User login
Accountable-Care Organizations on the Horizon for Hospitalists
Every HM group should look into transitioning from a fee-for-service model to an accountable-care organization (ACO), a leading hospitalist told conference attendees recently at the Third National Accountable Care Organization Congress.
"You need to be tackling it now, but that doesn't mean you need to be aggressively doing it now," Edward Murphy, MD, chairman of Sound Physicians, told eWire days before he spoke at the ACO Congress on Oct. 31 in Los Angeles. "By tackling it, you need to be doing a hard-nosed assessment of what's best for your group and your patients."
Question: Why is the ACO model so difficult in some instances?
Answer: The problem with the healthcare system today is we’ve spent 100 years building up a system that is designed around, and competent at, delivering services for fees. We're really not set up to manage care.
Q: What is the No. 1 thing you want hospitalists to know about ACOs today?
A: Figure out every single day how to improve the care of your patients at a lower cost. And then, how you can demonstrate it in a quantitative and clear way. ACO-style payments are really only a value proposition centered on providing superior outcomes for patients at higher satisfaction for lower cost. That’s a fundamental value that will always be noteworthy.
Q: Is a hospitalist's job to lead the charge toward ACOs, or support those who do?
A: That's the sort of thing that people on the ground don't have to be told. They just know. If I were the leader of a hospitalist group someplace and really thought the smart thing to do was to think about how to move to an accountable-care model … I would know from my discussions with my colleagues, my discussions with hospital executives where everybody was.
Visit our website for more information about ACOs.
Every HM group should look into transitioning from a fee-for-service model to an accountable-care organization (ACO), a leading hospitalist told conference attendees recently at the Third National Accountable Care Organization Congress.
"You need to be tackling it now, but that doesn't mean you need to be aggressively doing it now," Edward Murphy, MD, chairman of Sound Physicians, told eWire days before he spoke at the ACO Congress on Oct. 31 in Los Angeles. "By tackling it, you need to be doing a hard-nosed assessment of what's best for your group and your patients."
Question: Why is the ACO model so difficult in some instances?
Answer: The problem with the healthcare system today is we’ve spent 100 years building up a system that is designed around, and competent at, delivering services for fees. We're really not set up to manage care.
Q: What is the No. 1 thing you want hospitalists to know about ACOs today?
A: Figure out every single day how to improve the care of your patients at a lower cost. And then, how you can demonstrate it in a quantitative and clear way. ACO-style payments are really only a value proposition centered on providing superior outcomes for patients at higher satisfaction for lower cost. That’s a fundamental value that will always be noteworthy.
Q: Is a hospitalist's job to lead the charge toward ACOs, or support those who do?
A: That's the sort of thing that people on the ground don't have to be told. They just know. If I were the leader of a hospitalist group someplace and really thought the smart thing to do was to think about how to move to an accountable-care model … I would know from my discussions with my colleagues, my discussions with hospital executives where everybody was.
Visit our website for more information about ACOs.
Every HM group should look into transitioning from a fee-for-service model to an accountable-care organization (ACO), a leading hospitalist told conference attendees recently at the Third National Accountable Care Organization Congress.
"You need to be tackling it now, but that doesn't mean you need to be aggressively doing it now," Edward Murphy, MD, chairman of Sound Physicians, told eWire days before he spoke at the ACO Congress on Oct. 31 in Los Angeles. "By tackling it, you need to be doing a hard-nosed assessment of what's best for your group and your patients."
Question: Why is the ACO model so difficult in some instances?
Answer: The problem with the healthcare system today is we’ve spent 100 years building up a system that is designed around, and competent at, delivering services for fees. We're really not set up to manage care.
Q: What is the No. 1 thing you want hospitalists to know about ACOs today?
A: Figure out every single day how to improve the care of your patients at a lower cost. And then, how you can demonstrate it in a quantitative and clear way. ACO-style payments are really only a value proposition centered on providing superior outcomes for patients at higher satisfaction for lower cost. That’s a fundamental value that will always be noteworthy.
Q: Is a hospitalist's job to lead the charge toward ACOs, or support those who do?
A: That's the sort of thing that people on the ground don't have to be told. They just know. If I were the leader of a hospitalist group someplace and really thought the smart thing to do was to think about how to move to an accountable-care model … I would know from my discussions with my colleagues, my discussions with hospital executives where everybody was.
Visit our website for more information about ACOs.
ONLINE EXCLUSIVE: SHM Board Member Eric Siegal Offers Advice to Manage Scope Creep
ONLINE EXCLUSIVE: Anticoagulant's Receives FDA Approval to Treat Deep Vein Thrombosis, Pulmonary Embolism
Rivaroxaban (Xarelto) has won another approval from the U.S. Food and Drug Administration (FDA). Already green-lighted for use to reduce the risk of DVT and pulmonary embolism (PE) after knee or hip replacement surgery—and reduce the risk of stroke in non-valvular atrial fibrillation patients—the anticoagulant therapy has been approved for use in the treatment of acute DVT and PE, and to reduce the risk of recurrent DVT and PE after initial treatment. It’s a landmark step that will likely have big implications for hospitalists.
“Xarelto is the first oral anti-clotting drug approved to treat and reduce the recurrence of blood clots since the approval of warfarin nearly 60 years ago,” Richard Pazdur, MD, director of the Office of Hematology and Oncology Products in the FDA’s Center for Drug Evaluation and Research, said in a news release.
—Hiren Shah, MD, assistant professor of medicine, Northwestern University Feinberg School of Medicine, medical director, hospital medicine, Northwestern Memorial Hospital, Chicago
“Single-drug therapy without the need for parental bridging treatment, or drug-level monitoring, is a breakthrough in the treatment of VTE, and represents a paradigm shift that we have not seen in a long time for a very common emergency room and hospital-based medical condition,” says Hiren Shah, MD, assistant professor of medicine at Northwestern University’s Feinberg School of Medicine and medical director of hospital medicine at Northwestern Memorial Hospital in Chicago.
Ian Jenkins, assistant professor in the Division of Hospital Medicine at the University of California at San Diego, says factors that will help determine whether a patient is a candidate for rivaroxaban include the ability to pay for it; compliance, because the duration of effect is shorter than it is for warfarin; and good and stable renal function.
“We now have the first approved oral warfarin alternative for VTE, and for appropriate candidates, it's a more convenient if not better treatment,” Dr. Jenkins says. “The main downside is that warfarin remains reversible, and the new drugs are minimally so.”
Dr. Shah predicts a more efficient discharge process, which, for rivaroxaban patients, will no longer include arranging for international normalized ratio (INR) monitoring or time-consuming counseling on taking injections and drug interactions with vitamin-K antagonists.
“That’s a very complex, 30-minute process,” says Dr. Shah, who also who runs Northwestern’s VTE-prevention program. “With a single agent, I think the value here is you don’t need that complex care coordination anymore, and that’s time-saving for a hospitalist.”
Dr. Shah notes coordination of care will still be very important with this indication, especially because the dose for rivaroxaban in the treatment of acute DVT changes from twice a day to once a day starting at Day 21. “Whatever education initiatives we undertake, they have to extend that entire spectrum,” he adds.
Visit our website for more information about treating acute DVT.
Rivaroxaban (Xarelto) has won another approval from the U.S. Food and Drug Administration (FDA). Already green-lighted for use to reduce the risk of DVT and pulmonary embolism (PE) after knee or hip replacement surgery—and reduce the risk of stroke in non-valvular atrial fibrillation patients—the anticoagulant therapy has been approved for use in the treatment of acute DVT and PE, and to reduce the risk of recurrent DVT and PE after initial treatment. It’s a landmark step that will likely have big implications for hospitalists.
“Xarelto is the first oral anti-clotting drug approved to treat and reduce the recurrence of blood clots since the approval of warfarin nearly 60 years ago,” Richard Pazdur, MD, director of the Office of Hematology and Oncology Products in the FDA’s Center for Drug Evaluation and Research, said in a news release.
—Hiren Shah, MD, assistant professor of medicine, Northwestern University Feinberg School of Medicine, medical director, hospital medicine, Northwestern Memorial Hospital, Chicago
“Single-drug therapy without the need for parental bridging treatment, or drug-level monitoring, is a breakthrough in the treatment of VTE, and represents a paradigm shift that we have not seen in a long time for a very common emergency room and hospital-based medical condition,” says Hiren Shah, MD, assistant professor of medicine at Northwestern University’s Feinberg School of Medicine and medical director of hospital medicine at Northwestern Memorial Hospital in Chicago.
Ian Jenkins, assistant professor in the Division of Hospital Medicine at the University of California at San Diego, says factors that will help determine whether a patient is a candidate for rivaroxaban include the ability to pay for it; compliance, because the duration of effect is shorter than it is for warfarin; and good and stable renal function.
“We now have the first approved oral warfarin alternative for VTE, and for appropriate candidates, it's a more convenient if not better treatment,” Dr. Jenkins says. “The main downside is that warfarin remains reversible, and the new drugs are minimally so.”
Dr. Shah predicts a more efficient discharge process, which, for rivaroxaban patients, will no longer include arranging for international normalized ratio (INR) monitoring or time-consuming counseling on taking injections and drug interactions with vitamin-K antagonists.
“That’s a very complex, 30-minute process,” says Dr. Shah, who also who runs Northwestern’s VTE-prevention program. “With a single agent, I think the value here is you don’t need that complex care coordination anymore, and that’s time-saving for a hospitalist.”
Dr. Shah notes coordination of care will still be very important with this indication, especially because the dose for rivaroxaban in the treatment of acute DVT changes from twice a day to once a day starting at Day 21. “Whatever education initiatives we undertake, they have to extend that entire spectrum,” he adds.
Visit our website for more information about treating acute DVT.
Rivaroxaban (Xarelto) has won another approval from the U.S. Food and Drug Administration (FDA). Already green-lighted for use to reduce the risk of DVT and pulmonary embolism (PE) after knee or hip replacement surgery—and reduce the risk of stroke in non-valvular atrial fibrillation patients—the anticoagulant therapy has been approved for use in the treatment of acute DVT and PE, and to reduce the risk of recurrent DVT and PE after initial treatment. It’s a landmark step that will likely have big implications for hospitalists.
“Xarelto is the first oral anti-clotting drug approved to treat and reduce the recurrence of blood clots since the approval of warfarin nearly 60 years ago,” Richard Pazdur, MD, director of the Office of Hematology and Oncology Products in the FDA’s Center for Drug Evaluation and Research, said in a news release.
—Hiren Shah, MD, assistant professor of medicine, Northwestern University Feinberg School of Medicine, medical director, hospital medicine, Northwestern Memorial Hospital, Chicago
“Single-drug therapy without the need for parental bridging treatment, or drug-level monitoring, is a breakthrough in the treatment of VTE, and represents a paradigm shift that we have not seen in a long time for a very common emergency room and hospital-based medical condition,” says Hiren Shah, MD, assistant professor of medicine at Northwestern University’s Feinberg School of Medicine and medical director of hospital medicine at Northwestern Memorial Hospital in Chicago.
Ian Jenkins, assistant professor in the Division of Hospital Medicine at the University of California at San Diego, says factors that will help determine whether a patient is a candidate for rivaroxaban include the ability to pay for it; compliance, because the duration of effect is shorter than it is for warfarin; and good and stable renal function.
“We now have the first approved oral warfarin alternative for VTE, and for appropriate candidates, it's a more convenient if not better treatment,” Dr. Jenkins says. “The main downside is that warfarin remains reversible, and the new drugs are minimally so.”
Dr. Shah predicts a more efficient discharge process, which, for rivaroxaban patients, will no longer include arranging for international normalized ratio (INR) monitoring or time-consuming counseling on taking injections and drug interactions with vitamin-K antagonists.
“That’s a very complex, 30-minute process,” says Dr. Shah, who also who runs Northwestern’s VTE-prevention program. “With a single agent, I think the value here is you don’t need that complex care coordination anymore, and that’s time-saving for a hospitalist.”
Dr. Shah notes coordination of care will still be very important with this indication, especially because the dose for rivaroxaban in the treatment of acute DVT changes from twice a day to once a day starting at Day 21. “Whatever education initiatives we undertake, they have to extend that entire spectrum,” he adds.
Visit our website for more information about treating acute DVT.
U.S. Army Supports Rapid Deployment of Hospital Practice



A U.S. military combat-support hospital team based at Fort Polk near Leesville, La., works hard year-round to remain ready to erect a temporary, fully functioning tent hospital within 72 hours whenever and wherever it’s needed. That could mean an overseas war zone or closer to home for Americans hit by a tornado or hurricane.
The 115th Forward Support Battalion, led by Col. Kevin J. Stevens, has practiced assembling the temporary hospital three times this year, with another exercise planned for October. In its last run-through, a 24-hour acute-care hospital of 84 beds was erected in 66 hours. It included two operating rooms, two 24-bed ICUs with ventilators, patient wards, a six-bay ED, specialty clinics, and lab, pathology, biomedical, pharmacy, and blood services.
All of the needed equipment can be moved by truck, airplane, or boat in 32 20-foot-long vehicles, Stevens says. The staging team lays out the perimeter, perhaps in a parking lot or an existing structure, such as a school. Heating and cooling systems, water, oxygen, and power generators are brought in, and the team establishes a landing pad for helicopters.
“We bring all that wherever we go. But setting it up is the easy part,” Stevens says, adding that staffing and managing an acute-care hospital is the hard part.
When fully operational, the temporary hospital employs a professional staff of 75 to 80, including medical specialists. Some are based year-round at Fort Polk, keeping the equipment maintained. Others practice at hospitals across the country but are on the “call list” when a deployment is ordered. A new set of up-to-date, interlocking equipment for the temporary hospital was issued in March.
“Getting better at this is my mission,” says Stevens, a soldier since 1974 who has deployed with Forward Support Hospitals in both Iraq and Afghanistan. “We work to keep medical and deployment skills sharp at all times. Everything we do is meant to save soldier and civilian lives.”
Larry Beresford is a freelance writer in Oakland, Calif.
A U.S. military combat-support hospital team based at Fort Polk near Leesville, La., works hard year-round to remain ready to erect a temporary, fully functioning tent hospital within 72 hours whenever and wherever it’s needed. That could mean an overseas war zone or closer to home for Americans hit by a tornado or hurricane.
The 115th Forward Support Battalion, led by Col. Kevin J. Stevens, has practiced assembling the temporary hospital three times this year, with another exercise planned for October. In its last run-through, a 24-hour acute-care hospital of 84 beds was erected in 66 hours. It included two operating rooms, two 24-bed ICUs with ventilators, patient wards, a six-bay ED, specialty clinics, and lab, pathology, biomedical, pharmacy, and blood services.
All of the needed equipment can be moved by truck, airplane, or boat in 32 20-foot-long vehicles, Stevens says. The staging team lays out the perimeter, perhaps in a parking lot or an existing structure, such as a school. Heating and cooling systems, water, oxygen, and power generators are brought in, and the team establishes a landing pad for helicopters.
“We bring all that wherever we go. But setting it up is the easy part,” Stevens says, adding that staffing and managing an acute-care hospital is the hard part.
When fully operational, the temporary hospital employs a professional staff of 75 to 80, including medical specialists. Some are based year-round at Fort Polk, keeping the equipment maintained. Others practice at hospitals across the country but are on the “call list” when a deployment is ordered. A new set of up-to-date, interlocking equipment for the temporary hospital was issued in March.
“Getting better at this is my mission,” says Stevens, a soldier since 1974 who has deployed with Forward Support Hospitals in both Iraq and Afghanistan. “We work to keep medical and deployment skills sharp at all times. Everything we do is meant to save soldier and civilian lives.”
Larry Beresford is a freelance writer in Oakland, Calif.
A U.S. military combat-support hospital team based at Fort Polk near Leesville, La., works hard year-round to remain ready to erect a temporary, fully functioning tent hospital within 72 hours whenever and wherever it’s needed. That could mean an overseas war zone or closer to home for Americans hit by a tornado or hurricane.
The 115th Forward Support Battalion, led by Col. Kevin J. Stevens, has practiced assembling the temporary hospital three times this year, with another exercise planned for October. In its last run-through, a 24-hour acute-care hospital of 84 beds was erected in 66 hours. It included two operating rooms, two 24-bed ICUs with ventilators, patient wards, a six-bay ED, specialty clinics, and lab, pathology, biomedical, pharmacy, and blood services.
All of the needed equipment can be moved by truck, airplane, or boat in 32 20-foot-long vehicles, Stevens says. The staging team lays out the perimeter, perhaps in a parking lot or an existing structure, such as a school. Heating and cooling systems, water, oxygen, and power generators are brought in, and the team establishes a landing pad for helicopters.
“We bring all that wherever we go. But setting it up is the easy part,” Stevens says, adding that staffing and managing an acute-care hospital is the hard part.
When fully operational, the temporary hospital employs a professional staff of 75 to 80, including medical specialists. Some are based year-round at Fort Polk, keeping the equipment maintained. Others practice at hospitals across the country but are on the “call list” when a deployment is ordered. A new set of up-to-date, interlocking equipment for the temporary hospital was issued in March.
“Getting better at this is my mission,” says Stevens, a soldier since 1974 who has deployed with Forward Support Hospitals in both Iraq and Afghanistan. “We work to keep medical and deployment skills sharp at all times. Everything we do is meant to save soldier and civilian lives.”
Larry Beresford is a freelance writer in Oakland, Calif.
Five Ways Hospitalists Can Prevent Overextending Their Services
1. Do not feel sorry for yourself; it can become a self-fulfilling prophecy.
“Most of what is happening in medicine is outside of our control,” Dr. Nelson says. “We need to realize that our role is going to change, and we should not perceive ourselves as the low person on the totem pole.”
2. Increase “face time” with your specialist colleagues.
Join them for lunch in the physician’s lounge, call your colleagues by their first names, engage in meaningful discussions about cases, and show empathy for them and their patients. Look for opportunities to do mutual education with other services.
3. Know when to draw the line.
“HM leaders should have the skills to analyze an opportunity and assess whether their program has the staffing capacity and clinical skills to successfully deliver a requested service,” Dr. Simone says. “‘No’ is an acceptable answer, if there are clear and reasonable reasons that support that decision.”
4. Make it about the patient.
Whenever your HM service is approached about comanagement, phrase your decision within the context of ensuring patient safety and delivering quality care. In that way, Dr. Siy says, you will be on solid footing.
5. Openly promote strategic “yes” answers.
Instead of digging in their heels, HM groups can periodically examine all requests, pick one or two to begin with, then promote successful outcomes to boost the group’s value.
1. Do not feel sorry for yourself; it can become a self-fulfilling prophecy.
“Most of what is happening in medicine is outside of our control,” Dr. Nelson says. “We need to realize that our role is going to change, and we should not perceive ourselves as the low person on the totem pole.”
2. Increase “face time” with your specialist colleagues.
Join them for lunch in the physician’s lounge, call your colleagues by their first names, engage in meaningful discussions about cases, and show empathy for them and their patients. Look for opportunities to do mutual education with other services.
3. Know when to draw the line.
“HM leaders should have the skills to analyze an opportunity and assess whether their program has the staffing capacity and clinical skills to successfully deliver a requested service,” Dr. Simone says. “‘No’ is an acceptable answer, if there are clear and reasonable reasons that support that decision.”
4. Make it about the patient.
Whenever your HM service is approached about comanagement, phrase your decision within the context of ensuring patient safety and delivering quality care. In that way, Dr. Siy says, you will be on solid footing.
5. Openly promote strategic “yes” answers.
Instead of digging in their heels, HM groups can periodically examine all requests, pick one or two to begin with, then promote successful outcomes to boost the group’s value.
1. Do not feel sorry for yourself; it can become a self-fulfilling prophecy.
“Most of what is happening in medicine is outside of our control,” Dr. Nelson says. “We need to realize that our role is going to change, and we should not perceive ourselves as the low person on the totem pole.”
2. Increase “face time” with your specialist colleagues.
Join them for lunch in the physician’s lounge, call your colleagues by their first names, engage in meaningful discussions about cases, and show empathy for them and their patients. Look for opportunities to do mutual education with other services.
3. Know when to draw the line.
“HM leaders should have the skills to analyze an opportunity and assess whether their program has the staffing capacity and clinical skills to successfully deliver a requested service,” Dr. Simone says. “‘No’ is an acceptable answer, if there are clear and reasonable reasons that support that decision.”
4. Make it about the patient.
Whenever your HM service is approached about comanagement, phrase your decision within the context of ensuring patient safety and delivering quality care. In that way, Dr. Siy says, you will be on solid footing.
5. Openly promote strategic “yes” answers.
Instead of digging in their heels, HM groups can periodically examine all requests, pick one or two to begin with, then promote successful outcomes to boost the group’s value.
John Nelson: Heavy Workloads
Now that HM is moving (or has moved?) from infancy to adolescence or even maturity, you might think that we would have reached some sort of consensus on what a reasonable workload—or patient volume—for a hospitalist is. My sense is that conventional wisdom says a reasonable average daily workload for a daytime rounding/admitting hospitalist is in the range of 12 to 17 billed encounters. And to average this volume, the doctor will have a number of days with more or fewer patients.
After thinking about average workload, the next question is: What is a reasonable upper limit for patient volume on a single day? Here, opinion seems to be a little fuzzier, but I think most would say a hospitalist should be expected to see more than 20 patients in a single day only on rare occasions and on, say, no more than 10 days annually. Keep in mind that a hospitalist who has 22 patients today still has a pretty good chance they will have 20 or more tomorrow, and the day after. High volumes are not a single-day phenomenon, either, because it usually takes a number of days for those patients to reach discharge—and the doctor to realize a decline in workload.
But these numbers are only conventional wisdom. There are little research data to guide our thinking about patient volumes, and thoughtful people sometimes arrive at very different conclusions. As I’ve written in this space previously, I think each individual hospitalist should have significant influence or autonomy to decide the appropriate or optimal patient volume for themselves or their group. This usually requires that doctors are connected to the economic and quality-of-care effects of their patient volume choices, something many hospitalists resist.
Divergence of Opinion
But given lots of autonomy, some hospitalists could make poor choices. I have had the experience of working with hospitalists in three practices around the country who are confident that, at least for themselves, very high patient volumes are safe and reasonable. These high-energy hospitalists see as many as 30 or 40 patients per day, day after day.
At one of these practices, I sat down with the doctors on duty that day at 1 p.m. and talked uninterrupted by pager or patient-care issues for nearly three hours. It was only at the end of the meeting that they explained each of them was seeing around 30 patients that day but had nearly finished rounds before our meeting started. I was stunned. (I probably wouldn’t stop for lunch, to say nothing of a three-hour meeting, to see just 20 patients in a day.)
So I asked just what they saw as an excessive daily patient volume. One of them seemed to deliberate carefully and said, “I probably need help when I have more than 35 patients to see in a day, but I’m OK with anything less than that.”
But the record goes to a really nice, spirited hospitalist who told me that, in addition to his usual workload, he occasionally covered weekends for an internal-medicine group. On a recent weekend, he had 88 patients to see each day, he said. Yes, you read that correctly: 88! (Fortunately, he did see that as a problem and was working to decrease the number.)
Potential Risks
I want to be clear that my own opinion is that the volumes above are unacceptable and dangerous. I think that, in most settings, routinely seeing more than 20 patients in a day probably degrades performance and increases the risk of burnout. While I think most knowledgeable people in our field share this opinion, none of us can point to compelling, generalizable research data to support our opinion.
The way I see it, excessively high workloads risk:
- Adverse patient outcomes due to increased potential for clinical errors and accompanying poor documentation;
- Failure of hospitalists to meet performance and citizenship expectations, such as length of stay (LOS), resource utilization, use of standardized order sets, attention to early discharge times, etc.;
- Lack of any excess capacity to handle transient increases in workload;
- Recruiting and/or retention challenges for hospitalists who might not want to work so hard;
- High risk of hospitalist stress and burnout, which over time could negatively impact a person’s well-being, as well as their attitudes and interactions with other members of the patient care team;
- Overdependence on a few very-hard-working doctors; if one doctor gets sick or has to stop working for a period of time, the hospital must find the equivalent of one-and-a-half doctors to replace him or her; and
- Increased malpractice risk.
Limited Data
There is some research to guide the thinking about workload. I recall one or two abstracts presented at past SHM annual meetings in which doctors in a single practice showed that LOS increased when their patient volume was high. And some sharp hospitalist researchers at Christiana Care Health System in Wilmington, Del., conducted a more robust retrospective cohort study of thousands of non-ICU adult admissions to their 1,100-bed hospital over a three-year period. Their data, which they intend to publish, showed LOS rises as hospitalist workload increases.
Others have assessed the connection between workload and well-being or burnout. Surprisingly, it has been hard to document in the peer-reviewed literature that increasing workloads are associated with increased burnout. Studies of hospitalists published in 2001 and 2011 failed to show a connection between self-reported workload and burnout.1,2 A 2009 systemic review of literature on all physician specialties concluded that “an imbalance between expected and experienced … workload is moderately associated with dissatisfaction, but there is less evidence of a significant association with objective workload.”3 (Emphasis mine.)
Rather than workload, both of the hospitalist studies found that such attributes as organizational solidarity, climate, and fairness; the feeling of being valued by the whole healthcare team; personal time; and compensation were more tightly correlated with whether hospitalists would thrive than workload.
Unfortunately, I’m not aware of any robust studies showing the relationship between hospitalist workload and quality of care (please email me if you know of any). I think the burden of proof is on those who support high workloads to show they don’t adversely affect patient incomes.
If you’d like to discuss workload further, I’ll be moderating a session titled “Who Says 15 is the Right Number?” during HM13, May 17-19, 2013, in Washington, D.C. (www.hospitalmedicine2013.org). I hope to see you there.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is course co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at john.nelson@nelsonflores.com.
References
2. Hinami K, Whelan CT, Wolosin RJ, Miller JA, Wetterneck TB. Worklife and satisfaction of hospitalists: toward flourishing careers. J Gen Intern Med. 2012;27(1):28-36.
3. Scheurer D, McKean S, Miller J, Wetterneck T. U.S. physician satisfaction: a systematic review. J Hosp Med. 2009;4(9):560-568.
Now that HM is moving (or has moved?) from infancy to adolescence or even maturity, you might think that we would have reached some sort of consensus on what a reasonable workload—or patient volume—for a hospitalist is. My sense is that conventional wisdom says a reasonable average daily workload for a daytime rounding/admitting hospitalist is in the range of 12 to 17 billed encounters. And to average this volume, the doctor will have a number of days with more or fewer patients.
After thinking about average workload, the next question is: What is a reasonable upper limit for patient volume on a single day? Here, opinion seems to be a little fuzzier, but I think most would say a hospitalist should be expected to see more than 20 patients in a single day only on rare occasions and on, say, no more than 10 days annually. Keep in mind that a hospitalist who has 22 patients today still has a pretty good chance they will have 20 or more tomorrow, and the day after. High volumes are not a single-day phenomenon, either, because it usually takes a number of days for those patients to reach discharge—and the doctor to realize a decline in workload.
But these numbers are only conventional wisdom. There are little research data to guide our thinking about patient volumes, and thoughtful people sometimes arrive at very different conclusions. As I’ve written in this space previously, I think each individual hospitalist should have significant influence or autonomy to decide the appropriate or optimal patient volume for themselves or their group. This usually requires that doctors are connected to the economic and quality-of-care effects of their patient volume choices, something many hospitalists resist.
Divergence of Opinion
But given lots of autonomy, some hospitalists could make poor choices. I have had the experience of working with hospitalists in three practices around the country who are confident that, at least for themselves, very high patient volumes are safe and reasonable. These high-energy hospitalists see as many as 30 or 40 patients per day, day after day.
At one of these practices, I sat down with the doctors on duty that day at 1 p.m. and talked uninterrupted by pager or patient-care issues for nearly three hours. It was only at the end of the meeting that they explained each of them was seeing around 30 patients that day but had nearly finished rounds before our meeting started. I was stunned. (I probably wouldn’t stop for lunch, to say nothing of a three-hour meeting, to see just 20 patients in a day.)
So I asked just what they saw as an excessive daily patient volume. One of them seemed to deliberate carefully and said, “I probably need help when I have more than 35 patients to see in a day, but I’m OK with anything less than that.”
But the record goes to a really nice, spirited hospitalist who told me that, in addition to his usual workload, he occasionally covered weekends for an internal-medicine group. On a recent weekend, he had 88 patients to see each day, he said. Yes, you read that correctly: 88! (Fortunately, he did see that as a problem and was working to decrease the number.)
Potential Risks
I want to be clear that my own opinion is that the volumes above are unacceptable and dangerous. I think that, in most settings, routinely seeing more than 20 patients in a day probably degrades performance and increases the risk of burnout. While I think most knowledgeable people in our field share this opinion, none of us can point to compelling, generalizable research data to support our opinion.
The way I see it, excessively high workloads risk:
- Adverse patient outcomes due to increased potential for clinical errors and accompanying poor documentation;
- Failure of hospitalists to meet performance and citizenship expectations, such as length of stay (LOS), resource utilization, use of standardized order sets, attention to early discharge times, etc.;
- Lack of any excess capacity to handle transient increases in workload;
- Recruiting and/or retention challenges for hospitalists who might not want to work so hard;
- High risk of hospitalist stress and burnout, which over time could negatively impact a person’s well-being, as well as their attitudes and interactions with other members of the patient care team;
- Overdependence on a few very-hard-working doctors; if one doctor gets sick or has to stop working for a period of time, the hospital must find the equivalent of one-and-a-half doctors to replace him or her; and
- Increased malpractice risk.
Limited Data
There is some research to guide the thinking about workload. I recall one or two abstracts presented at past SHM annual meetings in which doctors in a single practice showed that LOS increased when their patient volume was high. And some sharp hospitalist researchers at Christiana Care Health System in Wilmington, Del., conducted a more robust retrospective cohort study of thousands of non-ICU adult admissions to their 1,100-bed hospital over a three-year period. Their data, which they intend to publish, showed LOS rises as hospitalist workload increases.
Others have assessed the connection between workload and well-being or burnout. Surprisingly, it has been hard to document in the peer-reviewed literature that increasing workloads are associated with increased burnout. Studies of hospitalists published in 2001 and 2011 failed to show a connection between self-reported workload and burnout.1,2 A 2009 systemic review of literature on all physician specialties concluded that “an imbalance between expected and experienced … workload is moderately associated with dissatisfaction, but there is less evidence of a significant association with objective workload.”3 (Emphasis mine.)
Rather than workload, both of the hospitalist studies found that such attributes as organizational solidarity, climate, and fairness; the feeling of being valued by the whole healthcare team; personal time; and compensation were more tightly correlated with whether hospitalists would thrive than workload.
Unfortunately, I’m not aware of any robust studies showing the relationship between hospitalist workload and quality of care (please email me if you know of any). I think the burden of proof is on those who support high workloads to show they don’t adversely affect patient incomes.
If you’d like to discuss workload further, I’ll be moderating a session titled “Who Says 15 is the Right Number?” during HM13, May 17-19, 2013, in Washington, D.C. (www.hospitalmedicine2013.org). I hope to see you there.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is course co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at john.nelson@nelsonflores.com.
References
2. Hinami K, Whelan CT, Wolosin RJ, Miller JA, Wetterneck TB. Worklife and satisfaction of hospitalists: toward flourishing careers. J Gen Intern Med. 2012;27(1):28-36.
3. Scheurer D, McKean S, Miller J, Wetterneck T. U.S. physician satisfaction: a systematic review. J Hosp Med. 2009;4(9):560-568.
Now that HM is moving (or has moved?) from infancy to adolescence or even maturity, you might think that we would have reached some sort of consensus on what a reasonable workload—or patient volume—for a hospitalist is. My sense is that conventional wisdom says a reasonable average daily workload for a daytime rounding/admitting hospitalist is in the range of 12 to 17 billed encounters. And to average this volume, the doctor will have a number of days with more or fewer patients.
After thinking about average workload, the next question is: What is a reasonable upper limit for patient volume on a single day? Here, opinion seems to be a little fuzzier, but I think most would say a hospitalist should be expected to see more than 20 patients in a single day only on rare occasions and on, say, no more than 10 days annually. Keep in mind that a hospitalist who has 22 patients today still has a pretty good chance they will have 20 or more tomorrow, and the day after. High volumes are not a single-day phenomenon, either, because it usually takes a number of days for those patients to reach discharge—and the doctor to realize a decline in workload.
But these numbers are only conventional wisdom. There are little research data to guide our thinking about patient volumes, and thoughtful people sometimes arrive at very different conclusions. As I’ve written in this space previously, I think each individual hospitalist should have significant influence or autonomy to decide the appropriate or optimal patient volume for themselves or their group. This usually requires that doctors are connected to the economic and quality-of-care effects of their patient volume choices, something many hospitalists resist.
Divergence of Opinion
But given lots of autonomy, some hospitalists could make poor choices. I have had the experience of working with hospitalists in three practices around the country who are confident that, at least for themselves, very high patient volumes are safe and reasonable. These high-energy hospitalists see as many as 30 or 40 patients per day, day after day.
At one of these practices, I sat down with the doctors on duty that day at 1 p.m. and talked uninterrupted by pager or patient-care issues for nearly three hours. It was only at the end of the meeting that they explained each of them was seeing around 30 patients that day but had nearly finished rounds before our meeting started. I was stunned. (I probably wouldn’t stop for lunch, to say nothing of a three-hour meeting, to see just 20 patients in a day.)
So I asked just what they saw as an excessive daily patient volume. One of them seemed to deliberate carefully and said, “I probably need help when I have more than 35 patients to see in a day, but I’m OK with anything less than that.”
But the record goes to a really nice, spirited hospitalist who told me that, in addition to his usual workload, he occasionally covered weekends for an internal-medicine group. On a recent weekend, he had 88 patients to see each day, he said. Yes, you read that correctly: 88! (Fortunately, he did see that as a problem and was working to decrease the number.)
Potential Risks
I want to be clear that my own opinion is that the volumes above are unacceptable and dangerous. I think that, in most settings, routinely seeing more than 20 patients in a day probably degrades performance and increases the risk of burnout. While I think most knowledgeable people in our field share this opinion, none of us can point to compelling, generalizable research data to support our opinion.
The way I see it, excessively high workloads risk:
- Adverse patient outcomes due to increased potential for clinical errors and accompanying poor documentation;
- Failure of hospitalists to meet performance and citizenship expectations, such as length of stay (LOS), resource utilization, use of standardized order sets, attention to early discharge times, etc.;
- Lack of any excess capacity to handle transient increases in workload;
- Recruiting and/or retention challenges for hospitalists who might not want to work so hard;
- High risk of hospitalist stress and burnout, which over time could negatively impact a person’s well-being, as well as their attitudes and interactions with other members of the patient care team;
- Overdependence on a few very-hard-working doctors; if one doctor gets sick or has to stop working for a period of time, the hospital must find the equivalent of one-and-a-half doctors to replace him or her; and
- Increased malpractice risk.
Limited Data
There is some research to guide the thinking about workload. I recall one or two abstracts presented at past SHM annual meetings in which doctors in a single practice showed that LOS increased when their patient volume was high. And some sharp hospitalist researchers at Christiana Care Health System in Wilmington, Del., conducted a more robust retrospective cohort study of thousands of non-ICU adult admissions to their 1,100-bed hospital over a three-year period. Their data, which they intend to publish, showed LOS rises as hospitalist workload increases.
Others have assessed the connection between workload and well-being or burnout. Surprisingly, it has been hard to document in the peer-reviewed literature that increasing workloads are associated with increased burnout. Studies of hospitalists published in 2001 and 2011 failed to show a connection between self-reported workload and burnout.1,2 A 2009 systemic review of literature on all physician specialties concluded that “an imbalance between expected and experienced … workload is moderately associated with dissatisfaction, but there is less evidence of a significant association with objective workload.”3 (Emphasis mine.)
Rather than workload, both of the hospitalist studies found that such attributes as organizational solidarity, climate, and fairness; the feeling of being valued by the whole healthcare team; personal time; and compensation were more tightly correlated with whether hospitalists would thrive than workload.
Unfortunately, I’m not aware of any robust studies showing the relationship between hospitalist workload and quality of care (please email me if you know of any). I think the burden of proof is on those who support high workloads to show they don’t adversely affect patient incomes.
If you’d like to discuss workload further, I’ll be moderating a session titled “Who Says 15 is the Right Number?” during HM13, May 17-19, 2013, in Washington, D.C. (www.hospitalmedicine2013.org). I hope to see you there.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is course co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at john.nelson@nelsonflores.com.
References
2. Hinami K, Whelan CT, Wolosin RJ, Miller JA, Wetterneck TB. Worklife and satisfaction of hospitalists: toward flourishing careers. J Gen Intern Med. 2012;27(1):28-36.
3. Scheurer D, McKean S, Miller J, Wetterneck T. U.S. physician satisfaction: a systematic review. J Hosp Med. 2009;4(9):560-568.
Five Ways to Enhance Your Hospital Medicine Group's Efficiency

Is there a role in HM for industrial engineering or industrial efficiency models? Jonathan Turner, PhD, thinks so. He is an industrial-engineer-turned-hospital-engineer whose job is to help make hospital care safer, faster, less costly, and more satisfying. He has few peers in this role, although any hospitalist group in the vicinity of a college department of engineering could seek out similar expertise there. Real-world problems make the best research projects, he says.
“I wrote my thesis on how a vascular surgery department could use computer simulation models to help balance multiple objectives in scheduling residents,” says Turner, who earned his doctorate at Northwestern University in Evanston, Ill.
His thesis examined, among other things, the need for pre-operative continuity of care and resident exposure to a variety of surgical experiences. He also found himself hanging around Northwestern’s Feinberg School of Medicine in Chicago at a time when Mark Williams, MD, MHM, chief of the division of hospital medicine, was looking for ways to build collaboration between Northwestern’s medical school, hospital, and department of engineering.
“Our objectives were the same,” says Turner, who was hired by Dr. Williams in May 2011.
Turner says many of the challenges of managing an HM group—making patient rounds better, improving length of stay (LOS) and throughput, or deciding how to incorporate technology into practice—can be scrutinized with an efficiency lens. At Northwestern, he optimized the HM group schedule and made it more appealing to the physicians. He examined the incremental costs incurred by patient handoffs and the effectiveness of consultations with medical specialists. He tackled technology, teamwork, and wait-time issues. He even helped surgeons standardize their instrument trays.
But every hospitalist group—from the three-FTE teams covering rural hospitals to high-volume groups with dozens of moving parts—has developed inefficient habits. Experts say most groups have never even thought of the problems, let alone the solutions—for example, regularly inputting data into spreadsheets that no one ever looks at.
Efficiency is an essential target for quality initiatives in the hospital, although the word means different things to different people. It typically involves trade-offs that need to be balanced if the system as a whole is to benefit. What makes an individual practice more efficient could make a group’s less so—and vice versa. What helps one department’s bottom line can harm another’s. Enhancing hospitalists’ work-life balance through schedule modification could make life harder for nurses.
-Jonathan Turner, PhD
One current example that cuts across HM groups of all shapes and sizes is the discharge process. Hospitalist groups speeding up discharges might lead to inadequately prepared patients leaving the hospital, which could mean post-discharge crises, which could lead to unnecessary readmissions, which certainly will mean government penalties. Pure efficiency, in terms of maximizing caseloads, also can conflict with patient safety or patient satisfaction. In many healthcare settings, approaching 100% of capacity limits the ability to respond to surges in demand, Turner says. That usually leads to backups, long waits, dissatisfaction, and even diversions from the ED, he explains.
HM groups have pursued a variety of tools and strategies to enhance efficiency. “One of the things we try to show is that you use these methods every day—but you can be more systematic in how you apply them,” Turner says. The character and personality of practicing hospitalists, who tend to be more quality-minded and focused on systems, might make them more open to becoming efficiency experts and willing to try new approaches.
Still, when engineers talk about efficiency, hospital professionals might feel that it cramps their practice style. “I need to be willing to listen to their concerns,” says Turner, who in September began a new position as director of systems engineering at University Hospital in Augusta, Ga.
“I don’t want to turn patients into widgets. I’d rather be thought of as an axe sharpener—helping people do their work more easily,” he says. “You can’t satisfy everybody, but you at least need to listen to everybody when you try to make their work lives more efficient.”
Following are some examples of how hospitalist groups have improved the efficiency of important aspects of their practice.
1. Specialized Care Plans
It is well known that some of the most challenging hospital patients consume a disproportionate share of costs and resources, says Rick Hilger, MD, SFHM, a hospitalist with HealthPartners at Regions Hospital in St. Paul, Minn. It can be controversial to suggest that these difficult patients should receive special handling, but Dr. Hilger, who presented a poster on the topic at HM12, says the current system isn’t safe for patients or sustainable in the long run.3
At Regions, about 70 high-utilizing patients have been given an ongoing, specialized care plan that is easily accessible in their electronic health record (EHR) whenever they present at a HealthPartners clinic, ED, or hospital. Patients include those with a history of drug-seeking behaviors, antisocial behavior disorders, aggression or noncompliance in the hospital, and a variety of traumatic brain injuries or memory deficits that might cause them to give a different story to every medical provider. They also include patients who simply have very complex medical conditions.
Referrals for a specialized care plan can come from any hospital staff member. A care-planning committee representing HM, case management, social work, emergency medicine, and administrative staffs meets monthly to review cases and decide if each patient would benefit from a specialized care plan. It offers quick access in the EHR to a cover page with common clinical scenarios, recent tests and procedures, and a template for optimal care that can save a lot of time and prevent duplicative or uncoordinated treatments, Dr. Hilger says. It also ensures that clinicians give a consistent message to the patient.
“Our mantra is that we want care plans that are easy to create, easy to find, easy to use, and likely to lead to better coordination of care,” he says. “We also say that if everybody has a specialized care plan, then nobody does. We want the provider—whether physician, case manager, or nurse—to walk away saying that the care plan saved them time and led to safer care.”
In its first two months, Regions saw a 68% reduction in total ED visits and hospital admissions for the 43 patients with specialized care plans.
2. Scheduling Models
A number of scheduling models are used for deploying hospitalists in larger groups, including seven on/seven off, five on/five off, weekdays versus weekends, zoned staffing, and admitters versus rounders. Research has shown an incremental cost for every handoff, and creating a work schedule that results in fewer handoffs might make patients more satisfied. But that goal needs to be balanced against provider schedules with an eye toward keeping caseloads localized in the hospital.
Shalini Chandra, MD, MS, FHM, a hospitalist at Johns Hopkins Bayview Medical Center in Baltimore, was co-presenter of a HM12 workshop on how to use performance-improvement principles to improve HM group schedules. She says the schedule needs to account for such variables as when hospitalists are assigned new patients, are required to interact with the ED, and are devoted to patient contact versus paperwork, which normally is greater at admission and discharge.
“You need to find the sweet spot between the hospital’s needs, the patient’s needs, and the doctor’s needs,” she says. “Our physicians felt they were being penalized for discharging patients in a timely manner [by receiving more new cases]. We had to go back and say, ‘OK, if somebody is doing a four-day stretch, how can we distribute patients more equitably?’”
Dr. Chandra’s quality team mapped out the entire admissions process and identified key metrics, then devised a model called CICLE (Creating Incentives and Continuity Leading to Efficiency in Hospital Medicine) for its four-day shift. The first day, which can be a long one, is front-loaded with new admissions. But on Day Two and Day Three, the hospitalist is largely protected from new admissions, thereby preserving the incentive to discharge patients when they are ready.
CICLE also results in fewer handoffs, with a third of patients seen by only one hospitalist, Dr. Chandra explains. That in turn translates into decreased LOS and cost.
The four-day schedule at Hopkins is complicated by the need to respond to other demands on the system, and Dr. Chandra says only 60 percent of the hospitalist caseload is scheduled this way.

—Rick Hilger, MD, SFHM
3. Individual Flexibility
The best schedule in the world can be turned upside down by vacations, sickness, or an open position that goes unfilled for months. Accounting for the nuances can be a full-time job.
At Northwestern, the hospitalist group is converting to scheduling software called Lightning Bolt (www.lightning-bolt.com) that provides flexibility to respond to varying needs among the 70-plus members of the group, including such needs as attending their children’s soccer games, says Charlotta Weaver, MD, assistant professor of medicine.
“An enormous amount of time, both administrative and medical, gets devoted to scheduling,” she says.
Each hospital and HM group is different, and each physician has varying desires from the schedule. “Things are constantly changing,” Dr. Weaver says. “People come and go or need to change jobs, there are changes in FTE allocations, physicians may get research grants, and there can be changes in hospital structure or service lines.”
The schedule also needs to facilitate “day trading” between members of the group, and Northwestern is experimenting with some new approaches, including pairing up two physicians on one service line and letting them work out their own schedules.
The group also needs a way to respond to admission surges beyond the capacity of scheduled physicians, which can be hard to predict, and the days when physicians call in sick.
“We have tried to develop a robust system of ‘jeopardy’ for first- and second-line backup,” Dr. Weaver says. Everyone in the hospitalist group has jeopardy one or two weeks per year, where they are in line to be called in if needed.
Franziska Jovin, MD, FHM, a hospitalist at the University of Pittsburgh Medical Center, says her group struggles with predicting patient peaks and valleys.
“One of our hospitalist teams is responsible for the transitional-care unit, and not every patient on that unit has to be seen every day,” Dr. Jovin says. “This person is already scheduled to work, but the responsibilities are not time-dependent. So we can pull in that doctor as needed to cover higher demand on the acute side.”
As most hospitalists know the winter months are busier, “and we staff accordingly,” she says, in response to higher incidence of flu, pneumonia, and the like.
4. Structured Rounds
Another challenge to scheduling is the rounding model used for daily care planning in the hospital. Various models have tried to address competing concerns of geography, schedule efficiency, and the needs of hospitalists, nurses, and other staff. At Emory Healthcare in Atlanta, an approach called Structured Interdisciplinary Bedside Rounds (SIBR) was described during an HM12 workshop and in a prize-winning poster presented by Christina Payne, MD (see “The Innovation Express,” May 2012, p. 27).
Dr. Payne described how SIBR works with two teaching hospitalist services on a 24-bed “accountable-care unit” at Emory University Hospital. Each team has a resident, three interns, a social worker, and the patient’s nurse, with the attending standing by.
“We round on each patient every day—beginning and ending on time,” 12 patients per hour, with five brisk minutes to report on each patient, she says. Rounding starts when the patient’s primary intern and nurse are both present in the patient’s room, and only ends when a plan of care for the day has been articulated—using a standardized script with safety and discharge planning checklists. The second intern enters the plan, in real time, into the EHR.
In addition to the time efficiency, this approach has posted positive outcomes, namely a 53% reduction in in-hospital mortality on the unit and an 11% reduction in LOS. With new residents and interns rotating through the unit every month, “We acknowledge to them that this will be difficult and they will be uncomfortable at first,” Dr. Payne says, “but by Week Two, we’re a well-oiled machine.”
Similar approaches have been implemented at other Emory hospitals.
5. NPP Mobilization
Many hospitalist groups have integrated nonphysician providers (NPPs, or nurse practitioners and physician assistants) into the group’s practice or are considering such a move. Tracy Cardin, ACNP-BC, a nurse practitioner in hospital practice at the University of Chicago Medical Center, says it’s important to ask why a group is considering a role for NPPs.
“Is it to promote efficiency? Is it because you can’t attract enough physicians?” she says. “Clarify your hopes for the position and how you will define success.” She also says HM group leaders need to factor in the time needed to hire, orient, and train an NPP, with mentoring that includes structured teaching and feedback.
There are a lot of models for deploying NPPs, says Cardin, a Team Hospitalist member.
“We utilize shared billing and teams of a hospitalist and nurse practitioner. This allows the physician to see a larger number of patients and brings more than one set of eyes and ears to the complex patient,” she says. “We’ve developed a process over the past six years where the hospitalist and NPP together go over the patient list every day. Both will see the patient, but the NPP commonly writes the notes and orders.”
Cardin emphasizes NPPs cost less than physicians and “can do many of the same things,” but “they are not free.” The most resourceful HM group’s use NPPs to extend the physician’s practice. “They can carry a pager and respond to small crises that come up, or see the patient on discharge day,” she says. “In other settings, the NPP does admissions, serves on quality projects, takes on a patient cohort based on diagnosis, or calls the primary-care physician at discharge.”
Efficiency can be a tough nut to crack in the hospital. Turner, the engineer, says HM groups need to “remember that the hospital is a very complex environment, with cascades of reactions and downstream effects.”
Hospitalists need the support of other professionals, and quality-improvement (QI) initiatives need sufficient time and resources to succeed.
One way to start advancing the efficiency agenda is to look for bright spots among the hospitalist group’s members. “Talk to them,” Turner says. “Find out how they do their jobs. Learn from them.”
Larry Beresford is a freelance author in Oakland, Calif.
References
- Yu D, Sanches S. Lean inpatient unit base care model [abstract]. J Hosp Med. 2012;7(Suppl 2):S107.
- Payne C, Odetoyinbo D, Castle B, et al. A dual hospital care and training model: structured interdisciplinary team rounds in an accountable care unit [abstract]. J Hosp Med. 2012;7(Suppl 2):S125.
- Hilger R, Quirk R, Dahms R. Use of restriction care plans to decrease medically unnecessary admissions and emergency department visits [abstract]. J Hosp Med. 2012;7(Suppl 2):S2.
- Premier. Year Three: QUEST Collaborative Findings. Premier website. Available at: http://www.premierinc.com/quality-safety/tools-services/quest/year3/quest-year-3-collaborative-findings.pdf. Accessed Sept. 26, 2012.
Is there a role in HM for industrial engineering or industrial efficiency models? Jonathan Turner, PhD, thinks so. He is an industrial-engineer-turned-hospital-engineer whose job is to help make hospital care safer, faster, less costly, and more satisfying. He has few peers in this role, although any hospitalist group in the vicinity of a college department of engineering could seek out similar expertise there. Real-world problems make the best research projects, he says.
“I wrote my thesis on how a vascular surgery department could use computer simulation models to help balance multiple objectives in scheduling residents,” says Turner, who earned his doctorate at Northwestern University in Evanston, Ill.
His thesis examined, among other things, the need for pre-operative continuity of care and resident exposure to a variety of surgical experiences. He also found himself hanging around Northwestern’s Feinberg School of Medicine in Chicago at a time when Mark Williams, MD, MHM, chief of the division of hospital medicine, was looking for ways to build collaboration between Northwestern’s medical school, hospital, and department of engineering.
“Our objectives were the same,” says Turner, who was hired by Dr. Williams in May 2011.
Turner says many of the challenges of managing an HM group—making patient rounds better, improving length of stay (LOS) and throughput, or deciding how to incorporate technology into practice—can be scrutinized with an efficiency lens. At Northwestern, he optimized the HM group schedule and made it more appealing to the physicians. He examined the incremental costs incurred by patient handoffs and the effectiveness of consultations with medical specialists. He tackled technology, teamwork, and wait-time issues. He even helped surgeons standardize their instrument trays.
But every hospitalist group—from the three-FTE teams covering rural hospitals to high-volume groups with dozens of moving parts—has developed inefficient habits. Experts say most groups have never even thought of the problems, let alone the solutions—for example, regularly inputting data into spreadsheets that no one ever looks at.
Efficiency is an essential target for quality initiatives in the hospital, although the word means different things to different people. It typically involves trade-offs that need to be balanced if the system as a whole is to benefit. What makes an individual practice more efficient could make a group’s less so—and vice versa. What helps one department’s bottom line can harm another’s. Enhancing hospitalists’ work-life balance through schedule modification could make life harder for nurses.
-Jonathan Turner, PhD
One current example that cuts across HM groups of all shapes and sizes is the discharge process. Hospitalist groups speeding up discharges might lead to inadequately prepared patients leaving the hospital, which could mean post-discharge crises, which could lead to unnecessary readmissions, which certainly will mean government penalties. Pure efficiency, in terms of maximizing caseloads, also can conflict with patient safety or patient satisfaction. In many healthcare settings, approaching 100% of capacity limits the ability to respond to surges in demand, Turner says. That usually leads to backups, long waits, dissatisfaction, and even diversions from the ED, he explains.
HM groups have pursued a variety of tools and strategies to enhance efficiency. “One of the things we try to show is that you use these methods every day—but you can be more systematic in how you apply them,” Turner says. The character and personality of practicing hospitalists, who tend to be more quality-minded and focused on systems, might make them more open to becoming efficiency experts and willing to try new approaches.
Still, when engineers talk about efficiency, hospital professionals might feel that it cramps their practice style. “I need to be willing to listen to their concerns,” says Turner, who in September began a new position as director of systems engineering at University Hospital in Augusta, Ga.
“I don’t want to turn patients into widgets. I’d rather be thought of as an axe sharpener—helping people do their work more easily,” he says. “You can’t satisfy everybody, but you at least need to listen to everybody when you try to make their work lives more efficient.”
Following are some examples of how hospitalist groups have improved the efficiency of important aspects of their practice.
1. Specialized Care Plans
It is well known that some of the most challenging hospital patients consume a disproportionate share of costs and resources, says Rick Hilger, MD, SFHM, a hospitalist with HealthPartners at Regions Hospital in St. Paul, Minn. It can be controversial to suggest that these difficult patients should receive special handling, but Dr. Hilger, who presented a poster on the topic at HM12, says the current system isn’t safe for patients or sustainable in the long run.3
At Regions, about 70 high-utilizing patients have been given an ongoing, specialized care plan that is easily accessible in their electronic health record (EHR) whenever they present at a HealthPartners clinic, ED, or hospital. Patients include those with a history of drug-seeking behaviors, antisocial behavior disorders, aggression or noncompliance in the hospital, and a variety of traumatic brain injuries or memory deficits that might cause them to give a different story to every medical provider. They also include patients who simply have very complex medical conditions.
Referrals for a specialized care plan can come from any hospital staff member. A care-planning committee representing HM, case management, social work, emergency medicine, and administrative staffs meets monthly to review cases and decide if each patient would benefit from a specialized care plan. It offers quick access in the EHR to a cover page with common clinical scenarios, recent tests and procedures, and a template for optimal care that can save a lot of time and prevent duplicative or uncoordinated treatments, Dr. Hilger says. It also ensures that clinicians give a consistent message to the patient.
“Our mantra is that we want care plans that are easy to create, easy to find, easy to use, and likely to lead to better coordination of care,” he says. “We also say that if everybody has a specialized care plan, then nobody does. We want the provider—whether physician, case manager, or nurse—to walk away saying that the care plan saved them time and led to safer care.”
In its first two months, Regions saw a 68% reduction in total ED visits and hospital admissions for the 43 patients with specialized care plans.
2. Scheduling Models
A number of scheduling models are used for deploying hospitalists in larger groups, including seven on/seven off, five on/five off, weekdays versus weekends, zoned staffing, and admitters versus rounders. Research has shown an incremental cost for every handoff, and creating a work schedule that results in fewer handoffs might make patients more satisfied. But that goal needs to be balanced against provider schedules with an eye toward keeping caseloads localized in the hospital.
Shalini Chandra, MD, MS, FHM, a hospitalist at Johns Hopkins Bayview Medical Center in Baltimore, was co-presenter of a HM12 workshop on how to use performance-improvement principles to improve HM group schedules. She says the schedule needs to account for such variables as when hospitalists are assigned new patients, are required to interact with the ED, and are devoted to patient contact versus paperwork, which normally is greater at admission and discharge.
“You need to find the sweet spot between the hospital’s needs, the patient’s needs, and the doctor’s needs,” she says. “Our physicians felt they were being penalized for discharging patients in a timely manner [by receiving more new cases]. We had to go back and say, ‘OK, if somebody is doing a four-day stretch, how can we distribute patients more equitably?’”
Dr. Chandra’s quality team mapped out the entire admissions process and identified key metrics, then devised a model called CICLE (Creating Incentives and Continuity Leading to Efficiency in Hospital Medicine) for its four-day shift. The first day, which can be a long one, is front-loaded with new admissions. But on Day Two and Day Three, the hospitalist is largely protected from new admissions, thereby preserving the incentive to discharge patients when they are ready.
CICLE also results in fewer handoffs, with a third of patients seen by only one hospitalist, Dr. Chandra explains. That in turn translates into decreased LOS and cost.
The four-day schedule at Hopkins is complicated by the need to respond to other demands on the system, and Dr. Chandra says only 60 percent of the hospitalist caseload is scheduled this way.
—Rick Hilger, MD, SFHM
3. Individual Flexibility
The best schedule in the world can be turned upside down by vacations, sickness, or an open position that goes unfilled for months. Accounting for the nuances can be a full-time job.
At Northwestern, the hospitalist group is converting to scheduling software called Lightning Bolt (www.lightning-bolt.com) that provides flexibility to respond to varying needs among the 70-plus members of the group, including such needs as attending their children’s soccer games, says Charlotta Weaver, MD, assistant professor of medicine.
“An enormous amount of time, both administrative and medical, gets devoted to scheduling,” she says.
Each hospital and HM group is different, and each physician has varying desires from the schedule. “Things are constantly changing,” Dr. Weaver says. “People come and go or need to change jobs, there are changes in FTE allocations, physicians may get research grants, and there can be changes in hospital structure or service lines.”
The schedule also needs to facilitate “day trading” between members of the group, and Northwestern is experimenting with some new approaches, including pairing up two physicians on one service line and letting them work out their own schedules.
The group also needs a way to respond to admission surges beyond the capacity of scheduled physicians, which can be hard to predict, and the days when physicians call in sick.
“We have tried to develop a robust system of ‘jeopardy’ for first- and second-line backup,” Dr. Weaver says. Everyone in the hospitalist group has jeopardy one or two weeks per year, where they are in line to be called in if needed.
Franziska Jovin, MD, FHM, a hospitalist at the University of Pittsburgh Medical Center, says her group struggles with predicting patient peaks and valleys.
“One of our hospitalist teams is responsible for the transitional-care unit, and not every patient on that unit has to be seen every day,” Dr. Jovin says. “This person is already scheduled to work, but the responsibilities are not time-dependent. So we can pull in that doctor as needed to cover higher demand on the acute side.”
As most hospitalists know the winter months are busier, “and we staff accordingly,” she says, in response to higher incidence of flu, pneumonia, and the like.
4. Structured Rounds
Another challenge to scheduling is the rounding model used for daily care planning in the hospital. Various models have tried to address competing concerns of geography, schedule efficiency, and the needs of hospitalists, nurses, and other staff. At Emory Healthcare in Atlanta, an approach called Structured Interdisciplinary Bedside Rounds (SIBR) was described during an HM12 workshop and in a prize-winning poster presented by Christina Payne, MD (see “The Innovation Express,” May 2012, p. 27).
Dr. Payne described how SIBR works with two teaching hospitalist services on a 24-bed “accountable-care unit” at Emory University Hospital. Each team has a resident, three interns, a social worker, and the patient’s nurse, with the attending standing by.
“We round on each patient every day—beginning and ending on time,” 12 patients per hour, with five brisk minutes to report on each patient, she says. Rounding starts when the patient’s primary intern and nurse are both present in the patient’s room, and only ends when a plan of care for the day has been articulated—using a standardized script with safety and discharge planning checklists. The second intern enters the plan, in real time, into the EHR.
In addition to the time efficiency, this approach has posted positive outcomes, namely a 53% reduction in in-hospital mortality on the unit and an 11% reduction in LOS. With new residents and interns rotating through the unit every month, “We acknowledge to them that this will be difficult and they will be uncomfortable at first,” Dr. Payne says, “but by Week Two, we’re a well-oiled machine.”
Similar approaches have been implemented at other Emory hospitals.
5. NPP Mobilization
Many hospitalist groups have integrated nonphysician providers (NPPs, or nurse practitioners and physician assistants) into the group’s practice or are considering such a move. Tracy Cardin, ACNP-BC, a nurse practitioner in hospital practice at the University of Chicago Medical Center, says it’s important to ask why a group is considering a role for NPPs.
“Is it to promote efficiency? Is it because you can’t attract enough physicians?” she says. “Clarify your hopes for the position and how you will define success.” She also says HM group leaders need to factor in the time needed to hire, orient, and train an NPP, with mentoring that includes structured teaching and feedback.
There are a lot of models for deploying NPPs, says Cardin, a Team Hospitalist member.
“We utilize shared billing and teams of a hospitalist and nurse practitioner. This allows the physician to see a larger number of patients and brings more than one set of eyes and ears to the complex patient,” she says. “We’ve developed a process over the past six years where the hospitalist and NPP together go over the patient list every day. Both will see the patient, but the NPP commonly writes the notes and orders.”
Cardin emphasizes NPPs cost less than physicians and “can do many of the same things,” but “they are not free.” The most resourceful HM group’s use NPPs to extend the physician’s practice. “They can carry a pager and respond to small crises that come up, or see the patient on discharge day,” she says. “In other settings, the NPP does admissions, serves on quality projects, takes on a patient cohort based on diagnosis, or calls the primary-care physician at discharge.”
Efficiency can be a tough nut to crack in the hospital. Turner, the engineer, says HM groups need to “remember that the hospital is a very complex environment, with cascades of reactions and downstream effects.”
Hospitalists need the support of other professionals, and quality-improvement (QI) initiatives need sufficient time and resources to succeed.
One way to start advancing the efficiency agenda is to look for bright spots among the hospitalist group’s members. “Talk to them,” Turner says. “Find out how they do their jobs. Learn from them.”
Larry Beresford is a freelance author in Oakland, Calif.
References
- Yu D, Sanches S. Lean inpatient unit base care model [abstract]. J Hosp Med. 2012;7(Suppl 2):S107.
- Payne C, Odetoyinbo D, Castle B, et al. A dual hospital care and training model: structured interdisciplinary team rounds in an accountable care unit [abstract]. J Hosp Med. 2012;7(Suppl 2):S125.
- Hilger R, Quirk R, Dahms R. Use of restriction care plans to decrease medically unnecessary admissions and emergency department visits [abstract]. J Hosp Med. 2012;7(Suppl 2):S2.
- Premier. Year Three: QUEST Collaborative Findings. Premier website. Available at: http://www.premierinc.com/quality-safety/tools-services/quest/year3/quest-year-3-collaborative-findings.pdf. Accessed Sept. 26, 2012.
Is there a role in HM for industrial engineering or industrial efficiency models? Jonathan Turner, PhD, thinks so. He is an industrial-engineer-turned-hospital-engineer whose job is to help make hospital care safer, faster, less costly, and more satisfying. He has few peers in this role, although any hospitalist group in the vicinity of a college department of engineering could seek out similar expertise there. Real-world problems make the best research projects, he says.
“I wrote my thesis on how a vascular surgery department could use computer simulation models to help balance multiple objectives in scheduling residents,” says Turner, who earned his doctorate at Northwestern University in Evanston, Ill.
His thesis examined, among other things, the need for pre-operative continuity of care and resident exposure to a variety of surgical experiences. He also found himself hanging around Northwestern’s Feinberg School of Medicine in Chicago at a time when Mark Williams, MD, MHM, chief of the division of hospital medicine, was looking for ways to build collaboration between Northwestern’s medical school, hospital, and department of engineering.
“Our objectives were the same,” says Turner, who was hired by Dr. Williams in May 2011.
Turner says many of the challenges of managing an HM group—making patient rounds better, improving length of stay (LOS) and throughput, or deciding how to incorporate technology into practice—can be scrutinized with an efficiency lens. At Northwestern, he optimized the HM group schedule and made it more appealing to the physicians. He examined the incremental costs incurred by patient handoffs and the effectiveness of consultations with medical specialists. He tackled technology, teamwork, and wait-time issues. He even helped surgeons standardize their instrument trays.
But every hospitalist group—from the three-FTE teams covering rural hospitals to high-volume groups with dozens of moving parts—has developed inefficient habits. Experts say most groups have never even thought of the problems, let alone the solutions—for example, regularly inputting data into spreadsheets that no one ever looks at.
Efficiency is an essential target for quality initiatives in the hospital, although the word means different things to different people. It typically involves trade-offs that need to be balanced if the system as a whole is to benefit. What makes an individual practice more efficient could make a group’s less so—and vice versa. What helps one department’s bottom line can harm another’s. Enhancing hospitalists’ work-life balance through schedule modification could make life harder for nurses.
-Jonathan Turner, PhD
One current example that cuts across HM groups of all shapes and sizes is the discharge process. Hospitalist groups speeding up discharges might lead to inadequately prepared patients leaving the hospital, which could mean post-discharge crises, which could lead to unnecessary readmissions, which certainly will mean government penalties. Pure efficiency, in terms of maximizing caseloads, also can conflict with patient safety or patient satisfaction. In many healthcare settings, approaching 100% of capacity limits the ability to respond to surges in demand, Turner says. That usually leads to backups, long waits, dissatisfaction, and even diversions from the ED, he explains.
HM groups have pursued a variety of tools and strategies to enhance efficiency. “One of the things we try to show is that you use these methods every day—but you can be more systematic in how you apply them,” Turner says. The character and personality of practicing hospitalists, who tend to be more quality-minded and focused on systems, might make them more open to becoming efficiency experts and willing to try new approaches.
Still, when engineers talk about efficiency, hospital professionals might feel that it cramps their practice style. “I need to be willing to listen to their concerns,” says Turner, who in September began a new position as director of systems engineering at University Hospital in Augusta, Ga.
“I don’t want to turn patients into widgets. I’d rather be thought of as an axe sharpener—helping people do their work more easily,” he says. “You can’t satisfy everybody, but you at least need to listen to everybody when you try to make their work lives more efficient.”
Following are some examples of how hospitalist groups have improved the efficiency of important aspects of their practice.
1. Specialized Care Plans
It is well known that some of the most challenging hospital patients consume a disproportionate share of costs and resources, says Rick Hilger, MD, SFHM, a hospitalist with HealthPartners at Regions Hospital in St. Paul, Minn. It can be controversial to suggest that these difficult patients should receive special handling, but Dr. Hilger, who presented a poster on the topic at HM12, says the current system isn’t safe for patients or sustainable in the long run.3
At Regions, about 70 high-utilizing patients have been given an ongoing, specialized care plan that is easily accessible in their electronic health record (EHR) whenever they present at a HealthPartners clinic, ED, or hospital. Patients include those with a history of drug-seeking behaviors, antisocial behavior disorders, aggression or noncompliance in the hospital, and a variety of traumatic brain injuries or memory deficits that might cause them to give a different story to every medical provider. They also include patients who simply have very complex medical conditions.
Referrals for a specialized care plan can come from any hospital staff member. A care-planning committee representing HM, case management, social work, emergency medicine, and administrative staffs meets monthly to review cases and decide if each patient would benefit from a specialized care plan. It offers quick access in the EHR to a cover page with common clinical scenarios, recent tests and procedures, and a template for optimal care that can save a lot of time and prevent duplicative or uncoordinated treatments, Dr. Hilger says. It also ensures that clinicians give a consistent message to the patient.
“Our mantra is that we want care plans that are easy to create, easy to find, easy to use, and likely to lead to better coordination of care,” he says. “We also say that if everybody has a specialized care plan, then nobody does. We want the provider—whether physician, case manager, or nurse—to walk away saying that the care plan saved them time and led to safer care.”
In its first two months, Regions saw a 68% reduction in total ED visits and hospital admissions for the 43 patients with specialized care plans.
2. Scheduling Models
A number of scheduling models are used for deploying hospitalists in larger groups, including seven on/seven off, five on/five off, weekdays versus weekends, zoned staffing, and admitters versus rounders. Research has shown an incremental cost for every handoff, and creating a work schedule that results in fewer handoffs might make patients more satisfied. But that goal needs to be balanced against provider schedules with an eye toward keeping caseloads localized in the hospital.
Shalini Chandra, MD, MS, FHM, a hospitalist at Johns Hopkins Bayview Medical Center in Baltimore, was co-presenter of a HM12 workshop on how to use performance-improvement principles to improve HM group schedules. She says the schedule needs to account for such variables as when hospitalists are assigned new patients, are required to interact with the ED, and are devoted to patient contact versus paperwork, which normally is greater at admission and discharge.
“You need to find the sweet spot between the hospital’s needs, the patient’s needs, and the doctor’s needs,” she says. “Our physicians felt they were being penalized for discharging patients in a timely manner [by receiving more new cases]. We had to go back and say, ‘OK, if somebody is doing a four-day stretch, how can we distribute patients more equitably?’”
Dr. Chandra’s quality team mapped out the entire admissions process and identified key metrics, then devised a model called CICLE (Creating Incentives and Continuity Leading to Efficiency in Hospital Medicine) for its four-day shift. The first day, which can be a long one, is front-loaded with new admissions. But on Day Two and Day Three, the hospitalist is largely protected from new admissions, thereby preserving the incentive to discharge patients when they are ready.
CICLE also results in fewer handoffs, with a third of patients seen by only one hospitalist, Dr. Chandra explains. That in turn translates into decreased LOS and cost.
The four-day schedule at Hopkins is complicated by the need to respond to other demands on the system, and Dr. Chandra says only 60 percent of the hospitalist caseload is scheduled this way.
—Rick Hilger, MD, SFHM
3. Individual Flexibility
The best schedule in the world can be turned upside down by vacations, sickness, or an open position that goes unfilled for months. Accounting for the nuances can be a full-time job.
At Northwestern, the hospitalist group is converting to scheduling software called Lightning Bolt (www.lightning-bolt.com) that provides flexibility to respond to varying needs among the 70-plus members of the group, including such needs as attending their children’s soccer games, says Charlotta Weaver, MD, assistant professor of medicine.
“An enormous amount of time, both administrative and medical, gets devoted to scheduling,” she says.
Each hospital and HM group is different, and each physician has varying desires from the schedule. “Things are constantly changing,” Dr. Weaver says. “People come and go or need to change jobs, there are changes in FTE allocations, physicians may get research grants, and there can be changes in hospital structure or service lines.”
The schedule also needs to facilitate “day trading” between members of the group, and Northwestern is experimenting with some new approaches, including pairing up two physicians on one service line and letting them work out their own schedules.
The group also needs a way to respond to admission surges beyond the capacity of scheduled physicians, which can be hard to predict, and the days when physicians call in sick.
“We have tried to develop a robust system of ‘jeopardy’ for first- and second-line backup,” Dr. Weaver says. Everyone in the hospitalist group has jeopardy one or two weeks per year, where they are in line to be called in if needed.
Franziska Jovin, MD, FHM, a hospitalist at the University of Pittsburgh Medical Center, says her group struggles with predicting patient peaks and valleys.
“One of our hospitalist teams is responsible for the transitional-care unit, and not every patient on that unit has to be seen every day,” Dr. Jovin says. “This person is already scheduled to work, but the responsibilities are not time-dependent. So we can pull in that doctor as needed to cover higher demand on the acute side.”
As most hospitalists know the winter months are busier, “and we staff accordingly,” she says, in response to higher incidence of flu, pneumonia, and the like.
4. Structured Rounds
Another challenge to scheduling is the rounding model used for daily care planning in the hospital. Various models have tried to address competing concerns of geography, schedule efficiency, and the needs of hospitalists, nurses, and other staff. At Emory Healthcare in Atlanta, an approach called Structured Interdisciplinary Bedside Rounds (SIBR) was described during an HM12 workshop and in a prize-winning poster presented by Christina Payne, MD (see “The Innovation Express,” May 2012, p. 27).
Dr. Payne described how SIBR works with two teaching hospitalist services on a 24-bed “accountable-care unit” at Emory University Hospital. Each team has a resident, three interns, a social worker, and the patient’s nurse, with the attending standing by.
“We round on each patient every day—beginning and ending on time,” 12 patients per hour, with five brisk minutes to report on each patient, she says. Rounding starts when the patient’s primary intern and nurse are both present in the patient’s room, and only ends when a plan of care for the day has been articulated—using a standardized script with safety and discharge planning checklists. The second intern enters the plan, in real time, into the EHR.
In addition to the time efficiency, this approach has posted positive outcomes, namely a 53% reduction in in-hospital mortality on the unit and an 11% reduction in LOS. With new residents and interns rotating through the unit every month, “We acknowledge to them that this will be difficult and they will be uncomfortable at first,” Dr. Payne says, “but by Week Two, we’re a well-oiled machine.”
Similar approaches have been implemented at other Emory hospitals.
5. NPP Mobilization
Many hospitalist groups have integrated nonphysician providers (NPPs, or nurse practitioners and physician assistants) into the group’s practice or are considering such a move. Tracy Cardin, ACNP-BC, a nurse practitioner in hospital practice at the University of Chicago Medical Center, says it’s important to ask why a group is considering a role for NPPs.
“Is it to promote efficiency? Is it because you can’t attract enough physicians?” she says. “Clarify your hopes for the position and how you will define success.” She also says HM group leaders need to factor in the time needed to hire, orient, and train an NPP, with mentoring that includes structured teaching and feedback.
There are a lot of models for deploying NPPs, says Cardin, a Team Hospitalist member.
“We utilize shared billing and teams of a hospitalist and nurse practitioner. This allows the physician to see a larger number of patients and brings more than one set of eyes and ears to the complex patient,” she says. “We’ve developed a process over the past six years where the hospitalist and NPP together go over the patient list every day. Both will see the patient, but the NPP commonly writes the notes and orders.”
Cardin emphasizes NPPs cost less than physicians and “can do many of the same things,” but “they are not free.” The most resourceful HM group’s use NPPs to extend the physician’s practice. “They can carry a pager and respond to small crises that come up, or see the patient on discharge day,” she says. “In other settings, the NPP does admissions, serves on quality projects, takes on a patient cohort based on diagnosis, or calls the primary-care physician at discharge.”
Efficiency can be a tough nut to crack in the hospital. Turner, the engineer, says HM groups need to “remember that the hospital is a very complex environment, with cascades of reactions and downstream effects.”
Hospitalists need the support of other professionals, and quality-improvement (QI) initiatives need sufficient time and resources to succeed.
One way to start advancing the efficiency agenda is to look for bright spots among the hospitalist group’s members. “Talk to them,” Turner says. “Find out how they do their jobs. Learn from them.”
Larry Beresford is a freelance author in Oakland, Calif.
References
- Yu D, Sanches S. Lean inpatient unit base care model [abstract]. J Hosp Med. 2012;7(Suppl 2):S107.
- Payne C, Odetoyinbo D, Castle B, et al. A dual hospital care and training model: structured interdisciplinary team rounds in an accountable care unit [abstract]. J Hosp Med. 2012;7(Suppl 2):S125.
- Hilger R, Quirk R, Dahms R. Use of restriction care plans to decrease medically unnecessary admissions and emergency department visits [abstract]. J Hosp Med. 2012;7(Suppl 2):S2.
- Premier. Year Three: QUEST Collaborative Findings. Premier website. Available at: http://www.premierinc.com/quality-safety/tools-services/quest/year3/quest-year-3-collaborative-findings.pdf. Accessed Sept. 26, 2012.
Off-Label Use of Antipsychotics for Dementia Patients Discouraged
Hospitalists can play a major role in reducing deaths that come as a result of off-label prescriptions for antipsychotic drugs being given to dementia patients, according to the Centers for Medicare & Medicaid Services (CMS) and SHM.
In a letter to hospitalist leaders, SHM encouraged hospitalists to “partner with others in your clinical work environment to reduce the use of antipsychotics for treating behavioral problems in patients with dementia. We believe that hospitalists have an important role to play in this initiative; hospital-based clinicians frequently care for patients with dementia and are responsible for medications prescribed during a patient’s hospitalization and at discharge.”
The joint education effort by CMS and SHM is based on an April 2011 report from the U.S. Department of Health and Human Services’ Office of Inspector General (OIG) that found that antipsychotic medications sometimes are used to treat patients with dementia for off-label reasons (e.g. “behaviors”) or against black-box warnings despite potential dangers to patients’ health.
An earlier warning from the FDA in 2008 outlined the potential dangers as:
- Increased risk (60% to 70%) of death in older adults with dementia;
- Prolongation of the QT interval on electrocardiogram, particularly with intravenous haloperidol use;
- Increased risk of stroke and TIAs; and
- Worsening cognitive function.
The letter to hospitalists noted the necessary changes and the need for collaboration between SHM, its members, and hospital leaders. “Increased prescriber training and system practice changes will help reduce unnecessary antipsychotic drug prescribing,” the letter stated. “SHM looks forward to an ongoing collaboration with members and hospital leaders on this important patient safety concern.”
Hospitalists can play a major role in reducing deaths that come as a result of off-label prescriptions for antipsychotic drugs being given to dementia patients, according to the Centers for Medicare & Medicaid Services (CMS) and SHM.
In a letter to hospitalist leaders, SHM encouraged hospitalists to “partner with others in your clinical work environment to reduce the use of antipsychotics for treating behavioral problems in patients with dementia. We believe that hospitalists have an important role to play in this initiative; hospital-based clinicians frequently care for patients with dementia and are responsible for medications prescribed during a patient’s hospitalization and at discharge.”
The joint education effort by CMS and SHM is based on an April 2011 report from the U.S. Department of Health and Human Services’ Office of Inspector General (OIG) that found that antipsychotic medications sometimes are used to treat patients with dementia for off-label reasons (e.g. “behaviors”) or against black-box warnings despite potential dangers to patients’ health.
An earlier warning from the FDA in 2008 outlined the potential dangers as:
- Increased risk (60% to 70%) of death in older adults with dementia;
- Prolongation of the QT interval on electrocardiogram, particularly with intravenous haloperidol use;
- Increased risk of stroke and TIAs; and
- Worsening cognitive function.
The letter to hospitalists noted the necessary changes and the need for collaboration between SHM, its members, and hospital leaders. “Increased prescriber training and system practice changes will help reduce unnecessary antipsychotic drug prescribing,” the letter stated. “SHM looks forward to an ongoing collaboration with members and hospital leaders on this important patient safety concern.”
Hospitalists can play a major role in reducing deaths that come as a result of off-label prescriptions for antipsychotic drugs being given to dementia patients, according to the Centers for Medicare & Medicaid Services (CMS) and SHM.
In a letter to hospitalist leaders, SHM encouraged hospitalists to “partner with others in your clinical work environment to reduce the use of antipsychotics for treating behavioral problems in patients with dementia. We believe that hospitalists have an important role to play in this initiative; hospital-based clinicians frequently care for patients with dementia and are responsible for medications prescribed during a patient’s hospitalization and at discharge.”
The joint education effort by CMS and SHM is based on an April 2011 report from the U.S. Department of Health and Human Services’ Office of Inspector General (OIG) that found that antipsychotic medications sometimes are used to treat patients with dementia for off-label reasons (e.g. “behaviors”) or against black-box warnings despite potential dangers to patients’ health.
An earlier warning from the FDA in 2008 outlined the potential dangers as:
- Increased risk (60% to 70%) of death in older adults with dementia;
- Prolongation of the QT interval on electrocardiogram, particularly with intravenous haloperidol use;
- Increased risk of stroke and TIAs; and
- Worsening cognitive function.
The letter to hospitalists noted the necessary changes and the need for collaboration between SHM, its members, and hospital leaders. “Increased prescriber training and system practice changes will help reduce unnecessary antipsychotic drug prescribing,” the letter stated. “SHM looks forward to an ongoing collaboration with members and hospital leaders on this important patient safety concern.”
Relationship Between Red Blood Cells and Protein Levels in Cerebrospinal Fluid in Young Infants Defined

Clinical question: What is the association between cerebrospinal fluid (CSF) red blood cell (RBC) counts and protein concentrations in infants younger than 57 days of age?
Background: Lumbar puncture (LP) is commonly performed in young infants to evaluate for meningitis in the clinical scenario of fever without source. Traumatic LP is common in children, and higher RBC counts are associated with increased CSF protein concentrations. The dynamic nature of CSF composition in young infants makes determination of the exact relationship between RBC counts and protein concentration challenging, which then complicates interpretation of CSF.
Study design: Retrospective, cross-sectional study.
Setting: Tertiary-care children's hospital.
Synopsis: Over a four-year period, 1,241 infants younger than 57 days of age that underwent LP were studied, excluding infants with conditions known to increase CSF protein concentrations: ventricular shunt, serious bacterial infection, congenital infection, herpes simplex virus or enterovirus positive PCR in CSF, seizure, or elevated serum bilirubin. Grossly bloody specimens with RBC counts >150,000 cells/mm3 were also excluded. Linear regression was used to determine relationship between CSF RBCs and protein, with protein increasing at a rate of 1.9 mg/dL per 1,000 CSF RBCs.
This ratio is different from a more traditional correction factor of approximately 1 mg/dL CSF protein increase per 1,000 CSF RBCs, which is derived from older populations of children.
However, this study is limited by the exclusion of grossly bloody specimens, which if included would have resulted in a ratio similar to the more traditional values. Additionally, application of this specific correction factor to prediction rules for bacterial meningitis has not been studied. Nonetheless, this study provides a baseline by which clinicians may interpret protein concentrations in traumatically bloody CSF specimens in young infants.
Bottom line: CSF protein concentrations increase at roughly 2 mg/dL per 1,000 CSF RBCs.
Citation: Hines BA, Nigrovic LE, Neuman MI, Shah SS. Adjustment of cerebrospinal fluid protein for red blood cells in neonates and young infants. J Hosp Med. 2012;7:325-328.
Reviewed by Pediatric Editor Mark Shen, MD, SFHM, medical director of hospital medicine at Dell Children's Medical Center, Austin, Texas.
Clinical question: What is the association between cerebrospinal fluid (CSF) red blood cell (RBC) counts and protein concentrations in infants younger than 57 days of age?
Background: Lumbar puncture (LP) is commonly performed in young infants to evaluate for meningitis in the clinical scenario of fever without source. Traumatic LP is common in children, and higher RBC counts are associated with increased CSF protein concentrations. The dynamic nature of CSF composition in young infants makes determination of the exact relationship between RBC counts and protein concentration challenging, which then complicates interpretation of CSF.
Study design: Retrospective, cross-sectional study.
Setting: Tertiary-care children's hospital.
Synopsis: Over a four-year period, 1,241 infants younger than 57 days of age that underwent LP were studied, excluding infants with conditions known to increase CSF protein concentrations: ventricular shunt, serious bacterial infection, congenital infection, herpes simplex virus or enterovirus positive PCR in CSF, seizure, or elevated serum bilirubin. Grossly bloody specimens with RBC counts >150,000 cells/mm3 were also excluded. Linear regression was used to determine relationship between CSF RBCs and protein, with protein increasing at a rate of 1.9 mg/dL per 1,000 CSF RBCs.
This ratio is different from a more traditional correction factor of approximately 1 mg/dL CSF protein increase per 1,000 CSF RBCs, which is derived from older populations of children.
However, this study is limited by the exclusion of grossly bloody specimens, which if included would have resulted in a ratio similar to the more traditional values. Additionally, application of this specific correction factor to prediction rules for bacterial meningitis has not been studied. Nonetheless, this study provides a baseline by which clinicians may interpret protein concentrations in traumatically bloody CSF specimens in young infants.
Bottom line: CSF protein concentrations increase at roughly 2 mg/dL per 1,000 CSF RBCs.
Citation: Hines BA, Nigrovic LE, Neuman MI, Shah SS. Adjustment of cerebrospinal fluid protein for red blood cells in neonates and young infants. J Hosp Med. 2012;7:325-328.
Reviewed by Pediatric Editor Mark Shen, MD, SFHM, medical director of hospital medicine at Dell Children's Medical Center, Austin, Texas.
Clinical question: What is the association between cerebrospinal fluid (CSF) red blood cell (RBC) counts and protein concentrations in infants younger than 57 days of age?
Background: Lumbar puncture (LP) is commonly performed in young infants to evaluate for meningitis in the clinical scenario of fever without source. Traumatic LP is common in children, and higher RBC counts are associated with increased CSF protein concentrations. The dynamic nature of CSF composition in young infants makes determination of the exact relationship between RBC counts and protein concentration challenging, which then complicates interpretation of CSF.
Study design: Retrospective, cross-sectional study.
Setting: Tertiary-care children's hospital.
Synopsis: Over a four-year period, 1,241 infants younger than 57 days of age that underwent LP were studied, excluding infants with conditions known to increase CSF protein concentrations: ventricular shunt, serious bacterial infection, congenital infection, herpes simplex virus or enterovirus positive PCR in CSF, seizure, or elevated serum bilirubin. Grossly bloody specimens with RBC counts >150,000 cells/mm3 were also excluded. Linear regression was used to determine relationship between CSF RBCs and protein, with protein increasing at a rate of 1.9 mg/dL per 1,000 CSF RBCs.
This ratio is different from a more traditional correction factor of approximately 1 mg/dL CSF protein increase per 1,000 CSF RBCs, which is derived from older populations of children.
However, this study is limited by the exclusion of grossly bloody specimens, which if included would have resulted in a ratio similar to the more traditional values. Additionally, application of this specific correction factor to prediction rules for bacterial meningitis has not been studied. Nonetheless, this study provides a baseline by which clinicians may interpret protein concentrations in traumatically bloody CSF specimens in young infants.
Bottom line: CSF protein concentrations increase at roughly 2 mg/dL per 1,000 CSF RBCs.
Citation: Hines BA, Nigrovic LE, Neuman MI, Shah SS. Adjustment of cerebrospinal fluid protein for red blood cells in neonates and young infants. J Hosp Med. 2012;7:325-328.
Reviewed by Pediatric Editor Mark Shen, MD, SFHM, medical director of hospital medicine at Dell Children's Medical Center, Austin, Texas.
How is Acute Pericarditis Diagnosed and Treated?
Case
A 32-year-old female with no significant past medical history is evaluated for sharp, left-sided chest pain for five days. Her pain is intermittent, worse with deep inspiration and in the supine position. She denies any shortness of breath. Her temperature is 100.8ºF, but otherwise her vital signs are normal. The physical exam and chest radiograph are unremarkable, but an electrocardiogram shows diffuse ST-segment elevations. The initial troponin is mildly elevated at 0.35 ng/ml.
Could this patient have acute pericarditis? If so, how should she be managed?
Background
Pericarditis is the most common pericardial disease encountered by hospitalists. As many as 5% of chest pain cases unattributable to myocardial infarction (MI) are diagnosed with pericarditis.1 In immunocompetent individuals, as many as 90% of acute pericarditis cases are viral or idiopathic in etiology.1,2 Human immunodeficiency virus (HIV) and tuberculosis are common culprits in developing countries and immunocompromised hosts.3 Other specific etiologies of acute pericarditis include autoimmune diseases, neoplasms, chest irradiation, trauma, and metabolic disturbances (e.g. uremia). An etiologic classification of acute pericarditis is shown in Table 2 (p. 16).
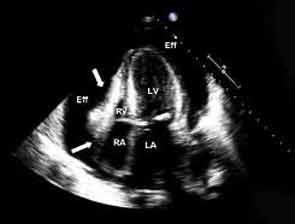
Pericarditis primarily is a clinical diagnosis. Most patients present with chest pain.4 A pericardial friction rub may or may not be heard (sensitivity 16% to 85%), but when present is nearly 100% specific for pericarditis.2,5 Diffuse ST-segment elevation on electrocardiogram (EKG) is present in 60% to 90% of cases, but it can be difficult to differentiate from ST-segment elevations in acute MI.4,6
Uncomplicated acute pericarditis often is treated successfully as an outpatient.4 However, patients with high-risk features (see Table 1, right) should be hospitalized for identification and treatment of specific underlying etiology and for monitoring of complications, such as tamponade.7
Our patient has features consistent with pericarditis. In the following sections, we will review the diagnosis and treatment of acute pericarditis.
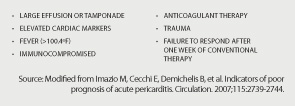
Review of the Data
How is acute pericarditis diagnosed?
Acute pericarditis is a clinical diagnosis supported by EKG and echocardiogram. At least two of the following four criteria must be present for the diagnosis: pleuritic chest pain, pericardial rub, diffuse ST-segment elevation on EKG, and pericardial effusion.8
History. Patients may report fever (46% in one small study of 69 patients) or a recent history of respiratory or gastrointestinal infection (40%).5 Most patients will report pleuritic chest pain. Typically, the pain is improved when sitting up and leaning forward, and gets worse when lying supine.4 Pain might radiate to the trapezius muscle ridge due to the common phrenic nerve innervation of pericardium and trapezius.9 However, pain might be minimal or absent in patients with uremic, neoplastic, tuberculous, or post-irradiation pericarditis.
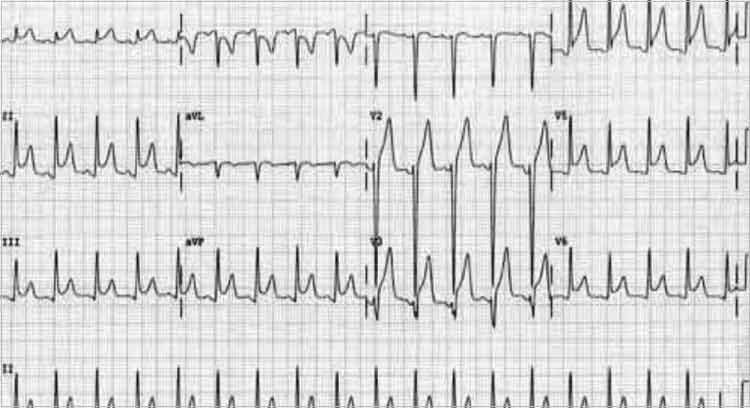
Physical exam. A pericardial friction rub is nearly 100% specific for a pericarditis diagnosis, but sensitivity can vary (16% to 85%) depending on the frequency of auscultation and underlying etiology.2,5 It is thought to be caused by friction between the parietal and visceral layers of inflamed pericardium. A pericardial rub classically is described as a superficial, high-pitched, scratchy, or squeaking sound best heard with the diaphragm of the stethoscope at the lower left sternal border with the patient leaning forward.
Laboratory data. A complete blood count, metabolic panel, and cardiac enzymes should be checked in all patients with suspected acute pericarditis. Troponin values are elevated in up to one-third of patients, indicating cardiac muscle injury or myopericarditis, but have not been shown to adversely impact hospital length of stay, readmission, or complication rates.5,10 Markers of inflammation (e.g. erythrocyte sedimentation rate or C-reactive protein) are frequently elevated but do not point to a specific underlying etiology. Routine viral cultures and antibody titers are not useful.11
Most cases of pericarditis are presumed idiopathic (viral); however, finding a specific etiology should be considered in patients who do not respond after one week of therapy. Anti-nuclear antibody, complement levels, and rheumatoid factor can serve as screening tests for autoimmune disease. Purified protein derivative or quantiferon testing and HIV testing might be indicated in patients with appropriate risk factors. In cases of suspected tuberculous or neoplastic pericarditis, pericardial fluid analysis and biopsy could be warranted.
Electrocardiography. The EKG is the most useful test in diagnosing acute pericarditis. EKG changes in acute pericarditis can progress over four stages:
- Stage 1: diffuse ST elevations with or without PR depressions, initially;
- Stage 2: normalization of ST and PR segments, typically after several days;
- Stage 3: diffuse T-wave inversions; and
- Stage 4: normalization of T-waves, typically after weeks or months.
While all four stages are unlikely to be present in a given case, 80% of patients with pericarditis will demonstrate diffuse ST-segment elevations and PR-segment depression (see Figure 2, above).12
Table 3 lists EKG features helpful in differentiating acute pericarditis from acute myocardial infarction.
Chest radiography. Because a pericardial effusion often accompanies pericarditis, a chest radiograph (CXR) should be performed in all suspected cases. The CXR might show enlargement of the cardiac silhouette if more than 250 ml of pericardial fluid is present.3 A CXR also is helpful to diagnose concomitant pulmonary infection, pleural effusion, or mediastinal mass—all findings that could point to an underlying specific etiology of pericarditis and/or pericardial effusion.
Echocardiography. An echocardiogram should be performed in all patients with suspected pericarditis to detect effusion, associated myocardial, or paracardial disease.13 The echocardiogram frequently is normal but could show an effusion in 60%, and tamponade (see Figure 1, p. 15) in 5%, of cases.4
Computed tomography (CT) and cardiac magnetic resonance imaging (CMR).CT or CMR are the imaging modalities of choice when an echocardiogram is inconclusive or in cases of pericarditis complicated by a hemorrhagic or localized effusion, pericardial thickening, or pericardial mass.14 They also help in precise imaging of neighboring structures, such as lungs or mediastinum.
Pericardial fluid analysis and pericardial biopsy. In cases of refractory pericarditis with effusion, pericardial fluid analysis might provide clues to the underlying etiology. Routine chemistry, cell count, gram and acid fast staining, culture, and cytology should be sent. In addition, acid-fast bacillus staining and culture, adenosine deaminase, and interferon-gamma testing should be ordered when tuberculous pericarditis is suspected. A pericardial biopsy may show granulomas or neoplastic cells. Overall, pericardial fluid analysis and biopsy reveal a diagnosis in roughly 20% of cases.11
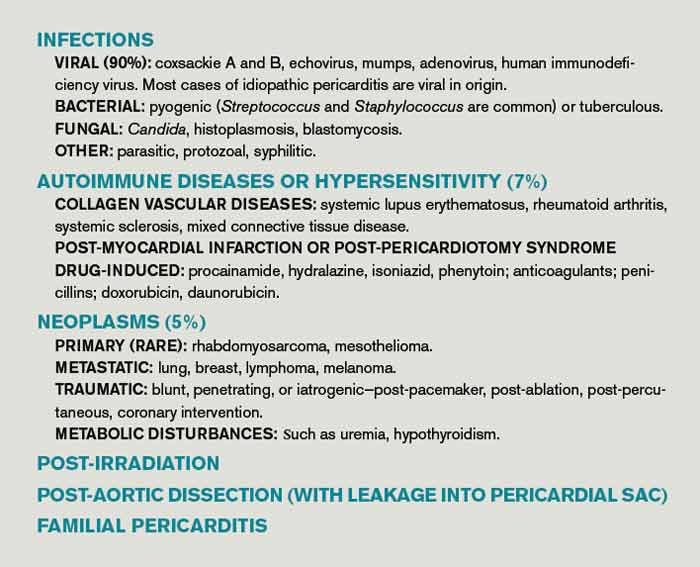
How is acute pericarditis treated?
Most cases of uncomplicated acute pericarditis are viral and respond well to NSAID plus colchicine therapy.2,4 Failure to respond to NSAIDs plus colchicine—evidenced by persistent fever, pericardial chest pain, new pericardial effusion, or worsening of general illness—within a week of treatment should prompt a search for an underlying systemic illness. If found, treatment should be aimed at the causative illness.
Bacterial pericarditis usually requires surgical drainage in addition to treatment with appropriate antibiotics.11 Tuberculous pericarditis is treated with multidrug therapy; when underlying HIV is present, patients should receive highly active anti-retroviral therapy as well. Steroids and immunosuppressants should be considered in addition to NSAIDs and colchicine in autoimmune pericarditis.10 Neoplastic pericarditis may resolve with chemotherapy but it has a high recurrence rate.13 Uremic pericarditis requires intensified dialysis.
Treatment options for uncomplicated idiopathic or viral pericarditis include:
NSAIDs. It is important to adequately dose NSAIDs when treating acute pericarditis. Initial treatment options include ibuprofen (1,600 to 3,200 mg daily), indomethacin (75 to 150 mg daily) or aspirin (2 to 4 gm daily) for one week.11,15 Aspirin is preferred in patients with ischemic heart disease. For patients with symptoms that persist longer than a week, NSAIDS may be continued, but investigation for an underlying etiology is indicated. Concomitant proton-pump-inhibitor therapy should be considered in patients at high risk for peptic ulcer disease to minimize gastric side effects.
Colchicine. Colchicine has a favorable risk-benefit profile as an adjunct treatment for acute and recurrent pericarditis. Patients experience better symptom relief when treated with both colchicine and an NSAID, compared with NSAIDs alone (88% versus 63%). Recurrence rates are lower with combined therapy (11% versus 32%).16 Colchicine treatment (0.6 mg twice daily after a loading dose of up to 2 mg) is recommended for several months to greater than one year.13,16,17
Glucocorticoids. Routine glucocorticoid use should be avoided in the treatment of acute pericarditis, as it has been associated with an increased risk for recurrence (OR 4.3).16,18 Glucocorticoid use should be considered in cases of pericarditis refractory to NSAIDs and colchicine, cases in which NSAIDs and or colchicine are contraindicated, and in autoimmune or connective-tissue-disease-related pericarditis. Prednisone should be dosed up to 1 mg/kg/day for at least one month, depending on symptom resolution, then tapered after either NSAIDs or colchicine have been started.13 Smaller prednisone doses of up to 0.5 mg/kg/day could be as effective, with the added benefit of reduced side effects and recurrences.19
Invasive treatment. Pericardiocentesis and/or pericardiectomy should be considered when pericarditis is complicated by a large effusion or tamponade, constrictive physiology, or recurrent effusion.11 Pericardiocentesis is the least invasive option and helps provide immediate relief in cases of tamponade or large symptomatic effusions. It is the preferred modality for obtaining pericardial fluid for diagnostic analysis. However, effusions can recur and in those cases pericardial window is preferred, as it provides continued outflow of pericardial fluid. Pericardiectomy is recommended in cases of symptomatic constrictive pericarditis unresponsive to medical therapy.15
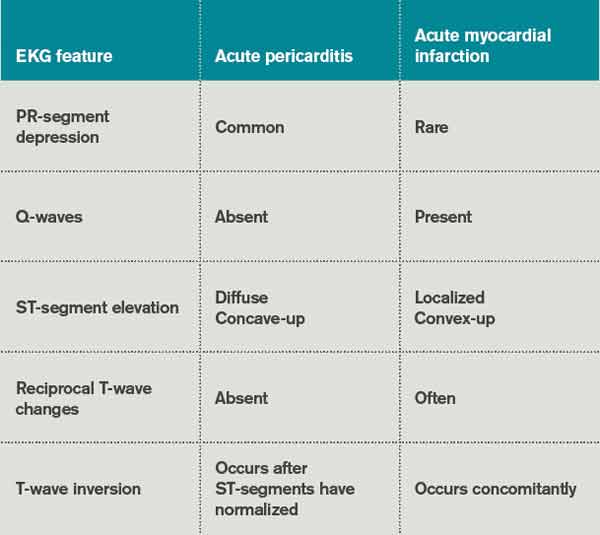
Back to the Case
The patient’s presentation—prodrome followed by fever and pleuritic chest pain—is characteristic of acute idiopathic pericarditis. No pericardial rub was heard, but EKG findings were typical. Troponin I elevation suggested underlying myopericarditis. An echocardiogram was unremarkable. Given the likely viral or idiopathic etiology, no further diagnostic tests were ordered to explore the possibility of an underlying systemic illness.
The patient was started on ibuprofen 600 mg every eight hours. She had significant relief of her symptoms within two days. A routine fever workup was negative. She was discharged the following day.
The patient was readmitted three months later with recurrent pleuritic chest pain, which did not improve with resumption of NSAID therapy. Initial troponin I was 0.22 ng/ml, electrocardiogram was unchanged, and an echocardiogram showed small effusion. She was started on ibuprofen 800 mg every eight hours, as well as colchicine 0.6 mg twice daily. Her symptoms resolved the next day and she was discharged with prescriptions for ibuprofen and colchicine. She was instructed to follow up with a primary-care doctor in one week.
At the clinic visit, ibuprofen was tapered but colchicine was continued for another six months. She remained asymptomatic at her six-month clinic follow-up.
Bottom Line
Acute pericarditis is a clinical diagnosis supported by EKG findings. Most cases are idiopathic or viral, and can be treated successfully with NSAIDs and colchicine. For cases that do not respond to initial therapy, or cases that present with high-risk features, a specific etiology should be sought.
Dr. Southern is chief of the division of hospital medicine at Montefiore Medical Center in Bronx, N.Y. Dr. Galhorta is an instructor and Drs. Martin, Korcak, and Stehlihova are assistant professors in the department of medicine at Albert Einstein.
References
- Lange RA, Hillis LD. Clinical practice. Acute pericarditis. N Engl J Med. 2004;351:2195-2202.
- Zayas R, Anguita M, Torres F, et al. Incidence of specific etiology and role of methods for specific etiologic diagnosis of primary acute pericarditis. Am J Cardiol. 1995;75:378-382.
- Troughton RW, Asher CR, Klein AL. Pericarditis. Lancet. 2004;363:717-727.
- Imazio M, Demichelis B, Parrini I, et al. Day-hospital treatment of acute pericarditis: a management program for outpatient therapy. J Am Coll Cardiol. 2004;43:1042-1046.
- Bonnefoy E, Godon P, Kirkorian G, et al. Serum cardiac troponin I and ST-segment elevation in patients with acute pericarditis. Eur Heart J. 2000;21:832-836.
- Salisbury AC, Olalla-Gomez C, Rihal CS, et al. Frequency and predictors of urgent coronary angiography in patients with acute pericarditis. Mayo Clin Proc. 2009;84(1):11-15.
- Imazio M, Cecchi E, Demichelis B, et al. Indicators of poor prognosis of acute pericarditis. Circulation. 2007;115:2739-2744.
- Imazio M, Spodick DH, Brucato A, et al. Diagnostic issues in the clinical management of pericarditis. Int J Clin Pract. 2010;64(10):1384-1392.
- Spodick DH. Acute pericarditis: current concepts and practice. JAMA. 2003;289:1150-1153.
- Imazio M, Demichelis B, Cecchi E. Cardiac troponin I in acute pericarditis. J Am Coll Cardiol. 2003;42(12):2144-2148.
- Sagristà Sauleda J, Permanyer Miralda G, Soler Soler J. Diagnosis and management of pericardial syndromes. Rev Esp Cardiol. 2005;58(7):830-841.
- Bruce MA, Spodick DH. Atypical electrocardiogram in acute pericarditis: characteristics and prevalence. J Electrocardiol. 1980;13:61-66.
- Maisch B, Seferovic PM, Ristic AD, et al. Guidelines on the diagnosis and management of pericardial diseases executive summary; the task force on the diagnosis and management of pericardial diseases of the European Society of Cardiology. Eur Heart J. 2004; 25(7):587-610.
- Verhaert D, Gabriel RS, Johnston D, et al. The role of multimodality imaging in the management of pericardial disease. Circ Cardiovasc Imaging. 2010;3:333-343.
- Imazio M, Spodick DH, Brucato A, et al. Controversial issues in the management of pericardial diseases. Circulation. 2010;121:916-928.
- Imazio M, Bobbio M, Cecchi E, et al. Colchicine in addition to conventional therapy for acute pericarditis: results of the colchicine for acute pericarditis (COPE) trial. Circulation. 2005;112(13):2012-2016.
- Adler Y, Finkelstein Y, Guindo J, et al. Colchicine treatment for recurrent pericarditis: a decade of experience. Circulation. 1998;97:2183-185.
- Imazio M, Bobbio M, Cecchi E, et al. Colchicine as first-choice therapy for recurrent pericarditis: results of the colchicine for recurrent pericarditis (CORE) trial. Arch Intern Med. 2005;165:1987-1991.
- Imazio M, Brucato A, Cumetti D, et al. Corticosteroids for recurrent pericarditis: high versus low doses: a nonrandomized observation. Circulation. 2008;118:667-771.
Case
A 32-year-old female with no significant past medical history is evaluated for sharp, left-sided chest pain for five days. Her pain is intermittent, worse with deep inspiration and in the supine position. She denies any shortness of breath. Her temperature is 100.8ºF, but otherwise her vital signs are normal. The physical exam and chest radiograph are unremarkable, but an electrocardiogram shows diffuse ST-segment elevations. The initial troponin is mildly elevated at 0.35 ng/ml.
Could this patient have acute pericarditis? If so, how should she be managed?
Background
Pericarditis is the most common pericardial disease encountered by hospitalists. As many as 5% of chest pain cases unattributable to myocardial infarction (MI) are diagnosed with pericarditis.1 In immunocompetent individuals, as many as 90% of acute pericarditis cases are viral or idiopathic in etiology.1,2 Human immunodeficiency virus (HIV) and tuberculosis are common culprits in developing countries and immunocompromised hosts.3 Other specific etiologies of acute pericarditis include autoimmune diseases, neoplasms, chest irradiation, trauma, and metabolic disturbances (e.g. uremia). An etiologic classification of acute pericarditis is shown in Table 2 (p. 16).
Pericarditis primarily is a clinical diagnosis. Most patients present with chest pain.4 A pericardial friction rub may or may not be heard (sensitivity 16% to 85%), but when present is nearly 100% specific for pericarditis.2,5 Diffuse ST-segment elevation on electrocardiogram (EKG) is present in 60% to 90% of cases, but it can be difficult to differentiate from ST-segment elevations in acute MI.4,6
Uncomplicated acute pericarditis often is treated successfully as an outpatient.4 However, patients with high-risk features (see Table 1, right) should be hospitalized for identification and treatment of specific underlying etiology and for monitoring of complications, such as tamponade.7
Our patient has features consistent with pericarditis. In the following sections, we will review the diagnosis and treatment of acute pericarditis.
Review of the Data
How is acute pericarditis diagnosed?
Acute pericarditis is a clinical diagnosis supported by EKG and echocardiogram. At least two of the following four criteria must be present for the diagnosis: pleuritic chest pain, pericardial rub, diffuse ST-segment elevation on EKG, and pericardial effusion.8
History. Patients may report fever (46% in one small study of 69 patients) or a recent history of respiratory or gastrointestinal infection (40%).5 Most patients will report pleuritic chest pain. Typically, the pain is improved when sitting up and leaning forward, and gets worse when lying supine.4 Pain might radiate to the trapezius muscle ridge due to the common phrenic nerve innervation of pericardium and trapezius.9 However, pain might be minimal or absent in patients with uremic, neoplastic, tuberculous, or post-irradiation pericarditis.
Physical exam. A pericardial friction rub is nearly 100% specific for a pericarditis diagnosis, but sensitivity can vary (16% to 85%) depending on the frequency of auscultation and underlying etiology.2,5 It is thought to be caused by friction between the parietal and visceral layers of inflamed pericardium. A pericardial rub classically is described as a superficial, high-pitched, scratchy, or squeaking sound best heard with the diaphragm of the stethoscope at the lower left sternal border with the patient leaning forward.
Laboratory data. A complete blood count, metabolic panel, and cardiac enzymes should be checked in all patients with suspected acute pericarditis. Troponin values are elevated in up to one-third of patients, indicating cardiac muscle injury or myopericarditis, but have not been shown to adversely impact hospital length of stay, readmission, or complication rates.5,10 Markers of inflammation (e.g. erythrocyte sedimentation rate or C-reactive protein) are frequently elevated but do not point to a specific underlying etiology. Routine viral cultures and antibody titers are not useful.11
Most cases of pericarditis are presumed idiopathic (viral); however, finding a specific etiology should be considered in patients who do not respond after one week of therapy. Anti-nuclear antibody, complement levels, and rheumatoid factor can serve as screening tests for autoimmune disease. Purified protein derivative or quantiferon testing and HIV testing might be indicated in patients with appropriate risk factors. In cases of suspected tuberculous or neoplastic pericarditis, pericardial fluid analysis and biopsy could be warranted.
Electrocardiography. The EKG is the most useful test in diagnosing acute pericarditis. EKG changes in acute pericarditis can progress over four stages:
- Stage 1: diffuse ST elevations with or without PR depressions, initially;
- Stage 2: normalization of ST and PR segments, typically after several days;
- Stage 3: diffuse T-wave inversions; and
- Stage 4: normalization of T-waves, typically after weeks or months.
While all four stages are unlikely to be present in a given case, 80% of patients with pericarditis will demonstrate diffuse ST-segment elevations and PR-segment depression (see Figure 2, above).12
Table 3 lists EKG features helpful in differentiating acute pericarditis from acute myocardial infarction.
Chest radiography. Because a pericardial effusion often accompanies pericarditis, a chest radiograph (CXR) should be performed in all suspected cases. The CXR might show enlargement of the cardiac silhouette if more than 250 ml of pericardial fluid is present.3 A CXR also is helpful to diagnose concomitant pulmonary infection, pleural effusion, or mediastinal mass—all findings that could point to an underlying specific etiology of pericarditis and/or pericardial effusion.
Echocardiography. An echocardiogram should be performed in all patients with suspected pericarditis to detect effusion, associated myocardial, or paracardial disease.13 The echocardiogram frequently is normal but could show an effusion in 60%, and tamponade (see Figure 1, p. 15) in 5%, of cases.4
Computed tomography (CT) and cardiac magnetic resonance imaging (CMR).CT or CMR are the imaging modalities of choice when an echocardiogram is inconclusive or in cases of pericarditis complicated by a hemorrhagic or localized effusion, pericardial thickening, or pericardial mass.14 They also help in precise imaging of neighboring structures, such as lungs or mediastinum.
Pericardial fluid analysis and pericardial biopsy. In cases of refractory pericarditis with effusion, pericardial fluid analysis might provide clues to the underlying etiology. Routine chemistry, cell count, gram and acid fast staining, culture, and cytology should be sent. In addition, acid-fast bacillus staining and culture, adenosine deaminase, and interferon-gamma testing should be ordered when tuberculous pericarditis is suspected. A pericardial biopsy may show granulomas or neoplastic cells. Overall, pericardial fluid analysis and biopsy reveal a diagnosis in roughly 20% of cases.11
How is acute pericarditis treated?
Most cases of uncomplicated acute pericarditis are viral and respond well to NSAID plus colchicine therapy.2,4 Failure to respond to NSAIDs plus colchicine—evidenced by persistent fever, pericardial chest pain, new pericardial effusion, or worsening of general illness—within a week of treatment should prompt a search for an underlying systemic illness. If found, treatment should be aimed at the causative illness.
Bacterial pericarditis usually requires surgical drainage in addition to treatment with appropriate antibiotics.11 Tuberculous pericarditis is treated with multidrug therapy; when underlying HIV is present, patients should receive highly active anti-retroviral therapy as well. Steroids and immunosuppressants should be considered in addition to NSAIDs and colchicine in autoimmune pericarditis.10 Neoplastic pericarditis may resolve with chemotherapy but it has a high recurrence rate.13 Uremic pericarditis requires intensified dialysis.
Treatment options for uncomplicated idiopathic or viral pericarditis include:
NSAIDs. It is important to adequately dose NSAIDs when treating acute pericarditis. Initial treatment options include ibuprofen (1,600 to 3,200 mg daily), indomethacin (75 to 150 mg daily) or aspirin (2 to 4 gm daily) for one week.11,15 Aspirin is preferred in patients with ischemic heart disease. For patients with symptoms that persist longer than a week, NSAIDS may be continued, but investigation for an underlying etiology is indicated. Concomitant proton-pump-inhibitor therapy should be considered in patients at high risk for peptic ulcer disease to minimize gastric side effects.
Colchicine. Colchicine has a favorable risk-benefit profile as an adjunct treatment for acute and recurrent pericarditis. Patients experience better symptom relief when treated with both colchicine and an NSAID, compared with NSAIDs alone (88% versus 63%). Recurrence rates are lower with combined therapy (11% versus 32%).16 Colchicine treatment (0.6 mg twice daily after a loading dose of up to 2 mg) is recommended for several months to greater than one year.13,16,17
Glucocorticoids. Routine glucocorticoid use should be avoided in the treatment of acute pericarditis, as it has been associated with an increased risk for recurrence (OR 4.3).16,18 Glucocorticoid use should be considered in cases of pericarditis refractory to NSAIDs and colchicine, cases in which NSAIDs and or colchicine are contraindicated, and in autoimmune or connective-tissue-disease-related pericarditis. Prednisone should be dosed up to 1 mg/kg/day for at least one month, depending on symptom resolution, then tapered after either NSAIDs or colchicine have been started.13 Smaller prednisone doses of up to 0.5 mg/kg/day could be as effective, with the added benefit of reduced side effects and recurrences.19
Invasive treatment. Pericardiocentesis and/or pericardiectomy should be considered when pericarditis is complicated by a large effusion or tamponade, constrictive physiology, or recurrent effusion.11 Pericardiocentesis is the least invasive option and helps provide immediate relief in cases of tamponade or large symptomatic effusions. It is the preferred modality for obtaining pericardial fluid for diagnostic analysis. However, effusions can recur and in those cases pericardial window is preferred, as it provides continued outflow of pericardial fluid. Pericardiectomy is recommended in cases of symptomatic constrictive pericarditis unresponsive to medical therapy.15
Back to the Case
The patient’s presentation—prodrome followed by fever and pleuritic chest pain—is characteristic of acute idiopathic pericarditis. No pericardial rub was heard, but EKG findings were typical. Troponin I elevation suggested underlying myopericarditis. An echocardiogram was unremarkable. Given the likely viral or idiopathic etiology, no further diagnostic tests were ordered to explore the possibility of an underlying systemic illness.
The patient was started on ibuprofen 600 mg every eight hours. She had significant relief of her symptoms within two days. A routine fever workup was negative. She was discharged the following day.
The patient was readmitted three months later with recurrent pleuritic chest pain, which did not improve with resumption of NSAID therapy. Initial troponin I was 0.22 ng/ml, electrocardiogram was unchanged, and an echocardiogram showed small effusion. She was started on ibuprofen 800 mg every eight hours, as well as colchicine 0.6 mg twice daily. Her symptoms resolved the next day and she was discharged with prescriptions for ibuprofen and colchicine. She was instructed to follow up with a primary-care doctor in one week.
At the clinic visit, ibuprofen was tapered but colchicine was continued for another six months. She remained asymptomatic at her six-month clinic follow-up.
Bottom Line
Acute pericarditis is a clinical diagnosis supported by EKG findings. Most cases are idiopathic or viral, and can be treated successfully with NSAIDs and colchicine. For cases that do not respond to initial therapy, or cases that present with high-risk features, a specific etiology should be sought.
Dr. Southern is chief of the division of hospital medicine at Montefiore Medical Center in Bronx, N.Y. Dr. Galhorta is an instructor and Drs. Martin, Korcak, and Stehlihova are assistant professors in the department of medicine at Albert Einstein.
References
- Lange RA, Hillis LD. Clinical practice. Acute pericarditis. N Engl J Med. 2004;351:2195-2202.
- Zayas R, Anguita M, Torres F, et al. Incidence of specific etiology and role of methods for specific etiologic diagnosis of primary acute pericarditis. Am J Cardiol. 1995;75:378-382.
- Troughton RW, Asher CR, Klein AL. Pericarditis. Lancet. 2004;363:717-727.
- Imazio M, Demichelis B, Parrini I, et al. Day-hospital treatment of acute pericarditis: a management program for outpatient therapy. J Am Coll Cardiol. 2004;43:1042-1046.
- Bonnefoy E, Godon P, Kirkorian G, et al. Serum cardiac troponin I and ST-segment elevation in patients with acute pericarditis. Eur Heart J. 2000;21:832-836.
- Salisbury AC, Olalla-Gomez C, Rihal CS, et al. Frequency and predictors of urgent coronary angiography in patients with acute pericarditis. Mayo Clin Proc. 2009;84(1):11-15.
- Imazio M, Cecchi E, Demichelis B, et al. Indicators of poor prognosis of acute pericarditis. Circulation. 2007;115:2739-2744.
- Imazio M, Spodick DH, Brucato A, et al. Diagnostic issues in the clinical management of pericarditis. Int J Clin Pract. 2010;64(10):1384-1392.
- Spodick DH. Acute pericarditis: current concepts and practice. JAMA. 2003;289:1150-1153.
- Imazio M, Demichelis B, Cecchi E. Cardiac troponin I in acute pericarditis. J Am Coll Cardiol. 2003;42(12):2144-2148.
- Sagristà Sauleda J, Permanyer Miralda G, Soler Soler J. Diagnosis and management of pericardial syndromes. Rev Esp Cardiol. 2005;58(7):830-841.
- Bruce MA, Spodick DH. Atypical electrocardiogram in acute pericarditis: characteristics and prevalence. J Electrocardiol. 1980;13:61-66.
- Maisch B, Seferovic PM, Ristic AD, et al. Guidelines on the diagnosis and management of pericardial diseases executive summary; the task force on the diagnosis and management of pericardial diseases of the European Society of Cardiology. Eur Heart J. 2004; 25(7):587-610.
- Verhaert D, Gabriel RS, Johnston D, et al. The role of multimodality imaging in the management of pericardial disease. Circ Cardiovasc Imaging. 2010;3:333-343.
- Imazio M, Spodick DH, Brucato A, et al. Controversial issues in the management of pericardial diseases. Circulation. 2010;121:916-928.
- Imazio M, Bobbio M, Cecchi E, et al. Colchicine in addition to conventional therapy for acute pericarditis: results of the colchicine for acute pericarditis (COPE) trial. Circulation. 2005;112(13):2012-2016.
- Adler Y, Finkelstein Y, Guindo J, et al. Colchicine treatment for recurrent pericarditis: a decade of experience. Circulation. 1998;97:2183-185.
- Imazio M, Bobbio M, Cecchi E, et al. Colchicine as first-choice therapy for recurrent pericarditis: results of the colchicine for recurrent pericarditis (CORE) trial. Arch Intern Med. 2005;165:1987-1991.
- Imazio M, Brucato A, Cumetti D, et al. Corticosteroids for recurrent pericarditis: high versus low doses: a nonrandomized observation. Circulation. 2008;118:667-771.
Case
A 32-year-old female with no significant past medical history is evaluated for sharp, left-sided chest pain for five days. Her pain is intermittent, worse with deep inspiration and in the supine position. She denies any shortness of breath. Her temperature is 100.8ºF, but otherwise her vital signs are normal. The physical exam and chest radiograph are unremarkable, but an electrocardiogram shows diffuse ST-segment elevations. The initial troponin is mildly elevated at 0.35 ng/ml.
Could this patient have acute pericarditis? If so, how should she be managed?
Background
Pericarditis is the most common pericardial disease encountered by hospitalists. As many as 5% of chest pain cases unattributable to myocardial infarction (MI) are diagnosed with pericarditis.1 In immunocompetent individuals, as many as 90% of acute pericarditis cases are viral or idiopathic in etiology.1,2 Human immunodeficiency virus (HIV) and tuberculosis are common culprits in developing countries and immunocompromised hosts.3 Other specific etiologies of acute pericarditis include autoimmune diseases, neoplasms, chest irradiation, trauma, and metabolic disturbances (e.g. uremia). An etiologic classification of acute pericarditis is shown in Table 2 (p. 16).
Pericarditis primarily is a clinical diagnosis. Most patients present with chest pain.4 A pericardial friction rub may or may not be heard (sensitivity 16% to 85%), but when present is nearly 100% specific for pericarditis.2,5 Diffuse ST-segment elevation on electrocardiogram (EKG) is present in 60% to 90% of cases, but it can be difficult to differentiate from ST-segment elevations in acute MI.4,6
Uncomplicated acute pericarditis often is treated successfully as an outpatient.4 However, patients with high-risk features (see Table 1, right) should be hospitalized for identification and treatment of specific underlying etiology and for monitoring of complications, such as tamponade.7
Our patient has features consistent with pericarditis. In the following sections, we will review the diagnosis and treatment of acute pericarditis.
Review of the Data
How is acute pericarditis diagnosed?
Acute pericarditis is a clinical diagnosis supported by EKG and echocardiogram. At least two of the following four criteria must be present for the diagnosis: pleuritic chest pain, pericardial rub, diffuse ST-segment elevation on EKG, and pericardial effusion.8
History. Patients may report fever (46% in one small study of 69 patients) or a recent history of respiratory or gastrointestinal infection (40%).5 Most patients will report pleuritic chest pain. Typically, the pain is improved when sitting up and leaning forward, and gets worse when lying supine.4 Pain might radiate to the trapezius muscle ridge due to the common phrenic nerve innervation of pericardium and trapezius.9 However, pain might be minimal or absent in patients with uremic, neoplastic, tuberculous, or post-irradiation pericarditis.
Physical exam. A pericardial friction rub is nearly 100% specific for a pericarditis diagnosis, but sensitivity can vary (16% to 85%) depending on the frequency of auscultation and underlying etiology.2,5 It is thought to be caused by friction between the parietal and visceral layers of inflamed pericardium. A pericardial rub classically is described as a superficial, high-pitched, scratchy, or squeaking sound best heard with the diaphragm of the stethoscope at the lower left sternal border with the patient leaning forward.
Laboratory data. A complete blood count, metabolic panel, and cardiac enzymes should be checked in all patients with suspected acute pericarditis. Troponin values are elevated in up to one-third of patients, indicating cardiac muscle injury or myopericarditis, but have not been shown to adversely impact hospital length of stay, readmission, or complication rates.5,10 Markers of inflammation (e.g. erythrocyte sedimentation rate or C-reactive protein) are frequently elevated but do not point to a specific underlying etiology. Routine viral cultures and antibody titers are not useful.11
Most cases of pericarditis are presumed idiopathic (viral); however, finding a specific etiology should be considered in patients who do not respond after one week of therapy. Anti-nuclear antibody, complement levels, and rheumatoid factor can serve as screening tests for autoimmune disease. Purified protein derivative or quantiferon testing and HIV testing might be indicated in patients with appropriate risk factors. In cases of suspected tuberculous or neoplastic pericarditis, pericardial fluid analysis and biopsy could be warranted.
Electrocardiography. The EKG is the most useful test in diagnosing acute pericarditis. EKG changes in acute pericarditis can progress over four stages:
- Stage 1: diffuse ST elevations with or without PR depressions, initially;
- Stage 2: normalization of ST and PR segments, typically after several days;
- Stage 3: diffuse T-wave inversions; and
- Stage 4: normalization of T-waves, typically after weeks or months.
While all four stages are unlikely to be present in a given case, 80% of patients with pericarditis will demonstrate diffuse ST-segment elevations and PR-segment depression (see Figure 2, above).12
Table 3 lists EKG features helpful in differentiating acute pericarditis from acute myocardial infarction.
Chest radiography. Because a pericardial effusion often accompanies pericarditis, a chest radiograph (CXR) should be performed in all suspected cases. The CXR might show enlargement of the cardiac silhouette if more than 250 ml of pericardial fluid is present.3 A CXR also is helpful to diagnose concomitant pulmonary infection, pleural effusion, or mediastinal mass—all findings that could point to an underlying specific etiology of pericarditis and/or pericardial effusion.
Echocardiography. An echocardiogram should be performed in all patients with suspected pericarditis to detect effusion, associated myocardial, or paracardial disease.13 The echocardiogram frequently is normal but could show an effusion in 60%, and tamponade (see Figure 1, p. 15) in 5%, of cases.4
Computed tomography (CT) and cardiac magnetic resonance imaging (CMR).CT or CMR are the imaging modalities of choice when an echocardiogram is inconclusive or in cases of pericarditis complicated by a hemorrhagic or localized effusion, pericardial thickening, or pericardial mass.14 They also help in precise imaging of neighboring structures, such as lungs or mediastinum.
Pericardial fluid analysis and pericardial biopsy. In cases of refractory pericarditis with effusion, pericardial fluid analysis might provide clues to the underlying etiology. Routine chemistry, cell count, gram and acid fast staining, culture, and cytology should be sent. In addition, acid-fast bacillus staining and culture, adenosine deaminase, and interferon-gamma testing should be ordered when tuberculous pericarditis is suspected. A pericardial biopsy may show granulomas or neoplastic cells. Overall, pericardial fluid analysis and biopsy reveal a diagnosis in roughly 20% of cases.11
How is acute pericarditis treated?
Most cases of uncomplicated acute pericarditis are viral and respond well to NSAID plus colchicine therapy.2,4 Failure to respond to NSAIDs plus colchicine—evidenced by persistent fever, pericardial chest pain, new pericardial effusion, or worsening of general illness—within a week of treatment should prompt a search for an underlying systemic illness. If found, treatment should be aimed at the causative illness.
Bacterial pericarditis usually requires surgical drainage in addition to treatment with appropriate antibiotics.11 Tuberculous pericarditis is treated with multidrug therapy; when underlying HIV is present, patients should receive highly active anti-retroviral therapy as well. Steroids and immunosuppressants should be considered in addition to NSAIDs and colchicine in autoimmune pericarditis.10 Neoplastic pericarditis may resolve with chemotherapy but it has a high recurrence rate.13 Uremic pericarditis requires intensified dialysis.
Treatment options for uncomplicated idiopathic or viral pericarditis include:
NSAIDs. It is important to adequately dose NSAIDs when treating acute pericarditis. Initial treatment options include ibuprofen (1,600 to 3,200 mg daily), indomethacin (75 to 150 mg daily) or aspirin (2 to 4 gm daily) for one week.11,15 Aspirin is preferred in patients with ischemic heart disease. For patients with symptoms that persist longer than a week, NSAIDS may be continued, but investigation for an underlying etiology is indicated. Concomitant proton-pump-inhibitor therapy should be considered in patients at high risk for peptic ulcer disease to minimize gastric side effects.
Colchicine. Colchicine has a favorable risk-benefit profile as an adjunct treatment for acute and recurrent pericarditis. Patients experience better symptom relief when treated with both colchicine and an NSAID, compared with NSAIDs alone (88% versus 63%). Recurrence rates are lower with combined therapy (11% versus 32%).16 Colchicine treatment (0.6 mg twice daily after a loading dose of up to 2 mg) is recommended for several months to greater than one year.13,16,17
Glucocorticoids. Routine glucocorticoid use should be avoided in the treatment of acute pericarditis, as it has been associated with an increased risk for recurrence (OR 4.3).16,18 Glucocorticoid use should be considered in cases of pericarditis refractory to NSAIDs and colchicine, cases in which NSAIDs and or colchicine are contraindicated, and in autoimmune or connective-tissue-disease-related pericarditis. Prednisone should be dosed up to 1 mg/kg/day for at least one month, depending on symptom resolution, then tapered after either NSAIDs or colchicine have been started.13 Smaller prednisone doses of up to 0.5 mg/kg/day could be as effective, with the added benefit of reduced side effects and recurrences.19
Invasive treatment. Pericardiocentesis and/or pericardiectomy should be considered when pericarditis is complicated by a large effusion or tamponade, constrictive physiology, or recurrent effusion.11 Pericardiocentesis is the least invasive option and helps provide immediate relief in cases of tamponade or large symptomatic effusions. It is the preferred modality for obtaining pericardial fluid for diagnostic analysis. However, effusions can recur and in those cases pericardial window is preferred, as it provides continued outflow of pericardial fluid. Pericardiectomy is recommended in cases of symptomatic constrictive pericarditis unresponsive to medical therapy.15
Back to the Case
The patient’s presentation—prodrome followed by fever and pleuritic chest pain—is characteristic of acute idiopathic pericarditis. No pericardial rub was heard, but EKG findings were typical. Troponin I elevation suggested underlying myopericarditis. An echocardiogram was unremarkable. Given the likely viral or idiopathic etiology, no further diagnostic tests were ordered to explore the possibility of an underlying systemic illness.
The patient was started on ibuprofen 600 mg every eight hours. She had significant relief of her symptoms within two days. A routine fever workup was negative. She was discharged the following day.
The patient was readmitted three months later with recurrent pleuritic chest pain, which did not improve with resumption of NSAID therapy. Initial troponin I was 0.22 ng/ml, electrocardiogram was unchanged, and an echocardiogram showed small effusion. She was started on ibuprofen 800 mg every eight hours, as well as colchicine 0.6 mg twice daily. Her symptoms resolved the next day and she was discharged with prescriptions for ibuprofen and colchicine. She was instructed to follow up with a primary-care doctor in one week.
At the clinic visit, ibuprofen was tapered but colchicine was continued for another six months. She remained asymptomatic at her six-month clinic follow-up.
Bottom Line
Acute pericarditis is a clinical diagnosis supported by EKG findings. Most cases are idiopathic or viral, and can be treated successfully with NSAIDs and colchicine. For cases that do not respond to initial therapy, or cases that present with high-risk features, a specific etiology should be sought.
Dr. Southern is chief of the division of hospital medicine at Montefiore Medical Center in Bronx, N.Y. Dr. Galhorta is an instructor and Drs. Martin, Korcak, and Stehlihova are assistant professors in the department of medicine at Albert Einstein.
References
- Lange RA, Hillis LD. Clinical practice. Acute pericarditis. N Engl J Med. 2004;351:2195-2202.
- Zayas R, Anguita M, Torres F, et al. Incidence of specific etiology and role of methods for specific etiologic diagnosis of primary acute pericarditis. Am J Cardiol. 1995;75:378-382.
- Troughton RW, Asher CR, Klein AL. Pericarditis. Lancet. 2004;363:717-727.
- Imazio M, Demichelis B, Parrini I, et al. Day-hospital treatment of acute pericarditis: a management program for outpatient therapy. J Am Coll Cardiol. 2004;43:1042-1046.
- Bonnefoy E, Godon P, Kirkorian G, et al. Serum cardiac troponin I and ST-segment elevation in patients with acute pericarditis. Eur Heart J. 2000;21:832-836.
- Salisbury AC, Olalla-Gomez C, Rihal CS, et al. Frequency and predictors of urgent coronary angiography in patients with acute pericarditis. Mayo Clin Proc. 2009;84(1):11-15.
- Imazio M, Cecchi E, Demichelis B, et al. Indicators of poor prognosis of acute pericarditis. Circulation. 2007;115:2739-2744.
- Imazio M, Spodick DH, Brucato A, et al. Diagnostic issues in the clinical management of pericarditis. Int J Clin Pract. 2010;64(10):1384-1392.
- Spodick DH. Acute pericarditis: current concepts and practice. JAMA. 2003;289:1150-1153.
- Imazio M, Demichelis B, Cecchi E. Cardiac troponin I in acute pericarditis. J Am Coll Cardiol. 2003;42(12):2144-2148.
- Sagristà Sauleda J, Permanyer Miralda G, Soler Soler J. Diagnosis and management of pericardial syndromes. Rev Esp Cardiol. 2005;58(7):830-841.
- Bruce MA, Spodick DH. Atypical electrocardiogram in acute pericarditis: characteristics and prevalence. J Electrocardiol. 1980;13:61-66.
- Maisch B, Seferovic PM, Ristic AD, et al. Guidelines on the diagnosis and management of pericardial diseases executive summary; the task force on the diagnosis and management of pericardial diseases of the European Society of Cardiology. Eur Heart J. 2004; 25(7):587-610.
- Verhaert D, Gabriel RS, Johnston D, et al. The role of multimodality imaging in the management of pericardial disease. Circ Cardiovasc Imaging. 2010;3:333-343.
- Imazio M, Spodick DH, Brucato A, et al. Controversial issues in the management of pericardial diseases. Circulation. 2010;121:916-928.
- Imazio M, Bobbio M, Cecchi E, et al. Colchicine in addition to conventional therapy for acute pericarditis: results of the colchicine for acute pericarditis (COPE) trial. Circulation. 2005;112(13):2012-2016.
- Adler Y, Finkelstein Y, Guindo J, et al. Colchicine treatment for recurrent pericarditis: a decade of experience. Circulation. 1998;97:2183-185.
- Imazio M, Bobbio M, Cecchi E, et al. Colchicine as first-choice therapy for recurrent pericarditis: results of the colchicine for recurrent pericarditis (CORE) trial. Arch Intern Med. 2005;165:1987-1991.
- Imazio M, Brucato A, Cumetti D, et al. Corticosteroids for recurrent pericarditis: high versus low doses: a nonrandomized observation. Circulation. 2008;118:667-771.