User login
Accountability in Action
“What we’ve got here is failure to communicate …”
(Cool Hand Luke)

Every three months, the personnel in my office get a little nervous as we send out the quarterly personal e-mails to physicians. These e-mails, titled “Quality Indicator Deficiency,” are generated from the quality department’s abstraction of quality measures. The e-mails are personally sent from me, the chief medical officer, to the attending physician. For each measure abstracted, an attending is assigned responsibility (some like to call it “blame”). Despite the fact that we are a teaching hospital, we focus on the attendings who oversee the residents, but residents are copied on the e-mail. The deficiency assignment is based on the physician deemed most critical to the delivery of the measure.
For example, for a patient with pneumonia admitted through the ED, the ED physician is assigned the correct antibiotics measure. If the patient was directly admitted to a nursing unit, the admitting attending is assigned the correct antibiotic measure. Similarly, the anesthesia attending, not the surgeon, is given the pre-operative antibiotic measure.
Why the anxiety from my office? Because when the letters go out, there usually is a very rapid response by many physicians, which results in significant scrutiny of the letters. I refer to this as “good conflict.” Not everyone in my office always agrees with the good part, but there is agreement that this leads to significant discussion and awareness. Prior to the letters, we were like many organizations: We reported aggregate data regularly in a variety of forums and formats in order to promote awareness. We had regular conversations with physicians, physician leaders, and hospital staff. There were numerous quality-improvement efforts in measure areas. We continue to do all of these things, but it is the letters that have turned it up a notch.
Assign Responsibility
Responses fall into three categories. First, “The data is wrong.” Second, “This is not my fault. It was so-and-so’s fault.” Third, “A hospital process prevented me from doing the right thing.” The responses have proven so predictable that I have developed standard scripting for my responses.
Occasionally, the data are wrong. All letters are sent after the charts are initially abstracted. The accuracy of a chart abstractor is close to 100%. Addition of a nurse reviewer and a physician reviewer will help us achieve perfection, but the cost of doing this is significant. I find that many physicians, including myself, want perfection when it gets personal, but I just can’t justify the expense. Moreover, when a physician states that the data are wrong, it is more likely that the data are correct, but the physician does not fully understand the specifications of the measure.
Fault is a more interesting response. Deliberately, our quality committee, which determines the assignment rules, has chosen to attach an attending to every single measure, even those driven by hospital staff. This is done because we feel the healthcare team needs to solve these deficiencies, and often this forces a discussion. For deficiencies that are more staff-related, we do send the letter to the physician and unit manager simultaneously. The usual response by the manager is to contact the physician, apologize, then work on a plan that will remedy the situation.
As a recent example, a nurse chose to give a medication prior to an antibiotic for pneumonia and thus missed the six-hour deadline. This resulted in a change in protocol in the ED.
The hospital process response is the most useful to me because for every quarter that we send letters, there are multiple hospital processes that are modified as a result of this response. It is always fascinating to me because almost all of these measures have had good quality-improvement teams, but there are always missed subtle issues or unintended consequences. Because physicians respond quickly and often passionately, the urgency to fix these processes is present, hence facilitating rapid change.
Kill Them with Kindness
When I suggested sending these letters a few years ago, many on the quality staff cringed. Their reluctance was not unfounded: My original letter was a tad abrasive. I have toned down the letter, even to the point that I am now asking for help rather than directly pointing the finger: “I need your help in reviewing the following patient’s chart. In an initial review of quality indicators, a deficiency is noted. This may be because of simple oversight, or the patient might have had a contraindication for therapy for which we cannot find documentation. A physician must document all contraindications. Please review this chart as soon as possible, and if you feel this deficiency is in error, please let me or one of the outcomes managers know immediately. This deficiency has not yet been reported to the federal quality-improvement organization. We may be able to correct the error prior to final submission.”
The last line of the response attaches responsibility: “If we do not hear from you, we will assume the deficiency stands.”
This whole plan is part of a campaign in our hospital to personalize quality data. Recently, several studies have shown that consumers do not review quality data. Other evidence is increasingly backing up the “embarrassment” approach, as some would like to label my methodology. I prefer to call it the “personalizing method.” Physician education these days is largely based on case studies and the evidence-based approach. Personalizing quality data combines both, and might be the ideal approach to taking great leaps in quality.
Some experts have lamented this approach, but I can tell you that when I received two letters regarding the omission of offering a patient with heart failure weight-monitoring instructions, I quickly changed my approach and now make sure that the residents and nurses are giving those instructions. Initially, I was a little defensive about it, but I did the right thing and made modifications. Personalizing does work, and we should embrace it more fully.
It is not easy to personalize. Our present systems—or lack thereof—require abstracting and the review of written notes to achieve high levels of accuracy in personalizing. Without these high levels of accuracy, it is difficult to engage physicians with this data. The future is in electronic capture, but none of this is perfect, either. Hospitals must develop and hone systems to catch physician assignment during multiple interventions of a typical patient stay.
The cost of all this is unknown and most likely significant. But one could easily imagine a tremendous improvement in quality.
My message to hospitalists and hospitalist leaders is “Make the data personal!” Start working on this today, so that within a few years, you, too, will have regular reports. Continue to aggregate quality data based on group performance and review it frequently. If you want more significant impact and greater physician engagement, make it personal. TH
Dr. Cawley is president of SHM.
“What we’ve got here is failure to communicate …”
(Cool Hand Luke)
Every three months, the personnel in my office get a little nervous as we send out the quarterly personal e-mails to physicians. These e-mails, titled “Quality Indicator Deficiency,” are generated from the quality department’s abstraction of quality measures. The e-mails are personally sent from me, the chief medical officer, to the attending physician. For each measure abstracted, an attending is assigned responsibility (some like to call it “blame”). Despite the fact that we are a teaching hospital, we focus on the attendings who oversee the residents, but residents are copied on the e-mail. The deficiency assignment is based on the physician deemed most critical to the delivery of the measure.
For example, for a patient with pneumonia admitted through the ED, the ED physician is assigned the correct antibiotics measure. If the patient was directly admitted to a nursing unit, the admitting attending is assigned the correct antibiotic measure. Similarly, the anesthesia attending, not the surgeon, is given the pre-operative antibiotic measure.
Why the anxiety from my office? Because when the letters go out, there usually is a very rapid response by many physicians, which results in significant scrutiny of the letters. I refer to this as “good conflict.” Not everyone in my office always agrees with the good part, but there is agreement that this leads to significant discussion and awareness. Prior to the letters, we were like many organizations: We reported aggregate data regularly in a variety of forums and formats in order to promote awareness. We had regular conversations with physicians, physician leaders, and hospital staff. There were numerous quality-improvement efforts in measure areas. We continue to do all of these things, but it is the letters that have turned it up a notch.
Assign Responsibility
Responses fall into three categories. First, “The data is wrong.” Second, “This is not my fault. It was so-and-so’s fault.” Third, “A hospital process prevented me from doing the right thing.” The responses have proven so predictable that I have developed standard scripting for my responses.
Occasionally, the data are wrong. All letters are sent after the charts are initially abstracted. The accuracy of a chart abstractor is close to 100%. Addition of a nurse reviewer and a physician reviewer will help us achieve perfection, but the cost of doing this is significant. I find that many physicians, including myself, want perfection when it gets personal, but I just can’t justify the expense. Moreover, when a physician states that the data are wrong, it is more likely that the data are correct, but the physician does not fully understand the specifications of the measure.
Fault is a more interesting response. Deliberately, our quality committee, which determines the assignment rules, has chosen to attach an attending to every single measure, even those driven by hospital staff. This is done because we feel the healthcare team needs to solve these deficiencies, and often this forces a discussion. For deficiencies that are more staff-related, we do send the letter to the physician and unit manager simultaneously. The usual response by the manager is to contact the physician, apologize, then work on a plan that will remedy the situation.
As a recent example, a nurse chose to give a medication prior to an antibiotic for pneumonia and thus missed the six-hour deadline. This resulted in a change in protocol in the ED.
The hospital process response is the most useful to me because for every quarter that we send letters, there are multiple hospital processes that are modified as a result of this response. It is always fascinating to me because almost all of these measures have had good quality-improvement teams, but there are always missed subtle issues or unintended consequences. Because physicians respond quickly and often passionately, the urgency to fix these processes is present, hence facilitating rapid change.
Kill Them with Kindness
When I suggested sending these letters a few years ago, many on the quality staff cringed. Their reluctance was not unfounded: My original letter was a tad abrasive. I have toned down the letter, even to the point that I am now asking for help rather than directly pointing the finger: “I need your help in reviewing the following patient’s chart. In an initial review of quality indicators, a deficiency is noted. This may be because of simple oversight, or the patient might have had a contraindication for therapy for which we cannot find documentation. A physician must document all contraindications. Please review this chart as soon as possible, and if you feel this deficiency is in error, please let me or one of the outcomes managers know immediately. This deficiency has not yet been reported to the federal quality-improvement organization. We may be able to correct the error prior to final submission.”
The last line of the response attaches responsibility: “If we do not hear from you, we will assume the deficiency stands.”
This whole plan is part of a campaign in our hospital to personalize quality data. Recently, several studies have shown that consumers do not review quality data. Other evidence is increasingly backing up the “embarrassment” approach, as some would like to label my methodology. I prefer to call it the “personalizing method.” Physician education these days is largely based on case studies and the evidence-based approach. Personalizing quality data combines both, and might be the ideal approach to taking great leaps in quality.
Some experts have lamented this approach, but I can tell you that when I received two letters regarding the omission of offering a patient with heart failure weight-monitoring instructions, I quickly changed my approach and now make sure that the residents and nurses are giving those instructions. Initially, I was a little defensive about it, but I did the right thing and made modifications. Personalizing does work, and we should embrace it more fully.
It is not easy to personalize. Our present systems—or lack thereof—require abstracting and the review of written notes to achieve high levels of accuracy in personalizing. Without these high levels of accuracy, it is difficult to engage physicians with this data. The future is in electronic capture, but none of this is perfect, either. Hospitals must develop and hone systems to catch physician assignment during multiple interventions of a typical patient stay.
The cost of all this is unknown and most likely significant. But one could easily imagine a tremendous improvement in quality.
My message to hospitalists and hospitalist leaders is “Make the data personal!” Start working on this today, so that within a few years, you, too, will have regular reports. Continue to aggregate quality data based on group performance and review it frequently. If you want more significant impact and greater physician engagement, make it personal. TH
Dr. Cawley is president of SHM.
“What we’ve got here is failure to communicate …”
(Cool Hand Luke)
Every three months, the personnel in my office get a little nervous as we send out the quarterly personal e-mails to physicians. These e-mails, titled “Quality Indicator Deficiency,” are generated from the quality department’s abstraction of quality measures. The e-mails are personally sent from me, the chief medical officer, to the attending physician. For each measure abstracted, an attending is assigned responsibility (some like to call it “blame”). Despite the fact that we are a teaching hospital, we focus on the attendings who oversee the residents, but residents are copied on the e-mail. The deficiency assignment is based on the physician deemed most critical to the delivery of the measure.
For example, for a patient with pneumonia admitted through the ED, the ED physician is assigned the correct antibiotics measure. If the patient was directly admitted to a nursing unit, the admitting attending is assigned the correct antibiotic measure. Similarly, the anesthesia attending, not the surgeon, is given the pre-operative antibiotic measure.
Why the anxiety from my office? Because when the letters go out, there usually is a very rapid response by many physicians, which results in significant scrutiny of the letters. I refer to this as “good conflict.” Not everyone in my office always agrees with the good part, but there is agreement that this leads to significant discussion and awareness. Prior to the letters, we were like many organizations: We reported aggregate data regularly in a variety of forums and formats in order to promote awareness. We had regular conversations with physicians, physician leaders, and hospital staff. There were numerous quality-improvement efforts in measure areas. We continue to do all of these things, but it is the letters that have turned it up a notch.
Assign Responsibility
Responses fall into three categories. First, “The data is wrong.” Second, “This is not my fault. It was so-and-so’s fault.” Third, “A hospital process prevented me from doing the right thing.” The responses have proven so predictable that I have developed standard scripting for my responses.
Occasionally, the data are wrong. All letters are sent after the charts are initially abstracted. The accuracy of a chart abstractor is close to 100%. Addition of a nurse reviewer and a physician reviewer will help us achieve perfection, but the cost of doing this is significant. I find that many physicians, including myself, want perfection when it gets personal, but I just can’t justify the expense. Moreover, when a physician states that the data are wrong, it is more likely that the data are correct, but the physician does not fully understand the specifications of the measure.
Fault is a more interesting response. Deliberately, our quality committee, which determines the assignment rules, has chosen to attach an attending to every single measure, even those driven by hospital staff. This is done because we feel the healthcare team needs to solve these deficiencies, and often this forces a discussion. For deficiencies that are more staff-related, we do send the letter to the physician and unit manager simultaneously. The usual response by the manager is to contact the physician, apologize, then work on a plan that will remedy the situation.
As a recent example, a nurse chose to give a medication prior to an antibiotic for pneumonia and thus missed the six-hour deadline. This resulted in a change in protocol in the ED.
The hospital process response is the most useful to me because for every quarter that we send letters, there are multiple hospital processes that are modified as a result of this response. It is always fascinating to me because almost all of these measures have had good quality-improvement teams, but there are always missed subtle issues or unintended consequences. Because physicians respond quickly and often passionately, the urgency to fix these processes is present, hence facilitating rapid change.
Kill Them with Kindness
When I suggested sending these letters a few years ago, many on the quality staff cringed. Their reluctance was not unfounded: My original letter was a tad abrasive. I have toned down the letter, even to the point that I am now asking for help rather than directly pointing the finger: “I need your help in reviewing the following patient’s chart. In an initial review of quality indicators, a deficiency is noted. This may be because of simple oversight, or the patient might have had a contraindication for therapy for which we cannot find documentation. A physician must document all contraindications. Please review this chart as soon as possible, and if you feel this deficiency is in error, please let me or one of the outcomes managers know immediately. This deficiency has not yet been reported to the federal quality-improvement organization. We may be able to correct the error prior to final submission.”
The last line of the response attaches responsibility: “If we do not hear from you, we will assume the deficiency stands.”
This whole plan is part of a campaign in our hospital to personalize quality data. Recently, several studies have shown that consumers do not review quality data. Other evidence is increasingly backing up the “embarrassment” approach, as some would like to label my methodology. I prefer to call it the “personalizing method.” Physician education these days is largely based on case studies and the evidence-based approach. Personalizing quality data combines both, and might be the ideal approach to taking great leaps in quality.
Some experts have lamented this approach, but I can tell you that when I received two letters regarding the omission of offering a patient with heart failure weight-monitoring instructions, I quickly changed my approach and now make sure that the residents and nurses are giving those instructions. Initially, I was a little defensive about it, but I did the right thing and made modifications. Personalizing does work, and we should embrace it more fully.
It is not easy to personalize. Our present systems—or lack thereof—require abstracting and the review of written notes to achieve high levels of accuracy in personalizing. Without these high levels of accuracy, it is difficult to engage physicians with this data. The future is in electronic capture, but none of this is perfect, either. Hospitals must develop and hone systems to catch physician assignment during multiple interventions of a typical patient stay.
The cost of all this is unknown and most likely significant. But one could easily imagine a tremendous improvement in quality.
My message to hospitalists and hospitalist leaders is “Make the data personal!” Start working on this today, so that within a few years, you, too, will have regular reports. Continue to aggregate quality data based on group performance and review it frequently. If you want more significant impact and greater physician engagement, make it personal. TH
Dr. Cawley is president of SHM.
One Hospital's Trash, Another Hospital's Treasure
The day after the Tepa District Hospital in Ghana, on the west coast of Africa, received its first sonogram machine, a life was saved. The scan picked up placenta previa in a young woman who was seven months pregnant, a complication that causes hundreds of maternal and fetal deaths each year in rural Africa.
Not this time. The ultrasound’s advance warning gave Isaac Boetang, MD, chief medical officer at Tepa District Hospital, the ability to plan ahead. Instead of facing a life-threatening hemorrhage at birth, which likely would tax his hospital’s limited resources, Dr. Boetang had time to prepare for a C-section and deliver a healthy baby to a healthy mother. In the seven months since the donated instrument arrived, Dr. Boetang estimates at least 30 more babies and mothers have been saved. Tepa’s sonogram machine was supplied by Doc to Dock, a non-profit organization working on a simple premise: Collect unused, surplus supplies from U.S. hospitals for distribution to needy hospitals in emerging countries.
Doc to Dock was born as the result of a call to charitable arms sounded by former President Bill Clinton in 2005 at his first summit meeting for the Clinton Global Initiative. He told the gathering his new foundation’s goal was “to help turn good intentions into good action and results.” Among the elite crowd of CEOs and celebrities in attendance that day was an unassuming New York cardiologist, Bruce Charash, MD, a clinical associate professor at New York University and former chief of cardiac care at Lenox Hospital in New York City. “It’s possible that year I was the only person who wasn’t a celebrity,” Dr. Charash says with a humble laugh. “They were asking us to do something to make an impact on the world, but until then my only developing world experience was spring break in 1975.”
As the former president challenged his guests to change the world, an idea Dr. Charash had long been mulling over crystallized. “I took it seriously and created a new charity,” he explains. “Send medical supplies to Africa.” When he was asked about a name, he thought slowly—and out loud. Doc, of course, his profession, to Dock, he says, as the image of a ship at a foreign port popped into his head. And that is how Dr. Charash made his own personal commitment to the Clinton Global Initiative. Doc to Dock was incorporated as a 501(c)(3) non-profit organization in February 2006. “We were the first charity formed under their umbrella,” he says. “and though we have no affiliation with them, they are an amazing support group.”

Good Deeds
The Greek poet Homer noted some 3,000 years ago, “the charity that is a trifle to us can be precious to others.” Dr. Charash knew American hospitals, doctors’ offices, pharmacies, and clinics, housed tons of unused medical supplies. In fact, the United Way estimates more than 7,000 tons of unused medical supplies and outdated equipment are discarded every day, either incinerated or carted off to landfills. At the same time in developing countries, thousands of patients are turned away from hospitals and medical centers due to a lack of medical supplies and equipment. Doc to Dock’s mission is to correct this imbalance.
Dr. Charash began conceiving a plan to somehow turn America’s trash—precious medical resources—into treasure, channeling the leftover sutures, scalpel blades, IV tubing, bandages, outdated equipment and machinery, old hospital beds and wheelchairs to hospitals in Africa.
Then Dr. Charash stumbled across a program, aptly named Merci, at The University of Virginia Medical Center, which collects its surplus supplies and used equipment for distribution to non-profit organizations, such as the Red Cross and Project Smile. The hospital invited Dr. Charash to take a look, and he was impressed by what he saw. Since its inception in 1992, Merci has collected more than 400 tons of medical materials worth more than $80 million.

Dr. Charash then set about soliciting donations from hospitals in his own backyard, New York City. It was a tall order. He and his small staff (one doctor, five staffers) needed to gather the surplus supplies and equipment, find a place to store it, recruit volunteers to inventory the items, and then enlist trucking and shipping companies to move the donations overseas. To find his supplies, he turned to hospitals, corporations, pharmaceutical companies, and even medical meetings. He found government and non-governmental organization partners willing to help him identify hospitals in need of and willing to receive the supplies. And, once identified, his team of volunteers began the process of matching the need with the goods collected, utilizing an online ordering system to supply the hospitals in Africa.
The Clinton name helped the cause enormously. In March, 2006, Dr. Charash reported to the Clinton Global Initiative (CGI) “the prestige of being a CGI commitment has opened many corporate doors that I do not necessarily believe would have opened without being identified with this effort.” Those open doors, coupled with Dr. Charash’s persistence, set Doc to Dock in motion.
It is proving a worthwhile voyage. One of the first partners to jump on board was Franklin Hospital in Valley Stream, N.Y., which is a part of the 305-bed North Shore Hospital System. Mary Hynes, a perioperative nurse educator, long had been discouraged by the waste of perfectly good supplies, some never even opened or routinely discarded from operating room packs. “I embraced it the nanosecond I heard it. We’d been wanting something for so long,” Hynes says. “For years, we had been throwing out stuff. It was almost criminal.”
Super Simple System
The Doc to Dock system is simple. Bright, electric-blue recycling barrels, emblazoned with the Doc to Dock logo, are stationed in the operating room and other easily accessible areas where hospital personnel can toss surplus supplies. Wrapped, sterile items, such as latex gloves, suture packs, scalpels, and bandages, routinely are overstocked in customized sterile packs as a bit of surgical “insurance.” Anything not used is discarded, still in a sterile wrap. “If a case is cancelled or something else happens,” Hynes says, “there is a sterile field with hundreds of dollars worth of supplies, which could not be reused. Everything has to be discarded and thrown away. You can’t reprocess it because there is too much liability involved.”
When Hynes switched jobs a few months ago, she transported her enthusiasm for Doc to Dock with her to the 371-bed Southside Hospital in Bay Shore, N.Y. Aided by a documentary DVD, which she showed her new colleagues, she instituted the Doc to Dock program at her new hospital. To date, the operating room and radiology department are donating excess supplies, and Hynes is planning to talk to the delivery room nurses soon.
“The barrels get filled right up,” Hynes explains. “This one hospital fills about six bins a week. Every two weeks, I call a trucker to pick them up.” Doc to Dock has arrangements with a dozen New York-area hospitals, thus far, including partnerships with the North Shore System and the Greater New York Hospital Association.
Make a Donation
The supplies may be donated, but it takes money to truck them, warehouse them and ship them to Africa. Doc to Dock relies on funding raised from corporations and philanthropic sources, plus in-kind donations from trucking and shipping companies who often move supplies for minimal or no cost.
In addition to supplies, Dr. Charash is looking for equipment. Many hospitals and clinics replace equipment, still in perfect working order, with newer models. Anesthesia machines, cryosurgery machines, mammogram machines, and cancer screening equipment, have found their way to African hospitals.
The sonogram traveled to Tepa District Hospital by way of a 40-foot shipping container, along with other supplies and equipment once destined for a U.S. scrap heap. The district serves about 100,000 villagers, and the hospital had been saving its nickels—one at a time—to purchase its own sonogram. The fundraising drive would have taken 10 years. One can only guess how many babies would have died in the meantime.
Through 2008, Doc to Dock had shipped nine containers to Ghana, Benin, Liberia, East Africa, Ethiopia, Kenya, and Uganda. Another container went to Haiti following a devastating hurricane. Four or five additional containers are just about ready to ship, Dr. Charash says. Each container costs about $25,000 per shipment. Dr. Charash estimates each shipment delivers approximately $500,000 worth of supplies and equipment.
Dr. Charash, who maintains privileges at Lenox and Mt. Sinai Medical Center in Manhattan, dreams big. He defines success by growing Doc to Dock to 100 containers per year within five years. He also wants to increase the number of hospitals donating goods, and the number of third-world hospitals receiving the supplies. Additionally, he wants to make the charity self-sustaining, as the need is always greater than the resources available.
“It’s a moral issue,” he says. “I have an obligation not to let it go to waste.” TH
Carol Berczuk is a freelance writer in New York CIty.
The day after the Tepa District Hospital in Ghana, on the west coast of Africa, received its first sonogram machine, a life was saved. The scan picked up placenta previa in a young woman who was seven months pregnant, a complication that causes hundreds of maternal and fetal deaths each year in rural Africa.
Not this time. The ultrasound’s advance warning gave Isaac Boetang, MD, chief medical officer at Tepa District Hospital, the ability to plan ahead. Instead of facing a life-threatening hemorrhage at birth, which likely would tax his hospital’s limited resources, Dr. Boetang had time to prepare for a C-section and deliver a healthy baby to a healthy mother. In the seven months since the donated instrument arrived, Dr. Boetang estimates at least 30 more babies and mothers have been saved. Tepa’s sonogram machine was supplied by Doc to Dock, a non-profit organization working on a simple premise: Collect unused, surplus supplies from U.S. hospitals for distribution to needy hospitals in emerging countries.
Doc to Dock was born as the result of a call to charitable arms sounded by former President Bill Clinton in 2005 at his first summit meeting for the Clinton Global Initiative. He told the gathering his new foundation’s goal was “to help turn good intentions into good action and results.” Among the elite crowd of CEOs and celebrities in attendance that day was an unassuming New York cardiologist, Bruce Charash, MD, a clinical associate professor at New York University and former chief of cardiac care at Lenox Hospital in New York City. “It’s possible that year I was the only person who wasn’t a celebrity,” Dr. Charash says with a humble laugh. “They were asking us to do something to make an impact on the world, but until then my only developing world experience was spring break in 1975.”
As the former president challenged his guests to change the world, an idea Dr. Charash had long been mulling over crystallized. “I took it seriously and created a new charity,” he explains. “Send medical supplies to Africa.” When he was asked about a name, he thought slowly—and out loud. Doc, of course, his profession, to Dock, he says, as the image of a ship at a foreign port popped into his head. And that is how Dr. Charash made his own personal commitment to the Clinton Global Initiative. Doc to Dock was incorporated as a 501(c)(3) non-profit organization in February 2006. “We were the first charity formed under their umbrella,” he says. “and though we have no affiliation with them, they are an amazing support group.”
Good Deeds
The Greek poet Homer noted some 3,000 years ago, “the charity that is a trifle to us can be precious to others.” Dr. Charash knew American hospitals, doctors’ offices, pharmacies, and clinics, housed tons of unused medical supplies. In fact, the United Way estimates more than 7,000 tons of unused medical supplies and outdated equipment are discarded every day, either incinerated or carted off to landfills. At the same time in developing countries, thousands of patients are turned away from hospitals and medical centers due to a lack of medical supplies and equipment. Doc to Dock’s mission is to correct this imbalance.
Dr. Charash began conceiving a plan to somehow turn America’s trash—precious medical resources—into treasure, channeling the leftover sutures, scalpel blades, IV tubing, bandages, outdated equipment and machinery, old hospital beds and wheelchairs to hospitals in Africa.
Then Dr. Charash stumbled across a program, aptly named Merci, at The University of Virginia Medical Center, which collects its surplus supplies and used equipment for distribution to non-profit organizations, such as the Red Cross and Project Smile. The hospital invited Dr. Charash to take a look, and he was impressed by what he saw. Since its inception in 1992, Merci has collected more than 400 tons of medical materials worth more than $80 million.
Dr. Charash then set about soliciting donations from hospitals in his own backyard, New York City. It was a tall order. He and his small staff (one doctor, five staffers) needed to gather the surplus supplies and equipment, find a place to store it, recruit volunteers to inventory the items, and then enlist trucking and shipping companies to move the donations overseas. To find his supplies, he turned to hospitals, corporations, pharmaceutical companies, and even medical meetings. He found government and non-governmental organization partners willing to help him identify hospitals in need of and willing to receive the supplies. And, once identified, his team of volunteers began the process of matching the need with the goods collected, utilizing an online ordering system to supply the hospitals in Africa.
The Clinton name helped the cause enormously. In March, 2006, Dr. Charash reported to the Clinton Global Initiative (CGI) “the prestige of being a CGI commitment has opened many corporate doors that I do not necessarily believe would have opened without being identified with this effort.” Those open doors, coupled with Dr. Charash’s persistence, set Doc to Dock in motion.
It is proving a worthwhile voyage. One of the first partners to jump on board was Franklin Hospital in Valley Stream, N.Y., which is a part of the 305-bed North Shore Hospital System. Mary Hynes, a perioperative nurse educator, long had been discouraged by the waste of perfectly good supplies, some never even opened or routinely discarded from operating room packs. “I embraced it the nanosecond I heard it. We’d been wanting something for so long,” Hynes says. “For years, we had been throwing out stuff. It was almost criminal.”
Super Simple System
The Doc to Dock system is simple. Bright, electric-blue recycling barrels, emblazoned with the Doc to Dock logo, are stationed in the operating room and other easily accessible areas where hospital personnel can toss surplus supplies. Wrapped, sterile items, such as latex gloves, suture packs, scalpels, and bandages, routinely are overstocked in customized sterile packs as a bit of surgical “insurance.” Anything not used is discarded, still in a sterile wrap. “If a case is cancelled or something else happens,” Hynes says, “there is a sterile field with hundreds of dollars worth of supplies, which could not be reused. Everything has to be discarded and thrown away. You can’t reprocess it because there is too much liability involved.”
When Hynes switched jobs a few months ago, she transported her enthusiasm for Doc to Dock with her to the 371-bed Southside Hospital in Bay Shore, N.Y. Aided by a documentary DVD, which she showed her new colleagues, she instituted the Doc to Dock program at her new hospital. To date, the operating room and radiology department are donating excess supplies, and Hynes is planning to talk to the delivery room nurses soon.
“The barrels get filled right up,” Hynes explains. “This one hospital fills about six bins a week. Every two weeks, I call a trucker to pick them up.” Doc to Dock has arrangements with a dozen New York-area hospitals, thus far, including partnerships with the North Shore System and the Greater New York Hospital Association.
Make a Donation
The supplies may be donated, but it takes money to truck them, warehouse them and ship them to Africa. Doc to Dock relies on funding raised from corporations and philanthropic sources, plus in-kind donations from trucking and shipping companies who often move supplies for minimal or no cost.
In addition to supplies, Dr. Charash is looking for equipment. Many hospitals and clinics replace equipment, still in perfect working order, with newer models. Anesthesia machines, cryosurgery machines, mammogram machines, and cancer screening equipment, have found their way to African hospitals.
The sonogram traveled to Tepa District Hospital by way of a 40-foot shipping container, along with other supplies and equipment once destined for a U.S. scrap heap. The district serves about 100,000 villagers, and the hospital had been saving its nickels—one at a time—to purchase its own sonogram. The fundraising drive would have taken 10 years. One can only guess how many babies would have died in the meantime.
Through 2008, Doc to Dock had shipped nine containers to Ghana, Benin, Liberia, East Africa, Ethiopia, Kenya, and Uganda. Another container went to Haiti following a devastating hurricane. Four or five additional containers are just about ready to ship, Dr. Charash says. Each container costs about $25,000 per shipment. Dr. Charash estimates each shipment delivers approximately $500,000 worth of supplies and equipment.
Dr. Charash, who maintains privileges at Lenox and Mt. Sinai Medical Center in Manhattan, dreams big. He defines success by growing Doc to Dock to 100 containers per year within five years. He also wants to increase the number of hospitals donating goods, and the number of third-world hospitals receiving the supplies. Additionally, he wants to make the charity self-sustaining, as the need is always greater than the resources available.
“It’s a moral issue,” he says. “I have an obligation not to let it go to waste.” TH
Carol Berczuk is a freelance writer in New York CIty.
The day after the Tepa District Hospital in Ghana, on the west coast of Africa, received its first sonogram machine, a life was saved. The scan picked up placenta previa in a young woman who was seven months pregnant, a complication that causes hundreds of maternal and fetal deaths each year in rural Africa.
Not this time. The ultrasound’s advance warning gave Isaac Boetang, MD, chief medical officer at Tepa District Hospital, the ability to plan ahead. Instead of facing a life-threatening hemorrhage at birth, which likely would tax his hospital’s limited resources, Dr. Boetang had time to prepare for a C-section and deliver a healthy baby to a healthy mother. In the seven months since the donated instrument arrived, Dr. Boetang estimates at least 30 more babies and mothers have been saved. Tepa’s sonogram machine was supplied by Doc to Dock, a non-profit organization working on a simple premise: Collect unused, surplus supplies from U.S. hospitals for distribution to needy hospitals in emerging countries.
Doc to Dock was born as the result of a call to charitable arms sounded by former President Bill Clinton in 2005 at his first summit meeting for the Clinton Global Initiative. He told the gathering his new foundation’s goal was “to help turn good intentions into good action and results.” Among the elite crowd of CEOs and celebrities in attendance that day was an unassuming New York cardiologist, Bruce Charash, MD, a clinical associate professor at New York University and former chief of cardiac care at Lenox Hospital in New York City. “It’s possible that year I was the only person who wasn’t a celebrity,” Dr. Charash says with a humble laugh. “They were asking us to do something to make an impact on the world, but until then my only developing world experience was spring break in 1975.”
As the former president challenged his guests to change the world, an idea Dr. Charash had long been mulling over crystallized. “I took it seriously and created a new charity,” he explains. “Send medical supplies to Africa.” When he was asked about a name, he thought slowly—and out loud. Doc, of course, his profession, to Dock, he says, as the image of a ship at a foreign port popped into his head. And that is how Dr. Charash made his own personal commitment to the Clinton Global Initiative. Doc to Dock was incorporated as a 501(c)(3) non-profit organization in February 2006. “We were the first charity formed under their umbrella,” he says. “and though we have no affiliation with them, they are an amazing support group.”
Good Deeds
The Greek poet Homer noted some 3,000 years ago, “the charity that is a trifle to us can be precious to others.” Dr. Charash knew American hospitals, doctors’ offices, pharmacies, and clinics, housed tons of unused medical supplies. In fact, the United Way estimates more than 7,000 tons of unused medical supplies and outdated equipment are discarded every day, either incinerated or carted off to landfills. At the same time in developing countries, thousands of patients are turned away from hospitals and medical centers due to a lack of medical supplies and equipment. Doc to Dock’s mission is to correct this imbalance.
Dr. Charash began conceiving a plan to somehow turn America’s trash—precious medical resources—into treasure, channeling the leftover sutures, scalpel blades, IV tubing, bandages, outdated equipment and machinery, old hospital beds and wheelchairs to hospitals in Africa.
Then Dr. Charash stumbled across a program, aptly named Merci, at The University of Virginia Medical Center, which collects its surplus supplies and used equipment for distribution to non-profit organizations, such as the Red Cross and Project Smile. The hospital invited Dr. Charash to take a look, and he was impressed by what he saw. Since its inception in 1992, Merci has collected more than 400 tons of medical materials worth more than $80 million.
Dr. Charash then set about soliciting donations from hospitals in his own backyard, New York City. It was a tall order. He and his small staff (one doctor, five staffers) needed to gather the surplus supplies and equipment, find a place to store it, recruit volunteers to inventory the items, and then enlist trucking and shipping companies to move the donations overseas. To find his supplies, he turned to hospitals, corporations, pharmaceutical companies, and even medical meetings. He found government and non-governmental organization partners willing to help him identify hospitals in need of and willing to receive the supplies. And, once identified, his team of volunteers began the process of matching the need with the goods collected, utilizing an online ordering system to supply the hospitals in Africa.
The Clinton name helped the cause enormously. In March, 2006, Dr. Charash reported to the Clinton Global Initiative (CGI) “the prestige of being a CGI commitment has opened many corporate doors that I do not necessarily believe would have opened without being identified with this effort.” Those open doors, coupled with Dr. Charash’s persistence, set Doc to Dock in motion.
It is proving a worthwhile voyage. One of the first partners to jump on board was Franklin Hospital in Valley Stream, N.Y., which is a part of the 305-bed North Shore Hospital System. Mary Hynes, a perioperative nurse educator, long had been discouraged by the waste of perfectly good supplies, some never even opened or routinely discarded from operating room packs. “I embraced it the nanosecond I heard it. We’d been wanting something for so long,” Hynes says. “For years, we had been throwing out stuff. It was almost criminal.”
Super Simple System
The Doc to Dock system is simple. Bright, electric-blue recycling barrels, emblazoned with the Doc to Dock logo, are stationed in the operating room and other easily accessible areas where hospital personnel can toss surplus supplies. Wrapped, sterile items, such as latex gloves, suture packs, scalpels, and bandages, routinely are overstocked in customized sterile packs as a bit of surgical “insurance.” Anything not used is discarded, still in a sterile wrap. “If a case is cancelled or something else happens,” Hynes says, “there is a sterile field with hundreds of dollars worth of supplies, which could not be reused. Everything has to be discarded and thrown away. You can’t reprocess it because there is too much liability involved.”
When Hynes switched jobs a few months ago, she transported her enthusiasm for Doc to Dock with her to the 371-bed Southside Hospital in Bay Shore, N.Y. Aided by a documentary DVD, which she showed her new colleagues, she instituted the Doc to Dock program at her new hospital. To date, the operating room and radiology department are donating excess supplies, and Hynes is planning to talk to the delivery room nurses soon.
“The barrels get filled right up,” Hynes explains. “This one hospital fills about six bins a week. Every two weeks, I call a trucker to pick them up.” Doc to Dock has arrangements with a dozen New York-area hospitals, thus far, including partnerships with the North Shore System and the Greater New York Hospital Association.
Make a Donation
The supplies may be donated, but it takes money to truck them, warehouse them and ship them to Africa. Doc to Dock relies on funding raised from corporations and philanthropic sources, plus in-kind donations from trucking and shipping companies who often move supplies for minimal or no cost.
In addition to supplies, Dr. Charash is looking for equipment. Many hospitals and clinics replace equipment, still in perfect working order, with newer models. Anesthesia machines, cryosurgery machines, mammogram machines, and cancer screening equipment, have found their way to African hospitals.
The sonogram traveled to Tepa District Hospital by way of a 40-foot shipping container, along with other supplies and equipment once destined for a U.S. scrap heap. The district serves about 100,000 villagers, and the hospital had been saving its nickels—one at a time—to purchase its own sonogram. The fundraising drive would have taken 10 years. One can only guess how many babies would have died in the meantime.
Through 2008, Doc to Dock had shipped nine containers to Ghana, Benin, Liberia, East Africa, Ethiopia, Kenya, and Uganda. Another container went to Haiti following a devastating hurricane. Four or five additional containers are just about ready to ship, Dr. Charash says. Each container costs about $25,000 per shipment. Dr. Charash estimates each shipment delivers approximately $500,000 worth of supplies and equipment.
Dr. Charash, who maintains privileges at Lenox and Mt. Sinai Medical Center in Manhattan, dreams big. He defines success by growing Doc to Dock to 100 containers per year within five years. He also wants to increase the number of hospitals donating goods, and the number of third-world hospitals receiving the supplies. Additionally, he wants to make the charity self-sustaining, as the need is always greater than the resources available.
“It’s a moral issue,” he says. “I have an obligation not to let it go to waste.” TH
Carol Berczuk is a freelance writer in New York CIty.
What is the proper duration of antibiotic treatment in adults hospitalized with community-acquired pneumonia?
Case
An 83-year-old male with hypertension, coronary artery disease, and obstructive sleep apnea presents with progressive shortness of breath, a productive cough, wheezing, and tachypnea. His blood pressure is 158/70 mm/Hg; temperature is 101.8; respirations are 26 breaths per minute; and oxygen saturation is 87% on room air. He has coarse breath sounds bilaterally, and decreased breath sounds over the right lower lung fields. His chest X-ray reveals a right lower lobe infiltrate. He is admitted to the hospital with a diagnosis of community-acquired pneumonia (CAP), and medical therapy is started. How should his antibiotic treatment be managed?
Overview
Community-acquired pneumonia is the most common infection-related cause of death in the U.S., and the eighth-leading cause of mortality overall.1 According to a 2006 survey, CAP results in more than 1.2 million hospital admissions annually, with an average length of stay of 5.1 days.2 Though less than 20% of CAP patients require hospitalization, cases necessitating admission contribute to more than 90% of the overall cost of pneumonia care.3
During the past several years, the availability of new antibiotics and the evolution of microbial resistance patterns have changed CAP treatment strategies. Furthermore, the development of prognostic scoring systems and increasing pressure to streamline resource utilization while improving quality of care have led to new treatment considerations, such as managing low-risk cases as outpatients.
More recently, attention has been directed to the optimal duration of antibiotic treatment, with a focus on shortening the duration of therapy. Historically, CAP treatment duration has been variable and not evidence-based. Shortening the course of antibiotics might limit antibiotic resistance, decrease costs, and improve patient adherence and tolerability.4 However, before defining the appropriate antibiotic duration for a patient hospitalized with CAP, other factors must be considered, such as the choice of empiric antibiotics, the patient’s initial response to treatment, severity of the disease, and presence of co-morbidities.
Review of the Data
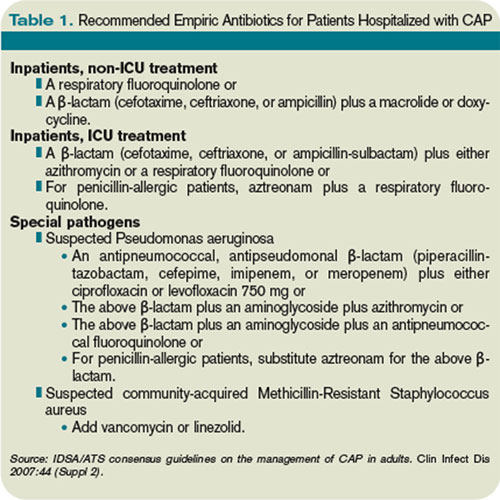
Antibiotic choice. The most widely referenced practice guidelines for the management of CAP patients were published in 2007 by representatives of the Infectious Diseases Society of America (IDSA) and the American Thoracic Society (ATS).5 Table 1 (above, right) summarizes the recommendations for empiric antibiotics for patients requiring inpatient treatment.
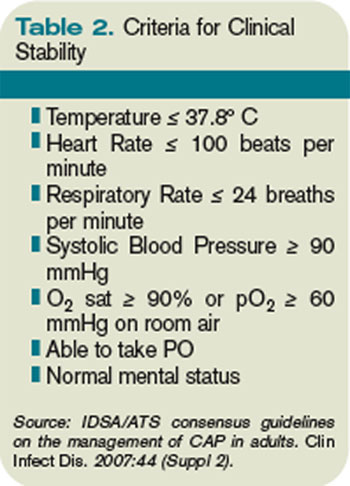
Time to clinical stability. A patient’s clinical response to empiric antibiotic therapy contributes heavily to the decision regarding treatment course and duration. The IDSA/ATS guidelines recommend patients be afebrile for 48 to 72 hours and have no more than one CAP-associated sign of clinical instability before discontinuation of therapy. Although studies have used different definitions of clinical stability, the consensus guidelines refer to six parameters, which are summarized in Table 2 (right).
With appropriate antibiotic therapy, most patients hospitalized with CAP achieve clinical stability in approximately three days.6,7 Providers should expect to see some improvement in vital signs within 48 to 72 hours of admission. Should a patient fail to demonstrate objective improvement during that time, providers should look for unusual pathogens, resistant organisms, nosocomial superinfections, or noninfectious conditions.5 Certain patients, such as those with multilobar pneumonia, associated pleural effusion, or higher pneumonia-severity index scores, also take longer to reach clinical stability.8
Switch to oral therapy. The ability to achieve clinical stability has important implications for hospital length of stay. Most patients hospitalized with CAP initially are treated with intravenous (IV) antibiotics and require transition to oral therapy in anticipation of discharge. Several studies have found there is no advantage to continuing IV medication once a patient is deemed clinically stable and is able to tolerate oral medication.9,10 There are no specific guidelines regarding choice of oral antibiotics, but it is common practice, supported by the IDSA/ATS recommendations, to use the same agent as the IV antibiotic or a medication in the same drug class. For patients started on β-lactam and macrolide combination therapy, it usually is appropriate to switch to a macrolide alone.5 In cases in which a pathogen has been identified, antibiotic selection should be based on the susceptibility profile.
Once patients are switched to oral antibiotics, it is not necessary for them to remain in the hospital for further observation, provided they have no other active medical problems or social needs. A retrospective analysis of 39,232 patients hospitalized with CAP compared those who were observed overnight after switching to oral antibiotics with those who were not and found no difference in 14-day readmission rate or 30-day mortality rate.11 These findings, in conjunction with the strategy of an early switch to oral therapy, suggest hospital length of stay may be safely reduced for many patients with uncomplicated CAP.
Duration of therapy. After a patient becomes clinically stable and a decision is made to switch to oral medication and a plan for hospital discharge, the question becomes how long to continue the course of antibiotics. Historically, clinical practice has extended treatment for up to two weeks, despite lack of evidence for this duration of therapy. The IDSA/ATS guidelines offer some general recommendations, noting patients should be treated for a minimum of five days, in addition to being afebrile for 48 to 72 hours and meet other criteria for clinical stability.5
Li and colleagues conducted a systematic review evaluating 15 randomized controlled trials comparing short-course (less than seven days) with extended (more than seven days) monotherapy for CAP in adults.4 Overall, the authors found no difference in the risk of treatment failure between short-course and extended-course antibiotic therapy, and they found no difference in bacteriologic eradication or mortality. It is important to note the studies included in this analysis enrolled patients with mild to moderate CAP, including those treated as outpatients, which limits the ability to extrapolate to exclusively inpatient populations and more severely ill patients.
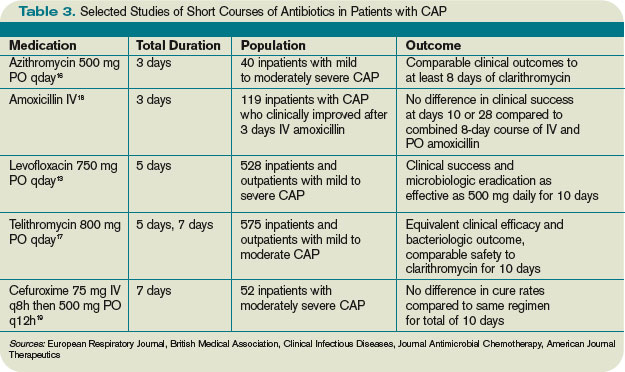
Another meta-analysis, published shortly thereafter, examined randomized controlled trials in outpatients and inpatients not requiring intensive care. It compared different durations of treatment with the same agent in the same dosage. The authors similarly found no difference in effectiveness or safety of short (less than seven days) versus longer (at least two additional days of therapy) courses.12 Table 3 (above) reviews selected trials of short courses of antibiotics, which have been studied in inpatient populations.
The trials summarized in these meta-analyses examined monotherapy with levofloxacin for five days; gemifloxacin for seven days, azithromycin for three to five days; ceftriaxone for five days; cefuroxime for seven days; amoxicillin for three days; or telithromycin for five to seven days. The variety of antibiotics in these studies contrasts the IDSA/ATS guidelines, which recommend only fluoroquinolones as monotherapy for inpatient CAP.
One important randomized, double-blind study of fluoroquinolones compared a five-day course of levofloxacin 750 mg daily, with a 10-day course of levofloxacin, 500 mg daily, in 528 patients with mild to severe CAP.13 The authors found no difference in clinical success or microbiologic eradication between the two groups, concluding high-dose levofloxacin for five days is an effective and well-tolerated alternative to a longer course of a lower dose, likely related to the drug’s concentration-dependent properties.

Azithromycin also offers potential for short courses of therapy, as pulmonary concentrations of azithromycin remain elevated for as many as five days following a single oral dose.14 Several small studies have demonstrated the safety, efficacy, and cost-effectiveness of three to five days of azithromycin, as summarized in a meta-analysis by Contopoulos-Ioannidis and colleagues.15 Most of these trials, however, were limited to outpatients or inpatients with mild disease or confirmed atypical pneumonia. One randomized trial of 40 inpatients with mild to moderately severe CAP found comparable clinical outcomes with a three-day course of oral azithromycin 500 mg daily versus clarithromycin for at least eight days.16 Larger studies in more severely ill patients must be completed before routinely recommending this approach in hospitalized patients. Furthermore, due to the rising prevalence of macrolide resistance, empiric therapy with a macrolide alone can only be used for the treatment of carefully selected hospitalized patients with nonsevere diseases and without risk factors for drug-resistant Streptococcus pneumoniae.5
Telithromycin is a ketolide antibiotic, which has been studied in mild to moderate CAP, including multidrug-resistant strains of S. pneumoniae, in courses of five to seven days.17 However, severe adverse reactions, including hepatotoxicity, have been reported. At the time of the 2007 guidelines, the IDSA/ATS committee waited for additional safety data before making any recommendations on its use.
One additional study of note was a trial of amoxicillin in adult inpatients with mild to moderately severe CAP.18 One hundred twenty-one patients who clinically improved (based on a composite score of pulmonary symptoms and general improvement) following three days of IV amoxicillin were randomized to oral amoxicillin for an additional five days or given a placebo. At days 10 and 28, there was no difference in clinical success between the two groups. The authors concluded that a total of three days of treatment was not inferior to eight days in patients who substantially improved after the first 72 hours of empiric treatment. This trial was conducted in the Netherlands, where amoxicillin is the preferred empiric antibiotic for CAP and patterns of antimicrobial resistance differ greatly from those found in the U.S.
Other considerations. While some evidence supports shorter courses of antibiotics, many of the existing studies are limited by their inclusion of outpatients, adults with mild to moderate CAP, or small sample size. Hence, clinical judgment continues to play an important role in determining the appropriate duration of therapy. Factors such as pre-existing co-morbidities, severity of illness, and occurrence of complications should be considered. Data is limited on the appropriate duration of antibiotics in CAP patients requiring intensive care. It also is important to note the IDSA/ATS recommendations and most of the studies reviewed exclude patients with human immunodeficiency virus (HIV), and it is unknown whether these shorter courses of antibiotics are appropriate in the HIV population.
Lastly, the IDSA/ATS guidelines note longer durations of treatment may be required if the initial therapy was not active against the identified pathogen, or in cases complicated by extrapulmonary infections, such as endocarditis or meningitis.
Back to the Case
Our patient with moderately severe CAP was hospitalized based on his age and hypoxia. He was immediately treated with supplemental oxygen by nasal cannula, IV fluids, and a dose of IV levofloxacin 750 mg. Within 48 hours he met criteria for clinical stability, including defervescence, a decline in his respiratory rate to 19 breaths per minute, and improvement in oxygen saturation to 95% on room air. At this point, he was changed from IV to oral antibiotics. He continued on levofloxacin 750 mg daily and later that day was discharged home in good condition to complete a five-day course.
Bottom Line
For hospitalized adults with mild to moderately severe CAP, five to seven days of treatment, depending on the antibiotic selected, appears to be effective in most cases. Patients should be afebrile for 48 to 72 hours and demonstrate signs of clinical stability before therapy is discontinued. TH
Kelly Cunningham, MD, and Shelley Ellis, MD, MPH, are members of the Section of Hospital Medicine at Vanderbilt University in Nashville, Tenn. Sunil Kripalani, MD, MSc, serves as the section chief.
References
1. Kung HC, Hoyert DL, Xu J, Murphy SL. Deaths: final data for 2005. Natl Vital Stat Rep. 2008;56.
2. DeFrances CJ, Lucas CA, Buie VC, Golosinskiy A. 2006 National Hospital Discharge Survey. Natl Health Stat Report. 2008;5.
3. Niederman MS. Recent advances in community-acquired pneumonia: inpatient and outpatient. Chest. 2007;131:1205-1215.
4. Li JZ, Winston LG, Moore DH, Bent S. Efficacy of short-course antibiotic regimens for community-acquired pneumonia: a meta-analysis. Am J Med. 2007;120:783-790.
5. Mandell LA, Wunderink RG, Anzueto A et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis. 2007;44(Suppl 2):S27-72.
6. Ramirez JA, Bordon J. Early switch from intravenous to oral antibiotics in hospitalized patients with bacteremic community-acquired Streptococcus pneumoniae pneumonia. Arch Intern Med. 2001;161:848-850.
7. Halm EA, Fine MJ, Marrie TJ et al. Time to clinical stability in patients hospitalized with community-acquired pneumonia: implications for practice guidelines. JAMA. 1998;279:1452-1457.
8. Menendez R, Torres A, Rodriguez de Castro F et al. Reaching stability in community-acquired pneumonia: the effects of the severity of disease, treatment, and the characteristics of patients. Clin Infect Dis. 2004;39:1783-1790.
9. Siegal RE, Halpern NA, Almenoff PL et al. A prospective randomised study of inpatient IV antibiotics for community-acquired pneumonia: the optimal duration of therapy. Chest. 1996;110:965-971.
10. Oosterheert JJ, Bonten MJ, Schneider MM et al. Effectiveness of early switch from intravenous to oral antibiotics in severe community acquired pneumonia: multicentre randomized trial. BMJ. 2006;333:1193-1197.
11. Nathan RV, Rhew DC, Murray C et al. In-hospital observation after antibiotic switch in pneumonia: a national evaluation. Am J Med. 2006;119:512-518.
12. Dimopoulos G, Matthaiou DK, Karageorgopoulos DE, et al. Short- versus long-course antibacterial therapy for community-acquired pneumonia: a meta-analysis. Drugs. 2008;68:1841-1854.
13. Dunbar LM, Wunderink RG, Habib MP et al. High-dose, short-course levofloxacin for community-acquired pneumonia: a new treatment paradigm. Clin Infect Dis. 2003;37:752-760.
14. Morris DL, De Souza A, Jones JA, Morgan WE. High and prolonged pulmonary tissue concentrations of azithromycin following a single oral dose. Eur J Clin Microbiol Infect Dis. 1991;10:859-861.
15. Contopoulos-Ioannidis DG, Ioannidis JPA, Chew P, Lau J. Meta-analysis of randomized controlled trials on the comparative efficacy and safety of azithromycin against other antibiotics for lower respiratory tract infections. J Antimicrob Chemother. 2001;48:691-703.
16. Rizzato G, Montemurro L, Fraioli P et al. Efficacy of a three-day course of azithromycin in moderately severe community-acquired pneumonia. Eur Respir J. 1995;8:398-402.
17. Tellier G, Niederman MS, Nusrat R et al. Clinical and bacteriological efficacy and safety of 5- and 7-day regimens of telithromycin once daily compared with a 10-day regimen of clarithromycin twice daily in patients with mild to moderate community-acquired pneumonia. J Antimicrob Chemother. 2004;54:515.
18. El Moussaoui R, de Borgie CA, van den Broek P et al. Effectiveness of discontinuing antibiotic treatment after three days versus eight days in mild to moderate-severe community acquired pneumonia: randomised, double blind study. BMJ. 2006;332:1355-1361.
19. Siegel RE, Alicea M, Lee A, Blaiklock R. Comparison of 7 versus 10 days of antibiotic therapy for hospitalized patients with uncomplicated community-acquired pneumonia: a prospective, randomized double-blind study. Am J Ther. 1999;6:217-222.
Case
An 83-year-old male with hypertension, coronary artery disease, and obstructive sleep apnea presents with progressive shortness of breath, a productive cough, wheezing, and tachypnea. His blood pressure is 158/70 mm/Hg; temperature is 101.8; respirations are 26 breaths per minute; and oxygen saturation is 87% on room air. He has coarse breath sounds bilaterally, and decreased breath sounds over the right lower lung fields. His chest X-ray reveals a right lower lobe infiltrate. He is admitted to the hospital with a diagnosis of community-acquired pneumonia (CAP), and medical therapy is started. How should his antibiotic treatment be managed?
Overview
Community-acquired pneumonia is the most common infection-related cause of death in the U.S., and the eighth-leading cause of mortality overall.1 According to a 2006 survey, CAP results in more than 1.2 million hospital admissions annually, with an average length of stay of 5.1 days.2 Though less than 20% of CAP patients require hospitalization, cases necessitating admission contribute to more than 90% of the overall cost of pneumonia care.3
During the past several years, the availability of new antibiotics and the evolution of microbial resistance patterns have changed CAP treatment strategies. Furthermore, the development of prognostic scoring systems and increasing pressure to streamline resource utilization while improving quality of care have led to new treatment considerations, such as managing low-risk cases as outpatients.
More recently, attention has been directed to the optimal duration of antibiotic treatment, with a focus on shortening the duration of therapy. Historically, CAP treatment duration has been variable and not evidence-based. Shortening the course of antibiotics might limit antibiotic resistance, decrease costs, and improve patient adherence and tolerability.4 However, before defining the appropriate antibiotic duration for a patient hospitalized with CAP, other factors must be considered, such as the choice of empiric antibiotics, the patient’s initial response to treatment, severity of the disease, and presence of co-morbidities.
Review of the Data
Antibiotic choice. The most widely referenced practice guidelines for the management of CAP patients were published in 2007 by representatives of the Infectious Diseases Society of America (IDSA) and the American Thoracic Society (ATS).5 Table 1 (above, right) summarizes the recommendations for empiric antibiotics for patients requiring inpatient treatment.
Time to clinical stability. A patient’s clinical response to empiric antibiotic therapy contributes heavily to the decision regarding treatment course and duration. The IDSA/ATS guidelines recommend patients be afebrile for 48 to 72 hours and have no more than one CAP-associated sign of clinical instability before discontinuation of therapy. Although studies have used different definitions of clinical stability, the consensus guidelines refer to six parameters, which are summarized in Table 2 (right).
With appropriate antibiotic therapy, most patients hospitalized with CAP achieve clinical stability in approximately three days.6,7 Providers should expect to see some improvement in vital signs within 48 to 72 hours of admission. Should a patient fail to demonstrate objective improvement during that time, providers should look for unusual pathogens, resistant organisms, nosocomial superinfections, or noninfectious conditions.5 Certain patients, such as those with multilobar pneumonia, associated pleural effusion, or higher pneumonia-severity index scores, also take longer to reach clinical stability.8
Switch to oral therapy. The ability to achieve clinical stability has important implications for hospital length of stay. Most patients hospitalized with CAP initially are treated with intravenous (IV) antibiotics and require transition to oral therapy in anticipation of discharge. Several studies have found there is no advantage to continuing IV medication once a patient is deemed clinically stable and is able to tolerate oral medication.9,10 There are no specific guidelines regarding choice of oral antibiotics, but it is common practice, supported by the IDSA/ATS recommendations, to use the same agent as the IV antibiotic or a medication in the same drug class. For patients started on β-lactam and macrolide combination therapy, it usually is appropriate to switch to a macrolide alone.5 In cases in which a pathogen has been identified, antibiotic selection should be based on the susceptibility profile.
Once patients are switched to oral antibiotics, it is not necessary for them to remain in the hospital for further observation, provided they have no other active medical problems or social needs. A retrospective analysis of 39,232 patients hospitalized with CAP compared those who were observed overnight after switching to oral antibiotics with those who were not and found no difference in 14-day readmission rate or 30-day mortality rate.11 These findings, in conjunction with the strategy of an early switch to oral therapy, suggest hospital length of stay may be safely reduced for many patients with uncomplicated CAP.
Duration of therapy. After a patient becomes clinically stable and a decision is made to switch to oral medication and a plan for hospital discharge, the question becomes how long to continue the course of antibiotics. Historically, clinical practice has extended treatment for up to two weeks, despite lack of evidence for this duration of therapy. The IDSA/ATS guidelines offer some general recommendations, noting patients should be treated for a minimum of five days, in addition to being afebrile for 48 to 72 hours and meet other criteria for clinical stability.5
Li and colleagues conducted a systematic review evaluating 15 randomized controlled trials comparing short-course (less than seven days) with extended (more than seven days) monotherapy for CAP in adults.4 Overall, the authors found no difference in the risk of treatment failure between short-course and extended-course antibiotic therapy, and they found no difference in bacteriologic eradication or mortality. It is important to note the studies included in this analysis enrolled patients with mild to moderate CAP, including those treated as outpatients, which limits the ability to extrapolate to exclusively inpatient populations and more severely ill patients.
Another meta-analysis, published shortly thereafter, examined randomized controlled trials in outpatients and inpatients not requiring intensive care. It compared different durations of treatment with the same agent in the same dosage. The authors similarly found no difference in effectiveness or safety of short (less than seven days) versus longer (at least two additional days of therapy) courses.12 Table 3 (above) reviews selected trials of short courses of antibiotics, which have been studied in inpatient populations.
The trials summarized in these meta-analyses examined monotherapy with levofloxacin for five days; gemifloxacin for seven days, azithromycin for three to five days; ceftriaxone for five days; cefuroxime for seven days; amoxicillin for three days; or telithromycin for five to seven days. The variety of antibiotics in these studies contrasts the IDSA/ATS guidelines, which recommend only fluoroquinolones as monotherapy for inpatient CAP.
One important randomized, double-blind study of fluoroquinolones compared a five-day course of levofloxacin 750 mg daily, with a 10-day course of levofloxacin, 500 mg daily, in 528 patients with mild to severe CAP.13 The authors found no difference in clinical success or microbiologic eradication between the two groups, concluding high-dose levofloxacin for five days is an effective and well-tolerated alternative to a longer course of a lower dose, likely related to the drug’s concentration-dependent properties.
Azithromycin also offers potential for short courses of therapy, as pulmonary concentrations of azithromycin remain elevated for as many as five days following a single oral dose.14 Several small studies have demonstrated the safety, efficacy, and cost-effectiveness of three to five days of azithromycin, as summarized in a meta-analysis by Contopoulos-Ioannidis and colleagues.15 Most of these trials, however, were limited to outpatients or inpatients with mild disease or confirmed atypical pneumonia. One randomized trial of 40 inpatients with mild to moderately severe CAP found comparable clinical outcomes with a three-day course of oral azithromycin 500 mg daily versus clarithromycin for at least eight days.16 Larger studies in more severely ill patients must be completed before routinely recommending this approach in hospitalized patients. Furthermore, due to the rising prevalence of macrolide resistance, empiric therapy with a macrolide alone can only be used for the treatment of carefully selected hospitalized patients with nonsevere diseases and without risk factors for drug-resistant Streptococcus pneumoniae.5
Telithromycin is a ketolide antibiotic, which has been studied in mild to moderate CAP, including multidrug-resistant strains of S. pneumoniae, in courses of five to seven days.17 However, severe adverse reactions, including hepatotoxicity, have been reported. At the time of the 2007 guidelines, the IDSA/ATS committee waited for additional safety data before making any recommendations on its use.
One additional study of note was a trial of amoxicillin in adult inpatients with mild to moderately severe CAP.18 One hundred twenty-one patients who clinically improved (based on a composite score of pulmonary symptoms and general improvement) following three days of IV amoxicillin were randomized to oral amoxicillin for an additional five days or given a placebo. At days 10 and 28, there was no difference in clinical success between the two groups. The authors concluded that a total of three days of treatment was not inferior to eight days in patients who substantially improved after the first 72 hours of empiric treatment. This trial was conducted in the Netherlands, where amoxicillin is the preferred empiric antibiotic for CAP and patterns of antimicrobial resistance differ greatly from those found in the U.S.
Other considerations. While some evidence supports shorter courses of antibiotics, many of the existing studies are limited by their inclusion of outpatients, adults with mild to moderate CAP, or small sample size. Hence, clinical judgment continues to play an important role in determining the appropriate duration of therapy. Factors such as pre-existing co-morbidities, severity of illness, and occurrence of complications should be considered. Data is limited on the appropriate duration of antibiotics in CAP patients requiring intensive care. It also is important to note the IDSA/ATS recommendations and most of the studies reviewed exclude patients with human immunodeficiency virus (HIV), and it is unknown whether these shorter courses of antibiotics are appropriate in the HIV population.
Lastly, the IDSA/ATS guidelines note longer durations of treatment may be required if the initial therapy was not active against the identified pathogen, or in cases complicated by extrapulmonary infections, such as endocarditis or meningitis.
Back to the Case
Our patient with moderately severe CAP was hospitalized based on his age and hypoxia. He was immediately treated with supplemental oxygen by nasal cannula, IV fluids, and a dose of IV levofloxacin 750 mg. Within 48 hours he met criteria for clinical stability, including defervescence, a decline in his respiratory rate to 19 breaths per minute, and improvement in oxygen saturation to 95% on room air. At this point, he was changed from IV to oral antibiotics. He continued on levofloxacin 750 mg daily and later that day was discharged home in good condition to complete a five-day course.
Bottom Line
For hospitalized adults with mild to moderately severe CAP, five to seven days of treatment, depending on the antibiotic selected, appears to be effective in most cases. Patients should be afebrile for 48 to 72 hours and demonstrate signs of clinical stability before therapy is discontinued. TH
Kelly Cunningham, MD, and Shelley Ellis, MD, MPH, are members of the Section of Hospital Medicine at Vanderbilt University in Nashville, Tenn. Sunil Kripalani, MD, MSc, serves as the section chief.
References
1. Kung HC, Hoyert DL, Xu J, Murphy SL. Deaths: final data for 2005. Natl Vital Stat Rep. 2008;56.
2. DeFrances CJ, Lucas CA, Buie VC, Golosinskiy A. 2006 National Hospital Discharge Survey. Natl Health Stat Report. 2008;5.
3. Niederman MS. Recent advances in community-acquired pneumonia: inpatient and outpatient. Chest. 2007;131:1205-1215.
4. Li JZ, Winston LG, Moore DH, Bent S. Efficacy of short-course antibiotic regimens for community-acquired pneumonia: a meta-analysis. Am J Med. 2007;120:783-790.
5. Mandell LA, Wunderink RG, Anzueto A et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis. 2007;44(Suppl 2):S27-72.
6. Ramirez JA, Bordon J. Early switch from intravenous to oral antibiotics in hospitalized patients with bacteremic community-acquired Streptococcus pneumoniae pneumonia. Arch Intern Med. 2001;161:848-850.
7. Halm EA, Fine MJ, Marrie TJ et al. Time to clinical stability in patients hospitalized with community-acquired pneumonia: implications for practice guidelines. JAMA. 1998;279:1452-1457.
8. Menendez R, Torres A, Rodriguez de Castro F et al. Reaching stability in community-acquired pneumonia: the effects of the severity of disease, treatment, and the characteristics of patients. Clin Infect Dis. 2004;39:1783-1790.
9. Siegal RE, Halpern NA, Almenoff PL et al. A prospective randomised study of inpatient IV antibiotics for community-acquired pneumonia: the optimal duration of therapy. Chest. 1996;110:965-971.
10. Oosterheert JJ, Bonten MJ, Schneider MM et al. Effectiveness of early switch from intravenous to oral antibiotics in severe community acquired pneumonia: multicentre randomized trial. BMJ. 2006;333:1193-1197.
11. Nathan RV, Rhew DC, Murray C et al. In-hospital observation after antibiotic switch in pneumonia: a national evaluation. Am J Med. 2006;119:512-518.
12. Dimopoulos G, Matthaiou DK, Karageorgopoulos DE, et al. Short- versus long-course antibacterial therapy for community-acquired pneumonia: a meta-analysis. Drugs. 2008;68:1841-1854.
13. Dunbar LM, Wunderink RG, Habib MP et al. High-dose, short-course levofloxacin for community-acquired pneumonia: a new treatment paradigm. Clin Infect Dis. 2003;37:752-760.
14. Morris DL, De Souza A, Jones JA, Morgan WE. High and prolonged pulmonary tissue concentrations of azithromycin following a single oral dose. Eur J Clin Microbiol Infect Dis. 1991;10:859-861.
15. Contopoulos-Ioannidis DG, Ioannidis JPA, Chew P, Lau J. Meta-analysis of randomized controlled trials on the comparative efficacy and safety of azithromycin against other antibiotics for lower respiratory tract infections. J Antimicrob Chemother. 2001;48:691-703.
16. Rizzato G, Montemurro L, Fraioli P et al. Efficacy of a three-day course of azithromycin in moderately severe community-acquired pneumonia. Eur Respir J. 1995;8:398-402.
17. Tellier G, Niederman MS, Nusrat R et al. Clinical and bacteriological efficacy and safety of 5- and 7-day regimens of telithromycin once daily compared with a 10-day regimen of clarithromycin twice daily in patients with mild to moderate community-acquired pneumonia. J Antimicrob Chemother. 2004;54:515.
18. El Moussaoui R, de Borgie CA, van den Broek P et al. Effectiveness of discontinuing antibiotic treatment after three days versus eight days in mild to moderate-severe community acquired pneumonia: randomised, double blind study. BMJ. 2006;332:1355-1361.
19. Siegel RE, Alicea M, Lee A, Blaiklock R. Comparison of 7 versus 10 days of antibiotic therapy for hospitalized patients with uncomplicated community-acquired pneumonia: a prospective, randomized double-blind study. Am J Ther. 1999;6:217-222.
Case
An 83-year-old male with hypertension, coronary artery disease, and obstructive sleep apnea presents with progressive shortness of breath, a productive cough, wheezing, and tachypnea. His blood pressure is 158/70 mm/Hg; temperature is 101.8; respirations are 26 breaths per minute; and oxygen saturation is 87% on room air. He has coarse breath sounds bilaterally, and decreased breath sounds over the right lower lung fields. His chest X-ray reveals a right lower lobe infiltrate. He is admitted to the hospital with a diagnosis of community-acquired pneumonia (CAP), and medical therapy is started. How should his antibiotic treatment be managed?
Overview
Community-acquired pneumonia is the most common infection-related cause of death in the U.S., and the eighth-leading cause of mortality overall.1 According to a 2006 survey, CAP results in more than 1.2 million hospital admissions annually, with an average length of stay of 5.1 days.2 Though less than 20% of CAP patients require hospitalization, cases necessitating admission contribute to more than 90% of the overall cost of pneumonia care.3
During the past several years, the availability of new antibiotics and the evolution of microbial resistance patterns have changed CAP treatment strategies. Furthermore, the development of prognostic scoring systems and increasing pressure to streamline resource utilization while improving quality of care have led to new treatment considerations, such as managing low-risk cases as outpatients.
More recently, attention has been directed to the optimal duration of antibiotic treatment, with a focus on shortening the duration of therapy. Historically, CAP treatment duration has been variable and not evidence-based. Shortening the course of antibiotics might limit antibiotic resistance, decrease costs, and improve patient adherence and tolerability.4 However, before defining the appropriate antibiotic duration for a patient hospitalized with CAP, other factors must be considered, such as the choice of empiric antibiotics, the patient’s initial response to treatment, severity of the disease, and presence of co-morbidities.
Review of the Data
Antibiotic choice. The most widely referenced practice guidelines for the management of CAP patients were published in 2007 by representatives of the Infectious Diseases Society of America (IDSA) and the American Thoracic Society (ATS).5 Table 1 (above, right) summarizes the recommendations for empiric antibiotics for patients requiring inpatient treatment.
Time to clinical stability. A patient’s clinical response to empiric antibiotic therapy contributes heavily to the decision regarding treatment course and duration. The IDSA/ATS guidelines recommend patients be afebrile for 48 to 72 hours and have no more than one CAP-associated sign of clinical instability before discontinuation of therapy. Although studies have used different definitions of clinical stability, the consensus guidelines refer to six parameters, which are summarized in Table 2 (right).
With appropriate antibiotic therapy, most patients hospitalized with CAP achieve clinical stability in approximately three days.6,7 Providers should expect to see some improvement in vital signs within 48 to 72 hours of admission. Should a patient fail to demonstrate objective improvement during that time, providers should look for unusual pathogens, resistant organisms, nosocomial superinfections, or noninfectious conditions.5 Certain patients, such as those with multilobar pneumonia, associated pleural effusion, or higher pneumonia-severity index scores, also take longer to reach clinical stability.8
Switch to oral therapy. The ability to achieve clinical stability has important implications for hospital length of stay. Most patients hospitalized with CAP initially are treated with intravenous (IV) antibiotics and require transition to oral therapy in anticipation of discharge. Several studies have found there is no advantage to continuing IV medication once a patient is deemed clinically stable and is able to tolerate oral medication.9,10 There are no specific guidelines regarding choice of oral antibiotics, but it is common practice, supported by the IDSA/ATS recommendations, to use the same agent as the IV antibiotic or a medication in the same drug class. For patients started on β-lactam and macrolide combination therapy, it usually is appropriate to switch to a macrolide alone.5 In cases in which a pathogen has been identified, antibiotic selection should be based on the susceptibility profile.
Once patients are switched to oral antibiotics, it is not necessary for them to remain in the hospital for further observation, provided they have no other active medical problems or social needs. A retrospective analysis of 39,232 patients hospitalized with CAP compared those who were observed overnight after switching to oral antibiotics with those who were not and found no difference in 14-day readmission rate or 30-day mortality rate.11 These findings, in conjunction with the strategy of an early switch to oral therapy, suggest hospital length of stay may be safely reduced for many patients with uncomplicated CAP.
Duration of therapy. After a patient becomes clinically stable and a decision is made to switch to oral medication and a plan for hospital discharge, the question becomes how long to continue the course of antibiotics. Historically, clinical practice has extended treatment for up to two weeks, despite lack of evidence for this duration of therapy. The IDSA/ATS guidelines offer some general recommendations, noting patients should be treated for a minimum of five days, in addition to being afebrile for 48 to 72 hours and meet other criteria for clinical stability.5
Li and colleagues conducted a systematic review evaluating 15 randomized controlled trials comparing short-course (less than seven days) with extended (more than seven days) monotherapy for CAP in adults.4 Overall, the authors found no difference in the risk of treatment failure between short-course and extended-course antibiotic therapy, and they found no difference in bacteriologic eradication or mortality. It is important to note the studies included in this analysis enrolled patients with mild to moderate CAP, including those treated as outpatients, which limits the ability to extrapolate to exclusively inpatient populations and more severely ill patients.
Another meta-analysis, published shortly thereafter, examined randomized controlled trials in outpatients and inpatients not requiring intensive care. It compared different durations of treatment with the same agent in the same dosage. The authors similarly found no difference in effectiveness or safety of short (less than seven days) versus longer (at least two additional days of therapy) courses.12 Table 3 (above) reviews selected trials of short courses of antibiotics, which have been studied in inpatient populations.
The trials summarized in these meta-analyses examined monotherapy with levofloxacin for five days; gemifloxacin for seven days, azithromycin for three to five days; ceftriaxone for five days; cefuroxime for seven days; amoxicillin for three days; or telithromycin for five to seven days. The variety of antibiotics in these studies contrasts the IDSA/ATS guidelines, which recommend only fluoroquinolones as monotherapy for inpatient CAP.
One important randomized, double-blind study of fluoroquinolones compared a five-day course of levofloxacin 750 mg daily, with a 10-day course of levofloxacin, 500 mg daily, in 528 patients with mild to severe CAP.13 The authors found no difference in clinical success or microbiologic eradication between the two groups, concluding high-dose levofloxacin for five days is an effective and well-tolerated alternative to a longer course of a lower dose, likely related to the drug’s concentration-dependent properties.
Azithromycin also offers potential for short courses of therapy, as pulmonary concentrations of azithromycin remain elevated for as many as five days following a single oral dose.14 Several small studies have demonstrated the safety, efficacy, and cost-effectiveness of three to five days of azithromycin, as summarized in a meta-analysis by Contopoulos-Ioannidis and colleagues.15 Most of these trials, however, were limited to outpatients or inpatients with mild disease or confirmed atypical pneumonia. One randomized trial of 40 inpatients with mild to moderately severe CAP found comparable clinical outcomes with a three-day course of oral azithromycin 500 mg daily versus clarithromycin for at least eight days.16 Larger studies in more severely ill patients must be completed before routinely recommending this approach in hospitalized patients. Furthermore, due to the rising prevalence of macrolide resistance, empiric therapy with a macrolide alone can only be used for the treatment of carefully selected hospitalized patients with nonsevere diseases and without risk factors for drug-resistant Streptococcus pneumoniae.5
Telithromycin is a ketolide antibiotic, which has been studied in mild to moderate CAP, including multidrug-resistant strains of S. pneumoniae, in courses of five to seven days.17 However, severe adverse reactions, including hepatotoxicity, have been reported. At the time of the 2007 guidelines, the IDSA/ATS committee waited for additional safety data before making any recommendations on its use.
One additional study of note was a trial of amoxicillin in adult inpatients with mild to moderately severe CAP.18 One hundred twenty-one patients who clinically improved (based on a composite score of pulmonary symptoms and general improvement) following three days of IV amoxicillin were randomized to oral amoxicillin for an additional five days or given a placebo. At days 10 and 28, there was no difference in clinical success between the two groups. The authors concluded that a total of three days of treatment was not inferior to eight days in patients who substantially improved after the first 72 hours of empiric treatment. This trial was conducted in the Netherlands, where amoxicillin is the preferred empiric antibiotic for CAP and patterns of antimicrobial resistance differ greatly from those found in the U.S.
Other considerations. While some evidence supports shorter courses of antibiotics, many of the existing studies are limited by their inclusion of outpatients, adults with mild to moderate CAP, or small sample size. Hence, clinical judgment continues to play an important role in determining the appropriate duration of therapy. Factors such as pre-existing co-morbidities, severity of illness, and occurrence of complications should be considered. Data is limited on the appropriate duration of antibiotics in CAP patients requiring intensive care. It also is important to note the IDSA/ATS recommendations and most of the studies reviewed exclude patients with human immunodeficiency virus (HIV), and it is unknown whether these shorter courses of antibiotics are appropriate in the HIV population.
Lastly, the IDSA/ATS guidelines note longer durations of treatment may be required if the initial therapy was not active against the identified pathogen, or in cases complicated by extrapulmonary infections, such as endocarditis or meningitis.
Back to the Case
Our patient with moderately severe CAP was hospitalized based on his age and hypoxia. He was immediately treated with supplemental oxygen by nasal cannula, IV fluids, and a dose of IV levofloxacin 750 mg. Within 48 hours he met criteria for clinical stability, including defervescence, a decline in his respiratory rate to 19 breaths per minute, and improvement in oxygen saturation to 95% on room air. At this point, he was changed from IV to oral antibiotics. He continued on levofloxacin 750 mg daily and later that day was discharged home in good condition to complete a five-day course.
Bottom Line
For hospitalized adults with mild to moderately severe CAP, five to seven days of treatment, depending on the antibiotic selected, appears to be effective in most cases. Patients should be afebrile for 48 to 72 hours and demonstrate signs of clinical stability before therapy is discontinued. TH
Kelly Cunningham, MD, and Shelley Ellis, MD, MPH, are members of the Section of Hospital Medicine at Vanderbilt University in Nashville, Tenn. Sunil Kripalani, MD, MSc, serves as the section chief.
References
1. Kung HC, Hoyert DL, Xu J, Murphy SL. Deaths: final data for 2005. Natl Vital Stat Rep. 2008;56.
2. DeFrances CJ, Lucas CA, Buie VC, Golosinskiy A. 2006 National Hospital Discharge Survey. Natl Health Stat Report. 2008;5.
3. Niederman MS. Recent advances in community-acquired pneumonia: inpatient and outpatient. Chest. 2007;131:1205-1215.
4. Li JZ, Winston LG, Moore DH, Bent S. Efficacy of short-course antibiotic regimens for community-acquired pneumonia: a meta-analysis. Am J Med. 2007;120:783-790.
5. Mandell LA, Wunderink RG, Anzueto A et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis. 2007;44(Suppl 2):S27-72.
6. Ramirez JA, Bordon J. Early switch from intravenous to oral antibiotics in hospitalized patients with bacteremic community-acquired Streptococcus pneumoniae pneumonia. Arch Intern Med. 2001;161:848-850.
7. Halm EA, Fine MJ, Marrie TJ et al. Time to clinical stability in patients hospitalized with community-acquired pneumonia: implications for practice guidelines. JAMA. 1998;279:1452-1457.
8. Menendez R, Torres A, Rodriguez de Castro F et al. Reaching stability in community-acquired pneumonia: the effects of the severity of disease, treatment, and the characteristics of patients. Clin Infect Dis. 2004;39:1783-1790.
9. Siegal RE, Halpern NA, Almenoff PL et al. A prospective randomised study of inpatient IV antibiotics for community-acquired pneumonia: the optimal duration of therapy. Chest. 1996;110:965-971.
10. Oosterheert JJ, Bonten MJ, Schneider MM et al. Effectiveness of early switch from intravenous to oral antibiotics in severe community acquired pneumonia: multicentre randomized trial. BMJ. 2006;333:1193-1197.
11. Nathan RV, Rhew DC, Murray C et al. In-hospital observation after antibiotic switch in pneumonia: a national evaluation. Am J Med. 2006;119:512-518.
12. Dimopoulos G, Matthaiou DK, Karageorgopoulos DE, et al. Short- versus long-course antibacterial therapy for community-acquired pneumonia: a meta-analysis. Drugs. 2008;68:1841-1854.
13. Dunbar LM, Wunderink RG, Habib MP et al. High-dose, short-course levofloxacin for community-acquired pneumonia: a new treatment paradigm. Clin Infect Dis. 2003;37:752-760.
14. Morris DL, De Souza A, Jones JA, Morgan WE. High and prolonged pulmonary tissue concentrations of azithromycin following a single oral dose. Eur J Clin Microbiol Infect Dis. 1991;10:859-861.
15. Contopoulos-Ioannidis DG, Ioannidis JPA, Chew P, Lau J. Meta-analysis of randomized controlled trials on the comparative efficacy and safety of azithromycin against other antibiotics for lower respiratory tract infections. J Antimicrob Chemother. 2001;48:691-703.
16. Rizzato G, Montemurro L, Fraioli P et al. Efficacy of a three-day course of azithromycin in moderately severe community-acquired pneumonia. Eur Respir J. 1995;8:398-402.
17. Tellier G, Niederman MS, Nusrat R et al. Clinical and bacteriological efficacy and safety of 5- and 7-day regimens of telithromycin once daily compared with a 10-day regimen of clarithromycin twice daily in patients with mild to moderate community-acquired pneumonia. J Antimicrob Chemother. 2004;54:515.
18. El Moussaoui R, de Borgie CA, van den Broek P et al. Effectiveness of discontinuing antibiotic treatment after three days versus eight days in mild to moderate-severe community acquired pneumonia: randomised, double blind study. BMJ. 2006;332:1355-1361.
19. Siegel RE, Alicea M, Lee A, Blaiklock R. Comparison of 7 versus 10 days of antibiotic therapy for hospitalized patients with uncomplicated community-acquired pneumonia: a prospective, randomized double-blind study. Am J Ther. 1999;6:217-222.
Safety in Numbers
Patient safety organizations, commonly referred to as PSOs, are about to take off. And when they do, PSOs should provide hospitalists with invaluable data on improving patient safety.
“PSOs are a great concept, but even though it’s been around since 2005, I haven’t seen it clinically,” says Janet Nagamine, RN, MD, hospitalist at Kaiser Permanente in Santa Clara, Calif., and chair of SHM’s Hospital Quality and Patient Safety Committee.
This calendar year, Nagamine and the rest of hospital medicine should start to see some movement—“PSO 1.0,” if you will.
Background
PSOs are public and private organizations approved by the Agency for Healthcare Research and Quality (AHRQ); they include such groups as Health Watch Inc., Human Performance Technology Group, and the Institute for Safe Medication Practices, which will collect, aggregate, and analyze data on patient safety events. Hospitals and other healthcare providers will voluntarily and confidentially report data. The ultimate goal is to advance changes in culture, processes, and systems to enhance patient safety.
PSOs grew out of the Patient Safety and Quality Improvement Act of 2005, which was a response to the Institute of Medicine’s landmark report “To Err Is Human: Building a Safer Health System.” But it wasn’t until last year that the U.S. Department of Health and Human Services issued a final rule outlining PSO requirements and procedures. The rule became effective Jan. 19, 2009.
AHRQ is responsible for coordinating the development of a set of common definitions and reporting formats, called common formats, for collecting the data. Eventually, AHRQ will create a network of patient safety databases to which PSOs, providers, and others can voluntarily contribute non-identifiable patient safety information. This network will serve as an interactive evidence-based management resource for providers, PSOs, and other entities. AHRQ will use data from the network to analyze national and regional statistics regarding patient safety events. Findings will be made public and will be included in AHRQ’s annual National Healthcare Quality Report.
IT Example
To date, the only comparable data-collection system is MedMarx, which compiles information on medication errors. The Joint Commission requires providers to supply a root-cause analysis on every Level 1 incident, “but that’s just scratching the surface of what occurs,” Dr. Nagamine says. “There are far many more Level 2 and Level 3 events with the same precursors, and that information would be very valuable.”
By collecting nationwide data on patient safety events, PSOs will be able to bridge the gaps in the reporting system and provide crucial patient safety information to the healthcare industry. “In general, the concept of aggregate information that allows us to compare events is incredibly important,” Dr. Nagamine says. “A hospitalist working in one hospital has only the information about events in that hospital, but 5,000 hospitals can provide more specific and actionable information. We just haven’t seen this operationalized yet.”
Dr. Nagamine uses a technology example to show the value PSOs could have in identifying patterns or problems that threaten patient safety: “Every hospital has a horror story of implementing a new information technology (IT) system, and we’re getting some very interesting feedback from hospitals about unintended consequences,” she says. “We’re hearing that patients are being hurt because of mistakes in systems—the use of dropdown menus (on computer screens) that don’t drop down far enough to reveal all options, or a screen where it’s easy to click the wrong item.”
Current systems might not allow problems like these to be highlighted. Even if staff knows of a problem, their hospital’s coding system might not allow them to detail it. “It may fall under ‘communications’ or ‘physician computerized order entry’ or something vague, so the data won’t show the specifics of what happened,” Dr. Nagamine points out. “If we had aggregate data on issues like this, we could address it. Right now, we just have word of mouth.”
An isolated event at a hospital is one thing, but similar data from around the nation is significant. “Drug companies or IT vendors confronted with (patterns) might make some changes,” she says. “That kind of data is powerful.”
Hospital Medicine on Board
When hospitals start reporting data to PSOs, where will hospitalists fit into the process? Hospitalists likely will be interviewed to answer some of the PSO’s questions, but they will not be the ones filling out the forms, Dr. Nagamine says. Hospitalists also will be among the ranks of healthcare professionals eagerly awaiting the release of the data. “The way that PSOs approach patient safety and quality—what’s near and dear to our hearts—is it gives us more data,” Dr. Nagamine says. This is crucial for hospitalists leading quality-improvement projects and similar tasks. “Without that data, it’s hard to get traction and movement. That data will help convince someone to invest more time and money in a particular problem area.”
Phase One: Participation
AHRQ has established a comprehensive Web site (www.pso.ahrq.gov) that includes information on the first draft of common formats for use with hospital inpatients. These are found on downloadable paper forms, available at the PSO Privacy Protection Center (PPC) Web site at www.psoppc.org/ web/patientsafety/paperforms.
“The forms are a first step,” Dr. Nagamine explains. “If we had these data points on every incident at every hospital, we’d know a lot more than we do now. We’d be able to harness that information.”
It will be a while before healthcare providers can search the data for patterns and possible solutions in patient safety, but the wait should be worth it. “You’ve got to start somewhere, and it’s not going to happen in one sweep,” Dr. Nagamine says. “This is simply a start. Hopefully, in a decade, we’ll have a lot more actionable information.” TH
Jane Jerrard is a medical writer based in Chicago.
Patient safety organizations, commonly referred to as PSOs, are about to take off. And when they do, PSOs should provide hospitalists with invaluable data on improving patient safety.
“PSOs are a great concept, but even though it’s been around since 2005, I haven’t seen it clinically,” says Janet Nagamine, RN, MD, hospitalist at Kaiser Permanente in Santa Clara, Calif., and chair of SHM’s Hospital Quality and Patient Safety Committee.
This calendar year, Nagamine and the rest of hospital medicine should start to see some movement—“PSO 1.0,” if you will.
Background
PSOs are public and private organizations approved by the Agency for Healthcare Research and Quality (AHRQ); they include such groups as Health Watch Inc., Human Performance Technology Group, and the Institute for Safe Medication Practices, which will collect, aggregate, and analyze data on patient safety events. Hospitals and other healthcare providers will voluntarily and confidentially report data. The ultimate goal is to advance changes in culture, processes, and systems to enhance patient safety.
PSOs grew out of the Patient Safety and Quality Improvement Act of 2005, which was a response to the Institute of Medicine’s landmark report “To Err Is Human: Building a Safer Health System.” But it wasn’t until last year that the U.S. Department of Health and Human Services issued a final rule outlining PSO requirements and procedures. The rule became effective Jan. 19, 2009.
AHRQ is responsible for coordinating the development of a set of common definitions and reporting formats, called common formats, for collecting the data. Eventually, AHRQ will create a network of patient safety databases to which PSOs, providers, and others can voluntarily contribute non-identifiable patient safety information. This network will serve as an interactive evidence-based management resource for providers, PSOs, and other entities. AHRQ will use data from the network to analyze national and regional statistics regarding patient safety events. Findings will be made public and will be included in AHRQ’s annual National Healthcare Quality Report.
IT Example
To date, the only comparable data-collection system is MedMarx, which compiles information on medication errors. The Joint Commission requires providers to supply a root-cause analysis on every Level 1 incident, “but that’s just scratching the surface of what occurs,” Dr. Nagamine says. “There are far many more Level 2 and Level 3 events with the same precursors, and that information would be very valuable.”
By collecting nationwide data on patient safety events, PSOs will be able to bridge the gaps in the reporting system and provide crucial patient safety information to the healthcare industry. “In general, the concept of aggregate information that allows us to compare events is incredibly important,” Dr. Nagamine says. “A hospitalist working in one hospital has only the information about events in that hospital, but 5,000 hospitals can provide more specific and actionable information. We just haven’t seen this operationalized yet.”
Dr. Nagamine uses a technology example to show the value PSOs could have in identifying patterns or problems that threaten patient safety: “Every hospital has a horror story of implementing a new information technology (IT) system, and we’re getting some very interesting feedback from hospitals about unintended consequences,” she says. “We’re hearing that patients are being hurt because of mistakes in systems—the use of dropdown menus (on computer screens) that don’t drop down far enough to reveal all options, or a screen where it’s easy to click the wrong item.”
Current systems might not allow problems like these to be highlighted. Even if staff knows of a problem, their hospital’s coding system might not allow them to detail it. “It may fall under ‘communications’ or ‘physician computerized order entry’ or something vague, so the data won’t show the specifics of what happened,” Dr. Nagamine points out. “If we had aggregate data on issues like this, we could address it. Right now, we just have word of mouth.”
An isolated event at a hospital is one thing, but similar data from around the nation is significant. “Drug companies or IT vendors confronted with (patterns) might make some changes,” she says. “That kind of data is powerful.”
Hospital Medicine on Board
When hospitals start reporting data to PSOs, where will hospitalists fit into the process? Hospitalists likely will be interviewed to answer some of the PSO’s questions, but they will not be the ones filling out the forms, Dr. Nagamine says. Hospitalists also will be among the ranks of healthcare professionals eagerly awaiting the release of the data. “The way that PSOs approach patient safety and quality—what’s near and dear to our hearts—is it gives us more data,” Dr. Nagamine says. This is crucial for hospitalists leading quality-improvement projects and similar tasks. “Without that data, it’s hard to get traction and movement. That data will help convince someone to invest more time and money in a particular problem area.”
Phase One: Participation
AHRQ has established a comprehensive Web site (www.pso.ahrq.gov) that includes information on the first draft of common formats for use with hospital inpatients. These are found on downloadable paper forms, available at the PSO Privacy Protection Center (PPC) Web site at www.psoppc.org/ web/patientsafety/paperforms.
“The forms are a first step,” Dr. Nagamine explains. “If we had these data points on every incident at every hospital, we’d know a lot more than we do now. We’d be able to harness that information.”
It will be a while before healthcare providers can search the data for patterns and possible solutions in patient safety, but the wait should be worth it. “You’ve got to start somewhere, and it’s not going to happen in one sweep,” Dr. Nagamine says. “This is simply a start. Hopefully, in a decade, we’ll have a lot more actionable information.” TH
Jane Jerrard is a medical writer based in Chicago.
Patient safety organizations, commonly referred to as PSOs, are about to take off. And when they do, PSOs should provide hospitalists with invaluable data on improving patient safety.
“PSOs are a great concept, but even though it’s been around since 2005, I haven’t seen it clinically,” says Janet Nagamine, RN, MD, hospitalist at Kaiser Permanente in Santa Clara, Calif., and chair of SHM’s Hospital Quality and Patient Safety Committee.
This calendar year, Nagamine and the rest of hospital medicine should start to see some movement—“PSO 1.0,” if you will.
Background
PSOs are public and private organizations approved by the Agency for Healthcare Research and Quality (AHRQ); they include such groups as Health Watch Inc., Human Performance Technology Group, and the Institute for Safe Medication Practices, which will collect, aggregate, and analyze data on patient safety events. Hospitals and other healthcare providers will voluntarily and confidentially report data. The ultimate goal is to advance changes in culture, processes, and systems to enhance patient safety.
PSOs grew out of the Patient Safety and Quality Improvement Act of 2005, which was a response to the Institute of Medicine’s landmark report “To Err Is Human: Building a Safer Health System.” But it wasn’t until last year that the U.S. Department of Health and Human Services issued a final rule outlining PSO requirements and procedures. The rule became effective Jan. 19, 2009.
AHRQ is responsible for coordinating the development of a set of common definitions and reporting formats, called common formats, for collecting the data. Eventually, AHRQ will create a network of patient safety databases to which PSOs, providers, and others can voluntarily contribute non-identifiable patient safety information. This network will serve as an interactive evidence-based management resource for providers, PSOs, and other entities. AHRQ will use data from the network to analyze national and regional statistics regarding patient safety events. Findings will be made public and will be included in AHRQ’s annual National Healthcare Quality Report.
IT Example
To date, the only comparable data-collection system is MedMarx, which compiles information on medication errors. The Joint Commission requires providers to supply a root-cause analysis on every Level 1 incident, “but that’s just scratching the surface of what occurs,” Dr. Nagamine says. “There are far many more Level 2 and Level 3 events with the same precursors, and that information would be very valuable.”
By collecting nationwide data on patient safety events, PSOs will be able to bridge the gaps in the reporting system and provide crucial patient safety information to the healthcare industry. “In general, the concept of aggregate information that allows us to compare events is incredibly important,” Dr. Nagamine says. “A hospitalist working in one hospital has only the information about events in that hospital, but 5,000 hospitals can provide more specific and actionable information. We just haven’t seen this operationalized yet.”
Dr. Nagamine uses a technology example to show the value PSOs could have in identifying patterns or problems that threaten patient safety: “Every hospital has a horror story of implementing a new information technology (IT) system, and we’re getting some very interesting feedback from hospitals about unintended consequences,” she says. “We’re hearing that patients are being hurt because of mistakes in systems—the use of dropdown menus (on computer screens) that don’t drop down far enough to reveal all options, or a screen where it’s easy to click the wrong item.”
Current systems might not allow problems like these to be highlighted. Even if staff knows of a problem, their hospital’s coding system might not allow them to detail it. “It may fall under ‘communications’ or ‘physician computerized order entry’ or something vague, so the data won’t show the specifics of what happened,” Dr. Nagamine points out. “If we had aggregate data on issues like this, we could address it. Right now, we just have word of mouth.”
An isolated event at a hospital is one thing, but similar data from around the nation is significant. “Drug companies or IT vendors confronted with (patterns) might make some changes,” she says. “That kind of data is powerful.”
Hospital Medicine on Board
When hospitals start reporting data to PSOs, where will hospitalists fit into the process? Hospitalists likely will be interviewed to answer some of the PSO’s questions, but they will not be the ones filling out the forms, Dr. Nagamine says. Hospitalists also will be among the ranks of healthcare professionals eagerly awaiting the release of the data. “The way that PSOs approach patient safety and quality—what’s near and dear to our hearts—is it gives us more data,” Dr. Nagamine says. This is crucial for hospitalists leading quality-improvement projects and similar tasks. “Without that data, it’s hard to get traction and movement. That data will help convince someone to invest more time and money in a particular problem area.”
Phase One: Participation
AHRQ has established a comprehensive Web site (www.pso.ahrq.gov) that includes information on the first draft of common formats for use with hospital inpatients. These are found on downloadable paper forms, available at the PSO Privacy Protection Center (PPC) Web site at www.psoppc.org/ web/patientsafety/paperforms.
“The forms are a first step,” Dr. Nagamine explains. “If we had these data points on every incident at every hospital, we’d know a lot more than we do now. We’d be able to harness that information.”
It will be a while before healthcare providers can search the data for patterns and possible solutions in patient safety, but the wait should be worth it. “You’ve got to start somewhere, and it’s not going to happen in one sweep,” Dr. Nagamine says. “This is simply a start. Hopefully, in a decade, we’ll have a lot more actionable information.” TH
Jane Jerrard is a medical writer based in Chicago.
Converse Like a Leader
Communication is an integral part of a hospitalist’s job: from admission interviews to conveying orders to nursing staff, communicating clearly and precisely is part of numerous best practices. When a hospitalist assumes a leadership role, however, the types and styles of communication change. A committee chair or department head must be aware of the messages they send—both literally and in the most general sense of the term. This transition to leadership can be tough.
“Physician communication is focused on clinical outcome. That’s easy for someone trained in medicine. But in leadership communication, there may not be a defined outcome,” says Timothy J. Keogh, PhD, assistant professor at The Citadel School of Business Administration in Charleston, S.C. “That’s a difficult switch from clinician to leader; maybe half of the problems a leader faces can’t be solved.”
Dr. Keogh and William F. Martin, PsyD, MPH, summarized their research data in “Managing Medical Groups: 21st Century Challenges and the Impact of Physician Leadership Styles,” published in the September-October 2004 issue of Journal of Medical Practice Management.
The Basics
The most basic communication skill a hospitalist leader should practice, according to Dr. Keogh, is “being less direct than [he or she] would like to be.” Dr. Keogh, who teaches communication skills as part of SHM’s Leadership Academy, says, “Data shows that physicians prefer to be more precise and cover topics quickly. In a leadership role, the initial part of the communication or conversation needs to be chattier. Some physicians believe that this uses up too much time, but, in fact, it doesn’t take that long and it’s a necessary step.” Acknowledge others’ need for connection by making eye contact, pausing, and exchanging quick pleasantries. “Leaders need to be able to say things in passing, greet people, et cetera,” Dr. Keogh stresses.
But what about in-depth communication?
Management Topics
If you supervise hospitalists, you can condense discussions of your expectations—at least compared with managers in business fields. “Physicians are skilled, well-trained individuals, so you don’t have to do so much of this,” Dr. Keogh says. “They have an internal sense of quality and you don’t really need to motivate them. It’s a matter of adjusting the edges.”
A hospitalist supervisor might need to address a situation in which a physician on the team has been disruptive or needs a disciplinary talk. In these instances, Dr. Keogh says, “The leader has to somehow collect data on what the hospitalist has displayed that doesn’t fit in with teamwork. The hard part is that the data is likely to be hearsay—what was said by whom, when. That’s management.”
For example, you might receive complaints from nursing staff of abrupt or rude behavior from a hospitalist. “Physicians may not think of this as data, but it is. What someone said or did, or gestured,” Dr. Keogh points out. “You have to be able to say, ‘Here’s what we know happened on this date. Help me understand what happened, because we have to change this. This behavior is not acceptable.’”
The key to all official management communication is to carefully consider how to frame the conversation and keep it flowing for both parties: Speak with hospitalists, not to them. Here is an example: “In a performance appraisal, one suggestion we make is to have a conversation about data,” Dr. Keogh explains. “Look at some numbers on quality assurance, patient load, or whatever you’re discussing. Do your homework and allow the other person to have a look at the data before you sit down with them. That’s a sign of respect.”
Styles of Communication
Dr. Keogh’s training for physician executives—including what he teaches at the Leadership Academy—is based on the personality profile system developed by Carlson Learning Company (now Inscape Publishing).1 The DiSC model outlines behavior or characteristic leadership preferences in four dimensions:
- Dominance (D): People who score high in this category have behavioral characteristics that include being motivated by control over tasks and work environment, directing others, and achieving specific stretch goals. In general, physician managers who score high on dominance tend to be results-focused, fast-paced, and value autonomy.
- Influence (I): People who score high in this category are motivated by interacting with others, giving and receiving immediate feedback, and acknowledging emotions as well as facts.
- Steadiness (S): People who score high in this category are motivated by job security, predictability, and clearly defined expectations.
- Conscientiousness (C): People who score high in this category are motivated by needing to be right, working alone, and preferring to work on tasks rather than dealing with people.
“This model provides groundwork for seeing that other people have different ways, different preferences of communicating,” Dr. Keogh says. In his own research, he says, he has found “nearly half of all physicians are some combination of time-sensitive and perfectionist,” meaning they fit the dominance style.
The trick to effective communication is learning to modify your style when necessary. Task-focused individuals must practice taking a minute for a greeting or a pleasantry, even if it initially goes against their routine. “Someone who is extremely outgoing and open can have trouble, too,” Dr. Keogh points out. “You can’t start a conversation with a lot of chit-chat, if you’re addressing someone who is direct. … That won’t work, either.”
The solution is to practice stepping outside of your normal communication style. “You can learn how to adjust your style, how to flex to others’ styles,” Dr. Keogh says. “Depending on whom you’re communicating with, you can mirror the style of the other person.” This helps to ensure that what you’re saying is received and understood.
Practicing new ways to communicate means making a fundamental shift in your behavior. It sounds difficult, but Dr. Keogh promises it’s not.
“The transition is not as hard as you think, because hospitalists have been trained to do patient interviews,” he says. “They’re skilled at observation and listening. In the transition to leadership, they sometimes forget that they have these skills and can use these to be a great leader.”” TH
Jane Jerrard is a medical writer based in Chicago. She also writes “Public Policy” for The Hospitalist.
Reference
1. Straw J. The 4-Dimensional Manager: DiSC Strategies for Managing Different People in the Best Ways. San Francisco: Berrett-Koehler Publishers, Inc.; 2002.
Communication is an integral part of a hospitalist’s job: from admission interviews to conveying orders to nursing staff, communicating clearly and precisely is part of numerous best practices. When a hospitalist assumes a leadership role, however, the types and styles of communication change. A committee chair or department head must be aware of the messages they send—both literally and in the most general sense of the term. This transition to leadership can be tough.
“Physician communication is focused on clinical outcome. That’s easy for someone trained in medicine. But in leadership communication, there may not be a defined outcome,” says Timothy J. Keogh, PhD, assistant professor at The Citadel School of Business Administration in Charleston, S.C. “That’s a difficult switch from clinician to leader; maybe half of the problems a leader faces can’t be solved.”
Dr. Keogh and William F. Martin, PsyD, MPH, summarized their research data in “Managing Medical Groups: 21st Century Challenges and the Impact of Physician Leadership Styles,” published in the September-October 2004 issue of Journal of Medical Practice Management.
The Basics
The most basic communication skill a hospitalist leader should practice, according to Dr. Keogh, is “being less direct than [he or she] would like to be.” Dr. Keogh, who teaches communication skills as part of SHM’s Leadership Academy, says, “Data shows that physicians prefer to be more precise and cover topics quickly. In a leadership role, the initial part of the communication or conversation needs to be chattier. Some physicians believe that this uses up too much time, but, in fact, it doesn’t take that long and it’s a necessary step.” Acknowledge others’ need for connection by making eye contact, pausing, and exchanging quick pleasantries. “Leaders need to be able to say things in passing, greet people, et cetera,” Dr. Keogh stresses.
But what about in-depth communication?
Management Topics
If you supervise hospitalists, you can condense discussions of your expectations—at least compared with managers in business fields. “Physicians are skilled, well-trained individuals, so you don’t have to do so much of this,” Dr. Keogh says. “They have an internal sense of quality and you don’t really need to motivate them. It’s a matter of adjusting the edges.”
A hospitalist supervisor might need to address a situation in which a physician on the team has been disruptive or needs a disciplinary talk. In these instances, Dr. Keogh says, “The leader has to somehow collect data on what the hospitalist has displayed that doesn’t fit in with teamwork. The hard part is that the data is likely to be hearsay—what was said by whom, when. That’s management.”
For example, you might receive complaints from nursing staff of abrupt or rude behavior from a hospitalist. “Physicians may not think of this as data, but it is. What someone said or did, or gestured,” Dr. Keogh points out. “You have to be able to say, ‘Here’s what we know happened on this date. Help me understand what happened, because we have to change this. This behavior is not acceptable.’”
The key to all official management communication is to carefully consider how to frame the conversation and keep it flowing for both parties: Speak with hospitalists, not to them. Here is an example: “In a performance appraisal, one suggestion we make is to have a conversation about data,” Dr. Keogh explains. “Look at some numbers on quality assurance, patient load, or whatever you’re discussing. Do your homework and allow the other person to have a look at the data before you sit down with them. That’s a sign of respect.”
Styles of Communication
Dr. Keogh’s training for physician executives—including what he teaches at the Leadership Academy—is based on the personality profile system developed by Carlson Learning Company (now Inscape Publishing).1 The DiSC model outlines behavior or characteristic leadership preferences in four dimensions:
- Dominance (D): People who score high in this category have behavioral characteristics that include being motivated by control over tasks and work environment, directing others, and achieving specific stretch goals. In general, physician managers who score high on dominance tend to be results-focused, fast-paced, and value autonomy.
- Influence (I): People who score high in this category are motivated by interacting with others, giving and receiving immediate feedback, and acknowledging emotions as well as facts.
- Steadiness (S): People who score high in this category are motivated by job security, predictability, and clearly defined expectations.
- Conscientiousness (C): People who score high in this category are motivated by needing to be right, working alone, and preferring to work on tasks rather than dealing with people.
“This model provides groundwork for seeing that other people have different ways, different preferences of communicating,” Dr. Keogh says. In his own research, he says, he has found “nearly half of all physicians are some combination of time-sensitive and perfectionist,” meaning they fit the dominance style.
The trick to effective communication is learning to modify your style when necessary. Task-focused individuals must practice taking a minute for a greeting or a pleasantry, even if it initially goes against their routine. “Someone who is extremely outgoing and open can have trouble, too,” Dr. Keogh points out. “You can’t start a conversation with a lot of chit-chat, if you’re addressing someone who is direct. … That won’t work, either.”
The solution is to practice stepping outside of your normal communication style. “You can learn how to adjust your style, how to flex to others’ styles,” Dr. Keogh says. “Depending on whom you’re communicating with, you can mirror the style of the other person.” This helps to ensure that what you’re saying is received and understood.
Practicing new ways to communicate means making a fundamental shift in your behavior. It sounds difficult, but Dr. Keogh promises it’s not.
“The transition is not as hard as you think, because hospitalists have been trained to do patient interviews,” he says. “They’re skilled at observation and listening. In the transition to leadership, they sometimes forget that they have these skills and can use these to be a great leader.”” TH
Jane Jerrard is a medical writer based in Chicago. She also writes “Public Policy” for The Hospitalist.
Reference
1. Straw J. The 4-Dimensional Manager: DiSC Strategies for Managing Different People in the Best Ways. San Francisco: Berrett-Koehler Publishers, Inc.; 2002.
Communication is an integral part of a hospitalist’s job: from admission interviews to conveying orders to nursing staff, communicating clearly and precisely is part of numerous best practices. When a hospitalist assumes a leadership role, however, the types and styles of communication change. A committee chair or department head must be aware of the messages they send—both literally and in the most general sense of the term. This transition to leadership can be tough.
“Physician communication is focused on clinical outcome. That’s easy for someone trained in medicine. But in leadership communication, there may not be a defined outcome,” says Timothy J. Keogh, PhD, assistant professor at The Citadel School of Business Administration in Charleston, S.C. “That’s a difficult switch from clinician to leader; maybe half of the problems a leader faces can’t be solved.”
Dr. Keogh and William F. Martin, PsyD, MPH, summarized their research data in “Managing Medical Groups: 21st Century Challenges and the Impact of Physician Leadership Styles,” published in the September-October 2004 issue of Journal of Medical Practice Management.
The Basics
The most basic communication skill a hospitalist leader should practice, according to Dr. Keogh, is “being less direct than [he or she] would like to be.” Dr. Keogh, who teaches communication skills as part of SHM’s Leadership Academy, says, “Data shows that physicians prefer to be more precise and cover topics quickly. In a leadership role, the initial part of the communication or conversation needs to be chattier. Some physicians believe that this uses up too much time, but, in fact, it doesn’t take that long and it’s a necessary step.” Acknowledge others’ need for connection by making eye contact, pausing, and exchanging quick pleasantries. “Leaders need to be able to say things in passing, greet people, et cetera,” Dr. Keogh stresses.
But what about in-depth communication?
Management Topics
If you supervise hospitalists, you can condense discussions of your expectations—at least compared with managers in business fields. “Physicians are skilled, well-trained individuals, so you don’t have to do so much of this,” Dr. Keogh says. “They have an internal sense of quality and you don’t really need to motivate them. It’s a matter of adjusting the edges.”
A hospitalist supervisor might need to address a situation in which a physician on the team has been disruptive or needs a disciplinary talk. In these instances, Dr. Keogh says, “The leader has to somehow collect data on what the hospitalist has displayed that doesn’t fit in with teamwork. The hard part is that the data is likely to be hearsay—what was said by whom, when. That’s management.”
For example, you might receive complaints from nursing staff of abrupt or rude behavior from a hospitalist. “Physicians may not think of this as data, but it is. What someone said or did, or gestured,” Dr. Keogh points out. “You have to be able to say, ‘Here’s what we know happened on this date. Help me understand what happened, because we have to change this. This behavior is not acceptable.’”
The key to all official management communication is to carefully consider how to frame the conversation and keep it flowing for both parties: Speak with hospitalists, not to them. Here is an example: “In a performance appraisal, one suggestion we make is to have a conversation about data,” Dr. Keogh explains. “Look at some numbers on quality assurance, patient load, or whatever you’re discussing. Do your homework and allow the other person to have a look at the data before you sit down with them. That’s a sign of respect.”
Styles of Communication
Dr. Keogh’s training for physician executives—including what he teaches at the Leadership Academy—is based on the personality profile system developed by Carlson Learning Company (now Inscape Publishing).1 The DiSC model outlines behavior or characteristic leadership preferences in four dimensions:
- Dominance (D): People who score high in this category have behavioral characteristics that include being motivated by control over tasks and work environment, directing others, and achieving specific stretch goals. In general, physician managers who score high on dominance tend to be results-focused, fast-paced, and value autonomy.
- Influence (I): People who score high in this category are motivated by interacting with others, giving and receiving immediate feedback, and acknowledging emotions as well as facts.
- Steadiness (S): People who score high in this category are motivated by job security, predictability, and clearly defined expectations.
- Conscientiousness (C): People who score high in this category are motivated by needing to be right, working alone, and preferring to work on tasks rather than dealing with people.
“This model provides groundwork for seeing that other people have different ways, different preferences of communicating,” Dr. Keogh says. In his own research, he says, he has found “nearly half of all physicians are some combination of time-sensitive and perfectionist,” meaning they fit the dominance style.
The trick to effective communication is learning to modify your style when necessary. Task-focused individuals must practice taking a minute for a greeting or a pleasantry, even if it initially goes against their routine. “Someone who is extremely outgoing and open can have trouble, too,” Dr. Keogh points out. “You can’t start a conversation with a lot of chit-chat, if you’re addressing someone who is direct. … That won’t work, either.”
The solution is to practice stepping outside of your normal communication style. “You can learn how to adjust your style, how to flex to others’ styles,” Dr. Keogh says. “Depending on whom you’re communicating with, you can mirror the style of the other person.” This helps to ensure that what you’re saying is received and understood.
Practicing new ways to communicate means making a fundamental shift in your behavior. It sounds difficult, but Dr. Keogh promises it’s not.
“The transition is not as hard as you think, because hospitalists have been trained to do patient interviews,” he says. “They’re skilled at observation and listening. In the transition to leadership, they sometimes forget that they have these skills and can use these to be a great leader.”” TH
Jane Jerrard is a medical writer based in Chicago. She also writes “Public Policy” for The Hospitalist.
Reference
1. Straw J. The 4-Dimensional Manager: DiSC Strategies for Managing Different People in the Best Ways. San Francisco: Berrett-Koehler Publishers, Inc.; 2002.
Never-Event Implications
The Center for Medicare and Medicaid Services (CMS) recently announced federal payor programs no longer reimburses for medical services rendered to treat certain complications of care. Although CMS chose the majority of these complications because they are “reasonably preventable by following evidence-based guidelines,” the national media and patient advocacy groups have adopted the term “never events” to describe them.
Aside from the payment implications, CMS’ new policy affects the liability risk of any person providing inpatient care, regardless of whether a federal payor is involved.
In its press release announcing the new payment policy, CMS stated, “when you enter the hospital for treatment of one medical problem, you don’t expect to leave with additional injuries, infections, or serious conditions that occur during the course of your stay.” Recognizing “some of these complications may not be avoidable,” CMS found “too often patients suffer from injuries or illnesses that could have been prevented if the hospital had taken proper precautions.”
Consequently, “as part of its commitment to improve the quality of care [patients] receive during a hospital stay,” CMS policy is targeted at reducing “hospital-acquired conditions like certain infections, advanced bed sores, or fractures;” and “preventable medical errors, like performing surgery on the wrong side of the body, that should never happen.”
The list of “never events” covered under the CMS payment policy can be organized into three categories: surgical events, medical products and devices, and case management. The following breaks down each category:
Case Management
- Stage III and Stage IV pressure ulcers;
- Air embolism;
- Manifestations of poor control of blood sugar levels; and
- Fracture, burns, joint dislocations, and other injuries occurring from falls or other trauma suffered while an inpatient.
Surgical Events
- Surgery on wrong body part;
- Surgery on the wrong patient;
- Wrong surgery on a patient;
- Retention of a foreign object, such as a sponge or needle, inadvertently left in a patient after surgery;
- Surgical site infection following a coronary artery bypass graft;
- Surgical site infection following bariatric surgery;
- Surgical site infection following certain orthopedic procedures; and
- Deep vein thrombosis or pulmonary embolism following certain orthopedic procedures.
Medical Products and Devices
- Transfusion of wrong blood type;
- Catheter associated urinary tract infection; and
- Vascular catheter associated infections.
It’s easy to see why some of the complications made the list. Wrong-side surgery or surgery on the wrong patient are the quintessential cases where liability is generally uncontested. There is not much one can do to satisfactorily explain to a patient, or a jury, why a surgeon and surgical team operated on the wrong body part.
In other cases, however, such as fatal pulmonary embolus, death can occur even when a patient has been appropriately managed. In fact, medical literature demonstrates a small percentage of patients will develop deep vein thrombosis or pulmonary embolus even after having received therapeutic doses of heparin.
Reasonable Expectations
In any case involving a “never event,” we expect plaintiffs’ attorneys to argue CMS’ reimbursement determination is tantamount to a finding of substandard care. In other words, plaintiffs’ attorneys will argue a physician acted negligently simply because the patient incurred one of the proscribed complications. It’s a compelling argument because the federal government has essentially concluded these complications do not occur if physicians and hospitals pay attention while providing care.
You may have heard the Latin phrase res ipsa loquitur; it translates to “the thing speaks for itself.” Legally, res ipsa loquitur states a rule of law where a jury must presume a defendant was negligent when a certain type of injury occurs. The burden then shifts to the defendant to prove the injury occurred in the absence of negligence. The res ipsa rule originated in 1863 when a plaintiff was struck by a barrel of flour falling from a second-story window. The barrel caused the judge hearing the case to remark, “It is the duty of persons who keep barrels in a warehouse to take care that they do not roll out, and I think that such a case would, beyond all doubt, afford prima facie evidence of negligence. A barrel could not roll out of a warehouse without some negligence. … [I]f there are any facts inconsistent with negligence, it is for the defendant to prove them.” Thus, res ipsa is grounded in the notion everyone knows barrels aren’t supposed to fall from second-floor windows.
Traditionally, res ipsa applied only in a small class of medical malpractice cases, such as retained objects following surgery. In such cases, jurors are just as capable as medical professionals in understanding someone was negligent. For example, it does not take expert testimony to establish there has been negligence when a surgical instrument is left in a patient. There’s simply no compelling medical reason for a surgeon to leave an instrument in a patient’s abdomen.
In contrast, res ipsa generally has not applied in cases involving pulmonary embolus because the process of thromboembolic disease is beyond the average juror’s understanding and death by pulmonary embolus would not give rise to a presumption of negligence.
Where res ipsa applies, it’s a powerful concept. If res ipsa were found to apply to pulmonary embolus cases, the jury would be instructed it is the duty of a physician caring for a post-surgical patient to take care that the patient does not develop pulmonary embolus. Thus, a jury would begin with the presumption a patient would not develop pulmonary embolus absent negligence. The physician would then be left with the burden to prove otherwise. Given such a charge, it is foreseeable a jury could return a verdict against a physician, even if the physician managed the patient’s care appropriately and ordered appropriate prophylaxis.
Take Extra Precaution
To prevent CMS' reimbursement decisions from becoming the functional equivalent of a res ipsa instruction, physicians need to raise the level of precaution they employ against “never event” complications. At the heart of CMS' decision is its statement “never event” complications are “reasonably preventable by following evidence-based guidelines.” When a condition is only “reasonably preventable,” instead of “absolutely preventable,” a defense lawyer retains the ability to argue some patients will develop the condition even when the care was entirely appropriate.
We believe most jurors understand the inherent difficulties of caring for sick patients, and the risks that exist every time a patient undergoes a surgical procedure. The defense lawyer’s challenge is convincing a jury the patient received appropriate care, notwithstanding the complication.
Because CMS refers to “evidence-based guidelines,” physicians must know and follow the guidelines. The first step is becoming familiar with the complications CMS will deny reimbursement, and then regularly review the available guidelines to identify practices to reduce or eliminate the complication. Re-evaluate and update your practice whenever new information becomes available.
A consistent cycle of evaluating and responding to complications will afford the defense lawyer the ability to argue the physician and hospital complied with “evidence-based guidelines” and the patient’s case represents one of the unfortunate incidents where a patient suffers a complication despite receiving the highest-level of care.
In our experience, many providers initially create good systems, but run into trouble in the follow up. Make sure you respond to new or additional information or methods of practice. Without this follow up, CMS’ reimbursement decisions have the potential to create malpractice liabilities for all inpatient providers. TH
Patrick O’Rourke works in the Office of University Counsel, Department of Litigation, University of Colorado Denver.
The Center for Medicare and Medicaid Services (CMS) recently announced federal payor programs no longer reimburses for medical services rendered to treat certain complications of care. Although CMS chose the majority of these complications because they are “reasonably preventable by following evidence-based guidelines,” the national media and patient advocacy groups have adopted the term “never events” to describe them.
Aside from the payment implications, CMS’ new policy affects the liability risk of any person providing inpatient care, regardless of whether a federal payor is involved.
In its press release announcing the new payment policy, CMS stated, “when you enter the hospital for treatment of one medical problem, you don’t expect to leave with additional injuries, infections, or serious conditions that occur during the course of your stay.” Recognizing “some of these complications may not be avoidable,” CMS found “too often patients suffer from injuries or illnesses that could have been prevented if the hospital had taken proper precautions.”
Consequently, “as part of its commitment to improve the quality of care [patients] receive during a hospital stay,” CMS policy is targeted at reducing “hospital-acquired conditions like certain infections, advanced bed sores, or fractures;” and “preventable medical errors, like performing surgery on the wrong side of the body, that should never happen.”
The list of “never events” covered under the CMS payment policy can be organized into three categories: surgical events, medical products and devices, and case management. The following breaks down each category:
Case Management
- Stage III and Stage IV pressure ulcers;
- Air embolism;
- Manifestations of poor control of blood sugar levels; and
- Fracture, burns, joint dislocations, and other injuries occurring from falls or other trauma suffered while an inpatient.
Surgical Events
- Surgery on wrong body part;
- Surgery on the wrong patient;
- Wrong surgery on a patient;
- Retention of a foreign object, such as a sponge or needle, inadvertently left in a patient after surgery;
- Surgical site infection following a coronary artery bypass graft;
- Surgical site infection following bariatric surgery;
- Surgical site infection following certain orthopedic procedures; and
- Deep vein thrombosis or pulmonary embolism following certain orthopedic procedures.
Medical Products and Devices
- Transfusion of wrong blood type;
- Catheter associated urinary tract infection; and
- Vascular catheter associated infections.
It’s easy to see why some of the complications made the list. Wrong-side surgery or surgery on the wrong patient are the quintessential cases where liability is generally uncontested. There is not much one can do to satisfactorily explain to a patient, or a jury, why a surgeon and surgical team operated on the wrong body part.
In other cases, however, such as fatal pulmonary embolus, death can occur even when a patient has been appropriately managed. In fact, medical literature demonstrates a small percentage of patients will develop deep vein thrombosis or pulmonary embolus even after having received therapeutic doses of heparin.
Reasonable Expectations
In any case involving a “never event,” we expect plaintiffs’ attorneys to argue CMS’ reimbursement determination is tantamount to a finding of substandard care. In other words, plaintiffs’ attorneys will argue a physician acted negligently simply because the patient incurred one of the proscribed complications. It’s a compelling argument because the federal government has essentially concluded these complications do not occur if physicians and hospitals pay attention while providing care.
You may have heard the Latin phrase res ipsa loquitur; it translates to “the thing speaks for itself.” Legally, res ipsa loquitur states a rule of law where a jury must presume a defendant was negligent when a certain type of injury occurs. The burden then shifts to the defendant to prove the injury occurred in the absence of negligence. The res ipsa rule originated in 1863 when a plaintiff was struck by a barrel of flour falling from a second-story window. The barrel caused the judge hearing the case to remark, “It is the duty of persons who keep barrels in a warehouse to take care that they do not roll out, and I think that such a case would, beyond all doubt, afford prima facie evidence of negligence. A barrel could not roll out of a warehouse without some negligence. … [I]f there are any facts inconsistent with negligence, it is for the defendant to prove them.” Thus, res ipsa is grounded in the notion everyone knows barrels aren’t supposed to fall from second-floor windows.
Traditionally, res ipsa applied only in a small class of medical malpractice cases, such as retained objects following surgery. In such cases, jurors are just as capable as medical professionals in understanding someone was negligent. For example, it does not take expert testimony to establish there has been negligence when a surgical instrument is left in a patient. There’s simply no compelling medical reason for a surgeon to leave an instrument in a patient’s abdomen.
In contrast, res ipsa generally has not applied in cases involving pulmonary embolus because the process of thromboembolic disease is beyond the average juror’s understanding and death by pulmonary embolus would not give rise to a presumption of negligence.
Where res ipsa applies, it’s a powerful concept. If res ipsa were found to apply to pulmonary embolus cases, the jury would be instructed it is the duty of a physician caring for a post-surgical patient to take care that the patient does not develop pulmonary embolus. Thus, a jury would begin with the presumption a patient would not develop pulmonary embolus absent negligence. The physician would then be left with the burden to prove otherwise. Given such a charge, it is foreseeable a jury could return a verdict against a physician, even if the physician managed the patient’s care appropriately and ordered appropriate prophylaxis.
Take Extra Precaution
To prevent CMS' reimbursement decisions from becoming the functional equivalent of a res ipsa instruction, physicians need to raise the level of precaution they employ against “never event” complications. At the heart of CMS' decision is its statement “never event” complications are “reasonably preventable by following evidence-based guidelines.” When a condition is only “reasonably preventable,” instead of “absolutely preventable,” a defense lawyer retains the ability to argue some patients will develop the condition even when the care was entirely appropriate.
We believe most jurors understand the inherent difficulties of caring for sick patients, and the risks that exist every time a patient undergoes a surgical procedure. The defense lawyer’s challenge is convincing a jury the patient received appropriate care, notwithstanding the complication.
Because CMS refers to “evidence-based guidelines,” physicians must know and follow the guidelines. The first step is becoming familiar with the complications CMS will deny reimbursement, and then regularly review the available guidelines to identify practices to reduce or eliminate the complication. Re-evaluate and update your practice whenever new information becomes available.
A consistent cycle of evaluating and responding to complications will afford the defense lawyer the ability to argue the physician and hospital complied with “evidence-based guidelines” and the patient’s case represents one of the unfortunate incidents where a patient suffers a complication despite receiving the highest-level of care.
In our experience, many providers initially create good systems, but run into trouble in the follow up. Make sure you respond to new or additional information or methods of practice. Without this follow up, CMS’ reimbursement decisions have the potential to create malpractice liabilities for all inpatient providers. TH
Patrick O’Rourke works in the Office of University Counsel, Department of Litigation, University of Colorado Denver.
The Center for Medicare and Medicaid Services (CMS) recently announced federal payor programs no longer reimburses for medical services rendered to treat certain complications of care. Although CMS chose the majority of these complications because they are “reasonably preventable by following evidence-based guidelines,” the national media and patient advocacy groups have adopted the term “never events” to describe them.
Aside from the payment implications, CMS’ new policy affects the liability risk of any person providing inpatient care, regardless of whether a federal payor is involved.
In its press release announcing the new payment policy, CMS stated, “when you enter the hospital for treatment of one medical problem, you don’t expect to leave with additional injuries, infections, or serious conditions that occur during the course of your stay.” Recognizing “some of these complications may not be avoidable,” CMS found “too often patients suffer from injuries or illnesses that could have been prevented if the hospital had taken proper precautions.”
Consequently, “as part of its commitment to improve the quality of care [patients] receive during a hospital stay,” CMS policy is targeted at reducing “hospital-acquired conditions like certain infections, advanced bed sores, or fractures;” and “preventable medical errors, like performing surgery on the wrong side of the body, that should never happen.”
The list of “never events” covered under the CMS payment policy can be organized into three categories: surgical events, medical products and devices, and case management. The following breaks down each category:
Case Management
- Stage III and Stage IV pressure ulcers;
- Air embolism;
- Manifestations of poor control of blood sugar levels; and
- Fracture, burns, joint dislocations, and other injuries occurring from falls or other trauma suffered while an inpatient.
Surgical Events
- Surgery on wrong body part;
- Surgery on the wrong patient;
- Wrong surgery on a patient;
- Retention of a foreign object, such as a sponge or needle, inadvertently left in a patient after surgery;
- Surgical site infection following a coronary artery bypass graft;
- Surgical site infection following bariatric surgery;
- Surgical site infection following certain orthopedic procedures; and
- Deep vein thrombosis or pulmonary embolism following certain orthopedic procedures.
Medical Products and Devices
- Transfusion of wrong blood type;
- Catheter associated urinary tract infection; and
- Vascular catheter associated infections.
It’s easy to see why some of the complications made the list. Wrong-side surgery or surgery on the wrong patient are the quintessential cases where liability is generally uncontested. There is not much one can do to satisfactorily explain to a patient, or a jury, why a surgeon and surgical team operated on the wrong body part.
In other cases, however, such as fatal pulmonary embolus, death can occur even when a patient has been appropriately managed. In fact, medical literature demonstrates a small percentage of patients will develop deep vein thrombosis or pulmonary embolus even after having received therapeutic doses of heparin.
Reasonable Expectations
In any case involving a “never event,” we expect plaintiffs’ attorneys to argue CMS’ reimbursement determination is tantamount to a finding of substandard care. In other words, plaintiffs’ attorneys will argue a physician acted negligently simply because the patient incurred one of the proscribed complications. It’s a compelling argument because the federal government has essentially concluded these complications do not occur if physicians and hospitals pay attention while providing care.
You may have heard the Latin phrase res ipsa loquitur; it translates to “the thing speaks for itself.” Legally, res ipsa loquitur states a rule of law where a jury must presume a defendant was negligent when a certain type of injury occurs. The burden then shifts to the defendant to prove the injury occurred in the absence of negligence. The res ipsa rule originated in 1863 when a plaintiff was struck by a barrel of flour falling from a second-story window. The barrel caused the judge hearing the case to remark, “It is the duty of persons who keep barrels in a warehouse to take care that they do not roll out, and I think that such a case would, beyond all doubt, afford prima facie evidence of negligence. A barrel could not roll out of a warehouse without some negligence. … [I]f there are any facts inconsistent with negligence, it is for the defendant to prove them.” Thus, res ipsa is grounded in the notion everyone knows barrels aren’t supposed to fall from second-floor windows.
Traditionally, res ipsa applied only in a small class of medical malpractice cases, such as retained objects following surgery. In such cases, jurors are just as capable as medical professionals in understanding someone was negligent. For example, it does not take expert testimony to establish there has been negligence when a surgical instrument is left in a patient. There’s simply no compelling medical reason for a surgeon to leave an instrument in a patient’s abdomen.
In contrast, res ipsa generally has not applied in cases involving pulmonary embolus because the process of thromboembolic disease is beyond the average juror’s understanding and death by pulmonary embolus would not give rise to a presumption of negligence.
Where res ipsa applies, it’s a powerful concept. If res ipsa were found to apply to pulmonary embolus cases, the jury would be instructed it is the duty of a physician caring for a post-surgical patient to take care that the patient does not develop pulmonary embolus. Thus, a jury would begin with the presumption a patient would not develop pulmonary embolus absent negligence. The physician would then be left with the burden to prove otherwise. Given such a charge, it is foreseeable a jury could return a verdict against a physician, even if the physician managed the patient’s care appropriately and ordered appropriate prophylaxis.
Take Extra Precaution
To prevent CMS' reimbursement decisions from becoming the functional equivalent of a res ipsa instruction, physicians need to raise the level of precaution they employ against “never event” complications. At the heart of CMS' decision is its statement “never event” complications are “reasonably preventable by following evidence-based guidelines.” When a condition is only “reasonably preventable,” instead of “absolutely preventable,” a defense lawyer retains the ability to argue some patients will develop the condition even when the care was entirely appropriate.
We believe most jurors understand the inherent difficulties of caring for sick patients, and the risks that exist every time a patient undergoes a surgical procedure. The defense lawyer’s challenge is convincing a jury the patient received appropriate care, notwithstanding the complication.
Because CMS refers to “evidence-based guidelines,” physicians must know and follow the guidelines. The first step is becoming familiar with the complications CMS will deny reimbursement, and then regularly review the available guidelines to identify practices to reduce or eliminate the complication. Re-evaluate and update your practice whenever new information becomes available.
A consistent cycle of evaluating and responding to complications will afford the defense lawyer the ability to argue the physician and hospital complied with “evidence-based guidelines” and the patient’s case represents one of the unfortunate incidents where a patient suffers a complication despite receiving the highest-level of care.
In our experience, many providers initially create good systems, but run into trouble in the follow up. Make sure you respond to new or additional information or methods of practice. Without this follow up, CMS’ reimbursement decisions have the potential to create malpractice liabilities for all inpatient providers. TH
Patrick O’Rourke works in the Office of University Counsel, Department of Litigation, University of Colorado Denver.
Focused on Patient Care
Julia S. Wright, MD, spent 10 years in traditional practice before joining the University of Wisconsin School of Medicine and Public Health in Madison. Now a clinical associate professor and section head of hospital medicine, the title has changed and the professional demands have intensified. The mission, however, remains the same.
Every decision she’s made in her career—whether it be medical, managerial, financial, or even her seemingly curious choice of college majors—has been guided by one basic question: What will this mean for the quality of patient care? “It may sound cliché, but that’s always the bottom line,” Dr. Wright says. “It’s why I do what I do.”
You spent 10 years in traditional practice before becoming a hospitalist. How did that prepare you for what you’re doing now?
Answer: That experience is a tremendous asset. I made the switch to inpatient medicine because that was the arena I enjoyed the most. But having had experience in the outpatient setting gives me a better understanding of the continuum of care, and my clinical skills have been honed by that experience. I also have an understanding of the strengths of the primary care physicians (PCP), as well as the breadth of the problems they are able to take on.
How does that help you?
A: It really helps in the patient transition, especially on the return side, when patients go back to their PCP after hospitalization. Having an understanding of what resources are available to PCPs helps to determine an appropriate time to discharge a patient. Someone without that experience may have a tendency to think every loose end has to be tied up, or they may make changes that wind up making things more difficult for PCP. But if you have an understanding of a PCP’s capabilities, maybe the patient can be discharged a little earlier.
The University of Wisconsin’s hospitalist program started in 2005. You were named director in 2006. How exciting is it to guide a new program and help it develop?
A: It’s been a tremendous experience. When I joined, we had six hospitalists. Now we have 19. But it was strategic growth; it wasn’t haphazard.
What do you mean by strategic growth?
A: We didn’t simply say, ‘We need more people.’ Every time we brought somebody on, we really made sure it was going to be someone who would add value to the program and be beneficial to the hospital. We were worried, as we got bigger, that it’d be hard to keep the same cohesiveness and that same espirit de corps. During the interviews and the search process, we’re not just asking, ‘Are they qualified?’ We’re asking, ‘Are they a really good fit?’ And everybody has different areas of interest within the group. Some are more research-inclined; one developed a curriculum; some are more clinically oriented. That allows each hospitalist to have an identity in the group. That translated into a good expansion, and it’s been a win-win for us.
What makes someone a good fit for your program?
A: It sounds cliché, but I think the key to a strong developing program is to have a strong sense of what the group values. For us, we value the academic experience. For people going into academic medicine, the struggle is to be able to provide value to the hospital and yet stay academic. Our hospitalists are very clear—that’s our vision. With the support of the hospital and the department, we were able to do both at the same time.
Can you pinpoint one experience that you’ve had that made you realize you’re doing what you’re meant to do?
A: The biggest reward is always patient care. I enjoy the direct patient experience as much as I always have, and that’s what keeps me in the game.
What have you enjoyed most about your transition to a leadership role?
A: I really enjoy the position, not because of the hierarchy, but because of the opportunities afforded by it. I get to interact with hospital medicine staff and the department of medicine chair, and the vice chairs. I’ve been able to interact with others in hospital medicine across the country, and that has been a great experience.
Some hospitalists enjoy what they do because they don’t have to handle the business side of operations or deal with the administrative hassles that private physicians face. In your role, though, you do have to face those challenges. Is that a drawback?
A: I do have to pay attention to the numbers. That’s the bottom line. But it’s something I actually really enjoy. When it comes to awareness of the balance sheet, there’s a division between the leadership level and the clinician level. It’s hard to bridge that chasm of, ‘I’m here for patient care and I don’t necessarily focus on the numbers.’
How do you bridge the chasm?
A: It’s something we should be emphasizing more in hospital medicine. Some people may think it’s distasteful to think about, but it’s something hospitals do need to care about. There’s not enough of that trickling down. This is a huge area for potential growth. It’s important to have an understanding of the importance of the bottom line without feeling too much like it’s threatening the quality of the practice or getting in the way of what we want to be doing.
What other changes are in store for hospital medicine?
A: If you look at the traditional role of a hospitalist, you do a few things on the side of quality, but basically you’re seeing patients. The theory is there could be market saturation, because there are only a certain number of patients you can see in a hospital. But now hospitalists are seen as a physician resource that didn’t exist before. You have a group of doctors that understand patient care very well and are available to make changes and implement initiatives within a hospital. That’s going to lead to more roles besides direct patient care role. Hospitalists are going to be in charge of a number of administrative duties or assume administrative positions within hospitals. Because we’re branching out into other areas of hospital-based care, we’ll see more growth and still see high demand.
One of your primary medical interests is healthcare for Spanish-speaking families. Why is that so important to you?
A: My interest in working with the Latino population comes from my own background. I was a Spanish literature major at Northwestern University, and I’ve had a lot of opportunities to travel. When I started practicing, a large number of the patients were Latino. It became clear how important it is for us to understand what’s happening in our communities. We need to know what patients are coming in, what their demographics are, what their experiences have been, and what their needs are. Everything we do in a hospital translates to what’s happening outside the hospital.
Hospital medicine is quite a switch from Spanish literature. How’d that come about?
A: Actually, it was planned. I always knew I was going to medical school, but I really enjoy linguistics and language. I kept that balance. I didn’t want to be too science-oriented. It was one of those left brain-right brain things.
What is the biggest challenge facing hospital medicine?
A: The challenge is going to be retaining hospitalists and trying to avoid burnout.
How do you address the retention issue?
A: A big part of retention is making people feel happy in their field. It’s about allowing them to feel like they’re contributing in their particular area of physician interest, making them feel like their contributions are valued, making them feel like they can effect change, and making them feel like they’re really part of a team. We’ve been able to keep those as priorities.
How about the risk of burnout?
A: We have to find ways to balance our professions with our personal lives. Everybody’s looking for that balance. I have a husband and three children, so I want it, too. We really have to be reasonable. An important part of being good doctors is being good human beings.
What’s next for you personally?
A: Expanding research and developing a fellowship are two of the primary areas of focus. We also want to focus on triage and flow, and improving the throughput. Beyond that, it’s going to be program expansion, just like it’s been. That’s going to keep me busy. TH
Mark Leiser is a freelance writer in New Jersey.
Julia S. Wright, MD, spent 10 years in traditional practice before joining the University of Wisconsin School of Medicine and Public Health in Madison. Now a clinical associate professor and section head of hospital medicine, the title has changed and the professional demands have intensified. The mission, however, remains the same.
Every decision she’s made in her career—whether it be medical, managerial, financial, or even her seemingly curious choice of college majors—has been guided by one basic question: What will this mean for the quality of patient care? “It may sound cliché, but that’s always the bottom line,” Dr. Wright says. “It’s why I do what I do.”
You spent 10 years in traditional practice before becoming a hospitalist. How did that prepare you for what you’re doing now?
Answer: That experience is a tremendous asset. I made the switch to inpatient medicine because that was the arena I enjoyed the most. But having had experience in the outpatient setting gives me a better understanding of the continuum of care, and my clinical skills have been honed by that experience. I also have an understanding of the strengths of the primary care physicians (PCP), as well as the breadth of the problems they are able to take on.
How does that help you?
A: It really helps in the patient transition, especially on the return side, when patients go back to their PCP after hospitalization. Having an understanding of what resources are available to PCPs helps to determine an appropriate time to discharge a patient. Someone without that experience may have a tendency to think every loose end has to be tied up, or they may make changes that wind up making things more difficult for PCP. But if you have an understanding of a PCP’s capabilities, maybe the patient can be discharged a little earlier.
The University of Wisconsin’s hospitalist program started in 2005. You were named director in 2006. How exciting is it to guide a new program and help it develop?
A: It’s been a tremendous experience. When I joined, we had six hospitalists. Now we have 19. But it was strategic growth; it wasn’t haphazard.
What do you mean by strategic growth?
A: We didn’t simply say, ‘We need more people.’ Every time we brought somebody on, we really made sure it was going to be someone who would add value to the program and be beneficial to the hospital. We were worried, as we got bigger, that it’d be hard to keep the same cohesiveness and that same espirit de corps. During the interviews and the search process, we’re not just asking, ‘Are they qualified?’ We’re asking, ‘Are they a really good fit?’ And everybody has different areas of interest within the group. Some are more research-inclined; one developed a curriculum; some are more clinically oriented. That allows each hospitalist to have an identity in the group. That translated into a good expansion, and it’s been a win-win for us.
What makes someone a good fit for your program?
A: It sounds cliché, but I think the key to a strong developing program is to have a strong sense of what the group values. For us, we value the academic experience. For people going into academic medicine, the struggle is to be able to provide value to the hospital and yet stay academic. Our hospitalists are very clear—that’s our vision. With the support of the hospital and the department, we were able to do both at the same time.
Can you pinpoint one experience that you’ve had that made you realize you’re doing what you’re meant to do?
A: The biggest reward is always patient care. I enjoy the direct patient experience as much as I always have, and that’s what keeps me in the game.
What have you enjoyed most about your transition to a leadership role?
A: I really enjoy the position, not because of the hierarchy, but because of the opportunities afforded by it. I get to interact with hospital medicine staff and the department of medicine chair, and the vice chairs. I’ve been able to interact with others in hospital medicine across the country, and that has been a great experience.
Some hospitalists enjoy what they do because they don’t have to handle the business side of operations or deal with the administrative hassles that private physicians face. In your role, though, you do have to face those challenges. Is that a drawback?
A: I do have to pay attention to the numbers. That’s the bottom line. But it’s something I actually really enjoy. When it comes to awareness of the balance sheet, there’s a division between the leadership level and the clinician level. It’s hard to bridge that chasm of, ‘I’m here for patient care and I don’t necessarily focus on the numbers.’
How do you bridge the chasm?
A: It’s something we should be emphasizing more in hospital medicine. Some people may think it’s distasteful to think about, but it’s something hospitals do need to care about. There’s not enough of that trickling down. This is a huge area for potential growth. It’s important to have an understanding of the importance of the bottom line without feeling too much like it’s threatening the quality of the practice or getting in the way of what we want to be doing.
What other changes are in store for hospital medicine?
A: If you look at the traditional role of a hospitalist, you do a few things on the side of quality, but basically you’re seeing patients. The theory is there could be market saturation, because there are only a certain number of patients you can see in a hospital. But now hospitalists are seen as a physician resource that didn’t exist before. You have a group of doctors that understand patient care very well and are available to make changes and implement initiatives within a hospital. That’s going to lead to more roles besides direct patient care role. Hospitalists are going to be in charge of a number of administrative duties or assume administrative positions within hospitals. Because we’re branching out into other areas of hospital-based care, we’ll see more growth and still see high demand.
One of your primary medical interests is healthcare for Spanish-speaking families. Why is that so important to you?
A: My interest in working with the Latino population comes from my own background. I was a Spanish literature major at Northwestern University, and I’ve had a lot of opportunities to travel. When I started practicing, a large number of the patients were Latino. It became clear how important it is for us to understand what’s happening in our communities. We need to know what patients are coming in, what their demographics are, what their experiences have been, and what their needs are. Everything we do in a hospital translates to what’s happening outside the hospital.
Hospital medicine is quite a switch from Spanish literature. How’d that come about?
A: Actually, it was planned. I always knew I was going to medical school, but I really enjoy linguistics and language. I kept that balance. I didn’t want to be too science-oriented. It was one of those left brain-right brain things.
What is the biggest challenge facing hospital medicine?
A: The challenge is going to be retaining hospitalists and trying to avoid burnout.
How do you address the retention issue?
A: A big part of retention is making people feel happy in their field. It’s about allowing them to feel like they’re contributing in their particular area of physician interest, making them feel like their contributions are valued, making them feel like they can effect change, and making them feel like they’re really part of a team. We’ve been able to keep those as priorities.
How about the risk of burnout?
A: We have to find ways to balance our professions with our personal lives. Everybody’s looking for that balance. I have a husband and three children, so I want it, too. We really have to be reasonable. An important part of being good doctors is being good human beings.
What’s next for you personally?
A: Expanding research and developing a fellowship are two of the primary areas of focus. We also want to focus on triage and flow, and improving the throughput. Beyond that, it’s going to be program expansion, just like it’s been. That’s going to keep me busy. TH
Mark Leiser is a freelance writer in New Jersey.
Julia S. Wright, MD, spent 10 years in traditional practice before joining the University of Wisconsin School of Medicine and Public Health in Madison. Now a clinical associate professor and section head of hospital medicine, the title has changed and the professional demands have intensified. The mission, however, remains the same.
Every decision she’s made in her career—whether it be medical, managerial, financial, or even her seemingly curious choice of college majors—has been guided by one basic question: What will this mean for the quality of patient care? “It may sound cliché, but that’s always the bottom line,” Dr. Wright says. “It’s why I do what I do.”
You spent 10 years in traditional practice before becoming a hospitalist. How did that prepare you for what you’re doing now?
Answer: That experience is a tremendous asset. I made the switch to inpatient medicine because that was the arena I enjoyed the most. But having had experience in the outpatient setting gives me a better understanding of the continuum of care, and my clinical skills have been honed by that experience. I also have an understanding of the strengths of the primary care physicians (PCP), as well as the breadth of the problems they are able to take on.
How does that help you?
A: It really helps in the patient transition, especially on the return side, when patients go back to their PCP after hospitalization. Having an understanding of what resources are available to PCPs helps to determine an appropriate time to discharge a patient. Someone without that experience may have a tendency to think every loose end has to be tied up, or they may make changes that wind up making things more difficult for PCP. But if you have an understanding of a PCP’s capabilities, maybe the patient can be discharged a little earlier.
The University of Wisconsin’s hospitalist program started in 2005. You were named director in 2006. How exciting is it to guide a new program and help it develop?
A: It’s been a tremendous experience. When I joined, we had six hospitalists. Now we have 19. But it was strategic growth; it wasn’t haphazard.
What do you mean by strategic growth?
A: We didn’t simply say, ‘We need more people.’ Every time we brought somebody on, we really made sure it was going to be someone who would add value to the program and be beneficial to the hospital. We were worried, as we got bigger, that it’d be hard to keep the same cohesiveness and that same espirit de corps. During the interviews and the search process, we’re not just asking, ‘Are they qualified?’ We’re asking, ‘Are they a really good fit?’ And everybody has different areas of interest within the group. Some are more research-inclined; one developed a curriculum; some are more clinically oriented. That allows each hospitalist to have an identity in the group. That translated into a good expansion, and it’s been a win-win for us.
What makes someone a good fit for your program?
A: It sounds cliché, but I think the key to a strong developing program is to have a strong sense of what the group values. For us, we value the academic experience. For people going into academic medicine, the struggle is to be able to provide value to the hospital and yet stay academic. Our hospitalists are very clear—that’s our vision. With the support of the hospital and the department, we were able to do both at the same time.
Can you pinpoint one experience that you’ve had that made you realize you’re doing what you’re meant to do?
A: The biggest reward is always patient care. I enjoy the direct patient experience as much as I always have, and that’s what keeps me in the game.
What have you enjoyed most about your transition to a leadership role?
A: I really enjoy the position, not because of the hierarchy, but because of the opportunities afforded by it. I get to interact with hospital medicine staff and the department of medicine chair, and the vice chairs. I’ve been able to interact with others in hospital medicine across the country, and that has been a great experience.
Some hospitalists enjoy what they do because they don’t have to handle the business side of operations or deal with the administrative hassles that private physicians face. In your role, though, you do have to face those challenges. Is that a drawback?
A: I do have to pay attention to the numbers. That’s the bottom line. But it’s something I actually really enjoy. When it comes to awareness of the balance sheet, there’s a division between the leadership level and the clinician level. It’s hard to bridge that chasm of, ‘I’m here for patient care and I don’t necessarily focus on the numbers.’
How do you bridge the chasm?
A: It’s something we should be emphasizing more in hospital medicine. Some people may think it’s distasteful to think about, but it’s something hospitals do need to care about. There’s not enough of that trickling down. This is a huge area for potential growth. It’s important to have an understanding of the importance of the bottom line without feeling too much like it’s threatening the quality of the practice or getting in the way of what we want to be doing.
What other changes are in store for hospital medicine?
A: If you look at the traditional role of a hospitalist, you do a few things on the side of quality, but basically you’re seeing patients. The theory is there could be market saturation, because there are only a certain number of patients you can see in a hospital. But now hospitalists are seen as a physician resource that didn’t exist before. You have a group of doctors that understand patient care very well and are available to make changes and implement initiatives within a hospital. That’s going to lead to more roles besides direct patient care role. Hospitalists are going to be in charge of a number of administrative duties or assume administrative positions within hospitals. Because we’re branching out into other areas of hospital-based care, we’ll see more growth and still see high demand.
One of your primary medical interests is healthcare for Spanish-speaking families. Why is that so important to you?
A: My interest in working with the Latino population comes from my own background. I was a Spanish literature major at Northwestern University, and I’ve had a lot of opportunities to travel. When I started practicing, a large number of the patients were Latino. It became clear how important it is for us to understand what’s happening in our communities. We need to know what patients are coming in, what their demographics are, what their experiences have been, and what their needs are. Everything we do in a hospital translates to what’s happening outside the hospital.
Hospital medicine is quite a switch from Spanish literature. How’d that come about?
A: Actually, it was planned. I always knew I was going to medical school, but I really enjoy linguistics and language. I kept that balance. I didn’t want to be too science-oriented. It was one of those left brain-right brain things.
What is the biggest challenge facing hospital medicine?
A: The challenge is going to be retaining hospitalists and trying to avoid burnout.
How do you address the retention issue?
A: A big part of retention is making people feel happy in their field. It’s about allowing them to feel like they’re contributing in their particular area of physician interest, making them feel like their contributions are valued, making them feel like they can effect change, and making them feel like they’re really part of a team. We’ve been able to keep those as priorities.
How about the risk of burnout?
A: We have to find ways to balance our professions with our personal lives. Everybody’s looking for that balance. I have a husband and three children, so I want it, too. We really have to be reasonable. An important part of being good doctors is being good human beings.
What’s next for you personally?
A: Expanding research and developing a fellowship are two of the primary areas of focus. We also want to focus on triage and flow, and improving the throughput. Beyond that, it’s going to be program expansion, just like it’s been. That’s going to keep me busy. TH
Mark Leiser is a freelance writer in New Jersey.
“Caregiver Culture” and End-of-Life Discussions
When it comes to discussing a patient’s wishes for code status care, practices at the institution play a more important role than almost any other factor, according to a new study, “Factors Associated with Discussion of Care Plans and Code Status at the Time of Hospital Admission: Results from the Multicenter Hospitalist Study,” in the Journal of Hospital Medicine.
“What was most surprising to me was how variable the discussion rate was,” lead author Andrew Auerbach, MD, tells The Hospitalist. “It had little or nothing to do with how sick the patient was, or with the type of institution in which the discussion took place.”
Hospitalists are no more or less likely to document such discussions than doctors in any other specialty, says Dr. Auerbach, a hospitalist and associate professor of medicine at the University of California San Francisco. He and his colleagues analyzed data from patients admitted to the general medicine services at six academic medical centers as part of the Multicenter Hospitalist Study. Each site complied with requirements established by the Patient Self-Determination Act (PSDA), which says patients must be informed of their right to create an advance directive.
None of the hospitals in the study had established guidelines or formal policies regarding physician-patient discussions about code status or end-of-life care. Patients were interviewed immediately after informed consent was obtained, usually within 24 hours of admission. In each case, the authors determined whether or not the patient had had a care discussion, defined as a documented discussion “between patients (or family) and at least one physician … during the first 24 hours of hospitalization,” the authors write. “Care discussions needed to specify that the person who wrote the note had actually spoken with the patient or their family for the purposes of determining preferences for care, and that this discussion resulted in a specific care plan.”
A notation, such as “the patient continues to want full efforts,” qualified as a care discussion. Less-specific comments, such as “DNR/DNI” or “spoke with family, questions answered,” did not qualify. “These were all really, really sick people, and it was important to assess their wishes for care,” Dr. Auerbach says. Individually, PSDA or durable power of attorney may not adequately convey a patient’s true wishes, because often times the measures involve nothing more than having the patient or family complete a form. “The true marker is a conversation,” he says.
—Andrew Auerbach, MD, University of California San Francisco
By the Numbers
Of 17,097 patients interviewed, only 1,776 (10.4%) had a documented care discussion within 24 hours of hospital admission. The frequency of discussions varied from a low of 2.8% at one institution, to a high of 24.9% at another.
On unadjusted analysis, patients with documented care discussions were more likely to have living wills, durable powers of attorney, or the names of surrogate decision-makers in their charts (P<0.0001 for all categories). These patients were older, more likely to be white, and more likely to be on Medicare, compared to patients without documented care discussions.
The unadjusted analysis also showed patients with care discussions were more likely to be married, but less likely to be living in their own home or apartment, and, not surprisingly, more likely to have been hospitalized at least once within the previous 12 months. Overall, the general health of patients with care discussions was poorer than those without. Patients with documented discussions were more likely to report needing help within the past month with chores or bathing or dressing themselves, than were patients who did not have care discussions. Cancer, depression, and a history of stroke were common among patients with care discussions. Compared to patients without documented discussions, those who did have the discussion appear to want more of a say in their care: they were less likely to agree with the study statements, “I prefer my doctor give me choices regarding my care,” and “I prefer to leave care decisions to my physician.”
The authors found multivariate analysis showed many of these factors turn out to have only a moderate association with a documented care discussion, with adjusted odds ratios of less than 2.0. The strongest predictors were the existence of informal notations describing pre-hospital care wishes, with odds ratios ranging from 3.22 to 11.32, compared to people with no such documentation, and site of enrollment, with odds ratios of 1.74 to 5.14.
The Caregiver Culture
These findings suggest the “caregiver culture” at any given institution is a stronger determinant of a patient participating in a documented care discussion than other, more intuitive factors, such as medical condition or socioeconomic characteristics, or even whether or not the patient has a pre-existing advance directive or durable power of attorney, Dr. Auerbach explains. “It may just be a part of what some hospitals do. It’s driven by what your peers are doing and by local practices.”
Based on the results of the study, Dr. Auerbach and his co-authors suggest simply establishing mandates to document code status on admission probably will not encourage more conversations of this nature, “unless sites also develop an approach to using this newly documented information as a prompt for subsequent discussions.” The Patient Self-Determination Act went into effect in 1991, but its effect on improving communication around end-of-life care remains uncertain, the authors note. It might be why California passed a new law, effective as of January 2009, requiring physicians and health care organizations in the state to provide terminally ill patients who ask about their end-of-life care options with comprehensive information and counseling. Such discussions must cover advance directives, hospice care, and the right to receive palliative care. The new law is the first of its kind in the nation, but proponents of the legislation hope it will serve as a model for other states to adopt.1
“Documentation has an impact on quality of care. Lots of errors are driven by code status,” Dr. Auerbach points out. “If a patient is admitted in the middle of the night, when the doctor checks in on him the next day, he can look at the chart and see that his partner documented the care discussion the night before. That is incredibly helpful.” TH
Norra MacReady is a medical writer based in California.
Reference
1. O’Reilly KB. California law mandates discussing end-of-life options. Am Med News Web site. Available at amaassn.org/amednews/2008/11/10/prsc1110.htm. Last accessed November 6, 2008.
When it comes to discussing a patient’s wishes for code status care, practices at the institution play a more important role than almost any other factor, according to a new study, “Factors Associated with Discussion of Care Plans and Code Status at the Time of Hospital Admission: Results from the Multicenter Hospitalist Study,” in the Journal of Hospital Medicine.
“What was most surprising to me was how variable the discussion rate was,” lead author Andrew Auerbach, MD, tells The Hospitalist. “It had little or nothing to do with how sick the patient was, or with the type of institution in which the discussion took place.”
Hospitalists are no more or less likely to document such discussions than doctors in any other specialty, says Dr. Auerbach, a hospitalist and associate professor of medicine at the University of California San Francisco. He and his colleagues analyzed data from patients admitted to the general medicine services at six academic medical centers as part of the Multicenter Hospitalist Study. Each site complied with requirements established by the Patient Self-Determination Act (PSDA), which says patients must be informed of their right to create an advance directive.
None of the hospitals in the study had established guidelines or formal policies regarding physician-patient discussions about code status or end-of-life care. Patients were interviewed immediately after informed consent was obtained, usually within 24 hours of admission. In each case, the authors determined whether or not the patient had had a care discussion, defined as a documented discussion “between patients (or family) and at least one physician … during the first 24 hours of hospitalization,” the authors write. “Care discussions needed to specify that the person who wrote the note had actually spoken with the patient or their family for the purposes of determining preferences for care, and that this discussion resulted in a specific care plan.”
A notation, such as “the patient continues to want full efforts,” qualified as a care discussion. Less-specific comments, such as “DNR/DNI” or “spoke with family, questions answered,” did not qualify. “These were all really, really sick people, and it was important to assess their wishes for care,” Dr. Auerbach says. Individually, PSDA or durable power of attorney may not adequately convey a patient’s true wishes, because often times the measures involve nothing more than having the patient or family complete a form. “The true marker is a conversation,” he says.
—Andrew Auerbach, MD, University of California San Francisco
By the Numbers
Of 17,097 patients interviewed, only 1,776 (10.4%) had a documented care discussion within 24 hours of hospital admission. The frequency of discussions varied from a low of 2.8% at one institution, to a high of 24.9% at another.
On unadjusted analysis, patients with documented care discussions were more likely to have living wills, durable powers of attorney, or the names of surrogate decision-makers in their charts (P<0.0001 for all categories). These patients were older, more likely to be white, and more likely to be on Medicare, compared to patients without documented care discussions.
The unadjusted analysis also showed patients with care discussions were more likely to be married, but less likely to be living in their own home or apartment, and, not surprisingly, more likely to have been hospitalized at least once within the previous 12 months. Overall, the general health of patients with care discussions was poorer than those without. Patients with documented discussions were more likely to report needing help within the past month with chores or bathing or dressing themselves, than were patients who did not have care discussions. Cancer, depression, and a history of stroke were common among patients with care discussions. Compared to patients without documented discussions, those who did have the discussion appear to want more of a say in their care: they were less likely to agree with the study statements, “I prefer my doctor give me choices regarding my care,” and “I prefer to leave care decisions to my physician.”
The authors found multivariate analysis showed many of these factors turn out to have only a moderate association with a documented care discussion, with adjusted odds ratios of less than 2.0. The strongest predictors were the existence of informal notations describing pre-hospital care wishes, with odds ratios ranging from 3.22 to 11.32, compared to people with no such documentation, and site of enrollment, with odds ratios of 1.74 to 5.14.
The Caregiver Culture
These findings suggest the “caregiver culture” at any given institution is a stronger determinant of a patient participating in a documented care discussion than other, more intuitive factors, such as medical condition or socioeconomic characteristics, or even whether or not the patient has a pre-existing advance directive or durable power of attorney, Dr. Auerbach explains. “It may just be a part of what some hospitals do. It’s driven by what your peers are doing and by local practices.”
Based on the results of the study, Dr. Auerbach and his co-authors suggest simply establishing mandates to document code status on admission probably will not encourage more conversations of this nature, “unless sites also develop an approach to using this newly documented information as a prompt for subsequent discussions.” The Patient Self-Determination Act went into effect in 1991, but its effect on improving communication around end-of-life care remains uncertain, the authors note. It might be why California passed a new law, effective as of January 2009, requiring physicians and health care organizations in the state to provide terminally ill patients who ask about their end-of-life care options with comprehensive information and counseling. Such discussions must cover advance directives, hospice care, and the right to receive palliative care. The new law is the first of its kind in the nation, but proponents of the legislation hope it will serve as a model for other states to adopt.1
“Documentation has an impact on quality of care. Lots of errors are driven by code status,” Dr. Auerbach points out. “If a patient is admitted in the middle of the night, when the doctor checks in on him the next day, he can look at the chart and see that his partner documented the care discussion the night before. That is incredibly helpful.” TH
Norra MacReady is a medical writer based in California.
Reference
1. O’Reilly KB. California law mandates discussing end-of-life options. Am Med News Web site. Available at amaassn.org/amednews/2008/11/10/prsc1110.htm. Last accessed November 6, 2008.
When it comes to discussing a patient’s wishes for code status care, practices at the institution play a more important role than almost any other factor, according to a new study, “Factors Associated with Discussion of Care Plans and Code Status at the Time of Hospital Admission: Results from the Multicenter Hospitalist Study,” in the Journal of Hospital Medicine.
“What was most surprising to me was how variable the discussion rate was,” lead author Andrew Auerbach, MD, tells The Hospitalist. “It had little or nothing to do with how sick the patient was, or with the type of institution in which the discussion took place.”
Hospitalists are no more or less likely to document such discussions than doctors in any other specialty, says Dr. Auerbach, a hospitalist and associate professor of medicine at the University of California San Francisco. He and his colleagues analyzed data from patients admitted to the general medicine services at six academic medical centers as part of the Multicenter Hospitalist Study. Each site complied with requirements established by the Patient Self-Determination Act (PSDA), which says patients must be informed of their right to create an advance directive.
None of the hospitals in the study had established guidelines or formal policies regarding physician-patient discussions about code status or end-of-life care. Patients were interviewed immediately after informed consent was obtained, usually within 24 hours of admission. In each case, the authors determined whether or not the patient had had a care discussion, defined as a documented discussion “between patients (or family) and at least one physician … during the first 24 hours of hospitalization,” the authors write. “Care discussions needed to specify that the person who wrote the note had actually spoken with the patient or their family for the purposes of determining preferences for care, and that this discussion resulted in a specific care plan.”
A notation, such as “the patient continues to want full efforts,” qualified as a care discussion. Less-specific comments, such as “DNR/DNI” or “spoke with family, questions answered,” did not qualify. “These were all really, really sick people, and it was important to assess their wishes for care,” Dr. Auerbach says. Individually, PSDA or durable power of attorney may not adequately convey a patient’s true wishes, because often times the measures involve nothing more than having the patient or family complete a form. “The true marker is a conversation,” he says.
—Andrew Auerbach, MD, University of California San Francisco
By the Numbers
Of 17,097 patients interviewed, only 1,776 (10.4%) had a documented care discussion within 24 hours of hospital admission. The frequency of discussions varied from a low of 2.8% at one institution, to a high of 24.9% at another.
On unadjusted analysis, patients with documented care discussions were more likely to have living wills, durable powers of attorney, or the names of surrogate decision-makers in their charts (P<0.0001 for all categories). These patients were older, more likely to be white, and more likely to be on Medicare, compared to patients without documented care discussions.
The unadjusted analysis also showed patients with care discussions were more likely to be married, but less likely to be living in their own home or apartment, and, not surprisingly, more likely to have been hospitalized at least once within the previous 12 months. Overall, the general health of patients with care discussions was poorer than those without. Patients with documented discussions were more likely to report needing help within the past month with chores or bathing or dressing themselves, than were patients who did not have care discussions. Cancer, depression, and a history of stroke were common among patients with care discussions. Compared to patients without documented discussions, those who did have the discussion appear to want more of a say in their care: they were less likely to agree with the study statements, “I prefer my doctor give me choices regarding my care,” and “I prefer to leave care decisions to my physician.”
The authors found multivariate analysis showed many of these factors turn out to have only a moderate association with a documented care discussion, with adjusted odds ratios of less than 2.0. The strongest predictors were the existence of informal notations describing pre-hospital care wishes, with odds ratios ranging from 3.22 to 11.32, compared to people with no such documentation, and site of enrollment, with odds ratios of 1.74 to 5.14.
The Caregiver Culture
These findings suggest the “caregiver culture” at any given institution is a stronger determinant of a patient participating in a documented care discussion than other, more intuitive factors, such as medical condition or socioeconomic characteristics, or even whether or not the patient has a pre-existing advance directive or durable power of attorney, Dr. Auerbach explains. “It may just be a part of what some hospitals do. It’s driven by what your peers are doing and by local practices.”
Based on the results of the study, Dr. Auerbach and his co-authors suggest simply establishing mandates to document code status on admission probably will not encourage more conversations of this nature, “unless sites also develop an approach to using this newly documented information as a prompt for subsequent discussions.” The Patient Self-Determination Act went into effect in 1991, but its effect on improving communication around end-of-life care remains uncertain, the authors note. It might be why California passed a new law, effective as of January 2009, requiring physicians and health care organizations in the state to provide terminally ill patients who ask about their end-of-life care options with comprehensive information and counseling. Such discussions must cover advance directives, hospice care, and the right to receive palliative care. The new law is the first of its kind in the nation, but proponents of the legislation hope it will serve as a model for other states to adopt.1
“Documentation has an impact on quality of care. Lots of errors are driven by code status,” Dr. Auerbach points out. “If a patient is admitted in the middle of the night, when the doctor checks in on him the next day, he can look at the chart and see that his partner documented the care discussion the night before. That is incredibly helpful.” TH
Norra MacReady is a medical writer based in California.
Reference
1. O’Reilly KB. California law mandates discussing end-of-life options. Am Med News Web site. Available at amaassn.org/amednews/2008/11/10/prsc1110.htm. Last accessed November 6, 2008.
QTc Interval Prolongation
Terfenadine, cisapride, astemizole … do you remember these drugs? They all were removed from the U.S. market subsequent to adverse outcomes related to QTc interval prolongation, including ventricular arrhythmias.1-3 Many drugs prolong the QTc interval, particularly if a drug is combined with others that affect its metabolism.
QTc interval prolongation can lead to torsades de pointes (TdP). Certain individuals are particularly predisposed to developing TdP, including: women, people with hypokalemia or hypomagnesemia, and those with a history of congenital or idiopathic QTc syndrome, cardiac arrest, syncope, congestive heart failure, bradycardia, baseline QT prolongation, renal failure, or cardiac failure.4 Some agents can prolong the QTc interval by five to 10 milliseconds and cause TdP, while others require a 50-millisecond increase or more.
Drugs that confer a risk of ventricular arrhythmias include: disopyramide, dofetilide, ibutilide, procainamide, quinidine, sotalol, and amiodarone (antiarrhythmic agents); clarithromycin, erythromycin, levofloxacin, gatifloxacin, gemifloxacin, moxifloxacin, telithromycin (anti-infectives); domperidone and droperidol antiemetics; chlorpromazine, haloperidol, mesoridazine, thioridazine, and pimozide (antipsychotics); amitriptyline, desipramine, doxepin, fluoxetine, imipramine, sertraline, and venlafaxine (antidepressants); fluconazole, itraconazole, and ketoconazole (antifungals); naratriptan, sumatriptan, and zolmitriptan; and methadone.4-8 Other related agents, such as voriconazole and ondansetron, have been reported to cause QTc prolongation.
Drugs of special concern are those that frequently inhibit the metabolism of other agents, including erythromycin, clarithromycin, ketoconazole, itraconazole, amiodarone, and quinidine, and many antidepressants and antiretroviral agents. Of the deaths associated with drug-induced QTc prolongation related to the prokinetic agent cisapride, many were due to drug interactions with an imidazole or macrolide antibiotic. In these cases, increased serum concentrations of cisapride occurred due to inhibition of the cytochrome P450 CYP3A4 isoenzyme.9
If treatment with a drug that has the potential for causing QTc prolongation is begun, tell your patient to report any “potential cardiac” symptoms, such as palpitations, syncope, or near-syncope with or without palpitations, to a member of the healthcare team. Always be on the lookout for any concomitant conditions or treatments that can cause hypokalemia (e.g., diuretic use, gastroenteritis, diarrhea, excessive vomiting), or other agents that inhibit drug metabolism.
Obtaining a complete medication history, including the use of herbal products and over-the-counter medications, can help identify and prevent QTc prolongation from a drug interaction. A routine, 12-lead electrocardiogram (EKG) should be utilized during treatment to detect asymptomatic QTc prolongation or abnormal postectopic QTc intervals. Additionally, any patient predisposed to QTc prolongation should have an EKG performed before commencing treatment as well as after treatment is complete. If a drug prolongs the QTc interval beyond normal limits, the benefit of continuing the drug should be weighed against the risk of serious adverse cardiac events.10 TH
Michele B Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City.
References
1. Kupec IF. Seldane and generic terfenadine withdrawn from market. Food and Drug Administration Web site. Available at: www.fda.gov/bbs/topics/answers/ ans00853.html. Accessed Nov. 7, 2008.
2. Zalewski JM. Cisapride withdrawal requires alternate therapy. Cleveland Clinic Web site. Available at: www.clevelandclinicmeded.com/medicalpubs/pharmacy/mayjune2000/cisapride.htm. Accessed Nov. 7, 2008.
3. Drugs removed from or restricted in the U.S. market because of drug interactions. Food and Drug Administration Web site. Available at: www.fda.gov/cder/drug/drugReactions/CERT%20Educational%20Module%201/sld013.htm. Updated Dec. 22, 2008. Accessed Nov. 7, 2008.
4. Roden DM. Drug-induced prolongation of the QT interval. N Engl J Med. 2004;350:1013-1022.
5. Pham CP, de Feiter PW, van der Kuy PHM, van Mook WN. Long QTc interval and torsades de pointes caused by fluconazole. Ann Pharmacother. 2006;40:1456-1461.
6. Nykamp DL, Blackmon CL, Schmidt PE, Roberson AG. QTc prolongation associated with combination therapy of levofloxacin, imipramine, and fluoxetine. Ann Pharmacother. 1005;39:543-546.
7. Philips JA, Marty FM, Stone RM et al. Torsades de pointes associated with voriconazole use. Transpl Infect Dis. 2007;9:33-36.
8. Charbit B, Alvarez JC, Dasque E, Abe E, Démolis JL, Funck-Brentano C. Droperidol and ondansetron-induced QT interval prolongation. Anesthesiol. 2008;109:206-212.
9. Yap YG, Camm AJ. Drug induced qt prolongation and torsades de pointes. Heart. 2003;89:1363-1372.
10. Jayasinghe R, Registrar S, Kovoor P. Drugs and the QTc interval. Aust Prescr. 2002;25:63-65.
11. Atacand HCT 32/25 mg gives patients and physicians more treatment flexibility. Available at: www.pharmacitelink.com/news/2008/08/14_az.pdf. Accessed Nov. 4, 2008.
12. FDA approves astellas’ vaprisol (conivaptan hydrochloride injection) premixed in 5% dextrose for the treatment of hyponatremia. Sandoz Web site. Available at: sandoz.yellowbrix.com/pages/sandoz/Story.nsp?story_id=122559939. Accessed Nov. 4, 2008.
13. U.S. FDA drug shortages. Available at: www.fda.gov/cder/drug/shortages/default.htm#Foscavir. Accessed Nov. 3, 2008.
14. FDA Drug Shortages. Food and Drug Administration Web site. Available at: www.fda.gov/cder/drug/ shortages/discontinuation.pdf. Accessed Nov. 6, 2008.
15. Waknine Y. FDA safety changes: mirena, zyvox, orencia. Medscape Web site. Available at: www.medscape.com/viewarticle/580101. Accessed Nov. 3, 2008.
16. MannKind and Pfizer announce collaboration for certain exubera patients to transition to Mannkind’s inhaled insulin therapy. Drugs.com Web site. Available at: www.drugs.com/news/mannkind-pfizer-announce-collaboration-certain-exubera-patients-transition-mannkind-s-inhaled-13677.html. Accessed Nov. 3, 2008.
17. MannKind reports positive data from a phase 3 clinical study of technosphere insulin in Type 1 diabetics. Drugs.com Web site. Available at: www.drugs.com/ clinical_trials/mannkind-reports-positive-data-phase-3-clinical-study-technosphere-insulin-type-1-diabetes-5554.html. Accessed Nov. 3, 2008.
18. Bratulic A. Sanofi-aventis to halt all Acomplia trials. FirstWord Web site. Available at: www.firstwordplus.com/Fws.do?articleid=34DAB2DC3D7A48939A1D24AB97204CB4&logRowId=263560. Accessed Nov. 6, 2008.
Terfenadine, cisapride, astemizole … do you remember these drugs? They all were removed from the U.S. market subsequent to adverse outcomes related to QTc interval prolongation, including ventricular arrhythmias.1-3 Many drugs prolong the QTc interval, particularly if a drug is combined with others that affect its metabolism.
QTc interval prolongation can lead to torsades de pointes (TdP). Certain individuals are particularly predisposed to developing TdP, including: women, people with hypokalemia or hypomagnesemia, and those with a history of congenital or idiopathic QTc syndrome, cardiac arrest, syncope, congestive heart failure, bradycardia, baseline QT prolongation, renal failure, or cardiac failure.4 Some agents can prolong the QTc interval by five to 10 milliseconds and cause TdP, while others require a 50-millisecond increase or more.
Drugs that confer a risk of ventricular arrhythmias include: disopyramide, dofetilide, ibutilide, procainamide, quinidine, sotalol, and amiodarone (antiarrhythmic agents); clarithromycin, erythromycin, levofloxacin, gatifloxacin, gemifloxacin, moxifloxacin, telithromycin (anti-infectives); domperidone and droperidol antiemetics; chlorpromazine, haloperidol, mesoridazine, thioridazine, and pimozide (antipsychotics); amitriptyline, desipramine, doxepin, fluoxetine, imipramine, sertraline, and venlafaxine (antidepressants); fluconazole, itraconazole, and ketoconazole (antifungals); naratriptan, sumatriptan, and zolmitriptan; and methadone.4-8 Other related agents, such as voriconazole and ondansetron, have been reported to cause QTc prolongation.
Drugs of special concern are those that frequently inhibit the metabolism of other agents, including erythromycin, clarithromycin, ketoconazole, itraconazole, amiodarone, and quinidine, and many antidepressants and antiretroviral agents. Of the deaths associated with drug-induced QTc prolongation related to the prokinetic agent cisapride, many were due to drug interactions with an imidazole or macrolide antibiotic. In these cases, increased serum concentrations of cisapride occurred due to inhibition of the cytochrome P450 CYP3A4 isoenzyme.9
If treatment with a drug that has the potential for causing QTc prolongation is begun, tell your patient to report any “potential cardiac” symptoms, such as palpitations, syncope, or near-syncope with or without palpitations, to a member of the healthcare team. Always be on the lookout for any concomitant conditions or treatments that can cause hypokalemia (e.g., diuretic use, gastroenteritis, diarrhea, excessive vomiting), or other agents that inhibit drug metabolism.
Obtaining a complete medication history, including the use of herbal products and over-the-counter medications, can help identify and prevent QTc prolongation from a drug interaction. A routine, 12-lead electrocardiogram (EKG) should be utilized during treatment to detect asymptomatic QTc prolongation or abnormal postectopic QTc intervals. Additionally, any patient predisposed to QTc prolongation should have an EKG performed before commencing treatment as well as after treatment is complete. If a drug prolongs the QTc interval beyond normal limits, the benefit of continuing the drug should be weighed against the risk of serious adverse cardiac events.10 TH
Michele B Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City.
References
1. Kupec IF. Seldane and generic terfenadine withdrawn from market. Food and Drug Administration Web site. Available at: www.fda.gov/bbs/topics/answers/ ans00853.html. Accessed Nov. 7, 2008.
2. Zalewski JM. Cisapride withdrawal requires alternate therapy. Cleveland Clinic Web site. Available at: www.clevelandclinicmeded.com/medicalpubs/pharmacy/mayjune2000/cisapride.htm. Accessed Nov. 7, 2008.
3. Drugs removed from or restricted in the U.S. market because of drug interactions. Food and Drug Administration Web site. Available at: www.fda.gov/cder/drug/drugReactions/CERT%20Educational%20Module%201/sld013.htm. Updated Dec. 22, 2008. Accessed Nov. 7, 2008.
4. Roden DM. Drug-induced prolongation of the QT interval. N Engl J Med. 2004;350:1013-1022.
5. Pham CP, de Feiter PW, van der Kuy PHM, van Mook WN. Long QTc interval and torsades de pointes caused by fluconazole. Ann Pharmacother. 2006;40:1456-1461.
6. Nykamp DL, Blackmon CL, Schmidt PE, Roberson AG. QTc prolongation associated with combination therapy of levofloxacin, imipramine, and fluoxetine. Ann Pharmacother. 1005;39:543-546.
7. Philips JA, Marty FM, Stone RM et al. Torsades de pointes associated with voriconazole use. Transpl Infect Dis. 2007;9:33-36.
8. Charbit B, Alvarez JC, Dasque E, Abe E, Démolis JL, Funck-Brentano C. Droperidol and ondansetron-induced QT interval prolongation. Anesthesiol. 2008;109:206-212.
9. Yap YG, Camm AJ. Drug induced qt prolongation and torsades de pointes. Heart. 2003;89:1363-1372.
10. Jayasinghe R, Registrar S, Kovoor P. Drugs and the QTc interval. Aust Prescr. 2002;25:63-65.
11. Atacand HCT 32/25 mg gives patients and physicians more treatment flexibility. Available at: www.pharmacitelink.com/news/2008/08/14_az.pdf. Accessed Nov. 4, 2008.
12. FDA approves astellas’ vaprisol (conivaptan hydrochloride injection) premixed in 5% dextrose for the treatment of hyponatremia. Sandoz Web site. Available at: sandoz.yellowbrix.com/pages/sandoz/Story.nsp?story_id=122559939. Accessed Nov. 4, 2008.
13. U.S. FDA drug shortages. Available at: www.fda.gov/cder/drug/shortages/default.htm#Foscavir. Accessed Nov. 3, 2008.
14. FDA Drug Shortages. Food and Drug Administration Web site. Available at: www.fda.gov/cder/drug/ shortages/discontinuation.pdf. Accessed Nov. 6, 2008.
15. Waknine Y. FDA safety changes: mirena, zyvox, orencia. Medscape Web site. Available at: www.medscape.com/viewarticle/580101. Accessed Nov. 3, 2008.
16. MannKind and Pfizer announce collaboration for certain exubera patients to transition to Mannkind’s inhaled insulin therapy. Drugs.com Web site. Available at: www.drugs.com/news/mannkind-pfizer-announce-collaboration-certain-exubera-patients-transition-mannkind-s-inhaled-13677.html. Accessed Nov. 3, 2008.
17. MannKind reports positive data from a phase 3 clinical study of technosphere insulin in Type 1 diabetics. Drugs.com Web site. Available at: www.drugs.com/ clinical_trials/mannkind-reports-positive-data-phase-3-clinical-study-technosphere-insulin-type-1-diabetes-5554.html. Accessed Nov. 3, 2008.
18. Bratulic A. Sanofi-aventis to halt all Acomplia trials. FirstWord Web site. Available at: www.firstwordplus.com/Fws.do?articleid=34DAB2DC3D7A48939A1D24AB97204CB4&logRowId=263560. Accessed Nov. 6, 2008.
Terfenadine, cisapride, astemizole … do you remember these drugs? They all were removed from the U.S. market subsequent to adverse outcomes related to QTc interval prolongation, including ventricular arrhythmias.1-3 Many drugs prolong the QTc interval, particularly if a drug is combined with others that affect its metabolism.
QTc interval prolongation can lead to torsades de pointes (TdP). Certain individuals are particularly predisposed to developing TdP, including: women, people with hypokalemia or hypomagnesemia, and those with a history of congenital or idiopathic QTc syndrome, cardiac arrest, syncope, congestive heart failure, bradycardia, baseline QT prolongation, renal failure, or cardiac failure.4 Some agents can prolong the QTc interval by five to 10 milliseconds and cause TdP, while others require a 50-millisecond increase or more.
Drugs that confer a risk of ventricular arrhythmias include: disopyramide, dofetilide, ibutilide, procainamide, quinidine, sotalol, and amiodarone (antiarrhythmic agents); clarithromycin, erythromycin, levofloxacin, gatifloxacin, gemifloxacin, moxifloxacin, telithromycin (anti-infectives); domperidone and droperidol antiemetics; chlorpromazine, haloperidol, mesoridazine, thioridazine, and pimozide (antipsychotics); amitriptyline, desipramine, doxepin, fluoxetine, imipramine, sertraline, and venlafaxine (antidepressants); fluconazole, itraconazole, and ketoconazole (antifungals); naratriptan, sumatriptan, and zolmitriptan; and methadone.4-8 Other related agents, such as voriconazole and ondansetron, have been reported to cause QTc prolongation.
Drugs of special concern are those that frequently inhibit the metabolism of other agents, including erythromycin, clarithromycin, ketoconazole, itraconazole, amiodarone, and quinidine, and many antidepressants and antiretroviral agents. Of the deaths associated with drug-induced QTc prolongation related to the prokinetic agent cisapride, many were due to drug interactions with an imidazole or macrolide antibiotic. In these cases, increased serum concentrations of cisapride occurred due to inhibition of the cytochrome P450 CYP3A4 isoenzyme.9
If treatment with a drug that has the potential for causing QTc prolongation is begun, tell your patient to report any “potential cardiac” symptoms, such as palpitations, syncope, or near-syncope with or without palpitations, to a member of the healthcare team. Always be on the lookout for any concomitant conditions or treatments that can cause hypokalemia (e.g., diuretic use, gastroenteritis, diarrhea, excessive vomiting), or other agents that inhibit drug metabolism.
Obtaining a complete medication history, including the use of herbal products and over-the-counter medications, can help identify and prevent QTc prolongation from a drug interaction. A routine, 12-lead electrocardiogram (EKG) should be utilized during treatment to detect asymptomatic QTc prolongation or abnormal postectopic QTc intervals. Additionally, any patient predisposed to QTc prolongation should have an EKG performed before commencing treatment as well as after treatment is complete. If a drug prolongs the QTc interval beyond normal limits, the benefit of continuing the drug should be weighed against the risk of serious adverse cardiac events.10 TH
Michele B Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City.
References
1. Kupec IF. Seldane and generic terfenadine withdrawn from market. Food and Drug Administration Web site. Available at: www.fda.gov/bbs/topics/answers/ ans00853.html. Accessed Nov. 7, 2008.
2. Zalewski JM. Cisapride withdrawal requires alternate therapy. Cleveland Clinic Web site. Available at: www.clevelandclinicmeded.com/medicalpubs/pharmacy/mayjune2000/cisapride.htm. Accessed Nov. 7, 2008.
3. Drugs removed from or restricted in the U.S. market because of drug interactions. Food and Drug Administration Web site. Available at: www.fda.gov/cder/drug/drugReactions/CERT%20Educational%20Module%201/sld013.htm. Updated Dec. 22, 2008. Accessed Nov. 7, 2008.
4. Roden DM. Drug-induced prolongation of the QT interval. N Engl J Med. 2004;350:1013-1022.
5. Pham CP, de Feiter PW, van der Kuy PHM, van Mook WN. Long QTc interval and torsades de pointes caused by fluconazole. Ann Pharmacother. 2006;40:1456-1461.
6. Nykamp DL, Blackmon CL, Schmidt PE, Roberson AG. QTc prolongation associated with combination therapy of levofloxacin, imipramine, and fluoxetine. Ann Pharmacother. 1005;39:543-546.
7. Philips JA, Marty FM, Stone RM et al. Torsades de pointes associated with voriconazole use. Transpl Infect Dis. 2007;9:33-36.
8. Charbit B, Alvarez JC, Dasque E, Abe E, Démolis JL, Funck-Brentano C. Droperidol and ondansetron-induced QT interval prolongation. Anesthesiol. 2008;109:206-212.
9. Yap YG, Camm AJ. Drug induced qt prolongation and torsades de pointes. Heart. 2003;89:1363-1372.
10. Jayasinghe R, Registrar S, Kovoor P. Drugs and the QTc interval. Aust Prescr. 2002;25:63-65.
11. Atacand HCT 32/25 mg gives patients and physicians more treatment flexibility. Available at: www.pharmacitelink.com/news/2008/08/14_az.pdf. Accessed Nov. 4, 2008.
12. FDA approves astellas’ vaprisol (conivaptan hydrochloride injection) premixed in 5% dextrose for the treatment of hyponatremia. Sandoz Web site. Available at: sandoz.yellowbrix.com/pages/sandoz/Story.nsp?story_id=122559939. Accessed Nov. 4, 2008.
13. U.S. FDA drug shortages. Available at: www.fda.gov/cder/drug/shortages/default.htm#Foscavir. Accessed Nov. 3, 2008.
14. FDA Drug Shortages. Food and Drug Administration Web site. Available at: www.fda.gov/cder/drug/ shortages/discontinuation.pdf. Accessed Nov. 6, 2008.
15. Waknine Y. FDA safety changes: mirena, zyvox, orencia. Medscape Web site. Available at: www.medscape.com/viewarticle/580101. Accessed Nov. 3, 2008.
16. MannKind and Pfizer announce collaboration for certain exubera patients to transition to Mannkind’s inhaled insulin therapy. Drugs.com Web site. Available at: www.drugs.com/news/mannkind-pfizer-announce-collaboration-certain-exubera-patients-transition-mannkind-s-inhaled-13677.html. Accessed Nov. 3, 2008.
17. MannKind reports positive data from a phase 3 clinical study of technosphere insulin in Type 1 diabetics. Drugs.com Web site. Available at: www.drugs.com/ clinical_trials/mannkind-reports-positive-data-phase-3-clinical-study-technosphere-insulin-type-1-diabetes-5554.html. Accessed Nov. 3, 2008.
18. Bratulic A. Sanofi-aventis to halt all Acomplia trials. FirstWord Web site. Available at: www.firstwordplus.com/Fws.do?articleid=34DAB2DC3D7A48939A1D24AB97204CB4&logRowId=263560. Accessed Nov. 6, 2008.
You Asked, We Delivered

When the groundhog pops out of the ground and sees his shadow, what does it mean again? Snow, rain, global warming? Better check Google.
One thing I don’t need a search engine to find out is that readers of The Hospitalist want more pediatric HM coverage. In fact, more than 40% of respondents to our recent reader survey specifically asked for it. More than 500 readers responded, which leads me to think the numbers are pretty accurate.
In response to the overwhelming demand, I’m pleased to announce a new addition to The Hospitalist’s editorial staff. Beginning this month, Mark Shen, MD, medical director of hospital medicine at Dell Children’s Medical Center in Austin, Texas, will become pediatric editor for The Hospitalist. A leading authority on pediatric issues in hospital medicine, Dr. Shen has practiced as a pediatric hospitalist in the seven years since he completed his medical training and pediatric residency at the University of Texas’ Southwestern Medical School in Dallas. With Dr. Shen serving as our guide, the editorial team will expand coverage of pediatric HM with:
- A monthly, pediatric-focused “In the Literature” review;
- More features focusing on trends in pediatric HM; and
- Dr. Shen’s semiannual column, in which he’ll concentrate on pediatric issues relevant to the entire HM community.
We’re glad to have Dr. Shen join us.
Digital Fever
What do a football star shooting himself in the leg, excessive and erroneous asthma diagnoses, and a respected hospitalist admitting to “being a slow learner” have in common? Each has been a lead story in eWire, our weekly e-newsletter that launched in October and appears in your inbox every Tuesday.
In “Taking the Pulse of Hospital Medicine,” we keep you apprised of the latest news and trends in HM in quick news “pieces,” providing you with useful tools, facts, and links to make your day a little easier. In response to your demand for more brief clinical updates, we recently added exclusive “In the Literature” reviews of clinical research and an HM blogosphere roundup. Keep a lookout online and on your phone, as more digital products are in the works.
HM 2009
Yes, SHM’s annual meeting is right around the corner. Early registration ends April 5, which might seem a long way off, but it really isn’t. For the record, I’m totally stoked. Not only will it be my first HM convention, but it will be a homecoming of sorts. I was raised outside of Chicago, in the long shadow of the Sears Tower, and have suffered as a diehard Cubs baseball fan. Sigh. The Cubbies will be in town that week, and I invite convention-goers to visit the hallowed brick house known as Wrigley Field (it’s 15 minutes from the HM09 hotel base).
But back to work. Our editorial staff is conjuring up some exciting HM09 coverage plans. In addition to previews of the big event, we’re planning special daily—yes, daily—news, features, and multimedia offerings from Chicago. Stay tuned.
And, for the record, Google directed me to a Web site that explained everything you need to know about woodchucks—er, groundhogs. When Punxsutawney Phil sees his shadow, it means six more weeks of winter. Let’s hope it doesn’t. TH
Jason Carris is editor of The Hospitalist.
When the groundhog pops out of the ground and sees his shadow, what does it mean again? Snow, rain, global warming? Better check Google.
One thing I don’t need a search engine to find out is that readers of The Hospitalist want more pediatric HM coverage. In fact, more than 40% of respondents to our recent reader survey specifically asked for it. More than 500 readers responded, which leads me to think the numbers are pretty accurate.
In response to the overwhelming demand, I’m pleased to announce a new addition to The Hospitalist’s editorial staff. Beginning this month, Mark Shen, MD, medical director of hospital medicine at Dell Children’s Medical Center in Austin, Texas, will become pediatric editor for The Hospitalist. A leading authority on pediatric issues in hospital medicine, Dr. Shen has practiced as a pediatric hospitalist in the seven years since he completed his medical training and pediatric residency at the University of Texas’ Southwestern Medical School in Dallas. With Dr. Shen serving as our guide, the editorial team will expand coverage of pediatric HM with:
- A monthly, pediatric-focused “In the Literature” review;
- More features focusing on trends in pediatric HM; and
- Dr. Shen’s semiannual column, in which he’ll concentrate on pediatric issues relevant to the entire HM community.
We’re glad to have Dr. Shen join us.
Digital Fever
What do a football star shooting himself in the leg, excessive and erroneous asthma diagnoses, and a respected hospitalist admitting to “being a slow learner” have in common? Each has been a lead story in eWire, our weekly e-newsletter that launched in October and appears in your inbox every Tuesday.
In “Taking the Pulse of Hospital Medicine,” we keep you apprised of the latest news and trends in HM in quick news “pieces,” providing you with useful tools, facts, and links to make your day a little easier. In response to your demand for more brief clinical updates, we recently added exclusive “In the Literature” reviews of clinical research and an HM blogosphere roundup. Keep a lookout online and on your phone, as more digital products are in the works.
HM 2009
Yes, SHM’s annual meeting is right around the corner. Early registration ends April 5, which might seem a long way off, but it really isn’t. For the record, I’m totally stoked. Not only will it be my first HM convention, but it will be a homecoming of sorts. I was raised outside of Chicago, in the long shadow of the Sears Tower, and have suffered as a diehard Cubs baseball fan. Sigh. The Cubbies will be in town that week, and I invite convention-goers to visit the hallowed brick house known as Wrigley Field (it’s 15 minutes from the HM09 hotel base).
But back to work. Our editorial staff is conjuring up some exciting HM09 coverage plans. In addition to previews of the big event, we’re planning special daily—yes, daily—news, features, and multimedia offerings from Chicago. Stay tuned.
And, for the record, Google directed me to a Web site that explained everything you need to know about woodchucks—er, groundhogs. When Punxsutawney Phil sees his shadow, it means six more weeks of winter. Let’s hope it doesn’t. TH
Jason Carris is editor of The Hospitalist.
When the groundhog pops out of the ground and sees his shadow, what does it mean again? Snow, rain, global warming? Better check Google.
One thing I don’t need a search engine to find out is that readers of The Hospitalist want more pediatric HM coverage. In fact, more than 40% of respondents to our recent reader survey specifically asked for it. More than 500 readers responded, which leads me to think the numbers are pretty accurate.
In response to the overwhelming demand, I’m pleased to announce a new addition to The Hospitalist’s editorial staff. Beginning this month, Mark Shen, MD, medical director of hospital medicine at Dell Children’s Medical Center in Austin, Texas, will become pediatric editor for The Hospitalist. A leading authority on pediatric issues in hospital medicine, Dr. Shen has practiced as a pediatric hospitalist in the seven years since he completed his medical training and pediatric residency at the University of Texas’ Southwestern Medical School in Dallas. With Dr. Shen serving as our guide, the editorial team will expand coverage of pediatric HM with:
- A monthly, pediatric-focused “In the Literature” review;
- More features focusing on trends in pediatric HM; and
- Dr. Shen’s semiannual column, in which he’ll concentrate on pediatric issues relevant to the entire HM community.
We’re glad to have Dr. Shen join us.
Digital Fever
What do a football star shooting himself in the leg, excessive and erroneous asthma diagnoses, and a respected hospitalist admitting to “being a slow learner” have in common? Each has been a lead story in eWire, our weekly e-newsletter that launched in October and appears in your inbox every Tuesday.
In “Taking the Pulse of Hospital Medicine,” we keep you apprised of the latest news and trends in HM in quick news “pieces,” providing you with useful tools, facts, and links to make your day a little easier. In response to your demand for more brief clinical updates, we recently added exclusive “In the Literature” reviews of clinical research and an HM blogosphere roundup. Keep a lookout online and on your phone, as more digital products are in the works.
HM 2009
Yes, SHM’s annual meeting is right around the corner. Early registration ends April 5, which might seem a long way off, but it really isn’t. For the record, I’m totally stoked. Not only will it be my first HM convention, but it will be a homecoming of sorts. I was raised outside of Chicago, in the long shadow of the Sears Tower, and have suffered as a diehard Cubs baseball fan. Sigh. The Cubbies will be in town that week, and I invite convention-goers to visit the hallowed brick house known as Wrigley Field (it’s 15 minutes from the HM09 hotel base).
But back to work. Our editorial staff is conjuring up some exciting HM09 coverage plans. In addition to previews of the big event, we’re planning special daily—yes, daily—news, features, and multimedia offerings from Chicago. Stay tuned.
And, for the record, Google directed me to a Web site that explained everything you need to know about woodchucks—er, groundhogs. When Punxsutawney Phil sees his shadow, it means six more weeks of winter. Let’s hope it doesn’t. TH
Jason Carris is editor of The Hospitalist.