A 32-year-old woman presents with a history of pelvic pain, dysmenorrhea, dyspareunia, dyschezia, and dysuria, with exacerbation of the symptoms during her menstrual cycles. Her menarche occurred at the age of 13 and her menses are regular. She has never undergone surgery and has no relevant pathologic processes. She also reports that for the past 18 months she has been unsuccessfully trying to conceive.
Two months ago, she went to the emergency department because of an acute episode of severe pelvic pain associated with abdominal cramps, vomiting, and dyschezia, occurring at the beginning of her menstrual cycle. At that time, her vital signs were within normal limits, but deep palpation of the right iliac fossa was painful. On that occasion, acute abdomen and bowel obstruction were excluded.
Now, vaginal examination reveals a bluish, painful, bulky induration in the posterior fornix. Digital rectal examination reveals a circular infiltrated area in the anterior rectal wall. Her cancer antigen 125 (CA 125) level is 230 U/mL (normal range 0–35 U/mL).
MENSES-RELATED SYMPTOMS AND THE DIAGNOSIS OF ENDOMETRIOSIS
The diagnosis of endometriosis should be considered in the patient described above. Many of her signs and symptoms can be associated with several diseases. However, the diagnostic hypothesis points strongly toward endometriosis, since her symptoms recur at the beginning of every menstrual cycle.1
Endometriosis is the presence of endometrial tissue outside the uterine cavity. The affected organs usually include the ovaries, fallopian tubes,2 peritoneal surface, vagina, cervix, abdominal wall,3 scar tissue, pouch of Douglas, urinary tract, and bowel. However, any organ can be involved.
So-called deeply infiltrating endometriosis is an endometriotic lesion penetrating into the retroperitoneal space (most often affecting the uterosacral ligaments and the rectovaginal septum) or the pelvic-organ wall to a depth of at least 5 mm and involving structures such as the rectum, vagina, ureters, and bladder.4 Its clinical presentation is highly variable, ranging from no symptoms to severe pain and dysfunction of pelvic organs.
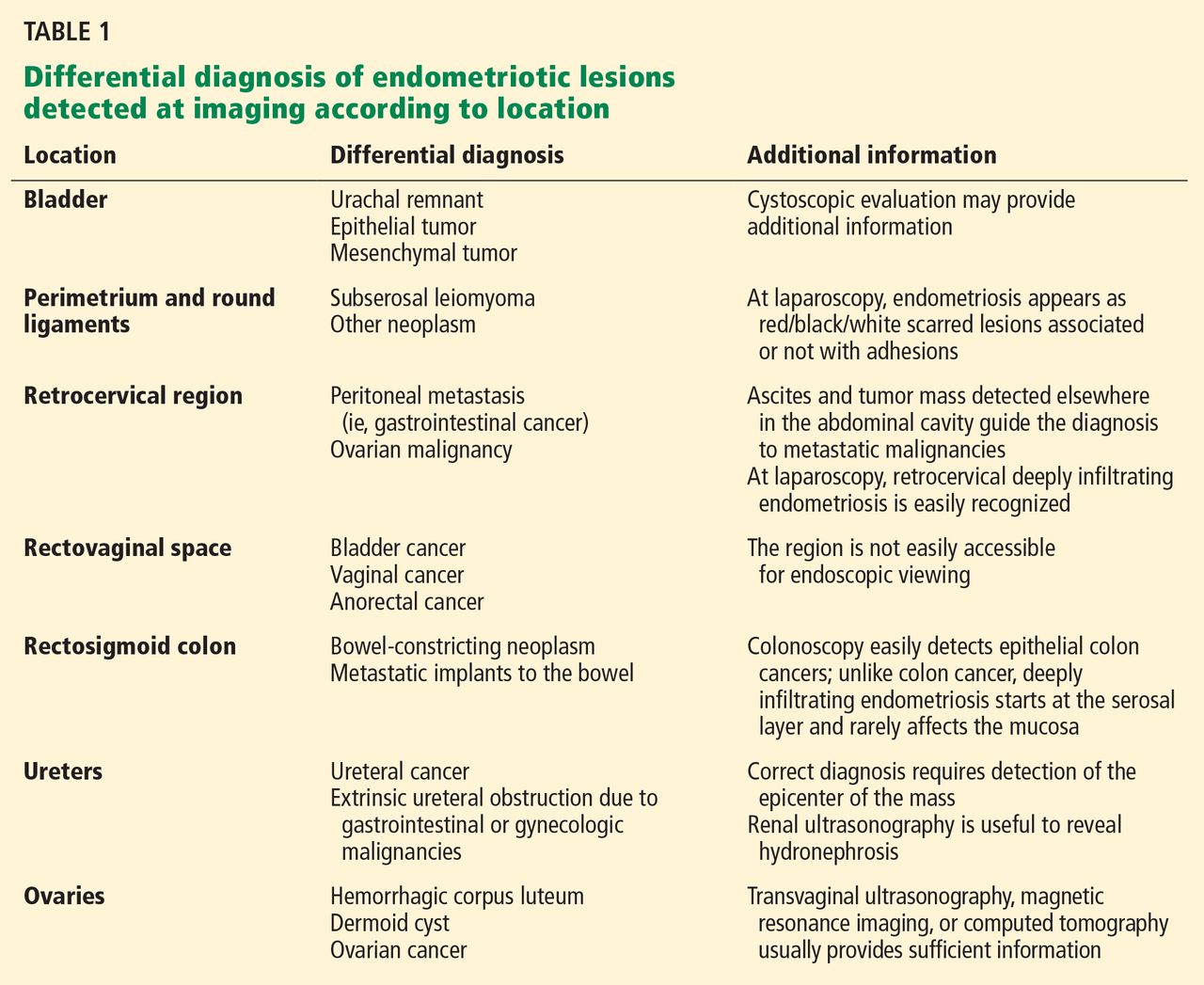
Endometriosis can be diagnosed with certainty only when the endometriotic lesions are observed by laparoscopy or laparotomy and after the histologic examination of surgically resected lesions (Figure 1).1 However, a presumptive diagnosis can be made on the basis of imaging findings, which can be useful in the differential diagnostic process (Table 1).
Figure 1. Diagnostic algorithm for endometriosis.
EXAMINATION AND BLOOD MARKERS PROVIDE LIMITED INFORMATION
Knowing the history of the patient, along with a physical examination that includes speculum and bimanual vaginal and rectal examination, can be helpful in the diagnostic process even if nothing abnormal is found.
Pelvic examination has a poor predictive value, as demonstrated in a study conducted by Nezhat et al5 in 91 patients with surgically confirmed endometriosis, 47% of whom had a normal bimanual examination.
CA 125 is the serologic marker most often used for diagnosing endometriosis. Levels are usually high in the sera of patients with endometriosis, especially in the advanced stages.6 However, levels increase both in the physiologic menstrual cycle and in epithelial ovarian cancers.7 Thus, the diagnostic value of CA 125 is limited in terms of both sensitivity and specificity.
INCLUDE IMAGING IN THE DIAGNOSTIC WORKUP
Surgical treatment is frequently offered to patients who have severe pelvic pain that does not respond to medical treatment, or in cases of infertility. Imaging investigations are mandatory both to ascertain the diagnosis and to assess involvement of internal organs before surgery. Moreover, imaging helps minimize the surgical risks.
The primary aim of the radiologic examination is to describe the precise location, the depth, and the number of pelvic endometriotic lesions. Furthermore, imaging is useful to check for endometriotic foci in pelvic organs such as the bowel, ureters, and bladder, which are often involved in the pathologic process.
Transvaginal ultrasonography and magnetic resonance imaging (MRI) can accurately delineate deeply infiltrating lesions of endometriosis that are not easily accessible laparoscopically.
Transvaginal ultrasonography
Transvaginal ultrasonography is the first-line imaging study when endometriosis is suspected: it is powerful, simple, widely available, and cost-effective. In particular, it is recommended for diagnosing endometriotic ovarian cysts (endometriomas)8,9 and endometriosis of the bladder.10 However, its value for the assessment of superficial peritoneal lesions, ovarian foci, and deeply infiltrating endometriosis is questionable.
Although uncomfortable for the patient, transvaginal ultrasonography should be performed during menses, or when the pain reaches its highest level. In fact, during menstrual bleeding the endometrial implants grow and become easier to detect.
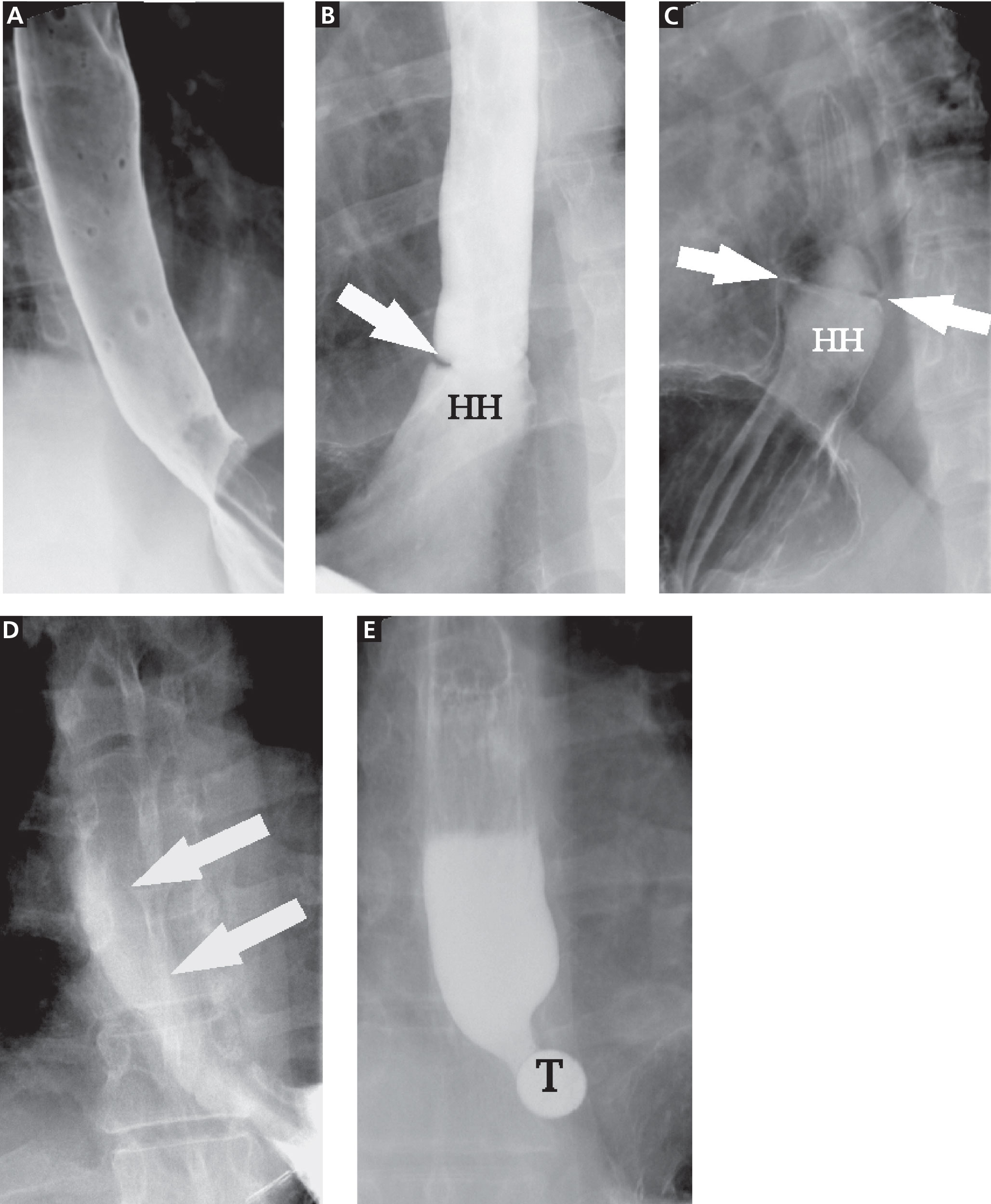
Mais et al8 reported that transvaginal ultrasonography has a sensitivity of 88% in differentiating endometriomas from other ovarian masses, and a specificity of 90% (Figure 2). Furthermore, its specificity is as high as that of MRI.8,9
Figure 2. Endometriotic ovarian cysts (endometriomas) (arrow) on transvaginal ultrasonography.
Endometriotic nodules detected in the uterosacral ligaments, rectovaginal septum, vagina, vesicouterine pouch, bladder (Figure 3), and ureters can be signs of deeply infiltrating endometriosis. Pelvic adhesions can be suspected when pelvic organs appear fixed to each other, when hyperechogenic plaques are found between the serosal surfaces of the different organs, and when the pouch of Douglas is partially or completely obliterated.
Figure 3. Transvaginal ultrasonography in the sagittal plane shows an endometriotic nodule in the posterior wall of the bladder (arrow).
The accuracy of transvaginal ultrasonography strongly depends on the operator’s skill. Furthermore, lesions of the sigmoid colon are impossible to visualize by transvaginal ultrasonography; hence, further diagnostic procedures are required. Transvaginal ultrasonography is the most accurate technique in detecting endometriotic nodules of the bladder wall in patients with urinary symptoms.
Transvaginal ultrasonography combined with color Doppler can also demonstrate the flow of urine through the ureters to the bladder, thereby ascertaining the patency of the ureters and clarifying the anatomic relationship between the ureters and any endometriotic lesions in the detrusors.10 Hydronephrosis can arise from ureteral restriction caused by endometriotic nodules. Thus, transabdominal ultrasonography of the kidneys is always recommended when deeply infiltrating endometriosis is suspected.
Some centers use a bowel-preparation protocol consisting of a laxative taken 24 hours before the procedure, combined with a low-residue diet and an enema 1 hour before the examination to cleanse the rectosigmoid colon of fecal content and gas, which can interfere with the visual examination of the pelvic structures.11
Transabdominal ultrasonography
Transabdominal ultrasonography can be used instead of transvaginal ultrasonography, eg, in young girls and women who have never been sexually active. When transabdominal ultrasonography is selected, the patient should have a full bladder to maximize the visualization of the pelvic structures. However, transvaginal ultrasonography is generally more sensitive than transabdominal in detecting adnexal masses and pelvic nodules.12
Magnetic resonance imaging
MRI has been recently introduced in the diagnosis of endometriosis. MRI is less operator-dependent than transvaginal ultrasonography and is more sensitive for detecting foci of deeply infiltrating endometriosis, because of its ability to completely survey the anterior and posterior compartments of the pelvis. However, its diagnostic value in cases of bladder endometriosis, superficial peritoneal lesions, and ovarian foci is still controversial.13–16
On MRI, lesions of deeply infiltrating endometriosis mainly appear as areas or nodules with regular, irregular, indistinct, or stellate margins. A distortion of the normal pelvic anatomy or the detection of a loculated fluid collection can indirectly signal the presence of adhesions.
MRI has high specificity for the diagnosis of endometriomas as a result of its ability to detect aged hemorrhagic content (Figure 4).17 Despite the many studies that point to the limits of MRI in detecting small endometriotic lesions, recent studies demonstrated that MRI also has good sensitivity for small peritoneal implants and adhesions.18,19 The injection of gadolinium contrast is still a debatable measure, because contrast-enhanced imaging cannot differentiate infiltrating lesions from other normal fibromuscular pelvic anatomic structures.15,20
Figure 4. Ovarian endometrioma on magnetic resonance imaging. (A) On a fat-saturation transverse T1-weighted image, the endometrioma has high signal intensity. (B) On transverse T2-weighted image, blood-degraded product content has intermediate to low signal intensity.
Bowel preparation can be done with an oral laxative the day before imaging, complemented by a low-residue diet. A single dose of a ready-to-use enema is given 30 minutes before the examination to cleanse the terminal section of the intestinal tract. To avoid motion artifacts caused by bowel peristalsis, images are obtained after intramuscular injections of a myorelaxant are given, if there is no contraindication. Bowel preparation is useful to eliminate fecal residue and gas, thereby allowing proper visualization of lesions of deeply infiltrating endometriosis, but it is not routinely prescribed in all centers.11
In most cases, endometriotic lesions have an MRI signal intensity that comes very close to that of the surrounding fibromuscular structures. In this regard, vaginal and rectal distention and opacification using ultrasonographic gel clearly help to delineate the cervix, vaginal fornices, and vaginal wall, as well as the rectum and wall of the rectosigmoid junction (Figure 5).20
Figure 5. Posterior deep infiltrating endometriotic nodule on magnetic resonance imaging. (A) On a T2- weighted image with no opacification of the vagina and rectum with ultrasonographic gel, a retrocervical endometriotic nodule (white oval) has a signal intensity very close to that of the surrounding fibromuscular anatomic structures such as the rectal wall (arrow), vagina, and cervical stroma (asterisk). (B) A T2- weighted image shows the endometriotic nodule (oval) extending downward to the vaginal fornix, which appears obliterated. Only the right vaginal fornix (asterisk) is distended. Between the nodule and the anterior rectal wall, interposing fat tissue (arrowhead) is likely to represent a safety margin and a plane of dissection.
PRESURGICAL IMAGING
Rectal endoscopic ultrasonography
Even though it should not be included in the routine diagnostic workup, rectal endoscopic ultrasonography, using a flexible echoendoscope, is suitable in certain presurgical cases. The aim of this imaging technique is to assess the depth of bowel wall infiltration thanks to the visualization of the different layers.21
Double-contrast barium enema and multislice computed tomography
Double-contrast barium enema is extensively used for the diagnosis of bowel endometriosis, once the decision to perform surgery has been made. It allows evaluation of the degree and length of the bowel occlusion at the level of the sigmoid or high rectosigmoid tract, but it does not permit differentiation of bowel endometriosis from other pathologies.
Multislice computed tomography offers the opportunity to evaluate the depth of the lesions with excellent precision. 22
The most relevant disadvantage of both procedures is the exposure of women of reproductive age to ionizing radiation. In addition, multislice computed tomography requires the administration of an intravenous iodinated contrast medium and a retrograde colonic distention with about 2 L of water.
References
Attaran M, Falcone T, Goldberg J. Endometriosis: still tough to diagnose and treat. Cleve Clin J Med2002; 69:647–653.
Wenger JM, Soave I, Lo Monte G, Petignat P, Marci R. Tubal endometrioma within a twisted fallopian tube: a clinically complex diagnosis. J Pediatr Adolesc Gynecol2013; 26:e1–e4.
Marci R, Lo Monte G, Soave I, Bianchi A, Patella A, Wenger JM. Rectus abdominis muscle endometriotic mass in a woman affected by multiple sclerosis. J Obstet Gynaecol Res2013; 39:462–465.
Vercellini P, Frontino G, Pietropaolo G, Gattei U, Daguati R, Crosignani PG. Deep endometriosis: definition, pathogenesis, and clinical management. J Am Assoc Gynecol Laparosc2004; 11:153–161.
Nezhat C, Santolaya J, Nezhat FR. Comparison of transvaginal sonography and bimanual pelvic examination in patients with laparoscopically confirmed endometriosis. J Am Assoc Gynecol Laparosc1994; 1:127–130.
Barbieri RL, Niloff JM, Bast RC, Scaetzl E, Kistner RW, Knapp RC. Elevated serum concentrations of CA-125 in patients with advanced endometriosis. Fertil Steril1986; 45:630–634.
Bon GG, Kenemans P, Dekker JJ, et al. Fluctuations in CA 125 and CA 15-3 serum concentrations during spontaneous ovulatory cycles. Hum Reprod1999; 14:566–570.
Mais V, Guerriero S, Ajossa S, Angiolucci M, Paoletti AM, Melis GB. The efficiency of transvaginal ultrasonography in the diagnosis of endometrioma. Fertil Steril1993; 60:776–780.
Guerriero S, Mais V, Ajossa S, et al. The role of endovaginal ultrasound in differentiating endometriomas from other ovarian cysts. Clin Exp Obstet Gynecol1995; 22:20–22.
Fedele L, Bianchi S, Raffaelli R, Portuese A. Pre-operative assessment of bladder endometriosis. Hum Reprod1997; 12:2519–2522.
Chamié LP, Blasbalg R, Pereira RM, Warmbrand G, Serafini PC. Findings of pelvic endometriosis at transvaginal US, MR imaging, and laparoscopy. Radiographics2011; 31:E77–E100.
Fleischer AC. Transabdominal and transvaginal sonography of ovarian masses. Clin Obstet Gynecol1991; 34:433–442.
Zawin M, McCarthy S, Scoutt L, Comite F. Endometriosis: appearance and detection at MR imaging. Radiology1989; 171:693–696.
Togashi K, Nishimura K, Kimura I, et al. Endometrial cysts: diagnosis with MR imaging. Radiology1991; 180:73–78.
Balleyguier C, Chapron C, Dubuisson JB, et al. Comparison of magnetic resonance imaging and transvaginal ultrasonography in diagnosing bladder endometriosis. J Am Assoc Gynecol Laparosc2002; 9:15–23.
Siegelman ES, Oliver ER. MR imaging of endometriosis: ten imaging pearls. Radiographics2012; 32:1675–1691.
Takeuchi M, Matsuzaki K, Kubo H, Nishitani H. Magnetic resonance manifestations of endometrial cysts at 3 T compared with 1.5 T. J Comput Assist Tomogr2008; 32:369–271.
Zanardi R, Del Frate C, Zuiani C, Del Frate G, Bazzocchi M. Staging of pelvic endometriosis using magnetic resonance imaging compared with the laparoscopic classification of the American Fertility Society: a prospective study. Radiol Med2003; 105:326–338.
Takahashi K, Okada M, Okada S, Kitao M, Imaoka I, Sugimura K. Studies on the detection of small endometrial implants by magnetic resonance imaging using a fat saturation technique. Gynecol Obstet Invest1996; 41:203–206.
Loubeyre P, Copercini M, Frossard JL, Wenger JM, Petignat P. Pictorial review: rectosigmoid endometriosis on MRI with gel opacification after rectosigmoid colon cleansing. Clin Imaging2012; 36:295–300.
Bahr A, de Parades V, Gadonneix P, et al. Endorectal ultrasonography in predicting rectal wall infiltration in patients with deep pelvic endometriosis: a modern tool for an ancient disease. Dis Colon Rectum2006; 49:869–875.
Giuseppe Lo Monte, MD Department of Morphology, Surgery and Experimental Medicine, University of Ferrara, Ferrara, Italy
Jean Marie Wenger, MD Department of Gynecology and Obstetrics, Division of Gynecology, Geneva University Hospitals, Geneva, Switzerland
Patrick Petignat, MD Department of Gynecology and Obstetrics, Division of Gynecology, Geneva University Hospitals, Geneva, Switzerland
Roberto Marci, PhD Department of Morphology, Surgery and Experimental Medicine, University of Ferrara, Ferrara, Italy
Address: Roberto Marci, PhD, Department of Morphology, Surgery and Experimental Medicine, University of Ferrara, Corso Giovecca 183, 44100, Ferrara, Italy; e-mail: roberto.marci@unife.it
Giuseppe Lo Monte, MD Department of Morphology, Surgery and Experimental Medicine, University of Ferrara, Ferrara, Italy
Jean Marie Wenger, MD Department of Gynecology and Obstetrics, Division of Gynecology, Geneva University Hospitals, Geneva, Switzerland
Patrick Petignat, MD Department of Gynecology and Obstetrics, Division of Gynecology, Geneva University Hospitals, Geneva, Switzerland
Roberto Marci, PhD Department of Morphology, Surgery and Experimental Medicine, University of Ferrara, Ferrara, Italy
Address: Roberto Marci, PhD, Department of Morphology, Surgery and Experimental Medicine, University of Ferrara, Corso Giovecca 183, 44100, Ferrara, Italy; e-mail: roberto.marci@unife.it
Author and Disclosure Information
Giuseppe Lo Monte, MD Department of Morphology, Surgery and Experimental Medicine, University of Ferrara, Ferrara, Italy
Jean Marie Wenger, MD Department of Gynecology and Obstetrics, Division of Gynecology, Geneva University Hospitals, Geneva, Switzerland
Patrick Petignat, MD Department of Gynecology and Obstetrics, Division of Gynecology, Geneva University Hospitals, Geneva, Switzerland
Roberto Marci, PhD Department of Morphology, Surgery and Experimental Medicine, University of Ferrara, Ferrara, Italy
Address: Roberto Marci, PhD, Department of Morphology, Surgery and Experimental Medicine, University of Ferrara, Corso Giovecca 183, 44100, Ferrara, Italy; e-mail: roberto.marci@unife.it
A 32-year-old woman presents with a history of pelvic pain, dysmenorrhea, dyspareunia, dyschezia, and dysuria, with exacerbation of the symptoms during her menstrual cycles. Her menarche occurred at the age of 13 and her menses are regular. She has never undergone surgery and has no relevant pathologic processes. She also reports that for the past 18 months she has been unsuccessfully trying to conceive.
Two months ago, she went to the emergency department because of an acute episode of severe pelvic pain associated with abdominal cramps, vomiting, and dyschezia, occurring at the beginning of her menstrual cycle. At that time, her vital signs were within normal limits, but deep palpation of the right iliac fossa was painful. On that occasion, acute abdomen and bowel obstruction were excluded.
Now, vaginal examination reveals a bluish, painful, bulky induration in the posterior fornix. Digital rectal examination reveals a circular infiltrated area in the anterior rectal wall. Her cancer antigen 125 (CA 125) level is 230 U/mL (normal range 0–35 U/mL).
MENSES-RELATED SYMPTOMS AND THE DIAGNOSIS OF ENDOMETRIOSIS
The diagnosis of endometriosis should be considered in the patient described above. Many of her signs and symptoms can be associated with several diseases. However, the diagnostic hypothesis points strongly toward endometriosis, since her symptoms recur at the beginning of every menstrual cycle.1
Endometriosis is the presence of endometrial tissue outside the uterine cavity. The affected organs usually include the ovaries, fallopian tubes,2 peritoneal surface, vagina, cervix, abdominal wall,3 scar tissue, pouch of Douglas, urinary tract, and bowel. However, any organ can be involved.
So-called deeply infiltrating endometriosis is an endometriotic lesion penetrating into the retroperitoneal space (most often affecting the uterosacral ligaments and the rectovaginal septum) or the pelvic-organ wall to a depth of at least 5 mm and involving structures such as the rectum, vagina, ureters, and bladder.4 Its clinical presentation is highly variable, ranging from no symptoms to severe pain and dysfunction of pelvic organs.
Endometriosis can be diagnosed with certainty only when the endometriotic lesions are observed by laparoscopy or laparotomy and after the histologic examination of surgically resected lesions (Figure 1).1 However, a presumptive diagnosis can be made on the basis of imaging findings, which can be useful in the differential diagnostic process (Table 1).
Figure 1. Diagnostic algorithm for endometriosis.
EXAMINATION AND BLOOD MARKERS PROVIDE LIMITED INFORMATION
Knowing the history of the patient, along with a physical examination that includes speculum and bimanual vaginal and rectal examination, can be helpful in the diagnostic process even if nothing abnormal is found.
Pelvic examination has a poor predictive value, as demonstrated in a study conducted by Nezhat et al5 in 91 patients with surgically confirmed endometriosis, 47% of whom had a normal bimanual examination.
CA 125 is the serologic marker most often used for diagnosing endometriosis. Levels are usually high in the sera of patients with endometriosis, especially in the advanced stages.6 However, levels increase both in the physiologic menstrual cycle and in epithelial ovarian cancers.7 Thus, the diagnostic value of CA 125 is limited in terms of both sensitivity and specificity.
INCLUDE IMAGING IN THE DIAGNOSTIC WORKUP
Surgical treatment is frequently offered to patients who have severe pelvic pain that does not respond to medical treatment, or in cases of infertility. Imaging investigations are mandatory both to ascertain the diagnosis and to assess involvement of internal organs before surgery. Moreover, imaging helps minimize the surgical risks.
The primary aim of the radiologic examination is to describe the precise location, the depth, and the number of pelvic endometriotic lesions. Furthermore, imaging is useful to check for endometriotic foci in pelvic organs such as the bowel, ureters, and bladder, which are often involved in the pathologic process.
Transvaginal ultrasonography and magnetic resonance imaging (MRI) can accurately delineate deeply infiltrating lesions of endometriosis that are not easily accessible laparoscopically.
Transvaginal ultrasonography
Transvaginal ultrasonography is the first-line imaging study when endometriosis is suspected: it is powerful, simple, widely available, and cost-effective. In particular, it is recommended for diagnosing endometriotic ovarian cysts (endometriomas)8,9 and endometriosis of the bladder.10 However, its value for the assessment of superficial peritoneal lesions, ovarian foci, and deeply infiltrating endometriosis is questionable.
Although uncomfortable for the patient, transvaginal ultrasonography should be performed during menses, or when the pain reaches its highest level. In fact, during menstrual bleeding the endometrial implants grow and become easier to detect.
Mais et al8 reported that transvaginal ultrasonography has a sensitivity of 88% in differentiating endometriomas from other ovarian masses, and a specificity of 90% (Figure 2). Furthermore, its specificity is as high as that of MRI.8,9
Figure 2. Endometriotic ovarian cysts (endometriomas) (arrow) on transvaginal ultrasonography.
Endometriotic nodules detected in the uterosacral ligaments, rectovaginal septum, vagina, vesicouterine pouch, bladder (Figure 3), and ureters can be signs of deeply infiltrating endometriosis. Pelvic adhesions can be suspected when pelvic organs appear fixed to each other, when hyperechogenic plaques are found between the serosal surfaces of the different organs, and when the pouch of Douglas is partially or completely obliterated.
Figure 3. Transvaginal ultrasonography in the sagittal plane shows an endometriotic nodule in the posterior wall of the bladder (arrow).
The accuracy of transvaginal ultrasonography strongly depends on the operator’s skill. Furthermore, lesions of the sigmoid colon are impossible to visualize by transvaginal ultrasonography; hence, further diagnostic procedures are required. Transvaginal ultrasonography is the most accurate technique in detecting endometriotic nodules of the bladder wall in patients with urinary symptoms.
Transvaginal ultrasonography combined with color Doppler can also demonstrate the flow of urine through the ureters to the bladder, thereby ascertaining the patency of the ureters and clarifying the anatomic relationship between the ureters and any endometriotic lesions in the detrusors.10 Hydronephrosis can arise from ureteral restriction caused by endometriotic nodules. Thus, transabdominal ultrasonography of the kidneys is always recommended when deeply infiltrating endometriosis is suspected.
Some centers use a bowel-preparation protocol consisting of a laxative taken 24 hours before the procedure, combined with a low-residue diet and an enema 1 hour before the examination to cleanse the rectosigmoid colon of fecal content and gas, which can interfere with the visual examination of the pelvic structures.11
Transabdominal ultrasonography
Transabdominal ultrasonography can be used instead of transvaginal ultrasonography, eg, in young girls and women who have never been sexually active. When transabdominal ultrasonography is selected, the patient should have a full bladder to maximize the visualization of the pelvic structures. However, transvaginal ultrasonography is generally more sensitive than transabdominal in detecting adnexal masses and pelvic nodules.12
Magnetic resonance imaging
MRI has been recently introduced in the diagnosis of endometriosis. MRI is less operator-dependent than transvaginal ultrasonography and is more sensitive for detecting foci of deeply infiltrating endometriosis, because of its ability to completely survey the anterior and posterior compartments of the pelvis. However, its diagnostic value in cases of bladder endometriosis, superficial peritoneal lesions, and ovarian foci is still controversial.13–16
On MRI, lesions of deeply infiltrating endometriosis mainly appear as areas or nodules with regular, irregular, indistinct, or stellate margins. A distortion of the normal pelvic anatomy or the detection of a loculated fluid collection can indirectly signal the presence of adhesions.
MRI has high specificity for the diagnosis of endometriomas as a result of its ability to detect aged hemorrhagic content (Figure 4).17 Despite the many studies that point to the limits of MRI in detecting small endometriotic lesions, recent studies demonstrated that MRI also has good sensitivity for small peritoneal implants and adhesions.18,19 The injection of gadolinium contrast is still a debatable measure, because contrast-enhanced imaging cannot differentiate infiltrating lesions from other normal fibromuscular pelvic anatomic structures.15,20
Figure 4. Ovarian endometrioma on magnetic resonance imaging. (A) On a fat-saturation transverse T1-weighted image, the endometrioma has high signal intensity. (B) On transverse T2-weighted image, blood-degraded product content has intermediate to low signal intensity.
Bowel preparation can be done with an oral laxative the day before imaging, complemented by a low-residue diet. A single dose of a ready-to-use enema is given 30 minutes before the examination to cleanse the terminal section of the intestinal tract. To avoid motion artifacts caused by bowel peristalsis, images are obtained after intramuscular injections of a myorelaxant are given, if there is no contraindication. Bowel preparation is useful to eliminate fecal residue and gas, thereby allowing proper visualization of lesions of deeply infiltrating endometriosis, but it is not routinely prescribed in all centers.11
In most cases, endometriotic lesions have an MRI signal intensity that comes very close to that of the surrounding fibromuscular structures. In this regard, vaginal and rectal distention and opacification using ultrasonographic gel clearly help to delineate the cervix, vaginal fornices, and vaginal wall, as well as the rectum and wall of the rectosigmoid junction (Figure 5).20
Figure 5. Posterior deep infiltrating endometriotic nodule on magnetic resonance imaging. (A) On a T2- weighted image with no opacification of the vagina and rectum with ultrasonographic gel, a retrocervical endometriotic nodule (white oval) has a signal intensity very close to that of the surrounding fibromuscular anatomic structures such as the rectal wall (arrow), vagina, and cervical stroma (asterisk). (B) A T2- weighted image shows the endometriotic nodule (oval) extending downward to the vaginal fornix, which appears obliterated. Only the right vaginal fornix (asterisk) is distended. Between the nodule and the anterior rectal wall, interposing fat tissue (arrowhead) is likely to represent a safety margin and a plane of dissection.
PRESURGICAL IMAGING
Rectal endoscopic ultrasonography
Even though it should not be included in the routine diagnostic workup, rectal endoscopic ultrasonography, using a flexible echoendoscope, is suitable in certain presurgical cases. The aim of this imaging technique is to assess the depth of bowel wall infiltration thanks to the visualization of the different layers.21
Double-contrast barium enema and multislice computed tomography
Double-contrast barium enema is extensively used for the diagnosis of bowel endometriosis, once the decision to perform surgery has been made. It allows evaluation of the degree and length of the bowel occlusion at the level of the sigmoid or high rectosigmoid tract, but it does not permit differentiation of bowel endometriosis from other pathologies.
Multislice computed tomography offers the opportunity to evaluate the depth of the lesions with excellent precision. 22
The most relevant disadvantage of both procedures is the exposure of women of reproductive age to ionizing radiation. In addition, multislice computed tomography requires the administration of an intravenous iodinated contrast medium and a retrograde colonic distention with about 2 L of water.
A 32-year-old woman presents with a history of pelvic pain, dysmenorrhea, dyspareunia, dyschezia, and dysuria, with exacerbation of the symptoms during her menstrual cycles. Her menarche occurred at the age of 13 and her menses are regular. She has never undergone surgery and has no relevant pathologic processes. She also reports that for the past 18 months she has been unsuccessfully trying to conceive.
Two months ago, she went to the emergency department because of an acute episode of severe pelvic pain associated with abdominal cramps, vomiting, and dyschezia, occurring at the beginning of her menstrual cycle. At that time, her vital signs were within normal limits, but deep palpation of the right iliac fossa was painful. On that occasion, acute abdomen and bowel obstruction were excluded.
Now, vaginal examination reveals a bluish, painful, bulky induration in the posterior fornix. Digital rectal examination reveals a circular infiltrated area in the anterior rectal wall. Her cancer antigen 125 (CA 125) level is 230 U/mL (normal range 0–35 U/mL).
MENSES-RELATED SYMPTOMS AND THE DIAGNOSIS OF ENDOMETRIOSIS
The diagnosis of endometriosis should be considered in the patient described above. Many of her signs and symptoms can be associated with several diseases. However, the diagnostic hypothesis points strongly toward endometriosis, since her symptoms recur at the beginning of every menstrual cycle.1
Endometriosis is the presence of endometrial tissue outside the uterine cavity. The affected organs usually include the ovaries, fallopian tubes,2 peritoneal surface, vagina, cervix, abdominal wall,3 scar tissue, pouch of Douglas, urinary tract, and bowel. However, any organ can be involved.
So-called deeply infiltrating endometriosis is an endometriotic lesion penetrating into the retroperitoneal space (most often affecting the uterosacral ligaments and the rectovaginal septum) or the pelvic-organ wall to a depth of at least 5 mm and involving structures such as the rectum, vagina, ureters, and bladder.4 Its clinical presentation is highly variable, ranging from no symptoms to severe pain and dysfunction of pelvic organs.
Endometriosis can be diagnosed with certainty only when the endometriotic lesions are observed by laparoscopy or laparotomy and after the histologic examination of surgically resected lesions (Figure 1).1 However, a presumptive diagnosis can be made on the basis of imaging findings, which can be useful in the differential diagnostic process (Table 1).
Figure 1. Diagnostic algorithm for endometriosis.
EXAMINATION AND BLOOD MARKERS PROVIDE LIMITED INFORMATION
Knowing the history of the patient, along with a physical examination that includes speculum and bimanual vaginal and rectal examination, can be helpful in the diagnostic process even if nothing abnormal is found.
Pelvic examination has a poor predictive value, as demonstrated in a study conducted by Nezhat et al5 in 91 patients with surgically confirmed endometriosis, 47% of whom had a normal bimanual examination.
CA 125 is the serologic marker most often used for diagnosing endometriosis. Levels are usually high in the sera of patients with endometriosis, especially in the advanced stages.6 However, levels increase both in the physiologic menstrual cycle and in epithelial ovarian cancers.7 Thus, the diagnostic value of CA 125 is limited in terms of both sensitivity and specificity.
INCLUDE IMAGING IN THE DIAGNOSTIC WORKUP
Surgical treatment is frequently offered to patients who have severe pelvic pain that does not respond to medical treatment, or in cases of infertility. Imaging investigations are mandatory both to ascertain the diagnosis and to assess involvement of internal organs before surgery. Moreover, imaging helps minimize the surgical risks.
The primary aim of the radiologic examination is to describe the precise location, the depth, and the number of pelvic endometriotic lesions. Furthermore, imaging is useful to check for endometriotic foci in pelvic organs such as the bowel, ureters, and bladder, which are often involved in the pathologic process.
Transvaginal ultrasonography and magnetic resonance imaging (MRI) can accurately delineate deeply infiltrating lesions of endometriosis that are not easily accessible laparoscopically.
Transvaginal ultrasonography
Transvaginal ultrasonography is the first-line imaging study when endometriosis is suspected: it is powerful, simple, widely available, and cost-effective. In particular, it is recommended for diagnosing endometriotic ovarian cysts (endometriomas)8,9 and endometriosis of the bladder.10 However, its value for the assessment of superficial peritoneal lesions, ovarian foci, and deeply infiltrating endometriosis is questionable.
Although uncomfortable for the patient, transvaginal ultrasonography should be performed during menses, or when the pain reaches its highest level. In fact, during menstrual bleeding the endometrial implants grow and become easier to detect.
Mais et al8 reported that transvaginal ultrasonography has a sensitivity of 88% in differentiating endometriomas from other ovarian masses, and a specificity of 90% (Figure 2). Furthermore, its specificity is as high as that of MRI.8,9
Figure 2. Endometriotic ovarian cysts (endometriomas) (arrow) on transvaginal ultrasonography.
Endometriotic nodules detected in the uterosacral ligaments, rectovaginal septum, vagina, vesicouterine pouch, bladder (Figure 3), and ureters can be signs of deeply infiltrating endometriosis. Pelvic adhesions can be suspected when pelvic organs appear fixed to each other, when hyperechogenic plaques are found between the serosal surfaces of the different organs, and when the pouch of Douglas is partially or completely obliterated.
Figure 3. Transvaginal ultrasonography in the sagittal plane shows an endometriotic nodule in the posterior wall of the bladder (arrow).
The accuracy of transvaginal ultrasonography strongly depends on the operator’s skill. Furthermore, lesions of the sigmoid colon are impossible to visualize by transvaginal ultrasonography; hence, further diagnostic procedures are required. Transvaginal ultrasonography is the most accurate technique in detecting endometriotic nodules of the bladder wall in patients with urinary symptoms.
Transvaginal ultrasonography combined with color Doppler can also demonstrate the flow of urine through the ureters to the bladder, thereby ascertaining the patency of the ureters and clarifying the anatomic relationship between the ureters and any endometriotic lesions in the detrusors.10 Hydronephrosis can arise from ureteral restriction caused by endometriotic nodules. Thus, transabdominal ultrasonography of the kidneys is always recommended when deeply infiltrating endometriosis is suspected.
Some centers use a bowel-preparation protocol consisting of a laxative taken 24 hours before the procedure, combined with a low-residue diet and an enema 1 hour before the examination to cleanse the rectosigmoid colon of fecal content and gas, which can interfere with the visual examination of the pelvic structures.11
Transabdominal ultrasonography
Transabdominal ultrasonography can be used instead of transvaginal ultrasonography, eg, in young girls and women who have never been sexually active. When transabdominal ultrasonography is selected, the patient should have a full bladder to maximize the visualization of the pelvic structures. However, transvaginal ultrasonography is generally more sensitive than transabdominal in detecting adnexal masses and pelvic nodules.12
Magnetic resonance imaging
MRI has been recently introduced in the diagnosis of endometriosis. MRI is less operator-dependent than transvaginal ultrasonography and is more sensitive for detecting foci of deeply infiltrating endometriosis, because of its ability to completely survey the anterior and posterior compartments of the pelvis. However, its diagnostic value in cases of bladder endometriosis, superficial peritoneal lesions, and ovarian foci is still controversial.13–16
On MRI, lesions of deeply infiltrating endometriosis mainly appear as areas or nodules with regular, irregular, indistinct, or stellate margins. A distortion of the normal pelvic anatomy or the detection of a loculated fluid collection can indirectly signal the presence of adhesions.
MRI has high specificity for the diagnosis of endometriomas as a result of its ability to detect aged hemorrhagic content (Figure 4).17 Despite the many studies that point to the limits of MRI in detecting small endometriotic lesions, recent studies demonstrated that MRI also has good sensitivity for small peritoneal implants and adhesions.18,19 The injection of gadolinium contrast is still a debatable measure, because contrast-enhanced imaging cannot differentiate infiltrating lesions from other normal fibromuscular pelvic anatomic structures.15,20
Figure 4. Ovarian endometrioma on magnetic resonance imaging. (A) On a fat-saturation transverse T1-weighted image, the endometrioma has high signal intensity. (B) On transverse T2-weighted image, blood-degraded product content has intermediate to low signal intensity.
Bowel preparation can be done with an oral laxative the day before imaging, complemented by a low-residue diet. A single dose of a ready-to-use enema is given 30 minutes before the examination to cleanse the terminal section of the intestinal tract. To avoid motion artifacts caused by bowel peristalsis, images are obtained after intramuscular injections of a myorelaxant are given, if there is no contraindication. Bowel preparation is useful to eliminate fecal residue and gas, thereby allowing proper visualization of lesions of deeply infiltrating endometriosis, but it is not routinely prescribed in all centers.11
In most cases, endometriotic lesions have an MRI signal intensity that comes very close to that of the surrounding fibromuscular structures. In this regard, vaginal and rectal distention and opacification using ultrasonographic gel clearly help to delineate the cervix, vaginal fornices, and vaginal wall, as well as the rectum and wall of the rectosigmoid junction (Figure 5).20
Figure 5. Posterior deep infiltrating endometriotic nodule on magnetic resonance imaging. (A) On a T2- weighted image with no opacification of the vagina and rectum with ultrasonographic gel, a retrocervical endometriotic nodule (white oval) has a signal intensity very close to that of the surrounding fibromuscular anatomic structures such as the rectal wall (arrow), vagina, and cervical stroma (asterisk). (B) A T2- weighted image shows the endometriotic nodule (oval) extending downward to the vaginal fornix, which appears obliterated. Only the right vaginal fornix (asterisk) is distended. Between the nodule and the anterior rectal wall, interposing fat tissue (arrowhead) is likely to represent a safety margin and a plane of dissection.
PRESURGICAL IMAGING
Rectal endoscopic ultrasonography
Even though it should not be included in the routine diagnostic workup, rectal endoscopic ultrasonography, using a flexible echoendoscope, is suitable in certain presurgical cases. The aim of this imaging technique is to assess the depth of bowel wall infiltration thanks to the visualization of the different layers.21
Double-contrast barium enema and multislice computed tomography
Double-contrast barium enema is extensively used for the diagnosis of bowel endometriosis, once the decision to perform surgery has been made. It allows evaluation of the degree and length of the bowel occlusion at the level of the sigmoid or high rectosigmoid tract, but it does not permit differentiation of bowel endometriosis from other pathologies.
Multislice computed tomography offers the opportunity to evaluate the depth of the lesions with excellent precision. 22
The most relevant disadvantage of both procedures is the exposure of women of reproductive age to ionizing radiation. In addition, multislice computed tomography requires the administration of an intravenous iodinated contrast medium and a retrograde colonic distention with about 2 L of water.
References
Attaran M, Falcone T, Goldberg J. Endometriosis: still tough to diagnose and treat. Cleve Clin J Med2002; 69:647–653.
Wenger JM, Soave I, Lo Monte G, Petignat P, Marci R. Tubal endometrioma within a twisted fallopian tube: a clinically complex diagnosis. J Pediatr Adolesc Gynecol2013; 26:e1–e4.
Marci R, Lo Monte G, Soave I, Bianchi A, Patella A, Wenger JM. Rectus abdominis muscle endometriotic mass in a woman affected by multiple sclerosis. J Obstet Gynaecol Res2013; 39:462–465.
Vercellini P, Frontino G, Pietropaolo G, Gattei U, Daguati R, Crosignani PG. Deep endometriosis: definition, pathogenesis, and clinical management. J Am Assoc Gynecol Laparosc2004; 11:153–161.
Nezhat C, Santolaya J, Nezhat FR. Comparison of transvaginal sonography and bimanual pelvic examination in patients with laparoscopically confirmed endometriosis. J Am Assoc Gynecol Laparosc1994; 1:127–130.
Barbieri RL, Niloff JM, Bast RC, Scaetzl E, Kistner RW, Knapp RC. Elevated serum concentrations of CA-125 in patients with advanced endometriosis. Fertil Steril1986; 45:630–634.
Bon GG, Kenemans P, Dekker JJ, et al. Fluctuations in CA 125 and CA 15-3 serum concentrations during spontaneous ovulatory cycles. Hum Reprod1999; 14:566–570.
Mais V, Guerriero S, Ajossa S, Angiolucci M, Paoletti AM, Melis GB. The efficiency of transvaginal ultrasonography in the diagnosis of endometrioma. Fertil Steril1993; 60:776–780.
Guerriero S, Mais V, Ajossa S, et al. The role of endovaginal ultrasound in differentiating endometriomas from other ovarian cysts. Clin Exp Obstet Gynecol1995; 22:20–22.
Fedele L, Bianchi S, Raffaelli R, Portuese A. Pre-operative assessment of bladder endometriosis. Hum Reprod1997; 12:2519–2522.
Chamié LP, Blasbalg R, Pereira RM, Warmbrand G, Serafini PC. Findings of pelvic endometriosis at transvaginal US, MR imaging, and laparoscopy. Radiographics2011; 31:E77–E100.
Fleischer AC. Transabdominal and transvaginal sonography of ovarian masses. Clin Obstet Gynecol1991; 34:433–442.
Zawin M, McCarthy S, Scoutt L, Comite F. Endometriosis: appearance and detection at MR imaging. Radiology1989; 171:693–696.
Togashi K, Nishimura K, Kimura I, et al. Endometrial cysts: diagnosis with MR imaging. Radiology1991; 180:73–78.
Balleyguier C, Chapron C, Dubuisson JB, et al. Comparison of magnetic resonance imaging and transvaginal ultrasonography in diagnosing bladder endometriosis. J Am Assoc Gynecol Laparosc2002; 9:15–23.
Siegelman ES, Oliver ER. MR imaging of endometriosis: ten imaging pearls. Radiographics2012; 32:1675–1691.
Takeuchi M, Matsuzaki K, Kubo H, Nishitani H. Magnetic resonance manifestations of endometrial cysts at 3 T compared with 1.5 T. J Comput Assist Tomogr2008; 32:369–271.
Zanardi R, Del Frate C, Zuiani C, Del Frate G, Bazzocchi M. Staging of pelvic endometriosis using magnetic resonance imaging compared with the laparoscopic classification of the American Fertility Society: a prospective study. Radiol Med2003; 105:326–338.
Takahashi K, Okada M, Okada S, Kitao M, Imaoka I, Sugimura K. Studies on the detection of small endometrial implants by magnetic resonance imaging using a fat saturation technique. Gynecol Obstet Invest1996; 41:203–206.
Loubeyre P, Copercini M, Frossard JL, Wenger JM, Petignat P. Pictorial review: rectosigmoid endometriosis on MRI with gel opacification after rectosigmoid colon cleansing. Clin Imaging2012; 36:295–300.
Bahr A, de Parades V, Gadonneix P, et al. Endorectal ultrasonography in predicting rectal wall infiltration in patients with deep pelvic endometriosis: a modern tool for an ancient disease. Dis Colon Rectum2006; 49:869–875.
Attaran M, Falcone T, Goldberg J. Endometriosis: still tough to diagnose and treat. Cleve Clin J Med2002; 69:647–653.
Wenger JM, Soave I, Lo Monte G, Petignat P, Marci R. Tubal endometrioma within a twisted fallopian tube: a clinically complex diagnosis. J Pediatr Adolesc Gynecol2013; 26:e1–e4.
Marci R, Lo Monte G, Soave I, Bianchi A, Patella A, Wenger JM. Rectus abdominis muscle endometriotic mass in a woman affected by multiple sclerosis. J Obstet Gynaecol Res2013; 39:462–465.
Vercellini P, Frontino G, Pietropaolo G, Gattei U, Daguati R, Crosignani PG. Deep endometriosis: definition, pathogenesis, and clinical management. J Am Assoc Gynecol Laparosc2004; 11:153–161.
Nezhat C, Santolaya J, Nezhat FR. Comparison of transvaginal sonography and bimanual pelvic examination in patients with laparoscopically confirmed endometriosis. J Am Assoc Gynecol Laparosc1994; 1:127–130.
Barbieri RL, Niloff JM, Bast RC, Scaetzl E, Kistner RW, Knapp RC. Elevated serum concentrations of CA-125 in patients with advanced endometriosis. Fertil Steril1986; 45:630–634.
Bon GG, Kenemans P, Dekker JJ, et al. Fluctuations in CA 125 and CA 15-3 serum concentrations during spontaneous ovulatory cycles. Hum Reprod1999; 14:566–570.
Mais V, Guerriero S, Ajossa S, Angiolucci M, Paoletti AM, Melis GB. The efficiency of transvaginal ultrasonography in the diagnosis of endometrioma. Fertil Steril1993; 60:776–780.
Guerriero S, Mais V, Ajossa S, et al. The role of endovaginal ultrasound in differentiating endometriomas from other ovarian cysts. Clin Exp Obstet Gynecol1995; 22:20–22.
Fedele L, Bianchi S, Raffaelli R, Portuese A. Pre-operative assessment of bladder endometriosis. Hum Reprod1997; 12:2519–2522.
Chamié LP, Blasbalg R, Pereira RM, Warmbrand G, Serafini PC. Findings of pelvic endometriosis at transvaginal US, MR imaging, and laparoscopy. Radiographics2011; 31:E77–E100.
Fleischer AC. Transabdominal and transvaginal sonography of ovarian masses. Clin Obstet Gynecol1991; 34:433–442.
Zawin M, McCarthy S, Scoutt L, Comite F. Endometriosis: appearance and detection at MR imaging. Radiology1989; 171:693–696.
Togashi K, Nishimura K, Kimura I, et al. Endometrial cysts: diagnosis with MR imaging. Radiology1991; 180:73–78.
Balleyguier C, Chapron C, Dubuisson JB, et al. Comparison of magnetic resonance imaging and transvaginal ultrasonography in diagnosing bladder endometriosis. J Am Assoc Gynecol Laparosc2002; 9:15–23.
Siegelman ES, Oliver ER. MR imaging of endometriosis: ten imaging pearls. Radiographics2012; 32:1675–1691.
Takeuchi M, Matsuzaki K, Kubo H, Nishitani H. Magnetic resonance manifestations of endometrial cysts at 3 T compared with 1.5 T. J Comput Assist Tomogr2008; 32:369–271.
Zanardi R, Del Frate C, Zuiani C, Del Frate G, Bazzocchi M. Staging of pelvic endometriosis using magnetic resonance imaging compared with the laparoscopic classification of the American Fertility Society: a prospective study. Radiol Med2003; 105:326–338.
Takahashi K, Okada M, Okada S, Kitao M, Imaoka I, Sugimura K. Studies on the detection of small endometrial implants by magnetic resonance imaging using a fat saturation technique. Gynecol Obstet Invest1996; 41:203–206.
Loubeyre P, Copercini M, Frossard JL, Wenger JM, Petignat P. Pictorial review: rectosigmoid endometriosis on MRI with gel opacification after rectosigmoid colon cleansing. Clin Imaging2012; 36:295–300.
Bahr A, de Parades V, Gadonneix P, et al. Endorectal ultrasonography in predicting rectal wall infiltration in patients with deep pelvic endometriosis: a modern tool for an ancient disease. Dis Colon Rectum2006; 49:869–875.
The diagnostic evaluation should always start with transvaginal ultrasonography of the pelvic structures followed by magnetic resonance imaging, especially if deeply infiltrating endometriosis is suspected.
An inaccurate imaging evaluation may lead to an incomplete excision of lesions if the patient undergoes surgery.
Transvaginal ultrasonography and magnetic resonance imaging allow the assessment of the size, location, and extent of the lesions.
Given the multifocal nature of the disease, a thorough evaluation of all pelvic structures, including the bowel, the bladder, and the ureters, is always recommended.
A 70-year-old man falls in his bathroom and subsequently presents to an urgent care clinic. Among his complaints is right-sided chest pain. On physical examination he has point tenderness over the lateral right thorax with some superficial swelling and bruising. The chest is normal on auscultation.
Should this patient undergo imaging to determine if he has a rib fracture? And which imaging study would be appropriate?
This article outlines the use of various imaging tests in the evaluation of suspected rib fractures and recommends an approach to management. This article does not address fractures in children.
MANY CAUSES OF RIB FRACTURES
Trauma, the most common cause of rib fractures, includes penetrating injuries and blunt injury to the chest wall. Between 10% and 66% of traumatic injuries result in rib fractures. 1 Traumatic injury can result from motor vehicle accidents, assault, sports, cardiopulmonary resuscitation, physical abuse (“nonaccidental” trauma), and, rarely, severe paroxysms of coughing.2
Cancer can cause pathologic fractures of the rib.
Stress fractures of the ribs are more likely to occur in high-level athletes whose activity involves repetitive musculoskeletal loading, although they can also occur in people with repetitive coughing paroxysms.3 Sports and activities that result in stress fractures include rowing, pitching or throwing, basketball, weight-lifting, ballet, golf, gymnastics, and swimming.4
WHICH RIB IS BROKEN?
The fourth through 10th ribs are the most often fractured. Fractures of the first through the third ribs can be associated with underlying nerve and vascular injuries, and fractures of the 10th through 12th ribs are associated with damage to abdominal organs,5 most commonly the liver, spleen, kidneys, and diaphragm.3
Fractures of the costal cartilage can occur by any of the mechanisms described above. The true incidence of costal cartilage fractures is not known because plain radiography, the traditional method of evaluation, does not reliably detect them.
WHY CONFIRM A RIB FRACTURE?
For many rib fractures without associated injury, a radiographic diagnosis has little impact on patient management, which consists mainly of pain control. But knowing whether a patient has a broken rib can often be important.
To detect associated injury. The rate of associated injury in patients with rib fractures is high.6 Potentially severe complications include:
Pneumothorax
Hemothorax
Pulmonary contusion
Flail chest
Pneumonia
Vascular and nerve damage (especially with trauma to the upper chest or the first through third ribs)
Abdominal organ injury (particularly with trauma to the lower thorax or lower ribs).
The absence of a rib fracture does not preclude these conditions, however.
To prevent complications. Even in the absence of associated injuries, radiographic confirmation of a rib fracture can help prevent complications such as atelectasis and is particularly important in patients with comorbidities such as chronic obstructive pulmonary disease, cardiac disease, hepatic disease, renal disease, dementia, and coagulopathy.1
To document the injury. Radiographic documentation of a rib fracture may be required for medical-legal issues in cases of assault, motor vehicle accident, occupational injury, and abuse.
To help manage pain. Confirmation of rib fracture can facilitate pain management, particularly in patients with undiagnosed fractures with long-standing refractory pain. For example, conservative pain control with nonsteroidal anti-inflammatory drugs may be sufficient for a soft-tissue injury but may not be enough for a rib fracture. Intravenous narcotics or nerve blocks might be preferable.3,7 Controlling pain helps limit the incidence of associated complications.
Figure 1. Oblique radiographic view shows an acute rib fracture in a patient with multiple myeloma.To detect pathologic fractures. Radiographic diagnosis can provide important information in cases of suspected pathologic fracture, as in multiple myeloma (Figure 1) or other malignancies.
To count how many ribs are broken. The more ribs broken, the greater the likelihood of illness and death in certain populations, such as the elderly. One study8 found that patients over age 45 with more than four broken ribs are at a significantly higher risk of prolonged stay in the intensive care unit, prolonged ventilator support, and prolonged overall hospital stay.
Knowing the number of ribs fractured may also influence other treatment decisions, such as whether to transfer the patient to a trauma center: a study showed that the more ribs broken, the greater the death rate, and that more than three rib fractures may indicate the need to transfer to a trauma center.6
HOW TO DIAGNOSE A BROKEN RIB
Signs and symptoms are unreliable but important
Clinical symptoms do not reliably tell us if a rib is broken.9,10 Nevertheless, the history and physical examination can uncover possible complications or associated injuries,10,11 such as flail chest, pneumothorax, or vascular injury.
Classic clinical signs and symptoms of rib fracture include point tenderness, focally referred pain with general chest compression, splinting, bony crepitus, and ecchymosis.9 A history of a motor vehicle accident (especially on a motorcycle) or other injury due to rapid deceleration, a fall from higher than 20 feet, a gunshot wound, assault, or a crushing injury would indicate a greater risk of complications.
Signs of complications may include decreased oxygen saturation, decreased or absent breath sounds, dullness or hyperresonance to percussion, tracheal deviation, hypotension, arrythmia, subcutaneous emphysema, neck vein distension, neck hematoma, a focal neurologic deficit below the clavicles or in the upper extremities, and flail chest.11 Flail chest results from multiple fractures in the same rib, so that a segment of chest wall does not contribute to breathing.
Further research is needed into the correlation of clinical symptoms with rib fractures. Much of the evidence that clinical symptoms correlate poorly with fractures comes from studies that used plain radiography to detect the fractures. However, ultrasonography and computed tomography (CT) can detect fractures that plain radiography cannot, and studies using these newer imaging tests may reveal a better correlation between clinical symptoms and rib fracture than previously thought.6
Chest radiography may miss 50% of rib fractures, but is still useful
Plain radiography of the chest with or without oblique views and optimized by the technologist for bony detail (“bone technique”) has historically been the imaging test of choice. However, it may miss up to 50% of fractures.10 Furthermore, it is not sensitive for costal cartilage3 or stress fractures.
Despite these limitations, plain radiography is vitally important in diagnosing complications and associated injuries such as a pneumothorax, hemothorax, pulmonary contusion, pneumomediastinum, or pneumoperitoneum. Also, a widened mediastinum could indicate aortic injury.
Currently, a standard chest x-ray is often the initial study of choice in the evaluation of chest pain and in cases of minor blunt trauma. If rib fractures are suspected clinically, a rib series can be of benefit. A rib series consists of a marker placed over the region of interest, oblique views, and optimization of the radiograph by the technologist to highlight bony detail. The decision to image a rib fracture in the absence of other underlying abnormalities or associated injuries depends on the clinical scenario.
Computed tomography provides more detail
Figure 2. Computed tomographic scan (zoomed axial image) shows an acute rib fracture.
CT is the primary study to fully evaluate for trauma-associated injuries and to evaluate bony detail (Figure 2). Its diagnostic capability is unsurpassed in this setting.11,12,13 It is also useful for diagnosing costal cartilage injury, whereas radiography is not.14 It can provide more details and new information when plain radiography indicates bone pathology: eg, a widened mediastinum suggesting vascular injury; pneumomediastinum or pneumoperitoneum of uncertain cause; cases of questionable pneumothorax; and locating foreign bodies or bony fragments, particularly in relation to vital vascular or nerve structures.
Figure 3. An axial image from a computed tomographic scan of the chest in a trauma patient shows a displaced fracture in a posterolateral right rib (arrow). There is an underlying effusion, the density of which indicates hemothorax. There is also a pulmonary contusion.
Additionally, CT may help elucidate nonspecific findings such as lung opacification, which may represent hemothorax or pulmonary contusion or both (Figure 3). It can also better characterize pathologic fractures related to cancer. Specific bone reconstruction algorithms and three-dimensional reconstructions further improve CT’s ability to detect rib pathology.
While CT appears to be the best imaging test for evaluating for rib fractures and associated injuries, it is relatively costly, is time-consuming, is not always available, and exposes the patient to a significant amount of radiation.
Also, while CT plays a vital role in major and penetrating trauma of the chest or abdomen, its use in other situations is more limited. Again, the issue of clinical impact of a diagnosis of rib fracture comes into play, and in this setting CT competes with plain radiography and ultrasonography, which are less costly and involve less or no radiation exposure.
Ultrasonography has advantages but is not widely used
Ultrasonography can be used to look for broken ribs and costal cartilage fractures. Associated injuries such as pneumothorax, hemothorax, and abdominal organ injury can also be evaluated. Studies have found it to be much more sensitive than plain radiography in detecting rib fractures,3,15 whereas other studies have suggested it is only equally sensitive or slightly better.7 It also has the advantage of not using radiation.
Because of a number of disadvantages, ultrasonography is rarely used in the evaluation of rib fracture. It is time-consuming and more costly than plain radiography. It is often not readily available. It can be painful, making it impractical for trauma patients. Its results depend greatly on the skill of the technician, and it is unable to adequately assess certain portions of the thorax (eg, the first rib under the clavicle, and the upper ribs under the scapula).7,15 Although able to detect some associated injuries, ultrasonography is not as sensitive and comprehensive as plain radiography and CT. Its role is therefore limited to situations in which the diagnosis of a rib fracture alone, in an accessible rib, is important.
Bone scan: Sensitive but not specific
Technetium Tc 99m methylene diphosphonate bone scanning can be used to look for bone pathology, including rib fractures. Bone scans are sensitive but not specific, and abnormal uptake generates an extensive differential diagnosis.16 Single-photon emission CT, or SPECT, can help localize the abnormality. 4 Because a hot spot on a bone scan can represent a number of conditions besides rib fractures, including cancer, focal sclerosis, and focal osteosclerosis, bone scanning is not routinely used for evaluating rib fractures, although it is very sensitive for stress fractures.
Occasionally, in a patient undergoing a bone scan as part of a workup for cancer, a scan shows a lesion that might be a rib fracture. In this case, one should correlate the results with those of plain radiography or CT.16
Magnetic resonance imaging: no role yet in rib fracture evaluation
MRI is not considered appropriate for evaluating rib fractures. It may be useful if there is concern about soft-tissue or vascular abnormalities. Beyond this, further research is needed to elucidate its role in rib fracture.
THE CHOICE OF TEST DEPENDS ON THE SITUATION
Figure 4. Recommended clinical management of patients with a history of chest trauma. In an asymptomatic patient, the key question is whether confirming a rib fracture with radiographic imaging will alter clinical management. In a symptomatic patient with a normal chest x-ray, one may consider CT to detect underlying injury as well as rib fractures.
Although several imaging tests can tell us if a patient has a rib fracture, in most cases the diagnosis of a rib fracture alone has little clinical relevance. The accurate and timely assessment of associated injuries and complications is more clinically useful, and for this, plain radiography and CT provide the most useful information. The choice of which test to use in a patient with a suspected rib fracture depends on the clinical circumstances (Figure 4).
In patients with penetrating or major chest or abdominal trauma, CT is the study of choice. It provides the most information about associated injuries, and it accurately detects rib fractures. This helps target treatment of associated injuries, and helps identify patients at higher risk, such as those with significant vascular, pulmonary, or abdominal injuries and those with a greater number of fractures. An unstable, critically injured patient would not be a candidate for CT because of the risk of transport to the scanner; chest radiography would have to suffice in these cases.
In cases of minor blunt trauma when there is little suspicion of associated injuries or complications, plain radiography is likely sufficient. If there is suspicion of a rib fracture alone and confirmation is of clinical importance (eg, in the elderly or those with long-standing refractory pain, or when certain pain management treatments are being considered), then oblique radiographic views, bone technique, and marker placement over the concerning region are recommended. The role of ultrasonography in this setting is still up for debate.
In cases of suspected rib fracture with longstanding pain refractory to conservative pain management, plain radiography with oblique views, bone technique, and marker placement is useful. If the radiograph is negative or if there is a high suspicion of cartilage fracture, CT or ultrasonography may be of benefit only if the diagnosis will alter clinical management.
If stress fracture is suspected, a nuclear bone scan may be helpful to first detect an abnormality, and CT may then be used for correlation if needed.
CASE CONCLUDED: LIVING WITH UNCERTAINTY
As for the 70-year-old man presented at the beginning of this article, the first question is whether we suspect an associated injury on the basis of clinical features. If we had clinical findings suspicious for pneumothorax or hemothorax, plain radiography of the chest would be indicated. Since the patient was not involved in major trauma, a CT scan is not indicated as the first study.
Our patient has clinical findings suggesting a rib fracture without associated injury. In this setting, routine posteroanterior and lateral chest radiography would be useful to rule out major associated injuries and, perhaps, to find a rib fracture. If the chest film is normal and rib fracture is still suspected, we must decide whether the diagnosis would alter our clinical management. Our patient would likely be treated the same regardless of whether or not he has a fracture; therefore, we would prescribe pain management.
Chest radiography was performed to rule out associated injuries, especially since the patient was elderly, but the chest x-ray did not reveal anything. On follow-up approximately 1 month later, he appeared improved, with less pain and tenderness. This may be due to healing of a rib fracture or healing of his soft-tissue injury. We will never know whether he truly had a fracture, but it is irrelevant to his care.
References
Bergeron E, Lavoie A, Clas D, et al. Elderly trauma patients with rib fractures are at greater risk of death and pneumonia. J Trauma2003; 54:478–485.
Lederer W, Mair D, Rabl W, Baubin M. Frequency of rib and sternum fractures associated with out-of-hospital cardiopulmonary resuscitation is underestimated by conventional chest x-ray. Resuscitation2004; 60:157–162.
Kara M, Dikmen E, Erdal HH, Simsir I, Kara SA. Disclosure of unnoticed rib fractures with the use of ultrasonography in minor blunt chest trauma. Eur J Cardiothorac Surg2003; 24:608–613.
Bansidhar BJ, Lagares-Garcia JA, Miller SL. Clinical rib fractures: are follow-up chest x-rays a waste of resources?Am Surg2002; 68:449–453.
Stawicki SP, Grossman MD, Hoey BA, Miller DL, Reed JF. Rib fractures in the elderly: a marker of injury severity. J Am Geriatr Soc2004; 52:805–808.
Hurley ME, Keye GD, Hamilton S. Is ultrasound really helpful in the detection of rib fractures?Injury2004; 35:562–566.
Holcomb JB, McMullin NR, Kozar RA, Lygas MH, Moore FA. Morbidity from rib fractures increases after age 45. J Am Coll Surg2003; 196:549–555.
Deluca SA, Rhea JT, O’Malley TO. Radiographic evaluation of rib fractures. AJR Am J Roentgenol1982; 138:91–92.
Dubinsky I, Low A. Non-life threatening blunt chest trauma: appropriate investigation and treatment. Am J Emerg Med1997; 15:240–243.
Sears BW, Luchette FA, Esposito TJ, et al. Old fashion clinical judgment in the era of protocols: is mandatory chest x-ray necessary in injured patients?J Trauma2005; 59:324–332.
Traub M, Stevenson M, McEvoy S, et al. The use of chest computed tomography versus chest x-ray in patients with major blunt trauma. Injury2007; 38:43–47.
Trupka A, Waydhas C, Hallfeldt KK, Nast-Kolb D, Pfeifer KJ, Schweiberer L. Value of thoracic computed tomography in the first assessment of severely injured patients with blunt chest trauma: results of a prospective study. J Trauma1997; 43:405–412.
Malghem J, Vande Berg B, Lecouvet F, Maldague B. Costal cartilage fractures as revealed on CT and sonography. AJR Am J Roentgenol2001; 176:429–432.
Griffith JF, Rainer TH, Ching AS, Law KL, Cocks RA, Metreweli C. Sonography compared with radiography in revealing acute rib fracture. AJR Am J Roentgenol1999; 173:1603–1609.
Niitsu M, Takeda T. Solitary hot spots in the ribs on bone scan: value of thin-section reformatted computed tomography to exclude radiography negative fractures. J Comput Assist Tomogr2003; 27:469–474.
A 70-year-old man falls in his bathroom and subsequently presents to an urgent care clinic. Among his complaints is right-sided chest pain. On physical examination he has point tenderness over the lateral right thorax with some superficial swelling and bruising. The chest is normal on auscultation.
Should this patient undergo imaging to determine if he has a rib fracture? And which imaging study would be appropriate?
This article outlines the use of various imaging tests in the evaluation of suspected rib fractures and recommends an approach to management. This article does not address fractures in children.
MANY CAUSES OF RIB FRACTURES
Trauma, the most common cause of rib fractures, includes penetrating injuries and blunt injury to the chest wall. Between 10% and 66% of traumatic injuries result in rib fractures. 1 Traumatic injury can result from motor vehicle accidents, assault, sports, cardiopulmonary resuscitation, physical abuse (“nonaccidental” trauma), and, rarely, severe paroxysms of coughing.2
Cancer can cause pathologic fractures of the rib.
Stress fractures of the ribs are more likely to occur in high-level athletes whose activity involves repetitive musculoskeletal loading, although they can also occur in people with repetitive coughing paroxysms.3 Sports and activities that result in stress fractures include rowing, pitching or throwing, basketball, weight-lifting, ballet, golf, gymnastics, and swimming.4
WHICH RIB IS BROKEN?
The fourth through 10th ribs are the most often fractured. Fractures of the first through the third ribs can be associated with underlying nerve and vascular injuries, and fractures of the 10th through 12th ribs are associated with damage to abdominal organs,5 most commonly the liver, spleen, kidneys, and diaphragm.3
Fractures of the costal cartilage can occur by any of the mechanisms described above. The true incidence of costal cartilage fractures is not known because plain radiography, the traditional method of evaluation, does not reliably detect them.
WHY CONFIRM A RIB FRACTURE?
For many rib fractures without associated injury, a radiographic diagnosis has little impact on patient management, which consists mainly of pain control. But knowing whether a patient has a broken rib can often be important.
To detect associated injury. The rate of associated injury in patients with rib fractures is high.6 Potentially severe complications include:
Pneumothorax
Hemothorax
Pulmonary contusion
Flail chest
Pneumonia
Vascular and nerve damage (especially with trauma to the upper chest or the first through third ribs)
Abdominal organ injury (particularly with trauma to the lower thorax or lower ribs).
The absence of a rib fracture does not preclude these conditions, however.
To prevent complications. Even in the absence of associated injuries, radiographic confirmation of a rib fracture can help prevent complications such as atelectasis and is particularly important in patients with comorbidities such as chronic obstructive pulmonary disease, cardiac disease, hepatic disease, renal disease, dementia, and coagulopathy.1
To document the injury. Radiographic documentation of a rib fracture may be required for medical-legal issues in cases of assault, motor vehicle accident, occupational injury, and abuse.
To help manage pain. Confirmation of rib fracture can facilitate pain management, particularly in patients with undiagnosed fractures with long-standing refractory pain. For example, conservative pain control with nonsteroidal anti-inflammatory drugs may be sufficient for a soft-tissue injury but may not be enough for a rib fracture. Intravenous narcotics or nerve blocks might be preferable.3,7 Controlling pain helps limit the incidence of associated complications.
Figure 1. Oblique radiographic view shows an acute rib fracture in a patient with multiple myeloma.To detect pathologic fractures. Radiographic diagnosis can provide important information in cases of suspected pathologic fracture, as in multiple myeloma (Figure 1) or other malignancies.
To count how many ribs are broken. The more ribs broken, the greater the likelihood of illness and death in certain populations, such as the elderly. One study8 found that patients over age 45 with more than four broken ribs are at a significantly higher risk of prolonged stay in the intensive care unit, prolonged ventilator support, and prolonged overall hospital stay.
Knowing the number of ribs fractured may also influence other treatment decisions, such as whether to transfer the patient to a trauma center: a study showed that the more ribs broken, the greater the death rate, and that more than three rib fractures may indicate the need to transfer to a trauma center.6
HOW TO DIAGNOSE A BROKEN RIB
Signs and symptoms are unreliable but important
Clinical symptoms do not reliably tell us if a rib is broken.9,10 Nevertheless, the history and physical examination can uncover possible complications or associated injuries,10,11 such as flail chest, pneumothorax, or vascular injury.
Classic clinical signs and symptoms of rib fracture include point tenderness, focally referred pain with general chest compression, splinting, bony crepitus, and ecchymosis.9 A history of a motor vehicle accident (especially on a motorcycle) or other injury due to rapid deceleration, a fall from higher than 20 feet, a gunshot wound, assault, or a crushing injury would indicate a greater risk of complications.
Signs of complications may include decreased oxygen saturation, decreased or absent breath sounds, dullness or hyperresonance to percussion, tracheal deviation, hypotension, arrythmia, subcutaneous emphysema, neck vein distension, neck hematoma, a focal neurologic deficit below the clavicles or in the upper extremities, and flail chest.11 Flail chest results from multiple fractures in the same rib, so that a segment of chest wall does not contribute to breathing.
Further research is needed into the correlation of clinical symptoms with rib fractures. Much of the evidence that clinical symptoms correlate poorly with fractures comes from studies that used plain radiography to detect the fractures. However, ultrasonography and computed tomography (CT) can detect fractures that plain radiography cannot, and studies using these newer imaging tests may reveal a better correlation between clinical symptoms and rib fracture than previously thought.6
Chest radiography may miss 50% of rib fractures, but is still useful
Plain radiography of the chest with or without oblique views and optimized by the technologist for bony detail (“bone technique”) has historically been the imaging test of choice. However, it may miss up to 50% of fractures.10 Furthermore, it is not sensitive for costal cartilage3 or stress fractures.
Despite these limitations, plain radiography is vitally important in diagnosing complications and associated injuries such as a pneumothorax, hemothorax, pulmonary contusion, pneumomediastinum, or pneumoperitoneum. Also, a widened mediastinum could indicate aortic injury.
Currently, a standard chest x-ray is often the initial study of choice in the evaluation of chest pain and in cases of minor blunt trauma. If rib fractures are suspected clinically, a rib series can be of benefit. A rib series consists of a marker placed over the region of interest, oblique views, and optimization of the radiograph by the technologist to highlight bony detail. The decision to image a rib fracture in the absence of other underlying abnormalities or associated injuries depends on the clinical scenario.
Computed tomography provides more detail
Figure 2. Computed tomographic scan (zoomed axial image) shows an acute rib fracture.
CT is the primary study to fully evaluate for trauma-associated injuries and to evaluate bony detail (Figure 2). Its diagnostic capability is unsurpassed in this setting.11,12,13 It is also useful for diagnosing costal cartilage injury, whereas radiography is not.14 It can provide more details and new information when plain radiography indicates bone pathology: eg, a widened mediastinum suggesting vascular injury; pneumomediastinum or pneumoperitoneum of uncertain cause; cases of questionable pneumothorax; and locating foreign bodies or bony fragments, particularly in relation to vital vascular or nerve structures.
Figure 3. An axial image from a computed tomographic scan of the chest in a trauma patient shows a displaced fracture in a posterolateral right rib (arrow). There is an underlying effusion, the density of which indicates hemothorax. There is also a pulmonary contusion.
Additionally, CT may help elucidate nonspecific findings such as lung opacification, which may represent hemothorax or pulmonary contusion or both (Figure 3). It can also better characterize pathologic fractures related to cancer. Specific bone reconstruction algorithms and three-dimensional reconstructions further improve CT’s ability to detect rib pathology.
While CT appears to be the best imaging test for evaluating for rib fractures and associated injuries, it is relatively costly, is time-consuming, is not always available, and exposes the patient to a significant amount of radiation.
Also, while CT plays a vital role in major and penetrating trauma of the chest or abdomen, its use in other situations is more limited. Again, the issue of clinical impact of a diagnosis of rib fracture comes into play, and in this setting CT competes with plain radiography and ultrasonography, which are less costly and involve less or no radiation exposure.
Ultrasonography has advantages but is not widely used
Ultrasonography can be used to look for broken ribs and costal cartilage fractures. Associated injuries such as pneumothorax, hemothorax, and abdominal organ injury can also be evaluated. Studies have found it to be much more sensitive than plain radiography in detecting rib fractures,3,15 whereas other studies have suggested it is only equally sensitive or slightly better.7 It also has the advantage of not using radiation.
Because of a number of disadvantages, ultrasonography is rarely used in the evaluation of rib fracture. It is time-consuming and more costly than plain radiography. It is often not readily available. It can be painful, making it impractical for trauma patients. Its results depend greatly on the skill of the technician, and it is unable to adequately assess certain portions of the thorax (eg, the first rib under the clavicle, and the upper ribs under the scapula).7,15 Although able to detect some associated injuries, ultrasonography is not as sensitive and comprehensive as plain radiography and CT. Its role is therefore limited to situations in which the diagnosis of a rib fracture alone, in an accessible rib, is important.
Bone scan: Sensitive but not specific
Technetium Tc 99m methylene diphosphonate bone scanning can be used to look for bone pathology, including rib fractures. Bone scans are sensitive but not specific, and abnormal uptake generates an extensive differential diagnosis.16 Single-photon emission CT, or SPECT, can help localize the abnormality. 4 Because a hot spot on a bone scan can represent a number of conditions besides rib fractures, including cancer, focal sclerosis, and focal osteosclerosis, bone scanning is not routinely used for evaluating rib fractures, although it is very sensitive for stress fractures.
Occasionally, in a patient undergoing a bone scan as part of a workup for cancer, a scan shows a lesion that might be a rib fracture. In this case, one should correlate the results with those of plain radiography or CT.16
Magnetic resonance imaging: no role yet in rib fracture evaluation
MRI is not considered appropriate for evaluating rib fractures. It may be useful if there is concern about soft-tissue or vascular abnormalities. Beyond this, further research is needed to elucidate its role in rib fracture.
THE CHOICE OF TEST DEPENDS ON THE SITUATION
Figure 4. Recommended clinical management of patients with a history of chest trauma. In an asymptomatic patient, the key question is whether confirming a rib fracture with radiographic imaging will alter clinical management. In a symptomatic patient with a normal chest x-ray, one may consider CT to detect underlying injury as well as rib fractures.
Although several imaging tests can tell us if a patient has a rib fracture, in most cases the diagnosis of a rib fracture alone has little clinical relevance. The accurate and timely assessment of associated injuries and complications is more clinically useful, and for this, plain radiography and CT provide the most useful information. The choice of which test to use in a patient with a suspected rib fracture depends on the clinical circumstances (Figure 4).
In patients with penetrating or major chest or abdominal trauma, CT is the study of choice. It provides the most information about associated injuries, and it accurately detects rib fractures. This helps target treatment of associated injuries, and helps identify patients at higher risk, such as those with significant vascular, pulmonary, or abdominal injuries and those with a greater number of fractures. An unstable, critically injured patient would not be a candidate for CT because of the risk of transport to the scanner; chest radiography would have to suffice in these cases.
In cases of minor blunt trauma when there is little suspicion of associated injuries or complications, plain radiography is likely sufficient. If there is suspicion of a rib fracture alone and confirmation is of clinical importance (eg, in the elderly or those with long-standing refractory pain, or when certain pain management treatments are being considered), then oblique radiographic views, bone technique, and marker placement over the concerning region are recommended. The role of ultrasonography in this setting is still up for debate.
In cases of suspected rib fracture with longstanding pain refractory to conservative pain management, plain radiography with oblique views, bone technique, and marker placement is useful. If the radiograph is negative or if there is a high suspicion of cartilage fracture, CT or ultrasonography may be of benefit only if the diagnosis will alter clinical management.
If stress fracture is suspected, a nuclear bone scan may be helpful to first detect an abnormality, and CT may then be used for correlation if needed.
CASE CONCLUDED: LIVING WITH UNCERTAINTY
As for the 70-year-old man presented at the beginning of this article, the first question is whether we suspect an associated injury on the basis of clinical features. If we had clinical findings suspicious for pneumothorax or hemothorax, plain radiography of the chest would be indicated. Since the patient was not involved in major trauma, a CT scan is not indicated as the first study.
Our patient has clinical findings suggesting a rib fracture without associated injury. In this setting, routine posteroanterior and lateral chest radiography would be useful to rule out major associated injuries and, perhaps, to find a rib fracture. If the chest film is normal and rib fracture is still suspected, we must decide whether the diagnosis would alter our clinical management. Our patient would likely be treated the same regardless of whether or not he has a fracture; therefore, we would prescribe pain management.
Chest radiography was performed to rule out associated injuries, especially since the patient was elderly, but the chest x-ray did not reveal anything. On follow-up approximately 1 month later, he appeared improved, with less pain and tenderness. This may be due to healing of a rib fracture or healing of his soft-tissue injury. We will never know whether he truly had a fracture, but it is irrelevant to his care.
A 70-year-old man falls in his bathroom and subsequently presents to an urgent care clinic. Among his complaints is right-sided chest pain. On physical examination he has point tenderness over the lateral right thorax with some superficial swelling and bruising. The chest is normal on auscultation.
Should this patient undergo imaging to determine if he has a rib fracture? And which imaging study would be appropriate?
This article outlines the use of various imaging tests in the evaluation of suspected rib fractures and recommends an approach to management. This article does not address fractures in children.
MANY CAUSES OF RIB FRACTURES
Trauma, the most common cause of rib fractures, includes penetrating injuries and blunt injury to the chest wall. Between 10% and 66% of traumatic injuries result in rib fractures. 1 Traumatic injury can result from motor vehicle accidents, assault, sports, cardiopulmonary resuscitation, physical abuse (“nonaccidental” trauma), and, rarely, severe paroxysms of coughing.2
Cancer can cause pathologic fractures of the rib.
Stress fractures of the ribs are more likely to occur in high-level athletes whose activity involves repetitive musculoskeletal loading, although they can also occur in people with repetitive coughing paroxysms.3 Sports and activities that result in stress fractures include rowing, pitching or throwing, basketball, weight-lifting, ballet, golf, gymnastics, and swimming.4
WHICH RIB IS BROKEN?
The fourth through 10th ribs are the most often fractured. Fractures of the first through the third ribs can be associated with underlying nerve and vascular injuries, and fractures of the 10th through 12th ribs are associated with damage to abdominal organs,5 most commonly the liver, spleen, kidneys, and diaphragm.3
Fractures of the costal cartilage can occur by any of the mechanisms described above. The true incidence of costal cartilage fractures is not known because plain radiography, the traditional method of evaluation, does not reliably detect them.
WHY CONFIRM A RIB FRACTURE?
For many rib fractures without associated injury, a radiographic diagnosis has little impact on patient management, which consists mainly of pain control. But knowing whether a patient has a broken rib can often be important.
To detect associated injury. The rate of associated injury in patients with rib fractures is high.6 Potentially severe complications include:
Pneumothorax
Hemothorax
Pulmonary contusion
Flail chest
Pneumonia
Vascular and nerve damage (especially with trauma to the upper chest or the first through third ribs)
Abdominal organ injury (particularly with trauma to the lower thorax or lower ribs).
The absence of a rib fracture does not preclude these conditions, however.
To prevent complications. Even in the absence of associated injuries, radiographic confirmation of a rib fracture can help prevent complications such as atelectasis and is particularly important in patients with comorbidities such as chronic obstructive pulmonary disease, cardiac disease, hepatic disease, renal disease, dementia, and coagulopathy.1
To document the injury. Radiographic documentation of a rib fracture may be required for medical-legal issues in cases of assault, motor vehicle accident, occupational injury, and abuse.
To help manage pain. Confirmation of rib fracture can facilitate pain management, particularly in patients with undiagnosed fractures with long-standing refractory pain. For example, conservative pain control with nonsteroidal anti-inflammatory drugs may be sufficient for a soft-tissue injury but may not be enough for a rib fracture. Intravenous narcotics or nerve blocks might be preferable.3,7 Controlling pain helps limit the incidence of associated complications.
Figure 1. Oblique radiographic view shows an acute rib fracture in a patient with multiple myeloma.To detect pathologic fractures. Radiographic diagnosis can provide important information in cases of suspected pathologic fracture, as in multiple myeloma (Figure 1) or other malignancies.
To count how many ribs are broken. The more ribs broken, the greater the likelihood of illness and death in certain populations, such as the elderly. One study8 found that patients over age 45 with more than four broken ribs are at a significantly higher risk of prolonged stay in the intensive care unit, prolonged ventilator support, and prolonged overall hospital stay.
Knowing the number of ribs fractured may also influence other treatment decisions, such as whether to transfer the patient to a trauma center: a study showed that the more ribs broken, the greater the death rate, and that more than three rib fractures may indicate the need to transfer to a trauma center.6
HOW TO DIAGNOSE A BROKEN RIB
Signs and symptoms are unreliable but important
Clinical symptoms do not reliably tell us if a rib is broken.9,10 Nevertheless, the history and physical examination can uncover possible complications or associated injuries,10,11 such as flail chest, pneumothorax, or vascular injury.
Classic clinical signs and symptoms of rib fracture include point tenderness, focally referred pain with general chest compression, splinting, bony crepitus, and ecchymosis.9 A history of a motor vehicle accident (especially on a motorcycle) or other injury due to rapid deceleration, a fall from higher than 20 feet, a gunshot wound, assault, or a crushing injury would indicate a greater risk of complications.
Signs of complications may include decreased oxygen saturation, decreased or absent breath sounds, dullness or hyperresonance to percussion, tracheal deviation, hypotension, arrythmia, subcutaneous emphysema, neck vein distension, neck hematoma, a focal neurologic deficit below the clavicles or in the upper extremities, and flail chest.11 Flail chest results from multiple fractures in the same rib, so that a segment of chest wall does not contribute to breathing.
Further research is needed into the correlation of clinical symptoms with rib fractures. Much of the evidence that clinical symptoms correlate poorly with fractures comes from studies that used plain radiography to detect the fractures. However, ultrasonography and computed tomography (CT) can detect fractures that plain radiography cannot, and studies using these newer imaging tests may reveal a better correlation between clinical symptoms and rib fracture than previously thought.6
Chest radiography may miss 50% of rib fractures, but is still useful
Plain radiography of the chest with or without oblique views and optimized by the technologist for bony detail (“bone technique”) has historically been the imaging test of choice. However, it may miss up to 50% of fractures.10 Furthermore, it is not sensitive for costal cartilage3 or stress fractures.
Despite these limitations, plain radiography is vitally important in diagnosing complications and associated injuries such as a pneumothorax, hemothorax, pulmonary contusion, pneumomediastinum, or pneumoperitoneum. Also, a widened mediastinum could indicate aortic injury.
Currently, a standard chest x-ray is often the initial study of choice in the evaluation of chest pain and in cases of minor blunt trauma. If rib fractures are suspected clinically, a rib series can be of benefit. A rib series consists of a marker placed over the region of interest, oblique views, and optimization of the radiograph by the technologist to highlight bony detail. The decision to image a rib fracture in the absence of other underlying abnormalities or associated injuries depends on the clinical scenario.
Computed tomography provides more detail
Figure 2. Computed tomographic scan (zoomed axial image) shows an acute rib fracture.
CT is the primary study to fully evaluate for trauma-associated injuries and to evaluate bony detail (Figure 2). Its diagnostic capability is unsurpassed in this setting.11,12,13 It is also useful for diagnosing costal cartilage injury, whereas radiography is not.14 It can provide more details and new information when plain radiography indicates bone pathology: eg, a widened mediastinum suggesting vascular injury; pneumomediastinum or pneumoperitoneum of uncertain cause; cases of questionable pneumothorax; and locating foreign bodies or bony fragments, particularly in relation to vital vascular or nerve structures.
Figure 3. An axial image from a computed tomographic scan of the chest in a trauma patient shows a displaced fracture in a posterolateral right rib (arrow). There is an underlying effusion, the density of which indicates hemothorax. There is also a pulmonary contusion.
Additionally, CT may help elucidate nonspecific findings such as lung opacification, which may represent hemothorax or pulmonary contusion or both (Figure 3). It can also better characterize pathologic fractures related to cancer. Specific bone reconstruction algorithms and three-dimensional reconstructions further improve CT’s ability to detect rib pathology.
While CT appears to be the best imaging test for evaluating for rib fractures and associated injuries, it is relatively costly, is time-consuming, is not always available, and exposes the patient to a significant amount of radiation.
Also, while CT plays a vital role in major and penetrating trauma of the chest or abdomen, its use in other situations is more limited. Again, the issue of clinical impact of a diagnosis of rib fracture comes into play, and in this setting CT competes with plain radiography and ultrasonography, which are less costly and involve less or no radiation exposure.
Ultrasonography has advantages but is not widely used
Ultrasonography can be used to look for broken ribs and costal cartilage fractures. Associated injuries such as pneumothorax, hemothorax, and abdominal organ injury can also be evaluated. Studies have found it to be much more sensitive than plain radiography in detecting rib fractures,3,15 whereas other studies have suggested it is only equally sensitive or slightly better.7 It also has the advantage of not using radiation.
Because of a number of disadvantages, ultrasonography is rarely used in the evaluation of rib fracture. It is time-consuming and more costly than plain radiography. It is often not readily available. It can be painful, making it impractical for trauma patients. Its results depend greatly on the skill of the technician, and it is unable to adequately assess certain portions of the thorax (eg, the first rib under the clavicle, and the upper ribs under the scapula).7,15 Although able to detect some associated injuries, ultrasonography is not as sensitive and comprehensive as plain radiography and CT. Its role is therefore limited to situations in which the diagnosis of a rib fracture alone, in an accessible rib, is important.
Bone scan: Sensitive but not specific
Technetium Tc 99m methylene diphosphonate bone scanning can be used to look for bone pathology, including rib fractures. Bone scans are sensitive but not specific, and abnormal uptake generates an extensive differential diagnosis.16 Single-photon emission CT, or SPECT, can help localize the abnormality. 4 Because a hot spot on a bone scan can represent a number of conditions besides rib fractures, including cancer, focal sclerosis, and focal osteosclerosis, bone scanning is not routinely used for evaluating rib fractures, although it is very sensitive for stress fractures.
Occasionally, in a patient undergoing a bone scan as part of a workup for cancer, a scan shows a lesion that might be a rib fracture. In this case, one should correlate the results with those of plain radiography or CT.16
Magnetic resonance imaging: no role yet in rib fracture evaluation
MRI is not considered appropriate for evaluating rib fractures. It may be useful if there is concern about soft-tissue or vascular abnormalities. Beyond this, further research is needed to elucidate its role in rib fracture.
THE CHOICE OF TEST DEPENDS ON THE SITUATION
Figure 4. Recommended clinical management of patients with a history of chest trauma. In an asymptomatic patient, the key question is whether confirming a rib fracture with radiographic imaging will alter clinical management. In a symptomatic patient with a normal chest x-ray, one may consider CT to detect underlying injury as well as rib fractures.
Although several imaging tests can tell us if a patient has a rib fracture, in most cases the diagnosis of a rib fracture alone has little clinical relevance. The accurate and timely assessment of associated injuries and complications is more clinically useful, and for this, plain radiography and CT provide the most useful information. The choice of which test to use in a patient with a suspected rib fracture depends on the clinical circumstances (Figure 4).
In patients with penetrating or major chest or abdominal trauma, CT is the study of choice. It provides the most information about associated injuries, and it accurately detects rib fractures. This helps target treatment of associated injuries, and helps identify patients at higher risk, such as those with significant vascular, pulmonary, or abdominal injuries and those with a greater number of fractures. An unstable, critically injured patient would not be a candidate for CT because of the risk of transport to the scanner; chest radiography would have to suffice in these cases.
In cases of minor blunt trauma when there is little suspicion of associated injuries or complications, plain radiography is likely sufficient. If there is suspicion of a rib fracture alone and confirmation is of clinical importance (eg, in the elderly or those with long-standing refractory pain, or when certain pain management treatments are being considered), then oblique radiographic views, bone technique, and marker placement over the concerning region are recommended. The role of ultrasonography in this setting is still up for debate.
In cases of suspected rib fracture with longstanding pain refractory to conservative pain management, plain radiography with oblique views, bone technique, and marker placement is useful. If the radiograph is negative or if there is a high suspicion of cartilage fracture, CT or ultrasonography may be of benefit only if the diagnosis will alter clinical management.
If stress fracture is suspected, a nuclear bone scan may be helpful to first detect an abnormality, and CT may then be used for correlation if needed.
CASE CONCLUDED: LIVING WITH UNCERTAINTY
As for the 70-year-old man presented at the beginning of this article, the first question is whether we suspect an associated injury on the basis of clinical features. If we had clinical findings suspicious for pneumothorax or hemothorax, plain radiography of the chest would be indicated. Since the patient was not involved in major trauma, a CT scan is not indicated as the first study.
Our patient has clinical findings suggesting a rib fracture without associated injury. In this setting, routine posteroanterior and lateral chest radiography would be useful to rule out major associated injuries and, perhaps, to find a rib fracture. If the chest film is normal and rib fracture is still suspected, we must decide whether the diagnosis would alter our clinical management. Our patient would likely be treated the same regardless of whether or not he has a fracture; therefore, we would prescribe pain management.
Chest radiography was performed to rule out associated injuries, especially since the patient was elderly, but the chest x-ray did not reveal anything. On follow-up approximately 1 month later, he appeared improved, with less pain and tenderness. This may be due to healing of a rib fracture or healing of his soft-tissue injury. We will never know whether he truly had a fracture, but it is irrelevant to his care.
References
Bergeron E, Lavoie A, Clas D, et al. Elderly trauma patients with rib fractures are at greater risk of death and pneumonia. J Trauma2003; 54:478–485.
Lederer W, Mair D, Rabl W, Baubin M. Frequency of rib and sternum fractures associated with out-of-hospital cardiopulmonary resuscitation is underestimated by conventional chest x-ray. Resuscitation2004; 60:157–162.
Kara M, Dikmen E, Erdal HH, Simsir I, Kara SA. Disclosure of unnoticed rib fractures with the use of ultrasonography in minor blunt chest trauma. Eur J Cardiothorac Surg2003; 24:608–613.
Bansidhar BJ, Lagares-Garcia JA, Miller SL. Clinical rib fractures: are follow-up chest x-rays a waste of resources?Am Surg2002; 68:449–453.
Stawicki SP, Grossman MD, Hoey BA, Miller DL, Reed JF. Rib fractures in the elderly: a marker of injury severity. J Am Geriatr Soc2004; 52:805–808.
Hurley ME, Keye GD, Hamilton S. Is ultrasound really helpful in the detection of rib fractures?Injury2004; 35:562–566.
Holcomb JB, McMullin NR, Kozar RA, Lygas MH, Moore FA. Morbidity from rib fractures increases after age 45. J Am Coll Surg2003; 196:549–555.
Deluca SA, Rhea JT, O’Malley TO. Radiographic evaluation of rib fractures. AJR Am J Roentgenol1982; 138:91–92.
Dubinsky I, Low A. Non-life threatening blunt chest trauma: appropriate investigation and treatment. Am J Emerg Med1997; 15:240–243.
Sears BW, Luchette FA, Esposito TJ, et al. Old fashion clinical judgment in the era of protocols: is mandatory chest x-ray necessary in injured patients?J Trauma2005; 59:324–332.
Traub M, Stevenson M, McEvoy S, et al. The use of chest computed tomography versus chest x-ray in patients with major blunt trauma. Injury2007; 38:43–47.
Trupka A, Waydhas C, Hallfeldt KK, Nast-Kolb D, Pfeifer KJ, Schweiberer L. Value of thoracic computed tomography in the first assessment of severely injured patients with blunt chest trauma: results of a prospective study. J Trauma1997; 43:405–412.
Malghem J, Vande Berg B, Lecouvet F, Maldague B. Costal cartilage fractures as revealed on CT and sonography. AJR Am J Roentgenol2001; 176:429–432.
Griffith JF, Rainer TH, Ching AS, Law KL, Cocks RA, Metreweli C. Sonography compared with radiography in revealing acute rib fracture. AJR Am J Roentgenol1999; 173:1603–1609.
Niitsu M, Takeda T. Solitary hot spots in the ribs on bone scan: value of thin-section reformatted computed tomography to exclude radiography negative fractures. J Comput Assist Tomogr2003; 27:469–474.
References
Bergeron E, Lavoie A, Clas D, et al. Elderly trauma patients with rib fractures are at greater risk of death and pneumonia. J Trauma2003; 54:478–485.
Lederer W, Mair D, Rabl W, Baubin M. Frequency of rib and sternum fractures associated with out-of-hospital cardiopulmonary resuscitation is underestimated by conventional chest x-ray. Resuscitation2004; 60:157–162.
Kara M, Dikmen E, Erdal HH, Simsir I, Kara SA. Disclosure of unnoticed rib fractures with the use of ultrasonography in minor blunt chest trauma. Eur J Cardiothorac Surg2003; 24:608–613.
Bansidhar BJ, Lagares-Garcia JA, Miller SL. Clinical rib fractures: are follow-up chest x-rays a waste of resources?Am Surg2002; 68:449–453.
Stawicki SP, Grossman MD, Hoey BA, Miller DL, Reed JF. Rib fractures in the elderly: a marker of injury severity. J Am Geriatr Soc2004; 52:805–808.
Hurley ME, Keye GD, Hamilton S. Is ultrasound really helpful in the detection of rib fractures?Injury2004; 35:562–566.
Holcomb JB, McMullin NR, Kozar RA, Lygas MH, Moore FA. Morbidity from rib fractures increases after age 45. J Am Coll Surg2003; 196:549–555.
Deluca SA, Rhea JT, O’Malley TO. Radiographic evaluation of rib fractures. AJR Am J Roentgenol1982; 138:91–92.
Dubinsky I, Low A. Non-life threatening blunt chest trauma: appropriate investigation and treatment. Am J Emerg Med1997; 15:240–243.
Sears BW, Luchette FA, Esposito TJ, et al. Old fashion clinical judgment in the era of protocols: is mandatory chest x-ray necessary in injured patients?J Trauma2005; 59:324–332.
Traub M, Stevenson M, McEvoy S, et al. The use of chest computed tomography versus chest x-ray in patients with major blunt trauma. Injury2007; 38:43–47.
Trupka A, Waydhas C, Hallfeldt KK, Nast-Kolb D, Pfeifer KJ, Schweiberer L. Value of thoracic computed tomography in the first assessment of severely injured patients with blunt chest trauma: results of a prospective study. J Trauma1997; 43:405–412.
Malghem J, Vande Berg B, Lecouvet F, Maldague B. Costal cartilage fractures as revealed on CT and sonography. AJR Am J Roentgenol2001; 176:429–432.
Griffith JF, Rainer TH, Ching AS, Law KL, Cocks RA, Metreweli C. Sonography compared with radiography in revealing acute rib fracture. AJR Am J Roentgenol1999; 173:1603–1609.
Niitsu M, Takeda T. Solitary hot spots in the ribs on bone scan: value of thin-section reformatted computed tomography to exclude radiography negative fractures. J Comput Assist Tomogr2003; 27:469–474.
Knowing the number of ribs fractured may influence treatment decisions, such as whether to transfer a patient to a trauma center.
Classic clinical signs and symptoms of rib fracture include point tenderness, focally referred pain with general chest compression, splinting, bony crepitus, and ecchymosis.
In a patient with minor blunt trauma, when there is little suspicion of associated injury or complication, plain radiography is likely sufficient.
Computed tomography is the imaging study of choice in patients with penetrating or major chest or abdominal trauma.
A 28-year-old woman comes in for her annual checkup. Her physician notices a palpable, painless, 1-cm, well-demarcated mass in the left breast at the 3 o’clock position 2 cm from the nipple, with no associated skin changes, nipple retraction, or discharge. The patient has no personal or family history of breast cancer.
Given the patient’s age, physical findings, and medical history, the clinician believes it unlikely that the patient has cancer. How should she proceed with the workup of this patient?
PHYSICAL FINDINGS OF A BREAST MASS ARE NOT EXCLUSIVE
Figure 1. A simple cyst in the left breast. All three mammographic views—craniocaudal (A), mediolateral oblique (B), and spot-compression (C)—show a round, well-circumscribed mass in the mid-breast. Ultrasonography (D) shows a round, well-circumscribed anechoic lesion with a sharply defined posterior wall and posterior acoustic enhancement.
Breast cancer is the most common female malignancy and the second-leading cause of cancer deaths in the United States.1 The incidence is low in young women and increases with advancing age. Benign breast disease is common in young women and less common in postmenopausal women.2,3 However, the discovery of a breast mass, whether by the woman herself or by a clinician, is a common occurrence and distressing for any woman.
Benign lesions tend to have discrete, well-defined margins and are typically mobile. Malignant lesions may be firm, may have indistinct borders, and are often immobile.2 Although most breast masses found by palpation are benign, imaging is the critical next step in the workup to help determine if the mass is benign or malignant.
Benign palpable masses include:
Figure 2. Fibroadenoma. On mammography, the craniocaudal (A) and mediolateral oblique (B) views with a bright metallic marker (arrows) show a round, well-circumscribed mass in the upper outer quadrant of the left breast. Ultrasonography (C) shows an oval, well-circumscribed, mildly heterogeneous, hypoechoic mass that is wider than tall, indicating a benign mass.
Cysts (Figure 1)
Fibroadenomas (Figure 2)
Prominent fat lobules
Lymph nodes
Oil cysts
Lipomas
Hamartomas (Figure 3)
Hematomas
Fat necrosis
Galactoceles.
Malignant palpable masses include:
Figure 3. Hamartoma. Craniocaudal (A) and mediolateral oblique (B) mammographic views of the left breast show an apparently encapsulated, heterogeneous mass that contains fat mixed with fibroglandular tissue.
Invasive ductal and lobular carcinoma (Figure 4)
Ductal carcinoma in situ (which rarely presents as a palpable mass.)
HISTORY AND PHYSICAL EXAMINATION
To ensure that imaging provides the most useful information about a palpable breast lump, it is important to first do a careful history and physical examination. Important aspects of the history include family history, personal history of breast cancer, and any previous breast biopsies. The onset and duration of the palpable mass, changes in its size, the relationship of these changes to the menstrual cycle, and the presence or lack of tenderness are additional important elements of the history.
Figure 4. Infiltrating ductal carcinoma. Craniocaudal (A) and mediolateral oblique (B) mammographic views of the right breast show an irregular, mildly spiculated, high-density lesion in the posterior, medial breast. Ultrasonography (C) shows an irregularly shaped hypoechoic mass which is taller than wide (a profile tending to indicate malignancy) and has mild posterior acoustic shadowing.
On examination, it is important to note the clock-face location, size, texture, tenderness, and mobility of the lump. Accompanying nipple discharge and skin erythema or retraction are also important to report. In addition to conveying the location of the mass to the radiologist, it is equally important that the patient know what features the physician feels. This way, if the clinical information from the ordering physician is not available at the time of the radiologic evaluation, the patient will be able to guide the radiologist to the region of concern.
IMAGING TECHNIQUES
Mammography and ultrasonography are the primary imaging studies for evaluating palpable breast masses. Typically, in women under age 30, ultrasonography is the first or the only test ordered to evaluate the abnormality.4 In women age 30 or older, diagnostic mammography is typically the first test ordered. If mammography indicates that the palpable mass is not benign, then ultrasonography is the next study to be done.3 Although a powerful tool, magnetic resonance imaging of the breast does not currently have a role in the workup of a palpable abnormality and should not be used as a decision-delaying tactic or in place of biopsy.
Screening or diagnostic mammography?
Mammography is used in both screening and diagnosis. Screening mammography consists of two standard views of each breast—craniocaudal and mediolateral oblique—and is appropriate for asymptomatic women.
Women age 30 or older who present with a palpable breast mass require diagnostic mammography, in which standard mammographic views are obtained, as well as additional views (eg, tangential or spot-compression views) to better define the area of clinical concern. In a tangential view, a metallic skin marker is placed on the skin overlying the site of the palpable abnormality.
On mammography, a suspicious palpable mass has an irregular shape with spiculated margins. A benign mass typically has a round shape with well-circumscribed margins. If the palpable abnormality is not mammographically benign (eg, if it does not look like a lymph node, lipoma, or degenerating fibroadenoma), then ultrasonography is performed.
Mammography is less sensitive in younger women (ie, under age 30) because their breast tissue tends to be dense and glandular, whereas the tissue becomes more “fat-replaced” with age.3
Ultrasonography plays a complementary role
Ultrasonography complements diagnostic mammography and can be used as a first imaging study to evaluate a palpable breast mass in a young woman (ie, under age 30) with dense breast tissue. Ultrasonography is helpful in distinguishing cystic lesions from solid masses. It helps the radiologist delineate the shape, borders, and acoustic properties of the mass. It is also performed when a palpable mass is mammographically occult. When a mass appears suspicious on either mammography or ultrasonography, ultrasonography can be used to guide biopsy.
A suspicious mass on ultrasonography classically appears “taller than wide” and has posterior acoustic shadowing. Microlobulations and a spiculated margin also raise concern for malignancy. A benign sonographic appearance of a palpable mass includes a “wider than tall” (ellipsoid) shape, with homogeneous echogenicity, and four or fewer gentle lobulations. A thin, echogenic capsule also suggests the mass is benign.
Core-needle biopsy with ultrasonographic guidance
Core-needle biopsy is performed with a large-diameter (14-gauge to 18-gauge) needle to obtain tissue cores for histologic analysis. It has gained popularity over fine-needle aspiration because it includes surrounding tissue architecture, thus providing a more definitive histologic diagnosis.
Pathologic information obtained from core-needle biopsy allows the radiologist and surgeon to counsel the patient and determine the best surgical management or follow-up imaging study. If a clinician performs fine-needle biopsy in the office, it should be preceded by an imaging workup of the palpable finding.
WHAT IS APPROPRIATE FOR OUR 28-YEAR-OLD PATIENT?
Because she is under age 30, ultrasonography is the initial study of choice to evaluate the mass. If a simple cyst is detected, she can be reassured that the lesion is benign, and no subsequent follow-up is required. If the lesion is a solid mass with benign features, mammography may be considered, the patient may be followed with short-interval imaging (every 6 months) depending on patient-specific factors such as family history, or the mass can be biopsied. If the lesion is a solid mass with suspicious or malignant features, mammography with spot-compression views should be performed, and the patient should undergo core-needle biopsy with ultrasonographic guidance.
In a patient age 30 or older, diagnostic mammography is the imaging study of first choice.3 If the mass is clearly benign on mammography, no additional imaging would be necessary. If mammography fails to image the mass or shows it to have benign features such as fat, then the patient can undergo ultrasonography for further evaluation and confirmation of the clinical and mammographic findings. If the mass appears suspicious or malignant on mammography, ultrasonography is the next step, as it can help characterize the lesion and be used to guide core-needle biopsy.
IF A PREGNANT WOMAN HAS A PALPABLE BREAST MASS
Most publications on breast cancer in pregnancy report a prevalence of 3 per 10,000 pregnancies, accounting for 3% of all breast cancers diagnosed.5 Therefore, imaging evaluation of a palpable mass should not be postponed.
Hormonal changes throughout pregnancy may increase the nodularity of breast tissue, raising the concern of palpable masses. Additionally, there is a higher prevalence of galactoceles and lactating adenomas in these patients. Because contrasting fatty breast tissue is lost during pregnancy and because of the need to minimize radiation exposure, ultrasonography is often the imaging test of first choice. If mammography is required, the radiation dose is very low and the patient’s abdomen and pelvis can be shielded.6 In this situation, the patient can be reassured that the imaging test is not jeopardizing her fetus.
WHAT WORKUP IS REQUIRED IN MEN?
Breast cancer in men is rare, accounting for less than 0.5% of all cases.7 Most often, a palpable breast mass in a man presents as unilateral gynecomastia. Gynecomastia occurs in a bimodal age distribution (in the 2nd and 7th decades) and has a variety of hormonal and drug-related causes. Despite the low prevalence of breast cancer in men, the combination of mammography and ultrasonography is recommended for evaluation at all ages.
References
Klein S. Evaluation of palpable breast masses. Am Fam Physician2005; 71:1731–1738.
Pruthi S. Detection and evaluation of a palpable breast mass. Mayo Clin Proc2001; 76:641–648.
Harvey JA. Sonography of palpable breast masses. Semin Ultrasound CT MR2006; 27:284–297.
Mehta TS. Current uses of ultrasound in the evaluation of the breast. Radiol Clin North Am2003; 41:841–856.
Gallenberg MM, Lopines CL. Breast cancer and pregnancy. Semin Oncol1989; 16:369–376.
Barnavon Y, Wallack MK. Management of the pregnant patient with carcinoma of the breast. Surg Gynecol Obstet1990; 171:347–352.
Cardenosa G. The Core Curriculum: Breast Imaging. Philadelphia: Lippincott Williams and Wilkins, 2003;304.
Lauren Stein, MD Imaging Institute, Cleveland Clinic
Melanie Chellman-Jeffers, MD Center for Specialized Women’s Health and Section of Breast Imaging, Department of Diagnostic Radiology, Imaging Institute, Cleveland Clinic
Address: Melanie Chellman-Jeffers, MD, Imaging Institute, Section of Breast Imaging, A10, Cleveland Clinic, 9500 Euclid Avenue, Cleveland, OH 44195; e-mail chellmm@ccf.org
Lauren Stein, MD Imaging Institute, Cleveland Clinic
Melanie Chellman-Jeffers, MD Center for Specialized Women’s Health and Section of Breast Imaging, Department of Diagnostic Radiology, Imaging Institute, Cleveland Clinic
Address: Melanie Chellman-Jeffers, MD, Imaging Institute, Section of Breast Imaging, A10, Cleveland Clinic, 9500 Euclid Avenue, Cleveland, OH 44195; e-mail chellmm@ccf.org
Author and Disclosure Information
Lauren Stein, MD Imaging Institute, Cleveland Clinic
Melanie Chellman-Jeffers, MD Center for Specialized Women’s Health and Section of Breast Imaging, Department of Diagnostic Radiology, Imaging Institute, Cleveland Clinic
Address: Melanie Chellman-Jeffers, MD, Imaging Institute, Section of Breast Imaging, A10, Cleveland Clinic, 9500 Euclid Avenue, Cleveland, OH 44195; e-mail chellmm@ccf.org
A 28-year-old woman comes in for her annual checkup. Her physician notices a palpable, painless, 1-cm, well-demarcated mass in the left breast at the 3 o’clock position 2 cm from the nipple, with no associated skin changes, nipple retraction, or discharge. The patient has no personal or family history of breast cancer.
Given the patient’s age, physical findings, and medical history, the clinician believes it unlikely that the patient has cancer. How should she proceed with the workup of this patient?
PHYSICAL FINDINGS OF A BREAST MASS ARE NOT EXCLUSIVE
Figure 1. A simple cyst in the left breast. All three mammographic views—craniocaudal (A), mediolateral oblique (B), and spot-compression (C)—show a round, well-circumscribed mass in the mid-breast. Ultrasonography (D) shows a round, well-circumscribed anechoic lesion with a sharply defined posterior wall and posterior acoustic enhancement.
Breast cancer is the most common female malignancy and the second-leading cause of cancer deaths in the United States.1 The incidence is low in young women and increases with advancing age. Benign breast disease is common in young women and less common in postmenopausal women.2,3 However, the discovery of a breast mass, whether by the woman herself or by a clinician, is a common occurrence and distressing for any woman.
Benign lesions tend to have discrete, well-defined margins and are typically mobile. Malignant lesions may be firm, may have indistinct borders, and are often immobile.2 Although most breast masses found by palpation are benign, imaging is the critical next step in the workup to help determine if the mass is benign or malignant.
Benign palpable masses include:
Figure 2. Fibroadenoma. On mammography, the craniocaudal (A) and mediolateral oblique (B) views with a bright metallic marker (arrows) show a round, well-circumscribed mass in the upper outer quadrant of the left breast. Ultrasonography (C) shows an oval, well-circumscribed, mildly heterogeneous, hypoechoic mass that is wider than tall, indicating a benign mass.
Cysts (Figure 1)
Fibroadenomas (Figure 2)
Prominent fat lobules
Lymph nodes
Oil cysts
Lipomas
Hamartomas (Figure 3)
Hematomas
Fat necrosis
Galactoceles.
Malignant palpable masses include:
Figure 3. Hamartoma. Craniocaudal (A) and mediolateral oblique (B) mammographic views of the left breast show an apparently encapsulated, heterogeneous mass that contains fat mixed with fibroglandular tissue.
Invasive ductal and lobular carcinoma (Figure 4)
Ductal carcinoma in situ (which rarely presents as a palpable mass.)
HISTORY AND PHYSICAL EXAMINATION
To ensure that imaging provides the most useful information about a palpable breast lump, it is important to first do a careful history and physical examination. Important aspects of the history include family history, personal history of breast cancer, and any previous breast biopsies. The onset and duration of the palpable mass, changes in its size, the relationship of these changes to the menstrual cycle, and the presence or lack of tenderness are additional important elements of the history.
Figure 4. Infiltrating ductal carcinoma. Craniocaudal (A) and mediolateral oblique (B) mammographic views of the right breast show an irregular, mildly spiculated, high-density lesion in the posterior, medial breast. Ultrasonography (C) shows an irregularly shaped hypoechoic mass which is taller than wide (a profile tending to indicate malignancy) and has mild posterior acoustic shadowing.
On examination, it is important to note the clock-face location, size, texture, tenderness, and mobility of the lump. Accompanying nipple discharge and skin erythema or retraction are also important to report. In addition to conveying the location of the mass to the radiologist, it is equally important that the patient know what features the physician feels. This way, if the clinical information from the ordering physician is not available at the time of the radiologic evaluation, the patient will be able to guide the radiologist to the region of concern.
IMAGING TECHNIQUES
Mammography and ultrasonography are the primary imaging studies for evaluating palpable breast masses. Typically, in women under age 30, ultrasonography is the first or the only test ordered to evaluate the abnormality.4 In women age 30 or older, diagnostic mammography is typically the first test ordered. If mammography indicates that the palpable mass is not benign, then ultrasonography is the next study to be done.3 Although a powerful tool, magnetic resonance imaging of the breast does not currently have a role in the workup of a palpable abnormality and should not be used as a decision-delaying tactic or in place of biopsy.
Screening or diagnostic mammography?
Mammography is used in both screening and diagnosis. Screening mammography consists of two standard views of each breast—craniocaudal and mediolateral oblique—and is appropriate for asymptomatic women.
Women age 30 or older who present with a palpable breast mass require diagnostic mammography, in which standard mammographic views are obtained, as well as additional views (eg, tangential or spot-compression views) to better define the area of clinical concern. In a tangential view, a metallic skin marker is placed on the skin overlying the site of the palpable abnormality.
On mammography, a suspicious palpable mass has an irregular shape with spiculated margins. A benign mass typically has a round shape with well-circumscribed margins. If the palpable abnormality is not mammographically benign (eg, if it does not look like a lymph node, lipoma, or degenerating fibroadenoma), then ultrasonography is performed.
Mammography is less sensitive in younger women (ie, under age 30) because their breast tissue tends to be dense and glandular, whereas the tissue becomes more “fat-replaced” with age.3
Ultrasonography plays a complementary role
Ultrasonography complements diagnostic mammography and can be used as a first imaging study to evaluate a palpable breast mass in a young woman (ie, under age 30) with dense breast tissue. Ultrasonography is helpful in distinguishing cystic lesions from solid masses. It helps the radiologist delineate the shape, borders, and acoustic properties of the mass. It is also performed when a palpable mass is mammographically occult. When a mass appears suspicious on either mammography or ultrasonography, ultrasonography can be used to guide biopsy.
A suspicious mass on ultrasonography classically appears “taller than wide” and has posterior acoustic shadowing. Microlobulations and a spiculated margin also raise concern for malignancy. A benign sonographic appearance of a palpable mass includes a “wider than tall” (ellipsoid) shape, with homogeneous echogenicity, and four or fewer gentle lobulations. A thin, echogenic capsule also suggests the mass is benign.
Core-needle biopsy with ultrasonographic guidance
Core-needle biopsy is performed with a large-diameter (14-gauge to 18-gauge) needle to obtain tissue cores for histologic analysis. It has gained popularity over fine-needle aspiration because it includes surrounding tissue architecture, thus providing a more definitive histologic diagnosis.
Pathologic information obtained from core-needle biopsy allows the radiologist and surgeon to counsel the patient and determine the best surgical management or follow-up imaging study. If a clinician performs fine-needle biopsy in the office, it should be preceded by an imaging workup of the palpable finding.
WHAT IS APPROPRIATE FOR OUR 28-YEAR-OLD PATIENT?
Because she is under age 30, ultrasonography is the initial study of choice to evaluate the mass. If a simple cyst is detected, she can be reassured that the lesion is benign, and no subsequent follow-up is required. If the lesion is a solid mass with benign features, mammography may be considered, the patient may be followed with short-interval imaging (every 6 months) depending on patient-specific factors such as family history, or the mass can be biopsied. If the lesion is a solid mass with suspicious or malignant features, mammography with spot-compression views should be performed, and the patient should undergo core-needle biopsy with ultrasonographic guidance.
In a patient age 30 or older, diagnostic mammography is the imaging study of first choice.3 If the mass is clearly benign on mammography, no additional imaging would be necessary. If mammography fails to image the mass or shows it to have benign features such as fat, then the patient can undergo ultrasonography for further evaluation and confirmation of the clinical and mammographic findings. If the mass appears suspicious or malignant on mammography, ultrasonography is the next step, as it can help characterize the lesion and be used to guide core-needle biopsy.
IF A PREGNANT WOMAN HAS A PALPABLE BREAST MASS
Most publications on breast cancer in pregnancy report a prevalence of 3 per 10,000 pregnancies, accounting for 3% of all breast cancers diagnosed.5 Therefore, imaging evaluation of a palpable mass should not be postponed.
Hormonal changes throughout pregnancy may increase the nodularity of breast tissue, raising the concern of palpable masses. Additionally, there is a higher prevalence of galactoceles and lactating adenomas in these patients. Because contrasting fatty breast tissue is lost during pregnancy and because of the need to minimize radiation exposure, ultrasonography is often the imaging test of first choice. If mammography is required, the radiation dose is very low and the patient’s abdomen and pelvis can be shielded.6 In this situation, the patient can be reassured that the imaging test is not jeopardizing her fetus.
WHAT WORKUP IS REQUIRED IN MEN?
Breast cancer in men is rare, accounting for less than 0.5% of all cases.7 Most often, a palpable breast mass in a man presents as unilateral gynecomastia. Gynecomastia occurs in a bimodal age distribution (in the 2nd and 7th decades) and has a variety of hormonal and drug-related causes. Despite the low prevalence of breast cancer in men, the combination of mammography and ultrasonography is recommended for evaluation at all ages.
A 28-year-old woman comes in for her annual checkup. Her physician notices a palpable, painless, 1-cm, well-demarcated mass in the left breast at the 3 o’clock position 2 cm from the nipple, with no associated skin changes, nipple retraction, or discharge. The patient has no personal or family history of breast cancer.
Given the patient’s age, physical findings, and medical history, the clinician believes it unlikely that the patient has cancer. How should she proceed with the workup of this patient?
PHYSICAL FINDINGS OF A BREAST MASS ARE NOT EXCLUSIVE
Figure 1. A simple cyst in the left breast. All three mammographic views—craniocaudal (A), mediolateral oblique (B), and spot-compression (C)—show a round, well-circumscribed mass in the mid-breast. Ultrasonography (D) shows a round, well-circumscribed anechoic lesion with a sharply defined posterior wall and posterior acoustic enhancement.
Breast cancer is the most common female malignancy and the second-leading cause of cancer deaths in the United States.1 The incidence is low in young women and increases with advancing age. Benign breast disease is common in young women and less common in postmenopausal women.2,3 However, the discovery of a breast mass, whether by the woman herself or by a clinician, is a common occurrence and distressing for any woman.
Benign lesions tend to have discrete, well-defined margins and are typically mobile. Malignant lesions may be firm, may have indistinct borders, and are often immobile.2 Although most breast masses found by palpation are benign, imaging is the critical next step in the workup to help determine if the mass is benign or malignant.
Benign palpable masses include:
Figure 2. Fibroadenoma. On mammography, the craniocaudal (A) and mediolateral oblique (B) views with a bright metallic marker (arrows) show a round, well-circumscribed mass in the upper outer quadrant of the left breast. Ultrasonography (C) shows an oval, well-circumscribed, mildly heterogeneous, hypoechoic mass that is wider than tall, indicating a benign mass.
Cysts (Figure 1)
Fibroadenomas (Figure 2)
Prominent fat lobules
Lymph nodes
Oil cysts
Lipomas
Hamartomas (Figure 3)
Hematomas
Fat necrosis
Galactoceles.
Malignant palpable masses include:
Figure 3. Hamartoma. Craniocaudal (A) and mediolateral oblique (B) mammographic views of the left breast show an apparently encapsulated, heterogeneous mass that contains fat mixed with fibroglandular tissue.
Invasive ductal and lobular carcinoma (Figure 4)
Ductal carcinoma in situ (which rarely presents as a palpable mass.)
HISTORY AND PHYSICAL EXAMINATION
To ensure that imaging provides the most useful information about a palpable breast lump, it is important to first do a careful history and physical examination. Important aspects of the history include family history, personal history of breast cancer, and any previous breast biopsies. The onset and duration of the palpable mass, changes in its size, the relationship of these changes to the menstrual cycle, and the presence or lack of tenderness are additional important elements of the history.
Figure 4. Infiltrating ductal carcinoma. Craniocaudal (A) and mediolateral oblique (B) mammographic views of the right breast show an irregular, mildly spiculated, high-density lesion in the posterior, medial breast. Ultrasonography (C) shows an irregularly shaped hypoechoic mass which is taller than wide (a profile tending to indicate malignancy) and has mild posterior acoustic shadowing.
On examination, it is important to note the clock-face location, size, texture, tenderness, and mobility of the lump. Accompanying nipple discharge and skin erythema or retraction are also important to report. In addition to conveying the location of the mass to the radiologist, it is equally important that the patient know what features the physician feels. This way, if the clinical information from the ordering physician is not available at the time of the radiologic evaluation, the patient will be able to guide the radiologist to the region of concern.
IMAGING TECHNIQUES
Mammography and ultrasonography are the primary imaging studies for evaluating palpable breast masses. Typically, in women under age 30, ultrasonography is the first or the only test ordered to evaluate the abnormality.4 In women age 30 or older, diagnostic mammography is typically the first test ordered. If mammography indicates that the palpable mass is not benign, then ultrasonography is the next study to be done.3 Although a powerful tool, magnetic resonance imaging of the breast does not currently have a role in the workup of a palpable abnormality and should not be used as a decision-delaying tactic or in place of biopsy.
Screening or diagnostic mammography?
Mammography is used in both screening and diagnosis. Screening mammography consists of two standard views of each breast—craniocaudal and mediolateral oblique—and is appropriate for asymptomatic women.
Women age 30 or older who present with a palpable breast mass require diagnostic mammography, in which standard mammographic views are obtained, as well as additional views (eg, tangential or spot-compression views) to better define the area of clinical concern. In a tangential view, a metallic skin marker is placed on the skin overlying the site of the palpable abnormality.
On mammography, a suspicious palpable mass has an irregular shape with spiculated margins. A benign mass typically has a round shape with well-circumscribed margins. If the palpable abnormality is not mammographically benign (eg, if it does not look like a lymph node, lipoma, or degenerating fibroadenoma), then ultrasonography is performed.
Mammography is less sensitive in younger women (ie, under age 30) because their breast tissue tends to be dense and glandular, whereas the tissue becomes more “fat-replaced” with age.3
Ultrasonography plays a complementary role
Ultrasonography complements diagnostic mammography and can be used as a first imaging study to evaluate a palpable breast mass in a young woman (ie, under age 30) with dense breast tissue. Ultrasonography is helpful in distinguishing cystic lesions from solid masses. It helps the radiologist delineate the shape, borders, and acoustic properties of the mass. It is also performed when a palpable mass is mammographically occult. When a mass appears suspicious on either mammography or ultrasonography, ultrasonography can be used to guide biopsy.
A suspicious mass on ultrasonography classically appears “taller than wide” and has posterior acoustic shadowing. Microlobulations and a spiculated margin also raise concern for malignancy. A benign sonographic appearance of a palpable mass includes a “wider than tall” (ellipsoid) shape, with homogeneous echogenicity, and four or fewer gentle lobulations. A thin, echogenic capsule also suggests the mass is benign.
Core-needle biopsy with ultrasonographic guidance
Core-needle biopsy is performed with a large-diameter (14-gauge to 18-gauge) needle to obtain tissue cores for histologic analysis. It has gained popularity over fine-needle aspiration because it includes surrounding tissue architecture, thus providing a more definitive histologic diagnosis.
Pathologic information obtained from core-needle biopsy allows the radiologist and surgeon to counsel the patient and determine the best surgical management or follow-up imaging study. If a clinician performs fine-needle biopsy in the office, it should be preceded by an imaging workup of the palpable finding.
WHAT IS APPROPRIATE FOR OUR 28-YEAR-OLD PATIENT?
Because she is under age 30, ultrasonography is the initial study of choice to evaluate the mass. If a simple cyst is detected, she can be reassured that the lesion is benign, and no subsequent follow-up is required. If the lesion is a solid mass with benign features, mammography may be considered, the patient may be followed with short-interval imaging (every 6 months) depending on patient-specific factors such as family history, or the mass can be biopsied. If the lesion is a solid mass with suspicious or malignant features, mammography with spot-compression views should be performed, and the patient should undergo core-needle biopsy with ultrasonographic guidance.
In a patient age 30 or older, diagnostic mammography is the imaging study of first choice.3 If the mass is clearly benign on mammography, no additional imaging would be necessary. If mammography fails to image the mass or shows it to have benign features such as fat, then the patient can undergo ultrasonography for further evaluation and confirmation of the clinical and mammographic findings. If the mass appears suspicious or malignant on mammography, ultrasonography is the next step, as it can help characterize the lesion and be used to guide core-needle biopsy.
IF A PREGNANT WOMAN HAS A PALPABLE BREAST MASS
Most publications on breast cancer in pregnancy report a prevalence of 3 per 10,000 pregnancies, accounting for 3% of all breast cancers diagnosed.5 Therefore, imaging evaluation of a palpable mass should not be postponed.
Hormonal changes throughout pregnancy may increase the nodularity of breast tissue, raising the concern of palpable masses. Additionally, there is a higher prevalence of galactoceles and lactating adenomas in these patients. Because contrasting fatty breast tissue is lost during pregnancy and because of the need to minimize radiation exposure, ultrasonography is often the imaging test of first choice. If mammography is required, the radiation dose is very low and the patient’s abdomen and pelvis can be shielded.6 In this situation, the patient can be reassured that the imaging test is not jeopardizing her fetus.
WHAT WORKUP IS REQUIRED IN MEN?
Breast cancer in men is rare, accounting for less than 0.5% of all cases.7 Most often, a palpable breast mass in a man presents as unilateral gynecomastia. Gynecomastia occurs in a bimodal age distribution (in the 2nd and 7th decades) and has a variety of hormonal and drug-related causes. Despite the low prevalence of breast cancer in men, the combination of mammography and ultrasonography is recommended for evaluation at all ages.
References
Klein S. Evaluation of palpable breast masses. Am Fam Physician2005; 71:1731–1738.
Pruthi S. Detection and evaluation of a palpable breast mass. Mayo Clin Proc2001; 76:641–648.
Harvey JA. Sonography of palpable breast masses. Semin Ultrasound CT MR2006; 27:284–297.
Mehta TS. Current uses of ultrasound in the evaluation of the breast. Radiol Clin North Am2003; 41:841–856.
Gallenberg MM, Lopines CL. Breast cancer and pregnancy. Semin Oncol1989; 16:369–376.
Barnavon Y, Wallack MK. Management of the pregnant patient with carcinoma of the breast. Surg Gynecol Obstet1990; 171:347–352.
Cardenosa G. The Core Curriculum: Breast Imaging. Philadelphia: Lippincott Williams and Wilkins, 2003;304.
References
Klein S. Evaluation of palpable breast masses. Am Fam Physician2005; 71:1731–1738.
Pruthi S. Detection and evaluation of a palpable breast mass. Mayo Clin Proc2001; 76:641–648.
Harvey JA. Sonography of palpable breast masses. Semin Ultrasound CT MR2006; 27:284–297.
Mehta TS. Current uses of ultrasound in the evaluation of the breast. Radiol Clin North Am2003; 41:841–856.
Gallenberg MM, Lopines CL. Breast cancer and pregnancy. Semin Oncol1989; 16:369–376.
Barnavon Y, Wallack MK. Management of the pregnant patient with carcinoma of the breast. Surg Gynecol Obstet1990; 171:347–352.
Cardenosa G. The Core Curriculum: Breast Imaging. Philadelphia: Lippincott Williams and Wilkins, 2003;304.
Typically, in women under age 30, ultrasonography is the first or the only test ordered to evaluate the abnormality. In women age 30 or older, diagnostic mammography is typically the first test ordered.
On mammography, a suspicious palpable mass has an irregular shape with spiculated margins. A benign mass typically has a round shape with well-circumscribed margins.
When mammography is required during pregnancy, the patient can be reassured that it will not jeopardize her fetus because the radiation dose is very low and the abdomen and pelvis can be shielded.
A 55-year-old woman presents with an intermittent sensation of food getting stuck in her mid to lower chest. The symptoms have occurred several times per year over the last 2 or 3 years and appear to be slowly worsening. She says she has no trouble swallowing liquids. She has a history of gastroesophageal reflux disease, for which she takes a proton pump inhibitor once a day. She says she has had no odynophagia, cough, regurgitation, or weight loss.
How should her symptoms best be evaluated?
DYSPHAGIA CAN BE OROPHARYNGEAL OR ESOPHAGEAL
Dysphagia is the subjective sensation of difficulty swallowing solids, liquids, or both. Symptoms can range from the inability to initiate a swallow to the sensation of esophageal obstruction. Other symptoms of esophageal disease may also be present, such as chest pain, heartburn, and regurgitation. There may also be nonesophageal symptoms related to the disease process causing the dysphagia.
Dysphagia can be separated into oropharyngeal and esophageal types.
Oropharyngeal dysphagia arises from problems in the oropharynx and cervical esophagus and is commonly caused by neurologic disorders of the central or peripheral nervous system (eg, stroke, myasthenia gravis), inflammatory myopathy, or a structural abnormality of the oropharynx, hypopharynx, or cervical esophagus such as a cricopharyngeal bar or tumor (Table 1). Patients typically complain of not being able to initiate a swallow or of food getting stuck in the cervical region immediately upon swallowing, accompanied by nasal regurgitation.1
Interestingly, many patients with symptoms of oropharyngeal dysphagia in fact have referred symptoms from primary esophageal dysphagia2; many patients with a distal mucosal ring describe a sense of something sticking in the cervical esophagus.
Esophageal dysphagia arises in the mid to distal esophagus or gastric cardia, and as a result, the symptoms are typically retrosternal.1 It can be caused by structural problems such as strictures, rings, webs, extrinsic compression, or a primary esophageal or gastroesophageal neoplasm, or by a primary motility abnormality such as achalasia (Table 1). Eosinophilic esophagitis is now a frequent cause of esophageal dysphagia, especially in white men.3
ESOPHAGOGRAPHY VS ENDOSCOPY IN EVALUATING DYSPHAGIA
Many gastroenterologists recommend endoscopy rather than barium esophagography as the initial examination in patients with dysphagia.4–8 Each test has certain advantages.
Advantages of endoscopy. Endoscopy is superior to esophagography in detecting milder grades of esophagitis. Further, interventions can be performed endoscopically (eg, dilation, biopsy, attachment of a wireless pH testing probe) that cannot be done during a radiographic procedure, and endoscopy does not expose the patient to radiation.
Advantages of esophagography. Endoscopy cannot detect evidence of gastroesophageal reflux disease unless mucosal injury is present. In dysphagia, the radiologic findings correlate well with endoscopic findings, including the detection of esophageal malignancy and moderate to severe esophagitis. Further, motility disorders can be detected with barium esophagography but not with endoscopy.9,10
Subtle abnormalities, especially rings and strictures, may be missed by narrow-diameter (9.8–10 mm) modern upper-endoscopic equipment. Further, esophagography is noninvasive, costs less, and may be more convenient (it does not require sedation and a chaperone for the patient after sedation). This examination also provides dynamic evaluation of the complex process of swallowing. Causes of dysphagia external to the esophagus can also be determined.
In view of the respective advantages and disadvantages of the two methods, we believe that in most instances barium esophagography should be the initial examination,1,9,11–15 and at our institution most patients presenting with dysphagia undergo barium esophagography before they undergo other examinations.14
OBTAIN A HISTORY BEFORE ORDERING ESOPHAGOGRAPHY
Before a barium examination of the esophagus is done, a focused medical history should be obtained, as it can guide the further workup as well as the esophageal study itself.
An attempt should be made to determine whether the dysphagia is oropharyngeal or if it is esophageal, as the former is generally best initially evaluated by a speech and language pathologist. Generally, the physician who orders the test judges whether the patient has oropharyngeal or esophageal dysphagia. Often, both an oropharyngeal examination, performed by a speech and language pathologist, and an esophageal examination, performed by a radiologist, are ordered.
Rapidly progressive symptoms, especially if accompanied by weight loss, should make one suspect cancer. Chronic symptoms usually point to gastroesophageal reflux disease or a motility disorder such as achalasia. Liquid dysphagia almost always means the patient has a motility disorder such as achalasia.
In view of the possibility of eosinophilic esophagitis, one should ask about food or seasonal allergies, especially in young patients with intermittent difficulty swallowing solids.3
BARIUM ESOPHAGOGRAPHY HAS EIGHT SEPARATE PHASES
Barium esophagography is tailored to the patient with dysphagia on the basis of his or her history. The standard examination is divided into eight separate phases (see below).14 Each phase addresses a specific question or questions concerning the structure and function of the esophagus.
At our institution, the first phase of the examination is determined by the presenting symptoms. If the patient has liquid dysphagia, we start with a timed barium swallow to assess esophageal emptying. If the patient does not have liquid dysphagia, we start with an air-contrast mucosal examination.
The patient must be cooperative and mobile to complete all phases of the examination.
Timed barium swallow to measure esophageal emptying
The timed barium swallow is an objective measure of esophageal emptying.16–18 This technique is essential in the initial evaluation of a patient with liquid dysphagia, a symptom common in patients with severe dysmotility, usually achalasia.
Figure 1. Timed barium swallow in a patient with achalasia. The patient consumed 140 mL of low-density barium. There is no emptying of barium between the 1-minute and 5-minute films.
In the upright position, the patient is asked to ingest up to 250 mL of low-density barium, as tolerated. The height and width of the barium column at 1 minute and 5 minutes are measured and recorded (Figure 1).
We use this examination in our patients with suspected or confirmed achalasia and to follow up patients who have been treated with pneumatic dilatation, botulinum toxin injection, and Heller myotomy.17,18 In addition, this timed test is an objective measure of emptying in patients who have undergone intervention but whose symptoms have not subjectively improved, and can suggest that further intervention may be required.
Air-contrast or mucosal phase
Figure 2. Esophagographic phases in a patient with solid-food dysphagia and a significant distal mucosal ring. A. The upright, mucosal phase of the examination shows no abnormalities. B. The distended or full-column phase of the examination shows the distal mucosal ring (arrow) as a sharply defined, ridge-like filling defect in the barium column above a small, sliding-type hiatal hernia (HH) (brought out by the increased intra-abdominal pressure with the patient in the semiprone position). C. The mucosal relief phase again shows the circumferential nature of the distal ring (arrows), as well as the hiatal hernia. D. Spontaneous reflux of gastric barium (arrows) with the patient in the supine position. The barium refluxed to the level of the thoracic inlet. E. Obstruction of the ingested 13-mm tablet (T) at the level of the distal mucosal ring. Barium above the tablet was given to precisely identify the location of the obstruction.
The air-contrast phase of the examination is designed to evaluate the esophageal mucosa and to determine if there is a fixed (nonreducible) hernia. In the upright position, the patient ingests CO2 gas-producing crystals with a small amount of water and then ingests high-density barium in order to coat the mucosa. Spot films are taken of the gas-distended, barium-coated esophagus (Figure 2A).
Although this phase is not as sensitive as endoscopy, it can detect masses, mucosal erosions, ulcers, and—most importantly in our experience—fixed hernias. Patients with a fixed hernia have a foreshortened esophagus, which is important to know about before repairing the hernia. Many esophageal surgeons believe that a foreshortened esophagus precludes a standard Nissen fundoplication and necessitates an esophageal lengthening procedure (ie, Collis gastroplasty with a Nissen fundoplication).14
Motility phase
The third phase examines esophageal motility. With the patient in a semiprone position, low-density barium is given in single swallows, separated by 25 to 30 seconds. The images are recorded on digital media to allow one to review them frame by frame.
The findings on this phase correlate well with those of manometry.19 This portion of the examination also uses impedance monitoring to assess bolus transfer, an aspect not evaluated by manometry.20,21 Impedance monitoring detects changes in resistance to current flow and correlates well with esophagraphic findings regarding bolus transfer.
While many patients with dysphagia also undergo esophageal manometry, the findings from this phase of the esophagographic examination may be the first indication of an esophageal motility disorder. In fact, this portion of the examination shows the distinct advantage of esophagography over endoscopy as the initial test in patients with dysphagia, as endoscopy may not identify patients with achalasia, especially early on.4
Single-contrast (full-column) phase to detect strictures, rings
The fourth phase of the esophagographic evaluation is the distended, single-contrast examination (Figure 2B). This is performed in the semiprone position with the patient rapidly drinking thin barium. It is done to detect esophageal strictures, rings, and contour abnormalities caused by extrinsic processes. Subtle abnormalities shown by this technique, including benign strictures and rings, are often not visualized with endoscopy.
Mucosal relief phase
The fifth phase is performed with a collapsed esophagus immediately after the distended, single-contrast phase, where spot films are taken of the barium-coated, collapsed esophagus (Figure 2C). This phase is used to evaluate thickened mucosal folds, a common finding in moderate to severe reflux esophagitis.
Reflux evaluation
Provocative maneuvers are used in the sixth phase to elicit gastroesophageal reflux (Figure 2D). With the patient supine, he or she is asked to roll side to side, do a Valsalva maneuver, and do a straight-leg raise. The patient then sips water in the supine position to assess for reflux (the water siphon test). If reflux is seen, the cause, the height of the reflux, and the duration of reflux retention are recorded.
Solid-bolus phase to assess strictures
In the seventh phase, the patient swallows a 13-mm barium tablet (Figure 2E). This allows one to assess the significance of a ring or stricture and to assess if dysphagia symptoms recur as a result of tablet obstruction. Subtle strictures that were not detected during the prior phases can also be detected using a tablet. If obstruction or impaired passage occurs, the site of obstruction and the presence or absence of symptoms are recorded.
Modified esophagography to assess the oropharynx
The final or eighth phase of barium esophagography is called “modified barium esophagography” or the modified barium swallow. However, it may be the first phase of the examination performed or the only portion of the examination performed, or it may not be performed at all.
Modified barium esophagography is used to define the anatomy of the oropharynx and to assess its function in swallowing.12 It may also guide rehabilitation strategies aimed at eliminating a patient’s swallowing symptoms.
Most patients referred for this test have sustained damage to the central nervous system or structures of the oropharynx, such as stroke or radiation therapy for laryngeal cancer. Many have difficulty in starting to swallow, aspirate when they try to swallow, or both.
In this test, thin liquids are given to the patient in escalating amounts. The patient is then given thicker foods, including thick liquids, purees, and food requiring chewing. If the patient has difficulty swallowing, intervention and therapeutic strategies are initiated. If the test is done by itself and the speech pathologist cannot find a cause of the patient’s symptoms, then barium esophagography should be performed by a radiologist.
The final esophagographic report should document the findings of each phase of the examination (Table 2).
WHAT HAPPENED TO OUR PATIENT?
Our patient underwent barium esophagography (Figure 2). A distal mucosal ring that transiently obstructed a 13-mm tablet was found. The patient underwent endoscopy and the ring was dilated. No biopsies were necessary.
References
Levine MS, Rubesin SE. Radiologic investigation of dysphagia. AJR Am J Roentgenol1990; 154:1157–1163.
Smith DF, Ott DJ, Gelfand DW, Chen MY. Lower esophageal mucosal ring: correlation of referred symptoms with radiographic findings using a marshmallow bolus. AJR Am J Roentgenol1998; 171:1361–1365.
Furuta GT, Liacouras CA, Collins MH, et al. Eosinophilic esophagitis in children and adults: a systematic review and consensus recommendations for diagnosis and treatment. Gastroenterology2007; 133:1342–1363.
Spechler SJ. American Gastroenterological Association medical position statement on treatment of patients with dysphagia caused by benign disorders of the distal esophagus. Gastroenterology1999; 117:229–233.
American Society for Gastrointestinal Endoscopy. Appropriate use of gastrointestinal endoscopy. Gastrointest Endosc2000; 52:831–837.
Esfandyari T, Potter JW, Vaezi MF. Dysphagia: a cost analysis of the diagnostic approach. Am J Gastroenterol2002; 97:2733–2737.
Varadarajulu S, Eloubeidi MA, Patel RS, et al. The yield and the predictors of esophageal pathology when upper endoscopy is used for the initial evaluation of dysphagia. Gastrointest Endosc2005; 61:804–808.
Standards of Practice Committee. Role of endoscopy in the management of GERD. Gastrointest Endosc2007; 66:219–224.
Halpert RD, Feczko PJ, Spickler EM, Ackerman LV. Radiological assessment of dysphagia with endoscopic correlation. Radiology1985; 157:599–602.
Ott DJ. Gastroesophageal reflux disease. Radiol Clin North Am1994; 32:1147–1166.
Ekberg O, Pokieser P. Radiologic evaluation of the dysphagic patient. Eur Radiol1997; 7:1285–1295.
Logemann JA. Role of the modified barium swallow in management of patients with dysphagia. Otolaryngol Head Neck Surg1997; 116:335–338.
Baker ME, Rice TW. Radiologic evaluation of the esophagus: methods and value in motility disorders and GERD. Semin Thorac Cardiovasc Surg2001; 13:201–225.
Baker ME, Einstein DM, Herts BR, et al. Gastroesophageal reflux disease: integrating the barium esophagram before and after antire-flux surgery. Radiology2007; 243:329–339.
Levine MS, Rubesin SE, Laufer I. Barium esophagography: a study for all seasons. Clin Gastroenterol Hepatol2008; 6:11–25.
deOliveira JM, Birgisson S, Doinoff C, et al. Timed barium swallow: a simple technique for evaluating esophageal emptying in patients with achalasia. AJR Am J Roentgenol1997; 169:473–479.
Kostic SV, Rice TW, Baker ME, et al. Time barium esophagram: a simple physiologic assessment for achalasia. J Thorac Cardiovasc Surg2000; 120:935–943.
Vaezi MF, Baker ME, Achkar E, Richter JE. Timed barium oesophagram: better predictor of long term success after pneumatic dilation in achalasia than symptom assessment. Gut2002; 50:765–770.
Hewson EG, Ott DJ, Dalton CB, Chen YM, Wu WC, Richter JE. Manometry and radiology. Complementary studies in the assessment of esophageal motility disorders. Gastroenterology1990; 98:626–632.
Imam H, Shay S, Ali A, Baker M. Bolus transit patterns in healthy subjects: a study using simultaneous impedance monitoring, video-esophagram, and esophageal manometry. Am J Physiol Gastrointest Liver Physiol2005;G1000–G1006.
Imam H, Baker M, Shay S. Simultaneous barium esophagram, impedance monitoring and manometry in patients with dysphagia due to a tight fundoplication [abstract]. Gastroenterology2004; 126:A-639.
Brian C. Allen, MD Imaging Institute, Cleveland Clinic
Mark E. Baker, MD Imaging Institute and Taussig Cancer Institute, Cleveland Clinic
Gary W. Falk, MD, MS Center for Swallowing and Esophageal Disorders, Digestive Disease Institute, and Taussig Cancer Institute, Cleveland Clinic; Professor of Medicine, Cleveland Clinic Lerner College of Medicine of Case, Western Reserve University
Address: Brian C. Allen, MD, Imaging Institute, Hb6, Cleveland Clinic, 9500 Euclid Avenue, Cleveland, OH; e-mail allenb@ccf.org
Brian C. Allen, MD Imaging Institute, Cleveland Clinic
Mark E. Baker, MD Imaging Institute and Taussig Cancer Institute, Cleveland Clinic
Gary W. Falk, MD, MS Center for Swallowing and Esophageal Disorders, Digestive Disease Institute, and Taussig Cancer Institute, Cleveland Clinic; Professor of Medicine, Cleveland Clinic Lerner College of Medicine of Case, Western Reserve University
Address: Brian C. Allen, MD, Imaging Institute, Hb6, Cleveland Clinic, 9500 Euclid Avenue, Cleveland, OH; e-mail allenb@ccf.org
Author and Disclosure Information
Brian C. Allen, MD Imaging Institute, Cleveland Clinic
Mark E. Baker, MD Imaging Institute and Taussig Cancer Institute, Cleveland Clinic
Gary W. Falk, MD, MS Center for Swallowing and Esophageal Disorders, Digestive Disease Institute, and Taussig Cancer Institute, Cleveland Clinic; Professor of Medicine, Cleveland Clinic Lerner College of Medicine of Case, Western Reserve University
Address: Brian C. Allen, MD, Imaging Institute, Hb6, Cleveland Clinic, 9500 Euclid Avenue, Cleveland, OH; e-mail allenb@ccf.org
A 55-year-old woman presents with an intermittent sensation of food getting stuck in her mid to lower chest. The symptoms have occurred several times per year over the last 2 or 3 years and appear to be slowly worsening. She says she has no trouble swallowing liquids. She has a history of gastroesophageal reflux disease, for which she takes a proton pump inhibitor once a day. She says she has had no odynophagia, cough, regurgitation, or weight loss.
How should her symptoms best be evaluated?
DYSPHAGIA CAN BE OROPHARYNGEAL OR ESOPHAGEAL
Dysphagia is the subjective sensation of difficulty swallowing solids, liquids, or both. Symptoms can range from the inability to initiate a swallow to the sensation of esophageal obstruction. Other symptoms of esophageal disease may also be present, such as chest pain, heartburn, and regurgitation. There may also be nonesophageal symptoms related to the disease process causing the dysphagia.
Dysphagia can be separated into oropharyngeal and esophageal types.
Oropharyngeal dysphagia arises from problems in the oropharynx and cervical esophagus and is commonly caused by neurologic disorders of the central or peripheral nervous system (eg, stroke, myasthenia gravis), inflammatory myopathy, or a structural abnormality of the oropharynx, hypopharynx, or cervical esophagus such as a cricopharyngeal bar or tumor (Table 1). Patients typically complain of not being able to initiate a swallow or of food getting stuck in the cervical region immediately upon swallowing, accompanied by nasal regurgitation.1
Interestingly, many patients with symptoms of oropharyngeal dysphagia in fact have referred symptoms from primary esophageal dysphagia2; many patients with a distal mucosal ring describe a sense of something sticking in the cervical esophagus.
Esophageal dysphagia arises in the mid to distal esophagus or gastric cardia, and as a result, the symptoms are typically retrosternal.1 It can be caused by structural problems such as strictures, rings, webs, extrinsic compression, or a primary esophageal or gastroesophageal neoplasm, or by a primary motility abnormality such as achalasia (Table 1). Eosinophilic esophagitis is now a frequent cause of esophageal dysphagia, especially in white men.3
ESOPHAGOGRAPHY VS ENDOSCOPY IN EVALUATING DYSPHAGIA
Many gastroenterologists recommend endoscopy rather than barium esophagography as the initial examination in patients with dysphagia.4–8 Each test has certain advantages.
Advantages of endoscopy. Endoscopy is superior to esophagography in detecting milder grades of esophagitis. Further, interventions can be performed endoscopically (eg, dilation, biopsy, attachment of a wireless pH testing probe) that cannot be done during a radiographic procedure, and endoscopy does not expose the patient to radiation.
Advantages of esophagography. Endoscopy cannot detect evidence of gastroesophageal reflux disease unless mucosal injury is present. In dysphagia, the radiologic findings correlate well with endoscopic findings, including the detection of esophageal malignancy and moderate to severe esophagitis. Further, motility disorders can be detected with barium esophagography but not with endoscopy.9,10
Subtle abnormalities, especially rings and strictures, may be missed by narrow-diameter (9.8–10 mm) modern upper-endoscopic equipment. Further, esophagography is noninvasive, costs less, and may be more convenient (it does not require sedation and a chaperone for the patient after sedation). This examination also provides dynamic evaluation of the complex process of swallowing. Causes of dysphagia external to the esophagus can also be determined.
In view of the respective advantages and disadvantages of the two methods, we believe that in most instances barium esophagography should be the initial examination,1,9,11–15 and at our institution most patients presenting with dysphagia undergo barium esophagography before they undergo other examinations.14
OBTAIN A HISTORY BEFORE ORDERING ESOPHAGOGRAPHY
Before a barium examination of the esophagus is done, a focused medical history should be obtained, as it can guide the further workup as well as the esophageal study itself.
An attempt should be made to determine whether the dysphagia is oropharyngeal or if it is esophageal, as the former is generally best initially evaluated by a speech and language pathologist. Generally, the physician who orders the test judges whether the patient has oropharyngeal or esophageal dysphagia. Often, both an oropharyngeal examination, performed by a speech and language pathologist, and an esophageal examination, performed by a radiologist, are ordered.
Rapidly progressive symptoms, especially if accompanied by weight loss, should make one suspect cancer. Chronic symptoms usually point to gastroesophageal reflux disease or a motility disorder such as achalasia. Liquid dysphagia almost always means the patient has a motility disorder such as achalasia.
In view of the possibility of eosinophilic esophagitis, one should ask about food or seasonal allergies, especially in young patients with intermittent difficulty swallowing solids.3
BARIUM ESOPHAGOGRAPHY HAS EIGHT SEPARATE PHASES
Barium esophagography is tailored to the patient with dysphagia on the basis of his or her history. The standard examination is divided into eight separate phases (see below).14 Each phase addresses a specific question or questions concerning the structure and function of the esophagus.
At our institution, the first phase of the examination is determined by the presenting symptoms. If the patient has liquid dysphagia, we start with a timed barium swallow to assess esophageal emptying. If the patient does not have liquid dysphagia, we start with an air-contrast mucosal examination.
The patient must be cooperative and mobile to complete all phases of the examination.
Timed barium swallow to measure esophageal emptying
The timed barium swallow is an objective measure of esophageal emptying.16–18 This technique is essential in the initial evaluation of a patient with liquid dysphagia, a symptom common in patients with severe dysmotility, usually achalasia.
Figure 1. Timed barium swallow in a patient with achalasia. The patient consumed 140 mL of low-density barium. There is no emptying of barium between the 1-minute and 5-minute films.
In the upright position, the patient is asked to ingest up to 250 mL of low-density barium, as tolerated. The height and width of the barium column at 1 minute and 5 minutes are measured and recorded (Figure 1).
We use this examination in our patients with suspected or confirmed achalasia and to follow up patients who have been treated with pneumatic dilatation, botulinum toxin injection, and Heller myotomy.17,18 In addition, this timed test is an objective measure of emptying in patients who have undergone intervention but whose symptoms have not subjectively improved, and can suggest that further intervention may be required.
Air-contrast or mucosal phase
Figure 2. Esophagographic phases in a patient with solid-food dysphagia and a significant distal mucosal ring. A. The upright, mucosal phase of the examination shows no abnormalities. B. The distended or full-column phase of the examination shows the distal mucosal ring (arrow) as a sharply defined, ridge-like filling defect in the barium column above a small, sliding-type hiatal hernia (HH) (brought out by the increased intra-abdominal pressure with the patient in the semiprone position). C. The mucosal relief phase again shows the circumferential nature of the distal ring (arrows), as well as the hiatal hernia. D. Spontaneous reflux of gastric barium (arrows) with the patient in the supine position. The barium refluxed to the level of the thoracic inlet. E. Obstruction of the ingested 13-mm tablet (T) at the level of the distal mucosal ring. Barium above the tablet was given to precisely identify the location of the obstruction.
The air-contrast phase of the examination is designed to evaluate the esophageal mucosa and to determine if there is a fixed (nonreducible) hernia. In the upright position, the patient ingests CO2 gas-producing crystals with a small amount of water and then ingests high-density barium in order to coat the mucosa. Spot films are taken of the gas-distended, barium-coated esophagus (Figure 2A).
Although this phase is not as sensitive as endoscopy, it can detect masses, mucosal erosions, ulcers, and—most importantly in our experience—fixed hernias. Patients with a fixed hernia have a foreshortened esophagus, which is important to know about before repairing the hernia. Many esophageal surgeons believe that a foreshortened esophagus precludes a standard Nissen fundoplication and necessitates an esophageal lengthening procedure (ie, Collis gastroplasty with a Nissen fundoplication).14
Motility phase
The third phase examines esophageal motility. With the patient in a semiprone position, low-density barium is given in single swallows, separated by 25 to 30 seconds. The images are recorded on digital media to allow one to review them frame by frame.
The findings on this phase correlate well with those of manometry.19 This portion of the examination also uses impedance monitoring to assess bolus transfer, an aspect not evaluated by manometry.20,21 Impedance monitoring detects changes in resistance to current flow and correlates well with esophagraphic findings regarding bolus transfer.
While many patients with dysphagia also undergo esophageal manometry, the findings from this phase of the esophagographic examination may be the first indication of an esophageal motility disorder. In fact, this portion of the examination shows the distinct advantage of esophagography over endoscopy as the initial test in patients with dysphagia, as endoscopy may not identify patients with achalasia, especially early on.4
Single-contrast (full-column) phase to detect strictures, rings
The fourth phase of the esophagographic evaluation is the distended, single-contrast examination (Figure 2B). This is performed in the semiprone position with the patient rapidly drinking thin barium. It is done to detect esophageal strictures, rings, and contour abnormalities caused by extrinsic processes. Subtle abnormalities shown by this technique, including benign strictures and rings, are often not visualized with endoscopy.
Mucosal relief phase
The fifth phase is performed with a collapsed esophagus immediately after the distended, single-contrast phase, where spot films are taken of the barium-coated, collapsed esophagus (Figure 2C). This phase is used to evaluate thickened mucosal folds, a common finding in moderate to severe reflux esophagitis.
Reflux evaluation
Provocative maneuvers are used in the sixth phase to elicit gastroesophageal reflux (Figure 2D). With the patient supine, he or she is asked to roll side to side, do a Valsalva maneuver, and do a straight-leg raise. The patient then sips water in the supine position to assess for reflux (the water siphon test). If reflux is seen, the cause, the height of the reflux, and the duration of reflux retention are recorded.
Solid-bolus phase to assess strictures
In the seventh phase, the patient swallows a 13-mm barium tablet (Figure 2E). This allows one to assess the significance of a ring or stricture and to assess if dysphagia symptoms recur as a result of tablet obstruction. Subtle strictures that were not detected during the prior phases can also be detected using a tablet. If obstruction or impaired passage occurs, the site of obstruction and the presence or absence of symptoms are recorded.
Modified esophagography to assess the oropharynx
The final or eighth phase of barium esophagography is called “modified barium esophagography” or the modified barium swallow. However, it may be the first phase of the examination performed or the only portion of the examination performed, or it may not be performed at all.
Modified barium esophagography is used to define the anatomy of the oropharynx and to assess its function in swallowing.12 It may also guide rehabilitation strategies aimed at eliminating a patient’s swallowing symptoms.
Most patients referred for this test have sustained damage to the central nervous system or structures of the oropharynx, such as stroke or radiation therapy for laryngeal cancer. Many have difficulty in starting to swallow, aspirate when they try to swallow, or both.
In this test, thin liquids are given to the patient in escalating amounts. The patient is then given thicker foods, including thick liquids, purees, and food requiring chewing. If the patient has difficulty swallowing, intervention and therapeutic strategies are initiated. If the test is done by itself and the speech pathologist cannot find a cause of the patient’s symptoms, then barium esophagography should be performed by a radiologist.
The final esophagographic report should document the findings of each phase of the examination (Table 2).
WHAT HAPPENED TO OUR PATIENT?
Our patient underwent barium esophagography (Figure 2). A distal mucosal ring that transiently obstructed a 13-mm tablet was found. The patient underwent endoscopy and the ring was dilated. No biopsies were necessary.
A 55-year-old woman presents with an intermittent sensation of food getting stuck in her mid to lower chest. The symptoms have occurred several times per year over the last 2 or 3 years and appear to be slowly worsening. She says she has no trouble swallowing liquids. She has a history of gastroesophageal reflux disease, for which she takes a proton pump inhibitor once a day. She says she has had no odynophagia, cough, regurgitation, or weight loss.
How should her symptoms best be evaluated?
DYSPHAGIA CAN BE OROPHARYNGEAL OR ESOPHAGEAL
Dysphagia is the subjective sensation of difficulty swallowing solids, liquids, or both. Symptoms can range from the inability to initiate a swallow to the sensation of esophageal obstruction. Other symptoms of esophageal disease may also be present, such as chest pain, heartburn, and regurgitation. There may also be nonesophageal symptoms related to the disease process causing the dysphagia.
Dysphagia can be separated into oropharyngeal and esophageal types.
Oropharyngeal dysphagia arises from problems in the oropharynx and cervical esophagus and is commonly caused by neurologic disorders of the central or peripheral nervous system (eg, stroke, myasthenia gravis), inflammatory myopathy, or a structural abnormality of the oropharynx, hypopharynx, or cervical esophagus such as a cricopharyngeal bar or tumor (Table 1). Patients typically complain of not being able to initiate a swallow or of food getting stuck in the cervical region immediately upon swallowing, accompanied by nasal regurgitation.1
Interestingly, many patients with symptoms of oropharyngeal dysphagia in fact have referred symptoms from primary esophageal dysphagia2; many patients with a distal mucosal ring describe a sense of something sticking in the cervical esophagus.
Esophageal dysphagia arises in the mid to distal esophagus or gastric cardia, and as a result, the symptoms are typically retrosternal.1 It can be caused by structural problems such as strictures, rings, webs, extrinsic compression, or a primary esophageal or gastroesophageal neoplasm, or by a primary motility abnormality such as achalasia (Table 1). Eosinophilic esophagitis is now a frequent cause of esophageal dysphagia, especially in white men.3
ESOPHAGOGRAPHY VS ENDOSCOPY IN EVALUATING DYSPHAGIA
Many gastroenterologists recommend endoscopy rather than barium esophagography as the initial examination in patients with dysphagia.4–8 Each test has certain advantages.
Advantages of endoscopy. Endoscopy is superior to esophagography in detecting milder grades of esophagitis. Further, interventions can be performed endoscopically (eg, dilation, biopsy, attachment of a wireless pH testing probe) that cannot be done during a radiographic procedure, and endoscopy does not expose the patient to radiation.
Advantages of esophagography. Endoscopy cannot detect evidence of gastroesophageal reflux disease unless mucosal injury is present. In dysphagia, the radiologic findings correlate well with endoscopic findings, including the detection of esophageal malignancy and moderate to severe esophagitis. Further, motility disorders can be detected with barium esophagography but not with endoscopy.9,10
Subtle abnormalities, especially rings and strictures, may be missed by narrow-diameter (9.8–10 mm) modern upper-endoscopic equipment. Further, esophagography is noninvasive, costs less, and may be more convenient (it does not require sedation and a chaperone for the patient after sedation). This examination also provides dynamic evaluation of the complex process of swallowing. Causes of dysphagia external to the esophagus can also be determined.
In view of the respective advantages and disadvantages of the two methods, we believe that in most instances barium esophagography should be the initial examination,1,9,11–15 and at our institution most patients presenting with dysphagia undergo barium esophagography before they undergo other examinations.14
OBTAIN A HISTORY BEFORE ORDERING ESOPHAGOGRAPHY
Before a barium examination of the esophagus is done, a focused medical history should be obtained, as it can guide the further workup as well as the esophageal study itself.
An attempt should be made to determine whether the dysphagia is oropharyngeal or if it is esophageal, as the former is generally best initially evaluated by a speech and language pathologist. Generally, the physician who orders the test judges whether the patient has oropharyngeal or esophageal dysphagia. Often, both an oropharyngeal examination, performed by a speech and language pathologist, and an esophageal examination, performed by a radiologist, are ordered.
Rapidly progressive symptoms, especially if accompanied by weight loss, should make one suspect cancer. Chronic symptoms usually point to gastroesophageal reflux disease or a motility disorder such as achalasia. Liquid dysphagia almost always means the patient has a motility disorder such as achalasia.
In view of the possibility of eosinophilic esophagitis, one should ask about food or seasonal allergies, especially in young patients with intermittent difficulty swallowing solids.3
BARIUM ESOPHAGOGRAPHY HAS EIGHT SEPARATE PHASES
Barium esophagography is tailored to the patient with dysphagia on the basis of his or her history. The standard examination is divided into eight separate phases (see below).14 Each phase addresses a specific question or questions concerning the structure and function of the esophagus.
At our institution, the first phase of the examination is determined by the presenting symptoms. If the patient has liquid dysphagia, we start with a timed barium swallow to assess esophageal emptying. If the patient does not have liquid dysphagia, we start with an air-contrast mucosal examination.
The patient must be cooperative and mobile to complete all phases of the examination.
Timed barium swallow to measure esophageal emptying
The timed barium swallow is an objective measure of esophageal emptying.16–18 This technique is essential in the initial evaluation of a patient with liquid dysphagia, a symptom common in patients with severe dysmotility, usually achalasia.
Figure 1. Timed barium swallow in a patient with achalasia. The patient consumed 140 mL of low-density barium. There is no emptying of barium between the 1-minute and 5-minute films.
In the upright position, the patient is asked to ingest up to 250 mL of low-density barium, as tolerated. The height and width of the barium column at 1 minute and 5 minutes are measured and recorded (Figure 1).
We use this examination in our patients with suspected or confirmed achalasia and to follow up patients who have been treated with pneumatic dilatation, botulinum toxin injection, and Heller myotomy.17,18 In addition, this timed test is an objective measure of emptying in patients who have undergone intervention but whose symptoms have not subjectively improved, and can suggest that further intervention may be required.
Air-contrast or mucosal phase
Figure 2. Esophagographic phases in a patient with solid-food dysphagia and a significant distal mucosal ring. A. The upright, mucosal phase of the examination shows no abnormalities. B. The distended or full-column phase of the examination shows the distal mucosal ring (arrow) as a sharply defined, ridge-like filling defect in the barium column above a small, sliding-type hiatal hernia (HH) (brought out by the increased intra-abdominal pressure with the patient in the semiprone position). C. The mucosal relief phase again shows the circumferential nature of the distal ring (arrows), as well as the hiatal hernia. D. Spontaneous reflux of gastric barium (arrows) with the patient in the supine position. The barium refluxed to the level of the thoracic inlet. E. Obstruction of the ingested 13-mm tablet (T) at the level of the distal mucosal ring. Barium above the tablet was given to precisely identify the location of the obstruction.
The air-contrast phase of the examination is designed to evaluate the esophageal mucosa and to determine if there is a fixed (nonreducible) hernia. In the upright position, the patient ingests CO2 gas-producing crystals with a small amount of water and then ingests high-density barium in order to coat the mucosa. Spot films are taken of the gas-distended, barium-coated esophagus (Figure 2A).
Although this phase is not as sensitive as endoscopy, it can detect masses, mucosal erosions, ulcers, and—most importantly in our experience—fixed hernias. Patients with a fixed hernia have a foreshortened esophagus, which is important to know about before repairing the hernia. Many esophageal surgeons believe that a foreshortened esophagus precludes a standard Nissen fundoplication and necessitates an esophageal lengthening procedure (ie, Collis gastroplasty with a Nissen fundoplication).14
Motility phase
The third phase examines esophageal motility. With the patient in a semiprone position, low-density barium is given in single swallows, separated by 25 to 30 seconds. The images are recorded on digital media to allow one to review them frame by frame.
The findings on this phase correlate well with those of manometry.19 This portion of the examination also uses impedance monitoring to assess bolus transfer, an aspect not evaluated by manometry.20,21 Impedance monitoring detects changes in resistance to current flow and correlates well with esophagraphic findings regarding bolus transfer.
While many patients with dysphagia also undergo esophageal manometry, the findings from this phase of the esophagographic examination may be the first indication of an esophageal motility disorder. In fact, this portion of the examination shows the distinct advantage of esophagography over endoscopy as the initial test in patients with dysphagia, as endoscopy may not identify patients with achalasia, especially early on.4
Single-contrast (full-column) phase to detect strictures, rings
The fourth phase of the esophagographic evaluation is the distended, single-contrast examination (Figure 2B). This is performed in the semiprone position with the patient rapidly drinking thin barium. It is done to detect esophageal strictures, rings, and contour abnormalities caused by extrinsic processes. Subtle abnormalities shown by this technique, including benign strictures and rings, are often not visualized with endoscopy.
Mucosal relief phase
The fifth phase is performed with a collapsed esophagus immediately after the distended, single-contrast phase, where spot films are taken of the barium-coated, collapsed esophagus (Figure 2C). This phase is used to evaluate thickened mucosal folds, a common finding in moderate to severe reflux esophagitis.
Reflux evaluation
Provocative maneuvers are used in the sixth phase to elicit gastroesophageal reflux (Figure 2D). With the patient supine, he or she is asked to roll side to side, do a Valsalva maneuver, and do a straight-leg raise. The patient then sips water in the supine position to assess for reflux (the water siphon test). If reflux is seen, the cause, the height of the reflux, and the duration of reflux retention are recorded.
Solid-bolus phase to assess strictures
In the seventh phase, the patient swallows a 13-mm barium tablet (Figure 2E). This allows one to assess the significance of a ring or stricture and to assess if dysphagia symptoms recur as a result of tablet obstruction. Subtle strictures that were not detected during the prior phases can also be detected using a tablet. If obstruction or impaired passage occurs, the site of obstruction and the presence or absence of symptoms are recorded.
Modified esophagography to assess the oropharynx
The final or eighth phase of barium esophagography is called “modified barium esophagography” or the modified barium swallow. However, it may be the first phase of the examination performed or the only portion of the examination performed, or it may not be performed at all.
Modified barium esophagography is used to define the anatomy of the oropharynx and to assess its function in swallowing.12 It may also guide rehabilitation strategies aimed at eliminating a patient’s swallowing symptoms.
Most patients referred for this test have sustained damage to the central nervous system or structures of the oropharynx, such as stroke or radiation therapy for laryngeal cancer. Many have difficulty in starting to swallow, aspirate when they try to swallow, or both.
In this test, thin liquids are given to the patient in escalating amounts. The patient is then given thicker foods, including thick liquids, purees, and food requiring chewing. If the patient has difficulty swallowing, intervention and therapeutic strategies are initiated. If the test is done by itself and the speech pathologist cannot find a cause of the patient’s symptoms, then barium esophagography should be performed by a radiologist.
The final esophagographic report should document the findings of each phase of the examination (Table 2).
WHAT HAPPENED TO OUR PATIENT?
Our patient underwent barium esophagography (Figure 2). A distal mucosal ring that transiently obstructed a 13-mm tablet was found. The patient underwent endoscopy and the ring was dilated. No biopsies were necessary.
References
Levine MS, Rubesin SE. Radiologic investigation of dysphagia. AJR Am J Roentgenol1990; 154:1157–1163.
Smith DF, Ott DJ, Gelfand DW, Chen MY. Lower esophageal mucosal ring: correlation of referred symptoms with radiographic findings using a marshmallow bolus. AJR Am J Roentgenol1998; 171:1361–1365.
Furuta GT, Liacouras CA, Collins MH, et al. Eosinophilic esophagitis in children and adults: a systematic review and consensus recommendations for diagnosis and treatment. Gastroenterology2007; 133:1342–1363.
Spechler SJ. American Gastroenterological Association medical position statement on treatment of patients with dysphagia caused by benign disorders of the distal esophagus. Gastroenterology1999; 117:229–233.
American Society for Gastrointestinal Endoscopy. Appropriate use of gastrointestinal endoscopy. Gastrointest Endosc2000; 52:831–837.
Esfandyari T, Potter JW, Vaezi MF. Dysphagia: a cost analysis of the diagnostic approach. Am J Gastroenterol2002; 97:2733–2737.
Varadarajulu S, Eloubeidi MA, Patel RS, et al. The yield and the predictors of esophageal pathology when upper endoscopy is used for the initial evaluation of dysphagia. Gastrointest Endosc2005; 61:804–808.
Standards of Practice Committee. Role of endoscopy in the management of GERD. Gastrointest Endosc2007; 66:219–224.
Halpert RD, Feczko PJ, Spickler EM, Ackerman LV. Radiological assessment of dysphagia with endoscopic correlation. Radiology1985; 157:599–602.
Ott DJ. Gastroesophageal reflux disease. Radiol Clin North Am1994; 32:1147–1166.
Ekberg O, Pokieser P. Radiologic evaluation of the dysphagic patient. Eur Radiol1997; 7:1285–1295.
Logemann JA. Role of the modified barium swallow in management of patients with dysphagia. Otolaryngol Head Neck Surg1997; 116:335–338.
Baker ME, Rice TW. Radiologic evaluation of the esophagus: methods and value in motility disorders and GERD. Semin Thorac Cardiovasc Surg2001; 13:201–225.
Baker ME, Einstein DM, Herts BR, et al. Gastroesophageal reflux disease: integrating the barium esophagram before and after antire-flux surgery. Radiology2007; 243:329–339.
Levine MS, Rubesin SE, Laufer I. Barium esophagography: a study for all seasons. Clin Gastroenterol Hepatol2008; 6:11–25.
deOliveira JM, Birgisson S, Doinoff C, et al. Timed barium swallow: a simple technique for evaluating esophageal emptying in patients with achalasia. AJR Am J Roentgenol1997; 169:473–479.
Kostic SV, Rice TW, Baker ME, et al. Time barium esophagram: a simple physiologic assessment for achalasia. J Thorac Cardiovasc Surg2000; 120:935–943.
Vaezi MF, Baker ME, Achkar E, Richter JE. Timed barium oesophagram: better predictor of long term success after pneumatic dilation in achalasia than symptom assessment. Gut2002; 50:765–770.
Hewson EG, Ott DJ, Dalton CB, Chen YM, Wu WC, Richter JE. Manometry and radiology. Complementary studies in the assessment of esophageal motility disorders. Gastroenterology1990; 98:626–632.
Imam H, Shay S, Ali A, Baker M. Bolus transit patterns in healthy subjects: a study using simultaneous impedance monitoring, video-esophagram, and esophageal manometry. Am J Physiol Gastrointest Liver Physiol2005;G1000–G1006.
Imam H, Baker M, Shay S. Simultaneous barium esophagram, impedance monitoring and manometry in patients with dysphagia due to a tight fundoplication [abstract]. Gastroenterology2004; 126:A-639.
References
Levine MS, Rubesin SE. Radiologic investigation of dysphagia. AJR Am J Roentgenol1990; 154:1157–1163.
Smith DF, Ott DJ, Gelfand DW, Chen MY. Lower esophageal mucosal ring: correlation of referred symptoms with radiographic findings using a marshmallow bolus. AJR Am J Roentgenol1998; 171:1361–1365.
Furuta GT, Liacouras CA, Collins MH, et al. Eosinophilic esophagitis in children and adults: a systematic review and consensus recommendations for diagnosis and treatment. Gastroenterology2007; 133:1342–1363.
Spechler SJ. American Gastroenterological Association medical position statement on treatment of patients with dysphagia caused by benign disorders of the distal esophagus. Gastroenterology1999; 117:229–233.
American Society for Gastrointestinal Endoscopy. Appropriate use of gastrointestinal endoscopy. Gastrointest Endosc2000; 52:831–837.
Esfandyari T, Potter JW, Vaezi MF. Dysphagia: a cost analysis of the diagnostic approach. Am J Gastroenterol2002; 97:2733–2737.
Varadarajulu S, Eloubeidi MA, Patel RS, et al. The yield and the predictors of esophageal pathology when upper endoscopy is used for the initial evaluation of dysphagia. Gastrointest Endosc2005; 61:804–808.
Standards of Practice Committee. Role of endoscopy in the management of GERD. Gastrointest Endosc2007; 66:219–224.
Halpert RD, Feczko PJ, Spickler EM, Ackerman LV. Radiological assessment of dysphagia with endoscopic correlation. Radiology1985; 157:599–602.
Ott DJ. Gastroesophageal reflux disease. Radiol Clin North Am1994; 32:1147–1166.
Ekberg O, Pokieser P. Radiologic evaluation of the dysphagic patient. Eur Radiol1997; 7:1285–1295.
Logemann JA. Role of the modified barium swallow in management of patients with dysphagia. Otolaryngol Head Neck Surg1997; 116:335–338.
Baker ME, Rice TW. Radiologic evaluation of the esophagus: methods and value in motility disorders and GERD. Semin Thorac Cardiovasc Surg2001; 13:201–225.
Baker ME, Einstein DM, Herts BR, et al. Gastroesophageal reflux disease: integrating the barium esophagram before and after antire-flux surgery. Radiology2007; 243:329–339.
Levine MS, Rubesin SE, Laufer I. Barium esophagography: a study for all seasons. Clin Gastroenterol Hepatol2008; 6:11–25.
deOliveira JM, Birgisson S, Doinoff C, et al. Timed barium swallow: a simple technique for evaluating esophageal emptying in patients with achalasia. AJR Am J Roentgenol1997; 169:473–479.
Kostic SV, Rice TW, Baker ME, et al. Time barium esophagram: a simple physiologic assessment for achalasia. J Thorac Cardiovasc Surg2000; 120:935–943.
Vaezi MF, Baker ME, Achkar E, Richter JE. Timed barium oesophagram: better predictor of long term success after pneumatic dilation in achalasia than symptom assessment. Gut2002; 50:765–770.
Hewson EG, Ott DJ, Dalton CB, Chen YM, Wu WC, Richter JE. Manometry and radiology. Complementary studies in the assessment of esophageal motility disorders. Gastroenterology1990; 98:626–632.
Imam H, Shay S, Ali A, Baker M. Bolus transit patterns in healthy subjects: a study using simultaneous impedance monitoring, video-esophagram, and esophageal manometry. Am J Physiol Gastrointest Liver Physiol2005;G1000–G1006.
Imam H, Baker M, Shay S. Simultaneous barium esophagram, impedance monitoring and manometry in patients with dysphagia due to a tight fundoplication [abstract]. Gastroenterology2004; 126:A-639.
Dysphagia can be due to problems in the oropharynx and cervical esophagus or in the distal esophagus.
Radiologic evaluation of dysphagia has distinct advantages over endoscopy, including its ability to diagnose both structural changes and motility disorders.
A barium evaluation can include a modified barium-swallowing study to evaluate the oropharynx, barium esophagography to evaluate the esophagus, and a timed study to evaluate esophageal emptying.
Often, the true cause of dysphagia is best approached with a combination of radiographic and endoscopic studies.
A 44-year-old man comes to the emergency room because of light-headedness and fatigue. He says he has had several similar but milder episodes in the last several months. He also mentions that he thinks he has been coughing up blood. He says he has no major medical or surgical problems of which he is aware, but he appears confused and unable to give an accurate history. No family members can be contacted for further history at the moment.
Physical examination reveals nothing remarkable, but the patient does cough up some blood during the examination. His hemoglobin level is 6.0 g/dL (reference range 13.5–17.5).
What imaging tests would be helpful in this patient’s evaluation?
HEMOPTYSIS HAS MANY CAUSES
Hemoptysis is defined as the expectoration of blood originating from the tracheobronchial tree or the pulmonary parenchyma.
Most cases of hemoptysis are benign and self-limited; life-threatening hemoptysis is rare.1–3 However, hemoptysis can be a sign of serious tracheopulmonary disease.
The bleeding can be from the large (Table 1)or the small (Table 2) pulmonary vessels. Bleeding from the small vessels is known as diffuse alveolar hemorrhage, and it characteristically presents as alveolar infiltrates on chest radiography. In these cases, further imaging studies provide little benefit.4 This paper will focus on the imaging of and radiographic interventions for large-vessel bleeding.
The causes of hemoptysis are numerous; common causes of bleeding from the large vessels nowadays include bronchiectasis, fungal infections, tuberculosis, and cancer.1,5,6 Still, no cause is identified in 15% to 30% of all cases,1,2,5 even after extensive evaluation.
Definition of ‘massive’ hemoptysis can vary
Various definitions of the severity of hemoptysis have been proposed. The threshold of “massive” hemoptysis has been defined as as low as 100 mL/24 hours and as high as 1 L/24 hours; the most common definition is 300 mL, or about 1 cup.2,3,5–10
However, the patient’s cardiorespiratory status must also be considered.5,6,9 If the patient cannot maintain his or her airway, a small amount of bleeding could be life-threatening and should be considered significant or massive. Thus, we define massive hemoptysis as more than 300 mL of blood within 24 hours or any amount of blood with concurrent cardiorespiratory compromise.
It is important to recognize massive hemoptysis quickly, because without urgent treatment, up to 80% of patients may die.5,6,11 This can sometimes pose a challenge, as the history may not always be helpful and the patient’s perception of massive hemoptysis may differ from the clinically accepted definition. For example, in a patient without respiratory compromise, we would not consider bloodtinged sputum or small amounts of blood that add up to 1 to 2 teaspoons (5–10 mL) to be massive, although the patient might. On the other hand, hemoptysis with cardiorespiratory compromise must be considered significant (and very possibly massive) until proven otherwise, even if the amount of blood is small.
Massive hemoptysis is usually the result of erosion of systemic (rather than pulmonary) arteries by bronchial neoplasm, active tuberculosis, or aspergilloma.6,9,12,13 Arteriovenous malformations and pulmonary artery aneurysms are much less common causes.5,11,13
IMAGING AND DIAGNOSTIC OPTIONS
Figure 1.
Most cases of hemoptysis have an identifiable source and cause of the bleeding at the time of initial diagnosis.14 Currently, there is no consensus on what is the best workup for hemoptysis. Still, a complete evaluation includes patient history, physical examination, bronchoscopy, laboratory tests, and imaging studies (Figure 1). Imaging studies that can be helpful include chest radiography, conventional computed tomography (CT), multi-detector CT angiography, and conventional angiography.
Chest radiography
Figure 2. Chest radiograph in a 52-year-old man with cough and hemoptysis. The ill-defined mass in the right lower lobe was found to be squamous cell carcinoma.
Chest radiography is an excellent initial imaging test for evaluating hemoptysis. It is quick and inexpensive and can provide insight into acute chest problems. As mentioned above, in cases of alveolar hemorrhage, radiography typically reveals alveolar infiltrates.4 In cases of hemoptysis due to large-vessel bleeding, radiography can reveal a variety of pertinent findings, such as a mass, pneumonia, chronic lung disease, atelectasis, or a cavitary lesion (FIGURE 2). Even if the findings are nonspecific (such as in pneumonia), radiography can narrow the location of the problem to a single lobe or at least to a single lung, and this information can guide further evaluation by bronchoscopy.4,9
In as many as 40% of cases of hemoptysis, however, the findings on chest radiography are normal or do not reveal the source of the bleeding.15,16 Approximately 5% to 6% of patients with hemoptysis and normal results on radiography are eventually found to have lung cancer.14 Thus, while a localizing finding on radiography is helpful, a normal or nonlocalizing finding warrants further evaluation by other means, including conventional CT, multidetector CT angiography, or bronchoscopy.
Computed tomography
Figure 3. A computed tomographic scan shows cystic dilatation of the bronchi bilaterally, consistent with cystic bronchiectasis.
Both conventional CT and multidetector CT angiography are quick and noninvasive ways to locate the site of bleeding, determine the cause of bleeding (Figure 3, Figure 4), and create a map to guide further therapy.5,6,11,13
Figure 4. A computed tomographic scan in a 44-year-old man with hemoptysis. The solid mass on the left is a mycetoma within a thin-walled cavity in the left upper lobe.
CT is superior to fiberoptic bronchoscopy in finding a cause of hemoptysis, its main advantage being its ability to show distal airways beyond the reach of the bronchoscope, and the lung parenchyma surrounding these distal airways.5,15,16 In locating the site of bleeding, CT performs about as well as fiberoptic bronchoscopy.5
However, while CT imaging is extremely useful in evaluating bleeding from larger vessels, it adds little information beyond that obtained by chest radiography in cases of diffuse alveolar hemorrhage.4
Multidetector CT angiography is the optimal CT study for evaluating hemoptysis. In addition to showing the lung parenchyma and airways, it allows one to evaluate the integrity of pulmonary, bronchial, and nonbronchial systemic arteries within the chest. It is at least as good as (and, with multiplanar reformatted images, possibly even better than) conventional angiography in evaluating bronchial and nonbronchial systemic arteries. Multidetector CT angiography is recommended before bronchial artery embolization to help one plan the procedure and shorten the procedure time, if the patient is stable enough that this imaging study can be done first.6,12,13
The iodinated contrast material used in CT angiography can cause contrast nephropathy in patients with renal failure. At Cleveland Clinic, we avoid using contrast if the patient’s serum creatinine level is 2.0 mg/dL or greater or if it is rapidly rising, even if it is in the normal range or only slightly elevated; a rapid rise would indicate acute renal failure (eg, in glomerulonephritis). In these cases, we recommend CT without contrast.
CT of the chest has revealed malignancies in cases of hemoptysis in which radiography and bronchoscopy did not.15,17 Although CT is more than 90% sensitive in detecting endobronchial lesions, it has limitations: a blood clot within the bronchus can look like a tumor, and acute bleeding can obscure an endobronchial lesion.5 Thus, bronchoscopy remains an important, complementary diagnostic tool in the evaluation of acute hemoptysis.
Bronchoscopy
Bronchoscopy is overall much less sensitive than CT in detecting the cause of the bleeding,15,16,18 but, if performed early it as useful as CT in finding the site of bleeding,5,9 information that can be helpful in planning further therapy.19 It may be more useful than CT in evaluating endobronchial lesions during acute hemoptysis, as active bleeding can obscure an endobronchial lesion on CT.5 However, the distal airways are often filled with blood, making them difficult to evaluate via bronchoscopy.
In approximately 10% of cases of massive hemoptysis, rigid bronchoscopy is preferred over fiberoptic bronchoscopy, and it is often used in a perioperative setting. However, its use is not usually possible in unstable patients receiving intensive care. Instead, flexible fiberoptic bronchoscopy can be used in patients whose condition is too unstable to allow them to leave the intensive care unit to undergo CT. Flexible fiberoptic bronchoscopy does not require an operating room or anesthesia,19 and can be done in the intensive care unit itself.
Not only can bronchoscopy accurately locate the site of bleeding, it can also aid in controlling the airway in patients with catastrophic hemorrhage and temporarily control bleeding through Fogarty balloon tamponade, direct application of a mixture of epinephrine and cold saline, or topical hemostatic tamponade therapy with a solution of thrombin or fibrinogen and thrombin.2,3,19 It also provides complementary information about endobronchial lesions and is valuable in providing samples for tissue diagnosis and microbial cultures.
Diagnostic angiography has limitations
Although it is possible to bypass radiography, CT, and bronchoscopy in a case of massive hemoptysis and to rush the patient to the angiography suite for combined diagnostic angiography and therapeutic bronchial artery embolization, this approach has limitations. Diagnostic angiography does not identify the source of bleeding as well as CT does.6 It is important to locate the bleeding site first via CT, multidetector CT angiography, or bronchoscopy. Diagnostic angiography can be time-consuming. The procedure time can be significantly shorter if CT, bronchoscopy, or both are done first to ascertain the site of bleeding before bronchial artery embolization.1,6 Another reason that performing CT first is important is that it can rule out situations in which surgery would be preferred over bronchial artery embolization.6
In more than 90% of cases of hemoptysis requiring embolization or surgery, the bleeding is from the bronchial arteries.5,6,9,11–13 However, bronchoscopy before bronchial artery embolization is unnecessary in patients with hemoptysis of known cause if the site of bleeding can be determined from radiography or CT and if no bronchoscopic airway management is needed.18
BRONCHIAL ARTERY EMBOLIZATION: AN ALTERNATIVE TO SURGERY
After a cause of the hemoptysis has been established by radiography, CT, or bronchoscopy, bronchial artery embolization is an effective first-line therapy to control massive, life-threatening bleeding.6 It is an alternative in patients who cannot undergo surgery because of bilateral or extensive disease that renders them unable to tolerate life after a lobectomy.6,12,18
Indications for bronchial artery embolization include failure of conservative management, massive hemoptysis, recurrent hemoptysis, and poor surgical risk. It is also done to control bleeding temporarily before surgery.1
Another indication for this therapy is peripheral pulmonary artery pseudoaneurysm, which is found in up to 11% of patients undergoing bronchial angiography for hemoptysis. These patients typically present with recurrent hemoptysis (sometimes massive) and occasionally with both hemoptysis and clubbing. Most of these patients have either chronic active pulmonary tuberculosis or a mycetoma complicating sarcoidosis or tuberculosis. Occlusion of the pulmonary artery pseudoaneurysm may require embolization of bronchial arteries, nonbronchial systemic arteries, or pulmonary artery branches.20
Surgery, however, is still the definitive treatment of choice for thoracic vascular injury, bronchial adenoma, aspergilloma resistant to other therapies, and hydatid cyst.6 A cardiothoracic surgeon should be consulted in these cases.
Outcomes of embolization
Images courtesy of Abraham Levitin, MD.
Figure 5. A pathologic bronchial artery to a mediastinal tumor before (left) and after (right) embolization with polyvinyl alcohol particles.
Aside from the cases in which surgery is indicated, bronchial artery embolization (Figure 5) is a very successful minimally invasive therapy that controls bleeding immediately in 66% to 90% of patients.1,7,21 It is the preferred emergency treatment for massive hemoptysis, as the death rate is 7.1% to 18.2%, which, though high, is considerably less than the 40% seen in emergency surgery for massive hemoptysis.6
If a patient with massive hemoptysis undergoes successful bronchial artery embolization but the bleeding recurs 1 to 6 months later, the cause is likely an undetected nonbronchial systemic arterial supply and incomplete embolization.1,22 Late rebleeding (6–12 months after the procedure) occurs in 20% to 40% of patients and is likely to be from disease progression.1,7
Common complications of bronchial artery embolization are transient chest pain and dysphagia. Very rare complications include subintimal dissection and spinal cord ischemia due to inadvertent occlusion of the spinal arteries.6 Another complication in patients with renal failure is contrast nephropathy, the risk of which must be weighed against the possible consequences—including death—of not performing bronchial artery embolization in a patient who cannot undergo surgery.
CASE REVISITED: CLINICAL COURSE
In the patient described at the beginning of this article, a chest radiograph obtained in the emergency room showed an area of nonspecific consolidation in the left upper lung. Conventional chest CT was then ordered (Figure 4), and it revealed a cavitary lesion in the left upper lobe, consistent with aspergilloma. Bronchoscopy was then performed, and it too indicated that the bleeding was coming from the left upper lobe. Samples obtained during the procedure were sent to the laboratory for bacterial and fungal cultures.
In the meantime, family members were contacted, and they revealed that the patient had a history of sarcoidosis.
The patient went on to develop massive hemoptysis. Although the treatment of choice for mycetoma is primary resection, our patient’s respiratory status was poor as a result of extensive pulmonary sarcoidosis, and he was not considered a candidate for emergency surgery at that time. He was rushed to the angiography suite and successfully underwent emergency bronchial artery embolization.
References
Andersen PE. Imaging and interventional radiological treatment of hemoptysis. Acta Radiologica2006; 47:780–792.
Corder R. Hemoptysis. Emerg Med Clin North Am2003; 21:421–435.
Valipour A, Kreuzer A, Koller H, Koessler W, Burghuber OC. Bronchoscopy-guided topical hemostatic tamponade therapy for the management of life-threatening hemoptysis. Chest2005; 127:2113–2118.
Khalil A, Soussan M, Mangiapan G, Fartoukh M, Parrot A, Carette MF. Utility of high-resolution chest CT scan in the emergency management of haemoptysis in the intensive care unit: severity, localization and aetiology. Br J Radiol2007; 80:21–25.
Yoon W, Kim JK, Kim YH, Chung TW, Kang HK. Bronchial and nonbronchial systemic artery embolization for life-threatening hemoptysis: a comprehensive review. Radiographics2002; 22:1395–1409.
Johnson JL. Manifestations of hemoptysis. How to manage minor, moderate, and massive bleeding. Postgrad Med2002; 1124:101–113.
Bidwell JL, Pachner RW. Hemoptysis: diagnosis and management. Am Fam Phys2005; 72:1253–1260.
Bruzzi JF, Remy-Jardin M, Delhaye D, Teisseire A, Khalil C, Remy J. Multi-detector row CT of hemoptysis. Radiographics2006; 26:3–22.
Ozgul MA, Turna A, Yildiz P, Ertan E, Kahraman S, Yilmaz V. Risk factors and recurrence patterns in 203 patients with hemoptysis. Tuberk Toraks2006; 54:243–248.
Khalil A, Fartoukh M, Tassart M, Parrot A, Marsault C, Carette MF. Role of MDCT in identification of the bleeding site and the vessels causing hemoptysis. AJR Am J Roentgenol2007; 188:W117–W125.
Remy-Jardin M, Bouaziz N, Dumont P, Brillet PY, Bruzzi J, Remy J. Bronchial and nonbronchial systemic arteries at multi-detector row CT angiography: comparison with conventional angiography. Radiology2004; 233:741–749.
Yoon YC, Lee KS, Jeong YJ, Shin SW, Chung MJ, Kwon OJ. Hemoptysis: bronchial and nonbronchial systemic arteries at 16-detector row CT. Radiology2005; 234:292–298.
Herth F, Ernst A, Becker HD. Long-term outcome and lung cancer incidence in patients with hemoptysis of unknown origin. Chest2001; 120:1592–1594.
Naidich DP, Funt S, Ettenger NA, Arranda C. Hemoptysis: CT-bronchoscopic correlations in 58 cases. Radiology1990; 177:357–362.
Revel MP, Fournier LS, Hennebicque AS, et al. Can CT replace bronchoscopy in the detection of the site and cause of bleeding in patients with large or massive hemoptysis?AJR Am J Roentgenol2002; 179:1217–1224.
Hsiao EI, Kirsch CM, Kagawa FT, Wehner JH, Jensen WA, Baxter RB. Utility of fiberoptic bronchoscopy before bronchial artery embolization for massive hemoptysis. AJR Am J Roentgenol2001; 177:861–867.
Raoof S, Mehrishi S, Prakash UB. Role of bronchoscopy in modern medical intensive care unit. Clin Chest Med2001; 22:241–261.
Sbano H, Mitchell AW, Ind PW, Jackson JE. Peripheral pulmonary artery pseudoaneurysms and massive hemoptysis. AJR Am J Roentgenol2005; 184:1253–1259.
Swanson KL, Johnson CM, Prakash UB, McKusick MA, Andrews JC, Stanson AW. Bronchial artery embolization: experience with 54 patients. Chest2002; 121:789–795.
Yoon W, Kim YH, Kim JK, Kim YC, Park JG, Kang HK. Massive hemoptysis: prediction of nonbronchial systemic arterial supply with chest CT. Radiology2003; 227:232–238.
A 44-year-old man comes to the emergency room because of light-headedness and fatigue. He says he has had several similar but milder episodes in the last several months. He also mentions that he thinks he has been coughing up blood. He says he has no major medical or surgical problems of which he is aware, but he appears confused and unable to give an accurate history. No family members can be contacted for further history at the moment.
Physical examination reveals nothing remarkable, but the patient does cough up some blood during the examination. His hemoglobin level is 6.0 g/dL (reference range 13.5–17.5).
What imaging tests would be helpful in this patient’s evaluation?
HEMOPTYSIS HAS MANY CAUSES
Hemoptysis is defined as the expectoration of blood originating from the tracheobronchial tree or the pulmonary parenchyma.
Most cases of hemoptysis are benign and self-limited; life-threatening hemoptysis is rare.1–3 However, hemoptysis can be a sign of serious tracheopulmonary disease.
The bleeding can be from the large (Table 1)or the small (Table 2) pulmonary vessels. Bleeding from the small vessels is known as diffuse alveolar hemorrhage, and it characteristically presents as alveolar infiltrates on chest radiography. In these cases, further imaging studies provide little benefit.4 This paper will focus on the imaging of and radiographic interventions for large-vessel bleeding.
The causes of hemoptysis are numerous; common causes of bleeding from the large vessels nowadays include bronchiectasis, fungal infections, tuberculosis, and cancer.1,5,6 Still, no cause is identified in 15% to 30% of all cases,1,2,5 even after extensive evaluation.
Definition of ‘massive’ hemoptysis can vary
Various definitions of the severity of hemoptysis have been proposed. The threshold of “massive” hemoptysis has been defined as as low as 100 mL/24 hours and as high as 1 L/24 hours; the most common definition is 300 mL, or about 1 cup.2,3,5–10
However, the patient’s cardiorespiratory status must also be considered.5,6,9 If the patient cannot maintain his or her airway, a small amount of bleeding could be life-threatening and should be considered significant or massive. Thus, we define massive hemoptysis as more than 300 mL of blood within 24 hours or any amount of blood with concurrent cardiorespiratory compromise.
It is important to recognize massive hemoptysis quickly, because without urgent treatment, up to 80% of patients may die.5,6,11 This can sometimes pose a challenge, as the history may not always be helpful and the patient’s perception of massive hemoptysis may differ from the clinically accepted definition. For example, in a patient without respiratory compromise, we would not consider bloodtinged sputum or small amounts of blood that add up to 1 to 2 teaspoons (5–10 mL) to be massive, although the patient might. On the other hand, hemoptysis with cardiorespiratory compromise must be considered significant (and very possibly massive) until proven otherwise, even if the amount of blood is small.
Massive hemoptysis is usually the result of erosion of systemic (rather than pulmonary) arteries by bronchial neoplasm, active tuberculosis, or aspergilloma.6,9,12,13 Arteriovenous malformations and pulmonary artery aneurysms are much less common causes.5,11,13
IMAGING AND DIAGNOSTIC OPTIONS
Figure 1.
Most cases of hemoptysis have an identifiable source and cause of the bleeding at the time of initial diagnosis.14 Currently, there is no consensus on what is the best workup for hemoptysis. Still, a complete evaluation includes patient history, physical examination, bronchoscopy, laboratory tests, and imaging studies (Figure 1). Imaging studies that can be helpful include chest radiography, conventional computed tomography (CT), multi-detector CT angiography, and conventional angiography.
Chest radiography
Figure 2. Chest radiograph in a 52-year-old man with cough and hemoptysis. The ill-defined mass in the right lower lobe was found to be squamous cell carcinoma.
Chest radiography is an excellent initial imaging test for evaluating hemoptysis. It is quick and inexpensive and can provide insight into acute chest problems. As mentioned above, in cases of alveolar hemorrhage, radiography typically reveals alveolar infiltrates.4 In cases of hemoptysis due to large-vessel bleeding, radiography can reveal a variety of pertinent findings, such as a mass, pneumonia, chronic lung disease, atelectasis, or a cavitary lesion (FIGURE 2). Even if the findings are nonspecific (such as in pneumonia), radiography can narrow the location of the problem to a single lobe or at least to a single lung, and this information can guide further evaluation by bronchoscopy.4,9
In as many as 40% of cases of hemoptysis, however, the findings on chest radiography are normal or do not reveal the source of the bleeding.15,16 Approximately 5% to 6% of patients with hemoptysis and normal results on radiography are eventually found to have lung cancer.14 Thus, while a localizing finding on radiography is helpful, a normal or nonlocalizing finding warrants further evaluation by other means, including conventional CT, multidetector CT angiography, or bronchoscopy.
Computed tomography
Figure 3. A computed tomographic scan shows cystic dilatation of the bronchi bilaterally, consistent with cystic bronchiectasis.
Both conventional CT and multidetector CT angiography are quick and noninvasive ways to locate the site of bleeding, determine the cause of bleeding (Figure 3, Figure 4), and create a map to guide further therapy.5,6,11,13
Figure 4. A computed tomographic scan in a 44-year-old man with hemoptysis. The solid mass on the left is a mycetoma within a thin-walled cavity in the left upper lobe.
CT is superior to fiberoptic bronchoscopy in finding a cause of hemoptysis, its main advantage being its ability to show distal airways beyond the reach of the bronchoscope, and the lung parenchyma surrounding these distal airways.5,15,16 In locating the site of bleeding, CT performs about as well as fiberoptic bronchoscopy.5
However, while CT imaging is extremely useful in evaluating bleeding from larger vessels, it adds little information beyond that obtained by chest radiography in cases of diffuse alveolar hemorrhage.4
Multidetector CT angiography is the optimal CT study for evaluating hemoptysis. In addition to showing the lung parenchyma and airways, it allows one to evaluate the integrity of pulmonary, bronchial, and nonbronchial systemic arteries within the chest. It is at least as good as (and, with multiplanar reformatted images, possibly even better than) conventional angiography in evaluating bronchial and nonbronchial systemic arteries. Multidetector CT angiography is recommended before bronchial artery embolization to help one plan the procedure and shorten the procedure time, if the patient is stable enough that this imaging study can be done first.6,12,13
The iodinated contrast material used in CT angiography can cause contrast nephropathy in patients with renal failure. At Cleveland Clinic, we avoid using contrast if the patient’s serum creatinine level is 2.0 mg/dL or greater or if it is rapidly rising, even if it is in the normal range or only slightly elevated; a rapid rise would indicate acute renal failure (eg, in glomerulonephritis). In these cases, we recommend CT without contrast.
CT of the chest has revealed malignancies in cases of hemoptysis in which radiography and bronchoscopy did not.15,17 Although CT is more than 90% sensitive in detecting endobronchial lesions, it has limitations: a blood clot within the bronchus can look like a tumor, and acute bleeding can obscure an endobronchial lesion.5 Thus, bronchoscopy remains an important, complementary diagnostic tool in the evaluation of acute hemoptysis.
Bronchoscopy
Bronchoscopy is overall much less sensitive than CT in detecting the cause of the bleeding,15,16,18 but, if performed early it as useful as CT in finding the site of bleeding,5,9 information that can be helpful in planning further therapy.19 It may be more useful than CT in evaluating endobronchial lesions during acute hemoptysis, as active bleeding can obscure an endobronchial lesion on CT.5 However, the distal airways are often filled with blood, making them difficult to evaluate via bronchoscopy.
In approximately 10% of cases of massive hemoptysis, rigid bronchoscopy is preferred over fiberoptic bronchoscopy, and it is often used in a perioperative setting. However, its use is not usually possible in unstable patients receiving intensive care. Instead, flexible fiberoptic bronchoscopy can be used in patients whose condition is too unstable to allow them to leave the intensive care unit to undergo CT. Flexible fiberoptic bronchoscopy does not require an operating room or anesthesia,19 and can be done in the intensive care unit itself.
Not only can bronchoscopy accurately locate the site of bleeding, it can also aid in controlling the airway in patients with catastrophic hemorrhage and temporarily control bleeding through Fogarty balloon tamponade, direct application of a mixture of epinephrine and cold saline, or topical hemostatic tamponade therapy with a solution of thrombin or fibrinogen and thrombin.2,3,19 It also provides complementary information about endobronchial lesions and is valuable in providing samples for tissue diagnosis and microbial cultures.
Diagnostic angiography has limitations
Although it is possible to bypass radiography, CT, and bronchoscopy in a case of massive hemoptysis and to rush the patient to the angiography suite for combined diagnostic angiography and therapeutic bronchial artery embolization, this approach has limitations. Diagnostic angiography does not identify the source of bleeding as well as CT does.6 It is important to locate the bleeding site first via CT, multidetector CT angiography, or bronchoscopy. Diagnostic angiography can be time-consuming. The procedure time can be significantly shorter if CT, bronchoscopy, or both are done first to ascertain the site of bleeding before bronchial artery embolization.1,6 Another reason that performing CT first is important is that it can rule out situations in which surgery would be preferred over bronchial artery embolization.6
In more than 90% of cases of hemoptysis requiring embolization or surgery, the bleeding is from the bronchial arteries.5,6,9,11–13 However, bronchoscopy before bronchial artery embolization is unnecessary in patients with hemoptysis of known cause if the site of bleeding can be determined from radiography or CT and if no bronchoscopic airway management is needed.18
BRONCHIAL ARTERY EMBOLIZATION: AN ALTERNATIVE TO SURGERY
After a cause of the hemoptysis has been established by radiography, CT, or bronchoscopy, bronchial artery embolization is an effective first-line therapy to control massive, life-threatening bleeding.6 It is an alternative in patients who cannot undergo surgery because of bilateral or extensive disease that renders them unable to tolerate life after a lobectomy.6,12,18
Indications for bronchial artery embolization include failure of conservative management, massive hemoptysis, recurrent hemoptysis, and poor surgical risk. It is also done to control bleeding temporarily before surgery.1
Another indication for this therapy is peripheral pulmonary artery pseudoaneurysm, which is found in up to 11% of patients undergoing bronchial angiography for hemoptysis. These patients typically present with recurrent hemoptysis (sometimes massive) and occasionally with both hemoptysis and clubbing. Most of these patients have either chronic active pulmonary tuberculosis or a mycetoma complicating sarcoidosis or tuberculosis. Occlusion of the pulmonary artery pseudoaneurysm may require embolization of bronchial arteries, nonbronchial systemic arteries, or pulmonary artery branches.20
Surgery, however, is still the definitive treatment of choice for thoracic vascular injury, bronchial adenoma, aspergilloma resistant to other therapies, and hydatid cyst.6 A cardiothoracic surgeon should be consulted in these cases.
Outcomes of embolization
Images courtesy of Abraham Levitin, MD.
Figure 5. A pathologic bronchial artery to a mediastinal tumor before (left) and after (right) embolization with polyvinyl alcohol particles.
Aside from the cases in which surgery is indicated, bronchial artery embolization (Figure 5) is a very successful minimally invasive therapy that controls bleeding immediately in 66% to 90% of patients.1,7,21 It is the preferred emergency treatment for massive hemoptysis, as the death rate is 7.1% to 18.2%, which, though high, is considerably less than the 40% seen in emergency surgery for massive hemoptysis.6
If a patient with massive hemoptysis undergoes successful bronchial artery embolization but the bleeding recurs 1 to 6 months later, the cause is likely an undetected nonbronchial systemic arterial supply and incomplete embolization.1,22 Late rebleeding (6–12 months after the procedure) occurs in 20% to 40% of patients and is likely to be from disease progression.1,7
Common complications of bronchial artery embolization are transient chest pain and dysphagia. Very rare complications include subintimal dissection and spinal cord ischemia due to inadvertent occlusion of the spinal arteries.6 Another complication in patients with renal failure is contrast nephropathy, the risk of which must be weighed against the possible consequences—including death—of not performing bronchial artery embolization in a patient who cannot undergo surgery.
CASE REVISITED: CLINICAL COURSE
In the patient described at the beginning of this article, a chest radiograph obtained in the emergency room showed an area of nonspecific consolidation in the left upper lung. Conventional chest CT was then ordered (Figure 4), and it revealed a cavitary lesion in the left upper lobe, consistent with aspergilloma. Bronchoscopy was then performed, and it too indicated that the bleeding was coming from the left upper lobe. Samples obtained during the procedure were sent to the laboratory for bacterial and fungal cultures.
In the meantime, family members were contacted, and they revealed that the patient had a history of sarcoidosis.
The patient went on to develop massive hemoptysis. Although the treatment of choice for mycetoma is primary resection, our patient’s respiratory status was poor as a result of extensive pulmonary sarcoidosis, and he was not considered a candidate for emergency surgery at that time. He was rushed to the angiography suite and successfully underwent emergency bronchial artery embolization.
A 44-year-old man comes to the emergency room because of light-headedness and fatigue. He says he has had several similar but milder episodes in the last several months. He also mentions that he thinks he has been coughing up blood. He says he has no major medical or surgical problems of which he is aware, but he appears confused and unable to give an accurate history. No family members can be contacted for further history at the moment.
Physical examination reveals nothing remarkable, but the patient does cough up some blood during the examination. His hemoglobin level is 6.0 g/dL (reference range 13.5–17.5).
What imaging tests would be helpful in this patient’s evaluation?
HEMOPTYSIS HAS MANY CAUSES
Hemoptysis is defined as the expectoration of blood originating from the tracheobronchial tree or the pulmonary parenchyma.
Most cases of hemoptysis are benign and self-limited; life-threatening hemoptysis is rare.1–3 However, hemoptysis can be a sign of serious tracheopulmonary disease.
The bleeding can be from the large (Table 1)or the small (Table 2) pulmonary vessels. Bleeding from the small vessels is known as diffuse alveolar hemorrhage, and it characteristically presents as alveolar infiltrates on chest radiography. In these cases, further imaging studies provide little benefit.4 This paper will focus on the imaging of and radiographic interventions for large-vessel bleeding.
The causes of hemoptysis are numerous; common causes of bleeding from the large vessels nowadays include bronchiectasis, fungal infections, tuberculosis, and cancer.1,5,6 Still, no cause is identified in 15% to 30% of all cases,1,2,5 even after extensive evaluation.
Definition of ‘massive’ hemoptysis can vary
Various definitions of the severity of hemoptysis have been proposed. The threshold of “massive” hemoptysis has been defined as as low as 100 mL/24 hours and as high as 1 L/24 hours; the most common definition is 300 mL, or about 1 cup.2,3,5–10
However, the patient’s cardiorespiratory status must also be considered.5,6,9 If the patient cannot maintain his or her airway, a small amount of bleeding could be life-threatening and should be considered significant or massive. Thus, we define massive hemoptysis as more than 300 mL of blood within 24 hours or any amount of blood with concurrent cardiorespiratory compromise.
It is important to recognize massive hemoptysis quickly, because without urgent treatment, up to 80% of patients may die.5,6,11 This can sometimes pose a challenge, as the history may not always be helpful and the patient’s perception of massive hemoptysis may differ from the clinically accepted definition. For example, in a patient without respiratory compromise, we would not consider bloodtinged sputum or small amounts of blood that add up to 1 to 2 teaspoons (5–10 mL) to be massive, although the patient might. On the other hand, hemoptysis with cardiorespiratory compromise must be considered significant (and very possibly massive) until proven otherwise, even if the amount of blood is small.
Massive hemoptysis is usually the result of erosion of systemic (rather than pulmonary) arteries by bronchial neoplasm, active tuberculosis, or aspergilloma.6,9,12,13 Arteriovenous malformations and pulmonary artery aneurysms are much less common causes.5,11,13
IMAGING AND DIAGNOSTIC OPTIONS
Figure 1.
Most cases of hemoptysis have an identifiable source and cause of the bleeding at the time of initial diagnosis.14 Currently, there is no consensus on what is the best workup for hemoptysis. Still, a complete evaluation includes patient history, physical examination, bronchoscopy, laboratory tests, and imaging studies (Figure 1). Imaging studies that can be helpful include chest radiography, conventional computed tomography (CT), multi-detector CT angiography, and conventional angiography.
Chest radiography
Figure 2. Chest radiograph in a 52-year-old man with cough and hemoptysis. The ill-defined mass in the right lower lobe was found to be squamous cell carcinoma.
Chest radiography is an excellent initial imaging test for evaluating hemoptysis. It is quick and inexpensive and can provide insight into acute chest problems. As mentioned above, in cases of alveolar hemorrhage, radiography typically reveals alveolar infiltrates.4 In cases of hemoptysis due to large-vessel bleeding, radiography can reveal a variety of pertinent findings, such as a mass, pneumonia, chronic lung disease, atelectasis, or a cavitary lesion (FIGURE 2). Even if the findings are nonspecific (such as in pneumonia), radiography can narrow the location of the problem to a single lobe or at least to a single lung, and this information can guide further evaluation by bronchoscopy.4,9
In as many as 40% of cases of hemoptysis, however, the findings on chest radiography are normal or do not reveal the source of the bleeding.15,16 Approximately 5% to 6% of patients with hemoptysis and normal results on radiography are eventually found to have lung cancer.14 Thus, while a localizing finding on radiography is helpful, a normal or nonlocalizing finding warrants further evaluation by other means, including conventional CT, multidetector CT angiography, or bronchoscopy.
Computed tomography
Figure 3. A computed tomographic scan shows cystic dilatation of the bronchi bilaterally, consistent with cystic bronchiectasis.
Both conventional CT and multidetector CT angiography are quick and noninvasive ways to locate the site of bleeding, determine the cause of bleeding (Figure 3, Figure 4), and create a map to guide further therapy.5,6,11,13
Figure 4. A computed tomographic scan in a 44-year-old man with hemoptysis. The solid mass on the left is a mycetoma within a thin-walled cavity in the left upper lobe.
CT is superior to fiberoptic bronchoscopy in finding a cause of hemoptysis, its main advantage being its ability to show distal airways beyond the reach of the bronchoscope, and the lung parenchyma surrounding these distal airways.5,15,16 In locating the site of bleeding, CT performs about as well as fiberoptic bronchoscopy.5
However, while CT imaging is extremely useful in evaluating bleeding from larger vessels, it adds little information beyond that obtained by chest radiography in cases of diffuse alveolar hemorrhage.4
Multidetector CT angiography is the optimal CT study for evaluating hemoptysis. In addition to showing the lung parenchyma and airways, it allows one to evaluate the integrity of pulmonary, bronchial, and nonbronchial systemic arteries within the chest. It is at least as good as (and, with multiplanar reformatted images, possibly even better than) conventional angiography in evaluating bronchial and nonbronchial systemic arteries. Multidetector CT angiography is recommended before bronchial artery embolization to help one plan the procedure and shorten the procedure time, if the patient is stable enough that this imaging study can be done first.6,12,13
The iodinated contrast material used in CT angiography can cause contrast nephropathy in patients with renal failure. At Cleveland Clinic, we avoid using contrast if the patient’s serum creatinine level is 2.0 mg/dL or greater or if it is rapidly rising, even if it is in the normal range or only slightly elevated; a rapid rise would indicate acute renal failure (eg, in glomerulonephritis). In these cases, we recommend CT without contrast.
CT of the chest has revealed malignancies in cases of hemoptysis in which radiography and bronchoscopy did not.15,17 Although CT is more than 90% sensitive in detecting endobronchial lesions, it has limitations: a blood clot within the bronchus can look like a tumor, and acute bleeding can obscure an endobronchial lesion.5 Thus, bronchoscopy remains an important, complementary diagnostic tool in the evaluation of acute hemoptysis.
Bronchoscopy
Bronchoscopy is overall much less sensitive than CT in detecting the cause of the bleeding,15,16,18 but, if performed early it as useful as CT in finding the site of bleeding,5,9 information that can be helpful in planning further therapy.19 It may be more useful than CT in evaluating endobronchial lesions during acute hemoptysis, as active bleeding can obscure an endobronchial lesion on CT.5 However, the distal airways are often filled with blood, making them difficult to evaluate via bronchoscopy.
In approximately 10% of cases of massive hemoptysis, rigid bronchoscopy is preferred over fiberoptic bronchoscopy, and it is often used in a perioperative setting. However, its use is not usually possible in unstable patients receiving intensive care. Instead, flexible fiberoptic bronchoscopy can be used in patients whose condition is too unstable to allow them to leave the intensive care unit to undergo CT. Flexible fiberoptic bronchoscopy does not require an operating room or anesthesia,19 and can be done in the intensive care unit itself.
Not only can bronchoscopy accurately locate the site of bleeding, it can also aid in controlling the airway in patients with catastrophic hemorrhage and temporarily control bleeding through Fogarty balloon tamponade, direct application of a mixture of epinephrine and cold saline, or topical hemostatic tamponade therapy with a solution of thrombin or fibrinogen and thrombin.2,3,19 It also provides complementary information about endobronchial lesions and is valuable in providing samples for tissue diagnosis and microbial cultures.
Diagnostic angiography has limitations
Although it is possible to bypass radiography, CT, and bronchoscopy in a case of massive hemoptysis and to rush the patient to the angiography suite for combined diagnostic angiography and therapeutic bronchial artery embolization, this approach has limitations. Diagnostic angiography does not identify the source of bleeding as well as CT does.6 It is important to locate the bleeding site first via CT, multidetector CT angiography, or bronchoscopy. Diagnostic angiography can be time-consuming. The procedure time can be significantly shorter if CT, bronchoscopy, or both are done first to ascertain the site of bleeding before bronchial artery embolization.1,6 Another reason that performing CT first is important is that it can rule out situations in which surgery would be preferred over bronchial artery embolization.6
In more than 90% of cases of hemoptysis requiring embolization or surgery, the bleeding is from the bronchial arteries.5,6,9,11–13 However, bronchoscopy before bronchial artery embolization is unnecessary in patients with hemoptysis of known cause if the site of bleeding can be determined from radiography or CT and if no bronchoscopic airway management is needed.18
BRONCHIAL ARTERY EMBOLIZATION: AN ALTERNATIVE TO SURGERY
After a cause of the hemoptysis has been established by radiography, CT, or bronchoscopy, bronchial artery embolization is an effective first-line therapy to control massive, life-threatening bleeding.6 It is an alternative in patients who cannot undergo surgery because of bilateral or extensive disease that renders them unable to tolerate life after a lobectomy.6,12,18
Indications for bronchial artery embolization include failure of conservative management, massive hemoptysis, recurrent hemoptysis, and poor surgical risk. It is also done to control bleeding temporarily before surgery.1
Another indication for this therapy is peripheral pulmonary artery pseudoaneurysm, which is found in up to 11% of patients undergoing bronchial angiography for hemoptysis. These patients typically present with recurrent hemoptysis (sometimes massive) and occasionally with both hemoptysis and clubbing. Most of these patients have either chronic active pulmonary tuberculosis or a mycetoma complicating sarcoidosis or tuberculosis. Occlusion of the pulmonary artery pseudoaneurysm may require embolization of bronchial arteries, nonbronchial systemic arteries, or pulmonary artery branches.20
Surgery, however, is still the definitive treatment of choice for thoracic vascular injury, bronchial adenoma, aspergilloma resistant to other therapies, and hydatid cyst.6 A cardiothoracic surgeon should be consulted in these cases.
Outcomes of embolization
Images courtesy of Abraham Levitin, MD.
Figure 5. A pathologic bronchial artery to a mediastinal tumor before (left) and after (right) embolization with polyvinyl alcohol particles.
Aside from the cases in which surgery is indicated, bronchial artery embolization (Figure 5) is a very successful minimally invasive therapy that controls bleeding immediately in 66% to 90% of patients.1,7,21 It is the preferred emergency treatment for massive hemoptysis, as the death rate is 7.1% to 18.2%, which, though high, is considerably less than the 40% seen in emergency surgery for massive hemoptysis.6
If a patient with massive hemoptysis undergoes successful bronchial artery embolization but the bleeding recurs 1 to 6 months later, the cause is likely an undetected nonbronchial systemic arterial supply and incomplete embolization.1,22 Late rebleeding (6–12 months after the procedure) occurs in 20% to 40% of patients and is likely to be from disease progression.1,7
Common complications of bronchial artery embolization are transient chest pain and dysphagia. Very rare complications include subintimal dissection and spinal cord ischemia due to inadvertent occlusion of the spinal arteries.6 Another complication in patients with renal failure is contrast nephropathy, the risk of which must be weighed against the possible consequences—including death—of not performing bronchial artery embolization in a patient who cannot undergo surgery.
CASE REVISITED: CLINICAL COURSE
In the patient described at the beginning of this article, a chest radiograph obtained in the emergency room showed an area of nonspecific consolidation in the left upper lung. Conventional chest CT was then ordered (Figure 4), and it revealed a cavitary lesion in the left upper lobe, consistent with aspergilloma. Bronchoscopy was then performed, and it too indicated that the bleeding was coming from the left upper lobe. Samples obtained during the procedure were sent to the laboratory for bacterial and fungal cultures.
In the meantime, family members were contacted, and they revealed that the patient had a history of sarcoidosis.
The patient went on to develop massive hemoptysis. Although the treatment of choice for mycetoma is primary resection, our patient’s respiratory status was poor as a result of extensive pulmonary sarcoidosis, and he was not considered a candidate for emergency surgery at that time. He was rushed to the angiography suite and successfully underwent emergency bronchial artery embolization.
References
Andersen PE. Imaging and interventional radiological treatment of hemoptysis. Acta Radiologica2006; 47:780–792.
Corder R. Hemoptysis. Emerg Med Clin North Am2003; 21:421–435.
Valipour A, Kreuzer A, Koller H, Koessler W, Burghuber OC. Bronchoscopy-guided topical hemostatic tamponade therapy for the management of life-threatening hemoptysis. Chest2005; 127:2113–2118.
Khalil A, Soussan M, Mangiapan G, Fartoukh M, Parrot A, Carette MF. Utility of high-resolution chest CT scan in the emergency management of haemoptysis in the intensive care unit: severity, localization and aetiology. Br J Radiol2007; 80:21–25.
Yoon W, Kim JK, Kim YH, Chung TW, Kang HK. Bronchial and nonbronchial systemic artery embolization for life-threatening hemoptysis: a comprehensive review. Radiographics2002; 22:1395–1409.
Johnson JL. Manifestations of hemoptysis. How to manage minor, moderate, and massive bleeding. Postgrad Med2002; 1124:101–113.
Bidwell JL, Pachner RW. Hemoptysis: diagnosis and management. Am Fam Phys2005; 72:1253–1260.
Bruzzi JF, Remy-Jardin M, Delhaye D, Teisseire A, Khalil C, Remy J. Multi-detector row CT of hemoptysis. Radiographics2006; 26:3–22.
Ozgul MA, Turna A, Yildiz P, Ertan E, Kahraman S, Yilmaz V. Risk factors and recurrence patterns in 203 patients with hemoptysis. Tuberk Toraks2006; 54:243–248.
Khalil A, Fartoukh M, Tassart M, Parrot A, Marsault C, Carette MF. Role of MDCT in identification of the bleeding site and the vessels causing hemoptysis. AJR Am J Roentgenol2007; 188:W117–W125.
Remy-Jardin M, Bouaziz N, Dumont P, Brillet PY, Bruzzi J, Remy J. Bronchial and nonbronchial systemic arteries at multi-detector row CT angiography: comparison with conventional angiography. Radiology2004; 233:741–749.
Yoon YC, Lee KS, Jeong YJ, Shin SW, Chung MJ, Kwon OJ. Hemoptysis: bronchial and nonbronchial systemic arteries at 16-detector row CT. Radiology2005; 234:292–298.
Herth F, Ernst A, Becker HD. Long-term outcome and lung cancer incidence in patients with hemoptysis of unknown origin. Chest2001; 120:1592–1594.
Naidich DP, Funt S, Ettenger NA, Arranda C. Hemoptysis: CT-bronchoscopic correlations in 58 cases. Radiology1990; 177:357–362.
Revel MP, Fournier LS, Hennebicque AS, et al. Can CT replace bronchoscopy in the detection of the site and cause of bleeding in patients with large or massive hemoptysis?AJR Am J Roentgenol2002; 179:1217–1224.
Hsiao EI, Kirsch CM, Kagawa FT, Wehner JH, Jensen WA, Baxter RB. Utility of fiberoptic bronchoscopy before bronchial artery embolization for massive hemoptysis. AJR Am J Roentgenol2001; 177:861–867.
Raoof S, Mehrishi S, Prakash UB. Role of bronchoscopy in modern medical intensive care unit. Clin Chest Med2001; 22:241–261.
Sbano H, Mitchell AW, Ind PW, Jackson JE. Peripheral pulmonary artery pseudoaneurysms and massive hemoptysis. AJR Am J Roentgenol2005; 184:1253–1259.
Swanson KL, Johnson CM, Prakash UB, McKusick MA, Andrews JC, Stanson AW. Bronchial artery embolization: experience with 54 patients. Chest2002; 121:789–795.
Yoon W, Kim YH, Kim JK, Kim YC, Park JG, Kang HK. Massive hemoptysis: prediction of nonbronchial systemic arterial supply with chest CT. Radiology2003; 227:232–238.
References
Andersen PE. Imaging and interventional radiological treatment of hemoptysis. Acta Radiologica2006; 47:780–792.
Corder R. Hemoptysis. Emerg Med Clin North Am2003; 21:421–435.
Valipour A, Kreuzer A, Koller H, Koessler W, Burghuber OC. Bronchoscopy-guided topical hemostatic tamponade therapy for the management of life-threatening hemoptysis. Chest2005; 127:2113–2118.
Khalil A, Soussan M, Mangiapan G, Fartoukh M, Parrot A, Carette MF. Utility of high-resolution chest CT scan in the emergency management of haemoptysis in the intensive care unit: severity, localization and aetiology. Br J Radiol2007; 80:21–25.
Yoon W, Kim JK, Kim YH, Chung TW, Kang HK. Bronchial and nonbronchial systemic artery embolization for life-threatening hemoptysis: a comprehensive review. Radiographics2002; 22:1395–1409.
Johnson JL. Manifestations of hemoptysis. How to manage minor, moderate, and massive bleeding. Postgrad Med2002; 1124:101–113.
Bidwell JL, Pachner RW. Hemoptysis: diagnosis and management. Am Fam Phys2005; 72:1253–1260.
Bruzzi JF, Remy-Jardin M, Delhaye D, Teisseire A, Khalil C, Remy J. Multi-detector row CT of hemoptysis. Radiographics2006; 26:3–22.
Ozgul MA, Turna A, Yildiz P, Ertan E, Kahraman S, Yilmaz V. Risk factors and recurrence patterns in 203 patients with hemoptysis. Tuberk Toraks2006; 54:243–248.
Khalil A, Fartoukh M, Tassart M, Parrot A, Marsault C, Carette MF. Role of MDCT in identification of the bleeding site and the vessels causing hemoptysis. AJR Am J Roentgenol2007; 188:W117–W125.
Remy-Jardin M, Bouaziz N, Dumont P, Brillet PY, Bruzzi J, Remy J. Bronchial and nonbronchial systemic arteries at multi-detector row CT angiography: comparison with conventional angiography. Radiology2004; 233:741–749.
Yoon YC, Lee KS, Jeong YJ, Shin SW, Chung MJ, Kwon OJ. Hemoptysis: bronchial and nonbronchial systemic arteries at 16-detector row CT. Radiology2005; 234:292–298.
Herth F, Ernst A, Becker HD. Long-term outcome and lung cancer incidence in patients with hemoptysis of unknown origin. Chest2001; 120:1592–1594.
Naidich DP, Funt S, Ettenger NA, Arranda C. Hemoptysis: CT-bronchoscopic correlations in 58 cases. Radiology1990; 177:357–362.
Revel MP, Fournier LS, Hennebicque AS, et al. Can CT replace bronchoscopy in the detection of the site and cause of bleeding in patients with large or massive hemoptysis?AJR Am J Roentgenol2002; 179:1217–1224.
Hsiao EI, Kirsch CM, Kagawa FT, Wehner JH, Jensen WA, Baxter RB. Utility of fiberoptic bronchoscopy before bronchial artery embolization for massive hemoptysis. AJR Am J Roentgenol2001; 177:861–867.
Raoof S, Mehrishi S, Prakash UB. Role of bronchoscopy in modern medical intensive care unit. Clin Chest Med2001; 22:241–261.
Sbano H, Mitchell AW, Ind PW, Jackson JE. Peripheral pulmonary artery pseudoaneurysms and massive hemoptysis. AJR Am J Roentgenol2005; 184:1253–1259.
Swanson KL, Johnson CM, Prakash UB, McKusick MA, Andrews JC, Stanson AW. Bronchial artery embolization: experience with 54 patients. Chest2002; 121:789–795.
Yoon W, Kim YH, Kim JK, Kim YC, Park JG, Kang HK. Massive hemoptysis: prediction of nonbronchial systemic arterial supply with chest CT. Radiology2003; 227:232–238.
We recommend chest radiography in the initial stages of evaluation of hemoptysis, whether the hemoptysis is massive or nonmassive.
In cases of hemoptysis that is intermittent (whether massive or nonmassive) in patients whose condition is stable, CT, multidetector CT angiography, and bronchoscopy are all useful.
In cases of hemoptysis that is active, persistent, and massive, multidetector CT angiography, bronchoscopy, and conventional bronchial angiography are all useful, depending on the hemodynamic stability of the patient.
Bronchial artery embolization is the preferred noninvasive first-line treatment for hemoptysis and offers an excellent alternative to surgery for patients who are poor candidates for surgery.
Disallow All Ads
Alternative CME
Consolidated Pubs: Do Not Show Source Publication Logo
Radiography plays a key role in the initial evaluation of acute knee pain in adults. Yet conflicting studies and the absence of clear guidelines may leave the primary care physician uncertain as to which imaging test to order—ie, whether radiography is sufficient, and when computed tomography (CT) or magnetic resonance imaging (MRI) is needed. This article reviews the indications for radiologic examination of the knee and discusses indications for cross-sectional imaging studies. Imaging in oncology patients is not discussed here.
ACUTE KNEE PAIN: A TYPICAL SCENARIO
A 47-year-old woman presents to the emergency department with left knee pain after a motor vehicle accident that occurred the day before. The car she was driving hit a tree, and she hit her knee on the dashboard. She was wearing a seatbelt at the time of the accident. She says she was unable to walk immediately after the accident because of knee pain.
The initial examination in the emergency room reveals swelling and pain throughout the range of motion. The anterior drawer test and the Lachman test are negative (see below).
Figure 1. This anteroposterior radiograph of a 47-year-old woman who was in a motor vehicle accident shows focal ossification adjacent to the medial femoral condyle (arrow) but no evidence of acute fracture.
Initial radiographs (Figure 1) reveal no acute fracture or effusion, but focal ossification adjacent to the proximal medial femoral condyle may indicate a past injury to the medial collateral ligament.
The patient is discharged home with a knee immobilizer, pain medication, and crutches, with instructions for a follow-up visit in the orthopedics clinic.
Five days later, she returns to the emergency department complaining of continuing knee pain. She says the knee gives way when she puts weight on it. The physical findings are unchanged, and she is discharged home with a follow-up appointment with orthopedics in 3 days.
At the follow-up visit, she complains of persistent knee pain in the medial aspect of the knee joint. Physical examination is difficult because of pain and swelling, and it reveals mild joint effusion with no gross instability. She has pain on the medial side with valgus stress, but there appears to be a hard end point. There is no posterior sag, and the Lachman test is negative.
Based on the physical examination and the patient’s complaints, she receives a diagnosis of medial collateral ligament strain and injury. She is given a hinged brace and is instructed to undergo a physical rehabilitation program.
Three weeks after the initial evaluation, she returns to the orthopedics clinic with continuing knee problems. Mild knee effusion persists, but she has less pain and swelling, allowing a more complete examination. The examination reveals less limitation of range of motion and a hint of positivity on the Lachman test. The knee is diffusely tender, and the pain seems out of proportion with the maneuvers used during the examination. She requests more pain medication. You suspect internal derangement of the knee. Which imaging test should you order to further evaluate this patient?
A SYSTEMATIC AND COST-EFFECTIVE APPROACH IS NEEDED
The case presented above represents a typical scenario for the presentation of acute knee pain and illustrates the diagnostic challenges.
Knee pain is a common reason for emergency room visits, and it accounts for approximately 1.9 million visits to primary care clinics annually.1 In the emergency department, most patients undergo plain radiography to assess for fracture, yet approximately 92% of radiographic studies do not show a fracture.2 Clearly, the evaluation of knee pain requires a systematic, accurate, and cost-effective approach.
Key elements of the physical examination
In acute knee pain, accurate diagnosis begins with a detailed history and physical examination.
The anterior drawer test is done to evaluate the anterior cruciate ligament. With the relaxed knee flexed to approximately 80° and the foot stabilized in a neutral position, the examiner grasps the proximal tibia in a firm yet gentle grip, and then applies anterior force, noting the degree of anterior displacement compared with the other knee.
The Lachman test, a variation of the anterior drawer test, is more definitive for the anterior cruciate ligament and is carried out with the knee in 15° of flexion and external rotation, in order to relax the iliotibial band. The upper hand grasps the distal thigh, and the lower hand, with the thumb on the tibial tubercle, pulls the tibia forward. The degree of anterior motion in millimeters is noted and compared with that on the other side, and the end point is graded as “soft” or “hard.” An end point is considered hard when a ligament abruptly halts the motion of the bone being tested against the stabilized bone. An end point is considered soft when the ligament is disrupted and the restraints are the more elastic secondary stabilizers.
Debate continues
Some authors contend that in skilled hands a thorough history, physical examination, and radiographic examination are sufficient to diagnose trauma-related intra-articular knee disorders.3 Others contend that MRI plays a key role in the initial evaluation. A number of studies4–8 have shown that using MRI in the initial evaluation not only identifies key lesions, but also may eliminate the need for an invasive diagnostic procedure (ie, arthroscopy).
For example, MRI can reveal fracture, stress fracture, insufficiency fracture, and transient patellar dislocation—conditions that may satisfactorily explain knee symptoms.
PLAIN RADIOGRAPHY STILL THE FIRST STEP IN KNEE EVALUATION
Radiography is the first step in the evaluation of knee pain. It is quick and inexpensive and can yield many diagnostic clues. It can readily reveal fractures, osteochondral defects, bony lesions, joint effusions, joint space narrowing, and bone misalignment.
In patients with knee trauma, supine anteroposterior and cross-table lateral radiographic images are generally obtained. In patients whose knee pain is not due to trauma, standing projections are done, as well as dedicated projection of the patellofemoral articulation. A standing series is most helpful for evaluating joint space and alignment.
Applying the Ottawa rules
When a patient presents to the emergency room with acute knee pain, the immediate concern is whether he or she has a fracture. The Ottawa knee rules9 for when to order radiography in adults with knee pain are highly sensitive for detecting a clinically important fracture. If any one of the five Ottawa criteria applies—ie, the patient is age 55 or older, has tenderness at the head of the fibula, has patellar tenderness, is unable to flex the knee to 90°, or is unable to bear weight—then radiography is indicated.
While studies have validated the ability of the Ottawa rules to detect important fractures in acute knee injury,2,10 fracture is the cause of only a small percentage of knee complaints in the primary care setting. More common causes include osteoarthritis, meniscal injury, ligamental injury, and crystal arthropathy, and these account for approximately half of all diagnoses. Sprain and strain account for most of the rest of knee injuries.1
Acute exacerbations of osteoarthritis
Osteoarthritis is a chronic problem, yet it is not unusual for a patient to present to the primary care physician with an acute exacerbation of joint pain. The clinical hallmarks include age over 50, stiffness lasting less than 30 minutes, bony enlargement and tenderness, and crepitus. The radiographic hallmarks, according to the Kellgren-Lawrence grading scale, are joint space narrowing, osteophytes, subchondral cysts, and sclerosis. These radiographic findings correlate well with clinical findings in these patients.11
Situations in which radiography is less helpful
In some cases the radiographic findings may not explain the patient’s clinical signs and symptoms. For example, in suspected crystalline and septic arthritis, the clinical presentation may include warmth, erythema, and effusion. Arthrocentesis would be indicated in such a patient. Indeed, in the case of suspected pseudogout, chondrocalcinosis may be radiographically evident. However, it is also present in many patients without symptoms or with osteoarthritis, so radiographic evidence does not provide a definite diagnosis.
While radiography may not always identify the cause of knee pain, it is useful in excluding serious problems such as fractures, advanced degenerative changes, and neoplasms, and it may help direct further management. Radiography is not useful in the evaluation of the cruciate and collateral ligaments, the menisci, and the hyaline cartilage of the knee and may fail to show an insufficiency or stress fracture. To evaluate these structures and associated soft tissues, MRI is preferable.
COMPUTED TOMOGRAPHY IN ACUTE KNEE PAIN
Figure 2. A 56-year-old woman with left knee pain after a fall. (A) Anteroposterior radiograph shows fracture of the tibial eminence (short arrow). The subchondral bone of the lateral tibial plateau is indistinct (long arrow), leading to suspicion of tibial plateau fracture. (B) A lateral radiograph shows joint effusion (short arrow). The lateral tibial plateau is depressed posteriorly (long arrow). (C) Sagittal computed tomography (CT) shows fracture of the tibial eminence (arrows) extending to the lateral tibial plateau. (D) Sagittal CT shows depression of the lateral tibial plateau (arrow). (E) Coronal CT shows fracture of the tibial eminence (short arrow) and tibial plateau (long arrow). The fibular head (arrowhead) is intact.
CT is the imaging method of choice when patients have knee trauma but radiographs are negative for fracture. CT can detect and help analyze fracture better, and it can better define fractures seen on conventional radiographs (Figure 2). CT is fast, the procedure lasting only a few minutes. It costs less than MRI and provides a better picture of bony detail. Because of this, CT is generally recommended in patients with knee trauma, since it can show fractures too subtle for radiography.
CURRENT USES OF MRI TO EVALUATE ACUTE KNEE PAIN
As mentioned above, MRI is useful in evaluating suspected meniscal and ligamentous injuries.
Figure 3. T2-weighted MRI of the left knee of the 47-year-old woman who was in a motor vehicle accident. (A) A coronal image reveals a fragment of the lateral meniscus displaced into the notch (long arrow). The medial meniscus is also shortened (short arrow). Edema (arrowhead) of the tibial plateau is consistent with bone bruise. (B) A sagittal image through the intercondylar notch shows absence of the anterior cruciate ligament (red arrow). The patella (short white arrow) and intact extensor mechanism (long white arrows) are also seen. (C) A sagittal image through the medial compartment shows the medial tibial plateau (short arrow) and the medial femoral condyle (long arrow). There is a tear of the posterior aspect of the medial meniscus, which appears shortened (red arrow). (D) A sagittal image of the lateral compartment shows the lateral tibial plateau (short white arrow) and the lateral femoral condyle (long white arrow). The posterior horn of the lateral meniscus (red arrow) is missing. The fibula (white arrowhead) is intact.
Patients with meniscal injury may report a history of twisting injury while bearing weight. Symptoms may include locking or catching, with loss of motion related to a mechanical block. Ligamentous injury may be due to a direct blow or forceful stress while the patient is bearing weight. In tearing of the anterior cruciate ligament, the patient may report having heard a pop at the time of injury, followed by swelling. Valgus and varus stresses may lead to collateral ligament injury. Often, more than one injury coexists: more than a third of meniscal tears are associated with anterior cruciate ligament injury.12
Figure 3 shows how T2-weighted MRI was used to evaluate for suspected meniscal injury in our 47-year-old female patient with left knee pain after a motor vehicle accident.
Figure 4. A 35-year-old man with intermittent locking of the right knee following a snowboarding injury underwent sagittal T2-weighted MRI of the right knee. (A) An image through the intercondylar notch shows the femur (long white arrow), proximal tibia (short white arrow), and patella (white arrowhead), as well as a “double posterior cruciate ligament” sign (red arrows), representing a “bucket-handle” tear of the medial meniscus, which is displaced into the intercondylar notch. The normal posterior cruciate ligament is the most posterior structure, denoted by the arrow on the right, and the smaller, inferior structure that resembles the ligament is the displaced meniscus. (B) An image of the medial compartment shows the medial tibial plateau (long white arrow), with a focal region of full-thickness loss of the articular cartilage (short red arrow) on the weight-bearing surface of the medial femoral condyle, likely representing an acute chondral fracture. Note the large knee effusion (long red arrow) and shortening of the medial meniscus (short white arrow). An anterior cruciate ligament tear, not shown, was also identified.Figure 4 shows how sagittal T2-weighted MRI was used in a 35-year-old man with intermittent locking of the right knee following a snowboarding injury. In this patient, MRI was able to uncover coexisting injuries.
Still a matter of debate
MRI’s role in the diagnosis of knee pain is still a contentious issue.
Advantages of MRI are that it is noninvasive, it does not use ionizing radiation, it gives multiplanar images, and it provides images of soft-tissue structures, which other imaging methods cannot.12 It is a well-proven and widely accepted test. Its sensitivity for detecting meniscal and cruciate ligament injury ranges from 75% to 88%,1 and it can help in the evaluation of other injuries for which radiography is not useful, including synovitis, bone bruise, stress or insufficiency fracture, osteochondral defects, and osteonecrosis.
In addition, several studies show that using MRI to establish the diagnosis in acute knee pain can mean that 22% to 42% fewer arthroscopic procedures need to be performed.4–8 Authors of a prospective double-blind study8 recommended that MRI be used in patients with acute knee injury when the findings of the clinical history and examination by orthopedic surgeons prove equivocal.8 MRI evaluation is especially desirable for young, active patients who wish to resume activity as soon as possible.
A routine MRI examination consists of T1- and T2-weighted images in three planes, although the number of sequences and planes varies from hospital to hospital. The use of gadolinium contrast is indicated only when osteomyelitis, septic arthritis, or a mass is suspected.
Disadvantages of MRI include its cost: Medicare reimbursement for knee MRI is around $400, compared with $200 for knee CT and $50 for knee radiography with four views. Also, while studies have shown MRI to have a high sensitivity and specificity in the diagnosis of acute knee injury, some have reported a high false-positive rate for the detection of meniscal tear.13,14 MRI has also been shown to have a lower sensitivity than arthroscopy for lesions of the articular cartilage.13 Furthermore, MRI has been shown to reveal cartilage lesions, osteophytes, and meniscal abnormalities in asymptomatic study volunteers with no history of pain, trauma or knee disease.14 Therefore, findings on MRI must closely correlate with findings on the history and physical examination.
Additional indications for knee MRI
Cartilage can be assessed on routine MRI sequences of the knee. Since closed MRI systems have more powerful magnets than open systems, closed MRI systems provide greater anatomic detail.
MRI can identify other lesions, such as spontaneous osteonecrosis of the knee, usually seen in elderly women who may present with sudden knee pain. In such patients, MRI findings of focal replacement of the bone marrow and surrounding edema are specific for osteonecrosis.
Opinions vary as to whether bone marrow edema is always associated with pain. Sequential MRI studies have shown persistence of bone marrow edema for 2 years in patients with degenerative arthritis whose symptoms have waned. Bone marrow edema may be associated with pain but may be absent or inconsequential in the presence of pain.
Because fluid-sensitive T2-weighted MRI is exquisitely sensitive for mobile water protons (ie, in bone marrow edema), it is important that a cause for the edema-like signal be sought on the MRI scan, since this finding is nonspecific and may be associated with articular disease, trauma, osteonecrosis, infection, or bone tumors. Additionally, clinicians need to be aware that the findings on MRI depend on the quality of the study, and are influenced by technical factors such as magnet strength, imaging planes, and use of surface coils.
MRI should be used in patients in whom surgical treatment, ie, arthroscopy, is being considered. As discussed above, several studies have shown that a significant number of unnecessary arthroscopies may be prevented when preceded by an MRI examination.
Figure 5. A 45-year-old man with left knee pain after a motorcycle accident. (A) Lateral radiograph shows an osseous fragment at the posterior aspect of the knee joint (long arrow). This was thought to represent an avulsion fracture of the posterior cruciate ligament. There is also a knee effusion (short arrow). (B) Sagittal proton-density-weighted MRI through the intercondylar notch shows an intact anterior cruciate ligament (white arrow). There is an avulsion fracture of the posterior proximal tibia (red arrow) at the attachment of the posterior cruciate ligament. The fragment, which is displaced proximally, is attached to the posterior cruciate ligament, which remains intact.
Other indications include cases in which clinical findings are equivocal in the setting of acute injury, in competitive athletes in whom an immediate diagnosis and treatment is required, and in patients who present a high surgical risk. MRI should not be routinely used to diagnose the painful or injured knee,13 and if the skilled physical examination does not indicate findings of ligamentous or meniscal injury, conservative therapy should be prescribed.1 MRI is also not useful and offers little for patients in whom changes of degenerative joint disease are evident on radiographs.
Figure 5 shows the use of MRI in the evaluation of a 45-year-old man with left knee pain after a motorcycle accident.
ULTRASONOGRAPHY HAS ONLY A LIMITED ROLE
Ultrasonography does not play a major role in the evaluation of acute knee pain in the United States, in part because the accuracy of the results depend much on the technical skills and experience of the operator.
Ultrasonography can be useful in evaluating for rupture of the quadriceps and patellar tendon, or to assess a repaired tendon after surgery,15 and it is a quick and reliable way to determine the presence of joint effusion and popliteal cyst. It is also used to guide needle placement for joint aspiration and injection.
References
Jackson JL, O’Malley PG, Kroenke K. Evaluation of acute knee pain in primary care. Ann Intern Med2003; 139:575–588.
Steill IG, Greenberg GH, Wells GA, et al. Prospective validation of a decision rule for the use of radiographs in acute knee injuries. JAMA1996; 275:611–615.
O’Shea KJ, Murphy DP, Heekin RD, Herzwurm PJ. The diagnostic accuracy of history, physical examination, and radiographs in the evaluation of traumatic knee disorders. Am J Sports Med1996; 24:164–167.
Spiers AS, Meagher T, Ostlere SJ, Wilson DJ, Dodd CA. Can MRI of the knee affect arthroscopic practice?J Bone Joint Surg1993; 75:49–52.
Bui-Mansfield LT, Youngberg RA, Warme W, Pitcher JD, Nguyen PL. Potential cost savings of MR imaging obtained before arthroscopy of the knee: evaluation of 50 consecutive patients. AJR Am J Roentgenol1997; 168:913–918.
Rangger C, Klestil T, Kathrein A, Inderster A, Hamid L. Influence of magnetic resonance imaging on indications for arthroscopy of the knee. Clin Orthop Rel Res1996; 330:133–142.
Mackenzie R, Dixon AK, Keene GS, Hollingsworth W, Lomas DJ, Villar RN. Magnetic resonance imaging of the knee: assessment of effectiveness. Clin Radiol1996; 51:245–250.
Munshi M, Davidson M, MacDonald PB, Froese W, Sutherland K. The efficacy of magnetic resonance imaging in acute knee injuries. Clin J Sport Med2000; 10:34–39.
Steill IG, Wells GA, Hoag RH, et al. Implementation of the Ottawa knee rule for the use of radiography in acute knee injuries. JAMA1997; 278:2075–2079.
Tigges S, Pitts S, Mukundan S, Morrison D, Olson M, Shahriara A. External validation of the Ottawa knee rules in an urban trauma center in the United States. AJR Am J Roentgenol1999; 172:1069–1071.
Claessens AA, Schouten JS, van den Ouweland FA, Valkenburg HA. Do clinical findings associate with radiographic osteoarthritis of the knee?Ann Rheum Dis1990; 49:771–774.
Gries PE, Bardana DE, Holmstrom MC, Burks RT. Meniscal injury: basic science and evaluation. J Am Acad Orthop Surg2002; 10:168–176.
Gelb HJ, Glasgow SG, Sapega AA, Torg JS. Magnetic resonance imaging of knee disorders. Clinical value and cost-effectiveness in a sports medicine practice. Am J Sports Med1996; 24:99–103.
Beattie KA, Boulos P, Pui M, et al. Abnormalities identified in the knees of asymptomatic volunteers using peripheral magnetic resonance imaging. Osteoarthritis Cartilage2005; 13:181–186.
Ilan DI, Tejwani N, Keschner M, Leibman M. Quadriceps tendon rupture. J Am Acad Orthop Surg2003; 11:192–200.
Monica Koplas, MD Imaging Institute, Cleveland Clinic
Jean Schils, MD Head, Section of Emergency Radiology and Musculoskeletal Radiology, Imaging Institute, Cleveland Clinic
Murali Sundaram, MD, MBBS Section of Musculoskeletal Radiology, Imaging Institute, Cleveland Clinic, and Professor of Radiology, Cleveland Clinic Lerner School of Medicine of Case Western Reserve University
Address: Jean Schils, MD, Imaging Institute, A21, Cleveland Clinic, 9500 Euclid Avenue, Cleveland, OH 44195.
Monica Koplas, MD Imaging Institute, Cleveland Clinic
Jean Schils, MD Head, Section of Emergency Radiology and Musculoskeletal Radiology, Imaging Institute, Cleveland Clinic
Murali Sundaram, MD, MBBS Section of Musculoskeletal Radiology, Imaging Institute, Cleveland Clinic, and Professor of Radiology, Cleveland Clinic Lerner School of Medicine of Case Western Reserve University
Address: Jean Schils, MD, Imaging Institute, A21, Cleveland Clinic, 9500 Euclid Avenue, Cleveland, OH 44195.
Author and Disclosure Information
Monica Koplas, MD Imaging Institute, Cleveland Clinic
Jean Schils, MD Head, Section of Emergency Radiology and Musculoskeletal Radiology, Imaging Institute, Cleveland Clinic
Murali Sundaram, MD, MBBS Section of Musculoskeletal Radiology, Imaging Institute, Cleveland Clinic, and Professor of Radiology, Cleveland Clinic Lerner School of Medicine of Case Western Reserve University
Address: Jean Schils, MD, Imaging Institute, A21, Cleveland Clinic, 9500 Euclid Avenue, Cleveland, OH 44195.
Radiography plays a key role in the initial evaluation of acute knee pain in adults. Yet conflicting studies and the absence of clear guidelines may leave the primary care physician uncertain as to which imaging test to order—ie, whether radiography is sufficient, and when computed tomography (CT) or magnetic resonance imaging (MRI) is needed. This article reviews the indications for radiologic examination of the knee and discusses indications for cross-sectional imaging studies. Imaging in oncology patients is not discussed here.
ACUTE KNEE PAIN: A TYPICAL SCENARIO
A 47-year-old woman presents to the emergency department with left knee pain after a motor vehicle accident that occurred the day before. The car she was driving hit a tree, and she hit her knee on the dashboard. She was wearing a seatbelt at the time of the accident. She says she was unable to walk immediately after the accident because of knee pain.
The initial examination in the emergency room reveals swelling and pain throughout the range of motion. The anterior drawer test and the Lachman test are negative (see below).
Figure 1. This anteroposterior radiograph of a 47-year-old woman who was in a motor vehicle accident shows focal ossification adjacent to the medial femoral condyle (arrow) but no evidence of acute fracture.
Initial radiographs (Figure 1) reveal no acute fracture or effusion, but focal ossification adjacent to the proximal medial femoral condyle may indicate a past injury to the medial collateral ligament.
The patient is discharged home with a knee immobilizer, pain medication, and crutches, with instructions for a follow-up visit in the orthopedics clinic.
Five days later, she returns to the emergency department complaining of continuing knee pain. She says the knee gives way when she puts weight on it. The physical findings are unchanged, and she is discharged home with a follow-up appointment with orthopedics in 3 days.
At the follow-up visit, she complains of persistent knee pain in the medial aspect of the knee joint. Physical examination is difficult because of pain and swelling, and it reveals mild joint effusion with no gross instability. She has pain on the medial side with valgus stress, but there appears to be a hard end point. There is no posterior sag, and the Lachman test is negative.
Based on the physical examination and the patient’s complaints, she receives a diagnosis of medial collateral ligament strain and injury. She is given a hinged brace and is instructed to undergo a physical rehabilitation program.
Three weeks after the initial evaluation, she returns to the orthopedics clinic with continuing knee problems. Mild knee effusion persists, but she has less pain and swelling, allowing a more complete examination. The examination reveals less limitation of range of motion and a hint of positivity on the Lachman test. The knee is diffusely tender, and the pain seems out of proportion with the maneuvers used during the examination. She requests more pain medication. You suspect internal derangement of the knee. Which imaging test should you order to further evaluate this patient?
A SYSTEMATIC AND COST-EFFECTIVE APPROACH IS NEEDED
The case presented above represents a typical scenario for the presentation of acute knee pain and illustrates the diagnostic challenges.
Knee pain is a common reason for emergency room visits, and it accounts for approximately 1.9 million visits to primary care clinics annually.1 In the emergency department, most patients undergo plain radiography to assess for fracture, yet approximately 92% of radiographic studies do not show a fracture.2 Clearly, the evaluation of knee pain requires a systematic, accurate, and cost-effective approach.
Key elements of the physical examination
In acute knee pain, accurate diagnosis begins with a detailed history and physical examination.
The anterior drawer test is done to evaluate the anterior cruciate ligament. With the relaxed knee flexed to approximately 80° and the foot stabilized in a neutral position, the examiner grasps the proximal tibia in a firm yet gentle grip, and then applies anterior force, noting the degree of anterior displacement compared with the other knee.
The Lachman test, a variation of the anterior drawer test, is more definitive for the anterior cruciate ligament and is carried out with the knee in 15° of flexion and external rotation, in order to relax the iliotibial band. The upper hand grasps the distal thigh, and the lower hand, with the thumb on the tibial tubercle, pulls the tibia forward. The degree of anterior motion in millimeters is noted and compared with that on the other side, and the end point is graded as “soft” or “hard.” An end point is considered hard when a ligament abruptly halts the motion of the bone being tested against the stabilized bone. An end point is considered soft when the ligament is disrupted and the restraints are the more elastic secondary stabilizers.
Debate continues
Some authors contend that in skilled hands a thorough history, physical examination, and radiographic examination are sufficient to diagnose trauma-related intra-articular knee disorders.3 Others contend that MRI plays a key role in the initial evaluation. A number of studies4–8 have shown that using MRI in the initial evaluation not only identifies key lesions, but also may eliminate the need for an invasive diagnostic procedure (ie, arthroscopy).
For example, MRI can reveal fracture, stress fracture, insufficiency fracture, and transient patellar dislocation—conditions that may satisfactorily explain knee symptoms.
PLAIN RADIOGRAPHY STILL THE FIRST STEP IN KNEE EVALUATION
Radiography is the first step in the evaluation of knee pain. It is quick and inexpensive and can yield many diagnostic clues. It can readily reveal fractures, osteochondral defects, bony lesions, joint effusions, joint space narrowing, and bone misalignment.
In patients with knee trauma, supine anteroposterior and cross-table lateral radiographic images are generally obtained. In patients whose knee pain is not due to trauma, standing projections are done, as well as dedicated projection of the patellofemoral articulation. A standing series is most helpful for evaluating joint space and alignment.
Applying the Ottawa rules
When a patient presents to the emergency room with acute knee pain, the immediate concern is whether he or she has a fracture. The Ottawa knee rules9 for when to order radiography in adults with knee pain are highly sensitive for detecting a clinically important fracture. If any one of the five Ottawa criteria applies—ie, the patient is age 55 or older, has tenderness at the head of the fibula, has patellar tenderness, is unable to flex the knee to 90°, or is unable to bear weight—then radiography is indicated.
While studies have validated the ability of the Ottawa rules to detect important fractures in acute knee injury,2,10 fracture is the cause of only a small percentage of knee complaints in the primary care setting. More common causes include osteoarthritis, meniscal injury, ligamental injury, and crystal arthropathy, and these account for approximately half of all diagnoses. Sprain and strain account for most of the rest of knee injuries.1
Acute exacerbations of osteoarthritis
Osteoarthritis is a chronic problem, yet it is not unusual for a patient to present to the primary care physician with an acute exacerbation of joint pain. The clinical hallmarks include age over 50, stiffness lasting less than 30 minutes, bony enlargement and tenderness, and crepitus. The radiographic hallmarks, according to the Kellgren-Lawrence grading scale, are joint space narrowing, osteophytes, subchondral cysts, and sclerosis. These radiographic findings correlate well with clinical findings in these patients.11
Situations in which radiography is less helpful
In some cases the radiographic findings may not explain the patient’s clinical signs and symptoms. For example, in suspected crystalline and septic arthritis, the clinical presentation may include warmth, erythema, and effusion. Arthrocentesis would be indicated in such a patient. Indeed, in the case of suspected pseudogout, chondrocalcinosis may be radiographically evident. However, it is also present in many patients without symptoms or with osteoarthritis, so radiographic evidence does not provide a definite diagnosis.
While radiography may not always identify the cause of knee pain, it is useful in excluding serious problems such as fractures, advanced degenerative changes, and neoplasms, and it may help direct further management. Radiography is not useful in the evaluation of the cruciate and collateral ligaments, the menisci, and the hyaline cartilage of the knee and may fail to show an insufficiency or stress fracture. To evaluate these structures and associated soft tissues, MRI is preferable.
COMPUTED TOMOGRAPHY IN ACUTE KNEE PAIN
Figure 2. A 56-year-old woman with left knee pain after a fall. (A) Anteroposterior radiograph shows fracture of the tibial eminence (short arrow). The subchondral bone of the lateral tibial plateau is indistinct (long arrow), leading to suspicion of tibial plateau fracture. (B) A lateral radiograph shows joint effusion (short arrow). The lateral tibial plateau is depressed posteriorly (long arrow). (C) Sagittal computed tomography (CT) shows fracture of the tibial eminence (arrows) extending to the lateral tibial plateau. (D) Sagittal CT shows depression of the lateral tibial plateau (arrow). (E) Coronal CT shows fracture of the tibial eminence (short arrow) and tibial plateau (long arrow). The fibular head (arrowhead) is intact.
CT is the imaging method of choice when patients have knee trauma but radiographs are negative for fracture. CT can detect and help analyze fracture better, and it can better define fractures seen on conventional radiographs (Figure 2). CT is fast, the procedure lasting only a few minutes. It costs less than MRI and provides a better picture of bony detail. Because of this, CT is generally recommended in patients with knee trauma, since it can show fractures too subtle for radiography.
CURRENT USES OF MRI TO EVALUATE ACUTE KNEE PAIN
As mentioned above, MRI is useful in evaluating suspected meniscal and ligamentous injuries.
Figure 3. T2-weighted MRI of the left knee of the 47-year-old woman who was in a motor vehicle accident. (A) A coronal image reveals a fragment of the lateral meniscus displaced into the notch (long arrow). The medial meniscus is also shortened (short arrow). Edema (arrowhead) of the tibial plateau is consistent with bone bruise. (B) A sagittal image through the intercondylar notch shows absence of the anterior cruciate ligament (red arrow). The patella (short white arrow) and intact extensor mechanism (long white arrows) are also seen. (C) A sagittal image through the medial compartment shows the medial tibial plateau (short arrow) and the medial femoral condyle (long arrow). There is a tear of the posterior aspect of the medial meniscus, which appears shortened (red arrow). (D) A sagittal image of the lateral compartment shows the lateral tibial plateau (short white arrow) and the lateral femoral condyle (long white arrow). The posterior horn of the lateral meniscus (red arrow) is missing. The fibula (white arrowhead) is intact.
Patients with meniscal injury may report a history of twisting injury while bearing weight. Symptoms may include locking or catching, with loss of motion related to a mechanical block. Ligamentous injury may be due to a direct blow or forceful stress while the patient is bearing weight. In tearing of the anterior cruciate ligament, the patient may report having heard a pop at the time of injury, followed by swelling. Valgus and varus stresses may lead to collateral ligament injury. Often, more than one injury coexists: more than a third of meniscal tears are associated with anterior cruciate ligament injury.12
Figure 3 shows how T2-weighted MRI was used to evaluate for suspected meniscal injury in our 47-year-old female patient with left knee pain after a motor vehicle accident.
Figure 4. A 35-year-old man with intermittent locking of the right knee following a snowboarding injury underwent sagittal T2-weighted MRI of the right knee. (A) An image through the intercondylar notch shows the femur (long white arrow), proximal tibia (short white arrow), and patella (white arrowhead), as well as a “double posterior cruciate ligament” sign (red arrows), representing a “bucket-handle” tear of the medial meniscus, which is displaced into the intercondylar notch. The normal posterior cruciate ligament is the most posterior structure, denoted by the arrow on the right, and the smaller, inferior structure that resembles the ligament is the displaced meniscus. (B) An image of the medial compartment shows the medial tibial plateau (long white arrow), with a focal region of full-thickness loss of the articular cartilage (short red arrow) on the weight-bearing surface of the medial femoral condyle, likely representing an acute chondral fracture. Note the large knee effusion (long red arrow) and shortening of the medial meniscus (short white arrow). An anterior cruciate ligament tear, not shown, was also identified.Figure 4 shows how sagittal T2-weighted MRI was used in a 35-year-old man with intermittent locking of the right knee following a snowboarding injury. In this patient, MRI was able to uncover coexisting injuries.
Still a matter of debate
MRI’s role in the diagnosis of knee pain is still a contentious issue.
Advantages of MRI are that it is noninvasive, it does not use ionizing radiation, it gives multiplanar images, and it provides images of soft-tissue structures, which other imaging methods cannot.12 It is a well-proven and widely accepted test. Its sensitivity for detecting meniscal and cruciate ligament injury ranges from 75% to 88%,1 and it can help in the evaluation of other injuries for which radiography is not useful, including synovitis, bone bruise, stress or insufficiency fracture, osteochondral defects, and osteonecrosis.
In addition, several studies show that using MRI to establish the diagnosis in acute knee pain can mean that 22% to 42% fewer arthroscopic procedures need to be performed.4–8 Authors of a prospective double-blind study8 recommended that MRI be used in patients with acute knee injury when the findings of the clinical history and examination by orthopedic surgeons prove equivocal.8 MRI evaluation is especially desirable for young, active patients who wish to resume activity as soon as possible.
A routine MRI examination consists of T1- and T2-weighted images in three planes, although the number of sequences and planes varies from hospital to hospital. The use of gadolinium contrast is indicated only when osteomyelitis, septic arthritis, or a mass is suspected.
Disadvantages of MRI include its cost: Medicare reimbursement for knee MRI is around $400, compared with $200 for knee CT and $50 for knee radiography with four views. Also, while studies have shown MRI to have a high sensitivity and specificity in the diagnosis of acute knee injury, some have reported a high false-positive rate for the detection of meniscal tear.13,14 MRI has also been shown to have a lower sensitivity than arthroscopy for lesions of the articular cartilage.13 Furthermore, MRI has been shown to reveal cartilage lesions, osteophytes, and meniscal abnormalities in asymptomatic study volunteers with no history of pain, trauma or knee disease.14 Therefore, findings on MRI must closely correlate with findings on the history and physical examination.
Additional indications for knee MRI
Cartilage can be assessed on routine MRI sequences of the knee. Since closed MRI systems have more powerful magnets than open systems, closed MRI systems provide greater anatomic detail.
MRI can identify other lesions, such as spontaneous osteonecrosis of the knee, usually seen in elderly women who may present with sudden knee pain. In such patients, MRI findings of focal replacement of the bone marrow and surrounding edema are specific for osteonecrosis.
Opinions vary as to whether bone marrow edema is always associated with pain. Sequential MRI studies have shown persistence of bone marrow edema for 2 years in patients with degenerative arthritis whose symptoms have waned. Bone marrow edema may be associated with pain but may be absent or inconsequential in the presence of pain.
Because fluid-sensitive T2-weighted MRI is exquisitely sensitive for mobile water protons (ie, in bone marrow edema), it is important that a cause for the edema-like signal be sought on the MRI scan, since this finding is nonspecific and may be associated with articular disease, trauma, osteonecrosis, infection, or bone tumors. Additionally, clinicians need to be aware that the findings on MRI depend on the quality of the study, and are influenced by technical factors such as magnet strength, imaging planes, and use of surface coils.
MRI should be used in patients in whom surgical treatment, ie, arthroscopy, is being considered. As discussed above, several studies have shown that a significant number of unnecessary arthroscopies may be prevented when preceded by an MRI examination.
Figure 5. A 45-year-old man with left knee pain after a motorcycle accident. (A) Lateral radiograph shows an osseous fragment at the posterior aspect of the knee joint (long arrow). This was thought to represent an avulsion fracture of the posterior cruciate ligament. There is also a knee effusion (short arrow). (B) Sagittal proton-density-weighted MRI through the intercondylar notch shows an intact anterior cruciate ligament (white arrow). There is an avulsion fracture of the posterior proximal tibia (red arrow) at the attachment of the posterior cruciate ligament. The fragment, which is displaced proximally, is attached to the posterior cruciate ligament, which remains intact.
Other indications include cases in which clinical findings are equivocal in the setting of acute injury, in competitive athletes in whom an immediate diagnosis and treatment is required, and in patients who present a high surgical risk. MRI should not be routinely used to diagnose the painful or injured knee,13 and if the skilled physical examination does not indicate findings of ligamentous or meniscal injury, conservative therapy should be prescribed.1 MRI is also not useful and offers little for patients in whom changes of degenerative joint disease are evident on radiographs.
Figure 5 shows the use of MRI in the evaluation of a 45-year-old man with left knee pain after a motorcycle accident.
ULTRASONOGRAPHY HAS ONLY A LIMITED ROLE
Ultrasonography does not play a major role in the evaluation of acute knee pain in the United States, in part because the accuracy of the results depend much on the technical skills and experience of the operator.
Ultrasonography can be useful in evaluating for rupture of the quadriceps and patellar tendon, or to assess a repaired tendon after surgery,15 and it is a quick and reliable way to determine the presence of joint effusion and popliteal cyst. It is also used to guide needle placement for joint aspiration and injection.
Radiography plays a key role in the initial evaluation of acute knee pain in adults. Yet conflicting studies and the absence of clear guidelines may leave the primary care physician uncertain as to which imaging test to order—ie, whether radiography is sufficient, and when computed tomography (CT) or magnetic resonance imaging (MRI) is needed. This article reviews the indications for radiologic examination of the knee and discusses indications for cross-sectional imaging studies. Imaging in oncology patients is not discussed here.
ACUTE KNEE PAIN: A TYPICAL SCENARIO
A 47-year-old woman presents to the emergency department with left knee pain after a motor vehicle accident that occurred the day before. The car she was driving hit a tree, and she hit her knee on the dashboard. She was wearing a seatbelt at the time of the accident. She says she was unable to walk immediately after the accident because of knee pain.
The initial examination in the emergency room reveals swelling and pain throughout the range of motion. The anterior drawer test and the Lachman test are negative (see below).
Figure 1. This anteroposterior radiograph of a 47-year-old woman who was in a motor vehicle accident shows focal ossification adjacent to the medial femoral condyle (arrow) but no evidence of acute fracture.
Initial radiographs (Figure 1) reveal no acute fracture or effusion, but focal ossification adjacent to the proximal medial femoral condyle may indicate a past injury to the medial collateral ligament.
The patient is discharged home with a knee immobilizer, pain medication, and crutches, with instructions for a follow-up visit in the orthopedics clinic.
Five days later, she returns to the emergency department complaining of continuing knee pain. She says the knee gives way when she puts weight on it. The physical findings are unchanged, and she is discharged home with a follow-up appointment with orthopedics in 3 days.
At the follow-up visit, she complains of persistent knee pain in the medial aspect of the knee joint. Physical examination is difficult because of pain and swelling, and it reveals mild joint effusion with no gross instability. She has pain on the medial side with valgus stress, but there appears to be a hard end point. There is no posterior sag, and the Lachman test is negative.
Based on the physical examination and the patient’s complaints, she receives a diagnosis of medial collateral ligament strain and injury. She is given a hinged brace and is instructed to undergo a physical rehabilitation program.
Three weeks after the initial evaluation, she returns to the orthopedics clinic with continuing knee problems. Mild knee effusion persists, but she has less pain and swelling, allowing a more complete examination. The examination reveals less limitation of range of motion and a hint of positivity on the Lachman test. The knee is diffusely tender, and the pain seems out of proportion with the maneuvers used during the examination. She requests more pain medication. You suspect internal derangement of the knee. Which imaging test should you order to further evaluate this patient?
A SYSTEMATIC AND COST-EFFECTIVE APPROACH IS NEEDED
The case presented above represents a typical scenario for the presentation of acute knee pain and illustrates the diagnostic challenges.
Knee pain is a common reason for emergency room visits, and it accounts for approximately 1.9 million visits to primary care clinics annually.1 In the emergency department, most patients undergo plain radiography to assess for fracture, yet approximately 92% of radiographic studies do not show a fracture.2 Clearly, the evaluation of knee pain requires a systematic, accurate, and cost-effective approach.
Key elements of the physical examination
In acute knee pain, accurate diagnosis begins with a detailed history and physical examination.
The anterior drawer test is done to evaluate the anterior cruciate ligament. With the relaxed knee flexed to approximately 80° and the foot stabilized in a neutral position, the examiner grasps the proximal tibia in a firm yet gentle grip, and then applies anterior force, noting the degree of anterior displacement compared with the other knee.
The Lachman test, a variation of the anterior drawer test, is more definitive for the anterior cruciate ligament and is carried out with the knee in 15° of flexion and external rotation, in order to relax the iliotibial band. The upper hand grasps the distal thigh, and the lower hand, with the thumb on the tibial tubercle, pulls the tibia forward. The degree of anterior motion in millimeters is noted and compared with that on the other side, and the end point is graded as “soft” or “hard.” An end point is considered hard when a ligament abruptly halts the motion of the bone being tested against the stabilized bone. An end point is considered soft when the ligament is disrupted and the restraints are the more elastic secondary stabilizers.
Debate continues
Some authors contend that in skilled hands a thorough history, physical examination, and radiographic examination are sufficient to diagnose trauma-related intra-articular knee disorders.3 Others contend that MRI plays a key role in the initial evaluation. A number of studies4–8 have shown that using MRI in the initial evaluation not only identifies key lesions, but also may eliminate the need for an invasive diagnostic procedure (ie, arthroscopy).
For example, MRI can reveal fracture, stress fracture, insufficiency fracture, and transient patellar dislocation—conditions that may satisfactorily explain knee symptoms.
PLAIN RADIOGRAPHY STILL THE FIRST STEP IN KNEE EVALUATION
Radiography is the first step in the evaluation of knee pain. It is quick and inexpensive and can yield many diagnostic clues. It can readily reveal fractures, osteochondral defects, bony lesions, joint effusions, joint space narrowing, and bone misalignment.
In patients with knee trauma, supine anteroposterior and cross-table lateral radiographic images are generally obtained. In patients whose knee pain is not due to trauma, standing projections are done, as well as dedicated projection of the patellofemoral articulation. A standing series is most helpful for evaluating joint space and alignment.
Applying the Ottawa rules
When a patient presents to the emergency room with acute knee pain, the immediate concern is whether he or she has a fracture. The Ottawa knee rules9 for when to order radiography in adults with knee pain are highly sensitive for detecting a clinically important fracture. If any one of the five Ottawa criteria applies—ie, the patient is age 55 or older, has tenderness at the head of the fibula, has patellar tenderness, is unable to flex the knee to 90°, or is unable to bear weight—then radiography is indicated.
While studies have validated the ability of the Ottawa rules to detect important fractures in acute knee injury,2,10 fracture is the cause of only a small percentage of knee complaints in the primary care setting. More common causes include osteoarthritis, meniscal injury, ligamental injury, and crystal arthropathy, and these account for approximately half of all diagnoses. Sprain and strain account for most of the rest of knee injuries.1
Acute exacerbations of osteoarthritis
Osteoarthritis is a chronic problem, yet it is not unusual for a patient to present to the primary care physician with an acute exacerbation of joint pain. The clinical hallmarks include age over 50, stiffness lasting less than 30 minutes, bony enlargement and tenderness, and crepitus. The radiographic hallmarks, according to the Kellgren-Lawrence grading scale, are joint space narrowing, osteophytes, subchondral cysts, and sclerosis. These radiographic findings correlate well with clinical findings in these patients.11
Situations in which radiography is less helpful
In some cases the radiographic findings may not explain the patient’s clinical signs and symptoms. For example, in suspected crystalline and septic arthritis, the clinical presentation may include warmth, erythema, and effusion. Arthrocentesis would be indicated in such a patient. Indeed, in the case of suspected pseudogout, chondrocalcinosis may be radiographically evident. However, it is also present in many patients without symptoms or with osteoarthritis, so radiographic evidence does not provide a definite diagnosis.
While radiography may not always identify the cause of knee pain, it is useful in excluding serious problems such as fractures, advanced degenerative changes, and neoplasms, and it may help direct further management. Radiography is not useful in the evaluation of the cruciate and collateral ligaments, the menisci, and the hyaline cartilage of the knee and may fail to show an insufficiency or stress fracture. To evaluate these structures and associated soft tissues, MRI is preferable.
COMPUTED TOMOGRAPHY IN ACUTE KNEE PAIN
Figure 2. A 56-year-old woman with left knee pain after a fall. (A) Anteroposterior radiograph shows fracture of the tibial eminence (short arrow). The subchondral bone of the lateral tibial plateau is indistinct (long arrow), leading to suspicion of tibial plateau fracture. (B) A lateral radiograph shows joint effusion (short arrow). The lateral tibial plateau is depressed posteriorly (long arrow). (C) Sagittal computed tomography (CT) shows fracture of the tibial eminence (arrows) extending to the lateral tibial plateau. (D) Sagittal CT shows depression of the lateral tibial plateau (arrow). (E) Coronal CT shows fracture of the tibial eminence (short arrow) and tibial plateau (long arrow). The fibular head (arrowhead) is intact.
CT is the imaging method of choice when patients have knee trauma but radiographs are negative for fracture. CT can detect and help analyze fracture better, and it can better define fractures seen on conventional radiographs (Figure 2). CT is fast, the procedure lasting only a few minutes. It costs less than MRI and provides a better picture of bony detail. Because of this, CT is generally recommended in patients with knee trauma, since it can show fractures too subtle for radiography.
CURRENT USES OF MRI TO EVALUATE ACUTE KNEE PAIN
As mentioned above, MRI is useful in evaluating suspected meniscal and ligamentous injuries.
Figure 3. T2-weighted MRI of the left knee of the 47-year-old woman who was in a motor vehicle accident. (A) A coronal image reveals a fragment of the lateral meniscus displaced into the notch (long arrow). The medial meniscus is also shortened (short arrow). Edema (arrowhead) of the tibial plateau is consistent with bone bruise. (B) A sagittal image through the intercondylar notch shows absence of the anterior cruciate ligament (red arrow). The patella (short white arrow) and intact extensor mechanism (long white arrows) are also seen. (C) A sagittal image through the medial compartment shows the medial tibial plateau (short arrow) and the medial femoral condyle (long arrow). There is a tear of the posterior aspect of the medial meniscus, which appears shortened (red arrow). (D) A sagittal image of the lateral compartment shows the lateral tibial plateau (short white arrow) and the lateral femoral condyle (long white arrow). The posterior horn of the lateral meniscus (red arrow) is missing. The fibula (white arrowhead) is intact.
Patients with meniscal injury may report a history of twisting injury while bearing weight. Symptoms may include locking or catching, with loss of motion related to a mechanical block. Ligamentous injury may be due to a direct blow or forceful stress while the patient is bearing weight. In tearing of the anterior cruciate ligament, the patient may report having heard a pop at the time of injury, followed by swelling. Valgus and varus stresses may lead to collateral ligament injury. Often, more than one injury coexists: more than a third of meniscal tears are associated with anterior cruciate ligament injury.12
Figure 3 shows how T2-weighted MRI was used to evaluate for suspected meniscal injury in our 47-year-old female patient with left knee pain after a motor vehicle accident.
Figure 4. A 35-year-old man with intermittent locking of the right knee following a snowboarding injury underwent sagittal T2-weighted MRI of the right knee. (A) An image through the intercondylar notch shows the femur (long white arrow), proximal tibia (short white arrow), and patella (white arrowhead), as well as a “double posterior cruciate ligament” sign (red arrows), representing a “bucket-handle” tear of the medial meniscus, which is displaced into the intercondylar notch. The normal posterior cruciate ligament is the most posterior structure, denoted by the arrow on the right, and the smaller, inferior structure that resembles the ligament is the displaced meniscus. (B) An image of the medial compartment shows the medial tibial plateau (long white arrow), with a focal region of full-thickness loss of the articular cartilage (short red arrow) on the weight-bearing surface of the medial femoral condyle, likely representing an acute chondral fracture. Note the large knee effusion (long red arrow) and shortening of the medial meniscus (short white arrow). An anterior cruciate ligament tear, not shown, was also identified.Figure 4 shows how sagittal T2-weighted MRI was used in a 35-year-old man with intermittent locking of the right knee following a snowboarding injury. In this patient, MRI was able to uncover coexisting injuries.
Still a matter of debate
MRI’s role in the diagnosis of knee pain is still a contentious issue.
Advantages of MRI are that it is noninvasive, it does not use ionizing radiation, it gives multiplanar images, and it provides images of soft-tissue structures, which other imaging methods cannot.12 It is a well-proven and widely accepted test. Its sensitivity for detecting meniscal and cruciate ligament injury ranges from 75% to 88%,1 and it can help in the evaluation of other injuries for which radiography is not useful, including synovitis, bone bruise, stress or insufficiency fracture, osteochondral defects, and osteonecrosis.
In addition, several studies show that using MRI to establish the diagnosis in acute knee pain can mean that 22% to 42% fewer arthroscopic procedures need to be performed.4–8 Authors of a prospective double-blind study8 recommended that MRI be used in patients with acute knee injury when the findings of the clinical history and examination by orthopedic surgeons prove equivocal.8 MRI evaluation is especially desirable for young, active patients who wish to resume activity as soon as possible.
A routine MRI examination consists of T1- and T2-weighted images in three planes, although the number of sequences and planes varies from hospital to hospital. The use of gadolinium contrast is indicated only when osteomyelitis, septic arthritis, or a mass is suspected.
Disadvantages of MRI include its cost: Medicare reimbursement for knee MRI is around $400, compared with $200 for knee CT and $50 for knee radiography with four views. Also, while studies have shown MRI to have a high sensitivity and specificity in the diagnosis of acute knee injury, some have reported a high false-positive rate for the detection of meniscal tear.13,14 MRI has also been shown to have a lower sensitivity than arthroscopy for lesions of the articular cartilage.13 Furthermore, MRI has been shown to reveal cartilage lesions, osteophytes, and meniscal abnormalities in asymptomatic study volunteers with no history of pain, trauma or knee disease.14 Therefore, findings on MRI must closely correlate with findings on the history and physical examination.
Additional indications for knee MRI
Cartilage can be assessed on routine MRI sequences of the knee. Since closed MRI systems have more powerful magnets than open systems, closed MRI systems provide greater anatomic detail.
MRI can identify other lesions, such as spontaneous osteonecrosis of the knee, usually seen in elderly women who may present with sudden knee pain. In such patients, MRI findings of focal replacement of the bone marrow and surrounding edema are specific for osteonecrosis.
Opinions vary as to whether bone marrow edema is always associated with pain. Sequential MRI studies have shown persistence of bone marrow edema for 2 years in patients with degenerative arthritis whose symptoms have waned. Bone marrow edema may be associated with pain but may be absent or inconsequential in the presence of pain.
Because fluid-sensitive T2-weighted MRI is exquisitely sensitive for mobile water protons (ie, in bone marrow edema), it is important that a cause for the edema-like signal be sought on the MRI scan, since this finding is nonspecific and may be associated with articular disease, trauma, osteonecrosis, infection, or bone tumors. Additionally, clinicians need to be aware that the findings on MRI depend on the quality of the study, and are influenced by technical factors such as magnet strength, imaging planes, and use of surface coils.
MRI should be used in patients in whom surgical treatment, ie, arthroscopy, is being considered. As discussed above, several studies have shown that a significant number of unnecessary arthroscopies may be prevented when preceded by an MRI examination.
Figure 5. A 45-year-old man with left knee pain after a motorcycle accident. (A) Lateral radiograph shows an osseous fragment at the posterior aspect of the knee joint (long arrow). This was thought to represent an avulsion fracture of the posterior cruciate ligament. There is also a knee effusion (short arrow). (B) Sagittal proton-density-weighted MRI through the intercondylar notch shows an intact anterior cruciate ligament (white arrow). There is an avulsion fracture of the posterior proximal tibia (red arrow) at the attachment of the posterior cruciate ligament. The fragment, which is displaced proximally, is attached to the posterior cruciate ligament, which remains intact.
Other indications include cases in which clinical findings are equivocal in the setting of acute injury, in competitive athletes in whom an immediate diagnosis and treatment is required, and in patients who present a high surgical risk. MRI should not be routinely used to diagnose the painful or injured knee,13 and if the skilled physical examination does not indicate findings of ligamentous or meniscal injury, conservative therapy should be prescribed.1 MRI is also not useful and offers little for patients in whom changes of degenerative joint disease are evident on radiographs.
Figure 5 shows the use of MRI in the evaluation of a 45-year-old man with left knee pain after a motorcycle accident.
ULTRASONOGRAPHY HAS ONLY A LIMITED ROLE
Ultrasonography does not play a major role in the evaluation of acute knee pain in the United States, in part because the accuracy of the results depend much on the technical skills and experience of the operator.
Ultrasonography can be useful in evaluating for rupture of the quadriceps and patellar tendon, or to assess a repaired tendon after surgery,15 and it is a quick and reliable way to determine the presence of joint effusion and popliteal cyst. It is also used to guide needle placement for joint aspiration and injection.
References
Jackson JL, O’Malley PG, Kroenke K. Evaluation of acute knee pain in primary care. Ann Intern Med2003; 139:575–588.
Steill IG, Greenberg GH, Wells GA, et al. Prospective validation of a decision rule for the use of radiographs in acute knee injuries. JAMA1996; 275:611–615.
O’Shea KJ, Murphy DP, Heekin RD, Herzwurm PJ. The diagnostic accuracy of history, physical examination, and radiographs in the evaluation of traumatic knee disorders. Am J Sports Med1996; 24:164–167.
Spiers AS, Meagher T, Ostlere SJ, Wilson DJ, Dodd CA. Can MRI of the knee affect arthroscopic practice?J Bone Joint Surg1993; 75:49–52.
Bui-Mansfield LT, Youngberg RA, Warme W, Pitcher JD, Nguyen PL. Potential cost savings of MR imaging obtained before arthroscopy of the knee: evaluation of 50 consecutive patients. AJR Am J Roentgenol1997; 168:913–918.
Rangger C, Klestil T, Kathrein A, Inderster A, Hamid L. Influence of magnetic resonance imaging on indications for arthroscopy of the knee. Clin Orthop Rel Res1996; 330:133–142.
Mackenzie R, Dixon AK, Keene GS, Hollingsworth W, Lomas DJ, Villar RN. Magnetic resonance imaging of the knee: assessment of effectiveness. Clin Radiol1996; 51:245–250.
Munshi M, Davidson M, MacDonald PB, Froese W, Sutherland K. The efficacy of magnetic resonance imaging in acute knee injuries. Clin J Sport Med2000; 10:34–39.
Steill IG, Wells GA, Hoag RH, et al. Implementation of the Ottawa knee rule for the use of radiography in acute knee injuries. JAMA1997; 278:2075–2079.
Tigges S, Pitts S, Mukundan S, Morrison D, Olson M, Shahriara A. External validation of the Ottawa knee rules in an urban trauma center in the United States. AJR Am J Roentgenol1999; 172:1069–1071.
Claessens AA, Schouten JS, van den Ouweland FA, Valkenburg HA. Do clinical findings associate with radiographic osteoarthritis of the knee?Ann Rheum Dis1990; 49:771–774.
Gries PE, Bardana DE, Holmstrom MC, Burks RT. Meniscal injury: basic science and evaluation. J Am Acad Orthop Surg2002; 10:168–176.
Gelb HJ, Glasgow SG, Sapega AA, Torg JS. Magnetic resonance imaging of knee disorders. Clinical value and cost-effectiveness in a sports medicine practice. Am J Sports Med1996; 24:99–103.
Beattie KA, Boulos P, Pui M, et al. Abnormalities identified in the knees of asymptomatic volunteers using peripheral magnetic resonance imaging. Osteoarthritis Cartilage2005; 13:181–186.
Ilan DI, Tejwani N, Keschner M, Leibman M. Quadriceps tendon rupture. J Am Acad Orthop Surg2003; 11:192–200.
References
Jackson JL, O’Malley PG, Kroenke K. Evaluation of acute knee pain in primary care. Ann Intern Med2003; 139:575–588.
Steill IG, Greenberg GH, Wells GA, et al. Prospective validation of a decision rule for the use of radiographs in acute knee injuries. JAMA1996; 275:611–615.
O’Shea KJ, Murphy DP, Heekin RD, Herzwurm PJ. The diagnostic accuracy of history, physical examination, and radiographs in the evaluation of traumatic knee disorders. Am J Sports Med1996; 24:164–167.
Spiers AS, Meagher T, Ostlere SJ, Wilson DJ, Dodd CA. Can MRI of the knee affect arthroscopic practice?J Bone Joint Surg1993; 75:49–52.
Bui-Mansfield LT, Youngberg RA, Warme W, Pitcher JD, Nguyen PL. Potential cost savings of MR imaging obtained before arthroscopy of the knee: evaluation of 50 consecutive patients. AJR Am J Roentgenol1997; 168:913–918.
Rangger C, Klestil T, Kathrein A, Inderster A, Hamid L. Influence of magnetic resonance imaging on indications for arthroscopy of the knee. Clin Orthop Rel Res1996; 330:133–142.
Mackenzie R, Dixon AK, Keene GS, Hollingsworth W, Lomas DJ, Villar RN. Magnetic resonance imaging of the knee: assessment of effectiveness. Clin Radiol1996; 51:245–250.
Munshi M, Davidson M, MacDonald PB, Froese W, Sutherland K. The efficacy of magnetic resonance imaging in acute knee injuries. Clin J Sport Med2000; 10:34–39.
Steill IG, Wells GA, Hoag RH, et al. Implementation of the Ottawa knee rule for the use of radiography in acute knee injuries. JAMA1997; 278:2075–2079.
Tigges S, Pitts S, Mukundan S, Morrison D, Olson M, Shahriara A. External validation of the Ottawa knee rules in an urban trauma center in the United States. AJR Am J Roentgenol1999; 172:1069–1071.
Claessens AA, Schouten JS, van den Ouweland FA, Valkenburg HA. Do clinical findings associate with radiographic osteoarthritis of the knee?Ann Rheum Dis1990; 49:771–774.
Gries PE, Bardana DE, Holmstrom MC, Burks RT. Meniscal injury: basic science and evaluation. J Am Acad Orthop Surg2002; 10:168–176.
Gelb HJ, Glasgow SG, Sapega AA, Torg JS. Magnetic resonance imaging of knee disorders. Clinical value and cost-effectiveness in a sports medicine practice. Am J Sports Med1996; 24:99–103.
Beattie KA, Boulos P, Pui M, et al. Abnormalities identified in the knees of asymptomatic volunteers using peripheral magnetic resonance imaging. Osteoarthritis Cartilage2005; 13:181–186.
Ilan DI, Tejwani N, Keschner M, Leibman M. Quadriceps tendon rupture. J Am Acad Orthop Surg2003; 11:192–200.
In the emergency department, most patients undergo plain radiography to assess for fracture, yet more than 90% of these studies do not show a fracture.
CT is useful in patients with knee trauma but normal radiographs.
MRI is the imaging modality for internal derangement of the knee.
Ultrasonography’s role in the evaluation of acute knee pain is generally limited to assessment of the extensor mechanism, joint effusion, and popliteal cyst.
Disallow All Ads
Alternative CME
Consolidated Pubs: Do Not Show Source Publication Logo