User login
Time-Restricted Eating Is Not a Metabolic Magic Bullet
This transcript has been edited for clarity.
One out of three American adults — about 100 million people in this country — have the metabolic syndrome. I’m showing you the official criteria here, but essentially this is a syndrome of insulin resistance and visceral adiposity that predisposes us to a host of chronic diseases such as diabetes, heart disease, and even dementia. 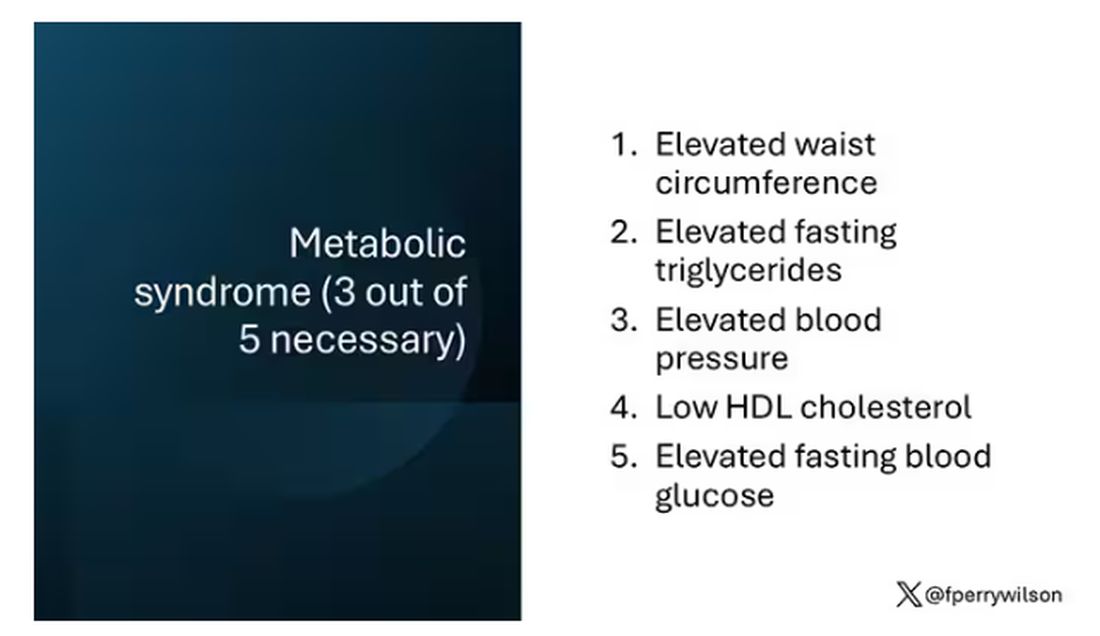
The metabolic syndrome is, fundamentally, a lifestyle disease. There is a direct line between our dietary habits and the wide availability of carbohydrate-rich, highly processed foods, and the rise in the syndrome in the population.
A saying I learned from one of my epidemiology teachers comes to mind: “Lifestyle diseases require lifestyle reinterventions.” But you know what? I’m not so sure anymore.
I’ve been around long enough to see multiple dietary fads come and go with varying efficacy. I grew up in the low-fat era, probably the most detrimental time to our national health as food manufacturers started replacing fats with carbohydrates, driving much of the problem we’re faced with today.
But I was also around for the Atkins diet and the low-carb craze — a healthier approach, all things being equal. And I’ve seen variants of these: the paleo diet (essentially a low-carb, high-protein diet based on minimally processed foods) and the Mediterranean diet, which sought to replace some percentage of fats with healthier fats.
And, of course, there is time-restricted eating.
Time-restricted eating, a variant of intermittent fasting, has the advantage of being very simple. No cookbooks, no recipes. Eat what you want — but limit it to certain hours in the day, ideally a window of less than 10 hours, such as 8 a.m. to 6 p.m.
When it comes to weight loss, the diets that work tend to work because they reduce calorie intake. I know, people will get angry about this, but thermodynamics is not just a good idea, it’s the law.
But weight loss is not the only reason we need to eat healthier. What we eat can impact our health in multiple ways; certain foods lead to more atherosclerosis, more inflammation, increased strain on the kidney and liver, and can affect our glucose homeostasis.
So I was really interested when I saw this article, “Time-Restricted Eating in Adults With Metabolic Syndrome,” appearing in Annals of Internal Medicine October 1, which examined the effect of time-restricted eating on the metabolic syndrome itself. Could this lifestyle intervention cure this lifestyle disease?
In the study, 108 individuals, all of whom had the metabolic syndrome but not full-blown diabetes, were randomized to usual care — basically, nutrition education — vs time-restricted eating. In that group, participants were instructed to reduce their window of eating by at least 4 hours to achieve an 8- to 10-hour eating window. The groups were followed for 3 months.
Now, before we get to the results, it’s important to remember that the success of a lifestyle intervention trial is quite dependent on how well people adhere to the lifestyle intervention. Time-restricted eating is not as easy as taking a pill once a day.
The researchers had participants log their consumption using a smartphone app to confirm whether they were adhering to that restricted eating window.
Broadly speaking, they did. At baseline, both groups had an eating window of about 14 hours a day — think 7 a.m. to 9 p.m. The intervention group reduced that to just under 10 hours, with 10% of days falling outside of the target window.
Lifestyle change achieved, the primary outcome was the change in hemoglobin A1c at 3 months. A1c integrates the serum glucose over time and is thus a good indicator of the success of the intervention in terms of insulin resistance. But the effect was, honestly, disappointing.
Technically, the time-restricted-eating group had a greater A1c change than the control group — by 0.1 percentage points. On average, they went from a baseline A1c of 5.87 to a 3-month A1c of 5.75.
Other metabolic syndrome markers were equally lackluster: no difference in fasting glucose, mean glucose, or fasting insulin.
There was some weight change. The control group, which got that dietary education, lost 1.5% of body weight over the 3 months. The time-restricted-eating group lost 3.3% — about 7 pounds, which is reasonable.
With that weight loss came statistically significant, albeit modest improvements in BMI, body fat percentage, and LDL cholesterol.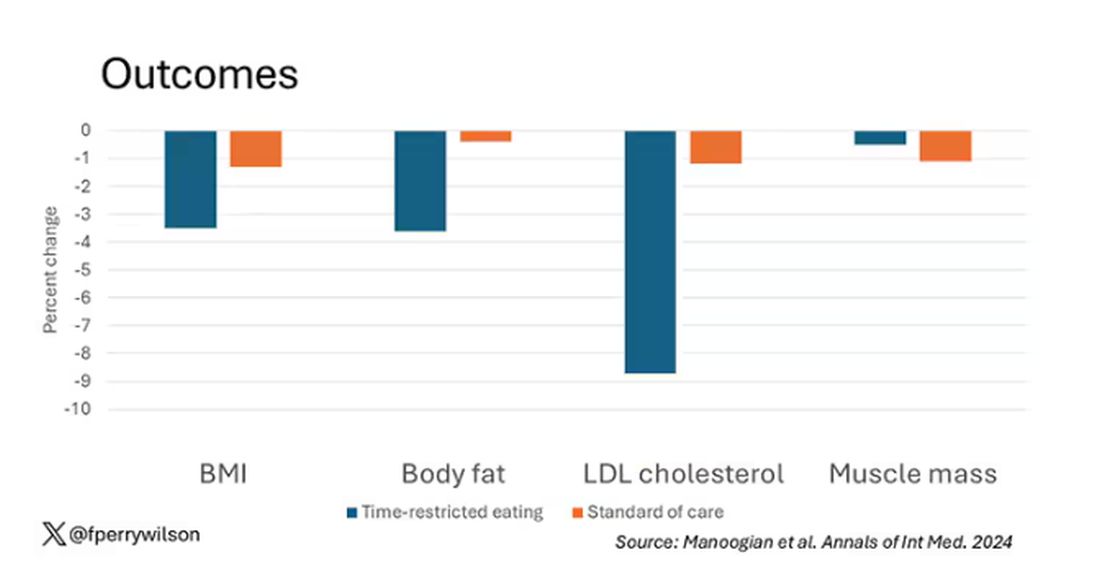
Of interest, despite the larger weight loss in the intermittent-fasting group, there was no difference in muscle mass loss, which is encouraging.
Taken together, we can say that, yes, it seems like time-restricted eating can help people lose some weight. This is essentially due to the fact that people eat fewer calories when they do time-restricted eating, as you can see here.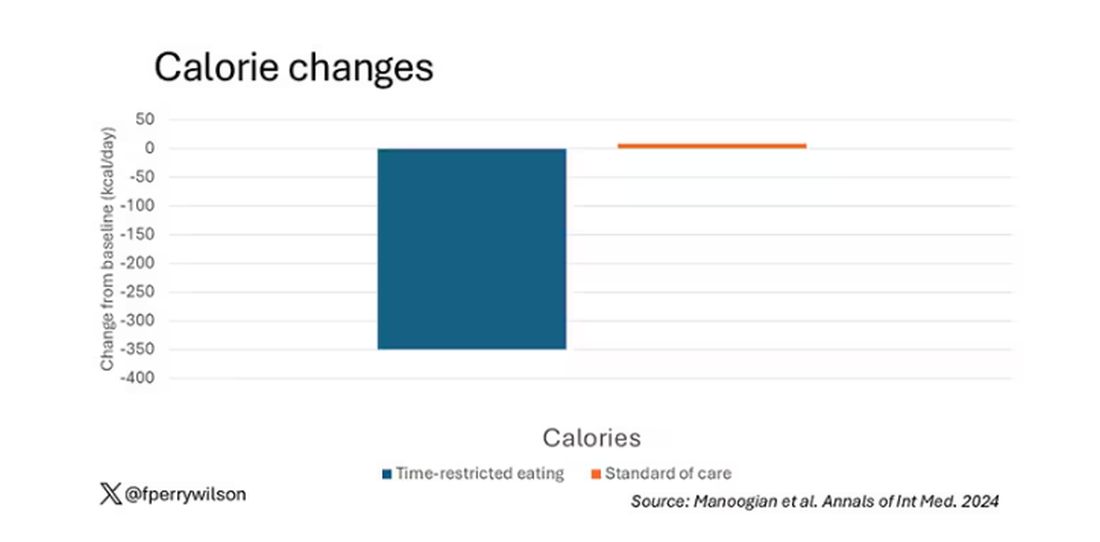
But, in the end, this trial examined whether this relatively straightforward lifestyle intervention would move the needle in terms of metabolic syndrome, and the data are not very compelling for that.
This graph shows how many of those five factors for metabolic syndrome the individuals in this trial had from the start to the end. You see that, over the 3 months, seven people in the time-restricted-eating group moved from having three criteria to two or one — being “cured” of metabolic syndrome, if you will. Nine people in the standard group were cured by that definition. Remember, they had to have at least three to have the syndrome and thus be eligible for the trial. 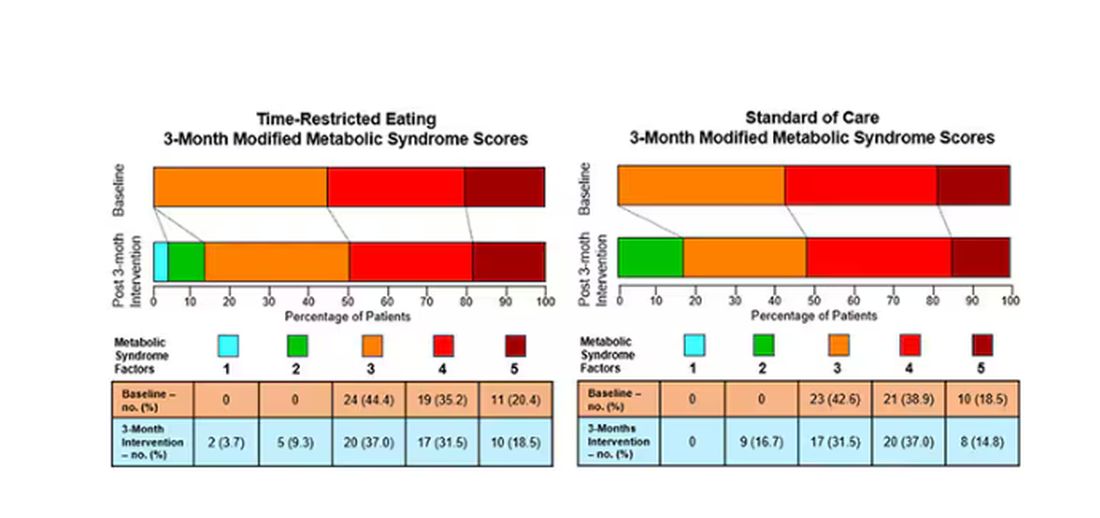
So If it just leads to weight loss by forcing people to consume less calories, then we need to acknowledge that we probably have better methods to achieve this same end. Ten years ago, I would have said that lifestyle change is the only way to end the epidemic of the metabolic syndrome in this country. Today, well, we live in a world of GLP-1 weight loss drugs. It is simply a different world now. Yes, they are expensive. Yes, they have side effects. But we need to evaluate them against the comparison. And so far, lifestyle changes alone are really no comparison.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
One out of three American adults — about 100 million people in this country — have the metabolic syndrome. I’m showing you the official criteria here, but essentially this is a syndrome of insulin resistance and visceral adiposity that predisposes us to a host of chronic diseases such as diabetes, heart disease, and even dementia.
The metabolic syndrome is, fundamentally, a lifestyle disease. There is a direct line between our dietary habits and the wide availability of carbohydrate-rich, highly processed foods, and the rise in the syndrome in the population.
A saying I learned from one of my epidemiology teachers comes to mind: “Lifestyle diseases require lifestyle reinterventions.” But you know what? I’m not so sure anymore.
I’ve been around long enough to see multiple dietary fads come and go with varying efficacy. I grew up in the low-fat era, probably the most detrimental time to our national health as food manufacturers started replacing fats with carbohydrates, driving much of the problem we’re faced with today.
But I was also around for the Atkins diet and the low-carb craze — a healthier approach, all things being equal. And I’ve seen variants of these: the paleo diet (essentially a low-carb, high-protein diet based on minimally processed foods) and the Mediterranean diet, which sought to replace some percentage of fats with healthier fats.
And, of course, there is time-restricted eating.
Time-restricted eating, a variant of intermittent fasting, has the advantage of being very simple. No cookbooks, no recipes. Eat what you want — but limit it to certain hours in the day, ideally a window of less than 10 hours, such as 8 a.m. to 6 p.m.
When it comes to weight loss, the diets that work tend to work because they reduce calorie intake. I know, people will get angry about this, but thermodynamics is not just a good idea, it’s the law.
But weight loss is not the only reason we need to eat healthier. What we eat can impact our health in multiple ways; certain foods lead to more atherosclerosis, more inflammation, increased strain on the kidney and liver, and can affect our glucose homeostasis.
So I was really interested when I saw this article, “Time-Restricted Eating in Adults With Metabolic Syndrome,” appearing in Annals of Internal Medicine October 1, which examined the effect of time-restricted eating on the metabolic syndrome itself. Could this lifestyle intervention cure this lifestyle disease?
In the study, 108 individuals, all of whom had the metabolic syndrome but not full-blown diabetes, were randomized to usual care — basically, nutrition education — vs time-restricted eating. In that group, participants were instructed to reduce their window of eating by at least 4 hours to achieve an 8- to 10-hour eating window. The groups were followed for 3 months.
Now, before we get to the results, it’s important to remember that the success of a lifestyle intervention trial is quite dependent on how well people adhere to the lifestyle intervention. Time-restricted eating is not as easy as taking a pill once a day.
The researchers had participants log their consumption using a smartphone app to confirm whether they were adhering to that restricted eating window.
Broadly speaking, they did. At baseline, both groups had an eating window of about 14 hours a day — think 7 a.m. to 9 p.m. The intervention group reduced that to just under 10 hours, with 10% of days falling outside of the target window.
Lifestyle change achieved, the primary outcome was the change in hemoglobin A1c at 3 months. A1c integrates the serum glucose over time and is thus a good indicator of the success of the intervention in terms of insulin resistance. But the effect was, honestly, disappointing.
Technically, the time-restricted-eating group had a greater A1c change than the control group — by 0.1 percentage points. On average, they went from a baseline A1c of 5.87 to a 3-month A1c of 5.75.
Other metabolic syndrome markers were equally lackluster: no difference in fasting glucose, mean glucose, or fasting insulin.
There was some weight change. The control group, which got that dietary education, lost 1.5% of body weight over the 3 months. The time-restricted-eating group lost 3.3% — about 7 pounds, which is reasonable.
With that weight loss came statistically significant, albeit modest improvements in BMI, body fat percentage, and LDL cholesterol.
Of interest, despite the larger weight loss in the intermittent-fasting group, there was no difference in muscle mass loss, which is encouraging.
Taken together, we can say that, yes, it seems like time-restricted eating can help people lose some weight. This is essentially due to the fact that people eat fewer calories when they do time-restricted eating, as you can see here.
But, in the end, this trial examined whether this relatively straightforward lifestyle intervention would move the needle in terms of metabolic syndrome, and the data are not very compelling for that.
This graph shows how many of those five factors for metabolic syndrome the individuals in this trial had from the start to the end. You see that, over the 3 months, seven people in the time-restricted-eating group moved from having three criteria to two or one — being “cured” of metabolic syndrome, if you will. Nine people in the standard group were cured by that definition. Remember, they had to have at least three to have the syndrome and thus be eligible for the trial.
So If it just leads to weight loss by forcing people to consume less calories, then we need to acknowledge that we probably have better methods to achieve this same end. Ten years ago, I would have said that lifestyle change is the only way to end the epidemic of the metabolic syndrome in this country. Today, well, we live in a world of GLP-1 weight loss drugs. It is simply a different world now. Yes, they are expensive. Yes, they have side effects. But we need to evaluate them against the comparison. And so far, lifestyle changes alone are really no comparison.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
One out of three American adults — about 100 million people in this country — have the metabolic syndrome. I’m showing you the official criteria here, but essentially this is a syndrome of insulin resistance and visceral adiposity that predisposes us to a host of chronic diseases such as diabetes, heart disease, and even dementia.
The metabolic syndrome is, fundamentally, a lifestyle disease. There is a direct line between our dietary habits and the wide availability of carbohydrate-rich, highly processed foods, and the rise in the syndrome in the population.
A saying I learned from one of my epidemiology teachers comes to mind: “Lifestyle diseases require lifestyle reinterventions.” But you know what? I’m not so sure anymore.
I’ve been around long enough to see multiple dietary fads come and go with varying efficacy. I grew up in the low-fat era, probably the most detrimental time to our national health as food manufacturers started replacing fats with carbohydrates, driving much of the problem we’re faced with today.
But I was also around for the Atkins diet and the low-carb craze — a healthier approach, all things being equal. And I’ve seen variants of these: the paleo diet (essentially a low-carb, high-protein diet based on minimally processed foods) and the Mediterranean diet, which sought to replace some percentage of fats with healthier fats.
And, of course, there is time-restricted eating.
Time-restricted eating, a variant of intermittent fasting, has the advantage of being very simple. No cookbooks, no recipes. Eat what you want — but limit it to certain hours in the day, ideally a window of less than 10 hours, such as 8 a.m. to 6 p.m.
When it comes to weight loss, the diets that work tend to work because they reduce calorie intake. I know, people will get angry about this, but thermodynamics is not just a good idea, it’s the law.
But weight loss is not the only reason we need to eat healthier. What we eat can impact our health in multiple ways; certain foods lead to more atherosclerosis, more inflammation, increased strain on the kidney and liver, and can affect our glucose homeostasis.
So I was really interested when I saw this article, “Time-Restricted Eating in Adults With Metabolic Syndrome,” appearing in Annals of Internal Medicine October 1, which examined the effect of time-restricted eating on the metabolic syndrome itself. Could this lifestyle intervention cure this lifestyle disease?
In the study, 108 individuals, all of whom had the metabolic syndrome but not full-blown diabetes, were randomized to usual care — basically, nutrition education — vs time-restricted eating. In that group, participants were instructed to reduce their window of eating by at least 4 hours to achieve an 8- to 10-hour eating window. The groups were followed for 3 months.
Now, before we get to the results, it’s important to remember that the success of a lifestyle intervention trial is quite dependent on how well people adhere to the lifestyle intervention. Time-restricted eating is not as easy as taking a pill once a day.
The researchers had participants log their consumption using a smartphone app to confirm whether they were adhering to that restricted eating window.
Broadly speaking, they did. At baseline, both groups had an eating window of about 14 hours a day — think 7 a.m. to 9 p.m. The intervention group reduced that to just under 10 hours, with 10% of days falling outside of the target window.
Lifestyle change achieved, the primary outcome was the change in hemoglobin A1c at 3 months. A1c integrates the serum glucose over time and is thus a good indicator of the success of the intervention in terms of insulin resistance. But the effect was, honestly, disappointing.
Technically, the time-restricted-eating group had a greater A1c change than the control group — by 0.1 percentage points. On average, they went from a baseline A1c of 5.87 to a 3-month A1c of 5.75.
Other metabolic syndrome markers were equally lackluster: no difference in fasting glucose, mean glucose, or fasting insulin.
There was some weight change. The control group, which got that dietary education, lost 1.5% of body weight over the 3 months. The time-restricted-eating group lost 3.3% — about 7 pounds, which is reasonable.
With that weight loss came statistically significant, albeit modest improvements in BMI, body fat percentage, and LDL cholesterol.
Of interest, despite the larger weight loss in the intermittent-fasting group, there was no difference in muscle mass loss, which is encouraging.
Taken together, we can say that, yes, it seems like time-restricted eating can help people lose some weight. This is essentially due to the fact that people eat fewer calories when they do time-restricted eating, as you can see here.
But, in the end, this trial examined whether this relatively straightforward lifestyle intervention would move the needle in terms of metabolic syndrome, and the data are not very compelling for that.
This graph shows how many of those five factors for metabolic syndrome the individuals in this trial had from the start to the end. You see that, over the 3 months, seven people in the time-restricted-eating group moved from having three criteria to two or one — being “cured” of metabolic syndrome, if you will. Nine people in the standard group were cured by that definition. Remember, they had to have at least three to have the syndrome and thus be eligible for the trial.
So If it just leads to weight loss by forcing people to consume less calories, then we need to acknowledge that we probably have better methods to achieve this same end. Ten years ago, I would have said that lifestyle change is the only way to end the epidemic of the metabolic syndrome in this country. Today, well, we live in a world of GLP-1 weight loss drugs. It is simply a different world now. Yes, they are expensive. Yes, they have side effects. But we need to evaluate them against the comparison. And so far, lifestyle changes alone are really no comparison.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Detecting Type 2 Diabetes Through Voice: How Does It Work?
An international study, Colive Voice, presented at the European Association for the Study of Diabetes (EASD) 2024 conference, shows that These results “open up possibilities for developing a first-line, noninvasive, and rapid screening tool for T2D, feasible with just a few seconds of voice recording on a smartphone or during consultations,” explained the study’s principal investigator Guy Fagherazzi, PhD, a diabetes epidemiologist at the Luxembourg Institute of Health, in an interview with this news organization.
How did the idea of detecting diabetes through voice come about?
During the COVID-19 pandemic, we began analyzing voice recordings from patients with chronic diseases. We wanted to find solutions to assess people’s health remotely, without physical contact. We quickly realized that this approach could be extended to other diseases. Because my main research focus has always been diabetes, I looked into how voice characteristics might correlate with diabetes. Previous studies had indicated that patients with diabetes have distinct voices compared with the general population, and this insight formed the starting point.
What mechanism could explain why patients with T2D have different voice characteristics?
It’s challenging to pinpoint a single factor that would explain why patients with T2D have different voices from those without diabetes. Several factors are involved.
Some biological mechanisms, especially those affecting the vascular system, influence symptoms in people with metabolic diseases such as diabetes. For example, people with T2D have more frequent cardiorespiratory fatigue. Obesity and overweight are also key factors, as these conditions can slightly alter vocal parameters compared with people of normal weight. Hypertension, common in patients with T2D, adds to the complexity.
Neurologic complications can affect the nerves and muscles involved in voice production, particularly the vocal cords.
Therefore, respiratory fatigue, neuropathies, and other conditions such as dehydration and gastric acid reflux, which are more common in patients with diabetes, can contribute to differences in voice.
These differences might not be noticeable to the human ear. That’s why we often don’t notice the link between voice and diabetes. However, technological advancements in signal processing and artificial intelligence allow us to extract a large amount of information from these subtle variations. By analyzing these small differences, we can detect diabetes with a reasonable degree of accuracy.
In your study, you mention that voice tone can indicate diabetic status. Could you elaborate?
Yes, voice tone can be affected, though it’s a complex, multidimensional phenomenon.
Patients who have had diabetes for 5-10 years, or longer, tend to have a rougher voice than those without diabetes of the same age and gender. In our study, we were able to extract many voice characteristics from the raw audio signal, which is why it’s difficult to isolate one specific factor that stands out.
Is there a difference in voice changes between patients with well-managed diabetes and those whose disease is uncontrolled?
The roughness of the voice tends to increase with the duration of diabetes. It’s more noticeable in people with poorly controlled diabetes. Our hypothesis, based on the results we presented at the EASD conference, is that fluctuations in blood sugar levels, both hypo- and hyperglycemia, may cause short-term changes in the voice. There are also many subtle, rapid changes that could potentially be detected, though we haven’t confirmed this yet. We’re currently conducting additional studies to explore this.
Why did you ask participants to read a passage from the Universal Declaration of Human Rights?
We used a highly standardized approach. Participants completed several recordings, including holding the sound “Aaaaaa” for as long as possible in one breath. They also read a passage, which helps us better distinguish between patients with and those without diabetes. This method works slightly better than other sounds typically used for analyzing diseases. We chose this particular text in the participant’s native language because it’s neutral and doesn’t trigger emotional fluctuations. Because Colive Voice is an international, multilingual study, we use official translations in various languages.
Your research focuses on T2D. Do you plan to study type 1 diabetes (T1D) as well?
We believe that individuals with T1D also exhibit voice changes over time. However, our current focus is on T2D because our goal is to develop large-scale screening methods. T1D, typically diagnosed in childhood, requires different screening approaches. For now, our research mainly involves adults.
Were there any gender differences in the accuracy of your voice analysis?
Yes, voice studies generally show that women have different vocal signatures from men, partly owing to hormonal fluctuations that affect pitch and tone. Detecting differences between healthy individuals and those with diabetes can sometimes be more challenging in women, depending on the condition. In our study, we achieved about 70% accuracy for women compared with 75% for men.
The EASD results focused on a US-based population. When can we expect data from France?
We started with the US because we could quickly gather a large number of patients. Now, we’re expanding to global and language-specific analyses. French data are certainly a priority, and we’re working on it. We encourage people to participate — it takes only 20 minutes and contributes to innovative research on noninvasive diabetes detection. Participants can sign up at www.colivevoice.org
Dr. Fagherazzi heads the Deep Digital Phenotyping laboratory and the Department of Precision Health at the Luxembourg Institute of Health. His research focuses on integrating new technologies and digital data into diabetes research. He has declared no relevant financial relationships.
This story was translated from the Medscape French edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
An international study, Colive Voice, presented at the European Association for the Study of Diabetes (EASD) 2024 conference, shows that These results “open up possibilities for developing a first-line, noninvasive, and rapid screening tool for T2D, feasible with just a few seconds of voice recording on a smartphone or during consultations,” explained the study’s principal investigator Guy Fagherazzi, PhD, a diabetes epidemiologist at the Luxembourg Institute of Health, in an interview with this news organization.
How did the idea of detecting diabetes through voice come about?
During the COVID-19 pandemic, we began analyzing voice recordings from patients with chronic diseases. We wanted to find solutions to assess people’s health remotely, without physical contact. We quickly realized that this approach could be extended to other diseases. Because my main research focus has always been diabetes, I looked into how voice characteristics might correlate with diabetes. Previous studies had indicated that patients with diabetes have distinct voices compared with the general population, and this insight formed the starting point.
What mechanism could explain why patients with T2D have different voice characteristics?
It’s challenging to pinpoint a single factor that would explain why patients with T2D have different voices from those without diabetes. Several factors are involved.
Some biological mechanisms, especially those affecting the vascular system, influence symptoms in people with metabolic diseases such as diabetes. For example, people with T2D have more frequent cardiorespiratory fatigue. Obesity and overweight are also key factors, as these conditions can slightly alter vocal parameters compared with people of normal weight. Hypertension, common in patients with T2D, adds to the complexity.
Neurologic complications can affect the nerves and muscles involved in voice production, particularly the vocal cords.
Therefore, respiratory fatigue, neuropathies, and other conditions such as dehydration and gastric acid reflux, which are more common in patients with diabetes, can contribute to differences in voice.
These differences might not be noticeable to the human ear. That’s why we often don’t notice the link between voice and diabetes. However, technological advancements in signal processing and artificial intelligence allow us to extract a large amount of information from these subtle variations. By analyzing these small differences, we can detect diabetes with a reasonable degree of accuracy.
In your study, you mention that voice tone can indicate diabetic status. Could you elaborate?
Yes, voice tone can be affected, though it’s a complex, multidimensional phenomenon.
Patients who have had diabetes for 5-10 years, or longer, tend to have a rougher voice than those without diabetes of the same age and gender. In our study, we were able to extract many voice characteristics from the raw audio signal, which is why it’s difficult to isolate one specific factor that stands out.
Is there a difference in voice changes between patients with well-managed diabetes and those whose disease is uncontrolled?
The roughness of the voice tends to increase with the duration of diabetes. It’s more noticeable in people with poorly controlled diabetes. Our hypothesis, based on the results we presented at the EASD conference, is that fluctuations in blood sugar levels, both hypo- and hyperglycemia, may cause short-term changes in the voice. There are also many subtle, rapid changes that could potentially be detected, though we haven’t confirmed this yet. We’re currently conducting additional studies to explore this.
Why did you ask participants to read a passage from the Universal Declaration of Human Rights?
We used a highly standardized approach. Participants completed several recordings, including holding the sound “Aaaaaa” for as long as possible in one breath. They also read a passage, which helps us better distinguish between patients with and those without diabetes. This method works slightly better than other sounds typically used for analyzing diseases. We chose this particular text in the participant’s native language because it’s neutral and doesn’t trigger emotional fluctuations. Because Colive Voice is an international, multilingual study, we use official translations in various languages.
Your research focuses on T2D. Do you plan to study type 1 diabetes (T1D) as well?
We believe that individuals with T1D also exhibit voice changes over time. However, our current focus is on T2D because our goal is to develop large-scale screening methods. T1D, typically diagnosed in childhood, requires different screening approaches. For now, our research mainly involves adults.
Were there any gender differences in the accuracy of your voice analysis?
Yes, voice studies generally show that women have different vocal signatures from men, partly owing to hormonal fluctuations that affect pitch and tone. Detecting differences between healthy individuals and those with diabetes can sometimes be more challenging in women, depending on the condition. In our study, we achieved about 70% accuracy for women compared with 75% for men.
The EASD results focused on a US-based population. When can we expect data from France?
We started with the US because we could quickly gather a large number of patients. Now, we’re expanding to global and language-specific analyses. French data are certainly a priority, and we’re working on it. We encourage people to participate — it takes only 20 minutes and contributes to innovative research on noninvasive diabetes detection. Participants can sign up at www.colivevoice.org
Dr. Fagherazzi heads the Deep Digital Phenotyping laboratory and the Department of Precision Health at the Luxembourg Institute of Health. His research focuses on integrating new technologies and digital data into diabetes research. He has declared no relevant financial relationships.
This story was translated from the Medscape French edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
An international study, Colive Voice, presented at the European Association for the Study of Diabetes (EASD) 2024 conference, shows that These results “open up possibilities for developing a first-line, noninvasive, and rapid screening tool for T2D, feasible with just a few seconds of voice recording on a smartphone or during consultations,” explained the study’s principal investigator Guy Fagherazzi, PhD, a diabetes epidemiologist at the Luxembourg Institute of Health, in an interview with this news organization.
How did the idea of detecting diabetes through voice come about?
During the COVID-19 pandemic, we began analyzing voice recordings from patients with chronic diseases. We wanted to find solutions to assess people’s health remotely, without physical contact. We quickly realized that this approach could be extended to other diseases. Because my main research focus has always been diabetes, I looked into how voice characteristics might correlate with diabetes. Previous studies had indicated that patients with diabetes have distinct voices compared with the general population, and this insight formed the starting point.
What mechanism could explain why patients with T2D have different voice characteristics?
It’s challenging to pinpoint a single factor that would explain why patients with T2D have different voices from those without diabetes. Several factors are involved.
Some biological mechanisms, especially those affecting the vascular system, influence symptoms in people with metabolic diseases such as diabetes. For example, people with T2D have more frequent cardiorespiratory fatigue. Obesity and overweight are also key factors, as these conditions can slightly alter vocal parameters compared with people of normal weight. Hypertension, common in patients with T2D, adds to the complexity.
Neurologic complications can affect the nerves and muscles involved in voice production, particularly the vocal cords.
Therefore, respiratory fatigue, neuropathies, and other conditions such as dehydration and gastric acid reflux, which are more common in patients with diabetes, can contribute to differences in voice.
These differences might not be noticeable to the human ear. That’s why we often don’t notice the link between voice and diabetes. However, technological advancements in signal processing and artificial intelligence allow us to extract a large amount of information from these subtle variations. By analyzing these small differences, we can detect diabetes with a reasonable degree of accuracy.
In your study, you mention that voice tone can indicate diabetic status. Could you elaborate?
Yes, voice tone can be affected, though it’s a complex, multidimensional phenomenon.
Patients who have had diabetes for 5-10 years, or longer, tend to have a rougher voice than those without diabetes of the same age and gender. In our study, we were able to extract many voice characteristics from the raw audio signal, which is why it’s difficult to isolate one specific factor that stands out.
Is there a difference in voice changes between patients with well-managed diabetes and those whose disease is uncontrolled?
The roughness of the voice tends to increase with the duration of diabetes. It’s more noticeable in people with poorly controlled diabetes. Our hypothesis, based on the results we presented at the EASD conference, is that fluctuations in blood sugar levels, both hypo- and hyperglycemia, may cause short-term changes in the voice. There are also many subtle, rapid changes that could potentially be detected, though we haven’t confirmed this yet. We’re currently conducting additional studies to explore this.
Why did you ask participants to read a passage from the Universal Declaration of Human Rights?
We used a highly standardized approach. Participants completed several recordings, including holding the sound “Aaaaaa” for as long as possible in one breath. They also read a passage, which helps us better distinguish between patients with and those without diabetes. This method works slightly better than other sounds typically used for analyzing diseases. We chose this particular text in the participant’s native language because it’s neutral and doesn’t trigger emotional fluctuations. Because Colive Voice is an international, multilingual study, we use official translations in various languages.
Your research focuses on T2D. Do you plan to study type 1 diabetes (T1D) as well?
We believe that individuals with T1D also exhibit voice changes over time. However, our current focus is on T2D because our goal is to develop large-scale screening methods. T1D, typically diagnosed in childhood, requires different screening approaches. For now, our research mainly involves adults.
Were there any gender differences in the accuracy of your voice analysis?
Yes, voice studies generally show that women have different vocal signatures from men, partly owing to hormonal fluctuations that affect pitch and tone. Detecting differences between healthy individuals and those with diabetes can sometimes be more challenging in women, depending on the condition. In our study, we achieved about 70% accuracy for women compared with 75% for men.
The EASD results focused on a US-based population. When can we expect data from France?
We started with the US because we could quickly gather a large number of patients. Now, we’re expanding to global and language-specific analyses. French data are certainly a priority, and we’re working on it. We encourage people to participate — it takes only 20 minutes and contributes to innovative research on noninvasive diabetes detection. Participants can sign up at www.colivevoice.org
Dr. Fagherazzi heads the Deep Digital Phenotyping laboratory and the Department of Precision Health at the Luxembourg Institute of Health. His research focuses on integrating new technologies and digital data into diabetes research. He has declared no relevant financial relationships.
This story was translated from the Medscape French edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
FROM EASD 2024
Cannabis Use Rising in Diabetes: What Do Endos Need to Know?
A recent US prevalence study estimated that 9% adults with diabetes used cannabis in the last month, a 33.7% increase between 2021 and 2022. Nearly half (48.9%) of users were younger than 50 years.
Cannabis use is also increasing sharply among those aged 65 years or older, many of whom have diabetes and other chronic conditions. In this demographic, the perceived risk surrounding regular cannabis use has dropped significantly, even as the data tell another story — that they are particularly at risk from emergency department visits for cannabis poisoning.
As legalization continues and cannabis products proliferate, endocrinologists will likely face more patients of all ages seeking advice about its use. Yet with few evidence-based resources to turn to, endocrinologists advising patients in this area are mostly left fending for themselves.
Evidence ‘Limited’
“The evidence on cannabis is limited mainly because of its scheduling in the United States,” Jay Shubrook, DO, a professor and diabetologist at College of Osteopathic Medicine, Touro University California, in Vallejo, California, told this news organization.
“It was declared to be a schedule I drug in the 1970s, which meant it was ‘dangerous’ and ‘had no medical benefit.’ This made it hard to access and study in human trials.”
That will likely change soon. On May 16, 2024, the US Department of Justice submitted a proposal to move marijuana from a schedule I to a schedule III drug under the Controlled Substances Act, emphasizing its accepted medical use. If approved, the door will open to more investigators seeking to study the effects of cannabis.
Yet, even in Canada, where recreational use has been legal since 2018 and cannabis is sold widely with government support, there are little hard data to guide practice. In 2019, Diabetes Canada issued a position statement on recreational cannabis use in people with type 1 diabetes (T1D) and type 2 diabetes (T2D). It sought to evaluate the effects of cannabis on metabolic factors and diabetes complications, as well as self-management behaviors in those aged 13 years or older.
The authors noted that five of the six studies upon which the statement was based did not consider or report the routes of cannabis administration, which have differing risks. In addition, their recommendations were based on grade D evidence and consensus.
What Patients Are Taking
Cannabis — also known as marijuana, weed, pot, or bud — refers to the dried flowers, leaves, stems, and seeds of the cannabis plant. The plant contains more than 100 compounds, including tetrahydrocannabinol (THC), which is responsible for the euphoric “high,” and other active compounds, including cannabidiol (CBD), which by itself is not mind-altering.
Cannabis can be ingested in several ways. It can be smoked (ie, joints, blunts, pipes, and water pipes), ingested in edible form (mixed or infused into foods), and inhaled using electronic vaporizing devices (ie, e-cigarettes or vape pens).
Compounds in cannabis can also be extracted to make oils and concentrates that can be vaped or inhaled. Smoking oils, concentrates, and extracts from the cannabis plant, known as “dabbing,” are on the rise in the United States.
There are no validated or standard dosage recommendations for cannabis strains and formulations, THC/CBD ratios, or modes of administration. Therefore, the Canadian Pharmacists Association prepared a guide for finding a safe and effective dose for medical purposes. GoodRx, a website with information on prescription drug prices, says that larger doses of THC pose greater risks, noting that the potency of cannabis has increased from 4% in 1995 to about 14% in 2019.
Potential Risks and Benefits: Canadian and US Perspectives
Health and safety risks vary with each of the different ways of using cannabis for individuals with and without diabetes, depending on a host of patient- and product-specific factors.
In a recent article proposing a “THC unit” for Canada’s legal cannabis market, researchers reported that consumers lack familiarity with THC levels, don’t know what constitutes a “low” or “high” THC amount, have trouble dosing, overconsume, and commonly experience adverse health events from cannabis use.
A recent study suggested that most clinicians are similarly uninformed, with “a lack of knowledge of beneficial effects, adverse effects, and of how to advise patients,” even for medical cannabis.
Diabetes Canada takes a stab at summarizing what’s known with respect to cannabis and diabetes, stating that:
“Research on recreational cannabis use suggests it may negatively impact diabetes metabolic factors and self-management behaviors. The safety of recreational cannabis use has not been demonstrated, whereas regular cannabis use is associated with worsening glycemic control, more diabetes-related complications, and poorer self-care behaviors, such as adequate glucose monitoring, adherence to medications, and compliance with dietary and physical activity recommendations for people living with both type 1 and type 2 diabetes.”
The American Diabetes Association’s information on cannabis consists of a patient-oriented article on CBD oil. The article stated:
“There’s a lot of hype surrounding CBD oil and diabetes. There is no noticeable effect on blood glucose (blood sugar) or insulin levels in people with type 2 diabetes. Researchers continue to study the effects of CBD on diabetes in animal studies.”
It concludes that:
“Although many claims continue to be made about CBD oil, there is little evidence of any benefit. It’s certainly not an alternative to traditional diabetes management. The safety of CBD is also unknown — it may have dangerous side effects that we won’t know about unless further research is done.”
A Roundup of Recent Studies
A smattering of recent studies have touched on various aspects of cannabis consumption and diabetes.
Angela Bryan, PhD, professor and co-director of CUChange at the University of Colorado Boulder, has been evaluating cannabis use in young adults (ages 21-40 years) in the SONIC study. Dr. Bryan reported at the American Diabetes Association (ADA) 84th Scientific Sessions that cannabis users were more likely to have a lower body mass index and less likely to develop T2D. Furthermore, chronic cannabis users were less likely to have measures of inflammation and no loss of insulin sensitivity.
Another study by Dr. Bryan’s group found that CBD-dominant forms of cannabis were associated with acute tension reduction, which might lead to longer-term reductions in anxiety. Bryan said the findings could be relevant in the context of diabetes distress.
Similarly positive results were found in a 15-week, double-blind, randomized, placebo-controlled, parallel-group study of THC/CBD spray for neuropathic pain among treatment-resistant patients. The investigators reported that “clinically important improvements” were seen in pain, sleep quality, and subjective impressions of pain. Another small study of inhaled cannabis in treatment-refractory patients found a dose-dependent reduction in diabetic peripheral neuropathy pain.
Findings from a 9-year longitudinal study of approximately 18,000 Swedish men and women suggested no association between cannabis and subsequent T2D development after controlling for age, although these authors also called for longer follow-up and more detailed information about cannabis use to make “more robust” conclusions.
On the other side of the spectrum, a “rapid” review of recreational cannabis use in people with T1D and T2D found that recreational cannabis use may negatively impact diabetes metabolic factors and self-management behaviors and may increase risks for peripheral arterial occlusion, myocardial infarction, and renal disease. However, the authors cautioned that more robust research is needed to confirm the potential impact of cannabis on diabetes.
How to Advise Patients
When Dr. Shubrook was working with patients with diabetes in his family medicine practice in Ohio, cannabis wasn’t legal.
“’Don’t ask, don’t tell’ was the way we handled it then,” he said.
By contrast, in California, where he’s currently located, “it’s pretty well accepted and legal, and patients volunteer information about use, even if it’s recreational,” he said. “Realizing this was something we could talk about was really eye-opening to me.”
Talking to patients about cannabis use is a “20-minute conversation that details what they’re doing,” he said. He proceeds by asking questions: Are you using for recreational or medicinal purposes? What do you take? What do you take it for? Does it work?
“People will tell you,” Dr. Shubrook said. “They know exactly what it works or doesn’t work for and how it affects their glucose control, which in most cases is only minimally.”
He tells patients he would prefer they don’t inhale cannabis, given the risks posed to the lungs.
“Edibles may have a slower onset of effect, but depending on what they’re adding it to, glucose might be affected,” he noted. “And I have seen that chronic use can lead to hyperemesis syndrome.”
Overall, he said, “Take the time to talk to your patients about cannabis — it will allow them to be honest with you, and you can improve the specificity and safety of its use. If cannabis is legal in your state, encourage people to go to legal dispensaries, which will reduce the risk of it being laced with another drug that could increase the danger of use.”
A recent US prevalence study found that people with diabetes who use cannabis likely engage in other substance and psychoactive substance use, including tobacco use, binge drinking, and misuse of opioids and stimulants.
“Use of these additional substances could further exacerbate the health risks associated with diabetes and also emphasizes the importance of addressing polysubstance use among adults with diabetes,” the study’s author Benjamin H. Han, MD, Division of Geriatrics, Gerontology and Palliative Care, Department of Medicine, US San Diego School of Medicine in La Jolla, California, told this news organization.
“We were surprised at how strong the associations were, especially with use of substances that can increase cardiovascular risk,” Dr. Han added. “And given the strong association we found between cannabis use and use of other psychoactive substances in diabetes, clinicians must screen all their patients for psychoactive substance use.”
Diabetes Canada’s position paper states that despite the limited evidence, “there were sufficient data to begin developing recommendations for type 1 and type 2 diabetes about education, counseling, and management related to recreational cannabis use.”
Their recommendations include the following:
- Healthcare professionals should engage their patients in discussions about substance use on a regular basis, with a nonjudgmental approach.
- The use of recreational cannabis is not recommended for adolescents and adults with diabetes.
- People with T1D should avoid recreational cannabis use because of the increased risk for diabetic ketoacidosis.
- For adults with T1D or T2D who intend to use cannabis recreationally, individualized assessment and counseling should be offered to inform them of the general risks of cannabis, with a focus on harm reduction and reduction of the risk for potential adverse effects on diabetes management and complications.
- People with T1D or T2D should be offered education on and encouraged to read public information available through resources from various Canadian health authorities about the general risks of cannabis use to reduce the risk for nondiabetes-related adverse effects of cannabis consumption.
Of note, in 2018, the Canadian government produced an exhaustive compendium of information on cannabis for healthcare professionals that includes information relevant to managing patients with diabetes.
Dr. Shubrook and Dr. Han reported no competing interests.
A version of this article appeared on Medscape.com.
A recent US prevalence study estimated that 9% adults with diabetes used cannabis in the last month, a 33.7% increase between 2021 and 2022. Nearly half (48.9%) of users were younger than 50 years.
Cannabis use is also increasing sharply among those aged 65 years or older, many of whom have diabetes and other chronic conditions. In this demographic, the perceived risk surrounding regular cannabis use has dropped significantly, even as the data tell another story — that they are particularly at risk from emergency department visits for cannabis poisoning.
As legalization continues and cannabis products proliferate, endocrinologists will likely face more patients of all ages seeking advice about its use. Yet with few evidence-based resources to turn to, endocrinologists advising patients in this area are mostly left fending for themselves.
Evidence ‘Limited’
“The evidence on cannabis is limited mainly because of its scheduling in the United States,” Jay Shubrook, DO, a professor and diabetologist at College of Osteopathic Medicine, Touro University California, in Vallejo, California, told this news organization.
“It was declared to be a schedule I drug in the 1970s, which meant it was ‘dangerous’ and ‘had no medical benefit.’ This made it hard to access and study in human trials.”
That will likely change soon. On May 16, 2024, the US Department of Justice submitted a proposal to move marijuana from a schedule I to a schedule III drug under the Controlled Substances Act, emphasizing its accepted medical use. If approved, the door will open to more investigators seeking to study the effects of cannabis.
Yet, even in Canada, where recreational use has been legal since 2018 and cannabis is sold widely with government support, there are little hard data to guide practice. In 2019, Diabetes Canada issued a position statement on recreational cannabis use in people with type 1 diabetes (T1D) and type 2 diabetes (T2D). It sought to evaluate the effects of cannabis on metabolic factors and diabetes complications, as well as self-management behaviors in those aged 13 years or older.
The authors noted that five of the six studies upon which the statement was based did not consider or report the routes of cannabis administration, which have differing risks. In addition, their recommendations were based on grade D evidence and consensus.
What Patients Are Taking
Cannabis — also known as marijuana, weed, pot, or bud — refers to the dried flowers, leaves, stems, and seeds of the cannabis plant. The plant contains more than 100 compounds, including tetrahydrocannabinol (THC), which is responsible for the euphoric “high,” and other active compounds, including cannabidiol (CBD), which by itself is not mind-altering.
Cannabis can be ingested in several ways. It can be smoked (ie, joints, blunts, pipes, and water pipes), ingested in edible form (mixed or infused into foods), and inhaled using electronic vaporizing devices (ie, e-cigarettes or vape pens).
Compounds in cannabis can also be extracted to make oils and concentrates that can be vaped or inhaled. Smoking oils, concentrates, and extracts from the cannabis plant, known as “dabbing,” are on the rise in the United States.
There are no validated or standard dosage recommendations for cannabis strains and formulations, THC/CBD ratios, or modes of administration. Therefore, the Canadian Pharmacists Association prepared a guide for finding a safe and effective dose for medical purposes. GoodRx, a website with information on prescription drug prices, says that larger doses of THC pose greater risks, noting that the potency of cannabis has increased from 4% in 1995 to about 14% in 2019.
Potential Risks and Benefits: Canadian and US Perspectives
Health and safety risks vary with each of the different ways of using cannabis for individuals with and without diabetes, depending on a host of patient- and product-specific factors.
In a recent article proposing a “THC unit” for Canada’s legal cannabis market, researchers reported that consumers lack familiarity with THC levels, don’t know what constitutes a “low” or “high” THC amount, have trouble dosing, overconsume, and commonly experience adverse health events from cannabis use.
A recent study suggested that most clinicians are similarly uninformed, with “a lack of knowledge of beneficial effects, adverse effects, and of how to advise patients,” even for medical cannabis.
Diabetes Canada takes a stab at summarizing what’s known with respect to cannabis and diabetes, stating that:
“Research on recreational cannabis use suggests it may negatively impact diabetes metabolic factors and self-management behaviors. The safety of recreational cannabis use has not been demonstrated, whereas regular cannabis use is associated with worsening glycemic control, more diabetes-related complications, and poorer self-care behaviors, such as adequate glucose monitoring, adherence to medications, and compliance with dietary and physical activity recommendations for people living with both type 1 and type 2 diabetes.”
The American Diabetes Association’s information on cannabis consists of a patient-oriented article on CBD oil. The article stated:
“There’s a lot of hype surrounding CBD oil and diabetes. There is no noticeable effect on blood glucose (blood sugar) or insulin levels in people with type 2 diabetes. Researchers continue to study the effects of CBD on diabetes in animal studies.”
It concludes that:
“Although many claims continue to be made about CBD oil, there is little evidence of any benefit. It’s certainly not an alternative to traditional diabetes management. The safety of CBD is also unknown — it may have dangerous side effects that we won’t know about unless further research is done.”
A Roundup of Recent Studies
A smattering of recent studies have touched on various aspects of cannabis consumption and diabetes.
Angela Bryan, PhD, professor and co-director of CUChange at the University of Colorado Boulder, has been evaluating cannabis use in young adults (ages 21-40 years) in the SONIC study. Dr. Bryan reported at the American Diabetes Association (ADA) 84th Scientific Sessions that cannabis users were more likely to have a lower body mass index and less likely to develop T2D. Furthermore, chronic cannabis users were less likely to have measures of inflammation and no loss of insulin sensitivity.
Another study by Dr. Bryan’s group found that CBD-dominant forms of cannabis were associated with acute tension reduction, which might lead to longer-term reductions in anxiety. Bryan said the findings could be relevant in the context of diabetes distress.
Similarly positive results were found in a 15-week, double-blind, randomized, placebo-controlled, parallel-group study of THC/CBD spray for neuropathic pain among treatment-resistant patients. The investigators reported that “clinically important improvements” were seen in pain, sleep quality, and subjective impressions of pain. Another small study of inhaled cannabis in treatment-refractory patients found a dose-dependent reduction in diabetic peripheral neuropathy pain.
Findings from a 9-year longitudinal study of approximately 18,000 Swedish men and women suggested no association between cannabis and subsequent T2D development after controlling for age, although these authors also called for longer follow-up and more detailed information about cannabis use to make “more robust” conclusions.
On the other side of the spectrum, a “rapid” review of recreational cannabis use in people with T1D and T2D found that recreational cannabis use may negatively impact diabetes metabolic factors and self-management behaviors and may increase risks for peripheral arterial occlusion, myocardial infarction, and renal disease. However, the authors cautioned that more robust research is needed to confirm the potential impact of cannabis on diabetes.
How to Advise Patients
When Dr. Shubrook was working with patients with diabetes in his family medicine practice in Ohio, cannabis wasn’t legal.
“’Don’t ask, don’t tell’ was the way we handled it then,” he said.
By contrast, in California, where he’s currently located, “it’s pretty well accepted and legal, and patients volunteer information about use, even if it’s recreational,” he said. “Realizing this was something we could talk about was really eye-opening to me.”
Talking to patients about cannabis use is a “20-minute conversation that details what they’re doing,” he said. He proceeds by asking questions: Are you using for recreational or medicinal purposes? What do you take? What do you take it for? Does it work?
“People will tell you,” Dr. Shubrook said. “They know exactly what it works or doesn’t work for and how it affects their glucose control, which in most cases is only minimally.”
He tells patients he would prefer they don’t inhale cannabis, given the risks posed to the lungs.
“Edibles may have a slower onset of effect, but depending on what they’re adding it to, glucose might be affected,” he noted. “And I have seen that chronic use can lead to hyperemesis syndrome.”
Overall, he said, “Take the time to talk to your patients about cannabis — it will allow them to be honest with you, and you can improve the specificity and safety of its use. If cannabis is legal in your state, encourage people to go to legal dispensaries, which will reduce the risk of it being laced with another drug that could increase the danger of use.”
A recent US prevalence study found that people with diabetes who use cannabis likely engage in other substance and psychoactive substance use, including tobacco use, binge drinking, and misuse of opioids and stimulants.
“Use of these additional substances could further exacerbate the health risks associated with diabetes and also emphasizes the importance of addressing polysubstance use among adults with diabetes,” the study’s author Benjamin H. Han, MD, Division of Geriatrics, Gerontology and Palliative Care, Department of Medicine, US San Diego School of Medicine in La Jolla, California, told this news organization.
“We were surprised at how strong the associations were, especially with use of substances that can increase cardiovascular risk,” Dr. Han added. “And given the strong association we found between cannabis use and use of other psychoactive substances in diabetes, clinicians must screen all their patients for psychoactive substance use.”
Diabetes Canada’s position paper states that despite the limited evidence, “there were sufficient data to begin developing recommendations for type 1 and type 2 diabetes about education, counseling, and management related to recreational cannabis use.”
Their recommendations include the following:
- Healthcare professionals should engage their patients in discussions about substance use on a regular basis, with a nonjudgmental approach.
- The use of recreational cannabis is not recommended for adolescents and adults with diabetes.
- People with T1D should avoid recreational cannabis use because of the increased risk for diabetic ketoacidosis.
- For adults with T1D or T2D who intend to use cannabis recreationally, individualized assessment and counseling should be offered to inform them of the general risks of cannabis, with a focus on harm reduction and reduction of the risk for potential adverse effects on diabetes management and complications.
- People with T1D or T2D should be offered education on and encouraged to read public information available through resources from various Canadian health authorities about the general risks of cannabis use to reduce the risk for nondiabetes-related adverse effects of cannabis consumption.
Of note, in 2018, the Canadian government produced an exhaustive compendium of information on cannabis for healthcare professionals that includes information relevant to managing patients with diabetes.
Dr. Shubrook and Dr. Han reported no competing interests.
A version of this article appeared on Medscape.com.
A recent US prevalence study estimated that 9% adults with diabetes used cannabis in the last month, a 33.7% increase between 2021 and 2022. Nearly half (48.9%) of users were younger than 50 years.
Cannabis use is also increasing sharply among those aged 65 years or older, many of whom have diabetes and other chronic conditions. In this demographic, the perceived risk surrounding regular cannabis use has dropped significantly, even as the data tell another story — that they are particularly at risk from emergency department visits for cannabis poisoning.
As legalization continues and cannabis products proliferate, endocrinologists will likely face more patients of all ages seeking advice about its use. Yet with few evidence-based resources to turn to, endocrinologists advising patients in this area are mostly left fending for themselves.
Evidence ‘Limited’
“The evidence on cannabis is limited mainly because of its scheduling in the United States,” Jay Shubrook, DO, a professor and diabetologist at College of Osteopathic Medicine, Touro University California, in Vallejo, California, told this news organization.
“It was declared to be a schedule I drug in the 1970s, which meant it was ‘dangerous’ and ‘had no medical benefit.’ This made it hard to access and study in human trials.”
That will likely change soon. On May 16, 2024, the US Department of Justice submitted a proposal to move marijuana from a schedule I to a schedule III drug under the Controlled Substances Act, emphasizing its accepted medical use. If approved, the door will open to more investigators seeking to study the effects of cannabis.
Yet, even in Canada, where recreational use has been legal since 2018 and cannabis is sold widely with government support, there are little hard data to guide practice. In 2019, Diabetes Canada issued a position statement on recreational cannabis use in people with type 1 diabetes (T1D) and type 2 diabetes (T2D). It sought to evaluate the effects of cannabis on metabolic factors and diabetes complications, as well as self-management behaviors in those aged 13 years or older.
The authors noted that five of the six studies upon which the statement was based did not consider or report the routes of cannabis administration, which have differing risks. In addition, their recommendations were based on grade D evidence and consensus.
What Patients Are Taking
Cannabis — also known as marijuana, weed, pot, or bud — refers to the dried flowers, leaves, stems, and seeds of the cannabis plant. The plant contains more than 100 compounds, including tetrahydrocannabinol (THC), which is responsible for the euphoric “high,” and other active compounds, including cannabidiol (CBD), which by itself is not mind-altering.
Cannabis can be ingested in several ways. It can be smoked (ie, joints, blunts, pipes, and water pipes), ingested in edible form (mixed or infused into foods), and inhaled using electronic vaporizing devices (ie, e-cigarettes or vape pens).
Compounds in cannabis can also be extracted to make oils and concentrates that can be vaped or inhaled. Smoking oils, concentrates, and extracts from the cannabis plant, known as “dabbing,” are on the rise in the United States.
There are no validated or standard dosage recommendations for cannabis strains and formulations, THC/CBD ratios, or modes of administration. Therefore, the Canadian Pharmacists Association prepared a guide for finding a safe and effective dose for medical purposes. GoodRx, a website with information on prescription drug prices, says that larger doses of THC pose greater risks, noting that the potency of cannabis has increased from 4% in 1995 to about 14% in 2019.
Potential Risks and Benefits: Canadian and US Perspectives
Health and safety risks vary with each of the different ways of using cannabis for individuals with and without diabetes, depending on a host of patient- and product-specific factors.
In a recent article proposing a “THC unit” for Canada’s legal cannabis market, researchers reported that consumers lack familiarity with THC levels, don’t know what constitutes a “low” or “high” THC amount, have trouble dosing, overconsume, and commonly experience adverse health events from cannabis use.
A recent study suggested that most clinicians are similarly uninformed, with “a lack of knowledge of beneficial effects, adverse effects, and of how to advise patients,” even for medical cannabis.
Diabetes Canada takes a stab at summarizing what’s known with respect to cannabis and diabetes, stating that:
“Research on recreational cannabis use suggests it may negatively impact diabetes metabolic factors and self-management behaviors. The safety of recreational cannabis use has not been demonstrated, whereas regular cannabis use is associated with worsening glycemic control, more diabetes-related complications, and poorer self-care behaviors, such as adequate glucose monitoring, adherence to medications, and compliance with dietary and physical activity recommendations for people living with both type 1 and type 2 diabetes.”
The American Diabetes Association’s information on cannabis consists of a patient-oriented article on CBD oil. The article stated:
“There’s a lot of hype surrounding CBD oil and diabetes. There is no noticeable effect on blood glucose (blood sugar) or insulin levels in people with type 2 diabetes. Researchers continue to study the effects of CBD on diabetes in animal studies.”
It concludes that:
“Although many claims continue to be made about CBD oil, there is little evidence of any benefit. It’s certainly not an alternative to traditional diabetes management. The safety of CBD is also unknown — it may have dangerous side effects that we won’t know about unless further research is done.”
A Roundup of Recent Studies
A smattering of recent studies have touched on various aspects of cannabis consumption and diabetes.
Angela Bryan, PhD, professor and co-director of CUChange at the University of Colorado Boulder, has been evaluating cannabis use in young adults (ages 21-40 years) in the SONIC study. Dr. Bryan reported at the American Diabetes Association (ADA) 84th Scientific Sessions that cannabis users were more likely to have a lower body mass index and less likely to develop T2D. Furthermore, chronic cannabis users were less likely to have measures of inflammation and no loss of insulin sensitivity.
Another study by Dr. Bryan’s group found that CBD-dominant forms of cannabis were associated with acute tension reduction, which might lead to longer-term reductions in anxiety. Bryan said the findings could be relevant in the context of diabetes distress.
Similarly positive results were found in a 15-week, double-blind, randomized, placebo-controlled, parallel-group study of THC/CBD spray for neuropathic pain among treatment-resistant patients. The investigators reported that “clinically important improvements” were seen in pain, sleep quality, and subjective impressions of pain. Another small study of inhaled cannabis in treatment-refractory patients found a dose-dependent reduction in diabetic peripheral neuropathy pain.
Findings from a 9-year longitudinal study of approximately 18,000 Swedish men and women suggested no association between cannabis and subsequent T2D development after controlling for age, although these authors also called for longer follow-up and more detailed information about cannabis use to make “more robust” conclusions.
On the other side of the spectrum, a “rapid” review of recreational cannabis use in people with T1D and T2D found that recreational cannabis use may negatively impact diabetes metabolic factors and self-management behaviors and may increase risks for peripheral arterial occlusion, myocardial infarction, and renal disease. However, the authors cautioned that more robust research is needed to confirm the potential impact of cannabis on diabetes.
How to Advise Patients
When Dr. Shubrook was working with patients with diabetes in his family medicine practice in Ohio, cannabis wasn’t legal.
“’Don’t ask, don’t tell’ was the way we handled it then,” he said.
By contrast, in California, where he’s currently located, “it’s pretty well accepted and legal, and patients volunteer information about use, even if it’s recreational,” he said. “Realizing this was something we could talk about was really eye-opening to me.”
Talking to patients about cannabis use is a “20-minute conversation that details what they’re doing,” he said. He proceeds by asking questions: Are you using for recreational or medicinal purposes? What do you take? What do you take it for? Does it work?
“People will tell you,” Dr. Shubrook said. “They know exactly what it works or doesn’t work for and how it affects their glucose control, which in most cases is only minimally.”
He tells patients he would prefer they don’t inhale cannabis, given the risks posed to the lungs.
“Edibles may have a slower onset of effect, but depending on what they’re adding it to, glucose might be affected,” he noted. “And I have seen that chronic use can lead to hyperemesis syndrome.”
Overall, he said, “Take the time to talk to your patients about cannabis — it will allow them to be honest with you, and you can improve the specificity and safety of its use. If cannabis is legal in your state, encourage people to go to legal dispensaries, which will reduce the risk of it being laced with another drug that could increase the danger of use.”
A recent US prevalence study found that people with diabetes who use cannabis likely engage in other substance and psychoactive substance use, including tobacco use, binge drinking, and misuse of opioids and stimulants.
“Use of these additional substances could further exacerbate the health risks associated with diabetes and also emphasizes the importance of addressing polysubstance use among adults with diabetes,” the study’s author Benjamin H. Han, MD, Division of Geriatrics, Gerontology and Palliative Care, Department of Medicine, US San Diego School of Medicine in La Jolla, California, told this news organization.
“We were surprised at how strong the associations were, especially with use of substances that can increase cardiovascular risk,” Dr. Han added. “And given the strong association we found between cannabis use and use of other psychoactive substances in diabetes, clinicians must screen all their patients for psychoactive substance use.”
Diabetes Canada’s position paper states that despite the limited evidence, “there were sufficient data to begin developing recommendations for type 1 and type 2 diabetes about education, counseling, and management related to recreational cannabis use.”
Their recommendations include the following:
- Healthcare professionals should engage their patients in discussions about substance use on a regular basis, with a nonjudgmental approach.
- The use of recreational cannabis is not recommended for adolescents and adults with diabetes.
- People with T1D should avoid recreational cannabis use because of the increased risk for diabetic ketoacidosis.
- For adults with T1D or T2D who intend to use cannabis recreationally, individualized assessment and counseling should be offered to inform them of the general risks of cannabis, with a focus on harm reduction and reduction of the risk for potential adverse effects on diabetes management and complications.
- People with T1D or T2D should be offered education on and encouraged to read public information available through resources from various Canadian health authorities about the general risks of cannabis use to reduce the risk for nondiabetes-related adverse effects of cannabis consumption.
Of note, in 2018, the Canadian government produced an exhaustive compendium of information on cannabis for healthcare professionals that includes information relevant to managing patients with diabetes.
Dr. Shubrook and Dr. Han reported no competing interests.
A version of this article appeared on Medscape.com.
First Patient-Derived Stem Cell Transplant a Success in T1D
The chemically induced pluripotent stem cell–derived islets came from the somatic cells of the patient, a 25-year-old woman who had lived for 11 years with unstable T1D with less than 50% time-in-target glucose range despite intensive insulin therapy. By 1 year following the transplantation of the cells into her abdomen, her glucose levels were nearly 100% in range, and her hemoglobin A1c had come down from 7.4%-8.0% to nondiabetic range (~5%).
Of note, she was already under immunosuppression for a prior liver transplant and remained on it throughout. There were no major safety concerns.
“We are very encouraged by the positive clinical findings seen in this first patient using this combination of technologies. These findings set a strong foundation for further development of stem cell–derived islet transplantation as a feasible treatment modality for diabetes,” study authors Soon Yi Liew, PhD, and Hongkui Deng, PhD, both of Peking University Health Science Center, Beijing, China, told this news organization in an email. Dr. Deng, the lead author, is the director of the university’s Institute of Stem Cell Research.
The findings were published in Cell.
What’s New With This Approach?
The use of the patient’s own cells is one of several ways in which this approach differs from other ongoing efforts in treating T1D with pluripotent stem cell–derived islets, such as those of the companies Vertex and Sernova, Dr. Liew and Dr. Deng explained.
Another difference is that “the patient-specific stem cell–derived islets used in this study were produced from induced pluripotent stem cells generated using chemical reprogramming, which is a nontransgenic approach to inducing pluripotent stem cells from somatic cells that uses only small molecules, different from the conventional method of viral transduction of transcription factors. ... Employing small molecules as reprogramming factors provides a greater degree of control — small molecules have defined structures easily manufactured and standardized, are not genome integrating, and are cost effective,” Dr. Liew and Dr. Deng said.
A third difference, they noted, is the placement of the stem cell–derived islets underneath the abdominal anterior rectus sheath of the patient, as opposed to the more commonly used hepatic portal vein. In addition to better ease of visualization, prior evidence suggested that this approach could lead to an improved engraftment and graft function and could circumvent graft loss from blood-mediated inflammatory responses associated with the liver site.
Moreover, they added, “to our knowledge, the rapidity with which insulin-independence was achieved post transplantation of stem cell–derived islets, 75 days post-transplantation, is also a first.”
Immunosuppression Remains a Challenge
Asked to comment, David M. Harlan, MD, the William and Doris Krupp professor of medicine and codirector of the Diabetes Center of Excellence at the University of Massachusetts Chan Medical School, Worcester, told this news organization, “on the one hand, it seems like a great breakthrough that you could take each individual cells and use those to make islets, but ... that process takes a long time, is very, very expensive, and then the T1D recipient still needs to be immunosuppressed. From a business point of view, I just don’t see it as getting any legs.”
Dr. Harlan, who had been involved in the islet transplantation field for several decades, pointed out that the additional autoimmunity of T1D poses a challenge beyond that of the body’s immune reaction to foreign tissue. “Because transplants have been around since the 1950s, we know a lot about how to prevent allogeneic rejection, from one person to another, but we know very little about how to prevent autoimmunity, so that’s still a very difficult nut to crack. I actually think the major effort should be focused on making the beta cells more hardy [via genetic modification] as opposed to focusing on the immune system. And there’s a lot of data to support that now, and that’s what we’re working on.”
Indeed, Dr. Liew and Dr. Deng said, “New immunomodulatory strategies to address graft longevity without immunosuppression remain to be established and tested. With reports of therapeutic efficacy of stem cell–derived islet transplantation such as with our study, stem cell–derived therapy without need for immunosuppression would be a meaningful next step in the treatment of this disease.”
The team has now performed the same procedure in two more patients and will report their data “in due course.”
Dr. Liew had no disclosures. Dr. Deng is a scientific adviser at Hangzhou Reprogenix Bioscience. Two coauthors are employees of Hangzhou Reprogenix Bioscience. Another is a former employee of Hangzhou Reprogenix Bioscience and is now affiliated with the Hangzhou Institute of Medicine, Chinese Academy of Sciences. Four coauthors have patent applications related to this work. Dr. Harlan is chief scientific officer and cofounder of Stability Health. He had no other disclosures.
A version of this article first appeared on Medscape.com.
The chemically induced pluripotent stem cell–derived islets came from the somatic cells of the patient, a 25-year-old woman who had lived for 11 years with unstable T1D with less than 50% time-in-target glucose range despite intensive insulin therapy. By 1 year following the transplantation of the cells into her abdomen, her glucose levels were nearly 100% in range, and her hemoglobin A1c had come down from 7.4%-8.0% to nondiabetic range (~5%).
Of note, she was already under immunosuppression for a prior liver transplant and remained on it throughout. There were no major safety concerns.
“We are very encouraged by the positive clinical findings seen in this first patient using this combination of technologies. These findings set a strong foundation for further development of stem cell–derived islet transplantation as a feasible treatment modality for diabetes,” study authors Soon Yi Liew, PhD, and Hongkui Deng, PhD, both of Peking University Health Science Center, Beijing, China, told this news organization in an email. Dr. Deng, the lead author, is the director of the university’s Institute of Stem Cell Research.
The findings were published in Cell.
What’s New With This Approach?
The use of the patient’s own cells is one of several ways in which this approach differs from other ongoing efforts in treating T1D with pluripotent stem cell–derived islets, such as those of the companies Vertex and Sernova, Dr. Liew and Dr. Deng explained.
Another difference is that “the patient-specific stem cell–derived islets used in this study were produced from induced pluripotent stem cells generated using chemical reprogramming, which is a nontransgenic approach to inducing pluripotent stem cells from somatic cells that uses only small molecules, different from the conventional method of viral transduction of transcription factors. ... Employing small molecules as reprogramming factors provides a greater degree of control — small molecules have defined structures easily manufactured and standardized, are not genome integrating, and are cost effective,” Dr. Liew and Dr. Deng said.
A third difference, they noted, is the placement of the stem cell–derived islets underneath the abdominal anterior rectus sheath of the patient, as opposed to the more commonly used hepatic portal vein. In addition to better ease of visualization, prior evidence suggested that this approach could lead to an improved engraftment and graft function and could circumvent graft loss from blood-mediated inflammatory responses associated with the liver site.
Moreover, they added, “to our knowledge, the rapidity with which insulin-independence was achieved post transplantation of stem cell–derived islets, 75 days post-transplantation, is also a first.”
Immunosuppression Remains a Challenge
Asked to comment, David M. Harlan, MD, the William and Doris Krupp professor of medicine and codirector of the Diabetes Center of Excellence at the University of Massachusetts Chan Medical School, Worcester, told this news organization, “on the one hand, it seems like a great breakthrough that you could take each individual cells and use those to make islets, but ... that process takes a long time, is very, very expensive, and then the T1D recipient still needs to be immunosuppressed. From a business point of view, I just don’t see it as getting any legs.”
Dr. Harlan, who had been involved in the islet transplantation field for several decades, pointed out that the additional autoimmunity of T1D poses a challenge beyond that of the body’s immune reaction to foreign tissue. “Because transplants have been around since the 1950s, we know a lot about how to prevent allogeneic rejection, from one person to another, but we know very little about how to prevent autoimmunity, so that’s still a very difficult nut to crack. I actually think the major effort should be focused on making the beta cells more hardy [via genetic modification] as opposed to focusing on the immune system. And there’s a lot of data to support that now, and that’s what we’re working on.”
Indeed, Dr. Liew and Dr. Deng said, “New immunomodulatory strategies to address graft longevity without immunosuppression remain to be established and tested. With reports of therapeutic efficacy of stem cell–derived islet transplantation such as with our study, stem cell–derived therapy without need for immunosuppression would be a meaningful next step in the treatment of this disease.”
The team has now performed the same procedure in two more patients and will report their data “in due course.”
Dr. Liew had no disclosures. Dr. Deng is a scientific adviser at Hangzhou Reprogenix Bioscience. Two coauthors are employees of Hangzhou Reprogenix Bioscience. Another is a former employee of Hangzhou Reprogenix Bioscience and is now affiliated with the Hangzhou Institute of Medicine, Chinese Academy of Sciences. Four coauthors have patent applications related to this work. Dr. Harlan is chief scientific officer and cofounder of Stability Health. He had no other disclosures.
A version of this article first appeared on Medscape.com.
The chemically induced pluripotent stem cell–derived islets came from the somatic cells of the patient, a 25-year-old woman who had lived for 11 years with unstable T1D with less than 50% time-in-target glucose range despite intensive insulin therapy. By 1 year following the transplantation of the cells into her abdomen, her glucose levels were nearly 100% in range, and her hemoglobin A1c had come down from 7.4%-8.0% to nondiabetic range (~5%).
Of note, she was already under immunosuppression for a prior liver transplant and remained on it throughout. There were no major safety concerns.
“We are very encouraged by the positive clinical findings seen in this first patient using this combination of technologies. These findings set a strong foundation for further development of stem cell–derived islet transplantation as a feasible treatment modality for diabetes,” study authors Soon Yi Liew, PhD, and Hongkui Deng, PhD, both of Peking University Health Science Center, Beijing, China, told this news organization in an email. Dr. Deng, the lead author, is the director of the university’s Institute of Stem Cell Research.
The findings were published in Cell.
What’s New With This Approach?
The use of the patient’s own cells is one of several ways in which this approach differs from other ongoing efforts in treating T1D with pluripotent stem cell–derived islets, such as those of the companies Vertex and Sernova, Dr. Liew and Dr. Deng explained.
Another difference is that “the patient-specific stem cell–derived islets used in this study were produced from induced pluripotent stem cells generated using chemical reprogramming, which is a nontransgenic approach to inducing pluripotent stem cells from somatic cells that uses only small molecules, different from the conventional method of viral transduction of transcription factors. ... Employing small molecules as reprogramming factors provides a greater degree of control — small molecules have defined structures easily manufactured and standardized, are not genome integrating, and are cost effective,” Dr. Liew and Dr. Deng said.
A third difference, they noted, is the placement of the stem cell–derived islets underneath the abdominal anterior rectus sheath of the patient, as opposed to the more commonly used hepatic portal vein. In addition to better ease of visualization, prior evidence suggested that this approach could lead to an improved engraftment and graft function and could circumvent graft loss from blood-mediated inflammatory responses associated with the liver site.
Moreover, they added, “to our knowledge, the rapidity with which insulin-independence was achieved post transplantation of stem cell–derived islets, 75 days post-transplantation, is also a first.”
Immunosuppression Remains a Challenge
Asked to comment, David M. Harlan, MD, the William and Doris Krupp professor of medicine and codirector of the Diabetes Center of Excellence at the University of Massachusetts Chan Medical School, Worcester, told this news organization, “on the one hand, it seems like a great breakthrough that you could take each individual cells and use those to make islets, but ... that process takes a long time, is very, very expensive, and then the T1D recipient still needs to be immunosuppressed. From a business point of view, I just don’t see it as getting any legs.”
Dr. Harlan, who had been involved in the islet transplantation field for several decades, pointed out that the additional autoimmunity of T1D poses a challenge beyond that of the body’s immune reaction to foreign tissue. “Because transplants have been around since the 1950s, we know a lot about how to prevent allogeneic rejection, from one person to another, but we know very little about how to prevent autoimmunity, so that’s still a very difficult nut to crack. I actually think the major effort should be focused on making the beta cells more hardy [via genetic modification] as opposed to focusing on the immune system. And there’s a lot of data to support that now, and that’s what we’re working on.”
Indeed, Dr. Liew and Dr. Deng said, “New immunomodulatory strategies to address graft longevity without immunosuppression remain to be established and tested. With reports of therapeutic efficacy of stem cell–derived islet transplantation such as with our study, stem cell–derived therapy without need for immunosuppression would be a meaningful next step in the treatment of this disease.”
The team has now performed the same procedure in two more patients and will report their data “in due course.”
Dr. Liew had no disclosures. Dr. Deng is a scientific adviser at Hangzhou Reprogenix Bioscience. Two coauthors are employees of Hangzhou Reprogenix Bioscience. Another is a former employee of Hangzhou Reprogenix Bioscience and is now affiliated with the Hangzhou Institute of Medicine, Chinese Academy of Sciences. Four coauthors have patent applications related to this work. Dr. Harlan is chief scientific officer and cofounder of Stability Health. He had no other disclosures.
A version of this article first appeared on Medscape.com.
FROM CELL
New Guidelines Emphasize Liver Care in T2D, Obesity
MADRID — Individuals with type 2 diabetes and/or obesity plus one or more metabolic risk factors are at a higher risk for metabolic dysfunction–associated steatotic liver disease (MASLD) with fibrosis and progression to more severe liver disease, stated new European guidelines that provide recommendations for diagnosis and management.
“The availability of improved treatment options underlines the need to identify at-risk individuals with MASLD early, as we now possess the tools to positively influence the course of the diseases, which is expected to prevent relevant clinical events,” stated the clinical practice guidelines, updated for the first time since 2016.
“Now we have guidelines that tell clinicians how to monitor the liver,” said Amalia Gastaldelli, PhD, research director at the Institute of Clinical Physiology of the National Research Council in Pisa, Italy, and a member of the panel that developed the guidelines.
Dr. Gastaldelli moderated a session focused on the guidelines at the annual meeting of the European Association for the Study of Diabetes (EASD). In an interview after the session, Dr. Gastaldelli, who leads a cardiometabolic risk research group, stressed the importance of the liver’s role in the body and the need for diabetes specialists to start paying more attention to this vital organ.
“It’s an important organ for monitoring because liver disease is silent, and the patient doesn’t feel unwell until disease is severe,” she said. “Diabetologists already monitor the eye, the heart, the kidney, and so on, but the liver is often neglected,” she said. A 2024 study found that the global pooled prevalence of MASLD among patients with type 2 diabetes was 65.33%.
Dr. Gastaldelli noted the importance of liver status in diabetes care. The liver makes triglycerides and very-low-density lipoprotein cholesterol, which are all major risk factors for atherosclerosis and cardiovascular disease (CVD), she said, as well as producing glucose, which in excess can lead to hyperglycemia.
The guidelines were jointly written by EASD, the European Association for the Study of the Liver, and the European Association for the Study of Obesity, and published in Diabetologia, The Journal of Hepatology, and Obesity Facts.
A Metabolic Condition
In the EASD meeting session, Dr. Gastaldelli discussed the reasons for, and implications of, shifting the name from nonalcoholic fatty liver disease (NAFLD) to MASLD.
“The name change focuses on the fact that this is a metabolic disease, while NAFLD had no mention of this and was considered stigmatizing by patients, especially in relation to the words ‘fatty’ and ‘nonalcoholic,’” she said.
According to the guidelines, MASLD is defined as liver steatosis in the presence of one or more cardiometabolic risk factor(s) and the absence of excess alcohol intake.
MASLD has become the most common chronic liver disease and includes isolated steatosis, metabolic dysfunction-associated steatohepatitis (MASH, previously NASH), MASH-related fibrosis, and cirrhosis.
In the overarching group of steatotic liver disease, a totally new intermediate category has been added: MASLD with moderate (increased) alcohol intake (MetALD), which represents MASLD in people who consume greater amounts of alcohol per week (140-350 g/week and 210-420 g/week for women and men, respectively).
The change in the nomenclature has been incremental and regional, Dr. Gastaldelli said. “The definition first changed from NAFLD to MAFLD, which recognizes the importance of metabolism in the pathophysiology of this disease but does not take into account alcohol intake. MAFLD is still used in Asia, Australasia, and North Africa, while Europe and the Americas have endorsed MASLD.”
Case-Finding and Diagnosis
Identifying MASLD cases in people at risk remains incidental, largely because it is a silent disease and is symptom-free until it becomes severe, said Dr. Gastaldelli.
The guideline recognizes that individuals with type 2 diabetes or obesity with additional metabolic risk factor(s) are at a higher risk for MASLD with fibrosis and progression to MASH.
Assessment strategies for severe liver fibrosis in MASLD include the use of noninvasive tests in people who have cardiometabolic risk factors, abnormal liver enzymes, and/or radiological signs of hepatic steatosis, particularly in the presence of type 2 diabetes or obesity or in the presence of one or more metabolic risk factors.
Dr. Gastaldelli noted that type 2 diabetes, metabolic syndrome, and obesity, including abdominal obesity identified by large waist circumference, are the major risk factors and should be warning signs.
“We need to consider abdominal obesity too — we’ve published data in relatively lean people, body mass index < 25, with MASH but without diabetes. Most of the patients accumulated fat viscerally and in the liver and had hypertriglyceridemia and hypercholesterolemia,” she said.
“The guidelines reflect this because the definition of MASLD includes steatosis plus at least one metabolic factor — waist circumference, for example, which is related to visceral fat, hyperlipidemia, or hyperglycemia. Of note, in both pharmacological and diet-induced weight loss, the decrease in liver fat was associated with the decrease in visceral fat.”
The noninvasive biomarker test, Fibrosis-4 (FIB-4) may be used to assess the risk for liver fibrosis. The FIB-4 index is calculated using a patient’s age and results of three blood tests — aspartate aminotransferase, alanine aminotransferase, and platelet count.
Advanced fibrosis (grade F3-F4) “is a major risk factor for severe outcomes,” said Dr. Gastaldelli. A FIB-4 test result below 1.3 indicates low risk for advanced liver fibrosis, 1.30-2.67 indicates intermediate risk, and above 2.67 indicates high risk.
“When fibrosis increases, then liver enzymes increase and the platelets decrease,” said Dr. Gastaldelli. “It is not a perfect tool, and we need to add in age because at a young age, it is prone to false negatives and when very old — false positives. It’s important to take a global view, especially if the patient has persistent high liver enzymes, but FIB-4 is low.”
“And if they have more than one metabolic risk factor, proceed with more tests, for example, transient elastography,” she advised. Imaging techniques such as transient elastography may rule out or rule in advanced fibrosis, which is predictive of liver-related outcomes.
“However, imaging techniques only diagnose steatosis and fibrosis, and right now, MASH can only be diagnosed with liver biopsy because we do not have any markers of liver inflammation and ballooning. In the future, noninvasive tests based on imaging and blood tests will be used to identify patients with MASH,” she added.
Management of MASLD — Lifestyle and Treatment
“Pharmacological treatments are designed for [patients] with MASH and fibrosis grade F2 or F3, but not MASLD,” Dr. Gastaldelli said. As such, lifestyle interventions are the mainstay of management — including weight loss, dietary changes, physical exercise, and low to no alcohol consumption. “Eating good-quality food and reducing calories are both important because the metabolism responds differently to different nutrients,” Dr. Gastaldelli said.
“In particular, the guidelines advise dietary management because some foods carry liver toxicity, for example, sugary foods with sucrose/fructose especially,” she said, adding that, “complex carbohydrates are less harmful than refined carbohydrates. Processed foods should be avoided if possible because they contain sugars, [as well as] saturated fats and hydrogenated fat, which is particularly bad for the liver. Olive oil is better than butter or margarine, which are rich in saturated fat, and fish and white meat are preferable.”
She added that a diet to help manage type 2 diabetes was not so dissimilar because sugar again needs to be reduced.
If a patient has severe obesity (and MASLD), data show that bariatric surgery is beneficial. “It not only helps weight loss, but it improves liver histology and has been shown to improve or resolve type 2 diabetes and reduce CVD risk. Importantly, regarding fibrosis, nutritional management after the bariatric surgery is the most important thing,” said Dr. Gastaldelli.
Optimal management of comorbidities — including the use of incretin-based therapies such as semaglutide or tirzepatide for type 2 diabetes or obesity, if indicated — is advised, according to the guidelines.
Glucagon-like peptide 1 receptor agonists (GLP-1 RAs) have been shown to have a beneficial effect on MASH, said Dr. Gastaldelli. “They have not shown effectiveness in the resolution of fibrosis, but this might take longer to manifest. However, if the medication is started early enough, it may prevent severe fibrosis. Significant weight loss, both with lifestyle and pharmacological treatment, should lead to an improvement in the liver too.”
There are currently no drugs available in Europe for the treatment of noncirrhotic MASH and severe fibrosis (stage ≥ 2). Resmetirom is the first approved MASH-targeted treatment in noncirrhotic MASH and significant liver fibrosis, with histological effectiveness on steatohepatitis and fibrosis, together with an acceptable safety and tolerability profile, but, for the moment, this agent is only available in United States.
Finally, turning to MASH-related cirrhosis, the guidelines advise adaptations of metabolic drugs, nutritional counseling, and surveillance for portal hypertension and hepatocellular carcinoma, as well as liver transplantation in decompensated cirrhosis.
After the session, this news organization spoke to Tushy Kailayanathan, MBBS BSc, medical director of the liver MRI company, Perspectum, who reviewed the limitations of the FIB-4 test. The FIB-4 test identifies those with advanced fibrosis in the liver, for example, patients with hepatitis C, she noted; however, “it performs worse in type 2 diabetic patients and in the elderly. There is little clinical guidance on the adjustment of FIB-4 thresholds needed for these high cardiometabolic risk groups. The priority patients are missed by FIB-4 because those individuals with early and active disease may not yet have progressed to advanced disease detected by FIB-4.”
These individuals are exactly those amenable to primary care prevention strategies, said Dr. Kailayanathan. Because of the nature of early and active liver disease in patients with high cardiometabolic risk, it would make sense to shift some diagnostic protocols into primary care.
“These individuals are exactly those amenable to primary care prevention strategies at annual diabetic review because they are likely to have modifiable cardiometabolic risk factors such as metabolic syndrome and would benefit from lifestyle and therapeutic intervention, including GLP-1 RAs and SGLT2is [sodium-glucose cotransporter-2 inhibitors],” she said. “Case-finding and detection of early-stage MASLD is a priority in diabetics, and there is an unmet need for accurate biomarkers to measure liver fat and inflammation early.”
Dr. Gastaldelli has been on the advisory board or consulting for Boehringer Ingelheim, Novo Nordisk, Eli Lilly, Fractyl, Pfizer, Merck-MSD, MetaDeq and a speaker for Eli Lilly, Novo Nordisk, and Pfizer. Dr. Kailayanathan is medical director at Perspectum, a UK-based company involved in liver imaging technology.
A version of this article first appeared on Medscape.com.
MADRID — Individuals with type 2 diabetes and/or obesity plus one or more metabolic risk factors are at a higher risk for metabolic dysfunction–associated steatotic liver disease (MASLD) with fibrosis and progression to more severe liver disease, stated new European guidelines that provide recommendations for diagnosis and management.
“The availability of improved treatment options underlines the need to identify at-risk individuals with MASLD early, as we now possess the tools to positively influence the course of the diseases, which is expected to prevent relevant clinical events,” stated the clinical practice guidelines, updated for the first time since 2016.
“Now we have guidelines that tell clinicians how to monitor the liver,” said Amalia Gastaldelli, PhD, research director at the Institute of Clinical Physiology of the National Research Council in Pisa, Italy, and a member of the panel that developed the guidelines.
Dr. Gastaldelli moderated a session focused on the guidelines at the annual meeting of the European Association for the Study of Diabetes (EASD). In an interview after the session, Dr. Gastaldelli, who leads a cardiometabolic risk research group, stressed the importance of the liver’s role in the body and the need for diabetes specialists to start paying more attention to this vital organ.
“It’s an important organ for monitoring because liver disease is silent, and the patient doesn’t feel unwell until disease is severe,” she said. “Diabetologists already monitor the eye, the heart, the kidney, and so on, but the liver is often neglected,” she said. A 2024 study found that the global pooled prevalence of MASLD among patients with type 2 diabetes was 65.33%.
Dr. Gastaldelli noted the importance of liver status in diabetes care. The liver makes triglycerides and very-low-density lipoprotein cholesterol, which are all major risk factors for atherosclerosis and cardiovascular disease (CVD), she said, as well as producing glucose, which in excess can lead to hyperglycemia.
The guidelines were jointly written by EASD, the European Association for the Study of the Liver, and the European Association for the Study of Obesity, and published in Diabetologia, The Journal of Hepatology, and Obesity Facts.
A Metabolic Condition
In the EASD meeting session, Dr. Gastaldelli discussed the reasons for, and implications of, shifting the name from nonalcoholic fatty liver disease (NAFLD) to MASLD.
“The name change focuses on the fact that this is a metabolic disease, while NAFLD had no mention of this and was considered stigmatizing by patients, especially in relation to the words ‘fatty’ and ‘nonalcoholic,’” she said.
According to the guidelines, MASLD is defined as liver steatosis in the presence of one or more cardiometabolic risk factor(s) and the absence of excess alcohol intake.
MASLD has become the most common chronic liver disease and includes isolated steatosis, metabolic dysfunction-associated steatohepatitis (MASH, previously NASH), MASH-related fibrosis, and cirrhosis.
In the overarching group of steatotic liver disease, a totally new intermediate category has been added: MASLD with moderate (increased) alcohol intake (MetALD), which represents MASLD in people who consume greater amounts of alcohol per week (140-350 g/week and 210-420 g/week for women and men, respectively).
The change in the nomenclature has been incremental and regional, Dr. Gastaldelli said. “The definition first changed from NAFLD to MAFLD, which recognizes the importance of metabolism in the pathophysiology of this disease but does not take into account alcohol intake. MAFLD is still used in Asia, Australasia, and North Africa, while Europe and the Americas have endorsed MASLD.”
Case-Finding and Diagnosis
Identifying MASLD cases in people at risk remains incidental, largely because it is a silent disease and is symptom-free until it becomes severe, said Dr. Gastaldelli.
The guideline recognizes that individuals with type 2 diabetes or obesity with additional metabolic risk factor(s) are at a higher risk for MASLD with fibrosis and progression to MASH.
Assessment strategies for severe liver fibrosis in MASLD include the use of noninvasive tests in people who have cardiometabolic risk factors, abnormal liver enzymes, and/or radiological signs of hepatic steatosis, particularly in the presence of type 2 diabetes or obesity or in the presence of one or more metabolic risk factors.
Dr. Gastaldelli noted that type 2 diabetes, metabolic syndrome, and obesity, including abdominal obesity identified by large waist circumference, are the major risk factors and should be warning signs.
“We need to consider abdominal obesity too — we’ve published data in relatively lean people, body mass index < 25, with MASH but without diabetes. Most of the patients accumulated fat viscerally and in the liver and had hypertriglyceridemia and hypercholesterolemia,” she said.
“The guidelines reflect this because the definition of MASLD includes steatosis plus at least one metabolic factor — waist circumference, for example, which is related to visceral fat, hyperlipidemia, or hyperglycemia. Of note, in both pharmacological and diet-induced weight loss, the decrease in liver fat was associated with the decrease in visceral fat.”
The noninvasive biomarker test, Fibrosis-4 (FIB-4) may be used to assess the risk for liver fibrosis. The FIB-4 index is calculated using a patient’s age and results of three blood tests — aspartate aminotransferase, alanine aminotransferase, and platelet count.
Advanced fibrosis (grade F3-F4) “is a major risk factor for severe outcomes,” said Dr. Gastaldelli. A FIB-4 test result below 1.3 indicates low risk for advanced liver fibrosis, 1.30-2.67 indicates intermediate risk, and above 2.67 indicates high risk.
“When fibrosis increases, then liver enzymes increase and the platelets decrease,” said Dr. Gastaldelli. “It is not a perfect tool, and we need to add in age because at a young age, it is prone to false negatives and when very old — false positives. It’s important to take a global view, especially if the patient has persistent high liver enzymes, but FIB-4 is low.”
“And if they have more than one metabolic risk factor, proceed with more tests, for example, transient elastography,” she advised. Imaging techniques such as transient elastography may rule out or rule in advanced fibrosis, which is predictive of liver-related outcomes.
“However, imaging techniques only diagnose steatosis and fibrosis, and right now, MASH can only be diagnosed with liver biopsy because we do not have any markers of liver inflammation and ballooning. In the future, noninvasive tests based on imaging and blood tests will be used to identify patients with MASH,” she added.
Management of MASLD — Lifestyle and Treatment
“Pharmacological treatments are designed for [patients] with MASH and fibrosis grade F2 or F3, but not MASLD,” Dr. Gastaldelli said. As such, lifestyle interventions are the mainstay of management — including weight loss, dietary changes, physical exercise, and low to no alcohol consumption. “Eating good-quality food and reducing calories are both important because the metabolism responds differently to different nutrients,” Dr. Gastaldelli said.
“In particular, the guidelines advise dietary management because some foods carry liver toxicity, for example, sugary foods with sucrose/fructose especially,” she said, adding that, “complex carbohydrates are less harmful than refined carbohydrates. Processed foods should be avoided if possible because they contain sugars, [as well as] saturated fats and hydrogenated fat, which is particularly bad for the liver. Olive oil is better than butter or margarine, which are rich in saturated fat, and fish and white meat are preferable.”
She added that a diet to help manage type 2 diabetes was not so dissimilar because sugar again needs to be reduced.
If a patient has severe obesity (and MASLD), data show that bariatric surgery is beneficial. “It not only helps weight loss, but it improves liver histology and has been shown to improve or resolve type 2 diabetes and reduce CVD risk. Importantly, regarding fibrosis, nutritional management after the bariatric surgery is the most important thing,” said Dr. Gastaldelli.
Optimal management of comorbidities — including the use of incretin-based therapies such as semaglutide or tirzepatide for type 2 diabetes or obesity, if indicated — is advised, according to the guidelines.
Glucagon-like peptide 1 receptor agonists (GLP-1 RAs) have been shown to have a beneficial effect on MASH, said Dr. Gastaldelli. “They have not shown effectiveness in the resolution of fibrosis, but this might take longer to manifest. However, if the medication is started early enough, it may prevent severe fibrosis. Significant weight loss, both with lifestyle and pharmacological treatment, should lead to an improvement in the liver too.”
There are currently no drugs available in Europe for the treatment of noncirrhotic MASH and severe fibrosis (stage ≥ 2). Resmetirom is the first approved MASH-targeted treatment in noncirrhotic MASH and significant liver fibrosis, with histological effectiveness on steatohepatitis and fibrosis, together with an acceptable safety and tolerability profile, but, for the moment, this agent is only available in United States.
Finally, turning to MASH-related cirrhosis, the guidelines advise adaptations of metabolic drugs, nutritional counseling, and surveillance for portal hypertension and hepatocellular carcinoma, as well as liver transplantation in decompensated cirrhosis.
After the session, this news organization spoke to Tushy Kailayanathan, MBBS BSc, medical director of the liver MRI company, Perspectum, who reviewed the limitations of the FIB-4 test. The FIB-4 test identifies those with advanced fibrosis in the liver, for example, patients with hepatitis C, she noted; however, “it performs worse in type 2 diabetic patients and in the elderly. There is little clinical guidance on the adjustment of FIB-4 thresholds needed for these high cardiometabolic risk groups. The priority patients are missed by FIB-4 because those individuals with early and active disease may not yet have progressed to advanced disease detected by FIB-4.”
These individuals are exactly those amenable to primary care prevention strategies, said Dr. Kailayanathan. Because of the nature of early and active liver disease in patients with high cardiometabolic risk, it would make sense to shift some diagnostic protocols into primary care.
“These individuals are exactly those amenable to primary care prevention strategies at annual diabetic review because they are likely to have modifiable cardiometabolic risk factors such as metabolic syndrome and would benefit from lifestyle and therapeutic intervention, including GLP-1 RAs and SGLT2is [sodium-glucose cotransporter-2 inhibitors],” she said. “Case-finding and detection of early-stage MASLD is a priority in diabetics, and there is an unmet need for accurate biomarkers to measure liver fat and inflammation early.”
Dr. Gastaldelli has been on the advisory board or consulting for Boehringer Ingelheim, Novo Nordisk, Eli Lilly, Fractyl, Pfizer, Merck-MSD, MetaDeq and a speaker for Eli Lilly, Novo Nordisk, and Pfizer. Dr. Kailayanathan is medical director at Perspectum, a UK-based company involved in liver imaging technology.
A version of this article first appeared on Medscape.com.
MADRID — Individuals with type 2 diabetes and/or obesity plus one or more metabolic risk factors are at a higher risk for metabolic dysfunction–associated steatotic liver disease (MASLD) with fibrosis and progression to more severe liver disease, stated new European guidelines that provide recommendations for diagnosis and management.
“The availability of improved treatment options underlines the need to identify at-risk individuals with MASLD early, as we now possess the tools to positively influence the course of the diseases, which is expected to prevent relevant clinical events,” stated the clinical practice guidelines, updated for the first time since 2016.
“Now we have guidelines that tell clinicians how to monitor the liver,” said Amalia Gastaldelli, PhD, research director at the Institute of Clinical Physiology of the National Research Council in Pisa, Italy, and a member of the panel that developed the guidelines.
Dr. Gastaldelli moderated a session focused on the guidelines at the annual meeting of the European Association for the Study of Diabetes (EASD). In an interview after the session, Dr. Gastaldelli, who leads a cardiometabolic risk research group, stressed the importance of the liver’s role in the body and the need for diabetes specialists to start paying more attention to this vital organ.
“It’s an important organ for monitoring because liver disease is silent, and the patient doesn’t feel unwell until disease is severe,” she said. “Diabetologists already monitor the eye, the heart, the kidney, and so on, but the liver is often neglected,” she said. A 2024 study found that the global pooled prevalence of MASLD among patients with type 2 diabetes was 65.33%.
Dr. Gastaldelli noted the importance of liver status in diabetes care. The liver makes triglycerides and very-low-density lipoprotein cholesterol, which are all major risk factors for atherosclerosis and cardiovascular disease (CVD), she said, as well as producing glucose, which in excess can lead to hyperglycemia.
The guidelines were jointly written by EASD, the European Association for the Study of the Liver, and the European Association for the Study of Obesity, and published in Diabetologia, The Journal of Hepatology, and Obesity Facts.
A Metabolic Condition
In the EASD meeting session, Dr. Gastaldelli discussed the reasons for, and implications of, shifting the name from nonalcoholic fatty liver disease (NAFLD) to MASLD.
“The name change focuses on the fact that this is a metabolic disease, while NAFLD had no mention of this and was considered stigmatizing by patients, especially in relation to the words ‘fatty’ and ‘nonalcoholic,’” she said.
According to the guidelines, MASLD is defined as liver steatosis in the presence of one or more cardiometabolic risk factor(s) and the absence of excess alcohol intake.
MASLD has become the most common chronic liver disease and includes isolated steatosis, metabolic dysfunction-associated steatohepatitis (MASH, previously NASH), MASH-related fibrosis, and cirrhosis.
In the overarching group of steatotic liver disease, a totally new intermediate category has been added: MASLD with moderate (increased) alcohol intake (MetALD), which represents MASLD in people who consume greater amounts of alcohol per week (140-350 g/week and 210-420 g/week for women and men, respectively).
The change in the nomenclature has been incremental and regional, Dr. Gastaldelli said. “The definition first changed from NAFLD to MAFLD, which recognizes the importance of metabolism in the pathophysiology of this disease but does not take into account alcohol intake. MAFLD is still used in Asia, Australasia, and North Africa, while Europe and the Americas have endorsed MASLD.”
Case-Finding and Diagnosis
Identifying MASLD cases in people at risk remains incidental, largely because it is a silent disease and is symptom-free until it becomes severe, said Dr. Gastaldelli.
The guideline recognizes that individuals with type 2 diabetes or obesity with additional metabolic risk factor(s) are at a higher risk for MASLD with fibrosis and progression to MASH.
Assessment strategies for severe liver fibrosis in MASLD include the use of noninvasive tests in people who have cardiometabolic risk factors, abnormal liver enzymes, and/or radiological signs of hepatic steatosis, particularly in the presence of type 2 diabetes or obesity or in the presence of one or more metabolic risk factors.
Dr. Gastaldelli noted that type 2 diabetes, metabolic syndrome, and obesity, including abdominal obesity identified by large waist circumference, are the major risk factors and should be warning signs.
“We need to consider abdominal obesity too — we’ve published data in relatively lean people, body mass index < 25, with MASH but without diabetes. Most of the patients accumulated fat viscerally and in the liver and had hypertriglyceridemia and hypercholesterolemia,” she said.
“The guidelines reflect this because the definition of MASLD includes steatosis plus at least one metabolic factor — waist circumference, for example, which is related to visceral fat, hyperlipidemia, or hyperglycemia. Of note, in both pharmacological and diet-induced weight loss, the decrease in liver fat was associated with the decrease in visceral fat.”
The noninvasive biomarker test, Fibrosis-4 (FIB-4) may be used to assess the risk for liver fibrosis. The FIB-4 index is calculated using a patient’s age and results of three blood tests — aspartate aminotransferase, alanine aminotransferase, and platelet count.
Advanced fibrosis (grade F3-F4) “is a major risk factor for severe outcomes,” said Dr. Gastaldelli. A FIB-4 test result below 1.3 indicates low risk for advanced liver fibrosis, 1.30-2.67 indicates intermediate risk, and above 2.67 indicates high risk.
“When fibrosis increases, then liver enzymes increase and the platelets decrease,” said Dr. Gastaldelli. “It is not a perfect tool, and we need to add in age because at a young age, it is prone to false negatives and when very old — false positives. It’s important to take a global view, especially if the patient has persistent high liver enzymes, but FIB-4 is low.”
“And if they have more than one metabolic risk factor, proceed with more tests, for example, transient elastography,” she advised. Imaging techniques such as transient elastography may rule out or rule in advanced fibrosis, which is predictive of liver-related outcomes.
“However, imaging techniques only diagnose steatosis and fibrosis, and right now, MASH can only be diagnosed with liver biopsy because we do not have any markers of liver inflammation and ballooning. In the future, noninvasive tests based on imaging and blood tests will be used to identify patients with MASH,” she added.
Management of MASLD — Lifestyle and Treatment
“Pharmacological treatments are designed for [patients] with MASH and fibrosis grade F2 or F3, but not MASLD,” Dr. Gastaldelli said. As such, lifestyle interventions are the mainstay of management — including weight loss, dietary changes, physical exercise, and low to no alcohol consumption. “Eating good-quality food and reducing calories are both important because the metabolism responds differently to different nutrients,” Dr. Gastaldelli said.
“In particular, the guidelines advise dietary management because some foods carry liver toxicity, for example, sugary foods with sucrose/fructose especially,” she said, adding that, “complex carbohydrates are less harmful than refined carbohydrates. Processed foods should be avoided if possible because they contain sugars, [as well as] saturated fats and hydrogenated fat, which is particularly bad for the liver. Olive oil is better than butter or margarine, which are rich in saturated fat, and fish and white meat are preferable.”
She added that a diet to help manage type 2 diabetes was not so dissimilar because sugar again needs to be reduced.
If a patient has severe obesity (and MASLD), data show that bariatric surgery is beneficial. “It not only helps weight loss, but it improves liver histology and has been shown to improve or resolve type 2 diabetes and reduce CVD risk. Importantly, regarding fibrosis, nutritional management after the bariatric surgery is the most important thing,” said Dr. Gastaldelli.
Optimal management of comorbidities — including the use of incretin-based therapies such as semaglutide or tirzepatide for type 2 diabetes or obesity, if indicated — is advised, according to the guidelines.
Glucagon-like peptide 1 receptor agonists (GLP-1 RAs) have been shown to have a beneficial effect on MASH, said Dr. Gastaldelli. “They have not shown effectiveness in the resolution of fibrosis, but this might take longer to manifest. However, if the medication is started early enough, it may prevent severe fibrosis. Significant weight loss, both with lifestyle and pharmacological treatment, should lead to an improvement in the liver too.”
There are currently no drugs available in Europe for the treatment of noncirrhotic MASH and severe fibrosis (stage ≥ 2). Resmetirom is the first approved MASH-targeted treatment in noncirrhotic MASH and significant liver fibrosis, with histological effectiveness on steatohepatitis and fibrosis, together with an acceptable safety and tolerability profile, but, for the moment, this agent is only available in United States.
Finally, turning to MASH-related cirrhosis, the guidelines advise adaptations of metabolic drugs, nutritional counseling, and surveillance for portal hypertension and hepatocellular carcinoma, as well as liver transplantation in decompensated cirrhosis.
After the session, this news organization spoke to Tushy Kailayanathan, MBBS BSc, medical director of the liver MRI company, Perspectum, who reviewed the limitations of the FIB-4 test. The FIB-4 test identifies those with advanced fibrosis in the liver, for example, patients with hepatitis C, she noted; however, “it performs worse in type 2 diabetic patients and in the elderly. There is little clinical guidance on the adjustment of FIB-4 thresholds needed for these high cardiometabolic risk groups. The priority patients are missed by FIB-4 because those individuals with early and active disease may not yet have progressed to advanced disease detected by FIB-4.”
These individuals are exactly those amenable to primary care prevention strategies, said Dr. Kailayanathan. Because of the nature of early and active liver disease in patients with high cardiometabolic risk, it would make sense to shift some diagnostic protocols into primary care.
“These individuals are exactly those amenable to primary care prevention strategies at annual diabetic review because they are likely to have modifiable cardiometabolic risk factors such as metabolic syndrome and would benefit from lifestyle and therapeutic intervention, including GLP-1 RAs and SGLT2is [sodium-glucose cotransporter-2 inhibitors],” she said. “Case-finding and detection of early-stage MASLD is a priority in diabetics, and there is an unmet need for accurate biomarkers to measure liver fat and inflammation early.”
Dr. Gastaldelli has been on the advisory board or consulting for Boehringer Ingelheim, Novo Nordisk, Eli Lilly, Fractyl, Pfizer, Merck-MSD, MetaDeq and a speaker for Eli Lilly, Novo Nordisk, and Pfizer. Dr. Kailayanathan is medical director at Perspectum, a UK-based company involved in liver imaging technology.
A version of this article first appeared on Medscape.com.
FROM EASD 2024
Diabetic Kidney Disease Therapies Keep on FLOWing
Further data from the FLOW study were presented during the 2024 congress of the European Association for the Study of Diabetes (EASD) in Madrid. The FLOW study was originally presented in May at the European Renal Association’s 2024 congress in Stockholm. It was the first dedicated kidney outcomes trial to examine a GLP-1 receptor agonist.
The FLOW study demonstrated significant kidney, cardiovascular, and mortality benefits with semaglutide 1 mg once weekly in patients with type 2 diabetes and chronic kidney disease (CKD). This study has elevated semaglutide to a new pillar of care for the management of diabetic kidney disease (DKD) alongside RAAS inhibitors, SGLT2 inhibitors, and finerenone.
At first, whether the benefits of semaglutide were independent of baseline SGLT2 inhibitor use was uncertain. The data presented at the EASD congress, however, appeared to confirm the additive benefits of semaglutide, when combined with SGLT2 inhibitor use, in patients with DKD. The authors did acknowledge that study power was limited, given the low use of SGLT2 inhibitors at trial recruitment (no licensed SGLT2 inhibitor was available for CKD at that point), so small, clinically relevant interactions may not have been detected.
So, what are the implications of the FLOW study for primary care?
DKD is a common clinical challenge in primary care; a national diabetes audit in the United Kingdom suggested that over 40% of patients with type 2 diabetes had kidney disease. Moreover, DKD is the most common cause of kidney failure in adults starting renal replacement therapy in the United Kingdom.
Residual renal risk in patients with DKD persists despite optimal use of guideline-directed medical therapy (GDMT) with RAAS inhibitors, SGLT2 inhibitors, and finerenone, as demonstrated in the many landmark kidney outcomes trials over the past 25 years.
So, a new pillar of GDMT is welcome, but I am worried that this widened choice of therapies may worsen therapeutic inertia; baseline use of the newer DKD therapies (specifically SGLT2 inhibitors and finerenone) remains low.
In addition, during the EASD FLOW session, Katherine Tuttle, MD, executive director for research at Providence Inland Northwest Health Services in Spokane, Washington, presented data from the US CURE-CKD registry study showing that baseline ACE inhibitor/ARB use of about 70% dropped to 50% after just 90 days. Baseline use of SGLT2 inhibitors was only about 6% and dropped to 5% after 90 days.
I suspect that much of this reduction in prescribing of ACE inhibitors/ARBs will have been in response to an acute dip in estimated glomerular filtration rate (eGFR) or hyperkalemia, which has been a perennial challenge with RAAS inhibitor use in primary care. Ongoing education in primary care is required to manage hyperkalemia and reductions in eGFR after RAAS inhibitor initiation to prevent premature cessation of these foundational therapies.
On a positive note, there was no acute dip in eGFR after prescribing semaglutide in DKD. This observation will be reassuring for primary care and hopefully prevent unnecessary cessation of therapy.
Also reassuring was the lack of difference in diabetic retinopathy adverse events between the semaglutide and placebo groups. These events raised concerns about semaglutide following the SUSTAIN-6 CVOT study and have affected attitudes in primary care. But the rapidity and magnitude of improvement in glycemic control with semaglutide was believed to be the underlying issue, rather than semaglutide itself. A similar phenomenon has been observed with insulin. The ongoing FOCUS study is exploring the long-term effects of semaglutide on diabetic retinopathy in patients with type 2 diabetes. This study will hopefully provide a definite answer to this issue.
Another useful message from the FLOW study for primary care is the utility of semaglutide for glucose-lowering in the context of CKD. A1c was 0.81% lower in the semaglutide group compared with the placebo group in participants with eGFRs as low as 25 mL/min/1.73 m2. It is well established that SGLT2 inhibitors have negligible glucose-lowering effects once eGFR drops below 45 mL/min/1.73 m2. Indeed, my usual practice in CKD, if additional glucose-lowering is required once renal protection has been established with an SGLT2 inhibitor, was to add a GLP-1 receptor agonist. It is reassuring to have my clinical practice ratified by the FLOW study.
Semaglutide also helpfully provides an alternative therapeutic option for patients who do not tolerate SGLT2 inhibitors because of, for example, recurrent mycotic genital infections or polyuria, or for those in whom SGLT2 inhibitors are contraindicated, such as patients who have experienced an unprovoked episode of diabetic ketoacidosis. Many of these patients still require cardiovascular and kidney protection, so the FLOW study gives me a viable evidence-based alternative.
As a class, semaglutide and GLP-1 receptor agonists are, of course, not without side effects. Gastrointestinal side effects are the most common, and this finding was echoed in the FLOW study. Gastrointestinal disorders led to permanent treatment discontinuation in 4.5% of the semaglutide group compared with 1.1% of the placebo group. The overall safety profile of semaglutide was favorable, however.
Gastrointestinal side effects can be particularly concerning in the context of CKD because of the possibility of clinical dehydration and acute kidney injury with persistent vomiting or diarrhea. Patient education is particularly important when using GLP-1 receptor agonists in this group of individuals. Reassuringly, there was no imbalance in dehydration and acute kidney injury between trial arms in the FLOW study.
Notably, past studies have suggested that patients with CKD are more likely to experience gastrointestinal side effects with GLP-1 receptor agonists; in these patients, the usual mantra of GLP-1 receptor agonist prescribing is particularly important: Start low, go slow.
Finally, medication adherence is a challenge with multiple pillars of GDMT: These evidence-based disease-modifying therapies work only if our patients take them regularly. My senior partner had a lovely turn of phrase when reviewing patients with multiple long-term conditions; he would always start the consultation by asking individuals which medications they were not taking regularly.
Overall, the FLOW study confirms semaglutide’s position as a new therapeutic pillar for DKD. This treatment will help address the residual renal risk for patients with DKD despite optimal use of GDMT. However, education and support will be required in primary care to prevent worsening therapeutic inertia.
Kevin Fernando, general practitioner partner, North Berwick Health Centre, North Berwick, UK, has disclosed the following relevant financial relationships: Received speaker fees from: Amarin; Amgen; AstraZeneca; Bayer; Boehringer Ingelheim; Dexcom; Daiichi Sankyo; Lilly; Menarini; Novartis; Novo Nordisk; Roche Diagnostics; Embecta; Roche Diabetes Care. Received honoraria for participation in advisory boards from: Amarin; Amgen; AstraZen
A version of this article first appeared on Medscape.com.
Further data from the FLOW study were presented during the 2024 congress of the European Association for the Study of Diabetes (EASD) in Madrid. The FLOW study was originally presented in May at the European Renal Association’s 2024 congress in Stockholm. It was the first dedicated kidney outcomes trial to examine a GLP-1 receptor agonist.
The FLOW study demonstrated significant kidney, cardiovascular, and mortality benefits with semaglutide 1 mg once weekly in patients with type 2 diabetes and chronic kidney disease (CKD). This study has elevated semaglutide to a new pillar of care for the management of diabetic kidney disease (DKD) alongside RAAS inhibitors, SGLT2 inhibitors, and finerenone.
At first, whether the benefits of semaglutide were independent of baseline SGLT2 inhibitor use was uncertain. The data presented at the EASD congress, however, appeared to confirm the additive benefits of semaglutide, when combined with SGLT2 inhibitor use, in patients with DKD. The authors did acknowledge that study power was limited, given the low use of SGLT2 inhibitors at trial recruitment (no licensed SGLT2 inhibitor was available for CKD at that point), so small, clinically relevant interactions may not have been detected.
So, what are the implications of the FLOW study for primary care?
DKD is a common clinical challenge in primary care; a national diabetes audit in the United Kingdom suggested that over 40% of patients with type 2 diabetes had kidney disease. Moreover, DKD is the most common cause of kidney failure in adults starting renal replacement therapy in the United Kingdom.
Residual renal risk in patients with DKD persists despite optimal use of guideline-directed medical therapy (GDMT) with RAAS inhibitors, SGLT2 inhibitors, and finerenone, as demonstrated in the many landmark kidney outcomes trials over the past 25 years.
So, a new pillar of GDMT is welcome, but I am worried that this widened choice of therapies may worsen therapeutic inertia; baseline use of the newer DKD therapies (specifically SGLT2 inhibitors and finerenone) remains low.
In addition, during the EASD FLOW session, Katherine Tuttle, MD, executive director for research at Providence Inland Northwest Health Services in Spokane, Washington, presented data from the US CURE-CKD registry study showing that baseline ACE inhibitor/ARB use of about 70% dropped to 50% after just 90 days. Baseline use of SGLT2 inhibitors was only about 6% and dropped to 5% after 90 days.
I suspect that much of this reduction in prescribing of ACE inhibitors/ARBs will have been in response to an acute dip in estimated glomerular filtration rate (eGFR) or hyperkalemia, which has been a perennial challenge with RAAS inhibitor use in primary care. Ongoing education in primary care is required to manage hyperkalemia and reductions in eGFR after RAAS inhibitor initiation to prevent premature cessation of these foundational therapies.
On a positive note, there was no acute dip in eGFR after prescribing semaglutide in DKD. This observation will be reassuring for primary care and hopefully prevent unnecessary cessation of therapy.
Also reassuring was the lack of difference in diabetic retinopathy adverse events between the semaglutide and placebo groups. These events raised concerns about semaglutide following the SUSTAIN-6 CVOT study and have affected attitudes in primary care. But the rapidity and magnitude of improvement in glycemic control with semaglutide was believed to be the underlying issue, rather than semaglutide itself. A similar phenomenon has been observed with insulin. The ongoing FOCUS study is exploring the long-term effects of semaglutide on diabetic retinopathy in patients with type 2 diabetes. This study will hopefully provide a definite answer to this issue.
Another useful message from the FLOW study for primary care is the utility of semaglutide for glucose-lowering in the context of CKD. A1c was 0.81% lower in the semaglutide group compared with the placebo group in participants with eGFRs as low as 25 mL/min/1.73 m2. It is well established that SGLT2 inhibitors have negligible glucose-lowering effects once eGFR drops below 45 mL/min/1.73 m2. Indeed, my usual practice in CKD, if additional glucose-lowering is required once renal protection has been established with an SGLT2 inhibitor, was to add a GLP-1 receptor agonist. It is reassuring to have my clinical practice ratified by the FLOW study.
Semaglutide also helpfully provides an alternative therapeutic option for patients who do not tolerate SGLT2 inhibitors because of, for example, recurrent mycotic genital infections or polyuria, or for those in whom SGLT2 inhibitors are contraindicated, such as patients who have experienced an unprovoked episode of diabetic ketoacidosis. Many of these patients still require cardiovascular and kidney protection, so the FLOW study gives me a viable evidence-based alternative.
As a class, semaglutide and GLP-1 receptor agonists are, of course, not without side effects. Gastrointestinal side effects are the most common, and this finding was echoed in the FLOW study. Gastrointestinal disorders led to permanent treatment discontinuation in 4.5% of the semaglutide group compared with 1.1% of the placebo group. The overall safety profile of semaglutide was favorable, however.
Gastrointestinal side effects can be particularly concerning in the context of CKD because of the possibility of clinical dehydration and acute kidney injury with persistent vomiting or diarrhea. Patient education is particularly important when using GLP-1 receptor agonists in this group of individuals. Reassuringly, there was no imbalance in dehydration and acute kidney injury between trial arms in the FLOW study.
Notably, past studies have suggested that patients with CKD are more likely to experience gastrointestinal side effects with GLP-1 receptor agonists; in these patients, the usual mantra of GLP-1 receptor agonist prescribing is particularly important: Start low, go slow.
Finally, medication adherence is a challenge with multiple pillars of GDMT: These evidence-based disease-modifying therapies work only if our patients take them regularly. My senior partner had a lovely turn of phrase when reviewing patients with multiple long-term conditions; he would always start the consultation by asking individuals which medications they were not taking regularly.
Overall, the FLOW study confirms semaglutide’s position as a new therapeutic pillar for DKD. This treatment will help address the residual renal risk for patients with DKD despite optimal use of GDMT. However, education and support will be required in primary care to prevent worsening therapeutic inertia.
Kevin Fernando, general practitioner partner, North Berwick Health Centre, North Berwick, UK, has disclosed the following relevant financial relationships: Received speaker fees from: Amarin; Amgen; AstraZeneca; Bayer; Boehringer Ingelheim; Dexcom; Daiichi Sankyo; Lilly; Menarini; Novartis; Novo Nordisk; Roche Diagnostics; Embecta; Roche Diabetes Care. Received honoraria for participation in advisory boards from: Amarin; Amgen; AstraZen
A version of this article first appeared on Medscape.com.
Further data from the FLOW study were presented during the 2024 congress of the European Association for the Study of Diabetes (EASD) in Madrid. The FLOW study was originally presented in May at the European Renal Association’s 2024 congress in Stockholm. It was the first dedicated kidney outcomes trial to examine a GLP-1 receptor agonist.
The FLOW study demonstrated significant kidney, cardiovascular, and mortality benefits with semaglutide 1 mg once weekly in patients with type 2 diabetes and chronic kidney disease (CKD). This study has elevated semaglutide to a new pillar of care for the management of diabetic kidney disease (DKD) alongside RAAS inhibitors, SGLT2 inhibitors, and finerenone.
At first, whether the benefits of semaglutide were independent of baseline SGLT2 inhibitor use was uncertain. The data presented at the EASD congress, however, appeared to confirm the additive benefits of semaglutide, when combined with SGLT2 inhibitor use, in patients with DKD. The authors did acknowledge that study power was limited, given the low use of SGLT2 inhibitors at trial recruitment (no licensed SGLT2 inhibitor was available for CKD at that point), so small, clinically relevant interactions may not have been detected.
So, what are the implications of the FLOW study for primary care?
DKD is a common clinical challenge in primary care; a national diabetes audit in the United Kingdom suggested that over 40% of patients with type 2 diabetes had kidney disease. Moreover, DKD is the most common cause of kidney failure in adults starting renal replacement therapy in the United Kingdom.
Residual renal risk in patients with DKD persists despite optimal use of guideline-directed medical therapy (GDMT) with RAAS inhibitors, SGLT2 inhibitors, and finerenone, as demonstrated in the many landmark kidney outcomes trials over the past 25 years.
So, a new pillar of GDMT is welcome, but I am worried that this widened choice of therapies may worsen therapeutic inertia; baseline use of the newer DKD therapies (specifically SGLT2 inhibitors and finerenone) remains low.
In addition, during the EASD FLOW session, Katherine Tuttle, MD, executive director for research at Providence Inland Northwest Health Services in Spokane, Washington, presented data from the US CURE-CKD registry study showing that baseline ACE inhibitor/ARB use of about 70% dropped to 50% after just 90 days. Baseline use of SGLT2 inhibitors was only about 6% and dropped to 5% after 90 days.
I suspect that much of this reduction in prescribing of ACE inhibitors/ARBs will have been in response to an acute dip in estimated glomerular filtration rate (eGFR) or hyperkalemia, which has been a perennial challenge with RAAS inhibitor use in primary care. Ongoing education in primary care is required to manage hyperkalemia and reductions in eGFR after RAAS inhibitor initiation to prevent premature cessation of these foundational therapies.
On a positive note, there was no acute dip in eGFR after prescribing semaglutide in DKD. This observation will be reassuring for primary care and hopefully prevent unnecessary cessation of therapy.
Also reassuring was the lack of difference in diabetic retinopathy adverse events between the semaglutide and placebo groups. These events raised concerns about semaglutide following the SUSTAIN-6 CVOT study and have affected attitudes in primary care. But the rapidity and magnitude of improvement in glycemic control with semaglutide was believed to be the underlying issue, rather than semaglutide itself. A similar phenomenon has been observed with insulin. The ongoing FOCUS study is exploring the long-term effects of semaglutide on diabetic retinopathy in patients with type 2 diabetes. This study will hopefully provide a definite answer to this issue.
Another useful message from the FLOW study for primary care is the utility of semaglutide for glucose-lowering in the context of CKD. A1c was 0.81% lower in the semaglutide group compared with the placebo group in participants with eGFRs as low as 25 mL/min/1.73 m2. It is well established that SGLT2 inhibitors have negligible glucose-lowering effects once eGFR drops below 45 mL/min/1.73 m2. Indeed, my usual practice in CKD, if additional glucose-lowering is required once renal protection has been established with an SGLT2 inhibitor, was to add a GLP-1 receptor agonist. It is reassuring to have my clinical practice ratified by the FLOW study.
Semaglutide also helpfully provides an alternative therapeutic option for patients who do not tolerate SGLT2 inhibitors because of, for example, recurrent mycotic genital infections or polyuria, or for those in whom SGLT2 inhibitors are contraindicated, such as patients who have experienced an unprovoked episode of diabetic ketoacidosis. Many of these patients still require cardiovascular and kidney protection, so the FLOW study gives me a viable evidence-based alternative.
As a class, semaglutide and GLP-1 receptor agonists are, of course, not without side effects. Gastrointestinal side effects are the most common, and this finding was echoed in the FLOW study. Gastrointestinal disorders led to permanent treatment discontinuation in 4.5% of the semaglutide group compared with 1.1% of the placebo group. The overall safety profile of semaglutide was favorable, however.
Gastrointestinal side effects can be particularly concerning in the context of CKD because of the possibility of clinical dehydration and acute kidney injury with persistent vomiting or diarrhea. Patient education is particularly important when using GLP-1 receptor agonists in this group of individuals. Reassuringly, there was no imbalance in dehydration and acute kidney injury between trial arms in the FLOW study.
Notably, past studies have suggested that patients with CKD are more likely to experience gastrointestinal side effects with GLP-1 receptor agonists; in these patients, the usual mantra of GLP-1 receptor agonist prescribing is particularly important: Start low, go slow.
Finally, medication adherence is a challenge with multiple pillars of GDMT: These evidence-based disease-modifying therapies work only if our patients take them regularly. My senior partner had a lovely turn of phrase when reviewing patients with multiple long-term conditions; he would always start the consultation by asking individuals which medications they were not taking regularly.
Overall, the FLOW study confirms semaglutide’s position as a new therapeutic pillar for DKD. This treatment will help address the residual renal risk for patients with DKD despite optimal use of GDMT. However, education and support will be required in primary care to prevent worsening therapeutic inertia.
Kevin Fernando, general practitioner partner, North Berwick Health Centre, North Berwick, UK, has disclosed the following relevant financial relationships: Received speaker fees from: Amarin; Amgen; AstraZeneca; Bayer; Boehringer Ingelheim; Dexcom; Daiichi Sankyo; Lilly; Menarini; Novartis; Novo Nordisk; Roche Diagnostics; Embecta; Roche Diabetes Care. Received honoraria for participation in advisory boards from: Amarin; Amgen; AstraZen
A version of this article first appeared on Medscape.com.
FROM EASD 2024
Diabetes Treatment May Lower Incidence of Uterine Fibroids
TOPLINE:
Diabetes is associated with a lower incidence of uterine fibroids in midlife women receiving diabetes treatment, especially metformin. The association between diabetes and the risk for uterine fibroids may vary based on menopausal status.
METHODOLOGY:
- Previous studies have provided inconsistent evidence regarding associations between the risk for uterine fibroids and markers of cardiometabolic health, such as fasting insulin, fasting glucose, and diabetes.
- Researchers conducted a prospective cohort study to examine the association of fasting levels of cardiometabolic blood biomarkers, diabetes, and diabetes treatment with the incidence of new fibroid diagnoses in midlife women.
- They included participants from the Study of Women’s Health Across the Nation cohort who reported fibroid diagnoses at enrollment and during 13 follow-up visits.
- At all visits, levels of glucose, insulin, and sex hormone–binding globulin (SHBG) were measured in fasting blood samples, and homeostatic model assessment for insulin resistance (HOMA-IR) was calculated.
- Discrete-time survival models were used to estimate the hazard ratios (HRs) for the associations of biomarkers and diabetes with fibroid diagnoses, adjusted for demographics and healthcare utilization.
TAKEAWAY:
- Researchers identified 2570 eligible women (median age, 45 years; 45% perimenopausal women), among whom approximately 3% had diabetes at baseline.
- Diabetes was associated with a 28% lower incidence of new fibroid diagnosis (adjusted HR, 0.72).
- This association was particularly strong among participants with treated diabetes, especially those on metformin, who had a 51% lower incidence of self-reported fibroids than those without diabetes. The estimates, however, had wide CIs suggesting uncertainty.
- Time-varying HOMA-IR and SHBG, insulin, and glucose levels were not significantly associated with the new fibroid diagnosis.
- When stratified by menopausal status, higher HOMA-IR and insulin levels were associated with a greater incidence of fibroid diagnosis during premenopause but not during perimenopause.
IN PRACTICE:
“Our findings contribute to preliminary evidence indicating a protective association between diabetes and risk of incident fibroids,” the authors wrote.
SOURCE:
The study was led by Susanna D. Mitro, Division of Research, Kaiser Permanente, Pleasanton, California, and was published online in The Journal of Clinical Endocrinology & Metabolism.
LIMITATIONS:
The study relied on self-reported fibroid diagnoses, which may result in the misclassification of cases. The sample size of participants with diabetes was small, which resulted in reduced precision and confidence in the findings. The baseline eligibility criteria (midlife participants with an intact uterus and no history of fibroid incidence) may have limited the generalizability of the findings to the wider population at risk for fibroids.
DISCLOSURES:
This study was supported by the National Institutes of Health (NIH), through the National Institute on Aging, the National Institute of Nursing Research, and the NIH Office of Research on Women’s Health. One author reported being a consultant and adviser for various pharmaceutical companies. Two other authors reported receiving salary support and royalties from various pharmaceutical companies and organizations.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Diabetes is associated with a lower incidence of uterine fibroids in midlife women receiving diabetes treatment, especially metformin. The association between diabetes and the risk for uterine fibroids may vary based on menopausal status.
METHODOLOGY:
- Previous studies have provided inconsistent evidence regarding associations between the risk for uterine fibroids and markers of cardiometabolic health, such as fasting insulin, fasting glucose, and diabetes.
- Researchers conducted a prospective cohort study to examine the association of fasting levels of cardiometabolic blood biomarkers, diabetes, and diabetes treatment with the incidence of new fibroid diagnoses in midlife women.
- They included participants from the Study of Women’s Health Across the Nation cohort who reported fibroid diagnoses at enrollment and during 13 follow-up visits.
- At all visits, levels of glucose, insulin, and sex hormone–binding globulin (SHBG) were measured in fasting blood samples, and homeostatic model assessment for insulin resistance (HOMA-IR) was calculated.
- Discrete-time survival models were used to estimate the hazard ratios (HRs) for the associations of biomarkers and diabetes with fibroid diagnoses, adjusted for demographics and healthcare utilization.
TAKEAWAY:
- Researchers identified 2570 eligible women (median age, 45 years; 45% perimenopausal women), among whom approximately 3% had diabetes at baseline.
- Diabetes was associated with a 28% lower incidence of new fibroid diagnosis (adjusted HR, 0.72).
- This association was particularly strong among participants with treated diabetes, especially those on metformin, who had a 51% lower incidence of self-reported fibroids than those without diabetes. The estimates, however, had wide CIs suggesting uncertainty.
- Time-varying HOMA-IR and SHBG, insulin, and glucose levels were not significantly associated with the new fibroid diagnosis.
- When stratified by menopausal status, higher HOMA-IR and insulin levels were associated with a greater incidence of fibroid diagnosis during premenopause but not during perimenopause.
IN PRACTICE:
“Our findings contribute to preliminary evidence indicating a protective association between diabetes and risk of incident fibroids,” the authors wrote.
SOURCE:
The study was led by Susanna D. Mitro, Division of Research, Kaiser Permanente, Pleasanton, California, and was published online in The Journal of Clinical Endocrinology & Metabolism.
LIMITATIONS:
The study relied on self-reported fibroid diagnoses, which may result in the misclassification of cases. The sample size of participants with diabetes was small, which resulted in reduced precision and confidence in the findings. The baseline eligibility criteria (midlife participants with an intact uterus and no history of fibroid incidence) may have limited the generalizability of the findings to the wider population at risk for fibroids.
DISCLOSURES:
This study was supported by the National Institutes of Health (NIH), through the National Institute on Aging, the National Institute of Nursing Research, and the NIH Office of Research on Women’s Health. One author reported being a consultant and adviser for various pharmaceutical companies. Two other authors reported receiving salary support and royalties from various pharmaceutical companies and organizations.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Diabetes is associated with a lower incidence of uterine fibroids in midlife women receiving diabetes treatment, especially metformin. The association between diabetes and the risk for uterine fibroids may vary based on menopausal status.
METHODOLOGY:
- Previous studies have provided inconsistent evidence regarding associations between the risk for uterine fibroids and markers of cardiometabolic health, such as fasting insulin, fasting glucose, and diabetes.
- Researchers conducted a prospective cohort study to examine the association of fasting levels of cardiometabolic blood biomarkers, diabetes, and diabetes treatment with the incidence of new fibroid diagnoses in midlife women.
- They included participants from the Study of Women’s Health Across the Nation cohort who reported fibroid diagnoses at enrollment and during 13 follow-up visits.
- At all visits, levels of glucose, insulin, and sex hormone–binding globulin (SHBG) were measured in fasting blood samples, and homeostatic model assessment for insulin resistance (HOMA-IR) was calculated.
- Discrete-time survival models were used to estimate the hazard ratios (HRs) for the associations of biomarkers and diabetes with fibroid diagnoses, adjusted for demographics and healthcare utilization.
TAKEAWAY:
- Researchers identified 2570 eligible women (median age, 45 years; 45% perimenopausal women), among whom approximately 3% had diabetes at baseline.
- Diabetes was associated with a 28% lower incidence of new fibroid diagnosis (adjusted HR, 0.72).
- This association was particularly strong among participants with treated diabetes, especially those on metformin, who had a 51% lower incidence of self-reported fibroids than those without diabetes. The estimates, however, had wide CIs suggesting uncertainty.
- Time-varying HOMA-IR and SHBG, insulin, and glucose levels were not significantly associated with the new fibroid diagnosis.
- When stratified by menopausal status, higher HOMA-IR and insulin levels were associated with a greater incidence of fibroid diagnosis during premenopause but not during perimenopause.
IN PRACTICE:
“Our findings contribute to preliminary evidence indicating a protective association between diabetes and risk of incident fibroids,” the authors wrote.
SOURCE:
The study was led by Susanna D. Mitro, Division of Research, Kaiser Permanente, Pleasanton, California, and was published online in The Journal of Clinical Endocrinology & Metabolism.
LIMITATIONS:
The study relied on self-reported fibroid diagnoses, which may result in the misclassification of cases. The sample size of participants with diabetes was small, which resulted in reduced precision and confidence in the findings. The baseline eligibility criteria (midlife participants with an intact uterus and no history of fibroid incidence) may have limited the generalizability of the findings to the wider population at risk for fibroids.
DISCLOSURES:
This study was supported by the National Institutes of Health (NIH), through the National Institute on Aging, the National Institute of Nursing Research, and the NIH Office of Research on Women’s Health. One author reported being a consultant and adviser for various pharmaceutical companies. Two other authors reported receiving salary support and royalties from various pharmaceutical companies and organizations.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
Air Travel Alters Insulin Pump Delivery on Takeoff, Landing
MADRID —
This phenomenon is due to air bubble formation and reabsorption in the insulin caused by ambient pressure changes in the airplane’s cabin. It has nothing to do with the pump itself and happens with all insulin pumps, including those in hybrid closed-loop systems, Bruce King, MD, said at the European Association for the Study of Diabetes (EASD) 2024 Annual Meeting.
The extent to which this affects people with diabetes who use insulin pumps depends on their dose and insulin sensitivity among other factors, but all who fly should be aware of the possibility and take precautions, particularly with children, Dr. King, a pediatric endocrinologist at John Hunter Children’s Hospital, Newcastle, Australia, told this news organization.
“Basically, the pumps are very safe in flight, but they deliver a little bit of extra insulin when you go up and stop delivery when you come back down again. There are a couple of simple steps that people can take to make sure that they don’t have problems during the flight,” he said.
Specifically, he advised that for pumps with tubing, wearers can disconnect just prior to takeoff and reconnect when the plane reaches cruising altitude, about 20 minutes into the flight. The insulin will still come out, but it won’t be delivered to the person, Dr. King said.
On descent, they can disconnect after landing and prime the line to remove the insulin deficit.
With the Omnipod, which can’t be disconnected, the only solution is to eat a small snack on takeoff. And on landing, eat another small snack such as a banana, and give a bolus for it to overcome the blockage of insulin delivery.
In any case, Dr. King said, “One of the most important things is informing people with diabetes about this effect so they’re aware of it and can act appropriately when they fly.”
Asked to comment, Nicholas B. Argento, MD, a practicing endocrinologist in Columbia, Maryland, and author of the American Diabetes Association’s book, “Putting Your Patients on the Pump,” called the issue a “minor effect,” adding, “While I think it would be reasonable to make those changes ... it seems like a lot of effort for a difference of 0.6 units extra on ascent and 0.5 units less on descent.”
He noted there is a risk that the individual might forget to reattach the pump after 20 minutes, leading to hyperglycemia and even diabetic ketoacidosis. Instead, “one could put the pump on suspend for 1 hour on ascent. That would not stop the extra insulin but would net less insulin during that time period.”
And after descent, “you have to walk a lot in most cases, so I don’t think they need to take this into consideration. So many other factors change in air travel that I don’t think this is a significant enough effect to make the effort.”
A Known Phenomenon, the Manufacturers Are Aware
This phenomenon has been described previously, including by Dr. King in a 2011 Diabetes Care paper. The new research is among a series of experiments funded by the European Union Aviation Safety Agency in collaboration with the pump manufacturers Medtronic (MiniMed), Tandem (t:slim), and Insulet (Omnipod), primarily aimed at establishing safety parameters for airline pilots with insulin-treated diabetes.
Both the Omnipod DASH and Omnipod 5 User Guides include warnings about unintended insulin delivery during flight, and both advise users to check their blood glucose levels frequently while flying.
In a statement, Jordan Pinsker, MD, Chief Medical Officer at Tandem Diabetes Care, told this news organization, “While it has long been known that routine air travel pressure changes can cause minor fluctuations in insulin pump delivery, the impact of these variations have been found to be generally minor as it relates to glycemic control.”
Dr. Pinsker added that the Tandem Mobi user manual includes a warning related to significant pressure changes in specific air travel situations and offers guidance to disconnect. However, “the t:slim X2 pump’s microdelivery technology limits how much extra insulin can get delivered from air pressure changes due to a mechanism between the tubing and the contents of the bag inside the cartridge.”
Medtronic’s user guide says that the 780G system has not been tested at altitudes higher than 10,150 feet.
Hypobaric Chamber Used to Simulate Flight
The study was conducted in vitro, in a hypobaric chamber designed to mimic atmospheric changes during commercial flight. A total of 10 Medtronic MiniMed 780G, 10 Tandem t:slim X2, and six Insulet Omnipod DASH pumps were tested.
The hypobaric chamber was depressurized to 550 mm Hg over a 20-minute ascent, maintained at a 30-minute cruise, followed by a 20-minute descent to ground (750 mm Hg). During the simulated flights, insulin infusion was set at 0.6 units per hour, a rate typical for both adults and children, to allow accurate measurements with multiple flights.
Insulin delivery rates and bubble formation were recorded by attaching infusion sets to open-ended 100 µL capillary tubes against 1-mm grid paper.
Full cartridges — Medtronic: 3 mL, t:slim: 3 mL, and Omnipod: 2 mL — all over-delivered 0.60 units of insulin over a 20-minute ascent compared with delivery at ground level. And during descent, the cartridges under-delivered 0.51 units of insulin.
But if There’s Rapid Decompression…
In a separate protocol, insulin infusion sets without pumps were tested in a simulation of rapid decompression. Insulin delivery during both ascent and descent showed statistically significant differences compared with delivery at ground level (both P < .001). In this scenario, fluid delivery was equivalent to 5.6 units of excess insulin.
Dr. King pointed out that while these are rare events, about 40-50 occur annually. One was the widely publicized Alaska Airlines flight in January 2024 when the door fell off in midair.
Dr. Argento said, “The catastrophic decompression is of note, and I would want patients to be aware of this, but it is asking a lot for someone thinking they are going to die to remember to disconnect as it starts.”
The researchers are investigating this phenomenon further in people, including airline pilots.
Dr. King’s research group has been involved in research with Medtronic, Tandem, and Insulet. Dr. Argento has consulted or been on advisory boards for Eli Lilly Diabetes, Dexcom, Diabeloop, Convatec, and Senseonics and served on the speakers’ bureaus for Boehringer Ingelheim, Dexcom, Eli Lilly Diabetes, MannKind, Novo Nordisk, Xeris, and Zealand Pharma.
A version of this article appeared on Medscape.com.
MADRID —
This phenomenon is due to air bubble formation and reabsorption in the insulin caused by ambient pressure changes in the airplane’s cabin. It has nothing to do with the pump itself and happens with all insulin pumps, including those in hybrid closed-loop systems, Bruce King, MD, said at the European Association for the Study of Diabetes (EASD) 2024 Annual Meeting.
The extent to which this affects people with diabetes who use insulin pumps depends on their dose and insulin sensitivity among other factors, but all who fly should be aware of the possibility and take precautions, particularly with children, Dr. King, a pediatric endocrinologist at John Hunter Children’s Hospital, Newcastle, Australia, told this news organization.
“Basically, the pumps are very safe in flight, but they deliver a little bit of extra insulin when you go up and stop delivery when you come back down again. There are a couple of simple steps that people can take to make sure that they don’t have problems during the flight,” he said.
Specifically, he advised that for pumps with tubing, wearers can disconnect just prior to takeoff and reconnect when the plane reaches cruising altitude, about 20 minutes into the flight. The insulin will still come out, but it won’t be delivered to the person, Dr. King said.
On descent, they can disconnect after landing and prime the line to remove the insulin deficit.
With the Omnipod, which can’t be disconnected, the only solution is to eat a small snack on takeoff. And on landing, eat another small snack such as a banana, and give a bolus for it to overcome the blockage of insulin delivery.
In any case, Dr. King said, “One of the most important things is informing people with diabetes about this effect so they’re aware of it and can act appropriately when they fly.”
Asked to comment, Nicholas B. Argento, MD, a practicing endocrinologist in Columbia, Maryland, and author of the American Diabetes Association’s book, “Putting Your Patients on the Pump,” called the issue a “minor effect,” adding, “While I think it would be reasonable to make those changes ... it seems like a lot of effort for a difference of 0.6 units extra on ascent and 0.5 units less on descent.”
He noted there is a risk that the individual might forget to reattach the pump after 20 minutes, leading to hyperglycemia and even diabetic ketoacidosis. Instead, “one could put the pump on suspend for 1 hour on ascent. That would not stop the extra insulin but would net less insulin during that time period.”
And after descent, “you have to walk a lot in most cases, so I don’t think they need to take this into consideration. So many other factors change in air travel that I don’t think this is a significant enough effect to make the effort.”
A Known Phenomenon, the Manufacturers Are Aware
This phenomenon has been described previously, including by Dr. King in a 2011 Diabetes Care paper. The new research is among a series of experiments funded by the European Union Aviation Safety Agency in collaboration with the pump manufacturers Medtronic (MiniMed), Tandem (t:slim), and Insulet (Omnipod), primarily aimed at establishing safety parameters for airline pilots with insulin-treated diabetes.
Both the Omnipod DASH and Omnipod 5 User Guides include warnings about unintended insulin delivery during flight, and both advise users to check their blood glucose levels frequently while flying.
In a statement, Jordan Pinsker, MD, Chief Medical Officer at Tandem Diabetes Care, told this news organization, “While it has long been known that routine air travel pressure changes can cause minor fluctuations in insulin pump delivery, the impact of these variations have been found to be generally minor as it relates to glycemic control.”
Dr. Pinsker added that the Tandem Mobi user manual includes a warning related to significant pressure changes in specific air travel situations and offers guidance to disconnect. However, “the t:slim X2 pump’s microdelivery technology limits how much extra insulin can get delivered from air pressure changes due to a mechanism between the tubing and the contents of the bag inside the cartridge.”
Medtronic’s user guide says that the 780G system has not been tested at altitudes higher than 10,150 feet.
Hypobaric Chamber Used to Simulate Flight
The study was conducted in vitro, in a hypobaric chamber designed to mimic atmospheric changes during commercial flight. A total of 10 Medtronic MiniMed 780G, 10 Tandem t:slim X2, and six Insulet Omnipod DASH pumps were tested.
The hypobaric chamber was depressurized to 550 mm Hg over a 20-minute ascent, maintained at a 30-minute cruise, followed by a 20-minute descent to ground (750 mm Hg). During the simulated flights, insulin infusion was set at 0.6 units per hour, a rate typical for both adults and children, to allow accurate measurements with multiple flights.
Insulin delivery rates and bubble formation were recorded by attaching infusion sets to open-ended 100 µL capillary tubes against 1-mm grid paper.
Full cartridges — Medtronic: 3 mL, t:slim: 3 mL, and Omnipod: 2 mL — all over-delivered 0.60 units of insulin over a 20-minute ascent compared with delivery at ground level. And during descent, the cartridges under-delivered 0.51 units of insulin.
But if There’s Rapid Decompression…
In a separate protocol, insulin infusion sets without pumps were tested in a simulation of rapid decompression. Insulin delivery during both ascent and descent showed statistically significant differences compared with delivery at ground level (both P < .001). In this scenario, fluid delivery was equivalent to 5.6 units of excess insulin.
Dr. King pointed out that while these are rare events, about 40-50 occur annually. One was the widely publicized Alaska Airlines flight in January 2024 when the door fell off in midair.
Dr. Argento said, “The catastrophic decompression is of note, and I would want patients to be aware of this, but it is asking a lot for someone thinking they are going to die to remember to disconnect as it starts.”
The researchers are investigating this phenomenon further in people, including airline pilots.
Dr. King’s research group has been involved in research with Medtronic, Tandem, and Insulet. Dr. Argento has consulted or been on advisory boards for Eli Lilly Diabetes, Dexcom, Diabeloop, Convatec, and Senseonics and served on the speakers’ bureaus for Boehringer Ingelheim, Dexcom, Eli Lilly Diabetes, MannKind, Novo Nordisk, Xeris, and Zealand Pharma.
A version of this article appeared on Medscape.com.
MADRID —
This phenomenon is due to air bubble formation and reabsorption in the insulin caused by ambient pressure changes in the airplane’s cabin. It has nothing to do with the pump itself and happens with all insulin pumps, including those in hybrid closed-loop systems, Bruce King, MD, said at the European Association for the Study of Diabetes (EASD) 2024 Annual Meeting.
The extent to which this affects people with diabetes who use insulin pumps depends on their dose and insulin sensitivity among other factors, but all who fly should be aware of the possibility and take precautions, particularly with children, Dr. King, a pediatric endocrinologist at John Hunter Children’s Hospital, Newcastle, Australia, told this news organization.
“Basically, the pumps are very safe in flight, but they deliver a little bit of extra insulin when you go up and stop delivery when you come back down again. There are a couple of simple steps that people can take to make sure that they don’t have problems during the flight,” he said.
Specifically, he advised that for pumps with tubing, wearers can disconnect just prior to takeoff and reconnect when the plane reaches cruising altitude, about 20 minutes into the flight. The insulin will still come out, but it won’t be delivered to the person, Dr. King said.
On descent, they can disconnect after landing and prime the line to remove the insulin deficit.
With the Omnipod, which can’t be disconnected, the only solution is to eat a small snack on takeoff. And on landing, eat another small snack such as a banana, and give a bolus for it to overcome the blockage of insulin delivery.
In any case, Dr. King said, “One of the most important things is informing people with diabetes about this effect so they’re aware of it and can act appropriately when they fly.”
Asked to comment, Nicholas B. Argento, MD, a practicing endocrinologist in Columbia, Maryland, and author of the American Diabetes Association’s book, “Putting Your Patients on the Pump,” called the issue a “minor effect,” adding, “While I think it would be reasonable to make those changes ... it seems like a lot of effort for a difference of 0.6 units extra on ascent and 0.5 units less on descent.”
He noted there is a risk that the individual might forget to reattach the pump after 20 minutes, leading to hyperglycemia and even diabetic ketoacidosis. Instead, “one could put the pump on suspend for 1 hour on ascent. That would not stop the extra insulin but would net less insulin during that time period.”
And after descent, “you have to walk a lot in most cases, so I don’t think they need to take this into consideration. So many other factors change in air travel that I don’t think this is a significant enough effect to make the effort.”
A Known Phenomenon, the Manufacturers Are Aware
This phenomenon has been described previously, including by Dr. King in a 2011 Diabetes Care paper. The new research is among a series of experiments funded by the European Union Aviation Safety Agency in collaboration with the pump manufacturers Medtronic (MiniMed), Tandem (t:slim), and Insulet (Omnipod), primarily aimed at establishing safety parameters for airline pilots with insulin-treated diabetes.
Both the Omnipod DASH and Omnipod 5 User Guides include warnings about unintended insulin delivery during flight, and both advise users to check their blood glucose levels frequently while flying.
In a statement, Jordan Pinsker, MD, Chief Medical Officer at Tandem Diabetes Care, told this news organization, “While it has long been known that routine air travel pressure changes can cause minor fluctuations in insulin pump delivery, the impact of these variations have been found to be generally minor as it relates to glycemic control.”
Dr. Pinsker added that the Tandem Mobi user manual includes a warning related to significant pressure changes in specific air travel situations and offers guidance to disconnect. However, “the t:slim X2 pump’s microdelivery technology limits how much extra insulin can get delivered from air pressure changes due to a mechanism between the tubing and the contents of the bag inside the cartridge.”
Medtronic’s user guide says that the 780G system has not been tested at altitudes higher than 10,150 feet.
Hypobaric Chamber Used to Simulate Flight
The study was conducted in vitro, in a hypobaric chamber designed to mimic atmospheric changes during commercial flight. A total of 10 Medtronic MiniMed 780G, 10 Tandem t:slim X2, and six Insulet Omnipod DASH pumps were tested.
The hypobaric chamber was depressurized to 550 mm Hg over a 20-minute ascent, maintained at a 30-minute cruise, followed by a 20-minute descent to ground (750 mm Hg). During the simulated flights, insulin infusion was set at 0.6 units per hour, a rate typical for both adults and children, to allow accurate measurements with multiple flights.
Insulin delivery rates and bubble formation were recorded by attaching infusion sets to open-ended 100 µL capillary tubes against 1-mm grid paper.
Full cartridges — Medtronic: 3 mL, t:slim: 3 mL, and Omnipod: 2 mL — all over-delivered 0.60 units of insulin over a 20-minute ascent compared with delivery at ground level. And during descent, the cartridges under-delivered 0.51 units of insulin.
But if There’s Rapid Decompression…
In a separate protocol, insulin infusion sets without pumps were tested in a simulation of rapid decompression. Insulin delivery during both ascent and descent showed statistically significant differences compared with delivery at ground level (both P < .001). In this scenario, fluid delivery was equivalent to 5.6 units of excess insulin.
Dr. King pointed out that while these are rare events, about 40-50 occur annually. One was the widely publicized Alaska Airlines flight in January 2024 when the door fell off in midair.
Dr. Argento said, “The catastrophic decompression is of note, and I would want patients to be aware of this, but it is asking a lot for someone thinking they are going to die to remember to disconnect as it starts.”
The researchers are investigating this phenomenon further in people, including airline pilots.
Dr. King’s research group has been involved in research with Medtronic, Tandem, and Insulet. Dr. Argento has consulted or been on advisory boards for Eli Lilly Diabetes, Dexcom, Diabeloop, Convatec, and Senseonics and served on the speakers’ bureaus for Boehringer Ingelheim, Dexcom, Eli Lilly Diabetes, MannKind, Novo Nordisk, Xeris, and Zealand Pharma.
A version of this article appeared on Medscape.com.
FROM EASD 2024
Walking App Works Only if Users Think It Does
TOPLINE:
Apps designed to increase physical activity may be useful in increasing daily step counts for users who believe the intervention beneficial, but not for those who do not. The app’s effectiveness is notably influenced by how users perceive its utility.
METHODOLOGY:
- Researchers conducted a randomized controlled trial from February 2021 to May 2022 to evaluate the effectiveness of SNapp, an adaptive app designed to promote walking through tailored coaching content.
- Overall, 176 adults (76% women; mean age, 56 years) were randomly assigned to use the app plus tailored coaching content (SNapp group; n = 87) or only the step counter app (control group; n = 89).
- SNapp’s coaching content provided personalized feedback on step counts and recommendations for increasing walking, while also considering individual preferences for behavior change techniques.
- The primary outcome was the daily step count recorded by the app, which was updated on an hourly basis in a database over an intervention period of 12 months.
- Perceptions of ease of use and usefulness were assessed to determine their effect on the effectiveness of the app.
TAKEAWAY:
- Intervention group participants used the app nearly 30% of days, while those using the app alone showed almost identical use.
- The SNapp intervention did not significantly affect the step counts on average over time (B, −202.30; 95% CI, −889.7 to 485.1).
- Perceived usefulness significantly moderated the intervention effect of SNapp (B, 344.38; 90% CI, 40.4-648.3), but perceived ease of use did not (B, 38.60; 90% CI, −276.5 to 353.7).
- Among participants with a high perceived usefulness, the SNapp group had a higher median step count than the control group (median difference, 1260 steps; 90% CI, −3243.7 to 1298.2); however, this difference was not statistically significant.
IN PRACTICE:
“This study shows that perceived usefulness is also an important factor influencing behavioral effects. Hence, it is essential for apps to be perceived as useful to effectively improve users’ activity levels,” the authors wrote.
SOURCE:
The study was led by Anne L. Vos, PhD, of the Amsterdam School of Communication Research at the University of Amsterdam, in the Netherlands. It was published online on September 16, 2024, in the American Journal of Preventive Medicine.
LIMITATIONS:
The study’s recruitment strategy primarily attracted highly educated individuals, limiting generalizability. The app’s accuracy in measuring steps could be improved, as it sometimes underestimated step counts. Researchers also were unable to check if participants read messages from coaches.
DISCLOSURES:
The study was supported by grants from the Dutch Heart Foundation and the Netherlands Organisation for Health Research and Development. No relevant conflicts of interest were disclosed by the authors.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Apps designed to increase physical activity may be useful in increasing daily step counts for users who believe the intervention beneficial, but not for those who do not. The app’s effectiveness is notably influenced by how users perceive its utility.
METHODOLOGY:
- Researchers conducted a randomized controlled trial from February 2021 to May 2022 to evaluate the effectiveness of SNapp, an adaptive app designed to promote walking through tailored coaching content.
- Overall, 176 adults (76% women; mean age, 56 years) were randomly assigned to use the app plus tailored coaching content (SNapp group; n = 87) or only the step counter app (control group; n = 89).
- SNapp’s coaching content provided personalized feedback on step counts and recommendations for increasing walking, while also considering individual preferences for behavior change techniques.
- The primary outcome was the daily step count recorded by the app, which was updated on an hourly basis in a database over an intervention period of 12 months.
- Perceptions of ease of use and usefulness were assessed to determine their effect on the effectiveness of the app.
TAKEAWAY:
- Intervention group participants used the app nearly 30% of days, while those using the app alone showed almost identical use.
- The SNapp intervention did not significantly affect the step counts on average over time (B, −202.30; 95% CI, −889.7 to 485.1).
- Perceived usefulness significantly moderated the intervention effect of SNapp (B, 344.38; 90% CI, 40.4-648.3), but perceived ease of use did not (B, 38.60; 90% CI, −276.5 to 353.7).
- Among participants with a high perceived usefulness, the SNapp group had a higher median step count than the control group (median difference, 1260 steps; 90% CI, −3243.7 to 1298.2); however, this difference was not statistically significant.
IN PRACTICE:
“This study shows that perceived usefulness is also an important factor influencing behavioral effects. Hence, it is essential for apps to be perceived as useful to effectively improve users’ activity levels,” the authors wrote.
SOURCE:
The study was led by Anne L. Vos, PhD, of the Amsterdam School of Communication Research at the University of Amsterdam, in the Netherlands. It was published online on September 16, 2024, in the American Journal of Preventive Medicine.
LIMITATIONS:
The study’s recruitment strategy primarily attracted highly educated individuals, limiting generalizability. The app’s accuracy in measuring steps could be improved, as it sometimes underestimated step counts. Researchers also were unable to check if participants read messages from coaches.
DISCLOSURES:
The study was supported by grants from the Dutch Heart Foundation and the Netherlands Organisation for Health Research and Development. No relevant conflicts of interest were disclosed by the authors.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Apps designed to increase physical activity may be useful in increasing daily step counts for users who believe the intervention beneficial, but not for those who do not. The app’s effectiveness is notably influenced by how users perceive its utility.
METHODOLOGY:
- Researchers conducted a randomized controlled trial from February 2021 to May 2022 to evaluate the effectiveness of SNapp, an adaptive app designed to promote walking through tailored coaching content.
- Overall, 176 adults (76% women; mean age, 56 years) were randomly assigned to use the app plus tailored coaching content (SNapp group; n = 87) or only the step counter app (control group; n = 89).
- SNapp’s coaching content provided personalized feedback on step counts and recommendations for increasing walking, while also considering individual preferences for behavior change techniques.
- The primary outcome was the daily step count recorded by the app, which was updated on an hourly basis in a database over an intervention period of 12 months.
- Perceptions of ease of use and usefulness were assessed to determine their effect on the effectiveness of the app.
TAKEAWAY:
- Intervention group participants used the app nearly 30% of days, while those using the app alone showed almost identical use.
- The SNapp intervention did not significantly affect the step counts on average over time (B, −202.30; 95% CI, −889.7 to 485.1).
- Perceived usefulness significantly moderated the intervention effect of SNapp (B, 344.38; 90% CI, 40.4-648.3), but perceived ease of use did not (B, 38.60; 90% CI, −276.5 to 353.7).
- Among participants with a high perceived usefulness, the SNapp group had a higher median step count than the control group (median difference, 1260 steps; 90% CI, −3243.7 to 1298.2); however, this difference was not statistically significant.
IN PRACTICE:
“This study shows that perceived usefulness is also an important factor influencing behavioral effects. Hence, it is essential for apps to be perceived as useful to effectively improve users’ activity levels,” the authors wrote.
SOURCE:
The study was led by Anne L. Vos, PhD, of the Amsterdam School of Communication Research at the University of Amsterdam, in the Netherlands. It was published online on September 16, 2024, in the American Journal of Preventive Medicine.
LIMITATIONS:
The study’s recruitment strategy primarily attracted highly educated individuals, limiting generalizability. The app’s accuracy in measuring steps could be improved, as it sometimes underestimated step counts. Researchers also were unable to check if participants read messages from coaches.
DISCLOSURES:
The study was supported by grants from the Dutch Heart Foundation and the Netherlands Organisation for Health Research and Development. No relevant conflicts of interest were disclosed by the authors.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
‘Call to Action’: Greater CVD Focus Urged for Type 1 Diabetes
MADRID — Emerging data points to the urgent need for cardiovascular risk reduction in all adults with type 1 diabetes (T1D), including those who are young and those diagnosed in adulthood.
At the European Association for the Study of Diabetes (EASD) 2024 Annual Meeting, two entire oral abstract sessions were devoted to research examining cardiovascular risk specifically in people with T1D. There is increasing evidence that as with type 2 diabetes (T2D), clinical visits need to focus on other cardiovascular risk factors and glucose.
Findings included the evidence of severe coronary artery disease (CAD) in asymptomatic adults with T1D, increased risks for mortality and cardiac events in people diagnosed with T1D in adulthood, and a greater cardiovascular risk for those with overweight/obesity and among those with more cumulative exposure to both hyperglycemia and dyslipidemia.
One speaker, Dr. Rebecka Johanna Bergdal, of the Folkhälsan Research Center and the University of Helsinki, Finland, issued a “call to action,” saying, “We call on healthcare professionals to continue supporting and encouraging individuals with T1D towards better management of diabetes, including both glucose and lipid management.”
Session Moderator Krzysztof Strojek, MD, PhD, head of the Department of Internal Medicine, Diabetology and Cardiometabolic Diseases at the Medical University of Silesia, Katowice, Poland, told this news organization that all the data point in the same direction for T1D management, to “look not only at A1c and blood glucose control but also lipids, hypertension, smoking status, all these risk factors recognized in type 2 ... are also important in T1D.”
The ‘Alarming’ Finding of CAD in Asymptomatic Patients
Michal Dubsky, MD, PhD, of the Diabetes Centre, Institute for Clinical and Experimental Medicine, Prague, Czech Republic, presented findings from 62 asymptomatic patients with T1D for > 10 years (mean, 36 years), with a mean A1c of 7.5% (58 mmol/mol), and no prior history of cardiovascular disease (CVD). They had slightly elevated CVD biomarkers, including a mean low-density lipoprotein (LDL) cholesterol level of 2.33 mmol/L, lipoprotein (a) level of 15 nmol/L, and N-terminal pro-B-type natriuretic peptide level of 125.3 ng/L.
All underwent a noninvasive carotid ultrasound and coronary artery calcium (CAC) scoring. Of those, 12 patients had a CAC score > 400 and/or presence of two or more carotid plaques identified as high-risk.
Those 12 patients underwent coronary angiography and had a total of 29 vessels examined by optical coherence tomography (OCT), “an invasive intravascular method for assessing coronary atherosclerosis that is far more sensitive than standard coronary angiography, especially for the detection of high-risk vulnerable plaques without a hemodynamically significant stenosis,” Dr. Dubsky explained.
Coronary angiography showed obstructive CAD in 5 of the 12 patients. Their mean calcium score was 950 and mean number of carotid plaques was 2.8. Features associated with plaque vulnerability included microphage accumulation in 24 vessels, lipid-rich plaques in 23, spotty calcium in 19, and neovascularizations in 13.
Thin-cap fibroatheroma, a strong predictor of plaque rupture, was present in 7 of the 12 patients (58.3%), and four had features of very high-risk plaques, defined as thin-cap fibroatheroma with a minimal lumen area < 3.5 mm2, a lipid arch > 180 degrees, and macrophages.
“Our study showed that asymptomatic T1D patients with high CAC score and carotid plaques had very severe OCT findings. We observed a significant proportion of high-risk lesions potentially associated with plaque rupture and risk of CV death. Therefore, we believe these patients should be treated as very high-risk with target LDL below 1.4 mmol/L (55 mg/dL), even though they are completely asymptomatic,” Dr. Dubsky concluded.
He added that because OCT is invasive and costly, the CAC score can be used to guide the decision for statin use, with any score above 100 considered elevated risk.
Study coauthor Martin Haluzik, MD, professor of internal medicine in the Charles University, Prague, Czech Republic, told this news organization, “I think it’s very alarming because some of these are basically very healthy-looking young people, so you don’t really expect them to have significant cardiovascular complications already or significant plaques. I think it shows that we should be more proactive in looking into the risk of cardiovascular complications and in looking into the early cardiovascular changes.”
Later Diagnosis Doesn’t Always Protect: Risk Seen in Adult-Onset T1D
Yuxia Wei, a PhD student at the Institute of Environmental Medicine, Karolinska Institutet, Stockholm, Sweden, presented an analysis of data from Sweden’s national health databases comparing cardiovascular outcomes between 10,184 people diagnosed with T1D at ages 18-29 years, 30-39 years, and ≥ 40 years; another 375,523 people diagnosed with T2D at those ages; and 509,172 population controls matched for age, sex, and county.
Those diagnosed after age 40 years had higher A1c levels and were less likely to be using insulin pumps than those diagnosed at younger adult ages.
Compared with population controls, at a median of about 7 years of follow-up, people with T1D had significantly higher all-cause mortality at all diagnosis age groups, with a hazard ratio of 1.71. This rose to 2.78 for those diagnosed at age 30-39 years.
Compared with those with T2D, the mortality risks weren’t significantly different at any age, but the risks for non-cardiovascular death, including from cancer and infection, were significantly higher among those diagnosed after age 40 years (1.31 overall). Those diagnosed with T1D at any adult age had lower risks for major cardiovascular events than those diagnosed with T2D. Hazard ratios ranged from 0.27 for those diagnosed at age 18-29 years to 0.78 for those diagnosed after the age of 40 years.
Smoking and A1c above target were the greatest contributors to mortality. Those two factors, along with body mass index (BMI), were the strongest contributors to major adverse cardiovascular events (MACE).
“Adult-onset T1D carries excess risk of death and cardiovascular disease, without obvious attenuation over age at diagnosis…Smoking, A1c, and BMI are the key factors to be managed to improve prognosis in adult-onset T1D,” Ms. Wei concluded.
BMI: Often Overlooked in T1D, but a Major CVD Risk Factor
Two studies examined the link between overweight/obesity and cardiovascular risk in T1D. One, by Laurence Salle, MCU PH, of the Endocrinology, Diabetes and Metabolic Diseases Department at CHU Limoges, France, was a prospective, longitudinal cohort study of 2367 people with T1D at 68 centers in France who didn’t have a cardiovascular history at baseline.
Of those, 51% had normal BMI (18.5-24.9), 31% had overweight (25-29.9), and 18% had obesity (≥ 30). Cardiovascular risk factors, including LDL cholesterol, triglycerides, and hypertension increased with an increasing BMI. The 10-year CVD risk was significantly higher for those with overweight (9.61%) and obesity (9.93%) than for those with normal weight (7.24%), in both men and women.
However, BMI was found to be an independent predictor of 10-year high cardiovascular risk in men but not women, while waist:height ratio independently predicted risk in both men and women, Dr. Salle reported.
The second BMI study, from Enrique Soto-Pedre, MBBS, of the Division of Population Health and Genomics at the University of Dundee, Scotland, presented data on a retrospective follow-up from 1995 to 2019 of 1973 people with T1D aged > 18 years at diagnosis (42% women; mean age, 34.2 years; 18.9% had obesity.
After 10 years of follow-up, those with overweight and obesity had significantly higher odds of developing arterial hypertension, even among those taking angiotensin-converting enzyme inhibitors/angiotensin receptor blockers, with statistically significant adjusted hazard ratios of 1.73 and 3.37 for the obese and overweight groups, respectively.
MACE were significantly more common among those with obesity, with an adjusted hazard ratio of 2.95, as was acute myocardial infarction, 3.33.
“These results emphasize the importance of incorporating weight management into the overall management of individuals with T1D. No one has doubts about weight management in T2D, but in type 1, it’s not so clear. One of the main [concerns] would be safety [in terms of hypoglycemia],” Dr. Soto-Pedre concluded.
Call for Action: Cumulative Glucose and Lipid Exposures Increase Risk
Dr. Bergdal presented data on the effects of cumulative glycemia and lipids on the risk for CAD in 3495 adults with T1D who had been diagnosed prior to the age of 40 years. The history of CAD or stroke was exclusion criteria. There were a total of 534 CAD events within a median follow-up of 19.4 years.
Cumulative glycemia, LDL cholesterol, triglycerides, and non–high-density lipoprotein cholesterol exposures were all significantly associated with CAD risk (P < .001 for all). With an adjustment for confounders, the highest tertile of glycemia was associated with a twofold increased risk for CAD. Both hyperglycemia and dyslipidemia were independently associated with CAD risk, Dr. Bergdal reported.
“It’s important to minimize the time spent above A1c 7%, and lipid management in T1D must not be forgotten,” she said, prior to issuing her call for action.
Dr. Haluzik reported receiving honoraria for talks and/or consultancy and/or research funding from Eli Lilly, Novo Nordisk, Sanofi, AstraZeneca, Mundipharma, Bristol Myers Squibb, Amgen, Boehringer Ingelheim, Janssen, Ypsomed, and Johnson & Johnson. The presenters had no disclosures.
A version of this article first appeared on Medscape.com.
MADRID — Emerging data points to the urgent need for cardiovascular risk reduction in all adults with type 1 diabetes (T1D), including those who are young and those diagnosed in adulthood.
At the European Association for the Study of Diabetes (EASD) 2024 Annual Meeting, two entire oral abstract sessions were devoted to research examining cardiovascular risk specifically in people with T1D. There is increasing evidence that as with type 2 diabetes (T2D), clinical visits need to focus on other cardiovascular risk factors and glucose.
Findings included the evidence of severe coronary artery disease (CAD) in asymptomatic adults with T1D, increased risks for mortality and cardiac events in people diagnosed with T1D in adulthood, and a greater cardiovascular risk for those with overweight/obesity and among those with more cumulative exposure to both hyperglycemia and dyslipidemia.
One speaker, Dr. Rebecka Johanna Bergdal, of the Folkhälsan Research Center and the University of Helsinki, Finland, issued a “call to action,” saying, “We call on healthcare professionals to continue supporting and encouraging individuals with T1D towards better management of diabetes, including both glucose and lipid management.”
Session Moderator Krzysztof Strojek, MD, PhD, head of the Department of Internal Medicine, Diabetology and Cardiometabolic Diseases at the Medical University of Silesia, Katowice, Poland, told this news organization that all the data point in the same direction for T1D management, to “look not only at A1c and blood glucose control but also lipids, hypertension, smoking status, all these risk factors recognized in type 2 ... are also important in T1D.”
The ‘Alarming’ Finding of CAD in Asymptomatic Patients
Michal Dubsky, MD, PhD, of the Diabetes Centre, Institute for Clinical and Experimental Medicine, Prague, Czech Republic, presented findings from 62 asymptomatic patients with T1D for > 10 years (mean, 36 years), with a mean A1c of 7.5% (58 mmol/mol), and no prior history of cardiovascular disease (CVD). They had slightly elevated CVD biomarkers, including a mean low-density lipoprotein (LDL) cholesterol level of 2.33 mmol/L, lipoprotein (a) level of 15 nmol/L, and N-terminal pro-B-type natriuretic peptide level of 125.3 ng/L.
All underwent a noninvasive carotid ultrasound and coronary artery calcium (CAC) scoring. Of those, 12 patients had a CAC score > 400 and/or presence of two or more carotid plaques identified as high-risk.
Those 12 patients underwent coronary angiography and had a total of 29 vessels examined by optical coherence tomography (OCT), “an invasive intravascular method for assessing coronary atherosclerosis that is far more sensitive than standard coronary angiography, especially for the detection of high-risk vulnerable plaques without a hemodynamically significant stenosis,” Dr. Dubsky explained.
Coronary angiography showed obstructive CAD in 5 of the 12 patients. Their mean calcium score was 950 and mean number of carotid plaques was 2.8. Features associated with plaque vulnerability included microphage accumulation in 24 vessels, lipid-rich plaques in 23, spotty calcium in 19, and neovascularizations in 13.
Thin-cap fibroatheroma, a strong predictor of plaque rupture, was present in 7 of the 12 patients (58.3%), and four had features of very high-risk plaques, defined as thin-cap fibroatheroma with a minimal lumen area < 3.5 mm2, a lipid arch > 180 degrees, and macrophages.
“Our study showed that asymptomatic T1D patients with high CAC score and carotid plaques had very severe OCT findings. We observed a significant proportion of high-risk lesions potentially associated with plaque rupture and risk of CV death. Therefore, we believe these patients should be treated as very high-risk with target LDL below 1.4 mmol/L (55 mg/dL), even though they are completely asymptomatic,” Dr. Dubsky concluded.
He added that because OCT is invasive and costly, the CAC score can be used to guide the decision for statin use, with any score above 100 considered elevated risk.
Study coauthor Martin Haluzik, MD, professor of internal medicine in the Charles University, Prague, Czech Republic, told this news organization, “I think it’s very alarming because some of these are basically very healthy-looking young people, so you don’t really expect them to have significant cardiovascular complications already or significant plaques. I think it shows that we should be more proactive in looking into the risk of cardiovascular complications and in looking into the early cardiovascular changes.”
Later Diagnosis Doesn’t Always Protect: Risk Seen in Adult-Onset T1D
Yuxia Wei, a PhD student at the Institute of Environmental Medicine, Karolinska Institutet, Stockholm, Sweden, presented an analysis of data from Sweden’s national health databases comparing cardiovascular outcomes between 10,184 people diagnosed with T1D at ages 18-29 years, 30-39 years, and ≥ 40 years; another 375,523 people diagnosed with T2D at those ages; and 509,172 population controls matched for age, sex, and county.
Those diagnosed after age 40 years had higher A1c levels and were less likely to be using insulin pumps than those diagnosed at younger adult ages.
Compared with population controls, at a median of about 7 years of follow-up, people with T1D had significantly higher all-cause mortality at all diagnosis age groups, with a hazard ratio of 1.71. This rose to 2.78 for those diagnosed at age 30-39 years.
Compared with those with T2D, the mortality risks weren’t significantly different at any age, but the risks for non-cardiovascular death, including from cancer and infection, were significantly higher among those diagnosed after age 40 years (1.31 overall). Those diagnosed with T1D at any adult age had lower risks for major cardiovascular events than those diagnosed with T2D. Hazard ratios ranged from 0.27 for those diagnosed at age 18-29 years to 0.78 for those diagnosed after the age of 40 years.
Smoking and A1c above target were the greatest contributors to mortality. Those two factors, along with body mass index (BMI), were the strongest contributors to major adverse cardiovascular events (MACE).
“Adult-onset T1D carries excess risk of death and cardiovascular disease, without obvious attenuation over age at diagnosis…Smoking, A1c, and BMI are the key factors to be managed to improve prognosis in adult-onset T1D,” Ms. Wei concluded.
BMI: Often Overlooked in T1D, but a Major CVD Risk Factor
Two studies examined the link between overweight/obesity and cardiovascular risk in T1D. One, by Laurence Salle, MCU PH, of the Endocrinology, Diabetes and Metabolic Diseases Department at CHU Limoges, France, was a prospective, longitudinal cohort study of 2367 people with T1D at 68 centers in France who didn’t have a cardiovascular history at baseline.
Of those, 51% had normal BMI (18.5-24.9), 31% had overweight (25-29.9), and 18% had obesity (≥ 30). Cardiovascular risk factors, including LDL cholesterol, triglycerides, and hypertension increased with an increasing BMI. The 10-year CVD risk was significantly higher for those with overweight (9.61%) and obesity (9.93%) than for those with normal weight (7.24%), in both men and women.
However, BMI was found to be an independent predictor of 10-year high cardiovascular risk in men but not women, while waist:height ratio independently predicted risk in both men and women, Dr. Salle reported.
The second BMI study, from Enrique Soto-Pedre, MBBS, of the Division of Population Health and Genomics at the University of Dundee, Scotland, presented data on a retrospective follow-up from 1995 to 2019 of 1973 people with T1D aged > 18 years at diagnosis (42% women; mean age, 34.2 years; 18.9% had obesity.
After 10 years of follow-up, those with overweight and obesity had significantly higher odds of developing arterial hypertension, even among those taking angiotensin-converting enzyme inhibitors/angiotensin receptor blockers, with statistically significant adjusted hazard ratios of 1.73 and 3.37 for the obese and overweight groups, respectively.
MACE were significantly more common among those with obesity, with an adjusted hazard ratio of 2.95, as was acute myocardial infarction, 3.33.
“These results emphasize the importance of incorporating weight management into the overall management of individuals with T1D. No one has doubts about weight management in T2D, but in type 1, it’s not so clear. One of the main [concerns] would be safety [in terms of hypoglycemia],” Dr. Soto-Pedre concluded.
Call for Action: Cumulative Glucose and Lipid Exposures Increase Risk
Dr. Bergdal presented data on the effects of cumulative glycemia and lipids on the risk for CAD in 3495 adults with T1D who had been diagnosed prior to the age of 40 years. The history of CAD or stroke was exclusion criteria. There were a total of 534 CAD events within a median follow-up of 19.4 years.
Cumulative glycemia, LDL cholesterol, triglycerides, and non–high-density lipoprotein cholesterol exposures were all significantly associated with CAD risk (P < .001 for all). With an adjustment for confounders, the highest tertile of glycemia was associated with a twofold increased risk for CAD. Both hyperglycemia and dyslipidemia were independently associated with CAD risk, Dr. Bergdal reported.
“It’s important to minimize the time spent above A1c 7%, and lipid management in T1D must not be forgotten,” she said, prior to issuing her call for action.
Dr. Haluzik reported receiving honoraria for talks and/or consultancy and/or research funding from Eli Lilly, Novo Nordisk, Sanofi, AstraZeneca, Mundipharma, Bristol Myers Squibb, Amgen, Boehringer Ingelheim, Janssen, Ypsomed, and Johnson & Johnson. The presenters had no disclosures.
A version of this article first appeared on Medscape.com.
MADRID — Emerging data points to the urgent need for cardiovascular risk reduction in all adults with type 1 diabetes (T1D), including those who are young and those diagnosed in adulthood.
At the European Association for the Study of Diabetes (EASD) 2024 Annual Meeting, two entire oral abstract sessions were devoted to research examining cardiovascular risk specifically in people with T1D. There is increasing evidence that as with type 2 diabetes (T2D), clinical visits need to focus on other cardiovascular risk factors and glucose.
Findings included the evidence of severe coronary artery disease (CAD) in asymptomatic adults with T1D, increased risks for mortality and cardiac events in people diagnosed with T1D in adulthood, and a greater cardiovascular risk for those with overweight/obesity and among those with more cumulative exposure to both hyperglycemia and dyslipidemia.
One speaker, Dr. Rebecka Johanna Bergdal, of the Folkhälsan Research Center and the University of Helsinki, Finland, issued a “call to action,” saying, “We call on healthcare professionals to continue supporting and encouraging individuals with T1D towards better management of diabetes, including both glucose and lipid management.”
Session Moderator Krzysztof Strojek, MD, PhD, head of the Department of Internal Medicine, Diabetology and Cardiometabolic Diseases at the Medical University of Silesia, Katowice, Poland, told this news organization that all the data point in the same direction for T1D management, to “look not only at A1c and blood glucose control but also lipids, hypertension, smoking status, all these risk factors recognized in type 2 ... are also important in T1D.”
The ‘Alarming’ Finding of CAD in Asymptomatic Patients
Michal Dubsky, MD, PhD, of the Diabetes Centre, Institute for Clinical and Experimental Medicine, Prague, Czech Republic, presented findings from 62 asymptomatic patients with T1D for > 10 years (mean, 36 years), with a mean A1c of 7.5% (58 mmol/mol), and no prior history of cardiovascular disease (CVD). They had slightly elevated CVD biomarkers, including a mean low-density lipoprotein (LDL) cholesterol level of 2.33 mmol/L, lipoprotein (a) level of 15 nmol/L, and N-terminal pro-B-type natriuretic peptide level of 125.3 ng/L.
All underwent a noninvasive carotid ultrasound and coronary artery calcium (CAC) scoring. Of those, 12 patients had a CAC score > 400 and/or presence of two or more carotid plaques identified as high-risk.
Those 12 patients underwent coronary angiography and had a total of 29 vessels examined by optical coherence tomography (OCT), “an invasive intravascular method for assessing coronary atherosclerosis that is far more sensitive than standard coronary angiography, especially for the detection of high-risk vulnerable plaques without a hemodynamically significant stenosis,” Dr. Dubsky explained.
Coronary angiography showed obstructive CAD in 5 of the 12 patients. Their mean calcium score was 950 and mean number of carotid plaques was 2.8. Features associated with plaque vulnerability included microphage accumulation in 24 vessels, lipid-rich plaques in 23, spotty calcium in 19, and neovascularizations in 13.
Thin-cap fibroatheroma, a strong predictor of plaque rupture, was present in 7 of the 12 patients (58.3%), and four had features of very high-risk plaques, defined as thin-cap fibroatheroma with a minimal lumen area < 3.5 mm2, a lipid arch > 180 degrees, and macrophages.
“Our study showed that asymptomatic T1D patients with high CAC score and carotid plaques had very severe OCT findings. We observed a significant proportion of high-risk lesions potentially associated with plaque rupture and risk of CV death. Therefore, we believe these patients should be treated as very high-risk with target LDL below 1.4 mmol/L (55 mg/dL), even though they are completely asymptomatic,” Dr. Dubsky concluded.
He added that because OCT is invasive and costly, the CAC score can be used to guide the decision for statin use, with any score above 100 considered elevated risk.
Study coauthor Martin Haluzik, MD, professor of internal medicine in the Charles University, Prague, Czech Republic, told this news organization, “I think it’s very alarming because some of these are basically very healthy-looking young people, so you don’t really expect them to have significant cardiovascular complications already or significant plaques. I think it shows that we should be more proactive in looking into the risk of cardiovascular complications and in looking into the early cardiovascular changes.”
Later Diagnosis Doesn’t Always Protect: Risk Seen in Adult-Onset T1D
Yuxia Wei, a PhD student at the Institute of Environmental Medicine, Karolinska Institutet, Stockholm, Sweden, presented an analysis of data from Sweden’s national health databases comparing cardiovascular outcomes between 10,184 people diagnosed with T1D at ages 18-29 years, 30-39 years, and ≥ 40 years; another 375,523 people diagnosed with T2D at those ages; and 509,172 population controls matched for age, sex, and county.
Those diagnosed after age 40 years had higher A1c levels and were less likely to be using insulin pumps than those diagnosed at younger adult ages.
Compared with population controls, at a median of about 7 years of follow-up, people with T1D had significantly higher all-cause mortality at all diagnosis age groups, with a hazard ratio of 1.71. This rose to 2.78 for those diagnosed at age 30-39 years.
Compared with those with T2D, the mortality risks weren’t significantly different at any age, but the risks for non-cardiovascular death, including from cancer and infection, were significantly higher among those diagnosed after age 40 years (1.31 overall). Those diagnosed with T1D at any adult age had lower risks for major cardiovascular events than those diagnosed with T2D. Hazard ratios ranged from 0.27 for those diagnosed at age 18-29 years to 0.78 for those diagnosed after the age of 40 years.
Smoking and A1c above target were the greatest contributors to mortality. Those two factors, along with body mass index (BMI), were the strongest contributors to major adverse cardiovascular events (MACE).
“Adult-onset T1D carries excess risk of death and cardiovascular disease, without obvious attenuation over age at diagnosis…Smoking, A1c, and BMI are the key factors to be managed to improve prognosis in adult-onset T1D,” Ms. Wei concluded.
BMI: Often Overlooked in T1D, but a Major CVD Risk Factor
Two studies examined the link between overweight/obesity and cardiovascular risk in T1D. One, by Laurence Salle, MCU PH, of the Endocrinology, Diabetes and Metabolic Diseases Department at CHU Limoges, France, was a prospective, longitudinal cohort study of 2367 people with T1D at 68 centers in France who didn’t have a cardiovascular history at baseline.
Of those, 51% had normal BMI (18.5-24.9), 31% had overweight (25-29.9), and 18% had obesity (≥ 30). Cardiovascular risk factors, including LDL cholesterol, triglycerides, and hypertension increased with an increasing BMI. The 10-year CVD risk was significantly higher for those with overweight (9.61%) and obesity (9.93%) than for those with normal weight (7.24%), in both men and women.
However, BMI was found to be an independent predictor of 10-year high cardiovascular risk in men but not women, while waist:height ratio independently predicted risk in both men and women, Dr. Salle reported.
The second BMI study, from Enrique Soto-Pedre, MBBS, of the Division of Population Health and Genomics at the University of Dundee, Scotland, presented data on a retrospective follow-up from 1995 to 2019 of 1973 people with T1D aged > 18 years at diagnosis (42% women; mean age, 34.2 years; 18.9% had obesity.
After 10 years of follow-up, those with overweight and obesity had significantly higher odds of developing arterial hypertension, even among those taking angiotensin-converting enzyme inhibitors/angiotensin receptor blockers, with statistically significant adjusted hazard ratios of 1.73 and 3.37 for the obese and overweight groups, respectively.
MACE were significantly more common among those with obesity, with an adjusted hazard ratio of 2.95, as was acute myocardial infarction, 3.33.
“These results emphasize the importance of incorporating weight management into the overall management of individuals with T1D. No one has doubts about weight management in T2D, but in type 1, it’s not so clear. One of the main [concerns] would be safety [in terms of hypoglycemia],” Dr. Soto-Pedre concluded.
Call for Action: Cumulative Glucose and Lipid Exposures Increase Risk
Dr. Bergdal presented data on the effects of cumulative glycemia and lipids on the risk for CAD in 3495 adults with T1D who had been diagnosed prior to the age of 40 years. The history of CAD or stroke was exclusion criteria. There were a total of 534 CAD events within a median follow-up of 19.4 years.
Cumulative glycemia, LDL cholesterol, triglycerides, and non–high-density lipoprotein cholesterol exposures were all significantly associated with CAD risk (P < .001 for all). With an adjustment for confounders, the highest tertile of glycemia was associated with a twofold increased risk for CAD. Both hyperglycemia and dyslipidemia were independently associated with CAD risk, Dr. Bergdal reported.
“It’s important to minimize the time spent above A1c 7%, and lipid management in T1D must not be forgotten,” she said, prior to issuing her call for action.
Dr. Haluzik reported receiving honoraria for talks and/or consultancy and/or research funding from Eli Lilly, Novo Nordisk, Sanofi, AstraZeneca, Mundipharma, Bristol Myers Squibb, Amgen, Boehringer Ingelheim, Janssen, Ypsomed, and Johnson & Johnson. The presenters had no disclosures.
A version of this article first appeared on Medscape.com.
FROM EASD 2024