User login
ONLINE EXCLUSIVE: Audio interview with SHM President Jeff Wiese, MD, FACP, SFHM
ONLINE EXCLUSIVE: Focused Practice in Hospital Medicine audio interview with SHM President Jeff Wiese, MD, FACP, SFHM
Market Watch
New Generic
- Perindopril erbumine tablets (generic Aceon)1
New Drugs, Indications, Dosage Forms, and Approval Recommendations
- Collagenase clostridium histolytica injection (Xiaflex) has been approved by the FDA for treating the hand disease Dupuytren’s contracture. The agent breaks down excessive collagen in the hand, allowing patients to straighten the arm and have proper use of their fingers. The agent is also being studied to treat Peyronie’s disease.2
- Dalfampridine tablets (Ampyra) have been approved by the FDA to improve walking in patients with multiple sclerosis (MS).3 Seizures might occur in patients who exceed the recommended daily dose of 10 mg twice daily, or in patients with moderate to severe kidney disease. Therefore, caution is advised in these patients.
- Iloperidone tablets (Fanapt) have been approved by the FDA for the acute treatment of schizophrenia in adults.4 An atypical antipsychotic, it is a mixed dopamine D2/serotonin 5HT2A receptor antagonist.
- Lamotrigine extended-release tablets (Lamictal XR) have received a new FDA-approved indication for once-daily, add-on therapy for epilepsy in patients 13 years and older, with primary, generalized tonic-clonic seizures.5
- Liraglutide (Victoza) has been approved by the FDA as a once-daily injection for the treatment of Type 2 diabetes mellitus.6 Liraglutide is a glucagon-like peptide-1 (GLP-1) receptor agonist, which is similar to exenatide. There is a label warning related to thyroid tumors that occurred in rats and mice. It is unclear whether medullary thyroid cancer will occur in adults; therefore, the agent should not be used in patients who already have this cancer or those with a family history of thyroid cancer.
- Trazodone extended-release tablets (Oleptro) have been approved by the FDA for treating major depressive disorder in adults.7 This product is formulated using Labopharm’s proprietary Contramid long-acting drug delivery system. The product will be available later this year.
Safety Information
- Didanosine (Videx/Videx EC) has undergone a label change in the warning and precautions sections related to the rare but serious complication of noncirrhotic portal hypertension. The label change was added because of the potential severity of portal hypertension, including death from hemorrhaging esophageal varices. A number of well-documented, postmarketing reports of this reaction were made following exclusion of other portal hypertension causes.8
- Long-acting beta-agonists (LABAs), formoterol (Foradil), and salmeterol (Sereven) are required to have a risk management strategy (REMS) and a revised medication guide written specifically for patients. The goal is to educate patients about the appropriate use of LABAs. There also is a plan to educate healthcare professionals about the appropriate use of LABAs.9,10 This update is due to continued analysis of studies that show increased risk of severe asthma exacerbations, which lead to hospitalizations in adult and pediatric patients, including deaths in some LABA-utilizing patients. To safely use LABAs, the following need to be considered:
- Single-ingredient LABAs should not be used as monotherapy; they should only be used in combination with an asthma controller;
- LABAs should only be used long-term in patients whose asthma cannot be adequately controlled on asthma controllers;
- Use an LABA for the shortest duration required to achieve asthma control and discontinue it, if possible, once asthma control is achieved. Patients should then be maintained on an asthma controller; and
- Use a combination product containing both an inhaled corticosteroid and an LABA to enhance adherence in pediatric and adolescent patients who require both of these classes to manage their asthma.
- Olanzapine (Zyprexa) has undergone a label change related to its indications for use in adolescents ages 13-17 for treating schizophrenia and bipolar I disorder (manic or mixed episodes).11 The new label asks providers to consider alternative treatments in this patient population due to the increased potential for weight gain and hyperlipidemia. Additionally, the effectiveness and safety of this agent have not been determined in patients under 13.
- Sibutramine (Meridia), marketed for weight loss, continues to be evaluated for safety.12 A recent review found it poses an increased risk of heart attack and stroke in patients with a history of cardiovascular disease. Although the product label already had a warning related to use in patients with cardiovascular disease, the manufacturer has added a new contraindication to the sibutramine label for patients with cardiovascular disease and a history of: 1) coronary artery disease; 2) stroke or transient ischemic attack; 3) arrhythmias; 4) congestive heart failure; 5) peripheral arterial disease; and/or 6) uncontrolled hypertension (e.g., >145/90 mmHg). Providers should monitor blood pressure and heart rate regularly. If there is an unremitting increase in blood pressure and/or heart rate, sibutramine should be discontinued. Sibutramine should also be stopped in patients who do not lose at least 5% of their baseline body weight within the first three to six months of treatment.13TH
Michele B. Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City and a clinical pharmacist at New York Downtown Hospital.
References
- Lupin receives US FDA approval for Perindopril erbumine tablets. Lupin Web site. Available at: http://www.lupinworld.com/28jan10.htm. Accessed Feb. 22, 2010.
- US FDA approves Auxilium drug for hand disease. Reuters Web site. Available at: http://www.reuters.com/article/idUSN0211921420100203. Accessed Feb. 22, 2010.
- Petrochko C. MS walking drug gets FDA nod. MedPage Today Web site. Available at: http://www.medpagetoday.com/Neurology/MultipleSclerosis/18112. Accessed Feb. 22, 2010.
- Fanapt available for acute schizophrenia. Monthly Prescribing Reference Web site. Available at: http://www.empr.com/fanapt-available-for-acute-schizophrenia/article/160985/. Accessed Feb. 22, 2010.
- FDA approves once-a-day Lamictal XR as add-on epilepsy therapy for primary generalized tonic-clonic seizures. Available at: http://www.medicalnewstoday.com/articles/177796.php. Accessed Feb. 22, 2010.
- FDA approves new treatment for Type 2 diabetes. U.S. Food and Drug Administration Web site. Available at: http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm198638.htm. Accessed Feb. 22, 2010.
- Labopharm receives FDA approval for Oleptro. PR Newswire Web site. Available at: http://www.prnewswire.com/news-releases/labopharm-receives-fda-approval-for-oleptrotm-83429037.html. Accessed Feb. 22, 2010.
- Videx/Videx EC (didanosine): Labeling revision—risk of non-cirrhotic portal hypertension. U.S. Food and Drug Administration Web site. Available at: http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm199343.htm. Accessed Feb. 22, 2010.
- Long-acting beta-agonists (LABAs): new safe use requirements. U.S. Food and Drug Administration Web site. Available at: http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm201003.htm. Accessed Feb. 22, 2010.
- Gever J. FDA says LABA asthma drugs not safe for solo use. MedPage Today Web site. Available at: http://www.medpagetoday.com/tbprint.cfm?tbid=18552. Accessed Feb. 22, 2010.
- Zyprexa (olanzapine): use in adolescents. U.S. Food and Drug Administration Web site. Available at: http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm198402.htm. Accessed Feb. 22, 2010.
- Follow-up to the November 2009 early communication about an ongoing safety review of sibutramine, marketed as Meridia. U.S. Food and Drug Administration Web site. Available at: http://www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/DrugSafetyInformationforHeathcareProfessionals/ucm198206.htm. Accessed Feb. 21, 2010.
- Petrochko C. FDA adds cardio warnings to weight-loss drug. MedPage Today Web site. Available at: http://www.medpagetoday.com/tbprint.cfm?tbid=18088?. Accessed Feb. 22, 2010.
New Generic
- Perindopril erbumine tablets (generic Aceon)1
New Drugs, Indications, Dosage Forms, and Approval Recommendations
- Collagenase clostridium histolytica injection (Xiaflex) has been approved by the FDA for treating the hand disease Dupuytren’s contracture. The agent breaks down excessive collagen in the hand, allowing patients to straighten the arm and have proper use of their fingers. The agent is also being studied to treat Peyronie’s disease.2
- Dalfampridine tablets (Ampyra) have been approved by the FDA to improve walking in patients with multiple sclerosis (MS).3 Seizures might occur in patients who exceed the recommended daily dose of 10 mg twice daily, or in patients with moderate to severe kidney disease. Therefore, caution is advised in these patients.
- Iloperidone tablets (Fanapt) have been approved by the FDA for the acute treatment of schizophrenia in adults.4 An atypical antipsychotic, it is a mixed dopamine D2/serotonin 5HT2A receptor antagonist.
- Lamotrigine extended-release tablets (Lamictal XR) have received a new FDA-approved indication for once-daily, add-on therapy for epilepsy in patients 13 years and older, with primary, generalized tonic-clonic seizures.5
- Liraglutide (Victoza) has been approved by the FDA as a once-daily injection for the treatment of Type 2 diabetes mellitus.6 Liraglutide is a glucagon-like peptide-1 (GLP-1) receptor agonist, which is similar to exenatide. There is a label warning related to thyroid tumors that occurred in rats and mice. It is unclear whether medullary thyroid cancer will occur in adults; therefore, the agent should not be used in patients who already have this cancer or those with a family history of thyroid cancer.
- Trazodone extended-release tablets (Oleptro) have been approved by the FDA for treating major depressive disorder in adults.7 This product is formulated using Labopharm’s proprietary Contramid long-acting drug delivery system. The product will be available later this year.
Safety Information
- Didanosine (Videx/Videx EC) has undergone a label change in the warning and precautions sections related to the rare but serious complication of noncirrhotic portal hypertension. The label change was added because of the potential severity of portal hypertension, including death from hemorrhaging esophageal varices. A number of well-documented, postmarketing reports of this reaction were made following exclusion of other portal hypertension causes.8
- Long-acting beta-agonists (LABAs), formoterol (Foradil), and salmeterol (Sereven) are required to have a risk management strategy (REMS) and a revised medication guide written specifically for patients. The goal is to educate patients about the appropriate use of LABAs. There also is a plan to educate healthcare professionals about the appropriate use of LABAs.9,10 This update is due to continued analysis of studies that show increased risk of severe asthma exacerbations, which lead to hospitalizations in adult and pediatric patients, including deaths in some LABA-utilizing patients. To safely use LABAs, the following need to be considered:
- Single-ingredient LABAs should not be used as monotherapy; they should only be used in combination with an asthma controller;
- LABAs should only be used long-term in patients whose asthma cannot be adequately controlled on asthma controllers;
- Use an LABA for the shortest duration required to achieve asthma control and discontinue it, if possible, once asthma control is achieved. Patients should then be maintained on an asthma controller; and
- Use a combination product containing both an inhaled corticosteroid and an LABA to enhance adherence in pediatric and adolescent patients who require both of these classes to manage their asthma.
- Olanzapine (Zyprexa) has undergone a label change related to its indications for use in adolescents ages 13-17 for treating schizophrenia and bipolar I disorder (manic or mixed episodes).11 The new label asks providers to consider alternative treatments in this patient population due to the increased potential for weight gain and hyperlipidemia. Additionally, the effectiveness and safety of this agent have not been determined in patients under 13.
- Sibutramine (Meridia), marketed for weight loss, continues to be evaluated for safety.12 A recent review found it poses an increased risk of heart attack and stroke in patients with a history of cardiovascular disease. Although the product label already had a warning related to use in patients with cardiovascular disease, the manufacturer has added a new contraindication to the sibutramine label for patients with cardiovascular disease and a history of: 1) coronary artery disease; 2) stroke or transient ischemic attack; 3) arrhythmias; 4) congestive heart failure; 5) peripheral arterial disease; and/or 6) uncontrolled hypertension (e.g., >145/90 mmHg). Providers should monitor blood pressure and heart rate regularly. If there is an unremitting increase in blood pressure and/or heart rate, sibutramine should be discontinued. Sibutramine should also be stopped in patients who do not lose at least 5% of their baseline body weight within the first three to six months of treatment.13TH
Michele B. Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City and a clinical pharmacist at New York Downtown Hospital.
References
- Lupin receives US FDA approval for Perindopril erbumine tablets. Lupin Web site. Available at: http://www.lupinworld.com/28jan10.htm. Accessed Feb. 22, 2010.
- US FDA approves Auxilium drug for hand disease. Reuters Web site. Available at: http://www.reuters.com/article/idUSN0211921420100203. Accessed Feb. 22, 2010.
- Petrochko C. MS walking drug gets FDA nod. MedPage Today Web site. Available at: http://www.medpagetoday.com/Neurology/MultipleSclerosis/18112. Accessed Feb. 22, 2010.
- Fanapt available for acute schizophrenia. Monthly Prescribing Reference Web site. Available at: http://www.empr.com/fanapt-available-for-acute-schizophrenia/article/160985/. Accessed Feb. 22, 2010.
- FDA approves once-a-day Lamictal XR as add-on epilepsy therapy for primary generalized tonic-clonic seizures. Available at: http://www.medicalnewstoday.com/articles/177796.php. Accessed Feb. 22, 2010.
- FDA approves new treatment for Type 2 diabetes. U.S. Food and Drug Administration Web site. Available at: http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm198638.htm. Accessed Feb. 22, 2010.
- Labopharm receives FDA approval for Oleptro. PR Newswire Web site. Available at: http://www.prnewswire.com/news-releases/labopharm-receives-fda-approval-for-oleptrotm-83429037.html. Accessed Feb. 22, 2010.
- Videx/Videx EC (didanosine): Labeling revision—risk of non-cirrhotic portal hypertension. U.S. Food and Drug Administration Web site. Available at: http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm199343.htm. Accessed Feb. 22, 2010.
- Long-acting beta-agonists (LABAs): new safe use requirements. U.S. Food and Drug Administration Web site. Available at: http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm201003.htm. Accessed Feb. 22, 2010.
- Gever J. FDA says LABA asthma drugs not safe for solo use. MedPage Today Web site. Available at: http://www.medpagetoday.com/tbprint.cfm?tbid=18552. Accessed Feb. 22, 2010.
- Zyprexa (olanzapine): use in adolescents. U.S. Food and Drug Administration Web site. Available at: http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm198402.htm. Accessed Feb. 22, 2010.
- Follow-up to the November 2009 early communication about an ongoing safety review of sibutramine, marketed as Meridia. U.S. Food and Drug Administration Web site. Available at: http://www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/DrugSafetyInformationforHeathcareProfessionals/ucm198206.htm. Accessed Feb. 21, 2010.
- Petrochko C. FDA adds cardio warnings to weight-loss drug. MedPage Today Web site. Available at: http://www.medpagetoday.com/tbprint.cfm?tbid=18088?. Accessed Feb. 22, 2010.
New Generic
- Perindopril erbumine tablets (generic Aceon)1
New Drugs, Indications, Dosage Forms, and Approval Recommendations
- Collagenase clostridium histolytica injection (Xiaflex) has been approved by the FDA for treating the hand disease Dupuytren’s contracture. The agent breaks down excessive collagen in the hand, allowing patients to straighten the arm and have proper use of their fingers. The agent is also being studied to treat Peyronie’s disease.2
- Dalfampridine tablets (Ampyra) have been approved by the FDA to improve walking in patients with multiple sclerosis (MS).3 Seizures might occur in patients who exceed the recommended daily dose of 10 mg twice daily, or in patients with moderate to severe kidney disease. Therefore, caution is advised in these patients.
- Iloperidone tablets (Fanapt) have been approved by the FDA for the acute treatment of schizophrenia in adults.4 An atypical antipsychotic, it is a mixed dopamine D2/serotonin 5HT2A receptor antagonist.
- Lamotrigine extended-release tablets (Lamictal XR) have received a new FDA-approved indication for once-daily, add-on therapy for epilepsy in patients 13 years and older, with primary, generalized tonic-clonic seizures.5
- Liraglutide (Victoza) has been approved by the FDA as a once-daily injection for the treatment of Type 2 diabetes mellitus.6 Liraglutide is a glucagon-like peptide-1 (GLP-1) receptor agonist, which is similar to exenatide. There is a label warning related to thyroid tumors that occurred in rats and mice. It is unclear whether medullary thyroid cancer will occur in adults; therefore, the agent should not be used in patients who already have this cancer or those with a family history of thyroid cancer.
- Trazodone extended-release tablets (Oleptro) have been approved by the FDA for treating major depressive disorder in adults.7 This product is formulated using Labopharm’s proprietary Contramid long-acting drug delivery system. The product will be available later this year.
Safety Information
- Didanosine (Videx/Videx EC) has undergone a label change in the warning and precautions sections related to the rare but serious complication of noncirrhotic portal hypertension. The label change was added because of the potential severity of portal hypertension, including death from hemorrhaging esophageal varices. A number of well-documented, postmarketing reports of this reaction were made following exclusion of other portal hypertension causes.8
- Long-acting beta-agonists (LABAs), formoterol (Foradil), and salmeterol (Sereven) are required to have a risk management strategy (REMS) and a revised medication guide written specifically for patients. The goal is to educate patients about the appropriate use of LABAs. There also is a plan to educate healthcare professionals about the appropriate use of LABAs.9,10 This update is due to continued analysis of studies that show increased risk of severe asthma exacerbations, which lead to hospitalizations in adult and pediatric patients, including deaths in some LABA-utilizing patients. To safely use LABAs, the following need to be considered:
- Single-ingredient LABAs should not be used as monotherapy; they should only be used in combination with an asthma controller;
- LABAs should only be used long-term in patients whose asthma cannot be adequately controlled on asthma controllers;
- Use an LABA for the shortest duration required to achieve asthma control and discontinue it, if possible, once asthma control is achieved. Patients should then be maintained on an asthma controller; and
- Use a combination product containing both an inhaled corticosteroid and an LABA to enhance adherence in pediatric and adolescent patients who require both of these classes to manage their asthma.
- Olanzapine (Zyprexa) has undergone a label change related to its indications for use in adolescents ages 13-17 for treating schizophrenia and bipolar I disorder (manic or mixed episodes).11 The new label asks providers to consider alternative treatments in this patient population due to the increased potential for weight gain and hyperlipidemia. Additionally, the effectiveness and safety of this agent have not been determined in patients under 13.
- Sibutramine (Meridia), marketed for weight loss, continues to be evaluated for safety.12 A recent review found it poses an increased risk of heart attack and stroke in patients with a history of cardiovascular disease. Although the product label already had a warning related to use in patients with cardiovascular disease, the manufacturer has added a new contraindication to the sibutramine label for patients with cardiovascular disease and a history of: 1) coronary artery disease; 2) stroke or transient ischemic attack; 3) arrhythmias; 4) congestive heart failure; 5) peripheral arterial disease; and/or 6) uncontrolled hypertension (e.g., >145/90 mmHg). Providers should monitor blood pressure and heart rate regularly. If there is an unremitting increase in blood pressure and/or heart rate, sibutramine should be discontinued. Sibutramine should also be stopped in patients who do not lose at least 5% of their baseline body weight within the first three to six months of treatment.13TH
Michele B. Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City and a clinical pharmacist at New York Downtown Hospital.
References
- Lupin receives US FDA approval for Perindopril erbumine tablets. Lupin Web site. Available at: http://www.lupinworld.com/28jan10.htm. Accessed Feb. 22, 2010.
- US FDA approves Auxilium drug for hand disease. Reuters Web site. Available at: http://www.reuters.com/article/idUSN0211921420100203. Accessed Feb. 22, 2010.
- Petrochko C. MS walking drug gets FDA nod. MedPage Today Web site. Available at: http://www.medpagetoday.com/Neurology/MultipleSclerosis/18112. Accessed Feb. 22, 2010.
- Fanapt available for acute schizophrenia. Monthly Prescribing Reference Web site. Available at: http://www.empr.com/fanapt-available-for-acute-schizophrenia/article/160985/. Accessed Feb. 22, 2010.
- FDA approves once-a-day Lamictal XR as add-on epilepsy therapy for primary generalized tonic-clonic seizures. Available at: http://www.medicalnewstoday.com/articles/177796.php. Accessed Feb. 22, 2010.
- FDA approves new treatment for Type 2 diabetes. U.S. Food and Drug Administration Web site. Available at: http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm198638.htm. Accessed Feb. 22, 2010.
- Labopharm receives FDA approval for Oleptro. PR Newswire Web site. Available at: http://www.prnewswire.com/news-releases/labopharm-receives-fda-approval-for-oleptrotm-83429037.html. Accessed Feb. 22, 2010.
- Videx/Videx EC (didanosine): Labeling revision—risk of non-cirrhotic portal hypertension. U.S. Food and Drug Administration Web site. Available at: http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm199343.htm. Accessed Feb. 22, 2010.
- Long-acting beta-agonists (LABAs): new safe use requirements. U.S. Food and Drug Administration Web site. Available at: http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm201003.htm. Accessed Feb. 22, 2010.
- Gever J. FDA says LABA asthma drugs not safe for solo use. MedPage Today Web site. Available at: http://www.medpagetoday.com/tbprint.cfm?tbid=18552. Accessed Feb. 22, 2010.
- Zyprexa (olanzapine): use in adolescents. U.S. Food and Drug Administration Web site. Available at: http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm198402.htm. Accessed Feb. 22, 2010.
- Follow-up to the November 2009 early communication about an ongoing safety review of sibutramine, marketed as Meridia. U.S. Food and Drug Administration Web site. Available at: http://www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/DrugSafetyInformationforHeathcareProfessionals/ucm198206.htm. Accessed Feb. 21, 2010.
- Petrochko C. FDA adds cardio warnings to weight-loss drug. MedPage Today Web site. Available at: http://www.medpagetoday.com/tbprint.cfm?tbid=18088?. Accessed Feb. 22, 2010.
In the Literature
In This Edition
Literature at a Glance
A guide to this month’s studies
- ICU volume and outcomes
- Bicarbonate and contrast-induced nephropathy
- Rate of incidental findings in chest CT angiography
- Consequences of adverse-event reporting by physicians
- Hip fracture comanagement
- Niacin vs. ezetimibe in atherosclerosis
- Effect of hospital pharmacists on readmission rates
- Antibiotics in acute exacerbations of COPD
Higher Patient ICU Inflow Volumes Are Associated with Unplanned Readmissions to ICU
Clinical question: Do higher rates of unplanned ICU readmissions occur on days with high patient inflow volumes?
Background: Patients readmitted to ICUs have longer lengths of stay (LOS) and higher rates of in-hospital mortality. Previous studies suggest many ICU readmissions might be due to premature discharge, but there is little evidence evaluating the impact of patient inflow volumes on the incidence of ICU readmissions.
Study design: Retrospective, cohort study.
Setting: Large, urban, tertiary-care academic medical center in Baltimore.
Synopsis: A retrospective review of 3,233 discharges from a neurosciences critical-care unit revealed 95 unplanned readmissions to the ICU setting within 72 hours of discharge to lower level of care. The odds of one or more discharges becoming an unplanned readmission became significantly higher on days when ≥8 patients were admitted to the ICU (OR, 1.66; 95% CI, 1.03-2.68), and the odds of an unplanned readmission were almost five times higher on days when ≥10 patients were admitted, compared with days when ≤9 patients were admitted (OR, 4.99; 95% CI, 2.45-10.17).
After adjusting for patient complexity, patients discharged on days with ≥10 admissions had higher than twice the odds of becoming an unplanned readmission than patients discharged on days with ≤9 admissions (OR, 2.34; 95% CI, 1.27-4.34).
This study was limited to patients in a neurosciences critical-care unit at a single academic medical center. Further research is needed to better understand how high admission volumes lead to increased unplanned readmission rates.
Bottom line: Days with high patient inflow volumes to the ICU are associated with higher rates of unplanned readmissions to the ICU, and the rate of unplanned readmissions becomes significant once a daily threshold of eight admissions is reached.
Citation: Baker DR, Pronovost PJ, Morlock LL, Geocadin RG, Holzmueller CG. Patient flow variability and unplanned readmissions to an intensive care unit. Crit Care Med. 2009;37(11):2882-2887.
Effectiveness of Sodium Bicarbonate in Contrast-Induced Nephropathy Prevention
Clinical question: Is IV sodium bicarbonate effective for prevention of contrast-induced nephropathy (CIN) in high-risk patients?
Background: CIN is a leading cause of acute kidney injury in the hospital setting. Some studies have suggested IV sodium bicarbonate might reduce risk for CIN; other studies challenge this conclusion.
Study design: Systematic review.
Setting: Published and unpublished randomized, controlled trials performed worldwide.
Synopsis: The research examined in this study was composed of randomized, controlled trials that investigated CIN prevention and included IV sodium bicarbonate in one of the treatment groups. Nine published and 15 unpublished trials were selected for a total of 3,563 patients studied. The overall pooled relative risk of CIN in patients treated with IV sodium bicarbonate compared with normal saline was 0.62 (95% CI, 0.45-0.86), though the strength of this evidence was questioned.
Significant heterogeneity across studies was found (I2=49.1%; P=0.004), partially related to substantially greater treatment effect in published (RR 0.43, 95% CI, 0.25-0.75) versus unpublished (RR 0.78, 95% CI, 0.52-1.17) studies. Publication bias was confirmed statistically. Among the published studies, greater treatment effect favoring bicarbonate over saline tended to be reported in those published before 2008, had fewer patients (<200) and events (<15), had measured events within 48 hours, and were studies of lower quality.
No effects regarding the risk of heart failure, the need for dialysis, or mortality were found, though the studies were not specifically designed to investigate those clinical outcomes. Larger studies are needed to better assess these questions.
Bottom line: IV sodium bicarbonate for CIN prevention in high-risk patients could be less effective than previous reports have suggested.
Citation: Zoungas S, Ninomiya T, Huxley R, et al. Systematic review: sodium bicarbonate treatment regimens for the prevention of contrast-induced nephropathy. Ann Intern Med. 2009;151(9):631-638.
Incidental Findings More Frequent than PE in Chest CT Angiograms
Clinical question: What is the prevalence of incidental findings on chest-computed tomographic angiograms (CTAs) ordered by an ED to evaluate for pulmonary embolism (PE)?
Background: CTAs commonly are ordered by ED physicians to assess for PE. While CTAs might yield findings to support an alternate diagnosis to PE, incidental findings might be found that often require further radiographic or clinical followup. The workup of these incidental findings can be burdensome and low-yield.
Study design: Retrospective chart review.
Setting: Single, academic, tertiary-care hospital in North Carolina.
Synopsis: All patients who underwent CTA evaluation for PE in the ED over two enrollment periods were selected; radiographic findings were compiled and their medical records reviewed. Fifty-five of 589 CTAs (9%) were positive for PE. New incidental findings requiring radiographic or clinical followup were found in 141 cases (24%).
Overall, pulmonary nodules were most common, requiring followup in 73 (13%) cases. Adenopathy requiring followup was seen in 51 cases (9%), and new masses requiring followup were found in 12 cases (2%). Findings to support alternate diagnoses for shortness of breath, hypoxemia, or tachycardia were found in 195 patients (33%), most commonly pleural effusion (19%) and infiltrates (11%). Other incidental findings that required less-urgent clinical attention were common with 615 total findings, most frequently nonmalignant bone findings in 144 cases (24%), mild dependent atelectasis in 137 cases (23%), and emphysema in 69 cases (12%).
Bottom line: Incidental findings requiring followup were more than twice as common as PE (24% vs. 9%) in CTAs ordered to evaluate for PE in an ED.
Citation: Hall WB, Truitt SG, Scheunemann LP, et al. The prevalence of clinically relevant incidental findings on chest computed tomographic angiograms ordered to diagnose pulmonary embolism. Arch Intern Med. 2009;169(21):1961-1965.
Patients Don’t Penalize for Adverse-Outcome Disclosure
Clinical question: What patient or clinical characteristics affect the likelihood of physician reporting of an adverse outcome, and how does adverse-outcome disclosure affect patient perceptions of quality of care?
Background: Harmful adverse events (AE), injuries caused by medical management rather than by the underlying condition of the patient, are common in the U.S. Previous studies have focused on physician and provider attitudes about disclosure. Little is known about how characteristics of the AE affect disclosure, and how disclosure affects patients’ perceptions of quality of care.
Study design: Retrospective cohort study.
Setting: Acute-care hospitals in Massachusetts.
Synopsis: Of 4,143 eligible patients, 2,582 (62%) agreed to a telephone interview that asked about patient experiences with adverse events during their hospital stay. Respondents reporting an AE were asked about disclosure by medical staff, effects of adverse events on their hospital course, and the quality of their hospital care.
Of the 845 AEs reported by 608 patients, only 40% were disclosed, defined as “anyone from the hospital explaining why the negative effects occurred.” The majority of the AEs were related to newly prescribed medications (40%) and surgical procedures (34%). Researchers determined that 31% of the AEs were preventable and 75% were severe. In multivariate analysis, disclosure was less likely if the AE was preventable or if patients had long-term effects from the AE. Patients with an AE were more likely to rate the quality of their hospitalization higher if there had been disclosure.
Bottom line: Disclosure of adverse events by medical personnel is low (40%) in hospitalized patients, even though disclosure of adverse events increases patients’ ratings of quality of care.
Citation: López L, Weismann JS, Schneider EC, Weingart SN, Cohen AP, Epstein AM. Disclosure of hospital adverse events and its association with patients’ ratings of the quality of care. Arch Intern Med. 2009;169(20):1888-1894.
Comanagement of Hip-Fracture Patients by Geriatricians Decreases Time to Surgery, LOS, and Complications
Clinical question: Does comanagement of hip-fracture patients by geriatricians and orthopedic surgeons improve short-term outcomes?
Background: Hip fractures in older adults are associated with considerable morbidity and mortality. A model at a single center, where hip fracture patients are comanaged by geriatricians and orthopedic surgeons, demonstrated decreased LOS, readmission rates, and mortality when compared with national data. This study compares results to a usual-care site.
Study design: Retrospective cohort study.
Setting: Community-based teaching hospital and a tertiary-care hospital in Rochester, N.Y.
Synopsis: Researchers enrolled 314 patients with hip fractures. The 193 patients in the intervention group were comanaged by geriatricians and orthopedic surgeons. The 121 patients in the usual-care group were admitted under the care of orthopedic surgeons, and hospitalists were consulted when deemed necessary. Retrospective chart reviews were performed; complications were defined a priori.
When compared with usual care, patients in the intervention group had significantly shorter times to surgery (24.1 hours vs. 37.4 hours), shorter LOS (4.6 days vs. 8.3 days), fewer complications (30.6% vs. 46.3%), including fewer postoperative infections (2.3% vs. 19.8%), cardiac complications (1.0% vs. 7.4%), cases of thromboembolism (0.5% vs. 5.0%), episodes of bleeding (0% vs. 3.3%), and episodes of hypoxia (6.7% vs. 14.1%). There was no difference in inpatient mortality or 30-day readmission rates.
Further assessment comanagement by hospitalists and comanagement by geriatricians is needed.
Bottom line: Perioperative comanagement of hip-fracture patients by geriatricians and orthopedic surgeons significantly improves short-term outcomes.
Citation: Friedman SM, Mendelson DA, Bingham KW, Kates SL. Impact of a comanaged geriatric fracture center on short-term hip fracture outcomes. Arch Intern Med. 2009;169 (18):1712-1717.
Niacin Is Superior to Ezetimibe in Causing Significant Regression of Carotid Intima-Media Thickness when Combined with a Statin
Clinical question: Is ezetimibe superior to niacin for reducing carotid intima-media thickness (CIMT) in patients with coronary artery disease (CAD) already on statin monotherapy?
Background: Statin montherapy significantly reduces the risk of cardiovascular events, and further lowering of this risk can be achieved by reducing the LDL, using statin intensification, or adding ezetimibe, or by raising the HDL levels by adding niacin therapy. This comparative-effectiveness trial compared the efficacy of these two approaches.
Study design: Prospective, randomized, parallel-group, open-label study.
Setting: Tertiary-care military medical center, and private tertiary-care hospital in Washington, D.C.
Synopsis: Three hundred sixty-three patients with known CAD or CAD equivalent were enrolled, and all of the patients were maintained on statin therapy with LDL <100 and HDL <50. Patients were randomized to ezetimibe 10 mg/day or niacin, starting at 500 mg at bedtime and titrated to 2 g/day. Primary endpoint was a mean change in CIMT after 14 months. Secondary endpoints were change in lipid levels, composite of major cardiovascular events, drug discontinuation, and quality of life.
The trial was terminated early after 208 patients had completed the trial. Although ezetimibe showed greater reduction of LDL, niacin showed significantly greater reduction in the progression of CIMT. Patients receiving niacin experienced fewer cardiovascular events (1% vs. 5%) but had higher rates of withdrawal (15% vs. 9%) due to flushing.
Limitations of the study are small sample size, short follow-up period, and use of CIMT as a surrogate marker for clinical endpoint.
Bottom line: Niacin is superior to ezetimibe in reducing CIMT and raising HDL levels and might be more efficacious in reducing cardiovascular risk.
Citation: Taylor AJ, Villines TC, Stanek EJ, et al. Extended-release niacin or ezetimibe and carotid intima-media thickness. N Engl J Med. 2009;361(22):2113-2122.
Pharmacist-Facilitated Hospital Discharge Program Didn’t Reduce Post-Discharge Healthcare Resource Utilization
Clinical question: Does pharmacist-facilitated hospital discharge reduce hospital readmission rates?
Background: Medication discrepancies at the time of discharge often lead to confusion, medical errors, and readmission to the hospital. Patients who are at high risk of medication errors often are on multiple medications and experience adverse drug events upon discharge.
Study design: Prospective cohort study.
Setting: Tertiary-care, academic teaching hospital in Michigan.
Synopsis: One pharmacist alternated between the resident service and hospitalist service every month. The pharmacist monitored the patients being discharged for appropriateness and accuracy of medications. The pharmacist assessed medication therapy, reconciled medications, screened for adherence concerns, counseled and educated patients, and performed post-discharge telephone follow-up.
Primary outcomes were ED visits within 72 hours and readmission rates by day 14 and day 30.
The study found high numbers of medication discrepancies in the control (33.5%) and intervention (59.6%) groups, and these discrepancies were resolved prior to discharge; however, there was no significant impact on post-discharge ED visits, or 14- and 30-day readmission rates. Post-discharge telephone calls reduced 14-day readmission rates.
Bottom line: Pharmacist-facilitated hospital discharge did not significantly reduce post-discharge ED visits or readmissions.
Citation: Walker PC, Bernstein SJ, Jones JN, et al. Impact of a pharmacist-facilitated hospital discharge program. Arch Intern Med. 2009;169(21):2003-2010.
Questionable Antibiotic Benefit for Patients with Acute COPD Exacerbations
Clinical question: Does the addition of antibiotics to systemic corticosteroids provide additional benefits for patients hospitalized with acute exacerbations of chronic obstructive pulmonary disease (AECOPD)?
Background: The role of antibiotics in the treatment of AECOPD is unclear, particularly in addition to systemic corticosteroids. Many of the studies demonstrating the benefit of antibiotics were conducted several decades before systemic steroids were used routinely for the treatment of AECOPD.
Study design: Randomized, double-blinded, placebo-controlled study.
Setting: Two academic teaching hospitals in the Netherlands.
Synopsis: Two hundred sixty-five acute exacerbations of COPD were enrolled in the study, and patients were randomized to a seven-day course of 200 mg/day of doxycycline or placebo. All patients received systemic corticosteroids, nebulized bronchodilator therapy, and physiotherapy. The study found that doxycycline was equivalent to placebo for the primary endpoint of clinical success on day 30; however, doxycycline was superior to placebo for secondary outcomes of clinical success, clinical cure, symptomatic improvement, microbiological success, and reducing open label antibiotic use on day 10, but not on day 30.
Because the population studied had low levels of advanced antimicrobial resistance, the findings might not be generalizable. Results suggested a difference of treatment effect between subgroups based on C-reactive protein values, but further research is needed.
Bottom line: Patients treated with doxycycline for acute exacerbation of COPD had improved clinical outcomes at day 10, but the benefits were not significant at day 30. Data are still equivocal regarding benefits of antibiotics in patients with acute exacerbations of COPD.
Citation: Daniels JM, Snijders D, de Graaff CS, Vlaspolder F, Jansen HM, Boersma WG. Antibiotics in addition to systemic corticosteroids for acute exacerbations of chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2010;181(2):150-157. TH
PEDIATRIC HM LITERATURE
By Mark Shen, MD

Less Is More in the Management of Acute Gastroenteritis
Clinical question: What is the effect of a guideline-training program for pediatricians on the management of acute gastroenteritis (AGE)?
Background: Guidelines recommending oral rehydration, early refeeding, and limited interventions have been developed for AGE management, but uptake by pediatricians has been slow. While individual components of these guidelines have been shown to be effective in comparison to other resource-intensive interventions, outcomes of global guideline implementation have not been studied well.
Study design: Prospective, randomized, controlled trial.
Setting: One hundred forty-nine primary-care pediatricians in Italy.
Synopsis: Pediatricians from the Italian national healthcare system were randomized to AGE guideline training or no training (usual practice; control group). The physicians enrolled 1,309 children in the study. Parents completed daily forms documenting the interventions for, and outcomes of, each illness.
Management by the trained group of pediatricians was in full compliance with the guidelines 66% of the time, as opposed to 33% of the time in the untrained group.
Significant differences between the groups were noted for each basic tenet of the guidelines: oral rehydration use, restrictive diets, medication use, and microbiologic testing. Notably, by both intention-to-treat and per-protocol analysis, the mean duration of diarrhea was shorter in children managed by the trained group of pediatricians.
As underadherence to evidence-based guidelines remains commonplace, effective implementation will become a greater area of focus. Despite a modest effect in an ambulatory population, these investigators demonstrated a clear improvement in outcomes with a simple, two-hour training program. While not studied, it is likely that the cost of care was significantly lower in the guideline group, given the dramatic differences in medication use and testing.
Bottom line: Effective implementation of AGE guidelines will improve outcomes and reduce costs.
Citation: Albano F, Lo Vecchio A, Guarino A. The applicability and efficacy of guidelines for the management of acute gastroenteritis in outpatient children: a field-randomized trial on primary care pediatricians. J Pediatr. 2010;156(2):226-230.
In This Edition
Literature at a Glance
A guide to this month’s studies
- ICU volume and outcomes
- Bicarbonate and contrast-induced nephropathy
- Rate of incidental findings in chest CT angiography
- Consequences of adverse-event reporting by physicians
- Hip fracture comanagement
- Niacin vs. ezetimibe in atherosclerosis
- Effect of hospital pharmacists on readmission rates
- Antibiotics in acute exacerbations of COPD
Higher Patient ICU Inflow Volumes Are Associated with Unplanned Readmissions to ICU
Clinical question: Do higher rates of unplanned ICU readmissions occur on days with high patient inflow volumes?
Background: Patients readmitted to ICUs have longer lengths of stay (LOS) and higher rates of in-hospital mortality. Previous studies suggest many ICU readmissions might be due to premature discharge, but there is little evidence evaluating the impact of patient inflow volumes on the incidence of ICU readmissions.
Study design: Retrospective, cohort study.
Setting: Large, urban, tertiary-care academic medical center in Baltimore.
Synopsis: A retrospective review of 3,233 discharges from a neurosciences critical-care unit revealed 95 unplanned readmissions to the ICU setting within 72 hours of discharge to lower level of care. The odds of one or more discharges becoming an unplanned readmission became significantly higher on days when ≥8 patients were admitted to the ICU (OR, 1.66; 95% CI, 1.03-2.68), and the odds of an unplanned readmission were almost five times higher on days when ≥10 patients were admitted, compared with days when ≤9 patients were admitted (OR, 4.99; 95% CI, 2.45-10.17).
After adjusting for patient complexity, patients discharged on days with ≥10 admissions had higher than twice the odds of becoming an unplanned readmission than patients discharged on days with ≤9 admissions (OR, 2.34; 95% CI, 1.27-4.34).
This study was limited to patients in a neurosciences critical-care unit at a single academic medical center. Further research is needed to better understand how high admission volumes lead to increased unplanned readmission rates.
Bottom line: Days with high patient inflow volumes to the ICU are associated with higher rates of unplanned readmissions to the ICU, and the rate of unplanned readmissions becomes significant once a daily threshold of eight admissions is reached.
Citation: Baker DR, Pronovost PJ, Morlock LL, Geocadin RG, Holzmueller CG. Patient flow variability and unplanned readmissions to an intensive care unit. Crit Care Med. 2009;37(11):2882-2887.
Effectiveness of Sodium Bicarbonate in Contrast-Induced Nephropathy Prevention
Clinical question: Is IV sodium bicarbonate effective for prevention of contrast-induced nephropathy (CIN) in high-risk patients?
Background: CIN is a leading cause of acute kidney injury in the hospital setting. Some studies have suggested IV sodium bicarbonate might reduce risk for CIN; other studies challenge this conclusion.
Study design: Systematic review.
Setting: Published and unpublished randomized, controlled trials performed worldwide.
Synopsis: The research examined in this study was composed of randomized, controlled trials that investigated CIN prevention and included IV sodium bicarbonate in one of the treatment groups. Nine published and 15 unpublished trials were selected for a total of 3,563 patients studied. The overall pooled relative risk of CIN in patients treated with IV sodium bicarbonate compared with normal saline was 0.62 (95% CI, 0.45-0.86), though the strength of this evidence was questioned.
Significant heterogeneity across studies was found (I2=49.1%; P=0.004), partially related to substantially greater treatment effect in published (RR 0.43, 95% CI, 0.25-0.75) versus unpublished (RR 0.78, 95% CI, 0.52-1.17) studies. Publication bias was confirmed statistically. Among the published studies, greater treatment effect favoring bicarbonate over saline tended to be reported in those published before 2008, had fewer patients (<200) and events (<15), had measured events within 48 hours, and were studies of lower quality.
No effects regarding the risk of heart failure, the need for dialysis, or mortality were found, though the studies were not specifically designed to investigate those clinical outcomes. Larger studies are needed to better assess these questions.
Bottom line: IV sodium bicarbonate for CIN prevention in high-risk patients could be less effective than previous reports have suggested.
Citation: Zoungas S, Ninomiya T, Huxley R, et al. Systematic review: sodium bicarbonate treatment regimens for the prevention of contrast-induced nephropathy. Ann Intern Med. 2009;151(9):631-638.
Incidental Findings More Frequent than PE in Chest CT Angiograms
Clinical question: What is the prevalence of incidental findings on chest-computed tomographic angiograms (CTAs) ordered by an ED to evaluate for pulmonary embolism (PE)?
Background: CTAs commonly are ordered by ED physicians to assess for PE. While CTAs might yield findings to support an alternate diagnosis to PE, incidental findings might be found that often require further radiographic or clinical followup. The workup of these incidental findings can be burdensome and low-yield.
Study design: Retrospective chart review.
Setting: Single, academic, tertiary-care hospital in North Carolina.
Synopsis: All patients who underwent CTA evaluation for PE in the ED over two enrollment periods were selected; radiographic findings were compiled and their medical records reviewed. Fifty-five of 589 CTAs (9%) were positive for PE. New incidental findings requiring radiographic or clinical followup were found in 141 cases (24%).
Overall, pulmonary nodules were most common, requiring followup in 73 (13%) cases. Adenopathy requiring followup was seen in 51 cases (9%), and new masses requiring followup were found in 12 cases (2%). Findings to support alternate diagnoses for shortness of breath, hypoxemia, or tachycardia were found in 195 patients (33%), most commonly pleural effusion (19%) and infiltrates (11%). Other incidental findings that required less-urgent clinical attention were common with 615 total findings, most frequently nonmalignant bone findings in 144 cases (24%), mild dependent atelectasis in 137 cases (23%), and emphysema in 69 cases (12%).
Bottom line: Incidental findings requiring followup were more than twice as common as PE (24% vs. 9%) in CTAs ordered to evaluate for PE in an ED.
Citation: Hall WB, Truitt SG, Scheunemann LP, et al. The prevalence of clinically relevant incidental findings on chest computed tomographic angiograms ordered to diagnose pulmonary embolism. Arch Intern Med. 2009;169(21):1961-1965.
Patients Don’t Penalize for Adverse-Outcome Disclosure
Clinical question: What patient or clinical characteristics affect the likelihood of physician reporting of an adverse outcome, and how does adverse-outcome disclosure affect patient perceptions of quality of care?
Background: Harmful adverse events (AE), injuries caused by medical management rather than by the underlying condition of the patient, are common in the U.S. Previous studies have focused on physician and provider attitudes about disclosure. Little is known about how characteristics of the AE affect disclosure, and how disclosure affects patients’ perceptions of quality of care.
Study design: Retrospective cohort study.
Setting: Acute-care hospitals in Massachusetts.
Synopsis: Of 4,143 eligible patients, 2,582 (62%) agreed to a telephone interview that asked about patient experiences with adverse events during their hospital stay. Respondents reporting an AE were asked about disclosure by medical staff, effects of adverse events on their hospital course, and the quality of their hospital care.
Of the 845 AEs reported by 608 patients, only 40% were disclosed, defined as “anyone from the hospital explaining why the negative effects occurred.” The majority of the AEs were related to newly prescribed medications (40%) and surgical procedures (34%). Researchers determined that 31% of the AEs were preventable and 75% were severe. In multivariate analysis, disclosure was less likely if the AE was preventable or if patients had long-term effects from the AE. Patients with an AE were more likely to rate the quality of their hospitalization higher if there had been disclosure.
Bottom line: Disclosure of adverse events by medical personnel is low (40%) in hospitalized patients, even though disclosure of adverse events increases patients’ ratings of quality of care.
Citation: López L, Weismann JS, Schneider EC, Weingart SN, Cohen AP, Epstein AM. Disclosure of hospital adverse events and its association with patients’ ratings of the quality of care. Arch Intern Med. 2009;169(20):1888-1894.
Comanagement of Hip-Fracture Patients by Geriatricians Decreases Time to Surgery, LOS, and Complications
Clinical question: Does comanagement of hip-fracture patients by geriatricians and orthopedic surgeons improve short-term outcomes?
Background: Hip fractures in older adults are associated with considerable morbidity and mortality. A model at a single center, where hip fracture patients are comanaged by geriatricians and orthopedic surgeons, demonstrated decreased LOS, readmission rates, and mortality when compared with national data. This study compares results to a usual-care site.
Study design: Retrospective cohort study.
Setting: Community-based teaching hospital and a tertiary-care hospital in Rochester, N.Y.
Synopsis: Researchers enrolled 314 patients with hip fractures. The 193 patients in the intervention group were comanaged by geriatricians and orthopedic surgeons. The 121 patients in the usual-care group were admitted under the care of orthopedic surgeons, and hospitalists were consulted when deemed necessary. Retrospective chart reviews were performed; complications were defined a priori.
When compared with usual care, patients in the intervention group had significantly shorter times to surgery (24.1 hours vs. 37.4 hours), shorter LOS (4.6 days vs. 8.3 days), fewer complications (30.6% vs. 46.3%), including fewer postoperative infections (2.3% vs. 19.8%), cardiac complications (1.0% vs. 7.4%), cases of thromboembolism (0.5% vs. 5.0%), episodes of bleeding (0% vs. 3.3%), and episodes of hypoxia (6.7% vs. 14.1%). There was no difference in inpatient mortality or 30-day readmission rates.
Further assessment comanagement by hospitalists and comanagement by geriatricians is needed.
Bottom line: Perioperative comanagement of hip-fracture patients by geriatricians and orthopedic surgeons significantly improves short-term outcomes.
Citation: Friedman SM, Mendelson DA, Bingham KW, Kates SL. Impact of a comanaged geriatric fracture center on short-term hip fracture outcomes. Arch Intern Med. 2009;169 (18):1712-1717.
Niacin Is Superior to Ezetimibe in Causing Significant Regression of Carotid Intima-Media Thickness when Combined with a Statin
Clinical question: Is ezetimibe superior to niacin for reducing carotid intima-media thickness (CIMT) in patients with coronary artery disease (CAD) already on statin monotherapy?
Background: Statin montherapy significantly reduces the risk of cardiovascular events, and further lowering of this risk can be achieved by reducing the LDL, using statin intensification, or adding ezetimibe, or by raising the HDL levels by adding niacin therapy. This comparative-effectiveness trial compared the efficacy of these two approaches.
Study design: Prospective, randomized, parallel-group, open-label study.
Setting: Tertiary-care military medical center, and private tertiary-care hospital in Washington, D.C.
Synopsis: Three hundred sixty-three patients with known CAD or CAD equivalent were enrolled, and all of the patients were maintained on statin therapy with LDL <100 and HDL <50. Patients were randomized to ezetimibe 10 mg/day or niacin, starting at 500 mg at bedtime and titrated to 2 g/day. Primary endpoint was a mean change in CIMT after 14 months. Secondary endpoints were change in lipid levels, composite of major cardiovascular events, drug discontinuation, and quality of life.
The trial was terminated early after 208 patients had completed the trial. Although ezetimibe showed greater reduction of LDL, niacin showed significantly greater reduction in the progression of CIMT. Patients receiving niacin experienced fewer cardiovascular events (1% vs. 5%) but had higher rates of withdrawal (15% vs. 9%) due to flushing.
Limitations of the study are small sample size, short follow-up period, and use of CIMT as a surrogate marker for clinical endpoint.
Bottom line: Niacin is superior to ezetimibe in reducing CIMT and raising HDL levels and might be more efficacious in reducing cardiovascular risk.
Citation: Taylor AJ, Villines TC, Stanek EJ, et al. Extended-release niacin or ezetimibe and carotid intima-media thickness. N Engl J Med. 2009;361(22):2113-2122.
Pharmacist-Facilitated Hospital Discharge Program Didn’t Reduce Post-Discharge Healthcare Resource Utilization
Clinical question: Does pharmacist-facilitated hospital discharge reduce hospital readmission rates?
Background: Medication discrepancies at the time of discharge often lead to confusion, medical errors, and readmission to the hospital. Patients who are at high risk of medication errors often are on multiple medications and experience adverse drug events upon discharge.
Study design: Prospective cohort study.
Setting: Tertiary-care, academic teaching hospital in Michigan.
Synopsis: One pharmacist alternated between the resident service and hospitalist service every month. The pharmacist monitored the patients being discharged for appropriateness and accuracy of medications. The pharmacist assessed medication therapy, reconciled medications, screened for adherence concerns, counseled and educated patients, and performed post-discharge telephone follow-up.
Primary outcomes were ED visits within 72 hours and readmission rates by day 14 and day 30.
The study found high numbers of medication discrepancies in the control (33.5%) and intervention (59.6%) groups, and these discrepancies were resolved prior to discharge; however, there was no significant impact on post-discharge ED visits, or 14- and 30-day readmission rates. Post-discharge telephone calls reduced 14-day readmission rates.
Bottom line: Pharmacist-facilitated hospital discharge did not significantly reduce post-discharge ED visits or readmissions.
Citation: Walker PC, Bernstein SJ, Jones JN, et al. Impact of a pharmacist-facilitated hospital discharge program. Arch Intern Med. 2009;169(21):2003-2010.
Questionable Antibiotic Benefit for Patients with Acute COPD Exacerbations
Clinical question: Does the addition of antibiotics to systemic corticosteroids provide additional benefits for patients hospitalized with acute exacerbations of chronic obstructive pulmonary disease (AECOPD)?
Background: The role of antibiotics in the treatment of AECOPD is unclear, particularly in addition to systemic corticosteroids. Many of the studies demonstrating the benefit of antibiotics were conducted several decades before systemic steroids were used routinely for the treatment of AECOPD.
Study design: Randomized, double-blinded, placebo-controlled study.
Setting: Two academic teaching hospitals in the Netherlands.
Synopsis: Two hundred sixty-five acute exacerbations of COPD were enrolled in the study, and patients were randomized to a seven-day course of 200 mg/day of doxycycline or placebo. All patients received systemic corticosteroids, nebulized bronchodilator therapy, and physiotherapy. The study found that doxycycline was equivalent to placebo for the primary endpoint of clinical success on day 30; however, doxycycline was superior to placebo for secondary outcomes of clinical success, clinical cure, symptomatic improvement, microbiological success, and reducing open label antibiotic use on day 10, but not on day 30.
Because the population studied had low levels of advanced antimicrobial resistance, the findings might not be generalizable. Results suggested a difference of treatment effect between subgroups based on C-reactive protein values, but further research is needed.
Bottom line: Patients treated with doxycycline for acute exacerbation of COPD had improved clinical outcomes at day 10, but the benefits were not significant at day 30. Data are still equivocal regarding benefits of antibiotics in patients with acute exacerbations of COPD.
Citation: Daniels JM, Snijders D, de Graaff CS, Vlaspolder F, Jansen HM, Boersma WG. Antibiotics in addition to systemic corticosteroids for acute exacerbations of chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2010;181(2):150-157. TH
PEDIATRIC HM LITERATURE
By Mark Shen, MD
Less Is More in the Management of Acute Gastroenteritis
Clinical question: What is the effect of a guideline-training program for pediatricians on the management of acute gastroenteritis (AGE)?
Background: Guidelines recommending oral rehydration, early refeeding, and limited interventions have been developed for AGE management, but uptake by pediatricians has been slow. While individual components of these guidelines have been shown to be effective in comparison to other resource-intensive interventions, outcomes of global guideline implementation have not been studied well.
Study design: Prospective, randomized, controlled trial.
Setting: One hundred forty-nine primary-care pediatricians in Italy.
Synopsis: Pediatricians from the Italian national healthcare system were randomized to AGE guideline training or no training (usual practice; control group). The physicians enrolled 1,309 children in the study. Parents completed daily forms documenting the interventions for, and outcomes of, each illness.
Management by the trained group of pediatricians was in full compliance with the guidelines 66% of the time, as opposed to 33% of the time in the untrained group.
Significant differences between the groups were noted for each basic tenet of the guidelines: oral rehydration use, restrictive diets, medication use, and microbiologic testing. Notably, by both intention-to-treat and per-protocol analysis, the mean duration of diarrhea was shorter in children managed by the trained group of pediatricians.
As underadherence to evidence-based guidelines remains commonplace, effective implementation will become a greater area of focus. Despite a modest effect in an ambulatory population, these investigators demonstrated a clear improvement in outcomes with a simple, two-hour training program. While not studied, it is likely that the cost of care was significantly lower in the guideline group, given the dramatic differences in medication use and testing.
Bottom line: Effective implementation of AGE guidelines will improve outcomes and reduce costs.
Citation: Albano F, Lo Vecchio A, Guarino A. The applicability and efficacy of guidelines for the management of acute gastroenteritis in outpatient children: a field-randomized trial on primary care pediatricians. J Pediatr. 2010;156(2):226-230.
In This Edition
Literature at a Glance
A guide to this month’s studies
- ICU volume and outcomes
- Bicarbonate and contrast-induced nephropathy
- Rate of incidental findings in chest CT angiography
- Consequences of adverse-event reporting by physicians
- Hip fracture comanagement
- Niacin vs. ezetimibe in atherosclerosis
- Effect of hospital pharmacists on readmission rates
- Antibiotics in acute exacerbations of COPD
Higher Patient ICU Inflow Volumes Are Associated with Unplanned Readmissions to ICU
Clinical question: Do higher rates of unplanned ICU readmissions occur on days with high patient inflow volumes?
Background: Patients readmitted to ICUs have longer lengths of stay (LOS) and higher rates of in-hospital mortality. Previous studies suggest many ICU readmissions might be due to premature discharge, but there is little evidence evaluating the impact of patient inflow volumes on the incidence of ICU readmissions.
Study design: Retrospective, cohort study.
Setting: Large, urban, tertiary-care academic medical center in Baltimore.
Synopsis: A retrospective review of 3,233 discharges from a neurosciences critical-care unit revealed 95 unplanned readmissions to the ICU setting within 72 hours of discharge to lower level of care. The odds of one or more discharges becoming an unplanned readmission became significantly higher on days when ≥8 patients were admitted to the ICU (OR, 1.66; 95% CI, 1.03-2.68), and the odds of an unplanned readmission were almost five times higher on days when ≥10 patients were admitted, compared with days when ≤9 patients were admitted (OR, 4.99; 95% CI, 2.45-10.17).
After adjusting for patient complexity, patients discharged on days with ≥10 admissions had higher than twice the odds of becoming an unplanned readmission than patients discharged on days with ≤9 admissions (OR, 2.34; 95% CI, 1.27-4.34).
This study was limited to patients in a neurosciences critical-care unit at a single academic medical center. Further research is needed to better understand how high admission volumes lead to increased unplanned readmission rates.
Bottom line: Days with high patient inflow volumes to the ICU are associated with higher rates of unplanned readmissions to the ICU, and the rate of unplanned readmissions becomes significant once a daily threshold of eight admissions is reached.
Citation: Baker DR, Pronovost PJ, Morlock LL, Geocadin RG, Holzmueller CG. Patient flow variability and unplanned readmissions to an intensive care unit. Crit Care Med. 2009;37(11):2882-2887.
Effectiveness of Sodium Bicarbonate in Contrast-Induced Nephropathy Prevention
Clinical question: Is IV sodium bicarbonate effective for prevention of contrast-induced nephropathy (CIN) in high-risk patients?
Background: CIN is a leading cause of acute kidney injury in the hospital setting. Some studies have suggested IV sodium bicarbonate might reduce risk for CIN; other studies challenge this conclusion.
Study design: Systematic review.
Setting: Published and unpublished randomized, controlled trials performed worldwide.
Synopsis: The research examined in this study was composed of randomized, controlled trials that investigated CIN prevention and included IV sodium bicarbonate in one of the treatment groups. Nine published and 15 unpublished trials were selected for a total of 3,563 patients studied. The overall pooled relative risk of CIN in patients treated with IV sodium bicarbonate compared with normal saline was 0.62 (95% CI, 0.45-0.86), though the strength of this evidence was questioned.
Significant heterogeneity across studies was found (I2=49.1%; P=0.004), partially related to substantially greater treatment effect in published (RR 0.43, 95% CI, 0.25-0.75) versus unpublished (RR 0.78, 95% CI, 0.52-1.17) studies. Publication bias was confirmed statistically. Among the published studies, greater treatment effect favoring bicarbonate over saline tended to be reported in those published before 2008, had fewer patients (<200) and events (<15), had measured events within 48 hours, and were studies of lower quality.
No effects regarding the risk of heart failure, the need for dialysis, or mortality were found, though the studies were not specifically designed to investigate those clinical outcomes. Larger studies are needed to better assess these questions.
Bottom line: IV sodium bicarbonate for CIN prevention in high-risk patients could be less effective than previous reports have suggested.
Citation: Zoungas S, Ninomiya T, Huxley R, et al. Systematic review: sodium bicarbonate treatment regimens for the prevention of contrast-induced nephropathy. Ann Intern Med. 2009;151(9):631-638.
Incidental Findings More Frequent than PE in Chest CT Angiograms
Clinical question: What is the prevalence of incidental findings on chest-computed tomographic angiograms (CTAs) ordered by an ED to evaluate for pulmonary embolism (PE)?
Background: CTAs commonly are ordered by ED physicians to assess for PE. While CTAs might yield findings to support an alternate diagnosis to PE, incidental findings might be found that often require further radiographic or clinical followup. The workup of these incidental findings can be burdensome and low-yield.
Study design: Retrospective chart review.
Setting: Single, academic, tertiary-care hospital in North Carolina.
Synopsis: All patients who underwent CTA evaluation for PE in the ED over two enrollment periods were selected; radiographic findings were compiled and their medical records reviewed. Fifty-five of 589 CTAs (9%) were positive for PE. New incidental findings requiring radiographic or clinical followup were found in 141 cases (24%).
Overall, pulmonary nodules were most common, requiring followup in 73 (13%) cases. Adenopathy requiring followup was seen in 51 cases (9%), and new masses requiring followup were found in 12 cases (2%). Findings to support alternate diagnoses for shortness of breath, hypoxemia, or tachycardia were found in 195 patients (33%), most commonly pleural effusion (19%) and infiltrates (11%). Other incidental findings that required less-urgent clinical attention were common with 615 total findings, most frequently nonmalignant bone findings in 144 cases (24%), mild dependent atelectasis in 137 cases (23%), and emphysema in 69 cases (12%).
Bottom line: Incidental findings requiring followup were more than twice as common as PE (24% vs. 9%) in CTAs ordered to evaluate for PE in an ED.
Citation: Hall WB, Truitt SG, Scheunemann LP, et al. The prevalence of clinically relevant incidental findings on chest computed tomographic angiograms ordered to diagnose pulmonary embolism. Arch Intern Med. 2009;169(21):1961-1965.
Patients Don’t Penalize for Adverse-Outcome Disclosure
Clinical question: What patient or clinical characteristics affect the likelihood of physician reporting of an adverse outcome, and how does adverse-outcome disclosure affect patient perceptions of quality of care?
Background: Harmful adverse events (AE), injuries caused by medical management rather than by the underlying condition of the patient, are common in the U.S. Previous studies have focused on physician and provider attitudes about disclosure. Little is known about how characteristics of the AE affect disclosure, and how disclosure affects patients’ perceptions of quality of care.
Study design: Retrospective cohort study.
Setting: Acute-care hospitals in Massachusetts.
Synopsis: Of 4,143 eligible patients, 2,582 (62%) agreed to a telephone interview that asked about patient experiences with adverse events during their hospital stay. Respondents reporting an AE were asked about disclosure by medical staff, effects of adverse events on their hospital course, and the quality of their hospital care.
Of the 845 AEs reported by 608 patients, only 40% were disclosed, defined as “anyone from the hospital explaining why the negative effects occurred.” The majority of the AEs were related to newly prescribed medications (40%) and surgical procedures (34%). Researchers determined that 31% of the AEs were preventable and 75% were severe. In multivariate analysis, disclosure was less likely if the AE was preventable or if patients had long-term effects from the AE. Patients with an AE were more likely to rate the quality of their hospitalization higher if there had been disclosure.
Bottom line: Disclosure of adverse events by medical personnel is low (40%) in hospitalized patients, even though disclosure of adverse events increases patients’ ratings of quality of care.
Citation: López L, Weismann JS, Schneider EC, Weingart SN, Cohen AP, Epstein AM. Disclosure of hospital adverse events and its association with patients’ ratings of the quality of care. Arch Intern Med. 2009;169(20):1888-1894.
Comanagement of Hip-Fracture Patients by Geriatricians Decreases Time to Surgery, LOS, and Complications
Clinical question: Does comanagement of hip-fracture patients by geriatricians and orthopedic surgeons improve short-term outcomes?
Background: Hip fractures in older adults are associated with considerable morbidity and mortality. A model at a single center, where hip fracture patients are comanaged by geriatricians and orthopedic surgeons, demonstrated decreased LOS, readmission rates, and mortality when compared with national data. This study compares results to a usual-care site.
Study design: Retrospective cohort study.
Setting: Community-based teaching hospital and a tertiary-care hospital in Rochester, N.Y.
Synopsis: Researchers enrolled 314 patients with hip fractures. The 193 patients in the intervention group were comanaged by geriatricians and orthopedic surgeons. The 121 patients in the usual-care group were admitted under the care of orthopedic surgeons, and hospitalists were consulted when deemed necessary. Retrospective chart reviews were performed; complications were defined a priori.
When compared with usual care, patients in the intervention group had significantly shorter times to surgery (24.1 hours vs. 37.4 hours), shorter LOS (4.6 days vs. 8.3 days), fewer complications (30.6% vs. 46.3%), including fewer postoperative infections (2.3% vs. 19.8%), cardiac complications (1.0% vs. 7.4%), cases of thromboembolism (0.5% vs. 5.0%), episodes of bleeding (0% vs. 3.3%), and episodes of hypoxia (6.7% vs. 14.1%). There was no difference in inpatient mortality or 30-day readmission rates.
Further assessment comanagement by hospitalists and comanagement by geriatricians is needed.
Bottom line: Perioperative comanagement of hip-fracture patients by geriatricians and orthopedic surgeons significantly improves short-term outcomes.
Citation: Friedman SM, Mendelson DA, Bingham KW, Kates SL. Impact of a comanaged geriatric fracture center on short-term hip fracture outcomes. Arch Intern Med. 2009;169 (18):1712-1717.
Niacin Is Superior to Ezetimibe in Causing Significant Regression of Carotid Intima-Media Thickness when Combined with a Statin
Clinical question: Is ezetimibe superior to niacin for reducing carotid intima-media thickness (CIMT) in patients with coronary artery disease (CAD) already on statin monotherapy?
Background: Statin montherapy significantly reduces the risk of cardiovascular events, and further lowering of this risk can be achieved by reducing the LDL, using statin intensification, or adding ezetimibe, or by raising the HDL levels by adding niacin therapy. This comparative-effectiveness trial compared the efficacy of these two approaches.
Study design: Prospective, randomized, parallel-group, open-label study.
Setting: Tertiary-care military medical center, and private tertiary-care hospital in Washington, D.C.
Synopsis: Three hundred sixty-three patients with known CAD or CAD equivalent were enrolled, and all of the patients were maintained on statin therapy with LDL <100 and HDL <50. Patients were randomized to ezetimibe 10 mg/day or niacin, starting at 500 mg at bedtime and titrated to 2 g/day. Primary endpoint was a mean change in CIMT after 14 months. Secondary endpoints were change in lipid levels, composite of major cardiovascular events, drug discontinuation, and quality of life.
The trial was terminated early after 208 patients had completed the trial. Although ezetimibe showed greater reduction of LDL, niacin showed significantly greater reduction in the progression of CIMT. Patients receiving niacin experienced fewer cardiovascular events (1% vs. 5%) but had higher rates of withdrawal (15% vs. 9%) due to flushing.
Limitations of the study are small sample size, short follow-up period, and use of CIMT as a surrogate marker for clinical endpoint.
Bottom line: Niacin is superior to ezetimibe in reducing CIMT and raising HDL levels and might be more efficacious in reducing cardiovascular risk.
Citation: Taylor AJ, Villines TC, Stanek EJ, et al. Extended-release niacin or ezetimibe and carotid intima-media thickness. N Engl J Med. 2009;361(22):2113-2122.
Pharmacist-Facilitated Hospital Discharge Program Didn’t Reduce Post-Discharge Healthcare Resource Utilization
Clinical question: Does pharmacist-facilitated hospital discharge reduce hospital readmission rates?
Background: Medication discrepancies at the time of discharge often lead to confusion, medical errors, and readmission to the hospital. Patients who are at high risk of medication errors often are on multiple medications and experience adverse drug events upon discharge.
Study design: Prospective cohort study.
Setting: Tertiary-care, academic teaching hospital in Michigan.
Synopsis: One pharmacist alternated between the resident service and hospitalist service every month. The pharmacist monitored the patients being discharged for appropriateness and accuracy of medications. The pharmacist assessed medication therapy, reconciled medications, screened for adherence concerns, counseled and educated patients, and performed post-discharge telephone follow-up.
Primary outcomes were ED visits within 72 hours and readmission rates by day 14 and day 30.
The study found high numbers of medication discrepancies in the control (33.5%) and intervention (59.6%) groups, and these discrepancies were resolved prior to discharge; however, there was no significant impact on post-discharge ED visits, or 14- and 30-day readmission rates. Post-discharge telephone calls reduced 14-day readmission rates.
Bottom line: Pharmacist-facilitated hospital discharge did not significantly reduce post-discharge ED visits or readmissions.
Citation: Walker PC, Bernstein SJ, Jones JN, et al. Impact of a pharmacist-facilitated hospital discharge program. Arch Intern Med. 2009;169(21):2003-2010.
Questionable Antibiotic Benefit for Patients with Acute COPD Exacerbations
Clinical question: Does the addition of antibiotics to systemic corticosteroids provide additional benefits for patients hospitalized with acute exacerbations of chronic obstructive pulmonary disease (AECOPD)?
Background: The role of antibiotics in the treatment of AECOPD is unclear, particularly in addition to systemic corticosteroids. Many of the studies demonstrating the benefit of antibiotics were conducted several decades before systemic steroids were used routinely for the treatment of AECOPD.
Study design: Randomized, double-blinded, placebo-controlled study.
Setting: Two academic teaching hospitals in the Netherlands.
Synopsis: Two hundred sixty-five acute exacerbations of COPD were enrolled in the study, and patients were randomized to a seven-day course of 200 mg/day of doxycycline or placebo. All patients received systemic corticosteroids, nebulized bronchodilator therapy, and physiotherapy. The study found that doxycycline was equivalent to placebo for the primary endpoint of clinical success on day 30; however, doxycycline was superior to placebo for secondary outcomes of clinical success, clinical cure, symptomatic improvement, microbiological success, and reducing open label antibiotic use on day 10, but not on day 30.
Because the population studied had low levels of advanced antimicrobial resistance, the findings might not be generalizable. Results suggested a difference of treatment effect between subgroups based on C-reactive protein values, but further research is needed.
Bottom line: Patients treated with doxycycline for acute exacerbation of COPD had improved clinical outcomes at day 10, but the benefits were not significant at day 30. Data are still equivocal regarding benefits of antibiotics in patients with acute exacerbations of COPD.
Citation: Daniels JM, Snijders D, de Graaff CS, Vlaspolder F, Jansen HM, Boersma WG. Antibiotics in addition to systemic corticosteroids for acute exacerbations of chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2010;181(2):150-157. TH
PEDIATRIC HM LITERATURE
By Mark Shen, MD
Less Is More in the Management of Acute Gastroenteritis
Clinical question: What is the effect of a guideline-training program for pediatricians on the management of acute gastroenteritis (AGE)?
Background: Guidelines recommending oral rehydration, early refeeding, and limited interventions have been developed for AGE management, but uptake by pediatricians has been slow. While individual components of these guidelines have been shown to be effective in comparison to other resource-intensive interventions, outcomes of global guideline implementation have not been studied well.
Study design: Prospective, randomized, controlled trial.
Setting: One hundred forty-nine primary-care pediatricians in Italy.
Synopsis: Pediatricians from the Italian national healthcare system were randomized to AGE guideline training or no training (usual practice; control group). The physicians enrolled 1,309 children in the study. Parents completed daily forms documenting the interventions for, and outcomes of, each illness.
Management by the trained group of pediatricians was in full compliance with the guidelines 66% of the time, as opposed to 33% of the time in the untrained group.
Significant differences between the groups were noted for each basic tenet of the guidelines: oral rehydration use, restrictive diets, medication use, and microbiologic testing. Notably, by both intention-to-treat and per-protocol analysis, the mean duration of diarrhea was shorter in children managed by the trained group of pediatricians.
As underadherence to evidence-based guidelines remains commonplace, effective implementation will become a greater area of focus. Despite a modest effect in an ambulatory population, these investigators demonstrated a clear improvement in outcomes with a simple, two-hour training program. While not studied, it is likely that the cost of care was significantly lower in the guideline group, given the dramatic differences in medication use and testing.
Bottom line: Effective implementation of AGE guidelines will improve outcomes and reduce costs.
Citation: Albano F, Lo Vecchio A, Guarino A. The applicability and efficacy of guidelines for the management of acute gastroenteritis in outpatient children: a field-randomized trial on primary care pediatricians. J Pediatr. 2010;156(2):226-230.
What Is the Appropriate Treatment of Cancer-Associated Venous Thromboembolic Disease?
Case
A 70-year-old woman with recently diagnosed pancreatic cancer is admitted with worsening abdominal pain and new right-lower-extremity edema. A CT scan of the abdomen and pelvis reveals occlusive IVC and common iliac thromboses. A right-common-femoral DVT appears on Doppler ultrasound. A CT angiogram of her chest is negative for pulmonary emboli. What is the appropriate treatment for this patient’s thromboembolic disease?
Overview
VTE in the setting of malignancy is common, and the incidence of VTE among cancer patients is increasing for unclear reasons.1,2,3 VTE occurs in an estimated 4% to 20% of all malignancy patients. Overall, cancer patients are at a sixfold increased risk of developing VTE compared with the general population, and these patients represent approximately 20% of all VTE cases.4,5
VTE is a leading cause of mortality among hospitalized cancer patients; evidence of VTE exists in up to 50% of cancer patients at autopsy.3,4 VTE complications lead to significant morbidity, including recurrent VTE, pulmonary hypertension, post-thrombophlebitic syndrome, bleeding, and decreased quality of life.6,7
The risk is greatest for hospitalized cancer patients and those receiving active chemotherapy, particularly with such antiangiogenic agents as thalidomide and bevacizumab.4,6 Certain malignancies are more frequently associated with VTE; these include gastrointestinal, gynecologic, brain, lung, renal, and hematologic cancers.4 Table 1 (p. 50) summarizes risk factors associated with VTE in cancer patients.4
Patients with malignancy are hypercoagulable, primarily because of tumor-related alterations in the coagulation cascade.8 Tumors contain cell-surface proteins (e.g., tissue factor and cancer procoagulant) that lead to activation of the clotting cascade via interactions with factors IX and/or X. In addition, tumor-released cytokines cause prothrombotic changes in the vascular endothelium.8
This hypercoagulability is exacerbated by cancer-associated treatment events, including immobility, central venous catheters, erythropoiesis-stimulating agents, and packed red-blood-cell and platelet transfusions.5,9
Cancer-related therapy complications further confound VTE management. Drug interactions, chemotherapy-induced thrombocytopenia, malnutrition, bleeding risk from surgery or tumor location, and liver dysfunction make safe management of cancer-associated VTE a challenge.
Review of the Data
Low-molecular-weight heparin (LMWH) vs. vitamin K antagonists (VKA): There is significant evidence that LMWH is the preferred pharmacologic therapy for the initial and long-term treatment of cancer-related VTE. The most convincing data were published as the CLOT trial, and is supported by several smaller studies.10 Recommendations for the preferred use of LMWH are consistent among several national and international guidelines.6,7
In the CLOT (Randomized Comparison of Low-Molecular-Weight Heparin Versus Oral Anticoagulant Therapy for the Prevention of Recurrent Venous Thromboembolism in Patients with Cancer) trial, six months of treatment with an oral VKA preceded by five to seven days of LMWH was compared with six months of treatment with LMWH (dalteparin). Patients with the diagnosis of acute symptomatic VTE were evaluated. After six months of treatment, 53 of 336 patients in the oral anticoagulant group had recurrent VTE, compared with 27 of 336 patients in the LMWH group—a relative risk reduction of 52% and an absolute risk reduction of 8% (P=0.002). Complication rates (major and minor bleeding) and overall mortality were similar between the two groups.7,10

Two smaller trials compared LMWHs with warfarin in the treatment of VTE in the setting of cancer. In one trial, seven of 67 enoxaparin-treated patients developed bleeding or recurrent VTE, compared with 15 of 71 warfarin-treated subjects; however, this reduction was not statistically significant (P=0.09).11 In another trial, seven of 100 tinzaparin-treated patients developed recurrent VTE, compared with 16 of 100 warfarin-treated patients (P=0.044).12
Thus, LMWH is the preferred therapeutic agent for both DVT and PE in the setting of malignancy.5 Even so, although the clinical evidence supports LMWH use in the treatment of cancer-associated VTE, it’s worth noting that many of the authors of the cited papers received compensation from large pharmaceutical companies. In addition, the CLOT trial was funded by Pharmacia, which supplied the study drug.
Initial treatment (5-10 days): The American Society of Clinical Oncology (ASCO) guidelines advocate the use of LMWH during the initial five to 10 days following VTE diagnosis. Four other cancer research organization guidelines, National Comprehensive Cancer Network (NCCN), the Italian Association of Medical Oncology (AIOM), the European Society of Medical Oncology (ESMO), and the French National Federation of the League of Centers Against Cancer (FNCLCC), echo this approach, with unfractionated heparin (UFH) or fondaparinux as additional initial treatment depending on the clinical situation—i.e., renal failure, heparin-induced thrombocytopenia (HIT), or bleeding risk.6
Table 2 (below) summarizes recommendations for VTE treatment in cancer patients from all five guideline panels.6
Long-term treatment and duration (3-6 months): All of the panels agree LMWH is the preferred agent for long-term therapy of cancer-related VTE. ASCO supports treatment with LMWH for at least six months; oral VKAs with a targeted INR of 2 to 3 are acceptable when LMWH is not feasible. NCCN, AIOM, ESMO, and FNCLCC recommend an LMWH treatment duration from three to six months (ASCO recommends at least six months).
All of the panels, however, advocate indefinite duration of anticoagulation in patients with such continuing risk factors as active (metastatic, recurrent, or persistent) cancer or chemotherapy treatment.6 AIOM and ESMO specify indefinite LMWH, whereas ASCO does not specify oral VKA or LMWH use. Given the difficulties of managing VKA in the setting of advanced malignancy or chemotherapy, LMWH is the most practical choice, if it’s available and isn’t cost-prohibitive.
LMWH availability: Dalteparin, tinzaparin, and enoxaparin are LMWHs currently available in the U.S. for VTE treatment. Dalteparin is the only FDA-approved LMWH drug for long-term use to treat cancer-associated VTE, although enoxaparin and tinzaparin are used in practice. All three are supplied in prefilled syringes, which make self-administration easier and significantly reduce the risk of dosage error.6
LMWH vs. UFH: LMWH is safer and more efficacious than UFH. A summary of 22 clinical trials (including cancer patients and noncancer patients) by a Cochrane systematic review showed that treatment with LMWH in comparison with UFH results in decreased recurrent VTE, bleeding, mortality, HIT, and osteoporosis.7,13
Other agents: Fondaparinux is a factor Xa inhibitor rarely associated with heparin-induced thrombocytopenia (HIT), which makes it an attractive alternate anticoagulant for HIT patients. Its use in comparison with other parenteral anticoagulants has not been established in patients with malignancy.
Fondaparinux is FDA-approved for initial VTE treatment, and is used in practice as an alternative prophylactic anticoagulant for patients with HIT history or heparin allergy.7 However, no randomized clinical trials have evaluated its efficacy in patients with HIT.
Several new oral anticoagulants, including direct thrombin and factor Xa inhibitors, are being investigated; efficacy has not been established in cancer patients.7
Inferior vena cava (IVC) filters: Limited data surround the use of IVC filters, and most consensus guidelines recommend their use only in specific settings. One randomized controlled study (not limited to patients with cancer) showed no difference in overall short-term or long-term survival among patients receiving IVC filters for VTE treatment. However, there was a decrease in symptomatic PE in the filter group 12 days after placement. The tradeoff was significantly more recurrent DVTs at two years’ followup. The authors concluded that systematic use of IVC filters is not recommended.14
Because all of the study participants in this trial were receiving concomitant anticoagulation, it is difficult to generalize results to patients who have contraindications to anticoagulation. Nonetheless, ASCO, NCCN, and several other guideline panels recommend IVC filters only for patients with contraindications to anticoagulation or failure of long-term anticoagulation. NCCN broadens these recommendations for IVC filter placement to include patients with severe cardiac or pulmonary dysfunction.6 However, this recommendation is controversial, given the lack of supporting data, cost, and invasiveness of the procedure.7
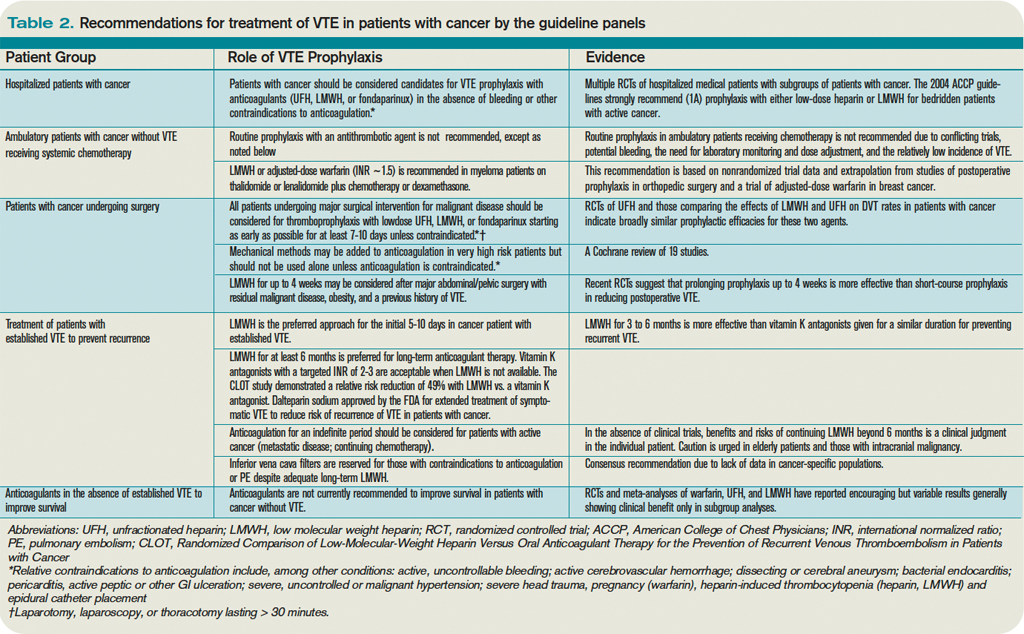
All patients with IVC filters without contraindication to anticoagulation should be anticoagulated.9
Prophylaxis: The importance of VTE prophylaxis in all hospitalized patients, including patients with cancer, is under close scrutiny in an attempt to improve patient safety and quality. The Centers for Medicare & Medicaid Services (CMS), in conjunction with the Joint Commission, has added VTE to its list of conditions that are reasonably preventable, and hospitals will no longer be reimbursed for the cost of treatment if acquired during a hospital stay. This rule currently is in effect for knee and hip replacements.15
The need for improvement in aggressive and appropriate prophylaxis of hospitalized patients was demonstrated by a single study in which just one-third of hospitalized patients received appropriate prophylaxis, according to American College of Chest Physicians (ACCP) guidelines.16
Despite a lack of robust data regarding VTE prophylaxis in patients with malignancy, strong data exist for VTE prophylaxis in hospitalized patients. All patients with cancer, and without contraindications to anticoagulation, should receive pharmacologic VTE prophylaxis while hospitalized. In the absence of supporting data, guidelines do not suggest VTE prophylaxis for ambulatory patients with cancer, except in certain multiple myeloma patients.6
Intracranial malignancies: Patients with intracranial malignancies are at risk for VTE, and the presence of intracranial tumors or metastases are not absolute contraindications to anticoagulation. However, data are sparse regarding VTE therapy in this subgroup. Active intracranial bleeding is an absolute contraindication to anticoagulation, and it should be avoided in patients with recent intracranial surgery or thrombocytopenia (e.g., platelet count < 50 x 109).4 In general, the presence of intracranial lesions without high-risk features should not deter the use of prophylactic anticoagulation.
Thrombocytopenia: Cancer patients frequently have chemotherapy-induced cytopenias, including thrombocytopenia. There is a paucity of data regarding anticoagulation in the setting of thrombocytopenia. In a recent review of VTE in the setting of cancer, Lee suggests dose reduction of LMWH by half in patients with platelet counts between 20 and 50 x 109/L.7 At our institution, hematologists suggest halving treatment-dose LMWH at platelet counts between 30 and 50 x 109/L, and discontinuing pharmacologic prophylaxis at platelet counts of less than 50 x 109/L—although there are little data to support these recommendations. Anticoagulation should be discontinued in patients with platelet counts below 20-30 x 109/L, as the risk of bleeding becomes too high.7
Thrombolytic therapy: Catheter-directed thrombolysis or systemic thrombolytic therapy might be appropriate treatment options for acute VTE. Presence of extensive proximal DVT, symptom duration of less than two weeks, life expectancy of greater than one year, good functional status, and low bleeding risk are prerequisites. Anticoagulation recommendations do not change following thrombolytic therapy.17
In the setting of PE, hemodynamic instability is the primary indication for thrombolysis. ACCP does not recommend thrombolytic therapy for the majority of VTE patients.17
Back to the Case
Our patient’s lower-extremity ultrasound and CT of the abdomen and pelvis both revealed extensive clot burden, which likely is related to her underlying pancreatic cancer. She should be started on an LMWH. Given the low likelihood of cure from her cancer, anticoagulation should be continued indefinitely, and an LMWH should be given for at least the first six months. Whether she should be switched to an oral VKA after six months depends on several factors: cost considerations, nutritional status, chemotherapy, presence of cytopenias, and bleeding risk.
IVC filter placement is not indicated at this time, as the patient does not have any contraindications to anticoagulation, has not failed anticoagulation, and does not have impending cardiac or pulmonary compromise. She is not a candidate for thrombolytic therapy due to her poor functional status and limited life expectancy.
Bottom Line
Cancer-associated VTE is increasingly common, and optimally is treated with LMWH for at least six months—indefinitely in the setting of active cancer or treatment. IVC filters have limited and specific indications in the setting of cancer-associated VTE, and should be reserved for situations when anticoagulation is contraindicated. TH
Dr. Weaver is an instructor in the division of hospital medicine at Northwestern University’s Feinberg School of Medicine in Chicago. Dr. Barsuk is an assistant professor in the division of hospital medicine at Feinberg.
References
- Khorana AA, Francis CW, Culakova E, Kuderer NM, Lyman GH. Frequency, risk factors, and trends for venous thromboembolism among hospitalized cancer patients. Cancer. 2007;110(10): 2339-2346.
- Stein PD, Beemath A, Meyers FA, Skaf E, Sanchez J, Olsen RE. Incidence of venous thromboembolism in patients hospitalized with cancer. Am J Med. 2006(1);119:60-68.
- Khorana AA, Francis CW, Culakova E, Kuderer NM, Lyman GH. Thromboembolism is a leading cause of death in cancer patients receiving outpatient chemotherapy. J Thromb Haemost. 2007;5(3):632-634.
- Lyman GA, Khorana AA, Falanga A, et al. American Society of Clinical Oncology guideline: recommendations for venous thromboembolism prophylaxis and treatment in patients with cancer. J Clin Oncol. 2007;25(34):5490-5505.
- Lyman GH, Khorana AA. Cancer, clots and consensus: new understanding of an old problem. J Clin Oncol. 2009;27(29):4821-4826.
- Khorana AA, Streiff MB, Farge D, et al. Venous thromboembolism prophylaxis and treatment in cancer: a consensus statement of major guidelines panels and call to action. J Clin Oncol. 2009;27(29):4919-4926.
- Lee, AY. Anticoagulation in the treatment of established venous thromboembolism in patients with cancer. J Clin Oncol. 2009;27(29):4895-4901.
- Kuderer NM, Ortel TL, Francis CW. Impact of venous thromboembolism and anticoagulation on cancer and cancer survival. J Clin Oncol. 2009;27(29):4902-4911.
- Prandoni, P. How I treat venous thromboembolism in patients with cancer. Blood. 2005;106(13):4027-4033.
- Lee AY, Levine MN, Baker RI, et al. Low-molecular-weight heparin versus a coumarin for the prevention of recurrent venous thromboembolism in patients with cancer. N Engl J Med. 2003;349(2):146-153.
- Meyer G, Marjanovic Z, Valcke J, et al. Comparison of low-molecular-weight heparin and warfarin for the secondary prevention of venous thromboembolism in patients with cancer: a randomized controlled study. Arch Intern Med. 2002;162(15):1729-1735.
- Hull RD, Pineo GF, Brant RF, et al. Long-term low-molecular-weight heparin versus usual care in proximal-vein thrombosis patients with cancer. Am J Med. 2006;119(12):1062-1072.
- Van Dongen CJ, van den Belt AG, Prins MH, Lensing AW. Fixed dose subcutaneous low molecular weight heparins versus adjusted dose unfractionated heparin for venous thromboembolism. Cochrane Database Syst Rev. 2004:18(4);CD001100.
- Decousus H, Leizorovicz A, Parent F, et al. A clinical trial of vena caval filters in the prevention of pulmonary embolism in patients with proximal deep-vein thrombosis. Prévention du Risque d’Embolie Pulmonaire par Interruption Cave Study Group. N Engl J Med. 1998;338(7): 409-415.
- Amin AN, Deitelzweig SB. Optimizing the prevention of venous thromboembolism: recent quality initiatives and strategies to drive improvement. Jt Comm J Qual Patient Saf. 2009;35(11):558-564.
- Amin A, Stemkowski S, Lin J, Yang G. Thromboprophylaxis rates in US medical centers: success or failure? J Thromb Haemost. 2007;5(8):1610-1616.
- Hirsch J, Guyatt G, Albers W, et al. Executive summary: American College of Chest Physicians evidence-based clinical practice guidelines (8th ed.). Chest. 2008:133(6 Suppl);71S-105S.
Case
A 70-year-old woman with recently diagnosed pancreatic cancer is admitted with worsening abdominal pain and new right-lower-extremity edema. A CT scan of the abdomen and pelvis reveals occlusive IVC and common iliac thromboses. A right-common-femoral DVT appears on Doppler ultrasound. A CT angiogram of her chest is negative for pulmonary emboli. What is the appropriate treatment for this patient’s thromboembolic disease?
Overview
VTE in the setting of malignancy is common, and the incidence of VTE among cancer patients is increasing for unclear reasons.1,2,3 VTE occurs in an estimated 4% to 20% of all malignancy patients. Overall, cancer patients are at a sixfold increased risk of developing VTE compared with the general population, and these patients represent approximately 20% of all VTE cases.4,5
VTE is a leading cause of mortality among hospitalized cancer patients; evidence of VTE exists in up to 50% of cancer patients at autopsy.3,4 VTE complications lead to significant morbidity, including recurrent VTE, pulmonary hypertension, post-thrombophlebitic syndrome, bleeding, and decreased quality of life.6,7
The risk is greatest for hospitalized cancer patients and those receiving active chemotherapy, particularly with such antiangiogenic agents as thalidomide and bevacizumab.4,6 Certain malignancies are more frequently associated with VTE; these include gastrointestinal, gynecologic, brain, lung, renal, and hematologic cancers.4 Table 1 (p. 50) summarizes risk factors associated with VTE in cancer patients.4
Patients with malignancy are hypercoagulable, primarily because of tumor-related alterations in the coagulation cascade.8 Tumors contain cell-surface proteins (e.g., tissue factor and cancer procoagulant) that lead to activation of the clotting cascade via interactions with factors IX and/or X. In addition, tumor-released cytokines cause prothrombotic changes in the vascular endothelium.8
This hypercoagulability is exacerbated by cancer-associated treatment events, including immobility, central venous catheters, erythropoiesis-stimulating agents, and packed red-blood-cell and platelet transfusions.5,9
Cancer-related therapy complications further confound VTE management. Drug interactions, chemotherapy-induced thrombocytopenia, malnutrition, bleeding risk from surgery or tumor location, and liver dysfunction make safe management of cancer-associated VTE a challenge.
Review of the Data
Low-molecular-weight heparin (LMWH) vs. vitamin K antagonists (VKA): There is significant evidence that LMWH is the preferred pharmacologic therapy for the initial and long-term treatment of cancer-related VTE. The most convincing data were published as the CLOT trial, and is supported by several smaller studies.10 Recommendations for the preferred use of LMWH are consistent among several national and international guidelines.6,7
In the CLOT (Randomized Comparison of Low-Molecular-Weight Heparin Versus Oral Anticoagulant Therapy for the Prevention of Recurrent Venous Thromboembolism in Patients with Cancer) trial, six months of treatment with an oral VKA preceded by five to seven days of LMWH was compared with six months of treatment with LMWH (dalteparin). Patients with the diagnosis of acute symptomatic VTE were evaluated. After six months of treatment, 53 of 336 patients in the oral anticoagulant group had recurrent VTE, compared with 27 of 336 patients in the LMWH group—a relative risk reduction of 52% and an absolute risk reduction of 8% (P=0.002). Complication rates (major and minor bleeding) and overall mortality were similar between the two groups.7,10
Two smaller trials compared LMWHs with warfarin in the treatment of VTE in the setting of cancer. In one trial, seven of 67 enoxaparin-treated patients developed bleeding or recurrent VTE, compared with 15 of 71 warfarin-treated subjects; however, this reduction was not statistically significant (P=0.09).11 In another trial, seven of 100 tinzaparin-treated patients developed recurrent VTE, compared with 16 of 100 warfarin-treated patients (P=0.044).12
Thus, LMWH is the preferred therapeutic agent for both DVT and PE in the setting of malignancy.5 Even so, although the clinical evidence supports LMWH use in the treatment of cancer-associated VTE, it’s worth noting that many of the authors of the cited papers received compensation from large pharmaceutical companies. In addition, the CLOT trial was funded by Pharmacia, which supplied the study drug.
Initial treatment (5-10 days): The American Society of Clinical Oncology (ASCO) guidelines advocate the use of LMWH during the initial five to 10 days following VTE diagnosis. Four other cancer research organization guidelines, National Comprehensive Cancer Network (NCCN), the Italian Association of Medical Oncology (AIOM), the European Society of Medical Oncology (ESMO), and the French National Federation of the League of Centers Against Cancer (FNCLCC), echo this approach, with unfractionated heparin (UFH) or fondaparinux as additional initial treatment depending on the clinical situation—i.e., renal failure, heparin-induced thrombocytopenia (HIT), or bleeding risk.6
Table 2 (below) summarizes recommendations for VTE treatment in cancer patients from all five guideline panels.6
Long-term treatment and duration (3-6 months): All of the panels agree LMWH is the preferred agent for long-term therapy of cancer-related VTE. ASCO supports treatment with LMWH for at least six months; oral VKAs with a targeted INR of 2 to 3 are acceptable when LMWH is not feasible. NCCN, AIOM, ESMO, and FNCLCC recommend an LMWH treatment duration from three to six months (ASCO recommends at least six months).
All of the panels, however, advocate indefinite duration of anticoagulation in patients with such continuing risk factors as active (metastatic, recurrent, or persistent) cancer or chemotherapy treatment.6 AIOM and ESMO specify indefinite LMWH, whereas ASCO does not specify oral VKA or LMWH use. Given the difficulties of managing VKA in the setting of advanced malignancy or chemotherapy, LMWH is the most practical choice, if it’s available and isn’t cost-prohibitive.
LMWH availability: Dalteparin, tinzaparin, and enoxaparin are LMWHs currently available in the U.S. for VTE treatment. Dalteparin is the only FDA-approved LMWH drug for long-term use to treat cancer-associated VTE, although enoxaparin and tinzaparin are used in practice. All three are supplied in prefilled syringes, which make self-administration easier and significantly reduce the risk of dosage error.6
LMWH vs. UFH: LMWH is safer and more efficacious than UFH. A summary of 22 clinical trials (including cancer patients and noncancer patients) by a Cochrane systematic review showed that treatment with LMWH in comparison with UFH results in decreased recurrent VTE, bleeding, mortality, HIT, and osteoporosis.7,13
Other agents: Fondaparinux is a factor Xa inhibitor rarely associated with heparin-induced thrombocytopenia (HIT), which makes it an attractive alternate anticoagulant for HIT patients. Its use in comparison with other parenteral anticoagulants has not been established in patients with malignancy.
Fondaparinux is FDA-approved for initial VTE treatment, and is used in practice as an alternative prophylactic anticoagulant for patients with HIT history or heparin allergy.7 However, no randomized clinical trials have evaluated its efficacy in patients with HIT.
Several new oral anticoagulants, including direct thrombin and factor Xa inhibitors, are being investigated; efficacy has not been established in cancer patients.7
Inferior vena cava (IVC) filters: Limited data surround the use of IVC filters, and most consensus guidelines recommend their use only in specific settings. One randomized controlled study (not limited to patients with cancer) showed no difference in overall short-term or long-term survival among patients receiving IVC filters for VTE treatment. However, there was a decrease in symptomatic PE in the filter group 12 days after placement. The tradeoff was significantly more recurrent DVTs at two years’ followup. The authors concluded that systematic use of IVC filters is not recommended.14
Because all of the study participants in this trial were receiving concomitant anticoagulation, it is difficult to generalize results to patients who have contraindications to anticoagulation. Nonetheless, ASCO, NCCN, and several other guideline panels recommend IVC filters only for patients with contraindications to anticoagulation or failure of long-term anticoagulation. NCCN broadens these recommendations for IVC filter placement to include patients with severe cardiac or pulmonary dysfunction.6 However, this recommendation is controversial, given the lack of supporting data, cost, and invasiveness of the procedure.7
All patients with IVC filters without contraindication to anticoagulation should be anticoagulated.9
Prophylaxis: The importance of VTE prophylaxis in all hospitalized patients, including patients with cancer, is under close scrutiny in an attempt to improve patient safety and quality. The Centers for Medicare & Medicaid Services (CMS), in conjunction with the Joint Commission, has added VTE to its list of conditions that are reasonably preventable, and hospitals will no longer be reimbursed for the cost of treatment if acquired during a hospital stay. This rule currently is in effect for knee and hip replacements.15
The need for improvement in aggressive and appropriate prophylaxis of hospitalized patients was demonstrated by a single study in which just one-third of hospitalized patients received appropriate prophylaxis, according to American College of Chest Physicians (ACCP) guidelines.16
Despite a lack of robust data regarding VTE prophylaxis in patients with malignancy, strong data exist for VTE prophylaxis in hospitalized patients. All patients with cancer, and without contraindications to anticoagulation, should receive pharmacologic VTE prophylaxis while hospitalized. In the absence of supporting data, guidelines do not suggest VTE prophylaxis for ambulatory patients with cancer, except in certain multiple myeloma patients.6
Intracranial malignancies: Patients with intracranial malignancies are at risk for VTE, and the presence of intracranial tumors or metastases are not absolute contraindications to anticoagulation. However, data are sparse regarding VTE therapy in this subgroup. Active intracranial bleeding is an absolute contraindication to anticoagulation, and it should be avoided in patients with recent intracranial surgery or thrombocytopenia (e.g., platelet count < 50 x 109).4 In general, the presence of intracranial lesions without high-risk features should not deter the use of prophylactic anticoagulation.
Thrombocytopenia: Cancer patients frequently have chemotherapy-induced cytopenias, including thrombocytopenia. There is a paucity of data regarding anticoagulation in the setting of thrombocytopenia. In a recent review of VTE in the setting of cancer, Lee suggests dose reduction of LMWH by half in patients with platelet counts between 20 and 50 x 109/L.7 At our institution, hematologists suggest halving treatment-dose LMWH at platelet counts between 30 and 50 x 109/L, and discontinuing pharmacologic prophylaxis at platelet counts of less than 50 x 109/L—although there are little data to support these recommendations. Anticoagulation should be discontinued in patients with platelet counts below 20-30 x 109/L, as the risk of bleeding becomes too high.7
Thrombolytic therapy: Catheter-directed thrombolysis or systemic thrombolytic therapy might be appropriate treatment options for acute VTE. Presence of extensive proximal DVT, symptom duration of less than two weeks, life expectancy of greater than one year, good functional status, and low bleeding risk are prerequisites. Anticoagulation recommendations do not change following thrombolytic therapy.17
In the setting of PE, hemodynamic instability is the primary indication for thrombolysis. ACCP does not recommend thrombolytic therapy for the majority of VTE patients.17
Back to the Case
Our patient’s lower-extremity ultrasound and CT of the abdomen and pelvis both revealed extensive clot burden, which likely is related to her underlying pancreatic cancer. She should be started on an LMWH. Given the low likelihood of cure from her cancer, anticoagulation should be continued indefinitely, and an LMWH should be given for at least the first six months. Whether she should be switched to an oral VKA after six months depends on several factors: cost considerations, nutritional status, chemotherapy, presence of cytopenias, and bleeding risk.
IVC filter placement is not indicated at this time, as the patient does not have any contraindications to anticoagulation, has not failed anticoagulation, and does not have impending cardiac or pulmonary compromise. She is not a candidate for thrombolytic therapy due to her poor functional status and limited life expectancy.
Bottom Line
Cancer-associated VTE is increasingly common, and optimally is treated with LMWH for at least six months—indefinitely in the setting of active cancer or treatment. IVC filters have limited and specific indications in the setting of cancer-associated VTE, and should be reserved for situations when anticoagulation is contraindicated. TH
Dr. Weaver is an instructor in the division of hospital medicine at Northwestern University’s Feinberg School of Medicine in Chicago. Dr. Barsuk is an assistant professor in the division of hospital medicine at Feinberg.
References
- Khorana AA, Francis CW, Culakova E, Kuderer NM, Lyman GH. Frequency, risk factors, and trends for venous thromboembolism among hospitalized cancer patients. Cancer. 2007;110(10): 2339-2346.
- Stein PD, Beemath A, Meyers FA, Skaf E, Sanchez J, Olsen RE. Incidence of venous thromboembolism in patients hospitalized with cancer. Am J Med. 2006(1);119:60-68.
- Khorana AA, Francis CW, Culakova E, Kuderer NM, Lyman GH. Thromboembolism is a leading cause of death in cancer patients receiving outpatient chemotherapy. J Thromb Haemost. 2007;5(3):632-634.
- Lyman GA, Khorana AA, Falanga A, et al. American Society of Clinical Oncology guideline: recommendations for venous thromboembolism prophylaxis and treatment in patients with cancer. J Clin Oncol. 2007;25(34):5490-5505.
- Lyman GH, Khorana AA. Cancer, clots and consensus: new understanding of an old problem. J Clin Oncol. 2009;27(29):4821-4826.
- Khorana AA, Streiff MB, Farge D, et al. Venous thromboembolism prophylaxis and treatment in cancer: a consensus statement of major guidelines panels and call to action. J Clin Oncol. 2009;27(29):4919-4926.
- Lee, AY. Anticoagulation in the treatment of established venous thromboembolism in patients with cancer. J Clin Oncol. 2009;27(29):4895-4901.
- Kuderer NM, Ortel TL, Francis CW. Impact of venous thromboembolism and anticoagulation on cancer and cancer survival. J Clin Oncol. 2009;27(29):4902-4911.
- Prandoni, P. How I treat venous thromboembolism in patients with cancer. Blood. 2005;106(13):4027-4033.
- Lee AY, Levine MN, Baker RI, et al. Low-molecular-weight heparin versus a coumarin for the prevention of recurrent venous thromboembolism in patients with cancer. N Engl J Med. 2003;349(2):146-153.
- Meyer G, Marjanovic Z, Valcke J, et al. Comparison of low-molecular-weight heparin and warfarin for the secondary prevention of venous thromboembolism in patients with cancer: a randomized controlled study. Arch Intern Med. 2002;162(15):1729-1735.
- Hull RD, Pineo GF, Brant RF, et al. Long-term low-molecular-weight heparin versus usual care in proximal-vein thrombosis patients with cancer. Am J Med. 2006;119(12):1062-1072.
- Van Dongen CJ, van den Belt AG, Prins MH, Lensing AW. Fixed dose subcutaneous low molecular weight heparins versus adjusted dose unfractionated heparin for venous thromboembolism. Cochrane Database Syst Rev. 2004:18(4);CD001100.
- Decousus H, Leizorovicz A, Parent F, et al. A clinical trial of vena caval filters in the prevention of pulmonary embolism in patients with proximal deep-vein thrombosis. Prévention du Risque d’Embolie Pulmonaire par Interruption Cave Study Group. N Engl J Med. 1998;338(7): 409-415.
- Amin AN, Deitelzweig SB. Optimizing the prevention of venous thromboembolism: recent quality initiatives and strategies to drive improvement. Jt Comm J Qual Patient Saf. 2009;35(11):558-564.
- Amin A, Stemkowski S, Lin J, Yang G. Thromboprophylaxis rates in US medical centers: success or failure? J Thromb Haemost. 2007;5(8):1610-1616.
- Hirsch J, Guyatt G, Albers W, et al. Executive summary: American College of Chest Physicians evidence-based clinical practice guidelines (8th ed.). Chest. 2008:133(6 Suppl);71S-105S.
Case
A 70-year-old woman with recently diagnosed pancreatic cancer is admitted with worsening abdominal pain and new right-lower-extremity edema. A CT scan of the abdomen and pelvis reveals occlusive IVC and common iliac thromboses. A right-common-femoral DVT appears on Doppler ultrasound. A CT angiogram of her chest is negative for pulmonary emboli. What is the appropriate treatment for this patient’s thromboembolic disease?
Overview
VTE in the setting of malignancy is common, and the incidence of VTE among cancer patients is increasing for unclear reasons.1,2,3 VTE occurs in an estimated 4% to 20% of all malignancy patients. Overall, cancer patients are at a sixfold increased risk of developing VTE compared with the general population, and these patients represent approximately 20% of all VTE cases.4,5
VTE is a leading cause of mortality among hospitalized cancer patients; evidence of VTE exists in up to 50% of cancer patients at autopsy.3,4 VTE complications lead to significant morbidity, including recurrent VTE, pulmonary hypertension, post-thrombophlebitic syndrome, bleeding, and decreased quality of life.6,7
The risk is greatest for hospitalized cancer patients and those receiving active chemotherapy, particularly with such antiangiogenic agents as thalidomide and bevacizumab.4,6 Certain malignancies are more frequently associated with VTE; these include gastrointestinal, gynecologic, brain, lung, renal, and hematologic cancers.4 Table 1 (p. 50) summarizes risk factors associated with VTE in cancer patients.4
Patients with malignancy are hypercoagulable, primarily because of tumor-related alterations in the coagulation cascade.8 Tumors contain cell-surface proteins (e.g., tissue factor and cancer procoagulant) that lead to activation of the clotting cascade via interactions with factors IX and/or X. In addition, tumor-released cytokines cause prothrombotic changes in the vascular endothelium.8
This hypercoagulability is exacerbated by cancer-associated treatment events, including immobility, central venous catheters, erythropoiesis-stimulating agents, and packed red-blood-cell and platelet transfusions.5,9
Cancer-related therapy complications further confound VTE management. Drug interactions, chemotherapy-induced thrombocytopenia, malnutrition, bleeding risk from surgery or tumor location, and liver dysfunction make safe management of cancer-associated VTE a challenge.
Review of the Data
Low-molecular-weight heparin (LMWH) vs. vitamin K antagonists (VKA): There is significant evidence that LMWH is the preferred pharmacologic therapy for the initial and long-term treatment of cancer-related VTE. The most convincing data were published as the CLOT trial, and is supported by several smaller studies.10 Recommendations for the preferred use of LMWH are consistent among several national and international guidelines.6,7
In the CLOT (Randomized Comparison of Low-Molecular-Weight Heparin Versus Oral Anticoagulant Therapy for the Prevention of Recurrent Venous Thromboembolism in Patients with Cancer) trial, six months of treatment with an oral VKA preceded by five to seven days of LMWH was compared with six months of treatment with LMWH (dalteparin). Patients with the diagnosis of acute symptomatic VTE were evaluated. After six months of treatment, 53 of 336 patients in the oral anticoagulant group had recurrent VTE, compared with 27 of 336 patients in the LMWH group—a relative risk reduction of 52% and an absolute risk reduction of 8% (P=0.002). Complication rates (major and minor bleeding) and overall mortality were similar between the two groups.7,10
Two smaller trials compared LMWHs with warfarin in the treatment of VTE in the setting of cancer. In one trial, seven of 67 enoxaparin-treated patients developed bleeding or recurrent VTE, compared with 15 of 71 warfarin-treated subjects; however, this reduction was not statistically significant (P=0.09).11 In another trial, seven of 100 tinzaparin-treated patients developed recurrent VTE, compared with 16 of 100 warfarin-treated patients (P=0.044).12
Thus, LMWH is the preferred therapeutic agent for both DVT and PE in the setting of malignancy.5 Even so, although the clinical evidence supports LMWH use in the treatment of cancer-associated VTE, it’s worth noting that many of the authors of the cited papers received compensation from large pharmaceutical companies. In addition, the CLOT trial was funded by Pharmacia, which supplied the study drug.
Initial treatment (5-10 days): The American Society of Clinical Oncology (ASCO) guidelines advocate the use of LMWH during the initial five to 10 days following VTE diagnosis. Four other cancer research organization guidelines, National Comprehensive Cancer Network (NCCN), the Italian Association of Medical Oncology (AIOM), the European Society of Medical Oncology (ESMO), and the French National Federation of the League of Centers Against Cancer (FNCLCC), echo this approach, with unfractionated heparin (UFH) or fondaparinux as additional initial treatment depending on the clinical situation—i.e., renal failure, heparin-induced thrombocytopenia (HIT), or bleeding risk.6
Table 2 (below) summarizes recommendations for VTE treatment in cancer patients from all five guideline panels.6
Long-term treatment and duration (3-6 months): All of the panels agree LMWH is the preferred agent for long-term therapy of cancer-related VTE. ASCO supports treatment with LMWH for at least six months; oral VKAs with a targeted INR of 2 to 3 are acceptable when LMWH is not feasible. NCCN, AIOM, ESMO, and FNCLCC recommend an LMWH treatment duration from three to six months (ASCO recommends at least six months).
All of the panels, however, advocate indefinite duration of anticoagulation in patients with such continuing risk factors as active (metastatic, recurrent, or persistent) cancer or chemotherapy treatment.6 AIOM and ESMO specify indefinite LMWH, whereas ASCO does not specify oral VKA or LMWH use. Given the difficulties of managing VKA in the setting of advanced malignancy or chemotherapy, LMWH is the most practical choice, if it’s available and isn’t cost-prohibitive.
LMWH availability: Dalteparin, tinzaparin, and enoxaparin are LMWHs currently available in the U.S. for VTE treatment. Dalteparin is the only FDA-approved LMWH drug for long-term use to treat cancer-associated VTE, although enoxaparin and tinzaparin are used in practice. All three are supplied in prefilled syringes, which make self-administration easier and significantly reduce the risk of dosage error.6
LMWH vs. UFH: LMWH is safer and more efficacious than UFH. A summary of 22 clinical trials (including cancer patients and noncancer patients) by a Cochrane systematic review showed that treatment with LMWH in comparison with UFH results in decreased recurrent VTE, bleeding, mortality, HIT, and osteoporosis.7,13
Other agents: Fondaparinux is a factor Xa inhibitor rarely associated with heparin-induced thrombocytopenia (HIT), which makes it an attractive alternate anticoagulant for HIT patients. Its use in comparison with other parenteral anticoagulants has not been established in patients with malignancy.
Fondaparinux is FDA-approved for initial VTE treatment, and is used in practice as an alternative prophylactic anticoagulant for patients with HIT history or heparin allergy.7 However, no randomized clinical trials have evaluated its efficacy in patients with HIT.
Several new oral anticoagulants, including direct thrombin and factor Xa inhibitors, are being investigated; efficacy has not been established in cancer patients.7
Inferior vena cava (IVC) filters: Limited data surround the use of IVC filters, and most consensus guidelines recommend their use only in specific settings. One randomized controlled study (not limited to patients with cancer) showed no difference in overall short-term or long-term survival among patients receiving IVC filters for VTE treatment. However, there was a decrease in symptomatic PE in the filter group 12 days after placement. The tradeoff was significantly more recurrent DVTs at two years’ followup. The authors concluded that systematic use of IVC filters is not recommended.14
Because all of the study participants in this trial were receiving concomitant anticoagulation, it is difficult to generalize results to patients who have contraindications to anticoagulation. Nonetheless, ASCO, NCCN, and several other guideline panels recommend IVC filters only for patients with contraindications to anticoagulation or failure of long-term anticoagulation. NCCN broadens these recommendations for IVC filter placement to include patients with severe cardiac or pulmonary dysfunction.6 However, this recommendation is controversial, given the lack of supporting data, cost, and invasiveness of the procedure.7
All patients with IVC filters without contraindication to anticoagulation should be anticoagulated.9
Prophylaxis: The importance of VTE prophylaxis in all hospitalized patients, including patients with cancer, is under close scrutiny in an attempt to improve patient safety and quality. The Centers for Medicare & Medicaid Services (CMS), in conjunction with the Joint Commission, has added VTE to its list of conditions that are reasonably preventable, and hospitals will no longer be reimbursed for the cost of treatment if acquired during a hospital stay. This rule currently is in effect for knee and hip replacements.15
The need for improvement in aggressive and appropriate prophylaxis of hospitalized patients was demonstrated by a single study in which just one-third of hospitalized patients received appropriate prophylaxis, according to American College of Chest Physicians (ACCP) guidelines.16
Despite a lack of robust data regarding VTE prophylaxis in patients with malignancy, strong data exist for VTE prophylaxis in hospitalized patients. All patients with cancer, and without contraindications to anticoagulation, should receive pharmacologic VTE prophylaxis while hospitalized. In the absence of supporting data, guidelines do not suggest VTE prophylaxis for ambulatory patients with cancer, except in certain multiple myeloma patients.6
Intracranial malignancies: Patients with intracranial malignancies are at risk for VTE, and the presence of intracranial tumors or metastases are not absolute contraindications to anticoagulation. However, data are sparse regarding VTE therapy in this subgroup. Active intracranial bleeding is an absolute contraindication to anticoagulation, and it should be avoided in patients with recent intracranial surgery or thrombocytopenia (e.g., platelet count < 50 x 109).4 In general, the presence of intracranial lesions without high-risk features should not deter the use of prophylactic anticoagulation.
Thrombocytopenia: Cancer patients frequently have chemotherapy-induced cytopenias, including thrombocytopenia. There is a paucity of data regarding anticoagulation in the setting of thrombocytopenia. In a recent review of VTE in the setting of cancer, Lee suggests dose reduction of LMWH by half in patients with platelet counts between 20 and 50 x 109/L.7 At our institution, hematologists suggest halving treatment-dose LMWH at platelet counts between 30 and 50 x 109/L, and discontinuing pharmacologic prophylaxis at platelet counts of less than 50 x 109/L—although there are little data to support these recommendations. Anticoagulation should be discontinued in patients with platelet counts below 20-30 x 109/L, as the risk of bleeding becomes too high.7
Thrombolytic therapy: Catheter-directed thrombolysis or systemic thrombolytic therapy might be appropriate treatment options for acute VTE. Presence of extensive proximal DVT, symptom duration of less than two weeks, life expectancy of greater than one year, good functional status, and low bleeding risk are prerequisites. Anticoagulation recommendations do not change following thrombolytic therapy.17
In the setting of PE, hemodynamic instability is the primary indication for thrombolysis. ACCP does not recommend thrombolytic therapy for the majority of VTE patients.17
Back to the Case
Our patient’s lower-extremity ultrasound and CT of the abdomen and pelvis both revealed extensive clot burden, which likely is related to her underlying pancreatic cancer. She should be started on an LMWH. Given the low likelihood of cure from her cancer, anticoagulation should be continued indefinitely, and an LMWH should be given for at least the first six months. Whether she should be switched to an oral VKA after six months depends on several factors: cost considerations, nutritional status, chemotherapy, presence of cytopenias, and bleeding risk.
IVC filter placement is not indicated at this time, as the patient does not have any contraindications to anticoagulation, has not failed anticoagulation, and does not have impending cardiac or pulmonary compromise. She is not a candidate for thrombolytic therapy due to her poor functional status and limited life expectancy.
Bottom Line
Cancer-associated VTE is increasingly common, and optimally is treated with LMWH for at least six months—indefinitely in the setting of active cancer or treatment. IVC filters have limited and specific indications in the setting of cancer-associated VTE, and should be reserved for situations when anticoagulation is contraindicated. TH
Dr. Weaver is an instructor in the division of hospital medicine at Northwestern University’s Feinberg School of Medicine in Chicago. Dr. Barsuk is an assistant professor in the division of hospital medicine at Feinberg.
References
- Khorana AA, Francis CW, Culakova E, Kuderer NM, Lyman GH. Frequency, risk factors, and trends for venous thromboembolism among hospitalized cancer patients. Cancer. 2007;110(10): 2339-2346.
- Stein PD, Beemath A, Meyers FA, Skaf E, Sanchez J, Olsen RE. Incidence of venous thromboembolism in patients hospitalized with cancer. Am J Med. 2006(1);119:60-68.
- Khorana AA, Francis CW, Culakova E, Kuderer NM, Lyman GH. Thromboembolism is a leading cause of death in cancer patients receiving outpatient chemotherapy. J Thromb Haemost. 2007;5(3):632-634.
- Lyman GA, Khorana AA, Falanga A, et al. American Society of Clinical Oncology guideline: recommendations for venous thromboembolism prophylaxis and treatment in patients with cancer. J Clin Oncol. 2007;25(34):5490-5505.
- Lyman GH, Khorana AA. Cancer, clots and consensus: new understanding of an old problem. J Clin Oncol. 2009;27(29):4821-4826.
- Khorana AA, Streiff MB, Farge D, et al. Venous thromboembolism prophylaxis and treatment in cancer: a consensus statement of major guidelines panels and call to action. J Clin Oncol. 2009;27(29):4919-4926.
- Lee, AY. Anticoagulation in the treatment of established venous thromboembolism in patients with cancer. J Clin Oncol. 2009;27(29):4895-4901.
- Kuderer NM, Ortel TL, Francis CW. Impact of venous thromboembolism and anticoagulation on cancer and cancer survival. J Clin Oncol. 2009;27(29):4902-4911.
- Prandoni, P. How I treat venous thromboembolism in patients with cancer. Blood. 2005;106(13):4027-4033.
- Lee AY, Levine MN, Baker RI, et al. Low-molecular-weight heparin versus a coumarin for the prevention of recurrent venous thromboembolism in patients with cancer. N Engl J Med. 2003;349(2):146-153.
- Meyer G, Marjanovic Z, Valcke J, et al. Comparison of low-molecular-weight heparin and warfarin for the secondary prevention of venous thromboembolism in patients with cancer: a randomized controlled study. Arch Intern Med. 2002;162(15):1729-1735.
- Hull RD, Pineo GF, Brant RF, et al. Long-term low-molecular-weight heparin versus usual care in proximal-vein thrombosis patients with cancer. Am J Med. 2006;119(12):1062-1072.
- Van Dongen CJ, van den Belt AG, Prins MH, Lensing AW. Fixed dose subcutaneous low molecular weight heparins versus adjusted dose unfractionated heparin for venous thromboembolism. Cochrane Database Syst Rev. 2004:18(4);CD001100.
- Decousus H, Leizorovicz A, Parent F, et al. A clinical trial of vena caval filters in the prevention of pulmonary embolism in patients with proximal deep-vein thrombosis. Prévention du Risque d’Embolie Pulmonaire par Interruption Cave Study Group. N Engl J Med. 1998;338(7): 409-415.
- Amin AN, Deitelzweig SB. Optimizing the prevention of venous thromboembolism: recent quality initiatives and strategies to drive improvement. Jt Comm J Qual Patient Saf. 2009;35(11):558-564.
- Amin A, Stemkowski S, Lin J, Yang G. Thromboprophylaxis rates in US medical centers: success or failure? J Thromb Haemost. 2007;5(8):1610-1616.
- Hirsch J, Guyatt G, Albers W, et al. Executive summary: American College of Chest Physicians evidence-based clinical practice guidelines (8th ed.). Chest. 2008:133(6 Suppl);71S-105S.
Spousal Consent
When recruiting a hospitalist for his company, Jason Stuckey makes it a point to call the candidate’s home. His goal isn’t to speak with the hospitalist the company is interested in hiring—it’s to talk with the candidate’s spouse.
“One of the top five mistakes recruiters make is to not involve the spouse in the [recruitment] process,” says Stuckey, who directs HM recruiting for TeamHealth, a Knoxville, Tenn.-based company that provides healthcare staffing and administrative services to hospitals in 14 states.
Hospitalists are generally so busy with work that the spouse is often the person in the family who takes the lead in the job search, says Tim Lary, vice president of profession staffing for IPC: The Hospitalist Co., a national physician group practice based in North Hollywood, Calif.
The spouse often gives final approval on a decision to accept a job offer, adds Peggy Fricke, director of physician staffing for Eagle Hospital Physicians, an Atlanta-based company that manages hospitalist practices for hospitals in the Southeast and Mid-Atlantic regions.
“The physician could be making the most money, but if their spouse and family are not happy, then they won’t stay in the position long,” Stuckey explains. “I’ve also found that if the spouse is not on board with moving and uprooting the family to a new location, then it’s not going to happen.”
As a result, recruiters and prospective employers often spend just as much time engaging the spouse as they do the actual job candidate, the recruiters say. For this reason, hospitalists who are searching for a new job would be wise to include their husband or wife as early as possible in the job hunt in order to get the most out of the recruiting process.
For example, while the hospitalist focuses on determining if the work is the right fit professionally and financially, the spouse can appraise the community to see if it meets the family’s needs in such areas as schools, neighborhoods, religious services, community groups, and entertainment/cultural outlets. If the hospitalist is invited for an on-site interview, it’s important that their spouse makes the trip as well.
“We always do a community tour, and we will do school tours when asked,” Fricke says of Eagle’s recruiting efforts. “We can introduce the families of the other hospitalists in the practice so a spouse can meet and get to know them.”
—Jason Stuckey, director, HM recruitment, TeamHealth, Knoxville, Tenn.
Upfront Inclusion
When the spouse is involved in the process, they usually are more receptive to receiving information about what opportunities exist in other communities and more open to the idea of moving to a new place, Stuckey says.
For instances in which children are involved, the spouse is most often interested in learning about the location’s school districts and private schools, and determining if the community has a good quality of life for families, Fricke says. For situations in which there are no children or the children are grown, the spouse often focuses on job prospects in their own profession.
Hospitalists with a husband or wife who works and whose career is important to them should see if the HM recruiter can help put their spouse in touch with potential employers in the community, because many times they will, says Fricke, who has connected spouses in IT and engineering fields with people who could assist them in their job search.
“It goes back to making sure everyone is happy. If the spouse can’t find work, that is going to affect their happiness,” says Darren Swenson, MD, medical affairs director for IPC of Nevada and regional chair of IPC’s national advisory board.
Aside from schools, quality of life, and their own job opportunities, spouses also ask about what their hospitalist husband or wife’s work schedule would be and how much vacation and holiday time they would have in the prospective job, Dr. Swenson says.
“It’s extremely important that we look at our hospitalists and their spouses being happy in their home life, because if they’re not, that is going to spill over into in their work life,” IPC’s Lary says.
Good Partnership, Bad Partnership
Times arise when the spouse takes a proactive role in evaluating the actual HM job offer, the recruiters say. “In all couples, there is someone who is dominant and someone who is not,” says Fricke, who has seen spouses participate in job interviews with hospital administrators. “If the spouse is dominant, we try to understand them and listen to what is important to them.”
Sometimes the spouse is an attorney or other type of professional who wants to review the hospitalist contract and has the most questions about it, Dr. Swenson says. When that happens, recruiters will often have group members sit in to answer their questions, he says.
“Absolutely, without question, the spouse has to be involved. But if the spouse is too demanding and everything has to be run through them, to an employer, that can be a big turnoff,” Stuckey says.
When it comes to business matters, the physician—not the spouse—has to take the lead, he says. If the physician doesn’t, it could make the prospective employer wonder what challenges could be ahead should the candidate be hired, Stuckey says.
Two-Physician Families
One time when it is acceptable for a spouse to get intimately involved in the contract and negotiations is when he or she is a hospitalist who also is being recruited by the same prospective employer.
“It’s a unique situation. It’s great to have two for the price of one, so to speak,” Stuckey says. “But there are challenges from the employer’s perspective—for example, scheduling—that have to be resolved on the front end rather than when they get there.”
While still relatively rare, husband-wife hospitalist couples are becoming more prevalent because there are more hospitalists, Fricke says. They tend to meet each other in medical school or residency, she says.
“Even though they are a couple, we treat them as individuals during the recruiting process,” Fricke says. “I think the most important thing is we try to do anything we can—within reason, of course—to help the hospitalist and their spouse make the best decision for themselves and their family.” TH
Lisa Ryan is a freelance writer based in New Jersey.
When recruiting a hospitalist for his company, Jason Stuckey makes it a point to call the candidate’s home. His goal isn’t to speak with the hospitalist the company is interested in hiring—it’s to talk with the candidate’s spouse.
“One of the top five mistakes recruiters make is to not involve the spouse in the [recruitment] process,” says Stuckey, who directs HM recruiting for TeamHealth, a Knoxville, Tenn.-based company that provides healthcare staffing and administrative services to hospitals in 14 states.
Hospitalists are generally so busy with work that the spouse is often the person in the family who takes the lead in the job search, says Tim Lary, vice president of profession staffing for IPC: The Hospitalist Co., a national physician group practice based in North Hollywood, Calif.
The spouse often gives final approval on a decision to accept a job offer, adds Peggy Fricke, director of physician staffing for Eagle Hospital Physicians, an Atlanta-based company that manages hospitalist practices for hospitals in the Southeast and Mid-Atlantic regions.
“The physician could be making the most money, but if their spouse and family are not happy, then they won’t stay in the position long,” Stuckey explains. “I’ve also found that if the spouse is not on board with moving and uprooting the family to a new location, then it’s not going to happen.”
As a result, recruiters and prospective employers often spend just as much time engaging the spouse as they do the actual job candidate, the recruiters say. For this reason, hospitalists who are searching for a new job would be wise to include their husband or wife as early as possible in the job hunt in order to get the most out of the recruiting process.
For example, while the hospitalist focuses on determining if the work is the right fit professionally and financially, the spouse can appraise the community to see if it meets the family’s needs in such areas as schools, neighborhoods, religious services, community groups, and entertainment/cultural outlets. If the hospitalist is invited for an on-site interview, it’s important that their spouse makes the trip as well.
“We always do a community tour, and we will do school tours when asked,” Fricke says of Eagle’s recruiting efforts. “We can introduce the families of the other hospitalists in the practice so a spouse can meet and get to know them.”
—Jason Stuckey, director, HM recruitment, TeamHealth, Knoxville, Tenn.
Upfront Inclusion
When the spouse is involved in the process, they usually are more receptive to receiving information about what opportunities exist in other communities and more open to the idea of moving to a new place, Stuckey says.
For instances in which children are involved, the spouse is most often interested in learning about the location’s school districts and private schools, and determining if the community has a good quality of life for families, Fricke says. For situations in which there are no children or the children are grown, the spouse often focuses on job prospects in their own profession.
Hospitalists with a husband or wife who works and whose career is important to them should see if the HM recruiter can help put their spouse in touch with potential employers in the community, because many times they will, says Fricke, who has connected spouses in IT and engineering fields with people who could assist them in their job search.
“It goes back to making sure everyone is happy. If the spouse can’t find work, that is going to affect their happiness,” says Darren Swenson, MD, medical affairs director for IPC of Nevada and regional chair of IPC’s national advisory board.
Aside from schools, quality of life, and their own job opportunities, spouses also ask about what their hospitalist husband or wife’s work schedule would be and how much vacation and holiday time they would have in the prospective job, Dr. Swenson says.
“It’s extremely important that we look at our hospitalists and their spouses being happy in their home life, because if they’re not, that is going to spill over into in their work life,” IPC’s Lary says.
Good Partnership, Bad Partnership
Times arise when the spouse takes a proactive role in evaluating the actual HM job offer, the recruiters say. “In all couples, there is someone who is dominant and someone who is not,” says Fricke, who has seen spouses participate in job interviews with hospital administrators. “If the spouse is dominant, we try to understand them and listen to what is important to them.”
Sometimes the spouse is an attorney or other type of professional who wants to review the hospitalist contract and has the most questions about it, Dr. Swenson says. When that happens, recruiters will often have group members sit in to answer their questions, he says.
“Absolutely, without question, the spouse has to be involved. But if the spouse is too demanding and everything has to be run through them, to an employer, that can be a big turnoff,” Stuckey says.
When it comes to business matters, the physician—not the spouse—has to take the lead, he says. If the physician doesn’t, it could make the prospective employer wonder what challenges could be ahead should the candidate be hired, Stuckey says.
Two-Physician Families
One time when it is acceptable for a spouse to get intimately involved in the contract and negotiations is when he or she is a hospitalist who also is being recruited by the same prospective employer.
“It’s a unique situation. It’s great to have two for the price of one, so to speak,” Stuckey says. “But there are challenges from the employer’s perspective—for example, scheduling—that have to be resolved on the front end rather than when they get there.”
While still relatively rare, husband-wife hospitalist couples are becoming more prevalent because there are more hospitalists, Fricke says. They tend to meet each other in medical school or residency, she says.
“Even though they are a couple, we treat them as individuals during the recruiting process,” Fricke says. “I think the most important thing is we try to do anything we can—within reason, of course—to help the hospitalist and their spouse make the best decision for themselves and their family.” TH
Lisa Ryan is a freelance writer based in New Jersey.
When recruiting a hospitalist for his company, Jason Stuckey makes it a point to call the candidate’s home. His goal isn’t to speak with the hospitalist the company is interested in hiring—it’s to talk with the candidate’s spouse.
“One of the top five mistakes recruiters make is to not involve the spouse in the [recruitment] process,” says Stuckey, who directs HM recruiting for TeamHealth, a Knoxville, Tenn.-based company that provides healthcare staffing and administrative services to hospitals in 14 states.
Hospitalists are generally so busy with work that the spouse is often the person in the family who takes the lead in the job search, says Tim Lary, vice president of profession staffing for IPC: The Hospitalist Co., a national physician group practice based in North Hollywood, Calif.
The spouse often gives final approval on a decision to accept a job offer, adds Peggy Fricke, director of physician staffing for Eagle Hospital Physicians, an Atlanta-based company that manages hospitalist practices for hospitals in the Southeast and Mid-Atlantic regions.
“The physician could be making the most money, but if their spouse and family are not happy, then they won’t stay in the position long,” Stuckey explains. “I’ve also found that if the spouse is not on board with moving and uprooting the family to a new location, then it’s not going to happen.”
As a result, recruiters and prospective employers often spend just as much time engaging the spouse as they do the actual job candidate, the recruiters say. For this reason, hospitalists who are searching for a new job would be wise to include their husband or wife as early as possible in the job hunt in order to get the most out of the recruiting process.
For example, while the hospitalist focuses on determining if the work is the right fit professionally and financially, the spouse can appraise the community to see if it meets the family’s needs in such areas as schools, neighborhoods, religious services, community groups, and entertainment/cultural outlets. If the hospitalist is invited for an on-site interview, it’s important that their spouse makes the trip as well.
“We always do a community tour, and we will do school tours when asked,” Fricke says of Eagle’s recruiting efforts. “We can introduce the families of the other hospitalists in the practice so a spouse can meet and get to know them.”
—Jason Stuckey, director, HM recruitment, TeamHealth, Knoxville, Tenn.
Upfront Inclusion
When the spouse is involved in the process, they usually are more receptive to receiving information about what opportunities exist in other communities and more open to the idea of moving to a new place, Stuckey says.
For instances in which children are involved, the spouse is most often interested in learning about the location’s school districts and private schools, and determining if the community has a good quality of life for families, Fricke says. For situations in which there are no children or the children are grown, the spouse often focuses on job prospects in their own profession.
Hospitalists with a husband or wife who works and whose career is important to them should see if the HM recruiter can help put their spouse in touch with potential employers in the community, because many times they will, says Fricke, who has connected spouses in IT and engineering fields with people who could assist them in their job search.
“It goes back to making sure everyone is happy. If the spouse can’t find work, that is going to affect their happiness,” says Darren Swenson, MD, medical affairs director for IPC of Nevada and regional chair of IPC’s national advisory board.
Aside from schools, quality of life, and their own job opportunities, spouses also ask about what their hospitalist husband or wife’s work schedule would be and how much vacation and holiday time they would have in the prospective job, Dr. Swenson says.
“It’s extremely important that we look at our hospitalists and their spouses being happy in their home life, because if they’re not, that is going to spill over into in their work life,” IPC’s Lary says.
Good Partnership, Bad Partnership
Times arise when the spouse takes a proactive role in evaluating the actual HM job offer, the recruiters say. “In all couples, there is someone who is dominant and someone who is not,” says Fricke, who has seen spouses participate in job interviews with hospital administrators. “If the spouse is dominant, we try to understand them and listen to what is important to them.”
Sometimes the spouse is an attorney or other type of professional who wants to review the hospitalist contract and has the most questions about it, Dr. Swenson says. When that happens, recruiters will often have group members sit in to answer their questions, he says.
“Absolutely, without question, the spouse has to be involved. But if the spouse is too demanding and everything has to be run through them, to an employer, that can be a big turnoff,” Stuckey says.
When it comes to business matters, the physician—not the spouse—has to take the lead, he says. If the physician doesn’t, it could make the prospective employer wonder what challenges could be ahead should the candidate be hired, Stuckey says.
Two-Physician Families
One time when it is acceptable for a spouse to get intimately involved in the contract and negotiations is when he or she is a hospitalist who also is being recruited by the same prospective employer.
“It’s a unique situation. It’s great to have two for the price of one, so to speak,” Stuckey says. “But there are challenges from the employer’s perspective—for example, scheduling—that have to be resolved on the front end rather than when they get there.”
While still relatively rare, husband-wife hospitalist couples are becoming more prevalent because there are more hospitalists, Fricke says. They tend to meet each other in medical school or residency, she says.
“Even though they are a couple, we treat them as individuals during the recruiting process,” Fricke says. “I think the most important thing is we try to do anything we can—within reason, of course—to help the hospitalist and their spouse make the best decision for themselves and their family.” TH
Lisa Ryan is a freelance writer based in New Jersey.
Discharge Services
Discharge day management services (99238-99239) seem unlikely to cause confusion in the physician community; however, continued requests for documentation involving these CPT codes prove the opposite.
Here’s an example of how a billing error might be made for discharge day management services. A patient with diabetes mellitus, hypertension, and chronic kidney disease is stable for discharge. The patient is being transferred to a skilled nursing facility (SNF). Dr. Aardsma prepares the patient for hospital discharge, and Dr. Broxton admits the patient to the SNF later that day. Dr. Aardsma and Dr. Broxton are members of the same group practice, with the same specialty designation. Can both physicians report their services?
Key Elements
Consider the basic billing principles of discharge services: what, who, and when.
Hospital discharge day management codes are used to report the physician’s total duration of time spent preparing the patient for discharge. These codes include, as appropriate:
- Final examination of the patient;
- Discussion of the hospital stay, even if the time spent by the physician on that date is not continuous;
- Instructions for continuing care to all relevant caregivers; and
- Preparation of discharge records, prescriptions, and referral forms.1
Hospitalists should report one discharge code per hospitalization, but only when the service occurs after the initial date of admission: 99238, hospital discharge day management, 30 minutes or less; or 99239, hospital discharge day management, more than 30 minutes.1,2 Select one of the two codes, depending upon the cumulative discharge service time provided on the patient’s hospital unit/floor during a single calendar day. Do not count time for services performed outside of the patient’s unit or floor (i.e., calls to the receiving physician/facility made from the physician’s private office) or services performed after the patient physically leaves the hospital.
Physician documentation must refer to the discharge status, as well as other clinically relevant information. Don’t be misled into believing that the presence of a discharge summary alone satisfies documentation requirements. In addition to the discharge groundwork, hospitalists must physically see the patient on the day he or she reports discharge management. Discharge summaries are not always useful in noting the physician’s required face-to-face encounter with the patient. Simply state, “Patient seen and examined by me on discharge day.”
Alternatively, hospitalists can elect to include details of a discharge day exam. Although a final exam isn’t mandatory for billing 99238-99239, it is the best justification of a face-to-face encounter on discharge day. Documentation of the time is required when reporting 99239 (e.g., discharge time >30 minutes). Time isn’t typically included in a discharge summary, and upon post-payment payor review, a claim involving 99239 without documented time in the patient’s medical record might result in either a service reduction to the lower level of care (99238) or a request for payment refund.3 Physicians can document all necessary details in the formal summary or a progress note.
Transfers of Care
The admitting physician or group is responsible for performing discharge services unless a formal transfer of care occurs, such as the patient’s transfer from the ICU to the standard medical floor as the patient’s condition improves. Without this transfer of care, comanaging physicians should merely report subsequent hospital-care codes (99231-99233) for the final patient encounter. An example of this is surgical comanagement: If a surgeon is identified as the attending of record, they are responsible for postoperative management of the patient, including discharge services.4,5 Providers in a different group or specialty report 99231-99233 for their medically necessary care.
As with all other time-based services, only the billing provider’s time counts. Discharge-related services performed by residents, students, or ancillary staff (i.e., RNs) do not count toward the physician’s discharge service time. Report the date of the physician’s actual discharge visit even if the patient leaves the facility on a different calendar date—for example, if a patient leaves the next day due to availability of the receiving facility.
Pronouncement of Death
Physicians might not realize that they can report discharge day management codes for pronouncement of death.7 Only the hospitalist who performs the pronouncement is allowed to report this service on the date pronouncement occurred, even if the paperwork is delayed to a subsequent date. Completion of the death certificate alone is not sufficient for billing. Hospitalists must “examine” the patient, thus satisfying the “face to face” visit requirement.
Additional services (e.g., speaking with family members, speaking with healthcare providers, filling out the necessary documentation) count toward the cumulative discharge service time, if performed on the patient’s unit or floor. Document the cumulative time when reporting 99239.
Back to the Case
Typical billing and payment rules mandate the reporting of only one E/M service per specialty, per patient, per day. One of the few exceptions involves reporting a hospital discharge code (99238-99239) with initial nursing facility care (99304-99306). Either the same physician or different physicians from the same group and specialty can report the hospital discharge and the nursing facility admission on the same day. When the same physician or group discharges the patient from any other location (e.g., observation unit) on the same day, report only one service: either the observation discharge (99217) or the initial nursing facility care (99304-99306).
When the same physician or group discharges a patient from the hospital and admits the patient to a facility other than a nursing facility on the same day, report only one service: either the hospital discharge (99228-99239) or the admission care (e.g., long-term acute-care hospital: 99221-99223). TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Abraham M, Beebe M, Dalton J, Evans D, Glenn R. Current Procedural Terminology Professional Edition. Chicago: American Medical Association Press; 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.9.1C. Centers for Medicare & Medicaid Services Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed March 3, 2010.
- Highmark Medicare Services Provider Bulletins: Hospital Discharge Day Management Codes 99238 and 99239. Highmark Medicare Services Web site. Available at: www.highmarkmedicareservices.com/bulletins/partb/news02212008a.html. Accessed March 4, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 40.1A. Centers for Medicare & Medicaid Services Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed March 5, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 40.3B. Centers for Medicare & Medicaid Services Web site, Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed March 5, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.9.2E. Centers for Medicare & Medicaid Services Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed March 5, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.9.1d. Centers for Medicare & Medicaid Services Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed March 5, 2010.
- Reporting inpatient hospital evaluation and management (E/M) services that could be described by current procedural terminology (CPT) consultation codes. Cigna Government Services Web site. Available at: www.cignagovernmentservices.com/partb/pubs/news/2010/0210/cope11694.html. Accessed March 5, 2010.
Discharge day management services (99238-99239) seem unlikely to cause confusion in the physician community; however, continued requests for documentation involving these CPT codes prove the opposite.
Here’s an example of how a billing error might be made for discharge day management services. A patient with diabetes mellitus, hypertension, and chronic kidney disease is stable for discharge. The patient is being transferred to a skilled nursing facility (SNF). Dr. Aardsma prepares the patient for hospital discharge, and Dr. Broxton admits the patient to the SNF later that day. Dr. Aardsma and Dr. Broxton are members of the same group practice, with the same specialty designation. Can both physicians report their services?
Key Elements
Consider the basic billing principles of discharge services: what, who, and when.
Hospital discharge day management codes are used to report the physician’s total duration of time spent preparing the patient for discharge. These codes include, as appropriate:
- Final examination of the patient;
- Discussion of the hospital stay, even if the time spent by the physician on that date is not continuous;
- Instructions for continuing care to all relevant caregivers; and
- Preparation of discharge records, prescriptions, and referral forms.1
Hospitalists should report one discharge code per hospitalization, but only when the service occurs after the initial date of admission: 99238, hospital discharge day management, 30 minutes or less; or 99239, hospital discharge day management, more than 30 minutes.1,2 Select one of the two codes, depending upon the cumulative discharge service time provided on the patient’s hospital unit/floor during a single calendar day. Do not count time for services performed outside of the patient’s unit or floor (i.e., calls to the receiving physician/facility made from the physician’s private office) or services performed after the patient physically leaves the hospital.
Physician documentation must refer to the discharge status, as well as other clinically relevant information. Don’t be misled into believing that the presence of a discharge summary alone satisfies documentation requirements. In addition to the discharge groundwork, hospitalists must physically see the patient on the day he or she reports discharge management. Discharge summaries are not always useful in noting the physician’s required face-to-face encounter with the patient. Simply state, “Patient seen and examined by me on discharge day.”
Alternatively, hospitalists can elect to include details of a discharge day exam. Although a final exam isn’t mandatory for billing 99238-99239, it is the best justification of a face-to-face encounter on discharge day. Documentation of the time is required when reporting 99239 (e.g., discharge time >30 minutes). Time isn’t typically included in a discharge summary, and upon post-payment payor review, a claim involving 99239 without documented time in the patient’s medical record might result in either a service reduction to the lower level of care (99238) or a request for payment refund.3 Physicians can document all necessary details in the formal summary or a progress note.
Transfers of Care
The admitting physician or group is responsible for performing discharge services unless a formal transfer of care occurs, such as the patient’s transfer from the ICU to the standard medical floor as the patient’s condition improves. Without this transfer of care, comanaging physicians should merely report subsequent hospital-care codes (99231-99233) for the final patient encounter. An example of this is surgical comanagement: If a surgeon is identified as the attending of record, they are responsible for postoperative management of the patient, including discharge services.4,5 Providers in a different group or specialty report 99231-99233 for their medically necessary care.
As with all other time-based services, only the billing provider’s time counts. Discharge-related services performed by residents, students, or ancillary staff (i.e., RNs) do not count toward the physician’s discharge service time. Report the date of the physician’s actual discharge visit even if the patient leaves the facility on a different calendar date—for example, if a patient leaves the next day due to availability of the receiving facility.
Pronouncement of Death
Physicians might not realize that they can report discharge day management codes for pronouncement of death.7 Only the hospitalist who performs the pronouncement is allowed to report this service on the date pronouncement occurred, even if the paperwork is delayed to a subsequent date. Completion of the death certificate alone is not sufficient for billing. Hospitalists must “examine” the patient, thus satisfying the “face to face” visit requirement.
Additional services (e.g., speaking with family members, speaking with healthcare providers, filling out the necessary documentation) count toward the cumulative discharge service time, if performed on the patient’s unit or floor. Document the cumulative time when reporting 99239.
Back to the Case
Typical billing and payment rules mandate the reporting of only one E/M service per specialty, per patient, per day. One of the few exceptions involves reporting a hospital discharge code (99238-99239) with initial nursing facility care (99304-99306). Either the same physician or different physicians from the same group and specialty can report the hospital discharge and the nursing facility admission on the same day. When the same physician or group discharges the patient from any other location (e.g., observation unit) on the same day, report only one service: either the observation discharge (99217) or the initial nursing facility care (99304-99306).
When the same physician or group discharges a patient from the hospital and admits the patient to a facility other than a nursing facility on the same day, report only one service: either the hospital discharge (99228-99239) or the admission care (e.g., long-term acute-care hospital: 99221-99223). TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Abraham M, Beebe M, Dalton J, Evans D, Glenn R. Current Procedural Terminology Professional Edition. Chicago: American Medical Association Press; 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.9.1C. Centers for Medicare & Medicaid Services Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed March 3, 2010.
- Highmark Medicare Services Provider Bulletins: Hospital Discharge Day Management Codes 99238 and 99239. Highmark Medicare Services Web site. Available at: www.highmarkmedicareservices.com/bulletins/partb/news02212008a.html. Accessed March 4, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 40.1A. Centers for Medicare & Medicaid Services Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed March 5, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 40.3B. Centers for Medicare & Medicaid Services Web site, Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed March 5, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.9.2E. Centers for Medicare & Medicaid Services Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed March 5, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.9.1d. Centers for Medicare & Medicaid Services Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed March 5, 2010.
- Reporting inpatient hospital evaluation and management (E/M) services that could be described by current procedural terminology (CPT) consultation codes. Cigna Government Services Web site. Available at: www.cignagovernmentservices.com/partb/pubs/news/2010/0210/cope11694.html. Accessed March 5, 2010.
Discharge day management services (99238-99239) seem unlikely to cause confusion in the physician community; however, continued requests for documentation involving these CPT codes prove the opposite.
Here’s an example of how a billing error might be made for discharge day management services. A patient with diabetes mellitus, hypertension, and chronic kidney disease is stable for discharge. The patient is being transferred to a skilled nursing facility (SNF). Dr. Aardsma prepares the patient for hospital discharge, and Dr. Broxton admits the patient to the SNF later that day. Dr. Aardsma and Dr. Broxton are members of the same group practice, with the same specialty designation. Can both physicians report their services?
Key Elements
Consider the basic billing principles of discharge services: what, who, and when.
Hospital discharge day management codes are used to report the physician’s total duration of time spent preparing the patient for discharge. These codes include, as appropriate:
- Final examination of the patient;
- Discussion of the hospital stay, even if the time spent by the physician on that date is not continuous;
- Instructions for continuing care to all relevant caregivers; and
- Preparation of discharge records, prescriptions, and referral forms.1
Hospitalists should report one discharge code per hospitalization, but only when the service occurs after the initial date of admission: 99238, hospital discharge day management, 30 minutes or less; or 99239, hospital discharge day management, more than 30 minutes.1,2 Select one of the two codes, depending upon the cumulative discharge service time provided on the patient’s hospital unit/floor during a single calendar day. Do not count time for services performed outside of the patient’s unit or floor (i.e., calls to the receiving physician/facility made from the physician’s private office) or services performed after the patient physically leaves the hospital.
Physician documentation must refer to the discharge status, as well as other clinically relevant information. Don’t be misled into believing that the presence of a discharge summary alone satisfies documentation requirements. In addition to the discharge groundwork, hospitalists must physically see the patient on the day he or she reports discharge management. Discharge summaries are not always useful in noting the physician’s required face-to-face encounter with the patient. Simply state, “Patient seen and examined by me on discharge day.”
Alternatively, hospitalists can elect to include details of a discharge day exam. Although a final exam isn’t mandatory for billing 99238-99239, it is the best justification of a face-to-face encounter on discharge day. Documentation of the time is required when reporting 99239 (e.g., discharge time >30 minutes). Time isn’t typically included in a discharge summary, and upon post-payment payor review, a claim involving 99239 without documented time in the patient’s medical record might result in either a service reduction to the lower level of care (99238) or a request for payment refund.3 Physicians can document all necessary details in the formal summary or a progress note.
Transfers of Care
The admitting physician or group is responsible for performing discharge services unless a formal transfer of care occurs, such as the patient’s transfer from the ICU to the standard medical floor as the patient’s condition improves. Without this transfer of care, comanaging physicians should merely report subsequent hospital-care codes (99231-99233) for the final patient encounter. An example of this is surgical comanagement: If a surgeon is identified as the attending of record, they are responsible for postoperative management of the patient, including discharge services.4,5 Providers in a different group or specialty report 99231-99233 for their medically necessary care.
As with all other time-based services, only the billing provider’s time counts. Discharge-related services performed by residents, students, or ancillary staff (i.e., RNs) do not count toward the physician’s discharge service time. Report the date of the physician’s actual discharge visit even if the patient leaves the facility on a different calendar date—for example, if a patient leaves the next day due to availability of the receiving facility.
Pronouncement of Death
Physicians might not realize that they can report discharge day management codes for pronouncement of death.7 Only the hospitalist who performs the pronouncement is allowed to report this service on the date pronouncement occurred, even if the paperwork is delayed to a subsequent date. Completion of the death certificate alone is not sufficient for billing. Hospitalists must “examine” the patient, thus satisfying the “face to face” visit requirement.
Additional services (e.g., speaking with family members, speaking with healthcare providers, filling out the necessary documentation) count toward the cumulative discharge service time, if performed on the patient’s unit or floor. Document the cumulative time when reporting 99239.
Back to the Case
Typical billing and payment rules mandate the reporting of only one E/M service per specialty, per patient, per day. One of the few exceptions involves reporting a hospital discharge code (99238-99239) with initial nursing facility care (99304-99306). Either the same physician or different physicians from the same group and specialty can report the hospital discharge and the nursing facility admission on the same day. When the same physician or group discharges the patient from any other location (e.g., observation unit) on the same day, report only one service: either the observation discharge (99217) or the initial nursing facility care (99304-99306).
When the same physician or group discharges a patient from the hospital and admits the patient to a facility other than a nursing facility on the same day, report only one service: either the hospital discharge (99228-99239) or the admission care (e.g., long-term acute-care hospital: 99221-99223). TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Abraham M, Beebe M, Dalton J, Evans D, Glenn R. Current Procedural Terminology Professional Edition. Chicago: American Medical Association Press; 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.9.1C. Centers for Medicare & Medicaid Services Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed March 3, 2010.
- Highmark Medicare Services Provider Bulletins: Hospital Discharge Day Management Codes 99238 and 99239. Highmark Medicare Services Web site. Available at: www.highmarkmedicareservices.com/bulletins/partb/news02212008a.html. Accessed March 4, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 40.1A. Centers for Medicare & Medicaid Services Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed March 5, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 40.3B. Centers for Medicare & Medicaid Services Web site, Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed March 5, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.9.2E. Centers for Medicare & Medicaid Services Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed March 5, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.9.1d. Centers for Medicare & Medicaid Services Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed March 5, 2010.
- Reporting inpatient hospital evaluation and management (E/M) services that could be described by current procedural terminology (CPT) consultation codes. Cigna Government Services Web site. Available at: www.cignagovernmentservices.com/partb/pubs/news/2010/0210/cope11694.html. Accessed March 5, 2010.
Satisfaction Challenge
In 1973, a survey was conducted to evaluate physician satisfaction. Less than 15% of physicians reported any doubt that they had made the right career choice, with 3.7% stating that they were “not happy.”1 Twenty years later, surveys revealed a different story: Forty percent of physicians stated that they would not choose the medical profession if they had to choose a career again.2
Dissatisfaction in medicine has been reported in diverse age groups, different areas of the country, and various medical specialties.3 When dissatisfied, physicians often leave their jobs and, consequently, the patient-physician relationship is disrupted. This turnover is quite costly to the healthcare system. In primary care, the cost of replacing a physician is estimated at $250,000.4
Here are some of the factors that contribute to burnout, as well as solutions for ensuring job satisfaction.
Challenges Ahead
Burnout is an interesting phenomenon in the medical profession. Unlike many other professionals, physicians often experience extreme fatigue and emotional exhaustion at an early stage in their careers—during medical school and residency. By midcareer, the momentum is maintained as colleagues recognize their hard work, and they continue to place service to others before themselves. Physicians who encounter burnout often experience emotional exhaustion, impaired job performance, relationship difficulties, and poor health, including irritability, sleep disturbances, headaches, depression, and drug addictions.
Increased rates of burnout have been linked to several internal and external factors. Internal factors—management style in a workplace, multiple demands at work, social support from colleagues, lack of control over the work environment—have been illustrated to correlate with higher rates of burnout. The ever-increasing demand on physicians’ time leads to higher rates of dissatisfaction. There are an exponentially increasing number of medications, tests, and procedures to discuss with patients and families. This is complicated by the rise of e-mail and the Internet, as some patients expect immediate responses to their concerns.
Some studies have shown that personality factors can lead to burnout. Compulsiveness, a trait often seen in physicians, is an adaptive behavior for the demands of medical education and practice. However, it can lead to chronic feelings of inadequacy, an exaggerated sense of responsibility, and difficulty setting limits. Furthermore, physicians often are conditioned in the psychology of postponement. It takes root in the early years of medical education and leads to habitually delaying various sources of renewal, such as vacations and relationships.
External factors include payment reductions, managing various insurers, and increasing malpractice cases.1,2,5 Evaluating the changing landscape of managed-care organizations reveals that while a small fraction of physicians are employed by them, more than 90% contract with them. Commonly cited reasons for dissatisfaction with managed care include “trafficking” of patients in and out of care, administrative paperwork, limitations on referring patients to specialists, financial incentives to curb medical workups, and pressure to evaluate increasing numbers of patients.6
Malpractice cases have increased in the past 30 years. The American Medical Association (AMA) has identified 18 states where providers are finding it challenging to purchase affordable insurance.7 An additional 26 states have been placed on “orange alert,” indicating a worsening situation in availability and affordability of insurance. Physicians who are not personally burdened by malpractice suits feel its repercussions. They practice “defensive medicine” by ordering increasing numbers of tests and procedures to avoid potential litigation. Physicians involved in lawsuits, regardless of the outcome, describe feeling shame, self-doubt, and disillusionment with medical practice.
What Makes You Happy?
In the December 2006 issue of The Hospitalist (see “Are You Satisfied?” p. 4), Mary Jo Gorman, MD, MBA, FHM, then president of SHM, pointed out five factors that contribute to physician satisfaction:
- Stimulation and challenge at work. It’s critical to have a job that requires technically difficult tasks, procedures, or intellectual challenges. The ability to interact and collaborate with other physicians further adds depth and richness to hospitalists’ clinical practice. However, it’s important to realize that overstimulation can lead to discomfort and unhappiness.
- Feeling appreciated. Recog-nition for your performance leads to feeling valued at work and has a strong correlation with overall job satisfaction. It keeps hospitalists interested and motivated. However, recognition should be personalized; otherwise, it can have a detrimental effect.
- Control over work. Auto-nomy and control over work is important to ensuring job satisfaction. This includes actively participating in the design of your work schedule and other work-related matters. When decisions are imposed on physicians, it creates tension and stress.
- Work environment. This includes the type of work, support, and opportunities for growth and development, as well as interactions with colleagues and staff.
- Income. Compensation is often fourth or fifth on the list of priorities for physicians. While all of us seek fair compensation for our work, it often is not the main reason we choose an employment.
Solutions
Burnout prevention is the responsibility of all healthcare professionals. It’s critical to promote well-being on all levels: physical, emotional, psychological, and spiritual. The following recommendations are based on various interventions established nationally to address physician burnout:
Establish realistic goals. Identify realistic goals for your professional and personal life, and actively work on balancing the two. Emphasize these goals throughout your professional career, avoiding the natural tendency for postponement.
Improve your work environment. Involve physicians in the design and management of the practice; build flexible schedules that allow coverage during important life events (i.e., graduations, births, weddings); minimize paperwork and improve efficiency; and establish a committee for open discussion of physician wellness issues.
Take care of yourself. Mentorship programs support junior members in their career development and help them balance the challenges of their personal and professional lives. Mentors can detect dissatisfaction and help physicians re-evaluate their interests and career paths. Require physicians to have their own primary-care physician (PCP) to ensure their physical and mental well-being. Offer memberships to fitness centers.
Provide opportunities to grow. Seek opportunities for medical education; address personal goals and aspirations, such as hobbies and interests; and establish sabbatical programs to gain perspective and broaden your horizons.
Fortunately, medicine has an enthusiastic applicant pool. There is hope that highly motivated and qualified students will continue to apply and enter the medical profession. However, there is concern that the dissatisfaction in medicine might influence the caliber of applicants who apply.
Medical education and training needs to address the challenges of practicing medicine. Students should be taught about the challenges of delivering high-quality care, risk management, cost containment, and utilization review. During the clinical years in medical school and residency, trainees need to experience the fast pace of medicine, the realities of payment dilemmas, and increased paperwork. It ultimately is the responsibility of educators in the medical profession to encourage students and residents to establish more accurate expectations of the practice of medicine. TH
Dr. Afsarmanesh is director of hospital medicine quality initiatives at Ronald Reagan UCLA Medical Center in Los Angeles.
References
- Mello MM, Studdert DM, Brennan TA. The new medical malpractice crisis. N Engl J Med. 2003;348(23):2281-2284.
- Hadley J, Cantor JC, Willke RJ, Feder J, Cohen AB. Young physicians most and least likely to have second thoughts about a career in medicine. Acad Med. 1992;67:180-190.
- Harvey LK, Shubat SC. AMA Public Opinion on Healthcare Issues. Chicago: American Medical Association Press; 1988.
- Leigh JP, Tancredi DJ, Kravitz RL. Physician career satisfaction within specialties. BMC Health Serv Res. 2009;9:166.
- Buchbinder SB, Wilson M, Melick CF, Powe NR. Estimates of costs of primary care physician turnover. Am J Manag Care. 1999;5(11):1431-1438.
- Reams HR, Dunstone DC. Professional satisfaction of physicians. Arch Intern Med. 1989;149:1951-1956.
- McMurray JE, Williams E, Schwartz MD, et al. Developing a model using qualitative data. J Gen Intern Med. 1997;12(11):711–714.
In 1973, a survey was conducted to evaluate physician satisfaction. Less than 15% of physicians reported any doubt that they had made the right career choice, with 3.7% stating that they were “not happy.”1 Twenty years later, surveys revealed a different story: Forty percent of physicians stated that they would not choose the medical profession if they had to choose a career again.2
Dissatisfaction in medicine has been reported in diverse age groups, different areas of the country, and various medical specialties.3 When dissatisfied, physicians often leave their jobs and, consequently, the patient-physician relationship is disrupted. This turnover is quite costly to the healthcare system. In primary care, the cost of replacing a physician is estimated at $250,000.4
Here are some of the factors that contribute to burnout, as well as solutions for ensuring job satisfaction.
Challenges Ahead
Burnout is an interesting phenomenon in the medical profession. Unlike many other professionals, physicians often experience extreme fatigue and emotional exhaustion at an early stage in their careers—during medical school and residency. By midcareer, the momentum is maintained as colleagues recognize their hard work, and they continue to place service to others before themselves. Physicians who encounter burnout often experience emotional exhaustion, impaired job performance, relationship difficulties, and poor health, including irritability, sleep disturbances, headaches, depression, and drug addictions.
Increased rates of burnout have been linked to several internal and external factors. Internal factors—management style in a workplace, multiple demands at work, social support from colleagues, lack of control over the work environment—have been illustrated to correlate with higher rates of burnout. The ever-increasing demand on physicians’ time leads to higher rates of dissatisfaction. There are an exponentially increasing number of medications, tests, and procedures to discuss with patients and families. This is complicated by the rise of e-mail and the Internet, as some patients expect immediate responses to their concerns.
Some studies have shown that personality factors can lead to burnout. Compulsiveness, a trait often seen in physicians, is an adaptive behavior for the demands of medical education and practice. However, it can lead to chronic feelings of inadequacy, an exaggerated sense of responsibility, and difficulty setting limits. Furthermore, physicians often are conditioned in the psychology of postponement. It takes root in the early years of medical education and leads to habitually delaying various sources of renewal, such as vacations and relationships.
External factors include payment reductions, managing various insurers, and increasing malpractice cases.1,2,5 Evaluating the changing landscape of managed-care organizations reveals that while a small fraction of physicians are employed by them, more than 90% contract with them. Commonly cited reasons for dissatisfaction with managed care include “trafficking” of patients in and out of care, administrative paperwork, limitations on referring patients to specialists, financial incentives to curb medical workups, and pressure to evaluate increasing numbers of patients.6
Malpractice cases have increased in the past 30 years. The American Medical Association (AMA) has identified 18 states where providers are finding it challenging to purchase affordable insurance.7 An additional 26 states have been placed on “orange alert,” indicating a worsening situation in availability and affordability of insurance. Physicians who are not personally burdened by malpractice suits feel its repercussions. They practice “defensive medicine” by ordering increasing numbers of tests and procedures to avoid potential litigation. Physicians involved in lawsuits, regardless of the outcome, describe feeling shame, self-doubt, and disillusionment with medical practice.
What Makes You Happy?
In the December 2006 issue of The Hospitalist (see “Are You Satisfied?” p. 4), Mary Jo Gorman, MD, MBA, FHM, then president of SHM, pointed out five factors that contribute to physician satisfaction:
- Stimulation and challenge at work. It’s critical to have a job that requires technically difficult tasks, procedures, or intellectual challenges. The ability to interact and collaborate with other physicians further adds depth and richness to hospitalists’ clinical practice. However, it’s important to realize that overstimulation can lead to discomfort and unhappiness.
- Feeling appreciated. Recog-nition for your performance leads to feeling valued at work and has a strong correlation with overall job satisfaction. It keeps hospitalists interested and motivated. However, recognition should be personalized; otherwise, it can have a detrimental effect.
- Control over work. Auto-nomy and control over work is important to ensuring job satisfaction. This includes actively participating in the design of your work schedule and other work-related matters. When decisions are imposed on physicians, it creates tension and stress.
- Work environment. This includes the type of work, support, and opportunities for growth and development, as well as interactions with colleagues and staff.
- Income. Compensation is often fourth or fifth on the list of priorities for physicians. While all of us seek fair compensation for our work, it often is not the main reason we choose an employment.
Solutions
Burnout prevention is the responsibility of all healthcare professionals. It’s critical to promote well-being on all levels: physical, emotional, psychological, and spiritual. The following recommendations are based on various interventions established nationally to address physician burnout:
Establish realistic goals. Identify realistic goals for your professional and personal life, and actively work on balancing the two. Emphasize these goals throughout your professional career, avoiding the natural tendency for postponement.
Improve your work environment. Involve physicians in the design and management of the practice; build flexible schedules that allow coverage during important life events (i.e., graduations, births, weddings); minimize paperwork and improve efficiency; and establish a committee for open discussion of physician wellness issues.
Take care of yourself. Mentorship programs support junior members in their career development and help them balance the challenges of their personal and professional lives. Mentors can detect dissatisfaction and help physicians re-evaluate their interests and career paths. Require physicians to have their own primary-care physician (PCP) to ensure their physical and mental well-being. Offer memberships to fitness centers.
Provide opportunities to grow. Seek opportunities for medical education; address personal goals and aspirations, such as hobbies and interests; and establish sabbatical programs to gain perspective and broaden your horizons.
Fortunately, medicine has an enthusiastic applicant pool. There is hope that highly motivated and qualified students will continue to apply and enter the medical profession. However, there is concern that the dissatisfaction in medicine might influence the caliber of applicants who apply.
Medical education and training needs to address the challenges of practicing medicine. Students should be taught about the challenges of delivering high-quality care, risk management, cost containment, and utilization review. During the clinical years in medical school and residency, trainees need to experience the fast pace of medicine, the realities of payment dilemmas, and increased paperwork. It ultimately is the responsibility of educators in the medical profession to encourage students and residents to establish more accurate expectations of the practice of medicine. TH
Dr. Afsarmanesh is director of hospital medicine quality initiatives at Ronald Reagan UCLA Medical Center in Los Angeles.
References
- Mello MM, Studdert DM, Brennan TA. The new medical malpractice crisis. N Engl J Med. 2003;348(23):2281-2284.
- Hadley J, Cantor JC, Willke RJ, Feder J, Cohen AB. Young physicians most and least likely to have second thoughts about a career in medicine. Acad Med. 1992;67:180-190.
- Harvey LK, Shubat SC. AMA Public Opinion on Healthcare Issues. Chicago: American Medical Association Press; 1988.
- Leigh JP, Tancredi DJ, Kravitz RL. Physician career satisfaction within specialties. BMC Health Serv Res. 2009;9:166.
- Buchbinder SB, Wilson M, Melick CF, Powe NR. Estimates of costs of primary care physician turnover. Am J Manag Care. 1999;5(11):1431-1438.
- Reams HR, Dunstone DC. Professional satisfaction of physicians. Arch Intern Med. 1989;149:1951-1956.
- McMurray JE, Williams E, Schwartz MD, et al. Developing a model using qualitative data. J Gen Intern Med. 1997;12(11):711–714.
In 1973, a survey was conducted to evaluate physician satisfaction. Less than 15% of physicians reported any doubt that they had made the right career choice, with 3.7% stating that they were “not happy.”1 Twenty years later, surveys revealed a different story: Forty percent of physicians stated that they would not choose the medical profession if they had to choose a career again.2
Dissatisfaction in medicine has been reported in diverse age groups, different areas of the country, and various medical specialties.3 When dissatisfied, physicians often leave their jobs and, consequently, the patient-physician relationship is disrupted. This turnover is quite costly to the healthcare system. In primary care, the cost of replacing a physician is estimated at $250,000.4
Here are some of the factors that contribute to burnout, as well as solutions for ensuring job satisfaction.
Challenges Ahead
Burnout is an interesting phenomenon in the medical profession. Unlike many other professionals, physicians often experience extreme fatigue and emotional exhaustion at an early stage in their careers—during medical school and residency. By midcareer, the momentum is maintained as colleagues recognize their hard work, and they continue to place service to others before themselves. Physicians who encounter burnout often experience emotional exhaustion, impaired job performance, relationship difficulties, and poor health, including irritability, sleep disturbances, headaches, depression, and drug addictions.
Increased rates of burnout have been linked to several internal and external factors. Internal factors—management style in a workplace, multiple demands at work, social support from colleagues, lack of control over the work environment—have been illustrated to correlate with higher rates of burnout. The ever-increasing demand on physicians’ time leads to higher rates of dissatisfaction. There are an exponentially increasing number of medications, tests, and procedures to discuss with patients and families. This is complicated by the rise of e-mail and the Internet, as some patients expect immediate responses to their concerns.
Some studies have shown that personality factors can lead to burnout. Compulsiveness, a trait often seen in physicians, is an adaptive behavior for the demands of medical education and practice. However, it can lead to chronic feelings of inadequacy, an exaggerated sense of responsibility, and difficulty setting limits. Furthermore, physicians often are conditioned in the psychology of postponement. It takes root in the early years of medical education and leads to habitually delaying various sources of renewal, such as vacations and relationships.
External factors include payment reductions, managing various insurers, and increasing malpractice cases.1,2,5 Evaluating the changing landscape of managed-care organizations reveals that while a small fraction of physicians are employed by them, more than 90% contract with them. Commonly cited reasons for dissatisfaction with managed care include “trafficking” of patients in and out of care, administrative paperwork, limitations on referring patients to specialists, financial incentives to curb medical workups, and pressure to evaluate increasing numbers of patients.6
Malpractice cases have increased in the past 30 years. The American Medical Association (AMA) has identified 18 states where providers are finding it challenging to purchase affordable insurance.7 An additional 26 states have been placed on “orange alert,” indicating a worsening situation in availability and affordability of insurance. Physicians who are not personally burdened by malpractice suits feel its repercussions. They practice “defensive medicine” by ordering increasing numbers of tests and procedures to avoid potential litigation. Physicians involved in lawsuits, regardless of the outcome, describe feeling shame, self-doubt, and disillusionment with medical practice.
What Makes You Happy?
In the December 2006 issue of The Hospitalist (see “Are You Satisfied?” p. 4), Mary Jo Gorman, MD, MBA, FHM, then president of SHM, pointed out five factors that contribute to physician satisfaction:
- Stimulation and challenge at work. It’s critical to have a job that requires technically difficult tasks, procedures, or intellectual challenges. The ability to interact and collaborate with other physicians further adds depth and richness to hospitalists’ clinical practice. However, it’s important to realize that overstimulation can lead to discomfort and unhappiness.
- Feeling appreciated. Recog-nition for your performance leads to feeling valued at work and has a strong correlation with overall job satisfaction. It keeps hospitalists interested and motivated. However, recognition should be personalized; otherwise, it can have a detrimental effect.
- Control over work. Auto-nomy and control over work is important to ensuring job satisfaction. This includes actively participating in the design of your work schedule and other work-related matters. When decisions are imposed on physicians, it creates tension and stress.
- Work environment. This includes the type of work, support, and opportunities for growth and development, as well as interactions with colleagues and staff.
- Income. Compensation is often fourth or fifth on the list of priorities for physicians. While all of us seek fair compensation for our work, it often is not the main reason we choose an employment.
Solutions
Burnout prevention is the responsibility of all healthcare professionals. It’s critical to promote well-being on all levels: physical, emotional, psychological, and spiritual. The following recommendations are based on various interventions established nationally to address physician burnout:
Establish realistic goals. Identify realistic goals for your professional and personal life, and actively work on balancing the two. Emphasize these goals throughout your professional career, avoiding the natural tendency for postponement.
Improve your work environment. Involve physicians in the design and management of the practice; build flexible schedules that allow coverage during important life events (i.e., graduations, births, weddings); minimize paperwork and improve efficiency; and establish a committee for open discussion of physician wellness issues.
Take care of yourself. Mentorship programs support junior members in their career development and help them balance the challenges of their personal and professional lives. Mentors can detect dissatisfaction and help physicians re-evaluate their interests and career paths. Require physicians to have their own primary-care physician (PCP) to ensure their physical and mental well-being. Offer memberships to fitness centers.
Provide opportunities to grow. Seek opportunities for medical education; address personal goals and aspirations, such as hobbies and interests; and establish sabbatical programs to gain perspective and broaden your horizons.
Fortunately, medicine has an enthusiastic applicant pool. There is hope that highly motivated and qualified students will continue to apply and enter the medical profession. However, there is concern that the dissatisfaction in medicine might influence the caliber of applicants who apply.
Medical education and training needs to address the challenges of practicing medicine. Students should be taught about the challenges of delivering high-quality care, risk management, cost containment, and utilization review. During the clinical years in medical school and residency, trainees need to experience the fast pace of medicine, the realities of payment dilemmas, and increased paperwork. It ultimately is the responsibility of educators in the medical profession to encourage students and residents to establish more accurate expectations of the practice of medicine. TH
Dr. Afsarmanesh is director of hospital medicine quality initiatives at Ronald Reagan UCLA Medical Center in Los Angeles.
References
- Mello MM, Studdert DM, Brennan TA. The new medical malpractice crisis. N Engl J Med. 2003;348(23):2281-2284.
- Hadley J, Cantor JC, Willke RJ, Feder J, Cohen AB. Young physicians most and least likely to have second thoughts about a career in medicine. Acad Med. 1992;67:180-190.
- Harvey LK, Shubat SC. AMA Public Opinion on Healthcare Issues. Chicago: American Medical Association Press; 1988.
- Leigh JP, Tancredi DJ, Kravitz RL. Physician career satisfaction within specialties. BMC Health Serv Res. 2009;9:166.
- Buchbinder SB, Wilson M, Melick CF, Powe NR. Estimates of costs of primary care physician turnover. Am J Manag Care. 1999;5(11):1431-1438.
- Reams HR, Dunstone DC. Professional satisfaction of physicians. Arch Intern Med. 1989;149:1951-1956.
- McMurray JE, Williams E, Schwartz MD, et al. Developing a model using qualitative data. J Gen Intern Med. 1997;12(11):711–714.
The Humble Approach
Bijo Chacko, MD, FHM, says the varied resources available in the multispecialty medical group in which he practices help to ensure patients receive the best possible care. The structure at Preferred Health Partners in Brooklyn, N.Y., which offers primary and specialty medical services under one roof, requires hospitalists to collaborate frequently with primary-care physicians (PCPs).
That interaction breaks down barriers, fosters communication, promotes the exchange of ideas, and ultimately improves the transition of care from outpatient to inpatient and vice versa, Dr. Chacko says.
His affinity for that environment might explain his passion for the work done by SHM’s Young Physician Task Force, and why “resources” is the word he repeats most often when describing the value of the group’s efforts. Just as experienced hospitalists can learn by interacting with PCPs and other specialists, those who are new to HM can benefit from those who have established themselves in the profession and cleared the hurdles physicians encounter early in a career, he says.
“The advantage of youth is the inherent energy that comes with it,” says Dr. Chacko, hospitalist program medical director with Preferred Health Partners, medical director of the hospitalist program at Good Samaritan Hospital in Suffern, N.Y., and a member of Team Hospitalist. “You really need that energy in your daily work routine, especially early in a career. The disadvantage is, depending on your training, you may not have the experience or been exposed to resources required to take on some of the challenges you’ll face. Hence, expanding the number of resources available to early-career hospitalists—and encouraging them to utilize what is available to them—becomes pivotal.”
Question: Two years after residency, you made the transition to hospitalist program medical director. What advice would you give to an aspiring HM leader?
Answer: Coming out of medical school or residency, you’re not provided all the tools you need to be a successful leader. Some people may achieve those skills during their training or in their first job. But going through some of the unique courses provided by SHM, such as the Leadership Academy, has been invaluable. The information, as well as the connections you make with others throughout the country, really prepares you for a leadership role and some of the challenges you may not have been taught to face in medical school.
Q: What are some of the challenges you aren’t necessarily taught how to handle?
A: Leadership roles take on a complexity of their own. You’re dealing with communications issues; you’re dealing with conflict resolution. Those are unique areas that have to be approached delicately. And one of the fundamental aspects of being a good leader is to define a shared organizational vision and set of shared values for your group that should be supported and promoted.
Q: Can you describe the vision and values you set for your group?
A: Our vision is to be the hospitalist program of choice for patients and physicians in the region. But the key aspect is, we want to provide high-quality patient care with a touch of humility. A physician who demonstrates his or her empathetic side goes a long way in what we do. Research has shown hospitalists provide efficient care—outcomes on cost savings are good. But the other issue is the patient experience, and that’s where the humility factor comes into play.
Q: How do you teach the physicians in your group to be more humble?
A: One thing we emphasize with the team is to imagine themselves or a family member in the patient’s shoes when they are communicating with them. This hits home the importance of bedside manners, and it has to be revisited at times.
Q: Any other techniques?
A: Positive feedback always translates well. We use examples from patients who say they generally had a great experience. In many cases, it amounts to a patient saying, “The doctor was able to explain things to me in a simpler language than anyone has been able to do before, or even attempted to do.” That positive reinforcement resonates well with the doctors. We also share patient scenarios where there were opportunities for improvement.
Q: Considering the demands of your leadership roles at Preferred Health Partners and Good Samaritan Hospital, why is it still a priority for you to provide inpatient clinical care?
A: The old adage is, if you don’t use it, you lose it. Because clinical care is so broad and diverse, and because it is changing so rapidly, it behooves one to stay abreast of it. Also, when you are leading members of a group, I think it’s important to walk in the trenches with them.
Q: You joined SHM’s Young Physician Task Force and served as chairman for two years. What prompted you to participate?
A: When I joined, I had already begun my leadership role as medical director and I was an early-career hospitalist, so I felt it made sense for my professional growth. I wanted an opportunity to collaborate with leading young hospitalists in the country and help shape some of the programs the (group) was working on.
Q: What issues has the group addressed?
A: Initially, the task force was focused on getting information out to early-career hospitalists and providing resources they could utilize. It redefined its section of the SHM website (www.hospitalmedicine .org/youngphysician), which now serves as a portal with information about everything from careers in hospital medicine to how to approach residency. It also introduced the Resident’s Corner (a quarterly column in The Hospitalist, see p. 25), which caters to residents and helps them make a smooth transition to a possible career in hospital medicine. The group has developed programs for early-career hospitalists at the annual SHM meetings.
Q: What major issues are on the agenda now?
A: The group is working on developing a mentorship program for early-career hospitalists, which would be a really valuable resource. The group also is working on projects to reach medical students and residents. The goal is to get them more engaged, and help them realize the diversity and rewards that accompany a career in hospital medicine.
Q: What do you see as the benefit of the mentor program?
A: The beauty of hospital medicine is there is a lot of diversity. If you have an interest in academia, quality initiatives, or research, that’s available. If you have a leadership interest, that can definitely be attained. …
But when you have someone who has had some experience in hospital medicine and can share that experience, and you can get their insights and hear about the challenges they faced and how they faced them, it can make the transition much easier. This will provide young hospitalists with pearls of wisdom and information they may not have been able to access elsewhere.
Q: So it comes back to the idea that there’s still a lot to learn, even after medical school and residency.
A: That’s exactly right. The scope of questions that can be posed or issues that can be addressed is infinite. Beyond that, someone who has already walked that pathway can help establish the fact that hospital medicine should be looked upon as a career with many opportunities, as opposed to a transition point to an alternative career. TH
Mark Leiser is a freelance writer in New Jersey.
Bijo Chacko, MD, FHM, says the varied resources available in the multispecialty medical group in which he practices help to ensure patients receive the best possible care. The structure at Preferred Health Partners in Brooklyn, N.Y., which offers primary and specialty medical services under one roof, requires hospitalists to collaborate frequently with primary-care physicians (PCPs).
That interaction breaks down barriers, fosters communication, promotes the exchange of ideas, and ultimately improves the transition of care from outpatient to inpatient and vice versa, Dr. Chacko says.
His affinity for that environment might explain his passion for the work done by SHM’s Young Physician Task Force, and why “resources” is the word he repeats most often when describing the value of the group’s efforts. Just as experienced hospitalists can learn by interacting with PCPs and other specialists, those who are new to HM can benefit from those who have established themselves in the profession and cleared the hurdles physicians encounter early in a career, he says.
“The advantage of youth is the inherent energy that comes with it,” says Dr. Chacko, hospitalist program medical director with Preferred Health Partners, medical director of the hospitalist program at Good Samaritan Hospital in Suffern, N.Y., and a member of Team Hospitalist. “You really need that energy in your daily work routine, especially early in a career. The disadvantage is, depending on your training, you may not have the experience or been exposed to resources required to take on some of the challenges you’ll face. Hence, expanding the number of resources available to early-career hospitalists—and encouraging them to utilize what is available to them—becomes pivotal.”
Question: Two years after residency, you made the transition to hospitalist program medical director. What advice would you give to an aspiring HM leader?
Answer: Coming out of medical school or residency, you’re not provided all the tools you need to be a successful leader. Some people may achieve those skills during their training or in their first job. But going through some of the unique courses provided by SHM, such as the Leadership Academy, has been invaluable. The information, as well as the connections you make with others throughout the country, really prepares you for a leadership role and some of the challenges you may not have been taught to face in medical school.
Q: What are some of the challenges you aren’t necessarily taught how to handle?
A: Leadership roles take on a complexity of their own. You’re dealing with communications issues; you’re dealing with conflict resolution. Those are unique areas that have to be approached delicately. And one of the fundamental aspects of being a good leader is to define a shared organizational vision and set of shared values for your group that should be supported and promoted.
Q: Can you describe the vision and values you set for your group?
A: Our vision is to be the hospitalist program of choice for patients and physicians in the region. But the key aspect is, we want to provide high-quality patient care with a touch of humility. A physician who demonstrates his or her empathetic side goes a long way in what we do. Research has shown hospitalists provide efficient care—outcomes on cost savings are good. But the other issue is the patient experience, and that’s where the humility factor comes into play.
Q: How do you teach the physicians in your group to be more humble?
A: One thing we emphasize with the team is to imagine themselves or a family member in the patient’s shoes when they are communicating with them. This hits home the importance of bedside manners, and it has to be revisited at times.
Q: Any other techniques?
A: Positive feedback always translates well. We use examples from patients who say they generally had a great experience. In many cases, it amounts to a patient saying, “The doctor was able to explain things to me in a simpler language than anyone has been able to do before, or even attempted to do.” That positive reinforcement resonates well with the doctors. We also share patient scenarios where there were opportunities for improvement.
Q: Considering the demands of your leadership roles at Preferred Health Partners and Good Samaritan Hospital, why is it still a priority for you to provide inpatient clinical care?
A: The old adage is, if you don’t use it, you lose it. Because clinical care is so broad and diverse, and because it is changing so rapidly, it behooves one to stay abreast of it. Also, when you are leading members of a group, I think it’s important to walk in the trenches with them.
Q: You joined SHM’s Young Physician Task Force and served as chairman for two years. What prompted you to participate?
A: When I joined, I had already begun my leadership role as medical director and I was an early-career hospitalist, so I felt it made sense for my professional growth. I wanted an opportunity to collaborate with leading young hospitalists in the country and help shape some of the programs the (group) was working on.
Q: What issues has the group addressed?
A: Initially, the task force was focused on getting information out to early-career hospitalists and providing resources they could utilize. It redefined its section of the SHM website (www.hospitalmedicine .org/youngphysician), which now serves as a portal with information about everything from careers in hospital medicine to how to approach residency. It also introduced the Resident’s Corner (a quarterly column in The Hospitalist, see p. 25), which caters to residents and helps them make a smooth transition to a possible career in hospital medicine. The group has developed programs for early-career hospitalists at the annual SHM meetings.
Q: What major issues are on the agenda now?
A: The group is working on developing a mentorship program for early-career hospitalists, which would be a really valuable resource. The group also is working on projects to reach medical students and residents. The goal is to get them more engaged, and help them realize the diversity and rewards that accompany a career in hospital medicine.
Q: What do you see as the benefit of the mentor program?
A: The beauty of hospital medicine is there is a lot of diversity. If you have an interest in academia, quality initiatives, or research, that’s available. If you have a leadership interest, that can definitely be attained. …
But when you have someone who has had some experience in hospital medicine and can share that experience, and you can get their insights and hear about the challenges they faced and how they faced them, it can make the transition much easier. This will provide young hospitalists with pearls of wisdom and information they may not have been able to access elsewhere.
Q: So it comes back to the idea that there’s still a lot to learn, even after medical school and residency.
A: That’s exactly right. The scope of questions that can be posed or issues that can be addressed is infinite. Beyond that, someone who has already walked that pathway can help establish the fact that hospital medicine should be looked upon as a career with many opportunities, as opposed to a transition point to an alternative career. TH
Mark Leiser is a freelance writer in New Jersey.
Bijo Chacko, MD, FHM, says the varied resources available in the multispecialty medical group in which he practices help to ensure patients receive the best possible care. The structure at Preferred Health Partners in Brooklyn, N.Y., which offers primary and specialty medical services under one roof, requires hospitalists to collaborate frequently with primary-care physicians (PCPs).
That interaction breaks down barriers, fosters communication, promotes the exchange of ideas, and ultimately improves the transition of care from outpatient to inpatient and vice versa, Dr. Chacko says.
His affinity for that environment might explain his passion for the work done by SHM’s Young Physician Task Force, and why “resources” is the word he repeats most often when describing the value of the group’s efforts. Just as experienced hospitalists can learn by interacting with PCPs and other specialists, those who are new to HM can benefit from those who have established themselves in the profession and cleared the hurdles physicians encounter early in a career, he says.
“The advantage of youth is the inherent energy that comes with it,” says Dr. Chacko, hospitalist program medical director with Preferred Health Partners, medical director of the hospitalist program at Good Samaritan Hospital in Suffern, N.Y., and a member of Team Hospitalist. “You really need that energy in your daily work routine, especially early in a career. The disadvantage is, depending on your training, you may not have the experience or been exposed to resources required to take on some of the challenges you’ll face. Hence, expanding the number of resources available to early-career hospitalists—and encouraging them to utilize what is available to them—becomes pivotal.”
Question: Two years after residency, you made the transition to hospitalist program medical director. What advice would you give to an aspiring HM leader?
Answer: Coming out of medical school or residency, you’re not provided all the tools you need to be a successful leader. Some people may achieve those skills during their training or in their first job. But going through some of the unique courses provided by SHM, such as the Leadership Academy, has been invaluable. The information, as well as the connections you make with others throughout the country, really prepares you for a leadership role and some of the challenges you may not have been taught to face in medical school.
Q: What are some of the challenges you aren’t necessarily taught how to handle?
A: Leadership roles take on a complexity of their own. You’re dealing with communications issues; you’re dealing with conflict resolution. Those are unique areas that have to be approached delicately. And one of the fundamental aspects of being a good leader is to define a shared organizational vision and set of shared values for your group that should be supported and promoted.
Q: Can you describe the vision and values you set for your group?
A: Our vision is to be the hospitalist program of choice for patients and physicians in the region. But the key aspect is, we want to provide high-quality patient care with a touch of humility. A physician who demonstrates his or her empathetic side goes a long way in what we do. Research has shown hospitalists provide efficient care—outcomes on cost savings are good. But the other issue is the patient experience, and that’s where the humility factor comes into play.
Q: How do you teach the physicians in your group to be more humble?
A: One thing we emphasize with the team is to imagine themselves or a family member in the patient’s shoes when they are communicating with them. This hits home the importance of bedside manners, and it has to be revisited at times.
Q: Any other techniques?
A: Positive feedback always translates well. We use examples from patients who say they generally had a great experience. In many cases, it amounts to a patient saying, “The doctor was able to explain things to me in a simpler language than anyone has been able to do before, or even attempted to do.” That positive reinforcement resonates well with the doctors. We also share patient scenarios where there were opportunities for improvement.
Q: Considering the demands of your leadership roles at Preferred Health Partners and Good Samaritan Hospital, why is it still a priority for you to provide inpatient clinical care?
A: The old adage is, if you don’t use it, you lose it. Because clinical care is so broad and diverse, and because it is changing so rapidly, it behooves one to stay abreast of it. Also, when you are leading members of a group, I think it’s important to walk in the trenches with them.
Q: You joined SHM’s Young Physician Task Force and served as chairman for two years. What prompted you to participate?
A: When I joined, I had already begun my leadership role as medical director and I was an early-career hospitalist, so I felt it made sense for my professional growth. I wanted an opportunity to collaborate with leading young hospitalists in the country and help shape some of the programs the (group) was working on.
Q: What issues has the group addressed?
A: Initially, the task force was focused on getting information out to early-career hospitalists and providing resources they could utilize. It redefined its section of the SHM website (www.hospitalmedicine .org/youngphysician), which now serves as a portal with information about everything from careers in hospital medicine to how to approach residency. It also introduced the Resident’s Corner (a quarterly column in The Hospitalist, see p. 25), which caters to residents and helps them make a smooth transition to a possible career in hospital medicine. The group has developed programs for early-career hospitalists at the annual SHM meetings.
Q: What major issues are on the agenda now?
A: The group is working on developing a mentorship program for early-career hospitalists, which would be a really valuable resource. The group also is working on projects to reach medical students and residents. The goal is to get them more engaged, and help them realize the diversity and rewards that accompany a career in hospital medicine.
Q: What do you see as the benefit of the mentor program?
A: The beauty of hospital medicine is there is a lot of diversity. If you have an interest in academia, quality initiatives, or research, that’s available. If you have a leadership interest, that can definitely be attained. …
But when you have someone who has had some experience in hospital medicine and can share that experience, and you can get their insights and hear about the challenges they faced and how they faced them, it can make the transition much easier. This will provide young hospitalists with pearls of wisdom and information they may not have been able to access elsewhere.
Q: So it comes back to the idea that there’s still a lot to learn, even after medical school and residency.
A: That’s exactly right. The scope of questions that can be posed or issues that can be addressed is infinite. Beyond that, someone who has already walked that pathway can help establish the fact that hospital medicine should be looked upon as a career with many opportunities, as opposed to a transition point to an alternative career. TH
Mark Leiser is a freelance writer in New Jersey.
Esse Est Percipi

You’re a what?” he asked over the noise of the passing Mardi Gras parade.
“I’m a hospitalist,” I replied.
“Oh.” There was an extended pause. I could tell he was searching his mental database to determine if he had a family member who was a hospitalist. Nope, nothing there. Then it came: “What is that exactly?” I followed with a general description of “what a hospitalist does,” but his response made it apparent that my description hadn’t stuck: “So you’re like a generalist, but you work in the hospital?”
I let it go. Mardi Gras wasn’t the time to launch into all that a hospitalist truly embodies: quality improvement, systems redesign, patient safety, effective transitions of care. And he probably wouldn’t remember it tomorrow anyway. But my reveler friend’s summary statement stayed with me through the night, for it returned me to a core philosophical tenet: Esse est percipi. We are who we appear to be.
There are 30,000 of us now, all facing the same problem: How do we match who we are perceived to be with who we are? The hospitalist is much more than a “generalist who works in a hospital,” but what is perceived to be is equally as important as what is. At the root of the problem is a question of accountability: How do we hold ourselves out to the public as a specialty that possesses the knowledge and skills necessary to advance quality and safety for the hospitalized patient?
This question of public accountability is not new to the profession. The heterogeneity of physicians in the early 1900s, from the authentic to the snake-oil salesmen, prompted the need for independent validation of physicians’ qualifications. Dr. Derrick Vail introduced the concept of a board certification in 1908, with the goal of “issuing credentials that would assure the public of the specialist’s qualifications.” The American Board of Medical Specialties was formed in 1933, and continues to this day to be the entity responsible for ensuring this accountability.
While there are no “snake-oil salesmen” in HM, there is heterogeneity. There are many of us answering the call to advance quality and patient safety, but there are many more of us who are not yet there. And there are some (i.e., those practicing medicine in the hospital while awaiting a subspecialty fellowship) who, while referred to as “hospitalists,” do not embrace the central tenets of the career hospitalist. Thirty-thousand hospitalists is a spectacular achievement, but with that growth comes the new problem of dilution: Without some measure of distinguishing those who are authentic in the value-added services of quality and patient safety from those who have not embraced these tenets, the perception of us all will be merely “physicians who practice in the hospital.”
To my mind, the American Board of Internal Medicine’s (ABIM) Maintenance of Certification (MOC) Focused Practice in Hospital Medicine (FPHM) program answers this question of public accountability. This new MOC process provides an objective way of establishing that hospitalists who claim to be competent in their field have, in fact, demonstrated this competence. Paradoxically, it is even more compelling than a board certification following a residency or fellowship; skills and knowledge fade over time, and new knowledge consistently is added. The MOC certification assures the public that despite these challenges, the certified hospitalist has continued to maintain competence in the field.
Further, the components of the FPHM (www.abim.org/specialty/fphm.aspx) provide assurance that the certified hospitalist has the expertise to practice HM, and has the knowledge and skills necessary to offer the value-added services of quality, patient safety, and performance improvement.
Why Is It Important to Recertify?
Registration for the MOC in FPHM opened March 15, and more than 100 hospitalists enrolled in the program in the first two weeks. While exciting, this number is not enough; here I share with you my reflections on why this MOC is so important to our field.
As with all things SHM, the rationale begins with, “What is the best thing for the patient?” I completed my first recertification in 2008, and I can honestly say that this was the first “test” in my career that actually made me a better physician for my patients. I was skeptical at first, seeing the MOC as another bureaucratic hurdle for which I would have the opportunity to pay $1,000. But the reality was that it was much more than that; it made me a better physician. It alerted me to blind spots in my clinical repertoire: some topics I had never learned, some I had forgotten, and some that were new knowledge.
Preparing for the examination isn’t onerous, perhaps a couple extra hours a week of reading. Since the examination focused on the practical aspects of diagnosis and management, and not the basic- science minutiae that had characterized the earlier examinations in my career, I found that the preparation for the MOC exam improved my practice of medicine. The only downside was that I did not have the luxury of an HM-focused exam in 2008, and there were content areas on the standard internal medicine (IM) MOC that were not a part of my inpatient practice.
But it was the Practice Improvement Module (PIM) component of the MOC process, a shared feature of both the FPHM and the IM MOC processes, that most benefited my patients. As a hospitalist, this too was not onerous, as practice improvement is what I do on a daily basis. Moreover, it was the external discipline of completing the PIM that made it truly valuable: collecting data, reflecting on methods of improvement, enacting an intervention, and then reassessing the results. The process forced me to reflect on my practice, and it heightened my sensitivity to other parts of my practice, and the hospital system, that needed to be improved.
Further benefit came through collaboration with other physicians in my group, as encouraged by the ABIM, to complete the PIM. This teamwork fostered a heightened spirit of QI within our team, further augmenting quality of care and sensitivity to needed systems improvements. True, at the end of the process, I was $1,000 lighter … but my conscience was richer. I had improved as a physician, and I think it has translated into a benefit for my patients.
What Recertification Means to HM
Although the virtue of improving patient care is sufficient to justify participation in the MOC in FPHM, the passage of healthcare reform legislation raises the stakes for hospitalists. The Physician Quality Reporting Initiative (PQRI) is an ongoing reality, further voicing the public’s need for accountability.
The final impact will hinge on the Center for Medicare & Medicaid Services’ (CMS) interpretation and execution of the language in the final bill, but it is clear that physicians who participate in the PQRI (through claims-based or registry reporting) have the opportunity to receive an additional 0.5% bonus on their total allowable Medicare charges in 2011 through 2014, if they also meet MOC program requirements. (The health reform bill provides a 1.0% bonus in 2011 for PQRI participation and a 0.5% bonus through 2014.)
Subsequently, physicians who do not participate in the PQRI will face a 1.5% payment penalty in 2015, and a 2% payment penalty in 2016 and thereafter. With these incentives, it appears the day-to-day finances of practice will offset the cost of MOC participation.
The importance of FPHM extends to the remainder of the PQRI as well. Currently, HM is not recognized by CMS as its own specialty, which means that it does not have its own CMS specialty code. In turn, this means that the core measures CMS will apply to the hospitalist in fulfilling the PQRI standards will be those of the general internist, and these might or might not apply to HM practice. For those to whom the standards do not apply, PQRI becomes a practical impossibility, though the financial penalty remains an unfortunate reality.
The extent to which the core measures for general medicine do not apply to the inpatient environment is the extent to which PQRI will be less effective in incentivizing the advancement of inpatient healthcare quality. This is an opportunity missed. Preventing this systematic exclusion begins with recognizing HM as a specialty. In convincing CMS that HM is its own specialty, deserving of its own code and its own PQRI indices, I can think of no argument as compelling as pointing to 10,000 hospitalists certified in the MOC in FPHM program.
Financial incentives aside, the ultimate success of HM will be in our ability to change the healthcare system such that it provides safe, timely, equitable, efficient, and patient-centered care. We’ve spent more than 10 years trying to get into the conversation, and now we have a seat at the table. But to be effective in this audacious goal, we must speak with a stentorian voice—a timbre that comes only from the chords of the sincere. Society must know of our sincerity—not by our words, but by our actions.
As president of SHM, I am calling on you to join me in meeting this standard of public accountability. Let us prove to the world that our talk of quality and patient safety is much more than talk. Let us establish that we are willing to engage in the ongoing self-improvement necessary to reach this wished-for goal.
Esse est percipi. We are as we are perceived. Now is our time to make one with the other—fulfilling a covenant that promises that we will, eventually, close this quality chasm. TH
Dr. Wiese is president of SHM.
You’re a what?” he asked over the noise of the passing Mardi Gras parade.
“I’m a hospitalist,” I replied.
“Oh.” There was an extended pause. I could tell he was searching his mental database to determine if he had a family member who was a hospitalist. Nope, nothing there. Then it came: “What is that exactly?” I followed with a general description of “what a hospitalist does,” but his response made it apparent that my description hadn’t stuck: “So you’re like a generalist, but you work in the hospital?”
I let it go. Mardi Gras wasn’t the time to launch into all that a hospitalist truly embodies: quality improvement, systems redesign, patient safety, effective transitions of care. And he probably wouldn’t remember it tomorrow anyway. But my reveler friend’s summary statement stayed with me through the night, for it returned me to a core philosophical tenet: Esse est percipi. We are who we appear to be.
There are 30,000 of us now, all facing the same problem: How do we match who we are perceived to be with who we are? The hospitalist is much more than a “generalist who works in a hospital,” but what is perceived to be is equally as important as what is. At the root of the problem is a question of accountability: How do we hold ourselves out to the public as a specialty that possesses the knowledge and skills necessary to advance quality and safety for the hospitalized patient?
This question of public accountability is not new to the profession. The heterogeneity of physicians in the early 1900s, from the authentic to the snake-oil salesmen, prompted the need for independent validation of physicians’ qualifications. Dr. Derrick Vail introduced the concept of a board certification in 1908, with the goal of “issuing credentials that would assure the public of the specialist’s qualifications.” The American Board of Medical Specialties was formed in 1933, and continues to this day to be the entity responsible for ensuring this accountability.
While there are no “snake-oil salesmen” in HM, there is heterogeneity. There are many of us answering the call to advance quality and patient safety, but there are many more of us who are not yet there. And there are some (i.e., those practicing medicine in the hospital while awaiting a subspecialty fellowship) who, while referred to as “hospitalists,” do not embrace the central tenets of the career hospitalist. Thirty-thousand hospitalists is a spectacular achievement, but with that growth comes the new problem of dilution: Without some measure of distinguishing those who are authentic in the value-added services of quality and patient safety from those who have not embraced these tenets, the perception of us all will be merely “physicians who practice in the hospital.”
To my mind, the American Board of Internal Medicine’s (ABIM) Maintenance of Certification (MOC) Focused Practice in Hospital Medicine (FPHM) program answers this question of public accountability. This new MOC process provides an objective way of establishing that hospitalists who claim to be competent in their field have, in fact, demonstrated this competence. Paradoxically, it is even more compelling than a board certification following a residency or fellowship; skills and knowledge fade over time, and new knowledge consistently is added. The MOC certification assures the public that despite these challenges, the certified hospitalist has continued to maintain competence in the field.
Further, the components of the FPHM (www.abim.org/specialty/fphm.aspx) provide assurance that the certified hospitalist has the expertise to practice HM, and has the knowledge and skills necessary to offer the value-added services of quality, patient safety, and performance improvement.
Why Is It Important to Recertify?
Registration for the MOC in FPHM opened March 15, and more than 100 hospitalists enrolled in the program in the first two weeks. While exciting, this number is not enough; here I share with you my reflections on why this MOC is so important to our field.
As with all things SHM, the rationale begins with, “What is the best thing for the patient?” I completed my first recertification in 2008, and I can honestly say that this was the first “test” in my career that actually made me a better physician for my patients. I was skeptical at first, seeing the MOC as another bureaucratic hurdle for which I would have the opportunity to pay $1,000. But the reality was that it was much more than that; it made me a better physician. It alerted me to blind spots in my clinical repertoire: some topics I had never learned, some I had forgotten, and some that were new knowledge.
Preparing for the examination isn’t onerous, perhaps a couple extra hours a week of reading. Since the examination focused on the practical aspects of diagnosis and management, and not the basic- science minutiae that had characterized the earlier examinations in my career, I found that the preparation for the MOC exam improved my practice of medicine. The only downside was that I did not have the luxury of an HM-focused exam in 2008, and there were content areas on the standard internal medicine (IM) MOC that were not a part of my inpatient practice.
But it was the Practice Improvement Module (PIM) component of the MOC process, a shared feature of both the FPHM and the IM MOC processes, that most benefited my patients. As a hospitalist, this too was not onerous, as practice improvement is what I do on a daily basis. Moreover, it was the external discipline of completing the PIM that made it truly valuable: collecting data, reflecting on methods of improvement, enacting an intervention, and then reassessing the results. The process forced me to reflect on my practice, and it heightened my sensitivity to other parts of my practice, and the hospital system, that needed to be improved.
Further benefit came through collaboration with other physicians in my group, as encouraged by the ABIM, to complete the PIM. This teamwork fostered a heightened spirit of QI within our team, further augmenting quality of care and sensitivity to needed systems improvements. True, at the end of the process, I was $1,000 lighter … but my conscience was richer. I had improved as a physician, and I think it has translated into a benefit for my patients.
What Recertification Means to HM
Although the virtue of improving patient care is sufficient to justify participation in the MOC in FPHM, the passage of healthcare reform legislation raises the stakes for hospitalists. The Physician Quality Reporting Initiative (PQRI) is an ongoing reality, further voicing the public’s need for accountability.
The final impact will hinge on the Center for Medicare & Medicaid Services’ (CMS) interpretation and execution of the language in the final bill, but it is clear that physicians who participate in the PQRI (through claims-based or registry reporting) have the opportunity to receive an additional 0.5% bonus on their total allowable Medicare charges in 2011 through 2014, if they also meet MOC program requirements. (The health reform bill provides a 1.0% bonus in 2011 for PQRI participation and a 0.5% bonus through 2014.)
Subsequently, physicians who do not participate in the PQRI will face a 1.5% payment penalty in 2015, and a 2% payment penalty in 2016 and thereafter. With these incentives, it appears the day-to-day finances of practice will offset the cost of MOC participation.
The importance of FPHM extends to the remainder of the PQRI as well. Currently, HM is not recognized by CMS as its own specialty, which means that it does not have its own CMS specialty code. In turn, this means that the core measures CMS will apply to the hospitalist in fulfilling the PQRI standards will be those of the general internist, and these might or might not apply to HM practice. For those to whom the standards do not apply, PQRI becomes a practical impossibility, though the financial penalty remains an unfortunate reality.
The extent to which the core measures for general medicine do not apply to the inpatient environment is the extent to which PQRI will be less effective in incentivizing the advancement of inpatient healthcare quality. This is an opportunity missed. Preventing this systematic exclusion begins with recognizing HM as a specialty. In convincing CMS that HM is its own specialty, deserving of its own code and its own PQRI indices, I can think of no argument as compelling as pointing to 10,000 hospitalists certified in the MOC in FPHM program.
Financial incentives aside, the ultimate success of HM will be in our ability to change the healthcare system such that it provides safe, timely, equitable, efficient, and patient-centered care. We’ve spent more than 10 years trying to get into the conversation, and now we have a seat at the table. But to be effective in this audacious goal, we must speak with a stentorian voice—a timbre that comes only from the chords of the sincere. Society must know of our sincerity—not by our words, but by our actions.
As president of SHM, I am calling on you to join me in meeting this standard of public accountability. Let us prove to the world that our talk of quality and patient safety is much more than talk. Let us establish that we are willing to engage in the ongoing self-improvement necessary to reach this wished-for goal.
Esse est percipi. We are as we are perceived. Now is our time to make one with the other—fulfilling a covenant that promises that we will, eventually, close this quality chasm. TH
Dr. Wiese is president of SHM.
You’re a what?” he asked over the noise of the passing Mardi Gras parade.
“I’m a hospitalist,” I replied.
“Oh.” There was an extended pause. I could tell he was searching his mental database to determine if he had a family member who was a hospitalist. Nope, nothing there. Then it came: “What is that exactly?” I followed with a general description of “what a hospitalist does,” but his response made it apparent that my description hadn’t stuck: “So you’re like a generalist, but you work in the hospital?”
I let it go. Mardi Gras wasn’t the time to launch into all that a hospitalist truly embodies: quality improvement, systems redesign, patient safety, effective transitions of care. And he probably wouldn’t remember it tomorrow anyway. But my reveler friend’s summary statement stayed with me through the night, for it returned me to a core philosophical tenet: Esse est percipi. We are who we appear to be.
There are 30,000 of us now, all facing the same problem: How do we match who we are perceived to be with who we are? The hospitalist is much more than a “generalist who works in a hospital,” but what is perceived to be is equally as important as what is. At the root of the problem is a question of accountability: How do we hold ourselves out to the public as a specialty that possesses the knowledge and skills necessary to advance quality and safety for the hospitalized patient?
This question of public accountability is not new to the profession. The heterogeneity of physicians in the early 1900s, from the authentic to the snake-oil salesmen, prompted the need for independent validation of physicians’ qualifications. Dr. Derrick Vail introduced the concept of a board certification in 1908, with the goal of “issuing credentials that would assure the public of the specialist’s qualifications.” The American Board of Medical Specialties was formed in 1933, and continues to this day to be the entity responsible for ensuring this accountability.
While there are no “snake-oil salesmen” in HM, there is heterogeneity. There are many of us answering the call to advance quality and patient safety, but there are many more of us who are not yet there. And there are some (i.e., those practicing medicine in the hospital while awaiting a subspecialty fellowship) who, while referred to as “hospitalists,” do not embrace the central tenets of the career hospitalist. Thirty-thousand hospitalists is a spectacular achievement, but with that growth comes the new problem of dilution: Without some measure of distinguishing those who are authentic in the value-added services of quality and patient safety from those who have not embraced these tenets, the perception of us all will be merely “physicians who practice in the hospital.”
To my mind, the American Board of Internal Medicine’s (ABIM) Maintenance of Certification (MOC) Focused Practice in Hospital Medicine (FPHM) program answers this question of public accountability. This new MOC process provides an objective way of establishing that hospitalists who claim to be competent in their field have, in fact, demonstrated this competence. Paradoxically, it is even more compelling than a board certification following a residency or fellowship; skills and knowledge fade over time, and new knowledge consistently is added. The MOC certification assures the public that despite these challenges, the certified hospitalist has continued to maintain competence in the field.
Further, the components of the FPHM (www.abim.org/specialty/fphm.aspx) provide assurance that the certified hospitalist has the expertise to practice HM, and has the knowledge and skills necessary to offer the value-added services of quality, patient safety, and performance improvement.
Why Is It Important to Recertify?
Registration for the MOC in FPHM opened March 15, and more than 100 hospitalists enrolled in the program in the first two weeks. While exciting, this number is not enough; here I share with you my reflections on why this MOC is so important to our field.
As with all things SHM, the rationale begins with, “What is the best thing for the patient?” I completed my first recertification in 2008, and I can honestly say that this was the first “test” in my career that actually made me a better physician for my patients. I was skeptical at first, seeing the MOC as another bureaucratic hurdle for which I would have the opportunity to pay $1,000. But the reality was that it was much more than that; it made me a better physician. It alerted me to blind spots in my clinical repertoire: some topics I had never learned, some I had forgotten, and some that were new knowledge.
Preparing for the examination isn’t onerous, perhaps a couple extra hours a week of reading. Since the examination focused on the practical aspects of diagnosis and management, and not the basic- science minutiae that had characterized the earlier examinations in my career, I found that the preparation for the MOC exam improved my practice of medicine. The only downside was that I did not have the luxury of an HM-focused exam in 2008, and there were content areas on the standard internal medicine (IM) MOC that were not a part of my inpatient practice.
But it was the Practice Improvement Module (PIM) component of the MOC process, a shared feature of both the FPHM and the IM MOC processes, that most benefited my patients. As a hospitalist, this too was not onerous, as practice improvement is what I do on a daily basis. Moreover, it was the external discipline of completing the PIM that made it truly valuable: collecting data, reflecting on methods of improvement, enacting an intervention, and then reassessing the results. The process forced me to reflect on my practice, and it heightened my sensitivity to other parts of my practice, and the hospital system, that needed to be improved.
Further benefit came through collaboration with other physicians in my group, as encouraged by the ABIM, to complete the PIM. This teamwork fostered a heightened spirit of QI within our team, further augmenting quality of care and sensitivity to needed systems improvements. True, at the end of the process, I was $1,000 lighter … but my conscience was richer. I had improved as a physician, and I think it has translated into a benefit for my patients.
What Recertification Means to HM
Although the virtue of improving patient care is sufficient to justify participation in the MOC in FPHM, the passage of healthcare reform legislation raises the stakes for hospitalists. The Physician Quality Reporting Initiative (PQRI) is an ongoing reality, further voicing the public’s need for accountability.
The final impact will hinge on the Center for Medicare & Medicaid Services’ (CMS) interpretation and execution of the language in the final bill, but it is clear that physicians who participate in the PQRI (through claims-based or registry reporting) have the opportunity to receive an additional 0.5% bonus on their total allowable Medicare charges in 2011 through 2014, if they also meet MOC program requirements. (The health reform bill provides a 1.0% bonus in 2011 for PQRI participation and a 0.5% bonus through 2014.)
Subsequently, physicians who do not participate in the PQRI will face a 1.5% payment penalty in 2015, and a 2% payment penalty in 2016 and thereafter. With these incentives, it appears the day-to-day finances of practice will offset the cost of MOC participation.
The importance of FPHM extends to the remainder of the PQRI as well. Currently, HM is not recognized by CMS as its own specialty, which means that it does not have its own CMS specialty code. In turn, this means that the core measures CMS will apply to the hospitalist in fulfilling the PQRI standards will be those of the general internist, and these might or might not apply to HM practice. For those to whom the standards do not apply, PQRI becomes a practical impossibility, though the financial penalty remains an unfortunate reality.
The extent to which the core measures for general medicine do not apply to the inpatient environment is the extent to which PQRI will be less effective in incentivizing the advancement of inpatient healthcare quality. This is an opportunity missed. Preventing this systematic exclusion begins with recognizing HM as a specialty. In convincing CMS that HM is its own specialty, deserving of its own code and its own PQRI indices, I can think of no argument as compelling as pointing to 10,000 hospitalists certified in the MOC in FPHM program.
Financial incentives aside, the ultimate success of HM will be in our ability to change the healthcare system such that it provides safe, timely, equitable, efficient, and patient-centered care. We’ve spent more than 10 years trying to get into the conversation, and now we have a seat at the table. But to be effective in this audacious goal, we must speak with a stentorian voice—a timbre that comes only from the chords of the sincere. Society must know of our sincerity—not by our words, but by our actions.
As president of SHM, I am calling on you to join me in meeting this standard of public accountability. Let us prove to the world that our talk of quality and patient safety is much more than talk. Let us establish that we are willing to engage in the ongoing self-improvement necessary to reach this wished-for goal.
Esse est percipi. We are as we are perceived. Now is our time to make one with the other—fulfilling a covenant that promises that we will, eventually, close this quality chasm. TH
Dr. Wiese is president of SHM.