User login
Distinguished CHEST Educators
In keeping with the commitment of the American College of Chest Physicians (CHEST) to be the home of the clinician educator, and supporting CHEST’s strategic vision of advancing best patient outcomes through innovative chest medicine education, a new designation intended to provide national-level recognition of excellence in continuing medical education has been established—the innovation award-winning Distinguished CHEST Educator.
Distinguished CHEST Educators are within the top 5% of CHEST’s faculty and are recognized for their achievements in making significant and long-term contributions to the design and delivery of CHEST education. With more than 108 ways to educate, these faculty members have exceeded expectations by serving as CHEST committee chairs, vice-chairs, faculty, and peer reviewers for programs such as the CHEST Annual Meeting.
“The greatest achievement I can imagine is seen in the people we train—as that lives on. Real values in medicine live only by being handed down to others. Over the past decade, CHEST has afforded me the privilege to represent the organization on a national platform, and, in doing so, I have been able to refine my own skills and those of my peers, as well as adding both quality and detail to my understanding of how young physicians learn,” says Nader Kamangar, MD, FCCP, of UCLA, CHEST member since 2000, and Distinguished CHEST Educator.
This designation will be granted to select clinical educators each year. The inaugural class of Distinguished CHEST Educators was honored at the end of October at CHEST 2017 in Toronto, as will be the tradition for the classes that follow.
Distinguished CHEST Educator
Congratulations to the inaugural class of Distinguished CHEST Educators.
Sandra Adams, MD, MS, FCCP
Doreen Addrizzo-Harris, MD, FCCP
A. Christine Argento, MD, FCCP
Robert Arntfield, MD, FCCP
Anthony Asciutto, RRT
Olivier Axler, MD, PhD, FCCP
Meyer Balter, MD, FCCP
Gisela Banauch, MD, MS, FCCP
Robert Baughman, MD, FCCP
David Bell, MD, FCCP
Michel Boivin, MD, FCCP
Gabriel Bosslet, MD, FCCP
Jean Bourbeau, MD, MS, FCCP
David Bowton, MD, FCCP
Kevin Brown, MD, FCCP
Jack Buckley, MD, MPH, FCCP
Kristin Burkart, MD, MS, FCCP
Brian Carlin, MD, FCCP
Christopher Carroll, MD, FCCP
Roberto Casal, MD
Richard Castriotta, MD, FCCP
Kevin Chan, MD, FCCP
Alexander Chen, MD
Michael Christian, MD, FCCP
Nancy Collop, MD, FCCP
Clayton Cowl, MD, MS, FCCP
Angel Coz Yataco, MD, FCCP
Gerard Criner, MD, FCCP
Carolyn D’Ambrosio, MD, FCCP
Mauricio Danckers, MD, FCCP
Aneesa Das, MD, FCCP
John Davies, RRT, MA, FCCP
Frank Detterbeck, MD, FCCP
Emily Diederich, MD, FCCP
Kevin Doerschug, MD, MS, FCCP
Meagan Dubosky, RRT-ACCS
Kevin Dushay, MD, FCCP
Eric Edell, MD, FCCP
William Enfinger
Michael Ezzie, MD, FCCP
David Feller-Kopman, MD, FCCP
Kevin Felner, MD, FCCP
Neil Freedman, MD, FCCP
Thomas Fuhrman, MD, MS, FCCP
John Gaillard, MD, FCCP
Colin Gillespie, MD
Maritza Groth, MD, FCCP
Mark Hall, MD
Jesse Hall, MD, FCCP
Nicola Hanania, MD, MBBS, FCCP
D. Kyle Hogarth, MD, FCCP
Steven Hollenberg, MD, FCCP
Robert Hyzy, MD, FCCP
Richard Irwin, MD, Master FCCP
Nader Kamangar, MD, MS, FCCP
Carl Kaplan, MD, FCCP
Brian Kaufman, MD, FCCP
William Kelly, MD, FCCP
Seth Koenig, MD, FCCP
Anastassios Koumbourlis, MD, MPH, FCCP
Lindsey Kreisher, RRT
Karol Kremens, MD, FCCP
Sunita Kumar, MD, MBBS, FCCP
Viera Lakticova, MD
Carla Lamb, MD, FCCP
Hans Lee, MD, FCCP
Peter Lenz, MD, MEd, FCCP
Stephanie Levine, MD, FCCP
Deborah Levine, MD, MS, FCCP
Kenneth Lyn-Kew, MD
Joao Alberto de Andrade, MD, FCCP
Neil MacIntyre, MD, FCCP
Donald Mahler, MD, FCCP
Fabien Maldonado, MD, FCCP
Atul Malhotra, MD, FCCP
Haney Mallemat, MD
Darcy Marciniuk, MD, FCCP
Diego Maselli Caceres, MD, FCCP
Paul Mayo, MD, FCCP
Peter Mazzone, MD, MPH, FCCP
John McIlwaine, DO, MBA, FCCP
Mark Metersky, MD, FCCP
Scott Millington, MD
Taro Minami, MD, FCCP
Lisa Moores, MD, FCCP
Amy Morris, MD
John Mullon, MD, FCCP
Septimiu Murgu, MD, FCCP
Mangala Narasimhan, DO, FCCP
Michael Niederman, MD, FCCP
Alexander Niven, MD, FCCP
Anne O’Donnell, MD, FCCP
Erik Osborn, MD
David Ost, MD, MPH, FCCP
Ronald Oudiz, MD, FCCP
Daniel Ouellette, MD, MS, FCCP
Nicholas Pastis, MD, FCCP
Paru Patrawalla, MD, FCCP
Jay Peters, MD, FCCP
Barbara Phillips, MD, MSPH, FCCP
Margaret Pisani, MD, MS, FCCP
Janos Porszasz, MD, PhD
Whitney Prince, MD, FCCP
Suhail Raoof, MBBS, FCCP
Marcos Restrepo, MD, MSc, FCCP
Otis Rickman, DO, FCCP
Roy Ridgeway
Mary Ried, RN, CCRN
Antoni Rosell, MD
Mark Rosen, MD, Master FCCP
Bernard Roth, MD, FCCP
Anthony Saleh, MD, FCCP
Juan Sanchez, MD, FCCP
Pralay Sarkar, MBBS, FCCP
Lewis Satterwhite, MD, FCCP
Paul Scanlon, MD, FCCP
Gregory Schmidt, MD, FCCP
David Schulman, MD, MPH, FCCP
Brady Scott, RRT, MS
Bernardo Selim, MD, FCCP
Curtis Sessler, MD, FCCP
Rakesh Shah, MD, FCCP
Ray Wes Shepherd, MD, FCCP
John Sherner, MD, FCCP
Ariel Shiloh, MD
Samira Shojaee, MD, FCCP
Gerard Silvestri, MD, MS, FCCP
Steven Simpson, MD, FCCP
James Stoller, MD, MS, FCCP
Mary Strek, MD, FCCP
William Stringer, MD, FCCP
Eleanor Summerhill, MD, FCCP
Lynn Tanoue, MD, FCCP
Victor Test, MD, FCCP
Arthur Tokarczyk, MD, FCCP
Anil Vachani, MD, FCCP
Momen Wahidi, MD, MBA, FCCP
Keith Wille, MD, FCCP
Lisa Wolfe, MD, FCCP
Richard Wunderink, MD, FCCP
Lonny Yarmus, DO, FCCP
Kazuhiro Yasufuku, MD, PhD, FCCP
Gulrukh Zaidi, MD
In keeping with the commitment of the American College of Chest Physicians (CHEST) to be the home of the clinician educator, and supporting CHEST’s strategic vision of advancing best patient outcomes through innovative chest medicine education, a new designation intended to provide national-level recognition of excellence in continuing medical education has been established—the innovation award-winning Distinguished CHEST Educator.
Distinguished CHEST Educators are within the top 5% of CHEST’s faculty and are recognized for their achievements in making significant and long-term contributions to the design and delivery of CHEST education. With more than 108 ways to educate, these faculty members have exceeded expectations by serving as CHEST committee chairs, vice-chairs, faculty, and peer reviewers for programs such as the CHEST Annual Meeting.
“The greatest achievement I can imagine is seen in the people we train—as that lives on. Real values in medicine live only by being handed down to others. Over the past decade, CHEST has afforded me the privilege to represent the organization on a national platform, and, in doing so, I have been able to refine my own skills and those of my peers, as well as adding both quality and detail to my understanding of how young physicians learn,” says Nader Kamangar, MD, FCCP, of UCLA, CHEST member since 2000, and Distinguished CHEST Educator.
This designation will be granted to select clinical educators each year. The inaugural class of Distinguished CHEST Educators was honored at the end of October at CHEST 2017 in Toronto, as will be the tradition for the classes that follow.
Distinguished CHEST Educator
Congratulations to the inaugural class of Distinguished CHEST Educators.
Sandra Adams, MD, MS, FCCP
Doreen Addrizzo-Harris, MD, FCCP
A. Christine Argento, MD, FCCP
Robert Arntfield, MD, FCCP
Anthony Asciutto, RRT
Olivier Axler, MD, PhD, FCCP
Meyer Balter, MD, FCCP
Gisela Banauch, MD, MS, FCCP
Robert Baughman, MD, FCCP
David Bell, MD, FCCP
Michel Boivin, MD, FCCP
Gabriel Bosslet, MD, FCCP
Jean Bourbeau, MD, MS, FCCP
David Bowton, MD, FCCP
Kevin Brown, MD, FCCP
Jack Buckley, MD, MPH, FCCP
Kristin Burkart, MD, MS, FCCP
Brian Carlin, MD, FCCP
Christopher Carroll, MD, FCCP
Roberto Casal, MD
Richard Castriotta, MD, FCCP
Kevin Chan, MD, FCCP
Alexander Chen, MD
Michael Christian, MD, FCCP
Nancy Collop, MD, FCCP
Clayton Cowl, MD, MS, FCCP
Angel Coz Yataco, MD, FCCP
Gerard Criner, MD, FCCP
Carolyn D’Ambrosio, MD, FCCP
Mauricio Danckers, MD, FCCP
Aneesa Das, MD, FCCP
John Davies, RRT, MA, FCCP
Frank Detterbeck, MD, FCCP
Emily Diederich, MD, FCCP
Kevin Doerschug, MD, MS, FCCP
Meagan Dubosky, RRT-ACCS
Kevin Dushay, MD, FCCP
Eric Edell, MD, FCCP
William Enfinger
Michael Ezzie, MD, FCCP
David Feller-Kopman, MD, FCCP
Kevin Felner, MD, FCCP
Neil Freedman, MD, FCCP
Thomas Fuhrman, MD, MS, FCCP
John Gaillard, MD, FCCP
Colin Gillespie, MD
Maritza Groth, MD, FCCP
Mark Hall, MD
Jesse Hall, MD, FCCP
Nicola Hanania, MD, MBBS, FCCP
D. Kyle Hogarth, MD, FCCP
Steven Hollenberg, MD, FCCP
Robert Hyzy, MD, FCCP
Richard Irwin, MD, Master FCCP
Nader Kamangar, MD, MS, FCCP
Carl Kaplan, MD, FCCP
Brian Kaufman, MD, FCCP
William Kelly, MD, FCCP
Seth Koenig, MD, FCCP
Anastassios Koumbourlis, MD, MPH, FCCP
Lindsey Kreisher, RRT
Karol Kremens, MD, FCCP
Sunita Kumar, MD, MBBS, FCCP
Viera Lakticova, MD
Carla Lamb, MD, FCCP
Hans Lee, MD, FCCP
Peter Lenz, MD, MEd, FCCP
Stephanie Levine, MD, FCCP
Deborah Levine, MD, MS, FCCP
Kenneth Lyn-Kew, MD
Joao Alberto de Andrade, MD, FCCP
Neil MacIntyre, MD, FCCP
Donald Mahler, MD, FCCP
Fabien Maldonado, MD, FCCP
Atul Malhotra, MD, FCCP
Haney Mallemat, MD
Darcy Marciniuk, MD, FCCP
Diego Maselli Caceres, MD, FCCP
Paul Mayo, MD, FCCP
Peter Mazzone, MD, MPH, FCCP
John McIlwaine, DO, MBA, FCCP
Mark Metersky, MD, FCCP
Scott Millington, MD
Taro Minami, MD, FCCP
Lisa Moores, MD, FCCP
Amy Morris, MD
John Mullon, MD, FCCP
Septimiu Murgu, MD, FCCP
Mangala Narasimhan, DO, FCCP
Michael Niederman, MD, FCCP
Alexander Niven, MD, FCCP
Anne O’Donnell, MD, FCCP
Erik Osborn, MD
David Ost, MD, MPH, FCCP
Ronald Oudiz, MD, FCCP
Daniel Ouellette, MD, MS, FCCP
Nicholas Pastis, MD, FCCP
Paru Patrawalla, MD, FCCP
Jay Peters, MD, FCCP
Barbara Phillips, MD, MSPH, FCCP
Margaret Pisani, MD, MS, FCCP
Janos Porszasz, MD, PhD
Whitney Prince, MD, FCCP
Suhail Raoof, MBBS, FCCP
Marcos Restrepo, MD, MSc, FCCP
Otis Rickman, DO, FCCP
Roy Ridgeway
Mary Ried, RN, CCRN
Antoni Rosell, MD
Mark Rosen, MD, Master FCCP
Bernard Roth, MD, FCCP
Anthony Saleh, MD, FCCP
Juan Sanchez, MD, FCCP
Pralay Sarkar, MBBS, FCCP
Lewis Satterwhite, MD, FCCP
Paul Scanlon, MD, FCCP
Gregory Schmidt, MD, FCCP
David Schulman, MD, MPH, FCCP
Brady Scott, RRT, MS
Bernardo Selim, MD, FCCP
Curtis Sessler, MD, FCCP
Rakesh Shah, MD, FCCP
Ray Wes Shepherd, MD, FCCP
John Sherner, MD, FCCP
Ariel Shiloh, MD
Samira Shojaee, MD, FCCP
Gerard Silvestri, MD, MS, FCCP
Steven Simpson, MD, FCCP
James Stoller, MD, MS, FCCP
Mary Strek, MD, FCCP
William Stringer, MD, FCCP
Eleanor Summerhill, MD, FCCP
Lynn Tanoue, MD, FCCP
Victor Test, MD, FCCP
Arthur Tokarczyk, MD, FCCP
Anil Vachani, MD, FCCP
Momen Wahidi, MD, MBA, FCCP
Keith Wille, MD, FCCP
Lisa Wolfe, MD, FCCP
Richard Wunderink, MD, FCCP
Lonny Yarmus, DO, FCCP
Kazuhiro Yasufuku, MD, PhD, FCCP
Gulrukh Zaidi, MD
In keeping with the commitment of the American College of Chest Physicians (CHEST) to be the home of the clinician educator, and supporting CHEST’s strategic vision of advancing best patient outcomes through innovative chest medicine education, a new designation intended to provide national-level recognition of excellence in continuing medical education has been established—the innovation award-winning Distinguished CHEST Educator.
Distinguished CHEST Educators are within the top 5% of CHEST’s faculty and are recognized for their achievements in making significant and long-term contributions to the design and delivery of CHEST education. With more than 108 ways to educate, these faculty members have exceeded expectations by serving as CHEST committee chairs, vice-chairs, faculty, and peer reviewers for programs such as the CHEST Annual Meeting.
“The greatest achievement I can imagine is seen in the people we train—as that lives on. Real values in medicine live only by being handed down to others. Over the past decade, CHEST has afforded me the privilege to represent the organization on a national platform, and, in doing so, I have been able to refine my own skills and those of my peers, as well as adding both quality and detail to my understanding of how young physicians learn,” says Nader Kamangar, MD, FCCP, of UCLA, CHEST member since 2000, and Distinguished CHEST Educator.
This designation will be granted to select clinical educators each year. The inaugural class of Distinguished CHEST Educators was honored at the end of October at CHEST 2017 in Toronto, as will be the tradition for the classes that follow.
Distinguished CHEST Educator
Congratulations to the inaugural class of Distinguished CHEST Educators.
Sandra Adams, MD, MS, FCCP
Doreen Addrizzo-Harris, MD, FCCP
A. Christine Argento, MD, FCCP
Robert Arntfield, MD, FCCP
Anthony Asciutto, RRT
Olivier Axler, MD, PhD, FCCP
Meyer Balter, MD, FCCP
Gisela Banauch, MD, MS, FCCP
Robert Baughman, MD, FCCP
David Bell, MD, FCCP
Michel Boivin, MD, FCCP
Gabriel Bosslet, MD, FCCP
Jean Bourbeau, MD, MS, FCCP
David Bowton, MD, FCCP
Kevin Brown, MD, FCCP
Jack Buckley, MD, MPH, FCCP
Kristin Burkart, MD, MS, FCCP
Brian Carlin, MD, FCCP
Christopher Carroll, MD, FCCP
Roberto Casal, MD
Richard Castriotta, MD, FCCP
Kevin Chan, MD, FCCP
Alexander Chen, MD
Michael Christian, MD, FCCP
Nancy Collop, MD, FCCP
Clayton Cowl, MD, MS, FCCP
Angel Coz Yataco, MD, FCCP
Gerard Criner, MD, FCCP
Carolyn D’Ambrosio, MD, FCCP
Mauricio Danckers, MD, FCCP
Aneesa Das, MD, FCCP
John Davies, RRT, MA, FCCP
Frank Detterbeck, MD, FCCP
Emily Diederich, MD, FCCP
Kevin Doerschug, MD, MS, FCCP
Meagan Dubosky, RRT-ACCS
Kevin Dushay, MD, FCCP
Eric Edell, MD, FCCP
William Enfinger
Michael Ezzie, MD, FCCP
David Feller-Kopman, MD, FCCP
Kevin Felner, MD, FCCP
Neil Freedman, MD, FCCP
Thomas Fuhrman, MD, MS, FCCP
John Gaillard, MD, FCCP
Colin Gillespie, MD
Maritza Groth, MD, FCCP
Mark Hall, MD
Jesse Hall, MD, FCCP
Nicola Hanania, MD, MBBS, FCCP
D. Kyle Hogarth, MD, FCCP
Steven Hollenberg, MD, FCCP
Robert Hyzy, MD, FCCP
Richard Irwin, MD, Master FCCP
Nader Kamangar, MD, MS, FCCP
Carl Kaplan, MD, FCCP
Brian Kaufman, MD, FCCP
William Kelly, MD, FCCP
Seth Koenig, MD, FCCP
Anastassios Koumbourlis, MD, MPH, FCCP
Lindsey Kreisher, RRT
Karol Kremens, MD, FCCP
Sunita Kumar, MD, MBBS, FCCP
Viera Lakticova, MD
Carla Lamb, MD, FCCP
Hans Lee, MD, FCCP
Peter Lenz, MD, MEd, FCCP
Stephanie Levine, MD, FCCP
Deborah Levine, MD, MS, FCCP
Kenneth Lyn-Kew, MD
Joao Alberto de Andrade, MD, FCCP
Neil MacIntyre, MD, FCCP
Donald Mahler, MD, FCCP
Fabien Maldonado, MD, FCCP
Atul Malhotra, MD, FCCP
Haney Mallemat, MD
Darcy Marciniuk, MD, FCCP
Diego Maselli Caceres, MD, FCCP
Paul Mayo, MD, FCCP
Peter Mazzone, MD, MPH, FCCP
John McIlwaine, DO, MBA, FCCP
Mark Metersky, MD, FCCP
Scott Millington, MD
Taro Minami, MD, FCCP
Lisa Moores, MD, FCCP
Amy Morris, MD
John Mullon, MD, FCCP
Septimiu Murgu, MD, FCCP
Mangala Narasimhan, DO, FCCP
Michael Niederman, MD, FCCP
Alexander Niven, MD, FCCP
Anne O’Donnell, MD, FCCP
Erik Osborn, MD
David Ost, MD, MPH, FCCP
Ronald Oudiz, MD, FCCP
Daniel Ouellette, MD, MS, FCCP
Nicholas Pastis, MD, FCCP
Paru Patrawalla, MD, FCCP
Jay Peters, MD, FCCP
Barbara Phillips, MD, MSPH, FCCP
Margaret Pisani, MD, MS, FCCP
Janos Porszasz, MD, PhD
Whitney Prince, MD, FCCP
Suhail Raoof, MBBS, FCCP
Marcos Restrepo, MD, MSc, FCCP
Otis Rickman, DO, FCCP
Roy Ridgeway
Mary Ried, RN, CCRN
Antoni Rosell, MD
Mark Rosen, MD, Master FCCP
Bernard Roth, MD, FCCP
Anthony Saleh, MD, FCCP
Juan Sanchez, MD, FCCP
Pralay Sarkar, MBBS, FCCP
Lewis Satterwhite, MD, FCCP
Paul Scanlon, MD, FCCP
Gregory Schmidt, MD, FCCP
David Schulman, MD, MPH, FCCP
Brady Scott, RRT, MS
Bernardo Selim, MD, FCCP
Curtis Sessler, MD, FCCP
Rakesh Shah, MD, FCCP
Ray Wes Shepherd, MD, FCCP
John Sherner, MD, FCCP
Ariel Shiloh, MD
Samira Shojaee, MD, FCCP
Gerard Silvestri, MD, MS, FCCP
Steven Simpson, MD, FCCP
James Stoller, MD, MS, FCCP
Mary Strek, MD, FCCP
William Stringer, MD, FCCP
Eleanor Summerhill, MD, FCCP
Lynn Tanoue, MD, FCCP
Victor Test, MD, FCCP
Arthur Tokarczyk, MD, FCCP
Anil Vachani, MD, FCCP
Momen Wahidi, MD, MBA, FCCP
Keith Wille, MD, FCCP
Lisa Wolfe, MD, FCCP
Richard Wunderink, MD, FCCP
Lonny Yarmus, DO, FCCP
Kazuhiro Yasufuku, MD, PhD, FCCP
Gulrukh Zaidi, MD
A Visit With Stephen J. Welch
Stephen J. Welch was officially appointed Executive Vice President and CEO in April after serving as the interim for both positions since May 2016. Here’s a little “inside look” at what Steve is all about.
What is one major accomplishment you hope to achieve as Executive Vice President & Chief Executive Officer?
My goal as EVP/CEO is fairly simple and straightforward: to ensure the organization remains relevant and viable as a leader in providing clinically focused, innovative educational programs and content. I don’t really have one accomplishment that I’m focused on, but I do want to ensure that we achieve our annual organizational goals that support CHEST’s strategic plan. That may sound a little vague, but it’s true. We have so many outstanding programs and initiatives that I’d be doing a disservice to identify a single goal.
How does your previous experience with CHEST help you successfully lead the organization?
With CHEST being a not-for-profit organization, which relies on volunteer leadership and faculty, I think the relationships I’ve built over the past 23 years within the organization and the chest medicine community are invaluable. I personally know so many of our leadership because I’ve been part of the organization at the executive level working with them for those 23 years. They know me and how I approach opportunities, address issues, and handle challenges, which has helped build an immediate level of mutual respect, trust, and confidence between the staff and leadership. In addition, there was no disruption from having someone come in from the outside and have to get up to speed. It made the transition pretty seamless for the staff, as well.
During my time at CHEST, I’ve seen how the organization operates, from the journal, to the annual meeting and board reviews, to the simulation and hands-on skills training, to operational activities like the management of our finances and new global headquarters and training center. I’ve also had the opportunity to meet with many of our international members and sister societies. Those experiences have allowed me to work closely with many of our faculty, authors, and educators to understand their educational and professional needs, so we can ensure that we meet them.
CHEST is only as good as the education we provide, and it’s our subject matter experts who drive that content engine. In my previous role leading the Publishing Division and working on our journal CHEST® and programs like SEEK, I’ve had the honor and pleasure of working with some of the greatest minds in pulmonary, critical care, and sleep medicine. It’s humbling.
What will be some of the underlying themes as you work to outline the strategic plan for the next 5 years?
We are in the final stages of planning for 2018 and beyond, and although our proposed roadmap isn’t significantly different than what we have been doing, there’s some greater emphasis on a few key areas. For example, we’re looking at innovations in educational delivery. We’ve got some very forward thinking faculty educators and staff who are collaborating to develop innovations like gamification of educational and simulation programs, and augmented reality. Globalization and growth are also a key part of our strategic plan, and we are committed to the broad delivery of our educational programs and content both here and around the world. Finally, we have invested in a data analytics project that is maturing, and we’ll be leveraging that information to provide more personalized education plans – not just for the physician but for the entire health-care team. It’s important for us to stay relevant and viable.

Why has CHEST shifted to an interdisciplinary, team-focused approach?
I look at it as simply an evolution that reflects how health care is changing. It’s a team sport now, and our advanced practice providers (APPs) play a huge role in patient management and care. To be as effective and efficient as possible, and ensure the best patient outcomes, the whole team needs to be on the same page, and we believe that providing education for the interdisciplinary care team will help ensure that the best patient care is delivered.
There’s also a need for this education, and we want to fill it. Our APPs tell us that there is no formal pulmonary training or post-masters fellowship in pulmonary medicine for them. They are often left on their own to fill any gaps in knowledge and skills. That’s where our CHEST programs, such as our CHEST Annual Meeting, come in. We have an Interprofessional NetWork made up of APPs and physicians, and they were integral in working with the CHEST 2017 Program Committee to ensure plenty of relevant content was offered. Moving forward, we will continue to offer and build interdisciplinary programs designed for the entire team, as well as programs that address clinical issues across disciplines.
What are some of the critical skills CHEST physicians need to keep the population healthy during the ever-evolving field?
Educationally, we recognize that conferences like the annual CHEST meeting must provide more than just talking heads. We’ve invested heavily in high-fidelity medical simulation through small group, hands-on skill training in critical care techniques, airway management, EBUS, critical care ultrasound, bronchoscopy, and other chest medicine content. It’s like the old adage about fishing: instead of telling people how to fish, we teach them to fish.
Any final thoughts?
I always encourage our members to get involved with CHEST and experience the camaraderie and connectivity of the CHEST family. Ask any of our leadership, and you will surely hear their story of that special person who first introduced them to the College. Reach out and tell a colleague about CHEST. We are focused on clinically relevant education that our members can take back and put into action immediately. At the end of the day, it’s about providing state-of-the-art education via high fidelity medical simulation, hands-on skills training, clinically focused courses, case-based programming, and more—all intended to be immediately implemented to improve patient care and patient outcomes. That’s what the CHEST organization is all about.
Stephen J. Welch was officially appointed Executive Vice President and CEO in April after serving as the interim for both positions since May 2016. Here’s a little “inside look” at what Steve is all about.
What is one major accomplishment you hope to achieve as Executive Vice President & Chief Executive Officer?
My goal as EVP/CEO is fairly simple and straightforward: to ensure the organization remains relevant and viable as a leader in providing clinically focused, innovative educational programs and content. I don’t really have one accomplishment that I’m focused on, but I do want to ensure that we achieve our annual organizational goals that support CHEST’s strategic plan. That may sound a little vague, but it’s true. We have so many outstanding programs and initiatives that I’d be doing a disservice to identify a single goal.
How does your previous experience with CHEST help you successfully lead the organization?
With CHEST being a not-for-profit organization, which relies on volunteer leadership and faculty, I think the relationships I’ve built over the past 23 years within the organization and the chest medicine community are invaluable. I personally know so many of our leadership because I’ve been part of the organization at the executive level working with them for those 23 years. They know me and how I approach opportunities, address issues, and handle challenges, which has helped build an immediate level of mutual respect, trust, and confidence between the staff and leadership. In addition, there was no disruption from having someone come in from the outside and have to get up to speed. It made the transition pretty seamless for the staff, as well.
During my time at CHEST, I’ve seen how the organization operates, from the journal, to the annual meeting and board reviews, to the simulation and hands-on skills training, to operational activities like the management of our finances and new global headquarters and training center. I’ve also had the opportunity to meet with many of our international members and sister societies. Those experiences have allowed me to work closely with many of our faculty, authors, and educators to understand their educational and professional needs, so we can ensure that we meet them.
CHEST is only as good as the education we provide, and it’s our subject matter experts who drive that content engine. In my previous role leading the Publishing Division and working on our journal CHEST® and programs like SEEK, I’ve had the honor and pleasure of working with some of the greatest minds in pulmonary, critical care, and sleep medicine. It’s humbling.
What will be some of the underlying themes as you work to outline the strategic plan for the next 5 years?
We are in the final stages of planning for 2018 and beyond, and although our proposed roadmap isn’t significantly different than what we have been doing, there’s some greater emphasis on a few key areas. For example, we’re looking at innovations in educational delivery. We’ve got some very forward thinking faculty educators and staff who are collaborating to develop innovations like gamification of educational and simulation programs, and augmented reality. Globalization and growth are also a key part of our strategic plan, and we are committed to the broad delivery of our educational programs and content both here and around the world. Finally, we have invested in a data analytics project that is maturing, and we’ll be leveraging that information to provide more personalized education plans – not just for the physician but for the entire health-care team. It’s important for us to stay relevant and viable.
Why has CHEST shifted to an interdisciplinary, team-focused approach?
I look at it as simply an evolution that reflects how health care is changing. It’s a team sport now, and our advanced practice providers (APPs) play a huge role in patient management and care. To be as effective and efficient as possible, and ensure the best patient outcomes, the whole team needs to be on the same page, and we believe that providing education for the interdisciplinary care team will help ensure that the best patient care is delivered.
There’s also a need for this education, and we want to fill it. Our APPs tell us that there is no formal pulmonary training or post-masters fellowship in pulmonary medicine for them. They are often left on their own to fill any gaps in knowledge and skills. That’s where our CHEST programs, such as our CHEST Annual Meeting, come in. We have an Interprofessional NetWork made up of APPs and physicians, and they were integral in working with the CHEST 2017 Program Committee to ensure plenty of relevant content was offered. Moving forward, we will continue to offer and build interdisciplinary programs designed for the entire team, as well as programs that address clinical issues across disciplines.
What are some of the critical skills CHEST physicians need to keep the population healthy during the ever-evolving field?
Educationally, we recognize that conferences like the annual CHEST meeting must provide more than just talking heads. We’ve invested heavily in high-fidelity medical simulation through small group, hands-on skill training in critical care techniques, airway management, EBUS, critical care ultrasound, bronchoscopy, and other chest medicine content. It’s like the old adage about fishing: instead of telling people how to fish, we teach them to fish.
Any final thoughts?
I always encourage our members to get involved with CHEST and experience the camaraderie and connectivity of the CHEST family. Ask any of our leadership, and you will surely hear their story of that special person who first introduced them to the College. Reach out and tell a colleague about CHEST. We are focused on clinically relevant education that our members can take back and put into action immediately. At the end of the day, it’s about providing state-of-the-art education via high fidelity medical simulation, hands-on skills training, clinically focused courses, case-based programming, and more—all intended to be immediately implemented to improve patient care and patient outcomes. That’s what the CHEST organization is all about.
Stephen J. Welch was officially appointed Executive Vice President and CEO in April after serving as the interim for both positions since May 2016. Here’s a little “inside look” at what Steve is all about.
What is one major accomplishment you hope to achieve as Executive Vice President & Chief Executive Officer?
My goal as EVP/CEO is fairly simple and straightforward: to ensure the organization remains relevant and viable as a leader in providing clinically focused, innovative educational programs and content. I don’t really have one accomplishment that I’m focused on, but I do want to ensure that we achieve our annual organizational goals that support CHEST’s strategic plan. That may sound a little vague, but it’s true. We have so many outstanding programs and initiatives that I’d be doing a disservice to identify a single goal.
How does your previous experience with CHEST help you successfully lead the organization?
With CHEST being a not-for-profit organization, which relies on volunteer leadership and faculty, I think the relationships I’ve built over the past 23 years within the organization and the chest medicine community are invaluable. I personally know so many of our leadership because I’ve been part of the organization at the executive level working with them for those 23 years. They know me and how I approach opportunities, address issues, and handle challenges, which has helped build an immediate level of mutual respect, trust, and confidence between the staff and leadership. In addition, there was no disruption from having someone come in from the outside and have to get up to speed. It made the transition pretty seamless for the staff, as well.
During my time at CHEST, I’ve seen how the organization operates, from the journal, to the annual meeting and board reviews, to the simulation and hands-on skills training, to operational activities like the management of our finances and new global headquarters and training center. I’ve also had the opportunity to meet with many of our international members and sister societies. Those experiences have allowed me to work closely with many of our faculty, authors, and educators to understand their educational and professional needs, so we can ensure that we meet them.
CHEST is only as good as the education we provide, and it’s our subject matter experts who drive that content engine. In my previous role leading the Publishing Division and working on our journal CHEST® and programs like SEEK, I’ve had the honor and pleasure of working with some of the greatest minds in pulmonary, critical care, and sleep medicine. It’s humbling.
What will be some of the underlying themes as you work to outline the strategic plan for the next 5 years?
We are in the final stages of planning for 2018 and beyond, and although our proposed roadmap isn’t significantly different than what we have been doing, there’s some greater emphasis on a few key areas. For example, we’re looking at innovations in educational delivery. We’ve got some very forward thinking faculty educators and staff who are collaborating to develop innovations like gamification of educational and simulation programs, and augmented reality. Globalization and growth are also a key part of our strategic plan, and we are committed to the broad delivery of our educational programs and content both here and around the world. Finally, we have invested in a data analytics project that is maturing, and we’ll be leveraging that information to provide more personalized education plans – not just for the physician but for the entire health-care team. It’s important for us to stay relevant and viable.
Why has CHEST shifted to an interdisciplinary, team-focused approach?
I look at it as simply an evolution that reflects how health care is changing. It’s a team sport now, and our advanced practice providers (APPs) play a huge role in patient management and care. To be as effective and efficient as possible, and ensure the best patient outcomes, the whole team needs to be on the same page, and we believe that providing education for the interdisciplinary care team will help ensure that the best patient care is delivered.
There’s also a need for this education, and we want to fill it. Our APPs tell us that there is no formal pulmonary training or post-masters fellowship in pulmonary medicine for them. They are often left on their own to fill any gaps in knowledge and skills. That’s where our CHEST programs, such as our CHEST Annual Meeting, come in. We have an Interprofessional NetWork made up of APPs and physicians, and they were integral in working with the CHEST 2017 Program Committee to ensure plenty of relevant content was offered. Moving forward, we will continue to offer and build interdisciplinary programs designed for the entire team, as well as programs that address clinical issues across disciplines.
What are some of the critical skills CHEST physicians need to keep the population healthy during the ever-evolving field?
Educationally, we recognize that conferences like the annual CHEST meeting must provide more than just talking heads. We’ve invested heavily in high-fidelity medical simulation through small group, hands-on skill training in critical care techniques, airway management, EBUS, critical care ultrasound, bronchoscopy, and other chest medicine content. It’s like the old adage about fishing: instead of telling people how to fish, we teach them to fish.
Any final thoughts?
I always encourage our members to get involved with CHEST and experience the camaraderie and connectivity of the CHEST family. Ask any of our leadership, and you will surely hear their story of that special person who first introduced them to the College. Reach out and tell a colleague about CHEST. We are focused on clinically relevant education that our members can take back and put into action immediately. At the end of the day, it’s about providing state-of-the-art education via high fidelity medical simulation, hands-on skills training, clinically focused courses, case-based programming, and more—all intended to be immediately implemented to improve patient care and patient outcomes. That’s what the CHEST organization is all about.
This Month in CHEST: Editor’s Picks
Original Research
Burden of Adult Community-Acquired, Health-care-Associated, Hospital-Acquired, and Ventilator-Associated Pneumonia: New York City, 2010 to 2014. By R. E. Corrado, et al.
Hyperbaric Oxygen Therapy Is Associated With Lower Short- and Long-Term Mortality in Patients With Carbon Monoxide Poisoning. By C-C Huang, et al.
Evidence-Based Medicine
Pharmacologic and Nonpharmacologic Treatment for Acute Cough Associated With the Common Cold: CHEST Expert Panel Report. By M. A. Malesker, et al, on behalf of the CHEST Expert Cough Panel.
Cough in Ambulatory Immunocompromised Adults: CHEST Expert Panel Report. By M. J. Rosen, et al, on behalf of the CHEST Expert Cough Panel.
Original Research
Burden of Adult Community-Acquired, Health-care-Associated, Hospital-Acquired, and Ventilator-Associated Pneumonia: New York City, 2010 to 2014. By R. E. Corrado, et al.
Hyperbaric Oxygen Therapy Is Associated With Lower Short- and Long-Term Mortality in Patients With Carbon Monoxide Poisoning. By C-C Huang, et al.
Evidence-Based Medicine
Pharmacologic and Nonpharmacologic Treatment for Acute Cough Associated With the Common Cold: CHEST Expert Panel Report. By M. A. Malesker, et al, on behalf of the CHEST Expert Cough Panel.
Cough in Ambulatory Immunocompromised Adults: CHEST Expert Panel Report. By M. J. Rosen, et al, on behalf of the CHEST Expert Cough Panel.
Original Research
Burden of Adult Community-Acquired, Health-care-Associated, Hospital-Acquired, and Ventilator-Associated Pneumonia: New York City, 2010 to 2014. By R. E. Corrado, et al.
Hyperbaric Oxygen Therapy Is Associated With Lower Short- and Long-Term Mortality in Patients With Carbon Monoxide Poisoning. By C-C Huang, et al.
Evidence-Based Medicine
Pharmacologic and Nonpharmacologic Treatment for Acute Cough Associated With the Common Cold: CHEST Expert Panel Report. By M. A. Malesker, et al, on behalf of the CHEST Expert Cough Panel.
Cough in Ambulatory Immunocompromised Adults: CHEST Expert Panel Report. By M. J. Rosen, et al, on behalf of the CHEST Expert Cough Panel.

Lessons Learned From SERVE-HF
Great attention has been paid to the SERVE-HF trial (“Treatment of Sleep-disordered Breathing with Predominant Central Sleep Apnea by Adaptive Servo Ventilation in Patients with Heart Failure”), which showed increased all-cause mortality and cardiovascular mortality in the Adaptive Servo-ventilation (ASV) group compared with the control group of conventional heart failure management alone. The results of this trial led to the recommendation by multiple ASV manufacturers and medical societies to withdraw clinical use of ASV from patients with heart failure and a reduced ejection fraction (HFrEF) less than 45%.
Sleep-disordered breathing is common in patients with HFrEF with prevalence rates of 50% to 75%. Central sleep apnea (CSA) is associated with increased mortality in heart failure (HF) and is found in 25% to 40% of this subpopulation. It is estimated that the severity of CSA increases in parallel with the severity of the HF. For several years, treatment of CSA with positive pressure ventilation was believed to favor outcomes in HFrEF with a protective effect.
In the Canadian Positive Airway Pressure for Patients with CSA and HF (CANPAP) trial, subjects were randomized to treatment with CPAP or no CPAP. This trial was terminated early; it did not show an advantage of CPAP in morbidity or mortality. A post-hoc analysis suggested that mortality might be reduced if the frequency of respiratory events per hour or apnea hypopnea index (AHI) is reduced to 15/hour or less while using CPAP.

Hoping to improve the outcomes of HF, SERVE-HF was the first randomized, large scale, multinational trial directed to treat CSA in patients with HFrEF < 45% and concomitant clinically significant sleep apnea with AHI > 15/hour of central predominance (CSA index >10/hour). Treatment arms compared the addition the ASV, one of the most effective noninvasive positive pressure ventilation technologies for central apneas that offers automated inspiratory pressure support in addition to expiratory positive pressure vs conventional medical treatment alone in the control group.
The study published in the New England Journal of Medicine in September 2015 was designed in an intention-to-treat basis with the primary end point of time to first event, a composite of death from any cause, lifesaving cardiovascular intervention (heart transplant, implantation of LVAD, resuscitation after sudden cardiac arrest, or defibrillation for ventricular arrhythmia), or unplanned hospitalization for heart failure. The study did not show significant differences in the primary end point between the ASV and control group (54.1% and 50.8%, respectively; hazard ratio, 1.13; 95% confidence interval, 0.97 to 1.31; P=.10).1
The most interesting and unexpected outcome was an increase in the all cause mortality and cardiovascular mortality in the ASV group (hazard ratio for death from any cause, 1.28; 95% CI, 1.06 to 1.55; P=.01; and hazard ratio from cardiovascular death, 1.34; 95% CI, 1.09 to 1.65; P=.006).1 These findings led to the above recommendations from manufacturers, as well as a position statement from the American Academy of Sleep Medicine. These findings cannot be extrapolated to the obstructive sleep apnea population with concomitant HFrEF or to patients with HF with preserved ejection fraction, where positive pressure ventilation has offered an advantage1 likely by a different physiologic mechanism not fully uncovered at this time, believed to be an overall effect of afterload reduction.
Selection and self-selection bias in this study was addressed in a new analysis by the same SERVE-HF investigator group published August 2017, where a time-dependent model of on-treatment analysis (done to tease out if the original results were related to the treatment assignment or to poor adherence) was conducted to understand potential causes of the initial findings in the original study. It showed patients randomized to ASV who crossed over to the control group were at higher risk of cardiovascular death than control subjects; also the control patients with crossover to ASV had a signal of lower risk of cardiovascular death risk compared with patients assigned to ASV.2 Reduced adherence to ASV treatment during SERVE-HF was a concern, since it resulted in a reduced exposure to the treatment. The on-treatment analysis showed again an increase of cardiovascular death in HFrEF patients with predominant CSA treated with ASV in addition to conventional heart failure treatment compared with the control group.2 There was no increase in cardiovascular death risk associated with ASV use intervals (dose effect). This effect is not related to the amount of hours used per night.
The effect of the recommended withdrawal of treatment in HFrEF patients with EF<45% and moderate to severe central predominant sleep apnea is being addressed in smaller studies. A single center retrospective analysis observed the effects after ASV discontinuation in this population. Thirteen out of 126 patients treated with ASV who met SERVE-HF criteria were followed for at least a year; 93% of the subjects who met criteria had ASV removed; immediate recurrence of the central apnea was observed in most (except two patients), while adverse events were not identified (defined as need for emergency hospitalization). Day and nighttime symptoms were reported by 61% of the group, and they were started on alternative treatments.3 At 1 year after ASV removal, 88% of patients were still alive, overall cardiac function did not change in 1 year (P=0.17), and seven patients required adjustment of medications for heart failure. Symptomatic patients were treated with oxygen supplementation for nocturnal symptoms or CPAP if they had daytime sleepiness. None was treated with bi-level PAP, acetazolamide, or phrenic nerve stimulation. Four patients insisted on continuation of ASV despite understanding physician concerns. 3 This study helps to demonstrate that ASV discontinuation is feasible but requires close follow-up. However, larger, long-term prospective reviews are required to draw statistically meaningful conclusions about the consequences and safety of ASV removal; these studies will be difficult to conduct under the current indications for ASV in the interest group.
At this time, investigators have shifted to further understand the causes of the increase in cardiovascular mortality, overall mortality, and the understanding of the pathophysiologic processes associated with ASV use in HFrEF. It is not known whether the effect in mortality is related to the specific ASV device/algorithm used to suppress CSA or is related to the ASV principle itself. Upcoming studies will assist in clarifying these details. Currently, there is an ongoing trial looking at the effect of ASV on survival and hospital admissions in heart failure (ADVENT–HF) using a different ASV device; this study will hopefully elucidate the impact of class effect vs device effect. It may also provide better insight of the etiology of mortality and the impact of improved ASV compliance, first addressed by the on-treatment analysis of the SERVE-HF.4
Although the reasons for increased mortality related to ASV are unclear, proposed hypotheses include: central apnea is an adaptive mechanism to HFrEF and the reversal of central apneas might adversely affect the underlying disease process,1 low adherence to ASV may impact outcomes, and specific devices may induce hyper-/hypoventilation generated by the algorithm designs of the specific ASV device and this may result in electrolyte abnormalities that generate arrhythmias.
The ADVENT-HF trial, although similar in design, has significant differences from SERVE-HF: different ASV devices may have a different impact on cardiac output and ventilation, recruited patients included those with less daytime sleepiness, and the potential to assess the effect of ASV in patients with OSA and low daytime sleepiness in patients with reduced EF.5,6 This ongoing study may help us to further understand why there is increased mortality and what effect ASV has on the treatment of sleep apnea in patients with HFrEF.
References
1. Cowie MR, et al. N Engl J Med. 2015;373(12):1095-1105.
2. Woehrle H, et al. Eur Respir J. 2017; 50:1601.
3. Brill AK, et al. Sleep Med. 2017;37:201-207.
4. Bradley TD, et al. Can Respir. 2015;22(6):313.
5. Lyons OD, et al. Eur J Heart Fail. 2017;19(4):579-587.
6. Haruki N, et al. Can J Cardiol. 2016;32(12):1402-1410.
Dr. Barrantes is an assistant professor, Department of Pulmonary, Critical Care, and Sleep Medicine, Baylor College of Medicine, Houston, Texas.
Great attention has been paid to the SERVE-HF trial (“Treatment of Sleep-disordered Breathing with Predominant Central Sleep Apnea by Adaptive Servo Ventilation in Patients with Heart Failure”), which showed increased all-cause mortality and cardiovascular mortality in the Adaptive Servo-ventilation (ASV) group compared with the control group of conventional heart failure management alone. The results of this trial led to the recommendation by multiple ASV manufacturers and medical societies to withdraw clinical use of ASV from patients with heart failure and a reduced ejection fraction (HFrEF) less than 45%.
Sleep-disordered breathing is common in patients with HFrEF with prevalence rates of 50% to 75%. Central sleep apnea (CSA) is associated with increased mortality in heart failure (HF) and is found in 25% to 40% of this subpopulation. It is estimated that the severity of CSA increases in parallel with the severity of the HF. For several years, treatment of CSA with positive pressure ventilation was believed to favor outcomes in HFrEF with a protective effect.
In the Canadian Positive Airway Pressure for Patients with CSA and HF (CANPAP) trial, subjects were randomized to treatment with CPAP or no CPAP. This trial was terminated early; it did not show an advantage of CPAP in morbidity or mortality. A post-hoc analysis suggested that mortality might be reduced if the frequency of respiratory events per hour or apnea hypopnea index (AHI) is reduced to 15/hour or less while using CPAP.
Hoping to improve the outcomes of HF, SERVE-HF was the first randomized, large scale, multinational trial directed to treat CSA in patients with HFrEF < 45% and concomitant clinically significant sleep apnea with AHI > 15/hour of central predominance (CSA index >10/hour). Treatment arms compared the addition the ASV, one of the most effective noninvasive positive pressure ventilation technologies for central apneas that offers automated inspiratory pressure support in addition to expiratory positive pressure vs conventional medical treatment alone in the control group.
The study published in the New England Journal of Medicine in September 2015 was designed in an intention-to-treat basis with the primary end point of time to first event, a composite of death from any cause, lifesaving cardiovascular intervention (heart transplant, implantation of LVAD, resuscitation after sudden cardiac arrest, or defibrillation for ventricular arrhythmia), or unplanned hospitalization for heart failure. The study did not show significant differences in the primary end point between the ASV and control group (54.1% and 50.8%, respectively; hazard ratio, 1.13; 95% confidence interval, 0.97 to 1.31; P=.10).1
The most interesting and unexpected outcome was an increase in the all cause mortality and cardiovascular mortality in the ASV group (hazard ratio for death from any cause, 1.28; 95% CI, 1.06 to 1.55; P=.01; and hazard ratio from cardiovascular death, 1.34; 95% CI, 1.09 to 1.65; P=.006).1 These findings led to the above recommendations from manufacturers, as well as a position statement from the American Academy of Sleep Medicine. These findings cannot be extrapolated to the obstructive sleep apnea population with concomitant HFrEF or to patients with HF with preserved ejection fraction, where positive pressure ventilation has offered an advantage1 likely by a different physiologic mechanism not fully uncovered at this time, believed to be an overall effect of afterload reduction.
Selection and self-selection bias in this study was addressed in a new analysis by the same SERVE-HF investigator group published August 2017, where a time-dependent model of on-treatment analysis (done to tease out if the original results were related to the treatment assignment or to poor adherence) was conducted to understand potential causes of the initial findings in the original study. It showed patients randomized to ASV who crossed over to the control group were at higher risk of cardiovascular death than control subjects; also the control patients with crossover to ASV had a signal of lower risk of cardiovascular death risk compared with patients assigned to ASV.2 Reduced adherence to ASV treatment during SERVE-HF was a concern, since it resulted in a reduced exposure to the treatment. The on-treatment analysis showed again an increase of cardiovascular death in HFrEF patients with predominant CSA treated with ASV in addition to conventional heart failure treatment compared with the control group.2 There was no increase in cardiovascular death risk associated with ASV use intervals (dose effect). This effect is not related to the amount of hours used per night.
The effect of the recommended withdrawal of treatment in HFrEF patients with EF<45% and moderate to severe central predominant sleep apnea is being addressed in smaller studies. A single center retrospective analysis observed the effects after ASV discontinuation in this population. Thirteen out of 126 patients treated with ASV who met SERVE-HF criteria were followed for at least a year; 93% of the subjects who met criteria had ASV removed; immediate recurrence of the central apnea was observed in most (except two patients), while adverse events were not identified (defined as need for emergency hospitalization). Day and nighttime symptoms were reported by 61% of the group, and they were started on alternative treatments.3 At 1 year after ASV removal, 88% of patients were still alive, overall cardiac function did not change in 1 year (P=0.17), and seven patients required adjustment of medications for heart failure. Symptomatic patients were treated with oxygen supplementation for nocturnal symptoms or CPAP if they had daytime sleepiness. None was treated with bi-level PAP, acetazolamide, or phrenic nerve stimulation. Four patients insisted on continuation of ASV despite understanding physician concerns. 3 This study helps to demonstrate that ASV discontinuation is feasible but requires close follow-up. However, larger, long-term prospective reviews are required to draw statistically meaningful conclusions about the consequences and safety of ASV removal; these studies will be difficult to conduct under the current indications for ASV in the interest group.
At this time, investigators have shifted to further understand the causes of the increase in cardiovascular mortality, overall mortality, and the understanding of the pathophysiologic processes associated with ASV use in HFrEF. It is not known whether the effect in mortality is related to the specific ASV device/algorithm used to suppress CSA or is related to the ASV principle itself. Upcoming studies will assist in clarifying these details. Currently, there is an ongoing trial looking at the effect of ASV on survival and hospital admissions in heart failure (ADVENT–HF) using a different ASV device; this study will hopefully elucidate the impact of class effect vs device effect. It may also provide better insight of the etiology of mortality and the impact of improved ASV compliance, first addressed by the on-treatment analysis of the SERVE-HF.4
Although the reasons for increased mortality related to ASV are unclear, proposed hypotheses include: central apnea is an adaptive mechanism to HFrEF and the reversal of central apneas might adversely affect the underlying disease process,1 low adherence to ASV may impact outcomes, and specific devices may induce hyper-/hypoventilation generated by the algorithm designs of the specific ASV device and this may result in electrolyte abnormalities that generate arrhythmias.
The ADVENT-HF trial, although similar in design, has significant differences from SERVE-HF: different ASV devices may have a different impact on cardiac output and ventilation, recruited patients included those with less daytime sleepiness, and the potential to assess the effect of ASV in patients with OSA and low daytime sleepiness in patients with reduced EF.5,6 This ongoing study may help us to further understand why there is increased mortality and what effect ASV has on the treatment of sleep apnea in patients with HFrEF.
References
1. Cowie MR, et al. N Engl J Med. 2015;373(12):1095-1105.
2. Woehrle H, et al. Eur Respir J. 2017; 50:1601.
3. Brill AK, et al. Sleep Med. 2017;37:201-207.
4. Bradley TD, et al. Can Respir. 2015;22(6):313.
5. Lyons OD, et al. Eur J Heart Fail. 2017;19(4):579-587.
6. Haruki N, et al. Can J Cardiol. 2016;32(12):1402-1410.
Dr. Barrantes is an assistant professor, Department of Pulmonary, Critical Care, and Sleep Medicine, Baylor College of Medicine, Houston, Texas.
Great attention has been paid to the SERVE-HF trial (“Treatment of Sleep-disordered Breathing with Predominant Central Sleep Apnea by Adaptive Servo Ventilation in Patients with Heart Failure”), which showed increased all-cause mortality and cardiovascular mortality in the Adaptive Servo-ventilation (ASV) group compared with the control group of conventional heart failure management alone. The results of this trial led to the recommendation by multiple ASV manufacturers and medical societies to withdraw clinical use of ASV from patients with heart failure and a reduced ejection fraction (HFrEF) less than 45%.
Sleep-disordered breathing is common in patients with HFrEF with prevalence rates of 50% to 75%. Central sleep apnea (CSA) is associated with increased mortality in heart failure (HF) and is found in 25% to 40% of this subpopulation. It is estimated that the severity of CSA increases in parallel with the severity of the HF. For several years, treatment of CSA with positive pressure ventilation was believed to favor outcomes in HFrEF with a protective effect.
In the Canadian Positive Airway Pressure for Patients with CSA and HF (CANPAP) trial, subjects were randomized to treatment with CPAP or no CPAP. This trial was terminated early; it did not show an advantage of CPAP in morbidity or mortality. A post-hoc analysis suggested that mortality might be reduced if the frequency of respiratory events per hour or apnea hypopnea index (AHI) is reduced to 15/hour or less while using CPAP.
Hoping to improve the outcomes of HF, SERVE-HF was the first randomized, large scale, multinational trial directed to treat CSA in patients with HFrEF < 45% and concomitant clinically significant sleep apnea with AHI > 15/hour of central predominance (CSA index >10/hour). Treatment arms compared the addition the ASV, one of the most effective noninvasive positive pressure ventilation technologies for central apneas that offers automated inspiratory pressure support in addition to expiratory positive pressure vs conventional medical treatment alone in the control group.
The study published in the New England Journal of Medicine in September 2015 was designed in an intention-to-treat basis with the primary end point of time to first event, a composite of death from any cause, lifesaving cardiovascular intervention (heart transplant, implantation of LVAD, resuscitation after sudden cardiac arrest, or defibrillation for ventricular arrhythmia), or unplanned hospitalization for heart failure. The study did not show significant differences in the primary end point between the ASV and control group (54.1% and 50.8%, respectively; hazard ratio, 1.13; 95% confidence interval, 0.97 to 1.31; P=.10).1
The most interesting and unexpected outcome was an increase in the all cause mortality and cardiovascular mortality in the ASV group (hazard ratio for death from any cause, 1.28; 95% CI, 1.06 to 1.55; P=.01; and hazard ratio from cardiovascular death, 1.34; 95% CI, 1.09 to 1.65; P=.006).1 These findings led to the above recommendations from manufacturers, as well as a position statement from the American Academy of Sleep Medicine. These findings cannot be extrapolated to the obstructive sleep apnea population with concomitant HFrEF or to patients with HF with preserved ejection fraction, where positive pressure ventilation has offered an advantage1 likely by a different physiologic mechanism not fully uncovered at this time, believed to be an overall effect of afterload reduction.
Selection and self-selection bias in this study was addressed in a new analysis by the same SERVE-HF investigator group published August 2017, where a time-dependent model of on-treatment analysis (done to tease out if the original results were related to the treatment assignment or to poor adherence) was conducted to understand potential causes of the initial findings in the original study. It showed patients randomized to ASV who crossed over to the control group were at higher risk of cardiovascular death than control subjects; also the control patients with crossover to ASV had a signal of lower risk of cardiovascular death risk compared with patients assigned to ASV.2 Reduced adherence to ASV treatment during SERVE-HF was a concern, since it resulted in a reduced exposure to the treatment. The on-treatment analysis showed again an increase of cardiovascular death in HFrEF patients with predominant CSA treated with ASV in addition to conventional heart failure treatment compared with the control group.2 There was no increase in cardiovascular death risk associated with ASV use intervals (dose effect). This effect is not related to the amount of hours used per night.
The effect of the recommended withdrawal of treatment in HFrEF patients with EF<45% and moderate to severe central predominant sleep apnea is being addressed in smaller studies. A single center retrospective analysis observed the effects after ASV discontinuation in this population. Thirteen out of 126 patients treated with ASV who met SERVE-HF criteria were followed for at least a year; 93% of the subjects who met criteria had ASV removed; immediate recurrence of the central apnea was observed in most (except two patients), while adverse events were not identified (defined as need for emergency hospitalization). Day and nighttime symptoms were reported by 61% of the group, and they were started on alternative treatments.3 At 1 year after ASV removal, 88% of patients were still alive, overall cardiac function did not change in 1 year (P=0.17), and seven patients required adjustment of medications for heart failure. Symptomatic patients were treated with oxygen supplementation for nocturnal symptoms or CPAP if they had daytime sleepiness. None was treated with bi-level PAP, acetazolamide, or phrenic nerve stimulation. Four patients insisted on continuation of ASV despite understanding physician concerns. 3 This study helps to demonstrate that ASV discontinuation is feasible but requires close follow-up. However, larger, long-term prospective reviews are required to draw statistically meaningful conclusions about the consequences and safety of ASV removal; these studies will be difficult to conduct under the current indications for ASV in the interest group.
At this time, investigators have shifted to further understand the causes of the increase in cardiovascular mortality, overall mortality, and the understanding of the pathophysiologic processes associated with ASV use in HFrEF. It is not known whether the effect in mortality is related to the specific ASV device/algorithm used to suppress CSA or is related to the ASV principle itself. Upcoming studies will assist in clarifying these details. Currently, there is an ongoing trial looking at the effect of ASV on survival and hospital admissions in heart failure (ADVENT–HF) using a different ASV device; this study will hopefully elucidate the impact of class effect vs device effect. It may also provide better insight of the etiology of mortality and the impact of improved ASV compliance, first addressed by the on-treatment analysis of the SERVE-HF.4
Although the reasons for increased mortality related to ASV are unclear, proposed hypotheses include: central apnea is an adaptive mechanism to HFrEF and the reversal of central apneas might adversely affect the underlying disease process,1 low adherence to ASV may impact outcomes, and specific devices may induce hyper-/hypoventilation generated by the algorithm designs of the specific ASV device and this may result in electrolyte abnormalities that generate arrhythmias.
The ADVENT-HF trial, although similar in design, has significant differences from SERVE-HF: different ASV devices may have a different impact on cardiac output and ventilation, recruited patients included those with less daytime sleepiness, and the potential to assess the effect of ASV in patients with OSA and low daytime sleepiness in patients with reduced EF.5,6 This ongoing study may help us to further understand why there is increased mortality and what effect ASV has on the treatment of sleep apnea in patients with HFrEF.
References
1. Cowie MR, et al. N Engl J Med. 2015;373(12):1095-1105.
2. Woehrle H, et al. Eur Respir J. 2017; 50:1601.
3. Brill AK, et al. Sleep Med. 2017;37:201-207.
4. Bradley TD, et al. Can Respir. 2015;22(6):313.
5. Lyons OD, et al. Eur J Heart Fail. 2017;19(4):579-587.
6. Haruki N, et al. Can J Cardiol. 2016;32(12):1402-1410.
Dr. Barrantes is an assistant professor, Department of Pulmonary, Critical Care, and Sleep Medicine, Baylor College of Medicine, Houston, Texas.
Former pharma exec nominated for top HHS post
Alex M. Azar II, a former pharmaceutical executive and member of the George W. Bush administration, has been selected by President Donald Trump to lead the Department of Health & Human Services.
Mr. Azar served as president of Eli Lilly in the United States for 5 years from 2012 to 2017, after joining the company in 2007. Prior to that, he served President Bush at HHS from 2001 to 2007, serving first as general counsel and later as deputy secretary under Secretary Michael O. Leavitt.

“The challenges plaguing the American health care system are serious. For too long, hardworking, middle-class families have been forced to bear the brunt of Obamacare’s failures in the form of higher premiums and fewer choices,” Senate Finance Committee Chairman Orrin Hatch (R-Utah) said in a statement. “The leader of HHS will be at the tip of the spear, working to not only right the wrongs of this deeply flawed law but also ensure the long-term sustainability of both Medicare and Medicaid.”
The Senate Finance Committee must first approve the nomination before it is considered by the full chamber.
“We commend President Trump for nominating Alex Azar for secretary of Health & Human Services,” House Energy & Commerce Committee Chairman Greg Walden (R-Ore.) and Health Subcommittee Chairman Michael Burgess, MD, (R-Texas) said in a joint statement. “He is a veteran of HHS, bringing with him a wealth of institutional knowledge that will be instrumental in delivering patient-centered health care and combating the opioid crisis. We look forward to working with Mr. Azar on these critical issues and many others in the future.”
The Campaign for Sustainable Rx Pricing, a coalition of physicians and other stakeholders across the health care industry, was more measured in its reaction to the news.
“We sincerely hope that Secretary-nominee Azar will follow through on the President’s commitment to achieve lower drug prices for all Americans,” according to a statement from CSRxP. “We look forward to working with him, once confirmed, to end anticompetitive practices that artificially inflate drug prices, restore a functioning prescription drug market, and rein in the exorbitant price hikes that harm patients, job creators, and taxpayers alike.”
The nomination process could be bumpy, as Mr. Azar has made statements in the news in the past that were in support the dismantling of the Affordable Care Act. But keeping him from the post will be difficult, as he would only need a simple majority vote in the Senate to gain approval. With Republicans holding 52 seats, it would only require three dissenting GOP senators, assuming the Democrats vote against the appointment. If two crossed the aisle, Vice President Mike Pence would cast the deciding vote.
Finance Committee Democrats boycotted the committee vote on Mr. Azar’s predecessor, Secretary Tom Price, MD, forcing committee Chairman Hatch to suspend rules in order to move the appointment to the full chamber for consideration.
Alex M. Azar II, a former pharmaceutical executive and member of the George W. Bush administration, has been selected by President Donald Trump to lead the Department of Health & Human Services.
Mr. Azar served as president of Eli Lilly in the United States for 5 years from 2012 to 2017, after joining the company in 2007. Prior to that, he served President Bush at HHS from 2001 to 2007, serving first as general counsel and later as deputy secretary under Secretary Michael O. Leavitt.
“The challenges plaguing the American health care system are serious. For too long, hardworking, middle-class families have been forced to bear the brunt of Obamacare’s failures in the form of higher premiums and fewer choices,” Senate Finance Committee Chairman Orrin Hatch (R-Utah) said in a statement. “The leader of HHS will be at the tip of the spear, working to not only right the wrongs of this deeply flawed law but also ensure the long-term sustainability of both Medicare and Medicaid.”
The Senate Finance Committee must first approve the nomination before it is considered by the full chamber.
“We commend President Trump for nominating Alex Azar for secretary of Health & Human Services,” House Energy & Commerce Committee Chairman Greg Walden (R-Ore.) and Health Subcommittee Chairman Michael Burgess, MD, (R-Texas) said in a joint statement. “He is a veteran of HHS, bringing with him a wealth of institutional knowledge that will be instrumental in delivering patient-centered health care and combating the opioid crisis. We look forward to working with Mr. Azar on these critical issues and many others in the future.”
The Campaign for Sustainable Rx Pricing, a coalition of physicians and other stakeholders across the health care industry, was more measured in its reaction to the news.
“We sincerely hope that Secretary-nominee Azar will follow through on the President’s commitment to achieve lower drug prices for all Americans,” according to a statement from CSRxP. “We look forward to working with him, once confirmed, to end anticompetitive practices that artificially inflate drug prices, restore a functioning prescription drug market, and rein in the exorbitant price hikes that harm patients, job creators, and taxpayers alike.”
The nomination process could be bumpy, as Mr. Azar has made statements in the news in the past that were in support the dismantling of the Affordable Care Act. But keeping him from the post will be difficult, as he would only need a simple majority vote in the Senate to gain approval. With Republicans holding 52 seats, it would only require three dissenting GOP senators, assuming the Democrats vote against the appointment. If two crossed the aisle, Vice President Mike Pence would cast the deciding vote.
Finance Committee Democrats boycotted the committee vote on Mr. Azar’s predecessor, Secretary Tom Price, MD, forcing committee Chairman Hatch to suspend rules in order to move the appointment to the full chamber for consideration.
Alex M. Azar II, a former pharmaceutical executive and member of the George W. Bush administration, has been selected by President Donald Trump to lead the Department of Health & Human Services.
Mr. Azar served as president of Eli Lilly in the United States for 5 years from 2012 to 2017, after joining the company in 2007. Prior to that, he served President Bush at HHS from 2001 to 2007, serving first as general counsel and later as deputy secretary under Secretary Michael O. Leavitt.
“The challenges plaguing the American health care system are serious. For too long, hardworking, middle-class families have been forced to bear the brunt of Obamacare’s failures in the form of higher premiums and fewer choices,” Senate Finance Committee Chairman Orrin Hatch (R-Utah) said in a statement. “The leader of HHS will be at the tip of the spear, working to not only right the wrongs of this deeply flawed law but also ensure the long-term sustainability of both Medicare and Medicaid.”
The Senate Finance Committee must first approve the nomination before it is considered by the full chamber.
“We commend President Trump for nominating Alex Azar for secretary of Health & Human Services,” House Energy & Commerce Committee Chairman Greg Walden (R-Ore.) and Health Subcommittee Chairman Michael Burgess, MD, (R-Texas) said in a joint statement. “He is a veteran of HHS, bringing with him a wealth of institutional knowledge that will be instrumental in delivering patient-centered health care and combating the opioid crisis. We look forward to working with Mr. Azar on these critical issues and many others in the future.”
The Campaign for Sustainable Rx Pricing, a coalition of physicians and other stakeholders across the health care industry, was more measured in its reaction to the news.
“We sincerely hope that Secretary-nominee Azar will follow through on the President’s commitment to achieve lower drug prices for all Americans,” according to a statement from CSRxP. “We look forward to working with him, once confirmed, to end anticompetitive practices that artificially inflate drug prices, restore a functioning prescription drug market, and rein in the exorbitant price hikes that harm patients, job creators, and taxpayers alike.”
The nomination process could be bumpy, as Mr. Azar has made statements in the news in the past that were in support the dismantling of the Affordable Care Act. But keeping him from the post will be difficult, as he would only need a simple majority vote in the Senate to gain approval. With Republicans holding 52 seats, it would only require three dissenting GOP senators, assuming the Democrats vote against the appointment. If two crossed the aisle, Vice President Mike Pence would cast the deciding vote.
Finance Committee Democrats boycotted the committee vote on Mr. Azar’s predecessor, Secretary Tom Price, MD, forcing committee Chairman Hatch to suspend rules in order to move the appointment to the full chamber for consideration.
New standard classification, pathophysiology of rosacea announced
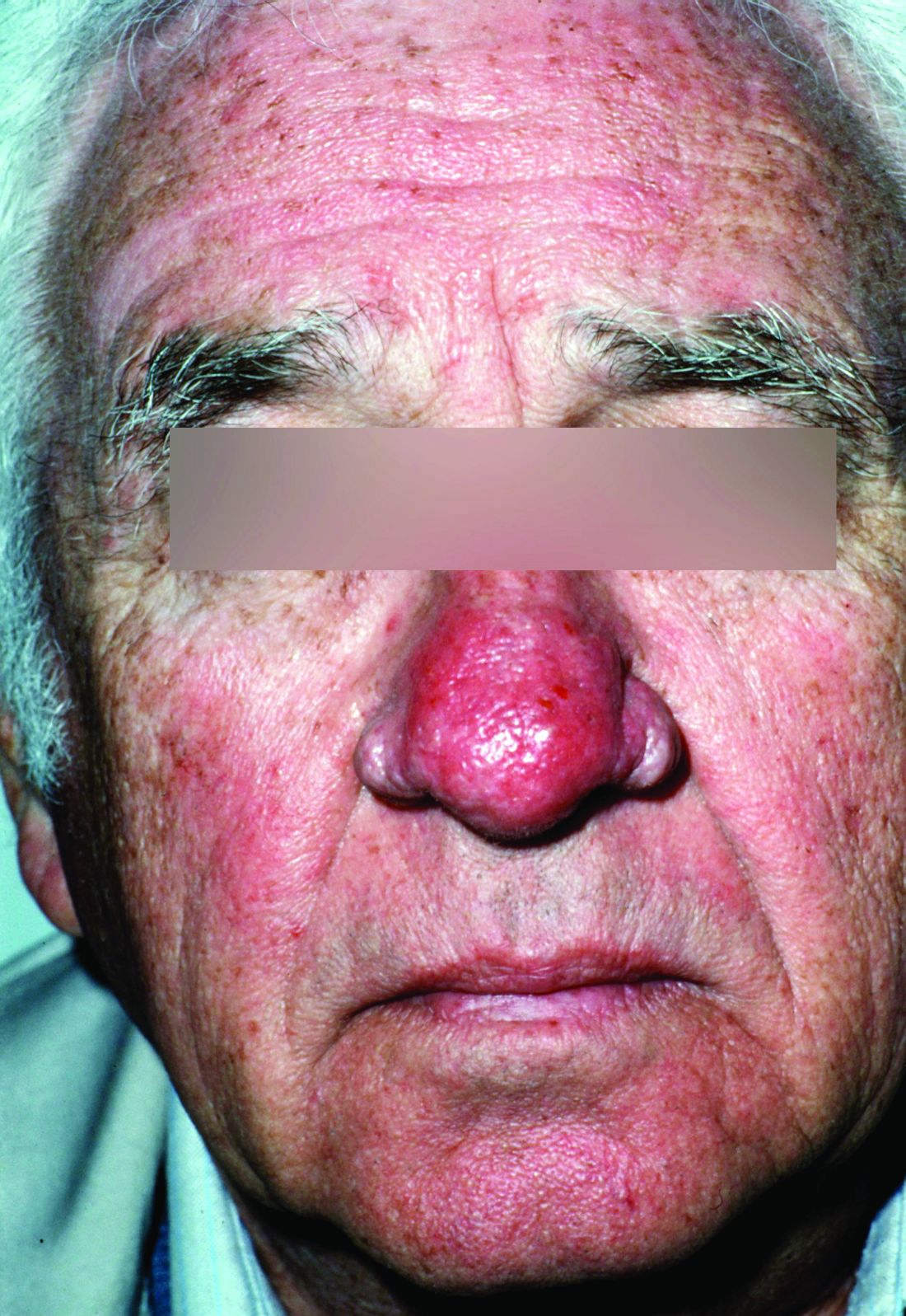
Rosacea’s phenotypes may occur in different combinations and at different times, but all are considered to be “manifestations of the same underlying inflammatory continuum,” the expert panel wrote (J Am Acad Dermatol. 2017. doi: 10.1016/j.jaad.2017.08.037).

Rosacea’s phenotypes may occur in different combinations and at different times, but all are considered to be “manifestations of the same underlying inflammatory continuum,” the expert panel wrote (J Am Acad Dermatol. 2017. doi: 10.1016/j.jaad.2017.08.037).
Rosacea’s phenotypes may occur in different combinations and at different times, but all are considered to be “manifestations of the same underlying inflammatory continuum,” the expert panel wrote (J Am Acad Dermatol. 2017. doi: 10.1016/j.jaad.2017.08.037).
FROM THE JOURNAL OF THE AMERICAN ACADEMY OF DERMATOLOGY

Delay predicting outcome in comatose cardiac arrest
ANAHEIM, CALIF. – Withdrawal of life-sustaining systemic therapies in comatose patients after out-of-hospital cardiac arrest as advised in current guidelines often occurs too early, resulting in the death of many patients who could potentially survive with good outcome, according to the results of NORCAST, the Norwegian Cardiorespiratory Arrest Study.
“The take-home message is to be patient and wait. Three days may be too early to make decisions on the patient,” Kjetil Sunde, MD, said in presenting the study findings at the Resuscitation Science Symposium held during the American Heart Association scientific sessions.

The European Resuscitation Council and European Society of Intensive Care Medicine have jointly recommended a prognostic algorithm in which a multimodal assessment is made on patients who are still comatose on day 3 after cardiac arrest. But this advice is based on expert opinion and has never been validated. This was the impetus for the prospective NORCAST study.
Current practice in the management of out-of-hospital cardiac arrest patients who are comatose upon hospital admission is to induce therapeutic hypothermia, with targeted temperature management to 33° C for 24 hours under deep sedation. The study hypothesis was that this strategy delays the time to awakening and that, as a consequence, the recommended prognostic tests that are usually done on day 3 after withdrawal of sedation are rendered insufficiently reliable. Thus, decisions to withdraw life-supporting therapies at that point will reduce the survival potential of this population, Dr. Sunde explained.
NORCAST was a prospective observational study that included 259 patients admitted to Oslo University Hospital in a comatose state after out-of-hospital cardiac arrest. In this unselected group, 81% had a cardiac cause for their arrest; the remainder had hypoxic arrest. All patients underwent therapeutic hypothermia, then a period of nonhypothermia followed by sedation withdrawal.
All of the widely used multimodal prognostic tests were ordered, including serial measurement of serum neuron-specific enolase; neurophysiologic testing using EEG and sensory-evoked potential readings obtained both during hypothermia and again at least 3 days after sedation withdrawal; a standardized clinical neurologic exam including assessment of brainstem reflexes and a Glasgow Coma Scale rating 3 days after sedation withdrawal; and a transcranial Doppler study and cerebral MRI on day 5-7. However, the treatment team was blinded to the results of these tests and was encouraged to delay withdrawal of life-supporting therapies as long as possible.
Key findings
Out of 259 patients who were comatose upon admission, 54% were alive at 6 months – and 91% of them had a CPC of 1 or 2.
The final tally at 6 months: 44% of patients were CPC 1, 5.5% were CPC 2, 4% were CPC 3, meaning severely disabled, and 46.5% were CPC 5, which is brain dead.
Withdrawal of life-supporting therapies occurred in 73 patients, or 28%, and 71% of those patients died, few of them in the early days.
Among patients with a CPC score of 1 or 2 at 6 months, only 20% were awake on day 1-3 following admission. Fifty-seven percent awoke on day 4-7, but importantly, 23% of patients with a good outcome at 6 months were not yet awake on day 8.
Three days after withdrawal of sedation, 49% of patients were rated as having a Glasgow Coma Scale score of 3-8, while 51% were Glasgow Coma Scale 9-15. Moreover, at that time 26% of patients with a good outcome as defined by a CPC of 1 or 2 at 6 months were still in a coma.
“So a lot of patients were still affected by their disease or by sedation at that point. That’s an important finding,” Dr. Sunde said.
Some prognostic tests were highly unreliable
A standout in poor performance was the widely utilized standard of a time to return of spontaneous circulation greater than 25 minutes as a predictor of poor cerebral outcome. In fact, it had a 34% false-positive rate.
“I think it’s really useless to use that. I would rather have return to spontaneous circulation after 40 minutes of good-quality CPR than not have it with 25 minutes of lesser-quality CPR,” he commented.
Similarly, a Glasgow Coma Scale score of 9 or less or a Glasgow Coma Scale-Motor score of 1-3 upon assessment 3 days after sedation withdrawal had false-positive rates of 30% and 34%, respectively.
During hypothermia, EEG abnormalities had a high false-positive rate, and sensory-evoked potential findings were difficult to interpret.
Predictors showing utility
Several clinical factors predicted poor cerebral outcome with low false-positive rates: Unwitnessed cardiac arrest had a false-positive rate of only 4%; initial presentation in asystole or with pulseless electrical activity had a false-positive rate of 6%; and no bystander CPR had a false-positive rate of 13%.
Abnormal sensory-evoked potential or EEG findings 3 days after sedation withdrawal had low false-positive rates as prognosticators of poor cerebral outcome. An EEG showing burst suppression or epileptiform activity had a “pretty good” false-positive rate of only 7%, Dr. Sunde noted. Bilaterally absent N20 sensory-evoked potential findings, while uncommon, had a false-positive rate of zero. A serum neuron-specific enolase level greater than 80 mcg/mL had a 3% false-positive rate, in sharp contrast to the previously recommended cutoff of more than 33 mcg/mL, which had an unacceptable 38% false-positive rate.
“We should avoid using single predictors in decision making and be patient, especially if we have a witnessed ventricular fibrillation with bystander CPR, independent of time to return of spontaneous circulation,” he concluded.
Dr. Sunde and his coinvestigators plan to present numerous further follow-up studies from NORCAST, including the results of comprehensive cognitive function testing 6-9 months after cardiac arrest in all survivors, coupled with interviews with their close relatives, as well as cognitive function and quality-of-life measurements 3-6 years after cardiac arrest along with interviews with relatives.
Several audience members rose to declare that they’ve been waiting for data such as this for a long time. Session chair Karl B. Kern, MD, professor of medicine at the University of Arizona, Tucson, and codirector of the University of Arizona Sarver Heart Center, commented, “We’ve been talking about whether 3 days is too early for a number of years, and clearly from your data it is. It was twice as long before most of them woke up.”
Dr. Sunde reported having no financial conflicts of interest regarding the NORCAST study, which was sponsored by Oslo University Hospital.
ANAHEIM, CALIF. – Withdrawal of life-sustaining systemic therapies in comatose patients after out-of-hospital cardiac arrest as advised in current guidelines often occurs too early, resulting in the death of many patients who could potentially survive with good outcome, according to the results of NORCAST, the Norwegian Cardiorespiratory Arrest Study.
“The take-home message is to be patient and wait. Three days may be too early to make decisions on the patient,” Kjetil Sunde, MD, said in presenting the study findings at the Resuscitation Science Symposium held during the American Heart Association scientific sessions.
The European Resuscitation Council and European Society of Intensive Care Medicine have jointly recommended a prognostic algorithm in which a multimodal assessment is made on patients who are still comatose on day 3 after cardiac arrest. But this advice is based on expert opinion and has never been validated. This was the impetus for the prospective NORCAST study.
Current practice in the management of out-of-hospital cardiac arrest patients who are comatose upon hospital admission is to induce therapeutic hypothermia, with targeted temperature management to 33° C for 24 hours under deep sedation. The study hypothesis was that this strategy delays the time to awakening and that, as a consequence, the recommended prognostic tests that are usually done on day 3 after withdrawal of sedation are rendered insufficiently reliable. Thus, decisions to withdraw life-supporting therapies at that point will reduce the survival potential of this population, Dr. Sunde explained.
NORCAST was a prospective observational study that included 259 patients admitted to Oslo University Hospital in a comatose state after out-of-hospital cardiac arrest. In this unselected group, 81% had a cardiac cause for their arrest; the remainder had hypoxic arrest. All patients underwent therapeutic hypothermia, then a period of nonhypothermia followed by sedation withdrawal.
All of the widely used multimodal prognostic tests were ordered, including serial measurement of serum neuron-specific enolase; neurophysiologic testing using EEG and sensory-evoked potential readings obtained both during hypothermia and again at least 3 days after sedation withdrawal; a standardized clinical neurologic exam including assessment of brainstem reflexes and a Glasgow Coma Scale rating 3 days after sedation withdrawal; and a transcranial Doppler study and cerebral MRI on day 5-7. However, the treatment team was blinded to the results of these tests and was encouraged to delay withdrawal of life-supporting therapies as long as possible.
Key findings
Out of 259 patients who were comatose upon admission, 54% were alive at 6 months – and 91% of them had a CPC of 1 or 2.
The final tally at 6 months: 44% of patients were CPC 1, 5.5% were CPC 2, 4% were CPC 3, meaning severely disabled, and 46.5% were CPC 5, which is brain dead.
Withdrawal of life-supporting therapies occurred in 73 patients, or 28%, and 71% of those patients died, few of them in the early days.
Among patients with a CPC score of 1 or 2 at 6 months, only 20% were awake on day 1-3 following admission. Fifty-seven percent awoke on day 4-7, but importantly, 23% of patients with a good outcome at 6 months were not yet awake on day 8.
Three days after withdrawal of sedation, 49% of patients were rated as having a Glasgow Coma Scale score of 3-8, while 51% were Glasgow Coma Scale 9-15. Moreover, at that time 26% of patients with a good outcome as defined by a CPC of 1 or 2 at 6 months were still in a coma.
“So a lot of patients were still affected by their disease or by sedation at that point. That’s an important finding,” Dr. Sunde said.
Some prognostic tests were highly unreliable
A standout in poor performance was the widely utilized standard of a time to return of spontaneous circulation greater than 25 minutes as a predictor of poor cerebral outcome. In fact, it had a 34% false-positive rate.
“I think it’s really useless to use that. I would rather have return to spontaneous circulation after 40 minutes of good-quality CPR than not have it with 25 minutes of lesser-quality CPR,” he commented.
Similarly, a Glasgow Coma Scale score of 9 or less or a Glasgow Coma Scale-Motor score of 1-3 upon assessment 3 days after sedation withdrawal had false-positive rates of 30% and 34%, respectively.
During hypothermia, EEG abnormalities had a high false-positive rate, and sensory-evoked potential findings were difficult to interpret.
Predictors showing utility
Several clinical factors predicted poor cerebral outcome with low false-positive rates: Unwitnessed cardiac arrest had a false-positive rate of only 4%; initial presentation in asystole or with pulseless electrical activity had a false-positive rate of 6%; and no bystander CPR had a false-positive rate of 13%.
Abnormal sensory-evoked potential or EEG findings 3 days after sedation withdrawal had low false-positive rates as prognosticators of poor cerebral outcome. An EEG showing burst suppression or epileptiform activity had a “pretty good” false-positive rate of only 7%, Dr. Sunde noted. Bilaterally absent N20 sensory-evoked potential findings, while uncommon, had a false-positive rate of zero. A serum neuron-specific enolase level greater than 80 mcg/mL had a 3% false-positive rate, in sharp contrast to the previously recommended cutoff of more than 33 mcg/mL, which had an unacceptable 38% false-positive rate.
“We should avoid using single predictors in decision making and be patient, especially if we have a witnessed ventricular fibrillation with bystander CPR, independent of time to return of spontaneous circulation,” he concluded.
Dr. Sunde and his coinvestigators plan to present numerous further follow-up studies from NORCAST, including the results of comprehensive cognitive function testing 6-9 months after cardiac arrest in all survivors, coupled with interviews with their close relatives, as well as cognitive function and quality-of-life measurements 3-6 years after cardiac arrest along with interviews with relatives.
Several audience members rose to declare that they’ve been waiting for data such as this for a long time. Session chair Karl B. Kern, MD, professor of medicine at the University of Arizona, Tucson, and codirector of the University of Arizona Sarver Heart Center, commented, “We’ve been talking about whether 3 days is too early for a number of years, and clearly from your data it is. It was twice as long before most of them woke up.”
Dr. Sunde reported having no financial conflicts of interest regarding the NORCAST study, which was sponsored by Oslo University Hospital.
ANAHEIM, CALIF. – Withdrawal of life-sustaining systemic therapies in comatose patients after out-of-hospital cardiac arrest as advised in current guidelines often occurs too early, resulting in the death of many patients who could potentially survive with good outcome, according to the results of NORCAST, the Norwegian Cardiorespiratory Arrest Study.
“The take-home message is to be patient and wait. Three days may be too early to make decisions on the patient,” Kjetil Sunde, MD, said in presenting the study findings at the Resuscitation Science Symposium held during the American Heart Association scientific sessions.
The European Resuscitation Council and European Society of Intensive Care Medicine have jointly recommended a prognostic algorithm in which a multimodal assessment is made on patients who are still comatose on day 3 after cardiac arrest. But this advice is based on expert opinion and has never been validated. This was the impetus for the prospective NORCAST study.
Current practice in the management of out-of-hospital cardiac arrest patients who are comatose upon hospital admission is to induce therapeutic hypothermia, with targeted temperature management to 33° C for 24 hours under deep sedation. The study hypothesis was that this strategy delays the time to awakening and that, as a consequence, the recommended prognostic tests that are usually done on day 3 after withdrawal of sedation are rendered insufficiently reliable. Thus, decisions to withdraw life-supporting therapies at that point will reduce the survival potential of this population, Dr. Sunde explained.
NORCAST was a prospective observational study that included 259 patients admitted to Oslo University Hospital in a comatose state after out-of-hospital cardiac arrest. In this unselected group, 81% had a cardiac cause for their arrest; the remainder had hypoxic arrest. All patients underwent therapeutic hypothermia, then a period of nonhypothermia followed by sedation withdrawal.
All of the widely used multimodal prognostic tests were ordered, including serial measurement of serum neuron-specific enolase; neurophysiologic testing using EEG and sensory-evoked potential readings obtained both during hypothermia and again at least 3 days after sedation withdrawal; a standardized clinical neurologic exam including assessment of brainstem reflexes and a Glasgow Coma Scale rating 3 days after sedation withdrawal; and a transcranial Doppler study and cerebral MRI on day 5-7. However, the treatment team was blinded to the results of these tests and was encouraged to delay withdrawal of life-supporting therapies as long as possible.
Key findings
Out of 259 patients who were comatose upon admission, 54% were alive at 6 months – and 91% of them had a CPC of 1 or 2.
The final tally at 6 months: 44% of patients were CPC 1, 5.5% were CPC 2, 4% were CPC 3, meaning severely disabled, and 46.5% were CPC 5, which is brain dead.
Withdrawal of life-supporting therapies occurred in 73 patients, or 28%, and 71% of those patients died, few of them in the early days.
Among patients with a CPC score of 1 or 2 at 6 months, only 20% were awake on day 1-3 following admission. Fifty-seven percent awoke on day 4-7, but importantly, 23% of patients with a good outcome at 6 months were not yet awake on day 8.
Three days after withdrawal of sedation, 49% of patients were rated as having a Glasgow Coma Scale score of 3-8, while 51% were Glasgow Coma Scale 9-15. Moreover, at that time 26% of patients with a good outcome as defined by a CPC of 1 or 2 at 6 months were still in a coma.
“So a lot of patients were still affected by their disease or by sedation at that point. That’s an important finding,” Dr. Sunde said.
Some prognostic tests were highly unreliable
A standout in poor performance was the widely utilized standard of a time to return of spontaneous circulation greater than 25 minutes as a predictor of poor cerebral outcome. In fact, it had a 34% false-positive rate.
“I think it’s really useless to use that. I would rather have return to spontaneous circulation after 40 minutes of good-quality CPR than not have it with 25 minutes of lesser-quality CPR,” he commented.
Similarly, a Glasgow Coma Scale score of 9 or less or a Glasgow Coma Scale-Motor score of 1-3 upon assessment 3 days after sedation withdrawal had false-positive rates of 30% and 34%, respectively.
During hypothermia, EEG abnormalities had a high false-positive rate, and sensory-evoked potential findings were difficult to interpret.
Predictors showing utility
Several clinical factors predicted poor cerebral outcome with low false-positive rates: Unwitnessed cardiac arrest had a false-positive rate of only 4%; initial presentation in asystole or with pulseless electrical activity had a false-positive rate of 6%; and no bystander CPR had a false-positive rate of 13%.
Abnormal sensory-evoked potential or EEG findings 3 days after sedation withdrawal had low false-positive rates as prognosticators of poor cerebral outcome. An EEG showing burst suppression or epileptiform activity had a “pretty good” false-positive rate of only 7%, Dr. Sunde noted. Bilaterally absent N20 sensory-evoked potential findings, while uncommon, had a false-positive rate of zero. A serum neuron-specific enolase level greater than 80 mcg/mL had a 3% false-positive rate, in sharp contrast to the previously recommended cutoff of more than 33 mcg/mL, which had an unacceptable 38% false-positive rate.
“We should avoid using single predictors in decision making and be patient, especially if we have a witnessed ventricular fibrillation with bystander CPR, independent of time to return of spontaneous circulation,” he concluded.
Dr. Sunde and his coinvestigators plan to present numerous further follow-up studies from NORCAST, including the results of comprehensive cognitive function testing 6-9 months after cardiac arrest in all survivors, coupled with interviews with their close relatives, as well as cognitive function and quality-of-life measurements 3-6 years after cardiac arrest along with interviews with relatives.
Several audience members rose to declare that they’ve been waiting for data such as this for a long time. Session chair Karl B. Kern, MD, professor of medicine at the University of Arizona, Tucson, and codirector of the University of Arizona Sarver Heart Center, commented, “We’ve been talking about whether 3 days is too early for a number of years, and clearly from your data it is. It was twice as long before most of them woke up.”
Dr. Sunde reported having no financial conflicts of interest regarding the NORCAST study, which was sponsored by Oslo University Hospital.
AT THE AHA SCIENTIFIC SESSIONS
Key clinical point:
Major finding: Patients with good cerebral function 6 months after admission in a comatose state stemming from out-of-hospital cardiac arrest awoke a mean of 6.2 days post cardiac arrest, far later than most prognostic assessments take place.
Data source: NORCAST, a prospective observational study, included 259 patients who were comatose upon hospital admission after out-of-hospital cardiac arrest.
Disclosures: NORCAST was sponsored by Oslo University Hospital. The presenter reported having no financial conflicts.
Frailty, not age, predicted complications after ambulatory surgery
Frailty was associated with a significant increase in 30-day complications after ambulatory hernia repair or ambulatory surgery of the breast, thyroid, or parathyroid, according to the results of a large retrospective cohort study.
The findings reinforce prior work indicating that frailty, not chronologic age, should be a primary factor when deciding about and preparing for surgery, Carolyn D. Seib, MD, and her associates at the University of California, San Francisco, wrote in JAMA Surgery. “Informed consent should be adjusted based on frailty to ensure that patients have an accurate assessment of their risk when making decisions about whether to undergo surgery,” the researchers said.
To test the hypothesis that frailty predicts morbidity and mortality after ambulatory general surgery, the researchers studied 140,828 patients older than 40 years from the 2007-2010 American College of Surgeons National Surgical Quality Improvement Program (JAMA Surg. 2017 Oct 11. doi: 10.1001/jamasurg.2017.4007). Nearly 2,500 (1.7%) patients experienced perioperative complications, and 0.7% had serious complications, the researchers said. After controlling for age sex, race or ethnicity, smoking, type of anesthesia, and corticosteroid use, patients with an intermediate (0.18-0.35) frailty score had a 70% higher odds of any complication (odds ratio, 1.7; 95% confidence interval, 1.5-1.9) and a 100% higher odds of serious complications (OR, 2.0; 95% CI, 1.7-2.3), compared with patients with a low frailty score.
An intermediate score reflected the presence of two to three frailty traits, such as impaired functional status, history of diabetes, pneumonia, chronic cardiovascular or lung disease, or impaired sensorium, the investigators noted. Notably, having a high modified frailty index (four or more frailty traits) was associated with 3.3-fold higher odds of any complication and with nearly 4-fold higher odds of serious complications, even after controlling for potential confounders.
Among modifiable risk factors, only the use of local and monitored anesthesia was associated with a significant decrease in the likelihood of serious 30-day complications (adjusted OR, 0.66; 95% CI, 0.53-0.81). Single-center studies of elderly patients undergoing inguinal hernia repair have reported similar findings, the researchers said. “For frail patients who choose to undergo hernia repair, local and monitored anesthesia care should be used whenever possible,” they wrote. “The use of local with monitored anesthesia care may be challenging in complex surgical procedures for breast cancer, such as modified radical mastectomy or axillary dissection, but it should be considered for patients with increased anesthesia risk who are undergoing ambulatory breast surgery.”
The National Institute on Aging provided partial funding. The investigators reported having no conflicts of interest.
Frailty was associated with a significant increase in 30-day complications after ambulatory hernia repair or ambulatory surgery of the breast, thyroid, or parathyroid, according to the results of a large retrospective cohort study.
The findings reinforce prior work indicating that frailty, not chronologic age, should be a primary factor when deciding about and preparing for surgery, Carolyn D. Seib, MD, and her associates at the University of California, San Francisco, wrote in JAMA Surgery. “Informed consent should be adjusted based on frailty to ensure that patients have an accurate assessment of their risk when making decisions about whether to undergo surgery,” the researchers said.
To test the hypothesis that frailty predicts morbidity and mortality after ambulatory general surgery, the researchers studied 140,828 patients older than 40 years from the 2007-2010 American College of Surgeons National Surgical Quality Improvement Program (JAMA Surg. 2017 Oct 11. doi: 10.1001/jamasurg.2017.4007). Nearly 2,500 (1.7%) patients experienced perioperative complications, and 0.7% had serious complications, the researchers said. After controlling for age sex, race or ethnicity, smoking, type of anesthesia, and corticosteroid use, patients with an intermediate (0.18-0.35) frailty score had a 70% higher odds of any complication (odds ratio, 1.7; 95% confidence interval, 1.5-1.9) and a 100% higher odds of serious complications (OR, 2.0; 95% CI, 1.7-2.3), compared with patients with a low frailty score.
An intermediate score reflected the presence of two to three frailty traits, such as impaired functional status, history of diabetes, pneumonia, chronic cardiovascular or lung disease, or impaired sensorium, the investigators noted. Notably, having a high modified frailty index (four or more frailty traits) was associated with 3.3-fold higher odds of any complication and with nearly 4-fold higher odds of serious complications, even after controlling for potential confounders.
Among modifiable risk factors, only the use of local and monitored anesthesia was associated with a significant decrease in the likelihood of serious 30-day complications (adjusted OR, 0.66; 95% CI, 0.53-0.81). Single-center studies of elderly patients undergoing inguinal hernia repair have reported similar findings, the researchers said. “For frail patients who choose to undergo hernia repair, local and monitored anesthesia care should be used whenever possible,” they wrote. “The use of local with monitored anesthesia care may be challenging in complex surgical procedures for breast cancer, such as modified radical mastectomy or axillary dissection, but it should be considered for patients with increased anesthesia risk who are undergoing ambulatory breast surgery.”
The National Institute on Aging provided partial funding. The investigators reported having no conflicts of interest.
Frailty was associated with a significant increase in 30-day complications after ambulatory hernia repair or ambulatory surgery of the breast, thyroid, or parathyroid, according to the results of a large retrospective cohort study.
The findings reinforce prior work indicating that frailty, not chronologic age, should be a primary factor when deciding about and preparing for surgery, Carolyn D. Seib, MD, and her associates at the University of California, San Francisco, wrote in JAMA Surgery. “Informed consent should be adjusted based on frailty to ensure that patients have an accurate assessment of their risk when making decisions about whether to undergo surgery,” the researchers said.
To test the hypothesis that frailty predicts morbidity and mortality after ambulatory general surgery, the researchers studied 140,828 patients older than 40 years from the 2007-2010 American College of Surgeons National Surgical Quality Improvement Program (JAMA Surg. 2017 Oct 11. doi: 10.1001/jamasurg.2017.4007). Nearly 2,500 (1.7%) patients experienced perioperative complications, and 0.7% had serious complications, the researchers said. After controlling for age sex, race or ethnicity, smoking, type of anesthesia, and corticosteroid use, patients with an intermediate (0.18-0.35) frailty score had a 70% higher odds of any complication (odds ratio, 1.7; 95% confidence interval, 1.5-1.9) and a 100% higher odds of serious complications (OR, 2.0; 95% CI, 1.7-2.3), compared with patients with a low frailty score.
An intermediate score reflected the presence of two to three frailty traits, such as impaired functional status, history of diabetes, pneumonia, chronic cardiovascular or lung disease, or impaired sensorium, the investigators noted. Notably, having a high modified frailty index (four or more frailty traits) was associated with 3.3-fold higher odds of any complication and with nearly 4-fold higher odds of serious complications, even after controlling for potential confounders.
Among modifiable risk factors, only the use of local and monitored anesthesia was associated with a significant decrease in the likelihood of serious 30-day complications (adjusted OR, 0.66; 95% CI, 0.53-0.81). Single-center studies of elderly patients undergoing inguinal hernia repair have reported similar findings, the researchers said. “For frail patients who choose to undergo hernia repair, local and monitored anesthesia care should be used whenever possible,” they wrote. “The use of local with monitored anesthesia care may be challenging in complex surgical procedures for breast cancer, such as modified radical mastectomy or axillary dissection, but it should be considered for patients with increased anesthesia risk who are undergoing ambulatory breast surgery.”
The National Institute on Aging provided partial funding. The investigators reported having no conflicts of interest.
FROM JAMA SURGERY
Key clinical point: Frailty was an independent risk factor for 30-day complications of ambulatory surgery, independent of age and other correlates.
Major finding: Having an intermediate (0.18-0.35) frailty score increased the odds of any complication by 70% (OR, 1.7).
Data source: A single-center retrospective cohort study of 140,828 patients older than 40 years from the 2007-2010 American College of Surgeons National Surgical Quality Improvement Program.
Disclosures: The investigators had no disclosures.
Low-sodium DASH benefits increase with higher blood pressures
ANAHEIM, CALIF. – The low-sodium DASH diet lowered systolic BP a mean of 20.8 mm Hg among patients with a baseline systolic pressure of 150-159 mm Hg, and did so in just 4 weeks, according to a new analysis of the DASH-Sodium trial.
The original 2001 study found that combining low sodium and the DASH [Dietary Approaches to Stop Hypertension] diet lowered blood pressure more than either alone, but results were not broken out by hypertension severity (N Engl J Med. 2001 Jan 4;344[1]:3-10).

It found that there were “progressively greater reductions at higher levels of baseline systolic BP (SBP). Among participants with baseline SBP at or above 150 mm Hg, “mean SBP reduction was striking,” said Dr. Juraschek, of Harvard Medical School/Beth Israel Deaconess Medical Center, Boston.
The original trial randomized 208 subjects to the DASH diet and 204 to a control diet similar to what most Americans eat. While on their diets, the subjects cycled through three sodium levels for 4 weeks each: 1.5 g/d, 2.4 g/d, and 3.3 g/d. Although deemed high sodium in the study, 3.3 g/d is typical of the American diet.
The new study analyzed outcomes according to four baseline SBP categories: 120-129, 130-139, 140-149, and 150-159 mm Hg.
Among subjects on the control diet, reducing sodium from high to low intake reduced SBP 3.20, 8.56, 8.99, and 7.04 mm Hg across the four baseline SBP categories (P = .004). Among patients consuming high sodium, the DASH diet, compared with the control diet, reduced SBP 4.5, 4.3, 4.7, and 10.6 mm Hg, but the trend was not statistically significant.
The low-sodium DASH diet, versus the high-sodium control diet, reduced SBP 5.3, 7.5, 9.7, and 20.8 mm Hg in subjects with baseline SBP at or above 150 mmHg (P < .001).
“The DASH diet with low sodium, compared with the control diet with high sodium, lowered SBP by nearly 10 mm Hg among those with a baseline SBP of 140-149 mm Hg and [greater than] 20 mm Hg among those with a baseline systolic BP [at or above] 150 mm Hg. SBP levels between 140 and 159 mm Hg represent the majority of patients with hypertension. Thus, our findings suggest that most adults with uncontrolled BP can experience substantial reductions in SBP from dietary changes alone,” the investigator said.
“To place our results in context, compared to placebo, angiotensin-converting enzyme inhibitors reduce SBP by 12 mm Hg, beta-blockers reduce SBP by 13 mm Hg, and calcium-channel blockers reduce SBP by 16 mm Hg,” he said.
“For many patients, it’s hard to take that step to be on a chronic medication. A lot of them want to talk about diet, but” find it hard to believe that something as simple as changing what you eat could beat drugs. “It’s important for both patients and physicians to realize that if you take this seriously, you can have significant reductions in your blood pressure. We should take it seriously as the first step. That’s the key take away,” Dr. Juraschek said in an interview.
None of the participants were on blood pressure medications; 57% were women, and 57% were black. The mean age was 48 years, and mean baseline BP was 135/86 mm Hg. The DASH diet includes whole grains, poultry, fish, and nuts, with reductions in red meat, sweets, and sugary drinks.
The results were published, online simultaneously with Dr. Juraschek’s presentation (J Am Coll Cardiol. 2017 Nov 12;doi: 10.1016/j.jacc.2017.10.011).
The original study was funded by the National Institutes of Health. Dr. Juraschek had no relevant disclosures.
ANAHEIM, CALIF. – The low-sodium DASH diet lowered systolic BP a mean of 20.8 mm Hg among patients with a baseline systolic pressure of 150-159 mm Hg, and did so in just 4 weeks, according to a new analysis of the DASH-Sodium trial.
The original 2001 study found that combining low sodium and the DASH [Dietary Approaches to Stop Hypertension] diet lowered blood pressure more than either alone, but results were not broken out by hypertension severity (N Engl J Med. 2001 Jan 4;344[1]:3-10).
It found that there were “progressively greater reductions at higher levels of baseline systolic BP (SBP). Among participants with baseline SBP at or above 150 mm Hg, “mean SBP reduction was striking,” said Dr. Juraschek, of Harvard Medical School/Beth Israel Deaconess Medical Center, Boston.
The original trial randomized 208 subjects to the DASH diet and 204 to a control diet similar to what most Americans eat. While on their diets, the subjects cycled through three sodium levels for 4 weeks each: 1.5 g/d, 2.4 g/d, and 3.3 g/d. Although deemed high sodium in the study, 3.3 g/d is typical of the American diet.
The new study analyzed outcomes according to four baseline SBP categories: 120-129, 130-139, 140-149, and 150-159 mm Hg.
Among subjects on the control diet, reducing sodium from high to low intake reduced SBP 3.20, 8.56, 8.99, and 7.04 mm Hg across the four baseline SBP categories (P = .004). Among patients consuming high sodium, the DASH diet, compared with the control diet, reduced SBP 4.5, 4.3, 4.7, and 10.6 mm Hg, but the trend was not statistically significant.
The low-sodium DASH diet, versus the high-sodium control diet, reduced SBP 5.3, 7.5, 9.7, and 20.8 mm Hg in subjects with baseline SBP at or above 150 mmHg (P < .001).
“The DASH diet with low sodium, compared with the control diet with high sodium, lowered SBP by nearly 10 mm Hg among those with a baseline SBP of 140-149 mm Hg and [greater than] 20 mm Hg among those with a baseline systolic BP [at or above] 150 mm Hg. SBP levels between 140 and 159 mm Hg represent the majority of patients with hypertension. Thus, our findings suggest that most adults with uncontrolled BP can experience substantial reductions in SBP from dietary changes alone,” the investigator said.
“To place our results in context, compared to placebo, angiotensin-converting enzyme inhibitors reduce SBP by 12 mm Hg, beta-blockers reduce SBP by 13 mm Hg, and calcium-channel blockers reduce SBP by 16 mm Hg,” he said.
“For many patients, it’s hard to take that step to be on a chronic medication. A lot of them want to talk about diet, but” find it hard to believe that something as simple as changing what you eat could beat drugs. “It’s important for both patients and physicians to realize that if you take this seriously, you can have significant reductions in your blood pressure. We should take it seriously as the first step. That’s the key take away,” Dr. Juraschek said in an interview.
None of the participants were on blood pressure medications; 57% were women, and 57% were black. The mean age was 48 years, and mean baseline BP was 135/86 mm Hg. The DASH diet includes whole grains, poultry, fish, and nuts, with reductions in red meat, sweets, and sugary drinks.
The results were published, online simultaneously with Dr. Juraschek’s presentation (J Am Coll Cardiol. 2017 Nov 12;doi: 10.1016/j.jacc.2017.10.011).
The original study was funded by the National Institutes of Health. Dr. Juraschek had no relevant disclosures.
ANAHEIM, CALIF. – The low-sodium DASH diet lowered systolic BP a mean of 20.8 mm Hg among patients with a baseline systolic pressure of 150-159 mm Hg, and did so in just 4 weeks, according to a new analysis of the DASH-Sodium trial.
The original 2001 study found that combining low sodium and the DASH [Dietary Approaches to Stop Hypertension] diet lowered blood pressure more than either alone, but results were not broken out by hypertension severity (N Engl J Med. 2001 Jan 4;344[1]:3-10).
It found that there were “progressively greater reductions at higher levels of baseline systolic BP (SBP). Among participants with baseline SBP at or above 150 mm Hg, “mean SBP reduction was striking,” said Dr. Juraschek, of Harvard Medical School/Beth Israel Deaconess Medical Center, Boston.
The original trial randomized 208 subjects to the DASH diet and 204 to a control diet similar to what most Americans eat. While on their diets, the subjects cycled through three sodium levels for 4 weeks each: 1.5 g/d, 2.4 g/d, and 3.3 g/d. Although deemed high sodium in the study, 3.3 g/d is typical of the American diet.
The new study analyzed outcomes according to four baseline SBP categories: 120-129, 130-139, 140-149, and 150-159 mm Hg.
Among subjects on the control diet, reducing sodium from high to low intake reduced SBP 3.20, 8.56, 8.99, and 7.04 mm Hg across the four baseline SBP categories (P = .004). Among patients consuming high sodium, the DASH diet, compared with the control diet, reduced SBP 4.5, 4.3, 4.7, and 10.6 mm Hg, but the trend was not statistically significant.
The low-sodium DASH diet, versus the high-sodium control diet, reduced SBP 5.3, 7.5, 9.7, and 20.8 mm Hg in subjects with baseline SBP at or above 150 mmHg (P < .001).
“The DASH diet with low sodium, compared with the control diet with high sodium, lowered SBP by nearly 10 mm Hg among those with a baseline SBP of 140-149 mm Hg and [greater than] 20 mm Hg among those with a baseline systolic BP [at or above] 150 mm Hg. SBP levels between 140 and 159 mm Hg represent the majority of patients with hypertension. Thus, our findings suggest that most adults with uncontrolled BP can experience substantial reductions in SBP from dietary changes alone,” the investigator said.
“To place our results in context, compared to placebo, angiotensin-converting enzyme inhibitors reduce SBP by 12 mm Hg, beta-blockers reduce SBP by 13 mm Hg, and calcium-channel blockers reduce SBP by 16 mm Hg,” he said.
“For many patients, it’s hard to take that step to be on a chronic medication. A lot of them want to talk about diet, but” find it hard to believe that something as simple as changing what you eat could beat drugs. “It’s important for both patients and physicians to realize that if you take this seriously, you can have significant reductions in your blood pressure. We should take it seriously as the first step. That’s the key take away,” Dr. Juraschek said in an interview.
None of the participants were on blood pressure medications; 57% were women, and 57% were black. The mean age was 48 years, and mean baseline BP was 135/86 mm Hg. The DASH diet includes whole grains, poultry, fish, and nuts, with reductions in red meat, sweets, and sugary drinks.
The results were published, online simultaneously with Dr. Juraschek’s presentation (J Am Coll Cardiol. 2017 Nov 12;doi: 10.1016/j.jacc.2017.10.011).
The original study was funded by the National Institutes of Health. Dr. Juraschek had no relevant disclosures.
AT THE AHA SCIENTIFIC SESSIONS
Key clinical point:
Major finding: The low-sodium DASH diet lowered systolic BP a mean of 20.8 mm Hg among patients with a baseline systolic pressure of 150-159 mm Hg, and did so in just 4 weeks.
Data source: New analysis of the landmark DASH-Sodium trial.
Disclosures: The original study was funded by the National Institutes of Health. The lead investigator in the new analysis didn’t have any relevant disclosures.
Virtual House Calls Are Feasible for Patients With Parkinson’s Disease
Providing remote neurologic care directly into the homes of patients with Parkinson’s disease is feasible and is neither more nor less efficacious than usual in-person care, according to research published in the September 12 issue of

Virtual house calls are becoming increasingly common for episodic conditions, but limited evidence supports their use for chronic conditions, according to the researchers. Approximately 40% of patients with Parkinson’s disease never receive care from a neurologist. These patients are more likely to have increased morbidity, to lose independence, and to die prematurely, they said.
Standard Care Versus Virtual House Calls
To determine whether providing virtual house calls is feasible, valuable, and beneficial, Dr. Beck and colleagues conducted a one-year randomized controlled study. Eligible participants had a clinical diagnosis of Parkinson’s disease; had a private, Internet-enabled device; and lived in a state where a site investigator was licensed to practice. Patients currently hospitalized, who had a condition that would preclude study participation in the judgment of the site investigator, or who were currently enrolled in another telemedicine study were excluded.
Investigators compared usual care to usual care supplemented with four virtual visits via video conferencing from a remote specialist into patients’ homes. Primary outcome measures were feasibility, measured by the proportion of participants who completed at least one virtual visit and the proportion of virtual visits completed on time, and efficacy, measured by change in the Parkinson’s Disease Questionnaire-39, a quality of life scale. Secondary outcomes included quality of care, caregiver burden, and time and travel savings.
Most Participants Were Satisfied With Virtual Visits
A total of 927 patients indicated interest in the study. Of these, 732 were excluded because they did not meet eligibility requirements, did not consent, or withdrew prior to randomization. A total of 210 patients were enrolled, and 195 were randomized. In all, 73% of participants had recently visited a specialist, 73% were college-educated, and 96% were white. The mean age of participants was 66. Ninety-eight percent of participants randomized to the intervention arm completed at least one virtual visit; 91% of 388 virtual visits were completed.
Quality of life did not improve for patients who received virtual house calls, nor did quality of care or caregiver burden. However, each virtual house call saved patients a median of 88 minutes per visit and 38 miles per visit. Ninety-seven percent of patients and 86% of physicians were satisfied or very satisfied with virtual visits.
One limitation of this study was that the majority of participants were white, well educated, and more familiar with the Internet than the general population. “Dedicated outreach to underserved populations, including those with advanced disease and from underserved demographic groups, especially women, rural residents, minorities, the homebound, or those in assisted living facilities, will help determine if the results are more generalizable and whether the benefits are potentially greater for those with historically less access to care,” said Dr. Beck and colleagues.
“Virtual house calls generated great interest and provided substantial convenience,” the researchers said. “Future efforts must address the digital divide and policy barriers to ensure that this new care model can address inequities in access to care.”
—Erica Tricarico
Suggested Reading
Beck CA, Beran DB, Biglan KM, et al. National randomized controlled trial of virtual house calls for Parkinson disease. Neurology. 2017;89(11):1152-1161.
Providing remote neurologic care directly into the homes of patients with Parkinson’s disease is feasible and is neither more nor less efficacious than usual in-person care, according to research published in the September 12 issue of
Virtual house calls are becoming increasingly common for episodic conditions, but limited evidence supports their use for chronic conditions, according to the researchers. Approximately 40% of patients with Parkinson’s disease never receive care from a neurologist. These patients are more likely to have increased morbidity, to lose independence, and to die prematurely, they said.
Standard Care Versus Virtual House Calls
To determine whether providing virtual house calls is feasible, valuable, and beneficial, Dr. Beck and colleagues conducted a one-year randomized controlled study. Eligible participants had a clinical diagnosis of Parkinson’s disease; had a private, Internet-enabled device; and lived in a state where a site investigator was licensed to practice. Patients currently hospitalized, who had a condition that would preclude study participation in the judgment of the site investigator, or who were currently enrolled in another telemedicine study were excluded.
Investigators compared usual care to usual care supplemented with four virtual visits via video conferencing from a remote specialist into patients’ homes. Primary outcome measures were feasibility, measured by the proportion of participants who completed at least one virtual visit and the proportion of virtual visits completed on time, and efficacy, measured by change in the Parkinson’s Disease Questionnaire-39, a quality of life scale. Secondary outcomes included quality of care, caregiver burden, and time and travel savings.
Most Participants Were Satisfied With Virtual Visits
A total of 927 patients indicated interest in the study. Of these, 732 were excluded because they did not meet eligibility requirements, did not consent, or withdrew prior to randomization. A total of 210 patients were enrolled, and 195 were randomized. In all, 73% of participants had recently visited a specialist, 73% were college-educated, and 96% were white. The mean age of participants was 66. Ninety-eight percent of participants randomized to the intervention arm completed at least one virtual visit; 91% of 388 virtual visits were completed.
Quality of life did not improve for patients who received virtual house calls, nor did quality of care or caregiver burden. However, each virtual house call saved patients a median of 88 minutes per visit and 38 miles per visit. Ninety-seven percent of patients and 86% of physicians were satisfied or very satisfied with virtual visits.
One limitation of this study was that the majority of participants were white, well educated, and more familiar with the Internet than the general population. “Dedicated outreach to underserved populations, including those with advanced disease and from underserved demographic groups, especially women, rural residents, minorities, the homebound, or those in assisted living facilities, will help determine if the results are more generalizable and whether the benefits are potentially greater for those with historically less access to care,” said Dr. Beck and colleagues.
“Virtual house calls generated great interest and provided substantial convenience,” the researchers said. “Future efforts must address the digital divide and policy barriers to ensure that this new care model can address inequities in access to care.”
—Erica Tricarico
Suggested Reading
Beck CA, Beran DB, Biglan KM, et al. National randomized controlled trial of virtual house calls for Parkinson disease. Neurology. 2017;89(11):1152-1161.
Providing remote neurologic care directly into the homes of patients with Parkinson’s disease is feasible and is neither more nor less efficacious than usual in-person care, according to research published in the September 12 issue of
Virtual house calls are becoming increasingly common for episodic conditions, but limited evidence supports their use for chronic conditions, according to the researchers. Approximately 40% of patients with Parkinson’s disease never receive care from a neurologist. These patients are more likely to have increased morbidity, to lose independence, and to die prematurely, they said.
Standard Care Versus Virtual House Calls
To determine whether providing virtual house calls is feasible, valuable, and beneficial, Dr. Beck and colleagues conducted a one-year randomized controlled study. Eligible participants had a clinical diagnosis of Parkinson’s disease; had a private, Internet-enabled device; and lived in a state where a site investigator was licensed to practice. Patients currently hospitalized, who had a condition that would preclude study participation in the judgment of the site investigator, or who were currently enrolled in another telemedicine study were excluded.
Investigators compared usual care to usual care supplemented with four virtual visits via video conferencing from a remote specialist into patients’ homes. Primary outcome measures were feasibility, measured by the proportion of participants who completed at least one virtual visit and the proportion of virtual visits completed on time, and efficacy, measured by change in the Parkinson’s Disease Questionnaire-39, a quality of life scale. Secondary outcomes included quality of care, caregiver burden, and time and travel savings.
Most Participants Were Satisfied With Virtual Visits
A total of 927 patients indicated interest in the study. Of these, 732 were excluded because they did not meet eligibility requirements, did not consent, or withdrew prior to randomization. A total of 210 patients were enrolled, and 195 were randomized. In all, 73% of participants had recently visited a specialist, 73% were college-educated, and 96% were white. The mean age of participants was 66. Ninety-eight percent of participants randomized to the intervention arm completed at least one virtual visit; 91% of 388 virtual visits were completed.
Quality of life did not improve for patients who received virtual house calls, nor did quality of care or caregiver burden. However, each virtual house call saved patients a median of 88 minutes per visit and 38 miles per visit. Ninety-seven percent of patients and 86% of physicians were satisfied or very satisfied with virtual visits.
One limitation of this study was that the majority of participants were white, well educated, and more familiar with the Internet than the general population. “Dedicated outreach to underserved populations, including those with advanced disease and from underserved demographic groups, especially women, rural residents, minorities, the homebound, or those in assisted living facilities, will help determine if the results are more generalizable and whether the benefits are potentially greater for those with historically less access to care,” said Dr. Beck and colleagues.
“Virtual house calls generated great interest and provided substantial convenience,” the researchers said. “Future efforts must address the digital divide and policy barriers to ensure that this new care model can address inequities in access to care.”
—Erica Tricarico
Suggested Reading
Beck CA, Beran DB, Biglan KM, et al. National randomized controlled trial of virtual house calls for Parkinson disease. Neurology. 2017;89(11):1152-1161.