User login
Ten reasons airborne transmission of SARS-CoV-2 appears airtight
The scientific evidence for airborne transmission of the SARS-CoV-2 virus from different researchers all point in the same direction – that infectious aerosols are the principal means of person-to-person transmission, according to experts.
Not that it’s without controversy.
The science backing aerosol transmission “is clear-cut, but it is not accepted in many circles,” Trisha Greenhalgh, PhD, said in an interview.
“In particular, some in the evidence-based medicine movement and some infectious diseases clinicians are remarkably resistant to the evidence,” added Dr. Greenhalgh, professor of primary care health sciences at the University of Oxford (England).
“It’s very hard to see why, since the evidence all stacks up,” Dr. Greenhalgh said.
“The scientific evidence on spread from both near-field and far-field aerosols has been clear since early on in the pandemic, but there was resistance to acknowledging this in some circles, including the medical journals,” Joseph G. Allen, DSc, MPH, told this news organization when asked to comment.
“This is the week the dam broke. Three new commentaries came out … in top medical journals – BMJ, The Lancet, JAMA – all making the same point that aerosols are the dominant mode of transmission,” added Dr. Allen, associate professor of exposure assessment science at the Harvard T.H. Chan School of Public Health in Boston.
Dr. Greenhalgh and colleagues point to an increase in COVID-19 cases in the aftermath of so-called “super-spreader” events, spread of SARS-CoV-2 to people across different hotel rooms, and the relatively lower transmission detected after outdoor events.
Top 10 reasons
They outlined 10 scientific reasons backing airborne transmission in a commentary published online April 15 in The Lancet:
- The dominance of airborne transmission is supported by long-range transmission observed at super-spreader events.
- Long-range transmission has been reported among rooms at COVID-19 quarantine hotels, settings where infected people never spent time in the same room.
- Asymptomatic individuals account for an estimated 33%-59% of SARS-CoV-2 transmission, and could be spreading the virus through speaking, which produces thousands of aerosol particles and few large droplets.
- Transmission outdoors and in well-ventilated indoor spaces is lower than in enclosed spaces.
- Nosocomial infections are reported in health care settings where protective measures address large droplets but not aerosols.
- Viable SARS-CoV-2 has been detected in the air of hospital rooms and in the car of an infected person.
- Investigators found SARS-CoV-2 in hospital air filters and building ducts.
- It’s not just humans – infected animals can infect animals in other cages connected only through an air duct.
- No strong evidence refutes airborne transmission, and contact tracing supports secondary transmission in crowded, poorly ventilated indoor spaces.
- Only limited evidence supports other means of SARS-CoV-2 transmission, including through fomites or large droplets.
“We thought we’d summarize [the evidence] to clarify the arguments for and against. We looked hard for evidence against but found none,” Dr. Greenhalgh said.
“Although other routes can contribute, we believe that the airborne route is likely to be dominant,” the authors note.
The evidence on airborne transmission was there very early on but the Centers for Disease Control and Prevention, World Health Organization, and others repeated the message that the primary concern was droplets and fomites.
Response to a review
The top 10 list is also part rebuttal of a systematic review funded by the WHO and published last month that points to inconclusive evidence for airborne transmission. The researchers involved with that review state that “the lack of recoverable viral culture samples of SARS-CoV-2 prevents firm conclusions to be drawn about airborne transmission.”
However, Dr. Greenhalgh and colleagues note that “this conclusion, and the wide circulation of the review’s findings, is concerning because of the public health implications.”
The current authors also argue that enough evidence already exists on airborne transmission. “Policy should change. We don’t need more research on this topic; we need different policy,” Dr. Greenhalgh said. “We need ventilation front and center, air filtration when necessary, and better-fitting masks worn whenever indoors.”
Dr. Allen agreed that guidance hasn’t always kept pace with the science. “With all of the new evidence accumulated on airborne transmission since last winter, there is still widespread confusion in the public about modes of transmission,” he said. Dr. Allen also serves as commissioner of The Lancet COVID-19 Commission and is chair of the commission’s Task Force on Safe Work, Safe Schools, and Safe Travel.
“It was only just last week that CDC pulled back on guidance on ‘deep cleaning’ and in its place correctly said that the risk from touching surfaces is low,” he added. “The science has been clear on this for over a year, but official guidance was only recently updated.”
As a result, many companies and organizations continued to focus on “hygiene theatre,” Dr. Allen said, “wasting resources on overcleaning surfaces. Unbelievably, many schools still close for an entire day each week for deep cleaning and some still quarantine library books. The message that shared air is the problem, not shared surfaces, is a message that still needs to be reinforced.”
The National Institute for Health Research, Economic and Social Research Council, and Wellcome support Dr. Greenhalgh’s research. Dr. Greenhalgh and Dr. Allen had no relevant financial relationships to disclose.
A version of this article first appeared on Medscape.com.
The scientific evidence for airborne transmission of the SARS-CoV-2 virus from different researchers all point in the same direction – that infectious aerosols are the principal means of person-to-person transmission, according to experts.
Not that it’s without controversy.
The science backing aerosol transmission “is clear-cut, but it is not accepted in many circles,” Trisha Greenhalgh, PhD, said in an interview.
“In particular, some in the evidence-based medicine movement and some infectious diseases clinicians are remarkably resistant to the evidence,” added Dr. Greenhalgh, professor of primary care health sciences at the University of Oxford (England).
“It’s very hard to see why, since the evidence all stacks up,” Dr. Greenhalgh said.
“The scientific evidence on spread from both near-field and far-field aerosols has been clear since early on in the pandemic, but there was resistance to acknowledging this in some circles, including the medical journals,” Joseph G. Allen, DSc, MPH, told this news organization when asked to comment.
“This is the week the dam broke. Three new commentaries came out … in top medical journals – BMJ, The Lancet, JAMA – all making the same point that aerosols are the dominant mode of transmission,” added Dr. Allen, associate professor of exposure assessment science at the Harvard T.H. Chan School of Public Health in Boston.
Dr. Greenhalgh and colleagues point to an increase in COVID-19 cases in the aftermath of so-called “super-spreader” events, spread of SARS-CoV-2 to people across different hotel rooms, and the relatively lower transmission detected after outdoor events.
Top 10 reasons
They outlined 10 scientific reasons backing airborne transmission in a commentary published online April 15 in The Lancet:
- The dominance of airborne transmission is supported by long-range transmission observed at super-spreader events.
- Long-range transmission has been reported among rooms at COVID-19 quarantine hotels, settings where infected people never spent time in the same room.
- Asymptomatic individuals account for an estimated 33%-59% of SARS-CoV-2 transmission, and could be spreading the virus through speaking, which produces thousands of aerosol particles and few large droplets.
- Transmission outdoors and in well-ventilated indoor spaces is lower than in enclosed spaces.
- Nosocomial infections are reported in health care settings where protective measures address large droplets but not aerosols.
- Viable SARS-CoV-2 has been detected in the air of hospital rooms and in the car of an infected person.
- Investigators found SARS-CoV-2 in hospital air filters and building ducts.
- It’s not just humans – infected animals can infect animals in other cages connected only through an air duct.
- No strong evidence refutes airborne transmission, and contact tracing supports secondary transmission in crowded, poorly ventilated indoor spaces.
- Only limited evidence supports other means of SARS-CoV-2 transmission, including through fomites or large droplets.
“We thought we’d summarize [the evidence] to clarify the arguments for and against. We looked hard for evidence against but found none,” Dr. Greenhalgh said.
“Although other routes can contribute, we believe that the airborne route is likely to be dominant,” the authors note.
The evidence on airborne transmission was there very early on but the Centers for Disease Control and Prevention, World Health Organization, and others repeated the message that the primary concern was droplets and fomites.
Response to a review
The top 10 list is also part rebuttal of a systematic review funded by the WHO and published last month that points to inconclusive evidence for airborne transmission. The researchers involved with that review state that “the lack of recoverable viral culture samples of SARS-CoV-2 prevents firm conclusions to be drawn about airborne transmission.”
However, Dr. Greenhalgh and colleagues note that “this conclusion, and the wide circulation of the review’s findings, is concerning because of the public health implications.”
The current authors also argue that enough evidence already exists on airborne transmission. “Policy should change. We don’t need more research on this topic; we need different policy,” Dr. Greenhalgh said. “We need ventilation front and center, air filtration when necessary, and better-fitting masks worn whenever indoors.”
Dr. Allen agreed that guidance hasn’t always kept pace with the science. “With all of the new evidence accumulated on airborne transmission since last winter, there is still widespread confusion in the public about modes of transmission,” he said. Dr. Allen also serves as commissioner of The Lancet COVID-19 Commission and is chair of the commission’s Task Force on Safe Work, Safe Schools, and Safe Travel.
“It was only just last week that CDC pulled back on guidance on ‘deep cleaning’ and in its place correctly said that the risk from touching surfaces is low,” he added. “The science has been clear on this for over a year, but official guidance was only recently updated.”
As a result, many companies and organizations continued to focus on “hygiene theatre,” Dr. Allen said, “wasting resources on overcleaning surfaces. Unbelievably, many schools still close for an entire day each week for deep cleaning and some still quarantine library books. The message that shared air is the problem, not shared surfaces, is a message that still needs to be reinforced.”
The National Institute for Health Research, Economic and Social Research Council, and Wellcome support Dr. Greenhalgh’s research. Dr. Greenhalgh and Dr. Allen had no relevant financial relationships to disclose.
A version of this article first appeared on Medscape.com.
The scientific evidence for airborne transmission of the SARS-CoV-2 virus from different researchers all point in the same direction – that infectious aerosols are the principal means of person-to-person transmission, according to experts.
Not that it’s without controversy.
The science backing aerosol transmission “is clear-cut, but it is not accepted in many circles,” Trisha Greenhalgh, PhD, said in an interview.
“In particular, some in the evidence-based medicine movement and some infectious diseases clinicians are remarkably resistant to the evidence,” added Dr. Greenhalgh, professor of primary care health sciences at the University of Oxford (England).
“It’s very hard to see why, since the evidence all stacks up,” Dr. Greenhalgh said.
“The scientific evidence on spread from both near-field and far-field aerosols has been clear since early on in the pandemic, but there was resistance to acknowledging this in some circles, including the medical journals,” Joseph G. Allen, DSc, MPH, told this news organization when asked to comment.
“This is the week the dam broke. Three new commentaries came out … in top medical journals – BMJ, The Lancet, JAMA – all making the same point that aerosols are the dominant mode of transmission,” added Dr. Allen, associate professor of exposure assessment science at the Harvard T.H. Chan School of Public Health in Boston.
Dr. Greenhalgh and colleagues point to an increase in COVID-19 cases in the aftermath of so-called “super-spreader” events, spread of SARS-CoV-2 to people across different hotel rooms, and the relatively lower transmission detected after outdoor events.
Top 10 reasons
They outlined 10 scientific reasons backing airborne transmission in a commentary published online April 15 in The Lancet:
- The dominance of airborne transmission is supported by long-range transmission observed at super-spreader events.
- Long-range transmission has been reported among rooms at COVID-19 quarantine hotels, settings where infected people never spent time in the same room.
- Asymptomatic individuals account for an estimated 33%-59% of SARS-CoV-2 transmission, and could be spreading the virus through speaking, which produces thousands of aerosol particles and few large droplets.
- Transmission outdoors and in well-ventilated indoor spaces is lower than in enclosed spaces.
- Nosocomial infections are reported in health care settings where protective measures address large droplets but not aerosols.
- Viable SARS-CoV-2 has been detected in the air of hospital rooms and in the car of an infected person.
- Investigators found SARS-CoV-2 in hospital air filters and building ducts.
- It’s not just humans – infected animals can infect animals in other cages connected only through an air duct.
- No strong evidence refutes airborne transmission, and contact tracing supports secondary transmission in crowded, poorly ventilated indoor spaces.
- Only limited evidence supports other means of SARS-CoV-2 transmission, including through fomites or large droplets.
“We thought we’d summarize [the evidence] to clarify the arguments for and against. We looked hard for evidence against but found none,” Dr. Greenhalgh said.
“Although other routes can contribute, we believe that the airborne route is likely to be dominant,” the authors note.
The evidence on airborne transmission was there very early on but the Centers for Disease Control and Prevention, World Health Organization, and others repeated the message that the primary concern was droplets and fomites.
Response to a review
The top 10 list is also part rebuttal of a systematic review funded by the WHO and published last month that points to inconclusive evidence for airborne transmission. The researchers involved with that review state that “the lack of recoverable viral culture samples of SARS-CoV-2 prevents firm conclusions to be drawn about airborne transmission.”
However, Dr. Greenhalgh and colleagues note that “this conclusion, and the wide circulation of the review’s findings, is concerning because of the public health implications.”
The current authors also argue that enough evidence already exists on airborne transmission. “Policy should change. We don’t need more research on this topic; we need different policy,” Dr. Greenhalgh said. “We need ventilation front and center, air filtration when necessary, and better-fitting masks worn whenever indoors.”
Dr. Allen agreed that guidance hasn’t always kept pace with the science. “With all of the new evidence accumulated on airborne transmission since last winter, there is still widespread confusion in the public about modes of transmission,” he said. Dr. Allen also serves as commissioner of The Lancet COVID-19 Commission and is chair of the commission’s Task Force on Safe Work, Safe Schools, and Safe Travel.
“It was only just last week that CDC pulled back on guidance on ‘deep cleaning’ and in its place correctly said that the risk from touching surfaces is low,” he added. “The science has been clear on this for over a year, but official guidance was only recently updated.”
As a result, many companies and organizations continued to focus on “hygiene theatre,” Dr. Allen said, “wasting resources on overcleaning surfaces. Unbelievably, many schools still close for an entire day each week for deep cleaning and some still quarantine library books. The message that shared air is the problem, not shared surfaces, is a message that still needs to be reinforced.”
The National Institute for Health Research, Economic and Social Research Council, and Wellcome support Dr. Greenhalgh’s research. Dr. Greenhalgh and Dr. Allen had no relevant financial relationships to disclose.
A version of this article first appeared on Medscape.com.
Children’s share of COVID-19 burden has never been higher
For the first time since the pandemic began, children’s share of weekly COVID-19 cases topped 20% in the United States, according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.
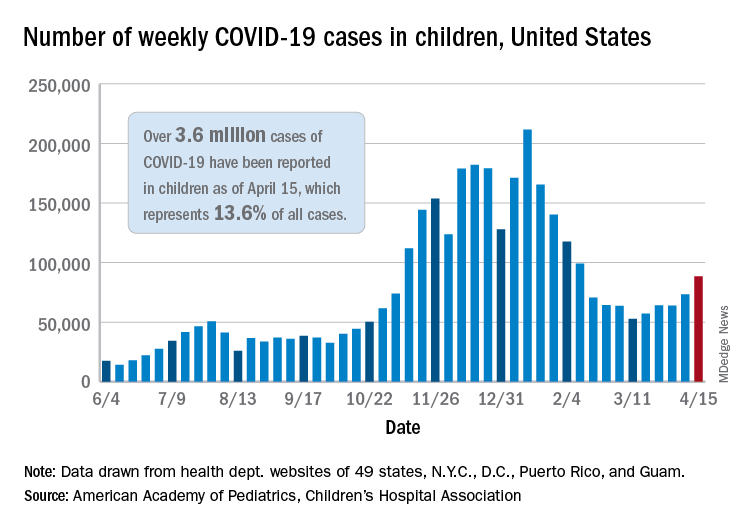
That represented 20.6% of all new cases for the week, eclipsing the previous high of 19.1% recorded just 3 weeks ago, based on data collected by the AAP and CHA from 49 states, the District of Columbia, New York City, Puerto Rico, and Guam.
Cumulative cases of COVID-19 in children exceed 3.6 million in those jurisdictions, which is 13.6% of the total reported among all ages, and the overall rate of coronavirus infection is 4,824 cases per 100,000 children in the population, the AAP and CHA said in their weekly COVID-19 report.
Among the 53 reporting jurisdictions, North Dakota has the highest cumulative rate, 9,167 per 100,000 children, followed by Tennessee (8,580), South Carolina (7,948), South Dakota (7,938), and Connecticut (7,707). Children’s share of cumulative cases is highest in Vermont, at 21.9%, with Alaska next at 20.0% and Wyoming at 19.2%, the AAP and CHA said.
Since the beginning of April, the largest local increases in cases reported came in Michigan (21.6%), Vermont (15.9%), and Maine (15.6%). Nationally, the increase over those same 2 weeks is just under 5%, the two organizations noted.
There were 5 deaths among children during the week of April 9-15, bringing the total to 297, but the recent increases in cases have not affected the long-term trends for serious illness. The death rate for children with COVID-19 has been 0.01% since early November – 43 states, New York City, Puerto Rico, and Guam are reporting such data – and the hospitalization rate has been 0.8% since mid-January in 24 states and New York City, the AAP/CHA data show.
For the first time since the pandemic began, children’s share of weekly COVID-19 cases topped 20% in the United States, according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.
That represented 20.6% of all new cases for the week, eclipsing the previous high of 19.1% recorded just 3 weeks ago, based on data collected by the AAP and CHA from 49 states, the District of Columbia, New York City, Puerto Rico, and Guam.
Cumulative cases of COVID-19 in children exceed 3.6 million in those jurisdictions, which is 13.6% of the total reported among all ages, and the overall rate of coronavirus infection is 4,824 cases per 100,000 children in the population, the AAP and CHA said in their weekly COVID-19 report.
Among the 53 reporting jurisdictions, North Dakota has the highest cumulative rate, 9,167 per 100,000 children, followed by Tennessee (8,580), South Carolina (7,948), South Dakota (7,938), and Connecticut (7,707). Children’s share of cumulative cases is highest in Vermont, at 21.9%, with Alaska next at 20.0% and Wyoming at 19.2%, the AAP and CHA said.
Since the beginning of April, the largest local increases in cases reported came in Michigan (21.6%), Vermont (15.9%), and Maine (15.6%). Nationally, the increase over those same 2 weeks is just under 5%, the two organizations noted.
There were 5 deaths among children during the week of April 9-15, bringing the total to 297, but the recent increases in cases have not affected the long-term trends for serious illness. The death rate for children with COVID-19 has been 0.01% since early November – 43 states, New York City, Puerto Rico, and Guam are reporting such data – and the hospitalization rate has been 0.8% since mid-January in 24 states and New York City, the AAP/CHA data show.
For the first time since the pandemic began, children’s share of weekly COVID-19 cases topped 20% in the United States, according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.
That represented 20.6% of all new cases for the week, eclipsing the previous high of 19.1% recorded just 3 weeks ago, based on data collected by the AAP and CHA from 49 states, the District of Columbia, New York City, Puerto Rico, and Guam.
Cumulative cases of COVID-19 in children exceed 3.6 million in those jurisdictions, which is 13.6% of the total reported among all ages, and the overall rate of coronavirus infection is 4,824 cases per 100,000 children in the population, the AAP and CHA said in their weekly COVID-19 report.
Among the 53 reporting jurisdictions, North Dakota has the highest cumulative rate, 9,167 per 100,000 children, followed by Tennessee (8,580), South Carolina (7,948), South Dakota (7,938), and Connecticut (7,707). Children’s share of cumulative cases is highest in Vermont, at 21.9%, with Alaska next at 20.0% and Wyoming at 19.2%, the AAP and CHA said.
Since the beginning of April, the largest local increases in cases reported came in Michigan (21.6%), Vermont (15.9%), and Maine (15.6%). Nationally, the increase over those same 2 weeks is just under 5%, the two organizations noted.
There were 5 deaths among children during the week of April 9-15, bringing the total to 297, but the recent increases in cases have not affected the long-term trends for serious illness. The death rate for children with COVID-19 has been 0.01% since early November – 43 states, New York City, Puerto Rico, and Guam are reporting such data – and the hospitalization rate has been 0.8% since mid-January in 24 states and New York City, the AAP/CHA data show.
Watch for abnormal movements in hospitalized COVID-19 patients
Myoclonus was diagnosed in about half of hospitalized COVID-19 patients who were evaluated for movement disorders, data from 50 cases show.
Abnormal movements often occur as complications from critical illness, and neurologic consultation can determine whether patients have experienced a seizure or stroke. However, restriction of bedside assessment in the wake of the COVID-19 pandemic increases the risk that abnormal movements will be missed, Jeffrey R. Clark and Eric M. Liotta, MD, of Northwestern University, Chicago, and colleagues wrote.
“Given the limited reports of abnormal movements in hospitalized COVID-19 patients and increased recognition of neurologic manifestations of COVID-19, we sought to examine the frequency and etiology of this finding as an indication of neurologic consultation,” they said.
In a study published in the Journal of the Neurological Sciences, the researchers reviewed data from the first 50 consecutive patients with COVID-19 symptoms who were hospitalized at a single center and underwent neurologic consultation between March 17, 2020, and May 18, 2020.
Overall, 11 patients (22.0%) of patients experienced abnormal movement, and all were admitted to the ICU within 7 days of meeting criteria for severe COVID-19. These patients included nine men and two women with an age range of 36-78 years. The most common comorbidities were obesity, hypertension, diabetes, chronic kidney disease, and coronary artery disease.
Myoclonus (generalized and focal) was the most common abnormal movement, and present in 6 of the 11 patients. Three cases were attributed to high-intensity sedation, and three to toxic-metabolic disturbances. In two patients, abnormal movements were attributed to focal seizures in the setting of encephalopathy, with focal facial twitching. An additional two patients experienced tremors; one showed an acute subdural hemorrhage on CT imaging. The second patient showed no sign of stroke or other abnormality on MRI and the tremor improved during the hospital stay. One patient who experienced abnormal high-amplitude nonrhythmic movements of the lower extremities was diagnosed with serotonin syndrome that resolved after discontinuing high-dose fentanyl.
The study findings were limited by several factors, including the small study population and limited availability of MRI, the researchers noted. Assessing severe COVID-19 cases in the ICU setting presents a challenge because of limited patient participation and the potentially confounding effects of sedation and mechanical ventilation.
However, the researchers said.
“A heightened awareness of abnormal eye movements, or subtle facial tremoring, may be the first steps in recognizing potentially dangerous neurologic manifestations,” and clinicians caring for patients with severe COVID-19 should be able to recognize abnormal movements and seek neurologic consultation when indicated, they emphasized.
The study was supported in part by grants to coauthors Nicholas J. Reish, MD, and Dr. Liotta from the National Institutes of Health. The researchers had no financial conflicts to disclose.
Myoclonus was diagnosed in about half of hospitalized COVID-19 patients who were evaluated for movement disorders, data from 50 cases show.
Abnormal movements often occur as complications from critical illness, and neurologic consultation can determine whether patients have experienced a seizure or stroke. However, restriction of bedside assessment in the wake of the COVID-19 pandemic increases the risk that abnormal movements will be missed, Jeffrey R. Clark and Eric M. Liotta, MD, of Northwestern University, Chicago, and colleagues wrote.
“Given the limited reports of abnormal movements in hospitalized COVID-19 patients and increased recognition of neurologic manifestations of COVID-19, we sought to examine the frequency and etiology of this finding as an indication of neurologic consultation,” they said.
In a study published in the Journal of the Neurological Sciences, the researchers reviewed data from the first 50 consecutive patients with COVID-19 symptoms who were hospitalized at a single center and underwent neurologic consultation between March 17, 2020, and May 18, 2020.
Overall, 11 patients (22.0%) of patients experienced abnormal movement, and all were admitted to the ICU within 7 days of meeting criteria for severe COVID-19. These patients included nine men and two women with an age range of 36-78 years. The most common comorbidities were obesity, hypertension, diabetes, chronic kidney disease, and coronary artery disease.
Myoclonus (generalized and focal) was the most common abnormal movement, and present in 6 of the 11 patients. Three cases were attributed to high-intensity sedation, and three to toxic-metabolic disturbances. In two patients, abnormal movements were attributed to focal seizures in the setting of encephalopathy, with focal facial twitching. An additional two patients experienced tremors; one showed an acute subdural hemorrhage on CT imaging. The second patient showed no sign of stroke or other abnormality on MRI and the tremor improved during the hospital stay. One patient who experienced abnormal high-amplitude nonrhythmic movements of the lower extremities was diagnosed with serotonin syndrome that resolved after discontinuing high-dose fentanyl.
The study findings were limited by several factors, including the small study population and limited availability of MRI, the researchers noted. Assessing severe COVID-19 cases in the ICU setting presents a challenge because of limited patient participation and the potentially confounding effects of sedation and mechanical ventilation.
However, the researchers said.
“A heightened awareness of abnormal eye movements, or subtle facial tremoring, may be the first steps in recognizing potentially dangerous neurologic manifestations,” and clinicians caring for patients with severe COVID-19 should be able to recognize abnormal movements and seek neurologic consultation when indicated, they emphasized.
The study was supported in part by grants to coauthors Nicholas J. Reish, MD, and Dr. Liotta from the National Institutes of Health. The researchers had no financial conflicts to disclose.
Myoclonus was diagnosed in about half of hospitalized COVID-19 patients who were evaluated for movement disorders, data from 50 cases show.
Abnormal movements often occur as complications from critical illness, and neurologic consultation can determine whether patients have experienced a seizure or stroke. However, restriction of bedside assessment in the wake of the COVID-19 pandemic increases the risk that abnormal movements will be missed, Jeffrey R. Clark and Eric M. Liotta, MD, of Northwestern University, Chicago, and colleagues wrote.
“Given the limited reports of abnormal movements in hospitalized COVID-19 patients and increased recognition of neurologic manifestations of COVID-19, we sought to examine the frequency and etiology of this finding as an indication of neurologic consultation,” they said.
In a study published in the Journal of the Neurological Sciences, the researchers reviewed data from the first 50 consecutive patients with COVID-19 symptoms who were hospitalized at a single center and underwent neurologic consultation between March 17, 2020, and May 18, 2020.
Overall, 11 patients (22.0%) of patients experienced abnormal movement, and all were admitted to the ICU within 7 days of meeting criteria for severe COVID-19. These patients included nine men and two women with an age range of 36-78 years. The most common comorbidities were obesity, hypertension, diabetes, chronic kidney disease, and coronary artery disease.
Myoclonus (generalized and focal) was the most common abnormal movement, and present in 6 of the 11 patients. Three cases were attributed to high-intensity sedation, and three to toxic-metabolic disturbances. In two patients, abnormal movements were attributed to focal seizures in the setting of encephalopathy, with focal facial twitching. An additional two patients experienced tremors; one showed an acute subdural hemorrhage on CT imaging. The second patient showed no sign of stroke or other abnormality on MRI and the tremor improved during the hospital stay. One patient who experienced abnormal high-amplitude nonrhythmic movements of the lower extremities was diagnosed with serotonin syndrome that resolved after discontinuing high-dose fentanyl.
The study findings were limited by several factors, including the small study population and limited availability of MRI, the researchers noted. Assessing severe COVID-19 cases in the ICU setting presents a challenge because of limited patient participation and the potentially confounding effects of sedation and mechanical ventilation.
However, the researchers said.
“A heightened awareness of abnormal eye movements, or subtle facial tremoring, may be the first steps in recognizing potentially dangerous neurologic manifestations,” and clinicians caring for patients with severe COVID-19 should be able to recognize abnormal movements and seek neurologic consultation when indicated, they emphasized.
The study was supported in part by grants to coauthors Nicholas J. Reish, MD, and Dr. Liotta from the National Institutes of Health. The researchers had no financial conflicts to disclose.
FROM THE JOURNAL OF THE NEUROLOGICAL SCIENCES
Twenty percent of dialysis patients are hesitant about COVID-19 vaccine
Among U.S. patients who regularly undergo hemodialysis, 20% had some degree of hesitancy about receiving a COVID-19 vaccine in a survey of 1,515 patients conducted during January and February 2021.
The most frequently cited concern associated with hesitancy over vaccination against the SARS-CoV-2 virus was with regard to possible adverse effects. This was cited by more than half of the patients who were concerned about being vaccinated.
Hesitancy rates were highest among people aged 44 years or younger, women, people who identified as non-Hispanic Black or non-Hispanic other (generally Native American or Pacific Islander), those with less than some college education, and those without a history of influenza vaccination, Pablo Garcia, MD, reported at the National Kidney Foundation (NKF) 2021 Spring Clinical Meetings.
Hesitancy or access?
Overall, however, the findings suggest that the main barrier to COVID-19 vaccine uptake is “access rather than hesitancy,” explained Dr. Garcia, a nephrologist at Stanford (Calif.) University. He predicts that this barrier will soon resolve, in part because of a Centers for Disease Control and Prevention program launched in March 2021 that is supplying COVID-19 vaccine to U.S. dialysis centers to administer to their patients.
“This will facilitate access to the vaccine” for patients who regularly receive hemodialysis, Dr. Garcia said during his presentation.
“Administering vaccines in dialysis clinics will help. Patients are already accustomed to receiving influenza vaccine in the clinic,” said Joseph A. Vassalotti, MD, a nephrologist at Mount Sinai Hospital, New York, and chief medical officer for the NKF.
Dr. Vassalotti cited the importance of protecting the vulnerable population of people who regularly receive hemodialysis. Among those patients, there was a 37% spike in all-cause mortality during peak weeks of the pandemic compared with similar periods during 2017-2019.
Any level of vaccine hesitancy is concerning
In an interview, he said, “Vaccination is the key to reducing this burden, so any level of vaccine hesitancy is concerning” with regard to patients who regularly undergo dialysis.
Hesitancy among patients who undergo dialysis appears to be less than in the general U.S. population, according to a series of surveys conducted from April through December 2020. In that series, hesitancy rates approached 50% in a sample of more than 8,000 people.
Hesitancy among people overall may have recently increased, at least for the short term, because of concerns over rare thrombotic events among people who receive certain types of COVID-19 vaccine, Dr. Vassalotti noted.
Dr. Garcia and associates conducted their survey from Jan. 8 to Feb. 11, 2021, among patients who regularly received hemodialysis at any of 150 randomly selected dialysis clinics that treat 30 or more patients and are managed by U.S. Renal Care. The study enrolled patients in 22 states. Most of the patients were aged 45-79 years; 30% were non-Hispanic White; 30% were Black, and 24% were Hispanic. The survey included 24 questions and took about 10 minutes to complete.
In reply to the statement, “If COVID-19 vaccine was proven safe and effective for the general population I would seek to get it,” 20% gave a reply of definitely not, probably not, or unsure; 79% answered either probably or definitely yes.
Another question asked about willingness to receive a vaccine if it was shown to be safe and effective for people receiving dialysis. In answer to that question, 19% said definitely not, probably not, or unsure.
Possible adverse effects an issue
Asked the reason why they were hesitant to receive the vaccine, 53% cited possible adverse effects; 19% cited general unease about vaccines; 19% said they did not think the COVID-19 vaccines would work; 17% said they did not think they needed a COVID-19 vaccine; and 15% said they had read or heard that COVID-19 vaccines were dangerous.
A set of questions asked survey respondents about their primary source of information about COVID-19 vaccines. About three-quarters cited television news; about 35% cited members of their dialysis clinic staff; about 30% cited friends and family; 20% cited social media; 20% cited their nephrologists; and roughly 15% cited newspapers.
The results suggest that potentially effective interventions to promote vaccine uptake include showing informational videos to patients during dialysis sessions and encouraging the staff at dialysis centers to proactively educate patients about COVID-19 vaccines and to promote uptake, suggest Dr. Garcia and Dr. Vassalotti.
Dr. Vassalotti noted that in a recent single-center survey of 90 U.S. patients undergoing hemodialysis that included 75 (85%) Black persons, the prevalence of hesitancy about COVID-19 vaccines was 50%. Hesitancy was often linked with gaps in patient education.
“We need broad educational measures, as well as targeting specific demographic groups” among whom the level of hesitancy is high, said Dr. Vassalotti.
He noted that patients who undergo dialysis are receptive to messages from dialysis clinic staff members and that this offers an “opportunity to understand misconceptions that underlie hesitancy and address them on an individual basis.”
The NKF has prepared a fact sheet for educating patients with kidney disease about the efficacy and safety of COVID-19 vaccines, Dr. Vassalotti noted.
Dr. Garcia has disclosed no relevant financial relationships. Dr. Vassalotti is an adviser and consultant to Renalytix AI and is a consultant to Janssen.
A version of this article first appeared on Medscape.com.
Among U.S. patients who regularly undergo hemodialysis, 20% had some degree of hesitancy about receiving a COVID-19 vaccine in a survey of 1,515 patients conducted during January and February 2021.
The most frequently cited concern associated with hesitancy over vaccination against the SARS-CoV-2 virus was with regard to possible adverse effects. This was cited by more than half of the patients who were concerned about being vaccinated.
Hesitancy rates were highest among people aged 44 years or younger, women, people who identified as non-Hispanic Black or non-Hispanic other (generally Native American or Pacific Islander), those with less than some college education, and those without a history of influenza vaccination, Pablo Garcia, MD, reported at the National Kidney Foundation (NKF) 2021 Spring Clinical Meetings.
Hesitancy or access?
Overall, however, the findings suggest that the main barrier to COVID-19 vaccine uptake is “access rather than hesitancy,” explained Dr. Garcia, a nephrologist at Stanford (Calif.) University. He predicts that this barrier will soon resolve, in part because of a Centers for Disease Control and Prevention program launched in March 2021 that is supplying COVID-19 vaccine to U.S. dialysis centers to administer to their patients.
“This will facilitate access to the vaccine” for patients who regularly receive hemodialysis, Dr. Garcia said during his presentation.
“Administering vaccines in dialysis clinics will help. Patients are already accustomed to receiving influenza vaccine in the clinic,” said Joseph A. Vassalotti, MD, a nephrologist at Mount Sinai Hospital, New York, and chief medical officer for the NKF.
Dr. Vassalotti cited the importance of protecting the vulnerable population of people who regularly receive hemodialysis. Among those patients, there was a 37% spike in all-cause mortality during peak weeks of the pandemic compared with similar periods during 2017-2019.
Any level of vaccine hesitancy is concerning
In an interview, he said, “Vaccination is the key to reducing this burden, so any level of vaccine hesitancy is concerning” with regard to patients who regularly undergo dialysis.
Hesitancy among patients who undergo dialysis appears to be less than in the general U.S. population, according to a series of surveys conducted from April through December 2020. In that series, hesitancy rates approached 50% in a sample of more than 8,000 people.
Hesitancy among people overall may have recently increased, at least for the short term, because of concerns over rare thrombotic events among people who receive certain types of COVID-19 vaccine, Dr. Vassalotti noted.
Dr. Garcia and associates conducted their survey from Jan. 8 to Feb. 11, 2021, among patients who regularly received hemodialysis at any of 150 randomly selected dialysis clinics that treat 30 or more patients and are managed by U.S. Renal Care. The study enrolled patients in 22 states. Most of the patients were aged 45-79 years; 30% were non-Hispanic White; 30% were Black, and 24% were Hispanic. The survey included 24 questions and took about 10 minutes to complete.
In reply to the statement, “If COVID-19 vaccine was proven safe and effective for the general population I would seek to get it,” 20% gave a reply of definitely not, probably not, or unsure; 79% answered either probably or definitely yes.
Another question asked about willingness to receive a vaccine if it was shown to be safe and effective for people receiving dialysis. In answer to that question, 19% said definitely not, probably not, or unsure.
Possible adverse effects an issue
Asked the reason why they were hesitant to receive the vaccine, 53% cited possible adverse effects; 19% cited general unease about vaccines; 19% said they did not think the COVID-19 vaccines would work; 17% said they did not think they needed a COVID-19 vaccine; and 15% said they had read or heard that COVID-19 vaccines were dangerous.
A set of questions asked survey respondents about their primary source of information about COVID-19 vaccines. About three-quarters cited television news; about 35% cited members of their dialysis clinic staff; about 30% cited friends and family; 20% cited social media; 20% cited their nephrologists; and roughly 15% cited newspapers.
The results suggest that potentially effective interventions to promote vaccine uptake include showing informational videos to patients during dialysis sessions and encouraging the staff at dialysis centers to proactively educate patients about COVID-19 vaccines and to promote uptake, suggest Dr. Garcia and Dr. Vassalotti.
Dr. Vassalotti noted that in a recent single-center survey of 90 U.S. patients undergoing hemodialysis that included 75 (85%) Black persons, the prevalence of hesitancy about COVID-19 vaccines was 50%. Hesitancy was often linked with gaps in patient education.
“We need broad educational measures, as well as targeting specific demographic groups” among whom the level of hesitancy is high, said Dr. Vassalotti.
He noted that patients who undergo dialysis are receptive to messages from dialysis clinic staff members and that this offers an “opportunity to understand misconceptions that underlie hesitancy and address them on an individual basis.”
The NKF has prepared a fact sheet for educating patients with kidney disease about the efficacy and safety of COVID-19 vaccines, Dr. Vassalotti noted.
Dr. Garcia has disclosed no relevant financial relationships. Dr. Vassalotti is an adviser and consultant to Renalytix AI and is a consultant to Janssen.
A version of this article first appeared on Medscape.com.
Among U.S. patients who regularly undergo hemodialysis, 20% had some degree of hesitancy about receiving a COVID-19 vaccine in a survey of 1,515 patients conducted during January and February 2021.
The most frequently cited concern associated with hesitancy over vaccination against the SARS-CoV-2 virus was with regard to possible adverse effects. This was cited by more than half of the patients who were concerned about being vaccinated.
Hesitancy rates were highest among people aged 44 years or younger, women, people who identified as non-Hispanic Black or non-Hispanic other (generally Native American or Pacific Islander), those with less than some college education, and those without a history of influenza vaccination, Pablo Garcia, MD, reported at the National Kidney Foundation (NKF) 2021 Spring Clinical Meetings.
Hesitancy or access?
Overall, however, the findings suggest that the main barrier to COVID-19 vaccine uptake is “access rather than hesitancy,” explained Dr. Garcia, a nephrologist at Stanford (Calif.) University. He predicts that this barrier will soon resolve, in part because of a Centers for Disease Control and Prevention program launched in March 2021 that is supplying COVID-19 vaccine to U.S. dialysis centers to administer to their patients.
“This will facilitate access to the vaccine” for patients who regularly receive hemodialysis, Dr. Garcia said during his presentation.
“Administering vaccines in dialysis clinics will help. Patients are already accustomed to receiving influenza vaccine in the clinic,” said Joseph A. Vassalotti, MD, a nephrologist at Mount Sinai Hospital, New York, and chief medical officer for the NKF.
Dr. Vassalotti cited the importance of protecting the vulnerable population of people who regularly receive hemodialysis. Among those patients, there was a 37% spike in all-cause mortality during peak weeks of the pandemic compared with similar periods during 2017-2019.
Any level of vaccine hesitancy is concerning
In an interview, he said, “Vaccination is the key to reducing this burden, so any level of vaccine hesitancy is concerning” with regard to patients who regularly undergo dialysis.
Hesitancy among patients who undergo dialysis appears to be less than in the general U.S. population, according to a series of surveys conducted from April through December 2020. In that series, hesitancy rates approached 50% in a sample of more than 8,000 people.
Hesitancy among people overall may have recently increased, at least for the short term, because of concerns over rare thrombotic events among people who receive certain types of COVID-19 vaccine, Dr. Vassalotti noted.
Dr. Garcia and associates conducted their survey from Jan. 8 to Feb. 11, 2021, among patients who regularly received hemodialysis at any of 150 randomly selected dialysis clinics that treat 30 or more patients and are managed by U.S. Renal Care. The study enrolled patients in 22 states. Most of the patients were aged 45-79 years; 30% were non-Hispanic White; 30% were Black, and 24% were Hispanic. The survey included 24 questions and took about 10 minutes to complete.
In reply to the statement, “If COVID-19 vaccine was proven safe and effective for the general population I would seek to get it,” 20% gave a reply of definitely not, probably not, or unsure; 79% answered either probably or definitely yes.
Another question asked about willingness to receive a vaccine if it was shown to be safe and effective for people receiving dialysis. In answer to that question, 19% said definitely not, probably not, or unsure.
Possible adverse effects an issue
Asked the reason why they were hesitant to receive the vaccine, 53% cited possible adverse effects; 19% cited general unease about vaccines; 19% said they did not think the COVID-19 vaccines would work; 17% said they did not think they needed a COVID-19 vaccine; and 15% said they had read or heard that COVID-19 vaccines were dangerous.
A set of questions asked survey respondents about their primary source of information about COVID-19 vaccines. About three-quarters cited television news; about 35% cited members of their dialysis clinic staff; about 30% cited friends and family; 20% cited social media; 20% cited their nephrologists; and roughly 15% cited newspapers.
The results suggest that potentially effective interventions to promote vaccine uptake include showing informational videos to patients during dialysis sessions and encouraging the staff at dialysis centers to proactively educate patients about COVID-19 vaccines and to promote uptake, suggest Dr. Garcia and Dr. Vassalotti.
Dr. Vassalotti noted that in a recent single-center survey of 90 U.S. patients undergoing hemodialysis that included 75 (85%) Black persons, the prevalence of hesitancy about COVID-19 vaccines was 50%. Hesitancy was often linked with gaps in patient education.
“We need broad educational measures, as well as targeting specific demographic groups” among whom the level of hesitancy is high, said Dr. Vassalotti.
He noted that patients who undergo dialysis are receptive to messages from dialysis clinic staff members and that this offers an “opportunity to understand misconceptions that underlie hesitancy and address them on an individual basis.”
The NKF has prepared a fact sheet for educating patients with kidney disease about the efficacy and safety of COVID-19 vaccines, Dr. Vassalotti noted.
Dr. Garcia has disclosed no relevant financial relationships. Dr. Vassalotti is an adviser and consultant to Renalytix AI and is a consultant to Janssen.
A version of this article first appeared on Medscape.com.
Addressing women’s concerns about the J&J vaccine
A rare form of venous thromboembolism (VTE) has developed in premenopausal women who have received the Johnson & Johnson (J&J) SARS-CoV-2 vaccine.

This week we learned that of the more than 6.8 million individuals in the United States who received the single-dose J&J vaccine, six women aged 18-48 years have been diagnosed with cerebral venous sinus thrombosis, and all had thrombocytopenia. In each case, symptoms were first noted 1-2 weeks after vaccination. The Food and Drug Administration and Centers for Disease Control and Prevention have recommended a pause in the administration of this vaccine.
Women’s health clinicians are already hearing from concerned patients, who understandably have questions about what this news means for them.
If they have already received the J&J vaccine within the past 3 weeks, I advise them that, although risks for any vaccine-related problems are extremely low, they should be mindful of new-onset leg or abdominal pain, or an unusual or severe headache. Such patients should contact their physician as soon as possible, and if they cannot be seen quickly, it would be appropriate to visit a hospital ED. When seeking medical care, patients should specify details of their vaccination history. Depending on the individual issues present, women with suggestive symptoms should receive blood work, Doppler venous studies (if there is a suspicion of lower-extremity deep vein thrombosis), and appropriate imaging (if there is concern for cerebral venous sinus thrombosis or pulmonary embolism).
As physicians and scientists at the CDC and FDA dig into this issue, I assume they are asking questions to determine whether the affected women have any factors that might increase their baseline risk for VTE, such as:
- A body mass index of at least 30 kg/m2
- Use of combination estrogen-progestin contraceptives (pill, ring, or patch)
- Known or suspected chronic inflammatory conditions such as rheumatoid arthritis, systemic lupus erythematosus, or
- Known familial or other thrombophilic conditions or chronic
- Recent prolonged immobility, such as a long airplane or automobile trip, which might increase risk for VTE

Experts say that the risk for a serious adverse event following receipt of the J&J vaccine is outweighed by the benefits of vaccination against COVID disease. However, that may not be enough to allay concerns among some premenopausal women.
Even if the “pause” in the administration of the vaccine is lifted, some women may be asking whether they should receive J&J’s viral vector vaccine or request one of the messenger RNA vaccines. I will be looking to the expert opinions of Anthony S. Fauci, MD, and advice from the CDC and FDA for guidance here. However, it may be reasonable to steer high-risk reproductive-age women away from the J&J vaccine in favor of the Moderna and Pfizer vaccines, if these options are available.
A version of this article first appeared on Medscape.com.
A rare form of venous thromboembolism (VTE) has developed in premenopausal women who have received the Johnson & Johnson (J&J) SARS-CoV-2 vaccine.
This week we learned that of the more than 6.8 million individuals in the United States who received the single-dose J&J vaccine, six women aged 18-48 years have been diagnosed with cerebral venous sinus thrombosis, and all had thrombocytopenia. In each case, symptoms were first noted 1-2 weeks after vaccination. The Food and Drug Administration and Centers for Disease Control and Prevention have recommended a pause in the administration of this vaccine.
Women’s health clinicians are already hearing from concerned patients, who understandably have questions about what this news means for them.
If they have already received the J&J vaccine within the past 3 weeks, I advise them that, although risks for any vaccine-related problems are extremely low, they should be mindful of new-onset leg or abdominal pain, or an unusual or severe headache. Such patients should contact their physician as soon as possible, and if they cannot be seen quickly, it would be appropriate to visit a hospital ED. When seeking medical care, patients should specify details of their vaccination history. Depending on the individual issues present, women with suggestive symptoms should receive blood work, Doppler venous studies (if there is a suspicion of lower-extremity deep vein thrombosis), and appropriate imaging (if there is concern for cerebral venous sinus thrombosis or pulmonary embolism).
As physicians and scientists at the CDC and FDA dig into this issue, I assume they are asking questions to determine whether the affected women have any factors that might increase their baseline risk for VTE, such as:
- A body mass index of at least 30 kg/m2
- Use of combination estrogen-progestin contraceptives (pill, ring, or patch)
- Known or suspected chronic inflammatory conditions such as rheumatoid arthritis, systemic lupus erythematosus, or
- Known familial or other thrombophilic conditions or chronic
- Recent prolonged immobility, such as a long airplane or automobile trip, which might increase risk for VTE
Experts say that the risk for a serious adverse event following receipt of the J&J vaccine is outweighed by the benefits of vaccination against COVID disease. However, that may not be enough to allay concerns among some premenopausal women.
Even if the “pause” in the administration of the vaccine is lifted, some women may be asking whether they should receive J&J’s viral vector vaccine or request one of the messenger RNA vaccines. I will be looking to the expert opinions of Anthony S. Fauci, MD, and advice from the CDC and FDA for guidance here. However, it may be reasonable to steer high-risk reproductive-age women away from the J&J vaccine in favor of the Moderna and Pfizer vaccines, if these options are available.
A version of this article first appeared on Medscape.com.
A rare form of venous thromboembolism (VTE) has developed in premenopausal women who have received the Johnson & Johnson (J&J) SARS-CoV-2 vaccine.
This week we learned that of the more than 6.8 million individuals in the United States who received the single-dose J&J vaccine, six women aged 18-48 years have been diagnosed with cerebral venous sinus thrombosis, and all had thrombocytopenia. In each case, symptoms were first noted 1-2 weeks after vaccination. The Food and Drug Administration and Centers for Disease Control and Prevention have recommended a pause in the administration of this vaccine.
Women’s health clinicians are already hearing from concerned patients, who understandably have questions about what this news means for them.
If they have already received the J&J vaccine within the past 3 weeks, I advise them that, although risks for any vaccine-related problems are extremely low, they should be mindful of new-onset leg or abdominal pain, or an unusual or severe headache. Such patients should contact their physician as soon as possible, and if they cannot be seen quickly, it would be appropriate to visit a hospital ED. When seeking medical care, patients should specify details of their vaccination history. Depending on the individual issues present, women with suggestive symptoms should receive blood work, Doppler venous studies (if there is a suspicion of lower-extremity deep vein thrombosis), and appropriate imaging (if there is concern for cerebral venous sinus thrombosis or pulmonary embolism).
As physicians and scientists at the CDC and FDA dig into this issue, I assume they are asking questions to determine whether the affected women have any factors that might increase their baseline risk for VTE, such as:
- A body mass index of at least 30 kg/m2
- Use of combination estrogen-progestin contraceptives (pill, ring, or patch)
- Known or suspected chronic inflammatory conditions such as rheumatoid arthritis, systemic lupus erythematosus, or
- Known familial or other thrombophilic conditions or chronic
- Recent prolonged immobility, such as a long airplane or automobile trip, which might increase risk for VTE
Experts say that the risk for a serious adverse event following receipt of the J&J vaccine is outweighed by the benefits of vaccination against COVID disease. However, that may not be enough to allay concerns among some premenopausal women.
Even if the “pause” in the administration of the vaccine is lifted, some women may be asking whether they should receive J&J’s viral vector vaccine or request one of the messenger RNA vaccines. I will be looking to the expert opinions of Anthony S. Fauci, MD, and advice from the CDC and FDA for guidance here. However, it may be reasonable to steer high-risk reproductive-age women away from the J&J vaccine in favor of the Moderna and Pfizer vaccines, if these options are available.
A version of this article first appeared on Medscape.com.
Pneumonia risk soars in heart failure patients, especially HFpEF
Patients with heart failure get pneumonia at a rate almost three times greater than expected and, once they do get pneumonia, have about a fourfold greater risk of death, investigators for a retrospective analysis of 13,000 patients from two landmark randomized HF trials have found.

The investigators also found that HF patients with preserved ejection fraction (HFpEF) are at the highest risk of developing pneumonia. The findings underscore the importance of patients with HF getting a pneumonia vaccination, they found.
The analysis showed that 6.3% of patients in the PARADIGM-HF trial and 10.6% of those in the PARAGON-HF trial developed pneumonia, reported the study authors, led by John J.V. McMurray, MD, of the British Heart Foundation Cardiovascular Research Center at the University of Glasgow in Scotland (J Am Coll Cardiol. 2021;77:1961-73).
“The main reason for doing this study was the fact that many heart failure patients are not vaccinated, as they should be, against pneumonia – both pneumococcus and influenza vaccination,” Dr. McMurray said in an interview. “We wanted to document the frequency and consequences of pneumonia in patients with heart failure to help highlight this deficiency in care.”
Dr. McMurray said he believes this is the first study to document the incidence of pneumonia and pneumonia-related outcomes according to the two major ejection fraction phenotypes.
PARADIGM-HF and PARAGON-HF
The post hoc analysis consisted of 8,399 patients with HF with reduced ejection fraction (HFrEF) in PARADIGM-HF (Eur J Heart Fail. 2013 Sep;15[9]:1062-73) and 4,796 patients with HFpEF in PARAGON-HF (N Engl J Med. 2014 Sep 11;371[11]:993-1004). The analysis focused on the 528 and 510 patients in each study, respectively, who developed pneumonia. Those rates translated to an incidence rate of 29 per 1,000 patient-years (95% confidence interval, 27-31) in PARADIGM-HF and 39 per 1,000 patient-years (95% CI, 36-42) in PARAGON-HF.
After pneumonia, the risk of death in patients increased substantially. In PARADIGM-HF, the adjusted hazard ratio for the risk of death from any cause after pneumonia was 4.34 (95% CI, 3.73-5.05). In PARAGON-HF, it was 3.76 (95% CI, 3.09-4.58). HF patients who contracted pneumonia also tended to have HF longer than their counterparts who didn’t develop pneumonia, but the frequency of previous hospitalization for HF didn’t vary between the pneumonia and no-pneumonia groups.
Patients who developed pneumonia tended to be older (average age of 66.9 years vs. 64.6 years, P < .001) and male (83.9% vs. 77.8%, P < .001). The mean age of patients in PARADIGM-HF was almost a decade younger than those in PARAGON-HF, 64 vs. 73 years.
Pneumonia patients also had worse Kansas City Cardiomyopathy Questionnaire scores (76 vs. 80 on average), but no difference in New York Heart Association functional class. “In general, patients who developed pneumonia had more symptoms and signs and HF than those who did not develop pneumonia,” Dr. McMurray and colleagues wrote.
Pneumonia patients also had higher rates of chronic obstructive pulmonary disease (26% vs. 12%), diabetes (43% vs. 34%), and atrial fibrillation (46% vs. 36%).
Another reason for conducting the study, Dr. McMurray said, “was the prior findings in patients with coronary disease and acute myocardial infarction that the risk associated with an episode of pneumonia [e.g., in subsequent vascular events and deaths] persisted long after the acute event. We wanted to see if this was also the case for heart failure, and indeed it was.”
For example, the adjusted HR for cardiovascular death or hospitalization in the first month following an episode of pneumonia was 9.48 (range of 6.85-13.12, P < .001), leveling off to 1.59 after 3 months or more.
Vaccination crucial in HF patients
Dr. McMurray noted that this study emphasizes the importance of pneumonia vaccination for patients with HF. “Given that we have so few treatments to offer patients with HFpEF, this makes the potential value of vaccination in these patients all the greater,” he said.
The COVID-19 pandemic, Dr. McMurray said, is a “good reminder of the dangers of a respiratory infection and the importance of vaccination in these patients. COVID-19 has interesting parallels in being a systemic disease and one with postacute, persisting effects.”
The persistent risk for adverse cardiovascular events 3 months and later after pneumonia is a novel finding of the study, wrote Donna Mancini, MD, and Gregory Gibson, MD, in an invited commentary (J Am Coll Cardiol. 2021;77:1974-6). Both are with the Icahn School of Medicine at Mt. Sinai in New York. The post hoc study also “serves as an important reminder” of pneumonia risk in patients with HF, especially during the pandemic, they wrote.
“Although vaccination alone appears unlikely to be a panacea, it is a readily accessible tool for mitigating disease severity and improving outcomes,” Dr. Mancini and Dr. Gibson wrote. “After all, an ounce of prevention is worth a pound of cure.”
Novartis provided funding for the PARADIGM-HF and PARAGON-HF trials, and Dr. McMurray and coauthors disclosed financial relationships with Novartis. Dr. Mancini and Dr. Gibson have no relevant financial relationships to disclose.
Patients with heart failure get pneumonia at a rate almost three times greater than expected and, once they do get pneumonia, have about a fourfold greater risk of death, investigators for a retrospective analysis of 13,000 patients from two landmark randomized HF trials have found.
The investigators also found that HF patients with preserved ejection fraction (HFpEF) are at the highest risk of developing pneumonia. The findings underscore the importance of patients with HF getting a pneumonia vaccination, they found.
The analysis showed that 6.3% of patients in the PARADIGM-HF trial and 10.6% of those in the PARAGON-HF trial developed pneumonia, reported the study authors, led by John J.V. McMurray, MD, of the British Heart Foundation Cardiovascular Research Center at the University of Glasgow in Scotland (J Am Coll Cardiol. 2021;77:1961-73).
“The main reason for doing this study was the fact that many heart failure patients are not vaccinated, as they should be, against pneumonia – both pneumococcus and influenza vaccination,” Dr. McMurray said in an interview. “We wanted to document the frequency and consequences of pneumonia in patients with heart failure to help highlight this deficiency in care.”
Dr. McMurray said he believes this is the first study to document the incidence of pneumonia and pneumonia-related outcomes according to the two major ejection fraction phenotypes.
PARADIGM-HF and PARAGON-HF
The post hoc analysis consisted of 8,399 patients with HF with reduced ejection fraction (HFrEF) in PARADIGM-HF (Eur J Heart Fail. 2013 Sep;15[9]:1062-73) and 4,796 patients with HFpEF in PARAGON-HF (N Engl J Med. 2014 Sep 11;371[11]:993-1004). The analysis focused on the 528 and 510 patients in each study, respectively, who developed pneumonia. Those rates translated to an incidence rate of 29 per 1,000 patient-years (95% confidence interval, 27-31) in PARADIGM-HF and 39 per 1,000 patient-years (95% CI, 36-42) in PARAGON-HF.
After pneumonia, the risk of death in patients increased substantially. In PARADIGM-HF, the adjusted hazard ratio for the risk of death from any cause after pneumonia was 4.34 (95% CI, 3.73-5.05). In PARAGON-HF, it was 3.76 (95% CI, 3.09-4.58). HF patients who contracted pneumonia also tended to have HF longer than their counterparts who didn’t develop pneumonia, but the frequency of previous hospitalization for HF didn’t vary between the pneumonia and no-pneumonia groups.
Patients who developed pneumonia tended to be older (average age of 66.9 years vs. 64.6 years, P < .001) and male (83.9% vs. 77.8%, P < .001). The mean age of patients in PARADIGM-HF was almost a decade younger than those in PARAGON-HF, 64 vs. 73 years.
Pneumonia patients also had worse Kansas City Cardiomyopathy Questionnaire scores (76 vs. 80 on average), but no difference in New York Heart Association functional class. “In general, patients who developed pneumonia had more symptoms and signs and HF than those who did not develop pneumonia,” Dr. McMurray and colleagues wrote.
Pneumonia patients also had higher rates of chronic obstructive pulmonary disease (26% vs. 12%), diabetes (43% vs. 34%), and atrial fibrillation (46% vs. 36%).
Another reason for conducting the study, Dr. McMurray said, “was the prior findings in patients with coronary disease and acute myocardial infarction that the risk associated with an episode of pneumonia [e.g., in subsequent vascular events and deaths] persisted long after the acute event. We wanted to see if this was also the case for heart failure, and indeed it was.”
For example, the adjusted HR for cardiovascular death or hospitalization in the first month following an episode of pneumonia was 9.48 (range of 6.85-13.12, P < .001), leveling off to 1.59 after 3 months or more.
Vaccination crucial in HF patients
Dr. McMurray noted that this study emphasizes the importance of pneumonia vaccination for patients with HF. “Given that we have so few treatments to offer patients with HFpEF, this makes the potential value of vaccination in these patients all the greater,” he said.
The COVID-19 pandemic, Dr. McMurray said, is a “good reminder of the dangers of a respiratory infection and the importance of vaccination in these patients. COVID-19 has interesting parallels in being a systemic disease and one with postacute, persisting effects.”
The persistent risk for adverse cardiovascular events 3 months and later after pneumonia is a novel finding of the study, wrote Donna Mancini, MD, and Gregory Gibson, MD, in an invited commentary (J Am Coll Cardiol. 2021;77:1974-6). Both are with the Icahn School of Medicine at Mt. Sinai in New York. The post hoc study also “serves as an important reminder” of pneumonia risk in patients with HF, especially during the pandemic, they wrote.
“Although vaccination alone appears unlikely to be a panacea, it is a readily accessible tool for mitigating disease severity and improving outcomes,” Dr. Mancini and Dr. Gibson wrote. “After all, an ounce of prevention is worth a pound of cure.”
Novartis provided funding for the PARADIGM-HF and PARAGON-HF trials, and Dr. McMurray and coauthors disclosed financial relationships with Novartis. Dr. Mancini and Dr. Gibson have no relevant financial relationships to disclose.
Patients with heart failure get pneumonia at a rate almost three times greater than expected and, once they do get pneumonia, have about a fourfold greater risk of death, investigators for a retrospective analysis of 13,000 patients from two landmark randomized HF trials have found.
The investigators also found that HF patients with preserved ejection fraction (HFpEF) are at the highest risk of developing pneumonia. The findings underscore the importance of patients with HF getting a pneumonia vaccination, they found.
The analysis showed that 6.3% of patients in the PARADIGM-HF trial and 10.6% of those in the PARAGON-HF trial developed pneumonia, reported the study authors, led by John J.V. McMurray, MD, of the British Heart Foundation Cardiovascular Research Center at the University of Glasgow in Scotland (J Am Coll Cardiol. 2021;77:1961-73).
“The main reason for doing this study was the fact that many heart failure patients are not vaccinated, as they should be, against pneumonia – both pneumococcus and influenza vaccination,” Dr. McMurray said in an interview. “We wanted to document the frequency and consequences of pneumonia in patients with heart failure to help highlight this deficiency in care.”
Dr. McMurray said he believes this is the first study to document the incidence of pneumonia and pneumonia-related outcomes according to the two major ejection fraction phenotypes.
PARADIGM-HF and PARAGON-HF
The post hoc analysis consisted of 8,399 patients with HF with reduced ejection fraction (HFrEF) in PARADIGM-HF (Eur J Heart Fail. 2013 Sep;15[9]:1062-73) and 4,796 patients with HFpEF in PARAGON-HF (N Engl J Med. 2014 Sep 11;371[11]:993-1004). The analysis focused on the 528 and 510 patients in each study, respectively, who developed pneumonia. Those rates translated to an incidence rate of 29 per 1,000 patient-years (95% confidence interval, 27-31) in PARADIGM-HF and 39 per 1,000 patient-years (95% CI, 36-42) in PARAGON-HF.
After pneumonia, the risk of death in patients increased substantially. In PARADIGM-HF, the adjusted hazard ratio for the risk of death from any cause after pneumonia was 4.34 (95% CI, 3.73-5.05). In PARAGON-HF, it was 3.76 (95% CI, 3.09-4.58). HF patients who contracted pneumonia also tended to have HF longer than their counterparts who didn’t develop pneumonia, but the frequency of previous hospitalization for HF didn’t vary between the pneumonia and no-pneumonia groups.
Patients who developed pneumonia tended to be older (average age of 66.9 years vs. 64.6 years, P < .001) and male (83.9% vs. 77.8%, P < .001). The mean age of patients in PARADIGM-HF was almost a decade younger than those in PARAGON-HF, 64 vs. 73 years.
Pneumonia patients also had worse Kansas City Cardiomyopathy Questionnaire scores (76 vs. 80 on average), but no difference in New York Heart Association functional class. “In general, patients who developed pneumonia had more symptoms and signs and HF than those who did not develop pneumonia,” Dr. McMurray and colleagues wrote.
Pneumonia patients also had higher rates of chronic obstructive pulmonary disease (26% vs. 12%), diabetes (43% vs. 34%), and atrial fibrillation (46% vs. 36%).
Another reason for conducting the study, Dr. McMurray said, “was the prior findings in patients with coronary disease and acute myocardial infarction that the risk associated with an episode of pneumonia [e.g., in subsequent vascular events and deaths] persisted long after the acute event. We wanted to see if this was also the case for heart failure, and indeed it was.”
For example, the adjusted HR for cardiovascular death or hospitalization in the first month following an episode of pneumonia was 9.48 (range of 6.85-13.12, P < .001), leveling off to 1.59 after 3 months or more.
Vaccination crucial in HF patients
Dr. McMurray noted that this study emphasizes the importance of pneumonia vaccination for patients with HF. “Given that we have so few treatments to offer patients with HFpEF, this makes the potential value of vaccination in these patients all the greater,” he said.
The COVID-19 pandemic, Dr. McMurray said, is a “good reminder of the dangers of a respiratory infection and the importance of vaccination in these patients. COVID-19 has interesting parallels in being a systemic disease and one with postacute, persisting effects.”
The persistent risk for adverse cardiovascular events 3 months and later after pneumonia is a novel finding of the study, wrote Donna Mancini, MD, and Gregory Gibson, MD, in an invited commentary (J Am Coll Cardiol. 2021;77:1974-6). Both are with the Icahn School of Medicine at Mt. Sinai in New York. The post hoc study also “serves as an important reminder” of pneumonia risk in patients with HF, especially during the pandemic, they wrote.
“Although vaccination alone appears unlikely to be a panacea, it is a readily accessible tool for mitigating disease severity and improving outcomes,” Dr. Mancini and Dr. Gibson wrote. “After all, an ounce of prevention is worth a pound of cure.”
Novartis provided funding for the PARADIGM-HF and PARAGON-HF trials, and Dr. McMurray and coauthors disclosed financial relationships with Novartis. Dr. Mancini and Dr. Gibson have no relevant financial relationships to disclose.
FROM JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY
CLL patients: Diagnostic difficulties, treatment confusion with COVID-19
Chronic lymphocytic leukemia (CLL) patients present significant problems with regard to COVID-19 disease, according to a literature review by Yousef Roosta, MD, of Urmia (Iran) University of Medical Sciences, and colleagues.
Diagnostic interaction between CLL and COVID-19 provides a major challenge. CLL patients have a lower rate of anti–SARS-CoV-2 IgG development, and evidence shows worse therapeutic outcomes in these patients, according to study published in Leukemia Research Reports.
The researchers assessed 20 retrieved articles, 11 of which examined patients with CLL and with concomitant COVID-19; and 9 articles were designed as prospective or retrospective case series of such patients. The studies were assessed qualitatively by the QUADAS-2 tool.
Troubling results
Although the overall prevalence of CLL and COVID-19 concurrence was low, at 0.6% (95% confidence interval 0.5%-0.7%) according to the meta-analysis, the results showed some special challenges in the diagnosis and care of these patients.
Diagnostic difficulties are a unique problem. Lymphopenia is common in patients with COVID-19, while lymphocytosis may be considered a transient or even rare finding. The interplay between the two diseases is sometimes very misleading for specialists, and in patients with lymphocytosis, the diagnosis of CLL may be completely ignored, according to the researchers. They added that when performing a diagnostic approach for concurrent COVID-19 and CLL, due to differences in the amount and type of immune response, “relying on serological testing, and especially the evaluation of the anti–SARS-CoV-2 IgG levels may not be beneficial,” they indicated.
In addition, studies showed unacceptable therapeutic outcome in patients with concurrent CLL and COVID-19, with mortality ranging from 33% to 41.7%, showing a need to revise current treatment protocols, according to the authors. In one study, 85.7% of surviving patients showed a considerable decrease in functional class and significant fatigue, with such a poor prognosis occurring more commonly in the elderly.
With regard to treatment, “it is quite obvious that despite the use of current standard protocols, the prognosis of these patients will be much worse than the prognosis of CLL patients with no evidence of COVID-19. Even in the first-line treatment protocol for these patients, there is no agreement in combination therapy with selected CLL drugs along with management protocols of COVID-19 patients,” the researchers stated.
“[The] different hematological behaviors of two diseases might mimic the detection of COVID-19 in the CLL state and vise versa. Also, due to the low level of immune response against SARS-CoV-2 in CLL patients, both scheduled immunological-based diagnosis and treatment may fail,” the researchers added.
The authors reported that they had no disclosures.
Chronic lymphocytic leukemia (CLL) patients present significant problems with regard to COVID-19 disease, according to a literature review by Yousef Roosta, MD, of Urmia (Iran) University of Medical Sciences, and colleagues.
Diagnostic interaction between CLL and COVID-19 provides a major challenge. CLL patients have a lower rate of anti–SARS-CoV-2 IgG development, and evidence shows worse therapeutic outcomes in these patients, according to study published in Leukemia Research Reports.
The researchers assessed 20 retrieved articles, 11 of which examined patients with CLL and with concomitant COVID-19; and 9 articles were designed as prospective or retrospective case series of such patients. The studies were assessed qualitatively by the QUADAS-2 tool.
Troubling results
Although the overall prevalence of CLL and COVID-19 concurrence was low, at 0.6% (95% confidence interval 0.5%-0.7%) according to the meta-analysis, the results showed some special challenges in the diagnosis and care of these patients.
Diagnostic difficulties are a unique problem. Lymphopenia is common in patients with COVID-19, while lymphocytosis may be considered a transient or even rare finding. The interplay between the two diseases is sometimes very misleading for specialists, and in patients with lymphocytosis, the diagnosis of CLL may be completely ignored, according to the researchers. They added that when performing a diagnostic approach for concurrent COVID-19 and CLL, due to differences in the amount and type of immune response, “relying on serological testing, and especially the evaluation of the anti–SARS-CoV-2 IgG levels may not be beneficial,” they indicated.
In addition, studies showed unacceptable therapeutic outcome in patients with concurrent CLL and COVID-19, with mortality ranging from 33% to 41.7%, showing a need to revise current treatment protocols, according to the authors. In one study, 85.7% of surviving patients showed a considerable decrease in functional class and significant fatigue, with such a poor prognosis occurring more commonly in the elderly.
With regard to treatment, “it is quite obvious that despite the use of current standard protocols, the prognosis of these patients will be much worse than the prognosis of CLL patients with no evidence of COVID-19. Even in the first-line treatment protocol for these patients, there is no agreement in combination therapy with selected CLL drugs along with management protocols of COVID-19 patients,” the researchers stated.
“[The] different hematological behaviors of two diseases might mimic the detection of COVID-19 in the CLL state and vise versa. Also, due to the low level of immune response against SARS-CoV-2 in CLL patients, both scheduled immunological-based diagnosis and treatment may fail,” the researchers added.
The authors reported that they had no disclosures.
Chronic lymphocytic leukemia (CLL) patients present significant problems with regard to COVID-19 disease, according to a literature review by Yousef Roosta, MD, of Urmia (Iran) University of Medical Sciences, and colleagues.
Diagnostic interaction between CLL and COVID-19 provides a major challenge. CLL patients have a lower rate of anti–SARS-CoV-2 IgG development, and evidence shows worse therapeutic outcomes in these patients, according to study published in Leukemia Research Reports.
The researchers assessed 20 retrieved articles, 11 of which examined patients with CLL and with concomitant COVID-19; and 9 articles were designed as prospective or retrospective case series of such patients. The studies were assessed qualitatively by the QUADAS-2 tool.
Troubling results
Although the overall prevalence of CLL and COVID-19 concurrence was low, at 0.6% (95% confidence interval 0.5%-0.7%) according to the meta-analysis, the results showed some special challenges in the diagnosis and care of these patients.
Diagnostic difficulties are a unique problem. Lymphopenia is common in patients with COVID-19, while lymphocytosis may be considered a transient or even rare finding. The interplay between the two diseases is sometimes very misleading for specialists, and in patients with lymphocytosis, the diagnosis of CLL may be completely ignored, according to the researchers. They added that when performing a diagnostic approach for concurrent COVID-19 and CLL, due to differences in the amount and type of immune response, “relying on serological testing, and especially the evaluation of the anti–SARS-CoV-2 IgG levels may not be beneficial,” they indicated.
In addition, studies showed unacceptable therapeutic outcome in patients with concurrent CLL and COVID-19, with mortality ranging from 33% to 41.7%, showing a need to revise current treatment protocols, according to the authors. In one study, 85.7% of surviving patients showed a considerable decrease in functional class and significant fatigue, with such a poor prognosis occurring more commonly in the elderly.
With regard to treatment, “it is quite obvious that despite the use of current standard protocols, the prognosis of these patients will be much worse than the prognosis of CLL patients with no evidence of COVID-19. Even in the first-line treatment protocol for these patients, there is no agreement in combination therapy with selected CLL drugs along with management protocols of COVID-19 patients,” the researchers stated.
“[The] different hematological behaviors of two diseases might mimic the detection of COVID-19 in the CLL state and vise versa. Also, due to the low level of immune response against SARS-CoV-2 in CLL patients, both scheduled immunological-based diagnosis and treatment may fail,” the researchers added.
The authors reported that they had no disclosures.
FROM LEUKEMIA RESEARCH REPORTS
COVID-19–related inflammatory syndrome tied to neurologic symptoms in children
About half of children with pediatric inflammatory multisystem syndrome temporally associated with SARS-CoV-2 (PIMS-TS) have new-onset neurologic symptoms, research shows.
These symptoms involve the central and peripheral nervous systems but do not always affect the respiratory system. In addition, neurologic symptoms appear to be more common in severe presentations of this syndrome.
“These new data consolidate the initial findings in our JAMA Neurology publication on the neurological problems that children with PIMS-TS can present with, even in the absence of respiratory systems,” study investigator Omar Abdel-Mannan, MD, clinical research fellow at University College London Institute of Neurology and senior resident at Great Ormond Street Hospital for children in London, said in an interview.
He added that the findings are in keeping with other recent research studies on PIMS-TS, which is known more commonly in the United States as multisystem inflammatory syndrome in children (MIS-C).
The findings will be presented April 18 at the American Academy of Neurology (AAN) 2021 Annual Meeting.
Neurologic manifestations common
Many children and adults with COVID-19 have developed neurologic manifestations. PIMS-TS is a severe, postinfectious, immune-mediated disorder characterized by persistent fever and extreme inflammation.
Patients may have acute diarrhea or vomiting, rash or bilateral conjunctivitis, and low blood pressure. They should be examined by a pediatric specialist, and most children with this disorder need intensive care.
To report the neurologic manifestations in children with PIMS-TS, the researchers retrospectively examined data for children and adolescents younger than 18 years who had the disorder and presented to a single center between April 4, 2020, and Sept. 1, 2020.
Forty-six patients (median age, 10.2 years) were included in the analysis. Thirty (65.2%) were male, and 37 (80.4%) were of non-White ethnicities.
Twenty-four (52.2%) patients had new-onset neurologic symptoms, which included headache (n = 24), encephalopathy (n = 14 patients), dysarthria/dysphonia (n = 6), hallucinations (n = 6), ataxia (n = 4), peripheral nerve involvement (n = 3), and seizures (n=1).
Laboratory and imaging results provided further information. One patient had 118 leukocytes in cerebrospinal fluid. Children with neurologic involvement had higher levels of peak inflammatory markers and were more likely to be ventilated and require inotropic support in the PICU (P < .05).
Four of 16 patients who underwent brain MRI had splenium signal changes. Of 15 patients who underwent electroencephalogram (EEG), 14 had an excess of slow activity. Four of 7 patients who underwent nerve conduction studies and electromyography (EMG) had myopathic and neuropathic changes.
Response to SARS-CoV-2
Central neurologic problems of the brain and peripheral nerve involvement rarely occur at the same time in children.
“This makes it highly possible that the syndrome is secondary to cytokine release in response to the SARS-CoV-2 virus, as there is significant clinical overlap with both genetic and acquired forms of another immune-mediated condition known as hemophagocytic lymphohistiocytosis,” said Dr. Abdel-Mannan.
The researchers found no demographic differences between children with neurologic involvement at presentation and those without.
“However, the numbers are small given the rarity of this condition, which makes it difficult to extrapolate associations and differences between the two groups, and will require future collaborative larger scale studies to look at what potentially makes some children more susceptible to neurologic involvement than others,” said Dr. Abdel-Mannan.
Excluding potential causes of the symptoms other than COVID-19 also is important, he added.
The preponderance of ethnic minorities in the current study population mirrors that in other PIMS-TS cohorts in other countries, said Dr. Abdel-Mannan. It reflects the higher incidence of COVID-19 in ethnic minority groups. However, presentation, investigations, and management did not differ between White and non-White children in the current study.
“Although PIMS-TS patients with neurologic involvement are initially sicker, our center’s preliminary follow-up data up to 6 months post discharge from hospital demonstrates that most of these children make an almost complete functional recovery, which is reassuring,” said Dr. Abdel-Mannan.
The data underscore how important it is that clinicians be aware that children with PIMS-TS can present with neurologic symptoms, even in the absence of respiratory involvement, he added.
The researchers will soon begin a multicenter research study that will involve longitudinal clinical and cognitive assessments and advanced neuroimaging. The objective will be to determine whether all children with PIMS-TS, or only those with neurologic symptoms, are at risk of chronic longer-term neurocognitive and psychiatric outcomes.
Unanswered questions
John B. Bodensteiner, MD, professor of neurology and pediatrics at Mayo Clinic, Rochester, Minn., said in an interview that the findings help flesh out the range of neurologic involvement that PIMS-TS entails.
“It’s not a surprise to us as neurologists, but it’s not been emphasized in the general literature and in the public health sector,” he said.
The study’s most important implication is that neurologic conditions are not uncommon among children with PIMS-TS, Dr. Bodensteiner added.
“We have no idea how long or what the long-term effects of that are,” he said. Not enough time has elapsed to enable a clear understanding of the syndrome’s lasting effects on cognition, he said, “but I think this certainly raises a flag that this is a real entity. This is nothing to sniff at.”
He noted that the study has the limitations of any retrospective case series. The researchers did not perform prospective and systematic evaluations of children with the syndrome
The findings also raise unanswered questions.
“They had 14 kids with encephalopathy, but not all of them got the same evaluation,” said Dr. Bodensteiner. Although the researchers mention peripheral nerve involvement in three children, they do not describe it. “They said that the EMG showed myopathic and neuropathic changes, but peripheral nerve involvement wouldn’t give you myopathic changes, so maybe there’s some direct involvement of the muscle in this inflammatory process.”
The study also focused on a select group of patients, said Dr. Bodensteiner. “These are all patients admitted to Great Ormond Street Hospital, and we don’t know what percentage of kids who get COVID are hospitalized, which is an important issue.”
It is necessary to know what proportion of children with COVID-19 develop encephalopathy and MRI changes, he added. The findings do confirm that this coronavirus-related inflammatory condition is real and may have long-term sequelae. “We should be careful about kids getting this disease,” said Dr. Bodensteiner
The study had no funding. Dr. Abdel-Mannan and Dr. Bodensteiner have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
About half of children with pediatric inflammatory multisystem syndrome temporally associated with SARS-CoV-2 (PIMS-TS) have new-onset neurologic symptoms, research shows.
These symptoms involve the central and peripheral nervous systems but do not always affect the respiratory system. In addition, neurologic symptoms appear to be more common in severe presentations of this syndrome.
“These new data consolidate the initial findings in our JAMA Neurology publication on the neurological problems that children with PIMS-TS can present with, even in the absence of respiratory systems,” study investigator Omar Abdel-Mannan, MD, clinical research fellow at University College London Institute of Neurology and senior resident at Great Ormond Street Hospital for children in London, said in an interview.
He added that the findings are in keeping with other recent research studies on PIMS-TS, which is known more commonly in the United States as multisystem inflammatory syndrome in children (MIS-C).
The findings will be presented April 18 at the American Academy of Neurology (AAN) 2021 Annual Meeting.
Neurologic manifestations common
Many children and adults with COVID-19 have developed neurologic manifestations. PIMS-TS is a severe, postinfectious, immune-mediated disorder characterized by persistent fever and extreme inflammation.
Patients may have acute diarrhea or vomiting, rash or bilateral conjunctivitis, and low blood pressure. They should be examined by a pediatric specialist, and most children with this disorder need intensive care.
To report the neurologic manifestations in children with PIMS-TS, the researchers retrospectively examined data for children and adolescents younger than 18 years who had the disorder and presented to a single center between April 4, 2020, and Sept. 1, 2020.
Forty-six patients (median age, 10.2 years) were included in the analysis. Thirty (65.2%) were male, and 37 (80.4%) were of non-White ethnicities.
Twenty-four (52.2%) patients had new-onset neurologic symptoms, which included headache (n = 24), encephalopathy (n = 14 patients), dysarthria/dysphonia (n = 6), hallucinations (n = 6), ataxia (n = 4), peripheral nerve involvement (n = 3), and seizures (n=1).
Laboratory and imaging results provided further information. One patient had 118 leukocytes in cerebrospinal fluid. Children with neurologic involvement had higher levels of peak inflammatory markers and were more likely to be ventilated and require inotropic support in the PICU (P < .05).
Four of 16 patients who underwent brain MRI had splenium signal changes. Of 15 patients who underwent electroencephalogram (EEG), 14 had an excess of slow activity. Four of 7 patients who underwent nerve conduction studies and electromyography (EMG) had myopathic and neuropathic changes.
Response to SARS-CoV-2
Central neurologic problems of the brain and peripheral nerve involvement rarely occur at the same time in children.
“This makes it highly possible that the syndrome is secondary to cytokine release in response to the SARS-CoV-2 virus, as there is significant clinical overlap with both genetic and acquired forms of another immune-mediated condition known as hemophagocytic lymphohistiocytosis,” said Dr. Abdel-Mannan.
The researchers found no demographic differences between children with neurologic involvement at presentation and those without.
“However, the numbers are small given the rarity of this condition, which makes it difficult to extrapolate associations and differences between the two groups, and will require future collaborative larger scale studies to look at what potentially makes some children more susceptible to neurologic involvement than others,” said Dr. Abdel-Mannan.
Excluding potential causes of the symptoms other than COVID-19 also is important, he added.
The preponderance of ethnic minorities in the current study population mirrors that in other PIMS-TS cohorts in other countries, said Dr. Abdel-Mannan. It reflects the higher incidence of COVID-19 in ethnic minority groups. However, presentation, investigations, and management did not differ between White and non-White children in the current study.
“Although PIMS-TS patients with neurologic involvement are initially sicker, our center’s preliminary follow-up data up to 6 months post discharge from hospital demonstrates that most of these children make an almost complete functional recovery, which is reassuring,” said Dr. Abdel-Mannan.
The data underscore how important it is that clinicians be aware that children with PIMS-TS can present with neurologic symptoms, even in the absence of respiratory involvement, he added.
The researchers will soon begin a multicenter research study that will involve longitudinal clinical and cognitive assessments and advanced neuroimaging. The objective will be to determine whether all children with PIMS-TS, or only those with neurologic symptoms, are at risk of chronic longer-term neurocognitive and psychiatric outcomes.
Unanswered questions
John B. Bodensteiner, MD, professor of neurology and pediatrics at Mayo Clinic, Rochester, Minn., said in an interview that the findings help flesh out the range of neurologic involvement that PIMS-TS entails.
“It’s not a surprise to us as neurologists, but it’s not been emphasized in the general literature and in the public health sector,” he said.
The study’s most important implication is that neurologic conditions are not uncommon among children with PIMS-TS, Dr. Bodensteiner added.
“We have no idea how long or what the long-term effects of that are,” he said. Not enough time has elapsed to enable a clear understanding of the syndrome’s lasting effects on cognition, he said, “but I think this certainly raises a flag that this is a real entity. This is nothing to sniff at.”
He noted that the study has the limitations of any retrospective case series. The researchers did not perform prospective and systematic evaluations of children with the syndrome
The findings also raise unanswered questions.
“They had 14 kids with encephalopathy, but not all of them got the same evaluation,” said Dr. Bodensteiner. Although the researchers mention peripheral nerve involvement in three children, they do not describe it. “They said that the EMG showed myopathic and neuropathic changes, but peripheral nerve involvement wouldn’t give you myopathic changes, so maybe there’s some direct involvement of the muscle in this inflammatory process.”
The study also focused on a select group of patients, said Dr. Bodensteiner. “These are all patients admitted to Great Ormond Street Hospital, and we don’t know what percentage of kids who get COVID are hospitalized, which is an important issue.”
It is necessary to know what proportion of children with COVID-19 develop encephalopathy and MRI changes, he added. The findings do confirm that this coronavirus-related inflammatory condition is real and may have long-term sequelae. “We should be careful about kids getting this disease,” said Dr. Bodensteiner
The study had no funding. Dr. Abdel-Mannan and Dr. Bodensteiner have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
About half of children with pediatric inflammatory multisystem syndrome temporally associated with SARS-CoV-2 (PIMS-TS) have new-onset neurologic symptoms, research shows.
These symptoms involve the central and peripheral nervous systems but do not always affect the respiratory system. In addition, neurologic symptoms appear to be more common in severe presentations of this syndrome.
“These new data consolidate the initial findings in our JAMA Neurology publication on the neurological problems that children with PIMS-TS can present with, even in the absence of respiratory systems,” study investigator Omar Abdel-Mannan, MD, clinical research fellow at University College London Institute of Neurology and senior resident at Great Ormond Street Hospital for children in London, said in an interview.
He added that the findings are in keeping with other recent research studies on PIMS-TS, which is known more commonly in the United States as multisystem inflammatory syndrome in children (MIS-C).
The findings will be presented April 18 at the American Academy of Neurology (AAN) 2021 Annual Meeting.
Neurologic manifestations common
Many children and adults with COVID-19 have developed neurologic manifestations. PIMS-TS is a severe, postinfectious, immune-mediated disorder characterized by persistent fever and extreme inflammation.
Patients may have acute diarrhea or vomiting, rash or bilateral conjunctivitis, and low blood pressure. They should be examined by a pediatric specialist, and most children with this disorder need intensive care.
To report the neurologic manifestations in children with PIMS-TS, the researchers retrospectively examined data for children and adolescents younger than 18 years who had the disorder and presented to a single center between April 4, 2020, and Sept. 1, 2020.
Forty-six patients (median age, 10.2 years) were included in the analysis. Thirty (65.2%) were male, and 37 (80.4%) were of non-White ethnicities.
Twenty-four (52.2%) patients had new-onset neurologic symptoms, which included headache (n = 24), encephalopathy (n = 14 patients), dysarthria/dysphonia (n = 6), hallucinations (n = 6), ataxia (n = 4), peripheral nerve involvement (n = 3), and seizures (n=1).
Laboratory and imaging results provided further information. One patient had 118 leukocytes in cerebrospinal fluid. Children with neurologic involvement had higher levels of peak inflammatory markers and were more likely to be ventilated and require inotropic support in the PICU (P < .05).
Four of 16 patients who underwent brain MRI had splenium signal changes. Of 15 patients who underwent electroencephalogram (EEG), 14 had an excess of slow activity. Four of 7 patients who underwent nerve conduction studies and electromyography (EMG) had myopathic and neuropathic changes.
Response to SARS-CoV-2
Central neurologic problems of the brain and peripheral nerve involvement rarely occur at the same time in children.
“This makes it highly possible that the syndrome is secondary to cytokine release in response to the SARS-CoV-2 virus, as there is significant clinical overlap with both genetic and acquired forms of another immune-mediated condition known as hemophagocytic lymphohistiocytosis,” said Dr. Abdel-Mannan.
The researchers found no demographic differences between children with neurologic involvement at presentation and those without.
“However, the numbers are small given the rarity of this condition, which makes it difficult to extrapolate associations and differences between the two groups, and will require future collaborative larger scale studies to look at what potentially makes some children more susceptible to neurologic involvement than others,” said Dr. Abdel-Mannan.
Excluding potential causes of the symptoms other than COVID-19 also is important, he added.
The preponderance of ethnic minorities in the current study population mirrors that in other PIMS-TS cohorts in other countries, said Dr. Abdel-Mannan. It reflects the higher incidence of COVID-19 in ethnic minority groups. However, presentation, investigations, and management did not differ between White and non-White children in the current study.
“Although PIMS-TS patients with neurologic involvement are initially sicker, our center’s preliminary follow-up data up to 6 months post discharge from hospital demonstrates that most of these children make an almost complete functional recovery, which is reassuring,” said Dr. Abdel-Mannan.
The data underscore how important it is that clinicians be aware that children with PIMS-TS can present with neurologic symptoms, even in the absence of respiratory involvement, he added.
The researchers will soon begin a multicenter research study that will involve longitudinal clinical and cognitive assessments and advanced neuroimaging. The objective will be to determine whether all children with PIMS-TS, or only those with neurologic symptoms, are at risk of chronic longer-term neurocognitive and psychiatric outcomes.
Unanswered questions
John B. Bodensteiner, MD, professor of neurology and pediatrics at Mayo Clinic, Rochester, Minn., said in an interview that the findings help flesh out the range of neurologic involvement that PIMS-TS entails.
“It’s not a surprise to us as neurologists, but it’s not been emphasized in the general literature and in the public health sector,” he said.
The study’s most important implication is that neurologic conditions are not uncommon among children with PIMS-TS, Dr. Bodensteiner added.
“We have no idea how long or what the long-term effects of that are,” he said. Not enough time has elapsed to enable a clear understanding of the syndrome’s lasting effects on cognition, he said, “but I think this certainly raises a flag that this is a real entity. This is nothing to sniff at.”
He noted that the study has the limitations of any retrospective case series. The researchers did not perform prospective and systematic evaluations of children with the syndrome
The findings also raise unanswered questions.
“They had 14 kids with encephalopathy, but not all of them got the same evaluation,” said Dr. Bodensteiner. Although the researchers mention peripheral nerve involvement in three children, they do not describe it. “They said that the EMG showed myopathic and neuropathic changes, but peripheral nerve involvement wouldn’t give you myopathic changes, so maybe there’s some direct involvement of the muscle in this inflammatory process.”
The study also focused on a select group of patients, said Dr. Bodensteiner. “These are all patients admitted to Great Ormond Street Hospital, and we don’t know what percentage of kids who get COVID are hospitalized, which is an important issue.”
It is necessary to know what proportion of children with COVID-19 develop encephalopathy and MRI changes, he added. The findings do confirm that this coronavirus-related inflammatory condition is real and may have long-term sequelae. “We should be careful about kids getting this disease,” said Dr. Bodensteiner
The study had no funding. Dr. Abdel-Mannan and Dr. Bodensteiner have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Preventing the psychosocial effects of adult ADHD during the pandemic
As some countries brace for yet another possible surge in the COVID-19 pandemic – particularly among young adults who have not yet been vaccinated – clinicians should remain wary of the cardinal symptoms of adult ADHD.
Research from an Israeli study shows that individuals with unmedicated ADHD are 52% more likely to test positive for the virus.1,2

The symptoms of ADHD, including impulsiveness and inability to follow directions, combined with the tendency to leave adults with ADHD on their own to sort out COVID-19–related protocols – make these individuals susceptible to exposure.
As we know, ADHD is a condition characterized by a pervasive pattern of impulsivity and/or inattention, which greatly reduces organizational capabilities by interfering at the developmental level.3 Other key symptoms include short attention span, hyperactivity, restlessness, difficulty in prioritizing tasks, and an absence of time awareness. Symptom presentation of ADHD is contingent upon the nature of the individual’s overall mental health and etiologic issues that may be traced back to the brain’s development.4

Diagnosing ADHD in adults is relatively difficult, because a formal diagnosis generally requires symptoms to show up between the ages of 6 and 12.5 Also, clinicians can interview parents and family members to assess whether the classical features of ADHD were present in childhood for those suspected of having the condition.
Early vs. late presentation
Among the preschool population, it has been observed that emerging ADHD symptoms may progress with time or remain relatively constant with respect to the activities that children partake in. In some instances, impulsive behavior, especially compared with other symptoms, might be identified quickly by the attentive parent or caregiver. However, when ADHD appears in adulthood, it is possible that prior ADHD symptoms escaped detection – only to be diagnosed later in life because of varying presentations and the increased organizational demands of adulthood.
Meanwhile, diagnosis in adolescence can bring a different set of challenges to the forefront as teenagers face problems with self-management and responsibilities of daily living. These young people must cope with academic6 and social pressures – and a host of new societal expectations.
It is essential to understand how all of those societal factors have affected ADHD and its aspects, especially within the context of COVID-19. The coronavirus has introduced myriad challenges at the global level. Individuals with ADHD exhibit neurodevelopmental and corollary attention deficit issues that make them more susceptible to environmental stressors. Physical distancing practices might aggravate existing behavioral problems.
Distance forced by pandemic offers challenges
Despite the widespread adoption of telemedicine during the pandemic, some physicians think that the delivery of optimal care and the ability to adequately address patients’ health-related concerns have been compromised. Certainly, in the case of addressing the needs of patients with ADHD or related learning disorders, in-person examinations and clinical visits are best.
That is also the case for ADHD patients with comorbid sleep disorders. For those patients, it might be prudent to explore lifestyle changes (for example, improvements in sleep hygiene practices) before resorting to the use of pharmacologic agents such as hypnotics and melatonin. Along similar lines, the European ADHD Guideline Group (EAGG) advises the use of pharmacotherapy after the successful completion of a physical exam; patients already adhering to a treatment plan should continue therapy without interruption. Clinicians caring for patients with adult ADHD have faced a dilemma because treatment breaks increase the likelihood of illnesses resulting from the pandemic. Also, the inability to conduct treatment in person because of the pandemic raises concerns about pharmacotherapy.
The pandemic has affected the course of pediatric care and also has presented new challenges for adolescents as they begin to tackle unique problems related to their health concerns. In prepandemic times, teachers played integral roles in the diagnostic process, because they were able to readily identify children and teenagers with mental and physical challenges. In stark contrast, connecting with students online may not allow teachers to identify skill deficits in young patients or in adults with ADHD.
Furthermore, adults with ADHD and medical comorbidities may be at increased risk of disease exposure directly resulting from an inability to address their social and/or emotional well-being adequately. The social distancing and other mitigation measures advised by public health experts ensure safety and protection but also can present numerous hurdles for children, teenagers, adults – and their respective families.
Individuals with adult ADHD and other psychiatric disorders may downplay their psychological distress7 [for example, sleep dysfunction, issues concerning activities of daily living], and view it as being the natural product of the COVID-19 environment. As a result of their misconceptions, they may avoid increasing their medication dose to control emergent symptoms of hyperactivity and impulsivity, instead opting to manage stress without aid from health care professionals. The absence of patient-provider interactivity and the integration of telemedicine has introduced unnecessary obstacles with respect to medication management and therapy as well as general access to expert advice. It is of utmost importance for clinicians to identify at-risk patients and reeducate the adult ADHD patient on issues concerning medication intake and psychological wellness.
Individuals with developmental disorders may experience numerous setbacks when trying to navigate their environments. The lack of correct feedback, supervision, and guidance may adversely affect adults with ADHD, contributing toward a lack of self-esteem and social awareness.
Individuals with adult ADHD are more likely than are their younger counterparts to have medical comorbidities, such as cardiovascular disease8 and type 2 diabetes,9 so it is crucial to prescribe dietary instructions to patients. Sometimes patients with adult ADHD lack support in the form of acceptance by family and peers, so it is critical for the patient to come to terms with his/her condition and seek professional help, incorporating effective strategies wherever needed to maintain day-to-day functioning.
Other possible comorbidities
There can be risk factors associated with isolation of adults who have depression and/or anxiety, poor eating habits, and maladaptive behaviors. Other adverse health-related issues may include substance use disorder.10 Drug use suppresses developmental growth and may induce ADHD symptom exacerbation. Consistent with Khantzian’s self-medication hypothesis, among individuals with ADHD, including those who lack a formal diagnosis, there is a tendency to gravitate toward illicit substances, in particular, stimulants.11
We also know that adolescents are known to engage in normal risk-taking and social experimentation. Given that, the notion of boundary setting becomes a complicated affair during a pandemic. Adults may no longer be involved in the same types of risk-taking behaviors, but enforced self-isolation coupled with unchecked consumption of various social medial platforms continue to take a toll on personal development. Socialization plays an enormous role in maintaining psychological health, and social media is no substitute for in-person interactions. Such platforms can reduce mental growth opportunities and affect ADHD adults unfavorably.
For instance, it has been reported that women with adult ADHD are more likely to present with negative cognitive biases and symptoms of anxiety as a function of social media use.12,13 As clinicians, we should recommend introducing activities with the aim of enhancing self-acceptance, mindfulness, and the ability to engage in healthy lifestyles. A holistic framework that focuses on psychological wellness and physical fitness will ensure treatment success. Medication management may prove to be a challenge because of differences in dosing, response schedules, and agreed-upon diagnostic criteria used for young patients, compared with those needed for adults.
Treatment strategies
Before the pandemic, researchers were observing an increase globally in the ADHD diagnosis,14 and clinicians have been exploring the efficacy of select medications, sometimes with limited success.15 Stimulant medication, combined with behavioral interventions, is supported by evidenced-based medicine and is the treatment of choice for childhood ADHD.
The stimulant remedy considered to be the most efficacious for adult ADHD is methylphenidate or dextroamphetamine.
However, be sure to proceed with caution and prepare a thorough work-up, because there can be cardiovascular risk factors associated with these medications with a pronounced increase in heart rate and blood pressure.
Stimulant medications are known to increase the risk of stroke or myocardial infarction for individuals with preexisting cardiovascular anomalies or structural anomalies. The American Heart Association no longer recommends a baseline EKG before commencing stimulant therapy with the exception of preexisting cardiac risk. Nonstimulant medications such as atomoxetine are available as alternatives.
The process of finding therapies that will reduce symptoms of ADHD takes considerable time, and individuals may fail to notice improvements, at least initially.
Before prescribing any medicine or therapies, it is important to evaluate for factors that are specific to ADHD and rule out the presence of other learning or developmental disorders, to prevent negative consequences.
Health care professionals can introduce nonspecific interventions as a means of tackling complicated cases of adult ADHD, especially those that coincide with underlying medical conditions (for example, cardiovascular disease, seizure disorders, and/or eating disorders). In such cases, stimulant medications may lead to symptom exacerbation, and the health care professional should carry out a systematic evaluation (risks vs. benefits of drug classes), despite the limitations of online appointments over the course of the pandemic.
Moreover, ADHD symptoms can take on a more severe form within the context of preexisting mood and anxiety disorders. Unfortunately, these comorbidities may have a negative prognostic outcome, too, thereby increasing other health-related risk factors. Psychological interventions can be implemented via online assessments because of recent technological advances worldwide, providing a new level of confidence and social engagement. EEG-assisted biofeedback is an example of new technological modalities that may help improve the overall performance and functionality of individuals with adult ADHD.16 Numerous services and resources are available to patients and their families that can improve mental health and well-being.
Other nonpharmacologic choices also play an instrumental role in bringing harmony and organization into a patient’s life through the use of daily planners, alarms, and to-do lists. In addition, therapists can provide treatment that helps individuals get motivated and reduce their anxiety levels. Behavioral therapies support patient initiatives by increasing their productivity, activity management, and satisfaction. Cognitive-behavioral therapy (CBT), and marriage counseling and family therapy are modalities that may help adults with ADHD change underlying thoughts and perceptions and develop coping skills and self-esteem.
Appropriate to the pandemic situation is another treatment, e-therapy, which includes text-based communication, video calling, and phone calls. It is a low-cost and convenient alternative for people. For some patients, traveling to a particular clinic or counseling center can be difficult, and there is a shortage of counselors worldwide, so it is beneficial to talk with a counselor on a video/phone call or through social media. It is crucial for the ADHD coach to be trained with relevant knowledge to make plans, set goals, and manage a patient’s schedule of activities. For the counselor, sharing tips based on personal experience and making the appropriate suggestions allows adults with ADHD to stay motivated and focus on the task at hand. It should be noted that counselors play an important role in reducing stress levels for those diagnosed with ADHD, allowing patients to lead productive lives and achieve career goals.
Various online support communities can provide patients and their parents with educational resources, to address issues connected to ADHD in a professional manner.17
The road to treatment success
Any delays in treating adults with ADHD can lead to a frustrating situation in which the entire family will be affected. As stated earlier, numerous support groups are available to adults with ADHD, and some of those groups can offer valuable tips about addressing stress management and the diverse roles that parents and family members may play in patient care.18 These groups provide a network for people to exchange ideas and recommend strategies. Online support groups may connect patients directly with key opinion leaders and health care providers.
Individuals with ADHD often experience problems with organization and concentration – especially within the context of the pandemic – and receiving guidance from counselors will provide an opportunity to learn valuable coping strategies and manage symptoms, recognizing and mitigating any mood swings associated with anxiety or depression that emerge alongside their ADHD. Psychotherapy is instrumental in patient care, and individuals with adult ADHD should be taught to acknowledge the role of medications (for example, neglect, divert, or self-medicate). A holistic approach to managing ADHD symptoms is necessary for optimal functioning and independence.
Dr. Aman is a faculty member in the biology department of City Colleges of Chicago. She is a postdoctoral researcher at the International Maternal and Child Health Foundation (IMCHF), Montreal; a fellow, medical staff development, from the American Academy of Medical Management; and a Masters Online Teacher, University of Illinois at Chicago. Dr. Aman disclosed no relevant financial relationships. Dr. Islam is a medical adviser for the IMCHF, Montreal, and is based in New York. He is a postdoctoral fellow, psychopharmacologist, and a board-certified medical affairs specialist. Dr. Islam disclosed no relevant financial relationships. Dr. Karama is a psychiatrist at the Douglas Mental Health University Institute, Montreal. He is an assistant professor at the department of psychiatry, McGill University, also in Montreal. He has no disclosures. Dr. Choudhry is the chief scientific officer and head of the department of mental health and clinical research at the IMCHF. He has no disclosures.
References
1. J Atten Disord. 2020. doi: 10.1177/1087054720943271.
2. ADDitude Magazine. 2020 Jul 23.
3. Management of ADHD in Adults: What the Science Says. 2007 Oct 9. Guilford Press.
4. N Engl J Med. 2013 Nov 14;369(20):1935-44.
5. J Clin Psychiatry. 2002;63 Suppl 12:29-35.
6. J Atten Dis. 2015 Jan 12. doi: 10.1177/1087054144566076.
7. Psychiatry Res. 2020 Oct;292. doi: 10.1016/j.psychres.2020.113345.
8. Case Rep Cardiol. 2016. doi: 10.1155/2016/2343691.
9. Curr Diab Rep. 2019 Jun 27;19(8):46. doi: 10.1007/s11892-019-1174-x.
10. Curr Psychiatry Rep. 2014 Mar;16(3):436. doi: 10.1007/s/11920-013-0436-6.
11. Current Psychiatry. 2014 Dec;13(12):e3-4.
12. BMC Psychiatry. 2020;20(40). doi: 10.1186/s/12888-020-02707-9.
13. Psychol Addict Behav. 2016 Mar;30(2):252–62.
14. ADDitude Magazine. 2017 Apr 6.
15. Harv Mental Health Letter. 2009 Nov.
16. MGM J Med Sci. 2020 Jul 17(3):161-2.
17. J Child Psychol Psychiatry. 2020 Jul 7.
18. Int J Disaster Risk Reduct. 2020 Dec;51. doi: 10.1016/j.ijdrr.2020.101845.
As some countries brace for yet another possible surge in the COVID-19 pandemic – particularly among young adults who have not yet been vaccinated – clinicians should remain wary of the cardinal symptoms of adult ADHD.
Research from an Israeli study shows that individuals with unmedicated ADHD are 52% more likely to test positive for the virus.1,2
The symptoms of ADHD, including impulsiveness and inability to follow directions, combined with the tendency to leave adults with ADHD on their own to sort out COVID-19–related protocols – make these individuals susceptible to exposure.
As we know, ADHD is a condition characterized by a pervasive pattern of impulsivity and/or inattention, which greatly reduces organizational capabilities by interfering at the developmental level.3 Other key symptoms include short attention span, hyperactivity, restlessness, difficulty in prioritizing tasks, and an absence of time awareness. Symptom presentation of ADHD is contingent upon the nature of the individual’s overall mental health and etiologic issues that may be traced back to the brain’s development.4
Diagnosing ADHD in adults is relatively difficult, because a formal diagnosis generally requires symptoms to show up between the ages of 6 and 12.5 Also, clinicians can interview parents and family members to assess whether the classical features of ADHD were present in childhood for those suspected of having the condition.
Early vs. late presentation
Among the preschool population, it has been observed that emerging ADHD symptoms may progress with time or remain relatively constant with respect to the activities that children partake in. In some instances, impulsive behavior, especially compared with other symptoms, might be identified quickly by the attentive parent or caregiver. However, when ADHD appears in adulthood, it is possible that prior ADHD symptoms escaped detection – only to be diagnosed later in life because of varying presentations and the increased organizational demands of adulthood.
Meanwhile, diagnosis in adolescence can bring a different set of challenges to the forefront as teenagers face problems with self-management and responsibilities of daily living. These young people must cope with academic6 and social pressures – and a host of new societal expectations.
It is essential to understand how all of those societal factors have affected ADHD and its aspects, especially within the context of COVID-19. The coronavirus has introduced myriad challenges at the global level. Individuals with ADHD exhibit neurodevelopmental and corollary attention deficit issues that make them more susceptible to environmental stressors. Physical distancing practices might aggravate existing behavioral problems.
Distance forced by pandemic offers challenges
Despite the widespread adoption of telemedicine during the pandemic, some physicians think that the delivery of optimal care and the ability to adequately address patients’ health-related concerns have been compromised. Certainly, in the case of addressing the needs of patients with ADHD or related learning disorders, in-person examinations and clinical visits are best.
That is also the case for ADHD patients with comorbid sleep disorders. For those patients, it might be prudent to explore lifestyle changes (for example, improvements in sleep hygiene practices) before resorting to the use of pharmacologic agents such as hypnotics and melatonin. Along similar lines, the European ADHD Guideline Group (EAGG) advises the use of pharmacotherapy after the successful completion of a physical exam; patients already adhering to a treatment plan should continue therapy without interruption. Clinicians caring for patients with adult ADHD have faced a dilemma because treatment breaks increase the likelihood of illnesses resulting from the pandemic. Also, the inability to conduct treatment in person because of the pandemic raises concerns about pharmacotherapy.
The pandemic has affected the course of pediatric care and also has presented new challenges for adolescents as they begin to tackle unique problems related to their health concerns. In prepandemic times, teachers played integral roles in the diagnostic process, because they were able to readily identify children and teenagers with mental and physical challenges. In stark contrast, connecting with students online may not allow teachers to identify skill deficits in young patients or in adults with ADHD.
Furthermore, adults with ADHD and medical comorbidities may be at increased risk of disease exposure directly resulting from an inability to address their social and/or emotional well-being adequately. The social distancing and other mitigation measures advised by public health experts ensure safety and protection but also can present numerous hurdles for children, teenagers, adults – and their respective families.
Individuals with adult ADHD and other psychiatric disorders may downplay their psychological distress7 [for example, sleep dysfunction, issues concerning activities of daily living], and view it as being the natural product of the COVID-19 environment. As a result of their misconceptions, they may avoid increasing their medication dose to control emergent symptoms of hyperactivity and impulsivity, instead opting to manage stress without aid from health care professionals. The absence of patient-provider interactivity and the integration of telemedicine has introduced unnecessary obstacles with respect to medication management and therapy as well as general access to expert advice. It is of utmost importance for clinicians to identify at-risk patients and reeducate the adult ADHD patient on issues concerning medication intake and psychological wellness.
Individuals with developmental disorders may experience numerous setbacks when trying to navigate their environments. The lack of correct feedback, supervision, and guidance may adversely affect adults with ADHD, contributing toward a lack of self-esteem and social awareness.
Individuals with adult ADHD are more likely than are their younger counterparts to have medical comorbidities, such as cardiovascular disease8 and type 2 diabetes,9 so it is crucial to prescribe dietary instructions to patients. Sometimes patients with adult ADHD lack support in the form of acceptance by family and peers, so it is critical for the patient to come to terms with his/her condition and seek professional help, incorporating effective strategies wherever needed to maintain day-to-day functioning.
Other possible comorbidities
There can be risk factors associated with isolation of adults who have depression and/or anxiety, poor eating habits, and maladaptive behaviors. Other adverse health-related issues may include substance use disorder.10 Drug use suppresses developmental growth and may induce ADHD symptom exacerbation. Consistent with Khantzian’s self-medication hypothesis, among individuals with ADHD, including those who lack a formal diagnosis, there is a tendency to gravitate toward illicit substances, in particular, stimulants.11
We also know that adolescents are known to engage in normal risk-taking and social experimentation. Given that, the notion of boundary setting becomes a complicated affair during a pandemic. Adults may no longer be involved in the same types of risk-taking behaviors, but enforced self-isolation coupled with unchecked consumption of various social medial platforms continue to take a toll on personal development. Socialization plays an enormous role in maintaining psychological health, and social media is no substitute for in-person interactions. Such platforms can reduce mental growth opportunities and affect ADHD adults unfavorably.
For instance, it has been reported that women with adult ADHD are more likely to present with negative cognitive biases and symptoms of anxiety as a function of social media use.12,13 As clinicians, we should recommend introducing activities with the aim of enhancing self-acceptance, mindfulness, and the ability to engage in healthy lifestyles. A holistic framework that focuses on psychological wellness and physical fitness will ensure treatment success. Medication management may prove to be a challenge because of differences in dosing, response schedules, and agreed-upon diagnostic criteria used for young patients, compared with those needed for adults.
Treatment strategies
Before the pandemic, researchers were observing an increase globally in the ADHD diagnosis,14 and clinicians have been exploring the efficacy of select medications, sometimes with limited success.15 Stimulant medication, combined with behavioral interventions, is supported by evidenced-based medicine and is the treatment of choice for childhood ADHD.
The stimulant remedy considered to be the most efficacious for adult ADHD is methylphenidate or dextroamphetamine.
However, be sure to proceed with caution and prepare a thorough work-up, because there can be cardiovascular risk factors associated with these medications with a pronounced increase in heart rate and blood pressure.
Stimulant medications are known to increase the risk of stroke or myocardial infarction for individuals with preexisting cardiovascular anomalies or structural anomalies. The American Heart Association no longer recommends a baseline EKG before commencing stimulant therapy with the exception of preexisting cardiac risk. Nonstimulant medications such as atomoxetine are available as alternatives.
The process of finding therapies that will reduce symptoms of ADHD takes considerable time, and individuals may fail to notice improvements, at least initially.
Before prescribing any medicine or therapies, it is important to evaluate for factors that are specific to ADHD and rule out the presence of other learning or developmental disorders, to prevent negative consequences.
Health care professionals can introduce nonspecific interventions as a means of tackling complicated cases of adult ADHD, especially those that coincide with underlying medical conditions (for example, cardiovascular disease, seizure disorders, and/or eating disorders). In such cases, stimulant medications may lead to symptom exacerbation, and the health care professional should carry out a systematic evaluation (risks vs. benefits of drug classes), despite the limitations of online appointments over the course of the pandemic.
Moreover, ADHD symptoms can take on a more severe form within the context of preexisting mood and anxiety disorders. Unfortunately, these comorbidities may have a negative prognostic outcome, too, thereby increasing other health-related risk factors. Psychological interventions can be implemented via online assessments because of recent technological advances worldwide, providing a new level of confidence and social engagement. EEG-assisted biofeedback is an example of new technological modalities that may help improve the overall performance and functionality of individuals with adult ADHD.16 Numerous services and resources are available to patients and their families that can improve mental health and well-being.
Other nonpharmacologic choices also play an instrumental role in bringing harmony and organization into a patient’s life through the use of daily planners, alarms, and to-do lists. In addition, therapists can provide treatment that helps individuals get motivated and reduce their anxiety levels. Behavioral therapies support patient initiatives by increasing their productivity, activity management, and satisfaction. Cognitive-behavioral therapy (CBT), and marriage counseling and family therapy are modalities that may help adults with ADHD change underlying thoughts and perceptions and develop coping skills and self-esteem.
Appropriate to the pandemic situation is another treatment, e-therapy, which includes text-based communication, video calling, and phone calls. It is a low-cost and convenient alternative for people. For some patients, traveling to a particular clinic or counseling center can be difficult, and there is a shortage of counselors worldwide, so it is beneficial to talk with a counselor on a video/phone call or through social media. It is crucial for the ADHD coach to be trained with relevant knowledge to make plans, set goals, and manage a patient’s schedule of activities. For the counselor, sharing tips based on personal experience and making the appropriate suggestions allows adults with ADHD to stay motivated and focus on the task at hand. It should be noted that counselors play an important role in reducing stress levels for those diagnosed with ADHD, allowing patients to lead productive lives and achieve career goals.
Various online support communities can provide patients and their parents with educational resources, to address issues connected to ADHD in a professional manner.17
The road to treatment success
Any delays in treating adults with ADHD can lead to a frustrating situation in which the entire family will be affected. As stated earlier, numerous support groups are available to adults with ADHD, and some of those groups can offer valuable tips about addressing stress management and the diverse roles that parents and family members may play in patient care.18 These groups provide a network for people to exchange ideas and recommend strategies. Online support groups may connect patients directly with key opinion leaders and health care providers.
Individuals with ADHD often experience problems with organization and concentration – especially within the context of the pandemic – and receiving guidance from counselors will provide an opportunity to learn valuable coping strategies and manage symptoms, recognizing and mitigating any mood swings associated with anxiety or depression that emerge alongside their ADHD. Psychotherapy is instrumental in patient care, and individuals with adult ADHD should be taught to acknowledge the role of medications (for example, neglect, divert, or self-medicate). A holistic approach to managing ADHD symptoms is necessary for optimal functioning and independence.
Dr. Aman is a faculty member in the biology department of City Colleges of Chicago. She is a postdoctoral researcher at the International Maternal and Child Health Foundation (IMCHF), Montreal; a fellow, medical staff development, from the American Academy of Medical Management; and a Masters Online Teacher, University of Illinois at Chicago. Dr. Aman disclosed no relevant financial relationships. Dr. Islam is a medical adviser for the IMCHF, Montreal, and is based in New York. He is a postdoctoral fellow, psychopharmacologist, and a board-certified medical affairs specialist. Dr. Islam disclosed no relevant financial relationships. Dr. Karama is a psychiatrist at the Douglas Mental Health University Institute, Montreal. He is an assistant professor at the department of psychiatry, McGill University, also in Montreal. He has no disclosures. Dr. Choudhry is the chief scientific officer and head of the department of mental health and clinical research at the IMCHF. He has no disclosures.
References
1. J Atten Disord. 2020. doi: 10.1177/1087054720943271.
2. ADDitude Magazine. 2020 Jul 23.
3. Management of ADHD in Adults: What the Science Says. 2007 Oct 9. Guilford Press.
4. N Engl J Med. 2013 Nov 14;369(20):1935-44.
5. J Clin Psychiatry. 2002;63 Suppl 12:29-35.
6. J Atten Dis. 2015 Jan 12. doi: 10.1177/1087054144566076.
7. Psychiatry Res. 2020 Oct;292. doi: 10.1016/j.psychres.2020.113345.
8. Case Rep Cardiol. 2016. doi: 10.1155/2016/2343691.
9. Curr Diab Rep. 2019 Jun 27;19(8):46. doi: 10.1007/s11892-019-1174-x.
10. Curr Psychiatry Rep. 2014 Mar;16(3):436. doi: 10.1007/s/11920-013-0436-6.
11. Current Psychiatry. 2014 Dec;13(12):e3-4.
12. BMC Psychiatry. 2020;20(40). doi: 10.1186/s/12888-020-02707-9.
13. Psychol Addict Behav. 2016 Mar;30(2):252–62.
14. ADDitude Magazine. 2017 Apr 6.
15. Harv Mental Health Letter. 2009 Nov.
16. MGM J Med Sci. 2020 Jul 17(3):161-2.
17. J Child Psychol Psychiatry. 2020 Jul 7.
18. Int J Disaster Risk Reduct. 2020 Dec;51. doi: 10.1016/j.ijdrr.2020.101845.
As some countries brace for yet another possible surge in the COVID-19 pandemic – particularly among young adults who have not yet been vaccinated – clinicians should remain wary of the cardinal symptoms of adult ADHD.
Research from an Israeli study shows that individuals with unmedicated ADHD are 52% more likely to test positive for the virus.1,2
The symptoms of ADHD, including impulsiveness and inability to follow directions, combined with the tendency to leave adults with ADHD on their own to sort out COVID-19–related protocols – make these individuals susceptible to exposure.
As we know, ADHD is a condition characterized by a pervasive pattern of impulsivity and/or inattention, which greatly reduces organizational capabilities by interfering at the developmental level.3 Other key symptoms include short attention span, hyperactivity, restlessness, difficulty in prioritizing tasks, and an absence of time awareness. Symptom presentation of ADHD is contingent upon the nature of the individual’s overall mental health and etiologic issues that may be traced back to the brain’s development.4
Diagnosing ADHD in adults is relatively difficult, because a formal diagnosis generally requires symptoms to show up between the ages of 6 and 12.5 Also, clinicians can interview parents and family members to assess whether the classical features of ADHD were present in childhood for those suspected of having the condition.
Early vs. late presentation
Among the preschool population, it has been observed that emerging ADHD symptoms may progress with time or remain relatively constant with respect to the activities that children partake in. In some instances, impulsive behavior, especially compared with other symptoms, might be identified quickly by the attentive parent or caregiver. However, when ADHD appears in adulthood, it is possible that prior ADHD symptoms escaped detection – only to be diagnosed later in life because of varying presentations and the increased organizational demands of adulthood.
Meanwhile, diagnosis in adolescence can bring a different set of challenges to the forefront as teenagers face problems with self-management and responsibilities of daily living. These young people must cope with academic6 and social pressures – and a host of new societal expectations.
It is essential to understand how all of those societal factors have affected ADHD and its aspects, especially within the context of COVID-19. The coronavirus has introduced myriad challenges at the global level. Individuals with ADHD exhibit neurodevelopmental and corollary attention deficit issues that make them more susceptible to environmental stressors. Physical distancing practices might aggravate existing behavioral problems.
Distance forced by pandemic offers challenges
Despite the widespread adoption of telemedicine during the pandemic, some physicians think that the delivery of optimal care and the ability to adequately address patients’ health-related concerns have been compromised. Certainly, in the case of addressing the needs of patients with ADHD or related learning disorders, in-person examinations and clinical visits are best.
That is also the case for ADHD patients with comorbid sleep disorders. For those patients, it might be prudent to explore lifestyle changes (for example, improvements in sleep hygiene practices) before resorting to the use of pharmacologic agents such as hypnotics and melatonin. Along similar lines, the European ADHD Guideline Group (EAGG) advises the use of pharmacotherapy after the successful completion of a physical exam; patients already adhering to a treatment plan should continue therapy without interruption. Clinicians caring for patients with adult ADHD have faced a dilemma because treatment breaks increase the likelihood of illnesses resulting from the pandemic. Also, the inability to conduct treatment in person because of the pandemic raises concerns about pharmacotherapy.
The pandemic has affected the course of pediatric care and also has presented new challenges for adolescents as they begin to tackle unique problems related to their health concerns. In prepandemic times, teachers played integral roles in the diagnostic process, because they were able to readily identify children and teenagers with mental and physical challenges. In stark contrast, connecting with students online may not allow teachers to identify skill deficits in young patients or in adults with ADHD.
Furthermore, adults with ADHD and medical comorbidities may be at increased risk of disease exposure directly resulting from an inability to address their social and/or emotional well-being adequately. The social distancing and other mitigation measures advised by public health experts ensure safety and protection but also can present numerous hurdles for children, teenagers, adults – and their respective families.
Individuals with adult ADHD and other psychiatric disorders may downplay their psychological distress7 [for example, sleep dysfunction, issues concerning activities of daily living], and view it as being the natural product of the COVID-19 environment. As a result of their misconceptions, they may avoid increasing their medication dose to control emergent symptoms of hyperactivity and impulsivity, instead opting to manage stress without aid from health care professionals. The absence of patient-provider interactivity and the integration of telemedicine has introduced unnecessary obstacles with respect to medication management and therapy as well as general access to expert advice. It is of utmost importance for clinicians to identify at-risk patients and reeducate the adult ADHD patient on issues concerning medication intake and psychological wellness.
Individuals with developmental disorders may experience numerous setbacks when trying to navigate their environments. The lack of correct feedback, supervision, and guidance may adversely affect adults with ADHD, contributing toward a lack of self-esteem and social awareness.
Individuals with adult ADHD are more likely than are their younger counterparts to have medical comorbidities, such as cardiovascular disease8 and type 2 diabetes,9 so it is crucial to prescribe dietary instructions to patients. Sometimes patients with adult ADHD lack support in the form of acceptance by family and peers, so it is critical for the patient to come to terms with his/her condition and seek professional help, incorporating effective strategies wherever needed to maintain day-to-day functioning.
Other possible comorbidities
There can be risk factors associated with isolation of adults who have depression and/or anxiety, poor eating habits, and maladaptive behaviors. Other adverse health-related issues may include substance use disorder.10 Drug use suppresses developmental growth and may induce ADHD symptom exacerbation. Consistent with Khantzian’s self-medication hypothesis, among individuals with ADHD, including those who lack a formal diagnosis, there is a tendency to gravitate toward illicit substances, in particular, stimulants.11
We also know that adolescents are known to engage in normal risk-taking and social experimentation. Given that, the notion of boundary setting becomes a complicated affair during a pandemic. Adults may no longer be involved in the same types of risk-taking behaviors, but enforced self-isolation coupled with unchecked consumption of various social medial platforms continue to take a toll on personal development. Socialization plays an enormous role in maintaining psychological health, and social media is no substitute for in-person interactions. Such platforms can reduce mental growth opportunities and affect ADHD adults unfavorably.
For instance, it has been reported that women with adult ADHD are more likely to present with negative cognitive biases and symptoms of anxiety as a function of social media use.12,13 As clinicians, we should recommend introducing activities with the aim of enhancing self-acceptance, mindfulness, and the ability to engage in healthy lifestyles. A holistic framework that focuses on psychological wellness and physical fitness will ensure treatment success. Medication management may prove to be a challenge because of differences in dosing, response schedules, and agreed-upon diagnostic criteria used for young patients, compared with those needed for adults.
Treatment strategies
Before the pandemic, researchers were observing an increase globally in the ADHD diagnosis,14 and clinicians have been exploring the efficacy of select medications, sometimes with limited success.15 Stimulant medication, combined with behavioral interventions, is supported by evidenced-based medicine and is the treatment of choice for childhood ADHD.
The stimulant remedy considered to be the most efficacious for adult ADHD is methylphenidate or dextroamphetamine.
However, be sure to proceed with caution and prepare a thorough work-up, because there can be cardiovascular risk factors associated with these medications with a pronounced increase in heart rate and blood pressure.
Stimulant medications are known to increase the risk of stroke or myocardial infarction for individuals with preexisting cardiovascular anomalies or structural anomalies. The American Heart Association no longer recommends a baseline EKG before commencing stimulant therapy with the exception of preexisting cardiac risk. Nonstimulant medications such as atomoxetine are available as alternatives.
The process of finding therapies that will reduce symptoms of ADHD takes considerable time, and individuals may fail to notice improvements, at least initially.
Before prescribing any medicine or therapies, it is important to evaluate for factors that are specific to ADHD and rule out the presence of other learning or developmental disorders, to prevent negative consequences.
Health care professionals can introduce nonspecific interventions as a means of tackling complicated cases of adult ADHD, especially those that coincide with underlying medical conditions (for example, cardiovascular disease, seizure disorders, and/or eating disorders). In such cases, stimulant medications may lead to symptom exacerbation, and the health care professional should carry out a systematic evaluation (risks vs. benefits of drug classes), despite the limitations of online appointments over the course of the pandemic.
Moreover, ADHD symptoms can take on a more severe form within the context of preexisting mood and anxiety disorders. Unfortunately, these comorbidities may have a negative prognostic outcome, too, thereby increasing other health-related risk factors. Psychological interventions can be implemented via online assessments because of recent technological advances worldwide, providing a new level of confidence and social engagement. EEG-assisted biofeedback is an example of new technological modalities that may help improve the overall performance and functionality of individuals with adult ADHD.16 Numerous services and resources are available to patients and their families that can improve mental health and well-being.
Other nonpharmacologic choices also play an instrumental role in bringing harmony and organization into a patient’s life through the use of daily planners, alarms, and to-do lists. In addition, therapists can provide treatment that helps individuals get motivated and reduce their anxiety levels. Behavioral therapies support patient initiatives by increasing their productivity, activity management, and satisfaction. Cognitive-behavioral therapy (CBT), and marriage counseling and family therapy are modalities that may help adults with ADHD change underlying thoughts and perceptions and develop coping skills and self-esteem.
Appropriate to the pandemic situation is another treatment, e-therapy, which includes text-based communication, video calling, and phone calls. It is a low-cost and convenient alternative for people. For some patients, traveling to a particular clinic or counseling center can be difficult, and there is a shortage of counselors worldwide, so it is beneficial to talk with a counselor on a video/phone call or through social media. It is crucial for the ADHD coach to be trained with relevant knowledge to make plans, set goals, and manage a patient’s schedule of activities. For the counselor, sharing tips based on personal experience and making the appropriate suggestions allows adults with ADHD to stay motivated and focus on the task at hand. It should be noted that counselors play an important role in reducing stress levels for those diagnosed with ADHD, allowing patients to lead productive lives and achieve career goals.
Various online support communities can provide patients and their parents with educational resources, to address issues connected to ADHD in a professional manner.17
The road to treatment success
Any delays in treating adults with ADHD can lead to a frustrating situation in which the entire family will be affected. As stated earlier, numerous support groups are available to adults with ADHD, and some of those groups can offer valuable tips about addressing stress management and the diverse roles that parents and family members may play in patient care.18 These groups provide a network for people to exchange ideas and recommend strategies. Online support groups may connect patients directly with key opinion leaders and health care providers.
Individuals with ADHD often experience problems with organization and concentration – especially within the context of the pandemic – and receiving guidance from counselors will provide an opportunity to learn valuable coping strategies and manage symptoms, recognizing and mitigating any mood swings associated with anxiety or depression that emerge alongside their ADHD. Psychotherapy is instrumental in patient care, and individuals with adult ADHD should be taught to acknowledge the role of medications (for example, neglect, divert, or self-medicate). A holistic approach to managing ADHD symptoms is necessary for optimal functioning and independence.
Dr. Aman is a faculty member in the biology department of City Colleges of Chicago. She is a postdoctoral researcher at the International Maternal and Child Health Foundation (IMCHF), Montreal; a fellow, medical staff development, from the American Academy of Medical Management; and a Masters Online Teacher, University of Illinois at Chicago. Dr. Aman disclosed no relevant financial relationships. Dr. Islam is a medical adviser for the IMCHF, Montreal, and is based in New York. He is a postdoctoral fellow, psychopharmacologist, and a board-certified medical affairs specialist. Dr. Islam disclosed no relevant financial relationships. Dr. Karama is a psychiatrist at the Douglas Mental Health University Institute, Montreal. He is an assistant professor at the department of psychiatry, McGill University, also in Montreal. He has no disclosures. Dr. Choudhry is the chief scientific officer and head of the department of mental health and clinical research at the IMCHF. He has no disclosures.
References
1. J Atten Disord. 2020. doi: 10.1177/1087054720943271.
2. ADDitude Magazine. 2020 Jul 23.
3. Management of ADHD in Adults: What the Science Says. 2007 Oct 9. Guilford Press.
4. N Engl J Med. 2013 Nov 14;369(20):1935-44.
5. J Clin Psychiatry. 2002;63 Suppl 12:29-35.
6. J Atten Dis. 2015 Jan 12. doi: 10.1177/1087054144566076.
7. Psychiatry Res. 2020 Oct;292. doi: 10.1016/j.psychres.2020.113345.
8. Case Rep Cardiol. 2016. doi: 10.1155/2016/2343691.
9. Curr Diab Rep. 2019 Jun 27;19(8):46. doi: 10.1007/s11892-019-1174-x.
10. Curr Psychiatry Rep. 2014 Mar;16(3):436. doi: 10.1007/s/11920-013-0436-6.
11. Current Psychiatry. 2014 Dec;13(12):e3-4.
12. BMC Psychiatry. 2020;20(40). doi: 10.1186/s/12888-020-02707-9.
13. Psychol Addict Behav. 2016 Mar;30(2):252–62.
14. ADDitude Magazine. 2017 Apr 6.
15. Harv Mental Health Letter. 2009 Nov.
16. MGM J Med Sci. 2020 Jul 17(3):161-2.
17. J Child Psychol Psychiatry. 2020 Jul 7.
18. Int J Disaster Risk Reduct. 2020 Dec;51. doi: 10.1016/j.ijdrr.2020.101845.
Antipsychotics protective against COVID-19?
Antipsychotics may protect against SARS-CoV-2 infection or lead to a milder course of illness, new research suggests.
“Counterintuitively,” the investigators noted, vulnerable people with severe mental illness “on antipsychotic treatment showed a lower risk of SARS-CoV-2 infection and a likely better COVID-19 prognosis.”
“These are very interesting findings that reflect a clinical reality where we see few patients with severe COVID-19, despite the presence of various risk factors,” study investigator Manuel Canal-Rivero, PhD, clinical psychologist, Virgen del Rocio University Hospital, Sevilla, Spain, said in a news release.
“The number of COVID-19 patients is lower than expected among this group of people and in cases where a proven infection does occur, the evolution is benign and does not reach a life-threatening clinical situation. These data as a whole seem to point to the protective effect of the medication,” Dr. Canal-Rivero added.
The study was published online as a letter to the editor February 19, 2021, in Schizophrenia Research.
A ‘striking’ finding
The researchers assessed the prevalence and prognosis of COVID-19 in 698 patients with serious mental disorders (SMDs) receiving treatment with long-acting injectable antipsychotic medication. The non-SMD population included the catchment area population of 557,576 individuals.
From February to November 2020, 4.1% of the non-SMD population were infected with SARS-CoV-2 versus just 1.3% of the SMD population (9 of 698 patients). All but one patient with SMD had asymptomatic illness (8 of 9, 89%). Accurate information on asymptomatic illness in the non-SMD population was not available.
There were also fewer hospital admissions in the SMD population (0% vs. 8.5%), ICU admissions (0% vs. 0.9%) and deaths because of COVID-19 (0% vs. 1.1%), although the differences were not statistically significant.
In related research, the same investigators found that many of the genes whose expression is altered by SARS-CoV-2 infection are significantly down-regulated by antipsychotic drugs.
“In a striking way, we have shown how antipsychotics reduce the activation of genes involved in many of the inflammatory and immunological pathways associated with the severity of COVID-19 infection,” Benedicto Crespo-Facorro, MD, PhD, University of Sevilla, who led the study, said in the news release.
“Although this finding requires replication, the discovery could be very significant because the treatment of COVID-19 with drugs originally indicated for unrelated clinical situations, that is to say drug repositioning, has been shown to be an interesting source of effective treatments for COVID-19 patients,” he added.
Antiviral properties?
In a comment, Samoon Ahmad, MD, professor, department of psychiatry, New York University, said the findings are “fascinating” and should be explored further.

While the findings on long-acting injectable antipsychotic treatment “seem counterintuitive at first, they are in line with other studies,” said Dr. Ahmad, who heads the inpatient psychiatry unit at Bellevue Hospital Center and is founder of the Integrative Center for Wellness in New York.
“ and antidepressant medications appear to activate key cellular proteins that the SARS-CoV-2 virus uses for replication,” explained Dr. Ahmad, who was not associated with the study.
For example, as reported by this news organization, a preliminary study published in 2020 showed that early treatment with the antidepressant fluvoxamine prevented clinical deterioration in adult outpatients with confirmed COVID-19.
The antipsychotic aripiprazole has also shown potential to treat severe COVID-19 infection.
“Consequently, there appears to be a possible explanation as to why these drugs afford patients with severe mental disorders increased protection against the SARS-CoV-2 virus,” Dr. Ahmad said in an interview.
However, he cautioned, there are several factors at play that could influence the results. Therefore, more research is needed before drawing any firm conclusions.
“Still, the possibility that psychiatric medications may have antiviral properties is a tremendous development and I really hope that additional studies confirm the preliminary findings,” Dr. Ahmad said.
The study had no specific funding. The authors and Dr. Ahmad disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Antipsychotics may protect against SARS-CoV-2 infection or lead to a milder course of illness, new research suggests.
“Counterintuitively,” the investigators noted, vulnerable people with severe mental illness “on antipsychotic treatment showed a lower risk of SARS-CoV-2 infection and a likely better COVID-19 prognosis.”
“These are very interesting findings that reflect a clinical reality where we see few patients with severe COVID-19, despite the presence of various risk factors,” study investigator Manuel Canal-Rivero, PhD, clinical psychologist, Virgen del Rocio University Hospital, Sevilla, Spain, said in a news release.
“The number of COVID-19 patients is lower than expected among this group of people and in cases where a proven infection does occur, the evolution is benign and does not reach a life-threatening clinical situation. These data as a whole seem to point to the protective effect of the medication,” Dr. Canal-Rivero added.
The study was published online as a letter to the editor February 19, 2021, in Schizophrenia Research.
A ‘striking’ finding
The researchers assessed the prevalence and prognosis of COVID-19 in 698 patients with serious mental disorders (SMDs) receiving treatment with long-acting injectable antipsychotic medication. The non-SMD population included the catchment area population of 557,576 individuals.
From February to November 2020, 4.1% of the non-SMD population were infected with SARS-CoV-2 versus just 1.3% of the SMD population (9 of 698 patients). All but one patient with SMD had asymptomatic illness (8 of 9, 89%). Accurate information on asymptomatic illness in the non-SMD population was not available.
There were also fewer hospital admissions in the SMD population (0% vs. 8.5%), ICU admissions (0% vs. 0.9%) and deaths because of COVID-19 (0% vs. 1.1%), although the differences were not statistically significant.
In related research, the same investigators found that many of the genes whose expression is altered by SARS-CoV-2 infection are significantly down-regulated by antipsychotic drugs.
“In a striking way, we have shown how antipsychotics reduce the activation of genes involved in many of the inflammatory and immunological pathways associated with the severity of COVID-19 infection,” Benedicto Crespo-Facorro, MD, PhD, University of Sevilla, who led the study, said in the news release.
“Although this finding requires replication, the discovery could be very significant because the treatment of COVID-19 with drugs originally indicated for unrelated clinical situations, that is to say drug repositioning, has been shown to be an interesting source of effective treatments for COVID-19 patients,” he added.
Antiviral properties?
In a comment, Samoon Ahmad, MD, professor, department of psychiatry, New York University, said the findings are “fascinating” and should be explored further.
While the findings on long-acting injectable antipsychotic treatment “seem counterintuitive at first, they are in line with other studies,” said Dr. Ahmad, who heads the inpatient psychiatry unit at Bellevue Hospital Center and is founder of the Integrative Center for Wellness in New York.
“ and antidepressant medications appear to activate key cellular proteins that the SARS-CoV-2 virus uses for replication,” explained Dr. Ahmad, who was not associated with the study.
For example, as reported by this news organization, a preliminary study published in 2020 showed that early treatment with the antidepressant fluvoxamine prevented clinical deterioration in adult outpatients with confirmed COVID-19.
The antipsychotic aripiprazole has also shown potential to treat severe COVID-19 infection.
“Consequently, there appears to be a possible explanation as to why these drugs afford patients with severe mental disorders increased protection against the SARS-CoV-2 virus,” Dr. Ahmad said in an interview.
However, he cautioned, there are several factors at play that could influence the results. Therefore, more research is needed before drawing any firm conclusions.
“Still, the possibility that psychiatric medications may have antiviral properties is a tremendous development and I really hope that additional studies confirm the preliminary findings,” Dr. Ahmad said.
The study had no specific funding. The authors and Dr. Ahmad disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Antipsychotics may protect against SARS-CoV-2 infection or lead to a milder course of illness, new research suggests.
“Counterintuitively,” the investigators noted, vulnerable people with severe mental illness “on antipsychotic treatment showed a lower risk of SARS-CoV-2 infection and a likely better COVID-19 prognosis.”
“These are very interesting findings that reflect a clinical reality where we see few patients with severe COVID-19, despite the presence of various risk factors,” study investigator Manuel Canal-Rivero, PhD, clinical psychologist, Virgen del Rocio University Hospital, Sevilla, Spain, said in a news release.
“The number of COVID-19 patients is lower than expected among this group of people and in cases where a proven infection does occur, the evolution is benign and does not reach a life-threatening clinical situation. These data as a whole seem to point to the protective effect of the medication,” Dr. Canal-Rivero added.
The study was published online as a letter to the editor February 19, 2021, in Schizophrenia Research.
A ‘striking’ finding
The researchers assessed the prevalence and prognosis of COVID-19 in 698 patients with serious mental disorders (SMDs) receiving treatment with long-acting injectable antipsychotic medication. The non-SMD population included the catchment area population of 557,576 individuals.
From February to November 2020, 4.1% of the non-SMD population were infected with SARS-CoV-2 versus just 1.3% of the SMD population (9 of 698 patients). All but one patient with SMD had asymptomatic illness (8 of 9, 89%). Accurate information on asymptomatic illness in the non-SMD population was not available.
There were also fewer hospital admissions in the SMD population (0% vs. 8.5%), ICU admissions (0% vs. 0.9%) and deaths because of COVID-19 (0% vs. 1.1%), although the differences were not statistically significant.
In related research, the same investigators found that many of the genes whose expression is altered by SARS-CoV-2 infection are significantly down-regulated by antipsychotic drugs.
“In a striking way, we have shown how antipsychotics reduce the activation of genes involved in many of the inflammatory and immunological pathways associated with the severity of COVID-19 infection,” Benedicto Crespo-Facorro, MD, PhD, University of Sevilla, who led the study, said in the news release.
“Although this finding requires replication, the discovery could be very significant because the treatment of COVID-19 with drugs originally indicated for unrelated clinical situations, that is to say drug repositioning, has been shown to be an interesting source of effective treatments for COVID-19 patients,” he added.
Antiviral properties?
In a comment, Samoon Ahmad, MD, professor, department of psychiatry, New York University, said the findings are “fascinating” and should be explored further.
While the findings on long-acting injectable antipsychotic treatment “seem counterintuitive at first, they are in line with other studies,” said Dr. Ahmad, who heads the inpatient psychiatry unit at Bellevue Hospital Center and is founder of the Integrative Center for Wellness in New York.
“ and antidepressant medications appear to activate key cellular proteins that the SARS-CoV-2 virus uses for replication,” explained Dr. Ahmad, who was not associated with the study.
For example, as reported by this news organization, a preliminary study published in 2020 showed that early treatment with the antidepressant fluvoxamine prevented clinical deterioration in adult outpatients with confirmed COVID-19.
The antipsychotic aripiprazole has also shown potential to treat severe COVID-19 infection.
“Consequently, there appears to be a possible explanation as to why these drugs afford patients with severe mental disorders increased protection against the SARS-CoV-2 virus,” Dr. Ahmad said in an interview.
However, he cautioned, there are several factors at play that could influence the results. Therefore, more research is needed before drawing any firm conclusions.
“Still, the possibility that psychiatric medications may have antiviral properties is a tremendous development and I really hope that additional studies confirm the preliminary findings,” Dr. Ahmad said.
The study had no specific funding. The authors and Dr. Ahmad disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.