User login
MDedge conference coverage features onsite reporting of the latest study results and expert perspectives from leading researchers.
Normal-weight prediabetes patients also benefit from lifestyle intervention
Adults with prediabetes of normal weight may derive at least as much benefit from lifestyle health coaching programs as adults who are overweight or obese, results of a recent nonrandomized, real-world study show.
Fasting plasma glucose (FPG) normalized in about 63% of prediabetic adults with normal body mass index (BMI) participating in a personalized coaching program that emphasized exercise, nutrition, and weight management, according to researcher Mandy Salmon, MS.
By contrast, FPG normalized in about 52% of overweight and 44% of obese prediabetic individuals participating in the program, according to Ms. Salmon, a medical student at the University of Pennsylvania, Philadelphia.
The normal-weight individuals didn’t lose any weight after participating in the coaching program, but they did significantly increase exercise, as did their overweight and obese counterparts, Ms. Salmon said in a presentation of her findings at virtual annual scientific sessions of the American Diabetes Association.
That means not only that normal-weight individuals shouldn’t be excluded from coaching interventions for diabetes prevention, but also that the success of such programs shouldn’t be judged solely on the magnitude of weight loss, according to the researcher.
“It is interesting to note that, although the normal weight group lost the least amount of weight, they still benefited from the lifestyle health coaching program, but having a resultant greatest decrease in fasting plasma glucose and normalization to a range of someone without prediabetes,” Ms. Salmon said.
The fact that most of those patients experienced normalization of FPG despite no weight loss emphasizes the importance of physical activity as a lifestyle intervention, according to Mark Schutta, MD, medical director of Penn Rodebaugh Diabetes Center in Philadelphia, who was not involved in the study.
“You hear these axioms that say things like, ‘you can never outexercise a bad diet,’ and that’s probably true. But all the studies will tell us that a fit, overweight diabetic has much lower risk of cardiovascular disease than an unfit overweight diabetic,” Dr. Schutta said in an interview.
Benefits in normal-weight individuals
One in three Americans has prediabetes, and of those individuals, one in five have a normal BMI, Ms. Salmon said in her virtual ADA presentation.
It’s thought that diabetes may develop in those normal-weight individuals through different pathological mechanisms than in overweight or obese individuals. In turn, that could mean that standard methods for staving off diabetes prevention may not be as effective for them, she said.
Those mechanisms are not well understood; even so, normal BMI is currently an exclusion criterion for many diabetes prevention programs, she added, including the Center for Disease Control and Prevention’s National Diabetes Prevention Program, which specifically requires that individuals have an elevated BMI to be eligible for referral.
To evaluate the potential benefits of coaching in normal-weight individuals, the investigators studied a cohort of 1,897 adults with prediabetes, defined as a baseline FPG of 100-125 mg/dL, who were participating in a lifestyle health coaching program. Of those participants, 188, or about 10% had a normal BMI of 18.5-24.9 mg/m2. Another 495 participants were overweight, with BMIs between 25 and 29.9, while 1,214 were obese, with a BMI of at least 30.
The intervention included an initial assessment to generate goals and a personalized action plan based on the individual’s risk factors, according to Ms. Salmon, along with an action plan that included one-on-one, behaviorally oriented, technology-enabled lifestyle health coaching focused on exercise and physical activity, weight management, and nutrition.
Key findings
With a mean follow-up of 145 days, weight loss in the obese group was greater than that of the overweight group, with mean BMI changes of –1.3 and –0.6, respectively, while there was no significant change in weight for the normal-weight individuals, according to Ms. Salmon.
By contrast, weekly aerobic activity increased significantly in all three groups, she added, with average increases of 95 minutes in the obese group, 98 minutes in the overweight group, and 77 minutes in the normal-weight group.
Likewise, significant decreases in FPG were seen in all 3 groups, with average changes of –6 mg/dL for the obese participants, –7 mg/dL for overweight participants, and –9 mg/dL for normal-weight participants, Ms. Salmon said.
The proportion of individuals whose FPG normalized was highest in the normal-weight group, at 62%, compared with 51.7% for overweight and 44% for obese individuals, she added.
Most previous studies of lifestyle interventions for prediabetes have excluded normal-weight individuals, according to Ms. Salmon, who said one strength of her study was that the subjects were already participating in the established lifestyle health coaching program and didn’t interact with the team of researchers.
“It was an effectiveness study in which we could see the real-world benefits of the program, rather than a theoretical efficacy study,” she said.
Ms. Salmon said she had no potential conflicts of interest to disclose. The coinvestigators of the study were members or employees of a privately held population health management company called INTERVENT International.
SOURCE: Salmon MK et al. ADA 2020, Abstract 273-OR.
Adults with prediabetes of normal weight may derive at least as much benefit from lifestyle health coaching programs as adults who are overweight or obese, results of a recent nonrandomized, real-world study show.
Fasting plasma glucose (FPG) normalized in about 63% of prediabetic adults with normal body mass index (BMI) participating in a personalized coaching program that emphasized exercise, nutrition, and weight management, according to researcher Mandy Salmon, MS.
By contrast, FPG normalized in about 52% of overweight and 44% of obese prediabetic individuals participating in the program, according to Ms. Salmon, a medical student at the University of Pennsylvania, Philadelphia.
The normal-weight individuals didn’t lose any weight after participating in the coaching program, but they did significantly increase exercise, as did their overweight and obese counterparts, Ms. Salmon said in a presentation of her findings at virtual annual scientific sessions of the American Diabetes Association.
That means not only that normal-weight individuals shouldn’t be excluded from coaching interventions for diabetes prevention, but also that the success of such programs shouldn’t be judged solely on the magnitude of weight loss, according to the researcher.
“It is interesting to note that, although the normal weight group lost the least amount of weight, they still benefited from the lifestyle health coaching program, but having a resultant greatest decrease in fasting plasma glucose and normalization to a range of someone without prediabetes,” Ms. Salmon said.
The fact that most of those patients experienced normalization of FPG despite no weight loss emphasizes the importance of physical activity as a lifestyle intervention, according to Mark Schutta, MD, medical director of Penn Rodebaugh Diabetes Center in Philadelphia, who was not involved in the study.
“You hear these axioms that say things like, ‘you can never outexercise a bad diet,’ and that’s probably true. But all the studies will tell us that a fit, overweight diabetic has much lower risk of cardiovascular disease than an unfit overweight diabetic,” Dr. Schutta said in an interview.
Benefits in normal-weight individuals
One in three Americans has prediabetes, and of those individuals, one in five have a normal BMI, Ms. Salmon said in her virtual ADA presentation.
It’s thought that diabetes may develop in those normal-weight individuals through different pathological mechanisms than in overweight or obese individuals. In turn, that could mean that standard methods for staving off diabetes prevention may not be as effective for them, she said.
Those mechanisms are not well understood; even so, normal BMI is currently an exclusion criterion for many diabetes prevention programs, she added, including the Center for Disease Control and Prevention’s National Diabetes Prevention Program, which specifically requires that individuals have an elevated BMI to be eligible for referral.
To evaluate the potential benefits of coaching in normal-weight individuals, the investigators studied a cohort of 1,897 adults with prediabetes, defined as a baseline FPG of 100-125 mg/dL, who were participating in a lifestyle health coaching program. Of those participants, 188, or about 10% had a normal BMI of 18.5-24.9 mg/m2. Another 495 participants were overweight, with BMIs between 25 and 29.9, while 1,214 were obese, with a BMI of at least 30.
The intervention included an initial assessment to generate goals and a personalized action plan based on the individual’s risk factors, according to Ms. Salmon, along with an action plan that included one-on-one, behaviorally oriented, technology-enabled lifestyle health coaching focused on exercise and physical activity, weight management, and nutrition.
Key findings
With a mean follow-up of 145 days, weight loss in the obese group was greater than that of the overweight group, with mean BMI changes of –1.3 and –0.6, respectively, while there was no significant change in weight for the normal-weight individuals, according to Ms. Salmon.
By contrast, weekly aerobic activity increased significantly in all three groups, she added, with average increases of 95 minutes in the obese group, 98 minutes in the overweight group, and 77 minutes in the normal-weight group.
Likewise, significant decreases in FPG were seen in all 3 groups, with average changes of –6 mg/dL for the obese participants, –7 mg/dL for overweight participants, and –9 mg/dL for normal-weight participants, Ms. Salmon said.
The proportion of individuals whose FPG normalized was highest in the normal-weight group, at 62%, compared with 51.7% for overweight and 44% for obese individuals, she added.
Most previous studies of lifestyle interventions for prediabetes have excluded normal-weight individuals, according to Ms. Salmon, who said one strength of her study was that the subjects were already participating in the established lifestyle health coaching program and didn’t interact with the team of researchers.
“It was an effectiveness study in which we could see the real-world benefits of the program, rather than a theoretical efficacy study,” she said.
Ms. Salmon said she had no potential conflicts of interest to disclose. The coinvestigators of the study were members or employees of a privately held population health management company called INTERVENT International.
SOURCE: Salmon MK et al. ADA 2020, Abstract 273-OR.
Adults with prediabetes of normal weight may derive at least as much benefit from lifestyle health coaching programs as adults who are overweight or obese, results of a recent nonrandomized, real-world study show.
Fasting plasma glucose (FPG) normalized in about 63% of prediabetic adults with normal body mass index (BMI) participating in a personalized coaching program that emphasized exercise, nutrition, and weight management, according to researcher Mandy Salmon, MS.
By contrast, FPG normalized in about 52% of overweight and 44% of obese prediabetic individuals participating in the program, according to Ms. Salmon, a medical student at the University of Pennsylvania, Philadelphia.
The normal-weight individuals didn’t lose any weight after participating in the coaching program, but they did significantly increase exercise, as did their overweight and obese counterparts, Ms. Salmon said in a presentation of her findings at virtual annual scientific sessions of the American Diabetes Association.
That means not only that normal-weight individuals shouldn’t be excluded from coaching interventions for diabetes prevention, but also that the success of such programs shouldn’t be judged solely on the magnitude of weight loss, according to the researcher.
“It is interesting to note that, although the normal weight group lost the least amount of weight, they still benefited from the lifestyle health coaching program, but having a resultant greatest decrease in fasting plasma glucose and normalization to a range of someone without prediabetes,” Ms. Salmon said.
The fact that most of those patients experienced normalization of FPG despite no weight loss emphasizes the importance of physical activity as a lifestyle intervention, according to Mark Schutta, MD, medical director of Penn Rodebaugh Diabetes Center in Philadelphia, who was not involved in the study.
“You hear these axioms that say things like, ‘you can never outexercise a bad diet,’ and that’s probably true. But all the studies will tell us that a fit, overweight diabetic has much lower risk of cardiovascular disease than an unfit overweight diabetic,” Dr. Schutta said in an interview.
Benefits in normal-weight individuals
One in three Americans has prediabetes, and of those individuals, one in five have a normal BMI, Ms. Salmon said in her virtual ADA presentation.
It’s thought that diabetes may develop in those normal-weight individuals through different pathological mechanisms than in overweight or obese individuals. In turn, that could mean that standard methods for staving off diabetes prevention may not be as effective for them, she said.
Those mechanisms are not well understood; even so, normal BMI is currently an exclusion criterion for many diabetes prevention programs, she added, including the Center for Disease Control and Prevention’s National Diabetes Prevention Program, which specifically requires that individuals have an elevated BMI to be eligible for referral.
To evaluate the potential benefits of coaching in normal-weight individuals, the investigators studied a cohort of 1,897 adults with prediabetes, defined as a baseline FPG of 100-125 mg/dL, who were participating in a lifestyle health coaching program. Of those participants, 188, or about 10% had a normal BMI of 18.5-24.9 mg/m2. Another 495 participants were overweight, with BMIs between 25 and 29.9, while 1,214 were obese, with a BMI of at least 30.
The intervention included an initial assessment to generate goals and a personalized action plan based on the individual’s risk factors, according to Ms. Salmon, along with an action plan that included one-on-one, behaviorally oriented, technology-enabled lifestyle health coaching focused on exercise and physical activity, weight management, and nutrition.
Key findings
With a mean follow-up of 145 days, weight loss in the obese group was greater than that of the overweight group, with mean BMI changes of –1.3 and –0.6, respectively, while there was no significant change in weight for the normal-weight individuals, according to Ms. Salmon.
By contrast, weekly aerobic activity increased significantly in all three groups, she added, with average increases of 95 minutes in the obese group, 98 minutes in the overweight group, and 77 minutes in the normal-weight group.
Likewise, significant decreases in FPG were seen in all 3 groups, with average changes of –6 mg/dL for the obese participants, –7 mg/dL for overweight participants, and –9 mg/dL for normal-weight participants, Ms. Salmon said.
The proportion of individuals whose FPG normalized was highest in the normal-weight group, at 62%, compared with 51.7% for overweight and 44% for obese individuals, she added.
Most previous studies of lifestyle interventions for prediabetes have excluded normal-weight individuals, according to Ms. Salmon, who said one strength of her study was that the subjects were already participating in the established lifestyle health coaching program and didn’t interact with the team of researchers.
“It was an effectiveness study in which we could see the real-world benefits of the program, rather than a theoretical efficacy study,” she said.
Ms. Salmon said she had no potential conflicts of interest to disclose. The coinvestigators of the study were members or employees of a privately held population health management company called INTERVENT International.
SOURCE: Salmon MK et al. ADA 2020, Abstract 273-OR.
FROM ADA 2020
EULAR gives pointers on intra-articular injection best practices
New EULAR recommendations for the intra-articular (IA) treatment of arthropathies aim to facilitate uniformity and quality of care for this mainstay of rheumatologic practice, according to a report on the new guidance that was presented at the annual European Congress of Rheumatology, held online this year due to COVID-19.
Until now there were no official recommendations on how best to use it in everyday practice. “This is the first time that there’s been a joint effort to develop evidence-based recommendations,” Jacqueline Usón, MD, PhD, associate professor medicine at Rey Juan Carlos University in Madrid, said in an interview. “Everything that we are saying is pretty logical, but it’s nice to see it put in recommendations based on evidence.”
IA therapy has been around for decades and is key for treating adults with a number of different conditions where synovitis, effusion, pain, or all three, are present, such as inflammatory arthritis and osteoarthritis, Dr. Usón observed during her presentation.
“Today, commonly used injectables are not only corticosteroids but also local anesthetics, hyaluronic acid, blood products, and maybe pharmaceuticals,” she said, adding that “there is a wide variation in the way intra-articular therapies are used and delivered to patients.” Health professionals also have very different views and habits depending on geographic locations and health care systems, she observed. Ironing out the variation was one of the main objectives of the recommendations.
As one of the two conveners of the EULAR task force behind the recommendations, Dr. Usón, herself a rheumatologist at University Hospital of Móstoles, pointed out that the task force brought together a range of specialties – rheumatologists, orthopedic surgeons, radiologists, nuclear medicine specialists, among others, as well as patients – to ensure that the best advice could be given.
The task force followed EULAR standard operating procedures for developing recommendations, with discussion groups, systematic literature reviews, and Delphi technique-based consensus all being employed. The literature search considered publications from 1946 up until 2019.
“We agreed on the need for more background information from health professionals and patients, so we developed two surveys: One for health professionals with 160 items, [for which] we obtained 186 responses from 26 countries; and the patient survey was made up of 44 items, translated into 10 different languages, and we obtained 200 responses,” she said.
The results of the systematic literature review and surveys were used to help form expert consensus, leading to 5 overarching principles and 11 recommendations that look at before, during, and after intra-articular therapy.
Five overarching principles
The first overarching principle recognizes the widespread use of IA therapies and that their use is specific to the disease that is being treated and “may not be interchangeable across indications,” Dr. Usón said. The second principle concerns improving patient-centered outcomes, which are “those that are relevant to the patient,” and include the benefits, harms, preferences, or implications for self-management.
“Contextual factors are important and contribute to the effect of IAT [intra-articular treatment],” she said, discussing the third principle. “These include effective communication, patient expectations, or settings [where the procedure takes place]. In addition, one should take into account that the route of delivery has in itself a placebo effect. We found that in different RCTs [randomized controlled trials], the pooled placebo effect of IA saline is moderate to large.”
The fourth principle looks at ensuring that patients and clinicians make an informed and shared decision, which is again highlighted by the first recommendation. The fifth, and last, overarching principle acknowledges that IA injections may be given by a range of health care professionals.
Advice for before, during, and after injection
Patients need to be “fully informed of the nature of the procedure, the injectable used, and potential effects – benefits and risks – [and] informed consent should be obtained and documented,” said Dr. Usón, outlining the first recommendation. “That seems common,” she said in the interview, “but when we did the survey, we realize that many patients didn’t [give consent], and the doctors didn’t even ask for it. This is why it’s a very general statement, and it’s our first recommendation. The agreement was 99%!”
The recommendations also look at the optimal settings for performing injections, such as providing a professional and private, well-lighted room, and having a resuscitation kit nearby in case patients faint. Accuracy is important, Dr. Usón said, and imaging, such as ultrasound, should be used where available to ensure accurate injection into the joint. This is an area where further research could be performed, she said, urging young rheumatologists and health professionals to consider this. “Intra-articular therapy is something that you learn and do, but you never really investigate in it,” she said.
One recommendation states that when intra-articular injections are being given to pregnant patients, the safety of injected compound must be considered, both for the mother and for the fetus. There is another recommendation on the need to perform IA injections under aseptic conditions, and another stating that patients should be offered local anesthetics, after explaining the pros and cons.
Special populations of patients are also considered, Dr. Usón said. For example, the guidance advises warning patients with diabetes of the risk of transient glycemia after IA glucocorticoids and the need to monitor their blood glucose levels carefully for a couple of days afterward.
As a rule, “IAT is not a contraindication to people with clotting or bleeding disorders, or taking antithrombotic medications,” she said, unless they are at a high risk of bleeding.
Importantly, the recommendations cover when IAT can be performed after joint replacement surgery (after at least 3 months), and the need to “avoid overuse of injected joints” while also avoiding complete immobilization for at least 24 hours afterward. The recommendations very generally cover re-injections, but not how long intervals between injections should be. When asked about interval duration after her presentation, Dr. Usón said that the usual advice is to give IA injections no more than 2-3 times a year, but it depends on the injectable.
“It wasn’t our intention to review the efficacy and the safety of the different injectables, nor to review the use of IAT in different types of joint diseases,” she said. “We do lack a lot of information, a lot of evidence in this, and I really would hope that new rheumatologists start looking into and start investigating in this topic,” she added.
Recommendations will increase awareness of good clinical practice
“IA injections are commonly administered in the rheumatology setting. This is because [IA injection] is often a useful treatment for acute flare of arthritis, particularly when it is limited to a few joints,” observed Ai Lyn Tan, MD, associate professor and honorary consultant rheumatologist at the Leeds (England) Institute of Rheumatic and Musculoskeletal Medicine.
IA injection “also relieves symptoms relatively quickly for patients; however, the response can be variable, and there are side effects associated with IA injections,” Dr. Tan added in an interview.
There is a lack of universally accepted recommendations, Dr. Tan observed, noting that while there might be some local guidelines on how to safely perform IA injections these were often not standardized and were subject to being continually updated to try to improve the experience for patients.
“It is therefore timely to learn about the new EULAR recommendations for IA injections. The advantage of this will be to increase awareness of good clinical practice for performing IA injections.”
Dr. Tan had no relevant conflicts of interest.
SOURCE: EULAR COVID-19 Recommendations. E-congress content available until Sept. 1, 2020.
New EULAR recommendations for the intra-articular (IA) treatment of arthropathies aim to facilitate uniformity and quality of care for this mainstay of rheumatologic practice, according to a report on the new guidance that was presented at the annual European Congress of Rheumatology, held online this year due to COVID-19.
Until now there were no official recommendations on how best to use it in everyday practice. “This is the first time that there’s been a joint effort to develop evidence-based recommendations,” Jacqueline Usón, MD, PhD, associate professor medicine at Rey Juan Carlos University in Madrid, said in an interview. “Everything that we are saying is pretty logical, but it’s nice to see it put in recommendations based on evidence.”
IA therapy has been around for decades and is key for treating adults with a number of different conditions where synovitis, effusion, pain, or all three, are present, such as inflammatory arthritis and osteoarthritis, Dr. Usón observed during her presentation.
“Today, commonly used injectables are not only corticosteroids but also local anesthetics, hyaluronic acid, blood products, and maybe pharmaceuticals,” she said, adding that “there is a wide variation in the way intra-articular therapies are used and delivered to patients.” Health professionals also have very different views and habits depending on geographic locations and health care systems, she observed. Ironing out the variation was one of the main objectives of the recommendations.
As one of the two conveners of the EULAR task force behind the recommendations, Dr. Usón, herself a rheumatologist at University Hospital of Móstoles, pointed out that the task force brought together a range of specialties – rheumatologists, orthopedic surgeons, radiologists, nuclear medicine specialists, among others, as well as patients – to ensure that the best advice could be given.
The task force followed EULAR standard operating procedures for developing recommendations, with discussion groups, systematic literature reviews, and Delphi technique-based consensus all being employed. The literature search considered publications from 1946 up until 2019.
“We agreed on the need for more background information from health professionals and patients, so we developed two surveys: One for health professionals with 160 items, [for which] we obtained 186 responses from 26 countries; and the patient survey was made up of 44 items, translated into 10 different languages, and we obtained 200 responses,” she said.
The results of the systematic literature review and surveys were used to help form expert consensus, leading to 5 overarching principles and 11 recommendations that look at before, during, and after intra-articular therapy.
Five overarching principles
The first overarching principle recognizes the widespread use of IA therapies and that their use is specific to the disease that is being treated and “may not be interchangeable across indications,” Dr. Usón said. The second principle concerns improving patient-centered outcomes, which are “those that are relevant to the patient,” and include the benefits, harms, preferences, or implications for self-management.
“Contextual factors are important and contribute to the effect of IAT [intra-articular treatment],” she said, discussing the third principle. “These include effective communication, patient expectations, or settings [where the procedure takes place]. In addition, one should take into account that the route of delivery has in itself a placebo effect. We found that in different RCTs [randomized controlled trials], the pooled placebo effect of IA saline is moderate to large.”
The fourth principle looks at ensuring that patients and clinicians make an informed and shared decision, which is again highlighted by the first recommendation. The fifth, and last, overarching principle acknowledges that IA injections may be given by a range of health care professionals.
Advice for before, during, and after injection
Patients need to be “fully informed of the nature of the procedure, the injectable used, and potential effects – benefits and risks – [and] informed consent should be obtained and documented,” said Dr. Usón, outlining the first recommendation. “That seems common,” she said in the interview, “but when we did the survey, we realize that many patients didn’t [give consent], and the doctors didn’t even ask for it. This is why it’s a very general statement, and it’s our first recommendation. The agreement was 99%!”
The recommendations also look at the optimal settings for performing injections, such as providing a professional and private, well-lighted room, and having a resuscitation kit nearby in case patients faint. Accuracy is important, Dr. Usón said, and imaging, such as ultrasound, should be used where available to ensure accurate injection into the joint. This is an area where further research could be performed, she said, urging young rheumatologists and health professionals to consider this. “Intra-articular therapy is something that you learn and do, but you never really investigate in it,” she said.
One recommendation states that when intra-articular injections are being given to pregnant patients, the safety of injected compound must be considered, both for the mother and for the fetus. There is another recommendation on the need to perform IA injections under aseptic conditions, and another stating that patients should be offered local anesthetics, after explaining the pros and cons.
Special populations of patients are also considered, Dr. Usón said. For example, the guidance advises warning patients with diabetes of the risk of transient glycemia after IA glucocorticoids and the need to monitor their blood glucose levels carefully for a couple of days afterward.
As a rule, “IAT is not a contraindication to people with clotting or bleeding disorders, or taking antithrombotic medications,” she said, unless they are at a high risk of bleeding.
Importantly, the recommendations cover when IAT can be performed after joint replacement surgery (after at least 3 months), and the need to “avoid overuse of injected joints” while also avoiding complete immobilization for at least 24 hours afterward. The recommendations very generally cover re-injections, but not how long intervals between injections should be. When asked about interval duration after her presentation, Dr. Usón said that the usual advice is to give IA injections no more than 2-3 times a year, but it depends on the injectable.
“It wasn’t our intention to review the efficacy and the safety of the different injectables, nor to review the use of IAT in different types of joint diseases,” she said. “We do lack a lot of information, a lot of evidence in this, and I really would hope that new rheumatologists start looking into and start investigating in this topic,” she added.
Recommendations will increase awareness of good clinical practice
“IA injections are commonly administered in the rheumatology setting. This is because [IA injection] is often a useful treatment for acute flare of arthritis, particularly when it is limited to a few joints,” observed Ai Lyn Tan, MD, associate professor and honorary consultant rheumatologist at the Leeds (England) Institute of Rheumatic and Musculoskeletal Medicine.
IA injection “also relieves symptoms relatively quickly for patients; however, the response can be variable, and there are side effects associated with IA injections,” Dr. Tan added in an interview.
There is a lack of universally accepted recommendations, Dr. Tan observed, noting that while there might be some local guidelines on how to safely perform IA injections these were often not standardized and were subject to being continually updated to try to improve the experience for patients.
“It is therefore timely to learn about the new EULAR recommendations for IA injections. The advantage of this will be to increase awareness of good clinical practice for performing IA injections.”
Dr. Tan had no relevant conflicts of interest.
SOURCE: EULAR COVID-19 Recommendations. E-congress content available until Sept. 1, 2020.
New EULAR recommendations for the intra-articular (IA) treatment of arthropathies aim to facilitate uniformity and quality of care for this mainstay of rheumatologic practice, according to a report on the new guidance that was presented at the annual European Congress of Rheumatology, held online this year due to COVID-19.
Until now there were no official recommendations on how best to use it in everyday practice. “This is the first time that there’s been a joint effort to develop evidence-based recommendations,” Jacqueline Usón, MD, PhD, associate professor medicine at Rey Juan Carlos University in Madrid, said in an interview. “Everything that we are saying is pretty logical, but it’s nice to see it put in recommendations based on evidence.”
IA therapy has been around for decades and is key for treating adults with a number of different conditions where synovitis, effusion, pain, or all three, are present, such as inflammatory arthritis and osteoarthritis, Dr. Usón observed during her presentation.
“Today, commonly used injectables are not only corticosteroids but also local anesthetics, hyaluronic acid, blood products, and maybe pharmaceuticals,” she said, adding that “there is a wide variation in the way intra-articular therapies are used and delivered to patients.” Health professionals also have very different views and habits depending on geographic locations and health care systems, she observed. Ironing out the variation was one of the main objectives of the recommendations.
As one of the two conveners of the EULAR task force behind the recommendations, Dr. Usón, herself a rheumatologist at University Hospital of Móstoles, pointed out that the task force brought together a range of specialties – rheumatologists, orthopedic surgeons, radiologists, nuclear medicine specialists, among others, as well as patients – to ensure that the best advice could be given.
The task force followed EULAR standard operating procedures for developing recommendations, with discussion groups, systematic literature reviews, and Delphi technique-based consensus all being employed. The literature search considered publications from 1946 up until 2019.
“We agreed on the need for more background information from health professionals and patients, so we developed two surveys: One for health professionals with 160 items, [for which] we obtained 186 responses from 26 countries; and the patient survey was made up of 44 items, translated into 10 different languages, and we obtained 200 responses,” she said.
The results of the systematic literature review and surveys were used to help form expert consensus, leading to 5 overarching principles and 11 recommendations that look at before, during, and after intra-articular therapy.
Five overarching principles
The first overarching principle recognizes the widespread use of IA therapies and that their use is specific to the disease that is being treated and “may not be interchangeable across indications,” Dr. Usón said. The second principle concerns improving patient-centered outcomes, which are “those that are relevant to the patient,” and include the benefits, harms, preferences, or implications for self-management.
“Contextual factors are important and contribute to the effect of IAT [intra-articular treatment],” she said, discussing the third principle. “These include effective communication, patient expectations, or settings [where the procedure takes place]. In addition, one should take into account that the route of delivery has in itself a placebo effect. We found that in different RCTs [randomized controlled trials], the pooled placebo effect of IA saline is moderate to large.”
The fourth principle looks at ensuring that patients and clinicians make an informed and shared decision, which is again highlighted by the first recommendation. The fifth, and last, overarching principle acknowledges that IA injections may be given by a range of health care professionals.
Advice for before, during, and after injection
Patients need to be “fully informed of the nature of the procedure, the injectable used, and potential effects – benefits and risks – [and] informed consent should be obtained and documented,” said Dr. Usón, outlining the first recommendation. “That seems common,” she said in the interview, “but when we did the survey, we realize that many patients didn’t [give consent], and the doctors didn’t even ask for it. This is why it’s a very general statement, and it’s our first recommendation. The agreement was 99%!”
The recommendations also look at the optimal settings for performing injections, such as providing a professional and private, well-lighted room, and having a resuscitation kit nearby in case patients faint. Accuracy is important, Dr. Usón said, and imaging, such as ultrasound, should be used where available to ensure accurate injection into the joint. This is an area where further research could be performed, she said, urging young rheumatologists and health professionals to consider this. “Intra-articular therapy is something that you learn and do, but you never really investigate in it,” she said.
One recommendation states that when intra-articular injections are being given to pregnant patients, the safety of injected compound must be considered, both for the mother and for the fetus. There is another recommendation on the need to perform IA injections under aseptic conditions, and another stating that patients should be offered local anesthetics, after explaining the pros and cons.
Special populations of patients are also considered, Dr. Usón said. For example, the guidance advises warning patients with diabetes of the risk of transient glycemia after IA glucocorticoids and the need to monitor their blood glucose levels carefully for a couple of days afterward.
As a rule, “IAT is not a contraindication to people with clotting or bleeding disorders, or taking antithrombotic medications,” she said, unless they are at a high risk of bleeding.
Importantly, the recommendations cover when IAT can be performed after joint replacement surgery (after at least 3 months), and the need to “avoid overuse of injected joints” while also avoiding complete immobilization for at least 24 hours afterward. The recommendations very generally cover re-injections, but not how long intervals between injections should be. When asked about interval duration after her presentation, Dr. Usón said that the usual advice is to give IA injections no more than 2-3 times a year, but it depends on the injectable.
“It wasn’t our intention to review the efficacy and the safety of the different injectables, nor to review the use of IAT in different types of joint diseases,” she said. “We do lack a lot of information, a lot of evidence in this, and I really would hope that new rheumatologists start looking into and start investigating in this topic,” she added.
Recommendations will increase awareness of good clinical practice
“IA injections are commonly administered in the rheumatology setting. This is because [IA injection] is often a useful treatment for acute flare of arthritis, particularly when it is limited to a few joints,” observed Ai Lyn Tan, MD, associate professor and honorary consultant rheumatologist at the Leeds (England) Institute of Rheumatic and Musculoskeletal Medicine.
IA injection “also relieves symptoms relatively quickly for patients; however, the response can be variable, and there are side effects associated with IA injections,” Dr. Tan added in an interview.
There is a lack of universally accepted recommendations, Dr. Tan observed, noting that while there might be some local guidelines on how to safely perform IA injections these were often not standardized and were subject to being continually updated to try to improve the experience for patients.
“It is therefore timely to learn about the new EULAR recommendations for IA injections. The advantage of this will be to increase awareness of good clinical practice for performing IA injections.”
Dr. Tan had no relevant conflicts of interest.
SOURCE: EULAR COVID-19 Recommendations. E-congress content available until Sept. 1, 2020.
FROM THE EULAR 2020 E-CONGRESS
Trifarotene sails through 52-week acne trial
James Q. Del Rosso, MD, reported at the virtual annual meeting of the American Academy of Dermatology.
The study is noteworthy because, even though roughly half of patients with facial acne also have truncal acne, there is actually very little clinical trial data on the treatment of truncal acne other than this new long-term study and the two earlier pivotal phase 3, 12-week trials which led to the October 2019 approval of trifarotene 50 mcg/g cream (Aklief) as the first novel retinoid for acne to reach the market in 20 years, observed Dr. Del Rosso, research director at JDR Research in Las Vegas and a member of the dermatology faculty at Touro University in Henderson, Nev.
The 52-week study, known as SATISFY, began with 454 patients with moderate facial and truncal acne who treated themselves with trifarotene once daily. Among the 348 patients who completed the full year, 67% achieved a score of 0 or 1 – clear or almost clear – with at least a 2-grade improvement from baseline by Investigator’s Global Assessment on their facial acne, and 65% met the same measure of success on the trunk. Moreover, 58% of patients met that standard at both acne sites.
The IGA success rate rose throughout the study period without ever reaching a plateau. However, it should be noted that 23% of participants dropped out of the study over the course of the year.
Mean tolerability scores reflecting redness, scaling, stinging or burning, and skin dryness remained well below the threshold for mild severity, peaking at weeks 2-4 of the study. The most common treatment-related adverse events were mild to moderate itching and irritation, each occurring in less than 5% of subjects.
Trifarotene is a first-in-class retinoid that specifically targets the retinoic acid receptor gamma, the most common cutaneous retinoic acid receptor.
Dr. Del Rosso reported serving as an investigator and consultant for Galderma, which sponsored the study and markets trifarotene cream.
James Q. Del Rosso, MD, reported at the virtual annual meeting of the American Academy of Dermatology.
The study is noteworthy because, even though roughly half of patients with facial acne also have truncal acne, there is actually very little clinical trial data on the treatment of truncal acne other than this new long-term study and the two earlier pivotal phase 3, 12-week trials which led to the October 2019 approval of trifarotene 50 mcg/g cream (Aklief) as the first novel retinoid for acne to reach the market in 20 years, observed Dr. Del Rosso, research director at JDR Research in Las Vegas and a member of the dermatology faculty at Touro University in Henderson, Nev.
The 52-week study, known as SATISFY, began with 454 patients with moderate facial and truncal acne who treated themselves with trifarotene once daily. Among the 348 patients who completed the full year, 67% achieved a score of 0 or 1 – clear or almost clear – with at least a 2-grade improvement from baseline by Investigator’s Global Assessment on their facial acne, and 65% met the same measure of success on the trunk. Moreover, 58% of patients met that standard at both acne sites.
The IGA success rate rose throughout the study period without ever reaching a plateau. However, it should be noted that 23% of participants dropped out of the study over the course of the year.
Mean tolerability scores reflecting redness, scaling, stinging or burning, and skin dryness remained well below the threshold for mild severity, peaking at weeks 2-4 of the study. The most common treatment-related adverse events were mild to moderate itching and irritation, each occurring in less than 5% of subjects.
Trifarotene is a first-in-class retinoid that specifically targets the retinoic acid receptor gamma, the most common cutaneous retinoic acid receptor.
Dr. Del Rosso reported serving as an investigator and consultant for Galderma, which sponsored the study and markets trifarotene cream.
James Q. Del Rosso, MD, reported at the virtual annual meeting of the American Academy of Dermatology.
The study is noteworthy because, even though roughly half of patients with facial acne also have truncal acne, there is actually very little clinical trial data on the treatment of truncal acne other than this new long-term study and the two earlier pivotal phase 3, 12-week trials which led to the October 2019 approval of trifarotene 50 mcg/g cream (Aklief) as the first novel retinoid for acne to reach the market in 20 years, observed Dr. Del Rosso, research director at JDR Research in Las Vegas and a member of the dermatology faculty at Touro University in Henderson, Nev.
The 52-week study, known as SATISFY, began with 454 patients with moderate facial and truncal acne who treated themselves with trifarotene once daily. Among the 348 patients who completed the full year, 67% achieved a score of 0 or 1 – clear or almost clear – with at least a 2-grade improvement from baseline by Investigator’s Global Assessment on their facial acne, and 65% met the same measure of success on the trunk. Moreover, 58% of patients met that standard at both acne sites.
The IGA success rate rose throughout the study period without ever reaching a plateau. However, it should be noted that 23% of participants dropped out of the study over the course of the year.
Mean tolerability scores reflecting redness, scaling, stinging or burning, and skin dryness remained well below the threshold for mild severity, peaking at weeks 2-4 of the study. The most common treatment-related adverse events were mild to moderate itching and irritation, each occurring in less than 5% of subjects.
Trifarotene is a first-in-class retinoid that specifically targets the retinoic acid receptor gamma, the most common cutaneous retinoic acid receptor.
Dr. Del Rosso reported serving as an investigator and consultant for Galderma, which sponsored the study and markets trifarotene cream.
FROM AAD 2020
Ibrutinib-venetoclax produces high MRD-negative rates in CLL/SLL
In patients with previously untreated chronic lymphocytic leukemia (CLL) or small lymphocytic lymphoma (SLL), a once-daily oral regimen of ibrutinib and venetoclax was associated with deep molecular remissions in both bone marrow and peripheral blood, including in patients with high-risk disease, according to investigators in the phase 2 CAPTIVATE MRD trial.
An intention-to-treat analysis of 164 patients with CLL/SLL treated with the combination of ibrutinib (Imbruvica) and venetoclax (Venclexta) showed a 75% rate of minimal residual disease (MRD) negativity in peripheral blood, and a 68% rate of MRD negativity in bone marrow among patients who received up to 12 cycles of the combination, reported Tanya Siddiqi, MD, of City of Hope National Medical Center, Duarte, Calif., and colleagues.
“This phase 2 study supports synergistic antitumor activity of the combination with notable deep responses across multiple compartments,” she said in an oral presentation during the virtual annual congress of the European Hematology Association.
Not ready to change practice
A hematologist/oncologist who was not involved in the study said that the data from CAPTIVATE MRD look good, but it’s still not known whether concurrent or sequential administration of the agents is optimal, and whether other regimens may be more effective in the first line.
“I think this is promising, but the informative and practice-changing study would be to compare this combination to ibrutinib monotherapy or to venetoclax and obinutuzumab, and that’s actually the subject of the next large German cooperative group study, CLL17,” said Catherine C. Coombs, MD, assistant professor of medicine at the University of North Carolina, and the UNC Lineberger Cancer Center, Chapel Hill.
She noted that the combination of venetoclax and obinutuzumab (Gazyva) is also associated with high rates of MRD negativity in the first-line setting, and that use of this regimen allows clinicians to reserve ibrutinib or acalabrutinib (Calquence) for patients in the relapsed setting.
Prerandomization results
Dr. Siddiqi presented prerandomization results from the MRD cohort of the CAPTIVATE trial (NCT02910583), which is evaluating the combination of ibrutinib and venetoclax for depth of MRD response. Following 12 cycles of the combinations, patients in this cohort are then randomized based on confirmed MRD status, with patients who are MRD negative randomized to maintenance with either ibrutinib or placebo, and patients with residual disease (MRD positive) randomized to maintenance with either ibrutinib alone or with venetoclax.
A total of 164 patients with previously untreated CLL/SLL and active disease requiring treatment who were under age 70 and had good performance status were enrolled. Following an ibrutinib lead-in period with the drug given at 420 mg once daily for three cycles of 28 days, the patients were continued on ibrutinib, and were started on venetoclax with a ramp up to 400 mg once daily, for 12 additional cycles.
As planned, patients were assessed after 15 cycles for tumor lysis syndrome (TLS) risk assessment, MRD, and hematologic, clinical, imaging, and bone marrow exams for response.
The median patient age was 58, with poor-risk features such as deletion 17p seen in 16%, complex karyotype in 19%, and unmutated immunoglobulin heavy chain variable (IGHV) in 59%.
A total of 152 patients (90%) completed all 12 cycles of the combined agents, with a median treatment duration of 14.7 months on ibrutinib and 12 months on venetoclax. Eight patients had adverse events leading to discontinuation, but there were no treatment-related deaths.
A majority of patients had reductions in lymph node burden after the three-cycle ibrutinib lead in. TLS risk also decreased during the lead-in period, with 90% of patients who had a high baseline TLS risk shifting to medium or low-risk categories, and no patients moved into the high-risk category.
“Hospitalization because of this was no longer required in 66% of at-risk patients after three cycles of ibrutinib lead in, and 82% of patients initiated venetoclax ramp up without the need for hospitalization,” Dr. Siddiqi said.
The best response of undetectable MRD was seen in peripheral blood of 75% of 163 evaluable patients, and in bone marrow of 72% of 155 patients. As noted before, the respective rates of MRD negativity in the intention-to-treat population were 75% and 68%. The proportion of patients with undetectable MRD in peripheral blood increased over time, from 57% after six cycles of the combination, she said.
The overall response rate was 97%, including 51% complete responses (CR) or CR with incomplete bone marrow recovery (CRi), and 46% partial (PR) or nodular PR (nPR). Among patients with CR/CRi, 85% had undetectable MRD in peripheral blood and 80% were MRD negative in bone marrow. In patients with PR/nPR, the respective rates were 69% and 59%. The high rates of undetectable MRD were seen irrespective of baseline disease characteristics, including bulky disease, cytogenetic risk category, del(17p) or TP53 mutation, and complex karyotype.
The most common adverse events with the combination were grade 1 or 2 diarrhea, arthralgia, fatigue, headache, and nausea. Grade 3 neutropenia was seen in 17% of patients, and grade 4 neutropenia was seen in 16%. Grade 3 febrile neutropenia and laboratory confirmed TLS occurred in 2 patients each (1%), and there were no grade 4 instances of either adverse event.
Postrandomization follow-up and analyses are currently being conducted, and results will be reported at a future meeting, real or virtual. An analysis of data on a separate cohort of 159 patients treated with the ibrutinib-venetoclax combination for a fixed duration is currently ongoing.
Dr. Siddiqi disclosed research funding and speakers bureau activity for Pharmacyclics, which sponsored the study, and others, as well as consulting/advising for several companies. Dr. Coombs disclosed consulting for AbbVie.
SOURCE: Siddiqi T et al. EHA25. Abstract S158.
In patients with previously untreated chronic lymphocytic leukemia (CLL) or small lymphocytic lymphoma (SLL), a once-daily oral regimen of ibrutinib and venetoclax was associated with deep molecular remissions in both bone marrow and peripheral blood, including in patients with high-risk disease, according to investigators in the phase 2 CAPTIVATE MRD trial.
An intention-to-treat analysis of 164 patients with CLL/SLL treated with the combination of ibrutinib (Imbruvica) and venetoclax (Venclexta) showed a 75% rate of minimal residual disease (MRD) negativity in peripheral blood, and a 68% rate of MRD negativity in bone marrow among patients who received up to 12 cycles of the combination, reported Tanya Siddiqi, MD, of City of Hope National Medical Center, Duarte, Calif., and colleagues.
“This phase 2 study supports synergistic antitumor activity of the combination with notable deep responses across multiple compartments,” she said in an oral presentation during the virtual annual congress of the European Hematology Association.
Not ready to change practice
A hematologist/oncologist who was not involved in the study said that the data from CAPTIVATE MRD look good, but it’s still not known whether concurrent or sequential administration of the agents is optimal, and whether other regimens may be more effective in the first line.
“I think this is promising, but the informative and practice-changing study would be to compare this combination to ibrutinib monotherapy or to venetoclax and obinutuzumab, and that’s actually the subject of the next large German cooperative group study, CLL17,” said Catherine C. Coombs, MD, assistant professor of medicine at the University of North Carolina, and the UNC Lineberger Cancer Center, Chapel Hill.
She noted that the combination of venetoclax and obinutuzumab (Gazyva) is also associated with high rates of MRD negativity in the first-line setting, and that use of this regimen allows clinicians to reserve ibrutinib or acalabrutinib (Calquence) for patients in the relapsed setting.
Prerandomization results
Dr. Siddiqi presented prerandomization results from the MRD cohort of the CAPTIVATE trial (NCT02910583), which is evaluating the combination of ibrutinib and venetoclax for depth of MRD response. Following 12 cycles of the combinations, patients in this cohort are then randomized based on confirmed MRD status, with patients who are MRD negative randomized to maintenance with either ibrutinib or placebo, and patients with residual disease (MRD positive) randomized to maintenance with either ibrutinib alone or with venetoclax.
A total of 164 patients with previously untreated CLL/SLL and active disease requiring treatment who were under age 70 and had good performance status were enrolled. Following an ibrutinib lead-in period with the drug given at 420 mg once daily for three cycles of 28 days, the patients were continued on ibrutinib, and were started on venetoclax with a ramp up to 400 mg once daily, for 12 additional cycles.
As planned, patients were assessed after 15 cycles for tumor lysis syndrome (TLS) risk assessment, MRD, and hematologic, clinical, imaging, and bone marrow exams for response.
The median patient age was 58, with poor-risk features such as deletion 17p seen in 16%, complex karyotype in 19%, and unmutated immunoglobulin heavy chain variable (IGHV) in 59%.
A total of 152 patients (90%) completed all 12 cycles of the combined agents, with a median treatment duration of 14.7 months on ibrutinib and 12 months on venetoclax. Eight patients had adverse events leading to discontinuation, but there were no treatment-related deaths.
A majority of patients had reductions in lymph node burden after the three-cycle ibrutinib lead in. TLS risk also decreased during the lead-in period, with 90% of patients who had a high baseline TLS risk shifting to medium or low-risk categories, and no patients moved into the high-risk category.
“Hospitalization because of this was no longer required in 66% of at-risk patients after three cycles of ibrutinib lead in, and 82% of patients initiated venetoclax ramp up without the need for hospitalization,” Dr. Siddiqi said.
The best response of undetectable MRD was seen in peripheral blood of 75% of 163 evaluable patients, and in bone marrow of 72% of 155 patients. As noted before, the respective rates of MRD negativity in the intention-to-treat population were 75% and 68%. The proportion of patients with undetectable MRD in peripheral blood increased over time, from 57% after six cycles of the combination, she said.
The overall response rate was 97%, including 51% complete responses (CR) or CR with incomplete bone marrow recovery (CRi), and 46% partial (PR) or nodular PR (nPR). Among patients with CR/CRi, 85% had undetectable MRD in peripheral blood and 80% were MRD negative in bone marrow. In patients with PR/nPR, the respective rates were 69% and 59%. The high rates of undetectable MRD were seen irrespective of baseline disease characteristics, including bulky disease, cytogenetic risk category, del(17p) or TP53 mutation, and complex karyotype.
The most common adverse events with the combination were grade 1 or 2 diarrhea, arthralgia, fatigue, headache, and nausea. Grade 3 neutropenia was seen in 17% of patients, and grade 4 neutropenia was seen in 16%. Grade 3 febrile neutropenia and laboratory confirmed TLS occurred in 2 patients each (1%), and there were no grade 4 instances of either adverse event.
Postrandomization follow-up and analyses are currently being conducted, and results will be reported at a future meeting, real or virtual. An analysis of data on a separate cohort of 159 patients treated with the ibrutinib-venetoclax combination for a fixed duration is currently ongoing.
Dr. Siddiqi disclosed research funding and speakers bureau activity for Pharmacyclics, which sponsored the study, and others, as well as consulting/advising for several companies. Dr. Coombs disclosed consulting for AbbVie.
SOURCE: Siddiqi T et al. EHA25. Abstract S158.
In patients with previously untreated chronic lymphocytic leukemia (CLL) or small lymphocytic lymphoma (SLL), a once-daily oral regimen of ibrutinib and venetoclax was associated with deep molecular remissions in both bone marrow and peripheral blood, including in patients with high-risk disease, according to investigators in the phase 2 CAPTIVATE MRD trial.
An intention-to-treat analysis of 164 patients with CLL/SLL treated with the combination of ibrutinib (Imbruvica) and venetoclax (Venclexta) showed a 75% rate of minimal residual disease (MRD) negativity in peripheral blood, and a 68% rate of MRD negativity in bone marrow among patients who received up to 12 cycles of the combination, reported Tanya Siddiqi, MD, of City of Hope National Medical Center, Duarte, Calif., and colleagues.
“This phase 2 study supports synergistic antitumor activity of the combination with notable deep responses across multiple compartments,” she said in an oral presentation during the virtual annual congress of the European Hematology Association.
Not ready to change practice
A hematologist/oncologist who was not involved in the study said that the data from CAPTIVATE MRD look good, but it’s still not known whether concurrent or sequential administration of the agents is optimal, and whether other regimens may be more effective in the first line.
“I think this is promising, but the informative and practice-changing study would be to compare this combination to ibrutinib monotherapy or to venetoclax and obinutuzumab, and that’s actually the subject of the next large German cooperative group study, CLL17,” said Catherine C. Coombs, MD, assistant professor of medicine at the University of North Carolina, and the UNC Lineberger Cancer Center, Chapel Hill.
She noted that the combination of venetoclax and obinutuzumab (Gazyva) is also associated with high rates of MRD negativity in the first-line setting, and that use of this regimen allows clinicians to reserve ibrutinib or acalabrutinib (Calquence) for patients in the relapsed setting.
Prerandomization results
Dr. Siddiqi presented prerandomization results from the MRD cohort of the CAPTIVATE trial (NCT02910583), which is evaluating the combination of ibrutinib and venetoclax for depth of MRD response. Following 12 cycles of the combinations, patients in this cohort are then randomized based on confirmed MRD status, with patients who are MRD negative randomized to maintenance with either ibrutinib or placebo, and patients with residual disease (MRD positive) randomized to maintenance with either ibrutinib alone or with venetoclax.
A total of 164 patients with previously untreated CLL/SLL and active disease requiring treatment who were under age 70 and had good performance status were enrolled. Following an ibrutinib lead-in period with the drug given at 420 mg once daily for three cycles of 28 days, the patients were continued on ibrutinib, and were started on venetoclax with a ramp up to 400 mg once daily, for 12 additional cycles.
As planned, patients were assessed after 15 cycles for tumor lysis syndrome (TLS) risk assessment, MRD, and hematologic, clinical, imaging, and bone marrow exams for response.
The median patient age was 58, with poor-risk features such as deletion 17p seen in 16%, complex karyotype in 19%, and unmutated immunoglobulin heavy chain variable (IGHV) in 59%.
A total of 152 patients (90%) completed all 12 cycles of the combined agents, with a median treatment duration of 14.7 months on ibrutinib and 12 months on venetoclax. Eight patients had adverse events leading to discontinuation, but there were no treatment-related deaths.
A majority of patients had reductions in lymph node burden after the three-cycle ibrutinib lead in. TLS risk also decreased during the lead-in period, with 90% of patients who had a high baseline TLS risk shifting to medium or low-risk categories, and no patients moved into the high-risk category.
“Hospitalization because of this was no longer required in 66% of at-risk patients after three cycles of ibrutinib lead in, and 82% of patients initiated venetoclax ramp up without the need for hospitalization,” Dr. Siddiqi said.
The best response of undetectable MRD was seen in peripheral blood of 75% of 163 evaluable patients, and in bone marrow of 72% of 155 patients. As noted before, the respective rates of MRD negativity in the intention-to-treat population were 75% and 68%. The proportion of patients with undetectable MRD in peripheral blood increased over time, from 57% after six cycles of the combination, she said.
The overall response rate was 97%, including 51% complete responses (CR) or CR with incomplete bone marrow recovery (CRi), and 46% partial (PR) or nodular PR (nPR). Among patients with CR/CRi, 85% had undetectable MRD in peripheral blood and 80% were MRD negative in bone marrow. In patients with PR/nPR, the respective rates were 69% and 59%. The high rates of undetectable MRD were seen irrespective of baseline disease characteristics, including bulky disease, cytogenetic risk category, del(17p) or TP53 mutation, and complex karyotype.
The most common adverse events with the combination were grade 1 or 2 diarrhea, arthralgia, fatigue, headache, and nausea. Grade 3 neutropenia was seen in 17% of patients, and grade 4 neutropenia was seen in 16%. Grade 3 febrile neutropenia and laboratory confirmed TLS occurred in 2 patients each (1%), and there were no grade 4 instances of either adverse event.
Postrandomization follow-up and analyses are currently being conducted, and results will be reported at a future meeting, real or virtual. An analysis of data on a separate cohort of 159 patients treated with the ibrutinib-venetoclax combination for a fixed duration is currently ongoing.
Dr. Siddiqi disclosed research funding and speakers bureau activity for Pharmacyclics, which sponsored the study, and others, as well as consulting/advising for several companies. Dr. Coombs disclosed consulting for AbbVie.
SOURCE: Siddiqi T et al. EHA25. Abstract S158.
FROM EHA 2020
What’s pushing cannabis use in first-episode psychosis?
The desire to feel better is a major driver for patients with first-episode psychosis (FEP) to turn to cannabis, new research shows.

An analysis of more than 1,300 individuals from six European countries showed patients with FEP were four times more likely than their healthy peers to start smoking cannabis in order to make themselves feel better.
The results also revealed that initiating cannabis use to feel better was associated with a more than tripled risk of being a daily user.
as well as offer an opportunity for psychoeducation – particularly as the reasons for starting cannabis appear to influence frequency of use, study investigator Edoardo Spinazzola, MD, Institute of Psychiatry, Psychology, and Neuroscience at King’s College London, said in an interview.
Patients who start smoking cannabis because their friends or family partakes may benefit from therapies that encourage more “assertiveness” and being “socially comfortable without the substance,” Dr. Spinazzola said, noting that it might also be beneficial to identify the specific cause of the psychological discomfort driving cannabis use, such as depression, and specifically treat that issue.
The results were scheduled to be presented at the Congress of the Schizophrenia International Research Society 2020, but the meeting was canceled because of the coronavirus pandemic.
Answering the skeptics
Previous studies suggest that cannabis use can increase risk for psychosis up to 290%, with both frequency of use and potency playing a role, the researchers noted.
However, they added that “skeptics” argue the association could be caused by individuals with psychosis using cannabis as a form of self-medication, the comorbid effect of other psychogenic drugs, or a common genetic vulnerability between cannabis use and psychosis.
The reasons for starting cannabis use remain “largely unexplored,” so the researchers examined records from the European network of national schizophrenia networks studying Gene-Environment Interactions (EU-GEI) database, which includes patients with FEP and healthy individuals acting as controls from France, Italy, the Netherlands, Spain, United Kingdom, and Brazil.
The analysis included 1,347 individuals, of whom 446 had a diagnosis of nonaffective psychosis, 89 had bipolar disorder, and 58 had psychotic depression.
Reasons to start smoking cannabis and patterns of use were determined using the modified version of the Cannabis Experiences Questionnaire.
Results showed that participants who started cannabis to feel better were significantly more likely to be younger, have fewer years of education, to be black or of mixed ethnicity, to be single, or to not be living independently than those who started it because their friends or family were using it (P < .001 for all comparisons).
In addition, 68% of the patients with FEP and 85% of the healthy controls started using cannabis because friends or family were using it. In contrast, 18% of those with FEP versus 5% of controls starting using cannabis to feel better; 13% versus 10%, respectively, started using for “other reasons.”
After taking into account gender, age, ethnicity, and study site, the patients with FEP were significantly more likely than their healthy peers to have started using cannabis to feel better (relative risk ratio, 4.67; P < .001).
Starting to smoke cannabis to feel better versus any other reason was associated with an increased frequency of use in both those with and without FEP, with an RRR of 2.9 for using the drug more than once a week (P = .001) and an RRR of 3.13 for daily use (P < .001). However, the association was stronger in the healthy controls than in those with FEP, with an RRR for daily use of 4.45 versus 3.11, respectively.
The investigators also examined whether there was a link between reasons to start smoking and an individual’s polygenic risk score (PRS) for developing schizophrenia.
Multinomial regression indicated that PRS was not associated with starting cannabis to feel better or because friends were using it. However, there was an association between PRS score and starting the drug because family members were using it (RRR, 0.68; P < .05).
Complex association
Gabriella Gobbi, MD, PhD, professor in the neurobiological psychiatry unit, department of psychiatry, at McGill University, Montreal, said the data confirm “what we already know about cannabis.”
She noted that one of the “major causes” of young people starting cannabis is the social environment, while the desire to use the drug to feel better is linked to “the fact that cannabis, in a lot of cases, is used as a self-medication” in order to be calmer and as a relief from anxiety.
There is a “very complex” association between using cannabis to feel better and the self-medication seen with cigarette smoking and alcohol in patients with schizophrenia, said Dr. Gobbi, who was not involved with the research.
“When we talk about [patients using] cannabis, alcohol, and cigarettes, actually we’re talking about the same group of people,” she said.
Although “it is true they say that people look to cigarettes, tobacco, and alcohol to feel happier because they are depressed, the risk of psychosis is only for cannabis,” she added. “It is very low for alcohol and tobacco.”
As a result, Dr. Gobbi said she and her colleagues are “very worried” about the consequences for mental health of the legalization of cannabis consumption in Canada in October 2018 with the passing of the Cannabis Act.
Although there are no firm statistics yet, she has observed that since the law was passed, cannabis use has stabilized at a lower level among adolescents. “But now we have another population of people aged 34 and older that consume cannabis,” she said.
Particularly when considering the impact of higher strength cannabis on psychosis risk, Dr. Gobbi believes the increase in consumption in this age group will result in a “more elevated” risk for mental health issues.
Dr. Spinazzola and Dr. Gobbi have reported no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
The desire to feel better is a major driver for patients with first-episode psychosis (FEP) to turn to cannabis, new research shows.
An analysis of more than 1,300 individuals from six European countries showed patients with FEP were four times more likely than their healthy peers to start smoking cannabis in order to make themselves feel better.
The results also revealed that initiating cannabis use to feel better was associated with a more than tripled risk of being a daily user.
as well as offer an opportunity for psychoeducation – particularly as the reasons for starting cannabis appear to influence frequency of use, study investigator Edoardo Spinazzola, MD, Institute of Psychiatry, Psychology, and Neuroscience at King’s College London, said in an interview.
Patients who start smoking cannabis because their friends or family partakes may benefit from therapies that encourage more “assertiveness” and being “socially comfortable without the substance,” Dr. Spinazzola said, noting that it might also be beneficial to identify the specific cause of the psychological discomfort driving cannabis use, such as depression, and specifically treat that issue.
The results were scheduled to be presented at the Congress of the Schizophrenia International Research Society 2020, but the meeting was canceled because of the coronavirus pandemic.
Answering the skeptics
Previous studies suggest that cannabis use can increase risk for psychosis up to 290%, with both frequency of use and potency playing a role, the researchers noted.
However, they added that “skeptics” argue the association could be caused by individuals with psychosis using cannabis as a form of self-medication, the comorbid effect of other psychogenic drugs, or a common genetic vulnerability between cannabis use and psychosis.
The reasons for starting cannabis use remain “largely unexplored,” so the researchers examined records from the European network of national schizophrenia networks studying Gene-Environment Interactions (EU-GEI) database, which includes patients with FEP and healthy individuals acting as controls from France, Italy, the Netherlands, Spain, United Kingdom, and Brazil.
The analysis included 1,347 individuals, of whom 446 had a diagnosis of nonaffective psychosis, 89 had bipolar disorder, and 58 had psychotic depression.
Reasons to start smoking cannabis and patterns of use were determined using the modified version of the Cannabis Experiences Questionnaire.
Results showed that participants who started cannabis to feel better were significantly more likely to be younger, have fewer years of education, to be black or of mixed ethnicity, to be single, or to not be living independently than those who started it because their friends or family were using it (P < .001 for all comparisons).
In addition, 68% of the patients with FEP and 85% of the healthy controls started using cannabis because friends or family were using it. In contrast, 18% of those with FEP versus 5% of controls starting using cannabis to feel better; 13% versus 10%, respectively, started using for “other reasons.”
After taking into account gender, age, ethnicity, and study site, the patients with FEP were significantly more likely than their healthy peers to have started using cannabis to feel better (relative risk ratio, 4.67; P < .001).
Starting to smoke cannabis to feel better versus any other reason was associated with an increased frequency of use in both those with and without FEP, with an RRR of 2.9 for using the drug more than once a week (P = .001) and an RRR of 3.13 for daily use (P < .001). However, the association was stronger in the healthy controls than in those with FEP, with an RRR for daily use of 4.45 versus 3.11, respectively.
The investigators also examined whether there was a link between reasons to start smoking and an individual’s polygenic risk score (PRS) for developing schizophrenia.
Multinomial regression indicated that PRS was not associated with starting cannabis to feel better or because friends were using it. However, there was an association between PRS score and starting the drug because family members were using it (RRR, 0.68; P < .05).
Complex association
Gabriella Gobbi, MD, PhD, professor in the neurobiological psychiatry unit, department of psychiatry, at McGill University, Montreal, said the data confirm “what we already know about cannabis.”
She noted that one of the “major causes” of young people starting cannabis is the social environment, while the desire to use the drug to feel better is linked to “the fact that cannabis, in a lot of cases, is used as a self-medication” in order to be calmer and as a relief from anxiety.
There is a “very complex” association between using cannabis to feel better and the self-medication seen with cigarette smoking and alcohol in patients with schizophrenia, said Dr. Gobbi, who was not involved with the research.
“When we talk about [patients using] cannabis, alcohol, and cigarettes, actually we’re talking about the same group of people,” she said.
Although “it is true they say that people look to cigarettes, tobacco, and alcohol to feel happier because they are depressed, the risk of psychosis is only for cannabis,” she added. “It is very low for alcohol and tobacco.”
As a result, Dr. Gobbi said she and her colleagues are “very worried” about the consequences for mental health of the legalization of cannabis consumption in Canada in October 2018 with the passing of the Cannabis Act.
Although there are no firm statistics yet, she has observed that since the law was passed, cannabis use has stabilized at a lower level among adolescents. “But now we have another population of people aged 34 and older that consume cannabis,” she said.
Particularly when considering the impact of higher strength cannabis on psychosis risk, Dr. Gobbi believes the increase in consumption in this age group will result in a “more elevated” risk for mental health issues.
Dr. Spinazzola and Dr. Gobbi have reported no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
The desire to feel better is a major driver for patients with first-episode psychosis (FEP) to turn to cannabis, new research shows.
An analysis of more than 1,300 individuals from six European countries showed patients with FEP were four times more likely than their healthy peers to start smoking cannabis in order to make themselves feel better.
The results also revealed that initiating cannabis use to feel better was associated with a more than tripled risk of being a daily user.
as well as offer an opportunity for psychoeducation – particularly as the reasons for starting cannabis appear to influence frequency of use, study investigator Edoardo Spinazzola, MD, Institute of Psychiatry, Psychology, and Neuroscience at King’s College London, said in an interview.
Patients who start smoking cannabis because their friends or family partakes may benefit from therapies that encourage more “assertiveness” and being “socially comfortable without the substance,” Dr. Spinazzola said, noting that it might also be beneficial to identify the specific cause of the psychological discomfort driving cannabis use, such as depression, and specifically treat that issue.
The results were scheduled to be presented at the Congress of the Schizophrenia International Research Society 2020, but the meeting was canceled because of the coronavirus pandemic.
Answering the skeptics
Previous studies suggest that cannabis use can increase risk for psychosis up to 290%, with both frequency of use and potency playing a role, the researchers noted.
However, they added that “skeptics” argue the association could be caused by individuals with psychosis using cannabis as a form of self-medication, the comorbid effect of other psychogenic drugs, or a common genetic vulnerability between cannabis use and psychosis.
The reasons for starting cannabis use remain “largely unexplored,” so the researchers examined records from the European network of national schizophrenia networks studying Gene-Environment Interactions (EU-GEI) database, which includes patients with FEP and healthy individuals acting as controls from France, Italy, the Netherlands, Spain, United Kingdom, and Brazil.
The analysis included 1,347 individuals, of whom 446 had a diagnosis of nonaffective psychosis, 89 had bipolar disorder, and 58 had psychotic depression.
Reasons to start smoking cannabis and patterns of use were determined using the modified version of the Cannabis Experiences Questionnaire.
Results showed that participants who started cannabis to feel better were significantly more likely to be younger, have fewer years of education, to be black or of mixed ethnicity, to be single, or to not be living independently than those who started it because their friends or family were using it (P < .001 for all comparisons).
In addition, 68% of the patients with FEP and 85% of the healthy controls started using cannabis because friends or family were using it. In contrast, 18% of those with FEP versus 5% of controls starting using cannabis to feel better; 13% versus 10%, respectively, started using for “other reasons.”
After taking into account gender, age, ethnicity, and study site, the patients with FEP were significantly more likely than their healthy peers to have started using cannabis to feel better (relative risk ratio, 4.67; P < .001).
Starting to smoke cannabis to feel better versus any other reason was associated with an increased frequency of use in both those with and without FEP, with an RRR of 2.9 for using the drug more than once a week (P = .001) and an RRR of 3.13 for daily use (P < .001). However, the association was stronger in the healthy controls than in those with FEP, with an RRR for daily use of 4.45 versus 3.11, respectively.
The investigators also examined whether there was a link between reasons to start smoking and an individual’s polygenic risk score (PRS) for developing schizophrenia.
Multinomial regression indicated that PRS was not associated with starting cannabis to feel better or because friends were using it. However, there was an association between PRS score and starting the drug because family members were using it (RRR, 0.68; P < .05).
Complex association
Gabriella Gobbi, MD, PhD, professor in the neurobiological psychiatry unit, department of psychiatry, at McGill University, Montreal, said the data confirm “what we already know about cannabis.”
She noted that one of the “major causes” of young people starting cannabis is the social environment, while the desire to use the drug to feel better is linked to “the fact that cannabis, in a lot of cases, is used as a self-medication” in order to be calmer and as a relief from anxiety.
There is a “very complex” association between using cannabis to feel better and the self-medication seen with cigarette smoking and alcohol in patients with schizophrenia, said Dr. Gobbi, who was not involved with the research.
“When we talk about [patients using] cannabis, alcohol, and cigarettes, actually we’re talking about the same group of people,” she said.
Although “it is true they say that people look to cigarettes, tobacco, and alcohol to feel happier because they are depressed, the risk of psychosis is only for cannabis,” she added. “It is very low for alcohol and tobacco.”
As a result, Dr. Gobbi said she and her colleagues are “very worried” about the consequences for mental health of the legalization of cannabis consumption in Canada in October 2018 with the passing of the Cannabis Act.
Although there are no firm statistics yet, she has observed that since the law was passed, cannabis use has stabilized at a lower level among adolescents. “But now we have another population of people aged 34 and older that consume cannabis,” she said.
Particularly when considering the impact of higher strength cannabis on psychosis risk, Dr. Gobbi believes the increase in consumption in this age group will result in a “more elevated” risk for mental health issues.
Dr. Spinazzola and Dr. Gobbi have reported no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
FROM SIRS 2020
T2D plus heart failure packs a deadly punch
It’s bad news for patients with newly diagnosed type 2 diabetes when they then develop heart failure during the next few years.

Patients with incident type 2 diabetes (T2D) who soon after also had heart failure appear faced a dramatically elevated mortality risk, higher than the incremental risk from any other cardiovascular or renal comorbidity that appeared following diabetes onset, in an analysis of more than 150,000 Danish patients with incident type 2 diabetes during 1998-2015.
The 5-year risk of death in patients who developed heart failure during the first 5 years following an initial diagnosis of T2D was about 48%, about threefold higher than in patients with newly diagnosed T2D who remained free of heart failure or any of the other studied comorbidities, Bochra Zareini, MD, and associates reported in a study published in Circulation: Cardiovascular Quality and Outcomes. The studied patients had no known cardiovascular or renal disease at the time of their first T2D diagnosis.
“Our study reports not only on the absolute 5-year risk” of mortality, “but also takes into consideration when patients developed” a comorbidity. “What is surprising and worrying is the very high risk of death following heart failure and the potential life years lost when compared to T2D patients who do not develop heart failure,” said Dr. Zareini, a cardiologist at Herlev and Gentofte University Hospital in Copenhagen. “The implications of our study are to create awareness and highlight the importance of early detection of heart failure development in patients with T2D.” The results also showed that “heart failure is a common cardiovascular disease” in patients with newly diagnosed T2D, she added in an interview.
The data she and her associates reported came from a retrospective analysis of 153,403 Danish citizens in national health records who received a prescription for an antidiabetes drug for the first time during 1998-2015, excluding patients with a prior diagnosis of heart failure, ischemic heart disease (IHD), stroke, peripheral artery disease (PAD), chronic kidney disease (CKD), or gestational diabetes. They followed these patients for a median of just under 10 years, during which time 45% of the cohort had an incident diagnosis of at least one of these cardiovascular and renal conditions, based on medical-record entries from hospitalization discharges or ambulatory contacts.
Nearly two-thirds of the T2D patients with an incident comorbidity during follow-up had a single new diagnosis, a quarter had two new comorbidities appear during follow-up, and 13% developed at least three new comorbidities.
Heart failure, least common but deadliest comorbidity
The most common of the tracked comorbidities was IHD, which appeared in 8% of the T2D patients within 5 years and in 13% after 10 years. Next most common was stroke, affecting 3% of patients after 5 years and 5% after 10 years. CKD occurred in 2.2% after 5 years and in 4.0% after 10 years, PAD occurred in 2.1% after 5 years and in 3.0% at 10 years, and heart failure occurred in 1.6% at 5 years and in 2.2% after 10 years.
But despite being the least common of the studied comorbidities, heart failure was by far the most deadly, roughly tripling the 5-year mortality rate, compared with T2D patients with no comorbidities, regardless of exactly when it first appeared during the first 5 years after the initial T2D diagnosis. The next most deadly comorbidities were stroke and PAD, which each roughly doubled mortality, compared with the patients who remained free of any studied comorbidity. CKD boosted mortality by 70%-110%, depending on exactly when it appeared during the first 5 years of follow-up, and IHD, while the most frequent comorbidity was also the most benign, increasing mortality by about 30%.
The most deadly combinations of two comorbidities were when heart failure appeared with either CKD or with PAD; each of these combinations boosted mortality by 300%-400% when it occurred during the first few years after a T2D diagnosis.
The findings came from “a very big and unselected patient group of patients, making our results highly generalizable in terms of assessing the prognostic consequences of heart failure,” Dr. Zareini stressed.
Management implications
The dangerous combination of T2D and heart failure has been documented for several years, and prompted a focused statement in 2019 about best practices for managing these patients (Circulation. 2019 Aug 3;140[7]:e294-324). “Heart failure has been known for some time to predict poorer outcomes in patients with T2D. Not much surprising” in the new findings reported by Dr. Zareini and associates, commented Robert H. Eckel, MD, a cardiovascular endocrinologist at the University of Colorado at Denver, Aurora. Heart failure “rarely acts alone, but in combination with other forms of heart or renal disease,” he noted in an interview.

Earlier studies may have “overlooked” heart failure’s importance compared with other comorbidities because they often “only investigated one cardiovascular disease in patients with T2D,” Dr. Zareini noted. In recent years the importance of heart failure occurring in patients with T2D also gained heightened significance because of the growing role of the sodium-glucose cotransporter 2 (SGLT2) inhibitor drug class in treating patients with T2D and the documented ability of these drugs to significantly reduce hospitalizations for heart failure (J Am Coll Cardiol. 2020 Apr 28;75[16]:1956-74). Dr. Zareini and associates put it this way in their report: “Heart failure has in recent years been recognized as an important clinical endpoint ... in patients with T2D, in particular, after the results from randomized, controlled trials of SGLT2 inhibitors showed benefit on cardiovascular death and heart failure hospitalizations.”
Despite this, the new findings “do not address treatment with SGLT2 inhibitors in patients with T2D, nor can we use our data to address which patients should not be treated,” with this drug class, which instead should rely on “current evidence and expert consensus,” she said.
“Guidelines favor SGLT2 inhibitors or [glucagonlike peptide–1] receptor agonists in patients with a history of or high risk for major adverse coronary events,” and SGLT2 inhibitors are also “preferable in patients with renal disease,” Dr. Eckel noted.
Other avenues also exist for minimizing the onset of heart failure and other cardiovascular diseases in patients with T2D, Dr. Zareini said, citing modifiable risks that lead to heart failure that include hypertension, “diabetic cardiomyopathy,” and ISD. “Clinicians must treat all modifiable risk factors in patients with T2D in order to improve prognosis and limit development of cardiovascular and renal disease.”
The study received no commercial funding. Dr. Zareini and Dr. Eckel had no disclosures.
SOURCE: Zareini B et al. Circ Cardiovasc Qual Outcomes. 2020 Jun 23. doi: 10.1161/CIRCOUTCOMES.119.006260.
It’s bad news for patients with newly diagnosed type 2 diabetes when they then develop heart failure during the next few years.
Patients with incident type 2 diabetes (T2D) who soon after also had heart failure appear faced a dramatically elevated mortality risk, higher than the incremental risk from any other cardiovascular or renal comorbidity that appeared following diabetes onset, in an analysis of more than 150,000 Danish patients with incident type 2 diabetes during 1998-2015.
The 5-year risk of death in patients who developed heart failure during the first 5 years following an initial diagnosis of T2D was about 48%, about threefold higher than in patients with newly diagnosed T2D who remained free of heart failure or any of the other studied comorbidities, Bochra Zareini, MD, and associates reported in a study published in Circulation: Cardiovascular Quality and Outcomes. The studied patients had no known cardiovascular or renal disease at the time of their first T2D diagnosis.
“Our study reports not only on the absolute 5-year risk” of mortality, “but also takes into consideration when patients developed” a comorbidity. “What is surprising and worrying is the very high risk of death following heart failure and the potential life years lost when compared to T2D patients who do not develop heart failure,” said Dr. Zareini, a cardiologist at Herlev and Gentofte University Hospital in Copenhagen. “The implications of our study are to create awareness and highlight the importance of early detection of heart failure development in patients with T2D.” The results also showed that “heart failure is a common cardiovascular disease” in patients with newly diagnosed T2D, she added in an interview.
The data she and her associates reported came from a retrospective analysis of 153,403 Danish citizens in national health records who received a prescription for an antidiabetes drug for the first time during 1998-2015, excluding patients with a prior diagnosis of heart failure, ischemic heart disease (IHD), stroke, peripheral artery disease (PAD), chronic kidney disease (CKD), or gestational diabetes. They followed these patients for a median of just under 10 years, during which time 45% of the cohort had an incident diagnosis of at least one of these cardiovascular and renal conditions, based on medical-record entries from hospitalization discharges or ambulatory contacts.
Nearly two-thirds of the T2D patients with an incident comorbidity during follow-up had a single new diagnosis, a quarter had two new comorbidities appear during follow-up, and 13% developed at least three new comorbidities.
Heart failure, least common but deadliest comorbidity
The most common of the tracked comorbidities was IHD, which appeared in 8% of the T2D patients within 5 years and in 13% after 10 years. Next most common was stroke, affecting 3% of patients after 5 years and 5% after 10 years. CKD occurred in 2.2% after 5 years and in 4.0% after 10 years, PAD occurred in 2.1% after 5 years and in 3.0% at 10 years, and heart failure occurred in 1.6% at 5 years and in 2.2% after 10 years.
But despite being the least common of the studied comorbidities, heart failure was by far the most deadly, roughly tripling the 5-year mortality rate, compared with T2D patients with no comorbidities, regardless of exactly when it first appeared during the first 5 years after the initial T2D diagnosis. The next most deadly comorbidities were stroke and PAD, which each roughly doubled mortality, compared with the patients who remained free of any studied comorbidity. CKD boosted mortality by 70%-110%, depending on exactly when it appeared during the first 5 years of follow-up, and IHD, while the most frequent comorbidity was also the most benign, increasing mortality by about 30%.
The most deadly combinations of two comorbidities were when heart failure appeared with either CKD or with PAD; each of these combinations boosted mortality by 300%-400% when it occurred during the first few years after a T2D diagnosis.
The findings came from “a very big and unselected patient group of patients, making our results highly generalizable in terms of assessing the prognostic consequences of heart failure,” Dr. Zareini stressed.
Management implications
The dangerous combination of T2D and heart failure has been documented for several years, and prompted a focused statement in 2019 about best practices for managing these patients (Circulation. 2019 Aug 3;140[7]:e294-324). “Heart failure has been known for some time to predict poorer outcomes in patients with T2D. Not much surprising” in the new findings reported by Dr. Zareini and associates, commented Robert H. Eckel, MD, a cardiovascular endocrinologist at the University of Colorado at Denver, Aurora. Heart failure “rarely acts alone, but in combination with other forms of heart or renal disease,” he noted in an interview.
Earlier studies may have “overlooked” heart failure’s importance compared with other comorbidities because they often “only investigated one cardiovascular disease in patients with T2D,” Dr. Zareini noted. In recent years the importance of heart failure occurring in patients with T2D also gained heightened significance because of the growing role of the sodium-glucose cotransporter 2 (SGLT2) inhibitor drug class in treating patients with T2D and the documented ability of these drugs to significantly reduce hospitalizations for heart failure (J Am Coll Cardiol. 2020 Apr 28;75[16]:1956-74). Dr. Zareini and associates put it this way in their report: “Heart failure has in recent years been recognized as an important clinical endpoint ... in patients with T2D, in particular, after the results from randomized, controlled trials of SGLT2 inhibitors showed benefit on cardiovascular death and heart failure hospitalizations.”
Despite this, the new findings “do not address treatment with SGLT2 inhibitors in patients with T2D, nor can we use our data to address which patients should not be treated,” with this drug class, which instead should rely on “current evidence and expert consensus,” she said.
“Guidelines favor SGLT2 inhibitors or [glucagonlike peptide–1] receptor agonists in patients with a history of or high risk for major adverse coronary events,” and SGLT2 inhibitors are also “preferable in patients with renal disease,” Dr. Eckel noted.
Other avenues also exist for minimizing the onset of heart failure and other cardiovascular diseases in patients with T2D, Dr. Zareini said, citing modifiable risks that lead to heart failure that include hypertension, “diabetic cardiomyopathy,” and ISD. “Clinicians must treat all modifiable risk factors in patients with T2D in order to improve prognosis and limit development of cardiovascular and renal disease.”
The study received no commercial funding. Dr. Zareini and Dr. Eckel had no disclosures.
SOURCE: Zareini B et al. Circ Cardiovasc Qual Outcomes. 2020 Jun 23. doi: 10.1161/CIRCOUTCOMES.119.006260.
It’s bad news for patients with newly diagnosed type 2 diabetes when they then develop heart failure during the next few years.
Patients with incident type 2 diabetes (T2D) who soon after also had heart failure appear faced a dramatically elevated mortality risk, higher than the incremental risk from any other cardiovascular or renal comorbidity that appeared following diabetes onset, in an analysis of more than 150,000 Danish patients with incident type 2 diabetes during 1998-2015.
The 5-year risk of death in patients who developed heart failure during the first 5 years following an initial diagnosis of T2D was about 48%, about threefold higher than in patients with newly diagnosed T2D who remained free of heart failure or any of the other studied comorbidities, Bochra Zareini, MD, and associates reported in a study published in Circulation: Cardiovascular Quality and Outcomes. The studied patients had no known cardiovascular or renal disease at the time of their first T2D diagnosis.
“Our study reports not only on the absolute 5-year risk” of mortality, “but also takes into consideration when patients developed” a comorbidity. “What is surprising and worrying is the very high risk of death following heart failure and the potential life years lost when compared to T2D patients who do not develop heart failure,” said Dr. Zareini, a cardiologist at Herlev and Gentofte University Hospital in Copenhagen. “The implications of our study are to create awareness and highlight the importance of early detection of heart failure development in patients with T2D.” The results also showed that “heart failure is a common cardiovascular disease” in patients with newly diagnosed T2D, she added in an interview.
The data she and her associates reported came from a retrospective analysis of 153,403 Danish citizens in national health records who received a prescription for an antidiabetes drug for the first time during 1998-2015, excluding patients with a prior diagnosis of heart failure, ischemic heart disease (IHD), stroke, peripheral artery disease (PAD), chronic kidney disease (CKD), or gestational diabetes. They followed these patients for a median of just under 10 years, during which time 45% of the cohort had an incident diagnosis of at least one of these cardiovascular and renal conditions, based on medical-record entries from hospitalization discharges or ambulatory contacts.
Nearly two-thirds of the T2D patients with an incident comorbidity during follow-up had a single new diagnosis, a quarter had two new comorbidities appear during follow-up, and 13% developed at least three new comorbidities.
Heart failure, least common but deadliest comorbidity
The most common of the tracked comorbidities was IHD, which appeared in 8% of the T2D patients within 5 years and in 13% after 10 years. Next most common was stroke, affecting 3% of patients after 5 years and 5% after 10 years. CKD occurred in 2.2% after 5 years and in 4.0% after 10 years, PAD occurred in 2.1% after 5 years and in 3.0% at 10 years, and heart failure occurred in 1.6% at 5 years and in 2.2% after 10 years.
But despite being the least common of the studied comorbidities, heart failure was by far the most deadly, roughly tripling the 5-year mortality rate, compared with T2D patients with no comorbidities, regardless of exactly when it first appeared during the first 5 years after the initial T2D diagnosis. The next most deadly comorbidities were stroke and PAD, which each roughly doubled mortality, compared with the patients who remained free of any studied comorbidity. CKD boosted mortality by 70%-110%, depending on exactly when it appeared during the first 5 years of follow-up, and IHD, while the most frequent comorbidity was also the most benign, increasing mortality by about 30%.
The most deadly combinations of two comorbidities were when heart failure appeared with either CKD or with PAD; each of these combinations boosted mortality by 300%-400% when it occurred during the first few years after a T2D diagnosis.
The findings came from “a very big and unselected patient group of patients, making our results highly generalizable in terms of assessing the prognostic consequences of heart failure,” Dr. Zareini stressed.
Management implications
The dangerous combination of T2D and heart failure has been documented for several years, and prompted a focused statement in 2019 about best practices for managing these patients (Circulation. 2019 Aug 3;140[7]:e294-324). “Heart failure has been known for some time to predict poorer outcomes in patients with T2D. Not much surprising” in the new findings reported by Dr. Zareini and associates, commented Robert H. Eckel, MD, a cardiovascular endocrinologist at the University of Colorado at Denver, Aurora. Heart failure “rarely acts alone, but in combination with other forms of heart or renal disease,” he noted in an interview.
Earlier studies may have “overlooked” heart failure’s importance compared with other comorbidities because they often “only investigated one cardiovascular disease in patients with T2D,” Dr. Zareini noted. In recent years the importance of heart failure occurring in patients with T2D also gained heightened significance because of the growing role of the sodium-glucose cotransporter 2 (SGLT2) inhibitor drug class in treating patients with T2D and the documented ability of these drugs to significantly reduce hospitalizations for heart failure (J Am Coll Cardiol. 2020 Apr 28;75[16]:1956-74). Dr. Zareini and associates put it this way in their report: “Heart failure has in recent years been recognized as an important clinical endpoint ... in patients with T2D, in particular, after the results from randomized, controlled trials of SGLT2 inhibitors showed benefit on cardiovascular death and heart failure hospitalizations.”
Despite this, the new findings “do not address treatment with SGLT2 inhibitors in patients with T2D, nor can we use our data to address which patients should not be treated,” with this drug class, which instead should rely on “current evidence and expert consensus,” she said.
“Guidelines favor SGLT2 inhibitors or [glucagonlike peptide–1] receptor agonists in patients with a history of or high risk for major adverse coronary events,” and SGLT2 inhibitors are also “preferable in patients with renal disease,” Dr. Eckel noted.
Other avenues also exist for minimizing the onset of heart failure and other cardiovascular diseases in patients with T2D, Dr. Zareini said, citing modifiable risks that lead to heart failure that include hypertension, “diabetic cardiomyopathy,” and ISD. “Clinicians must treat all modifiable risk factors in patients with T2D in order to improve prognosis and limit development of cardiovascular and renal disease.”
The study received no commercial funding. Dr. Zareini and Dr. Eckel had no disclosures.
SOURCE: Zareini B et al. Circ Cardiovasc Qual Outcomes. 2020 Jun 23. doi: 10.1161/CIRCOUTCOMES.119.006260.
FROM CIRCULATION: CARDIOVASCULAR QUALITY AND OUTCOMES
Study evaluates number of needed to refer, biopsy for diagnosing a melanoma
At the same time, the number needed to refer to diagnose non-melanoma skin cancer was 4 and the number needed to biopsy was 1.5.

The findings come from a retrospective review of 707 patients referred to a tertiary medical center dermatology practice for suspicious lesions, presented in a poster session at the virtual annual meeting of the American Academy of Dermatology
“Multiple studies in the dermatology literature have looked at the number needed to treat (NNT) as a quality metric for dermatology clinics, where a lower number is ‘better,’” the study’s first author, Nikolai Klebanov, MD, said in an interview following the virtual meeting. “Our particular study is unique in that we estimated both the number needed to refer and number needed to biopsy to closely examine the process of referrals for suspicious lesions from primary care settings to specialists. We also looked closely at the underlying patient-centered characteristics, which could be used by all clinicians to streamline the referral process by reducing the volume of low-risk referrals.”
Dr. Klebanov, of the department of dermatology at Massachusetts General Hospital, Boston, and his associates reviewed 707 unique patient visits to the department during July 2015–February 2016. They calculated the number needed to refer and biopsy for melanoma as the ratio of biopsy-proven melanoma diagnoses among benign and dysplastic nevi and seborrheic keratoses. For nonmelanoma skin cancer, they used the ratio of basal and squamous cell carcinoma among actinic keratoses and seborrheic keratoses.
Of the 707 patients, 54% were female, and males were slightly older than females (a mean of 58 vs. 54 years, respectively). The researchers found that lesions were more commonly benign among all age groups, while the frequency of premalignant and malignant lesions such as actinic keratoses, nonmelanoma skin cancer, and melanoma was highest for males and increased with age. Nevi were the most common benign diagnosis among patients 39 years of age and younger, while seborrheic keratoses were more common among patients aged 40 years and older.
The researchers found that the number needed to treat for melanoma was 31.5 and the number needed to biopsy was 7.5, which represents a 4.2-fold difference. Meanwhile, the number needed to refer for nonmelanoma skin cancer was 4, and the number needed to biopsy was 1.5, which represents a 2.7-fold difference. Despite variable rates of skin cancer between demographics, the biopsy rate ranged between 18% and 30%, for a mean of 23.4%.
“We found that most young patients referred for a ‘suspicious lesion’ on clinical prebiopsy assessment by the dermatologist were determined to actually have a benign nevus, and that older patients were most likely to have a seborrheic keratosis as the underlying lesion,” Dr. Klebanov said. “Among the minority of patients in each demographic group who were selected for biopsy, those lesions which were found to be benign were also largely nevi and keratoses. Even by being mindful of just the patient’s age, primary care providers can follow patients clinically with a tailored differential diagnosis in mind before referral, and dermatologists can reduce the number of biopsies they perform on patients who are being referred.”
He added that he and his colleagues were surprised that despite very low rates of skin cancer in young patients, and thus different pretest probabilities of cancer, biopsy rates across demographics were consistently around 20%. “We also found a disproportionate number of female patients younger than age 40 who were referred for suspicious lesions, while in the older age groups, the ratio of males to females was approximately equal.”
Dr. Klebanov acknowledged certain limitations of the study, including its single-center, retrospective design, and that information was not collected on patients’ family history of skin cancer, Fitzpatrick skin type, nor the clinical course of the lesion while it was followed by the primary care office. “The nuanced differences in these factors may certainly play a role in decisions for individual patients,” he said.
The study’s principal investigator was Hensin Tsao MD, PhD, clinical director of the MGH Melanoma & Pigmented Lesion Center The work was supported by the Alpha Omega Alpha Carolyn Kuckein Research Fellowship. The researchers reported having no financial disclosures.
SOURCE: Klebanov N et al. AAD 20. Abstract 15881.
At the same time, the number needed to refer to diagnose non-melanoma skin cancer was 4 and the number needed to biopsy was 1.5.
The findings come from a retrospective review of 707 patients referred to a tertiary medical center dermatology practice for suspicious lesions, presented in a poster session at the virtual annual meeting of the American Academy of Dermatology
“Multiple studies in the dermatology literature have looked at the number needed to treat (NNT) as a quality metric for dermatology clinics, where a lower number is ‘better,’” the study’s first author, Nikolai Klebanov, MD, said in an interview following the virtual meeting. “Our particular study is unique in that we estimated both the number needed to refer and number needed to biopsy to closely examine the process of referrals for suspicious lesions from primary care settings to specialists. We also looked closely at the underlying patient-centered characteristics, which could be used by all clinicians to streamline the referral process by reducing the volume of low-risk referrals.”
Dr. Klebanov, of the department of dermatology at Massachusetts General Hospital, Boston, and his associates reviewed 707 unique patient visits to the department during July 2015–February 2016. They calculated the number needed to refer and biopsy for melanoma as the ratio of biopsy-proven melanoma diagnoses among benign and dysplastic nevi and seborrheic keratoses. For nonmelanoma skin cancer, they used the ratio of basal and squamous cell carcinoma among actinic keratoses and seborrheic keratoses.
Of the 707 patients, 54% were female, and males were slightly older than females (a mean of 58 vs. 54 years, respectively). The researchers found that lesions were more commonly benign among all age groups, while the frequency of premalignant and malignant lesions such as actinic keratoses, nonmelanoma skin cancer, and melanoma was highest for males and increased with age. Nevi were the most common benign diagnosis among patients 39 years of age and younger, while seborrheic keratoses were more common among patients aged 40 years and older.
The researchers found that the number needed to treat for melanoma was 31.5 and the number needed to biopsy was 7.5, which represents a 4.2-fold difference. Meanwhile, the number needed to refer for nonmelanoma skin cancer was 4, and the number needed to biopsy was 1.5, which represents a 2.7-fold difference. Despite variable rates of skin cancer between demographics, the biopsy rate ranged between 18% and 30%, for a mean of 23.4%.
“We found that most young patients referred for a ‘suspicious lesion’ on clinical prebiopsy assessment by the dermatologist were determined to actually have a benign nevus, and that older patients were most likely to have a seborrheic keratosis as the underlying lesion,” Dr. Klebanov said. “Among the minority of patients in each demographic group who were selected for biopsy, those lesions which were found to be benign were also largely nevi and keratoses. Even by being mindful of just the patient’s age, primary care providers can follow patients clinically with a tailored differential diagnosis in mind before referral, and dermatologists can reduce the number of biopsies they perform on patients who are being referred.”
He added that he and his colleagues were surprised that despite very low rates of skin cancer in young patients, and thus different pretest probabilities of cancer, biopsy rates across demographics were consistently around 20%. “We also found a disproportionate number of female patients younger than age 40 who were referred for suspicious lesions, while in the older age groups, the ratio of males to females was approximately equal.”
Dr. Klebanov acknowledged certain limitations of the study, including its single-center, retrospective design, and that information was not collected on patients’ family history of skin cancer, Fitzpatrick skin type, nor the clinical course of the lesion while it was followed by the primary care office. “The nuanced differences in these factors may certainly play a role in decisions for individual patients,” he said.
The study’s principal investigator was Hensin Tsao MD, PhD, clinical director of the MGH Melanoma & Pigmented Lesion Center The work was supported by the Alpha Omega Alpha Carolyn Kuckein Research Fellowship. The researchers reported having no financial disclosures.
SOURCE: Klebanov N et al. AAD 20. Abstract 15881.
At the same time, the number needed to refer to diagnose non-melanoma skin cancer was 4 and the number needed to biopsy was 1.5.
The findings come from a retrospective review of 707 patients referred to a tertiary medical center dermatology practice for suspicious lesions, presented in a poster session at the virtual annual meeting of the American Academy of Dermatology
“Multiple studies in the dermatology literature have looked at the number needed to treat (NNT) as a quality metric for dermatology clinics, where a lower number is ‘better,’” the study’s first author, Nikolai Klebanov, MD, said in an interview following the virtual meeting. “Our particular study is unique in that we estimated both the number needed to refer and number needed to biopsy to closely examine the process of referrals for suspicious lesions from primary care settings to specialists. We also looked closely at the underlying patient-centered characteristics, which could be used by all clinicians to streamline the referral process by reducing the volume of low-risk referrals.”
Dr. Klebanov, of the department of dermatology at Massachusetts General Hospital, Boston, and his associates reviewed 707 unique patient visits to the department during July 2015–February 2016. They calculated the number needed to refer and biopsy for melanoma as the ratio of biopsy-proven melanoma diagnoses among benign and dysplastic nevi and seborrheic keratoses. For nonmelanoma skin cancer, they used the ratio of basal and squamous cell carcinoma among actinic keratoses and seborrheic keratoses.
Of the 707 patients, 54% were female, and males were slightly older than females (a mean of 58 vs. 54 years, respectively). The researchers found that lesions were more commonly benign among all age groups, while the frequency of premalignant and malignant lesions such as actinic keratoses, nonmelanoma skin cancer, and melanoma was highest for males and increased with age. Nevi were the most common benign diagnosis among patients 39 years of age and younger, while seborrheic keratoses were more common among patients aged 40 years and older.
The researchers found that the number needed to treat for melanoma was 31.5 and the number needed to biopsy was 7.5, which represents a 4.2-fold difference. Meanwhile, the number needed to refer for nonmelanoma skin cancer was 4, and the number needed to biopsy was 1.5, which represents a 2.7-fold difference. Despite variable rates of skin cancer between demographics, the biopsy rate ranged between 18% and 30%, for a mean of 23.4%.
“We found that most young patients referred for a ‘suspicious lesion’ on clinical prebiopsy assessment by the dermatologist were determined to actually have a benign nevus, and that older patients were most likely to have a seborrheic keratosis as the underlying lesion,” Dr. Klebanov said. “Among the minority of patients in each demographic group who were selected for biopsy, those lesions which were found to be benign were also largely nevi and keratoses. Even by being mindful of just the patient’s age, primary care providers can follow patients clinically with a tailored differential diagnosis in mind before referral, and dermatologists can reduce the number of biopsies they perform on patients who are being referred.”
He added that he and his colleagues were surprised that despite very low rates of skin cancer in young patients, and thus different pretest probabilities of cancer, biopsy rates across demographics were consistently around 20%. “We also found a disproportionate number of female patients younger than age 40 who were referred for suspicious lesions, while in the older age groups, the ratio of males to females was approximately equal.”
Dr. Klebanov acknowledged certain limitations of the study, including its single-center, retrospective design, and that information was not collected on patients’ family history of skin cancer, Fitzpatrick skin type, nor the clinical course of the lesion while it was followed by the primary care office. “The nuanced differences in these factors may certainly play a role in decisions for individual patients,” he said.
The study’s principal investigator was Hensin Tsao MD, PhD, clinical director of the MGH Melanoma & Pigmented Lesion Center The work was supported by the Alpha Omega Alpha Carolyn Kuckein Research Fellowship. The researchers reported having no financial disclosures.
SOURCE: Klebanov N et al. AAD 20. Abstract 15881.
FROM AAD 20
Headache may predict clinical evolution of COVID-19
new research suggests. An observational study of more than 100 patients showed that headache onset could occur during the presymptomatic or symptomatic phase of COVID-19 and could resemble tension-type or migraine headache.
Headache itself was associated with a shorter symptomatic period, while headache and anosmia were associated with a shorter hospitalization period. In a subgroup of participants, headache persisted even after the symptoms of COVID-19 had been resolved.
Investigators noted that understanding the pathophysiology of headache in COVID-19 could improve understanding of migraine and other headache disorders. “It seems that those patients who start early on, during the asymptomatic or early symptomatic period of COVID-19, with headache have a more localized inflammatory response that may reflect the ability of the body to better control and respond to the infection by SARS-CoV-2,” lead investigator Patricia Pozo-Rosich, MD, PhD, head of the headache and craniofacial pain unit at Vall d’Hebron University Hospital, Barcelona, said in an interview.
She presented the findings at the virtual annual meeting of the American Headache Society.
Systemic inflammation
Headache is one of the main symptoms of COVID-19. A recent study of 214 patients with COVID-19 showed that approximately 13% of the participants had headache and 5% had anosmia.
SARS-CoV-2 penetrates the cells through the ACE2 receptor, which is present throughout the body. “SARS-CoV-2 enters the body through the nasal cavity and it probably penetrates the nervous system in the periphery through afferent branches of the olfactory and trigeminal nerve,” Dr. Pozo-Rosich said. It travels to the lungs and, later, the bloodstream. This generates systemic inflammation that may turn into a cytokine storm. Evidence has identified cortical hyperintensities and olfactory bulb hyperintensities in patients with COVID-19, suggesting that the virus directly infects the CNS.
Interleukin-6, one of the main inflammatory molecules, has been proven to be related to COVID-19 and has become a therapeutic target. Levels of IL-6 may be lower and tend to be more stable in patients with both COVID-19 and headache than in patients with COVID-19 only.
The researchers observed 130 patients (51% women; mean age, 54 years) with COVID-19 who were attended by neurologists at Vall d’Hebron. In this group, 74.4% had headache. Patients with headache tended to be younger than those without headache (mean age, 50 years vs. 63 years, respectively) and tended to be women (58.6% vs. 29.4%).
Approximately one-third of patients with headache had a history of migraine. Most reported mild to moderate pain that resembled tension-type headache. In participants with severe pain and migraine-like features, headache more often began during the asymptomatic phase of COVID-19.
Disease evolution predictor?
The investigators followed up on 100 of the 130 patients with COVID-19, of whom 74 had headache. About 38% of these patients had ongoing headache after 6 weeks, which suggests that some patients may develop a new daily persistent headache once a 3-month period has elapsed. Half of this group had no previous headache history. Headache had been the prodromal symptom of COVID-19 for 21.4% of these patients.
Results showed that headache predicted the clinical evolution of COVID-19. The symptomatic phase of COVID-19 was 7 days shorter for patients with headache than for those without headache. In addition, the period of hospitalization was 7 days shorter for patients with headache and anosmia, compared with patients who had neither headache nor anosmia.
Most therapies, including ibuprofen, candesartan, and anti–calcitonin gene–related peptide (CGRP) monoclonal antibodies, are safe for treating headache in COVID-19, the investigators noted. “We should just try to initially avoid steroids to avoid interference with the body’s reaction to SARS-CoV-2,” Dr. Pozo-Rosich said.
Researchers at Sidney Kimmel Medical College, Philadelphia, are currently studying intranasal vazegepant, an anti-CGRP therapy, as a way to potentially blunt the severe inflammatory response in the lungs of patients with COVID-19, she noted, adding that this peptide may have a future role not only in headache, but also in COVID-19.
Historical link to viral infections
Commenting on the study, Matthew S. Robbins, MD, associate professor of neurology at Weill Cornell Medicine, New York, said the findings associating headache with a shorter symptomatic phase of COVID-19 were “interesting.”
“Headache is common with mild viral infections. More severe viral infections may simply feature more overwhelming respiratory symptoms and fever that lead to underreporting or underascertainment of headache,” said Dr. Robbins, who was not involved with the research.
He noted that the finding showing an association of headache and COVID-19 with a younger age and in women “may be related to a higher prevalence of migraine biology in such patients, and being triggered by the virus or the psychological stress associated with it.”
Dr. Robbins added that viral illnesses have long been associated with new daily persistent headache, “dating back to the early 1980s,” when it was first described in association with Epstein-Barr virus. These infections have also been implicated in the progression of migraine to chronic migraine in adolescents.
“In my view, treatment should be aimed at the symptomatic headache type for which new daily persistent headache resembles, regardless of the potential inciting factor,” Dr. Robbins said.
Dr. Pozo-Rosich has received consulting fees from Allergan, Amgen, Almirall, Biohaven, Chiesi, Eli Lilly, Medscape, Novartis, and Teva Pharmaceuticals. Dr. Robbins has disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
new research suggests. An observational study of more than 100 patients showed that headache onset could occur during the presymptomatic or symptomatic phase of COVID-19 and could resemble tension-type or migraine headache.
Headache itself was associated with a shorter symptomatic period, while headache and anosmia were associated with a shorter hospitalization period. In a subgroup of participants, headache persisted even after the symptoms of COVID-19 had been resolved.
Investigators noted that understanding the pathophysiology of headache in COVID-19 could improve understanding of migraine and other headache disorders. “It seems that those patients who start early on, during the asymptomatic or early symptomatic period of COVID-19, with headache have a more localized inflammatory response that may reflect the ability of the body to better control and respond to the infection by SARS-CoV-2,” lead investigator Patricia Pozo-Rosich, MD, PhD, head of the headache and craniofacial pain unit at Vall d’Hebron University Hospital, Barcelona, said in an interview.
She presented the findings at the virtual annual meeting of the American Headache Society.
Systemic inflammation
Headache is one of the main symptoms of COVID-19. A recent study of 214 patients with COVID-19 showed that approximately 13% of the participants had headache and 5% had anosmia.
SARS-CoV-2 penetrates the cells through the ACE2 receptor, which is present throughout the body. “SARS-CoV-2 enters the body through the nasal cavity and it probably penetrates the nervous system in the periphery through afferent branches of the olfactory and trigeminal nerve,” Dr. Pozo-Rosich said. It travels to the lungs and, later, the bloodstream. This generates systemic inflammation that may turn into a cytokine storm. Evidence has identified cortical hyperintensities and olfactory bulb hyperintensities in patients with COVID-19, suggesting that the virus directly infects the CNS.
Interleukin-6, one of the main inflammatory molecules, has been proven to be related to COVID-19 and has become a therapeutic target. Levels of IL-6 may be lower and tend to be more stable in patients with both COVID-19 and headache than in patients with COVID-19 only.
The researchers observed 130 patients (51% women; mean age, 54 years) with COVID-19 who were attended by neurologists at Vall d’Hebron. In this group, 74.4% had headache. Patients with headache tended to be younger than those without headache (mean age, 50 years vs. 63 years, respectively) and tended to be women (58.6% vs. 29.4%).
Approximately one-third of patients with headache had a history of migraine. Most reported mild to moderate pain that resembled tension-type headache. In participants with severe pain and migraine-like features, headache more often began during the asymptomatic phase of COVID-19.
Disease evolution predictor?
The investigators followed up on 100 of the 130 patients with COVID-19, of whom 74 had headache. About 38% of these patients had ongoing headache after 6 weeks, which suggests that some patients may develop a new daily persistent headache once a 3-month period has elapsed. Half of this group had no previous headache history. Headache had been the prodromal symptom of COVID-19 for 21.4% of these patients.
Results showed that headache predicted the clinical evolution of COVID-19. The symptomatic phase of COVID-19 was 7 days shorter for patients with headache than for those without headache. In addition, the period of hospitalization was 7 days shorter for patients with headache and anosmia, compared with patients who had neither headache nor anosmia.
Most therapies, including ibuprofen, candesartan, and anti–calcitonin gene–related peptide (CGRP) monoclonal antibodies, are safe for treating headache in COVID-19, the investigators noted. “We should just try to initially avoid steroids to avoid interference with the body’s reaction to SARS-CoV-2,” Dr. Pozo-Rosich said.
Researchers at Sidney Kimmel Medical College, Philadelphia, are currently studying intranasal vazegepant, an anti-CGRP therapy, as a way to potentially blunt the severe inflammatory response in the lungs of patients with COVID-19, she noted, adding that this peptide may have a future role not only in headache, but also in COVID-19.
Historical link to viral infections
Commenting on the study, Matthew S. Robbins, MD, associate professor of neurology at Weill Cornell Medicine, New York, said the findings associating headache with a shorter symptomatic phase of COVID-19 were “interesting.”
“Headache is common with mild viral infections. More severe viral infections may simply feature more overwhelming respiratory symptoms and fever that lead to underreporting or underascertainment of headache,” said Dr. Robbins, who was not involved with the research.
He noted that the finding showing an association of headache and COVID-19 with a younger age and in women “may be related to a higher prevalence of migraine biology in such patients, and being triggered by the virus or the psychological stress associated with it.”
Dr. Robbins added that viral illnesses have long been associated with new daily persistent headache, “dating back to the early 1980s,” when it was first described in association with Epstein-Barr virus. These infections have also been implicated in the progression of migraine to chronic migraine in adolescents.
“In my view, treatment should be aimed at the symptomatic headache type for which new daily persistent headache resembles, regardless of the potential inciting factor,” Dr. Robbins said.
Dr. Pozo-Rosich has received consulting fees from Allergan, Amgen, Almirall, Biohaven, Chiesi, Eli Lilly, Medscape, Novartis, and Teva Pharmaceuticals. Dr. Robbins has disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
new research suggests. An observational study of more than 100 patients showed that headache onset could occur during the presymptomatic or symptomatic phase of COVID-19 and could resemble tension-type or migraine headache.
Headache itself was associated with a shorter symptomatic period, while headache and anosmia were associated with a shorter hospitalization period. In a subgroup of participants, headache persisted even after the symptoms of COVID-19 had been resolved.
Investigators noted that understanding the pathophysiology of headache in COVID-19 could improve understanding of migraine and other headache disorders. “It seems that those patients who start early on, during the asymptomatic or early symptomatic period of COVID-19, with headache have a more localized inflammatory response that may reflect the ability of the body to better control and respond to the infection by SARS-CoV-2,” lead investigator Patricia Pozo-Rosich, MD, PhD, head of the headache and craniofacial pain unit at Vall d’Hebron University Hospital, Barcelona, said in an interview.
She presented the findings at the virtual annual meeting of the American Headache Society.
Systemic inflammation
Headache is one of the main symptoms of COVID-19. A recent study of 214 patients with COVID-19 showed that approximately 13% of the participants had headache and 5% had anosmia.
SARS-CoV-2 penetrates the cells through the ACE2 receptor, which is present throughout the body. “SARS-CoV-2 enters the body through the nasal cavity and it probably penetrates the nervous system in the periphery through afferent branches of the olfactory and trigeminal nerve,” Dr. Pozo-Rosich said. It travels to the lungs and, later, the bloodstream. This generates systemic inflammation that may turn into a cytokine storm. Evidence has identified cortical hyperintensities and olfactory bulb hyperintensities in patients with COVID-19, suggesting that the virus directly infects the CNS.
Interleukin-6, one of the main inflammatory molecules, has been proven to be related to COVID-19 and has become a therapeutic target. Levels of IL-6 may be lower and tend to be more stable in patients with both COVID-19 and headache than in patients with COVID-19 only.
The researchers observed 130 patients (51% women; mean age, 54 years) with COVID-19 who were attended by neurologists at Vall d’Hebron. In this group, 74.4% had headache. Patients with headache tended to be younger than those without headache (mean age, 50 years vs. 63 years, respectively) and tended to be women (58.6% vs. 29.4%).
Approximately one-third of patients with headache had a history of migraine. Most reported mild to moderate pain that resembled tension-type headache. In participants with severe pain and migraine-like features, headache more often began during the asymptomatic phase of COVID-19.
Disease evolution predictor?
The investigators followed up on 100 of the 130 patients with COVID-19, of whom 74 had headache. About 38% of these patients had ongoing headache after 6 weeks, which suggests that some patients may develop a new daily persistent headache once a 3-month period has elapsed. Half of this group had no previous headache history. Headache had been the prodromal symptom of COVID-19 for 21.4% of these patients.
Results showed that headache predicted the clinical evolution of COVID-19. The symptomatic phase of COVID-19 was 7 days shorter for patients with headache than for those without headache. In addition, the period of hospitalization was 7 days shorter for patients with headache and anosmia, compared with patients who had neither headache nor anosmia.
Most therapies, including ibuprofen, candesartan, and anti–calcitonin gene–related peptide (CGRP) monoclonal antibodies, are safe for treating headache in COVID-19, the investigators noted. “We should just try to initially avoid steroids to avoid interference with the body’s reaction to SARS-CoV-2,” Dr. Pozo-Rosich said.
Researchers at Sidney Kimmel Medical College, Philadelphia, are currently studying intranasal vazegepant, an anti-CGRP therapy, as a way to potentially blunt the severe inflammatory response in the lungs of patients with COVID-19, she noted, adding that this peptide may have a future role not only in headache, but also in COVID-19.
Historical link to viral infections
Commenting on the study, Matthew S. Robbins, MD, associate professor of neurology at Weill Cornell Medicine, New York, said the findings associating headache with a shorter symptomatic phase of COVID-19 were “interesting.”
“Headache is common with mild viral infections. More severe viral infections may simply feature more overwhelming respiratory symptoms and fever that lead to underreporting or underascertainment of headache,” said Dr. Robbins, who was not involved with the research.
He noted that the finding showing an association of headache and COVID-19 with a younger age and in women “may be related to a higher prevalence of migraine biology in such patients, and being triggered by the virus or the psychological stress associated with it.”
Dr. Robbins added that viral illnesses have long been associated with new daily persistent headache, “dating back to the early 1980s,” when it was first described in association with Epstein-Barr virus. These infections have also been implicated in the progression of migraine to chronic migraine in adolescents.
“In my view, treatment should be aimed at the symptomatic headache type for which new daily persistent headache resembles, regardless of the potential inciting factor,” Dr. Robbins said.
Dr. Pozo-Rosich has received consulting fees from Allergan, Amgen, Almirall, Biohaven, Chiesi, Eli Lilly, Medscape, Novartis, and Teva Pharmaceuticals. Dr. Robbins has disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
FROM AHS 2020
Lipid-lowering bempedoic acid does not hasten or worsen diabetes
In an analysis of four phase 3 trials, the oral lipid-lowering drug bempedoic acid (Nexletol; Esperion) did not worsen glycemic control or increase the incidence of type 2 diabetes.
As previously reported, this first-in-class drug, which acts by inhibiting ATP-citrate lyase, was approved by the Food and Drug Administration in February 2020.
Lawrence A. Leiter MD, from the University of Toronto, delivered the findings of this latest analysis in an oral presentation at the virtual American Diabetes Association 80th Scientific Sessions.
“The current study is important as it shows overall consistent efficacy and safety regardless of glycemic status and no increase in new-onset diabetes,” Dr. Leiter said in an interview.
There is interest in how lipid-lowering drugs might affect glycemia because “meta-analyses have shown about a 10% increased risk of new-onset diabetes in statin users, although the absolute increased risk is 1 extra case per 255 treated patients [in whom one would expect 5.4 cardiovascular events to be prevented by the statin],” he noted.
In a comment, John R. Guyton, MD, from Duke University Medical Center, Durham, N.C., agreed that the new study demonstrates that “patients with diabetes and prediabetes respond to bempedoic acid with LDL cholesterol lowering that is similar to that in patients with normal glucose tolerance.”
Although “statins have a slight effect of worsening glucose tolerance and a modest effect of increasing cases of new-onset diabetes,” the current research shows that “bempedoic acid appears to be free of these effects,” said Dr. Guyton, who discussed this drug in another symposium at the meeting where he also discussed how the agent will “fit” into prescribing patterns.
How do patients with diabetes, prediabetes fare?
“Current guidelines support aggressive LDL cholesterol lowering in patients with diabetes, given the increased risk of cardiovascular morbidity and mortality,” said Dr. Leiter.
Bempedoic acid was approved as an adjunct to diet and maximally tolerated statin therapy to treat adults with atherosclerotic cardiovascular disease (ASCVD) and/or heterozygous familial hypercholesterolemia (HeFH) who require additional lowering of LDL cholesterol, although its effect on cardiovascular morbidity and mortality has not been determined, the prescribing information states.
However, it has been unknown how bempedoic acid affects LDL cholesterol or hemoglobin A1c levels in patients with diabetes, prediabetes, or normoglycemia.
To examine this, the researchers pooled data from four phase 3 trials in 3623 patients with ASCVD or HeFH who had been randomized 2:1 to bempedoic acid 180 mg/day or placebo for 12 or 24 weeks (if they were statin intolerant) or 52 weeks (if they were also on statins).
In the pooled sample, about half the patients had prediabetes (52%), and the rest had diabetes (31%) or normoglycemia (17%). Overall, 75%-84% of patients had a history of ASCVD.
Mean LDL cholesterol levels were higher in patients with normoglycemia (119 mg/dL) or prediabetes (115 mg/dL) than in patients with diabetes (110 mg/dL).
The primary outcome was percent change in LDL cholesterol from baseline to week 12.
In the two types of patients (all with ASCVD or HeFH) – those on statins and those with statin intolerance – LDL cholesterol at 12 weeks was significantly lower in patients who received bempedoic acid, compared with placebo, regardless of whether they had no diabetes, prediabetes, or diabetes (all P < .001).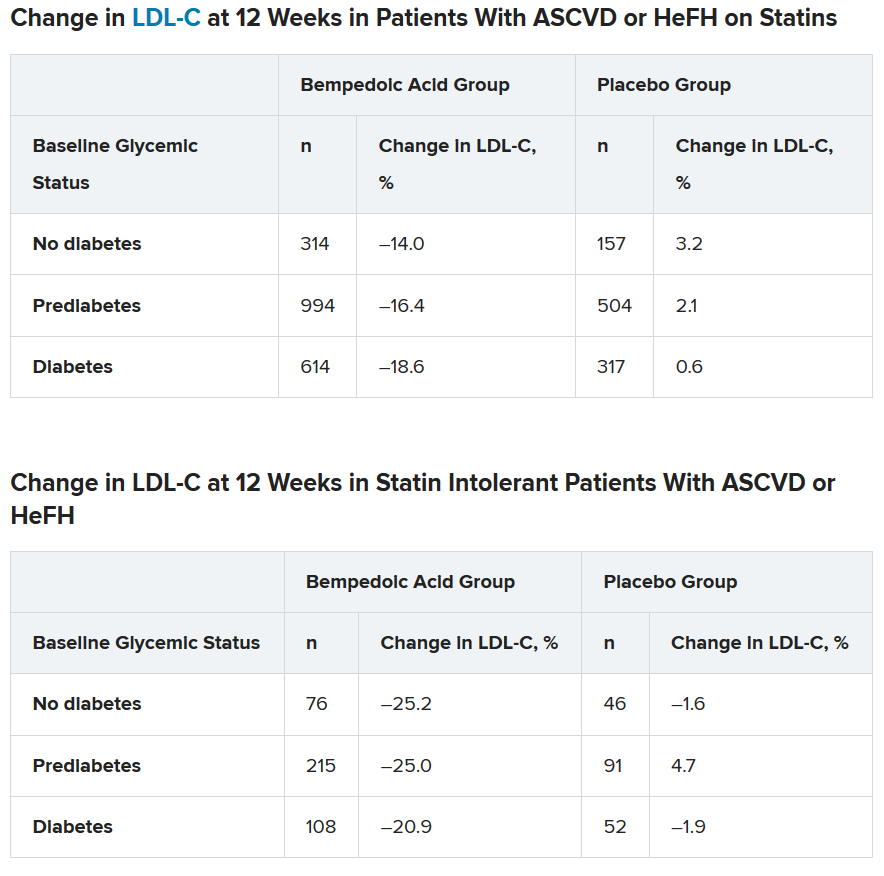
Similarly, patients who received bempedoic acid also had significant reductions in total cholesterol, non–HDL cholesterol, apolipoprotein B, and high-sensitivity C-reactive protein (hsCRP) at 12 weeks, compared with patients who received placebo (all P < .01).
The safety profile of bempedoic acid was similar to placebo and did not vary by glycemic status.
“Of course, with any lipid-lowering therapy, there’s lots of interest in changes in glycemic parameters,” said Dr. Leiter. “A1c did not increase. In fact, it was significantly lower in patients with prediabetes and diabetes on bempedoic acid versus placebo.”
In addition, “statin trials have shown small increases in body weight. We did not observe this,” he reported.
Where does bempedoic acid ‘fit?’
“Bempedoic acid will be a useful add-on to any patient who requires additional LDL cholesterol lowering,” according to Dr. Leiter. “It will typically be used as an add-on to statins, but will also be very useful in the statin-intolerant patient, especially when used in combination with ezetimib.”
The fixed-dose combination of bempedoic acid plus ezetimibe (Nexlizet; Esperion), was also approved in the United States in February, just days after bempedoic acid as a solo agent was cleared for marketing.
“Bempedoic acid would not be chosen in preference to a statin, ezetimibe, or PCSK9 inhibitor,” Dr. Guyton said. Rather, “its chief use will be in patients with statin intolerance and either FH or ASCVD when LDL-cholesterol is poorly controlled despite maximum tolerated lipid-lowering therapy.”
According to Dr. Guyton, “use of bempedoic acid should be undertaken only when provider-patient discussion acknowledges that it has not been shown to reduce cardiovascular events, although preliminary evidence from genetic analysis [Mendelian randomization study] suggests that it will,” as previously reported.
The CLEAR Outcomes cardiovascular outcomes trial of bempedoic acid completed enrollment in August 2019, involving 14,032 patients with hypercholesterolemia and high CVD risk according to a company statement.
The study was funded by Esperion. Dr. Leiter has reported being on advisory panels for Abbott, Amgen, AstraZeneca, Boehringer Ingelheim, Eli Lilly, HLS Therapeutics, Janssen, Merck, Novo Nordisk, Sanofi, and Servier, receiving research support from Amgen, AstraZeneca, Kowa Pharmaceuticals, and the Medicines Company, and being on speakers bureaus for Amgen, AstraZeneca, Boehringer Ingelheim, Eli Lilly, HLS Therapeutics, Janssen, Medscape, Merck, Novo Nordisk, Sanofi, and Servier. Disclosures for the other authors are listed with the abstract. Dr. Guyton has reported being a consultant for Amarin and receiving research support form Regeneron.
A version of this article originally appeared on Medscape.com.
In an analysis of four phase 3 trials, the oral lipid-lowering drug bempedoic acid (Nexletol; Esperion) did not worsen glycemic control or increase the incidence of type 2 diabetes.
As previously reported, this first-in-class drug, which acts by inhibiting ATP-citrate lyase, was approved by the Food and Drug Administration in February 2020.
Lawrence A. Leiter MD, from the University of Toronto, delivered the findings of this latest analysis in an oral presentation at the virtual American Diabetes Association 80th Scientific Sessions.
“The current study is important as it shows overall consistent efficacy and safety regardless of glycemic status and no increase in new-onset diabetes,” Dr. Leiter said in an interview.
There is interest in how lipid-lowering drugs might affect glycemia because “meta-analyses have shown about a 10% increased risk of new-onset diabetes in statin users, although the absolute increased risk is 1 extra case per 255 treated patients [in whom one would expect 5.4 cardiovascular events to be prevented by the statin],” he noted.
In a comment, John R. Guyton, MD, from Duke University Medical Center, Durham, N.C., agreed that the new study demonstrates that “patients with diabetes and prediabetes respond to bempedoic acid with LDL cholesterol lowering that is similar to that in patients with normal glucose tolerance.”
Although “statins have a slight effect of worsening glucose tolerance and a modest effect of increasing cases of new-onset diabetes,” the current research shows that “bempedoic acid appears to be free of these effects,” said Dr. Guyton, who discussed this drug in another symposium at the meeting where he also discussed how the agent will “fit” into prescribing patterns.
How do patients with diabetes, prediabetes fare?
“Current guidelines support aggressive LDL cholesterol lowering in patients with diabetes, given the increased risk of cardiovascular morbidity and mortality,” said Dr. Leiter.
Bempedoic acid was approved as an adjunct to diet and maximally tolerated statin therapy to treat adults with atherosclerotic cardiovascular disease (ASCVD) and/or heterozygous familial hypercholesterolemia (HeFH) who require additional lowering of LDL cholesterol, although its effect on cardiovascular morbidity and mortality has not been determined, the prescribing information states.
However, it has been unknown how bempedoic acid affects LDL cholesterol or hemoglobin A1c levels in patients with diabetes, prediabetes, or normoglycemia.
To examine this, the researchers pooled data from four phase 3 trials in 3623 patients with ASCVD or HeFH who had been randomized 2:1 to bempedoic acid 180 mg/day or placebo for 12 or 24 weeks (if they were statin intolerant) or 52 weeks (if they were also on statins).
In the pooled sample, about half the patients had prediabetes (52%), and the rest had diabetes (31%) or normoglycemia (17%). Overall, 75%-84% of patients had a history of ASCVD.
Mean LDL cholesterol levels were higher in patients with normoglycemia (119 mg/dL) or prediabetes (115 mg/dL) than in patients with diabetes (110 mg/dL).
The primary outcome was percent change in LDL cholesterol from baseline to week 12.
In the two types of patients (all with ASCVD or HeFH) – those on statins and those with statin intolerance – LDL cholesterol at 12 weeks was significantly lower in patients who received bempedoic acid, compared with placebo, regardless of whether they had no diabetes, prediabetes, or diabetes (all P < .001).
Similarly, patients who received bempedoic acid also had significant reductions in total cholesterol, non–HDL cholesterol, apolipoprotein B, and high-sensitivity C-reactive protein (hsCRP) at 12 weeks, compared with patients who received placebo (all P < .01).
The safety profile of bempedoic acid was similar to placebo and did not vary by glycemic status.
“Of course, with any lipid-lowering therapy, there’s lots of interest in changes in glycemic parameters,” said Dr. Leiter. “A1c did not increase. In fact, it was significantly lower in patients with prediabetes and diabetes on bempedoic acid versus placebo.”
In addition, “statin trials have shown small increases in body weight. We did not observe this,” he reported.
Where does bempedoic acid ‘fit?’
“Bempedoic acid will be a useful add-on to any patient who requires additional LDL cholesterol lowering,” according to Dr. Leiter. “It will typically be used as an add-on to statins, but will also be very useful in the statin-intolerant patient, especially when used in combination with ezetimib.”
The fixed-dose combination of bempedoic acid plus ezetimibe (Nexlizet; Esperion), was also approved in the United States in February, just days after bempedoic acid as a solo agent was cleared for marketing.
“Bempedoic acid would not be chosen in preference to a statin, ezetimibe, or PCSK9 inhibitor,” Dr. Guyton said. Rather, “its chief use will be in patients with statin intolerance and either FH or ASCVD when LDL-cholesterol is poorly controlled despite maximum tolerated lipid-lowering therapy.”
According to Dr. Guyton, “use of bempedoic acid should be undertaken only when provider-patient discussion acknowledges that it has not been shown to reduce cardiovascular events, although preliminary evidence from genetic analysis [Mendelian randomization study] suggests that it will,” as previously reported.
The CLEAR Outcomes cardiovascular outcomes trial of bempedoic acid completed enrollment in August 2019, involving 14,032 patients with hypercholesterolemia and high CVD risk according to a company statement.
The study was funded by Esperion. Dr. Leiter has reported being on advisory panels for Abbott, Amgen, AstraZeneca, Boehringer Ingelheim, Eli Lilly, HLS Therapeutics, Janssen, Merck, Novo Nordisk, Sanofi, and Servier, receiving research support from Amgen, AstraZeneca, Kowa Pharmaceuticals, and the Medicines Company, and being on speakers bureaus for Amgen, AstraZeneca, Boehringer Ingelheim, Eli Lilly, HLS Therapeutics, Janssen, Medscape, Merck, Novo Nordisk, Sanofi, and Servier. Disclosures for the other authors are listed with the abstract. Dr. Guyton has reported being a consultant for Amarin and receiving research support form Regeneron.
A version of this article originally appeared on Medscape.com.
In an analysis of four phase 3 trials, the oral lipid-lowering drug bempedoic acid (Nexletol; Esperion) did not worsen glycemic control or increase the incidence of type 2 diabetes.
As previously reported, this first-in-class drug, which acts by inhibiting ATP-citrate lyase, was approved by the Food and Drug Administration in February 2020.
Lawrence A. Leiter MD, from the University of Toronto, delivered the findings of this latest analysis in an oral presentation at the virtual American Diabetes Association 80th Scientific Sessions.
“The current study is important as it shows overall consistent efficacy and safety regardless of glycemic status and no increase in new-onset diabetes,” Dr. Leiter said in an interview.
There is interest in how lipid-lowering drugs might affect glycemia because “meta-analyses have shown about a 10% increased risk of new-onset diabetes in statin users, although the absolute increased risk is 1 extra case per 255 treated patients [in whom one would expect 5.4 cardiovascular events to be prevented by the statin],” he noted.
In a comment, John R. Guyton, MD, from Duke University Medical Center, Durham, N.C., agreed that the new study demonstrates that “patients with diabetes and prediabetes respond to bempedoic acid with LDL cholesterol lowering that is similar to that in patients with normal glucose tolerance.”
Although “statins have a slight effect of worsening glucose tolerance and a modest effect of increasing cases of new-onset diabetes,” the current research shows that “bempedoic acid appears to be free of these effects,” said Dr. Guyton, who discussed this drug in another symposium at the meeting where he also discussed how the agent will “fit” into prescribing patterns.
How do patients with diabetes, prediabetes fare?
“Current guidelines support aggressive LDL cholesterol lowering in patients with diabetes, given the increased risk of cardiovascular morbidity and mortality,” said Dr. Leiter.
Bempedoic acid was approved as an adjunct to diet and maximally tolerated statin therapy to treat adults with atherosclerotic cardiovascular disease (ASCVD) and/or heterozygous familial hypercholesterolemia (HeFH) who require additional lowering of LDL cholesterol, although its effect on cardiovascular morbidity and mortality has not been determined, the prescribing information states.
However, it has been unknown how bempedoic acid affects LDL cholesterol or hemoglobin A1c levels in patients with diabetes, prediabetes, or normoglycemia.
To examine this, the researchers pooled data from four phase 3 trials in 3623 patients with ASCVD or HeFH who had been randomized 2:1 to bempedoic acid 180 mg/day or placebo for 12 or 24 weeks (if they were statin intolerant) or 52 weeks (if they were also on statins).
In the pooled sample, about half the patients had prediabetes (52%), and the rest had diabetes (31%) or normoglycemia (17%). Overall, 75%-84% of patients had a history of ASCVD.
Mean LDL cholesterol levels were higher in patients with normoglycemia (119 mg/dL) or prediabetes (115 mg/dL) than in patients with diabetes (110 mg/dL).
The primary outcome was percent change in LDL cholesterol from baseline to week 12.
In the two types of patients (all with ASCVD or HeFH) – those on statins and those with statin intolerance – LDL cholesterol at 12 weeks was significantly lower in patients who received bempedoic acid, compared with placebo, regardless of whether they had no diabetes, prediabetes, or diabetes (all P < .001).
Similarly, patients who received bempedoic acid also had significant reductions in total cholesterol, non–HDL cholesterol, apolipoprotein B, and high-sensitivity C-reactive protein (hsCRP) at 12 weeks, compared with patients who received placebo (all P < .01).
The safety profile of bempedoic acid was similar to placebo and did not vary by glycemic status.
“Of course, with any lipid-lowering therapy, there’s lots of interest in changes in glycemic parameters,” said Dr. Leiter. “A1c did not increase. In fact, it was significantly lower in patients with prediabetes and diabetes on bempedoic acid versus placebo.”
In addition, “statin trials have shown small increases in body weight. We did not observe this,” he reported.
Where does bempedoic acid ‘fit?’
“Bempedoic acid will be a useful add-on to any patient who requires additional LDL cholesterol lowering,” according to Dr. Leiter. “It will typically be used as an add-on to statins, but will also be very useful in the statin-intolerant patient, especially when used in combination with ezetimib.”
The fixed-dose combination of bempedoic acid plus ezetimibe (Nexlizet; Esperion), was also approved in the United States in February, just days after bempedoic acid as a solo agent was cleared for marketing.
“Bempedoic acid would not be chosen in preference to a statin, ezetimibe, or PCSK9 inhibitor,” Dr. Guyton said. Rather, “its chief use will be in patients with statin intolerance and either FH or ASCVD when LDL-cholesterol is poorly controlled despite maximum tolerated lipid-lowering therapy.”
According to Dr. Guyton, “use of bempedoic acid should be undertaken only when provider-patient discussion acknowledges that it has not been shown to reduce cardiovascular events, although preliminary evidence from genetic analysis [Mendelian randomization study] suggests that it will,” as previously reported.
The CLEAR Outcomes cardiovascular outcomes trial of bempedoic acid completed enrollment in August 2019, involving 14,032 patients with hypercholesterolemia and high CVD risk according to a company statement.
The study was funded by Esperion. Dr. Leiter has reported being on advisory panels for Abbott, Amgen, AstraZeneca, Boehringer Ingelheim, Eli Lilly, HLS Therapeutics, Janssen, Merck, Novo Nordisk, Sanofi, and Servier, receiving research support from Amgen, AstraZeneca, Kowa Pharmaceuticals, and the Medicines Company, and being on speakers bureaus for Amgen, AstraZeneca, Boehringer Ingelheim, Eli Lilly, HLS Therapeutics, Janssen, Medscape, Merck, Novo Nordisk, Sanofi, and Servier. Disclosures for the other authors are listed with the abstract. Dr. Guyton has reported being a consultant for Amarin and receiving research support form Regeneron.
A version of this article originally appeared on Medscape.com.
Pilot study shows apremilast effective for severe recurrent canker sores
showed.

“Canker sores [aphthous ulcers] are very common, yet are often not well managed as the diagnosis is not always correctly made,” lead study author Alison J. Bruce, MB, ChB, said in an interview following the virtual annual meeting of the American Academy of Dermatology. “They’re often mistaken for herpes infection and therefore treated with antiviral therapy. Of the available therapies, several have common side effects or require lab monitoring or are not uniformly effective.”
In their poster abstract, Dr. Bruce, of the division of dermatology at the Mayo Clinic, Jacksonville, Fla., and colleagues noted that, while no principal etiology has been established for recurrent aphthous stomatitis (RAS), immune up-regulation plays a role in the pathogenesis of the condition. “Attacks of RAS may be precipitated by local trauma, stress, food intake, drugs, hormonal changes and vitamin and trace element deficiencies,” they wrote. “Local and systemic conditions and genetic, immunological and microbial factors all may play a role in the pathogenesis.”
Apremilast, a phosphodiesterase-4 inhibitor, down-regulates inflammatory response by modulating expression of tumor necrosis factor–alpha; interferon-gamma; and interleukin-2, IL-12, IL-17, and IL-23. It is approved by the Food and Drug Administration for treating plaque psoriasis and psoriatic arthritis, and in July 2019, was approved for treating ulcers associated with Behçet’s disease, in adults.*
For the pilot study, the researchers enrolled 15 patients with RAS to receive apremilast 30 mg twice daily for 15 weeks after 1 week titration. To be eligible for the trial, patients must have had monthly oral ulcers in preceding 6 months, at least two ulcers in previous 4 weeks prior to enrollment at baseline, at least three ulcers during flares, inadequate control with topical therapy, and no evidence of systemic disease. They excluded patients on immune-modulating therapy or systemic steroids, pregnant or breastfeeding women, those with a systemic infection, those with a history of recurrent bacterial, viral, fungal, or mycobacterial infection, those with a history of depression, as well as those with a known malignancy or vitamin deficiencies. Patients were assessed monthly, evaluating number of ulcers, visual analog pain scale, physician’s global assessment and Chronic Oral Mucosal Disease Questionnaire (COMDQ).
Dr. Bruce and colleagues found that, within 4 weeks of therapy, complete clearance of RAS lesions occurred in all patients except one in whom ulcers were reported to be less severe. That patient had considerable reduction in number, size, and duration of oral ulcers. Remission in all patients was sustained during 16 weeks of treatment. COMDQ responses improved considerably from baseline to week 8, and this was continued until week 16.
“Onset of response [to apremilast] was rapid,” Dr. Bruce said. “For many other therapies, patients are counseled that [they] may take several weeks to become effective. Response was also dramatic. Almost all patients had complete remission from their ulcers, compared with other therapies where oftentimes reduction or attenuation is achieved, as opposed to complete resolution. There was a suggestion that a lower dose [of apremilast] may still be effective. This adds to our ‘toolbox’ of therapeutic options.”
The most common adverse effects were nausea/vomiting and headache, but these were mild and tolerable and generally resolved by week 4.
The researchers acknowledged certain limitations of the study, including its small sample size. “The challenge will most likely be insurance coverage,” Dr. Bruce said. “This is unfortunate, as it would be ideal to offer a safe treatment without the need for monitoring.”
The investigator-initiated study was supported by Celgene. The researchers reported having no financial disclosures.
SOURCE: Bruce AJ et al. AAD 20, Abstract 17701.
*Correction 6/23/2020: An earlier version of this story misstated the approved indications for apremilast.
showed.
“Canker sores [aphthous ulcers] are very common, yet are often not well managed as the diagnosis is not always correctly made,” lead study author Alison J. Bruce, MB, ChB, said in an interview following the virtual annual meeting of the American Academy of Dermatology. “They’re often mistaken for herpes infection and therefore treated with antiviral therapy. Of the available therapies, several have common side effects or require lab monitoring or are not uniformly effective.”
In their poster abstract, Dr. Bruce, of the division of dermatology at the Mayo Clinic, Jacksonville, Fla., and colleagues noted that, while no principal etiology has been established for recurrent aphthous stomatitis (RAS), immune up-regulation plays a role in the pathogenesis of the condition. “Attacks of RAS may be precipitated by local trauma, stress, food intake, drugs, hormonal changes and vitamin and trace element deficiencies,” they wrote. “Local and systemic conditions and genetic, immunological and microbial factors all may play a role in the pathogenesis.”
Apremilast, a phosphodiesterase-4 inhibitor, down-regulates inflammatory response by modulating expression of tumor necrosis factor–alpha; interferon-gamma; and interleukin-2, IL-12, IL-17, and IL-23. It is approved by the Food and Drug Administration for treating plaque psoriasis and psoriatic arthritis, and in July 2019, was approved for treating ulcers associated with Behçet’s disease, in adults.*
For the pilot study, the researchers enrolled 15 patients with RAS to receive apremilast 30 mg twice daily for 15 weeks after 1 week titration. To be eligible for the trial, patients must have had monthly oral ulcers in preceding 6 months, at least two ulcers in previous 4 weeks prior to enrollment at baseline, at least three ulcers during flares, inadequate control with topical therapy, and no evidence of systemic disease. They excluded patients on immune-modulating therapy or systemic steroids, pregnant or breastfeeding women, those with a systemic infection, those with a history of recurrent bacterial, viral, fungal, or mycobacterial infection, those with a history of depression, as well as those with a known malignancy or vitamin deficiencies. Patients were assessed monthly, evaluating number of ulcers, visual analog pain scale, physician’s global assessment and Chronic Oral Mucosal Disease Questionnaire (COMDQ).
Dr. Bruce and colleagues found that, within 4 weeks of therapy, complete clearance of RAS lesions occurred in all patients except one in whom ulcers were reported to be less severe. That patient had considerable reduction in number, size, and duration of oral ulcers. Remission in all patients was sustained during 16 weeks of treatment. COMDQ responses improved considerably from baseline to week 8, and this was continued until week 16.
“Onset of response [to apremilast] was rapid,” Dr. Bruce said. “For many other therapies, patients are counseled that [they] may take several weeks to become effective. Response was also dramatic. Almost all patients had complete remission from their ulcers, compared with other therapies where oftentimes reduction or attenuation is achieved, as opposed to complete resolution. There was a suggestion that a lower dose [of apremilast] may still be effective. This adds to our ‘toolbox’ of therapeutic options.”
The most common adverse effects were nausea/vomiting and headache, but these were mild and tolerable and generally resolved by week 4.
The researchers acknowledged certain limitations of the study, including its small sample size. “The challenge will most likely be insurance coverage,” Dr. Bruce said. “This is unfortunate, as it would be ideal to offer a safe treatment without the need for monitoring.”
The investigator-initiated study was supported by Celgene. The researchers reported having no financial disclosures.
SOURCE: Bruce AJ et al. AAD 20, Abstract 17701.
*Correction 6/23/2020: An earlier version of this story misstated the approved indications for apremilast.
showed.
“Canker sores [aphthous ulcers] are very common, yet are often not well managed as the diagnosis is not always correctly made,” lead study author Alison J. Bruce, MB, ChB, said in an interview following the virtual annual meeting of the American Academy of Dermatology. “They’re often mistaken for herpes infection and therefore treated with antiviral therapy. Of the available therapies, several have common side effects or require lab monitoring or are not uniformly effective.”
In their poster abstract, Dr. Bruce, of the division of dermatology at the Mayo Clinic, Jacksonville, Fla., and colleagues noted that, while no principal etiology has been established for recurrent aphthous stomatitis (RAS), immune up-regulation plays a role in the pathogenesis of the condition. “Attacks of RAS may be precipitated by local trauma, stress, food intake, drugs, hormonal changes and vitamin and trace element deficiencies,” they wrote. “Local and systemic conditions and genetic, immunological and microbial factors all may play a role in the pathogenesis.”
Apremilast, a phosphodiesterase-4 inhibitor, down-regulates inflammatory response by modulating expression of tumor necrosis factor–alpha; interferon-gamma; and interleukin-2, IL-12, IL-17, and IL-23. It is approved by the Food and Drug Administration for treating plaque psoriasis and psoriatic arthritis, and in July 2019, was approved for treating ulcers associated with Behçet’s disease, in adults.*
For the pilot study, the researchers enrolled 15 patients with RAS to receive apremilast 30 mg twice daily for 15 weeks after 1 week titration. To be eligible for the trial, patients must have had monthly oral ulcers in preceding 6 months, at least two ulcers in previous 4 weeks prior to enrollment at baseline, at least three ulcers during flares, inadequate control with topical therapy, and no evidence of systemic disease. They excluded patients on immune-modulating therapy or systemic steroids, pregnant or breastfeeding women, those with a systemic infection, those with a history of recurrent bacterial, viral, fungal, or mycobacterial infection, those with a history of depression, as well as those with a known malignancy or vitamin deficiencies. Patients were assessed monthly, evaluating number of ulcers, visual analog pain scale, physician’s global assessment and Chronic Oral Mucosal Disease Questionnaire (COMDQ).
Dr. Bruce and colleagues found that, within 4 weeks of therapy, complete clearance of RAS lesions occurred in all patients except one in whom ulcers were reported to be less severe. That patient had considerable reduction in number, size, and duration of oral ulcers. Remission in all patients was sustained during 16 weeks of treatment. COMDQ responses improved considerably from baseline to week 8, and this was continued until week 16.
“Onset of response [to apremilast] was rapid,” Dr. Bruce said. “For many other therapies, patients are counseled that [they] may take several weeks to become effective. Response was also dramatic. Almost all patients had complete remission from their ulcers, compared with other therapies where oftentimes reduction or attenuation is achieved, as opposed to complete resolution. There was a suggestion that a lower dose [of apremilast] may still be effective. This adds to our ‘toolbox’ of therapeutic options.”
The most common adverse effects were nausea/vomiting and headache, but these were mild and tolerable and generally resolved by week 4.
The researchers acknowledged certain limitations of the study, including its small sample size. “The challenge will most likely be insurance coverage,” Dr. Bruce said. “This is unfortunate, as it would be ideal to offer a safe treatment without the need for monitoring.”
The investigator-initiated study was supported by Celgene. The researchers reported having no financial disclosures.
SOURCE: Bruce AJ et al. AAD 20, Abstract 17701.
*Correction 6/23/2020: An earlier version of this story misstated the approved indications for apremilast.
FROM AAD 20