User login
More Hospitals Report Zero Central-Line-Associated Bloodstream Infections (CLABSIs)
Percentage of hospitals participating in the Agency for Healthcare Research and Quality’s Comprehensive Unit-Based Safety Program (CUSP) that reported zero central-line-associated bloodstream infections (CLABSIs) during a quarter of 2011. That figure is up from 27.3% the year before. CUSP (www.OnTheCuspStopHAI.org) was launched in 2009 to promote the use of customizable, standardized checklists of evidence-based interventions to prevent hospital-acquired infections. It now includes 1,055 hospitals in 44 states, and the program collectively charted a decrease from 1.87 CLABSIs per 1,000 central-line days to 1.25, a 33% reduction.
Percentage of hospitals participating in the Agency for Healthcare Research and Quality’s Comprehensive Unit-Based Safety Program (CUSP) that reported zero central-line-associated bloodstream infections (CLABSIs) during a quarter of 2011. That figure is up from 27.3% the year before. CUSP (www.OnTheCuspStopHAI.org) was launched in 2009 to promote the use of customizable, standardized checklists of evidence-based interventions to prevent hospital-acquired infections. It now includes 1,055 hospitals in 44 states, and the program collectively charted a decrease from 1.87 CLABSIs per 1,000 central-line days to 1.25, a 33% reduction.
Percentage of hospitals participating in the Agency for Healthcare Research and Quality’s Comprehensive Unit-Based Safety Program (CUSP) that reported zero central-line-associated bloodstream infections (CLABSIs) during a quarter of 2011. That figure is up from 27.3% the year before. CUSP (www.OnTheCuspStopHAI.org) was launched in 2009 to promote the use of customizable, standardized checklists of evidence-based interventions to prevent hospital-acquired infections. It now includes 1,055 hospitals in 44 states, and the program collectively charted a decrease from 1.87 CLABSIs per 1,000 central-line days to 1.25, a 33% reduction.
Innovator of Care Transitions Model for Hospital Patients Honored
University of Colorado at Denver geriatrician Eric Coleman, MD, MPH—who pioneered the celebrated Care Transitions Model (www.caretransitions.org), which sends “coaches” on home visits and has them make phone calls to patients in an effort to smooth post-hospital discharge transitions and enhance self-care—has been honored with a MacArthur Foundation “genius” award.
Dr. Coleman also co-chairs the advisory board for SHM’s Project BOOST (Better Outcomes for Older Adults through Safe Transitions) national quality initiative.
The MacArthur Fellowship is known for honoring individuals who have shown exceptional originality and creativity, bestowing them with a $500,000 award—no strings attached. Dr. Coleman says the award “promotes the opportunity for approaching complex problems in new light—taking risks with new approaches and serving in the role of a ‘change agent.’”
“I look forward to working collaboratively with hospitalists and hospitals on finding new strategies and solutions for improving the discharge experience,” he says.
University of Colorado at Denver geriatrician Eric Coleman, MD, MPH—who pioneered the celebrated Care Transitions Model (www.caretransitions.org), which sends “coaches” on home visits and has them make phone calls to patients in an effort to smooth post-hospital discharge transitions and enhance self-care—has been honored with a MacArthur Foundation “genius” award.
Dr. Coleman also co-chairs the advisory board for SHM’s Project BOOST (Better Outcomes for Older Adults through Safe Transitions) national quality initiative.
The MacArthur Fellowship is known for honoring individuals who have shown exceptional originality and creativity, bestowing them with a $500,000 award—no strings attached. Dr. Coleman says the award “promotes the opportunity for approaching complex problems in new light—taking risks with new approaches and serving in the role of a ‘change agent.’”
“I look forward to working collaboratively with hospitalists and hospitals on finding new strategies and solutions for improving the discharge experience,” he says.
University of Colorado at Denver geriatrician Eric Coleman, MD, MPH—who pioneered the celebrated Care Transitions Model (www.caretransitions.org), which sends “coaches” on home visits and has them make phone calls to patients in an effort to smooth post-hospital discharge transitions and enhance self-care—has been honored with a MacArthur Foundation “genius” award.
Dr. Coleman also co-chairs the advisory board for SHM’s Project BOOST (Better Outcomes for Older Adults through Safe Transitions) national quality initiative.
The MacArthur Fellowship is known for honoring individuals who have shown exceptional originality and creativity, bestowing them with a $500,000 award—no strings attached. Dr. Coleman says the award “promotes the opportunity for approaching complex problems in new light—taking risks with new approaches and serving in the role of a ‘change agent.’”
“I look forward to working collaboratively with hospitalists and hospitals on finding new strategies and solutions for improving the discharge experience,” he says.
Win Whitcomb: Introducing Neuroquality and Neurosafety

The prefix “neuro” has become quite popular the last couple of years. We have neuroeconomics, neuroplasticity, neuroergonomics, and, of course, neurohospitalist. The explosion of interest in the brain can be seen in the popular press, television, blogs, and the Journal of the American Medical Association.
I predict that recent breakthroughs in brain science and related fields (cognitive psychology, neurobiology, molecular biology, linguistics, and artificial intelligence, among others) will have a profound impact on the fields of quality improvement (QI) and patient safety, and, consequently on HM. To date, the patient safety movement has focused on systems issues in an effort to reduce harm induced by the healthcare system. I submit that for healthcare to be reliable and error-free in the future, we must leverage the innate strengths of the brain. Here I mention four areas where brain science breakthroughs can enable us to improve patient safety practices.
Diagnostic Error
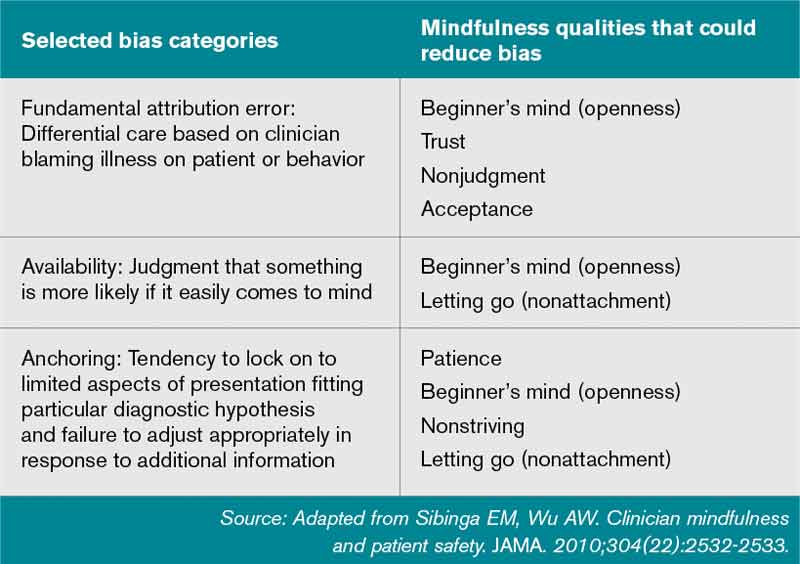
Patrick Croskerry, an emergency physician and researcher, has described errors in diagnosis as stemming in part from cognitive bias. He offers “de-biasing strategies” as an approach to decreasing diagnostic error.
One of the most powerful de-biasing strategies is metacognition, or awareness of one’s own thinking processes. Closely related to metacognition is mindfulness, defined as the “nonjudgmental awareness of the present moment.” A growing body of literature makes the case that enhancing mindfulness might reduce the impact bias has on diagnostic error.1 Table 1 (right) mentions a subset of bias types and how mindfulness might mitigate them. I’m sure you can think of cases you’ve encountered where bias has affected the diagnostic outcome.
Empathy and Patient Experience
As the focus on patient experience grows, approaches to improving performance on patient satisfaction surveys are proliferating. Whatever technical components you choose to employ, a capacity for caregiver empathy is a crucial underlying factor to a better patient experience. Harvard psychiatrist Helen Riess, MD, points out that we are now beginning to understand the neurobiological basis of empathy. She and others present evidence that we may be able to “up-regulate” empathy through education or cognitive practices.2 Several studies suggest we might be able to realize improved therapeutic relationships between physicians and patients, and they have led to programs, such as the ones at Stanford and Emory universities, that train caregivers to enhance empathy and compassion.
Interruptions and Cognitive Error
It has been customary in high-risk industries to ensure that certain procedures are free of interruptions. There is recognition that disturbances during high-stakes tasks, such as airline takeoff, carry disastrous consequences. We now know that multitasking is a myth and that the brain instead switches between tasks sequentially. But task-switching comes at the high cost of a marked increase in the rate of cognitive error.3 As we learn more, decreasing interruptions or delineating “interruption-free” zones in healthcare could be a way to mitigate an inherent vulnerability in our cognitive abilities.
Fatigue and Medical Error
It is well documented that sleep deprivation correlates with a decline in cognitive
performance in a number of classes of healthcare workers. Fatigue has also increased diagnostic error among residents. A 2011 Sentinel Alert from The Joint Commission creates a standard that healthcare organizations implement a fatigue-management plan to mitigate the potential harm caused by tired professionals.
Most of the approaches to improving outcomes in the hospital have focused on process improvement and systems thinking. But errors also occur due to the thinking process of clinicians. In the book “Brain Rules,” author John Medina argues that schools and businesses create an environment that is less than friendly to the brain, citing current classroom design and cubicles for office workers. As a result, he states, we often have poor educational and business performance. I have little doubt that if Medina spent a few hours in a hospital, he would come to a similar conclusion: We don’t do the brain any favors when it comes to creating a healthy environment for providing safe and reliable care to our patients.
References
- Sibinga EM, Wu AW. Clinician mindfulness and patient safety. JAMA. 2010;304(22):2532-2533.
- Riess H. Empathy in medicine─a neurobiological perspective. JAMA. 2010;304(14):1604-1605.
- Rogers RD, Monsell S. The costs of a predictable switch between simple cognitive tasks. J Exper Psychol. 1995;124(2):207–231.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at wfwhit@comcast.net.
The prefix “neuro” has become quite popular the last couple of years. We have neuroeconomics, neuroplasticity, neuroergonomics, and, of course, neurohospitalist. The explosion of interest in the brain can be seen in the popular press, television, blogs, and the Journal of the American Medical Association.
I predict that recent breakthroughs in brain science and related fields (cognitive psychology, neurobiology, molecular biology, linguistics, and artificial intelligence, among others) will have a profound impact on the fields of quality improvement (QI) and patient safety, and, consequently on HM. To date, the patient safety movement has focused on systems issues in an effort to reduce harm induced by the healthcare system. I submit that for healthcare to be reliable and error-free in the future, we must leverage the innate strengths of the brain. Here I mention four areas where brain science breakthroughs can enable us to improve patient safety practices.
Diagnostic Error
Patrick Croskerry, an emergency physician and researcher, has described errors in diagnosis as stemming in part from cognitive bias. He offers “de-biasing strategies” as an approach to decreasing diagnostic error.
One of the most powerful de-biasing strategies is metacognition, or awareness of one’s own thinking processes. Closely related to metacognition is mindfulness, defined as the “nonjudgmental awareness of the present moment.” A growing body of literature makes the case that enhancing mindfulness might reduce the impact bias has on diagnostic error.1 Table 1 (right) mentions a subset of bias types and how mindfulness might mitigate them. I’m sure you can think of cases you’ve encountered where bias has affected the diagnostic outcome.
Empathy and Patient Experience
As the focus on patient experience grows, approaches to improving performance on patient satisfaction surveys are proliferating. Whatever technical components you choose to employ, a capacity for caregiver empathy is a crucial underlying factor to a better patient experience. Harvard psychiatrist Helen Riess, MD, points out that we are now beginning to understand the neurobiological basis of empathy. She and others present evidence that we may be able to “up-regulate” empathy through education or cognitive practices.2 Several studies suggest we might be able to realize improved therapeutic relationships between physicians and patients, and they have led to programs, such as the ones at Stanford and Emory universities, that train caregivers to enhance empathy and compassion.
Interruptions and Cognitive Error
It has been customary in high-risk industries to ensure that certain procedures are free of interruptions. There is recognition that disturbances during high-stakes tasks, such as airline takeoff, carry disastrous consequences. We now know that multitasking is a myth and that the brain instead switches between tasks sequentially. But task-switching comes at the high cost of a marked increase in the rate of cognitive error.3 As we learn more, decreasing interruptions or delineating “interruption-free” zones in healthcare could be a way to mitigate an inherent vulnerability in our cognitive abilities.
Fatigue and Medical Error
It is well documented that sleep deprivation correlates with a decline in cognitive
performance in a number of classes of healthcare workers. Fatigue has also increased diagnostic error among residents. A 2011 Sentinel Alert from The Joint Commission creates a standard that healthcare organizations implement a fatigue-management plan to mitigate the potential harm caused by tired professionals.
Most of the approaches to improving outcomes in the hospital have focused on process improvement and systems thinking. But errors also occur due to the thinking process of clinicians. In the book “Brain Rules,” author John Medina argues that schools and businesses create an environment that is less than friendly to the brain, citing current classroom design and cubicles for office workers. As a result, he states, we often have poor educational and business performance. I have little doubt that if Medina spent a few hours in a hospital, he would come to a similar conclusion: We don’t do the brain any favors when it comes to creating a healthy environment for providing safe and reliable care to our patients.
References
- Sibinga EM, Wu AW. Clinician mindfulness and patient safety. JAMA. 2010;304(22):2532-2533.
- Riess H. Empathy in medicine─a neurobiological perspective. JAMA. 2010;304(14):1604-1605.
- Rogers RD, Monsell S. The costs of a predictable switch between simple cognitive tasks. J Exper Psychol. 1995;124(2):207–231.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at wfwhit@comcast.net.
The prefix “neuro” has become quite popular the last couple of years. We have neuroeconomics, neuroplasticity, neuroergonomics, and, of course, neurohospitalist. The explosion of interest in the brain can be seen in the popular press, television, blogs, and the Journal of the American Medical Association.
I predict that recent breakthroughs in brain science and related fields (cognitive psychology, neurobiology, molecular biology, linguistics, and artificial intelligence, among others) will have a profound impact on the fields of quality improvement (QI) and patient safety, and, consequently on HM. To date, the patient safety movement has focused on systems issues in an effort to reduce harm induced by the healthcare system. I submit that for healthcare to be reliable and error-free in the future, we must leverage the innate strengths of the brain. Here I mention four areas where brain science breakthroughs can enable us to improve patient safety practices.
Diagnostic Error
Patrick Croskerry, an emergency physician and researcher, has described errors in diagnosis as stemming in part from cognitive bias. He offers “de-biasing strategies” as an approach to decreasing diagnostic error.
One of the most powerful de-biasing strategies is metacognition, or awareness of one’s own thinking processes. Closely related to metacognition is mindfulness, defined as the “nonjudgmental awareness of the present moment.” A growing body of literature makes the case that enhancing mindfulness might reduce the impact bias has on diagnostic error.1 Table 1 (right) mentions a subset of bias types and how mindfulness might mitigate them. I’m sure you can think of cases you’ve encountered where bias has affected the diagnostic outcome.
Empathy and Patient Experience
As the focus on patient experience grows, approaches to improving performance on patient satisfaction surveys are proliferating. Whatever technical components you choose to employ, a capacity for caregiver empathy is a crucial underlying factor to a better patient experience. Harvard psychiatrist Helen Riess, MD, points out that we are now beginning to understand the neurobiological basis of empathy. She and others present evidence that we may be able to “up-regulate” empathy through education or cognitive practices.2 Several studies suggest we might be able to realize improved therapeutic relationships between physicians and patients, and they have led to programs, such as the ones at Stanford and Emory universities, that train caregivers to enhance empathy and compassion.
Interruptions and Cognitive Error
It has been customary in high-risk industries to ensure that certain procedures are free of interruptions. There is recognition that disturbances during high-stakes tasks, such as airline takeoff, carry disastrous consequences. We now know that multitasking is a myth and that the brain instead switches between tasks sequentially. But task-switching comes at the high cost of a marked increase in the rate of cognitive error.3 As we learn more, decreasing interruptions or delineating “interruption-free” zones in healthcare could be a way to mitigate an inherent vulnerability in our cognitive abilities.
Fatigue and Medical Error
It is well documented that sleep deprivation correlates with a decline in cognitive
performance in a number of classes of healthcare workers. Fatigue has also increased diagnostic error among residents. A 2011 Sentinel Alert from The Joint Commission creates a standard that healthcare organizations implement a fatigue-management plan to mitigate the potential harm caused by tired professionals.
Most of the approaches to improving outcomes in the hospital have focused on process improvement and systems thinking. But errors also occur due to the thinking process of clinicians. In the book “Brain Rules,” author John Medina argues that schools and businesses create an environment that is less than friendly to the brain, citing current classroom design and cubicles for office workers. As a result, he states, we often have poor educational and business performance. I have little doubt that if Medina spent a few hours in a hospital, he would come to a similar conclusion: We don’t do the brain any favors when it comes to creating a healthy environment for providing safe and reliable care to our patients.
References
- Sibinga EM, Wu AW. Clinician mindfulness and patient safety. JAMA. 2010;304(22):2532-2533.
- Riess H. Empathy in medicine─a neurobiological perspective. JAMA. 2010;304(14):1604-1605.
- Rogers RD, Monsell S. The costs of a predictable switch between simple cognitive tasks. J Exper Psychol. 1995;124(2):207–231.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at wfwhit@comcast.net.
12 Things Hospitalists Need to Know About Nephrology
One number alone should be enough for hospitalists to want to know everything they can about kidney disease: 26 million. It’s the number of Americans that the National Kidney Foundation estimates to have chronic kidney disease (CKD). That’s about the same number as the American Diabetes Association’s estimate for Americans battling diabetes.
And a lot of people who have CKD don’t even know they have it, kidney specialists warn, making it that much more important to be a knowledgeable watchdog looking out for people admitted to the hospital.
The Hospitalist talked to a half-dozen experts on kidney disease, requesting their words of wisdom for hospitalists. The following are 12 things the experts believe hospitalists should keep in mind as they care for patients with kidney disease.
1) Coordination is key, especially with regard to medications and dialysis after discharge.
A goal should be to develop a “tacit understanding of who does what and just trying to see each day that everyone’s working toward the same goal, so I’m not stopping fluids and then you’re starting fluids, or vice versa,” says Ted Shaikewitz, MD, attending nephrologist at Durham (N.C.) Regional Medical Center and a nephrologist at Durham Nephrology Associates.
A key component of hospitalist-nephrologist collaboration is examining and reconciling medications.
“If it looks like they’re on too many medications, then call the specialist, as opposed to each of you expecting the other one to do it,” he says. “Just pare things down and get rid of things that are unnecessary.”
Often, Dr. Shaikewitz says, the hospitalist and the nephrologist both are reluctant to stop or tweak a medication because someone else started the patient on it. He stresses that the more a medication regimen can be simplified, the better.
Coordination is especially important for dialysis patients who are being sent home, says Ruben Velez, MD, president of the Renal Physicians Association (RPA) and president of Dallas Nephrology Associates. If a nephrologist hasn’t been contacted at discharge, the nephrologist hasn’t contacted the patient’s dialysis center to arrange treatment after the hospitalization. And that treatment likely needs to be altered from what it was before the hospitalization, Dr. Velez explains.
The dialysis center needs to get a small discharge summary, so it’s important to get that ball rolling right away, he adds.
“It’s not uncommon for a nephrologist to round in the morning and suddenly realize that the patient was sent home last night,” he says. “We go, ‘Oops. Did somebody call the dialysis center?’ and we don’t know.”
Informing the nephrologist about discharge helps them do their jobs better, he says.
“My job and my clinical responsibility is, I need to contact the treating nephrologist. I need to contact the dialysis clinic,” he says. “I need to tell them, ‘Change your medications.’ I need to tell them there’s been added antibiotics or other things. I need to tell them what they came in with and what was done. And I need to tell them if there has been a change in their weight....The dialysis clinic has difficulty in dialyzing that patient unless they get this information.”

2) Acknowledge the significance of small, early changes.
A jump in serum creatinine levels at the lower end of the range is far more serious than jumps when the creatinine already is at higher levels, says Lynda Szczech, MD, president of the National Kidney Foundation and medical director at Pharmaceutical Product Development.
“The amount of kidney function that’s described by a [serum creatinine] change of 0.1 when that 0.1” is between 1 and 2, “meaning going from 1.1 to 1.2 or 1.3 to 1.4, is huge compared to the amount of kidney function that is described by a change of 0.1 when you’re higher, when you’re going from 3.0 to 3.1,” Dr. Szczech says. “That’s important, because the earlier changes of going from 0.9 to 1.1 might not trigger a cause for concern, but they actually should be the biggest concern. When you go from a creatinine of 1 to 2, you’ve lost 50 percent of your kidney function. When you go from a creatinine of 3 to 4, you’ve probably lost about 10 percent.”
Hospitalists need to understand both the significance of the change and know “how to jump on something,” Dr. Szczech says. “That is probably the most important thing.”
3) Avoid NSAIDs in patients with advanced CKD and transplant patients.
“The nonsteroidal anti-inflammatory drugs can make your renal function much worse,” Dr. Velez says. “Those can finish your kidneys off, and you end up on dialysis.”
That concept is so simple that it’s commonly forgotten, he adds. Patients come to the hospital and are put on an NSAID and the kidneys are damaged.
“It’s horrible,” Dr. Velez says. “That’s one of the worst, and we want to avoid more damage to their kidney function.”
It’s such a common occurrence that the American Society of Nephrology (ASN) included it on their short list of suggestions for the American Board of Internal Medicine’s (ABIM) Choosing Wisely campaign, which aims to arm patients and providers with better information, promote evidence-based care, and reduce unnecessary testing and cost.
4) Don’t place PICC lines in advanced CKD and ESRD patients.
Placement of peripheral intravenous central catheter (PICC) lines in advanced CKD and end-stage renal disease (ESRD) patients is something hospitalists should “avoid as much as possible,” Dr. Velez says, “or forever.”
“PICC lines will destroy veins that we will need to use to create fistulas” needed for dialysis or potential dialysis, he explains.
This item also appears on the Choosing Wisely list.
—Michael Shapiro, MD, MBA, FACP, CPE, president, Denver Nephrology
5) Take basic steps in cases of acute kidney injury (AKI), but be careful about ordering too many tests.
Dr. Shaikewitz says there is little point in hospitalists “ordering everything they can” before the nephrologist is even consulted. That said, certain basic steps—ultrasound, urinalysis, stopping NSAIDs, stopping angiotensin-converting enzyme inhibitors, and hydration—should be taken very early, he says.
But hydrating the patient really means achieving a “euvolemic state,” he explains.
“You don’t want to drown the patient,” Dr. Shaikewitz says. Once patients “clearly have enough fluid on board, then you can stop.”
Plus, while it might sound basic, looking back at old creatinine levels is crucial.
“Oftentimes, a lot of what is going on with a patient will become obvious, and the differential will become obvious, when you have more data,” he says.
He also says it’s important to keep in mind that “patients who are in flux with kidney issues often times can tolerate higher blood pressures,” and the goal should be to get it going in the right direction, not necessarily hitting a specific number.
6) Don’t wait for AKI to progress to needing dialysis before consulting the nephrologist.
As Michael Shapiro, MD, MBA, FACP, CPE, president of Denver Nephrology, puts it, “it doesn’t have to be a catastrophe or an emergency for us to be there within a very quick period of time.”
Nephrologists would rather help out earlier than later.
“What we hate to do is have [hospitalists] spend most of the day trying to manage a problem and then calling us late in the day or in the evening, especially if a procedure like dialysis would be needed at that point in time,” he says. “It’s a lot harder to manage those troops, so to speak, once we let the day go. It’s a little bit more of a crash as opposed to a nice plan.”
Hospitalists should adopt the “earlier is better” mantra for cases of electrolyte problems, such as hypokalemia, hyperkalemia, and significant hyponatremia, or low salt levels, he notes.
“We don’t mind being curb-sided,” Dr. Shapiro says. If the specialist gets a simple heads-up about a patient on the fourth floor—even if it doesn’t require immediate action—he can then pop in and check on the status of that patient when he’s there on his rounds, he says.
Dr. Shaikewitz admits that some kidney specialists prefer not to be called in very early; therefore, it’s important for hospitalists to develop relationships and understand individual preferences. But in his case, an early referral is favorable.
“When in doubt, refer a little bit on the early side,” he says. “It’s actually kind of a fun teamwork with the hospitalists, trying to manage the patient and doing everything as a group.”
—Ruben Velez, MD, president, Renal Physicians Association, president, Dallas Nephrology Associates
7) Always call a nephrologist when a kidney transplant patient is admitted.
Robert Kossmann, MD, president-elect of the RPA, and other experts agree that it’s a good idea to at least call and inform a nephrologist that a transplant patient has been admitted. The call can go something like, “I have this patient coming in to the hospital, their kidney transplant function is fine, but they’re here with X, Y, or Z,” he says. “Is there something that we should be paying particular attention to or do you need to come see that patient?”
Dr. Kossmann says hospitalists don’t need to automatically consult a nephrologist every time, but “it’s probably a good idea to call and talk to the nephrologist every time.”
Dr. Velez says he’s seen a lot of unnecessary mistakes around transplant patients.
“There’s a lot of drug interactions with immunosuppressive drugs that these patients take that could have been prevented or avoided,” he says. “Even on patients that have fantastic renal function up to transplant … these patients can turn sour on a dime.”
8) Don’t forget the power of a simple urinalysis.
You can get a lot of diagnostic information from the urinalysis—“from a simple dipstick,” Dr. Szczech says. She points out the value of the specific gravity reading.
“A specific gravity of 1.010 in the setting of a rising creatinine [level] probably means you’ve got injury to the tubule,” she says.
The power of this simple tool can sometimes be overlooked, she says, as clinicians seek to understand how to use the newer biomarkers.
“In nephrology, we can make things quite complicated,” she adds. “We can’t forget about the low-tech stuff that we just take for granted.”
9) Simply looking at serum creatinine level is not enough.
It’s extremely important to calculate the glomerular filtration rate (GFR), says Katherine Tuttle, MD, clinical professor of medicine in the University of Washington’s division of nephrology. Some hospital labs will do this, but hospitalists need to “make sure they review the GFR values, not just the serum creatinine,” she says.
And those readings have important ripple effects.
“Everything from need for adjustment of drugs for low GFR to drug interactions to caution about, for example, using iodinated contrasts because of risk of acute kidney injury, increased risk of infection, increased risk of cardiovascular complications,” she says. “So it’s a very important part of the clinical assessment.”
10) Know the potential benefits of isolated ultrafiltration.
This dialysis-like procedure is becoming more widely recognized as helpful for patients with congestive heart failure who have recurrent readmissions.
“This is a very small group, but a very complicated group,” Dr. Kossmann says. “You can’t keep them out of the hospital.”
Isolated ultrafiltration can help “pull off quite a lot of fluid while they’re in the hospital or in a setting where you can do that,” he adds. “That’s something that I think hospitalists may be seeing more of as this unfolds into the future. It’s a small group of people, but there’s so much heart disease in this country that it winds up being a significant increase in number.”
11) Avoid using low-molecular-weight heparins, especially Lovenox, in advanced kidney disease and dialysis patients.
Don’t just follow the protocols for preventing thromboembolic events, says Dr. Velez, who adds it’s done “very frequently.”
“In this day and age of preventing thromboembolic [events], they have protocols where they just put them on it and they don’t realize they have advanced kidney disease or end-stage renal disease,” he says. “Heparin is fine. Lovenox should be avoided.”
Such mistakes are, in part, a product of operating within a protocol-driven environment.
“Dealing with a lot of protocols and algorithms and pressure from the hospital and you name it—and we’re all busy—we want to do the right thing,” Dr. Velez says. “But we don’t apply it to individual patients, and that’s a concern of having too many protocols and trying to treat everybody the same.”
Dr. Tuttle says the risk of “over-reliance” on protocols and guidelines is real.
“The problem with guidelines is people extrapolate them too far and they overinterpret them,” she says. “That happens in the hospital all the time.”
12) Take a moment and ask: Am I really comfortable handling this patient?
“It’s worth pausing at some point with yourself and sort of taking a self-assessment and saying—whether it’s nephrology, cardiology, or something else—‘Where do I feel confident and strong?’” Dr. Kossmann says. “Although it sounds overly basic, that’s an important starting point.”
He says he’s witnessed hospitalists with a wide range of comfort levels handle cases involving kidney dysfunction.
“There’s no one-size-fits-all,” he says. “Sometimes the question I get asked is, ‘Rob, what’s the general rule? When should a nephrologist be called for a consult?’ And that’s a terrible question, because it depends on the doctor who’s seeing the patient.”
Thomas Collins is a freelance writer in South Florida.
One number alone should be enough for hospitalists to want to know everything they can about kidney disease: 26 million. It’s the number of Americans that the National Kidney Foundation estimates to have chronic kidney disease (CKD). That’s about the same number as the American Diabetes Association’s estimate for Americans battling diabetes.
And a lot of people who have CKD don’t even know they have it, kidney specialists warn, making it that much more important to be a knowledgeable watchdog looking out for people admitted to the hospital.
The Hospitalist talked to a half-dozen experts on kidney disease, requesting their words of wisdom for hospitalists. The following are 12 things the experts believe hospitalists should keep in mind as they care for patients with kidney disease.
1) Coordination is key, especially with regard to medications and dialysis after discharge.
A goal should be to develop a “tacit understanding of who does what and just trying to see each day that everyone’s working toward the same goal, so I’m not stopping fluids and then you’re starting fluids, or vice versa,” says Ted Shaikewitz, MD, attending nephrologist at Durham (N.C.) Regional Medical Center and a nephrologist at Durham Nephrology Associates.
A key component of hospitalist-nephrologist collaboration is examining and reconciling medications.
“If it looks like they’re on too many medications, then call the specialist, as opposed to each of you expecting the other one to do it,” he says. “Just pare things down and get rid of things that are unnecessary.”
Often, Dr. Shaikewitz says, the hospitalist and the nephrologist both are reluctant to stop or tweak a medication because someone else started the patient on it. He stresses that the more a medication regimen can be simplified, the better.
Coordination is especially important for dialysis patients who are being sent home, says Ruben Velez, MD, president of the Renal Physicians Association (RPA) and president of Dallas Nephrology Associates. If a nephrologist hasn’t been contacted at discharge, the nephrologist hasn’t contacted the patient’s dialysis center to arrange treatment after the hospitalization. And that treatment likely needs to be altered from what it was before the hospitalization, Dr. Velez explains.
The dialysis center needs to get a small discharge summary, so it’s important to get that ball rolling right away, he adds.
“It’s not uncommon for a nephrologist to round in the morning and suddenly realize that the patient was sent home last night,” he says. “We go, ‘Oops. Did somebody call the dialysis center?’ and we don’t know.”
Informing the nephrologist about discharge helps them do their jobs better, he says.
“My job and my clinical responsibility is, I need to contact the treating nephrologist. I need to contact the dialysis clinic,” he says. “I need to tell them, ‘Change your medications.’ I need to tell them there’s been added antibiotics or other things. I need to tell them what they came in with and what was done. And I need to tell them if there has been a change in their weight....The dialysis clinic has difficulty in dialyzing that patient unless they get this information.”
2) Acknowledge the significance of small, early changes.
A jump in serum creatinine levels at the lower end of the range is far more serious than jumps when the creatinine already is at higher levels, says Lynda Szczech, MD, president of the National Kidney Foundation and medical director at Pharmaceutical Product Development.
“The amount of kidney function that’s described by a [serum creatinine] change of 0.1 when that 0.1” is between 1 and 2, “meaning going from 1.1 to 1.2 or 1.3 to 1.4, is huge compared to the amount of kidney function that is described by a change of 0.1 when you’re higher, when you’re going from 3.0 to 3.1,” Dr. Szczech says. “That’s important, because the earlier changes of going from 0.9 to 1.1 might not trigger a cause for concern, but they actually should be the biggest concern. When you go from a creatinine of 1 to 2, you’ve lost 50 percent of your kidney function. When you go from a creatinine of 3 to 4, you’ve probably lost about 10 percent.”
Hospitalists need to understand both the significance of the change and know “how to jump on something,” Dr. Szczech says. “That is probably the most important thing.”
3) Avoid NSAIDs in patients with advanced CKD and transplant patients.
“The nonsteroidal anti-inflammatory drugs can make your renal function much worse,” Dr. Velez says. “Those can finish your kidneys off, and you end up on dialysis.”
That concept is so simple that it’s commonly forgotten, he adds. Patients come to the hospital and are put on an NSAID and the kidneys are damaged.
“It’s horrible,” Dr. Velez says. “That’s one of the worst, and we want to avoid more damage to their kidney function.”
It’s such a common occurrence that the American Society of Nephrology (ASN) included it on their short list of suggestions for the American Board of Internal Medicine’s (ABIM) Choosing Wisely campaign, which aims to arm patients and providers with better information, promote evidence-based care, and reduce unnecessary testing and cost.
4) Don’t place PICC lines in advanced CKD and ESRD patients.
Placement of peripheral intravenous central catheter (PICC) lines in advanced CKD and end-stage renal disease (ESRD) patients is something hospitalists should “avoid as much as possible,” Dr. Velez says, “or forever.”
“PICC lines will destroy veins that we will need to use to create fistulas” needed for dialysis or potential dialysis, he explains.
This item also appears on the Choosing Wisely list.
—Michael Shapiro, MD, MBA, FACP, CPE, president, Denver Nephrology
5) Take basic steps in cases of acute kidney injury (AKI), but be careful about ordering too many tests.
Dr. Shaikewitz says there is little point in hospitalists “ordering everything they can” before the nephrologist is even consulted. That said, certain basic steps—ultrasound, urinalysis, stopping NSAIDs, stopping angiotensin-converting enzyme inhibitors, and hydration—should be taken very early, he says.
But hydrating the patient really means achieving a “euvolemic state,” he explains.
“You don’t want to drown the patient,” Dr. Shaikewitz says. Once patients “clearly have enough fluid on board, then you can stop.”
Plus, while it might sound basic, looking back at old creatinine levels is crucial.
“Oftentimes, a lot of what is going on with a patient will become obvious, and the differential will become obvious, when you have more data,” he says.
He also says it’s important to keep in mind that “patients who are in flux with kidney issues often times can tolerate higher blood pressures,” and the goal should be to get it going in the right direction, not necessarily hitting a specific number.
6) Don’t wait for AKI to progress to needing dialysis before consulting the nephrologist.
As Michael Shapiro, MD, MBA, FACP, CPE, president of Denver Nephrology, puts it, “it doesn’t have to be a catastrophe or an emergency for us to be there within a very quick period of time.”
Nephrologists would rather help out earlier than later.
“What we hate to do is have [hospitalists] spend most of the day trying to manage a problem and then calling us late in the day or in the evening, especially if a procedure like dialysis would be needed at that point in time,” he says. “It’s a lot harder to manage those troops, so to speak, once we let the day go. It’s a little bit more of a crash as opposed to a nice plan.”
Hospitalists should adopt the “earlier is better” mantra for cases of electrolyte problems, such as hypokalemia, hyperkalemia, and significant hyponatremia, or low salt levels, he notes.
“We don’t mind being curb-sided,” Dr. Shapiro says. If the specialist gets a simple heads-up about a patient on the fourth floor—even if it doesn’t require immediate action—he can then pop in and check on the status of that patient when he’s there on his rounds, he says.
Dr. Shaikewitz admits that some kidney specialists prefer not to be called in very early; therefore, it’s important for hospitalists to develop relationships and understand individual preferences. But in his case, an early referral is favorable.
“When in doubt, refer a little bit on the early side,” he says. “It’s actually kind of a fun teamwork with the hospitalists, trying to manage the patient and doing everything as a group.”
—Ruben Velez, MD, president, Renal Physicians Association, president, Dallas Nephrology Associates
7) Always call a nephrologist when a kidney transplant patient is admitted.
Robert Kossmann, MD, president-elect of the RPA, and other experts agree that it’s a good idea to at least call and inform a nephrologist that a transplant patient has been admitted. The call can go something like, “I have this patient coming in to the hospital, their kidney transplant function is fine, but they’re here with X, Y, or Z,” he says. “Is there something that we should be paying particular attention to or do you need to come see that patient?”
Dr. Kossmann says hospitalists don’t need to automatically consult a nephrologist every time, but “it’s probably a good idea to call and talk to the nephrologist every time.”
Dr. Velez says he’s seen a lot of unnecessary mistakes around transplant patients.
“There’s a lot of drug interactions with immunosuppressive drugs that these patients take that could have been prevented or avoided,” he says. “Even on patients that have fantastic renal function up to transplant … these patients can turn sour on a dime.”
8) Don’t forget the power of a simple urinalysis.
You can get a lot of diagnostic information from the urinalysis—“from a simple dipstick,” Dr. Szczech says. She points out the value of the specific gravity reading.
“A specific gravity of 1.010 in the setting of a rising creatinine [level] probably means you’ve got injury to the tubule,” she says.
The power of this simple tool can sometimes be overlooked, she says, as clinicians seek to understand how to use the newer biomarkers.
“In nephrology, we can make things quite complicated,” she adds. “We can’t forget about the low-tech stuff that we just take for granted.”
9) Simply looking at serum creatinine level is not enough.
It’s extremely important to calculate the glomerular filtration rate (GFR), says Katherine Tuttle, MD, clinical professor of medicine in the University of Washington’s division of nephrology. Some hospital labs will do this, but hospitalists need to “make sure they review the GFR values, not just the serum creatinine,” she says.
And those readings have important ripple effects.
“Everything from need for adjustment of drugs for low GFR to drug interactions to caution about, for example, using iodinated contrasts because of risk of acute kidney injury, increased risk of infection, increased risk of cardiovascular complications,” she says. “So it’s a very important part of the clinical assessment.”
10) Know the potential benefits of isolated ultrafiltration.
This dialysis-like procedure is becoming more widely recognized as helpful for patients with congestive heart failure who have recurrent readmissions.
“This is a very small group, but a very complicated group,” Dr. Kossmann says. “You can’t keep them out of the hospital.”
Isolated ultrafiltration can help “pull off quite a lot of fluid while they’re in the hospital or in a setting where you can do that,” he adds. “That’s something that I think hospitalists may be seeing more of as this unfolds into the future. It’s a small group of people, but there’s so much heart disease in this country that it winds up being a significant increase in number.”
11) Avoid using low-molecular-weight heparins, especially Lovenox, in advanced kidney disease and dialysis patients.
Don’t just follow the protocols for preventing thromboembolic events, says Dr. Velez, who adds it’s done “very frequently.”
“In this day and age of preventing thromboembolic [events], they have protocols where they just put them on it and they don’t realize they have advanced kidney disease or end-stage renal disease,” he says. “Heparin is fine. Lovenox should be avoided.”
Such mistakes are, in part, a product of operating within a protocol-driven environment.
“Dealing with a lot of protocols and algorithms and pressure from the hospital and you name it—and we’re all busy—we want to do the right thing,” Dr. Velez says. “But we don’t apply it to individual patients, and that’s a concern of having too many protocols and trying to treat everybody the same.”
Dr. Tuttle says the risk of “over-reliance” on protocols and guidelines is real.
“The problem with guidelines is people extrapolate them too far and they overinterpret them,” she says. “That happens in the hospital all the time.”
12) Take a moment and ask: Am I really comfortable handling this patient?
“It’s worth pausing at some point with yourself and sort of taking a self-assessment and saying—whether it’s nephrology, cardiology, or something else—‘Where do I feel confident and strong?’” Dr. Kossmann says. “Although it sounds overly basic, that’s an important starting point.”
He says he’s witnessed hospitalists with a wide range of comfort levels handle cases involving kidney dysfunction.
“There’s no one-size-fits-all,” he says. “Sometimes the question I get asked is, ‘Rob, what’s the general rule? When should a nephrologist be called for a consult?’ And that’s a terrible question, because it depends on the doctor who’s seeing the patient.”
Thomas Collins is a freelance writer in South Florida.
One number alone should be enough for hospitalists to want to know everything they can about kidney disease: 26 million. It’s the number of Americans that the National Kidney Foundation estimates to have chronic kidney disease (CKD). That’s about the same number as the American Diabetes Association’s estimate for Americans battling diabetes.
And a lot of people who have CKD don’t even know they have it, kidney specialists warn, making it that much more important to be a knowledgeable watchdog looking out for people admitted to the hospital.
The Hospitalist talked to a half-dozen experts on kidney disease, requesting their words of wisdom for hospitalists. The following are 12 things the experts believe hospitalists should keep in mind as they care for patients with kidney disease.
1) Coordination is key, especially with regard to medications and dialysis after discharge.
A goal should be to develop a “tacit understanding of who does what and just trying to see each day that everyone’s working toward the same goal, so I’m not stopping fluids and then you’re starting fluids, or vice versa,” says Ted Shaikewitz, MD, attending nephrologist at Durham (N.C.) Regional Medical Center and a nephrologist at Durham Nephrology Associates.
A key component of hospitalist-nephrologist collaboration is examining and reconciling medications.
“If it looks like they’re on too many medications, then call the specialist, as opposed to each of you expecting the other one to do it,” he says. “Just pare things down and get rid of things that are unnecessary.”
Often, Dr. Shaikewitz says, the hospitalist and the nephrologist both are reluctant to stop or tweak a medication because someone else started the patient on it. He stresses that the more a medication regimen can be simplified, the better.
Coordination is especially important for dialysis patients who are being sent home, says Ruben Velez, MD, president of the Renal Physicians Association (RPA) and president of Dallas Nephrology Associates. If a nephrologist hasn’t been contacted at discharge, the nephrologist hasn’t contacted the patient’s dialysis center to arrange treatment after the hospitalization. And that treatment likely needs to be altered from what it was before the hospitalization, Dr. Velez explains.
The dialysis center needs to get a small discharge summary, so it’s important to get that ball rolling right away, he adds.
“It’s not uncommon for a nephrologist to round in the morning and suddenly realize that the patient was sent home last night,” he says. “We go, ‘Oops. Did somebody call the dialysis center?’ and we don’t know.”
Informing the nephrologist about discharge helps them do their jobs better, he says.
“My job and my clinical responsibility is, I need to contact the treating nephrologist. I need to contact the dialysis clinic,” he says. “I need to tell them, ‘Change your medications.’ I need to tell them there’s been added antibiotics or other things. I need to tell them what they came in with and what was done. And I need to tell them if there has been a change in their weight....The dialysis clinic has difficulty in dialyzing that patient unless they get this information.”
2) Acknowledge the significance of small, early changes.
A jump in serum creatinine levels at the lower end of the range is far more serious than jumps when the creatinine already is at higher levels, says Lynda Szczech, MD, president of the National Kidney Foundation and medical director at Pharmaceutical Product Development.
“The amount of kidney function that’s described by a [serum creatinine] change of 0.1 when that 0.1” is between 1 and 2, “meaning going from 1.1 to 1.2 or 1.3 to 1.4, is huge compared to the amount of kidney function that is described by a change of 0.1 when you’re higher, when you’re going from 3.0 to 3.1,” Dr. Szczech says. “That’s important, because the earlier changes of going from 0.9 to 1.1 might not trigger a cause for concern, but they actually should be the biggest concern. When you go from a creatinine of 1 to 2, you’ve lost 50 percent of your kidney function. When you go from a creatinine of 3 to 4, you’ve probably lost about 10 percent.”
Hospitalists need to understand both the significance of the change and know “how to jump on something,” Dr. Szczech says. “That is probably the most important thing.”
3) Avoid NSAIDs in patients with advanced CKD and transplant patients.
“The nonsteroidal anti-inflammatory drugs can make your renal function much worse,” Dr. Velez says. “Those can finish your kidneys off, and you end up on dialysis.”
That concept is so simple that it’s commonly forgotten, he adds. Patients come to the hospital and are put on an NSAID and the kidneys are damaged.
“It’s horrible,” Dr. Velez says. “That’s one of the worst, and we want to avoid more damage to their kidney function.”
It’s such a common occurrence that the American Society of Nephrology (ASN) included it on their short list of suggestions for the American Board of Internal Medicine’s (ABIM) Choosing Wisely campaign, which aims to arm patients and providers with better information, promote evidence-based care, and reduce unnecessary testing and cost.
4) Don’t place PICC lines in advanced CKD and ESRD patients.
Placement of peripheral intravenous central catheter (PICC) lines in advanced CKD and end-stage renal disease (ESRD) patients is something hospitalists should “avoid as much as possible,” Dr. Velez says, “or forever.”
“PICC lines will destroy veins that we will need to use to create fistulas” needed for dialysis or potential dialysis, he explains.
This item also appears on the Choosing Wisely list.
—Michael Shapiro, MD, MBA, FACP, CPE, president, Denver Nephrology
5) Take basic steps in cases of acute kidney injury (AKI), but be careful about ordering too many tests.
Dr. Shaikewitz says there is little point in hospitalists “ordering everything they can” before the nephrologist is even consulted. That said, certain basic steps—ultrasound, urinalysis, stopping NSAIDs, stopping angiotensin-converting enzyme inhibitors, and hydration—should be taken very early, he says.
But hydrating the patient really means achieving a “euvolemic state,” he explains.
“You don’t want to drown the patient,” Dr. Shaikewitz says. Once patients “clearly have enough fluid on board, then you can stop.”
Plus, while it might sound basic, looking back at old creatinine levels is crucial.
“Oftentimes, a lot of what is going on with a patient will become obvious, and the differential will become obvious, when you have more data,” he says.
He also says it’s important to keep in mind that “patients who are in flux with kidney issues often times can tolerate higher blood pressures,” and the goal should be to get it going in the right direction, not necessarily hitting a specific number.
6) Don’t wait for AKI to progress to needing dialysis before consulting the nephrologist.
As Michael Shapiro, MD, MBA, FACP, CPE, president of Denver Nephrology, puts it, “it doesn’t have to be a catastrophe or an emergency for us to be there within a very quick period of time.”
Nephrologists would rather help out earlier than later.
“What we hate to do is have [hospitalists] spend most of the day trying to manage a problem and then calling us late in the day or in the evening, especially if a procedure like dialysis would be needed at that point in time,” he says. “It’s a lot harder to manage those troops, so to speak, once we let the day go. It’s a little bit more of a crash as opposed to a nice plan.”
Hospitalists should adopt the “earlier is better” mantra for cases of electrolyte problems, such as hypokalemia, hyperkalemia, and significant hyponatremia, or low salt levels, he notes.
“We don’t mind being curb-sided,” Dr. Shapiro says. If the specialist gets a simple heads-up about a patient on the fourth floor—even if it doesn’t require immediate action—he can then pop in and check on the status of that patient when he’s there on his rounds, he says.
Dr. Shaikewitz admits that some kidney specialists prefer not to be called in very early; therefore, it’s important for hospitalists to develop relationships and understand individual preferences. But in his case, an early referral is favorable.
“When in doubt, refer a little bit on the early side,” he says. “It’s actually kind of a fun teamwork with the hospitalists, trying to manage the patient and doing everything as a group.”
—Ruben Velez, MD, president, Renal Physicians Association, president, Dallas Nephrology Associates
7) Always call a nephrologist when a kidney transplant patient is admitted.
Robert Kossmann, MD, president-elect of the RPA, and other experts agree that it’s a good idea to at least call and inform a nephrologist that a transplant patient has been admitted. The call can go something like, “I have this patient coming in to the hospital, their kidney transplant function is fine, but they’re here with X, Y, or Z,” he says. “Is there something that we should be paying particular attention to or do you need to come see that patient?”
Dr. Kossmann says hospitalists don’t need to automatically consult a nephrologist every time, but “it’s probably a good idea to call and talk to the nephrologist every time.”
Dr. Velez says he’s seen a lot of unnecessary mistakes around transplant patients.
“There’s a lot of drug interactions with immunosuppressive drugs that these patients take that could have been prevented or avoided,” he says. “Even on patients that have fantastic renal function up to transplant … these patients can turn sour on a dime.”
8) Don’t forget the power of a simple urinalysis.
You can get a lot of diagnostic information from the urinalysis—“from a simple dipstick,” Dr. Szczech says. She points out the value of the specific gravity reading.
“A specific gravity of 1.010 in the setting of a rising creatinine [level] probably means you’ve got injury to the tubule,” she says.
The power of this simple tool can sometimes be overlooked, she says, as clinicians seek to understand how to use the newer biomarkers.
“In nephrology, we can make things quite complicated,” she adds. “We can’t forget about the low-tech stuff that we just take for granted.”
9) Simply looking at serum creatinine level is not enough.
It’s extremely important to calculate the glomerular filtration rate (GFR), says Katherine Tuttle, MD, clinical professor of medicine in the University of Washington’s division of nephrology. Some hospital labs will do this, but hospitalists need to “make sure they review the GFR values, not just the serum creatinine,” she says.
And those readings have important ripple effects.
“Everything from need for adjustment of drugs for low GFR to drug interactions to caution about, for example, using iodinated contrasts because of risk of acute kidney injury, increased risk of infection, increased risk of cardiovascular complications,” she says. “So it’s a very important part of the clinical assessment.”
10) Know the potential benefits of isolated ultrafiltration.
This dialysis-like procedure is becoming more widely recognized as helpful for patients with congestive heart failure who have recurrent readmissions.
“This is a very small group, but a very complicated group,” Dr. Kossmann says. “You can’t keep them out of the hospital.”
Isolated ultrafiltration can help “pull off quite a lot of fluid while they’re in the hospital or in a setting where you can do that,” he adds. “That’s something that I think hospitalists may be seeing more of as this unfolds into the future. It’s a small group of people, but there’s so much heart disease in this country that it winds up being a significant increase in number.”
11) Avoid using low-molecular-weight heparins, especially Lovenox, in advanced kidney disease and dialysis patients.
Don’t just follow the protocols for preventing thromboembolic events, says Dr. Velez, who adds it’s done “very frequently.”
“In this day and age of preventing thromboembolic [events], they have protocols where they just put them on it and they don’t realize they have advanced kidney disease or end-stage renal disease,” he says. “Heparin is fine. Lovenox should be avoided.”
Such mistakes are, in part, a product of operating within a protocol-driven environment.
“Dealing with a lot of protocols and algorithms and pressure from the hospital and you name it—and we’re all busy—we want to do the right thing,” Dr. Velez says. “But we don’t apply it to individual patients, and that’s a concern of having too many protocols and trying to treat everybody the same.”
Dr. Tuttle says the risk of “over-reliance” on protocols and guidelines is real.
“The problem with guidelines is people extrapolate them too far and they overinterpret them,” she says. “That happens in the hospital all the time.”
12) Take a moment and ask: Am I really comfortable handling this patient?
“It’s worth pausing at some point with yourself and sort of taking a self-assessment and saying—whether it’s nephrology, cardiology, or something else—‘Where do I feel confident and strong?’” Dr. Kossmann says. “Although it sounds overly basic, that’s an important starting point.”
He says he’s witnessed hospitalists with a wide range of comfort levels handle cases involving kidney dysfunction.
“There’s no one-size-fits-all,” he says. “Sometimes the question I get asked is, ‘Rob, what’s the general rule? When should a nephrologist be called for a consult?’ And that’s a terrible question, because it depends on the doctor who’s seeing the patient.”
Thomas Collins is a freelance writer in South Florida.
Guidelines Help Hospitalists Manage Acute Coronary Syndrome Patients

Acute coronary syndrome (ACS) accounts for more than 1.4 million hospital admissions per year, and as many as 1 in 5 ACS patients die in the first six months after diagnosis, according to the American Academy of Family Physicians. With that in mind, Bruce Darrow, MD, PhD, presented the seminar “Acute Coronary Syndrome (ACS): Keys to Treatment and New Advances” for more than 150 hospitalists at the seventh annual Mid-Atlantic Hospital Medicine Symposium in October at Mount Sinai Medical Center in New York City.
“ACS patients are being admitted to a hospitalist’s care, although these physicians are not coronary service-line providers,” said Dr. Darrow, Mount Sinai’s director of telemetry services. “Often they work with cardiologists, but there are things hospitalists should be comfortable doing without consulting a specialist.”
Dr. Darrow spent the majority of his presentation reviewing the American College of Cardiology Foundation/American Heart Association (ACCF/AHA) 2012 update of the 2007 guidelines for managing patients with myocardial infarction (MI).
Three Phases of Treatment
To achieve the comfort level he believes hospitalists require, Dr. Darrow explained three phases of ACS care: initial medical treatment, reperfusion therapy, and transitional management.1,2 Hospitalists who see patients within the first 24 hours of their hospital stay are providing
initial treatment.
Once the physician determines that the patient is experiencing an acute myocardial infarction, treatment should begin with:
- Aspirin;
- Low-molecular-weight heparin (or heparin if the patient will be heading to the cath lab); and
- Antiplatelet agents (clopidogrel or ticagrelor for this “upstream” portion of therapy).
—Bruce Darrow, MD, PhD, director of telemetry services, Mount Sinai Medical Center, New York
Other medications to consider are intravenous IIb/IIIa inhibitors, such as abciximab, that often were used for patients going to the cath lab. Beta-blockers, although no longer required, can be included in the arsenal. Similarly, anti-ischemics may be employed, despite a lack of evidence to support their use (e.g. oxygen can be a good idea, and morphine will certainly benefit someone in pain).
In cases with ST elevation, after initial treatment, the patient is generally sent to reperfusion therapy, unless it is contraindicated. Primary percutaneous coronary intervention (PCI) is recommended in facilities with a 24/7 cath lab, or in cases for which the patient can be transferred to a hospital with an available cath lab within three hours. Otherwise, thrombolysis is the route to take, and all hospitals should be capable of that procedure, Dr. Darrow said.
After reperfusion or conservative management measures are taken, the patient is transitioned to post-MI care, which includes:
- Aspirin (except where contraindicated);
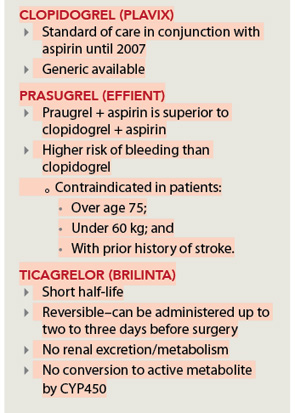
- Antiplatelet agents (clopidogrel, ticagrelor, and prasugruel, depending on patient risk factors; see Figure 1, right);
- Beta-blockers;
- Statins;
- ACE inhibitors (for patients with systolic dysfunction); and
- Eplerenone/spironolactone (for patients with systolic dysfunction and respiratory conditions).
Core Measures
Dr. Darrow also addressed the ACS Core Measures, performance measurement, and improvement initiatives set by The Joint Commission and the Centers for Medicare & Medicaid Services (CMS).3
Upon arrival, patients should be given:
- Aspirin (Joint Commission-required; voluntary according to CMS);
- Thrombolyis within 30 minutes (if applicable); and
- Primary PCI within 90 minutes (if applicable).
At discharge, patients should be given:
- Aspirin;
- Beta-blockers (Joint Commission-required; voluntary according to CMS);
- ACE/ARB for systolic heart failure (Joint Commission-required;
- voluntary according to CMS); and
- Statins.
Maybelle Cowan-Lincoln is a freelance writer in New Jersey.
References
- Jneid H, Anderson JL, Wright RS, et al. 2012 ACCF/AHA focused update of the guideline for the management of patients with unstable angina/non–ST-elevation myocardial infarction (updating the 2007 guideline and replacing the 2011 focused update). a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2012;60(7):645-681.
- Darrow B. Acute coronary syndrome (ACS): Keys to treatment and new advances. Paper presented at the seventh annual Mid-Atlantic Hospital Medicine Symposium; Oct. 19, 2012; New York, NY.
- Joint Commission and the Centers for Medicare & Medicaid Services. Specifications Manual for National Hospital Inpatient Quality Measures. The Joint Commission website. Available at: http://www.jointcommission.org/specifications_manual_for_national_hospital_inpatient_quality_measures.aspx. Accessed Oct. 22, 2012.
Acute coronary syndrome (ACS) accounts for more than 1.4 million hospital admissions per year, and as many as 1 in 5 ACS patients die in the first six months after diagnosis, according to the American Academy of Family Physicians. With that in mind, Bruce Darrow, MD, PhD, presented the seminar “Acute Coronary Syndrome (ACS): Keys to Treatment and New Advances” for more than 150 hospitalists at the seventh annual Mid-Atlantic Hospital Medicine Symposium in October at Mount Sinai Medical Center in New York City.
“ACS patients are being admitted to a hospitalist’s care, although these physicians are not coronary service-line providers,” said Dr. Darrow, Mount Sinai’s director of telemetry services. “Often they work with cardiologists, but there are things hospitalists should be comfortable doing without consulting a specialist.”
Dr. Darrow spent the majority of his presentation reviewing the American College of Cardiology Foundation/American Heart Association (ACCF/AHA) 2012 update of the 2007 guidelines for managing patients with myocardial infarction (MI).
Three Phases of Treatment
To achieve the comfort level he believes hospitalists require, Dr. Darrow explained three phases of ACS care: initial medical treatment, reperfusion therapy, and transitional management.1,2 Hospitalists who see patients within the first 24 hours of their hospital stay are providing
initial treatment.
Once the physician determines that the patient is experiencing an acute myocardial infarction, treatment should begin with:
- Aspirin;
- Low-molecular-weight heparin (or heparin if the patient will be heading to the cath lab); and
- Antiplatelet agents (clopidogrel or ticagrelor for this “upstream” portion of therapy).
—Bruce Darrow, MD, PhD, director of telemetry services, Mount Sinai Medical Center, New York
Other medications to consider are intravenous IIb/IIIa inhibitors, such as abciximab, that often were used for patients going to the cath lab. Beta-blockers, although no longer required, can be included in the arsenal. Similarly, anti-ischemics may be employed, despite a lack of evidence to support their use (e.g. oxygen can be a good idea, and morphine will certainly benefit someone in pain).
In cases with ST elevation, after initial treatment, the patient is generally sent to reperfusion therapy, unless it is contraindicated. Primary percutaneous coronary intervention (PCI) is recommended in facilities with a 24/7 cath lab, or in cases for which the patient can be transferred to a hospital with an available cath lab within three hours. Otherwise, thrombolysis is the route to take, and all hospitals should be capable of that procedure, Dr. Darrow said.
After reperfusion or conservative management measures are taken, the patient is transitioned to post-MI care, which includes:
- Aspirin (except where contraindicated);
- Antiplatelet agents (clopidogrel, ticagrelor, and prasugruel, depending on patient risk factors; see Figure 1, right);
- Beta-blockers;
- Statins;
- ACE inhibitors (for patients with systolic dysfunction); and
- Eplerenone/spironolactone (for patients with systolic dysfunction and respiratory conditions).
Core Measures
Dr. Darrow also addressed the ACS Core Measures, performance measurement, and improvement initiatives set by The Joint Commission and the Centers for Medicare & Medicaid Services (CMS).3
Upon arrival, patients should be given:
- Aspirin (Joint Commission-required; voluntary according to CMS);
- Thrombolyis within 30 minutes (if applicable); and
- Primary PCI within 90 minutes (if applicable).
At discharge, patients should be given:
- Aspirin;
- Beta-blockers (Joint Commission-required; voluntary according to CMS);
- ACE/ARB for systolic heart failure (Joint Commission-required;
- voluntary according to CMS); and
- Statins.
Maybelle Cowan-Lincoln is a freelance writer in New Jersey.
References
- Jneid H, Anderson JL, Wright RS, et al. 2012 ACCF/AHA focused update of the guideline for the management of patients with unstable angina/non–ST-elevation myocardial infarction (updating the 2007 guideline and replacing the 2011 focused update). a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2012;60(7):645-681.
- Darrow B. Acute coronary syndrome (ACS): Keys to treatment and new advances. Paper presented at the seventh annual Mid-Atlantic Hospital Medicine Symposium; Oct. 19, 2012; New York, NY.
- Joint Commission and the Centers for Medicare & Medicaid Services. Specifications Manual for National Hospital Inpatient Quality Measures. The Joint Commission website. Available at: http://www.jointcommission.org/specifications_manual_for_national_hospital_inpatient_quality_measures.aspx. Accessed Oct. 22, 2012.
Acute coronary syndrome (ACS) accounts for more than 1.4 million hospital admissions per year, and as many as 1 in 5 ACS patients die in the first six months after diagnosis, according to the American Academy of Family Physicians. With that in mind, Bruce Darrow, MD, PhD, presented the seminar “Acute Coronary Syndrome (ACS): Keys to Treatment and New Advances” for more than 150 hospitalists at the seventh annual Mid-Atlantic Hospital Medicine Symposium in October at Mount Sinai Medical Center in New York City.
“ACS patients are being admitted to a hospitalist’s care, although these physicians are not coronary service-line providers,” said Dr. Darrow, Mount Sinai’s director of telemetry services. “Often they work with cardiologists, but there are things hospitalists should be comfortable doing without consulting a specialist.”
Dr. Darrow spent the majority of his presentation reviewing the American College of Cardiology Foundation/American Heart Association (ACCF/AHA) 2012 update of the 2007 guidelines for managing patients with myocardial infarction (MI).
Three Phases of Treatment
To achieve the comfort level he believes hospitalists require, Dr. Darrow explained three phases of ACS care: initial medical treatment, reperfusion therapy, and transitional management.1,2 Hospitalists who see patients within the first 24 hours of their hospital stay are providing
initial treatment.
Once the physician determines that the patient is experiencing an acute myocardial infarction, treatment should begin with:
- Aspirin;
- Low-molecular-weight heparin (or heparin if the patient will be heading to the cath lab); and
- Antiplatelet agents (clopidogrel or ticagrelor for this “upstream” portion of therapy).
—Bruce Darrow, MD, PhD, director of telemetry services, Mount Sinai Medical Center, New York
Other medications to consider are intravenous IIb/IIIa inhibitors, such as abciximab, that often were used for patients going to the cath lab. Beta-blockers, although no longer required, can be included in the arsenal. Similarly, anti-ischemics may be employed, despite a lack of evidence to support their use (e.g. oxygen can be a good idea, and morphine will certainly benefit someone in pain).
In cases with ST elevation, after initial treatment, the patient is generally sent to reperfusion therapy, unless it is contraindicated. Primary percutaneous coronary intervention (PCI) is recommended in facilities with a 24/7 cath lab, or in cases for which the patient can be transferred to a hospital with an available cath lab within three hours. Otherwise, thrombolysis is the route to take, and all hospitals should be capable of that procedure, Dr. Darrow said.
After reperfusion or conservative management measures are taken, the patient is transitioned to post-MI care, which includes:
- Aspirin (except where contraindicated);
- Antiplatelet agents (clopidogrel, ticagrelor, and prasugruel, depending on patient risk factors; see Figure 1, right);
- Beta-blockers;
- Statins;
- ACE inhibitors (for patients with systolic dysfunction); and
- Eplerenone/spironolactone (for patients with systolic dysfunction and respiratory conditions).
Core Measures
Dr. Darrow also addressed the ACS Core Measures, performance measurement, and improvement initiatives set by The Joint Commission and the Centers for Medicare & Medicaid Services (CMS).3
Upon arrival, patients should be given:
- Aspirin (Joint Commission-required; voluntary according to CMS);
- Thrombolyis within 30 minutes (if applicable); and
- Primary PCI within 90 minutes (if applicable).
At discharge, patients should be given:
- Aspirin;
- Beta-blockers (Joint Commission-required; voluntary according to CMS);
- ACE/ARB for systolic heart failure (Joint Commission-required;
- voluntary according to CMS); and
- Statins.
Maybelle Cowan-Lincoln is a freelance writer in New Jersey.
References
- Jneid H, Anderson JL, Wright RS, et al. 2012 ACCF/AHA focused update of the guideline for the management of patients with unstable angina/non–ST-elevation myocardial infarction (updating the 2007 guideline and replacing the 2011 focused update). a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2012;60(7):645-681.
- Darrow B. Acute coronary syndrome (ACS): Keys to treatment and new advances. Paper presented at the seventh annual Mid-Atlantic Hospital Medicine Symposium; Oct. 19, 2012; New York, NY.
- Joint Commission and the Centers for Medicare & Medicaid Services. Specifications Manual for National Hospital Inpatient Quality Measures. The Joint Commission website. Available at: http://www.jointcommission.org/specifications_manual_for_national_hospital_inpatient_quality_measures.aspx. Accessed Oct. 22, 2012.
The Hospital Home Team: Physicians Increase Focus on Inpatient Care

For most of my medical career, the hospital functioned more as a swap meet, where every physician had his or her own booth, than as an integrated, community health resource with a focused mission. Although the innovation of HM might be counted as the beginning of a new, more aligned approach between physicians and the hospital as an institution, the rapidly evolving employment of physicians by hospitals and the focusing of physician practice primarily on inpatient care has taken this to another level.
The New Paradigm
A number of recent surveys by physician recruitment firms and physician management companies have found that less than 25% of physicians are self-employed. Planned changes to insurance and Medicare reimbursement for healthcare have driven cardiologists, orthopedists, surgeons, and many other physicians, who want to protect their flow of patients and dollars, to readily become hospital or large-group-practice employees. The entrance of accountable-care organizations (ACOs) to the landscape and the greater need for physician and hospital alignment have only accelerated this trend.
At the same time, the growth of all sorts of hospitalist specialties has further changed the medical staff of the hospital. Internal-medicine and family-practice hospitalists now number more than 35,000. There are probably more than 2,000 pediatric hospitalists. The newly formed Society of OB/GYN Hospitalists (SOGH) estimates there are more than 1,500 so-called laborists in the U.S., and there are several hundred neurohospitalists, orthopedic hospitalists, and acute-care surgeons.
It is clear to me that a “home team” for the hospital of the future is developing, and it includes hospitalists, ED physicians, critical-care physicians, and the growing panoply of hospital-employed cardiologists and surgeons. There is an opportunity for alignment and integration in what has been a fragmented delivery of healthcare.
On the commercial side of the equation, this new opportunity for physician-hospital alignment might allow for a new distribution of compensation. It already is common for hospitals to be transferring some of “their” Medicare Part A dollars to hospitalists. With penalties or additional payments in the ACO model (e.g. shared savings) or in value-based purchasing, there certainly are mechanisms to redistribute funding to new physician compensation models, based more on performance than on volume of services (i.e. the old productivity model).
On another level, where compensation and performance merge, the new medical staff has the ability to deliver a safer hospital experience to our patients and to improve performance. This could take the form of reduction in hospital-acquired infections (HAIs) or reducing unnecessary DVTs and PEs. It could take the form of a better discharge process that leads to fewer unnecessary readmissions or fewer preventable ED visits. On the OB side, 24-hour on-site availability of OB hospitalists has been shown to reduce adverse birth events and, therefore, reduce liability risk and malpractice premiums. On-site availability for patients with fractures and trauma cases by orthopedic hospitalists or hospital-employed orthopedists also can reduce expenses and adverse events for these acutely ill patients.
HM’s Role
With all these changes occurring so rapidly and with all these new players being thrown into the stew at the hospital, it may be worth a few minutes for the “traditional” hospitalist on the medical service to step back and see how our role may evolve. We already have an increasing role in comanagement of surgical and subspecialty patients, as well as a more integrated role at the ED-hospitalist interface. As hospitals look for hospital-focused physicians, there is a potential for scope creep that must be thoughtfully managed.
This may require “rules of engagement” with other key services. While it may be appropriate for a patient with an acute abdomen to be admitted to the hospitalist service, if the hospitalist determines that this patient needs surgery sooner rather than later, there needs to be a straightforward way to get the surgeon in house and on the case and the patient to the operating room. To this point, medical hospitalists can help manage the medical aspects of a neurosurgical case, but we don’t do burr holes. And if there is to be pushback from the surgeon, this can’t happen at 2 a.m. over the telephone; it must be handled by the service leaders at their weekly meeting.
On another level, hospitalists need to be careful that the hospital doesn’t just hand us the administrative functions of other physicians’ care. Hospitalists are not the default to do H&Ps on surgical cases or handle their discharges, even if this falls into the hospital strategy to be able to employ fewer high-priced surgeons and subspecialists by handing off some of their work to their hospitalists.
On the other hand, it is totally appropriate for many of the hospital-focused physicians to come together, possibly under the leadership of the hospital CMO, to look at the workflow and to set up a new way to deliver healthcare that not only redefines the workload, but also involves the rest of the team, including nursing, pharmacy, case management, and social services. Medical hospitalists will need to consider whether we should be the hub of the new physician enterprise and what that would mean for workload, FTEs, and scope of practice.
Such organizations as SHM and the American Hospital Association (AHA) are thinking how best to support and convene the hospital-based physician. AHA has developed a Physician Forum with more than 6,000 members who now have their practices aligned with their hospital. SHM has held meetings of the leaders of hospital-focused practice and is developing virtual forums on Hospital Medicine Exchange to keep the discussion going. Through the Hospital Care Collaborative (HCC), SHM is engaging the leadership of pharmacy, nursing, case management, social services, and respiratory therapy.
Although we are still early in creating the direction for the new medical staff, the water is rising and the current is moving rapidly. The strong forces that are driving new payment paradigms are leading to changes in compensation and an emphasis on definable, measureable outcomes of performance and safety. Hospitalists, who have been thinking in this way and who have some experience in the new ways, should be well positioned to lead and participate actively in the formation of the new hospital home team.
When opportunity knocks, you still have to get up and answer the door. It’s time to get ready to step up.
Dr. Wellikson is CEO of SHM.
For most of my medical career, the hospital functioned more as a swap meet, where every physician had his or her own booth, than as an integrated, community health resource with a focused mission. Although the innovation of HM might be counted as the beginning of a new, more aligned approach between physicians and the hospital as an institution, the rapidly evolving employment of physicians by hospitals and the focusing of physician practice primarily on inpatient care has taken this to another level.
The New Paradigm
A number of recent surveys by physician recruitment firms and physician management companies have found that less than 25% of physicians are self-employed. Planned changes to insurance and Medicare reimbursement for healthcare have driven cardiologists, orthopedists, surgeons, and many other physicians, who want to protect their flow of patients and dollars, to readily become hospital or large-group-practice employees. The entrance of accountable-care organizations (ACOs) to the landscape and the greater need for physician and hospital alignment have only accelerated this trend.
At the same time, the growth of all sorts of hospitalist specialties has further changed the medical staff of the hospital. Internal-medicine and family-practice hospitalists now number more than 35,000. There are probably more than 2,000 pediatric hospitalists. The newly formed Society of OB/GYN Hospitalists (SOGH) estimates there are more than 1,500 so-called laborists in the U.S., and there are several hundred neurohospitalists, orthopedic hospitalists, and acute-care surgeons.
It is clear to me that a “home team” for the hospital of the future is developing, and it includes hospitalists, ED physicians, critical-care physicians, and the growing panoply of hospital-employed cardiologists and surgeons. There is an opportunity for alignment and integration in what has been a fragmented delivery of healthcare.
On the commercial side of the equation, this new opportunity for physician-hospital alignment might allow for a new distribution of compensation. It already is common for hospitals to be transferring some of “their” Medicare Part A dollars to hospitalists. With penalties or additional payments in the ACO model (e.g. shared savings) or in value-based purchasing, there certainly are mechanisms to redistribute funding to new physician compensation models, based more on performance than on volume of services (i.e. the old productivity model).
On another level, where compensation and performance merge, the new medical staff has the ability to deliver a safer hospital experience to our patients and to improve performance. This could take the form of reduction in hospital-acquired infections (HAIs) or reducing unnecessary DVTs and PEs. It could take the form of a better discharge process that leads to fewer unnecessary readmissions or fewer preventable ED visits. On the OB side, 24-hour on-site availability of OB hospitalists has been shown to reduce adverse birth events and, therefore, reduce liability risk and malpractice premiums. On-site availability for patients with fractures and trauma cases by orthopedic hospitalists or hospital-employed orthopedists also can reduce expenses and adverse events for these acutely ill patients.
HM’s Role
With all these changes occurring so rapidly and with all these new players being thrown into the stew at the hospital, it may be worth a few minutes for the “traditional” hospitalist on the medical service to step back and see how our role may evolve. We already have an increasing role in comanagement of surgical and subspecialty patients, as well as a more integrated role at the ED-hospitalist interface. As hospitals look for hospital-focused physicians, there is a potential for scope creep that must be thoughtfully managed.
This may require “rules of engagement” with other key services. While it may be appropriate for a patient with an acute abdomen to be admitted to the hospitalist service, if the hospitalist determines that this patient needs surgery sooner rather than later, there needs to be a straightforward way to get the surgeon in house and on the case and the patient to the operating room. To this point, medical hospitalists can help manage the medical aspects of a neurosurgical case, but we don’t do burr holes. And if there is to be pushback from the surgeon, this can’t happen at 2 a.m. over the telephone; it must be handled by the service leaders at their weekly meeting.
On another level, hospitalists need to be careful that the hospital doesn’t just hand us the administrative functions of other physicians’ care. Hospitalists are not the default to do H&Ps on surgical cases or handle their discharges, even if this falls into the hospital strategy to be able to employ fewer high-priced surgeons and subspecialists by handing off some of their work to their hospitalists.
On the other hand, it is totally appropriate for many of the hospital-focused physicians to come together, possibly under the leadership of the hospital CMO, to look at the workflow and to set up a new way to deliver healthcare that not only redefines the workload, but also involves the rest of the team, including nursing, pharmacy, case management, and social services. Medical hospitalists will need to consider whether we should be the hub of the new physician enterprise and what that would mean for workload, FTEs, and scope of practice.
Such organizations as SHM and the American Hospital Association (AHA) are thinking how best to support and convene the hospital-based physician. AHA has developed a Physician Forum with more than 6,000 members who now have their practices aligned with their hospital. SHM has held meetings of the leaders of hospital-focused practice and is developing virtual forums on Hospital Medicine Exchange to keep the discussion going. Through the Hospital Care Collaborative (HCC), SHM is engaging the leadership of pharmacy, nursing, case management, social services, and respiratory therapy.
Although we are still early in creating the direction for the new medical staff, the water is rising and the current is moving rapidly. The strong forces that are driving new payment paradigms are leading to changes in compensation and an emphasis on definable, measureable outcomes of performance and safety. Hospitalists, who have been thinking in this way and who have some experience in the new ways, should be well positioned to lead and participate actively in the formation of the new hospital home team.
When opportunity knocks, you still have to get up and answer the door. It’s time to get ready to step up.
Dr. Wellikson is CEO of SHM.
For most of my medical career, the hospital functioned more as a swap meet, where every physician had his or her own booth, than as an integrated, community health resource with a focused mission. Although the innovation of HM might be counted as the beginning of a new, more aligned approach between physicians and the hospital as an institution, the rapidly evolving employment of physicians by hospitals and the focusing of physician practice primarily on inpatient care has taken this to another level.
The New Paradigm
A number of recent surveys by physician recruitment firms and physician management companies have found that less than 25% of physicians are self-employed. Planned changes to insurance and Medicare reimbursement for healthcare have driven cardiologists, orthopedists, surgeons, and many other physicians, who want to protect their flow of patients and dollars, to readily become hospital or large-group-practice employees. The entrance of accountable-care organizations (ACOs) to the landscape and the greater need for physician and hospital alignment have only accelerated this trend.
At the same time, the growth of all sorts of hospitalist specialties has further changed the medical staff of the hospital. Internal-medicine and family-practice hospitalists now number more than 35,000. There are probably more than 2,000 pediatric hospitalists. The newly formed Society of OB/GYN Hospitalists (SOGH) estimates there are more than 1,500 so-called laborists in the U.S., and there are several hundred neurohospitalists, orthopedic hospitalists, and acute-care surgeons.
It is clear to me that a “home team” for the hospital of the future is developing, and it includes hospitalists, ED physicians, critical-care physicians, and the growing panoply of hospital-employed cardiologists and surgeons. There is an opportunity for alignment and integration in what has been a fragmented delivery of healthcare.
On the commercial side of the equation, this new opportunity for physician-hospital alignment might allow for a new distribution of compensation. It already is common for hospitals to be transferring some of “their” Medicare Part A dollars to hospitalists. With penalties or additional payments in the ACO model (e.g. shared savings) or in value-based purchasing, there certainly are mechanisms to redistribute funding to new physician compensation models, based more on performance than on volume of services (i.e. the old productivity model).
On another level, where compensation and performance merge, the new medical staff has the ability to deliver a safer hospital experience to our patients and to improve performance. This could take the form of reduction in hospital-acquired infections (HAIs) or reducing unnecessary DVTs and PEs. It could take the form of a better discharge process that leads to fewer unnecessary readmissions or fewer preventable ED visits. On the OB side, 24-hour on-site availability of OB hospitalists has been shown to reduce adverse birth events and, therefore, reduce liability risk and malpractice premiums. On-site availability for patients with fractures and trauma cases by orthopedic hospitalists or hospital-employed orthopedists also can reduce expenses and adverse events for these acutely ill patients.
HM’s Role
With all these changes occurring so rapidly and with all these new players being thrown into the stew at the hospital, it may be worth a few minutes for the “traditional” hospitalist on the medical service to step back and see how our role may evolve. We already have an increasing role in comanagement of surgical and subspecialty patients, as well as a more integrated role at the ED-hospitalist interface. As hospitals look for hospital-focused physicians, there is a potential for scope creep that must be thoughtfully managed.
This may require “rules of engagement” with other key services. While it may be appropriate for a patient with an acute abdomen to be admitted to the hospitalist service, if the hospitalist determines that this patient needs surgery sooner rather than later, there needs to be a straightforward way to get the surgeon in house and on the case and the patient to the operating room. To this point, medical hospitalists can help manage the medical aspects of a neurosurgical case, but we don’t do burr holes. And if there is to be pushback from the surgeon, this can’t happen at 2 a.m. over the telephone; it must be handled by the service leaders at their weekly meeting.
On another level, hospitalists need to be careful that the hospital doesn’t just hand us the administrative functions of other physicians’ care. Hospitalists are not the default to do H&Ps on surgical cases or handle their discharges, even if this falls into the hospital strategy to be able to employ fewer high-priced surgeons and subspecialists by handing off some of their work to their hospitalists.
On the other hand, it is totally appropriate for many of the hospital-focused physicians to come together, possibly under the leadership of the hospital CMO, to look at the workflow and to set up a new way to deliver healthcare that not only redefines the workload, but also involves the rest of the team, including nursing, pharmacy, case management, and social services. Medical hospitalists will need to consider whether we should be the hub of the new physician enterprise and what that would mean for workload, FTEs, and scope of practice.
Such organizations as SHM and the American Hospital Association (AHA) are thinking how best to support and convene the hospital-based physician. AHA has developed a Physician Forum with more than 6,000 members who now have their practices aligned with their hospital. SHM has held meetings of the leaders of hospital-focused practice and is developing virtual forums on Hospital Medicine Exchange to keep the discussion going. Through the Hospital Care Collaborative (HCC), SHM is engaging the leadership of pharmacy, nursing, case management, social services, and respiratory therapy.
Although we are still early in creating the direction for the new medical staff, the water is rising and the current is moving rapidly. The strong forces that are driving new payment paradigms are leading to changes in compensation and an emphasis on definable, measureable outcomes of performance and safety. Hospitalists, who have been thinking in this way and who have some experience in the new ways, should be well positioned to lead and participate actively in the formation of the new hospital home team.
When opportunity knocks, you still have to get up and answer the door. It’s time to get ready to step up.
Dr. Wellikson is CEO of SHM.
The Numerators: Treating Noncompliant, Medically Complicated Hospital Patients

We hospitalists are scientifically minded. We understand basic statistics, including percentages, percentiles, numerators, denominators (see Figure 1, right). In healthcare, we see a lot of patients we call denominators; these denominators are generally the types of patients to whom not much happens. They come in “pre-” and they leave “post-.” They generally pass through our walls, and our lives, according to plan, without leaving an impenetrable memory of who they were or what they experienced.
The numerators, on the other hand, do have something happen to them—something unexpected, untoward, unanticipated, unlikely. Sometimes we describe numerators as “noncompliant” or “medically complicated” or “refractory to treatment.” We often find ways to rationalize and explain how the patient turned from a denominator into a numerator—something they did, or didn’t do, to nudge them above the line. They smoked, they ate too much, they didn’t take their medications “as prescribed.” Often there is a less robust discussion about what we could have done to reduce the nudge: understand their background, their literacy, their finances, their physical/cognitive limitations, their understanding of risks and benefits.
I read a powerful piece about “numerators” written by Kerry O’Connell. In this piece, she describes what it was like to cross over the line into being a numerator after acquiring a hospital-acquired infection:
Five years ago this summer while under deep anesthesia for arm surgery number 3, I drifted above the line and joined the group called Numerators. … Numerators have lost a lot to join this group; many have lost organs, and some have lost all their limbs, all have many kinds of scars from their journey. It was not our choice to leave the world of Denominators … and many will struggle the rest of their lives to understand why...
There are lots of silly rules for not counting some infected souls, as if by not counting us we might not exist. Numerators that are identified are then divided by the Denominators to create a nameless, faceless, mysteriously small number called infection rates. “Rates,” like their cousin “odds,” claim to portray hope while predicting doom for some of us. Denominators are in love with rates, for no matter how many Numerators they have sired, someone else has sired more. Rates soothe the Denominator conscious and allow them to sleep peacefully at night ...
Numerators don’t ask for much from the world. We ask that Denominators look behind the numbers to see the people, to love us, count us, respect our suffering, and help keep us out of bankruptcy, for once we were Denominators just like you. Our greatest dream is that you find the daily strength to truly care. To care enough to follow the checklists, to care enough to wash your hands, to care enough to only use virgin needles, for the saddest day for all Numerators is when another unsuspecting Denominator rises above the line to join our group.1
CB’s Story
Now think of all the numerators you have met. I am going to repeat that phrase. Think of all the numerators you have met. I have met quite a few. Now I am going to tell you about my most memorable numerator.
CB was a 36-year-old white female admitted to the hospital with a recent diagnosis of ulcerative colitis. She had a protracted hospital course on various immunosuppressant drugs, none of which relieved her symptoms. During her hospital stay, her family, including her 2-year-old twins, visited every single day. After several weeks with no improvement, the decision was made to proceed to a colectomy. The surgical procedure itself was uncomplicated, a true denominator.
Then, on post-op Day 5, the day of her anticipated discharge, a pulmonary embolus thrust her into the numerator position. A preventable, eventually fatal numerator—a numerator who “just would not keep her compression devices on” and whom the staff tried to get out of bed, “but she just wouldn’t do it.” A numerator who just so happened to be my sister.
Every year on April 2, when I call my niece and nephew to wish them a happy birthday, I think about numerators. And I think about how incredibly different life would be for those 10-year-old twins, had their mom just stayed a denominator. And every day, when I sit in conference rooms and hear from countless people about how difficult it is to prevent this and reduce that, and how zero is not feasible, I think about numerators. I don’t look at their bar chart, or their run chart, or their red line, or their blue line, or whether their line is within the control limits, or what their P-value is. I think about who represents that black dot, and about how we are going to actually convince ourselves to “First, do no harm.”
When I find myself amongst a crowd quibbling about finances, lunch breaks, workflows, accountability, and about who is going to check the box or fill out the form, I think about the numerators, and how we are truly wasting their time, their livelihood, and their ability to stay below the line.
And someday, when my niece and nephew are old enough to understand, I will try to help them tolerate and accept the fact that “preventable” and “prevented” are not interchangeable. At least not in the medical industry. At least not yet.
In memory of Colleen Conlin Bowen, May 14, 2004
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at scheured@musc.edu.
Reference
We hospitalists are scientifically minded. We understand basic statistics, including percentages, percentiles, numerators, denominators (see Figure 1, right). In healthcare, we see a lot of patients we call denominators; these denominators are generally the types of patients to whom not much happens. They come in “pre-” and they leave “post-.” They generally pass through our walls, and our lives, according to plan, without leaving an impenetrable memory of who they were or what they experienced.
The numerators, on the other hand, do have something happen to them—something unexpected, untoward, unanticipated, unlikely. Sometimes we describe numerators as “noncompliant” or “medically complicated” or “refractory to treatment.” We often find ways to rationalize and explain how the patient turned from a denominator into a numerator—something they did, or didn’t do, to nudge them above the line. They smoked, they ate too much, they didn’t take their medications “as prescribed.” Often there is a less robust discussion about what we could have done to reduce the nudge: understand their background, their literacy, their finances, their physical/cognitive limitations, their understanding of risks and benefits.
I read a powerful piece about “numerators” written by Kerry O’Connell. In this piece, she describes what it was like to cross over the line into being a numerator after acquiring a hospital-acquired infection:
Five years ago this summer while under deep anesthesia for arm surgery number 3, I drifted above the line and joined the group called Numerators. … Numerators have lost a lot to join this group; many have lost organs, and some have lost all their limbs, all have many kinds of scars from their journey. It was not our choice to leave the world of Denominators … and many will struggle the rest of their lives to understand why...
There are lots of silly rules for not counting some infected souls, as if by not counting us we might not exist. Numerators that are identified are then divided by the Denominators to create a nameless, faceless, mysteriously small number called infection rates. “Rates,” like their cousin “odds,” claim to portray hope while predicting doom for some of us. Denominators are in love with rates, for no matter how many Numerators they have sired, someone else has sired more. Rates soothe the Denominator conscious and allow them to sleep peacefully at night ...
Numerators don’t ask for much from the world. We ask that Denominators look behind the numbers to see the people, to love us, count us, respect our suffering, and help keep us out of bankruptcy, for once we were Denominators just like you. Our greatest dream is that you find the daily strength to truly care. To care enough to follow the checklists, to care enough to wash your hands, to care enough to only use virgin needles, for the saddest day for all Numerators is when another unsuspecting Denominator rises above the line to join our group.1
CB’s Story
Now think of all the numerators you have met. I am going to repeat that phrase. Think of all the numerators you have met. I have met quite a few. Now I am going to tell you about my most memorable numerator.
CB was a 36-year-old white female admitted to the hospital with a recent diagnosis of ulcerative colitis. She had a protracted hospital course on various immunosuppressant drugs, none of which relieved her symptoms. During her hospital stay, her family, including her 2-year-old twins, visited every single day. After several weeks with no improvement, the decision was made to proceed to a colectomy. The surgical procedure itself was uncomplicated, a true denominator.
Then, on post-op Day 5, the day of her anticipated discharge, a pulmonary embolus thrust her into the numerator position. A preventable, eventually fatal numerator—a numerator who “just would not keep her compression devices on” and whom the staff tried to get out of bed, “but she just wouldn’t do it.” A numerator who just so happened to be my sister.
Every year on April 2, when I call my niece and nephew to wish them a happy birthday, I think about numerators. And I think about how incredibly different life would be for those 10-year-old twins, had their mom just stayed a denominator. And every day, when I sit in conference rooms and hear from countless people about how difficult it is to prevent this and reduce that, and how zero is not feasible, I think about numerators. I don’t look at their bar chart, or their run chart, or their red line, or their blue line, or whether their line is within the control limits, or what their P-value is. I think about who represents that black dot, and about how we are going to actually convince ourselves to “First, do no harm.”
When I find myself amongst a crowd quibbling about finances, lunch breaks, workflows, accountability, and about who is going to check the box or fill out the form, I think about the numerators, and how we are truly wasting their time, their livelihood, and their ability to stay below the line.
And someday, when my niece and nephew are old enough to understand, I will try to help them tolerate and accept the fact that “preventable” and “prevented” are not interchangeable. At least not in the medical industry. At least not yet.
In memory of Colleen Conlin Bowen, May 14, 2004
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at scheured@musc.edu.
Reference
We hospitalists are scientifically minded. We understand basic statistics, including percentages, percentiles, numerators, denominators (see Figure 1, right). In healthcare, we see a lot of patients we call denominators; these denominators are generally the types of patients to whom not much happens. They come in “pre-” and they leave “post-.” They generally pass through our walls, and our lives, according to plan, without leaving an impenetrable memory of who they were or what they experienced.
The numerators, on the other hand, do have something happen to them—something unexpected, untoward, unanticipated, unlikely. Sometimes we describe numerators as “noncompliant” or “medically complicated” or “refractory to treatment.” We often find ways to rationalize and explain how the patient turned from a denominator into a numerator—something they did, or didn’t do, to nudge them above the line. They smoked, they ate too much, they didn’t take their medications “as prescribed.” Often there is a less robust discussion about what we could have done to reduce the nudge: understand their background, their literacy, their finances, their physical/cognitive limitations, their understanding of risks and benefits.
I read a powerful piece about “numerators” written by Kerry O’Connell. In this piece, she describes what it was like to cross over the line into being a numerator after acquiring a hospital-acquired infection:
Five years ago this summer while under deep anesthesia for arm surgery number 3, I drifted above the line and joined the group called Numerators. … Numerators have lost a lot to join this group; many have lost organs, and some have lost all their limbs, all have many kinds of scars from their journey. It was not our choice to leave the world of Denominators … and many will struggle the rest of their lives to understand why...
There are lots of silly rules for not counting some infected souls, as if by not counting us we might not exist. Numerators that are identified are then divided by the Denominators to create a nameless, faceless, mysteriously small number called infection rates. “Rates,” like their cousin “odds,” claim to portray hope while predicting doom for some of us. Denominators are in love with rates, for no matter how many Numerators they have sired, someone else has sired more. Rates soothe the Denominator conscious and allow them to sleep peacefully at night ...
Numerators don’t ask for much from the world. We ask that Denominators look behind the numbers to see the people, to love us, count us, respect our suffering, and help keep us out of bankruptcy, for once we were Denominators just like you. Our greatest dream is that you find the daily strength to truly care. To care enough to follow the checklists, to care enough to wash your hands, to care enough to only use virgin needles, for the saddest day for all Numerators is when another unsuspecting Denominator rises above the line to join our group.1
CB’s Story
Now think of all the numerators you have met. I am going to repeat that phrase. Think of all the numerators you have met. I have met quite a few. Now I am going to tell you about my most memorable numerator.
CB was a 36-year-old white female admitted to the hospital with a recent diagnosis of ulcerative colitis. She had a protracted hospital course on various immunosuppressant drugs, none of which relieved her symptoms. During her hospital stay, her family, including her 2-year-old twins, visited every single day. After several weeks with no improvement, the decision was made to proceed to a colectomy. The surgical procedure itself was uncomplicated, a true denominator.
Then, on post-op Day 5, the day of her anticipated discharge, a pulmonary embolus thrust her into the numerator position. A preventable, eventually fatal numerator—a numerator who “just would not keep her compression devices on” and whom the staff tried to get out of bed, “but she just wouldn’t do it.” A numerator who just so happened to be my sister.
Every year on April 2, when I call my niece and nephew to wish them a happy birthday, I think about numerators. And I think about how incredibly different life would be for those 10-year-old twins, had their mom just stayed a denominator. And every day, when I sit in conference rooms and hear from countless people about how difficult it is to prevent this and reduce that, and how zero is not feasible, I think about numerators. I don’t look at their bar chart, or their run chart, or their red line, or their blue line, or whether their line is within the control limits, or what their P-value is. I think about who represents that black dot, and about how we are going to actually convince ourselves to “First, do no harm.”
When I find myself amongst a crowd quibbling about finances, lunch breaks, workflows, accountability, and about who is going to check the box or fill out the form, I think about the numerators, and how we are truly wasting their time, their livelihood, and their ability to stay below the line.
And someday, when my niece and nephew are old enough to understand, I will try to help them tolerate and accept the fact that “preventable” and “prevented” are not interchangeable. At least not in the medical industry. At least not yet.
In memory of Colleen Conlin Bowen, May 14, 2004
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at scheured@musc.edu.
Reference
Recommendations for Antithrombotic and Thrombolytic Therapy
Background
Each year, 1 million people are hospitalized with a diagnosis of stroke; it was the fourth-leading cause of death in the U.S. in 2009 and 2010.1 The majority of strokes (80%) are caused by focal cerebral ischemia, and the remainder are caused by hemorrhage.1 In 2008, the direct medical costs of stroke were approximately $18.8 billion, with almost half of this amount directed toward hospitalization.1 Although stroke inpatients make up only 3% of total hospitalizations, the mortality rate is more than twice that of other patients’.1
Over the past several decades, much has been learned about the pathophysiology and treatment for ischemic stroke. The mainstays of therapies include restoring perfusion in a timely manner and targeting both clot formation and hemostasis. These therapies improve patient outcomes and reduce the risk of recurrence in appropriately selected populations.
Guideline Update
In February, the American College of Chest Physicians (ACCP) published new practice guidelines for medical patients regarding antithrombotic and thrombolytic therapy in acute ischemic stroke.2 These evidence-based guidelines are the result of new clinical trial data and a review of previous studies. They address three aspects of management decisions for stroke, including acute treatment, VTE prevention, and secondary prevention, as well as specifically address the treatment of cerebral venous sinus thrombosis.
In the management of acute ischemic stroke, several recommendations were made. In terms of IV recombinant tissue plasminogen activator (r-tPA) administration, the guidelines were expanded and allow for a less restrictive time threshold for administration. Previous recommendations limited the usage of IV r-tPA to within three hours of symptom onset in acute ischemic stroke. A science advisory from the American Heart Association/American Stroke Association (AHA/ASA) from 2009 extended that window to 4.5 hours. The 2012 ACCP guidelines have followed suit to extend this time to 4.5 hours from symptom onset as well.
In addition, intrarterial r-tPA can be given in patients not eligible for IV r-tPA within six hours of presentation of acute ischemic stroke due to proximal cerebral artery occlusion.
These updated acute stroke guidelines recommend against the use of mechanical thrombectomy based mostly on lack of data rather than lack of benefit.2
The new guidelines continue to recommend early aspirin therapy at a dosage of 160 mg to 325 mg within the first 48 hours of acute ischemic stroke. Therapeutic parenteral anticoagulation with heparin or related drugs was not recommended in patients with noncardioembolic stroke due to atrial fibrillation (afib) or in patients with stroke due to large artery stenosis or arterial dissection. In this updated analysis, there was no benefit of anticoagulation compared with antiplatelet therapy, and the risk for extracranial hemorrhage was increased. No specific recommendation regarding anticoagulation was made in patients with mechanical heart valves or intracardiac thrombus.
Updates have been made for VTE prophylaxis in patients hospitalized for acute stroke. In stroke patients with restricted mobility, prophylactic unfractionated heparin (UFH) or low-molecular-weight heparin (LMWH) and/or intermittent pneumatic compression devices should be initiated as early as possible. The panel is no longer recommending elastic compression stockings as VTE prevention given the risk of skin damage and no clear benefit in symptomatic VTE prevention. For patients with hemorrhagic stroke and restricted mobility, similar recommendations were made for VTE prevention, except to start pharmacologic treatment between days 2 and 4 of the hospital stay. However, if there is a bleeding concern, intermittent pneumatic compression devices are favored over pharmacologic prophylaxis. In all patients for whom pharmacologic prevention is utilized, prophylactic LMWH is preferred over UFH.
Secondary stroke prevention is addressed, with 2012 guidelines outlining a preference for clopidogrel or aspirin/extended-release dipyridamole rather than aspirin or cilostazol in patients with a history of noncardioembolic ischemic stroke or TIA. Oral anticoagulation is preferred in patients with a history of stroke or TIA with afib over aspirin alone, aspirin plus clopidogrel, or no antithrombotic therapy. Of the available anticoagulants, the panel recommended dabigatran 150 mg twice daily over adjusted-dose warfarin.2 This recommendation is based on results from the RE-LY trial, which showed dabigatran as noninferior to warfarin in patients with nonvalvular afib without severe renal failure or advanced liver disease.3
For patients who have contraindications or choose not to initiate anticoagulation, the combination of aspirin (ASA) and clopidogrel is a reasonable alternative. Timing of the initiation of oral anticoagulation should be between one and two weeks after the stroke. Patients with extensive infarction or hemorrhagic transformation should delay starting oral anticoagulation, with no exact timeline. Long-term antithrombotic therapy is contraindicated in patients with history of a symptomatic primary intracerebral hemorrhage.2 New guidelines also recommend full anticoagulation for patients with symptomatic cerebral venous sinus thrombosis.
The panel did not make any recommendations regarding statin usage. In several studies, findings showed that statins reduced infarct size and had improved outcome in all stroke types.4
Analysis
Prior to the 2012 update, the last guideline for antithrombotic and thrombolytic therapy for ischemic stroke was published by the ACCP in the June 2008 issue of Chest.5 Dating back to 2001, medications included r-tPA administration within three hours of stroke symptom onset, and aspirin, clopidogrel, or a com bination of aspirin and extended-release dipyridamole for stroke prophylaxis.
The management of stroke continues to focus on early intervention and secondary prevention. Thrombolytic therapy is an effective treatment of acute ischemic stroke if given within the narrow window from onset of stroke symptoms up to 4.5 hours, with the goal of treatment within a three-hour window. Beyond this time constraint, the risk outweighs the benefit of using r-tPA except in the case of intra-arterial r-tPA administration for proximal cerebral artery occlusion.
In 2010, a meta-analysis supported this by showing that the risk of death increased significantly in patients receiving r-tPA beyond 4.5 hours. Therefore, antiplatelet therapy is the best alternative for patients ineligible for thrombolytic therapy.6 Even so, that study offered little data for patients with mechanical heart valves or intracardiac thrombi. Thus, the choice for acute anticoagulation therapy is variable and uncertain. If the hemorrhagic risk is low, anticoagulation can be considered in this subgroup, but no specific guideline endorsement was made.
In 2011, the AHA/ASA published an updated treatment guideline for patients with stroke or TIA. This was an update to 2007 guidelines that outlined the early management of ischemic stroke and affirmed the benefit of IV r-tPA at 4.5 hours for the treatment of stroke.7 Of note, IV r-tPA is only FDA-approved for treatment of acute ischemic stroke within the previously recommended three-hour period from symptom onset.
Aspirin has been found to be effective in both early treatment of acute ischemic stroke and secondary prevention. The CAST trial showed a statistically significant rate of reduction of nonfatal strokes with the use of aspirin. Other antiplatelet agents, including clopidogrel and dipyridamole, can be used. The FASTER trial compared aspirin alone versus aspirin plus clopidogrel, with no difference in outcome measures, although the MATCH trial found a larger risk of hemorrhagic and bleeding complications in the acetylsalicylic acid (ASA)-plus-clopidogrel group.6,7
In TIA or stroke patients, clopidogrel is not superior to ASA in preventing recurrent stroke. However, patients who have peripheral artery disease (PAD), previous coronary artery bypass grafting (CABG), insulin dependent diabetes mellitus (IDDM), or recurrent vascular events show a benefit of transitioning from ASA to clopidogrel for secondary long-term prevention. Clopidogrel or aspirin/extended-release dipyridamole is preferred over aspirin alone or cilostazol for long-term treatment in patients with a history of noncardioembolic ischemic stroke or TIA based on the PROFESS trial.2,7
HM Takeaways
The 2012 guidelines are a resource available to hospitalists for treating acute ischemic stroke either alone or with neurology consultation. These guidelines further define the timing of r-tPA and the use of both anticoagulation and antiplatelet therapy in the proper clinical settings.
In terms of VTE prevention, the guidelines recommend using LMWH preferentially over UH, except in patients at risk for rebleeding. The clinician should be aware of the treatment considerations for secondary prevention, noting the primary role of aspirin therapy in ischemic stroke with consideration of other agents (i.e. clopidogrel) in select populations.
Drs. Barr and Schumacher are hospitalists and assistant professors in the division of hospital medicine at The Ohio State University College of Medicine in Columbus.
References
Available at the-hospitalist.org.
Background
Each year, 1 million people are hospitalized with a diagnosis of stroke; it was the fourth-leading cause of death in the U.S. in 2009 and 2010.1 The majority of strokes (80%) are caused by focal cerebral ischemia, and the remainder are caused by hemorrhage.1 In 2008, the direct medical costs of stroke were approximately $18.8 billion, with almost half of this amount directed toward hospitalization.1 Although stroke inpatients make up only 3% of total hospitalizations, the mortality rate is more than twice that of other patients’.1
Over the past several decades, much has been learned about the pathophysiology and treatment for ischemic stroke. The mainstays of therapies include restoring perfusion in a timely manner and targeting both clot formation and hemostasis. These therapies improve patient outcomes and reduce the risk of recurrence in appropriately selected populations.
Guideline Update
In February, the American College of Chest Physicians (ACCP) published new practice guidelines for medical patients regarding antithrombotic and thrombolytic therapy in acute ischemic stroke.2 These evidence-based guidelines are the result of new clinical trial data and a review of previous studies. They address three aspects of management decisions for stroke, including acute treatment, VTE prevention, and secondary prevention, as well as specifically address the treatment of cerebral venous sinus thrombosis.
In the management of acute ischemic stroke, several recommendations were made. In terms of IV recombinant tissue plasminogen activator (r-tPA) administration, the guidelines were expanded and allow for a less restrictive time threshold for administration. Previous recommendations limited the usage of IV r-tPA to within three hours of symptom onset in acute ischemic stroke. A science advisory from the American Heart Association/American Stroke Association (AHA/ASA) from 2009 extended that window to 4.5 hours. The 2012 ACCP guidelines have followed suit to extend this time to 4.5 hours from symptom onset as well.
In addition, intrarterial r-tPA can be given in patients not eligible for IV r-tPA within six hours of presentation of acute ischemic stroke due to proximal cerebral artery occlusion.
These updated acute stroke guidelines recommend against the use of mechanical thrombectomy based mostly on lack of data rather than lack of benefit.2
The new guidelines continue to recommend early aspirin therapy at a dosage of 160 mg to 325 mg within the first 48 hours of acute ischemic stroke. Therapeutic parenteral anticoagulation with heparin or related drugs was not recommended in patients with noncardioembolic stroke due to atrial fibrillation (afib) or in patients with stroke due to large artery stenosis or arterial dissection. In this updated analysis, there was no benefit of anticoagulation compared with antiplatelet therapy, and the risk for extracranial hemorrhage was increased. No specific recommendation regarding anticoagulation was made in patients with mechanical heart valves or intracardiac thrombus.
Updates have been made for VTE prophylaxis in patients hospitalized for acute stroke. In stroke patients with restricted mobility, prophylactic unfractionated heparin (UFH) or low-molecular-weight heparin (LMWH) and/or intermittent pneumatic compression devices should be initiated as early as possible. The panel is no longer recommending elastic compression stockings as VTE prevention given the risk of skin damage and no clear benefit in symptomatic VTE prevention. For patients with hemorrhagic stroke and restricted mobility, similar recommendations were made for VTE prevention, except to start pharmacologic treatment between days 2 and 4 of the hospital stay. However, if there is a bleeding concern, intermittent pneumatic compression devices are favored over pharmacologic prophylaxis. In all patients for whom pharmacologic prevention is utilized, prophylactic LMWH is preferred over UFH.
Secondary stroke prevention is addressed, with 2012 guidelines outlining a preference for clopidogrel or aspirin/extended-release dipyridamole rather than aspirin or cilostazol in patients with a history of noncardioembolic ischemic stroke or TIA. Oral anticoagulation is preferred in patients with a history of stroke or TIA with afib over aspirin alone, aspirin plus clopidogrel, or no antithrombotic therapy. Of the available anticoagulants, the panel recommended dabigatran 150 mg twice daily over adjusted-dose warfarin.2 This recommendation is based on results from the RE-LY trial, which showed dabigatran as noninferior to warfarin in patients with nonvalvular afib without severe renal failure or advanced liver disease.3
For patients who have contraindications or choose not to initiate anticoagulation, the combination of aspirin (ASA) and clopidogrel is a reasonable alternative. Timing of the initiation of oral anticoagulation should be between one and two weeks after the stroke. Patients with extensive infarction or hemorrhagic transformation should delay starting oral anticoagulation, with no exact timeline. Long-term antithrombotic therapy is contraindicated in patients with history of a symptomatic primary intracerebral hemorrhage.2 New guidelines also recommend full anticoagulation for patients with symptomatic cerebral venous sinus thrombosis.
The panel did not make any recommendations regarding statin usage. In several studies, findings showed that statins reduced infarct size and had improved outcome in all stroke types.4
Analysis
Prior to the 2012 update, the last guideline for antithrombotic and thrombolytic therapy for ischemic stroke was published by the ACCP in the June 2008 issue of Chest.5 Dating back to 2001, medications included r-tPA administration within three hours of stroke symptom onset, and aspirin, clopidogrel, or a com bination of aspirin and extended-release dipyridamole for stroke prophylaxis.
The management of stroke continues to focus on early intervention and secondary prevention. Thrombolytic therapy is an effective treatment of acute ischemic stroke if given within the narrow window from onset of stroke symptoms up to 4.5 hours, with the goal of treatment within a three-hour window. Beyond this time constraint, the risk outweighs the benefit of using r-tPA except in the case of intra-arterial r-tPA administration for proximal cerebral artery occlusion.
In 2010, a meta-analysis supported this by showing that the risk of death increased significantly in patients receiving r-tPA beyond 4.5 hours. Therefore, antiplatelet therapy is the best alternative for patients ineligible for thrombolytic therapy.6 Even so, that study offered little data for patients with mechanical heart valves or intracardiac thrombi. Thus, the choice for acute anticoagulation therapy is variable and uncertain. If the hemorrhagic risk is low, anticoagulation can be considered in this subgroup, but no specific guideline endorsement was made.
In 2011, the AHA/ASA published an updated treatment guideline for patients with stroke or TIA. This was an update to 2007 guidelines that outlined the early management of ischemic stroke and affirmed the benefit of IV r-tPA at 4.5 hours for the treatment of stroke.7 Of note, IV r-tPA is only FDA-approved for treatment of acute ischemic stroke within the previously recommended three-hour period from symptom onset.
Aspirin has been found to be effective in both early treatment of acute ischemic stroke and secondary prevention. The CAST trial showed a statistically significant rate of reduction of nonfatal strokes with the use of aspirin. Other antiplatelet agents, including clopidogrel and dipyridamole, can be used. The FASTER trial compared aspirin alone versus aspirin plus clopidogrel, with no difference in outcome measures, although the MATCH trial found a larger risk of hemorrhagic and bleeding complications in the acetylsalicylic acid (ASA)-plus-clopidogrel group.6,7
In TIA or stroke patients, clopidogrel is not superior to ASA in preventing recurrent stroke. However, patients who have peripheral artery disease (PAD), previous coronary artery bypass grafting (CABG), insulin dependent diabetes mellitus (IDDM), or recurrent vascular events show a benefit of transitioning from ASA to clopidogrel for secondary long-term prevention. Clopidogrel or aspirin/extended-release dipyridamole is preferred over aspirin alone or cilostazol for long-term treatment in patients with a history of noncardioembolic ischemic stroke or TIA based on the PROFESS trial.2,7
HM Takeaways
The 2012 guidelines are a resource available to hospitalists for treating acute ischemic stroke either alone or with neurology consultation. These guidelines further define the timing of r-tPA and the use of both anticoagulation and antiplatelet therapy in the proper clinical settings.
In terms of VTE prevention, the guidelines recommend using LMWH preferentially over UH, except in patients at risk for rebleeding. The clinician should be aware of the treatment considerations for secondary prevention, noting the primary role of aspirin therapy in ischemic stroke with consideration of other agents (i.e. clopidogrel) in select populations.
Drs. Barr and Schumacher are hospitalists and assistant professors in the division of hospital medicine at The Ohio State University College of Medicine in Columbus.
References
Available at the-hospitalist.org.
Background
Each year, 1 million people are hospitalized with a diagnosis of stroke; it was the fourth-leading cause of death in the U.S. in 2009 and 2010.1 The majority of strokes (80%) are caused by focal cerebral ischemia, and the remainder are caused by hemorrhage.1 In 2008, the direct medical costs of stroke were approximately $18.8 billion, with almost half of this amount directed toward hospitalization.1 Although stroke inpatients make up only 3% of total hospitalizations, the mortality rate is more than twice that of other patients’.1
Over the past several decades, much has been learned about the pathophysiology and treatment for ischemic stroke. The mainstays of therapies include restoring perfusion in a timely manner and targeting both clot formation and hemostasis. These therapies improve patient outcomes and reduce the risk of recurrence in appropriately selected populations.
Guideline Update
In February, the American College of Chest Physicians (ACCP) published new practice guidelines for medical patients regarding antithrombotic and thrombolytic therapy in acute ischemic stroke.2 These evidence-based guidelines are the result of new clinical trial data and a review of previous studies. They address three aspects of management decisions for stroke, including acute treatment, VTE prevention, and secondary prevention, as well as specifically address the treatment of cerebral venous sinus thrombosis.
In the management of acute ischemic stroke, several recommendations were made. In terms of IV recombinant tissue plasminogen activator (r-tPA) administration, the guidelines were expanded and allow for a less restrictive time threshold for administration. Previous recommendations limited the usage of IV r-tPA to within three hours of symptom onset in acute ischemic stroke. A science advisory from the American Heart Association/American Stroke Association (AHA/ASA) from 2009 extended that window to 4.5 hours. The 2012 ACCP guidelines have followed suit to extend this time to 4.5 hours from symptom onset as well.
In addition, intrarterial r-tPA can be given in patients not eligible for IV r-tPA within six hours of presentation of acute ischemic stroke due to proximal cerebral artery occlusion.
These updated acute stroke guidelines recommend against the use of mechanical thrombectomy based mostly on lack of data rather than lack of benefit.2
The new guidelines continue to recommend early aspirin therapy at a dosage of 160 mg to 325 mg within the first 48 hours of acute ischemic stroke. Therapeutic parenteral anticoagulation with heparin or related drugs was not recommended in patients with noncardioembolic stroke due to atrial fibrillation (afib) or in patients with stroke due to large artery stenosis or arterial dissection. In this updated analysis, there was no benefit of anticoagulation compared with antiplatelet therapy, and the risk for extracranial hemorrhage was increased. No specific recommendation regarding anticoagulation was made in patients with mechanical heart valves or intracardiac thrombus.
Updates have been made for VTE prophylaxis in patients hospitalized for acute stroke. In stroke patients with restricted mobility, prophylactic unfractionated heparin (UFH) or low-molecular-weight heparin (LMWH) and/or intermittent pneumatic compression devices should be initiated as early as possible. The panel is no longer recommending elastic compression stockings as VTE prevention given the risk of skin damage and no clear benefit in symptomatic VTE prevention. For patients with hemorrhagic stroke and restricted mobility, similar recommendations were made for VTE prevention, except to start pharmacologic treatment between days 2 and 4 of the hospital stay. However, if there is a bleeding concern, intermittent pneumatic compression devices are favored over pharmacologic prophylaxis. In all patients for whom pharmacologic prevention is utilized, prophylactic LMWH is preferred over UFH.
Secondary stroke prevention is addressed, with 2012 guidelines outlining a preference for clopidogrel or aspirin/extended-release dipyridamole rather than aspirin or cilostazol in patients with a history of noncardioembolic ischemic stroke or TIA. Oral anticoagulation is preferred in patients with a history of stroke or TIA with afib over aspirin alone, aspirin plus clopidogrel, or no antithrombotic therapy. Of the available anticoagulants, the panel recommended dabigatran 150 mg twice daily over adjusted-dose warfarin.2 This recommendation is based on results from the RE-LY trial, which showed dabigatran as noninferior to warfarin in patients with nonvalvular afib without severe renal failure or advanced liver disease.3
For patients who have contraindications or choose not to initiate anticoagulation, the combination of aspirin (ASA) and clopidogrel is a reasonable alternative. Timing of the initiation of oral anticoagulation should be between one and two weeks after the stroke. Patients with extensive infarction or hemorrhagic transformation should delay starting oral anticoagulation, with no exact timeline. Long-term antithrombotic therapy is contraindicated in patients with history of a symptomatic primary intracerebral hemorrhage.2 New guidelines also recommend full anticoagulation for patients with symptomatic cerebral venous sinus thrombosis.
The panel did not make any recommendations regarding statin usage. In several studies, findings showed that statins reduced infarct size and had improved outcome in all stroke types.4
Analysis
Prior to the 2012 update, the last guideline for antithrombotic and thrombolytic therapy for ischemic stroke was published by the ACCP in the June 2008 issue of Chest.5 Dating back to 2001, medications included r-tPA administration within three hours of stroke symptom onset, and aspirin, clopidogrel, or a com bination of aspirin and extended-release dipyridamole for stroke prophylaxis.
The management of stroke continues to focus on early intervention and secondary prevention. Thrombolytic therapy is an effective treatment of acute ischemic stroke if given within the narrow window from onset of stroke symptoms up to 4.5 hours, with the goal of treatment within a three-hour window. Beyond this time constraint, the risk outweighs the benefit of using r-tPA except in the case of intra-arterial r-tPA administration for proximal cerebral artery occlusion.
In 2010, a meta-analysis supported this by showing that the risk of death increased significantly in patients receiving r-tPA beyond 4.5 hours. Therefore, antiplatelet therapy is the best alternative for patients ineligible for thrombolytic therapy.6 Even so, that study offered little data for patients with mechanical heart valves or intracardiac thrombi. Thus, the choice for acute anticoagulation therapy is variable and uncertain. If the hemorrhagic risk is low, anticoagulation can be considered in this subgroup, but no specific guideline endorsement was made.
In 2011, the AHA/ASA published an updated treatment guideline for patients with stroke or TIA. This was an update to 2007 guidelines that outlined the early management of ischemic stroke and affirmed the benefit of IV r-tPA at 4.5 hours for the treatment of stroke.7 Of note, IV r-tPA is only FDA-approved for treatment of acute ischemic stroke within the previously recommended three-hour period from symptom onset.
Aspirin has been found to be effective in both early treatment of acute ischemic stroke and secondary prevention. The CAST trial showed a statistically significant rate of reduction of nonfatal strokes with the use of aspirin. Other antiplatelet agents, including clopidogrel and dipyridamole, can be used. The FASTER trial compared aspirin alone versus aspirin plus clopidogrel, with no difference in outcome measures, although the MATCH trial found a larger risk of hemorrhagic and bleeding complications in the acetylsalicylic acid (ASA)-plus-clopidogrel group.6,7
In TIA or stroke patients, clopidogrel is not superior to ASA in preventing recurrent stroke. However, patients who have peripheral artery disease (PAD), previous coronary artery bypass grafting (CABG), insulin dependent diabetes mellitus (IDDM), or recurrent vascular events show a benefit of transitioning from ASA to clopidogrel for secondary long-term prevention. Clopidogrel or aspirin/extended-release dipyridamole is preferred over aspirin alone or cilostazol for long-term treatment in patients with a history of noncardioembolic ischemic stroke or TIA based on the PROFESS trial.2,7
HM Takeaways
The 2012 guidelines are a resource available to hospitalists for treating acute ischemic stroke either alone or with neurology consultation. These guidelines further define the timing of r-tPA and the use of both anticoagulation and antiplatelet therapy in the proper clinical settings.
In terms of VTE prevention, the guidelines recommend using LMWH preferentially over UH, except in patients at risk for rebleeding. The clinician should be aware of the treatment considerations for secondary prevention, noting the primary role of aspirin therapy in ischemic stroke with consideration of other agents (i.e. clopidogrel) in select populations.
Drs. Barr and Schumacher are hospitalists and assistant professors in the division of hospital medicine at The Ohio State University College of Medicine in Columbus.
References
Available at the-hospitalist.org.
Consider Patient Safety, Outcomes Risk before Prescribing Off-Label Drugs

Consider Patient Safety, Outcomes Risk before Prescribing “Off-Label”
What is the story with off-label drug use? I have seen some other physicians in my group use dabigatran for VTE prophylaxis, which I know it is not an approved indication. Am I taking on risk by continuing this treatment?
—Fabian Harris, Tuscaloosa, Ala.
Dr. Hospitalist responds:
Our friends at the FDA are in the business of approving drugs for use, but they do not regulate medical practice. So the short answer to your question is that off-label drug use is perfectly acceptable. Once a drug has been approved for use, if, in your clinical judgment, there are other indications for which it could be beneficial, then you are well within your rights to prescribe it. The FDA does not dictate how you practice medicine.
However, you will still be held to the community standard when it comes to your medical practice. As an example, gabapentin is used all the time for neuropathic pain syndromes, though technically it is only approved for seizures and post-herpetic neuralgia. Although the FDA won’t restrict your prescribing, it does prohibit pharmaceutical companies from marketing their drugs for anything other than their approved indications. In fact, Pfizer settled a case in 2004 on this very drug due to the promotion of prescribing it for nonapproved indications. I think at this point it’s fairly well accepted that lots of physicians use gabapentin for neuropathic pain, so you would not be too far out on a limb in prescribing it yourself in this manner.
For newer drugs, I might proceed with a little more caution. Anyone out there remember trovofloxacin (Trovan)? It was a new antibiotic approved in the late 1990s, with a coverage spectrum similar to levofloxacin, but with even more weight toward the gram positives. A wonder drug! Oral! As a result, it got prescribed like water, but not for the serious infections it was designed for: It got prescribed “off label” for common URIs and sinusitis. Unfortunately, it also caused a fair amount of liver failure and was summarily pulled from the market.
Does this mean dabigatran is a bad drug? No, but we don’t have much history with it, either. So while it might seem to be an innocuous extension to prescribe it for VTE prevention when it has already been approved for stroke prevention in afib, I think you carry some risk by doing this. In addition, some insurers will not cover a drug being prescribed in this manner, so you might be exposing your patient to added costs as well. Additionally, there’s nothing about off-label prescribing that says you have to tell the patient that’s what you’re doing. However, if you put together the factors of not informing a patient about an off-label use, and a patient having to pay out of pocket for that medicine, with an adverse outcome ... well, let’s just say that might not end too well.
Ultimately, I think you will need to consider the safety profile of the drug, the risk for an adverse outcome, your own risk tolerance, and the current state of medical practice before you consistently agree to use a drug “off label.” Given the slow-moving jungle of FDA approval, I can understand the desire to use a newer drug in an off-label manner, but it’s probably best to stop and think about the alternatives before proceeding. If you’re practicing in a group, then it’s just as important to come to a consensus with your partners about which drugs you will comfortably use off-label and which ones you won’t, especially as newer drugs come into the marketplace.
Consider Patient Safety, Outcomes Risk before Prescribing “Off-Label”
What is the story with off-label drug use? I have seen some other physicians in my group use dabigatran for VTE prophylaxis, which I know it is not an approved indication. Am I taking on risk by continuing this treatment?
—Fabian Harris, Tuscaloosa, Ala.
Dr. Hospitalist responds:
Our friends at the FDA are in the business of approving drugs for use, but they do not regulate medical practice. So the short answer to your question is that off-label drug use is perfectly acceptable. Once a drug has been approved for use, if, in your clinical judgment, there are other indications for which it could be beneficial, then you are well within your rights to prescribe it. The FDA does not dictate how you practice medicine.
However, you will still be held to the community standard when it comes to your medical practice. As an example, gabapentin is used all the time for neuropathic pain syndromes, though technically it is only approved for seizures and post-herpetic neuralgia. Although the FDA won’t restrict your prescribing, it does prohibit pharmaceutical companies from marketing their drugs for anything other than their approved indications. In fact, Pfizer settled a case in 2004 on this very drug due to the promotion of prescribing it for nonapproved indications. I think at this point it’s fairly well accepted that lots of physicians use gabapentin for neuropathic pain, so you would not be too far out on a limb in prescribing it yourself in this manner.
For newer drugs, I might proceed with a little more caution. Anyone out there remember trovofloxacin (Trovan)? It was a new antibiotic approved in the late 1990s, with a coverage spectrum similar to levofloxacin, but with even more weight toward the gram positives. A wonder drug! Oral! As a result, it got prescribed like water, but not for the serious infections it was designed for: It got prescribed “off label” for common URIs and sinusitis. Unfortunately, it also caused a fair amount of liver failure and was summarily pulled from the market.
Does this mean dabigatran is a bad drug? No, but we don’t have much history with it, either. So while it might seem to be an innocuous extension to prescribe it for VTE prevention when it has already been approved for stroke prevention in afib, I think you carry some risk by doing this. In addition, some insurers will not cover a drug being prescribed in this manner, so you might be exposing your patient to added costs as well. Additionally, there’s nothing about off-label prescribing that says you have to tell the patient that’s what you’re doing. However, if you put together the factors of not informing a patient about an off-label use, and a patient having to pay out of pocket for that medicine, with an adverse outcome ... well, let’s just say that might not end too well.
Ultimately, I think you will need to consider the safety profile of the drug, the risk for an adverse outcome, your own risk tolerance, and the current state of medical practice before you consistently agree to use a drug “off label.” Given the slow-moving jungle of FDA approval, I can understand the desire to use a newer drug in an off-label manner, but it’s probably best to stop and think about the alternatives before proceeding. If you’re practicing in a group, then it’s just as important to come to a consensus with your partners about which drugs you will comfortably use off-label and which ones you won’t, especially as newer drugs come into the marketplace.
Consider Patient Safety, Outcomes Risk before Prescribing “Off-Label”
What is the story with off-label drug use? I have seen some other physicians in my group use dabigatran for VTE prophylaxis, which I know it is not an approved indication. Am I taking on risk by continuing this treatment?
—Fabian Harris, Tuscaloosa, Ala.
Dr. Hospitalist responds:
Our friends at the FDA are in the business of approving drugs for use, but they do not regulate medical practice. So the short answer to your question is that off-label drug use is perfectly acceptable. Once a drug has been approved for use, if, in your clinical judgment, there are other indications for which it could be beneficial, then you are well within your rights to prescribe it. The FDA does not dictate how you practice medicine.
However, you will still be held to the community standard when it comes to your medical practice. As an example, gabapentin is used all the time for neuropathic pain syndromes, though technically it is only approved for seizures and post-herpetic neuralgia. Although the FDA won’t restrict your prescribing, it does prohibit pharmaceutical companies from marketing their drugs for anything other than their approved indications. In fact, Pfizer settled a case in 2004 on this very drug due to the promotion of prescribing it for nonapproved indications. I think at this point it’s fairly well accepted that lots of physicians use gabapentin for neuropathic pain, so you would not be too far out on a limb in prescribing it yourself in this manner.
For newer drugs, I might proceed with a little more caution. Anyone out there remember trovofloxacin (Trovan)? It was a new antibiotic approved in the late 1990s, with a coverage spectrum similar to levofloxacin, but with even more weight toward the gram positives. A wonder drug! Oral! As a result, it got prescribed like water, but not for the serious infections it was designed for: It got prescribed “off label” for common URIs and sinusitis. Unfortunately, it also caused a fair amount of liver failure and was summarily pulled from the market.
Does this mean dabigatran is a bad drug? No, but we don’t have much history with it, either. So while it might seem to be an innocuous extension to prescribe it for VTE prevention when it has already been approved for stroke prevention in afib, I think you carry some risk by doing this. In addition, some insurers will not cover a drug being prescribed in this manner, so you might be exposing your patient to added costs as well. Additionally, there’s nothing about off-label prescribing that says you have to tell the patient that’s what you’re doing. However, if you put together the factors of not informing a patient about an off-label use, and a patient having to pay out of pocket for that medicine, with an adverse outcome ... well, let’s just say that might not end too well.
Ultimately, I think you will need to consider the safety profile of the drug, the risk for an adverse outcome, your own risk tolerance, and the current state of medical practice before you consistently agree to use a drug “off label.” Given the slow-moving jungle of FDA approval, I can understand the desire to use a newer drug in an off-label manner, but it’s probably best to stop and think about the alternatives before proceeding. If you’re practicing in a group, then it’s just as important to come to a consensus with your partners about which drugs you will comfortably use off-label and which ones you won’t, especially as newer drugs come into the marketplace.
Federal Grant Supports "eHospitalist" Pilot Program in Wisconsin
John Almquist, MD, FHM, director of hospitalist services for Ministry Health Care, a 15-hospital system serving rural Wisconsin, believes that an "e-hospitalist" pilot project now being tested at Ministry St. Mary's Hospital in Rhinelander, Wis., could be a boon for rural communities that have difficulty recruiting primary-care physicians (PCPs).
When the hospitals in those communities are unable to offer hospitalist coverage, it makes the setting less attractive to PCPs because they might have to follow their patients in the hospital day and night, he explains.
Ministry recruited and trained two nurse practitioners who will soon be deployed at a critical-access hospital in Eagle River, population 1,443, supported remotely by the eight-member HM group in Rhinelander for consultations, supervision, and multidisciplinary rounds. The training is bolstered by written order sets focused on 30 common medical conditions that lead to admissions to rural hospitals.
"The hospitalist in Rhinelander is also able to talk directly to the patient at the remote site," Dr. Almquist says.
The e-hospitalist program uses a telehealth network developed by Marshfield Clinic, a multispecialty physician group practice based in Marshfield, Wis. The clinic recently received a $1 million grant from the federal government to expand its 15-year-old telemedicine program. Part of the grant money is being used to expand the ehospitalist approach to new sites.
Visit our website for more information about hospitalists and telemedicine.
John Almquist, MD, FHM, director of hospitalist services for Ministry Health Care, a 15-hospital system serving rural Wisconsin, believes that an "e-hospitalist" pilot project now being tested at Ministry St. Mary's Hospital in Rhinelander, Wis., could be a boon for rural communities that have difficulty recruiting primary-care physicians (PCPs).
When the hospitals in those communities are unable to offer hospitalist coverage, it makes the setting less attractive to PCPs because they might have to follow their patients in the hospital day and night, he explains.
Ministry recruited and trained two nurse practitioners who will soon be deployed at a critical-access hospital in Eagle River, population 1,443, supported remotely by the eight-member HM group in Rhinelander for consultations, supervision, and multidisciplinary rounds. The training is bolstered by written order sets focused on 30 common medical conditions that lead to admissions to rural hospitals.
"The hospitalist in Rhinelander is also able to talk directly to the patient at the remote site," Dr. Almquist says.
The e-hospitalist program uses a telehealth network developed by Marshfield Clinic, a multispecialty physician group practice based in Marshfield, Wis. The clinic recently received a $1 million grant from the federal government to expand its 15-year-old telemedicine program. Part of the grant money is being used to expand the ehospitalist approach to new sites.
Visit our website for more information about hospitalists and telemedicine.
John Almquist, MD, FHM, director of hospitalist services for Ministry Health Care, a 15-hospital system serving rural Wisconsin, believes that an "e-hospitalist" pilot project now being tested at Ministry St. Mary's Hospital in Rhinelander, Wis., could be a boon for rural communities that have difficulty recruiting primary-care physicians (PCPs).
When the hospitals in those communities are unable to offer hospitalist coverage, it makes the setting less attractive to PCPs because they might have to follow their patients in the hospital day and night, he explains.
Ministry recruited and trained two nurse practitioners who will soon be deployed at a critical-access hospital in Eagle River, population 1,443, supported remotely by the eight-member HM group in Rhinelander for consultations, supervision, and multidisciplinary rounds. The training is bolstered by written order sets focused on 30 common medical conditions that lead to admissions to rural hospitals.
"The hospitalist in Rhinelander is also able to talk directly to the patient at the remote site," Dr. Almquist says.
The e-hospitalist program uses a telehealth network developed by Marshfield Clinic, a multispecialty physician group practice based in Marshfield, Wis. The clinic recently received a $1 million grant from the federal government to expand its 15-year-old telemedicine program. Part of the grant money is being used to expand the ehospitalist approach to new sites.
Visit our website for more information about hospitalists and telemedicine.