User login
Stem cells restore lost function after traumatic brain injury
, results from a phase 2 trial indicate. “We proved for the first time that we can affect outcomes in moderately to severely disabled patients with TBI using stem cells,” said study investigator Peter McAllister, MD, cofounder and medical director of the New England Center for Neurology and Headache, Stamford, Conn.
“I think the potential of regenerative medicine was always out there, but we are now getting to the point where we’re living up to that potential,” said Dr. McAllister, associate professor of neurology at Yale University, New Haven, Conn.
The findings were presented at the 2022 annual meeting of the American Academy of Neurology.
No effective treatment to date
TBI can lead to motor deficits and chronic disability and currently there are no effective drugs to treat these deficits.
Researchers are increasingly focused on using somatic stem cells to restore lost function. Stem cells can differentiate or proliferate into different types of cells and are thought to promote repair and regeneration of tissues or organs damaged due to illness or injury.
The study included 61 patients with TBI with an average age of 34 years (70% were male and 69% were White). The mean time from injury was 8 years and Glasgow Outcome Scale Extended (GOS-E) ranged from 3 to 6.
Forty-six participants were randomly assigned to receive the stem cell therapy and 15 a sham procedure. In the treatment group, there were three different doses of cells (2.5 x 106, 5 x 106, and 10 x 106).
The treatment involved an investigational regenerative cell medicine comprised of bone marrow-derived mesenchymal stem cells (SB623). The allogeneic cells came from a male donor.
For the 20-minute procedure, a neurosurgeon drilled a tiny hole in the skull and, guided by MRI, injected the stem cells into the area of the lesion.
Patients receiving a surgical sham procedure were brought to the operating room, anesthetized, and had a hole drilled into the head over the area of the lesion. However, the surgeon went only halfway through the skull bone.
Participants were instructed to do specific physiotherapy exercises at home every morning and afternoon for the first 6 months of the study.
The primary efficacy endpoint was change in the Fugl-Meyer Motor Scale score (FMMS). This scale is widely used for clinical assessment of motor function, including range of motion, walking, lower limb movement, and dexterity.
At 24 weeks, the change in FMMS score for SB623-treated patients (least square [LS] mean increase 8.3) compared with controls (LS increase 2.3) was significant (P = .04).
“When we looked at all the data at 6 months, the folks who got the stem cells did statistically significantly better than the group that got the sham,” and that improvement began within the first week or two, said Dr. McAllister.
‘A real impact’
The treatment had a real impact on people’s lives, he said. “Some who couldn’t move their arm at all were able to put a nut on a bolt or brush their teeth, and some were able to button and unbutton where they couldn’t do that before.”
One teenager who was previously completely aphasic spoke an entire sentence.
The middle dose (5 x 106) had “by far” the best outcome, said Dr. McAllister. It’s not yet known whether the improvements will be permanent, he added.
At 48 weeks, treated patients experienced improvement over controls in secondary endpoints of the Action Research Arm Test (ARAT), which assesses grasp, grip, pinch, and gross movements; Gait Velocity (walking 10 meters); and NeuroQOL, a self-report measure of ability to carry out various activities.
However, although these endpoints were all numerically better in the stem cell groups, none reached statistical significance. This is likely because of the small study size and the fact the control group improved so much, said Dr. McAllister.
The exact mechanism of stem cell therapy is unclear, but researchers believe it “establishes a milieu of growth” for cells in the brain and promotes anti-inflammatory properties, said Dr. McAllister.
By 48 weeks, all study subjects had experienced at least one adverse event, with no differences between groups and no patient withdrawing as a result of adverse events. “There was no safety signal at all related to the stem cells,” said Dr. McAllister.
A larger phase 3 study of SB623 is planned.
The treatment may be useful in other conditions. A study of stroke survivors “just barely missed statistical significance” likely for methodological reasons and an older, sicker population, but the company plans to do another study in patients who were affected by stroke, said Dr. McAllister.
In addition, there may be potential for this approach with brain hemorrhage, Parkinson’s disease, multiple sclerosis, and other brain-related disorders, he said.
‘Modern-day holy grail’
Reached for a comment, TBI specialist Frank Conidi, MD, director of the Florida Center for Headache and Sports Neurology, said stem cell therapy is the most promising potential treatment for brain injury. “It’s the modern-day ‘holy grail.’ “
In this study, “to see a modest improvement in gait in the primary outcome is impressive,” he said.
In addition, the fact the study didn’t have any significant or severe adverse outcomes “is promising,” he added.
Studies like this “are going to help to lay the groundwork for future studies and hopefully one day result in a safe, noninvasive treatment” for Parkinson’s disease, Alzheimer’s disease, and disorders that affect the central nervous system such as spinal cord injury, Dr. Conidi said.
This therapy involves an invasive procedure requiring implantation directly into the brain, he noted. “At present, there’s no way to get stem cells to cross the blood-brain barrier.”
In addition, although motor impairment is definitely a component of TBI, it’s not as prevalent as cognitive impairment, said Dr. Conidi.
The study was supported by SanBio Co Ltd. Dr. McAllister and Dr. Conidi have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, results from a phase 2 trial indicate. “We proved for the first time that we can affect outcomes in moderately to severely disabled patients with TBI using stem cells,” said study investigator Peter McAllister, MD, cofounder and medical director of the New England Center for Neurology and Headache, Stamford, Conn.
“I think the potential of regenerative medicine was always out there, but we are now getting to the point where we’re living up to that potential,” said Dr. McAllister, associate professor of neurology at Yale University, New Haven, Conn.
The findings were presented at the 2022 annual meeting of the American Academy of Neurology.
No effective treatment to date
TBI can lead to motor deficits and chronic disability and currently there are no effective drugs to treat these deficits.
Researchers are increasingly focused on using somatic stem cells to restore lost function. Stem cells can differentiate or proliferate into different types of cells and are thought to promote repair and regeneration of tissues or organs damaged due to illness or injury.
The study included 61 patients with TBI with an average age of 34 years (70% were male and 69% were White). The mean time from injury was 8 years and Glasgow Outcome Scale Extended (GOS-E) ranged from 3 to 6.
Forty-six participants were randomly assigned to receive the stem cell therapy and 15 a sham procedure. In the treatment group, there were three different doses of cells (2.5 x 106, 5 x 106, and 10 x 106).
The treatment involved an investigational regenerative cell medicine comprised of bone marrow-derived mesenchymal stem cells (SB623). The allogeneic cells came from a male donor.
For the 20-minute procedure, a neurosurgeon drilled a tiny hole in the skull and, guided by MRI, injected the stem cells into the area of the lesion.
Patients receiving a surgical sham procedure were brought to the operating room, anesthetized, and had a hole drilled into the head over the area of the lesion. However, the surgeon went only halfway through the skull bone.
Participants were instructed to do specific physiotherapy exercises at home every morning and afternoon for the first 6 months of the study.
The primary efficacy endpoint was change in the Fugl-Meyer Motor Scale score (FMMS). This scale is widely used for clinical assessment of motor function, including range of motion, walking, lower limb movement, and dexterity.
At 24 weeks, the change in FMMS score for SB623-treated patients (least square [LS] mean increase 8.3) compared with controls (LS increase 2.3) was significant (P = .04).
“When we looked at all the data at 6 months, the folks who got the stem cells did statistically significantly better than the group that got the sham,” and that improvement began within the first week or two, said Dr. McAllister.
‘A real impact’
The treatment had a real impact on people’s lives, he said. “Some who couldn’t move their arm at all were able to put a nut on a bolt or brush their teeth, and some were able to button and unbutton where they couldn’t do that before.”
One teenager who was previously completely aphasic spoke an entire sentence.
The middle dose (5 x 106) had “by far” the best outcome, said Dr. McAllister. It’s not yet known whether the improvements will be permanent, he added.
At 48 weeks, treated patients experienced improvement over controls in secondary endpoints of the Action Research Arm Test (ARAT), which assesses grasp, grip, pinch, and gross movements; Gait Velocity (walking 10 meters); and NeuroQOL, a self-report measure of ability to carry out various activities.
However, although these endpoints were all numerically better in the stem cell groups, none reached statistical significance. This is likely because of the small study size and the fact the control group improved so much, said Dr. McAllister.
The exact mechanism of stem cell therapy is unclear, but researchers believe it “establishes a milieu of growth” for cells in the brain and promotes anti-inflammatory properties, said Dr. McAllister.
By 48 weeks, all study subjects had experienced at least one adverse event, with no differences between groups and no patient withdrawing as a result of adverse events. “There was no safety signal at all related to the stem cells,” said Dr. McAllister.
A larger phase 3 study of SB623 is planned.
The treatment may be useful in other conditions. A study of stroke survivors “just barely missed statistical significance” likely for methodological reasons and an older, sicker population, but the company plans to do another study in patients who were affected by stroke, said Dr. McAllister.
In addition, there may be potential for this approach with brain hemorrhage, Parkinson’s disease, multiple sclerosis, and other brain-related disorders, he said.
‘Modern-day holy grail’
Reached for a comment, TBI specialist Frank Conidi, MD, director of the Florida Center for Headache and Sports Neurology, said stem cell therapy is the most promising potential treatment for brain injury. “It’s the modern-day ‘holy grail.’ “
In this study, “to see a modest improvement in gait in the primary outcome is impressive,” he said.
In addition, the fact the study didn’t have any significant or severe adverse outcomes “is promising,” he added.
Studies like this “are going to help to lay the groundwork for future studies and hopefully one day result in a safe, noninvasive treatment” for Parkinson’s disease, Alzheimer’s disease, and disorders that affect the central nervous system such as spinal cord injury, Dr. Conidi said.
This therapy involves an invasive procedure requiring implantation directly into the brain, he noted. “At present, there’s no way to get stem cells to cross the blood-brain barrier.”
In addition, although motor impairment is definitely a component of TBI, it’s not as prevalent as cognitive impairment, said Dr. Conidi.
The study was supported by SanBio Co Ltd. Dr. McAllister and Dr. Conidi have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, results from a phase 2 trial indicate. “We proved for the first time that we can affect outcomes in moderately to severely disabled patients with TBI using stem cells,” said study investigator Peter McAllister, MD, cofounder and medical director of the New England Center for Neurology and Headache, Stamford, Conn.
“I think the potential of regenerative medicine was always out there, but we are now getting to the point where we’re living up to that potential,” said Dr. McAllister, associate professor of neurology at Yale University, New Haven, Conn.
The findings were presented at the 2022 annual meeting of the American Academy of Neurology.
No effective treatment to date
TBI can lead to motor deficits and chronic disability and currently there are no effective drugs to treat these deficits.
Researchers are increasingly focused on using somatic stem cells to restore lost function. Stem cells can differentiate or proliferate into different types of cells and are thought to promote repair and regeneration of tissues or organs damaged due to illness or injury.
The study included 61 patients with TBI with an average age of 34 years (70% were male and 69% were White). The mean time from injury was 8 years and Glasgow Outcome Scale Extended (GOS-E) ranged from 3 to 6.
Forty-six participants were randomly assigned to receive the stem cell therapy and 15 a sham procedure. In the treatment group, there were three different doses of cells (2.5 x 106, 5 x 106, and 10 x 106).
The treatment involved an investigational regenerative cell medicine comprised of bone marrow-derived mesenchymal stem cells (SB623). The allogeneic cells came from a male donor.
For the 20-minute procedure, a neurosurgeon drilled a tiny hole in the skull and, guided by MRI, injected the stem cells into the area of the lesion.
Patients receiving a surgical sham procedure were brought to the operating room, anesthetized, and had a hole drilled into the head over the area of the lesion. However, the surgeon went only halfway through the skull bone.
Participants were instructed to do specific physiotherapy exercises at home every morning and afternoon for the first 6 months of the study.
The primary efficacy endpoint was change in the Fugl-Meyer Motor Scale score (FMMS). This scale is widely used for clinical assessment of motor function, including range of motion, walking, lower limb movement, and dexterity.
At 24 weeks, the change in FMMS score for SB623-treated patients (least square [LS] mean increase 8.3) compared with controls (LS increase 2.3) was significant (P = .04).
“When we looked at all the data at 6 months, the folks who got the stem cells did statistically significantly better than the group that got the sham,” and that improvement began within the first week or two, said Dr. McAllister.
‘A real impact’
The treatment had a real impact on people’s lives, he said. “Some who couldn’t move their arm at all were able to put a nut on a bolt or brush their teeth, and some were able to button and unbutton where they couldn’t do that before.”
One teenager who was previously completely aphasic spoke an entire sentence.
The middle dose (5 x 106) had “by far” the best outcome, said Dr. McAllister. It’s not yet known whether the improvements will be permanent, he added.
At 48 weeks, treated patients experienced improvement over controls in secondary endpoints of the Action Research Arm Test (ARAT), which assesses grasp, grip, pinch, and gross movements; Gait Velocity (walking 10 meters); and NeuroQOL, a self-report measure of ability to carry out various activities.
However, although these endpoints were all numerically better in the stem cell groups, none reached statistical significance. This is likely because of the small study size and the fact the control group improved so much, said Dr. McAllister.
The exact mechanism of stem cell therapy is unclear, but researchers believe it “establishes a milieu of growth” for cells in the brain and promotes anti-inflammatory properties, said Dr. McAllister.
By 48 weeks, all study subjects had experienced at least one adverse event, with no differences between groups and no patient withdrawing as a result of adverse events. “There was no safety signal at all related to the stem cells,” said Dr. McAllister.
A larger phase 3 study of SB623 is planned.
The treatment may be useful in other conditions. A study of stroke survivors “just barely missed statistical significance” likely for methodological reasons and an older, sicker population, but the company plans to do another study in patients who were affected by stroke, said Dr. McAllister.
In addition, there may be potential for this approach with brain hemorrhage, Parkinson’s disease, multiple sclerosis, and other brain-related disorders, he said.
‘Modern-day holy grail’
Reached for a comment, TBI specialist Frank Conidi, MD, director of the Florida Center for Headache and Sports Neurology, said stem cell therapy is the most promising potential treatment for brain injury. “It’s the modern-day ‘holy grail.’ “
In this study, “to see a modest improvement in gait in the primary outcome is impressive,” he said.
In addition, the fact the study didn’t have any significant or severe adverse outcomes “is promising,” he added.
Studies like this “are going to help to lay the groundwork for future studies and hopefully one day result in a safe, noninvasive treatment” for Parkinson’s disease, Alzheimer’s disease, and disorders that affect the central nervous system such as spinal cord injury, Dr. Conidi said.
This therapy involves an invasive procedure requiring implantation directly into the brain, he noted. “At present, there’s no way to get stem cells to cross the blood-brain barrier.”
In addition, although motor impairment is definitely a component of TBI, it’s not as prevalent as cognitive impairment, said Dr. Conidi.
The study was supported by SanBio Co Ltd. Dr. McAllister and Dr. Conidi have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM AAN 2022
Novel combo drug shows promise as first-line Parkinson’s disease treatment
, new research suggests. Results from a phase 3 trial of P2B001, a combination of pramipexole and rasagiline at currently unavailable low doses, showed the drug was more effective than its individual components and as effective as higher-dose pramipexole ER – with far less daytime sleepiness.
The combination drug is taken once per day and does not require titration, which investigators say make it a good option for first-line treatment of Parkinson’s disease.
“I don’t think people, including me, expected intuitively that if you used small doses and combined it with a little rasagiline it would be equal to full doses of pramipexole, but it appears that it is,” said lead investigator Warren Olanow, MD, professor and chair emeritus of neurology and professor emeritus of neuroscience at Icahn School of Medicine at Mount Sinai, New York.
The findings were presented at the 2022 annual meeting of the American Academy of Neurology.
‘Synergistic effects’
Levodopa is considered to be the most effective treatment for Parkinson’s disease, but long-term use is associated with increased risk for motor complications, such as dyskinesia. Dopamine agonists such as pramipexole have been linked in previous research to excessive daytime sleepiness and impulse control disorders. In addition, monoamine oxidase-B inhibitors such as rasagiline are not as effective at controlling Parkinson’s disease as other treatment options.
“There is no consistent agreement on how to initiate treatment because no one treatment is ideal,” Dr. Olanow said.
P2B001, developed by Pharma Two B, is a combination of 0.6 mg of pramipexole and 0.75 mg of rasagiline. The drugs work by dual mechanisms, which investigators suspected might have “synergistic effects.”
Following promising results from an earlier trial, researches launched a phase 3, 12-week, international, randomized, double-blind trial to study the efficacy, safety, and tolerability of P2B001, compared with its individual components and with a calibration arm of pramipexole ER in 519 patients with early Parkinson’s disease.
Participants received P2B001, 0.6 mg of pramipexole ER, 0.75 mg of rasagiline ER, or pramipexole ER titrated to an optimal dose for each patient (1.5-4.5 mg).
New first-line treatment?
Results showed that the adjusted mean change from baseline in total Unified Parkinson’s Disease Rating Scale (UPDRS) score was -2.66 points for P2B001 versus pramipexole (P = .0018) and -3.30 points for P2B001 versus rasagiline (P = .0001).
There was no significant difference in UPDRS scores between P2B001 and pramipexole ER, but patients who received P2B001 reported significantly less daytime sleepiness.
The adjusted mean change from baseline in Epworth Sleepiness Scale score for P2B001 versus pramipexole ER was -2.66 points (P < .0001).
In addition, fewer dopaminergic adverse events were reported with the combination drug versus pramipexole ER (44.7% vs. 66.2%), including somnolence (14.7% vs. 31.1%) and orthostatic hypotension (2.7% vs. 12.2%).
As a first-line treatment, P2B001 could offer an effective option instead of levodopa, Dr. Olanow said. “It could be really good for patients because it would delay the introduction of levodopa and allow levodopa to be used in lower doses when the time comes and hopefully reduce the risk of complications,” he added.
Questions, cost concerns
Commenting on the study, Alfonso Fasano, MD, PhD, professor of neurology and chair in neuromodulation, University of Toronto, agreed that better therapeutic options are needed for Parkinson’s disease.
Combining available treatments into one pill “might help patients’ adherence, although this can compromise our ability to dose each compound individually,” said Dr. Fasano, who was not involved with the research.
He added that there are also questions about dosage modification as a patient’s disease progresses and whether a higher dose might pose safety problems. There is also the issue of cost. “Conducting large clinical trials like this one is expensive, and I wonder about the cost of the drug when approved,” Dr. Fasano noted. “Do we really need to invest in combination pills containing two already well-known compounds?”
Dr. Olanow, who is not directly involved with Pharma Two B, the developer of P2B001, said he has no information on what the drug might cost or how it might be marketed if approved for use.
“The advantage of the combination is the component doses are not replicable, they are both in an extended-release formulation, it doesn’t require titration, and it has been tested and proven to work,” he said.
The study was funded by Pharma Two B. Dr. Olanow is employed by Clintrex Research Corporation and owns stock in Clintrex Research Corporation. Dr. Fasano reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, new research suggests. Results from a phase 3 trial of P2B001, a combination of pramipexole and rasagiline at currently unavailable low doses, showed the drug was more effective than its individual components and as effective as higher-dose pramipexole ER – with far less daytime sleepiness.
The combination drug is taken once per day and does not require titration, which investigators say make it a good option for first-line treatment of Parkinson’s disease.
“I don’t think people, including me, expected intuitively that if you used small doses and combined it with a little rasagiline it would be equal to full doses of pramipexole, but it appears that it is,” said lead investigator Warren Olanow, MD, professor and chair emeritus of neurology and professor emeritus of neuroscience at Icahn School of Medicine at Mount Sinai, New York.
The findings were presented at the 2022 annual meeting of the American Academy of Neurology.
‘Synergistic effects’
Levodopa is considered to be the most effective treatment for Parkinson’s disease, but long-term use is associated with increased risk for motor complications, such as dyskinesia. Dopamine agonists such as pramipexole have been linked in previous research to excessive daytime sleepiness and impulse control disorders. In addition, monoamine oxidase-B inhibitors such as rasagiline are not as effective at controlling Parkinson’s disease as other treatment options.
“There is no consistent agreement on how to initiate treatment because no one treatment is ideal,” Dr. Olanow said.
P2B001, developed by Pharma Two B, is a combination of 0.6 mg of pramipexole and 0.75 mg of rasagiline. The drugs work by dual mechanisms, which investigators suspected might have “synergistic effects.”
Following promising results from an earlier trial, researches launched a phase 3, 12-week, international, randomized, double-blind trial to study the efficacy, safety, and tolerability of P2B001, compared with its individual components and with a calibration arm of pramipexole ER in 519 patients with early Parkinson’s disease.
Participants received P2B001, 0.6 mg of pramipexole ER, 0.75 mg of rasagiline ER, or pramipexole ER titrated to an optimal dose for each patient (1.5-4.5 mg).
New first-line treatment?
Results showed that the adjusted mean change from baseline in total Unified Parkinson’s Disease Rating Scale (UPDRS) score was -2.66 points for P2B001 versus pramipexole (P = .0018) and -3.30 points for P2B001 versus rasagiline (P = .0001).
There was no significant difference in UPDRS scores between P2B001 and pramipexole ER, but patients who received P2B001 reported significantly less daytime sleepiness.
The adjusted mean change from baseline in Epworth Sleepiness Scale score for P2B001 versus pramipexole ER was -2.66 points (P < .0001).
In addition, fewer dopaminergic adverse events were reported with the combination drug versus pramipexole ER (44.7% vs. 66.2%), including somnolence (14.7% vs. 31.1%) and orthostatic hypotension (2.7% vs. 12.2%).
As a first-line treatment, P2B001 could offer an effective option instead of levodopa, Dr. Olanow said. “It could be really good for patients because it would delay the introduction of levodopa and allow levodopa to be used in lower doses when the time comes and hopefully reduce the risk of complications,” he added.
Questions, cost concerns
Commenting on the study, Alfonso Fasano, MD, PhD, professor of neurology and chair in neuromodulation, University of Toronto, agreed that better therapeutic options are needed for Parkinson’s disease.
Combining available treatments into one pill “might help patients’ adherence, although this can compromise our ability to dose each compound individually,” said Dr. Fasano, who was not involved with the research.
He added that there are also questions about dosage modification as a patient’s disease progresses and whether a higher dose might pose safety problems. There is also the issue of cost. “Conducting large clinical trials like this one is expensive, and I wonder about the cost of the drug when approved,” Dr. Fasano noted. “Do we really need to invest in combination pills containing two already well-known compounds?”
Dr. Olanow, who is not directly involved with Pharma Two B, the developer of P2B001, said he has no information on what the drug might cost or how it might be marketed if approved for use.
“The advantage of the combination is the component doses are not replicable, they are both in an extended-release formulation, it doesn’t require titration, and it has been tested and proven to work,” he said.
The study was funded by Pharma Two B. Dr. Olanow is employed by Clintrex Research Corporation and owns stock in Clintrex Research Corporation. Dr. Fasano reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, new research suggests. Results from a phase 3 trial of P2B001, a combination of pramipexole and rasagiline at currently unavailable low doses, showed the drug was more effective than its individual components and as effective as higher-dose pramipexole ER – with far less daytime sleepiness.
The combination drug is taken once per day and does not require titration, which investigators say make it a good option for first-line treatment of Parkinson’s disease.
“I don’t think people, including me, expected intuitively that if you used small doses and combined it with a little rasagiline it would be equal to full doses of pramipexole, but it appears that it is,” said lead investigator Warren Olanow, MD, professor and chair emeritus of neurology and professor emeritus of neuroscience at Icahn School of Medicine at Mount Sinai, New York.
The findings were presented at the 2022 annual meeting of the American Academy of Neurology.
‘Synergistic effects’
Levodopa is considered to be the most effective treatment for Parkinson’s disease, but long-term use is associated with increased risk for motor complications, such as dyskinesia. Dopamine agonists such as pramipexole have been linked in previous research to excessive daytime sleepiness and impulse control disorders. In addition, monoamine oxidase-B inhibitors such as rasagiline are not as effective at controlling Parkinson’s disease as other treatment options.
“There is no consistent agreement on how to initiate treatment because no one treatment is ideal,” Dr. Olanow said.
P2B001, developed by Pharma Two B, is a combination of 0.6 mg of pramipexole and 0.75 mg of rasagiline. The drugs work by dual mechanisms, which investigators suspected might have “synergistic effects.”
Following promising results from an earlier trial, researches launched a phase 3, 12-week, international, randomized, double-blind trial to study the efficacy, safety, and tolerability of P2B001, compared with its individual components and with a calibration arm of pramipexole ER in 519 patients with early Parkinson’s disease.
Participants received P2B001, 0.6 mg of pramipexole ER, 0.75 mg of rasagiline ER, or pramipexole ER titrated to an optimal dose for each patient (1.5-4.5 mg).
New first-line treatment?
Results showed that the adjusted mean change from baseline in total Unified Parkinson’s Disease Rating Scale (UPDRS) score was -2.66 points for P2B001 versus pramipexole (P = .0018) and -3.30 points for P2B001 versus rasagiline (P = .0001).
There was no significant difference in UPDRS scores between P2B001 and pramipexole ER, but patients who received P2B001 reported significantly less daytime sleepiness.
The adjusted mean change from baseline in Epworth Sleepiness Scale score for P2B001 versus pramipexole ER was -2.66 points (P < .0001).
In addition, fewer dopaminergic adverse events were reported with the combination drug versus pramipexole ER (44.7% vs. 66.2%), including somnolence (14.7% vs. 31.1%) and orthostatic hypotension (2.7% vs. 12.2%).
As a first-line treatment, P2B001 could offer an effective option instead of levodopa, Dr. Olanow said. “It could be really good for patients because it would delay the introduction of levodopa and allow levodopa to be used in lower doses when the time comes and hopefully reduce the risk of complications,” he added.
Questions, cost concerns
Commenting on the study, Alfonso Fasano, MD, PhD, professor of neurology and chair in neuromodulation, University of Toronto, agreed that better therapeutic options are needed for Parkinson’s disease.
Combining available treatments into one pill “might help patients’ adherence, although this can compromise our ability to dose each compound individually,” said Dr. Fasano, who was not involved with the research.
He added that there are also questions about dosage modification as a patient’s disease progresses and whether a higher dose might pose safety problems. There is also the issue of cost. “Conducting large clinical trials like this one is expensive, and I wonder about the cost of the drug when approved,” Dr. Fasano noted. “Do we really need to invest in combination pills containing two already well-known compounds?”
Dr. Olanow, who is not directly involved with Pharma Two B, the developer of P2B001, said he has no information on what the drug might cost or how it might be marketed if approved for use.
“The advantage of the combination is the component doses are not replicable, they are both in an extended-release formulation, it doesn’t require titration, and it has been tested and proven to work,” he said.
The study was funded by Pharma Two B. Dr. Olanow is employed by Clintrex Research Corporation and owns stock in Clintrex Research Corporation. Dr. Fasano reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM AAN 2022
Antibody reduces amyloid, induces symptom decline
SEATTLE – The researchers identified two plasma biomarkers that correlate well with established amyloid PET standard uptake value ratio (SUVr) changes, potentially paving the way for monitoring lecanemab treatment effects. The researchers also found evidence that the plasma biomarker could be used to allow dose frequency reduction after initial reduction in amyloid plaques.
Lecanemab preferably targets aggregated species of amyloid called protofibrils, which is unique among anti-amyloid antibodies, and these are also among the most toxic manifestations of amyloid, according to Chad Swanson, PhD, who presented the study at the 2022 annual meeting of the American Academy of Neurology.
Are amyloid plaques a key driver of Alzheimer’s disease?
The study could help answer the question of whether amyloid plaques drive the cognitive decline seen in Alzheimer’s disease, in part because the antibody is so effective at what it was designed to do, according to Fernando Testai, MD, PhD, who comoderated the session where the study was presented. “The effect on amyloid content that they measured was persistent over a number of months. Cognition may follow along, so more studies have to be done, but the medication seems to be quite effective doing what it’s supposed to do. If it has something to do with disease, these treatments actually should give us the answer, because the effect on amyloid is pretty significant. After so many years of thinking amyloid probably has nothing to do (with Alzheimer’s symptoms, these results suggest) it may have something to do with the disease,” Dr. Testai said in an interview. He is a professor of neurology at the University of Illinois at Chicago.
Dr. Swanson is confident that amyloid plaques are a key driver of disease. “I’d say a number of companies now with anti-amyloid agents have shown that targeting amyloid can produce some slowing of clinical decline, as well as a robust reduction in amyloid, supporting this idea that that amyloid is meaningful. And it’s very clear that amyloid [deposition] tends to trigger tau pathology,” said Dr. Swanson in an interview. He is executive director of the neurology business group at Eisai Pharmaceuticals, which is developing the anti-amyloid antibody, called lecanemab.
Searching for the best dose and dose frequency
Dr. Swanson noted that Eisai has already conducted a large phase 2b study which informed the current phase 3 ClarityAD study design. The phase 2b study utilized a Bayesian adaptive design, which allocated more patients in a fully blinded way to doses that had the most potential for slowing clinical decline. “The intent was to maximize the efficiency of the design so that more subjects would go to a dose that looks like it could be the best dose according to the Bayesian algorithm,” said Dr. Swanson.
The study also included a gap period that followed the randomized phase of the trial, where subjects were not being dosed with the antibody from 9 to 59 months (mean, 2 years), before reinitiation at the start of the open-label extension phase. “[That] allowed us to answer some really important questions about what happens when you remove lecanemab after reducing amyloid, and then what happens when you reintroduce lecanemab in the open-label extension,” said Dr. Swanson.
The researchers found that amyloid reaccumulated during the treatment gap, and soluble biomarkers were potentially the most sensitive to the change. “Taking all of this information together with clinical data that suggest potential disease-modifying effects, it suggests that we need to continue to treat these individuals, but we may be able to treat with a less-frequent dosing interval once amyloid is removed from the brain. It’s a biweekly infusion. Following 18 months of treatment, we may be able to go in once every month or once every 3 months to maintain low levels of amyloid. We’re going to be testing that soon in the current phase 2 open-label extension,” said Dr. Swanson.
The study included 856 patients who were randomized to biweekly placebo or lecanemab 2.5 mg/kg biweekly, 5 mg/kg monthly, 5 mg/kg biweekly, 10 mg/kg monthly, or 10 mg/kg biweekly. The primary endpoint was the Alzheimer’s disease composite score at 12 months; secondary endpoints included ADCOMS and various biomarker levels at 18 months.
At 18 months, the 10-mg/kg biweekly group had an adjusted mean change from placebo in brain amyloid of –0.31 SUVr units, with more than 80% of the subjects converting from amyloid positive to amyloid negative by visual read. Most subjects remained amyloid negative at open-label extension baseline following the gap period despite a slow reaccumulation of amyloid plaque in the treated group. Out to 18 months in the core study, the same group had a 30% reduction in cognitive decline, compared with placebo, as measured by ADCOMS (P < .05).
There was a correlation between PET SUVr, clinical outcomes, and the Abeta42/40 ratio and plasma p-tau181. During the gap period, treatment discontinuation was associated with changes in the plasma biomarkers that echoed amyloid re-accumulation and clinical decline. Change from baseline in both plasma biomarkers were associated with a change from baseline in PET SUVr at 18 months.
Amyloid-related imaging abnormalities related to brain edema or sulcal effusion (ARIA-E) occurred in 9.9% of patients during the randomized phase of the trial, and 7.8% during the open-label extension phase. About 2% were symptomatic in both the randomization and open-label extension phases. The majority of ARIA-E cases appeared within 3 months of treatment initiation, and generally resolved in 4-16 weeks. 80% were mild to moderate by radiography.
Dr. Swanson is an employee of Eisai Pharmaceuticals, which sponsored the study. Dr. Testai has no relevant financial disclosures.
SEATTLE – The researchers identified two plasma biomarkers that correlate well with established amyloid PET standard uptake value ratio (SUVr) changes, potentially paving the way for monitoring lecanemab treatment effects. The researchers also found evidence that the plasma biomarker could be used to allow dose frequency reduction after initial reduction in amyloid plaques.
Lecanemab preferably targets aggregated species of amyloid called protofibrils, which is unique among anti-amyloid antibodies, and these are also among the most toxic manifestations of amyloid, according to Chad Swanson, PhD, who presented the study at the 2022 annual meeting of the American Academy of Neurology.
Are amyloid plaques a key driver of Alzheimer’s disease?
The study could help answer the question of whether amyloid plaques drive the cognitive decline seen in Alzheimer’s disease, in part because the antibody is so effective at what it was designed to do, according to Fernando Testai, MD, PhD, who comoderated the session where the study was presented. “The effect on amyloid content that they measured was persistent over a number of months. Cognition may follow along, so more studies have to be done, but the medication seems to be quite effective doing what it’s supposed to do. If it has something to do with disease, these treatments actually should give us the answer, because the effect on amyloid is pretty significant. After so many years of thinking amyloid probably has nothing to do (with Alzheimer’s symptoms, these results suggest) it may have something to do with the disease,” Dr. Testai said in an interview. He is a professor of neurology at the University of Illinois at Chicago.
Dr. Swanson is confident that amyloid plaques are a key driver of disease. “I’d say a number of companies now with anti-amyloid agents have shown that targeting amyloid can produce some slowing of clinical decline, as well as a robust reduction in amyloid, supporting this idea that that amyloid is meaningful. And it’s very clear that amyloid [deposition] tends to trigger tau pathology,” said Dr. Swanson in an interview. He is executive director of the neurology business group at Eisai Pharmaceuticals, which is developing the anti-amyloid antibody, called lecanemab.
Searching for the best dose and dose frequency
Dr. Swanson noted that Eisai has already conducted a large phase 2b study which informed the current phase 3 ClarityAD study design. The phase 2b study utilized a Bayesian adaptive design, which allocated more patients in a fully blinded way to doses that had the most potential for slowing clinical decline. “The intent was to maximize the efficiency of the design so that more subjects would go to a dose that looks like it could be the best dose according to the Bayesian algorithm,” said Dr. Swanson.
The study also included a gap period that followed the randomized phase of the trial, where subjects were not being dosed with the antibody from 9 to 59 months (mean, 2 years), before reinitiation at the start of the open-label extension phase. “[That] allowed us to answer some really important questions about what happens when you remove lecanemab after reducing amyloid, and then what happens when you reintroduce lecanemab in the open-label extension,” said Dr. Swanson.
The researchers found that amyloid reaccumulated during the treatment gap, and soluble biomarkers were potentially the most sensitive to the change. “Taking all of this information together with clinical data that suggest potential disease-modifying effects, it suggests that we need to continue to treat these individuals, but we may be able to treat with a less-frequent dosing interval once amyloid is removed from the brain. It’s a biweekly infusion. Following 18 months of treatment, we may be able to go in once every month or once every 3 months to maintain low levels of amyloid. We’re going to be testing that soon in the current phase 2 open-label extension,” said Dr. Swanson.
The study included 856 patients who were randomized to biweekly placebo or lecanemab 2.5 mg/kg biweekly, 5 mg/kg monthly, 5 mg/kg biweekly, 10 mg/kg monthly, or 10 mg/kg biweekly. The primary endpoint was the Alzheimer’s disease composite score at 12 months; secondary endpoints included ADCOMS and various biomarker levels at 18 months.
At 18 months, the 10-mg/kg biweekly group had an adjusted mean change from placebo in brain amyloid of –0.31 SUVr units, with more than 80% of the subjects converting from amyloid positive to amyloid negative by visual read. Most subjects remained amyloid negative at open-label extension baseline following the gap period despite a slow reaccumulation of amyloid plaque in the treated group. Out to 18 months in the core study, the same group had a 30% reduction in cognitive decline, compared with placebo, as measured by ADCOMS (P < .05).
There was a correlation between PET SUVr, clinical outcomes, and the Abeta42/40 ratio and plasma p-tau181. During the gap period, treatment discontinuation was associated with changes in the plasma biomarkers that echoed amyloid re-accumulation and clinical decline. Change from baseline in both plasma biomarkers were associated with a change from baseline in PET SUVr at 18 months.
Amyloid-related imaging abnormalities related to brain edema or sulcal effusion (ARIA-E) occurred in 9.9% of patients during the randomized phase of the trial, and 7.8% during the open-label extension phase. About 2% were symptomatic in both the randomization and open-label extension phases. The majority of ARIA-E cases appeared within 3 months of treatment initiation, and generally resolved in 4-16 weeks. 80% were mild to moderate by radiography.
Dr. Swanson is an employee of Eisai Pharmaceuticals, which sponsored the study. Dr. Testai has no relevant financial disclosures.
SEATTLE – The researchers identified two plasma biomarkers that correlate well with established amyloid PET standard uptake value ratio (SUVr) changes, potentially paving the way for monitoring lecanemab treatment effects. The researchers also found evidence that the plasma biomarker could be used to allow dose frequency reduction after initial reduction in amyloid plaques.
Lecanemab preferably targets aggregated species of amyloid called protofibrils, which is unique among anti-amyloid antibodies, and these are also among the most toxic manifestations of amyloid, according to Chad Swanson, PhD, who presented the study at the 2022 annual meeting of the American Academy of Neurology.
Are amyloid plaques a key driver of Alzheimer’s disease?
The study could help answer the question of whether amyloid plaques drive the cognitive decline seen in Alzheimer’s disease, in part because the antibody is so effective at what it was designed to do, according to Fernando Testai, MD, PhD, who comoderated the session where the study was presented. “The effect on amyloid content that they measured was persistent over a number of months. Cognition may follow along, so more studies have to be done, but the medication seems to be quite effective doing what it’s supposed to do. If it has something to do with disease, these treatments actually should give us the answer, because the effect on amyloid is pretty significant. After so many years of thinking amyloid probably has nothing to do (with Alzheimer’s symptoms, these results suggest) it may have something to do with the disease,” Dr. Testai said in an interview. He is a professor of neurology at the University of Illinois at Chicago.
Dr. Swanson is confident that amyloid plaques are a key driver of disease. “I’d say a number of companies now with anti-amyloid agents have shown that targeting amyloid can produce some slowing of clinical decline, as well as a robust reduction in amyloid, supporting this idea that that amyloid is meaningful. And it’s very clear that amyloid [deposition] tends to trigger tau pathology,” said Dr. Swanson in an interview. He is executive director of the neurology business group at Eisai Pharmaceuticals, which is developing the anti-amyloid antibody, called lecanemab.
Searching for the best dose and dose frequency
Dr. Swanson noted that Eisai has already conducted a large phase 2b study which informed the current phase 3 ClarityAD study design. The phase 2b study utilized a Bayesian adaptive design, which allocated more patients in a fully blinded way to doses that had the most potential for slowing clinical decline. “The intent was to maximize the efficiency of the design so that more subjects would go to a dose that looks like it could be the best dose according to the Bayesian algorithm,” said Dr. Swanson.
The study also included a gap period that followed the randomized phase of the trial, where subjects were not being dosed with the antibody from 9 to 59 months (mean, 2 years), before reinitiation at the start of the open-label extension phase. “[That] allowed us to answer some really important questions about what happens when you remove lecanemab after reducing amyloid, and then what happens when you reintroduce lecanemab in the open-label extension,” said Dr. Swanson.
The researchers found that amyloid reaccumulated during the treatment gap, and soluble biomarkers were potentially the most sensitive to the change. “Taking all of this information together with clinical data that suggest potential disease-modifying effects, it suggests that we need to continue to treat these individuals, but we may be able to treat with a less-frequent dosing interval once amyloid is removed from the brain. It’s a biweekly infusion. Following 18 months of treatment, we may be able to go in once every month or once every 3 months to maintain low levels of amyloid. We’re going to be testing that soon in the current phase 2 open-label extension,” said Dr. Swanson.
The study included 856 patients who were randomized to biweekly placebo or lecanemab 2.5 mg/kg biweekly, 5 mg/kg monthly, 5 mg/kg biweekly, 10 mg/kg monthly, or 10 mg/kg biweekly. The primary endpoint was the Alzheimer’s disease composite score at 12 months; secondary endpoints included ADCOMS and various biomarker levels at 18 months.
At 18 months, the 10-mg/kg biweekly group had an adjusted mean change from placebo in brain amyloid of –0.31 SUVr units, with more than 80% of the subjects converting from amyloid positive to amyloid negative by visual read. Most subjects remained amyloid negative at open-label extension baseline following the gap period despite a slow reaccumulation of amyloid plaque in the treated group. Out to 18 months in the core study, the same group had a 30% reduction in cognitive decline, compared with placebo, as measured by ADCOMS (P < .05).
There was a correlation between PET SUVr, clinical outcomes, and the Abeta42/40 ratio and plasma p-tau181. During the gap period, treatment discontinuation was associated with changes in the plasma biomarkers that echoed amyloid re-accumulation and clinical decline. Change from baseline in both plasma biomarkers were associated with a change from baseline in PET SUVr at 18 months.
Amyloid-related imaging abnormalities related to brain edema or sulcal effusion (ARIA-E) occurred in 9.9% of patients during the randomized phase of the trial, and 7.8% during the open-label extension phase. About 2% were symptomatic in both the randomization and open-label extension phases. The majority of ARIA-E cases appeared within 3 months of treatment initiation, and generally resolved in 4-16 weeks. 80% were mild to moderate by radiography.
Dr. Swanson is an employee of Eisai Pharmaceuticals, which sponsored the study. Dr. Testai has no relevant financial disclosures.
AT AAN 2022
Neighborhood-level data sheds new light on racial and ethnic diversity in MS
SEATTLE – These populations often have more severe disease, likely driven by socioeconomic factors and health care access, according to a new study that examined neighborhood-level data and disease severity in the United States.
“It has previously been thought that MS is less common among non-European Caucasian White populations, driven partly by the well-known association of incidence with latitude. It is abundantly clear at this point that this idea is not true,” said Christopher Orlando, MD, during a presentation at the 2022 annual meeting of the American Academy of Neurology.
He noted that several U.S. studies with large sample sizes have shown greater disease severity and a higher disability burden among Hispanic and Black patients. “Black patients in particular appear to have a higher incidence of disease and a greater proportion of progressive disease phenotypes,” said Dr. Orlando.
Race and ethnicity are unlikely explanations for this disparity, according to Dr. Orlando. “While much remains to be discovered of the genetic underpinnings of MS, what we do know does not support the idea that minorities would have a predilection to more severe disease. For example, the well-known high-risk allele HLA DRB1*1501 appears to have a lower frequency in African populations, compared with European [populations].”
Instead, evidence suggests that interrelated social causes include access to resources, environmental exposures, and psychosocial stress. “These affect health via a number of pathways including direct physical injury, allostatic load, and access to health care,” said Dr. Orlando.
Probing racial and ethnic disparities
Previous studies that corrected for social determinants of health such as socioeconomic and insurance status reduce the association between MS disability and race, but they do not completely explain it.
To get a better understanding of the impacts of these factors, researchers have used neighborhood-level data combined with information on socioeconomic status and social deprivation to identify associations with MS severity.
At the conference, Dr. Orlando presented a new study that is the first to use this methodology in the United States, and it is the first to apply it to the study of racial and ethnic disparities in MS.
The study confirmed more severe disability in Hispanic and Black patients than in White patients. Clinical factors associated with more severe disease were similar across the three groups, with some small differences among individual traits. “More stark differences appeared when we compared social determinants of health. Hispanic patients were less likely to speak English as a primary language or to complete 12 years of education. Black patients were less likely to live in a rural county and more likely to be unemployed. One particularly stark difference was in the number of unemployed specifically due to their MS, with only 1 White patient [1.1%], 7 Hispanic patients [7.8%] and 27 Black patients [31.0%],” said Dr. Orlando.
The researchers found that Black and Hispanic patients tend to live in more vulnerable neighborhoods than White patients. The researchers found no significant association between social vulnerability index (SVI) values and MS severity, though there was an association in a separate analysis that only included White patients. The SVI uses 15 measures taken from the U.S. Census to identify communities that might require additional support during natural disasters.
“It would appear that the sheer complexity both in variety and magnitude of the social determinants of health are such that by far the stronger association is with race and ethnicity, which are surrogates for any number of social determinants and societal inequities,” said Dr. Orlando.
What drives the inequity?
Dr. Orlando acknowledged that some might wonder if these results indicate a true biologically intrinsic factor such as genetic predisposition. “I want to warn against that kind of thinking in the strongest possible terms. It is implausible on several levels. It’s not biologically plausible based on our understanding that race and ethnicity are not genetic constructs. And it’s also not numerically plausible based on these data,” said Dr. Orlando.
While some of the drivers of this inequity have been partially examined, many have not been studied. “As long as this is the case, our ability to fulfill our roles as physicians will be limited in several important ways. Our ability to assess our patients’ individual risk will be missing key information, which will limit the efficacy of shared decision-making, which of course is the cornerstone of MS treatment. In addition, we will continue to struggle to include minority patients in our research studies, and the very design and results of those studies may be misguided, as we will either fail to include these populations, or we will fail to adjust for important confounders,” he said.
New answers, new questions
The neighborhood-level data examined by Dr. Orlando’s group “brings extra information in terms of the negative impact of social determinants of health. The disparity seen in neighborhood living is quite striking,” said Lilyana Amezcua, MD, who served as a discussant for Dr. Orlando’s presentation. The study reinforces findings of her own group in Hispanic and Latinx individuals with MS. Some comorbidities are more common among these groups, which is exacerbated by poor health access.
“We have noted that almost 30% of them also have this comorbidity of hypertension, but what is also observed is that only 7% of them are aware [that they have hypertension],” said Dr. Amezcua, who is an associate professor of neurology at the University of Southern California, Los Angeles.
The findings should prompt further research to understand the impact of systemic racism and neighborhood factors, such as disinvestment in the public and private sectors, underresourced hospitals and clinics, and negative infrastructure. “We need to start discussing the (patient’s) environment so we can better understand the community resources they may have available, as well as create innovative transitional care services. We need to also recognize and accept that structural racism and imbalanced distribution of resources and neighborhoods does restrict educational and economic opportunities, as well as health care access and the safety of these marginalized communities,” said Dr. Amezcua.
Dr. Amezcua has consulted for, received speaking fees from, or served on steering committees or advisory boards for Biogen Idec, Novartis, Genentech, and EMD Serono. She has received research support from the Bristol-Myers Squibb Foundation and Biogen Idec. Dr. Orlando has no relevant financial disclosures.
SEATTLE – These populations often have more severe disease, likely driven by socioeconomic factors and health care access, according to a new study that examined neighborhood-level data and disease severity in the United States.
“It has previously been thought that MS is less common among non-European Caucasian White populations, driven partly by the well-known association of incidence with latitude. It is abundantly clear at this point that this idea is not true,” said Christopher Orlando, MD, during a presentation at the 2022 annual meeting of the American Academy of Neurology.
He noted that several U.S. studies with large sample sizes have shown greater disease severity and a higher disability burden among Hispanic and Black patients. “Black patients in particular appear to have a higher incidence of disease and a greater proportion of progressive disease phenotypes,” said Dr. Orlando.
Race and ethnicity are unlikely explanations for this disparity, according to Dr. Orlando. “While much remains to be discovered of the genetic underpinnings of MS, what we do know does not support the idea that minorities would have a predilection to more severe disease. For example, the well-known high-risk allele HLA DRB1*1501 appears to have a lower frequency in African populations, compared with European [populations].”
Instead, evidence suggests that interrelated social causes include access to resources, environmental exposures, and psychosocial stress. “These affect health via a number of pathways including direct physical injury, allostatic load, and access to health care,” said Dr. Orlando.
Probing racial and ethnic disparities
Previous studies that corrected for social determinants of health such as socioeconomic and insurance status reduce the association between MS disability and race, but they do not completely explain it.
To get a better understanding of the impacts of these factors, researchers have used neighborhood-level data combined with information on socioeconomic status and social deprivation to identify associations with MS severity.
At the conference, Dr. Orlando presented a new study that is the first to use this methodology in the United States, and it is the first to apply it to the study of racial and ethnic disparities in MS.
The study confirmed more severe disability in Hispanic and Black patients than in White patients. Clinical factors associated with more severe disease were similar across the three groups, with some small differences among individual traits. “More stark differences appeared when we compared social determinants of health. Hispanic patients were less likely to speak English as a primary language or to complete 12 years of education. Black patients were less likely to live in a rural county and more likely to be unemployed. One particularly stark difference was in the number of unemployed specifically due to their MS, with only 1 White patient [1.1%], 7 Hispanic patients [7.8%] and 27 Black patients [31.0%],” said Dr. Orlando.
The researchers found that Black and Hispanic patients tend to live in more vulnerable neighborhoods than White patients. The researchers found no significant association between social vulnerability index (SVI) values and MS severity, though there was an association in a separate analysis that only included White patients. The SVI uses 15 measures taken from the U.S. Census to identify communities that might require additional support during natural disasters.
“It would appear that the sheer complexity both in variety and magnitude of the social determinants of health are such that by far the stronger association is with race and ethnicity, which are surrogates for any number of social determinants and societal inequities,” said Dr. Orlando.
What drives the inequity?
Dr. Orlando acknowledged that some might wonder if these results indicate a true biologically intrinsic factor such as genetic predisposition. “I want to warn against that kind of thinking in the strongest possible terms. It is implausible on several levels. It’s not biologically plausible based on our understanding that race and ethnicity are not genetic constructs. And it’s also not numerically plausible based on these data,” said Dr. Orlando.
While some of the drivers of this inequity have been partially examined, many have not been studied. “As long as this is the case, our ability to fulfill our roles as physicians will be limited in several important ways. Our ability to assess our patients’ individual risk will be missing key information, which will limit the efficacy of shared decision-making, which of course is the cornerstone of MS treatment. In addition, we will continue to struggle to include minority patients in our research studies, and the very design and results of those studies may be misguided, as we will either fail to include these populations, or we will fail to adjust for important confounders,” he said.
New answers, new questions
The neighborhood-level data examined by Dr. Orlando’s group “brings extra information in terms of the negative impact of social determinants of health. The disparity seen in neighborhood living is quite striking,” said Lilyana Amezcua, MD, who served as a discussant for Dr. Orlando’s presentation. The study reinforces findings of her own group in Hispanic and Latinx individuals with MS. Some comorbidities are more common among these groups, which is exacerbated by poor health access.
“We have noted that almost 30% of them also have this comorbidity of hypertension, but what is also observed is that only 7% of them are aware [that they have hypertension],” said Dr. Amezcua, who is an associate professor of neurology at the University of Southern California, Los Angeles.
The findings should prompt further research to understand the impact of systemic racism and neighborhood factors, such as disinvestment in the public and private sectors, underresourced hospitals and clinics, and negative infrastructure. “We need to start discussing the (patient’s) environment so we can better understand the community resources they may have available, as well as create innovative transitional care services. We need to also recognize and accept that structural racism and imbalanced distribution of resources and neighborhoods does restrict educational and economic opportunities, as well as health care access and the safety of these marginalized communities,” said Dr. Amezcua.
Dr. Amezcua has consulted for, received speaking fees from, or served on steering committees or advisory boards for Biogen Idec, Novartis, Genentech, and EMD Serono. She has received research support from the Bristol-Myers Squibb Foundation and Biogen Idec. Dr. Orlando has no relevant financial disclosures.
SEATTLE – These populations often have more severe disease, likely driven by socioeconomic factors and health care access, according to a new study that examined neighborhood-level data and disease severity in the United States.
“It has previously been thought that MS is less common among non-European Caucasian White populations, driven partly by the well-known association of incidence with latitude. It is abundantly clear at this point that this idea is not true,” said Christopher Orlando, MD, during a presentation at the 2022 annual meeting of the American Academy of Neurology.
He noted that several U.S. studies with large sample sizes have shown greater disease severity and a higher disability burden among Hispanic and Black patients. “Black patients in particular appear to have a higher incidence of disease and a greater proportion of progressive disease phenotypes,” said Dr. Orlando.
Race and ethnicity are unlikely explanations for this disparity, according to Dr. Orlando. “While much remains to be discovered of the genetic underpinnings of MS, what we do know does not support the idea that minorities would have a predilection to more severe disease. For example, the well-known high-risk allele HLA DRB1*1501 appears to have a lower frequency in African populations, compared with European [populations].”
Instead, evidence suggests that interrelated social causes include access to resources, environmental exposures, and psychosocial stress. “These affect health via a number of pathways including direct physical injury, allostatic load, and access to health care,” said Dr. Orlando.
Probing racial and ethnic disparities
Previous studies that corrected for social determinants of health such as socioeconomic and insurance status reduce the association between MS disability and race, but they do not completely explain it.
To get a better understanding of the impacts of these factors, researchers have used neighborhood-level data combined with information on socioeconomic status and social deprivation to identify associations with MS severity.
At the conference, Dr. Orlando presented a new study that is the first to use this methodology in the United States, and it is the first to apply it to the study of racial and ethnic disparities in MS.
The study confirmed more severe disability in Hispanic and Black patients than in White patients. Clinical factors associated with more severe disease were similar across the three groups, with some small differences among individual traits. “More stark differences appeared when we compared social determinants of health. Hispanic patients were less likely to speak English as a primary language or to complete 12 years of education. Black patients were less likely to live in a rural county and more likely to be unemployed. One particularly stark difference was in the number of unemployed specifically due to their MS, with only 1 White patient [1.1%], 7 Hispanic patients [7.8%] and 27 Black patients [31.0%],” said Dr. Orlando.
The researchers found that Black and Hispanic patients tend to live in more vulnerable neighborhoods than White patients. The researchers found no significant association between social vulnerability index (SVI) values and MS severity, though there was an association in a separate analysis that only included White patients. The SVI uses 15 measures taken from the U.S. Census to identify communities that might require additional support during natural disasters.
“It would appear that the sheer complexity both in variety and magnitude of the social determinants of health are such that by far the stronger association is with race and ethnicity, which are surrogates for any number of social determinants and societal inequities,” said Dr. Orlando.
What drives the inequity?
Dr. Orlando acknowledged that some might wonder if these results indicate a true biologically intrinsic factor such as genetic predisposition. “I want to warn against that kind of thinking in the strongest possible terms. It is implausible on several levels. It’s not biologically plausible based on our understanding that race and ethnicity are not genetic constructs. And it’s also not numerically plausible based on these data,” said Dr. Orlando.
While some of the drivers of this inequity have been partially examined, many have not been studied. “As long as this is the case, our ability to fulfill our roles as physicians will be limited in several important ways. Our ability to assess our patients’ individual risk will be missing key information, which will limit the efficacy of shared decision-making, which of course is the cornerstone of MS treatment. In addition, we will continue to struggle to include minority patients in our research studies, and the very design and results of those studies may be misguided, as we will either fail to include these populations, or we will fail to adjust for important confounders,” he said.
New answers, new questions
The neighborhood-level data examined by Dr. Orlando’s group “brings extra information in terms of the negative impact of social determinants of health. The disparity seen in neighborhood living is quite striking,” said Lilyana Amezcua, MD, who served as a discussant for Dr. Orlando’s presentation. The study reinforces findings of her own group in Hispanic and Latinx individuals with MS. Some comorbidities are more common among these groups, which is exacerbated by poor health access.
“We have noted that almost 30% of them also have this comorbidity of hypertension, but what is also observed is that only 7% of them are aware [that they have hypertension],” said Dr. Amezcua, who is an associate professor of neurology at the University of Southern California, Los Angeles.
The findings should prompt further research to understand the impact of systemic racism and neighborhood factors, such as disinvestment in the public and private sectors, underresourced hospitals and clinics, and negative infrastructure. “We need to start discussing the (patient’s) environment so we can better understand the community resources they may have available, as well as create innovative transitional care services. We need to also recognize and accept that structural racism and imbalanced distribution of resources and neighborhoods does restrict educational and economic opportunities, as well as health care access and the safety of these marginalized communities,” said Dr. Amezcua.
Dr. Amezcua has consulted for, received speaking fees from, or served on steering committees or advisory boards for Biogen Idec, Novartis, Genentech, and EMD Serono. She has received research support from the Bristol-Myers Squibb Foundation and Biogen Idec. Dr. Orlando has no relevant financial disclosures.
AT AAN 2022
Steroids counter ataxia telangiectasia
SEATTLE –
The disease is an autosomal recessive disorder caused by mutations in the ATM gene, which is critical to the response to cellular insults such as DNA breaks, oxidative damage, and other forms of stress. The result is clinical manifestations that range from a suppressed immune system to organ damage and neurological symptoms that typically lead patients to be wheelchair bound by their teenage years.
“It’s really multisystem and a very, very difficult disease for people to live with,” Howard M. Lederman, MD, PhD, said in an interview. Dr. Lederman is a coauthor of the study, which was presented by Stefan Zielen, PhD, professor at the University of Goethe, at the 2022 annual meeting of the American Academy of Neurology.
Various therapies have been developed to improve immunodeficiency, lung disease, and some of the other clinical aspects of the condition, but there is no treatment for its neurological effects. “There’s not really been a good animal model, which has been a big problem in trying to test drugs and design treatment trials,” said Dr. Lederman, professor of pediatrics and medicine at Johns Hopkins University, Baltimore.
The new results may change that. “In the children under the age of 9, there was really a very clear slowdown in the neurodegeneration, and specifically the time that it took for them to lose the ability to ambulate. It’s very exciting, because it’s the first time that anybody has really shown in a double-blind, placebo-controlled, large phase 3 study that any drug has been able to do this. And there were really no steroid side effects, which is the other really remarkable thing about this study,” said Dr. Lederman.
The therapy grew out of a study by researchers in Italy who treated pediatric ataxia telangiectasia patients with corticosteroids and found some transitory improvements in gross motor function, but concerns about long-term exposure to steroids limited its application. EryDel, which specializes in encapsulating therapeutics in red blood cells, became interested and developed a formulation using the patient’s own red blood cells infused with DSP. Reinfused to the patients, the red blood cells slowly release the steroid.
It isn’t clear how dexamethasone works. There are data suggesting that it might lead to transcription of small pieces of the ATM protein, “but that has really not been nailed down in any way at this point. Corticosteroids act on all kinds of cells in all kinds of ways, and so there might be a little bit of this so-called mini-ATM that’s produced, but that may or may not be related to the way in which corticosteroids have a beneficial effect on the rate of neurodegeneration,” said Dr. Lederman.
The treatment process is not easy. Children must have 50-60 cc of blood removed. Red blood cells treated to become porous are exposed to DSP, and then resealed. Then the cells are reinfused. “The whole process takes from beginning to end probably about 3 hours, with a really experienced team of people doing it. And it’s limiting because it’s not easy to put in an IV and take 50 or 60 cc of blood out of children much younger than 5 or 6. The process is now being modified to see whether we could do it with 20 to 30 cc instead,” said Dr. Lederman.
A ‘promising and impressive’ study
The study is promising, according to Nicholas Johnson, MD, who comoderated the session where the study was presented. “They were able to show a slower rate of neurological degeneration or duration on both the lower and higher dose compared with the placebo. This is promising and impressive, in the sense that it’s a really large (trial) for a rare condition,” Dr. Johnson, vice chair of research at Virginia Commonwealth University, Richmond, said in an interview.
The study included 164 patients Europe, Australia, Israel, Tunisia, India, and the United States, who received 5-10 mg dexamethasone, 14-22 mg DSP, or placebo. Mean ages in each group ranged from 9.6 to 10.4 years.
In an intention-to-treat analysis, modified International Cooperative Ataxia Rating Scale (mICARS) scores trended toward improvement in the low-dose (–1.37; P = .0847) and high-dose groups (–1.40; P = .0765) when determined by central raters during the COVID-19 pandemic. There was also a trend toward improvement when determined by local raters in the low dose group (–1.73; P = .0720) and a statistically significant change in the high dose group (–2.11; P = .0277). The researchers noted some inconsistency between local and central raters, due to inconsistency of videography and language challenges for central raters.
An intention-to-treat analysis of a subgroup of 89 patients age 6-9, who were compared with natural history data from 245 patients, found a deterioration of mICARS of 3.7 per year, compared with 0.92 in the high-dose group, for a reduction of 75% (P = .020). In the high-dose group, 51.7% had a minimal or significant improvement compared with baseline according to the Clinical Global Impression of Change, as did 29.0% on low dose, and 27.6% in the placebo group.
SEATTLE –
The disease is an autosomal recessive disorder caused by mutations in the ATM gene, which is critical to the response to cellular insults such as DNA breaks, oxidative damage, and other forms of stress. The result is clinical manifestations that range from a suppressed immune system to organ damage and neurological symptoms that typically lead patients to be wheelchair bound by their teenage years.
“It’s really multisystem and a very, very difficult disease for people to live with,” Howard M. Lederman, MD, PhD, said in an interview. Dr. Lederman is a coauthor of the study, which was presented by Stefan Zielen, PhD, professor at the University of Goethe, at the 2022 annual meeting of the American Academy of Neurology.
Various therapies have been developed to improve immunodeficiency, lung disease, and some of the other clinical aspects of the condition, but there is no treatment for its neurological effects. “There’s not really been a good animal model, which has been a big problem in trying to test drugs and design treatment trials,” said Dr. Lederman, professor of pediatrics and medicine at Johns Hopkins University, Baltimore.
The new results may change that. “In the children under the age of 9, there was really a very clear slowdown in the neurodegeneration, and specifically the time that it took for them to lose the ability to ambulate. It’s very exciting, because it’s the first time that anybody has really shown in a double-blind, placebo-controlled, large phase 3 study that any drug has been able to do this. And there were really no steroid side effects, which is the other really remarkable thing about this study,” said Dr. Lederman.
The therapy grew out of a study by researchers in Italy who treated pediatric ataxia telangiectasia patients with corticosteroids and found some transitory improvements in gross motor function, but concerns about long-term exposure to steroids limited its application. EryDel, which specializes in encapsulating therapeutics in red blood cells, became interested and developed a formulation using the patient’s own red blood cells infused with DSP. Reinfused to the patients, the red blood cells slowly release the steroid.
It isn’t clear how dexamethasone works. There are data suggesting that it might lead to transcription of small pieces of the ATM protein, “but that has really not been nailed down in any way at this point. Corticosteroids act on all kinds of cells in all kinds of ways, and so there might be a little bit of this so-called mini-ATM that’s produced, but that may or may not be related to the way in which corticosteroids have a beneficial effect on the rate of neurodegeneration,” said Dr. Lederman.
The treatment process is not easy. Children must have 50-60 cc of blood removed. Red blood cells treated to become porous are exposed to DSP, and then resealed. Then the cells are reinfused. “The whole process takes from beginning to end probably about 3 hours, with a really experienced team of people doing it. And it’s limiting because it’s not easy to put in an IV and take 50 or 60 cc of blood out of children much younger than 5 or 6. The process is now being modified to see whether we could do it with 20 to 30 cc instead,” said Dr. Lederman.
A ‘promising and impressive’ study
The study is promising, according to Nicholas Johnson, MD, who comoderated the session where the study was presented. “They were able to show a slower rate of neurological degeneration or duration on both the lower and higher dose compared with the placebo. This is promising and impressive, in the sense that it’s a really large (trial) for a rare condition,” Dr. Johnson, vice chair of research at Virginia Commonwealth University, Richmond, said in an interview.
The study included 164 patients Europe, Australia, Israel, Tunisia, India, and the United States, who received 5-10 mg dexamethasone, 14-22 mg DSP, or placebo. Mean ages in each group ranged from 9.6 to 10.4 years.
In an intention-to-treat analysis, modified International Cooperative Ataxia Rating Scale (mICARS) scores trended toward improvement in the low-dose (–1.37; P = .0847) and high-dose groups (–1.40; P = .0765) when determined by central raters during the COVID-19 pandemic. There was also a trend toward improvement when determined by local raters in the low dose group (–1.73; P = .0720) and a statistically significant change in the high dose group (–2.11; P = .0277). The researchers noted some inconsistency between local and central raters, due to inconsistency of videography and language challenges for central raters.
An intention-to-treat analysis of a subgroup of 89 patients age 6-9, who were compared with natural history data from 245 patients, found a deterioration of mICARS of 3.7 per year, compared with 0.92 in the high-dose group, for a reduction of 75% (P = .020). In the high-dose group, 51.7% had a minimal or significant improvement compared with baseline according to the Clinical Global Impression of Change, as did 29.0% on low dose, and 27.6% in the placebo group.
SEATTLE –
The disease is an autosomal recessive disorder caused by mutations in the ATM gene, which is critical to the response to cellular insults such as DNA breaks, oxidative damage, and other forms of stress. The result is clinical manifestations that range from a suppressed immune system to organ damage and neurological symptoms that typically lead patients to be wheelchair bound by their teenage years.
“It’s really multisystem and a very, very difficult disease for people to live with,” Howard M. Lederman, MD, PhD, said in an interview. Dr. Lederman is a coauthor of the study, which was presented by Stefan Zielen, PhD, professor at the University of Goethe, at the 2022 annual meeting of the American Academy of Neurology.
Various therapies have been developed to improve immunodeficiency, lung disease, and some of the other clinical aspects of the condition, but there is no treatment for its neurological effects. “There’s not really been a good animal model, which has been a big problem in trying to test drugs and design treatment trials,” said Dr. Lederman, professor of pediatrics and medicine at Johns Hopkins University, Baltimore.
The new results may change that. “In the children under the age of 9, there was really a very clear slowdown in the neurodegeneration, and specifically the time that it took for them to lose the ability to ambulate. It’s very exciting, because it’s the first time that anybody has really shown in a double-blind, placebo-controlled, large phase 3 study that any drug has been able to do this. And there were really no steroid side effects, which is the other really remarkable thing about this study,” said Dr. Lederman.
The therapy grew out of a study by researchers in Italy who treated pediatric ataxia telangiectasia patients with corticosteroids and found some transitory improvements in gross motor function, but concerns about long-term exposure to steroids limited its application. EryDel, which specializes in encapsulating therapeutics in red blood cells, became interested and developed a formulation using the patient’s own red blood cells infused with DSP. Reinfused to the patients, the red blood cells slowly release the steroid.
It isn’t clear how dexamethasone works. There are data suggesting that it might lead to transcription of small pieces of the ATM protein, “but that has really not been nailed down in any way at this point. Corticosteroids act on all kinds of cells in all kinds of ways, and so there might be a little bit of this so-called mini-ATM that’s produced, but that may or may not be related to the way in which corticosteroids have a beneficial effect on the rate of neurodegeneration,” said Dr. Lederman.
The treatment process is not easy. Children must have 50-60 cc of blood removed. Red blood cells treated to become porous are exposed to DSP, and then resealed. Then the cells are reinfused. “The whole process takes from beginning to end probably about 3 hours, with a really experienced team of people doing it. And it’s limiting because it’s not easy to put in an IV and take 50 or 60 cc of blood out of children much younger than 5 or 6. The process is now being modified to see whether we could do it with 20 to 30 cc instead,” said Dr. Lederman.
A ‘promising and impressive’ study
The study is promising, according to Nicholas Johnson, MD, who comoderated the session where the study was presented. “They were able to show a slower rate of neurological degeneration or duration on both the lower and higher dose compared with the placebo. This is promising and impressive, in the sense that it’s a really large (trial) for a rare condition,” Dr. Johnson, vice chair of research at Virginia Commonwealth University, Richmond, said in an interview.
The study included 164 patients Europe, Australia, Israel, Tunisia, India, and the United States, who received 5-10 mg dexamethasone, 14-22 mg DSP, or placebo. Mean ages in each group ranged from 9.6 to 10.4 years.
In an intention-to-treat analysis, modified International Cooperative Ataxia Rating Scale (mICARS) scores trended toward improvement in the low-dose (–1.37; P = .0847) and high-dose groups (–1.40; P = .0765) when determined by central raters during the COVID-19 pandemic. There was also a trend toward improvement when determined by local raters in the low dose group (–1.73; P = .0720) and a statistically significant change in the high dose group (–2.11; P = .0277). The researchers noted some inconsistency between local and central raters, due to inconsistency of videography and language challenges for central raters.
An intention-to-treat analysis of a subgroup of 89 patients age 6-9, who were compared with natural history data from 245 patients, found a deterioration of mICARS of 3.7 per year, compared with 0.92 in the high-dose group, for a reduction of 75% (P = .020). In the high-dose group, 51.7% had a minimal or significant improvement compared with baseline according to the Clinical Global Impression of Change, as did 29.0% on low dose, and 27.6% in the placebo group.
AT AAN 2022
Nanoparticle shows promise for ALS
SEATTLE – , which was the change in the summated motor unit index (MUNIX) from baseline to week 36.
The drug, CNM-Au8, is being developed by Clene, and would represent a novel mechanism of action. “This is a brand-new approach. We used it complementary with riluzole and it was well tolerated, so I see this as an add-on therapy. I think if we can show some more positivity and longer-term results, it’s going to be a game changer for ALS,” Matthew Kiernan, MBBS, PhD, said in an interview. Dr. Kiernan presented the results at the 2022 annual meeting of the American Academy of Neurology.

Riluzole (Rilutek), which received Food and Drug Administration approval in 1995, inhibits glutamate release to counter excitotoxicity, which is believed to play a role in ALS, Huntington’s disease, ischemia, and other acute and chronic neurodegenerative diseases. The other FDA-approved agent for ALS is the neuroprotective agent and free-radical scavenger edaravone (Radicava), approved in 2017.
CNM-Au8 is made up of catalytically active gold nanocrystals that cross the blood-brain barrier, but lacks the toxicity associated with other synthetic gold compounds, according to the company. The formulation is also being investigated for the treatment of Parkinson’s disease and multiple sclerosis. Basic research has shown that it stabilizes mitochondria and reduces accumulation of the TDP-43 protein, which is linked to spread of ALS through the brain, Dr. Kiernan said during his presentation.
The treatment is well tolerated. “Normally in an ALS trial, we see about a 25% dropout rate. There were no dropouts on the active compound in the clinical trial. There are less deaths, so improved survival,” said Dr. Kiernan, the Bushell chair of neurology at the University of Sydney and codirector of the Brain and Mind Center in Sydney.
Good safety signal
The fact that the trial missed its primary endpoint isn’t too concerning, according to Nicholas Johnson, MD, who comoderated the session where the study was presented. “ALS clinical trials are incredibly difficult to conduct, especially a phase 2 learning-phase clinical trial. At this phase, I’m much more buoyed by the fact that they have a good safety signal, and that they’re willing to move forward to that phase 3 clinical trial,” Dr. Johnson said in an interview. He is vice chair of research at Virginia Commonwealth University, Richmond.
A phase 3 clinical trial is in development in the United States and Europe. The drug also is included as part of the HEALEY ALS Platform Trial, which is testing multiple ALS therapies simultaneously. “The results from that should be available by the second half of this year and it will also inform us as to what the approach should be,” said Dr. Kiernan.
Dr. Johnson also was enthusiastic. “I’m excited to see the results in terms of the primary endpoints for that next phase 3 clinical trial,” he said.
Ongoing research
In September 2021, Clene announced a second expanded access program for people with ALS.
The study included a 36-week double-blind treatment period followed by long-term, open-label follow-up. Twenty-three patients received 30 mg CNM-Au8, and 22 received placebo. In the first 36 weeks, the treatment group was more likely to have no disease progression, defined as death, tracheostomy, noninvasive ventilation, or a gastronomy tube (P = .0125). The researchers compared the probability of experiencing a less than 6-point decline in the Revised Amyotrophic Lateral Sclerosis Functional Rating Scale. At 12 weeks, it was about 85% in both groups. At 24 weeks, it was about 60% to 50% in favor of the CNM-Au8 group, and at 36 weeks it was about 50% to 20% (P = .0350).
At 36 weeks, quality of life as measured by the ALS Specific Quality of Life–Short Form was better in the treatment group at 36 weeks (mean change, 0.9; P = .0177).
Survival was better in the treatment group at 96 weeks than the mortality derived from a European Network for the Cure of ALS prediction model (hazard ratio [HR], 0.2974; P = .0068). This benefit also was experienced by patients who received drug throughout the study (HR, 0.36; 95% confidence interval [CI], 0.12-1.1) and those who started out on placebo and converted to active drug during the open-label period (HR, 0.24; 95% CI, 0.064-0.88).
The study was funded by Clene and FightMND. Dr. Kiernan and Dr. Johnson have no relevant financial disclosures.
SEATTLE – , which was the change in the summated motor unit index (MUNIX) from baseline to week 36.
The drug, CNM-Au8, is being developed by Clene, and would represent a novel mechanism of action. “This is a brand-new approach. We used it complementary with riluzole and it was well tolerated, so I see this as an add-on therapy. I think if we can show some more positivity and longer-term results, it’s going to be a game changer for ALS,” Matthew Kiernan, MBBS, PhD, said in an interview. Dr. Kiernan presented the results at the 2022 annual meeting of the American Academy of Neurology.
Riluzole (Rilutek), which received Food and Drug Administration approval in 1995, inhibits glutamate release to counter excitotoxicity, which is believed to play a role in ALS, Huntington’s disease, ischemia, and other acute and chronic neurodegenerative diseases. The other FDA-approved agent for ALS is the neuroprotective agent and free-radical scavenger edaravone (Radicava), approved in 2017.
CNM-Au8 is made up of catalytically active gold nanocrystals that cross the blood-brain barrier, but lacks the toxicity associated with other synthetic gold compounds, according to the company. The formulation is also being investigated for the treatment of Parkinson’s disease and multiple sclerosis. Basic research has shown that it stabilizes mitochondria and reduces accumulation of the TDP-43 protein, which is linked to spread of ALS through the brain, Dr. Kiernan said during his presentation.
The treatment is well tolerated. “Normally in an ALS trial, we see about a 25% dropout rate. There were no dropouts on the active compound in the clinical trial. There are less deaths, so improved survival,” said Dr. Kiernan, the Bushell chair of neurology at the University of Sydney and codirector of the Brain and Mind Center in Sydney.
Good safety signal
The fact that the trial missed its primary endpoint isn’t too concerning, according to Nicholas Johnson, MD, who comoderated the session where the study was presented. “ALS clinical trials are incredibly difficult to conduct, especially a phase 2 learning-phase clinical trial. At this phase, I’m much more buoyed by the fact that they have a good safety signal, and that they’re willing to move forward to that phase 3 clinical trial,” Dr. Johnson said in an interview. He is vice chair of research at Virginia Commonwealth University, Richmond.
A phase 3 clinical trial is in development in the United States and Europe. The drug also is included as part of the HEALEY ALS Platform Trial, which is testing multiple ALS therapies simultaneously. “The results from that should be available by the second half of this year and it will also inform us as to what the approach should be,” said Dr. Kiernan.
Dr. Johnson also was enthusiastic. “I’m excited to see the results in terms of the primary endpoints for that next phase 3 clinical trial,” he said.
Ongoing research
In September 2021, Clene announced a second expanded access program for people with ALS.
The study included a 36-week double-blind treatment period followed by long-term, open-label follow-up. Twenty-three patients received 30 mg CNM-Au8, and 22 received placebo. In the first 36 weeks, the treatment group was more likely to have no disease progression, defined as death, tracheostomy, noninvasive ventilation, or a gastronomy tube (P = .0125). The researchers compared the probability of experiencing a less than 6-point decline in the Revised Amyotrophic Lateral Sclerosis Functional Rating Scale. At 12 weeks, it was about 85% in both groups. At 24 weeks, it was about 60% to 50% in favor of the CNM-Au8 group, and at 36 weeks it was about 50% to 20% (P = .0350).
At 36 weeks, quality of life as measured by the ALS Specific Quality of Life–Short Form was better in the treatment group at 36 weeks (mean change, 0.9; P = .0177).
Survival was better in the treatment group at 96 weeks than the mortality derived from a European Network for the Cure of ALS prediction model (hazard ratio [HR], 0.2974; P = .0068). This benefit also was experienced by patients who received drug throughout the study (HR, 0.36; 95% confidence interval [CI], 0.12-1.1) and those who started out on placebo and converted to active drug during the open-label period (HR, 0.24; 95% CI, 0.064-0.88).
The study was funded by Clene and FightMND. Dr. Kiernan and Dr. Johnson have no relevant financial disclosures.
SEATTLE – , which was the change in the summated motor unit index (MUNIX) from baseline to week 36.
The drug, CNM-Au8, is being developed by Clene, and would represent a novel mechanism of action. “This is a brand-new approach. We used it complementary with riluzole and it was well tolerated, so I see this as an add-on therapy. I think if we can show some more positivity and longer-term results, it’s going to be a game changer for ALS,” Matthew Kiernan, MBBS, PhD, said in an interview. Dr. Kiernan presented the results at the 2022 annual meeting of the American Academy of Neurology.
Riluzole (Rilutek), which received Food and Drug Administration approval in 1995, inhibits glutamate release to counter excitotoxicity, which is believed to play a role in ALS, Huntington’s disease, ischemia, and other acute and chronic neurodegenerative diseases. The other FDA-approved agent for ALS is the neuroprotective agent and free-radical scavenger edaravone (Radicava), approved in 2017.
CNM-Au8 is made up of catalytically active gold nanocrystals that cross the blood-brain barrier, but lacks the toxicity associated with other synthetic gold compounds, according to the company. The formulation is also being investigated for the treatment of Parkinson’s disease and multiple sclerosis. Basic research has shown that it stabilizes mitochondria and reduces accumulation of the TDP-43 protein, which is linked to spread of ALS through the brain, Dr. Kiernan said during his presentation.
The treatment is well tolerated. “Normally in an ALS trial, we see about a 25% dropout rate. There were no dropouts on the active compound in the clinical trial. There are less deaths, so improved survival,” said Dr. Kiernan, the Bushell chair of neurology at the University of Sydney and codirector of the Brain and Mind Center in Sydney.
Good safety signal
The fact that the trial missed its primary endpoint isn’t too concerning, according to Nicholas Johnson, MD, who comoderated the session where the study was presented. “ALS clinical trials are incredibly difficult to conduct, especially a phase 2 learning-phase clinical trial. At this phase, I’m much more buoyed by the fact that they have a good safety signal, and that they’re willing to move forward to that phase 3 clinical trial,” Dr. Johnson said in an interview. He is vice chair of research at Virginia Commonwealth University, Richmond.
A phase 3 clinical trial is in development in the United States and Europe. The drug also is included as part of the HEALEY ALS Platform Trial, which is testing multiple ALS therapies simultaneously. “The results from that should be available by the second half of this year and it will also inform us as to what the approach should be,” said Dr. Kiernan.
Dr. Johnson also was enthusiastic. “I’m excited to see the results in terms of the primary endpoints for that next phase 3 clinical trial,” he said.
Ongoing research
In September 2021, Clene announced a second expanded access program for people with ALS.
The study included a 36-week double-blind treatment period followed by long-term, open-label follow-up. Twenty-three patients received 30 mg CNM-Au8, and 22 received placebo. In the first 36 weeks, the treatment group was more likely to have no disease progression, defined as death, tracheostomy, noninvasive ventilation, or a gastronomy tube (P = .0125). The researchers compared the probability of experiencing a less than 6-point decline in the Revised Amyotrophic Lateral Sclerosis Functional Rating Scale. At 12 weeks, it was about 85% in both groups. At 24 weeks, it was about 60% to 50% in favor of the CNM-Au8 group, and at 36 weeks it was about 50% to 20% (P = .0350).
At 36 weeks, quality of life as measured by the ALS Specific Quality of Life–Short Form was better in the treatment group at 36 weeks (mean change, 0.9; P = .0177).
Survival was better in the treatment group at 96 weeks than the mortality derived from a European Network for the Cure of ALS prediction model (hazard ratio [HR], 0.2974; P = .0068). This benefit also was experienced by patients who received drug throughout the study (HR, 0.36; 95% confidence interval [CI], 0.12-1.1) and those who started out on placebo and converted to active drug during the open-label period (HR, 0.24; 95% CI, 0.064-0.88).
The study was funded by Clene and FightMND. Dr. Kiernan and Dr. Johnson have no relevant financial disclosures.
AT AAN 2022
Physical fitness tied to lower risk of Alzheimer’s disease
, new findings suggest. “One exciting finding of this study is that as people’s fitness improved, their risk of Alzheimer’s disease decreased – it was not an all-or-nothing proposition,” study investigator Edward Zamrini, MD, of the Washington DC VA Medical Center, said in a news release.
The findings suggest that people can work toward making incremental changes and improvements in their physical fitness, which may help decrease their risk of dementia, Dr. Zamrini added.
The findings were presented at the 2022 annual meeting of the American Academy of Neurology.
Effective prevention strategy
Using the Veterans Health Administration database, Dr. Zamrini and colleagues identified 649,605 veterans (mean age, 61 years) free of Alzheimer’s disease and related disorders (ADRD) when they completed standardized exercise treadmill tests between 2000 and 2017.
They divided participants into five age-specific fitness groups, from least fit to most fit, based on peak metabolic equivalents (METs) achieved during the treadmill test: lowest-fit (METs, ±3.8), low-fit (METs, ±5.8), moderate-fit (METs, ±7.5), fit (METs, ±9.2), and highest-fit (METs, ±11.7).
In unadjusted analysis, veterans with the lowest cardiorespiratory fitness developed ADRD at a rate of 9.5 cases per 1,000 person-years, compared with a rate of 6.4 cases per 1,000 person-years for the most fit group (P < .001).
After adjusting for factors that could affect risk of ADRD, compared with the lowest-fit group, the highest-fit and fit groups were 33% and 26% less likely to develop ADRD, respectively, while the moderate-fit and low-fit groups were 20% and 13% less likely to develop the disease, respectively.
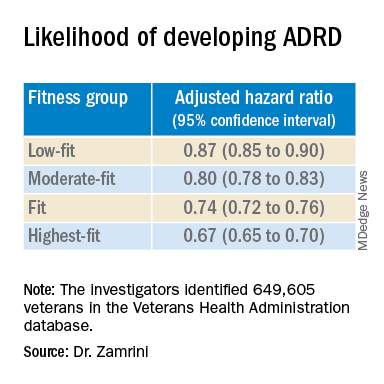
The findings suggest that the association between cardiorespiratory fitness and ADRD risk is “inverse, independent, and graded,” the researchers said in their conference abstract.
“The idea that you can reduce your risk for Alzheimer’s disease by simply increasing your activity is very promising, especially since there are no adequate treatments to prevent or stop the progression of the disease,” Dr. Zamrini added in the news release.
“We hope to develop a simple scale that can be individualized so people can see the benefits that even incremental improvements in fitness can deliver,” he said.
The next vital sign?
Commenting on the study, Shaheen E. Lakhan, MD, PhD, a neurologist in Boston, noted that “for decades and with increasing body of support from studies like this, we have known that preventing dementia is based on healthy behaviors for the brain including a proper diet (NASH and/or Mediterranean), exercise regimen (aerobic/cardio more than anaerobic/weight-lifting), sleep hygiene, and social and intellectual engagements.”
“Frankly, what’s good for the body is good for the brain,” said Dr. Lakhan.
“It should be noted that the measure studied here is cardiorespiratory fitness, which has been associated with heart disease and resulting death, death from any cause, and now brain health,” Dr. Lakhan said.
“This powerful predictor may in fact be the next vital sign, after your heart rate and blood pressure, from which your primary care provider can make a personalized treatment plan,” he added.
“Accelerating this process, the ability to measure cardiorespiratory fitness traditionally from huge stationary machines down to wearables like a watch or ring, or even your iPhone or Android, is just on the horizon,” Dr. Lakhan said.
“Instead of tracking just your weight, shape, and BMI, personal fitness may be tailored to optimizing this indicator and further empowering individuals to take charge of their health,” he said.
The study was supported by the National Institute on Aging, the National Institutes of Health, the U.S. Department of Veterans Affairs, the Washington DC VA Medical Center, and George Washington University. Dr. Zamrini and Dr. Lakhan have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, new findings suggest. “One exciting finding of this study is that as people’s fitness improved, their risk of Alzheimer’s disease decreased – it was not an all-or-nothing proposition,” study investigator Edward Zamrini, MD, of the Washington DC VA Medical Center, said in a news release.
The findings suggest that people can work toward making incremental changes and improvements in their physical fitness, which may help decrease their risk of dementia, Dr. Zamrini added.
The findings were presented at the 2022 annual meeting of the American Academy of Neurology.
Effective prevention strategy
Using the Veterans Health Administration database, Dr. Zamrini and colleagues identified 649,605 veterans (mean age, 61 years) free of Alzheimer’s disease and related disorders (ADRD) when they completed standardized exercise treadmill tests between 2000 and 2017.
They divided participants into five age-specific fitness groups, from least fit to most fit, based on peak metabolic equivalents (METs) achieved during the treadmill test: lowest-fit (METs, ±3.8), low-fit (METs, ±5.8), moderate-fit (METs, ±7.5), fit (METs, ±9.2), and highest-fit (METs, ±11.7).
In unadjusted analysis, veterans with the lowest cardiorespiratory fitness developed ADRD at a rate of 9.5 cases per 1,000 person-years, compared with a rate of 6.4 cases per 1,000 person-years for the most fit group (P < .001).
After adjusting for factors that could affect risk of ADRD, compared with the lowest-fit group, the highest-fit and fit groups were 33% and 26% less likely to develop ADRD, respectively, while the moderate-fit and low-fit groups were 20% and 13% less likely to develop the disease, respectively.
The findings suggest that the association between cardiorespiratory fitness and ADRD risk is “inverse, independent, and graded,” the researchers said in their conference abstract.
“The idea that you can reduce your risk for Alzheimer’s disease by simply increasing your activity is very promising, especially since there are no adequate treatments to prevent or stop the progression of the disease,” Dr. Zamrini added in the news release.
“We hope to develop a simple scale that can be individualized so people can see the benefits that even incremental improvements in fitness can deliver,” he said.
The next vital sign?
Commenting on the study, Shaheen E. Lakhan, MD, PhD, a neurologist in Boston, noted that “for decades and with increasing body of support from studies like this, we have known that preventing dementia is based on healthy behaviors for the brain including a proper diet (NASH and/or Mediterranean), exercise regimen (aerobic/cardio more than anaerobic/weight-lifting), sleep hygiene, and social and intellectual engagements.”
“Frankly, what’s good for the body is good for the brain,” said Dr. Lakhan.
“It should be noted that the measure studied here is cardiorespiratory fitness, which has been associated with heart disease and resulting death, death from any cause, and now brain health,” Dr. Lakhan said.
“This powerful predictor may in fact be the next vital sign, after your heart rate and blood pressure, from which your primary care provider can make a personalized treatment plan,” he added.
“Accelerating this process, the ability to measure cardiorespiratory fitness traditionally from huge stationary machines down to wearables like a watch or ring, or even your iPhone or Android, is just on the horizon,” Dr. Lakhan said.
“Instead of tracking just your weight, shape, and BMI, personal fitness may be tailored to optimizing this indicator and further empowering individuals to take charge of their health,” he said.
The study was supported by the National Institute on Aging, the National Institutes of Health, the U.S. Department of Veterans Affairs, the Washington DC VA Medical Center, and George Washington University. Dr. Zamrini and Dr. Lakhan have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, new findings suggest. “One exciting finding of this study is that as people’s fitness improved, their risk of Alzheimer’s disease decreased – it was not an all-or-nothing proposition,” study investigator Edward Zamrini, MD, of the Washington DC VA Medical Center, said in a news release.
The findings suggest that people can work toward making incremental changes and improvements in their physical fitness, which may help decrease their risk of dementia, Dr. Zamrini added.
The findings were presented at the 2022 annual meeting of the American Academy of Neurology.
Effective prevention strategy
Using the Veterans Health Administration database, Dr. Zamrini and colleagues identified 649,605 veterans (mean age, 61 years) free of Alzheimer’s disease and related disorders (ADRD) when they completed standardized exercise treadmill tests between 2000 and 2017.
They divided participants into five age-specific fitness groups, from least fit to most fit, based on peak metabolic equivalents (METs) achieved during the treadmill test: lowest-fit (METs, ±3.8), low-fit (METs, ±5.8), moderate-fit (METs, ±7.5), fit (METs, ±9.2), and highest-fit (METs, ±11.7).
In unadjusted analysis, veterans with the lowest cardiorespiratory fitness developed ADRD at a rate of 9.5 cases per 1,000 person-years, compared with a rate of 6.4 cases per 1,000 person-years for the most fit group (P < .001).
After adjusting for factors that could affect risk of ADRD, compared with the lowest-fit group, the highest-fit and fit groups were 33% and 26% less likely to develop ADRD, respectively, while the moderate-fit and low-fit groups were 20% and 13% less likely to develop the disease, respectively.
The findings suggest that the association between cardiorespiratory fitness and ADRD risk is “inverse, independent, and graded,” the researchers said in their conference abstract.
“The idea that you can reduce your risk for Alzheimer’s disease by simply increasing your activity is very promising, especially since there are no adequate treatments to prevent or stop the progression of the disease,” Dr. Zamrini added in the news release.
“We hope to develop a simple scale that can be individualized so people can see the benefits that even incremental improvements in fitness can deliver,” he said.
The next vital sign?
Commenting on the study, Shaheen E. Lakhan, MD, PhD, a neurologist in Boston, noted that “for decades and with increasing body of support from studies like this, we have known that preventing dementia is based on healthy behaviors for the brain including a proper diet (NASH and/or Mediterranean), exercise regimen (aerobic/cardio more than anaerobic/weight-lifting), sleep hygiene, and social and intellectual engagements.”
“Frankly, what’s good for the body is good for the brain,” said Dr. Lakhan.
“It should be noted that the measure studied here is cardiorespiratory fitness, which has been associated with heart disease and resulting death, death from any cause, and now brain health,” Dr. Lakhan said.
“This powerful predictor may in fact be the next vital sign, after your heart rate and blood pressure, from which your primary care provider can make a personalized treatment plan,” he added.
“Accelerating this process, the ability to measure cardiorespiratory fitness traditionally from huge stationary machines down to wearables like a watch or ring, or even your iPhone or Android, is just on the horizon,” Dr. Lakhan said.
“Instead of tracking just your weight, shape, and BMI, personal fitness may be tailored to optimizing this indicator and further empowering individuals to take charge of their health,” he said.
The study was supported by the National Institute on Aging, the National Institutes of Health, the U.S. Department of Veterans Affairs, the Washington DC VA Medical Center, and George Washington University. Dr. Zamrini and Dr. Lakhan have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM AAN 2022
More years of ice hockey play tied to higher CTE risk
new research suggests. Early results from a study that examined donor brains showed that each additional year of ice hockey play increased the risk for CTE by 23%.
This information should be on the “radar” of all clinicians, said coinvestigator Jesse Mez, MD, associate professor of neurology at Boston University. “When they’re talking to kids and families and parents about playing contact sports, they should discuss the benefits as well as the risks so all that information can be taken into consideration.”
Dr. Mez noted that clinicians should also consider the amount of hockey played when assessing patients for thinking and memory trouble later in life. “CTE could be in the differential diagnosis,” he said.
The study findings were presented at the 2022 annual meeting of the American Academy of Neurology.
Football data
CTE is a neurodegenerative disease associated with repetitive hits to the head. In previous research, the investigators showed that the more that athletes play American football, the more likely they are to develop CTE.
“Hockey, like football, involves repetitive head impacts as part of the game,” said Dr. Mez. “So we hypothesized that we would see a similar type of dose-response relationship in hockey.”
From two brain banks – the Veterans Affairs–Boston University–Concussion Legacy Foundation and the Framingham Heart Study – the researchers accessed 74 consecutive brains from donors who had played ice hockey. They collected information about hockey play during “pretty comprehensive” interviews with next of kin, Dr. Mez reported.
The study participants ranged in age from 13 to 91 years. The cause of death varied; most died with end-stage dementia and neurodegenerative disease, but some died of cardiovascular disease, and others from accidents.
For 9% of the individuals, the highest level of play was a youth league; 34% had reached the high school level, 30% reached the juniors/college level, and 26% played professionally. In addition, 46% played another contact sport – including 43% who played American football.
Primary outcomes included evidence of CTE from stage 0 (no CTE) to stage IV and severity of CTE, which was defined by the amount of neurofibrillary tangle (NFT) burden in 11 brain regions. For this burden, the score ranged from 0 (absent) to 3 (severe) in each region for a total range of 0-33.
Dr. Mez noted that, in CTE, tau protein accumulates abnormally. “It typically begins in the cortex in the frontal lobe and then spreads to other parts of the brain, including to the medial temporal structures, and is widespread by stage IV.”
The researchers estimated the association of duration of ice hockey play in years with each neuropathologic outcome and adjusted for age at death and duration of football play.
Consistent findings
Results showed that, of the 74 donors, 40 (54%) had CTE. Each additional year of hockey play corresponded to increased chances for having CTE (odds ratio, 1.23; 95% confidence interval, 11%-36%; P < .01). This increase in risk is similar to that which was found with football players, Dr. Mez noted. This was somewhat surprising, as hockey involves fewer “hits” than football.
“Hits are not as quintessential to the game of hockey as they are in football, where contacts occur with nearly every play,” he said. “In football, you have several hundred impacts over the course of a season.”
Researchers also found a 15% increase in odds for increasing one CTE stage (95% CI, 8%-22%; P < .01), and a .03 standard deviation increase in cumulative NFT burden (95% CI, 0.01-0.05; P < .01).
Dr. Mez noted that the fact that the results were consistent across different outcomes “improves the validity” of the findings.
In a sensitivity analysis that excluded participants who also played football, estimates “were pretty similar” to those in the full analysis, said Dr. Mez.
The investigators have not yet examined the effect of level of hockey play, such as professionally or at the college level, on CTE risk. However, in football players, they found that level of play is another “valuable predictor of CTE pathology,” Dr. Mez said, adding that level of play, position played, and years of play “are all probably contributing” to CTE risk.
Asking about years of play is useful in a clinical setting. “It’s very easy for a clinician to ask patients how many years of hockey they played,” said Dr. Mez.
Overall, the new results are important, as “millions of individuals” play contact sports, whether that is hockey, football, or European soccer, he added. “And for all sports, there seems to be this relationship between more play and risk of this disease.”
‘Skewed’ population?
Commenting on the findings, Frank Conidi, MD, director, Florida Center for Health and Sports Neurology, Port St. Lucie, said he was surprised the investigators found a 23% per year increase in risk for CTE among hockey players.
Dr. Conidi has played hockey himself and works with the Florida Panthers of the National Hockey League. In his practice, he treats retired professional football players who have neurodegenerative disorders. From his experience, the number of repetitive direct head impacts in football is significantly higher than in hockey. “Most of the forces seen in hockey are from hits to the body, where the force is transferred to the head,” said Dr. Conidi, who was not involved with the research.
He noted differences in the way hockey is played around the world. In European countries, for example, the ice surface is relatively large and the emphasis tends to be more on skill than hitting.
“It would have been interesting to have the study group analyze the data based on where the athlete grew up,” he said. Dr. Conidi would also like to know when the participants played hockey. “The game is vastly different now than it was in the 1970s, ‘80s, and early ‘90s, when there was more fighting, less protective gear, and more hitting in general.”
As is the case for most studies of CTE in athletes, the study population is “skewed” because the participants likely had neurocognitive and other problems that led to their decision to donate their brain, said Dr. Conidi.
He also doesn’t believe the study should be the sole factor in a decision to continue or stop playing hockey. “We are still in the infancy stages of understanding the effects of high-impact sports on athletes’ brains.”
The study received funding from the National Institute of Neurological Diseases and Stroke and the National Institute on Aging. Dr. Mez and Dr. Conidi have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
new research suggests. Early results from a study that examined donor brains showed that each additional year of ice hockey play increased the risk for CTE by 23%.
This information should be on the “radar” of all clinicians, said coinvestigator Jesse Mez, MD, associate professor of neurology at Boston University. “When they’re talking to kids and families and parents about playing contact sports, they should discuss the benefits as well as the risks so all that information can be taken into consideration.”
Dr. Mez noted that clinicians should also consider the amount of hockey played when assessing patients for thinking and memory trouble later in life. “CTE could be in the differential diagnosis,” he said.
The study findings were presented at the 2022 annual meeting of the American Academy of Neurology.
Football data
CTE is a neurodegenerative disease associated with repetitive hits to the head. In previous research, the investigators showed that the more that athletes play American football, the more likely they are to develop CTE.
“Hockey, like football, involves repetitive head impacts as part of the game,” said Dr. Mez. “So we hypothesized that we would see a similar type of dose-response relationship in hockey.”
From two brain banks – the Veterans Affairs–Boston University–Concussion Legacy Foundation and the Framingham Heart Study – the researchers accessed 74 consecutive brains from donors who had played ice hockey. They collected information about hockey play during “pretty comprehensive” interviews with next of kin, Dr. Mez reported.
The study participants ranged in age from 13 to 91 years. The cause of death varied; most died with end-stage dementia and neurodegenerative disease, but some died of cardiovascular disease, and others from accidents.
For 9% of the individuals, the highest level of play was a youth league; 34% had reached the high school level, 30% reached the juniors/college level, and 26% played professionally. In addition, 46% played another contact sport – including 43% who played American football.
Primary outcomes included evidence of CTE from stage 0 (no CTE) to stage IV and severity of CTE, which was defined by the amount of neurofibrillary tangle (NFT) burden in 11 brain regions. For this burden, the score ranged from 0 (absent) to 3 (severe) in each region for a total range of 0-33.
Dr. Mez noted that, in CTE, tau protein accumulates abnormally. “It typically begins in the cortex in the frontal lobe and then spreads to other parts of the brain, including to the medial temporal structures, and is widespread by stage IV.”
The researchers estimated the association of duration of ice hockey play in years with each neuropathologic outcome and adjusted for age at death and duration of football play.
Consistent findings
Results showed that, of the 74 donors, 40 (54%) had CTE. Each additional year of hockey play corresponded to increased chances for having CTE (odds ratio, 1.23; 95% confidence interval, 11%-36%; P < .01). This increase in risk is similar to that which was found with football players, Dr. Mez noted. This was somewhat surprising, as hockey involves fewer “hits” than football.
“Hits are not as quintessential to the game of hockey as they are in football, where contacts occur with nearly every play,” he said. “In football, you have several hundred impacts over the course of a season.”
Researchers also found a 15% increase in odds for increasing one CTE stage (95% CI, 8%-22%; P < .01), and a .03 standard deviation increase in cumulative NFT burden (95% CI, 0.01-0.05; P < .01).
Dr. Mez noted that the fact that the results were consistent across different outcomes “improves the validity” of the findings.
In a sensitivity analysis that excluded participants who also played football, estimates “were pretty similar” to those in the full analysis, said Dr. Mez.
The investigators have not yet examined the effect of level of hockey play, such as professionally or at the college level, on CTE risk. However, in football players, they found that level of play is another “valuable predictor of CTE pathology,” Dr. Mez said, adding that level of play, position played, and years of play “are all probably contributing” to CTE risk.
Asking about years of play is useful in a clinical setting. “It’s very easy for a clinician to ask patients how many years of hockey they played,” said Dr. Mez.
Overall, the new results are important, as “millions of individuals” play contact sports, whether that is hockey, football, or European soccer, he added. “And for all sports, there seems to be this relationship between more play and risk of this disease.”
‘Skewed’ population?
Commenting on the findings, Frank Conidi, MD, director, Florida Center for Health and Sports Neurology, Port St. Lucie, said he was surprised the investigators found a 23% per year increase in risk for CTE among hockey players.
Dr. Conidi has played hockey himself and works with the Florida Panthers of the National Hockey League. In his practice, he treats retired professional football players who have neurodegenerative disorders. From his experience, the number of repetitive direct head impacts in football is significantly higher than in hockey. “Most of the forces seen in hockey are from hits to the body, where the force is transferred to the head,” said Dr. Conidi, who was not involved with the research.
He noted differences in the way hockey is played around the world. In European countries, for example, the ice surface is relatively large and the emphasis tends to be more on skill than hitting.
“It would have been interesting to have the study group analyze the data based on where the athlete grew up,” he said. Dr. Conidi would also like to know when the participants played hockey. “The game is vastly different now than it was in the 1970s, ‘80s, and early ‘90s, when there was more fighting, less protective gear, and more hitting in general.”
As is the case for most studies of CTE in athletes, the study population is “skewed” because the participants likely had neurocognitive and other problems that led to their decision to donate their brain, said Dr. Conidi.
He also doesn’t believe the study should be the sole factor in a decision to continue or stop playing hockey. “We are still in the infancy stages of understanding the effects of high-impact sports on athletes’ brains.”
The study received funding from the National Institute of Neurological Diseases and Stroke and the National Institute on Aging. Dr. Mez and Dr. Conidi have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
new research suggests. Early results from a study that examined donor brains showed that each additional year of ice hockey play increased the risk for CTE by 23%.
This information should be on the “radar” of all clinicians, said coinvestigator Jesse Mez, MD, associate professor of neurology at Boston University. “When they’re talking to kids and families and parents about playing contact sports, they should discuss the benefits as well as the risks so all that information can be taken into consideration.”
Dr. Mez noted that clinicians should also consider the amount of hockey played when assessing patients for thinking and memory trouble later in life. “CTE could be in the differential diagnosis,” he said.
The study findings were presented at the 2022 annual meeting of the American Academy of Neurology.
Football data
CTE is a neurodegenerative disease associated with repetitive hits to the head. In previous research, the investigators showed that the more that athletes play American football, the more likely they are to develop CTE.
“Hockey, like football, involves repetitive head impacts as part of the game,” said Dr. Mez. “So we hypothesized that we would see a similar type of dose-response relationship in hockey.”
From two brain banks – the Veterans Affairs–Boston University–Concussion Legacy Foundation and the Framingham Heart Study – the researchers accessed 74 consecutive brains from donors who had played ice hockey. They collected information about hockey play during “pretty comprehensive” interviews with next of kin, Dr. Mez reported.
The study participants ranged in age from 13 to 91 years. The cause of death varied; most died with end-stage dementia and neurodegenerative disease, but some died of cardiovascular disease, and others from accidents.
For 9% of the individuals, the highest level of play was a youth league; 34% had reached the high school level, 30% reached the juniors/college level, and 26% played professionally. In addition, 46% played another contact sport – including 43% who played American football.
Primary outcomes included evidence of CTE from stage 0 (no CTE) to stage IV and severity of CTE, which was defined by the amount of neurofibrillary tangle (NFT) burden in 11 brain regions. For this burden, the score ranged from 0 (absent) to 3 (severe) in each region for a total range of 0-33.
Dr. Mez noted that, in CTE, tau protein accumulates abnormally. “It typically begins in the cortex in the frontal lobe and then spreads to other parts of the brain, including to the medial temporal structures, and is widespread by stage IV.”
The researchers estimated the association of duration of ice hockey play in years with each neuropathologic outcome and adjusted for age at death and duration of football play.
Consistent findings
Results showed that, of the 74 donors, 40 (54%) had CTE. Each additional year of hockey play corresponded to increased chances for having CTE (odds ratio, 1.23; 95% confidence interval, 11%-36%; P < .01). This increase in risk is similar to that which was found with football players, Dr. Mez noted. This was somewhat surprising, as hockey involves fewer “hits” than football.
“Hits are not as quintessential to the game of hockey as they are in football, where contacts occur with nearly every play,” he said. “In football, you have several hundred impacts over the course of a season.”
Researchers also found a 15% increase in odds for increasing one CTE stage (95% CI, 8%-22%; P < .01), and a .03 standard deviation increase in cumulative NFT burden (95% CI, 0.01-0.05; P < .01).
Dr. Mez noted that the fact that the results were consistent across different outcomes “improves the validity” of the findings.
In a sensitivity analysis that excluded participants who also played football, estimates “were pretty similar” to those in the full analysis, said Dr. Mez.
The investigators have not yet examined the effect of level of hockey play, such as professionally or at the college level, on CTE risk. However, in football players, they found that level of play is another “valuable predictor of CTE pathology,” Dr. Mez said, adding that level of play, position played, and years of play “are all probably contributing” to CTE risk.
Asking about years of play is useful in a clinical setting. “It’s very easy for a clinician to ask patients how many years of hockey they played,” said Dr. Mez.
Overall, the new results are important, as “millions of individuals” play contact sports, whether that is hockey, football, or European soccer, he added. “And for all sports, there seems to be this relationship between more play and risk of this disease.”
‘Skewed’ population?
Commenting on the findings, Frank Conidi, MD, director, Florida Center for Health and Sports Neurology, Port St. Lucie, said he was surprised the investigators found a 23% per year increase in risk for CTE among hockey players.
Dr. Conidi has played hockey himself and works with the Florida Panthers of the National Hockey League. In his practice, he treats retired professional football players who have neurodegenerative disorders. From his experience, the number of repetitive direct head impacts in football is significantly higher than in hockey. “Most of the forces seen in hockey are from hits to the body, where the force is transferred to the head,” said Dr. Conidi, who was not involved with the research.
He noted differences in the way hockey is played around the world. In European countries, for example, the ice surface is relatively large and the emphasis tends to be more on skill than hitting.
“It would have been interesting to have the study group analyze the data based on where the athlete grew up,” he said. Dr. Conidi would also like to know when the participants played hockey. “The game is vastly different now than it was in the 1970s, ‘80s, and early ‘90s, when there was more fighting, less protective gear, and more hitting in general.”
As is the case for most studies of CTE in athletes, the study population is “skewed” because the participants likely had neurocognitive and other problems that led to their decision to donate their brain, said Dr. Conidi.
He also doesn’t believe the study should be the sole factor in a decision to continue or stop playing hockey. “We are still in the infancy stages of understanding the effects of high-impact sports on athletes’ brains.”
The study received funding from the National Institute of Neurological Diseases and Stroke and the National Institute on Aging. Dr. Mez and Dr. Conidi have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM AAN 2022
Brain implant is a potential life-changer for paralyzed patients
, results of a small, first-in-human study show.
A potential life changer for patients with amyotrophic lateral sclerosis (ALS), the minimally invasive device enables patients to carry out important activities of daily living.
“Our participants are able to use the device to perform tasks like sending email, texting loved ones and caregivers, browsing the web, and doing personal finances such as online banking,” study investigator Douglas J. Weber, PhD, professor of mechanical engineering and neuroscience, Carnegie Mellon University, Pittsburgh, told a press briefing.
The technology allowed one patient to write a book (due out later this year) and another patient to maintain communication despite losing his ability to speak, said the study’s lead investigator, Bruce Campbell, MBBS, PhD, professor of neurology, Royal Melbourne Hospital, University of Melbourne.
“In addition to providing patients with communicative capabilities not possible as a result of their disease, it is our goal to enable patients to be more independently involved in their care going forward, by enabling effective and faster communication directly with their caregiver and physician,” said Dr. Campbell.
The findings were presented at the 2022 annual meeting of the American Academy of Neurology.
Minimally invasive
ALS, also known as Lou Gehrig’s disease, is a progressive neurodegenerative disease that affects nerve cells in the brain and spinal cord. Patients with ALS eventually lose the ability to control muscle movement, often leading to total paralysis.
“Extending the period in which patients are able to communicate with loved ones and caregivers could provide a very meaningful benefit to patients with ALS,” said Dr. Weber.
Brain-computer interfaces measure and translate brain signals, with some functioning as motor neuro-prostheses. These devices provide direct communication between the brain and an external device by recording and decoding signals from the precentral gyrus as the result of movement intention.
“The technology has potential to empower the more than five million people in the U.S. who are severely paralyzed to once again perform important activities of daily living independently,” said Dr. Weber.
Until now, motor neuro-prostheses required surgery to remove a portion of the skull and place electrodes on to the brain. However, the new minimally invasive motor neuro-prostheses reach the brain by vascular access, dispensing with the need for a craniotomy.
“The brain-computer interface device used in our study is unique in that it does not require invasive open surgery to implant,” said Dr. Weber. “Instead this is an endovascular brain-computer interface.”
Using a catheter, surgeons feed the BCI through one of two jugular veins in the neck. They position an array of 16 sensors or electrodes on a stent-like scaffold that deploys against the walls of the superior sagittal sinus.
No adverse events
Describing the device, Dr. Weber said the electrodes or sensing elements are tiny and the body of the stent, which serves as a scaffold to support the electrodes, resembles a standard endovascular stent.
“It’s very small at the time of delivery because it’s held within the body of a catheter, but then when deployed it expands to contact the wall of the vein.”
The device transmits brain signals from the motor cortex to an electronics unit, located in a subcutaneous pocket that decodes movement signals. The machine-learning decoder is programmed as follows: When a trainer asked participants to attempt certain movements, like tapping their foot or extending their knee, the decoder analyzes nerve cell signals from those movement attempts. The decoder is able to translate movement signals into computer navigation.
The study included four patients with ALS who were paralyzed because of the disease and were trained to use the device.
A key safety endpoint was device-related serious adverse events resulting in death or increased disability during the post-implant evaluation period. Results showed all four participants successfully completed the 12-month follow-up with no serious adverse events.
Researchers also assessed target vessel patency and incidence of device migration at 3 and 12 months. Postoperative imaging showed that in all participants, the blood vessel that held the implanted device remained open and stayed in place.
Addressing the potential for blood clots, Dr. Weber said that so far there has been no sign of clotting or vascular occlusion.
“The device itself integrates well into the walls of the blood vessel over time,” he said. “Within the acute period after implantation, there’s time where the device is exposed to the blood stream, but once it becomes encapsulated and fully integrated into the blood vessel wall, the risks of thrombosis diminish.”
Greater independence
Researchers also recorded signal fidelity and stability over 12 months and use of the brain-computer interface to perform routine tasks. All participants learned to use the motor neuro-prostheses with eye tracking for computer use. Eye tracking technology helps a computer determine what a person is looking at.
Using the system, patients were able to complete tasks without help. These included text messaging and managing finances. “Since the device is fully implanted and easy for patients to use, they can use the technology independently and in their own home,” said Dr. Weber.
Although the study started with patients with ALS, those paralyzed from other causes, such as an upper spinal cord injury or brain-stem stroke could also benefit from this technology, Dr. Weber said. In addition, the technology could be expanded to broaden brain communication capabilities potentially to include robotic limbs, he said.
There’s even the potential to use this minimally invasive brain interface technology to deliver therapies like deep brain stimulation, which Dr. Weber noted is a growing field. “It’s [the] early days, but it’s a very exciting new direction for brain interface technology,” he said.
Researchers are now recruiting patients for the first U.S.-based feasibility trial of the device that will be funded by the NIH, said Dr. Weber. A limitation of the research was the study’s small size.
Advancing the field
Reached for a comment, Kevin C. Davis, an MD and PhD student in the department of biomedical engineering, University of Miami Miller School of Medicine, said this new work moves the field forward in an important way.
Dr. Davis and colleagues have shown the effectiveness of another technology used to overcome paralysis – a small portable system that facilitates hand grasp of a patient with a spinal cord injury. He reported on this DBS-based BCI system at the American Association of Neurological Surgeons (AANS) 2021 Annual Meeting.
Developing effective brain-computer interfaces, and motor neural prosthetics that avoid surgery, as the team did in this new study, is “worth exploring,” said Dr. Davis.
However, although the device used in this new study avoids cranial surgery, “sole vascular access may limit the device’s ability to reach other areas of the brain more suitable for upper-limb motor prosthetics,” he said.
“Determining how much function such a device could provide to individuals with locked-in syndrome or paralysis will be important in determining its viability as an eventual clinical tool for patients.”
The study was supported by Synchron, the maker of the device, the U.S. Defense Advanced Research Projects Agency, the Office of Naval Research, the National Health and Medical Research Council of Australia, the Australian Federal Government Foundation, and the Motor Neuron Disease Research Institute of Australia.
A version of this article first appeared on Medscape.com.
, results of a small, first-in-human study show.
A potential life changer for patients with amyotrophic lateral sclerosis (ALS), the minimally invasive device enables patients to carry out important activities of daily living.
“Our participants are able to use the device to perform tasks like sending email, texting loved ones and caregivers, browsing the web, and doing personal finances such as online banking,” study investigator Douglas J. Weber, PhD, professor of mechanical engineering and neuroscience, Carnegie Mellon University, Pittsburgh, told a press briefing.
The technology allowed one patient to write a book (due out later this year) and another patient to maintain communication despite losing his ability to speak, said the study’s lead investigator, Bruce Campbell, MBBS, PhD, professor of neurology, Royal Melbourne Hospital, University of Melbourne.
“In addition to providing patients with communicative capabilities not possible as a result of their disease, it is our goal to enable patients to be more independently involved in their care going forward, by enabling effective and faster communication directly with their caregiver and physician,” said Dr. Campbell.
The findings were presented at the 2022 annual meeting of the American Academy of Neurology.
Minimally invasive
ALS, also known as Lou Gehrig’s disease, is a progressive neurodegenerative disease that affects nerve cells in the brain and spinal cord. Patients with ALS eventually lose the ability to control muscle movement, often leading to total paralysis.
“Extending the period in which patients are able to communicate with loved ones and caregivers could provide a very meaningful benefit to patients with ALS,” said Dr. Weber.
Brain-computer interfaces measure and translate brain signals, with some functioning as motor neuro-prostheses. These devices provide direct communication between the brain and an external device by recording and decoding signals from the precentral gyrus as the result of movement intention.
“The technology has potential to empower the more than five million people in the U.S. who are severely paralyzed to once again perform important activities of daily living independently,” said Dr. Weber.
Until now, motor neuro-prostheses required surgery to remove a portion of the skull and place electrodes on to the brain. However, the new minimally invasive motor neuro-prostheses reach the brain by vascular access, dispensing with the need for a craniotomy.
“The brain-computer interface device used in our study is unique in that it does not require invasive open surgery to implant,” said Dr. Weber. “Instead this is an endovascular brain-computer interface.”
Using a catheter, surgeons feed the BCI through one of two jugular veins in the neck. They position an array of 16 sensors or electrodes on a stent-like scaffold that deploys against the walls of the superior sagittal sinus.
No adverse events
Describing the device, Dr. Weber said the electrodes or sensing elements are tiny and the body of the stent, which serves as a scaffold to support the electrodes, resembles a standard endovascular stent.
“It’s very small at the time of delivery because it’s held within the body of a catheter, but then when deployed it expands to contact the wall of the vein.”
The device transmits brain signals from the motor cortex to an electronics unit, located in a subcutaneous pocket that decodes movement signals. The machine-learning decoder is programmed as follows: When a trainer asked participants to attempt certain movements, like tapping their foot or extending their knee, the decoder analyzes nerve cell signals from those movement attempts. The decoder is able to translate movement signals into computer navigation.
The study included four patients with ALS who were paralyzed because of the disease and were trained to use the device.
A key safety endpoint was device-related serious adverse events resulting in death or increased disability during the post-implant evaluation period. Results showed all four participants successfully completed the 12-month follow-up with no serious adverse events.
Researchers also assessed target vessel patency and incidence of device migration at 3 and 12 months. Postoperative imaging showed that in all participants, the blood vessel that held the implanted device remained open and stayed in place.
Addressing the potential for blood clots, Dr. Weber said that so far there has been no sign of clotting or vascular occlusion.
“The device itself integrates well into the walls of the blood vessel over time,” he said. “Within the acute period after implantation, there’s time where the device is exposed to the blood stream, but once it becomes encapsulated and fully integrated into the blood vessel wall, the risks of thrombosis diminish.”
Greater independence
Researchers also recorded signal fidelity and stability over 12 months and use of the brain-computer interface to perform routine tasks. All participants learned to use the motor neuro-prostheses with eye tracking for computer use. Eye tracking technology helps a computer determine what a person is looking at.
Using the system, patients were able to complete tasks without help. These included text messaging and managing finances. “Since the device is fully implanted and easy for patients to use, they can use the technology independently and in their own home,” said Dr. Weber.
Although the study started with patients with ALS, those paralyzed from other causes, such as an upper spinal cord injury or brain-stem stroke could also benefit from this technology, Dr. Weber said. In addition, the technology could be expanded to broaden brain communication capabilities potentially to include robotic limbs, he said.
There’s even the potential to use this minimally invasive brain interface technology to deliver therapies like deep brain stimulation, which Dr. Weber noted is a growing field. “It’s [the] early days, but it’s a very exciting new direction for brain interface technology,” he said.
Researchers are now recruiting patients for the first U.S.-based feasibility trial of the device that will be funded by the NIH, said Dr. Weber. A limitation of the research was the study’s small size.
Advancing the field
Reached for a comment, Kevin C. Davis, an MD and PhD student in the department of biomedical engineering, University of Miami Miller School of Medicine, said this new work moves the field forward in an important way.
Dr. Davis and colleagues have shown the effectiveness of another technology used to overcome paralysis – a small portable system that facilitates hand grasp of a patient with a spinal cord injury. He reported on this DBS-based BCI system at the American Association of Neurological Surgeons (AANS) 2021 Annual Meeting.
Developing effective brain-computer interfaces, and motor neural prosthetics that avoid surgery, as the team did in this new study, is “worth exploring,” said Dr. Davis.
However, although the device used in this new study avoids cranial surgery, “sole vascular access may limit the device’s ability to reach other areas of the brain more suitable for upper-limb motor prosthetics,” he said.
“Determining how much function such a device could provide to individuals with locked-in syndrome or paralysis will be important in determining its viability as an eventual clinical tool for patients.”
The study was supported by Synchron, the maker of the device, the U.S. Defense Advanced Research Projects Agency, the Office of Naval Research, the National Health and Medical Research Council of Australia, the Australian Federal Government Foundation, and the Motor Neuron Disease Research Institute of Australia.
A version of this article first appeared on Medscape.com.
, results of a small, first-in-human study show.
A potential life changer for patients with amyotrophic lateral sclerosis (ALS), the minimally invasive device enables patients to carry out important activities of daily living.
“Our participants are able to use the device to perform tasks like sending email, texting loved ones and caregivers, browsing the web, and doing personal finances such as online banking,” study investigator Douglas J. Weber, PhD, professor of mechanical engineering and neuroscience, Carnegie Mellon University, Pittsburgh, told a press briefing.
The technology allowed one patient to write a book (due out later this year) and another patient to maintain communication despite losing his ability to speak, said the study’s lead investigator, Bruce Campbell, MBBS, PhD, professor of neurology, Royal Melbourne Hospital, University of Melbourne.
“In addition to providing patients with communicative capabilities not possible as a result of their disease, it is our goal to enable patients to be more independently involved in their care going forward, by enabling effective and faster communication directly with their caregiver and physician,” said Dr. Campbell.
The findings were presented at the 2022 annual meeting of the American Academy of Neurology.
Minimally invasive
ALS, also known as Lou Gehrig’s disease, is a progressive neurodegenerative disease that affects nerve cells in the brain and spinal cord. Patients with ALS eventually lose the ability to control muscle movement, often leading to total paralysis.
“Extending the period in which patients are able to communicate with loved ones and caregivers could provide a very meaningful benefit to patients with ALS,” said Dr. Weber.
Brain-computer interfaces measure and translate brain signals, with some functioning as motor neuro-prostheses. These devices provide direct communication between the brain and an external device by recording and decoding signals from the precentral gyrus as the result of movement intention.
“The technology has potential to empower the more than five million people in the U.S. who are severely paralyzed to once again perform important activities of daily living independently,” said Dr. Weber.
Until now, motor neuro-prostheses required surgery to remove a portion of the skull and place electrodes on to the brain. However, the new minimally invasive motor neuro-prostheses reach the brain by vascular access, dispensing with the need for a craniotomy.
“The brain-computer interface device used in our study is unique in that it does not require invasive open surgery to implant,” said Dr. Weber. “Instead this is an endovascular brain-computer interface.”
Using a catheter, surgeons feed the BCI through one of two jugular veins in the neck. They position an array of 16 sensors or electrodes on a stent-like scaffold that deploys against the walls of the superior sagittal sinus.
No adverse events
Describing the device, Dr. Weber said the electrodes or sensing elements are tiny and the body of the stent, which serves as a scaffold to support the electrodes, resembles a standard endovascular stent.
“It’s very small at the time of delivery because it’s held within the body of a catheter, but then when deployed it expands to contact the wall of the vein.”
The device transmits brain signals from the motor cortex to an electronics unit, located in a subcutaneous pocket that decodes movement signals. The machine-learning decoder is programmed as follows: When a trainer asked participants to attempt certain movements, like tapping their foot or extending their knee, the decoder analyzes nerve cell signals from those movement attempts. The decoder is able to translate movement signals into computer navigation.
The study included four patients with ALS who were paralyzed because of the disease and were trained to use the device.
A key safety endpoint was device-related serious adverse events resulting in death or increased disability during the post-implant evaluation period. Results showed all four participants successfully completed the 12-month follow-up with no serious adverse events.
Researchers also assessed target vessel patency and incidence of device migration at 3 and 12 months. Postoperative imaging showed that in all participants, the blood vessel that held the implanted device remained open and stayed in place.
Addressing the potential for blood clots, Dr. Weber said that so far there has been no sign of clotting or vascular occlusion.
“The device itself integrates well into the walls of the blood vessel over time,” he said. “Within the acute period after implantation, there’s time where the device is exposed to the blood stream, but once it becomes encapsulated and fully integrated into the blood vessel wall, the risks of thrombosis diminish.”
Greater independence
Researchers also recorded signal fidelity and stability over 12 months and use of the brain-computer interface to perform routine tasks. All participants learned to use the motor neuro-prostheses with eye tracking for computer use. Eye tracking technology helps a computer determine what a person is looking at.
Using the system, patients were able to complete tasks without help. These included text messaging and managing finances. “Since the device is fully implanted and easy for patients to use, they can use the technology independently and in their own home,” said Dr. Weber.
Although the study started with patients with ALS, those paralyzed from other causes, such as an upper spinal cord injury or brain-stem stroke could also benefit from this technology, Dr. Weber said. In addition, the technology could be expanded to broaden brain communication capabilities potentially to include robotic limbs, he said.
There’s even the potential to use this minimally invasive brain interface technology to deliver therapies like deep brain stimulation, which Dr. Weber noted is a growing field. “It’s [the] early days, but it’s a very exciting new direction for brain interface technology,” he said.
Researchers are now recruiting patients for the first U.S.-based feasibility trial of the device that will be funded by the NIH, said Dr. Weber. A limitation of the research was the study’s small size.
Advancing the field
Reached for a comment, Kevin C. Davis, an MD and PhD student in the department of biomedical engineering, University of Miami Miller School of Medicine, said this new work moves the field forward in an important way.
Dr. Davis and colleagues have shown the effectiveness of another technology used to overcome paralysis – a small portable system that facilitates hand grasp of a patient with a spinal cord injury. He reported on this DBS-based BCI system at the American Association of Neurological Surgeons (AANS) 2021 Annual Meeting.
Developing effective brain-computer interfaces, and motor neural prosthetics that avoid surgery, as the team did in this new study, is “worth exploring,” said Dr. Davis.
However, although the device used in this new study avoids cranial surgery, “sole vascular access may limit the device’s ability to reach other areas of the brain more suitable for upper-limb motor prosthetics,” he said.
“Determining how much function such a device could provide to individuals with locked-in syndrome or paralysis will be important in determining its viability as an eventual clinical tool for patients.”
The study was supported by Synchron, the maker of the device, the U.S. Defense Advanced Research Projects Agency, the Office of Naval Research, the National Health and Medical Research Council of Australia, the Australian Federal Government Foundation, and the Motor Neuron Disease Research Institute of Australia.
A version of this article first appeared on Medscape.com.
FROM AAN 2022
Antiseizure medication appears safe in pregnancy
SEATTLE – , according to new results from the Maternal Outcomes and Neurodevelopmental Effects of Antiepileptic Drugs (MONEAD) study.
The study follows results from the Neurodevelopmental Effects of Antiepileptic Drugs (NEAD) study, which found no evidence of cognitive harm in children who were exposed in utero to antiepileptic drugs. “[In the NEAD study] we followed our cohort to age 6 and found them to have actually an improvement in cognition by about 4 IQ points by the time they got to age 6,” Kimford J. Meador, MD, said during a presentation of the results of the MONEAD study at the 2022 annual meeting of the American Academy of Neurology.

Breastfeeding has health benefits for both mothers and children, including reduced risk of respiratory tract infections, atopic dermatitis, asthma, and diabetes in children, and reduced risk of diabetes, breast cancer, ovarian cancer, and postpartum depression in mothers. Despite those benefits, concerns about harms from exposure to antiepileptic drugs may prompt some women to avoid breastfeeding.
The results of NEAD and MONEAD should reassure patients, according to Dr. Meador, professor of neurology at Stanford (Calif.) University. “Given the known multiple benefits of breastfeeding … women with epilepsy should be encouraged to breastfeed,” he said.
A responsibility to ‘engage and educate’ patients
Jennifer Hopp, MD, who served as a discussant for the presentation, underscored the need for neurologists to address pregnancy with female patients of childbearing agents. “The issues may include fertility, peripartum management, and outcomes that really go through the lifespan to also include issues of menopause,” Dr. Hopp, associate professor of neurology at the University of Maryland, Baltimore, said during her presentation.
Dr. Hopp noted one study showing lower rates of breastfeeding among mothers with epilepsy. “Breastfeeding rates in women with epilepsy are strikingly lower than in women who do not have epilepsy,” said Dr. Hopp. Another study showed that women with epilepsy were less likely to sustain breastfeeding after 6 weeks.
Dr. Hopp implored neurologists to address this. “It’s our responsibility to engage and educate our patients. These data provide us messaging to our patients that the newer drugs do not adversely affect outcome independently of their other exposure, and really support well-informed choices in breastfeeding,” said Dr. Hopp.
Outdated attitudes still persist
Dr. Meador referred to the stigma that surrounds epilepsy, including some state laws that called for sterilization of women with epilepsy that lasted until the 1960s. One might think that such attitudes are gone, “but it’s still there,” said Dr. Meador, who recounted a story a colleague told him about a woman on antiseizure medication. In the hospital, the nurse told her not to breastfeed. The neurological consult told her not to breastfeed. She breastfed anyway. “Then they reported her for child neglect, and that was just a few years ago. So I think the message needs to be loud and clear that we encourage [women with epilepsy] to breastfeed because we have the known benefits, and now several studies showing clearly no adverse effects of breastfeeding while taking antiseizure medications,” said Dr. Meador.
MONEAD findings
The MONEAD study included women from 20 different sites, with 145 participating investigators. The researchers compared outcomes in 284 women with epilepsy and 87 healthy women. The maternal mean IQ was 98 among women with epilepsy (95% confidence interval [CI], 96-99), and 105 (95% CI, 102-107) among healthy women. Seventy-six percent of women with epilepsy breastfed, versus 89% of controls.
Among the study cohort, 79% of women with epilepsy were on monotherapy, and 21% were on polytherapy. Thirty-five percent received lamotrigine, 28% levetiracetam, 16% were on another monotherapy, 10% received a combination of lamotrigine and levetiracetam, and 11% received a different combination.
At age 3, there was no association between the verbal index score of the child and whether the mother had epilepsy or not (difference, 0.4; P = .770). The researchers did find associations with the mother’s IQ (0.3; P < .001), male versus female child sex (–4.9; P < .001), Hispanic or Latino ethnicity (vs. Non-Hispanic, –5.5; P < .001), mother without college degree (–7.0; P < .001), average Beck Anxiety Inventory score after birth (–0.4; P < .001), and weeks of gestational age at enrollment.
The researchers found no association between third trimester antiseizure medication blood levels and verbal index score after adjustment (–2.9; P = .149), with the exception of levetiracetam (–9.0; P = .033). “This is interesting (but) not to be overblown, because overall the children on levetiracetam did well. But it must be remembered that teratogens act in an exposure dependent manner, so we’re constantly in this balancing act of trying to make sure you get enough medication on board to stop the seizures and protect the mother and the child, and at the same time, not too much on board where we increase the risk of teratogenicity in the child,” said Dr. Meador.
The study was funded by the National Institutes of Health. Dr. Meador and Dr. Hopp have no relevant financial disclosures.
SEATTLE – , according to new results from the Maternal Outcomes and Neurodevelopmental Effects of Antiepileptic Drugs (MONEAD) study.
The study follows results from the Neurodevelopmental Effects of Antiepileptic Drugs (NEAD) study, which found no evidence of cognitive harm in children who were exposed in utero to antiepileptic drugs. “[In the NEAD study] we followed our cohort to age 6 and found them to have actually an improvement in cognition by about 4 IQ points by the time they got to age 6,” Kimford J. Meador, MD, said during a presentation of the results of the MONEAD study at the 2022 annual meeting of the American Academy of Neurology.
Breastfeeding has health benefits for both mothers and children, including reduced risk of respiratory tract infections, atopic dermatitis, asthma, and diabetes in children, and reduced risk of diabetes, breast cancer, ovarian cancer, and postpartum depression in mothers. Despite those benefits, concerns about harms from exposure to antiepileptic drugs may prompt some women to avoid breastfeeding.
The results of NEAD and MONEAD should reassure patients, according to Dr. Meador, professor of neurology at Stanford (Calif.) University. “Given the known multiple benefits of breastfeeding … women with epilepsy should be encouraged to breastfeed,” he said.
A responsibility to ‘engage and educate’ patients
Jennifer Hopp, MD, who served as a discussant for the presentation, underscored the need for neurologists to address pregnancy with female patients of childbearing agents. “The issues may include fertility, peripartum management, and outcomes that really go through the lifespan to also include issues of menopause,” Dr. Hopp, associate professor of neurology at the University of Maryland, Baltimore, said during her presentation.
Dr. Hopp noted one study showing lower rates of breastfeeding among mothers with epilepsy. “Breastfeeding rates in women with epilepsy are strikingly lower than in women who do not have epilepsy,” said Dr. Hopp. Another study showed that women with epilepsy were less likely to sustain breastfeeding after 6 weeks.
Dr. Hopp implored neurologists to address this. “It’s our responsibility to engage and educate our patients. These data provide us messaging to our patients that the newer drugs do not adversely affect outcome independently of their other exposure, and really support well-informed choices in breastfeeding,” said Dr. Hopp.
Outdated attitudes still persist
Dr. Meador referred to the stigma that surrounds epilepsy, including some state laws that called for sterilization of women with epilepsy that lasted until the 1960s. One might think that such attitudes are gone, “but it’s still there,” said Dr. Meador, who recounted a story a colleague told him about a woman on antiseizure medication. In the hospital, the nurse told her not to breastfeed. The neurological consult told her not to breastfeed. She breastfed anyway. “Then they reported her for child neglect, and that was just a few years ago. So I think the message needs to be loud and clear that we encourage [women with epilepsy] to breastfeed because we have the known benefits, and now several studies showing clearly no adverse effects of breastfeeding while taking antiseizure medications,” said Dr. Meador.
MONEAD findings
The MONEAD study included women from 20 different sites, with 145 participating investigators. The researchers compared outcomes in 284 women with epilepsy and 87 healthy women. The maternal mean IQ was 98 among women with epilepsy (95% confidence interval [CI], 96-99), and 105 (95% CI, 102-107) among healthy women. Seventy-six percent of women with epilepsy breastfed, versus 89% of controls.
Among the study cohort, 79% of women with epilepsy were on monotherapy, and 21% were on polytherapy. Thirty-five percent received lamotrigine, 28% levetiracetam, 16% were on another monotherapy, 10% received a combination of lamotrigine and levetiracetam, and 11% received a different combination.
At age 3, there was no association between the verbal index score of the child and whether the mother had epilepsy or not (difference, 0.4; P = .770). The researchers did find associations with the mother’s IQ (0.3; P < .001), male versus female child sex (–4.9; P < .001), Hispanic or Latino ethnicity (vs. Non-Hispanic, –5.5; P < .001), mother without college degree (–7.0; P < .001), average Beck Anxiety Inventory score after birth (–0.4; P < .001), and weeks of gestational age at enrollment.
The researchers found no association between third trimester antiseizure medication blood levels and verbal index score after adjustment (–2.9; P = .149), with the exception of levetiracetam (–9.0; P = .033). “This is interesting (but) not to be overblown, because overall the children on levetiracetam did well. But it must be remembered that teratogens act in an exposure dependent manner, so we’re constantly in this balancing act of trying to make sure you get enough medication on board to stop the seizures and protect the mother and the child, and at the same time, not too much on board where we increase the risk of teratogenicity in the child,” said Dr. Meador.
The study was funded by the National Institutes of Health. Dr. Meador and Dr. Hopp have no relevant financial disclosures.
SEATTLE – , according to new results from the Maternal Outcomes and Neurodevelopmental Effects of Antiepileptic Drugs (MONEAD) study.
The study follows results from the Neurodevelopmental Effects of Antiepileptic Drugs (NEAD) study, which found no evidence of cognitive harm in children who were exposed in utero to antiepileptic drugs. “[In the NEAD study] we followed our cohort to age 6 and found them to have actually an improvement in cognition by about 4 IQ points by the time they got to age 6,” Kimford J. Meador, MD, said during a presentation of the results of the MONEAD study at the 2022 annual meeting of the American Academy of Neurology.
Breastfeeding has health benefits for both mothers and children, including reduced risk of respiratory tract infections, atopic dermatitis, asthma, and diabetes in children, and reduced risk of diabetes, breast cancer, ovarian cancer, and postpartum depression in mothers. Despite those benefits, concerns about harms from exposure to antiepileptic drugs may prompt some women to avoid breastfeeding.
The results of NEAD and MONEAD should reassure patients, according to Dr. Meador, professor of neurology at Stanford (Calif.) University. “Given the known multiple benefits of breastfeeding … women with epilepsy should be encouraged to breastfeed,” he said.
A responsibility to ‘engage and educate’ patients
Jennifer Hopp, MD, who served as a discussant for the presentation, underscored the need for neurologists to address pregnancy with female patients of childbearing agents. “The issues may include fertility, peripartum management, and outcomes that really go through the lifespan to also include issues of menopause,” Dr. Hopp, associate professor of neurology at the University of Maryland, Baltimore, said during her presentation.
Dr. Hopp noted one study showing lower rates of breastfeeding among mothers with epilepsy. “Breastfeeding rates in women with epilepsy are strikingly lower than in women who do not have epilepsy,” said Dr. Hopp. Another study showed that women with epilepsy were less likely to sustain breastfeeding after 6 weeks.
Dr. Hopp implored neurologists to address this. “It’s our responsibility to engage and educate our patients. These data provide us messaging to our patients that the newer drugs do not adversely affect outcome independently of their other exposure, and really support well-informed choices in breastfeeding,” said Dr. Hopp.
Outdated attitudes still persist
Dr. Meador referred to the stigma that surrounds epilepsy, including some state laws that called for sterilization of women with epilepsy that lasted until the 1960s. One might think that such attitudes are gone, “but it’s still there,” said Dr. Meador, who recounted a story a colleague told him about a woman on antiseizure medication. In the hospital, the nurse told her not to breastfeed. The neurological consult told her not to breastfeed. She breastfed anyway. “Then they reported her for child neglect, and that was just a few years ago. So I think the message needs to be loud and clear that we encourage [women with epilepsy] to breastfeed because we have the known benefits, and now several studies showing clearly no adverse effects of breastfeeding while taking antiseizure medications,” said Dr. Meador.
MONEAD findings
The MONEAD study included women from 20 different sites, with 145 participating investigators. The researchers compared outcomes in 284 women with epilepsy and 87 healthy women. The maternal mean IQ was 98 among women with epilepsy (95% confidence interval [CI], 96-99), and 105 (95% CI, 102-107) among healthy women. Seventy-six percent of women with epilepsy breastfed, versus 89% of controls.
Among the study cohort, 79% of women with epilepsy were on monotherapy, and 21% were on polytherapy. Thirty-five percent received lamotrigine, 28% levetiracetam, 16% were on another monotherapy, 10% received a combination of lamotrigine and levetiracetam, and 11% received a different combination.
At age 3, there was no association between the verbal index score of the child and whether the mother had epilepsy or not (difference, 0.4; P = .770). The researchers did find associations with the mother’s IQ (0.3; P < .001), male versus female child sex (–4.9; P < .001), Hispanic or Latino ethnicity (vs. Non-Hispanic, –5.5; P < .001), mother without college degree (–7.0; P < .001), average Beck Anxiety Inventory score after birth (–0.4; P < .001), and weeks of gestational age at enrollment.
The researchers found no association between third trimester antiseizure medication blood levels and verbal index score after adjustment (–2.9; P = .149), with the exception of levetiracetam (–9.0; P = .033). “This is interesting (but) not to be overblown, because overall the children on levetiracetam did well. But it must be remembered that teratogens act in an exposure dependent manner, so we’re constantly in this balancing act of trying to make sure you get enough medication on board to stop the seizures and protect the mother and the child, and at the same time, not too much on board where we increase the risk of teratogenicity in the child,” said Dr. Meador.
The study was funded by the National Institutes of Health. Dr. Meador and Dr. Hopp have no relevant financial disclosures.
AT AAN 2022