User login
Learning to Share
GRAPEVINE, Texas — Sitting in the third row of a large meeting room, Robin Buckley, MD, FHM, was soaking in the morning portion of the "ABIM Maintenance of Certification (MOC) Learning Session" pre-course, clicking her keypad with answers to questions and making mental notes this morning at HM11.
Dr. Buckley, medical director of hospitalist services at 72-bed Scott & White Healthcare in Round Rock, Texas, has to recertify in 2012, so she is getting an early start. One of nine pre-courses held annually, the learning session offers 6.5 CME credits.
"I'm really excited about sharing the information with my group, especially the questions focused on quality," says Dr. Buckley, who has been a hospitalist since 2004 and joined her expanding HM group in 2008. "I want to apply the information to our clinical practice, because I think it’s going to make us better."
She's also considering the Focused Practice in Hospital Medicine (FPHM) pathway, and used the pre-course to understand the specialized MOC pathway better. The main concerns, she says, are the added cost and the every-three-year requirement of the Performance Improvement Modules (PIM).
"The three-year PIM cycle makes a lot of sense," Dr. Buckley says, noting she is "encouraged" to learn ABIM has approved three of SHM's quality projects to count toward the MOC requirement. Although she might still recertify through the traditional internal-medicine MOC next year, she definitely has the FPHM on the radar.
"Maybe in a couple years," Dr. Buckley says. "The PIM templates will be extremely helpful and encourage me to do it even more. The FPHM shows dedication to the field."
GRAPEVINE, Texas — Sitting in the third row of a large meeting room, Robin Buckley, MD, FHM, was soaking in the morning portion of the "ABIM Maintenance of Certification (MOC) Learning Session" pre-course, clicking her keypad with answers to questions and making mental notes this morning at HM11.
Dr. Buckley, medical director of hospitalist services at 72-bed Scott & White Healthcare in Round Rock, Texas, has to recertify in 2012, so she is getting an early start. One of nine pre-courses held annually, the learning session offers 6.5 CME credits.
"I'm really excited about sharing the information with my group, especially the questions focused on quality," says Dr. Buckley, who has been a hospitalist since 2004 and joined her expanding HM group in 2008. "I want to apply the information to our clinical practice, because I think it’s going to make us better."
She's also considering the Focused Practice in Hospital Medicine (FPHM) pathway, and used the pre-course to understand the specialized MOC pathway better. The main concerns, she says, are the added cost and the every-three-year requirement of the Performance Improvement Modules (PIM).
"The three-year PIM cycle makes a lot of sense," Dr. Buckley says, noting she is "encouraged" to learn ABIM has approved three of SHM's quality projects to count toward the MOC requirement. Although she might still recertify through the traditional internal-medicine MOC next year, she definitely has the FPHM on the radar.
"Maybe in a couple years," Dr. Buckley says. "The PIM templates will be extremely helpful and encourage me to do it even more. The FPHM shows dedication to the field."
GRAPEVINE, Texas — Sitting in the third row of a large meeting room, Robin Buckley, MD, FHM, was soaking in the morning portion of the "ABIM Maintenance of Certification (MOC) Learning Session" pre-course, clicking her keypad with answers to questions and making mental notes this morning at HM11.
Dr. Buckley, medical director of hospitalist services at 72-bed Scott & White Healthcare in Round Rock, Texas, has to recertify in 2012, so she is getting an early start. One of nine pre-courses held annually, the learning session offers 6.5 CME credits.
"I'm really excited about sharing the information with my group, especially the questions focused on quality," says Dr. Buckley, who has been a hospitalist since 2004 and joined her expanding HM group in 2008. "I want to apply the information to our clinical practice, because I think it’s going to make us better."
She's also considering the Focused Practice in Hospital Medicine (FPHM) pathway, and used the pre-course to understand the specialized MOC pathway better. The main concerns, she says, are the added cost and the every-three-year requirement of the Performance Improvement Modules (PIM).
"The three-year PIM cycle makes a lot of sense," Dr. Buckley says, noting she is "encouraged" to learn ABIM has approved three of SHM's quality projects to count toward the MOC requirement. Although she might still recertify through the traditional internal-medicine MOC next year, she definitely has the FPHM on the radar.
"Maybe in a couple years," Dr. Buckley says. "The PIM templates will be extremely helpful and encourage me to do it even more. The FPHM shows dedication to the field."
Critical Lessons in Care
GRAPEVINE, Texas – Hospitalist Gilbert Asomaning, MB, ChB, walked into a post-anesthesia care unit (PACU) this morning and was confronted with a 55-year-old male in shock. The monitor presented a myriad of issues: He was making lactate, had trouble urinating–and the familiar PACU beeping was incessant.
But no one knew why. Colleagues screamed out questions: Is he responsive? How are his extremities? Is he on oxygen? Still, the cause of what turned out to be hypovolemic shock was a mystery until someone said it: a pinned iliac artery. The case wasn't real; it was a simulation that was part of an HM11 pre-course at the Gaylord Texan Resort & Convention Center. But the value of the daylong session, "Advanced Interactive Critical Care," was quite real.
"This is a great session...it seems like the real thing, but here you know, you are hear to learn," says Dr. Asomaning, who has been to previous SHM meetings, but this year trekked out a day early from Capital Medical Center in Olympia, Wash., specifically to attend the critical care pre-course. "You go through it and when you make your mistakes, you are corrected. And then you sort of reorganize things in your mind again and you are more prepared when the real thing happens."
The simulation was led by course co-director Kevin Felner, MD, of New York University School of Medicine, who says supplementing lectures with hands-on situations is key to increased comprehension.
"Most people are learners by doing…and learn more from doing something than 45 minutes of lecture with a chalkboard," he says. "We push people, take them out of their comfort zone. That’s how you learn."
GRAPEVINE, Texas – Hospitalist Gilbert Asomaning, MB, ChB, walked into a post-anesthesia care unit (PACU) this morning and was confronted with a 55-year-old male in shock. The monitor presented a myriad of issues: He was making lactate, had trouble urinating–and the familiar PACU beeping was incessant.
But no one knew why. Colleagues screamed out questions: Is he responsive? How are his extremities? Is he on oxygen? Still, the cause of what turned out to be hypovolemic shock was a mystery until someone said it: a pinned iliac artery. The case wasn't real; it was a simulation that was part of an HM11 pre-course at the Gaylord Texan Resort & Convention Center. But the value of the daylong session, "Advanced Interactive Critical Care," was quite real.
"This is a great session...it seems like the real thing, but here you know, you are hear to learn," says Dr. Asomaning, who has been to previous SHM meetings, but this year trekked out a day early from Capital Medical Center in Olympia, Wash., specifically to attend the critical care pre-course. "You go through it and when you make your mistakes, you are corrected. And then you sort of reorganize things in your mind again and you are more prepared when the real thing happens."
The simulation was led by course co-director Kevin Felner, MD, of New York University School of Medicine, who says supplementing lectures with hands-on situations is key to increased comprehension.
"Most people are learners by doing…and learn more from doing something than 45 minutes of lecture with a chalkboard," he says. "We push people, take them out of their comfort zone. That’s how you learn."
GRAPEVINE, Texas – Hospitalist Gilbert Asomaning, MB, ChB, walked into a post-anesthesia care unit (PACU) this morning and was confronted with a 55-year-old male in shock. The monitor presented a myriad of issues: He was making lactate, had trouble urinating–and the familiar PACU beeping was incessant.
But no one knew why. Colleagues screamed out questions: Is he responsive? How are his extremities? Is he on oxygen? Still, the cause of what turned out to be hypovolemic shock was a mystery until someone said it: a pinned iliac artery. The case wasn't real; it was a simulation that was part of an HM11 pre-course at the Gaylord Texan Resort & Convention Center. But the value of the daylong session, "Advanced Interactive Critical Care," was quite real.
"This is a great session...it seems like the real thing, but here you know, you are hear to learn," says Dr. Asomaning, who has been to previous SHM meetings, but this year trekked out a day early from Capital Medical Center in Olympia, Wash., specifically to attend the critical care pre-course. "You go through it and when you make your mistakes, you are corrected. And then you sort of reorganize things in your mind again and you are more prepared when the real thing happens."
The simulation was led by course co-director Kevin Felner, MD, of New York University School of Medicine, who says supplementing lectures with hands-on situations is key to increased comprehension.
"Most people are learners by doing…and learn more from doing something than 45 minutes of lecture with a chalkboard," he says. "We push people, take them out of their comfort zone. That’s how you learn."
Facilitating Hospice Discussions: A Six-Step Roadmap
How we do it
Jennifer Shin MD![]()
![]()
Abstract
Hospice programs provide comprehensive, compassionate care to dying patients and their families. However, many patients do not enroll in hospice, and those who do generally receive hospice care only in the last weeks of life. Although patients and families rely on their physicians to discuss hospice, there is often inadequate communication between patients and physicians about end-of-life issues. We describe a Six-Step Roadmap for navigating discussions about hospice adapted from the SPIKES protocol for delivering bad news: setting up the discussion, assessing the patient’s perception, inviting a patient to discuss individual goals and needs, sharing knowledge, empathizing with the patient’s emotions, and summarizing and strategizing the next steps.
Article Outline
- A Six-Step Roadmap
- Step 1: Set Up the Discussion About Hospice
- Step 2: Assess the Patient's Perception
- Step 3: Invite the Patient to Discuss Goals of Care and Needs for Care
- Step 4: Share Knowledge
- Step 5: Empathize With the Patient's Emotion
- Step 6: Summarize the Discussion and Strategize Next Steps
Case
Mr. C is a 54-year-old man with metastatic lung adenocarcinoma who presented 1 year ago with multiple lung nodules and hepatic metastases. His tumor responded to initial treatment with four cycles of carboplatin and pemetrexed, and he was treated with maintenance pemetrexed for 5 months before his liver lesions progressed. Despite treatment with docetaxel and then erlotinib, his liver and lung tumors progressed rapidly. He has lost 10 pounds in the last few weeks and is now so fatigued that he spends most of his day resting in his recliner. He has been admitted to the hospital twice in the last month for worsening dyspnea in the setting of progressive pulmonary metastases.
Introduction
Hospice programs provide high-quality, compassionate care to dying patients and their families through an interdisciplinary team specializing in pain and symptom management.[1] and [2] These patients also receive medications and supplies, durable medical equipment, and home health aide services. Patients and their families receive support from a chaplain, social worker, physician, nurse, and volunteer. Families are offered bereavement services for at least 13 months following the patient's death (Table 1).3
| Services |
| • Pain and symptom management |
| • 24-hour telephone access to a clinician |
| • Assistance with personal care needs |
| • Help with errands and light housework |
| • Spiritual support |
| • Companionship for the patient and family |
| • Bereavement counseling before and after the patient's death |
| • Patient and family education and counseling |
| • Case management and coordination |
| • Advance care planning |
| • Medications and supplies related to the hospice diagnosis |
| • Durable medical equipment |
| • Child bereavement services |
| • Respite services (up to 5 consecutive days of inpatient care to allow families a needed break) |
| • Inpatient hospice (for treatment of severe symptoms that cannot be managed at home) |
| Team members |
| • Physician |
| • Nurse |
| • Social worker |
| • Home health aide |
| • Chaplain |
| • Bereavement counselor |
| • Physical therapist |
| • Occupational therapist |
| • Volunteer |
National Hospice and Palliative Care Organization. NHPCO Facts and Figures: Hospice Care in America.3
Families report high levels of satisfaction with hospice and are more likely to describe high-quality care.1 Despite this, only 40% of people in the United States die while receiving hospice care.3 Although longer hospice stays are associated with better quality of life in patients and less depression in bereaved family members,[4] and [5] many patients enroll very late in the course of illness. In fact, the median length of stay is just over 3 weeks, and a third of patients die or are discharged within 1 week of hospice enrollment.3 The result is that brief exposures to hospice at the end of life do not allow patients and families to take full advantage of the benefits.6
There are several explanations for why people enroll in hospice so late. The Medicare Hospice Benefit requires hospice patients to choose a plan of comfort care, which means that they must usually forgo disease-directed therapies unless they provide a specific palliative benefit. Furthermore, the financial per diem payment structure of hospice means that patients may need to forgo palliative treatments that cannot be covered under the typical hospice reimbursement (approximately $150/day for routine home care). Patients may not be willing to give up these therapies or may be reluctant to transition from a model of care focusing on disease-directed therapies to one with palliation as the goal.
Patients may also enroll in hospice later if their physicians do not discuss hospice or if they have these discussions in the last few weeks of the patient's life.[7] and [8] Physicians may delay hospice discussions because they are unsure of the patient's prognosis,9 although the disease trajectory in patients with cancer is often more straightforward than in patients with non-oncologic diagnoses. Studies have documented deficiencies in doctor–patient communication regarding prognosis and end-of-life issues,10 and patients report inadequate communication with physicians about shared decision making at the end of life.1 Another study found that about half of patients diagnosed with metastatic lung cancer reported not having discussed hospice with a provider within 4–7 months after diagnosis.11
Although these discussions may be delayed or avoided altogether, seriously ill patients value the ability to prepare for the end of life.[12] and [13] Patients rely on their physicians to discuss hospice and other end-of-life care options. Furthermore, most family caregivers report that communication with their oncologists was important in helping them to understand the patient's prognosis and to see the role that hospice could play as a treatment alternative.7
These conversations are often difficult for patients and families and can also be challenging for physicians. Nevertheless, communication skills in discussing transitions to palliative care can be learned.[14] and [15] Although these discussions are not nearly as straightforward as a medical or surgical procedure, one can approach them with the same methodical preparation and careful consideration of the steps involved.
When Is a Hospice Discussion Appropriate?
To be eligible for the Medicare Hospice Benefit, a patient must have a prognosis of 6 months or less if his or her illness runs its usual course; also, the patient needs to be willing to accept the hospice philosophy of comfort care. This second criterion is not formally defined but is generally accepted to mean that the patient must be willing to forgo disease-directed therapies related to the hospice admitting diagnosis.
These eligibility criteria should not be used to define the patients for whom a hospice discussion is appropriate however. When a patient's goals and values reflect a desire to focus on palliation, it is time for the physician to initiate a hospice discussion. Other triggers for early hospice discussions can include a change in clinical status, recent hospitalization, decline in performance status, new weight loss, or complication of treatment. Although these factors may prompt a discussion of options for care, including hospice,[16] and [17] not all discussions will lead to a hospice enrollment decision. Nevertheless, earlier discussions that prompt conversations about a patient's needs, goals, and preferences can facilitate later decisions about hospice and other treatment options.
A Six-Step Roadmap
We provide a Six-Step Roadmap for navigating discussions about hospice adapted from the SPIKES protocol for delivering bad news.18 This strategy is comprised of six communication steps that can be remembered by using the mnemonic SPIKES: setting up the discussion, assessing the patient's perception, inviting a patient to discuss individual goals and needs, sharing knowledge, empathizing with the patient's emotions, and summarizing and strategizing the next steps.
Step 1: Set Up the Discussion About Hospice
Before discussing hospice with a patient and family, it is important to communicate with other members of the medical team to ensure an understanding of the patient's prognosis and treatment options. It is also helpful to find out what the patient and family may have expressed to other providers regarding these issues and how they have been coping. Any provider who has been in contact with the patient may be able to contribute to this consensus, including the medical oncologist, radiation oncologist, palliative care physician, primary care physician, home nurse, and social worker. A clear, unified message from the team decreases confusion for the patient and family.
Once a common agreement has been established regarding the patient's prognosis and treatment options, physicians can schedule a time and arrange for a place to allow for an uninterrupted conversation. Scheduling a patient at the end of a clinic day or visiting a patient in the hospital during an admission are potential ways to do this. Before scheduling a meeting, however, it is essential to know who the patient would like to be present at the meeting. One approach may be to tell the patient that there are important options to discuss regarding the next steps in his or her care and find out who may be able to help the patient with such decisions (Table 2). Additionally, a palliative care physician may cofacilitate these discussions. If the patient already has a palliative care physician, it may be helpful to have him or her involved in the meeting. If the patient has not yet been evaluated by a palliative care team, it may be possible to consult a palliative care specialist who can attend the meeting or follow up with the patient afterward.
Adapted from Cassett et al8 and Baille et al15
| Invite other decision makers | “Who do you usually rely on to help you make important decisions?” “When we discuss your results, who would you like to be present?” |
| Assess understanding of prognosis | “Tell me about your understanding of the most recent tests/studies.” “Can you share with me what you think is happening with your cancer and the treatments?” |
| Identify goals of care | “What is most important to you right now?” “What are your biggest concerns right now?” “What are your hopes for the coming weeks/months?” “What do you enjoy doing now?” “What is most important to you now?” “What are you worried about now? In the future?” |
| Reframe goals (“wish” statements) | “I wish I could promise you that you will be able to make it to your daughter's wedding, but unfortunately I can't. What do you think about writing a letter for her to read on her wedding day? We can also think about other ways to let her know that you will always be with her, even if you cannot physically be there.” “I wish that we could find a new chemotherapy that could cure your cancer. Even though cure is not possible, I think that we can meet some of your other goals, like staying at home to spend time with your children.” |
| Identify needs for care | “What has been hard for you and your family?” “What is your life like when you are at home? How are you and your family managing?” “Are you experiencing pain or other symptoms that are bothering you?” “Have you been feeling sad or anxious lately?” “Would it be helpful to have a visiting nurse come to your home to assist you with your medications?” |
| Introduce hospice | “One of the best ways to give you the help that you need to stay at home is through hospice.” “The hospice team specializes in caring for seriously ill patients at home.” “Hospice can provide you and your family with more services and support.” |
| Recommend hospice | “From what you have shared with me today, I recommend hospice as a way of helping you meet the goals that are important to you.” “I feel that hospice is the best option for you and your family. I know this is a big decision, and I want you to know that the decision is yours.” |
Mr. C's medical oncologist, Dr. A, contacted Mr. C's radiation oncologist as well as his primary care physician. They all agreed that his prognosis could be measured in weeks to months and that his performance status precluded any further chemotherapy. Dr. A also spoke with the hospital social worker who met Mr. C and his wife during his most recent hospitalization. The social worker said that Mr. C's wife has been very distressed, particularly about his increasing debility and her difficulty in caring for him at home. When Dr. A visited Mr. C during his hospitalization, Dr. A explained to Mr. C that they would be making some decisions about the next steps in his care and asked who might be able to help with these decisions. When Mr. C said his wife would be this person, Dr. A asked that she come to his next visit. Dr. A decided to schedule Mr. C for an appointment at the end of his clinic session the following week.
Step 2: Assess the Patient's Perception
The physician can begin this discussion by asking the patient to describe his or her current medical situation (Table 2). Although the physician may have provided this information on prior occasions, it is important to hear the patient's perception of the diagnosis and prognosis. Patients with advanced cancer often overestimate their prognosis and are more likely to favor life-extending therapies over hospice.19 These questions provide an opportunity to address any misconceptions or gaps in understanding that the patient may have. When the physician, patient, and family are in agreement with the patient's current medical situation it allows for further exploration of the patient's hopes and concerns.
This part of the discussion should rely on open-ended questions designed to elicit the patient's perspective. In particular, an invitation to “tell me more” encourages patients to explore how they are thinking or feeling and can yield more information than closed-ended or leading questions. This phrase can also help redirect the conversation when necessary (“You mentioned before that you are worried that the chemotherapy is not working anymore. Tell me more about your concerns.”).
Dr. A asked Mr. C how he was doing overall and to describe his understanding of whether the erlotinib had been working. In response, Mr. C expressed his concern about his recent weight loss and lethargy. Dr. A asked Mr. C to tell him more about these concerns, and Mr. C said that he thought his symptoms were a sign that the erlotinib was not helping him. He said he knew that the CT scans showed progression of disease, and he wondered whether chemotherapy could help. Dr. A confirmed there was progression of cancer in his lungs and liver. Dr. A also expressed his concern that more chemotherapy would not provide additional benefit for him and may harm him. Mr. C and his wife were tearful and agreed that he was too weak for more chemotherapy. Dr. A acknowledged that the disease had progressed quickly and must be very upsetting to them.
Step 3: Invite the Patient to Discuss Goals of Care and Needs for Care
Before sharing information about hospice with a patient, it is important to understand the patient's hopes and fears about the future, goals of care, and needs for care. It is helpful to start with learning about the patient's perspectives on the future and linking that to the patient's goals of care. Once the goals are clear, it is easier to match the patient's needs with his or her goals.
One way to elicit patients' goals of care is by asking them to describe their hopes and fears about their cancer in the context of their life (Table 2). Patients may volunteer information about their hopes (eg, attending their daughter's wedding) or fears (eg, worrying about pain) that provide insight into their more global goals of care. Again, the “tell me more” phrase can be helpful (“Tell me more about what you mean when you say you are a burden on your family.”).
Once the patient and family express their thoughts, it is useful to restate the patient's goals by asking a question that summarizes the patient's statements (“From what you and your family have just shared with me, I hear that the most important thing to you is … . Did I understand you correctly?”). It is often challenging for patients to specifically articulate their goals of care. Asking a question allows the patient and family the chance to elaborate or offer corrections.
If a patient expresses unrealistic expectations (eg, a cure, years of life), “wish” statements can be helpful in providing gentle redirection. These statements express empathy while also communicating that the wished-for outcome is unlikely (“I wish that we could guarantee that … but unfortunately we can't.”). These statements can explain the reality of the situation in a compassionate manner (Table 2). Patients and families who have unrealistic goals of care may need time to readjust their expectations, and in these cases it may be prudent to revisit the discussion of hospice at a later date.
Once the goals of care have been established, it is important to further explore the needs for care. Although some of these needs may have been mentioned during the goals discussion, it is helpful to directly ask the patient and family about their needs. General questions about what has been hard for the patient and the family can be useful in eliciting needs, as are questions about what life has been like at home and how they are managing (Table 2). It is also important to ask more specific questions that pertain to the patient's symptoms such as pain or depression and those that address the family's needs for help around the house (Table 2). Once this information has been shared, it is often useful to repeat a summary back to the patient and family (“From what we have just discussed, it may be helpful to have a visiting nurse to assist with his medications and a home health aide to dress and bathe him … . Does it sound like this could be helpful to you?”). Often, these needs can be addressed by the multidisciplinary hospice team, and it is important to understand what needs exist in preparation for a discussion about how hospice might be helpful.
Mr. C shares with you that his two hospitalizations for dyspnea have been frustrating because he feels that they have prevented him from spending quality time with his daughters. Although he did not want to be admitted to the hospital, he tearfully expressed that he was worried about “suffocating to death” and did not want to die at home in front of his wife and children. Mr. C's wife also shares that it has been harder to bathe and dress him because he is becoming so weak. Mr. and Mrs. C agree that it would be helpful to have the support of a visiting nurse and a home health aide.
Step 4: Share Knowledge
Once the patient's goals and needs for care have been clarified, physicians can introduce hospice as a way of achieving their goals and meeting their needs. In presenting hospice in this transparent manner, patients and families can better understand how hospice is part of a plan of care that addresses their individualized goals and needs. Most family caregivers report that communication with their oncologists was critical in their understanding the patient's prognosis and hospice as a treatment alternative.7 In one survey, the majority of caregivers did not realize that their loved ones could benefit from hospice until their physicians first discussed it with them.7
A discussion of hospice should offer concrete information about the services provided to patients and their families (Table 1). Many patients and families do not understand the benefits, such as a visiting nurse for frequent symptom management or a home health aide to assist with daily patient care, until after enrollment. Many say they wish they had known sooner.20 By providing this information earlier, patients and families may make more informed decisions about hospice. This description also makes clear to the patient and family that hospice is not simply a generic recommendation but rather the physician's recommendation of a program that is the best fit for their specific goals and needs.
Given the emotional nature of these discussions and the large amount of information involved, it is important to ask the patient to explain in his or her own words how hospice could help (“To make sure I did a good job of explaining things, can you tell me what we just talked about in your own words?” and “How do you think hospice might help you?”). This provides the opportunity to assess understanding and clarify any confusion.
Since not all patients are best served by hospice, the discussion may also be expanded to include other options for palliative care. For example, hospice is not equipped to care for debilitated patients at home who do not have a caretaker, nor is it usually able to absorb the costs of expensive palliative treatments. Sometimes, larger hospices may be able to make exceptions on a case-by-case basis, but it is helpful to be aware of other options for palliative care like bridge-to-hospice home care and outpatient palliative care programs.
Dr. A explained that hospice could provide intensive management of his dyspnea with the assistance of a visiting nurse and a 24-hour phone line to call for assistance. With these measures in place, Dr. A said that he hoped hospitalizations could be avoided, allowing him more time at home with his family. Dr. A addressed Mr. C's concern about dying at home and shared with him that he could be transferred to an inpatient hospice if death seemed imminent. Dr. A shared with Mrs. C that hospice could provide the services of a home health aide, which seemed to reduce her concerns about being able to care for her husband as he became weaker.
Step 5: Empathize With the Patient's Emotion
In discussions regarding end-of-life care, patients and families value empathy, compassion, and honesty balanced with sensitivity and hope.21 Throughout the conversation, it is likely that the patient and family will express a range of emotions. Rather than providing immediate reassurance or trying to “fix” the emotion, it can be helpful to use an empathic statement to let the patient know that his or her emotions are recognized.15 Empathic responses address and validate a patient's emotions and encourage further disclosure.22 The NURSE mnemonic summarizes ways in which to respond to emotions: naming, understanding, respecting, supporting, and exploring the feelings the patient has shared (Table 3).[15] and [23]
Adapted from Back et al[15] and [23]
| N = Naming | “It sounds like you are worried about how fast the cancer has been progressing.” “Some people in this situation would feel frustrated.” |
| U = Understanding | “My understanding of what you have told me is that you are worried about being able to live independently at home.” “I can see how difficult this has been for you and your family.” |
| R = Respecting | “It is very clear to me how supportive your family has been.” “I can see how hard you have worked to understand the treatment options for your cancer.” |
| S = Supporting | “I will support the decisions that you make, no matter what you decide.” “I will always be your doctor.” |
| E = Exploring | “Could you tell me more about what you mean when you say that you don't want to give up?” “I sense that you may be feeling anxious about stopping chemotherapy. Can you share with me what you are feeling?” |
Some of the emotions arising during a hospice discussion may stem from preconceived notions or a prior experience. Therefore, it may be helpful to specifically ask patients and families about these perceptions and experiences. Common misperceptions may include the concern that hospice hastens death. Other patients view hospice as “giving up” and worry about being abandoned by their physicians. A hospice discussion provides the opportunity to directly address these concerns and provide clarification (“No, hospice does not hasten death. Hospice helps you have the best quality of life for whatever time you have.”).
Ultimately, some patients and families may decide that hospice is not the right choice for them. It is important to recognize that the time invested has not been wasted. Instead, if done well, these discussions offer an opportunity for the physician to align his or her goals and understanding with those of the patient and family. Specifically, these discussions are a chance to demonstrate a desire to understand the patient's individualized goals and to share concerns about disease progression. In essence, it is a valuable opportunity to establish a collective understanding about the patient's current situation while also laying important groundwork for future discussions.
Mr. C tearfully shared his concern about being a burden to his wife and about how his daughters would handle his progressive decline. Dr. A sat quietly, allowed Mr. C to fully detail his worries, and then said, “I can see how worried you are about your family and understand that you want to make sure that their needs are also addressed.”
Step 6: Summarize the Discussion and Strategize Next Steps
In all stages of cancer, patients and families rely on their oncologist for information about treatment options. This is particularly important when a patient's cancer has progressed despite therapy and when the focus of care may be shifting from disease-directed therapies to palliation. Just as a physician may have previously recommended a chemotherapeutic option for a patient, so should he or she recommend the therapeutic option of focusing on quality of life. If hospice appears consistent with the patient's and family's goals and needs, the physician should make this recommendation. It may be helpful for the patient and family to hear a summary of how hospice will meet their needs. If the patient is amenable to learning more about hospice but is not yet ready to enroll, the physician can arrange for an informational visit with the hospice team.
Dr. A recommends hospice and emphasizes that hospice would provide services that meet Mr. C's goals of symptom management, avoiding hospitalizations, and providing support for his family. Mr. C and his wife agree that hospice is the best option for them. They would like to enroll after they have spoken with their children about their decision.
Conclusion
Discussions about goals of care and hospice are not easy. They are rarely as straightforward as presented in this case, and an oncologist may face numerous barriers when attempting to have these discussions. For instance, treating physicians may have differing opinions on therapeutic options. Patients and family members may have different goals and may be in different stages of accepting a life-limiting cancer diagnosis. Additionally, these discussions take preparation, time, and skill. Although there are no easy solutions to these issues, the general guidance provided in this article focuses on suggesting tools and techniques that can make these discussions easier for oncologists, patients, and families. By increasing our competence and comfort with these conversations, we can reduce delays in offering patients the benefits of hospice as they near the end of life.
Although no algorithm will fully address the complexities and nuances of these conversations, this approach provides a general framework and offers tools to use while speaking with patients and families. Conversations about hospice do not begin with the recommendation of hospice but rather with an honest discussion of the goals and needs of a patient and family. If these goals and needs can be met with the services that hospice can provide, the physician has the opportunity to educate the patient and to make the recommendation as they would for any other therapeutic option.
Patients and families consider communication to be one of the most important facets of end-of-life care.24 Seriously ill patients value being able to prepare for death,13 and physicians have the duty to help patients and families prepare for the end of life.25 Physicians can help increase the time patients have to plan for the last phase of their lives by having honest and open discussions about hospice and other alternatives. Oncologists have the responsibility to present patients with the benefits and burdens of therapies throughout the trajectory of their illness, and it is critically important during the transition from disease-directed to palliative care. By exploring the option of hospice, patients and families can make informed decisions about whether hospice may meet their needs. Equally important, patients are given the control to choose how they would like to live the final phase of their lives.
References1
1 J.M. Teno, B.R. Clarridge, V. Casey, L.C. Welch, T. Wetle, R. Shield and V. Mor, Family perspectives on end-of-life care at the last place of care, JAMA 291 (1) (2004), pp. 88–93. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (411)
2 S.C. Miller, V. Mor and J. Teno, Hospice enrollment and pain assessment and management in nursing homes, J Pain Symptom Manage 26 (3) (2003), pp. 791–799. Article |

3 National Hospice and Palliative Care Organization, NHPCO Facts and Figures: Hospice Care in America www.nhpco.org/files/public/Statistics_Research/Hospice_Facts_Figures_Oct-2010.pdf+NHPCO+Facts+and+Figures:+Hospice+Care+in+America.+National+Hospice+and+Palliative+Care+Organization&hl=en&gl=us&pid=bl&srcid=ADGEESgPEeCPa2C7KZ3zQT0yldBWHrCAHY4UemVw6R1Odl2VxMKsjrMnNridOO3qiHrvN9cAfwCzkIY3Mc28JRgBLdvCaN3nQXt7EUNL6H-PTkYYaVAl4-VECDAsh16DvmofChWiLRfa&sig=AHIEtbTMY3LallQ5V2Ceyd_ACIQfUh-ggA (2010).
4 A.A. Wright, B. Zhang, A. Ray, J.W. Mack, E. Trice, T. Balboni, S.L. Mitchell, V.A. Jackson, S.D. Block, P.K. Maciejewski and H.G. Prigerson, Associations between end-of-life discussions, patient mental health, medical care near death, and caregiver bereavement adjustment, JAMA 300 (14) (2008), pp. 1665–1673. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (131)
5 E.H. Bradley, H. Prigerson, M.D.A. Carlson, E. Cherlin, R. Johnson-Hurzeler and S.V. Kasl, Depression among surviving caregivers: does length of hospice enrollment matter?, Am J Psychiatry 161 (12) (2004), pp. 2257–2262. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (29)
6 I.R. Byock, W.B. Forman and M. Appleton, Academy of hospice physicians' position statement on access to hospice and palliative care, J Pain Symptom Manage 11 (2) (1996), pp. 69–70. Article |
7 E. Cherlin, T. Fried, H.G. Prigerson, D. Schulman-Green, R. Johnson-Hurzeler and E.H. Bradley, Communication between physicians and family caregivers about care at the end of life: when do discussions occur and what is said?, J Palliat Med 8 (6) (2005), pp. 1176–1185. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (51)
8 D.J. Casarett and T.E. Quill, “I'm not ready for hospice”: strategies for timely and effective hospice discussions, Ann Intern Med 146 (6) (2007), pp. 443–449. View Record in Scopus | Cited By in Scopus (36)
9 E.B. Lamont and N.A. Christakis, Prognostic disclosure to patients with cancer near the end of life, Ann Intern Med 134 (12) (2001), pp. 1096–1105. View Record in Scopus | Cited By in Scopus (166)
10 M. Gysels, A. Richardson and I.J. Higginson, Communication training for health professionals who care for patients with cancer: a systematic review of effectiveness, Support Care Cancer 12 (10) (2004), pp. 692–700. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (41)
11 H.A. Huskamp, N.L. Keating, J.L. Malin, A.M. Zaslavsky, J.C. Weeks, C.C. Earle, J.M. Teno, B.A. Virnig, K.L. Kahn, Y. He and J.Z. Ayanian, Discussions with physicians about hospice among patients with metastatic lung cancer, Arch Intern Med 169 (10) (2009), pp. 954–962. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (4)
12 K.E. Steinhauser, N.A. Christakis, E.C. Clipp, M. McNeilly, S. Grambow, J. Parker and J.A. Tulsky, Preparing for the end of life: preferences of patients, families, physicians, and other care providers, J Pain Symptom Manage 22 (3) (2001), pp. 727–737. Article |
13 K.E. Steinhauser, N.A. Christakis, E.C. Clipp, M. McNeilly, L. McIntyre and J.A. Tulsky, Factors considered important at the end of life by patients, family, physicians, and other care providers, JAMA 284 (19) (2000), pp. 2476–2482. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (615)
14 A.L. Back, R.M. Arnold, W.F. Baile, K.A. Fryer-Edwards, S.C. Alexander, G.E. Barley, T.A. Gooley and J.A. Tulsky, Efficacy of communication skills training for giving bad news and discussing transitions to palliative care, Arch Intern Med 167 (5) (2007), pp. 453–460. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (94)
15 A.L. Back, R.M. Arnold, W.F. Baile, J.A. Tulsky and K. Fryer-Edwards, Approaching difficult communication tasks in oncology, CA Cancer J Clin 55 (3) (2005), pp. 164–177. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (103)
16 C. Conill, E. Verger and M. Salamero, Performance status assessment in cancer patients, Cancer 65 (8) (1990), pp. 1864–1866. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (81)
17 V. Mor, L. Laliberte, J.N. Morris and M. Wiemann, The Karnofsky Performance Status Scale: An examination of its reliability and validity in a research setting, Cancer 53 (9) (1984), pp. 2002–2007. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (314)
18 W.F. Baile, R. Buckman, R. Lenzi, G. Glober, E.A. Beale and A.P. Kudelka, SPIKES—a six-step protocol for delivering bad news: application to the patient with cancer, Oncologist 5 (4) (2000), pp. 302–311. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (293)
19 J.C. Weeks, E.F. Cook, S.J. O'Day, L.M. Peterson, N. Wenger, D. Reding, F.E. Harrell, P. Kussin, N.V. Dawson, A.F. Connors, J. Lynn and R.S. Phillips, Relationship between cancer patients' predictions of prognosis and their treatment preferences, JAMA 279 (21) (1998), pp. 1709–1714. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (350)
20 D.J. Casarett, R.L. Crowley and K.B. Hirschman, How should clinicians describe hospice to patients and families?, J Am Geriatr Soc 52 (11) (2004), pp. 1923–1928. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (46)
21 S.M. Parker, J.M. Clayton, K. Hancock, S. Walder, P.N. Butow, S. Carrick, D. Currow, D. Ghersi, P. Glare, R. Hagerty and M.H. Tattersall, A systematic review of prognostic/end-of-life communication with adults in the advanced stages of a life-limiting illness: patient/caregiver preferences for the content, style, and timing of information, J Pain Symptom Manage 34 (1) (2007), pp. 81–93. Article |
22 K.I. Pollak, R.M. Arnold, A.S. Jeffreys, S.C. Alexander, M.K. Olsen, A.P. Abernethy, C. Sugg Skinner, K.L. Rodriguez and J.A. Tulsky, Oncologist communication about emotion during visits with patients with advanced cancer, J Clin Oncol 25 (36) (2007), pp. 5748–5752. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (47)
23 A.L. Back, W.G. Anderson, L. Bunch, L.A. Marr, J.A. Wallace, H.B. Yang and R.M. Arnold, Communication about cancer near the end of life, Cancer 113 (suppl 7) (2008), pp. 1897–1910. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (12)
24 M.D. Wenrich, J.R. Curtis, S.E. Shannon, J.D. Carline, D.M. Ambrozy and P.G. Ramsey, Communicating with dying patients within the spectrum of medical care from terminal diagnosis to death, Arch Intern Med 161 (6) (2001), pp. 868–874. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (114)
25 J. Lynn, Perspectives on care at the close of life: Serving patients who may die soon and their families: the role of hospice and other services, JAMA 285 (7) (2001), pp. 925–932. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (124)

Vitae
Dr. Shin is from the Division of Hematology–Oncology, University of Pennsylvania School of Medicine, Philadelphia
Dr. Casarett is from the Division of Geriatric Medicine and the Penn-Wissahickon Hospice, University of Pennsylvania School of Medicine, Philadelphia
How we do it
Jennifer Shin MD![]()
![]()
Abstract
Hospice programs provide comprehensive, compassionate care to dying patients and their families. However, many patients do not enroll in hospice, and those who do generally receive hospice care only in the last weeks of life. Although patients and families rely on their physicians to discuss hospice, there is often inadequate communication between patients and physicians about end-of-life issues. We describe a Six-Step Roadmap for navigating discussions about hospice adapted from the SPIKES protocol for delivering bad news: setting up the discussion, assessing the patient’s perception, inviting a patient to discuss individual goals and needs, sharing knowledge, empathizing with the patient’s emotions, and summarizing and strategizing the next steps.
Article Outline
- A Six-Step Roadmap
- Step 1: Set Up the Discussion About Hospice
- Step 2: Assess the Patient's Perception
- Step 3: Invite the Patient to Discuss Goals of Care and Needs for Care
- Step 4: Share Knowledge
- Step 5: Empathize With the Patient's Emotion
- Step 6: Summarize the Discussion and Strategize Next Steps
Case
Mr. C is a 54-year-old man with metastatic lung adenocarcinoma who presented 1 year ago with multiple lung nodules and hepatic metastases. His tumor responded to initial treatment with four cycles of carboplatin and pemetrexed, and he was treated with maintenance pemetrexed for 5 months before his liver lesions progressed. Despite treatment with docetaxel and then erlotinib, his liver and lung tumors progressed rapidly. He has lost 10 pounds in the last few weeks and is now so fatigued that he spends most of his day resting in his recliner. He has been admitted to the hospital twice in the last month for worsening dyspnea in the setting of progressive pulmonary metastases.
Introduction
Hospice programs provide high-quality, compassionate care to dying patients and their families through an interdisciplinary team specializing in pain and symptom management.[1] and [2] These patients also receive medications and supplies, durable medical equipment, and home health aide services. Patients and their families receive support from a chaplain, social worker, physician, nurse, and volunteer. Families are offered bereavement services for at least 13 months following the patient's death (Table 1).3
| Services |
| • Pain and symptom management |
| • 24-hour telephone access to a clinician |
| • Assistance with personal care needs |
| • Help with errands and light housework |
| • Spiritual support |
| • Companionship for the patient and family |
| • Bereavement counseling before and after the patient's death |
| • Patient and family education and counseling |
| • Case management and coordination |
| • Advance care planning |
| • Medications and supplies related to the hospice diagnosis |
| • Durable medical equipment |
| • Child bereavement services |
| • Respite services (up to 5 consecutive days of inpatient care to allow families a needed break) |
| • Inpatient hospice (for treatment of severe symptoms that cannot be managed at home) |
| Team members |
| • Physician |
| • Nurse |
| • Social worker |
| • Home health aide |
| • Chaplain |
| • Bereavement counselor |
| • Physical therapist |
| • Occupational therapist |
| • Volunteer |
National Hospice and Palliative Care Organization. NHPCO Facts and Figures: Hospice Care in America.3
Families report high levels of satisfaction with hospice and are more likely to describe high-quality care.1 Despite this, only 40% of people in the United States die while receiving hospice care.3 Although longer hospice stays are associated with better quality of life in patients and less depression in bereaved family members,[4] and [5] many patients enroll very late in the course of illness. In fact, the median length of stay is just over 3 weeks, and a third of patients die or are discharged within 1 week of hospice enrollment.3 The result is that brief exposures to hospice at the end of life do not allow patients and families to take full advantage of the benefits.6
There are several explanations for why people enroll in hospice so late. The Medicare Hospice Benefit requires hospice patients to choose a plan of comfort care, which means that they must usually forgo disease-directed therapies unless they provide a specific palliative benefit. Furthermore, the financial per diem payment structure of hospice means that patients may need to forgo palliative treatments that cannot be covered under the typical hospice reimbursement (approximately $150/day for routine home care). Patients may not be willing to give up these therapies or may be reluctant to transition from a model of care focusing on disease-directed therapies to one with palliation as the goal.
Patients may also enroll in hospice later if their physicians do not discuss hospice or if they have these discussions in the last few weeks of the patient's life.[7] and [8] Physicians may delay hospice discussions because they are unsure of the patient's prognosis,9 although the disease trajectory in patients with cancer is often more straightforward than in patients with non-oncologic diagnoses. Studies have documented deficiencies in doctor–patient communication regarding prognosis and end-of-life issues,10 and patients report inadequate communication with physicians about shared decision making at the end of life.1 Another study found that about half of patients diagnosed with metastatic lung cancer reported not having discussed hospice with a provider within 4–7 months after diagnosis.11
Although these discussions may be delayed or avoided altogether, seriously ill patients value the ability to prepare for the end of life.[12] and [13] Patients rely on their physicians to discuss hospice and other end-of-life care options. Furthermore, most family caregivers report that communication with their oncologists was important in helping them to understand the patient's prognosis and to see the role that hospice could play as a treatment alternative.7
These conversations are often difficult for patients and families and can also be challenging for physicians. Nevertheless, communication skills in discussing transitions to palliative care can be learned.[14] and [15] Although these discussions are not nearly as straightforward as a medical or surgical procedure, one can approach them with the same methodical preparation and careful consideration of the steps involved.
When Is a Hospice Discussion Appropriate?
To be eligible for the Medicare Hospice Benefit, a patient must have a prognosis of 6 months or less if his or her illness runs its usual course; also, the patient needs to be willing to accept the hospice philosophy of comfort care. This second criterion is not formally defined but is generally accepted to mean that the patient must be willing to forgo disease-directed therapies related to the hospice admitting diagnosis.
These eligibility criteria should not be used to define the patients for whom a hospice discussion is appropriate however. When a patient's goals and values reflect a desire to focus on palliation, it is time for the physician to initiate a hospice discussion. Other triggers for early hospice discussions can include a change in clinical status, recent hospitalization, decline in performance status, new weight loss, or complication of treatment. Although these factors may prompt a discussion of options for care, including hospice,[16] and [17] not all discussions will lead to a hospice enrollment decision. Nevertheless, earlier discussions that prompt conversations about a patient's needs, goals, and preferences can facilitate later decisions about hospice and other treatment options.
A Six-Step Roadmap
We provide a Six-Step Roadmap for navigating discussions about hospice adapted from the SPIKES protocol for delivering bad news.18 This strategy is comprised of six communication steps that can be remembered by using the mnemonic SPIKES: setting up the discussion, assessing the patient's perception, inviting a patient to discuss individual goals and needs, sharing knowledge, empathizing with the patient's emotions, and summarizing and strategizing the next steps.
Step 1: Set Up the Discussion About Hospice
Before discussing hospice with a patient and family, it is important to communicate with other members of the medical team to ensure an understanding of the patient's prognosis and treatment options. It is also helpful to find out what the patient and family may have expressed to other providers regarding these issues and how they have been coping. Any provider who has been in contact with the patient may be able to contribute to this consensus, including the medical oncologist, radiation oncologist, palliative care physician, primary care physician, home nurse, and social worker. A clear, unified message from the team decreases confusion for the patient and family.
Once a common agreement has been established regarding the patient's prognosis and treatment options, physicians can schedule a time and arrange for a place to allow for an uninterrupted conversation. Scheduling a patient at the end of a clinic day or visiting a patient in the hospital during an admission are potential ways to do this. Before scheduling a meeting, however, it is essential to know who the patient would like to be present at the meeting. One approach may be to tell the patient that there are important options to discuss regarding the next steps in his or her care and find out who may be able to help the patient with such decisions (Table 2). Additionally, a palliative care physician may cofacilitate these discussions. If the patient already has a palliative care physician, it may be helpful to have him or her involved in the meeting. If the patient has not yet been evaluated by a palliative care team, it may be possible to consult a palliative care specialist who can attend the meeting or follow up with the patient afterward.
Adapted from Cassett et al8 and Baille et al15
| Invite other decision makers | “Who do you usually rely on to help you make important decisions?” “When we discuss your results, who would you like to be present?” |
| Assess understanding of prognosis | “Tell me about your understanding of the most recent tests/studies.” “Can you share with me what you think is happening with your cancer and the treatments?” |
| Identify goals of care | “What is most important to you right now?” “What are your biggest concerns right now?” “What are your hopes for the coming weeks/months?” “What do you enjoy doing now?” “What is most important to you now?” “What are you worried about now? In the future?” |
| Reframe goals (“wish” statements) | “I wish I could promise you that you will be able to make it to your daughter's wedding, but unfortunately I can't. What do you think about writing a letter for her to read on her wedding day? We can also think about other ways to let her know that you will always be with her, even if you cannot physically be there.” “I wish that we could find a new chemotherapy that could cure your cancer. Even though cure is not possible, I think that we can meet some of your other goals, like staying at home to spend time with your children.” |
| Identify needs for care | “What has been hard for you and your family?” “What is your life like when you are at home? How are you and your family managing?” “Are you experiencing pain or other symptoms that are bothering you?” “Have you been feeling sad or anxious lately?” “Would it be helpful to have a visiting nurse come to your home to assist you with your medications?” |
| Introduce hospice | “One of the best ways to give you the help that you need to stay at home is through hospice.” “The hospice team specializes in caring for seriously ill patients at home.” “Hospice can provide you and your family with more services and support.” |
| Recommend hospice | “From what you have shared with me today, I recommend hospice as a way of helping you meet the goals that are important to you.” “I feel that hospice is the best option for you and your family. I know this is a big decision, and I want you to know that the decision is yours.” |
Mr. C's medical oncologist, Dr. A, contacted Mr. C's radiation oncologist as well as his primary care physician. They all agreed that his prognosis could be measured in weeks to months and that his performance status precluded any further chemotherapy. Dr. A also spoke with the hospital social worker who met Mr. C and his wife during his most recent hospitalization. The social worker said that Mr. C's wife has been very distressed, particularly about his increasing debility and her difficulty in caring for him at home. When Dr. A visited Mr. C during his hospitalization, Dr. A explained to Mr. C that they would be making some decisions about the next steps in his care and asked who might be able to help with these decisions. When Mr. C said his wife would be this person, Dr. A asked that she come to his next visit. Dr. A decided to schedule Mr. C for an appointment at the end of his clinic session the following week.
Step 2: Assess the Patient's Perception
The physician can begin this discussion by asking the patient to describe his or her current medical situation (Table 2). Although the physician may have provided this information on prior occasions, it is important to hear the patient's perception of the diagnosis and prognosis. Patients with advanced cancer often overestimate their prognosis and are more likely to favor life-extending therapies over hospice.19 These questions provide an opportunity to address any misconceptions or gaps in understanding that the patient may have. When the physician, patient, and family are in agreement with the patient's current medical situation it allows for further exploration of the patient's hopes and concerns.
This part of the discussion should rely on open-ended questions designed to elicit the patient's perspective. In particular, an invitation to “tell me more” encourages patients to explore how they are thinking or feeling and can yield more information than closed-ended or leading questions. This phrase can also help redirect the conversation when necessary (“You mentioned before that you are worried that the chemotherapy is not working anymore. Tell me more about your concerns.”).
Dr. A asked Mr. C how he was doing overall and to describe his understanding of whether the erlotinib had been working. In response, Mr. C expressed his concern about his recent weight loss and lethargy. Dr. A asked Mr. C to tell him more about these concerns, and Mr. C said that he thought his symptoms were a sign that the erlotinib was not helping him. He said he knew that the CT scans showed progression of disease, and he wondered whether chemotherapy could help. Dr. A confirmed there was progression of cancer in his lungs and liver. Dr. A also expressed his concern that more chemotherapy would not provide additional benefit for him and may harm him. Mr. C and his wife were tearful and agreed that he was too weak for more chemotherapy. Dr. A acknowledged that the disease had progressed quickly and must be very upsetting to them.
Step 3: Invite the Patient to Discuss Goals of Care and Needs for Care
Before sharing information about hospice with a patient, it is important to understand the patient's hopes and fears about the future, goals of care, and needs for care. It is helpful to start with learning about the patient's perspectives on the future and linking that to the patient's goals of care. Once the goals are clear, it is easier to match the patient's needs with his or her goals.
One way to elicit patients' goals of care is by asking them to describe their hopes and fears about their cancer in the context of their life (Table 2). Patients may volunteer information about their hopes (eg, attending their daughter's wedding) or fears (eg, worrying about pain) that provide insight into their more global goals of care. Again, the “tell me more” phrase can be helpful (“Tell me more about what you mean when you say you are a burden on your family.”).
Once the patient and family express their thoughts, it is useful to restate the patient's goals by asking a question that summarizes the patient's statements (“From what you and your family have just shared with me, I hear that the most important thing to you is … . Did I understand you correctly?”). It is often challenging for patients to specifically articulate their goals of care. Asking a question allows the patient and family the chance to elaborate or offer corrections.
If a patient expresses unrealistic expectations (eg, a cure, years of life), “wish” statements can be helpful in providing gentle redirection. These statements express empathy while also communicating that the wished-for outcome is unlikely (“I wish that we could guarantee that … but unfortunately we can't.”). These statements can explain the reality of the situation in a compassionate manner (Table 2). Patients and families who have unrealistic goals of care may need time to readjust their expectations, and in these cases it may be prudent to revisit the discussion of hospice at a later date.
Once the goals of care have been established, it is important to further explore the needs for care. Although some of these needs may have been mentioned during the goals discussion, it is helpful to directly ask the patient and family about their needs. General questions about what has been hard for the patient and the family can be useful in eliciting needs, as are questions about what life has been like at home and how they are managing (Table 2). It is also important to ask more specific questions that pertain to the patient's symptoms such as pain or depression and those that address the family's needs for help around the house (Table 2). Once this information has been shared, it is often useful to repeat a summary back to the patient and family (“From what we have just discussed, it may be helpful to have a visiting nurse to assist with his medications and a home health aide to dress and bathe him … . Does it sound like this could be helpful to you?”). Often, these needs can be addressed by the multidisciplinary hospice team, and it is important to understand what needs exist in preparation for a discussion about how hospice might be helpful.
Mr. C shares with you that his two hospitalizations for dyspnea have been frustrating because he feels that they have prevented him from spending quality time with his daughters. Although he did not want to be admitted to the hospital, he tearfully expressed that he was worried about “suffocating to death” and did not want to die at home in front of his wife and children. Mr. C's wife also shares that it has been harder to bathe and dress him because he is becoming so weak. Mr. and Mrs. C agree that it would be helpful to have the support of a visiting nurse and a home health aide.
Step 4: Share Knowledge
Once the patient's goals and needs for care have been clarified, physicians can introduce hospice as a way of achieving their goals and meeting their needs. In presenting hospice in this transparent manner, patients and families can better understand how hospice is part of a plan of care that addresses their individualized goals and needs. Most family caregivers report that communication with their oncologists was critical in their understanding the patient's prognosis and hospice as a treatment alternative.7 In one survey, the majority of caregivers did not realize that their loved ones could benefit from hospice until their physicians first discussed it with them.7
A discussion of hospice should offer concrete information about the services provided to patients and their families (Table 1). Many patients and families do not understand the benefits, such as a visiting nurse for frequent symptom management or a home health aide to assist with daily patient care, until after enrollment. Many say they wish they had known sooner.20 By providing this information earlier, patients and families may make more informed decisions about hospice. This description also makes clear to the patient and family that hospice is not simply a generic recommendation but rather the physician's recommendation of a program that is the best fit for their specific goals and needs.
Given the emotional nature of these discussions and the large amount of information involved, it is important to ask the patient to explain in his or her own words how hospice could help (“To make sure I did a good job of explaining things, can you tell me what we just talked about in your own words?” and “How do you think hospice might help you?”). This provides the opportunity to assess understanding and clarify any confusion.
Since not all patients are best served by hospice, the discussion may also be expanded to include other options for palliative care. For example, hospice is not equipped to care for debilitated patients at home who do not have a caretaker, nor is it usually able to absorb the costs of expensive palliative treatments. Sometimes, larger hospices may be able to make exceptions on a case-by-case basis, but it is helpful to be aware of other options for palliative care like bridge-to-hospice home care and outpatient palliative care programs.
Dr. A explained that hospice could provide intensive management of his dyspnea with the assistance of a visiting nurse and a 24-hour phone line to call for assistance. With these measures in place, Dr. A said that he hoped hospitalizations could be avoided, allowing him more time at home with his family. Dr. A addressed Mr. C's concern about dying at home and shared with him that he could be transferred to an inpatient hospice if death seemed imminent. Dr. A shared with Mrs. C that hospice could provide the services of a home health aide, which seemed to reduce her concerns about being able to care for her husband as he became weaker.
Step 5: Empathize With the Patient's Emotion
In discussions regarding end-of-life care, patients and families value empathy, compassion, and honesty balanced with sensitivity and hope.21 Throughout the conversation, it is likely that the patient and family will express a range of emotions. Rather than providing immediate reassurance or trying to “fix” the emotion, it can be helpful to use an empathic statement to let the patient know that his or her emotions are recognized.15 Empathic responses address and validate a patient's emotions and encourage further disclosure.22 The NURSE mnemonic summarizes ways in which to respond to emotions: naming, understanding, respecting, supporting, and exploring the feelings the patient has shared (Table 3).[15] and [23]
Adapted from Back et al[15] and [23]
| N = Naming | “It sounds like you are worried about how fast the cancer has been progressing.” “Some people in this situation would feel frustrated.” |
| U = Understanding | “My understanding of what you have told me is that you are worried about being able to live independently at home.” “I can see how difficult this has been for you and your family.” |
| R = Respecting | “It is very clear to me how supportive your family has been.” “I can see how hard you have worked to understand the treatment options for your cancer.” |
| S = Supporting | “I will support the decisions that you make, no matter what you decide.” “I will always be your doctor.” |
| E = Exploring | “Could you tell me more about what you mean when you say that you don't want to give up?” “I sense that you may be feeling anxious about stopping chemotherapy. Can you share with me what you are feeling?” |
Some of the emotions arising during a hospice discussion may stem from preconceived notions or a prior experience. Therefore, it may be helpful to specifically ask patients and families about these perceptions and experiences. Common misperceptions may include the concern that hospice hastens death. Other patients view hospice as “giving up” and worry about being abandoned by their physicians. A hospice discussion provides the opportunity to directly address these concerns and provide clarification (“No, hospice does not hasten death. Hospice helps you have the best quality of life for whatever time you have.”).
Ultimately, some patients and families may decide that hospice is not the right choice for them. It is important to recognize that the time invested has not been wasted. Instead, if done well, these discussions offer an opportunity for the physician to align his or her goals and understanding with those of the patient and family. Specifically, these discussions are a chance to demonstrate a desire to understand the patient's individualized goals and to share concerns about disease progression. In essence, it is a valuable opportunity to establish a collective understanding about the patient's current situation while also laying important groundwork for future discussions.
Mr. C tearfully shared his concern about being a burden to his wife and about how his daughters would handle his progressive decline. Dr. A sat quietly, allowed Mr. C to fully detail his worries, and then said, “I can see how worried you are about your family and understand that you want to make sure that their needs are also addressed.”
Step 6: Summarize the Discussion and Strategize Next Steps
In all stages of cancer, patients and families rely on their oncologist for information about treatment options. This is particularly important when a patient's cancer has progressed despite therapy and when the focus of care may be shifting from disease-directed therapies to palliation. Just as a physician may have previously recommended a chemotherapeutic option for a patient, so should he or she recommend the therapeutic option of focusing on quality of life. If hospice appears consistent with the patient's and family's goals and needs, the physician should make this recommendation. It may be helpful for the patient and family to hear a summary of how hospice will meet their needs. If the patient is amenable to learning more about hospice but is not yet ready to enroll, the physician can arrange for an informational visit with the hospice team.
Dr. A recommends hospice and emphasizes that hospice would provide services that meet Mr. C's goals of symptom management, avoiding hospitalizations, and providing support for his family. Mr. C and his wife agree that hospice is the best option for them. They would like to enroll after they have spoken with their children about their decision.
Conclusion
Discussions about goals of care and hospice are not easy. They are rarely as straightforward as presented in this case, and an oncologist may face numerous barriers when attempting to have these discussions. For instance, treating physicians may have differing opinions on therapeutic options. Patients and family members may have different goals and may be in different stages of accepting a life-limiting cancer diagnosis. Additionally, these discussions take preparation, time, and skill. Although there are no easy solutions to these issues, the general guidance provided in this article focuses on suggesting tools and techniques that can make these discussions easier for oncologists, patients, and families. By increasing our competence and comfort with these conversations, we can reduce delays in offering patients the benefits of hospice as they near the end of life.
Although no algorithm will fully address the complexities and nuances of these conversations, this approach provides a general framework and offers tools to use while speaking with patients and families. Conversations about hospice do not begin with the recommendation of hospice but rather with an honest discussion of the goals and needs of a patient and family. If these goals and needs can be met with the services that hospice can provide, the physician has the opportunity to educate the patient and to make the recommendation as they would for any other therapeutic option.
Patients and families consider communication to be one of the most important facets of end-of-life care.24 Seriously ill patients value being able to prepare for death,13 and physicians have the duty to help patients and families prepare for the end of life.25 Physicians can help increase the time patients have to plan for the last phase of their lives by having honest and open discussions about hospice and other alternatives. Oncologists have the responsibility to present patients with the benefits and burdens of therapies throughout the trajectory of their illness, and it is critically important during the transition from disease-directed to palliative care. By exploring the option of hospice, patients and families can make informed decisions about whether hospice may meet their needs. Equally important, patients are given the control to choose how they would like to live the final phase of their lives.
References1
1 J.M. Teno, B.R. Clarridge, V. Casey, L.C. Welch, T. Wetle, R. Shield and V. Mor, Family perspectives on end-of-life care at the last place of care, JAMA 291 (1) (2004), pp. 88–93. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (411)
2 S.C. Miller, V. Mor and J. Teno, Hospice enrollment and pain assessment and management in nursing homes, J Pain Symptom Manage 26 (3) (2003), pp. 791–799. Article |
3 National Hospice and Palliative Care Organization, NHPCO Facts and Figures: Hospice Care in America www.nhpco.org/files/public/Statistics_Research/Hospice_Facts_Figures_Oct-2010.pdf+NHPCO+Facts+and+Figures:+Hospice+Care+in+America.+National+Hospice+and+Palliative+Care+Organization&hl=en&gl=us&pid=bl&srcid=ADGEESgPEeCPa2C7KZ3zQT0yldBWHrCAHY4UemVw6R1Odl2VxMKsjrMnNridOO3qiHrvN9cAfwCzkIY3Mc28JRgBLdvCaN3nQXt7EUNL6H-PTkYYaVAl4-VECDAsh16DvmofChWiLRfa&sig=AHIEtbTMY3LallQ5V2Ceyd_ACIQfUh-ggA (2010).
4 A.A. Wright, B. Zhang, A. Ray, J.W. Mack, E. Trice, T. Balboni, S.L. Mitchell, V.A. Jackson, S.D. Block, P.K. Maciejewski and H.G. Prigerson, Associations between end-of-life discussions, patient mental health, medical care near death, and caregiver bereavement adjustment, JAMA 300 (14) (2008), pp. 1665–1673. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (131)
5 E.H. Bradley, H. Prigerson, M.D.A. Carlson, E. Cherlin, R. Johnson-Hurzeler and S.V. Kasl, Depression among surviving caregivers: does length of hospice enrollment matter?, Am J Psychiatry 161 (12) (2004), pp. 2257–2262. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (29)
6 I.R. Byock, W.B. Forman and M. Appleton, Academy of hospice physicians' position statement on access to hospice and palliative care, J Pain Symptom Manage 11 (2) (1996), pp. 69–70. Article |
7 E. Cherlin, T. Fried, H.G. Prigerson, D. Schulman-Green, R. Johnson-Hurzeler and E.H. Bradley, Communication between physicians and family caregivers about care at the end of life: when do discussions occur and what is said?, J Palliat Med 8 (6) (2005), pp. 1176–1185. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (51)
8 D.J. Casarett and T.E. Quill, “I'm not ready for hospice”: strategies for timely and effective hospice discussions, Ann Intern Med 146 (6) (2007), pp. 443–449. View Record in Scopus | Cited By in Scopus (36)
9 E.B. Lamont and N.A. Christakis, Prognostic disclosure to patients with cancer near the end of life, Ann Intern Med 134 (12) (2001), pp. 1096–1105. View Record in Scopus | Cited By in Scopus (166)
10 M. Gysels, A. Richardson and I.J. Higginson, Communication training for health professionals who care for patients with cancer: a systematic review of effectiveness, Support Care Cancer 12 (10) (2004), pp. 692–700. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (41)
11 H.A. Huskamp, N.L. Keating, J.L. Malin, A.M. Zaslavsky, J.C. Weeks, C.C. Earle, J.M. Teno, B.A. Virnig, K.L. Kahn, Y. He and J.Z. Ayanian, Discussions with physicians about hospice among patients with metastatic lung cancer, Arch Intern Med 169 (10) (2009), pp. 954–962. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (4)
12 K.E. Steinhauser, N.A. Christakis, E.C. Clipp, M. McNeilly, S. Grambow, J. Parker and J.A. Tulsky, Preparing for the end of life: preferences of patients, families, physicians, and other care providers, J Pain Symptom Manage 22 (3) (2001), pp. 727–737. Article |
13 K.E. Steinhauser, N.A. Christakis, E.C. Clipp, M. McNeilly, L. McIntyre and J.A. Tulsky, Factors considered important at the end of life by patients, family, physicians, and other care providers, JAMA 284 (19) (2000), pp. 2476–2482. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (615)
14 A.L. Back, R.M. Arnold, W.F. Baile, K.A. Fryer-Edwards, S.C. Alexander, G.E. Barley, T.A. Gooley and J.A. Tulsky, Efficacy of communication skills training for giving bad news and discussing transitions to palliative care, Arch Intern Med 167 (5) (2007), pp. 453–460. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (94)
15 A.L. Back, R.M. Arnold, W.F. Baile, J.A. Tulsky and K. Fryer-Edwards, Approaching difficult communication tasks in oncology, CA Cancer J Clin 55 (3) (2005), pp. 164–177. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (103)
16 C. Conill, E. Verger and M. Salamero, Performance status assessment in cancer patients, Cancer 65 (8) (1990), pp. 1864–1866. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (81)
17 V. Mor, L. Laliberte, J.N. Morris and M. Wiemann, The Karnofsky Performance Status Scale: An examination of its reliability and validity in a research setting, Cancer 53 (9) (1984), pp. 2002–2007. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (314)
18 W.F. Baile, R. Buckman, R. Lenzi, G. Glober, E.A. Beale and A.P. Kudelka, SPIKES—a six-step protocol for delivering bad news: application to the patient with cancer, Oncologist 5 (4) (2000), pp. 302–311. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (293)
19 J.C. Weeks, E.F. Cook, S.J. O'Day, L.M. Peterson, N. Wenger, D. Reding, F.E. Harrell, P. Kussin, N.V. Dawson, A.F. Connors, J. Lynn and R.S. Phillips, Relationship between cancer patients' predictions of prognosis and their treatment preferences, JAMA 279 (21) (1998), pp. 1709–1714. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (350)
20 D.J. Casarett, R.L. Crowley and K.B. Hirschman, How should clinicians describe hospice to patients and families?, J Am Geriatr Soc 52 (11) (2004), pp. 1923–1928. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (46)
21 S.M. Parker, J.M. Clayton, K. Hancock, S. Walder, P.N. Butow, S. Carrick, D. Currow, D. Ghersi, P. Glare, R. Hagerty and M.H. Tattersall, A systematic review of prognostic/end-of-life communication with adults in the advanced stages of a life-limiting illness: patient/caregiver preferences for the content, style, and timing of information, J Pain Symptom Manage 34 (1) (2007), pp. 81–93. Article |
22 K.I. Pollak, R.M. Arnold, A.S. Jeffreys, S.C. Alexander, M.K. Olsen, A.P. Abernethy, C. Sugg Skinner, K.L. Rodriguez and J.A. Tulsky, Oncologist communication about emotion during visits with patients with advanced cancer, J Clin Oncol 25 (36) (2007), pp. 5748–5752. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (47)
23 A.L. Back, W.G. Anderson, L. Bunch, L.A. Marr, J.A. Wallace, H.B. Yang and R.M. Arnold, Communication about cancer near the end of life, Cancer 113 (suppl 7) (2008), pp. 1897–1910. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (12)
24 M.D. Wenrich, J.R. Curtis, S.E. Shannon, J.D. Carline, D.M. Ambrozy and P.G. Ramsey, Communicating with dying patients within the spectrum of medical care from terminal diagnosis to death, Arch Intern Med 161 (6) (2001), pp. 868–874. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (114)
25 J. Lynn, Perspectives on care at the close of life: Serving patients who may die soon and their families: the role of hospice and other services, JAMA 285 (7) (2001), pp. 925–932. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (124)
Vitae
Dr. Shin is from the Division of Hematology–Oncology, University of Pennsylvania School of Medicine, Philadelphia
Dr. Casarett is from the Division of Geriatric Medicine and the Penn-Wissahickon Hospice, University of Pennsylvania School of Medicine, Philadelphia
How we do it
Jennifer Shin MD![]()
![]()
Abstract
Hospice programs provide comprehensive, compassionate care to dying patients and their families. However, many patients do not enroll in hospice, and those who do generally receive hospice care only in the last weeks of life. Although patients and families rely on their physicians to discuss hospice, there is often inadequate communication between patients and physicians about end-of-life issues. We describe a Six-Step Roadmap for navigating discussions about hospice adapted from the SPIKES protocol for delivering bad news: setting up the discussion, assessing the patient’s perception, inviting a patient to discuss individual goals and needs, sharing knowledge, empathizing with the patient’s emotions, and summarizing and strategizing the next steps.
Article Outline
- A Six-Step Roadmap
- Step 1: Set Up the Discussion About Hospice
- Step 2: Assess the Patient's Perception
- Step 3: Invite the Patient to Discuss Goals of Care and Needs for Care
- Step 4: Share Knowledge
- Step 5: Empathize With the Patient's Emotion
- Step 6: Summarize the Discussion and Strategize Next Steps
Case
Mr. C is a 54-year-old man with metastatic lung adenocarcinoma who presented 1 year ago with multiple lung nodules and hepatic metastases. His tumor responded to initial treatment with four cycles of carboplatin and pemetrexed, and he was treated with maintenance pemetrexed for 5 months before his liver lesions progressed. Despite treatment with docetaxel and then erlotinib, his liver and lung tumors progressed rapidly. He has lost 10 pounds in the last few weeks and is now so fatigued that he spends most of his day resting in his recliner. He has been admitted to the hospital twice in the last month for worsening dyspnea in the setting of progressive pulmonary metastases.
Introduction
Hospice programs provide high-quality, compassionate care to dying patients and their families through an interdisciplinary team specializing in pain and symptom management.[1] and [2] These patients also receive medications and supplies, durable medical equipment, and home health aide services. Patients and their families receive support from a chaplain, social worker, physician, nurse, and volunteer. Families are offered bereavement services for at least 13 months following the patient's death (Table 1).3
| Services |
| • Pain and symptom management |
| • 24-hour telephone access to a clinician |
| • Assistance with personal care needs |
| • Help with errands and light housework |
| • Spiritual support |
| • Companionship for the patient and family |
| • Bereavement counseling before and after the patient's death |
| • Patient and family education and counseling |
| • Case management and coordination |
| • Advance care planning |
| • Medications and supplies related to the hospice diagnosis |
| • Durable medical equipment |
| • Child bereavement services |
| • Respite services (up to 5 consecutive days of inpatient care to allow families a needed break) |
| • Inpatient hospice (for treatment of severe symptoms that cannot be managed at home) |
| Team members |
| • Physician |
| • Nurse |
| • Social worker |
| • Home health aide |
| • Chaplain |
| • Bereavement counselor |
| • Physical therapist |
| • Occupational therapist |
| • Volunteer |
National Hospice and Palliative Care Organization. NHPCO Facts and Figures: Hospice Care in America.3
Families report high levels of satisfaction with hospice and are more likely to describe high-quality care.1 Despite this, only 40% of people in the United States die while receiving hospice care.3 Although longer hospice stays are associated with better quality of life in patients and less depression in bereaved family members,[4] and [5] many patients enroll very late in the course of illness. In fact, the median length of stay is just over 3 weeks, and a third of patients die or are discharged within 1 week of hospice enrollment.3 The result is that brief exposures to hospice at the end of life do not allow patients and families to take full advantage of the benefits.6
There are several explanations for why people enroll in hospice so late. The Medicare Hospice Benefit requires hospice patients to choose a plan of comfort care, which means that they must usually forgo disease-directed therapies unless they provide a specific palliative benefit. Furthermore, the financial per diem payment structure of hospice means that patients may need to forgo palliative treatments that cannot be covered under the typical hospice reimbursement (approximately $150/day for routine home care). Patients may not be willing to give up these therapies or may be reluctant to transition from a model of care focusing on disease-directed therapies to one with palliation as the goal.
Patients may also enroll in hospice later if their physicians do not discuss hospice or if they have these discussions in the last few weeks of the patient's life.[7] and [8] Physicians may delay hospice discussions because they are unsure of the patient's prognosis,9 although the disease trajectory in patients with cancer is often more straightforward than in patients with non-oncologic diagnoses. Studies have documented deficiencies in doctor–patient communication regarding prognosis and end-of-life issues,10 and patients report inadequate communication with physicians about shared decision making at the end of life.1 Another study found that about half of patients diagnosed with metastatic lung cancer reported not having discussed hospice with a provider within 4–7 months after diagnosis.11
Although these discussions may be delayed or avoided altogether, seriously ill patients value the ability to prepare for the end of life.[12] and [13] Patients rely on their physicians to discuss hospice and other end-of-life care options. Furthermore, most family caregivers report that communication with their oncologists was important in helping them to understand the patient's prognosis and to see the role that hospice could play as a treatment alternative.7
These conversations are often difficult for patients and families and can also be challenging for physicians. Nevertheless, communication skills in discussing transitions to palliative care can be learned.[14] and [15] Although these discussions are not nearly as straightforward as a medical or surgical procedure, one can approach them with the same methodical preparation and careful consideration of the steps involved.
When Is a Hospice Discussion Appropriate?
To be eligible for the Medicare Hospice Benefit, a patient must have a prognosis of 6 months or less if his or her illness runs its usual course; also, the patient needs to be willing to accept the hospice philosophy of comfort care. This second criterion is not formally defined but is generally accepted to mean that the patient must be willing to forgo disease-directed therapies related to the hospice admitting diagnosis.
These eligibility criteria should not be used to define the patients for whom a hospice discussion is appropriate however. When a patient's goals and values reflect a desire to focus on palliation, it is time for the physician to initiate a hospice discussion. Other triggers for early hospice discussions can include a change in clinical status, recent hospitalization, decline in performance status, new weight loss, or complication of treatment. Although these factors may prompt a discussion of options for care, including hospice,[16] and [17] not all discussions will lead to a hospice enrollment decision. Nevertheless, earlier discussions that prompt conversations about a patient's needs, goals, and preferences can facilitate later decisions about hospice and other treatment options.
A Six-Step Roadmap
We provide a Six-Step Roadmap for navigating discussions about hospice adapted from the SPIKES protocol for delivering bad news.18 This strategy is comprised of six communication steps that can be remembered by using the mnemonic SPIKES: setting up the discussion, assessing the patient's perception, inviting a patient to discuss individual goals and needs, sharing knowledge, empathizing with the patient's emotions, and summarizing and strategizing the next steps.
Step 1: Set Up the Discussion About Hospice
Before discussing hospice with a patient and family, it is important to communicate with other members of the medical team to ensure an understanding of the patient's prognosis and treatment options. It is also helpful to find out what the patient and family may have expressed to other providers regarding these issues and how they have been coping. Any provider who has been in contact with the patient may be able to contribute to this consensus, including the medical oncologist, radiation oncologist, palliative care physician, primary care physician, home nurse, and social worker. A clear, unified message from the team decreases confusion for the patient and family.
Once a common agreement has been established regarding the patient's prognosis and treatment options, physicians can schedule a time and arrange for a place to allow for an uninterrupted conversation. Scheduling a patient at the end of a clinic day or visiting a patient in the hospital during an admission are potential ways to do this. Before scheduling a meeting, however, it is essential to know who the patient would like to be present at the meeting. One approach may be to tell the patient that there are important options to discuss regarding the next steps in his or her care and find out who may be able to help the patient with such decisions (Table 2). Additionally, a palliative care physician may cofacilitate these discussions. If the patient already has a palliative care physician, it may be helpful to have him or her involved in the meeting. If the patient has not yet been evaluated by a palliative care team, it may be possible to consult a palliative care specialist who can attend the meeting or follow up with the patient afterward.
Adapted from Cassett et al8 and Baille et al15
| Invite other decision makers | “Who do you usually rely on to help you make important decisions?” “When we discuss your results, who would you like to be present?” |
| Assess understanding of prognosis | “Tell me about your understanding of the most recent tests/studies.” “Can you share with me what you think is happening with your cancer and the treatments?” |
| Identify goals of care | “What is most important to you right now?” “What are your biggest concerns right now?” “What are your hopes for the coming weeks/months?” “What do you enjoy doing now?” “What is most important to you now?” “What are you worried about now? In the future?” |
| Reframe goals (“wish” statements) | “I wish I could promise you that you will be able to make it to your daughter's wedding, but unfortunately I can't. What do you think about writing a letter for her to read on her wedding day? We can also think about other ways to let her know that you will always be with her, even if you cannot physically be there.” “I wish that we could find a new chemotherapy that could cure your cancer. Even though cure is not possible, I think that we can meet some of your other goals, like staying at home to spend time with your children.” |
| Identify needs for care | “What has been hard for you and your family?” “What is your life like when you are at home? How are you and your family managing?” “Are you experiencing pain or other symptoms that are bothering you?” “Have you been feeling sad or anxious lately?” “Would it be helpful to have a visiting nurse come to your home to assist you with your medications?” |
| Introduce hospice | “One of the best ways to give you the help that you need to stay at home is through hospice.” “The hospice team specializes in caring for seriously ill patients at home.” “Hospice can provide you and your family with more services and support.” |
| Recommend hospice | “From what you have shared with me today, I recommend hospice as a way of helping you meet the goals that are important to you.” “I feel that hospice is the best option for you and your family. I know this is a big decision, and I want you to know that the decision is yours.” |
Mr. C's medical oncologist, Dr. A, contacted Mr. C's radiation oncologist as well as his primary care physician. They all agreed that his prognosis could be measured in weeks to months and that his performance status precluded any further chemotherapy. Dr. A also spoke with the hospital social worker who met Mr. C and his wife during his most recent hospitalization. The social worker said that Mr. C's wife has been very distressed, particularly about his increasing debility and her difficulty in caring for him at home. When Dr. A visited Mr. C during his hospitalization, Dr. A explained to Mr. C that they would be making some decisions about the next steps in his care and asked who might be able to help with these decisions. When Mr. C said his wife would be this person, Dr. A asked that she come to his next visit. Dr. A decided to schedule Mr. C for an appointment at the end of his clinic session the following week.
Step 2: Assess the Patient's Perception
The physician can begin this discussion by asking the patient to describe his or her current medical situation (Table 2). Although the physician may have provided this information on prior occasions, it is important to hear the patient's perception of the diagnosis and prognosis. Patients with advanced cancer often overestimate their prognosis and are more likely to favor life-extending therapies over hospice.19 These questions provide an opportunity to address any misconceptions or gaps in understanding that the patient may have. When the physician, patient, and family are in agreement with the patient's current medical situation it allows for further exploration of the patient's hopes and concerns.
This part of the discussion should rely on open-ended questions designed to elicit the patient's perspective. In particular, an invitation to “tell me more” encourages patients to explore how they are thinking or feeling and can yield more information than closed-ended or leading questions. This phrase can also help redirect the conversation when necessary (“You mentioned before that you are worried that the chemotherapy is not working anymore. Tell me more about your concerns.”).
Dr. A asked Mr. C how he was doing overall and to describe his understanding of whether the erlotinib had been working. In response, Mr. C expressed his concern about his recent weight loss and lethargy. Dr. A asked Mr. C to tell him more about these concerns, and Mr. C said that he thought his symptoms were a sign that the erlotinib was not helping him. He said he knew that the CT scans showed progression of disease, and he wondered whether chemotherapy could help. Dr. A confirmed there was progression of cancer in his lungs and liver. Dr. A also expressed his concern that more chemotherapy would not provide additional benefit for him and may harm him. Mr. C and his wife were tearful and agreed that he was too weak for more chemotherapy. Dr. A acknowledged that the disease had progressed quickly and must be very upsetting to them.
Step 3: Invite the Patient to Discuss Goals of Care and Needs for Care
Before sharing information about hospice with a patient, it is important to understand the patient's hopes and fears about the future, goals of care, and needs for care. It is helpful to start with learning about the patient's perspectives on the future and linking that to the patient's goals of care. Once the goals are clear, it is easier to match the patient's needs with his or her goals.
One way to elicit patients' goals of care is by asking them to describe their hopes and fears about their cancer in the context of their life (Table 2). Patients may volunteer information about their hopes (eg, attending their daughter's wedding) or fears (eg, worrying about pain) that provide insight into their more global goals of care. Again, the “tell me more” phrase can be helpful (“Tell me more about what you mean when you say you are a burden on your family.”).
Once the patient and family express their thoughts, it is useful to restate the patient's goals by asking a question that summarizes the patient's statements (“From what you and your family have just shared with me, I hear that the most important thing to you is … . Did I understand you correctly?”). It is often challenging for patients to specifically articulate their goals of care. Asking a question allows the patient and family the chance to elaborate or offer corrections.
If a patient expresses unrealistic expectations (eg, a cure, years of life), “wish” statements can be helpful in providing gentle redirection. These statements express empathy while also communicating that the wished-for outcome is unlikely (“I wish that we could guarantee that … but unfortunately we can't.”). These statements can explain the reality of the situation in a compassionate manner (Table 2). Patients and families who have unrealistic goals of care may need time to readjust their expectations, and in these cases it may be prudent to revisit the discussion of hospice at a later date.
Once the goals of care have been established, it is important to further explore the needs for care. Although some of these needs may have been mentioned during the goals discussion, it is helpful to directly ask the patient and family about their needs. General questions about what has been hard for the patient and the family can be useful in eliciting needs, as are questions about what life has been like at home and how they are managing (Table 2). It is also important to ask more specific questions that pertain to the patient's symptoms such as pain or depression and those that address the family's needs for help around the house (Table 2). Once this information has been shared, it is often useful to repeat a summary back to the patient and family (“From what we have just discussed, it may be helpful to have a visiting nurse to assist with his medications and a home health aide to dress and bathe him … . Does it sound like this could be helpful to you?”). Often, these needs can be addressed by the multidisciplinary hospice team, and it is important to understand what needs exist in preparation for a discussion about how hospice might be helpful.
Mr. C shares with you that his two hospitalizations for dyspnea have been frustrating because he feels that they have prevented him from spending quality time with his daughters. Although he did not want to be admitted to the hospital, he tearfully expressed that he was worried about “suffocating to death” and did not want to die at home in front of his wife and children. Mr. C's wife also shares that it has been harder to bathe and dress him because he is becoming so weak. Mr. and Mrs. C agree that it would be helpful to have the support of a visiting nurse and a home health aide.
Step 4: Share Knowledge
Once the patient's goals and needs for care have been clarified, physicians can introduce hospice as a way of achieving their goals and meeting their needs. In presenting hospice in this transparent manner, patients and families can better understand how hospice is part of a plan of care that addresses their individualized goals and needs. Most family caregivers report that communication with their oncologists was critical in their understanding the patient's prognosis and hospice as a treatment alternative.7 In one survey, the majority of caregivers did not realize that their loved ones could benefit from hospice until their physicians first discussed it with them.7
A discussion of hospice should offer concrete information about the services provided to patients and their families (Table 1). Many patients and families do not understand the benefits, such as a visiting nurse for frequent symptom management or a home health aide to assist with daily patient care, until after enrollment. Many say they wish they had known sooner.20 By providing this information earlier, patients and families may make more informed decisions about hospice. This description also makes clear to the patient and family that hospice is not simply a generic recommendation but rather the physician's recommendation of a program that is the best fit for their specific goals and needs.
Given the emotional nature of these discussions and the large amount of information involved, it is important to ask the patient to explain in his or her own words how hospice could help (“To make sure I did a good job of explaining things, can you tell me what we just talked about in your own words?” and “How do you think hospice might help you?”). This provides the opportunity to assess understanding and clarify any confusion.
Since not all patients are best served by hospice, the discussion may also be expanded to include other options for palliative care. For example, hospice is not equipped to care for debilitated patients at home who do not have a caretaker, nor is it usually able to absorb the costs of expensive palliative treatments. Sometimes, larger hospices may be able to make exceptions on a case-by-case basis, but it is helpful to be aware of other options for palliative care like bridge-to-hospice home care and outpatient palliative care programs.
Dr. A explained that hospice could provide intensive management of his dyspnea with the assistance of a visiting nurse and a 24-hour phone line to call for assistance. With these measures in place, Dr. A said that he hoped hospitalizations could be avoided, allowing him more time at home with his family. Dr. A addressed Mr. C's concern about dying at home and shared with him that he could be transferred to an inpatient hospice if death seemed imminent. Dr. A shared with Mrs. C that hospice could provide the services of a home health aide, which seemed to reduce her concerns about being able to care for her husband as he became weaker.
Step 5: Empathize With the Patient's Emotion
In discussions regarding end-of-life care, patients and families value empathy, compassion, and honesty balanced with sensitivity and hope.21 Throughout the conversation, it is likely that the patient and family will express a range of emotions. Rather than providing immediate reassurance or trying to “fix” the emotion, it can be helpful to use an empathic statement to let the patient know that his or her emotions are recognized.15 Empathic responses address and validate a patient's emotions and encourage further disclosure.22 The NURSE mnemonic summarizes ways in which to respond to emotions: naming, understanding, respecting, supporting, and exploring the feelings the patient has shared (Table 3).[15] and [23]
Adapted from Back et al[15] and [23]
| N = Naming | “It sounds like you are worried about how fast the cancer has been progressing.” “Some people in this situation would feel frustrated.” |
| U = Understanding | “My understanding of what you have told me is that you are worried about being able to live independently at home.” “I can see how difficult this has been for you and your family.” |
| R = Respecting | “It is very clear to me how supportive your family has been.” “I can see how hard you have worked to understand the treatment options for your cancer.” |
| S = Supporting | “I will support the decisions that you make, no matter what you decide.” “I will always be your doctor.” |
| E = Exploring | “Could you tell me more about what you mean when you say that you don't want to give up?” “I sense that you may be feeling anxious about stopping chemotherapy. Can you share with me what you are feeling?” |
Some of the emotions arising during a hospice discussion may stem from preconceived notions or a prior experience. Therefore, it may be helpful to specifically ask patients and families about these perceptions and experiences. Common misperceptions may include the concern that hospice hastens death. Other patients view hospice as “giving up” and worry about being abandoned by their physicians. A hospice discussion provides the opportunity to directly address these concerns and provide clarification (“No, hospice does not hasten death. Hospice helps you have the best quality of life for whatever time you have.”).
Ultimately, some patients and families may decide that hospice is not the right choice for them. It is important to recognize that the time invested has not been wasted. Instead, if done well, these discussions offer an opportunity for the physician to align his or her goals and understanding with those of the patient and family. Specifically, these discussions are a chance to demonstrate a desire to understand the patient's individualized goals and to share concerns about disease progression. In essence, it is a valuable opportunity to establish a collective understanding about the patient's current situation while also laying important groundwork for future discussions.
Mr. C tearfully shared his concern about being a burden to his wife and about how his daughters would handle his progressive decline. Dr. A sat quietly, allowed Mr. C to fully detail his worries, and then said, “I can see how worried you are about your family and understand that you want to make sure that their needs are also addressed.”
Step 6: Summarize the Discussion and Strategize Next Steps
In all stages of cancer, patients and families rely on their oncologist for information about treatment options. This is particularly important when a patient's cancer has progressed despite therapy and when the focus of care may be shifting from disease-directed therapies to palliation. Just as a physician may have previously recommended a chemotherapeutic option for a patient, so should he or she recommend the therapeutic option of focusing on quality of life. If hospice appears consistent with the patient's and family's goals and needs, the physician should make this recommendation. It may be helpful for the patient and family to hear a summary of how hospice will meet their needs. If the patient is amenable to learning more about hospice but is not yet ready to enroll, the physician can arrange for an informational visit with the hospice team.
Dr. A recommends hospice and emphasizes that hospice would provide services that meet Mr. C's goals of symptom management, avoiding hospitalizations, and providing support for his family. Mr. C and his wife agree that hospice is the best option for them. They would like to enroll after they have spoken with their children about their decision.
Conclusion
Discussions about goals of care and hospice are not easy. They are rarely as straightforward as presented in this case, and an oncologist may face numerous barriers when attempting to have these discussions. For instance, treating physicians may have differing opinions on therapeutic options. Patients and family members may have different goals and may be in different stages of accepting a life-limiting cancer diagnosis. Additionally, these discussions take preparation, time, and skill. Although there are no easy solutions to these issues, the general guidance provided in this article focuses on suggesting tools and techniques that can make these discussions easier for oncologists, patients, and families. By increasing our competence and comfort with these conversations, we can reduce delays in offering patients the benefits of hospice as they near the end of life.
Although no algorithm will fully address the complexities and nuances of these conversations, this approach provides a general framework and offers tools to use while speaking with patients and families. Conversations about hospice do not begin with the recommendation of hospice but rather with an honest discussion of the goals and needs of a patient and family. If these goals and needs can be met with the services that hospice can provide, the physician has the opportunity to educate the patient and to make the recommendation as they would for any other therapeutic option.
Patients and families consider communication to be one of the most important facets of end-of-life care.24 Seriously ill patients value being able to prepare for death,13 and physicians have the duty to help patients and families prepare for the end of life.25 Physicians can help increase the time patients have to plan for the last phase of their lives by having honest and open discussions about hospice and other alternatives. Oncologists have the responsibility to present patients with the benefits and burdens of therapies throughout the trajectory of their illness, and it is critically important during the transition from disease-directed to palliative care. By exploring the option of hospice, patients and families can make informed decisions about whether hospice may meet their needs. Equally important, patients are given the control to choose how they would like to live the final phase of their lives.
References1
1 J.M. Teno, B.R. Clarridge, V. Casey, L.C. Welch, T. Wetle, R. Shield and V. Mor, Family perspectives on end-of-life care at the last place of care, JAMA 291 (1) (2004), pp. 88–93. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (411)
2 S.C. Miller, V. Mor and J. Teno, Hospice enrollment and pain assessment and management in nursing homes, J Pain Symptom Manage 26 (3) (2003), pp. 791–799. Article |
3 National Hospice and Palliative Care Organization, NHPCO Facts and Figures: Hospice Care in America www.nhpco.org/files/public/Statistics_Research/Hospice_Facts_Figures_Oct-2010.pdf+NHPCO+Facts+and+Figures:+Hospice+Care+in+America.+National+Hospice+and+Palliative+Care+Organization&hl=en&gl=us&pid=bl&srcid=ADGEESgPEeCPa2C7KZ3zQT0yldBWHrCAHY4UemVw6R1Odl2VxMKsjrMnNridOO3qiHrvN9cAfwCzkIY3Mc28JRgBLdvCaN3nQXt7EUNL6H-PTkYYaVAl4-VECDAsh16DvmofChWiLRfa&sig=AHIEtbTMY3LallQ5V2Ceyd_ACIQfUh-ggA (2010).
4 A.A. Wright, B. Zhang, A. Ray, J.W. Mack, E. Trice, T. Balboni, S.L. Mitchell, V.A. Jackson, S.D. Block, P.K. Maciejewski and H.G. Prigerson, Associations between end-of-life discussions, patient mental health, medical care near death, and caregiver bereavement adjustment, JAMA 300 (14) (2008), pp. 1665–1673. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (131)
5 E.H. Bradley, H. Prigerson, M.D.A. Carlson, E. Cherlin, R. Johnson-Hurzeler and S.V. Kasl, Depression among surviving caregivers: does length of hospice enrollment matter?, Am J Psychiatry 161 (12) (2004), pp. 2257–2262. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (29)
6 I.R. Byock, W.B. Forman and M. Appleton, Academy of hospice physicians' position statement on access to hospice and palliative care, J Pain Symptom Manage 11 (2) (1996), pp. 69–70. Article |
7 E. Cherlin, T. Fried, H.G. Prigerson, D. Schulman-Green, R. Johnson-Hurzeler and E.H. Bradley, Communication between physicians and family caregivers about care at the end of life: when do discussions occur and what is said?, J Palliat Med 8 (6) (2005), pp. 1176–1185. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (51)
8 D.J. Casarett and T.E. Quill, “I'm not ready for hospice”: strategies for timely and effective hospice discussions, Ann Intern Med 146 (6) (2007), pp. 443–449. View Record in Scopus | Cited By in Scopus (36)
9 E.B. Lamont and N.A. Christakis, Prognostic disclosure to patients with cancer near the end of life, Ann Intern Med 134 (12) (2001), pp. 1096–1105. View Record in Scopus | Cited By in Scopus (166)
10 M. Gysels, A. Richardson and I.J. Higginson, Communication training for health professionals who care for patients with cancer: a systematic review of effectiveness, Support Care Cancer 12 (10) (2004), pp. 692–700. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (41)
11 H.A. Huskamp, N.L. Keating, J.L. Malin, A.M. Zaslavsky, J.C. Weeks, C.C. Earle, J.M. Teno, B.A. Virnig, K.L. Kahn, Y. He and J.Z. Ayanian, Discussions with physicians about hospice among patients with metastatic lung cancer, Arch Intern Med 169 (10) (2009), pp. 954–962. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (4)
12 K.E. Steinhauser, N.A. Christakis, E.C. Clipp, M. McNeilly, S. Grambow, J. Parker and J.A. Tulsky, Preparing for the end of life: preferences of patients, families, physicians, and other care providers, J Pain Symptom Manage 22 (3) (2001), pp. 727–737. Article |
13 K.E. Steinhauser, N.A. Christakis, E.C. Clipp, M. McNeilly, L. McIntyre and J.A. Tulsky, Factors considered important at the end of life by patients, family, physicians, and other care providers, JAMA 284 (19) (2000), pp. 2476–2482. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (615)
14 A.L. Back, R.M. Arnold, W.F. Baile, K.A. Fryer-Edwards, S.C. Alexander, G.E. Barley, T.A. Gooley and J.A. Tulsky, Efficacy of communication skills training for giving bad news and discussing transitions to palliative care, Arch Intern Med 167 (5) (2007), pp. 453–460. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (94)
15 A.L. Back, R.M. Arnold, W.F. Baile, J.A. Tulsky and K. Fryer-Edwards, Approaching difficult communication tasks in oncology, CA Cancer J Clin 55 (3) (2005), pp. 164–177. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (103)
16 C. Conill, E. Verger and M. Salamero, Performance status assessment in cancer patients, Cancer 65 (8) (1990), pp. 1864–1866. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (81)
17 V. Mor, L. Laliberte, J.N. Morris and M. Wiemann, The Karnofsky Performance Status Scale: An examination of its reliability and validity in a research setting, Cancer 53 (9) (1984), pp. 2002–2007. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (314)
18 W.F. Baile, R. Buckman, R. Lenzi, G. Glober, E.A. Beale and A.P. Kudelka, SPIKES—a six-step protocol for delivering bad news: application to the patient with cancer, Oncologist 5 (4) (2000), pp. 302–311. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (293)
19 J.C. Weeks, E.F. Cook, S.J. O'Day, L.M. Peterson, N. Wenger, D. Reding, F.E. Harrell, P. Kussin, N.V. Dawson, A.F. Connors, J. Lynn and R.S. Phillips, Relationship between cancer patients' predictions of prognosis and their treatment preferences, JAMA 279 (21) (1998), pp. 1709–1714. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (350)
20 D.J. Casarett, R.L. Crowley and K.B. Hirschman, How should clinicians describe hospice to patients and families?, J Am Geriatr Soc 52 (11) (2004), pp. 1923–1928. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (46)
21 S.M. Parker, J.M. Clayton, K. Hancock, S. Walder, P.N. Butow, S. Carrick, D. Currow, D. Ghersi, P. Glare, R. Hagerty and M.H. Tattersall, A systematic review of prognostic/end-of-life communication with adults in the advanced stages of a life-limiting illness: patient/caregiver preferences for the content, style, and timing of information, J Pain Symptom Manage 34 (1) (2007), pp. 81–93. Article |
22 K.I. Pollak, R.M. Arnold, A.S. Jeffreys, S.C. Alexander, M.K. Olsen, A.P. Abernethy, C. Sugg Skinner, K.L. Rodriguez and J.A. Tulsky, Oncologist communication about emotion during visits with patients with advanced cancer, J Clin Oncol 25 (36) (2007), pp. 5748–5752. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (47)
23 A.L. Back, W.G. Anderson, L. Bunch, L.A. Marr, J.A. Wallace, H.B. Yang and R.M. Arnold, Communication about cancer near the end of life, Cancer 113 (suppl 7) (2008), pp. 1897–1910. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (12)
24 M.D. Wenrich, J.R. Curtis, S.E. Shannon, J.D. Carline, D.M. Ambrozy and P.G. Ramsey, Communicating with dying patients within the spectrum of medical care from terminal diagnosis to death, Arch Intern Med 161 (6) (2001), pp. 868–874. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (114)
25 J. Lynn, Perspectives on care at the close of life: Serving patients who may die soon and their families: the role of hospice and other services, JAMA 285 (7) (2001), pp. 925–932. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (124)
Vitae
Dr. Shin is from the Division of Hematology–Oncology, University of Pennsylvania School of Medicine, Philadelphia
Dr. Casarett is from the Division of Geriatric Medicine and the Penn-Wissahickon Hospice, University of Pennsylvania School of Medicine, Philadelphia
Pediatric Hospitalist Takes CMS Leadership Position
Patrick Conway, MD, MSc, SFHM, a pediatric hospitalist and director of hospital medicine at Cincinnati Children’s Hospital Medical Center, has been appointed chief medical officer of the Centers for Medicare & Medicaid Services (CMS). Dr. Conway’s key responsibilities will be administering federal healthcare quality initiatives and setting the government’s quality agenda.

— Patrick Conway, MD, MSc, SFHM, chief medical officer, Centers for Medicare & Medicaid Services
Dr. Conway, who previously served as CMO of the Policy Division of the Office of Secretary of Health and Human Services and was a 2007-2008 White House fellow assigned to the Agency for Healthcare Research and Quality (AHRQ), is a leader in safety, quality, and outcomes initiatives at Cincinnati Children’s, holds a voluntary faculty appointment at the University of Cincinnati, and is chair of SHM’s Public Policy Committee. In his new job, starting May 9, he will direct CMS’ Office of Clinical Standards and Quality.
“Dr. Conway’s passion for improving healthcare delivery systems, his day-to-day experience as a hospitalist physician, and his accomplishments in quality-improvement research, such as implementing evidence-based healthcare for all children, provide a strong background for his critical role at CMS as chief medical officer,” says colleague Arnold W. Strauss, MD, chair of pediatrics at the University of Cincinnati. “Dr. Conway and our colleagues at Cincinnati Children’s have demonstrated that improving patient outcomes at lower cost—the goal of healthcare reform—is feasible.”
At Cincinnati Children’s, Dr. Conway is an associate professor, associate vice president of outcomes performance, and director of Rapid Evidence Adoption in the James M. Anderson Center. He will give up these roles and his SHM committee chair to assume the federal position. He will maintain his position at the University of Cincinnati and will work some weekends seeing patients at Children’s National Medical Center in Washington, D.C. “I love patient care, so I don’t want to stop doing that. Plus, it helps me connect to the front lines of providing medical care,” Dr. Conway says.
Larry Wellikson, MD, SFHM, CEO of SHM, calls Dr. Conway a leader in the society and the field of HM. “Having Pat as the new CMO of CMS just further confirms the importance of hospital medicine to being central to the changes in our health system at a national level,” he says.
Dr. Conway’s role at CMS will include major components of surveys, certification, and accreditation issues for hospitals and other Medicare providers; healthcare information technology; and hospital value-based purchasing initiatives. But his initial priorities will focus on quality-measures development, illustrated by CMS’ Hospital Compare website, and quality improvement. Another major issue involves care transitions and readmissions, “which I try to frame positively—how can we have the most effective care transitions possible?” he says. “SHM and its publications have done a good job of stressing how hospitals and hospitalists can add value.”
Married with two children, Dr. Conway says he was not looking to move back inside the Beltway, even though he believes his experience at both the macro and micro levels of healthcare will benefit the overall system. “I actually think if we realign incentives, the system can perform better,” he says. “So I see it as an opportunity to perform a public service. But we also need front-line clinicians, including hospitalists, working to improve our healthcare system. … We need frontline providers that are measuring the quality of their care and improving it.”
Larry Beresford is a freelance writer based in California.
Patrick Conway, MD, MSc, SFHM, a pediatric hospitalist and director of hospital medicine at Cincinnati Children’s Hospital Medical Center, has been appointed chief medical officer of the Centers for Medicare & Medicaid Services (CMS). Dr. Conway’s key responsibilities will be administering federal healthcare quality initiatives and setting the government’s quality agenda.
— Patrick Conway, MD, MSc, SFHM, chief medical officer, Centers for Medicare & Medicaid Services
Dr. Conway, who previously served as CMO of the Policy Division of the Office of Secretary of Health and Human Services and was a 2007-2008 White House fellow assigned to the Agency for Healthcare Research and Quality (AHRQ), is a leader in safety, quality, and outcomes initiatives at Cincinnati Children’s, holds a voluntary faculty appointment at the University of Cincinnati, and is chair of SHM’s Public Policy Committee. In his new job, starting May 9, he will direct CMS’ Office of Clinical Standards and Quality.
“Dr. Conway’s passion for improving healthcare delivery systems, his day-to-day experience as a hospitalist physician, and his accomplishments in quality-improvement research, such as implementing evidence-based healthcare for all children, provide a strong background for his critical role at CMS as chief medical officer,” says colleague Arnold W. Strauss, MD, chair of pediatrics at the University of Cincinnati. “Dr. Conway and our colleagues at Cincinnati Children’s have demonstrated that improving patient outcomes at lower cost—the goal of healthcare reform—is feasible.”
At Cincinnati Children’s, Dr. Conway is an associate professor, associate vice president of outcomes performance, and director of Rapid Evidence Adoption in the James M. Anderson Center. He will give up these roles and his SHM committee chair to assume the federal position. He will maintain his position at the University of Cincinnati and will work some weekends seeing patients at Children’s National Medical Center in Washington, D.C. “I love patient care, so I don’t want to stop doing that. Plus, it helps me connect to the front lines of providing medical care,” Dr. Conway says.
Larry Wellikson, MD, SFHM, CEO of SHM, calls Dr. Conway a leader in the society and the field of HM. “Having Pat as the new CMO of CMS just further confirms the importance of hospital medicine to being central to the changes in our health system at a national level,” he says.
Dr. Conway’s role at CMS will include major components of surveys, certification, and accreditation issues for hospitals and other Medicare providers; healthcare information technology; and hospital value-based purchasing initiatives. But his initial priorities will focus on quality-measures development, illustrated by CMS’ Hospital Compare website, and quality improvement. Another major issue involves care transitions and readmissions, “which I try to frame positively—how can we have the most effective care transitions possible?” he says. “SHM and its publications have done a good job of stressing how hospitals and hospitalists can add value.”
Married with two children, Dr. Conway says he was not looking to move back inside the Beltway, even though he believes his experience at both the macro and micro levels of healthcare will benefit the overall system. “I actually think if we realign incentives, the system can perform better,” he says. “So I see it as an opportunity to perform a public service. But we also need front-line clinicians, including hospitalists, working to improve our healthcare system. … We need frontline providers that are measuring the quality of their care and improving it.”
Larry Beresford is a freelance writer based in California.
Patrick Conway, MD, MSc, SFHM, a pediatric hospitalist and director of hospital medicine at Cincinnati Children’s Hospital Medical Center, has been appointed chief medical officer of the Centers for Medicare & Medicaid Services (CMS). Dr. Conway’s key responsibilities will be administering federal healthcare quality initiatives and setting the government’s quality agenda.
— Patrick Conway, MD, MSc, SFHM, chief medical officer, Centers for Medicare & Medicaid Services
Dr. Conway, who previously served as CMO of the Policy Division of the Office of Secretary of Health and Human Services and was a 2007-2008 White House fellow assigned to the Agency for Healthcare Research and Quality (AHRQ), is a leader in safety, quality, and outcomes initiatives at Cincinnati Children’s, holds a voluntary faculty appointment at the University of Cincinnati, and is chair of SHM’s Public Policy Committee. In his new job, starting May 9, he will direct CMS’ Office of Clinical Standards and Quality.
“Dr. Conway’s passion for improving healthcare delivery systems, his day-to-day experience as a hospitalist physician, and his accomplishments in quality-improvement research, such as implementing evidence-based healthcare for all children, provide a strong background for his critical role at CMS as chief medical officer,” says colleague Arnold W. Strauss, MD, chair of pediatrics at the University of Cincinnati. “Dr. Conway and our colleagues at Cincinnati Children’s have demonstrated that improving patient outcomes at lower cost—the goal of healthcare reform—is feasible.”
At Cincinnati Children’s, Dr. Conway is an associate professor, associate vice president of outcomes performance, and director of Rapid Evidence Adoption in the James M. Anderson Center. He will give up these roles and his SHM committee chair to assume the federal position. He will maintain his position at the University of Cincinnati and will work some weekends seeing patients at Children’s National Medical Center in Washington, D.C. “I love patient care, so I don’t want to stop doing that. Plus, it helps me connect to the front lines of providing medical care,” Dr. Conway says.
Larry Wellikson, MD, SFHM, CEO of SHM, calls Dr. Conway a leader in the society and the field of HM. “Having Pat as the new CMO of CMS just further confirms the importance of hospital medicine to being central to the changes in our health system at a national level,” he says.
Dr. Conway’s role at CMS will include major components of surveys, certification, and accreditation issues for hospitals and other Medicare providers; healthcare information technology; and hospital value-based purchasing initiatives. But his initial priorities will focus on quality-measures development, illustrated by CMS’ Hospital Compare website, and quality improvement. Another major issue involves care transitions and readmissions, “which I try to frame positively—how can we have the most effective care transitions possible?” he says. “SHM and its publications have done a good job of stressing how hospitals and hospitalists can add value.”
Married with two children, Dr. Conway says he was not looking to move back inside the Beltway, even though he believes his experience at both the macro and micro levels of healthcare will benefit the overall system. “I actually think if we realign incentives, the system can perform better,” he says. “So I see it as an opportunity to perform a public service. But we also need front-line clinicians, including hospitalists, working to improve our healthcare system. … We need frontline providers that are measuring the quality of their care and improving it.”
Larry Beresford is a freelance writer based in California.
Confusion Clouds New Documentation Rule
A newly implemented rule (PDF) requiring hospitalists and others who order home health services for Medicare patients to document face-to-face encounters has left SHM and other physician groups searching for clarity.
Under a Centers for Medicare & Medicaid Services (CMS) guideline that took effect April 1, physicians need to show proof of documentation before a patient can receive home care services. The documentation is known as a "certification form," and, either on the form or as an addendum to it, physicians must show that they either they saw the patient or allowed a nonphysician provider to do so. CMS is allowing such documentation (PDF) to be generated from an electronic health record.
Some industry watchers say that despite the deadline, many hospitalists are unaware of the rule. And many of those who are aware are confused as to whether any additional paperwork is required of them, creating the potential for an overwhelming paperwork burden being placed on hospitalists.
SHM and other professional societies, including the American Medical Association (AMA) and the American Hospital Association (AHA), asked CMS to delay the implementation until July 1, in the hopes that more time would help clear up any confusion. CMS declined.
In a letter to CMS Administrator Donald Berwick, MD, last month the AMA wrote, "it is our hope that CMS will reconsider its decision not to further delay the home health requirement and that in the future, imposition of policies … would be discussed with the medical profession BEFORE they turn up in a proposed rule." In addition, CMS needs to significantly improve its education efforts for physicians."
Ryan Genzink, PA-C, of IPC/Hospitalists of West Michigan in Grand Rapids says his hospital began using a new form just to document face-to-face encounters, until he learned from SHM that adding the information to existing documentation could satisfy the new rule. Genzink fears hospitalists around the country are operating under a patchwork of forms and guidelines, which can be a waste of time and money.
"The primary barrier to compliance is the paperwork burden on physicians," SHM and other trade groups wrote to CMS in March. "...The solution to the documentation concerns lies within CMS authority."
A newly implemented rule (PDF) requiring hospitalists and others who order home health services for Medicare patients to document face-to-face encounters has left SHM and other physician groups searching for clarity.
Under a Centers for Medicare & Medicaid Services (CMS) guideline that took effect April 1, physicians need to show proof of documentation before a patient can receive home care services. The documentation is known as a "certification form," and, either on the form or as an addendum to it, physicians must show that they either they saw the patient or allowed a nonphysician provider to do so. CMS is allowing such documentation (PDF) to be generated from an electronic health record.
Some industry watchers say that despite the deadline, many hospitalists are unaware of the rule. And many of those who are aware are confused as to whether any additional paperwork is required of them, creating the potential for an overwhelming paperwork burden being placed on hospitalists.
SHM and other professional societies, including the American Medical Association (AMA) and the American Hospital Association (AHA), asked CMS to delay the implementation until July 1, in the hopes that more time would help clear up any confusion. CMS declined.
In a letter to CMS Administrator Donald Berwick, MD, last month the AMA wrote, "it is our hope that CMS will reconsider its decision not to further delay the home health requirement and that in the future, imposition of policies … would be discussed with the medical profession BEFORE they turn up in a proposed rule." In addition, CMS needs to significantly improve its education efforts for physicians."
Ryan Genzink, PA-C, of IPC/Hospitalists of West Michigan in Grand Rapids says his hospital began using a new form just to document face-to-face encounters, until he learned from SHM that adding the information to existing documentation could satisfy the new rule. Genzink fears hospitalists around the country are operating under a patchwork of forms and guidelines, which can be a waste of time and money.
"The primary barrier to compliance is the paperwork burden on physicians," SHM and other trade groups wrote to CMS in March. "...The solution to the documentation concerns lies within CMS authority."
A newly implemented rule (PDF) requiring hospitalists and others who order home health services for Medicare patients to document face-to-face encounters has left SHM and other physician groups searching for clarity.
Under a Centers for Medicare & Medicaid Services (CMS) guideline that took effect April 1, physicians need to show proof of documentation before a patient can receive home care services. The documentation is known as a "certification form," and, either on the form or as an addendum to it, physicians must show that they either they saw the patient or allowed a nonphysician provider to do so. CMS is allowing such documentation (PDF) to be generated from an electronic health record.
Some industry watchers say that despite the deadline, many hospitalists are unaware of the rule. And many of those who are aware are confused as to whether any additional paperwork is required of them, creating the potential for an overwhelming paperwork burden being placed on hospitalists.
SHM and other professional societies, including the American Medical Association (AMA) and the American Hospital Association (AHA), asked CMS to delay the implementation until July 1, in the hopes that more time would help clear up any confusion. CMS declined.
In a letter to CMS Administrator Donald Berwick, MD, last month the AMA wrote, "it is our hope that CMS will reconsider its decision not to further delay the home health requirement and that in the future, imposition of policies … would be discussed with the medical profession BEFORE they turn up in a proposed rule." In addition, CMS needs to significantly improve its education efforts for physicians."
Ryan Genzink, PA-C, of IPC/Hospitalists of West Michigan in Grand Rapids says his hospital began using a new form just to document face-to-face encounters, until he learned from SHM that adding the information to existing documentation could satisfy the new rule. Genzink fears hospitalists around the country are operating under a patchwork of forms and guidelines, which can be a waste of time and money.
"The primary barrier to compliance is the paperwork burden on physicians," SHM and other trade groups wrote to CMS in March. "...The solution to the documentation concerns lies within CMS authority."
Millions Available to Transitions-Focused Hospitalists
CMS clearly has care transitions on its radar, having made $500 million in grant opportunities available to help hospitals, their hospitalists, and community partners work collaboratively to improve transitions and prevent rehospitalizations, observes hospitalist Matthew Schreiber, MD, chief medical officer of Piedmont Hospital in Atlanta.
"But for me, there is little question that today's carrot will turn into tomorrow's stick, so now is the time to get this right," Dr. Schreiber says.
Piedmont was one of six initial sites for SHM's Project BOOST care transitions initiative, and the hospital also participated with a coalition of Atlanta-area community providers that served as one of 14 test sites for the Community-Based Care Transitions Program (CCTP) federal demonstration project. Based on the success of those demos, $500 million in funds were earmarked for CCTP through the Affordable Care Act to support care-transitions projects by community-based organizations partnering with hospitals and by eligible hospitals with community-based partners.
CCTP and its $500 million recently were rolled into a five-year, $1 billion federal reform initiative called Partnership for Patients, which was announced last month by Health and Human Services Secretary Kathleen Sebelius. Its goals are to save 63,000 lives and $35 billion in healthcare costs by reducing preventable hospital-associated injuries by 40% and reducing overall hospital readmissions by 20%, both targets to be achieved by the end of 2013.
In announcing the national Partnership for Patients, CMS administrator Donald Berwick, MD, pledged to "focus first on a set of well-established, evidence-based interventions.” Such interventions, which explicitly include Project BOOST and Boston University's Project RED (Re-Engineered Discharge), will be given preference in CCTP applications. That means hospitals that already are Project BOOST sites or participating in one of the other recognized care-transitions programs and collaborating with other health providers in their communities to enhance the care patients receive following hospital discharge will have a big leg up in qualifying for CCTP funding.
Hospitalists can't obtain these grants by themselves but can be major collaborators in the care-transitions coalitions that can. Long-awaited CCTP application criteria were made available last month.
CMS clearly has care transitions on its radar, having made $500 million in grant opportunities available to help hospitals, their hospitalists, and community partners work collaboratively to improve transitions and prevent rehospitalizations, observes hospitalist Matthew Schreiber, MD, chief medical officer of Piedmont Hospital in Atlanta.
"But for me, there is little question that today's carrot will turn into tomorrow's stick, so now is the time to get this right," Dr. Schreiber says.
Piedmont was one of six initial sites for SHM's Project BOOST care transitions initiative, and the hospital also participated with a coalition of Atlanta-area community providers that served as one of 14 test sites for the Community-Based Care Transitions Program (CCTP) federal demonstration project. Based on the success of those demos, $500 million in funds were earmarked for CCTP through the Affordable Care Act to support care-transitions projects by community-based organizations partnering with hospitals and by eligible hospitals with community-based partners.
CCTP and its $500 million recently were rolled into a five-year, $1 billion federal reform initiative called Partnership for Patients, which was announced last month by Health and Human Services Secretary Kathleen Sebelius. Its goals are to save 63,000 lives and $35 billion in healthcare costs by reducing preventable hospital-associated injuries by 40% and reducing overall hospital readmissions by 20%, both targets to be achieved by the end of 2013.
In announcing the national Partnership for Patients, CMS administrator Donald Berwick, MD, pledged to "focus first on a set of well-established, evidence-based interventions.” Such interventions, which explicitly include Project BOOST and Boston University's Project RED (Re-Engineered Discharge), will be given preference in CCTP applications. That means hospitals that already are Project BOOST sites or participating in one of the other recognized care-transitions programs and collaborating with other health providers in their communities to enhance the care patients receive following hospital discharge will have a big leg up in qualifying for CCTP funding.
Hospitalists can't obtain these grants by themselves but can be major collaborators in the care-transitions coalitions that can. Long-awaited CCTP application criteria were made available last month.
CMS clearly has care transitions on its radar, having made $500 million in grant opportunities available to help hospitals, their hospitalists, and community partners work collaboratively to improve transitions and prevent rehospitalizations, observes hospitalist Matthew Schreiber, MD, chief medical officer of Piedmont Hospital in Atlanta.
"But for me, there is little question that today's carrot will turn into tomorrow's stick, so now is the time to get this right," Dr. Schreiber says.
Piedmont was one of six initial sites for SHM's Project BOOST care transitions initiative, and the hospital also participated with a coalition of Atlanta-area community providers that served as one of 14 test sites for the Community-Based Care Transitions Program (CCTP) federal demonstration project. Based on the success of those demos, $500 million in funds were earmarked for CCTP through the Affordable Care Act to support care-transitions projects by community-based organizations partnering with hospitals and by eligible hospitals with community-based partners.
CCTP and its $500 million recently were rolled into a five-year, $1 billion federal reform initiative called Partnership for Patients, which was announced last month by Health and Human Services Secretary Kathleen Sebelius. Its goals are to save 63,000 lives and $35 billion in healthcare costs by reducing preventable hospital-associated injuries by 40% and reducing overall hospital readmissions by 20%, both targets to be achieved by the end of 2013.
In announcing the national Partnership for Patients, CMS administrator Donald Berwick, MD, pledged to "focus first on a set of well-established, evidence-based interventions.” Such interventions, which explicitly include Project BOOST and Boston University's Project RED (Re-Engineered Discharge), will be given preference in CCTP applications. That means hospitals that already are Project BOOST sites or participating in one of the other recognized care-transitions programs and collaborating with other health providers in their communities to enhance the care patients receive following hospital discharge will have a big leg up in qualifying for CCTP funding.
Hospitalists can't obtain these grants by themselves but can be major collaborators in the care-transitions coalitions that can. Long-awaited CCTP application criteria were made available last month.
Value-Based Purchasing Raises the Stakes

Mock scorecards, interactive blueprints, quality dashboards: Hospitals are frantically seeking out any advantage that might help them excel in a fast-approaching, mandatory competition with millions of dollars on the line. Value-based purchasing (VBP), a program authorized by the Patient Protection and Accountable Care Act of 2010, gives the Centers for Medicare & Medicaid Services (CMS) the power to base a portion of hospital reimbursement payments on how well hospitals perform in 25 core measures.
The move is intended to help CMS flex its muscles and move from being a passive bystander to an active buyer of what its officials have deemed higher-quality healthcare. Analysts and healthcare experts warn that if hospitalists aren’t paying attention, however, they could put themselves at unnecessary risk or lose out on a major opportunity to demonstrate their value in what Patrick Torcson, MD, SFHM, is calling a “team sport.”
Dr. Torcson, chair of SHM’s Performance and Standards Committee, says every hospitalist should be aware of the core-measures concept, which has been around since 2003 in what’s now called the Hospital Inpatient Quality Reporting (IQR) Program. “We’re not reinventing the wheel; we’re just transforming the program from pay-for-reporting to actual pay-for-performance,” he says. Value-based purchasing, though, is raising the stakes considerably. “It’s really significant because it marks the beginning of an era of accountability and true pay-for-performance at the hospital level.”
A major reason for the heightened concern is the structure of the program. In other quality demonstration projects, CMS has established a score to beat: “Anyone above that threshold is in the money. If you didn’t make it, there was no harm, no foul,” says Trent Haywood, MD, JD, chief medical officer of the Irving, Tex.-based for-profit healthcare cooperative VHA Inc.

—Laura Dietzel, PeaceHealth’s program director for High-Tech Meaningful Use
What’s different this time is that value-based purchasing is not a collaboration but a competition in which every hospital is pitted against the entire market, says Dr. Haywood, the former deputy chief medical officer at CMS. It’s also a zero-sum game. That means there will be winners and losers, with the entire cost-neutral program funded by extracting money from the worst performers to financially reward the best. “In this competition-type model, you need to know who you can beat,” he says.
Race to the Top
That new reality has set off a mad scramble among hospitals hoping to gain any edge they can and spawned a cottage industry of consultants, lawyers, and quality specialists advising them on how to maximize their points. The drive to achieve and maintain a high level of performance is also spurring hospitals to seek more individual accountability as they look to minimize their financial risk.
Hospitals’ baseline scores already have been set, and the initial nine-month performance evaluation period begins July 1. Beginning with discharges on Oct. 1, 2012 (fiscal year 2013), the payment phase will kick in. CMS will start by withholding 1% of the base DRG reimbursement paid to hospitals. That money can be earned back based on how well each hospital scores on the performance measures during the evaluation period. The amount initially withheld will rise by 0.25 percentage points per year until it is capped at 2% in 2017 and beyond.
Think of the competition as an annual decathlon with a pool of prize money funded by the participants, except that hospitals will be evaluated on far more measures. So far, the program includes 17 core Clinical Process of Care measures and eight measures based on Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) surveys. Twenty other potential measures are waiting in the wings, including ones related to hospital-acquired conditions, patient safety, inpatient quality, and mortality, some of which likely will be introduced in fiscal year 2014.
CMS intends to monitor and evaluate the program’s impact on access and quality of care, especially for “vulnerable populations,” the percentage of patients who receive appropriate care, the rates of hospital-acquired conditions, and the best practices of high-performing hospitals.
The complicated nature of the rules and scoring, and significant money attached to the competition, have generated deep concern. In October and again in February, healthcare providers bombarded CMS representatives with questions and suggestions during open phone forums, when the regulations were still in flux. Would the rules be fair? Would CMS provide an early warning of impending losses? Was the agency giving too much weight to patient satisfaction scores?
SHM supports the program, stating, “We believe that the Medicare reimbursement system must be changed to promote value, and we strongly support policies that link quality measurement to performance-based payment.”
Other observers, though, have warned of the potential for unintended consequences. If doctors avoid complicated medical cases in order to increase a hospital’s score, for example, are they really improving care? Will poorly performing hospitals get caught in a vicious circle due to declining financial resources?
Some critics have complained that by scoring on a curve rather than on an absolute point system, the value-based purchasing program might not be a quality initiative so much as an opportunity for CMS to reduce hospital payments. “I believe that this is largely a shell game played by the Centers for Medicare & Medicaid Services to give hospitals the idea that they can win at this game, when all but a few will lose,” wrote Richard Rohr, MD, FHM, in his Feb. 1 entry at the Medical Staff Leader blog (http://blogs.hcpro.com/medicalstaff/). Hospitalist subsidies could be a prime target as the cost-reduction pressures rise, wrote Dr. Rohr, who directs HM programs for Guthrie Healthcare System in Sayre, Pa. Enhancing productivity, he stressed, could be the best defense against a rollback in salaries.
Most experts agree that investing in a quality infrastructure will be essential for success, though other hospitalists differ on the potential effects that VBP might have on their profession. “I think a big part of a quality infrastructure is a hospital medicine program,” Dr. Torcson says. In fact, he recommends that hospitalists approach a hospital CFO or CEO and offer their assistance with the program. “I really think that’s the right direction and the right attitude, kind of the way the Samurai used to serve the Japanese emperor,” he explains.
A major reason for taking the initiative, he says, is that value-based purchasing could become the new business case for HM. In the 1990s, hospitalists could put a real number on how much they saved hospitals by reducing length of stay, sparking an investment in HM programs. “I think value-based purchasing is now in the same position,” Dr. Torcson says, “and the savings is actually going to be even more quantifiable for the hospital in terms of their success or failure.”
continued below...
Expectations on the Rise
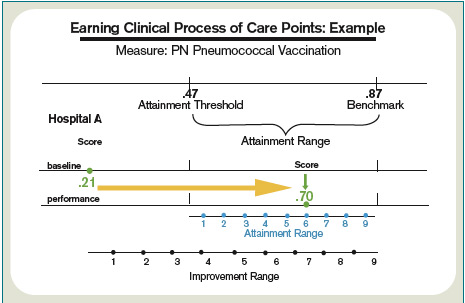
SHM’s annual meeting this month in Grapevine, Texas (www.hospitalmedicine2011.org), will feature a session on improving HCAHPS scores, and Dr. Torcson has been working on a society task force educating members about how to be successful amid the coming changes. A Web-based toolkit in the works, he says, will highlight best practices for myocardial infarctions, heart failure, surgical care, pneumonia, and patient satisfaction to help hospitalists ensure they have the necessary skill sets. (SHM will offer a full platform of VBP courses by end of 2011.)
“At the individual hospitalist level, once you’ve decided to commit to serving that hospital-level performance agenda, we want SHM to be the place to turn to get the information on best practices and what you need,” Dr. Torcson says.
But first, says Bill Darling, a Washington, D.C., and Austin, Tex.-based partner with Strasburger Attorneys at Law, hospitalists will need a much stronger understanding of hospital expectations. Many hospital officials already are indicating that they’re leaning toward their own pay-for-performance programs to put individual doctors on the hook for negative financial incentives and penalties.
“Ultimately, in these value-based systems,” says Darling, a specialist in healthcare contracts and regulations, “the quality scores for physicians may affect their medical staff privileges or their membership in their group, or their ability to even move to another hospital.”
Moreover, hospital administrators are trying to instill a sense of shared responsibility in maintaining high value-based purchasing scores. “I cannot make a physician prescribe an ACE inhibitor when it’s appropriate to deal with heart failure, but the hospital takes a hit for that,” says Dee Rogers, RN, director of quality and risk management at Magnolia Regional Medical Center in Magnolia, Ark. “Not that I want to see people get their hands slapped—I want to see equal accountability.”
Like other hospitals, Rogers’ 49-bed rural facility is tracking doctors’ performance on quality measures and guidelines as part of its credentialing process. Many facilities are starting to include more comprehensive evaluations as part of their contract renegotiations. Magnolia has one weekend hospitalist and is conducting a feasibility study on whether to launch a full-time hospitalist program on weekdays. If the hospital pursues that program, Rogers says, she’d like to see upfront expectations built into the doctors’ contracts.
Seven Tips to Prepare for Value-Based Purchasing
- Pick your partners carefully. Lawyer Bill Darling says hospitalists must understand the terms of any contractual arrangement they enter and who their teammates will be for value-based purchasing. Are others likely to hold up their end of the bargain? If not, how much risk will fall upon hospitalists?
- Accept personal accountability. The reality is that more hospitals are demanding responsibility from individual physicians and posting their performance on key measures. Hospitalists might not be able to control how others respond, but embracing their own responsibility now will help ease the transition to an era of more public accountability. Become board-certified. Doing so, says Patrick Torcson, MD, will augment the disease-specific knowledge and quality-improvement skills necessary to be successful with value-based purchasing.
- Talk to your nurses. Not being on the same page can drag down both doctor-communication and nurse-communication scores in the eyes of patients who assume a medical team is regularly sharing information, says VHA Inc.’s Trent Haywood, MD.
- Make eye contact with your patients. If doctors sit with patients and make direct eye contact, even if only for five minutes, “it makes the patient feel like they’re being validated,” says Dee Rogers, RN. Satisfaction rates will “go through the roof,” she says.
- Establish upfront expectations. Remind-ing patients of what they should expect during their hospital stay, says Patricia Richardson, RN, RCP, director of quality and risk at Samaritan Hospital in Moses Lake, Wis., might help them put their experience in the proper context and not hold the facility to the same standards as their own homes.
- Pay attention to details and be adaptable. PeaceHealth’s Laura Dietzel says a two-sentence section in CMS’s proposed rules spurred her healthcare system to quickly adapt. PeaceHealth shifted away from several measures it had been focusing on after it became clear they would be retired from the competition “in the near future,” according to the rules.—BN


PeaceHealth, a faith-based nonprofit healthcare system that operates eight hospitals in Oregon, Washington, and Alaska, is moving in the same direction. “I think we’re getting pretty close—certainly within the next year, probably sooner—of creating a reliable mechanism for physician accountability related to the measures that are included in value-based purchasing,” says Laura Dietzel, PeaceHealth’s program director for High-Tech Meaningful Use. That mechanism will connect specific core measures with specific physicians, not just roles or departments.
“We are really honing in on that kind of a quality dashboard, and [VBP’s arrival] is definitely going to be a big boost toward doing that,” says Dietzel, the health system’s former program manager for core measures. “We are talking about making it part of our credentialing process, part of our privileging process, and part of our physician reimbursement and pay schedule process.”
Dietzel concedes that the health system will need to develop a valid method for ensuring that it correctly records who had the responsibility for key decisions. Apart from the concern over proper credit and blame, Darling warns that doctors who haven’t been paying attention could be left holding the bag.
If a hospitalist contract doesn’t discuss how payments will be handled with bundling, value-based purchasing, accountable care, and other models coming down the pike, Darling says, “it may be that you’ve bought a pig in a poke and that you’re just hoping for the kindness of strangers.” Likewise, if a hospital underperforms on its VBP scores due to a lack of investment or training, he asks, will its physicians also look bad on paper? The perceived guilt by association might hurt their chances at finding employment elsewhere if other hospital administrators fear that doctors from poorly performing facilities will hurt their scores as well.
To avoid the most dire “What if?” scenarios, hospitals are enlisting their staff and trying out new tools to help them identify and address trouble spots. At Dr. Torcson’s own hospital, 237-bed St. Tammany Parish Hospital in Covington, La., hospitalists and other staff members are scrutinizing the core measures and tweaking guidelines and best practices to make sure the facility is in top form. Based on initial modeling, the hospital expects to earn back all of its withheld reimbursements, though Dr. Torcson says the push is still on to increase the cushion.
A few QI organizations that contract with CMS, including Seattle-based Qualis Health, have developed interactive calculators or mock scorecards to help hospitals determine where they stand in the value-based purchasing scrum. Patricia Richardson, MA, RCP, director of quality and risk for 50-bed Samaritan Hospital in Moses Lake, Wash., says the hospital has worked with Qualis (www.qualishealth.org) on a scorecard to help staff understand which measures need attention and what the financial repercussions would be if the hospital doesn’t improve.
After earlier pushback from doctors on some core measures, quality-review specialist Rebecca Johnson says Samaritan began posting how individual doctors were performing. “And, over time, that motivated them,” she says. “Nobody wants to be the guy in the red.” Johnson says the hospital’s four hospitalists, though, have been fully engaged. “Our hospitalists are very interested in how we’re doing,” she says. “When I’m on the floor doing my reviews, they consistently ask—all of them—‘How are we doing on the core measures?’ ”
Although Richardson concedes that Samaritan still has work to do to increase its patient-satisfaction scores, she’s hopeful that more education and engagement of both patients and staff will begin to pay off. Initiatives that have recruited patients as active participants in helping the hospital improve might help boost patient satisfaction scores, and internal competitions could help motivate the medical staff.
Setting upfront expectations about the hospital stay during the admissions process also can help. Richardson says patients naturally compare a hospital’s noise level to that of their own homes unless a doctor or other staff member provides the proper context. Letting patients know what to expect and reminding them that they’ll likely have to be awakened a few times during the night can make a big difference in whether they rate the hospital as being sufficiently quiet, she says.
Competition Breeds Cooperation
Hospitals likely will be able to differentiate themselves the most through the national competition’s patient perception of care scores, VHA Inc.’s Dr. Haywood says, largely because the contenders have had less time to prepare for them than for the clinical process-of-care measures. Among the eight HCAHPS measures, Dr. Haywood says, focusing on doctor communication, nurse communication, hospital staff responsiveness, and a quiet room might provide the biggest return on investment.
“If physicians don’t communicate effectively with the nurses, then the nurse communication score goes down because the patients assume that the nurses know the care plan,” he says. “A typical question that we see all the time is that the nurse will ask the patient, ‘Did the doctor come and see you today?’ And if the patient says yes, then the nurse will ask, ‘Well, what did the doctor say?’ because the nurse doesn’t know.”
With VBP in mind, Dr. Haywood’s health system repurposed part of its catalogue of Web-based blueprints designed to help hospitals improve their clinical practices (see Figure 2, below). The cooperative is now making its collection of more than 100 blueprints available to its members to help them prop up sagging core measure scores. All depict best-practice solutions in an easy-to-remember visual format, based on weeklong site visits to exemplary hospitals from a clinical team that includes a cultural anthropologist and graphic artist.
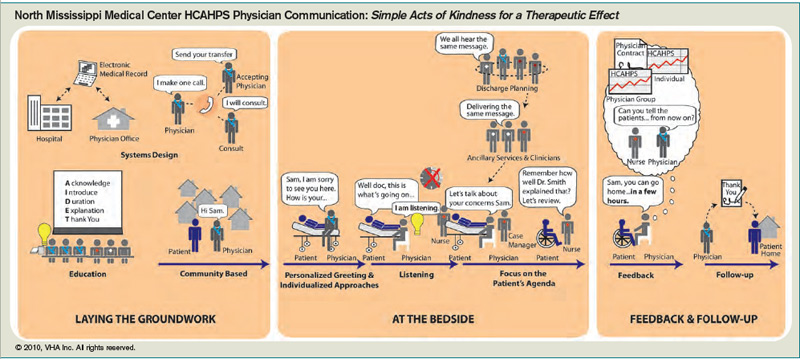
Arkansas’ Magnolia already exceeds the national average for every HCAHPS score except the overall rating, a score that will likely increase because most patient evaluations were conducted before a new facility replaced the previous, aging hospital in February 2010. Rogers says Magnolia’s weekend hospitalist has helped with continuity of care—an important factor for maintaining high satisfaction in a small, rural community where doctors tend to see the same elderly patients on a frequent basis. The patients know the hospitalist by name, she says, “so they almost have as much of a relationship to him as they do with their primary-care physician.”
Rogers says the weekend hospitalist also has helped improve some of the hospital’s lagging pneumonia-related scores by educating and communicating with other members of the medical staff about their respective responsibilities. Because he has gained the trust of his peers, Rogers says, he’s helped the hospital get more buy-in from them as well.
Embracing the role of VBP champion, Dr. Torcson says, could help further define the worth of hospitalists to their employers. And with a trend toward more individual physician accountability, rising to the occasion now could help hospitalists stay on top of their own game. TH
Bryn Nelson is a freelance medical writer in Seattle.
Scorecards and Price Tags: VBP’s Bottom Line
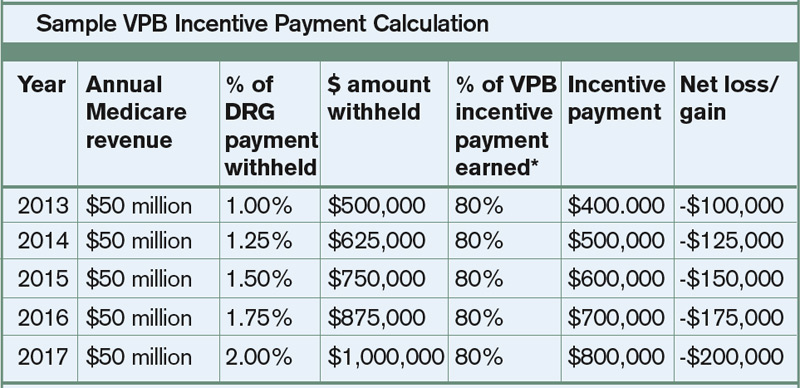
Hospitalists likely won’t be involved in calculating exactly how much hospitals stand to lose or gain with value-based purchasing. Nonetheless, knowing a little about how the scoring system works can help put your facility’s potential scores and their impact on the bottom line into perspective. Consider the example of patients’ perception of doctor communication, one of eight measures in the HCAHPS surveys.
In this case, Hospital A initially struggles with its baseline score, ranking only in the 42nd percentile among all hospitals. In order to receive any achievement points, the hospital would have to climb to at least the 50th percentile.
Fortunately, Hospital A improves to the 64th percentile during the performance period (which begins July 1). Based on the CMS scoring system, it would receive 3 achievement points or 4 improvement points. The latter score is higher, so the hospital gains 4 out of 10 possible points, giving it a final score of 40%.
Let’s say this same hospital is eligible for 23 of the 25 measures, and gets a total performance average of 57% (or 5.7 out of 10 possible points on all measures). Based on the current exchange function, that hospital would get back about 80% of its withheld DRG reimbursements from CMS. What does that mean in terms of money? The table below offers a sample calculation, revealing that Hospital A could lose about $100,000 next year, and up to $200,000 in 2017.
Mock scorecards, interactive blueprints, quality dashboards: Hospitals are frantically seeking out any advantage that might help them excel in a fast-approaching, mandatory competition with millions of dollars on the line. Value-based purchasing (VBP), a program authorized by the Patient Protection and Accountable Care Act of 2010, gives the Centers for Medicare & Medicaid Services (CMS) the power to base a portion of hospital reimbursement payments on how well hospitals perform in 25 core measures.
The move is intended to help CMS flex its muscles and move from being a passive bystander to an active buyer of what its officials have deemed higher-quality healthcare. Analysts and healthcare experts warn that if hospitalists aren’t paying attention, however, they could put themselves at unnecessary risk or lose out on a major opportunity to demonstrate their value in what Patrick Torcson, MD, SFHM, is calling a “team sport.”
Dr. Torcson, chair of SHM’s Performance and Standards Committee, says every hospitalist should be aware of the core-measures concept, which has been around since 2003 in what’s now called the Hospital Inpatient Quality Reporting (IQR) Program. “We’re not reinventing the wheel; we’re just transforming the program from pay-for-reporting to actual pay-for-performance,” he says. Value-based purchasing, though, is raising the stakes considerably. “It’s really significant because it marks the beginning of an era of accountability and true pay-for-performance at the hospital level.”
A major reason for the heightened concern is the structure of the program. In other quality demonstration projects, CMS has established a score to beat: “Anyone above that threshold is in the money. If you didn’t make it, there was no harm, no foul,” says Trent Haywood, MD, JD, chief medical officer of the Irving, Tex.-based for-profit healthcare cooperative VHA Inc.
—Laura Dietzel, PeaceHealth’s program director for High-Tech Meaningful Use
What’s different this time is that value-based purchasing is not a collaboration but a competition in which every hospital is pitted against the entire market, says Dr. Haywood, the former deputy chief medical officer at CMS. It’s also a zero-sum game. That means there will be winners and losers, with the entire cost-neutral program funded by extracting money from the worst performers to financially reward the best. “In this competition-type model, you need to know who you can beat,” he says.
Race to the Top
That new reality has set off a mad scramble among hospitals hoping to gain any edge they can and spawned a cottage industry of consultants, lawyers, and quality specialists advising them on how to maximize their points. The drive to achieve and maintain a high level of performance is also spurring hospitals to seek more individual accountability as they look to minimize their financial risk.
Hospitals’ baseline scores already have been set, and the initial nine-month performance evaluation period begins July 1. Beginning with discharges on Oct. 1, 2012 (fiscal year 2013), the payment phase will kick in. CMS will start by withholding 1% of the base DRG reimbursement paid to hospitals. That money can be earned back based on how well each hospital scores on the performance measures during the evaluation period. The amount initially withheld will rise by 0.25 percentage points per year until it is capped at 2% in 2017 and beyond.
Think of the competition as an annual decathlon with a pool of prize money funded by the participants, except that hospitals will be evaluated on far more measures. So far, the program includes 17 core Clinical Process of Care measures and eight measures based on Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) surveys. Twenty other potential measures are waiting in the wings, including ones related to hospital-acquired conditions, patient safety, inpatient quality, and mortality, some of which likely will be introduced in fiscal year 2014.
CMS intends to monitor and evaluate the program’s impact on access and quality of care, especially for “vulnerable populations,” the percentage of patients who receive appropriate care, the rates of hospital-acquired conditions, and the best practices of high-performing hospitals.
The complicated nature of the rules and scoring, and significant money attached to the competition, have generated deep concern. In October and again in February, healthcare providers bombarded CMS representatives with questions and suggestions during open phone forums, when the regulations were still in flux. Would the rules be fair? Would CMS provide an early warning of impending losses? Was the agency giving too much weight to patient satisfaction scores?
SHM supports the program, stating, “We believe that the Medicare reimbursement system must be changed to promote value, and we strongly support policies that link quality measurement to performance-based payment.”
Other observers, though, have warned of the potential for unintended consequences. If doctors avoid complicated medical cases in order to increase a hospital’s score, for example, are they really improving care? Will poorly performing hospitals get caught in a vicious circle due to declining financial resources?
Some critics have complained that by scoring on a curve rather than on an absolute point system, the value-based purchasing program might not be a quality initiative so much as an opportunity for CMS to reduce hospital payments. “I believe that this is largely a shell game played by the Centers for Medicare & Medicaid Services to give hospitals the idea that they can win at this game, when all but a few will lose,” wrote Richard Rohr, MD, FHM, in his Feb. 1 entry at the Medical Staff Leader blog (http://blogs.hcpro.com/medicalstaff/). Hospitalist subsidies could be a prime target as the cost-reduction pressures rise, wrote Dr. Rohr, who directs HM programs for Guthrie Healthcare System in Sayre, Pa. Enhancing productivity, he stressed, could be the best defense against a rollback in salaries.
Most experts agree that investing in a quality infrastructure will be essential for success, though other hospitalists differ on the potential effects that VBP might have on their profession. “I think a big part of a quality infrastructure is a hospital medicine program,” Dr. Torcson says. In fact, he recommends that hospitalists approach a hospital CFO or CEO and offer their assistance with the program. “I really think that’s the right direction and the right attitude, kind of the way the Samurai used to serve the Japanese emperor,” he explains.
A major reason for taking the initiative, he says, is that value-based purchasing could become the new business case for HM. In the 1990s, hospitalists could put a real number on how much they saved hospitals by reducing length of stay, sparking an investment in HM programs. “I think value-based purchasing is now in the same position,” Dr. Torcson says, “and the savings is actually going to be even more quantifiable for the hospital in terms of their success or failure.”
continued below...
Expectations on the Rise
SHM’s annual meeting this month in Grapevine, Texas (www.hospitalmedicine2011.org), will feature a session on improving HCAHPS scores, and Dr. Torcson has been working on a society task force educating members about how to be successful amid the coming changes. A Web-based toolkit in the works, he says, will highlight best practices for myocardial infarctions, heart failure, surgical care, pneumonia, and patient satisfaction to help hospitalists ensure they have the necessary skill sets. (SHM will offer a full platform of VBP courses by end of 2011.)
“At the individual hospitalist level, once you’ve decided to commit to serving that hospital-level performance agenda, we want SHM to be the place to turn to get the information on best practices and what you need,” Dr. Torcson says.
But first, says Bill Darling, a Washington, D.C., and Austin, Tex.-based partner with Strasburger Attorneys at Law, hospitalists will need a much stronger understanding of hospital expectations. Many hospital officials already are indicating that they’re leaning toward their own pay-for-performance programs to put individual doctors on the hook for negative financial incentives and penalties.
“Ultimately, in these value-based systems,” says Darling, a specialist in healthcare contracts and regulations, “the quality scores for physicians may affect their medical staff privileges or their membership in their group, or their ability to even move to another hospital.”
Moreover, hospital administrators are trying to instill a sense of shared responsibility in maintaining high value-based purchasing scores. “I cannot make a physician prescribe an ACE inhibitor when it’s appropriate to deal with heart failure, but the hospital takes a hit for that,” says Dee Rogers, RN, director of quality and risk management at Magnolia Regional Medical Center in Magnolia, Ark. “Not that I want to see people get their hands slapped—I want to see equal accountability.”
Like other hospitals, Rogers’ 49-bed rural facility is tracking doctors’ performance on quality measures and guidelines as part of its credentialing process. Many facilities are starting to include more comprehensive evaluations as part of their contract renegotiations. Magnolia has one weekend hospitalist and is conducting a feasibility study on whether to launch a full-time hospitalist program on weekdays. If the hospital pursues that program, Rogers says, she’d like to see upfront expectations built into the doctors’ contracts.
Seven Tips to Prepare for Value-Based Purchasing
- Pick your partners carefully. Lawyer Bill Darling says hospitalists must understand the terms of any contractual arrangement they enter and who their teammates will be for value-based purchasing. Are others likely to hold up their end of the bargain? If not, how much risk will fall upon hospitalists?
- Accept personal accountability. The reality is that more hospitals are demanding responsibility from individual physicians and posting their performance on key measures. Hospitalists might not be able to control how others respond, but embracing their own responsibility now will help ease the transition to an era of more public accountability. Become board-certified. Doing so, says Patrick Torcson, MD, will augment the disease-specific knowledge and quality-improvement skills necessary to be successful with value-based purchasing.
- Talk to your nurses. Not being on the same page can drag down both doctor-communication and nurse-communication scores in the eyes of patients who assume a medical team is regularly sharing information, says VHA Inc.’s Trent Haywood, MD.
- Make eye contact with your patients. If doctors sit with patients and make direct eye contact, even if only for five minutes, “it makes the patient feel like they’re being validated,” says Dee Rogers, RN. Satisfaction rates will “go through the roof,” she says.
- Establish upfront expectations. Remind-ing patients of what they should expect during their hospital stay, says Patricia Richardson, RN, RCP, director of quality and risk at Samaritan Hospital in Moses Lake, Wis., might help them put their experience in the proper context and not hold the facility to the same standards as their own homes.
- Pay attention to details and be adaptable. PeaceHealth’s Laura Dietzel says a two-sentence section in CMS’s proposed rules spurred her healthcare system to quickly adapt. PeaceHealth shifted away from several measures it had been focusing on after it became clear they would be retired from the competition “in the near future,” according to the rules.—BN
PeaceHealth, a faith-based nonprofit healthcare system that operates eight hospitals in Oregon, Washington, and Alaska, is moving in the same direction. “I think we’re getting pretty close—certainly within the next year, probably sooner—of creating a reliable mechanism for physician accountability related to the measures that are included in value-based purchasing,” says Laura Dietzel, PeaceHealth’s program director for High-Tech Meaningful Use. That mechanism will connect specific core measures with specific physicians, not just roles or departments.
“We are really honing in on that kind of a quality dashboard, and [VBP’s arrival] is definitely going to be a big boost toward doing that,” says Dietzel, the health system’s former program manager for core measures. “We are talking about making it part of our credentialing process, part of our privileging process, and part of our physician reimbursement and pay schedule process.”
Dietzel concedes that the health system will need to develop a valid method for ensuring that it correctly records who had the responsibility for key decisions. Apart from the concern over proper credit and blame, Darling warns that doctors who haven’t been paying attention could be left holding the bag.
If a hospitalist contract doesn’t discuss how payments will be handled with bundling, value-based purchasing, accountable care, and other models coming down the pike, Darling says, “it may be that you’ve bought a pig in a poke and that you’re just hoping for the kindness of strangers.” Likewise, if a hospital underperforms on its VBP scores due to a lack of investment or training, he asks, will its physicians also look bad on paper? The perceived guilt by association might hurt their chances at finding employment elsewhere if other hospital administrators fear that doctors from poorly performing facilities will hurt their scores as well.
To avoid the most dire “What if?” scenarios, hospitals are enlisting their staff and trying out new tools to help them identify and address trouble spots. At Dr. Torcson’s own hospital, 237-bed St. Tammany Parish Hospital in Covington, La., hospitalists and other staff members are scrutinizing the core measures and tweaking guidelines and best practices to make sure the facility is in top form. Based on initial modeling, the hospital expects to earn back all of its withheld reimbursements, though Dr. Torcson says the push is still on to increase the cushion.
A few QI organizations that contract with CMS, including Seattle-based Qualis Health, have developed interactive calculators or mock scorecards to help hospitals determine where they stand in the value-based purchasing scrum. Patricia Richardson, MA, RCP, director of quality and risk for 50-bed Samaritan Hospital in Moses Lake, Wash., says the hospital has worked with Qualis (www.qualishealth.org) on a scorecard to help staff understand which measures need attention and what the financial repercussions would be if the hospital doesn’t improve.
After earlier pushback from doctors on some core measures, quality-review specialist Rebecca Johnson says Samaritan began posting how individual doctors were performing. “And, over time, that motivated them,” she says. “Nobody wants to be the guy in the red.” Johnson says the hospital’s four hospitalists, though, have been fully engaged. “Our hospitalists are very interested in how we’re doing,” she says. “When I’m on the floor doing my reviews, they consistently ask—all of them—‘How are we doing on the core measures?’ ”
Although Richardson concedes that Samaritan still has work to do to increase its patient-satisfaction scores, she’s hopeful that more education and engagement of both patients and staff will begin to pay off. Initiatives that have recruited patients as active participants in helping the hospital improve might help boost patient satisfaction scores, and internal competitions could help motivate the medical staff.
Setting upfront expectations about the hospital stay during the admissions process also can help. Richardson says patients naturally compare a hospital’s noise level to that of their own homes unless a doctor or other staff member provides the proper context. Letting patients know what to expect and reminding them that they’ll likely have to be awakened a few times during the night can make a big difference in whether they rate the hospital as being sufficiently quiet, she says.
Competition Breeds Cooperation
Hospitals likely will be able to differentiate themselves the most through the national competition’s patient perception of care scores, VHA Inc.’s Dr. Haywood says, largely because the contenders have had less time to prepare for them than for the clinical process-of-care measures. Among the eight HCAHPS measures, Dr. Haywood says, focusing on doctor communication, nurse communication, hospital staff responsiveness, and a quiet room might provide the biggest return on investment.
“If physicians don’t communicate effectively with the nurses, then the nurse communication score goes down because the patients assume that the nurses know the care plan,” he says. “A typical question that we see all the time is that the nurse will ask the patient, ‘Did the doctor come and see you today?’ And if the patient says yes, then the nurse will ask, ‘Well, what did the doctor say?’ because the nurse doesn’t know.”
With VBP in mind, Dr. Haywood’s health system repurposed part of its catalogue of Web-based blueprints designed to help hospitals improve their clinical practices (see Figure 2, below). The cooperative is now making its collection of more than 100 blueprints available to its members to help them prop up sagging core measure scores. All depict best-practice solutions in an easy-to-remember visual format, based on weeklong site visits to exemplary hospitals from a clinical team that includes a cultural anthropologist and graphic artist.
Arkansas’ Magnolia already exceeds the national average for every HCAHPS score except the overall rating, a score that will likely increase because most patient evaluations were conducted before a new facility replaced the previous, aging hospital in February 2010. Rogers says Magnolia’s weekend hospitalist has helped with continuity of care—an important factor for maintaining high satisfaction in a small, rural community where doctors tend to see the same elderly patients on a frequent basis. The patients know the hospitalist by name, she says, “so they almost have as much of a relationship to him as they do with their primary-care physician.”
Rogers says the weekend hospitalist also has helped improve some of the hospital’s lagging pneumonia-related scores by educating and communicating with other members of the medical staff about their respective responsibilities. Because he has gained the trust of his peers, Rogers says, he’s helped the hospital get more buy-in from them as well.
Embracing the role of VBP champion, Dr. Torcson says, could help further define the worth of hospitalists to their employers. And with a trend toward more individual physician accountability, rising to the occasion now could help hospitalists stay on top of their own game. TH
Bryn Nelson is a freelance medical writer in Seattle.
Scorecards and Price Tags: VBP’s Bottom Line
Hospitalists likely won’t be involved in calculating exactly how much hospitals stand to lose or gain with value-based purchasing. Nonetheless, knowing a little about how the scoring system works can help put your facility’s potential scores and their impact on the bottom line into perspective. Consider the example of patients’ perception of doctor communication, one of eight measures in the HCAHPS surveys.
In this case, Hospital A initially struggles with its baseline score, ranking only in the 42nd percentile among all hospitals. In order to receive any achievement points, the hospital would have to climb to at least the 50th percentile.
Fortunately, Hospital A improves to the 64th percentile during the performance period (which begins July 1). Based on the CMS scoring system, it would receive 3 achievement points or 4 improvement points. The latter score is higher, so the hospital gains 4 out of 10 possible points, giving it a final score of 40%.
Let’s say this same hospital is eligible for 23 of the 25 measures, and gets a total performance average of 57% (or 5.7 out of 10 possible points on all measures). Based on the current exchange function, that hospital would get back about 80% of its withheld DRG reimbursements from CMS. What does that mean in terms of money? The table below offers a sample calculation, revealing that Hospital A could lose about $100,000 next year, and up to $200,000 in 2017.
Mock scorecards, interactive blueprints, quality dashboards: Hospitals are frantically seeking out any advantage that might help them excel in a fast-approaching, mandatory competition with millions of dollars on the line. Value-based purchasing (VBP), a program authorized by the Patient Protection and Accountable Care Act of 2010, gives the Centers for Medicare & Medicaid Services (CMS) the power to base a portion of hospital reimbursement payments on how well hospitals perform in 25 core measures.
The move is intended to help CMS flex its muscles and move from being a passive bystander to an active buyer of what its officials have deemed higher-quality healthcare. Analysts and healthcare experts warn that if hospitalists aren’t paying attention, however, they could put themselves at unnecessary risk or lose out on a major opportunity to demonstrate their value in what Patrick Torcson, MD, SFHM, is calling a “team sport.”
Dr. Torcson, chair of SHM’s Performance and Standards Committee, says every hospitalist should be aware of the core-measures concept, which has been around since 2003 in what’s now called the Hospital Inpatient Quality Reporting (IQR) Program. “We’re not reinventing the wheel; we’re just transforming the program from pay-for-reporting to actual pay-for-performance,” he says. Value-based purchasing, though, is raising the stakes considerably. “It’s really significant because it marks the beginning of an era of accountability and true pay-for-performance at the hospital level.”
A major reason for the heightened concern is the structure of the program. In other quality demonstration projects, CMS has established a score to beat: “Anyone above that threshold is in the money. If you didn’t make it, there was no harm, no foul,” says Trent Haywood, MD, JD, chief medical officer of the Irving, Tex.-based for-profit healthcare cooperative VHA Inc.
—Laura Dietzel, PeaceHealth’s program director for High-Tech Meaningful Use
What’s different this time is that value-based purchasing is not a collaboration but a competition in which every hospital is pitted against the entire market, says Dr. Haywood, the former deputy chief medical officer at CMS. It’s also a zero-sum game. That means there will be winners and losers, with the entire cost-neutral program funded by extracting money from the worst performers to financially reward the best. “In this competition-type model, you need to know who you can beat,” he says.
Race to the Top
That new reality has set off a mad scramble among hospitals hoping to gain any edge they can and spawned a cottage industry of consultants, lawyers, and quality specialists advising them on how to maximize their points. The drive to achieve and maintain a high level of performance is also spurring hospitals to seek more individual accountability as they look to minimize their financial risk.
Hospitals’ baseline scores already have been set, and the initial nine-month performance evaluation period begins July 1. Beginning with discharges on Oct. 1, 2012 (fiscal year 2013), the payment phase will kick in. CMS will start by withholding 1% of the base DRG reimbursement paid to hospitals. That money can be earned back based on how well each hospital scores on the performance measures during the evaluation period. The amount initially withheld will rise by 0.25 percentage points per year until it is capped at 2% in 2017 and beyond.
Think of the competition as an annual decathlon with a pool of prize money funded by the participants, except that hospitals will be evaluated on far more measures. So far, the program includes 17 core Clinical Process of Care measures and eight measures based on Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) surveys. Twenty other potential measures are waiting in the wings, including ones related to hospital-acquired conditions, patient safety, inpatient quality, and mortality, some of which likely will be introduced in fiscal year 2014.
CMS intends to monitor and evaluate the program’s impact on access and quality of care, especially for “vulnerable populations,” the percentage of patients who receive appropriate care, the rates of hospital-acquired conditions, and the best practices of high-performing hospitals.
The complicated nature of the rules and scoring, and significant money attached to the competition, have generated deep concern. In October and again in February, healthcare providers bombarded CMS representatives with questions and suggestions during open phone forums, when the regulations were still in flux. Would the rules be fair? Would CMS provide an early warning of impending losses? Was the agency giving too much weight to patient satisfaction scores?
SHM supports the program, stating, “We believe that the Medicare reimbursement system must be changed to promote value, and we strongly support policies that link quality measurement to performance-based payment.”
Other observers, though, have warned of the potential for unintended consequences. If doctors avoid complicated medical cases in order to increase a hospital’s score, for example, are they really improving care? Will poorly performing hospitals get caught in a vicious circle due to declining financial resources?
Some critics have complained that by scoring on a curve rather than on an absolute point system, the value-based purchasing program might not be a quality initiative so much as an opportunity for CMS to reduce hospital payments. “I believe that this is largely a shell game played by the Centers for Medicare & Medicaid Services to give hospitals the idea that they can win at this game, when all but a few will lose,” wrote Richard Rohr, MD, FHM, in his Feb. 1 entry at the Medical Staff Leader blog (http://blogs.hcpro.com/medicalstaff/). Hospitalist subsidies could be a prime target as the cost-reduction pressures rise, wrote Dr. Rohr, who directs HM programs for Guthrie Healthcare System in Sayre, Pa. Enhancing productivity, he stressed, could be the best defense against a rollback in salaries.
Most experts agree that investing in a quality infrastructure will be essential for success, though other hospitalists differ on the potential effects that VBP might have on their profession. “I think a big part of a quality infrastructure is a hospital medicine program,” Dr. Torcson says. In fact, he recommends that hospitalists approach a hospital CFO or CEO and offer their assistance with the program. “I really think that’s the right direction and the right attitude, kind of the way the Samurai used to serve the Japanese emperor,” he explains.
A major reason for taking the initiative, he says, is that value-based purchasing could become the new business case for HM. In the 1990s, hospitalists could put a real number on how much they saved hospitals by reducing length of stay, sparking an investment in HM programs. “I think value-based purchasing is now in the same position,” Dr. Torcson says, “and the savings is actually going to be even more quantifiable for the hospital in terms of their success or failure.”
continued below...
Expectations on the Rise
SHM’s annual meeting this month in Grapevine, Texas (www.hospitalmedicine2011.org), will feature a session on improving HCAHPS scores, and Dr. Torcson has been working on a society task force educating members about how to be successful amid the coming changes. A Web-based toolkit in the works, he says, will highlight best practices for myocardial infarctions, heart failure, surgical care, pneumonia, and patient satisfaction to help hospitalists ensure they have the necessary skill sets. (SHM will offer a full platform of VBP courses by end of 2011.)
“At the individual hospitalist level, once you’ve decided to commit to serving that hospital-level performance agenda, we want SHM to be the place to turn to get the information on best practices and what you need,” Dr. Torcson says.
But first, says Bill Darling, a Washington, D.C., and Austin, Tex.-based partner with Strasburger Attorneys at Law, hospitalists will need a much stronger understanding of hospital expectations. Many hospital officials already are indicating that they’re leaning toward their own pay-for-performance programs to put individual doctors on the hook for negative financial incentives and penalties.
“Ultimately, in these value-based systems,” says Darling, a specialist in healthcare contracts and regulations, “the quality scores for physicians may affect their medical staff privileges or their membership in their group, or their ability to even move to another hospital.”
Moreover, hospital administrators are trying to instill a sense of shared responsibility in maintaining high value-based purchasing scores. “I cannot make a physician prescribe an ACE inhibitor when it’s appropriate to deal with heart failure, but the hospital takes a hit for that,” says Dee Rogers, RN, director of quality and risk management at Magnolia Regional Medical Center in Magnolia, Ark. “Not that I want to see people get their hands slapped—I want to see equal accountability.”
Like other hospitals, Rogers’ 49-bed rural facility is tracking doctors’ performance on quality measures and guidelines as part of its credentialing process. Many facilities are starting to include more comprehensive evaluations as part of their contract renegotiations. Magnolia has one weekend hospitalist and is conducting a feasibility study on whether to launch a full-time hospitalist program on weekdays. If the hospital pursues that program, Rogers says, she’d like to see upfront expectations built into the doctors’ contracts.
Seven Tips to Prepare for Value-Based Purchasing
- Pick your partners carefully. Lawyer Bill Darling says hospitalists must understand the terms of any contractual arrangement they enter and who their teammates will be for value-based purchasing. Are others likely to hold up their end of the bargain? If not, how much risk will fall upon hospitalists?
- Accept personal accountability. The reality is that more hospitals are demanding responsibility from individual physicians and posting their performance on key measures. Hospitalists might not be able to control how others respond, but embracing their own responsibility now will help ease the transition to an era of more public accountability. Become board-certified. Doing so, says Patrick Torcson, MD, will augment the disease-specific knowledge and quality-improvement skills necessary to be successful with value-based purchasing.
- Talk to your nurses. Not being on the same page can drag down both doctor-communication and nurse-communication scores in the eyes of patients who assume a medical team is regularly sharing information, says VHA Inc.’s Trent Haywood, MD.
- Make eye contact with your patients. If doctors sit with patients and make direct eye contact, even if only for five minutes, “it makes the patient feel like they’re being validated,” says Dee Rogers, RN. Satisfaction rates will “go through the roof,” she says.
- Establish upfront expectations. Remind-ing patients of what they should expect during their hospital stay, says Patricia Richardson, RN, RCP, director of quality and risk at Samaritan Hospital in Moses Lake, Wis., might help them put their experience in the proper context and not hold the facility to the same standards as their own homes.
- Pay attention to details and be adaptable. PeaceHealth’s Laura Dietzel says a two-sentence section in CMS’s proposed rules spurred her healthcare system to quickly adapt. PeaceHealth shifted away from several measures it had been focusing on after it became clear they would be retired from the competition “in the near future,” according to the rules.—BN
PeaceHealth, a faith-based nonprofit healthcare system that operates eight hospitals in Oregon, Washington, and Alaska, is moving in the same direction. “I think we’re getting pretty close—certainly within the next year, probably sooner—of creating a reliable mechanism for physician accountability related to the measures that are included in value-based purchasing,” says Laura Dietzel, PeaceHealth’s program director for High-Tech Meaningful Use. That mechanism will connect specific core measures with specific physicians, not just roles or departments.
“We are really honing in on that kind of a quality dashboard, and [VBP’s arrival] is definitely going to be a big boost toward doing that,” says Dietzel, the health system’s former program manager for core measures. “We are talking about making it part of our credentialing process, part of our privileging process, and part of our physician reimbursement and pay schedule process.”
Dietzel concedes that the health system will need to develop a valid method for ensuring that it correctly records who had the responsibility for key decisions. Apart from the concern over proper credit and blame, Darling warns that doctors who haven’t been paying attention could be left holding the bag.
If a hospitalist contract doesn’t discuss how payments will be handled with bundling, value-based purchasing, accountable care, and other models coming down the pike, Darling says, “it may be that you’ve bought a pig in a poke and that you’re just hoping for the kindness of strangers.” Likewise, if a hospital underperforms on its VBP scores due to a lack of investment or training, he asks, will its physicians also look bad on paper? The perceived guilt by association might hurt their chances at finding employment elsewhere if other hospital administrators fear that doctors from poorly performing facilities will hurt their scores as well.
To avoid the most dire “What if?” scenarios, hospitals are enlisting their staff and trying out new tools to help them identify and address trouble spots. At Dr. Torcson’s own hospital, 237-bed St. Tammany Parish Hospital in Covington, La., hospitalists and other staff members are scrutinizing the core measures and tweaking guidelines and best practices to make sure the facility is in top form. Based on initial modeling, the hospital expects to earn back all of its withheld reimbursements, though Dr. Torcson says the push is still on to increase the cushion.
A few QI organizations that contract with CMS, including Seattle-based Qualis Health, have developed interactive calculators or mock scorecards to help hospitals determine where they stand in the value-based purchasing scrum. Patricia Richardson, MA, RCP, director of quality and risk for 50-bed Samaritan Hospital in Moses Lake, Wash., says the hospital has worked with Qualis (www.qualishealth.org) on a scorecard to help staff understand which measures need attention and what the financial repercussions would be if the hospital doesn’t improve.
After earlier pushback from doctors on some core measures, quality-review specialist Rebecca Johnson says Samaritan began posting how individual doctors were performing. “And, over time, that motivated them,” she says. “Nobody wants to be the guy in the red.” Johnson says the hospital’s four hospitalists, though, have been fully engaged. “Our hospitalists are very interested in how we’re doing,” she says. “When I’m on the floor doing my reviews, they consistently ask—all of them—‘How are we doing on the core measures?’ ”
Although Richardson concedes that Samaritan still has work to do to increase its patient-satisfaction scores, she’s hopeful that more education and engagement of both patients and staff will begin to pay off. Initiatives that have recruited patients as active participants in helping the hospital improve might help boost patient satisfaction scores, and internal competitions could help motivate the medical staff.
Setting upfront expectations about the hospital stay during the admissions process also can help. Richardson says patients naturally compare a hospital’s noise level to that of their own homes unless a doctor or other staff member provides the proper context. Letting patients know what to expect and reminding them that they’ll likely have to be awakened a few times during the night can make a big difference in whether they rate the hospital as being sufficiently quiet, she says.
Competition Breeds Cooperation
Hospitals likely will be able to differentiate themselves the most through the national competition’s patient perception of care scores, VHA Inc.’s Dr. Haywood says, largely because the contenders have had less time to prepare for them than for the clinical process-of-care measures. Among the eight HCAHPS measures, Dr. Haywood says, focusing on doctor communication, nurse communication, hospital staff responsiveness, and a quiet room might provide the biggest return on investment.
“If physicians don’t communicate effectively with the nurses, then the nurse communication score goes down because the patients assume that the nurses know the care plan,” he says. “A typical question that we see all the time is that the nurse will ask the patient, ‘Did the doctor come and see you today?’ And if the patient says yes, then the nurse will ask, ‘Well, what did the doctor say?’ because the nurse doesn’t know.”
With VBP in mind, Dr. Haywood’s health system repurposed part of its catalogue of Web-based blueprints designed to help hospitals improve their clinical practices (see Figure 2, below). The cooperative is now making its collection of more than 100 blueprints available to its members to help them prop up sagging core measure scores. All depict best-practice solutions in an easy-to-remember visual format, based on weeklong site visits to exemplary hospitals from a clinical team that includes a cultural anthropologist and graphic artist.
Arkansas’ Magnolia already exceeds the national average for every HCAHPS score except the overall rating, a score that will likely increase because most patient evaluations were conducted before a new facility replaced the previous, aging hospital in February 2010. Rogers says Magnolia’s weekend hospitalist has helped with continuity of care—an important factor for maintaining high satisfaction in a small, rural community where doctors tend to see the same elderly patients on a frequent basis. The patients know the hospitalist by name, she says, “so they almost have as much of a relationship to him as they do with their primary-care physician.”
Rogers says the weekend hospitalist also has helped improve some of the hospital’s lagging pneumonia-related scores by educating and communicating with other members of the medical staff about their respective responsibilities. Because he has gained the trust of his peers, Rogers says, he’s helped the hospital get more buy-in from them as well.
Embracing the role of VBP champion, Dr. Torcson says, could help further define the worth of hospitalists to their employers. And with a trend toward more individual physician accountability, rising to the occasion now could help hospitalists stay on top of their own game. TH
Bryn Nelson is a freelance medical writer in Seattle.
Scorecards and Price Tags: VBP’s Bottom Line
Hospitalists likely won’t be involved in calculating exactly how much hospitals stand to lose or gain with value-based purchasing. Nonetheless, knowing a little about how the scoring system works can help put your facility’s potential scores and their impact on the bottom line into perspective. Consider the example of patients’ perception of doctor communication, one of eight measures in the HCAHPS surveys.
In this case, Hospital A initially struggles with its baseline score, ranking only in the 42nd percentile among all hospitals. In order to receive any achievement points, the hospital would have to climb to at least the 50th percentile.
Fortunately, Hospital A improves to the 64th percentile during the performance period (which begins July 1). Based on the CMS scoring system, it would receive 3 achievement points or 4 improvement points. The latter score is higher, so the hospital gains 4 out of 10 possible points, giving it a final score of 40%.
Let’s say this same hospital is eligible for 23 of the 25 measures, and gets a total performance average of 57% (or 5.7 out of 10 possible points on all measures). Based on the current exchange function, that hospital would get back about 80% of its withheld DRG reimbursements from CMS. What does that mean in terms of money? The table below offers a sample calculation, revealing that Hospital A could lose about $100,000 next year, and up to $200,000 in 2017.
NEW DEPARTMENT: Innovations
No one becomes a doctor to make a fashion statement, but a new study (http://onlinelibrary.wiley.com/doi/10.1002/jhm.864/abstract) in the Journal of Hospital Medicine reports that the choice between long-sleeved white coats and freshly laundered scrubs might be a question of taste, not safety.
The report, “Newly Cleaned Physician Uniforms and Infrequently Washed White Coats Have Similar Rates of Bacterial Contamination After an 8-Hour Workday: A Randomized Controlled Trial,” found no statistically significant differences in bacterial or methicillin-resistant Staphylococcus aureus (MRSA) contamination of physicians’ white coats compared with scrubs or in contamination of the skin at the wrists of physicians wearing either garment.
In an email interview, Marisha Burden, MD, interim chief of hospital medicine at the Denver Health and Hospital Authority, says that the topic area came up during a review of research regarding MRSA and infection-control policies. Dr. Burden found references to the so-called “bare below the elbows” policy in the United Kingdom, a reference to 2007 rules from the British Department of Health banning long-sleeved coats in an attempt to stop nosocomial bacterial transmission.
“This policy was interesting to us secondary to the fact that there was no literature to support the measures being implemented,” Dr. Burden says. “ … Our data show that bacterial contamination of work clothes occurs within hours of putting them on, as well that at the end of an eight-hour workday, there is no difference in bacterial or MRSA contamination of either dress.”
Dr. Burden says the data do not support discarding white coats for uniforms that are changed on a daily basis, or for “requiring healthcare workers to avoid long-sleeved garments.” She also says that white coats have traditional lures as well as practical ones: Most of the physicians who declined to participate in the study did so because they refused to work without the pockets that came with their lab coats.
“I think we also have to consider the professional image that our physicians portray,” she adds. “Our patients expect their physicians to appear professional with clean, white coats.”—RQ
Technology
App Allows CT, MRI, PET Diagnoses Via iPhone, iPad
What can a hospitalist do the next time someone in the group has no immediate access to a work station but needs to make a medical diagnoses based on computed tomography (CT), magnetic resonance imaging (MRI), or positron emission tomography (PET)?
Grab the nearest iPhone.
The FDA recently approved an application from MIM Software Inc. of Cleveland to let doctors review medical images on the iPhone and iPad via a secure network transfer. The application, Mobile MIM, is the first with the FDA’s imprimatur. It allows hospitalists and other physicians to measure distance on the image and image intensity values and display measurement lines, annotations, and regions of interest, according to the FDA.
“Think of how cell phones were perceived a few decades ago; many dismissed ‘anytime access’ as not necessary,” MIM chief technology officer Mark Cain says in an email. “Yet now we know myriad of cases where the cell phone has proven immensely valuable. The same can be said of diagnostic medical image access. How many ways can this improve healthcare? More ways than I can predict.”—RQ
Quality Research
Research Confirms Benefits of ICU Safety Checklists
The value of checklists containing evidence-supported QI interventions to improve ICU outcomes, pioneered at Johns Hopkins in Baltimore, has been confirmed by several recent studies. The Keystone ICU Project, which sought to replicate the Hopkins experience in hospitals across Michigan, succeeded in nearly eliminating bloodstream infections and reducing mortality.1
Based on Medicare claims from 95 study hospitals and comparison data from 11 surrounding states, patients in hospitals using the checklist were significantly more likely to survive a hospital stay. The project was not, however, sufficiently powered to show a significant difference in length of stay.
A second Keystone Project study showed that five simple therapies aimed at lessening the time spent on ventilators, including elevating the head of the bed 30 degrees, giving anticoagulants, and lessening sedation, combined with education and a hospital culture supporting patient safety, reduced cases of ventilator-associated pneumonia by more than 70%.2
A comprehensive, video-conference-based intervention to support implementing six evidence-based quality practices in 15 community hospital ICUs in Canada improved the adoption of these practices. Expert-led forums and educational sessions promoted the sequential dissemination of treatment algorhythms, with a new practice targeted every four months.3—LB
References
- Lipitz-Snyderman A, Steinwachs D, Needham DM, Colantuoni E, Morlock LL, Pronovost PJ. Impact of a statewide intensive care unit quality improvement initiative on hospital mortality and length of stay: retrospective comparative analysis. BMJ. 2011;342:d219.
- Berenholtz SM, Pham JC, Thompson DA, Needhamm et al. Collaborative cohort study of an intervention to reduce ventilator-associated pneumonia in the intensive care unit. Infect Control Hosp Epidemiol. 2011;(4):305-314.
- Scales DC, Dainty K, Hales B. A multifaceted intervention for quality improvement in a network of intensive care units: a cluster randomized trial. JAMA. 2011;305:363-372.
HM-Based Quality Research
Homeless Respite Helps Avoid Rehospitalizations
Some readmissions come about because things fall apart when patients are discharged with a follow-up plan that is not realistic to their circumstances. This is especially true for homeless patients, says Audrey Kuang, MD, a hospitalist at Santa Clara Valley Medical Center (SCVMC) in San Jose, Calif., and medical director of the Santa Clara County Medical Respite Program, a shelter for homeless patients following discharge from seven San Jose area hospitals.
Dr. Kuang described the collaborative program in a plenary presentation for the Research, Innovations, and Clinical Vignettes competition at HM10.
SCVMC is a county safety net hospital, and Dr. Kuang says the hospitalists “see a fair amount of homeless patients with recurrent exacerbations.” Patients given prescriptions for medications they can’t afford, special diets, or instructions for bed rest are then discharged to the street; inevitably, they are readmitted.
Dr. Kuang began tracking patients who had prolonged hospital stays because of homelessness or unsafe social situations. Her presentation to administrators led to participating hospitals contributing $25,000 each to launch the program with a multidisciplinary team, which included Dr. Kuang.
In its first year, 200 referrals were made to the respite program; 60% were accepted. The most common diagnoses were foot fractures, foot infections, and cancer. Quantified clinical outcomes are still being compiled, Dr. Kuang said, although the participating hospitals have reported decreased rehospitalizations and bed days—results documented in other studies of respite programs.1
“The main idea is post-acute medical care and support for homeless patients in need,” she explained. “Hospitalists may feel this is beyond our scope of practice, but it is our responsibility to know what’s going on out there.”—LB
Reference
- Buchanan D, Doblin B, Sai T, Garcia P. The effects of respite care for homeless patients: a cohort study. Am J Public Health. 2006;96:1278-1281.
By The Numbers
$44,000, $46,659, $120,000: EHR Implementation Costs Higher than Medicare Reimbursement
A new study in Health Affairs on the first-year costs of implementing electronic health records (EHR) in a 450-physician North Texas primary-care network doesn’t translate directly to HM, but figures showing that the installation cost is more for an average five-physician practice than Medicare is offering in incentive pay might serve as a warning sign for HM groups looking to build EHR into their practice:
- EHR incentive payments from Medicare over five years: $44,000;
- EHR implementation cost per doctor after first year: $46,659;
- EHR adoption costs per physician, estimated: $120,000.—RQ TH
No one becomes a doctor to make a fashion statement, but a new study (http://onlinelibrary.wiley.com/doi/10.1002/jhm.864/abstract) in the Journal of Hospital Medicine reports that the choice between long-sleeved white coats and freshly laundered scrubs might be a question of taste, not safety.
The report, “Newly Cleaned Physician Uniforms and Infrequently Washed White Coats Have Similar Rates of Bacterial Contamination After an 8-Hour Workday: A Randomized Controlled Trial,” found no statistically significant differences in bacterial or methicillin-resistant Staphylococcus aureus (MRSA) contamination of physicians’ white coats compared with scrubs or in contamination of the skin at the wrists of physicians wearing either garment.
In an email interview, Marisha Burden, MD, interim chief of hospital medicine at the Denver Health and Hospital Authority, says that the topic area came up during a review of research regarding MRSA and infection-control policies. Dr. Burden found references to the so-called “bare below the elbows” policy in the United Kingdom, a reference to 2007 rules from the British Department of Health banning long-sleeved coats in an attempt to stop nosocomial bacterial transmission.
“This policy was interesting to us secondary to the fact that there was no literature to support the measures being implemented,” Dr. Burden says. “ … Our data show that bacterial contamination of work clothes occurs within hours of putting them on, as well that at the end of an eight-hour workday, there is no difference in bacterial or MRSA contamination of either dress.”
Dr. Burden says the data do not support discarding white coats for uniforms that are changed on a daily basis, or for “requiring healthcare workers to avoid long-sleeved garments.” She also says that white coats have traditional lures as well as practical ones: Most of the physicians who declined to participate in the study did so because they refused to work without the pockets that came with their lab coats.
“I think we also have to consider the professional image that our physicians portray,” she adds. “Our patients expect their physicians to appear professional with clean, white coats.”—RQ
Technology
App Allows CT, MRI, PET Diagnoses Via iPhone, iPad
What can a hospitalist do the next time someone in the group has no immediate access to a work station but needs to make a medical diagnoses based on computed tomography (CT), magnetic resonance imaging (MRI), or positron emission tomography (PET)?
Grab the nearest iPhone.
The FDA recently approved an application from MIM Software Inc. of Cleveland to let doctors review medical images on the iPhone and iPad via a secure network transfer. The application, Mobile MIM, is the first with the FDA’s imprimatur. It allows hospitalists and other physicians to measure distance on the image and image intensity values and display measurement lines, annotations, and regions of interest, according to the FDA.
“Think of how cell phones were perceived a few decades ago; many dismissed ‘anytime access’ as not necessary,” MIM chief technology officer Mark Cain says in an email. “Yet now we know myriad of cases where the cell phone has proven immensely valuable. The same can be said of diagnostic medical image access. How many ways can this improve healthcare? More ways than I can predict.”—RQ
Quality Research
Research Confirms Benefits of ICU Safety Checklists
The value of checklists containing evidence-supported QI interventions to improve ICU outcomes, pioneered at Johns Hopkins in Baltimore, has been confirmed by several recent studies. The Keystone ICU Project, which sought to replicate the Hopkins experience in hospitals across Michigan, succeeded in nearly eliminating bloodstream infections and reducing mortality.1
Based on Medicare claims from 95 study hospitals and comparison data from 11 surrounding states, patients in hospitals using the checklist were significantly more likely to survive a hospital stay. The project was not, however, sufficiently powered to show a significant difference in length of stay.
A second Keystone Project study showed that five simple therapies aimed at lessening the time spent on ventilators, including elevating the head of the bed 30 degrees, giving anticoagulants, and lessening sedation, combined with education and a hospital culture supporting patient safety, reduced cases of ventilator-associated pneumonia by more than 70%.2
A comprehensive, video-conference-based intervention to support implementing six evidence-based quality practices in 15 community hospital ICUs in Canada improved the adoption of these practices. Expert-led forums and educational sessions promoted the sequential dissemination of treatment algorhythms, with a new practice targeted every four months.3—LB
References
- Lipitz-Snyderman A, Steinwachs D, Needham DM, Colantuoni E, Morlock LL, Pronovost PJ. Impact of a statewide intensive care unit quality improvement initiative on hospital mortality and length of stay: retrospective comparative analysis. BMJ. 2011;342:d219.
- Berenholtz SM, Pham JC, Thompson DA, Needhamm et al. Collaborative cohort study of an intervention to reduce ventilator-associated pneumonia in the intensive care unit. Infect Control Hosp Epidemiol. 2011;(4):305-314.
- Scales DC, Dainty K, Hales B. A multifaceted intervention for quality improvement in a network of intensive care units: a cluster randomized trial. JAMA. 2011;305:363-372.
HM-Based Quality Research
Homeless Respite Helps Avoid Rehospitalizations
Some readmissions come about because things fall apart when patients are discharged with a follow-up plan that is not realistic to their circumstances. This is especially true for homeless patients, says Audrey Kuang, MD, a hospitalist at Santa Clara Valley Medical Center (SCVMC) in San Jose, Calif., and medical director of the Santa Clara County Medical Respite Program, a shelter for homeless patients following discharge from seven San Jose area hospitals.
Dr. Kuang described the collaborative program in a plenary presentation for the Research, Innovations, and Clinical Vignettes competition at HM10.
SCVMC is a county safety net hospital, and Dr. Kuang says the hospitalists “see a fair amount of homeless patients with recurrent exacerbations.” Patients given prescriptions for medications they can’t afford, special diets, or instructions for bed rest are then discharged to the street; inevitably, they are readmitted.
Dr. Kuang began tracking patients who had prolonged hospital stays because of homelessness or unsafe social situations. Her presentation to administrators led to participating hospitals contributing $25,000 each to launch the program with a multidisciplinary team, which included Dr. Kuang.
In its first year, 200 referrals were made to the respite program; 60% were accepted. The most common diagnoses were foot fractures, foot infections, and cancer. Quantified clinical outcomes are still being compiled, Dr. Kuang said, although the participating hospitals have reported decreased rehospitalizations and bed days—results documented in other studies of respite programs.1
“The main idea is post-acute medical care and support for homeless patients in need,” she explained. “Hospitalists may feel this is beyond our scope of practice, but it is our responsibility to know what’s going on out there.”—LB
Reference
- Buchanan D, Doblin B, Sai T, Garcia P. The effects of respite care for homeless patients: a cohort study. Am J Public Health. 2006;96:1278-1281.
By The Numbers
$44,000, $46,659, $120,000: EHR Implementation Costs Higher than Medicare Reimbursement
A new study in Health Affairs on the first-year costs of implementing electronic health records (EHR) in a 450-physician North Texas primary-care network doesn’t translate directly to HM, but figures showing that the installation cost is more for an average five-physician practice than Medicare is offering in incentive pay might serve as a warning sign for HM groups looking to build EHR into their practice:
- EHR incentive payments from Medicare over five years: $44,000;
- EHR implementation cost per doctor after first year: $46,659;
- EHR adoption costs per physician, estimated: $120,000.—RQ TH
No one becomes a doctor to make a fashion statement, but a new study (http://onlinelibrary.wiley.com/doi/10.1002/jhm.864/abstract) in the Journal of Hospital Medicine reports that the choice between long-sleeved white coats and freshly laundered scrubs might be a question of taste, not safety.
The report, “Newly Cleaned Physician Uniforms and Infrequently Washed White Coats Have Similar Rates of Bacterial Contamination After an 8-Hour Workday: A Randomized Controlled Trial,” found no statistically significant differences in bacterial or methicillin-resistant Staphylococcus aureus (MRSA) contamination of physicians’ white coats compared with scrubs or in contamination of the skin at the wrists of physicians wearing either garment.
In an email interview, Marisha Burden, MD, interim chief of hospital medicine at the Denver Health and Hospital Authority, says that the topic area came up during a review of research regarding MRSA and infection-control policies. Dr. Burden found references to the so-called “bare below the elbows” policy in the United Kingdom, a reference to 2007 rules from the British Department of Health banning long-sleeved coats in an attempt to stop nosocomial bacterial transmission.
“This policy was interesting to us secondary to the fact that there was no literature to support the measures being implemented,” Dr. Burden says. “ … Our data show that bacterial contamination of work clothes occurs within hours of putting them on, as well that at the end of an eight-hour workday, there is no difference in bacterial or MRSA contamination of either dress.”
Dr. Burden says the data do not support discarding white coats for uniforms that are changed on a daily basis, or for “requiring healthcare workers to avoid long-sleeved garments.” She also says that white coats have traditional lures as well as practical ones: Most of the physicians who declined to participate in the study did so because they refused to work without the pockets that came with their lab coats.
“I think we also have to consider the professional image that our physicians portray,” she adds. “Our patients expect their physicians to appear professional with clean, white coats.”—RQ
Technology
App Allows CT, MRI, PET Diagnoses Via iPhone, iPad
What can a hospitalist do the next time someone in the group has no immediate access to a work station but needs to make a medical diagnoses based on computed tomography (CT), magnetic resonance imaging (MRI), or positron emission tomography (PET)?
Grab the nearest iPhone.
The FDA recently approved an application from MIM Software Inc. of Cleveland to let doctors review medical images on the iPhone and iPad via a secure network transfer. The application, Mobile MIM, is the first with the FDA’s imprimatur. It allows hospitalists and other physicians to measure distance on the image and image intensity values and display measurement lines, annotations, and regions of interest, according to the FDA.
“Think of how cell phones were perceived a few decades ago; many dismissed ‘anytime access’ as not necessary,” MIM chief technology officer Mark Cain says in an email. “Yet now we know myriad of cases where the cell phone has proven immensely valuable. The same can be said of diagnostic medical image access. How many ways can this improve healthcare? More ways than I can predict.”—RQ
Quality Research
Research Confirms Benefits of ICU Safety Checklists
The value of checklists containing evidence-supported QI interventions to improve ICU outcomes, pioneered at Johns Hopkins in Baltimore, has been confirmed by several recent studies. The Keystone ICU Project, which sought to replicate the Hopkins experience in hospitals across Michigan, succeeded in nearly eliminating bloodstream infections and reducing mortality.1
Based on Medicare claims from 95 study hospitals and comparison data from 11 surrounding states, patients in hospitals using the checklist were significantly more likely to survive a hospital stay. The project was not, however, sufficiently powered to show a significant difference in length of stay.
A second Keystone Project study showed that five simple therapies aimed at lessening the time spent on ventilators, including elevating the head of the bed 30 degrees, giving anticoagulants, and lessening sedation, combined with education and a hospital culture supporting patient safety, reduced cases of ventilator-associated pneumonia by more than 70%.2
A comprehensive, video-conference-based intervention to support implementing six evidence-based quality practices in 15 community hospital ICUs in Canada improved the adoption of these practices. Expert-led forums and educational sessions promoted the sequential dissemination of treatment algorhythms, with a new practice targeted every four months.3—LB
References
- Lipitz-Snyderman A, Steinwachs D, Needham DM, Colantuoni E, Morlock LL, Pronovost PJ. Impact of a statewide intensive care unit quality improvement initiative on hospital mortality and length of stay: retrospective comparative analysis. BMJ. 2011;342:d219.
- Berenholtz SM, Pham JC, Thompson DA, Needhamm et al. Collaborative cohort study of an intervention to reduce ventilator-associated pneumonia in the intensive care unit. Infect Control Hosp Epidemiol. 2011;(4):305-314.
- Scales DC, Dainty K, Hales B. A multifaceted intervention for quality improvement in a network of intensive care units: a cluster randomized trial. JAMA. 2011;305:363-372.
HM-Based Quality Research
Homeless Respite Helps Avoid Rehospitalizations
Some readmissions come about because things fall apart when patients are discharged with a follow-up plan that is not realistic to their circumstances. This is especially true for homeless patients, says Audrey Kuang, MD, a hospitalist at Santa Clara Valley Medical Center (SCVMC) in San Jose, Calif., and medical director of the Santa Clara County Medical Respite Program, a shelter for homeless patients following discharge from seven San Jose area hospitals.
Dr. Kuang described the collaborative program in a plenary presentation for the Research, Innovations, and Clinical Vignettes competition at HM10.
SCVMC is a county safety net hospital, and Dr. Kuang says the hospitalists “see a fair amount of homeless patients with recurrent exacerbations.” Patients given prescriptions for medications they can’t afford, special diets, or instructions for bed rest are then discharged to the street; inevitably, they are readmitted.
Dr. Kuang began tracking patients who had prolonged hospital stays because of homelessness or unsafe social situations. Her presentation to administrators led to participating hospitals contributing $25,000 each to launch the program with a multidisciplinary team, which included Dr. Kuang.
In its first year, 200 referrals were made to the respite program; 60% were accepted. The most common diagnoses were foot fractures, foot infections, and cancer. Quantified clinical outcomes are still being compiled, Dr. Kuang said, although the participating hospitals have reported decreased rehospitalizations and bed days—results documented in other studies of respite programs.1
“The main idea is post-acute medical care and support for homeless patients in need,” she explained. “Hospitalists may feel this is beyond our scope of practice, but it is our responsibility to know what’s going on out there.”—LB
Reference
- Buchanan D, Doblin B, Sai T, Garcia P. The effects of respite care for homeless patients: a cohort study. Am J Public Health. 2006;96:1278-1281.
By The Numbers
$44,000, $46,659, $120,000: EHR Implementation Costs Higher than Medicare Reimbursement
A new study in Health Affairs on the first-year costs of implementing electronic health records (EHR) in a 450-physician North Texas primary-care network doesn’t translate directly to HM, but figures showing that the installation cost is more for an average five-physician practice than Medicare is offering in incentive pay might serve as a warning sign for HM groups looking to build EHR into their practice:
- EHR incentive payments from Medicare over five years: $44,000;
- EHR implementation cost per doctor after first year: $46,659;
- EHR adoption costs per physician, estimated: $120,000.—RQ TH
The Billing & Coding Bandwagon

It’s no secret that documenting and coding one’s work is not the average hospitalist’s favorite thing to do. It’s probably not even in the top 10 or 20. In fact, many consider the whole documentation process a “thorn in the side.”
“When I first started working, I couldn’t believe that I could get audited and fined just because I didn’t add ‘10-point’ or ‘12-point’ to my note of ‘review of systems: negative,’ ” says hospitalist Amaka Nweke, MD, assistant director with Hospitalists Management Group (HMG) at Kenosha Medical Center in Kenosha, Wis. “I had a lot of frustration, because I had to repackage and re-present my notes in a manner that makes sense to Medicare but makes no sense to physicians.”
Like it or not, healthcare providers live in a highly regulated world, says Richard D. Pinson, MD, FACP, CCS, who became a certified coding specialist and formed his own consulting company, Houston-based HCQ Consulting, to help hospitals and physicians achieve diagnostic accuracy for inpatient care. Documentation and coding have become a serious, high-stakes word game, he says. “Perfectly good clinical documentation, especially with some important diagnoses, may not correspond at all to what is required by the strict coding rules that govern code assignments,” he says.
A hospitalist’s documentation is at the heart of accurate coding, whether it’s for the hospital’s DRG reimbursement, quality and performance scores, or for assigning current procedural terminology (CPT) and evaluation and management (E/M) codes for billing for their own professional services. And if hospitalists don’t buy into the coding mindset, they risk decreased reimbursement for their services, monetary losses for the hospital, Medicare audits, compromised quality scores for both the hospital and themselves, and noncompliance.
“If your documentation is not up to par, then the hospital may get fined and lose money, and you can’t prove your worth as a hospitalist,” Dr. Nweke says.
What’s at Stake?

Inadequate documentation results in “undercoding” a patient’s condition and underpayment to your hospital (see Table 1, right). Undercoding also can result in inadequate representation of the severity of a patient’s illness, complexity, and cost of care. If a patient gets worse in the hospital, then that initial lower severity of illness might show up in poor performance scores on outcome measures. If a patient’s severity of illness is miscoded, Medicare might question the medical necessity for inpatient admission and deny payment.
On the other hand, if overcoding occurs because the clinical criteria for a specific diagnosis have not been met, Medicare will take action to recover the overpayment, leveling penalties and sanctions. (For more information on Medicare’s Recovery Audit Contractor program, dubbed “Medicare’s repo men” by Dr. Pinson, see “Take Proactive Approach to Recovery Audit Contractors,” p. 28.)
Lack of specificity also hampers reimbursement for professional fees, says Barb Pierce, CCS-P, ACS-EM, president of Barb Pierce Coding and Consulting Inc. of West Des Moines, Iowa. “Unfortunately,” she observes, “the code isn’t just based on decision-making, which is why physicians went to school for all those years. The guidelines [Documentation Guidelines for Evaluation and Management Services] mandate that if you forget one little bullet in history or examination, even if you’ve got the riskiest, highest-level, decision-making patient in front of you, that could pull down the whole code selection.”1
How costly might such small mistakes be for an HM group? According to the State of Hospital Medicine: 2010 Report Based on 2009 Data survey, internal-medicine hospitalists generate a median of 1.86 work relative value units (wRVUs) per encounter, and collect $45.57 per wRVU.2 If a hospitalist has 2,200 encounters per year and averages only 1.65 wRVUs per encounter, improving documentation and coding performance could add an additional 0.21 wRVUs, meeting the national average. Multiplying those 2,200 encounters by the national average of 1.86, the hospitalist could potentially add an additional 462 wRVUs for the year. Such documentation improvement—up to the national average—would equate to $21,053 in additional billed revenue without increasing the physician’s overall workload.
Dr. Pinson explains that physicians often perceive their time constraints as so severe that they’d be hard pressed to find the time to learn about documentation and coding. But he maintains that even short seminars yield “a huge amount of information that would astound [hospitalists], in terms of usefulness for their own clinical practices.”
Barriers to the Coding Mindset

Most hospitalists receive little or no training in documentation and coding during medical school or residency. The lack of education is further complicated because there are several coding sets healthcare providers must master, each with different rules governing assignment of diagnoses and levels of care (see “Coding Sets: Separate but Overlapping,” above).
Inexperience with coding guidelines can lead to mismatches. Nelly Leon-Chisen, RHIA, director of coding and classification for the American Hospital Association (AHA), gives one example: The ICD-9-CM Official Coding Guideline stipulates that coders cannot assign diagnosis codes based on lab results.3 So although it might appear intuitive to a physician that repeated blood sugars and monitoring of insulin levels indicate a patient has diabetes, the coder cannot assign the diagnosis unless it’s explicitly stated in the record.
Some physicians could simply be using outmoded terminology, such as “renal insufficiency” instead of “acute renal failure,” Dr. Pinson notes. If hospitalists learn to focus on evidence-based clinical criteria to support the codes, it leads to more effective care, he says.
The nature of hospitalist programs might not lend itself to efficient revenue-cycle processes for their own professional billing, says Jeri Leong, RN, CPC, CPC-H, president and CEO of Honolulu-based Healthcare Coding Consultants of Hawaii. If the HM group contracts with several hospitals, the hospitalists will be together rarely as a group, “so they don’t have the luxury of sitting down together with their billers to get important feedback and coding updates,” she says.
Leong’s company identifies missed charges, for instance, when charge tags from different shifts do not get married together (Hospitalist A might round on the patient in the morning and turn in a charge tag; Hospitalist B might do a procedure in the afternoon, but the two tags do not get combined). Examples such as these, she says, “can be an issue from a compliance perspective, and can leave money on the table.”
One of the problems Kathy DeVault, RHIA, CCS, CCS-P, manager of professional practice resources for the American Health Information Management Association (AHIMA), sees is a lack of continuity between initial admitting diagnosis and discharge summaries. For example, a hospitalist might admit a patient for acute renal failure—the correct diagnosis—and be able to reverse the condition fairly quickly, especially if the failure is due to dehydration.
The patient, whose issue is resolved, could be discharged by an attending physician who does not note the acute diagnosis in the summary. “That acute condition disappears, and the RAC auditor may then challenge the claim for payment,” DeVault says.
The Remedies
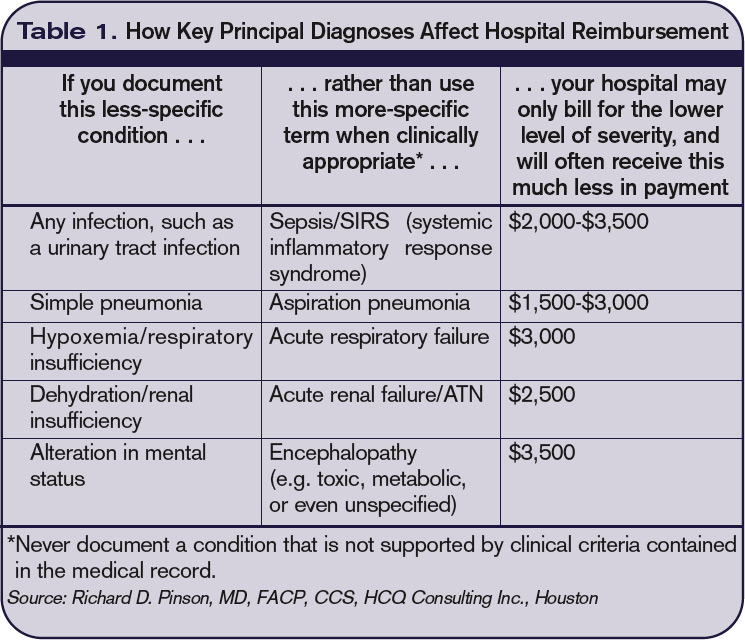
While physicians might think that they don’t have the time to acquire coding education, there could be other incentives coming down the pike. Dr. Pinson has noticed that hospitals are beginning to incorporate documentation accuracy into their contractual reimbursement formulas.
Documentation fixes vary according to domain. A hospital’s clinical documentation specialists can query physicians for clarity and detail in their notes; for instance, a diagnosis of congestive heart failure (CHF) must be accompanied by additional documentation stating whether the CHF is acute or chronic, and whether it is systolic or diastolic.
Many hospitals have instituted clinical documentation improvement (CDI) programs, sometimes called clinical documentation integrity programs, to address documentation discrepancies. CDI programs are essential to hospitals’ financial survival, Dr. Pinson says, and hospitalists are ideally positioned to join those efforts.
“[The hospitalists] are the most important people to the hospital in all of this,” he says. “They’re at the center of this whirlpool. If you have these skills, your value to the hospital and to your group is greatly enhanced.” (Visit the-hospitalist.org to listen to Dr. Pinson discuss HM’s role in documentation improvement.)
Leon-Chisen also says that the relationship between coders and physicians should be collaborative. “If it’s adversarial, nobody wins,” she points out, adding that CDI programs present an opportunity for mutual education.
Conducting audits of the practice’s documentation and coding can identify coding strengths and weaknesses, says Pierce, who is faculty for SHM’s billing and coding pre-course and regularly consults with hospitalist groups. Audits are helpful, she says, not just for increasing group revenue, but for compliance reasons as well. “You need to know what you’re doing well, and what you’re not doing quite so well, and get it fixed internally before an entity like Medicare discovers it,” she says.
It’s no doubt difficult for a busy HM group to stay on top of annual coding updates and changes to guidelines for reporting their services, Leong notes. Her company has worked with many hospitalist groups over the years, offering coding workshops, “back end” audits, and real-time feedback of E/M and CPT coding choices. If all of the hospitalists in a group cannot convene simultaneously, Leong provides the feedback (in the form of a scorecard) to the group’s physician champion, who becomes the lead contact to help those physicians who struggle more with their coding. (Leong talks more about real-time feedback and capturing CPT and E/M codes at the-hospitalist.org.)
In lieu of hiring professional coders, some HM groups use electronic coding devices. The software could be a standalone product, or it could interface with other products, such as electronic medical records (EMRs). These programs assist with a variety of coding-related activities, such as CPT or ICD-9 lookups, or calculation of E/M key components with assignment of an appropriate level of billing. Leong, however, cautions too much reliance on technology.
“While these devices can be accurate, compact, and convenient, it’s important to maintain a current [software] subscription to keep abreast of updates to the code sets, which occur sometimes as often as quarterly,” she says.
Pierce adds that coding tools should be double-checked against an audit tool. She has sometimes found discrepancies when auditing against an EMR product that assigns the E/M level.

Attitude Adjustment
Coding experts emphasize that physicians need not worry about mastering coding manuals, but they should forge relationships with both their hospital’s billers and the coders for their practice.
Dr. Nweke took advantage of coding and billing workshops offered by her group, HMG, and through the seminars began to understand what a DRG meant not just for her hospital but for her own evaluations and the expansion of her HM group, too. “Now, when I get questions from billers and coders, I try to answer them quickly,” she says. “I don’t look upon them as the enemy, but rather as people who are helping me document appropriately, so I don’t get audited by Medicare. I think the way you view the coders and billers definitely affects your willingness to learn.”
Dr. Nweke also takes a broader view of her role as a hospitalist. “You are there to take care of patients and assist with transitioning them in and out of the hospital, but you’re also there to ensure that the hospital remains afloat financially,” she says. “Your documentation plays a huge role in that. We have a huge contribution to make.”
The patient gains, too, says Leon-Chisen, who explains that documentation should be as accurate as possible “because someone else—the patient’s primary physician—will be taking over care of that patient and needs to understand what happened in the hospital.”
“The bottom line,” Dr. Pinson says, “is that we need accurate documentation that can be correctly coded to reflect the true complexity of care and severity of illness. If we do that, good things will follow.” TH
Gretchen Henkel is a freelance writer based in California.
References
- 1997 Documentation Guidelines for Evaluation and Management Services. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/MLNProducts/Downloads/MASTER1.pdf. Accessed April 11, 2011.
- State of Hospital Medicine: 2010 Report Based on 2009 Data. Society of Hospital Medicine and Medical Group Management Association; Philadelphia and Englewood, Colo.; 2010.
- ICD-9-CM Official Coding Guidelines. CMS and National Center for Health Statistics; Washington, D.C.; 2008. Available at: www.ama-assn.org/resources/doc/cpt/icd9cm_coding_guidelines_08_09_full.pdf. Accessed April 10, 2011.
Take Proactive Approach to Recovery Audit Contractors
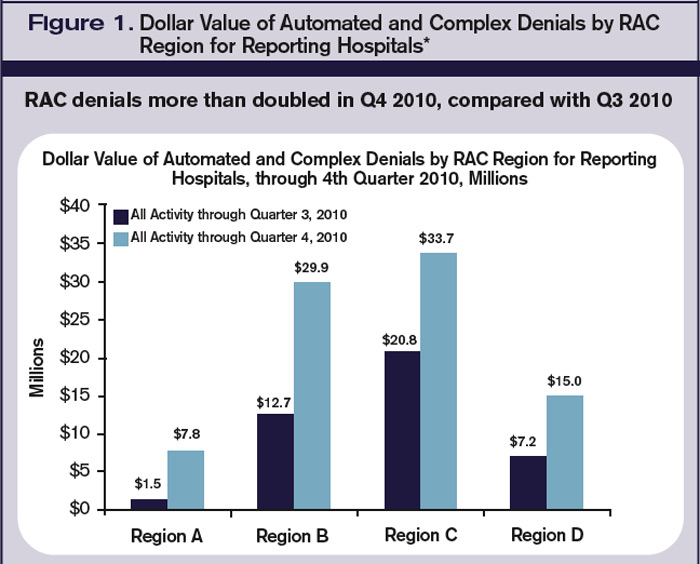
The congressionally authorized Medicare Recovery Audit Contractor (RAC) program began with a three-year demonstration pilot project in 2005. In August 2010, the program expanded to the entire country. The RAC’s main objective is to identify improper Medicare payments, both overpayments and underpayments, to providers. CMS, which administrates Medicare and the RAC program, has agreements with contractors who are authorized to audit and review claims that are up to three years old.
According to Elizabeth Baskett, senior associate director of policy at the AHA, medical necessity review was a big focus of the RAC demonstration project and now is “under way in the permanent RAC program. We are bracing ourselves for a significant amount of denials.”
The AHA has created a free, Web-based survey called RAC Trac (www.aha.org/aha/issues/RAC/ractrac.html) to assess the nationwide impact the RAC program has on U.S. hospitals. In a report released Feb. 24, the RAC Trac survey shows that $82 million in denials were reported, more than double the dollar amount of denials reported in the third quarter of 2010 (see Figure 1, below). It also shows 57% of the more than 1,850 participating hospitals cited “medically unnecessary” as a reason for a denial of a claim.
Nearly 80% of the participating hospitals reported RAC activity in 2010, with general medical and surgical hospitals reporting the most activity. Fifty percent of reporting hospitals noted that their administrative burden—in the form of hiring consultants, copying medical records, hiring legal counsel, and the like—had increased as a result of RAC activity.
Most importantly, the report shows the average dollar value of automated denials was $399. But when a complex review—one involving a human review of requested records—was conducted, the average value of the denial was $5,281. Additionally, inpatient facilities were most likely to experience complex denials, which account for 90% of the value of denied claims.
Leong says RAC audits are just one area of “exposure to review for hospitals and providers. Other third-party payers, including individual commercial insurance companies,” she says, “also do routine post-payment review and recoupment, several years after payment.”—GH
It’s no secret that documenting and coding one’s work is not the average hospitalist’s favorite thing to do. It’s probably not even in the top 10 or 20. In fact, many consider the whole documentation process a “thorn in the side.”
“When I first started working, I couldn’t believe that I could get audited and fined just because I didn’t add ‘10-point’ or ‘12-point’ to my note of ‘review of systems: negative,’ ” says hospitalist Amaka Nweke, MD, assistant director with Hospitalists Management Group (HMG) at Kenosha Medical Center in Kenosha, Wis. “I had a lot of frustration, because I had to repackage and re-present my notes in a manner that makes sense to Medicare but makes no sense to physicians.”
Like it or not, healthcare providers live in a highly regulated world, says Richard D. Pinson, MD, FACP, CCS, who became a certified coding specialist and formed his own consulting company, Houston-based HCQ Consulting, to help hospitals and physicians achieve diagnostic accuracy for inpatient care. Documentation and coding have become a serious, high-stakes word game, he says. “Perfectly good clinical documentation, especially with some important diagnoses, may not correspond at all to what is required by the strict coding rules that govern code assignments,” he says.
A hospitalist’s documentation is at the heart of accurate coding, whether it’s for the hospital’s DRG reimbursement, quality and performance scores, or for assigning current procedural terminology (CPT) and evaluation and management (E/M) codes for billing for their own professional services. And if hospitalists don’t buy into the coding mindset, they risk decreased reimbursement for their services, monetary losses for the hospital, Medicare audits, compromised quality scores for both the hospital and themselves, and noncompliance.
“If your documentation is not up to par, then the hospital may get fined and lose money, and you can’t prove your worth as a hospitalist,” Dr. Nweke says.
What’s at Stake?
Inadequate documentation results in “undercoding” a patient’s condition and underpayment to your hospital (see Table 1, right). Undercoding also can result in inadequate representation of the severity of a patient’s illness, complexity, and cost of care. If a patient gets worse in the hospital, then that initial lower severity of illness might show up in poor performance scores on outcome measures. If a patient’s severity of illness is miscoded, Medicare might question the medical necessity for inpatient admission and deny payment.
On the other hand, if overcoding occurs because the clinical criteria for a specific diagnosis have not been met, Medicare will take action to recover the overpayment, leveling penalties and sanctions. (For more information on Medicare’s Recovery Audit Contractor program, dubbed “Medicare’s repo men” by Dr. Pinson, see “Take Proactive Approach to Recovery Audit Contractors,” p. 28.)
Lack of specificity also hampers reimbursement for professional fees, says Barb Pierce, CCS-P, ACS-EM, president of Barb Pierce Coding and Consulting Inc. of West Des Moines, Iowa. “Unfortunately,” she observes, “the code isn’t just based on decision-making, which is why physicians went to school for all those years. The guidelines [Documentation Guidelines for Evaluation and Management Services] mandate that if you forget one little bullet in history or examination, even if you’ve got the riskiest, highest-level, decision-making patient in front of you, that could pull down the whole code selection.”1
How costly might such small mistakes be for an HM group? According to the State of Hospital Medicine: 2010 Report Based on 2009 Data survey, internal-medicine hospitalists generate a median of 1.86 work relative value units (wRVUs) per encounter, and collect $45.57 per wRVU.2 If a hospitalist has 2,200 encounters per year and averages only 1.65 wRVUs per encounter, improving documentation and coding performance could add an additional 0.21 wRVUs, meeting the national average. Multiplying those 2,200 encounters by the national average of 1.86, the hospitalist could potentially add an additional 462 wRVUs for the year. Such documentation improvement—up to the national average—would equate to $21,053 in additional billed revenue without increasing the physician’s overall workload.
Dr. Pinson explains that physicians often perceive their time constraints as so severe that they’d be hard pressed to find the time to learn about documentation and coding. But he maintains that even short seminars yield “a huge amount of information that would astound [hospitalists], in terms of usefulness for their own clinical practices.”
Barriers to the Coding Mindset
Most hospitalists receive little or no training in documentation and coding during medical school or residency. The lack of education is further complicated because there are several coding sets healthcare providers must master, each with different rules governing assignment of diagnoses and levels of care (see “Coding Sets: Separate but Overlapping,” above).
Inexperience with coding guidelines can lead to mismatches. Nelly Leon-Chisen, RHIA, director of coding and classification for the American Hospital Association (AHA), gives one example: The ICD-9-CM Official Coding Guideline stipulates that coders cannot assign diagnosis codes based on lab results.3 So although it might appear intuitive to a physician that repeated blood sugars and monitoring of insulin levels indicate a patient has diabetes, the coder cannot assign the diagnosis unless it’s explicitly stated in the record.
Some physicians could simply be using outmoded terminology, such as “renal insufficiency” instead of “acute renal failure,” Dr. Pinson notes. If hospitalists learn to focus on evidence-based clinical criteria to support the codes, it leads to more effective care, he says.
The nature of hospitalist programs might not lend itself to efficient revenue-cycle processes for their own professional billing, says Jeri Leong, RN, CPC, CPC-H, president and CEO of Honolulu-based Healthcare Coding Consultants of Hawaii. If the HM group contracts with several hospitals, the hospitalists will be together rarely as a group, “so they don’t have the luxury of sitting down together with their billers to get important feedback and coding updates,” she says.
Leong’s company identifies missed charges, for instance, when charge tags from different shifts do not get married together (Hospitalist A might round on the patient in the morning and turn in a charge tag; Hospitalist B might do a procedure in the afternoon, but the two tags do not get combined). Examples such as these, she says, “can be an issue from a compliance perspective, and can leave money on the table.”
One of the problems Kathy DeVault, RHIA, CCS, CCS-P, manager of professional practice resources for the American Health Information Management Association (AHIMA), sees is a lack of continuity between initial admitting diagnosis and discharge summaries. For example, a hospitalist might admit a patient for acute renal failure—the correct diagnosis—and be able to reverse the condition fairly quickly, especially if the failure is due to dehydration.
The patient, whose issue is resolved, could be discharged by an attending physician who does not note the acute diagnosis in the summary. “That acute condition disappears, and the RAC auditor may then challenge the claim for payment,” DeVault says.
The Remedies
While physicians might think that they don’t have the time to acquire coding education, there could be other incentives coming down the pike. Dr. Pinson has noticed that hospitals are beginning to incorporate documentation accuracy into their contractual reimbursement formulas.
Documentation fixes vary according to domain. A hospital’s clinical documentation specialists can query physicians for clarity and detail in their notes; for instance, a diagnosis of congestive heart failure (CHF) must be accompanied by additional documentation stating whether the CHF is acute or chronic, and whether it is systolic or diastolic.
Many hospitals have instituted clinical documentation improvement (CDI) programs, sometimes called clinical documentation integrity programs, to address documentation discrepancies. CDI programs are essential to hospitals’ financial survival, Dr. Pinson says, and hospitalists are ideally positioned to join those efforts.
“[The hospitalists] are the most important people to the hospital in all of this,” he says. “They’re at the center of this whirlpool. If you have these skills, your value to the hospital and to your group is greatly enhanced.” (Visit the-hospitalist.org to listen to Dr. Pinson discuss HM’s role in documentation improvement.)
Leon-Chisen also says that the relationship between coders and physicians should be collaborative. “If it’s adversarial, nobody wins,” she points out, adding that CDI programs present an opportunity for mutual education.
Conducting audits of the practice’s documentation and coding can identify coding strengths and weaknesses, says Pierce, who is faculty for SHM’s billing and coding pre-course and regularly consults with hospitalist groups. Audits are helpful, she says, not just for increasing group revenue, but for compliance reasons as well. “You need to know what you’re doing well, and what you’re not doing quite so well, and get it fixed internally before an entity like Medicare discovers it,” she says.
It’s no doubt difficult for a busy HM group to stay on top of annual coding updates and changes to guidelines for reporting their services, Leong notes. Her company has worked with many hospitalist groups over the years, offering coding workshops, “back end” audits, and real-time feedback of E/M and CPT coding choices. If all of the hospitalists in a group cannot convene simultaneously, Leong provides the feedback (in the form of a scorecard) to the group’s physician champion, who becomes the lead contact to help those physicians who struggle more with their coding. (Leong talks more about real-time feedback and capturing CPT and E/M codes at the-hospitalist.org.)
In lieu of hiring professional coders, some HM groups use electronic coding devices. The software could be a standalone product, or it could interface with other products, such as electronic medical records (EMRs). These programs assist with a variety of coding-related activities, such as CPT or ICD-9 lookups, or calculation of E/M key components with assignment of an appropriate level of billing. Leong, however, cautions too much reliance on technology.
“While these devices can be accurate, compact, and convenient, it’s important to maintain a current [software] subscription to keep abreast of updates to the code sets, which occur sometimes as often as quarterly,” she says.
Pierce adds that coding tools should be double-checked against an audit tool. She has sometimes found discrepancies when auditing against an EMR product that assigns the E/M level.
Attitude Adjustment
Coding experts emphasize that physicians need not worry about mastering coding manuals, but they should forge relationships with both their hospital’s billers and the coders for their practice.
Dr. Nweke took advantage of coding and billing workshops offered by her group, HMG, and through the seminars began to understand what a DRG meant not just for her hospital but for her own evaluations and the expansion of her HM group, too. “Now, when I get questions from billers and coders, I try to answer them quickly,” she says. “I don’t look upon them as the enemy, but rather as people who are helping me document appropriately, so I don’t get audited by Medicare. I think the way you view the coders and billers definitely affects your willingness to learn.”
Dr. Nweke also takes a broader view of her role as a hospitalist. “You are there to take care of patients and assist with transitioning them in and out of the hospital, but you’re also there to ensure that the hospital remains afloat financially,” she says. “Your documentation plays a huge role in that. We have a huge contribution to make.”
The patient gains, too, says Leon-Chisen, who explains that documentation should be as accurate as possible “because someone else—the patient’s primary physician—will be taking over care of that patient and needs to understand what happened in the hospital.”
“The bottom line,” Dr. Pinson says, “is that we need accurate documentation that can be correctly coded to reflect the true complexity of care and severity of illness. If we do that, good things will follow.” TH
Gretchen Henkel is a freelance writer based in California.
References
- 1997 Documentation Guidelines for Evaluation and Management Services. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/MLNProducts/Downloads/MASTER1.pdf. Accessed April 11, 2011.
- State of Hospital Medicine: 2010 Report Based on 2009 Data. Society of Hospital Medicine and Medical Group Management Association; Philadelphia and Englewood, Colo.; 2010.
- ICD-9-CM Official Coding Guidelines. CMS and National Center for Health Statistics; Washington, D.C.; 2008. Available at: www.ama-assn.org/resources/doc/cpt/icd9cm_coding_guidelines_08_09_full.pdf. Accessed April 10, 2011.
Take Proactive Approach to Recovery Audit Contractors
The congressionally authorized Medicare Recovery Audit Contractor (RAC) program began with a three-year demonstration pilot project in 2005. In August 2010, the program expanded to the entire country. The RAC’s main objective is to identify improper Medicare payments, both overpayments and underpayments, to providers. CMS, which administrates Medicare and the RAC program, has agreements with contractors who are authorized to audit and review claims that are up to three years old.
According to Elizabeth Baskett, senior associate director of policy at the AHA, medical necessity review was a big focus of the RAC demonstration project and now is “under way in the permanent RAC program. We are bracing ourselves for a significant amount of denials.”
The AHA has created a free, Web-based survey called RAC Trac (www.aha.org/aha/issues/RAC/ractrac.html) to assess the nationwide impact the RAC program has on U.S. hospitals. In a report released Feb. 24, the RAC Trac survey shows that $82 million in denials were reported, more than double the dollar amount of denials reported in the third quarter of 2010 (see Figure 1, below). It also shows 57% of the more than 1,850 participating hospitals cited “medically unnecessary” as a reason for a denial of a claim.
Nearly 80% of the participating hospitals reported RAC activity in 2010, with general medical and surgical hospitals reporting the most activity. Fifty percent of reporting hospitals noted that their administrative burden—in the form of hiring consultants, copying medical records, hiring legal counsel, and the like—had increased as a result of RAC activity.
Most importantly, the report shows the average dollar value of automated denials was $399. But when a complex review—one involving a human review of requested records—was conducted, the average value of the denial was $5,281. Additionally, inpatient facilities were most likely to experience complex denials, which account for 90% of the value of denied claims.
Leong says RAC audits are just one area of “exposure to review for hospitals and providers. Other third-party payers, including individual commercial insurance companies,” she says, “also do routine post-payment review and recoupment, several years after payment.”—GH
It’s no secret that documenting and coding one’s work is not the average hospitalist’s favorite thing to do. It’s probably not even in the top 10 or 20. In fact, many consider the whole documentation process a “thorn in the side.”
“When I first started working, I couldn’t believe that I could get audited and fined just because I didn’t add ‘10-point’ or ‘12-point’ to my note of ‘review of systems: negative,’ ” says hospitalist Amaka Nweke, MD, assistant director with Hospitalists Management Group (HMG) at Kenosha Medical Center in Kenosha, Wis. “I had a lot of frustration, because I had to repackage and re-present my notes in a manner that makes sense to Medicare but makes no sense to physicians.”
Like it or not, healthcare providers live in a highly regulated world, says Richard D. Pinson, MD, FACP, CCS, who became a certified coding specialist and formed his own consulting company, Houston-based HCQ Consulting, to help hospitals and physicians achieve diagnostic accuracy for inpatient care. Documentation and coding have become a serious, high-stakes word game, he says. “Perfectly good clinical documentation, especially with some important diagnoses, may not correspond at all to what is required by the strict coding rules that govern code assignments,” he says.
A hospitalist’s documentation is at the heart of accurate coding, whether it’s for the hospital’s DRG reimbursement, quality and performance scores, or for assigning current procedural terminology (CPT) and evaluation and management (E/M) codes for billing for their own professional services. And if hospitalists don’t buy into the coding mindset, they risk decreased reimbursement for their services, monetary losses for the hospital, Medicare audits, compromised quality scores for both the hospital and themselves, and noncompliance.
“If your documentation is not up to par, then the hospital may get fined and lose money, and you can’t prove your worth as a hospitalist,” Dr. Nweke says.
What’s at Stake?
Inadequate documentation results in “undercoding” a patient’s condition and underpayment to your hospital (see Table 1, right). Undercoding also can result in inadequate representation of the severity of a patient’s illness, complexity, and cost of care. If a patient gets worse in the hospital, then that initial lower severity of illness might show up in poor performance scores on outcome measures. If a patient’s severity of illness is miscoded, Medicare might question the medical necessity for inpatient admission and deny payment.
On the other hand, if overcoding occurs because the clinical criteria for a specific diagnosis have not been met, Medicare will take action to recover the overpayment, leveling penalties and sanctions. (For more information on Medicare’s Recovery Audit Contractor program, dubbed “Medicare’s repo men” by Dr. Pinson, see “Take Proactive Approach to Recovery Audit Contractors,” p. 28.)
Lack of specificity also hampers reimbursement for professional fees, says Barb Pierce, CCS-P, ACS-EM, president of Barb Pierce Coding and Consulting Inc. of West Des Moines, Iowa. “Unfortunately,” she observes, “the code isn’t just based on decision-making, which is why physicians went to school for all those years. The guidelines [Documentation Guidelines for Evaluation and Management Services] mandate that if you forget one little bullet in history or examination, even if you’ve got the riskiest, highest-level, decision-making patient in front of you, that could pull down the whole code selection.”1
How costly might such small mistakes be for an HM group? According to the State of Hospital Medicine: 2010 Report Based on 2009 Data survey, internal-medicine hospitalists generate a median of 1.86 work relative value units (wRVUs) per encounter, and collect $45.57 per wRVU.2 If a hospitalist has 2,200 encounters per year and averages only 1.65 wRVUs per encounter, improving documentation and coding performance could add an additional 0.21 wRVUs, meeting the national average. Multiplying those 2,200 encounters by the national average of 1.86, the hospitalist could potentially add an additional 462 wRVUs for the year. Such documentation improvement—up to the national average—would equate to $21,053 in additional billed revenue without increasing the physician’s overall workload.
Dr. Pinson explains that physicians often perceive their time constraints as so severe that they’d be hard pressed to find the time to learn about documentation and coding. But he maintains that even short seminars yield “a huge amount of information that would astound [hospitalists], in terms of usefulness for their own clinical practices.”
Barriers to the Coding Mindset
Most hospitalists receive little or no training in documentation and coding during medical school or residency. The lack of education is further complicated because there are several coding sets healthcare providers must master, each with different rules governing assignment of diagnoses and levels of care (see “Coding Sets: Separate but Overlapping,” above).
Inexperience with coding guidelines can lead to mismatches. Nelly Leon-Chisen, RHIA, director of coding and classification for the American Hospital Association (AHA), gives one example: The ICD-9-CM Official Coding Guideline stipulates that coders cannot assign diagnosis codes based on lab results.3 So although it might appear intuitive to a physician that repeated blood sugars and monitoring of insulin levels indicate a patient has diabetes, the coder cannot assign the diagnosis unless it’s explicitly stated in the record.
Some physicians could simply be using outmoded terminology, such as “renal insufficiency” instead of “acute renal failure,” Dr. Pinson notes. If hospitalists learn to focus on evidence-based clinical criteria to support the codes, it leads to more effective care, he says.
The nature of hospitalist programs might not lend itself to efficient revenue-cycle processes for their own professional billing, says Jeri Leong, RN, CPC, CPC-H, president and CEO of Honolulu-based Healthcare Coding Consultants of Hawaii. If the HM group contracts with several hospitals, the hospitalists will be together rarely as a group, “so they don’t have the luxury of sitting down together with their billers to get important feedback and coding updates,” she says.
Leong’s company identifies missed charges, for instance, when charge tags from different shifts do not get married together (Hospitalist A might round on the patient in the morning and turn in a charge tag; Hospitalist B might do a procedure in the afternoon, but the two tags do not get combined). Examples such as these, she says, “can be an issue from a compliance perspective, and can leave money on the table.”
One of the problems Kathy DeVault, RHIA, CCS, CCS-P, manager of professional practice resources for the American Health Information Management Association (AHIMA), sees is a lack of continuity between initial admitting diagnosis and discharge summaries. For example, a hospitalist might admit a patient for acute renal failure—the correct diagnosis—and be able to reverse the condition fairly quickly, especially if the failure is due to dehydration.
The patient, whose issue is resolved, could be discharged by an attending physician who does not note the acute diagnosis in the summary. “That acute condition disappears, and the RAC auditor may then challenge the claim for payment,” DeVault says.
The Remedies
While physicians might think that they don’t have the time to acquire coding education, there could be other incentives coming down the pike. Dr. Pinson has noticed that hospitals are beginning to incorporate documentation accuracy into their contractual reimbursement formulas.
Documentation fixes vary according to domain. A hospital’s clinical documentation specialists can query physicians for clarity and detail in their notes; for instance, a diagnosis of congestive heart failure (CHF) must be accompanied by additional documentation stating whether the CHF is acute or chronic, and whether it is systolic or diastolic.
Many hospitals have instituted clinical documentation improvement (CDI) programs, sometimes called clinical documentation integrity programs, to address documentation discrepancies. CDI programs are essential to hospitals’ financial survival, Dr. Pinson says, and hospitalists are ideally positioned to join those efforts.
“[The hospitalists] are the most important people to the hospital in all of this,” he says. “They’re at the center of this whirlpool. If you have these skills, your value to the hospital and to your group is greatly enhanced.” (Visit the-hospitalist.org to listen to Dr. Pinson discuss HM’s role in documentation improvement.)
Leon-Chisen also says that the relationship between coders and physicians should be collaborative. “If it’s adversarial, nobody wins,” she points out, adding that CDI programs present an opportunity for mutual education.
Conducting audits of the practice’s documentation and coding can identify coding strengths and weaknesses, says Pierce, who is faculty for SHM’s billing and coding pre-course and regularly consults with hospitalist groups. Audits are helpful, she says, not just for increasing group revenue, but for compliance reasons as well. “You need to know what you’re doing well, and what you’re not doing quite so well, and get it fixed internally before an entity like Medicare discovers it,” she says.
It’s no doubt difficult for a busy HM group to stay on top of annual coding updates and changes to guidelines for reporting their services, Leong notes. Her company has worked with many hospitalist groups over the years, offering coding workshops, “back end” audits, and real-time feedback of E/M and CPT coding choices. If all of the hospitalists in a group cannot convene simultaneously, Leong provides the feedback (in the form of a scorecard) to the group’s physician champion, who becomes the lead contact to help those physicians who struggle more with their coding. (Leong talks more about real-time feedback and capturing CPT and E/M codes at the-hospitalist.org.)
In lieu of hiring professional coders, some HM groups use electronic coding devices. The software could be a standalone product, or it could interface with other products, such as electronic medical records (EMRs). These programs assist with a variety of coding-related activities, such as CPT or ICD-9 lookups, or calculation of E/M key components with assignment of an appropriate level of billing. Leong, however, cautions too much reliance on technology.
“While these devices can be accurate, compact, and convenient, it’s important to maintain a current [software] subscription to keep abreast of updates to the code sets, which occur sometimes as often as quarterly,” she says.
Pierce adds that coding tools should be double-checked against an audit tool. She has sometimes found discrepancies when auditing against an EMR product that assigns the E/M level.
Attitude Adjustment
Coding experts emphasize that physicians need not worry about mastering coding manuals, but they should forge relationships with both their hospital’s billers and the coders for their practice.
Dr. Nweke took advantage of coding and billing workshops offered by her group, HMG, and through the seminars began to understand what a DRG meant not just for her hospital but for her own evaluations and the expansion of her HM group, too. “Now, when I get questions from billers and coders, I try to answer them quickly,” she says. “I don’t look upon them as the enemy, but rather as people who are helping me document appropriately, so I don’t get audited by Medicare. I think the way you view the coders and billers definitely affects your willingness to learn.”
Dr. Nweke also takes a broader view of her role as a hospitalist. “You are there to take care of patients and assist with transitioning them in and out of the hospital, but you’re also there to ensure that the hospital remains afloat financially,” she says. “Your documentation plays a huge role in that. We have a huge contribution to make.”
The patient gains, too, says Leon-Chisen, who explains that documentation should be as accurate as possible “because someone else—the patient’s primary physician—will be taking over care of that patient and needs to understand what happened in the hospital.”
“The bottom line,” Dr. Pinson says, “is that we need accurate documentation that can be correctly coded to reflect the true complexity of care and severity of illness. If we do that, good things will follow.” TH
Gretchen Henkel is a freelance writer based in California.
References
- 1997 Documentation Guidelines for Evaluation and Management Services. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/MLNProducts/Downloads/MASTER1.pdf. Accessed April 11, 2011.
- State of Hospital Medicine: 2010 Report Based on 2009 Data. Society of Hospital Medicine and Medical Group Management Association; Philadelphia and Englewood, Colo.; 2010.
- ICD-9-CM Official Coding Guidelines. CMS and National Center for Health Statistics; Washington, D.C.; 2008. Available at: www.ama-assn.org/resources/doc/cpt/icd9cm_coding_guidelines_08_09_full.pdf. Accessed April 10, 2011.
Take Proactive Approach to Recovery Audit Contractors
The congressionally authorized Medicare Recovery Audit Contractor (RAC) program began with a three-year demonstration pilot project in 2005. In August 2010, the program expanded to the entire country. The RAC’s main objective is to identify improper Medicare payments, both overpayments and underpayments, to providers. CMS, which administrates Medicare and the RAC program, has agreements with contractors who are authorized to audit and review claims that are up to three years old.
According to Elizabeth Baskett, senior associate director of policy at the AHA, medical necessity review was a big focus of the RAC demonstration project and now is “under way in the permanent RAC program. We are bracing ourselves for a significant amount of denials.”
The AHA has created a free, Web-based survey called RAC Trac (www.aha.org/aha/issues/RAC/ractrac.html) to assess the nationwide impact the RAC program has on U.S. hospitals. In a report released Feb. 24, the RAC Trac survey shows that $82 million in denials were reported, more than double the dollar amount of denials reported in the third quarter of 2010 (see Figure 1, below). It also shows 57% of the more than 1,850 participating hospitals cited “medically unnecessary” as a reason for a denial of a claim.
Nearly 80% of the participating hospitals reported RAC activity in 2010, with general medical and surgical hospitals reporting the most activity. Fifty percent of reporting hospitals noted that their administrative burden—in the form of hiring consultants, copying medical records, hiring legal counsel, and the like—had increased as a result of RAC activity.
Most importantly, the report shows the average dollar value of automated denials was $399. But when a complex review—one involving a human review of requested records—was conducted, the average value of the denial was $5,281. Additionally, inpatient facilities were most likely to experience complex denials, which account for 90% of the value of denied claims.
Leong says RAC audits are just one area of “exposure to review for hospitals and providers. Other third-party payers, including individual commercial insurance companies,” she says, “also do routine post-payment review and recoupment, several years after payment.”—GH
Rural Hospitals Choose ED-HM Combination
For 10-bed Carilion Tazewell Community Hospital in Tazewell, Va. (population 44,000), mounting financial pressure recently prompted staff redeployment, equipment upgrades, and other efforts to rebuild patient volume that had been siphoned by hospitals in communities 25 or more miles away.
Central to the reorganization, says John H. Burton, MD, chair of emergency medicine for Tazewell’s seven-hospital parent company, Carilion Clinic, was to combine the ED with HM. One physician now covers both the ED, which averages about a visit an hour, and HM, reducing the number of physician FTEs employed by the hospital.
“Traditionally, we think of the emergency department doctor and the hospitalist, who are both paid by the hospital on a fixed basis, as separate roles and separate skill sets,” Dr. Burton says. In larger hospitals, ED docs generally need to be board-certified. “But doctors from family medicine and internal medicine, if trained, can practice very good emergency medicine,” Dr. Burton says. “It dawned on us we could fuse the positions. Caseload has to be manageable; this wouldn’t work in larger hospitals. But for us, it’s easily manageable by one physician doing both roles with the support of a midlevel provider.”
—John H. Burton, MD, chair of emergency medicine, Carilion Tazewell (Va.) Community Hospital
The fused service was launched in February. Long-range plans include a small onsite clinic for post-discharge follow-up, also staffed by the ED/HM physician on duty. “Our dream candidate is internal-medicine-trained and -boarded, but has also practiced in emergency medicine,” Dr. Burton says. “Hospitalists in many settings don’t have the emergency medical skill set—particularly pediatrics. What makes this approach a good fit for us is we already had physicians able to do both.”
A similar approach—combining the ED and HM on a single shift—was implemented earlier this year at Broaddus Hospital in Philippi, W.Va. (population 3,000), which has 12 acute beds and about 8,000 ED visits per year. “We don’t exactly have an abundance of family practice doctors in this area,” says hospital CEO Jeff Powelson.
In many cases, the PCPs continue to round in the hospital, but the ED/HM is able to pick up those who can’t, as well as unassigned patients. Powelson says the new structure helps PCPs who practice at multiple hospitals and can’t be everywhere at once. But if the ED/hospitalist had to cover all of the inpatients, the volume would become unsustainable for a single physician, he admits.
Six physicians are filling the new combined role (four FTEs) and rotating through 24-hour or split shifts. Powelson says communication has improved. In cases where the admitting ED physician also is the hospitalist, there is one less handoff to manage.
“We had to tweak our physician personnel a bit,” hospitalist Randy Turner, DO, says. “Some are not interested in doing this; others are very comfortable wearing both hats, maybe because they’ve done both before. We had to make sure the type of patients we care for wasn’t more than we can handle, and did we have the right personnel.”
John Nelson, MD, MHM, a hospitalist group director, practice management consultant, co-founder of SHM, and columnist for The Hospitalist, sees combined positions as “great ideas” for very small, low-volume hospitals. “[It’s] probably very good for patient care in those facilities,” he says.
Dr. Burton considers his hospitals new plan “innovative.”
“Unfortunately, working at a rural hospital that doesn’t meet federal qualifications for a critical-access hospital, we’re increasingly challenged by changes in the healthcare system,” he says. “We don’t want rural hospitals to go away. We want to serve patients in the same way, with the same level of quality, as urban hospitals. But practical problems in the healthcare system make that difficult.
“This model achieves the best of what we could hope for in this community, enabling us to pay higher rates and attract better physicians,” he says.
Larry Beresford is a freelance writer based in Oakland, Calif.
For 10-bed Carilion Tazewell Community Hospital in Tazewell, Va. (population 44,000), mounting financial pressure recently prompted staff redeployment, equipment upgrades, and other efforts to rebuild patient volume that had been siphoned by hospitals in communities 25 or more miles away.
Central to the reorganization, says John H. Burton, MD, chair of emergency medicine for Tazewell’s seven-hospital parent company, Carilion Clinic, was to combine the ED with HM. One physician now covers both the ED, which averages about a visit an hour, and HM, reducing the number of physician FTEs employed by the hospital.
“Traditionally, we think of the emergency department doctor and the hospitalist, who are both paid by the hospital on a fixed basis, as separate roles and separate skill sets,” Dr. Burton says. In larger hospitals, ED docs generally need to be board-certified. “But doctors from family medicine and internal medicine, if trained, can practice very good emergency medicine,” Dr. Burton says. “It dawned on us we could fuse the positions. Caseload has to be manageable; this wouldn’t work in larger hospitals. But for us, it’s easily manageable by one physician doing both roles with the support of a midlevel provider.”
—John H. Burton, MD, chair of emergency medicine, Carilion Tazewell (Va.) Community Hospital
The fused service was launched in February. Long-range plans include a small onsite clinic for post-discharge follow-up, also staffed by the ED/HM physician on duty. “Our dream candidate is internal-medicine-trained and -boarded, but has also practiced in emergency medicine,” Dr. Burton says. “Hospitalists in many settings don’t have the emergency medical skill set—particularly pediatrics. What makes this approach a good fit for us is we already had physicians able to do both.”
A similar approach—combining the ED and HM on a single shift—was implemented earlier this year at Broaddus Hospital in Philippi, W.Va. (population 3,000), which has 12 acute beds and about 8,000 ED visits per year. “We don’t exactly have an abundance of family practice doctors in this area,” says hospital CEO Jeff Powelson.
In many cases, the PCPs continue to round in the hospital, but the ED/HM is able to pick up those who can’t, as well as unassigned patients. Powelson says the new structure helps PCPs who practice at multiple hospitals and can’t be everywhere at once. But if the ED/hospitalist had to cover all of the inpatients, the volume would become unsustainable for a single physician, he admits.
Six physicians are filling the new combined role (four FTEs) and rotating through 24-hour or split shifts. Powelson says communication has improved. In cases where the admitting ED physician also is the hospitalist, there is one less handoff to manage.
“We had to tweak our physician personnel a bit,” hospitalist Randy Turner, DO, says. “Some are not interested in doing this; others are very comfortable wearing both hats, maybe because they’ve done both before. We had to make sure the type of patients we care for wasn’t more than we can handle, and did we have the right personnel.”
John Nelson, MD, MHM, a hospitalist group director, practice management consultant, co-founder of SHM, and columnist for The Hospitalist, sees combined positions as “great ideas” for very small, low-volume hospitals. “[It’s] probably very good for patient care in those facilities,” he says.
Dr. Burton considers his hospitals new plan “innovative.”
“Unfortunately, working at a rural hospital that doesn’t meet federal qualifications for a critical-access hospital, we’re increasingly challenged by changes in the healthcare system,” he says. “We don’t want rural hospitals to go away. We want to serve patients in the same way, with the same level of quality, as urban hospitals. But practical problems in the healthcare system make that difficult.
“This model achieves the best of what we could hope for in this community, enabling us to pay higher rates and attract better physicians,” he says.
Larry Beresford is a freelance writer based in Oakland, Calif.
For 10-bed Carilion Tazewell Community Hospital in Tazewell, Va. (population 44,000), mounting financial pressure recently prompted staff redeployment, equipment upgrades, and other efforts to rebuild patient volume that had been siphoned by hospitals in communities 25 or more miles away.
Central to the reorganization, says John H. Burton, MD, chair of emergency medicine for Tazewell’s seven-hospital parent company, Carilion Clinic, was to combine the ED with HM. One physician now covers both the ED, which averages about a visit an hour, and HM, reducing the number of physician FTEs employed by the hospital.
“Traditionally, we think of the emergency department doctor and the hospitalist, who are both paid by the hospital on a fixed basis, as separate roles and separate skill sets,” Dr. Burton says. In larger hospitals, ED docs generally need to be board-certified. “But doctors from family medicine and internal medicine, if trained, can practice very good emergency medicine,” Dr. Burton says. “It dawned on us we could fuse the positions. Caseload has to be manageable; this wouldn’t work in larger hospitals. But for us, it’s easily manageable by one physician doing both roles with the support of a midlevel provider.”
—John H. Burton, MD, chair of emergency medicine, Carilion Tazewell (Va.) Community Hospital
The fused service was launched in February. Long-range plans include a small onsite clinic for post-discharge follow-up, also staffed by the ED/HM physician on duty. “Our dream candidate is internal-medicine-trained and -boarded, but has also practiced in emergency medicine,” Dr. Burton says. “Hospitalists in many settings don’t have the emergency medical skill set—particularly pediatrics. What makes this approach a good fit for us is we already had physicians able to do both.”
A similar approach—combining the ED and HM on a single shift—was implemented earlier this year at Broaddus Hospital in Philippi, W.Va. (population 3,000), which has 12 acute beds and about 8,000 ED visits per year. “We don’t exactly have an abundance of family practice doctors in this area,” says hospital CEO Jeff Powelson.
In many cases, the PCPs continue to round in the hospital, but the ED/HM is able to pick up those who can’t, as well as unassigned patients. Powelson says the new structure helps PCPs who practice at multiple hospitals and can’t be everywhere at once. But if the ED/hospitalist had to cover all of the inpatients, the volume would become unsustainable for a single physician, he admits.
Six physicians are filling the new combined role (four FTEs) and rotating through 24-hour or split shifts. Powelson says communication has improved. In cases where the admitting ED physician also is the hospitalist, there is one less handoff to manage.
“We had to tweak our physician personnel a bit,” hospitalist Randy Turner, DO, says. “Some are not interested in doing this; others are very comfortable wearing both hats, maybe because they’ve done both before. We had to make sure the type of patients we care for wasn’t more than we can handle, and did we have the right personnel.”
John Nelson, MD, MHM, a hospitalist group director, practice management consultant, co-founder of SHM, and columnist for The Hospitalist, sees combined positions as “great ideas” for very small, low-volume hospitals. “[It’s] probably very good for patient care in those facilities,” he says.
Dr. Burton considers his hospitals new plan “innovative.”
“Unfortunately, working at a rural hospital that doesn’t meet federal qualifications for a critical-access hospital, we’re increasingly challenged by changes in the healthcare system,” he says. “We don’t want rural hospitals to go away. We want to serve patients in the same way, with the same level of quality, as urban hospitals. But practical problems in the healthcare system make that difficult.
“This model achieves the best of what we could hope for in this community, enabling us to pay higher rates and attract better physicians,” he says.
Larry Beresford is a freelance writer based in Oakland, Calif.