User login
How mental health care would look under a Trump vs. Biden administration
The COVID-19 pandemic is one of the most pressing public health challenges the United States has ever faced, and the resulting financial ruin and social isolation are creating a mental health pandemic that will continue well after COVID-19 lockdowns end. To understand which presidential candidate would best lead the mental health recovery, we identified three of the most critical issues in mental health and compared the plans of the two candidates.
Fighting the opioid epidemic

Over the last several years, the opioid epidemic has devastated American families and communities. Prior to the pandemic, drug overdoses were the leading cause of death for American adults under 50 years of age. The effects of COVID-19–enabled overdose deaths to rise even higher. Multiple elements of the pandemic – isolation, unemployment, and increased anxiety and depression – make those struggling with substance use even more vulnerable, and immediate and comprehensive action is needed to address this national tragedy.
Donald J. Trump: President Trump has been vocal and active in addressing this problem since he took office. One of the Trump administration’s successes is launching the Opioid and Drug Abuse Commission and rolling out a five-point strategy built around improving services, data, research, overdose-reversing drugs, and pain management. Last year, the Trump administration funded $10 billion over 5 years to combat both the opioid epidemic and mental health issues by building upon the 21st Century CURES Act. However, in this same budget, the administration proposed cutting funding by $600 million for SAMHSA, the Substance Abuse and Mental Health Services Administration, which is the top government agency for addressing and providing care for substance use.
President Trump also created an assistant secretary for mental health and substance use position in the Department of Health & Human Services, and appointed Elinore F. McCance-Katz, MD, PhD, a psychiatrist with a strong track record on fighting opioid abuse in Rhode Island, to the post.
Joe Biden: Former Vice President Biden emphasizes that substance use is “a disease of the brain,” refuting the long-held misconception that addiction is an issue of willpower. This stigmatization is very personal given that his own son Hunter reportedly suffered through mental health and substance use issues since his teenage years. However, Biden also had a major role in pushing forward the federal “war on drugs,” including his role in crafting the “Len Bias law.”

Mr. Biden has since released a multifaceted plan for reducing substance use, aiming to make prevention and treatment services more available through a $125 billion federal investment. There are also measures to hold pharmaceutical companies accountable for triggering the crisis, stop the flow of fentanyl to the United States, and restrict incentive payments from manufacturers to doctors so as to limit the dosing and usage of powerful opioids.
Accessing health care
One of the main dividing lines in this election has been the battle to either gut or build upon the Affordable Care Act (ACA). This will have deep ramifications on people’s access to health mental health services. Since COVID-19 started, more than 50% of Americans have reported worsening mental health. This makes it crucial that each candidate’s mental health plan is judged by how they would expand access to insurance, address unenforced parity laws, and protect those who have a mental health disorder as a preexisting condition.
Mr. Trump: Following a failed Senate vote to repeal this law, the Trump administration took a piecemeal approach to dismantling the ACA that included removing the individual mandate, enabling states to introduce Medicaid work requirements, and reducing cost-sharing subsidies to insurers.
If a re-elected Trump administration pursued a complete repeal of the ACA law, many individuals with previous access to mental health and substance abuse treatment via Medicaid expansion may lose access altogether. In addition, key mechanisms aimed at making sure that mental health services are covered by private health plans may be lost, which could undermine policies to address opioids and suicide. On the other hand, the Trump administration’s move during the pandemic to expand telemedicine services has also expanded access to mental health services.
Mr. Biden: Mr. Biden’s plan would build upon the ACA by working to achieve parity between the treatment of mental health and physical health. The ACA itself strengthened the Mental Health Parity and Addiction Equity Act (federal parity law), which Mr. Biden championed as vice president, by mandating that all private insurance cover mental health and substance abuse treatment. This act still exempts some health plans, such as larger employers; and many insurers have used loopholes in the policy to illegally deny what could be life-saving coverage.
It follows that those who can afford Mr. Biden’s proposed public option Medicare buy-in would receive more comprehensive mental health benefits. He also says he would invest in school and college mental health professionals, an important opportunity for early intervention given 75% of lifetime mental illness starts by age 24 years. While Mr. Biden has not stated a specific plan for addressing minority groups, whose mental health has been disproportionately affected by COVID-19, he has acknowledged that this unmet need should be targeted.
Addressing suicide
More than 3,000 Americans attempt suicide every day. Suicide is the second leading cause of death for America’s youth and one of the top 10 leading causes of death across the population. Numerous strategies are necessary to address suicide, but one of the most decisive is gun control. Gun violence is inextricably tied to suicide: States where gun prevalence is higher see about four times the number of suicides because of guns, whereas nonfirearm suicide rates are the same as those seen elsewhere. In 2017, of the nearly 40,000 people who died of gun violence, 60% were attributable to suicides. Since the pandemic started, there have been increases in reported suicidal thoughts and a nearly 1,000% increase in use of the national crisis hotline. This is especially concerning given the uptick during the pandemic of gun purchases; as of September, more guns have been purchased this year than any year before.
Mr. Trump: Prior to coronavirus, the Trump administration was unwilling to enact gun control legislation. In early 2017, Mr. Trump removed an Obama-era bill that would have expanded the background check database. It would have added those deemed legally unfit to handle their own funds and those who received Social Security funds for mental health reasons. During the lockdown, the administration made an advisory ruling declaring gun shops as essential businesses that states should keep open.
Mr. Biden: The former vice president has a history of supporting gun control measures in his time as a senator and vice president. In the Senate, Mr. Biden supported both the Brady handgun bill in 1993 and a ban on assault weapons in 1994. As vice president, he was tasked by President Obama to push for a renewed assault weapons ban and a background check bill (Manchin-Toomey bill).
During his 2020 presidential campaign, Mr. Biden has suggested creating universal background checks and reinstating bans on assault rifle sales. He has said that he is also open to having a federal buyback program for assault rifles from gun owners.
Why this matters
The winner of the 2020 election will lead an electorate that is reeling from the health, economic, and social consequences COVID-19. The next administration needs to act swiftly to address the mental health pandemic and have a keen awareness of what is ahead. As Americans make their voting decision, consider who has the best plans not only to contain the virus but also the mental health crises that are ravaging our nation.
Dr. Vasan is a clinical assistant professor of psychiatry at Stanford (Calif.) University, where she is founder and executive director of Brainstorm: The Stanford Lab for Mental Health Innovation. She also serves as chief medical officer of Real, and chair of the American Psychiatric Association Committee on Innovation. Dr. Vasan has no conflicts of interest. Mr. Agbafe is a fellow at Stanford Brainstorm and a first-year medical student at the University of Michigan, Ann Arbor. He has no conflicts of interest. Ms. Li is a policy intern at Stanford Brainstorm and an undergraduate student in the department of economics at the University of California, Berkeley. She has no conflicts of interest.
The COVID-19 pandemic is one of the most pressing public health challenges the United States has ever faced, and the resulting financial ruin and social isolation are creating a mental health pandemic that will continue well after COVID-19 lockdowns end. To understand which presidential candidate would best lead the mental health recovery, we identified three of the most critical issues in mental health and compared the plans of the two candidates.
Fighting the opioid epidemic
Over the last several years, the opioid epidemic has devastated American families and communities. Prior to the pandemic, drug overdoses were the leading cause of death for American adults under 50 years of age. The effects of COVID-19–enabled overdose deaths to rise even higher. Multiple elements of the pandemic – isolation, unemployment, and increased anxiety and depression – make those struggling with substance use even more vulnerable, and immediate and comprehensive action is needed to address this national tragedy.
Donald J. Trump: President Trump has been vocal and active in addressing this problem since he took office. One of the Trump administration’s successes is launching the Opioid and Drug Abuse Commission and rolling out a five-point strategy built around improving services, data, research, overdose-reversing drugs, and pain management. Last year, the Trump administration funded $10 billion over 5 years to combat both the opioid epidemic and mental health issues by building upon the 21st Century CURES Act. However, in this same budget, the administration proposed cutting funding by $600 million for SAMHSA, the Substance Abuse and Mental Health Services Administration, which is the top government agency for addressing and providing care for substance use.
President Trump also created an assistant secretary for mental health and substance use position in the Department of Health & Human Services, and appointed Elinore F. McCance-Katz, MD, PhD, a psychiatrist with a strong track record on fighting opioid abuse in Rhode Island, to the post.
Joe Biden: Former Vice President Biden emphasizes that substance use is “a disease of the brain,” refuting the long-held misconception that addiction is an issue of willpower. This stigmatization is very personal given that his own son Hunter reportedly suffered through mental health and substance use issues since his teenage years. However, Biden also had a major role in pushing forward the federal “war on drugs,” including his role in crafting the “Len Bias law.”
Mr. Biden has since released a multifaceted plan for reducing substance use, aiming to make prevention and treatment services more available through a $125 billion federal investment. There are also measures to hold pharmaceutical companies accountable for triggering the crisis, stop the flow of fentanyl to the United States, and restrict incentive payments from manufacturers to doctors so as to limit the dosing and usage of powerful opioids.
Accessing health care
One of the main dividing lines in this election has been the battle to either gut or build upon the Affordable Care Act (ACA). This will have deep ramifications on people’s access to health mental health services. Since COVID-19 started, more than 50% of Americans have reported worsening mental health. This makes it crucial that each candidate’s mental health plan is judged by how they would expand access to insurance, address unenforced parity laws, and protect those who have a mental health disorder as a preexisting condition.
Mr. Trump: Following a failed Senate vote to repeal this law, the Trump administration took a piecemeal approach to dismantling the ACA that included removing the individual mandate, enabling states to introduce Medicaid work requirements, and reducing cost-sharing subsidies to insurers.
If a re-elected Trump administration pursued a complete repeal of the ACA law, many individuals with previous access to mental health and substance abuse treatment via Medicaid expansion may lose access altogether. In addition, key mechanisms aimed at making sure that mental health services are covered by private health plans may be lost, which could undermine policies to address opioids and suicide. On the other hand, the Trump administration’s move during the pandemic to expand telemedicine services has also expanded access to mental health services.
Mr. Biden: Mr. Biden’s plan would build upon the ACA by working to achieve parity between the treatment of mental health and physical health. The ACA itself strengthened the Mental Health Parity and Addiction Equity Act (federal parity law), which Mr. Biden championed as vice president, by mandating that all private insurance cover mental health and substance abuse treatment. This act still exempts some health plans, such as larger employers; and many insurers have used loopholes in the policy to illegally deny what could be life-saving coverage.
It follows that those who can afford Mr. Biden’s proposed public option Medicare buy-in would receive more comprehensive mental health benefits. He also says he would invest in school and college mental health professionals, an important opportunity for early intervention given 75% of lifetime mental illness starts by age 24 years. While Mr. Biden has not stated a specific plan for addressing minority groups, whose mental health has been disproportionately affected by COVID-19, he has acknowledged that this unmet need should be targeted.
Addressing suicide
More than 3,000 Americans attempt suicide every day. Suicide is the second leading cause of death for America’s youth and one of the top 10 leading causes of death across the population. Numerous strategies are necessary to address suicide, but one of the most decisive is gun control. Gun violence is inextricably tied to suicide: States where gun prevalence is higher see about four times the number of suicides because of guns, whereas nonfirearm suicide rates are the same as those seen elsewhere. In 2017, of the nearly 40,000 people who died of gun violence, 60% were attributable to suicides. Since the pandemic started, there have been increases in reported suicidal thoughts and a nearly 1,000% increase in use of the national crisis hotline. This is especially concerning given the uptick during the pandemic of gun purchases; as of September, more guns have been purchased this year than any year before.
Mr. Trump: Prior to coronavirus, the Trump administration was unwilling to enact gun control legislation. In early 2017, Mr. Trump removed an Obama-era bill that would have expanded the background check database. It would have added those deemed legally unfit to handle their own funds and those who received Social Security funds for mental health reasons. During the lockdown, the administration made an advisory ruling declaring gun shops as essential businesses that states should keep open.
Mr. Biden: The former vice president has a history of supporting gun control measures in his time as a senator and vice president. In the Senate, Mr. Biden supported both the Brady handgun bill in 1993 and a ban on assault weapons in 1994. As vice president, he was tasked by President Obama to push for a renewed assault weapons ban and a background check bill (Manchin-Toomey bill).
During his 2020 presidential campaign, Mr. Biden has suggested creating universal background checks and reinstating bans on assault rifle sales. He has said that he is also open to having a federal buyback program for assault rifles from gun owners.
Why this matters
The winner of the 2020 election will lead an electorate that is reeling from the health, economic, and social consequences COVID-19. The next administration needs to act swiftly to address the mental health pandemic and have a keen awareness of what is ahead. As Americans make their voting decision, consider who has the best plans not only to contain the virus but also the mental health crises that are ravaging our nation.
Dr. Vasan is a clinical assistant professor of psychiatry at Stanford (Calif.) University, where she is founder and executive director of Brainstorm: The Stanford Lab for Mental Health Innovation. She also serves as chief medical officer of Real, and chair of the American Psychiatric Association Committee on Innovation. Dr. Vasan has no conflicts of interest. Mr. Agbafe is a fellow at Stanford Brainstorm and a first-year medical student at the University of Michigan, Ann Arbor. He has no conflicts of interest. Ms. Li is a policy intern at Stanford Brainstorm and an undergraduate student in the department of economics at the University of California, Berkeley. She has no conflicts of interest.
The COVID-19 pandemic is one of the most pressing public health challenges the United States has ever faced, and the resulting financial ruin and social isolation are creating a mental health pandemic that will continue well after COVID-19 lockdowns end. To understand which presidential candidate would best lead the mental health recovery, we identified three of the most critical issues in mental health and compared the plans of the two candidates.
Fighting the opioid epidemic
Over the last several years, the opioid epidemic has devastated American families and communities. Prior to the pandemic, drug overdoses were the leading cause of death for American adults under 50 years of age. The effects of COVID-19–enabled overdose deaths to rise even higher. Multiple elements of the pandemic – isolation, unemployment, and increased anxiety and depression – make those struggling with substance use even more vulnerable, and immediate and comprehensive action is needed to address this national tragedy.
Donald J. Trump: President Trump has been vocal and active in addressing this problem since he took office. One of the Trump administration’s successes is launching the Opioid and Drug Abuse Commission and rolling out a five-point strategy built around improving services, data, research, overdose-reversing drugs, and pain management. Last year, the Trump administration funded $10 billion over 5 years to combat both the opioid epidemic and mental health issues by building upon the 21st Century CURES Act. However, in this same budget, the administration proposed cutting funding by $600 million for SAMHSA, the Substance Abuse and Mental Health Services Administration, which is the top government agency for addressing and providing care for substance use.
President Trump also created an assistant secretary for mental health and substance use position in the Department of Health & Human Services, and appointed Elinore F. McCance-Katz, MD, PhD, a psychiatrist with a strong track record on fighting opioid abuse in Rhode Island, to the post.
Joe Biden: Former Vice President Biden emphasizes that substance use is “a disease of the brain,” refuting the long-held misconception that addiction is an issue of willpower. This stigmatization is very personal given that his own son Hunter reportedly suffered through mental health and substance use issues since his teenage years. However, Biden also had a major role in pushing forward the federal “war on drugs,” including his role in crafting the “Len Bias law.”
Mr. Biden has since released a multifaceted plan for reducing substance use, aiming to make prevention and treatment services more available through a $125 billion federal investment. There are also measures to hold pharmaceutical companies accountable for triggering the crisis, stop the flow of fentanyl to the United States, and restrict incentive payments from manufacturers to doctors so as to limit the dosing and usage of powerful opioids.
Accessing health care
One of the main dividing lines in this election has been the battle to either gut or build upon the Affordable Care Act (ACA). This will have deep ramifications on people’s access to health mental health services. Since COVID-19 started, more than 50% of Americans have reported worsening mental health. This makes it crucial that each candidate’s mental health plan is judged by how they would expand access to insurance, address unenforced parity laws, and protect those who have a mental health disorder as a preexisting condition.
Mr. Trump: Following a failed Senate vote to repeal this law, the Trump administration took a piecemeal approach to dismantling the ACA that included removing the individual mandate, enabling states to introduce Medicaid work requirements, and reducing cost-sharing subsidies to insurers.
If a re-elected Trump administration pursued a complete repeal of the ACA law, many individuals with previous access to mental health and substance abuse treatment via Medicaid expansion may lose access altogether. In addition, key mechanisms aimed at making sure that mental health services are covered by private health plans may be lost, which could undermine policies to address opioids and suicide. On the other hand, the Trump administration’s move during the pandemic to expand telemedicine services has also expanded access to mental health services.
Mr. Biden: Mr. Biden’s plan would build upon the ACA by working to achieve parity between the treatment of mental health and physical health. The ACA itself strengthened the Mental Health Parity and Addiction Equity Act (federal parity law), which Mr. Biden championed as vice president, by mandating that all private insurance cover mental health and substance abuse treatment. This act still exempts some health plans, such as larger employers; and many insurers have used loopholes in the policy to illegally deny what could be life-saving coverage.
It follows that those who can afford Mr. Biden’s proposed public option Medicare buy-in would receive more comprehensive mental health benefits. He also says he would invest in school and college mental health professionals, an important opportunity for early intervention given 75% of lifetime mental illness starts by age 24 years. While Mr. Biden has not stated a specific plan for addressing minority groups, whose mental health has been disproportionately affected by COVID-19, he has acknowledged that this unmet need should be targeted.
Addressing suicide
More than 3,000 Americans attempt suicide every day. Suicide is the second leading cause of death for America’s youth and one of the top 10 leading causes of death across the population. Numerous strategies are necessary to address suicide, but one of the most decisive is gun control. Gun violence is inextricably tied to suicide: States where gun prevalence is higher see about four times the number of suicides because of guns, whereas nonfirearm suicide rates are the same as those seen elsewhere. In 2017, of the nearly 40,000 people who died of gun violence, 60% were attributable to suicides. Since the pandemic started, there have been increases in reported suicidal thoughts and a nearly 1,000% increase in use of the national crisis hotline. This is especially concerning given the uptick during the pandemic of gun purchases; as of September, more guns have been purchased this year than any year before.
Mr. Trump: Prior to coronavirus, the Trump administration was unwilling to enact gun control legislation. In early 2017, Mr. Trump removed an Obama-era bill that would have expanded the background check database. It would have added those deemed legally unfit to handle their own funds and those who received Social Security funds for mental health reasons. During the lockdown, the administration made an advisory ruling declaring gun shops as essential businesses that states should keep open.
Mr. Biden: The former vice president has a history of supporting gun control measures in his time as a senator and vice president. In the Senate, Mr. Biden supported both the Brady handgun bill in 1993 and a ban on assault weapons in 1994. As vice president, he was tasked by President Obama to push for a renewed assault weapons ban and a background check bill (Manchin-Toomey bill).
During his 2020 presidential campaign, Mr. Biden has suggested creating universal background checks and reinstating bans on assault rifle sales. He has said that he is also open to having a federal buyback program for assault rifles from gun owners.
Why this matters
The winner of the 2020 election will lead an electorate that is reeling from the health, economic, and social consequences COVID-19. The next administration needs to act swiftly to address the mental health pandemic and have a keen awareness of what is ahead. As Americans make their voting decision, consider who has the best plans not only to contain the virus but also the mental health crises that are ravaging our nation.
Dr. Vasan is a clinical assistant professor of psychiatry at Stanford (Calif.) University, where she is founder and executive director of Brainstorm: The Stanford Lab for Mental Health Innovation. She also serves as chief medical officer of Real, and chair of the American Psychiatric Association Committee on Innovation. Dr. Vasan has no conflicts of interest. Mr. Agbafe is a fellow at Stanford Brainstorm and a first-year medical student at the University of Michigan, Ann Arbor. He has no conflicts of interest. Ms. Li is a policy intern at Stanford Brainstorm and an undergraduate student in the department of economics at the University of California, Berkeley. She has no conflicts of interest.
New technologies aim to improve ovarian cancer detection
Encouraging trends abound in the management of ovarian cancer. As rates of ovarian disease continue to decline, there has also been a notable increase in tools for detecting it earlier in its course.
To better understand these developments, this news organization reached out to Rebecca Stone, MD, an ovarian cancer expert and associate professor of gynecologic oncology at Johns Hopkins University, in Baltimore, Maryland. This interview has been edited for length and clarity.
There has been a decline in the rates of ovarian cancer in recent years. What are the possible causes of this?Dr. Stone: The number of new cases in the United States has actually been declining over the past 2 decades. This is thought to be attributable to the increased prescribing of oral contraceptive pills in the late 1990s and the uptake of preventive measures, such as risk-reducing gynecologic surgery for women with genetic predisposition to ovarian cancer, as well as opportunistic salpingectomy in the general population. Opportunistic salpingectomy was introduced about 10 years ago. It is a surgical means for primary prevention of tubo-ovarian cancer by removing both fallopian tubes at the time of elective surgery for women who have completed childbearing or in lieu of “tying the tubes” for women who desire permanent surgical sterility.
What can you tell us about a recent study suggesting that high-grade serous epithelial ovarian cancer may be detected earlier in the course of the disease by testing for TP53 clonal variants in DNA from Papanicolaou (Pap) tests performed during cervical cancer screening?
The idea here is that early mutational events that ultimately result in the development of epithelial ovarian cancer can be detected by performing gene sequencing on genetic material collected at the time of routine Pap smear screening done for cervical cancer. Pap tests are known to contain cells and genetic material shed from the fallopian tubes, where the precancerous lesions thought to give rise to epithelial ovarian cancer, predominantly serous epithelial ovarian cancers, start.
p53 gene mutations are thought to occur early in the evolution of ovarian cancer. There are data indicating that these mutations actually occur in cells lining the fallopian tubes. Polymerase chain reaction–based DNA/gene sequencing performed on cervical fluid collected by Pap smears could detect these p53-mutated cells shed from the fallopian tubes.
A strength of this study is that it included healthy controls. None of their Pap smears screened positive for the p53 mutations, unlike the Pap smears of women predating their diagnosis of ovarian cancer. Limitations of the study include the fact that it had a small sample size. Findings will need to be confirmed in a larger patient population.
Also, the study only looked for p53 gene mutations. Ovarian cancers, like other cancers, are largely thought to occur when there is a buildup of mutations in critical genes that result in uncontrolled cell growth and division. These genetic changes/mutations are acquired during a person’s lifetime. Thus, there are likely early genetic changes/mutations that occur in addition to p53 mutations that ultimately lead to the development of ovarian cancer. Detecting these along with p53 mutations could improve the sensitivity/detection rate of the screening strategy that the authors are investigating.
Finally, this screening strategy may not prove effective for the early detection of all histologic subtypes of epithelial ovarian cancer or for nonepithelial ovarian cancers.
What other recent developments in the diagnosis of ovarian cancer should clinicians be aware of?
Liquid biopsies using circulating tumor DNA (ctDNA) have shown promising results for cancer detection and management, including ovarian cancer. However, further clarification is needed to define the minimum tumor size/burden detectable using ctDNA-based approaches. Moreover, large prospective studies are needed to determine the clinical utility of ctDNA detection for early diagnosis of ovarian cancer and its impact on patient outcomes.
DNA methylation is an early event in carcinogenesis and can be detected in blood plasma samples from cancer patients. Data related to the discovery and validation of discriminated methylated DNA marker candidates extracted from ovarian cancer tissues were presented at the American Society of Clinical Oncology meeting this year. Findings were subsequently evaluated in plasma from women with and without ovarian cancer.
In addition to blood, peritoneal fluid and uterine lavage have been used to obtain cell pellets that are used for the identification of common mutant genes – TP53, BRCA1, and BRCA2. These body fluids have also been shown as the source of tumor-derived material that can be used to differentiate between ovarian cancer patients and healthy individuals.
Further studies are needed to determine the sensitivity and specificity of other noninvasive tests for the diagnosis of ovarian cancer.
The American Cancer Society issued a statement that the human papillomavirus (HPV) test is the preferred cervical cancer screening tool. Why do they prefer the HPV test over the Pap test?
The American Cancer Society recommends that cervical cancer testing (screening) begin at age 25 years. Women aged 25-65 years should have a primary HPV test every 5 years. If primary HPV testing is not available, screening may be done with either a co-test that combines an HPV test with a Pap test every 5 years or a Pap test alone every 3 years.
The HPV test is widely available. The cost of an HPV test is approximately $44 (unit cost, 2014 USD). The cost of a Pap test is approximately $30 (unit cost, 2014 USD).
The HPV test is preferred over cytologic testing (Pap) for several reasons.
Firstly, in well-designed studies, the sensitivity of a single Pap smear for detecting high-grade precancer of the cervix is around 50%, which is less than optimal for a cancer screening test. Sensitivity means the chance that, if you have the disease (in this case, high-grade precancer of the cervix), the test will detect it. In particular, cytology is known to have an even more limited ability to detect glandular precancers, which arise in the endocervical canal rather than on or in close proximity to the exterior surface of the cervix (ectocervix). Thus, HPV-based screening programs hold the promise of improving detection of cervical adenocarcinoma.
Secondly, to function reliably, cytology programs require substantial infrastructure, highly qualified human resources, and a well‐defined quality-control system, which have proved to be costly and difficult to implement. This results in global disparities in cytology-based cervical cancer screening programs.
Thirdly, although co‐testing with both cytology and HPV tests is an option for screening programs, studies have confirmed that there is limited benefit from adding cytology to HPV screening. Long‐term studies from Kaiser Permanente that included over 1 million women found that HPV testing has a very high negative predictive value for precancerous lesions. Women with negative HPV tests were very unlikely to develop precancerous lesions in the following 5 years. The 5‐year risk of high-grade precancer or cancer of the cervix following a negative HPV test was 0.14%, whereas for women with a negative cytology, it was 0.31%. The screening benefit of co‐testing is largely driven by HPV testing and not cytology.
So, in summary, HPV testing is preferred over cytologic screening for cervical cancer, given its improved sensitivity and quality assurance, the opportunity to automate testing, and ultimately, its prospect of reducing the overall number of lifetime screenings for women.
Dr. Stone has disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Encouraging trends abound in the management of ovarian cancer. As rates of ovarian disease continue to decline, there has also been a notable increase in tools for detecting it earlier in its course.
To better understand these developments, this news organization reached out to Rebecca Stone, MD, an ovarian cancer expert and associate professor of gynecologic oncology at Johns Hopkins University, in Baltimore, Maryland. This interview has been edited for length and clarity.
There has been a decline in the rates of ovarian cancer in recent years. What are the possible causes of this?Dr. Stone: The number of new cases in the United States has actually been declining over the past 2 decades. This is thought to be attributable to the increased prescribing of oral contraceptive pills in the late 1990s and the uptake of preventive measures, such as risk-reducing gynecologic surgery for women with genetic predisposition to ovarian cancer, as well as opportunistic salpingectomy in the general population. Opportunistic salpingectomy was introduced about 10 years ago. It is a surgical means for primary prevention of tubo-ovarian cancer by removing both fallopian tubes at the time of elective surgery for women who have completed childbearing or in lieu of “tying the tubes” for women who desire permanent surgical sterility.
What can you tell us about a recent study suggesting that high-grade serous epithelial ovarian cancer may be detected earlier in the course of the disease by testing for TP53 clonal variants in DNA from Papanicolaou (Pap) tests performed during cervical cancer screening?
The idea here is that early mutational events that ultimately result in the development of epithelial ovarian cancer can be detected by performing gene sequencing on genetic material collected at the time of routine Pap smear screening done for cervical cancer. Pap tests are known to contain cells and genetic material shed from the fallopian tubes, where the precancerous lesions thought to give rise to epithelial ovarian cancer, predominantly serous epithelial ovarian cancers, start.
p53 gene mutations are thought to occur early in the evolution of ovarian cancer. There are data indicating that these mutations actually occur in cells lining the fallopian tubes. Polymerase chain reaction–based DNA/gene sequencing performed on cervical fluid collected by Pap smears could detect these p53-mutated cells shed from the fallopian tubes.
A strength of this study is that it included healthy controls. None of their Pap smears screened positive for the p53 mutations, unlike the Pap smears of women predating their diagnosis of ovarian cancer. Limitations of the study include the fact that it had a small sample size. Findings will need to be confirmed in a larger patient population.
Also, the study only looked for p53 gene mutations. Ovarian cancers, like other cancers, are largely thought to occur when there is a buildup of mutations in critical genes that result in uncontrolled cell growth and division. These genetic changes/mutations are acquired during a person’s lifetime. Thus, there are likely early genetic changes/mutations that occur in addition to p53 mutations that ultimately lead to the development of ovarian cancer. Detecting these along with p53 mutations could improve the sensitivity/detection rate of the screening strategy that the authors are investigating.
Finally, this screening strategy may not prove effective for the early detection of all histologic subtypes of epithelial ovarian cancer or for nonepithelial ovarian cancers.
What other recent developments in the diagnosis of ovarian cancer should clinicians be aware of?
Liquid biopsies using circulating tumor DNA (ctDNA) have shown promising results for cancer detection and management, including ovarian cancer. However, further clarification is needed to define the minimum tumor size/burden detectable using ctDNA-based approaches. Moreover, large prospective studies are needed to determine the clinical utility of ctDNA detection for early diagnosis of ovarian cancer and its impact on patient outcomes.
DNA methylation is an early event in carcinogenesis and can be detected in blood plasma samples from cancer patients. Data related to the discovery and validation of discriminated methylated DNA marker candidates extracted from ovarian cancer tissues were presented at the American Society of Clinical Oncology meeting this year. Findings were subsequently evaluated in plasma from women with and without ovarian cancer.
In addition to blood, peritoneal fluid and uterine lavage have been used to obtain cell pellets that are used for the identification of common mutant genes – TP53, BRCA1, and BRCA2. These body fluids have also been shown as the source of tumor-derived material that can be used to differentiate between ovarian cancer patients and healthy individuals.
Further studies are needed to determine the sensitivity and specificity of other noninvasive tests for the diagnosis of ovarian cancer.
The American Cancer Society issued a statement that the human papillomavirus (HPV) test is the preferred cervical cancer screening tool. Why do they prefer the HPV test over the Pap test?
The American Cancer Society recommends that cervical cancer testing (screening) begin at age 25 years. Women aged 25-65 years should have a primary HPV test every 5 years. If primary HPV testing is not available, screening may be done with either a co-test that combines an HPV test with a Pap test every 5 years or a Pap test alone every 3 years.
The HPV test is widely available. The cost of an HPV test is approximately $44 (unit cost, 2014 USD). The cost of a Pap test is approximately $30 (unit cost, 2014 USD).
The HPV test is preferred over cytologic testing (Pap) for several reasons.
Firstly, in well-designed studies, the sensitivity of a single Pap smear for detecting high-grade precancer of the cervix is around 50%, which is less than optimal for a cancer screening test. Sensitivity means the chance that, if you have the disease (in this case, high-grade precancer of the cervix), the test will detect it. In particular, cytology is known to have an even more limited ability to detect glandular precancers, which arise in the endocervical canal rather than on or in close proximity to the exterior surface of the cervix (ectocervix). Thus, HPV-based screening programs hold the promise of improving detection of cervical adenocarcinoma.
Secondly, to function reliably, cytology programs require substantial infrastructure, highly qualified human resources, and a well‐defined quality-control system, which have proved to be costly and difficult to implement. This results in global disparities in cytology-based cervical cancer screening programs.
Thirdly, although co‐testing with both cytology and HPV tests is an option for screening programs, studies have confirmed that there is limited benefit from adding cytology to HPV screening. Long‐term studies from Kaiser Permanente that included over 1 million women found that HPV testing has a very high negative predictive value for precancerous lesions. Women with negative HPV tests were very unlikely to develop precancerous lesions in the following 5 years. The 5‐year risk of high-grade precancer or cancer of the cervix following a negative HPV test was 0.14%, whereas for women with a negative cytology, it was 0.31%. The screening benefit of co‐testing is largely driven by HPV testing and not cytology.
So, in summary, HPV testing is preferred over cytologic screening for cervical cancer, given its improved sensitivity and quality assurance, the opportunity to automate testing, and ultimately, its prospect of reducing the overall number of lifetime screenings for women.
Dr. Stone has disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Encouraging trends abound in the management of ovarian cancer. As rates of ovarian disease continue to decline, there has also been a notable increase in tools for detecting it earlier in its course.
To better understand these developments, this news organization reached out to Rebecca Stone, MD, an ovarian cancer expert and associate professor of gynecologic oncology at Johns Hopkins University, in Baltimore, Maryland. This interview has been edited for length and clarity.
There has been a decline in the rates of ovarian cancer in recent years. What are the possible causes of this?Dr. Stone: The number of new cases in the United States has actually been declining over the past 2 decades. This is thought to be attributable to the increased prescribing of oral contraceptive pills in the late 1990s and the uptake of preventive measures, such as risk-reducing gynecologic surgery for women with genetic predisposition to ovarian cancer, as well as opportunistic salpingectomy in the general population. Opportunistic salpingectomy was introduced about 10 years ago. It is a surgical means for primary prevention of tubo-ovarian cancer by removing both fallopian tubes at the time of elective surgery for women who have completed childbearing or in lieu of “tying the tubes” for women who desire permanent surgical sterility.
What can you tell us about a recent study suggesting that high-grade serous epithelial ovarian cancer may be detected earlier in the course of the disease by testing for TP53 clonal variants in DNA from Papanicolaou (Pap) tests performed during cervical cancer screening?
The idea here is that early mutational events that ultimately result in the development of epithelial ovarian cancer can be detected by performing gene sequencing on genetic material collected at the time of routine Pap smear screening done for cervical cancer. Pap tests are known to contain cells and genetic material shed from the fallopian tubes, where the precancerous lesions thought to give rise to epithelial ovarian cancer, predominantly serous epithelial ovarian cancers, start.
p53 gene mutations are thought to occur early in the evolution of ovarian cancer. There are data indicating that these mutations actually occur in cells lining the fallopian tubes. Polymerase chain reaction–based DNA/gene sequencing performed on cervical fluid collected by Pap smears could detect these p53-mutated cells shed from the fallopian tubes.
A strength of this study is that it included healthy controls. None of their Pap smears screened positive for the p53 mutations, unlike the Pap smears of women predating their diagnosis of ovarian cancer. Limitations of the study include the fact that it had a small sample size. Findings will need to be confirmed in a larger patient population.
Also, the study only looked for p53 gene mutations. Ovarian cancers, like other cancers, are largely thought to occur when there is a buildup of mutations in critical genes that result in uncontrolled cell growth and division. These genetic changes/mutations are acquired during a person’s lifetime. Thus, there are likely early genetic changes/mutations that occur in addition to p53 mutations that ultimately lead to the development of ovarian cancer. Detecting these along with p53 mutations could improve the sensitivity/detection rate of the screening strategy that the authors are investigating.
Finally, this screening strategy may not prove effective for the early detection of all histologic subtypes of epithelial ovarian cancer or for nonepithelial ovarian cancers.
What other recent developments in the diagnosis of ovarian cancer should clinicians be aware of?
Liquid biopsies using circulating tumor DNA (ctDNA) have shown promising results for cancer detection and management, including ovarian cancer. However, further clarification is needed to define the minimum tumor size/burden detectable using ctDNA-based approaches. Moreover, large prospective studies are needed to determine the clinical utility of ctDNA detection for early diagnosis of ovarian cancer and its impact on patient outcomes.
DNA methylation is an early event in carcinogenesis and can be detected in blood plasma samples from cancer patients. Data related to the discovery and validation of discriminated methylated DNA marker candidates extracted from ovarian cancer tissues were presented at the American Society of Clinical Oncology meeting this year. Findings were subsequently evaluated in plasma from women with and without ovarian cancer.
In addition to blood, peritoneal fluid and uterine lavage have been used to obtain cell pellets that are used for the identification of common mutant genes – TP53, BRCA1, and BRCA2. These body fluids have also been shown as the source of tumor-derived material that can be used to differentiate between ovarian cancer patients and healthy individuals.
Further studies are needed to determine the sensitivity and specificity of other noninvasive tests for the diagnosis of ovarian cancer.
The American Cancer Society issued a statement that the human papillomavirus (HPV) test is the preferred cervical cancer screening tool. Why do they prefer the HPV test over the Pap test?
The American Cancer Society recommends that cervical cancer testing (screening) begin at age 25 years. Women aged 25-65 years should have a primary HPV test every 5 years. If primary HPV testing is not available, screening may be done with either a co-test that combines an HPV test with a Pap test every 5 years or a Pap test alone every 3 years.
The HPV test is widely available. The cost of an HPV test is approximately $44 (unit cost, 2014 USD). The cost of a Pap test is approximately $30 (unit cost, 2014 USD).
The HPV test is preferred over cytologic testing (Pap) for several reasons.
Firstly, in well-designed studies, the sensitivity of a single Pap smear for detecting high-grade precancer of the cervix is around 50%, which is less than optimal for a cancer screening test. Sensitivity means the chance that, if you have the disease (in this case, high-grade precancer of the cervix), the test will detect it. In particular, cytology is known to have an even more limited ability to detect glandular precancers, which arise in the endocervical canal rather than on or in close proximity to the exterior surface of the cervix (ectocervix). Thus, HPV-based screening programs hold the promise of improving detection of cervical adenocarcinoma.
Secondly, to function reliably, cytology programs require substantial infrastructure, highly qualified human resources, and a well‐defined quality-control system, which have proved to be costly and difficult to implement. This results in global disparities in cytology-based cervical cancer screening programs.
Thirdly, although co‐testing with both cytology and HPV tests is an option for screening programs, studies have confirmed that there is limited benefit from adding cytology to HPV screening. Long‐term studies from Kaiser Permanente that included over 1 million women found that HPV testing has a very high negative predictive value for precancerous lesions. Women with negative HPV tests were very unlikely to develop precancerous lesions in the following 5 years. The 5‐year risk of high-grade precancer or cancer of the cervix following a negative HPV test was 0.14%, whereas for women with a negative cytology, it was 0.31%. The screening benefit of co‐testing is largely driven by HPV testing and not cytology.
So, in summary, HPV testing is preferred over cytologic screening for cervical cancer, given its improved sensitivity and quality assurance, the opportunity to automate testing, and ultimately, its prospect of reducing the overall number of lifetime screenings for women.
Dr. Stone has disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
A guide to the new agents reshaping ovarian cancer treatment
The treatment of ovarian cancer has evolved considerably in the last few years, with the approval of several PARP inhibitors, antiangiogenic agents, and other therapies for a multitude of indications. Additional treatments are likely to soon join this already diverse spectrum of available options, if their promising efficacy and safety continues to be borne out in ongoing research.
To better understand the individual merits and potential drawbacks of these treatments, Medscape recently spoke with Rebecca Stone, MD, an ovarian cancer expert and associate professor of gynecologic oncology at Johns Hopkins University, Baltimore. This interview has been edited for length and clarity.
Medscape: We’re starting to see preliminary data on pamiparib , an investigational inhibitor of PARP1 and PARP2, for the treatment of ovarian cancer. What is the evidence supporting this drug?
Dr. Stone: Currently, six different PARP inhibitors – olaparib, rucaparib, veliparib, niraparib, talazoparib, and pamiparib – have been in clinical development at different stages. In clinical applications, PARP inhibitors, including olaparib, rucaparib, niraparib, and talazoparib, have demonstrated sustained antitumor responses as single agents in patients with BRCA1 or BRCA2 mutations. Those with Food and Drug Administration indications in ovarian cancer include olaparib, rucaparib, and niraparib. The preclinical and clinical data with pamiparib is limited as of now. But, in a xenograft breast cancer model, it was found to be over 10 times more potent than olaparib.
If approved, where would pamiparib fit in the treatment paradigm for ovarian cancer?
It would potentially fit as monotherapy as well as in combination with agents other than standard chemotherapy for the treatment of BRCA mutated ovarian cancer. It could also be considered for maintenance therapy at the conclusion of chemotherapy treatment of newly diagnosed or recurrent BRCA-mutated ovarian cancer.
What adverse events are associated with pamiparib? How does the toxicity profile compare with other drugs for ovarian cancer?
With respect to PARP inhibitors, the differences in potency (PARP trapping) correlate with their toxicity profiles. The most common adverse events are gastrointestinal, hematologic, and constitutional (fatigue). Even though it is difficult to compare toxicities across different trials with heterogeneous patient populations, there are a few points worth noting.
Rucaparib leads to inhibition of renal transporter proteins involved in secretion of creatinine and can lead to increased creatinine (any grade: 15%; grade 3: ≤1%). Transaminitis is generally self-limiting and highest with rucaparib (any grade: 34%; grade 3: 10%). Hematologic toxicities are the highest with niraparib (any grade: thrombocytopenia 61%, anemia 50%, neutropenia 30%; grade ≥3: thrombocytopenia 34%, anemia 25%, neutropenia 20%).
Toxicities are more common in the first few cycles of treatment, warranting closer early monitoring. This differs somewhat from the gastrointestinal, hematological, and constitutional (fatigue) adverse events that we see with common chemotherapeutic agents used to treat ovarian cancer, which are generally cumulative.
PARP inhibitor treatment is also associated with an increased risk of developing myelodysplastic syndrome/acute myeloid leukemia (MDS/AML). That being said, therapy-related MDS/AML is a well-recognized complication of conventional chemotherapy used to treat a variety of primary malignancies, including ovarian cancer.
The expected toxicity profile for pamiparib is based on what we have seen with the other PARP inhibitors. This includes any grade nausea (50%), fatigue (33%), anemia (20%), vomiting (15%), and neutropenia (13%). Toxicity of grade 3 or higher includes anemia (13%), neutropenia (8%), and fatigue (5%).
Where do the newest drugs to be approved for ovarian cancer in recent years fit within the treatment paradigm? What do the research findings show about their efficacy and safety?
Data from phase 2/3 trials support the use of PARP inhibitors as monotherapy as well as in combination with other agents (most commonly agents other than standard chemotherapy) for the treatment of BRCA mutated or otherwise homologous recombination-deficient (HRD) ovarian cancer. They can also be considered for maintenance therapy at the conclusion of treatment of newly diagnosed or recurrent BRCA-mutated/HRD ovarian cancer.
Large phase 3 studies have resulted in the approval of the antiangiogenic agent bevacizumab in combination with chemotherapy for the treatment of newly diagnosed and recurrent ovarian cancer, as well as for maintenance therapy at the conclusion of combination chemotherapy plus bevacizumab treatment of newly diagnosed (GOG 218 and ICON 7 trials) or recurrent ovarian cancer (GOG 218, OCEANS, and AURELIA trials). The most common toxicity with antiangiogenic agents is hypertension. Women also commonly experience arthralgia/myalgia. There is an increased risk of proteinuria, blood clots, bleeding, and serious gastrointestinal events such as fistula and bowel perforation.
Data from the phase 2 KEYNOTE 158 trial support pembrolizumab for microsatellite high or mismatch repair-deficient ovarian cancers. Common side effects associated with the use of pembrolizumab include fatigue, itchy skin, diarrhea, nausea, decreased appetite, rash, fever, cough, difficulty breathing, musculoskeletal pain, constipation, and joint pain. Pembrolizumab can cause the immune system to attack normal organs and tissues in the body resulting in serious side effects, including inflammation of such organs as the lungs, colon, liver, endocrine glands, and kidneys.
Evidence for hormonal therapy (i.e., aromatase inhibitors like letrozole) for the treatment of newly diagnosed and recurrent low-grade serous/endometrioid epithelial ovarian cancer comes from largely retrospective cohort studies. A large phase 3 study, now enrolling, will examine if letrozole monotherapy/maintenance is non-inferior to intravenous paclitaxel/carboplatin and maintenance letrozole with respect to progression-free survival in women with stage II-IV primary low-grade serous carcinoma of the ovary or peritoneum after primary surgical cytoreduction.
Hormonal therapies are generally very well tolerated. Common side effects may include hot flashes, warmth or redness in the face or chest, headache, dizziness, weakness, bone pain, muscle or joint pain, swelling, weight gain, increased sweating, or increased cholesterol in the blood.
What other drugs are in development for ovarian cancer?
VEGF receptor tyrosine kinase inhibitors, such as cediranib, are in development. Anlotinib is another drug being investigated. It is a new multi-target tyrosine kinase inhibitor that targets VEGFR, PDGFR, and FGFR. Drugs targeting folate-alpha receptor, such as mirvetuximab, are under investigation, particularly for patients with high folate-alpha receptor membrane staining by immunohistochemistry. Drugs targeting cell cycle arrest, such as CDK4/6 inhibitors, are also being considered.
Can you provide some of the highlights of ovarian cancer research presented at this year’s American Society of Clinical Oncology meeting ?
My take is that we have gone from a monotonous landscape of platinum doublet chemotherapy to an exciting, diversified landscape over the past several years. All of this activity has driven median overall survival up from 3 years to 5 years and progression-free survival following first platinum sensitive recurrence to well beyond 6 months.
Since last year’s meeting, we have seen several new approvals, including niraparib for the treatment of BRCA mutated and HRD disease, as well as for first-line maintenance in all comers. In May, the FDA expanded the indication for olaparib to include its combination with bevacizumab as first-line maintenance for BRCA-mutated and HRD disease based on the results of PAOLA-1. With certainty, our treatment paradigms will continue to evolve in response to these and other new data.
At this year’s meeting, the SOLO-2 investigators revealed the first overall survival data for second-line PARP inhibitor maintenance, which is the first suggestion that PARP inhibitor maintenance improves overall survival.
We have a new understanding about the genetics of long-term responders to rucaparib on ARIEL-2.
We also understand how the role of secondary cytoreductive surgery and how nonchemotherapy options for the treatment of platinum sensitive relapse compare in terms of efficacy and toxicity (i.e., AVANOVA-2 and GY004 trials). We see again the importance of R0 cytoreduction when surgery is pursued. Achieving anything less than R0 cytoreduction for the treatment of first platinum sensitive recurrence may translate into shorter survival, compared with chemotherapy alone.
We are also becoming increasingly familiar with the limited therapeutic benefit of single-agent anti-PD-1/PD-L1, which is so different from our experience in mismatch repair-deficient endometrial cancer. In the small percentage of responders, there are some durable responses and a suggestion of particular efficacy among women with clear cell ovarian cancer.
What other recent findings in ovarian cancer research should oncologists be aware of?
Data supporting improved efficacy of a gastrointestinal-type chemotherapy regimen for mucinous epithelial ovarian cancers come from a retrospective cohort study of patients with ovarian mucinous carcinoma who received postoperative adjuvant chemotherapy at two academic centers.
Identification of inactivating SMARCA4 mutations as the driver of small cell carcinoma of the ovary, hypercalcemic type, and the idea that CDK4/6 inhibitors could be effectively repurposed to treat this rare but highly aggressive type of ovarian cancer is also new and exciting.
Dr. Stone has disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
The treatment of ovarian cancer has evolved considerably in the last few years, with the approval of several PARP inhibitors, antiangiogenic agents, and other therapies for a multitude of indications. Additional treatments are likely to soon join this already diverse spectrum of available options, if their promising efficacy and safety continues to be borne out in ongoing research.
To better understand the individual merits and potential drawbacks of these treatments, Medscape recently spoke with Rebecca Stone, MD, an ovarian cancer expert and associate professor of gynecologic oncology at Johns Hopkins University, Baltimore. This interview has been edited for length and clarity.
Medscape: We’re starting to see preliminary data on pamiparib , an investigational inhibitor of PARP1 and PARP2, for the treatment of ovarian cancer. What is the evidence supporting this drug?
Dr. Stone: Currently, six different PARP inhibitors – olaparib, rucaparib, veliparib, niraparib, talazoparib, and pamiparib – have been in clinical development at different stages. In clinical applications, PARP inhibitors, including olaparib, rucaparib, niraparib, and talazoparib, have demonstrated sustained antitumor responses as single agents in patients with BRCA1 or BRCA2 mutations. Those with Food and Drug Administration indications in ovarian cancer include olaparib, rucaparib, and niraparib. The preclinical and clinical data with pamiparib is limited as of now. But, in a xenograft breast cancer model, it was found to be over 10 times more potent than olaparib.
If approved, where would pamiparib fit in the treatment paradigm for ovarian cancer?
It would potentially fit as monotherapy as well as in combination with agents other than standard chemotherapy for the treatment of BRCA mutated ovarian cancer. It could also be considered for maintenance therapy at the conclusion of chemotherapy treatment of newly diagnosed or recurrent BRCA-mutated ovarian cancer.
What adverse events are associated with pamiparib? How does the toxicity profile compare with other drugs for ovarian cancer?
With respect to PARP inhibitors, the differences in potency (PARP trapping) correlate with their toxicity profiles. The most common adverse events are gastrointestinal, hematologic, and constitutional (fatigue). Even though it is difficult to compare toxicities across different trials with heterogeneous patient populations, there are a few points worth noting.
Rucaparib leads to inhibition of renal transporter proteins involved in secretion of creatinine and can lead to increased creatinine (any grade: 15%; grade 3: ≤1%). Transaminitis is generally self-limiting and highest with rucaparib (any grade: 34%; grade 3: 10%). Hematologic toxicities are the highest with niraparib (any grade: thrombocytopenia 61%, anemia 50%, neutropenia 30%; grade ≥3: thrombocytopenia 34%, anemia 25%, neutropenia 20%).
Toxicities are more common in the first few cycles of treatment, warranting closer early monitoring. This differs somewhat from the gastrointestinal, hematological, and constitutional (fatigue) adverse events that we see with common chemotherapeutic agents used to treat ovarian cancer, which are generally cumulative.
PARP inhibitor treatment is also associated with an increased risk of developing myelodysplastic syndrome/acute myeloid leukemia (MDS/AML). That being said, therapy-related MDS/AML is a well-recognized complication of conventional chemotherapy used to treat a variety of primary malignancies, including ovarian cancer.
The expected toxicity profile for pamiparib is based on what we have seen with the other PARP inhibitors. This includes any grade nausea (50%), fatigue (33%), anemia (20%), vomiting (15%), and neutropenia (13%). Toxicity of grade 3 or higher includes anemia (13%), neutropenia (8%), and fatigue (5%).
Where do the newest drugs to be approved for ovarian cancer in recent years fit within the treatment paradigm? What do the research findings show about their efficacy and safety?
Data from phase 2/3 trials support the use of PARP inhibitors as monotherapy as well as in combination with other agents (most commonly agents other than standard chemotherapy) for the treatment of BRCA mutated or otherwise homologous recombination-deficient (HRD) ovarian cancer. They can also be considered for maintenance therapy at the conclusion of treatment of newly diagnosed or recurrent BRCA-mutated/HRD ovarian cancer.
Large phase 3 studies have resulted in the approval of the antiangiogenic agent bevacizumab in combination with chemotherapy for the treatment of newly diagnosed and recurrent ovarian cancer, as well as for maintenance therapy at the conclusion of combination chemotherapy plus bevacizumab treatment of newly diagnosed (GOG 218 and ICON 7 trials) or recurrent ovarian cancer (GOG 218, OCEANS, and AURELIA trials). The most common toxicity with antiangiogenic agents is hypertension. Women also commonly experience arthralgia/myalgia. There is an increased risk of proteinuria, blood clots, bleeding, and serious gastrointestinal events such as fistula and bowel perforation.
Data from the phase 2 KEYNOTE 158 trial support pembrolizumab for microsatellite high or mismatch repair-deficient ovarian cancers. Common side effects associated with the use of pembrolizumab include fatigue, itchy skin, diarrhea, nausea, decreased appetite, rash, fever, cough, difficulty breathing, musculoskeletal pain, constipation, and joint pain. Pembrolizumab can cause the immune system to attack normal organs and tissues in the body resulting in serious side effects, including inflammation of such organs as the lungs, colon, liver, endocrine glands, and kidneys.
Evidence for hormonal therapy (i.e., aromatase inhibitors like letrozole) for the treatment of newly diagnosed and recurrent low-grade serous/endometrioid epithelial ovarian cancer comes from largely retrospective cohort studies. A large phase 3 study, now enrolling, will examine if letrozole monotherapy/maintenance is non-inferior to intravenous paclitaxel/carboplatin and maintenance letrozole with respect to progression-free survival in women with stage II-IV primary low-grade serous carcinoma of the ovary or peritoneum after primary surgical cytoreduction.
Hormonal therapies are generally very well tolerated. Common side effects may include hot flashes, warmth or redness in the face or chest, headache, dizziness, weakness, bone pain, muscle or joint pain, swelling, weight gain, increased sweating, or increased cholesterol in the blood.
What other drugs are in development for ovarian cancer?
VEGF receptor tyrosine kinase inhibitors, such as cediranib, are in development. Anlotinib is another drug being investigated. It is a new multi-target tyrosine kinase inhibitor that targets VEGFR, PDGFR, and FGFR. Drugs targeting folate-alpha receptor, such as mirvetuximab, are under investigation, particularly for patients with high folate-alpha receptor membrane staining by immunohistochemistry. Drugs targeting cell cycle arrest, such as CDK4/6 inhibitors, are also being considered.
Can you provide some of the highlights of ovarian cancer research presented at this year’s American Society of Clinical Oncology meeting ?
My take is that we have gone from a monotonous landscape of platinum doublet chemotherapy to an exciting, diversified landscape over the past several years. All of this activity has driven median overall survival up from 3 years to 5 years and progression-free survival following first platinum sensitive recurrence to well beyond 6 months.
Since last year’s meeting, we have seen several new approvals, including niraparib for the treatment of BRCA mutated and HRD disease, as well as for first-line maintenance in all comers. In May, the FDA expanded the indication for olaparib to include its combination with bevacizumab as first-line maintenance for BRCA-mutated and HRD disease based on the results of PAOLA-1. With certainty, our treatment paradigms will continue to evolve in response to these and other new data.
At this year’s meeting, the SOLO-2 investigators revealed the first overall survival data for second-line PARP inhibitor maintenance, which is the first suggestion that PARP inhibitor maintenance improves overall survival.
We have a new understanding about the genetics of long-term responders to rucaparib on ARIEL-2.
We also understand how the role of secondary cytoreductive surgery and how nonchemotherapy options for the treatment of platinum sensitive relapse compare in terms of efficacy and toxicity (i.e., AVANOVA-2 and GY004 trials). We see again the importance of R0 cytoreduction when surgery is pursued. Achieving anything less than R0 cytoreduction for the treatment of first platinum sensitive recurrence may translate into shorter survival, compared with chemotherapy alone.
We are also becoming increasingly familiar with the limited therapeutic benefit of single-agent anti-PD-1/PD-L1, which is so different from our experience in mismatch repair-deficient endometrial cancer. In the small percentage of responders, there are some durable responses and a suggestion of particular efficacy among women with clear cell ovarian cancer.
What other recent findings in ovarian cancer research should oncologists be aware of?
Data supporting improved efficacy of a gastrointestinal-type chemotherapy regimen for mucinous epithelial ovarian cancers come from a retrospective cohort study of patients with ovarian mucinous carcinoma who received postoperative adjuvant chemotherapy at two academic centers.
Identification of inactivating SMARCA4 mutations as the driver of small cell carcinoma of the ovary, hypercalcemic type, and the idea that CDK4/6 inhibitors could be effectively repurposed to treat this rare but highly aggressive type of ovarian cancer is also new and exciting.
Dr. Stone has disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
The treatment of ovarian cancer has evolved considerably in the last few years, with the approval of several PARP inhibitors, antiangiogenic agents, and other therapies for a multitude of indications. Additional treatments are likely to soon join this already diverse spectrum of available options, if their promising efficacy and safety continues to be borne out in ongoing research.
To better understand the individual merits and potential drawbacks of these treatments, Medscape recently spoke with Rebecca Stone, MD, an ovarian cancer expert and associate professor of gynecologic oncology at Johns Hopkins University, Baltimore. This interview has been edited for length and clarity.
Medscape: We’re starting to see preliminary data on pamiparib , an investigational inhibitor of PARP1 and PARP2, for the treatment of ovarian cancer. What is the evidence supporting this drug?
Dr. Stone: Currently, six different PARP inhibitors – olaparib, rucaparib, veliparib, niraparib, talazoparib, and pamiparib – have been in clinical development at different stages. In clinical applications, PARP inhibitors, including olaparib, rucaparib, niraparib, and talazoparib, have demonstrated sustained antitumor responses as single agents in patients with BRCA1 or BRCA2 mutations. Those with Food and Drug Administration indications in ovarian cancer include olaparib, rucaparib, and niraparib. The preclinical and clinical data with pamiparib is limited as of now. But, in a xenograft breast cancer model, it was found to be over 10 times more potent than olaparib.
If approved, where would pamiparib fit in the treatment paradigm for ovarian cancer?
It would potentially fit as monotherapy as well as in combination with agents other than standard chemotherapy for the treatment of BRCA mutated ovarian cancer. It could also be considered for maintenance therapy at the conclusion of chemotherapy treatment of newly diagnosed or recurrent BRCA-mutated ovarian cancer.
What adverse events are associated with pamiparib? How does the toxicity profile compare with other drugs for ovarian cancer?
With respect to PARP inhibitors, the differences in potency (PARP trapping) correlate with their toxicity profiles. The most common adverse events are gastrointestinal, hematologic, and constitutional (fatigue). Even though it is difficult to compare toxicities across different trials with heterogeneous patient populations, there are a few points worth noting.
Rucaparib leads to inhibition of renal transporter proteins involved in secretion of creatinine and can lead to increased creatinine (any grade: 15%; grade 3: ≤1%). Transaminitis is generally self-limiting and highest with rucaparib (any grade: 34%; grade 3: 10%). Hematologic toxicities are the highest with niraparib (any grade: thrombocytopenia 61%, anemia 50%, neutropenia 30%; grade ≥3: thrombocytopenia 34%, anemia 25%, neutropenia 20%).
Toxicities are more common in the first few cycles of treatment, warranting closer early monitoring. This differs somewhat from the gastrointestinal, hematological, and constitutional (fatigue) adverse events that we see with common chemotherapeutic agents used to treat ovarian cancer, which are generally cumulative.
PARP inhibitor treatment is also associated with an increased risk of developing myelodysplastic syndrome/acute myeloid leukemia (MDS/AML). That being said, therapy-related MDS/AML is a well-recognized complication of conventional chemotherapy used to treat a variety of primary malignancies, including ovarian cancer.
The expected toxicity profile for pamiparib is based on what we have seen with the other PARP inhibitors. This includes any grade nausea (50%), fatigue (33%), anemia (20%), vomiting (15%), and neutropenia (13%). Toxicity of grade 3 or higher includes anemia (13%), neutropenia (8%), and fatigue (5%).
Where do the newest drugs to be approved for ovarian cancer in recent years fit within the treatment paradigm? What do the research findings show about their efficacy and safety?
Data from phase 2/3 trials support the use of PARP inhibitors as monotherapy as well as in combination with other agents (most commonly agents other than standard chemotherapy) for the treatment of BRCA mutated or otherwise homologous recombination-deficient (HRD) ovarian cancer. They can also be considered for maintenance therapy at the conclusion of treatment of newly diagnosed or recurrent BRCA-mutated/HRD ovarian cancer.
Large phase 3 studies have resulted in the approval of the antiangiogenic agent bevacizumab in combination with chemotherapy for the treatment of newly diagnosed and recurrent ovarian cancer, as well as for maintenance therapy at the conclusion of combination chemotherapy plus bevacizumab treatment of newly diagnosed (GOG 218 and ICON 7 trials) or recurrent ovarian cancer (GOG 218, OCEANS, and AURELIA trials). The most common toxicity with antiangiogenic agents is hypertension. Women also commonly experience arthralgia/myalgia. There is an increased risk of proteinuria, blood clots, bleeding, and serious gastrointestinal events such as fistula and bowel perforation.
Data from the phase 2 KEYNOTE 158 trial support pembrolizumab for microsatellite high or mismatch repair-deficient ovarian cancers. Common side effects associated with the use of pembrolizumab include fatigue, itchy skin, diarrhea, nausea, decreased appetite, rash, fever, cough, difficulty breathing, musculoskeletal pain, constipation, and joint pain. Pembrolizumab can cause the immune system to attack normal organs and tissues in the body resulting in serious side effects, including inflammation of such organs as the lungs, colon, liver, endocrine glands, and kidneys.
Evidence for hormonal therapy (i.e., aromatase inhibitors like letrozole) for the treatment of newly diagnosed and recurrent low-grade serous/endometrioid epithelial ovarian cancer comes from largely retrospective cohort studies. A large phase 3 study, now enrolling, will examine if letrozole monotherapy/maintenance is non-inferior to intravenous paclitaxel/carboplatin and maintenance letrozole with respect to progression-free survival in women with stage II-IV primary low-grade serous carcinoma of the ovary or peritoneum after primary surgical cytoreduction.
Hormonal therapies are generally very well tolerated. Common side effects may include hot flashes, warmth or redness in the face or chest, headache, dizziness, weakness, bone pain, muscle or joint pain, swelling, weight gain, increased sweating, or increased cholesterol in the blood.
What other drugs are in development for ovarian cancer?
VEGF receptor tyrosine kinase inhibitors, such as cediranib, are in development. Anlotinib is another drug being investigated. It is a new multi-target tyrosine kinase inhibitor that targets VEGFR, PDGFR, and FGFR. Drugs targeting folate-alpha receptor, such as mirvetuximab, are under investigation, particularly for patients with high folate-alpha receptor membrane staining by immunohistochemistry. Drugs targeting cell cycle arrest, such as CDK4/6 inhibitors, are also being considered.
Can you provide some of the highlights of ovarian cancer research presented at this year’s American Society of Clinical Oncology meeting ?
My take is that we have gone from a monotonous landscape of platinum doublet chemotherapy to an exciting, diversified landscape over the past several years. All of this activity has driven median overall survival up from 3 years to 5 years and progression-free survival following first platinum sensitive recurrence to well beyond 6 months.
Since last year’s meeting, we have seen several new approvals, including niraparib for the treatment of BRCA mutated and HRD disease, as well as for first-line maintenance in all comers. In May, the FDA expanded the indication for olaparib to include its combination with bevacizumab as first-line maintenance for BRCA-mutated and HRD disease based on the results of PAOLA-1. With certainty, our treatment paradigms will continue to evolve in response to these and other new data.
At this year’s meeting, the SOLO-2 investigators revealed the first overall survival data for second-line PARP inhibitor maintenance, which is the first suggestion that PARP inhibitor maintenance improves overall survival.
We have a new understanding about the genetics of long-term responders to rucaparib on ARIEL-2.
We also understand how the role of secondary cytoreductive surgery and how nonchemotherapy options for the treatment of platinum sensitive relapse compare in terms of efficacy and toxicity (i.e., AVANOVA-2 and GY004 trials). We see again the importance of R0 cytoreduction when surgery is pursued. Achieving anything less than R0 cytoreduction for the treatment of first platinum sensitive recurrence may translate into shorter survival, compared with chemotherapy alone.
We are also becoming increasingly familiar with the limited therapeutic benefit of single-agent anti-PD-1/PD-L1, which is so different from our experience in mismatch repair-deficient endometrial cancer. In the small percentage of responders, there are some durable responses and a suggestion of particular efficacy among women with clear cell ovarian cancer.
What other recent findings in ovarian cancer research should oncologists be aware of?
Data supporting improved efficacy of a gastrointestinal-type chemotherapy regimen for mucinous epithelial ovarian cancers come from a retrospective cohort study of patients with ovarian mucinous carcinoma who received postoperative adjuvant chemotherapy at two academic centers.
Identification of inactivating SMARCA4 mutations as the driver of small cell carcinoma of the ovary, hypercalcemic type, and the idea that CDK4/6 inhibitors could be effectively repurposed to treat this rare but highly aggressive type of ovarian cancer is also new and exciting.
Dr. Stone has disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Is ketamine living up to the promise for depression?
After years of dormancy, psychiatric drug development is showing signs of life. There is the novel antipsychotic lumateperone, recently approved for adults with schizophrenia. Brexanolone was approved last year for postpartum depression. And perhaps generating the most attention lately among psychiatrists – and people with depression – is the use of ketamine and esketamine for depression.

Columbia psychiatrist J. John Mann, MD, a professor of translational neuroscience and a mood disorder specialist, has been involved in several notable studies of ketamine in patients with depression. He and his colleagues’ recent research efforts include a randomized study into ketamine’s ability to reduce suicidal thoughts in bipolar depression and an MRI analysis illuminating the role that dosing plays in antidepressant effects.
Dr. Sederer: Nearly 20 million people in this country alone suffer from clinical depression every year. That means they have a functional impairment in addition to their suffering and are at risk of taking their own lives. Depression is a very prevalent, painful, and disabling condition. The psychopharmacologic treatments we’ve had have been more or less the same for the past 20 or 30 years.

We’ve asked Dr. Mann to … talk to us about ketamine and its nasal preparation esketamine, which is a novel psychopharmacologic treatment. Dr. Mann, please tell us about ketamine, its utility, and the yet-to-be-answered questions.
Dr. Mann: Ketamine and esketamine, which is a component of ketamine itself, is different from traditional antidepressant medications in three fundamental ways.
The first is that it acts very quickly. Traditional antidepressants take 4, 6, 8 weeks to work. This means that the patient has to put up with a great deal of suffering while waiting for a response. And the probability of the medication working isn’t that high. About 50%-70% of individuals will respond eventually at the end of this ride. But ketamine, when it works, does so in 2 hours. That’s a totally different timescale.
The second aspect is that, when it does work, it often works very robustly, even though it’s a quick-acting antidepressant. The patient often quickly feels distinctly better.
Very often when you’re using traditional antidepressants, it takes a while for the improvement to reach the point that the patient is confident that they are clearly better, and too often that does not happen.
Dr. Sederer: As the treating doctor, you’re trying to keep that patient’s hope alive, even though we don’t have substantial evidence that they’re going to respond.
Dr. Mann: Exactly. One of the difficulties of keeping patients on track with traditional antidepressants is that, after the first dose or two, they have all the side effects and yet no benefit has emerged. In many ways patients sometimes feel that they’re going backwards. They have all of their depression plus the side effects of the medication.
But with ketamine, it’s rather different. You come in, you have the treatment, and many patients feel improved in a couple of hours. And not just a bit improved, but in many cases distinctly improved.
It’s very important for clinicians to appreciate that ketamine will work in patients who have a classically described treatment-resistant depression, meaning they’ve tried several other types of antidepressant medications that haven’t worked.
A prerequisite for treatment with ketamine is that they have had a number of treatment failures. The labeling for the intranasal esketamine states that you should try the other antidepressants first and then use this if they don’t work. The fact that ketamine can work even when the other medications have failed is a huge advantage.
Dr. Sederer: There is another feature of ketamine, in that it also has a pronounced benefit for suicidal ideation, which your research has reported on.
Dr. Mann: Yes, we’ve learned over the years that depression and suicidality are in some ways comorbid conditions. That both have to be addressed in order to keep somebody alive so that they can respond to treatment.
That’s a very important point. If the patient is suffering from depression and the antidepressant takes weeks to work, they may lose hope during that time. They may become overwhelmed by the suicidal ideation, no longer able to control or resist the impulse to take their life. A lot of the management is therefore to try to help support the patient (and family) so that these thoughts never become too compelling. Often we have to consider hospitalization to protect these patients so that they can stay alive long enough for the antidepressant to work. But ketamine not only has this very rapid effect for their depression, it also has a partly independent effect on suicidal ideation that is equally rapid and robust, which can render the patient safer.
Dr. Sederer: In other words, it’s effective and rapidly so for depression, with a bonus of reducing suicidality? This sounds almost too good to be true.
Dr. Mann: There are some limitations that we have to keep in mind. One limitation is that a single administration of ketamine will produce this robust improvement but it will only persist for most people for 5-7 days.
Dr. Sederer: Is the same duration true for scheduling the next treatment as well?
Dr. Mann: Yes, it is. The patient will gradually begin to deteriorate if you do not repeat the treatment. But as we showed in our randomized controlled clinical study, with ketamine for suicidal ideation, if you continue to deliver the medication, you can sustain the benefit.
Dr. Sederer: Can a person receive both ketamine and a conventional antidepressant at the same time?
Dr. Mann: Yes. In this study, half of the patients were actually continued on their previous medication while we added the ketamine on top of that. It worked very well.
In practice, people use two approaches. One approach used by most ketamine clinics is to give six doses of ketamine at a frequency of about two per week. Then they will reduce the frequency down to once a week for a few more doses and then once a month.
Dr. Sederer:: And this is a ketamine infusion?
Dr. Mann: Yes, this generally has been a ketamine infusion. This approach seems to work quite well. But that may not be necessary.
Another strategy is to give one, two, or three doses of ketamine. If the patient doesn’t respond robustly to two or three doses, they’re not going to respond to subsequent doses.
Dr. Sederer: So, initial responses are a predictor of future response?
Dr. Mann: Exactly. Now, if they haven’t done well with two or three doses, then you’ve got to use other treatments. But if they do well with the two or three, then you’ve got a choice: You can either complete the treatment course with ketamine and then continue them on antidepressant medications, or simply treat them with ketamine alone. What we tend to do is to treat with only antidepressant medications after a small number of ketamine treatments. We also use ketamine as a kind of “rescue medication” if they relapse into severe depression, though this is true for only a minority of patients.
Dr. Sederer: One of the things that we’ve learned is that antidepressants have a very beneficial effect for some people, but then they wear out and the person starts to relapse. Should ketamine be studied as an intervention for people who are no longer responding to the antidepressant(s) that they are on?
Dr. Mann: We do not really know the answer to that question. My experience treating very seriously ill patients is that sometimes the ketamine will work very well the first time or the second time but then in the future, if you try to use it as a rescue medication, it might not work that well. There is some clinical experience that suggests that that may be true for some people. But we have no idea about the frequency or timing with which this might happen. That’s all uncertain.
Moreover, most of our control clinical trial data come from either one dose of ketamine or from a few trials where people have received multiple doses of ketamine, followed by a bit of a taper. But there are very, very few of those types of studies. We’re still learning about the use of this medication.
Dr. Sederer: Importantly, you referenced the side effects of antidepressants. What are the side effects and risks of ketamine?
Dr. Mann: We know a lot more about the immediate short-term side effects of a single dose or a few doses of ketamine. Most people will get a kind of tripping experience. They’ll feel a bit unreal, or their circumstances or experiences of the world feel a bit distorted.
Some patients develop strange ideas. Most patients don’t enjoy those symptoms, even though I know ketamine is used as a party drug, and so on and so forth.
Dr. Sederer: It seems that the context is what matters.
Dr. Mann: Yes. And in a clinic context, most patients simply don’t enjoy these types of dissociative experiences, but they put up with them. They’re not severe, in general.
Dr. Sederer: Is part of the preparation of the patient telling them that this may happen?
Dr. Mann: Yes. We try to explain the potential for these symptoms and that most people get them. These side effects almost invariably terminate with the cessation of the administration.
Dr. Sederer: What’s the typical duration of the infusion you use?
Dr. Mann: Traditionally, infusion is 40 minutes and always in a clinic setting.
Dr. Sederer: And that’s because of the concern that a patient may have these symptoms?
Dr. Mann: Exactly. They may have dissociative effects that they’re disturbed by, and we need to monitor that. They’re probably going to remain under observation in the clinic for about the same amount of time because it takes about the same time for these effects to wear off.
The other consideration is that some people get a little nausea. In our experience with the intravenous ketamine, there’s also a problematic side effect that their blood pressure will be slightly raised. Therefore, it’s good to know that the person’s blood pressure is under control before they begin the treatments and that you’re monitoring it during administration.
Dr. Sederer: What are the differences you’re discovering between esketamine and ketamine?
Dr. Mann: It is a bit different. We’ve just completed a very important National Institutes of Health–funded clinical trial here at Columbia showing that with esketamine or ketamine itself, the dose and the blood levels are very closely related to the robustness of the clinical response.
When you give a drug intravenously, you give a very reliable dose. When you give the drug over 40 minutes, you’re spreading the dose administration over a period of time so that it doesn’t peak very high. The side effects appear to be proportional to the peak dose.
When you give it intranasally, you give the drug over a much shorter period of time. Even if you use more than one intranasal administration to give the whole dose, it’s still a relatively shorter time, compared with the 40 minutes.
Dr. Sederer: This means that to get the equivalent dose intranasally, the patient is going to have to experience a higher peak. Can you predict that those patients who are treated intranasally are going to have more side effects?
Dr. Mann: Right. And that should be explained to the patient. You will not need an intravenous line inserted, which some people might find highly appealing and advantageous, but you will probably have more side effects.
Also, in general, intranasal absorption of drugs is more variable. The predictability of the blood level and, therefore, the degree of antidepressant effect is not as good intranasally as intravenously.
Now, all of this is anecdotal clinical experience, based on theoretical pharmacology, because nobody has actually done a head-to-head control comparison.
Dr. Sederer: What about the cost of both of these preparations?
Dr. Mann: There is a bit of a range in pricing between ketamine clinics around the country. It’s always important to find out what they charge per administration. And then it makes a difference whether you have two or three administrations versus six plus further tapered administration. Clearly, the cost can vary a great deal.
Dr. Sederer: But it’s generally not covered by insurance, so most people are paying out of pocket.
Dr. Mann: Yes. The intranasal ketamine is still in negotiation at the moment, but it should be resolved before it’s fully marketed.
Dr. Sederer: Ketamine is used for major depression. Does it have utility in bipolar depression?
Dr. Mann: We and some others have done initial studies in bipolar depression. In our view, it’s probably going to be as effective in bipolar disorder as it is in major depressive disorder, unipolar depression.
We haven’t seen any manic episodes triggered, but we don’t give repeated doses. We allow research patients to stay on anticonvulsants or mood stabilizers, so that’s helpful. Generally, people with bipolar disorder who come for ketamine treatment for their depression are coming on a mood stabilizer, because that and perhaps other conventional antidepressants have not proven to be effective. So, I think that ketamine plus mood stabilizers seems to be very promising.
Dr. Sederer: I want to return to the antisuicidal properties that you had previously mentioned. I heard from a colleague about a patient who had been admitted to a psychiatric inpatient unit. The patient was in her 20s; she did not have major depression but was persistently suicidal, constantly trying to hurt herself in any way she could. But that seemed to be more a product of borderline personality disorder, with its impulsive and self-destructive problems.
In the end, they tried intranasal ketamine. The response was, just as you described, robust. Her self-injurious behavior dropped in a very pronounced way within a day or two. But she then did require administrations a couple of times a week in order to keep that suicidality at bay.
Based on that example, I’m wondering whether there is an application here for people who are suicidal yet who may not have features of major depression or bipolar depression.
Dr. Mann: It’s a very interesting suggestion for which we have no data-based answer. However, we have a clue from the study that we published in the American Journal of Psychiatry and have since published further analyses on.
The reasons that people die by suicide, or make suicide attempts, are not entirely attributable to the fact that they suffer from a mood disorder.
Dr. Sederer: Yes, because only a minority of individuals with a mood disorder ever make suicide attempts. But there is a subgroup at risk.
Dr. Mann: Here at Columbia, we’ve promulgated the stress-diathesis model for suicidal behavior. A stressor could be external life events, but the internal stressor would be something like an acute episode of depression.
But predisposition also plays an important role, which has several elements to it. One is decision-making. These are patients with a propensity to go for a short-term, quick relief. In other words, a patient would be seeking immediate relief rather than waiting for the delayed improvement from an antidepressant. They’re more prone to act on the pain of the depression and terminate their lives – to try to end their pain – rather than wait and hope that, in time, there’s a chance that the antidepressant will work.
Dr. Sederer: What else do you want to share with our viewers about this medication and how it’s used?
Dr. Mann: My goal in treating patients is to try to use the least amount of medication possible. We do not really know yet the long-term safety of ketamine treatment.
It’s been used for many decades in anesthesia, but people don’t get repeated anesthetic doses of ketamine. And higher doses of ketamine given repeatedly have been shown in preclinical studies to produce little lesions in the brain, which is not good. But we’re using much lower doses.
As we potentially move into a time when we could be giving multiple doses of ketamine to patients, we should remember that we need to be cautious about that. If we don’t need to give them more doses, we shouldn’t. We should know that there is a potential downside that we don’t fully understand yet to giving ketamine repeatedly.
And that’s aside from its abuse potential. We know that people have employed ketamine for physical and emotional pain, and when they administer it themselves, they tend to get dependent on it. In a clinic setting it’s given in a very formal and structured fashion, a bit like the administration of opioids. In that setting, it is much safer and the risk for abuse and diversion is minimized. But we need to remember that this drug does have abuse potential and perhaps not yet fully measurable neurotoxic effects.
Dr. Sederer: If physicians, nurses, and other professional clinicians want to learn more about this medication, what are the accurate, reliable sources of information to which you suggest they turn?
Dr. Mann: The National Institute of Mental Health’s website offers good and reliable information for patients and their families. It is an unbiased, scientific, and thoughtful source of information, and better than just trolling the Internet for information.
People are much more sophisticated now than they were 20 years ago in these matters, and scientific papers are much more accessible to the public. Reading papers in recognized journals is also a useful way to gain information.
For example, one of the major papers that we published in the American Journal of Psychiatry is available to anybody on the Internet to read. So, I encourage people to make their own inquiries and talk to more than one doctor. Informed patients and families are the best partners a doctor can ever have. We encourage that in all of our patients.
Dr. Sederer: I want to thank you very much, Dr. Mann, for your work in this area and for joining us here at Medscape and Columbia Psychiatry to teach us so much about what is truly a novel psychopharmacologic agent, yet one where we still have a lot more to learn.
A version of this article originally appeared on Medscape.com.
After years of dormancy, psychiatric drug development is showing signs of life. There is the novel antipsychotic lumateperone, recently approved for adults with schizophrenia. Brexanolone was approved last year for postpartum depression. And perhaps generating the most attention lately among psychiatrists – and people with depression – is the use of ketamine and esketamine for depression.
Columbia psychiatrist J. John Mann, MD, a professor of translational neuroscience and a mood disorder specialist, has been involved in several notable studies of ketamine in patients with depression. He and his colleagues’ recent research efforts include a randomized study into ketamine’s ability to reduce suicidal thoughts in bipolar depression and an MRI analysis illuminating the role that dosing plays in antidepressant effects.
Dr. Sederer: Nearly 20 million people in this country alone suffer from clinical depression every year. That means they have a functional impairment in addition to their suffering and are at risk of taking their own lives. Depression is a very prevalent, painful, and disabling condition. The psychopharmacologic treatments we’ve had have been more or less the same for the past 20 or 30 years.
We’ve asked Dr. Mann to … talk to us about ketamine and its nasal preparation esketamine, which is a novel psychopharmacologic treatment. Dr. Mann, please tell us about ketamine, its utility, and the yet-to-be-answered questions.
Dr. Mann: Ketamine and esketamine, which is a component of ketamine itself, is different from traditional antidepressant medications in three fundamental ways.
The first is that it acts very quickly. Traditional antidepressants take 4, 6, 8 weeks to work. This means that the patient has to put up with a great deal of suffering while waiting for a response. And the probability of the medication working isn’t that high. About 50%-70% of individuals will respond eventually at the end of this ride. But ketamine, when it works, does so in 2 hours. That’s a totally different timescale.
The second aspect is that, when it does work, it often works very robustly, even though it’s a quick-acting antidepressant. The patient often quickly feels distinctly better.
Very often when you’re using traditional antidepressants, it takes a while for the improvement to reach the point that the patient is confident that they are clearly better, and too often that does not happen.
Dr. Sederer: As the treating doctor, you’re trying to keep that patient’s hope alive, even though we don’t have substantial evidence that they’re going to respond.
Dr. Mann: Exactly. One of the difficulties of keeping patients on track with traditional antidepressants is that, after the first dose or two, they have all the side effects and yet no benefit has emerged. In many ways patients sometimes feel that they’re going backwards. They have all of their depression plus the side effects of the medication.
But with ketamine, it’s rather different. You come in, you have the treatment, and many patients feel improved in a couple of hours. And not just a bit improved, but in many cases distinctly improved.
It’s very important for clinicians to appreciate that ketamine will work in patients who have a classically described treatment-resistant depression, meaning they’ve tried several other types of antidepressant medications that haven’t worked.
A prerequisite for treatment with ketamine is that they have had a number of treatment failures. The labeling for the intranasal esketamine states that you should try the other antidepressants first and then use this if they don’t work. The fact that ketamine can work even when the other medications have failed is a huge advantage.
Dr. Sederer: There is another feature of ketamine, in that it also has a pronounced benefit for suicidal ideation, which your research has reported on.
Dr. Mann: Yes, we’ve learned over the years that depression and suicidality are in some ways comorbid conditions. That both have to be addressed in order to keep somebody alive so that they can respond to treatment.
That’s a very important point. If the patient is suffering from depression and the antidepressant takes weeks to work, they may lose hope during that time. They may become overwhelmed by the suicidal ideation, no longer able to control or resist the impulse to take their life. A lot of the management is therefore to try to help support the patient (and family) so that these thoughts never become too compelling. Often we have to consider hospitalization to protect these patients so that they can stay alive long enough for the antidepressant to work. But ketamine not only has this very rapid effect for their depression, it also has a partly independent effect on suicidal ideation that is equally rapid and robust, which can render the patient safer.
Dr. Sederer: In other words, it’s effective and rapidly so for depression, with a bonus of reducing suicidality? This sounds almost too good to be true.
Dr. Mann: There are some limitations that we have to keep in mind. One limitation is that a single administration of ketamine will produce this robust improvement but it will only persist for most people for 5-7 days.
Dr. Sederer: Is the same duration true for scheduling the next treatment as well?
Dr. Mann: Yes, it is. The patient will gradually begin to deteriorate if you do not repeat the treatment. But as we showed in our randomized controlled clinical study, with ketamine for suicidal ideation, if you continue to deliver the medication, you can sustain the benefit.
Dr. Sederer: Can a person receive both ketamine and a conventional antidepressant at the same time?
Dr. Mann: Yes. In this study, half of the patients were actually continued on their previous medication while we added the ketamine on top of that. It worked very well.
In practice, people use two approaches. One approach used by most ketamine clinics is to give six doses of ketamine at a frequency of about two per week. Then they will reduce the frequency down to once a week for a few more doses and then once a month.
Dr. Sederer:: And this is a ketamine infusion?
Dr. Mann: Yes, this generally has been a ketamine infusion. This approach seems to work quite well. But that may not be necessary.
Another strategy is to give one, two, or three doses of ketamine. If the patient doesn’t respond robustly to two or three doses, they’re not going to respond to subsequent doses.
Dr. Sederer: So, initial responses are a predictor of future response?
Dr. Mann: Exactly. Now, if they haven’t done well with two or three doses, then you’ve got to use other treatments. But if they do well with the two or three, then you’ve got a choice: You can either complete the treatment course with ketamine and then continue them on antidepressant medications, or simply treat them with ketamine alone. What we tend to do is to treat with only antidepressant medications after a small number of ketamine treatments. We also use ketamine as a kind of “rescue medication” if they relapse into severe depression, though this is true for only a minority of patients.
Dr. Sederer: One of the things that we’ve learned is that antidepressants have a very beneficial effect for some people, but then they wear out and the person starts to relapse. Should ketamine be studied as an intervention for people who are no longer responding to the antidepressant(s) that they are on?
Dr. Mann: We do not really know the answer to that question. My experience treating very seriously ill patients is that sometimes the ketamine will work very well the first time or the second time but then in the future, if you try to use it as a rescue medication, it might not work that well. There is some clinical experience that suggests that that may be true for some people. But we have no idea about the frequency or timing with which this might happen. That’s all uncertain.
Moreover, most of our control clinical trial data come from either one dose of ketamine or from a few trials where people have received multiple doses of ketamine, followed by a bit of a taper. But there are very, very few of those types of studies. We’re still learning about the use of this medication.
Dr. Sederer: Importantly, you referenced the side effects of antidepressants. What are the side effects and risks of ketamine?
Dr. Mann: We know a lot more about the immediate short-term side effects of a single dose or a few doses of ketamine. Most people will get a kind of tripping experience. They’ll feel a bit unreal, or their circumstances or experiences of the world feel a bit distorted.
Some patients develop strange ideas. Most patients don’t enjoy those symptoms, even though I know ketamine is used as a party drug, and so on and so forth.
Dr. Sederer: It seems that the context is what matters.
Dr. Mann: Yes. And in a clinic context, most patients simply don’t enjoy these types of dissociative experiences, but they put up with them. They’re not severe, in general.
Dr. Sederer: Is part of the preparation of the patient telling them that this may happen?
Dr. Mann: Yes. We try to explain the potential for these symptoms and that most people get them. These side effects almost invariably terminate with the cessation of the administration.
Dr. Sederer: What’s the typical duration of the infusion you use?
Dr. Mann: Traditionally, infusion is 40 minutes and always in a clinic setting.
Dr. Sederer: And that’s because of the concern that a patient may have these symptoms?
Dr. Mann: Exactly. They may have dissociative effects that they’re disturbed by, and we need to monitor that. They’re probably going to remain under observation in the clinic for about the same amount of time because it takes about the same time for these effects to wear off.
The other consideration is that some people get a little nausea. In our experience with the intravenous ketamine, there’s also a problematic side effect that their blood pressure will be slightly raised. Therefore, it’s good to know that the person’s blood pressure is under control before they begin the treatments and that you’re monitoring it during administration.
Dr. Sederer: What are the differences you’re discovering between esketamine and ketamine?
Dr. Mann: It is a bit different. We’ve just completed a very important National Institutes of Health–funded clinical trial here at Columbia showing that with esketamine or ketamine itself, the dose and the blood levels are very closely related to the robustness of the clinical response.
When you give a drug intravenously, you give a very reliable dose. When you give the drug over 40 minutes, you’re spreading the dose administration over a period of time so that it doesn’t peak very high. The side effects appear to be proportional to the peak dose.
When you give it intranasally, you give the drug over a much shorter period of time. Even if you use more than one intranasal administration to give the whole dose, it’s still a relatively shorter time, compared with the 40 minutes.
Dr. Sederer: This means that to get the equivalent dose intranasally, the patient is going to have to experience a higher peak. Can you predict that those patients who are treated intranasally are going to have more side effects?
Dr. Mann: Right. And that should be explained to the patient. You will not need an intravenous line inserted, which some people might find highly appealing and advantageous, but you will probably have more side effects.
Also, in general, intranasal absorption of drugs is more variable. The predictability of the blood level and, therefore, the degree of antidepressant effect is not as good intranasally as intravenously.
Now, all of this is anecdotal clinical experience, based on theoretical pharmacology, because nobody has actually done a head-to-head control comparison.
Dr. Sederer: What about the cost of both of these preparations?
Dr. Mann: There is a bit of a range in pricing between ketamine clinics around the country. It’s always important to find out what they charge per administration. And then it makes a difference whether you have two or three administrations versus six plus further tapered administration. Clearly, the cost can vary a great deal.
Dr. Sederer: But it’s generally not covered by insurance, so most people are paying out of pocket.
Dr. Mann: Yes. The intranasal ketamine is still in negotiation at the moment, but it should be resolved before it’s fully marketed.
Dr. Sederer: Ketamine is used for major depression. Does it have utility in bipolar depression?
Dr. Mann: We and some others have done initial studies in bipolar depression. In our view, it’s probably going to be as effective in bipolar disorder as it is in major depressive disorder, unipolar depression.
We haven’t seen any manic episodes triggered, but we don’t give repeated doses. We allow research patients to stay on anticonvulsants or mood stabilizers, so that’s helpful. Generally, people with bipolar disorder who come for ketamine treatment for their depression are coming on a mood stabilizer, because that and perhaps other conventional antidepressants have not proven to be effective. So, I think that ketamine plus mood stabilizers seems to be very promising.
Dr. Sederer: I want to return to the antisuicidal properties that you had previously mentioned. I heard from a colleague about a patient who had been admitted to a psychiatric inpatient unit. The patient was in her 20s; she did not have major depression but was persistently suicidal, constantly trying to hurt herself in any way she could. But that seemed to be more a product of borderline personality disorder, with its impulsive and self-destructive problems.
In the end, they tried intranasal ketamine. The response was, just as you described, robust. Her self-injurious behavior dropped in a very pronounced way within a day or two. But she then did require administrations a couple of times a week in order to keep that suicidality at bay.
Based on that example, I’m wondering whether there is an application here for people who are suicidal yet who may not have features of major depression or bipolar depression.
Dr. Mann: It’s a very interesting suggestion for which we have no data-based answer. However, we have a clue from the study that we published in the American Journal of Psychiatry and have since published further analyses on.
The reasons that people die by suicide, or make suicide attempts, are not entirely attributable to the fact that they suffer from a mood disorder.
Dr. Sederer: Yes, because only a minority of individuals with a mood disorder ever make suicide attempts. But there is a subgroup at risk.
Dr. Mann: Here at Columbia, we’ve promulgated the stress-diathesis model for suicidal behavior. A stressor could be external life events, but the internal stressor would be something like an acute episode of depression.
But predisposition also plays an important role, which has several elements to it. One is decision-making. These are patients with a propensity to go for a short-term, quick relief. In other words, a patient would be seeking immediate relief rather than waiting for the delayed improvement from an antidepressant. They’re more prone to act on the pain of the depression and terminate their lives – to try to end their pain – rather than wait and hope that, in time, there’s a chance that the antidepressant will work.
Dr. Sederer: What else do you want to share with our viewers about this medication and how it’s used?
Dr. Mann: My goal in treating patients is to try to use the least amount of medication possible. We do not really know yet the long-term safety of ketamine treatment.
It’s been used for many decades in anesthesia, but people don’t get repeated anesthetic doses of ketamine. And higher doses of ketamine given repeatedly have been shown in preclinical studies to produce little lesions in the brain, which is not good. But we’re using much lower doses.
As we potentially move into a time when we could be giving multiple doses of ketamine to patients, we should remember that we need to be cautious about that. If we don’t need to give them more doses, we shouldn’t. We should know that there is a potential downside that we don’t fully understand yet to giving ketamine repeatedly.
And that’s aside from its abuse potential. We know that people have employed ketamine for physical and emotional pain, and when they administer it themselves, they tend to get dependent on it. In a clinic setting it’s given in a very formal and structured fashion, a bit like the administration of opioids. In that setting, it is much safer and the risk for abuse and diversion is minimized. But we need to remember that this drug does have abuse potential and perhaps not yet fully measurable neurotoxic effects.
Dr. Sederer: If physicians, nurses, and other professional clinicians want to learn more about this medication, what are the accurate, reliable sources of information to which you suggest they turn?
Dr. Mann: The National Institute of Mental Health’s website offers good and reliable information for patients and their families. It is an unbiased, scientific, and thoughtful source of information, and better than just trolling the Internet for information.
People are much more sophisticated now than they were 20 years ago in these matters, and scientific papers are much more accessible to the public. Reading papers in recognized journals is also a useful way to gain information.
For example, one of the major papers that we published in the American Journal of Psychiatry is available to anybody on the Internet to read. So, I encourage people to make their own inquiries and talk to more than one doctor. Informed patients and families are the best partners a doctor can ever have. We encourage that in all of our patients.
Dr. Sederer: I want to thank you very much, Dr. Mann, for your work in this area and for joining us here at Medscape and Columbia Psychiatry to teach us so much about what is truly a novel psychopharmacologic agent, yet one where we still have a lot more to learn.
A version of this article originally appeared on Medscape.com.
After years of dormancy, psychiatric drug development is showing signs of life. There is the novel antipsychotic lumateperone, recently approved for adults with schizophrenia. Brexanolone was approved last year for postpartum depression. And perhaps generating the most attention lately among psychiatrists – and people with depression – is the use of ketamine and esketamine for depression.
Columbia psychiatrist J. John Mann, MD, a professor of translational neuroscience and a mood disorder specialist, has been involved in several notable studies of ketamine in patients with depression. He and his colleagues’ recent research efforts include a randomized study into ketamine’s ability to reduce suicidal thoughts in bipolar depression and an MRI analysis illuminating the role that dosing plays in antidepressant effects.
Dr. Sederer: Nearly 20 million people in this country alone suffer from clinical depression every year. That means they have a functional impairment in addition to their suffering and are at risk of taking their own lives. Depression is a very prevalent, painful, and disabling condition. The psychopharmacologic treatments we’ve had have been more or less the same for the past 20 or 30 years.
We’ve asked Dr. Mann to … talk to us about ketamine and its nasal preparation esketamine, which is a novel psychopharmacologic treatment. Dr. Mann, please tell us about ketamine, its utility, and the yet-to-be-answered questions.
Dr. Mann: Ketamine and esketamine, which is a component of ketamine itself, is different from traditional antidepressant medications in three fundamental ways.
The first is that it acts very quickly. Traditional antidepressants take 4, 6, 8 weeks to work. This means that the patient has to put up with a great deal of suffering while waiting for a response. And the probability of the medication working isn’t that high. About 50%-70% of individuals will respond eventually at the end of this ride. But ketamine, when it works, does so in 2 hours. That’s a totally different timescale.
The second aspect is that, when it does work, it often works very robustly, even though it’s a quick-acting antidepressant. The patient often quickly feels distinctly better.
Very often when you’re using traditional antidepressants, it takes a while for the improvement to reach the point that the patient is confident that they are clearly better, and too often that does not happen.
Dr. Sederer: As the treating doctor, you’re trying to keep that patient’s hope alive, even though we don’t have substantial evidence that they’re going to respond.
Dr. Mann: Exactly. One of the difficulties of keeping patients on track with traditional antidepressants is that, after the first dose or two, they have all the side effects and yet no benefit has emerged. In many ways patients sometimes feel that they’re going backwards. They have all of their depression plus the side effects of the medication.
But with ketamine, it’s rather different. You come in, you have the treatment, and many patients feel improved in a couple of hours. And not just a bit improved, but in many cases distinctly improved.
It’s very important for clinicians to appreciate that ketamine will work in patients who have a classically described treatment-resistant depression, meaning they’ve tried several other types of antidepressant medications that haven’t worked.
A prerequisite for treatment with ketamine is that they have had a number of treatment failures. The labeling for the intranasal esketamine states that you should try the other antidepressants first and then use this if they don’t work. The fact that ketamine can work even when the other medications have failed is a huge advantage.
Dr. Sederer: There is another feature of ketamine, in that it also has a pronounced benefit for suicidal ideation, which your research has reported on.
Dr. Mann: Yes, we’ve learned over the years that depression and suicidality are in some ways comorbid conditions. That both have to be addressed in order to keep somebody alive so that they can respond to treatment.
That’s a very important point. If the patient is suffering from depression and the antidepressant takes weeks to work, they may lose hope during that time. They may become overwhelmed by the suicidal ideation, no longer able to control or resist the impulse to take their life. A lot of the management is therefore to try to help support the patient (and family) so that these thoughts never become too compelling. Often we have to consider hospitalization to protect these patients so that they can stay alive long enough for the antidepressant to work. But ketamine not only has this very rapid effect for their depression, it also has a partly independent effect on suicidal ideation that is equally rapid and robust, which can render the patient safer.
Dr. Sederer: In other words, it’s effective and rapidly so for depression, with a bonus of reducing suicidality? This sounds almost too good to be true.
Dr. Mann: There are some limitations that we have to keep in mind. One limitation is that a single administration of ketamine will produce this robust improvement but it will only persist for most people for 5-7 days.
Dr. Sederer: Is the same duration true for scheduling the next treatment as well?
Dr. Mann: Yes, it is. The patient will gradually begin to deteriorate if you do not repeat the treatment. But as we showed in our randomized controlled clinical study, with ketamine for suicidal ideation, if you continue to deliver the medication, you can sustain the benefit.
Dr. Sederer: Can a person receive both ketamine and a conventional antidepressant at the same time?
Dr. Mann: Yes. In this study, half of the patients were actually continued on their previous medication while we added the ketamine on top of that. It worked very well.
In practice, people use two approaches. One approach used by most ketamine clinics is to give six doses of ketamine at a frequency of about two per week. Then they will reduce the frequency down to once a week for a few more doses and then once a month.
Dr. Sederer:: And this is a ketamine infusion?
Dr. Mann: Yes, this generally has been a ketamine infusion. This approach seems to work quite well. But that may not be necessary.
Another strategy is to give one, two, or three doses of ketamine. If the patient doesn’t respond robustly to two or three doses, they’re not going to respond to subsequent doses.
Dr. Sederer: So, initial responses are a predictor of future response?
Dr. Mann: Exactly. Now, if they haven’t done well with two or three doses, then you’ve got to use other treatments. But if they do well with the two or three, then you’ve got a choice: You can either complete the treatment course with ketamine and then continue them on antidepressant medications, or simply treat them with ketamine alone. What we tend to do is to treat with only antidepressant medications after a small number of ketamine treatments. We also use ketamine as a kind of “rescue medication” if they relapse into severe depression, though this is true for only a minority of patients.
Dr. Sederer: One of the things that we’ve learned is that antidepressants have a very beneficial effect for some people, but then they wear out and the person starts to relapse. Should ketamine be studied as an intervention for people who are no longer responding to the antidepressant(s) that they are on?
Dr. Mann: We do not really know the answer to that question. My experience treating very seriously ill patients is that sometimes the ketamine will work very well the first time or the second time but then in the future, if you try to use it as a rescue medication, it might not work that well. There is some clinical experience that suggests that that may be true for some people. But we have no idea about the frequency or timing with which this might happen. That’s all uncertain.
Moreover, most of our control clinical trial data come from either one dose of ketamine or from a few trials where people have received multiple doses of ketamine, followed by a bit of a taper. But there are very, very few of those types of studies. We’re still learning about the use of this medication.
Dr. Sederer: Importantly, you referenced the side effects of antidepressants. What are the side effects and risks of ketamine?
Dr. Mann: We know a lot more about the immediate short-term side effects of a single dose or a few doses of ketamine. Most people will get a kind of tripping experience. They’ll feel a bit unreal, or their circumstances or experiences of the world feel a bit distorted.
Some patients develop strange ideas. Most patients don’t enjoy those symptoms, even though I know ketamine is used as a party drug, and so on and so forth.
Dr. Sederer: It seems that the context is what matters.
Dr. Mann: Yes. And in a clinic context, most patients simply don’t enjoy these types of dissociative experiences, but they put up with them. They’re not severe, in general.
Dr. Sederer: Is part of the preparation of the patient telling them that this may happen?
Dr. Mann: Yes. We try to explain the potential for these symptoms and that most people get them. These side effects almost invariably terminate with the cessation of the administration.
Dr. Sederer: What’s the typical duration of the infusion you use?
Dr. Mann: Traditionally, infusion is 40 minutes and always in a clinic setting.
Dr. Sederer: And that’s because of the concern that a patient may have these symptoms?
Dr. Mann: Exactly. They may have dissociative effects that they’re disturbed by, and we need to monitor that. They’re probably going to remain under observation in the clinic for about the same amount of time because it takes about the same time for these effects to wear off.
The other consideration is that some people get a little nausea. In our experience with the intravenous ketamine, there’s also a problematic side effect that their blood pressure will be slightly raised. Therefore, it’s good to know that the person’s blood pressure is under control before they begin the treatments and that you’re monitoring it during administration.
Dr. Sederer: What are the differences you’re discovering between esketamine and ketamine?
Dr. Mann: It is a bit different. We’ve just completed a very important National Institutes of Health–funded clinical trial here at Columbia showing that with esketamine or ketamine itself, the dose and the blood levels are very closely related to the robustness of the clinical response.
When you give a drug intravenously, you give a very reliable dose. When you give the drug over 40 minutes, you’re spreading the dose administration over a period of time so that it doesn’t peak very high. The side effects appear to be proportional to the peak dose.
When you give it intranasally, you give the drug over a much shorter period of time. Even if you use more than one intranasal administration to give the whole dose, it’s still a relatively shorter time, compared with the 40 minutes.
Dr. Sederer: This means that to get the equivalent dose intranasally, the patient is going to have to experience a higher peak. Can you predict that those patients who are treated intranasally are going to have more side effects?
Dr. Mann: Right. And that should be explained to the patient. You will not need an intravenous line inserted, which some people might find highly appealing and advantageous, but you will probably have more side effects.
Also, in general, intranasal absorption of drugs is more variable. The predictability of the blood level and, therefore, the degree of antidepressant effect is not as good intranasally as intravenously.
Now, all of this is anecdotal clinical experience, based on theoretical pharmacology, because nobody has actually done a head-to-head control comparison.
Dr. Sederer: What about the cost of both of these preparations?
Dr. Mann: There is a bit of a range in pricing between ketamine clinics around the country. It’s always important to find out what they charge per administration. And then it makes a difference whether you have two or three administrations versus six plus further tapered administration. Clearly, the cost can vary a great deal.
Dr. Sederer: But it’s generally not covered by insurance, so most people are paying out of pocket.
Dr. Mann: Yes. The intranasal ketamine is still in negotiation at the moment, but it should be resolved before it’s fully marketed.
Dr. Sederer: Ketamine is used for major depression. Does it have utility in bipolar depression?
Dr. Mann: We and some others have done initial studies in bipolar depression. In our view, it’s probably going to be as effective in bipolar disorder as it is in major depressive disorder, unipolar depression.
We haven’t seen any manic episodes triggered, but we don’t give repeated doses. We allow research patients to stay on anticonvulsants or mood stabilizers, so that’s helpful. Generally, people with bipolar disorder who come for ketamine treatment for their depression are coming on a mood stabilizer, because that and perhaps other conventional antidepressants have not proven to be effective. So, I think that ketamine plus mood stabilizers seems to be very promising.
Dr. Sederer: I want to return to the antisuicidal properties that you had previously mentioned. I heard from a colleague about a patient who had been admitted to a psychiatric inpatient unit. The patient was in her 20s; she did not have major depression but was persistently suicidal, constantly trying to hurt herself in any way she could. But that seemed to be more a product of borderline personality disorder, with its impulsive and self-destructive problems.
In the end, they tried intranasal ketamine. The response was, just as you described, robust. Her self-injurious behavior dropped in a very pronounced way within a day or two. But she then did require administrations a couple of times a week in order to keep that suicidality at bay.
Based on that example, I’m wondering whether there is an application here for people who are suicidal yet who may not have features of major depression or bipolar depression.
Dr. Mann: It’s a very interesting suggestion for which we have no data-based answer. However, we have a clue from the study that we published in the American Journal of Psychiatry and have since published further analyses on.
The reasons that people die by suicide, or make suicide attempts, are not entirely attributable to the fact that they suffer from a mood disorder.
Dr. Sederer: Yes, because only a minority of individuals with a mood disorder ever make suicide attempts. But there is a subgroup at risk.
Dr. Mann: Here at Columbia, we’ve promulgated the stress-diathesis model for suicidal behavior. A stressor could be external life events, but the internal stressor would be something like an acute episode of depression.
But predisposition also plays an important role, which has several elements to it. One is decision-making. These are patients with a propensity to go for a short-term, quick relief. In other words, a patient would be seeking immediate relief rather than waiting for the delayed improvement from an antidepressant. They’re more prone to act on the pain of the depression and terminate their lives – to try to end their pain – rather than wait and hope that, in time, there’s a chance that the antidepressant will work.
Dr. Sederer: What else do you want to share with our viewers about this medication and how it’s used?
Dr. Mann: My goal in treating patients is to try to use the least amount of medication possible. We do not really know yet the long-term safety of ketamine treatment.
It’s been used for many decades in anesthesia, but people don’t get repeated anesthetic doses of ketamine. And higher doses of ketamine given repeatedly have been shown in preclinical studies to produce little lesions in the brain, which is not good. But we’re using much lower doses.
As we potentially move into a time when we could be giving multiple doses of ketamine to patients, we should remember that we need to be cautious about that. If we don’t need to give them more doses, we shouldn’t. We should know that there is a potential downside that we don’t fully understand yet to giving ketamine repeatedly.
And that’s aside from its abuse potential. We know that people have employed ketamine for physical and emotional pain, and when they administer it themselves, they tend to get dependent on it. In a clinic setting it’s given in a very formal and structured fashion, a bit like the administration of opioids. In that setting, it is much safer and the risk for abuse and diversion is minimized. But we need to remember that this drug does have abuse potential and perhaps not yet fully measurable neurotoxic effects.
Dr. Sederer: If physicians, nurses, and other professional clinicians want to learn more about this medication, what are the accurate, reliable sources of information to which you suggest they turn?
Dr. Mann: The National Institute of Mental Health’s website offers good and reliable information for patients and their families. It is an unbiased, scientific, and thoughtful source of information, and better than just trolling the Internet for information.
People are much more sophisticated now than they were 20 years ago in these matters, and scientific papers are much more accessible to the public. Reading papers in recognized journals is also a useful way to gain information.
For example, one of the major papers that we published in the American Journal of Psychiatry is available to anybody on the Internet to read. So, I encourage people to make their own inquiries and talk to more than one doctor. Informed patients and families are the best partners a doctor can ever have. We encourage that in all of our patients.
Dr. Sederer: I want to thank you very much, Dr. Mann, for your work in this area and for joining us here at Medscape and Columbia Psychiatry to teach us so much about what is truly a novel psychopharmacologic agent, yet one where we still have a lot more to learn.
A version of this article originally appeared on Medscape.com.
Issues with the Maintenance of Certification program; Overcoming a ‘quadruple threat’
Issues with the MOC
In Dr. Nasrallah’s editorial “Revamp the MOC” (From the Editor,
I was not so fortunate to have been grandfathered with lifetime certification, so I have been forced to recertify twice now. I will be 70 years old when I will need to decide whether to recertify once again. It is my belief that the MOC process is cumbersome and nonsensical, having little, if any, relevance in assessing one’s competency. Again, the ABPN’s purpose is not to “protect the public” and ensure safe and competent care, but to generate tremendous revenue for the Board. How can any rational individual believe that this exam is a legitimate test of one’s knowledge and competency when the pass rates are so stratospherically high year after year? I do not know of a single individual who has failed the recertification exam, so it would appear that if you pay the fees and sit for the exam, you will pass. It saddens me that the Board can perpetrate such a hoax on the public, leading them to believe that the MOC actually means something.
The cost to recertify is not inexpensive. Apparently, in a desire to add to its coffers, the ABPN has recently implemented the Physician Folios portal, whereby psychiatrists are forced to pay an annual fee. Its purpose, according to the Board, is to provide“a dynamic conduit for important data exchange such as making updates to personal contact information, updating medical license information, and applying and paying for an examination.”1 Give me a break!
It is my hope that a better, less expensive, more appropriate system is developed, allowing the psychiatrist to focus his/her efforts on treating patients.
Terrence Boyadjis, MD
Private psychiatric practice
West Chester, Pennsylvania
Reference
1. American Board of Psychiatry and Neurology. ABPN Physician Folios. https://application.abpn.com/webclient/landing_page.asp. Accessed October 20, 2020.
Dr. Nasrallah’s editorial about the MOC process is another addition to his collection of many of the best editorials I’ve ever read. I related fondly to his experiences taking the oral exam, which I took in 1972. I also became an examiner during the mid-1970s. Dr. Nasrallah continues to be a source of down-to-earth wisdom for our beloved profession.
Richard W. Worst, MD
Twin Falls, Idaho
Continue to: Overcoming a ‘quadruple threat’
Overcoming a ‘quadruple threat’
Dr. Nasrallah’s editorial “Enduring the ordeal of a quadruple threat is especially arduous for psychiatric patients” (From the Editor,
Robert W. Pollack, MD
Founder/COO
Psychiatric Associates of Southwest Florida
Fort Myers, Florida
Disclosures: The authors report no financial relationships with any companies whose products are mentioned in this article, or with manufacturers of competing products.
Issues with the MOC
In Dr. Nasrallah’s editorial “Revamp the MOC” (From the Editor,
I was not so fortunate to have been grandfathered with lifetime certification, so I have been forced to recertify twice now. I will be 70 years old when I will need to decide whether to recertify once again. It is my belief that the MOC process is cumbersome and nonsensical, having little, if any, relevance in assessing one’s competency. Again, the ABPN’s purpose is not to “protect the public” and ensure safe and competent care, but to generate tremendous revenue for the Board. How can any rational individual believe that this exam is a legitimate test of one’s knowledge and competency when the pass rates are so stratospherically high year after year? I do not know of a single individual who has failed the recertification exam, so it would appear that if you pay the fees and sit for the exam, you will pass. It saddens me that the Board can perpetrate such a hoax on the public, leading them to believe that the MOC actually means something.
The cost to recertify is not inexpensive. Apparently, in a desire to add to its coffers, the ABPN has recently implemented the Physician Folios portal, whereby psychiatrists are forced to pay an annual fee. Its purpose, according to the Board, is to provide“a dynamic conduit for important data exchange such as making updates to personal contact information, updating medical license information, and applying and paying for an examination.”1 Give me a break!
It is my hope that a better, less expensive, more appropriate system is developed, allowing the psychiatrist to focus his/her efforts on treating patients.
Terrence Boyadjis, MD
Private psychiatric practice
West Chester, Pennsylvania
Reference
1. American Board of Psychiatry and Neurology. ABPN Physician Folios. https://application.abpn.com/webclient/landing_page.asp. Accessed October 20, 2020.
Dr. Nasrallah’s editorial about the MOC process is another addition to his collection of many of the best editorials I’ve ever read. I related fondly to his experiences taking the oral exam, which I took in 1972. I also became an examiner during the mid-1970s. Dr. Nasrallah continues to be a source of down-to-earth wisdom for our beloved profession.
Richard W. Worst, MD
Twin Falls, Idaho
Continue to: Overcoming a ‘quadruple threat’
Overcoming a ‘quadruple threat’
Dr. Nasrallah’s editorial “Enduring the ordeal of a quadruple threat is especially arduous for psychiatric patients” (From the Editor,
Robert W. Pollack, MD
Founder/COO
Psychiatric Associates of Southwest Florida
Fort Myers, Florida
Disclosures: The authors report no financial relationships with any companies whose products are mentioned in this article, or with manufacturers of competing products.
Issues with the MOC
In Dr. Nasrallah’s editorial “Revamp the MOC” (From the Editor,
I was not so fortunate to have been grandfathered with lifetime certification, so I have been forced to recertify twice now. I will be 70 years old when I will need to decide whether to recertify once again. It is my belief that the MOC process is cumbersome and nonsensical, having little, if any, relevance in assessing one’s competency. Again, the ABPN’s purpose is not to “protect the public” and ensure safe and competent care, but to generate tremendous revenue for the Board. How can any rational individual believe that this exam is a legitimate test of one’s knowledge and competency when the pass rates are so stratospherically high year after year? I do not know of a single individual who has failed the recertification exam, so it would appear that if you pay the fees and sit for the exam, you will pass. It saddens me that the Board can perpetrate such a hoax on the public, leading them to believe that the MOC actually means something.
The cost to recertify is not inexpensive. Apparently, in a desire to add to its coffers, the ABPN has recently implemented the Physician Folios portal, whereby psychiatrists are forced to pay an annual fee. Its purpose, according to the Board, is to provide“a dynamic conduit for important data exchange such as making updates to personal contact information, updating medical license information, and applying and paying for an examination.”1 Give me a break!
It is my hope that a better, less expensive, more appropriate system is developed, allowing the psychiatrist to focus his/her efforts on treating patients.
Terrence Boyadjis, MD
Private psychiatric practice
West Chester, Pennsylvania
Reference
1. American Board of Psychiatry and Neurology. ABPN Physician Folios. https://application.abpn.com/webclient/landing_page.asp. Accessed October 20, 2020.
Dr. Nasrallah’s editorial about the MOC process is another addition to his collection of many of the best editorials I’ve ever read. I related fondly to his experiences taking the oral exam, which I took in 1972. I also became an examiner during the mid-1970s. Dr. Nasrallah continues to be a source of down-to-earth wisdom for our beloved profession.
Richard W. Worst, MD
Twin Falls, Idaho
Continue to: Overcoming a ‘quadruple threat’
Overcoming a ‘quadruple threat’
Dr. Nasrallah’s editorial “Enduring the ordeal of a quadruple threat is especially arduous for psychiatric patients” (From the Editor,
Robert W. Pollack, MD
Founder/COO
Psychiatric Associates of Southwest Florida
Fort Myers, Florida
Disclosures: The authors report no financial relationships with any companies whose products are mentioned in this article, or with manufacturers of competing products.
Unmet needs in the pharmacotherapy of psychiatric brain syndromes
Let’s face it: The greatest unmet need in psychiatry is discovering a treatment for the infamous syndrome of toxic political extremism. Its ugly symptoms include blind hatred, visceral malice, bigotry, vandalism, hypocrisy, racism, hubris, intransigence, narcissism, demagoguery, mutual contempt, and intense schadenfreude.
This corrosive affliction has engulfed and polluted our society, and compromised our well-being and quality of life. Treating this malignant syndrome is beyond the reach of psychopharmacology!
Thus, we psychiatrists should focus on the mood, psychotic, anxiety, and addiction syndromes that we encounter daily in our hospitals, clinics, and private offices. They affect tens of millions of patients. We currently have many psychotropic medications for these conditions. When combined with psychotherapy, the resulting synergy can be magical and immensely gratifying. However, some of those agents have limited efficacy due to the extensive heterogeneity of syndromes such as schizophrenia or depression, which are often confounded with comorbidities. A perfect balance between efficacy, tolerability, and safety are often hard to come by in pharmacotherapy.
The most glaring psychopharmacologic unmet need is that 80% of DSM disorders still do not have a single FDA-approved (evidence-based) medication.1 It will take decades, hundreds of billions of dollars, and the motivation of the often-maligned pharmaceutical industry (indispensable, because they are the only entity with the large R&D infrastructure to develop medications for psychiatry). Both academic and clinical psychiatrists must advise pharmaceutical companies about the unmet needs in our field and urge them to develop novel pharmacotherapies to address the gaps in the clinical care of psychiatric patients.
An inventory of unmet needs
With that in mind, here is a list of unmet needs I have been thinking about lately, and hoping that they will be resolved to help our patients achieve better clinical and functional outcomes.
Rapid-onset antipsychotics. The discovery that ketamine can rapidly convert refractory patients who are chronically depressed or suicidal to normal mood within a few hours shattered the dogma that weeks and months are needed for severe depression to improve, let alone achieve full remission. There is a similar dogma about psychosis requiring a protracted duration of antipsychotic treatment to attain significant impact. A rapid-acting antipsychotic agent would represent a major advance in psychiatry and its pharmaco-economic benefits would be substantial, given the high cost of inpatient hospitalization. Just as neurobiologic research guided the discovery of ketamine as a dramatic paradigm shift in treating depression, targeted research, especially focusing on glutamate pathways, may help identify a rapid-onset agent, whether oral, intranasal, IV, or even (why not) intrathecal. Research is known to enhance serendipity, which has been kind to psychiatry and has led to the discovery of several pharmacologic therapies in psychiatry, such as chlorpromazine, monoamine oxidase inhibitor antidepressants, and lithium.
Long-acting antidepressants and anxiolytics. This can be regarded as low-hanging fruit. Several technologies have been developed for long-acting formulations, yet they have been exploited mainly for antipsychotic medications. Some of these technologies can be employed to convert commonly used antidepressants (such as selective serotonin reuptake inhibitors) into long-acting antidepressants that can also reduce anxiety. Nonadherence among patients with depression is quite common, and relapses may lead to suicide attempts. The use of injectable, long-acting antidepressants can also reduce the incidence of overdoses because the patient will not have possession of potentially fatal pills.
Continue to: Long-acting mood stabilizers
Long-acting mood stabilizers. The rationale for long-acting mood stabilizers is the same as for long-acting antidepressants. Patients with bipolar disorder are known to stop taking their medications because they miss their “highs.” Some long-acting antipsychotics are approved for bipolar disorder, but these are often associated with adverse effects, such as metabolic dysregulation, extrapyramidal symptoms, and tardive dyskinesia. Mood stabilizers are essential for the bipolar spectrum.
A “real” treatment for alcohol use disorders that eliminates craving for alcohol. Alcoholism is associated with more than 100 medical complications and is one of the leading causes of disability in the world. It is frustrating that very few drug companies have focused on this widely prevalent brain disorder, which is also a common comorbid condition in many psychiatric syndromes.
Treatment-resistance pharmacotherapy solutions. All psychiatric syndromes are heterogeneous and contain ≥1 subgroups (biotypes) that fail to respond to what is considered the “standard” psychopharmacologic treatment (such as antipsychotics, antidepressants, mood stabilizers, or anti-obsessive medications). Technically, those so-called treatment-resistant subtypes need medications with a different mechanism of action. For example, clozapine for treatment-resistant schizophrenia and ketamine for treatment-resistant depression provide proof that treatment resistance is treatable but by a mechanism of action that is completely different from that of standard therapies, such as N-methyl-
Negative symptoms of schizophrenia cause significant functional disability and are well known to be a major unmet need. Some promising data are emerging on agents such as pimavanserin, cariprazine, and roluperidone, which is encouraging, but nothing is approved yet.
Cognitive deficits of schizophrenia, both neurocognition and social cognition, are another major unmet need that impair function in many patients. Many attempts to develop a pharmacologic treatment for these serious cognitive impairments have been made, but several candidates that initially appeared promising have bitten the dust. A focus on modulating the glutamate NMDA receptor may eventually lead to a breakthrough, and that may also help patients with bipolar disorder and major depressive disorder, both of whom also have cognitive deficits in several domains, albeit less severe than those experienced by patients with schizophrenia.
Continue to: Personality disorders
Personality disorders, especially borderline personality disorder, are very challenging to treat pharmacologically despite their prevalence and serious disruption to people’s lives. Hardly any FDA clinical trials have been conducted on any personality disorder. It is an unmet need that all psychiatrists would love to see addressed. But the mythical notion that personality disorders are untreatable may be an impediment in the pursuit of novel pharmacotherapy for borderline, narcissistic, antisocial, or schizotypal personality disorders, and other disorders. Heart attacks and religious conversion often change the baseline personality dramatically.
Childhood disorders. Apart from attention-deficit/hyperactivity disorder (ADHD), very few childhood psychiatric disorders have an FDA-approved medication. Why do drug companies avoid conducting controlled clinical trials in children age <10 who have autism, spectrum disorders, conduct disorder, oppositional defiant disorder, and other disorders? Effective pharmacotherapy for these children can be regarded as a desirable early intervention that may short-circuit their progression to serious adult psychopathology.
Parsimonious psychopharmacology for the treatment of trans-diagnostic psychiatric disorders. Recent research strongly suggests there is a strong overlap among psychiatric conditions, genetically, clinically, and biologically.2,3 For example, bipolar disorder is frequently accompanied by anxiety or substance use, patients with schizophrenia often experience anxiety, depression, or substance use, and ADHD has been found to share genes with autism.4,5
Eating disorders. There are no truly efficacious pharmacologic treatments for anorexia or bulimia nervosa. Research in this area is thin, and needs to be beefed up.
Sexual disorders. A huge unmet need exists for the pharmacotherapy of many sexual disorders that can have serious legal consequences (paraphilias) or quality-of-life repercussions (low sexual desire and orgasm disorders).
Continue to: A coordinated effort
A coordinated effort
It will take a massive collaboration among multiple stakeholders to launch the herculean process of addressing the unmet needs of all the above psychiatric disorders. This includes:
- the pharmaceutical industry (to provide the massive financial investment and R&D expertise)
- the federal government (to provide incentives)
- the FDA (to allow novel clinical trial designs)
- academic psychiatrists (to conduct research to discover the pathophysiology of psychiatric diseases)
- clinical psychiatrists (to provide consultations and advise about the clinical gaps in current psychopharmacological treatments)
- psychiatric patients (who are needed to volunteer for large-scale clinical trials).
This will be a veritable “psychiatric Manhattan Project” to advance the treatment of numerous psychiatric illnesses. The greatest benefit of discovering cures for disabling mental disorders is the evaporation of the virulent stigma that continues to plague our patients.
As for the political extremism that has corroded our society, it may be beyond pharmacologic redemption. An antidote to the “kool aid” has not yet been invented…
1. Devulapalli KK, Nasrallah HA. An analysis of the high psychotropic off-label use in psychiatric disorders: the majority of psychiatric diagnoses have no approved drug. Asian J Psychiatr. 2009;2(1):29-36.
2. Nasrallah HA. Is there only 1 neurobiologic disorder, with different clinical expressions? Current Psychiatry. 2015;14(7):10-12.
3. Nasrallah HA. Pleiotropy of psychiatric disorders will reinvent DSM. Current Psychiatry. 2013;12(4):6-7.
4. Caspi A, Moffitt TE. All for one and one for all: mental disorders in one dimension. Am J Psychiatry. 2018;175(9):831-844.
5. Marshall M. Roots of mental illness. Nature. 2020;581:19-21.
Let’s face it: The greatest unmet need in psychiatry is discovering a treatment for the infamous syndrome of toxic political extremism. Its ugly symptoms include blind hatred, visceral malice, bigotry, vandalism, hypocrisy, racism, hubris, intransigence, narcissism, demagoguery, mutual contempt, and intense schadenfreude.
This corrosive affliction has engulfed and polluted our society, and compromised our well-being and quality of life. Treating this malignant syndrome is beyond the reach of psychopharmacology!
Thus, we psychiatrists should focus on the mood, psychotic, anxiety, and addiction syndromes that we encounter daily in our hospitals, clinics, and private offices. They affect tens of millions of patients. We currently have many psychotropic medications for these conditions. When combined with psychotherapy, the resulting synergy can be magical and immensely gratifying. However, some of those agents have limited efficacy due to the extensive heterogeneity of syndromes such as schizophrenia or depression, which are often confounded with comorbidities. A perfect balance between efficacy, tolerability, and safety are often hard to come by in pharmacotherapy.
The most glaring psychopharmacologic unmet need is that 80% of DSM disorders still do not have a single FDA-approved (evidence-based) medication.1 It will take decades, hundreds of billions of dollars, and the motivation of the often-maligned pharmaceutical industry (indispensable, because they are the only entity with the large R&D infrastructure to develop medications for psychiatry). Both academic and clinical psychiatrists must advise pharmaceutical companies about the unmet needs in our field and urge them to develop novel pharmacotherapies to address the gaps in the clinical care of psychiatric patients.
An inventory of unmet needs
With that in mind, here is a list of unmet needs I have been thinking about lately, and hoping that they will be resolved to help our patients achieve better clinical and functional outcomes.
Rapid-onset antipsychotics. The discovery that ketamine can rapidly convert refractory patients who are chronically depressed or suicidal to normal mood within a few hours shattered the dogma that weeks and months are needed for severe depression to improve, let alone achieve full remission. There is a similar dogma about psychosis requiring a protracted duration of antipsychotic treatment to attain significant impact. A rapid-acting antipsychotic agent would represent a major advance in psychiatry and its pharmaco-economic benefits would be substantial, given the high cost of inpatient hospitalization. Just as neurobiologic research guided the discovery of ketamine as a dramatic paradigm shift in treating depression, targeted research, especially focusing on glutamate pathways, may help identify a rapid-onset agent, whether oral, intranasal, IV, or even (why not) intrathecal. Research is known to enhance serendipity, which has been kind to psychiatry and has led to the discovery of several pharmacologic therapies in psychiatry, such as chlorpromazine, monoamine oxidase inhibitor antidepressants, and lithium.
Long-acting antidepressants and anxiolytics. This can be regarded as low-hanging fruit. Several technologies have been developed for long-acting formulations, yet they have been exploited mainly for antipsychotic medications. Some of these technologies can be employed to convert commonly used antidepressants (such as selective serotonin reuptake inhibitors) into long-acting antidepressants that can also reduce anxiety. Nonadherence among patients with depression is quite common, and relapses may lead to suicide attempts. The use of injectable, long-acting antidepressants can also reduce the incidence of overdoses because the patient will not have possession of potentially fatal pills.
Continue to: Long-acting mood stabilizers
Long-acting mood stabilizers. The rationale for long-acting mood stabilizers is the same as for long-acting antidepressants. Patients with bipolar disorder are known to stop taking their medications because they miss their “highs.” Some long-acting antipsychotics are approved for bipolar disorder, but these are often associated with adverse effects, such as metabolic dysregulation, extrapyramidal symptoms, and tardive dyskinesia. Mood stabilizers are essential for the bipolar spectrum.
A “real” treatment for alcohol use disorders that eliminates craving for alcohol. Alcoholism is associated with more than 100 medical complications and is one of the leading causes of disability in the world. It is frustrating that very few drug companies have focused on this widely prevalent brain disorder, which is also a common comorbid condition in many psychiatric syndromes.
Treatment-resistance pharmacotherapy solutions. All psychiatric syndromes are heterogeneous and contain ≥1 subgroups (biotypes) that fail to respond to what is considered the “standard” psychopharmacologic treatment (such as antipsychotics, antidepressants, mood stabilizers, or anti-obsessive medications). Technically, those so-called treatment-resistant subtypes need medications with a different mechanism of action. For example, clozapine for treatment-resistant schizophrenia and ketamine for treatment-resistant depression provide proof that treatment resistance is treatable but by a mechanism of action that is completely different from that of standard therapies, such as N-methyl-
Negative symptoms of schizophrenia cause significant functional disability and are well known to be a major unmet need. Some promising data are emerging on agents such as pimavanserin, cariprazine, and roluperidone, which is encouraging, but nothing is approved yet.
Cognitive deficits of schizophrenia, both neurocognition and social cognition, are another major unmet need that impair function in many patients. Many attempts to develop a pharmacologic treatment for these serious cognitive impairments have been made, but several candidates that initially appeared promising have bitten the dust. A focus on modulating the glutamate NMDA receptor may eventually lead to a breakthrough, and that may also help patients with bipolar disorder and major depressive disorder, both of whom also have cognitive deficits in several domains, albeit less severe than those experienced by patients with schizophrenia.
Continue to: Personality disorders
Personality disorders, especially borderline personality disorder, are very challenging to treat pharmacologically despite their prevalence and serious disruption to people’s lives. Hardly any FDA clinical trials have been conducted on any personality disorder. It is an unmet need that all psychiatrists would love to see addressed. But the mythical notion that personality disorders are untreatable may be an impediment in the pursuit of novel pharmacotherapy for borderline, narcissistic, antisocial, or schizotypal personality disorders, and other disorders. Heart attacks and religious conversion often change the baseline personality dramatically.
Childhood disorders. Apart from attention-deficit/hyperactivity disorder (ADHD), very few childhood psychiatric disorders have an FDA-approved medication. Why do drug companies avoid conducting controlled clinical trials in children age <10 who have autism, spectrum disorders, conduct disorder, oppositional defiant disorder, and other disorders? Effective pharmacotherapy for these children can be regarded as a desirable early intervention that may short-circuit their progression to serious adult psychopathology.
Parsimonious psychopharmacology for the treatment of trans-diagnostic psychiatric disorders. Recent research strongly suggests there is a strong overlap among psychiatric conditions, genetically, clinically, and biologically.2,3 For example, bipolar disorder is frequently accompanied by anxiety or substance use, patients with schizophrenia often experience anxiety, depression, or substance use, and ADHD has been found to share genes with autism.4,5
Eating disorders. There are no truly efficacious pharmacologic treatments for anorexia or bulimia nervosa. Research in this area is thin, and needs to be beefed up.
Sexual disorders. A huge unmet need exists for the pharmacotherapy of many sexual disorders that can have serious legal consequences (paraphilias) or quality-of-life repercussions (low sexual desire and orgasm disorders).
Continue to: A coordinated effort
A coordinated effort
It will take a massive collaboration among multiple stakeholders to launch the herculean process of addressing the unmet needs of all the above psychiatric disorders. This includes:
- the pharmaceutical industry (to provide the massive financial investment and R&D expertise)
- the federal government (to provide incentives)
- the FDA (to allow novel clinical trial designs)
- academic psychiatrists (to conduct research to discover the pathophysiology of psychiatric diseases)
- clinical psychiatrists (to provide consultations and advise about the clinical gaps in current psychopharmacological treatments)
- psychiatric patients (who are needed to volunteer for large-scale clinical trials).
This will be a veritable “psychiatric Manhattan Project” to advance the treatment of numerous psychiatric illnesses. The greatest benefit of discovering cures for disabling mental disorders is the evaporation of the virulent stigma that continues to plague our patients.
As for the political extremism that has corroded our society, it may be beyond pharmacologic redemption. An antidote to the “kool aid” has not yet been invented…
Let’s face it: The greatest unmet need in psychiatry is discovering a treatment for the infamous syndrome of toxic political extremism. Its ugly symptoms include blind hatred, visceral malice, bigotry, vandalism, hypocrisy, racism, hubris, intransigence, narcissism, demagoguery, mutual contempt, and intense schadenfreude.
This corrosive affliction has engulfed and polluted our society, and compromised our well-being and quality of life. Treating this malignant syndrome is beyond the reach of psychopharmacology!
Thus, we psychiatrists should focus on the mood, psychotic, anxiety, and addiction syndromes that we encounter daily in our hospitals, clinics, and private offices. They affect tens of millions of patients. We currently have many psychotropic medications for these conditions. When combined with psychotherapy, the resulting synergy can be magical and immensely gratifying. However, some of those agents have limited efficacy due to the extensive heterogeneity of syndromes such as schizophrenia or depression, which are often confounded with comorbidities. A perfect balance between efficacy, tolerability, and safety are often hard to come by in pharmacotherapy.
The most glaring psychopharmacologic unmet need is that 80% of DSM disorders still do not have a single FDA-approved (evidence-based) medication.1 It will take decades, hundreds of billions of dollars, and the motivation of the often-maligned pharmaceutical industry (indispensable, because they are the only entity with the large R&D infrastructure to develop medications for psychiatry). Both academic and clinical psychiatrists must advise pharmaceutical companies about the unmet needs in our field and urge them to develop novel pharmacotherapies to address the gaps in the clinical care of psychiatric patients.
An inventory of unmet needs
With that in mind, here is a list of unmet needs I have been thinking about lately, and hoping that they will be resolved to help our patients achieve better clinical and functional outcomes.
Rapid-onset antipsychotics. The discovery that ketamine can rapidly convert refractory patients who are chronically depressed or suicidal to normal mood within a few hours shattered the dogma that weeks and months are needed for severe depression to improve, let alone achieve full remission. There is a similar dogma about psychosis requiring a protracted duration of antipsychotic treatment to attain significant impact. A rapid-acting antipsychotic agent would represent a major advance in psychiatry and its pharmaco-economic benefits would be substantial, given the high cost of inpatient hospitalization. Just as neurobiologic research guided the discovery of ketamine as a dramatic paradigm shift in treating depression, targeted research, especially focusing on glutamate pathways, may help identify a rapid-onset agent, whether oral, intranasal, IV, or even (why not) intrathecal. Research is known to enhance serendipity, which has been kind to psychiatry and has led to the discovery of several pharmacologic therapies in psychiatry, such as chlorpromazine, monoamine oxidase inhibitor antidepressants, and lithium.
Long-acting antidepressants and anxiolytics. This can be regarded as low-hanging fruit. Several technologies have been developed for long-acting formulations, yet they have been exploited mainly for antipsychotic medications. Some of these technologies can be employed to convert commonly used antidepressants (such as selective serotonin reuptake inhibitors) into long-acting antidepressants that can also reduce anxiety. Nonadherence among patients with depression is quite common, and relapses may lead to suicide attempts. The use of injectable, long-acting antidepressants can also reduce the incidence of overdoses because the patient will not have possession of potentially fatal pills.
Continue to: Long-acting mood stabilizers
Long-acting mood stabilizers. The rationale for long-acting mood stabilizers is the same as for long-acting antidepressants. Patients with bipolar disorder are known to stop taking their medications because they miss their “highs.” Some long-acting antipsychotics are approved for bipolar disorder, but these are often associated with adverse effects, such as metabolic dysregulation, extrapyramidal symptoms, and tardive dyskinesia. Mood stabilizers are essential for the bipolar spectrum.
A “real” treatment for alcohol use disorders that eliminates craving for alcohol. Alcoholism is associated with more than 100 medical complications and is one of the leading causes of disability in the world. It is frustrating that very few drug companies have focused on this widely prevalent brain disorder, which is also a common comorbid condition in many psychiatric syndromes.
Treatment-resistance pharmacotherapy solutions. All psychiatric syndromes are heterogeneous and contain ≥1 subgroups (biotypes) that fail to respond to what is considered the “standard” psychopharmacologic treatment (such as antipsychotics, antidepressants, mood stabilizers, or anti-obsessive medications). Technically, those so-called treatment-resistant subtypes need medications with a different mechanism of action. For example, clozapine for treatment-resistant schizophrenia and ketamine for treatment-resistant depression provide proof that treatment resistance is treatable but by a mechanism of action that is completely different from that of standard therapies, such as N-methyl-
Negative symptoms of schizophrenia cause significant functional disability and are well known to be a major unmet need. Some promising data are emerging on agents such as pimavanserin, cariprazine, and roluperidone, which is encouraging, but nothing is approved yet.
Cognitive deficits of schizophrenia, both neurocognition and social cognition, are another major unmet need that impair function in many patients. Many attempts to develop a pharmacologic treatment for these serious cognitive impairments have been made, but several candidates that initially appeared promising have bitten the dust. A focus on modulating the glutamate NMDA receptor may eventually lead to a breakthrough, and that may also help patients with bipolar disorder and major depressive disorder, both of whom also have cognitive deficits in several domains, albeit less severe than those experienced by patients with schizophrenia.
Continue to: Personality disorders
Personality disorders, especially borderline personality disorder, are very challenging to treat pharmacologically despite their prevalence and serious disruption to people’s lives. Hardly any FDA clinical trials have been conducted on any personality disorder. It is an unmet need that all psychiatrists would love to see addressed. But the mythical notion that personality disorders are untreatable may be an impediment in the pursuit of novel pharmacotherapy for borderline, narcissistic, antisocial, or schizotypal personality disorders, and other disorders. Heart attacks and religious conversion often change the baseline personality dramatically.
Childhood disorders. Apart from attention-deficit/hyperactivity disorder (ADHD), very few childhood psychiatric disorders have an FDA-approved medication. Why do drug companies avoid conducting controlled clinical trials in children age <10 who have autism, spectrum disorders, conduct disorder, oppositional defiant disorder, and other disorders? Effective pharmacotherapy for these children can be regarded as a desirable early intervention that may short-circuit their progression to serious adult psychopathology.
Parsimonious psychopharmacology for the treatment of trans-diagnostic psychiatric disorders. Recent research strongly suggests there is a strong overlap among psychiatric conditions, genetically, clinically, and biologically.2,3 For example, bipolar disorder is frequently accompanied by anxiety or substance use, patients with schizophrenia often experience anxiety, depression, or substance use, and ADHD has been found to share genes with autism.4,5
Eating disorders. There are no truly efficacious pharmacologic treatments for anorexia or bulimia nervosa. Research in this area is thin, and needs to be beefed up.
Sexual disorders. A huge unmet need exists for the pharmacotherapy of many sexual disorders that can have serious legal consequences (paraphilias) or quality-of-life repercussions (low sexual desire and orgasm disorders).
Continue to: A coordinated effort
A coordinated effort
It will take a massive collaboration among multiple stakeholders to launch the herculean process of addressing the unmet needs of all the above psychiatric disorders. This includes:
- the pharmaceutical industry (to provide the massive financial investment and R&D expertise)
- the federal government (to provide incentives)
- the FDA (to allow novel clinical trial designs)
- academic psychiatrists (to conduct research to discover the pathophysiology of psychiatric diseases)
- clinical psychiatrists (to provide consultations and advise about the clinical gaps in current psychopharmacological treatments)
- psychiatric patients (who are needed to volunteer for large-scale clinical trials).
This will be a veritable “psychiatric Manhattan Project” to advance the treatment of numerous psychiatric illnesses. The greatest benefit of discovering cures for disabling mental disorders is the evaporation of the virulent stigma that continues to plague our patients.
As for the political extremism that has corroded our society, it may be beyond pharmacologic redemption. An antidote to the “kool aid” has not yet been invented…
1. Devulapalli KK, Nasrallah HA. An analysis of the high psychotropic off-label use in psychiatric disorders: the majority of psychiatric diagnoses have no approved drug. Asian J Psychiatr. 2009;2(1):29-36.
2. Nasrallah HA. Is there only 1 neurobiologic disorder, with different clinical expressions? Current Psychiatry. 2015;14(7):10-12.
3. Nasrallah HA. Pleiotropy of psychiatric disorders will reinvent DSM. Current Psychiatry. 2013;12(4):6-7.
4. Caspi A, Moffitt TE. All for one and one for all: mental disorders in one dimension. Am J Psychiatry. 2018;175(9):831-844.
5. Marshall M. Roots of mental illness. Nature. 2020;581:19-21.
1. Devulapalli KK, Nasrallah HA. An analysis of the high psychotropic off-label use in psychiatric disorders: the majority of psychiatric diagnoses have no approved drug. Asian J Psychiatr. 2009;2(1):29-36.
2. Nasrallah HA. Is there only 1 neurobiologic disorder, with different clinical expressions? Current Psychiatry. 2015;14(7):10-12.
3. Nasrallah HA. Pleiotropy of psychiatric disorders will reinvent DSM. Current Psychiatry. 2013;12(4):6-7.
4. Caspi A, Moffitt TE. All for one and one for all: mental disorders in one dimension. Am J Psychiatry. 2018;175(9):831-844.
5. Marshall M. Roots of mental illness. Nature. 2020;581:19-21.

Infected with COVID-19: One psychiatrist’s story
Emil: Coronavirus disease 2019 (COVID-19) wasn’t really on my mind until the first weekend in March, specifically Sunday, March 8, 2020. That weekend had us traveling from Chicago to Berwyn, Pennsylvania to attend the funeral of one of my older cousins. Though we were the only ones from his side at the graveside, his funeral had drawn numerous relatives, none of whom were “socially distanced.”
On our way home, I received an e-mail from a colleague in Brazil who had invited me to speak at a conference in São Paulo. He told me that several of my American colleagues had contacted him and informed him that their universities had banned travel because of COVID. “I’m coming,” I replied. “I don’t think COVID’s going to be a big deal here.” He said COVID wasn’t a “big deal” in Brazil, either. Famous last words.
The next weekend, I left early on Saturday morning to start my call duty at the hospital. After finishing rounds at one hospital and going to the next, I got a text from my wife, Anne, asking “What’s wrong with your people over there? What kind of doctors would take a 65-year-old colleague with a history of asthma, and history of an ICU stay with 10 days on a respirator with acute respiratory distress syndrome 10 years ago, and have him exposed to this lethal virus? Are they trying to kill you?”
It stopped me in my tracks. She was right. A lot had changed in a week. In that single week, it had become clear that COVID was a real threat, and I was vulnerable. I finished my call duty but made it clear to the “powers that be” I was going to stay home and isolate for the next few weeks, until we knew more. I was ahead of the curve, but not by much: within days, Chicago shut down with a “stay-at-home” order.
Anne: When the threat of COVID first became known, I said to family and friends, “If Emil gets this, it’s going to be very, very bad.” After that, we made certain to wear masks and gloves when we went out, which wasn’t often.
Emil: We stayed in for the next 3 months until we moved to Columbus, Ohio for my new position as Vice Chair for Research in the Department of Psychiatry and Behavioral Health at The Ohio State University Wexner Medical Center (OSUMC).
The day after arriving, I went to the emergency dental clinic because of a severe toothache. While they couldn’t save my tooth, I got something in return: COVID. The clinic took more than appropriate precautions, but I was in a very large room, not a private office, with many patients having their teeth drilled and whatever it is dentists do (actually, I do know; my father was a dentist).
Continue to: All was fine until 2 days later...
All was fine until 2 days later, when I began to feel a bit “unwell” on late Friday afternoon. I went out to do some chores the next morning, but soon returned home exhausted. The rest of the weekend was more of the same, and I was surprised at how I just couldn’t get anything done. On Monday, I felt a chill and thought I might have COVID.
The next morning, I went to OSUMC for a COVID test, but by then I already knew the result. The night before, Anne started complaining of a dry cough that would not stop.
Anne: When I realized Emil had COVID, I wrote to a friend, “If he gets bad and has to go to the hospital, or worse … he goes on a ventilator, I may need to be admitted to a psych ward!” I was still upset from the memory of sitting by Emil’s bedside when he was sick, and on a ventilator, 10 years ago, with his doctors talking with me about when, not if, he died.
Emil: My test came back within 8 hours on Tuesday. It was positive, as was the one for Anne the next day. The doctor I spoke to that evening thought I was only having a mild case and that I should just stay isolated. We immediately got a thermometer and a pulse oximeter to follow our symptoms. Anne’s oxygen saturation levels were always above 95%, but mine were lower, and by Friday, 3 days later and 1 week after my first symptoms, they were down to 92% or less. At that point, we both went to the ER at OSUMC.
Anne: We went to different places in the ER to be evaluated. As Emil was being wheeled away in the ER for his evaluation, I ran over for a kiss—with our masks on.
Continue to: As my ER evaluation...
As my ER evaluation was concluding, my doctor said, “I want someone, preferably the same person, to check in on you every day.” I replied I had a friend who is a critical care nurse. He smiled and said, “Excellent.” My friend called every day, and when she didn’t like how I sounded, on some days, she found an excuse to call again.
Emil: I barely recall my ER evaluation, except that I was to be admitted for observation and supplemental oxygen. I accepted this with aplomb, knowing I was in good hands and hoping I’d be home soon.
Anne: Because we were in the same ER, I thought I’d be able to see Emil once they decided to admit him. No. They wouldn’t even let me go to him to get his wallet for safekeeping. Instead, it was brought to me in a hazmat bag. Thus began our forced separation for the next 5 weeks.
Emil: I had to wait hours for a bed and was wheeled up late in the evening to a double room with one other patient, also with COVID, I supposed. While I had an oxygen mask on, we were only separated by a curtain. I had no idea I wouldn’t see Anne for weeks.
Anne: I returned “home” to a house I had spent less than 5 days in. We had barely moved in and it only had a bed, a couch, a TV, and a kitchen chair. I didn’t even know my neighbors to wave at, and … I was in quarantine. No one could come to me. Our eldest daughter was alone near Burlington, Vermont (where she had escaped to from New York City when it was the national epicenter for COVID back in March). Our youngest daughter was alone in Los Angeles, and our son, a newly minted First Lieutenant in the Army, was stationed in Afghanistan. “Good for him,” I thought. He could safely interact with his army buddies. It was so ironic; the one in the war zone was the only one of us who was safe from COVID.
Continue to: I reached out to family and friends...
I reached out to family and friends and asked for prayers. Emil was prayed for by all of our Catholic, Methodist, Jewish, Muslim, and Buddhist friends. As I told him later, he was prayed for from Afghanistan to Alaska. My extended family activated a text chain so all I had to do was reply and everyone on the chain would have the same information. I also received many notes and cards of support from friends and Emil’s family. Many told me how strong I was and how I would be fine. Later, I realized how many of these were from widows who were telling me I would survive bereavement, should that be the outcome.
Emil: The next day, the doctors started me on a 5-day course of the newly “approved” antiviral remdesivir, and the day after that, I received 2 units of convalescent plasma on “compassionate use” from the Mayo Clinic. It didn’t matter. I kept getting worse.
Anne: I received twice-daily updates from the nurses. When the updates were late in coming, I crawled the walls, waiting at least 2 hours before reaching out. One day, the nurse who answered said she couldn’t talk because his nurse was dealing with an emergency with him. I didn’t take a deep breath until his nurse called back to say he was stable. Regardless, he just kept getting sicker and sicker, and I began to fear he would not make it.
Emil: By Day 5, my X-ray showed clear evidence of a bilateral pneumonia (it had appeared “normal” on admission) and I was transferred to a “step-up unit.” The next day, I was transferred to the ICU and placed on a ventilator, in the prone position, for 16 hours a day.
Anne: The day Emil was transferred to the ICU, he told me he was worried about his fate. He called and asked me to stay on the phone with him while waiting to go to the ICU. We were both so weak we couldn’t do more than say “I love you” and listen to the other’s labored breathing. That was our last phone call until he was off the ventilator 10 days later.
Continue to: Emil's reply
Emil: At this point I had no idea what was going on. I was on a ventilator and I was “out.”
Anne: In the meantime, my family made sure I knew they were thinking of us. Every day I woke up with a text from one cousin asking how the night was while my sister checked in every afternoon. They sent flowers and baskets of goodies. Knowing how difficult it was waiting for updates, they sent me a jigsaw puzzle with a thousand pieces. I was surprised at how important that was for binding my anxiety. A friend sent books from my favorite writers.
Despite all this, I was absolutely beside myself the night Emil was placed on the ventilator. I cleaned and scrubbed the house; not that it needed it, I needed it. In the bedroom I saw a bottle under the bed. I retrieved it but couldn’t get up off the floor. I was weak and had tremendous muscle pain each time I moved. I had my phone, so knew I wouldn’t be stranded, but … I didn’t relish the idea of calling 911 and have them break down the front door in their hazmat suits. After more than 30 minutes, and much effort, I was able to get myself up; soon after, I put a house key outside.
When a friend who was taking care of our 2 dogs in Chicago heard that Emil was on the ventilator, she drove through the night to bring them to me so I would have them for solace. She couldn’t even come in the house. She stayed at a nearby hotel and visited with me from outside with masks on waiting for the updates.
Emil: Being an elder lawyer married to a physician, Anne knows a thing or 2 about medicine (because she’s seen a thing or 2 about medicine). She’s even been known to give her elderly clients Mini-Mental State Exams. In addition to talking with members of her support system, Anne was also talking with friends and relatives who are physicians. One exclaimed, “He’s having a cytokine storm!” and said I needed steroids. Another said, yes, that and serious “anti-inflammatory” drugs. At that moment, data supporting the use of steroids or “anti-inflammatories” in COVID hadn’t yet become public. The data on steroids came out early the next week in the Lancet and the data on “anti-inflammatories” was still in process until a few weeks later.
Continue to: Anne was ahead of the curve...
Anne was ahead of the curve and advocated hard for both treatments. At the same time, my OSUMC physicians were considering other options for me. They were checking on my inflammatory status by following my levels of C-reactive protein (CRP) and interleukin-6 (IL-6). On Days 2 and 3, my CRP level was 64 mg/L and my IL-6 level was 32 pg/mL (neither should be higher than 1).
While I don’t recall much before being on the ventilator, I do recall my alarm at seeing my CRP/IL-6 levels go up in real time on alerts from “My Chart” (my CRP/IL-6 levels were 149/123 within 4 days of admission, and reached a high of about 250/190 as I entered the ICU). I knew what those numbers meant. It was surreal; like watching myself die off in the distance, emotionally disconnected from the whole scene.
The decision to give steroids was relatively easy, and I was started on dexamethasone, a very inexpensive steroid, on Day 7 (ICU Day 2). The decision of which “antiinflammatory” to give was more difficult, as OSUMC had over 40 treatment protocols for COVID. Anne suggested 2 drugs based on recommendations from our physician friends—tocilizumab and acalabrutinib— both were on the market for other conditions and very expensive. The first is an IL-6 antagonist, while the second shuts down cytokine production in B cells, an effect also observed in lung tissue. While tocilizumab was not included in any of the OSUMC COVID protocols, acalabrutinib was, and I started on that medication on Day 8 (ICU Day 3).
Anne: My experience being the advocate was different than the first time 10 years before. That time, Emil had a community-acquired pneumonia, with which our doctors had much experience. This time, I was more active because no one had much information about how to deal with COVID and, thus, there was no standard of care. In fact, Emil was only the second patient to receive acalabrutinib at OSUMC; later, we found out that that patient did well.
Emil: The “anti-inflammatory” strategy worked. Within 5 days of starting the 2 drugs, my CRP and IL-6 levels were down to 10 and 5, respectively; a reduction of >95%. As these levels dropped, so did my oxygen requirements.
Continue to: Anne's reply
Anne: Emil was finally on the upswing. I woke up the next morning and, surprisingly, found that my first emotion wasn’t one of terror. His ICU doctor, a real booster for Emil, made it her mission to get him off the ventilator before the end of her ICU service week. She succeeded.
Emil: Five days after coming off the ventilator, I went to a rehab unit for reconditioning and to begin the long process of recovering my strength and stamina.
Most people say to me, “How awful for you! How terrible!” I smile and say, “Yeah, well, I missed all the excitement. It was really much worse for Anne.” I told them that, although you don’t recall anything while on the ventilator, you get retrograde amnesia for the several days prior to artificial ventilation. I have texts on my cell phone, written by me in those first few days, I don’t recall writing. Anne says we had conversations all the way up to my admission to the ICU; I recall none of those. Frankly, that’s for the best.
One thing to highlight is that your brain doesn’t stop working while you’re “out.” I had numerous vivid dreams, or whatever they were, while on the ventilator and after. Many were “bizarre and dark,” others were “dark and bizarre.” A few were amusing— in the end. I recall watching a TV news program segment describing how we donated our 2 little dogs to the Queen of England, who then gave them to her youngest son, Edward. I swear, I actually “saw” this TV program and watched the Queen and her son (and his wife) playing with our dogs. I was so convinced, I asked Anne where our dogs were; with her, of course. No, she assured me, we hadn’t given them to Queen Elizabeth II. Another conversation I swore I had with Anne was one in which she was telling me she was starting the vetting process to be a VP candidate for Joe Biden (Anne had been involved in Chicago politics so … not totally “crazy”). Nevertheless, I was quickly disabused of this one by my eldest daughter, also a lawyer.
Anne: This time, like the last time he was on a ventilator, Emil took a few more days to clear all the drugs keeping him sedated. Last time, his medical center sent his colleague, the Chair of Neurology, to check on him because there was a concern that he wasn’t “clearing” fast enough. This time, I was the one reassuring the doctors and nurses to be “patient.” At the same time, I was disabusing him of his far-fetched idea that he was head of all research at OSUMC and head of the ICU. He told me, “I don’t understand it. Don’t these people know they work for me?” “No,” I told him. “You are a patient there, and you need to behave.” Aside from that, Emil was fairly lucid. As one of his nurses said, “He’s oriented, he’s just wrong!”
Continue to: Emil's reply
Emil: Some people have asked me if this experience has changed my perspective. It could have, but I went through something worse 10 years ago when I was first brought back from the “mostly dead.” After that, I realized the most important things in life are the people you love and the people who love you; the good stuff is “gravy” and everything else isn’t worth spending much time or energy on. The first thing I said to Anne when we were face-to-face, as I entered the rehab facility (with masks on, of course), was “I can’t do this to you again.”
Anne: One of the most inhumane aspects of COVID is that you can’t be with your loved one while they are sick. Last time I spent 10 to 12 hours a day at the bedside. This time I couldn’t be there at all. It was especially hard because I knew from the last time how much my presence meant to him. If I left, he would get agitated. His heart rate would come down by 10 beats when I sat next to him.
When we had our first post-ventilator conversation on Father’s Day, he was surprised I was so excited to talk to him. Somehow, he thought I had abandoned him. What he didn’t know was that I was thinking about getting a job in Housekeeping at the hospital just so I could go see him!
Emil: In the end, I’m now back to baseline and grateful I’m alive. I still have things I want to do professionally and personally, and am appreciative I’ll have more time for those. However, I am appalled at how a serious public health issue has been turned into a political weapon by “science deniers” and that this is continuing to kill our citizens. That’s not a nightmare from when I was ill. It’s the “day-mare” we are living now.
Emil: Coronavirus disease 2019 (COVID-19) wasn’t really on my mind until the first weekend in March, specifically Sunday, March 8, 2020. That weekend had us traveling from Chicago to Berwyn, Pennsylvania to attend the funeral of one of my older cousins. Though we were the only ones from his side at the graveside, his funeral had drawn numerous relatives, none of whom were “socially distanced.”
On our way home, I received an e-mail from a colleague in Brazil who had invited me to speak at a conference in São Paulo. He told me that several of my American colleagues had contacted him and informed him that their universities had banned travel because of COVID. “I’m coming,” I replied. “I don’t think COVID’s going to be a big deal here.” He said COVID wasn’t a “big deal” in Brazil, either. Famous last words.
The next weekend, I left early on Saturday morning to start my call duty at the hospital. After finishing rounds at one hospital and going to the next, I got a text from my wife, Anne, asking “What’s wrong with your people over there? What kind of doctors would take a 65-year-old colleague with a history of asthma, and history of an ICU stay with 10 days on a respirator with acute respiratory distress syndrome 10 years ago, and have him exposed to this lethal virus? Are they trying to kill you?”
It stopped me in my tracks. She was right. A lot had changed in a week. In that single week, it had become clear that COVID was a real threat, and I was vulnerable. I finished my call duty but made it clear to the “powers that be” I was going to stay home and isolate for the next few weeks, until we knew more. I was ahead of the curve, but not by much: within days, Chicago shut down with a “stay-at-home” order.
Anne: When the threat of COVID first became known, I said to family and friends, “If Emil gets this, it’s going to be very, very bad.” After that, we made certain to wear masks and gloves when we went out, which wasn’t often.
Emil: We stayed in for the next 3 months until we moved to Columbus, Ohio for my new position as Vice Chair for Research in the Department of Psychiatry and Behavioral Health at The Ohio State University Wexner Medical Center (OSUMC).
The day after arriving, I went to the emergency dental clinic because of a severe toothache. While they couldn’t save my tooth, I got something in return: COVID. The clinic took more than appropriate precautions, but I was in a very large room, not a private office, with many patients having their teeth drilled and whatever it is dentists do (actually, I do know; my father was a dentist).
Continue to: All was fine until 2 days later...
All was fine until 2 days later, when I began to feel a bit “unwell” on late Friday afternoon. I went out to do some chores the next morning, but soon returned home exhausted. The rest of the weekend was more of the same, and I was surprised at how I just couldn’t get anything done. On Monday, I felt a chill and thought I might have COVID.
The next morning, I went to OSUMC for a COVID test, but by then I already knew the result. The night before, Anne started complaining of a dry cough that would not stop.
Anne: When I realized Emil had COVID, I wrote to a friend, “If he gets bad and has to go to the hospital, or worse … he goes on a ventilator, I may need to be admitted to a psych ward!” I was still upset from the memory of sitting by Emil’s bedside when he was sick, and on a ventilator, 10 years ago, with his doctors talking with me about when, not if, he died.
Emil: My test came back within 8 hours on Tuesday. It was positive, as was the one for Anne the next day. The doctor I spoke to that evening thought I was only having a mild case and that I should just stay isolated. We immediately got a thermometer and a pulse oximeter to follow our symptoms. Anne’s oxygen saturation levels were always above 95%, but mine were lower, and by Friday, 3 days later and 1 week after my first symptoms, they were down to 92% or less. At that point, we both went to the ER at OSUMC.
Anne: We went to different places in the ER to be evaluated. As Emil was being wheeled away in the ER for his evaluation, I ran over for a kiss—with our masks on.
Continue to: As my ER evaluation...
As my ER evaluation was concluding, my doctor said, “I want someone, preferably the same person, to check in on you every day.” I replied I had a friend who is a critical care nurse. He smiled and said, “Excellent.” My friend called every day, and when she didn’t like how I sounded, on some days, she found an excuse to call again.
Emil: I barely recall my ER evaluation, except that I was to be admitted for observation and supplemental oxygen. I accepted this with aplomb, knowing I was in good hands and hoping I’d be home soon.
Anne: Because we were in the same ER, I thought I’d be able to see Emil once they decided to admit him. No. They wouldn’t even let me go to him to get his wallet for safekeeping. Instead, it was brought to me in a hazmat bag. Thus began our forced separation for the next 5 weeks.
Emil: I had to wait hours for a bed and was wheeled up late in the evening to a double room with one other patient, also with COVID, I supposed. While I had an oxygen mask on, we were only separated by a curtain. I had no idea I wouldn’t see Anne for weeks.
Anne: I returned “home” to a house I had spent less than 5 days in. We had barely moved in and it only had a bed, a couch, a TV, and a kitchen chair. I didn’t even know my neighbors to wave at, and … I was in quarantine. No one could come to me. Our eldest daughter was alone near Burlington, Vermont (where she had escaped to from New York City when it was the national epicenter for COVID back in March). Our youngest daughter was alone in Los Angeles, and our son, a newly minted First Lieutenant in the Army, was stationed in Afghanistan. “Good for him,” I thought. He could safely interact with his army buddies. It was so ironic; the one in the war zone was the only one of us who was safe from COVID.
Continue to: I reached out to family and friends...
I reached out to family and friends and asked for prayers. Emil was prayed for by all of our Catholic, Methodist, Jewish, Muslim, and Buddhist friends. As I told him later, he was prayed for from Afghanistan to Alaska. My extended family activated a text chain so all I had to do was reply and everyone on the chain would have the same information. I also received many notes and cards of support from friends and Emil’s family. Many told me how strong I was and how I would be fine. Later, I realized how many of these were from widows who were telling me I would survive bereavement, should that be the outcome.
Emil: The next day, the doctors started me on a 5-day course of the newly “approved” antiviral remdesivir, and the day after that, I received 2 units of convalescent plasma on “compassionate use” from the Mayo Clinic. It didn’t matter. I kept getting worse.
Anne: I received twice-daily updates from the nurses. When the updates were late in coming, I crawled the walls, waiting at least 2 hours before reaching out. One day, the nurse who answered said she couldn’t talk because his nurse was dealing with an emergency with him. I didn’t take a deep breath until his nurse called back to say he was stable. Regardless, he just kept getting sicker and sicker, and I began to fear he would not make it.
Emil: By Day 5, my X-ray showed clear evidence of a bilateral pneumonia (it had appeared “normal” on admission) and I was transferred to a “step-up unit.” The next day, I was transferred to the ICU and placed on a ventilator, in the prone position, for 16 hours a day.
Anne: The day Emil was transferred to the ICU, he told me he was worried about his fate. He called and asked me to stay on the phone with him while waiting to go to the ICU. We were both so weak we couldn’t do more than say “I love you” and listen to the other’s labored breathing. That was our last phone call until he was off the ventilator 10 days later.
Continue to: Emil's reply
Emil: At this point I had no idea what was going on. I was on a ventilator and I was “out.”
Anne: In the meantime, my family made sure I knew they were thinking of us. Every day I woke up with a text from one cousin asking how the night was while my sister checked in every afternoon. They sent flowers and baskets of goodies. Knowing how difficult it was waiting for updates, they sent me a jigsaw puzzle with a thousand pieces. I was surprised at how important that was for binding my anxiety. A friend sent books from my favorite writers.
Despite all this, I was absolutely beside myself the night Emil was placed on the ventilator. I cleaned and scrubbed the house; not that it needed it, I needed it. In the bedroom I saw a bottle under the bed. I retrieved it but couldn’t get up off the floor. I was weak and had tremendous muscle pain each time I moved. I had my phone, so knew I wouldn’t be stranded, but … I didn’t relish the idea of calling 911 and have them break down the front door in their hazmat suits. After more than 30 minutes, and much effort, I was able to get myself up; soon after, I put a house key outside.
When a friend who was taking care of our 2 dogs in Chicago heard that Emil was on the ventilator, she drove through the night to bring them to me so I would have them for solace. She couldn’t even come in the house. She stayed at a nearby hotel and visited with me from outside with masks on waiting for the updates.
Emil: Being an elder lawyer married to a physician, Anne knows a thing or 2 about medicine (because she’s seen a thing or 2 about medicine). She’s even been known to give her elderly clients Mini-Mental State Exams. In addition to talking with members of her support system, Anne was also talking with friends and relatives who are physicians. One exclaimed, “He’s having a cytokine storm!” and said I needed steroids. Another said, yes, that and serious “anti-inflammatory” drugs. At that moment, data supporting the use of steroids or “anti-inflammatories” in COVID hadn’t yet become public. The data on steroids came out early the next week in the Lancet and the data on “anti-inflammatories” was still in process until a few weeks later.
Continue to: Anne was ahead of the curve...
Anne was ahead of the curve and advocated hard for both treatments. At the same time, my OSUMC physicians were considering other options for me. They were checking on my inflammatory status by following my levels of C-reactive protein (CRP) and interleukin-6 (IL-6). On Days 2 and 3, my CRP level was 64 mg/L and my IL-6 level was 32 pg/mL (neither should be higher than 1).
While I don’t recall much before being on the ventilator, I do recall my alarm at seeing my CRP/IL-6 levels go up in real time on alerts from “My Chart” (my CRP/IL-6 levels were 149/123 within 4 days of admission, and reached a high of about 250/190 as I entered the ICU). I knew what those numbers meant. It was surreal; like watching myself die off in the distance, emotionally disconnected from the whole scene.
The decision to give steroids was relatively easy, and I was started on dexamethasone, a very inexpensive steroid, on Day 7 (ICU Day 2). The decision of which “antiinflammatory” to give was more difficult, as OSUMC had over 40 treatment protocols for COVID. Anne suggested 2 drugs based on recommendations from our physician friends—tocilizumab and acalabrutinib— both were on the market for other conditions and very expensive. The first is an IL-6 antagonist, while the second shuts down cytokine production in B cells, an effect also observed in lung tissue. While tocilizumab was not included in any of the OSUMC COVID protocols, acalabrutinib was, and I started on that medication on Day 8 (ICU Day 3).
Anne: My experience being the advocate was different than the first time 10 years before. That time, Emil had a community-acquired pneumonia, with which our doctors had much experience. This time, I was more active because no one had much information about how to deal with COVID and, thus, there was no standard of care. In fact, Emil was only the second patient to receive acalabrutinib at OSUMC; later, we found out that that patient did well.
Emil: The “anti-inflammatory” strategy worked. Within 5 days of starting the 2 drugs, my CRP and IL-6 levels were down to 10 and 5, respectively; a reduction of >95%. As these levels dropped, so did my oxygen requirements.
Continue to: Anne's reply
Anne: Emil was finally on the upswing. I woke up the next morning and, surprisingly, found that my first emotion wasn’t one of terror. His ICU doctor, a real booster for Emil, made it her mission to get him off the ventilator before the end of her ICU service week. She succeeded.
Emil: Five days after coming off the ventilator, I went to a rehab unit for reconditioning and to begin the long process of recovering my strength and stamina.
Most people say to me, “How awful for you! How terrible!” I smile and say, “Yeah, well, I missed all the excitement. It was really much worse for Anne.” I told them that, although you don’t recall anything while on the ventilator, you get retrograde amnesia for the several days prior to artificial ventilation. I have texts on my cell phone, written by me in those first few days, I don’t recall writing. Anne says we had conversations all the way up to my admission to the ICU; I recall none of those. Frankly, that’s for the best.
One thing to highlight is that your brain doesn’t stop working while you’re “out.” I had numerous vivid dreams, or whatever they were, while on the ventilator and after. Many were “bizarre and dark,” others were “dark and bizarre.” A few were amusing— in the end. I recall watching a TV news program segment describing how we donated our 2 little dogs to the Queen of England, who then gave them to her youngest son, Edward. I swear, I actually “saw” this TV program and watched the Queen and her son (and his wife) playing with our dogs. I was so convinced, I asked Anne where our dogs were; with her, of course. No, she assured me, we hadn’t given them to Queen Elizabeth II. Another conversation I swore I had with Anne was one in which she was telling me she was starting the vetting process to be a VP candidate for Joe Biden (Anne had been involved in Chicago politics so … not totally “crazy”). Nevertheless, I was quickly disabused of this one by my eldest daughter, also a lawyer.
Anne: This time, like the last time he was on a ventilator, Emil took a few more days to clear all the drugs keeping him sedated. Last time, his medical center sent his colleague, the Chair of Neurology, to check on him because there was a concern that he wasn’t “clearing” fast enough. This time, I was the one reassuring the doctors and nurses to be “patient.” At the same time, I was disabusing him of his far-fetched idea that he was head of all research at OSUMC and head of the ICU. He told me, “I don’t understand it. Don’t these people know they work for me?” “No,” I told him. “You are a patient there, and you need to behave.” Aside from that, Emil was fairly lucid. As one of his nurses said, “He’s oriented, he’s just wrong!”
Continue to: Emil's reply
Emil: Some people have asked me if this experience has changed my perspective. It could have, but I went through something worse 10 years ago when I was first brought back from the “mostly dead.” After that, I realized the most important things in life are the people you love and the people who love you; the good stuff is “gravy” and everything else isn’t worth spending much time or energy on. The first thing I said to Anne when we were face-to-face, as I entered the rehab facility (with masks on, of course), was “I can’t do this to you again.”
Anne: One of the most inhumane aspects of COVID is that you can’t be with your loved one while they are sick. Last time I spent 10 to 12 hours a day at the bedside. This time I couldn’t be there at all. It was especially hard because I knew from the last time how much my presence meant to him. If I left, he would get agitated. His heart rate would come down by 10 beats when I sat next to him.
When we had our first post-ventilator conversation on Father’s Day, he was surprised I was so excited to talk to him. Somehow, he thought I had abandoned him. What he didn’t know was that I was thinking about getting a job in Housekeeping at the hospital just so I could go see him!
Emil: In the end, I’m now back to baseline and grateful I’m alive. I still have things I want to do professionally and personally, and am appreciative I’ll have more time for those. However, I am appalled at how a serious public health issue has been turned into a political weapon by “science deniers” and that this is continuing to kill our citizens. That’s not a nightmare from when I was ill. It’s the “day-mare” we are living now.
Emil: Coronavirus disease 2019 (COVID-19) wasn’t really on my mind until the first weekend in March, specifically Sunday, March 8, 2020. That weekend had us traveling from Chicago to Berwyn, Pennsylvania to attend the funeral of one of my older cousins. Though we were the only ones from his side at the graveside, his funeral had drawn numerous relatives, none of whom were “socially distanced.”
On our way home, I received an e-mail from a colleague in Brazil who had invited me to speak at a conference in São Paulo. He told me that several of my American colleagues had contacted him and informed him that their universities had banned travel because of COVID. “I’m coming,” I replied. “I don’t think COVID’s going to be a big deal here.” He said COVID wasn’t a “big deal” in Brazil, either. Famous last words.
The next weekend, I left early on Saturday morning to start my call duty at the hospital. After finishing rounds at one hospital and going to the next, I got a text from my wife, Anne, asking “What’s wrong with your people over there? What kind of doctors would take a 65-year-old colleague with a history of asthma, and history of an ICU stay with 10 days on a respirator with acute respiratory distress syndrome 10 years ago, and have him exposed to this lethal virus? Are they trying to kill you?”
It stopped me in my tracks. She was right. A lot had changed in a week. In that single week, it had become clear that COVID was a real threat, and I was vulnerable. I finished my call duty but made it clear to the “powers that be” I was going to stay home and isolate for the next few weeks, until we knew more. I was ahead of the curve, but not by much: within days, Chicago shut down with a “stay-at-home” order.
Anne: When the threat of COVID first became known, I said to family and friends, “If Emil gets this, it’s going to be very, very bad.” After that, we made certain to wear masks and gloves when we went out, which wasn’t often.
Emil: We stayed in for the next 3 months until we moved to Columbus, Ohio for my new position as Vice Chair for Research in the Department of Psychiatry and Behavioral Health at The Ohio State University Wexner Medical Center (OSUMC).
The day after arriving, I went to the emergency dental clinic because of a severe toothache. While they couldn’t save my tooth, I got something in return: COVID. The clinic took more than appropriate precautions, but I was in a very large room, not a private office, with many patients having their teeth drilled and whatever it is dentists do (actually, I do know; my father was a dentist).
Continue to: All was fine until 2 days later...
All was fine until 2 days later, when I began to feel a bit “unwell” on late Friday afternoon. I went out to do some chores the next morning, but soon returned home exhausted. The rest of the weekend was more of the same, and I was surprised at how I just couldn’t get anything done. On Monday, I felt a chill and thought I might have COVID.
The next morning, I went to OSUMC for a COVID test, but by then I already knew the result. The night before, Anne started complaining of a dry cough that would not stop.
Anne: When I realized Emil had COVID, I wrote to a friend, “If he gets bad and has to go to the hospital, or worse … he goes on a ventilator, I may need to be admitted to a psych ward!” I was still upset from the memory of sitting by Emil’s bedside when he was sick, and on a ventilator, 10 years ago, with his doctors talking with me about when, not if, he died.
Emil: My test came back within 8 hours on Tuesday. It was positive, as was the one for Anne the next day. The doctor I spoke to that evening thought I was only having a mild case and that I should just stay isolated. We immediately got a thermometer and a pulse oximeter to follow our symptoms. Anne’s oxygen saturation levels were always above 95%, but mine were lower, and by Friday, 3 days later and 1 week after my first symptoms, they were down to 92% or less. At that point, we both went to the ER at OSUMC.
Anne: We went to different places in the ER to be evaluated. As Emil was being wheeled away in the ER for his evaluation, I ran over for a kiss—with our masks on.
Continue to: As my ER evaluation...
As my ER evaluation was concluding, my doctor said, “I want someone, preferably the same person, to check in on you every day.” I replied I had a friend who is a critical care nurse. He smiled and said, “Excellent.” My friend called every day, and when she didn’t like how I sounded, on some days, she found an excuse to call again.
Emil: I barely recall my ER evaluation, except that I was to be admitted for observation and supplemental oxygen. I accepted this with aplomb, knowing I was in good hands and hoping I’d be home soon.
Anne: Because we were in the same ER, I thought I’d be able to see Emil once they decided to admit him. No. They wouldn’t even let me go to him to get his wallet for safekeeping. Instead, it was brought to me in a hazmat bag. Thus began our forced separation for the next 5 weeks.
Emil: I had to wait hours for a bed and was wheeled up late in the evening to a double room with one other patient, also with COVID, I supposed. While I had an oxygen mask on, we were only separated by a curtain. I had no idea I wouldn’t see Anne for weeks.
Anne: I returned “home” to a house I had spent less than 5 days in. We had barely moved in and it only had a bed, a couch, a TV, and a kitchen chair. I didn’t even know my neighbors to wave at, and … I was in quarantine. No one could come to me. Our eldest daughter was alone near Burlington, Vermont (where she had escaped to from New York City when it was the national epicenter for COVID back in March). Our youngest daughter was alone in Los Angeles, and our son, a newly minted First Lieutenant in the Army, was stationed in Afghanistan. “Good for him,” I thought. He could safely interact with his army buddies. It was so ironic; the one in the war zone was the only one of us who was safe from COVID.
Continue to: I reached out to family and friends...
I reached out to family and friends and asked for prayers. Emil was prayed for by all of our Catholic, Methodist, Jewish, Muslim, and Buddhist friends. As I told him later, he was prayed for from Afghanistan to Alaska. My extended family activated a text chain so all I had to do was reply and everyone on the chain would have the same information. I also received many notes and cards of support from friends and Emil’s family. Many told me how strong I was and how I would be fine. Later, I realized how many of these were from widows who were telling me I would survive bereavement, should that be the outcome.
Emil: The next day, the doctors started me on a 5-day course of the newly “approved” antiviral remdesivir, and the day after that, I received 2 units of convalescent plasma on “compassionate use” from the Mayo Clinic. It didn’t matter. I kept getting worse.
Anne: I received twice-daily updates from the nurses. When the updates were late in coming, I crawled the walls, waiting at least 2 hours before reaching out. One day, the nurse who answered said she couldn’t talk because his nurse was dealing with an emergency with him. I didn’t take a deep breath until his nurse called back to say he was stable. Regardless, he just kept getting sicker and sicker, and I began to fear he would not make it.
Emil: By Day 5, my X-ray showed clear evidence of a bilateral pneumonia (it had appeared “normal” on admission) and I was transferred to a “step-up unit.” The next day, I was transferred to the ICU and placed on a ventilator, in the prone position, for 16 hours a day.
Anne: The day Emil was transferred to the ICU, he told me he was worried about his fate. He called and asked me to stay on the phone with him while waiting to go to the ICU. We were both so weak we couldn’t do more than say “I love you” and listen to the other’s labored breathing. That was our last phone call until he was off the ventilator 10 days later.
Continue to: Emil's reply
Emil: At this point I had no idea what was going on. I was on a ventilator and I was “out.”
Anne: In the meantime, my family made sure I knew they were thinking of us. Every day I woke up with a text from one cousin asking how the night was while my sister checked in every afternoon. They sent flowers and baskets of goodies. Knowing how difficult it was waiting for updates, they sent me a jigsaw puzzle with a thousand pieces. I was surprised at how important that was for binding my anxiety. A friend sent books from my favorite writers.
Despite all this, I was absolutely beside myself the night Emil was placed on the ventilator. I cleaned and scrubbed the house; not that it needed it, I needed it. In the bedroom I saw a bottle under the bed. I retrieved it but couldn’t get up off the floor. I was weak and had tremendous muscle pain each time I moved. I had my phone, so knew I wouldn’t be stranded, but … I didn’t relish the idea of calling 911 and have them break down the front door in their hazmat suits. After more than 30 minutes, and much effort, I was able to get myself up; soon after, I put a house key outside.
When a friend who was taking care of our 2 dogs in Chicago heard that Emil was on the ventilator, she drove through the night to bring them to me so I would have them for solace. She couldn’t even come in the house. She stayed at a nearby hotel and visited with me from outside with masks on waiting for the updates.
Emil: Being an elder lawyer married to a physician, Anne knows a thing or 2 about medicine (because she’s seen a thing or 2 about medicine). She’s even been known to give her elderly clients Mini-Mental State Exams. In addition to talking with members of her support system, Anne was also talking with friends and relatives who are physicians. One exclaimed, “He’s having a cytokine storm!” and said I needed steroids. Another said, yes, that and serious “anti-inflammatory” drugs. At that moment, data supporting the use of steroids or “anti-inflammatories” in COVID hadn’t yet become public. The data on steroids came out early the next week in the Lancet and the data on “anti-inflammatories” was still in process until a few weeks later.
Continue to: Anne was ahead of the curve...
Anne was ahead of the curve and advocated hard for both treatments. At the same time, my OSUMC physicians were considering other options for me. They were checking on my inflammatory status by following my levels of C-reactive protein (CRP) and interleukin-6 (IL-6). On Days 2 and 3, my CRP level was 64 mg/L and my IL-6 level was 32 pg/mL (neither should be higher than 1).
While I don’t recall much before being on the ventilator, I do recall my alarm at seeing my CRP/IL-6 levels go up in real time on alerts from “My Chart” (my CRP/IL-6 levels were 149/123 within 4 days of admission, and reached a high of about 250/190 as I entered the ICU). I knew what those numbers meant. It was surreal; like watching myself die off in the distance, emotionally disconnected from the whole scene.
The decision to give steroids was relatively easy, and I was started on dexamethasone, a very inexpensive steroid, on Day 7 (ICU Day 2). The decision of which “antiinflammatory” to give was more difficult, as OSUMC had over 40 treatment protocols for COVID. Anne suggested 2 drugs based on recommendations from our physician friends—tocilizumab and acalabrutinib— both were on the market for other conditions and very expensive. The first is an IL-6 antagonist, while the second shuts down cytokine production in B cells, an effect also observed in lung tissue. While tocilizumab was not included in any of the OSUMC COVID protocols, acalabrutinib was, and I started on that medication on Day 8 (ICU Day 3).
Anne: My experience being the advocate was different than the first time 10 years before. That time, Emil had a community-acquired pneumonia, with which our doctors had much experience. This time, I was more active because no one had much information about how to deal with COVID and, thus, there was no standard of care. In fact, Emil was only the second patient to receive acalabrutinib at OSUMC; later, we found out that that patient did well.
Emil: The “anti-inflammatory” strategy worked. Within 5 days of starting the 2 drugs, my CRP and IL-6 levels were down to 10 and 5, respectively; a reduction of >95%. As these levels dropped, so did my oxygen requirements.
Continue to: Anne's reply
Anne: Emil was finally on the upswing. I woke up the next morning and, surprisingly, found that my first emotion wasn’t one of terror. His ICU doctor, a real booster for Emil, made it her mission to get him off the ventilator before the end of her ICU service week. She succeeded.
Emil: Five days after coming off the ventilator, I went to a rehab unit for reconditioning and to begin the long process of recovering my strength and stamina.
Most people say to me, “How awful for you! How terrible!” I smile and say, “Yeah, well, I missed all the excitement. It was really much worse for Anne.” I told them that, although you don’t recall anything while on the ventilator, you get retrograde amnesia for the several days prior to artificial ventilation. I have texts on my cell phone, written by me in those first few days, I don’t recall writing. Anne says we had conversations all the way up to my admission to the ICU; I recall none of those. Frankly, that’s for the best.
One thing to highlight is that your brain doesn’t stop working while you’re “out.” I had numerous vivid dreams, or whatever they were, while on the ventilator and after. Many were “bizarre and dark,” others were “dark and bizarre.” A few were amusing— in the end. I recall watching a TV news program segment describing how we donated our 2 little dogs to the Queen of England, who then gave them to her youngest son, Edward. I swear, I actually “saw” this TV program and watched the Queen and her son (and his wife) playing with our dogs. I was so convinced, I asked Anne where our dogs were; with her, of course. No, she assured me, we hadn’t given them to Queen Elizabeth II. Another conversation I swore I had with Anne was one in which she was telling me she was starting the vetting process to be a VP candidate for Joe Biden (Anne had been involved in Chicago politics so … not totally “crazy”). Nevertheless, I was quickly disabused of this one by my eldest daughter, also a lawyer.
Anne: This time, like the last time he was on a ventilator, Emil took a few more days to clear all the drugs keeping him sedated. Last time, his medical center sent his colleague, the Chair of Neurology, to check on him because there was a concern that he wasn’t “clearing” fast enough. This time, I was the one reassuring the doctors and nurses to be “patient.” At the same time, I was disabusing him of his far-fetched idea that he was head of all research at OSUMC and head of the ICU. He told me, “I don’t understand it. Don’t these people know they work for me?” “No,” I told him. “You are a patient there, and you need to behave.” Aside from that, Emil was fairly lucid. As one of his nurses said, “He’s oriented, he’s just wrong!”
Continue to: Emil's reply
Emil: Some people have asked me if this experience has changed my perspective. It could have, but I went through something worse 10 years ago when I was first brought back from the “mostly dead.” After that, I realized the most important things in life are the people you love and the people who love you; the good stuff is “gravy” and everything else isn’t worth spending much time or energy on. The first thing I said to Anne when we were face-to-face, as I entered the rehab facility (with masks on, of course), was “I can’t do this to you again.”
Anne: One of the most inhumane aspects of COVID is that you can’t be with your loved one while they are sick. Last time I spent 10 to 12 hours a day at the bedside. This time I couldn’t be there at all. It was especially hard because I knew from the last time how much my presence meant to him. If I left, he would get agitated. His heart rate would come down by 10 beats when I sat next to him.
When we had our first post-ventilator conversation on Father’s Day, he was surprised I was so excited to talk to him. Somehow, he thought I had abandoned him. What he didn’t know was that I was thinking about getting a job in Housekeeping at the hospital just so I could go see him!
Emil: In the end, I’m now back to baseline and grateful I’m alive. I still have things I want to do professionally and personally, and am appreciative I’ll have more time for those. However, I am appalled at how a serious public health issue has been turned into a political weapon by “science deniers” and that this is continuing to kill our citizens. That’s not a nightmare from when I was ill. It’s the “day-mare” we are living now.

Disruption of postpandemic world will precipitate innovation
When this editorial is published, we will know the results of the national election (hopefully) and whether there will be a smooth transition of power. We should know whether the Affordable Care Act will remain intact, and we will have indications about the impact of a COVID/flu combination. Health care will never be the same.

According to a recent Medscape survey, 62% of U.S. physicians saw a reduction of monthly income (12% saw a reduction of over 70%) in the first 6 months of this year. Almost a third of the physician workforce is contemplating retirement earlier than anticipated. As worrisome, according to a JAMA article (Aug 4, 2020;324:510-3) the United States saw a 35% increase in excess deaths because of non-COVID etiologies, an indication of health care deferral and avoidance. We all are scrambling to catch up and accommodate an enormous demand.
We are witnessing a “K” shaped recovery for both individuals and GI practices. If your health care is covered by Medicare, you own a mortgage-free home and your wealth is based on a balanced equity/bond portfolio, then all of your assets increased in value compared to last year’s peak valuations. For the other 90% of Americans, the recovery is modest, neutral, or more often nonexistent. Gastroenterologists who work in academic centers or large health systems did not lose income this year and were protected by billion-dollar credit lines and cash-on-hand accounts from robust days available to these entities. Independent practices (critically dependent on monthly cash flow) were decimated, furthering the trend towards consolidation, retirement, and acquisitions. With the new CMS E/M valuations we will see further reduction in procedural reimbursement.
However, disruption always precipitates innovation. Challenges are great but opportunities are clearly evident for those willing to risk.
John I. Allen, MD, MBA, AGAF
Editor in Chief
When this editorial is published, we will know the results of the national election (hopefully) and whether there will be a smooth transition of power. We should know whether the Affordable Care Act will remain intact, and we will have indications about the impact of a COVID/flu combination. Health care will never be the same.
According to a recent Medscape survey, 62% of U.S. physicians saw a reduction of monthly income (12% saw a reduction of over 70%) in the first 6 months of this year. Almost a third of the physician workforce is contemplating retirement earlier than anticipated. As worrisome, according to a JAMA article (Aug 4, 2020;324:510-3) the United States saw a 35% increase in excess deaths because of non-COVID etiologies, an indication of health care deferral and avoidance. We all are scrambling to catch up and accommodate an enormous demand.
We are witnessing a “K” shaped recovery for both individuals and GI practices. If your health care is covered by Medicare, you own a mortgage-free home and your wealth is based on a balanced equity/bond portfolio, then all of your assets increased in value compared to last year’s peak valuations. For the other 90% of Americans, the recovery is modest, neutral, or more often nonexistent. Gastroenterologists who work in academic centers or large health systems did not lose income this year and were protected by billion-dollar credit lines and cash-on-hand accounts from robust days available to these entities. Independent practices (critically dependent on monthly cash flow) were decimated, furthering the trend towards consolidation, retirement, and acquisitions. With the new CMS E/M valuations we will see further reduction in procedural reimbursement.
However, disruption always precipitates innovation. Challenges are great but opportunities are clearly evident for those willing to risk.
John I. Allen, MD, MBA, AGAF
Editor in Chief
When this editorial is published, we will know the results of the national election (hopefully) and whether there will be a smooth transition of power. We should know whether the Affordable Care Act will remain intact, and we will have indications about the impact of a COVID/flu combination. Health care will never be the same.
According to a recent Medscape survey, 62% of U.S. physicians saw a reduction of monthly income (12% saw a reduction of over 70%) in the first 6 months of this year. Almost a third of the physician workforce is contemplating retirement earlier than anticipated. As worrisome, according to a JAMA article (Aug 4, 2020;324:510-3) the United States saw a 35% increase in excess deaths because of non-COVID etiologies, an indication of health care deferral and avoidance. We all are scrambling to catch up and accommodate an enormous demand.
We are witnessing a “K” shaped recovery for both individuals and GI practices. If your health care is covered by Medicare, you own a mortgage-free home and your wealth is based on a balanced equity/bond portfolio, then all of your assets increased in value compared to last year’s peak valuations. For the other 90% of Americans, the recovery is modest, neutral, or more often nonexistent. Gastroenterologists who work in academic centers or large health systems did not lose income this year and were protected by billion-dollar credit lines and cash-on-hand accounts from robust days available to these entities. Independent practices (critically dependent on monthly cash flow) were decimated, furthering the trend towards consolidation, retirement, and acquisitions. With the new CMS E/M valuations we will see further reduction in procedural reimbursement.
However, disruption always precipitates innovation. Challenges are great but opportunities are clearly evident for those willing to risk.
John I. Allen, MD, MBA, AGAF
Editor in Chief
Adenomyosis: An update on imaging, medical, and surgical treatment
Adenomyosis is a benign disorder, present in 20%-35% of women and characterized by the presence of endometrial glands and stroma within the myometrium. The ectopic endometrial tissue appears to cause hypertrophy in the myometrium, resulting in an enlarged globular uterus.

Adenomyosis may present as diffuse or focal involvement within the uterus. When the focal lesion appears to be well defined, it is referred to as an adenomyoma. It is not encapsulated like a fibroid. There may be involvement of the junctional zone of the myometrium – the area between the subendometrial myometrium and the outer myometrium. While the pathogenesis of adenomyosis is unknown, two rigorous theories exist: endomyometrial invagination of the endometrium and de novo from Müllerian rests.
For this installment of the Master Class in Gynecologic Surgery, I have enlisted Keith B. Isaacson, MD, to discuss the clinical presentation, diagnosis, and medical and surgical treatment of adenomyosis.
Dr. Isaacson is the director of minimally invasive gynecologic surgery and infertility at Newton-Wellesley Hospital, Newton, Mass., and associate professor of obstetrics and gynecology at Harvard Medical School, Boston. He is currently in practice specializing in minimally invasive gynecologic surgery and infertility at Newton-Wellesley Hospital, where he is the director of the AAGL Fellowship in Minimally Invasive Gynecologic Surgery. Dr. Isaacson is a past president of both the AAGL and the Society of Reproductive Surgeons, as well as a published clinical researcher and surgical innovator.
It is a true honor to welcome Dr. Isaacson to this edition of the Master Class in Gynecologic Surgery.
Dr. Miller is professor of obstetrics & gynecology in the Department of Clinical Sciences, Rosalind Franklin University, North Chicago, and director of minimally invasive gynecologic surgery at Advocate Lutheran General Hospital, Park Ridge, both in Illinois. Dr. Miller reported that he has no relevant disclosures. Email him at obnews@mdedge.com.
Adenomyosis is a benign disorder, present in 20%-35% of women and characterized by the presence of endometrial glands and stroma within the myometrium. The ectopic endometrial tissue appears to cause hypertrophy in the myometrium, resulting in an enlarged globular uterus.
Adenomyosis may present as diffuse or focal involvement within the uterus. When the focal lesion appears to be well defined, it is referred to as an adenomyoma. It is not encapsulated like a fibroid. There may be involvement of the junctional zone of the myometrium – the area between the subendometrial myometrium and the outer myometrium. While the pathogenesis of adenomyosis is unknown, two rigorous theories exist: endomyometrial invagination of the endometrium and de novo from Müllerian rests.
For this installment of the Master Class in Gynecologic Surgery, I have enlisted Keith B. Isaacson, MD, to discuss the clinical presentation, diagnosis, and medical and surgical treatment of adenomyosis.
Dr. Isaacson is the director of minimally invasive gynecologic surgery and infertility at Newton-Wellesley Hospital, Newton, Mass., and associate professor of obstetrics and gynecology at Harvard Medical School, Boston. He is currently in practice specializing in minimally invasive gynecologic surgery and infertility at Newton-Wellesley Hospital, where he is the director of the AAGL Fellowship in Minimally Invasive Gynecologic Surgery. Dr. Isaacson is a past president of both the AAGL and the Society of Reproductive Surgeons, as well as a published clinical researcher and surgical innovator.
It is a true honor to welcome Dr. Isaacson to this edition of the Master Class in Gynecologic Surgery.
Dr. Miller is professor of obstetrics & gynecology in the Department of Clinical Sciences, Rosalind Franklin University, North Chicago, and director of minimally invasive gynecologic surgery at Advocate Lutheran General Hospital, Park Ridge, both in Illinois. Dr. Miller reported that he has no relevant disclosures. Email him at obnews@mdedge.com.
Adenomyosis is a benign disorder, present in 20%-35% of women and characterized by the presence of endometrial glands and stroma within the myometrium. The ectopic endometrial tissue appears to cause hypertrophy in the myometrium, resulting in an enlarged globular uterus.
Adenomyosis may present as diffuse or focal involvement within the uterus. When the focal lesion appears to be well defined, it is referred to as an adenomyoma. It is not encapsulated like a fibroid. There may be involvement of the junctional zone of the myometrium – the area between the subendometrial myometrium and the outer myometrium. While the pathogenesis of adenomyosis is unknown, two rigorous theories exist: endomyometrial invagination of the endometrium and de novo from Müllerian rests.
For this installment of the Master Class in Gynecologic Surgery, I have enlisted Keith B. Isaacson, MD, to discuss the clinical presentation, diagnosis, and medical and surgical treatment of adenomyosis.
Dr. Isaacson is the director of minimally invasive gynecologic surgery and infertility at Newton-Wellesley Hospital, Newton, Mass., and associate professor of obstetrics and gynecology at Harvard Medical School, Boston. He is currently in practice specializing in minimally invasive gynecologic surgery and infertility at Newton-Wellesley Hospital, where he is the director of the AAGL Fellowship in Minimally Invasive Gynecologic Surgery. Dr. Isaacson is a past president of both the AAGL and the Society of Reproductive Surgeons, as well as a published clinical researcher and surgical innovator.
It is a true honor to welcome Dr. Isaacson to this edition of the Master Class in Gynecologic Surgery.
Dr. Miller is professor of obstetrics & gynecology in the Department of Clinical Sciences, Rosalind Franklin University, North Chicago, and director of minimally invasive gynecologic surgery at Advocate Lutheran General Hospital, Park Ridge, both in Illinois. Dr. Miller reported that he has no relevant disclosures. Email him at obnews@mdedge.com.

Adenomyosis: While a last resort, surgery remains an option
Adenomyosis causing severe dysmenorrhea, dyspareunia, and heavy menstrual bleeding has been thought to affect primarily multiparous women in their mid- to late 40s. Often women who experience pain and heavy bleeding will tolerate their symptoms until they are done with childbearing, at which point they often go on to have a hysterectomy to relieve them of these symptoms. Tissue histology obtained at the time of hysterectomy confirms the diagnosis of adenomyosis.

Because the diagnosis is made at the time of hysterectomy, the published incidence and prevalence of adenomyosis is more a reflection of a risk for hysterectomy and not for the disease itself. MRI has been used to evaluate the junctional zone in patients with symptoms of endometriosis. This screen tool is an expensive one, however, and has not been used extensively to evaluate women with symptoms of adenomyosis who are not candidates for a hysterectomy.
Ultrasound studies
Over the past 5-7 years, numerous studies have been performed that demonstrate ultrasound changes consistent with adenomyosis within the uterus. These changes include asymmetry and heterogeneity of the anterior and posterior myometrium, cystic lesions in the myometrium, ultrasound striations, and streaking and irregular junctional zone thickening seen on 3-D scans.
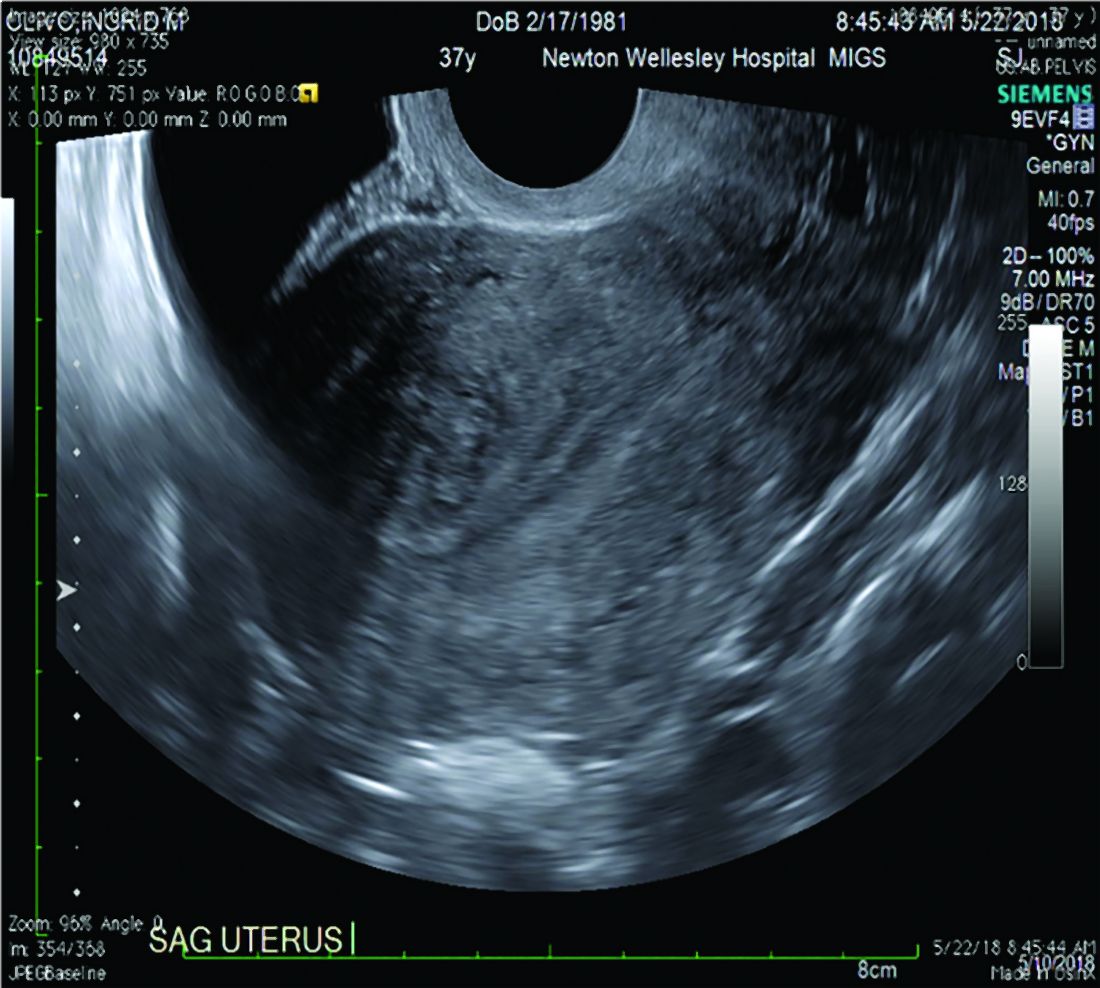
Our newfound ability to demonstrate changes consistent with adenomyosis by ultrasound – a tool that is much less expensive than MRI and more available to patients – means that we can and should consider adenomyosis in patients suffering from dysmenorrhea, heavy menstrual bleeding, back pain, dyspareunia, and infertility – regardless of the patient’s age.
In the last 5 years, adenomyosis has been increasingly recognized as a disorder affecting women of all reproductive ages, including teenagers whose dysmenorrhea disrupts their education and young women undergoing infertility evaluations. In one study, 12% of adolescent girls and young women aged 14–20 years lost days of school or work each month because of dysmenorrhea.1 This disruption is not “normal.”
Several meta-analyses have also demonstrated that ultrasound and MRI changes consistent with adenomyosis can affect embryo implantation rates in women undergoing in vitro fertilization. The implantation rates can be as low as one half the expected rate without adenomyosis. Additionally, adenomyosis has been shown to increase the risk of miscarriage and preterm delivery.2,3
The clinicians who order and carefully look at the ultrasound themselves, rather than rely on the radiologist to make the diagnosis, will be able to see the changes consistent with adenomyosis. Over time – I anticipate the next several years – a standardized radiologic definition for adenomyosis will evolve, and radiologists will become more familiar with these changes. In the meantime, our patients should not have missed diagnoses.
Considerations for surgery
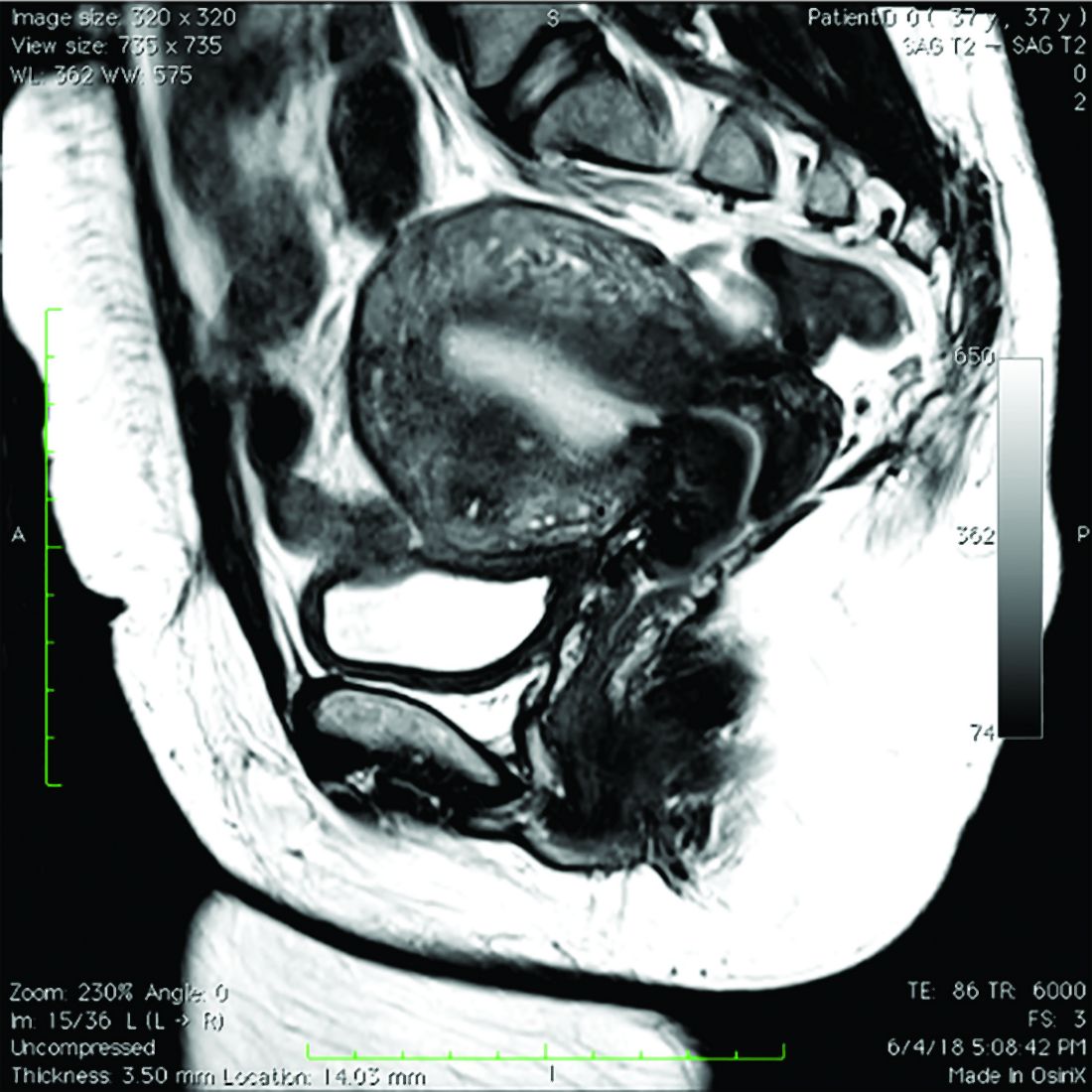
For the majority of younger patients who are not trying to conceive but want to maintain their fertility, medical treatment with oral contraceptives, progestins, or the levonorgestrel-releasing intrauterine device (Mirena) will relieve symptoms. The Mirena IUD has been found in studies of 6-36 months’ treatment duration to decrease the size of the uterus by 25%4 and improve dysmenorrhea and menorrhagia with a low profile of adverse effects in most women.
The Mirena IUD should be considered as a first-line therapy for all women with heavy menstrual bleeding and dyspareunia who want to preserve their fertility.
Patients who do not respond to or cannot tolerate medical therapy, and do not want to preserve their fertility, may consider hysterectomy, long regarded as the preferred method of treatment. Endometrial ablation can also be considered in those who no longer desire to preserve fertility and are experiencing heavy menstrual bleeding. Those with extensive adenomyosis, however, often experience poor results with endometrial ablation and may ultimately require hysterectomy. Endometrial ablation has a history of a high failure rate in women younger than 45 years old.
Patients with adenomyosis who wish to preserve their fertility and cannot tolerate or are unresponsive to hormonal therapy, or those with infertility thought to be caused by adenomyosis, should consider these three management options:
- Do nothing. The embryo implantation rate is not zero with adenomyosis, and we have no data on the number of patients who conceive with adenomyotic changes detected by MRI or ultrasound.
- Pretreat with a GnRH agonist for 2-3 months prior to a frozen embryo transfer (FET). Suppressing the disease prior to an FET seems to increase the implantation rate to what is expected for that patient given her age and other fertility factors.3 While this approach is often successful, an estimated 15%-20% of patients are unable to tolerate GnRH agonist treatment because of its side effects.
- Seek surgical resection of adenomyosis. Unlike uterine fibroids, adenomyosis has no pseudocapsule. When resecting the disease via laparotomy, laparoscopy, or hysteroscopy, the process is more of a debulking procedure. Surgical resection should be reserved for those who cannot tolerate hormonal suppression or have failed the other two options.
Surgical approaches
Surgical excision can be challenging because adenomyosis burrows its way through the muscle, is often diffuse, and cannot necessarily be resected with clean margins as can a fibroid. Yet, as demonstrated in a systematic review of 27 observational studies of conservative surgery for adenomyosis – 10 prospective and 17 retrospective studies with a total of almost 1,400 patients and all with adenomyosis confirmed histopathologically – surgery can improve pain, menorrhagia, and adenomyosis-related infertility in a significant number of cases.5
Disease may be resected through laparotomy, laparoscopy, or as we are currently doing with focal disease that is close to the endometrium, hysteroscopy. The type of surgery will depend on the location and characteristics of the disease, and on the surgeon’s skills. The principles are the same with all three approaches: to remove as much diseased tissue – and preserve as much healthy myometrial tissue – as possible and to reconstruct the uterine wall so that it maintains its integrity and can sustain a pregnancy.
The open approach known as the Osada procedure, after Hisao Osada, MD, PhD, in Tokyo, is well described in the literature, with a relatively large number of cases reported in prospective studies. Dr. Osada performs a radical adenomyosis excision with a triple flap method of uterine wall reconstruction. The uterus is bisected in the mid-sagittal plane all the way down through the adenomyosis until the uterine cavity is reached. Excision of the adenomyotic tissue is guided by palpation with the index finger, and a myometrial thickness of 1 cm from the serosa and the endometrium is preserved.
The endometrium is closed, and the myometrial defect is closed with a triple flap method that avoids overlapping suture lines. On one side of the uterus, the myometrium and serosa are sutured in the antero-posterior plane. The seromuscular layer of the opposite side of the uterine wall is then brought over the first seromuscular suture line.6
Others, such as Grigoris H. Grimbizis, MD, PhD, in Greece, have used a laparoscopic approach and closed the myometrium in layers similar to those of a myomectomy.7 There are no comparative trials that demonstrate one technique is superior to the other.
While there are no textbook techniques published for resecting adenomyotic tissue laparoscopically or hysteroscopically from the normal myometrium, there are some general principals the surgeon should keep in mind. Adenomyosis is defined as the presence of endometrial glands and stroma within myometrium, but biopsy studies have demonstrated that there are relatively few glands and stroma within the diseased tissue. Mostly, the adenomyotic tissue we encounter comprises smooth muscle hyperplasia and fibrosis.
Since there is no pseudocapsule surrounding adenomyotic tissue, the visual cue for the cytoreductive procedure is the presence of normal-appearing myometrium. The normal myometrium can be delineated by palpation with laparoscopic instruments or hysteroscopic loops as it clearly feels less fibrotic and firm than the adenomyotic tissue. For this reason, the adenomyotic tissue is removed in a piecemeal fashion until normal tissue is encountered. (This same philosophy can be applied to removing fibrotic, glandular, or cystic tissue hysteroscopically.)
If the disease involves the inner myometrium, it should resected as this may be very important to restoring normal uterine contractions needed for embryo implantation and development, even if it means entering the cavity laparoscopically.
Hysteroscopically, there is no ability to suture a myometrial defect. This limitation is concerning because the adenomyosis is thought to invade the myometrium and not displace it as seen with monoclonal uterine fibroids. There are no case reports of uterine rupture after hysteroscopic resection of adenomyosis, but the number of cases reported with this type of resection in general is very small.
Laparoscopically, the myometrial defect should be repaired similarly to a myomectomy defect. Chromic or polydioxanone (PDS) suture is appropriate. We have used 2-0 PDS V-loc and a 2-3 layer closure in our laparoscopic cases.
Diffuse adenomyosis can involve the entire anterior or posterior wall of the uterus or both. The surgeon should not attempt to remove all of the disease in this situation and must leave enough tissue, even diseased, to allow for structural integrity during pregnancy. Uterine rupture has not been reported in all published case series and studies, but overall, it is a concern with surgical excision of adenomyosis. An analysis of over 2,000 cases of adenomyomectomies reported worldwide since 1990 shows a uterine rupture rate in the 6% rate, with a pregnancy rate ranging from 7%-72%.8
When the disease is focal and close to the endometrium, as opposed to diffuse and affecting the entire back wall of the uterus, hysteroscopic excision may be an appropriate, less invasive approach.
One of the patients for whom we’ve taken this approach was a 37-year-old patient who presented with a history of six miscarriages, a negative work-up for recurrent pregnancy loss, an enlarged uterus, 8 years of heavy menstrual bleeding, and only mild dysmenorrhea. She had undergone in vitro fertilization with failed embryo transfers but normal genetic screens of the embryos. She was referred with a suspicion of fibroids. An MRI and ultrasound showed heterogeneous myometrium adjacent to the endometrium. This tissue was resected using a bipolar loop electrode until normal myometrium was encountered.
Hysteroscopic resections are currently described in the literature through case reports rather than larger prospective or retrospective studies, and much more research is needed to demonstrate the efficacy and safety of this approach.
At this point in time, while surgery to excise adenomyosis is a last resort and best methods are deliberated, it is still important to appreciate that surgery is an option. Continued infertility is not the only choice, nor is hysterectomy.
References
1. J Pediatr Adolesc Gynecol 2014;27:258-65.
2. Minerva Ginecol. 2018 Jun;70(3):295-302.
3. Fertil Steril. 2017;108(3):483-490.e3.
4. Am J Obstet Gynecol. 2008;198(4):373.e1-7.
5. J. Minim Invasive Gynecol. 2018 Feb;25:265-76.
6. Reproductive BioMed Online. 2011 Jan;22(1):94-9.
7. Fertil Steril. 2014 Feb;101(2):472-87.
8. Fertil Steril. 2018 Mar;109(3):406-17.
Adenomyosis causing severe dysmenorrhea, dyspareunia, and heavy menstrual bleeding has been thought to affect primarily multiparous women in their mid- to late 40s. Often women who experience pain and heavy bleeding will tolerate their symptoms until they are done with childbearing, at which point they often go on to have a hysterectomy to relieve them of these symptoms. Tissue histology obtained at the time of hysterectomy confirms the diagnosis of adenomyosis.
Because the diagnosis is made at the time of hysterectomy, the published incidence and prevalence of adenomyosis is more a reflection of a risk for hysterectomy and not for the disease itself. MRI has been used to evaluate the junctional zone in patients with symptoms of endometriosis. This screen tool is an expensive one, however, and has not been used extensively to evaluate women with symptoms of adenomyosis who are not candidates for a hysterectomy.
Ultrasound studies
Over the past 5-7 years, numerous studies have been performed that demonstrate ultrasound changes consistent with adenomyosis within the uterus. These changes include asymmetry and heterogeneity of the anterior and posterior myometrium, cystic lesions in the myometrium, ultrasound striations, and streaking and irregular junctional zone thickening seen on 3-D scans.
Our newfound ability to demonstrate changes consistent with adenomyosis by ultrasound – a tool that is much less expensive than MRI and more available to patients – means that we can and should consider adenomyosis in patients suffering from dysmenorrhea, heavy menstrual bleeding, back pain, dyspareunia, and infertility – regardless of the patient’s age.
In the last 5 years, adenomyosis has been increasingly recognized as a disorder affecting women of all reproductive ages, including teenagers whose dysmenorrhea disrupts their education and young women undergoing infertility evaluations. In one study, 12% of adolescent girls and young women aged 14–20 years lost days of school or work each month because of dysmenorrhea.1 This disruption is not “normal.”
Several meta-analyses have also demonstrated that ultrasound and MRI changes consistent with adenomyosis can affect embryo implantation rates in women undergoing in vitro fertilization. The implantation rates can be as low as one half the expected rate without adenomyosis. Additionally, adenomyosis has been shown to increase the risk of miscarriage and preterm delivery.2,3
The clinicians who order and carefully look at the ultrasound themselves, rather than rely on the radiologist to make the diagnosis, will be able to see the changes consistent with adenomyosis. Over time – I anticipate the next several years – a standardized radiologic definition for adenomyosis will evolve, and radiologists will become more familiar with these changes. In the meantime, our patients should not have missed diagnoses.
Considerations for surgery
For the majority of younger patients who are not trying to conceive but want to maintain their fertility, medical treatment with oral contraceptives, progestins, or the levonorgestrel-releasing intrauterine device (Mirena) will relieve symptoms. The Mirena IUD has been found in studies of 6-36 months’ treatment duration to decrease the size of the uterus by 25%4 and improve dysmenorrhea and menorrhagia with a low profile of adverse effects in most women.
The Mirena IUD should be considered as a first-line therapy for all women with heavy menstrual bleeding and dyspareunia who want to preserve their fertility.
Patients who do not respond to or cannot tolerate medical therapy, and do not want to preserve their fertility, may consider hysterectomy, long regarded as the preferred method of treatment. Endometrial ablation can also be considered in those who no longer desire to preserve fertility and are experiencing heavy menstrual bleeding. Those with extensive adenomyosis, however, often experience poor results with endometrial ablation and may ultimately require hysterectomy. Endometrial ablation has a history of a high failure rate in women younger than 45 years old.
Patients with adenomyosis who wish to preserve their fertility and cannot tolerate or are unresponsive to hormonal therapy, or those with infertility thought to be caused by adenomyosis, should consider these three management options:
- Do nothing. The embryo implantation rate is not zero with adenomyosis, and we have no data on the number of patients who conceive with adenomyotic changes detected by MRI or ultrasound.
- Pretreat with a GnRH agonist for 2-3 months prior to a frozen embryo transfer (FET). Suppressing the disease prior to an FET seems to increase the implantation rate to what is expected for that patient given her age and other fertility factors.3 While this approach is often successful, an estimated 15%-20% of patients are unable to tolerate GnRH agonist treatment because of its side effects.
- Seek surgical resection of adenomyosis. Unlike uterine fibroids, adenomyosis has no pseudocapsule. When resecting the disease via laparotomy, laparoscopy, or hysteroscopy, the process is more of a debulking procedure. Surgical resection should be reserved for those who cannot tolerate hormonal suppression or have failed the other two options.
Surgical approaches
Surgical excision can be challenging because adenomyosis burrows its way through the muscle, is often diffuse, and cannot necessarily be resected with clean margins as can a fibroid. Yet, as demonstrated in a systematic review of 27 observational studies of conservative surgery for adenomyosis – 10 prospective and 17 retrospective studies with a total of almost 1,400 patients and all with adenomyosis confirmed histopathologically – surgery can improve pain, menorrhagia, and adenomyosis-related infertility in a significant number of cases.5
Disease may be resected through laparotomy, laparoscopy, or as we are currently doing with focal disease that is close to the endometrium, hysteroscopy. The type of surgery will depend on the location and characteristics of the disease, and on the surgeon’s skills. The principles are the same with all three approaches: to remove as much diseased tissue – and preserve as much healthy myometrial tissue – as possible and to reconstruct the uterine wall so that it maintains its integrity and can sustain a pregnancy.
The open approach known as the Osada procedure, after Hisao Osada, MD, PhD, in Tokyo, is well described in the literature, with a relatively large number of cases reported in prospective studies. Dr. Osada performs a radical adenomyosis excision with a triple flap method of uterine wall reconstruction. The uterus is bisected in the mid-sagittal plane all the way down through the adenomyosis until the uterine cavity is reached. Excision of the adenomyotic tissue is guided by palpation with the index finger, and a myometrial thickness of 1 cm from the serosa and the endometrium is preserved.
The endometrium is closed, and the myometrial defect is closed with a triple flap method that avoids overlapping suture lines. On one side of the uterus, the myometrium and serosa are sutured in the antero-posterior plane. The seromuscular layer of the opposite side of the uterine wall is then brought over the first seromuscular suture line.6
Others, such as Grigoris H. Grimbizis, MD, PhD, in Greece, have used a laparoscopic approach and closed the myometrium in layers similar to those of a myomectomy.7 There are no comparative trials that demonstrate one technique is superior to the other.
While there are no textbook techniques published for resecting adenomyotic tissue laparoscopically or hysteroscopically from the normal myometrium, there are some general principals the surgeon should keep in mind. Adenomyosis is defined as the presence of endometrial glands and stroma within myometrium, but biopsy studies have demonstrated that there are relatively few glands and stroma within the diseased tissue. Mostly, the adenomyotic tissue we encounter comprises smooth muscle hyperplasia and fibrosis.
Since there is no pseudocapsule surrounding adenomyotic tissue, the visual cue for the cytoreductive procedure is the presence of normal-appearing myometrium. The normal myometrium can be delineated by palpation with laparoscopic instruments or hysteroscopic loops as it clearly feels less fibrotic and firm than the adenomyotic tissue. For this reason, the adenomyotic tissue is removed in a piecemeal fashion until normal tissue is encountered. (This same philosophy can be applied to removing fibrotic, glandular, or cystic tissue hysteroscopically.)
If the disease involves the inner myometrium, it should resected as this may be very important to restoring normal uterine contractions needed for embryo implantation and development, even if it means entering the cavity laparoscopically.
Hysteroscopically, there is no ability to suture a myometrial defect. This limitation is concerning because the adenomyosis is thought to invade the myometrium and not displace it as seen with monoclonal uterine fibroids. There are no case reports of uterine rupture after hysteroscopic resection of adenomyosis, but the number of cases reported with this type of resection in general is very small.
Laparoscopically, the myometrial defect should be repaired similarly to a myomectomy defect. Chromic or polydioxanone (PDS) suture is appropriate. We have used 2-0 PDS V-loc and a 2-3 layer closure in our laparoscopic cases.
Diffuse adenomyosis can involve the entire anterior or posterior wall of the uterus or both. The surgeon should not attempt to remove all of the disease in this situation and must leave enough tissue, even diseased, to allow for structural integrity during pregnancy. Uterine rupture has not been reported in all published case series and studies, but overall, it is a concern with surgical excision of adenomyosis. An analysis of over 2,000 cases of adenomyomectomies reported worldwide since 1990 shows a uterine rupture rate in the 6% rate, with a pregnancy rate ranging from 7%-72%.8
When the disease is focal and close to the endometrium, as opposed to diffuse and affecting the entire back wall of the uterus, hysteroscopic excision may be an appropriate, less invasive approach.
One of the patients for whom we’ve taken this approach was a 37-year-old patient who presented with a history of six miscarriages, a negative work-up for recurrent pregnancy loss, an enlarged uterus, 8 years of heavy menstrual bleeding, and only mild dysmenorrhea. She had undergone in vitro fertilization with failed embryo transfers but normal genetic screens of the embryos. She was referred with a suspicion of fibroids. An MRI and ultrasound showed heterogeneous myometrium adjacent to the endometrium. This tissue was resected using a bipolar loop electrode until normal myometrium was encountered.
Hysteroscopic resections are currently described in the literature through case reports rather than larger prospective or retrospective studies, and much more research is needed to demonstrate the efficacy and safety of this approach.
At this point in time, while surgery to excise adenomyosis is a last resort and best methods are deliberated, it is still important to appreciate that surgery is an option. Continued infertility is not the only choice, nor is hysterectomy.
References
1. J Pediatr Adolesc Gynecol 2014;27:258-65.
2. Minerva Ginecol. 2018 Jun;70(3):295-302.
3. Fertil Steril. 2017;108(3):483-490.e3.
4. Am J Obstet Gynecol. 2008;198(4):373.e1-7.
5. J. Minim Invasive Gynecol. 2018 Feb;25:265-76.
6. Reproductive BioMed Online. 2011 Jan;22(1):94-9.
7. Fertil Steril. 2014 Feb;101(2):472-87.
8. Fertil Steril. 2018 Mar;109(3):406-17.
Adenomyosis causing severe dysmenorrhea, dyspareunia, and heavy menstrual bleeding has been thought to affect primarily multiparous women in their mid- to late 40s. Often women who experience pain and heavy bleeding will tolerate their symptoms until they are done with childbearing, at which point they often go on to have a hysterectomy to relieve them of these symptoms. Tissue histology obtained at the time of hysterectomy confirms the diagnosis of adenomyosis.
Because the diagnosis is made at the time of hysterectomy, the published incidence and prevalence of adenomyosis is more a reflection of a risk for hysterectomy and not for the disease itself. MRI has been used to evaluate the junctional zone in patients with symptoms of endometriosis. This screen tool is an expensive one, however, and has not been used extensively to evaluate women with symptoms of adenomyosis who are not candidates for a hysterectomy.
Ultrasound studies
Over the past 5-7 years, numerous studies have been performed that demonstrate ultrasound changes consistent with adenomyosis within the uterus. These changes include asymmetry and heterogeneity of the anterior and posterior myometrium, cystic lesions in the myometrium, ultrasound striations, and streaking and irregular junctional zone thickening seen on 3-D scans.
Our newfound ability to demonstrate changes consistent with adenomyosis by ultrasound – a tool that is much less expensive than MRI and more available to patients – means that we can and should consider adenomyosis in patients suffering from dysmenorrhea, heavy menstrual bleeding, back pain, dyspareunia, and infertility – regardless of the patient’s age.
In the last 5 years, adenomyosis has been increasingly recognized as a disorder affecting women of all reproductive ages, including teenagers whose dysmenorrhea disrupts their education and young women undergoing infertility evaluations. In one study, 12% of adolescent girls and young women aged 14–20 years lost days of school or work each month because of dysmenorrhea.1 This disruption is not “normal.”
Several meta-analyses have also demonstrated that ultrasound and MRI changes consistent with adenomyosis can affect embryo implantation rates in women undergoing in vitro fertilization. The implantation rates can be as low as one half the expected rate without adenomyosis. Additionally, adenomyosis has been shown to increase the risk of miscarriage and preterm delivery.2,3
The clinicians who order and carefully look at the ultrasound themselves, rather than rely on the radiologist to make the diagnosis, will be able to see the changes consistent with adenomyosis. Over time – I anticipate the next several years – a standardized radiologic definition for adenomyosis will evolve, and radiologists will become more familiar with these changes. In the meantime, our patients should not have missed diagnoses.
Considerations for surgery
For the majority of younger patients who are not trying to conceive but want to maintain their fertility, medical treatment with oral contraceptives, progestins, or the levonorgestrel-releasing intrauterine device (Mirena) will relieve symptoms. The Mirena IUD has been found in studies of 6-36 months’ treatment duration to decrease the size of the uterus by 25%4 and improve dysmenorrhea and menorrhagia with a low profile of adverse effects in most women.
The Mirena IUD should be considered as a first-line therapy for all women with heavy menstrual bleeding and dyspareunia who want to preserve their fertility.
Patients who do not respond to or cannot tolerate medical therapy, and do not want to preserve their fertility, may consider hysterectomy, long regarded as the preferred method of treatment. Endometrial ablation can also be considered in those who no longer desire to preserve fertility and are experiencing heavy menstrual bleeding. Those with extensive adenomyosis, however, often experience poor results with endometrial ablation and may ultimately require hysterectomy. Endometrial ablation has a history of a high failure rate in women younger than 45 years old.
Patients with adenomyosis who wish to preserve their fertility and cannot tolerate or are unresponsive to hormonal therapy, or those with infertility thought to be caused by adenomyosis, should consider these three management options:
- Do nothing. The embryo implantation rate is not zero with adenomyosis, and we have no data on the number of patients who conceive with adenomyotic changes detected by MRI or ultrasound.
- Pretreat with a GnRH agonist for 2-3 months prior to a frozen embryo transfer (FET). Suppressing the disease prior to an FET seems to increase the implantation rate to what is expected for that patient given her age and other fertility factors.3 While this approach is often successful, an estimated 15%-20% of patients are unable to tolerate GnRH agonist treatment because of its side effects.
- Seek surgical resection of adenomyosis. Unlike uterine fibroids, adenomyosis has no pseudocapsule. When resecting the disease via laparotomy, laparoscopy, or hysteroscopy, the process is more of a debulking procedure. Surgical resection should be reserved for those who cannot tolerate hormonal suppression or have failed the other two options.
Surgical approaches
Surgical excision can be challenging because adenomyosis burrows its way through the muscle, is often diffuse, and cannot necessarily be resected with clean margins as can a fibroid. Yet, as demonstrated in a systematic review of 27 observational studies of conservative surgery for adenomyosis – 10 prospective and 17 retrospective studies with a total of almost 1,400 patients and all with adenomyosis confirmed histopathologically – surgery can improve pain, menorrhagia, and adenomyosis-related infertility in a significant number of cases.5
Disease may be resected through laparotomy, laparoscopy, or as we are currently doing with focal disease that is close to the endometrium, hysteroscopy. The type of surgery will depend on the location and characteristics of the disease, and on the surgeon’s skills. The principles are the same with all three approaches: to remove as much diseased tissue – and preserve as much healthy myometrial tissue – as possible and to reconstruct the uterine wall so that it maintains its integrity and can sustain a pregnancy.
The open approach known as the Osada procedure, after Hisao Osada, MD, PhD, in Tokyo, is well described in the literature, with a relatively large number of cases reported in prospective studies. Dr. Osada performs a radical adenomyosis excision with a triple flap method of uterine wall reconstruction. The uterus is bisected in the mid-sagittal plane all the way down through the adenomyosis until the uterine cavity is reached. Excision of the adenomyotic tissue is guided by palpation with the index finger, and a myometrial thickness of 1 cm from the serosa and the endometrium is preserved.
The endometrium is closed, and the myometrial defect is closed with a triple flap method that avoids overlapping suture lines. On one side of the uterus, the myometrium and serosa are sutured in the antero-posterior plane. The seromuscular layer of the opposite side of the uterine wall is then brought over the first seromuscular suture line.6
Others, such as Grigoris H. Grimbizis, MD, PhD, in Greece, have used a laparoscopic approach and closed the myometrium in layers similar to those of a myomectomy.7 There are no comparative trials that demonstrate one technique is superior to the other.
While there are no textbook techniques published for resecting adenomyotic tissue laparoscopically or hysteroscopically from the normal myometrium, there are some general principals the surgeon should keep in mind. Adenomyosis is defined as the presence of endometrial glands and stroma within myometrium, but biopsy studies have demonstrated that there are relatively few glands and stroma within the diseased tissue. Mostly, the adenomyotic tissue we encounter comprises smooth muscle hyperplasia and fibrosis.
Since there is no pseudocapsule surrounding adenomyotic tissue, the visual cue for the cytoreductive procedure is the presence of normal-appearing myometrium. The normal myometrium can be delineated by palpation with laparoscopic instruments or hysteroscopic loops as it clearly feels less fibrotic and firm than the adenomyotic tissue. For this reason, the adenomyotic tissue is removed in a piecemeal fashion until normal tissue is encountered. (This same philosophy can be applied to removing fibrotic, glandular, or cystic tissue hysteroscopically.)
If the disease involves the inner myometrium, it should resected as this may be very important to restoring normal uterine contractions needed for embryo implantation and development, even if it means entering the cavity laparoscopically.
Hysteroscopically, there is no ability to suture a myometrial defect. This limitation is concerning because the adenomyosis is thought to invade the myometrium and not displace it as seen with monoclonal uterine fibroids. There are no case reports of uterine rupture after hysteroscopic resection of adenomyosis, but the number of cases reported with this type of resection in general is very small.
Laparoscopically, the myometrial defect should be repaired similarly to a myomectomy defect. Chromic or polydioxanone (PDS) suture is appropriate. We have used 2-0 PDS V-loc and a 2-3 layer closure in our laparoscopic cases.
Diffuse adenomyosis can involve the entire anterior or posterior wall of the uterus or both. The surgeon should not attempt to remove all of the disease in this situation and must leave enough tissue, even diseased, to allow for structural integrity during pregnancy. Uterine rupture has not been reported in all published case series and studies, but overall, it is a concern with surgical excision of adenomyosis. An analysis of over 2,000 cases of adenomyomectomies reported worldwide since 1990 shows a uterine rupture rate in the 6% rate, with a pregnancy rate ranging from 7%-72%.8
When the disease is focal and close to the endometrium, as opposed to diffuse and affecting the entire back wall of the uterus, hysteroscopic excision may be an appropriate, less invasive approach.
One of the patients for whom we’ve taken this approach was a 37-year-old patient who presented with a history of six miscarriages, a negative work-up for recurrent pregnancy loss, an enlarged uterus, 8 years of heavy menstrual bleeding, and only mild dysmenorrhea. She had undergone in vitro fertilization with failed embryo transfers but normal genetic screens of the embryos. She was referred with a suspicion of fibroids. An MRI and ultrasound showed heterogeneous myometrium adjacent to the endometrium. This tissue was resected using a bipolar loop electrode until normal myometrium was encountered.
Hysteroscopic resections are currently described in the literature through case reports rather than larger prospective or retrospective studies, and much more research is needed to demonstrate the efficacy and safety of this approach.
At this point in time, while surgery to excise adenomyosis is a last resort and best methods are deliberated, it is still important to appreciate that surgery is an option. Continued infertility is not the only choice, nor is hysterectomy.
References
1. J Pediatr Adolesc Gynecol 2014;27:258-65.
2. Minerva Ginecol. 2018 Jun;70(3):295-302.
3. Fertil Steril. 2017;108(3):483-490.e3.
4. Am J Obstet Gynecol. 2008;198(4):373.e1-7.
5. J. Minim Invasive Gynecol. 2018 Feb;25:265-76.
6. Reproductive BioMed Online. 2011 Jan;22(1):94-9.
7. Fertil Steril. 2014 Feb;101(2):472-87.
8. Fertil Steril. 2018 Mar;109(3):406-17.