User login
The Official Newspaper of the American Association for Thoracic Surgery
Burning the midnight oil does not impact surgical outcomes
Attending physicians who work through the wee hours of the night do not have measurably different short-term outcomes for elective surgeries performed the next day, according to a population-based, matched-control study published online Aug. 26.
The primary composite outcome of death, readmission, or complications within 30 days occurred in 22.2% of patients undergoing elective daytime surgery by an attending who treated patients from midnight to 7 a.m. and in 22.4% of those undergoing the same procedure by the same attending, but after a night when no clinical work had been performed (P = .66).

There was no significant between-group difference in the primary outcome in adjusted analyses (adjusted odds ratio, 0.99; P = .65).
Secondary outcomes also were similar between the postmidnight and control groups: death within 30 days (both 1.1%), readmission within 30 days (6.6% vs. 7.1%), complications within 30 days (18.1% vs. 18.2%), median length of stay (both 3 days), and median duration of surgery (both 2.6 hours).
“These data suggest that calls for broad-based policy shifts in duty hours and practices of attending surgeons may not be necessary at this time,” wrote surgical oncologist Dr. Anand Govindarajan of Mount Sinai Hospital, Toronto, and his associates (N Engl J Med. 2015;373:845-53. doi: 10.1056/NEJMsa1415994).
The current study addresses a gap in the literature on the effects of sleep deprivation and may help inform policy discussions on this issue, the authors suggested.
Most studies of physicians suggesting that sleep deprivation may affect mood, cognition, and psycho-motor function have focused on medical trainees, but few studies have examined the effects of sleep deprivation in attending physicians and the results have been conflicting.
A 2009 single-center study prompted calls for policy-level changes regarding sleep deprivation in surgeons after showing a higher rate of complications for procedures performed by attending physicians with sleep opportunities of less than 6 hours (JAMA. 2009 Oct 14;302[14]:1565-72), but the findings have not been replicated by other groups, Dr. Govindarajan and his associates observed.
In the current study, a small but significant increase in complications was observed in the subset of patients whose physician had performed two or more procedures the night before (adjusted OR, 1.14; P = .05). Importantly, this isolated finding was from a post-hoc subgroup analysis and may be the result of random error, they suggested.
Further, three a priori analyses found no significant difference in outcomes after stratification for academic vs. nonacademic center, physician age, or type of procedure.
The current study involved 38,978 patients who underwent 1 of 12 elective daytime procedures performed by 1,448 physicians at 147 hospitals in Ontario. Patients undergoing procedures performed by a physician who had treated patients from midnight to 7 a.m. were matched in a 1:1 ratio to patients undergoing the same procedure by the same physician on a day when the physician had not treated patients after midnight.
The physicians had been in practice for a median of 20 years, and 40.6% of procedures were performed at academic institutions. Physicians who treated patients after midnight performed a mean of 1.25 procedures during that time.
The elective procedures (cholecystectomy, gastric bypass, colon resection, coronary artery bypass grafting, coronary angioplasty, knee replacement, hip replacement, hip fracture repair, hysterectomy, spinal surgery, craniotomy, and lung resection) were all performed on weekdays.
The investigators selected procedures that varied in duration and were associated with a range of complication rates because sleep studies have suggested that tasks requiring longer periods of concentration may be more affected by sleep deprivation.
“The broad scope of the study enhances its generalizability, a particularly relevant consideration if policy changes are being contemplated with respect to duty hours,” Dr. Govindarajan and his associates noted.
Other strengths of the study are the matched study groups and sufficiently sized cohorts and event rates to provide adequate power to show clinically meaningful differences.
Limitations of the study are the inability to quantify the number of hours that a physician was deprived of sleep and to determine whether there was a difference in outcomes between daytime procedures performed later in the day and those performed earlier in the day or whether procedures may have been postponed till later in the day because of substantial sleep deprivation. “However, given the constraints of operating room schedules in Ontario, it would not usually be feasible to postpone an operation until later in the day on short notice,” the investigators wrote.
Dr. Govindarajan reported grant support from the Canadian Institutes for Health Research and the University of Toronto Dean’s Fund while conducting the study.
On Twitter @pwendl
Attending physicians who work through the wee hours of the night do not have measurably different short-term outcomes for elective surgeries performed the next day, according to a population-based, matched-control study published online Aug. 26.
The primary composite outcome of death, readmission, or complications within 30 days occurred in 22.2% of patients undergoing elective daytime surgery by an attending who treated patients from midnight to 7 a.m. and in 22.4% of those undergoing the same procedure by the same attending, but after a night when no clinical work had been performed (P = .66).
There was no significant between-group difference in the primary outcome in adjusted analyses (adjusted odds ratio, 0.99; P = .65).
Secondary outcomes also were similar between the postmidnight and control groups: death within 30 days (both 1.1%), readmission within 30 days (6.6% vs. 7.1%), complications within 30 days (18.1% vs. 18.2%), median length of stay (both 3 days), and median duration of surgery (both 2.6 hours).
“These data suggest that calls for broad-based policy shifts in duty hours and practices of attending surgeons may not be necessary at this time,” wrote surgical oncologist Dr. Anand Govindarajan of Mount Sinai Hospital, Toronto, and his associates (N Engl J Med. 2015;373:845-53. doi: 10.1056/NEJMsa1415994).
The current study addresses a gap in the literature on the effects of sleep deprivation and may help inform policy discussions on this issue, the authors suggested.
Most studies of physicians suggesting that sleep deprivation may affect mood, cognition, and psycho-motor function have focused on medical trainees, but few studies have examined the effects of sleep deprivation in attending physicians and the results have been conflicting.
A 2009 single-center study prompted calls for policy-level changes regarding sleep deprivation in surgeons after showing a higher rate of complications for procedures performed by attending physicians with sleep opportunities of less than 6 hours (JAMA. 2009 Oct 14;302[14]:1565-72), but the findings have not been replicated by other groups, Dr. Govindarajan and his associates observed.
In the current study, a small but significant increase in complications was observed in the subset of patients whose physician had performed two or more procedures the night before (adjusted OR, 1.14; P = .05). Importantly, this isolated finding was from a post-hoc subgroup analysis and may be the result of random error, they suggested.
Further, three a priori analyses found no significant difference in outcomes after stratification for academic vs. nonacademic center, physician age, or type of procedure.
The current study involved 38,978 patients who underwent 1 of 12 elective daytime procedures performed by 1,448 physicians at 147 hospitals in Ontario. Patients undergoing procedures performed by a physician who had treated patients from midnight to 7 a.m. were matched in a 1:1 ratio to patients undergoing the same procedure by the same physician on a day when the physician had not treated patients after midnight.
The physicians had been in practice for a median of 20 years, and 40.6% of procedures were performed at academic institutions. Physicians who treated patients after midnight performed a mean of 1.25 procedures during that time.
The elective procedures (cholecystectomy, gastric bypass, colon resection, coronary artery bypass grafting, coronary angioplasty, knee replacement, hip replacement, hip fracture repair, hysterectomy, spinal surgery, craniotomy, and lung resection) were all performed on weekdays.
The investigators selected procedures that varied in duration and were associated with a range of complication rates because sleep studies have suggested that tasks requiring longer periods of concentration may be more affected by sleep deprivation.
“The broad scope of the study enhances its generalizability, a particularly relevant consideration if policy changes are being contemplated with respect to duty hours,” Dr. Govindarajan and his associates noted.
Other strengths of the study are the matched study groups and sufficiently sized cohorts and event rates to provide adequate power to show clinically meaningful differences.
Limitations of the study are the inability to quantify the number of hours that a physician was deprived of sleep and to determine whether there was a difference in outcomes between daytime procedures performed later in the day and those performed earlier in the day or whether procedures may have been postponed till later in the day because of substantial sleep deprivation. “However, given the constraints of operating room schedules in Ontario, it would not usually be feasible to postpone an operation until later in the day on short notice,” the investigators wrote.
Dr. Govindarajan reported grant support from the Canadian Institutes for Health Research and the University of Toronto Dean’s Fund while conducting the study.
On Twitter @pwendl
Attending physicians who work through the wee hours of the night do not have measurably different short-term outcomes for elective surgeries performed the next day, according to a population-based, matched-control study published online Aug. 26.
The primary composite outcome of death, readmission, or complications within 30 days occurred in 22.2% of patients undergoing elective daytime surgery by an attending who treated patients from midnight to 7 a.m. and in 22.4% of those undergoing the same procedure by the same attending, but after a night when no clinical work had been performed (P = .66).
There was no significant between-group difference in the primary outcome in adjusted analyses (adjusted odds ratio, 0.99; P = .65).
Secondary outcomes also were similar between the postmidnight and control groups: death within 30 days (both 1.1%), readmission within 30 days (6.6% vs. 7.1%), complications within 30 days (18.1% vs. 18.2%), median length of stay (both 3 days), and median duration of surgery (both 2.6 hours).
“These data suggest that calls for broad-based policy shifts in duty hours and practices of attending surgeons may not be necessary at this time,” wrote surgical oncologist Dr. Anand Govindarajan of Mount Sinai Hospital, Toronto, and his associates (N Engl J Med. 2015;373:845-53. doi: 10.1056/NEJMsa1415994).
The current study addresses a gap in the literature on the effects of sleep deprivation and may help inform policy discussions on this issue, the authors suggested.
Most studies of physicians suggesting that sleep deprivation may affect mood, cognition, and psycho-motor function have focused on medical trainees, but few studies have examined the effects of sleep deprivation in attending physicians and the results have been conflicting.
A 2009 single-center study prompted calls for policy-level changes regarding sleep deprivation in surgeons after showing a higher rate of complications for procedures performed by attending physicians with sleep opportunities of less than 6 hours (JAMA. 2009 Oct 14;302[14]:1565-72), but the findings have not been replicated by other groups, Dr. Govindarajan and his associates observed.
In the current study, a small but significant increase in complications was observed in the subset of patients whose physician had performed two or more procedures the night before (adjusted OR, 1.14; P = .05). Importantly, this isolated finding was from a post-hoc subgroup analysis and may be the result of random error, they suggested.
Further, three a priori analyses found no significant difference in outcomes after stratification for academic vs. nonacademic center, physician age, or type of procedure.
The current study involved 38,978 patients who underwent 1 of 12 elective daytime procedures performed by 1,448 physicians at 147 hospitals in Ontario. Patients undergoing procedures performed by a physician who had treated patients from midnight to 7 a.m. were matched in a 1:1 ratio to patients undergoing the same procedure by the same physician on a day when the physician had not treated patients after midnight.
The physicians had been in practice for a median of 20 years, and 40.6% of procedures were performed at academic institutions. Physicians who treated patients after midnight performed a mean of 1.25 procedures during that time.
The elective procedures (cholecystectomy, gastric bypass, colon resection, coronary artery bypass grafting, coronary angioplasty, knee replacement, hip replacement, hip fracture repair, hysterectomy, spinal surgery, craniotomy, and lung resection) were all performed on weekdays.
The investigators selected procedures that varied in duration and were associated with a range of complication rates because sleep studies have suggested that tasks requiring longer periods of concentration may be more affected by sleep deprivation.
“The broad scope of the study enhances its generalizability, a particularly relevant consideration if policy changes are being contemplated with respect to duty hours,” Dr. Govindarajan and his associates noted.
Other strengths of the study are the matched study groups and sufficiently sized cohorts and event rates to provide adequate power to show clinically meaningful differences.
Limitations of the study are the inability to quantify the number of hours that a physician was deprived of sleep and to determine whether there was a difference in outcomes between daytime procedures performed later in the day and those performed earlier in the day or whether procedures may have been postponed till later in the day because of substantial sleep deprivation. “However, given the constraints of operating room schedules in Ontario, it would not usually be feasible to postpone an operation until later in the day on short notice,” the investigators wrote.
Dr. Govindarajan reported grant support from the Canadian Institutes for Health Research and the University of Toronto Dean’s Fund while conducting the study.
On Twitter @pwendl
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point: The risks of adverse outcomes of elective daytime surgical procedures were similar whether or not the attending physician had provided medical care the previous night.
Major finding: The primary composite endpoint was similar between the postmidnight and control groups (22.2% vs. 22.4%; P = .66).
Data source: Population-based, retrospective, matched cohort study in 38,978 patients.
Disclosures: Dr. Govindarajan reported grant support from the Canadian Institutes for Health Research and the University of Toronto Dean’s Fund while conducting the study.

3-D–printed devices mitigate pediatric tracheobronchomalacia
Immediate and continued life-sustaining improvement was seen in three pediatric patients implanted with 3-D–printed tracheobronchial splints as a treatment for terminal tracheobronchomalacia (TBM), a condition of excessive collapse of the airways during respiration leading to cardiopulmonary arrest.
The particular value of such 3-D–printable biomaterials to pediatric surgery is their ability to adopt a 4-D modality – to exhibit specifically engineered shape changes in response to surrounding tissue growth over a defined time period. In addition to their malleability, these devices also are designed to biodegrade. These features have proven especially useful as seen in this medical device emergency use exemption study performed at the University of Michigan, according to a report published in Science Translational Medicine (2015 Apr 29. [doi: 10.1126/scitranslmed.3010825]).
“Our multidisciplinary team designed an archetype device to allow radial expansion of the affected airway over the critical growth period while resisting external compression and intrinsic collapse,” wrote Dr. Robert J. Morrison of the University of Michigan, Ann Arbor, and his colleagues.
The study population involved three infant boys, aged 3 months, 5 months, and 16 months at time of treatment. In each patient, a sternotomy exposed their affected airways. The 3-D–printed splint, consisting of conjoined rib-like C-shaped arches was placed around the affected airway and secured with polypropylene sutures. The splint counters external pressure on the airway and holds it open. Because the splint is malleable, with an expandable opening placed opposite to the main collapsing pressure, it is capable of expanding as the airway grows.
Examination of the airway immediately after placement demonstrated patency, which was confirmed 1 month later. Results showed the benefit of the splints for all three patients, although total results were complicated by additional comorbidities:
• Patient 1: Blood gases returned to normal immediately after implantation and remained normal at 3 months’ follow-up. A week after implantation, weaning from mechanical ventilation was initiated and, 3 weeks after the procedure, the child was discharged to home. Repeat imaging at 1, 3, 6, 12, and 39 months postoperatively demonstrated continued resolution of the TBM, with evidence of fragmentation and degradation of the splint at 39 months.
• Patient 2: Immediately after implantation of the device, blood gases improved greatly and the left lung perfused. The patient had opioid and benzodiazepine dependence from long-term ventilator support, requiring a longer controlled wean from the ventilator. Four weeks after surgery, the patient was transitioned to a portable ventilator system, completely weaned at 15 weeks, and discharged from the hospital to home for the first time in his life.
• Patient 3: After implantation, the patient ceased experiencing life-threatening desaturation episodes and showed sustained improvement in blood gases. Imaging showed continued patency of the left main bronchus with resolution of left-lung air trapping. However, at 14 months post implantation, he remained on permanent ventilator support, “presumably because of distal left segmental bronchomalacia beyond what the splint was designed to address,” according to Dr. Morrison and his colleagues.
“We report successful implantation of patient-specific bioresorbable airway splints for the treatment of severe TBM. The personalized splints conformed to the patients’ individual geometries and expanded with airway growth (in the ‘fourth dimension’),” the researchers summarized.
“The three pediatric patients implanted with these 3-D–printed airway splints had a terminal form of TBM. The clinical improvement in each case was immediate and sustained, suggesting that improvement is not attributable to the natural history of the disease alone,” they concluded.
The study was funded by the National Institutes of Health. Two of the study authors were coinventors of the device for which they have filed a patent. There were no other disclosures.
As illustrated in this article, the investigators demonstrate the potential for the future of 3-D–printing in medicine. While there have been numerous reports of utilizing 3-D–printing for a generation of personalized prostheses, these have been used in static circumstances in which the prosthesis is not required to change over time. In pediatric applications, as the child grows, the prosthesis also needs to adapt to this growth, thereby necessitating “4-D” printing.

|
Dr. Sai Yendamuri |
In three patients, the authors have applied this 4-D–printing paradigm to devise external bronchial splints to alleviate life-threatening tracheobronchomalacia using a novel design and a bioresorbable material, resulting in superb medium-term outcomes for patients with an otherwise dire prognosis.
Dr. Sai Yendamuri is an attending surgeon at the department of thoracic surgery, and director, Thoracic Surgery Research Laboratory, and an associate professor of oncology at Roswell Park Cancer Institute, Buffalo, N.Y. He is also an associate medical editor for Thoracic Surgery News.
As illustrated in this article, the investigators demonstrate the potential for the future of 3-D–printing in medicine. While there have been numerous reports of utilizing 3-D–printing for a generation of personalized prostheses, these have been used in static circumstances in which the prosthesis is not required to change over time. In pediatric applications, as the child grows, the prosthesis also needs to adapt to this growth, thereby necessitating “4-D” printing.
|
|
Dr. Sai Yendamuri |
In three patients, the authors have applied this 4-D–printing paradigm to devise external bronchial splints to alleviate life-threatening tracheobronchomalacia using a novel design and a bioresorbable material, resulting in superb medium-term outcomes for patients with an otherwise dire prognosis.
Dr. Sai Yendamuri is an attending surgeon at the department of thoracic surgery, and director, Thoracic Surgery Research Laboratory, and an associate professor of oncology at Roswell Park Cancer Institute, Buffalo, N.Y. He is also an associate medical editor for Thoracic Surgery News.
As illustrated in this article, the investigators demonstrate the potential for the future of 3-D–printing in medicine. While there have been numerous reports of utilizing 3-D–printing for a generation of personalized prostheses, these have been used in static circumstances in which the prosthesis is not required to change over time. In pediatric applications, as the child grows, the prosthesis also needs to adapt to this growth, thereby necessitating “4-D” printing.
|
|
Dr. Sai Yendamuri |
In three patients, the authors have applied this 4-D–printing paradigm to devise external bronchial splints to alleviate life-threatening tracheobronchomalacia using a novel design and a bioresorbable material, resulting in superb medium-term outcomes for patients with an otherwise dire prognosis.
Dr. Sai Yendamuri is an attending surgeon at the department of thoracic surgery, and director, Thoracic Surgery Research Laboratory, and an associate professor of oncology at Roswell Park Cancer Institute, Buffalo, N.Y. He is also an associate medical editor for Thoracic Surgery News.
Immediate and continued life-sustaining improvement was seen in three pediatric patients implanted with 3-D–printed tracheobronchial splints as a treatment for terminal tracheobronchomalacia (TBM), a condition of excessive collapse of the airways during respiration leading to cardiopulmonary arrest.
The particular value of such 3-D–printable biomaterials to pediatric surgery is their ability to adopt a 4-D modality – to exhibit specifically engineered shape changes in response to surrounding tissue growth over a defined time period. In addition to their malleability, these devices also are designed to biodegrade. These features have proven especially useful as seen in this medical device emergency use exemption study performed at the University of Michigan, according to a report published in Science Translational Medicine (2015 Apr 29. [doi: 10.1126/scitranslmed.3010825]).
“Our multidisciplinary team designed an archetype device to allow radial expansion of the affected airway over the critical growth period while resisting external compression and intrinsic collapse,” wrote Dr. Robert J. Morrison of the University of Michigan, Ann Arbor, and his colleagues.
The study population involved three infant boys, aged 3 months, 5 months, and 16 months at time of treatment. In each patient, a sternotomy exposed their affected airways. The 3-D–printed splint, consisting of conjoined rib-like C-shaped arches was placed around the affected airway and secured with polypropylene sutures. The splint counters external pressure on the airway and holds it open. Because the splint is malleable, with an expandable opening placed opposite to the main collapsing pressure, it is capable of expanding as the airway grows.
Examination of the airway immediately after placement demonstrated patency, which was confirmed 1 month later. Results showed the benefit of the splints for all three patients, although total results were complicated by additional comorbidities:
• Patient 1: Blood gases returned to normal immediately after implantation and remained normal at 3 months’ follow-up. A week after implantation, weaning from mechanical ventilation was initiated and, 3 weeks after the procedure, the child was discharged to home. Repeat imaging at 1, 3, 6, 12, and 39 months postoperatively demonstrated continued resolution of the TBM, with evidence of fragmentation and degradation of the splint at 39 months.
• Patient 2: Immediately after implantation of the device, blood gases improved greatly and the left lung perfused. The patient had opioid and benzodiazepine dependence from long-term ventilator support, requiring a longer controlled wean from the ventilator. Four weeks after surgery, the patient was transitioned to a portable ventilator system, completely weaned at 15 weeks, and discharged from the hospital to home for the first time in his life.
• Patient 3: After implantation, the patient ceased experiencing life-threatening desaturation episodes and showed sustained improvement in blood gases. Imaging showed continued patency of the left main bronchus with resolution of left-lung air trapping. However, at 14 months post implantation, he remained on permanent ventilator support, “presumably because of distal left segmental bronchomalacia beyond what the splint was designed to address,” according to Dr. Morrison and his colleagues.
“We report successful implantation of patient-specific bioresorbable airway splints for the treatment of severe TBM. The personalized splints conformed to the patients’ individual geometries and expanded with airway growth (in the ‘fourth dimension’),” the researchers summarized.
“The three pediatric patients implanted with these 3-D–printed airway splints had a terminal form of TBM. The clinical improvement in each case was immediate and sustained, suggesting that improvement is not attributable to the natural history of the disease alone,” they concluded.
The study was funded by the National Institutes of Health. Two of the study authors were coinventors of the device for which they have filed a patent. There were no other disclosures.
Immediate and continued life-sustaining improvement was seen in three pediatric patients implanted with 3-D–printed tracheobronchial splints as a treatment for terminal tracheobronchomalacia (TBM), a condition of excessive collapse of the airways during respiration leading to cardiopulmonary arrest.
The particular value of such 3-D–printable biomaterials to pediatric surgery is their ability to adopt a 4-D modality – to exhibit specifically engineered shape changes in response to surrounding tissue growth over a defined time period. In addition to their malleability, these devices also are designed to biodegrade. These features have proven especially useful as seen in this medical device emergency use exemption study performed at the University of Michigan, according to a report published in Science Translational Medicine (2015 Apr 29. [doi: 10.1126/scitranslmed.3010825]).
“Our multidisciplinary team designed an archetype device to allow radial expansion of the affected airway over the critical growth period while resisting external compression and intrinsic collapse,” wrote Dr. Robert J. Morrison of the University of Michigan, Ann Arbor, and his colleagues.
The study population involved three infant boys, aged 3 months, 5 months, and 16 months at time of treatment. In each patient, a sternotomy exposed their affected airways. The 3-D–printed splint, consisting of conjoined rib-like C-shaped arches was placed around the affected airway and secured with polypropylene sutures. The splint counters external pressure on the airway and holds it open. Because the splint is malleable, with an expandable opening placed opposite to the main collapsing pressure, it is capable of expanding as the airway grows.
Examination of the airway immediately after placement demonstrated patency, which was confirmed 1 month later. Results showed the benefit of the splints for all three patients, although total results were complicated by additional comorbidities:
• Patient 1: Blood gases returned to normal immediately after implantation and remained normal at 3 months’ follow-up. A week after implantation, weaning from mechanical ventilation was initiated and, 3 weeks after the procedure, the child was discharged to home. Repeat imaging at 1, 3, 6, 12, and 39 months postoperatively demonstrated continued resolution of the TBM, with evidence of fragmentation and degradation of the splint at 39 months.
• Patient 2: Immediately after implantation of the device, blood gases improved greatly and the left lung perfused. The patient had opioid and benzodiazepine dependence from long-term ventilator support, requiring a longer controlled wean from the ventilator. Four weeks after surgery, the patient was transitioned to a portable ventilator system, completely weaned at 15 weeks, and discharged from the hospital to home for the first time in his life.
• Patient 3: After implantation, the patient ceased experiencing life-threatening desaturation episodes and showed sustained improvement in blood gases. Imaging showed continued patency of the left main bronchus with resolution of left-lung air trapping. However, at 14 months post implantation, he remained on permanent ventilator support, “presumably because of distal left segmental bronchomalacia beyond what the splint was designed to address,” according to Dr. Morrison and his colleagues.
“We report successful implantation of patient-specific bioresorbable airway splints for the treatment of severe TBM. The personalized splints conformed to the patients’ individual geometries and expanded with airway growth (in the ‘fourth dimension’),” the researchers summarized.
“The three pediatric patients implanted with these 3-D–printed airway splints had a terminal form of TBM. The clinical improvement in each case was immediate and sustained, suggesting that improvement is not attributable to the natural history of the disease alone,” they concluded.
The study was funded by the National Institutes of Health. Two of the study authors were coinventors of the device for which they have filed a patent. There were no other disclosures.
FROM SCIENCE TRANSLATIONAL MEDICINE
Key clinical point: The use of 3-D–printed airway implants mitigated life-threatening tracheobronchomalacia (TBM) in three infants.
Major finding: Three infants with a terminal form of TBM ceased exhibiting life-threatening airway disease and showed continued growth of pulmonary airways after 3-D tracheal implants.
Data source: A study performed at the University of Michigan, Ann Arbor, of three infants with terminal TBM who received a medical device emergency use exemption for a 3-D tracheal implant.
Disclosures: The study was funded by the National Institutes of Health. Two of the study authors were coinventors of the device for which they have filed a patent. There were no other disclosures.

Surgeon volume may affect choice of surgery type for NSCLC
A surgeon’s comfort level with a favored operation for non–small cell lung cancer can strongly influence whether the patient will have that operation, which, in turn, can affect the patient’s outcome and long-term survival, according to an analysis of a population-linked database. For patients whose surgeons have lower levels of experience, that could mean a greater chance they will have more invasive total lung removal rather than more difficult operations that spare part of the affected lung, according to investigators at McMaster University in Hamilton, Ontario.
“If a surgeon with high surgical volumes is less likely to perform higher-risk pneumonectomy procedures than one with lower volumes, this may translate to a significant reduction in adverse events,” said lead author Dr. Christian Finley and coauthors online in the Journal of Thoracic and Cardiovascular Surgery (2015 Jun 30 [doi: 10.1016/j.jtcvs.2015.04.060]). “Surgeon volume should be considered an important component in how care is delivered in this population.”
The McMaster investigators evaluated 8,070 patients in an Ontario population-based linked database who underwent surgical resection for non–small cell lung cancer during 2004-2011, including pneumonectomy, or total lung removal (842 patients), lobectomy (6,212 patients), and wedge resection (1,002 patients). Over the years of the study, the proportion of patients who underwent pneumonectomy fell by more than half, from 14.8% in 2004 to 7.6% in 2011.
Of the three procedures, pneumonectomy carries a threefold greater mortality and while the procedure is often avoidable, there may be cases where it’s necessary because of the location of the tumor, Dr. Finley and his colleagues said. Lobectomy is desirable because it spares the parenchyma and has lower recurrence rates than laser resections.
The study investigators aimed to explore the hypothesis that surgeons with less expertise are more inclined to perform the higher-risk pneumonectomy or sublobar resections such as a segmentectomy or a wedge resection than a lobectomy, the rationale being that these procedures can be less challenging than a standard or sleeve lobectomy. The study analyzed results from 124 different physicians at 45 institutions in Ontario.
Data analysis showed that physician volume, age, year of procedure, sex, and comorbidities were predictive of the surgeon performing a pneumonectomy. “Adjusting for these variables, the results indicated that for each 10-unit increase in physician volume, the relative risk of performing a pneumonectomy decreased by 9.1%,” Dr. Finley and his colleagues wrote. They also found no significant difference in stage distribution among low-, medium-, and high-volume surgeons.
“This is meaningful as pneumonectomy is known to have the highest mortality rate of lung cancer resection, found in this study to be 12.6%, demonstrating a potentially large impact on patient survival,” Dr. Finley and his colleagues said.
This analysis cites an earlier study that surgeon volume for many procedures was a key determinant in the link between hospital volume and operative mortality (N Engl J Med. 2003 Nov 27;349[2]:2117-27.). “This study suggests that a patient may improve their chance of survival substantially, even at high-volume institutions, by selecting surgeons who perform operations more frequently,” Dr. Finley and his colleagues said.
They said that despite their study’s limitations, the findings on how surgeon experience can influence the choice of lung resection for cancer warrant further study.
McMaster University, Division of Thoracic Surgery, provided funding for the study. The study authors had no disclosures.
Because the McMaster University study derived the reported outcomes from registry data, determining the reasons that influenced surgeons’ choices of lung resection is impossible, Dr. Eric Lim of the Imperial College of Medicine, London, said in his invited commentary (J Thorac Cardiovasc Surg. 2015 May 21 [doi:10.1016/j.jtcvs.2015.05.048]).
The study authors noted that lower-volume surgeons were more inclined to perform pneumonectomy, and, Dr. Lim noted, previous studies have found that higher-volume centers tended to see more patients with advanced-stage cancers and increased morbidities. “An alternative explanation is that higher-volume surgeons have better skill sets to undertake procedures such as sleeve lobectomies that would lower the pneumonectomy rates and possibly more segmentectomies to lower the wedge-resection rate,” Dr. Lim said.
Until better evidence exists on what procedure is best for central and peripheral tumors, “surgeons can argue either way,” Dr. Lim said. The questions that follow from the study should concentrate on the relative harm of each procedure and the level of practice variation that’s unacceptable.
“As a surgical community, it is incumbent on us to continue to evaluate surgical treatments generating the highest levels of evidence possible (randomized trials) and have sufficient humility to cross refer to colleagues when appropriate to ensure the best care for our patients,” Dr. Lim concluded.
Because the McMaster University study derived the reported outcomes from registry data, determining the reasons that influenced surgeons’ choices of lung resection is impossible, Dr. Eric Lim of the Imperial College of Medicine, London, said in his invited commentary (J Thorac Cardiovasc Surg. 2015 May 21 [doi:10.1016/j.jtcvs.2015.05.048]).
The study authors noted that lower-volume surgeons were more inclined to perform pneumonectomy, and, Dr. Lim noted, previous studies have found that higher-volume centers tended to see more patients with advanced-stage cancers and increased morbidities. “An alternative explanation is that higher-volume surgeons have better skill sets to undertake procedures such as sleeve lobectomies that would lower the pneumonectomy rates and possibly more segmentectomies to lower the wedge-resection rate,” Dr. Lim said.
Until better evidence exists on what procedure is best for central and peripheral tumors, “surgeons can argue either way,” Dr. Lim said. The questions that follow from the study should concentrate on the relative harm of each procedure and the level of practice variation that’s unacceptable.
“As a surgical community, it is incumbent on us to continue to evaluate surgical treatments generating the highest levels of evidence possible (randomized trials) and have sufficient humility to cross refer to colleagues when appropriate to ensure the best care for our patients,” Dr. Lim concluded.
Because the McMaster University study derived the reported outcomes from registry data, determining the reasons that influenced surgeons’ choices of lung resection is impossible, Dr. Eric Lim of the Imperial College of Medicine, London, said in his invited commentary (J Thorac Cardiovasc Surg. 2015 May 21 [doi:10.1016/j.jtcvs.2015.05.048]).
The study authors noted that lower-volume surgeons were more inclined to perform pneumonectomy, and, Dr. Lim noted, previous studies have found that higher-volume centers tended to see more patients with advanced-stage cancers and increased morbidities. “An alternative explanation is that higher-volume surgeons have better skill sets to undertake procedures such as sleeve lobectomies that would lower the pneumonectomy rates and possibly more segmentectomies to lower the wedge-resection rate,” Dr. Lim said.
Until better evidence exists on what procedure is best for central and peripheral tumors, “surgeons can argue either way,” Dr. Lim said. The questions that follow from the study should concentrate on the relative harm of each procedure and the level of practice variation that’s unacceptable.
“As a surgical community, it is incumbent on us to continue to evaluate surgical treatments generating the highest levels of evidence possible (randomized trials) and have sufficient humility to cross refer to colleagues when appropriate to ensure the best care for our patients,” Dr. Lim concluded.
A surgeon’s comfort level with a favored operation for non–small cell lung cancer can strongly influence whether the patient will have that operation, which, in turn, can affect the patient’s outcome and long-term survival, according to an analysis of a population-linked database. For patients whose surgeons have lower levels of experience, that could mean a greater chance they will have more invasive total lung removal rather than more difficult operations that spare part of the affected lung, according to investigators at McMaster University in Hamilton, Ontario.
“If a surgeon with high surgical volumes is less likely to perform higher-risk pneumonectomy procedures than one with lower volumes, this may translate to a significant reduction in adverse events,” said lead author Dr. Christian Finley and coauthors online in the Journal of Thoracic and Cardiovascular Surgery (2015 Jun 30 [doi: 10.1016/j.jtcvs.2015.04.060]). “Surgeon volume should be considered an important component in how care is delivered in this population.”
The McMaster investigators evaluated 8,070 patients in an Ontario population-based linked database who underwent surgical resection for non–small cell lung cancer during 2004-2011, including pneumonectomy, or total lung removal (842 patients), lobectomy (6,212 patients), and wedge resection (1,002 patients). Over the years of the study, the proportion of patients who underwent pneumonectomy fell by more than half, from 14.8% in 2004 to 7.6% in 2011.
Of the three procedures, pneumonectomy carries a threefold greater mortality and while the procedure is often avoidable, there may be cases where it’s necessary because of the location of the tumor, Dr. Finley and his colleagues said. Lobectomy is desirable because it spares the parenchyma and has lower recurrence rates than laser resections.
The study investigators aimed to explore the hypothesis that surgeons with less expertise are more inclined to perform the higher-risk pneumonectomy or sublobar resections such as a segmentectomy or a wedge resection than a lobectomy, the rationale being that these procedures can be less challenging than a standard or sleeve lobectomy. The study analyzed results from 124 different physicians at 45 institutions in Ontario.
Data analysis showed that physician volume, age, year of procedure, sex, and comorbidities were predictive of the surgeon performing a pneumonectomy. “Adjusting for these variables, the results indicated that for each 10-unit increase in physician volume, the relative risk of performing a pneumonectomy decreased by 9.1%,” Dr. Finley and his colleagues wrote. They also found no significant difference in stage distribution among low-, medium-, and high-volume surgeons.
“This is meaningful as pneumonectomy is known to have the highest mortality rate of lung cancer resection, found in this study to be 12.6%, demonstrating a potentially large impact on patient survival,” Dr. Finley and his colleagues said.
This analysis cites an earlier study that surgeon volume for many procedures was a key determinant in the link between hospital volume and operative mortality (N Engl J Med. 2003 Nov 27;349[2]:2117-27.). “This study suggests that a patient may improve their chance of survival substantially, even at high-volume institutions, by selecting surgeons who perform operations more frequently,” Dr. Finley and his colleagues said.
They said that despite their study’s limitations, the findings on how surgeon experience can influence the choice of lung resection for cancer warrant further study.
McMaster University, Division of Thoracic Surgery, provided funding for the study. The study authors had no disclosures.
A surgeon’s comfort level with a favored operation for non–small cell lung cancer can strongly influence whether the patient will have that operation, which, in turn, can affect the patient’s outcome and long-term survival, according to an analysis of a population-linked database. For patients whose surgeons have lower levels of experience, that could mean a greater chance they will have more invasive total lung removal rather than more difficult operations that spare part of the affected lung, according to investigators at McMaster University in Hamilton, Ontario.
“If a surgeon with high surgical volumes is less likely to perform higher-risk pneumonectomy procedures than one with lower volumes, this may translate to a significant reduction in adverse events,” said lead author Dr. Christian Finley and coauthors online in the Journal of Thoracic and Cardiovascular Surgery (2015 Jun 30 [doi: 10.1016/j.jtcvs.2015.04.060]). “Surgeon volume should be considered an important component in how care is delivered in this population.”
The McMaster investigators evaluated 8,070 patients in an Ontario population-based linked database who underwent surgical resection for non–small cell lung cancer during 2004-2011, including pneumonectomy, or total lung removal (842 patients), lobectomy (6,212 patients), and wedge resection (1,002 patients). Over the years of the study, the proportion of patients who underwent pneumonectomy fell by more than half, from 14.8% in 2004 to 7.6% in 2011.
Of the three procedures, pneumonectomy carries a threefold greater mortality and while the procedure is often avoidable, there may be cases where it’s necessary because of the location of the tumor, Dr. Finley and his colleagues said. Lobectomy is desirable because it spares the parenchyma and has lower recurrence rates than laser resections.
The study investigators aimed to explore the hypothesis that surgeons with less expertise are more inclined to perform the higher-risk pneumonectomy or sublobar resections such as a segmentectomy or a wedge resection than a lobectomy, the rationale being that these procedures can be less challenging than a standard or sleeve lobectomy. The study analyzed results from 124 different physicians at 45 institutions in Ontario.
Data analysis showed that physician volume, age, year of procedure, sex, and comorbidities were predictive of the surgeon performing a pneumonectomy. “Adjusting for these variables, the results indicated that for each 10-unit increase in physician volume, the relative risk of performing a pneumonectomy decreased by 9.1%,” Dr. Finley and his colleagues wrote. They also found no significant difference in stage distribution among low-, medium-, and high-volume surgeons.
“This is meaningful as pneumonectomy is known to have the highest mortality rate of lung cancer resection, found in this study to be 12.6%, demonstrating a potentially large impact on patient survival,” Dr. Finley and his colleagues said.
This analysis cites an earlier study that surgeon volume for many procedures was a key determinant in the link between hospital volume and operative mortality (N Engl J Med. 2003 Nov 27;349[2]:2117-27.). “This study suggests that a patient may improve their chance of survival substantially, even at high-volume institutions, by selecting surgeons who perform operations more frequently,” Dr. Finley and his colleagues said.
They said that despite their study’s limitations, the findings on how surgeon experience can influence the choice of lung resection for cancer warrant further study.
McMaster University, Division of Thoracic Surgery, provided funding for the study. The study authors had no disclosures.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: Surgeon volume is a predictor of procedure selection for lung cancer surgery and has implications on outcomes.
Major finding: For each 10 unit increase in physician volume, the relative risk of performing a pneumonectomy decreased by 9.1%.
Data source: Dataset of 8,070 patients constructed from Ontario population-based linked databases accessed via the Institute for Clinical Evaluate Sciences.
Disclosures: McMaster University, Division of Thoracic Surgery, provided study funding. The authors had no disclosures.
How patient-reported outcomes may alter care
As Medicare and commercial payers rely increasingly on quality outcomes to determine reimbursement levels, clinicians focused on traditional clinical outcomes like length of hospital stay and readmission may be missing the point if they don’t take into consideration more patient-centric outcome. A team of investigators at MD Anderson Cancer Center in Houston recently evaluated that institution’s tool for measuring patient-reported outcomes in tracking results after thoracic surgery for lung cancer.
Christopher P. Fagundes, Ph.D., led the research team that reported their findings in the September issue of the Journal of Thoracic and Cardiovascular Surgery (2015 [doi:10.1016/j.jtcvs.2015.05.057]).
“We used the MD Anderson Symptom Inventory (MDASI) to elicit patient reports of the worst symptoms experienced after thoracic surgery,” Dr. Fagundes and his colleagues said in what may be the first study to use patient-reported outcomes to chart a recovery course after surgery. “This study demonstrates that the MDASI is a sensitive tool for detecting symptomatic recovery with an expected relationship among surgery type, preoperative performance status, and comorbid conditions,” the authors stated.
The MDASI measures the severity of 13 common cancer-related symptoms over the previous 24 hours and rates each on a scale from 0-10, with 10 as most severe. Patients in the study completed a written MDASI questionnaire, 60 upon enrollment, and 77 patients 3 and 5 days after surgery in the hospital. After discharge and for 3 months after surgery, patients received weekly calls from a computer/telephone interactive voice-response system that asked them to rate their symptoms.
All patients were newly diagnosed and treatment naive with early-stage non–small cell lung cancer (NSCLC) who had either standard open thoracotomy or video-assisted thoracoscopic surgery (VATS) lobectomy.
The investigators used a two-pronged approach to define recovery after surgery: symptoms returning to their baseline levels or to a mild level of severity. In the first week after surgery, pain, fatigue, and shortness of breath were “highly prevalent,” perhaps a combined effect from surgical insult and care during and after surgery. After a month, ratings for most symptoms returned to baseline, but fatigue remained the most-persistent symptom during the 3-month study.
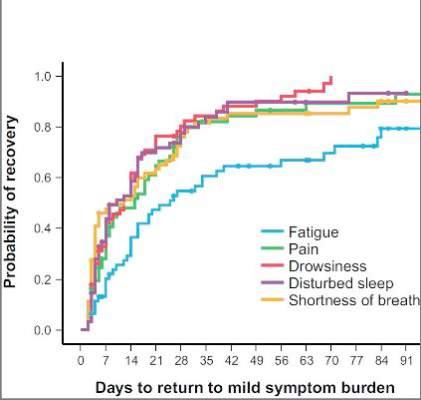
NSCLC patients typically have a host of symptoms after major surgery, including inflammation, organ stress, and reaction to medications. In addition, up to a quarter have postsurgical complications that can amplify their symptoms and even delay their course of cancer treatment. The five most-severe postoperative symptoms patients in the study reported were fatigue, pain, shortness of breath, disturbed sleep, and drowsiness.
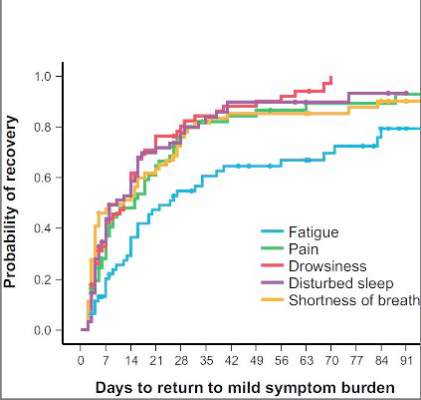
The median time to return to mild symptom severity for these five symptoms was shorter than return to baseline severity, with fatigue taking longer. Pain recovered significantly faster for patients who underwent VATS lobectomy vs. standard open thoracotomy (8 vs. 18 days, respectively; P = .022), according to the researchers. In addition, the researchers found that patients who had poor preoperative performance status or comorbidities reported significantly higher postoperative pain (P less than .05).
Having the ability to measure patient-reported outcomes allows physicians to identify patients at greatest risk for symptoms after surgery and to help caregivers develop pathways to speed up recovery and get patients to chemotherapy or other cancer treatments on schedule, Dr. Fagundes and his coauthors said.
“Using a straightforward, concise tool like the MDASI to obtain the patient’s perspective on how well he or she is recovering is a clinically relevant and user-friendly method for optimizing perioperative care,” the authors added.
Minimally invasive surgical techniques along with opioid-sparing analgesia have been incorporated into enhanced recovery programs to aim for better objective postoperative outcomes like fewer complications and shorter hospital stays. “Missing from these metrics is the voice of the patient, who is arguably the best source of information about what ‘recovery’ from surgery means,” Dr. Fagundes and colleagues said. “Lack of research on how to define and measure symptomatic and functional recovery after major cancer surgery from the patent’s perspective is an important gap in comprehensive postoperative care; it also compromises any comparison of ERP [enhanced recovery program] innovations against standard care.”
Study coauthors received funding from the National Cancer Institute of the National Institutes of Health, the MD Anderson Cancer Center Support Grant program and the American Cancer Society Research Scholar Grant program. The coauthors reported no conflicts of interest in this work.
“Whether ‘subjective’ or not, the measurements of five common postoperative symptoms appear to reflect the real world experience of many,” Dr. Robert B. Cameron of the University of California, Los Angeles, said in his invited commentary (J. Thorac. Cardiovasc. Surg. 2015 [doi: 10.1016/j.jtcvs.2015.06.017]).
What’s more, because the study investigators collected patient data after discharge, they eliminated opportunities to “game the system,” in Dr. Cameron’s words. One example of gaming the outcome measures would be to discharge patients early after surgery with a Heimlich chest tube, subjecting them to problems at home and requiring physicians visits and even emergency department care that can go unrecorded.
“Subjective” patient experiences are “real issues,” Dr. Cameron said. “After all, patients are the customers that the health care system serves.”
Patient-reported outcome measures could dramatically influence how physicians and health systems report patient outcomes. “While length of stay (LOS) and hospital complication rates appear to be valid outcome measures to report, in reality, they are outcomes only in a world when hospitals are the ‘customers,’ ” Dr. Cameron said. “In a patient-centric system, when patient outcomes matter, [patient-reported outcomes], such as those proposed by the MD Anderson investigators, are what truly matter.”
“Whether ‘subjective’ or not, the measurements of five common postoperative symptoms appear to reflect the real world experience of many,” Dr. Robert B. Cameron of the University of California, Los Angeles, said in his invited commentary (J. Thorac. Cardiovasc. Surg. 2015 [doi: 10.1016/j.jtcvs.2015.06.017]).
What’s more, because the study investigators collected patient data after discharge, they eliminated opportunities to “game the system,” in Dr. Cameron’s words. One example of gaming the outcome measures would be to discharge patients early after surgery with a Heimlich chest tube, subjecting them to problems at home and requiring physicians visits and even emergency department care that can go unrecorded.
“Subjective” patient experiences are “real issues,” Dr. Cameron said. “After all, patients are the customers that the health care system serves.”
Patient-reported outcome measures could dramatically influence how physicians and health systems report patient outcomes. “While length of stay (LOS) and hospital complication rates appear to be valid outcome measures to report, in reality, they are outcomes only in a world when hospitals are the ‘customers,’ ” Dr. Cameron said. “In a patient-centric system, when patient outcomes matter, [patient-reported outcomes], such as those proposed by the MD Anderson investigators, are what truly matter.”
“Whether ‘subjective’ or not, the measurements of five common postoperative symptoms appear to reflect the real world experience of many,” Dr. Robert B. Cameron of the University of California, Los Angeles, said in his invited commentary (J. Thorac. Cardiovasc. Surg. 2015 [doi: 10.1016/j.jtcvs.2015.06.017]).
What’s more, because the study investigators collected patient data after discharge, they eliminated opportunities to “game the system,” in Dr. Cameron’s words. One example of gaming the outcome measures would be to discharge patients early after surgery with a Heimlich chest tube, subjecting them to problems at home and requiring physicians visits and even emergency department care that can go unrecorded.
“Subjective” patient experiences are “real issues,” Dr. Cameron said. “After all, patients are the customers that the health care system serves.”
Patient-reported outcome measures could dramatically influence how physicians and health systems report patient outcomes. “While length of stay (LOS) and hospital complication rates appear to be valid outcome measures to report, in reality, they are outcomes only in a world when hospitals are the ‘customers,’ ” Dr. Cameron said. “In a patient-centric system, when patient outcomes matter, [patient-reported outcomes], such as those proposed by the MD Anderson investigators, are what truly matter.”
As Medicare and commercial payers rely increasingly on quality outcomes to determine reimbursement levels, clinicians focused on traditional clinical outcomes like length of hospital stay and readmission may be missing the point if they don’t take into consideration more patient-centric outcome. A team of investigators at MD Anderson Cancer Center in Houston recently evaluated that institution’s tool for measuring patient-reported outcomes in tracking results after thoracic surgery for lung cancer.
Christopher P. Fagundes, Ph.D., led the research team that reported their findings in the September issue of the Journal of Thoracic and Cardiovascular Surgery (2015 [doi:10.1016/j.jtcvs.2015.05.057]).
“We used the MD Anderson Symptom Inventory (MDASI) to elicit patient reports of the worst symptoms experienced after thoracic surgery,” Dr. Fagundes and his colleagues said in what may be the first study to use patient-reported outcomes to chart a recovery course after surgery. “This study demonstrates that the MDASI is a sensitive tool for detecting symptomatic recovery with an expected relationship among surgery type, preoperative performance status, and comorbid conditions,” the authors stated.
The MDASI measures the severity of 13 common cancer-related symptoms over the previous 24 hours and rates each on a scale from 0-10, with 10 as most severe. Patients in the study completed a written MDASI questionnaire, 60 upon enrollment, and 77 patients 3 and 5 days after surgery in the hospital. After discharge and for 3 months after surgery, patients received weekly calls from a computer/telephone interactive voice-response system that asked them to rate their symptoms.
All patients were newly diagnosed and treatment naive with early-stage non–small cell lung cancer (NSCLC) who had either standard open thoracotomy or video-assisted thoracoscopic surgery (VATS) lobectomy.
The investigators used a two-pronged approach to define recovery after surgery: symptoms returning to their baseline levels or to a mild level of severity. In the first week after surgery, pain, fatigue, and shortness of breath were “highly prevalent,” perhaps a combined effect from surgical insult and care during and after surgery. After a month, ratings for most symptoms returned to baseline, but fatigue remained the most-persistent symptom during the 3-month study.
NSCLC patients typically have a host of symptoms after major surgery, including inflammation, organ stress, and reaction to medications. In addition, up to a quarter have postsurgical complications that can amplify their symptoms and even delay their course of cancer treatment. The five most-severe postoperative symptoms patients in the study reported were fatigue, pain, shortness of breath, disturbed sleep, and drowsiness.
The median time to return to mild symptom severity for these five symptoms was shorter than return to baseline severity, with fatigue taking longer. Pain recovered significantly faster for patients who underwent VATS lobectomy vs. standard open thoracotomy (8 vs. 18 days, respectively; P = .022), according to the researchers. In addition, the researchers found that patients who had poor preoperative performance status or comorbidities reported significantly higher postoperative pain (P less than .05).
Having the ability to measure patient-reported outcomes allows physicians to identify patients at greatest risk for symptoms after surgery and to help caregivers develop pathways to speed up recovery and get patients to chemotherapy or other cancer treatments on schedule, Dr. Fagundes and his coauthors said.
“Using a straightforward, concise tool like the MDASI to obtain the patient’s perspective on how well he or she is recovering is a clinically relevant and user-friendly method for optimizing perioperative care,” the authors added.
Minimally invasive surgical techniques along with opioid-sparing analgesia have been incorporated into enhanced recovery programs to aim for better objective postoperative outcomes like fewer complications and shorter hospital stays. “Missing from these metrics is the voice of the patient, who is arguably the best source of information about what ‘recovery’ from surgery means,” Dr. Fagundes and colleagues said. “Lack of research on how to define and measure symptomatic and functional recovery after major cancer surgery from the patent’s perspective is an important gap in comprehensive postoperative care; it also compromises any comparison of ERP [enhanced recovery program] innovations against standard care.”
Study coauthors received funding from the National Cancer Institute of the National Institutes of Health, the MD Anderson Cancer Center Support Grant program and the American Cancer Society Research Scholar Grant program. The coauthors reported no conflicts of interest in this work.
As Medicare and commercial payers rely increasingly on quality outcomes to determine reimbursement levels, clinicians focused on traditional clinical outcomes like length of hospital stay and readmission may be missing the point if they don’t take into consideration more patient-centric outcome. A team of investigators at MD Anderson Cancer Center in Houston recently evaluated that institution’s tool for measuring patient-reported outcomes in tracking results after thoracic surgery for lung cancer.
Christopher P. Fagundes, Ph.D., led the research team that reported their findings in the September issue of the Journal of Thoracic and Cardiovascular Surgery (2015 [doi:10.1016/j.jtcvs.2015.05.057]).
“We used the MD Anderson Symptom Inventory (MDASI) to elicit patient reports of the worst symptoms experienced after thoracic surgery,” Dr. Fagundes and his colleagues said in what may be the first study to use patient-reported outcomes to chart a recovery course after surgery. “This study demonstrates that the MDASI is a sensitive tool for detecting symptomatic recovery with an expected relationship among surgery type, preoperative performance status, and comorbid conditions,” the authors stated.
The MDASI measures the severity of 13 common cancer-related symptoms over the previous 24 hours and rates each on a scale from 0-10, with 10 as most severe. Patients in the study completed a written MDASI questionnaire, 60 upon enrollment, and 77 patients 3 and 5 days after surgery in the hospital. After discharge and for 3 months after surgery, patients received weekly calls from a computer/telephone interactive voice-response system that asked them to rate their symptoms.
All patients were newly diagnosed and treatment naive with early-stage non–small cell lung cancer (NSCLC) who had either standard open thoracotomy or video-assisted thoracoscopic surgery (VATS) lobectomy.
The investigators used a two-pronged approach to define recovery after surgery: symptoms returning to their baseline levels or to a mild level of severity. In the first week after surgery, pain, fatigue, and shortness of breath were “highly prevalent,” perhaps a combined effect from surgical insult and care during and after surgery. After a month, ratings for most symptoms returned to baseline, but fatigue remained the most-persistent symptom during the 3-month study.
NSCLC patients typically have a host of symptoms after major surgery, including inflammation, organ stress, and reaction to medications. In addition, up to a quarter have postsurgical complications that can amplify their symptoms and even delay their course of cancer treatment. The five most-severe postoperative symptoms patients in the study reported were fatigue, pain, shortness of breath, disturbed sleep, and drowsiness.
The median time to return to mild symptom severity for these five symptoms was shorter than return to baseline severity, with fatigue taking longer. Pain recovered significantly faster for patients who underwent VATS lobectomy vs. standard open thoracotomy (8 vs. 18 days, respectively; P = .022), according to the researchers. In addition, the researchers found that patients who had poor preoperative performance status or comorbidities reported significantly higher postoperative pain (P less than .05).
Having the ability to measure patient-reported outcomes allows physicians to identify patients at greatest risk for symptoms after surgery and to help caregivers develop pathways to speed up recovery and get patients to chemotherapy or other cancer treatments on schedule, Dr. Fagundes and his coauthors said.
“Using a straightforward, concise tool like the MDASI to obtain the patient’s perspective on how well he or she is recovering is a clinically relevant and user-friendly method for optimizing perioperative care,” the authors added.
Minimally invasive surgical techniques along with opioid-sparing analgesia have been incorporated into enhanced recovery programs to aim for better objective postoperative outcomes like fewer complications and shorter hospital stays. “Missing from these metrics is the voice of the patient, who is arguably the best source of information about what ‘recovery’ from surgery means,” Dr. Fagundes and colleagues said. “Lack of research on how to define and measure symptomatic and functional recovery after major cancer surgery from the patent’s perspective is an important gap in comprehensive postoperative care; it also compromises any comparison of ERP [enhanced recovery program] innovations against standard care.”
Study coauthors received funding from the National Cancer Institute of the National Institutes of Health, the MD Anderson Cancer Center Support Grant program and the American Cancer Society Research Scholar Grant program. The coauthors reported no conflicts of interest in this work.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: Using the MD Anderson Symptom Inventory to elicit patient-reported symptom burden is a simple, clinically relevant way to optimize care after thoracic surgery for lung cancer.
Major finding: Assessing symptoms from the patient’s perspective throughout the postoperative recovery period is an effective strategy for evaluating perioperative care.
Data source: Sixty newly diagnosed patients with early-stage non–small cell lung cancer scheduled for thoracic surgery prospectively were recruited for evaluation.
Disclosures: Study coauthors received funding from the National Cancer Institute of the National Institutes of Health, the MD Anderson Cancer Center Support Grant program, and the American Cancer Society Research Scholar Grant program. The coauthors reported no conflicts of interest in this work.
CTS Innovation: The promise of tissue engineering for heart valve replacement and repair
Bioengineered tissues are showing promise in the treatment of valvular heart disease, according to the results of several early clinical and preclinical studies demonstrating the benefits of using heterologous substrates as scaffolding capable of promoting in vivo cell infiltration and remodeling.
Ultimately, cardiac tissue engineering seeks to develop the ideal material for replacement and repair of a variety of heart components – a material able to integrate, function, and, when necessary, grow and develop in a manner undifferentiated from normal cellular structures.
One of the most important areas of focus for such efforts is the development of heart valves and valve patches suitable for use in replacement or repair. The need is obvious: “The fact that literature continues to be published debating the best type of valve prosthesis is proof that, to date, the ideal valve substitute has not been found,” according to Cristian Rosu, Ph.D. and Dr. Edward G. Soltesz of the Cleveland Clinic (Semin Thorac Cardiovasc Surg. 2015 June 30 [doi: 10.1053/j.semtcvs.2015.06.007]).
Dr. Roşu and Dr. Soltesz go on to say that this lack of an ideal prosthetic heart valve leaves surgeons and their patients with a difficult choice at the time of valve surgery. The focus of their concern relates to how current bioprostheses are being used in younger and younger patients, and how these devices have a finite lifespan – requiring eventual reoperation and replacement, perhaps multiple times. In addition, calcification is a prominent and well-known risk of bioprosthetic valves, especially in children (Circulation. 2014 Jul 1;130[1]:51-60).
As for mechanical valves, although durable, they require a lifetime of anticoagulation therapy to prevent thrombosis. And the lack of growth potential found in both mechanical and current bioprosthetic devices is obviously a bane to pediatric valve therapy.
The latest efforts in tissue engineering therefore seek to develop valves and valve components that may be more permanent solutions by better mimicking natural valves.
But better mimicking of a natural valve is not an easy task, when such valves exist in “a near-perfect correlation of structure and function, enabling the valve to avoid excess stress on the cusps while simultaneously withstanding the wear and tear of 40-million repetitive deformations per year, equivalent to some 3 billion over a 75-year lifetime.” (“Principles of Tissue Engineering,” 4th ed. [London: Academic Press 2014, p. 813]).
The “holy grail” of tissue engineering, therefore, is to provide a completely in vitro–developed, autologous, fully cellularized, functional scaffolding for implantation that can live up to these requirements. In order to do this, extensive research into the search for the best cell sources and growth matrices and methods is underway, as illustrated by several recent reviews (Front Cell Dev Biol. 30 June 2015 [doi.org/10.3389/fcell.2015.00039] and Mater Sci Eng C. 2015 March 1;48:556-65).
Candidate cell types include a variety of embryonic stem cells, as well as adult cell types that have proven amenable to rejuvenation and redifferentiation (Adv Drug Deliv Rev. 2014;69-70:254-69).
In one example of the quest for completely in vitro human-tissue designed valves, Dr. Jean Dubé of Laval University, Quebec, and his colleagues reported research on a human tissue–engineered trileaflet heart valve assembled in vitro using human fibroblasts. These cells self-assembled into living tissue sheets when cultured in the presence of sodium ascorbate. These sheets could be layered together to create a thick construct, with the ultimate goal of replacing the use of bovine pericardium tissue implants with ones made of autologous cells from the patient (Acta Biomater. 2014 Aug;10[8]:3563-70).
Currently, however, many of the preclinical studies of fully tissue engineered heart valves have shown retraction of the heart valve leaflets as a major mechanism of functional failure. This retraction is caused by both passive and active cell stress and passive matrix stress, according to a review by Inge A.E.W. van Loosdregt, Ph.D., and her colleagues at the Eindhoven (the Netherlands) University of Technology (J Biomech. 2014 Jun 27;47[9]:2064-9).
While all of these developmental issues regarding the use of fully tissue-engineered valves are being worked out, early clinical applications are already being found for a new generation of valve prostheses that take an intermediate approach, one that uses an implanted scaffolding material that allows autologous cell infiltration and replacement in vivo.
Two of the most prominent examples of these scaffoldings currently in investigation and in early clinical use for heart valve repair or replacement are the bovine pericardium-derived CardioCel (Admedus, Brisbane, Australia) and the porcine intestinal submucosa-derived CorMatrix ECM(CorMatrix Cardiovascular, Roswell, Ga.). CorMatrix ECM was approved by the Food and Drug Administration in 2005 for pericardial repair and reconstruction, and in 2007 for cardiac tissue repair. The FDA approved CardioCel in 2014 for use in the United States in pericardial closure and for the repair of cardiac and vascular defects in both adults and children.
Both technologies rely on the concept of matrix infiltration by autologous cells after implantation in order to create a living mimic of the patient’s own tissues.
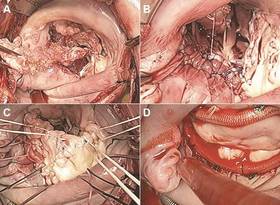
CardioCel is a highly treated, bovine pericardium-derived, decellularized collagen matrix. It showed significant resistance to calcification in mitral and pulmonary implants in a juvenile sheep model as reported by Dr. Christian P. Brizard at Royal Children’s Hospital, Melbourne, and his colleagues (J Thorac Cardiovasc Surg. 2014 Dec;148[6]:3194-201). These investigators replaced the posterior leaflet of the mitral valve and one of the pulmonary valve cusps with patches in 10-month-old ewes. They compared the use of CardioCel in six ewes to a control group of four ewes repaired with autologous pericardium that was treated intraoperatively with glutaraldehyde, which is the standard default used at their institution for more than 2 decades as the best material for valve repair in their pediatric patients.

The primary end points of the study were thickening and calcium content. They found that all animals survived with normal valve echocardiography until sacrifice at 7 months. They reported that the bovine pericardium patches allowed accurate valve repair at both systemic and pulmonary pressure with preserved mechanical properties and more-controlled healing and without calcification as compared with the controls. (Calcification is a known major risk factor for the eventual failure of bioprosthetic valves.) Additionally, the bovine pericardium patched valves showed the in vivo development of dense but thin cellularized outer layers of mature collagen I, compared with the controls, which had outer layers that were much less dense and showed the presence of immature collagen III.
In another case of valvular use of the CardioCel material, at the recent American Association for Thoracic Surgery Mitral Conclave 2015, M. Bonnie Ghosh-Dastidar, Ph.D., and her colleagues from the Royal Brompton Hospital, London, reported on a severely ill patient with significant mitral regurgitation and an infected mitral valve with large vegetations on the anterior leaflets. The infected tissue was resected and a large patch of CardioCel bovine pericardium was used to reconstruct the leaflets. Postoperative assessment showed a competent mitral valve with good area of leaflet coaptation, according to Dr. Ghosh-Dastidar.
In his invited commentary on the animal-model research by Dr. Brizard, Dr. Niv Ad, director of cardiac surgery research at Inova Heart and Vascular Institute, Falls Church, Va., said that despite the promise of the CardioCel patches, there were a number of alternative approaches being investigated. “Other engineered materials currently being study include processes such as lyophilization, which has shown promising results in reducing inflammation. Another proposed approach is the use of decellularized vessels and patches with the promise of normal remodeling and growth, such as extracellular matrix and its potential for tissue regeneration.”
Dr. Ad also stated that, “the key bioengineering challenge is to determine how biologic, structural, and mechanical factors interact and function in vivo. The understanding of these factors will prove critical to the development of a clinically viable tissue-engineered heart valve,” (J Thorac Cardiovasc Surg. 2014 Dec;148[6]:3202-3).
An example of the use of extracellular matrix material referred to by Dr. Ad is the CorMatrix ECM, which is an extracellular matrix material derived from porcine small-intestinal submucosa, processed and decellularized.
Dr. Marc W. Gerdisch and his colleagues from the Franciscan St. Francis Heart Center, Indianapolis, reported on the results of treating 19 patients with mitral valve disease using the CorMatrix patch material for partial or subtotal leaflet repair or extension. There were three deaths unrelated to the repair and no instances of perioperative or late stroke. Two patients with a history of cancer and cancer therapy experienced failure of the initial repair, requiring reintervention. However, the other mitral valve repair patients continued to show good valvular function and no calcification on echocardiographic follow-up of 4 days to 48 months (Thorac Cardiovasc Surg. 2014 Oct;148[4]:1370-8).
And in 2015, CorMatrix Cardiovascular announced FDA approval of an investigational device exemption for an early feasibility study of their CorMatrix ECM Tricuspid Heart Valve in up to 15 patients at 5 U.S. centers (NCT02397668). Indications are for the surgical management of tricuspid valve disease not amenable to annuloplasty or repair, including tricuspid valve disease secondary to congenital heart disease in pediatric patients and adult endocarditis patients. The CorMatrix ECM Tricuspid Valve is a flexible, unstented valve acting as a 3‐D scaffold designed to function immediately as a prosthetic, but one constructed to permit native cellular infiltration and remodeling.
Ultimately, both the CardioCel and the CorMatrix materials are just the tip of an iceberg of research into tissue engineering as a clinical tool. And success and the wider adoption of any current or developing technologies will require the results of far-more-extensive studies and long-term clinical results.
At some future date, engineered total organ substitutes or the routine injection of genetically engineered stem cells may provide a practical alternative for treating a diseased or damaged heart. But for now, the most-likely scenario is the continued exploration of tissue engineering to develop the most durable, growth-, stress-, and biologically compatible patches, valves, and vasculatures possible – defined tools that can be adapted to current surgical techniques, designed to obtain the best repair of congenital or acquired heart disease conditions.
As with any transformative technology in medicine, the path from laboratory success and optimistic short-term clinical results to durable, long-term postoperative benefits may be a rocky one. But given the current enthusiasm, it certainly looks as if it will be a well-traveled road.
Dr. Brizard reported consulting and lecturing fees from Admedus. His research was supported with the assistance of a grant from Admedus. Dr. Gerdisch reported consulting fees and equity ownership in CorMatrix Cardiovascular.
Bioengineered tissues are showing promise in the treatment of valvular heart disease, according to the results of several early clinical and preclinical studies demonstrating the benefits of using heterologous substrates as scaffolding capable of promoting in vivo cell infiltration and remodeling.
Ultimately, cardiac tissue engineering seeks to develop the ideal material for replacement and repair of a variety of heart components – a material able to integrate, function, and, when necessary, grow and develop in a manner undifferentiated from normal cellular structures.
One of the most important areas of focus for such efforts is the development of heart valves and valve patches suitable for use in replacement or repair. The need is obvious: “The fact that literature continues to be published debating the best type of valve prosthesis is proof that, to date, the ideal valve substitute has not been found,” according to Cristian Rosu, Ph.D. and Dr. Edward G. Soltesz of the Cleveland Clinic (Semin Thorac Cardiovasc Surg. 2015 June 30 [doi: 10.1053/j.semtcvs.2015.06.007]).
Dr. Roşu and Dr. Soltesz go on to say that this lack of an ideal prosthetic heart valve leaves surgeons and their patients with a difficult choice at the time of valve surgery. The focus of their concern relates to how current bioprostheses are being used in younger and younger patients, and how these devices have a finite lifespan – requiring eventual reoperation and replacement, perhaps multiple times. In addition, calcification is a prominent and well-known risk of bioprosthetic valves, especially in children (Circulation. 2014 Jul 1;130[1]:51-60).
As for mechanical valves, although durable, they require a lifetime of anticoagulation therapy to prevent thrombosis. And the lack of growth potential found in both mechanical and current bioprosthetic devices is obviously a bane to pediatric valve therapy.
The latest efforts in tissue engineering therefore seek to develop valves and valve components that may be more permanent solutions by better mimicking natural valves.
But better mimicking of a natural valve is not an easy task, when such valves exist in “a near-perfect correlation of structure and function, enabling the valve to avoid excess stress on the cusps while simultaneously withstanding the wear and tear of 40-million repetitive deformations per year, equivalent to some 3 billion over a 75-year lifetime.” (“Principles of Tissue Engineering,” 4th ed. [London: Academic Press 2014, p. 813]).
The “holy grail” of tissue engineering, therefore, is to provide a completely in vitro–developed, autologous, fully cellularized, functional scaffolding for implantation that can live up to these requirements. In order to do this, extensive research into the search for the best cell sources and growth matrices and methods is underway, as illustrated by several recent reviews (Front Cell Dev Biol. 30 June 2015 [doi.org/10.3389/fcell.2015.00039] and Mater Sci Eng C. 2015 March 1;48:556-65).
Candidate cell types include a variety of embryonic stem cells, as well as adult cell types that have proven amenable to rejuvenation and redifferentiation (Adv Drug Deliv Rev. 2014;69-70:254-69).
In one example of the quest for completely in vitro human-tissue designed valves, Dr. Jean Dubé of Laval University, Quebec, and his colleagues reported research on a human tissue–engineered trileaflet heart valve assembled in vitro using human fibroblasts. These cells self-assembled into living tissue sheets when cultured in the presence of sodium ascorbate. These sheets could be layered together to create a thick construct, with the ultimate goal of replacing the use of bovine pericardium tissue implants with ones made of autologous cells from the patient (Acta Biomater. 2014 Aug;10[8]:3563-70).
Currently, however, many of the preclinical studies of fully tissue engineered heart valves have shown retraction of the heart valve leaflets as a major mechanism of functional failure. This retraction is caused by both passive and active cell stress and passive matrix stress, according to a review by Inge A.E.W. van Loosdregt, Ph.D., and her colleagues at the Eindhoven (the Netherlands) University of Technology (J Biomech. 2014 Jun 27;47[9]:2064-9).
While all of these developmental issues regarding the use of fully tissue-engineered valves are being worked out, early clinical applications are already being found for a new generation of valve prostheses that take an intermediate approach, one that uses an implanted scaffolding material that allows autologous cell infiltration and replacement in vivo.
Two of the most prominent examples of these scaffoldings currently in investigation and in early clinical use for heart valve repair or replacement are the bovine pericardium-derived CardioCel (Admedus, Brisbane, Australia) and the porcine intestinal submucosa-derived CorMatrix ECM(CorMatrix Cardiovascular, Roswell, Ga.). CorMatrix ECM was approved by the Food and Drug Administration in 2005 for pericardial repair and reconstruction, and in 2007 for cardiac tissue repair. The FDA approved CardioCel in 2014 for use in the United States in pericardial closure and for the repair of cardiac and vascular defects in both adults and children.
Both technologies rely on the concept of matrix infiltration by autologous cells after implantation in order to create a living mimic of the patient’s own tissues.
CardioCel is a highly treated, bovine pericardium-derived, decellularized collagen matrix. It showed significant resistance to calcification in mitral and pulmonary implants in a juvenile sheep model as reported by Dr. Christian P. Brizard at Royal Children’s Hospital, Melbourne, and his colleagues (J Thorac Cardiovasc Surg. 2014 Dec;148[6]:3194-201). These investigators replaced the posterior leaflet of the mitral valve and one of the pulmonary valve cusps with patches in 10-month-old ewes. They compared the use of CardioCel in six ewes to a control group of four ewes repaired with autologous pericardium that was treated intraoperatively with glutaraldehyde, which is the standard default used at their institution for more than 2 decades as the best material for valve repair in their pediatric patients.
The primary end points of the study were thickening and calcium content. They found that all animals survived with normal valve echocardiography until sacrifice at 7 months. They reported that the bovine pericardium patches allowed accurate valve repair at both systemic and pulmonary pressure with preserved mechanical properties and more-controlled healing and without calcification as compared with the controls. (Calcification is a known major risk factor for the eventual failure of bioprosthetic valves.) Additionally, the bovine pericardium patched valves showed the in vivo development of dense but thin cellularized outer layers of mature collagen I, compared with the controls, which had outer layers that were much less dense and showed the presence of immature collagen III.
In another case of valvular use of the CardioCel material, at the recent American Association for Thoracic Surgery Mitral Conclave 2015, M. Bonnie Ghosh-Dastidar, Ph.D., and her colleagues from the Royal Brompton Hospital, London, reported on a severely ill patient with significant mitral regurgitation and an infected mitral valve with large vegetations on the anterior leaflets. The infected tissue was resected and a large patch of CardioCel bovine pericardium was used to reconstruct the leaflets. Postoperative assessment showed a competent mitral valve with good area of leaflet coaptation, according to Dr. Ghosh-Dastidar.
In his invited commentary on the animal-model research by Dr. Brizard, Dr. Niv Ad, director of cardiac surgery research at Inova Heart and Vascular Institute, Falls Church, Va., said that despite the promise of the CardioCel patches, there were a number of alternative approaches being investigated. “Other engineered materials currently being study include processes such as lyophilization, which has shown promising results in reducing inflammation. Another proposed approach is the use of decellularized vessels and patches with the promise of normal remodeling and growth, such as extracellular matrix and its potential for tissue regeneration.”
Dr. Ad also stated that, “the key bioengineering challenge is to determine how biologic, structural, and mechanical factors interact and function in vivo. The understanding of these factors will prove critical to the development of a clinically viable tissue-engineered heart valve,” (J Thorac Cardiovasc Surg. 2014 Dec;148[6]:3202-3).
An example of the use of extracellular matrix material referred to by Dr. Ad is the CorMatrix ECM, which is an extracellular matrix material derived from porcine small-intestinal submucosa, processed and decellularized.
Dr. Marc W. Gerdisch and his colleagues from the Franciscan St. Francis Heart Center, Indianapolis, reported on the results of treating 19 patients with mitral valve disease using the CorMatrix patch material for partial or subtotal leaflet repair or extension. There were three deaths unrelated to the repair and no instances of perioperative or late stroke. Two patients with a history of cancer and cancer therapy experienced failure of the initial repair, requiring reintervention. However, the other mitral valve repair patients continued to show good valvular function and no calcification on echocardiographic follow-up of 4 days to 48 months (Thorac Cardiovasc Surg. 2014 Oct;148[4]:1370-8).
And in 2015, CorMatrix Cardiovascular announced FDA approval of an investigational device exemption for an early feasibility study of their CorMatrix ECM Tricuspid Heart Valve in up to 15 patients at 5 U.S. centers (NCT02397668). Indications are for the surgical management of tricuspid valve disease not amenable to annuloplasty or repair, including tricuspid valve disease secondary to congenital heart disease in pediatric patients and adult endocarditis patients. The CorMatrix ECM Tricuspid Valve is a flexible, unstented valve acting as a 3‐D scaffold designed to function immediately as a prosthetic, but one constructed to permit native cellular infiltration and remodeling.
Ultimately, both the CardioCel and the CorMatrix materials are just the tip of an iceberg of research into tissue engineering as a clinical tool. And success and the wider adoption of any current or developing technologies will require the results of far-more-extensive studies and long-term clinical results.
At some future date, engineered total organ substitutes or the routine injection of genetically engineered stem cells may provide a practical alternative for treating a diseased or damaged heart. But for now, the most-likely scenario is the continued exploration of tissue engineering to develop the most durable, growth-, stress-, and biologically compatible patches, valves, and vasculatures possible – defined tools that can be adapted to current surgical techniques, designed to obtain the best repair of congenital or acquired heart disease conditions.
As with any transformative technology in medicine, the path from laboratory success and optimistic short-term clinical results to durable, long-term postoperative benefits may be a rocky one. But given the current enthusiasm, it certainly looks as if it will be a well-traveled road.
Dr. Brizard reported consulting and lecturing fees from Admedus. His research was supported with the assistance of a grant from Admedus. Dr. Gerdisch reported consulting fees and equity ownership in CorMatrix Cardiovascular.
Bioengineered tissues are showing promise in the treatment of valvular heart disease, according to the results of several early clinical and preclinical studies demonstrating the benefits of using heterologous substrates as scaffolding capable of promoting in vivo cell infiltration and remodeling.
Ultimately, cardiac tissue engineering seeks to develop the ideal material for replacement and repair of a variety of heart components – a material able to integrate, function, and, when necessary, grow and develop in a manner undifferentiated from normal cellular structures.
One of the most important areas of focus for such efforts is the development of heart valves and valve patches suitable for use in replacement or repair. The need is obvious: “The fact that literature continues to be published debating the best type of valve prosthesis is proof that, to date, the ideal valve substitute has not been found,” according to Cristian Rosu, Ph.D. and Dr. Edward G. Soltesz of the Cleveland Clinic (Semin Thorac Cardiovasc Surg. 2015 June 30 [doi: 10.1053/j.semtcvs.2015.06.007]).
Dr. Roşu and Dr. Soltesz go on to say that this lack of an ideal prosthetic heart valve leaves surgeons and their patients with a difficult choice at the time of valve surgery. The focus of their concern relates to how current bioprostheses are being used in younger and younger patients, and how these devices have a finite lifespan – requiring eventual reoperation and replacement, perhaps multiple times. In addition, calcification is a prominent and well-known risk of bioprosthetic valves, especially in children (Circulation. 2014 Jul 1;130[1]:51-60).
As for mechanical valves, although durable, they require a lifetime of anticoagulation therapy to prevent thrombosis. And the lack of growth potential found in both mechanical and current bioprosthetic devices is obviously a bane to pediatric valve therapy.
The latest efforts in tissue engineering therefore seek to develop valves and valve components that may be more permanent solutions by better mimicking natural valves.
But better mimicking of a natural valve is not an easy task, when such valves exist in “a near-perfect correlation of structure and function, enabling the valve to avoid excess stress on the cusps while simultaneously withstanding the wear and tear of 40-million repetitive deformations per year, equivalent to some 3 billion over a 75-year lifetime.” (“Principles of Tissue Engineering,” 4th ed. [London: Academic Press 2014, p. 813]).
The “holy grail” of tissue engineering, therefore, is to provide a completely in vitro–developed, autologous, fully cellularized, functional scaffolding for implantation that can live up to these requirements. In order to do this, extensive research into the search for the best cell sources and growth matrices and methods is underway, as illustrated by several recent reviews (Front Cell Dev Biol. 30 June 2015 [doi.org/10.3389/fcell.2015.00039] and Mater Sci Eng C. 2015 March 1;48:556-65).
Candidate cell types include a variety of embryonic stem cells, as well as adult cell types that have proven amenable to rejuvenation and redifferentiation (Adv Drug Deliv Rev. 2014;69-70:254-69).
In one example of the quest for completely in vitro human-tissue designed valves, Dr. Jean Dubé of Laval University, Quebec, and his colleagues reported research on a human tissue–engineered trileaflet heart valve assembled in vitro using human fibroblasts. These cells self-assembled into living tissue sheets when cultured in the presence of sodium ascorbate. These sheets could be layered together to create a thick construct, with the ultimate goal of replacing the use of bovine pericardium tissue implants with ones made of autologous cells from the patient (Acta Biomater. 2014 Aug;10[8]:3563-70).
Currently, however, many of the preclinical studies of fully tissue engineered heart valves have shown retraction of the heart valve leaflets as a major mechanism of functional failure. This retraction is caused by both passive and active cell stress and passive matrix stress, according to a review by Inge A.E.W. van Loosdregt, Ph.D., and her colleagues at the Eindhoven (the Netherlands) University of Technology (J Biomech. 2014 Jun 27;47[9]:2064-9).
While all of these developmental issues regarding the use of fully tissue-engineered valves are being worked out, early clinical applications are already being found for a new generation of valve prostheses that take an intermediate approach, one that uses an implanted scaffolding material that allows autologous cell infiltration and replacement in vivo.
Two of the most prominent examples of these scaffoldings currently in investigation and in early clinical use for heart valve repair or replacement are the bovine pericardium-derived CardioCel (Admedus, Brisbane, Australia) and the porcine intestinal submucosa-derived CorMatrix ECM(CorMatrix Cardiovascular, Roswell, Ga.). CorMatrix ECM was approved by the Food and Drug Administration in 2005 for pericardial repair and reconstruction, and in 2007 for cardiac tissue repair. The FDA approved CardioCel in 2014 for use in the United States in pericardial closure and for the repair of cardiac and vascular defects in both adults and children.
Both technologies rely on the concept of matrix infiltration by autologous cells after implantation in order to create a living mimic of the patient’s own tissues.
CardioCel is a highly treated, bovine pericardium-derived, decellularized collagen matrix. It showed significant resistance to calcification in mitral and pulmonary implants in a juvenile sheep model as reported by Dr. Christian P. Brizard at Royal Children’s Hospital, Melbourne, and his colleagues (J Thorac Cardiovasc Surg. 2014 Dec;148[6]:3194-201). These investigators replaced the posterior leaflet of the mitral valve and one of the pulmonary valve cusps with patches in 10-month-old ewes. They compared the use of CardioCel in six ewes to a control group of four ewes repaired with autologous pericardium that was treated intraoperatively with glutaraldehyde, which is the standard default used at their institution for more than 2 decades as the best material for valve repair in their pediatric patients.
The primary end points of the study were thickening and calcium content. They found that all animals survived with normal valve echocardiography until sacrifice at 7 months. They reported that the bovine pericardium patches allowed accurate valve repair at both systemic and pulmonary pressure with preserved mechanical properties and more-controlled healing and without calcification as compared with the controls. (Calcification is a known major risk factor for the eventual failure of bioprosthetic valves.) Additionally, the bovine pericardium patched valves showed the in vivo development of dense but thin cellularized outer layers of mature collagen I, compared with the controls, which had outer layers that were much less dense and showed the presence of immature collagen III.
In another case of valvular use of the CardioCel material, at the recent American Association for Thoracic Surgery Mitral Conclave 2015, M. Bonnie Ghosh-Dastidar, Ph.D., and her colleagues from the Royal Brompton Hospital, London, reported on a severely ill patient with significant mitral regurgitation and an infected mitral valve with large vegetations on the anterior leaflets. The infected tissue was resected and a large patch of CardioCel bovine pericardium was used to reconstruct the leaflets. Postoperative assessment showed a competent mitral valve with good area of leaflet coaptation, according to Dr. Ghosh-Dastidar.
In his invited commentary on the animal-model research by Dr. Brizard, Dr. Niv Ad, director of cardiac surgery research at Inova Heart and Vascular Institute, Falls Church, Va., said that despite the promise of the CardioCel patches, there were a number of alternative approaches being investigated. “Other engineered materials currently being study include processes such as lyophilization, which has shown promising results in reducing inflammation. Another proposed approach is the use of decellularized vessels and patches with the promise of normal remodeling and growth, such as extracellular matrix and its potential for tissue regeneration.”
Dr. Ad also stated that, “the key bioengineering challenge is to determine how biologic, structural, and mechanical factors interact and function in vivo. The understanding of these factors will prove critical to the development of a clinically viable tissue-engineered heart valve,” (J Thorac Cardiovasc Surg. 2014 Dec;148[6]:3202-3).
An example of the use of extracellular matrix material referred to by Dr. Ad is the CorMatrix ECM, which is an extracellular matrix material derived from porcine small-intestinal submucosa, processed and decellularized.
Dr. Marc W. Gerdisch and his colleagues from the Franciscan St. Francis Heart Center, Indianapolis, reported on the results of treating 19 patients with mitral valve disease using the CorMatrix patch material for partial or subtotal leaflet repair or extension. There were three deaths unrelated to the repair and no instances of perioperative or late stroke. Two patients with a history of cancer and cancer therapy experienced failure of the initial repair, requiring reintervention. However, the other mitral valve repair patients continued to show good valvular function and no calcification on echocardiographic follow-up of 4 days to 48 months (Thorac Cardiovasc Surg. 2014 Oct;148[4]:1370-8).
And in 2015, CorMatrix Cardiovascular announced FDA approval of an investigational device exemption for an early feasibility study of their CorMatrix ECM Tricuspid Heart Valve in up to 15 patients at 5 U.S. centers (NCT02397668). Indications are for the surgical management of tricuspid valve disease not amenable to annuloplasty or repair, including tricuspid valve disease secondary to congenital heart disease in pediatric patients and adult endocarditis patients. The CorMatrix ECM Tricuspid Valve is a flexible, unstented valve acting as a 3‐D scaffold designed to function immediately as a prosthetic, but one constructed to permit native cellular infiltration and remodeling.
Ultimately, both the CardioCel and the CorMatrix materials are just the tip of an iceberg of research into tissue engineering as a clinical tool. And success and the wider adoption of any current or developing technologies will require the results of far-more-extensive studies and long-term clinical results.
At some future date, engineered total organ substitutes or the routine injection of genetically engineered stem cells may provide a practical alternative for treating a diseased or damaged heart. But for now, the most-likely scenario is the continued exploration of tissue engineering to develop the most durable, growth-, stress-, and biologically compatible patches, valves, and vasculatures possible – defined tools that can be adapted to current surgical techniques, designed to obtain the best repair of congenital or acquired heart disease conditions.
As with any transformative technology in medicine, the path from laboratory success and optimistic short-term clinical results to durable, long-term postoperative benefits may be a rocky one. But given the current enthusiasm, it certainly looks as if it will be a well-traveled road.
Dr. Brizard reported consulting and lecturing fees from Admedus. His research was supported with the assistance of a grant from Admedus. Dr. Gerdisch reported consulting fees and equity ownership in CorMatrix Cardiovascular.

More lawsuits against doctors? Overpayment ruling could be bad news
In a novel decision, the U.S. District Court for the Southern District of New York has ruled that the 60-day clock to return overpayments to the government begins ticking when a health provider receives notice a potential overpayment exists, not when an overpayment is conclusively ascertained.
Doctors should be concerned about the ruling, said Houston health law attorney Michael E. Clark, immediate past chair for the American Bar Association Health Law Section.

“This is a very troubling development because the judge has embraced the theory that certainty is not required as to what constitutes an identified overpayment,” Mr. Clark said in an interview. “Rather, knowledge can be established by recklessness under the facts. In short, practitioners must set up systems to alert them about potential overpayments so they can move quickly to avoid potentially ruinous False Claims Act liability.”
The Aug. 3 ruling in Kane v. Healthfirst is the first published decision to address the 60-day overpayment rule imposed under the Affordable Care Act and the Fraud Enforcement and Recovery Act (FERA). The rule requires that an overpayment be reported and returned by health providers within 60 days of the “date on which the overpayment was identified.” Health providers who retain an overpayment beyond that point are subject to liability under the False Claims Act (FCA).
In the Kane case, the federal government contends that three hospitals operated by Continuum Health Partners failed to report and return overpayments to Medicaid within 60 days of identification. Because of a computer glitch, Continuum billed both the government and a managed care organization for the same services, according to court documents. After the New York State Comptroller’s Office alerted Continuum to a possible overbilling, Continuum hired an employee, Robert P. Kane, to conduct an internal investigation into its billing. Mr. Kane – who was later fired – allegedly found 900 potentially improper Medicaid claims totaling $1 million, according to court documents. The government claims Continuum failed to repay the overpayments within 60 days and instead repaid only “small batches” of the affected claims over the next 2 years. Mr. Kane filed a whistleblower suit against Continuum, and the government intervened as a plaintiff.
But Continuum argued that the hospitals did not knowingly conceal the overpayments from the government, and that the overbillings had not been officially “identified.” The defendants were provided only notice of potential overpayments and did not identify actual overpayments so as to trigger the 60-day report and return clock, Continuum said in court documents. The health system requested the court throw out the government’s suit for lack of merit.
District Judge Edgardo Ramos agreed with the federal government and allowed the lawsuit to continue. Judge Ramos said the legislative history indicates that Congress intended for FCA liability to attach in circumstances where there is an established duty to pay money to the government, even if the precise amount due has yet to be determined.
“Here, after the comptroller alerted defendants to the software glitch and approached them with specific wrongful claims, and after Kane put defendants on notice of a set of claims likely to contain numerous overpayments, defendants had an established duty to report and return wrongly collected money,” Judge Ramos said in his opinion. “To allow defendants to evade liability because Kane’s email did not conclusively establish each erroneous claim and did not provide the specific amount owed to the government would contradict Congress’s intentions as expressed during the passage of the FERA.”

In an email, a spokesperson for the defendants said the hospitals are disappointed with the judge’s decision and will continue to vigorously defend its case in court. Attorneys for the government did not return messages seeking comment.
The judge’s ruling is encouraging to the federal government and for plaintiffs who wish to sue health providers for overbilling violations, said Joel M. Androphy, a Houston plaintiffs’ attorney.
“This is going to open the floodgates for lawyers now as part of their false claim and reporting practices to let the courts know about overpayment issues because they know the court and the government will be listening,” Mr. Androphy said in an interview. “It’s not going to be the sole basis for [a plaintiff’s] claim necessarily, but it could be an integral part.”
Mr. Androphy added that defendants can no longer complain they were confused by the 60-day overpayment rule and the meaning of “identification.” The judge’s ruling makes the regulation more clear and provides guidance to health providers about how the rule will be enforced, he said.
Washington health law attorney Robert T. Rhoad however, disagreed that the opinion clarifies application of the 60-day overpayment rule. The decision does not provide the bright lines for compliance that providers expect and need, said Mr. Rhoad.

“While the Kane decision provides an exposition of the etiology and perceived intent of the 60-day rule, its ultimate ruling was made through the narrow lens of the specific and arguably egregious [facts] alleged,” Mr. Rhoad said in an interview. “If anything, by finding that certainty is not required in identifying an overpayment triggering the 60-day rule, the decision may encourage the government and qui tam relators to come forward with expansive theories of what might constitute reckless disregard by a provider to identify an overpayment to invoke FCA liability by the running of the 60-day clock.”
To protect themselves from litigation, physicians should take prudent steps to conduct an appropriate investigation if faced with actual or constructive notice of a possible overpayment, Mr. Rhoad said. Showing that they acted with due diligence and without delay to investigate and, if identified, report an overpayment could help doctors withstand future governmental or judicial scrutiny.
On Twitter @legal_med
In a novel decision, the U.S. District Court for the Southern District of New York has ruled that the 60-day clock to return overpayments to the government begins ticking when a health provider receives notice a potential overpayment exists, not when an overpayment is conclusively ascertained.
Doctors should be concerned about the ruling, said Houston health law attorney Michael E. Clark, immediate past chair for the American Bar Association Health Law Section.
“This is a very troubling development because the judge has embraced the theory that certainty is not required as to what constitutes an identified overpayment,” Mr. Clark said in an interview. “Rather, knowledge can be established by recklessness under the facts. In short, practitioners must set up systems to alert them about potential overpayments so they can move quickly to avoid potentially ruinous False Claims Act liability.”
The Aug. 3 ruling in Kane v. Healthfirst is the first published decision to address the 60-day overpayment rule imposed under the Affordable Care Act and the Fraud Enforcement and Recovery Act (FERA). The rule requires that an overpayment be reported and returned by health providers within 60 days of the “date on which the overpayment was identified.” Health providers who retain an overpayment beyond that point are subject to liability under the False Claims Act (FCA).
In the Kane case, the federal government contends that three hospitals operated by Continuum Health Partners failed to report and return overpayments to Medicaid within 60 days of identification. Because of a computer glitch, Continuum billed both the government and a managed care organization for the same services, according to court documents. After the New York State Comptroller’s Office alerted Continuum to a possible overbilling, Continuum hired an employee, Robert P. Kane, to conduct an internal investigation into its billing. Mr. Kane – who was later fired – allegedly found 900 potentially improper Medicaid claims totaling $1 million, according to court documents. The government claims Continuum failed to repay the overpayments within 60 days and instead repaid only “small batches” of the affected claims over the next 2 years. Mr. Kane filed a whistleblower suit against Continuum, and the government intervened as a plaintiff.
But Continuum argued that the hospitals did not knowingly conceal the overpayments from the government, and that the overbillings had not been officially “identified.” The defendants were provided only notice of potential overpayments and did not identify actual overpayments so as to trigger the 60-day report and return clock, Continuum said in court documents. The health system requested the court throw out the government’s suit for lack of merit.
District Judge Edgardo Ramos agreed with the federal government and allowed the lawsuit to continue. Judge Ramos said the legislative history indicates that Congress intended for FCA liability to attach in circumstances where there is an established duty to pay money to the government, even if the precise amount due has yet to be determined.
“Here, after the comptroller alerted defendants to the software glitch and approached them with specific wrongful claims, and after Kane put defendants on notice of a set of claims likely to contain numerous overpayments, defendants had an established duty to report and return wrongly collected money,” Judge Ramos said in his opinion. “To allow defendants to evade liability because Kane’s email did not conclusively establish each erroneous claim and did not provide the specific amount owed to the government would contradict Congress’s intentions as expressed during the passage of the FERA.”
In an email, a spokesperson for the defendants said the hospitals are disappointed with the judge’s decision and will continue to vigorously defend its case in court. Attorneys for the government did not return messages seeking comment.
The judge’s ruling is encouraging to the federal government and for plaintiffs who wish to sue health providers for overbilling violations, said Joel M. Androphy, a Houston plaintiffs’ attorney.
“This is going to open the floodgates for lawyers now as part of their false claim and reporting practices to let the courts know about overpayment issues because they know the court and the government will be listening,” Mr. Androphy said in an interview. “It’s not going to be the sole basis for [a plaintiff’s] claim necessarily, but it could be an integral part.”
Mr. Androphy added that defendants can no longer complain they were confused by the 60-day overpayment rule and the meaning of “identification.” The judge’s ruling makes the regulation more clear and provides guidance to health providers about how the rule will be enforced, he said.
Washington health law attorney Robert T. Rhoad however, disagreed that the opinion clarifies application of the 60-day overpayment rule. The decision does not provide the bright lines for compliance that providers expect and need, said Mr. Rhoad.
“While the Kane decision provides an exposition of the etiology and perceived intent of the 60-day rule, its ultimate ruling was made through the narrow lens of the specific and arguably egregious [facts] alleged,” Mr. Rhoad said in an interview. “If anything, by finding that certainty is not required in identifying an overpayment triggering the 60-day rule, the decision may encourage the government and qui tam relators to come forward with expansive theories of what might constitute reckless disregard by a provider to identify an overpayment to invoke FCA liability by the running of the 60-day clock.”
To protect themselves from litigation, physicians should take prudent steps to conduct an appropriate investigation if faced with actual or constructive notice of a possible overpayment, Mr. Rhoad said. Showing that they acted with due diligence and without delay to investigate and, if identified, report an overpayment could help doctors withstand future governmental or judicial scrutiny.
On Twitter @legal_med
In a novel decision, the U.S. District Court for the Southern District of New York has ruled that the 60-day clock to return overpayments to the government begins ticking when a health provider receives notice a potential overpayment exists, not when an overpayment is conclusively ascertained.
Doctors should be concerned about the ruling, said Houston health law attorney Michael E. Clark, immediate past chair for the American Bar Association Health Law Section.
“This is a very troubling development because the judge has embraced the theory that certainty is not required as to what constitutes an identified overpayment,” Mr. Clark said in an interview. “Rather, knowledge can be established by recklessness under the facts. In short, practitioners must set up systems to alert them about potential overpayments so they can move quickly to avoid potentially ruinous False Claims Act liability.”
The Aug. 3 ruling in Kane v. Healthfirst is the first published decision to address the 60-day overpayment rule imposed under the Affordable Care Act and the Fraud Enforcement and Recovery Act (FERA). The rule requires that an overpayment be reported and returned by health providers within 60 days of the “date on which the overpayment was identified.” Health providers who retain an overpayment beyond that point are subject to liability under the False Claims Act (FCA).
In the Kane case, the federal government contends that three hospitals operated by Continuum Health Partners failed to report and return overpayments to Medicaid within 60 days of identification. Because of a computer glitch, Continuum billed both the government and a managed care organization for the same services, according to court documents. After the New York State Comptroller’s Office alerted Continuum to a possible overbilling, Continuum hired an employee, Robert P. Kane, to conduct an internal investigation into its billing. Mr. Kane – who was later fired – allegedly found 900 potentially improper Medicaid claims totaling $1 million, according to court documents. The government claims Continuum failed to repay the overpayments within 60 days and instead repaid only “small batches” of the affected claims over the next 2 years. Mr. Kane filed a whistleblower suit against Continuum, and the government intervened as a plaintiff.
But Continuum argued that the hospitals did not knowingly conceal the overpayments from the government, and that the overbillings had not been officially “identified.” The defendants were provided only notice of potential overpayments and did not identify actual overpayments so as to trigger the 60-day report and return clock, Continuum said in court documents. The health system requested the court throw out the government’s suit for lack of merit.
District Judge Edgardo Ramos agreed with the federal government and allowed the lawsuit to continue. Judge Ramos said the legislative history indicates that Congress intended for FCA liability to attach in circumstances where there is an established duty to pay money to the government, even if the precise amount due has yet to be determined.
“Here, after the comptroller alerted defendants to the software glitch and approached them with specific wrongful claims, and after Kane put defendants on notice of a set of claims likely to contain numerous overpayments, defendants had an established duty to report and return wrongly collected money,” Judge Ramos said in his opinion. “To allow defendants to evade liability because Kane’s email did not conclusively establish each erroneous claim and did not provide the specific amount owed to the government would contradict Congress’s intentions as expressed during the passage of the FERA.”
In an email, a spokesperson for the defendants said the hospitals are disappointed with the judge’s decision and will continue to vigorously defend its case in court. Attorneys for the government did not return messages seeking comment.
The judge’s ruling is encouraging to the federal government and for plaintiffs who wish to sue health providers for overbilling violations, said Joel M. Androphy, a Houston plaintiffs’ attorney.
“This is going to open the floodgates for lawyers now as part of their false claim and reporting practices to let the courts know about overpayment issues because they know the court and the government will be listening,” Mr. Androphy said in an interview. “It’s not going to be the sole basis for [a plaintiff’s] claim necessarily, but it could be an integral part.”
Mr. Androphy added that defendants can no longer complain they were confused by the 60-day overpayment rule and the meaning of “identification.” The judge’s ruling makes the regulation more clear and provides guidance to health providers about how the rule will be enforced, he said.
Washington health law attorney Robert T. Rhoad however, disagreed that the opinion clarifies application of the 60-day overpayment rule. The decision does not provide the bright lines for compliance that providers expect and need, said Mr. Rhoad.
“While the Kane decision provides an exposition of the etiology and perceived intent of the 60-day rule, its ultimate ruling was made through the narrow lens of the specific and arguably egregious [facts] alleged,” Mr. Rhoad said in an interview. “If anything, by finding that certainty is not required in identifying an overpayment triggering the 60-day rule, the decision may encourage the government and qui tam relators to come forward with expansive theories of what might constitute reckless disregard by a provider to identify an overpayment to invoke FCA liability by the running of the 60-day clock.”
To protect themselves from litigation, physicians should take prudent steps to conduct an appropriate investigation if faced with actual or constructive notice of a possible overpayment, Mr. Rhoad said. Showing that they acted with due diligence and without delay to investigate and, if identified, report an overpayment could help doctors withstand future governmental or judicial scrutiny.
On Twitter @legal_med

ACC to launch registries for atrial fibrillation treatments
The American College of Cardiology (ACC) will launch two registries to track the outcomes of treatments for atrial fibrillation, the medical society announced today.
The LAAO Registry will capture data on left atrial appendage occlusion procedures to assess real-world procedural indications and outcomes, as well as short- and long-term safety.

The AFib Ablation Registry will assess the prevalence, demographics, acute management, and outcomes of patients undergoing atrial fibrillation ablation procedures. This registry’s data will support the development of evidence-based guidelines and quality metrics for atrial fibrillation treatments that will improve outcomes, according to the ACC.
“With a growing prevalence of atrial fibrillation and growing options for treatment and stroke prevention in AFib patients, the ACC saw a need for real-world data to track and evaluate the use of these new technologies,” said Dr. Kim A. Williams Sr., ACC president.
The American College of Cardiology (ACC) will launch two registries to track the outcomes of treatments for atrial fibrillation, the medical society announced today.
The LAAO Registry will capture data on left atrial appendage occlusion procedures to assess real-world procedural indications and outcomes, as well as short- and long-term safety.
The AFib Ablation Registry will assess the prevalence, demographics, acute management, and outcomes of patients undergoing atrial fibrillation ablation procedures. This registry’s data will support the development of evidence-based guidelines and quality metrics for atrial fibrillation treatments that will improve outcomes, according to the ACC.
“With a growing prevalence of atrial fibrillation and growing options for treatment and stroke prevention in AFib patients, the ACC saw a need for real-world data to track and evaluate the use of these new technologies,” said Dr. Kim A. Williams Sr., ACC president.
The American College of Cardiology (ACC) will launch two registries to track the outcomes of treatments for atrial fibrillation, the medical society announced today.
The LAAO Registry will capture data on left atrial appendage occlusion procedures to assess real-world procedural indications and outcomes, as well as short- and long-term safety.
The AFib Ablation Registry will assess the prevalence, demographics, acute management, and outcomes of patients undergoing atrial fibrillation ablation procedures. This registry’s data will support the development of evidence-based guidelines and quality metrics for atrial fibrillation treatments that will improve outcomes, according to the ACC.
“With a growing prevalence of atrial fibrillation and growing options for treatment and stroke prevention in AFib patients, the ACC saw a need for real-world data to track and evaluate the use of these new technologies,” said Dr. Kim A. Williams Sr., ACC president.

James L. Cox Fellowship in Atrial Fibrillation Surgery: Deadline September 1
The AATS Graham Foundation invites applications for the James L. Cox Fellowship in Atrial Fibrillation sponsored by Atricure.
About
The fellowship allows newly graduated CT surgeons to spend up to three months improving their atrial fibrillation techniques at a host institution.
This hands-on immersive experience allows awardees to enhance their clinical understanding and surgical proficiency in treatming atrial fibrillation under the tutelage of top surgeon educators.
Stipend
Successful applicants will receive a $15,000 stipend to help offset their living expenses.
Deadline: September 1, 2015
The AATS Graham Foundation invites applications for the James L. Cox Fellowship in Atrial Fibrillation sponsored by Atricure.
About
The fellowship allows newly graduated CT surgeons to spend up to three months improving their atrial fibrillation techniques at a host institution.
This hands-on immersive experience allows awardees to enhance their clinical understanding and surgical proficiency in treatming atrial fibrillation under the tutelage of top surgeon educators.
Stipend
Successful applicants will receive a $15,000 stipend to help offset their living expenses.
Deadline: September 1, 2015
The AATS Graham Foundation invites applications for the James L. Cox Fellowship in Atrial Fibrillation sponsored by Atricure.
About
The fellowship allows newly graduated CT surgeons to spend up to three months improving their atrial fibrillation techniques at a host institution.
This hands-on immersive experience allows awardees to enhance their clinical understanding and surgical proficiency in treatming atrial fibrillation under the tutelage of top surgeon educators.
Stipend
Successful applicants will receive a $15,000 stipend to help offset their living expenses.
Deadline: September 1, 2015
Cardiothoracic Ethics Forum Scholarship: Deadline September 1
Applications Now Open for the Cardiothoracic Ethics Forum Scholarship
The Cardiothoracic Ethics Forum fosters future leaders in cardiothoracic (CT) ethics by offering up to $10,000 in grants, allowing surgeons to receive biomedical ethics education and training at leading North American ethics centers.
The Forum is the joint governance body of the American Associate for Thoracic Surgery (AATS) and Society of Thoracic Surgeons (STS) responsible for ethics education in CT surgery. It has sponsored 50 ethics sessions at CT surgery meetings and its members have published over 340 papers on ethics topics since its inception in 2000.
Academic period: August 2015 – August 2016
Purpose
The scholarship provides opportunities for intellectual development and participation for leadership roles in CT ethics, allowing recipients to obtain formal biomedical ethics education through several leading programs. Ethics centers include Columbia University, Georgetown University and the University of Washington, among others.
Application GuidelinesCandidates must:
**Be members of AATS or STS.
** Identify a specific educational program that will advance their ethics knowledge and skills in preparation for participation and leadership in CT ethics programs.
** Provide a curriculum vitae or resume that displays evidence of scholarly activity and leadership roles.
** Submit a proposed plan of study (500 words or less) clearly stating how the scholarship will provide educational insights and benefits advancing their professional careers and the CT surgery field.
Deadline: September 1, 2015
Questions: Contact Robert M. Sade, MD
Applications Now Open for the Cardiothoracic Ethics Forum Scholarship
The Cardiothoracic Ethics Forum fosters future leaders in cardiothoracic (CT) ethics by offering up to $10,000 in grants, allowing surgeons to receive biomedical ethics education and training at leading North American ethics centers.
The Forum is the joint governance body of the American Associate for Thoracic Surgery (AATS) and Society of Thoracic Surgeons (STS) responsible for ethics education in CT surgery. It has sponsored 50 ethics sessions at CT surgery meetings and its members have published over 340 papers on ethics topics since its inception in 2000.
Academic period: August 2015 – August 2016
Purpose
The scholarship provides opportunities for intellectual development and participation for leadership roles in CT ethics, allowing recipients to obtain formal biomedical ethics education through several leading programs. Ethics centers include Columbia University, Georgetown University and the University of Washington, among others.
Application GuidelinesCandidates must:
**Be members of AATS or STS.
** Identify a specific educational program that will advance their ethics knowledge and skills in preparation for participation and leadership in CT ethics programs.
** Provide a curriculum vitae or resume that displays evidence of scholarly activity and leadership roles.
** Submit a proposed plan of study (500 words or less) clearly stating how the scholarship will provide educational insights and benefits advancing their professional careers and the CT surgery field.
Deadline: September 1, 2015
Questions: Contact Robert M. Sade, MD
Applications Now Open for the Cardiothoracic Ethics Forum Scholarship
The Cardiothoracic Ethics Forum fosters future leaders in cardiothoracic (CT) ethics by offering up to $10,000 in grants, allowing surgeons to receive biomedical ethics education and training at leading North American ethics centers.
The Forum is the joint governance body of the American Associate for Thoracic Surgery (AATS) and Society of Thoracic Surgeons (STS) responsible for ethics education in CT surgery. It has sponsored 50 ethics sessions at CT surgery meetings and its members have published over 340 papers on ethics topics since its inception in 2000.
Academic period: August 2015 – August 2016
Purpose
The scholarship provides opportunities for intellectual development and participation for leadership roles in CT ethics, allowing recipients to obtain formal biomedical ethics education through several leading programs. Ethics centers include Columbia University, Georgetown University and the University of Washington, among others.
Application GuidelinesCandidates must:
**Be members of AATS or STS.
** Identify a specific educational program that will advance their ethics knowledge and skills in preparation for participation and leadership in CT ethics programs.
** Provide a curriculum vitae or resume that displays evidence of scholarly activity and leadership roles.
** Submit a proposed plan of study (500 words or less) clearly stating how the scholarship will provide educational insights and benefits advancing their professional careers and the CT surgery field.
Deadline: September 1, 2015
Questions: Contact Robert M. Sade, MD

View Preliminary Program & Register for AATS International Coronary Congress: State of the Art Surgical Coronary Revascularization - August 21-23
Be part of the International Coronary Congress focused on state-of-the-art coronary surgery.
August 21 – 23, 2015
Marriott Marquis, New York
New York City, NY
An international expert faculty will lead this highly practical interdisciplinary program. Topics will include the latest evidence, technologies, tips and tricks for all aspects of coronary revascularization — with a particular emphasis on safely and easily increasing use of arterial grafts.
This two and one-half day program is designed for surgeons, physicians, physician assistants and nurses from around the world. It will include a comprehensive simultaneous curriculum for physician assistants and surgical first assistants.
Surgeons are encouraged to attend with their entire operating team to maximize its unique benefits.
Program Directors
John Puskas
David Taggart
Robert Carlucci
Program Committee Members
Hirokuni Arai
Stephen Fremes
Joseph Sabik
James Tatoulis
Be part of the International Coronary Congress focused on state-of-the-art coronary surgery.
August 21 – 23, 2015
Marriott Marquis, New York
New York City, NY
An international expert faculty will lead this highly practical interdisciplinary program. Topics will include the latest evidence, technologies, tips and tricks for all aspects of coronary revascularization — with a particular emphasis on safely and easily increasing use of arterial grafts.
This two and one-half day program is designed for surgeons, physicians, physician assistants and nurses from around the world. It will include a comprehensive simultaneous curriculum for physician assistants and surgical first assistants.
Surgeons are encouraged to attend with their entire operating team to maximize its unique benefits.
Program Directors
John Puskas
David Taggart
Robert Carlucci
Program Committee Members
Hirokuni Arai
Stephen Fremes
Joseph Sabik
James Tatoulis
Be part of the International Coronary Congress focused on state-of-the-art coronary surgery.
August 21 – 23, 2015
Marriott Marquis, New York
New York City, NY
An international expert faculty will lead this highly practical interdisciplinary program. Topics will include the latest evidence, technologies, tips and tricks for all aspects of coronary revascularization — with a particular emphasis on safely and easily increasing use of arterial grafts.
This two and one-half day program is designed for surgeons, physicians, physician assistants and nurses from around the world. It will include a comprehensive simultaneous curriculum for physician assistants and surgical first assistants.
Surgeons are encouraged to attend with their entire operating team to maximize its unique benefits.
Program Directors
John Puskas
David Taggart
Robert Carlucci
Program Committee Members
Hirokuni Arai
Stephen Fremes
Joseph Sabik
James Tatoulis
