User login
MDedge conference coverage features onsite reporting of the latest study results and expert perspectives from leading researchers.
Rapid relief of opioid-induced constipation with MNTX
Subcutaneously administered methylnaltrexone (MNTX) (Relistor), a peripherally acting mu-opioid receptor antagonist, relieves opioid-induced constipation (OID) in both chronic, noncancer-related illness and cancer-related illness, a new analysis concludes.
“While these are two very different patient groups, the ability to have something to treat OIC in noncancer patients who stay on opioids for whatever reason helps, because [otherwise] these patients are not doing well,” said lead author Eric Shah, MD, motility director for the Dartmouth program at Dartmouth Hitchcock Health, Lebanon, N.H.
Importantly, peripherally acting mu-opioid receptor antagonists such as MNTX do not affect overall pain control to any significant extent, which is “reassuring,” he said in an interview.
These drugs decrease the constipating effects of opioids without reversing CNS-mediated opioid effects, he explained.
“Methylnaltrexone has already been approved for the treatment of OIC in adults with chronic noncancer pain as well as for OIC in adults with advanced illness who are receiving palliative care, which is often the case in patients with cancer-related pain,” he noted.
Dr. Shah discussed the new analysis during PAINWeek 2020, the American Society of Regional Anesthesia and Pain Medicine 19th Annual Pain Medicine Meeting.
The analysis was based on a review of data collected in two previously reported randomized, placebo-controlled studies (study 302 and 4000), which were used to gain approval.
The new analysis shows that “the drug works up front, and the effect is able to be maintained. I think the studies are clinically relevant in that patients are able to have a bowel movement quickly after you give them an injectable formulation when they are vomiting or otherwise can’t tolerate a pill and they are feeling miserable,” Dr. Shah commented. Many patients with OIC are constipated for reasons other than from opioid use. They often have other side effects from opioids, including bloating, nausea, and vomiting.
“When patients go to the emergency room, it’s not just that they are not able to have a bowel movement; they are often also vomiting, so it’s important to have agents that can be given in a manner that avoids the need for oral medication,” Dr. Shah said. MNTX is the only peripherally acting opioid antagonist available in a subcutaneous formulation.
Moreover, if patients are able to control these symptoms at home with an injectable formulation, they may not need to go to the ED for treatment of their gastrointestinal distress, he added.
Viable product
In a comment, Darren Brenner, MD, associate professor of medicine and surgery, Northwestern University, Chicago, who has worked with this subcutaneous formulation, said it is “definitely a viable product.
“The data presented here were in patients with advanced illness receiving palliative care when other laxatives have failed, and the difference and the potential benefit for MNTX is that it is the only peripherally acting mu-opioid receptor antagonist that is approved for advanced cancer,” he added. The other products that are currently approved, naloxegol (Movantik) and naldemedine (Symproic), are both indicated for chronic, noncancer pain.
The other potential benefit of subcutaneous MNTX is that it can work very rapidly for the patients who respond to it. “One of the things investigators did not mention in these two trials but which has been shown in previous studies is that almost half of patients who respond to this drug respond within the first 30 minutes of receiving the injection,” Dr. Brenner said in an interview.
This can be very beneficial in an emergency setting, because it may avoid having patients admitted to hospital. They can be discharged and sent home with enough drug to use on demand, Dr. Brenner suggested.
New analysis of data from studies 302 and 4000
Both studies were carried out in adults with advanced illness and OIC whose conditions were refractory to laxative use. Both of the studies were placebo controlled.
Study 302 involved 78 patients with cancer and 56 patients with noncancer-related OIC. MNTX was given at a dose of 0.15 mg/kg subcutaneously every other day for 2 weeks.
Study 4000 included 152 patients with cancer and OIC and 78 patients with noncancer-related OIC. In this study, the dose of MNTX was based on body weight. Seven or fewer doses of either 8 mg or 12 mg were given subcutaneously for 2 weeks.
The main endpoints of both studies was the proportion of patients who achieved a rescue-free laxation (RFL) response within 4 hours after the first dose and the proportion of patients with an RFL response within 4 hours for two or more of the first four doses within 24 hours.
Dr. Shah explained that RFL is a meaningful clinical endpoint. Patients could achieve a bowel movement with the two prespecified time endpoints in both studies.
Not all patients were hospitalized for OIC, Dr. Shah noted. Entry criteria were strict and included having fewer than three bowel movements during the previous week and no clinically significant laxation (defecation) within 48 hours of receiving the first dose of study drug.
“In both studies, a significantly greater proportion of patients treated with MNTX versus placebo achieved an RFL within 4 hours after the first dose among both cancer and noncancer patients,” the investigators reported.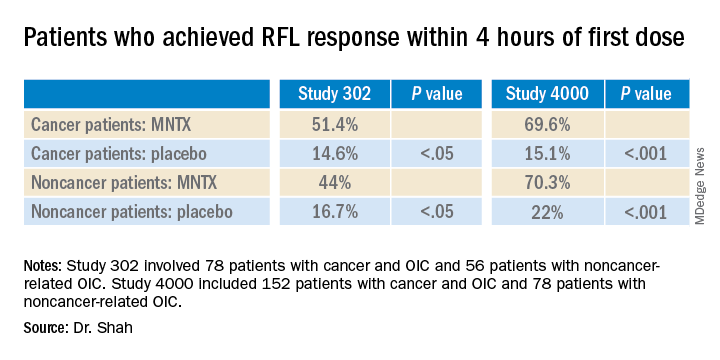
Results were relatively comparable between cancer and noncancer patients who were treated for OIC in study 4000, the investigators noted.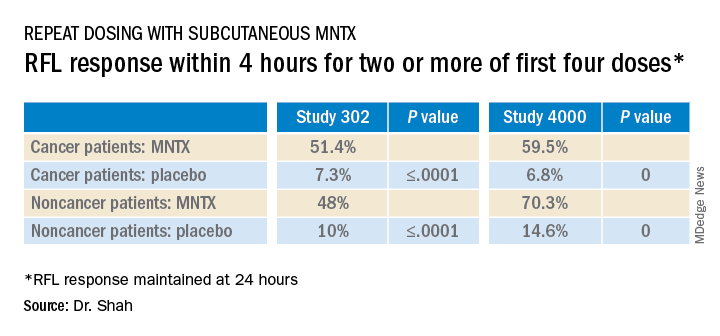
Both studies were sponsored by Salix Pharmaceuticals. Dr. Shah has received travel fees from Salix Pharmaceuticals. Dr. Brenner has served as a consultant for Salix Pharmaceuticals, AstraZeneca, and Purdue Pharma. AstraZeneca developed naloxegol.
This article first appeared on Medscape.com.
Subcutaneously administered methylnaltrexone (MNTX) (Relistor), a peripherally acting mu-opioid receptor antagonist, relieves opioid-induced constipation (OID) in both chronic, noncancer-related illness and cancer-related illness, a new analysis concludes.
“While these are two very different patient groups, the ability to have something to treat OIC in noncancer patients who stay on opioids for whatever reason helps, because [otherwise] these patients are not doing well,” said lead author Eric Shah, MD, motility director for the Dartmouth program at Dartmouth Hitchcock Health, Lebanon, N.H.
Importantly, peripherally acting mu-opioid receptor antagonists such as MNTX do not affect overall pain control to any significant extent, which is “reassuring,” he said in an interview.
These drugs decrease the constipating effects of opioids without reversing CNS-mediated opioid effects, he explained.
“Methylnaltrexone has already been approved for the treatment of OIC in adults with chronic noncancer pain as well as for OIC in adults with advanced illness who are receiving palliative care, which is often the case in patients with cancer-related pain,” he noted.
Dr. Shah discussed the new analysis during PAINWeek 2020, the American Society of Regional Anesthesia and Pain Medicine 19th Annual Pain Medicine Meeting.
The analysis was based on a review of data collected in two previously reported randomized, placebo-controlled studies (study 302 and 4000), which were used to gain approval.
The new analysis shows that “the drug works up front, and the effect is able to be maintained. I think the studies are clinically relevant in that patients are able to have a bowel movement quickly after you give them an injectable formulation when they are vomiting or otherwise can’t tolerate a pill and they are feeling miserable,” Dr. Shah commented. Many patients with OIC are constipated for reasons other than from opioid use. They often have other side effects from opioids, including bloating, nausea, and vomiting.
“When patients go to the emergency room, it’s not just that they are not able to have a bowel movement; they are often also vomiting, so it’s important to have agents that can be given in a manner that avoids the need for oral medication,” Dr. Shah said. MNTX is the only peripherally acting opioid antagonist available in a subcutaneous formulation.
Moreover, if patients are able to control these symptoms at home with an injectable formulation, they may not need to go to the ED for treatment of their gastrointestinal distress, he added.
Viable product
In a comment, Darren Brenner, MD, associate professor of medicine and surgery, Northwestern University, Chicago, who has worked with this subcutaneous formulation, said it is “definitely a viable product.
“The data presented here were in patients with advanced illness receiving palliative care when other laxatives have failed, and the difference and the potential benefit for MNTX is that it is the only peripherally acting mu-opioid receptor antagonist that is approved for advanced cancer,” he added. The other products that are currently approved, naloxegol (Movantik) and naldemedine (Symproic), are both indicated for chronic, noncancer pain.
The other potential benefit of subcutaneous MNTX is that it can work very rapidly for the patients who respond to it. “One of the things investigators did not mention in these two trials but which has been shown in previous studies is that almost half of patients who respond to this drug respond within the first 30 minutes of receiving the injection,” Dr. Brenner said in an interview.
This can be very beneficial in an emergency setting, because it may avoid having patients admitted to hospital. They can be discharged and sent home with enough drug to use on demand, Dr. Brenner suggested.
New analysis of data from studies 302 and 4000
Both studies were carried out in adults with advanced illness and OIC whose conditions were refractory to laxative use. Both of the studies were placebo controlled.
Study 302 involved 78 patients with cancer and 56 patients with noncancer-related OIC. MNTX was given at a dose of 0.15 mg/kg subcutaneously every other day for 2 weeks.
Study 4000 included 152 patients with cancer and OIC and 78 patients with noncancer-related OIC. In this study, the dose of MNTX was based on body weight. Seven or fewer doses of either 8 mg or 12 mg were given subcutaneously for 2 weeks.
The main endpoints of both studies was the proportion of patients who achieved a rescue-free laxation (RFL) response within 4 hours after the first dose and the proportion of patients with an RFL response within 4 hours for two or more of the first four doses within 24 hours.
Dr. Shah explained that RFL is a meaningful clinical endpoint. Patients could achieve a bowel movement with the two prespecified time endpoints in both studies.
Not all patients were hospitalized for OIC, Dr. Shah noted. Entry criteria were strict and included having fewer than three bowel movements during the previous week and no clinically significant laxation (defecation) within 48 hours of receiving the first dose of study drug.
“In both studies, a significantly greater proportion of patients treated with MNTX versus placebo achieved an RFL within 4 hours after the first dose among both cancer and noncancer patients,” the investigators reported.
Results were relatively comparable between cancer and noncancer patients who were treated for OIC in study 4000, the investigators noted.
Both studies were sponsored by Salix Pharmaceuticals. Dr. Shah has received travel fees from Salix Pharmaceuticals. Dr. Brenner has served as a consultant for Salix Pharmaceuticals, AstraZeneca, and Purdue Pharma. AstraZeneca developed naloxegol.
This article first appeared on Medscape.com.
Subcutaneously administered methylnaltrexone (MNTX) (Relistor), a peripherally acting mu-opioid receptor antagonist, relieves opioid-induced constipation (OID) in both chronic, noncancer-related illness and cancer-related illness, a new analysis concludes.
“While these are two very different patient groups, the ability to have something to treat OIC in noncancer patients who stay on opioids for whatever reason helps, because [otherwise] these patients are not doing well,” said lead author Eric Shah, MD, motility director for the Dartmouth program at Dartmouth Hitchcock Health, Lebanon, N.H.
Importantly, peripherally acting mu-opioid receptor antagonists such as MNTX do not affect overall pain control to any significant extent, which is “reassuring,” he said in an interview.
These drugs decrease the constipating effects of opioids without reversing CNS-mediated opioid effects, he explained.
“Methylnaltrexone has already been approved for the treatment of OIC in adults with chronic noncancer pain as well as for OIC in adults with advanced illness who are receiving palliative care, which is often the case in patients with cancer-related pain,” he noted.
Dr. Shah discussed the new analysis during PAINWeek 2020, the American Society of Regional Anesthesia and Pain Medicine 19th Annual Pain Medicine Meeting.
The analysis was based on a review of data collected in two previously reported randomized, placebo-controlled studies (study 302 and 4000), which were used to gain approval.
The new analysis shows that “the drug works up front, and the effect is able to be maintained. I think the studies are clinically relevant in that patients are able to have a bowel movement quickly after you give them an injectable formulation when they are vomiting or otherwise can’t tolerate a pill and they are feeling miserable,” Dr. Shah commented. Many patients with OIC are constipated for reasons other than from opioid use. They often have other side effects from opioids, including bloating, nausea, and vomiting.
“When patients go to the emergency room, it’s not just that they are not able to have a bowel movement; they are often also vomiting, so it’s important to have agents that can be given in a manner that avoids the need for oral medication,” Dr. Shah said. MNTX is the only peripherally acting opioid antagonist available in a subcutaneous formulation.
Moreover, if patients are able to control these symptoms at home with an injectable formulation, they may not need to go to the ED for treatment of their gastrointestinal distress, he added.
Viable product
In a comment, Darren Brenner, MD, associate professor of medicine and surgery, Northwestern University, Chicago, who has worked with this subcutaneous formulation, said it is “definitely a viable product.
“The data presented here were in patients with advanced illness receiving palliative care when other laxatives have failed, and the difference and the potential benefit for MNTX is that it is the only peripherally acting mu-opioid receptor antagonist that is approved for advanced cancer,” he added. The other products that are currently approved, naloxegol (Movantik) and naldemedine (Symproic), are both indicated for chronic, noncancer pain.
The other potential benefit of subcutaneous MNTX is that it can work very rapidly for the patients who respond to it. “One of the things investigators did not mention in these two trials but which has been shown in previous studies is that almost half of patients who respond to this drug respond within the first 30 minutes of receiving the injection,” Dr. Brenner said in an interview.
This can be very beneficial in an emergency setting, because it may avoid having patients admitted to hospital. They can be discharged and sent home with enough drug to use on demand, Dr. Brenner suggested.
New analysis of data from studies 302 and 4000
Both studies were carried out in adults with advanced illness and OIC whose conditions were refractory to laxative use. Both of the studies were placebo controlled.
Study 302 involved 78 patients with cancer and 56 patients with noncancer-related OIC. MNTX was given at a dose of 0.15 mg/kg subcutaneously every other day for 2 weeks.
Study 4000 included 152 patients with cancer and OIC and 78 patients with noncancer-related OIC. In this study, the dose of MNTX was based on body weight. Seven or fewer doses of either 8 mg or 12 mg were given subcutaneously for 2 weeks.
The main endpoints of both studies was the proportion of patients who achieved a rescue-free laxation (RFL) response within 4 hours after the first dose and the proportion of patients with an RFL response within 4 hours for two or more of the first four doses within 24 hours.
Dr. Shah explained that RFL is a meaningful clinical endpoint. Patients could achieve a bowel movement with the two prespecified time endpoints in both studies.
Not all patients were hospitalized for OIC, Dr. Shah noted. Entry criteria were strict and included having fewer than three bowel movements during the previous week and no clinically significant laxation (defecation) within 48 hours of receiving the first dose of study drug.
“In both studies, a significantly greater proportion of patients treated with MNTX versus placebo achieved an RFL within 4 hours after the first dose among both cancer and noncancer patients,” the investigators reported.
Results were relatively comparable between cancer and noncancer patients who were treated for OIC in study 4000, the investigators noted.
Both studies were sponsored by Salix Pharmaceuticals. Dr. Shah has received travel fees from Salix Pharmaceuticals. Dr. Brenner has served as a consultant for Salix Pharmaceuticals, AstraZeneca, and Purdue Pharma. AstraZeneca developed naloxegol.
This article first appeared on Medscape.com.
Role of lasers and light sources in medicine continue to expand
suggests R. Rox Anderson, MD.

“I’ve been doing this in my practice for a number of years and it’s quite gratifying,” Dr. Anderson, a dermatologist who directs the Wellman Center for Photomedicine at Massachusetts General Hospital, Boston, said during a virtual course on laser and aesthetic skin therapy. “You treat the periorbital skin, mostly under the eye, just as if you were treating telangiectasia rosacea. The meibomian glands under the upper eyelid that cause this disease are sebaceous glands, and most of the people with dry eye have rosacea.”
In a retrospective noncomparative, interventional case series, 78 patients with severe dry eye syndrome were treated with intense pulsed-light therapy and gland expression at a single outpatient clinic over 30 months. Physician-judged improvement in dry eye tear breakup time was found for 87% of patients with an average of seven treatment visits and four maintenance visits, while 93% of patients reported posttreatment satisfaction with the degree of dry eye syndrome symptoms. More information about the approach were published in Investigative Ophthalmology & Visual Science and Current Opinion in Ophthalmology.
“What’s gratifying here is that most patients will get about 2 months of relief after a single treatment,” Dr. Anderson said. “They are very happy – some of the happiest patients in my practice. Many ophthalmologists don’t have the technology, so I think you can do this depending on your local referral system.”
Light-based approaches are also making promising inroads in cancer treatment. A recent study led by Martin Purschke, PhD, at the Wellman Center evaluated the use of a novel radio-phototherapy approach for killing cancer cells. The center of solid tissue tumors that are treated with radiotherapy is hypoxic, Dr. Anderson explained, “and oxygen is typically located around the perimeter of the tumor. After a radiation therapy treatment, you kill only the outer portion of it, and then the remaining cells grow back, and you end up with the same tumor. This is why you have to do radiation therapy over and over again. In contrast, if you add scintillating nanoparticles, which are particles with a very high C number atoms in them that pick up the x-ray photon and then emit many UV photons from one x-ray photon, they are very efficient at converting x-ray energy to UV energy.” The x-ray, he added, “generates UV light, and the UV light kills the tumor. We’re hoping that we can make a dent in radiotherapy this way.”
Dr. Anderson predicted that fiber lasers, which are highly advanced for industrial applications, will play an increasing role in dermatology and in other areas of medicine. “There are not a new kid on the block anymore but fiber lasers are relatively new to medicine,” he said during the meeting, which was sponsored by Harvard Medical School, Massachusetts General Hospital, and the Wellman Center for Photomedicine. “We are seeing incredible capabilities with fiber lasers: essentially any wavelength, any power, any pulse duration you want. The lasers are efficient, small, rugged, and their lifetime exceeds your lifetime. They are likely to displace many of our old lasers in dermatology. I don’t know when, but I know it will happen.”
He reported having received research funding and/or consulting fees from numerous device and pharmaceutical companies.
suggests R. Rox Anderson, MD.
“I’ve been doing this in my practice for a number of years and it’s quite gratifying,” Dr. Anderson, a dermatologist who directs the Wellman Center for Photomedicine at Massachusetts General Hospital, Boston, said during a virtual course on laser and aesthetic skin therapy. “You treat the periorbital skin, mostly under the eye, just as if you were treating telangiectasia rosacea. The meibomian glands under the upper eyelid that cause this disease are sebaceous glands, and most of the people with dry eye have rosacea.”
In a retrospective noncomparative, interventional case series, 78 patients with severe dry eye syndrome were treated with intense pulsed-light therapy and gland expression at a single outpatient clinic over 30 months. Physician-judged improvement in dry eye tear breakup time was found for 87% of patients with an average of seven treatment visits and four maintenance visits, while 93% of patients reported posttreatment satisfaction with the degree of dry eye syndrome symptoms. More information about the approach were published in Investigative Ophthalmology & Visual Science and Current Opinion in Ophthalmology.
“What’s gratifying here is that most patients will get about 2 months of relief after a single treatment,” Dr. Anderson said. “They are very happy – some of the happiest patients in my practice. Many ophthalmologists don’t have the technology, so I think you can do this depending on your local referral system.”
Light-based approaches are also making promising inroads in cancer treatment. A recent study led by Martin Purschke, PhD, at the Wellman Center evaluated the use of a novel radio-phototherapy approach for killing cancer cells. The center of solid tissue tumors that are treated with radiotherapy is hypoxic, Dr. Anderson explained, “and oxygen is typically located around the perimeter of the tumor. After a radiation therapy treatment, you kill only the outer portion of it, and then the remaining cells grow back, and you end up with the same tumor. This is why you have to do radiation therapy over and over again. In contrast, if you add scintillating nanoparticles, which are particles with a very high C number atoms in them that pick up the x-ray photon and then emit many UV photons from one x-ray photon, they are very efficient at converting x-ray energy to UV energy.” The x-ray, he added, “generates UV light, and the UV light kills the tumor. We’re hoping that we can make a dent in radiotherapy this way.”
Dr. Anderson predicted that fiber lasers, which are highly advanced for industrial applications, will play an increasing role in dermatology and in other areas of medicine. “There are not a new kid on the block anymore but fiber lasers are relatively new to medicine,” he said during the meeting, which was sponsored by Harvard Medical School, Massachusetts General Hospital, and the Wellman Center for Photomedicine. “We are seeing incredible capabilities with fiber lasers: essentially any wavelength, any power, any pulse duration you want. The lasers are efficient, small, rugged, and their lifetime exceeds your lifetime. They are likely to displace many of our old lasers in dermatology. I don’t know when, but I know it will happen.”
He reported having received research funding and/or consulting fees from numerous device and pharmaceutical companies.
suggests R. Rox Anderson, MD.
“I’ve been doing this in my practice for a number of years and it’s quite gratifying,” Dr. Anderson, a dermatologist who directs the Wellman Center for Photomedicine at Massachusetts General Hospital, Boston, said during a virtual course on laser and aesthetic skin therapy. “You treat the periorbital skin, mostly under the eye, just as if you were treating telangiectasia rosacea. The meibomian glands under the upper eyelid that cause this disease are sebaceous glands, and most of the people with dry eye have rosacea.”
In a retrospective noncomparative, interventional case series, 78 patients with severe dry eye syndrome were treated with intense pulsed-light therapy and gland expression at a single outpatient clinic over 30 months. Physician-judged improvement in dry eye tear breakup time was found for 87% of patients with an average of seven treatment visits and four maintenance visits, while 93% of patients reported posttreatment satisfaction with the degree of dry eye syndrome symptoms. More information about the approach were published in Investigative Ophthalmology & Visual Science and Current Opinion in Ophthalmology.
“What’s gratifying here is that most patients will get about 2 months of relief after a single treatment,” Dr. Anderson said. “They are very happy – some of the happiest patients in my practice. Many ophthalmologists don’t have the technology, so I think you can do this depending on your local referral system.”
Light-based approaches are also making promising inroads in cancer treatment. A recent study led by Martin Purschke, PhD, at the Wellman Center evaluated the use of a novel radio-phototherapy approach for killing cancer cells. The center of solid tissue tumors that are treated with radiotherapy is hypoxic, Dr. Anderson explained, “and oxygen is typically located around the perimeter of the tumor. After a radiation therapy treatment, you kill only the outer portion of it, and then the remaining cells grow back, and you end up with the same tumor. This is why you have to do radiation therapy over and over again. In contrast, if you add scintillating nanoparticles, which are particles with a very high C number atoms in them that pick up the x-ray photon and then emit many UV photons from one x-ray photon, they are very efficient at converting x-ray energy to UV energy.” The x-ray, he added, “generates UV light, and the UV light kills the tumor. We’re hoping that we can make a dent in radiotherapy this way.”
Dr. Anderson predicted that fiber lasers, which are highly advanced for industrial applications, will play an increasing role in dermatology and in other areas of medicine. “There are not a new kid on the block anymore but fiber lasers are relatively new to medicine,” he said during the meeting, which was sponsored by Harvard Medical School, Massachusetts General Hospital, and the Wellman Center for Photomedicine. “We are seeing incredible capabilities with fiber lasers: essentially any wavelength, any power, any pulse duration you want. The lasers are efficient, small, rugged, and their lifetime exceeds your lifetime. They are likely to displace many of our old lasers in dermatology. I don’t know when, but I know it will happen.”
He reported having received research funding and/or consulting fees from numerous device and pharmaceutical companies.
FROM A LASER & AESTHETIC SKIN THERAPY COURSE
Chronic daily migraine from medication overuse: How worried should you be?
. Physicians worry about episodic migraine converting to chronic daily headache, but this worry can also lead to under-treatment and even stigmatization of patients who aggressively treat their symptoms.
These concerns and others were a topic of a debate at the Headache Cooperative of New England’s 20th Annual HCNE Boston Fall Headache Symposium, which was conducted virtually.
The International Classification of Headache-3 (ICHD-3) defines medication overuse headache as a headache that occurs on 15 or more days per month in a patient with pre-existing primary headache, and that develops because of regular overuse of acute or symptomatic headache medication. The ICHD-3 also says that headache usually resolves when overuse is stopped, though not always.
Paul Rizzoli, MD, took issue with that definition. “If you have a lot of headaches and you take medication for them, then you likely have medication overuse headache. They say the most common cause of symptoms suggestive of chronic migraine is medication overuse. That’s like saying, if you have a rash on your arm, then it is an allergic sun exposure rash. No need to characterize the rash,” said Dr. Rizzoli, who is clinical director of the John R. Graham Headache Center at Brigham and Women’s Faulkner Hospital in Boston, during the session.
Is medication overuse really the culprit?

Dr. Rizzoli began by emphasizing that taking a lot of medication is always a concern. “Significant hepatic and renal and GI toxicities can result from taking and overusing medication of all sorts. What (I am) questioning is whether or not this rather strange, arbitrary, fluidly-defined concept of abortive migraine medicine overuse is truly responsible for causing all of the ills of which it is accused – and just as importantly, if the proposed solution for it, which is to just stop the overused medication and all will be better – if that solution is the right or wrong advice to give to a patient,” he said.
Much of Dr. Rizzoli’s criticism rested on the definition of medication overuse syndrome. He believes that many concerns about medication overuse can be traced to the use of opiates or barbiturate-containing medications, which have known propensities to lead to headaches. Other cases are less well defined, and “it’s not quite clear what the pathophysiology of the condition is – whether or not it’s the same as rebound or withdrawal headache, or if it is the same as a pronociceptive effect of analgesics, also called medicine-induced headache. Both are well documented and accepted, and the idea of opioid-induced analgesia tolerance is well documented and has several plausible mechanisms attributed to it,” said Dr. Rizzoli.
He said that changes in structural imaging in the brain suggest there at least two subgroups of patients that are both labeled as having medication overuse headache, one from medication overuse and one from progression of migraine disease. “Based on physiology, medication overuse headache cannot be clearly seen as a unitary condition,” he said.
Dr. Rizzoli cited other research on triptans, opioids, and barbiturates that showed an overall conversion from episodic migraine to chronic migraine, with the lowest frequency occurring in patients taking acetaminophen, aspirin, and caffeine (2%), followed by NSAIDs (4%), triptans (4%), opioids (5%), and barbiturates (6%). A total of 52 patients who became chronic were taking triptans, on average 7 days per month. The 1,370 triptan-using patients who remained episodic took triptans on average 5 days per month. “Does this seem like a huge difference between these two groups? The transformation rate in just this triptan subgroup was about 3%-4%, suggesting that, compared with the overall transformation rate of 3%, use of triptans did not exert much force overall on the baseline rate,” he said. Similar patterns were visible with use of other classes of drugs.
Meanwhile, the higher rates of conversion seen with opioids and barbiturates suggests an effect from these drugs. “Perhaps this data suggests the previously known effect is at play here and argues against the need for a separate diagnosis of medication overuse headache,” Dr. Rizzoli said.
“The evidence that simple analgesics can cause medication overuse headache is especially weak, and the evidence that NSAIDs do is conflicting, with some evidence suggesting they’re protective at some doses.” Other population studies suggested most patients with daily headache do not overuse medications, and studies in India, where analgesics are rarely used, still showed a similar rate of conversion to daily headache. Other studies failed to show evidence that withdrawal of overused medication leads to improvement. “Studies of populations after aggressive management of medicine overuse headache indicate that, for the majority of the headaches, for the most part did not clear after treatment, except maybe for a short time,” said Dr. Rizzoli.
A systematic review of 18 population studies showed the prevalence of medical overuse headache ranged from 11% to 68%. “That indicates substantial uncertainty about the magnitude of the problem,” said Dr. Rizzoli.
He also noted potential harms to patients. Many patients come in experience between 10 and 20 headaches per month. “To see them out of medical overuse would have us advising not to treat half of their headaches monthly in order to avoid this evil. Many patients who have read or heard about this condition are themselves restricting treatment so as to avoid medication overuse headache. The harms of such undertreatment have not been fully investigated.”
To get at the issue, he recommended adapting the traditional number-needed-to-treat calculation. “You could calculate a number needed to overtreat. If medication use is assumed to be the sole cause of headache chronification, the calculations could suggest you would need to restrict therapy for about 4 people for each person you protect from going chronic. That’s a lot of undertreatment,” said Dr. Rizzoli.
He summed up by saying that some patients may have a progressive disorder with structure and physiological changes in the brain that result in chronic pain, and such patients should be identified and studied. In others with frequent headache, high medication use may simply be associated with the condition becoming chronic, but not causative. “These diagnostic groups may be mixed and may be difficult to untangle,” said Dr. Rizzoli.
Medication overuse is to blame

Dr. Rizzoli’s debate lecture was followed by Barbara Nye, MD, who argued that concerns over medication overuse headache are valid. She noted a more unifying definition in ICHD-3, which requires regular medication overuse for at least 3 months, along with primary headache disorder.
Dr. Nye, who is codirector of the Headache Clinic at Dartmouth-Hitchcock Medical Center in Lebanon, N.H., related her experience that medication overuse headache often occurs more quickly than the 3-month time frame contained in ICHD-3, especially in patients who were given pain medications after undergoing surgery. She echoed Dr. Rizzoli’s concerns about opiates and barbiturates. “Medicine overuse headache should be something we focus on, and we should be warning providers both in neurology and primary care about the frequent use of opiate and butalbital-containing medications, and frequent over-the-counter medicine use in high-frequency headache disorders,” Dr. Nye said during her talk.
She cited research showing risk factors for conversion from episodic to chronic daily headache. As well as medication overuse, these include White race, lower education status, previous marriage, obesity, diabetes, arthritis, top-quartile caffeine use, stressful life events, and higher headache frequency.
Risks vary by medication class. Opiates and narcotics used more than 2 or 3 times per week are of particular concern, as are short-acting over-the-counter medicines used more than three times per week or 10-15 days per month. She agreed that NSAIDs may have a protective effect, but only at much lower doses and when used about five (or fewer) times per month. One study showed a possible protection effect of NSAIDs, though when used more than 10 days/month, they were associated with medication overuse headache.
Fioricet and Fiorinal, used more than 1 day/week, have an early and robust medicine overuse effect. “Limiting that use is very important,” said Dr. Nye. Other medicines and doses of concern include Tramadol/Ultram used at a higher than 50 mg/day dose, which has a metabolite that causes headache, and triptans used more than 10 days/month.
These concerns came about after analysis of large trials in patients with other conditions who also suffer from episodic migraines. A study of patients with irritable bowel syndrome and migraine showed a risk of conversion with opioid treatment. Another study of patients with arthritis and episodic migraine showed an association between conversion and NSAIDs alone, NSAIDs combined with Tylenol, and NSAIDs combined with opioids.
Risks of medication overuse also included collateral damage to the gastrointestinal and kidney systems, development of dependence, exacerbation of depression, and opioid-induced hyperalgesia, according to Dr. Nye. The overused medication may also interfere with the use of preventive medication. Those concerns drive the conventional wisdom of weaning patients off the overused medication, Dr. Nye said.
Dr. Nye discussed some of the observations of structural changes in the brain found in episodic migraine and chronic migraine associated with medication overuse. Functional MRI showed changes in grey matter, both as a result of medication overuse headache and further changes after medication withdrawal. “A lot of neuroplasticity and neuroadaptation occurs, and these effects seem to be sustained anywhere from 4-6 months after (medicine) discontinuation,” said Dr. Nye.
Common ground
Dr. Nye emphasized the need to be aware of the dangers of medication overuse headache, but noted that clinicians should address the problem to ensure that patients are empowered, potentially providing preventive medications and encouraging more effective use of daily abortive medications.
In response, Dr. Rizzoli suggested that the two agreed on many issues. For her part, Dr. Nye agreed that medication overuse headache is a muddy concept that needs more research to understand the relationship between opiate use and chronic migraine, “but I do think there have been some good studies of fMRI evaluating the difference between those with medication overuse headache and seeing how they convert back to a different underlying network (following medication withdrawal). I do agree that there is probably a subpopulation that is not affected by medication overuse headache,” Dr. Nye said.
In the end, both expressed concerns for the patient. “I share Barbara’s concern that we need to be mindful and protect our patients from medication use, but on the other hand I think we also need to protect our patients from the complications of having a diagnosis of medical overuse and the stigmatization that goes with that. That particular issue goes both ways,” said Dr. Rizzoli.
“I absolutely agree with that,” responded Dr. Nye.
Dr. Nye is on the advisory boards for Biohaven, Upsher Smith, and Impel. She is a trial site principal investigator for Allergan, Amgen, and Satsuma. Dr. Rizzoli has been a consultant for Nestle and served on the scientific advisory or data safety monitoring board for Biohaven and Xoc Pharma. He has also received research support from Allergan.
. Physicians worry about episodic migraine converting to chronic daily headache, but this worry can also lead to under-treatment and even stigmatization of patients who aggressively treat their symptoms.
These concerns and others were a topic of a debate at the Headache Cooperative of New England’s 20th Annual HCNE Boston Fall Headache Symposium, which was conducted virtually.
The International Classification of Headache-3 (ICHD-3) defines medication overuse headache as a headache that occurs on 15 or more days per month in a patient with pre-existing primary headache, and that develops because of regular overuse of acute or symptomatic headache medication. The ICHD-3 also says that headache usually resolves when overuse is stopped, though not always.
Paul Rizzoli, MD, took issue with that definition. “If you have a lot of headaches and you take medication for them, then you likely have medication overuse headache. They say the most common cause of symptoms suggestive of chronic migraine is medication overuse. That’s like saying, if you have a rash on your arm, then it is an allergic sun exposure rash. No need to characterize the rash,” said Dr. Rizzoli, who is clinical director of the John R. Graham Headache Center at Brigham and Women’s Faulkner Hospital in Boston, during the session.
Is medication overuse really the culprit?
Dr. Rizzoli began by emphasizing that taking a lot of medication is always a concern. “Significant hepatic and renal and GI toxicities can result from taking and overusing medication of all sorts. What (I am) questioning is whether or not this rather strange, arbitrary, fluidly-defined concept of abortive migraine medicine overuse is truly responsible for causing all of the ills of which it is accused – and just as importantly, if the proposed solution for it, which is to just stop the overused medication and all will be better – if that solution is the right or wrong advice to give to a patient,” he said.
Much of Dr. Rizzoli’s criticism rested on the definition of medication overuse syndrome. He believes that many concerns about medication overuse can be traced to the use of opiates or barbiturate-containing medications, which have known propensities to lead to headaches. Other cases are less well defined, and “it’s not quite clear what the pathophysiology of the condition is – whether or not it’s the same as rebound or withdrawal headache, or if it is the same as a pronociceptive effect of analgesics, also called medicine-induced headache. Both are well documented and accepted, and the idea of opioid-induced analgesia tolerance is well documented and has several plausible mechanisms attributed to it,” said Dr. Rizzoli.
He said that changes in structural imaging in the brain suggest there at least two subgroups of patients that are both labeled as having medication overuse headache, one from medication overuse and one from progression of migraine disease. “Based on physiology, medication overuse headache cannot be clearly seen as a unitary condition,” he said.
Dr. Rizzoli cited other research on triptans, opioids, and barbiturates that showed an overall conversion from episodic migraine to chronic migraine, with the lowest frequency occurring in patients taking acetaminophen, aspirin, and caffeine (2%), followed by NSAIDs (4%), triptans (4%), opioids (5%), and barbiturates (6%). A total of 52 patients who became chronic were taking triptans, on average 7 days per month. The 1,370 triptan-using patients who remained episodic took triptans on average 5 days per month. “Does this seem like a huge difference between these two groups? The transformation rate in just this triptan subgroup was about 3%-4%, suggesting that, compared with the overall transformation rate of 3%, use of triptans did not exert much force overall on the baseline rate,” he said. Similar patterns were visible with use of other classes of drugs.
Meanwhile, the higher rates of conversion seen with opioids and barbiturates suggests an effect from these drugs. “Perhaps this data suggests the previously known effect is at play here and argues against the need for a separate diagnosis of medication overuse headache,” Dr. Rizzoli said.
“The evidence that simple analgesics can cause medication overuse headache is especially weak, and the evidence that NSAIDs do is conflicting, with some evidence suggesting they’re protective at some doses.” Other population studies suggested most patients with daily headache do not overuse medications, and studies in India, where analgesics are rarely used, still showed a similar rate of conversion to daily headache. Other studies failed to show evidence that withdrawal of overused medication leads to improvement. “Studies of populations after aggressive management of medicine overuse headache indicate that, for the majority of the headaches, for the most part did not clear after treatment, except maybe for a short time,” said Dr. Rizzoli.
A systematic review of 18 population studies showed the prevalence of medical overuse headache ranged from 11% to 68%. “That indicates substantial uncertainty about the magnitude of the problem,” said Dr. Rizzoli.
He also noted potential harms to patients. Many patients come in experience between 10 and 20 headaches per month. “To see them out of medical overuse would have us advising not to treat half of their headaches monthly in order to avoid this evil. Many patients who have read or heard about this condition are themselves restricting treatment so as to avoid medication overuse headache. The harms of such undertreatment have not been fully investigated.”
To get at the issue, he recommended adapting the traditional number-needed-to-treat calculation. “You could calculate a number needed to overtreat. If medication use is assumed to be the sole cause of headache chronification, the calculations could suggest you would need to restrict therapy for about 4 people for each person you protect from going chronic. That’s a lot of undertreatment,” said Dr. Rizzoli.
He summed up by saying that some patients may have a progressive disorder with structure and physiological changes in the brain that result in chronic pain, and such patients should be identified and studied. In others with frequent headache, high medication use may simply be associated with the condition becoming chronic, but not causative. “These diagnostic groups may be mixed and may be difficult to untangle,” said Dr. Rizzoli.
Medication overuse is to blame
Dr. Rizzoli’s debate lecture was followed by Barbara Nye, MD, who argued that concerns over medication overuse headache are valid. She noted a more unifying definition in ICHD-3, which requires regular medication overuse for at least 3 months, along with primary headache disorder.
Dr. Nye, who is codirector of the Headache Clinic at Dartmouth-Hitchcock Medical Center in Lebanon, N.H., related her experience that medication overuse headache often occurs more quickly than the 3-month time frame contained in ICHD-3, especially in patients who were given pain medications after undergoing surgery. She echoed Dr. Rizzoli’s concerns about opiates and barbiturates. “Medicine overuse headache should be something we focus on, and we should be warning providers both in neurology and primary care about the frequent use of opiate and butalbital-containing medications, and frequent over-the-counter medicine use in high-frequency headache disorders,” Dr. Nye said during her talk.
She cited research showing risk factors for conversion from episodic to chronic daily headache. As well as medication overuse, these include White race, lower education status, previous marriage, obesity, diabetes, arthritis, top-quartile caffeine use, stressful life events, and higher headache frequency.
Risks vary by medication class. Opiates and narcotics used more than 2 or 3 times per week are of particular concern, as are short-acting over-the-counter medicines used more than three times per week or 10-15 days per month. She agreed that NSAIDs may have a protective effect, but only at much lower doses and when used about five (or fewer) times per month. One study showed a possible protection effect of NSAIDs, though when used more than 10 days/month, they were associated with medication overuse headache.
Fioricet and Fiorinal, used more than 1 day/week, have an early and robust medicine overuse effect. “Limiting that use is very important,” said Dr. Nye. Other medicines and doses of concern include Tramadol/Ultram used at a higher than 50 mg/day dose, which has a metabolite that causes headache, and triptans used more than 10 days/month.
These concerns came about after analysis of large trials in patients with other conditions who also suffer from episodic migraines. A study of patients with irritable bowel syndrome and migraine showed a risk of conversion with opioid treatment. Another study of patients with arthritis and episodic migraine showed an association between conversion and NSAIDs alone, NSAIDs combined with Tylenol, and NSAIDs combined with opioids.
Risks of medication overuse also included collateral damage to the gastrointestinal and kidney systems, development of dependence, exacerbation of depression, and opioid-induced hyperalgesia, according to Dr. Nye. The overused medication may also interfere with the use of preventive medication. Those concerns drive the conventional wisdom of weaning patients off the overused medication, Dr. Nye said.
Dr. Nye discussed some of the observations of structural changes in the brain found in episodic migraine and chronic migraine associated with medication overuse. Functional MRI showed changes in grey matter, both as a result of medication overuse headache and further changes after medication withdrawal. “A lot of neuroplasticity and neuroadaptation occurs, and these effects seem to be sustained anywhere from 4-6 months after (medicine) discontinuation,” said Dr. Nye.
Common ground
Dr. Nye emphasized the need to be aware of the dangers of medication overuse headache, but noted that clinicians should address the problem to ensure that patients are empowered, potentially providing preventive medications and encouraging more effective use of daily abortive medications.
In response, Dr. Rizzoli suggested that the two agreed on many issues. For her part, Dr. Nye agreed that medication overuse headache is a muddy concept that needs more research to understand the relationship between opiate use and chronic migraine, “but I do think there have been some good studies of fMRI evaluating the difference between those with medication overuse headache and seeing how they convert back to a different underlying network (following medication withdrawal). I do agree that there is probably a subpopulation that is not affected by medication overuse headache,” Dr. Nye said.
In the end, both expressed concerns for the patient. “I share Barbara’s concern that we need to be mindful and protect our patients from medication use, but on the other hand I think we also need to protect our patients from the complications of having a diagnosis of medical overuse and the stigmatization that goes with that. That particular issue goes both ways,” said Dr. Rizzoli.
“I absolutely agree with that,” responded Dr. Nye.
Dr. Nye is on the advisory boards for Biohaven, Upsher Smith, and Impel. She is a trial site principal investigator for Allergan, Amgen, and Satsuma. Dr. Rizzoli has been a consultant for Nestle and served on the scientific advisory or data safety monitoring board for Biohaven and Xoc Pharma. He has also received research support from Allergan.
. Physicians worry about episodic migraine converting to chronic daily headache, but this worry can also lead to under-treatment and even stigmatization of patients who aggressively treat their symptoms.
These concerns and others were a topic of a debate at the Headache Cooperative of New England’s 20th Annual HCNE Boston Fall Headache Symposium, which was conducted virtually.
The International Classification of Headache-3 (ICHD-3) defines medication overuse headache as a headache that occurs on 15 or more days per month in a patient with pre-existing primary headache, and that develops because of regular overuse of acute or symptomatic headache medication. The ICHD-3 also says that headache usually resolves when overuse is stopped, though not always.
Paul Rizzoli, MD, took issue with that definition. “If you have a lot of headaches and you take medication for them, then you likely have medication overuse headache. They say the most common cause of symptoms suggestive of chronic migraine is medication overuse. That’s like saying, if you have a rash on your arm, then it is an allergic sun exposure rash. No need to characterize the rash,” said Dr. Rizzoli, who is clinical director of the John R. Graham Headache Center at Brigham and Women’s Faulkner Hospital in Boston, during the session.
Is medication overuse really the culprit?
Dr. Rizzoli began by emphasizing that taking a lot of medication is always a concern. “Significant hepatic and renal and GI toxicities can result from taking and overusing medication of all sorts. What (I am) questioning is whether or not this rather strange, arbitrary, fluidly-defined concept of abortive migraine medicine overuse is truly responsible for causing all of the ills of which it is accused – and just as importantly, if the proposed solution for it, which is to just stop the overused medication and all will be better – if that solution is the right or wrong advice to give to a patient,” he said.
Much of Dr. Rizzoli’s criticism rested on the definition of medication overuse syndrome. He believes that many concerns about medication overuse can be traced to the use of opiates or barbiturate-containing medications, which have known propensities to lead to headaches. Other cases are less well defined, and “it’s not quite clear what the pathophysiology of the condition is – whether or not it’s the same as rebound or withdrawal headache, or if it is the same as a pronociceptive effect of analgesics, also called medicine-induced headache. Both are well documented and accepted, and the idea of opioid-induced analgesia tolerance is well documented and has several plausible mechanisms attributed to it,” said Dr. Rizzoli.
He said that changes in structural imaging in the brain suggest there at least two subgroups of patients that are both labeled as having medication overuse headache, one from medication overuse and one from progression of migraine disease. “Based on physiology, medication overuse headache cannot be clearly seen as a unitary condition,” he said.
Dr. Rizzoli cited other research on triptans, opioids, and barbiturates that showed an overall conversion from episodic migraine to chronic migraine, with the lowest frequency occurring in patients taking acetaminophen, aspirin, and caffeine (2%), followed by NSAIDs (4%), triptans (4%), opioids (5%), and barbiturates (6%). A total of 52 patients who became chronic were taking triptans, on average 7 days per month. The 1,370 triptan-using patients who remained episodic took triptans on average 5 days per month. “Does this seem like a huge difference between these two groups? The transformation rate in just this triptan subgroup was about 3%-4%, suggesting that, compared with the overall transformation rate of 3%, use of triptans did not exert much force overall on the baseline rate,” he said. Similar patterns were visible with use of other classes of drugs.
Meanwhile, the higher rates of conversion seen with opioids and barbiturates suggests an effect from these drugs. “Perhaps this data suggests the previously known effect is at play here and argues against the need for a separate diagnosis of medication overuse headache,” Dr. Rizzoli said.
“The evidence that simple analgesics can cause medication overuse headache is especially weak, and the evidence that NSAIDs do is conflicting, with some evidence suggesting they’re protective at some doses.” Other population studies suggested most patients with daily headache do not overuse medications, and studies in India, where analgesics are rarely used, still showed a similar rate of conversion to daily headache. Other studies failed to show evidence that withdrawal of overused medication leads to improvement. “Studies of populations after aggressive management of medicine overuse headache indicate that, for the majority of the headaches, for the most part did not clear after treatment, except maybe for a short time,” said Dr. Rizzoli.
A systematic review of 18 population studies showed the prevalence of medical overuse headache ranged from 11% to 68%. “That indicates substantial uncertainty about the magnitude of the problem,” said Dr. Rizzoli.
He also noted potential harms to patients. Many patients come in experience between 10 and 20 headaches per month. “To see them out of medical overuse would have us advising not to treat half of their headaches monthly in order to avoid this evil. Many patients who have read or heard about this condition are themselves restricting treatment so as to avoid medication overuse headache. The harms of such undertreatment have not been fully investigated.”
To get at the issue, he recommended adapting the traditional number-needed-to-treat calculation. “You could calculate a number needed to overtreat. If medication use is assumed to be the sole cause of headache chronification, the calculations could suggest you would need to restrict therapy for about 4 people for each person you protect from going chronic. That’s a lot of undertreatment,” said Dr. Rizzoli.
He summed up by saying that some patients may have a progressive disorder with structure and physiological changes in the brain that result in chronic pain, and such patients should be identified and studied. In others with frequent headache, high medication use may simply be associated with the condition becoming chronic, but not causative. “These diagnostic groups may be mixed and may be difficult to untangle,” said Dr. Rizzoli.
Medication overuse is to blame
Dr. Rizzoli’s debate lecture was followed by Barbara Nye, MD, who argued that concerns over medication overuse headache are valid. She noted a more unifying definition in ICHD-3, which requires regular medication overuse for at least 3 months, along with primary headache disorder.
Dr. Nye, who is codirector of the Headache Clinic at Dartmouth-Hitchcock Medical Center in Lebanon, N.H., related her experience that medication overuse headache often occurs more quickly than the 3-month time frame contained in ICHD-3, especially in patients who were given pain medications after undergoing surgery. She echoed Dr. Rizzoli’s concerns about opiates and barbiturates. “Medicine overuse headache should be something we focus on, and we should be warning providers both in neurology and primary care about the frequent use of opiate and butalbital-containing medications, and frequent over-the-counter medicine use in high-frequency headache disorders,” Dr. Nye said during her talk.
She cited research showing risk factors for conversion from episodic to chronic daily headache. As well as medication overuse, these include White race, lower education status, previous marriage, obesity, diabetes, arthritis, top-quartile caffeine use, stressful life events, and higher headache frequency.
Risks vary by medication class. Opiates and narcotics used more than 2 or 3 times per week are of particular concern, as are short-acting over-the-counter medicines used more than three times per week or 10-15 days per month. She agreed that NSAIDs may have a protective effect, but only at much lower doses and when used about five (or fewer) times per month. One study showed a possible protection effect of NSAIDs, though when used more than 10 days/month, they were associated with medication overuse headache.
Fioricet and Fiorinal, used more than 1 day/week, have an early and robust medicine overuse effect. “Limiting that use is very important,” said Dr. Nye. Other medicines and doses of concern include Tramadol/Ultram used at a higher than 50 mg/day dose, which has a metabolite that causes headache, and triptans used more than 10 days/month.
These concerns came about after analysis of large trials in patients with other conditions who also suffer from episodic migraines. A study of patients with irritable bowel syndrome and migraine showed a risk of conversion with opioid treatment. Another study of patients with arthritis and episodic migraine showed an association between conversion and NSAIDs alone, NSAIDs combined with Tylenol, and NSAIDs combined with opioids.
Risks of medication overuse also included collateral damage to the gastrointestinal and kidney systems, development of dependence, exacerbation of depression, and opioid-induced hyperalgesia, according to Dr. Nye. The overused medication may also interfere with the use of preventive medication. Those concerns drive the conventional wisdom of weaning patients off the overused medication, Dr. Nye said.
Dr. Nye discussed some of the observations of structural changes in the brain found in episodic migraine and chronic migraine associated with medication overuse. Functional MRI showed changes in grey matter, both as a result of medication overuse headache and further changes after medication withdrawal. “A lot of neuroplasticity and neuroadaptation occurs, and these effects seem to be sustained anywhere from 4-6 months after (medicine) discontinuation,” said Dr. Nye.
Common ground
Dr. Nye emphasized the need to be aware of the dangers of medication overuse headache, but noted that clinicians should address the problem to ensure that patients are empowered, potentially providing preventive medications and encouraging more effective use of daily abortive medications.
In response, Dr. Rizzoli suggested that the two agreed on many issues. For her part, Dr. Nye agreed that medication overuse headache is a muddy concept that needs more research to understand the relationship between opiate use and chronic migraine, “but I do think there have been some good studies of fMRI evaluating the difference between those with medication overuse headache and seeing how they convert back to a different underlying network (following medication withdrawal). I do agree that there is probably a subpopulation that is not affected by medication overuse headache,” Dr. Nye said.
In the end, both expressed concerns for the patient. “I share Barbara’s concern that we need to be mindful and protect our patients from medication use, but on the other hand I think we also need to protect our patients from the complications of having a diagnosis of medical overuse and the stigmatization that goes with that. That particular issue goes both ways,” said Dr. Rizzoli.
“I absolutely agree with that,” responded Dr. Nye.
Dr. Nye is on the advisory boards for Biohaven, Upsher Smith, and Impel. She is a trial site principal investigator for Allergan, Amgen, and Satsuma. Dr. Rizzoli has been a consultant for Nestle and served on the scientific advisory or data safety monitoring board for Biohaven and Xoc Pharma. He has also received research support from Allergan.
FROM HCNE’S 20TH ANNUAL BOSTON FALL HEADACHE SYMPOSIUM
AASLD 2020: A clinical news roundup
Studies that address fundamental questions in hepatology and have the potential to change or improve clinical practice were the focus of a clinical debrief session from the virtual annual meeting of the American Association for the Study of Liver Diseases.
“We chose papers that had the highest level of evidence, such as randomized controlled trials, controlled studies, and large data sets – and some small data sets too,” said Tamar Taddei, MD, associate professor of medicine in the section of digestive disease at Yale University, New Haven, Conn.
Dr. Taddei and colleagues Silvia Vilarinho, MD, PhD; Simona Jakab, MD; and Ariel Jaffe, MD, all also from Yale, selected the papers from among 197 oral and 1,769 poster abstracts presented at AASLD 2020.
They highlighted the most important findings from presentations on autoimmune and cholestatic disease, transplantation, cirrhosis and portal hypertension, alcoholic liver disease, neoplasia, drug-induced liver injury, and COVID-19. They did not review studies focused primarily on nonalcoholic steatohepatitis or nonalcoholic fatty liver disease, viral hepatitis, or basic science, all of which were covered in separate debriefing sessions.
Cirrhosis and portal hypertension
A study from the Department of Veterans Affairs looked at the prevalence of liver disease risk factors and rates of subsequent testing for and diagnosis of cirrhosis in the Veterans Health Administration system (VHA).
The authors found that, among more than 6.65 million VHA users in 2018 with no prior diagnosis of cirrhosis, approximately half were at risk for cirrhosis, of whom about 75% were screened, and approximately 5% of those who were screened were positive for possible cirrhosis (133,636). Of the patients who screened positive, about 10% (12,566) received a diagnosis of cirrhosis, including 4,120 with liver decompensation.
“This paper underscores the importance of population-level screening in uncovering unrecognized cirrhosis, enabling intervention earlier in the course of disease,” Dr. Taddei said (Abstract #661).
A study looking at external validation of novel cirrhosis surgical risk models designed to improve prognostication for a range of common surgeries showed that the VOCAL-Penn score was superior to the Mayo Risk Score, Model for End-stage Liver Disease and MELD-sodium scores for discrimination of 30-day and 90-day postoperative mortality (Abstract #91).
“While these models are not a substitute for clinical acumen, they certainly improve our surgical risk prediction in patients with cirrhosis, a very common question in consultative hepatology,” Dr. Taddei said.
She also cited three abstracts that address the important questions regarding performing studies in patients with varices or ascites, including whether it’s safe to perform transesophageal echocardiography in patients with cirrhosis without first screening for varices, and whether nonselective beta-blockers should be continued in patients with refractory ascites.
A retrospective study of 191 patients with cirrhosis who underwent upper endoscopy within 4 years of transesophageal echocardiography had no overt gastrointestinal bleeding regardless of the presence of esophageal varices, suggesting that routine preprocedure esophagogastroduodenoscopy “is of no utility,” (Abstract #1872).
A study to determine risk of sepsis in 1,198 patients with cirrhosis found that 1-year risk of sepsis was reduced by 50% with the use of nonselective beta-blockers (Abstract #94).
The final abstract in this category touched on the use of an advance care planning video support tool to help transplant-ineligible patients with end-stage liver disease decide whether they want support measures such cardiopulmonary resuscitation or intubation. The authors found that the video decision tool was feasible and acceptable to patients, and improved their knowledge of end-of-life care. More patients randomized to the video arm opted against CPR or intubation, compared with those assigned to a verbal discussion of options (Abstract #712).
Alcohol
The reviewers highlighted two studies of alcohol use: The first was designed to determine the prevalence of early alcohol relapse (resumption within 3 months) in patients who presented with alcoholic hepatitis. The subjects included 478 patients enrolled in the STOPAH trial, and a validation set of 194 patients from the InTeam (Integrated Approaches for identifying Molecular Targets in Alcoholic Hepatitis) Consortium.
“They found that high-risk patients were younger, unemployed, and without a stable relationship. Intermediate risk were middle aged, employed, and in a stable relationship, and low-risk profiles were older, with known cirrhosis; they were mostly retired and in a stable relationship,” Dr. Taddei said.
The identification of nongenetic factors that predict early relapse may aid in personalization of treatment strategies, she said (Abstract #232).
The second study looked at fecal microbial transplant (FMT) for reducing cravings in adults with alcohol use disorder (AUD) and cirrhosis. The investigators saw a nonsignificant trend toward greater total abstinence at 6 months in patients randomized to FMT versus placebo.
“Future trials should be performed to determine the impact of FMT on altering the gut-brain axis in patients with AUD,” she said (Abstract #7).
Transplantation
The prospective controlled QUICKTRANS study by French and Belgian researchers found that patients who underwent early liver transplantation for severe alcoholic hepatitis had numerically but not significantly higher rates of relapse than patients who were transplanted after at least 6 months of abstinence, although heavy drinking was more frequent in patients who underwent early transplant.
The 2-year survival rates for both patients who underwent early transplant and those who underwent transplant after 6 months of sobriety were “identical, and excellent.” In addition, the 2-year survival rate for patients with severe alcoholic hepatitis who underwent transplant was 82.8%, compared with 28.2% for patients who were deemed ineligible for transplant according to a selection algorithm (P < .001).
“Perhaps most important is that studies in this population can be conducted in a controlled fashion across centers with reproducible transplant eligibility algorithms,” Dr. Taddei commented (Abstract #6).
The place of honor – Abstract # 1 – was reserved for a study looking at the effects on liver transplant practice of a new “safety net” policy from the Organ Procurement and Transplantation Network and United Network for Organ Sharing stating that patients awaiting liver transplantation who develop kidney failure may be given priority on the kidney transplant waiting list.
The investigators found that the new policy significantly increased the number of adult primary liver transplant alone candidates who where on dialysis at the time of listing, and did not affect either waiting list mortality or posttransplant outcomes.
The authors also saw a significant increase in kidney transplant listing after liver transplant, especially for patients who were on hemodialysis at the time of list.
In the period after implementation of the policy, there was a significantly higher probability of kidney transplant, and significant reduction in waiting list mortality.
Autoimmune & cholestatic diseases
Investigators performed an analysis of the phase 3 randomized controlled ENHANCE trial of seladelpar in patients with primary biliary cholangitis. The trial was stopped because of an adverse event ultimately deemed to be unrelated to the drug, so the analysis looked at the composite responder rate at month 3.
“The key takeaway from this study is that at the 10-mg dosage of seladelpar, 78% met a composite endpoint, 27% of patients normalized their alkaline phosphatase, and 50% normalized their ALT. There was significant improvement in pruritus,” Dr. Taddei said.
The drug was generally safe and well tolerated. A 52-week phase 3 global registration study will begin enrolling patients in early 2021 (Abstract #LO11).
In a pediatric study, investigators looked at differences in primary sclerosing cholangitis (PSC) among various population, and found that “Black and Hispanic patients have dramatically worse clinical outcomes, compared to White and Asian patients. They are more likely to be diagnosed with PSC at an advanced stage with extensive fibrosis and portal hypertensive manifestations.”
The authors suggested that the differences may be explained in part by socioeconomic disparities leading to delay in diagnosis, to a more aggressive phenotype, or both (Abstract #66).
A meta-analysis of maternal and fetal outcomes in women with autoimmune hepatitis showed that the disease is associated with increased risk of gestational diabetes, premature births, and small-for-gestational age or low-birth-weight babies.
“Pregnant women should be monitored closely before, during and after pregnancy. It’s important to know that, in the prevalence data, flares were most prevalent postpartum at 41%. These finds will help us counsel our patients with autoimmune hepatitis who become pregnant,” Dr. Taddei said (Abstract #97).
Drug-induced liver injury
A study of clinical outcomes following immune checkpoint inhibitor rechallenge in melanoma patients with resolved higher grade 3 or higher checkpoint inhibitor–induced hepatitis showed that 4 of 31 patients (13%) developed recurrence of grade 2 or greater hepatitis, and 15 of 31 (48%) developed an immune-related adverse event after rechallenge.
There was no difference in time to death between patients who were rechallenged and those who were not, and immune-related liver toxicities requiring drug discontinuation after rechallenge were uncommon.
“High-grade immune checkpoint inhibitor hepatitis should be reconsidered as an absolute contraindication for immune checkpoint inhibitor rechallenge,” Dr. Taddei said (Abstract # 116).
Neoplasia
The investigators also highlighted an abstract describing significant urban-rural and racial ethnic differences in hepatocellular carcinoma rates. A fuller description of this study can be found here (Abstract #136).
COVID-19
Finally, the reviewer highlighted a study of the clinical course of COVID-19 in patients with chronic liver disease, and to determine factors associated with adverse outcomes in patients with chronic liver disease who acquire COVID-19.
The investigators found that patients with chronic liver disease and COVID-19 have a 14% morality rate, and that alcohol-related liver disease, decompensated cirrhosis, and hepatocellular carcinoma are all risk factors for increased mortality from COVID-19.
They recommended emphasizing telemedicine, prioritizing patients with chronic liver disease for vaccination, and including these patients in prospective studies and drug trials for COVID-19 therapies.
Dr. Taddei reported having no disclosures.
Studies that address fundamental questions in hepatology and have the potential to change or improve clinical practice were the focus of a clinical debrief session from the virtual annual meeting of the American Association for the Study of Liver Diseases.
“We chose papers that had the highest level of evidence, such as randomized controlled trials, controlled studies, and large data sets – and some small data sets too,” said Tamar Taddei, MD, associate professor of medicine in the section of digestive disease at Yale University, New Haven, Conn.
Dr. Taddei and colleagues Silvia Vilarinho, MD, PhD; Simona Jakab, MD; and Ariel Jaffe, MD, all also from Yale, selected the papers from among 197 oral and 1,769 poster abstracts presented at AASLD 2020.
They highlighted the most important findings from presentations on autoimmune and cholestatic disease, transplantation, cirrhosis and portal hypertension, alcoholic liver disease, neoplasia, drug-induced liver injury, and COVID-19. They did not review studies focused primarily on nonalcoholic steatohepatitis or nonalcoholic fatty liver disease, viral hepatitis, or basic science, all of which were covered in separate debriefing sessions.
Cirrhosis and portal hypertension
A study from the Department of Veterans Affairs looked at the prevalence of liver disease risk factors and rates of subsequent testing for and diagnosis of cirrhosis in the Veterans Health Administration system (VHA).
The authors found that, among more than 6.65 million VHA users in 2018 with no prior diagnosis of cirrhosis, approximately half were at risk for cirrhosis, of whom about 75% were screened, and approximately 5% of those who were screened were positive for possible cirrhosis (133,636). Of the patients who screened positive, about 10% (12,566) received a diagnosis of cirrhosis, including 4,120 with liver decompensation.
“This paper underscores the importance of population-level screening in uncovering unrecognized cirrhosis, enabling intervention earlier in the course of disease,” Dr. Taddei said (Abstract #661).
A study looking at external validation of novel cirrhosis surgical risk models designed to improve prognostication for a range of common surgeries showed that the VOCAL-Penn score was superior to the Mayo Risk Score, Model for End-stage Liver Disease and MELD-sodium scores for discrimination of 30-day and 90-day postoperative mortality (Abstract #91).
“While these models are not a substitute for clinical acumen, they certainly improve our surgical risk prediction in patients with cirrhosis, a very common question in consultative hepatology,” Dr. Taddei said.
She also cited three abstracts that address the important questions regarding performing studies in patients with varices or ascites, including whether it’s safe to perform transesophageal echocardiography in patients with cirrhosis without first screening for varices, and whether nonselective beta-blockers should be continued in patients with refractory ascites.
A retrospective study of 191 patients with cirrhosis who underwent upper endoscopy within 4 years of transesophageal echocardiography had no overt gastrointestinal bleeding regardless of the presence of esophageal varices, suggesting that routine preprocedure esophagogastroduodenoscopy “is of no utility,” (Abstract #1872).
A study to determine risk of sepsis in 1,198 patients with cirrhosis found that 1-year risk of sepsis was reduced by 50% with the use of nonselective beta-blockers (Abstract #94).
The final abstract in this category touched on the use of an advance care planning video support tool to help transplant-ineligible patients with end-stage liver disease decide whether they want support measures such cardiopulmonary resuscitation or intubation. The authors found that the video decision tool was feasible and acceptable to patients, and improved their knowledge of end-of-life care. More patients randomized to the video arm opted against CPR or intubation, compared with those assigned to a verbal discussion of options (Abstract #712).
Alcohol
The reviewers highlighted two studies of alcohol use: The first was designed to determine the prevalence of early alcohol relapse (resumption within 3 months) in patients who presented with alcoholic hepatitis. The subjects included 478 patients enrolled in the STOPAH trial, and a validation set of 194 patients from the InTeam (Integrated Approaches for identifying Molecular Targets in Alcoholic Hepatitis) Consortium.
“They found that high-risk patients were younger, unemployed, and without a stable relationship. Intermediate risk were middle aged, employed, and in a stable relationship, and low-risk profiles were older, with known cirrhosis; they were mostly retired and in a stable relationship,” Dr. Taddei said.
The identification of nongenetic factors that predict early relapse may aid in personalization of treatment strategies, she said (Abstract #232).
The second study looked at fecal microbial transplant (FMT) for reducing cravings in adults with alcohol use disorder (AUD) and cirrhosis. The investigators saw a nonsignificant trend toward greater total abstinence at 6 months in patients randomized to FMT versus placebo.
“Future trials should be performed to determine the impact of FMT on altering the gut-brain axis in patients with AUD,” she said (Abstract #7).
Transplantation
The prospective controlled QUICKTRANS study by French and Belgian researchers found that patients who underwent early liver transplantation for severe alcoholic hepatitis had numerically but not significantly higher rates of relapse than patients who were transplanted after at least 6 months of abstinence, although heavy drinking was more frequent in patients who underwent early transplant.
The 2-year survival rates for both patients who underwent early transplant and those who underwent transplant after 6 months of sobriety were “identical, and excellent.” In addition, the 2-year survival rate for patients with severe alcoholic hepatitis who underwent transplant was 82.8%, compared with 28.2% for patients who were deemed ineligible for transplant according to a selection algorithm (P < .001).
“Perhaps most important is that studies in this population can be conducted in a controlled fashion across centers with reproducible transplant eligibility algorithms,” Dr. Taddei commented (Abstract #6).
The place of honor – Abstract # 1 – was reserved for a study looking at the effects on liver transplant practice of a new “safety net” policy from the Organ Procurement and Transplantation Network and United Network for Organ Sharing stating that patients awaiting liver transplantation who develop kidney failure may be given priority on the kidney transplant waiting list.
The investigators found that the new policy significantly increased the number of adult primary liver transplant alone candidates who where on dialysis at the time of listing, and did not affect either waiting list mortality or posttransplant outcomes.
The authors also saw a significant increase in kidney transplant listing after liver transplant, especially for patients who were on hemodialysis at the time of list.
In the period after implementation of the policy, there was a significantly higher probability of kidney transplant, and significant reduction in waiting list mortality.
Autoimmune & cholestatic diseases
Investigators performed an analysis of the phase 3 randomized controlled ENHANCE trial of seladelpar in patients with primary biliary cholangitis. The trial was stopped because of an adverse event ultimately deemed to be unrelated to the drug, so the analysis looked at the composite responder rate at month 3.
“The key takeaway from this study is that at the 10-mg dosage of seladelpar, 78% met a composite endpoint, 27% of patients normalized their alkaline phosphatase, and 50% normalized their ALT. There was significant improvement in pruritus,” Dr. Taddei said.
The drug was generally safe and well tolerated. A 52-week phase 3 global registration study will begin enrolling patients in early 2021 (Abstract #LO11).
In a pediatric study, investigators looked at differences in primary sclerosing cholangitis (PSC) among various population, and found that “Black and Hispanic patients have dramatically worse clinical outcomes, compared to White and Asian patients. They are more likely to be diagnosed with PSC at an advanced stage with extensive fibrosis and portal hypertensive manifestations.”
The authors suggested that the differences may be explained in part by socioeconomic disparities leading to delay in diagnosis, to a more aggressive phenotype, or both (Abstract #66).
A meta-analysis of maternal and fetal outcomes in women with autoimmune hepatitis showed that the disease is associated with increased risk of gestational diabetes, premature births, and small-for-gestational age or low-birth-weight babies.
“Pregnant women should be monitored closely before, during and after pregnancy. It’s important to know that, in the prevalence data, flares were most prevalent postpartum at 41%. These finds will help us counsel our patients with autoimmune hepatitis who become pregnant,” Dr. Taddei said (Abstract #97).
Drug-induced liver injury
A study of clinical outcomes following immune checkpoint inhibitor rechallenge in melanoma patients with resolved higher grade 3 or higher checkpoint inhibitor–induced hepatitis showed that 4 of 31 patients (13%) developed recurrence of grade 2 or greater hepatitis, and 15 of 31 (48%) developed an immune-related adverse event after rechallenge.
There was no difference in time to death between patients who were rechallenged and those who were not, and immune-related liver toxicities requiring drug discontinuation after rechallenge were uncommon.
“High-grade immune checkpoint inhibitor hepatitis should be reconsidered as an absolute contraindication for immune checkpoint inhibitor rechallenge,” Dr. Taddei said (Abstract # 116).
Neoplasia
The investigators also highlighted an abstract describing significant urban-rural and racial ethnic differences in hepatocellular carcinoma rates. A fuller description of this study can be found here (Abstract #136).
COVID-19
Finally, the reviewer highlighted a study of the clinical course of COVID-19 in patients with chronic liver disease, and to determine factors associated with adverse outcomes in patients with chronic liver disease who acquire COVID-19.
The investigators found that patients with chronic liver disease and COVID-19 have a 14% morality rate, and that alcohol-related liver disease, decompensated cirrhosis, and hepatocellular carcinoma are all risk factors for increased mortality from COVID-19.
They recommended emphasizing telemedicine, prioritizing patients with chronic liver disease for vaccination, and including these patients in prospective studies and drug trials for COVID-19 therapies.
Dr. Taddei reported having no disclosures.
Studies that address fundamental questions in hepatology and have the potential to change or improve clinical practice were the focus of a clinical debrief session from the virtual annual meeting of the American Association for the Study of Liver Diseases.
“We chose papers that had the highest level of evidence, such as randomized controlled trials, controlled studies, and large data sets – and some small data sets too,” said Tamar Taddei, MD, associate professor of medicine in the section of digestive disease at Yale University, New Haven, Conn.
Dr. Taddei and colleagues Silvia Vilarinho, MD, PhD; Simona Jakab, MD; and Ariel Jaffe, MD, all also from Yale, selected the papers from among 197 oral and 1,769 poster abstracts presented at AASLD 2020.
They highlighted the most important findings from presentations on autoimmune and cholestatic disease, transplantation, cirrhosis and portal hypertension, alcoholic liver disease, neoplasia, drug-induced liver injury, and COVID-19. They did not review studies focused primarily on nonalcoholic steatohepatitis or nonalcoholic fatty liver disease, viral hepatitis, or basic science, all of which were covered in separate debriefing sessions.
Cirrhosis and portal hypertension
A study from the Department of Veterans Affairs looked at the prevalence of liver disease risk factors and rates of subsequent testing for and diagnosis of cirrhosis in the Veterans Health Administration system (VHA).
The authors found that, among more than 6.65 million VHA users in 2018 with no prior diagnosis of cirrhosis, approximately half were at risk for cirrhosis, of whom about 75% were screened, and approximately 5% of those who were screened were positive for possible cirrhosis (133,636). Of the patients who screened positive, about 10% (12,566) received a diagnosis of cirrhosis, including 4,120 with liver decompensation.
“This paper underscores the importance of population-level screening in uncovering unrecognized cirrhosis, enabling intervention earlier in the course of disease,” Dr. Taddei said (Abstract #661).
A study looking at external validation of novel cirrhosis surgical risk models designed to improve prognostication for a range of common surgeries showed that the VOCAL-Penn score was superior to the Mayo Risk Score, Model for End-stage Liver Disease and MELD-sodium scores for discrimination of 30-day and 90-day postoperative mortality (Abstract #91).
“While these models are not a substitute for clinical acumen, they certainly improve our surgical risk prediction in patients with cirrhosis, a very common question in consultative hepatology,” Dr. Taddei said.
She also cited three abstracts that address the important questions regarding performing studies in patients with varices or ascites, including whether it’s safe to perform transesophageal echocardiography in patients with cirrhosis without first screening for varices, and whether nonselective beta-blockers should be continued in patients with refractory ascites.
A retrospective study of 191 patients with cirrhosis who underwent upper endoscopy within 4 years of transesophageal echocardiography had no overt gastrointestinal bleeding regardless of the presence of esophageal varices, suggesting that routine preprocedure esophagogastroduodenoscopy “is of no utility,” (Abstract #1872).
A study to determine risk of sepsis in 1,198 patients with cirrhosis found that 1-year risk of sepsis was reduced by 50% with the use of nonselective beta-blockers (Abstract #94).
The final abstract in this category touched on the use of an advance care planning video support tool to help transplant-ineligible patients with end-stage liver disease decide whether they want support measures such cardiopulmonary resuscitation or intubation. The authors found that the video decision tool was feasible and acceptable to patients, and improved their knowledge of end-of-life care. More patients randomized to the video arm opted against CPR or intubation, compared with those assigned to a verbal discussion of options (Abstract #712).
Alcohol
The reviewers highlighted two studies of alcohol use: The first was designed to determine the prevalence of early alcohol relapse (resumption within 3 months) in patients who presented with alcoholic hepatitis. The subjects included 478 patients enrolled in the STOPAH trial, and a validation set of 194 patients from the InTeam (Integrated Approaches for identifying Molecular Targets in Alcoholic Hepatitis) Consortium.
“They found that high-risk patients were younger, unemployed, and without a stable relationship. Intermediate risk were middle aged, employed, and in a stable relationship, and low-risk profiles were older, with known cirrhosis; they were mostly retired and in a stable relationship,” Dr. Taddei said.
The identification of nongenetic factors that predict early relapse may aid in personalization of treatment strategies, she said (Abstract #232).
The second study looked at fecal microbial transplant (FMT) for reducing cravings in adults with alcohol use disorder (AUD) and cirrhosis. The investigators saw a nonsignificant trend toward greater total abstinence at 6 months in patients randomized to FMT versus placebo.
“Future trials should be performed to determine the impact of FMT on altering the gut-brain axis in patients with AUD,” she said (Abstract #7).
Transplantation
The prospective controlled QUICKTRANS study by French and Belgian researchers found that patients who underwent early liver transplantation for severe alcoholic hepatitis had numerically but not significantly higher rates of relapse than patients who were transplanted after at least 6 months of abstinence, although heavy drinking was more frequent in patients who underwent early transplant.
The 2-year survival rates for both patients who underwent early transplant and those who underwent transplant after 6 months of sobriety were “identical, and excellent.” In addition, the 2-year survival rate for patients with severe alcoholic hepatitis who underwent transplant was 82.8%, compared with 28.2% for patients who were deemed ineligible for transplant according to a selection algorithm (P < .001).
“Perhaps most important is that studies in this population can be conducted in a controlled fashion across centers with reproducible transplant eligibility algorithms,” Dr. Taddei commented (Abstract #6).
The place of honor – Abstract # 1 – was reserved for a study looking at the effects on liver transplant practice of a new “safety net” policy from the Organ Procurement and Transplantation Network and United Network for Organ Sharing stating that patients awaiting liver transplantation who develop kidney failure may be given priority on the kidney transplant waiting list.
The investigators found that the new policy significantly increased the number of adult primary liver transplant alone candidates who where on dialysis at the time of listing, and did not affect either waiting list mortality or posttransplant outcomes.
The authors also saw a significant increase in kidney transplant listing after liver transplant, especially for patients who were on hemodialysis at the time of list.
In the period after implementation of the policy, there was a significantly higher probability of kidney transplant, and significant reduction in waiting list mortality.
Autoimmune & cholestatic diseases
Investigators performed an analysis of the phase 3 randomized controlled ENHANCE trial of seladelpar in patients with primary biliary cholangitis. The trial was stopped because of an adverse event ultimately deemed to be unrelated to the drug, so the analysis looked at the composite responder rate at month 3.
“The key takeaway from this study is that at the 10-mg dosage of seladelpar, 78% met a composite endpoint, 27% of patients normalized their alkaline phosphatase, and 50% normalized their ALT. There was significant improvement in pruritus,” Dr. Taddei said.
The drug was generally safe and well tolerated. A 52-week phase 3 global registration study will begin enrolling patients in early 2021 (Abstract #LO11).
In a pediatric study, investigators looked at differences in primary sclerosing cholangitis (PSC) among various population, and found that “Black and Hispanic patients have dramatically worse clinical outcomes, compared to White and Asian patients. They are more likely to be diagnosed with PSC at an advanced stage with extensive fibrosis and portal hypertensive manifestations.”
The authors suggested that the differences may be explained in part by socioeconomic disparities leading to delay in diagnosis, to a more aggressive phenotype, or both (Abstract #66).
A meta-analysis of maternal and fetal outcomes in women with autoimmune hepatitis showed that the disease is associated with increased risk of gestational diabetes, premature births, and small-for-gestational age or low-birth-weight babies.
“Pregnant women should be monitored closely before, during and after pregnancy. It’s important to know that, in the prevalence data, flares were most prevalent postpartum at 41%. These finds will help us counsel our patients with autoimmune hepatitis who become pregnant,” Dr. Taddei said (Abstract #97).
Drug-induced liver injury
A study of clinical outcomes following immune checkpoint inhibitor rechallenge in melanoma patients with resolved higher grade 3 or higher checkpoint inhibitor–induced hepatitis showed that 4 of 31 patients (13%) developed recurrence of grade 2 or greater hepatitis, and 15 of 31 (48%) developed an immune-related adverse event after rechallenge.
There was no difference in time to death between patients who were rechallenged and those who were not, and immune-related liver toxicities requiring drug discontinuation after rechallenge were uncommon.
“High-grade immune checkpoint inhibitor hepatitis should be reconsidered as an absolute contraindication for immune checkpoint inhibitor rechallenge,” Dr. Taddei said (Abstract # 116).
Neoplasia
The investigators also highlighted an abstract describing significant urban-rural and racial ethnic differences in hepatocellular carcinoma rates. A fuller description of this study can be found here (Abstract #136).
COVID-19
Finally, the reviewer highlighted a study of the clinical course of COVID-19 in patients with chronic liver disease, and to determine factors associated with adverse outcomes in patients with chronic liver disease who acquire COVID-19.
The investigators found that patients with chronic liver disease and COVID-19 have a 14% morality rate, and that alcohol-related liver disease, decompensated cirrhosis, and hepatocellular carcinoma are all risk factors for increased mortality from COVID-19.
They recommended emphasizing telemedicine, prioritizing patients with chronic liver disease for vaccination, and including these patients in prospective studies and drug trials for COVID-19 therapies.
Dr. Taddei reported having no disclosures.
FROM THE LIVER MEETING DIGITAL EXPERIENCE
A closer look at migraine aura
Migraine aura sometimes accompanies or precedes migraine pain, but the phenomenon is difficult to treat and poorly understood. However, some evidence points to potential neurological mechanisms, and migraine aura is associated with cardiovascular disease risk.

Andrea Harriott, MD, PhD, said at the Stowe Headache Symposium sponsored by the Headache Cooperative of New England, which was conducted virtually. Dr. Harriott is assistant professor of neurology at Massachusetts General Hospital in Boston.
Somewhere between 20% and 40% of patients with migraine experience aura. It is most often visual, though it can also include sensory, aphasic, and motor symptoms. Visual aura usually begins as a flickering zigzag pattern in the central visual field that moves slowly toward the periphery and often leaves a scotoma. Typical duration is 15-30 minutes. Aura symptoms are more common in females.
Research in the 1940s conducted by the Brazilian researcher Aristides de Azevedo Pacheco Leão, PhD, then at Harvard Medical School, Boston, showed evidence of CSD in rabbits after electrical or mechanical stimulation. He observed a wave of vasodilation and increased blood flow over the cortex that spread over nearly the entire dorsolateral cortex within 3-6 minutes.
In the 1940s and 1950s, researchers sketched on paper the visual disturbance over 10 minutes, tracking the expanding spectrum across the visual field, from the center toward the periphery. The resulting scotoma advanced across the visual cortex at a rate very similar to that of the cortical spreading observed by Dr. Leão, “potentially linking this electrical event that was described with the aura event of migraine,” said Dr. Harriott. Those researchers hypothesized that the aura was produced by a strong excitation phase, followed by a wave of total inhibition.
More recent functional magnetic resonance imaging studies have also shown that CSD-like disturbances occur when patients experience migraine aura. In one study, researchers observed an initial increase and then a decrease in the blood oxygenation level dependent (BOLD) signal, which spread slowly across the visual cortex and correlated with the aura event. “This study was really important in confirming that a CSD-like phenomenon was likely the underlying perturbation that produced the visual aura of migraine,” said Dr. Harriott.
Despite the evidence that CSD causes migraine aura, its connection to migraine pain hasn’t been firmly established. But Dr. Harriott presented some evidence linking the two. Migraine aura is usually followed by pain, and aura precedes migraine attacks 78%-93% of the time. Cephalic allodynia occurs in migraine about 70% to 80% of the time, and migraine with aura is more often associated with severe cutaneous allodynia than is migraine without aura. Finally, migraine patients with comorbidities have more severe disability, and more frequent cutaneous allodynia and aura than does the general migraine population (40% vs. 29%).
All of that suggests that activation of trigeminal nociceptors is involved with migraine aura, according to Dr. Harriott. Preclinical studies have also suggested links between CSD and activation of trigeminal nociceptors, with both immunohistochemical and electrophysiological lines of evidence. “These data suggest that spreading depression actually activates trigeminal nociceptors that we know are involved in signal pain in the head and neck, and that we know are involved in cephalic allodynia as well,” Dr. Harriott said.
The evidence impressed Allan Purdy, MD, professor of medicine at Dalhousie University, Halifax, N.S., who was the discussant for the presentation. “It’s an excellent case that CSD is a remarkably good correlate for aura,” he said during the session.
Along with potential impacts on migraine pain, aura is also associated with cardiovascular risk. “This is really important to know about in our clinical population,” said Dr. Harriott.
Meta-analyses of case control and cohort studies have shown associations between migraine aura and vascular disorders such as ischemic stroke. One meta-analysis showed about a twofold increased risk associated with migraine compared with the nonmigraine population. This difference was driven by migraine with aura (relative risk [RR], 2.25; 95% confidence interval [CI], 1.53-3.33) rather than migraine without aura (RR, 1.24; 95% CI, 0.86-1.79). Migraine generally is associated with greater risk of myocardial infarction (adjusted hazard ratio, 1.33; 95% CI, 1.08-1.64), and that association may be stronger in the aura phenotype.
There doesn’t appear to be evidence that traditional risk factors for heart disease – such as hypertension, diabetes, or high cholesterol – play a role in the association between aura and heart disease. One possibility is that variables like platelet activation, hypercoagulable state, or genetic susceptibility could be responsible.
The risks associated with migraine aura should be noted, but with a caveat, according to Dr. Purdy. “Even though the relative risk is high, the absolute risk is still relatively low, and patients with migraine with aura, who smoke or are female and over 45, those are the cases where the worry comes in.”
Dr. Harriott and Dr. Purdy have nothing to disclose.
Migraine aura sometimes accompanies or precedes migraine pain, but the phenomenon is difficult to treat and poorly understood. However, some evidence points to potential neurological mechanisms, and migraine aura is associated with cardiovascular disease risk.
Andrea Harriott, MD, PhD, said at the Stowe Headache Symposium sponsored by the Headache Cooperative of New England, which was conducted virtually. Dr. Harriott is assistant professor of neurology at Massachusetts General Hospital in Boston.
Somewhere between 20% and 40% of patients with migraine experience aura. It is most often visual, though it can also include sensory, aphasic, and motor symptoms. Visual aura usually begins as a flickering zigzag pattern in the central visual field that moves slowly toward the periphery and often leaves a scotoma. Typical duration is 15-30 minutes. Aura symptoms are more common in females.
Research in the 1940s conducted by the Brazilian researcher Aristides de Azevedo Pacheco Leão, PhD, then at Harvard Medical School, Boston, showed evidence of CSD in rabbits after electrical or mechanical stimulation. He observed a wave of vasodilation and increased blood flow over the cortex that spread over nearly the entire dorsolateral cortex within 3-6 minutes.
In the 1940s and 1950s, researchers sketched on paper the visual disturbance over 10 minutes, tracking the expanding spectrum across the visual field, from the center toward the periphery. The resulting scotoma advanced across the visual cortex at a rate very similar to that of the cortical spreading observed by Dr. Leão, “potentially linking this electrical event that was described with the aura event of migraine,” said Dr. Harriott. Those researchers hypothesized that the aura was produced by a strong excitation phase, followed by a wave of total inhibition.
More recent functional magnetic resonance imaging studies have also shown that CSD-like disturbances occur when patients experience migraine aura. In one study, researchers observed an initial increase and then a decrease in the blood oxygenation level dependent (BOLD) signal, which spread slowly across the visual cortex and correlated with the aura event. “This study was really important in confirming that a CSD-like phenomenon was likely the underlying perturbation that produced the visual aura of migraine,” said Dr. Harriott.
Despite the evidence that CSD causes migraine aura, its connection to migraine pain hasn’t been firmly established. But Dr. Harriott presented some evidence linking the two. Migraine aura is usually followed by pain, and aura precedes migraine attacks 78%-93% of the time. Cephalic allodynia occurs in migraine about 70% to 80% of the time, and migraine with aura is more often associated with severe cutaneous allodynia than is migraine without aura. Finally, migraine patients with comorbidities have more severe disability, and more frequent cutaneous allodynia and aura than does the general migraine population (40% vs. 29%).
All of that suggests that activation of trigeminal nociceptors is involved with migraine aura, according to Dr. Harriott. Preclinical studies have also suggested links between CSD and activation of trigeminal nociceptors, with both immunohistochemical and electrophysiological lines of evidence. “These data suggest that spreading depression actually activates trigeminal nociceptors that we know are involved in signal pain in the head and neck, and that we know are involved in cephalic allodynia as well,” Dr. Harriott said.
The evidence impressed Allan Purdy, MD, professor of medicine at Dalhousie University, Halifax, N.S., who was the discussant for the presentation. “It’s an excellent case that CSD is a remarkably good correlate for aura,” he said during the session.
Along with potential impacts on migraine pain, aura is also associated with cardiovascular risk. “This is really important to know about in our clinical population,” said Dr. Harriott.
Meta-analyses of case control and cohort studies have shown associations between migraine aura and vascular disorders such as ischemic stroke. One meta-analysis showed about a twofold increased risk associated with migraine compared with the nonmigraine population. This difference was driven by migraine with aura (relative risk [RR], 2.25; 95% confidence interval [CI], 1.53-3.33) rather than migraine without aura (RR, 1.24; 95% CI, 0.86-1.79). Migraine generally is associated with greater risk of myocardial infarction (adjusted hazard ratio, 1.33; 95% CI, 1.08-1.64), and that association may be stronger in the aura phenotype.
There doesn’t appear to be evidence that traditional risk factors for heart disease – such as hypertension, diabetes, or high cholesterol – play a role in the association between aura and heart disease. One possibility is that variables like platelet activation, hypercoagulable state, or genetic susceptibility could be responsible.
The risks associated with migraine aura should be noted, but with a caveat, according to Dr. Purdy. “Even though the relative risk is high, the absolute risk is still relatively low, and patients with migraine with aura, who smoke or are female and over 45, those are the cases where the worry comes in.”
Dr. Harriott and Dr. Purdy have nothing to disclose.
Migraine aura sometimes accompanies or precedes migraine pain, but the phenomenon is difficult to treat and poorly understood. However, some evidence points to potential neurological mechanisms, and migraine aura is associated with cardiovascular disease risk.
Andrea Harriott, MD, PhD, said at the Stowe Headache Symposium sponsored by the Headache Cooperative of New England, which was conducted virtually. Dr. Harriott is assistant professor of neurology at Massachusetts General Hospital in Boston.
Somewhere between 20% and 40% of patients with migraine experience aura. It is most often visual, though it can also include sensory, aphasic, and motor symptoms. Visual aura usually begins as a flickering zigzag pattern in the central visual field that moves slowly toward the periphery and often leaves a scotoma. Typical duration is 15-30 minutes. Aura symptoms are more common in females.
Research in the 1940s conducted by the Brazilian researcher Aristides de Azevedo Pacheco Leão, PhD, then at Harvard Medical School, Boston, showed evidence of CSD in rabbits after electrical or mechanical stimulation. He observed a wave of vasodilation and increased blood flow over the cortex that spread over nearly the entire dorsolateral cortex within 3-6 minutes.
In the 1940s and 1950s, researchers sketched on paper the visual disturbance over 10 minutes, tracking the expanding spectrum across the visual field, from the center toward the periphery. The resulting scotoma advanced across the visual cortex at a rate very similar to that of the cortical spreading observed by Dr. Leão, “potentially linking this electrical event that was described with the aura event of migraine,” said Dr. Harriott. Those researchers hypothesized that the aura was produced by a strong excitation phase, followed by a wave of total inhibition.
More recent functional magnetic resonance imaging studies have also shown that CSD-like disturbances occur when patients experience migraine aura. In one study, researchers observed an initial increase and then a decrease in the blood oxygenation level dependent (BOLD) signal, which spread slowly across the visual cortex and correlated with the aura event. “This study was really important in confirming that a CSD-like phenomenon was likely the underlying perturbation that produced the visual aura of migraine,” said Dr. Harriott.
Despite the evidence that CSD causes migraine aura, its connection to migraine pain hasn’t been firmly established. But Dr. Harriott presented some evidence linking the two. Migraine aura is usually followed by pain, and aura precedes migraine attacks 78%-93% of the time. Cephalic allodynia occurs in migraine about 70% to 80% of the time, and migraine with aura is more often associated with severe cutaneous allodynia than is migraine without aura. Finally, migraine patients with comorbidities have more severe disability, and more frequent cutaneous allodynia and aura than does the general migraine population (40% vs. 29%).
All of that suggests that activation of trigeminal nociceptors is involved with migraine aura, according to Dr. Harriott. Preclinical studies have also suggested links between CSD and activation of trigeminal nociceptors, with both immunohistochemical and electrophysiological lines of evidence. “These data suggest that spreading depression actually activates trigeminal nociceptors that we know are involved in signal pain in the head and neck, and that we know are involved in cephalic allodynia as well,” Dr. Harriott said.
The evidence impressed Allan Purdy, MD, professor of medicine at Dalhousie University, Halifax, N.S., who was the discussant for the presentation. “It’s an excellent case that CSD is a remarkably good correlate for aura,” he said during the session.
Along with potential impacts on migraine pain, aura is also associated with cardiovascular risk. “This is really important to know about in our clinical population,” said Dr. Harriott.
Meta-analyses of case control and cohort studies have shown associations between migraine aura and vascular disorders such as ischemic stroke. One meta-analysis showed about a twofold increased risk associated with migraine compared with the nonmigraine population. This difference was driven by migraine with aura (relative risk [RR], 2.25; 95% confidence interval [CI], 1.53-3.33) rather than migraine without aura (RR, 1.24; 95% CI, 0.86-1.79). Migraine generally is associated with greater risk of myocardial infarction (adjusted hazard ratio, 1.33; 95% CI, 1.08-1.64), and that association may be stronger in the aura phenotype.
There doesn’t appear to be evidence that traditional risk factors for heart disease – such as hypertension, diabetes, or high cholesterol – play a role in the association between aura and heart disease. One possibility is that variables like platelet activation, hypercoagulable state, or genetic susceptibility could be responsible.
The risks associated with migraine aura should be noted, but with a caveat, according to Dr. Purdy. “Even though the relative risk is high, the absolute risk is still relatively low, and patients with migraine with aura, who smoke or are female and over 45, those are the cases where the worry comes in.”
Dr. Harriott and Dr. Purdy have nothing to disclose.
FROM HCNE STOWE 2020
Microneedling: What’s the truth?
according to Catherine M. DiGiorgio, MD, MS.

During a virtual course on laser and aesthetic skin therapy, Dr. DiGiorgio, a laser and cosmetic dermatologist at the Boston Center for Facial Rejuvenation, provided a state-of-the-art update on microneedling, a procedure in which microneedles are rolled over the skin to create epidermal and dermal microwounds.
“The depths are adjustable and it’s purely mechanical: no energy is being delivered with these treatments,” she said. “The hypothesized mechanism of action is that microneedling creates microwounds which initiate wound healing to stimulate new collagen production. This breaks apart compact collagen in the superficial dermis while stimulating new collagen and elastin,” she explained, adding that it is also hypothesized that this “stimulates growth factors that directly impact collagen and elastin synthesis.”
Conditions that have been reported to be treatable with microneedling in the medical literature include scars – especially acne scars – as well as rhytides, skin laxity, striae, melasma, and enlarged pores. Microneedling can also be used for transdermal drug delivery, although it’s far inferior to microinjection of medications. Contraindications are similar to those with laser surgery, including active infection of the area, history of keloids, inflammatory acne, and immunosuppression; and it should not be performed on the same day as neuromodulator treatment, to avoid diffusion of the neuromodulator. Herpes simplex virus prophylaxis is also indicated prior to microneedling treatment.
Many devices are available for use, including fixed, manual needle rollers and electric-powered pens with single-use sterile cartridges. The devices vary by needle length, quantity, diameter, configuration, and material of which the microneedles are made of. The needle length is not reliable for penetration depth, especially when greater than 1 mm. Treatment guidelines vary based on the area being treated.
“You put tension on the skin and apply the device perpendicularly,” Dr. DiGiorgio said during the meeting, which was sponsored by Harvard Medical School, Massachusetts General Hospital, and the Wellman Center for Photomedicine. “It should be performed in quadrants, and I prefer to treat in cosmetic units. The endpoint is pinpoint bleeding versus deep purpura. Ice water–soaked sterile gauze can be applied after treatment and skin care can be resumed in 5-7 days.”
In an effort to compare the efficacy and safety of the 2940-nm Er:YAG laser and microneedling for the treatment of atrophic acne scars, researchers in Egypt performed a randomized, split-face study in 30 patients. Study participants were evaluated by two blinded physicians at baseline and at 3 months follow-up. Both modalities showed a significant improvement in acne scars, but those treated with the Er:YAG laser showed a statistically significant greater improvement (70% vs. 30%, respectively; P < .001). Histology revealed a significantly higher increase in the mean quantity of collagen fibers in the Er:YAG-treated patients, compared with those who underwent microneedling, but patients in the microneedling group experienced less erythema and edema. Pain scores were significantly higher in the microneedling group compared with the Er:YAG group.
In a more recent study, researchers performed a systematic review of 37 articles in the medical literature related to microneedling. They found that the procedure provides good results when used on its own, and is preferred by patients because of its minimal downtime and side effects. However, they concluded that, while microneedling is a safe and effective option, methodological shortcomings and further research is required to establish it as an evidence-based therapeutic option.
“There are a limited number of high-quality studies demonstrating the efficacy of microneedling,” Dr. DiGiorgio said. “It is a safe procedure, which could complement laser treatments, so you could perform it between expensive and high-downtime lasers. It is an option for patients who seek measurable results with little to no downtime, and it’s also an option for clinicians who do not use laser-resurfacing devices. Basically, further research is needed to establish microneedling as an evidence-based therapeutic option. Laser continues to remain the gold standard for treatment.”
Another treatment option is fractional microneedling with radiofrequency (RF). These are microneedles which deliver energy in the form of RF at the tip of the needle, which denatures collagen and creates thermal coagulative injury zones at temperatures greater than 65° C. The microneedles can be insulated or noninsulated. “Insulated tips are safer for darker skin types because the epidermis is protected from the heat damage,” Dr. DiGiorgio said.
These treatments are used for the improvement of rhytides and scars and for skin tightening. “The treatments are painful and require topical anesthesia,” she said. “Erythema can range from about 24 hours to 4 days depending on the device being used. Usually monthly treatments are recommended.”
A study by investigators in South Korea and China set out to analyze histometric changes of this approach in pigs. They treated the pigs with a fractional microneedle delivery system at various depths, conduction times, and energies, and performed punch biopsies immediately after treatment, 4 days post treatment, and at 2 weeks post treatment. They noted that depth and conduction time affected the height, width, and volume of the columns of coagulation, but that the energy only affected the level of tissue destruction. “They also noted that RF-induced coagulated columns had a mixed cellular infiltrate, neovascularization, granular tissue formation with fibroblasts, and neocollagenesis and elastogenesis in the dermis,” Dr. DiGiorgio said.
In another study, researchers in Thailand performed a study in two women who were going to undergo abdominoplasty. Participants received six treatments prior to abdominoplasty with biopsies at different time intervals following microneedling with radiofrequency. The researchers tested five energy levels and five test areas; no collagen denaturization was observed with microneedling alone.
“This supports the idea that heat is required to stimulate neocollagenesis, and needles alone do not denature collagen,” Dr. DiGiorgio said. “They also found that neocollagenesis and neoelastogenesis occurred at optimal heating levels.”
In a separate study, researchers from Denmark used a number of different imaging modalities to evaluate the impact of microneedle fractional RF-induced micropores. When they used reflectance confocal microscopy, they observed that the micropores showed a concentric shape. “They contained hyper-reflective granules, and the coagulated tissue was seen from the epidermis to the dermal-epidermal junction,” Dr. DiGiorgio said. “This was not seen in the low energy microneedle RF. On optical coherence tomography, they noted that high-energy needle RF showed deeper, more easily identifiable micropores versus low-energy microneedle RF.” On histology the researchers noted that tissue coagulation reached a depth of 1,500 mcm with high-energy microneedle RF, but low-energy microneedle RF only showed visible damage to the epidermis. “This also supports the idea that microneedles alone without energy do not reach the deeper layers of the dermis,” she said.
Dr. DiGiorgio concluded her presentation by discussing promising results from a split-face study of fractional microneedling RF for the treatment of rosacea. For the 12-week randomized study, researchers from South Korea performed two sessions 4 weeks apart, with no treatment to the control side. Erythema decreased 13.6% and results were maintained for about 2 months after treatment. The researchers also measured inflammatory markers and noticed decreased dermal inflammation and mast cell counts and decreased markers related to angiogenesis, inflammation, innate immunity, and neuronal cation channels. “This could be a promising treatment for inflammatory rosacea in the future,” Dr. DiGiorgio said.
She disclosed that she is a consultant for Allergan Aesthetics.
according to Catherine M. DiGiorgio, MD, MS.
During a virtual course on laser and aesthetic skin therapy, Dr. DiGiorgio, a laser and cosmetic dermatologist at the Boston Center for Facial Rejuvenation, provided a state-of-the-art update on microneedling, a procedure in which microneedles are rolled over the skin to create epidermal and dermal microwounds.
“The depths are adjustable and it’s purely mechanical: no energy is being delivered with these treatments,” she said. “The hypothesized mechanism of action is that microneedling creates microwounds which initiate wound healing to stimulate new collagen production. This breaks apart compact collagen in the superficial dermis while stimulating new collagen and elastin,” she explained, adding that it is also hypothesized that this “stimulates growth factors that directly impact collagen and elastin synthesis.”
Conditions that have been reported to be treatable with microneedling in the medical literature include scars – especially acne scars – as well as rhytides, skin laxity, striae, melasma, and enlarged pores. Microneedling can also be used for transdermal drug delivery, although it’s far inferior to microinjection of medications. Contraindications are similar to those with laser surgery, including active infection of the area, history of keloids, inflammatory acne, and immunosuppression; and it should not be performed on the same day as neuromodulator treatment, to avoid diffusion of the neuromodulator. Herpes simplex virus prophylaxis is also indicated prior to microneedling treatment.
Many devices are available for use, including fixed, manual needle rollers and electric-powered pens with single-use sterile cartridges. The devices vary by needle length, quantity, diameter, configuration, and material of which the microneedles are made of. The needle length is not reliable for penetration depth, especially when greater than 1 mm. Treatment guidelines vary based on the area being treated.
“You put tension on the skin and apply the device perpendicularly,” Dr. DiGiorgio said during the meeting, which was sponsored by Harvard Medical School, Massachusetts General Hospital, and the Wellman Center for Photomedicine. “It should be performed in quadrants, and I prefer to treat in cosmetic units. The endpoint is pinpoint bleeding versus deep purpura. Ice water–soaked sterile gauze can be applied after treatment and skin care can be resumed in 5-7 days.”
In an effort to compare the efficacy and safety of the 2940-nm Er:YAG laser and microneedling for the treatment of atrophic acne scars, researchers in Egypt performed a randomized, split-face study in 30 patients. Study participants were evaluated by two blinded physicians at baseline and at 3 months follow-up. Both modalities showed a significant improvement in acne scars, but those treated with the Er:YAG laser showed a statistically significant greater improvement (70% vs. 30%, respectively; P < .001). Histology revealed a significantly higher increase in the mean quantity of collagen fibers in the Er:YAG-treated patients, compared with those who underwent microneedling, but patients in the microneedling group experienced less erythema and edema. Pain scores were significantly higher in the microneedling group compared with the Er:YAG group.
In a more recent study, researchers performed a systematic review of 37 articles in the medical literature related to microneedling. They found that the procedure provides good results when used on its own, and is preferred by patients because of its minimal downtime and side effects. However, they concluded that, while microneedling is a safe and effective option, methodological shortcomings and further research is required to establish it as an evidence-based therapeutic option.
“There are a limited number of high-quality studies demonstrating the efficacy of microneedling,” Dr. DiGiorgio said. “It is a safe procedure, which could complement laser treatments, so you could perform it between expensive and high-downtime lasers. It is an option for patients who seek measurable results with little to no downtime, and it’s also an option for clinicians who do not use laser-resurfacing devices. Basically, further research is needed to establish microneedling as an evidence-based therapeutic option. Laser continues to remain the gold standard for treatment.”
Another treatment option is fractional microneedling with radiofrequency (RF). These are microneedles which deliver energy in the form of RF at the tip of the needle, which denatures collagen and creates thermal coagulative injury zones at temperatures greater than 65° C. The microneedles can be insulated or noninsulated. “Insulated tips are safer for darker skin types because the epidermis is protected from the heat damage,” Dr. DiGiorgio said.
These treatments are used for the improvement of rhytides and scars and for skin tightening. “The treatments are painful and require topical anesthesia,” she said. “Erythema can range from about 24 hours to 4 days depending on the device being used. Usually monthly treatments are recommended.”
A study by investigators in South Korea and China set out to analyze histometric changes of this approach in pigs. They treated the pigs with a fractional microneedle delivery system at various depths, conduction times, and energies, and performed punch biopsies immediately after treatment, 4 days post treatment, and at 2 weeks post treatment. They noted that depth and conduction time affected the height, width, and volume of the columns of coagulation, but that the energy only affected the level of tissue destruction. “They also noted that RF-induced coagulated columns had a mixed cellular infiltrate, neovascularization, granular tissue formation with fibroblasts, and neocollagenesis and elastogenesis in the dermis,” Dr. DiGiorgio said.
In another study, researchers in Thailand performed a study in two women who were going to undergo abdominoplasty. Participants received six treatments prior to abdominoplasty with biopsies at different time intervals following microneedling with radiofrequency. The researchers tested five energy levels and five test areas; no collagen denaturization was observed with microneedling alone.
“This supports the idea that heat is required to stimulate neocollagenesis, and needles alone do not denature collagen,” Dr. DiGiorgio said. “They also found that neocollagenesis and neoelastogenesis occurred at optimal heating levels.”
In a separate study, researchers from Denmark used a number of different imaging modalities to evaluate the impact of microneedle fractional RF-induced micropores. When they used reflectance confocal microscopy, they observed that the micropores showed a concentric shape. “They contained hyper-reflective granules, and the coagulated tissue was seen from the epidermis to the dermal-epidermal junction,” Dr. DiGiorgio said. “This was not seen in the low energy microneedle RF. On optical coherence tomography, they noted that high-energy needle RF showed deeper, more easily identifiable micropores versus low-energy microneedle RF.” On histology the researchers noted that tissue coagulation reached a depth of 1,500 mcm with high-energy microneedle RF, but low-energy microneedle RF only showed visible damage to the epidermis. “This also supports the idea that microneedles alone without energy do not reach the deeper layers of the dermis,” she said.
Dr. DiGiorgio concluded her presentation by discussing promising results from a split-face study of fractional microneedling RF for the treatment of rosacea. For the 12-week randomized study, researchers from South Korea performed two sessions 4 weeks apart, with no treatment to the control side. Erythema decreased 13.6% and results were maintained for about 2 months after treatment. The researchers also measured inflammatory markers and noticed decreased dermal inflammation and mast cell counts and decreased markers related to angiogenesis, inflammation, innate immunity, and neuronal cation channels. “This could be a promising treatment for inflammatory rosacea in the future,” Dr. DiGiorgio said.
She disclosed that she is a consultant for Allergan Aesthetics.
according to Catherine M. DiGiorgio, MD, MS.
During a virtual course on laser and aesthetic skin therapy, Dr. DiGiorgio, a laser and cosmetic dermatologist at the Boston Center for Facial Rejuvenation, provided a state-of-the-art update on microneedling, a procedure in which microneedles are rolled over the skin to create epidermal and dermal microwounds.
“The depths are adjustable and it’s purely mechanical: no energy is being delivered with these treatments,” she said. “The hypothesized mechanism of action is that microneedling creates microwounds which initiate wound healing to stimulate new collagen production. This breaks apart compact collagen in the superficial dermis while stimulating new collagen and elastin,” she explained, adding that it is also hypothesized that this “stimulates growth factors that directly impact collagen and elastin synthesis.”
Conditions that have been reported to be treatable with microneedling in the medical literature include scars – especially acne scars – as well as rhytides, skin laxity, striae, melasma, and enlarged pores. Microneedling can also be used for transdermal drug delivery, although it’s far inferior to microinjection of medications. Contraindications are similar to those with laser surgery, including active infection of the area, history of keloids, inflammatory acne, and immunosuppression; and it should not be performed on the same day as neuromodulator treatment, to avoid diffusion of the neuromodulator. Herpes simplex virus prophylaxis is also indicated prior to microneedling treatment.
Many devices are available for use, including fixed, manual needle rollers and electric-powered pens with single-use sterile cartridges. The devices vary by needle length, quantity, diameter, configuration, and material of which the microneedles are made of. The needle length is not reliable for penetration depth, especially when greater than 1 mm. Treatment guidelines vary based on the area being treated.
“You put tension on the skin and apply the device perpendicularly,” Dr. DiGiorgio said during the meeting, which was sponsored by Harvard Medical School, Massachusetts General Hospital, and the Wellman Center for Photomedicine. “It should be performed in quadrants, and I prefer to treat in cosmetic units. The endpoint is pinpoint bleeding versus deep purpura. Ice water–soaked sterile gauze can be applied after treatment and skin care can be resumed in 5-7 days.”
In an effort to compare the efficacy and safety of the 2940-nm Er:YAG laser and microneedling for the treatment of atrophic acne scars, researchers in Egypt performed a randomized, split-face study in 30 patients. Study participants were evaluated by two blinded physicians at baseline and at 3 months follow-up. Both modalities showed a significant improvement in acne scars, but those treated with the Er:YAG laser showed a statistically significant greater improvement (70% vs. 30%, respectively; P < .001). Histology revealed a significantly higher increase in the mean quantity of collagen fibers in the Er:YAG-treated patients, compared with those who underwent microneedling, but patients in the microneedling group experienced less erythema and edema. Pain scores were significantly higher in the microneedling group compared with the Er:YAG group.
In a more recent study, researchers performed a systematic review of 37 articles in the medical literature related to microneedling. They found that the procedure provides good results when used on its own, and is preferred by patients because of its minimal downtime and side effects. However, they concluded that, while microneedling is a safe and effective option, methodological shortcomings and further research is required to establish it as an evidence-based therapeutic option.
“There are a limited number of high-quality studies demonstrating the efficacy of microneedling,” Dr. DiGiorgio said. “It is a safe procedure, which could complement laser treatments, so you could perform it between expensive and high-downtime lasers. It is an option for patients who seek measurable results with little to no downtime, and it’s also an option for clinicians who do not use laser-resurfacing devices. Basically, further research is needed to establish microneedling as an evidence-based therapeutic option. Laser continues to remain the gold standard for treatment.”
Another treatment option is fractional microneedling with radiofrequency (RF). These are microneedles which deliver energy in the form of RF at the tip of the needle, which denatures collagen and creates thermal coagulative injury zones at temperatures greater than 65° C. The microneedles can be insulated or noninsulated. “Insulated tips are safer for darker skin types because the epidermis is protected from the heat damage,” Dr. DiGiorgio said.
These treatments are used for the improvement of rhytides and scars and for skin tightening. “The treatments are painful and require topical anesthesia,” she said. “Erythema can range from about 24 hours to 4 days depending on the device being used. Usually monthly treatments are recommended.”
A study by investigators in South Korea and China set out to analyze histometric changes of this approach in pigs. They treated the pigs with a fractional microneedle delivery system at various depths, conduction times, and energies, and performed punch biopsies immediately after treatment, 4 days post treatment, and at 2 weeks post treatment. They noted that depth and conduction time affected the height, width, and volume of the columns of coagulation, but that the energy only affected the level of tissue destruction. “They also noted that RF-induced coagulated columns had a mixed cellular infiltrate, neovascularization, granular tissue formation with fibroblasts, and neocollagenesis and elastogenesis in the dermis,” Dr. DiGiorgio said.
In another study, researchers in Thailand performed a study in two women who were going to undergo abdominoplasty. Participants received six treatments prior to abdominoplasty with biopsies at different time intervals following microneedling with radiofrequency. The researchers tested five energy levels and five test areas; no collagen denaturization was observed with microneedling alone.
“This supports the idea that heat is required to stimulate neocollagenesis, and needles alone do not denature collagen,” Dr. DiGiorgio said. “They also found that neocollagenesis and neoelastogenesis occurred at optimal heating levels.”
In a separate study, researchers from Denmark used a number of different imaging modalities to evaluate the impact of microneedle fractional RF-induced micropores. When they used reflectance confocal microscopy, they observed that the micropores showed a concentric shape. “They contained hyper-reflective granules, and the coagulated tissue was seen from the epidermis to the dermal-epidermal junction,” Dr. DiGiorgio said. “This was not seen in the low energy microneedle RF. On optical coherence tomography, they noted that high-energy needle RF showed deeper, more easily identifiable micropores versus low-energy microneedle RF.” On histology the researchers noted that tissue coagulation reached a depth of 1,500 mcm with high-energy microneedle RF, but low-energy microneedle RF only showed visible damage to the epidermis. “This also supports the idea that microneedles alone without energy do not reach the deeper layers of the dermis,” she said.
Dr. DiGiorgio concluded her presentation by discussing promising results from a split-face study of fractional microneedling RF for the treatment of rosacea. For the 12-week randomized study, researchers from South Korea performed two sessions 4 weeks apart, with no treatment to the control side. Erythema decreased 13.6% and results were maintained for about 2 months after treatment. The researchers also measured inflammatory markers and noticed decreased dermal inflammation and mast cell counts and decreased markers related to angiogenesis, inflammation, innate immunity, and neuronal cation channels. “This could be a promising treatment for inflammatory rosacea in the future,” Dr. DiGiorgio said.
She disclosed that she is a consultant for Allergan Aesthetics.
FROM A LASER & AESTHETIC SKIN THERAPY COURSE
Metformin improves most outcomes for T2D during pregnancy
including reduced weight gain, reduced insulin doses, and fewer large-for-gestational-age babies, suggest the results of a randomized controlled trial.
However, the drug was associated with an increased risk of small-for-gestational-age babies, which poses the question as to risk versus benefit of metformin on the health of offspring.
“Better understanding of the short- and long-term implications of these effects on infants will be important to properly advise patients with type 2 diabetes contemplating use of metformin during pregnancy,” said lead author Denice S. Feig, MD, Mount Sinai Hospital, Toronto.
The research was presented at the Diabetes UK Professional Conference: Online Series on Nov. 17 and recently published in The Lancet Diabetes & Endocrinology.
Summing up, Dr. Feig said that, on balance, she would be inclined to give metformin to most pregnant women with type 2 diabetes, perhaps with the exception of those who may have risk factors for small-for-gestational-age babies; for example, women who’ve had intrauterine growth restriction, who are smokers, and have significant renal disease, or have a lower body mass index.
Increased prevalence of type 2 diabetes in pregnancy
Dr. Feig said that across the developed world there have been huge increases in the prevalence of type 2 diabetes in pregnancy in recent years.
Insulin is the standard treatment for the management of type 2 diabetes in pregnancy, but these women have marked insulin resistance that worsens in pregnancy, which means their insulin requirements increase, leading to weight gain, painful injections, high cost, and noncompliance.
So despite treatment with insulin, these women continue to face increased rates of adverse maternal and fetal outcomes.
And although metformin is increasingly being used in women with type 2 diabetes during pregnancy, there is a scarcity of data on the benefits and harms of metformin use on pregnancy outcomes in these women.
The MiTy trial was therefore undertaken to determine whether metformin could improve outcomes.
The team recruited 502 women from 29 sites in Canada and Australia who had type 2 diabetes prior to pregnancy or were diagnosed during pregnancy, before 20 weeks’ gestation. The women were randomized to metformin 1 g twice daily or placebo, in addition to their usual insulin regimen, at between 6 and 28 weeks’ gestation.
Type 2 diabetes was diagnosed prior to pregnancy in 83% of women in the metformin group and in 90% of those assigned to placebo. The mean hemoglobin A1c level at randomization was 47 mmol/mol (6.5%) in both groups.
The average maternal age at baseline was approximately 35 years and mean gestational age at randomization was 16 weeks. Mean prepregnancy BMI was approximately 34 kg/m2.
Of note, only 30% were of European ethnicity.
Less weight gain, lower A1c, less insulin needed with metformin
Dr. Feig reported that there was no significant difference between the treatment groups in terms of the proportion of women with the composite primary outcome of pregnancy loss, preterm birth, birth injury, respiratory distress, neonatal hypoglycemia, or admission to neonatal intensive care lasting more than 24 hours (P = 0.86).
However, women in the metformin group had significantly less overall weight gain during pregnancy than did those in the placebo group, at –1.8 kg (P < .0001).
They also had a significantly lower last A1c level in pregnancy, at 41 mmol/mol (5.9%) versus 43.2 mmol/mol (6.1%) in those given placebo (P = .015), and required fewer insulin doses, at 1.1 versus 1.5 units/kg/day (P < .0001), which translated to a reduction of almost 44 units/day.
Women given metformin were also less likely to require Cesarean section delivery, at 53.4% versus 62.7% in the placebo group (P = .03), although there was no difference between groups in terms of gestational hypertension or preeclampsia.
The most common adverse events were gastrointestinal complications, which occurred in 27.3% of women in the metformin group and 22.3% of those given placebo.
There were no significant differences between the metformin and placebo groups in rates of pregnancy loss (P = .81), preterm birth (P = .16), birth injury (P = .37), respiratory distress (P = .49), and congenital anomalies (P = .16).
Average birth weight lower with metformin
However, Dr. Feig showed that the average birth weight was lower for offspring of women given metformin than those assigned to placebo, at 3.2 kg (7.05 lb) versus 3.4 kg (7.4 lb) (P = .002).
Women given metformin were also less likely to have a baby with a birth weight of 4 kg (8.8 lb) or more, at 12.1% versus 19.2%, or a relative risk of 0.65 (P = .046), and a baby that was extremely large for gestational age, at 8.6% versus 14.8%, or a relative risk of 0.58 (P = .046).
But of concern, metformin was associated with an increased risk of small-for-gestational-age babies, at 12.9% versus 6.6% with placebo, or a relative risk of 1.96 (P = .03).
Dr. Feig suggested that this may be due to a direct effect of metformin “because as we know metformin inhibits the mTOR pathway,” which is a “primary nutrient sensor in the placenta” and could “attenuate nutrient flux and fetal growth.”
She said it is not clear whether the small-for-gestational-age babies were “healthy or unhealthy.”
To investigate further, the team has launched the MiTy Kids study, which will follow the offspring in the MiTy trial to determine whether metformin during pregnancy is associated with a reduction in adiposity and improvement in insulin resistance in the babies at 2 years of age.
Who should be given metformin?
During the discussion, Helen R. Murphy, MD, PhD, Norwich Medical School, University of East Anglia, England, asked whether Dr. Feig would recommend continuing metformin in pregnancy if it was started preconception for fertility issues rather than diabetes.
She replied: “If they don’t have diabetes and it’s simply for PCOS [polycystic ovary syndrome], then I have either stopped it as soon as they got pregnant or sometimes continued it through the first trimester, and then stopped.
“If the person has diabetes, however, I think given this work, for most people I would continue it,” she said.
The study was funded by the Canadian Institutes of Health Research, Lunenfeld-Tanenbaum Research Institute, and the University of Toronto. The authors have reported no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
including reduced weight gain, reduced insulin doses, and fewer large-for-gestational-age babies, suggest the results of a randomized controlled trial.
However, the drug was associated with an increased risk of small-for-gestational-age babies, which poses the question as to risk versus benefit of metformin on the health of offspring.
“Better understanding of the short- and long-term implications of these effects on infants will be important to properly advise patients with type 2 diabetes contemplating use of metformin during pregnancy,” said lead author Denice S. Feig, MD, Mount Sinai Hospital, Toronto.
The research was presented at the Diabetes UK Professional Conference: Online Series on Nov. 17 and recently published in The Lancet Diabetes & Endocrinology.
Summing up, Dr. Feig said that, on balance, she would be inclined to give metformin to most pregnant women with type 2 diabetes, perhaps with the exception of those who may have risk factors for small-for-gestational-age babies; for example, women who’ve had intrauterine growth restriction, who are smokers, and have significant renal disease, or have a lower body mass index.
Increased prevalence of type 2 diabetes in pregnancy
Dr. Feig said that across the developed world there have been huge increases in the prevalence of type 2 diabetes in pregnancy in recent years.
Insulin is the standard treatment for the management of type 2 diabetes in pregnancy, but these women have marked insulin resistance that worsens in pregnancy, which means their insulin requirements increase, leading to weight gain, painful injections, high cost, and noncompliance.
So despite treatment with insulin, these women continue to face increased rates of adverse maternal and fetal outcomes.
And although metformin is increasingly being used in women with type 2 diabetes during pregnancy, there is a scarcity of data on the benefits and harms of metformin use on pregnancy outcomes in these women.
The MiTy trial was therefore undertaken to determine whether metformin could improve outcomes.
The team recruited 502 women from 29 sites in Canada and Australia who had type 2 diabetes prior to pregnancy or were diagnosed during pregnancy, before 20 weeks’ gestation. The women were randomized to metformin 1 g twice daily or placebo, in addition to their usual insulin regimen, at between 6 and 28 weeks’ gestation.
Type 2 diabetes was diagnosed prior to pregnancy in 83% of women in the metformin group and in 90% of those assigned to placebo. The mean hemoglobin A1c level at randomization was 47 mmol/mol (6.5%) in both groups.
The average maternal age at baseline was approximately 35 years and mean gestational age at randomization was 16 weeks. Mean prepregnancy BMI was approximately 34 kg/m2.
Of note, only 30% were of European ethnicity.
Less weight gain, lower A1c, less insulin needed with metformin
Dr. Feig reported that there was no significant difference between the treatment groups in terms of the proportion of women with the composite primary outcome of pregnancy loss, preterm birth, birth injury, respiratory distress, neonatal hypoglycemia, or admission to neonatal intensive care lasting more than 24 hours (P = 0.86).
However, women in the metformin group had significantly less overall weight gain during pregnancy than did those in the placebo group, at –1.8 kg (P < .0001).
They also had a significantly lower last A1c level in pregnancy, at 41 mmol/mol (5.9%) versus 43.2 mmol/mol (6.1%) in those given placebo (P = .015), and required fewer insulin doses, at 1.1 versus 1.5 units/kg/day (P < .0001), which translated to a reduction of almost 44 units/day.
Women given metformin were also less likely to require Cesarean section delivery, at 53.4% versus 62.7% in the placebo group (P = .03), although there was no difference between groups in terms of gestational hypertension or preeclampsia.
The most common adverse events were gastrointestinal complications, which occurred in 27.3% of women in the metformin group and 22.3% of those given placebo.
There were no significant differences between the metformin and placebo groups in rates of pregnancy loss (P = .81), preterm birth (P = .16), birth injury (P = .37), respiratory distress (P = .49), and congenital anomalies (P = .16).
Average birth weight lower with metformin
However, Dr. Feig showed that the average birth weight was lower for offspring of women given metformin than those assigned to placebo, at 3.2 kg (7.05 lb) versus 3.4 kg (7.4 lb) (P = .002).
Women given metformin were also less likely to have a baby with a birth weight of 4 kg (8.8 lb) or more, at 12.1% versus 19.2%, or a relative risk of 0.65 (P = .046), and a baby that was extremely large for gestational age, at 8.6% versus 14.8%, or a relative risk of 0.58 (P = .046).
But of concern, metformin was associated with an increased risk of small-for-gestational-age babies, at 12.9% versus 6.6% with placebo, or a relative risk of 1.96 (P = .03).
Dr. Feig suggested that this may be due to a direct effect of metformin “because as we know metformin inhibits the mTOR pathway,” which is a “primary nutrient sensor in the placenta” and could “attenuate nutrient flux and fetal growth.”
She said it is not clear whether the small-for-gestational-age babies were “healthy or unhealthy.”
To investigate further, the team has launched the MiTy Kids study, which will follow the offspring in the MiTy trial to determine whether metformin during pregnancy is associated with a reduction in adiposity and improvement in insulin resistance in the babies at 2 years of age.
Who should be given metformin?
During the discussion, Helen R. Murphy, MD, PhD, Norwich Medical School, University of East Anglia, England, asked whether Dr. Feig would recommend continuing metformin in pregnancy if it was started preconception for fertility issues rather than diabetes.
She replied: “If they don’t have diabetes and it’s simply for PCOS [polycystic ovary syndrome], then I have either stopped it as soon as they got pregnant or sometimes continued it through the first trimester, and then stopped.
“If the person has diabetes, however, I think given this work, for most people I would continue it,” she said.
The study was funded by the Canadian Institutes of Health Research, Lunenfeld-Tanenbaum Research Institute, and the University of Toronto. The authors have reported no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
including reduced weight gain, reduced insulin doses, and fewer large-for-gestational-age babies, suggest the results of a randomized controlled trial.
However, the drug was associated with an increased risk of small-for-gestational-age babies, which poses the question as to risk versus benefit of metformin on the health of offspring.
“Better understanding of the short- and long-term implications of these effects on infants will be important to properly advise patients with type 2 diabetes contemplating use of metformin during pregnancy,” said lead author Denice S. Feig, MD, Mount Sinai Hospital, Toronto.
The research was presented at the Diabetes UK Professional Conference: Online Series on Nov. 17 and recently published in The Lancet Diabetes & Endocrinology.
Summing up, Dr. Feig said that, on balance, she would be inclined to give metformin to most pregnant women with type 2 diabetes, perhaps with the exception of those who may have risk factors for small-for-gestational-age babies; for example, women who’ve had intrauterine growth restriction, who are smokers, and have significant renal disease, or have a lower body mass index.
Increased prevalence of type 2 diabetes in pregnancy
Dr. Feig said that across the developed world there have been huge increases in the prevalence of type 2 diabetes in pregnancy in recent years.
Insulin is the standard treatment for the management of type 2 diabetes in pregnancy, but these women have marked insulin resistance that worsens in pregnancy, which means their insulin requirements increase, leading to weight gain, painful injections, high cost, and noncompliance.
So despite treatment with insulin, these women continue to face increased rates of adverse maternal and fetal outcomes.
And although metformin is increasingly being used in women with type 2 diabetes during pregnancy, there is a scarcity of data on the benefits and harms of metformin use on pregnancy outcomes in these women.
The MiTy trial was therefore undertaken to determine whether metformin could improve outcomes.
The team recruited 502 women from 29 sites in Canada and Australia who had type 2 diabetes prior to pregnancy or were diagnosed during pregnancy, before 20 weeks’ gestation. The women were randomized to metformin 1 g twice daily or placebo, in addition to their usual insulin regimen, at between 6 and 28 weeks’ gestation.
Type 2 diabetes was diagnosed prior to pregnancy in 83% of women in the metformin group and in 90% of those assigned to placebo. The mean hemoglobin A1c level at randomization was 47 mmol/mol (6.5%) in both groups.
The average maternal age at baseline was approximately 35 years and mean gestational age at randomization was 16 weeks. Mean prepregnancy BMI was approximately 34 kg/m2.
Of note, only 30% were of European ethnicity.
Less weight gain, lower A1c, less insulin needed with metformin
Dr. Feig reported that there was no significant difference between the treatment groups in terms of the proportion of women with the composite primary outcome of pregnancy loss, preterm birth, birth injury, respiratory distress, neonatal hypoglycemia, or admission to neonatal intensive care lasting more than 24 hours (P = 0.86).
However, women in the metformin group had significantly less overall weight gain during pregnancy than did those in the placebo group, at –1.8 kg (P < .0001).
They also had a significantly lower last A1c level in pregnancy, at 41 mmol/mol (5.9%) versus 43.2 mmol/mol (6.1%) in those given placebo (P = .015), and required fewer insulin doses, at 1.1 versus 1.5 units/kg/day (P < .0001), which translated to a reduction of almost 44 units/day.
Women given metformin were also less likely to require Cesarean section delivery, at 53.4% versus 62.7% in the placebo group (P = .03), although there was no difference between groups in terms of gestational hypertension or preeclampsia.
The most common adverse events were gastrointestinal complications, which occurred in 27.3% of women in the metformin group and 22.3% of those given placebo.
There were no significant differences between the metformin and placebo groups in rates of pregnancy loss (P = .81), preterm birth (P = .16), birth injury (P = .37), respiratory distress (P = .49), and congenital anomalies (P = .16).
Average birth weight lower with metformin
However, Dr. Feig showed that the average birth weight was lower for offspring of women given metformin than those assigned to placebo, at 3.2 kg (7.05 lb) versus 3.4 kg (7.4 lb) (P = .002).
Women given metformin were also less likely to have a baby with a birth weight of 4 kg (8.8 lb) or more, at 12.1% versus 19.2%, or a relative risk of 0.65 (P = .046), and a baby that was extremely large for gestational age, at 8.6% versus 14.8%, or a relative risk of 0.58 (P = .046).
But of concern, metformin was associated with an increased risk of small-for-gestational-age babies, at 12.9% versus 6.6% with placebo, or a relative risk of 1.96 (P = .03).
Dr. Feig suggested that this may be due to a direct effect of metformin “because as we know metformin inhibits the mTOR pathway,” which is a “primary nutrient sensor in the placenta” and could “attenuate nutrient flux and fetal growth.”
She said it is not clear whether the small-for-gestational-age babies were “healthy or unhealthy.”
To investigate further, the team has launched the MiTy Kids study, which will follow the offspring in the MiTy trial to determine whether metformin during pregnancy is associated with a reduction in adiposity and improvement in insulin resistance in the babies at 2 years of age.
Who should be given metformin?
During the discussion, Helen R. Murphy, MD, PhD, Norwich Medical School, University of East Anglia, England, asked whether Dr. Feig would recommend continuing metformin in pregnancy if it was started preconception for fertility issues rather than diabetes.
She replied: “If they don’t have diabetes and it’s simply for PCOS [polycystic ovary syndrome], then I have either stopped it as soon as they got pregnant or sometimes continued it through the first trimester, and then stopped.
“If the person has diabetes, however, I think given this work, for most people I would continue it,” she said.
The study was funded by the Canadian Institutes of Health Research, Lunenfeld-Tanenbaum Research Institute, and the University of Toronto. The authors have reported no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Neoadjuvant immunotherapy combo produces high response rate in melanoma
A neoadjuvant strategy combining two immunostimulatory agents with differing mechanisms of action is efficacious and safe in patients with high-risk, resectable melanoma, according to final results of the phase 2 Neo-C-Nivo trial.
The two agents are the PD-1 inhibitor nivolumab and CMP-001, an investigational Toll-like receptor 9 agonist that activates tumor-associated plasmacytoid dendritic cells.
CMP-001 and nivolumab produced a major pathologic response in 60% of patients, and these patients had a 1-year relapse-free survival rate of 89%. About 23% of patients had grade 3 treatment-related adverse events, and there were no grade 4-5 treatment-related events.
These data were reported at the Society for Immunotherapy of Cancer’s 35th Anniversary Annual Meeting.
“Stage III melanoma is a very, very high risk disease. Despite appropriate management, which involves surgical resection followed by adjuvant immunotherapy, a large number of patients still relapse,” noted study author Diwakar Davar, MD, of the University of Pittsburgh Hillman Cancer Center.
“Neoadjuvant immunotherapy in this setting enhances the systemic T-cell response to tumor antigens,” he explained. “As a result, there is greater detection and killing of micrometastatic disease. And, indeed, neoadjuvant immunotherapy with anti–[programmed death–1] monotherapy or with anti-PD1 and anti-CTLA4 combination therapy produces high response rates, although the combination therapy is associated with significant toxicity.”
Patients, treatment, and response
The Neo-C-Nivo trial enrolled 31 patients with resectable stage IIIB/C/D melanoma having clinically apparent lymph node disease.
The patients were treated with three cycles of nivolumab given every 2 weeks. They also received seven weekly injections of CMP-001 subcutaneously and then intratumorally. After surgical resection, the patients received more of the same immunotherapy.
At a median follow-up of 15 months, 60% of patients had a major pathologic response, 50% had a complete response, and 10% had a major response. Some 70% of patients (after additionally including partial responders) had any pathologic response.
“More than half of the patients that we treated had more than one injectable lesion,” Dr. Davar noted. “I want to emphasize that only one lesion was injected, so the results we got illustrate that the rest of the patients who had more than one injectable lesion had regression in their injected and uninjected lesions.”
Biomarker analyses showed that response was associated with evidence of immune activation, both in the tumor and in the blood. With immunotherapy, the density of CD8 tumor-infiltrating lymphocytes increased by a median of 10.3-fold in pathologic responders as compared with only 0.8-fold in nonresponders (P < .05). In addition, responders had evidence of activated CD8-positive T cells peripherally, as well as presence of plasmacytoid dendritic cells within the tumor microenvironment.
Survival and safety
Patients had better median relapse-free survival if they attained a major pathologic response (not reached in either group, P = .0106) or any pathologic response (not reached vs. 5 months, P = .0001).
The landmark 1-year relapse-free survival rate was 89% for major pathologic responders and 90% for all pathologic responders.
Overall, 22.6% of patients experienced grade 3 treatment-related adverse events, the majority of which did not require medical intervention and none of which delayed planned surgery. There were no grade 4-5 treatment-related adverse events.
Cytokine release syndrome was uncommon, seen in 16.1% of patients, possibly because the cohort received prophylaxis, Dr. Davar proposed.
Another treatment option?
“Intratumoral CMP-001 increases clinical efficacy of PD-1 blockade with minimal additional toxicity in patients with regionally advanced melanoma. Further study of this combination in high-risk resectable melanoma is planned,” Dr. Davar concluded.
“This combination achieved high response rates and certainly should be considered for a larger trial,” agreed session cochair Brian Gastman, MD, of the Cleveland (Ohio) Clinic.
However, long-term outcomes are pending, and it is not clear how efficacy of the studied combination will ultimately stack up against that of other treatment options, Dr. Gastman cautioned in an interview. “For example, it’s hard to tell if this will lead to better results versus, say, T-VEC [talimogene laherparepvec] with an anti-PD-1 agent,” he elaborated.
Nonetheless, “the implication of these findings is that there is another potential injectable option that can be combined with checkpoint inhibitors, and it may be useful for patients with refractory disease,” Dr. Gastman concluded.
The trial was funded by Checkmate Pharmaceuticals. Dr. Davar disclosed relationships with Checkmate Pharmaceuticals, Array Biopharma, Merck, Shionogi, Vedanta, Bristol-Myers Squibb, CellSight Technologies, GlaxoSmithKline/Tesaro, and Medpacto. Dr. Gastman disclosed no relevant conflicts of interest.
SOURCE: Davar D et al. SITC 2020, Abstract 303.
A neoadjuvant strategy combining two immunostimulatory agents with differing mechanisms of action is efficacious and safe in patients with high-risk, resectable melanoma, according to final results of the phase 2 Neo-C-Nivo trial.
The two agents are the PD-1 inhibitor nivolumab and CMP-001, an investigational Toll-like receptor 9 agonist that activates tumor-associated plasmacytoid dendritic cells.
CMP-001 and nivolumab produced a major pathologic response in 60% of patients, and these patients had a 1-year relapse-free survival rate of 89%. About 23% of patients had grade 3 treatment-related adverse events, and there were no grade 4-5 treatment-related events.
These data were reported at the Society for Immunotherapy of Cancer’s 35th Anniversary Annual Meeting.
“Stage III melanoma is a very, very high risk disease. Despite appropriate management, which involves surgical resection followed by adjuvant immunotherapy, a large number of patients still relapse,” noted study author Diwakar Davar, MD, of the University of Pittsburgh Hillman Cancer Center.
“Neoadjuvant immunotherapy in this setting enhances the systemic T-cell response to tumor antigens,” he explained. “As a result, there is greater detection and killing of micrometastatic disease. And, indeed, neoadjuvant immunotherapy with anti–[programmed death–1] monotherapy or with anti-PD1 and anti-CTLA4 combination therapy produces high response rates, although the combination therapy is associated with significant toxicity.”
Patients, treatment, and response
The Neo-C-Nivo trial enrolled 31 patients with resectable stage IIIB/C/D melanoma having clinically apparent lymph node disease.
The patients were treated with three cycles of nivolumab given every 2 weeks. They also received seven weekly injections of CMP-001 subcutaneously and then intratumorally. After surgical resection, the patients received more of the same immunotherapy.
At a median follow-up of 15 months, 60% of patients had a major pathologic response, 50% had a complete response, and 10% had a major response. Some 70% of patients (after additionally including partial responders) had any pathologic response.
“More than half of the patients that we treated had more than one injectable lesion,” Dr. Davar noted. “I want to emphasize that only one lesion was injected, so the results we got illustrate that the rest of the patients who had more than one injectable lesion had regression in their injected and uninjected lesions.”
Biomarker analyses showed that response was associated with evidence of immune activation, both in the tumor and in the blood. With immunotherapy, the density of CD8 tumor-infiltrating lymphocytes increased by a median of 10.3-fold in pathologic responders as compared with only 0.8-fold in nonresponders (P < .05). In addition, responders had evidence of activated CD8-positive T cells peripherally, as well as presence of plasmacytoid dendritic cells within the tumor microenvironment.
Survival and safety
Patients had better median relapse-free survival if they attained a major pathologic response (not reached in either group, P = .0106) or any pathologic response (not reached vs. 5 months, P = .0001).
The landmark 1-year relapse-free survival rate was 89% for major pathologic responders and 90% for all pathologic responders.
Overall, 22.6% of patients experienced grade 3 treatment-related adverse events, the majority of which did not require medical intervention and none of which delayed planned surgery. There were no grade 4-5 treatment-related adverse events.
Cytokine release syndrome was uncommon, seen in 16.1% of patients, possibly because the cohort received prophylaxis, Dr. Davar proposed.
Another treatment option?
“Intratumoral CMP-001 increases clinical efficacy of PD-1 blockade with minimal additional toxicity in patients with regionally advanced melanoma. Further study of this combination in high-risk resectable melanoma is planned,” Dr. Davar concluded.
“This combination achieved high response rates and certainly should be considered for a larger trial,” agreed session cochair Brian Gastman, MD, of the Cleveland (Ohio) Clinic.
However, long-term outcomes are pending, and it is not clear how efficacy of the studied combination will ultimately stack up against that of other treatment options, Dr. Gastman cautioned in an interview. “For example, it’s hard to tell if this will lead to better results versus, say, T-VEC [talimogene laherparepvec] with an anti-PD-1 agent,” he elaborated.
Nonetheless, “the implication of these findings is that there is another potential injectable option that can be combined with checkpoint inhibitors, and it may be useful for patients with refractory disease,” Dr. Gastman concluded.
The trial was funded by Checkmate Pharmaceuticals. Dr. Davar disclosed relationships with Checkmate Pharmaceuticals, Array Biopharma, Merck, Shionogi, Vedanta, Bristol-Myers Squibb, CellSight Technologies, GlaxoSmithKline/Tesaro, and Medpacto. Dr. Gastman disclosed no relevant conflicts of interest.
SOURCE: Davar D et al. SITC 2020, Abstract 303.
A neoadjuvant strategy combining two immunostimulatory agents with differing mechanisms of action is efficacious and safe in patients with high-risk, resectable melanoma, according to final results of the phase 2 Neo-C-Nivo trial.
The two agents are the PD-1 inhibitor nivolumab and CMP-001, an investigational Toll-like receptor 9 agonist that activates tumor-associated plasmacytoid dendritic cells.
CMP-001 and nivolumab produced a major pathologic response in 60% of patients, and these patients had a 1-year relapse-free survival rate of 89%. About 23% of patients had grade 3 treatment-related adverse events, and there were no grade 4-5 treatment-related events.
These data were reported at the Society for Immunotherapy of Cancer’s 35th Anniversary Annual Meeting.
“Stage III melanoma is a very, very high risk disease. Despite appropriate management, which involves surgical resection followed by adjuvant immunotherapy, a large number of patients still relapse,” noted study author Diwakar Davar, MD, of the University of Pittsburgh Hillman Cancer Center.
“Neoadjuvant immunotherapy in this setting enhances the systemic T-cell response to tumor antigens,” he explained. “As a result, there is greater detection and killing of micrometastatic disease. And, indeed, neoadjuvant immunotherapy with anti–[programmed death–1] monotherapy or with anti-PD1 and anti-CTLA4 combination therapy produces high response rates, although the combination therapy is associated with significant toxicity.”
Patients, treatment, and response
The Neo-C-Nivo trial enrolled 31 patients with resectable stage IIIB/C/D melanoma having clinically apparent lymph node disease.
The patients were treated with three cycles of nivolumab given every 2 weeks. They also received seven weekly injections of CMP-001 subcutaneously and then intratumorally. After surgical resection, the patients received more of the same immunotherapy.
At a median follow-up of 15 months, 60% of patients had a major pathologic response, 50% had a complete response, and 10% had a major response. Some 70% of patients (after additionally including partial responders) had any pathologic response.
“More than half of the patients that we treated had more than one injectable lesion,” Dr. Davar noted. “I want to emphasize that only one lesion was injected, so the results we got illustrate that the rest of the patients who had more than one injectable lesion had regression in their injected and uninjected lesions.”
Biomarker analyses showed that response was associated with evidence of immune activation, both in the tumor and in the blood. With immunotherapy, the density of CD8 tumor-infiltrating lymphocytes increased by a median of 10.3-fold in pathologic responders as compared with only 0.8-fold in nonresponders (P < .05). In addition, responders had evidence of activated CD8-positive T cells peripherally, as well as presence of plasmacytoid dendritic cells within the tumor microenvironment.
Survival and safety
Patients had better median relapse-free survival if they attained a major pathologic response (not reached in either group, P = .0106) or any pathologic response (not reached vs. 5 months, P = .0001).
The landmark 1-year relapse-free survival rate was 89% for major pathologic responders and 90% for all pathologic responders.
Overall, 22.6% of patients experienced grade 3 treatment-related adverse events, the majority of which did not require medical intervention and none of which delayed planned surgery. There were no grade 4-5 treatment-related adverse events.
Cytokine release syndrome was uncommon, seen in 16.1% of patients, possibly because the cohort received prophylaxis, Dr. Davar proposed.
Another treatment option?
“Intratumoral CMP-001 increases clinical efficacy of PD-1 blockade with minimal additional toxicity in patients with regionally advanced melanoma. Further study of this combination in high-risk resectable melanoma is planned,” Dr. Davar concluded.
“This combination achieved high response rates and certainly should be considered for a larger trial,” agreed session cochair Brian Gastman, MD, of the Cleveland (Ohio) Clinic.
However, long-term outcomes are pending, and it is not clear how efficacy of the studied combination will ultimately stack up against that of other treatment options, Dr. Gastman cautioned in an interview. “For example, it’s hard to tell if this will lead to better results versus, say, T-VEC [talimogene laherparepvec] with an anti-PD-1 agent,” he elaborated.
Nonetheless, “the implication of these findings is that there is another potential injectable option that can be combined with checkpoint inhibitors, and it may be useful for patients with refractory disease,” Dr. Gastman concluded.
The trial was funded by Checkmate Pharmaceuticals. Dr. Davar disclosed relationships with Checkmate Pharmaceuticals, Array Biopharma, Merck, Shionogi, Vedanta, Bristol-Myers Squibb, CellSight Technologies, GlaxoSmithKline/Tesaro, and Medpacto. Dr. Gastman disclosed no relevant conflicts of interest.
SOURCE: Davar D et al. SITC 2020, Abstract 303.
FROM SITC 2020
Is a pelvic examination necessary 6 weeks after hysterectomy?
Doctors commonly perform pelvic examinations approximately 6 weeks following hysterectomy to assess the integrity of the vaginal cuff. But this practice may not be necessary if patients do not have symptoms, a study suggests.
“The 6-week posthysterectomy pelvic examination in asymptomatic women may not be necessary, as it neither detected cuff dehiscence nor negated future risk for dehiscence,” Ritchie Mae Delara, MD, said at the meeting sponsored by AAGL, held virtually this year.
Dr. Delara, of the Mayo Clinic in Phoenix, and colleagues conducted a retrospective cohort study of data from more than 2,000 patients to assess the utility of the 6-week posthysterectomy pelvic examination in detecting cuff dehiscence in asymptomatic women.
An unpredictable complication
Vaginal cuff dehiscence is a rare complication of hysterectomy that can occur days or decades after surgery, which makes “identifying an optimal time for cuff evaluation difficult,” Dr. Delara said. “Currently there is neither evidence demonstrating benefit of routine posthysterectomy examination in detecting vaginal cuff dehiscence, nor data demonstrating the best time to perform posthysterectomy examination.”
For their study, which was also published in the Journal of Minimally Invasive Gynecology, the researchers examined data from 2,051 women who underwent hysterectomy at a single institution during a 6-year period. Patients received at least one postoperative evaluation within 90 days of surgery. Examination of the vaginal cuff routinely was performed approximately 6 weeks after hysterectomy. Patients’ posthysterectomy symptoms and pelvic examination findings were recorded.
About 80% of patients were asymptomatic at the 6-week visit.
Asymptomatic patients were more likely to have normal pelvic examination findings, compared with patients with posthysterectomy symptoms (86.4% vs. 54.3%).
In all, 13 patients experienced complete cuff dehiscence. All of them had an intact vaginal cuff at their 6-week examination. Three had symptoms at that time, including vaginal bleeding in one patient and pelvic pain in two patients.
One patient experienced a complete cuff dehiscence that was provoked by intercourse prior to her examination. The patient subsequently developed two additional episodes of dehiscence provoked by intercourse.
Dehiscence may present differently after benign and oncologic hysterectomies, the study indicated.
Eight patients who experienced complete cuff dehiscence after benign hysterectomy had symptoms such as pelvic pain and vaginal bleeding at the time of presentation for dehiscence, which mainly occurred after intercourse.
Five patients who experienced dehiscence after oncologic hysterectomy were more likely to present without symptoms or provocation.
The median time to dehiscence after benign hysterectomy was about 19 weeks, whereas the median time to dehiscence after oncologic hysterectomy was about 81 weeks.
Surgeons should educate patients about symptoms of dehiscence and the potential for events such as coitus to provoke its occurrence, and patients should promptly seek evaluation if symptoms occur, Dr. Delara said.
Patients with risk factors such as malignancy may benefit from continued routine evaluation, she added.
Timely research
The findings may be especially relevant during the COVID-19 pandemic, when states have issued shelter-in-place orders and doctors have increased their use of telemedicine to reduce in-person visits, Dr. Delara noted.
In that sense, the study is “extremely timely” and may inform and support practice changes, commented Emad Mikhail, MD, in a discussion following the research presentation.
Whether the results generalize to other centers, including smaller centers that perform fewer surgeries, is unclear, said Dr. Mikhail, of the University of South Florida, Tampa.
“It takes vision and critical thinking to challenge these traditional practices,” he said. “I applaud Dr. Delara for challenging one of these.”
Dr. Delara and Dr. Mikhail had no relevant disclosures.
SOURCE: Delara RMM et al. J Minim Invasive Gynecol. 2020 Nov 1. doi: 10.1016/j.jmig.2020.08.306.
Doctors commonly perform pelvic examinations approximately 6 weeks following hysterectomy to assess the integrity of the vaginal cuff. But this practice may not be necessary if patients do not have symptoms, a study suggests.
“The 6-week posthysterectomy pelvic examination in asymptomatic women may not be necessary, as it neither detected cuff dehiscence nor negated future risk for dehiscence,” Ritchie Mae Delara, MD, said at the meeting sponsored by AAGL, held virtually this year.
Dr. Delara, of the Mayo Clinic in Phoenix, and colleagues conducted a retrospective cohort study of data from more than 2,000 patients to assess the utility of the 6-week posthysterectomy pelvic examination in detecting cuff dehiscence in asymptomatic women.
An unpredictable complication
Vaginal cuff dehiscence is a rare complication of hysterectomy that can occur days or decades after surgery, which makes “identifying an optimal time for cuff evaluation difficult,” Dr. Delara said. “Currently there is neither evidence demonstrating benefit of routine posthysterectomy examination in detecting vaginal cuff dehiscence, nor data demonstrating the best time to perform posthysterectomy examination.”
For their study, which was also published in the Journal of Minimally Invasive Gynecology, the researchers examined data from 2,051 women who underwent hysterectomy at a single institution during a 6-year period. Patients received at least one postoperative evaluation within 90 days of surgery. Examination of the vaginal cuff routinely was performed approximately 6 weeks after hysterectomy. Patients’ posthysterectomy symptoms and pelvic examination findings were recorded.
About 80% of patients were asymptomatic at the 6-week visit.
Asymptomatic patients were more likely to have normal pelvic examination findings, compared with patients with posthysterectomy symptoms (86.4% vs. 54.3%).
In all, 13 patients experienced complete cuff dehiscence. All of them had an intact vaginal cuff at their 6-week examination. Three had symptoms at that time, including vaginal bleeding in one patient and pelvic pain in two patients.
One patient experienced a complete cuff dehiscence that was provoked by intercourse prior to her examination. The patient subsequently developed two additional episodes of dehiscence provoked by intercourse.
Dehiscence may present differently after benign and oncologic hysterectomies, the study indicated.
Eight patients who experienced complete cuff dehiscence after benign hysterectomy had symptoms such as pelvic pain and vaginal bleeding at the time of presentation for dehiscence, which mainly occurred after intercourse.
Five patients who experienced dehiscence after oncologic hysterectomy were more likely to present without symptoms or provocation.
The median time to dehiscence after benign hysterectomy was about 19 weeks, whereas the median time to dehiscence after oncologic hysterectomy was about 81 weeks.
Surgeons should educate patients about symptoms of dehiscence and the potential for events such as coitus to provoke its occurrence, and patients should promptly seek evaluation if symptoms occur, Dr. Delara said.
Patients with risk factors such as malignancy may benefit from continued routine evaluation, she added.
Timely research
The findings may be especially relevant during the COVID-19 pandemic, when states have issued shelter-in-place orders and doctors have increased their use of telemedicine to reduce in-person visits, Dr. Delara noted.
In that sense, the study is “extremely timely” and may inform and support practice changes, commented Emad Mikhail, MD, in a discussion following the research presentation.
Whether the results generalize to other centers, including smaller centers that perform fewer surgeries, is unclear, said Dr. Mikhail, of the University of South Florida, Tampa.
“It takes vision and critical thinking to challenge these traditional practices,” he said. “I applaud Dr. Delara for challenging one of these.”
Dr. Delara and Dr. Mikhail had no relevant disclosures.
SOURCE: Delara RMM et al. J Minim Invasive Gynecol. 2020 Nov 1. doi: 10.1016/j.jmig.2020.08.306.
Doctors commonly perform pelvic examinations approximately 6 weeks following hysterectomy to assess the integrity of the vaginal cuff. But this practice may not be necessary if patients do not have symptoms, a study suggests.
“The 6-week posthysterectomy pelvic examination in asymptomatic women may not be necessary, as it neither detected cuff dehiscence nor negated future risk for dehiscence,” Ritchie Mae Delara, MD, said at the meeting sponsored by AAGL, held virtually this year.
Dr. Delara, of the Mayo Clinic in Phoenix, and colleagues conducted a retrospective cohort study of data from more than 2,000 patients to assess the utility of the 6-week posthysterectomy pelvic examination in detecting cuff dehiscence in asymptomatic women.
An unpredictable complication
Vaginal cuff dehiscence is a rare complication of hysterectomy that can occur days or decades after surgery, which makes “identifying an optimal time for cuff evaluation difficult,” Dr. Delara said. “Currently there is neither evidence demonstrating benefit of routine posthysterectomy examination in detecting vaginal cuff dehiscence, nor data demonstrating the best time to perform posthysterectomy examination.”
For their study, which was also published in the Journal of Minimally Invasive Gynecology, the researchers examined data from 2,051 women who underwent hysterectomy at a single institution during a 6-year period. Patients received at least one postoperative evaluation within 90 days of surgery. Examination of the vaginal cuff routinely was performed approximately 6 weeks after hysterectomy. Patients’ posthysterectomy symptoms and pelvic examination findings were recorded.
About 80% of patients were asymptomatic at the 6-week visit.
Asymptomatic patients were more likely to have normal pelvic examination findings, compared with patients with posthysterectomy symptoms (86.4% vs. 54.3%).
In all, 13 patients experienced complete cuff dehiscence. All of them had an intact vaginal cuff at their 6-week examination. Three had symptoms at that time, including vaginal bleeding in one patient and pelvic pain in two patients.
One patient experienced a complete cuff dehiscence that was provoked by intercourse prior to her examination. The patient subsequently developed two additional episodes of dehiscence provoked by intercourse.
Dehiscence may present differently after benign and oncologic hysterectomies, the study indicated.
Eight patients who experienced complete cuff dehiscence after benign hysterectomy had symptoms such as pelvic pain and vaginal bleeding at the time of presentation for dehiscence, which mainly occurred after intercourse.
Five patients who experienced dehiscence after oncologic hysterectomy were more likely to present without symptoms or provocation.
The median time to dehiscence after benign hysterectomy was about 19 weeks, whereas the median time to dehiscence after oncologic hysterectomy was about 81 weeks.
Surgeons should educate patients about symptoms of dehiscence and the potential for events such as coitus to provoke its occurrence, and patients should promptly seek evaluation if symptoms occur, Dr. Delara said.
Patients with risk factors such as malignancy may benefit from continued routine evaluation, she added.
Timely research
The findings may be especially relevant during the COVID-19 pandemic, when states have issued shelter-in-place orders and doctors have increased their use of telemedicine to reduce in-person visits, Dr. Delara noted.
In that sense, the study is “extremely timely” and may inform and support practice changes, commented Emad Mikhail, MD, in a discussion following the research presentation.
Whether the results generalize to other centers, including smaller centers that perform fewer surgeries, is unclear, said Dr. Mikhail, of the University of South Florida, Tampa.
“It takes vision and critical thinking to challenge these traditional practices,” he said. “I applaud Dr. Delara for challenging one of these.”
Dr. Delara and Dr. Mikhail had no relevant disclosures.
SOURCE: Delara RMM et al. J Minim Invasive Gynecol. 2020 Nov 1. doi: 10.1016/j.jmig.2020.08.306.
FROM AAGL GLOBAL CONGRESS
Blood pressure treatment reduces bleeding in ICH
a systematic review and meta-analysis shows, although it does reduce hematoma growth in these patients.
Despite the negative finding, the investigators observed broad variation in treatment effect among the studies they reviewed. They also found that target-based blood pressure treatment tended to improve function more than fixed-dose treatment.
“These data provide a strong message that early blood pressure–lowering treatment can control bleeding. This was not clear beforehand,” Craig Anderson, PhD, professor of neurology and epidemiology at the University of New South Wales, Sydney, said in an interview.
“But these data also indicate that the management of blood pressure in ICH is complex,” he added. Timing, type of drug, and type of patient must be considered, he said. “We need more data to allow better individualizing of such therapy.”
The results were presented at the European Stroke Organisation–World Stroke Organisation (ESO-WSO) Conference 2020.
Controversy about the efficacy of blood pressure reduction for patients with ICH continues, despite studies that have examined this question. In this analysis, Dr. Anderson and colleagues sought to examine the evidence from randomized controlled trials in this area and identify potentially overlooked heterogeneity among trials.
The investigators conducted a systematic review and meta-analysis of studies in the Cochrane Central Register of Controlled Trials, EMBASE, and MEDLINE databases. They searched for randomized controlled trials of blood pressure management for adults with acute ICH, focusing on studies in which patients were enrolled within 7 days of ICH onset. These studies compared intensive blood pressure management with guideline-based management.
Investigators chose function, defined as Modified Rankin Scale (mRS) score at 90 days, as their primary outcome. Radiologic outcomes included absolute (>6 mL) and proportional (>33%) hematoma growth at 24 hours. They used the intention to treat dataset from each trial in their statistical analyses and created generalized linear mixed models with prespecified covariables using a one-stage approach.
Variation by drug
A total of 7,094 studies were identified, of which 50 were eligible for inclusion. Their analysis encompassed 16 studies for which the respective investigators were willing to share patient-level data. The analysis included data on 6,221 patients. The mean age of the patients was 64.2 years, 36.4% were women, and the median time from symptom onset to randomization was 3.8 hours.
Mean National Institutes of Health Stroke Scale score was approximately 11. Mean systolic blood pressure at baseline was 177 mm Hg, and mean hematoma volume was approximately 10.6 mL.
The difference in blood pressure between the intensive and guideline groups was approximately 8 mm Hg at 1 hour and 12 mm Hg at 24 hours.
Intensive blood pressure management did not affect function at 90 days. The adjusted odds ratio for unfavorable shift in mRS scores was 0.97 (95% CI, 0.88-1.06; P = .503). Intensive blood pressure management did, however, reduce hematoma growth (absolute aOR, 0.75; 95% CI, 0.60-0.92; P = .007; relative aOR, 0.82; 95% CI, 0.68-0.99; P = .034).
In prespecified subgroup analyses, they found a trend toward adverse outcomes among patients who received renin-angiotensin blockers and a trend toward benefit for patients who received alpha- or beta-receptor antagonists or calcium channel blockers. They did not observe a clear association between time of treatment and outcome.
In addition to hematoma growth, other factors influence prognosis after ICH, such as the patient’s status before ICH (for example, cardiovascular risk factors, age, and hypertensive effects on the brain, kidneys, and heart), the location of ICH and its effects on surrounding structures, and complications of care in hospitals, such as infection and bleeding, said Dr. Anderson.
They are conducting two ongoing clinical trials in patients with ICH. One, INTERACT3, is evaluating a “care bundle” quality control package that includes early intensive blood pressure lowering for patients with large ICH who undergo surgery.
The other, INTERACT4, is evaluating early blood pressure control in the ambulance for patients with suspected acute stroke. At least one-fifth of those patients will have ICH, said Dr. Anderson.
Prevention is essential
Among patients with ICH, much of the bleeding occurs before presentation at the hospital, Louis R. Caplan, MD, a neurologist at Beth Israel Deaconess Medical Center, Boston, said in an interview. Furthermore, the bleeding mainly occurs in the deep part of the brain where most of the important motor tracts are. “If those tracts are already hit, a little extra blood isn’t going to change things,” said Dr. Caplan, who was not involved in the research.
In addition, blood is pushed from inside the brain to the periphery until the pressure outside the brain is equal to the pressure inside it. “You can decrease the amount of bleeding significantly, but it probably doesn’t affect the outcome,” said Dr. Caplan.
One factor in patients’ apparent lack of functional improvement is that the mRS is not sensitive to minor changes in disability, he said. “You have to show a pretty important change for it to make a difference,” said Dr. Caplan.
In addition, recovery from a hemorrhage takes much longer than recovery from an infarct. Examining the population at 6 months would have been preferable to examining them at 90 days, but the investigators might not have 6-month data, said Dr. Caplan.
“The main thing is really prevention,” he concluded.
The study was conducted with funding from Takeda. Dr. Anderson reported receiving funding from the National Health and Medical Research Council of Australia and speaker fees from Takeda. Dr. Caplan has disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
a systematic review and meta-analysis shows, although it does reduce hematoma growth in these patients.
Despite the negative finding, the investigators observed broad variation in treatment effect among the studies they reviewed. They also found that target-based blood pressure treatment tended to improve function more than fixed-dose treatment.
“These data provide a strong message that early blood pressure–lowering treatment can control bleeding. This was not clear beforehand,” Craig Anderson, PhD, professor of neurology and epidemiology at the University of New South Wales, Sydney, said in an interview.
“But these data also indicate that the management of blood pressure in ICH is complex,” he added. Timing, type of drug, and type of patient must be considered, he said. “We need more data to allow better individualizing of such therapy.”
The results were presented at the European Stroke Organisation–World Stroke Organisation (ESO-WSO) Conference 2020.
Controversy about the efficacy of blood pressure reduction for patients with ICH continues, despite studies that have examined this question. In this analysis, Dr. Anderson and colleagues sought to examine the evidence from randomized controlled trials in this area and identify potentially overlooked heterogeneity among trials.
The investigators conducted a systematic review and meta-analysis of studies in the Cochrane Central Register of Controlled Trials, EMBASE, and MEDLINE databases. They searched for randomized controlled trials of blood pressure management for adults with acute ICH, focusing on studies in which patients were enrolled within 7 days of ICH onset. These studies compared intensive blood pressure management with guideline-based management.
Investigators chose function, defined as Modified Rankin Scale (mRS) score at 90 days, as their primary outcome. Radiologic outcomes included absolute (>6 mL) and proportional (>33%) hematoma growth at 24 hours. They used the intention to treat dataset from each trial in their statistical analyses and created generalized linear mixed models with prespecified covariables using a one-stage approach.
Variation by drug
A total of 7,094 studies were identified, of which 50 were eligible for inclusion. Their analysis encompassed 16 studies for which the respective investigators were willing to share patient-level data. The analysis included data on 6,221 patients. The mean age of the patients was 64.2 years, 36.4% were women, and the median time from symptom onset to randomization was 3.8 hours.
Mean National Institutes of Health Stroke Scale score was approximately 11. Mean systolic blood pressure at baseline was 177 mm Hg, and mean hematoma volume was approximately 10.6 mL.
The difference in blood pressure between the intensive and guideline groups was approximately 8 mm Hg at 1 hour and 12 mm Hg at 24 hours.
Intensive blood pressure management did not affect function at 90 days. The adjusted odds ratio for unfavorable shift in mRS scores was 0.97 (95% CI, 0.88-1.06; P = .503). Intensive blood pressure management did, however, reduce hematoma growth (absolute aOR, 0.75; 95% CI, 0.60-0.92; P = .007; relative aOR, 0.82; 95% CI, 0.68-0.99; P = .034).
In prespecified subgroup analyses, they found a trend toward adverse outcomes among patients who received renin-angiotensin blockers and a trend toward benefit for patients who received alpha- or beta-receptor antagonists or calcium channel blockers. They did not observe a clear association between time of treatment and outcome.
In addition to hematoma growth, other factors influence prognosis after ICH, such as the patient’s status before ICH (for example, cardiovascular risk factors, age, and hypertensive effects on the brain, kidneys, and heart), the location of ICH and its effects on surrounding structures, and complications of care in hospitals, such as infection and bleeding, said Dr. Anderson.
They are conducting two ongoing clinical trials in patients with ICH. One, INTERACT3, is evaluating a “care bundle” quality control package that includes early intensive blood pressure lowering for patients with large ICH who undergo surgery.
The other, INTERACT4, is evaluating early blood pressure control in the ambulance for patients with suspected acute stroke. At least one-fifth of those patients will have ICH, said Dr. Anderson.
Prevention is essential
Among patients with ICH, much of the bleeding occurs before presentation at the hospital, Louis R. Caplan, MD, a neurologist at Beth Israel Deaconess Medical Center, Boston, said in an interview. Furthermore, the bleeding mainly occurs in the deep part of the brain where most of the important motor tracts are. “If those tracts are already hit, a little extra blood isn’t going to change things,” said Dr. Caplan, who was not involved in the research.
In addition, blood is pushed from inside the brain to the periphery until the pressure outside the brain is equal to the pressure inside it. “You can decrease the amount of bleeding significantly, but it probably doesn’t affect the outcome,” said Dr. Caplan.
One factor in patients’ apparent lack of functional improvement is that the mRS is not sensitive to minor changes in disability, he said. “You have to show a pretty important change for it to make a difference,” said Dr. Caplan.
In addition, recovery from a hemorrhage takes much longer than recovery from an infarct. Examining the population at 6 months would have been preferable to examining them at 90 days, but the investigators might not have 6-month data, said Dr. Caplan.
“The main thing is really prevention,” he concluded.
The study was conducted with funding from Takeda. Dr. Anderson reported receiving funding from the National Health and Medical Research Council of Australia and speaker fees from Takeda. Dr. Caplan has disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
a systematic review and meta-analysis shows, although it does reduce hematoma growth in these patients.
Despite the negative finding, the investigators observed broad variation in treatment effect among the studies they reviewed. They also found that target-based blood pressure treatment tended to improve function more than fixed-dose treatment.
“These data provide a strong message that early blood pressure–lowering treatment can control bleeding. This was not clear beforehand,” Craig Anderson, PhD, professor of neurology and epidemiology at the University of New South Wales, Sydney, said in an interview.
“But these data also indicate that the management of blood pressure in ICH is complex,” he added. Timing, type of drug, and type of patient must be considered, he said. “We need more data to allow better individualizing of such therapy.”
The results were presented at the European Stroke Organisation–World Stroke Organisation (ESO-WSO) Conference 2020.
Controversy about the efficacy of blood pressure reduction for patients with ICH continues, despite studies that have examined this question. In this analysis, Dr. Anderson and colleagues sought to examine the evidence from randomized controlled trials in this area and identify potentially overlooked heterogeneity among trials.
The investigators conducted a systematic review and meta-analysis of studies in the Cochrane Central Register of Controlled Trials, EMBASE, and MEDLINE databases. They searched for randomized controlled trials of blood pressure management for adults with acute ICH, focusing on studies in which patients were enrolled within 7 days of ICH onset. These studies compared intensive blood pressure management with guideline-based management.
Investigators chose function, defined as Modified Rankin Scale (mRS) score at 90 days, as their primary outcome. Radiologic outcomes included absolute (>6 mL) and proportional (>33%) hematoma growth at 24 hours. They used the intention to treat dataset from each trial in their statistical analyses and created generalized linear mixed models with prespecified covariables using a one-stage approach.
Variation by drug
A total of 7,094 studies were identified, of which 50 were eligible for inclusion. Their analysis encompassed 16 studies for which the respective investigators were willing to share patient-level data. The analysis included data on 6,221 patients. The mean age of the patients was 64.2 years, 36.4% were women, and the median time from symptom onset to randomization was 3.8 hours.
Mean National Institutes of Health Stroke Scale score was approximately 11. Mean systolic blood pressure at baseline was 177 mm Hg, and mean hematoma volume was approximately 10.6 mL.
The difference in blood pressure between the intensive and guideline groups was approximately 8 mm Hg at 1 hour and 12 mm Hg at 24 hours.
Intensive blood pressure management did not affect function at 90 days. The adjusted odds ratio for unfavorable shift in mRS scores was 0.97 (95% CI, 0.88-1.06; P = .503). Intensive blood pressure management did, however, reduce hematoma growth (absolute aOR, 0.75; 95% CI, 0.60-0.92; P = .007; relative aOR, 0.82; 95% CI, 0.68-0.99; P = .034).
In prespecified subgroup analyses, they found a trend toward adverse outcomes among patients who received renin-angiotensin blockers and a trend toward benefit for patients who received alpha- or beta-receptor antagonists or calcium channel blockers. They did not observe a clear association between time of treatment and outcome.
In addition to hematoma growth, other factors influence prognosis after ICH, such as the patient’s status before ICH (for example, cardiovascular risk factors, age, and hypertensive effects on the brain, kidneys, and heart), the location of ICH and its effects on surrounding structures, and complications of care in hospitals, such as infection and bleeding, said Dr. Anderson.
They are conducting two ongoing clinical trials in patients with ICH. One, INTERACT3, is evaluating a “care bundle” quality control package that includes early intensive blood pressure lowering for patients with large ICH who undergo surgery.
The other, INTERACT4, is evaluating early blood pressure control in the ambulance for patients with suspected acute stroke. At least one-fifth of those patients will have ICH, said Dr. Anderson.
Prevention is essential
Among patients with ICH, much of the bleeding occurs before presentation at the hospital, Louis R. Caplan, MD, a neurologist at Beth Israel Deaconess Medical Center, Boston, said in an interview. Furthermore, the bleeding mainly occurs in the deep part of the brain where most of the important motor tracts are. “If those tracts are already hit, a little extra blood isn’t going to change things,” said Dr. Caplan, who was not involved in the research.
In addition, blood is pushed from inside the brain to the periphery until the pressure outside the brain is equal to the pressure inside it. “You can decrease the amount of bleeding significantly, but it probably doesn’t affect the outcome,” said Dr. Caplan.
One factor in patients’ apparent lack of functional improvement is that the mRS is not sensitive to minor changes in disability, he said. “You have to show a pretty important change for it to make a difference,” said Dr. Caplan.
In addition, recovery from a hemorrhage takes much longer than recovery from an infarct. Examining the population at 6 months would have been preferable to examining them at 90 days, but the investigators might not have 6-month data, said Dr. Caplan.
“The main thing is really prevention,” he concluded.
The study was conducted with funding from Takeda. Dr. Anderson reported receiving funding from the National Health and Medical Research Council of Australia and speaker fees from Takeda. Dr. Caplan has disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
FROM ESO-WSO CONFERENCE 2020