User login
Primary cirrhotic prophylaxis of bacterial peritonitis falls short
WASHINGTON –
The mortality rate during follow-up of cirrhotic patients hospitalized while on primary prophylaxis against spontaneous bacterial peritonitis (SBP) was 19%, compared with a 9% death rate among cirrhotic patients hospitalized while on secondary prophylaxis, Jasmohan S. Bajaj, MD, said at the annual Digestive Disease Week®.

Although the findings raised questions about the value of primary prophylaxis with an antibiotic in cirrhotic patients for preventing a first episode of SBP, secondary prophylaxis remains an important precaution.
“There is clear benefit from secondary prophylaxis; please use it. The data supporting it are robust,” said Dr. Bajaj, a hepatologist at Virginia Commonwealth University, Richmond. In contrast, the evidence supporting benefits from primary prophylaxis is weaker, he said. The findings were also counterintuitive, because patients who experience repeat episodes of SBP might be expected to fare worse than those hit by SBP just once.
Dr. Bajaj also acknowledged the substantial confounding that distinguishes patients with cirrhosis receiving primary or secondary prophylaxis, and the difficulty of fully adjusting for all this confounding by statistical analyses. “There is selective bias for secondary prevention, and there is no way to correct for this,” he explained. Patients who need secondary prophylaxis have “weathered the storm” of a first episode of SBP, which might have exerted selection pressure, and might have triggered important immunologic changes, Dr. Bajaj suggested.
The findings also raised concerns about the appropriateness of existing antibiotic prophylaxis for SBP. The patients included in the study all received similar regimens regardless of whether they were on primary or secondary prophylaxis. Three-quarters of primary prophylaxis patients received a fluoroquinolone, as did 81% on secondary prophylaxis. All other patients received trimethoprim-sulfamethoxazole. These regimens are aimed at preventing gram-negative infections; however, an increasing number of SBP episodes are caused by either gram-positive pathogens or strains of gram-negative bacteria or fungi resistant to standard antibiotics.
Clinicians “absolutely” need to rethink their approach to both primary and secondary prophylaxis, Dr. Bajaj said. “As fast as treatment evolves, bacteria evolve 20 times faster. We need to find ways to prevent infections without antibiotic prophylaxis, whatever that might be.”
The study used data collected prospectively from patients with cirrhosis at any of 12 U.S. and 2 Canadian centers that belonged to the North American Consortium for the Study of End-Stage Liver Disease. Among 2,731 cirrhotic patients admitted nonelectively, 492 (18%) were on antibiotic prophylaxis at the time of their admission, 305 for primary prophylaxis and 187 for secondary prophylaxis. Dr. Bajaj and his associates used both the baseline model for end-stage liver disease score and serum albumin level of each patient to focus on a group of 154 primary prophylaxis and 154 secondary prophylaxis patients who were similar by these two criteria. Despite this matching, the two subgroups showed statistically significant differences at the time of their index hospitalization for several important clinical measures.
The secondary prophylaxis patients were significantly more likely to have been hospitalized within the previous 6 months, significantly more likely to be on treatment for hepatic encephalopathy at the time of their index admission, and significantly less likely to have systemic inflammatory response syndrome on admission.
Also, at the time of admission, secondary prophylaxis patients were significantly more likely to have an infection of any type at a rate of 40%, compared with 24% among those on primary prophylaxis, as well as a significantly higher rate of SBP at 16%, compared with a 9% rate among the primary prophylaxis patients. During hospitalization, nosocomial SBP occurred significantly more often among the secondary prophylaxis patients at a rate of 6%, compared with a 0.5% rate among those on primary prophylaxis.
Despite these between-group differences, the average duration of hospitalization, and the average incidence of acute-on-chronic liver failure during follow-up out to 30 days post discharge was similar in the two subgroups. And the patients on secondary prophylaxis showed better outcomes by two important parameters: mortality during hospitalization and 30 days post discharge; and the incidence of ICU admission during hospitalization, which was significantly greater for primary prophylaxis patients at 31%, compared with 21% among the secondary prophylaxis patients, Dr. Bajaj reported.
Dr. Bajaj has been a consultant for Norgine and Salix Pharmaceuticals and has received research support from Grifols and Salix Pharmaceuticals.
WASHINGTON –
The mortality rate during follow-up of cirrhotic patients hospitalized while on primary prophylaxis against spontaneous bacterial peritonitis (SBP) was 19%, compared with a 9% death rate among cirrhotic patients hospitalized while on secondary prophylaxis, Jasmohan S. Bajaj, MD, said at the annual Digestive Disease Week®.
Although the findings raised questions about the value of primary prophylaxis with an antibiotic in cirrhotic patients for preventing a first episode of SBP, secondary prophylaxis remains an important precaution.
“There is clear benefit from secondary prophylaxis; please use it. The data supporting it are robust,” said Dr. Bajaj, a hepatologist at Virginia Commonwealth University, Richmond. In contrast, the evidence supporting benefits from primary prophylaxis is weaker, he said. The findings were also counterintuitive, because patients who experience repeat episodes of SBP might be expected to fare worse than those hit by SBP just once.
Dr. Bajaj also acknowledged the substantial confounding that distinguishes patients with cirrhosis receiving primary or secondary prophylaxis, and the difficulty of fully adjusting for all this confounding by statistical analyses. “There is selective bias for secondary prevention, and there is no way to correct for this,” he explained. Patients who need secondary prophylaxis have “weathered the storm” of a first episode of SBP, which might have exerted selection pressure, and might have triggered important immunologic changes, Dr. Bajaj suggested.
The findings also raised concerns about the appropriateness of existing antibiotic prophylaxis for SBP. The patients included in the study all received similar regimens regardless of whether they were on primary or secondary prophylaxis. Three-quarters of primary prophylaxis patients received a fluoroquinolone, as did 81% on secondary prophylaxis. All other patients received trimethoprim-sulfamethoxazole. These regimens are aimed at preventing gram-negative infections; however, an increasing number of SBP episodes are caused by either gram-positive pathogens or strains of gram-negative bacteria or fungi resistant to standard antibiotics.
Clinicians “absolutely” need to rethink their approach to both primary and secondary prophylaxis, Dr. Bajaj said. “As fast as treatment evolves, bacteria evolve 20 times faster. We need to find ways to prevent infections without antibiotic prophylaxis, whatever that might be.”
The study used data collected prospectively from patients with cirrhosis at any of 12 U.S. and 2 Canadian centers that belonged to the North American Consortium for the Study of End-Stage Liver Disease. Among 2,731 cirrhotic patients admitted nonelectively, 492 (18%) were on antibiotic prophylaxis at the time of their admission, 305 for primary prophylaxis and 187 for secondary prophylaxis. Dr. Bajaj and his associates used both the baseline model for end-stage liver disease score and serum albumin level of each patient to focus on a group of 154 primary prophylaxis and 154 secondary prophylaxis patients who were similar by these two criteria. Despite this matching, the two subgroups showed statistically significant differences at the time of their index hospitalization for several important clinical measures.
The secondary prophylaxis patients were significantly more likely to have been hospitalized within the previous 6 months, significantly more likely to be on treatment for hepatic encephalopathy at the time of their index admission, and significantly less likely to have systemic inflammatory response syndrome on admission.
Also, at the time of admission, secondary prophylaxis patients were significantly more likely to have an infection of any type at a rate of 40%, compared with 24% among those on primary prophylaxis, as well as a significantly higher rate of SBP at 16%, compared with a 9% rate among the primary prophylaxis patients. During hospitalization, nosocomial SBP occurred significantly more often among the secondary prophylaxis patients at a rate of 6%, compared with a 0.5% rate among those on primary prophylaxis.
Despite these between-group differences, the average duration of hospitalization, and the average incidence of acute-on-chronic liver failure during follow-up out to 30 days post discharge was similar in the two subgroups. And the patients on secondary prophylaxis showed better outcomes by two important parameters: mortality during hospitalization and 30 days post discharge; and the incidence of ICU admission during hospitalization, which was significantly greater for primary prophylaxis patients at 31%, compared with 21% among the secondary prophylaxis patients, Dr. Bajaj reported.
Dr. Bajaj has been a consultant for Norgine and Salix Pharmaceuticals and has received research support from Grifols and Salix Pharmaceuticals.
WASHINGTON –
The mortality rate during follow-up of cirrhotic patients hospitalized while on primary prophylaxis against spontaneous bacterial peritonitis (SBP) was 19%, compared with a 9% death rate among cirrhotic patients hospitalized while on secondary prophylaxis, Jasmohan S. Bajaj, MD, said at the annual Digestive Disease Week®.
Although the findings raised questions about the value of primary prophylaxis with an antibiotic in cirrhotic patients for preventing a first episode of SBP, secondary prophylaxis remains an important precaution.
“There is clear benefit from secondary prophylaxis; please use it. The data supporting it are robust,” said Dr. Bajaj, a hepatologist at Virginia Commonwealth University, Richmond. In contrast, the evidence supporting benefits from primary prophylaxis is weaker, he said. The findings were also counterintuitive, because patients who experience repeat episodes of SBP might be expected to fare worse than those hit by SBP just once.
Dr. Bajaj also acknowledged the substantial confounding that distinguishes patients with cirrhosis receiving primary or secondary prophylaxis, and the difficulty of fully adjusting for all this confounding by statistical analyses. “There is selective bias for secondary prevention, and there is no way to correct for this,” he explained. Patients who need secondary prophylaxis have “weathered the storm” of a first episode of SBP, which might have exerted selection pressure, and might have triggered important immunologic changes, Dr. Bajaj suggested.
The findings also raised concerns about the appropriateness of existing antibiotic prophylaxis for SBP. The patients included in the study all received similar regimens regardless of whether they were on primary or secondary prophylaxis. Three-quarters of primary prophylaxis patients received a fluoroquinolone, as did 81% on secondary prophylaxis. All other patients received trimethoprim-sulfamethoxazole. These regimens are aimed at preventing gram-negative infections; however, an increasing number of SBP episodes are caused by either gram-positive pathogens or strains of gram-negative bacteria or fungi resistant to standard antibiotics.
Clinicians “absolutely” need to rethink their approach to both primary and secondary prophylaxis, Dr. Bajaj said. “As fast as treatment evolves, bacteria evolve 20 times faster. We need to find ways to prevent infections without antibiotic prophylaxis, whatever that might be.”
The study used data collected prospectively from patients with cirrhosis at any of 12 U.S. and 2 Canadian centers that belonged to the North American Consortium for the Study of End-Stage Liver Disease. Among 2,731 cirrhotic patients admitted nonelectively, 492 (18%) were on antibiotic prophylaxis at the time of their admission, 305 for primary prophylaxis and 187 for secondary prophylaxis. Dr. Bajaj and his associates used both the baseline model for end-stage liver disease score and serum albumin level of each patient to focus on a group of 154 primary prophylaxis and 154 secondary prophylaxis patients who were similar by these two criteria. Despite this matching, the two subgroups showed statistically significant differences at the time of their index hospitalization for several important clinical measures.
The secondary prophylaxis patients were significantly more likely to have been hospitalized within the previous 6 months, significantly more likely to be on treatment for hepatic encephalopathy at the time of their index admission, and significantly less likely to have systemic inflammatory response syndrome on admission.
Also, at the time of admission, secondary prophylaxis patients were significantly more likely to have an infection of any type at a rate of 40%, compared with 24% among those on primary prophylaxis, as well as a significantly higher rate of SBP at 16%, compared with a 9% rate among the primary prophylaxis patients. During hospitalization, nosocomial SBP occurred significantly more often among the secondary prophylaxis patients at a rate of 6%, compared with a 0.5% rate among those on primary prophylaxis.
Despite these between-group differences, the average duration of hospitalization, and the average incidence of acute-on-chronic liver failure during follow-up out to 30 days post discharge was similar in the two subgroups. And the patients on secondary prophylaxis showed better outcomes by two important parameters: mortality during hospitalization and 30 days post discharge; and the incidence of ICU admission during hospitalization, which was significantly greater for primary prophylaxis patients at 31%, compared with 21% among the secondary prophylaxis patients, Dr. Bajaj reported.
Dr. Bajaj has been a consultant for Norgine and Salix Pharmaceuticals and has received research support from Grifols and Salix Pharmaceuticals.
REPORTING FROM DDW 2018
Key clinical point: Antibiotic prophylaxis for bacterial peritonitis showed limitations, especially for primary prophylaxis.
Major finding: Mortality was 19% among primary prophylaxis patients and 9% among secondary prophylaxis patients during hospitalization and 30 days following.
Study details: An analysis of data from 308 cirrhotic patients on antibiotic prophylaxis at 14 North American centers.
Disclosures: Dr. Bajaj has been a consultant for Norgine and Salix Pharmaceuticals and has received research support from Grifols and Salix Pharmaceuticals.
25+ Years of Migraine
R. Allan Purdy, MD, FRCPC
Dr. Purdy is Professor of Medicine (Neurology) at Dalhousie University, Halifax, Nova Scotia.
Although migraine has been with humans since antiquity, it is truly amazing that over the past 25 years and a bit longer there have been remarkable advances in our clinical understanding of migraine and its variations, along with sophisticated epidemiologic evidence and basic research into the neurobiological basis of migraine. These advances have brought this disorder/disease to the forefront as a serious neurologic condition deserving of attention. Migraine is a major cause of neurologic disability in the world. This fact has only been fully recognized in recent years.

From the 1980s through the 1990s, a series of events led to a seminal study of a medication that would truly alter the vector for migraine in the future. Studies coming out of Glaxo in the United Kingdom, under the direction of Pat Humphrey, OBE, DSc, PhD, led to the discovery of sumatriptan, the first truly designer medication for the treatment of acute migraine. The story of how this medication biologically affects the brain serotonin receptors on blood vessels and brain tissue to abort a migraine attack is well known today. Early observations on patients receiving subcutaneous sumatriptan clearly showed how powerful this agent was in shutting down the migraine attack. Patients having migraine in extremis, with severe throbbing headache, pallor, nausea and vomiting, appearing markedly distressed and ill, within minutes to an hour would return to a normal state. Nothing that preceded sumatriptan demonstrated such a remarkable clinical response in patients with headache.
In the past century, sumatriptan came to be one of the most important therapeutic advances in neurology. After its discovery, six other triptans entered the market over time. All of them had minor tweaks on the original molecule’s pharmacology and pharmacokinetics, including various modes of delivery with different results in subgroups of patients. Nevertheless, on balance, the triptans acted in a similar manner to produce similar outcomes. Today, many patients take triptans regularly for help with acute migraine attacks; however, other patients with migraine remain undiagnosed and undertreated and do not receive optimal care.
In the past 20 years, sophisticated laboratory and neuroimaging research allowed in-depth analysis of the migraine attack and spectrum of the migraine disorder. The brain areas that subserve the migraine attack have been mapped neuroanatomically throughout the nervous system, with input from the brainstem, hypothalamus, thalamus, and cortical structures. Cortical-initiated electrical events possibly trigger the trigeminal vascular system, and/or peripheral or central activation mechanisms produce the symptoms of migraine. The migraine story is not complete, but evidence clearly shows migraine to be a valid neurobiological disorder and disease. For some people with migraine, it is occasional aggravation, but for others it can be life-altering and, rarely, life-threatening.
In the past few years, new targets for migraine therapy have been pursued. A CGRP receptor antagonist (or “gepant”) showed benefit in early trials; however, because of potential hepatic side effects, other gepants and CGRP monoclonal antibodies have been studied in clinical trials.
Results of recent trials—one in episodic migraine and the other in chronic migraine—show that anti-CGRP monoclonal antibodies appear to be quite efficacious, have few side effects, and are well tolerated. Time will determine whether there are long-term consequences of their use, and what is the effectiveness of using these large molecules to treat migraine, but current results appear promising. Another triptan-like agent, a ditan, which activates receptors of serotonin without vasoconstrictor properties, has shown promise in acute migraine. Neuromodulation devices are also showing promise in migraine therapy and appear to be safe and well tolerated. Nonpharmacological therapies are more often utilized with benefits and help to avoid problems with medications and their side effects.
Increasing knowledge of migraine epidemiology has shown that there is a transition from acute to more frequent, and from high frequency to subsequent chronic migraine attacks. This transformation, or chronification, appears unique in patients with migraine. This process appears to be bidirectional and reversible in migraine. Whether migraine becomes chronic as a process over time or whether migraine is a chronic disease with episodic fluctuations is something to be further explored in research and clinical practice. Nevertheless, these concepts can only lead to better understanding and, hopefully, new therapeutic interventions that will reduce the frequency and severity of this unique neurologic disease.
As migraine progresses or evolves it can be associated with multiple comorbid disorders, including stroke, depression, seizures, and medication overuse. New preventive therapies in development can be modifications of medications for other neurologic conditions, such as the antiepileptic medications, for example. There are many other potential targets that will be explored for the management of migraine in this century. The future looks promising in that regard.
For decades, and now centuries, neurologists have been interested in migraine and related disorders. Sumatriptan jump-started the modern revolution and evolution of therapeutic options to manage migraine pharmacologically. Since its discovery and use in clinical medicine, the world of migraine has changed dramatically. As headache clinicians are being trained in the latest advances in migraine and other headache disorders, they are showing increasing interest and knowledge,which is provided by some of the most unique and relevant research involving the brain in the world. A cure for migraine may not be possible, but a better understanding and control of all of migraine’s myriad of symptoms is probably within reach in this century.
Suggested Reading
Bigal ME, Lipton RB. Clinical course in migraine: conceptualizing migraine transformation. Neurology. 2008;71(11):848-855.
Deen M, Correnti E, Kamm K, et al. Blocking CGRP in migraine patients – a review of pros and cons. J Headache Pain. 2017;18(1):96.
Dodick DW. Migraine. Lancet. 2018;391(10127):1315-1330.
Färkkilä M, Diener HC, Géraud G, et al. Efficacy and tolerability of lasmiditan, an oral 5-HT(1F) receptor agonist, for the acute treatment of migraine: a phase 2 randomised, placebo-controlled, parallel-group, dose-ranging study. Lancet Neurology. 2012;11(5):405-413.
Goadsby PJ, Reuter U, Hallström Y, et al. A controlled trial of erenumab for episodic migraine. N Engl J Med. 2017;377(22):2123-2132.
Humphrey PP. The discovery and development of the triptans, a major therapeutic breakthrough. Headache. 2008;48(5):685-687.
Puledda F, Goadsby PJ. An update on non-pharmacological neuromodulation for the acute and preventive treatment of migraine. Headache. 2017;57(4):685-691.
Silberstein SD, Dodick DW, Bigal ME, et al. Fremanezumab for the preventive treatment of chronic migraine. N Engl J Med. 2017;377(22):2113-2122.
Wietecha LA, Kuca B, Case MG, et al. Phase 3 study (SPARTAN) of lasmiditan compared to placebo for acute treatment of migraine. Cephalalgia. 2017;37 (suppl 1):367-68 (abstr).
R. Allan Purdy, MD, FRCPC
Dr. Purdy is Professor of Medicine (Neurology) at Dalhousie University, Halifax, Nova Scotia.
Although migraine has been with humans since antiquity, it is truly amazing that over the past 25 years and a bit longer there have been remarkable advances in our clinical understanding of migraine and its variations, along with sophisticated epidemiologic evidence and basic research into the neurobiological basis of migraine. These advances have brought this disorder/disease to the forefront as a serious neurologic condition deserving of attention. Migraine is a major cause of neurologic disability in the world. This fact has only been fully recognized in recent years.
From the 1980s through the 1990s, a series of events led to a seminal study of a medication that would truly alter the vector for migraine in the future. Studies coming out of Glaxo in the United Kingdom, under the direction of Pat Humphrey, OBE, DSc, PhD, led to the discovery of sumatriptan, the first truly designer medication for the treatment of acute migraine. The story of how this medication biologically affects the brain serotonin receptors on blood vessels and brain tissue to abort a migraine attack is well known today. Early observations on patients receiving subcutaneous sumatriptan clearly showed how powerful this agent was in shutting down the migraine attack. Patients having migraine in extremis, with severe throbbing headache, pallor, nausea and vomiting, appearing markedly distressed and ill, within minutes to an hour would return to a normal state. Nothing that preceded sumatriptan demonstrated such a remarkable clinical response in patients with headache.
In the past century, sumatriptan came to be one of the most important therapeutic advances in neurology. After its discovery, six other triptans entered the market over time. All of them had minor tweaks on the original molecule’s pharmacology and pharmacokinetics, including various modes of delivery with different results in subgroups of patients. Nevertheless, on balance, the triptans acted in a similar manner to produce similar outcomes. Today, many patients take triptans regularly for help with acute migraine attacks; however, other patients with migraine remain undiagnosed and undertreated and do not receive optimal care.
In the past 20 years, sophisticated laboratory and neuroimaging research allowed in-depth analysis of the migraine attack and spectrum of the migraine disorder. The brain areas that subserve the migraine attack have been mapped neuroanatomically throughout the nervous system, with input from the brainstem, hypothalamus, thalamus, and cortical structures. Cortical-initiated electrical events possibly trigger the trigeminal vascular system, and/or peripheral or central activation mechanisms produce the symptoms of migraine. The migraine story is not complete, but evidence clearly shows migraine to be a valid neurobiological disorder and disease. For some people with migraine, it is occasional aggravation, but for others it can be life-altering and, rarely, life-threatening.
In the past few years, new targets for migraine therapy have been pursued. A CGRP receptor antagonist (or “gepant”) showed benefit in early trials; however, because of potential hepatic side effects, other gepants and CGRP monoclonal antibodies have been studied in clinical trials.
Results of recent trials—one in episodic migraine and the other in chronic migraine—show that anti-CGRP monoclonal antibodies appear to be quite efficacious, have few side effects, and are well tolerated. Time will determine whether there are long-term consequences of their use, and what is the effectiveness of using these large molecules to treat migraine, but current results appear promising. Another triptan-like agent, a ditan, which activates receptors of serotonin without vasoconstrictor properties, has shown promise in acute migraine. Neuromodulation devices are also showing promise in migraine therapy and appear to be safe and well tolerated. Nonpharmacological therapies are more often utilized with benefits and help to avoid problems with medications and their side effects.
Increasing knowledge of migraine epidemiology has shown that there is a transition from acute to more frequent, and from high frequency to subsequent chronic migraine attacks. This transformation, or chronification, appears unique in patients with migraine. This process appears to be bidirectional and reversible in migraine. Whether migraine becomes chronic as a process over time or whether migraine is a chronic disease with episodic fluctuations is something to be further explored in research and clinical practice. Nevertheless, these concepts can only lead to better understanding and, hopefully, new therapeutic interventions that will reduce the frequency and severity of this unique neurologic disease.
As migraine progresses or evolves it can be associated with multiple comorbid disorders, including stroke, depression, seizures, and medication overuse. New preventive therapies in development can be modifications of medications for other neurologic conditions, such as the antiepileptic medications, for example. There are many other potential targets that will be explored for the management of migraine in this century. The future looks promising in that regard.
For decades, and now centuries, neurologists have been interested in migraine and related disorders. Sumatriptan jump-started the modern revolution and evolution of therapeutic options to manage migraine pharmacologically. Since its discovery and use in clinical medicine, the world of migraine has changed dramatically. As headache clinicians are being trained in the latest advances in migraine and other headache disorders, they are showing increasing interest and knowledge,which is provided by some of the most unique and relevant research involving the brain in the world. A cure for migraine may not be possible, but a better understanding and control of all of migraine’s myriad of symptoms is probably within reach in this century.
Suggested Reading
Bigal ME, Lipton RB. Clinical course in migraine: conceptualizing migraine transformation. Neurology. 2008;71(11):848-855.
Deen M, Correnti E, Kamm K, et al. Blocking CGRP in migraine patients – a review of pros and cons. J Headache Pain. 2017;18(1):96.
Dodick DW. Migraine. Lancet. 2018;391(10127):1315-1330.
Färkkilä M, Diener HC, Géraud G, et al. Efficacy and tolerability of lasmiditan, an oral 5-HT(1F) receptor agonist, for the acute treatment of migraine: a phase 2 randomised, placebo-controlled, parallel-group, dose-ranging study. Lancet Neurology. 2012;11(5):405-413.
Goadsby PJ, Reuter U, Hallström Y, et al. A controlled trial of erenumab for episodic migraine. N Engl J Med. 2017;377(22):2123-2132.
Humphrey PP. The discovery and development of the triptans, a major therapeutic breakthrough. Headache. 2008;48(5):685-687.
Puledda F, Goadsby PJ. An update on non-pharmacological neuromodulation for the acute and preventive treatment of migraine. Headache. 2017;57(4):685-691.
Silberstein SD, Dodick DW, Bigal ME, et al. Fremanezumab for the preventive treatment of chronic migraine. N Engl J Med. 2017;377(22):2113-2122.
Wietecha LA, Kuca B, Case MG, et al. Phase 3 study (SPARTAN) of lasmiditan compared to placebo for acute treatment of migraine. Cephalalgia. 2017;37 (suppl 1):367-68 (abstr).
R. Allan Purdy, MD, FRCPC
Dr. Purdy is Professor of Medicine (Neurology) at Dalhousie University, Halifax, Nova Scotia.
Although migraine has been with humans since antiquity, it is truly amazing that over the past 25 years and a bit longer there have been remarkable advances in our clinical understanding of migraine and its variations, along with sophisticated epidemiologic evidence and basic research into the neurobiological basis of migraine. These advances have brought this disorder/disease to the forefront as a serious neurologic condition deserving of attention. Migraine is a major cause of neurologic disability in the world. This fact has only been fully recognized in recent years.
From the 1980s through the 1990s, a series of events led to a seminal study of a medication that would truly alter the vector for migraine in the future. Studies coming out of Glaxo in the United Kingdom, under the direction of Pat Humphrey, OBE, DSc, PhD, led to the discovery of sumatriptan, the first truly designer medication for the treatment of acute migraine. The story of how this medication biologically affects the brain serotonin receptors on blood vessels and brain tissue to abort a migraine attack is well known today. Early observations on patients receiving subcutaneous sumatriptan clearly showed how powerful this agent was in shutting down the migraine attack. Patients having migraine in extremis, with severe throbbing headache, pallor, nausea and vomiting, appearing markedly distressed and ill, within minutes to an hour would return to a normal state. Nothing that preceded sumatriptan demonstrated such a remarkable clinical response in patients with headache.
In the past century, sumatriptan came to be one of the most important therapeutic advances in neurology. After its discovery, six other triptans entered the market over time. All of them had minor tweaks on the original molecule’s pharmacology and pharmacokinetics, including various modes of delivery with different results in subgroups of patients. Nevertheless, on balance, the triptans acted in a similar manner to produce similar outcomes. Today, many patients take triptans regularly for help with acute migraine attacks; however, other patients with migraine remain undiagnosed and undertreated and do not receive optimal care.
In the past 20 years, sophisticated laboratory and neuroimaging research allowed in-depth analysis of the migraine attack and spectrum of the migraine disorder. The brain areas that subserve the migraine attack have been mapped neuroanatomically throughout the nervous system, with input from the brainstem, hypothalamus, thalamus, and cortical structures. Cortical-initiated electrical events possibly trigger the trigeminal vascular system, and/or peripheral or central activation mechanisms produce the symptoms of migraine. The migraine story is not complete, but evidence clearly shows migraine to be a valid neurobiological disorder and disease. For some people with migraine, it is occasional aggravation, but for others it can be life-altering and, rarely, life-threatening.
In the past few years, new targets for migraine therapy have been pursued. A CGRP receptor antagonist (or “gepant”) showed benefit in early trials; however, because of potential hepatic side effects, other gepants and CGRP monoclonal antibodies have been studied in clinical trials.
Results of recent trials—one in episodic migraine and the other in chronic migraine—show that anti-CGRP monoclonal antibodies appear to be quite efficacious, have few side effects, and are well tolerated. Time will determine whether there are long-term consequences of their use, and what is the effectiveness of using these large molecules to treat migraine, but current results appear promising. Another triptan-like agent, a ditan, which activates receptors of serotonin without vasoconstrictor properties, has shown promise in acute migraine. Neuromodulation devices are also showing promise in migraine therapy and appear to be safe and well tolerated. Nonpharmacological therapies are more often utilized with benefits and help to avoid problems with medications and their side effects.
Increasing knowledge of migraine epidemiology has shown that there is a transition from acute to more frequent, and from high frequency to subsequent chronic migraine attacks. This transformation, or chronification, appears unique in patients with migraine. This process appears to be bidirectional and reversible in migraine. Whether migraine becomes chronic as a process over time or whether migraine is a chronic disease with episodic fluctuations is something to be further explored in research and clinical practice. Nevertheless, these concepts can only lead to better understanding and, hopefully, new therapeutic interventions that will reduce the frequency and severity of this unique neurologic disease.
As migraine progresses or evolves it can be associated with multiple comorbid disorders, including stroke, depression, seizures, and medication overuse. New preventive therapies in development can be modifications of medications for other neurologic conditions, such as the antiepileptic medications, for example. There are many other potential targets that will be explored for the management of migraine in this century. The future looks promising in that regard.
For decades, and now centuries, neurologists have been interested in migraine and related disorders. Sumatriptan jump-started the modern revolution and evolution of therapeutic options to manage migraine pharmacologically. Since its discovery and use in clinical medicine, the world of migraine has changed dramatically. As headache clinicians are being trained in the latest advances in migraine and other headache disorders, they are showing increasing interest and knowledge,which is provided by some of the most unique and relevant research involving the brain in the world. A cure for migraine may not be possible, but a better understanding and control of all of migraine’s myriad of symptoms is probably within reach in this century.
Suggested Reading
Bigal ME, Lipton RB. Clinical course in migraine: conceptualizing migraine transformation. Neurology. 2008;71(11):848-855.
Deen M, Correnti E, Kamm K, et al. Blocking CGRP in migraine patients – a review of pros and cons. J Headache Pain. 2017;18(1):96.
Dodick DW. Migraine. Lancet. 2018;391(10127):1315-1330.
Färkkilä M, Diener HC, Géraud G, et al. Efficacy and tolerability of lasmiditan, an oral 5-HT(1F) receptor agonist, for the acute treatment of migraine: a phase 2 randomised, placebo-controlled, parallel-group, dose-ranging study. Lancet Neurology. 2012;11(5):405-413.
Goadsby PJ, Reuter U, Hallström Y, et al. A controlled trial of erenumab for episodic migraine. N Engl J Med. 2017;377(22):2123-2132.
Humphrey PP. The discovery and development of the triptans, a major therapeutic breakthrough. Headache. 2008;48(5):685-687.
Puledda F, Goadsby PJ. An update on non-pharmacological neuromodulation for the acute and preventive treatment of migraine. Headache. 2017;57(4):685-691.
Silberstein SD, Dodick DW, Bigal ME, et al. Fremanezumab for the preventive treatment of chronic migraine. N Engl J Med. 2017;377(22):2113-2122.
Wietecha LA, Kuca B, Case MG, et al. Phase 3 study (SPARTAN) of lasmiditan compared to placebo for acute treatment of migraine. Cephalalgia. 2017;37 (suppl 1):367-68 (abstr).
Drug price transparency laws gain ground
Connecticut is the latest state to enact a so-called drug price transparency law that imposes reporting requirements on drug makers, health insurers, and pharmacy benefit managers (PBMs).
The new requirements, signed into law by Connecticut Governor Dannel Malloy (D) on May 31, call on drug manufacturers to provide information about significant drug cost increases, including the factors that triggered the price hike and information about the drug’s development costs and capital expenditures. As part of the law, PBMs must report the volume of formulary rebates received from drug makers, including the portion provided to health insurers.
Connecticut’s law is the first to require that health insurers submit data about the most frequently prescribed and highest-cost drugs, as well as information about the impact of drug costs on the plan and its members.
Connecticut Comptroller Kevin Lembo called the law “groundbreaking” and said enactment of the measure is a victory for patients who pay outrageous prices while corporations are “enriched by big discounts.
“The extreme wealth exchange between corporate giants from pharmaceutical manufacturers to pharmacy benefit managers to insurance companies, will no longer happen in the dark,” Mr. Lembo said in a statement. “This legislative victory is a groundbreaking step, but the fight for fairness has only just begun as we continue the fight for relief at the pharmacy counter.”
Priscilla VanderVeer, a spokeswoman for Pharmaceutical Research and Manufacturers of America (PhRMA), said Connecticut’s law has some positive features, but does not go far enough in ensuring savings are passed along to patients.
“While we are glad that this legislation will require middlemen to report what portion of rebates are being passed on to consumers, we are disappointed that the final version of the legislation does not include provisions that would ensure steep rebates given to middlemen are passed on to consumers,” Ms. VanderVeer said in an interview. “Making sure that patients who share the cost of their prescription medicines also share the savings is one of the most important things we can do to provide relief for patients facing higher out-of-pocket costs at the pharmacy counter. We are committed to working with Connecticut lawmakers and other health care stakeholders to craft a solution that will provide patients with the solutions that matter the most to them.”
_web.jpg)
At least seven other states have passed similar laws that aim to expose questionable medication pricing and compel drug makers to provide the reasoning behind their cost decisions. Between 2016 and 2018, drug price transparency laws were enacted in California, Louisiana, Nevada, New York, Oregon, Maryland, and Vermont. Maine meanwhile, has enacted legislation that requires the development of a plan to collect data from manufacturers.
The majority of drug price transparency laws require drug makers to report and justify dramatic drug price increases to the state. Maryland however, went a step further by allowing the state attorney general to take legal action against drug makers that price gouge and to obtain restitution for state health programs and patients. In April, a federal appeals court struck down Maryland’s law as unconstitutional, ruling that the measure violates the federal commerce clause because it attempts to regulate price transactions. The law remains in limbo while the legal challenge continues.
The recent drug price transparency laws are necessary first steps to enable states to better understand and anticipate price increases, said Jennifer Reck, project director for the National Academy for State Health Policy.
“Faced with unsustainable prescription drug price increases, states are passing laws to create greater transparency and accountability around pricing,” Ms. Reck said in an interview.

However, with the exception of Maryland’s measure, the laws are limited because they do not empower states to take action when companies dramatically increase drug prices, she said. It’s also unclear what impact the greater transparency requirements will have on the marketplace, she added.
Gerard F. Anderson, PhD, a health policy and management professor at Johns Hopkins University in Baltimore, agreed that the drug price transparency laws are a good start. But a second component is needed so that states can take effective action, he said in an interview.
“Price transparency, alone, doesn’t do anything,” he said. “What you need to do is couple price transparency with some kind of other activity that would allow you to actually lower the price.”
Some of those other activities include prohibiting rebates by PBMs, rate setting, or establishing a maximum amount that patients should pay for certain drugs, he suggested.
Some states are already exploring policies that go beyond transparency to allow states to take action against overpricing of medications, Ms. Reck noted. New Jersey and Minnesota, for example, have introduced rate-setting bills that would create cost commissions with the authority to establish payment rates for drugs determined to be unjustifiably priced.
To truly lower drug costs for patients, state laws must be comprehensive and address the various rungs of the pharmaceutical supply chain, Ms. VanderVeer said. PhRMA supported Louisiana’s recent drug price transparency law, but has opposed laws in Vermont, California, and Nevada.
“If it is transparency legislation and other policies that actually help patients afford their medicines and make sure that they are getting access to the same discounts and rebates their insurers and PMBs are getting, then yes, we support it,” Ms. VanderVeer said in an interview. “Unfortunately, a lot of the so-called ‘transparency’ bills that have passed over the last few years do no such thing. All they do is look at one part of the supply chain – the inventors and manufacturers of the medicines – and completely leave out those in the middle and have no provisions in them that will help patients access or afford their medicines.”
Connecticut’s law goes into effect in January 2020.
Connecticut is the latest state to enact a so-called drug price transparency law that imposes reporting requirements on drug makers, health insurers, and pharmacy benefit managers (PBMs).
The new requirements, signed into law by Connecticut Governor Dannel Malloy (D) on May 31, call on drug manufacturers to provide information about significant drug cost increases, including the factors that triggered the price hike and information about the drug’s development costs and capital expenditures. As part of the law, PBMs must report the volume of formulary rebates received from drug makers, including the portion provided to health insurers.
Connecticut’s law is the first to require that health insurers submit data about the most frequently prescribed and highest-cost drugs, as well as information about the impact of drug costs on the plan and its members.
Connecticut Comptroller Kevin Lembo called the law “groundbreaking” and said enactment of the measure is a victory for patients who pay outrageous prices while corporations are “enriched by big discounts.
“The extreme wealth exchange between corporate giants from pharmaceutical manufacturers to pharmacy benefit managers to insurance companies, will no longer happen in the dark,” Mr. Lembo said in a statement. “This legislative victory is a groundbreaking step, but the fight for fairness has only just begun as we continue the fight for relief at the pharmacy counter.”
Priscilla VanderVeer, a spokeswoman for Pharmaceutical Research and Manufacturers of America (PhRMA), said Connecticut’s law has some positive features, but does not go far enough in ensuring savings are passed along to patients.
“While we are glad that this legislation will require middlemen to report what portion of rebates are being passed on to consumers, we are disappointed that the final version of the legislation does not include provisions that would ensure steep rebates given to middlemen are passed on to consumers,” Ms. VanderVeer said in an interview. “Making sure that patients who share the cost of their prescription medicines also share the savings is one of the most important things we can do to provide relief for patients facing higher out-of-pocket costs at the pharmacy counter. We are committed to working with Connecticut lawmakers and other health care stakeholders to craft a solution that will provide patients with the solutions that matter the most to them.”
At least seven other states have passed similar laws that aim to expose questionable medication pricing and compel drug makers to provide the reasoning behind their cost decisions. Between 2016 and 2018, drug price transparency laws were enacted in California, Louisiana, Nevada, New York, Oregon, Maryland, and Vermont. Maine meanwhile, has enacted legislation that requires the development of a plan to collect data from manufacturers.
The majority of drug price transparency laws require drug makers to report and justify dramatic drug price increases to the state. Maryland however, went a step further by allowing the state attorney general to take legal action against drug makers that price gouge and to obtain restitution for state health programs and patients. In April, a federal appeals court struck down Maryland’s law as unconstitutional, ruling that the measure violates the federal commerce clause because it attempts to regulate price transactions. The law remains in limbo while the legal challenge continues.
The recent drug price transparency laws are necessary first steps to enable states to better understand and anticipate price increases, said Jennifer Reck, project director for the National Academy for State Health Policy.
“Faced with unsustainable prescription drug price increases, states are passing laws to create greater transparency and accountability around pricing,” Ms. Reck said in an interview.
However, with the exception of Maryland’s measure, the laws are limited because they do not empower states to take action when companies dramatically increase drug prices, she said. It’s also unclear what impact the greater transparency requirements will have on the marketplace, she added.
Gerard F. Anderson, PhD, a health policy and management professor at Johns Hopkins University in Baltimore, agreed that the drug price transparency laws are a good start. But a second component is needed so that states can take effective action, he said in an interview.
“Price transparency, alone, doesn’t do anything,” he said. “What you need to do is couple price transparency with some kind of other activity that would allow you to actually lower the price.”
Some of those other activities include prohibiting rebates by PBMs, rate setting, or establishing a maximum amount that patients should pay for certain drugs, he suggested.
Some states are already exploring policies that go beyond transparency to allow states to take action against overpricing of medications, Ms. Reck noted. New Jersey and Minnesota, for example, have introduced rate-setting bills that would create cost commissions with the authority to establish payment rates for drugs determined to be unjustifiably priced.
To truly lower drug costs for patients, state laws must be comprehensive and address the various rungs of the pharmaceutical supply chain, Ms. VanderVeer said. PhRMA supported Louisiana’s recent drug price transparency law, but has opposed laws in Vermont, California, and Nevada.
“If it is transparency legislation and other policies that actually help patients afford their medicines and make sure that they are getting access to the same discounts and rebates their insurers and PMBs are getting, then yes, we support it,” Ms. VanderVeer said in an interview. “Unfortunately, a lot of the so-called ‘transparency’ bills that have passed over the last few years do no such thing. All they do is look at one part of the supply chain – the inventors and manufacturers of the medicines – and completely leave out those in the middle and have no provisions in them that will help patients access or afford their medicines.”
Connecticut’s law goes into effect in January 2020.
Connecticut is the latest state to enact a so-called drug price transparency law that imposes reporting requirements on drug makers, health insurers, and pharmacy benefit managers (PBMs).
The new requirements, signed into law by Connecticut Governor Dannel Malloy (D) on May 31, call on drug manufacturers to provide information about significant drug cost increases, including the factors that triggered the price hike and information about the drug’s development costs and capital expenditures. As part of the law, PBMs must report the volume of formulary rebates received from drug makers, including the portion provided to health insurers.
Connecticut’s law is the first to require that health insurers submit data about the most frequently prescribed and highest-cost drugs, as well as information about the impact of drug costs on the plan and its members.
Connecticut Comptroller Kevin Lembo called the law “groundbreaking” and said enactment of the measure is a victory for patients who pay outrageous prices while corporations are “enriched by big discounts.
“The extreme wealth exchange between corporate giants from pharmaceutical manufacturers to pharmacy benefit managers to insurance companies, will no longer happen in the dark,” Mr. Lembo said in a statement. “This legislative victory is a groundbreaking step, but the fight for fairness has only just begun as we continue the fight for relief at the pharmacy counter.”
Priscilla VanderVeer, a spokeswoman for Pharmaceutical Research and Manufacturers of America (PhRMA), said Connecticut’s law has some positive features, but does not go far enough in ensuring savings are passed along to patients.
“While we are glad that this legislation will require middlemen to report what portion of rebates are being passed on to consumers, we are disappointed that the final version of the legislation does not include provisions that would ensure steep rebates given to middlemen are passed on to consumers,” Ms. VanderVeer said in an interview. “Making sure that patients who share the cost of their prescription medicines also share the savings is one of the most important things we can do to provide relief for patients facing higher out-of-pocket costs at the pharmacy counter. We are committed to working with Connecticut lawmakers and other health care stakeholders to craft a solution that will provide patients with the solutions that matter the most to them.”
At least seven other states have passed similar laws that aim to expose questionable medication pricing and compel drug makers to provide the reasoning behind their cost decisions. Between 2016 and 2018, drug price transparency laws were enacted in California, Louisiana, Nevada, New York, Oregon, Maryland, and Vermont. Maine meanwhile, has enacted legislation that requires the development of a plan to collect data from manufacturers.
The majority of drug price transparency laws require drug makers to report and justify dramatic drug price increases to the state. Maryland however, went a step further by allowing the state attorney general to take legal action against drug makers that price gouge and to obtain restitution for state health programs and patients. In April, a federal appeals court struck down Maryland’s law as unconstitutional, ruling that the measure violates the federal commerce clause because it attempts to regulate price transactions. The law remains in limbo while the legal challenge continues.
The recent drug price transparency laws are necessary first steps to enable states to better understand and anticipate price increases, said Jennifer Reck, project director for the National Academy for State Health Policy.
“Faced with unsustainable prescription drug price increases, states are passing laws to create greater transparency and accountability around pricing,” Ms. Reck said in an interview.
However, with the exception of Maryland’s measure, the laws are limited because they do not empower states to take action when companies dramatically increase drug prices, she said. It’s also unclear what impact the greater transparency requirements will have on the marketplace, she added.
Gerard F. Anderson, PhD, a health policy and management professor at Johns Hopkins University in Baltimore, agreed that the drug price transparency laws are a good start. But a second component is needed so that states can take effective action, he said in an interview.
“Price transparency, alone, doesn’t do anything,” he said. “What you need to do is couple price transparency with some kind of other activity that would allow you to actually lower the price.”
Some of those other activities include prohibiting rebates by PBMs, rate setting, or establishing a maximum amount that patients should pay for certain drugs, he suggested.
Some states are already exploring policies that go beyond transparency to allow states to take action against overpricing of medications, Ms. Reck noted. New Jersey and Minnesota, for example, have introduced rate-setting bills that would create cost commissions with the authority to establish payment rates for drugs determined to be unjustifiably priced.
To truly lower drug costs for patients, state laws must be comprehensive and address the various rungs of the pharmaceutical supply chain, Ms. VanderVeer said. PhRMA supported Louisiana’s recent drug price transparency law, but has opposed laws in Vermont, California, and Nevada.
“If it is transparency legislation and other policies that actually help patients afford their medicines and make sure that they are getting access to the same discounts and rebates their insurers and PMBs are getting, then yes, we support it,” Ms. VanderVeer said in an interview. “Unfortunately, a lot of the so-called ‘transparency’ bills that have passed over the last few years do no such thing. All they do is look at one part of the supply chain – the inventors and manufacturers of the medicines – and completely leave out those in the middle and have no provisions in them that will help patients access or afford their medicines.”
Connecticut’s law goes into effect in January 2020.
Using Stroke Order Sets to Improve Compliance With Quality Measures for Ischemic Stroke Admissions
Stroke and cardiovascular disease (CVD) create a heavy economic burden on the health care system in the US.1 About 795,000 people have a stroke in the US each year. In 2013, stroke was the cause of 1 in every 20 deaths in the US.2 On average, someone in the US has a stroke every 40 seconds, and someone dies of one about every 4 minutes.3 Stroke also accounts for 889,000 hospitalizations per year.4,5
Stroke has been studied widely, and evidence-based guidelines have been created for the management of stroke. Despite these published guidelines for stroke care, inconsistencies in stroke management of veterans still exist. These inconsistencies led to the creation of guidelines that include quality measurements for the care of veterans with stroke.
Several campaigns have been mounted to bolster quality care for veterans with ischemic stroke. These include the Primary Stroke Center Certification by The Joint Commission (JC),6 Get With the Guidelines by the American Stroke Association,7 the Paul Coverdell Registry by the Centers for Disease Control and Prevention,8 and other efforts by the National Quality Forum (NQF) and the Centers for Medicare and Medicaid Services.9 These organizations have independently and collaboratively established quality metrics associated with health care delivery for the care of veterans with stroke. Some of these metrics have been distinguished as performance measures, or metrics that are suitable for public reporting, and may be used for comparing institutions and rewarding those who meet specific thresholds (ie, pay for performance).10
The aim of this project was to increase compliance at the Atlanta VA Medical Center (VAMC) in Decatur, Georgia, with JC National Quality Measures for the care of veterans with ischemic stroke, thus providing optimal care for veterans admitted for ischemic stroke management.
There are 3 phases in the management of a patient with a stroke: stroke presentation, admission/management, and discharge. This project focused on the admission/management phase. The stroke presentation phase is completed in the emergency department (ED), and the discharge phase has a check list for stroke, including atrial fibrillation (AF) and counseling prior to discharge. Data from the check list and counseling were not included in this project.
Specific attention was given to the following JC measures: stroke (STK) 1, STK 5, and STK 10 because the Atlanta VAMC was below the national average for these core measures for fiscal year 2015. Compliance was accomplished by creating order sets for the admission and subsequent care of veterans with ischemic stroke, tracking order set usage, and reporting regularly to the medicine/admitting team members on use rates and meeting quality measures. This project underwent the quality vs research review process and was determined to be a quality improvement (QI) project, so the project did not require institutional review board approval.
Methods
At the Atlanta VAMC, all patients admitted for stroke workup or management are admitted to the medicine service. The medicine admitting teams are composed of an attending physician, a medicine resident, a nurse practitioner (NP), a pharmacist, and 2 interns; and the hospitalist team composed of a hospitalist. The project began January 1, 2016, and ended December 31, 2016.
The hospitalist created evidence-based admission orders for all patients admitted for stroke or transient ischemic attack (TIA).The measures used were from the JC Specification Manual for Joint Commission National Quality as well as The American College of Cardiology/American Heart Association classification of care metrics.5
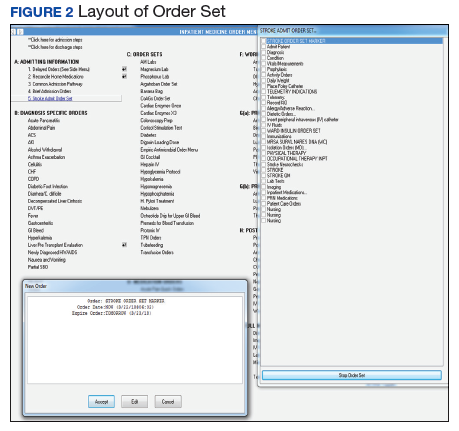
The order sets were reviewed and confirmed by a neurologist. The JC quality measures required for the care of patients admitted for stroke management were embedded in these order sets. These order sets were placed directly under the general admission orders in the Computerized Patient Record System (CPRS)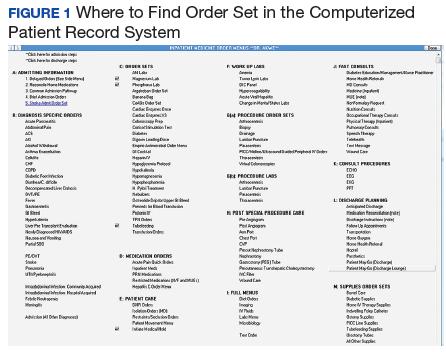
The quality measures included:
- STK 1: Veteran admitted for stroke received venous thromboembolic (VTE) prophylaxis in a timely manner. Pharmacologic management for VTE prophylaxis with subcutaneous low-molecular weight heparin and/or application of bilateral sequential compression devices were tracked.
- STK 5: Veteran admitted for stroke administered antithrombotic therapy by end of hospital day 2. Aspirin, aspirin/dipyridamole, and ticlopidine were tracked.
- STK 10: Veteran admitted for stroke assessed for rehabilitation services during admission. Physical therapy and occupational therapy consult placements were tracked. Quality measures, such as administration of tissue plasminogen activator (tPA), were not embedded in the order set because veterans who met the criteria for tPA were immediately administered tPA in the ED or transferred to the closest stroke center.
In this QI project, only quality measures that had to be completed in the inpatient setting were included. Quality measures such as tPA administration, National Institutes of Health (NIH) Stroke Scale timely documentation, swallow screen prior to po intake, and stroke transfers were completed in the ED prior to clearance for admission, so these were not included in the project. The Atlanta VAMC ED has protocols to care for these patients, but they do not have order sets with markers that could trace their usage.
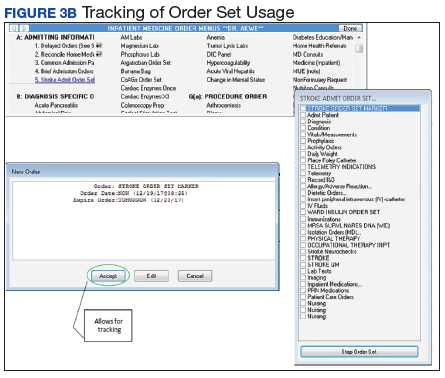
All admission orders placed were reviewed by a QI team to check whether the stroke order set had been used. The ability to determine order set use was accomplished by adding the unique identifier Stroke Order Set Marker, which allowed for querying using structured query language (SQL) within the Corporate Data Warehouse. 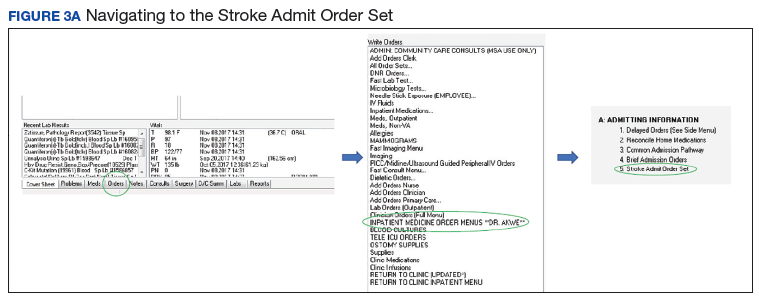
Next, all admissions were checked through chart review for compliance with quality measures. Admissions that had not been completed for all quality measures were identified, and the physicians or NPs caring for those veterans were alerted. These order sets were supposed to be used during admission of all patients admitted for stroke management or workup; however, some patients were admitted without the use of the order sets.
The successful completion of the quality measures were then compared between the groups of patients admitted using the order set and the group of patients in which the order set was not used at their admission. The physicians were provided acceptable reasons, including contraindications to certain medications such as patient history of allergy. The admitting physician made decisions on the antiplatelet medications to use or on neurology recommendations. The neurology department was consulted on all patients who had acute or subacute ischemic stroke findings on magnetic resonance imaging (MRI).
At the beginning of the month, internal medicine residents from Emory University and Morehouse School of Medicine received orientation on the use of the stroke order set from the team NP and chief resident. Tips on how to use the CPRS and how to access the stroke order sets also were created. 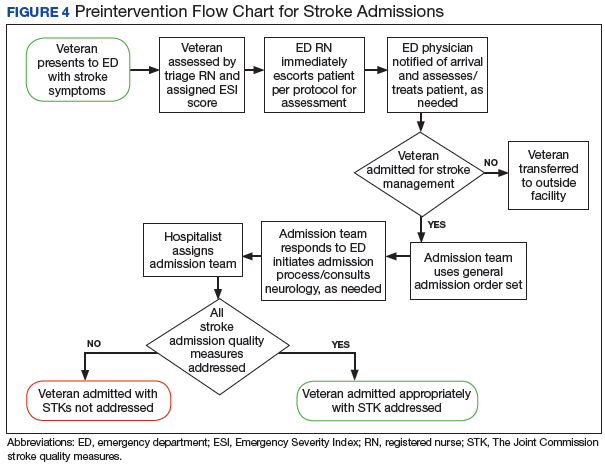
One challenge the project faced was the continuous change in the admitting team pool: Some residents did not remember to use the stroke order sets. 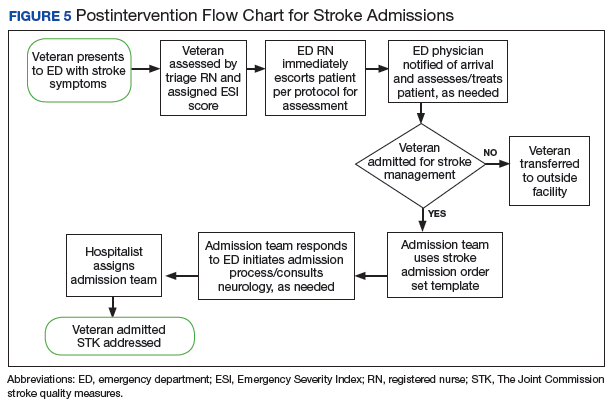
Results
Of 323 admitted patients with stroke, 93 admissions were entered using the stroke order set. Out of these completed orders, 85 (91%) veterans admitted for ischemic stroke or TIA management received timely VTE prophylaxis, and 8 (9%) veterans did not. Of the 230 admissions completed without using the stroke order set, 167 (73%) veterans received timely VTE prophylaxis, and 63 (28%) veterans did not. Additionally out of the 93 veterans admitted using the stroke order set, 74 (80%) veterans admitted for the management of ischemic stroke received antithrombotic therapy by end of hospital day 2, whereas 19 (20%) veterans did not, and there were no clear contraindications documented as to why.
For veterans admitted without using the order set, 167 (73%) veterans admitted for the management of ischemic stroke received antithrombotic therapy by the end of hospital day 2, whereas 76 (33%) veterans did not. Last, 90 (97%) of the 93 veterans admitted for stroke workup using the order set were assessed for rehabilitation services during admission, whereas 3 (3%) were not. For the veterans who were admitted without using the stroke order set, 162 (70%) were assessed for rehabilitation services during admission, whereas 68 (30%) were not.
Out of 969 compliance measures looked at, 237 measures were missed and 732 measures were appropriately completed irrespective of whether the stroke order set was used. Out of the 279 admissions where the stroke order set was used, 249 (89%) quality measures were met. 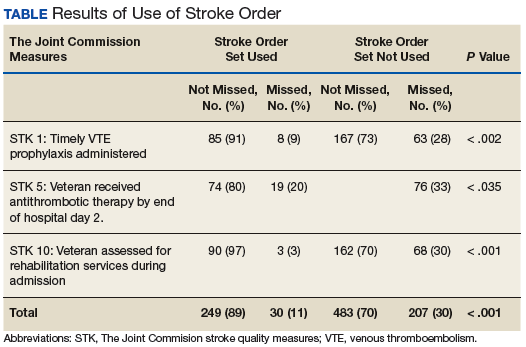
The study threshold for meeting the standards was the national average for 2015, which was 91.1% for the administration of VTE prophylaxis in a timely manner, 97.9% for administering antithrombotic therapy by end of hospital day 2, and 94.2% for assessment of the patient by rehabilitation services during the admission.
Discussion
Despite the repeated training and orientation, compliance to the order set usage was not optimal, likely secondary to a frequent change in the pool of admitting physicians using the order set. Also, the order set was new to staff, thus, admitting physicians sometimes forgot to use them. The next step in this project will be to create an order set for the ED with markers for tracing usage. These order sets will include all quality measures that need to be completed in the ED, such as the NIH Stroke Scale timely documentation, tPA administration data, swallow screen prior to po intake, and stroke transfers.
This QI project also streamlined the process for stroke admissions. With the creation of the order set, all orders needed for stroke were available to the admitting physician, resulting in less need for searching the order individually from a large pool of orders (Figures 3 and 4).
Several reputable institutions have quality metrics and performance measures typically focused on processes of care based on specific clinical guidelines recommendations. Clinical guidelines are usually based on sufficient evidence that failure to provide the recommended care is likely to result in suboptimal clinical outcomes. Stroke quality measure compliance is part of the Reporting Hospital Quality Data for Annual Payment Update (RHQDAPU) initiative, and most hospitals will be required to report these measures in order to receive full Medicare payments.11
Limitations
Limitations of this study relate to CPRS functions, which must be specifically activated at different VA sites in order to enable the use of these functions. Also, the successful creation of these order sets depended on the information specialist’s knowledge of the capabilities of the CPRS.
Conclusion
Gaps in practice and recommended guidelines can be bridged by creating standardized admission orders embedded with required quality measures. The Atlanta VAMC project showed that the use of a standardized stroke admission order set significantly improved compliance to quality measures for veterans admitted for ischemic stroke management. This is consistent with a study completed in the ED, which showed that for veterans hospitalized for acute ischemic stroke, electronic order set use was associated with increased use of IV tPA.12 Creating order sets can be challenging, but if these barriers can be overcome, with the first order set, similar templates can be used to create order sets for other clinical conditions, such as heart failure, sepsis, and chronic obstructive pulmonary disease exacerbation.
1. Writing Group Members, Mozaffarian D, Benjamin EJ, Go AS, et al; American Heart Association Statistics Committee; Stroke Statistics Subcommittee. Executive summary: heart disease and stroke statistics—2016 update: a report from the American Heart Association. Circulation. 2016;133(4):447-454.
2. Centers for Disease Control and Prevention. Vital signs: recent trends in stroke death rates–United States, 2000-2015. https://www.cdc.gov/mmwr/volumes/66/wr/mm6635e1.htm. Published September 8, 2017. Accessed June 14, 2018.
3. Benjamin EJ, Blaha MJ, Chiuve SE, et al; American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics—2017 update: a report from the American Heart Association. Circulation. 2017;135(10):e229-e445.
4. Lloyd-Jones D, Adams R, Carnethon M, et al; American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics—2009 update: a report from the American heart association statistics committee and stroke statistics subcommittee. Circulation. 2009;119(3):480-486.
5. Poisson SN, Josephson SA. Quality measures in stroke. Neurohospitalist. 2011;1(2):71-77.
6. The Joint Commission. Primary Stroke Centers—Stroke Performance Measurement. https://www.jointcommission.org/performance_ measurement.aspx. Accessed June 14, 2018.
7. American Stroke Association. Get with the guidelines–stroke. http://www.heart.org/HEARTORG/Professional/GetWithTheGuidelines/GetWithTheGuidelines-Stroke/Get-With-The-Guidelines-Stroke-Overview_UCM_308021_Article.jsp#.WyKre1VKiUk. Accessed June 14, 2018.
8. Centers for Disease Control and Prevention. The Paul Coverdell National Acute Stroke Registry. www.cdc.gov/DHDSP/stroke_registry.htm. Published March 13, 2008.
9. Reeves MJ, Parker C, Fonarow GC, Smith EE, Schwamm LH. Development of stroke performance measures: definitions, methods, and current measures. Stroke. 2010;41(7):1573-1578.
10. American College of Cardiology/American Heart Association Task Force on Performance Measures, Bonow RO, Masoudi FA, et al. ACC/AHA classification of care metrics: performance measures and quality metrics: a report of the American College of Cardiology/American Heart Association Task Force on performance measures. Circulation. 2008;118(24):2662-2666.
11. Centers for Medicare and Medicaid Services. Reporting Hospital Quality Data for Annual Payment Update https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/HospitalQualityInits/downloads/HospitalFactSheetAP.pdf. Published November 2004. Accessed June 14, 2018.
12. Ballard DW, Kim AS, Huang J, et al; KP CREST Network Investigators. Implementation of computerized physician order entry is associated with increased thrombolytic administration for emergency department veterans with acute ischemic stroke. Ann Emerg Med. 2015;66(6):601-610.
Stroke and cardiovascular disease (CVD) create a heavy economic burden on the health care system in the US.1 About 795,000 people have a stroke in the US each year. In 2013, stroke was the cause of 1 in every 20 deaths in the US.2 On average, someone in the US has a stroke every 40 seconds, and someone dies of one about every 4 minutes.3 Stroke also accounts for 889,000 hospitalizations per year.4,5
Stroke has been studied widely, and evidence-based guidelines have been created for the management of stroke. Despite these published guidelines for stroke care, inconsistencies in stroke management of veterans still exist. These inconsistencies led to the creation of guidelines that include quality measurements for the care of veterans with stroke.
Several campaigns have been mounted to bolster quality care for veterans with ischemic stroke. These include the Primary Stroke Center Certification by The Joint Commission (JC),6 Get With the Guidelines by the American Stroke Association,7 the Paul Coverdell Registry by the Centers for Disease Control and Prevention,8 and other efforts by the National Quality Forum (NQF) and the Centers for Medicare and Medicaid Services.9 These organizations have independently and collaboratively established quality metrics associated with health care delivery for the care of veterans with stroke. Some of these metrics have been distinguished as performance measures, or metrics that are suitable for public reporting, and may be used for comparing institutions and rewarding those who meet specific thresholds (ie, pay for performance).10
The aim of this project was to increase compliance at the Atlanta VA Medical Center (VAMC) in Decatur, Georgia, with JC National Quality Measures for the care of veterans with ischemic stroke, thus providing optimal care for veterans admitted for ischemic stroke management.
There are 3 phases in the management of a patient with a stroke: stroke presentation, admission/management, and discharge. This project focused on the admission/management phase. The stroke presentation phase is completed in the emergency department (ED), and the discharge phase has a check list for stroke, including atrial fibrillation (AF) and counseling prior to discharge. Data from the check list and counseling were not included in this project.
Specific attention was given to the following JC measures: stroke (STK) 1, STK 5, and STK 10 because the Atlanta VAMC was below the national average for these core measures for fiscal year 2015. Compliance was accomplished by creating order sets for the admission and subsequent care of veterans with ischemic stroke, tracking order set usage, and reporting regularly to the medicine/admitting team members on use rates and meeting quality measures. This project underwent the quality vs research review process and was determined to be a quality improvement (QI) project, so the project did not require institutional review board approval.
Methods
At the Atlanta VAMC, all patients admitted for stroke workup or management are admitted to the medicine service. The medicine admitting teams are composed of an attending physician, a medicine resident, a nurse practitioner (NP), a pharmacist, and 2 interns; and the hospitalist team composed of a hospitalist. The project began January 1, 2016, and ended December 31, 2016.
The hospitalist created evidence-based admission orders for all patients admitted for stroke or transient ischemic attack (TIA).The measures used were from the JC Specification Manual for Joint Commission National Quality as well as The American College of Cardiology/American Heart Association classification of care metrics.5
The order sets were reviewed and confirmed by a neurologist. The JC quality measures required for the care of patients admitted for stroke management were embedded in these order sets. These order sets were placed directly under the general admission orders in the Computerized Patient Record System (CPRS)
The quality measures included:
- STK 1: Veteran admitted for stroke received venous thromboembolic (VTE) prophylaxis in a timely manner. Pharmacologic management for VTE prophylaxis with subcutaneous low-molecular weight heparin and/or application of bilateral sequential compression devices were tracked.
- STK 5: Veteran admitted for stroke administered antithrombotic therapy by end of hospital day 2. Aspirin, aspirin/dipyridamole, and ticlopidine were tracked.
- STK 10: Veteran admitted for stroke assessed for rehabilitation services during admission. Physical therapy and occupational therapy consult placements were tracked. Quality measures, such as administration of tissue plasminogen activator (tPA), were not embedded in the order set because veterans who met the criteria for tPA were immediately administered tPA in the ED or transferred to the closest stroke center.
In this QI project, only quality measures that had to be completed in the inpatient setting were included. Quality measures such as tPA administration, National Institutes of Health (NIH) Stroke Scale timely documentation, swallow screen prior to po intake, and stroke transfers were completed in the ED prior to clearance for admission, so these were not included in the project. The Atlanta VAMC ED has protocols to care for these patients, but they do not have order sets with markers that could trace their usage.
All admission orders placed were reviewed by a QI team to check whether the stroke order set had been used. The ability to determine order set use was accomplished by adding the unique identifier Stroke Order Set Marker, which allowed for querying using structured query language (SQL) within the Corporate Data Warehouse.
Next, all admissions were checked through chart review for compliance with quality measures. Admissions that had not been completed for all quality measures were identified, and the physicians or NPs caring for those veterans were alerted. These order sets were supposed to be used during admission of all patients admitted for stroke management or workup; however, some patients were admitted without the use of the order sets.
The successful completion of the quality measures were then compared between the groups of patients admitted using the order set and the group of patients in which the order set was not used at their admission. The physicians were provided acceptable reasons, including contraindications to certain medications such as patient history of allergy. The admitting physician made decisions on the antiplatelet medications to use or on neurology recommendations. The neurology department was consulted on all patients who had acute or subacute ischemic stroke findings on magnetic resonance imaging (MRI).
At the beginning of the month, internal medicine residents from Emory University and Morehouse School of Medicine received orientation on the use of the stroke order set from the team NP and chief resident. Tips on how to use the CPRS and how to access the stroke order sets also were created.
One challenge the project faced was the continuous change in the admitting team pool: Some residents did not remember to use the stroke order sets.
Results
Of 323 admitted patients with stroke, 93 admissions were entered using the stroke order set. Out of these completed orders, 85 (91%) veterans admitted for ischemic stroke or TIA management received timely VTE prophylaxis, and 8 (9%) veterans did not. Of the 230 admissions completed without using the stroke order set, 167 (73%) veterans received timely VTE prophylaxis, and 63 (28%) veterans did not. Additionally out of the 93 veterans admitted using the stroke order set, 74 (80%) veterans admitted for the management of ischemic stroke received antithrombotic therapy by end of hospital day 2, whereas 19 (20%) veterans did not, and there were no clear contraindications documented as to why.
For veterans admitted without using the order set, 167 (73%) veterans admitted for the management of ischemic stroke received antithrombotic therapy by the end of hospital day 2, whereas 76 (33%) veterans did not. Last, 90 (97%) of the 93 veterans admitted for stroke workup using the order set were assessed for rehabilitation services during admission, whereas 3 (3%) were not. For the veterans who were admitted without using the stroke order set, 162 (70%) were assessed for rehabilitation services during admission, whereas 68 (30%) were not.
Out of 969 compliance measures looked at, 237 measures were missed and 732 measures were appropriately completed irrespective of whether the stroke order set was used. Out of the 279 admissions where the stroke order set was used, 249 (89%) quality measures were met.
The study threshold for meeting the standards was the national average for 2015, which was 91.1% for the administration of VTE prophylaxis in a timely manner, 97.9% for administering antithrombotic therapy by end of hospital day 2, and 94.2% for assessment of the patient by rehabilitation services during the admission.
Discussion
Despite the repeated training and orientation, compliance to the order set usage was not optimal, likely secondary to a frequent change in the pool of admitting physicians using the order set. Also, the order set was new to staff, thus, admitting physicians sometimes forgot to use them. The next step in this project will be to create an order set for the ED with markers for tracing usage. These order sets will include all quality measures that need to be completed in the ED, such as the NIH Stroke Scale timely documentation, tPA administration data, swallow screen prior to po intake, and stroke transfers.
This QI project also streamlined the process for stroke admissions. With the creation of the order set, all orders needed for stroke were available to the admitting physician, resulting in less need for searching the order individually from a large pool of orders (Figures 3 and 4).
Several reputable institutions have quality metrics and performance measures typically focused on processes of care based on specific clinical guidelines recommendations. Clinical guidelines are usually based on sufficient evidence that failure to provide the recommended care is likely to result in suboptimal clinical outcomes. Stroke quality measure compliance is part of the Reporting Hospital Quality Data for Annual Payment Update (RHQDAPU) initiative, and most hospitals will be required to report these measures in order to receive full Medicare payments.11
Limitations
Limitations of this study relate to CPRS functions, which must be specifically activated at different VA sites in order to enable the use of these functions. Also, the successful creation of these order sets depended on the information specialist’s knowledge of the capabilities of the CPRS.
Conclusion
Gaps in practice and recommended guidelines can be bridged by creating standardized admission orders embedded with required quality measures. The Atlanta VAMC project showed that the use of a standardized stroke admission order set significantly improved compliance to quality measures for veterans admitted for ischemic stroke management. This is consistent with a study completed in the ED, which showed that for veterans hospitalized for acute ischemic stroke, electronic order set use was associated with increased use of IV tPA.12 Creating order sets can be challenging, but if these barriers can be overcome, with the first order set, similar templates can be used to create order sets for other clinical conditions, such as heart failure, sepsis, and chronic obstructive pulmonary disease exacerbation.
Stroke and cardiovascular disease (CVD) create a heavy economic burden on the health care system in the US.1 About 795,000 people have a stroke in the US each year. In 2013, stroke was the cause of 1 in every 20 deaths in the US.2 On average, someone in the US has a stroke every 40 seconds, and someone dies of one about every 4 minutes.3 Stroke also accounts for 889,000 hospitalizations per year.4,5
Stroke has been studied widely, and evidence-based guidelines have been created for the management of stroke. Despite these published guidelines for stroke care, inconsistencies in stroke management of veterans still exist. These inconsistencies led to the creation of guidelines that include quality measurements for the care of veterans with stroke.
Several campaigns have been mounted to bolster quality care for veterans with ischemic stroke. These include the Primary Stroke Center Certification by The Joint Commission (JC),6 Get With the Guidelines by the American Stroke Association,7 the Paul Coverdell Registry by the Centers for Disease Control and Prevention,8 and other efforts by the National Quality Forum (NQF) and the Centers for Medicare and Medicaid Services.9 These organizations have independently and collaboratively established quality metrics associated with health care delivery for the care of veterans with stroke. Some of these metrics have been distinguished as performance measures, or metrics that are suitable for public reporting, and may be used for comparing institutions and rewarding those who meet specific thresholds (ie, pay for performance).10
The aim of this project was to increase compliance at the Atlanta VA Medical Center (VAMC) in Decatur, Georgia, with JC National Quality Measures for the care of veterans with ischemic stroke, thus providing optimal care for veterans admitted for ischemic stroke management.
There are 3 phases in the management of a patient with a stroke: stroke presentation, admission/management, and discharge. This project focused on the admission/management phase. The stroke presentation phase is completed in the emergency department (ED), and the discharge phase has a check list for stroke, including atrial fibrillation (AF) and counseling prior to discharge. Data from the check list and counseling were not included in this project.
Specific attention was given to the following JC measures: stroke (STK) 1, STK 5, and STK 10 because the Atlanta VAMC was below the national average for these core measures for fiscal year 2015. Compliance was accomplished by creating order sets for the admission and subsequent care of veterans with ischemic stroke, tracking order set usage, and reporting regularly to the medicine/admitting team members on use rates and meeting quality measures. This project underwent the quality vs research review process and was determined to be a quality improvement (QI) project, so the project did not require institutional review board approval.
Methods
At the Atlanta VAMC, all patients admitted for stroke workup or management are admitted to the medicine service. The medicine admitting teams are composed of an attending physician, a medicine resident, a nurse practitioner (NP), a pharmacist, and 2 interns; and the hospitalist team composed of a hospitalist. The project began January 1, 2016, and ended December 31, 2016.
The hospitalist created evidence-based admission orders for all patients admitted for stroke or transient ischemic attack (TIA).The measures used were from the JC Specification Manual for Joint Commission National Quality as well as The American College of Cardiology/American Heart Association classification of care metrics.5
The order sets were reviewed and confirmed by a neurologist. The JC quality measures required for the care of patients admitted for stroke management were embedded in these order sets. These order sets were placed directly under the general admission orders in the Computerized Patient Record System (CPRS)
The quality measures included:
- STK 1: Veteran admitted for stroke received venous thromboembolic (VTE) prophylaxis in a timely manner. Pharmacologic management for VTE prophylaxis with subcutaneous low-molecular weight heparin and/or application of bilateral sequential compression devices were tracked.
- STK 5: Veteran admitted for stroke administered antithrombotic therapy by end of hospital day 2. Aspirin, aspirin/dipyridamole, and ticlopidine were tracked.
- STK 10: Veteran admitted for stroke assessed for rehabilitation services during admission. Physical therapy and occupational therapy consult placements were tracked. Quality measures, such as administration of tissue plasminogen activator (tPA), were not embedded in the order set because veterans who met the criteria for tPA were immediately administered tPA in the ED or transferred to the closest stroke center.
In this QI project, only quality measures that had to be completed in the inpatient setting were included. Quality measures such as tPA administration, National Institutes of Health (NIH) Stroke Scale timely documentation, swallow screen prior to po intake, and stroke transfers were completed in the ED prior to clearance for admission, so these were not included in the project. The Atlanta VAMC ED has protocols to care for these patients, but they do not have order sets with markers that could trace their usage.
All admission orders placed were reviewed by a QI team to check whether the stroke order set had been used. The ability to determine order set use was accomplished by adding the unique identifier Stroke Order Set Marker, which allowed for querying using structured query language (SQL) within the Corporate Data Warehouse.
Next, all admissions were checked through chart review for compliance with quality measures. Admissions that had not been completed for all quality measures were identified, and the physicians or NPs caring for those veterans were alerted. These order sets were supposed to be used during admission of all patients admitted for stroke management or workup; however, some patients were admitted without the use of the order sets.
The successful completion of the quality measures were then compared between the groups of patients admitted using the order set and the group of patients in which the order set was not used at their admission. The physicians were provided acceptable reasons, including contraindications to certain medications such as patient history of allergy. The admitting physician made decisions on the antiplatelet medications to use or on neurology recommendations. The neurology department was consulted on all patients who had acute or subacute ischemic stroke findings on magnetic resonance imaging (MRI).
At the beginning of the month, internal medicine residents from Emory University and Morehouse School of Medicine received orientation on the use of the stroke order set from the team NP and chief resident. Tips on how to use the CPRS and how to access the stroke order sets also were created.
One challenge the project faced was the continuous change in the admitting team pool: Some residents did not remember to use the stroke order sets.
Results
Of 323 admitted patients with stroke, 93 admissions were entered using the stroke order set. Out of these completed orders, 85 (91%) veterans admitted for ischemic stroke or TIA management received timely VTE prophylaxis, and 8 (9%) veterans did not. Of the 230 admissions completed without using the stroke order set, 167 (73%) veterans received timely VTE prophylaxis, and 63 (28%) veterans did not. Additionally out of the 93 veterans admitted using the stroke order set, 74 (80%) veterans admitted for the management of ischemic stroke received antithrombotic therapy by end of hospital day 2, whereas 19 (20%) veterans did not, and there were no clear contraindications documented as to why.
For veterans admitted without using the order set, 167 (73%) veterans admitted for the management of ischemic stroke received antithrombotic therapy by the end of hospital day 2, whereas 76 (33%) veterans did not. Last, 90 (97%) of the 93 veterans admitted for stroke workup using the order set were assessed for rehabilitation services during admission, whereas 3 (3%) were not. For the veterans who were admitted without using the stroke order set, 162 (70%) were assessed for rehabilitation services during admission, whereas 68 (30%) were not.
Out of 969 compliance measures looked at, 237 measures were missed and 732 measures were appropriately completed irrespective of whether the stroke order set was used. Out of the 279 admissions where the stroke order set was used, 249 (89%) quality measures were met.
The study threshold for meeting the standards was the national average for 2015, which was 91.1% for the administration of VTE prophylaxis in a timely manner, 97.9% for administering antithrombotic therapy by end of hospital day 2, and 94.2% for assessment of the patient by rehabilitation services during the admission.
Discussion
Despite the repeated training and orientation, compliance to the order set usage was not optimal, likely secondary to a frequent change in the pool of admitting physicians using the order set. Also, the order set was new to staff, thus, admitting physicians sometimes forgot to use them. The next step in this project will be to create an order set for the ED with markers for tracing usage. These order sets will include all quality measures that need to be completed in the ED, such as the NIH Stroke Scale timely documentation, tPA administration data, swallow screen prior to po intake, and stroke transfers.
This QI project also streamlined the process for stroke admissions. With the creation of the order set, all orders needed for stroke were available to the admitting physician, resulting in less need for searching the order individually from a large pool of orders (Figures 3 and 4).
Several reputable institutions have quality metrics and performance measures typically focused on processes of care based on specific clinical guidelines recommendations. Clinical guidelines are usually based on sufficient evidence that failure to provide the recommended care is likely to result in suboptimal clinical outcomes. Stroke quality measure compliance is part of the Reporting Hospital Quality Data for Annual Payment Update (RHQDAPU) initiative, and most hospitals will be required to report these measures in order to receive full Medicare payments.11
Limitations
Limitations of this study relate to CPRS functions, which must be specifically activated at different VA sites in order to enable the use of these functions. Also, the successful creation of these order sets depended on the information specialist’s knowledge of the capabilities of the CPRS.
Conclusion
Gaps in practice and recommended guidelines can be bridged by creating standardized admission orders embedded with required quality measures. The Atlanta VAMC project showed that the use of a standardized stroke admission order set significantly improved compliance to quality measures for veterans admitted for ischemic stroke management. This is consistent with a study completed in the ED, which showed that for veterans hospitalized for acute ischemic stroke, electronic order set use was associated with increased use of IV tPA.12 Creating order sets can be challenging, but if these barriers can be overcome, with the first order set, similar templates can be used to create order sets for other clinical conditions, such as heart failure, sepsis, and chronic obstructive pulmonary disease exacerbation.
1. Writing Group Members, Mozaffarian D, Benjamin EJ, Go AS, et al; American Heart Association Statistics Committee; Stroke Statistics Subcommittee. Executive summary: heart disease and stroke statistics—2016 update: a report from the American Heart Association. Circulation. 2016;133(4):447-454.
2. Centers for Disease Control and Prevention. Vital signs: recent trends in stroke death rates–United States, 2000-2015. https://www.cdc.gov/mmwr/volumes/66/wr/mm6635e1.htm. Published September 8, 2017. Accessed June 14, 2018.
3. Benjamin EJ, Blaha MJ, Chiuve SE, et al; American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics—2017 update: a report from the American Heart Association. Circulation. 2017;135(10):e229-e445.
4. Lloyd-Jones D, Adams R, Carnethon M, et al; American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics—2009 update: a report from the American heart association statistics committee and stroke statistics subcommittee. Circulation. 2009;119(3):480-486.
5. Poisson SN, Josephson SA. Quality measures in stroke. Neurohospitalist. 2011;1(2):71-77.
6. The Joint Commission. Primary Stroke Centers—Stroke Performance Measurement. https://www.jointcommission.org/performance_ measurement.aspx. Accessed June 14, 2018.
7. American Stroke Association. Get with the guidelines–stroke. http://www.heart.org/HEARTORG/Professional/GetWithTheGuidelines/GetWithTheGuidelines-Stroke/Get-With-The-Guidelines-Stroke-Overview_UCM_308021_Article.jsp#.WyKre1VKiUk. Accessed June 14, 2018.
8. Centers for Disease Control and Prevention. The Paul Coverdell National Acute Stroke Registry. www.cdc.gov/DHDSP/stroke_registry.htm. Published March 13, 2008.
9. Reeves MJ, Parker C, Fonarow GC, Smith EE, Schwamm LH. Development of stroke performance measures: definitions, methods, and current measures. Stroke. 2010;41(7):1573-1578.
10. American College of Cardiology/American Heart Association Task Force on Performance Measures, Bonow RO, Masoudi FA, et al. ACC/AHA classification of care metrics: performance measures and quality metrics: a report of the American College of Cardiology/American Heart Association Task Force on performance measures. Circulation. 2008;118(24):2662-2666.
11. Centers for Medicare and Medicaid Services. Reporting Hospital Quality Data for Annual Payment Update https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/HospitalQualityInits/downloads/HospitalFactSheetAP.pdf. Published November 2004. Accessed June 14, 2018.
12. Ballard DW, Kim AS, Huang J, et al; KP CREST Network Investigators. Implementation of computerized physician order entry is associated with increased thrombolytic administration for emergency department veterans with acute ischemic stroke. Ann Emerg Med. 2015;66(6):601-610.
1. Writing Group Members, Mozaffarian D, Benjamin EJ, Go AS, et al; American Heart Association Statistics Committee; Stroke Statistics Subcommittee. Executive summary: heart disease and stroke statistics—2016 update: a report from the American Heart Association. Circulation. 2016;133(4):447-454.
2. Centers for Disease Control and Prevention. Vital signs: recent trends in stroke death rates–United States, 2000-2015. https://www.cdc.gov/mmwr/volumes/66/wr/mm6635e1.htm. Published September 8, 2017. Accessed June 14, 2018.
3. Benjamin EJ, Blaha MJ, Chiuve SE, et al; American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics—2017 update: a report from the American Heart Association. Circulation. 2017;135(10):e229-e445.
4. Lloyd-Jones D, Adams R, Carnethon M, et al; American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics—2009 update: a report from the American heart association statistics committee and stroke statistics subcommittee. Circulation. 2009;119(3):480-486.
5. Poisson SN, Josephson SA. Quality measures in stroke. Neurohospitalist. 2011;1(2):71-77.
6. The Joint Commission. Primary Stroke Centers—Stroke Performance Measurement. https://www.jointcommission.org/performance_ measurement.aspx. Accessed June 14, 2018.
7. American Stroke Association. Get with the guidelines–stroke. http://www.heart.org/HEARTORG/Professional/GetWithTheGuidelines/GetWithTheGuidelines-Stroke/Get-With-The-Guidelines-Stroke-Overview_UCM_308021_Article.jsp#.WyKre1VKiUk. Accessed June 14, 2018.
8. Centers for Disease Control and Prevention. The Paul Coverdell National Acute Stroke Registry. www.cdc.gov/DHDSP/stroke_registry.htm. Published March 13, 2008.
9. Reeves MJ, Parker C, Fonarow GC, Smith EE, Schwamm LH. Development of stroke performance measures: definitions, methods, and current measures. Stroke. 2010;41(7):1573-1578.
10. American College of Cardiology/American Heart Association Task Force on Performance Measures, Bonow RO, Masoudi FA, et al. ACC/AHA classification of care metrics: performance measures and quality metrics: a report of the American College of Cardiology/American Heart Association Task Force on performance measures. Circulation. 2008;118(24):2662-2666.
11. Centers for Medicare and Medicaid Services. Reporting Hospital Quality Data for Annual Payment Update https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/HospitalQualityInits/downloads/HospitalFactSheetAP.pdf. Published November 2004. Accessed June 14, 2018.
12. Ballard DW, Kim AS, Huang J, et al; KP CREST Network Investigators. Implementation of computerized physician order entry is associated with increased thrombolytic administration for emergency department veterans with acute ischemic stroke. Ann Emerg Med. 2015;66(6):601-610.
Federal Health Care Data Trends: Gulf War & Post-9/11 Veterans
Currently, the largest growing percentage of veterans are those who served during the Gulf War and Post-9/11 era. Over the next few years, nearly every state in the US can expect growth in this veteran population greater than 20%. Although this group of 4.1 million veterans tend to use their VA health benefits less than do the veterans of previous eras, these veterans also exhibit some unique qualities not previously seen in VA patient populations. These veterans already have been identified to be at an increased risk of acquiring several diseases, which include arthritis, chronic fatigue syndrome, and sleep apnea. But perhaps the biggest shift, and the one that could require the most change in the way the Veterans Health Administration provides care, is along gender lines.
Click here to continue reading.
Currently, the largest growing percentage of veterans are those who served during the Gulf War and Post-9/11 era. Over the next few years, nearly every state in the US can expect growth in this veteran population greater than 20%. Although this group of 4.1 million veterans tend to use their VA health benefits less than do the veterans of previous eras, these veterans also exhibit some unique qualities not previously seen in VA patient populations. These veterans already have been identified to be at an increased risk of acquiring several diseases, which include arthritis, chronic fatigue syndrome, and sleep apnea. But perhaps the biggest shift, and the one that could require the most change in the way the Veterans Health Administration provides care, is along gender lines.
Click here to continue reading.
Currently, the largest growing percentage of veterans are those who served during the Gulf War and Post-9/11 era. Over the next few years, nearly every state in the US can expect growth in this veteran population greater than 20%. Although this group of 4.1 million veterans tend to use their VA health benefits less than do the veterans of previous eras, these veterans also exhibit some unique qualities not previously seen in VA patient populations. These veterans already have been identified to be at an increased risk of acquiring several diseases, which include arthritis, chronic fatigue syndrome, and sleep apnea. But perhaps the biggest shift, and the one that could require the most change in the way the Veterans Health Administration provides care, is along gender lines.
Click here to continue reading.
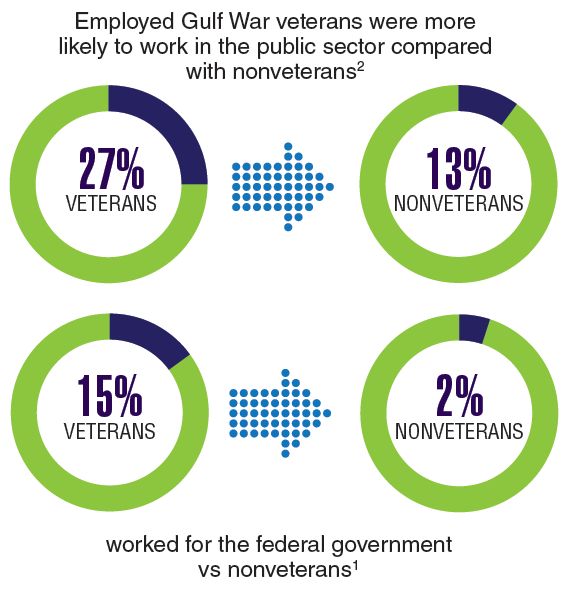
Inhibitor could be repurposed for MM

Tofacitinib, a pan-JAK inhibitor approved to treat rheumatoid arthritis, may advance as a potential treatment for multiple myeloma (MM) based on results from preclinical studies.
In these studies, tofacitinib was able to reverse proliferative effects in stromal-responsive human MM cell lines and reduce tumor growth in mouse models of MM.
Christine Lam, of University of California, San Francisco, and her colleagues conducted this research and reported the results in haematologica.
The researchers showed that, in co-cultures of MM cell lines and bone marrow stromal cells (BMSCs), tofacitinib inhibited the growth of MM cells in a dose-dependent manner.
RNA sequencing and phosphoproteonomics revealed an upregulation of 67 transcripts in MM cell lines co-cultured with BMSCs—most related to JAK-STAT and interleukin signaling.
Additional cell culture experiments showed that tofacitinib inhibited the downstream signaling molecule STAT3, which is responsible for proliferation through the JAK/STAT pathway.
The JAK1/2 inhibitor ruxolitinib did not replicate results seen with tofacitinib.
Further experiments showed that carfilzomib did not have synergistic effects with tofacitinib.
Venetoclax did demonstrate synergy with tofacitinib but only in MM cells cocultured with BMSCs, not in MM cells alone.
The researchers also tested tofacitinib in vivo. They injected mice with an MM cell line, and, after 2 weeks, mice were treated with tofacitinib for 4 weeks.
Mice treated with tofacitinib had lower tumor burden and a significant improvement in survival compared to untreated control mice.
Finally, the researchers tested tofacitinib in bone marrow mononuclear cells from patients. After stimulation with IL-6, the cells were exposed to tofacitinib.
The researchers observed “modest” viability against malignant plasma cells. They noted that because ex vivo MM plasma cells are minimally proliferative even with added cytokines or stromal stimulations, “these results may not fully reflect the potential therapeutic efficacy of tofacitinib in MM patients, where plasma cells are constantly proliferating within the [bone marrow].”
The researchers concluded that “tofacitinib is a promising agent to reverse the tumor-proliferative effects of the [bone marrow] microenvironment that can be rapidly repurposed to benefit MM patients.”
Tofacitinib, a pan-JAK inhibitor approved to treat rheumatoid arthritis, may advance as a potential treatment for multiple myeloma (MM) based on results from preclinical studies.
In these studies, tofacitinib was able to reverse proliferative effects in stromal-responsive human MM cell lines and reduce tumor growth in mouse models of MM.
Christine Lam, of University of California, San Francisco, and her colleagues conducted this research and reported the results in haematologica.
The researchers showed that, in co-cultures of MM cell lines and bone marrow stromal cells (BMSCs), tofacitinib inhibited the growth of MM cells in a dose-dependent manner.
RNA sequencing and phosphoproteonomics revealed an upregulation of 67 transcripts in MM cell lines co-cultured with BMSCs—most related to JAK-STAT and interleukin signaling.
Additional cell culture experiments showed that tofacitinib inhibited the downstream signaling molecule STAT3, which is responsible for proliferation through the JAK/STAT pathway.
The JAK1/2 inhibitor ruxolitinib did not replicate results seen with tofacitinib.
Further experiments showed that carfilzomib did not have synergistic effects with tofacitinib.
Venetoclax did demonstrate synergy with tofacitinib but only in MM cells cocultured with BMSCs, not in MM cells alone.
The researchers also tested tofacitinib in vivo. They injected mice with an MM cell line, and, after 2 weeks, mice were treated with tofacitinib for 4 weeks.
Mice treated with tofacitinib had lower tumor burden and a significant improvement in survival compared to untreated control mice.
Finally, the researchers tested tofacitinib in bone marrow mononuclear cells from patients. After stimulation with IL-6, the cells were exposed to tofacitinib.
The researchers observed “modest” viability against malignant plasma cells. They noted that because ex vivo MM plasma cells are minimally proliferative even with added cytokines or stromal stimulations, “these results may not fully reflect the potential therapeutic efficacy of tofacitinib in MM patients, where plasma cells are constantly proliferating within the [bone marrow].”
The researchers concluded that “tofacitinib is a promising agent to reverse the tumor-proliferative effects of the [bone marrow] microenvironment that can be rapidly repurposed to benefit MM patients.”
Tofacitinib, a pan-JAK inhibitor approved to treat rheumatoid arthritis, may advance as a potential treatment for multiple myeloma (MM) based on results from preclinical studies.
In these studies, tofacitinib was able to reverse proliferative effects in stromal-responsive human MM cell lines and reduce tumor growth in mouse models of MM.
Christine Lam, of University of California, San Francisco, and her colleagues conducted this research and reported the results in haematologica.
The researchers showed that, in co-cultures of MM cell lines and bone marrow stromal cells (BMSCs), tofacitinib inhibited the growth of MM cells in a dose-dependent manner.
RNA sequencing and phosphoproteonomics revealed an upregulation of 67 transcripts in MM cell lines co-cultured with BMSCs—most related to JAK-STAT and interleukin signaling.
Additional cell culture experiments showed that tofacitinib inhibited the downstream signaling molecule STAT3, which is responsible for proliferation through the JAK/STAT pathway.
The JAK1/2 inhibitor ruxolitinib did not replicate results seen with tofacitinib.
Further experiments showed that carfilzomib did not have synergistic effects with tofacitinib.
Venetoclax did demonstrate synergy with tofacitinib but only in MM cells cocultured with BMSCs, not in MM cells alone.
The researchers also tested tofacitinib in vivo. They injected mice with an MM cell line, and, after 2 weeks, mice were treated with tofacitinib for 4 weeks.
Mice treated with tofacitinib had lower tumor burden and a significant improvement in survival compared to untreated control mice.
Finally, the researchers tested tofacitinib in bone marrow mononuclear cells from patients. After stimulation with IL-6, the cells were exposed to tofacitinib.
The researchers observed “modest” viability against malignant plasma cells. They noted that because ex vivo MM plasma cells are minimally proliferative even with added cytokines or stromal stimulations, “these results may not fully reflect the potential therapeutic efficacy of tofacitinib in MM patients, where plasma cells are constantly proliferating within the [bone marrow].”
The researchers concluded that “tofacitinib is a promising agent to reverse the tumor-proliferative effects of the [bone marrow] microenvironment that can be rapidly repurposed to benefit MM patients.”
The Pop That Stopped the Soccer Game

ANSWER
The radiograph shows an avulsion fracture of the right iliac crest. While the patient does have a growth plate in this location, there is asymmetry between the right and left sides.
Pelvic avulsion fractures can be easy to overlook and are often misdiagnosed as strains. Providers must remember that the pelvis serves as an insertion site for multiple muscles; in both adolescent and adult patients, certain activities (eg, sprinting, jumping, kicking) can increase tension and result in a bone avulsion. Affected patients typically report a popping sensation, pain with range of motion, and point tenderness over the fracture.
Avulsion fractures can usually be identified on x-ray; CT and MRI are used only when definitive diagnosis is unclear. Treatment consists of conservative management—rest, protected weight bearing, and physical therapy. Surgery is typically reserved for those with > 2 cm displacement of the fracture fragment.
In athletes, a gradual return to sports is advised, with full participation at four to 12 weeks postinjury. Possible complications include recurrent symptoms, prolonged healing time, nonunion, malunion, or hip weakness.
This patient was placed on crutches with non-weight-bearing status for one week. She used OTC pain medication as needed. The patient completed a four-week course of physical therapy and returned to full weight-bearing status. After six weeks, the patient had returned to full activity with pain-free range of motion and full strength.
ANSWER
The radiograph shows an avulsion fracture of the right iliac crest. While the patient does have a growth plate in this location, there is asymmetry between the right and left sides.
Pelvic avulsion fractures can be easy to overlook and are often misdiagnosed as strains. Providers must remember that the pelvis serves as an insertion site for multiple muscles; in both adolescent and adult patients, certain activities (eg, sprinting, jumping, kicking) can increase tension and result in a bone avulsion. Affected patients typically report a popping sensation, pain with range of motion, and point tenderness over the fracture.
Avulsion fractures can usually be identified on x-ray; CT and MRI are used only when definitive diagnosis is unclear. Treatment consists of conservative management—rest, protected weight bearing, and physical therapy. Surgery is typically reserved for those with > 2 cm displacement of the fracture fragment.
In athletes, a gradual return to sports is advised, with full participation at four to 12 weeks postinjury. Possible complications include recurrent symptoms, prolonged healing time, nonunion, malunion, or hip weakness.
This patient was placed on crutches with non-weight-bearing status for one week. She used OTC pain medication as needed. The patient completed a four-week course of physical therapy and returned to full weight-bearing status. After six weeks, the patient had returned to full activity with pain-free range of motion and full strength.
ANSWER
The radiograph shows an avulsion fracture of the right iliac crest. While the patient does have a growth plate in this location, there is asymmetry between the right and left sides.
Pelvic avulsion fractures can be easy to overlook and are often misdiagnosed as strains. Providers must remember that the pelvis serves as an insertion site for multiple muscles; in both adolescent and adult patients, certain activities (eg, sprinting, jumping, kicking) can increase tension and result in a bone avulsion. Affected patients typically report a popping sensation, pain with range of motion, and point tenderness over the fracture.
Avulsion fractures can usually be identified on x-ray; CT and MRI are used only when definitive diagnosis is unclear. Treatment consists of conservative management—rest, protected weight bearing, and physical therapy. Surgery is typically reserved for those with > 2 cm displacement of the fracture fragment.
In athletes, a gradual return to sports is advised, with full participation at four to 12 weeks postinjury. Possible complications include recurrent symptoms, prolonged healing time, nonunion, malunion, or hip weakness.
This patient was placed on crutches with non-weight-bearing status for one week. She used OTC pain medication as needed. The patient completed a four-week course of physical therapy and returned to full weight-bearing status. After six weeks, the patient had returned to full activity with pain-free range of motion and full strength.

A 13-year-old girl presents with her mother for evaluation of right hip pain following a soccer game two days ago. The patient says she felt a “pop” in her right hip while running and kicking the ball. She was escorted off the field, unable to finish the game.
Since then, she has had pain over the right superior pelvic region. She rates the pain as a 1/10 at rest but 7/10 with ambulation. She is unwilling to bear weight secondary to discomfort and has been using crutches provided by her trainer. She has been using ice and ibuprofen without relief. Her medical history is unremarkable.
On physical exam, you note a well-developed, well-nourished female in no acute distress. No ecchymosis, erythema, or abrasions can be seen on skin exam. The patient has point tenderness over the right iliac crest. She has mild pain and weakness with hip flexion and significant pain with abduction. The extremity is neurovascularly intact.
A pelvic radiograph is obtained. What is your impression?

ESMO, ASCO seek improved cancer services

The European Society for Medical Oncology (ESMO) and the American Society of Clinical Oncology (ASCO) have called for renewed political commitment to improve cancer services and reduce cancer deaths.
ASCO and ESMO issued a joint statement in which they asked heads of state and health ministers to attend the United Nations Civil Society Hearing on Non-communicable Diseases (NCDs) in September and reconfirm their commitment to “pass legislation and invest in actions that will reduce the burden of NCDs, including cancer.”
Specifically, ESMO and ASCO said governments should:
- Implement the 2017 World Health Assembly Cancer Resolution
- Develop and strengthen educational programs that provide lifestyle recommendations to reduce cancer risk (eg, prevent tobacco use, encourage healthy weight control, etc.)
- Develop efficient and cost-effective primary prevention measures (eg, Helicobacter pylori eradication)
- Ensure timely access to screening, early stage diagnosis, and treatment for all stages of cancer
- Strengthen health systems so they can provide cancer services to all who need them
- Provide essential secondary healthcare services that ensure an adequate number of well-trained oncology professionals who have access to necessary resources
- Aim to reduce premature mortality by 25% by 2025 and by 33% by 2030 across all NCDs.
“Recent UN and WHO reports1,2,3,4 note that, unless countries significantly scale-up their actions and investments, they will not meet agreed targets to reduce deaths from non-communicable diseases,” said ESMO President Josep Tabernero, MD, PhD.
“We are concerned that governments may find it easier to achieve their targets by reducing deaths from only some NCDs, leaving cancer patients behind. We believe there are cost-effective ways to improve cancer care and stand ready to assist countries in doing this by providing our expertise in cancer management to support implementation of the 2017 World Health Assembly Cancer Resolution.”
“We urge member states to consider our joint call and amendments to strengthen the political declaration to be approved during the UN high-level meeting on 27 September and thus change the future outlook for cancer patients worldwide.”
1. United Nations Report by the Secretary General, Document A_72_662, 21 December 2017: http://www.who.int/ncds/governance/high-level-commission/A_72_662.pdf
2. World Health Assembly Report by the WHO Director General, Document WHA 71.2, 26 May 2018: http://apps.who.int/gb/ebwha/pdf_files/WHA71/A71_R2-en.pdf
3. WHO Independent High-Level Commission on NCDs Report, Time to Deliver, 1 June 2018: http://apps.who.int/iris/bitstream/handle/10665/272710/9789241514163-eng.pdf?ua=1
4. WHO Report Saving Lives, Spending Less, 21 May 2018: http://apps.who.int/iris/bitstream/handle/10665/272534/WHO-NMH-NVI-18.8-eng.pdf
The European Society for Medical Oncology (ESMO) and the American Society of Clinical Oncology (ASCO) have called for renewed political commitment to improve cancer services and reduce cancer deaths.
ASCO and ESMO issued a joint statement in which they asked heads of state and health ministers to attend the United Nations Civil Society Hearing on Non-communicable Diseases (NCDs) in September and reconfirm their commitment to “pass legislation and invest in actions that will reduce the burden of NCDs, including cancer.”
Specifically, ESMO and ASCO said governments should:
- Implement the 2017 World Health Assembly Cancer Resolution
- Develop and strengthen educational programs that provide lifestyle recommendations to reduce cancer risk (eg, prevent tobacco use, encourage healthy weight control, etc.)
- Develop efficient and cost-effective primary prevention measures (eg, Helicobacter pylori eradication)
- Ensure timely access to screening, early stage diagnosis, and treatment for all stages of cancer
- Strengthen health systems so they can provide cancer services to all who need them
- Provide essential secondary healthcare services that ensure an adequate number of well-trained oncology professionals who have access to necessary resources
- Aim to reduce premature mortality by 25% by 2025 and by 33% by 2030 across all NCDs.
“Recent UN and WHO reports1,2,3,4 note that, unless countries significantly scale-up their actions and investments, they will not meet agreed targets to reduce deaths from non-communicable diseases,” said ESMO President Josep Tabernero, MD, PhD.
“We are concerned that governments may find it easier to achieve their targets by reducing deaths from only some NCDs, leaving cancer patients behind. We believe there are cost-effective ways to improve cancer care and stand ready to assist countries in doing this by providing our expertise in cancer management to support implementation of the 2017 World Health Assembly Cancer Resolution.”
“We urge member states to consider our joint call and amendments to strengthen the political declaration to be approved during the UN high-level meeting on 27 September and thus change the future outlook for cancer patients worldwide.”
1. United Nations Report by the Secretary General, Document A_72_662, 21 December 2017: http://www.who.int/ncds/governance/high-level-commission/A_72_662.pdf
2. World Health Assembly Report by the WHO Director General, Document WHA 71.2, 26 May 2018: http://apps.who.int/gb/ebwha/pdf_files/WHA71/A71_R2-en.pdf
3. WHO Independent High-Level Commission on NCDs Report, Time to Deliver, 1 June 2018: http://apps.who.int/iris/bitstream/handle/10665/272710/9789241514163-eng.pdf?ua=1
4. WHO Report Saving Lives, Spending Less, 21 May 2018: http://apps.who.int/iris/bitstream/handle/10665/272534/WHO-NMH-NVI-18.8-eng.pdf
The European Society for Medical Oncology (ESMO) and the American Society of Clinical Oncology (ASCO) have called for renewed political commitment to improve cancer services and reduce cancer deaths.
ASCO and ESMO issued a joint statement in which they asked heads of state and health ministers to attend the United Nations Civil Society Hearing on Non-communicable Diseases (NCDs) in September and reconfirm their commitment to “pass legislation and invest in actions that will reduce the burden of NCDs, including cancer.”
Specifically, ESMO and ASCO said governments should:
- Implement the 2017 World Health Assembly Cancer Resolution
- Develop and strengthen educational programs that provide lifestyle recommendations to reduce cancer risk (eg, prevent tobacco use, encourage healthy weight control, etc.)
- Develop efficient and cost-effective primary prevention measures (eg, Helicobacter pylori eradication)
- Ensure timely access to screening, early stage diagnosis, and treatment for all stages of cancer
- Strengthen health systems so they can provide cancer services to all who need them
- Provide essential secondary healthcare services that ensure an adequate number of well-trained oncology professionals who have access to necessary resources
- Aim to reduce premature mortality by 25% by 2025 and by 33% by 2030 across all NCDs.
“Recent UN and WHO reports1,2,3,4 note that, unless countries significantly scale-up their actions and investments, they will not meet agreed targets to reduce deaths from non-communicable diseases,” said ESMO President Josep Tabernero, MD, PhD.
“We are concerned that governments may find it easier to achieve their targets by reducing deaths from only some NCDs, leaving cancer patients behind. We believe there are cost-effective ways to improve cancer care and stand ready to assist countries in doing this by providing our expertise in cancer management to support implementation of the 2017 World Health Assembly Cancer Resolution.”
“We urge member states to consider our joint call and amendments to strengthen the political declaration to be approved during the UN high-level meeting on 27 September and thus change the future outlook for cancer patients worldwide.”
1. United Nations Report by the Secretary General, Document A_72_662, 21 December 2017: http://www.who.int/ncds/governance/high-level-commission/A_72_662.pdf
2. World Health Assembly Report by the WHO Director General, Document WHA 71.2, 26 May 2018: http://apps.who.int/gb/ebwha/pdf_files/WHA71/A71_R2-en.pdf
3. WHO Independent High-Level Commission on NCDs Report, Time to Deliver, 1 June 2018: http://apps.who.int/iris/bitstream/handle/10665/272710/9789241514163-eng.pdf?ua=1
4. WHO Report Saving Lives, Spending Less, 21 May 2018: http://apps.who.int/iris/bitstream/handle/10665/272534/WHO-NMH-NVI-18.8-eng.pdf
FDA revises guidance on screening blood for Zika

The US Food and Drug Administration (FDA) has released a revised guidance on testing donated blood and blood components for Zika virus.
The revised guidance states that it is no longer necessary to screen every donation individually.
Pooled donations can be tested for Zika virus in most cases, although, in areas where there is an increased risk of mosquito-borne transmission of Zika, donations should be tested individually.
The FDA said the revised guidance is a result of careful consideration of all available scientific evidence, including consultation with other public health agencies, and following the recommendations of the December 2017 meeting of the Blood Products Advisory Committee.
“When Zika virus first emerged, the unknown course of the epidemic and the observed severe effects from the disease indicated that individual donor testing was needed to ensure the continued safety of the blood supply,” said Peter Marks, MD, PhD, director of the FDA’s Center for Biologics Evaluation and Research.
“Now, given the significant decrease in cases of Zika virus infection in the US and its territories, we are moving away from testing each individual donation to testing pooled donations. This is usually more cost-effective and less burdensome for blood establishments. However, the FDA will continue to monitor the situation closely, and as appropriate, reconsider what measures are needed to maintain the safety of the blood supply.”
The FDA’s revised guidance replaces the August 2016 guidance, which recommended universal nucleic acid testing of individual units of blood donated in US states and territories.
The revised guidance explains that, to comply with applicable testing regulations, blood establishments must continue to test all donated whole blood and blood components for Zika virus using a nucleic acid test.
However, in many cases, pooled testing of donations using an FDA-licensed screening test is a sufficient method for complying with these regulations. If there is an increased risk of local mosquito-borne transmission of Zika virus in a specific area, donations should be tested individually.
As an alternative to pooled or individual testing, blood establishments can use an FDA-approved pathogen-reduction device for plasma and certain platelet products.
The FDA said these recommendations will continue to ensure the safety of the US blood supply by reducing the risk of Zika virus transmission while also reducing the burden of testing for blood establishments.
The US Food and Drug Administration (FDA) has released a revised guidance on testing donated blood and blood components for Zika virus.
The revised guidance states that it is no longer necessary to screen every donation individually.
Pooled donations can be tested for Zika virus in most cases, although, in areas where there is an increased risk of mosquito-borne transmission of Zika, donations should be tested individually.
The FDA said the revised guidance is a result of careful consideration of all available scientific evidence, including consultation with other public health agencies, and following the recommendations of the December 2017 meeting of the Blood Products Advisory Committee.
“When Zika virus first emerged, the unknown course of the epidemic and the observed severe effects from the disease indicated that individual donor testing was needed to ensure the continued safety of the blood supply,” said Peter Marks, MD, PhD, director of the FDA’s Center for Biologics Evaluation and Research.
“Now, given the significant decrease in cases of Zika virus infection in the US and its territories, we are moving away from testing each individual donation to testing pooled donations. This is usually more cost-effective and less burdensome for blood establishments. However, the FDA will continue to monitor the situation closely, and as appropriate, reconsider what measures are needed to maintain the safety of the blood supply.”
The FDA’s revised guidance replaces the August 2016 guidance, which recommended universal nucleic acid testing of individual units of blood donated in US states and territories.
The revised guidance explains that, to comply with applicable testing regulations, blood establishments must continue to test all donated whole blood and blood components for Zika virus using a nucleic acid test.
However, in many cases, pooled testing of donations using an FDA-licensed screening test is a sufficient method for complying with these regulations. If there is an increased risk of local mosquito-borne transmission of Zika virus in a specific area, donations should be tested individually.
As an alternative to pooled or individual testing, blood establishments can use an FDA-approved pathogen-reduction device for plasma and certain platelet products.
The FDA said these recommendations will continue to ensure the safety of the US blood supply by reducing the risk of Zika virus transmission while also reducing the burden of testing for blood establishments.
The US Food and Drug Administration (FDA) has released a revised guidance on testing donated blood and blood components for Zika virus.
The revised guidance states that it is no longer necessary to screen every donation individually.
Pooled donations can be tested for Zika virus in most cases, although, in areas where there is an increased risk of mosquito-borne transmission of Zika, donations should be tested individually.
The FDA said the revised guidance is a result of careful consideration of all available scientific evidence, including consultation with other public health agencies, and following the recommendations of the December 2017 meeting of the Blood Products Advisory Committee.
“When Zika virus first emerged, the unknown course of the epidemic and the observed severe effects from the disease indicated that individual donor testing was needed to ensure the continued safety of the blood supply,” said Peter Marks, MD, PhD, director of the FDA’s Center for Biologics Evaluation and Research.
“Now, given the significant decrease in cases of Zika virus infection in the US and its territories, we are moving away from testing each individual donation to testing pooled donations. This is usually more cost-effective and less burdensome for blood establishments. However, the FDA will continue to monitor the situation closely, and as appropriate, reconsider what measures are needed to maintain the safety of the blood supply.”
The FDA’s revised guidance replaces the August 2016 guidance, which recommended universal nucleic acid testing of individual units of blood donated in US states and territories.
The revised guidance explains that, to comply with applicable testing regulations, blood establishments must continue to test all donated whole blood and blood components for Zika virus using a nucleic acid test.
However, in many cases, pooled testing of donations using an FDA-licensed screening test is a sufficient method for complying with these regulations. If there is an increased risk of local mosquito-borne transmission of Zika virus in a specific area, donations should be tested individually.
As an alternative to pooled or individual testing, blood establishments can use an FDA-approved pathogen-reduction device for plasma and certain platelet products.
The FDA said these recommendations will continue to ensure the safety of the US blood supply by reducing the risk of Zika virus transmission while also reducing the burden of testing for blood establishments.
GOP Doctors Caucus seeks lower MIPS threshold
The House GOP Doctors Caucus is pushing officials at the Centers for Medicare & Medicaid to lower the exclusion threshold for participation in the Merit-Based Incentive Payment System (MIPS).
In a letter to CMS Administrator Seema Verma, the lawmakers noted that about 60% of health care providers are excluded from MIPS – one track of the agency’s Quality Payment Program – mostly because of the high participation threshold set by the agency.
Since the program provides incentive payments to doctors by shifting Medicare Part B payments, the low participation is also lowering the payments available for high-level performance.
“The most notable ramification of the current threshold has been lower maximum positive updates on how MIPS ultimately adjusts Part B payments,” the lawmakers wrote. “For example, high performers are estimated to receive an aggregate payment adjustment in 2019 of 1.1% – based on their 2017 performance – even though adjustments of up to 4% are authorized.”
This payment trend “fails to incentivize meaningful participation in MIPS,” they wrote.
The current MIPS threshold excludes any physician or practice that generates $90,000 or less in Part B billing or sees 200 or fewer Medicare patients. The agency had initially set the threshold lower, at $30,000 or less in billing or 100 patients but created a larger exemption based on feedback from many physician groups.
The five members of the House GOP Doctors Caucus who signed on to the letter are Phil Roe (Tenn.), Andy Harris (Md.), Earl “Buddy” Carter (Ga.), Larry Bucshon (Ind.), and Scott DesJarlais (Tenn.).
The House GOP Doctors Caucus is pushing officials at the Centers for Medicare & Medicaid to lower the exclusion threshold for participation in the Merit-Based Incentive Payment System (MIPS).
In a letter to CMS Administrator Seema Verma, the lawmakers noted that about 60% of health care providers are excluded from MIPS – one track of the agency’s Quality Payment Program – mostly because of the high participation threshold set by the agency.
Since the program provides incentive payments to doctors by shifting Medicare Part B payments, the low participation is also lowering the payments available for high-level performance.
“The most notable ramification of the current threshold has been lower maximum positive updates on how MIPS ultimately adjusts Part B payments,” the lawmakers wrote. “For example, high performers are estimated to receive an aggregate payment adjustment in 2019 of 1.1% – based on their 2017 performance – even though adjustments of up to 4% are authorized.”
This payment trend “fails to incentivize meaningful participation in MIPS,” they wrote.
The current MIPS threshold excludes any physician or practice that generates $90,000 or less in Part B billing or sees 200 or fewer Medicare patients. The agency had initially set the threshold lower, at $30,000 or less in billing or 100 patients but created a larger exemption based on feedback from many physician groups.
The five members of the House GOP Doctors Caucus who signed on to the letter are Phil Roe (Tenn.), Andy Harris (Md.), Earl “Buddy” Carter (Ga.), Larry Bucshon (Ind.), and Scott DesJarlais (Tenn.).
The House GOP Doctors Caucus is pushing officials at the Centers for Medicare & Medicaid to lower the exclusion threshold for participation in the Merit-Based Incentive Payment System (MIPS).
In a letter to CMS Administrator Seema Verma, the lawmakers noted that about 60% of health care providers are excluded from MIPS – one track of the agency’s Quality Payment Program – mostly because of the high participation threshold set by the agency.
Since the program provides incentive payments to doctors by shifting Medicare Part B payments, the low participation is also lowering the payments available for high-level performance.
“The most notable ramification of the current threshold has been lower maximum positive updates on how MIPS ultimately adjusts Part B payments,” the lawmakers wrote. “For example, high performers are estimated to receive an aggregate payment adjustment in 2019 of 1.1% – based on their 2017 performance – even though adjustments of up to 4% are authorized.”
This payment trend “fails to incentivize meaningful participation in MIPS,” they wrote.
The current MIPS threshold excludes any physician or practice that generates $90,000 or less in Part B billing or sees 200 or fewer Medicare patients. The agency had initially set the threshold lower, at $30,000 or less in billing or 100 patients but created a larger exemption based on feedback from many physician groups.
The five members of the House GOP Doctors Caucus who signed on to the letter are Phil Roe (Tenn.), Andy Harris (Md.), Earl “Buddy” Carter (Ga.), Larry Bucshon (Ind.), and Scott DesJarlais (Tenn.).