User login
The Official Newspaper of the American Association for Thoracic Surgery
September 22: Early Registration Deadline For Focus on Thoracic Surgery
October 23-24, 2015
Seaport Hotel &
World Trade Center
Boston, MA
Complications remain one of the major challenges in treating patients. The 2015 Focus on Thoracic Surgery meeting will concentrate on the intraoperative challenges and management of complications facing thoracic surgeons in treating lung and esophageal cancers. This year’s course is particularly aimed at operating surgeons who are active and seek to learn innovative solutions to clinical problems during surgery.
This course will display new advanced diagnosis and prompt management approaches, allowing attendees to understand and readily translate them into daily practice.
This two-day conference will have a faculty of experts in the field who are leaders in the application of new technologies in surgical management. It will combine informational sessions, panel discussions, and complex case presentations.
Focus on Thoracic Surgery is a must for surgeons who specialize in the treatment of lung and esophageal cancers and want to enhance their skills so they can overcome challenges and complications in their surgical practices.
Program Focus
• Intraoperative Challenges during Thoracoscopic Lobectomy
• Intraoperative Challenges during Extended Pulmonary Resections
• Managing Complications after Pneumonectomy
• Intraoperative Challenges during Complex Esophageal Surgery
• Intraoperative Challenges during Esophagectomy
• Managing Complications after Esophageal Resection
• Intraoperative Challenges in Airway Surgery
• Complex Case Presentations
Register & Reserve Hotel Today & Save!Register and reserve housing before September 22, 2015 and benefit from lower registration fees and a guaranteed hotel room in Boston.
Program Directors
G. Alec Patterson
David J. Sugarbaker
Program Committee Members
Thomas A. D’Amico
Shaf Keshavjee
James D. Luketich
Bryan F. Meyers
Scott J. Swanson
October 23-24, 2015
Seaport Hotel &
World Trade Center
Boston, MA
Complications remain one of the major challenges in treating patients. The 2015 Focus on Thoracic Surgery meeting will concentrate on the intraoperative challenges and management of complications facing thoracic surgeons in treating lung and esophageal cancers. This year’s course is particularly aimed at operating surgeons who are active and seek to learn innovative solutions to clinical problems during surgery.
This course will display new advanced diagnosis and prompt management approaches, allowing attendees to understand and readily translate them into daily practice.
This two-day conference will have a faculty of experts in the field who are leaders in the application of new technologies in surgical management. It will combine informational sessions, panel discussions, and complex case presentations.
Focus on Thoracic Surgery is a must for surgeons who specialize in the treatment of lung and esophageal cancers and want to enhance their skills so they can overcome challenges and complications in their surgical practices.
Program Focus
• Intraoperative Challenges during Thoracoscopic Lobectomy
• Intraoperative Challenges during Extended Pulmonary Resections
• Managing Complications after Pneumonectomy
• Intraoperative Challenges during Complex Esophageal Surgery
• Intraoperative Challenges during Esophagectomy
• Managing Complications after Esophageal Resection
• Intraoperative Challenges in Airway Surgery
• Complex Case Presentations
Register & Reserve Hotel Today & Save!Register and reserve housing before September 22, 2015 and benefit from lower registration fees and a guaranteed hotel room in Boston.
Program Directors
G. Alec Patterson
David J. Sugarbaker
Program Committee Members
Thomas A. D’Amico
Shaf Keshavjee
James D. Luketich
Bryan F. Meyers
Scott J. Swanson
October 23-24, 2015
Seaport Hotel &
World Trade Center
Boston, MA
Complications remain one of the major challenges in treating patients. The 2015 Focus on Thoracic Surgery meeting will concentrate on the intraoperative challenges and management of complications facing thoracic surgeons in treating lung and esophageal cancers. This year’s course is particularly aimed at operating surgeons who are active and seek to learn innovative solutions to clinical problems during surgery.
This course will display new advanced diagnosis and prompt management approaches, allowing attendees to understand and readily translate them into daily practice.
This two-day conference will have a faculty of experts in the field who are leaders in the application of new technologies in surgical management. It will combine informational sessions, panel discussions, and complex case presentations.
Focus on Thoracic Surgery is a must for surgeons who specialize in the treatment of lung and esophageal cancers and want to enhance their skills so they can overcome challenges and complications in their surgical practices.
Program Focus
• Intraoperative Challenges during Thoracoscopic Lobectomy
• Intraoperative Challenges during Extended Pulmonary Resections
• Managing Complications after Pneumonectomy
• Intraoperative Challenges during Complex Esophageal Surgery
• Intraoperative Challenges during Esophagectomy
• Managing Complications after Esophageal Resection
• Intraoperative Challenges in Airway Surgery
• Complex Case Presentations
Register & Reserve Hotel Today & Save!Register and reserve housing before September 22, 2015 and benefit from lower registration fees and a guaranteed hotel room in Boston.
Program Directors
G. Alec Patterson
David J. Sugarbaker
Program Committee Members
Thomas A. D’Amico
Shaf Keshavjee
James D. Luketich
Bryan F. Meyers
Scott J. Swanson

North American Residents Eligible to Receive Free Subscriptions to AATS Publications
North American residents are eligible to receive complementary subscriptions to three (3) AATS publications thanks to educational grants from Edwards LifeSciences and the AATS Graham Foundation.
Publications included in this special offer include:
• Journal of Thoracic and Cardiovascular Surgery (JTCVS)
• Operative Techniques in Thoracic and Cardiovascular Surgery (Op-Techs)
• Seminars in Thoracic and Cardiovascular Surgery (Seminars)
North American residents are eligible to receive complementary subscriptions to three (3) AATS publications thanks to educational grants from Edwards LifeSciences and the AATS Graham Foundation.
Publications included in this special offer include:
• Journal of Thoracic and Cardiovascular Surgery (JTCVS)
• Operative Techniques in Thoracic and Cardiovascular Surgery (Op-Techs)
• Seminars in Thoracic and Cardiovascular Surgery (Seminars)
North American residents are eligible to receive complementary subscriptions to three (3) AATS publications thanks to educational grants from Edwards LifeSciences and the AATS Graham Foundation.
Publications included in this special offer include:
• Journal of Thoracic and Cardiovascular Surgery (JTCVS)
• Operative Techniques in Thoracic and Cardiovascular Surgery (Op-Techs)
• Seminars in Thoracic and Cardiovascular Surgery (Seminars)
Don’t Miss the Heart Valve Summit – Medical, Surgical & Interventional Decision Making
October 1-3, 2015
Radisson Blu Aqua Hotel
Chicago, IL
Course Directors
David H. Adams/Mount Sinai Medical Center
Steven F. Bolling/University of Michigan
Robert O. Bonow/Northwestern University
Howard C. Herrmann/University of Pennsylvania
Nurse Planner
Michele Mistovich, RN, MS/Northwestern Memorial Hospital
Focusing on interactivity and practical decision-making, the 2015 Heart Valve Summit will engage participants in discussions, debates, and potential controversies using real-world cases. Its faculty will include renowned experts, who are on the cutting edge of clinically relevant VHD data.
Course Highlights Include:
• Basics of Aortic Stenosis
• Decision Making: Less Than Severe Regurgitation
• Degenerative Mitral Anatomy & Physiology
• Guideline Controversies
• HOCM 2015
• My Most Interesting, Controversial, or Complicated TAVR Case
• Secondary Mitral Valve Regurgitation
• The Asymptomatic Patient
• The Cardiac Network Trials: Answers & More Questions
• NEW: Valve Disease in Young Patients
Target Audience
The 2015 Heart Valve Summit is intended for cardiologists, interventional cardiologists, cardiothoracic surgeons, internists, nurses, physician assistants, and all health care professionals involved in the evaluation, diagnosis, and/or management of VHD patients.
Accreditation
Physicians
This course has been approved for AMA PRA Category 1 Credits™.
Nurses
The American College of Cardiology Foundation is accredited as a provider of continuing nursing education by the American Nurses Credentialing Center’s Commission on Accreditation.
October 1-3, 2015
Radisson Blu Aqua Hotel
Chicago, IL
Course Directors
David H. Adams/Mount Sinai Medical Center
Steven F. Bolling/University of Michigan
Robert O. Bonow/Northwestern University
Howard C. Herrmann/University of Pennsylvania
Nurse Planner
Michele Mistovich, RN, MS/Northwestern Memorial Hospital
Focusing on interactivity and practical decision-making, the 2015 Heart Valve Summit will engage participants in discussions, debates, and potential controversies using real-world cases. Its faculty will include renowned experts, who are on the cutting edge of clinically relevant VHD data.
Course Highlights Include:
• Basics of Aortic Stenosis
• Decision Making: Less Than Severe Regurgitation
• Degenerative Mitral Anatomy & Physiology
• Guideline Controversies
• HOCM 2015
• My Most Interesting, Controversial, or Complicated TAVR Case
• Secondary Mitral Valve Regurgitation
• The Asymptomatic Patient
• The Cardiac Network Trials: Answers & More Questions
• NEW: Valve Disease in Young Patients
Target Audience
The 2015 Heart Valve Summit is intended for cardiologists, interventional cardiologists, cardiothoracic surgeons, internists, nurses, physician assistants, and all health care professionals involved in the evaluation, diagnosis, and/or management of VHD patients.
Accreditation
Physicians
This course has been approved for AMA PRA Category 1 Credits™.
Nurses
The American College of Cardiology Foundation is accredited as a provider of continuing nursing education by the American Nurses Credentialing Center’s Commission on Accreditation.
October 1-3, 2015
Radisson Blu Aqua Hotel
Chicago, IL
Course Directors
David H. Adams/Mount Sinai Medical Center
Steven F. Bolling/University of Michigan
Robert O. Bonow/Northwestern University
Howard C. Herrmann/University of Pennsylvania
Nurse Planner
Michele Mistovich, RN, MS/Northwestern Memorial Hospital
Focusing on interactivity and practical decision-making, the 2015 Heart Valve Summit will engage participants in discussions, debates, and potential controversies using real-world cases. Its faculty will include renowned experts, who are on the cutting edge of clinically relevant VHD data.
Course Highlights Include:
• Basics of Aortic Stenosis
• Decision Making: Less Than Severe Regurgitation
• Degenerative Mitral Anatomy & Physiology
• Guideline Controversies
• HOCM 2015
• My Most Interesting, Controversial, or Complicated TAVR Case
• Secondary Mitral Valve Regurgitation
• The Asymptomatic Patient
• The Cardiac Network Trials: Answers & More Questions
• NEW: Valve Disease in Young Patients
Target Audience
The 2015 Heart Valve Summit is intended for cardiologists, interventional cardiologists, cardiothoracic surgeons, internists, nurses, physician assistants, and all health care professionals involved in the evaluation, diagnosis, and/or management of VHD patients.
Accreditation
Physicians
This course has been approved for AMA PRA Category 1 Credits™.
Nurses
The American College of Cardiology Foundation is accredited as a provider of continuing nursing education by the American Nurses Credentialing Center’s Commission on Accreditation.
Call for Abstracts/Videos for 2016 AATS Annual Meeting
Submissions are now open for abstracts and case videos for the AATS Annual Meeting.
Presentation Types
• Regular Session (Plenary and Simultaneous Sessions)
• Laboratory Research Fora (Cardiac Surgery and General Thoracic Surgery)
• Emerging Technologies and Techniques Forum
• C. Walton Lillehei Resident Forum
• Case Videos
Plenary and Simultaneous Session Abstracts may be submitted for the following categories
• Adult Cardiac
• Congenital
• General Thoracic
• Perioperative Care
Case Videos may be submitted for the following categories
• Adult Cardiac
• Congenital
• General Thoracic
Waiver of mandatory manuscript submission for publication in JTCVS may be requested at the time of submission.
Deadline: Monday, October 19, 2014 at 11:59 p.m. EDT
Submissions are now open for abstracts and case videos for the AATS Annual Meeting.
Presentation Types
• Regular Session (Plenary and Simultaneous Sessions)
• Laboratory Research Fora (Cardiac Surgery and General Thoracic Surgery)
• Emerging Technologies and Techniques Forum
• C. Walton Lillehei Resident Forum
• Case Videos
Plenary and Simultaneous Session Abstracts may be submitted for the following categories
• Adult Cardiac
• Congenital
• General Thoracic
• Perioperative Care
Case Videos may be submitted for the following categories
• Adult Cardiac
• Congenital
• General Thoracic
Waiver of mandatory manuscript submission for publication in JTCVS may be requested at the time of submission.
Deadline: Monday, October 19, 2014 at 11:59 p.m. EDT
Submissions are now open for abstracts and case videos for the AATS Annual Meeting.
Presentation Types
• Regular Session (Plenary and Simultaneous Sessions)
• Laboratory Research Fora (Cardiac Surgery and General Thoracic Surgery)
• Emerging Technologies and Techniques Forum
• C. Walton Lillehei Resident Forum
• Case Videos
Plenary and Simultaneous Session Abstracts may be submitted for the following categories
• Adult Cardiac
• Congenital
• General Thoracic
• Perioperative Care
Case Videos may be submitted for the following categories
• Adult Cardiac
• Congenital
• General Thoracic
Waiver of mandatory manuscript submission for publication in JTCVS may be requested at the time of submission.
Deadline: Monday, October 19, 2014 at 11:59 p.m. EDT
Submit Abstracts/Videos for AATS Aortic Symposium 2016
Abstract and video submissions are now open for AATS Aortic Symposium 2016.
May 12-13, 2016
Sheraton New York Times Square Hotel
New York, NY, USA
Course Directors
Joseph S. Coselli
Steven L. Lansman
Co-Directors
Joseph E. Bavaria
Nicholas T. Kouchoukos
G. Chad Hughes
David Spielvogel
Thoralf M. Sundt, III
Lars G. Svensson
Submission of Abstracts & Videos
Specific instructions for abstract and video submission
Investigators are invited to submit original work to include BOTH of the following:
• Abstract (maximum of 200 words), accompanied by
• PowerPoint presentation of the material (maximum of 12 slides)
OR
• Abstract (maximum of 200 words), accompanied by
• Video (maximum of five minutes, for the Presentation On Demand (POD) system ONLY and must be narrated in English)
Submission Categories:
• Aortic Rootchever
• Descending/Thoracoabdominal Aorta
• Endoluminal Prostheses
• Natural History/ Follow-up
• Spinal Cord Protection
• Trauma
• Other
Abstract and video submissions are now open for AATS Aortic Symposium 2016.
May 12-13, 2016
Sheraton New York Times Square Hotel
New York, NY, USA
Course Directors
Joseph S. Coselli
Steven L. Lansman
Co-Directors
Joseph E. Bavaria
Nicholas T. Kouchoukos
G. Chad Hughes
David Spielvogel
Thoralf M. Sundt, III
Lars G. Svensson
Submission of Abstracts & Videos
Specific instructions for abstract and video submission
Investigators are invited to submit original work to include BOTH of the following:
• Abstract (maximum of 200 words), accompanied by
• PowerPoint presentation of the material (maximum of 12 slides)
OR
• Abstract (maximum of 200 words), accompanied by
• Video (maximum of five minutes, for the Presentation On Demand (POD) system ONLY and must be narrated in English)
Submission Categories:
• Aortic Rootchever
• Descending/Thoracoabdominal Aorta
• Endoluminal Prostheses
• Natural History/ Follow-up
• Spinal Cord Protection
• Trauma
• Other
Abstract and video submissions are now open for AATS Aortic Symposium 2016.
May 12-13, 2016
Sheraton New York Times Square Hotel
New York, NY, USA
Course Directors
Joseph S. Coselli
Steven L. Lansman
Co-Directors
Joseph E. Bavaria
Nicholas T. Kouchoukos
G. Chad Hughes
David Spielvogel
Thoralf M. Sundt, III
Lars G. Svensson
Submission of Abstracts & Videos
Specific instructions for abstract and video submission
Investigators are invited to submit original work to include BOTH of the following:
• Abstract (maximum of 200 words), accompanied by
• PowerPoint presentation of the material (maximum of 12 slides)
OR
• Abstract (maximum of 200 words), accompanied by
• Video (maximum of five minutes, for the Presentation On Demand (POD) system ONLY and must be narrated in English)
Submission Categories:
• Aortic Rootchever
• Descending/Thoracoabdominal Aorta
• Endoluminal Prostheses
• Natural History/ Follow-up
• Spinal Cord Protection
• Trauma
• Other

Assessing progression, impact of radiofrequency ablation in Barrett’s esophagus
Patients with Barrett’s esophagus have about a 0.2% annual chance of developing esophageal adenocarcinoma in the 5 years after initial diagnosis, but the likelihood then rises so that about 9% of all patients will develop cancer by 20 years out, according to a study in the September issue of Gastroenterology.
The modeled rates of progression for the early years after diagnosis are substantially lower than are those reported by prospective studies, which involve more intensive surveillance and therefore suffer from detection bias, said Dr. Sonja Kroep of Erasmus Medical Center, Rotterdam, the Netherlands, and her associates. “Clinicians informing their patients about their cancer risk can best use this clinical progression rate, which is not influenced by surveillance-detected cancers,” they wrote.
Past analyses have yielded varying results for the rate at which Barrett’s esophagus with low-grade dysplasia progresses to high-grade dysplasia and esophageal carcinoma. For their study, Dr. Kroep and her associates calibrated a model based on the annual rate of 0.18% reported by population-level studies, and used it to simulate prospective studies and to predict results from both population-based and prospective studies for various follow-up periods (Gastroenterology 2015 Apr 29. pii: S0016-5085(15)00601-0).
For the first 5 years of follow-up, the model predicted a 0.19% annual rate of transformation to esophageal adenocarcinoma for population-based studies and a 0.36% annual rate for prospective studies, the researchers reported. At 20 years, these rates rose to 0.63% and 0.65% annually, for a cumulative incidence rate of 9.1% to 9.5%. Between the 5-year and 20-year thresholds, the gap between rates of progression for the two types of studies narrowed from 91% to 5%. Taken together, the findings suggest that for the first 5 years after a diagnosis of Barrett’s esophagus, rates of progression to esophageal adenocarcinoma reflect those from population-level studies instead of surveillance-based prospective studies, the investigators said. “Clinicians should use this information to explain to patients their short-term and long-term risks if no action is taken, and then discuss the risks and benefits of surveillance,” they added.
In a separate retrospective study, radiofrequency ablation of low-grade esophageal dysplasia was linked to substantially lower rates of progression compared with watchful waiting in the form of endoscopic surveillance, said Dr. Aaron Small of the University of Pennsylvania, Philadelphia, and his associates. Their study included 125 patients with Barrett’s esophagus and low-grade dysplasia who underwent surveillance only, and 45 patients who underwent radiofrequency ablation at three university medical centers.
Over median follow-up periods of more than 2 years, the risk of progression with radiofrequency ablation was significantly lower than with endoscopic surveillance only, even after the researchers controlled for year of diagnosis (adjusted hazard ratio, 0.06; 95% confidence interval, 0.008-0.48; P = .008). The ablation group also had fewer visible macroscopic lesions, although the difference was not significant. “We estimate that for every three patients treated with radiofrequency ablation, one additional patient with low-grade dysplasia will avoid progression to high-grade dysplasia or esophageal adenocarcinoma within 3 years,” the researchers wrote. “Although selection bias cannot be excluded, these findings provide additional evidence for the use of endoscopic ablation therapy for low-grade dysplasia” (Gastroenterology 2015 Apr 24. pii: S0016-5085(15)00569-7).
The study by Dr. Kroep and her associates was funded by grant U01 CA152926, and the investigators reported having no conflicts of interest. The study by Dr. Small and his associates was supported by the National Institutes of Health/National Institute of Diabetes and Digestive and Kidney Diseases and by institutional funds. Dr. Small reported no conflicts of interest, but seven coauthors reported ties with a number of pharmaceutical companies.
These two studies highlight two different hot topics in the management of patients with a Barrett’s esophagus. The first is the low rate of neoplastic progression in patients undergoing surveillance for nondysplastic BE. The second relates to the management of patients with low-grade dysplasia (LG

|
| Dr. Jacques Bergman |
Population-based BE surveillance studies have shown lower progression rates than have prospective surveillance studies. The biggest difference between these two is that not all patients in population-based studies actually undergo subsequent surveillance endoscopies and/or surveillance is carried out less rigorously than in prospective surveillance studies. Patients who have undergone a baseline endoscopy showing no neoplasia first need to develop early neoplasia (which is generally asymptomatic) that then needs to progress to a symptomatic stage before they are diagnosed. During this interval they may die from other causes or may be lost to follow-up. Patients in strict surveillance programs will be diagnosed at an earlier stage and at a higher rate. This is especially true in the first years of follow-up, when the initial screening endoscopy has its largest effect. Over time, the difference then fades away as suggested by the 9% progression rate of both types of studies at 20 years of follow-up. Both perspectives are relevant for patients. For elderly patients with significant comorbidity, the 5-year data from population-based studies reassure them not to undergo surveillance endoscopies because even when an early cancer develops it is unlikely to bear any clinical relevance, whereas for patients with a long life expectancy, the 9% cancer risk at 20 years and the dismal prognosis of a symptomatic Barrett’s cancer may be strong arguments for participating in a surveillance program.
For patients with LGD, the situation is different: The rate of progression is much higher than that reported for nondysplastic BE, and with radiofrequency ablation (RFA), an effective and safe tool is at hand to significantly reduce this rate of neoplastic progression. Small et al. reported that only three patients need to be treated with RFA to prevent one patient from progressing to high-grade dysplasia or cancer. These data are in agreement with data from a prospective randomized study on the use of RFA for patients with a confirmed diagnosis of LGD. Most societies therefore consider a confirmed histologic diagnosis of LGD a justified indication for prophylactic ablation with RFA.
However, this does not imply that all patients with LGD should be ablated. First, only patients in whom the histologic diagnosis of LGD is confirmed by an expert BE pathologist should be considered for RFA. In approximately 75% of patients, the LGD diagnosis will be downstaged to nondysplastic BE upon expert review. Second, the lessons learned from the Kroep study also apply here: For an elderly LGD patient with or without significant comorbidity, the decision to proceed to RFA is different from the decision for patients with a longer life expectancy, especially if an intermediate solution – to continue endoscopic surveillance and proceed to endoscopic management in case neoplasia is diagnosed – is also considered.
Jacques Bergman, M.D., Ph.D., is professor of gastrointestinal endoscopy, director of endoscopy, at the Academic Medical Center, Amsterdam. He received research support for clinical studies and consulted for Covidien/Medtronic GI solutions.
These two studies highlight two different hot topics in the management of patients with a Barrett’s esophagus. The first is the low rate of neoplastic progression in patients undergoing surveillance for nondysplastic BE. The second relates to the management of patients with low-grade dysplasia (LG
|
|
| Dr. Jacques Bergman |
Population-based BE surveillance studies have shown lower progression rates than have prospective surveillance studies. The biggest difference between these two is that not all patients in population-based studies actually undergo subsequent surveillance endoscopies and/or surveillance is carried out less rigorously than in prospective surveillance studies. Patients who have undergone a baseline endoscopy showing no neoplasia first need to develop early neoplasia (which is generally asymptomatic) that then needs to progress to a symptomatic stage before they are diagnosed. During this interval they may die from other causes or may be lost to follow-up. Patients in strict surveillance programs will be diagnosed at an earlier stage and at a higher rate. This is especially true in the first years of follow-up, when the initial screening endoscopy has its largest effect. Over time, the difference then fades away as suggested by the 9% progression rate of both types of studies at 20 years of follow-up. Both perspectives are relevant for patients. For elderly patients with significant comorbidity, the 5-year data from population-based studies reassure them not to undergo surveillance endoscopies because even when an early cancer develops it is unlikely to bear any clinical relevance, whereas for patients with a long life expectancy, the 9% cancer risk at 20 years and the dismal prognosis of a symptomatic Barrett’s cancer may be strong arguments for participating in a surveillance program.
For patients with LGD, the situation is different: The rate of progression is much higher than that reported for nondysplastic BE, and with radiofrequency ablation (RFA), an effective and safe tool is at hand to significantly reduce this rate of neoplastic progression. Small et al. reported that only three patients need to be treated with RFA to prevent one patient from progressing to high-grade dysplasia or cancer. These data are in agreement with data from a prospective randomized study on the use of RFA for patients with a confirmed diagnosis of LGD. Most societies therefore consider a confirmed histologic diagnosis of LGD a justified indication for prophylactic ablation with RFA.
However, this does not imply that all patients with LGD should be ablated. First, only patients in whom the histologic diagnosis of LGD is confirmed by an expert BE pathologist should be considered for RFA. In approximately 75% of patients, the LGD diagnosis will be downstaged to nondysplastic BE upon expert review. Second, the lessons learned from the Kroep study also apply here: For an elderly LGD patient with or without significant comorbidity, the decision to proceed to RFA is different from the decision for patients with a longer life expectancy, especially if an intermediate solution – to continue endoscopic surveillance and proceed to endoscopic management in case neoplasia is diagnosed – is also considered.
Jacques Bergman, M.D., Ph.D., is professor of gastrointestinal endoscopy, director of endoscopy, at the Academic Medical Center, Amsterdam. He received research support for clinical studies and consulted for Covidien/Medtronic GI solutions.
These two studies highlight two different hot topics in the management of patients with a Barrett’s esophagus. The first is the low rate of neoplastic progression in patients undergoing surveillance for nondysplastic BE. The second relates to the management of patients with low-grade dysplasia (LG
|
|
| Dr. Jacques Bergman |
Population-based BE surveillance studies have shown lower progression rates than have prospective surveillance studies. The biggest difference between these two is that not all patients in population-based studies actually undergo subsequent surveillance endoscopies and/or surveillance is carried out less rigorously than in prospective surveillance studies. Patients who have undergone a baseline endoscopy showing no neoplasia first need to develop early neoplasia (which is generally asymptomatic) that then needs to progress to a symptomatic stage before they are diagnosed. During this interval they may die from other causes or may be lost to follow-up. Patients in strict surveillance programs will be diagnosed at an earlier stage and at a higher rate. This is especially true in the first years of follow-up, when the initial screening endoscopy has its largest effect. Over time, the difference then fades away as suggested by the 9% progression rate of both types of studies at 20 years of follow-up. Both perspectives are relevant for patients. For elderly patients with significant comorbidity, the 5-year data from population-based studies reassure them not to undergo surveillance endoscopies because even when an early cancer develops it is unlikely to bear any clinical relevance, whereas for patients with a long life expectancy, the 9% cancer risk at 20 years and the dismal prognosis of a symptomatic Barrett’s cancer may be strong arguments for participating in a surveillance program.
For patients with LGD, the situation is different: The rate of progression is much higher than that reported for nondysplastic BE, and with radiofrequency ablation (RFA), an effective and safe tool is at hand to significantly reduce this rate of neoplastic progression. Small et al. reported that only three patients need to be treated with RFA to prevent one patient from progressing to high-grade dysplasia or cancer. These data are in agreement with data from a prospective randomized study on the use of RFA for patients with a confirmed diagnosis of LGD. Most societies therefore consider a confirmed histologic diagnosis of LGD a justified indication for prophylactic ablation with RFA.
However, this does not imply that all patients with LGD should be ablated. First, only patients in whom the histologic diagnosis of LGD is confirmed by an expert BE pathologist should be considered for RFA. In approximately 75% of patients, the LGD diagnosis will be downstaged to nondysplastic BE upon expert review. Second, the lessons learned from the Kroep study also apply here: For an elderly LGD patient with or without significant comorbidity, the decision to proceed to RFA is different from the decision for patients with a longer life expectancy, especially if an intermediate solution – to continue endoscopic surveillance and proceed to endoscopic management in case neoplasia is diagnosed – is also considered.
Jacques Bergman, M.D., Ph.D., is professor of gastrointestinal endoscopy, director of endoscopy, at the Academic Medical Center, Amsterdam. He received research support for clinical studies and consulted for Covidien/Medtronic GI solutions.
Patients with Barrett’s esophagus have about a 0.2% annual chance of developing esophageal adenocarcinoma in the 5 years after initial diagnosis, but the likelihood then rises so that about 9% of all patients will develop cancer by 20 years out, according to a study in the September issue of Gastroenterology.
The modeled rates of progression for the early years after diagnosis are substantially lower than are those reported by prospective studies, which involve more intensive surveillance and therefore suffer from detection bias, said Dr. Sonja Kroep of Erasmus Medical Center, Rotterdam, the Netherlands, and her associates. “Clinicians informing their patients about their cancer risk can best use this clinical progression rate, which is not influenced by surveillance-detected cancers,” they wrote.
Past analyses have yielded varying results for the rate at which Barrett’s esophagus with low-grade dysplasia progresses to high-grade dysplasia and esophageal carcinoma. For their study, Dr. Kroep and her associates calibrated a model based on the annual rate of 0.18% reported by population-level studies, and used it to simulate prospective studies and to predict results from both population-based and prospective studies for various follow-up periods (Gastroenterology 2015 Apr 29. pii: S0016-5085(15)00601-0).
For the first 5 years of follow-up, the model predicted a 0.19% annual rate of transformation to esophageal adenocarcinoma for population-based studies and a 0.36% annual rate for prospective studies, the researchers reported. At 20 years, these rates rose to 0.63% and 0.65% annually, for a cumulative incidence rate of 9.1% to 9.5%. Between the 5-year and 20-year thresholds, the gap between rates of progression for the two types of studies narrowed from 91% to 5%. Taken together, the findings suggest that for the first 5 years after a diagnosis of Barrett’s esophagus, rates of progression to esophageal adenocarcinoma reflect those from population-level studies instead of surveillance-based prospective studies, the investigators said. “Clinicians should use this information to explain to patients their short-term and long-term risks if no action is taken, and then discuss the risks and benefits of surveillance,” they added.
In a separate retrospective study, radiofrequency ablation of low-grade esophageal dysplasia was linked to substantially lower rates of progression compared with watchful waiting in the form of endoscopic surveillance, said Dr. Aaron Small of the University of Pennsylvania, Philadelphia, and his associates. Their study included 125 patients with Barrett’s esophagus and low-grade dysplasia who underwent surveillance only, and 45 patients who underwent radiofrequency ablation at three university medical centers.
Over median follow-up periods of more than 2 years, the risk of progression with radiofrequency ablation was significantly lower than with endoscopic surveillance only, even after the researchers controlled for year of diagnosis (adjusted hazard ratio, 0.06; 95% confidence interval, 0.008-0.48; P = .008). The ablation group also had fewer visible macroscopic lesions, although the difference was not significant. “We estimate that for every three patients treated with radiofrequency ablation, one additional patient with low-grade dysplasia will avoid progression to high-grade dysplasia or esophageal adenocarcinoma within 3 years,” the researchers wrote. “Although selection bias cannot be excluded, these findings provide additional evidence for the use of endoscopic ablation therapy for low-grade dysplasia” (Gastroenterology 2015 Apr 24. pii: S0016-5085(15)00569-7).
The study by Dr. Kroep and her associates was funded by grant U01 CA152926, and the investigators reported having no conflicts of interest. The study by Dr. Small and his associates was supported by the National Institutes of Health/National Institute of Diabetes and Digestive and Kidney Diseases and by institutional funds. Dr. Small reported no conflicts of interest, but seven coauthors reported ties with a number of pharmaceutical companies.
Patients with Barrett’s esophagus have about a 0.2% annual chance of developing esophageal adenocarcinoma in the 5 years after initial diagnosis, but the likelihood then rises so that about 9% of all patients will develop cancer by 20 years out, according to a study in the September issue of Gastroenterology.
The modeled rates of progression for the early years after diagnosis are substantially lower than are those reported by prospective studies, which involve more intensive surveillance and therefore suffer from detection bias, said Dr. Sonja Kroep of Erasmus Medical Center, Rotterdam, the Netherlands, and her associates. “Clinicians informing their patients about their cancer risk can best use this clinical progression rate, which is not influenced by surveillance-detected cancers,” they wrote.
Past analyses have yielded varying results for the rate at which Barrett’s esophagus with low-grade dysplasia progresses to high-grade dysplasia and esophageal carcinoma. For their study, Dr. Kroep and her associates calibrated a model based on the annual rate of 0.18% reported by population-level studies, and used it to simulate prospective studies and to predict results from both population-based and prospective studies for various follow-up periods (Gastroenterology 2015 Apr 29. pii: S0016-5085(15)00601-0).
For the first 5 years of follow-up, the model predicted a 0.19% annual rate of transformation to esophageal adenocarcinoma for population-based studies and a 0.36% annual rate for prospective studies, the researchers reported. At 20 years, these rates rose to 0.63% and 0.65% annually, for a cumulative incidence rate of 9.1% to 9.5%. Between the 5-year and 20-year thresholds, the gap between rates of progression for the two types of studies narrowed from 91% to 5%. Taken together, the findings suggest that for the first 5 years after a diagnosis of Barrett’s esophagus, rates of progression to esophageal adenocarcinoma reflect those from population-level studies instead of surveillance-based prospective studies, the investigators said. “Clinicians should use this information to explain to patients their short-term and long-term risks if no action is taken, and then discuss the risks and benefits of surveillance,” they added.
In a separate retrospective study, radiofrequency ablation of low-grade esophageal dysplasia was linked to substantially lower rates of progression compared with watchful waiting in the form of endoscopic surveillance, said Dr. Aaron Small of the University of Pennsylvania, Philadelphia, and his associates. Their study included 125 patients with Barrett’s esophagus and low-grade dysplasia who underwent surveillance only, and 45 patients who underwent radiofrequency ablation at three university medical centers.
Over median follow-up periods of more than 2 years, the risk of progression with radiofrequency ablation was significantly lower than with endoscopic surveillance only, even after the researchers controlled for year of diagnosis (adjusted hazard ratio, 0.06; 95% confidence interval, 0.008-0.48; P = .008). The ablation group also had fewer visible macroscopic lesions, although the difference was not significant. “We estimate that for every three patients treated with radiofrequency ablation, one additional patient with low-grade dysplasia will avoid progression to high-grade dysplasia or esophageal adenocarcinoma within 3 years,” the researchers wrote. “Although selection bias cannot be excluded, these findings provide additional evidence for the use of endoscopic ablation therapy for low-grade dysplasia” (Gastroenterology 2015 Apr 24. pii: S0016-5085(15)00569-7).
The study by Dr. Kroep and her associates was funded by grant U01 CA152926, and the investigators reported having no conflicts of interest. The study by Dr. Small and his associates was supported by the National Institutes of Health/National Institute of Diabetes and Digestive and Kidney Diseases and by institutional funds. Dr. Small reported no conflicts of interest, but seven coauthors reported ties with a number of pharmaceutical companies.
FROM GASTROENTEROLOGY
Key clinical point: Barrett’s esophagus with low-grade dysplasia had a lower rate of progression to cancer than that suggested by prospective surveillance studies, but radiofrequency ablation might further cut the risk.
Major finding: About 0.2% of cases progress during the 5 years after diagnosis, and RFA might significantly decrease risk of progression (adjusted hazard ratio, 0.06).
Data source: A model of rates of progression based on population-level studies, and a multicenter retrospective study of 170 patients with Barrett’s esophagus and low-grade dysplasia.
Disclosures: The study by Dr. Small and associates was supported by the National Institutes of Health/National Institute of Diabetes and Digestive and Kidney Diseases and by institutional funds. Dr. Small reported no conflicts of interest; seven coauthors reported ties with a number of pharmaceutical companies. The study by Dr. Kroep and her associates was funded by grant U01 CA152926, and the investigators reported having no conflicts of interest.

Right-side mini-AVR an option for frail patients
Many patients with aortic valve disease still undergo conventional aortic valve replacement (AVR) with standard full sternotomy or seek out alternative treatments like transcatheter aortic valve insertion (TAVI). But a minimally invasive approach that uses a sutureless prostheses may reduce operation times and put AVR within reach of more frail patients.
Investigators from G. Pasquinucci Heart Hospital in Massa, Italy, reported on 593 patients who had AVR through right anterior minithoracotomy (RAMT) over 10 years at their institution (J Thorac Cardiovasc Surg. 2015. doi: 10.1016/j.jtcvs.2015.06.045). In 302 of the patients, the researchers used a sutureless or rapidly implantable biological prosthesis.
“More surgeons should enrich their armamentarium by RAMT AVR,” lead author Dr. Mattia Glauber and his coauthors said. “Sutureless prostheses can increase adoption of RAMT AVR.”
The authors acknowledged that minimally invasive approaches to AVR, including partial sternotomy, require longer operation times than open surgery despite reduced aortic cross-clamping and cardiopulmonary bypass times, but have resulted in better outcomes and lower death rates.
A new generation of aortic valve prostheses, including sutureless devices, have emerged in an attempt to further reduce operative times and improve outcomes, so the Italian investigators designed their study to compare early and midterm outcomes after minimally invasive AVR using sutured and sutureless repair at their institution between 2004 and 2014.
In 302 (50.9%) patients, sutureless or rapidly implantable biological prosthesis was used, 23 (3.9%) had a mechanical prosthesis, and the remainder received a conventional biological prosthesis.
The investigators determined patients were suitable for RAMT if CT scan showed specific anatomic features, including rightward positioning of the ascending aorta at the level of the main pulmonary artery. Once the sutureless prostheses became available in 2011, every patient undergoing AVR via RAMT was considered a potential candidate, although the investigators decided that patients with type 1 and 2 bicuspid aortic valves without raphe and asymmetric aortic root were not suitable for the sutureless approach.
The subgroup that underwent sutureless repair tended to be older and sicker than the overall study population and had a higher prevalence of tricuspid aortic valve and aortic stenosis, a slightly higher body mass index, and a higher propensity to be obese. The sutureless subgroup also had fewer smokers.
Cardiopulmonary bypass time averaged 88 minutes and aortic cross-clamping times 55 minutes in the sutureless subgroup vs. 107 and 74 minutes, respectively, in the overall RAMT study subgroup.
The death before discharge rate of patients who had RAMT repair was 1%, and the 30-day in-hospital death rate was 1.5%. Overall, 97% of patients who had RAMT did not require reoperation at 5 years.
Between the sutured and sutureless subgroups, hospital and intensive care unit lengths of stay were similar, as were bleeding rates and in-hospital mortality. One measure in which the two subgroups deviated was prolonged ICU stay – a rate of 11.3% in the sutureless subgroup and 6.6% in the sutured subgroup.
“To the best of our knowledge, this is the largest up-to-date single-center experience on minimally invasive AVR through RAMT,” Dr. Glauber and coauthors said. “Our data along with earlier reports confirm that minimally invasive AVR through RAMT is safe and reproducible. It is associated with low perioperative mortality and morbidity.”
Dr. Glauber and coauthor Dr. Marco Solinas disclosed a commercial/financial relationship with Sorin Group.
“Have we found the end of the road, and the future for isolated AVR is made up of RAMT with sutureless AVR?” asks Dr. Patrick M. McCarthy, chief of cardiac surgery at Northwestern University Feinberg School of Medicine in Chicago, in his invited commentary (J Thorac Cardiovasc Surg. 2015. doi: 10.1016/j.jtcvs.2015.07.007). “The cardiology literature serves as a reality check.”
He noted that results from the NOTION Trial of transaortic valve replacement (TAVR) vs. surgical AVR (J Am Coll Cardiol. 2015;65:2184-94) had 30-day results similar to the G. Pasquinucci Heart Hospital results. However, 34% in the TAVR group in NOTION needed pacemakers, and 16% had moderate or greater valvular regurgitation and higher rates of dyspnea.

|
Dr. Patrick M. McCarthy |
Right anterior minithoracotomy is different from other minimally invasive approaches, Dr. McCarthy said. “It’s more of a tunnel down to the aortic valve which is why patient selection based on anatomic factors determined by preoperative CT scan (which is an unnecessary expense for hemisternotomy) is so important,” he said.
The evolution of TAVR is still in the early stage, so the “flaws” involved in the approach can yet be eliminated, “but the message that TAVR outcomes today are still very different than [surgical] AVR in low-risk patients, the type that have a minimally invasive AVR, may be lost on many readers,” Dr. McCarthy said.
For isolated aortic stenosis, the era of minimally invasive procedures that involve bypass, cross-clamping and a difficult surgical approach may be fading, he said. “The handwriting is on the wall, or in the journals in this case.”
Dr. McCarthy disclosed relationships with Edwards Lifesciences and Abbott Vascular. He is the inventor of the Edwards MC3 Ring and dETlogix Ring and coinventor of the IMR ETlogix Ring.
“Have we found the end of the road, and the future for isolated AVR is made up of RAMT with sutureless AVR?” asks Dr. Patrick M. McCarthy, chief of cardiac surgery at Northwestern University Feinberg School of Medicine in Chicago, in his invited commentary (J Thorac Cardiovasc Surg. 2015. doi: 10.1016/j.jtcvs.2015.07.007). “The cardiology literature serves as a reality check.”
He noted that results from the NOTION Trial of transaortic valve replacement (TAVR) vs. surgical AVR (J Am Coll Cardiol. 2015;65:2184-94) had 30-day results similar to the G. Pasquinucci Heart Hospital results. However, 34% in the TAVR group in NOTION needed pacemakers, and 16% had moderate or greater valvular regurgitation and higher rates of dyspnea.
|
|
Dr. Patrick M. McCarthy |
Right anterior minithoracotomy is different from other minimally invasive approaches, Dr. McCarthy said. “It’s more of a tunnel down to the aortic valve which is why patient selection based on anatomic factors determined by preoperative CT scan (which is an unnecessary expense for hemisternotomy) is so important,” he said.
The evolution of TAVR is still in the early stage, so the “flaws” involved in the approach can yet be eliminated, “but the message that TAVR outcomes today are still very different than [surgical] AVR in low-risk patients, the type that have a minimally invasive AVR, may be lost on many readers,” Dr. McCarthy said.
For isolated aortic stenosis, the era of minimally invasive procedures that involve bypass, cross-clamping and a difficult surgical approach may be fading, he said. “The handwriting is on the wall, or in the journals in this case.”
Dr. McCarthy disclosed relationships with Edwards Lifesciences and Abbott Vascular. He is the inventor of the Edwards MC3 Ring and dETlogix Ring and coinventor of the IMR ETlogix Ring.
“Have we found the end of the road, and the future for isolated AVR is made up of RAMT with sutureless AVR?” asks Dr. Patrick M. McCarthy, chief of cardiac surgery at Northwestern University Feinberg School of Medicine in Chicago, in his invited commentary (J Thorac Cardiovasc Surg. 2015. doi: 10.1016/j.jtcvs.2015.07.007). “The cardiology literature serves as a reality check.”
He noted that results from the NOTION Trial of transaortic valve replacement (TAVR) vs. surgical AVR (J Am Coll Cardiol. 2015;65:2184-94) had 30-day results similar to the G. Pasquinucci Heart Hospital results. However, 34% in the TAVR group in NOTION needed pacemakers, and 16% had moderate or greater valvular regurgitation and higher rates of dyspnea.
|
|
Dr. Patrick M. McCarthy |
Right anterior minithoracotomy is different from other minimally invasive approaches, Dr. McCarthy said. “It’s more of a tunnel down to the aortic valve which is why patient selection based on anatomic factors determined by preoperative CT scan (which is an unnecessary expense for hemisternotomy) is so important,” he said.
The evolution of TAVR is still in the early stage, so the “flaws” involved in the approach can yet be eliminated, “but the message that TAVR outcomes today are still very different than [surgical] AVR in low-risk patients, the type that have a minimally invasive AVR, may be lost on many readers,” Dr. McCarthy said.
For isolated aortic stenosis, the era of minimally invasive procedures that involve bypass, cross-clamping and a difficult surgical approach may be fading, he said. “The handwriting is on the wall, or in the journals in this case.”
Dr. McCarthy disclosed relationships with Edwards Lifesciences and Abbott Vascular. He is the inventor of the Edwards MC3 Ring and dETlogix Ring and coinventor of the IMR ETlogix Ring.
Many patients with aortic valve disease still undergo conventional aortic valve replacement (AVR) with standard full sternotomy or seek out alternative treatments like transcatheter aortic valve insertion (TAVI). But a minimally invasive approach that uses a sutureless prostheses may reduce operation times and put AVR within reach of more frail patients.
Investigators from G. Pasquinucci Heart Hospital in Massa, Italy, reported on 593 patients who had AVR through right anterior minithoracotomy (RAMT) over 10 years at their institution (J Thorac Cardiovasc Surg. 2015. doi: 10.1016/j.jtcvs.2015.06.045). In 302 of the patients, the researchers used a sutureless or rapidly implantable biological prosthesis.
“More surgeons should enrich their armamentarium by RAMT AVR,” lead author Dr. Mattia Glauber and his coauthors said. “Sutureless prostheses can increase adoption of RAMT AVR.”
The authors acknowledged that minimally invasive approaches to AVR, including partial sternotomy, require longer operation times than open surgery despite reduced aortic cross-clamping and cardiopulmonary bypass times, but have resulted in better outcomes and lower death rates.
A new generation of aortic valve prostheses, including sutureless devices, have emerged in an attempt to further reduce operative times and improve outcomes, so the Italian investigators designed their study to compare early and midterm outcomes after minimally invasive AVR using sutured and sutureless repair at their institution between 2004 and 2014.
In 302 (50.9%) patients, sutureless or rapidly implantable biological prosthesis was used, 23 (3.9%) had a mechanical prosthesis, and the remainder received a conventional biological prosthesis.
The investigators determined patients were suitable for RAMT if CT scan showed specific anatomic features, including rightward positioning of the ascending aorta at the level of the main pulmonary artery. Once the sutureless prostheses became available in 2011, every patient undergoing AVR via RAMT was considered a potential candidate, although the investigators decided that patients with type 1 and 2 bicuspid aortic valves without raphe and asymmetric aortic root were not suitable for the sutureless approach.
The subgroup that underwent sutureless repair tended to be older and sicker than the overall study population and had a higher prevalence of tricuspid aortic valve and aortic stenosis, a slightly higher body mass index, and a higher propensity to be obese. The sutureless subgroup also had fewer smokers.
Cardiopulmonary bypass time averaged 88 minutes and aortic cross-clamping times 55 minutes in the sutureless subgroup vs. 107 and 74 minutes, respectively, in the overall RAMT study subgroup.
The death before discharge rate of patients who had RAMT repair was 1%, and the 30-day in-hospital death rate was 1.5%. Overall, 97% of patients who had RAMT did not require reoperation at 5 years.
Between the sutured and sutureless subgroups, hospital and intensive care unit lengths of stay were similar, as were bleeding rates and in-hospital mortality. One measure in which the two subgroups deviated was prolonged ICU stay – a rate of 11.3% in the sutureless subgroup and 6.6% in the sutured subgroup.
“To the best of our knowledge, this is the largest up-to-date single-center experience on minimally invasive AVR through RAMT,” Dr. Glauber and coauthors said. “Our data along with earlier reports confirm that minimally invasive AVR through RAMT is safe and reproducible. It is associated with low perioperative mortality and morbidity.”
Dr. Glauber and coauthor Dr. Marco Solinas disclosed a commercial/financial relationship with Sorin Group.
Many patients with aortic valve disease still undergo conventional aortic valve replacement (AVR) with standard full sternotomy or seek out alternative treatments like transcatheter aortic valve insertion (TAVI). But a minimally invasive approach that uses a sutureless prostheses may reduce operation times and put AVR within reach of more frail patients.
Investigators from G. Pasquinucci Heart Hospital in Massa, Italy, reported on 593 patients who had AVR through right anterior minithoracotomy (RAMT) over 10 years at their institution (J Thorac Cardiovasc Surg. 2015. doi: 10.1016/j.jtcvs.2015.06.045). In 302 of the patients, the researchers used a sutureless or rapidly implantable biological prosthesis.
“More surgeons should enrich their armamentarium by RAMT AVR,” lead author Dr. Mattia Glauber and his coauthors said. “Sutureless prostheses can increase adoption of RAMT AVR.”
The authors acknowledged that minimally invasive approaches to AVR, including partial sternotomy, require longer operation times than open surgery despite reduced aortic cross-clamping and cardiopulmonary bypass times, but have resulted in better outcomes and lower death rates.
A new generation of aortic valve prostheses, including sutureless devices, have emerged in an attempt to further reduce operative times and improve outcomes, so the Italian investigators designed their study to compare early and midterm outcomes after minimally invasive AVR using sutured and sutureless repair at their institution between 2004 and 2014.
In 302 (50.9%) patients, sutureless or rapidly implantable biological prosthesis was used, 23 (3.9%) had a mechanical prosthesis, and the remainder received a conventional biological prosthesis.
The investigators determined patients were suitable for RAMT if CT scan showed specific anatomic features, including rightward positioning of the ascending aorta at the level of the main pulmonary artery. Once the sutureless prostheses became available in 2011, every patient undergoing AVR via RAMT was considered a potential candidate, although the investigators decided that patients with type 1 and 2 bicuspid aortic valves without raphe and asymmetric aortic root were not suitable for the sutureless approach.
The subgroup that underwent sutureless repair tended to be older and sicker than the overall study population and had a higher prevalence of tricuspid aortic valve and aortic stenosis, a slightly higher body mass index, and a higher propensity to be obese. The sutureless subgroup also had fewer smokers.
Cardiopulmonary bypass time averaged 88 minutes and aortic cross-clamping times 55 minutes in the sutureless subgroup vs. 107 and 74 minutes, respectively, in the overall RAMT study subgroup.
The death before discharge rate of patients who had RAMT repair was 1%, and the 30-day in-hospital death rate was 1.5%. Overall, 97% of patients who had RAMT did not require reoperation at 5 years.
Between the sutured and sutureless subgroups, hospital and intensive care unit lengths of stay were similar, as were bleeding rates and in-hospital mortality. One measure in which the two subgroups deviated was prolonged ICU stay – a rate of 11.3% in the sutureless subgroup and 6.6% in the sutured subgroup.
“To the best of our knowledge, this is the largest up-to-date single-center experience on minimally invasive AVR through RAMT,” Dr. Glauber and coauthors said. “Our data along with earlier reports confirm that minimally invasive AVR through RAMT is safe and reproducible. It is associated with low perioperative mortality and morbidity.”
Dr. Glauber and coauthor Dr. Marco Solinas disclosed a commercial/financial relationship with Sorin Group.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: Aortic valve replacement through right anterior minithoracotomy provides excellent outcomes. Sutureless prostheses facilitate mini-AVR.
Major finding: Study subjects had a survival rate of 95% at 31.5 months follow-up on average, and operative times were significantly shorter with sutureless prostheses, compared with sutured prostheses.
Data source: A retrospective, observational cohort study with prospective data collection on 593 patients who had right anterior minithoracotomy for AVR at a single institution over a 10-yar period.
Disclosures: Study coauthors Mattia Glauber and Marco Solinas disclosed a commercial/financial relationship with Sorin Group.

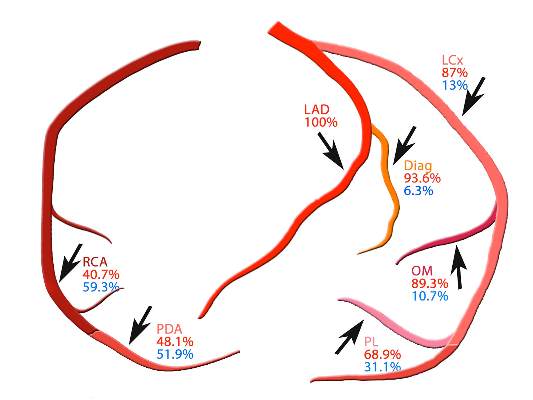
SYNTAX: Early CABG results with arterial grafts similar to venous in matched groups
While single-center studies have supported the advantages of multiple arterial grafts over venous grafts in coronary artery bypass surgery, an analysis of patients in the international and multicenter SYNTAX trial has shown that, on propensity matching, rates of cardiac events and death are actually similar between the two groups.
These findings of the SYNTAX investigators, led by Dr. Catalina Parasca of Erasmus University in Rotterdam, the Netherlands, were published online in the Journal of Thoracic and Cardiovascular Surgery (doi:10.1016/j.jtcvs.2015.05.010).
The SYNTAX trial compared percutaneous coronary intervention (PCI) with coronary artery bypass grafting (CABG) in patients with left main or three-vessel coronary artery disease (Lancet. 2013;381[9867]:629-38).
In the latest report, the SYNTAX investigators found that patients in unmatched groups who received arterial grafts in addition to an arterial graft of the left anterior descending artery (LAD) had noticeably lower rates of death and a composite endpoint of death-stroke-MI than did those who received a second venous graft. However, when the researchers applied propensity matching, the outcomes between the two groups were similar.
Because large randomized trials have yet to prove the superiority of multiarterial grafts, the adoption rate has been low, Dr. Parasca and colleagues said. “The objective of this study was to assess the effect of using a second arterial graft on 5-year outcomes in patients who underwent CABG in the SYNTAX trial and registry,” they said.
They looked at 1,322 SYNTAX trial patients who had CABG with 5-year follow-up. In unmatched groups, the safety endpoint of the death-stroke-MI composite was 13.3% in the multiarterial group vs. 18.7% in the vein graft group. Although the incidence of stroke, MI, and graft occlusion was similar between the unmatched groups, the second-graft arterial group had a higher revascularization rate at 5 years, 12.6% vs. 9.6%, mainly due to repeat PCI. The element of the composite where the two unmatched groups deviated was the all-cause death rate at 5 years: 8.9% in the second-graft arterial group and 13.1% in the venous group.
However, when the investigators applied propensity matching, the differences between the two groups were insignificant.
“The results of the present study must be seen in the light of a multicenter CABG cohort with complex coronary disease, where revascularization was performed according to surgeon’s personal experience and local practices,” Dr. Parasca and coauthors noted. “The result was a high heterogeneity of CABG techniques, which shows different understanding of the best ‘graft-target match’ across centers.”
While the SYNTAX analysis demonstrates the variation in patient selection and operator technique with regard to arterial revascularization typical of a multicenter study, “extended follow-up beyond 5 years is required to estimate its impact on long-term outcomes,” Dr. Parasca and colleagues said.
Boston Scientific supported the trial. Coauthor Keith Dawkins is employed by Boston Scientific and coauthor Ted Feldman has received consulting fees from the company. The other authors reported no disclosures.
That arterial grafts are a better long-term match in coronary bypass surgery has been a tenet in cardiac surgery, but multiple factors have prevented their more widespread acceptance, Dr. Davis C. Drinkwater Jr. said in his invited commentary (J Thorac Cardiovasc Surg. 2015.doi:10.1016/j.jtcvs.2015.06.014). Concerns about sternal wound healing, particularly in diabetic or obese patients, as well as the alternative generally good early and mid-term results in multivessel coronary artery disease using the left internal thoracic artery to LAD accompanied by saphenous vein grafts, have made surgeons hesitant to take up the approach more readily, said Dr. Drinkwater of Frist Cardiology, Tristar Centennial Medical Center, Nashville, Tenn.
The SYNTAX investigators’ main finding of no survival advantage among the matched groups at 5 years is in line with most reports comparing patency between arterial and venous grafts, “requiring between 5- and 10-year follow-up to show a divergence,” Dr. Drinkwater said.
He pointed out that the patients who had second arterial grafts in the unmatched group were younger and healthier – the average age was 62 years, and 27% of them had previous heart attacks, compared with 66 years of age and a heart attack rate of 35.6% in the venous graft group – and that may explain the higher reintervention rate in the former group. Another factor may be the younger and healthier patients had longer cardiopulmonary bypass and aortic cross clamp times despite a greater percentage having undergone the off-pump technique.
“This counterintuitive information underscores an inherent weakness of this multicenter trial that is without surgical randomization into the two arterial groups, and with potentially varied surgical experience using nonstandardized technical and management protocols,” Dr. Drinkwater said. “This is in stark contrast to the previous and well accepted single high-volume-center reports of the benefits of using multiple arterial bypass grafts.”
Because the report points out the technical challenges of achieving complete revascularization with multiple arterial grafting at “the early” interval of up to 5 years, the authors may be inappropriately discouraging centers that do not currently offer multiarterial grafting from embracing it, Dr. Drinkwater concluded.
He had no disclosures to report.
That arterial grafts are a better long-term match in coronary bypass surgery has been a tenet in cardiac surgery, but multiple factors have prevented their more widespread acceptance, Dr. Davis C. Drinkwater Jr. said in his invited commentary (J Thorac Cardiovasc Surg. 2015.doi:10.1016/j.jtcvs.2015.06.014). Concerns about sternal wound healing, particularly in diabetic or obese patients, as well as the alternative generally good early and mid-term results in multivessel coronary artery disease using the left internal thoracic artery to LAD accompanied by saphenous vein grafts, have made surgeons hesitant to take up the approach more readily, said Dr. Drinkwater of Frist Cardiology, Tristar Centennial Medical Center, Nashville, Tenn.
The SYNTAX investigators’ main finding of no survival advantage among the matched groups at 5 years is in line with most reports comparing patency between arterial and venous grafts, “requiring between 5- and 10-year follow-up to show a divergence,” Dr. Drinkwater said.
He pointed out that the patients who had second arterial grafts in the unmatched group were younger and healthier – the average age was 62 years, and 27% of them had previous heart attacks, compared with 66 years of age and a heart attack rate of 35.6% in the venous graft group – and that may explain the higher reintervention rate in the former group. Another factor may be the younger and healthier patients had longer cardiopulmonary bypass and aortic cross clamp times despite a greater percentage having undergone the off-pump technique.
“This counterintuitive information underscores an inherent weakness of this multicenter trial that is without surgical randomization into the two arterial groups, and with potentially varied surgical experience using nonstandardized technical and management protocols,” Dr. Drinkwater said. “This is in stark contrast to the previous and well accepted single high-volume-center reports of the benefits of using multiple arterial bypass grafts.”
Because the report points out the technical challenges of achieving complete revascularization with multiple arterial grafting at “the early” interval of up to 5 years, the authors may be inappropriately discouraging centers that do not currently offer multiarterial grafting from embracing it, Dr. Drinkwater concluded.
He had no disclosures to report.
That arterial grafts are a better long-term match in coronary bypass surgery has been a tenet in cardiac surgery, but multiple factors have prevented their more widespread acceptance, Dr. Davis C. Drinkwater Jr. said in his invited commentary (J Thorac Cardiovasc Surg. 2015.doi:10.1016/j.jtcvs.2015.06.014). Concerns about sternal wound healing, particularly in diabetic or obese patients, as well as the alternative generally good early and mid-term results in multivessel coronary artery disease using the left internal thoracic artery to LAD accompanied by saphenous vein grafts, have made surgeons hesitant to take up the approach more readily, said Dr. Drinkwater of Frist Cardiology, Tristar Centennial Medical Center, Nashville, Tenn.
The SYNTAX investigators’ main finding of no survival advantage among the matched groups at 5 years is in line with most reports comparing patency between arterial and venous grafts, “requiring between 5- and 10-year follow-up to show a divergence,” Dr. Drinkwater said.
He pointed out that the patients who had second arterial grafts in the unmatched group were younger and healthier – the average age was 62 years, and 27% of them had previous heart attacks, compared with 66 years of age and a heart attack rate of 35.6% in the venous graft group – and that may explain the higher reintervention rate in the former group. Another factor may be the younger and healthier patients had longer cardiopulmonary bypass and aortic cross clamp times despite a greater percentage having undergone the off-pump technique.
“This counterintuitive information underscores an inherent weakness of this multicenter trial that is without surgical randomization into the two arterial groups, and with potentially varied surgical experience using nonstandardized technical and management protocols,” Dr. Drinkwater said. “This is in stark contrast to the previous and well accepted single high-volume-center reports of the benefits of using multiple arterial bypass grafts.”
Because the report points out the technical challenges of achieving complete revascularization with multiple arterial grafting at “the early” interval of up to 5 years, the authors may be inappropriately discouraging centers that do not currently offer multiarterial grafting from embracing it, Dr. Drinkwater concluded.
He had no disclosures to report.
While single-center studies have supported the advantages of multiple arterial grafts over venous grafts in coronary artery bypass surgery, an analysis of patients in the international and multicenter SYNTAX trial has shown that, on propensity matching, rates of cardiac events and death are actually similar between the two groups.
These findings of the SYNTAX investigators, led by Dr. Catalina Parasca of Erasmus University in Rotterdam, the Netherlands, were published online in the Journal of Thoracic and Cardiovascular Surgery (doi:10.1016/j.jtcvs.2015.05.010).
The SYNTAX trial compared percutaneous coronary intervention (PCI) with coronary artery bypass grafting (CABG) in patients with left main or three-vessel coronary artery disease (Lancet. 2013;381[9867]:629-38).
In the latest report, the SYNTAX investigators found that patients in unmatched groups who received arterial grafts in addition to an arterial graft of the left anterior descending artery (LAD) had noticeably lower rates of death and a composite endpoint of death-stroke-MI than did those who received a second venous graft. However, when the researchers applied propensity matching, the outcomes between the two groups were similar.
Because large randomized trials have yet to prove the superiority of multiarterial grafts, the adoption rate has been low, Dr. Parasca and colleagues said. “The objective of this study was to assess the effect of using a second arterial graft on 5-year outcomes in patients who underwent CABG in the SYNTAX trial and registry,” they said.
They looked at 1,322 SYNTAX trial patients who had CABG with 5-year follow-up. In unmatched groups, the safety endpoint of the death-stroke-MI composite was 13.3% in the multiarterial group vs. 18.7% in the vein graft group. Although the incidence of stroke, MI, and graft occlusion was similar between the unmatched groups, the second-graft arterial group had a higher revascularization rate at 5 years, 12.6% vs. 9.6%, mainly due to repeat PCI. The element of the composite where the two unmatched groups deviated was the all-cause death rate at 5 years: 8.9% in the second-graft arterial group and 13.1% in the venous group.
However, when the investigators applied propensity matching, the differences between the two groups were insignificant.
“The results of the present study must be seen in the light of a multicenter CABG cohort with complex coronary disease, where revascularization was performed according to surgeon’s personal experience and local practices,” Dr. Parasca and coauthors noted. “The result was a high heterogeneity of CABG techniques, which shows different understanding of the best ‘graft-target match’ across centers.”
While the SYNTAX analysis demonstrates the variation in patient selection and operator technique with regard to arterial revascularization typical of a multicenter study, “extended follow-up beyond 5 years is required to estimate its impact on long-term outcomes,” Dr. Parasca and colleagues said.
Boston Scientific supported the trial. Coauthor Keith Dawkins is employed by Boston Scientific and coauthor Ted Feldman has received consulting fees from the company. The other authors reported no disclosures.
While single-center studies have supported the advantages of multiple arterial grafts over venous grafts in coronary artery bypass surgery, an analysis of patients in the international and multicenter SYNTAX trial has shown that, on propensity matching, rates of cardiac events and death are actually similar between the two groups.
These findings of the SYNTAX investigators, led by Dr. Catalina Parasca of Erasmus University in Rotterdam, the Netherlands, were published online in the Journal of Thoracic and Cardiovascular Surgery (doi:10.1016/j.jtcvs.2015.05.010).
The SYNTAX trial compared percutaneous coronary intervention (PCI) with coronary artery bypass grafting (CABG) in patients with left main or three-vessel coronary artery disease (Lancet. 2013;381[9867]:629-38).
In the latest report, the SYNTAX investigators found that patients in unmatched groups who received arterial grafts in addition to an arterial graft of the left anterior descending artery (LAD) had noticeably lower rates of death and a composite endpoint of death-stroke-MI than did those who received a second venous graft. However, when the researchers applied propensity matching, the outcomes between the two groups were similar.
Because large randomized trials have yet to prove the superiority of multiarterial grafts, the adoption rate has been low, Dr. Parasca and colleagues said. “The objective of this study was to assess the effect of using a second arterial graft on 5-year outcomes in patients who underwent CABG in the SYNTAX trial and registry,” they said.
They looked at 1,322 SYNTAX trial patients who had CABG with 5-year follow-up. In unmatched groups, the safety endpoint of the death-stroke-MI composite was 13.3% in the multiarterial group vs. 18.7% in the vein graft group. Although the incidence of stroke, MI, and graft occlusion was similar between the unmatched groups, the second-graft arterial group had a higher revascularization rate at 5 years, 12.6% vs. 9.6%, mainly due to repeat PCI. The element of the composite where the two unmatched groups deviated was the all-cause death rate at 5 years: 8.9% in the second-graft arterial group and 13.1% in the venous group.
However, when the investigators applied propensity matching, the differences between the two groups were insignificant.
“The results of the present study must be seen in the light of a multicenter CABG cohort with complex coronary disease, where revascularization was performed according to surgeon’s personal experience and local practices,” Dr. Parasca and coauthors noted. “The result was a high heterogeneity of CABG techniques, which shows different understanding of the best ‘graft-target match’ across centers.”
While the SYNTAX analysis demonstrates the variation in patient selection and operator technique with regard to arterial revascularization typical of a multicenter study, “extended follow-up beyond 5 years is required to estimate its impact on long-term outcomes,” Dr. Parasca and colleagues said.
Boston Scientific supported the trial. Coauthor Keith Dawkins is employed by Boston Scientific and coauthor Ted Feldman has received consulting fees from the company. The other authors reported no disclosures.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: Surgeons should choose arterial grafts for multigraft coronary artery bypass surgery when feasible.
Major finding: Patients who received multiple arterial graft had significantly lower rates of death and other problems than did those who received venous grafts in unmatched groups, but results were similar between propensity matched groups.
Data source: Registry of 1,322 patients who had 5-year follow-up after coronary artery bypass surgery within the SYNTAX trial.
Disclosures: Boston Scientific supported the trial. Coauthor Keith Dawkins is employed by Boston Scientific and coauthor Ted Feldman has received consulting fees from the company. The other authors reported no disclosures.
Adjuvant erlotinib showed no benefit in NSCLC patients
Among patients with completely resected non–small-cell lung cancer (NSCLC) whose tumors expressed epidermal growth factor receptor (EGFR), disease-free survival (DFS) rates were similar between erlotinib and placebo groups, according to results from the RADIANT phase III trial.
EGFR-activating mutations (EGFRm) were observed in a subgroup of patients (16.5%, 89 with del19 and 72 with L858R mutations) but these patients were not stratified by mutation status, which limited interpretation of the results. For the erlotinib vs. placebo arms of the EGFRm-positive subgroup, median DFS was 46.4 and 28.5 months, respectively, with 2-year DFS rates of 75% and 54%. The results were not statistically significant due to hierarchical testing. There were between-arm imbalances of disease characteristics, and the placebo arm of the EGFRm-positive subgroup had substantially worse DFS than the intention-to-treat population.

“The trend toward improvement in DFS with erlotinib in the EGFRm-positive subgroup warrants further evaluation,” wrote Dr. Karen Kelly of UC Davis Comprehensive Cancer Center, Sacramento, California, and colleagues (J Clin Oncol. 2015 Aug 31. doi:10.1200/JCO.2015.61.8918).
The randomized, double-blind, placebo-controlled RADIANT trial included 973 patients with completely resected stage IB to IIIA NSCLC with EGFR-expressing tumors by immunohistochemistry (IHC) and EGFR high copy number or amplification by fluorescence in situ hybridization (FISH). Previous studies indicated that EGFR protein expression detected by IHC and FISH may be predictive of prolonged survival with EGFR tyrosine kinase inhibitors (TKIs) such as erlotinib. However, subsequent to activation of the RADIANT trial, two phase III studies failed to show that IHC and FISH results were predictive of EGFR-TKI efficacy. Emerging data show that EGFRm-positive status is the strongest predictor of EFGR-TKI sensitivity.
The duration of treatment in the RADIANT trial was 2 years, but the authors speculate that, based on results from the recent SELECT trial in which only four patients experienced relapse while taking erlotinib, a longer treatment duration “may be needed to achieve the goal of increasing the cure rate of early-stage NSCLC in an EGFRm-positive population.”
KRAS mutation status, tested in 828 patient samples, was not prognostic and did not predict erlotinib benefit.
The study was supported by Astellas Pharma Global Development, F. Hoffmann-La Roche, and Genentech. Dr. Kelly reported having no disclosures. Several of her coauthors were employed by or reported consulting or advisory roles with industry sources.
Among patients with completely resected non–small-cell lung cancer (NSCLC) whose tumors expressed epidermal growth factor receptor (EGFR), disease-free survival (DFS) rates were similar between erlotinib and placebo groups, according to results from the RADIANT phase III trial.
EGFR-activating mutations (EGFRm) were observed in a subgroup of patients (16.5%, 89 with del19 and 72 with L858R mutations) but these patients were not stratified by mutation status, which limited interpretation of the results. For the erlotinib vs. placebo arms of the EGFRm-positive subgroup, median DFS was 46.4 and 28.5 months, respectively, with 2-year DFS rates of 75% and 54%. The results were not statistically significant due to hierarchical testing. There were between-arm imbalances of disease characteristics, and the placebo arm of the EGFRm-positive subgroup had substantially worse DFS than the intention-to-treat population.
“The trend toward improvement in DFS with erlotinib in the EGFRm-positive subgroup warrants further evaluation,” wrote Dr. Karen Kelly of UC Davis Comprehensive Cancer Center, Sacramento, California, and colleagues (J Clin Oncol. 2015 Aug 31. doi:10.1200/JCO.2015.61.8918).
The randomized, double-blind, placebo-controlled RADIANT trial included 973 patients with completely resected stage IB to IIIA NSCLC with EGFR-expressing tumors by immunohistochemistry (IHC) and EGFR high copy number or amplification by fluorescence in situ hybridization (FISH). Previous studies indicated that EGFR protein expression detected by IHC and FISH may be predictive of prolonged survival with EGFR tyrosine kinase inhibitors (TKIs) such as erlotinib. However, subsequent to activation of the RADIANT trial, two phase III studies failed to show that IHC and FISH results were predictive of EGFR-TKI efficacy. Emerging data show that EGFRm-positive status is the strongest predictor of EFGR-TKI sensitivity.
The duration of treatment in the RADIANT trial was 2 years, but the authors speculate that, based on results from the recent SELECT trial in which only four patients experienced relapse while taking erlotinib, a longer treatment duration “may be needed to achieve the goal of increasing the cure rate of early-stage NSCLC in an EGFRm-positive population.”
KRAS mutation status, tested in 828 patient samples, was not prognostic and did not predict erlotinib benefit.
The study was supported by Astellas Pharma Global Development, F. Hoffmann-La Roche, and Genentech. Dr. Kelly reported having no disclosures. Several of her coauthors were employed by or reported consulting or advisory roles with industry sources.
Among patients with completely resected non–small-cell lung cancer (NSCLC) whose tumors expressed epidermal growth factor receptor (EGFR), disease-free survival (DFS) rates were similar between erlotinib and placebo groups, according to results from the RADIANT phase III trial.
EGFR-activating mutations (EGFRm) were observed in a subgroup of patients (16.5%, 89 with del19 and 72 with L858R mutations) but these patients were not stratified by mutation status, which limited interpretation of the results. For the erlotinib vs. placebo arms of the EGFRm-positive subgroup, median DFS was 46.4 and 28.5 months, respectively, with 2-year DFS rates of 75% and 54%. The results were not statistically significant due to hierarchical testing. There were between-arm imbalances of disease characteristics, and the placebo arm of the EGFRm-positive subgroup had substantially worse DFS than the intention-to-treat population.
“The trend toward improvement in DFS with erlotinib in the EGFRm-positive subgroup warrants further evaluation,” wrote Dr. Karen Kelly of UC Davis Comprehensive Cancer Center, Sacramento, California, and colleagues (J Clin Oncol. 2015 Aug 31. doi:10.1200/JCO.2015.61.8918).
The randomized, double-blind, placebo-controlled RADIANT trial included 973 patients with completely resected stage IB to IIIA NSCLC with EGFR-expressing tumors by immunohistochemistry (IHC) and EGFR high copy number or amplification by fluorescence in situ hybridization (FISH). Previous studies indicated that EGFR protein expression detected by IHC and FISH may be predictive of prolonged survival with EGFR tyrosine kinase inhibitors (TKIs) such as erlotinib. However, subsequent to activation of the RADIANT trial, two phase III studies failed to show that IHC and FISH results were predictive of EGFR-TKI efficacy. Emerging data show that EGFRm-positive status is the strongest predictor of EFGR-TKI sensitivity.
The duration of treatment in the RADIANT trial was 2 years, but the authors speculate that, based on results from the recent SELECT trial in which only four patients experienced relapse while taking erlotinib, a longer treatment duration “may be needed to achieve the goal of increasing the cure rate of early-stage NSCLC in an EGFRm-positive population.”
KRAS mutation status, tested in 828 patient samples, was not prognostic and did not predict erlotinib benefit.
The study was supported by Astellas Pharma Global Development, F. Hoffmann-La Roche, and Genentech. Dr. Kelly reported having no disclosures. Several of her coauthors were employed by or reported consulting or advisory roles with industry sources.
Key clinical point: Adjuvant erlotinib demonstrated no DFS benefit in patients with non–small-cell lung cancer (NSCLC) whose tumors expressed epidermal growth factor receptor (EGFR).
Major finding: After a median follow up of 47 months, the median DFS for patients who received erlotinib was 50.5 months compared with 48.2 months for placebo.
Data source: The randomized, double-blind, placebo-controlled RADIANT trial included 973 patients with completely resected stage IB to IIIA NSCLC with EGFR-expressing tumors by immunohistochemistry and EGFR high copy number or amplification by fluorescence in situ hybridization.
Disclosures: The study was supported by Astellas Pharma Global Development, F. Hoffmann-La Roche, and Genentech. Dr. Kelly reported having no disclosures. Several coauthors were employed by or reported consulting or advisory roles with industry sources.
Heart failure readmission-reducing device debuts slowly
In an era when rehospitalization of patients with heart failure for episodes of acute decompensation has become a top target for reduction in the U.S. health care system via Medicare’s Readmissions Reduction Program CardioMEMS looks like the tool that every U.S. health care system and medical center has dreamed of having.
A wireless and battery-less implanted device, CardioMEMS guides management of stage III heart failure patients by allowing daily monitoring of patients’ pulmonary-artery pressure (PAP). Using these measures to fine-tune patient treatment with diuretics and vasodilators led to a statistically significant and clinically meaningful 37% relative reduction in heart failure rehospitalizations over an average 15-month follow-up, based on results from CardioMEMS’ pivotal U.S. trial as well as from subsequent secondary analyses. All-cause mortality was reduced and patients’ quality of life improved. And device-driven therapy yielded these benefits equally well in patients with either preserved or reduced left ventricular function as well as in a variety of other subgroups including patients with cardiac resynchronization devices or implantable cardioverter defibrillators, chronic obstructive pulmonary disease, chronic kidney disease, atrial fibrillation, pulmonary hypertension, or a history of myocardial infarction.
Yet in the first year after CardioMEMS received Food and Drug Administration approval and came onto the U.S. market, the device has taken a strikingly slow path into routine heart failure practice, according to heart failure cardiologists at several U.S. centers. A representative of St. Jude, the company that markets CardioMEMS, saidin July that sales of the device during the first half of 2015 had involved more than 200 U.S. customers and slightly surpassed earlier expectations, and the company now anticipated full 2015 sales to run roughly 25% ahead of projections made at the start of this year. Despite that, the company’s second quarter report acknowledged the challenges that CardioMEMS faced during its first year on the U.S. market.
Numbers show a slow rollout
“I belong to a consortium of academic heart failure physicians who come from many of the major U.S. academic medical centers, and a recent straw poll of the members showed that close to no one was using it [CardioMEMS] on a regular basis, and the majority said they were not yet using it at all or in the process of starting their program,” said Dr. Javed Butler, a heart failure specialist who is professor of medicine, chief of cardiology, and codirector of the Stony Brook (N.Y.) University Heart Center.

At Stony Brook, no heart failure patient had received the device as of July 2015, although Dr. Butler said that his program’s use of CardioMEMS will probably start soon. Cardiologists at a handful of other U.S. centers report similarly slow starts.
At Massachusetts General Hospital (MGH) in Boston not a single patient has received CardioMEMS, though the heart failure staff there hopes to soon launch pilot use in 10 patients, said Dr. Kimberly A. Parks, associate director of the resynchronization and advanced cardiac therapeutics program. At the University of Colorado Hospital in Aurora, three patients have received the device since their first implant in the late winter, and the program is now on track to place devices in another one or two patients each month, said Dr. Natasha L. Altman, a cardiologist who heads the center’s CardioMEMS program. At Brigham and Women’s Hospital in Boston, which participated in the CHAMPION (CardioMEMS Heart Sensor Allows Monitoring of Pressure to Improve Outcomes in NYHA Class III Heart Failure Patients) pivotal trial that led to CardioMEMS approval, so far a “handful, fewer than 10 patients” received the device since marketing began, said Dr. Akshay S. Desai, associate director of Brigham Cardiovascular Consultants. Even at Ohio State’s Wexner Medical Center in Columbus, the program run by Dr. William T. Abraham, coprincipal investigator for CHAMPION, a relatively modest number of roughly 50 patients had received CardioMEMS in routine practice since the first patient received a device there in June 2014 following the FDA’s approval, Dr. Abraham said in an interview.

Contrasting with this level of use is the substantial number of patients who meet the CHAMPION enrollment criteria of New York Heart Association class III heart failure and a heart failure hospitalization within the prior year. Experts estimate that throughout the United States this group must number at least a half-million patients, and at the level of individual medical centers that provide advanced heart failure care, the numbers likely reach several hundred patients at each site.
Several challenges slow CardioMEMS implantation
Why such a slow start for what seems to be such an attractive device that clinicians uniformly praise for having a strong evidence base in CHAMPION and a compelling medical rationale? The answer seems multifactorial, including the need to convince skeptical hospital administrators and insurance payers to provide and pay for the device and follow-up care, a requirement to ramp up the patient-monitoring and management infrastructure, and the challenge of transitioning a relatively complex therapeutic formula from a successful clinical trial model into routine care.
“If this was a pill that you could prescribe to patients at hospital discharge, people would jump on it. But CardioMEMS is not as simple as prescribing a pill. There are a lot of logistical issues that make it very difficult,” said Stony Brook’s Dr. Butler in an interview.
This sentiment was shared not only by other cardiologists but also by St. Jude itself, as a company spokesman itemized several challenges the company encountered once it began trying to sell CardioMEMS commercially. “Developing the market for CardioMEMS will continue to take time,” said the St. Jude staffer during a July webcast on the company’s second-quarter 2015 performance. CardioMEMS’ sales were affected by the need to educate multiple constituencies, satisfy new-technology review committees, address reimbursement, access capital budgets, and create consensus among disparate stakeholders, the webcast said. In addition, the early St. Jude experience selling CardioMEMS showed that once a new customer signs a contract, “we find that customers tend to introduce CardioMEMS ... [on] a pilot basis to gain experience with the technology and the reimbursement process.”

First is the challenge of selling a hospital’s administrative leadership on making an upfront capital investment in CardioMEMS equipment, giving the green light to performing procedures that just about break even relative to reimbursement, and then waiting to recoup the initial expenditure and perhaps make some money in the long term by avoiding readmissions and cutting lengths of stay. According to an analysis run by Dr. Parks of MGH, based on the CHAMPION results, for every 10 patients managed using CardioMEMS for 6 months, a center could expect to prevent nearly 15 patient-days in the hospital.
“Our administration is in support, but skeptical; I think that’s why it’s been slow to start,” said Dr. Parks. “The biggest limitation is the upfront cost of the device, and it’s not clear that the reimbursement will allow you to break even” when putting in devices, she said in an interview. “You could justify this by saying you’ll reduce hospitalizations, but the first impression from our administrators was that we were already doing a pretty good job limiting rehospitalizations so why do we need to add this?” The MGH leadership and clinicians eventually agreed on a plan to start the program with 10 implants and then analyze the results to decide if it makes sense to continue. Dr. Parks said she and her colleagues hope to have their first 10 patients implanted with a CardioMEMS before the end of this year.
Another hurdle at MGH was setting up the infrastructure so that a nurse could monitor patients and set in motion the alerts and treatment changes designed to normalize PAP normalized when it falls out of the target range. “It’s a lot of work to put the system in place to manage the devices,” Dr. Parks noted.
Dr. Butler echoed both these challenges. “You need to convince the hospital administrators and make a case based on the cost savings [later on during ongoing management] rather than positive revenue when you do the procedure. If you can expect future cost savings it’s a viable case to make, but a more difficult case to make,” he said. “You also take on the liability of monitoring patients” long term. “If you can follow several hundred patients there may be enough [follow-up] interventions to pay the salaries of staff ” who monitor the patients, but it is very difficult if you have a nurse who is monitoring five patients,” he said. Another issue complicating the economics is that the physicians who supervise monitoring are mostly not the same ones who performed the CardioMEMS placement procedure and received the procedure’s reimbursement. “These are the system barriers that are out there,” Dr. Butler said.
Dr. Altman in Colorado faced a different challenge. “We had good buy-in from our administration. Everyone is interested in reducing rehospitalizations so the administrators were very supportive. The major roadblock has been insurers. Medicare covers it, but so far Colorado Medicaid and several private insurers do not,” Dr. Altman said in an interview. The inconsistent pattern of insurance coverage has already meant that some heart failure patients in her program who were good clinical candidates for CardioMEMS could not receive the device. “I’ve had at least six or seven good candidates, but only three received the device because of insurance reimbursement issues,” she said.
But Dr. Altman expressed optimism that the coverage situation would improve as more programs start using CarioMEMS and insurers grow more familiar with daily PAP monitoring of heart failure patients. She noted that a new CardioMEMS program will soon start at a second Denver-based medical center, and she expressed confidence that ongoing pressure from physicians and administrators at both institutions will change the mind of officials at Colorado’s Medicaid program to provide reimbursement, and once that happens she expects the private insurers will change their policies as well.
To Dr. Abraham at Ohio State, one of the developers of the concept of using an implanted PAP monitor to guide management of heart failure patients, CardioMEMS slow take off is not surprising. “It provides physicians with daily information on a patient’s hemodynamics, which is something they never had before except in the catheterization laboratory, intensive care unit or cardiac care unit. Managing patients based on hemodynamics even in the absence of worsening signs and symptoms is a paradigm shift. It takes time to adopt new things.” He noted that most hospitals and health systems already have in place case managers or nurse navigators who run systems that have relied on the insensitive parameters of signs, symptoms, and patients’ weights. The same infrastructure should be able to fairly easily switch to focusing instead on PAP, said Dr. Abraham, professor and director of cardiovascular medicine at Wexner Medical Center.
He acknowledged that the upfront capital cost required to start a CardioMEMS program can poses a financial barrier at many U.S. centers, but once that start-up price is paid the actual implantation into each patient comes close to breaking even with existing reimbursements and the system should eventually result in a return on the investment in the form of reduced readmissions and keeping patients stable, he said. Dr. Abraham suggested that the possibility also exists that maintaining better stability in patients with class III heart failure and preventing episodes of acute decompensation through better-titrated fluid-volume control could produce a long-term change in the natural history of these patients, whose disease historically has been marked by progression to class IV heart failure and the eventual need for a left ventricular assist device, heart transplant, and death. Although this potential impact of refined treatment based on daily PAP monitoring remains to be proven, a secondary analysis from CHAMPION showing a 57% relative reduction in all-cause mortality over an average of 17 months of follow-up that Dr. Abraham reported at the American College of Cardiology annual meeting in March
The hurdle of routine practice
Transitioning CardioMEMS from its successful research track record to everyday clinical practice may pose the trickiest barrier of all. The consensus among heart failure experts seems to be that the best approach to do this successfully is to start slow, focus on the most rational patients within the broad enrollment criteria used in CHAMPION, and then gradually expand from that presuming the first wave of results from routine use at a particular site look similar to those from the trial.

“The next big question for PAP monitoring is can we replicate the trial’s success in routine practice? Can this be scaled up?” said Dr. Desai from Brigham and Women’s. “We’re still learning how to identify the right patients, the ones who’ll benefit,”
“The two types of patients we are primarily implanting now are those with classic class III heart failure who were hospitalized during the past 12 months and now are hospitalized again and are right in front of us. They are the lowest-hanging fruit because they are in the hospital today,” said Dr. Abraham. “The second group are the patients who come into the clinic complaining about their symptoms. What we are not yet doing is calling in all patients” with stage III heart failure and a history of at least one hospitalization.”
Other groups are taking a much more selective approach. Dr. Altman and her colleagues in Denver are only targeting patients who have been hospitalized at least twice within the past year, and more specifically patients recently rehospitalized within 30 days of their prior hospitalization. They are also focusing on patients expected to have a high level of compliance with the daily data-collection demands of PAP monitoring and the need to regularly adjust their medication dosages after receiving call backs from their clinicians. This criteria means that they are ruling out patients with a history of substance abuse, she said.
She also noted the need to tailor the target PAP to the specific clinical status of individual patients. Patients with mitral regurgitation, for example, will have a higher “normal” diastolic PAP and hence require a somewhat different target for stability maintenance. “You need to understand each patient’s baseline pressures and adjust their medications based on that,” Dr. Altman said.
“In real life patients tend to be older and sicker, so their benefit may be even greater than what was seen in CHAMPION, but perhaps the results will also be diluted because of comorbidities like renal failure or chronic obstructive pulmonary disease,” said Dr. Butler, although post hoc subanalyses of CHAMPION data showed that these comorbidities did not blunt the positive impact of PAP-guided treatment. “I don’t know if I’ll be successful in selecting the right patients, and whether my interventions in real life will produce the same good outcomes” seen in CHAMPION. “We’ll select patients who are close to the CHAMPION criteria, but not patients on dialysis [who were excluded from CHAMPION]; we’ll select patients with a modest degree of comorbidity and reasonable expected survival,” Dr. Butler said.
“If you had a drug that reduced rehospitalization rates it would be pretty clear how to proceed, but in this case it is not the device that reduces readmissions, it just gives you data and you need to act on the data,” Dr. Butler added. He acknowledged that the CHAMPION investigators used a relatively simple, straightforward management algorithm for patients whose PAP fell out of the target range, such as a diastolic PAP greater than 20 mm Hg or less than 8 mm Hg. The first management step is to raise or reduce the patient’s diuretic dosage, and if that fails to quickly normalize PAP the next step is to adjust the vasodilator dosage.
Managing patients in CHAMPION was “not totally an art” but neither was it “totally a science,” Dr. Butler said. Managing patients based on daily data collected using a CardioMEMS device will “require a little finesse,” he said. “It’s not straight science.”
Programs that have already used PAP monitoring on a routine basis, like those in Denver and at Brigham and Women’s, consider their experience too small in size and short in duration to draw any substantive conclusions regarding their success compared with the CHAMPION results. But Dr. Abraham, whose program has now placed CardioMEMS routinely in a few dozen patients and followed them for as long as a year, said that in his center’s patients the device and management system has produced outcomes that roughly match what he saw in the pivotal trial.
“The ongoing concern is that what was achieved in the CHAMPION trial may not be what is achieved in routine practice,” said Dr. Desai. The care that patients received in the trial is “a little of a black box,” he said, and during the FDA’s approval process some reviewers raised concerns that patients in the active-treatment arm simply received more intensive surveillance, although this concern eventually resolved. “There is not a lot of skepticism” among clinicians about this treatment, but there is uncertainly about exactly whom are the best patients to treat and whether their responses be as good as in CHAMPION, Dr. Desai said in an interview.
“The proof [of efficacy] will be in each individual center’s experience” using CardioMEMS, Dr. Altman said.
CHAMPION was initially funded by CardioMEMS, which then was acquired by St. Jude which is the company marketing the CardioMEMS device and associated hardware. Dr. Butler said that he had no current relevant disclosures, although in the past he had been a consultant to CardioMEMS (prior to its acquisition by St. Jude). Dr. Parks and Dr. Altman had no disclosures. Dr. Desai has been a consultant to and has received honoraria as a speaker on behalf of CardioMEMS and St. Jude. Dr. Abraham has been a consultant to CardioMEMS and St. Jude, was co-principal investigator on the CHAMPION trial, and is the principal investigator on a new St. Jude-funded trial studying CardioMEMS.
On Twitter @mitchelzoler
In an era when rehospitalization of patients with heart failure for episodes of acute decompensation has become a top target for reduction in the U.S. health care system via Medicare’s Readmissions Reduction Program CardioMEMS looks like the tool that every U.S. health care system and medical center has dreamed of having.
A wireless and battery-less implanted device, CardioMEMS guides management of stage III heart failure patients by allowing daily monitoring of patients’ pulmonary-artery pressure (PAP). Using these measures to fine-tune patient treatment with diuretics and vasodilators led to a statistically significant and clinically meaningful 37% relative reduction in heart failure rehospitalizations over an average 15-month follow-up, based on results from CardioMEMS’ pivotal U.S. trial as well as from subsequent secondary analyses. All-cause mortality was reduced and patients’ quality of life improved. And device-driven therapy yielded these benefits equally well in patients with either preserved or reduced left ventricular function as well as in a variety of other subgroups including patients with cardiac resynchronization devices or implantable cardioverter defibrillators, chronic obstructive pulmonary disease, chronic kidney disease, atrial fibrillation, pulmonary hypertension, or a history of myocardial infarction.
Yet in the first year after CardioMEMS received Food and Drug Administration approval and came onto the U.S. market, the device has taken a strikingly slow path into routine heart failure practice, according to heart failure cardiologists at several U.S. centers. A representative of St. Jude, the company that markets CardioMEMS, saidin July that sales of the device during the first half of 2015 had involved more than 200 U.S. customers and slightly surpassed earlier expectations, and the company now anticipated full 2015 sales to run roughly 25% ahead of projections made at the start of this year. Despite that, the company’s second quarter report acknowledged the challenges that CardioMEMS faced during its first year on the U.S. market.
Numbers show a slow rollout
“I belong to a consortium of academic heart failure physicians who come from many of the major U.S. academic medical centers, and a recent straw poll of the members showed that close to no one was using it [CardioMEMS] on a regular basis, and the majority said they were not yet using it at all or in the process of starting their program,” said Dr. Javed Butler, a heart failure specialist who is professor of medicine, chief of cardiology, and codirector of the Stony Brook (N.Y.) University Heart Center.
At Stony Brook, no heart failure patient had received the device as of July 2015, although Dr. Butler said that his program’s use of CardioMEMS will probably start soon. Cardiologists at a handful of other U.S. centers report similarly slow starts.
At Massachusetts General Hospital (MGH) in Boston not a single patient has received CardioMEMS, though the heart failure staff there hopes to soon launch pilot use in 10 patients, said Dr. Kimberly A. Parks, associate director of the resynchronization and advanced cardiac therapeutics program. At the University of Colorado Hospital in Aurora, three patients have received the device since their first implant in the late winter, and the program is now on track to place devices in another one or two patients each month, said Dr. Natasha L. Altman, a cardiologist who heads the center’s CardioMEMS program. At Brigham and Women’s Hospital in Boston, which participated in the CHAMPION (CardioMEMS Heart Sensor Allows Monitoring of Pressure to Improve Outcomes in NYHA Class III Heart Failure Patients) pivotal trial that led to CardioMEMS approval, so far a “handful, fewer than 10 patients” received the device since marketing began, said Dr. Akshay S. Desai, associate director of Brigham Cardiovascular Consultants. Even at Ohio State’s Wexner Medical Center in Columbus, the program run by Dr. William T. Abraham, coprincipal investigator for CHAMPION, a relatively modest number of roughly 50 patients had received CardioMEMS in routine practice since the first patient received a device there in June 2014 following the FDA’s approval, Dr. Abraham said in an interview.
Contrasting with this level of use is the substantial number of patients who meet the CHAMPION enrollment criteria of New York Heart Association class III heart failure and a heart failure hospitalization within the prior year. Experts estimate that throughout the United States this group must number at least a half-million patients, and at the level of individual medical centers that provide advanced heart failure care, the numbers likely reach several hundred patients at each site.
Several challenges slow CardioMEMS implantation
Why such a slow start for what seems to be such an attractive device that clinicians uniformly praise for having a strong evidence base in CHAMPION and a compelling medical rationale? The answer seems multifactorial, including the need to convince skeptical hospital administrators and insurance payers to provide and pay for the device and follow-up care, a requirement to ramp up the patient-monitoring and management infrastructure, and the challenge of transitioning a relatively complex therapeutic formula from a successful clinical trial model into routine care.
“If this was a pill that you could prescribe to patients at hospital discharge, people would jump on it. But CardioMEMS is not as simple as prescribing a pill. There are a lot of logistical issues that make it very difficult,” said Stony Brook’s Dr. Butler in an interview.
This sentiment was shared not only by other cardiologists but also by St. Jude itself, as a company spokesman itemized several challenges the company encountered once it began trying to sell CardioMEMS commercially. “Developing the market for CardioMEMS will continue to take time,” said the St. Jude staffer during a July webcast on the company’s second-quarter 2015 performance. CardioMEMS’ sales were affected by the need to educate multiple constituencies, satisfy new-technology review committees, address reimbursement, access capital budgets, and create consensus among disparate stakeholders, the webcast said. In addition, the early St. Jude experience selling CardioMEMS showed that once a new customer signs a contract, “we find that customers tend to introduce CardioMEMS ... [on] a pilot basis to gain experience with the technology and the reimbursement process.”
First is the challenge of selling a hospital’s administrative leadership on making an upfront capital investment in CardioMEMS equipment, giving the green light to performing procedures that just about break even relative to reimbursement, and then waiting to recoup the initial expenditure and perhaps make some money in the long term by avoiding readmissions and cutting lengths of stay. According to an analysis run by Dr. Parks of MGH, based on the CHAMPION results, for every 10 patients managed using CardioMEMS for 6 months, a center could expect to prevent nearly 15 patient-days in the hospital.
“Our administration is in support, but skeptical; I think that’s why it’s been slow to start,” said Dr. Parks. “The biggest limitation is the upfront cost of the device, and it’s not clear that the reimbursement will allow you to break even” when putting in devices, she said in an interview. “You could justify this by saying you’ll reduce hospitalizations, but the first impression from our administrators was that we were already doing a pretty good job limiting rehospitalizations so why do we need to add this?” The MGH leadership and clinicians eventually agreed on a plan to start the program with 10 implants and then analyze the results to decide if it makes sense to continue. Dr. Parks said she and her colleagues hope to have their first 10 patients implanted with a CardioMEMS before the end of this year.
Another hurdle at MGH was setting up the infrastructure so that a nurse could monitor patients and set in motion the alerts and treatment changes designed to normalize PAP normalized when it falls out of the target range. “It’s a lot of work to put the system in place to manage the devices,” Dr. Parks noted.
Dr. Butler echoed both these challenges. “You need to convince the hospital administrators and make a case based on the cost savings [later on during ongoing management] rather than positive revenue when you do the procedure. If you can expect future cost savings it’s a viable case to make, but a more difficult case to make,” he said. “You also take on the liability of monitoring patients” long term. “If you can follow several hundred patients there may be enough [follow-up] interventions to pay the salaries of staff ” who monitor the patients, but it is very difficult if you have a nurse who is monitoring five patients,” he said. Another issue complicating the economics is that the physicians who supervise monitoring are mostly not the same ones who performed the CardioMEMS placement procedure and received the procedure’s reimbursement. “These are the system barriers that are out there,” Dr. Butler said.
Dr. Altman in Colorado faced a different challenge. “We had good buy-in from our administration. Everyone is interested in reducing rehospitalizations so the administrators were very supportive. The major roadblock has been insurers. Medicare covers it, but so far Colorado Medicaid and several private insurers do not,” Dr. Altman said in an interview. The inconsistent pattern of insurance coverage has already meant that some heart failure patients in her program who were good clinical candidates for CardioMEMS could not receive the device. “I’ve had at least six or seven good candidates, but only three received the device because of insurance reimbursement issues,” she said.
But Dr. Altman expressed optimism that the coverage situation would improve as more programs start using CarioMEMS and insurers grow more familiar with daily PAP monitoring of heart failure patients. She noted that a new CardioMEMS program will soon start at a second Denver-based medical center, and she expressed confidence that ongoing pressure from physicians and administrators at both institutions will change the mind of officials at Colorado’s Medicaid program to provide reimbursement, and once that happens she expects the private insurers will change their policies as well.
To Dr. Abraham at Ohio State, one of the developers of the concept of using an implanted PAP monitor to guide management of heart failure patients, CardioMEMS slow take off is not surprising. “It provides physicians with daily information on a patient’s hemodynamics, which is something they never had before except in the catheterization laboratory, intensive care unit or cardiac care unit. Managing patients based on hemodynamics even in the absence of worsening signs and symptoms is a paradigm shift. It takes time to adopt new things.” He noted that most hospitals and health systems already have in place case managers or nurse navigators who run systems that have relied on the insensitive parameters of signs, symptoms, and patients’ weights. The same infrastructure should be able to fairly easily switch to focusing instead on PAP, said Dr. Abraham, professor and director of cardiovascular medicine at Wexner Medical Center.
He acknowledged that the upfront capital cost required to start a CardioMEMS program can poses a financial barrier at many U.S. centers, but once that start-up price is paid the actual implantation into each patient comes close to breaking even with existing reimbursements and the system should eventually result in a return on the investment in the form of reduced readmissions and keeping patients stable, he said. Dr. Abraham suggested that the possibility also exists that maintaining better stability in patients with class III heart failure and preventing episodes of acute decompensation through better-titrated fluid-volume control could produce a long-term change in the natural history of these patients, whose disease historically has been marked by progression to class IV heart failure and the eventual need for a left ventricular assist device, heart transplant, and death. Although this potential impact of refined treatment based on daily PAP monitoring remains to be proven, a secondary analysis from CHAMPION showing a 57% relative reduction in all-cause mortality over an average of 17 months of follow-up that Dr. Abraham reported at the American College of Cardiology annual meeting in March
The hurdle of routine practice
Transitioning CardioMEMS from its successful research track record to everyday clinical practice may pose the trickiest barrier of all. The consensus among heart failure experts seems to be that the best approach to do this successfully is to start slow, focus on the most rational patients within the broad enrollment criteria used in CHAMPION, and then gradually expand from that presuming the first wave of results from routine use at a particular site look similar to those from the trial.
“The next big question for PAP monitoring is can we replicate the trial’s success in routine practice? Can this be scaled up?” said Dr. Desai from Brigham and Women’s. “We’re still learning how to identify the right patients, the ones who’ll benefit,”
“The two types of patients we are primarily implanting now are those with classic class III heart failure who were hospitalized during the past 12 months and now are hospitalized again and are right in front of us. They are the lowest-hanging fruit because they are in the hospital today,” said Dr. Abraham. “The second group are the patients who come into the clinic complaining about their symptoms. What we are not yet doing is calling in all patients” with stage III heart failure and a history of at least one hospitalization.”
Other groups are taking a much more selective approach. Dr. Altman and her colleagues in Denver are only targeting patients who have been hospitalized at least twice within the past year, and more specifically patients recently rehospitalized within 30 days of their prior hospitalization. They are also focusing on patients expected to have a high level of compliance with the daily data-collection demands of PAP monitoring and the need to regularly adjust their medication dosages after receiving call backs from their clinicians. This criteria means that they are ruling out patients with a history of substance abuse, she said.
She also noted the need to tailor the target PAP to the specific clinical status of individual patients. Patients with mitral regurgitation, for example, will have a higher “normal” diastolic PAP and hence require a somewhat different target for stability maintenance. “You need to understand each patient’s baseline pressures and adjust their medications based on that,” Dr. Altman said.
“In real life patients tend to be older and sicker, so their benefit may be even greater than what was seen in CHAMPION, but perhaps the results will also be diluted because of comorbidities like renal failure or chronic obstructive pulmonary disease,” said Dr. Butler, although post hoc subanalyses of CHAMPION data showed that these comorbidities did not blunt the positive impact of PAP-guided treatment. “I don’t know if I’ll be successful in selecting the right patients, and whether my interventions in real life will produce the same good outcomes” seen in CHAMPION. “We’ll select patients who are close to the CHAMPION criteria, but not patients on dialysis [who were excluded from CHAMPION]; we’ll select patients with a modest degree of comorbidity and reasonable expected survival,” Dr. Butler said.
“If you had a drug that reduced rehospitalization rates it would be pretty clear how to proceed, but in this case it is not the device that reduces readmissions, it just gives you data and you need to act on the data,” Dr. Butler added. He acknowledged that the CHAMPION investigators used a relatively simple, straightforward management algorithm for patients whose PAP fell out of the target range, such as a diastolic PAP greater than 20 mm Hg or less than 8 mm Hg. The first management step is to raise or reduce the patient’s diuretic dosage, and if that fails to quickly normalize PAP the next step is to adjust the vasodilator dosage.
Managing patients in CHAMPION was “not totally an art” but neither was it “totally a science,” Dr. Butler said. Managing patients based on daily data collected using a CardioMEMS device will “require a little finesse,” he said. “It’s not straight science.”
Programs that have already used PAP monitoring on a routine basis, like those in Denver and at Brigham and Women’s, consider their experience too small in size and short in duration to draw any substantive conclusions regarding their success compared with the CHAMPION results. But Dr. Abraham, whose program has now placed CardioMEMS routinely in a few dozen patients and followed them for as long as a year, said that in his center’s patients the device and management system has produced outcomes that roughly match what he saw in the pivotal trial.
“The ongoing concern is that what was achieved in the CHAMPION trial may not be what is achieved in routine practice,” said Dr. Desai. The care that patients received in the trial is “a little of a black box,” he said, and during the FDA’s approval process some reviewers raised concerns that patients in the active-treatment arm simply received more intensive surveillance, although this concern eventually resolved. “There is not a lot of skepticism” among clinicians about this treatment, but there is uncertainly about exactly whom are the best patients to treat and whether their responses be as good as in CHAMPION, Dr. Desai said in an interview.
“The proof [of efficacy] will be in each individual center’s experience” using CardioMEMS, Dr. Altman said.
CHAMPION was initially funded by CardioMEMS, which then was acquired by St. Jude which is the company marketing the CardioMEMS device and associated hardware. Dr. Butler said that he had no current relevant disclosures, although in the past he had been a consultant to CardioMEMS (prior to its acquisition by St. Jude). Dr. Parks and Dr. Altman had no disclosures. Dr. Desai has been a consultant to and has received honoraria as a speaker on behalf of CardioMEMS and St. Jude. Dr. Abraham has been a consultant to CardioMEMS and St. Jude, was co-principal investigator on the CHAMPION trial, and is the principal investigator on a new St. Jude-funded trial studying CardioMEMS.
On Twitter @mitchelzoler
In an era when rehospitalization of patients with heart failure for episodes of acute decompensation has become a top target for reduction in the U.S. health care system via Medicare’s Readmissions Reduction Program CardioMEMS looks like the tool that every U.S. health care system and medical center has dreamed of having.
A wireless and battery-less implanted device, CardioMEMS guides management of stage III heart failure patients by allowing daily monitoring of patients’ pulmonary-artery pressure (PAP). Using these measures to fine-tune patient treatment with diuretics and vasodilators led to a statistically significant and clinically meaningful 37% relative reduction in heart failure rehospitalizations over an average 15-month follow-up, based on results from CardioMEMS’ pivotal U.S. trial as well as from subsequent secondary analyses. All-cause mortality was reduced and patients’ quality of life improved. And device-driven therapy yielded these benefits equally well in patients with either preserved or reduced left ventricular function as well as in a variety of other subgroups including patients with cardiac resynchronization devices or implantable cardioverter defibrillators, chronic obstructive pulmonary disease, chronic kidney disease, atrial fibrillation, pulmonary hypertension, or a history of myocardial infarction.
Yet in the first year after CardioMEMS received Food and Drug Administration approval and came onto the U.S. market, the device has taken a strikingly slow path into routine heart failure practice, according to heart failure cardiologists at several U.S. centers. A representative of St. Jude, the company that markets CardioMEMS, saidin July that sales of the device during the first half of 2015 had involved more than 200 U.S. customers and slightly surpassed earlier expectations, and the company now anticipated full 2015 sales to run roughly 25% ahead of projections made at the start of this year. Despite that, the company’s second quarter report acknowledged the challenges that CardioMEMS faced during its first year on the U.S. market.
Numbers show a slow rollout
“I belong to a consortium of academic heart failure physicians who come from many of the major U.S. academic medical centers, and a recent straw poll of the members showed that close to no one was using it [CardioMEMS] on a regular basis, and the majority said they were not yet using it at all or in the process of starting their program,” said Dr. Javed Butler, a heart failure specialist who is professor of medicine, chief of cardiology, and codirector of the Stony Brook (N.Y.) University Heart Center.
At Stony Brook, no heart failure patient had received the device as of July 2015, although Dr. Butler said that his program’s use of CardioMEMS will probably start soon. Cardiologists at a handful of other U.S. centers report similarly slow starts.
At Massachusetts General Hospital (MGH) in Boston not a single patient has received CardioMEMS, though the heart failure staff there hopes to soon launch pilot use in 10 patients, said Dr. Kimberly A. Parks, associate director of the resynchronization and advanced cardiac therapeutics program. At the University of Colorado Hospital in Aurora, three patients have received the device since their first implant in the late winter, and the program is now on track to place devices in another one or two patients each month, said Dr. Natasha L. Altman, a cardiologist who heads the center’s CardioMEMS program. At Brigham and Women’s Hospital in Boston, which participated in the CHAMPION (CardioMEMS Heart Sensor Allows Monitoring of Pressure to Improve Outcomes in NYHA Class III Heart Failure Patients) pivotal trial that led to CardioMEMS approval, so far a “handful, fewer than 10 patients” received the device since marketing began, said Dr. Akshay S. Desai, associate director of Brigham Cardiovascular Consultants. Even at Ohio State’s Wexner Medical Center in Columbus, the program run by Dr. William T. Abraham, coprincipal investigator for CHAMPION, a relatively modest number of roughly 50 patients had received CardioMEMS in routine practice since the first patient received a device there in June 2014 following the FDA’s approval, Dr. Abraham said in an interview.
Contrasting with this level of use is the substantial number of patients who meet the CHAMPION enrollment criteria of New York Heart Association class III heart failure and a heart failure hospitalization within the prior year. Experts estimate that throughout the United States this group must number at least a half-million patients, and at the level of individual medical centers that provide advanced heart failure care, the numbers likely reach several hundred patients at each site.
Several challenges slow CardioMEMS implantation
Why such a slow start for what seems to be such an attractive device that clinicians uniformly praise for having a strong evidence base in CHAMPION and a compelling medical rationale? The answer seems multifactorial, including the need to convince skeptical hospital administrators and insurance payers to provide and pay for the device and follow-up care, a requirement to ramp up the patient-monitoring and management infrastructure, and the challenge of transitioning a relatively complex therapeutic formula from a successful clinical trial model into routine care.
“If this was a pill that you could prescribe to patients at hospital discharge, people would jump on it. But CardioMEMS is not as simple as prescribing a pill. There are a lot of logistical issues that make it very difficult,” said Stony Brook’s Dr. Butler in an interview.
This sentiment was shared not only by other cardiologists but also by St. Jude itself, as a company spokesman itemized several challenges the company encountered once it began trying to sell CardioMEMS commercially. “Developing the market for CardioMEMS will continue to take time,” said the St. Jude staffer during a July webcast on the company’s second-quarter 2015 performance. CardioMEMS’ sales were affected by the need to educate multiple constituencies, satisfy new-technology review committees, address reimbursement, access capital budgets, and create consensus among disparate stakeholders, the webcast said. In addition, the early St. Jude experience selling CardioMEMS showed that once a new customer signs a contract, “we find that customers tend to introduce CardioMEMS ... [on] a pilot basis to gain experience with the technology and the reimbursement process.”
First is the challenge of selling a hospital’s administrative leadership on making an upfront capital investment in CardioMEMS equipment, giving the green light to performing procedures that just about break even relative to reimbursement, and then waiting to recoup the initial expenditure and perhaps make some money in the long term by avoiding readmissions and cutting lengths of stay. According to an analysis run by Dr. Parks of MGH, based on the CHAMPION results, for every 10 patients managed using CardioMEMS for 6 months, a center could expect to prevent nearly 15 patient-days in the hospital.
“Our administration is in support, but skeptical; I think that’s why it’s been slow to start,” said Dr. Parks. “The biggest limitation is the upfront cost of the device, and it’s not clear that the reimbursement will allow you to break even” when putting in devices, she said in an interview. “You could justify this by saying you’ll reduce hospitalizations, but the first impression from our administrators was that we were already doing a pretty good job limiting rehospitalizations so why do we need to add this?” The MGH leadership and clinicians eventually agreed on a plan to start the program with 10 implants and then analyze the results to decide if it makes sense to continue. Dr. Parks said she and her colleagues hope to have their first 10 patients implanted with a CardioMEMS before the end of this year.
Another hurdle at MGH was setting up the infrastructure so that a nurse could monitor patients and set in motion the alerts and treatment changes designed to normalize PAP normalized when it falls out of the target range. “It’s a lot of work to put the system in place to manage the devices,” Dr. Parks noted.
Dr. Butler echoed both these challenges. “You need to convince the hospital administrators and make a case based on the cost savings [later on during ongoing management] rather than positive revenue when you do the procedure. If you can expect future cost savings it’s a viable case to make, but a more difficult case to make,” he said. “You also take on the liability of monitoring patients” long term. “If you can follow several hundred patients there may be enough [follow-up] interventions to pay the salaries of staff ” who monitor the patients, but it is very difficult if you have a nurse who is monitoring five patients,” he said. Another issue complicating the economics is that the physicians who supervise monitoring are mostly not the same ones who performed the CardioMEMS placement procedure and received the procedure’s reimbursement. “These are the system barriers that are out there,” Dr. Butler said.
Dr. Altman in Colorado faced a different challenge. “We had good buy-in from our administration. Everyone is interested in reducing rehospitalizations so the administrators were very supportive. The major roadblock has been insurers. Medicare covers it, but so far Colorado Medicaid and several private insurers do not,” Dr. Altman said in an interview. The inconsistent pattern of insurance coverage has already meant that some heart failure patients in her program who were good clinical candidates for CardioMEMS could not receive the device. “I’ve had at least six or seven good candidates, but only three received the device because of insurance reimbursement issues,” she said.
But Dr. Altman expressed optimism that the coverage situation would improve as more programs start using CarioMEMS and insurers grow more familiar with daily PAP monitoring of heart failure patients. She noted that a new CardioMEMS program will soon start at a second Denver-based medical center, and she expressed confidence that ongoing pressure from physicians and administrators at both institutions will change the mind of officials at Colorado’s Medicaid program to provide reimbursement, and once that happens she expects the private insurers will change their policies as well.
To Dr. Abraham at Ohio State, one of the developers of the concept of using an implanted PAP monitor to guide management of heart failure patients, CardioMEMS slow take off is not surprising. “It provides physicians with daily information on a patient’s hemodynamics, which is something they never had before except in the catheterization laboratory, intensive care unit or cardiac care unit. Managing patients based on hemodynamics even in the absence of worsening signs and symptoms is a paradigm shift. It takes time to adopt new things.” He noted that most hospitals and health systems already have in place case managers or nurse navigators who run systems that have relied on the insensitive parameters of signs, symptoms, and patients’ weights. The same infrastructure should be able to fairly easily switch to focusing instead on PAP, said Dr. Abraham, professor and director of cardiovascular medicine at Wexner Medical Center.
He acknowledged that the upfront capital cost required to start a CardioMEMS program can poses a financial barrier at many U.S. centers, but once that start-up price is paid the actual implantation into each patient comes close to breaking even with existing reimbursements and the system should eventually result in a return on the investment in the form of reduced readmissions and keeping patients stable, he said. Dr. Abraham suggested that the possibility also exists that maintaining better stability in patients with class III heart failure and preventing episodes of acute decompensation through better-titrated fluid-volume control could produce a long-term change in the natural history of these patients, whose disease historically has been marked by progression to class IV heart failure and the eventual need for a left ventricular assist device, heart transplant, and death. Although this potential impact of refined treatment based on daily PAP monitoring remains to be proven, a secondary analysis from CHAMPION showing a 57% relative reduction in all-cause mortality over an average of 17 months of follow-up that Dr. Abraham reported at the American College of Cardiology annual meeting in March
The hurdle of routine practice
Transitioning CardioMEMS from its successful research track record to everyday clinical practice may pose the trickiest barrier of all. The consensus among heart failure experts seems to be that the best approach to do this successfully is to start slow, focus on the most rational patients within the broad enrollment criteria used in CHAMPION, and then gradually expand from that presuming the first wave of results from routine use at a particular site look similar to those from the trial.
“The next big question for PAP monitoring is can we replicate the trial’s success in routine practice? Can this be scaled up?” said Dr. Desai from Brigham and Women’s. “We’re still learning how to identify the right patients, the ones who’ll benefit,”
“The two types of patients we are primarily implanting now are those with classic class III heart failure who were hospitalized during the past 12 months and now are hospitalized again and are right in front of us. They are the lowest-hanging fruit because they are in the hospital today,” said Dr. Abraham. “The second group are the patients who come into the clinic complaining about their symptoms. What we are not yet doing is calling in all patients” with stage III heart failure and a history of at least one hospitalization.”
Other groups are taking a much more selective approach. Dr. Altman and her colleagues in Denver are only targeting patients who have been hospitalized at least twice within the past year, and more specifically patients recently rehospitalized within 30 days of their prior hospitalization. They are also focusing on patients expected to have a high level of compliance with the daily data-collection demands of PAP monitoring and the need to regularly adjust their medication dosages after receiving call backs from their clinicians. This criteria means that they are ruling out patients with a history of substance abuse, she said.
She also noted the need to tailor the target PAP to the specific clinical status of individual patients. Patients with mitral regurgitation, for example, will have a higher “normal” diastolic PAP and hence require a somewhat different target for stability maintenance. “You need to understand each patient’s baseline pressures and adjust their medications based on that,” Dr. Altman said.
“In real life patients tend to be older and sicker, so their benefit may be even greater than what was seen in CHAMPION, but perhaps the results will also be diluted because of comorbidities like renal failure or chronic obstructive pulmonary disease,” said Dr. Butler, although post hoc subanalyses of CHAMPION data showed that these comorbidities did not blunt the positive impact of PAP-guided treatment. “I don’t know if I’ll be successful in selecting the right patients, and whether my interventions in real life will produce the same good outcomes” seen in CHAMPION. “We’ll select patients who are close to the CHAMPION criteria, but not patients on dialysis [who were excluded from CHAMPION]; we’ll select patients with a modest degree of comorbidity and reasonable expected survival,” Dr. Butler said.
“If you had a drug that reduced rehospitalization rates it would be pretty clear how to proceed, but in this case it is not the device that reduces readmissions, it just gives you data and you need to act on the data,” Dr. Butler added. He acknowledged that the CHAMPION investigators used a relatively simple, straightforward management algorithm for patients whose PAP fell out of the target range, such as a diastolic PAP greater than 20 mm Hg or less than 8 mm Hg. The first management step is to raise or reduce the patient’s diuretic dosage, and if that fails to quickly normalize PAP the next step is to adjust the vasodilator dosage.
Managing patients in CHAMPION was “not totally an art” but neither was it “totally a science,” Dr. Butler said. Managing patients based on daily data collected using a CardioMEMS device will “require a little finesse,” he said. “It’s not straight science.”
Programs that have already used PAP monitoring on a routine basis, like those in Denver and at Brigham and Women’s, consider their experience too small in size and short in duration to draw any substantive conclusions regarding their success compared with the CHAMPION results. But Dr. Abraham, whose program has now placed CardioMEMS routinely in a few dozen patients and followed them for as long as a year, said that in his center’s patients the device and management system has produced outcomes that roughly match what he saw in the pivotal trial.
“The ongoing concern is that what was achieved in the CHAMPION trial may not be what is achieved in routine practice,” said Dr. Desai. The care that patients received in the trial is “a little of a black box,” he said, and during the FDA’s approval process some reviewers raised concerns that patients in the active-treatment arm simply received more intensive surveillance, although this concern eventually resolved. “There is not a lot of skepticism” among clinicians about this treatment, but there is uncertainly about exactly whom are the best patients to treat and whether their responses be as good as in CHAMPION, Dr. Desai said in an interview.
“The proof [of efficacy] will be in each individual center’s experience” using CardioMEMS, Dr. Altman said.
CHAMPION was initially funded by CardioMEMS, which then was acquired by St. Jude which is the company marketing the CardioMEMS device and associated hardware. Dr. Butler said that he had no current relevant disclosures, although in the past he had been a consultant to CardioMEMS (prior to its acquisition by St. Jude). Dr. Parks and Dr. Altman had no disclosures. Dr. Desai has been a consultant to and has received honoraria as a speaker on behalf of CardioMEMS and St. Jude. Dr. Abraham has been a consultant to CardioMEMS and St. Jude, was co-principal investigator on the CHAMPION trial, and is the principal investigator on a new St. Jude-funded trial studying CardioMEMS.
On Twitter @mitchelzoler
