User login
The Official Newspaper of the American Association for Thoracic Surgery
Hospital Privileging Faces New Challenges
Hospital privileges (credentials) are often treated as a footnote to board certification by new Thoracic graduates seeking the beginning of their procedural bliss. Without hospital privileges, though, new graduates cannot perform the technical accomplishments they have spent so long refining. In addition, these surgeons will not have access to the shared financial resources the hospital can afford.
Privileges are important not only from a revenue standpoint but they also play a role in defining the scope of one’s practice. As surgeons progress in their careers and want to expand their scope of clinical care, as well as gain new technologies, hospital privileges must be updated. In addition, continued and mandatory hospital review of the physician makes the process never ending.
Gaining hospital privileges efficiently requires understanding why they exist, the power privileges give and the complications that can occur with their use.
Hospital privileges are a method for the hospital to verify and maintain standards of the physicians working at the institution. The American College of Surgeons was the first to enact quality measures that hospitals voluntarily agreed to in 1917.
The Hill-Burton Act of 1946 caused states seeking federal funds for hospitals to maintain certain standards. Within the hospital it is the medical staff who must make up these standards for the credentialing process. The medical staff is made up of professionals, mainly doctors, guided by state regulations.
In the last decade a hospital’s Medical Staff has been under more scrutiny in dispensing privileges by certifying agencies such as The Joint Commission, CMS and the Healthcare Facility Accreditation Program among others.
One challenging aspect facing new graduates is that approval is based on the recommendations from outside institutions. For this reason, Medical Staff may require a more detailed case log, a review of case reports or even direct observation as part of their approval process.
For the majority of procedures, hospitals have umbrella approval dependent on specialty. Difficulties come into play when a new surgeon is bringing in new technologies. These new procedures must be individually approved. Medical staff must then rely on either industry-set guidelines or position papers written by organizations such as the American Association for Thoracic Surgery (AATS).
Examples of past guidelines include industry’s training program for endovascular stents and the position paper written by the AATS and Society of Thoracic Surgeons (STS) on credentialing for thoracoscopic procedures.
Graduates should review a hospital’s bylaws prior to beginning the process. Hospital bylaws will state policies, governance procedures, explain the privileging process, and give regulations for the hospital. Bylaws will vary between hospitals even in the same state and must be evaluated closely. Areas to focus on when reviewing them are: definitions, staff appointment categories, the privileging process, the bylaws amendment process, and the hearing process if privileges are denied.
Trouble often occurs when trying to gain privileges in overlapping fields. As technology allows and requires merging of previously separate fields, more and more "turf battles" are fought at the stage of gaining hospital privileges. For example, procedures such as percutaneous gastrostomy tubes, endovascular stents, and now endovascular valves can all technically be performed by multiple specialties. When and where these procedures are performed in the hospital is most commonly determined by hospital privileges. The medical staff therefore becomes entangled in maintaining medical credentials and settling disputes amongst specialties. Be prepared to state your case and prove your competence when embarking on such procedures!
More controversial is the ever-expanding role of so called economiccredentialing, which means the credentialing process is either directly or indirectly tied to economic rather than medical outcomes.
As physicians control approximately 80% of hospital spending, their economic role in the hospital is closely linked with their medical one. Hospitals are also increasingly linking anti-competition clauses limiting referral patterns and locations at which procedures may be performed with the credentialing process.
The increasing role of economics in credentialing is also seen at the oversight level in JCAHO’s Total Quality Management (TQM) initiative which takes efficiency of care delivered into consideration when making recommendations on physician recertification. State laws mirror this initiative with states such as Washington mandating that hospital’s Medical Staff are governed by certain "cost efficiencies".
Gaining credentials at a new hospital requires forethought and planning. Some tips on gaining an advantage in the process include:
1. Maintaining a private detailed procedural log even after graduation.
2. Enrolling in industry-sponsored training programs that give certification in new technologies.
3. Keep up to date on professional society training guidelines for specific procedures, especially procedures crossing specialties.
4. Maintain open lines of communication with your medical staff and those vested in the procedures you are performing.
Hospitals will continue to seek guidance in the process of physician certification and granting of privileges. Once gained by a new graduate, it is imperative to realize that rules are not formed in a vacuum and that the Medical Staff must be engaged to help guide decisions that in the end will benefit the patient.☐
Hospital privileges (credentials) are often treated as a footnote to board certification by new Thoracic graduates seeking the beginning of their procedural bliss. Without hospital privileges, though, new graduates cannot perform the technical accomplishments they have spent so long refining. In addition, these surgeons will not have access to the shared financial resources the hospital can afford.
Privileges are important not only from a revenue standpoint but they also play a role in defining the scope of one’s practice. As surgeons progress in their careers and want to expand their scope of clinical care, as well as gain new technologies, hospital privileges must be updated. In addition, continued and mandatory hospital review of the physician makes the process never ending.
Gaining hospital privileges efficiently requires understanding why they exist, the power privileges give and the complications that can occur with their use.
Hospital privileges are a method for the hospital to verify and maintain standards of the physicians working at the institution. The American College of Surgeons was the first to enact quality measures that hospitals voluntarily agreed to in 1917.
The Hill-Burton Act of 1946 caused states seeking federal funds for hospitals to maintain certain standards. Within the hospital it is the medical staff who must make up these standards for the credentialing process. The medical staff is made up of professionals, mainly doctors, guided by state regulations.
In the last decade a hospital’s Medical Staff has been under more scrutiny in dispensing privileges by certifying agencies such as The Joint Commission, CMS and the Healthcare Facility Accreditation Program among others.
One challenging aspect facing new graduates is that approval is based on the recommendations from outside institutions. For this reason, Medical Staff may require a more detailed case log, a review of case reports or even direct observation as part of their approval process.
For the majority of procedures, hospitals have umbrella approval dependent on specialty. Difficulties come into play when a new surgeon is bringing in new technologies. These new procedures must be individually approved. Medical staff must then rely on either industry-set guidelines or position papers written by organizations such as the American Association for Thoracic Surgery (AATS).
Examples of past guidelines include industry’s training program for endovascular stents and the position paper written by the AATS and Society of Thoracic Surgeons (STS) on credentialing for thoracoscopic procedures.
Graduates should review a hospital’s bylaws prior to beginning the process. Hospital bylaws will state policies, governance procedures, explain the privileging process, and give regulations for the hospital. Bylaws will vary between hospitals even in the same state and must be evaluated closely. Areas to focus on when reviewing them are: definitions, staff appointment categories, the privileging process, the bylaws amendment process, and the hearing process if privileges are denied.
Trouble often occurs when trying to gain privileges in overlapping fields. As technology allows and requires merging of previously separate fields, more and more "turf battles" are fought at the stage of gaining hospital privileges. For example, procedures such as percutaneous gastrostomy tubes, endovascular stents, and now endovascular valves can all technically be performed by multiple specialties. When and where these procedures are performed in the hospital is most commonly determined by hospital privileges. The medical staff therefore becomes entangled in maintaining medical credentials and settling disputes amongst specialties. Be prepared to state your case and prove your competence when embarking on such procedures!
More controversial is the ever-expanding role of so called economiccredentialing, which means the credentialing process is either directly or indirectly tied to economic rather than medical outcomes.
As physicians control approximately 80% of hospital spending, their economic role in the hospital is closely linked with their medical one. Hospitals are also increasingly linking anti-competition clauses limiting referral patterns and locations at which procedures may be performed with the credentialing process.
The increasing role of economics in credentialing is also seen at the oversight level in JCAHO’s Total Quality Management (TQM) initiative which takes efficiency of care delivered into consideration when making recommendations on physician recertification. State laws mirror this initiative with states such as Washington mandating that hospital’s Medical Staff are governed by certain "cost efficiencies".
Gaining credentials at a new hospital requires forethought and planning. Some tips on gaining an advantage in the process include:
1. Maintaining a private detailed procedural log even after graduation.
2. Enrolling in industry-sponsored training programs that give certification in new technologies.
3. Keep up to date on professional society training guidelines for specific procedures, especially procedures crossing specialties.
4. Maintain open lines of communication with your medical staff and those vested in the procedures you are performing.
Hospitals will continue to seek guidance in the process of physician certification and granting of privileges. Once gained by a new graduate, it is imperative to realize that rules are not formed in a vacuum and that the Medical Staff must be engaged to help guide decisions that in the end will benefit the patient.☐
Hospital privileges (credentials) are often treated as a footnote to board certification by new Thoracic graduates seeking the beginning of their procedural bliss. Without hospital privileges, though, new graduates cannot perform the technical accomplishments they have spent so long refining. In addition, these surgeons will not have access to the shared financial resources the hospital can afford.
Privileges are important not only from a revenue standpoint but they also play a role in defining the scope of one’s practice. As surgeons progress in their careers and want to expand their scope of clinical care, as well as gain new technologies, hospital privileges must be updated. In addition, continued and mandatory hospital review of the physician makes the process never ending.
Gaining hospital privileges efficiently requires understanding why they exist, the power privileges give and the complications that can occur with their use.
Hospital privileges are a method for the hospital to verify and maintain standards of the physicians working at the institution. The American College of Surgeons was the first to enact quality measures that hospitals voluntarily agreed to in 1917.
The Hill-Burton Act of 1946 caused states seeking federal funds for hospitals to maintain certain standards. Within the hospital it is the medical staff who must make up these standards for the credentialing process. The medical staff is made up of professionals, mainly doctors, guided by state regulations.
In the last decade a hospital’s Medical Staff has been under more scrutiny in dispensing privileges by certifying agencies such as The Joint Commission, CMS and the Healthcare Facility Accreditation Program among others.
One challenging aspect facing new graduates is that approval is based on the recommendations from outside institutions. For this reason, Medical Staff may require a more detailed case log, a review of case reports or even direct observation as part of their approval process.
For the majority of procedures, hospitals have umbrella approval dependent on specialty. Difficulties come into play when a new surgeon is bringing in new technologies. These new procedures must be individually approved. Medical staff must then rely on either industry-set guidelines or position papers written by organizations such as the American Association for Thoracic Surgery (AATS).
Examples of past guidelines include industry’s training program for endovascular stents and the position paper written by the AATS and Society of Thoracic Surgeons (STS) on credentialing for thoracoscopic procedures.
Graduates should review a hospital’s bylaws prior to beginning the process. Hospital bylaws will state policies, governance procedures, explain the privileging process, and give regulations for the hospital. Bylaws will vary between hospitals even in the same state and must be evaluated closely. Areas to focus on when reviewing them are: definitions, staff appointment categories, the privileging process, the bylaws amendment process, and the hearing process if privileges are denied.
Trouble often occurs when trying to gain privileges in overlapping fields. As technology allows and requires merging of previously separate fields, more and more "turf battles" are fought at the stage of gaining hospital privileges. For example, procedures such as percutaneous gastrostomy tubes, endovascular stents, and now endovascular valves can all technically be performed by multiple specialties. When and where these procedures are performed in the hospital is most commonly determined by hospital privileges. The medical staff therefore becomes entangled in maintaining medical credentials and settling disputes amongst specialties. Be prepared to state your case and prove your competence when embarking on such procedures!
More controversial is the ever-expanding role of so called economiccredentialing, which means the credentialing process is either directly or indirectly tied to economic rather than medical outcomes.
As physicians control approximately 80% of hospital spending, their economic role in the hospital is closely linked with their medical one. Hospitals are also increasingly linking anti-competition clauses limiting referral patterns and locations at which procedures may be performed with the credentialing process.
The increasing role of economics in credentialing is also seen at the oversight level in JCAHO’s Total Quality Management (TQM) initiative which takes efficiency of care delivered into consideration when making recommendations on physician recertification. State laws mirror this initiative with states such as Washington mandating that hospital’s Medical Staff are governed by certain "cost efficiencies".
Gaining credentials at a new hospital requires forethought and planning. Some tips on gaining an advantage in the process include:
1. Maintaining a private detailed procedural log even after graduation.
2. Enrolling in industry-sponsored training programs that give certification in new technologies.
3. Keep up to date on professional society training guidelines for specific procedures, especially procedures crossing specialties.
4. Maintain open lines of communication with your medical staff and those vested in the procedures you are performing.
Hospitals will continue to seek guidance in the process of physician certification and granting of privileges. Once gained by a new graduate, it is imperative to realize that rules are not formed in a vacuum and that the Medical Staff must be engaged to help guide decisions that in the end will benefit the patient.☐
Improving Resident Communication
SAN FRANCISCO – Training residents to notify attending surgeons of any significant change in a patient’s condition greatly reduced the proportion of critical events that were not communicated to attending surgeons, from 33% to 2%, in a prospective study of four hospitals.
The current study was undertaken in response to a previous study by the same research group showing that ambiguity about who is responsible for communications contributed to communication breakdowns between attending surgeons and other members of the team at any point in patient care, Dr. Caprice C. Greenberg said at the annual clinical congress of the American College of Surgeons.
In the previous study, 444 malpractice claims were reviewed, and this process identified 60 cases in which communication breakdown resulted in harm to a patient. Dr. Greenberg and colleagues found that communication breakdowns related to surgery are equally likely to happen during preoperative, intraoperative, and postoperative care, and most commonly involve communications attempted between an attending surgeon and another attending surgeon, a resident, or the patient or family.
Ambiguity about who is responsible for communicating played a role in 58% of communication breakdowns, said Dr. Greenberg, director of the Wisconsin Surgical Outcomes Research Program at the University of Wisconsin, Madison.
Handoffs of patient care from one provider to another contributed to 43% of communication breakdowns, and transferring a patient to a different location contributed to 39% of communication breakdowns. The data also showed that an asymmetry in status between the two communicating parties contributed to 74% of message breakdowns ( J. Am. Coll. Surg. 2007;204:533-40).
Dr. Greenberg and her associates identified "triggers" that should prompt residents or nurses to contact attending surgeons, including a patient’s admission to a hospital, discharge, or a visit to an emergency department, transfer into or out of the ICU, unplanned intubation, or the development of cardiac arrest, new arrhythmia, or hemodynamic instability.
Significant neurologic changes, major wound complications, unplanned blood transfusion, an invasive procedure or operation, or errors in medication or treatment necessitating an intervention also should trigger communication with the attending surgeon. Even simply concern by a surgical trainee or a request from a nurse or another physician to contact the attending surgeon were considered triggers for communication.
The triggers were included in guidelines created by representatives of the four hospitals in Harvard University’s system in a collaboration organized by the system’s malpractice insurers. Under the new guidelines, residents were to notify attending surgeons of any significant changes in a patient’s condition regardless of the day or time. The residents would be trained to understand what qualifies as "significant changes" based in part on specialty-specific definitions, she said.
"What a urologist cares about is probably a little bit different from what a neurosurgeon or cardiac surgeon cares about," she explained.
A study of previous practices found that residents thought that 61 of 80 critical patient events (76%) did not need to be communicated to attending surgeons for safe patient care, and 26 events were not communicated (33%). Of the 54 events that were communicated, discussions with the attending surgeons changed management in 18 cases (33%). Attending surgeons responded to calls 100% of the time ( Ann. Surg. 2009;250:861-5).
"It wasn’t that the attendings didn’t want to be called. It was that residents either felt unempowered to call or they felt that it wasn’t necessary," she said.
Breakdowns in communication are common and play a significant role in adverse events, prior data suggest. One study of 48 surgeries found that 31% of 421 attempted communications between surgical team members failed, and approximately a third of these communication failures potentially jeopardized patient safety (Qual. Saf. Health Care 2004;13:330-4).
Other strategies to reduce the risk of errors during surgery include "workload leveling," Dr. Greenberg added. This means the attending surgeon should communicate frequently to members of the interdisciplinary surgical team about the status of the case and expected progression of the case, so that team members can manage their time and plan to do auxiliary tasks at the appropriate times. It’s probably impossible to avoid all errors, so surgeons need to find the right balance of error prevention and error mitigation through "resilience" – the ability to anticipate, cope with, recover from, and learn from unforeseen developments, she added. "To start to increase resilience, we really need to teach people adaptability and flexibility," she said.
Dr. Mary Klingensmith, a professor of surgery at Washington University, St. Louis, and Dr. John Hanks, a professor of surgery at the University of Virginia, Charlottesville, commented, "The conclusion of this study may seem obvious to those of us no longer in training – namely that residents should communicate critical patient events to attendings. Yet the imperative nature of such communication is not stressed adequately in our surgical training culture. In many training programs, there are some time-honored but outdated concepts in play, such as it is a "sign of weakness" to call the attending. Dr. Greenberg describes residents in this position as feeling "unempowered" to place such a call.
"We need to debunk this myth and explicitly instruct our residents about what we want and expect. Under the new paradigm, this accountability must include rapid and accurate transmittal of information with confidence on both the sending and receiving ends.
"The intervention put into place by Dr. Greenberg’s group did just that, laying out for trainees the patient events that should trigger a call to the attending. Interestingly, they reported that change in patient management, as a result of attending input, occurred in only 33% of cases in which the attending was called – a result suggesting that information transfer was merely that of the "FYI" variety. Yet in all instances, the attending wanted to be called.
"If the patient safety aspect of these communication triggers can be stressed, we can more effectively shape trainee behavior." ☐
Effective communication continues to be a problem as medical teams become more modular in their approach to patient care. Although methods of communication for residents have become ubiquitous, communication to the attending often does not occur in a reliable manner.
This study is an excellent example of improving patient safety by removing potential communication breakdowns. This prospective study by Dr. Greenberg created clear, documented expectations on when the attending should be notified by either a resident or nurse. As such, critical patient events were more effectively delivered to the attending. In a third of these notifications, the patient care plan was then changed. An interesting component of this study was the setting of expectations on both ends; when to call and when to be open to receiving a call.
This study is also a microcosm of the dilemma surgical education finds itself in when attempting to merge ideals of graded resident autonomy with safe patient care. Grey-haired residency stories abound of feats of technical magnificence as their attending slept. Yet, over time, increased scrutiny on accountability and improved outcomes has shortened if not changed the leash trainees are given. Resident autonomy though is based on effective, bi-directional communication guided by an attending.
More hospitals are adopting critical pathways which cause a mandatory notification to the attending. Potential exists for the resident to be marginalized, becoming an outsider in patient care. It is imperative that safety measures implemented in hospital programs include an educational component. Integrating the resident into algorithms that emphasizes their role in diagnosis and implementing a treatment plan is crucial.
Dr. Robroy MacIver is a pediatric cardiothoracic surgery fellow at Seattle Children’s Hospital and a resident editor of Thoracic Surgery News.
Effective communication continues to be a problem as medical teams become more modular in their approach to patient care. Although methods of communication for residents have become ubiquitous, communication to the attending often does not occur in a reliable manner.
This study is an excellent example of improving patient safety by removing potential communication breakdowns. This prospective study by Dr. Greenberg created clear, documented expectations on when the attending should be notified by either a resident or nurse. As such, critical patient events were more effectively delivered to the attending. In a third of these notifications, the patient care plan was then changed. An interesting component of this study was the setting of expectations on both ends; when to call and when to be open to receiving a call.
This study is also a microcosm of the dilemma surgical education finds itself in when attempting to merge ideals of graded resident autonomy with safe patient care. Grey-haired residency stories abound of feats of technical magnificence as their attending slept. Yet, over time, increased scrutiny on accountability and improved outcomes has shortened if not changed the leash trainees are given. Resident autonomy though is based on effective, bi-directional communication guided by an attending.
More hospitals are adopting critical pathways which cause a mandatory notification to the attending. Potential exists for the resident to be marginalized, becoming an outsider in patient care. It is imperative that safety measures implemented in hospital programs include an educational component. Integrating the resident into algorithms that emphasizes their role in diagnosis and implementing a treatment plan is crucial.
Dr. Robroy MacIver is a pediatric cardiothoracic surgery fellow at Seattle Children’s Hospital and a resident editor of Thoracic Surgery News.
Effective communication continues to be a problem as medical teams become more modular in their approach to patient care. Although methods of communication for residents have become ubiquitous, communication to the attending often does not occur in a reliable manner.
This study is an excellent example of improving patient safety by removing potential communication breakdowns. This prospective study by Dr. Greenberg created clear, documented expectations on when the attending should be notified by either a resident or nurse. As such, critical patient events were more effectively delivered to the attending. In a third of these notifications, the patient care plan was then changed. An interesting component of this study was the setting of expectations on both ends; when to call and when to be open to receiving a call.
This study is also a microcosm of the dilemma surgical education finds itself in when attempting to merge ideals of graded resident autonomy with safe patient care. Grey-haired residency stories abound of feats of technical magnificence as their attending slept. Yet, over time, increased scrutiny on accountability and improved outcomes has shortened if not changed the leash trainees are given. Resident autonomy though is based on effective, bi-directional communication guided by an attending.
More hospitals are adopting critical pathways which cause a mandatory notification to the attending. Potential exists for the resident to be marginalized, becoming an outsider in patient care. It is imperative that safety measures implemented in hospital programs include an educational component. Integrating the resident into algorithms that emphasizes their role in diagnosis and implementing a treatment plan is crucial.
Dr. Robroy MacIver is a pediatric cardiothoracic surgery fellow at Seattle Children’s Hospital and a resident editor of Thoracic Surgery News.
SAN FRANCISCO – Training residents to notify attending surgeons of any significant change in a patient’s condition greatly reduced the proportion of critical events that were not communicated to attending surgeons, from 33% to 2%, in a prospective study of four hospitals.
The current study was undertaken in response to a previous study by the same research group showing that ambiguity about who is responsible for communications contributed to communication breakdowns between attending surgeons and other members of the team at any point in patient care, Dr. Caprice C. Greenberg said at the annual clinical congress of the American College of Surgeons.
In the previous study, 444 malpractice claims were reviewed, and this process identified 60 cases in which communication breakdown resulted in harm to a patient. Dr. Greenberg and colleagues found that communication breakdowns related to surgery are equally likely to happen during preoperative, intraoperative, and postoperative care, and most commonly involve communications attempted between an attending surgeon and another attending surgeon, a resident, or the patient or family.
Ambiguity about who is responsible for communicating played a role in 58% of communication breakdowns, said Dr. Greenberg, director of the Wisconsin Surgical Outcomes Research Program at the University of Wisconsin, Madison.
Handoffs of patient care from one provider to another contributed to 43% of communication breakdowns, and transferring a patient to a different location contributed to 39% of communication breakdowns. The data also showed that an asymmetry in status between the two communicating parties contributed to 74% of message breakdowns ( J. Am. Coll. Surg. 2007;204:533-40).
Dr. Greenberg and her associates identified "triggers" that should prompt residents or nurses to contact attending surgeons, including a patient’s admission to a hospital, discharge, or a visit to an emergency department, transfer into or out of the ICU, unplanned intubation, or the development of cardiac arrest, new arrhythmia, or hemodynamic instability.
Significant neurologic changes, major wound complications, unplanned blood transfusion, an invasive procedure or operation, or errors in medication or treatment necessitating an intervention also should trigger communication with the attending surgeon. Even simply concern by a surgical trainee or a request from a nurse or another physician to contact the attending surgeon were considered triggers for communication.
The triggers were included in guidelines created by representatives of the four hospitals in Harvard University’s system in a collaboration organized by the system’s malpractice insurers. Under the new guidelines, residents were to notify attending surgeons of any significant changes in a patient’s condition regardless of the day or time. The residents would be trained to understand what qualifies as "significant changes" based in part on specialty-specific definitions, she said.
"What a urologist cares about is probably a little bit different from what a neurosurgeon or cardiac surgeon cares about," she explained.
A study of previous practices found that residents thought that 61 of 80 critical patient events (76%) did not need to be communicated to attending surgeons for safe patient care, and 26 events were not communicated (33%). Of the 54 events that were communicated, discussions with the attending surgeons changed management in 18 cases (33%). Attending surgeons responded to calls 100% of the time ( Ann. Surg. 2009;250:861-5).
"It wasn’t that the attendings didn’t want to be called. It was that residents either felt unempowered to call or they felt that it wasn’t necessary," she said.
Breakdowns in communication are common and play a significant role in adverse events, prior data suggest. One study of 48 surgeries found that 31% of 421 attempted communications between surgical team members failed, and approximately a third of these communication failures potentially jeopardized patient safety (Qual. Saf. Health Care 2004;13:330-4).
Other strategies to reduce the risk of errors during surgery include "workload leveling," Dr. Greenberg added. This means the attending surgeon should communicate frequently to members of the interdisciplinary surgical team about the status of the case and expected progression of the case, so that team members can manage their time and plan to do auxiliary tasks at the appropriate times. It’s probably impossible to avoid all errors, so surgeons need to find the right balance of error prevention and error mitigation through "resilience" – the ability to anticipate, cope with, recover from, and learn from unforeseen developments, she added. "To start to increase resilience, we really need to teach people adaptability and flexibility," she said.
Dr. Mary Klingensmith, a professor of surgery at Washington University, St. Louis, and Dr. John Hanks, a professor of surgery at the University of Virginia, Charlottesville, commented, "The conclusion of this study may seem obvious to those of us no longer in training – namely that residents should communicate critical patient events to attendings. Yet the imperative nature of such communication is not stressed adequately in our surgical training culture. In many training programs, there are some time-honored but outdated concepts in play, such as it is a "sign of weakness" to call the attending. Dr. Greenberg describes residents in this position as feeling "unempowered" to place such a call.
"We need to debunk this myth and explicitly instruct our residents about what we want and expect. Under the new paradigm, this accountability must include rapid and accurate transmittal of information with confidence on both the sending and receiving ends.
"The intervention put into place by Dr. Greenberg’s group did just that, laying out for trainees the patient events that should trigger a call to the attending. Interestingly, they reported that change in patient management, as a result of attending input, occurred in only 33% of cases in which the attending was called – a result suggesting that information transfer was merely that of the "FYI" variety. Yet in all instances, the attending wanted to be called.
"If the patient safety aspect of these communication triggers can be stressed, we can more effectively shape trainee behavior." ☐
SAN FRANCISCO – Training residents to notify attending surgeons of any significant change in a patient’s condition greatly reduced the proportion of critical events that were not communicated to attending surgeons, from 33% to 2%, in a prospective study of four hospitals.
The current study was undertaken in response to a previous study by the same research group showing that ambiguity about who is responsible for communications contributed to communication breakdowns between attending surgeons and other members of the team at any point in patient care, Dr. Caprice C. Greenberg said at the annual clinical congress of the American College of Surgeons.
In the previous study, 444 malpractice claims were reviewed, and this process identified 60 cases in which communication breakdown resulted in harm to a patient. Dr. Greenberg and colleagues found that communication breakdowns related to surgery are equally likely to happen during preoperative, intraoperative, and postoperative care, and most commonly involve communications attempted between an attending surgeon and another attending surgeon, a resident, or the patient or family.
Ambiguity about who is responsible for communicating played a role in 58% of communication breakdowns, said Dr. Greenberg, director of the Wisconsin Surgical Outcomes Research Program at the University of Wisconsin, Madison.
Handoffs of patient care from one provider to another contributed to 43% of communication breakdowns, and transferring a patient to a different location contributed to 39% of communication breakdowns. The data also showed that an asymmetry in status between the two communicating parties contributed to 74% of message breakdowns ( J. Am. Coll. Surg. 2007;204:533-40).
Dr. Greenberg and her associates identified "triggers" that should prompt residents or nurses to contact attending surgeons, including a patient’s admission to a hospital, discharge, or a visit to an emergency department, transfer into or out of the ICU, unplanned intubation, or the development of cardiac arrest, new arrhythmia, or hemodynamic instability.
Significant neurologic changes, major wound complications, unplanned blood transfusion, an invasive procedure or operation, or errors in medication or treatment necessitating an intervention also should trigger communication with the attending surgeon. Even simply concern by a surgical trainee or a request from a nurse or another physician to contact the attending surgeon were considered triggers for communication.
The triggers were included in guidelines created by representatives of the four hospitals in Harvard University’s system in a collaboration organized by the system’s malpractice insurers. Under the new guidelines, residents were to notify attending surgeons of any significant changes in a patient’s condition regardless of the day or time. The residents would be trained to understand what qualifies as "significant changes" based in part on specialty-specific definitions, she said.
"What a urologist cares about is probably a little bit different from what a neurosurgeon or cardiac surgeon cares about," she explained.
A study of previous practices found that residents thought that 61 of 80 critical patient events (76%) did not need to be communicated to attending surgeons for safe patient care, and 26 events were not communicated (33%). Of the 54 events that were communicated, discussions with the attending surgeons changed management in 18 cases (33%). Attending surgeons responded to calls 100% of the time ( Ann. Surg. 2009;250:861-5).
"It wasn’t that the attendings didn’t want to be called. It was that residents either felt unempowered to call or they felt that it wasn’t necessary," she said.
Breakdowns in communication are common and play a significant role in adverse events, prior data suggest. One study of 48 surgeries found that 31% of 421 attempted communications between surgical team members failed, and approximately a third of these communication failures potentially jeopardized patient safety (Qual. Saf. Health Care 2004;13:330-4).
Other strategies to reduce the risk of errors during surgery include "workload leveling," Dr. Greenberg added. This means the attending surgeon should communicate frequently to members of the interdisciplinary surgical team about the status of the case and expected progression of the case, so that team members can manage their time and plan to do auxiliary tasks at the appropriate times. It’s probably impossible to avoid all errors, so surgeons need to find the right balance of error prevention and error mitigation through "resilience" – the ability to anticipate, cope with, recover from, and learn from unforeseen developments, she added. "To start to increase resilience, we really need to teach people adaptability and flexibility," she said.
Dr. Mary Klingensmith, a professor of surgery at Washington University, St. Louis, and Dr. John Hanks, a professor of surgery at the University of Virginia, Charlottesville, commented, "The conclusion of this study may seem obvious to those of us no longer in training – namely that residents should communicate critical patient events to attendings. Yet the imperative nature of such communication is not stressed adequately in our surgical training culture. In many training programs, there are some time-honored but outdated concepts in play, such as it is a "sign of weakness" to call the attending. Dr. Greenberg describes residents in this position as feeling "unempowered" to place such a call.
"We need to debunk this myth and explicitly instruct our residents about what we want and expect. Under the new paradigm, this accountability must include rapid and accurate transmittal of information with confidence on both the sending and receiving ends.
"The intervention put into place by Dr. Greenberg’s group did just that, laying out for trainees the patient events that should trigger a call to the attending. Interestingly, they reported that change in patient management, as a result of attending input, occurred in only 33% of cases in which the attending was called – a result suggesting that information transfer was merely that of the "FYI" variety. Yet in all instances, the attending wanted to be called.
"If the patient safety aspect of these communication triggers can be stressed, we can more effectively shape trainee behavior." ☐
Major Finding: Residents failed to inform attending surgeons of critical patient events in 26 of 80 cases (33%) before adoption of new guidelines, and in only 1 of 47 cases (2%) after the intervention.
Data Source: Prospective studies at four hospitals before and after adoption of guidelines requiring residents to inform attending surgeons of any significant change in patient status.
Disclosures: Dr. Greenberg said she has no relevant conflicts of interest.
Disclose and Discuss Errors; Don't Defend, Deny
SAN FRANCISCO – Changing the clinical culture so that physicians were more willing to talk with patients about medical and surgical errors increased the number of errors reported, decreased lawsuits and legal costs, and improved safety at one institution.
"It used to be a ‘defend and deny’ culture," said Dr. Darrell A. Campbell Jr., professor of surgery and chief of clinical affairs at the University of Michigan, Ann Arbor. "Now it’s ‘disclose and discuss.’ "
The University of Michigan Health System’s "Disclosure of Unanticipated Outcomes" policy requires physicians to give patients "full disclosure of results, including results that differ significantly from what was anticipated" to allow patients to make informed decisions about future medical care, he said at the annual clinical congress of the American College of Surgeons.
Under the policy’s driving principles, the health system will defend medically appropriate care vigorously but will compensate quickly and fairly when inappropriate medical care causes injury and will learn from mistakes to improve patient safety and communication. The health system can compensate quickly and fairly because it is a closed-staff model covered by a captive insurance company, he said.
Reports of errors and "risk management events" more than doubled since full implementation of the policy in February 2004, from 6,706 in 2004 to 15,650 in 2007, he said. "I think people feel much more comfortable reporting errors" now.
A comparison of data from 2001 (before the policy) and 2005 (after the policy) found that the number of claims and lawsuits fell from 262 to 114, the average time to resolve claims and lawsuits decreased from 21 months to 10 months, and annual litigation costs declined from $3 million to $1 million, he said.
A retrospective study by other investigators looked at the university’s experience from 1995 to 2007 and reported similar findings. The average monthly rate of new legal claims decreased from seven per 100,000 patient encounters to less than five per 100,000 patient encounters after adopting the new policy.
The median time to resolve claims decreased from 1.36 to 0.95 years, and costs decreased for total liability, patient compensation, and legal costs not related to compensation (Ann. Intern. Med. 2010;153:213-21).
Dr. Campbell, a transplantation surgeon, described a case that went awry to illustrate possible responses to the situation. A 9-month-old girl undergoing a liver transplant had a small-diameter hepatic artery. Although the surgeon communicated to the anesthesiologist that the patient should not be overtransfused, the message may have been lost during handoff. The first postoperative hematocrit was 50%, the hepatic artery thrombosed, and the patient required retransplantation.
Prior to the full-disclosure policy, it might have been tempting to tell the patient’s parents, "These things happen," he said. While this is true, and it may avoid litigation, it’s not the whole truth. Caregivers would feel bad about it, the clinical safety culture would suffer, nothing would be learned, and the same problem could happen again.
If the physician instead says to the parents, "I’m concerned about what just happened. Let’s talk," the conversation is more difficult and could lead to litigation, but it’s an honest approach that augments doctor-patient trust and the culture of safety, which should make caregivers feel better, he said.
"Let’s talk" does not mean the surgeon should make reckless comments, Dr. Campbell stressed. It would not be helpful to say, "Anesthesia is incompetent," or "The fellow dropped the ball," or "I should have been notified earlier," or "I did a perfect operation," or "Somebody’s head will roll," for example.
Disclosing an unanticipated outcome should sound something like the following, he suggested: "This was an unexpected result. I am going to investigate fully. You have the right to know the whole story – the facts. I will tell you what I learn, but not right now."
That provides a window for exploring other possible complications in the case he described, he said. There may have been a laboratory or transcription error. An artery may have been open at the time of reexploration and not seen on relatively insensitive ultrasound. A technical error could have been made, or the patient may have had a humorally mediated rejection of the organ.
Dr. Campbell reported he had no relevant conflicts.
Body text
Doctor’s Bio
Body text
Doctor’s Bio
Body text
Doctor’s Bio
SAN FRANCISCO – Changing the clinical culture so that physicians were more willing to talk with patients about medical and surgical errors increased the number of errors reported, decreased lawsuits and legal costs, and improved safety at one institution.
"It used to be a ‘defend and deny’ culture," said Dr. Darrell A. Campbell Jr., professor of surgery and chief of clinical affairs at the University of Michigan, Ann Arbor. "Now it’s ‘disclose and discuss.’ "
The University of Michigan Health System’s "Disclosure of Unanticipated Outcomes" policy requires physicians to give patients "full disclosure of results, including results that differ significantly from what was anticipated" to allow patients to make informed decisions about future medical care, he said at the annual clinical congress of the American College of Surgeons.
Under the policy’s driving principles, the health system will defend medically appropriate care vigorously but will compensate quickly and fairly when inappropriate medical care causes injury and will learn from mistakes to improve patient safety and communication. The health system can compensate quickly and fairly because it is a closed-staff model covered by a captive insurance company, he said.
Reports of errors and "risk management events" more than doubled since full implementation of the policy in February 2004, from 6,706 in 2004 to 15,650 in 2007, he said. "I think people feel much more comfortable reporting errors" now.
A comparison of data from 2001 (before the policy) and 2005 (after the policy) found that the number of claims and lawsuits fell from 262 to 114, the average time to resolve claims and lawsuits decreased from 21 months to 10 months, and annual litigation costs declined from $3 million to $1 million, he said.
A retrospective study by other investigators looked at the university’s experience from 1995 to 2007 and reported similar findings. The average monthly rate of new legal claims decreased from seven per 100,000 patient encounters to less than five per 100,000 patient encounters after adopting the new policy.
The median time to resolve claims decreased from 1.36 to 0.95 years, and costs decreased for total liability, patient compensation, and legal costs not related to compensation (Ann. Intern. Med. 2010;153:213-21).
Dr. Campbell, a transplantation surgeon, described a case that went awry to illustrate possible responses to the situation. A 9-month-old girl undergoing a liver transplant had a small-diameter hepatic artery. Although the surgeon communicated to the anesthesiologist that the patient should not be overtransfused, the message may have been lost during handoff. The first postoperative hematocrit was 50%, the hepatic artery thrombosed, and the patient required retransplantation.
Prior to the full-disclosure policy, it might have been tempting to tell the patient’s parents, "These things happen," he said. While this is true, and it may avoid litigation, it’s not the whole truth. Caregivers would feel bad about it, the clinical safety culture would suffer, nothing would be learned, and the same problem could happen again.
If the physician instead says to the parents, "I’m concerned about what just happened. Let’s talk," the conversation is more difficult and could lead to litigation, but it’s an honest approach that augments doctor-patient trust and the culture of safety, which should make caregivers feel better, he said.
"Let’s talk" does not mean the surgeon should make reckless comments, Dr. Campbell stressed. It would not be helpful to say, "Anesthesia is incompetent," or "The fellow dropped the ball," or "I should have been notified earlier," or "I did a perfect operation," or "Somebody’s head will roll," for example.
Disclosing an unanticipated outcome should sound something like the following, he suggested: "This was an unexpected result. I am going to investigate fully. You have the right to know the whole story – the facts. I will tell you what I learn, but not right now."
That provides a window for exploring other possible complications in the case he described, he said. There may have been a laboratory or transcription error. An artery may have been open at the time of reexploration and not seen on relatively insensitive ultrasound. A technical error could have been made, or the patient may have had a humorally mediated rejection of the organ.
Dr. Campbell reported he had no relevant conflicts.
SAN FRANCISCO – Changing the clinical culture so that physicians were more willing to talk with patients about medical and surgical errors increased the number of errors reported, decreased lawsuits and legal costs, and improved safety at one institution.
"It used to be a ‘defend and deny’ culture," said Dr. Darrell A. Campbell Jr., professor of surgery and chief of clinical affairs at the University of Michigan, Ann Arbor. "Now it’s ‘disclose and discuss.’ "
The University of Michigan Health System’s "Disclosure of Unanticipated Outcomes" policy requires physicians to give patients "full disclosure of results, including results that differ significantly from what was anticipated" to allow patients to make informed decisions about future medical care, he said at the annual clinical congress of the American College of Surgeons.
Under the policy’s driving principles, the health system will defend medically appropriate care vigorously but will compensate quickly and fairly when inappropriate medical care causes injury and will learn from mistakes to improve patient safety and communication. The health system can compensate quickly and fairly because it is a closed-staff model covered by a captive insurance company, he said.
Reports of errors and "risk management events" more than doubled since full implementation of the policy in February 2004, from 6,706 in 2004 to 15,650 in 2007, he said. "I think people feel much more comfortable reporting errors" now.
A comparison of data from 2001 (before the policy) and 2005 (after the policy) found that the number of claims and lawsuits fell from 262 to 114, the average time to resolve claims and lawsuits decreased from 21 months to 10 months, and annual litigation costs declined from $3 million to $1 million, he said.
A retrospective study by other investigators looked at the university’s experience from 1995 to 2007 and reported similar findings. The average monthly rate of new legal claims decreased from seven per 100,000 patient encounters to less than five per 100,000 patient encounters after adopting the new policy.
The median time to resolve claims decreased from 1.36 to 0.95 years, and costs decreased for total liability, patient compensation, and legal costs not related to compensation (Ann. Intern. Med. 2010;153:213-21).
Dr. Campbell, a transplantation surgeon, described a case that went awry to illustrate possible responses to the situation. A 9-month-old girl undergoing a liver transplant had a small-diameter hepatic artery. Although the surgeon communicated to the anesthesiologist that the patient should not be overtransfused, the message may have been lost during handoff. The first postoperative hematocrit was 50%, the hepatic artery thrombosed, and the patient required retransplantation.
Prior to the full-disclosure policy, it might have been tempting to tell the patient’s parents, "These things happen," he said. While this is true, and it may avoid litigation, it’s not the whole truth. Caregivers would feel bad about it, the clinical safety culture would suffer, nothing would be learned, and the same problem could happen again.
If the physician instead says to the parents, "I’m concerned about what just happened. Let’s talk," the conversation is more difficult and could lead to litigation, but it’s an honest approach that augments doctor-patient trust and the culture of safety, which should make caregivers feel better, he said.
"Let’s talk" does not mean the surgeon should make reckless comments, Dr. Campbell stressed. It would not be helpful to say, "Anesthesia is incompetent," or "The fellow dropped the ball," or "I should have been notified earlier," or "I did a perfect operation," or "Somebody’s head will roll," for example.
Disclosing an unanticipated outcome should sound something like the following, he suggested: "This was an unexpected result. I am going to investigate fully. You have the right to know the whole story – the facts. I will tell you what I learn, but not right now."
That provides a window for exploring other possible complications in the case he described, he said. There may have been a laboratory or transcription error. An artery may have been open at the time of reexploration and not seen on relatively insensitive ultrasound. A technical error could have been made, or the patient may have had a humorally mediated rejection of the organ.
Dr. Campbell reported he had no relevant conflicts.
Major Finding:
Data Source:
Disclosures:
Antiplatelet Use
Tthe other major message from the revised CABG guidelines is a new approach to dealing with antiplatelet therapies in the days leading up to cardiac surgery, said Dr. Peter K. Smith, vice-chairman of the CABG guidelines committee.
"There is a growing body of evidence that patients benefit from these agents," the P2Y12-receptor binding drug class of clopidogrel (Plavix), prasugrel (Effient), and ticagrelor (Brilinta). "Our guidelines emphasize that surgery can be safely done in the presence of some of these platelet inhibitors when necessary," he said in an interview. "There is reluctance against doing surgery in the presence of these drugs that is to the disadvantage of patients."
Specifically, the new guidelines say that in patients referred for urgent CABG, clopidogrel and ticagrelor should be discontinued to at least 24 hours to reduce major bleeding complications. Stoppage scheduled 1 day before surgery is a significant scaling down from the prior recommendation that clopidogrel be halted at least 5 days before surgery, he said. "Surgeons need to be more permissive about having this [antiplatelet] environment in place when surgery is performed."
The new guidelines add that for patients undergoing elective CABG, clopidogrel or ticagrelor treatment should stop at least 5 days before surgery, and prasugrel treatment should stop for at least 7 days. This more conservative approach makes sense when patients are not unstable and in a prothrombotic state, Dr. Smith said.
The guidelines also update the presurgical approach to aspirin treatment. Aspirin should be administered preoperatively, at 100-325 mg/day, right up to surgery. Prior guidelines called for stopping aspirin several days before. The new guidelines recommend if aspirin was not administered preoperatively, it should be initiated within 6 hours after surgery and then continued indefinitely. Clopidogrel should be used in patients allergic to or intolerant of aspirin.
–Mitchel L. Zoler
Tthe other major message from the revised CABG guidelines is a new approach to dealing with antiplatelet therapies in the days leading up to cardiac surgery, said Dr. Peter K. Smith, vice-chairman of the CABG guidelines committee.
"There is a growing body of evidence that patients benefit from these agents," the P2Y12-receptor binding drug class of clopidogrel (Plavix), prasugrel (Effient), and ticagrelor (Brilinta). "Our guidelines emphasize that surgery can be safely done in the presence of some of these platelet inhibitors when necessary," he said in an interview. "There is reluctance against doing surgery in the presence of these drugs that is to the disadvantage of patients."
Specifically, the new guidelines say that in patients referred for urgent CABG, clopidogrel and ticagrelor should be discontinued to at least 24 hours to reduce major bleeding complications. Stoppage scheduled 1 day before surgery is a significant scaling down from the prior recommendation that clopidogrel be halted at least 5 days before surgery, he said. "Surgeons need to be more permissive about having this [antiplatelet] environment in place when surgery is performed."
The new guidelines add that for patients undergoing elective CABG, clopidogrel or ticagrelor treatment should stop at least 5 days before surgery, and prasugrel treatment should stop for at least 7 days. This more conservative approach makes sense when patients are not unstable and in a prothrombotic state, Dr. Smith said.
The guidelines also update the presurgical approach to aspirin treatment. Aspirin should be administered preoperatively, at 100-325 mg/day, right up to surgery. Prior guidelines called for stopping aspirin several days before. The new guidelines recommend if aspirin was not administered preoperatively, it should be initiated within 6 hours after surgery and then continued indefinitely. Clopidogrel should be used in patients allergic to or intolerant of aspirin.
–Mitchel L. Zoler
Tthe other major message from the revised CABG guidelines is a new approach to dealing with antiplatelet therapies in the days leading up to cardiac surgery, said Dr. Peter K. Smith, vice-chairman of the CABG guidelines committee.
"There is a growing body of evidence that patients benefit from these agents," the P2Y12-receptor binding drug class of clopidogrel (Plavix), prasugrel (Effient), and ticagrelor (Brilinta). "Our guidelines emphasize that surgery can be safely done in the presence of some of these platelet inhibitors when necessary," he said in an interview. "There is reluctance against doing surgery in the presence of these drugs that is to the disadvantage of patients."
Specifically, the new guidelines say that in patients referred for urgent CABG, clopidogrel and ticagrelor should be discontinued to at least 24 hours to reduce major bleeding complications. Stoppage scheduled 1 day before surgery is a significant scaling down from the prior recommendation that clopidogrel be halted at least 5 days before surgery, he said. "Surgeons need to be more permissive about having this [antiplatelet] environment in place when surgery is performed."
The new guidelines add that for patients undergoing elective CABG, clopidogrel or ticagrelor treatment should stop at least 5 days before surgery, and prasugrel treatment should stop for at least 7 days. This more conservative approach makes sense when patients are not unstable and in a prothrombotic state, Dr. Smith said.
The guidelines also update the presurgical approach to aspirin treatment. Aspirin should be administered preoperatively, at 100-325 mg/day, right up to surgery. Prior guidelines called for stopping aspirin several days before. The new guidelines recommend if aspirin was not administered preoperatively, it should be initiated within 6 hours after surgery and then continued indefinitely. Clopidogrel should be used in patients allergic to or intolerant of aspirin.
–Mitchel L. Zoler
Noninvasive Scan Has Promise For Lung Cancer Genotyping
AMSTERDAM – An experimental combination of PET scanning and a positron-emitting form of erlotinib appeared to work as a noninvasive way of identifying patients with advanced non–small cell lung cancer tumors that have the right genotype to receive erlotinib therapy.
"[11C]erlotinib PET shows promise as a noninvasive, in vivo means of selecting patients who may benefit from thymidine kinase inhibitor therapy," Dr. Idris Bahce said, reporting on a pilot study of 10 patients. Erlotinib (Tarceva) is from the thymidine kinase inhibitor drug class.
In his study, uptake of 11C-labeled erlotinib was significantly linked to the patients’ having an activating mutation in their epidermal growth factor receptor (EGFR) gene, specifically an exon 19 deletion.
Patients positive for erlotinib uptake on the PET scan also showed a tendency for better clinical responses to a therapeutic erlotinib regimen, reported Dr. Bahce, a pulmonologist at VU University, Amsterdam, during the World Conference on Lung Cancer.
Until now, the only way to identify advanced non–small cell lung cancer (NSCLC) tumors that are candidates for treatment with a tyrosine kinase inhibitor has been to biopsy the tumor and run an in vitro genetic analysis on the tumor cells. That can be challenging in some patients, such as when the tumor is not easy to biopsy, a limited amount of tissue is available, or the tumor is genetically heterogeneous. To get a reliable result from biopsy and testing, at least 30% of the specimen must contain malignant cells, Dr. Bahce said at the conference, sponsored by the International Association for the Study of Lung Cancer.
"It is a very early study, but ... it’s important because personalized treatment [for cancer] has gone to the next level, where we use new agents and match them to the right patients by doing biopsies," commented Dr. Roy S. Herbst, chief of medical oncology at the Yale Cancer Center in New Haven. "The PET method also allows physicians to assess the volume of cancer carrying the EGFR mutation following treatment, a way to track treatment efficacy," said Dr. Herbst in an interview.
"Instead of getting tissue at one point in time, you can image more frequently. It’s a way to track the course of treatment noninvasively," and in real time, he said.
He also predicted that the [11C]erlotinib PET test will become commercialized, although currently Dr. Bahce’s studies do not have any commercial funding.
"This is a proof of concept study," commented Dr. Luis Paz-Ares, chief of medical oncology at University Hospital Virgin del Rocio in Seville, Spain. "We need to define the positive predictive value and the negative predictive value" of the test, he added. The long-term future of a test like this may also be limited because future testing will probably need to look at multiple biomarkers, Dr. Paz-Ares said.
The study enrolled five patients with advanced NSCLC who had exon 19 deletion EGFR mutations, and five advanced NSCLC patients with wild-type EGFR genes. Each patient underwent a pair of [11C]erlotinib PET scans, each preceded by a [15O]water PET scan to assess blood perfusion of the tumors. A 4-hour interval separated the two sets of scans.
The scan results showed that the volume of distribution of the tagged erlotinib in the patients with EGFR mutations ran about 50% higher than in the patients with wild-type tumors, a difference that was significant (P = .03). Clinically, two of the five wild-type patients had nonetheless received erlotinib treatment prior to testing, and neither patient responded, with both showing progressive disease.
Three of the five patients with an EGFR mutation began receiving erlotinib treatment after testing and responded. In one of these patients, the tumor remained in check for 13 months. In a second patient, the tumor began to progress after 17 months of no progression on treatment. In the third patient, the tumor began to progress again after about 4 weeks of no progression on erlotinib treatment, Dr. Bahce said. A fourth patient went on erlotinib treatment before testing, and did not respond and continued to have progressive disease.
The two patient subgroups showed no difference in blood perfusion into the tumors or in EGFR expression in cell membranes.
Dr. Bahce said he had no disclosures.☐
AMSTERDAM – An experimental combination of PET scanning and a positron-emitting form of erlotinib appeared to work as a noninvasive way of identifying patients with advanced non–small cell lung cancer tumors that have the right genotype to receive erlotinib therapy.
"[11C]erlotinib PET shows promise as a noninvasive, in vivo means of selecting patients who may benefit from thymidine kinase inhibitor therapy," Dr. Idris Bahce said, reporting on a pilot study of 10 patients. Erlotinib (Tarceva) is from the thymidine kinase inhibitor drug class.
In his study, uptake of 11C-labeled erlotinib was significantly linked to the patients’ having an activating mutation in their epidermal growth factor receptor (EGFR) gene, specifically an exon 19 deletion.
Patients positive for erlotinib uptake on the PET scan also showed a tendency for better clinical responses to a therapeutic erlotinib regimen, reported Dr. Bahce, a pulmonologist at VU University, Amsterdam, during the World Conference on Lung Cancer.
Until now, the only way to identify advanced non–small cell lung cancer (NSCLC) tumors that are candidates for treatment with a tyrosine kinase inhibitor has been to biopsy the tumor and run an in vitro genetic analysis on the tumor cells. That can be challenging in some patients, such as when the tumor is not easy to biopsy, a limited amount of tissue is available, or the tumor is genetically heterogeneous. To get a reliable result from biopsy and testing, at least 30% of the specimen must contain malignant cells, Dr. Bahce said at the conference, sponsored by the International Association for the Study of Lung Cancer.
"It is a very early study, but ... it’s important because personalized treatment [for cancer] has gone to the next level, where we use new agents and match them to the right patients by doing biopsies," commented Dr. Roy S. Herbst, chief of medical oncology at the Yale Cancer Center in New Haven. "The PET method also allows physicians to assess the volume of cancer carrying the EGFR mutation following treatment, a way to track treatment efficacy," said Dr. Herbst in an interview.
"Instead of getting tissue at one point in time, you can image more frequently. It’s a way to track the course of treatment noninvasively," and in real time, he said.
He also predicted that the [11C]erlotinib PET test will become commercialized, although currently Dr. Bahce’s studies do not have any commercial funding.
"This is a proof of concept study," commented Dr. Luis Paz-Ares, chief of medical oncology at University Hospital Virgin del Rocio in Seville, Spain. "We need to define the positive predictive value and the negative predictive value" of the test, he added. The long-term future of a test like this may also be limited because future testing will probably need to look at multiple biomarkers, Dr. Paz-Ares said.
The study enrolled five patients with advanced NSCLC who had exon 19 deletion EGFR mutations, and five advanced NSCLC patients with wild-type EGFR genes. Each patient underwent a pair of [11C]erlotinib PET scans, each preceded by a [15O]water PET scan to assess blood perfusion of the tumors. A 4-hour interval separated the two sets of scans.
The scan results showed that the volume of distribution of the tagged erlotinib in the patients with EGFR mutations ran about 50% higher than in the patients with wild-type tumors, a difference that was significant (P = .03). Clinically, two of the five wild-type patients had nonetheless received erlotinib treatment prior to testing, and neither patient responded, with both showing progressive disease.
Three of the five patients with an EGFR mutation began receiving erlotinib treatment after testing and responded. In one of these patients, the tumor remained in check for 13 months. In a second patient, the tumor began to progress after 17 months of no progression on treatment. In the third patient, the tumor began to progress again after about 4 weeks of no progression on erlotinib treatment, Dr. Bahce said. A fourth patient went on erlotinib treatment before testing, and did not respond and continued to have progressive disease.
The two patient subgroups showed no difference in blood perfusion into the tumors or in EGFR expression in cell membranes.
Dr. Bahce said he had no disclosures.☐
AMSTERDAM – An experimental combination of PET scanning and a positron-emitting form of erlotinib appeared to work as a noninvasive way of identifying patients with advanced non–small cell lung cancer tumors that have the right genotype to receive erlotinib therapy.
"[11C]erlotinib PET shows promise as a noninvasive, in vivo means of selecting patients who may benefit from thymidine kinase inhibitor therapy," Dr. Idris Bahce said, reporting on a pilot study of 10 patients. Erlotinib (Tarceva) is from the thymidine kinase inhibitor drug class.
In his study, uptake of 11C-labeled erlotinib was significantly linked to the patients’ having an activating mutation in their epidermal growth factor receptor (EGFR) gene, specifically an exon 19 deletion.
Patients positive for erlotinib uptake on the PET scan also showed a tendency for better clinical responses to a therapeutic erlotinib regimen, reported Dr. Bahce, a pulmonologist at VU University, Amsterdam, during the World Conference on Lung Cancer.
Until now, the only way to identify advanced non–small cell lung cancer (NSCLC) tumors that are candidates for treatment with a tyrosine kinase inhibitor has been to biopsy the tumor and run an in vitro genetic analysis on the tumor cells. That can be challenging in some patients, such as when the tumor is not easy to biopsy, a limited amount of tissue is available, or the tumor is genetically heterogeneous. To get a reliable result from biopsy and testing, at least 30% of the specimen must contain malignant cells, Dr. Bahce said at the conference, sponsored by the International Association for the Study of Lung Cancer.
"It is a very early study, but ... it’s important because personalized treatment [for cancer] has gone to the next level, where we use new agents and match them to the right patients by doing biopsies," commented Dr. Roy S. Herbst, chief of medical oncology at the Yale Cancer Center in New Haven. "The PET method also allows physicians to assess the volume of cancer carrying the EGFR mutation following treatment, a way to track treatment efficacy," said Dr. Herbst in an interview.
"Instead of getting tissue at one point in time, you can image more frequently. It’s a way to track the course of treatment noninvasively," and in real time, he said.
He also predicted that the [11C]erlotinib PET test will become commercialized, although currently Dr. Bahce’s studies do not have any commercial funding.
"This is a proof of concept study," commented Dr. Luis Paz-Ares, chief of medical oncology at University Hospital Virgin del Rocio in Seville, Spain. "We need to define the positive predictive value and the negative predictive value" of the test, he added. The long-term future of a test like this may also be limited because future testing will probably need to look at multiple biomarkers, Dr. Paz-Ares said.
The study enrolled five patients with advanced NSCLC who had exon 19 deletion EGFR mutations, and five advanced NSCLC patients with wild-type EGFR genes. Each patient underwent a pair of [11C]erlotinib PET scans, each preceded by a [15O]water PET scan to assess blood perfusion of the tumors. A 4-hour interval separated the two sets of scans.
The scan results showed that the volume of distribution of the tagged erlotinib in the patients with EGFR mutations ran about 50% higher than in the patients with wild-type tumors, a difference that was significant (P = .03). Clinically, two of the five wild-type patients had nonetheless received erlotinib treatment prior to testing, and neither patient responded, with both showing progressive disease.
Three of the five patients with an EGFR mutation began receiving erlotinib treatment after testing and responded. In one of these patients, the tumor remained in check for 13 months. In a second patient, the tumor began to progress after 17 months of no progression on treatment. In the third patient, the tumor began to progress again after about 4 weeks of no progression on erlotinib treatment, Dr. Bahce said. A fourth patient went on erlotinib treatment before testing, and did not respond and continued to have progressive disease.
The two patient subgroups showed no difference in blood perfusion into the tumors or in EGFR expression in cell membranes.
Dr. Bahce said he had no disclosures.☐
Major Finding: Advanced non–small cell lung cancer tumors with an epidermal growth factor receptor (EGFR)–activating mutation bound significantly more radiolabeled erlotinib than did tumors with wild-type EGFR genes (P = .03).
Data Source: A pilot study in 10 patients.
Disclosures: Dr. Bahce said he had no disclosures.
Policy Experts Parse Implications of Health Care Reform
SAN FRANCISCO – Societal trends will trump health reform in changing the health care system, and surgeons need to do their part to decrease costs, leaders in the American College of Surgeons said at their annual clinical congress.
"Change is happening in spite of, alongside, and with the Affordable Care Act [ACA]," said Thomas Ricketts, Ph.D., codirector of the American College of Surgeons Health Policy Research Institute. Change is being driven as much as or more by the economy along with institutional and professional decisions, he said.
Those forces are shifting the health care system from one that is dominated by independent physicians and surgeons to one in which physicians will be employees. Health insurers are linking up with clinician groups. Instead of community-based hospitals responsive to local needs, institutions are aggregating in large, geographically spread "empires" that are learning how to manage themselves, said Dr. Ricketts, professor of health policy and management at the University of North Carolina at Chapel Hill.
The pace of mergers accelerated after passage of the ACA in March 2010. In the first two quarters of 2011 there were 139 mergers or acquisitions involving hospitals, compared with 37-82 in each of the years from 2001 to 2010, he said.
The ACA will make health coverage accessible to an estimated 32 million currently uninsured Americans. Seven in 10 hospitals and health systems in the United States plan to hire more physicians in the next 1-3 years, but it’s unclear whether there will be enough physicians. "It’s a huge problem," Dr. Ricketts said.
Physicians and patients should brace themselves for what he called "simple complexity" in the evolving health system, which will define the individual roles of providers with specificity, yet add complexity as system structures evolve.
Major provisions of the ACA will roll out over time, but many of the provisions of particular concern to surgeons kick in by 2014, Dr. Don E. Detmer said in a separate presentation during the same session. Enactment began with 13 components in 2010 involving payment reform, workforce and quality-of-care improvements, access to care, and new insurance rules. Eight major provisions in 2011 affected physician quality reporting, new approaches to payment and delivery of care, and more, said Dr. Detmer, medical director of the ACS Division of Advocacy and Health Policy.
In 2012, four provisions kick in that involve reduced payments for preventable hospital readmissions, launch of Accountable Care Organizations, higher Medicare payments to hospitals with high-quality and outcomes data, and required reporting of data on health disparities.
Five major provisions starting in 2013 include bundled payments for episodes of postacute care, limits on flexible spending accounts, increased payroll taxes for Medicare, expansion of preventive services in Medicaid, and electronic simplification of some administrative functions.
The top four of nine provisions that start in 2014 include creation of an essential benefits package for insurers to offer, the start of insurance exchanges through employers or states to offer insurance to people who have no coverage, a requirement for uninsured individuals to buy coverage or pay a penalty, and creation of an independent payment advisory board to identify potentially wasteful spending in Medicare.
As enacted, the ACA is unlikely to produce sufficient reforms to significantly alter the curve of ever-increasing costs through overall system performance, "but the ACA plus physician payment reforms just might," predicted Dr. Detmer, professor emeritus at the University of Virginia, Charlottesville.
Another player besides the ACA could have had a drastic effect – the Congressional Joint Select Committee on Deficit Reduction (also called the Super Committee) was charged with decreasing federal budget deficits by $1.2 trillion between 2012 and 2021. They failed to agree on a plan, so, that will likely trigger massive, widespread cuts in federal spending starting in January 2013.
Policy-driven changes in health care make many physicians nervous, but any resulting changes are "probably not as scary as what we’ve got now," Dr. Detmer said.
A separate federal commission on government spending, known as the Debt Commission, has recommended a number of reductions in health care spending, including cutting $54 billion from graduate and indirect medical education between 2012 and 2020, Dr. George F. Sheldon said in a separate presentation during the session. Fifteen new U.S. medical schools currently are planned with no federal support, which may help supply the physicians and surgeons needed to meet growing demand for care, but the schools alone will not be sufficient, said Dr. Sheldon, codirector of the ACS Health Policy Research Institute.
Of the 26,769 active general surgeons in the United States, 42% are aged 55 years or older, 2008 data show. The number of active general surgeons decreased by 2% between 1996 and 2006, especially in rural areas, other studies report.
The regionalization of health systems offers an opportunity for different models of surgical care, he suggested. Surgeons and high-technology equipment may locate more in regional centers than individual practices.
Government programs could do more to increase the supply of surgeons, added Dr. Sheldon, professor of surgery at the University of North Carolina at Chapel Hill. The National Health Service Corps doesn’t include surgeons, "but it would be great if they did," he said.
Creating new medical schools – and somehow finding the residency programs to train the extra graduates – is a good long-term plan, but it doesn’t solve immediate workforce shortages, said Dr. Andrew L. Warshaw, chair of the ACS Health Policy Advisory Group. "If we have shortages now, it will be worse" as the ACA is implemented, he said in a presentation during the session. He noted that such shortages occurred in Massachusetts after the state adopted universal health care coverage.
Greater use of mid-level providers may help extend physicians’ reach, and regionalization models can either put more physicians where they’re needed or bring patients to physicians’ locations, he suggested.
But physicians need to tackle costs of health care, added Dr. Warshaw, of Harvard Medical School, Boston. If any solutions include a fix of the Sustainable Growth Rate (SGR) formula as requested by physicians, $1.6 trillion instead of $1.2 trillion would have to be cut from the federal deficit – cuts that could come from other parts of health care.
"What can surgeons do?" Dr. Warshaw said. "Every person in this room needs to do something, somewhere, somehow within your own practice to figure out what’s the right kind of care to give your patients. There’s good evidence that that can go a long way toward paying down the SGR."
If postoperative complications cost an average of $10,000, preventing just one postoperative complication per day at every U.S. hospital would reduce costs by $125-$250 billion over 10 years, he estimated.
Surgeons also need to figure out optimal care for patients and demand that other specialties do the same. One study at Massachusetts General Hospital found that physicians ordered between 1 and 30 CAT scans for patients seen in the emergency department for head trauma. Such a wide range in practices is "wrong," he said. "It’s our job to figure this out." Medical liability reform potentially could save another $62 billion in health care costs over 10 years, he added.
"I don’t think we can count on the ACA to reduce costs. We have to do a lot more," Dr. Warshaw said. "There’s a huge amount going on, and it’s way ahead of the Affordable Care Act in many ways."
Dr. Detmer has consulted for CS Placement. Dr. Ricketts, Dr. Sheldon, and Dr. Warshaw said that they had no financial conflicts. ☐
Body text
Doctor’s Bio
Body text
Doctor’s Bio
Body text
Doctor’s Bio
SAN FRANCISCO – Societal trends will trump health reform in changing the health care system, and surgeons need to do their part to decrease costs, leaders in the American College of Surgeons said at their annual clinical congress.
"Change is happening in spite of, alongside, and with the Affordable Care Act [ACA]," said Thomas Ricketts, Ph.D., codirector of the American College of Surgeons Health Policy Research Institute. Change is being driven as much as or more by the economy along with institutional and professional decisions, he said.
Those forces are shifting the health care system from one that is dominated by independent physicians and surgeons to one in which physicians will be employees. Health insurers are linking up with clinician groups. Instead of community-based hospitals responsive to local needs, institutions are aggregating in large, geographically spread "empires" that are learning how to manage themselves, said Dr. Ricketts, professor of health policy and management at the University of North Carolina at Chapel Hill.
The pace of mergers accelerated after passage of the ACA in March 2010. In the first two quarters of 2011 there were 139 mergers or acquisitions involving hospitals, compared with 37-82 in each of the years from 2001 to 2010, he said.
The ACA will make health coverage accessible to an estimated 32 million currently uninsured Americans. Seven in 10 hospitals and health systems in the United States plan to hire more physicians in the next 1-3 years, but it’s unclear whether there will be enough physicians. "It’s a huge problem," Dr. Ricketts said.
Physicians and patients should brace themselves for what he called "simple complexity" in the evolving health system, which will define the individual roles of providers with specificity, yet add complexity as system structures evolve.
Major provisions of the ACA will roll out over time, but many of the provisions of particular concern to surgeons kick in by 2014, Dr. Don E. Detmer said in a separate presentation during the same session. Enactment began with 13 components in 2010 involving payment reform, workforce and quality-of-care improvements, access to care, and new insurance rules. Eight major provisions in 2011 affected physician quality reporting, new approaches to payment and delivery of care, and more, said Dr. Detmer, medical director of the ACS Division of Advocacy and Health Policy.
In 2012, four provisions kick in that involve reduced payments for preventable hospital readmissions, launch of Accountable Care Organizations, higher Medicare payments to hospitals with high-quality and outcomes data, and required reporting of data on health disparities.
Five major provisions starting in 2013 include bundled payments for episodes of postacute care, limits on flexible spending accounts, increased payroll taxes for Medicare, expansion of preventive services in Medicaid, and electronic simplification of some administrative functions.
The top four of nine provisions that start in 2014 include creation of an essential benefits package for insurers to offer, the start of insurance exchanges through employers or states to offer insurance to people who have no coverage, a requirement for uninsured individuals to buy coverage or pay a penalty, and creation of an independent payment advisory board to identify potentially wasteful spending in Medicare.
As enacted, the ACA is unlikely to produce sufficient reforms to significantly alter the curve of ever-increasing costs through overall system performance, "but the ACA plus physician payment reforms just might," predicted Dr. Detmer, professor emeritus at the University of Virginia, Charlottesville.
Another player besides the ACA could have had a drastic effect – the Congressional Joint Select Committee on Deficit Reduction (also called the Super Committee) was charged with decreasing federal budget deficits by $1.2 trillion between 2012 and 2021. They failed to agree on a plan, so, that will likely trigger massive, widespread cuts in federal spending starting in January 2013.
Policy-driven changes in health care make many physicians nervous, but any resulting changes are "probably not as scary as what we’ve got now," Dr. Detmer said.
A separate federal commission on government spending, known as the Debt Commission, has recommended a number of reductions in health care spending, including cutting $54 billion from graduate and indirect medical education between 2012 and 2020, Dr. George F. Sheldon said in a separate presentation during the session. Fifteen new U.S. medical schools currently are planned with no federal support, which may help supply the physicians and surgeons needed to meet growing demand for care, but the schools alone will not be sufficient, said Dr. Sheldon, codirector of the ACS Health Policy Research Institute.
Of the 26,769 active general surgeons in the United States, 42% are aged 55 years or older, 2008 data show. The number of active general surgeons decreased by 2% between 1996 and 2006, especially in rural areas, other studies report.
The regionalization of health systems offers an opportunity for different models of surgical care, he suggested. Surgeons and high-technology equipment may locate more in regional centers than individual practices.
Government programs could do more to increase the supply of surgeons, added Dr. Sheldon, professor of surgery at the University of North Carolina at Chapel Hill. The National Health Service Corps doesn’t include surgeons, "but it would be great if they did," he said.
Creating new medical schools – and somehow finding the residency programs to train the extra graduates – is a good long-term plan, but it doesn’t solve immediate workforce shortages, said Dr. Andrew L. Warshaw, chair of the ACS Health Policy Advisory Group. "If we have shortages now, it will be worse" as the ACA is implemented, he said in a presentation during the session. He noted that such shortages occurred in Massachusetts after the state adopted universal health care coverage.
Greater use of mid-level providers may help extend physicians’ reach, and regionalization models can either put more physicians where they’re needed or bring patients to physicians’ locations, he suggested.
But physicians need to tackle costs of health care, added Dr. Warshaw, of Harvard Medical School, Boston. If any solutions include a fix of the Sustainable Growth Rate (SGR) formula as requested by physicians, $1.6 trillion instead of $1.2 trillion would have to be cut from the federal deficit – cuts that could come from other parts of health care.
"What can surgeons do?" Dr. Warshaw said. "Every person in this room needs to do something, somewhere, somehow within your own practice to figure out what’s the right kind of care to give your patients. There’s good evidence that that can go a long way toward paying down the SGR."
If postoperative complications cost an average of $10,000, preventing just one postoperative complication per day at every U.S. hospital would reduce costs by $125-$250 billion over 10 years, he estimated.
Surgeons also need to figure out optimal care for patients and demand that other specialties do the same. One study at Massachusetts General Hospital found that physicians ordered between 1 and 30 CAT scans for patients seen in the emergency department for head trauma. Such a wide range in practices is "wrong," he said. "It’s our job to figure this out." Medical liability reform potentially could save another $62 billion in health care costs over 10 years, he added.
"I don’t think we can count on the ACA to reduce costs. We have to do a lot more," Dr. Warshaw said. "There’s a huge amount going on, and it’s way ahead of the Affordable Care Act in many ways."
Dr. Detmer has consulted for CS Placement. Dr. Ricketts, Dr. Sheldon, and Dr. Warshaw said that they had no financial conflicts. ☐
SAN FRANCISCO – Societal trends will trump health reform in changing the health care system, and surgeons need to do their part to decrease costs, leaders in the American College of Surgeons said at their annual clinical congress.
"Change is happening in spite of, alongside, and with the Affordable Care Act [ACA]," said Thomas Ricketts, Ph.D., codirector of the American College of Surgeons Health Policy Research Institute. Change is being driven as much as or more by the economy along with institutional and professional decisions, he said.
Those forces are shifting the health care system from one that is dominated by independent physicians and surgeons to one in which physicians will be employees. Health insurers are linking up with clinician groups. Instead of community-based hospitals responsive to local needs, institutions are aggregating in large, geographically spread "empires" that are learning how to manage themselves, said Dr. Ricketts, professor of health policy and management at the University of North Carolina at Chapel Hill.
The pace of mergers accelerated after passage of the ACA in March 2010. In the first two quarters of 2011 there were 139 mergers or acquisitions involving hospitals, compared with 37-82 in each of the years from 2001 to 2010, he said.
The ACA will make health coverage accessible to an estimated 32 million currently uninsured Americans. Seven in 10 hospitals and health systems in the United States plan to hire more physicians in the next 1-3 years, but it’s unclear whether there will be enough physicians. "It’s a huge problem," Dr. Ricketts said.
Physicians and patients should brace themselves for what he called "simple complexity" in the evolving health system, which will define the individual roles of providers with specificity, yet add complexity as system structures evolve.
Major provisions of the ACA will roll out over time, but many of the provisions of particular concern to surgeons kick in by 2014, Dr. Don E. Detmer said in a separate presentation during the same session. Enactment began with 13 components in 2010 involving payment reform, workforce and quality-of-care improvements, access to care, and new insurance rules. Eight major provisions in 2011 affected physician quality reporting, new approaches to payment and delivery of care, and more, said Dr. Detmer, medical director of the ACS Division of Advocacy and Health Policy.
In 2012, four provisions kick in that involve reduced payments for preventable hospital readmissions, launch of Accountable Care Organizations, higher Medicare payments to hospitals with high-quality and outcomes data, and required reporting of data on health disparities.
Five major provisions starting in 2013 include bundled payments for episodes of postacute care, limits on flexible spending accounts, increased payroll taxes for Medicare, expansion of preventive services in Medicaid, and electronic simplification of some administrative functions.
The top four of nine provisions that start in 2014 include creation of an essential benefits package for insurers to offer, the start of insurance exchanges through employers or states to offer insurance to people who have no coverage, a requirement for uninsured individuals to buy coverage or pay a penalty, and creation of an independent payment advisory board to identify potentially wasteful spending in Medicare.
As enacted, the ACA is unlikely to produce sufficient reforms to significantly alter the curve of ever-increasing costs through overall system performance, "but the ACA plus physician payment reforms just might," predicted Dr. Detmer, professor emeritus at the University of Virginia, Charlottesville.
Another player besides the ACA could have had a drastic effect – the Congressional Joint Select Committee on Deficit Reduction (also called the Super Committee) was charged with decreasing federal budget deficits by $1.2 trillion between 2012 and 2021. They failed to agree on a plan, so, that will likely trigger massive, widespread cuts in federal spending starting in January 2013.
Policy-driven changes in health care make many physicians nervous, but any resulting changes are "probably not as scary as what we’ve got now," Dr. Detmer said.
A separate federal commission on government spending, known as the Debt Commission, has recommended a number of reductions in health care spending, including cutting $54 billion from graduate and indirect medical education between 2012 and 2020, Dr. George F. Sheldon said in a separate presentation during the session. Fifteen new U.S. medical schools currently are planned with no federal support, which may help supply the physicians and surgeons needed to meet growing demand for care, but the schools alone will not be sufficient, said Dr. Sheldon, codirector of the ACS Health Policy Research Institute.
Of the 26,769 active general surgeons in the United States, 42% are aged 55 years or older, 2008 data show. The number of active general surgeons decreased by 2% between 1996 and 2006, especially in rural areas, other studies report.
The regionalization of health systems offers an opportunity for different models of surgical care, he suggested. Surgeons and high-technology equipment may locate more in regional centers than individual practices.
Government programs could do more to increase the supply of surgeons, added Dr. Sheldon, professor of surgery at the University of North Carolina at Chapel Hill. The National Health Service Corps doesn’t include surgeons, "but it would be great if they did," he said.
Creating new medical schools – and somehow finding the residency programs to train the extra graduates – is a good long-term plan, but it doesn’t solve immediate workforce shortages, said Dr. Andrew L. Warshaw, chair of the ACS Health Policy Advisory Group. "If we have shortages now, it will be worse" as the ACA is implemented, he said in a presentation during the session. He noted that such shortages occurred in Massachusetts after the state adopted universal health care coverage.
Greater use of mid-level providers may help extend physicians’ reach, and regionalization models can either put more physicians where they’re needed or bring patients to physicians’ locations, he suggested.
But physicians need to tackle costs of health care, added Dr. Warshaw, of Harvard Medical School, Boston. If any solutions include a fix of the Sustainable Growth Rate (SGR) formula as requested by physicians, $1.6 trillion instead of $1.2 trillion would have to be cut from the federal deficit – cuts that could come from other parts of health care.
"What can surgeons do?" Dr. Warshaw said. "Every person in this room needs to do something, somewhere, somehow within your own practice to figure out what’s the right kind of care to give your patients. There’s good evidence that that can go a long way toward paying down the SGR."
If postoperative complications cost an average of $10,000, preventing just one postoperative complication per day at every U.S. hospital would reduce costs by $125-$250 billion over 10 years, he estimated.
Surgeons also need to figure out optimal care for patients and demand that other specialties do the same. One study at Massachusetts General Hospital found that physicians ordered between 1 and 30 CAT scans for patients seen in the emergency department for head trauma. Such a wide range in practices is "wrong," he said. "It’s our job to figure this out." Medical liability reform potentially could save another $62 billion in health care costs over 10 years, he added.
"I don’t think we can count on the ACA to reduce costs. We have to do a lot more," Dr. Warshaw said. "There’s a huge amount going on, and it’s way ahead of the Affordable Care Act in many ways."
Dr. Detmer has consulted for CS Placement. Dr. Ricketts, Dr. Sheldon, and Dr. Warshaw said that they had no financial conflicts. ☐
Major Finding:
Data Source:
Disclosures:
Noninvasive Scan Has Promise For Lung Cancer Genotyping
AMSTERDAM – An experimental combination of PET scanning and a positron-emitting form of erlotinib appeared to work as a noninvasive way of identifying patients with advanced non–small cell lung cancer tumors that have the right genotype to receive erlotinib therapy.
"[11C]erlotinib PET shows promise as a noninvasive, in vivo means of selecting patients who may benefit from thymidine kinase inhibitor therapy," Dr. Idris Bahce said, reporting on a pilot study of 10 patients. Erlotinib (Tarceva) is from the thymidine kinase inhibitor drug class.
In his study, uptake of 11C-labeled erlotinib was significantly linked to the patients’ having an activating mutation in their epidermal growth factor receptor (EGFR) gene, specifically an exon 19 deletion.
Patients positive for erlotinib uptake on the PET scan also showed a tendency for better clinical responses to a therapeutic erlotinib regimen, reported Dr. Bahce, a pulmonologist at VU University, Amsterdam, during the World Conference on Lung Cancer.
Until now, the only way to identify advanced non–small cell lung cancer (NSCLC) tumors that are candidates for treatment with a tyrosine kinase inhibitor has been to biopsy the tumor and run an in vitro genetic analysis on the tumor cells. That can be challenging in some patients, such as when the tumor is not easy to biopsy, a limited amount of tissue is available, or the tumor is genetically heterogeneous. To get a reliable result from biopsy and testing, at least 30% of the specimen must contain malignant cells, Dr. Bahce said at the conference, sponsored by the International Association for the Study of Lung Cancer.
"It is a very early study, but ... it’s important because personalized treatment [for cancer] has gone to the next level, where we use new agents and match them to the right patients by doing biopsies," commented Dr. Roy S. Herbst, chief of medical oncology at the Yale Cancer Center in New Haven. "The PET method also allows physicians to assess the volume of cancer carrying the EGFR mutation following treatment, a way to track treatment efficacy," said Dr. Herbst in an interview.
"Instead of getting tissue at one point in time, you can image more frequently. It’s a way to track the course of treatment noninvasively," and in real time, he said.
He also predicted that the [11C]erlotinib PET test will become commercialized, although currently Dr. Bahce’s studies do not have any commercial funding.
"This is a proof of concept study," commented Dr. Luis Paz-Ares, chief of medical oncology at University Hospital Virgin del Rocio in Seville, Spain. "We need to define the positive predictive value and the negative predictive value" of the test, he added. The long-term future of a test like this may also be limited because future testing will probably need to look at multiple biomarkers, Dr. Paz-Ares said.
The study enrolled five patients with advanced NSCLC who had exon 19 deletion EGFR mutations, and five advanced NSCLC patients with wild-type EGFR genes. Each patient underwent a pair of [11C]erlotinib PET scans, each preceded by a [15O]water PET scan to assess blood perfusion of the tumors. A 4-hour interval separated the two sets of scans.
The scan results showed that the volume of distribution of the tagged erlotinib in the patients with EGFR mutations ran about 50% higher than in the patients with wild-type tumors, a difference that was significant (P = .03). Clinically, two of the five wild-type patients had nonetheless received erlotinib treatment prior to testing, and neither patient responded, with both showing progressive disease.
Three of the five patients with an EGFR mutation began receiving erlotinib treatment after testing and responded. In one of these patients, the tumor remained in check for 13 months. In a second patient, the tumor began to progress after 17 months of no progression on treatment. In the third patient, the tumor began to progress again after about 4 weeks of no progression on erlotinib treatment, Dr. Bahce said. A fourth patient went on erlotinib treatment before testing, and did not respond and continued to have progressive disease.
The two patient subgroups showed no difference in blood perfusion into the tumors or in EGFR expression in cell membranes.
Dr. Bahce said he had no disclosures.☐
AMSTERDAM – An experimental combination of PET scanning and a positron-emitting form of erlotinib appeared to work as a noninvasive way of identifying patients with advanced non–small cell lung cancer tumors that have the right genotype to receive erlotinib therapy.
"[11C]erlotinib PET shows promise as a noninvasive, in vivo means of selecting patients who may benefit from thymidine kinase inhibitor therapy," Dr. Idris Bahce said, reporting on a pilot study of 10 patients. Erlotinib (Tarceva) is from the thymidine kinase inhibitor drug class.
In his study, uptake of 11C-labeled erlotinib was significantly linked to the patients’ having an activating mutation in their epidermal growth factor receptor (EGFR) gene, specifically an exon 19 deletion.
Patients positive for erlotinib uptake on the PET scan also showed a tendency for better clinical responses to a therapeutic erlotinib regimen, reported Dr. Bahce, a pulmonologist at VU University, Amsterdam, during the World Conference on Lung Cancer.
Until now, the only way to identify advanced non–small cell lung cancer (NSCLC) tumors that are candidates for treatment with a tyrosine kinase inhibitor has been to biopsy the tumor and run an in vitro genetic analysis on the tumor cells. That can be challenging in some patients, such as when the tumor is not easy to biopsy, a limited amount of tissue is available, or the tumor is genetically heterogeneous. To get a reliable result from biopsy and testing, at least 30% of the specimen must contain malignant cells, Dr. Bahce said at the conference, sponsored by the International Association for the Study of Lung Cancer.
"It is a very early study, but ... it’s important because personalized treatment [for cancer] has gone to the next level, where we use new agents and match them to the right patients by doing biopsies," commented Dr. Roy S. Herbst, chief of medical oncology at the Yale Cancer Center in New Haven. "The PET method also allows physicians to assess the volume of cancer carrying the EGFR mutation following treatment, a way to track treatment efficacy," said Dr. Herbst in an interview.
"Instead of getting tissue at one point in time, you can image more frequently. It’s a way to track the course of treatment noninvasively," and in real time, he said.
He also predicted that the [11C]erlotinib PET test will become commercialized, although currently Dr. Bahce’s studies do not have any commercial funding.
"This is a proof of concept study," commented Dr. Luis Paz-Ares, chief of medical oncology at University Hospital Virgin del Rocio in Seville, Spain. "We need to define the positive predictive value and the negative predictive value" of the test, he added. The long-term future of a test like this may also be limited because future testing will probably need to look at multiple biomarkers, Dr. Paz-Ares said.
The study enrolled five patients with advanced NSCLC who had exon 19 deletion EGFR mutations, and five advanced NSCLC patients with wild-type EGFR genes. Each patient underwent a pair of [11C]erlotinib PET scans, each preceded by a [15O]water PET scan to assess blood perfusion of the tumors. A 4-hour interval separated the two sets of scans.
The scan results showed that the volume of distribution of the tagged erlotinib in the patients with EGFR mutations ran about 50% higher than in the patients with wild-type tumors, a difference that was significant (P = .03). Clinically, two of the five wild-type patients had nonetheless received erlotinib treatment prior to testing, and neither patient responded, with both showing progressive disease.
Three of the five patients with an EGFR mutation began receiving erlotinib treatment after testing and responded. In one of these patients, the tumor remained in check for 13 months. In a second patient, the tumor began to progress after 17 months of no progression on treatment. In the third patient, the tumor began to progress again after about 4 weeks of no progression on erlotinib treatment, Dr. Bahce said. A fourth patient went on erlotinib treatment before testing, and did not respond and continued to have progressive disease.
The two patient subgroups showed no difference in blood perfusion into the tumors or in EGFR expression in cell membranes.
Dr. Bahce said he had no disclosures.☐
AMSTERDAM – An experimental combination of PET scanning and a positron-emitting form of erlotinib appeared to work as a noninvasive way of identifying patients with advanced non–small cell lung cancer tumors that have the right genotype to receive erlotinib therapy.
"[11C]erlotinib PET shows promise as a noninvasive, in vivo means of selecting patients who may benefit from thymidine kinase inhibitor therapy," Dr. Idris Bahce said, reporting on a pilot study of 10 patients. Erlotinib (Tarceva) is from the thymidine kinase inhibitor drug class.
In his study, uptake of 11C-labeled erlotinib was significantly linked to the patients’ having an activating mutation in their epidermal growth factor receptor (EGFR) gene, specifically an exon 19 deletion.
Patients positive for erlotinib uptake on the PET scan also showed a tendency for better clinical responses to a therapeutic erlotinib regimen, reported Dr. Bahce, a pulmonologist at VU University, Amsterdam, during the World Conference on Lung Cancer.
Until now, the only way to identify advanced non–small cell lung cancer (NSCLC) tumors that are candidates for treatment with a tyrosine kinase inhibitor has been to biopsy the tumor and run an in vitro genetic analysis on the tumor cells. That can be challenging in some patients, such as when the tumor is not easy to biopsy, a limited amount of tissue is available, or the tumor is genetically heterogeneous. To get a reliable result from biopsy and testing, at least 30% of the specimen must contain malignant cells, Dr. Bahce said at the conference, sponsored by the International Association for the Study of Lung Cancer.
"It is a very early study, but ... it’s important because personalized treatment [for cancer] has gone to the next level, where we use new agents and match them to the right patients by doing biopsies," commented Dr. Roy S. Herbst, chief of medical oncology at the Yale Cancer Center in New Haven. "The PET method also allows physicians to assess the volume of cancer carrying the EGFR mutation following treatment, a way to track treatment efficacy," said Dr. Herbst in an interview.
"Instead of getting tissue at one point in time, you can image more frequently. It’s a way to track the course of treatment noninvasively," and in real time, he said.
He also predicted that the [11C]erlotinib PET test will become commercialized, although currently Dr. Bahce’s studies do not have any commercial funding.
"This is a proof of concept study," commented Dr. Luis Paz-Ares, chief of medical oncology at University Hospital Virgin del Rocio in Seville, Spain. "We need to define the positive predictive value and the negative predictive value" of the test, he added. The long-term future of a test like this may also be limited because future testing will probably need to look at multiple biomarkers, Dr. Paz-Ares said.
The study enrolled five patients with advanced NSCLC who had exon 19 deletion EGFR mutations, and five advanced NSCLC patients with wild-type EGFR genes. Each patient underwent a pair of [11C]erlotinib PET scans, each preceded by a [15O]water PET scan to assess blood perfusion of the tumors. A 4-hour interval separated the two sets of scans.
The scan results showed that the volume of distribution of the tagged erlotinib in the patients with EGFR mutations ran about 50% higher than in the patients with wild-type tumors, a difference that was significant (P = .03). Clinically, two of the five wild-type patients had nonetheless received erlotinib treatment prior to testing, and neither patient responded, with both showing progressive disease.
Three of the five patients with an EGFR mutation began receiving erlotinib treatment after testing and responded. In one of these patients, the tumor remained in check for 13 months. In a second patient, the tumor began to progress after 17 months of no progression on treatment. In the third patient, the tumor began to progress again after about 4 weeks of no progression on erlotinib treatment, Dr. Bahce said. A fourth patient went on erlotinib treatment before testing, and did not respond and continued to have progressive disease.
The two patient subgroups showed no difference in blood perfusion into the tumors or in EGFR expression in cell membranes.
Dr. Bahce said he had no disclosures.☐
Major Finding: Advanced non–small cell lung cancer tumors with an epidermal growth factor receptor (EGFR)–activating mutation bound significantly more radiolabeled erlotinib than did tumors with wild-type EGFR genes (P = .03).
Data Source: A pilot study in 10 patients.
Disclosures: Dr. Bahce said he had no disclosures.
Antiplatelet Use
Tthe other major message from the revised CABG guidelines is a new approach to dealing with antiplatelet therapies in the days leading up to cardiac surgery, said Dr. Peter K. Smith, vice-chairman of the CABG guidelines committee.
"There is a growing body of evidence that patients benefit from these agents," the P2Y12-receptor binding drug class of clopidogrel (Plavix), prasugrel (Effient), and ticagrelor (Brilinta). "Our guidelines emphasize that surgery can be safely done in the presence of some of these platelet inhibitors when necessary," he said in an interview. "There is reluctance against doing surgery in the presence of these drugs that is to the disadvantage of patients."
Specifically, the new guidelines say that in patients referred for urgent CABG, clopidogrel and ticagrelor should be discontinued to at least 24 hours to reduce major bleeding complications. Stoppage scheduled 1 day before surgery is a significant scaling down from the prior recommendation that clopidogrel be halted at least 5 days before surgery, he said. "Surgeons need to be more permissive about having this [antiplatelet] environment in place when surgery is performed."
The new guidelines add that for patients undergoing elective CABG, clopidogrel or ticagrelor treatment should stop at least 5 days before surgery, and prasugrel treatment should stop for at least 7 days. This more conservative approach makes sense when patients are not unstable and in a prothrombotic state, Dr. Smith said.
The guidelines also update the presurgical approach to aspirin treatment. Aspirin should be administered preoperatively, at 100-325 mg/day, right up to surgery. Prior guidelines called for stopping aspirin several days before. The new guidelines recommend if aspirin was not administered preoperatively, it should be initiated within 6 hours after surgery and then continued indefinitely. Clopidogrel should be used in patients allergic to or intolerant of aspirin.
–Mitchel L. Zoler
Tthe other major message from the revised CABG guidelines is a new approach to dealing with antiplatelet therapies in the days leading up to cardiac surgery, said Dr. Peter K. Smith, vice-chairman of the CABG guidelines committee.
"There is a growing body of evidence that patients benefit from these agents," the P2Y12-receptor binding drug class of clopidogrel (Plavix), prasugrel (Effient), and ticagrelor (Brilinta). "Our guidelines emphasize that surgery can be safely done in the presence of some of these platelet inhibitors when necessary," he said in an interview. "There is reluctance against doing surgery in the presence of these drugs that is to the disadvantage of patients."
Specifically, the new guidelines say that in patients referred for urgent CABG, clopidogrel and ticagrelor should be discontinued to at least 24 hours to reduce major bleeding complications. Stoppage scheduled 1 day before surgery is a significant scaling down from the prior recommendation that clopidogrel be halted at least 5 days before surgery, he said. "Surgeons need to be more permissive about having this [antiplatelet] environment in place when surgery is performed."
The new guidelines add that for patients undergoing elective CABG, clopidogrel or ticagrelor treatment should stop at least 5 days before surgery, and prasugrel treatment should stop for at least 7 days. This more conservative approach makes sense when patients are not unstable and in a prothrombotic state, Dr. Smith said.
The guidelines also update the presurgical approach to aspirin treatment. Aspirin should be administered preoperatively, at 100-325 mg/day, right up to surgery. Prior guidelines called for stopping aspirin several days before. The new guidelines recommend if aspirin was not administered preoperatively, it should be initiated within 6 hours after surgery and then continued indefinitely. Clopidogrel should be used in patients allergic to or intolerant of aspirin.
–Mitchel L. Zoler
Tthe other major message from the revised CABG guidelines is a new approach to dealing with antiplatelet therapies in the days leading up to cardiac surgery, said Dr. Peter K. Smith, vice-chairman of the CABG guidelines committee.
"There is a growing body of evidence that patients benefit from these agents," the P2Y12-receptor binding drug class of clopidogrel (Plavix), prasugrel (Effient), and ticagrelor (Brilinta). "Our guidelines emphasize that surgery can be safely done in the presence of some of these platelet inhibitors when necessary," he said in an interview. "There is reluctance against doing surgery in the presence of these drugs that is to the disadvantage of patients."
Specifically, the new guidelines say that in patients referred for urgent CABG, clopidogrel and ticagrelor should be discontinued to at least 24 hours to reduce major bleeding complications. Stoppage scheduled 1 day before surgery is a significant scaling down from the prior recommendation that clopidogrel be halted at least 5 days before surgery, he said. "Surgeons need to be more permissive about having this [antiplatelet] environment in place when surgery is performed."
The new guidelines add that for patients undergoing elective CABG, clopidogrel or ticagrelor treatment should stop at least 5 days before surgery, and prasugrel treatment should stop for at least 7 days. This more conservative approach makes sense when patients are not unstable and in a prothrombotic state, Dr. Smith said.
The guidelines also update the presurgical approach to aspirin treatment. Aspirin should be administered preoperatively, at 100-325 mg/day, right up to surgery. Prior guidelines called for stopping aspirin several days before. The new guidelines recommend if aspirin was not administered preoperatively, it should be initiated within 6 hours after surgery and then continued indefinitely. Clopidogrel should be used in patients allergic to or intolerant of aspirin.
–Mitchel L. Zoler
Alter Surveillance for Barrett's Esophagus?
The incidence of esophageal adenocarcinoma among patients with Barrett’s esophagus was only 1.2 cases per 1,000 person-years in a study of the entire population of Denmark reported in the New England Journal of Medicine.
That rate is four to five times lower than rates reported previously, said Dr. Frederik Hvid-Jensen of the department of surgical gastroenterology at Aarhus (Denmark) University and his associates.
"Our study provides solid evidence that esophageal adenocarcinoma will develop in very few patients with Barrett’s esophagus. Together with another recent study, as well as studies of cost-effectiveness and patients’ quality of life, the results of our study suggest that the risk of esophageal adenocarcinoma among patients with Barrett’s esophagus is so minor that in the absence of dysplasia, routine surveillance of such patients is of doubtful value," the investigators said.
The relevance of such surveillance programs has been questioned before because they have never been shown to improve survival and because an estimated 95% of patients with a new diagnosis of esophageal adenocarcinoma do not have a previous diagnosis of Barrett’s esophagus, they noted.
Dr. Hvid-Jensen and his colleagues used data from Denmark’s nationwide pathology and cancer registries to calculate the incidence of adenocarcinoma among patients with Barrett’s esophagus and compare it with the expected incidence in the general population of 5.4 million people.
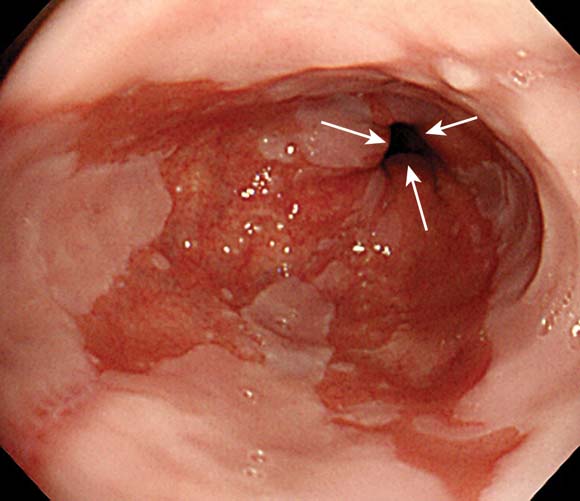
A total of 11,028 patients underwent endoscopic biopsy and received a diagnosis of Barrett’s esophagus during 1992-2009. The median age at baseline was 63 years, and patients were followed for a median of 5.2 years.
During that time, 197 of these patients with Barrett’s esophagus developed new esophageal adenocarcinomas, which comprised 7.6% of all the 2,602 incident esophageal adenocarcinomas diagnosed in the general Danish population during 1992-2009.
After excluding cancer cases that developed in the first year after a diagnosis of Barrett’s esophagus, the incidence of esophageal adenocarcinoma among patients with Barrett’s esophagus was found to be 1.2 cases per 1,000 person-years, the investigators said (N. Engl. J. Med. 2011;365:1375-83).
The annual risk of developing the malignancy was only 0.12%, or one case of adenocarcinoma per 860 patient-years.
In contrast, there were four reviews of the literature published in the past decade that pooled the results of numerous small studies conducted throughout the United States and Europe. These studies calculated the esophageal adenocarcinoma incidence as ranging from 5.2 to 7.0 cases per 1,000 person-years. In addition, two previous registry studies calculated similar incidences of 4.0 and 5.0 cases of esophogeal cardinoma per 1,000 person-years.
Current surveillance guidelines are based upon these earlier studies, which appear to have overstated the risks, Dr. Hvid-Jensen and his associates stated.
Their population-based, nationwide study is one of the largest studies of the issue; it included patients of all ages and both sexes and had almost no loss to follow-up. Because of Denmark’s universal health care plan, this study also had no referral bias or diagnostic bias.
"The generalizability of our results is therefore high," they noted.
Moreover, a recent population-based study in Northern Ireland found remarkably similar results: an incidence of 1.3 cases of esophageal adenocarcinoma per 1,000 patient-years among people with Barrett’s esophagus.
And another recent study "in which Markov models were used to evaluate available data on the incidence of adenocarcinoma supports our findings ... [and suggests] that surveillance is not beneficial," the researchers added.
This study was supported by the University of Aarhus Clinical Institute. No financial conflicts of interest were reported.☐
The "elegant" epidemiologic study by Dr. Hvid-Jensen and associates clearly shows that the relative risk of esophageal adenocarcinoma for a person with Barrett’s esophagus, as compared with the general population, is 11.3, "a substantial drop from the increase by a factor of 30 or 40 estimated in early reports," said Dr. Peter J. Kahrilas.
"As our knowledge of the biologic characteristics of Barrett’s esophagus has matured, the significance of the lesion has dwindled. In fact, patients with Barrett’s esophagus have the same life expectancy as does the general population, and esophageal cancer proves to be an uncommon cause of death in patients with Barrett’s esophagus regardless of surveillance," he noted.
Dr. Kahrilas is with the department of medicine at Northwestern University, Chicago. He reported ties to numerous industry sources. These remarks were taken from his editorial accompanying Dr. Hvid-Jensen’s report (N. Engl. J. Med. 2011;365:1437-8).
The "elegant" epidemiologic study by Dr. Hvid-Jensen and associates clearly shows that the relative risk of esophageal adenocarcinoma for a person with Barrett’s esophagus, as compared with the general population, is 11.3, "a substantial drop from the increase by a factor of 30 or 40 estimated in early reports," said Dr. Peter J. Kahrilas.
"As our knowledge of the biologic characteristics of Barrett’s esophagus has matured, the significance of the lesion has dwindled. In fact, patients with Barrett’s esophagus have the same life expectancy as does the general population, and esophageal cancer proves to be an uncommon cause of death in patients with Barrett’s esophagus regardless of surveillance," he noted.
Dr. Kahrilas is with the department of medicine at Northwestern University, Chicago. He reported ties to numerous industry sources. These remarks were taken from his editorial accompanying Dr. Hvid-Jensen’s report (N. Engl. J. Med. 2011;365:1437-8).
The "elegant" epidemiologic study by Dr. Hvid-Jensen and associates clearly shows that the relative risk of esophageal adenocarcinoma for a person with Barrett’s esophagus, as compared with the general population, is 11.3, "a substantial drop from the increase by a factor of 30 or 40 estimated in early reports," said Dr. Peter J. Kahrilas.
"As our knowledge of the biologic characteristics of Barrett’s esophagus has matured, the significance of the lesion has dwindled. In fact, patients with Barrett’s esophagus have the same life expectancy as does the general population, and esophageal cancer proves to be an uncommon cause of death in patients with Barrett’s esophagus regardless of surveillance," he noted.
Dr. Kahrilas is with the department of medicine at Northwestern University, Chicago. He reported ties to numerous industry sources. These remarks were taken from his editorial accompanying Dr. Hvid-Jensen’s report (N. Engl. J. Med. 2011;365:1437-8).
The incidence of esophageal adenocarcinoma among patients with Barrett’s esophagus was only 1.2 cases per 1,000 person-years in a study of the entire population of Denmark reported in the New England Journal of Medicine.
That rate is four to five times lower than rates reported previously, said Dr. Frederik Hvid-Jensen of the department of surgical gastroenterology at Aarhus (Denmark) University and his associates.
"Our study provides solid evidence that esophageal adenocarcinoma will develop in very few patients with Barrett’s esophagus. Together with another recent study, as well as studies of cost-effectiveness and patients’ quality of life, the results of our study suggest that the risk of esophageal adenocarcinoma among patients with Barrett’s esophagus is so minor that in the absence of dysplasia, routine surveillance of such patients is of doubtful value," the investigators said.
The relevance of such surveillance programs has been questioned before because they have never been shown to improve survival and because an estimated 95% of patients with a new diagnosis of esophageal adenocarcinoma do not have a previous diagnosis of Barrett’s esophagus, they noted.
Dr. Hvid-Jensen and his colleagues used data from Denmark’s nationwide pathology and cancer registries to calculate the incidence of adenocarcinoma among patients with Barrett’s esophagus and compare it with the expected incidence in the general population of 5.4 million people.
A total of 11,028 patients underwent endoscopic biopsy and received a diagnosis of Barrett’s esophagus during 1992-2009. The median age at baseline was 63 years, and patients were followed for a median of 5.2 years.
During that time, 197 of these patients with Barrett’s esophagus developed new esophageal adenocarcinomas, which comprised 7.6% of all the 2,602 incident esophageal adenocarcinomas diagnosed in the general Danish population during 1992-2009.
After excluding cancer cases that developed in the first year after a diagnosis of Barrett’s esophagus, the incidence of esophageal adenocarcinoma among patients with Barrett’s esophagus was found to be 1.2 cases per 1,000 person-years, the investigators said (N. Engl. J. Med. 2011;365:1375-83).
The annual risk of developing the malignancy was only 0.12%, or one case of adenocarcinoma per 860 patient-years.
In contrast, there were four reviews of the literature published in the past decade that pooled the results of numerous small studies conducted throughout the United States and Europe. These studies calculated the esophageal adenocarcinoma incidence as ranging from 5.2 to 7.0 cases per 1,000 person-years. In addition, two previous registry studies calculated similar incidences of 4.0 and 5.0 cases of esophogeal cardinoma per 1,000 person-years.
Current surveillance guidelines are based upon these earlier studies, which appear to have overstated the risks, Dr. Hvid-Jensen and his associates stated.
Their population-based, nationwide study is one of the largest studies of the issue; it included patients of all ages and both sexes and had almost no loss to follow-up. Because of Denmark’s universal health care plan, this study also had no referral bias or diagnostic bias.
"The generalizability of our results is therefore high," they noted.
Moreover, a recent population-based study in Northern Ireland found remarkably similar results: an incidence of 1.3 cases of esophageal adenocarcinoma per 1,000 patient-years among people with Barrett’s esophagus.
And another recent study "in which Markov models were used to evaluate available data on the incidence of adenocarcinoma supports our findings ... [and suggests] that surveillance is not beneficial," the researchers added.
This study was supported by the University of Aarhus Clinical Institute. No financial conflicts of interest were reported.☐
The incidence of esophageal adenocarcinoma among patients with Barrett’s esophagus was only 1.2 cases per 1,000 person-years in a study of the entire population of Denmark reported in the New England Journal of Medicine.
That rate is four to five times lower than rates reported previously, said Dr. Frederik Hvid-Jensen of the department of surgical gastroenterology at Aarhus (Denmark) University and his associates.
"Our study provides solid evidence that esophageal adenocarcinoma will develop in very few patients with Barrett’s esophagus. Together with another recent study, as well as studies of cost-effectiveness and patients’ quality of life, the results of our study suggest that the risk of esophageal adenocarcinoma among patients with Barrett’s esophagus is so minor that in the absence of dysplasia, routine surveillance of such patients is of doubtful value," the investigators said.
The relevance of such surveillance programs has been questioned before because they have never been shown to improve survival and because an estimated 95% of patients with a new diagnosis of esophageal adenocarcinoma do not have a previous diagnosis of Barrett’s esophagus, they noted.
Dr. Hvid-Jensen and his colleagues used data from Denmark’s nationwide pathology and cancer registries to calculate the incidence of adenocarcinoma among patients with Barrett’s esophagus and compare it with the expected incidence in the general population of 5.4 million people.
A total of 11,028 patients underwent endoscopic biopsy and received a diagnosis of Barrett’s esophagus during 1992-2009. The median age at baseline was 63 years, and patients were followed for a median of 5.2 years.
During that time, 197 of these patients with Barrett’s esophagus developed new esophageal adenocarcinomas, which comprised 7.6% of all the 2,602 incident esophageal adenocarcinomas diagnosed in the general Danish population during 1992-2009.
After excluding cancer cases that developed in the first year after a diagnosis of Barrett’s esophagus, the incidence of esophageal adenocarcinoma among patients with Barrett’s esophagus was found to be 1.2 cases per 1,000 person-years, the investigators said (N. Engl. J. Med. 2011;365:1375-83).
The annual risk of developing the malignancy was only 0.12%, or one case of adenocarcinoma per 860 patient-years.
In contrast, there were four reviews of the literature published in the past decade that pooled the results of numerous small studies conducted throughout the United States and Europe. These studies calculated the esophageal adenocarcinoma incidence as ranging from 5.2 to 7.0 cases per 1,000 person-years. In addition, two previous registry studies calculated similar incidences of 4.0 and 5.0 cases of esophogeal cardinoma per 1,000 person-years.
Current surveillance guidelines are based upon these earlier studies, which appear to have overstated the risks, Dr. Hvid-Jensen and his associates stated.
Their population-based, nationwide study is one of the largest studies of the issue; it included patients of all ages and both sexes and had almost no loss to follow-up. Because of Denmark’s universal health care plan, this study also had no referral bias or diagnostic bias.
"The generalizability of our results is therefore high," they noted.
Moreover, a recent population-based study in Northern Ireland found remarkably similar results: an incidence of 1.3 cases of esophageal adenocarcinoma per 1,000 patient-years among people with Barrett’s esophagus.
And another recent study "in which Markov models were used to evaluate available data on the incidence of adenocarcinoma supports our findings ... [and suggests] that surveillance is not beneficial," the researchers added.
This study was supported by the University of Aarhus Clinical Institute. No financial conflicts of interest were reported.☐
Major Finding: The incidence of esophageal adenocarcinoma among all patients in Denmark with Barrett’s esophagus was 1.2 cases per 1,000 person-years, which is four to five times lower than estimated in previous, smaller studies.
Data Source: An epidemiologic cohort study of esophageal adenocarcinoma among the 5.4 million residents of Denmark, including 11,028 with Barrett’s esophagus followed for a median of 5.2 years.
Disclosures: This study was supported by the University of Aarhus Clinical Institute. No financial conflicts of interest were reported.
Medicare Sets Measures for Hospital P4P
Medicare officials are expanding the list of quality measures that hospitals will be judged on as part of a new pay-for-performance program created under the Affordable Care Act.
In a final rule released Nov. 1, detailing Medicare payment rates for hospital outpatient departments, officials at the Centers for Medicare and Medicaid Services announced that they are adding a new clinical process of care measure related to urinary catheters to the Hospital Inpatient Value-Based Purchasing (VBP) Program. The new measure, which will go into effect in October 2013 for fiscal year 2014, will assess whether a urinary catheter inserted during surgery is removed on the first or second postsurgical day. Hospitals will begin reporting data to the CMS on the new measure in 2012.
The new measure will be added to 12 clinical process measures and 1 patient experience measure that were adopted for the first year of the program. The CMS also finalized plans to include three outcome measures related to 30-day mortality for acute myocardial infarction, heart failure, and pneumonia in the program for fiscal year 2014.
At the same time, the CMS is delaying plans to include other measures. The agency had planned to include eight measures on hospital-acquired conditions, two composite measures from the Agency for Healthcare Research and Quality, and a Medicare Spending per Beneficiary measure in the Hospital VBP program in fiscal year 2014. But after receiving public comments noting that performance data had not been publicly available long enough for hospitals to prepare to incorporate the measures, Medicare officials relented.
According to the final rule, the CMS will post hospital performance data on the measures to Medicare’s Hospital Compare website for at least 1 year before requiring hospitals to report data on them.
Under the Hospital VBP program, the CMS will begin making incentive payments to hospitals based on quality on Oct. 1, 2012. The payments are funded by reducing Medicare payments to hospitals by 1% during fiscal year 2013 and 1.25% in fiscal year 2014.
Hospital payments under the program will be based on performance on clinical process-of-care measures, patient satisfaction, and clinical outcomes. In fiscal year 2014, process-of-care measures will be weighted at 45% of the score, patient satisfaction at 30%, and outcomes at 25%. During the first year of the program, process-of-care measures will weighted at 70% and patient satisfaction measures at 30%.
Medicare officials are also moving ahead with plans to require ambulatory surgical centers (ASCs) to report on quality measures next year.
In the final rule, the CMS adopted four clinical outcome measures and one surgical infection control measure that ASCs must report on beginning in October 2012. The final list includes measures related to patient burns; patient falls; wrong site, wrong side, wrong patient, wrong procedure, and wrong implant surgery; rate of ASC admissions requiring a hospital transfer/admission upon discharge; and prophylactic intravenous antibiotic timing. The data reported will be used to determine payments for 2014, according to the final rule.
In 2013, ASCs will also have to report on their use of the safe surgery checklist and report data on their facility volume on selected procedures. That information will be used in setting payments for 2015. Additionally, hospitals will be required to report on influenza vaccination coverage among health care workers starting in 2014, which will affect their 2016 payments.
The more than 1,500-page final rule also outlines the 2012 payments to hospitals and ASCs for outpatient services. The CMS estimates that in 2012, it will spend about $41.1 billion to pay the more than 4,000 general acute care hospitals, inpatient rehabilitation facilities, inpatient psychiatric facilities, long-term acute care hospitals, children’s hospitals, and cancer hospitals under Medicare’s Outpatient Prospective Payment System. And the agency will pay another $3.5 billion to about 5,000 ASCs next year.
The final rule increased payments to hospital outpatient departments by 1.9% in 2012. Under the rule, payments to cancer hospitals will go up by 11.3% due to adjustments required under the Affordable Care Act. ACSs will also see their payments increase by 1.6% in 2012. ☐
Medicare officials are expanding the list of quality measures that hospitals will be judged on as part of a new pay-for-performance program created under the Affordable Care Act.
In a final rule released Nov. 1, detailing Medicare payment rates for hospital outpatient departments, officials at the Centers for Medicare and Medicaid Services announced that they are adding a new clinical process of care measure related to urinary catheters to the Hospital Inpatient Value-Based Purchasing (VBP) Program. The new measure, which will go into effect in October 2013 for fiscal year 2014, will assess whether a urinary catheter inserted during surgery is removed on the first or second postsurgical day. Hospitals will begin reporting data to the CMS on the new measure in 2012.
The new measure will be added to 12 clinical process measures and 1 patient experience measure that were adopted for the first year of the program. The CMS also finalized plans to include three outcome measures related to 30-day mortality for acute myocardial infarction, heart failure, and pneumonia in the program for fiscal year 2014.
At the same time, the CMS is delaying plans to include other measures. The agency had planned to include eight measures on hospital-acquired conditions, two composite measures from the Agency for Healthcare Research and Quality, and a Medicare Spending per Beneficiary measure in the Hospital VBP program in fiscal year 2014. But after receiving public comments noting that performance data had not been publicly available long enough for hospitals to prepare to incorporate the measures, Medicare officials relented.
According to the final rule, the CMS will post hospital performance data on the measures to Medicare’s Hospital Compare website for at least 1 year before requiring hospitals to report data on them.
Under the Hospital VBP program, the CMS will begin making incentive payments to hospitals based on quality on Oct. 1, 2012. The payments are funded by reducing Medicare payments to hospitals by 1% during fiscal year 2013 and 1.25% in fiscal year 2014.
Hospital payments under the program will be based on performance on clinical process-of-care measures, patient satisfaction, and clinical outcomes. In fiscal year 2014, process-of-care measures will be weighted at 45% of the score, patient satisfaction at 30%, and outcomes at 25%. During the first year of the program, process-of-care measures will weighted at 70% and patient satisfaction measures at 30%.
Medicare officials are also moving ahead with plans to require ambulatory surgical centers (ASCs) to report on quality measures next year.
In the final rule, the CMS adopted four clinical outcome measures and one surgical infection control measure that ASCs must report on beginning in October 2012. The final list includes measures related to patient burns; patient falls; wrong site, wrong side, wrong patient, wrong procedure, and wrong implant surgery; rate of ASC admissions requiring a hospital transfer/admission upon discharge; and prophylactic intravenous antibiotic timing. The data reported will be used to determine payments for 2014, according to the final rule.
In 2013, ASCs will also have to report on their use of the safe surgery checklist and report data on their facility volume on selected procedures. That information will be used in setting payments for 2015. Additionally, hospitals will be required to report on influenza vaccination coverage among health care workers starting in 2014, which will affect their 2016 payments.
The more than 1,500-page final rule also outlines the 2012 payments to hospitals and ASCs for outpatient services. The CMS estimates that in 2012, it will spend about $41.1 billion to pay the more than 4,000 general acute care hospitals, inpatient rehabilitation facilities, inpatient psychiatric facilities, long-term acute care hospitals, children’s hospitals, and cancer hospitals under Medicare’s Outpatient Prospective Payment System. And the agency will pay another $3.5 billion to about 5,000 ASCs next year.
The final rule increased payments to hospital outpatient departments by 1.9% in 2012. Under the rule, payments to cancer hospitals will go up by 11.3% due to adjustments required under the Affordable Care Act. ACSs will also see their payments increase by 1.6% in 2012. ☐
Medicare officials are expanding the list of quality measures that hospitals will be judged on as part of a new pay-for-performance program created under the Affordable Care Act.
In a final rule released Nov. 1, detailing Medicare payment rates for hospital outpatient departments, officials at the Centers for Medicare and Medicaid Services announced that they are adding a new clinical process of care measure related to urinary catheters to the Hospital Inpatient Value-Based Purchasing (VBP) Program. The new measure, which will go into effect in October 2013 for fiscal year 2014, will assess whether a urinary catheter inserted during surgery is removed on the first or second postsurgical day. Hospitals will begin reporting data to the CMS on the new measure in 2012.
The new measure will be added to 12 clinical process measures and 1 patient experience measure that were adopted for the first year of the program. The CMS also finalized plans to include three outcome measures related to 30-day mortality for acute myocardial infarction, heart failure, and pneumonia in the program for fiscal year 2014.
At the same time, the CMS is delaying plans to include other measures. The agency had planned to include eight measures on hospital-acquired conditions, two composite measures from the Agency for Healthcare Research and Quality, and a Medicare Spending per Beneficiary measure in the Hospital VBP program in fiscal year 2014. But after receiving public comments noting that performance data had not been publicly available long enough for hospitals to prepare to incorporate the measures, Medicare officials relented.
According to the final rule, the CMS will post hospital performance data on the measures to Medicare’s Hospital Compare website for at least 1 year before requiring hospitals to report data on them.
Under the Hospital VBP program, the CMS will begin making incentive payments to hospitals based on quality on Oct. 1, 2012. The payments are funded by reducing Medicare payments to hospitals by 1% during fiscal year 2013 and 1.25% in fiscal year 2014.
Hospital payments under the program will be based on performance on clinical process-of-care measures, patient satisfaction, and clinical outcomes. In fiscal year 2014, process-of-care measures will be weighted at 45% of the score, patient satisfaction at 30%, and outcomes at 25%. During the first year of the program, process-of-care measures will weighted at 70% and patient satisfaction measures at 30%.
Medicare officials are also moving ahead with plans to require ambulatory surgical centers (ASCs) to report on quality measures next year.
In the final rule, the CMS adopted four clinical outcome measures and one surgical infection control measure that ASCs must report on beginning in October 2012. The final list includes measures related to patient burns; patient falls; wrong site, wrong side, wrong patient, wrong procedure, and wrong implant surgery; rate of ASC admissions requiring a hospital transfer/admission upon discharge; and prophylactic intravenous antibiotic timing. The data reported will be used to determine payments for 2014, according to the final rule.
In 2013, ASCs will also have to report on their use of the safe surgery checklist and report data on their facility volume on selected procedures. That information will be used in setting payments for 2015. Additionally, hospitals will be required to report on influenza vaccination coverage among health care workers starting in 2014, which will affect their 2016 payments.
The more than 1,500-page final rule also outlines the 2012 payments to hospitals and ASCs for outpatient services. The CMS estimates that in 2012, it will spend about $41.1 billion to pay the more than 4,000 general acute care hospitals, inpatient rehabilitation facilities, inpatient psychiatric facilities, long-term acute care hospitals, children’s hospitals, and cancer hospitals under Medicare’s Outpatient Prospective Payment System. And the agency will pay another $3.5 billion to about 5,000 ASCs next year.
The final rule increased payments to hospital outpatient departments by 1.9% in 2012. Under the rule, payments to cancer hospitals will go up by 11.3% due to adjustments required under the Affordable Care Act. ACSs will also see their payments increase by 1.6% in 2012. ☐