User login
Study reveals germline variants in AML, other cancers

A study published in Nature Communications has shed light on the hereditary elements of 12 cancer types.
Investigators looked for rare germline mutations in genes known to be associated with cancer and found the frequency of these mutations varied widely, from 4% in the acute myeloid leukemia (AML) cases studied to 19% in cases of ovarian cancer.
The team’s analysis also revealed an unexpected inherited component to stomach cancer and provided some clarity on the consequences of certain mutations in the BRCA1 and BRCA2 genes.
Li Ding, PhD, of Washington University School of Medicine in St Louis, Missouri, and her colleagues conducted this study, analyzing genetic information from more than 4000 cancer cases included in The Cancer Genome Atlas project.
“In general, we have known that ovarian and breast cancers have a significant inherited component, and others, such as acute myeloid leukemia and lung cancer, have a much smaller inherited genetic contribution,” Dr Ding said. “But this is the first time, on a large scale, that we’ve been able to pinpoint gene culprits or even the actual mutations responsible for cancer susceptibility.”
To help tease out cancer’s inherited components, Dr Ding and her colleagues looked for germline truncations in 114 genes known to be associated with cancer.
“We looked for germline mutations in the tumor, but it was not enough for the mutations simply to be present,” Dr Ding said. “They needed to be enriched in the tumor—present at higher frequency. If a mutation is present in the germline and amplified in the tumor, there is a high likelihood it is playing a role in the cancer.”
The investigators found germline truncations in all 12 cancer types analyzed, but the mutations occurred in varying frequencies depending on the cancer.
The percentage of tumors with truncations in the germline was 4% for AML and glioblastoma; 5% for kidney cancer; 7% for lung adenocarcinoma and endometrial cancer; 8% for head and neck cancer, glioma, lung squamous cell carcinoma, and prostate cancer; 9% for breast cancer; 11% for stomach cancer; and 19% for ovarian cancer.
“We also found a significant number of germline truncations in the BRCA1 and BRCA2 genes present in tumor types other than breast cancer, including stomach and prostate cancers, for example,” Dr Ding said. “This suggests we should pay attention to the potential involvement of these 2 genes in other cancer types.”
The investigators said they identified 13 cancer genes with significant enrichment of rare truncations. Some of these were associated with specific cancers—for example, RAD51C in AML, PALB2 in stomach cancer, and MSH6 in endometrial cancer.
And the team observed significant, tumor-specific loss of heterozygosity in 9 genes—ATM, BAP1, BRCA1/2, BRIP1, FANCM, PALB2, and RAD51C/D.
Dr Ding said more research is needed to confirm these results before they can be used to advise patients making healthcare decisions.
“Our strategy of investigating germline-tumor interactions provides a good way to prioritize important mutations that we should focus on,” she said. “For the information to eventually be used in the clinic, we will need to perform this type of analysis on even larger numbers of patients.” ![]()
A study published in Nature Communications has shed light on the hereditary elements of 12 cancer types.
Investigators looked for rare germline mutations in genes known to be associated with cancer and found the frequency of these mutations varied widely, from 4% in the acute myeloid leukemia (AML) cases studied to 19% in cases of ovarian cancer.
The team’s analysis also revealed an unexpected inherited component to stomach cancer and provided some clarity on the consequences of certain mutations in the BRCA1 and BRCA2 genes.
Li Ding, PhD, of Washington University School of Medicine in St Louis, Missouri, and her colleagues conducted this study, analyzing genetic information from more than 4000 cancer cases included in The Cancer Genome Atlas project.
“In general, we have known that ovarian and breast cancers have a significant inherited component, and others, such as acute myeloid leukemia and lung cancer, have a much smaller inherited genetic contribution,” Dr Ding said. “But this is the first time, on a large scale, that we’ve been able to pinpoint gene culprits or even the actual mutations responsible for cancer susceptibility.”
To help tease out cancer’s inherited components, Dr Ding and her colleagues looked for germline truncations in 114 genes known to be associated with cancer.
“We looked for germline mutations in the tumor, but it was not enough for the mutations simply to be present,” Dr Ding said. “They needed to be enriched in the tumor—present at higher frequency. If a mutation is present in the germline and amplified in the tumor, there is a high likelihood it is playing a role in the cancer.”
The investigators found germline truncations in all 12 cancer types analyzed, but the mutations occurred in varying frequencies depending on the cancer.
The percentage of tumors with truncations in the germline was 4% for AML and glioblastoma; 5% for kidney cancer; 7% for lung adenocarcinoma and endometrial cancer; 8% for head and neck cancer, glioma, lung squamous cell carcinoma, and prostate cancer; 9% for breast cancer; 11% for stomach cancer; and 19% for ovarian cancer.
“We also found a significant number of germline truncations in the BRCA1 and BRCA2 genes present in tumor types other than breast cancer, including stomach and prostate cancers, for example,” Dr Ding said. “This suggests we should pay attention to the potential involvement of these 2 genes in other cancer types.”
The investigators said they identified 13 cancer genes with significant enrichment of rare truncations. Some of these were associated with specific cancers—for example, RAD51C in AML, PALB2 in stomach cancer, and MSH6 in endometrial cancer.
And the team observed significant, tumor-specific loss of heterozygosity in 9 genes—ATM, BAP1, BRCA1/2, BRIP1, FANCM, PALB2, and RAD51C/D.
Dr Ding said more research is needed to confirm these results before they can be used to advise patients making healthcare decisions.
“Our strategy of investigating germline-tumor interactions provides a good way to prioritize important mutations that we should focus on,” she said. “For the information to eventually be used in the clinic, we will need to perform this type of analysis on even larger numbers of patients.” ![]()
A study published in Nature Communications has shed light on the hereditary elements of 12 cancer types.
Investigators looked for rare germline mutations in genes known to be associated with cancer and found the frequency of these mutations varied widely, from 4% in the acute myeloid leukemia (AML) cases studied to 19% in cases of ovarian cancer.
The team’s analysis also revealed an unexpected inherited component to stomach cancer and provided some clarity on the consequences of certain mutations in the BRCA1 and BRCA2 genes.
Li Ding, PhD, of Washington University School of Medicine in St Louis, Missouri, and her colleagues conducted this study, analyzing genetic information from more than 4000 cancer cases included in The Cancer Genome Atlas project.
“In general, we have known that ovarian and breast cancers have a significant inherited component, and others, such as acute myeloid leukemia and lung cancer, have a much smaller inherited genetic contribution,” Dr Ding said. “But this is the first time, on a large scale, that we’ve been able to pinpoint gene culprits or even the actual mutations responsible for cancer susceptibility.”
To help tease out cancer’s inherited components, Dr Ding and her colleagues looked for germline truncations in 114 genes known to be associated with cancer.
“We looked for germline mutations in the tumor, but it was not enough for the mutations simply to be present,” Dr Ding said. “They needed to be enriched in the tumor—present at higher frequency. If a mutation is present in the germline and amplified in the tumor, there is a high likelihood it is playing a role in the cancer.”
The investigators found germline truncations in all 12 cancer types analyzed, but the mutations occurred in varying frequencies depending on the cancer.
The percentage of tumors with truncations in the germline was 4% for AML and glioblastoma; 5% for kidney cancer; 7% for lung adenocarcinoma and endometrial cancer; 8% for head and neck cancer, glioma, lung squamous cell carcinoma, and prostate cancer; 9% for breast cancer; 11% for stomach cancer; and 19% for ovarian cancer.
“We also found a significant number of germline truncations in the BRCA1 and BRCA2 genes present in tumor types other than breast cancer, including stomach and prostate cancers, for example,” Dr Ding said. “This suggests we should pay attention to the potential involvement of these 2 genes in other cancer types.”
The investigators said they identified 13 cancer genes with significant enrichment of rare truncations. Some of these were associated with specific cancers—for example, RAD51C in AML, PALB2 in stomach cancer, and MSH6 in endometrial cancer.
And the team observed significant, tumor-specific loss of heterozygosity in 9 genes—ATM, BAP1, BRCA1/2, BRIP1, FANCM, PALB2, and RAD51C/D.
Dr Ding said more research is needed to confirm these results before they can be used to advise patients making healthcare decisions.
“Our strategy of investigating germline-tumor interactions provides a good way to prioritize important mutations that we should focus on,” she said. “For the information to eventually be used in the clinic, we will need to perform this type of analysis on even larger numbers of patients.” ![]()
Protein discovery could have therapeutic implications

Photo courtesy of The
Scripps Research Institute
New research shows how NPM1—a protein implicated in non-Hodgkin lymphoma, acute myelogenous leukemia, and other cancers—twists and morphs into different structures.
This protein has many functions and, when mutated, has been shown to interfere with cells’ normal tumor suppressing ability.
Previous research showed that a section of NPM1, called the N-terminal domain, doesn’t have a defined, folded structure.
Instead, the protein morphs between 2 forms: a 1-subunit disordered monomer and a 5-subunit folded pentamer.
Until now, the mechanism behind this transformation was unknown, but researchers believed this monomer-pentamer equilibrium could be important for the protein’s location and functioning in the cell.
Ashok Deniz, PhD, of The Scripps Research Institute in La Jolla, California, and his colleagues conducted the current study to shed light on how this transformation occurs. They reported their findings in Angewandte Chemie.
The researchers used a combination of 3 techniques to analyze NPM1—single-molecule biophysics, fluorescence resonance energy transfer, and circular dichroism.
These techniques revealed that NPM1’s transformation can proceed through more than one pathway. In one pathway, the transformation begins when the cell sends signals to attach phosphoryl groups to NPM1.
This phosphorylation prompts the ordered pentamer to become disordered and likely causes NPM1 to shuttle outside the cell’s nucleus. A meeting with a binding partner can mediate the reverse transformation to a pentamer.
However, when NPM1 does become a pentamer again under these conditions, which likely causes it to move back to the nucleolus, it takes a different path instead of just retracing its earlier steps.
The study also revealed many intermediate states between monomer and pentamer structures. And it showed that these states can be manipulated or “tuned” by changing conditions such as salt levels, phosphorylation, and partner binding, which may explain how cells regulate NPM1’s multiple functions.
The researchers said future studies could shed more light on the biological functions of these different structures and how they might be used in future cancer therapies.
“We’re studying basic biophysics, but we believe the complexity and rules we uncover for the physics of protein disorder and folding could one day also be used for better designs of therapeutics,” Dr Deniz said.
He and his colleagues also believe that combining the 3 techniques used in this study, plus a novel protein-labeling technique for single-molecule fluorescence, could be a useful strategy for studying other unstructured, intrinsically disordered proteins. ![]()
Photo courtesy of The
Scripps Research Institute
New research shows how NPM1—a protein implicated in non-Hodgkin lymphoma, acute myelogenous leukemia, and other cancers—twists and morphs into different structures.
This protein has many functions and, when mutated, has been shown to interfere with cells’ normal tumor suppressing ability.
Previous research showed that a section of NPM1, called the N-terminal domain, doesn’t have a defined, folded structure.
Instead, the protein morphs between 2 forms: a 1-subunit disordered monomer and a 5-subunit folded pentamer.
Until now, the mechanism behind this transformation was unknown, but researchers believed this monomer-pentamer equilibrium could be important for the protein’s location and functioning in the cell.
Ashok Deniz, PhD, of The Scripps Research Institute in La Jolla, California, and his colleagues conducted the current study to shed light on how this transformation occurs. They reported their findings in Angewandte Chemie.
The researchers used a combination of 3 techniques to analyze NPM1—single-molecule biophysics, fluorescence resonance energy transfer, and circular dichroism.
These techniques revealed that NPM1’s transformation can proceed through more than one pathway. In one pathway, the transformation begins when the cell sends signals to attach phosphoryl groups to NPM1.
This phosphorylation prompts the ordered pentamer to become disordered and likely causes NPM1 to shuttle outside the cell’s nucleus. A meeting with a binding partner can mediate the reverse transformation to a pentamer.
However, when NPM1 does become a pentamer again under these conditions, which likely causes it to move back to the nucleolus, it takes a different path instead of just retracing its earlier steps.
The study also revealed many intermediate states between monomer and pentamer structures. And it showed that these states can be manipulated or “tuned” by changing conditions such as salt levels, phosphorylation, and partner binding, which may explain how cells regulate NPM1’s multiple functions.
The researchers said future studies could shed more light on the biological functions of these different structures and how they might be used in future cancer therapies.
“We’re studying basic biophysics, but we believe the complexity and rules we uncover for the physics of protein disorder and folding could one day also be used for better designs of therapeutics,” Dr Deniz said.
He and his colleagues also believe that combining the 3 techniques used in this study, plus a novel protein-labeling technique for single-molecule fluorescence, could be a useful strategy for studying other unstructured, intrinsically disordered proteins. ![]()
Photo courtesy of The
Scripps Research Institute
New research shows how NPM1—a protein implicated in non-Hodgkin lymphoma, acute myelogenous leukemia, and other cancers—twists and morphs into different structures.
This protein has many functions and, when mutated, has been shown to interfere with cells’ normal tumor suppressing ability.
Previous research showed that a section of NPM1, called the N-terminal domain, doesn’t have a defined, folded structure.
Instead, the protein morphs between 2 forms: a 1-subunit disordered monomer and a 5-subunit folded pentamer.
Until now, the mechanism behind this transformation was unknown, but researchers believed this monomer-pentamer equilibrium could be important for the protein’s location and functioning in the cell.
Ashok Deniz, PhD, of The Scripps Research Institute in La Jolla, California, and his colleagues conducted the current study to shed light on how this transformation occurs. They reported their findings in Angewandte Chemie.
The researchers used a combination of 3 techniques to analyze NPM1—single-molecule biophysics, fluorescence resonance energy transfer, and circular dichroism.
These techniques revealed that NPM1’s transformation can proceed through more than one pathway. In one pathway, the transformation begins when the cell sends signals to attach phosphoryl groups to NPM1.
This phosphorylation prompts the ordered pentamer to become disordered and likely causes NPM1 to shuttle outside the cell’s nucleus. A meeting with a binding partner can mediate the reverse transformation to a pentamer.
However, when NPM1 does become a pentamer again under these conditions, which likely causes it to move back to the nucleolus, it takes a different path instead of just retracing its earlier steps.
The study also revealed many intermediate states between monomer and pentamer structures. And it showed that these states can be manipulated or “tuned” by changing conditions such as salt levels, phosphorylation, and partner binding, which may explain how cells regulate NPM1’s multiple functions.
The researchers said future studies could shed more light on the biological functions of these different structures and how they might be used in future cancer therapies.
“We’re studying basic biophysics, but we believe the complexity and rules we uncover for the physics of protein disorder and folding could one day also be used for better designs of therapeutics,” Dr Deniz said.
He and his colleagues also believe that combining the 3 techniques used in this study, plus a novel protein-labeling technique for single-molecule fluorescence, could be a useful strategy for studying other unstructured, intrinsically disordered proteins. ![]()
Chemo quadruples risk for myeloid cancers
ORLANDO – Patients who undergo cytotoxic chemotherapy, even in the modern era, are at increased risk for developing myeloid neoplasms, based on data from a cohort of nearly 750,000 adults who were initially treated with chemotherapy and survived at least 1 year after diagnosis.
In the cohort, the standardized incidence ratio (SIR) for treatment-related acute myeloid leukemia (tAML) or myelodysplastic syndrome (MDS) was four times greater than would be expected in the general population, reported Lindsay M. Morton, Ph.D., of the division of cancer epidemiology and genetics at the National Cancer Institute in Bethesda, Md.

“We now demonstrate that there are elevated risks for treatment-related leukemia after treatment for a broad spectrum of first primary malignancies that are generally consistent with what we know about changing treatment practices,” she said at the American Society of Hematology annual meeting.
“The number of cancer survivors in the United States has increased dramatically, to reach nearly 14 million individuals today, and in just the next few years the number is expected to reach more than 18 million people, which means that the long-term health of this population is of great clinical importance as well as public health importance,” Dr. Morton emphasized.
The link between cytotoxic chemotherapy and leukemia risk has been known since the 1960s, with certain classes of agents carrying higher risks than others, including platinum-containing compounds, alkylating agents (for example, cyclophosphamide, melphalan, chlorambucil), topoisomerase II inhibitors (doxorubicin, daunorubicin, epirubicin, etc.), and antimetabolites (5-fluorauracil, capecitabine, gemcitabine, et al.).
Treatment-related leukemias are associated with higher doses of these agents, and the trend in contemporary medicine is to use more of these agents upfront for the treatment of primary malignancies. Yet estimates of the risk of tAML, MDS, or other malignancies have been hard to come by because of the relative rarity of cases and the sporadic reports in the literature, Dr. Morton said.
The investigators previously reported that risk for tAML and other myeloid neoplasms changed over time, and showed that since the 1990s there was an uptick in risk for patients treated with chemotherapy for cancers of bone, joints, and endometrium, and since 2000 for patients treated with chemotherapy for cancers of the esophagus, cervix and prostate.
For example, risks for tAML were higher in the 1970s for patients with ovarian cancer treated with melphalan, a highly leukemogenic agent, but dropped somewhat with the switch to platinum-based agents. Similarly, women with breast cancer had a comparatively high risk with the use of melphalan, a decline in risk with the introduction of cyclophosphamide, and then an increase with the addition of anthracyclines and dose-dense regimens.
Risk update
To get a better idea of the magnitude of risk in the modern era, Dr. Morton and colleagues sifted through Surveillance, Epidemiology, and End Results (SEER) data to identify a cohort of 746,007 adults who were initially treated with chemotherapy and survived for at least 1 year following a diagnosis with a first primary malignancy from 2000 through 2012. They calculated SIRs based on variables that included age, race, sex, malignancy type and treatment period.
They looked at four categories of myeloid neoplasms as defined by World Health Organization criteria: AML/MDS, chronic myeloid leukemia, myeloproliferative neoplasms (MPN) negative for BCR-ABL (Philadelphia-negative), and chronic myelomonocytic leukemia (CMML).
They found that 2,071 patients developed treatment-related AML/MDS, translating into a fourfold incidence compared with the general population (SIR 4.1, 95% confidence interval [CI] 3.9-4.2), 106 were diagnosed with CMML
They also identified novel risk for tAML/MDS after chemotherapy by malignancy (see table).
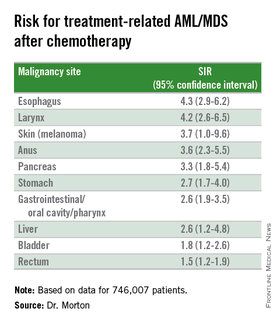
The investigators found that breast cancer, non-Hodgkin lymphoma, and lung cancer were most commonly associated with tAML/MDS (SIRs 4.1, 7.3, and 4.1, respectively, all significant).
In addition, although the overall numbers of cases were small, the investigators noted “strikingly elevated” risks for cancers of bone (SIR 35.1, CI. 16.9-64.6). testes (15.6, CI, 9.2-24.6), and soft tissue (12.6, CI=7.7-19.4),
Risk for tAML/MD was more modestly elevated for cancers of the brain, ovaries, endometrium, cervix, and prostate, and for Hodgkin lymphoma, chronic lymphocytic leukemia, and multiple myeloma.
Adding radiotherapy to chemotherapy for cancers of the breast, lung, and stomach cancers showed a trend toward heightened tAML/MDS risk, but this was not significant.
An elevated risk for CMML was also seen after chemotherapy for lung cancer (SIR 2.5, CI, 1.3-4.4), breast cancer (1.8, CI, 1.3-2.5), and non-Hodgkin lymphoma (2.1, CI, 1.2-3.4). There was elevated risk for CMML following chemotherapy for breast cancer (3.0, CI. 1.7-5.0) and non-Hodgkin lymphoma (4.2, CI, 2.4-6.9).
There were no increased risks for other myeloproliferative neoplasms after chemotherapy for any first primary cancer, however.
“This reminds us that with new uses of standard agents and introduction of new agents, it’s critical to carefully weigh the risks and benefits of systemic therapy,” Dr. Morton said.
The investigators plan to quantify risks associated with specific drugs and doses, she added.
The study was supported by the National Cancer Institute. Dr. Morton reported no relevant conflicts of interest to disclose.
ORLANDO – Patients who undergo cytotoxic chemotherapy, even in the modern era, are at increased risk for developing myeloid neoplasms, based on data from a cohort of nearly 750,000 adults who were initially treated with chemotherapy and survived at least 1 year after diagnosis.
In the cohort, the standardized incidence ratio (SIR) for treatment-related acute myeloid leukemia (tAML) or myelodysplastic syndrome (MDS) was four times greater than would be expected in the general population, reported Lindsay M. Morton, Ph.D., of the division of cancer epidemiology and genetics at the National Cancer Institute in Bethesda, Md.
“We now demonstrate that there are elevated risks for treatment-related leukemia after treatment for a broad spectrum of first primary malignancies that are generally consistent with what we know about changing treatment practices,” she said at the American Society of Hematology annual meeting.
“The number of cancer survivors in the United States has increased dramatically, to reach nearly 14 million individuals today, and in just the next few years the number is expected to reach more than 18 million people, which means that the long-term health of this population is of great clinical importance as well as public health importance,” Dr. Morton emphasized.
The link between cytotoxic chemotherapy and leukemia risk has been known since the 1960s, with certain classes of agents carrying higher risks than others, including platinum-containing compounds, alkylating agents (for example, cyclophosphamide, melphalan, chlorambucil), topoisomerase II inhibitors (doxorubicin, daunorubicin, epirubicin, etc.), and antimetabolites (5-fluorauracil, capecitabine, gemcitabine, et al.).
Treatment-related leukemias are associated with higher doses of these agents, and the trend in contemporary medicine is to use more of these agents upfront for the treatment of primary malignancies. Yet estimates of the risk of tAML, MDS, or other malignancies have been hard to come by because of the relative rarity of cases and the sporadic reports in the literature, Dr. Morton said.
The investigators previously reported that risk for tAML and other myeloid neoplasms changed over time, and showed that since the 1990s there was an uptick in risk for patients treated with chemotherapy for cancers of bone, joints, and endometrium, and since 2000 for patients treated with chemotherapy for cancers of the esophagus, cervix and prostate.
For example, risks for tAML were higher in the 1970s for patients with ovarian cancer treated with melphalan, a highly leukemogenic agent, but dropped somewhat with the switch to platinum-based agents. Similarly, women with breast cancer had a comparatively high risk with the use of melphalan, a decline in risk with the introduction of cyclophosphamide, and then an increase with the addition of anthracyclines and dose-dense regimens.
Risk update
To get a better idea of the magnitude of risk in the modern era, Dr. Morton and colleagues sifted through Surveillance, Epidemiology, and End Results (SEER) data to identify a cohort of 746,007 adults who were initially treated with chemotherapy and survived for at least 1 year following a diagnosis with a first primary malignancy from 2000 through 2012. They calculated SIRs based on variables that included age, race, sex, malignancy type and treatment period.
They looked at four categories of myeloid neoplasms as defined by World Health Organization criteria: AML/MDS, chronic myeloid leukemia, myeloproliferative neoplasms (MPN) negative for BCR-ABL (Philadelphia-negative), and chronic myelomonocytic leukemia (CMML).
They found that 2,071 patients developed treatment-related AML/MDS, translating into a fourfold incidence compared with the general population (SIR 4.1, 95% confidence interval [CI] 3.9-4.2), 106 were diagnosed with CMML
They also identified novel risk for tAML/MDS after chemotherapy by malignancy (see table).
The investigators found that breast cancer, non-Hodgkin lymphoma, and lung cancer were most commonly associated with tAML/MDS (SIRs 4.1, 7.3, and 4.1, respectively, all significant).
In addition, although the overall numbers of cases were small, the investigators noted “strikingly elevated” risks for cancers of bone (SIR 35.1, CI. 16.9-64.6). testes (15.6, CI, 9.2-24.6), and soft tissue (12.6, CI=7.7-19.4),
Risk for tAML/MD was more modestly elevated for cancers of the brain, ovaries, endometrium, cervix, and prostate, and for Hodgkin lymphoma, chronic lymphocytic leukemia, and multiple myeloma.
Adding radiotherapy to chemotherapy for cancers of the breast, lung, and stomach cancers showed a trend toward heightened tAML/MDS risk, but this was not significant.
An elevated risk for CMML was also seen after chemotherapy for lung cancer (SIR 2.5, CI, 1.3-4.4), breast cancer (1.8, CI, 1.3-2.5), and non-Hodgkin lymphoma (2.1, CI, 1.2-3.4). There was elevated risk for CMML following chemotherapy for breast cancer (3.0, CI. 1.7-5.0) and non-Hodgkin lymphoma (4.2, CI, 2.4-6.9).
There were no increased risks for other myeloproliferative neoplasms after chemotherapy for any first primary cancer, however.
“This reminds us that with new uses of standard agents and introduction of new agents, it’s critical to carefully weigh the risks and benefits of systemic therapy,” Dr. Morton said.
The investigators plan to quantify risks associated with specific drugs and doses, she added.
The study was supported by the National Cancer Institute. Dr. Morton reported no relevant conflicts of interest to disclose.
ORLANDO – Patients who undergo cytotoxic chemotherapy, even in the modern era, are at increased risk for developing myeloid neoplasms, based on data from a cohort of nearly 750,000 adults who were initially treated with chemotherapy and survived at least 1 year after diagnosis.
In the cohort, the standardized incidence ratio (SIR) for treatment-related acute myeloid leukemia (tAML) or myelodysplastic syndrome (MDS) was four times greater than would be expected in the general population, reported Lindsay M. Morton, Ph.D., of the division of cancer epidemiology and genetics at the National Cancer Institute in Bethesda, Md.
“We now demonstrate that there are elevated risks for treatment-related leukemia after treatment for a broad spectrum of first primary malignancies that are generally consistent with what we know about changing treatment practices,” she said at the American Society of Hematology annual meeting.
“The number of cancer survivors in the United States has increased dramatically, to reach nearly 14 million individuals today, and in just the next few years the number is expected to reach more than 18 million people, which means that the long-term health of this population is of great clinical importance as well as public health importance,” Dr. Morton emphasized.
The link between cytotoxic chemotherapy and leukemia risk has been known since the 1960s, with certain classes of agents carrying higher risks than others, including platinum-containing compounds, alkylating agents (for example, cyclophosphamide, melphalan, chlorambucil), topoisomerase II inhibitors (doxorubicin, daunorubicin, epirubicin, etc.), and antimetabolites (5-fluorauracil, capecitabine, gemcitabine, et al.).
Treatment-related leukemias are associated with higher doses of these agents, and the trend in contemporary medicine is to use more of these agents upfront for the treatment of primary malignancies. Yet estimates of the risk of tAML, MDS, or other malignancies have been hard to come by because of the relative rarity of cases and the sporadic reports in the literature, Dr. Morton said.
The investigators previously reported that risk for tAML and other myeloid neoplasms changed over time, and showed that since the 1990s there was an uptick in risk for patients treated with chemotherapy for cancers of bone, joints, and endometrium, and since 2000 for patients treated with chemotherapy for cancers of the esophagus, cervix and prostate.
For example, risks for tAML were higher in the 1970s for patients with ovarian cancer treated with melphalan, a highly leukemogenic agent, but dropped somewhat with the switch to platinum-based agents. Similarly, women with breast cancer had a comparatively high risk with the use of melphalan, a decline in risk with the introduction of cyclophosphamide, and then an increase with the addition of anthracyclines and dose-dense regimens.
Risk update
To get a better idea of the magnitude of risk in the modern era, Dr. Morton and colleagues sifted through Surveillance, Epidemiology, and End Results (SEER) data to identify a cohort of 746,007 adults who were initially treated with chemotherapy and survived for at least 1 year following a diagnosis with a first primary malignancy from 2000 through 2012. They calculated SIRs based on variables that included age, race, sex, malignancy type and treatment period.
They looked at four categories of myeloid neoplasms as defined by World Health Organization criteria: AML/MDS, chronic myeloid leukemia, myeloproliferative neoplasms (MPN) negative for BCR-ABL (Philadelphia-negative), and chronic myelomonocytic leukemia (CMML).
They found that 2,071 patients developed treatment-related AML/MDS, translating into a fourfold incidence compared with the general population (SIR 4.1, 95% confidence interval [CI] 3.9-4.2), 106 were diagnosed with CMML
They also identified novel risk for tAML/MDS after chemotherapy by malignancy (see table).
The investigators found that breast cancer, non-Hodgkin lymphoma, and lung cancer were most commonly associated with tAML/MDS (SIRs 4.1, 7.3, and 4.1, respectively, all significant).
In addition, although the overall numbers of cases were small, the investigators noted “strikingly elevated” risks for cancers of bone (SIR 35.1, CI. 16.9-64.6). testes (15.6, CI, 9.2-24.6), and soft tissue (12.6, CI=7.7-19.4),
Risk for tAML/MD was more modestly elevated for cancers of the brain, ovaries, endometrium, cervix, and prostate, and for Hodgkin lymphoma, chronic lymphocytic leukemia, and multiple myeloma.
Adding radiotherapy to chemotherapy for cancers of the breast, lung, and stomach cancers showed a trend toward heightened tAML/MDS risk, but this was not significant.
An elevated risk for CMML was also seen after chemotherapy for lung cancer (SIR 2.5, CI, 1.3-4.4), breast cancer (1.8, CI, 1.3-2.5), and non-Hodgkin lymphoma (2.1, CI, 1.2-3.4). There was elevated risk for CMML following chemotherapy for breast cancer (3.0, CI. 1.7-5.0) and non-Hodgkin lymphoma (4.2, CI, 2.4-6.9).
There were no increased risks for other myeloproliferative neoplasms after chemotherapy for any first primary cancer, however.
“This reminds us that with new uses of standard agents and introduction of new agents, it’s critical to carefully weigh the risks and benefits of systemic therapy,” Dr. Morton said.
The investigators plan to quantify risks associated with specific drugs and doses, she added.
The study was supported by the National Cancer Institute. Dr. Morton reported no relevant conflicts of interest to disclose.
AT ASH 2015
Key clinical point: This study quantifies the risks for treatment-related myeloid cancers after chemotherapy.
Major finding: Chemotherapy is associated with a fourfold risk for treatment-related AML/MDS, compared with the general population.
Data source: Retrospective review of data on 746,007 adults treated with chemotherapy for a first primary malignancy.
Disclosures: The National Cancer Institute supported the study. Dr. Morton reported having no conflicts of interest to disclose.

A potential target for IDH1-mutant cancers
acute myeloid leukemia
Researchers say they have identified a potential therapeutic target for IDH1-mutant malignancies.
Preclinical experiments showed that tumors characterized by IDH1 mutations are “extremely vulnerable” to depletion of NAD+, a metabolic cofactor.
“Our finding . . . supports the proposal that medications that can decrease levels of this metabolite, which are in development, have the potential to specifically treat these cancers,” said Daniel Cahill, MD, PhD, of Massachusetts General Hospital in Boston.
Dr Cahill and his colleagues described their research in Cancer Cell.
IDH1 and IDH2 are known to play essential roles in cellular metabolism, including the processes by which cells convert glucose and other nutrients into ATP, providing the energy needed for cellular survival.
In 2008, researchers discovered that IDH1 mutations are involved in several cancers. The gene is mutated in around 20% of adult gliomas, in more than 10% of acute myeloid leukemias, and in a smaller percentage of other cancers.
One clear result of IDH1 mutation is a 100-fold elevation in levels of the metabolite 2-HG, which is known to mediate several properties that lead to tumor development. Drugs that decrease levels of 2-HG are currently under development.
Dr Cahill and his colleagues wanted to find additional ways of blocking the mutation’s effects, so they inhibited mutant IDH1 in tumor cells. They were surprised to find that this reduced 2-HG levels, but, in many cases, that reduction did not halt cell growth.
Detailed metabolic profiling of IDH1-mutant cells revealed that inhibiting the mutated enzyme greatly increased levels of NAD+, a cofactor that plays a role in several cellular energy processes.
Additional experiments showed that depletion of NAD+ induced the death of IDH1-mutant tumor cells and inhibited tumor growth in an animal model of glioma.
“Accumulation of excess 2-HG is known to drive several changes leading to tumor development, but our results indicate that simply depleting 2-HG levels was not sufficient to halt the growth of several types of later-stage IDH1-mutant tumors,” said Hiroaki Wakimoto, MD, PhD, of Massachusetts General Hospital.
“In addition, we found that mutant IDH1 reduces expression of an enzyme that maintains NAD+ levels, rendering IDH1-mutant tumor cells highly sensitive to direct NAD+ depletion. Several drugs that inhibit the synthesis of NAD+ are already in clinical trials, and these agents may prove useful for patients with IDH-mutant cancers. While we primarily focused on IDH1-mutant gliomas, we also found evidence that NAD+ inhibition could slow the growth of other types of cancer with this mutation.” ![]()
acute myeloid leukemia
Researchers say they have identified a potential therapeutic target for IDH1-mutant malignancies.
Preclinical experiments showed that tumors characterized by IDH1 mutations are “extremely vulnerable” to depletion of NAD+, a metabolic cofactor.
“Our finding . . . supports the proposal that medications that can decrease levels of this metabolite, which are in development, have the potential to specifically treat these cancers,” said Daniel Cahill, MD, PhD, of Massachusetts General Hospital in Boston.
Dr Cahill and his colleagues described their research in Cancer Cell.
IDH1 and IDH2 are known to play essential roles in cellular metabolism, including the processes by which cells convert glucose and other nutrients into ATP, providing the energy needed for cellular survival.
In 2008, researchers discovered that IDH1 mutations are involved in several cancers. The gene is mutated in around 20% of adult gliomas, in more than 10% of acute myeloid leukemias, and in a smaller percentage of other cancers.
One clear result of IDH1 mutation is a 100-fold elevation in levels of the metabolite 2-HG, which is known to mediate several properties that lead to tumor development. Drugs that decrease levels of 2-HG are currently under development.
Dr Cahill and his colleagues wanted to find additional ways of blocking the mutation’s effects, so they inhibited mutant IDH1 in tumor cells. They were surprised to find that this reduced 2-HG levels, but, in many cases, that reduction did not halt cell growth.
Detailed metabolic profiling of IDH1-mutant cells revealed that inhibiting the mutated enzyme greatly increased levels of NAD+, a cofactor that plays a role in several cellular energy processes.
Additional experiments showed that depletion of NAD+ induced the death of IDH1-mutant tumor cells and inhibited tumor growth in an animal model of glioma.
“Accumulation of excess 2-HG is known to drive several changes leading to tumor development, but our results indicate that simply depleting 2-HG levels was not sufficient to halt the growth of several types of later-stage IDH1-mutant tumors,” said Hiroaki Wakimoto, MD, PhD, of Massachusetts General Hospital.
“In addition, we found that mutant IDH1 reduces expression of an enzyme that maintains NAD+ levels, rendering IDH1-mutant tumor cells highly sensitive to direct NAD+ depletion. Several drugs that inhibit the synthesis of NAD+ are already in clinical trials, and these agents may prove useful for patients with IDH-mutant cancers. While we primarily focused on IDH1-mutant gliomas, we also found evidence that NAD+ inhibition could slow the growth of other types of cancer with this mutation.” ![]()
acute myeloid leukemia
Researchers say they have identified a potential therapeutic target for IDH1-mutant malignancies.
Preclinical experiments showed that tumors characterized by IDH1 mutations are “extremely vulnerable” to depletion of NAD+, a metabolic cofactor.
“Our finding . . . supports the proposal that medications that can decrease levels of this metabolite, which are in development, have the potential to specifically treat these cancers,” said Daniel Cahill, MD, PhD, of Massachusetts General Hospital in Boston.
Dr Cahill and his colleagues described their research in Cancer Cell.
IDH1 and IDH2 are known to play essential roles in cellular metabolism, including the processes by which cells convert glucose and other nutrients into ATP, providing the energy needed for cellular survival.
In 2008, researchers discovered that IDH1 mutations are involved in several cancers. The gene is mutated in around 20% of adult gliomas, in more than 10% of acute myeloid leukemias, and in a smaller percentage of other cancers.
One clear result of IDH1 mutation is a 100-fold elevation in levels of the metabolite 2-HG, which is known to mediate several properties that lead to tumor development. Drugs that decrease levels of 2-HG are currently under development.
Dr Cahill and his colleagues wanted to find additional ways of blocking the mutation’s effects, so they inhibited mutant IDH1 in tumor cells. They were surprised to find that this reduced 2-HG levels, but, in many cases, that reduction did not halt cell growth.
Detailed metabolic profiling of IDH1-mutant cells revealed that inhibiting the mutated enzyme greatly increased levels of NAD+, a cofactor that plays a role in several cellular energy processes.
Additional experiments showed that depletion of NAD+ induced the death of IDH1-mutant tumor cells and inhibited tumor growth in an animal model of glioma.
“Accumulation of excess 2-HG is known to drive several changes leading to tumor development, but our results indicate that simply depleting 2-HG levels was not sufficient to halt the growth of several types of later-stage IDH1-mutant tumors,” said Hiroaki Wakimoto, MD, PhD, of Massachusetts General Hospital.
“In addition, we found that mutant IDH1 reduces expression of an enzyme that maintains NAD+ levels, rendering IDH1-mutant tumor cells highly sensitive to direct NAD+ depletion. Several drugs that inhibit the synthesis of NAD+ are already in clinical trials, and these agents may prove useful for patients with IDH-mutant cancers. While we primarily focused on IDH1-mutant gliomas, we also found evidence that NAD+ inhibition could slow the growth of other types of cancer with this mutation.” ![]()
Academic hospitals offer better AML survival
ORLANDO – Patients with acute myeloid leukemia (AML) initially treated at an academic center lived significantly longer than those treated at nonacademic centers, a database analysis shows.
Median overall survival increased from 7 months at a nonacademic center to 12.6 months at an academic center (P less than .001).
One-year overall survival rates were also significantly better at 51% vs. 39% (P less than .001).
The difference remained significant even after controlling for important confounders including age, comorbidity burden, receipt of chemotherapy, transplant, and delay between diagnosis and treatment, Mr. Smith Giri reported at the annual meeting of the American Society of Hematology.
“From a policy perspective, it may be useful to know whether these results are due to higher volume of cases, more advanced technology, expanded role of specialists, or greater, round-the-clock availability of resident physicians,” said Mr. Giri of the University of Tennessee Health Science Center in Memphis.
Prior studies in cancer have suggested better overall survival among breast cancer patients treated at academic centers, but this is the first study looking at outcomes in AML, the most common acute leukemia in adults.
Using the National Cancer Database Participant User File, the investigators identified 7,823 patients with AML who received their initial therapy at the reporting facility from 1998 to 2011. The database collects information from more than 1,500 Commission on Cancer (CoC)–accredited facilities. Of the 7,823 patients, 4,681 (60%) were treated at an AC (academic/research program) and 3,142 at a non-AC (community cancer program/comprehensive community cancer program).
Patients treated at an AC were significantly younger than those treated at a non-AC (median 62 years vs. 67 years), tended to be of nonwhite race, less educated, have a lower income, and more comorbidities.
Receipt of chemotherapy (97.4% vs. 94.5%) and transplant (9% vs. 2.4%) were significantly higher at an AC than a non-AC (both P less than .001).
Kaplan Meier survival curves suggested disparate survival curves between the two groups, mainly within the first 5 years of follow-up (P less than .001), Mr. Giri said.
In multivariate model analysis, the non-AC group had significantly worse risk adjusted 30-day mortality than the AC group (odds ratio, 1.52; 95% confidence interval 1.33-1.74; P less than .001) and worse overall survival (hazard ratio, 1.13; 95% CI 1.07-1.19; P less than .001).
The study (Ab. 533) findings should be interpreted with caution because of its limitations, including the lack of information on AML risk type in the database, the fact that administrative datasets are prone to coding errors, and because the analysis did not adjust for hospital volume, which has been shown to affect survival, he said. Also, because there are more than 3,500 non–Coc approved hospitals, the sample may not be representative of overall U.S. hospitals.
During a discussion of the results, Mr. Giri acknowledged that patients treated at academic centers may have greater access to clinical trials and experimental agents. Future analyses should also distinguish patients with a diagnosis of acute promyelocytic leukemia, a distinct subset of AML.
ORLANDO – Patients with acute myeloid leukemia (AML) initially treated at an academic center lived significantly longer than those treated at nonacademic centers, a database analysis shows.
Median overall survival increased from 7 months at a nonacademic center to 12.6 months at an academic center (P less than .001).
One-year overall survival rates were also significantly better at 51% vs. 39% (P less than .001).
The difference remained significant even after controlling for important confounders including age, comorbidity burden, receipt of chemotherapy, transplant, and delay between diagnosis and treatment, Mr. Smith Giri reported at the annual meeting of the American Society of Hematology.
“From a policy perspective, it may be useful to know whether these results are due to higher volume of cases, more advanced technology, expanded role of specialists, or greater, round-the-clock availability of resident physicians,” said Mr. Giri of the University of Tennessee Health Science Center in Memphis.
Prior studies in cancer have suggested better overall survival among breast cancer patients treated at academic centers, but this is the first study looking at outcomes in AML, the most common acute leukemia in adults.
Using the National Cancer Database Participant User File, the investigators identified 7,823 patients with AML who received their initial therapy at the reporting facility from 1998 to 2011. The database collects information from more than 1,500 Commission on Cancer (CoC)–accredited facilities. Of the 7,823 patients, 4,681 (60%) were treated at an AC (academic/research program) and 3,142 at a non-AC (community cancer program/comprehensive community cancer program).
Patients treated at an AC were significantly younger than those treated at a non-AC (median 62 years vs. 67 years), tended to be of nonwhite race, less educated, have a lower income, and more comorbidities.
Receipt of chemotherapy (97.4% vs. 94.5%) and transplant (9% vs. 2.4%) were significantly higher at an AC than a non-AC (both P less than .001).
Kaplan Meier survival curves suggested disparate survival curves between the two groups, mainly within the first 5 years of follow-up (P less than .001), Mr. Giri said.
In multivariate model analysis, the non-AC group had significantly worse risk adjusted 30-day mortality than the AC group (odds ratio, 1.52; 95% confidence interval 1.33-1.74; P less than .001) and worse overall survival (hazard ratio, 1.13; 95% CI 1.07-1.19; P less than .001).
The study (Ab. 533) findings should be interpreted with caution because of its limitations, including the lack of information on AML risk type in the database, the fact that administrative datasets are prone to coding errors, and because the analysis did not adjust for hospital volume, which has been shown to affect survival, he said. Also, because there are more than 3,500 non–Coc approved hospitals, the sample may not be representative of overall U.S. hospitals.
During a discussion of the results, Mr. Giri acknowledged that patients treated at academic centers may have greater access to clinical trials and experimental agents. Future analyses should also distinguish patients with a diagnosis of acute promyelocytic leukemia, a distinct subset of AML.
ORLANDO – Patients with acute myeloid leukemia (AML) initially treated at an academic center lived significantly longer than those treated at nonacademic centers, a database analysis shows.
Median overall survival increased from 7 months at a nonacademic center to 12.6 months at an academic center (P less than .001).
One-year overall survival rates were also significantly better at 51% vs. 39% (P less than .001).
The difference remained significant even after controlling for important confounders including age, comorbidity burden, receipt of chemotherapy, transplant, and delay between diagnosis and treatment, Mr. Smith Giri reported at the annual meeting of the American Society of Hematology.
“From a policy perspective, it may be useful to know whether these results are due to higher volume of cases, more advanced technology, expanded role of specialists, or greater, round-the-clock availability of resident physicians,” said Mr. Giri of the University of Tennessee Health Science Center in Memphis.
Prior studies in cancer have suggested better overall survival among breast cancer patients treated at academic centers, but this is the first study looking at outcomes in AML, the most common acute leukemia in adults.
Using the National Cancer Database Participant User File, the investigators identified 7,823 patients with AML who received their initial therapy at the reporting facility from 1998 to 2011. The database collects information from more than 1,500 Commission on Cancer (CoC)–accredited facilities. Of the 7,823 patients, 4,681 (60%) were treated at an AC (academic/research program) and 3,142 at a non-AC (community cancer program/comprehensive community cancer program).
Patients treated at an AC were significantly younger than those treated at a non-AC (median 62 years vs. 67 years), tended to be of nonwhite race, less educated, have a lower income, and more comorbidities.
Receipt of chemotherapy (97.4% vs. 94.5%) and transplant (9% vs. 2.4%) were significantly higher at an AC than a non-AC (both P less than .001).
Kaplan Meier survival curves suggested disparate survival curves between the two groups, mainly within the first 5 years of follow-up (P less than .001), Mr. Giri said.
In multivariate model analysis, the non-AC group had significantly worse risk adjusted 30-day mortality than the AC group (odds ratio, 1.52; 95% confidence interval 1.33-1.74; P less than .001) and worse overall survival (hazard ratio, 1.13; 95% CI 1.07-1.19; P less than .001).
The study (Ab. 533) findings should be interpreted with caution because of its limitations, including the lack of information on AML risk type in the database, the fact that administrative datasets are prone to coding errors, and because the analysis did not adjust for hospital volume, which has been shown to affect survival, he said. Also, because there are more than 3,500 non–Coc approved hospitals, the sample may not be representative of overall U.S. hospitals.
During a discussion of the results, Mr. Giri acknowledged that patients treated at academic centers may have greater access to clinical trials and experimental agents. Future analyses should also distinguish patients with a diagnosis of acute promyelocytic leukemia, a distinct subset of AML.
AT ASH 2015
Key clinical point: Academic hospitals tend to have better short- and long-term mortality for patients with AML than nonacademic hospitals.
Major finding: Median overall survival was 12.6 months at an academic center vs. 7 months at a nonacademic center (P less than .001).
Data source: Retrospective analysis of 7,823 patients with AML.
Disclosures: The research was supported in part by a grant from the University of Nebraska Medical Center. The National Cancer Database is jointly sponsored by the American College of Surgeons and American Cancer Society. Mr. Giri reported having no relevant conflicts of interest.

Genes can stop onset of AML, study suggests

Image by Lance Liotta
Two genes can stop the development of acute myeloid leukemia (AML), according to research published in the Journal of Experimental Medicine.
The work suggests that Hif-1α and Hif-2α work together to stop the formation of leukemic stem cells, and blocking either Hif-2α or both genes
accelerates AML development.
Investigators said these findings are surprising because previous research suggested that blocking Hif-1α or Hif-2α might stop AML progression.
But their study suggests that therapies designed to block these genes might worsen AML or at least have no impact on the disease.
Conversely, designing new therapies that promote the activity of Hif-1α and Hif-2α could help treat AML or stop relapse after chemotherapy.
“Our discovery that Hif-1α and Hif-2α molecules act together to stop leukemia development is a major milestone in our efforts to combat leukemia,” said study author Kamil R. Kranc, DPhil, of the University of Edinburgh in Scotland.
“We now intend to harness this knowledge to develop curative therapies that eliminate leukemic stem cells, which are the underlying cause of AML.” ![]()
Image by Lance Liotta
Two genes can stop the development of acute myeloid leukemia (AML), according to research published in the Journal of Experimental Medicine.
The work suggests that Hif-1α and Hif-2α work together to stop the formation of leukemic stem cells, and blocking either Hif-2α or both genes
accelerates AML development.
Investigators said these findings are surprising because previous research suggested that blocking Hif-1α or Hif-2α might stop AML progression.
But their study suggests that therapies designed to block these genes might worsen AML or at least have no impact on the disease.
Conversely, designing new therapies that promote the activity of Hif-1α and Hif-2α could help treat AML or stop relapse after chemotherapy.
“Our discovery that Hif-1α and Hif-2α molecules act together to stop leukemia development is a major milestone in our efforts to combat leukemia,” said study author Kamil R. Kranc, DPhil, of the University of Edinburgh in Scotland.
“We now intend to harness this knowledge to develop curative therapies that eliminate leukemic stem cells, which are the underlying cause of AML.” ![]()
Image by Lance Liotta
Two genes can stop the development of acute myeloid leukemia (AML), according to research published in the Journal of Experimental Medicine.
The work suggests that Hif-1α and Hif-2α work together to stop the formation of leukemic stem cells, and blocking either Hif-2α or both genes
accelerates AML development.
Investigators said these findings are surprising because previous research suggested that blocking Hif-1α or Hif-2α might stop AML progression.
But their study suggests that therapies designed to block these genes might worsen AML or at least have no impact on the disease.
Conversely, designing new therapies that promote the activity of Hif-1α and Hif-2α could help treat AML or stop relapse after chemotherapy.
“Our discovery that Hif-1α and Hif-2α molecules act together to stop leukemia development is a major milestone in our efforts to combat leukemia,” said study author Kamil R. Kranc, DPhil, of the University of Edinburgh in Scotland.
“We now intend to harness this knowledge to develop curative therapies that eliminate leukemic stem cells, which are the underlying cause of AML.” ![]()
Minimal residual disease predicts outcome of allogeneic HCT in acute myeloid leukemia
Patients with acute myeloid leukemia (AML) who are in remission but with minimal residual disease (MRD) detectable by multiparameter flow cytometry have outcomes similar to those of patients with morphologically detectable disease, and both groups have significantly worse outcomes than patients in MRD-negative remission.
“Is it time to move toward an MRD-based definition of CR [complete remission]? We believe so,” wrote Dr. Daisuke Araki of the University of Washington, Seattle, and colleagues. The researchers suggest that decision algorithms based on “the classic morphologic remission definition are not ideal. Our data support treatment algorithms that use MRD-based (i.e., patients in MRD-negative CR [versus] all other patients), rather than morphology-based disease assessments” (J Clin Oncol. 2015 Dec 12 [doi:10.1200/JCO.2015.63.3826]).
Three-year overall survival estimates for patients with active AML, patients in MRD-positive remission, and patients in MRD-negative remission were 23% (12%-35%), 26% (17%-37%), and 73% (66%-78%), respectively. Progression-free survival estimates showed a similar delineation between patients with morphologically detectable AML and MRD-positive remission compared with MRD-negative remission: 13% (5%-23%) for active AML, 12% (5%-21%) for MRD-positive remission, and 67% (61%-73%) for MRD-negative remission.
The retrospective analysis included 359 patients with AML treated with myeloablative hematopoietic cell transplantation (HCT) at the Fred Hutchinson Cancer Research Center from 2006 to 2014. In total, 311 patients (87%) had morphologically determined CR (less than 5% bone marrow blasts). Of these, 76 patients (24%) had MRD by multiparameter flow cytometry (MRD-positive remission) and 235 (76%) had no flow cytometric evidence of MRD (MRD-negative remission). In the pre-HCT assessment, 48 patients (13%) had 5% or more bone marrow blasts and were classified as having active AML.
Even patients with the lowest detectable amount of MRD had significantly worse outcomes than did patients with no MRD. Among the patients with evidence of leukemia (those in MRD-positive remission and with classified active AML), researchers found no statistically significant differences in outcomes based on MRD levels (less than 0.5%, 0.5%-5%, and greater than 5% abnormal blasts). Sensitivity analysis with different cut points yielded similar findings.
However, in line with previous findings, the data show that a small but significant subset of patients with active leukemia at the time of HCT can achieve long-term disease control with myeloablative conditioning.
No significant associations were found between disease status and non-relapse mortality.
The investigators caution that the results do not necessarily demonstrate that HCT outcomes for patients in MRD-positive remission and those with active disease are identical, because the preparative regimens, in general, were different for the two groups.
Dr. Araki reported having no disclosures. Several of his coauthors reported ties to industry.
For patients in complete remission, with a risk profile that suggests HCT to cure acute myeloid leukemia, MRD should not be ignored. The inexpensive, relatively easy-to-assess analysis provides a sensitive and patient-specific risk indicator, adding information beyond cytogenetic risk class and underlying genetic abnormalities. The results from Araki et al. prompt new clinical studies and, perhaps, a new transplantation strategy. Patients in MRD-positive remission could be combined with patients with active disease in trials aimed primarily at reducing the risk of post-transplant relapse.
In acute lymphoblastic leukemia (ALL), MRD refines individual risk assessment and is crucial to decision making regarding HCT. Its role in AML is similarly growing in importance.
HCT is a powerful therapy commonly prescribed for younger patients in CR with intermediate- and high-risk characteristics, but has significant downsides in terms of economic costs, acute and chronic toxicities, and above all, risk of transplant-related mortality, which averages just below 10%. Use of MRD may profoundly influence the treatment approach for AML by permitting a better definition of CR and risk class, and favoring better risk-adapted treatment strategies oriented to spared the risk of treatment-related mortality and transplant-related morbidity.
One additional note concerns the potential bias in positive results for successful late transplantation in MRD-negative patients (after 6-12 months from CR). Some of these patients may have been cured by prior chemotherapy, particularly if a patient tests negative for MRD soon after achieving CR and prior to HCT. New trials should address this bias by using predefined MRD time points from CR to HCT.
Dr. Renato Bassan is an oncologist at UOC Ematologia, Ospedale dell’Angelo, Mestre-Venezia, Italy. These remarks were part of an editorial accompanying a report in the Journal of Clinical Oncology (2015 Dec 12. doi: 10.1200/JCO.2015.64.8907). Dr. Bassan reported ties to Mundipharma, ARIAD, Roche, and Amgen.
For patients in complete remission, with a risk profile that suggests HCT to cure acute myeloid leukemia, MRD should not be ignored. The inexpensive, relatively easy-to-assess analysis provides a sensitive and patient-specific risk indicator, adding information beyond cytogenetic risk class and underlying genetic abnormalities. The results from Araki et al. prompt new clinical studies and, perhaps, a new transplantation strategy. Patients in MRD-positive remission could be combined with patients with active disease in trials aimed primarily at reducing the risk of post-transplant relapse.
In acute lymphoblastic leukemia (ALL), MRD refines individual risk assessment and is crucial to decision making regarding HCT. Its role in AML is similarly growing in importance.
HCT is a powerful therapy commonly prescribed for younger patients in CR with intermediate- and high-risk characteristics, but has significant downsides in terms of economic costs, acute and chronic toxicities, and above all, risk of transplant-related mortality, which averages just below 10%. Use of MRD may profoundly influence the treatment approach for AML by permitting a better definition of CR and risk class, and favoring better risk-adapted treatment strategies oriented to spared the risk of treatment-related mortality and transplant-related morbidity.
One additional note concerns the potential bias in positive results for successful late transplantation in MRD-negative patients (after 6-12 months from CR). Some of these patients may have been cured by prior chemotherapy, particularly if a patient tests negative for MRD soon after achieving CR and prior to HCT. New trials should address this bias by using predefined MRD time points from CR to HCT.
Dr. Renato Bassan is an oncologist at UOC Ematologia, Ospedale dell’Angelo, Mestre-Venezia, Italy. These remarks were part of an editorial accompanying a report in the Journal of Clinical Oncology (2015 Dec 12. doi: 10.1200/JCO.2015.64.8907). Dr. Bassan reported ties to Mundipharma, ARIAD, Roche, and Amgen.
For patients in complete remission, with a risk profile that suggests HCT to cure acute myeloid leukemia, MRD should not be ignored. The inexpensive, relatively easy-to-assess analysis provides a sensitive and patient-specific risk indicator, adding information beyond cytogenetic risk class and underlying genetic abnormalities. The results from Araki et al. prompt new clinical studies and, perhaps, a new transplantation strategy. Patients in MRD-positive remission could be combined with patients with active disease in trials aimed primarily at reducing the risk of post-transplant relapse.
In acute lymphoblastic leukemia (ALL), MRD refines individual risk assessment and is crucial to decision making regarding HCT. Its role in AML is similarly growing in importance.
HCT is a powerful therapy commonly prescribed for younger patients in CR with intermediate- and high-risk characteristics, but has significant downsides in terms of economic costs, acute and chronic toxicities, and above all, risk of transplant-related mortality, which averages just below 10%. Use of MRD may profoundly influence the treatment approach for AML by permitting a better definition of CR and risk class, and favoring better risk-adapted treatment strategies oriented to spared the risk of treatment-related mortality and transplant-related morbidity.
One additional note concerns the potential bias in positive results for successful late transplantation in MRD-negative patients (after 6-12 months from CR). Some of these patients may have been cured by prior chemotherapy, particularly if a patient tests negative for MRD soon after achieving CR and prior to HCT. New trials should address this bias by using predefined MRD time points from CR to HCT.
Dr. Renato Bassan is an oncologist at UOC Ematologia, Ospedale dell’Angelo, Mestre-Venezia, Italy. These remarks were part of an editorial accompanying a report in the Journal of Clinical Oncology (2015 Dec 12. doi: 10.1200/JCO.2015.64.8907). Dr. Bassan reported ties to Mundipharma, ARIAD, Roche, and Amgen.
Patients with acute myeloid leukemia (AML) who are in remission but with minimal residual disease (MRD) detectable by multiparameter flow cytometry have outcomes similar to those of patients with morphologically detectable disease, and both groups have significantly worse outcomes than patients in MRD-negative remission.
“Is it time to move toward an MRD-based definition of CR [complete remission]? We believe so,” wrote Dr. Daisuke Araki of the University of Washington, Seattle, and colleagues. The researchers suggest that decision algorithms based on “the classic morphologic remission definition are not ideal. Our data support treatment algorithms that use MRD-based (i.e., patients in MRD-negative CR [versus] all other patients), rather than morphology-based disease assessments” (J Clin Oncol. 2015 Dec 12 [doi:10.1200/JCO.2015.63.3826]).
Three-year overall survival estimates for patients with active AML, patients in MRD-positive remission, and patients in MRD-negative remission were 23% (12%-35%), 26% (17%-37%), and 73% (66%-78%), respectively. Progression-free survival estimates showed a similar delineation between patients with morphologically detectable AML and MRD-positive remission compared with MRD-negative remission: 13% (5%-23%) for active AML, 12% (5%-21%) for MRD-positive remission, and 67% (61%-73%) for MRD-negative remission.
The retrospective analysis included 359 patients with AML treated with myeloablative hematopoietic cell transplantation (HCT) at the Fred Hutchinson Cancer Research Center from 2006 to 2014. In total, 311 patients (87%) had morphologically determined CR (less than 5% bone marrow blasts). Of these, 76 patients (24%) had MRD by multiparameter flow cytometry (MRD-positive remission) and 235 (76%) had no flow cytometric evidence of MRD (MRD-negative remission). In the pre-HCT assessment, 48 patients (13%) had 5% or more bone marrow blasts and were classified as having active AML.
Even patients with the lowest detectable amount of MRD had significantly worse outcomes than did patients with no MRD. Among the patients with evidence of leukemia (those in MRD-positive remission and with classified active AML), researchers found no statistically significant differences in outcomes based on MRD levels (less than 0.5%, 0.5%-5%, and greater than 5% abnormal blasts). Sensitivity analysis with different cut points yielded similar findings.
However, in line with previous findings, the data show that a small but significant subset of patients with active leukemia at the time of HCT can achieve long-term disease control with myeloablative conditioning.
No significant associations were found between disease status and non-relapse mortality.
The investigators caution that the results do not necessarily demonstrate that HCT outcomes for patients in MRD-positive remission and those with active disease are identical, because the preparative regimens, in general, were different for the two groups.
Dr. Araki reported having no disclosures. Several of his coauthors reported ties to industry.
Patients with acute myeloid leukemia (AML) who are in remission but with minimal residual disease (MRD) detectable by multiparameter flow cytometry have outcomes similar to those of patients with morphologically detectable disease, and both groups have significantly worse outcomes than patients in MRD-negative remission.
“Is it time to move toward an MRD-based definition of CR [complete remission]? We believe so,” wrote Dr. Daisuke Araki of the University of Washington, Seattle, and colleagues. The researchers suggest that decision algorithms based on “the classic morphologic remission definition are not ideal. Our data support treatment algorithms that use MRD-based (i.e., patients in MRD-negative CR [versus] all other patients), rather than morphology-based disease assessments” (J Clin Oncol. 2015 Dec 12 [doi:10.1200/JCO.2015.63.3826]).
Three-year overall survival estimates for patients with active AML, patients in MRD-positive remission, and patients in MRD-negative remission were 23% (12%-35%), 26% (17%-37%), and 73% (66%-78%), respectively. Progression-free survival estimates showed a similar delineation between patients with morphologically detectable AML and MRD-positive remission compared with MRD-negative remission: 13% (5%-23%) for active AML, 12% (5%-21%) for MRD-positive remission, and 67% (61%-73%) for MRD-negative remission.
The retrospective analysis included 359 patients with AML treated with myeloablative hematopoietic cell transplantation (HCT) at the Fred Hutchinson Cancer Research Center from 2006 to 2014. In total, 311 patients (87%) had morphologically determined CR (less than 5% bone marrow blasts). Of these, 76 patients (24%) had MRD by multiparameter flow cytometry (MRD-positive remission) and 235 (76%) had no flow cytometric evidence of MRD (MRD-negative remission). In the pre-HCT assessment, 48 patients (13%) had 5% or more bone marrow blasts and were classified as having active AML.
Even patients with the lowest detectable amount of MRD had significantly worse outcomes than did patients with no MRD. Among the patients with evidence of leukemia (those in MRD-positive remission and with classified active AML), researchers found no statistically significant differences in outcomes based on MRD levels (less than 0.5%, 0.5%-5%, and greater than 5% abnormal blasts). Sensitivity analysis with different cut points yielded similar findings.
However, in line with previous findings, the data show that a small but significant subset of patients with active leukemia at the time of HCT can achieve long-term disease control with myeloablative conditioning.
No significant associations were found between disease status and non-relapse mortality.
The investigators caution that the results do not necessarily demonstrate that HCT outcomes for patients in MRD-positive remission and those with active disease are identical, because the preparative regimens, in general, were different for the two groups.
Dr. Araki reported having no disclosures. Several of his coauthors reported ties to industry.
Key clinical point: Allogeneic hematopoietic cell transplantation (HCT) outcomes for patients in minimal residual disease (MRD)–positive remission were similar to outcomes of patients with morphologically detectable acute myeloid leukemia (AML), and significantly worse than outcomes of patients in MRD-negative remission.
Major finding: Three-year overall survival estimates for patients with active AML, patients in MRD-positive remission, and patients in MRD-negative remission were 23% (12%-35%), 26% (17%-37%), and 73% (66%-78%), respectively.
Data sources: A retrospective analysis of 359 patients with AML treated with myeloablative HCT at the Fred Hutchinson Cancer Research Center from 2006 to 2014.
Disclosures: Dr. Araki reported having no disclosures. Several of his coauthors reported ties to industry.
RATIFY trial results available after almost 10 years in the making

Photo courtesy of ASH
ORLANDO, FL—After almost 10 years, during which time no new drug for acute myeloid leukemia (AML) has been approved, results of the RATIFY trial are available.
In this trial, investigators evaluated midostaurin in combination with chemotherapy for younger patients with FLT3-mutated AML.
Patients who received midostaurin in their regimen instead of placebo experienced significantly longer overall survival (OS) and event-free survival (EFS).
“The primary endpoint of the trial was overall survival—which was very important—uncensored for transplant,” said Richard Stone, MD, of Dana-Farber Cancer Institute in Boston, Massachusetts.
“This is very much a ‘real-world’ trial. We just took patients from the start and saw how they did until the end.”
Dr Stone presented results from the trial during the plenary session of the 2015 ASH Annual Meeting (abstract 6*).
Midostaurin (PKC412), developed as a VEGF and protein kinase C inhibitor, is a known FLT3 inhibitor that specifically inhibits the growth of leukemic cell lines.
As a multi-kinase inhibitor, its potency against FLT3 may be limited, but it is active against both ITD and TKD mutations. Because AML is polyclonal at diagnosis, a multi-targeted inhibitor may have an advantage in newly diagnosed AML.
As a single agent, Dr Stone explained, midostaurin produced few remissions in advanced, mutant AML. But when combined with chemotherapy in a phase 1B study in newly diagnosed patients, it produced encouraging results.
So members of the Alliance for Clinical Trials in Oncology, formerly CALGB, and many other cooperative groups around the world—the AMLSG, CETLAM, ECOG, EORTC, GIMEMA, NCIC, OSHO, PETHEMA, SAL, and SWOG—conducted a phase 3, randomized, double-blind trial of induction and consolidation with or without midostaurin in patients younger than 60 with newly diagnosed FLT3-mutated AML.
The primary endpoint was OS, and secondary endpoints were OS censored and uncensored at the time of transplant, complete remission (CR) rates, EFS, disease-free survival (DFS), and adverse events.
Mark Levis, MD, of Johns Hopkins Sidney Kimmel Comprehensive Cancer Center in Baltimore, Maryland, who introduced the plenary presentation, suggested that OS may not be the best primary endpoint for an AML trial, given the long time it takes to complete a trial like this.
He pointed out that, “while we waited for RATIFY to accrue and mature, our approach to the disease changed.” Allogeneic transplant is now often the favored consolidation.
Eligibility criteria
Patients aged 18 to 60 with normal end-organ function and documented AML were eligible to enroll. Patients could not have had acute promyelocytic leukemia.
Their FLT3 mutation had to be centrally determined prior to enrollment by 1 of 9 academic labs around the world, and results had to be obtainable within 48 hours of sample collection.
Patients could receive up to 5 days of hydroxyurea prior to the start of treatment while awaiting the results of the mutation analysis.
Trial design
Investigators randomized patients to induction of daunorubicin and cytarabine with either midostaurin or placebo.
Daunorubicin was administered at 60 mg/m2 by intravenous push on days 1-3, cytarabine at 200 mg/m2 per day on days 1-7, and midostaurin at 50 mg orally twice a day on days 8-21.
A second cycle of induction was given based on day 21 bone marrow biopsy.
When patients achieved CR, they went on to consolidation with high-dose cytarabine (3 g/m2 over 3 hours every 12 hours on days 1, 3, and 5) and either midostaurin at the same induction dose or placebo.
After up to 4 doses of consolidation, patients went on to maintenance therapy for 12 months. This consisted of placebo or midostaurin at the same dose twice daily on days 1-28.
Patient population
The investigators screened 3279 patients younger than 60 years with newly diagnosed AML and found 27% (n=887) to be FLT3-positive.
They randomized 717 patients—81% of the FLT3-positive patients—to either the midostaurin arm (n=360) or the placebo arm (n=357). These 717 patients were evaluable for the intent-to-treat analysis.
The median age was 47.1 (range, 19.0–59.8) in the midostaurin arm and 48.6 (range, 18.0–60.9) in the placebo arm. There were significantly more males in the midostaurin arm (48.1%) than in the placebo arm (40.6%, P=0.045).
And the arms were almost identical for FLT3 stratification. In the midostaurin group, 22.5% had FLT3 TKD (no ITD), 47.5% had an ITD allelic ratio (+/- FLT3 TKD) less than 0.7, and 30.0% had a ratio of 0.7 or more.
In the placebo arm, 22.7% had FLT3 TKD, and 47.6% and 29.7% had ITD allelic ratios less than and greater than 0.7, respectively.
Safety
Rash/desquamation was the only significant difference in grade 3-4 non-hematologic events between the arms, with 13% in the midostaurin arm and 8% in the placebo arm (P=0.02).
Other grade 3-4 non-hematologic events occurring in 10% of patients or more included, in the midostaurin and placebo arms, respectively: febrile neutropenia (81%, 82%), infection (40%, 38%), diarrhea (15%, 16%), hypokalemia (13%, 17%), pain (13%, 13%), other infection (12%, 12%), ALT/SGPT (12%, 9%), and fatigue (9%, 11%).
There were 18 deaths (5%) in the midostaurin arm and 19 (5.3%) in the placebo arm during induction and consolidation treatment.
Efficacy
OS was superior for patients randomized to midostaurin. The median survival was 74.7 months (range, 31.7-not estimable) in the midostaurin arm and 25.6 months (range,18.6-42.9) in the placebo arm (P=0.0076).
Overall, there were 357 deaths, 171 and 186 in the midostaurin and placebo arms, respectively.
The 5-year survival rate was 50.9% for midostaurin and 43.9% for placebo.
EFS was also superior for patients randomized to midostaurin (P=0.0032), at a median of 8.0 months for midostaurin and 3.6 months for placebo. The 5-year EFS was 27.5% for midostaurin and 19.3% for placebo.
The CR rates by day 60 were not significantly different between the arms, at 59% and 53% for midostaurin and placebo, respectively. And the median time to CR was the same in each group, at 35 days.
The survival benefit, both overall and event-free, was consistent regardless of whether the patients were FLT3-ITD high, low, or FLT3-TKD.
The OS and EFS benefits were also consistent in censored and uncensored analyses, despite the high stem cell transplant rate. Four hundred eight patients (57%) received a transplant, 212 in the midostaurin arm and 196 in the placebo arm.
“The trial was positive whether you censored the patients at transplant or you kept following them for the whole time,” Dr Stone said.
He concluded that this type of international collaborative AML study based on genotype at diagnosis is feasible to do. But it took “a lot of collaboration, a lot of cooperation, a lot of persistence, because the trial took a long time to conceive of, conduct, and analyze.” ![]()
*Data in the presentation differ from the abstract.
Photo courtesy of ASH
ORLANDO, FL—After almost 10 years, during which time no new drug for acute myeloid leukemia (AML) has been approved, results of the RATIFY trial are available.
In this trial, investigators evaluated midostaurin in combination with chemotherapy for younger patients with FLT3-mutated AML.
Patients who received midostaurin in their regimen instead of placebo experienced significantly longer overall survival (OS) and event-free survival (EFS).
“The primary endpoint of the trial was overall survival—which was very important—uncensored for transplant,” said Richard Stone, MD, of Dana-Farber Cancer Institute in Boston, Massachusetts.
“This is very much a ‘real-world’ trial. We just took patients from the start and saw how they did until the end.”
Dr Stone presented results from the trial during the plenary session of the 2015 ASH Annual Meeting (abstract 6*).
Midostaurin (PKC412), developed as a VEGF and protein kinase C inhibitor, is a known FLT3 inhibitor that specifically inhibits the growth of leukemic cell lines.
As a multi-kinase inhibitor, its potency against FLT3 may be limited, but it is active against both ITD and TKD mutations. Because AML is polyclonal at diagnosis, a multi-targeted inhibitor may have an advantage in newly diagnosed AML.
As a single agent, Dr Stone explained, midostaurin produced few remissions in advanced, mutant AML. But when combined with chemotherapy in a phase 1B study in newly diagnosed patients, it produced encouraging results.
So members of the Alliance for Clinical Trials in Oncology, formerly CALGB, and many other cooperative groups around the world—the AMLSG, CETLAM, ECOG, EORTC, GIMEMA, NCIC, OSHO, PETHEMA, SAL, and SWOG—conducted a phase 3, randomized, double-blind trial of induction and consolidation with or without midostaurin in patients younger than 60 with newly diagnosed FLT3-mutated AML.
The primary endpoint was OS, and secondary endpoints were OS censored and uncensored at the time of transplant, complete remission (CR) rates, EFS, disease-free survival (DFS), and adverse events.
Mark Levis, MD, of Johns Hopkins Sidney Kimmel Comprehensive Cancer Center in Baltimore, Maryland, who introduced the plenary presentation, suggested that OS may not be the best primary endpoint for an AML trial, given the long time it takes to complete a trial like this.
He pointed out that, “while we waited for RATIFY to accrue and mature, our approach to the disease changed.” Allogeneic transplant is now often the favored consolidation.
Eligibility criteria
Patients aged 18 to 60 with normal end-organ function and documented AML were eligible to enroll. Patients could not have had acute promyelocytic leukemia.
Their FLT3 mutation had to be centrally determined prior to enrollment by 1 of 9 academic labs around the world, and results had to be obtainable within 48 hours of sample collection.
Patients could receive up to 5 days of hydroxyurea prior to the start of treatment while awaiting the results of the mutation analysis.
Trial design
Investigators randomized patients to induction of daunorubicin and cytarabine with either midostaurin or placebo.
Daunorubicin was administered at 60 mg/m2 by intravenous push on days 1-3, cytarabine at 200 mg/m2 per day on days 1-7, and midostaurin at 50 mg orally twice a day on days 8-21.
A second cycle of induction was given based on day 21 bone marrow biopsy.
When patients achieved CR, they went on to consolidation with high-dose cytarabine (3 g/m2 over 3 hours every 12 hours on days 1, 3, and 5) and either midostaurin at the same induction dose or placebo.
After up to 4 doses of consolidation, patients went on to maintenance therapy for 12 months. This consisted of placebo or midostaurin at the same dose twice daily on days 1-28.
Patient population
The investigators screened 3279 patients younger than 60 years with newly diagnosed AML and found 27% (n=887) to be FLT3-positive.
They randomized 717 patients—81% of the FLT3-positive patients—to either the midostaurin arm (n=360) or the placebo arm (n=357). These 717 patients were evaluable for the intent-to-treat analysis.
The median age was 47.1 (range, 19.0–59.8) in the midostaurin arm and 48.6 (range, 18.0–60.9) in the placebo arm. There were significantly more males in the midostaurin arm (48.1%) than in the placebo arm (40.6%, P=0.045).
And the arms were almost identical for FLT3 stratification. In the midostaurin group, 22.5% had FLT3 TKD (no ITD), 47.5% had an ITD allelic ratio (+/- FLT3 TKD) less than 0.7, and 30.0% had a ratio of 0.7 or more.
In the placebo arm, 22.7% had FLT3 TKD, and 47.6% and 29.7% had ITD allelic ratios less than and greater than 0.7, respectively.
Safety
Rash/desquamation was the only significant difference in grade 3-4 non-hematologic events between the arms, with 13% in the midostaurin arm and 8% in the placebo arm (P=0.02).
Other grade 3-4 non-hematologic events occurring in 10% of patients or more included, in the midostaurin and placebo arms, respectively: febrile neutropenia (81%, 82%), infection (40%, 38%), diarrhea (15%, 16%), hypokalemia (13%, 17%), pain (13%, 13%), other infection (12%, 12%), ALT/SGPT (12%, 9%), and fatigue (9%, 11%).
There were 18 deaths (5%) in the midostaurin arm and 19 (5.3%) in the placebo arm during induction and consolidation treatment.
Efficacy
OS was superior for patients randomized to midostaurin. The median survival was 74.7 months (range, 31.7-not estimable) in the midostaurin arm and 25.6 months (range,18.6-42.9) in the placebo arm (P=0.0076).
Overall, there were 357 deaths, 171 and 186 in the midostaurin and placebo arms, respectively.
The 5-year survival rate was 50.9% for midostaurin and 43.9% for placebo.
EFS was also superior for patients randomized to midostaurin (P=0.0032), at a median of 8.0 months for midostaurin and 3.6 months for placebo. The 5-year EFS was 27.5% for midostaurin and 19.3% for placebo.
The CR rates by day 60 were not significantly different between the arms, at 59% and 53% for midostaurin and placebo, respectively. And the median time to CR was the same in each group, at 35 days.
The survival benefit, both overall and event-free, was consistent regardless of whether the patients were FLT3-ITD high, low, or FLT3-TKD.
The OS and EFS benefits were also consistent in censored and uncensored analyses, despite the high stem cell transplant rate. Four hundred eight patients (57%) received a transplant, 212 in the midostaurin arm and 196 in the placebo arm.
“The trial was positive whether you censored the patients at transplant or you kept following them for the whole time,” Dr Stone said.
He concluded that this type of international collaborative AML study based on genotype at diagnosis is feasible to do. But it took “a lot of collaboration, a lot of cooperation, a lot of persistence, because the trial took a long time to conceive of, conduct, and analyze.” ![]()
*Data in the presentation differ from the abstract.
Photo courtesy of ASH
ORLANDO, FL—After almost 10 years, during which time no new drug for acute myeloid leukemia (AML) has been approved, results of the RATIFY trial are available.
In this trial, investigators evaluated midostaurin in combination with chemotherapy for younger patients with FLT3-mutated AML.
Patients who received midostaurin in their regimen instead of placebo experienced significantly longer overall survival (OS) and event-free survival (EFS).
“The primary endpoint of the trial was overall survival—which was very important—uncensored for transplant,” said Richard Stone, MD, of Dana-Farber Cancer Institute in Boston, Massachusetts.
“This is very much a ‘real-world’ trial. We just took patients from the start and saw how they did until the end.”
Dr Stone presented results from the trial during the plenary session of the 2015 ASH Annual Meeting (abstract 6*).
Midostaurin (PKC412), developed as a VEGF and protein kinase C inhibitor, is a known FLT3 inhibitor that specifically inhibits the growth of leukemic cell lines.
As a multi-kinase inhibitor, its potency against FLT3 may be limited, but it is active against both ITD and TKD mutations. Because AML is polyclonal at diagnosis, a multi-targeted inhibitor may have an advantage in newly diagnosed AML.
As a single agent, Dr Stone explained, midostaurin produced few remissions in advanced, mutant AML. But when combined with chemotherapy in a phase 1B study in newly diagnosed patients, it produced encouraging results.
So members of the Alliance for Clinical Trials in Oncology, formerly CALGB, and many other cooperative groups around the world—the AMLSG, CETLAM, ECOG, EORTC, GIMEMA, NCIC, OSHO, PETHEMA, SAL, and SWOG—conducted a phase 3, randomized, double-blind trial of induction and consolidation with or without midostaurin in patients younger than 60 with newly diagnosed FLT3-mutated AML.
The primary endpoint was OS, and secondary endpoints were OS censored and uncensored at the time of transplant, complete remission (CR) rates, EFS, disease-free survival (DFS), and adverse events.
Mark Levis, MD, of Johns Hopkins Sidney Kimmel Comprehensive Cancer Center in Baltimore, Maryland, who introduced the plenary presentation, suggested that OS may not be the best primary endpoint for an AML trial, given the long time it takes to complete a trial like this.
He pointed out that, “while we waited for RATIFY to accrue and mature, our approach to the disease changed.” Allogeneic transplant is now often the favored consolidation.
Eligibility criteria
Patients aged 18 to 60 with normal end-organ function and documented AML were eligible to enroll. Patients could not have had acute promyelocytic leukemia.
Their FLT3 mutation had to be centrally determined prior to enrollment by 1 of 9 academic labs around the world, and results had to be obtainable within 48 hours of sample collection.
Patients could receive up to 5 days of hydroxyurea prior to the start of treatment while awaiting the results of the mutation analysis.
Trial design
Investigators randomized patients to induction of daunorubicin and cytarabine with either midostaurin or placebo.
Daunorubicin was administered at 60 mg/m2 by intravenous push on days 1-3, cytarabine at 200 mg/m2 per day on days 1-7, and midostaurin at 50 mg orally twice a day on days 8-21.
A second cycle of induction was given based on day 21 bone marrow biopsy.
When patients achieved CR, they went on to consolidation with high-dose cytarabine (3 g/m2 over 3 hours every 12 hours on days 1, 3, and 5) and either midostaurin at the same induction dose or placebo.
After up to 4 doses of consolidation, patients went on to maintenance therapy for 12 months. This consisted of placebo or midostaurin at the same dose twice daily on days 1-28.
Patient population
The investigators screened 3279 patients younger than 60 years with newly diagnosed AML and found 27% (n=887) to be FLT3-positive.
They randomized 717 patients—81% of the FLT3-positive patients—to either the midostaurin arm (n=360) or the placebo arm (n=357). These 717 patients were evaluable for the intent-to-treat analysis.
The median age was 47.1 (range, 19.0–59.8) in the midostaurin arm and 48.6 (range, 18.0–60.9) in the placebo arm. There were significantly more males in the midostaurin arm (48.1%) than in the placebo arm (40.6%, P=0.045).
And the arms were almost identical for FLT3 stratification. In the midostaurin group, 22.5% had FLT3 TKD (no ITD), 47.5% had an ITD allelic ratio (+/- FLT3 TKD) less than 0.7, and 30.0% had a ratio of 0.7 or more.
In the placebo arm, 22.7% had FLT3 TKD, and 47.6% and 29.7% had ITD allelic ratios less than and greater than 0.7, respectively.
Safety
Rash/desquamation was the only significant difference in grade 3-4 non-hematologic events between the arms, with 13% in the midostaurin arm and 8% in the placebo arm (P=0.02).
Other grade 3-4 non-hematologic events occurring in 10% of patients or more included, in the midostaurin and placebo arms, respectively: febrile neutropenia (81%, 82%), infection (40%, 38%), diarrhea (15%, 16%), hypokalemia (13%, 17%), pain (13%, 13%), other infection (12%, 12%), ALT/SGPT (12%, 9%), and fatigue (9%, 11%).
There were 18 deaths (5%) in the midostaurin arm and 19 (5.3%) in the placebo arm during induction and consolidation treatment.
Efficacy
OS was superior for patients randomized to midostaurin. The median survival was 74.7 months (range, 31.7-not estimable) in the midostaurin arm and 25.6 months (range,18.6-42.9) in the placebo arm (P=0.0076).
Overall, there were 357 deaths, 171 and 186 in the midostaurin and placebo arms, respectively.
The 5-year survival rate was 50.9% for midostaurin and 43.9% for placebo.
EFS was also superior for patients randomized to midostaurin (P=0.0032), at a median of 8.0 months for midostaurin and 3.6 months for placebo. The 5-year EFS was 27.5% for midostaurin and 19.3% for placebo.
The CR rates by day 60 were not significantly different between the arms, at 59% and 53% for midostaurin and placebo, respectively. And the median time to CR was the same in each group, at 35 days.
The survival benefit, both overall and event-free, was consistent regardless of whether the patients were FLT3-ITD high, low, or FLT3-TKD.
The OS and EFS benefits were also consistent in censored and uncensored analyses, despite the high stem cell transplant rate. Four hundred eight patients (57%) received a transplant, 212 in the midostaurin arm and 196 in the placebo arm.
“The trial was positive whether you censored the patients at transplant or you kept following them for the whole time,” Dr Stone said.
He concluded that this type of international collaborative AML study based on genotype at diagnosis is feasible to do. But it took “a lot of collaboration, a lot of cooperation, a lot of persistence, because the trial took a long time to conceive of, conduct, and analyze.” ![]()
*Data in the presentation differ from the abstract.
VIDEO: High-intensity conditioning stands ground in MDS, AML
ORLANDO – Reduced-intensity conditioning regimens failed to show a significant survival benefit over high-intensity regimens in myelodysplastic syndrome or acute myeloid leukemia in the phase III MAVERICK trial.
Pretransplant reduced intensity conditioning (RIC) also resulted in a significantly higher risk of relapse and inferior relapse-free survival vs. myeloablative conditioning (MAC).
The findings, reported in the late-breaking abstract (LBA-8) session at the annual meeting of the American Society of Hematology, generated a lively debate over the study construct and whether its conclusion that MAC remain “the treatment of choice” in appropriate candidates should be applied to both diseases.
Session comoderator Dr. David P. Steensma, a myelodysplasia physician at the Dana-Farber Cancer Institute in Boston, said in an interview that the data will not change his practice and that physicians should continue to “push the envelope” and provide as intense a conditioning regimen as their patients can tolerate.
“The take-home message is that using a reduced conditioning regimen whatever your choice might be, even though it is gentler on the patient and may be easier for them to go through the transplant, the biggest risk is still the disease, the underlying leukemia or myelodysplasia coming back. And the benefit from reduced intensity is not enough to outweigh that risk.”
To sort out this complex trial, we spoke with study author Dr. Bart L. Scott of the Fred Hutchinson Cancer Research Center at the University of Washington, Seattle.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
ORLANDO – Reduced-intensity conditioning regimens failed to show a significant survival benefit over high-intensity regimens in myelodysplastic syndrome or acute myeloid leukemia in the phase III MAVERICK trial.
Pretransplant reduced intensity conditioning (RIC) also resulted in a significantly higher risk of relapse and inferior relapse-free survival vs. myeloablative conditioning (MAC).
The findings, reported in the late-breaking abstract (LBA-8) session at the annual meeting of the American Society of Hematology, generated a lively debate over the study construct and whether its conclusion that MAC remain “the treatment of choice” in appropriate candidates should be applied to both diseases.
Session comoderator Dr. David P. Steensma, a myelodysplasia physician at the Dana-Farber Cancer Institute in Boston, said in an interview that the data will not change his practice and that physicians should continue to “push the envelope” and provide as intense a conditioning regimen as their patients can tolerate.
“The take-home message is that using a reduced conditioning regimen whatever your choice might be, even though it is gentler on the patient and may be easier for them to go through the transplant, the biggest risk is still the disease, the underlying leukemia or myelodysplasia coming back. And the benefit from reduced intensity is not enough to outweigh that risk.”
To sort out this complex trial, we spoke with study author Dr. Bart L. Scott of the Fred Hutchinson Cancer Research Center at the University of Washington, Seattle.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
ORLANDO – Reduced-intensity conditioning regimens failed to show a significant survival benefit over high-intensity regimens in myelodysplastic syndrome or acute myeloid leukemia in the phase III MAVERICK trial.
Pretransplant reduced intensity conditioning (RIC) also resulted in a significantly higher risk of relapse and inferior relapse-free survival vs. myeloablative conditioning (MAC).
The findings, reported in the late-breaking abstract (LBA-8) session at the annual meeting of the American Society of Hematology, generated a lively debate over the study construct and whether its conclusion that MAC remain “the treatment of choice” in appropriate candidates should be applied to both diseases.
Session comoderator Dr. David P. Steensma, a myelodysplasia physician at the Dana-Farber Cancer Institute in Boston, said in an interview that the data will not change his practice and that physicians should continue to “push the envelope” and provide as intense a conditioning regimen as their patients can tolerate.
“The take-home message is that using a reduced conditioning regimen whatever your choice might be, even though it is gentler on the patient and may be easier for them to go through the transplant, the biggest risk is still the disease, the underlying leukemia or myelodysplasia coming back. And the benefit from reduced intensity is not enough to outweigh that risk.”
To sort out this complex trial, we spoke with study author Dr. Bart L. Scott of the Fred Hutchinson Cancer Research Center at the University of Washington, Seattle.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
AT ASH 2015

VIDEO: Midostaurin hits mark in FLT3-mutated AML
ORLANDO – The oral multikinase inhibitor midostaurin improved overall survival by 23% when added to standard chemotherapy and given as maintenance therapy for 1 year in newly diagnosed patients with FLT3-mutated acute myeloid leukemia (AML) in the global phase III CALGB 10603/RATIFY trial.
The results struck a chord at the annual meeting of the American Society of Hematology because the benefits of targeted therapy have so far eluded AML patients despite transforming the treatment of other blood cancers. Currently, there are no approved, targeted treatments for AML.
CALGB 10603/RATIFY is the first large, controlled trial to show an overall survival benefit in the roughly 30% of AML patients with a mutation in the FLT3 gene.
“This is exciting because we haven’t had a new treatment in AML for 30 years,” Dr. Robert Hromas of the University of Florida, Gainesville, said while moderating a press conference highlighting the plenary abstract.
The results were a decade in the making after midostaurin failed previously when used in all AML patients rather than the subset with the FLT3 mutation. But the persistence of researchers, the international collaboration, and funding in cancer research paid off, Dr. Hromas said.
Study author Dr. Richard M. Stone, chief of staff at Dana-Farber Cancer Institute in Boston, reviewed the results of CALGB 10603/RATIFY in an interview.
CALGB 10603/RATIFY was sponsored by the Cancer Therapy Evaluation Program. Dr. Stone reported financial relationships with several drug companies including Novartis, which provided the study drug and sponsored the trial outside North America. Dr. Hromas disclosed serving as an uncompensated advisory board member without equity for Cloud Pharmaceuticals.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
ORLANDO – The oral multikinase inhibitor midostaurin improved overall survival by 23% when added to standard chemotherapy and given as maintenance therapy for 1 year in newly diagnosed patients with FLT3-mutated acute myeloid leukemia (AML) in the global phase III CALGB 10603/RATIFY trial.
The results struck a chord at the annual meeting of the American Society of Hematology because the benefits of targeted therapy have so far eluded AML patients despite transforming the treatment of other blood cancers. Currently, there are no approved, targeted treatments for AML.
CALGB 10603/RATIFY is the first large, controlled trial to show an overall survival benefit in the roughly 30% of AML patients with a mutation in the FLT3 gene.
“This is exciting because we haven’t had a new treatment in AML for 30 years,” Dr. Robert Hromas of the University of Florida, Gainesville, said while moderating a press conference highlighting the plenary abstract.
The results were a decade in the making after midostaurin failed previously when used in all AML patients rather than the subset with the FLT3 mutation. But the persistence of researchers, the international collaboration, and funding in cancer research paid off, Dr. Hromas said.
Study author Dr. Richard M. Stone, chief of staff at Dana-Farber Cancer Institute in Boston, reviewed the results of CALGB 10603/RATIFY in an interview.
CALGB 10603/RATIFY was sponsored by the Cancer Therapy Evaluation Program. Dr. Stone reported financial relationships with several drug companies including Novartis, which provided the study drug and sponsored the trial outside North America. Dr. Hromas disclosed serving as an uncompensated advisory board member without equity for Cloud Pharmaceuticals.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
ORLANDO – The oral multikinase inhibitor midostaurin improved overall survival by 23% when added to standard chemotherapy and given as maintenance therapy for 1 year in newly diagnosed patients with FLT3-mutated acute myeloid leukemia (AML) in the global phase III CALGB 10603/RATIFY trial.
The results struck a chord at the annual meeting of the American Society of Hematology because the benefits of targeted therapy have so far eluded AML patients despite transforming the treatment of other blood cancers. Currently, there are no approved, targeted treatments for AML.
CALGB 10603/RATIFY is the first large, controlled trial to show an overall survival benefit in the roughly 30% of AML patients with a mutation in the FLT3 gene.
“This is exciting because we haven’t had a new treatment in AML for 30 years,” Dr. Robert Hromas of the University of Florida, Gainesville, said while moderating a press conference highlighting the plenary abstract.
The results were a decade in the making after midostaurin failed previously when used in all AML patients rather than the subset with the FLT3 mutation. But the persistence of researchers, the international collaboration, and funding in cancer research paid off, Dr. Hromas said.
Study author Dr. Richard M. Stone, chief of staff at Dana-Farber Cancer Institute in Boston, reviewed the results of CALGB 10603/RATIFY in an interview.
CALGB 10603/RATIFY was sponsored by the Cancer Therapy Evaluation Program. Dr. Stone reported financial relationships with several drug companies including Novartis, which provided the study drug and sponsored the trial outside North America. Dr. Hromas disclosed serving as an uncompensated advisory board member without equity for Cloud Pharmaceuticals.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
AT ASH 2015
