. The investigators noted that results from this trial have already led to approval of a monthly dosing schedule in the United States and several other countries.
“This convenient regimen has the potential to improve the care of patients by decreasing their treatment burden, and increasing uptake and adherence to effective prophylaxis, which is known to decrease the development of debilitating secondary complications,” the investigators wrote. The report is in The Lancet Haematology.
The data were collected at 20 centers in 8 countries. Eligibility required that patients have severe congenital hemophilia A (less than 1% normal FVIII activity), or hemophilia A with FVIII inhibitors and concurrent treatment with bypassing agents or FVIII concentrates.
An initial run-in cohort that included seven patients assessed pharmacokinetics and safety. These patients received 6 mg/kg of emicizumab subcutaneously every 4 weeks for at least 24 weeks. After this group showed good responses, 41 additional patients were enrolled in an expansion cohort, which involved an initial loading phase of weekly doses at 3 mg/kg for the first month, followed by monthly dosing at 6 mg/kg for at least 6 months (24 weeks).
The efficacy endpoint of the study was bleed prevention, as measured by treated target joint bleeds, treated joint bleeds, treated spontaneous bleeds, all bleeds (untreated and treated), and annualized bleed rates for treated bleeds.
In the expansion cohort, the median number of bleeds in the 24-week period preceding enrollment was five. In the same group, five patients (12%) had FVIII inhibitors and 61% of patients exhibited at least one target joint.
After a median treatment of 25.6 weeks, the model-based annualized bleed rate for treated bleeds was 2.4, while the median annualized bleed rate was zero.
Slightly more than half of the patients (56.1%) reported no treated bleeds, 90% of patients reported 0-3 treated bleeds, and 85% of patients did not require treatment for targeted joint bleeds.
When untreated bleeds were included, the model-based annualized bleed rate was 4.5, while the median annualized bleed rate was 2.1. Almost one-third of patients (29%) had no bleeding events of any kind and most (80%) had 0-3 treated or untreated bleeds.
Overall, treatment was well tolerated, with no patients withdrawing from the study, discontinuing treatment, or requiring dose modifications. Laboratory parameters remained stable throughout. The most common treatment-related adverse event was injection-site reaction (22%), followed distantly by pre-syncope, chills, rash, and erythema, each of which occurred in 2% of patients.
“Overall, the results of HAVEN 4 are consistent with the findings of other HAVEN studies,” the investigators wrote. “The option of treatment with emicizumab every 4 weeks broadens the range of administration frequencies and allows clinicians to tailor treatment to each patient’s needs and preferences.”
F. Hoffman-La Roche and Chugai funded the study. The investigators reported financial relationships with the study sponsors and other companies.
SOURCE: Pipe SW et al. Lancet Haem. 2019 Apr 16. doi: 10.1016/S2352-3026(19)30054-7.
For many patients with hemophilia A, with or without inhibitors, a monthly emicizumab injection is enough to ensure a high level of bleed control, based on results from the ongoing HAVEN 4 trial.
Most patients reported three or fewer treated bleeds, while slightly more than half had no treated bleeds at all, according to lead author Steven W. Pipe, MD, of the University of Michigan, Ann Arbor, and his colleagues. The investigators noted that results from this trial have already led to approval of a monthly dosing schedule in the United States and several other countries.
“This convenient regimen has the potential to improve the care of patients by decreasing their treatment burden, and increasing uptake and adherence to effective prophylaxis, which is known to decrease the development of debilitating secondary complications,” the investigators wrote. The report is in The Lancet Haematology.
The data were collected at 20 centers in 8 countries. Eligibility required that patients have severe congenital hemophilia A (less than 1% normal FVIII activity), or hemophilia A with FVIII inhibitors and concurrent treatment with bypassing agents or FVIII concentrates.
An initial run-in cohort that included seven patients assessed pharmacokinetics and safety. These patients received 6 mg/kg of emicizumab subcutaneously every 4 weeks for at least 24 weeks. After this group showed good responses, 41 additional patients were enrolled in an expansion cohort, which involved an initial loading phase of weekly doses at 3 mg/kg for the first month, followed by monthly dosing at 6 mg/kg for at least 6 months (24 weeks).
The efficacy endpoint of the study was bleed prevention, as measured by treated target joint bleeds, treated joint bleeds, treated spontaneous bleeds, all bleeds (untreated and treated), and annualized bleed rates for treated bleeds.
In the expansion cohort, the median number of bleeds in the 24-week period preceding enrollment was five. In the same group, five patients (12%) had FVIII inhibitors and 61% of patients exhibited at least one target joint.
After a median treatment of 25.6 weeks, the model-based annualized bleed rate for treated bleeds was 2.4, while the median annualized bleed rate was zero.
Slightly more than half of the patients (56.1%) reported no treated bleeds, 90% of patients reported 0-3 treated bleeds, and 85% of patients did not require treatment for targeted joint bleeds.
When untreated bleeds were included, the model-based annualized bleed rate was 4.5, while the median annualized bleed rate was 2.1. Almost one-third of patients (29%) had no bleeding events of any kind and most (80%) had 0-3 treated or untreated bleeds.
Overall, treatment was well tolerated, with no patients withdrawing from the study, discontinuing treatment, or requiring dose modifications. Laboratory parameters remained stable throughout. The most common treatment-related adverse event was injection-site reaction (22%), followed distantly by pre-syncope, chills, rash, and erythema, each of which occurred in 2% of patients.
“Overall, the results of HAVEN 4 are consistent with the findings of other HAVEN studies,” the investigators wrote. “The option of treatment with emicizumab every 4 weeks broadens the range of administration frequencies and allows clinicians to tailor treatment to each patient’s needs and preferences.”
F. Hoffman-La Roche and Chugai funded the study. The investigators reported financial relationships with the study sponsors and other companies.
SOURCE: Pipe SW et al. Lancet Haem. 2019 Apr 16. doi: 10.1016/S2352-3026(19)30054-7.
For many patients with hemophilia A, with or without inhibitors, a monthly emicizumab injection is enough to ensure a high level of bleed control, based on results from the ongoing HAVEN 4 trial.
Most patients reported three or fewer treated bleeds, while slightly more than half had no treated bleeds at all, according to lead author Steven W. Pipe, MD, of the University of Michigan, Ann Arbor, and his colleagues. The investigators noted that results from this trial have already led to approval of a monthly dosing schedule in the United States and several other countries.
“This convenient regimen has the potential to improve the care of patients by decreasing their treatment burden, and increasing uptake and adherence to effective prophylaxis, which is known to decrease the development of debilitating secondary complications,” the investigators wrote. The report is in The Lancet Haematology.
The data were collected at 20 centers in 8 countries. Eligibility required that patients have severe congenital hemophilia A (less than 1% normal FVIII activity), or hemophilia A with FVIII inhibitors and concurrent treatment with bypassing agents or FVIII concentrates.
An initial run-in cohort that included seven patients assessed pharmacokinetics and safety. These patients received 6 mg/kg of emicizumab subcutaneously every 4 weeks for at least 24 weeks. After this group showed good responses, 41 additional patients were enrolled in an expansion cohort, which involved an initial loading phase of weekly doses at 3 mg/kg for the first month, followed by monthly dosing at 6 mg/kg for at least 6 months (24 weeks).
The efficacy endpoint of the study was bleed prevention, as measured by treated target joint bleeds, treated joint bleeds, treated spontaneous bleeds, all bleeds (untreated and treated), and annualized bleed rates for treated bleeds.
In the expansion cohort, the median number of bleeds in the 24-week period preceding enrollment was five. In the same group, five patients (12%) had FVIII inhibitors and 61% of patients exhibited at least one target joint.
After a median treatment of 25.6 weeks, the model-based annualized bleed rate for treated bleeds was 2.4, while the median annualized bleed rate was zero.
Slightly more than half of the patients (56.1%) reported no treated bleeds, 90% of patients reported 0-3 treated bleeds, and 85% of patients did not require treatment for targeted joint bleeds.
When untreated bleeds were included, the model-based annualized bleed rate was 4.5, while the median annualized bleed rate was 2.1. Almost one-third of patients (29%) had no bleeding events of any kind and most (80%) had 0-3 treated or untreated bleeds.
Overall, treatment was well tolerated, with no patients withdrawing from the study, discontinuing treatment, or requiring dose modifications. Laboratory parameters remained stable throughout. The most common treatment-related adverse event was injection-site reaction (22%), followed distantly by pre-syncope, chills, rash, and erythema, each of which occurred in 2% of patients.
“Overall, the results of HAVEN 4 are consistent with the findings of other HAVEN studies,” the investigators wrote. “The option of treatment with emicizumab every 4 weeks broadens the range of administration frequencies and allows clinicians to tailor treatment to each patient’s needs and preferences.”
F. Hoffman-La Roche and Chugai funded the study. The investigators reported financial relationships with the study sponsors and other companies.
SOURCE: Pipe SW et al. Lancet Haem. 2019 Apr 16. doi: 10.1016/S2352-3026(19)30054-7.
FROM THE LANCET HAEMATOLOGY
Factors emerge for mitigating CD19 CAR T toxicity
HOUSTON – Cytokine release syndrome and neurotoxicity frequently occur with CD19-directed chimeric antigen receptor (CAR) T-cell immunotherapies, but targetable factors for mitigating the risk and effects of these complications are emerging, according to Cameron Turtle, MBBS, PhD.

These factors include infused CAR T-cell dose, bone marrow disease burden, immune response, and the lymphodepletion regimen used, Dr. Turtle, of Fred Hutchinson Cancer Research Center, Seattle, said at the Transplantation & Cellular Therapies Meetings. This list is based on an analysis of several studies that included a total of 195 patients with B-cell malignancies who were treated with defined-composition CD19 CAR T cells.
In a 2016 study included in the analysis, for instance, Dr. Turtle and his colleagues found that CD19 CAR T cells administered to adults with B-cell acute lymphoblastic leukemia (B-ALL) after lymphodepletion chemotherapy were “remarkably potent.” Remission was achieved in 27 of 29 patients (J Clin Invest. 2016 Jun 1;126[6]:2123-38).
However, the study also established that high CAR T-cell doses and tumor burden increased the risk of severe cytokine release syndrome (CRS) and neurotoxicity, Dr. Turtle said at the meeting, held by the American Society for Blood and Marrow Transplantation and the Center for International Blood and Marrow Transplant Research. At its meeting, the American Society for Blood and Marrow Transplantation announced a new name for the society: American Society for Transplantation and Cellular Therapy (ASTCT).
“Importantly, we identified serum biomarkers that allow testing of early intervention strategies in the patients who have the highest risk of toxicity,” he said.
Dr. Turtle explained that significantly higher peak interleuken-6 (IL-6) and interferon (IFN)-gamma levels were seen after CAR T-cell infusion in patients with high bone marrow tumor burden and in patients requiring treatment in an intensive care unit (ICU).
ICU care correlated with a higher percentage of bone marrow blasts before lymphodepletion chemotherapy, he added.
Elevations of serum C-reactive protein (CRP) and ferritin also correlated with bone marrow disease burden and with the occurrence of severe CRS requiring ICU care, he said, noting that ferritin and CRP levels declined after tocilizumab or corticosteroid therapy.
In addition, all patients in the study who developed neurotoxicity had evidence of CRS. Peak levels of IL-6, IFN-gamma, ferritin, and CRP were significantly higher in those who developed grade 3 or higher neurotoxicity. Further, serum IL-6 and IFN-gamma concentrations on day 1 after infusion were significantly higher in those who required ICU care and in those who subsequently developed grade 4 neurotoxicity than in patients who developed grade 3 neurotoxicity.
Multivariate analysis indicated that serum IL-6 concentration of more than 30 pg/mL on day 1 and the total number of CD19+ cells in bone marrow before therapy were independent predictors of subsequent development of grade 3 or higher neurotoxicity.
Notably, serum IL-6 of more than 30 pg/mL on day 1 identified all patients in the study who subsequently developed grade 4 or higher neurotoxicity, Dr. Turtle and his colleagues noted.
“The findings suggested that evaluation of serum IL-6 concentration early after CAR T-cell infusion might be useful for identifying patients at high risk of severe neurotoxicity and to evaluate early intervention approaches,” he said.
Neurotoxicity
In a 2017 study from Juliane Gust, MD, PhD, and her colleagues, bone marrow disease burden, lymphodepletion regimen, and CAR T-cell dose were found to be significantly associated with neurotoxicity during multivariate analysis (Cancer Discov. 2017 Dec;7[12]:1404-19).
Patients with severe neurotoxicity in that study demonstrated evidence of endothelial activation, including disseminated intravascular coagulation, capillary leak, and increased blood-brain barrier permeability – with the latter leading to a failure to protect the cerebrospinal fluid from high concentrations of systemic cytokines, including IFN-gamma. These high levels of cytokines may cause vascular pericyte activation and stress, Dr. Turtle explained.
Patients who subsequently developed grade 4 or higher neurotoxicity had higher pretreatment levels of endothelial activation biomarkers.

“Endothelial cells and pericytes contribute to the integrity of the blood-brain barrier; this suggests a potential role for IL-6 and vascular endothelial growth factor from pericytes to augment endothelial permeability,” Dr. Turtle said.
CRS
In another 2017 study, from Kevin A. Hay, MD, and his colleagues, similar factors were found to be associated with CRS (Blood. 2017 Nov 23;130[21]:2295-306).
Multivariable analysis identified high marrow tumor burden, lymphodepletion using cyclophosphamide and fludarabine, higher CAR T-cell dose, thrombocytopenia before lymphodepletion, and manufacturing of CAR T cells without selection of CD8+ central memory T cells as independent predictors of CRS.
Severe CRS was characterized by hemodynamic instability, capillary leak, and consumptive coagulopathy. As in the study by Dr. Gust and her colleagues, biomarkers of endothelial activation, including angiopoietin-2 and von Willebrand factor, were increased during severe CRS and before lymphodepletion in patients who subsequently developed CRS.
Potential modifications
The findings to date suggest that risk stratification, prophylaxis, early intervention and therapeutic intervention are among potential strategies for mitigating the risk of CD19-directed CAR T toxicity, Dr. Turtle said. Steroids, tocilizumab, siltuximab, anakinra, anti-GM-CSF, small molecules, plasma exchange, angiopoietin-1, and hypertransfusion are among candidates under consideration for such interventions, he noted.
Other approaches that have been tested in small studies, and which may reduce toxicity and improve the therapeutic index of CD19 CAR T-cell therapy for B-ALL, include split dosing and risk-adapted dosing.
“These approaches do appear to mitigate toxicity, but larger studies are needed to confirm that treatment efficacy is maintained,” Dr. Turtle said.
Toxicity prediction and early intervention to maintain the CAR T-cell dose while avoiding grade 4 or greater toxicities would be helpful and is within reach, he said, noting that the findings by Dr. Hay and his colleagues led to the development of “day-1 cytokine combination algorithms that predict grade 4-5 CRS and could direct preemptive intervention.”
One algorithm based on three cytokines had high sensitivity and specificity, but would require screening of all patients.
Early intervention in patients in whom toxicity is predicted has not been extensively evaluated in clinical studies, he said.
Dr. Hay and his colleagues did, however, develop a “classification tree model of early intervention strategies” using their findings.
A complicating factor in predicting risk and intervening is that each CAR T-cell product is associated with differing levels of toxicity risk. The varying rates of toxicity suggest that promising approaches for addressing CAR T toxicity require validation for each product with respect to cutpoints, efficacy, and maintenance of response, Dr. Turtle said.
“The findings to date are encouraging and show that potentially targetable factors for mitigating the toxicity of CAR T-cell therapy can be identified,” he said. “But clinical studies have yet to convincingly establish the best approach.”
Dr. Turtle has served on advisory boards for Juno/Celgene, Kite/Gilead, Novartis, Precision Biosciences, Eureka Therapeutics, Caribou Biosciences, Nektar Therapeutics, Humanigen, and Aptevo; has intellectual property rights licensed to Juno; has stock options with Precision Biosciences, Eureka Therapeutics, and Caribou Biosciences; and has received research funding from Juno and Nektar Therapeutics.
HOUSTON – Cytokine release syndrome and neurotoxicity frequently occur with CD19-directed chimeric antigen receptor (CAR) T-cell immunotherapies, but targetable factors for mitigating the risk and effects of these complications are emerging, according to Cameron Turtle, MBBS, PhD.
These factors include infused CAR T-cell dose, bone marrow disease burden, immune response, and the lymphodepletion regimen used, Dr. Turtle, of Fred Hutchinson Cancer Research Center, Seattle, said at the Transplantation & Cellular Therapies Meetings. This list is based on an analysis of several studies that included a total of 195 patients with B-cell malignancies who were treated with defined-composition CD19 CAR T cells.
In a 2016 study included in the analysis, for instance, Dr. Turtle and his colleagues found that CD19 CAR T cells administered to adults with B-cell acute lymphoblastic leukemia (B-ALL) after lymphodepletion chemotherapy were “remarkably potent.” Remission was achieved in 27 of 29 patients (J Clin Invest. 2016 Jun 1;126[6]:2123-38).
However, the study also established that high CAR T-cell doses and tumor burden increased the risk of severe cytokine release syndrome (CRS) and neurotoxicity, Dr. Turtle said at the meeting, held by the American Society for Blood and Marrow Transplantation and the Center for International Blood and Marrow Transplant Research. At its meeting, the American Society for Blood and Marrow Transplantation announced a new name for the society: American Society for Transplantation and Cellular Therapy (ASTCT).
“Importantly, we identified serum biomarkers that allow testing of early intervention strategies in the patients who have the highest risk of toxicity,” he said.
Dr. Turtle explained that significantly higher peak interleuken-6 (IL-6) and interferon (IFN)-gamma levels were seen after CAR T-cell infusion in patients with high bone marrow tumor burden and in patients requiring treatment in an intensive care unit (ICU).
ICU care correlated with a higher percentage of bone marrow blasts before lymphodepletion chemotherapy, he added.
Elevations of serum C-reactive protein (CRP) and ferritin also correlated with bone marrow disease burden and with the occurrence of severe CRS requiring ICU care, he said, noting that ferritin and CRP levels declined after tocilizumab or corticosteroid therapy.
In addition, all patients in the study who developed neurotoxicity had evidence of CRS. Peak levels of IL-6, IFN-gamma, ferritin, and CRP were significantly higher in those who developed grade 3 or higher neurotoxicity. Further, serum IL-6 and IFN-gamma concentrations on day 1 after infusion were significantly higher in those who required ICU care and in those who subsequently developed grade 4 neurotoxicity than in patients who developed grade 3 neurotoxicity.
Multivariate analysis indicated that serum IL-6 concentration of more than 30 pg/mL on day 1 and the total number of CD19+ cells in bone marrow before therapy were independent predictors of subsequent development of grade 3 or higher neurotoxicity.
Notably, serum IL-6 of more than 30 pg/mL on day 1 identified all patients in the study who subsequently developed grade 4 or higher neurotoxicity, Dr. Turtle and his colleagues noted.
“The findings suggested that evaluation of serum IL-6 concentration early after CAR T-cell infusion might be useful for identifying patients at high risk of severe neurotoxicity and to evaluate early intervention approaches,” he said.
Neurotoxicity
In a 2017 study from Juliane Gust, MD, PhD, and her colleagues, bone marrow disease burden, lymphodepletion regimen, and CAR T-cell dose were found to be significantly associated with neurotoxicity during multivariate analysis (Cancer Discov. 2017 Dec;7[12]:1404-19).
Patients with severe neurotoxicity in that study demonstrated evidence of endothelial activation, including disseminated intravascular coagulation, capillary leak, and increased blood-brain barrier permeability – with the latter leading to a failure to protect the cerebrospinal fluid from high concentrations of systemic cytokines, including IFN-gamma. These high levels of cytokines may cause vascular pericyte activation and stress, Dr. Turtle explained.
Patients who subsequently developed grade 4 or higher neurotoxicity had higher pretreatment levels of endothelial activation biomarkers.
“Endothelial cells and pericytes contribute to the integrity of the blood-brain barrier; this suggests a potential role for IL-6 and vascular endothelial growth factor from pericytes to augment endothelial permeability,” Dr. Turtle said.
CRS
In another 2017 study, from Kevin A. Hay, MD, and his colleagues, similar factors were found to be associated with CRS (Blood. 2017 Nov 23;130[21]:2295-306).
Multivariable analysis identified high marrow tumor burden, lymphodepletion using cyclophosphamide and fludarabine, higher CAR T-cell dose, thrombocytopenia before lymphodepletion, and manufacturing of CAR T cells without selection of CD8+ central memory T cells as independent predictors of CRS.
Severe CRS was characterized by hemodynamic instability, capillary leak, and consumptive coagulopathy. As in the study by Dr. Gust and her colleagues, biomarkers of endothelial activation, including angiopoietin-2 and von Willebrand factor, were increased during severe CRS and before lymphodepletion in patients who subsequently developed CRS.
Potential modifications
The findings to date suggest that risk stratification, prophylaxis, early intervention and therapeutic intervention are among potential strategies for mitigating the risk of CD19-directed CAR T toxicity, Dr. Turtle said. Steroids, tocilizumab, siltuximab, anakinra, anti-GM-CSF, small molecules, plasma exchange, angiopoietin-1, and hypertransfusion are among candidates under consideration for such interventions, he noted.
Other approaches that have been tested in small studies, and which may reduce toxicity and improve the therapeutic index of CD19 CAR T-cell therapy for B-ALL, include split dosing and risk-adapted dosing.
“These approaches do appear to mitigate toxicity, but larger studies are needed to confirm that treatment efficacy is maintained,” Dr. Turtle said.
Toxicity prediction and early intervention to maintain the CAR T-cell dose while avoiding grade 4 or greater toxicities would be helpful and is within reach, he said, noting that the findings by Dr. Hay and his colleagues led to the development of “day-1 cytokine combination algorithms that predict grade 4-5 CRS and could direct preemptive intervention.”
One algorithm based on three cytokines had high sensitivity and specificity, but would require screening of all patients.
Early intervention in patients in whom toxicity is predicted has not been extensively evaluated in clinical studies, he said.
Dr. Hay and his colleagues did, however, develop a “classification tree model of early intervention strategies” using their findings.
A complicating factor in predicting risk and intervening is that each CAR T-cell product is associated with differing levels of toxicity risk. The varying rates of toxicity suggest that promising approaches for addressing CAR T toxicity require validation for each product with respect to cutpoints, efficacy, and maintenance of response, Dr. Turtle said.
“The findings to date are encouraging and show that potentially targetable factors for mitigating the toxicity of CAR T-cell therapy can be identified,” he said. “But clinical studies have yet to convincingly establish the best approach.”
Dr. Turtle has served on advisory boards for Juno/Celgene, Kite/Gilead, Novartis, Precision Biosciences, Eureka Therapeutics, Caribou Biosciences, Nektar Therapeutics, Humanigen, and Aptevo; has intellectual property rights licensed to Juno; has stock options with Precision Biosciences, Eureka Therapeutics, and Caribou Biosciences; and has received research funding from Juno and Nektar Therapeutics.
HOUSTON – Cytokine release syndrome and neurotoxicity frequently occur with CD19-directed chimeric antigen receptor (CAR) T-cell immunotherapies, but targetable factors for mitigating the risk and effects of these complications are emerging, according to Cameron Turtle, MBBS, PhD.
These factors include infused CAR T-cell dose, bone marrow disease burden, immune response, and the lymphodepletion regimen used, Dr. Turtle, of Fred Hutchinson Cancer Research Center, Seattle, said at the Transplantation & Cellular Therapies Meetings. This list is based on an analysis of several studies that included a total of 195 patients with B-cell malignancies who were treated with defined-composition CD19 CAR T cells.
In a 2016 study included in the analysis, for instance, Dr. Turtle and his colleagues found that CD19 CAR T cells administered to adults with B-cell acute lymphoblastic leukemia (B-ALL) after lymphodepletion chemotherapy were “remarkably potent.” Remission was achieved in 27 of 29 patients (J Clin Invest. 2016 Jun 1;126[6]:2123-38).
However, the study also established that high CAR T-cell doses and tumor burden increased the risk of severe cytokine release syndrome (CRS) and neurotoxicity, Dr. Turtle said at the meeting, held by the American Society for Blood and Marrow Transplantation and the Center for International Blood and Marrow Transplant Research. At its meeting, the American Society for Blood and Marrow Transplantation announced a new name for the society: American Society for Transplantation and Cellular Therapy (ASTCT).
“Importantly, we identified serum biomarkers that allow testing of early intervention strategies in the patients who have the highest risk of toxicity,” he said.
Dr. Turtle explained that significantly higher peak interleuken-6 (IL-6) and interferon (IFN)-gamma levels were seen after CAR T-cell infusion in patients with high bone marrow tumor burden and in patients requiring treatment in an intensive care unit (ICU).
ICU care correlated with a higher percentage of bone marrow blasts before lymphodepletion chemotherapy, he added.
Elevations of serum C-reactive protein (CRP) and ferritin also correlated with bone marrow disease burden and with the occurrence of severe CRS requiring ICU care, he said, noting that ferritin and CRP levels declined after tocilizumab or corticosteroid therapy.
In addition, all patients in the study who developed neurotoxicity had evidence of CRS. Peak levels of IL-6, IFN-gamma, ferritin, and CRP were significantly higher in those who developed grade 3 or higher neurotoxicity. Further, serum IL-6 and IFN-gamma concentrations on day 1 after infusion were significantly higher in those who required ICU care and in those who subsequently developed grade 4 neurotoxicity than in patients who developed grade 3 neurotoxicity.
Multivariate analysis indicated that serum IL-6 concentration of more than 30 pg/mL on day 1 and the total number of CD19+ cells in bone marrow before therapy were independent predictors of subsequent development of grade 3 or higher neurotoxicity.
Notably, serum IL-6 of more than 30 pg/mL on day 1 identified all patients in the study who subsequently developed grade 4 or higher neurotoxicity, Dr. Turtle and his colleagues noted.
“The findings suggested that evaluation of serum IL-6 concentration early after CAR T-cell infusion might be useful for identifying patients at high risk of severe neurotoxicity and to evaluate early intervention approaches,” he said.
Neurotoxicity
In a 2017 study from Juliane Gust, MD, PhD, and her colleagues, bone marrow disease burden, lymphodepletion regimen, and CAR T-cell dose were found to be significantly associated with neurotoxicity during multivariate analysis (Cancer Discov. 2017 Dec;7[12]:1404-19).
Patients with severe neurotoxicity in that study demonstrated evidence of endothelial activation, including disseminated intravascular coagulation, capillary leak, and increased blood-brain barrier permeability – with the latter leading to a failure to protect the cerebrospinal fluid from high concentrations of systemic cytokines, including IFN-gamma. These high levels of cytokines may cause vascular pericyte activation and stress, Dr. Turtle explained.
Patients who subsequently developed grade 4 or higher neurotoxicity had higher pretreatment levels of endothelial activation biomarkers.
“Endothelial cells and pericytes contribute to the integrity of the blood-brain barrier; this suggests a potential role for IL-6 and vascular endothelial growth factor from pericytes to augment endothelial permeability,” Dr. Turtle said.
CRS
In another 2017 study, from Kevin A. Hay, MD, and his colleagues, similar factors were found to be associated with CRS (Blood. 2017 Nov 23;130[21]:2295-306).
Multivariable analysis identified high marrow tumor burden, lymphodepletion using cyclophosphamide and fludarabine, higher CAR T-cell dose, thrombocytopenia before lymphodepletion, and manufacturing of CAR T cells without selection of CD8+ central memory T cells as independent predictors of CRS.
Severe CRS was characterized by hemodynamic instability, capillary leak, and consumptive coagulopathy. As in the study by Dr. Gust and her colleagues, biomarkers of endothelial activation, including angiopoietin-2 and von Willebrand factor, were increased during severe CRS and before lymphodepletion in patients who subsequently developed CRS.
Potential modifications
The findings to date suggest that risk stratification, prophylaxis, early intervention and therapeutic intervention are among potential strategies for mitigating the risk of CD19-directed CAR T toxicity, Dr. Turtle said. Steroids, tocilizumab, siltuximab, anakinra, anti-GM-CSF, small molecules, plasma exchange, angiopoietin-1, and hypertransfusion are among candidates under consideration for such interventions, he noted.
Other approaches that have been tested in small studies, and which may reduce toxicity and improve the therapeutic index of CD19 CAR T-cell therapy for B-ALL, include split dosing and risk-adapted dosing.
“These approaches do appear to mitigate toxicity, but larger studies are needed to confirm that treatment efficacy is maintained,” Dr. Turtle said.
Toxicity prediction and early intervention to maintain the CAR T-cell dose while avoiding grade 4 or greater toxicities would be helpful and is within reach, he said, noting that the findings by Dr. Hay and his colleagues led to the development of “day-1 cytokine combination algorithms that predict grade 4-5 CRS and could direct preemptive intervention.”
One algorithm based on three cytokines had high sensitivity and specificity, but would require screening of all patients.
Early intervention in patients in whom toxicity is predicted has not been extensively evaluated in clinical studies, he said.
Dr. Hay and his colleagues did, however, develop a “classification tree model of early intervention strategies” using their findings.
A complicating factor in predicting risk and intervening is that each CAR T-cell product is associated with differing levels of toxicity risk. The varying rates of toxicity suggest that promising approaches for addressing CAR T toxicity require validation for each product with respect to cutpoints, efficacy, and maintenance of response, Dr. Turtle said.
“The findings to date are encouraging and show that potentially targetable factors for mitigating the toxicity of CAR T-cell therapy can be identified,” he said. “But clinical studies have yet to convincingly establish the best approach.”
Dr. Turtle has served on advisory boards for Juno/Celgene, Kite/Gilead, Novartis, Precision Biosciences, Eureka Therapeutics, Caribou Biosciences, Nektar Therapeutics, Humanigen, and Aptevo; has intellectual property rights licensed to Juno; has stock options with Precision Biosciences, Eureka Therapeutics, and Caribou Biosciences; and has received research funding from Juno and Nektar Therapeutics.
REPORTING FROM TCT 2019

Study highlights lack of data on transgender leukemia patients
NEWPORT BEACH, CALIF. – Researchers have shown they can identify transgender leukemia patients by detecting gender-karyotype mismatches, but some transgender patients may be overlooked with this method.
The researchers’ work also highlights how little we know about transgender patients with leukemia and other cancers.
Alison Alpert, MD, of the University of Rochester (N.Y.) Medical Center, and her colleagues conducted this research and presented their findings in a poster at the Acute Leukemia Forum of Hemedicus.
“There’s almost no data about transgender people with cancer ... in terms of prevalence or anything else,” Dr. Alpert noted. “And because we don’t know which patients with cancer are transgender, we can’t begin to answer any of the other big questions for patients.”
Specifically, it’s unclear what kinds of cancer transgender patients have, if there are health disparities among transgender patients, if it is safe to continue hormone therapy during cancer treatment, and if it is possible to do transition-related surgeries in the context of cancer care.
With this in mind, Dr. Alpert and her colleagues set out to identify transgender patients by detecting gender-karyotype mismatches. The team analyzed data on patients with acute myeloid leukemia (AML) or myelodysplastic syndromes enrolled in five Southwest Oncology Group (SWOG) trials.
Of the 1,748 patients analyzed, six (0.3%) had a gender-karyotype mismatch. Five patients had a 46,XY karyotype and identified as female, and one patient had a 46,XX karyotype and identified as male.
“Some transgender patients have their gender identity accurately reflected in the electronic medical record, [but] some transgender patients probably don’t,” Dr. Alpert noted. “So we identified some, but probably not all, and probably not even most, transgender patients with leukemia in this cohort.”
All six of the transgender patients identified had AML, and all were white. They ranged in age from 18 to 57 years. Four patients had achieved a complete response to therapy, and two had refractory disease.
Four patients, including one who was refractory, were still alive at last follow-up. The remaining two patients, including one who had achieved a complete response, had died.
The transgender patients identified in this analysis represent a very small percentage of the population studied, Dr. Alpert noted. Therefore, the researchers could not draw any conclusions about transgender patients with AML.
“Mostly, what we did was, we pointed out how little information we have,” Dr. Alpert said. “Oncologists don’t routinely collect gender identity information, and this information doesn’t exist in cooperative group databases either.”
“But going forward, what probably really needs to happen is that oncologists need to ask their patients whether they are transgender or not. And then, ideally, consent forms for large cooperative groups like SWOG would include gender identity data, and then we would be able to answer some of our other questions and better counsel our patients.”
Dr. Alpert and her colleagues are hoping to gain insights regarding transgender patients with lymphoma as well. The researchers are analyzing the lymphoma database at the University of Rochester Medical Center, which includes about 2,200 patients.
The team is attempting to identify transgender lymphoma patients using gender-karyotype mismatch as well as other methods, including assessing patients’ medication and surgical histories, determining whether patients have any aliases, and looking for the word “transgender” in patient charts.
“Given that the country is finally starting to talk about transgender patients, their health disparities, and their needs and experiences, it’s really time that we start collecting this data,” Dr. Alpert said.
“[I]f we are able to start to collect this data, it can help us build relationships with our patients, improve their care and outcomes, and, hopefully, be able to better counsel them about hormones and surgery.”
Dr. Alpert and her colleagues did not disclose any conflicts of interest.
The Acute Leukemia Forum is organized by Hemedicus, which is owned by the same company as this news organization.
NEWPORT BEACH, CALIF. – Researchers have shown they can identify transgender leukemia patients by detecting gender-karyotype mismatches, but some transgender patients may be overlooked with this method.
The researchers’ work also highlights how little we know about transgender patients with leukemia and other cancers.
Alison Alpert, MD, of the University of Rochester (N.Y.) Medical Center, and her colleagues conducted this research and presented their findings in a poster at the Acute Leukemia Forum of Hemedicus.
“There’s almost no data about transgender people with cancer ... in terms of prevalence or anything else,” Dr. Alpert noted. “And because we don’t know which patients with cancer are transgender, we can’t begin to answer any of the other big questions for patients.”
Specifically, it’s unclear what kinds of cancer transgender patients have, if there are health disparities among transgender patients, if it is safe to continue hormone therapy during cancer treatment, and if it is possible to do transition-related surgeries in the context of cancer care.
With this in mind, Dr. Alpert and her colleagues set out to identify transgender patients by detecting gender-karyotype mismatches. The team analyzed data on patients with acute myeloid leukemia (AML) or myelodysplastic syndromes enrolled in five Southwest Oncology Group (SWOG) trials.
Of the 1,748 patients analyzed, six (0.3%) had a gender-karyotype mismatch. Five patients had a 46,XY karyotype and identified as female, and one patient had a 46,XX karyotype and identified as male.
“Some transgender patients have their gender identity accurately reflected in the electronic medical record, [but] some transgender patients probably don’t,” Dr. Alpert noted. “So we identified some, but probably not all, and probably not even most, transgender patients with leukemia in this cohort.”
All six of the transgender patients identified had AML, and all were white. They ranged in age from 18 to 57 years. Four patients had achieved a complete response to therapy, and two had refractory disease.
Four patients, including one who was refractory, were still alive at last follow-up. The remaining two patients, including one who had achieved a complete response, had died.
The transgender patients identified in this analysis represent a very small percentage of the population studied, Dr. Alpert noted. Therefore, the researchers could not draw any conclusions about transgender patients with AML.
“Mostly, what we did was, we pointed out how little information we have,” Dr. Alpert said. “Oncologists don’t routinely collect gender identity information, and this information doesn’t exist in cooperative group databases either.”
“But going forward, what probably really needs to happen is that oncologists need to ask their patients whether they are transgender or not. And then, ideally, consent forms for large cooperative groups like SWOG would include gender identity data, and then we would be able to answer some of our other questions and better counsel our patients.”
Dr. Alpert and her colleagues are hoping to gain insights regarding transgender patients with lymphoma as well. The researchers are analyzing the lymphoma database at the University of Rochester Medical Center, which includes about 2,200 patients.
The team is attempting to identify transgender lymphoma patients using gender-karyotype mismatch as well as other methods, including assessing patients’ medication and surgical histories, determining whether patients have any aliases, and looking for the word “transgender” in patient charts.
“Given that the country is finally starting to talk about transgender patients, their health disparities, and their needs and experiences, it’s really time that we start collecting this data,” Dr. Alpert said.
“[I]f we are able to start to collect this data, it can help us build relationships with our patients, improve their care and outcomes, and, hopefully, be able to better counsel them about hormones and surgery.”
Dr. Alpert and her colleagues did not disclose any conflicts of interest.
The Acute Leukemia Forum is organized by Hemedicus, which is owned by the same company as this news organization.
NEWPORT BEACH, CALIF. – Researchers have shown they can identify transgender leukemia patients by detecting gender-karyotype mismatches, but some transgender patients may be overlooked with this method.
The researchers’ work also highlights how little we know about transgender patients with leukemia and other cancers.
Alison Alpert, MD, of the University of Rochester (N.Y.) Medical Center, and her colleagues conducted this research and presented their findings in a poster at the Acute Leukemia Forum of Hemedicus.
“There’s almost no data about transgender people with cancer ... in terms of prevalence or anything else,” Dr. Alpert noted. “And because we don’t know which patients with cancer are transgender, we can’t begin to answer any of the other big questions for patients.”
Specifically, it’s unclear what kinds of cancer transgender patients have, if there are health disparities among transgender patients, if it is safe to continue hormone therapy during cancer treatment, and if it is possible to do transition-related surgeries in the context of cancer care.
With this in mind, Dr. Alpert and her colleagues set out to identify transgender patients by detecting gender-karyotype mismatches. The team analyzed data on patients with acute myeloid leukemia (AML) or myelodysplastic syndromes enrolled in five Southwest Oncology Group (SWOG) trials.
Of the 1,748 patients analyzed, six (0.3%) had a gender-karyotype mismatch. Five patients had a 46,XY karyotype and identified as female, and one patient had a 46,XX karyotype and identified as male.
“Some transgender patients have their gender identity accurately reflected in the electronic medical record, [but] some transgender patients probably don’t,” Dr. Alpert noted. “So we identified some, but probably not all, and probably not even most, transgender patients with leukemia in this cohort.”
All six of the transgender patients identified had AML, and all were white. They ranged in age from 18 to 57 years. Four patients had achieved a complete response to therapy, and two had refractory disease.
Four patients, including one who was refractory, were still alive at last follow-up. The remaining two patients, including one who had achieved a complete response, had died.
The transgender patients identified in this analysis represent a very small percentage of the population studied, Dr. Alpert noted. Therefore, the researchers could not draw any conclusions about transgender patients with AML.
“Mostly, what we did was, we pointed out how little information we have,” Dr. Alpert said. “Oncologists don’t routinely collect gender identity information, and this information doesn’t exist in cooperative group databases either.”
“But going forward, what probably really needs to happen is that oncologists need to ask their patients whether they are transgender or not. And then, ideally, consent forms for large cooperative groups like SWOG would include gender identity data, and then we would be able to answer some of our other questions and better counsel our patients.”
Dr. Alpert and her colleagues are hoping to gain insights regarding transgender patients with lymphoma as well. The researchers are analyzing the lymphoma database at the University of Rochester Medical Center, which includes about 2,200 patients.
The team is attempting to identify transgender lymphoma patients using gender-karyotype mismatch as well as other methods, including assessing patients’ medication and surgical histories, determining whether patients have any aliases, and looking for the word “transgender” in patient charts.
“Given that the country is finally starting to talk about transgender patients, their health disparities, and their needs and experiences, it’s really time that we start collecting this data,” Dr. Alpert said.
“[I]f we are able to start to collect this data, it can help us build relationships with our patients, improve their care and outcomes, and, hopefully, be able to better counsel them about hormones and surgery.”
Dr. Alpert and her colleagues did not disclose any conflicts of interest.
The Acute Leukemia Forum is organized by Hemedicus, which is owned by the same company as this news organization.
REPORTING FROM ALF 2019

2018 at a glance: Recently approved therapies in oncology
Advances in genomics and technology perpetually change and improve therapies in oncology. Enhanced comprehension of cellular signaling, division, and replication has created a platform to selectively restrict neoplastic growth while preserving the integrity of benign cells.
This article reviews therapies that were newly approved in 2018, as well as those previously approved whose indications were expanded this past year. The list highlights the most clinically important approvals, as well as adverse events that are unique or especially severe.
Click on the PDF above to download the full article and charts in an easy-to-print format.
Apalutamide (Erleada)
Class: Androgen receptor inhibitor.
Disease: Nonmetastatic castration-resistant prostate cancer.
Dose: 240 mg orally, once daily.
Adverse Events (AEs): Hyperkalemia and increased risks of seizures, falls, and fractures.
Phase 3 SPARTAN trial (NCT01946204): 40.5-month metastasis-free survival rate, compared with 16.2 months in the placebo group.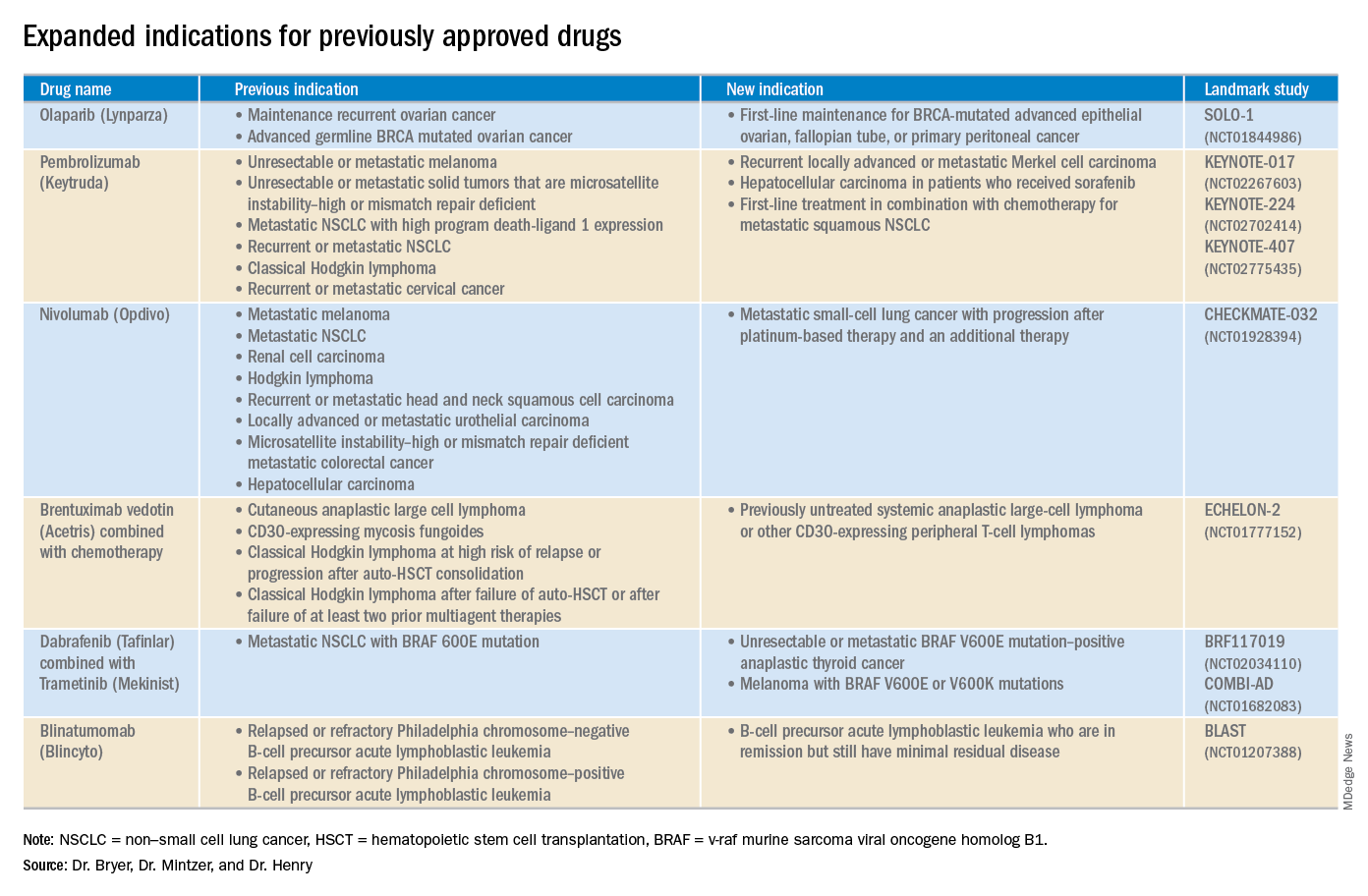
Cemiplimab (Libtayo)
Class: Antibody against programmed cell death protein-1 (PD-1).
Disease: Metastatic cutaneous squamous cell carcinoma (CSCC) or locally advanced CSCC that is ineligible for curative surgery/radiation.
Dose: 350 mg intravenous infusion every 3 weeks.
AEs: Pneumonitis, autoimmune myocarditis, hepatitis, and aseptic meningitis.
1423 and 1540 trials (NCT02383212 and NCT02760498): 47.2% of patients who received cemiplimab had complete disappearance of the tumor or a decrease in tumor size.
Dacomitinib (Vizimpro)
Class: Second-generation tyrosine kinase inhibitor.
Disease: Metastatic non–small cell lung cancer (NSCLC) with epidermal growth factor receptor (EGFR) exon 19 deletion or exon 21 L858R substitution mutation.
Dose: 45 mg orally once daily.
AEs: Dermatotoxicity and diarrhea.
ARCHER1050 trial (NCT01774721): Patients who received dacomitinib demonstrated an improved overall survival, with a median of 34.1 months, compared with 26.8 months with gefitinib.
Duvelisib (Copiktra)
Class: Dual inhibitor of phosphatidylinositol 3-kinase delta and gamma.
Disease: Relapsed or refractory chronic lymphocytic leukemia (CLL), small lymphocytic lymphoma, or relapsed or refractory follicular lymphoma after at least two prior systemic therapies.
Dose: 25 mg orally twice daily.
AEs: Infection, diarrhea or colitis, and pneumonia.
Phase 3 DUO trial (NCT02004522): Progression-free survival in the duvelisib arm was 7.3 months longer than that in the ofatumumab arm. The overall response rate for patients receiving duvelisib was 78%, compared with 39% for those receiving ofatumumab.
Gilteritinib (Xospata)
Class: Inhibits the FLT3 internal tandem duplication (ITD) and FLT3 tyrosine kinase domain (TKD).
Disease: Relapsed or refractory acute myeloid leukemia (AML) with an FLT3 mutation.
Dose: 120 mg orally daily.
ADMIRAL trial (NCT02421939): 21% of the patients who received gilteritinib exhibited complete remission or complete remission with partial hematologic recovery.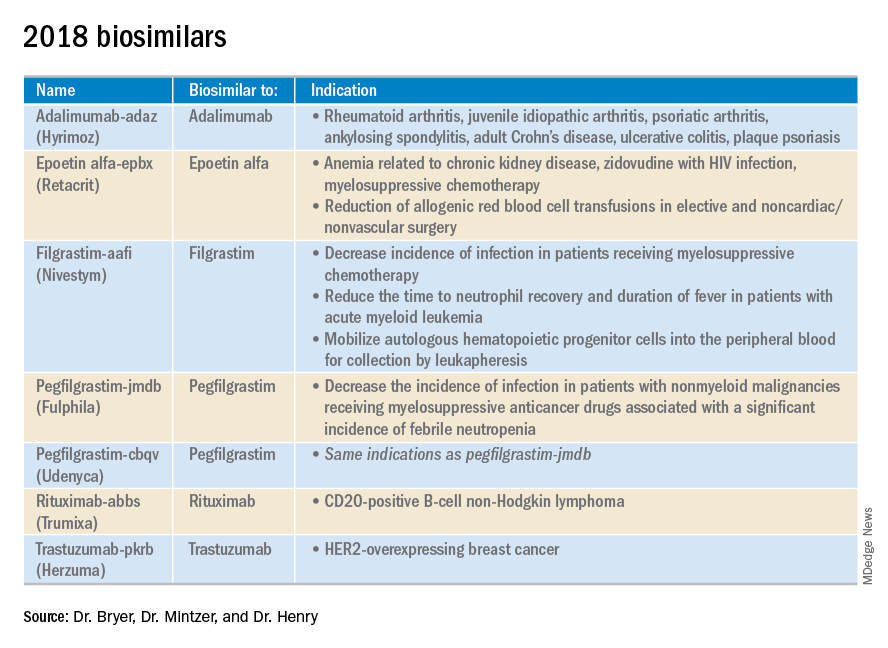
Glasdegib (Daurismo)
Class: Hedgehog pathway inhibitor.
Disease: Adults over age 75 years with newly diagnosed AML and other medical comorbidities that preclude them from intensive chemotherapy.
Dose: The recommended dose is 100 mg orally continuously in 28-day cycles.
AE: QT prolongation and embryo-fetal toxicity
Phase 2 BRIGHT 1003 trial (NCT01546038): 3.9-month overall survival advantage for glasdegib plus cytarabine, compared with cytarabine alone. Overall, 15% of the glasdegib plus low dose cytarabine arm achieved complete remission, compared with the 1% complete remission rate in patients who received cytarabine alone.
Iobenguane I 131 (Azedra)
Class: Radiopharmaceutical agent; induces cell death within the noradrenaline transporter.
Disease: Iobenguane scan–positive, unresectable, locally advanced or metastatic pheochromocytoma or paraganglioma
Dose: Initial intravenous dosimetric dose, followed by two therapeutic doses.
AE: Pancytopenia and elevated international normalized ratio (INR).
IB12B trial (NCT00874614): One-quarter of patients receiving this therapy had at least a 50% reduction in the dose and number of antihypertensives for at least 6 months; almost all patients had a tumor response.
Ivosidenib (Tibsovo)
Class: Small-molecule inhibitor of mutant isocitrate dehydrogenase (IDH1).
Disease: Refractory AML and an IDH1 mutation
Dose: 500 mg orally daily.
AG120-C-001 trial (NCT02074839): Overall response rate of 41.6% in patients who received ivosidenib, with a 30.4% rate of complete remission or complete remission with partial hematologic recovery.
Larotrectinib (Vitrakvi)
Class: Oral tyrosine kinase inhibitor.
Disease: Advanced solid tumors harboring a neurotrophic tyrosine receptor kinase (NTRK) gene fusion.
Dose: 100 mg orally twice daily.
LOXO-TRK-14001, SCOUT, and NAVIGATE trials (NCT02122913, NCT02637687, and NCT02576431): Patients who received larotrectinib had durable responses regardless of patient age, tumor type, and fusion status.
Lutetium Lu 177 dotatate (Lutathera)
Class: Radiolabeled somatostatin analogue.
Disease: Somatostatin receptor–positive gastroenteropancreatic neuroendocrine tumors (GEP-NETs).
Dose: Intravenous infusion 7.4 GBq (200 mCi) every 8 weeks for a total of four doses.
NETTER-1 trial (NCT01578239): 65% of adults who received lutetium Lu 177 showed improved progression-free survival at 20 months, compared with just 10.8% in the control group.
Mogamulizumab (Poteligeo)
Class: Monoclonal antibody that binds to a protein (CC chemokine receptor type 4).
Disease: Relapsed or refractory mycosis fungoides or Sézary syndrome.
Dose: Intravenous infusion 1 mg/kg.
AE: Dermatologic toxicity.
MAVORIC trial (NCT01728805): Patients who received mogamulizumab had improved progression-free survival (median 7.7 months), compared with those taking vorinostat (median 3.1 months).
Moxetumomab pasudotox-tdfk (Lumoxiti)
Class: CD22-directed cytotoxin fused with a fragment of Pseudomonas exotoxin A.
Disease: Relapsed or refractory hairy cell leukemia previously treated with at least two prior systemic therapies, including a purine nucleoside analogue.
Dose: Intravenously as 0.04 mg/kg.
AE: Hemolytic uremic syndrome.
1053 trial (NCT01829711): 30% of the patients who received moxetumomab pasudotox-tdfk had a durable complete response confirmed by maintenance hematologic remission.
Talazoparib (Talzenna)
Class: Poly (ADP-ribose) polymerase (PARP) inhibitor.
Disease: gBRCAm HER2-negative locally advanced or metastatic breast cancer.
Dose: 1 mg orally per day.
EMBRACA trial (NCT01945775): Patients who received talazoparib demonstrated significantly longer progression-free survival, with a median of 8.6 months versis 5.6 months in the control arm.
Dr. Bryer is a resident in the department of internal medicine at the University of Pennsylvania, Philadelphia. Dr. Mentzer is chief of hematology-oncology at Pennsylvania Hospital and professor of medicine at the University of Pennsylvania. Dr. Henry is a hematologist-oncologist at Pennsylvania Hospital and a professor of medicine at the University of Pennsylvania.
Advances in genomics and technology perpetually change and improve therapies in oncology. Enhanced comprehension of cellular signaling, division, and replication has created a platform to selectively restrict neoplastic growth while preserving the integrity of benign cells.
This article reviews therapies that were newly approved in 2018, as well as those previously approved whose indications were expanded this past year. The list highlights the most clinically important approvals, as well as adverse events that are unique or especially severe.
Click on the PDF above to download the full article and charts in an easy-to-print format.
Apalutamide (Erleada)
Class: Androgen receptor inhibitor.
Disease: Nonmetastatic castration-resistant prostate cancer.
Dose: 240 mg orally, once daily.
Adverse Events (AEs): Hyperkalemia and increased risks of seizures, falls, and fractures.
Phase 3 SPARTAN trial (NCT01946204): 40.5-month metastasis-free survival rate, compared with 16.2 months in the placebo group.
Cemiplimab (Libtayo)
Class: Antibody against programmed cell death protein-1 (PD-1).
Disease: Metastatic cutaneous squamous cell carcinoma (CSCC) or locally advanced CSCC that is ineligible for curative surgery/radiation.
Dose: 350 mg intravenous infusion every 3 weeks.
AEs: Pneumonitis, autoimmune myocarditis, hepatitis, and aseptic meningitis.
1423 and 1540 trials (NCT02383212 and NCT02760498): 47.2% of patients who received cemiplimab had complete disappearance of the tumor or a decrease in tumor size.
Dacomitinib (Vizimpro)
Class: Second-generation tyrosine kinase inhibitor.
Disease: Metastatic non–small cell lung cancer (NSCLC) with epidermal growth factor receptor (EGFR) exon 19 deletion or exon 21 L858R substitution mutation.
Dose: 45 mg orally once daily.
AEs: Dermatotoxicity and diarrhea.
ARCHER1050 trial (NCT01774721): Patients who received dacomitinib demonstrated an improved overall survival, with a median of 34.1 months, compared with 26.8 months with gefitinib.
Duvelisib (Copiktra)
Class: Dual inhibitor of phosphatidylinositol 3-kinase delta and gamma.
Disease: Relapsed or refractory chronic lymphocytic leukemia (CLL), small lymphocytic lymphoma, or relapsed or refractory follicular lymphoma after at least two prior systemic therapies.
Dose: 25 mg orally twice daily.
AEs: Infection, diarrhea or colitis, and pneumonia.
Phase 3 DUO trial (NCT02004522): Progression-free survival in the duvelisib arm was 7.3 months longer than that in the ofatumumab arm. The overall response rate for patients receiving duvelisib was 78%, compared with 39% for those receiving ofatumumab.
Gilteritinib (Xospata)
Class: Inhibits the FLT3 internal tandem duplication (ITD) and FLT3 tyrosine kinase domain (TKD).
Disease: Relapsed or refractory acute myeloid leukemia (AML) with an FLT3 mutation.
Dose: 120 mg orally daily.
ADMIRAL trial (NCT02421939): 21% of the patients who received gilteritinib exhibited complete remission or complete remission with partial hematologic recovery.
Glasdegib (Daurismo)
Class: Hedgehog pathway inhibitor.
Disease: Adults over age 75 years with newly diagnosed AML and other medical comorbidities that preclude them from intensive chemotherapy.
Dose: The recommended dose is 100 mg orally continuously in 28-day cycles.
AE: QT prolongation and embryo-fetal toxicity
Phase 2 BRIGHT 1003 trial (NCT01546038): 3.9-month overall survival advantage for glasdegib plus cytarabine, compared with cytarabine alone. Overall, 15% of the glasdegib plus low dose cytarabine arm achieved complete remission, compared with the 1% complete remission rate in patients who received cytarabine alone.
Iobenguane I 131 (Azedra)
Class: Radiopharmaceutical agent; induces cell death within the noradrenaline transporter.
Disease: Iobenguane scan–positive, unresectable, locally advanced or metastatic pheochromocytoma or paraganglioma
Dose: Initial intravenous dosimetric dose, followed by two therapeutic doses.
AE: Pancytopenia and elevated international normalized ratio (INR).
IB12B trial (NCT00874614): One-quarter of patients receiving this therapy had at least a 50% reduction in the dose and number of antihypertensives for at least 6 months; almost all patients had a tumor response.
Ivosidenib (Tibsovo)
Class: Small-molecule inhibitor of mutant isocitrate dehydrogenase (IDH1).
Disease: Refractory AML and an IDH1 mutation
Dose: 500 mg orally daily.
AG120-C-001 trial (NCT02074839): Overall response rate of 41.6% in patients who received ivosidenib, with a 30.4% rate of complete remission or complete remission with partial hematologic recovery.
Larotrectinib (Vitrakvi)
Class: Oral tyrosine kinase inhibitor.
Disease: Advanced solid tumors harboring a neurotrophic tyrosine receptor kinase (NTRK) gene fusion.
Dose: 100 mg orally twice daily.
LOXO-TRK-14001, SCOUT, and NAVIGATE trials (NCT02122913, NCT02637687, and NCT02576431): Patients who received larotrectinib had durable responses regardless of patient age, tumor type, and fusion status.
Lutetium Lu 177 dotatate (Lutathera)
Class: Radiolabeled somatostatin analogue.
Disease: Somatostatin receptor–positive gastroenteropancreatic neuroendocrine tumors (GEP-NETs).
Dose: Intravenous infusion 7.4 GBq (200 mCi) every 8 weeks for a total of four doses.
NETTER-1 trial (NCT01578239): 65% of adults who received lutetium Lu 177 showed improved progression-free survival at 20 months, compared with just 10.8% in the control group.
Mogamulizumab (Poteligeo)
Class: Monoclonal antibody that binds to a protein (CC chemokine receptor type 4).
Disease: Relapsed or refractory mycosis fungoides or Sézary syndrome.
Dose: Intravenous infusion 1 mg/kg.
AE: Dermatologic toxicity.
MAVORIC trial (NCT01728805): Patients who received mogamulizumab had improved progression-free survival (median 7.7 months), compared with those taking vorinostat (median 3.1 months).
Moxetumomab pasudotox-tdfk (Lumoxiti)
Class: CD22-directed cytotoxin fused with a fragment of Pseudomonas exotoxin A.
Disease: Relapsed or refractory hairy cell leukemia previously treated with at least two prior systemic therapies, including a purine nucleoside analogue.
Dose: Intravenously as 0.04 mg/kg.
AE: Hemolytic uremic syndrome.
1053 trial (NCT01829711): 30% of the patients who received moxetumomab pasudotox-tdfk had a durable complete response confirmed by maintenance hematologic remission.
Talazoparib (Talzenna)
Class: Poly (ADP-ribose) polymerase (PARP) inhibitor.
Disease: gBRCAm HER2-negative locally advanced or metastatic breast cancer.
Dose: 1 mg orally per day.
EMBRACA trial (NCT01945775): Patients who received talazoparib demonstrated significantly longer progression-free survival, with a median of 8.6 months versis 5.6 months in the control arm.
Dr. Bryer is a resident in the department of internal medicine at the University of Pennsylvania, Philadelphia. Dr. Mentzer is chief of hematology-oncology at Pennsylvania Hospital and professor of medicine at the University of Pennsylvania. Dr. Henry is a hematologist-oncologist at Pennsylvania Hospital and a professor of medicine at the University of Pennsylvania.
Advances in genomics and technology perpetually change and improve therapies in oncology. Enhanced comprehension of cellular signaling, division, and replication has created a platform to selectively restrict neoplastic growth while preserving the integrity of benign cells.
This article reviews therapies that were newly approved in 2018, as well as those previously approved whose indications were expanded this past year. The list highlights the most clinically important approvals, as well as adverse events that are unique or especially severe.
Click on the PDF above to download the full article and charts in an easy-to-print format.
Apalutamide (Erleada)
Class: Androgen receptor inhibitor.
Disease: Nonmetastatic castration-resistant prostate cancer.
Dose: 240 mg orally, once daily.
Adverse Events (AEs): Hyperkalemia and increased risks of seizures, falls, and fractures.
Phase 3 SPARTAN trial (NCT01946204): 40.5-month metastasis-free survival rate, compared with 16.2 months in the placebo group.
Cemiplimab (Libtayo)
Class: Antibody against programmed cell death protein-1 (PD-1).
Disease: Metastatic cutaneous squamous cell carcinoma (CSCC) or locally advanced CSCC that is ineligible for curative surgery/radiation.
Dose: 350 mg intravenous infusion every 3 weeks.
AEs: Pneumonitis, autoimmune myocarditis, hepatitis, and aseptic meningitis.
1423 and 1540 trials (NCT02383212 and NCT02760498): 47.2% of patients who received cemiplimab had complete disappearance of the tumor or a decrease in tumor size.
Dacomitinib (Vizimpro)
Class: Second-generation tyrosine kinase inhibitor.
Disease: Metastatic non–small cell lung cancer (NSCLC) with epidermal growth factor receptor (EGFR) exon 19 deletion or exon 21 L858R substitution mutation.
Dose: 45 mg orally once daily.
AEs: Dermatotoxicity and diarrhea.
ARCHER1050 trial (NCT01774721): Patients who received dacomitinib demonstrated an improved overall survival, with a median of 34.1 months, compared with 26.8 months with gefitinib.
Duvelisib (Copiktra)
Class: Dual inhibitor of phosphatidylinositol 3-kinase delta and gamma.
Disease: Relapsed or refractory chronic lymphocytic leukemia (CLL), small lymphocytic lymphoma, or relapsed or refractory follicular lymphoma after at least two prior systemic therapies.
Dose: 25 mg orally twice daily.
AEs: Infection, diarrhea or colitis, and pneumonia.
Phase 3 DUO trial (NCT02004522): Progression-free survival in the duvelisib arm was 7.3 months longer than that in the ofatumumab arm. The overall response rate for patients receiving duvelisib was 78%, compared with 39% for those receiving ofatumumab.
Gilteritinib (Xospata)
Class: Inhibits the FLT3 internal tandem duplication (ITD) and FLT3 tyrosine kinase domain (TKD).
Disease: Relapsed or refractory acute myeloid leukemia (AML) with an FLT3 mutation.
Dose: 120 mg orally daily.
ADMIRAL trial (NCT02421939): 21% of the patients who received gilteritinib exhibited complete remission or complete remission with partial hematologic recovery.
Glasdegib (Daurismo)
Class: Hedgehog pathway inhibitor.
Disease: Adults over age 75 years with newly diagnosed AML and other medical comorbidities that preclude them from intensive chemotherapy.
Dose: The recommended dose is 100 mg orally continuously in 28-day cycles.
AE: QT prolongation and embryo-fetal toxicity
Phase 2 BRIGHT 1003 trial (NCT01546038): 3.9-month overall survival advantage for glasdegib plus cytarabine, compared with cytarabine alone. Overall, 15% of the glasdegib plus low dose cytarabine arm achieved complete remission, compared with the 1% complete remission rate in patients who received cytarabine alone.
Iobenguane I 131 (Azedra)
Class: Radiopharmaceutical agent; induces cell death within the noradrenaline transporter.
Disease: Iobenguane scan–positive, unresectable, locally advanced or metastatic pheochromocytoma or paraganglioma
Dose: Initial intravenous dosimetric dose, followed by two therapeutic doses.
AE: Pancytopenia and elevated international normalized ratio (INR).
IB12B trial (NCT00874614): One-quarter of patients receiving this therapy had at least a 50% reduction in the dose and number of antihypertensives for at least 6 months; almost all patients had a tumor response.
Ivosidenib (Tibsovo)
Class: Small-molecule inhibitor of mutant isocitrate dehydrogenase (IDH1).
Disease: Refractory AML and an IDH1 mutation
Dose: 500 mg orally daily.
AG120-C-001 trial (NCT02074839): Overall response rate of 41.6% in patients who received ivosidenib, with a 30.4% rate of complete remission or complete remission with partial hematologic recovery.
Larotrectinib (Vitrakvi)
Class: Oral tyrosine kinase inhibitor.
Disease: Advanced solid tumors harboring a neurotrophic tyrosine receptor kinase (NTRK) gene fusion.
Dose: 100 mg orally twice daily.
LOXO-TRK-14001, SCOUT, and NAVIGATE trials (NCT02122913, NCT02637687, and NCT02576431): Patients who received larotrectinib had durable responses regardless of patient age, tumor type, and fusion status.
Lutetium Lu 177 dotatate (Lutathera)
Class: Radiolabeled somatostatin analogue.
Disease: Somatostatin receptor–positive gastroenteropancreatic neuroendocrine tumors (GEP-NETs).
Dose: Intravenous infusion 7.4 GBq (200 mCi) every 8 weeks for a total of four doses.
NETTER-1 trial (NCT01578239): 65% of adults who received lutetium Lu 177 showed improved progression-free survival at 20 months, compared with just 10.8% in the control group.
Mogamulizumab (Poteligeo)
Class: Monoclonal antibody that binds to a protein (CC chemokine receptor type 4).
Disease: Relapsed or refractory mycosis fungoides or Sézary syndrome.
Dose: Intravenous infusion 1 mg/kg.
AE: Dermatologic toxicity.
MAVORIC trial (NCT01728805): Patients who received mogamulizumab had improved progression-free survival (median 7.7 months), compared with those taking vorinostat (median 3.1 months).
Moxetumomab pasudotox-tdfk (Lumoxiti)
Class: CD22-directed cytotoxin fused with a fragment of Pseudomonas exotoxin A.
Disease: Relapsed or refractory hairy cell leukemia previously treated with at least two prior systemic therapies, including a purine nucleoside analogue.
Dose: Intravenously as 0.04 mg/kg.
AE: Hemolytic uremic syndrome.
1053 trial (NCT01829711): 30% of the patients who received moxetumomab pasudotox-tdfk had a durable complete response confirmed by maintenance hematologic remission.
Talazoparib (Talzenna)
Class: Poly (ADP-ribose) polymerase (PARP) inhibitor.
Disease: gBRCAm HER2-negative locally advanced or metastatic breast cancer.
Dose: 1 mg orally per day.
EMBRACA trial (NCT01945775): Patients who received talazoparib demonstrated significantly longer progression-free survival, with a median of 8.6 months versis 5.6 months in the control arm.
Dr. Bryer is a resident in the department of internal medicine at the University of Pennsylvania, Philadelphia. Dr. Mentzer is chief of hematology-oncology at Pennsylvania Hospital and professor of medicine at the University of Pennsylvania. Dr. Henry is a hematologist-oncologist at Pennsylvania Hospital and a professor of medicine at the University of Pennsylvania.
Mortality rates higher in affiliates, compared with top-ranked hospitals
The sharing of a top-ranked cancer hospital brand across affiliate hospitals doesn’t necessarily guarantee the same quality of care, a new study suggests.
In a paper published in JAMA Network Open, researchers presented the outcomes of a cross-sectional study of 29,228 patients aged over 65 years who underwent complex cancer surgery at either 59 top-ranked hospitals or 343 affiliated hospitals.
The researchers saw a significant 40% higher 90-day mortality rate among patients who underwent complex cancer surgery at one of the affiliate hospitals, compared with those who were treated at the top-ranked hospitals (P less than .001), even after adjusting for factors such as age, comorbidity score, procedure type, and admission type.
“This is not entirely surprising, as affiliated hospitals are generally smaller, less likely to be teaching hospitals, and perform complex surgical procedures with less frequency (lower volume) when compared with top-ranked hospitals,” wrote Jessica R. Hoag, PhD, from the department of surgery at Yale University, New Haven, Conn., and her coauthors. However, including hospital characteristics in the models attenuated but did not eliminate the differences in mortality rates between top-ranked and affiliate hospitals.
The difference in 90-day mortality was particularly evident for gastrectomy, where there was a 100% higher 90-day mortality rate in affiliate hospitals, compared with top-ranked hospitals (P less than .001). The mortality rate for pancreaticoduodenectomy was 59% higher in affiliate hospitals, compared with top-ranked hospitals (P = .009); for colectomy it was 32% higher (P = .001), and for lobectomy it was 34% higher (P = .03).
The only procedure where the mortality rate was not statistically significantly different between top-ranked and affiliate hospitals was esophagectomy (odds ratio, 1.48; P = .06).
When the authors looked at standardized mortality ratios for the top-ranked and affiliate hospitals, they found that 41 of the 49 top-ranked hospitals had lower mortality ratios than their collective affiliates. In 37 cases, the difference in standardized mortality ratios between the top-ranked hospital and its affiliates was statistically significant.
Overall, 39 of the 49 top-ranked hospitals had better standardized mortality ratios than the national average, compared with 17 of the affiliated networks.
The authors wrote that their findings were important because previous studies showed affiliation status played a significant role in which hospital patients choose for their treatment.
“As a result, there is cause for concern that a proportion of the U.S. public could misinterpret brand sharing as indicating equivalent care,” they wrote, suggesting that one way to reduce mortality might therefore be to direct patients with the most risky and complex surgical requirements to top-ranked hospitals rather than affiliates, although acknowledged this might be challenging to implement.
One author reported receiving funding from the Centers for Medicare & Medicaid Services, one reported advisory board and steering committee positions with the private medical sector, and one reported receiving nonfinancial support from private industry outside the submitted work. No other conflicts of interest were reported.
SOURCE: Hoag JR et al. JAMA Netw Open. 2019 Apr 12. doi: 10.1001/jamanetworkopen.2019.1912.
Network affiliations with top-ranked hospitals could help expand access to high-quality cancer care and reduce travel times for patients who live too far away to access the top-ranked hospital itself. However, this study shows that the outcomes and quality of the flagship hospital do not necessarily translate to the affiliate hospitals in the network.
While affiliate hospitals are likely to deal with smaller numbers of complex patients and are less likely to be teaching hospitals, they do offer a way to potentially leverage their affiliation with top-ranked hospitals to improve the overall quality of care for cancer patients. The challenge is to work out how best to do this and to identify which patients are likely to do just as well at an affiliate hospital and which patients will be optimally treated at the flagship hospital.
Lesly A. Dossett, MD, MPH, is from the department of surgery at the University of Michigan, Ann Arbor. These comments are adapted from an accompanying editorial (JAMA Netw Open. 2019 Apr 12. doi:10.1001/jamanetworkopen.2019.1910). No conflicts of interest were reported.
Network affiliations with top-ranked hospitals could help expand access to high-quality cancer care and reduce travel times for patients who live too far away to access the top-ranked hospital itself. However, this study shows that the outcomes and quality of the flagship hospital do not necessarily translate to the affiliate hospitals in the network.
While affiliate hospitals are likely to deal with smaller numbers of complex patients and are less likely to be teaching hospitals, they do offer a way to potentially leverage their affiliation with top-ranked hospitals to improve the overall quality of care for cancer patients. The challenge is to work out how best to do this and to identify which patients are likely to do just as well at an affiliate hospital and which patients will be optimally treated at the flagship hospital.
Lesly A. Dossett, MD, MPH, is from the department of surgery at the University of Michigan, Ann Arbor. These comments are adapted from an accompanying editorial (JAMA Netw Open. 2019 Apr 12. doi:10.1001/jamanetworkopen.2019.1910). No conflicts of interest were reported.
Network affiliations with top-ranked hospitals could help expand access to high-quality cancer care and reduce travel times for patients who live too far away to access the top-ranked hospital itself. However, this study shows that the outcomes and quality of the flagship hospital do not necessarily translate to the affiliate hospitals in the network.
While affiliate hospitals are likely to deal with smaller numbers of complex patients and are less likely to be teaching hospitals, they do offer a way to potentially leverage their affiliation with top-ranked hospitals to improve the overall quality of care for cancer patients. The challenge is to work out how best to do this and to identify which patients are likely to do just as well at an affiliate hospital and which patients will be optimally treated at the flagship hospital.
Lesly A. Dossett, MD, MPH, is from the department of surgery at the University of Michigan, Ann Arbor. These comments are adapted from an accompanying editorial (JAMA Netw Open. 2019 Apr 12. doi:10.1001/jamanetworkopen.2019.1910). No conflicts of interest were reported.
The sharing of a top-ranked cancer hospital brand across affiliate hospitals doesn’t necessarily guarantee the same quality of care, a new study suggests.
In a paper published in JAMA Network Open, researchers presented the outcomes of a cross-sectional study of 29,228 patients aged over 65 years who underwent complex cancer surgery at either 59 top-ranked hospitals or 343 affiliated hospitals.
The researchers saw a significant 40% higher 90-day mortality rate among patients who underwent complex cancer surgery at one of the affiliate hospitals, compared with those who were treated at the top-ranked hospitals (P less than .001), even after adjusting for factors such as age, comorbidity score, procedure type, and admission type.
“This is not entirely surprising, as affiliated hospitals are generally smaller, less likely to be teaching hospitals, and perform complex surgical procedures with less frequency (lower volume) when compared with top-ranked hospitals,” wrote Jessica R. Hoag, PhD, from the department of surgery at Yale University, New Haven, Conn., and her coauthors. However, including hospital characteristics in the models attenuated but did not eliminate the differences in mortality rates between top-ranked and affiliate hospitals.
The difference in 90-day mortality was particularly evident for gastrectomy, where there was a 100% higher 90-day mortality rate in affiliate hospitals, compared with top-ranked hospitals (P less than .001). The mortality rate for pancreaticoduodenectomy was 59% higher in affiliate hospitals, compared with top-ranked hospitals (P = .009); for colectomy it was 32% higher (P = .001), and for lobectomy it was 34% higher (P = .03).
The only procedure where the mortality rate was not statistically significantly different between top-ranked and affiliate hospitals was esophagectomy (odds ratio, 1.48; P = .06).
When the authors looked at standardized mortality ratios for the top-ranked and affiliate hospitals, they found that 41 of the 49 top-ranked hospitals had lower mortality ratios than their collective affiliates. In 37 cases, the difference in standardized mortality ratios between the top-ranked hospital and its affiliates was statistically significant.
Overall, 39 of the 49 top-ranked hospitals had better standardized mortality ratios than the national average, compared with 17 of the affiliated networks.
The authors wrote that their findings were important because previous studies showed affiliation status played a significant role in which hospital patients choose for their treatment.
“As a result, there is cause for concern that a proportion of the U.S. public could misinterpret brand sharing as indicating equivalent care,” they wrote, suggesting that one way to reduce mortality might therefore be to direct patients with the most risky and complex surgical requirements to top-ranked hospitals rather than affiliates, although acknowledged this might be challenging to implement.
One author reported receiving funding from the Centers for Medicare & Medicaid Services, one reported advisory board and steering committee positions with the private medical sector, and one reported receiving nonfinancial support from private industry outside the submitted work. No other conflicts of interest were reported.
SOURCE: Hoag JR et al. JAMA Netw Open. 2019 Apr 12. doi: 10.1001/jamanetworkopen.2019.1912.
The sharing of a top-ranked cancer hospital brand across affiliate hospitals doesn’t necessarily guarantee the same quality of care, a new study suggests.
In a paper published in JAMA Network Open, researchers presented the outcomes of a cross-sectional study of 29,228 patients aged over 65 years who underwent complex cancer surgery at either 59 top-ranked hospitals or 343 affiliated hospitals.
The researchers saw a significant 40% higher 90-day mortality rate among patients who underwent complex cancer surgery at one of the affiliate hospitals, compared with those who were treated at the top-ranked hospitals (P less than .001), even after adjusting for factors such as age, comorbidity score, procedure type, and admission type.
“This is not entirely surprising, as affiliated hospitals are generally smaller, less likely to be teaching hospitals, and perform complex surgical procedures with less frequency (lower volume) when compared with top-ranked hospitals,” wrote Jessica R. Hoag, PhD, from the department of surgery at Yale University, New Haven, Conn., and her coauthors. However, including hospital characteristics in the models attenuated but did not eliminate the differences in mortality rates between top-ranked and affiliate hospitals.
The difference in 90-day mortality was particularly evident for gastrectomy, where there was a 100% higher 90-day mortality rate in affiliate hospitals, compared with top-ranked hospitals (P less than .001). The mortality rate for pancreaticoduodenectomy was 59% higher in affiliate hospitals, compared with top-ranked hospitals (P = .009); for colectomy it was 32% higher (P = .001), and for lobectomy it was 34% higher (P = .03).
The only procedure where the mortality rate was not statistically significantly different between top-ranked and affiliate hospitals was esophagectomy (odds ratio, 1.48; P = .06).
When the authors looked at standardized mortality ratios for the top-ranked and affiliate hospitals, they found that 41 of the 49 top-ranked hospitals had lower mortality ratios than their collective affiliates. In 37 cases, the difference in standardized mortality ratios between the top-ranked hospital and its affiliates was statistically significant.
Overall, 39 of the 49 top-ranked hospitals had better standardized mortality ratios than the national average, compared with 17 of the affiliated networks.
The authors wrote that their findings were important because previous studies showed affiliation status played a significant role in which hospital patients choose for their treatment.
“As a result, there is cause for concern that a proportion of the U.S. public could misinterpret brand sharing as indicating equivalent care,” they wrote, suggesting that one way to reduce mortality might therefore be to direct patients with the most risky and complex surgical requirements to top-ranked hospitals rather than affiliates, although acknowledged this might be challenging to implement.
One author reported receiving funding from the Centers for Medicare & Medicaid Services, one reported advisory board and steering committee positions with the private medical sector, and one reported receiving nonfinancial support from private industry outside the submitted work. No other conflicts of interest were reported.
SOURCE: Hoag JR et al. JAMA Netw Open. 2019 Apr 12. doi: 10.1001/jamanetworkopen.2019.1912.
FROM JAMA NETWORK OPEN
Rash with hair loss

The FP had never seen a condition like this before, so he used some online resources to come up with a differential diagnosis that included sarcoidosis, leprosy, drug eruption, and mycosis fungoides. Aside from an occasional drug eruption, the other conditions were ones that he had seen in textbooks only.
Based on that differential diagnosis, the FP decided to do a punch biopsy of the largest nodule, which was near the patient’s mouth. (See the Watch & Learn video on “Punch biopsy.”)
The pathology report came back as folliculotropic mycosis fungoides. The FP researched the diagnosis and determined that this was a cutaneous T-cell lymphoma that involved hair follicles and tended to occur on the head and neck. This explained the patient’s hair loss in his beard and right eyebrow. While the prognosis for mycosis fungoides is quite good, the same cannot be said for the folliculotropic variant.
The FP referred the patient to Dermatology for further evaluation and treatment. In consultation with Hematology, the patient was treated with a potent topical steroid, chemotherapy, and narrowband ultraviolet B light therapy. His condition improved, but ongoing treatment and surveillance were needed.
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Chacon G, Nayar A. Cutaneous T-cell lymphoma. In: Usatine R, Smith M, Mayeaux EJ, et al. Color Atlas and Synopsis of Family Medicine. 3rd ed. New York, NY: McGraw-Hill;2019:1124-1131.
To learn more about the newest 3rd edition of the Color Atlas and Synopsis of Family Medicine, see: https://www.amazon.com/Color-Atlas-Synopsis-Family-Medicine/dp/1259862046/
You can get the Color Atlas of Family Medicine app by clicking on this link: usatinemedia.com
The FP had never seen a condition like this before, so he used some online resources to come up with a differential diagnosis that included sarcoidosis, leprosy, drug eruption, and mycosis fungoides. Aside from an occasional drug eruption, the other conditions were ones that he had seen in textbooks only.
Based on that differential diagnosis, the FP decided to do a punch biopsy of the largest nodule, which was near the patient’s mouth. (See the Watch & Learn video on “Punch biopsy.”)
The pathology report came back as folliculotropic mycosis fungoides. The FP researched the diagnosis and determined that this was a cutaneous T-cell lymphoma that involved hair follicles and tended to occur on the head and neck. This explained the patient’s hair loss in his beard and right eyebrow. While the prognosis for mycosis fungoides is quite good, the same cannot be said for the folliculotropic variant.
The FP referred the patient to Dermatology for further evaluation and treatment. In consultation with Hematology, the patient was treated with a potent topical steroid, chemotherapy, and narrowband ultraviolet B light therapy. His condition improved, but ongoing treatment and surveillance were needed.
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Chacon G, Nayar A. Cutaneous T-cell lymphoma. In: Usatine R, Smith M, Mayeaux EJ, et al. Color Atlas and Synopsis of Family Medicine. 3rd ed. New York, NY: McGraw-Hill;2019:1124-1131.
To learn more about the newest 3rd edition of the Color Atlas and Synopsis of Family Medicine, see: https://www.amazon.com/Color-Atlas-Synopsis-Family-Medicine/dp/1259862046/
You can get the Color Atlas of Family Medicine app by clicking on this link: usatinemedia.com
The FP had never seen a condition like this before, so he used some online resources to come up with a differential diagnosis that included sarcoidosis, leprosy, drug eruption, and mycosis fungoides. Aside from an occasional drug eruption, the other conditions were ones that he had seen in textbooks only.
Based on that differential diagnosis, the FP decided to do a punch biopsy of the largest nodule, which was near the patient’s mouth. (See the Watch & Learn video on “Punch biopsy.”)
The pathology report came back as folliculotropic mycosis fungoides. The FP researched the diagnosis and determined that this was a cutaneous T-cell lymphoma that involved hair follicles and tended to occur on the head and neck. This explained the patient’s hair loss in his beard and right eyebrow. While the prognosis for mycosis fungoides is quite good, the same cannot be said for the folliculotropic variant.
The FP referred the patient to Dermatology for further evaluation and treatment. In consultation with Hematology, the patient was treated with a potent topical steroid, chemotherapy, and narrowband ultraviolet B light therapy. His condition improved, but ongoing treatment and surveillance were needed.
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Chacon G, Nayar A. Cutaneous T-cell lymphoma. In: Usatine R, Smith M, Mayeaux EJ, et al. Color Atlas and Synopsis of Family Medicine. 3rd ed. New York, NY: McGraw-Hill;2019:1124-1131.
To learn more about the newest 3rd edition of the Color Atlas and Synopsis of Family Medicine, see: https://www.amazon.com/Color-Atlas-Synopsis-Family-Medicine/dp/1259862046/
You can get the Color Atlas of Family Medicine app by clicking on this link: usatinemedia.com
