User login
Prevent Defense
Three U.S. medical centers have been recognized for innovative approaches to preventing DVT and its potentially fatal complications, which include pulmonary embolism (PE). Central to each of the DVT prevention strategies is a risk assessment tool that is easy to use, built directly into routine care, and linked directly to guideline-recommended choices for prophylaxis.
The University of California at San Diego (UCSD) Medical Center, Johns Hopkins Hospital in Baltimore, and the Veterans Affairs (VA) Medical Center in Washington, D.C., each received the first DVTeamCare Hospital Award. The North American Thrombosis Forum (NATF), in conjunction with pharmaceutical company Eisai Inc., recognized each center’s accomplishment based upon an evaluation by an independent panel of expert judges.

—Gregory A. Maynard, MD, FHM, hospital medicine division chief, University of California at San Diego
The award reflects NATF’s goal of enhancing thrombosis education, prevention, diagnosis, and treatment to improve patient outcomes, says NATF Executive Director Ilene Sussman, PhD. Dr. Sussman notes that DVT affects more than 600,000 Americans annually, kills more than 100,000, and is one of the leading causes of preventable deaths in hospitals. Preventable DVT-related complication is on Medicare’s list of “never events,” for which hospitals will no longer be reimbursed.
UCSD, representing medical centers with more than 200 beds, imbedded its VTE prevention protocol into admission, transfer, and perioperative order sets across all medical and surgical services, says Gregory A. Maynard, MD, FHM, hospital medicine division chief. The protocol flags three levels of DVT risk, notes possible contraindications for a particular kind of patient, and presents a set of options for guideline-recommended prophylaxis. The protocol can be paper- or computer-based. Prompting concurrent intervention is a central component of UCSD’s implementation strategy, “identifying in real-time patients who are not receiving the right DVT prophylaxis and having a front-line nurse or pharmacist intervene appropriately,” Dr. Maynard explains.
The percent of UCSD’s patients on adequate prophylaxis rose to more than 98% in the past two years, up from about 50% before the intervention, while preventable VTE dropped by 85%—about 50 fewer cases per year in a hospital with fewer than 300 beds. “Having DVT prevention protocols such as these in place allows hospitalists to provide better care with less effort by leaving hospitalists free to focus on more complicated patient-care issues,” Dr. Maynard says.
UCSD has partnered with SHM to develop DVT prevention toolkits and mentored collaboratives, with which hospitalists can take the lead on QI projects at their local institutions. SHM’s online VTE Implementation Guide is available at www.hospitalmedicine.org/ResourceRoomRedesign/RR_VTE/VTE_Home.cfm.

Johns Hopkins Hospital, representing medical centers with more than 200 beds, developed a mandatory computer-based decision-support system to facilitate specialty-specific risk-factor assessment and the application of risk-appropriate VTE prophylaxis, says Michael Streiff, MD, FACP, director of Johns Hopkins’ Anticoagulation Management Service and Outpatient Clinic, and a member of its Evidence-Based Practice Center. Before a physician can issue any orders—medications, lab tests, nursing instructions, etc.—using a physician transfer order set, the computerized order-entry system automatically guides them through a concise set of questions about a patient’s DVT risk factors, contraindications for blood thinners, and guideline-recommended prophylaxis choices, Dr. Streiff says.

Since implementing the system, the percent of patients being DVT-risk-stratified within 24 hours of hospital admission rose to more than 90%, and nearly 9 in 10 of the appropriate patients are now receiving risk-appropriate, American College of Chest Physicians-approved DVT prophylaxis, up from about 26% before the intervention, Dr. Streiff notes.
The VA Medical Center in Washington, D.C., representing medical centers with fewer than 200 beds, participated in a mentorship collaborative with UCSD’s Dr. Maynard and designed a seven-step process that walks providers through an evidence-based risk-factor assessment to determine appropriate thromboprophylactic therapy, says Divya Shroff, MD, associate chief of staff, Informatics. The guideline-driven steps are integrated into the VA’s computerized patient medical record system and take no more than 60 seconds to follow, says pharmacy practice resident Jovonne H. Jones, PharmD. The steps include:
- Assess patient DVT risk level;
- Educate patient about the order;
- Identify contraindications, if any;
- Choose prophylaxis drug or device;
- Accept order for drug or device;
- Check if additional prophylactic method is needed; and
- Accept the final order.

After the intervention, the rate at which patients receive appropriate prophylaxis upon admission more than doubled. Twenty VA medical centers around the country are in the process of implementing the system, Jones says.
The award-winning protocols will be presented at an NATF-hosted program April 9 at Harvard Medical School. The protocols and implementation plans will be made available at www.DVTeamCareAward.com to help other hospitals enhance their efforts to prevent DVT. TH
Chris Guadagnino is a freelance medical writer based in Philadelphia.
Three U.S. medical centers have been recognized for innovative approaches to preventing DVT and its potentially fatal complications, which include pulmonary embolism (PE). Central to each of the DVT prevention strategies is a risk assessment tool that is easy to use, built directly into routine care, and linked directly to guideline-recommended choices for prophylaxis.
The University of California at San Diego (UCSD) Medical Center, Johns Hopkins Hospital in Baltimore, and the Veterans Affairs (VA) Medical Center in Washington, D.C., each received the first DVTeamCare Hospital Award. The North American Thrombosis Forum (NATF), in conjunction with pharmaceutical company Eisai Inc., recognized each center’s accomplishment based upon an evaluation by an independent panel of expert judges.
—Gregory A. Maynard, MD, FHM, hospital medicine division chief, University of California at San Diego
The award reflects NATF’s goal of enhancing thrombosis education, prevention, diagnosis, and treatment to improve patient outcomes, says NATF Executive Director Ilene Sussman, PhD. Dr. Sussman notes that DVT affects more than 600,000 Americans annually, kills more than 100,000, and is one of the leading causes of preventable deaths in hospitals. Preventable DVT-related complication is on Medicare’s list of “never events,” for which hospitals will no longer be reimbursed.
UCSD, representing medical centers with more than 200 beds, imbedded its VTE prevention protocol into admission, transfer, and perioperative order sets across all medical and surgical services, says Gregory A. Maynard, MD, FHM, hospital medicine division chief. The protocol flags three levels of DVT risk, notes possible contraindications for a particular kind of patient, and presents a set of options for guideline-recommended prophylaxis. The protocol can be paper- or computer-based. Prompting concurrent intervention is a central component of UCSD’s implementation strategy, “identifying in real-time patients who are not receiving the right DVT prophylaxis and having a front-line nurse or pharmacist intervene appropriately,” Dr. Maynard explains.
The percent of UCSD’s patients on adequate prophylaxis rose to more than 98% in the past two years, up from about 50% before the intervention, while preventable VTE dropped by 85%—about 50 fewer cases per year in a hospital with fewer than 300 beds. “Having DVT prevention protocols such as these in place allows hospitalists to provide better care with less effort by leaving hospitalists free to focus on more complicated patient-care issues,” Dr. Maynard says.
UCSD has partnered with SHM to develop DVT prevention toolkits and mentored collaboratives, with which hospitalists can take the lead on QI projects at their local institutions. SHM’s online VTE Implementation Guide is available at www.hospitalmedicine.org/ResourceRoomRedesign/RR_VTE/VTE_Home.cfm.
Johns Hopkins Hospital, representing medical centers with more than 200 beds, developed a mandatory computer-based decision-support system to facilitate specialty-specific risk-factor assessment and the application of risk-appropriate VTE prophylaxis, says Michael Streiff, MD, FACP, director of Johns Hopkins’ Anticoagulation Management Service and Outpatient Clinic, and a member of its Evidence-Based Practice Center. Before a physician can issue any orders—medications, lab tests, nursing instructions, etc.—using a physician transfer order set, the computerized order-entry system automatically guides them through a concise set of questions about a patient’s DVT risk factors, contraindications for blood thinners, and guideline-recommended prophylaxis choices, Dr. Streiff says.
Since implementing the system, the percent of patients being DVT-risk-stratified within 24 hours of hospital admission rose to more than 90%, and nearly 9 in 10 of the appropriate patients are now receiving risk-appropriate, American College of Chest Physicians-approved DVT prophylaxis, up from about 26% before the intervention, Dr. Streiff notes.
The VA Medical Center in Washington, D.C., representing medical centers with fewer than 200 beds, participated in a mentorship collaborative with UCSD’s Dr. Maynard and designed a seven-step process that walks providers through an evidence-based risk-factor assessment to determine appropriate thromboprophylactic therapy, says Divya Shroff, MD, associate chief of staff, Informatics. The guideline-driven steps are integrated into the VA’s computerized patient medical record system and take no more than 60 seconds to follow, says pharmacy practice resident Jovonne H. Jones, PharmD. The steps include:
- Assess patient DVT risk level;
- Educate patient about the order;
- Identify contraindications, if any;
- Choose prophylaxis drug or device;
- Accept order for drug or device;
- Check if additional prophylactic method is needed; and
- Accept the final order.
After the intervention, the rate at which patients receive appropriate prophylaxis upon admission more than doubled. Twenty VA medical centers around the country are in the process of implementing the system, Jones says.
The award-winning protocols will be presented at an NATF-hosted program April 9 at Harvard Medical School. The protocols and implementation plans will be made available at www.DVTeamCareAward.com to help other hospitals enhance their efforts to prevent DVT. TH
Chris Guadagnino is a freelance medical writer based in Philadelphia.
Three U.S. medical centers have been recognized for innovative approaches to preventing DVT and its potentially fatal complications, which include pulmonary embolism (PE). Central to each of the DVT prevention strategies is a risk assessment tool that is easy to use, built directly into routine care, and linked directly to guideline-recommended choices for prophylaxis.
The University of California at San Diego (UCSD) Medical Center, Johns Hopkins Hospital in Baltimore, and the Veterans Affairs (VA) Medical Center in Washington, D.C., each received the first DVTeamCare Hospital Award. The North American Thrombosis Forum (NATF), in conjunction with pharmaceutical company Eisai Inc., recognized each center’s accomplishment based upon an evaluation by an independent panel of expert judges.
—Gregory A. Maynard, MD, FHM, hospital medicine division chief, University of California at San Diego
The award reflects NATF’s goal of enhancing thrombosis education, prevention, diagnosis, and treatment to improve patient outcomes, says NATF Executive Director Ilene Sussman, PhD. Dr. Sussman notes that DVT affects more than 600,000 Americans annually, kills more than 100,000, and is one of the leading causes of preventable deaths in hospitals. Preventable DVT-related complication is on Medicare’s list of “never events,” for which hospitals will no longer be reimbursed.
UCSD, representing medical centers with more than 200 beds, imbedded its VTE prevention protocol into admission, transfer, and perioperative order sets across all medical and surgical services, says Gregory A. Maynard, MD, FHM, hospital medicine division chief. The protocol flags three levels of DVT risk, notes possible contraindications for a particular kind of patient, and presents a set of options for guideline-recommended prophylaxis. The protocol can be paper- or computer-based. Prompting concurrent intervention is a central component of UCSD’s implementation strategy, “identifying in real-time patients who are not receiving the right DVT prophylaxis and having a front-line nurse or pharmacist intervene appropriately,” Dr. Maynard explains.
The percent of UCSD’s patients on adequate prophylaxis rose to more than 98% in the past two years, up from about 50% before the intervention, while preventable VTE dropped by 85%—about 50 fewer cases per year in a hospital with fewer than 300 beds. “Having DVT prevention protocols such as these in place allows hospitalists to provide better care with less effort by leaving hospitalists free to focus on more complicated patient-care issues,” Dr. Maynard says.
UCSD has partnered with SHM to develop DVT prevention toolkits and mentored collaboratives, with which hospitalists can take the lead on QI projects at their local institutions. SHM’s online VTE Implementation Guide is available at www.hospitalmedicine.org/ResourceRoomRedesign/RR_VTE/VTE_Home.cfm.
Johns Hopkins Hospital, representing medical centers with more than 200 beds, developed a mandatory computer-based decision-support system to facilitate specialty-specific risk-factor assessment and the application of risk-appropriate VTE prophylaxis, says Michael Streiff, MD, FACP, director of Johns Hopkins’ Anticoagulation Management Service and Outpatient Clinic, and a member of its Evidence-Based Practice Center. Before a physician can issue any orders—medications, lab tests, nursing instructions, etc.—using a physician transfer order set, the computerized order-entry system automatically guides them through a concise set of questions about a patient’s DVT risk factors, contraindications for blood thinners, and guideline-recommended prophylaxis choices, Dr. Streiff says.
Since implementing the system, the percent of patients being DVT-risk-stratified within 24 hours of hospital admission rose to more than 90%, and nearly 9 in 10 of the appropriate patients are now receiving risk-appropriate, American College of Chest Physicians-approved DVT prophylaxis, up from about 26% before the intervention, Dr. Streiff notes.
The VA Medical Center in Washington, D.C., representing medical centers with fewer than 200 beds, participated in a mentorship collaborative with UCSD’s Dr. Maynard and designed a seven-step process that walks providers through an evidence-based risk-factor assessment to determine appropriate thromboprophylactic therapy, says Divya Shroff, MD, associate chief of staff, Informatics. The guideline-driven steps are integrated into the VA’s computerized patient medical record system and take no more than 60 seconds to follow, says pharmacy practice resident Jovonne H. Jones, PharmD. The steps include:
- Assess patient DVT risk level;
- Educate patient about the order;
- Identify contraindications, if any;
- Choose prophylaxis drug or device;
- Accept order for drug or device;
- Check if additional prophylactic method is needed; and
- Accept the final order.
After the intervention, the rate at which patients receive appropriate prophylaxis upon admission more than doubled. Twenty VA medical centers around the country are in the process of implementing the system, Jones says.
The award-winning protocols will be presented at an NATF-hosted program April 9 at Harvard Medical School. The protocols and implementation plans will be made available at www.DVTeamCareAward.com to help other hospitals enhance their efforts to prevent DVT. TH
Chris Guadagnino is a freelance medical writer based in Philadelphia.
Transitions of Care Integral to HM Patient Care

Transitions of Care Integral to HM Patient Care
I just finished my internal-medicine training and started a job as a hospitalist. We are a new hospitalist group, and I have been told that “transitions of care” is important to HM groups. I understand that getting information back to the patients’ primary-care physicians (PCPs) is important, but I am worried that I don’t have the whole picture. Is there something I am missing?
E. Parkhurst, MD
Tampa, Fla.
Dr. Hospitalist responds: Congrats on your new job. I am pleased to hear that you are motivated to learn more about transitions of care. It is important to hospitalist groups, but even more important to patients. I suspect your instincts are correct. You have an idea of what is meant by “transitions of care,” but probably do not appreciate all the nuances of the term. I certainly did not when I came out of training many years ago.
Transitions of care is a critical aspect of every patient’s care, and thus should be important to every healthcare provider. Our job is to care for the hospitalized patient and help them navigate through the complex systems of the hospital. How well we guide the patients through these transitions is reflected in their outcomes.
What is the definition of “transitions of care”? I find it useful to think about the patient’s journey when the decision is made to hospitalize the patient. When the patient is hospitalized, it is easy to recognize that the patient’s physical location is different; some, if not all, of the patient’s providers are different, too. The patient might have the same PCP caring for them in the hospital, but the nurses are different. The contrast is more evident if all of the patient’s providers are different. The ED is the point of entry for most patients. This is another location with another group of providers who do not have knowledge of all of the patient’s medical issues.
The hospital discharge is another inevitable transition. Most patients go home, but some will go to another healthcare facility (e.g., rehabilitation hospital) with another group of providers.
As you can see, the admission and discharge from the hospital involves multiple transitions. But multiple transitions also occur within the hospital. The patient could move from the general medical ward to the ICU and back; the patient might spend time in the surgical suite or operating room. Many patients go to radiology or other parts of the hospital for testing or procedures. At each location, the patient has a new group of providers.
But even if a physical location does not change, there could be a transition in care. During the day, one hospitalist or nurse might care for the patient. At night, another group of doctors and nurses are responsible for the patient’s care. Information must be transmitted and received between all of the parties at each transition in order for the appropriate care to proceed.
Effective transitions can improve provider efficiency. Think about how much easier it is to care for a patient whose care you assume when you have a clear understanding of the patient’s issues. Minimizing medical errors and increasing effective communication can reduce medical and legal risks. Effective transitions also minimize the length of hospital stay for the patient and minimize the risk of unnecessary readmission to the hospital. These can result in enhanced financial outcomes.
I think the key to effective and safe transitions of care is to create a mutually-agreed-upon process of communication and a level of expectation from all providers to carry out their role in the process. This is always easier said than done. In fact, the lack of an agreed-upon process often is a common barrier to effective transitions of care. Each participant’s role in the patient’s transitions might compete with another set of agendas.
As you can see, transitions of care is a complex topic, and I have only briefly reviewed it here. For more information, visit www.hospitalmedicine.org/boost. TH
Image Source: AMANE KANEKO
Transitions of Care Integral to HM Patient Care
I just finished my internal-medicine training and started a job as a hospitalist. We are a new hospitalist group, and I have been told that “transitions of care” is important to HM groups. I understand that getting information back to the patients’ primary-care physicians (PCPs) is important, but I am worried that I don’t have the whole picture. Is there something I am missing?
E. Parkhurst, MD
Tampa, Fla.
Dr. Hospitalist responds: Congrats on your new job. I am pleased to hear that you are motivated to learn more about transitions of care. It is important to hospitalist groups, but even more important to patients. I suspect your instincts are correct. You have an idea of what is meant by “transitions of care,” but probably do not appreciate all the nuances of the term. I certainly did not when I came out of training many years ago.
Transitions of care is a critical aspect of every patient’s care, and thus should be important to every healthcare provider. Our job is to care for the hospitalized patient and help them navigate through the complex systems of the hospital. How well we guide the patients through these transitions is reflected in their outcomes.
What is the definition of “transitions of care”? I find it useful to think about the patient’s journey when the decision is made to hospitalize the patient. When the patient is hospitalized, it is easy to recognize that the patient’s physical location is different; some, if not all, of the patient’s providers are different, too. The patient might have the same PCP caring for them in the hospital, but the nurses are different. The contrast is more evident if all of the patient’s providers are different. The ED is the point of entry for most patients. This is another location with another group of providers who do not have knowledge of all of the patient’s medical issues.
The hospital discharge is another inevitable transition. Most patients go home, but some will go to another healthcare facility (e.g., rehabilitation hospital) with another group of providers.
As you can see, the admission and discharge from the hospital involves multiple transitions. But multiple transitions also occur within the hospital. The patient could move from the general medical ward to the ICU and back; the patient might spend time in the surgical suite or operating room. Many patients go to radiology or other parts of the hospital for testing or procedures. At each location, the patient has a new group of providers.
But even if a physical location does not change, there could be a transition in care. During the day, one hospitalist or nurse might care for the patient. At night, another group of doctors and nurses are responsible for the patient’s care. Information must be transmitted and received between all of the parties at each transition in order for the appropriate care to proceed.
Effective transitions can improve provider efficiency. Think about how much easier it is to care for a patient whose care you assume when you have a clear understanding of the patient’s issues. Minimizing medical errors and increasing effective communication can reduce medical and legal risks. Effective transitions also minimize the length of hospital stay for the patient and minimize the risk of unnecessary readmission to the hospital. These can result in enhanced financial outcomes.
I think the key to effective and safe transitions of care is to create a mutually-agreed-upon process of communication and a level of expectation from all providers to carry out their role in the process. This is always easier said than done. In fact, the lack of an agreed-upon process often is a common barrier to effective transitions of care. Each participant’s role in the patient’s transitions might compete with another set of agendas.
As you can see, transitions of care is a complex topic, and I have only briefly reviewed it here. For more information, visit www.hospitalmedicine.org/boost. TH
Image Source: AMANE KANEKO
Transitions of Care Integral to HM Patient Care
I just finished my internal-medicine training and started a job as a hospitalist. We are a new hospitalist group, and I have been told that “transitions of care” is important to HM groups. I understand that getting information back to the patients’ primary-care physicians (PCPs) is important, but I am worried that I don’t have the whole picture. Is there something I am missing?
E. Parkhurst, MD
Tampa, Fla.
Dr. Hospitalist responds: Congrats on your new job. I am pleased to hear that you are motivated to learn more about transitions of care. It is important to hospitalist groups, but even more important to patients. I suspect your instincts are correct. You have an idea of what is meant by “transitions of care,” but probably do not appreciate all the nuances of the term. I certainly did not when I came out of training many years ago.
Transitions of care is a critical aspect of every patient’s care, and thus should be important to every healthcare provider. Our job is to care for the hospitalized patient and help them navigate through the complex systems of the hospital. How well we guide the patients through these transitions is reflected in their outcomes.
What is the definition of “transitions of care”? I find it useful to think about the patient’s journey when the decision is made to hospitalize the patient. When the patient is hospitalized, it is easy to recognize that the patient’s physical location is different; some, if not all, of the patient’s providers are different, too. The patient might have the same PCP caring for them in the hospital, but the nurses are different. The contrast is more evident if all of the patient’s providers are different. The ED is the point of entry for most patients. This is another location with another group of providers who do not have knowledge of all of the patient’s medical issues.
The hospital discharge is another inevitable transition. Most patients go home, but some will go to another healthcare facility (e.g., rehabilitation hospital) with another group of providers.
As you can see, the admission and discharge from the hospital involves multiple transitions. But multiple transitions also occur within the hospital. The patient could move from the general medical ward to the ICU and back; the patient might spend time in the surgical suite or operating room. Many patients go to radiology or other parts of the hospital for testing or procedures. At each location, the patient has a new group of providers.
But even if a physical location does not change, there could be a transition in care. During the day, one hospitalist or nurse might care for the patient. At night, another group of doctors and nurses are responsible for the patient’s care. Information must be transmitted and received between all of the parties at each transition in order for the appropriate care to proceed.
Effective transitions can improve provider efficiency. Think about how much easier it is to care for a patient whose care you assume when you have a clear understanding of the patient’s issues. Minimizing medical errors and increasing effective communication can reduce medical and legal risks. Effective transitions also minimize the length of hospital stay for the patient and minimize the risk of unnecessary readmission to the hospital. These can result in enhanced financial outcomes.
I think the key to effective and safe transitions of care is to create a mutually-agreed-upon process of communication and a level of expectation from all providers to carry out their role in the process. This is always easier said than done. In fact, the lack of an agreed-upon process often is a common barrier to effective transitions of care. Each participant’s role in the patient’s transitions might compete with another set of agendas.
As you can see, transitions of care is a complex topic, and I have only briefly reviewed it here. For more information, visit www.hospitalmedicine.org/boost. TH
Image Source: AMANE KANEKO
HM Growth: Phase 2

The growth of our medical specialty is old news. Yes, we now number about 30,000; yes, we now manage the medical care of 50% of hospitalized Medicare patients; yes, hospitalists are in two-thirds of U.S. hospitals. I could go on and on. But recently, I have observed a different type of growth altogether. It is the growth of stability.
In the recent history of HM, the focus was on the increasing number of hospitals that had hospitalists, the growth of SHM’s membership, the growth of our annual meeting, and the ever-increasing number of doctors who, at least when surveyed, called themselves hospitalists. It all looked so impressive.
Many of you know, however, that when you lifted up the hood of our field, it was not always as it seemed. HM actually was a bit unstable. Some doctors who called themselves hospitalists were, in reality, biding time until they moved on to a “real job” or went off to do a fellowship. Multiple groups competed for patients within any given hospital, and also competed for doctors. There were numerous jobs available for any given hospitalist, and, as a result, some groups had substantial turnover despite growth in numbers. In these programs, the group photo from one year to the next had an entirely new set of faces.
Instability did not just affect rank-and-file hospitalists; it also existed within programmatic leadership and entire programs. Annually in many hospitals, the hospitalists had to convince administration that the hospital needed hospitalists and that they were worthy of support. Unfortunately, it was not always successful, so some programs vanished.
Five years ago in Michigan, we were working to create a multihospital safety consortium. We had several participating institutions, all with hospitalist programs. One day, my secretary complained that every time she sent an e-mail to the consortium listserv, a handful would bounce back and indicate a handful of e-mail addresses no longer were in service, or note that an individual had “left the program.” Some of them were HM program directors. Follow-up calls showed that the program had a new director or had folded. In some cases, however, they were just too busy figuring out how to survive instead of focus on safety issues.
Fortunately, that all appears to be changing.
From Unknown to Accepted to Counted On
I have seen the change in my own institution. We, of course, continue to negotiate with hospital administration, but it is no longer about whether we should continue the program or not. Negotiations now center on line items in the budget, how much space we need, where we anticipate future growth, and what quality and safety initiatives we’re working on.
I like to think that the HM program is important infrastructure. Just as you can’t imagine a hospital without an ED or an ICU, the same holds true for the HM program.
Perhaps an even better analogy could be found in technologic innovation. Back when Al Gore invented the Internet, having an Internet connection at home was viewed as a luxury. Now, it nearly is a necessity. Just like HM programs! (OK, maybe that was a stretch.)
There also is stability within the faculty ranks. Many of our faculty have been here for years and plan to stay. Turnover has decreased dramatically. This is not unique to our program, but anecdotally is happening everywhere. In fact, we are in the process of launching additional multihospital HM-based safety projects and collaboratives. And when I reach out to programs to ask them to participate, the directors of these programs are the same ones when I last checked. If they have moved on, it has been to assume a local leadership role. The group photos also show all the same old faces, plus a few new ones. There really has been some stabilization in the field.
New Paradigm Here to Stay
The factors behind this newfound stability are numerous. Among them is the recognized importance of a well-managed HM program. In many institutions, the alternatives to hospitalists (primary-care physicians, surgeons managing all post-operative care, specialists admitting their own patients, etc.) have left the building. There is no going back, and there is no “plan B” if HM programs fold.
The recognition by prospective hospitalists—residents and students—that HM is a viable career path has increased interest in the field, and, in turn, has given many programs more choices among qualified applicants. Hospitalists currently employed in a reasonably functioning program are less likely to jump ship every year looking for something slightly better. And I expect the current economic climate has been a factor as well. As hospitals see operating margins erode, plans for infrastructure growth are delayed, funding for new programs shrinks, and hospitalist groups are asked to do more with less. In other words, they are not hiring as many new hospitalists.
In some sense, the perceived slowing in the growth of hospitalists might be concerning. I see it a different way. Slowing growth in overall numbers allows programs and the field to stabilize a bit, and this growth in stability creates enormous opportunity. Programs formerly struggling to survive can begin to innovate. We’ve seen that in Michigan, as the interest among hospitalist programs that want to participate in QI collaborations has grown. And when we hear what some programs are working on, it’s an impressive list of high-impact projects.
Hospitalists are taking ownership of care transitions, prevention of hospital-acquired complications, and disease-based QI initiatives centered on patients with heart failure, COPD, and diabetes.
Nationally, we have seen hospitalist programs coming together to successfully compete for federal research grants or foundation support targeting important national healthcare priorities. If the current healthcare reform legislation passes, it will better position HM to lead the transformation of healthcare in U.S. hospitals.
My big hope is that 10 to 20 years from now, HM is better known for its second phase of growth. Right now, we are more famous for our rapid growth and, to some extent, our impact on efficiency of care. Efficiency clearly is important; dollars saved from waste can be better put to use improving quality. But I want the field to be judged by our ability to innovate, improve the quality of hospital-care delivery, and to generate new knowledge that advances the care of all patients. Those accomplishments will have a more lasting impact on healthcare.
The stabilization of HM is making all of this possible. Our population expects and deserves great things from the nation’s fastest-growing “specialty,” and I am optimistic we will not let them down. TH
Dr. Flanders is president of SHM.
The growth of our medical specialty is old news. Yes, we now number about 30,000; yes, we now manage the medical care of 50% of hospitalized Medicare patients; yes, hospitalists are in two-thirds of U.S. hospitals. I could go on and on. But recently, I have observed a different type of growth altogether. It is the growth of stability.
In the recent history of HM, the focus was on the increasing number of hospitals that had hospitalists, the growth of SHM’s membership, the growth of our annual meeting, and the ever-increasing number of doctors who, at least when surveyed, called themselves hospitalists. It all looked so impressive.
Many of you know, however, that when you lifted up the hood of our field, it was not always as it seemed. HM actually was a bit unstable. Some doctors who called themselves hospitalists were, in reality, biding time until they moved on to a “real job” or went off to do a fellowship. Multiple groups competed for patients within any given hospital, and also competed for doctors. There were numerous jobs available for any given hospitalist, and, as a result, some groups had substantial turnover despite growth in numbers. In these programs, the group photo from one year to the next had an entirely new set of faces.
Instability did not just affect rank-and-file hospitalists; it also existed within programmatic leadership and entire programs. Annually in many hospitals, the hospitalists had to convince administration that the hospital needed hospitalists and that they were worthy of support. Unfortunately, it was not always successful, so some programs vanished.
Five years ago in Michigan, we were working to create a multihospital safety consortium. We had several participating institutions, all with hospitalist programs. One day, my secretary complained that every time she sent an e-mail to the consortium listserv, a handful would bounce back and indicate a handful of e-mail addresses no longer were in service, or note that an individual had “left the program.” Some of them were HM program directors. Follow-up calls showed that the program had a new director or had folded. In some cases, however, they were just too busy figuring out how to survive instead of focus on safety issues.
Fortunately, that all appears to be changing.
From Unknown to Accepted to Counted On
I have seen the change in my own institution. We, of course, continue to negotiate with hospital administration, but it is no longer about whether we should continue the program or not. Negotiations now center on line items in the budget, how much space we need, where we anticipate future growth, and what quality and safety initiatives we’re working on.
I like to think that the HM program is important infrastructure. Just as you can’t imagine a hospital without an ED or an ICU, the same holds true for the HM program.
Perhaps an even better analogy could be found in technologic innovation. Back when Al Gore invented the Internet, having an Internet connection at home was viewed as a luxury. Now, it nearly is a necessity. Just like HM programs! (OK, maybe that was a stretch.)
There also is stability within the faculty ranks. Many of our faculty have been here for years and plan to stay. Turnover has decreased dramatically. This is not unique to our program, but anecdotally is happening everywhere. In fact, we are in the process of launching additional multihospital HM-based safety projects and collaboratives. And when I reach out to programs to ask them to participate, the directors of these programs are the same ones when I last checked. If they have moved on, it has been to assume a local leadership role. The group photos also show all the same old faces, plus a few new ones. There really has been some stabilization in the field.
New Paradigm Here to Stay
The factors behind this newfound stability are numerous. Among them is the recognized importance of a well-managed HM program. In many institutions, the alternatives to hospitalists (primary-care physicians, surgeons managing all post-operative care, specialists admitting their own patients, etc.) have left the building. There is no going back, and there is no “plan B” if HM programs fold.
The recognition by prospective hospitalists—residents and students—that HM is a viable career path has increased interest in the field, and, in turn, has given many programs more choices among qualified applicants. Hospitalists currently employed in a reasonably functioning program are less likely to jump ship every year looking for something slightly better. And I expect the current economic climate has been a factor as well. As hospitals see operating margins erode, plans for infrastructure growth are delayed, funding for new programs shrinks, and hospitalist groups are asked to do more with less. In other words, they are not hiring as many new hospitalists.
In some sense, the perceived slowing in the growth of hospitalists might be concerning. I see it a different way. Slowing growth in overall numbers allows programs and the field to stabilize a bit, and this growth in stability creates enormous opportunity. Programs formerly struggling to survive can begin to innovate. We’ve seen that in Michigan, as the interest among hospitalist programs that want to participate in QI collaborations has grown. And when we hear what some programs are working on, it’s an impressive list of high-impact projects.
Hospitalists are taking ownership of care transitions, prevention of hospital-acquired complications, and disease-based QI initiatives centered on patients with heart failure, COPD, and diabetes.
Nationally, we have seen hospitalist programs coming together to successfully compete for federal research grants or foundation support targeting important national healthcare priorities. If the current healthcare reform legislation passes, it will better position HM to lead the transformation of healthcare in U.S. hospitals.
My big hope is that 10 to 20 years from now, HM is better known for its second phase of growth. Right now, we are more famous for our rapid growth and, to some extent, our impact on efficiency of care. Efficiency clearly is important; dollars saved from waste can be better put to use improving quality. But I want the field to be judged by our ability to innovate, improve the quality of hospital-care delivery, and to generate new knowledge that advances the care of all patients. Those accomplishments will have a more lasting impact on healthcare.
The stabilization of HM is making all of this possible. Our population expects and deserves great things from the nation’s fastest-growing “specialty,” and I am optimistic we will not let them down. TH
Dr. Flanders is president of SHM.
The growth of our medical specialty is old news. Yes, we now number about 30,000; yes, we now manage the medical care of 50% of hospitalized Medicare patients; yes, hospitalists are in two-thirds of U.S. hospitals. I could go on and on. But recently, I have observed a different type of growth altogether. It is the growth of stability.
In the recent history of HM, the focus was on the increasing number of hospitals that had hospitalists, the growth of SHM’s membership, the growth of our annual meeting, and the ever-increasing number of doctors who, at least when surveyed, called themselves hospitalists. It all looked so impressive.
Many of you know, however, that when you lifted up the hood of our field, it was not always as it seemed. HM actually was a bit unstable. Some doctors who called themselves hospitalists were, in reality, biding time until they moved on to a “real job” or went off to do a fellowship. Multiple groups competed for patients within any given hospital, and also competed for doctors. There were numerous jobs available for any given hospitalist, and, as a result, some groups had substantial turnover despite growth in numbers. In these programs, the group photo from one year to the next had an entirely new set of faces.
Instability did not just affect rank-and-file hospitalists; it also existed within programmatic leadership and entire programs. Annually in many hospitals, the hospitalists had to convince administration that the hospital needed hospitalists and that they were worthy of support. Unfortunately, it was not always successful, so some programs vanished.
Five years ago in Michigan, we were working to create a multihospital safety consortium. We had several participating institutions, all with hospitalist programs. One day, my secretary complained that every time she sent an e-mail to the consortium listserv, a handful would bounce back and indicate a handful of e-mail addresses no longer were in service, or note that an individual had “left the program.” Some of them were HM program directors. Follow-up calls showed that the program had a new director or had folded. In some cases, however, they were just too busy figuring out how to survive instead of focus on safety issues.
Fortunately, that all appears to be changing.
From Unknown to Accepted to Counted On
I have seen the change in my own institution. We, of course, continue to negotiate with hospital administration, but it is no longer about whether we should continue the program or not. Negotiations now center on line items in the budget, how much space we need, where we anticipate future growth, and what quality and safety initiatives we’re working on.
I like to think that the HM program is important infrastructure. Just as you can’t imagine a hospital without an ED or an ICU, the same holds true for the HM program.
Perhaps an even better analogy could be found in technologic innovation. Back when Al Gore invented the Internet, having an Internet connection at home was viewed as a luxury. Now, it nearly is a necessity. Just like HM programs! (OK, maybe that was a stretch.)
There also is stability within the faculty ranks. Many of our faculty have been here for years and plan to stay. Turnover has decreased dramatically. This is not unique to our program, but anecdotally is happening everywhere. In fact, we are in the process of launching additional multihospital HM-based safety projects and collaboratives. And when I reach out to programs to ask them to participate, the directors of these programs are the same ones when I last checked. If they have moved on, it has been to assume a local leadership role. The group photos also show all the same old faces, plus a few new ones. There really has been some stabilization in the field.
New Paradigm Here to Stay
The factors behind this newfound stability are numerous. Among them is the recognized importance of a well-managed HM program. In many institutions, the alternatives to hospitalists (primary-care physicians, surgeons managing all post-operative care, specialists admitting their own patients, etc.) have left the building. There is no going back, and there is no “plan B” if HM programs fold.
The recognition by prospective hospitalists—residents and students—that HM is a viable career path has increased interest in the field, and, in turn, has given many programs more choices among qualified applicants. Hospitalists currently employed in a reasonably functioning program are less likely to jump ship every year looking for something slightly better. And I expect the current economic climate has been a factor as well. As hospitals see operating margins erode, plans for infrastructure growth are delayed, funding for new programs shrinks, and hospitalist groups are asked to do more with less. In other words, they are not hiring as many new hospitalists.
In some sense, the perceived slowing in the growth of hospitalists might be concerning. I see it a different way. Slowing growth in overall numbers allows programs and the field to stabilize a bit, and this growth in stability creates enormous opportunity. Programs formerly struggling to survive can begin to innovate. We’ve seen that in Michigan, as the interest among hospitalist programs that want to participate in QI collaborations has grown. And when we hear what some programs are working on, it’s an impressive list of high-impact projects.
Hospitalists are taking ownership of care transitions, prevention of hospital-acquired complications, and disease-based QI initiatives centered on patients with heart failure, COPD, and diabetes.
Nationally, we have seen hospitalist programs coming together to successfully compete for federal research grants or foundation support targeting important national healthcare priorities. If the current healthcare reform legislation passes, it will better position HM to lead the transformation of healthcare in U.S. hospitals.
My big hope is that 10 to 20 years from now, HM is better known for its second phase of growth. Right now, we are more famous for our rapid growth and, to some extent, our impact on efficiency of care. Efficiency clearly is important; dollars saved from waste can be better put to use improving quality. But I want the field to be judged by our ability to innovate, improve the quality of hospital-care delivery, and to generate new knowledge that advances the care of all patients. Those accomplishments will have a more lasting impact on healthcare.
The stabilization of HM is making all of this possible. Our population expects and deserves great things from the nation’s fastest-growing “specialty,” and I am optimistic we will not let them down. TH
Dr. Flanders is president of SHM.
Market Watch
New Generics
- Fentanyl citrate troche/lozenge (generic Actiq) transmucosal lollipop1,2
- Perindopril erbumine (generic Aceon) tablets3
New Drugs, Indications, Label Changes, and Dosage Forms
- Capsaicin 8% patch (Qutenza) has been approved by the U.S. Food and Drug Administration (FDA) as a prescription medication to treat pain associated with post-herpetic neuralgia.4 The patch is a higher concentration than over-the-counter (OTC) products. The most common side effects in clinical trials were pain, swelling, itching, redness, and bumps at the application site, as well as blood pressure increases.5 Patch placement requires the use of a topical anesthetic and additional pain relief (ice or opioid pain relievers). Therefore, patch placement must be performed by a healthcare professional. Once the patch is applied, the patient must be observed for at least an hour, as there could be a significant increase in blood pressure.
- Diclofenac sodium topical (Pennsaid) has been approved by the FDA as a topical treatment to manage knee osteoarthritis.6 The transdermal carrier dimethylsulfoxide (DMSO) is utilized to deliver active diclofenac sodium through the skin to the pain site.7
- Exenatide injection (Byetta) has been approved by the FDA as monotherapy for treating patients with Type 2 diabetes mellitus, along with diet and exercise.8
- Human papilloma virus (HPV) vaccine (Gardasil) has been approved by the FDA for preventing condyloma acuminata due to HPV types 6 and 11 in males ages 9 to 26.9 The makers hope that this vaccine will decrease the need to treat genital warts. Clinical studies showed that in males not infected with HPV at the beginning of the study, the vaccine was close to 90% effective in preventing genital warts caused by infection of HPV types 6 and 11. The manufacturer plans to obtain additional safety and effectiveness information in this patient population.
- Lansoprazole 24HR (Prevacid OTC) 15-mg delayed-release capsules are available for treating frequent heartburn.10 The capsules will be available by prescription in both the 15-mg and 30-mg dosage strengths.
- Metoclopramide HCl orally disintegrating tablet (Metozolv ODT) has been approved by the FDA for treating both acute and recurrent diabetic gastroparesis and for the short-term management (four to 12 weeks) of adults with documented symptomatic gastroesophageal reflux disease who do not respond to conventional therapy.11
- Peramivir intravenous will be made available by the Centers for Disease Control (CDC) as an emergency treatment for children and adult patients who develop H1N1 influenza and are nonresponsive to oral or inhaled antiviral therapies.12
- Rosuvastatin (Crestor) has been approved by the FDA for treating heterozygous familial cholesterolemia in children ages 10-17.13
- Telmisartan 80-mg tablets (Micardis) have been approved by the FDA for risk reduction of myocardial infarction, stroke, or death from cardiovascular causes in patients 55 years and older who are at high risk for major cardiovascular events, or who are not able to take angiotensin-converting enzyme inhibitors.14
- Telmisartan/amlodipine tablets (Twynsta) have been approved by the FDA as a new combination for treating hypertension, either alone or in combination with other antihypertensive agents. This combination is not indicated for cardiovascular risk reduction. The tablets are available in the following strengths of telmisartan/amlodipine, respectively: 40 mg/5 mg, 40 mg/10 mg, 80 mg/5 mg, and 80 mg/10 mg.
- Tranexamic acid (Lysteda) has been approved by the FDA for the treatment of menorrhagia.15 This is the first nonhormonal, oral therapeutic agent approved to treat this condition.16
Pipeline
- Indacaterol is being investigated as a once-daily bronchodilator for treating adults with chronic obstructive pulmonary disease (COPD).17 Novartis has received a complete response letter from the FDA requesting additional data on the dosing of the agent. The company is working with the FDA to resolve these issues.
- Rituximab injection (Rituxan) is approved for treating moderate to severe rheumatoid arthritis after patients have been treated with methotrexate, as well as non-Hodgkin’s lymphoma.18 Genentech/Biogen is attempting to expand rituximab use to treat patients earlier in the course of their disease. The FDA recently rejected this application, citing the rare but serious safety risk of developing progressive multifocal leukoencephalopathy.
Safety Information
Use of omeprazole and clopidogrel combination therapy should be avoided, according to new data from the FDA.18 Current data suggest that clopidogrel’s antiplatelet effect may be hindered by 50% with concomitant omeprazole therapy. Omeprazole blocks the conversion of clopidogrel to its active, antiplatelet form, thus significantly decreasing its effectiveness. It is not known if other proton-pump inhibitors interfere with clopidogrel’s effectiveness. Other drugs that should not be used with clopidogrel include esomeprazole (Nexium), cimetidine (Tagamet and Tagamet HB), fluconazole (Diflucan), ketoconazole (Nizoral), voriconazole (VFEND), etravirine (Intelence), felbamate (Felbatol), fluoxetine (Prozac, Sarafem, and Symbyax), fluvoxamine (Luvox), and ticlopidine (Ticlid). TH
Michele B. Kaufman is a freelance medical writer based in New York City and a clinical pharmacist at New York Downtown Hospital.
References
- Orange Book: Approved Drug Products with Therapeutic Equivalence Evaluations. FDA Web site. Available at: www.accessdata.fda.gov/scripts/cder/ob/docs/obdetail.cfm?Appl_No=077312&TABLE1=OB_Rx. Accessed Nov. 19, 2009.
- Covidien gets approval of generic pain drug. Forbes.com Web site. Available at: http://www.forbes.com/feeds/ap/2009/10/30/business-health-care-us-covidien-actiq_7069457.html. Accessed Nov. 19, 2009.
- Orange Book: Approved Drug Products with Therapeutic Equivalence Evaluations. FDA Web site. Available at: www.accessdata.fda.gov/scripts/cder/ob/default.cfm Accessed Nov. 19, 2009.
- Riley K. FDA Approves New Drug Treatment for Long-Term Pain Relief after Shingles Attacks. FDA Web site. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm191003.htm. Accessed Nov. 19, 2009.
- Qutenza Approved for Post-Shingles Nerve Pain. U.S. News and World Report Web site. Available at: health.usnews.com/articles/health/healthday/2009/11/17/qutenza-approved-for-post-shingles-nerve-pain.html. Accessed Nov. 19, 2009.
- Nuvo shares surge on FDA pain cream approval. Reuters Web site. Available at: www.reuters.com/article/email/idUSN0543459820091105. Accessed Nov. 19, 2009.
- Pennsaid. Nuvo Web site. Available at: www.nuvoresearch.com/pipeline/pennsaid.asp. Accessed Nov. 19, 2009.
- BYETTA Approved For Expanded Use As First-Line Treatment For Type 2 Diabetes. Medical News Today Web site. Available at: www.medicalnewstoday.com/articles/169396.php. Accessed Nov. 19, 2009.
- Burgess S. FDA Approves New Indication for Gardasil to Prevent Genital Warts in Men and Boys. FDA Web site. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm187003.htm Accessed Nov. 19, 2009.
- Prevacid 24hr available over-the-counter. Monthly Prescribing Reference Web site. Available at: www.empr.com/prevacid-24hr-available-over-the-counter/article/157592/. Accessed Nov. 19, 2009.
- FDA Approves New Salix Product Exclusively in Catalent’s Zydis Fast Dissolve Technology. Catalent Web site. Available at: www.catalent.com/about-us/news/45. Accessed Nov. 19, 2009.
- Peramivir to be Used for Special Swine Flu Cases. Pharmaceutical-Technology.com Web site. Available at: www.pharmaceutical-technology.com/News/News68102.html. Accessed Nov. 19, 2009.
- Dennis M. AstraZeneca’s Crestor approved in US for paediatric use; Vimovo filed in Europe. FirstWord Web site. Available at: www.firstwordplus.com/Fws.do?articleid=41E54BF434C54C8E903A9EB4EF0839AA&logRowId=332380. Accessed Nov. 19, 2009.
- FDA Approves New Use for Micardis in Cardiovascular Risk Reduction and Twynsta as New Combination Treatment for High Blood Pressure. Boehringer Ingelheim Web site. Available at: us.boehringer-ingelheim.com/newsroom/2009/files/micardis_twynsta_approve_10-19-09.pdf. Accessed Nov. 19, 2009.
- Todoruk M. FDA approves Xanodyne’s Lysteda for menorrhaegia. FirstWord Web site. Available at: www.firstwordplus.com/Fws.do?articleid=8FCB424A8E7147A08CEC9BFCD8A450D2&logRowId=337054. Accessed Nov. 19, 2009.
- Xanodyne announces FDA approval of Lysteda for treatment of women with heavy menstrual bleeding. Xanodyne Web site. Available at: www.xanodyne.com/newsroom_details.asp?NewsId=61. Accessed Nov. 19, 2009.
- Todoruk M. FDA requests additional data for Novartis’ COPD drug indacaterol. FirstWord Web site. Available at: www.firstwordplus.com/Fws.do?articleid=B426F5ED30AB43A89338DAD0124168A7&logRowId=332718. Accessed Nov. 19, 2009.
- Genentech and Biogen Idec Receive a Complete Response from FDA for Earlier Use of Rituxan for Rheumatoid Arthritis. Genentech Web site. Available at: www.gene.com/gene/news/press-releases/display.do?method=detail&id=12407. Accessed Nov. 19, 2009.
- Walsh S. FDA Announces New Warning on Plavix: Avoid Use with Prilosec/Prilosec OTC. FDA Web site. Available at www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm191169.htm. Accessed Nov. 19, 2009.
New Generics
- Fentanyl citrate troche/lozenge (generic Actiq) transmucosal lollipop1,2
- Perindopril erbumine (generic Aceon) tablets3
New Drugs, Indications, Label Changes, and Dosage Forms
- Capsaicin 8% patch (Qutenza) has been approved by the U.S. Food and Drug Administration (FDA) as a prescription medication to treat pain associated with post-herpetic neuralgia.4 The patch is a higher concentration than over-the-counter (OTC) products. The most common side effects in clinical trials were pain, swelling, itching, redness, and bumps at the application site, as well as blood pressure increases.5 Patch placement requires the use of a topical anesthetic and additional pain relief (ice or opioid pain relievers). Therefore, patch placement must be performed by a healthcare professional. Once the patch is applied, the patient must be observed for at least an hour, as there could be a significant increase in blood pressure.
- Diclofenac sodium topical (Pennsaid) has been approved by the FDA as a topical treatment to manage knee osteoarthritis.6 The transdermal carrier dimethylsulfoxide (DMSO) is utilized to deliver active diclofenac sodium through the skin to the pain site.7
- Exenatide injection (Byetta) has been approved by the FDA as monotherapy for treating patients with Type 2 diabetes mellitus, along with diet and exercise.8
- Human papilloma virus (HPV) vaccine (Gardasil) has been approved by the FDA for preventing condyloma acuminata due to HPV types 6 and 11 in males ages 9 to 26.9 The makers hope that this vaccine will decrease the need to treat genital warts. Clinical studies showed that in males not infected with HPV at the beginning of the study, the vaccine was close to 90% effective in preventing genital warts caused by infection of HPV types 6 and 11. The manufacturer plans to obtain additional safety and effectiveness information in this patient population.
- Lansoprazole 24HR (Prevacid OTC) 15-mg delayed-release capsules are available for treating frequent heartburn.10 The capsules will be available by prescription in both the 15-mg and 30-mg dosage strengths.
- Metoclopramide HCl orally disintegrating tablet (Metozolv ODT) has been approved by the FDA for treating both acute and recurrent diabetic gastroparesis and for the short-term management (four to 12 weeks) of adults with documented symptomatic gastroesophageal reflux disease who do not respond to conventional therapy.11
- Peramivir intravenous will be made available by the Centers for Disease Control (CDC) as an emergency treatment for children and adult patients who develop H1N1 influenza and are nonresponsive to oral or inhaled antiviral therapies.12
- Rosuvastatin (Crestor) has been approved by the FDA for treating heterozygous familial cholesterolemia in children ages 10-17.13
- Telmisartan 80-mg tablets (Micardis) have been approved by the FDA for risk reduction of myocardial infarction, stroke, or death from cardiovascular causes in patients 55 years and older who are at high risk for major cardiovascular events, or who are not able to take angiotensin-converting enzyme inhibitors.14
- Telmisartan/amlodipine tablets (Twynsta) have been approved by the FDA as a new combination for treating hypertension, either alone or in combination with other antihypertensive agents. This combination is not indicated for cardiovascular risk reduction. The tablets are available in the following strengths of telmisartan/amlodipine, respectively: 40 mg/5 mg, 40 mg/10 mg, 80 mg/5 mg, and 80 mg/10 mg.
- Tranexamic acid (Lysteda) has been approved by the FDA for the treatment of menorrhagia.15 This is the first nonhormonal, oral therapeutic agent approved to treat this condition.16
Pipeline
- Indacaterol is being investigated as a once-daily bronchodilator for treating adults with chronic obstructive pulmonary disease (COPD).17 Novartis has received a complete response letter from the FDA requesting additional data on the dosing of the agent. The company is working with the FDA to resolve these issues.
- Rituximab injection (Rituxan) is approved for treating moderate to severe rheumatoid arthritis after patients have been treated with methotrexate, as well as non-Hodgkin’s lymphoma.18 Genentech/Biogen is attempting to expand rituximab use to treat patients earlier in the course of their disease. The FDA recently rejected this application, citing the rare but serious safety risk of developing progressive multifocal leukoencephalopathy.
Safety Information
Use of omeprazole and clopidogrel combination therapy should be avoided, according to new data from the FDA.18 Current data suggest that clopidogrel’s antiplatelet effect may be hindered by 50% with concomitant omeprazole therapy. Omeprazole blocks the conversion of clopidogrel to its active, antiplatelet form, thus significantly decreasing its effectiveness. It is not known if other proton-pump inhibitors interfere with clopidogrel’s effectiveness. Other drugs that should not be used with clopidogrel include esomeprazole (Nexium), cimetidine (Tagamet and Tagamet HB), fluconazole (Diflucan), ketoconazole (Nizoral), voriconazole (VFEND), etravirine (Intelence), felbamate (Felbatol), fluoxetine (Prozac, Sarafem, and Symbyax), fluvoxamine (Luvox), and ticlopidine (Ticlid). TH
Michele B. Kaufman is a freelance medical writer based in New York City and a clinical pharmacist at New York Downtown Hospital.
References
- Orange Book: Approved Drug Products with Therapeutic Equivalence Evaluations. FDA Web site. Available at: www.accessdata.fda.gov/scripts/cder/ob/docs/obdetail.cfm?Appl_No=077312&TABLE1=OB_Rx. Accessed Nov. 19, 2009.
- Covidien gets approval of generic pain drug. Forbes.com Web site. Available at: http://www.forbes.com/feeds/ap/2009/10/30/business-health-care-us-covidien-actiq_7069457.html. Accessed Nov. 19, 2009.
- Orange Book: Approved Drug Products with Therapeutic Equivalence Evaluations. FDA Web site. Available at: www.accessdata.fda.gov/scripts/cder/ob/default.cfm Accessed Nov. 19, 2009.
- Riley K. FDA Approves New Drug Treatment for Long-Term Pain Relief after Shingles Attacks. FDA Web site. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm191003.htm. Accessed Nov. 19, 2009.
- Qutenza Approved for Post-Shingles Nerve Pain. U.S. News and World Report Web site. Available at: health.usnews.com/articles/health/healthday/2009/11/17/qutenza-approved-for-post-shingles-nerve-pain.html. Accessed Nov. 19, 2009.
- Nuvo shares surge on FDA pain cream approval. Reuters Web site. Available at: www.reuters.com/article/email/idUSN0543459820091105. Accessed Nov. 19, 2009.
- Pennsaid. Nuvo Web site. Available at: www.nuvoresearch.com/pipeline/pennsaid.asp. Accessed Nov. 19, 2009.
- BYETTA Approved For Expanded Use As First-Line Treatment For Type 2 Diabetes. Medical News Today Web site. Available at: www.medicalnewstoday.com/articles/169396.php. Accessed Nov. 19, 2009.
- Burgess S. FDA Approves New Indication for Gardasil to Prevent Genital Warts in Men and Boys. FDA Web site. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm187003.htm Accessed Nov. 19, 2009.
- Prevacid 24hr available over-the-counter. Monthly Prescribing Reference Web site. Available at: www.empr.com/prevacid-24hr-available-over-the-counter/article/157592/. Accessed Nov. 19, 2009.
- FDA Approves New Salix Product Exclusively in Catalent’s Zydis Fast Dissolve Technology. Catalent Web site. Available at: www.catalent.com/about-us/news/45. Accessed Nov. 19, 2009.
- Peramivir to be Used for Special Swine Flu Cases. Pharmaceutical-Technology.com Web site. Available at: www.pharmaceutical-technology.com/News/News68102.html. Accessed Nov. 19, 2009.
- Dennis M. AstraZeneca’s Crestor approved in US for paediatric use; Vimovo filed in Europe. FirstWord Web site. Available at: www.firstwordplus.com/Fws.do?articleid=41E54BF434C54C8E903A9EB4EF0839AA&logRowId=332380. Accessed Nov. 19, 2009.
- FDA Approves New Use for Micardis in Cardiovascular Risk Reduction and Twynsta as New Combination Treatment for High Blood Pressure. Boehringer Ingelheim Web site. Available at: us.boehringer-ingelheim.com/newsroom/2009/files/micardis_twynsta_approve_10-19-09.pdf. Accessed Nov. 19, 2009.
- Todoruk M. FDA approves Xanodyne’s Lysteda for menorrhaegia. FirstWord Web site. Available at: www.firstwordplus.com/Fws.do?articleid=8FCB424A8E7147A08CEC9BFCD8A450D2&logRowId=337054. Accessed Nov. 19, 2009.
- Xanodyne announces FDA approval of Lysteda for treatment of women with heavy menstrual bleeding. Xanodyne Web site. Available at: www.xanodyne.com/newsroom_details.asp?NewsId=61. Accessed Nov. 19, 2009.
- Todoruk M. FDA requests additional data for Novartis’ COPD drug indacaterol. FirstWord Web site. Available at: www.firstwordplus.com/Fws.do?articleid=B426F5ED30AB43A89338DAD0124168A7&logRowId=332718. Accessed Nov. 19, 2009.
- Genentech and Biogen Idec Receive a Complete Response from FDA for Earlier Use of Rituxan for Rheumatoid Arthritis. Genentech Web site. Available at: www.gene.com/gene/news/press-releases/display.do?method=detail&id=12407. Accessed Nov. 19, 2009.
- Walsh S. FDA Announces New Warning on Plavix: Avoid Use with Prilosec/Prilosec OTC. FDA Web site. Available at www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm191169.htm. Accessed Nov. 19, 2009.
New Generics
- Fentanyl citrate troche/lozenge (generic Actiq) transmucosal lollipop1,2
- Perindopril erbumine (generic Aceon) tablets3
New Drugs, Indications, Label Changes, and Dosage Forms
- Capsaicin 8% patch (Qutenza) has been approved by the U.S. Food and Drug Administration (FDA) as a prescription medication to treat pain associated with post-herpetic neuralgia.4 The patch is a higher concentration than over-the-counter (OTC) products. The most common side effects in clinical trials were pain, swelling, itching, redness, and bumps at the application site, as well as blood pressure increases.5 Patch placement requires the use of a topical anesthetic and additional pain relief (ice or opioid pain relievers). Therefore, patch placement must be performed by a healthcare professional. Once the patch is applied, the patient must be observed for at least an hour, as there could be a significant increase in blood pressure.
- Diclofenac sodium topical (Pennsaid) has been approved by the FDA as a topical treatment to manage knee osteoarthritis.6 The transdermal carrier dimethylsulfoxide (DMSO) is utilized to deliver active diclofenac sodium through the skin to the pain site.7
- Exenatide injection (Byetta) has been approved by the FDA as monotherapy for treating patients with Type 2 diabetes mellitus, along with diet and exercise.8
- Human papilloma virus (HPV) vaccine (Gardasil) has been approved by the FDA for preventing condyloma acuminata due to HPV types 6 and 11 in males ages 9 to 26.9 The makers hope that this vaccine will decrease the need to treat genital warts. Clinical studies showed that in males not infected with HPV at the beginning of the study, the vaccine was close to 90% effective in preventing genital warts caused by infection of HPV types 6 and 11. The manufacturer plans to obtain additional safety and effectiveness information in this patient population.
- Lansoprazole 24HR (Prevacid OTC) 15-mg delayed-release capsules are available for treating frequent heartburn.10 The capsules will be available by prescription in both the 15-mg and 30-mg dosage strengths.
- Metoclopramide HCl orally disintegrating tablet (Metozolv ODT) has been approved by the FDA for treating both acute and recurrent diabetic gastroparesis and for the short-term management (four to 12 weeks) of adults with documented symptomatic gastroesophageal reflux disease who do not respond to conventional therapy.11
- Peramivir intravenous will be made available by the Centers for Disease Control (CDC) as an emergency treatment for children and adult patients who develop H1N1 influenza and are nonresponsive to oral or inhaled antiviral therapies.12
- Rosuvastatin (Crestor) has been approved by the FDA for treating heterozygous familial cholesterolemia in children ages 10-17.13
- Telmisartan 80-mg tablets (Micardis) have been approved by the FDA for risk reduction of myocardial infarction, stroke, or death from cardiovascular causes in patients 55 years and older who are at high risk for major cardiovascular events, or who are not able to take angiotensin-converting enzyme inhibitors.14
- Telmisartan/amlodipine tablets (Twynsta) have been approved by the FDA as a new combination for treating hypertension, either alone or in combination with other antihypertensive agents. This combination is not indicated for cardiovascular risk reduction. The tablets are available in the following strengths of telmisartan/amlodipine, respectively: 40 mg/5 mg, 40 mg/10 mg, 80 mg/5 mg, and 80 mg/10 mg.
- Tranexamic acid (Lysteda) has been approved by the FDA for the treatment of menorrhagia.15 This is the first nonhormonal, oral therapeutic agent approved to treat this condition.16
Pipeline
- Indacaterol is being investigated as a once-daily bronchodilator for treating adults with chronic obstructive pulmonary disease (COPD).17 Novartis has received a complete response letter from the FDA requesting additional data on the dosing of the agent. The company is working with the FDA to resolve these issues.
- Rituximab injection (Rituxan) is approved for treating moderate to severe rheumatoid arthritis after patients have been treated with methotrexate, as well as non-Hodgkin’s lymphoma.18 Genentech/Biogen is attempting to expand rituximab use to treat patients earlier in the course of their disease. The FDA recently rejected this application, citing the rare but serious safety risk of developing progressive multifocal leukoencephalopathy.
Safety Information
Use of omeprazole and clopidogrel combination therapy should be avoided, according to new data from the FDA.18 Current data suggest that clopidogrel’s antiplatelet effect may be hindered by 50% with concomitant omeprazole therapy. Omeprazole blocks the conversion of clopidogrel to its active, antiplatelet form, thus significantly decreasing its effectiveness. It is not known if other proton-pump inhibitors interfere with clopidogrel’s effectiveness. Other drugs that should not be used with clopidogrel include esomeprazole (Nexium), cimetidine (Tagamet and Tagamet HB), fluconazole (Diflucan), ketoconazole (Nizoral), voriconazole (VFEND), etravirine (Intelence), felbamate (Felbatol), fluoxetine (Prozac, Sarafem, and Symbyax), fluvoxamine (Luvox), and ticlopidine (Ticlid). TH
Michele B. Kaufman is a freelance medical writer based in New York City and a clinical pharmacist at New York Downtown Hospital.
References
- Orange Book: Approved Drug Products with Therapeutic Equivalence Evaluations. FDA Web site. Available at: www.accessdata.fda.gov/scripts/cder/ob/docs/obdetail.cfm?Appl_No=077312&TABLE1=OB_Rx. Accessed Nov. 19, 2009.
- Covidien gets approval of generic pain drug. Forbes.com Web site. Available at: http://www.forbes.com/feeds/ap/2009/10/30/business-health-care-us-covidien-actiq_7069457.html. Accessed Nov. 19, 2009.
- Orange Book: Approved Drug Products with Therapeutic Equivalence Evaluations. FDA Web site. Available at: www.accessdata.fda.gov/scripts/cder/ob/default.cfm Accessed Nov. 19, 2009.
- Riley K. FDA Approves New Drug Treatment for Long-Term Pain Relief after Shingles Attacks. FDA Web site. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm191003.htm. Accessed Nov. 19, 2009.
- Qutenza Approved for Post-Shingles Nerve Pain. U.S. News and World Report Web site. Available at: health.usnews.com/articles/health/healthday/2009/11/17/qutenza-approved-for-post-shingles-nerve-pain.html. Accessed Nov. 19, 2009.
- Nuvo shares surge on FDA pain cream approval. Reuters Web site. Available at: www.reuters.com/article/email/idUSN0543459820091105. Accessed Nov. 19, 2009.
- Pennsaid. Nuvo Web site. Available at: www.nuvoresearch.com/pipeline/pennsaid.asp. Accessed Nov. 19, 2009.
- BYETTA Approved For Expanded Use As First-Line Treatment For Type 2 Diabetes. Medical News Today Web site. Available at: www.medicalnewstoday.com/articles/169396.php. Accessed Nov. 19, 2009.
- Burgess S. FDA Approves New Indication for Gardasil to Prevent Genital Warts in Men and Boys. FDA Web site. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm187003.htm Accessed Nov. 19, 2009.
- Prevacid 24hr available over-the-counter. Monthly Prescribing Reference Web site. Available at: www.empr.com/prevacid-24hr-available-over-the-counter/article/157592/. Accessed Nov. 19, 2009.
- FDA Approves New Salix Product Exclusively in Catalent’s Zydis Fast Dissolve Technology. Catalent Web site. Available at: www.catalent.com/about-us/news/45. Accessed Nov. 19, 2009.
- Peramivir to be Used for Special Swine Flu Cases. Pharmaceutical-Technology.com Web site. Available at: www.pharmaceutical-technology.com/News/News68102.html. Accessed Nov. 19, 2009.
- Dennis M. AstraZeneca’s Crestor approved in US for paediatric use; Vimovo filed in Europe. FirstWord Web site. Available at: www.firstwordplus.com/Fws.do?articleid=41E54BF434C54C8E903A9EB4EF0839AA&logRowId=332380. Accessed Nov. 19, 2009.
- FDA Approves New Use for Micardis in Cardiovascular Risk Reduction and Twynsta as New Combination Treatment for High Blood Pressure. Boehringer Ingelheim Web site. Available at: us.boehringer-ingelheim.com/newsroom/2009/files/micardis_twynsta_approve_10-19-09.pdf. Accessed Nov. 19, 2009.
- Todoruk M. FDA approves Xanodyne’s Lysteda for menorrhaegia. FirstWord Web site. Available at: www.firstwordplus.com/Fws.do?articleid=8FCB424A8E7147A08CEC9BFCD8A450D2&logRowId=337054. Accessed Nov. 19, 2009.
- Xanodyne announces FDA approval of Lysteda for treatment of women with heavy menstrual bleeding. Xanodyne Web site. Available at: www.xanodyne.com/newsroom_details.asp?NewsId=61. Accessed Nov. 19, 2009.
- Todoruk M. FDA requests additional data for Novartis’ COPD drug indacaterol. FirstWord Web site. Available at: www.firstwordplus.com/Fws.do?articleid=B426F5ED30AB43A89338DAD0124168A7&logRowId=332718. Accessed Nov. 19, 2009.
- Genentech and Biogen Idec Receive a Complete Response from FDA for Earlier Use of Rituxan for Rheumatoid Arthritis. Genentech Web site. Available at: www.gene.com/gene/news/press-releases/display.do?method=detail&id=12407. Accessed Nov. 19, 2009.
- Walsh S. FDA Announces New Warning on Plavix: Avoid Use with Prilosec/Prilosec OTC. FDA Web site. Available at www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm191169.htm. Accessed Nov. 19, 2009.
ONLINE EXCLUSIVE: Audio interview with HM10 Course Director
Effective Communication Ensures Patient Safety

Effective Communication Ensures Patient Safety
Can you explain to me what is meant by SBAR? I heard this acronym mentioned during a session at HM09, but I did not understand the term.
S. East, MD
Pullman, Wash.
Dr. Hospitalist responds: SBAR (pronounced “ess-bar”) is a standardized method of communication that originated in the Navy’s nuclear submarine program. It stands for:
- Situation: What is happening presently?
- Background: What circumstances led to this situation?
- Assessment: What do I think is the problem?
- Recommendation: What should we do to correct the problem?
The SBAR system was developed to prevent simple communication errors that could lead to global disaster.
Kaiser Permanente of Colorado was among the first to adopt this model of communication among its staff and has since popularized its use in healthcare. Numerous hospitals and healthcare organizations have implemented SBAR as an approach to minimize communication errors between healthcare providers. The idea is that eliminating communication errors between healthcare providers improves patient safety. SBAR encourages all providers (doctors, nurses, pharmacists, etc.) to communicate with a shared mental model for information transfer.
SBAR requires providers to organize their thoughts, understand what it is they want to convey, and make requests in an organized fashion. Adherence to SBAR allows providers to transmit factual information in a concise manner.
Highly effective communication is essential to any hospitalist program. The SBAR approach should not be limited to nurse-doctor communication. I encourage you to implement this tool at your institution.
For more information, an SBAR toolkit is available at www.azhha.org/patient_safety/sbar.aspx. TH
Effective Communication Ensures Patient Safety
Can you explain to me what is meant by SBAR? I heard this acronym mentioned during a session at HM09, but I did not understand the term.
S. East, MD
Pullman, Wash.
Dr. Hospitalist responds: SBAR (pronounced “ess-bar”) is a standardized method of communication that originated in the Navy’s nuclear submarine program. It stands for:
- Situation: What is happening presently?
- Background: What circumstances led to this situation?
- Assessment: What do I think is the problem?
- Recommendation: What should we do to correct the problem?
The SBAR system was developed to prevent simple communication errors that could lead to global disaster.
Kaiser Permanente of Colorado was among the first to adopt this model of communication among its staff and has since popularized its use in healthcare. Numerous hospitals and healthcare organizations have implemented SBAR as an approach to minimize communication errors between healthcare providers. The idea is that eliminating communication errors between healthcare providers improves patient safety. SBAR encourages all providers (doctors, nurses, pharmacists, etc.) to communicate with a shared mental model for information transfer.
SBAR requires providers to organize their thoughts, understand what it is they want to convey, and make requests in an organized fashion. Adherence to SBAR allows providers to transmit factual information in a concise manner.
Highly effective communication is essential to any hospitalist program. The SBAR approach should not be limited to nurse-doctor communication. I encourage you to implement this tool at your institution.
For more information, an SBAR toolkit is available at www.azhha.org/patient_safety/sbar.aspx. TH
Effective Communication Ensures Patient Safety
Can you explain to me what is meant by SBAR? I heard this acronym mentioned during a session at HM09, but I did not understand the term.
S. East, MD
Pullman, Wash.
Dr. Hospitalist responds: SBAR (pronounced “ess-bar”) is a standardized method of communication that originated in the Navy’s nuclear submarine program. It stands for:
- Situation: What is happening presently?
- Background: What circumstances led to this situation?
- Assessment: What do I think is the problem?
- Recommendation: What should we do to correct the problem?
The SBAR system was developed to prevent simple communication errors that could lead to global disaster.
Kaiser Permanente of Colorado was among the first to adopt this model of communication among its staff and has since popularized its use in healthcare. Numerous hospitals and healthcare organizations have implemented SBAR as an approach to minimize communication errors between healthcare providers. The idea is that eliminating communication errors between healthcare providers improves patient safety. SBAR encourages all providers (doctors, nurses, pharmacists, etc.) to communicate with a shared mental model for information transfer.
SBAR requires providers to organize their thoughts, understand what it is they want to convey, and make requests in an organized fashion. Adherence to SBAR allows providers to transmit factual information in a concise manner.
Highly effective communication is essential to any hospitalist program. The SBAR approach should not be limited to nurse-doctor communication. I encourage you to implement this tool at your institution.
For more information, an SBAR toolkit is available at www.azhha.org/patient_safety/sbar.aspx. TH
Growth Spurt
Despite intravenous medication, a young boy in status epilepticus had the pediatric ICU team at the University of Wisconsin School of Medicine and Public Health in Madison stumped. The team called for a consult with the Integrative Medicine Program, which works with licensed acupuncturists and has been affiliated with the department of family medicine since 2001. Acupuncture’s efficacy in this setting has not been validated, but it has been shown to ease chemotherapy-induced nausea and vomiting, as well as radiation-induced xerostomia.1,2
Following several treatments by a licensed acupuncturist and continued conventional care, the boy’s seizures subsided and he was transitioned to the medical floor. Did the acupuncture contribute to bringing the seizures under control? “I can’t say that it was the acupuncture—it was probably a function of all the therapies working together,” says David P. Rakel, MD, assistant professor and director of UW’s Integrative Medicine Program.
The UW case illustrates both current trends and the constant conundrum that surrounds hospital-based complementary medicine: Complementary and alternative medicine’s use is increasing in some U.S. hospitals, yet the existing research evidence for the efficacy of its multiple modalities is decidedly mixed.
Even if your hospital does not offer complementary and alternative medicine (CAM), your patients are using CAM at ever-increasing rates. In 1993, 34% of Americans reported using some type of CAM (e.g., supplements, massage therapy, prayer, and so on). That number has almost doubled to 62%.3 Americans spend $47 billion a year—of their own money—for CAM therapies, chiropractors, acupuncturists, and massage therapists. And older patients with chronic conditions—the kind of patient hospitalists are most familiar with—tend to try CAM more than younger patients.4
These trends can directly affect hospitalists’ treatment decisions, but they also play a part in how you establish communication and trust with your patients, and how you keep your patients safe from adverse drug interactions. According to the National Academy of Sciences, in order to effectively counsel patients and ensure high-quality comprehensive care, conventional professionals need more CAM-related education.5
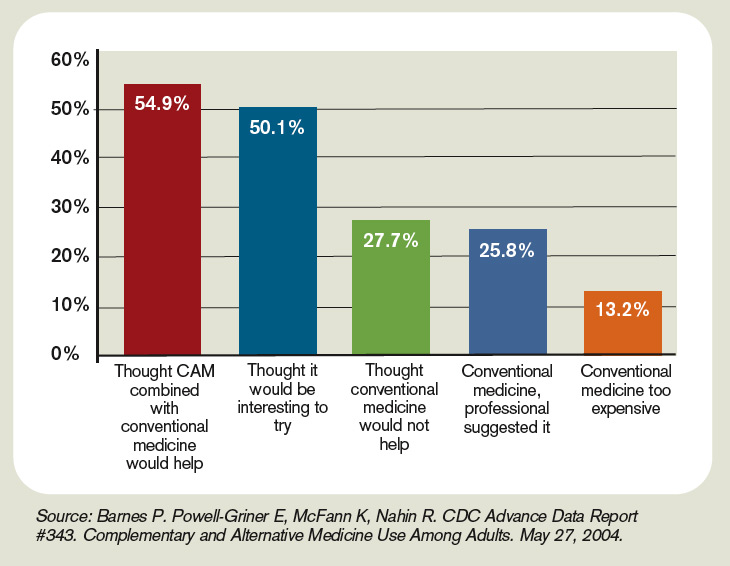

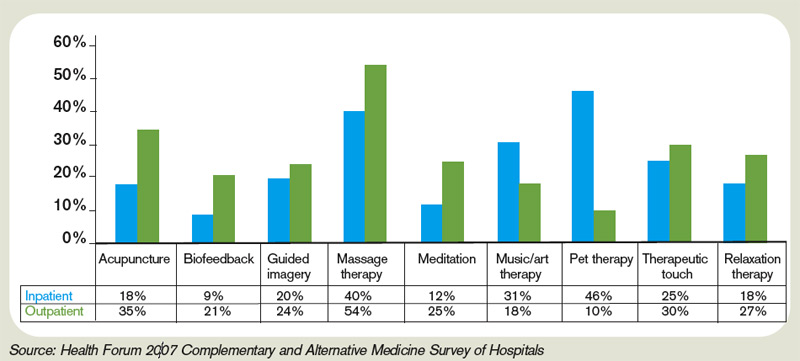
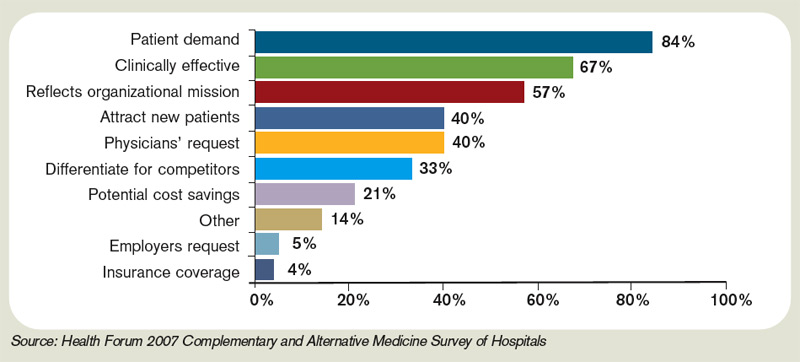
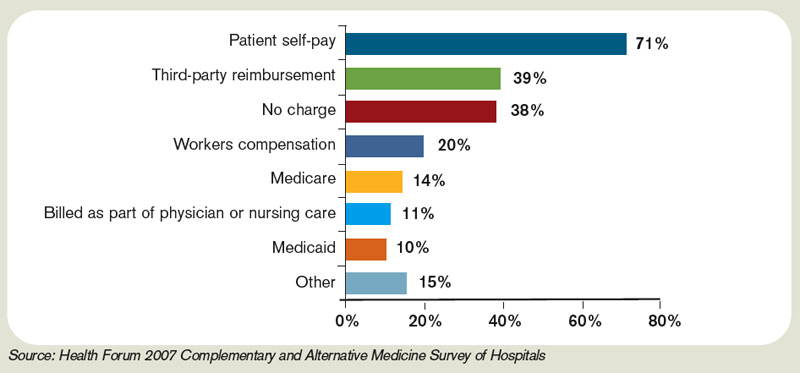

—Suzanne Bertisch, MD, MPH, fellow, Harvard Medical School’s Osher Research Center
Complementary Medicine: Online Resources

- National Center for Complementary and Alternative Medicine: http://nccam.nih.gov
- Integrative Medicine Service at Memorial Sloan-Kettering Cancer Center’s About Herbs: www.mskcc.org/mskcc/html/11570.cfm
- Natural Standard: www.naturalstandard.com
- The M.D. Anderson Cancer Center’s Complementary/Integrative Medicine Education Resources: www.mdanderson.org/departments/CIMER
What Trends Show
In 2007, according to the American Hospital Association, 20.8% of community hospitals offered some type of care or treatment not based on traditional Western allopathic medicine. That’s up from 8.6% of reporting hospitals that offered those services in 1998.
The 1990s saw rapid growth of integrative medicine centers at major research institutions, and the majority of U.S. cancer centers now offer some form of complementary therapy, says Barrie R. Cassileth, MS, PhD, the Laurance S. Rockefeller Chair in Integrative Medicine and chief of the Integrative Medicine Service at Memorial Sloan-Kettering Cancer Center in New York City.
The 2007 Health Forum/AHA Complementary and Alternative Medicine Survey of Hospitals reported that complementary programs are more common in urban rather than rural hospitals; services vary by hospital size (see Figure 2, above); and the top six modalities offered on an inpatient basis are pet therapy, massage therapy, music/art therapy, guided imagery, acupuncture, and reiki (see “Glossary of Complementary Terms,” above). Eighty-four percent of hospitals offer complementary services due to patient demand, the survey showed.
Joseph Ming-Wah Li, MD, FHM, SHM board member and assistant professor of medicine at Harvard Medical School and director of the hospital medicine program and associate chief of the division of general medicine and primary care at Beth Israel Deaconess Medical Center in Boston, doesn’t see a problem with modalities that can make his patients feel better. Patients at his hospital have access to pet therapy, massage, and acupuncture. “I don’t think these modalities hurt our patients, and there is very little downside, except for potential cost,” says Dr. Li, an SHM board member. “What’s not clear is whether these therapies work or not.”
What’s in a Name?
Numerous therapies and modalities crowd under the CAM umbrella, but most experts classify “complementary” modalities as those used in conjunction with conventional medicine to mitigate symptoms of disease or treatment, whereas “alternative” connotes therapies claiming to treat or cure the underlying disease. Some harmful, dangerous, and dishonest practices fall into the “alternative” category, such as Hulda Clark’s “Zapper” device, which was promoted as a cure for liver flukes, something she says cause everything from diabetes to heart disease. (For more on questionable practices, visit www.quackwatch.com or the National Council Against Health Fraud’s Web site at www.ncahf.org.)
The National Institutes of Health’s National Center for Complementary and Alternative Medicine (NCCAM) defines CAM as a group of “diverse medical and health care systems, practices, and products that are not presently considered to be part of conventional medicine.” Dr. Cassileth says the conflation of “complementary and alternative” into one neat acronym—CAM—causes confusion among patients and medical professionals. NCCAM will be changing its name soon, she says, to the National Center for Integrative Medicine, emphasizing the use of adjunctive modalities along with conventional medical treatments.
Hospitalist Suzanne Bertisch, MD, MPH, recently completed a research fellowship at Harvard Medical School’s Osher Research Center. She explains that integrative medicine uses a macro model of health, claiming a middle ground between the traditional, allopathic model of treating disease.
All Kinds of Evidence
Twenty years of complementary medicine research has yielded some information about safety—namely, what works and what doesn’t. For example, saw palmetto has not panned out as an effective treatment for benign prostatic hyperplasia; St. John’s wort, useful for mild depression, interferes with many medications, including cyclosporine and warfarin, and should be avoided at least five days prior to surgery.7,8
Since NCCAM’s inception in October 1998, its research portfolio has stirred debate in the scientific community. Part of the disagreement stems from the difficulty of fitting multidimensional interventions, some of which are provider-dependent (e.g., massage or acupuncture), into the gold standard of the randomized, double-blind, placebo-controlled trial, explains Darshan Mehta, MD, MPH, associate director of medical education at the Benson-Henry Institute for Mind Body Medicine at Massachusetts General Hospital in Boston. The manner in which the effectiveness of integrative techniques is assessed requires a higher sophistication of systems research, Dr. Mehta says.
“The way we construe evidence needs to change,” she adds.
Likely to Expand
Most private health plans do not cover complementary services, although Medicare and numerous insurance plans will reimburse treatment in conjunction with physical therapy (e.g., massage) in the outpatient setting. Twenty-three states cover chiropractic care under Medicaid, and Medicare has begun to assess the cost-effectiveness of including acupuncture—especially for postoperative and chemotherapy-associated nausea and vomiting—in its benefits package.9 Other modalities, ranging from aromatherapy to guided imagery training, are paid for largely out-of-pocket.10
Dr. Rakel notes that the delivery of integrative medicine services at UW entails conversations with patients about out-of-pocket payments. “It can pose a barrier to the clinician-patient relationship if you give them acupuncture to help with their chemotherapy-induced nausea and then ask for their credit card,” he says.
Hospitalist Preparation
Most complementary therapies are currently offered on an outpatient basis. Because of this trend, and because they deal with acute conditions, hospitalists are less likely to be involved with complementary or integrative medicine services, says Beth Israel Deaconess Medical Center hospitalist Andrew C. Ahn, MD, MPH. But that’s not to say complementary medicine is something hospitalists should ignore; patients arrive at the hospital with CAM regimens in tow. It’s the No. 1 reason, Dr. Ahn says, hospitalists should be knowledgeable and exposed to CAM therapies.
Physicians must understand patient patterns and preferences regarding allopathic and complementary medicine, says Sita Ananth, MHA, director of knowledge services and optimal healing environments at the Samueli Institute in Alexandria, Va., and author of the 2007 AHA report. She points to a 2006 survey conducted by AARP and NCCAM that found almost 70% of respondents did not tell their physicians about their complementary medicine approaches. These patients are within the age range most likely to be cared for by hospitalists, and failure to communicate about complementary treatment, such as supplemental vitamin use, could lead to safety issues. Moreover, without complete disclosure, the patient-physician relationship might not be as open as possible, Dr. Ananth says.
Many acute-care hospitalists do not have formal dietary supplement policies, and less than half of U.S. children’s hospitals require documentation of a check for drug or dietary supplement interaction.11,12 As a safety issue, it is always incumbent on hospitalists, says Dr. Li, to ask about any supplements or therapies patients are trying on their own as part of the history and physical examination. The policy at Memorial Sloan-Kettering Cancer Center, Dr. Cassileth says, is that patients on chemotherapy or who are undergoing radiation or facing surgery must avoid herbal dietary supplements.
Beyond Safety
Dr. Bertisch advises hospitalists to pose questions about complementary therapies in an open manner, avoiding antagonistic discussions. “Even when I disagree, I try to guide them to issues about safety and nonsafety, and coax in my concerns,” she says. “The most challenging part about complementary medicine is that patients’ beliefs in these therapies may be so strong that even if the doctor says it won’t work, that will not necessarily change that belief.” A 2001 study in the Archives of Internal Medicine revealed that 70% of respondents would continue to take supplements even if a major study or their physician told them they didn’t work.13
The attraction to complementary medicine often reflects patients’ preferences for a holistic approach to health, says Dr. Ahn, or it may emanate from traditions carried with them from their country of origin. “Once you do understand their reasons for using CAM, then the patient-physician relationship can be significantly strengthened,” he says. With nearly two-thirds of Americans using some form of CAM, hospitalists need to engage in this dialogue.
Dr. Rakel agrees understanding patient culture is vital to uncovering useful information. “Most clinicians would agree that if we can match a therapy to the patient culture and belief system, we are more likely to get buy-in from the patient,” he says.
Dr. Mehta also is a clinical instructor of medicine at Harvard Medical School. He teaches his residents to educate themselves about credentialing, certification, and licensure of complementary providers. He also asks them to maintain an open mind. He says the most important preparation for hospitalists right now is to help educate their patients to be more proactive in their own healthcare. “An engaged patient,” he says, “is better than a disengaged patient.” TH
Gretchen Henkel is a freelance writer based in California.
References
- Deng G, Cassileth BR, Yeung KS. Complementary therapies for cancer-related symptoms. J Support Oncol. 2004;2(5):419-426.
- Kahn ST, Johnstone PA. Management of xerostomia related to radiotherapy for head and neck cancer. Oncology. 2005;19(14):1827-1832.
- Barnes PM, Powell-Griner E, McFann K, Nahin RL. Complementary and alternative medicine use among adults: United States, 2002. Adv Data. 2004;27(343):1-19.
- Eisenberg DM, Davis RB, Ettner SL, et al. Trends in alternative medicine use in the United States, 1990-1997: results of a follow-up national survey. JAMA. 1998;280(18):1569-1575.
- Committee on the Use of Complementary and Alternative Medicine by the American Public. Complementary and Alternative Medicine in the United States. Washington, D.C: National Academies Press; 2005.
- Ananth S. 2007 Health Forum/AHA Complementary and Alternative Medicine Survey of Hospitals. Health Forum LLC. 2008.
- Bent S, Kane C, Shinohara K, et al. Saw palmetto for benign prostatic hyperplasia. N Engl J Med. 2006;354(6):557-566.
- Bauer BA. The herbal hospitalist. The Hospitalist. 2006;10(2);16-17.
- Ananth S. Applying integrative healthcare. Explore. 2009;5(2):119-120.
- Eisenberg DM, Kessler RC, Foster C, Norlock FE, Calkins DR, Delbanco TL. Unconventional medicine in the United States. Prevalence, costs, and patterns of use. N Engl J Med. 1993;328:246-52
- Bassie KL, Witmer DR, Pinto B, Bush C, Clark J, Deffenbaugh J Jr. National survey of dietary supplement policies in acute care facilities. Am J Health Syst Pharm. 2006;63(1):65-70.
- Gardiner P, Phillips RS, Kemper KJ, Legedza A, Henlon S, Woolf AD. Dietary supplements: inpatient policies in US children’s hospitals. Pediatrics. 2008;121(4):e775-781.
- Blendon RJ, DesRoches CM, Benson JM, Brodie M, Altman DE. Americans’ views on the use and regulation of dietary supplements. Arch Intern Med. 2001;161(6):805-810.
Top Image Source: TETRA IMAGES
Despite intravenous medication, a young boy in status epilepticus had the pediatric ICU team at the University of Wisconsin School of Medicine and Public Health in Madison stumped. The team called for a consult with the Integrative Medicine Program, which works with licensed acupuncturists and has been affiliated with the department of family medicine since 2001. Acupuncture’s efficacy in this setting has not been validated, but it has been shown to ease chemotherapy-induced nausea and vomiting, as well as radiation-induced xerostomia.1,2
Following several treatments by a licensed acupuncturist and continued conventional care, the boy’s seizures subsided and he was transitioned to the medical floor. Did the acupuncture contribute to bringing the seizures under control? “I can’t say that it was the acupuncture—it was probably a function of all the therapies working together,” says David P. Rakel, MD, assistant professor and director of UW’s Integrative Medicine Program.
The UW case illustrates both current trends and the constant conundrum that surrounds hospital-based complementary medicine: Complementary and alternative medicine’s use is increasing in some U.S. hospitals, yet the existing research evidence for the efficacy of its multiple modalities is decidedly mixed.
Even if your hospital does not offer complementary and alternative medicine (CAM), your patients are using CAM at ever-increasing rates. In 1993, 34% of Americans reported using some type of CAM (e.g., supplements, massage therapy, prayer, and so on). That number has almost doubled to 62%.3 Americans spend $47 billion a year—of their own money—for CAM therapies, chiropractors, acupuncturists, and massage therapists. And older patients with chronic conditions—the kind of patient hospitalists are most familiar with—tend to try CAM more than younger patients.4
These trends can directly affect hospitalists’ treatment decisions, but they also play a part in how you establish communication and trust with your patients, and how you keep your patients safe from adverse drug interactions. According to the National Academy of Sciences, in order to effectively counsel patients and ensure high-quality comprehensive care, conventional professionals need more CAM-related education.5
—Suzanne Bertisch, MD, MPH, fellow, Harvard Medical School’s Osher Research Center
Complementary Medicine: Online Resources
- National Center for Complementary and Alternative Medicine: http://nccam.nih.gov
- Integrative Medicine Service at Memorial Sloan-Kettering Cancer Center’s About Herbs: www.mskcc.org/mskcc/html/11570.cfm
- Natural Standard: www.naturalstandard.com
- The M.D. Anderson Cancer Center’s Complementary/Integrative Medicine Education Resources: www.mdanderson.org/departments/CIMER
What Trends Show
In 2007, according to the American Hospital Association, 20.8% of community hospitals offered some type of care or treatment not based on traditional Western allopathic medicine. That’s up from 8.6% of reporting hospitals that offered those services in 1998.
The 1990s saw rapid growth of integrative medicine centers at major research institutions, and the majority of U.S. cancer centers now offer some form of complementary therapy, says Barrie R. Cassileth, MS, PhD, the Laurance S. Rockefeller Chair in Integrative Medicine and chief of the Integrative Medicine Service at Memorial Sloan-Kettering Cancer Center in New York City.
The 2007 Health Forum/AHA Complementary and Alternative Medicine Survey of Hospitals reported that complementary programs are more common in urban rather than rural hospitals; services vary by hospital size (see Figure 2, above); and the top six modalities offered on an inpatient basis are pet therapy, massage therapy, music/art therapy, guided imagery, acupuncture, and reiki (see “Glossary of Complementary Terms,” above). Eighty-four percent of hospitals offer complementary services due to patient demand, the survey showed.
Joseph Ming-Wah Li, MD, FHM, SHM board member and assistant professor of medicine at Harvard Medical School and director of the hospital medicine program and associate chief of the division of general medicine and primary care at Beth Israel Deaconess Medical Center in Boston, doesn’t see a problem with modalities that can make his patients feel better. Patients at his hospital have access to pet therapy, massage, and acupuncture. “I don’t think these modalities hurt our patients, and there is very little downside, except for potential cost,” says Dr. Li, an SHM board member. “What’s not clear is whether these therapies work or not.”
What’s in a Name?
Numerous therapies and modalities crowd under the CAM umbrella, but most experts classify “complementary” modalities as those used in conjunction with conventional medicine to mitigate symptoms of disease or treatment, whereas “alternative” connotes therapies claiming to treat or cure the underlying disease. Some harmful, dangerous, and dishonest practices fall into the “alternative” category, such as Hulda Clark’s “Zapper” device, which was promoted as a cure for liver flukes, something she says cause everything from diabetes to heart disease. (For more on questionable practices, visit www.quackwatch.com or the National Council Against Health Fraud’s Web site at www.ncahf.org.)
The National Institutes of Health’s National Center for Complementary and Alternative Medicine (NCCAM) defines CAM as a group of “diverse medical and health care systems, practices, and products that are not presently considered to be part of conventional medicine.” Dr. Cassileth says the conflation of “complementary and alternative” into one neat acronym—CAM—causes confusion among patients and medical professionals. NCCAM will be changing its name soon, she says, to the National Center for Integrative Medicine, emphasizing the use of adjunctive modalities along with conventional medical treatments.
Hospitalist Suzanne Bertisch, MD, MPH, recently completed a research fellowship at Harvard Medical School’s Osher Research Center. She explains that integrative medicine uses a macro model of health, claiming a middle ground between the traditional, allopathic model of treating disease.
All Kinds of Evidence
Twenty years of complementary medicine research has yielded some information about safety—namely, what works and what doesn’t. For example, saw palmetto has not panned out as an effective treatment for benign prostatic hyperplasia; St. John’s wort, useful for mild depression, interferes with many medications, including cyclosporine and warfarin, and should be avoided at least five days prior to surgery.7,8
Since NCCAM’s inception in October 1998, its research portfolio has stirred debate in the scientific community. Part of the disagreement stems from the difficulty of fitting multidimensional interventions, some of which are provider-dependent (e.g., massage or acupuncture), into the gold standard of the randomized, double-blind, placebo-controlled trial, explains Darshan Mehta, MD, MPH, associate director of medical education at the Benson-Henry Institute for Mind Body Medicine at Massachusetts General Hospital in Boston. The manner in which the effectiveness of integrative techniques is assessed requires a higher sophistication of systems research, Dr. Mehta says.
“The way we construe evidence needs to change,” she adds.
Likely to Expand
Most private health plans do not cover complementary services, although Medicare and numerous insurance plans will reimburse treatment in conjunction with physical therapy (e.g., massage) in the outpatient setting. Twenty-three states cover chiropractic care under Medicaid, and Medicare has begun to assess the cost-effectiveness of including acupuncture—especially for postoperative and chemotherapy-associated nausea and vomiting—in its benefits package.9 Other modalities, ranging from aromatherapy to guided imagery training, are paid for largely out-of-pocket.10
Dr. Rakel notes that the delivery of integrative medicine services at UW entails conversations with patients about out-of-pocket payments. “It can pose a barrier to the clinician-patient relationship if you give them acupuncture to help with their chemotherapy-induced nausea and then ask for their credit card,” he says.
Hospitalist Preparation
Most complementary therapies are currently offered on an outpatient basis. Because of this trend, and because they deal with acute conditions, hospitalists are less likely to be involved with complementary or integrative medicine services, says Beth Israel Deaconess Medical Center hospitalist Andrew C. Ahn, MD, MPH. But that’s not to say complementary medicine is something hospitalists should ignore; patients arrive at the hospital with CAM regimens in tow. It’s the No. 1 reason, Dr. Ahn says, hospitalists should be knowledgeable and exposed to CAM therapies.
Physicians must understand patient patterns and preferences regarding allopathic and complementary medicine, says Sita Ananth, MHA, director of knowledge services and optimal healing environments at the Samueli Institute in Alexandria, Va., and author of the 2007 AHA report. She points to a 2006 survey conducted by AARP and NCCAM that found almost 70% of respondents did not tell their physicians about their complementary medicine approaches. These patients are within the age range most likely to be cared for by hospitalists, and failure to communicate about complementary treatment, such as supplemental vitamin use, could lead to safety issues. Moreover, without complete disclosure, the patient-physician relationship might not be as open as possible, Dr. Ananth says.
Many acute-care hospitalists do not have formal dietary supplement policies, and less than half of U.S. children’s hospitals require documentation of a check for drug or dietary supplement interaction.11,12 As a safety issue, it is always incumbent on hospitalists, says Dr. Li, to ask about any supplements or therapies patients are trying on their own as part of the history and physical examination. The policy at Memorial Sloan-Kettering Cancer Center, Dr. Cassileth says, is that patients on chemotherapy or who are undergoing radiation or facing surgery must avoid herbal dietary supplements.
Beyond Safety
Dr. Bertisch advises hospitalists to pose questions about complementary therapies in an open manner, avoiding antagonistic discussions. “Even when I disagree, I try to guide them to issues about safety and nonsafety, and coax in my concerns,” she says. “The most challenging part about complementary medicine is that patients’ beliefs in these therapies may be so strong that even if the doctor says it won’t work, that will not necessarily change that belief.” A 2001 study in the Archives of Internal Medicine revealed that 70% of respondents would continue to take supplements even if a major study or their physician told them they didn’t work.13
The attraction to complementary medicine often reflects patients’ preferences for a holistic approach to health, says Dr. Ahn, or it may emanate from traditions carried with them from their country of origin. “Once you do understand their reasons for using CAM, then the patient-physician relationship can be significantly strengthened,” he says. With nearly two-thirds of Americans using some form of CAM, hospitalists need to engage in this dialogue.
Dr. Rakel agrees understanding patient culture is vital to uncovering useful information. “Most clinicians would agree that if we can match a therapy to the patient culture and belief system, we are more likely to get buy-in from the patient,” he says.
Dr. Mehta also is a clinical instructor of medicine at Harvard Medical School. He teaches his residents to educate themselves about credentialing, certification, and licensure of complementary providers. He also asks them to maintain an open mind. He says the most important preparation for hospitalists right now is to help educate their patients to be more proactive in their own healthcare. “An engaged patient,” he says, “is better than a disengaged patient.” TH
Gretchen Henkel is a freelance writer based in California.
References
- Deng G, Cassileth BR, Yeung KS. Complementary therapies for cancer-related symptoms. J Support Oncol. 2004;2(5):419-426.
- Kahn ST, Johnstone PA. Management of xerostomia related to radiotherapy for head and neck cancer. Oncology. 2005;19(14):1827-1832.
- Barnes PM, Powell-Griner E, McFann K, Nahin RL. Complementary and alternative medicine use among adults: United States, 2002. Adv Data. 2004;27(343):1-19.
- Eisenberg DM, Davis RB, Ettner SL, et al. Trends in alternative medicine use in the United States, 1990-1997: results of a follow-up national survey. JAMA. 1998;280(18):1569-1575.
- Committee on the Use of Complementary and Alternative Medicine by the American Public. Complementary and Alternative Medicine in the United States. Washington, D.C: National Academies Press; 2005.
- Ananth S. 2007 Health Forum/AHA Complementary and Alternative Medicine Survey of Hospitals. Health Forum LLC. 2008.
- Bent S, Kane C, Shinohara K, et al. Saw palmetto for benign prostatic hyperplasia. N Engl J Med. 2006;354(6):557-566.
- Bauer BA. The herbal hospitalist. The Hospitalist. 2006;10(2);16-17.
- Ananth S. Applying integrative healthcare. Explore. 2009;5(2):119-120.
- Eisenberg DM, Kessler RC, Foster C, Norlock FE, Calkins DR, Delbanco TL. Unconventional medicine in the United States. Prevalence, costs, and patterns of use. N Engl J Med. 1993;328:246-52
- Bassie KL, Witmer DR, Pinto B, Bush C, Clark J, Deffenbaugh J Jr. National survey of dietary supplement policies in acute care facilities. Am J Health Syst Pharm. 2006;63(1):65-70.
- Gardiner P, Phillips RS, Kemper KJ, Legedza A, Henlon S, Woolf AD. Dietary supplements: inpatient policies in US children’s hospitals. Pediatrics. 2008;121(4):e775-781.
- Blendon RJ, DesRoches CM, Benson JM, Brodie M, Altman DE. Americans’ views on the use and regulation of dietary supplements. Arch Intern Med. 2001;161(6):805-810.
Top Image Source: TETRA IMAGES
Despite intravenous medication, a young boy in status epilepticus had the pediatric ICU team at the University of Wisconsin School of Medicine and Public Health in Madison stumped. The team called for a consult with the Integrative Medicine Program, which works with licensed acupuncturists and has been affiliated with the department of family medicine since 2001. Acupuncture’s efficacy in this setting has not been validated, but it has been shown to ease chemotherapy-induced nausea and vomiting, as well as radiation-induced xerostomia.1,2
Following several treatments by a licensed acupuncturist and continued conventional care, the boy’s seizures subsided and he was transitioned to the medical floor. Did the acupuncture contribute to bringing the seizures under control? “I can’t say that it was the acupuncture—it was probably a function of all the therapies working together,” says David P. Rakel, MD, assistant professor and director of UW’s Integrative Medicine Program.
The UW case illustrates both current trends and the constant conundrum that surrounds hospital-based complementary medicine: Complementary and alternative medicine’s use is increasing in some U.S. hospitals, yet the existing research evidence for the efficacy of its multiple modalities is decidedly mixed.
Even if your hospital does not offer complementary and alternative medicine (CAM), your patients are using CAM at ever-increasing rates. In 1993, 34% of Americans reported using some type of CAM (e.g., supplements, massage therapy, prayer, and so on). That number has almost doubled to 62%.3 Americans spend $47 billion a year—of their own money—for CAM therapies, chiropractors, acupuncturists, and massage therapists. And older patients with chronic conditions—the kind of patient hospitalists are most familiar with—tend to try CAM more than younger patients.4
These trends can directly affect hospitalists’ treatment decisions, but they also play a part in how you establish communication and trust with your patients, and how you keep your patients safe from adverse drug interactions. According to the National Academy of Sciences, in order to effectively counsel patients and ensure high-quality comprehensive care, conventional professionals need more CAM-related education.5
—Suzanne Bertisch, MD, MPH, fellow, Harvard Medical School’s Osher Research Center
Complementary Medicine: Online Resources
- National Center for Complementary and Alternative Medicine: http://nccam.nih.gov
- Integrative Medicine Service at Memorial Sloan-Kettering Cancer Center’s About Herbs: www.mskcc.org/mskcc/html/11570.cfm
- Natural Standard: www.naturalstandard.com
- The M.D. Anderson Cancer Center’s Complementary/Integrative Medicine Education Resources: www.mdanderson.org/departments/CIMER
What Trends Show
In 2007, according to the American Hospital Association, 20.8% of community hospitals offered some type of care or treatment not based on traditional Western allopathic medicine. That’s up from 8.6% of reporting hospitals that offered those services in 1998.
The 1990s saw rapid growth of integrative medicine centers at major research institutions, and the majority of U.S. cancer centers now offer some form of complementary therapy, says Barrie R. Cassileth, MS, PhD, the Laurance S. Rockefeller Chair in Integrative Medicine and chief of the Integrative Medicine Service at Memorial Sloan-Kettering Cancer Center in New York City.
The 2007 Health Forum/AHA Complementary and Alternative Medicine Survey of Hospitals reported that complementary programs are more common in urban rather than rural hospitals; services vary by hospital size (see Figure 2, above); and the top six modalities offered on an inpatient basis are pet therapy, massage therapy, music/art therapy, guided imagery, acupuncture, and reiki (see “Glossary of Complementary Terms,” above). Eighty-four percent of hospitals offer complementary services due to patient demand, the survey showed.
Joseph Ming-Wah Li, MD, FHM, SHM board member and assistant professor of medicine at Harvard Medical School and director of the hospital medicine program and associate chief of the division of general medicine and primary care at Beth Israel Deaconess Medical Center in Boston, doesn’t see a problem with modalities that can make his patients feel better. Patients at his hospital have access to pet therapy, massage, and acupuncture. “I don’t think these modalities hurt our patients, and there is very little downside, except for potential cost,” says Dr. Li, an SHM board member. “What’s not clear is whether these therapies work or not.”
What’s in a Name?
Numerous therapies and modalities crowd under the CAM umbrella, but most experts classify “complementary” modalities as those used in conjunction with conventional medicine to mitigate symptoms of disease or treatment, whereas “alternative” connotes therapies claiming to treat or cure the underlying disease. Some harmful, dangerous, and dishonest practices fall into the “alternative” category, such as Hulda Clark’s “Zapper” device, which was promoted as a cure for liver flukes, something she says cause everything from diabetes to heart disease. (For more on questionable practices, visit www.quackwatch.com or the National Council Against Health Fraud’s Web site at www.ncahf.org.)
The National Institutes of Health’s National Center for Complementary and Alternative Medicine (NCCAM) defines CAM as a group of “diverse medical and health care systems, practices, and products that are not presently considered to be part of conventional medicine.” Dr. Cassileth says the conflation of “complementary and alternative” into one neat acronym—CAM—causes confusion among patients and medical professionals. NCCAM will be changing its name soon, she says, to the National Center for Integrative Medicine, emphasizing the use of adjunctive modalities along with conventional medical treatments.
Hospitalist Suzanne Bertisch, MD, MPH, recently completed a research fellowship at Harvard Medical School’s Osher Research Center. She explains that integrative medicine uses a macro model of health, claiming a middle ground between the traditional, allopathic model of treating disease.
All Kinds of Evidence
Twenty years of complementary medicine research has yielded some information about safety—namely, what works and what doesn’t. For example, saw palmetto has not panned out as an effective treatment for benign prostatic hyperplasia; St. John’s wort, useful for mild depression, interferes with many medications, including cyclosporine and warfarin, and should be avoided at least five days prior to surgery.7,8
Since NCCAM’s inception in October 1998, its research portfolio has stirred debate in the scientific community. Part of the disagreement stems from the difficulty of fitting multidimensional interventions, some of which are provider-dependent (e.g., massage or acupuncture), into the gold standard of the randomized, double-blind, placebo-controlled trial, explains Darshan Mehta, MD, MPH, associate director of medical education at the Benson-Henry Institute for Mind Body Medicine at Massachusetts General Hospital in Boston. The manner in which the effectiveness of integrative techniques is assessed requires a higher sophistication of systems research, Dr. Mehta says.
“The way we construe evidence needs to change,” she adds.
Likely to Expand
Most private health plans do not cover complementary services, although Medicare and numerous insurance plans will reimburse treatment in conjunction with physical therapy (e.g., massage) in the outpatient setting. Twenty-three states cover chiropractic care under Medicaid, and Medicare has begun to assess the cost-effectiveness of including acupuncture—especially for postoperative and chemotherapy-associated nausea and vomiting—in its benefits package.9 Other modalities, ranging from aromatherapy to guided imagery training, are paid for largely out-of-pocket.10
Dr. Rakel notes that the delivery of integrative medicine services at UW entails conversations with patients about out-of-pocket payments. “It can pose a barrier to the clinician-patient relationship if you give them acupuncture to help with their chemotherapy-induced nausea and then ask for their credit card,” he says.
Hospitalist Preparation
Most complementary therapies are currently offered on an outpatient basis. Because of this trend, and because they deal with acute conditions, hospitalists are less likely to be involved with complementary or integrative medicine services, says Beth Israel Deaconess Medical Center hospitalist Andrew C. Ahn, MD, MPH. But that’s not to say complementary medicine is something hospitalists should ignore; patients arrive at the hospital with CAM regimens in tow. It’s the No. 1 reason, Dr. Ahn says, hospitalists should be knowledgeable and exposed to CAM therapies.
Physicians must understand patient patterns and preferences regarding allopathic and complementary medicine, says Sita Ananth, MHA, director of knowledge services and optimal healing environments at the Samueli Institute in Alexandria, Va., and author of the 2007 AHA report. She points to a 2006 survey conducted by AARP and NCCAM that found almost 70% of respondents did not tell their physicians about their complementary medicine approaches. These patients are within the age range most likely to be cared for by hospitalists, and failure to communicate about complementary treatment, such as supplemental vitamin use, could lead to safety issues. Moreover, without complete disclosure, the patient-physician relationship might not be as open as possible, Dr. Ananth says.
Many acute-care hospitalists do not have formal dietary supplement policies, and less than half of U.S. children’s hospitals require documentation of a check for drug or dietary supplement interaction.11,12 As a safety issue, it is always incumbent on hospitalists, says Dr. Li, to ask about any supplements or therapies patients are trying on their own as part of the history and physical examination. The policy at Memorial Sloan-Kettering Cancer Center, Dr. Cassileth says, is that patients on chemotherapy or who are undergoing radiation or facing surgery must avoid herbal dietary supplements.
Beyond Safety
Dr. Bertisch advises hospitalists to pose questions about complementary therapies in an open manner, avoiding antagonistic discussions. “Even when I disagree, I try to guide them to issues about safety and nonsafety, and coax in my concerns,” she says. “The most challenging part about complementary medicine is that patients’ beliefs in these therapies may be so strong that even if the doctor says it won’t work, that will not necessarily change that belief.” A 2001 study in the Archives of Internal Medicine revealed that 70% of respondents would continue to take supplements even if a major study or their physician told them they didn’t work.13
The attraction to complementary medicine often reflects patients’ preferences for a holistic approach to health, says Dr. Ahn, or it may emanate from traditions carried with them from their country of origin. “Once you do understand their reasons for using CAM, then the patient-physician relationship can be significantly strengthened,” he says. With nearly two-thirds of Americans using some form of CAM, hospitalists need to engage in this dialogue.
Dr. Rakel agrees understanding patient culture is vital to uncovering useful information. “Most clinicians would agree that if we can match a therapy to the patient culture and belief system, we are more likely to get buy-in from the patient,” he says.
Dr. Mehta also is a clinical instructor of medicine at Harvard Medical School. He teaches his residents to educate themselves about credentialing, certification, and licensure of complementary providers. He also asks them to maintain an open mind. He says the most important preparation for hospitalists right now is to help educate their patients to be more proactive in their own healthcare. “An engaged patient,” he says, “is better than a disengaged patient.” TH
Gretchen Henkel is a freelance writer based in California.
References
- Deng G, Cassileth BR, Yeung KS. Complementary therapies for cancer-related symptoms. J Support Oncol. 2004;2(5):419-426.
- Kahn ST, Johnstone PA. Management of xerostomia related to radiotherapy for head and neck cancer. Oncology. 2005;19(14):1827-1832.
- Barnes PM, Powell-Griner E, McFann K, Nahin RL. Complementary and alternative medicine use among adults: United States, 2002. Adv Data. 2004;27(343):1-19.
- Eisenberg DM, Davis RB, Ettner SL, et al. Trends in alternative medicine use in the United States, 1990-1997: results of a follow-up national survey. JAMA. 1998;280(18):1569-1575.
- Committee on the Use of Complementary and Alternative Medicine by the American Public. Complementary and Alternative Medicine in the United States. Washington, D.C: National Academies Press; 2005.
- Ananth S. 2007 Health Forum/AHA Complementary and Alternative Medicine Survey of Hospitals. Health Forum LLC. 2008.
- Bent S, Kane C, Shinohara K, et al. Saw palmetto for benign prostatic hyperplasia. N Engl J Med. 2006;354(6):557-566.
- Bauer BA. The herbal hospitalist. The Hospitalist. 2006;10(2);16-17.
- Ananth S. Applying integrative healthcare. Explore. 2009;5(2):119-120.
- Eisenberg DM, Kessler RC, Foster C, Norlock FE, Calkins DR, Delbanco TL. Unconventional medicine in the United States. Prevalence, costs, and patterns of use. N Engl J Med. 1993;328:246-52
- Bassie KL, Witmer DR, Pinto B, Bush C, Clark J, Deffenbaugh J Jr. National survey of dietary supplement policies in acute care facilities. Am J Health Syst Pharm. 2006;63(1):65-70.
- Gardiner P, Phillips RS, Kemper KJ, Legedza A, Henlon S, Woolf AD. Dietary supplements: inpatient policies in US children’s hospitals. Pediatrics. 2008;121(4):e775-781.
- Blendon RJ, DesRoches CM, Benson JM, Brodie M, Altman DE. Americans’ views on the use and regulation of dietary supplements. Arch Intern Med. 2001;161(6):805-810.
Top Image Source: TETRA IMAGES
Step-by-Step Medicine
Evidence-based practice guidelines are key tools to help hospitalists practice high-quality medicine and demonstrate the value of their inpatient care model. Guidelines are designed to produce superior care outcomes and resource utilization efficiencies by encouraging proven medical practices and discouraging ineffective or unproven ones. Yet inefficiencies, variation, and quality gaps persist in medical care—much to the chagrin of policymakers.
Is the answer more guidelines, and better implementation of existing ones?
Research experts and many HM leaders say yes.
In fact, HM is leading the way in an important new area for which there is little uniform guidance: optimal care transitions during patient handoffs. Care transitions are a pivotal time in the patient care process and are replete with avoidable service duplication, poor communication among providers, gaps in care reconciliation, and patient-safety issues.
SHM has joined five other organizations in issuing a Transitions of Care Consensus Policy Statement, which promises more systematic, safe, and efficient patient handoffs.1 SHM also is targeting care-transition improvement in a variety of other venues, all of which can help hospitalists demonstrate more persuasively the value they bring to healthcare delivery.
Guidelines Work
Practice guidelines work, in the sense that they help providers practice in ways consistent with what the best aggregate knowledge and expert opinion says is most effective. The evidence allows physicians to avoid expending scarce resources on ineffective clinical services. Their importance is magnified by the current urgency given to value-based purchasing in healthcare reform. “The right care, for the right patient, at the right time” is the new mantra of payors and policymakers, many of whom are demanding the best and most efficient healthcare delivery at the lowest cost.

“When providers are not providing the right care at the right time to patients, we find that the patient often gets more services … that they didn’t need. That oftentimes exposes them to potential harm and (services) that are wasteful of resources,” says Janet M. Corrigan, PhD, MBA, president and CEO of the National Quality Forum (NQF), a standard-setting organization that convenes national experts to apply “gold standard” endorsement of guidelines developed by professional medical societies and other entities. “Guidelines are a way of synthesizing evidence and translating it into action steps that providers can follow so that they get the best results that we know how to get for their patients.”
Clinicians and healthcare organizations have several sources for guidelines. The Agency for Healthcare Research and Quality (AHRQ) systematically reviews and vets guidelines submitted for inclusion in its National Guideline Clearinghouse (www.guideline.gov), and makes them available for evidence-based clinical decision-making, says Jean Slutsky, director of AHRQ’s Center for Outcomes and Evidence. AHRQ also offers public access to the National Quality Measure Clearinghouse and the Health Care Innovations Exchange, repositories of searchable quality measures and tools relevant to an array of diseases and conditions.
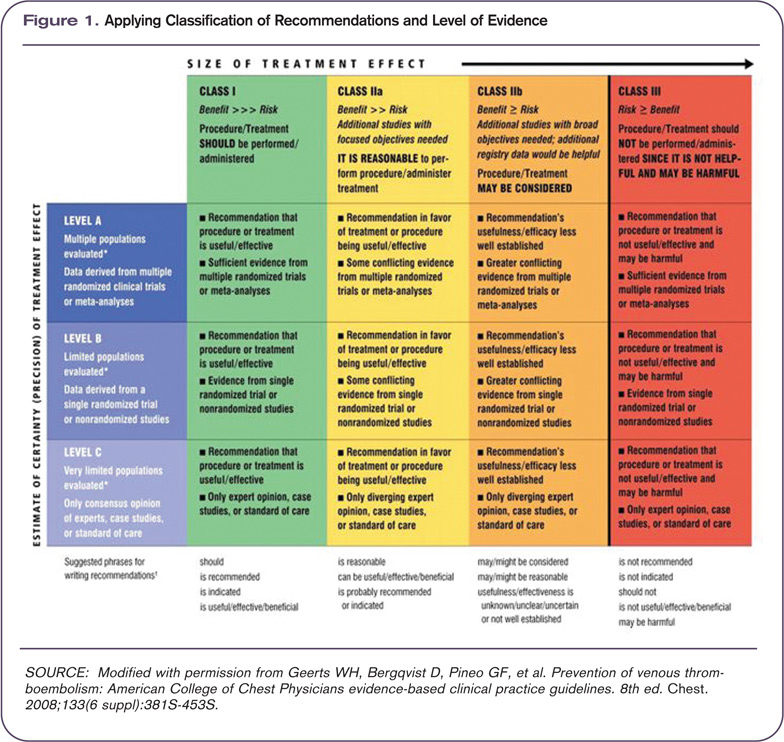
The Institute for Healthcare Improvement (IHI), an independent nonprofit organization, helps frontline physicians implement guidelines, and also helps provider teams decide which guidelines are most appropriate to achieve their desired outcomes, according to Amy E. Boutwell, MD, MPP, IHI’s director of health policy strategy.
Hospitalists use an array of disease-specific practice guidelines from different specialty societies for diagnoses they frequently encounter, such as chest pain, stroke, pneumonia, myocardial infarction, gastrointestinal bleeding, asthma, and chronic obstructive pulmonary disease (COPD). “Most hospitalists want to keep up with the best available evidence,” says Patrick J. Torcson, MD, MMM, FACP, director of hospital medicine at St. Tammany Parish Hospital in Covington, La., and chair of SHM’s Performance and Standards Committee. “The recently updated American College of Cardiology (ACC) and American Heart Association (AHA) guidelines on heart failure are exceptional. The American College of Chest Physicians has an extremely comprehensive set of guidelines on thrombosis, which is the bible for handling anticoagulation.”
Studies are published every month demonstrating that physicians who implement national guidelines at the local level improve such patient outcomes as mortality, length of stay, and time to clinical stability. Dr. Corrigan notes that there are abundant examples of guideline adherence boosting quality outcomes, and cites as a prime example the AHA’s Get With the Guidelines program (www.american heart.org/presenter.jhtml?identifier=1165), which has documented quality gains in coronary artery disease, stroke, and heart failure patients.

—William T. Ford, MD, FHM, section chief of hospital medicine, Temple University Hospital, Philadelphia
Barriers to Acceptance and Adherence
But there are obstacles to guideline adherence, and widespread practice pattern variation remains a huge national problem. Providers in some regions of the country can use twice the resources as their counterparts in other regions and bring no additional benefit to patients (see “Medicare Fee Inspection,” p. 30). The Dartmouth Atlas of Health Care says unwarranted practice variation is responsible for as much as 30% of wasted healthcare spending in the U.S.—a cost that reformers are anxious to eliminate.
The traditional culture of autonomy in the medical profession is perhaps the most difficult and enduring barrier to reducing unjustified practice variation: clinicians don’t automatically follow guidelines, many treat them more as options than as true standards, and organizations do not sufficiently enforce or reward adherence to guidelines, wrote researchers in a special 2005 issue of Health Affairs focusing on guidelines.2
“In an age of mandated cost control and resource limitation under managed care,” the researchers wrote, some physicians still regard practice guidelines as “cookbook medicine” that threatens the use of clinical judgment and encourages treating patients as essentially interchangeable. In the face of that perceived threat, the researchers added, many physicians continue to uphold a traditional view of medicine as an art “in which individual expertise and technique are allowed to shine through and ultimately result in a higher standard of patient care.”
Dr. Corrigan acknowledges the significant obstacles to successful practice guideline implementation:
- Guidelines are developed by various sources, particularly specialty societies, who do not always coordinate their activities. Physicians are left with overlapping and sometimes contradictory guidelines for managing the same disease or condition.
- Guidelines must be maintained and kept current, or physicians will lose confidence and not follow them.
- Guidelines are of varying quality. Some provide clear clinical direction; others are not written in a way that physicians can clearly translate into clinical practice.
- There are significant gaps in the evidence basis for guideline development. Much more comparative effectiveness research needs to be conducted to develop more valid and meaningful guidelines.
- Guidelines must be communicated effectively to physicians, making them available and convenient at the point of clinical care. Electronic health records with user-friendly decision support functions show great promise in “making the right thing the easy thing to do.”
- The fee-for-service payment system encourages greater volume of services, irrespective of guideline recommendations.
Physicians also recognize inherent limitations of guidelines. “Guidelines typically apply across populations. Adding levels of clinical complexity gets further away from a guideline’s applicability. Many physicians will tell you that the patient in front of them is a special case requiring a modification of the protocol,” Dr. Boutwell explains. For example, diabetic management guidelines are based on what is best for a population of diabetics, versus what is best for said hospitalist’s patient who has eight co-morbidities, one of which is diabetes, Boutwell notes. “Guidelines come disease-specific. Patients don’t,” she adds.
Nevertheless, Dr. Boutwell notes, there are robust guidelines and the IHI tries to help front-line physicians and care teams to implement them reliably and effectively.
An obstacle that inhibits hospitalists from implementing guidelines in an optimal fashion “is that we’re not one specialty—we deal with it all—and that complexity can be overwhelming. There is no central repository where all of the guidelines can be found in one place,” according to William T. Ford, MD, FHM, program medical director for Cogent Healthcare and section chief of hospital medicine for Temple University Hospital in Philadelphia.
Make Guidelines Work
Researchers say guidelines are most successful when they are well-supported and uncomplicated, backed by strong leadership and sufficient resources, and are used as “rallying points” to stimulate interdependent and collaborative care among physicians, nurses, pharmacists, equipment suppliers, administrators, and patients.
“Guidelines are really the foundation for determining best practices,” Dr. Torcson says. “There is no shortage of excellent guidelines, or proof that specific interventions do improve outcomes. The key is achieving more uniform implementation. We need tools like pre-printed orders in electronic health records (EHR) to effectively integrate these guidelines into hospitalists’ practice.”
More widespread EHR adoption with user-friendly medical decision-support systems will play a huge role in boosting guideline adoption and effectiveness, says Mary Nix, MS, MT(ASCP)SBB, health science administrator at AHRQ and project officer for the agency’s Center for Outcomes and Evidence.
Dr. Ford says HM groups must evaluate the top 10 to 15 diagnosis-related groups (DRGs) that they see each day (e.g., congestive heart failure, acute kidney failure, pneumonia, cellulitis, or acute coronary syndrome) and come to consensus on which guidelines best address them.
HM groups must then secure buy-in to those guidelines from everyone in the group; from the subspecialists they work with; and from their hospital’s chief medical, financial, and utilization officers.
Care-Transition Guidelines: Opportunity for Hospitalists
A particularly important HM opportunity is improving care transitions. Deficits in communication and information transfer between hospital-based and primary-care physicians (PCPs) are “substantial and ubiquitous,” while delays and omissions are consistently large, and traditional methods of completing and delivering discharge summaries are “suboptimal for communicating timely, accurate, and medically important data to the physicians who will be responsible for follow-up care,” according to a hospitalist-authored Feb. 28, 2007, article in the Journal of the American Medical Association.3 PCPs routinely are not notified about patient admissions or complications during the hospital stay, and some PCPs fail to provide sufficient information to hospitalists at admission, fail to visit or call hospitalized patients, or fail to participate in discharge planning, the study’s researchers noted. For patients with chronic illnesses and frequent hospitalization, those deficits are multiplied, making completeness of information handoffs particularly important.
Because patient handoffs have notoriously been fraught with miscommunication and poor information exchange between providers, adopting a professional consensus on what constitutes the best, safest, and most effective activities during these handoffs is sorely needed.
“Care-transition guidelines can have tremendous power because they affect every hospital patient—each of whom experiences care transitions,” says Rusty Holman, MD, FHM, chief operating officer of Brentwood, Tenn.-based Cogent Healthcare and past president of SHM. “It is an area undergoing rapid development, evolution, and discovery, and hospitalists have positioned themselves as leaders and owners of this particular scenario.”

As care-transition guidelines emerge and mature, Holman thinks they eventually will be tied to value-based healthcare purchasing programs that affect hospitalists’ reimbursement equations and further boost incentives to follow those guidelines. A prime example: Medicare calculated it could save $12 billion annually by reducing preventable 30-day hospital readmissions and will soon stop paying for them. Perhaps 3% to 5% of a hospital’s DRG reimbursement will be at risk under Medicare’s proposal, Dr. Torcson notes.
“Hospitals are going to be much more motivated to build systems and engage physicians, especially hospitalists, to lower readmission rates. Hospitalists will be focusing more and more on how care-transition process improvements can lower those rates,” Dr. Holman says. “That’s a huge opportunity for hospitalists to make a business case for the value they bring to their institutions, and will further justify the financial support they already receive.”
Dr. Ford is more cautious in his appraisal of the financial rewards of better guideline implementation. “We do not capture that much revenue per patient, and even a length-of-stay reduction is difficult for a hospital’s CFO to extrapolate how much money hospitalists save,” he says. “I don’t think hospitalists will be paid more, even if they save the hospital money. You’re just doing your job, but you’re going to keep your job, and you’ll have an enormous bargaining chip when renegotiating contracts with hospitals.”
Still, a prevented readmission might mean a bed for a revenue-generating elective surgery, something that adds to the reward equation.

—Patrick Torcson, MD, MMM, FACP, director of hospital medicine, St. Tammany Parish Hospital, Covington, La., SHM Performance and Standards Committee chair
Transition Evolution
SHM and other sources offer physicians and hospitals expert assistance in implementing care-transition guidelines (see “Care-Transition Guidance,” p. 7). The transitions-of-care policy statement jointly issued by the SHM and five other specialty societies further demonstrates that hospitalists play a key leadership role on this front.1
The policy statement emerged from a multi-stakeholder consensus conference convened by SHM, the American College of Physicians (ACP), and the Society of General Internal Medicine, which was attended by more than 30 medical specialty societies, governmental agencies, and performance measure developers. Participants focused on what standard pieces of information should be exchanged among providers during inpatient to outpatient transitions, and they issued a set of standards for improving those transitions (see “Managing Transitions in Care Between the Inpatient and Outpatient Settings,” p. 7).
“This consensus statement has enormous significance,” Dr. Ford says. “We’re finally shedding light on how to tackle patient handoff and hospital readmission issues, and we as a specialty have to take on care-transition improvement as our mantra. If we were to solve just that one piece, we can more easily start implementing other clinical guidelines. Care-transition guidelines are a fundamental tool to build consensus within your own group and with other clinicians in a team approach.”
Dr. Corrigan applauds the physician groups for publishing the transitions-of-care statement and encourages the societies to work together to “take it to the next step, which is to develop the measures and get them endorsed through the NQF process.”
SHM members are participating in workgroups convened by the NQF to identify standardized performance measures and to develop action plans over the next few months for several national priority areas—one of which is care coordination. “We have a ways to go to achieve better patient handoffs and information exchange between hospitals and other settings in the community. Hospitalists can drive the development of those guidelines and protocols,” Dr. Corrigan says. TH
Christopher Guadagnino, PhD, is a freelance medical writer based in Pennsylvania.
References
- Kripalani S, LeFevre F, Phillips CO, Williams MV; Basaviah P, Baker DW. Deficits in communication and information transfer between hospital-based and primary care physicians: implications for patient safety and continuity of care. JAMA. 2007;297:831-841.
- Timmermans S, Mauck A. The promises and pitfalls of evidence-based medicine. Health Affairs. 2005; 24(1):18-28.
- Snow V, Beck D, Budnitz T, et al. Transitions of care consensus policy statement: American College of Physicians, Society of General Internal Medicine, Society of Hospital Medicine, American Geriatrics Society, American College of Emergency Physicians, Society of Academic Emergency Medicine. J Hosp Med. 2009: 4(6)364-370.
Top Image Source: GOLDEN PIXELS LLC/ALAMY
Managing Transitions of Care Between the Inpatient and Outpatient Settings

The following are joint recommendations from SHM, ACP, SGIM, AGS, ACEP, and SAEM, based upon a multi-stakeholder consensus conference in July 2007 and published in the July/August Journal of Hospital Medicine (http://onlinelibrary.wiley.com/doi/10.1002/jhm.510/full):
- Communication and information exchange between the sending and receiving provider should be timely, as dictated by clinical presentation and urgency of follow-up care required.
- The transition record should always include at least these data elements: principal diagnosis, medication list, contact information of the transferring physician, patient’s cognitive status, test results or pending results. An ideal transition record would add six more elements.
- All communications need to be secure, private, HIPAA-compliant, and accessible to patients and their providers.
- Communities need to develop standard data transfer forms, with the ability to modify information as a patient’s condition changes.
- The sending provider maintains responsibility for the care of the patient until the receiving provider confirms that the transfer is complete. The sending provider should be available to clarify issues of care, and the patient should be able to identify the responsible provider.
- Information transfer should be timely, as determined by transition setting, patient circumstances, level of acuity, and clear transition responsibility.
- Medical institutions must adopt national standards and establish processes to promote effective transitions of care.
- Standardized and evidence-based metrics related to these standards should be used for monitoring and improving transitions.
Evidence-based practice guidelines are key tools to help hospitalists practice high-quality medicine and demonstrate the value of their inpatient care model. Guidelines are designed to produce superior care outcomes and resource utilization efficiencies by encouraging proven medical practices and discouraging ineffective or unproven ones. Yet inefficiencies, variation, and quality gaps persist in medical care—much to the chagrin of policymakers.
Is the answer more guidelines, and better implementation of existing ones?
Research experts and many HM leaders say yes.
In fact, HM is leading the way in an important new area for which there is little uniform guidance: optimal care transitions during patient handoffs. Care transitions are a pivotal time in the patient care process and are replete with avoidable service duplication, poor communication among providers, gaps in care reconciliation, and patient-safety issues.
SHM has joined five other organizations in issuing a Transitions of Care Consensus Policy Statement, which promises more systematic, safe, and efficient patient handoffs.1 SHM also is targeting care-transition improvement in a variety of other venues, all of which can help hospitalists demonstrate more persuasively the value they bring to healthcare delivery.
Guidelines Work
Practice guidelines work, in the sense that they help providers practice in ways consistent with what the best aggregate knowledge and expert opinion says is most effective. The evidence allows physicians to avoid expending scarce resources on ineffective clinical services. Their importance is magnified by the current urgency given to value-based purchasing in healthcare reform. “The right care, for the right patient, at the right time” is the new mantra of payors and policymakers, many of whom are demanding the best and most efficient healthcare delivery at the lowest cost.
“When providers are not providing the right care at the right time to patients, we find that the patient often gets more services … that they didn’t need. That oftentimes exposes them to potential harm and (services) that are wasteful of resources,” says Janet M. Corrigan, PhD, MBA, president and CEO of the National Quality Forum (NQF), a standard-setting organization that convenes national experts to apply “gold standard” endorsement of guidelines developed by professional medical societies and other entities. “Guidelines are a way of synthesizing evidence and translating it into action steps that providers can follow so that they get the best results that we know how to get for their patients.”
Clinicians and healthcare organizations have several sources for guidelines. The Agency for Healthcare Research and Quality (AHRQ) systematically reviews and vets guidelines submitted for inclusion in its National Guideline Clearinghouse (www.guideline.gov), and makes them available for evidence-based clinical decision-making, says Jean Slutsky, director of AHRQ’s Center for Outcomes and Evidence. AHRQ also offers public access to the National Quality Measure Clearinghouse and the Health Care Innovations Exchange, repositories of searchable quality measures and tools relevant to an array of diseases and conditions.
The Institute for Healthcare Improvement (IHI), an independent nonprofit organization, helps frontline physicians implement guidelines, and also helps provider teams decide which guidelines are most appropriate to achieve their desired outcomes, according to Amy E. Boutwell, MD, MPP, IHI’s director of health policy strategy.
Hospitalists use an array of disease-specific practice guidelines from different specialty societies for diagnoses they frequently encounter, such as chest pain, stroke, pneumonia, myocardial infarction, gastrointestinal bleeding, asthma, and chronic obstructive pulmonary disease (COPD). “Most hospitalists want to keep up with the best available evidence,” says Patrick J. Torcson, MD, MMM, FACP, director of hospital medicine at St. Tammany Parish Hospital in Covington, La., and chair of SHM’s Performance and Standards Committee. “The recently updated American College of Cardiology (ACC) and American Heart Association (AHA) guidelines on heart failure are exceptional. The American College of Chest Physicians has an extremely comprehensive set of guidelines on thrombosis, which is the bible for handling anticoagulation.”
Studies are published every month demonstrating that physicians who implement national guidelines at the local level improve such patient outcomes as mortality, length of stay, and time to clinical stability. Dr. Corrigan notes that there are abundant examples of guideline adherence boosting quality outcomes, and cites as a prime example the AHA’s Get With the Guidelines program (www.american heart.org/presenter.jhtml?identifier=1165), which has documented quality gains in coronary artery disease, stroke, and heart failure patients.
—William T. Ford, MD, FHM, section chief of hospital medicine, Temple University Hospital, Philadelphia
Barriers to Acceptance and Adherence
But there are obstacles to guideline adherence, and widespread practice pattern variation remains a huge national problem. Providers in some regions of the country can use twice the resources as their counterparts in other regions and bring no additional benefit to patients (see “Medicare Fee Inspection,” p. 30). The Dartmouth Atlas of Health Care says unwarranted practice variation is responsible for as much as 30% of wasted healthcare spending in the U.S.—a cost that reformers are anxious to eliminate.
The traditional culture of autonomy in the medical profession is perhaps the most difficult and enduring barrier to reducing unjustified practice variation: clinicians don’t automatically follow guidelines, many treat them more as options than as true standards, and organizations do not sufficiently enforce or reward adherence to guidelines, wrote researchers in a special 2005 issue of Health Affairs focusing on guidelines.2
“In an age of mandated cost control and resource limitation under managed care,” the researchers wrote, some physicians still regard practice guidelines as “cookbook medicine” that threatens the use of clinical judgment and encourages treating patients as essentially interchangeable. In the face of that perceived threat, the researchers added, many physicians continue to uphold a traditional view of medicine as an art “in which individual expertise and technique are allowed to shine through and ultimately result in a higher standard of patient care.”
Dr. Corrigan acknowledges the significant obstacles to successful practice guideline implementation:
- Guidelines are developed by various sources, particularly specialty societies, who do not always coordinate their activities. Physicians are left with overlapping and sometimes contradictory guidelines for managing the same disease or condition.
- Guidelines must be maintained and kept current, or physicians will lose confidence and not follow them.
- Guidelines are of varying quality. Some provide clear clinical direction; others are not written in a way that physicians can clearly translate into clinical practice.
- There are significant gaps in the evidence basis for guideline development. Much more comparative effectiveness research needs to be conducted to develop more valid and meaningful guidelines.
- Guidelines must be communicated effectively to physicians, making them available and convenient at the point of clinical care. Electronic health records with user-friendly decision support functions show great promise in “making the right thing the easy thing to do.”
- The fee-for-service payment system encourages greater volume of services, irrespective of guideline recommendations.
Physicians also recognize inherent limitations of guidelines. “Guidelines typically apply across populations. Adding levels of clinical complexity gets further away from a guideline’s applicability. Many physicians will tell you that the patient in front of them is a special case requiring a modification of the protocol,” Dr. Boutwell explains. For example, diabetic management guidelines are based on what is best for a population of diabetics, versus what is best for said hospitalist’s patient who has eight co-morbidities, one of which is diabetes, Boutwell notes. “Guidelines come disease-specific. Patients don’t,” she adds.
Nevertheless, Dr. Boutwell notes, there are robust guidelines and the IHI tries to help front-line physicians and care teams to implement them reliably and effectively.
An obstacle that inhibits hospitalists from implementing guidelines in an optimal fashion “is that we’re not one specialty—we deal with it all—and that complexity can be overwhelming. There is no central repository where all of the guidelines can be found in one place,” according to William T. Ford, MD, FHM, program medical director for Cogent Healthcare and section chief of hospital medicine for Temple University Hospital in Philadelphia.
Make Guidelines Work
Researchers say guidelines are most successful when they are well-supported and uncomplicated, backed by strong leadership and sufficient resources, and are used as “rallying points” to stimulate interdependent and collaborative care among physicians, nurses, pharmacists, equipment suppliers, administrators, and patients.
“Guidelines are really the foundation for determining best practices,” Dr. Torcson says. “There is no shortage of excellent guidelines, or proof that specific interventions do improve outcomes. The key is achieving more uniform implementation. We need tools like pre-printed orders in electronic health records (EHR) to effectively integrate these guidelines into hospitalists’ practice.”
More widespread EHR adoption with user-friendly medical decision-support systems will play a huge role in boosting guideline adoption and effectiveness, says Mary Nix, MS, MT(ASCP)SBB, health science administrator at AHRQ and project officer for the agency’s Center for Outcomes and Evidence.
Dr. Ford says HM groups must evaluate the top 10 to 15 diagnosis-related groups (DRGs) that they see each day (e.g., congestive heart failure, acute kidney failure, pneumonia, cellulitis, or acute coronary syndrome) and come to consensus on which guidelines best address them.
HM groups must then secure buy-in to those guidelines from everyone in the group; from the subspecialists they work with; and from their hospital’s chief medical, financial, and utilization officers.
Care-Transition Guidelines: Opportunity for Hospitalists
A particularly important HM opportunity is improving care transitions. Deficits in communication and information transfer between hospital-based and primary-care physicians (PCPs) are “substantial and ubiquitous,” while delays and omissions are consistently large, and traditional methods of completing and delivering discharge summaries are “suboptimal for communicating timely, accurate, and medically important data to the physicians who will be responsible for follow-up care,” according to a hospitalist-authored Feb. 28, 2007, article in the Journal of the American Medical Association.3 PCPs routinely are not notified about patient admissions or complications during the hospital stay, and some PCPs fail to provide sufficient information to hospitalists at admission, fail to visit or call hospitalized patients, or fail to participate in discharge planning, the study’s researchers noted. For patients with chronic illnesses and frequent hospitalization, those deficits are multiplied, making completeness of information handoffs particularly important.
Because patient handoffs have notoriously been fraught with miscommunication and poor information exchange between providers, adopting a professional consensus on what constitutes the best, safest, and most effective activities during these handoffs is sorely needed.
“Care-transition guidelines can have tremendous power because they affect every hospital patient—each of whom experiences care transitions,” says Rusty Holman, MD, FHM, chief operating officer of Brentwood, Tenn.-based Cogent Healthcare and past president of SHM. “It is an area undergoing rapid development, evolution, and discovery, and hospitalists have positioned themselves as leaders and owners of this particular scenario.”
As care-transition guidelines emerge and mature, Holman thinks they eventually will be tied to value-based healthcare purchasing programs that affect hospitalists’ reimbursement equations and further boost incentives to follow those guidelines. A prime example: Medicare calculated it could save $12 billion annually by reducing preventable 30-day hospital readmissions and will soon stop paying for them. Perhaps 3% to 5% of a hospital’s DRG reimbursement will be at risk under Medicare’s proposal, Dr. Torcson notes.
“Hospitals are going to be much more motivated to build systems and engage physicians, especially hospitalists, to lower readmission rates. Hospitalists will be focusing more and more on how care-transition process improvements can lower those rates,” Dr. Holman says. “That’s a huge opportunity for hospitalists to make a business case for the value they bring to their institutions, and will further justify the financial support they already receive.”
Dr. Ford is more cautious in his appraisal of the financial rewards of better guideline implementation. “We do not capture that much revenue per patient, and even a length-of-stay reduction is difficult for a hospital’s CFO to extrapolate how much money hospitalists save,” he says. “I don’t think hospitalists will be paid more, even if they save the hospital money. You’re just doing your job, but you’re going to keep your job, and you’ll have an enormous bargaining chip when renegotiating contracts with hospitals.”
Still, a prevented readmission might mean a bed for a revenue-generating elective surgery, something that adds to the reward equation.
—Patrick Torcson, MD, MMM, FACP, director of hospital medicine, St. Tammany Parish Hospital, Covington, La., SHM Performance and Standards Committee chair
Transition Evolution
SHM and other sources offer physicians and hospitals expert assistance in implementing care-transition guidelines (see “Care-Transition Guidance,” p. 7). The transitions-of-care policy statement jointly issued by the SHM and five other specialty societies further demonstrates that hospitalists play a key leadership role on this front.1
The policy statement emerged from a multi-stakeholder consensus conference convened by SHM, the American College of Physicians (ACP), and the Society of General Internal Medicine, which was attended by more than 30 medical specialty societies, governmental agencies, and performance measure developers. Participants focused on what standard pieces of information should be exchanged among providers during inpatient to outpatient transitions, and they issued a set of standards for improving those transitions (see “Managing Transitions in Care Between the Inpatient and Outpatient Settings,” p. 7).
“This consensus statement has enormous significance,” Dr. Ford says. “We’re finally shedding light on how to tackle patient handoff and hospital readmission issues, and we as a specialty have to take on care-transition improvement as our mantra. If we were to solve just that one piece, we can more easily start implementing other clinical guidelines. Care-transition guidelines are a fundamental tool to build consensus within your own group and with other clinicians in a team approach.”
Dr. Corrigan applauds the physician groups for publishing the transitions-of-care statement and encourages the societies to work together to “take it to the next step, which is to develop the measures and get them endorsed through the NQF process.”
SHM members are participating in workgroups convened by the NQF to identify standardized performance measures and to develop action plans over the next few months for several national priority areas—one of which is care coordination. “We have a ways to go to achieve better patient handoffs and information exchange between hospitals and other settings in the community. Hospitalists can drive the development of those guidelines and protocols,” Dr. Corrigan says. TH
Christopher Guadagnino, PhD, is a freelance medical writer based in Pennsylvania.
References
- Kripalani S, LeFevre F, Phillips CO, Williams MV; Basaviah P, Baker DW. Deficits in communication and information transfer between hospital-based and primary care physicians: implications for patient safety and continuity of care. JAMA. 2007;297:831-841.
- Timmermans S, Mauck A. The promises and pitfalls of evidence-based medicine. Health Affairs. 2005; 24(1):18-28.
- Snow V, Beck D, Budnitz T, et al. Transitions of care consensus policy statement: American College of Physicians, Society of General Internal Medicine, Society of Hospital Medicine, American Geriatrics Society, American College of Emergency Physicians, Society of Academic Emergency Medicine. J Hosp Med. 2009: 4(6)364-370.
Top Image Source: GOLDEN PIXELS LLC/ALAMY
Managing Transitions of Care Between the Inpatient and Outpatient Settings
The following are joint recommendations from SHM, ACP, SGIM, AGS, ACEP, and SAEM, based upon a multi-stakeholder consensus conference in July 2007 and published in the July/August Journal of Hospital Medicine (http://onlinelibrary.wiley.com/doi/10.1002/jhm.510/full):
- Communication and information exchange between the sending and receiving provider should be timely, as dictated by clinical presentation and urgency of follow-up care required.
- The transition record should always include at least these data elements: principal diagnosis, medication list, contact information of the transferring physician, patient’s cognitive status, test results or pending results. An ideal transition record would add six more elements.
- All communications need to be secure, private, HIPAA-compliant, and accessible to patients and their providers.
- Communities need to develop standard data transfer forms, with the ability to modify information as a patient’s condition changes.
- The sending provider maintains responsibility for the care of the patient until the receiving provider confirms that the transfer is complete. The sending provider should be available to clarify issues of care, and the patient should be able to identify the responsible provider.
- Information transfer should be timely, as determined by transition setting, patient circumstances, level of acuity, and clear transition responsibility.
- Medical institutions must adopt national standards and establish processes to promote effective transitions of care.
- Standardized and evidence-based metrics related to these standards should be used for monitoring and improving transitions.
Evidence-based practice guidelines are key tools to help hospitalists practice high-quality medicine and demonstrate the value of their inpatient care model. Guidelines are designed to produce superior care outcomes and resource utilization efficiencies by encouraging proven medical practices and discouraging ineffective or unproven ones. Yet inefficiencies, variation, and quality gaps persist in medical care—much to the chagrin of policymakers.
Is the answer more guidelines, and better implementation of existing ones?
Research experts and many HM leaders say yes.
In fact, HM is leading the way in an important new area for which there is little uniform guidance: optimal care transitions during patient handoffs. Care transitions are a pivotal time in the patient care process and are replete with avoidable service duplication, poor communication among providers, gaps in care reconciliation, and patient-safety issues.
SHM has joined five other organizations in issuing a Transitions of Care Consensus Policy Statement, which promises more systematic, safe, and efficient patient handoffs.1 SHM also is targeting care-transition improvement in a variety of other venues, all of which can help hospitalists demonstrate more persuasively the value they bring to healthcare delivery.
Guidelines Work
Practice guidelines work, in the sense that they help providers practice in ways consistent with what the best aggregate knowledge and expert opinion says is most effective. The evidence allows physicians to avoid expending scarce resources on ineffective clinical services. Their importance is magnified by the current urgency given to value-based purchasing in healthcare reform. “The right care, for the right patient, at the right time” is the new mantra of payors and policymakers, many of whom are demanding the best and most efficient healthcare delivery at the lowest cost.
“When providers are not providing the right care at the right time to patients, we find that the patient often gets more services … that they didn’t need. That oftentimes exposes them to potential harm and (services) that are wasteful of resources,” says Janet M. Corrigan, PhD, MBA, president and CEO of the National Quality Forum (NQF), a standard-setting organization that convenes national experts to apply “gold standard” endorsement of guidelines developed by professional medical societies and other entities. “Guidelines are a way of synthesizing evidence and translating it into action steps that providers can follow so that they get the best results that we know how to get for their patients.”
Clinicians and healthcare organizations have several sources for guidelines. The Agency for Healthcare Research and Quality (AHRQ) systematically reviews and vets guidelines submitted for inclusion in its National Guideline Clearinghouse (www.guideline.gov), and makes them available for evidence-based clinical decision-making, says Jean Slutsky, director of AHRQ’s Center for Outcomes and Evidence. AHRQ also offers public access to the National Quality Measure Clearinghouse and the Health Care Innovations Exchange, repositories of searchable quality measures and tools relevant to an array of diseases and conditions.
The Institute for Healthcare Improvement (IHI), an independent nonprofit organization, helps frontline physicians implement guidelines, and also helps provider teams decide which guidelines are most appropriate to achieve their desired outcomes, according to Amy E. Boutwell, MD, MPP, IHI’s director of health policy strategy.
Hospitalists use an array of disease-specific practice guidelines from different specialty societies for diagnoses they frequently encounter, such as chest pain, stroke, pneumonia, myocardial infarction, gastrointestinal bleeding, asthma, and chronic obstructive pulmonary disease (COPD). “Most hospitalists want to keep up with the best available evidence,” says Patrick J. Torcson, MD, MMM, FACP, director of hospital medicine at St. Tammany Parish Hospital in Covington, La., and chair of SHM’s Performance and Standards Committee. “The recently updated American College of Cardiology (ACC) and American Heart Association (AHA) guidelines on heart failure are exceptional. The American College of Chest Physicians has an extremely comprehensive set of guidelines on thrombosis, which is the bible for handling anticoagulation.”
Studies are published every month demonstrating that physicians who implement national guidelines at the local level improve such patient outcomes as mortality, length of stay, and time to clinical stability. Dr. Corrigan notes that there are abundant examples of guideline adherence boosting quality outcomes, and cites as a prime example the AHA’s Get With the Guidelines program (www.american heart.org/presenter.jhtml?identifier=1165), which has documented quality gains in coronary artery disease, stroke, and heart failure patients.
—William T. Ford, MD, FHM, section chief of hospital medicine, Temple University Hospital, Philadelphia
Barriers to Acceptance and Adherence
But there are obstacles to guideline adherence, and widespread practice pattern variation remains a huge national problem. Providers in some regions of the country can use twice the resources as their counterparts in other regions and bring no additional benefit to patients (see “Medicare Fee Inspection,” p. 30). The Dartmouth Atlas of Health Care says unwarranted practice variation is responsible for as much as 30% of wasted healthcare spending in the U.S.—a cost that reformers are anxious to eliminate.
The traditional culture of autonomy in the medical profession is perhaps the most difficult and enduring barrier to reducing unjustified practice variation: clinicians don’t automatically follow guidelines, many treat them more as options than as true standards, and organizations do not sufficiently enforce or reward adherence to guidelines, wrote researchers in a special 2005 issue of Health Affairs focusing on guidelines.2
“In an age of mandated cost control and resource limitation under managed care,” the researchers wrote, some physicians still regard practice guidelines as “cookbook medicine” that threatens the use of clinical judgment and encourages treating patients as essentially interchangeable. In the face of that perceived threat, the researchers added, many physicians continue to uphold a traditional view of medicine as an art “in which individual expertise and technique are allowed to shine through and ultimately result in a higher standard of patient care.”
Dr. Corrigan acknowledges the significant obstacles to successful practice guideline implementation:
- Guidelines are developed by various sources, particularly specialty societies, who do not always coordinate their activities. Physicians are left with overlapping and sometimes contradictory guidelines for managing the same disease or condition.
- Guidelines must be maintained and kept current, or physicians will lose confidence and not follow them.
- Guidelines are of varying quality. Some provide clear clinical direction; others are not written in a way that physicians can clearly translate into clinical practice.
- There are significant gaps in the evidence basis for guideline development. Much more comparative effectiveness research needs to be conducted to develop more valid and meaningful guidelines.
- Guidelines must be communicated effectively to physicians, making them available and convenient at the point of clinical care. Electronic health records with user-friendly decision support functions show great promise in “making the right thing the easy thing to do.”
- The fee-for-service payment system encourages greater volume of services, irrespective of guideline recommendations.
Physicians also recognize inherent limitations of guidelines. “Guidelines typically apply across populations. Adding levels of clinical complexity gets further away from a guideline’s applicability. Many physicians will tell you that the patient in front of them is a special case requiring a modification of the protocol,” Dr. Boutwell explains. For example, diabetic management guidelines are based on what is best for a population of diabetics, versus what is best for said hospitalist’s patient who has eight co-morbidities, one of which is diabetes, Boutwell notes. “Guidelines come disease-specific. Patients don’t,” she adds.
Nevertheless, Dr. Boutwell notes, there are robust guidelines and the IHI tries to help front-line physicians and care teams to implement them reliably and effectively.
An obstacle that inhibits hospitalists from implementing guidelines in an optimal fashion “is that we’re not one specialty—we deal with it all—and that complexity can be overwhelming. There is no central repository where all of the guidelines can be found in one place,” according to William T. Ford, MD, FHM, program medical director for Cogent Healthcare and section chief of hospital medicine for Temple University Hospital in Philadelphia.
Make Guidelines Work
Researchers say guidelines are most successful when they are well-supported and uncomplicated, backed by strong leadership and sufficient resources, and are used as “rallying points” to stimulate interdependent and collaborative care among physicians, nurses, pharmacists, equipment suppliers, administrators, and patients.
“Guidelines are really the foundation for determining best practices,” Dr. Torcson says. “There is no shortage of excellent guidelines, or proof that specific interventions do improve outcomes. The key is achieving more uniform implementation. We need tools like pre-printed orders in electronic health records (EHR) to effectively integrate these guidelines into hospitalists’ practice.”
More widespread EHR adoption with user-friendly medical decision-support systems will play a huge role in boosting guideline adoption and effectiveness, says Mary Nix, MS, MT(ASCP)SBB, health science administrator at AHRQ and project officer for the agency’s Center for Outcomes and Evidence.
Dr. Ford says HM groups must evaluate the top 10 to 15 diagnosis-related groups (DRGs) that they see each day (e.g., congestive heart failure, acute kidney failure, pneumonia, cellulitis, or acute coronary syndrome) and come to consensus on which guidelines best address them.
HM groups must then secure buy-in to those guidelines from everyone in the group; from the subspecialists they work with; and from their hospital’s chief medical, financial, and utilization officers.
Care-Transition Guidelines: Opportunity for Hospitalists
A particularly important HM opportunity is improving care transitions. Deficits in communication and information transfer between hospital-based and primary-care physicians (PCPs) are “substantial and ubiquitous,” while delays and omissions are consistently large, and traditional methods of completing and delivering discharge summaries are “suboptimal for communicating timely, accurate, and medically important data to the physicians who will be responsible for follow-up care,” according to a hospitalist-authored Feb. 28, 2007, article in the Journal of the American Medical Association.3 PCPs routinely are not notified about patient admissions or complications during the hospital stay, and some PCPs fail to provide sufficient information to hospitalists at admission, fail to visit or call hospitalized patients, or fail to participate in discharge planning, the study’s researchers noted. For patients with chronic illnesses and frequent hospitalization, those deficits are multiplied, making completeness of information handoffs particularly important.
Because patient handoffs have notoriously been fraught with miscommunication and poor information exchange between providers, adopting a professional consensus on what constitutes the best, safest, and most effective activities during these handoffs is sorely needed.
“Care-transition guidelines can have tremendous power because they affect every hospital patient—each of whom experiences care transitions,” says Rusty Holman, MD, FHM, chief operating officer of Brentwood, Tenn.-based Cogent Healthcare and past president of SHM. “It is an area undergoing rapid development, evolution, and discovery, and hospitalists have positioned themselves as leaders and owners of this particular scenario.”
As care-transition guidelines emerge and mature, Holman thinks they eventually will be tied to value-based healthcare purchasing programs that affect hospitalists’ reimbursement equations and further boost incentives to follow those guidelines. A prime example: Medicare calculated it could save $12 billion annually by reducing preventable 30-day hospital readmissions and will soon stop paying for them. Perhaps 3% to 5% of a hospital’s DRG reimbursement will be at risk under Medicare’s proposal, Dr. Torcson notes.
“Hospitals are going to be much more motivated to build systems and engage physicians, especially hospitalists, to lower readmission rates. Hospitalists will be focusing more and more on how care-transition process improvements can lower those rates,” Dr. Holman says. “That’s a huge opportunity for hospitalists to make a business case for the value they bring to their institutions, and will further justify the financial support they already receive.”
Dr. Ford is more cautious in his appraisal of the financial rewards of better guideline implementation. “We do not capture that much revenue per patient, and even a length-of-stay reduction is difficult for a hospital’s CFO to extrapolate how much money hospitalists save,” he says. “I don’t think hospitalists will be paid more, even if they save the hospital money. You’re just doing your job, but you’re going to keep your job, and you’ll have an enormous bargaining chip when renegotiating contracts with hospitals.”
Still, a prevented readmission might mean a bed for a revenue-generating elective surgery, something that adds to the reward equation.
—Patrick Torcson, MD, MMM, FACP, director of hospital medicine, St. Tammany Parish Hospital, Covington, La., SHM Performance and Standards Committee chair
Transition Evolution
SHM and other sources offer physicians and hospitals expert assistance in implementing care-transition guidelines (see “Care-Transition Guidance,” p. 7). The transitions-of-care policy statement jointly issued by the SHM and five other specialty societies further demonstrates that hospitalists play a key leadership role on this front.1
The policy statement emerged from a multi-stakeholder consensus conference convened by SHM, the American College of Physicians (ACP), and the Society of General Internal Medicine, which was attended by more than 30 medical specialty societies, governmental agencies, and performance measure developers. Participants focused on what standard pieces of information should be exchanged among providers during inpatient to outpatient transitions, and they issued a set of standards for improving those transitions (see “Managing Transitions in Care Between the Inpatient and Outpatient Settings,” p. 7).
“This consensus statement has enormous significance,” Dr. Ford says. “We’re finally shedding light on how to tackle patient handoff and hospital readmission issues, and we as a specialty have to take on care-transition improvement as our mantra. If we were to solve just that one piece, we can more easily start implementing other clinical guidelines. Care-transition guidelines are a fundamental tool to build consensus within your own group and with other clinicians in a team approach.”
Dr. Corrigan applauds the physician groups for publishing the transitions-of-care statement and encourages the societies to work together to “take it to the next step, which is to develop the measures and get them endorsed through the NQF process.”
SHM members are participating in workgroups convened by the NQF to identify standardized performance measures and to develop action plans over the next few months for several national priority areas—one of which is care coordination. “We have a ways to go to achieve better patient handoffs and information exchange between hospitals and other settings in the community. Hospitalists can drive the development of those guidelines and protocols,” Dr. Corrigan says. TH
Christopher Guadagnino, PhD, is a freelance medical writer based in Pennsylvania.
References
- Kripalani S, LeFevre F, Phillips CO, Williams MV; Basaviah P, Baker DW. Deficits in communication and information transfer between hospital-based and primary care physicians: implications for patient safety and continuity of care. JAMA. 2007;297:831-841.
- Timmermans S, Mauck A. The promises and pitfalls of evidence-based medicine. Health Affairs. 2005; 24(1):18-28.
- Snow V, Beck D, Budnitz T, et al. Transitions of care consensus policy statement: American College of Physicians, Society of General Internal Medicine, Society of Hospital Medicine, American Geriatrics Society, American College of Emergency Physicians, Society of Academic Emergency Medicine. J Hosp Med. 2009: 4(6)364-370.
Top Image Source: GOLDEN PIXELS LLC/ALAMY
Managing Transitions of Care Between the Inpatient and Outpatient Settings
The following are joint recommendations from SHM, ACP, SGIM, AGS, ACEP, and SAEM, based upon a multi-stakeholder consensus conference in July 2007 and published in the July/August Journal of Hospital Medicine (http://onlinelibrary.wiley.com/doi/10.1002/jhm.510/full):
- Communication and information exchange between the sending and receiving provider should be timely, as dictated by clinical presentation and urgency of follow-up care required.
- The transition record should always include at least these data elements: principal diagnosis, medication list, contact information of the transferring physician, patient’s cognitive status, test results or pending results. An ideal transition record would add six more elements.
- All communications need to be secure, private, HIPAA-compliant, and accessible to patients and their providers.
- Communities need to develop standard data transfer forms, with the ability to modify information as a patient’s condition changes.
- The sending provider maintains responsibility for the care of the patient until the receiving provider confirms that the transfer is complete. The sending provider should be available to clarify issues of care, and the patient should be able to identify the responsible provider.
- Information transfer should be timely, as determined by transition setting, patient circumstances, level of acuity, and clear transition responsibility.
- Medical institutions must adopt national standards and establish processes to promote effective transitions of care.
- Standardized and evidence-based metrics related to these standards should be used for monitoring and improving transitions.