User login
Subcutaneous Actemra approved for systemic JIA
The Food and Drug Administration has approved the subcutaneous formulation of Actemra (tocilizumab) for systemic juvenile idiopathic arthritis (SJIA) for patients aged 2 years and older, according to a press release from its developer, Genentech. The intravenous formulation was approved in 2011 for this indication.

The approval is based on data the JIGSAW-118 study. This 52-week, open-label, multicenter, phase 1b pharmacokinetic/pharmacodynamic bridging study was designed to determine the appropriate dosing regimen by treating 51 patients with SJIA according to body weight.
The safety profile of subcutaneous tocilizumab was similar to that seen with intravenous tocilizumab, although there were more injection-site reactions seen with the subcutaneous formulation. Its efficacy was extrapolated based on the drug’s pharmacokinetic profile seen with IV tocilizumab in SJIA patients and with subcutaneous tocilizumab in patients with rheumatoid arthritis.
SJIA is a rare disease with limited treatment options, according to the press release. In general, JIA affects almost 300,000 children in the United States, and about 10% of those cases are SJIA.
The Food and Drug Administration has approved the subcutaneous formulation of Actemra (tocilizumab) for systemic juvenile idiopathic arthritis (SJIA) for patients aged 2 years and older, according to a press release from its developer, Genentech. The intravenous formulation was approved in 2011 for this indication.
The approval is based on data the JIGSAW-118 study. This 52-week, open-label, multicenter, phase 1b pharmacokinetic/pharmacodynamic bridging study was designed to determine the appropriate dosing regimen by treating 51 patients with SJIA according to body weight.
The safety profile of subcutaneous tocilizumab was similar to that seen with intravenous tocilizumab, although there were more injection-site reactions seen with the subcutaneous formulation. Its efficacy was extrapolated based on the drug’s pharmacokinetic profile seen with IV tocilizumab in SJIA patients and with subcutaneous tocilizumab in patients with rheumatoid arthritis.
SJIA is a rare disease with limited treatment options, according to the press release. In general, JIA affects almost 300,000 children in the United States, and about 10% of those cases are SJIA.
The Food and Drug Administration has approved the subcutaneous formulation of Actemra (tocilizumab) for systemic juvenile idiopathic arthritis (SJIA) for patients aged 2 years and older, according to a press release from its developer, Genentech. The intravenous formulation was approved in 2011 for this indication.
The approval is based on data the JIGSAW-118 study. This 52-week, open-label, multicenter, phase 1b pharmacokinetic/pharmacodynamic bridging study was designed to determine the appropriate dosing regimen by treating 51 patients with SJIA according to body weight.
The safety profile of subcutaneous tocilizumab was similar to that seen with intravenous tocilizumab, although there were more injection-site reactions seen with the subcutaneous formulation. Its efficacy was extrapolated based on the drug’s pharmacokinetic profile seen with IV tocilizumab in SJIA patients and with subcutaneous tocilizumab in patients with rheumatoid arthritis.
SJIA is a rare disease with limited treatment options, according to the press release. In general, JIA affects almost 300,000 children in the United States, and about 10% of those cases are SJIA.
FDA approves new hairy cell leukemia drug
The Food and Drug Administration (FDA) has approved moxetumomab pasudotox-tdfk (Lumoxiti), a CD22-directed cytotoxin, to treat hairy cell leukemia (HCL).
Moxetumomab pasudotox is approved to treat adults with relapsed or refractory HCL who have received at least two prior systemic therapies, including treatment with a purine nucleoside analog.
The prescribing information for moxetumomab pasudotox includes a boxed warning noting that the drug poses risks of capillary leak syndrome and hemolytic uremic syndrome. Other serious warnings include the risk of decreased renal function, infusion-related reactions, and electrolyte abnormalities.
The FDA granted the application for moxetumomab pasudotox fast track, priority review, and an orphan drug designation.
The agency approved AstraZeneca’s moxetumomab pasudotox based on results from a phase 3 trial (NCT01829711). Data from this study were presented at the 2018 annual meeting of the American Society of Clinical Oncology (abstract 7004).
The trial included 80 patients with relapsed or refractory HCL who had received at least two prior lines of therapy.
At a median of 16.7 months of follow-up, the objective response rate was 75%, the complete response (CR) rate was 41%, and the durable CR rate was 30%. Durable CR was defined as CR with hematologic remission for more than 180 days.
Most patients with a CR achieved minimal residual disease negativity (82%; 27/33).
The median duration of response was not reached, nor was the median progression-free survival.
The most common treatment-related adverse events (AEs) were nausea, peripheral edema, headache, and pyrexia. Other treatment-related AEs included infections and neutropenia.
Treatment-related AEs that led to discontinuation included capillary leak syndrome, hemolytic uremic syndrome, and increased blood creatinine.
There were three deaths in this trial, but none of them were considered treatment related.
The Food and Drug Administration (FDA) has approved moxetumomab pasudotox-tdfk (Lumoxiti), a CD22-directed cytotoxin, to treat hairy cell leukemia (HCL).
Moxetumomab pasudotox is approved to treat adults with relapsed or refractory HCL who have received at least two prior systemic therapies, including treatment with a purine nucleoside analog.
The prescribing information for moxetumomab pasudotox includes a boxed warning noting that the drug poses risks of capillary leak syndrome and hemolytic uremic syndrome. Other serious warnings include the risk of decreased renal function, infusion-related reactions, and electrolyte abnormalities.
The FDA granted the application for moxetumomab pasudotox fast track, priority review, and an orphan drug designation.
The agency approved AstraZeneca’s moxetumomab pasudotox based on results from a phase 3 trial (NCT01829711). Data from this study were presented at the 2018 annual meeting of the American Society of Clinical Oncology (abstract 7004).
The trial included 80 patients with relapsed or refractory HCL who had received at least two prior lines of therapy.
At a median of 16.7 months of follow-up, the objective response rate was 75%, the complete response (CR) rate was 41%, and the durable CR rate was 30%. Durable CR was defined as CR with hematologic remission for more than 180 days.
Most patients with a CR achieved minimal residual disease negativity (82%; 27/33).
The median duration of response was not reached, nor was the median progression-free survival.
The most common treatment-related adverse events (AEs) were nausea, peripheral edema, headache, and pyrexia. Other treatment-related AEs included infections and neutropenia.
Treatment-related AEs that led to discontinuation included capillary leak syndrome, hemolytic uremic syndrome, and increased blood creatinine.
There were three deaths in this trial, but none of them were considered treatment related.
The Food and Drug Administration (FDA) has approved moxetumomab pasudotox-tdfk (Lumoxiti), a CD22-directed cytotoxin, to treat hairy cell leukemia (HCL).
Moxetumomab pasudotox is approved to treat adults with relapsed or refractory HCL who have received at least two prior systemic therapies, including treatment with a purine nucleoside analog.
The prescribing information for moxetumomab pasudotox includes a boxed warning noting that the drug poses risks of capillary leak syndrome and hemolytic uremic syndrome. Other serious warnings include the risk of decreased renal function, infusion-related reactions, and electrolyte abnormalities.
The FDA granted the application for moxetumomab pasudotox fast track, priority review, and an orphan drug designation.
The agency approved AstraZeneca’s moxetumomab pasudotox based on results from a phase 3 trial (NCT01829711). Data from this study were presented at the 2018 annual meeting of the American Society of Clinical Oncology (abstract 7004).
The trial included 80 patients with relapsed or refractory HCL who had received at least two prior lines of therapy.
At a median of 16.7 months of follow-up, the objective response rate was 75%, the complete response (CR) rate was 41%, and the durable CR rate was 30%. Durable CR was defined as CR with hematologic remission for more than 180 days.
Most patients with a CR achieved minimal residual disease negativity (82%; 27/33).
The median duration of response was not reached, nor was the median progression-free survival.
The most common treatment-related adverse events (AEs) were nausea, peripheral edema, headache, and pyrexia. Other treatment-related AEs included infections and neutropenia.
Treatment-related AEs that led to discontinuation included capillary leak syndrome, hemolytic uremic syndrome, and increased blood creatinine.
There were three deaths in this trial, but none of them were considered treatment related.
CDC opens Emergency Operations Center in advance of Hurricane Florence
The Centers for Disease Control and Prevention is activating its Emergency Operations Center (EOC) in advance of the landfall of Hurricane Florence, according to a CDC media statement.
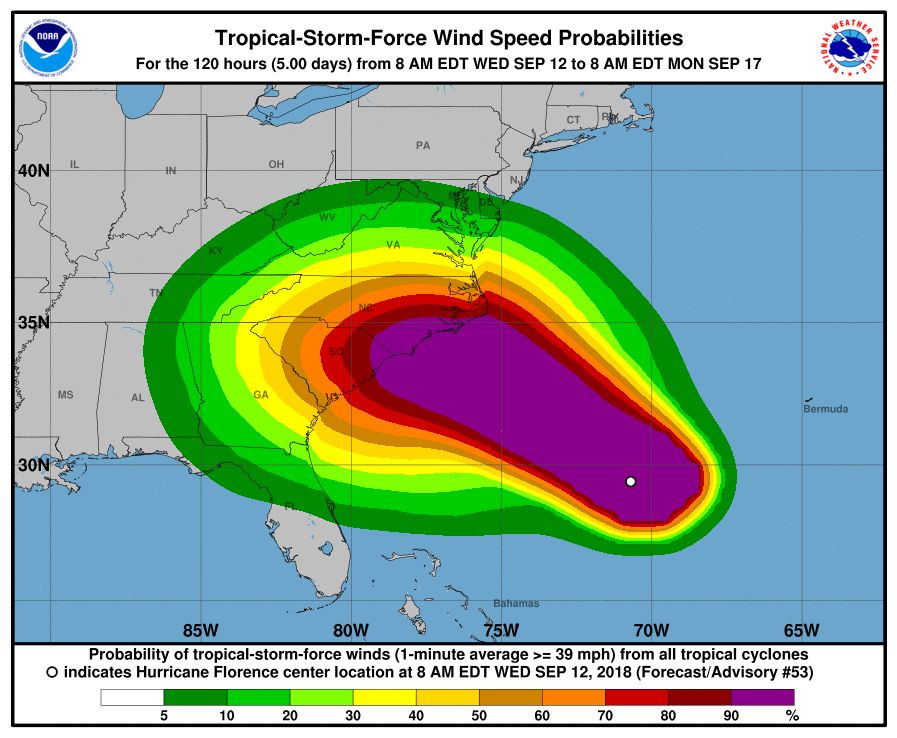
Activation of the center will allow for 24/7 management of all CDC activities before, during, and after the landfall of Hurricane Florence, including deployment of personnel and resources.
All CDC staff should be ready to provide infectious disease outbreak surveillance, public health messages, water/food safety evaluations, mold prevention and treatment, industrial contamination containment, and standing water control. The CDC is also sharing messages with the public on how to protect themselves from threats before, during, and after landfall, such as drowning and floodwater safety, carbon monoxide poisoning, downed power lines, unsafe food and water, and mold.
The EOC is the CDC’s command center for the coordination and monitoring of CDC activity with all other U.S. federal, state, and local agencies. The EOC also works with the Secretary of Health & Human Services Secretary’s Operations Center to ensure awareness and a coordinated public health and medical response, according to the statement.
Additional resources for interested parties can be found on the CDC website.
The Centers for Disease Control and Prevention is activating its Emergency Operations Center (EOC) in advance of the landfall of Hurricane Florence, according to a CDC media statement.
Activation of the center will allow for 24/7 management of all CDC activities before, during, and after the landfall of Hurricane Florence, including deployment of personnel and resources.
All CDC staff should be ready to provide infectious disease outbreak surveillance, public health messages, water/food safety evaluations, mold prevention and treatment, industrial contamination containment, and standing water control. The CDC is also sharing messages with the public on how to protect themselves from threats before, during, and after landfall, such as drowning and floodwater safety, carbon monoxide poisoning, downed power lines, unsafe food and water, and mold.
The EOC is the CDC’s command center for the coordination and monitoring of CDC activity with all other U.S. federal, state, and local agencies. The EOC also works with the Secretary of Health & Human Services Secretary’s Operations Center to ensure awareness and a coordinated public health and medical response, according to the statement.
Additional resources for interested parties can be found on the CDC website.
The Centers for Disease Control and Prevention is activating its Emergency Operations Center (EOC) in advance of the landfall of Hurricane Florence, according to a CDC media statement.
Activation of the center will allow for 24/7 management of all CDC activities before, during, and after the landfall of Hurricane Florence, including deployment of personnel and resources.
All CDC staff should be ready to provide infectious disease outbreak surveillance, public health messages, water/food safety evaluations, mold prevention and treatment, industrial contamination containment, and standing water control. The CDC is also sharing messages with the public on how to protect themselves from threats before, during, and after landfall, such as drowning and floodwater safety, carbon monoxide poisoning, downed power lines, unsafe food and water, and mold.
The EOC is the CDC’s command center for the coordination and monitoring of CDC activity with all other U.S. federal, state, and local agencies. The EOC also works with the Secretary of Health & Human Services Secretary’s Operations Center to ensure awareness and a coordinated public health and medical response, according to the statement.
Additional resources for interested parties can be found on the CDC website.
FDA warns kratom vendors about unproven claims
The Food and Drug Administration has issued letters of warning to – and therefore breaking federal law – according to a statement from FDA commissioner Scott Gottlieb, MD. These vendors both claimed that their kratom products could, among other things, “relieve” or “treat” opium/opioid withdrawal.

“To date, there have been no adequate and well-controlled studies involving the use of kratom as a treatment for opioid use withdrawal or other diseases in humans,” noted Dr. Gottlieb.
As Dr. Gottlieb pointed out in his statement, not only can fraudulent health claims pose direct health risks, they can also, in the case of kratom, deter or delay people who’re suffering from opioid use disorder from seeking FDA-approved treatments that have been demonstrated to be safe and effective.

Kratom, also known more formally as Mitragyna speciosa, is a plant native to Thailand, Malaysia, Indonesia, and Papua New Guinea. Some compounds in the plant are believed to be opioids, some of which may have the potential for abuse. As Dr. Gottlieb pointed out in his statement, the substance is illegal or controlled in several countries and banned in some states and municipalities in the United States.
Find out more in Dr. Gottlieb’s full statement on the FDA website.
The Food and Drug Administration has issued letters of warning to – and therefore breaking federal law – according to a statement from FDA commissioner Scott Gottlieb, MD. These vendors both claimed that their kratom products could, among other things, “relieve” or “treat” opium/opioid withdrawal.
“To date, there have been no adequate and well-controlled studies involving the use of kratom as a treatment for opioid use withdrawal or other diseases in humans,” noted Dr. Gottlieb.
As Dr. Gottlieb pointed out in his statement, not only can fraudulent health claims pose direct health risks, they can also, in the case of kratom, deter or delay people who’re suffering from opioid use disorder from seeking FDA-approved treatments that have been demonstrated to be safe and effective.
Kratom, also known more formally as Mitragyna speciosa, is a plant native to Thailand, Malaysia, Indonesia, and Papua New Guinea. Some compounds in the plant are believed to be opioids, some of which may have the potential for abuse. As Dr. Gottlieb pointed out in his statement, the substance is illegal or controlled in several countries and banned in some states and municipalities in the United States.
Find out more in Dr. Gottlieb’s full statement on the FDA website.
The Food and Drug Administration has issued letters of warning to – and therefore breaking federal law – according to a statement from FDA commissioner Scott Gottlieb, MD. These vendors both claimed that their kratom products could, among other things, “relieve” or “treat” opium/opioid withdrawal.
“To date, there have been no adequate and well-controlled studies involving the use of kratom as a treatment for opioid use withdrawal or other diseases in humans,” noted Dr. Gottlieb.
As Dr. Gottlieb pointed out in his statement, not only can fraudulent health claims pose direct health risks, they can also, in the case of kratom, deter or delay people who’re suffering from opioid use disorder from seeking FDA-approved treatments that have been demonstrated to be safe and effective.
Kratom, also known more formally as Mitragyna speciosa, is a plant native to Thailand, Malaysia, Indonesia, and Papua New Guinea. Some compounds in the plant are believed to be opioids, some of which may have the potential for abuse. As Dr. Gottlieb pointed out in his statement, the substance is illegal or controlled in several countries and banned in some states and municipalities in the United States.
Find out more in Dr. Gottlieb’s full statement on the FDA website.
FDA approves Cassipa for opioid dependence
Cassipa sublingual film, made by Teva Pharmaceuticals, is a 16 mg/4 mg dosage of buprenorphine and naloxone for the maintenance treatment of opioid dependence. Buprenorphine and naloxone sublingual film also is approved in both brand name and generic versions and in various strengths, the FDA said in a press release.
Cassipa should be used as part of a complete treatment plan that includes counseling and psychosocial support and should be used only after patient induction and stabilization up to a dose of 16 mg of buprenorphine using another marketed product. These products may only be prescribed by Drug Addiction Treatment Act (DATA)–certified prescribers.
“There’s an urgent need to ensure access to, and wider use and understanding of, medication-assisted treatment for opioid use disorder ... the FDA recently described a streamlined approach to drug development for certain medication-assisted treatments that are based on buprenorphine. This streamlined approach can reduce drug development costs, so products may be offered at a lower price to patients and we can broaden access to treatment,” FDA Commissioner Scott Gottlieb, MD, said in the statement.
He added that “individuals who successfully transition onto medication-assisted treatment are not swapping one addiction for another. Opioid replacement therapy can be an important part of effective treatment. Opioid use disorder should be viewed similarly to any other chronic condition that is treated with medication.”
Medication-assisted treatment (MAT) is a comprehensive approach that combines FDA-approved medications (currently methadone, buprenorphine, or naltrexone) with counseling and other behavioral therapies to treat patients with opioid use disorder. Regular adherence to MAT with buprenorphine reduces opioid withdrawal symptoms and the desire to use opioids. According to the Substance Abuse and Mental Health Services Administration, patients receiving MAT for treatment of their opioid use disorder cut their risk of death from all causes in half.
Improving access to prevention, treatment, and recovery services, including the full range of MAT, is part of the Department of Health and Human Services’ Five-Point Strategy to Combat the Opioid Crisis. Last month, the FDA issued draft guidance outlining new ways for drug developers to consider measuring and demonstrating the effectiveness and benefits of new or existing MAT products, building on another draft guidance issued in April outlining the agency’s current thinking about drug development and trial design issues relevant to the study of depot buprenorphine products (i.e., modified-release products for injection or implantation). In June, the agency also approved the first generic versions of Suboxone (buprenorphine and naloxone) sublingual film in multiple strengths, the statement said.
Cassipa was approved through the abbreviated 505(b)(2) approval pathway and its application relied, in part, on the FDA’s finding of safety and effectiveness for Suboxone sublingual film to support approval. The applicant demonstrated that reliance on the FDA’s finding of safety and effectiveness for Suboxone was scientifically justified and provided Cassipa-specific pharmacokinetic data to establish the drug’s safety and efficacy for its approved uses, according to the FDA.
Adverse events commonly observed with the buprenorphine and naloxone sublingual film are oral hypoesthesia, glossodynia, oral mucosal erythema, headache, nausea, vomiting, hyperhidrosis, constipation, signs and symptoms of withdrawal, insomnia, pain, and peripheral edema.
Cassipa sublingual film, made by Teva Pharmaceuticals, is a 16 mg/4 mg dosage of buprenorphine and naloxone for the maintenance treatment of opioid dependence. Buprenorphine and naloxone sublingual film also is approved in both brand name and generic versions and in various strengths, the FDA said in a press release.
Cassipa should be used as part of a complete treatment plan that includes counseling and psychosocial support and should be used only after patient induction and stabilization up to a dose of 16 mg of buprenorphine using another marketed product. These products may only be prescribed by Drug Addiction Treatment Act (DATA)–certified prescribers.
“There’s an urgent need to ensure access to, and wider use and understanding of, medication-assisted treatment for opioid use disorder ... the FDA recently described a streamlined approach to drug development for certain medication-assisted treatments that are based on buprenorphine. This streamlined approach can reduce drug development costs, so products may be offered at a lower price to patients and we can broaden access to treatment,” FDA Commissioner Scott Gottlieb, MD, said in the statement.
He added that “individuals who successfully transition onto medication-assisted treatment are not swapping one addiction for another. Opioid replacement therapy can be an important part of effective treatment. Opioid use disorder should be viewed similarly to any other chronic condition that is treated with medication.”
Medication-assisted treatment (MAT) is a comprehensive approach that combines FDA-approved medications (currently methadone, buprenorphine, or naltrexone) with counseling and other behavioral therapies to treat patients with opioid use disorder. Regular adherence to MAT with buprenorphine reduces opioid withdrawal symptoms and the desire to use opioids. According to the Substance Abuse and Mental Health Services Administration, patients receiving MAT for treatment of their opioid use disorder cut their risk of death from all causes in half.
Improving access to prevention, treatment, and recovery services, including the full range of MAT, is part of the Department of Health and Human Services’ Five-Point Strategy to Combat the Opioid Crisis. Last month, the FDA issued draft guidance outlining new ways for drug developers to consider measuring and demonstrating the effectiveness and benefits of new or existing MAT products, building on another draft guidance issued in April outlining the agency’s current thinking about drug development and trial design issues relevant to the study of depot buprenorphine products (i.e., modified-release products for injection or implantation). In June, the agency also approved the first generic versions of Suboxone (buprenorphine and naloxone) sublingual film in multiple strengths, the statement said.
Cassipa was approved through the abbreviated 505(b)(2) approval pathway and its application relied, in part, on the FDA’s finding of safety and effectiveness for Suboxone sublingual film to support approval. The applicant demonstrated that reliance on the FDA’s finding of safety and effectiveness for Suboxone was scientifically justified and provided Cassipa-specific pharmacokinetic data to establish the drug’s safety and efficacy for its approved uses, according to the FDA.
Adverse events commonly observed with the buprenorphine and naloxone sublingual film are oral hypoesthesia, glossodynia, oral mucosal erythema, headache, nausea, vomiting, hyperhidrosis, constipation, signs and symptoms of withdrawal, insomnia, pain, and peripheral edema.
Cassipa sublingual film, made by Teva Pharmaceuticals, is a 16 mg/4 mg dosage of buprenorphine and naloxone for the maintenance treatment of opioid dependence. Buprenorphine and naloxone sublingual film also is approved in both brand name and generic versions and in various strengths, the FDA said in a press release.
Cassipa should be used as part of a complete treatment plan that includes counseling and psychosocial support and should be used only after patient induction and stabilization up to a dose of 16 mg of buprenorphine using another marketed product. These products may only be prescribed by Drug Addiction Treatment Act (DATA)–certified prescribers.
“There’s an urgent need to ensure access to, and wider use and understanding of, medication-assisted treatment for opioid use disorder ... the FDA recently described a streamlined approach to drug development for certain medication-assisted treatments that are based on buprenorphine. This streamlined approach can reduce drug development costs, so products may be offered at a lower price to patients and we can broaden access to treatment,” FDA Commissioner Scott Gottlieb, MD, said in the statement.
He added that “individuals who successfully transition onto medication-assisted treatment are not swapping one addiction for another. Opioid replacement therapy can be an important part of effective treatment. Opioid use disorder should be viewed similarly to any other chronic condition that is treated with medication.”
Medication-assisted treatment (MAT) is a comprehensive approach that combines FDA-approved medications (currently methadone, buprenorphine, or naltrexone) with counseling and other behavioral therapies to treat patients with opioid use disorder. Regular adherence to MAT with buprenorphine reduces opioid withdrawal symptoms and the desire to use opioids. According to the Substance Abuse and Mental Health Services Administration, patients receiving MAT for treatment of their opioid use disorder cut their risk of death from all causes in half.
Improving access to prevention, treatment, and recovery services, including the full range of MAT, is part of the Department of Health and Human Services’ Five-Point Strategy to Combat the Opioid Crisis. Last month, the FDA issued draft guidance outlining new ways for drug developers to consider measuring and demonstrating the effectiveness and benefits of new or existing MAT products, building on another draft guidance issued in April outlining the agency’s current thinking about drug development and trial design issues relevant to the study of depot buprenorphine products (i.e., modified-release products for injection or implantation). In June, the agency also approved the first generic versions of Suboxone (buprenorphine and naloxone) sublingual film in multiple strengths, the statement said.
Cassipa was approved through the abbreviated 505(b)(2) approval pathway and its application relied, in part, on the FDA’s finding of safety and effectiveness for Suboxone sublingual film to support approval. The applicant demonstrated that reliance on the FDA’s finding of safety and effectiveness for Suboxone was scientifically justified and provided Cassipa-specific pharmacokinetic data to establish the drug’s safety and efficacy for its approved uses, according to the FDA.
Adverse events commonly observed with the buprenorphine and naloxone sublingual film are oral hypoesthesia, glossodynia, oral mucosal erythema, headache, nausea, vomiting, hyperhidrosis, constipation, signs and symptoms of withdrawal, insomnia, pain, and peripheral edema.
CDC releases guidelines for pediatric mTBI
and should base management and prognostication on clinical decision-making tools and symptom rating scales, according to new practice guidelines issued by a working group of the Centers for Disease Control and Prevention (JAMA Pediatrics. 2018 Sep 4. doi: 10.1001/jamapediatrics.2018.2853.
The guidelines were released simultaneously with a systematic review, conducted by the same authors, of the existing literature regarding pediatric mTBI (JAMA Pediatrics 2018 Sep 4. doi: 10.1001/jamapediatrics.2018.2847). As the evaluators sorted through the literature to find high-quality studies for this population, the funnel rapidly narrowed: From an initial pool of over 15,000 studies conducted between 1990 and 2015, findings from just 75 studies were eventually included in the systematic review.
The review’s findings formed the basis for the guidelines and allowed Angela Lumba-Brown, MD, a pediatric emergency medicine physician at Stanford (Calif.) University, and her coauthors to ascribe a level of confidence in the inference from study data for a given recommendation. Recommendations also are categorized by strength and accordingly indicate that clinicians “should” or “may” follow them. Exceptions are carved out for practices, such as the use of hypertonic 3% saline solution for acute headache in the ED, that should not be used outside research settings.
In the end, the guidelines cover 19 main topics, sorted into guidance regarding the diagnosis, prognosis, and management and treatment of mTBI in children.
Diagnosis
The recommendations regarding mTBI diagnosis center around determining which children are at risk for significant intracranial injury (ICI). The guidelines recommend, with moderate confidence, that clinicians usually should not obtain a head CT for children with mTBI. Validated clinical decision rules should be used for risk stratification to determine which children can safely avoid imaging and which children should be considered for head CT, wrote Dr. Lumba-Brown and her coauthors. Magnetic resonance imaging is not recommended for initial evaluation of mTBI, nor should skull radiographs be ordered in the absence of clinical suspicion for skull fracture.
From the systematic review, Dr. Lumba-Brown and her colleagues found that several risk factors taken together may mean that significant ICI is more likely. These include patient age younger than 2 years; any vomiting, loss of consciousness, or amnesia; a severe mechanism of injury, severe or worsening headache, or nonfrontal scalp hematoma; a Glasgow Coma Scale (GCS) score of less than 15; and clinical suspicion for skull fracture. Clinicians should give consideration to the risks of ionizing radiation to the head, and balance this against their assessment of risk for severe – and perhaps actionable – injury.
A validated symptom rating scale, used in an age-appropriate way, should be used as part of the evaluation of children with mTBI. For children aged 6 and older, the Graded Symptom Checklist is an appropriate tool within 2 days after injury, while the Post Concussion Symptom Scale as part of computerized neurocognitive testing can differentiate which high school athletes have mTBI when used within 4 days of injury, according to the guidelines, which also identify other validated symptom rating scales.
The guidelines authors recommend, with high confidence, that serum biomarkers should not be used outside of research settings in the diagnosis of mTBI in children at present.
Prognosis
Families should be counseled that symptoms mostly resolve within 1-3 months for up to 80% of children with mTBI, but families also should know that “each child’s recovery from mTBI is unique and will follow its own trajectory,” wrote Dr. Lumba-Brown and her coauthors, in a moderate-strength recommendation.
Some factors have been associated with slower recovery from mTBI, and either upon evaluation for mTBI or in routine sports examinations, families should be told about this potential if risk factors are present, said the guidelines, although the evidence supporting the associations is of “varying strength,” wrote Dr. Lumba-Brown and her coauthors. Children with previous mTBIs and those with a history of premorbid neurologic and psychiatric problems, learning problems, or family and social stress all may have delayed recovery. For children with ICI, lower cognitive ability also is associated with delayed recovery.
Demographic factors such as lower socioeconomic status and being of Hispanic ethnicity also may increase the risk for delayed mTBI recovery. Older children and adolescents may recover more slowly. Those with more severe initial presentation and more symptoms in the immediate post-mTBI phase also may have a slower recovery course, said Dr. Lumba-Brown and her coauthors.

A validated prediction rule can be used in the ED to gather information about these discrete risk factors to guide family counseling, according to the guidelines, which note that research has found that “an empirically derived set of risk factors predicted the risk of persistent post-concussion symptoms at 28 days” for children seen in the ED with mTBI.
During the recovery phase, a combination of tools should be used to track recovery from mTBI; these can include validated symptom scales, validated cognitive testing, reaction time measures, and, in adolescent athletes, balance testing. Using a combination of tools is a valuable strategy, the researchers wrote. “No single assessment tool is strongly predictive of outcome in children with mTBI,” they noted.
When prognosis is poor, or recovery is not proceeding as expected, clinicians should have a low threshold for initiating other interventions and referrals.
Management and treatment
Although the guideline authors acknowledged significant knowledge gaps in all areas of pediatric mTBI diagnosis and management, evidence is especially scant for best practices for treatment, rest, and return to play and school after a child sustains mTBI, said Dr. Lumba-Brown and her coauthors.
However, families should be given information about warning signs for serious head injury and how to monitor symptoms, as well as information about mTBI and the expected recovery course. Other forward-looking instructions should cover the importance of preventing new head injuries, managing the gradual return to normal cognitive and physical activities, and clear instructions regarding return to school and recreational activities. The guideline authors made a strong recommendation to provide this information, with high confidence in the data.
However, little strong evidence points the way to a clear set of criteria for when children are ready for school, play, and athletic participation. These decisions must be customized to the individual child, and decision making, particularly about return to school and academic activities, should be a collaborative affair, with schools, clinicians, and families all communicating to make sure the pace of return to normal life is keeping pace with the child’s recovery. “Because postconcussive symptoms resolve at different rates in different children after mTBI, individualization of return-to-school programming is necessary,” wrote Dr. Lumba-Brown and her coauthors.
The guideline authors cite evidence that “suggests that early rest (within the first 3 days) may be beneficial but that inactivity beyond this period for most children may worsen their self-reported symptoms.”
Psychosocial support may be beneficial for certain children, wrote the researchers, drawing on evidence showing that such support is beneficial in frank TBI, and is probably beneficial in mTBI.
Active rehabilitation as tolerated is recommended after an initial period of rest, with exertion kept to a level that does not exacerbate symptoms. Children should not participate in contact activities until symptoms are fully resolved.
A posttraumatic headache that is severe or worsens in the ED should prompt consideration of emergent neuroimaging, according to the guidelines. In the postacute phase, however, children can have nonopioid analgesia, although parents should know about such risks as rebound headache. When chronic headache follows a mTBI, the guidelines recommend that clinicians refer patients for a multidisciplinary evaluation that can assess the many factors – including analgesic overuse – that can be contributors.
Drawing on the larger body of adult TBI research, the authors recommend that insufficient or disordered sleep be addressed, because “the maintenance of appropriate sleep and the management of disrupted sleep may be a critical target of treatment for the child with mTBI.”
Children who suffer a mTBI may experience cognitive dysfunction as a direct result of injury to the brain or secondary to the effects of other symptoms such as sleep disruptions, headache pain, fatigue, or low tolerance of frustration. Clinicians may want to perform or refer their patients for a neuropsychological evaluation to determine what is causing the cognitive dysfunction, the authors said.
Dr. Lumba-Brown and her coauthors, who formed the CDC’s Pediatric Mild Traumatic Brain Injury Guideline Workgroup, also recommended that clinicians use the term “mild traumatic brain injury” to describe head injuries that cause confusion or disorientation, without loss of consciousness, or loss of consciousness of up to 30 minutes or less, or posttraumatic amnesia of less than 24 hours duration, and that are associated with a GCS of 13-15 by 30 minutes after injury or at the time of initial medical assessment. This practice, they said, may reduce the risk of misinterpretation by medical professionals and the public that can occur when the terms “mTBI,” “concussion,” and “minor head injury” all may refer to the same injury.
The CDC has developed a suite of materials to assist both health care providers and the public in guideline implementation. The agency also is using its HEADS UP campaign to publicize the guidelines and related materials, and plans ongoing evaluation of the guidelines and implementation materials.
Many study authors, including Dr. Lumba-Brown, had relationships with medical device or pharmaceutical companies. The systematic review and guideline development were funded by the CDC.
A growing realization that mTBI can have persistent and significant deleterious effects has informed medical and public attitudes toward concussion in children, which now results in almost 1 million annual ED visits.
Progress at the laboratory bench has elucidated much of the neurometabolic cascade that occurs with the insult of mTBI, and has allowed researchers to document the path of brain healing after injury. Neuroimaging now can go beyond static images to trace neural networks and detect previously unseen and subtle functional deficits engendered by mTBI.
In particular, 21st century magnetic resonance imaging (MRI) has shown increased sensitivity over CT alone. In the TRACK-TBI study, over one in four patients whose CTs were read as normal had MRI findings consistent with trauma-induced pathology. Both multimodal MRI and serum biomarkers show promise, although more research regarding their utility is needed, particularly in the case of proteomic biomarkers.
Still, high-quality studies of pediatric mTBI are scant, and translation of burgeoning research into clinical practice is severely impeded by the numerous knowledge gaps that exist in the field.
Dr. Lumba-Brown and her colleagues have synthesized research that supports a neurobiopsychosocial model of mTBI in children that comes into play most prominently in the postacute phase, when non–injury-related factors such as demographics, socioeconomic status, and premorbid psychological conditions are strong mediators of the recovery trajectory.
With children as with adults, scant research guides the path forward for treatment and recovery from mTBI. For children, clinicians are still grappling with issues surrounding return to full participation in the academic and recreational activities of the school environment.
Data from two currently active studies should help light the way forward, however. The TRACK-TBI study, funded by the National Institutes of Health, will include almost 200 children among its 2,700 enrollees who have sustained all levels of TBI.
The Concussion Assessment, Research, and Education (CARE) Consortium is funded jointly by the National College Athletic Association and the Department of Defense. Between student athletes and military cadets, over 40,000 individuals are now part of the study.
The two studies’ testing modalities and methodologies align, offering the opportunity for a powerful pooled analysis that includes civilians, athletes, and those in the military.
Until then, these guidelines provide a way forward to an individualized approach to the best care for a child with mTBI.
Michael McCrea, PhD, is professor of neurology and neurosurgery, and director of brain injury research at the Medical College of Wisconsin, Milwaukee. Geoff Manley, MD, PhD, is professor of neurologic surgery at the University of California, San Francisco. Neither author reported conflicts of interest. These remarks were drawn from an editorial accompanying the guidelines and systematic review (JAMA Pediatrics. 2018 Sep 4. doi: 10.1001/jamapediatrics.2018.2846).
A growing realization that mTBI can have persistent and significant deleterious effects has informed medical and public attitudes toward concussion in children, which now results in almost 1 million annual ED visits.
Progress at the laboratory bench has elucidated much of the neurometabolic cascade that occurs with the insult of mTBI, and has allowed researchers to document the path of brain healing after injury. Neuroimaging now can go beyond static images to trace neural networks and detect previously unseen and subtle functional deficits engendered by mTBI.
In particular, 21st century magnetic resonance imaging (MRI) has shown increased sensitivity over CT alone. In the TRACK-TBI study, over one in four patients whose CTs were read as normal had MRI findings consistent with trauma-induced pathology. Both multimodal MRI and serum biomarkers show promise, although more research regarding their utility is needed, particularly in the case of proteomic biomarkers.
Still, high-quality studies of pediatric mTBI are scant, and translation of burgeoning research into clinical practice is severely impeded by the numerous knowledge gaps that exist in the field.
Dr. Lumba-Brown and her colleagues have synthesized research that supports a neurobiopsychosocial model of mTBI in children that comes into play most prominently in the postacute phase, when non–injury-related factors such as demographics, socioeconomic status, and premorbid psychological conditions are strong mediators of the recovery trajectory.
With children as with adults, scant research guides the path forward for treatment and recovery from mTBI. For children, clinicians are still grappling with issues surrounding return to full participation in the academic and recreational activities of the school environment.
Data from two currently active studies should help light the way forward, however. The TRACK-TBI study, funded by the National Institutes of Health, will include almost 200 children among its 2,700 enrollees who have sustained all levels of TBI.
The Concussion Assessment, Research, and Education (CARE) Consortium is funded jointly by the National College Athletic Association and the Department of Defense. Between student athletes and military cadets, over 40,000 individuals are now part of the study.
The two studies’ testing modalities and methodologies align, offering the opportunity for a powerful pooled analysis that includes civilians, athletes, and those in the military.
Until then, these guidelines provide a way forward to an individualized approach to the best care for a child with mTBI.
Michael McCrea, PhD, is professor of neurology and neurosurgery, and director of brain injury research at the Medical College of Wisconsin, Milwaukee. Geoff Manley, MD, PhD, is professor of neurologic surgery at the University of California, San Francisco. Neither author reported conflicts of interest. These remarks were drawn from an editorial accompanying the guidelines and systematic review (JAMA Pediatrics. 2018 Sep 4. doi: 10.1001/jamapediatrics.2018.2846).
A growing realization that mTBI can have persistent and significant deleterious effects has informed medical and public attitudes toward concussion in children, which now results in almost 1 million annual ED visits.
Progress at the laboratory bench has elucidated much of the neurometabolic cascade that occurs with the insult of mTBI, and has allowed researchers to document the path of brain healing after injury. Neuroimaging now can go beyond static images to trace neural networks and detect previously unseen and subtle functional deficits engendered by mTBI.
In particular, 21st century magnetic resonance imaging (MRI) has shown increased sensitivity over CT alone. In the TRACK-TBI study, over one in four patients whose CTs were read as normal had MRI findings consistent with trauma-induced pathology. Both multimodal MRI and serum biomarkers show promise, although more research regarding their utility is needed, particularly in the case of proteomic biomarkers.
Still, high-quality studies of pediatric mTBI are scant, and translation of burgeoning research into clinical practice is severely impeded by the numerous knowledge gaps that exist in the field.
Dr. Lumba-Brown and her colleagues have synthesized research that supports a neurobiopsychosocial model of mTBI in children that comes into play most prominently in the postacute phase, when non–injury-related factors such as demographics, socioeconomic status, and premorbid psychological conditions are strong mediators of the recovery trajectory.
With children as with adults, scant research guides the path forward for treatment and recovery from mTBI. For children, clinicians are still grappling with issues surrounding return to full participation in the academic and recreational activities of the school environment.
Data from two currently active studies should help light the way forward, however. The TRACK-TBI study, funded by the National Institutes of Health, will include almost 200 children among its 2,700 enrollees who have sustained all levels of TBI.
The Concussion Assessment, Research, and Education (CARE) Consortium is funded jointly by the National College Athletic Association and the Department of Defense. Between student athletes and military cadets, over 40,000 individuals are now part of the study.
The two studies’ testing modalities and methodologies align, offering the opportunity for a powerful pooled analysis that includes civilians, athletes, and those in the military.
Until then, these guidelines provide a way forward to an individualized approach to the best care for a child with mTBI.
Michael McCrea, PhD, is professor of neurology and neurosurgery, and director of brain injury research at the Medical College of Wisconsin, Milwaukee. Geoff Manley, MD, PhD, is professor of neurologic surgery at the University of California, San Francisco. Neither author reported conflicts of interest. These remarks were drawn from an editorial accompanying the guidelines and systematic review (JAMA Pediatrics. 2018 Sep 4. doi: 10.1001/jamapediatrics.2018.2846).
and should base management and prognostication on clinical decision-making tools and symptom rating scales, according to new practice guidelines issued by a working group of the Centers for Disease Control and Prevention (JAMA Pediatrics. 2018 Sep 4. doi: 10.1001/jamapediatrics.2018.2853.
The guidelines were released simultaneously with a systematic review, conducted by the same authors, of the existing literature regarding pediatric mTBI (JAMA Pediatrics 2018 Sep 4. doi: 10.1001/jamapediatrics.2018.2847). As the evaluators sorted through the literature to find high-quality studies for this population, the funnel rapidly narrowed: From an initial pool of over 15,000 studies conducted between 1990 and 2015, findings from just 75 studies were eventually included in the systematic review.
The review’s findings formed the basis for the guidelines and allowed Angela Lumba-Brown, MD, a pediatric emergency medicine physician at Stanford (Calif.) University, and her coauthors to ascribe a level of confidence in the inference from study data for a given recommendation. Recommendations also are categorized by strength and accordingly indicate that clinicians “should” or “may” follow them. Exceptions are carved out for practices, such as the use of hypertonic 3% saline solution for acute headache in the ED, that should not be used outside research settings.
In the end, the guidelines cover 19 main topics, sorted into guidance regarding the diagnosis, prognosis, and management and treatment of mTBI in children.
Diagnosis
The recommendations regarding mTBI diagnosis center around determining which children are at risk for significant intracranial injury (ICI). The guidelines recommend, with moderate confidence, that clinicians usually should not obtain a head CT for children with mTBI. Validated clinical decision rules should be used for risk stratification to determine which children can safely avoid imaging and which children should be considered for head CT, wrote Dr. Lumba-Brown and her coauthors. Magnetic resonance imaging is not recommended for initial evaluation of mTBI, nor should skull radiographs be ordered in the absence of clinical suspicion for skull fracture.
From the systematic review, Dr. Lumba-Brown and her colleagues found that several risk factors taken together may mean that significant ICI is more likely. These include patient age younger than 2 years; any vomiting, loss of consciousness, or amnesia; a severe mechanism of injury, severe or worsening headache, or nonfrontal scalp hematoma; a Glasgow Coma Scale (GCS) score of less than 15; and clinical suspicion for skull fracture. Clinicians should give consideration to the risks of ionizing radiation to the head, and balance this against their assessment of risk for severe – and perhaps actionable – injury.
A validated symptom rating scale, used in an age-appropriate way, should be used as part of the evaluation of children with mTBI. For children aged 6 and older, the Graded Symptom Checklist is an appropriate tool within 2 days after injury, while the Post Concussion Symptom Scale as part of computerized neurocognitive testing can differentiate which high school athletes have mTBI when used within 4 days of injury, according to the guidelines, which also identify other validated symptom rating scales.
The guidelines authors recommend, with high confidence, that serum biomarkers should not be used outside of research settings in the diagnosis of mTBI in children at present.
Prognosis
Families should be counseled that symptoms mostly resolve within 1-3 months for up to 80% of children with mTBI, but families also should know that “each child’s recovery from mTBI is unique and will follow its own trajectory,” wrote Dr. Lumba-Brown and her coauthors, in a moderate-strength recommendation.
Some factors have been associated with slower recovery from mTBI, and either upon evaluation for mTBI or in routine sports examinations, families should be told about this potential if risk factors are present, said the guidelines, although the evidence supporting the associations is of “varying strength,” wrote Dr. Lumba-Brown and her coauthors. Children with previous mTBIs and those with a history of premorbid neurologic and psychiatric problems, learning problems, or family and social stress all may have delayed recovery. For children with ICI, lower cognitive ability also is associated with delayed recovery.
Demographic factors such as lower socioeconomic status and being of Hispanic ethnicity also may increase the risk for delayed mTBI recovery. Older children and adolescents may recover more slowly. Those with more severe initial presentation and more symptoms in the immediate post-mTBI phase also may have a slower recovery course, said Dr. Lumba-Brown and her coauthors.
A validated prediction rule can be used in the ED to gather information about these discrete risk factors to guide family counseling, according to the guidelines, which note that research has found that “an empirically derived set of risk factors predicted the risk of persistent post-concussion symptoms at 28 days” for children seen in the ED with mTBI.
During the recovery phase, a combination of tools should be used to track recovery from mTBI; these can include validated symptom scales, validated cognitive testing, reaction time measures, and, in adolescent athletes, balance testing. Using a combination of tools is a valuable strategy, the researchers wrote. “No single assessment tool is strongly predictive of outcome in children with mTBI,” they noted.
When prognosis is poor, or recovery is not proceeding as expected, clinicians should have a low threshold for initiating other interventions and referrals.
Management and treatment
Although the guideline authors acknowledged significant knowledge gaps in all areas of pediatric mTBI diagnosis and management, evidence is especially scant for best practices for treatment, rest, and return to play and school after a child sustains mTBI, said Dr. Lumba-Brown and her coauthors.
However, families should be given information about warning signs for serious head injury and how to monitor symptoms, as well as information about mTBI and the expected recovery course. Other forward-looking instructions should cover the importance of preventing new head injuries, managing the gradual return to normal cognitive and physical activities, and clear instructions regarding return to school and recreational activities. The guideline authors made a strong recommendation to provide this information, with high confidence in the data.
However, little strong evidence points the way to a clear set of criteria for when children are ready for school, play, and athletic participation. These decisions must be customized to the individual child, and decision making, particularly about return to school and academic activities, should be a collaborative affair, with schools, clinicians, and families all communicating to make sure the pace of return to normal life is keeping pace with the child’s recovery. “Because postconcussive symptoms resolve at different rates in different children after mTBI, individualization of return-to-school programming is necessary,” wrote Dr. Lumba-Brown and her coauthors.
The guideline authors cite evidence that “suggests that early rest (within the first 3 days) may be beneficial but that inactivity beyond this period for most children may worsen their self-reported symptoms.”
Psychosocial support may be beneficial for certain children, wrote the researchers, drawing on evidence showing that such support is beneficial in frank TBI, and is probably beneficial in mTBI.
Active rehabilitation as tolerated is recommended after an initial period of rest, with exertion kept to a level that does not exacerbate symptoms. Children should not participate in contact activities until symptoms are fully resolved.
A posttraumatic headache that is severe or worsens in the ED should prompt consideration of emergent neuroimaging, according to the guidelines. In the postacute phase, however, children can have nonopioid analgesia, although parents should know about such risks as rebound headache. When chronic headache follows a mTBI, the guidelines recommend that clinicians refer patients for a multidisciplinary evaluation that can assess the many factors – including analgesic overuse – that can be contributors.
Drawing on the larger body of adult TBI research, the authors recommend that insufficient or disordered sleep be addressed, because “the maintenance of appropriate sleep and the management of disrupted sleep may be a critical target of treatment for the child with mTBI.”
Children who suffer a mTBI may experience cognitive dysfunction as a direct result of injury to the brain or secondary to the effects of other symptoms such as sleep disruptions, headache pain, fatigue, or low tolerance of frustration. Clinicians may want to perform or refer their patients for a neuropsychological evaluation to determine what is causing the cognitive dysfunction, the authors said.
Dr. Lumba-Brown and her coauthors, who formed the CDC’s Pediatric Mild Traumatic Brain Injury Guideline Workgroup, also recommended that clinicians use the term “mild traumatic brain injury” to describe head injuries that cause confusion or disorientation, without loss of consciousness, or loss of consciousness of up to 30 minutes or less, or posttraumatic amnesia of less than 24 hours duration, and that are associated with a GCS of 13-15 by 30 minutes after injury or at the time of initial medical assessment. This practice, they said, may reduce the risk of misinterpretation by medical professionals and the public that can occur when the terms “mTBI,” “concussion,” and “minor head injury” all may refer to the same injury.
The CDC has developed a suite of materials to assist both health care providers and the public in guideline implementation. The agency also is using its HEADS UP campaign to publicize the guidelines and related materials, and plans ongoing evaluation of the guidelines and implementation materials.
Many study authors, including Dr. Lumba-Brown, had relationships with medical device or pharmaceutical companies. The systematic review and guideline development were funded by the CDC.
and should base management and prognostication on clinical decision-making tools and symptom rating scales, according to new practice guidelines issued by a working group of the Centers for Disease Control and Prevention (JAMA Pediatrics. 2018 Sep 4. doi: 10.1001/jamapediatrics.2018.2853.
The guidelines were released simultaneously with a systematic review, conducted by the same authors, of the existing literature regarding pediatric mTBI (JAMA Pediatrics 2018 Sep 4. doi: 10.1001/jamapediatrics.2018.2847). As the evaluators sorted through the literature to find high-quality studies for this population, the funnel rapidly narrowed: From an initial pool of over 15,000 studies conducted between 1990 and 2015, findings from just 75 studies were eventually included in the systematic review.
The review’s findings formed the basis for the guidelines and allowed Angela Lumba-Brown, MD, a pediatric emergency medicine physician at Stanford (Calif.) University, and her coauthors to ascribe a level of confidence in the inference from study data for a given recommendation. Recommendations also are categorized by strength and accordingly indicate that clinicians “should” or “may” follow them. Exceptions are carved out for practices, such as the use of hypertonic 3% saline solution for acute headache in the ED, that should not be used outside research settings.
In the end, the guidelines cover 19 main topics, sorted into guidance regarding the diagnosis, prognosis, and management and treatment of mTBI in children.
Diagnosis
The recommendations regarding mTBI diagnosis center around determining which children are at risk for significant intracranial injury (ICI). The guidelines recommend, with moderate confidence, that clinicians usually should not obtain a head CT for children with mTBI. Validated clinical decision rules should be used for risk stratification to determine which children can safely avoid imaging and which children should be considered for head CT, wrote Dr. Lumba-Brown and her coauthors. Magnetic resonance imaging is not recommended for initial evaluation of mTBI, nor should skull radiographs be ordered in the absence of clinical suspicion for skull fracture.
From the systematic review, Dr. Lumba-Brown and her colleagues found that several risk factors taken together may mean that significant ICI is more likely. These include patient age younger than 2 years; any vomiting, loss of consciousness, or amnesia; a severe mechanism of injury, severe or worsening headache, or nonfrontal scalp hematoma; a Glasgow Coma Scale (GCS) score of less than 15; and clinical suspicion for skull fracture. Clinicians should give consideration to the risks of ionizing radiation to the head, and balance this against their assessment of risk for severe – and perhaps actionable – injury.
A validated symptom rating scale, used in an age-appropriate way, should be used as part of the evaluation of children with mTBI. For children aged 6 and older, the Graded Symptom Checklist is an appropriate tool within 2 days after injury, while the Post Concussion Symptom Scale as part of computerized neurocognitive testing can differentiate which high school athletes have mTBI when used within 4 days of injury, according to the guidelines, which also identify other validated symptom rating scales.
The guidelines authors recommend, with high confidence, that serum biomarkers should not be used outside of research settings in the diagnosis of mTBI in children at present.
Prognosis
Families should be counseled that symptoms mostly resolve within 1-3 months for up to 80% of children with mTBI, but families also should know that “each child’s recovery from mTBI is unique and will follow its own trajectory,” wrote Dr. Lumba-Brown and her coauthors, in a moderate-strength recommendation.
Some factors have been associated with slower recovery from mTBI, and either upon evaluation for mTBI or in routine sports examinations, families should be told about this potential if risk factors are present, said the guidelines, although the evidence supporting the associations is of “varying strength,” wrote Dr. Lumba-Brown and her coauthors. Children with previous mTBIs and those with a history of premorbid neurologic and psychiatric problems, learning problems, or family and social stress all may have delayed recovery. For children with ICI, lower cognitive ability also is associated with delayed recovery.
Demographic factors such as lower socioeconomic status and being of Hispanic ethnicity also may increase the risk for delayed mTBI recovery. Older children and adolescents may recover more slowly. Those with more severe initial presentation and more symptoms in the immediate post-mTBI phase also may have a slower recovery course, said Dr. Lumba-Brown and her coauthors.
A validated prediction rule can be used in the ED to gather information about these discrete risk factors to guide family counseling, according to the guidelines, which note that research has found that “an empirically derived set of risk factors predicted the risk of persistent post-concussion symptoms at 28 days” for children seen in the ED with mTBI.
During the recovery phase, a combination of tools should be used to track recovery from mTBI; these can include validated symptom scales, validated cognitive testing, reaction time measures, and, in adolescent athletes, balance testing. Using a combination of tools is a valuable strategy, the researchers wrote. “No single assessment tool is strongly predictive of outcome in children with mTBI,” they noted.
When prognosis is poor, or recovery is not proceeding as expected, clinicians should have a low threshold for initiating other interventions and referrals.
Management and treatment
Although the guideline authors acknowledged significant knowledge gaps in all areas of pediatric mTBI diagnosis and management, evidence is especially scant for best practices for treatment, rest, and return to play and school after a child sustains mTBI, said Dr. Lumba-Brown and her coauthors.
However, families should be given information about warning signs for serious head injury and how to monitor symptoms, as well as information about mTBI and the expected recovery course. Other forward-looking instructions should cover the importance of preventing new head injuries, managing the gradual return to normal cognitive and physical activities, and clear instructions regarding return to school and recreational activities. The guideline authors made a strong recommendation to provide this information, with high confidence in the data.
However, little strong evidence points the way to a clear set of criteria for when children are ready for school, play, and athletic participation. These decisions must be customized to the individual child, and decision making, particularly about return to school and academic activities, should be a collaborative affair, with schools, clinicians, and families all communicating to make sure the pace of return to normal life is keeping pace with the child’s recovery. “Because postconcussive symptoms resolve at different rates in different children after mTBI, individualization of return-to-school programming is necessary,” wrote Dr. Lumba-Brown and her coauthors.
The guideline authors cite evidence that “suggests that early rest (within the first 3 days) may be beneficial but that inactivity beyond this period for most children may worsen their self-reported symptoms.”
Psychosocial support may be beneficial for certain children, wrote the researchers, drawing on evidence showing that such support is beneficial in frank TBI, and is probably beneficial in mTBI.
Active rehabilitation as tolerated is recommended after an initial period of rest, with exertion kept to a level that does not exacerbate symptoms. Children should not participate in contact activities until symptoms are fully resolved.
A posttraumatic headache that is severe or worsens in the ED should prompt consideration of emergent neuroimaging, according to the guidelines. In the postacute phase, however, children can have nonopioid analgesia, although parents should know about such risks as rebound headache. When chronic headache follows a mTBI, the guidelines recommend that clinicians refer patients for a multidisciplinary evaluation that can assess the many factors – including analgesic overuse – that can be contributors.
Drawing on the larger body of adult TBI research, the authors recommend that insufficient or disordered sleep be addressed, because “the maintenance of appropriate sleep and the management of disrupted sleep may be a critical target of treatment for the child with mTBI.”
Children who suffer a mTBI may experience cognitive dysfunction as a direct result of injury to the brain or secondary to the effects of other symptoms such as sleep disruptions, headache pain, fatigue, or low tolerance of frustration. Clinicians may want to perform or refer their patients for a neuropsychological evaluation to determine what is causing the cognitive dysfunction, the authors said.
Dr. Lumba-Brown and her coauthors, who formed the CDC’s Pediatric Mild Traumatic Brain Injury Guideline Workgroup, also recommended that clinicians use the term “mild traumatic brain injury” to describe head injuries that cause confusion or disorientation, without loss of consciousness, or loss of consciousness of up to 30 minutes or less, or posttraumatic amnesia of less than 24 hours duration, and that are associated with a GCS of 13-15 by 30 minutes after injury or at the time of initial medical assessment. This practice, they said, may reduce the risk of misinterpretation by medical professionals and the public that can occur when the terms “mTBI,” “concussion,” and “minor head injury” all may refer to the same injury.
The CDC has developed a suite of materials to assist both health care providers and the public in guideline implementation. The agency also is using its HEADS UP campaign to publicize the guidelines and related materials, and plans ongoing evaluation of the guidelines and implementation materials.
Many study authors, including Dr. Lumba-Brown, had relationships with medical device or pharmaceutical companies. The systematic review and guideline development were funded by the CDC.
FROM JAMA PEDIATRICS
Janssen submits NDA for esketamine nasal spray
Janssen has announced its submission of a new drug application to the Food and Drug Administration for esketamine nasal spray, which is intended for adult patients with treatment-resistant depression.
About 30% of people with depression do not respond to currently available interventions (Biol Psychiatry. 2016 Sep 15;80[6]:424-31). “This represents a major unmet public health need,” Mathai Mammen, MD, PhD, global head, Janssen Research & Development, said in a Sept. 4 press release announcing the NDA.
The application submitted by Janssen is based on data from five phase 3 trials, all of which demonstrated rapid reduction of depressive symptoms, as well as delayed time to relapse of symptoms, in patients with treatment-resistant depression, Janssen said in the release. Those studies compared treatment with esketamine plus a newly initiated oral antidepressant with that of placebo plus a newly initiated oral antidepressant. One of the studies evaluated long-term safety associated with esketamine treatment and found no new safety signals at 52 weeks of treatment, compared with those seen in short-term studies of the drug.
Previously, it received Breakthrough Therapy Designations for both treatment-resistant depression and major depressive disorder with imminent risk for suicide. Phase 3 clinical studies for the latter indication are ongoing. According to Janssen, the company plans to submit a Marketing Authorization Application to the European Medicines Agency later in 2018 for the treatment-resistant depression indication.
Janssen has announced its submission of a new drug application to the Food and Drug Administration for esketamine nasal spray, which is intended for adult patients with treatment-resistant depression.
About 30% of people with depression do not respond to currently available interventions (Biol Psychiatry. 2016 Sep 15;80[6]:424-31). “This represents a major unmet public health need,” Mathai Mammen, MD, PhD, global head, Janssen Research & Development, said in a Sept. 4 press release announcing the NDA.
The application submitted by Janssen is based on data from five phase 3 trials, all of which demonstrated rapid reduction of depressive symptoms, as well as delayed time to relapse of symptoms, in patients with treatment-resistant depression, Janssen said in the release. Those studies compared treatment with esketamine plus a newly initiated oral antidepressant with that of placebo plus a newly initiated oral antidepressant. One of the studies evaluated long-term safety associated with esketamine treatment and found no new safety signals at 52 weeks of treatment, compared with those seen in short-term studies of the drug.
Previously, it received Breakthrough Therapy Designations for both treatment-resistant depression and major depressive disorder with imminent risk for suicide. Phase 3 clinical studies for the latter indication are ongoing. According to Janssen, the company plans to submit a Marketing Authorization Application to the European Medicines Agency later in 2018 for the treatment-resistant depression indication.
Janssen has announced its submission of a new drug application to the Food and Drug Administration for esketamine nasal spray, which is intended for adult patients with treatment-resistant depression.
About 30% of people with depression do not respond to currently available interventions (Biol Psychiatry. 2016 Sep 15;80[6]:424-31). “This represents a major unmet public health need,” Mathai Mammen, MD, PhD, global head, Janssen Research & Development, said in a Sept. 4 press release announcing the NDA.
The application submitted by Janssen is based on data from five phase 3 trials, all of which demonstrated rapid reduction of depressive symptoms, as well as delayed time to relapse of symptoms, in patients with treatment-resistant depression, Janssen said in the release. Those studies compared treatment with esketamine plus a newly initiated oral antidepressant with that of placebo plus a newly initiated oral antidepressant. One of the studies evaluated long-term safety associated with esketamine treatment and found no new safety signals at 52 weeks of treatment, compared with those seen in short-term studies of the drug.
Previously, it received Breakthrough Therapy Designations for both treatment-resistant depression and major depressive disorder with imminent risk for suicide. Phase 3 clinical studies for the latter indication are ongoing. According to Janssen, the company plans to submit a Marketing Authorization Application to the European Medicines Agency later in 2018 for the treatment-resistant depression indication.
FDA fast-tracks CX-01 for newly diagnosed AML
The Food and Drug Administration has granted fast-track designation to CX-01 as a treatment for patients older than 60 years receiving induction therapy for newly diagnosed acute myeloid leukemia (AML).
CX-01 also has orphan drug designation from the FDA.
CX-01 is a polysaccharide derived from heparin thought to enhance chemotherapy by disrupting leukemia cell adhesion in bone marrow. Cantex Pharmaceuticals is conducting a randomized, phase 2b study to determine whether CX-01 can improve the efficacy of frontline chemotherapy in patients with AML.
This study builds upon results of a pilot study, which were published in Blood Advances (Blood Adv. 2018 Feb 27;2[4]:381-9). The pilot study enrolled 12 adults with newly diagnosed AML who received CX-01 as a continuous infusion for 7 days, along with standard induction chemotherapy (cytarabine and idarubicin).
A total of 11 patients achieved morphological complete remission after one cycle of induction. This included two patients who did not complete induction. All patients received subsequent therapy – consolidation, salvage, or transplant – on or off study.
At a median follow-up of 24 months, eight patients were still alive. Two patients died of transplant-related complications, one died of infectious complications, and one died of cerebral hemorrhage. The median disease-free survival was 14.8 months, and the median overall survival was not reached.
There were five serious adverse events in five patients; most were considered unrelated to CX-01, but a case of grade 4 sepsis was possibly related.
The FDA’s fast-track development program is designed to expedite clinical development and submission of applications for products with the potential to treat serious or life-threatening conditions and address unmet medical needs.
The Food and Drug Administration has granted fast-track designation to CX-01 as a treatment for patients older than 60 years receiving induction therapy for newly diagnosed acute myeloid leukemia (AML).
CX-01 also has orphan drug designation from the FDA.
CX-01 is a polysaccharide derived from heparin thought to enhance chemotherapy by disrupting leukemia cell adhesion in bone marrow. Cantex Pharmaceuticals is conducting a randomized, phase 2b study to determine whether CX-01 can improve the efficacy of frontline chemotherapy in patients with AML.
This study builds upon results of a pilot study, which were published in Blood Advances (Blood Adv. 2018 Feb 27;2[4]:381-9). The pilot study enrolled 12 adults with newly diagnosed AML who received CX-01 as a continuous infusion for 7 days, along with standard induction chemotherapy (cytarabine and idarubicin).
A total of 11 patients achieved morphological complete remission after one cycle of induction. This included two patients who did not complete induction. All patients received subsequent therapy – consolidation, salvage, or transplant – on or off study.
At a median follow-up of 24 months, eight patients were still alive. Two patients died of transplant-related complications, one died of infectious complications, and one died of cerebral hemorrhage. The median disease-free survival was 14.8 months, and the median overall survival was not reached.
There were five serious adverse events in five patients; most were considered unrelated to CX-01, but a case of grade 4 sepsis was possibly related.
The FDA’s fast-track development program is designed to expedite clinical development and submission of applications for products with the potential to treat serious or life-threatening conditions and address unmet medical needs.
The Food and Drug Administration has granted fast-track designation to CX-01 as a treatment for patients older than 60 years receiving induction therapy for newly diagnosed acute myeloid leukemia (AML).
CX-01 also has orphan drug designation from the FDA.
CX-01 is a polysaccharide derived from heparin thought to enhance chemotherapy by disrupting leukemia cell adhesion in bone marrow. Cantex Pharmaceuticals is conducting a randomized, phase 2b study to determine whether CX-01 can improve the efficacy of frontline chemotherapy in patients with AML.
This study builds upon results of a pilot study, which were published in Blood Advances (Blood Adv. 2018 Feb 27;2[4]:381-9). The pilot study enrolled 12 adults with newly diagnosed AML who received CX-01 as a continuous infusion for 7 days, along with standard induction chemotherapy (cytarabine and idarubicin).
A total of 11 patients achieved morphological complete remission after one cycle of induction. This included two patients who did not complete induction. All patients received subsequent therapy – consolidation, salvage, or transplant – on or off study.
At a median follow-up of 24 months, eight patients were still alive. Two patients died of transplant-related complications, one died of infectious complications, and one died of cerebral hemorrhage. The median disease-free survival was 14.8 months, and the median overall survival was not reached.
There were five serious adverse events in five patients; most were considered unrelated to CX-01, but a case of grade 4 sepsis was possibly related.
The FDA’s fast-track development program is designed to expedite clinical development and submission of applications for products with the potential to treat serious or life-threatening conditions and address unmet medical needs.
FDA approves two once-daily HIV drugs
Two once-daily oral HIV-1 medicines have been approved by the Food and Drug Administration, according to Merck: Delstrigo, a fixed-dose combination tablet of doravirine (100 mg), lamivudine (300 mg), and tenofovir disoproxil fumarate (300 mg), and Pifeltro (doravirine, 100 mg). Both drugs are indicated for treating HIV-1 infection in adult patients with no prior antiretroviral treatment.
Pifeltro is a nonnucleoside reverse transcriptase inhibitor to be used in combination with other antiretroviral medicines. Delstrigo contains a boxed warning regarding posttreatment acute exacerbation of hepatitis B infection.
Delstrigo and Pifeltro are not curative, according to the announcement by Merck, which manufactures both drugs.
The FDA approval of Delstrigo was based on findings from the DRIVE-AHEAD trial (NCT02403674), which randomized 728 participants with no history of antiretroviral treatment to receive once daily either Delstrigo or efavirenz/emtricitabine/tenofovir disoproxil fumarate (EFV 600 mg/FTC 200 mg/TDF 300 mg). Delstrigo was associated with sustained viral suppression through 48 weeks, meeting its primary endpoint of noninferior efficacy when compared with EFV/FTC/TDF (84% vs. 81%, respectively), according to Merck.
Pifeltro was approved based on the results of the DRIVE-FORWARD trial (NCT02275780), which randomized 766 participants with no history of antiretroviral treatment to receive either Pifeltro once daily or darunavir 800 mg plus ritonavir 100 mg (DRV+r) once daily, each in combination with either emtricitabine (FTC)/TDF or abacavir (ABC)/lamivudine (3TC), as selected by the investigator. Pifeltro was associated with sustained viral suppression through 48 weeks, meeting its primary endpoint of noninferior efficacy when compared with DRV+r, each in combination with FTC/TDF or ABC/3TC (84% vs. 80%, respectively), according to the Merck announcement.
Two once-daily oral HIV-1 medicines have been approved by the Food and Drug Administration, according to Merck: Delstrigo, a fixed-dose combination tablet of doravirine (100 mg), lamivudine (300 mg), and tenofovir disoproxil fumarate (300 mg), and Pifeltro (doravirine, 100 mg). Both drugs are indicated for treating HIV-1 infection in adult patients with no prior antiretroviral treatment.
Pifeltro is a nonnucleoside reverse transcriptase inhibitor to be used in combination with other antiretroviral medicines. Delstrigo contains a boxed warning regarding posttreatment acute exacerbation of hepatitis B infection.
Delstrigo and Pifeltro are not curative, according to the announcement by Merck, which manufactures both drugs.
The FDA approval of Delstrigo was based on findings from the DRIVE-AHEAD trial (NCT02403674), which randomized 728 participants with no history of antiretroviral treatment to receive once daily either Delstrigo or efavirenz/emtricitabine/tenofovir disoproxil fumarate (EFV 600 mg/FTC 200 mg/TDF 300 mg). Delstrigo was associated with sustained viral suppression through 48 weeks, meeting its primary endpoint of noninferior efficacy when compared with EFV/FTC/TDF (84% vs. 81%, respectively), according to Merck.
Pifeltro was approved based on the results of the DRIVE-FORWARD trial (NCT02275780), which randomized 766 participants with no history of antiretroviral treatment to receive either Pifeltro once daily or darunavir 800 mg plus ritonavir 100 mg (DRV+r) once daily, each in combination with either emtricitabine (FTC)/TDF or abacavir (ABC)/lamivudine (3TC), as selected by the investigator. Pifeltro was associated with sustained viral suppression through 48 weeks, meeting its primary endpoint of noninferior efficacy when compared with DRV+r, each in combination with FTC/TDF or ABC/3TC (84% vs. 80%, respectively), according to the Merck announcement.
Two once-daily oral HIV-1 medicines have been approved by the Food and Drug Administration, according to Merck: Delstrigo, a fixed-dose combination tablet of doravirine (100 mg), lamivudine (300 mg), and tenofovir disoproxil fumarate (300 mg), and Pifeltro (doravirine, 100 mg). Both drugs are indicated for treating HIV-1 infection in adult patients with no prior antiretroviral treatment.
Pifeltro is a nonnucleoside reverse transcriptase inhibitor to be used in combination with other antiretroviral medicines. Delstrigo contains a boxed warning regarding posttreatment acute exacerbation of hepatitis B infection.
Delstrigo and Pifeltro are not curative, according to the announcement by Merck, which manufactures both drugs.
The FDA approval of Delstrigo was based on findings from the DRIVE-AHEAD trial (NCT02403674), which randomized 728 participants with no history of antiretroviral treatment to receive once daily either Delstrigo or efavirenz/emtricitabine/tenofovir disoproxil fumarate (EFV 600 mg/FTC 200 mg/TDF 300 mg). Delstrigo was associated with sustained viral suppression through 48 weeks, meeting its primary endpoint of noninferior efficacy when compared with EFV/FTC/TDF (84% vs. 81%, respectively), according to Merck.
Pifeltro was approved based on the results of the DRIVE-FORWARD trial (NCT02275780), which randomized 766 participants with no history of antiretroviral treatment to receive either Pifeltro once daily or darunavir 800 mg plus ritonavir 100 mg (DRV+r) once daily, each in combination with either emtricitabine (FTC)/TDF or abacavir (ABC)/lamivudine (3TC), as selected by the investigator. Pifeltro was associated with sustained viral suppression through 48 weeks, meeting its primary endpoint of noninferior efficacy when compared with DRV+r, each in combination with FTC/TDF or ABC/3TC (84% vs. 80%, respectively), according to the Merck announcement.
FDA approves new factor VIII product for hemophilia A
Jivi (formerly BAY94-9027), a DNA-derived, factor VIII concentrate, is now approved for use in previously treated adults and adolescents – aged 12 years and older – with hemophilia A.
The product is also approved for on-demand treatment and control of bleeding episodes, for perioperative management of bleeding, and as routine prophylaxis to reduce the frequency of bleeding episodes.
The initial recommended prophylactic regimen is dosing twice weekly (30-40 IU/kg) with the ability to dose every 5 days (45-60 IU/kg) and to further individually adjust to less or more frequent dosing based on bleeding episodes.
The FDA’s approval of Jivi is based on results from the phase 2/3 PROTECT VIII trial. Some results from this trial were published in the Journal of Thrombosis and Haemostasis (2017 Mar;15[3]:411-419). Additional results are available in the prescribing information for Jivi. The product is marketed by Bayer.
PROTECT VIII enrolled previously treated adults and adolescents with severe hemophilia A. In part A, researchers evaluated different dosing regimens for Jivi used as prophylaxis and on-demand treatment. An optional extension study was available to patients who completed part A. In part B, researchers evaluated Jivi for perioperative management.
In part A, there were 132 patients in the intent‐to‐treat population – 112 in the prophylaxis group and 20 in the on-demand group.
Patients received Jivi for 36 weeks. For the first 10 weeks, patients in the prophylaxis group received twice-weekly dosing at 25 IU/kg.
Patients with more than one bleed during this time went on to receive 30-40 IU/kg twice weekly. Patients with one or fewer bleeds were eligible for randomization to dosing every 5 days (45-60 IU/kg) or every 7 days (60 IU/kg).
The median annualized bleeding rate (ABR) for the patients who were treated twice weekly and were not eligible for randomization (n = 13) improved after their dose increase. Their median ABR decreased from 17.4 to 4.1.
The median ABR for patients who were randomized to treatment every 5 days (n = 43) was 1.9. The median ABR was also 1.9 for patients who were eligible for randomization but continued on twice-weekly treatment (n = 11). The median ABR for patients who completed prophylaxis with dosing every 7 days (32/43) was 0.96. The median ABR for patients treated on demand was 24.1.
There were 388 treated bleeds in the on-demand group and 317 treated bleeds in the prophylaxis group.
The safety data in the prescribing information includes 221 patients from three studies. The 17 patients who received Jivi for perioperative management were excluded from the pooled safety analysis but included in the analysis for inhibitor development.
In the 148 patients aged 12 years and older who were exposed to Jivi, adverse events included abdominal pain, nausea, vomiting, injection site reactions, pyrexia, hypersensitivity, dizziness, headache, insomnia, cough, erythema, pruritus, rash, and flushing.
A factor VIII inhibitor was reported in one adult patient, but repeat testing did not confirm the report.
One adult patient with asthma had a clinical hypersensitivity reaction and a transient increase of IgM anti-PEG antibody titer, which was negative upon retesting.
Jivi (formerly BAY94-9027), a DNA-derived, factor VIII concentrate, is now approved for use in previously treated adults and adolescents – aged 12 years and older – with hemophilia A.
The product is also approved for on-demand treatment and control of bleeding episodes, for perioperative management of bleeding, and as routine prophylaxis to reduce the frequency of bleeding episodes.
The initial recommended prophylactic regimen is dosing twice weekly (30-40 IU/kg) with the ability to dose every 5 days (45-60 IU/kg) and to further individually adjust to less or more frequent dosing based on bleeding episodes.
The FDA’s approval of Jivi is based on results from the phase 2/3 PROTECT VIII trial. Some results from this trial were published in the Journal of Thrombosis and Haemostasis (2017 Mar;15[3]:411-419). Additional results are available in the prescribing information for Jivi. The product is marketed by Bayer.
PROTECT VIII enrolled previously treated adults and adolescents with severe hemophilia A. In part A, researchers evaluated different dosing regimens for Jivi used as prophylaxis and on-demand treatment. An optional extension study was available to patients who completed part A. In part B, researchers evaluated Jivi for perioperative management.
In part A, there were 132 patients in the intent‐to‐treat population – 112 in the prophylaxis group and 20 in the on-demand group.
Patients received Jivi for 36 weeks. For the first 10 weeks, patients in the prophylaxis group received twice-weekly dosing at 25 IU/kg.
Patients with more than one bleed during this time went on to receive 30-40 IU/kg twice weekly. Patients with one or fewer bleeds were eligible for randomization to dosing every 5 days (45-60 IU/kg) or every 7 days (60 IU/kg).
The median annualized bleeding rate (ABR) for the patients who were treated twice weekly and were not eligible for randomization (n = 13) improved after their dose increase. Their median ABR decreased from 17.4 to 4.1.
The median ABR for patients who were randomized to treatment every 5 days (n = 43) was 1.9. The median ABR was also 1.9 for patients who were eligible for randomization but continued on twice-weekly treatment (n = 11). The median ABR for patients who completed prophylaxis with dosing every 7 days (32/43) was 0.96. The median ABR for patients treated on demand was 24.1.
There were 388 treated bleeds in the on-demand group and 317 treated bleeds in the prophylaxis group.
The safety data in the prescribing information includes 221 patients from three studies. The 17 patients who received Jivi for perioperative management were excluded from the pooled safety analysis but included in the analysis for inhibitor development.
In the 148 patients aged 12 years and older who were exposed to Jivi, adverse events included abdominal pain, nausea, vomiting, injection site reactions, pyrexia, hypersensitivity, dizziness, headache, insomnia, cough, erythema, pruritus, rash, and flushing.
A factor VIII inhibitor was reported in one adult patient, but repeat testing did not confirm the report.
One adult patient with asthma had a clinical hypersensitivity reaction and a transient increase of IgM anti-PEG antibody titer, which was negative upon retesting.
Jivi (formerly BAY94-9027), a DNA-derived, factor VIII concentrate, is now approved for use in previously treated adults and adolescents – aged 12 years and older – with hemophilia A.
The product is also approved for on-demand treatment and control of bleeding episodes, for perioperative management of bleeding, and as routine prophylaxis to reduce the frequency of bleeding episodes.
The initial recommended prophylactic regimen is dosing twice weekly (30-40 IU/kg) with the ability to dose every 5 days (45-60 IU/kg) and to further individually adjust to less or more frequent dosing based on bleeding episodes.
The FDA’s approval of Jivi is based on results from the phase 2/3 PROTECT VIII trial. Some results from this trial were published in the Journal of Thrombosis and Haemostasis (2017 Mar;15[3]:411-419). Additional results are available in the prescribing information for Jivi. The product is marketed by Bayer.
PROTECT VIII enrolled previously treated adults and adolescents with severe hemophilia A. In part A, researchers evaluated different dosing regimens for Jivi used as prophylaxis and on-demand treatment. An optional extension study was available to patients who completed part A. In part B, researchers evaluated Jivi for perioperative management.
In part A, there were 132 patients in the intent‐to‐treat population – 112 in the prophylaxis group and 20 in the on-demand group.
Patients received Jivi for 36 weeks. For the first 10 weeks, patients in the prophylaxis group received twice-weekly dosing at 25 IU/kg.
Patients with more than one bleed during this time went on to receive 30-40 IU/kg twice weekly. Patients with one or fewer bleeds were eligible for randomization to dosing every 5 days (45-60 IU/kg) or every 7 days (60 IU/kg).
The median annualized bleeding rate (ABR) for the patients who were treated twice weekly and were not eligible for randomization (n = 13) improved after their dose increase. Their median ABR decreased from 17.4 to 4.1.
The median ABR for patients who were randomized to treatment every 5 days (n = 43) was 1.9. The median ABR was also 1.9 for patients who were eligible for randomization but continued on twice-weekly treatment (n = 11). The median ABR for patients who completed prophylaxis with dosing every 7 days (32/43) was 0.96. The median ABR for patients treated on demand was 24.1.
There were 388 treated bleeds in the on-demand group and 317 treated bleeds in the prophylaxis group.
The safety data in the prescribing information includes 221 patients from three studies. The 17 patients who received Jivi for perioperative management were excluded from the pooled safety analysis but included in the analysis for inhibitor development.
In the 148 patients aged 12 years and older who were exposed to Jivi, adverse events included abdominal pain, nausea, vomiting, injection site reactions, pyrexia, hypersensitivity, dizziness, headache, insomnia, cough, erythema, pruritus, rash, and flushing.
A factor VIII inhibitor was reported in one adult patient, but repeat testing did not confirm the report.
One adult patient with asthma had a clinical hypersensitivity reaction and a transient increase of IgM anti-PEG antibody titer, which was negative upon retesting.