User login
For MD-IQ use only
Erythema extent predicts death in cutaneous GVHD
“There is value in collecting erythema serially over time as a continuous variable on a scale of 0%-100%” to identify high-risk patients for prophylactic and preemptive treatment, say investigators led by dermatologist Emily Baumrin, MD, director of the GVHD clinic at the University of Pennsylvania, Philadelphia.
They report a study of more than 300 patients with ccGVHD, which found that the extent of skin erythema strongly predicted the risk for death from GVHD.
Of the 267 patients with cutaneous GVHD at baseline, 103 patients died, the majority without a relapse of their blood cancer.
With additional research, erythema body surface area (BSA) should be “introduced as an outcome measure in clinical practice and trials,” they conclude.
At the moment, the NIH Skin Score is commonly used for risk assessment in cutaneous GVHD, but the researchers found that erythema BSA out-predicts this score.
The investigators explain that the NIH Skin Score does incorporate erythema surface area, but it does so as a categorical variable, not a continuous variable. Among other additional factors, it also includes assessments of skin sclerosis, which the investigators found was not associated with GVHD mortality.
Overall, the composite score waters down the weight given to erythema BSA because the score is “driven by stable sclerotic features, and erythema changes are missed,” they explain.
The study was published online in JAMA Dermatology.
Study details
The study included 469 patients with chronic GVHD (cGVHD), of whom 267 (57%) had cutaneous cGVHD at enrollment and 89 (19%) developed skin involvement subsequently.
All of the patients were on systemic immunosuppression for GVHD after allogeneic stem cell transplants for various blood cancers.
They were enrolled from 2007 through 2012 at nine U.S. medical centers – all members of the Chronic Graft Versus Host Disease Consortium – and they were followed until 2018.
Erythema BSA and NIH Skin Score were assessed at baseline and then every 3-6 months. Erythema was the first manifestation of skin involvement in the majority of patients, with a median surface area involvement of 11% at baseline.
The study team found that the extent of erythema at first follow-up visit was associated with both nonrelapse mortality (hazard ratio, 1.33 per 10% BSA increase; P < .001) and overall survival (HR, 1.28 per 10% BSA increase; P < .001), whereas extent of sclerotic skin involvement was not associated with either.
Participants in the study were predominantly White. The investigators note that “BSA assessments of erythema may be less reliable in patients with darker skin.”
The work was funded by the Department of Veterans Affairs and the National Institutes of Health. Dr. Baumrin had no disclosures; one coauthor is an employee of CorEvitas, and two others reported grants/adviser fees from several companies, including Janssen, Mallinckrodt, and Pfizer.
A version of this article first appeared on Medscape.com.
“There is value in collecting erythema serially over time as a continuous variable on a scale of 0%-100%” to identify high-risk patients for prophylactic and preemptive treatment, say investigators led by dermatologist Emily Baumrin, MD, director of the GVHD clinic at the University of Pennsylvania, Philadelphia.
They report a study of more than 300 patients with ccGVHD, which found that the extent of skin erythema strongly predicted the risk for death from GVHD.
Of the 267 patients with cutaneous GVHD at baseline, 103 patients died, the majority without a relapse of their blood cancer.
With additional research, erythema body surface area (BSA) should be “introduced as an outcome measure in clinical practice and trials,” they conclude.
At the moment, the NIH Skin Score is commonly used for risk assessment in cutaneous GVHD, but the researchers found that erythema BSA out-predicts this score.
The investigators explain that the NIH Skin Score does incorporate erythema surface area, but it does so as a categorical variable, not a continuous variable. Among other additional factors, it also includes assessments of skin sclerosis, which the investigators found was not associated with GVHD mortality.
Overall, the composite score waters down the weight given to erythema BSA because the score is “driven by stable sclerotic features, and erythema changes are missed,” they explain.
The study was published online in JAMA Dermatology.
Study details
The study included 469 patients with chronic GVHD (cGVHD), of whom 267 (57%) had cutaneous cGVHD at enrollment and 89 (19%) developed skin involvement subsequently.
All of the patients were on systemic immunosuppression for GVHD after allogeneic stem cell transplants for various blood cancers.
They were enrolled from 2007 through 2012 at nine U.S. medical centers – all members of the Chronic Graft Versus Host Disease Consortium – and they were followed until 2018.
Erythema BSA and NIH Skin Score were assessed at baseline and then every 3-6 months. Erythema was the first manifestation of skin involvement in the majority of patients, with a median surface area involvement of 11% at baseline.
The study team found that the extent of erythema at first follow-up visit was associated with both nonrelapse mortality (hazard ratio, 1.33 per 10% BSA increase; P < .001) and overall survival (HR, 1.28 per 10% BSA increase; P < .001), whereas extent of sclerotic skin involvement was not associated with either.
Participants in the study were predominantly White. The investigators note that “BSA assessments of erythema may be less reliable in patients with darker skin.”
The work was funded by the Department of Veterans Affairs and the National Institutes of Health. Dr. Baumrin had no disclosures; one coauthor is an employee of CorEvitas, and two others reported grants/adviser fees from several companies, including Janssen, Mallinckrodt, and Pfizer.
A version of this article first appeared on Medscape.com.
“There is value in collecting erythema serially over time as a continuous variable on a scale of 0%-100%” to identify high-risk patients for prophylactic and preemptive treatment, say investigators led by dermatologist Emily Baumrin, MD, director of the GVHD clinic at the University of Pennsylvania, Philadelphia.
They report a study of more than 300 patients with ccGVHD, which found that the extent of skin erythema strongly predicted the risk for death from GVHD.
Of the 267 patients with cutaneous GVHD at baseline, 103 patients died, the majority without a relapse of their blood cancer.
With additional research, erythema body surface area (BSA) should be “introduced as an outcome measure in clinical practice and trials,” they conclude.
At the moment, the NIH Skin Score is commonly used for risk assessment in cutaneous GVHD, but the researchers found that erythema BSA out-predicts this score.
The investigators explain that the NIH Skin Score does incorporate erythema surface area, but it does so as a categorical variable, not a continuous variable. Among other additional factors, it also includes assessments of skin sclerosis, which the investigators found was not associated with GVHD mortality.
Overall, the composite score waters down the weight given to erythema BSA because the score is “driven by stable sclerotic features, and erythema changes are missed,” they explain.
The study was published online in JAMA Dermatology.
Study details
The study included 469 patients with chronic GVHD (cGVHD), of whom 267 (57%) had cutaneous cGVHD at enrollment and 89 (19%) developed skin involvement subsequently.
All of the patients were on systemic immunosuppression for GVHD after allogeneic stem cell transplants for various blood cancers.
They were enrolled from 2007 through 2012 at nine U.S. medical centers – all members of the Chronic Graft Versus Host Disease Consortium – and they were followed until 2018.
Erythema BSA and NIH Skin Score were assessed at baseline and then every 3-6 months. Erythema was the first manifestation of skin involvement in the majority of patients, with a median surface area involvement of 11% at baseline.
The study team found that the extent of erythema at first follow-up visit was associated with both nonrelapse mortality (hazard ratio, 1.33 per 10% BSA increase; P < .001) and overall survival (HR, 1.28 per 10% BSA increase; P < .001), whereas extent of sclerotic skin involvement was not associated with either.
Participants in the study were predominantly White. The investigators note that “BSA assessments of erythema may be less reliable in patients with darker skin.”
The work was funded by the Department of Veterans Affairs and the National Institutes of Health. Dr. Baumrin had no disclosures; one coauthor is an employee of CorEvitas, and two others reported grants/adviser fees from several companies, including Janssen, Mallinckrodt, and Pfizer.
A version of this article first appeared on Medscape.com.
Inspector General Finds Security Vulnerabilities and Risks at VA Medical Facilities
In 2022, the US Department of Veterans Affairs (VA) Office of Inspector General (OIG) received 36 separate serious incident reports involving 32 medical facilities—including a bomb threat. In response to those reports, OIG teams of auditors and criminal investigators visited 70 VA medical facilities in September 2022 to assess security and to issue a formal report.
Noting that VA policy includes an “extensive list of security safeguards” for medical facilities to implement, the OIG focused its review on those that “a person with a reasonable level of security knowledge could assess.” According to their report, released in February, they identified a variety of security vulnerabilities and deficiencies, ranging from shortages of police officers to radios with poor signal strength.
For one, the OIG says, the facilities were designed to provide a welcoming environment, which means the public can enter the grounds freely at many different points. But the open-campus design makes it more difficult to balance security with easy and prompt access for patients. Consequently, the OIG says, “threats may originate from many locations within the medical facility campus itself or in the nearby community.”
Walking around the perimeters of the facility buildings, the OIG teams assessed the security level of 2960 public and nonpublic access doors. They found that 87% of public doors did not have an active security presence, and of those, 23% also did not have a security camera. Moreover, 17% of nonpublic doors were unlocked; 97% of those did not have a security presence, and 43% did not have a security camera. Even more concerning: Some of those doors led to sensitive or restricted facility areas. For example, at one midwestern facility, an unlocked nonpublic access door led to the surgical intensive care unit.
The OIG teams also assessed training records for 170 police officers across the 70 facilities and found that nearly all officers were compliant with training requirements. Most respondents also reported they received adequate training to perform their job duties and provided numerous positive indicators. Well trained or not, though, a notable problem in maintaining security, the OIG teams found, was there simply weren’t enough officers.
The OIG has repeatedly issued reports on significant police officer staffing shortages since at least 2018. VA police officers are not only empowered to make arrests, carry firearms while on duty, and investigate criminal activity within VA’s jurisdiction, but also assist individuals on medical campuses “in myriad ways,” the OIG notes. Staffing shortages are likely to compromise overall facility security, morale, and staff retention and underscore the need for maintaining communication with local law enforcement agencies for assistance, the OIG report points out.
In the OIG surveys, security personnel often noted they were understaffed. Although VA guidance calls for at least 2 VA police officers on duty at all times, 21% of respondents said they were aware of a duty shift during which minimum police staffing requirements were not met. About 37% of respondents expressed concerns about the physical security at their facilities. Some pointed out that the lack of VA police on duty could make it difficult to respond to threats like an active shooter.
In May 2022, the VA issued a directive that established minimum police coverage at medical facilities, as well as a police officer staffing decision tool to help determine appropriate officer levels. It required facilities to have an active security presence in their emergency departments around-the-clock by May 2023. As of September 2022, 58% of the facilities’ emergency departments did not yet have a visible security presence.
The teams also found issues with security devices: 19% of all cameras were not functional; at 24 facilities, more than 20% of the cameras were not working. A few facilities had “highly functional” systems that allowed personnel to monitor the campus thoroughly and even search for specific individuals—but they weren’t always operable.
At one western facility, it came down to a problem that would be frustrating at any time, but alarming for security management: Security personnel could not access the monitoring system because the required security certificates had expired, and no one knew the administrative password. If the system went offline, the OIG team was told, no one could fix the problem without password access. Neither VA’s Office of Information and Technology nor the contractor for the facility’s cameras could override the administrative password.
On the bright side, the OIG teams found that camera video feeds were being actively surveilled by security personnel at 60 of 70 facilities. All but 1 site kept camera footage for an average of 2 weeks or more.
VA policy states that, in addition to at least 2 intermediate weapons (such as batons and pepper spray) uniformed officers must always be issued radios for use while on duty. Survey respondents generally indicated they received their equipment and that it was adequate, but 15% said theirs lacked functionality, such as battery life and signal strength.
Based on the teams’ findings, the OIG made 6 recommendations: (1) delegating a responsible official to monitor and report monthly on facilities’ security-related vacancies; (2) authorizing sufficient staff to inspect VA police forces per the OIG’s 2018 unimplemented recommendation; (3) ensuring medical facility directors appropriately assess VA police staffing needs, authorize associated positions, and leverage available mechanisms to fill vacancies; (4) committing sufficient resources to ensure that facility security measures are adequate, current, and operational; (5) directing Veterans Integrated Services Network police chiefs, in coordination with medical facility directors, facility police chiefs, and facility emergency management leaders, to present a plan to remedy identified security weaknesses; and (6) establishing policy that standardizes the review and retention requirements for facility security camera footage.
The VA concurred with all recommendations and submitted corrective action plans.
In 2022, the US Department of Veterans Affairs (VA) Office of Inspector General (OIG) received 36 separate serious incident reports involving 32 medical facilities—including a bomb threat. In response to those reports, OIG teams of auditors and criminal investigators visited 70 VA medical facilities in September 2022 to assess security and to issue a formal report.
Noting that VA policy includes an “extensive list of security safeguards” for medical facilities to implement, the OIG focused its review on those that “a person with a reasonable level of security knowledge could assess.” According to their report, released in February, they identified a variety of security vulnerabilities and deficiencies, ranging from shortages of police officers to radios with poor signal strength.
For one, the OIG says, the facilities were designed to provide a welcoming environment, which means the public can enter the grounds freely at many different points. But the open-campus design makes it more difficult to balance security with easy and prompt access for patients. Consequently, the OIG says, “threats may originate from many locations within the medical facility campus itself or in the nearby community.”
Walking around the perimeters of the facility buildings, the OIG teams assessed the security level of 2960 public and nonpublic access doors. They found that 87% of public doors did not have an active security presence, and of those, 23% also did not have a security camera. Moreover, 17% of nonpublic doors were unlocked; 97% of those did not have a security presence, and 43% did not have a security camera. Even more concerning: Some of those doors led to sensitive or restricted facility areas. For example, at one midwestern facility, an unlocked nonpublic access door led to the surgical intensive care unit.
The OIG teams also assessed training records for 170 police officers across the 70 facilities and found that nearly all officers were compliant with training requirements. Most respondents also reported they received adequate training to perform their job duties and provided numerous positive indicators. Well trained or not, though, a notable problem in maintaining security, the OIG teams found, was there simply weren’t enough officers.
The OIG has repeatedly issued reports on significant police officer staffing shortages since at least 2018. VA police officers are not only empowered to make arrests, carry firearms while on duty, and investigate criminal activity within VA’s jurisdiction, but also assist individuals on medical campuses “in myriad ways,” the OIG notes. Staffing shortages are likely to compromise overall facility security, morale, and staff retention and underscore the need for maintaining communication with local law enforcement agencies for assistance, the OIG report points out.
In the OIG surveys, security personnel often noted they were understaffed. Although VA guidance calls for at least 2 VA police officers on duty at all times, 21% of respondents said they were aware of a duty shift during which minimum police staffing requirements were not met. About 37% of respondents expressed concerns about the physical security at their facilities. Some pointed out that the lack of VA police on duty could make it difficult to respond to threats like an active shooter.
In May 2022, the VA issued a directive that established minimum police coverage at medical facilities, as well as a police officer staffing decision tool to help determine appropriate officer levels. It required facilities to have an active security presence in their emergency departments around-the-clock by May 2023. As of September 2022, 58% of the facilities’ emergency departments did not yet have a visible security presence.
The teams also found issues with security devices: 19% of all cameras were not functional; at 24 facilities, more than 20% of the cameras were not working. A few facilities had “highly functional” systems that allowed personnel to monitor the campus thoroughly and even search for specific individuals—but they weren’t always operable.
At one western facility, it came down to a problem that would be frustrating at any time, but alarming for security management: Security personnel could not access the monitoring system because the required security certificates had expired, and no one knew the administrative password. If the system went offline, the OIG team was told, no one could fix the problem without password access. Neither VA’s Office of Information and Technology nor the contractor for the facility’s cameras could override the administrative password.
On the bright side, the OIG teams found that camera video feeds were being actively surveilled by security personnel at 60 of 70 facilities. All but 1 site kept camera footage for an average of 2 weeks or more.
VA policy states that, in addition to at least 2 intermediate weapons (such as batons and pepper spray) uniformed officers must always be issued radios for use while on duty. Survey respondents generally indicated they received their equipment and that it was adequate, but 15% said theirs lacked functionality, such as battery life and signal strength.
Based on the teams’ findings, the OIG made 6 recommendations: (1) delegating a responsible official to monitor and report monthly on facilities’ security-related vacancies; (2) authorizing sufficient staff to inspect VA police forces per the OIG’s 2018 unimplemented recommendation; (3) ensuring medical facility directors appropriately assess VA police staffing needs, authorize associated positions, and leverage available mechanisms to fill vacancies; (4) committing sufficient resources to ensure that facility security measures are adequate, current, and operational; (5) directing Veterans Integrated Services Network police chiefs, in coordination with medical facility directors, facility police chiefs, and facility emergency management leaders, to present a plan to remedy identified security weaknesses; and (6) establishing policy that standardizes the review and retention requirements for facility security camera footage.
The VA concurred with all recommendations and submitted corrective action plans.
In 2022, the US Department of Veterans Affairs (VA) Office of Inspector General (OIG) received 36 separate serious incident reports involving 32 medical facilities—including a bomb threat. In response to those reports, OIG teams of auditors and criminal investigators visited 70 VA medical facilities in September 2022 to assess security and to issue a formal report.
Noting that VA policy includes an “extensive list of security safeguards” for medical facilities to implement, the OIG focused its review on those that “a person with a reasonable level of security knowledge could assess.” According to their report, released in February, they identified a variety of security vulnerabilities and deficiencies, ranging from shortages of police officers to radios with poor signal strength.
For one, the OIG says, the facilities were designed to provide a welcoming environment, which means the public can enter the grounds freely at many different points. But the open-campus design makes it more difficult to balance security with easy and prompt access for patients. Consequently, the OIG says, “threats may originate from many locations within the medical facility campus itself or in the nearby community.”
Walking around the perimeters of the facility buildings, the OIG teams assessed the security level of 2960 public and nonpublic access doors. They found that 87% of public doors did not have an active security presence, and of those, 23% also did not have a security camera. Moreover, 17% of nonpublic doors were unlocked; 97% of those did not have a security presence, and 43% did not have a security camera. Even more concerning: Some of those doors led to sensitive or restricted facility areas. For example, at one midwestern facility, an unlocked nonpublic access door led to the surgical intensive care unit.
The OIG teams also assessed training records for 170 police officers across the 70 facilities and found that nearly all officers were compliant with training requirements. Most respondents also reported they received adequate training to perform their job duties and provided numerous positive indicators. Well trained or not, though, a notable problem in maintaining security, the OIG teams found, was there simply weren’t enough officers.
The OIG has repeatedly issued reports on significant police officer staffing shortages since at least 2018. VA police officers are not only empowered to make arrests, carry firearms while on duty, and investigate criminal activity within VA’s jurisdiction, but also assist individuals on medical campuses “in myriad ways,” the OIG notes. Staffing shortages are likely to compromise overall facility security, morale, and staff retention and underscore the need for maintaining communication with local law enforcement agencies for assistance, the OIG report points out.
In the OIG surveys, security personnel often noted they were understaffed. Although VA guidance calls for at least 2 VA police officers on duty at all times, 21% of respondents said they were aware of a duty shift during which minimum police staffing requirements were not met. About 37% of respondents expressed concerns about the physical security at their facilities. Some pointed out that the lack of VA police on duty could make it difficult to respond to threats like an active shooter.
In May 2022, the VA issued a directive that established minimum police coverage at medical facilities, as well as a police officer staffing decision tool to help determine appropriate officer levels. It required facilities to have an active security presence in their emergency departments around-the-clock by May 2023. As of September 2022, 58% of the facilities’ emergency departments did not yet have a visible security presence.
The teams also found issues with security devices: 19% of all cameras were not functional; at 24 facilities, more than 20% of the cameras were not working. A few facilities had “highly functional” systems that allowed personnel to monitor the campus thoroughly and even search for specific individuals—but they weren’t always operable.
At one western facility, it came down to a problem that would be frustrating at any time, but alarming for security management: Security personnel could not access the monitoring system because the required security certificates had expired, and no one knew the administrative password. If the system went offline, the OIG team was told, no one could fix the problem without password access. Neither VA’s Office of Information and Technology nor the contractor for the facility’s cameras could override the administrative password.
On the bright side, the OIG teams found that camera video feeds were being actively surveilled by security personnel at 60 of 70 facilities. All but 1 site kept camera footage for an average of 2 weeks or more.
VA policy states that, in addition to at least 2 intermediate weapons (such as batons and pepper spray) uniformed officers must always be issued radios for use while on duty. Survey respondents generally indicated they received their equipment and that it was adequate, but 15% said theirs lacked functionality, such as battery life and signal strength.
Based on the teams’ findings, the OIG made 6 recommendations: (1) delegating a responsible official to monitor and report monthly on facilities’ security-related vacancies; (2) authorizing sufficient staff to inspect VA police forces per the OIG’s 2018 unimplemented recommendation; (3) ensuring medical facility directors appropriately assess VA police staffing needs, authorize associated positions, and leverage available mechanisms to fill vacancies; (4) committing sufficient resources to ensure that facility security measures are adequate, current, and operational; (5) directing Veterans Integrated Services Network police chiefs, in coordination with medical facility directors, facility police chiefs, and facility emergency management leaders, to present a plan to remedy identified security weaknesses; and (6) establishing policy that standardizes the review and retention requirements for facility security camera footage.
The VA concurred with all recommendations and submitted corrective action plans.
Venetoclax shows promise for r/r hairy cell leukemia
Venetoclax is already approved for adults with chronic lymphocytic leukemia, small lymphocytic leukemia, and as part of a treatment combination in certain patients with acute myeloid leukemia.
The new findings suggest that the drug could also be a chemotherapy-free treatment option for HCL patients after the failure of multiple prior lines of therapy, including vemurafenib plus rituximab, the investigators wrote in a letter to the editor published in the New England Journal of Medicine.
Treatment options for such patients are limited, they noted.
Enrico Tiacci, MD, of the University of Perugia (Italy), and colleagues decided to explore the use of venetoclax in this patient population after reports of in vitro findings showing a possible benefit.
The investigators administered the drug off-label to six patients who had received vemurafenib plus rituximab as their most recent prior therapy; one was resistant and five relapsed after that therapy, they reported. Venetoclax was delivered in 29-day cycles.
After 6 or 12 cycles, two patients experienced complete remission with minimal residual disease (MRD), and one had partial remission, although each had incomplete platelet recovery.
Adding rituximab at a dose of 375 mg per square meter of body-surface area for three to eight cycles improved the depth of response in a patient who had a previous minor response, further reduced MRD in one who had a complete remission to venetoclax, and led to hematologic remission in one who had no response to venetoclax, they noted.
Progression-free survival ranged from 23 to 53-plus months in all five patients who did not have early progression and was similar or better than PFS seen after vemurafenib plus rituximab.
The main toxic effect of venetoclax was worsening of baseline neutropenia, which was sometimes complicated by infections or febrile neutropenia and was managed by dose reductions and granulocyte colony-stimulating factor.
“Thus, venetoclax with or without rituximab may serve as a safe and effective salvage option after failure of vemurafenib plus rituximab treatment, especially in patients who do not require a rapid recovery of blood count,” they concluded.
The study was supported by grants from Fondazione Associazione Italiana per la Ricerca sul Cancro and the Italian Ministry of Health.
A version of this article first appeared on Medscape.com.
Venetoclax is already approved for adults with chronic lymphocytic leukemia, small lymphocytic leukemia, and as part of a treatment combination in certain patients with acute myeloid leukemia.
The new findings suggest that the drug could also be a chemotherapy-free treatment option for HCL patients after the failure of multiple prior lines of therapy, including vemurafenib plus rituximab, the investigators wrote in a letter to the editor published in the New England Journal of Medicine.
Treatment options for such patients are limited, they noted.
Enrico Tiacci, MD, of the University of Perugia (Italy), and colleagues decided to explore the use of venetoclax in this patient population after reports of in vitro findings showing a possible benefit.
The investigators administered the drug off-label to six patients who had received vemurafenib plus rituximab as their most recent prior therapy; one was resistant and five relapsed after that therapy, they reported. Venetoclax was delivered in 29-day cycles.
After 6 or 12 cycles, two patients experienced complete remission with minimal residual disease (MRD), and one had partial remission, although each had incomplete platelet recovery.
Adding rituximab at a dose of 375 mg per square meter of body-surface area for three to eight cycles improved the depth of response in a patient who had a previous minor response, further reduced MRD in one who had a complete remission to venetoclax, and led to hematologic remission in one who had no response to venetoclax, they noted.
Progression-free survival ranged from 23 to 53-plus months in all five patients who did not have early progression and was similar or better than PFS seen after vemurafenib plus rituximab.
The main toxic effect of venetoclax was worsening of baseline neutropenia, which was sometimes complicated by infections or febrile neutropenia and was managed by dose reductions and granulocyte colony-stimulating factor.
“Thus, venetoclax with or without rituximab may serve as a safe and effective salvage option after failure of vemurafenib plus rituximab treatment, especially in patients who do not require a rapid recovery of blood count,” they concluded.
The study was supported by grants from Fondazione Associazione Italiana per la Ricerca sul Cancro and the Italian Ministry of Health.
A version of this article first appeared on Medscape.com.
Venetoclax is already approved for adults with chronic lymphocytic leukemia, small lymphocytic leukemia, and as part of a treatment combination in certain patients with acute myeloid leukemia.
The new findings suggest that the drug could also be a chemotherapy-free treatment option for HCL patients after the failure of multiple prior lines of therapy, including vemurafenib plus rituximab, the investigators wrote in a letter to the editor published in the New England Journal of Medicine.
Treatment options for such patients are limited, they noted.
Enrico Tiacci, MD, of the University of Perugia (Italy), and colleagues decided to explore the use of venetoclax in this patient population after reports of in vitro findings showing a possible benefit.
The investigators administered the drug off-label to six patients who had received vemurafenib plus rituximab as their most recent prior therapy; one was resistant and five relapsed after that therapy, they reported. Venetoclax was delivered in 29-day cycles.
After 6 or 12 cycles, two patients experienced complete remission with minimal residual disease (MRD), and one had partial remission, although each had incomplete platelet recovery.
Adding rituximab at a dose of 375 mg per square meter of body-surface area for three to eight cycles improved the depth of response in a patient who had a previous minor response, further reduced MRD in one who had a complete remission to venetoclax, and led to hematologic remission in one who had no response to venetoclax, they noted.
Progression-free survival ranged from 23 to 53-plus months in all five patients who did not have early progression and was similar or better than PFS seen after vemurafenib plus rituximab.
The main toxic effect of venetoclax was worsening of baseline neutropenia, which was sometimes complicated by infections or febrile neutropenia and was managed by dose reductions and granulocyte colony-stimulating factor.
“Thus, venetoclax with or without rituximab may serve as a safe and effective salvage option after failure of vemurafenib plus rituximab treatment, especially in patients who do not require a rapid recovery of blood count,” they concluded.
The study was supported by grants from Fondazione Associazione Italiana per la Ricerca sul Cancro and the Italian Ministry of Health.
A version of this article first appeared on Medscape.com.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Cancer clinical trials: Can industry stack the deck?
A year before the COVID-19 pandemic began, a team of clinical statisticians at the University of Texas MD Anderson Cancer Center sat together in small office for a year, painstakingly hand coding data from the U.S. clinical trials database, www.clinicaltrials.gov.

“We found marked disparities across different disease sites. ... The patients that are enrolling on studies are markedly younger than the average patient seen in the population with those same conditions,” said team leader Ethan Ludmir, MD, assistant professor, Division of Radiation Oncology at the University of Texas.
And this age disparity was significantly greater in industry-funded trials.
Researchers have known for 20 years that cancer trial participants are not representative of the wider cancer population, and numerous government guidance documents have been issued on the matter. However, this Texas team’s findings were the first unambiguous evidence that pharmaceutical companies seem to be selecting younger patients to test their drugs.
“If we’re being generous then perhaps the answer is: They’re looking for some element of homogeneity, which is to say they don’t want competing risks to make the signal-to-noise ratio uninterpretable,” said Dr. Ludmir.
Dr. Laura Bothwell, PhD, assistant professor, Yale School of Public Health, recently coauthored a 259-page consensus report for the National Academies of Sciences, Engineering and Medicine on how to increase the research involvement of under-represented groups.
Dr. Bothwell said, “The problem with industry funded research is that ... it’s an inevitable conflict of interest that exists. They want the research to show that their products work. And older populations ... have a lot more complications, which leads to potentially less favorable results.”
The MD Anderson findings were published in JAMA Oncology. “That was the starting point in our journey,” said Dr. Ludmir. For the next 3 years, the researchers mined their painstakingly constructed database to understand what was preventing greater numbers of older patients from enrollment in cancer trials.
Meanwhile, answers were coming from elsewhere. In parallel with the work at MD Anderson, a team in California led by Mina Sedrak, MD, a medical oncologist at the City of Hope National Medical Center, had also started investigating age disparities in clinical trials.

Dr. Sedrak, who also serves as deputy director of Clinical Trials at the Center for Cancer and Aging, said he had become increasingly concerned that he did not have adequate information on new cancer therapies for his older patients.
“I was caring for a large number of people who were ... older adults,” said Dr. Sedrak, “But the data that was being used to get the standard-of-care treatment for cancer did not include older adults. And so there was this lack of applicability.”
He summed up the challenges in a 2021 review paper: “Most of what we know about cancer therapeutics is based on clinical trials conducted in younger, healthier patients.”
By 2030, it is estimated that 70% of all new cancer diagnoses will be in patients 65 years old and older. By contrast, patients over age 65 still account for only 40% of patients in cancer trials registered with the FDA (2015 figures) and older adults make up only 44% of participants in practice-changing cancer trials, according to a 2022 study.
So what is going on? Are studies specifically designed to squeeze out older patients?
Surprisingly, patients are not being kept out of trials by formal age limits, according to Dr. Ludmir. His team found that only 10% of phase 3 trials over the past 30 years had an upper limit for age, and age restrictions have been dropping by 1% a year. (For example, 16% of trials that enrolled in 2002-2005 had an upper age limit, compared with just 8% of trials that started in 2010-2014.)
Dr. Sedrak’s team found that “clinician bias” may be a factor, a situation in which trial investigators – particularly academic oncologists – are subconsciously picking younger, healthier patients for trials and excluding older, sicker patients to protect them from drug toxicities.
Dr. Ludmir said this was understandable, especially in the case of industry-driven trials, which tend to have demanding endpoints and “an overall posture of more treatment aggressiveness.”
“These are typically not trials where they’re saying, `Hey, if we add acupuncture ... are we going to see improved patient reported outcomes?’” Dr. Ludmir explained. “You’re asking ... I’ve got this cocktail of two pretty rough chemos: I want to see what happens if I add an immunotherapy to that. If I’m the clinician in clinic, I might reasonably, subconsciously, say, is the 75-year-old really who I want on this?”
What about patient bias? Perhaps fewer older patients wish to join clinical trials?
Not so, at least not at community cancer centers, said Dr. Sedrak. His team’s analysis of the National Cancer Institute Community Oncology Research Program database for 2016-2019 revealed that older patients were just as keen as the younger patients to participate in trials (68% of patients aged 50-69 years and 65% of patients 70+; P = .28).
However, drug companies may be excluding older patients by more subtle means. One-fifth of patients over 65 have had a prior cancer. Dr. Ludmir and coauthor Roshal Patel, MD, used their hand-coded www.clinicaltrials.gov database to look at prior malignancy exclusion criteria (PMEC). The analysis found “pervasive utilization” of PMEC in phase 3 trials, cropping up in 41% of studies over the past 30 years.
PMEC was significantly associated with age disparities and was significantly more common in industry-funded trials.
When asked whether PMEC are “age restriction by stealth” on the part of drug companies, Dr. Ludmir was reluctant to assign blame, but stood by his data: “The wider you restrict people in terms of having a prior cancer, the wider the age disparities in the subsequent studies, which to me is about as strong, in terms of causal understanding of these phenomena, as you can reasonably get at this level.”
In March the FDA released a guidance document titled Inclusion of Older Adults in Cancer Clinical Trials. However, its recommendations are “nonbinding” and “do not have the force and effect of law.”
To fix the issues, said Dr. Sedrak, the FDA must be given teeth.
“Okay, you write guidelines,” he said. “But if you don’t actually hold people accountable to following the guidelines, how are we going to implement and make sure that we’re transforming policy into action?”
Dr. Bothwell of Yale’s School of Public Health agreed. “Accountability has been the weakest link for decades now.”
She concluded, “In medicine there’s a tendency to believe that a therapy, because it exists and it has been tested and it’s shown some efficacy, it’s useful. But we don’t know the answer to that question unless we have statistically valid research in the population that we’re using it in.”
Dr. Bothwell and Dr. Ludmir report no conflicts of interest. In his publications, Dr. Sedrak reports industry grants from Seattle Genetics, Eli Lilly, Novartis, and Pfizer Foundation.
A year before the COVID-19 pandemic began, a team of clinical statisticians at the University of Texas MD Anderson Cancer Center sat together in small office for a year, painstakingly hand coding data from the U.S. clinical trials database, www.clinicaltrials.gov.
“We found marked disparities across different disease sites. ... The patients that are enrolling on studies are markedly younger than the average patient seen in the population with those same conditions,” said team leader Ethan Ludmir, MD, assistant professor, Division of Radiation Oncology at the University of Texas.
And this age disparity was significantly greater in industry-funded trials.
Researchers have known for 20 years that cancer trial participants are not representative of the wider cancer population, and numerous government guidance documents have been issued on the matter. However, this Texas team’s findings were the first unambiguous evidence that pharmaceutical companies seem to be selecting younger patients to test their drugs.
“If we’re being generous then perhaps the answer is: They’re looking for some element of homogeneity, which is to say they don’t want competing risks to make the signal-to-noise ratio uninterpretable,” said Dr. Ludmir.
Dr. Laura Bothwell, PhD, assistant professor, Yale School of Public Health, recently coauthored a 259-page consensus report for the National Academies of Sciences, Engineering and Medicine on how to increase the research involvement of under-represented groups.
Dr. Bothwell said, “The problem with industry funded research is that ... it’s an inevitable conflict of interest that exists. They want the research to show that their products work. And older populations ... have a lot more complications, which leads to potentially less favorable results.”
The MD Anderson findings were published in JAMA Oncology. “That was the starting point in our journey,” said Dr. Ludmir. For the next 3 years, the researchers mined their painstakingly constructed database to understand what was preventing greater numbers of older patients from enrollment in cancer trials.
Meanwhile, answers were coming from elsewhere. In parallel with the work at MD Anderson, a team in California led by Mina Sedrak, MD, a medical oncologist at the City of Hope National Medical Center, had also started investigating age disparities in clinical trials.
Dr. Sedrak, who also serves as deputy director of Clinical Trials at the Center for Cancer and Aging, said he had become increasingly concerned that he did not have adequate information on new cancer therapies for his older patients.
“I was caring for a large number of people who were ... older adults,” said Dr. Sedrak, “But the data that was being used to get the standard-of-care treatment for cancer did not include older adults. And so there was this lack of applicability.”
He summed up the challenges in a 2021 review paper: “Most of what we know about cancer therapeutics is based on clinical trials conducted in younger, healthier patients.”
By 2030, it is estimated that 70% of all new cancer diagnoses will be in patients 65 years old and older. By contrast, patients over age 65 still account for only 40% of patients in cancer trials registered with the FDA (2015 figures) and older adults make up only 44% of participants in practice-changing cancer trials, according to a 2022 study.
So what is going on? Are studies specifically designed to squeeze out older patients?
Surprisingly, patients are not being kept out of trials by formal age limits, according to Dr. Ludmir. His team found that only 10% of phase 3 trials over the past 30 years had an upper limit for age, and age restrictions have been dropping by 1% a year. (For example, 16% of trials that enrolled in 2002-2005 had an upper age limit, compared with just 8% of trials that started in 2010-2014.)
Dr. Sedrak’s team found that “clinician bias” may be a factor, a situation in which trial investigators – particularly academic oncologists – are subconsciously picking younger, healthier patients for trials and excluding older, sicker patients to protect them from drug toxicities.
Dr. Ludmir said this was understandable, especially in the case of industry-driven trials, which tend to have demanding endpoints and “an overall posture of more treatment aggressiveness.”
“These are typically not trials where they’re saying, `Hey, if we add acupuncture ... are we going to see improved patient reported outcomes?’” Dr. Ludmir explained. “You’re asking ... I’ve got this cocktail of two pretty rough chemos: I want to see what happens if I add an immunotherapy to that. If I’m the clinician in clinic, I might reasonably, subconsciously, say, is the 75-year-old really who I want on this?”
What about patient bias? Perhaps fewer older patients wish to join clinical trials?
Not so, at least not at community cancer centers, said Dr. Sedrak. His team’s analysis of the National Cancer Institute Community Oncology Research Program database for 2016-2019 revealed that older patients were just as keen as the younger patients to participate in trials (68% of patients aged 50-69 years and 65% of patients 70+; P = .28).
However, drug companies may be excluding older patients by more subtle means. One-fifth of patients over 65 have had a prior cancer. Dr. Ludmir and coauthor Roshal Patel, MD, used their hand-coded www.clinicaltrials.gov database to look at prior malignancy exclusion criteria (PMEC). The analysis found “pervasive utilization” of PMEC in phase 3 trials, cropping up in 41% of studies over the past 30 years.
PMEC was significantly associated with age disparities and was significantly more common in industry-funded trials.
When asked whether PMEC are “age restriction by stealth” on the part of drug companies, Dr. Ludmir was reluctant to assign blame, but stood by his data: “The wider you restrict people in terms of having a prior cancer, the wider the age disparities in the subsequent studies, which to me is about as strong, in terms of causal understanding of these phenomena, as you can reasonably get at this level.”
In March the FDA released a guidance document titled Inclusion of Older Adults in Cancer Clinical Trials. However, its recommendations are “nonbinding” and “do not have the force and effect of law.”
To fix the issues, said Dr. Sedrak, the FDA must be given teeth.
“Okay, you write guidelines,” he said. “But if you don’t actually hold people accountable to following the guidelines, how are we going to implement and make sure that we’re transforming policy into action?”
Dr. Bothwell of Yale’s School of Public Health agreed. “Accountability has been the weakest link for decades now.”
She concluded, “In medicine there’s a tendency to believe that a therapy, because it exists and it has been tested and it’s shown some efficacy, it’s useful. But we don’t know the answer to that question unless we have statistically valid research in the population that we’re using it in.”
Dr. Bothwell and Dr. Ludmir report no conflicts of interest. In his publications, Dr. Sedrak reports industry grants from Seattle Genetics, Eli Lilly, Novartis, and Pfizer Foundation.
A year before the COVID-19 pandemic began, a team of clinical statisticians at the University of Texas MD Anderson Cancer Center sat together in small office for a year, painstakingly hand coding data from the U.S. clinical trials database, www.clinicaltrials.gov.
“We found marked disparities across different disease sites. ... The patients that are enrolling on studies are markedly younger than the average patient seen in the population with those same conditions,” said team leader Ethan Ludmir, MD, assistant professor, Division of Radiation Oncology at the University of Texas.
And this age disparity was significantly greater in industry-funded trials.
Researchers have known for 20 years that cancer trial participants are not representative of the wider cancer population, and numerous government guidance documents have been issued on the matter. However, this Texas team’s findings were the first unambiguous evidence that pharmaceutical companies seem to be selecting younger patients to test their drugs.
“If we’re being generous then perhaps the answer is: They’re looking for some element of homogeneity, which is to say they don’t want competing risks to make the signal-to-noise ratio uninterpretable,” said Dr. Ludmir.
Dr. Laura Bothwell, PhD, assistant professor, Yale School of Public Health, recently coauthored a 259-page consensus report for the National Academies of Sciences, Engineering and Medicine on how to increase the research involvement of under-represented groups.
Dr. Bothwell said, “The problem with industry funded research is that ... it’s an inevitable conflict of interest that exists. They want the research to show that their products work. And older populations ... have a lot more complications, which leads to potentially less favorable results.”
The MD Anderson findings were published in JAMA Oncology. “That was the starting point in our journey,” said Dr. Ludmir. For the next 3 years, the researchers mined their painstakingly constructed database to understand what was preventing greater numbers of older patients from enrollment in cancer trials.
Meanwhile, answers were coming from elsewhere. In parallel with the work at MD Anderson, a team in California led by Mina Sedrak, MD, a medical oncologist at the City of Hope National Medical Center, had also started investigating age disparities in clinical trials.
Dr. Sedrak, who also serves as deputy director of Clinical Trials at the Center for Cancer and Aging, said he had become increasingly concerned that he did not have adequate information on new cancer therapies for his older patients.
“I was caring for a large number of people who were ... older adults,” said Dr. Sedrak, “But the data that was being used to get the standard-of-care treatment for cancer did not include older adults. And so there was this lack of applicability.”
He summed up the challenges in a 2021 review paper: “Most of what we know about cancer therapeutics is based on clinical trials conducted in younger, healthier patients.”
By 2030, it is estimated that 70% of all new cancer diagnoses will be in patients 65 years old and older. By contrast, patients over age 65 still account for only 40% of patients in cancer trials registered with the FDA (2015 figures) and older adults make up only 44% of participants in practice-changing cancer trials, according to a 2022 study.
So what is going on? Are studies specifically designed to squeeze out older patients?
Surprisingly, patients are not being kept out of trials by formal age limits, according to Dr. Ludmir. His team found that only 10% of phase 3 trials over the past 30 years had an upper limit for age, and age restrictions have been dropping by 1% a year. (For example, 16% of trials that enrolled in 2002-2005 had an upper age limit, compared with just 8% of trials that started in 2010-2014.)
Dr. Sedrak’s team found that “clinician bias” may be a factor, a situation in which trial investigators – particularly academic oncologists – are subconsciously picking younger, healthier patients for trials and excluding older, sicker patients to protect them from drug toxicities.
Dr. Ludmir said this was understandable, especially in the case of industry-driven trials, which tend to have demanding endpoints and “an overall posture of more treatment aggressiveness.”
“These are typically not trials where they’re saying, `Hey, if we add acupuncture ... are we going to see improved patient reported outcomes?’” Dr. Ludmir explained. “You’re asking ... I’ve got this cocktail of two pretty rough chemos: I want to see what happens if I add an immunotherapy to that. If I’m the clinician in clinic, I might reasonably, subconsciously, say, is the 75-year-old really who I want on this?”
What about patient bias? Perhaps fewer older patients wish to join clinical trials?
Not so, at least not at community cancer centers, said Dr. Sedrak. His team’s analysis of the National Cancer Institute Community Oncology Research Program database for 2016-2019 revealed that older patients were just as keen as the younger patients to participate in trials (68% of patients aged 50-69 years and 65% of patients 70+; P = .28).
However, drug companies may be excluding older patients by more subtle means. One-fifth of patients over 65 have had a prior cancer. Dr. Ludmir and coauthor Roshal Patel, MD, used their hand-coded www.clinicaltrials.gov database to look at prior malignancy exclusion criteria (PMEC). The analysis found “pervasive utilization” of PMEC in phase 3 trials, cropping up in 41% of studies over the past 30 years.
PMEC was significantly associated with age disparities and was significantly more common in industry-funded trials.
When asked whether PMEC are “age restriction by stealth” on the part of drug companies, Dr. Ludmir was reluctant to assign blame, but stood by his data: “The wider you restrict people in terms of having a prior cancer, the wider the age disparities in the subsequent studies, which to me is about as strong, in terms of causal understanding of these phenomena, as you can reasonably get at this level.”
In March the FDA released a guidance document titled Inclusion of Older Adults in Cancer Clinical Trials. However, its recommendations are “nonbinding” and “do not have the force and effect of law.”
To fix the issues, said Dr. Sedrak, the FDA must be given teeth.
“Okay, you write guidelines,” he said. “But if you don’t actually hold people accountable to following the guidelines, how are we going to implement and make sure that we’re transforming policy into action?”
Dr. Bothwell of Yale’s School of Public Health agreed. “Accountability has been the weakest link for decades now.”
She concluded, “In medicine there’s a tendency to believe that a therapy, because it exists and it has been tested and it’s shown some efficacy, it’s useful. But we don’t know the answer to that question unless we have statistically valid research in the population that we’re using it in.”
Dr. Bothwell and Dr. Ludmir report no conflicts of interest. In his publications, Dr. Sedrak reports industry grants from Seattle Genetics, Eli Lilly, Novartis, and Pfizer Foundation.

Should antenatal testing be performed in patients with a pre-pregnancy BMI ≥ 35?
Evidence summary
Association between higher maternal BMI and increased risk for stillbirth
The purpose of antenatal testing is to decrease the risk for stillbirth between visits. Because of the resources involved and the risk for false-positives when testing low-risk patients, antenatal testing is reserved for pregnant people with higher risk for stillbirth.
In a retrospective cohort study of more than 2.8 million singleton births including 9030 stillbirths, pregnant people with an elevated BMI had an increased risk for stillbirth compared to those with a normal BMI. The adjusted hazard ratio was 1.71 (95% CI, 1.62-1.83) for those with a BMI of 30.0 to 34.9; 2.04 (95% CI, 1.8-2.21) for those with a BMI of 35.0 to 39.9; and 2.50 (95% CI, 2.28-2.74) for those with a BMI ≥ 40.1
A meta-analysis of 38 studies, which included data on 16,274 stillbirths, found that a 5-unit increase in BMI was associated with an increased risk for stillbirth (relative risk, 1.24; 95% CI, 1.18-1.30).2
Another meta-analysis included 6 cohort studies involving more than 1 million pregnancies and 3 case-control studies involving 2530 stillbirths and 2837 controls from 1980-2005. There was an association between increasing BMI and stillbirth: the odds ratio (OR) was 1.47 (95% CI, 1.08-1.94) for those with a BMI of 25.0 to 29.9 and 2.07 (95% CI, 1.59-2.74) for those with a BMI ≥ 30.0, compared to those with a normal BMI.3
However, a retrospective cohort study of 182,362 singleton births including 442 stillbirths found no association between stillbirth and increasing BMI. The OR was 1.10 (95% CI, 0.90-1.36) for those with a BMI of 25.0 to 29.9 and 1.09 (95% CI, 0.87-1.37) for those with a BMI ≥ 30.0, compared to those with a normal BMI.4 However, this cohort study may have been underpowered to detect an association between stillbirth and BMI.
Recommendations from others
In 2021, ACOG suggested that weekly antenatal testing may be considered from 34w0d for pregnant people with a BMI ≥ 40.0 and from 37w0d for pregnant people with a BMI between 35.0 and 39.9.5 The 2021 ACOG Practice Bulletin on Obesity in Pregnancy rates this recommendation as Level C—based primarily on consensus and expert opinion.6
A 2018 Royal College of Obstetricians and Gynecologists Green-top Guideline recognizes “definitive recommendations for fetal surveillance are hampered by the lack of randomized controlled trials demonstrating that antepartum fetal surveillance decreases perinatal morbidity or mortality in late-term and post-term gestations…. There are no definitive studies determining the optimal type or frequency of such testing and no evidence specific for women with obesity.”7
A 2019 Society of Obstetricians and Gynecologists of Canada practice guideline states “stillbirth is more common with maternal obesity” and recommends “increased fetal surveillance … in the third trimester if reduced fetal movements are reported.” The guideline notes “the role for non-stress tests … in surveillance of well-being in this population is uncertain.” Also, for pregnant people with a BMI > 30, “assessment of fetal well-being is … recommended weekly from 37 weeks until delivery.” Finally, increased fetal surveillance is recommended in the setting of increased BMI and an abnormal pulsatility index of the umbilical artery and/or maternal uterine artery.8
Editor’s takeaway
Evidence demonstrates that increased maternal BMI is associated with increased stillbirths. However, evidence has not shown that third-trimester antenatal testing decreases this morbidity and mortality. Expert opinion varies, with ACOG recommending weekly antenatal testing from 34 and 37 weeks for pregnant people with a BMI ≥ 40 and of 35 to 39.9, respectively.
1. Yao R, Ananth C, Park B, et al; Perinatal Research Consortium. Obesity and the risk of stillbirth: a population-based cohort study. Am J Obstet Gynecol. 2014;210:e1-e9. doi: 10.1016/j.ajog. 2014.01.044
2. Aune D, Saugstad O, Henriksen T, et al. Maternal body mass index and the risk of fetal death, stillbirth, and infant death: a systematic review and meta-analysis. JAMA. 2014;311:1536-1546. doi: 10.1001/jama.2014.2269
3. Chu S, Kim S, Lau J, et al. Maternal obesity and risk of stillbirth: a meta-analysis. Am J Obstet Gynecol. 2007;197:223-228. doi: 10.1016/j.ajog.2007.03.027
4. Mahomed K, Chan G, Norton M. Obesity and the risk of stillbirth—a reappraisal—a retrospective cohort study. Eur J Obstet Gynecol Reprod Biol. 2020;255:25-28. doi: 10.1016/j.ejogrb. 2020.09.044
5. American College of Obstetricians and Gynecologists’ Committee on Obstetric Practice, Society for Maternal-Fetal Medicine. Indications for outpatient antenatal fetal surveillance: ACOG committee opinion, number 828. Obstet Gynecol. 2021;137:e177-e197. doi: 10.1097/AOG.0000000000004407
6. American College of Obstetricians and Gynecologists’ Committee on Practice Bulletins–Obstetrics. Obesity in pregnancy: ACOG practice bulletin, number 230. Obstet Gynecol. 2021;137:e128-e144. doi: 10.1097/AOG.0000000000004395
7. Denison F, Aedla N, Keag O, et al; Royal College of Obstetricians and Gynaecologists. Care of women with obesity in pregnancy: Green-top Guideline No. 72. BJOG. 2019;126:e62-e106. doi: 10.1111/1471-0528.15386
8. Maxwell C, Gaudet L, Cassir G, et al. Guideline No. 391–Pregnancy and maternal obesity part 1: pre-conception and prenatal care. J Obstet Gynaecol Can. 2019;41:1623-1640. doi: 10.1016/j.jogc. 2019.03.026
Evidence summary
Association between higher maternal BMI and increased risk for stillbirth
The purpose of antenatal testing is to decrease the risk for stillbirth between visits. Because of the resources involved and the risk for false-positives when testing low-risk patients, antenatal testing is reserved for pregnant people with higher risk for stillbirth.
In a retrospective cohort study of more than 2.8 million singleton births including 9030 stillbirths, pregnant people with an elevated BMI had an increased risk for stillbirth compared to those with a normal BMI. The adjusted hazard ratio was 1.71 (95% CI, 1.62-1.83) for those with a BMI of 30.0 to 34.9; 2.04 (95% CI, 1.8-2.21) for those with a BMI of 35.0 to 39.9; and 2.50 (95% CI, 2.28-2.74) for those with a BMI ≥ 40.1
A meta-analysis of 38 studies, which included data on 16,274 stillbirths, found that a 5-unit increase in BMI was associated with an increased risk for stillbirth (relative risk, 1.24; 95% CI, 1.18-1.30).2
Another meta-analysis included 6 cohort studies involving more than 1 million pregnancies and 3 case-control studies involving 2530 stillbirths and 2837 controls from 1980-2005. There was an association between increasing BMI and stillbirth: the odds ratio (OR) was 1.47 (95% CI, 1.08-1.94) for those with a BMI of 25.0 to 29.9 and 2.07 (95% CI, 1.59-2.74) for those with a BMI ≥ 30.0, compared to those with a normal BMI.3
However, a retrospective cohort study of 182,362 singleton births including 442 stillbirths found no association between stillbirth and increasing BMI. The OR was 1.10 (95% CI, 0.90-1.36) for those with a BMI of 25.0 to 29.9 and 1.09 (95% CI, 0.87-1.37) for those with a BMI ≥ 30.0, compared to those with a normal BMI.4 However, this cohort study may have been underpowered to detect an association between stillbirth and BMI.
Recommendations from others
In 2021, ACOG suggested that weekly antenatal testing may be considered from 34w0d for pregnant people with a BMI ≥ 40.0 and from 37w0d for pregnant people with a BMI between 35.0 and 39.9.5 The 2021 ACOG Practice Bulletin on Obesity in Pregnancy rates this recommendation as Level C—based primarily on consensus and expert opinion.6
A 2018 Royal College of Obstetricians and Gynecologists Green-top Guideline recognizes “definitive recommendations for fetal surveillance are hampered by the lack of randomized controlled trials demonstrating that antepartum fetal surveillance decreases perinatal morbidity or mortality in late-term and post-term gestations…. There are no definitive studies determining the optimal type or frequency of such testing and no evidence specific for women with obesity.”7
A 2019 Society of Obstetricians and Gynecologists of Canada practice guideline states “stillbirth is more common with maternal obesity” and recommends “increased fetal surveillance … in the third trimester if reduced fetal movements are reported.” The guideline notes “the role for non-stress tests … in surveillance of well-being in this population is uncertain.” Also, for pregnant people with a BMI > 30, “assessment of fetal well-being is … recommended weekly from 37 weeks until delivery.” Finally, increased fetal surveillance is recommended in the setting of increased BMI and an abnormal pulsatility index of the umbilical artery and/or maternal uterine artery.8
Editor’s takeaway
Evidence demonstrates that increased maternal BMI is associated with increased stillbirths. However, evidence has not shown that third-trimester antenatal testing decreases this morbidity and mortality. Expert opinion varies, with ACOG recommending weekly antenatal testing from 34 and 37 weeks for pregnant people with a BMI ≥ 40 and of 35 to 39.9, respectively.
Evidence summary
Association between higher maternal BMI and increased risk for stillbirth
The purpose of antenatal testing is to decrease the risk for stillbirth between visits. Because of the resources involved and the risk for false-positives when testing low-risk patients, antenatal testing is reserved for pregnant people with higher risk for stillbirth.
In a retrospective cohort study of more than 2.8 million singleton births including 9030 stillbirths, pregnant people with an elevated BMI had an increased risk for stillbirth compared to those with a normal BMI. The adjusted hazard ratio was 1.71 (95% CI, 1.62-1.83) for those with a BMI of 30.0 to 34.9; 2.04 (95% CI, 1.8-2.21) for those with a BMI of 35.0 to 39.9; and 2.50 (95% CI, 2.28-2.74) for those with a BMI ≥ 40.1
A meta-analysis of 38 studies, which included data on 16,274 stillbirths, found that a 5-unit increase in BMI was associated with an increased risk for stillbirth (relative risk, 1.24; 95% CI, 1.18-1.30).2
Another meta-analysis included 6 cohort studies involving more than 1 million pregnancies and 3 case-control studies involving 2530 stillbirths and 2837 controls from 1980-2005. There was an association between increasing BMI and stillbirth: the odds ratio (OR) was 1.47 (95% CI, 1.08-1.94) for those with a BMI of 25.0 to 29.9 and 2.07 (95% CI, 1.59-2.74) for those with a BMI ≥ 30.0, compared to those with a normal BMI.3
However, a retrospective cohort study of 182,362 singleton births including 442 stillbirths found no association between stillbirth and increasing BMI. The OR was 1.10 (95% CI, 0.90-1.36) for those with a BMI of 25.0 to 29.9 and 1.09 (95% CI, 0.87-1.37) for those with a BMI ≥ 30.0, compared to those with a normal BMI.4 However, this cohort study may have been underpowered to detect an association between stillbirth and BMI.
Recommendations from others
In 2021, ACOG suggested that weekly antenatal testing may be considered from 34w0d for pregnant people with a BMI ≥ 40.0 and from 37w0d for pregnant people with a BMI between 35.0 and 39.9.5 The 2021 ACOG Practice Bulletin on Obesity in Pregnancy rates this recommendation as Level C—based primarily on consensus and expert opinion.6
A 2018 Royal College of Obstetricians and Gynecologists Green-top Guideline recognizes “definitive recommendations for fetal surveillance are hampered by the lack of randomized controlled trials demonstrating that antepartum fetal surveillance decreases perinatal morbidity or mortality in late-term and post-term gestations…. There are no definitive studies determining the optimal type or frequency of such testing and no evidence specific for women with obesity.”7
A 2019 Society of Obstetricians and Gynecologists of Canada practice guideline states “stillbirth is more common with maternal obesity” and recommends “increased fetal surveillance … in the third trimester if reduced fetal movements are reported.” The guideline notes “the role for non-stress tests … in surveillance of well-being in this population is uncertain.” Also, for pregnant people with a BMI > 30, “assessment of fetal well-being is … recommended weekly from 37 weeks until delivery.” Finally, increased fetal surveillance is recommended in the setting of increased BMI and an abnormal pulsatility index of the umbilical artery and/or maternal uterine artery.8
Editor’s takeaway
Evidence demonstrates that increased maternal BMI is associated with increased stillbirths. However, evidence has not shown that third-trimester antenatal testing decreases this morbidity and mortality. Expert opinion varies, with ACOG recommending weekly antenatal testing from 34 and 37 weeks for pregnant people with a BMI ≥ 40 and of 35 to 39.9, respectively.
1. Yao R, Ananth C, Park B, et al; Perinatal Research Consortium. Obesity and the risk of stillbirth: a population-based cohort study. Am J Obstet Gynecol. 2014;210:e1-e9. doi: 10.1016/j.ajog. 2014.01.044
2. Aune D, Saugstad O, Henriksen T, et al. Maternal body mass index and the risk of fetal death, stillbirth, and infant death: a systematic review and meta-analysis. JAMA. 2014;311:1536-1546. doi: 10.1001/jama.2014.2269
3. Chu S, Kim S, Lau J, et al. Maternal obesity and risk of stillbirth: a meta-analysis. Am J Obstet Gynecol. 2007;197:223-228. doi: 10.1016/j.ajog.2007.03.027
4. Mahomed K, Chan G, Norton M. Obesity and the risk of stillbirth—a reappraisal—a retrospective cohort study. Eur J Obstet Gynecol Reprod Biol. 2020;255:25-28. doi: 10.1016/j.ejogrb. 2020.09.044
5. American College of Obstetricians and Gynecologists’ Committee on Obstetric Practice, Society for Maternal-Fetal Medicine. Indications for outpatient antenatal fetal surveillance: ACOG committee opinion, number 828. Obstet Gynecol. 2021;137:e177-e197. doi: 10.1097/AOG.0000000000004407
6. American College of Obstetricians and Gynecologists’ Committee on Practice Bulletins–Obstetrics. Obesity in pregnancy: ACOG practice bulletin, number 230. Obstet Gynecol. 2021;137:e128-e144. doi: 10.1097/AOG.0000000000004395
7. Denison F, Aedla N, Keag O, et al; Royal College of Obstetricians and Gynaecologists. Care of women with obesity in pregnancy: Green-top Guideline No. 72. BJOG. 2019;126:e62-e106. doi: 10.1111/1471-0528.15386
8. Maxwell C, Gaudet L, Cassir G, et al. Guideline No. 391–Pregnancy and maternal obesity part 1: pre-conception and prenatal care. J Obstet Gynaecol Can. 2019;41:1623-1640. doi: 10.1016/j.jogc. 2019.03.026
1. Yao R, Ananth C, Park B, et al; Perinatal Research Consortium. Obesity and the risk of stillbirth: a population-based cohort study. Am J Obstet Gynecol. 2014;210:e1-e9. doi: 10.1016/j.ajog. 2014.01.044
2. Aune D, Saugstad O, Henriksen T, et al. Maternal body mass index and the risk of fetal death, stillbirth, and infant death: a systematic review and meta-analysis. JAMA. 2014;311:1536-1546. doi: 10.1001/jama.2014.2269
3. Chu S, Kim S, Lau J, et al. Maternal obesity and risk of stillbirth: a meta-analysis. Am J Obstet Gynecol. 2007;197:223-228. doi: 10.1016/j.ajog.2007.03.027
4. Mahomed K, Chan G, Norton M. Obesity and the risk of stillbirth—a reappraisal—a retrospective cohort study. Eur J Obstet Gynecol Reprod Biol. 2020;255:25-28. doi: 10.1016/j.ejogrb. 2020.09.044
5. American College of Obstetricians and Gynecologists’ Committee on Obstetric Practice, Society for Maternal-Fetal Medicine. Indications for outpatient antenatal fetal surveillance: ACOG committee opinion, number 828. Obstet Gynecol. 2021;137:e177-e197. doi: 10.1097/AOG.0000000000004407
6. American College of Obstetricians and Gynecologists’ Committee on Practice Bulletins–Obstetrics. Obesity in pregnancy: ACOG practice bulletin, number 230. Obstet Gynecol. 2021;137:e128-e144. doi: 10.1097/AOG.0000000000004395
7. Denison F, Aedla N, Keag O, et al; Royal College of Obstetricians and Gynaecologists. Care of women with obesity in pregnancy: Green-top Guideline No. 72. BJOG. 2019;126:e62-e106. doi: 10.1111/1471-0528.15386
8. Maxwell C, Gaudet L, Cassir G, et al. Guideline No. 391–Pregnancy and maternal obesity part 1: pre-conception and prenatal care. J Obstet Gynaecol Can. 2019;41:1623-1640. doi: 10.1016/j.jogc. 2019.03.026
EVIDENCE-BASED REVIEW:
Possibly. Elevated BMI is associated with an increased risk for stillbirth (strength of recommendation [SOR], B; cohort studies and meta-analysis of cohort studies). Three studies found an association between elevated BMI and stillbirth and one did not. However, no studies demonstrate that antenatal testing in pregnant people with higher BMIs decreases stillbirth rates, or that no harm is caused by unnecessary testing or resultant interventions.
Still, in 2021, the American College of Obstetricians and Gynecologists (ACOG) suggested weekly antenatal testing may be considered from 34w0d for pregnant people with a BMI ≥ 40.0 and from 37w0d for pregnant people with a BMI between 35.0 and 39.9 (SOR, C; consensus guideline). Thus, doing the antenatal testing recommended in the ACOG guideline in an attempt to prevent stillbirth is reasonable, given evidence that elevated BMI is associated with stillbirth.

Isolated third nerve palsy: Lessons from the literature and 4 case studies
Of all the cranial nerve (CN) palsies that affect the eye, the third (oculomotor) nerve palsy (TNP) requires the most urgent evaluation.1 Third nerve dysfunction may signal an underlying neurologic emergency, such as ruptured cerebral aneurysm or giant cell arteritis. Early recognition and prompt treatment choices are key to reversing clinical and visual defects. The classic presentation of isolated TNP is a “down and out eye” deviation and ptosis with or without pupillary involvement.1
Recognize varying clinical presentations. TNPs, isolated or not, may be partial or complete, congenital or acquired, pupil involving or pupil sparing. In many cases, patients may have additional constitutional, ocular, or neurologic symptoms or signs, such as ataxia or hemiplegia.2 Recognition of these clinical findings, which at times can be subtle, is crucial. Appropriate clinical diagnosis and management rely on distinguishing isolated TNP from TNP that involves other CNs.2
Further clues to underlying pathology. Disruption of the third nerve can occur anywhere along its course from the oculomotor nucleus in the brain to its terminus at the extraocular muscles in the orbit.2 TNP’s effect on the pupil can often aid in diagnosis.3 Pupil-sparing TNP is usually due to microvascular ischemia, as may occur with diabetes or hypertension. Pupil involvement, though, may be the first sign of a compressive lesion.
Influence of age. Among individuals older than 60 years, the annual incidence of isolated TNP has been shown to be 12.5 per 100,000, compared with 1.7 per 100,000 in those younger than 60 years.4 In those older than 50 years, microvascular ischemia tends to be the dominant cause.4 Other possible causes include aneurysm, trauma, and neoplasm, particularly pituitary adenoma and metastatic tumor. In childhood and young adulthood, the most common cause of TNP is trauma.5
Use of vascular imaging is influenced by an individual’s age and clinical risk for an aneurysm. Isolated partial TNP or TNP with pupil involvement suggest compression of the third nerve and the need for immediate imaging. Given the dire implications of intracranial aneurysm, most physicians will focus their initial evaluation on vascular imaging, if available.2 If clinical findings instead suggest underlying microvascular ischemia, a delay of imaging may be possible.
In the text that follows, we present 4 patient cases describing the clinical investigative process and treatment determinations based on an individual’s history, clinical presentation, and neurologic findings.
CASE 1
Herpes zoster ophthalmicus
An 84-year-old man with no known medical illness presented to the emergency department (ED) with vesicular skin lesions that had appeared 4 days earlier over his scalp, right forehead, and periorbital region. The vesicles followed the distribution of the ophthalmic division of the trigeminal nerve (FIGURE 1). The patient was given a diagnosis of shingles. The only notable ocular features were the swollen right upper eyelid, injected conjunctiva, and reduced corneal sensation with otherwise normal right eye vision at 6/6. For right eye herpes zoster ophthalmicus (HZO), he was prescribed oral acyclovir 800 mg 5 times per day for 2 weeks.

Continue to: Two days later...
Two days later, he returned after experiencing a sudden onset of binocular diplopia and ptosis of the right eye. Partial ptosis was noted, with restricted adduction and elevation. Pupils were reactive and equal bilaterally. Hutchinson sign, which would indicate an impaired nasociliary nerve and increased risk for corneal and ocular sequelae,6 was absent. Relative afferent pupillary defect also was absent. All other CN functions were intact, with no systemic neurologic deficit. Contrast CT of the brain and orbit showed no radiologic evidence of meningitis, space-occupying lesion, or cerebral aneurysm.
Given the unremarkable imaging findings and lack of symptoms of meningism (eg, headache, vomiting, neck stiffness, or fever), we diagnosed right eye pupil-sparing partial TNP secondary to HZO. The patient continued taking oral acyclovir, which was tapered over 6 weeks. After 4 weeks of antiviral treatment, he recovered full extraocular movement and the ptosis subsided.
CASE 2
Posterior communicating artery aneurysm
A 71-year-old woman with hypercholesterolemia, hypertension, and ischemic heart disease presented to the ED with a 4-day history of headache, vomiting, and neck pain and a 2-day history of a drooping left eyelid. When asked if she had double vision, she said “No.” She had no other neurologic symptoms. Her blood pressure (BP) was 199/88 mm Hg. An initial plain CT of the brain ruled out ischemia, intracranial hemorrhage, and space-occupying lesion.
Once her BP was stabilized, she was referred to us for detailed eye assessment. Her best corrected visual acuity was 6/12 bilaterally. In contrast to her right eye pupil, which was 4 mm in diameter and reactive, her left eye pupil was 7 mm and poorly reactive to light. Optic nerve functions were preserved. There was complete ptosis of the left eye, with exotropia and total limitation of elevation, depression, and abduction (FIGURE 2). There was no proptosis; intraocular pressure was normal. Fundus examination of the left eye was unremarkable. All other CN and neurologic examinations were normal. We diagnosed left eye pupil-involving TNP.

Further assessment of the brain with magnetic resonance imaging (MRI) revealed a left posterior communicating artery aneurysm. We performed cerebral angiography (FIGURE 3) with coiling. Postoperatively, her ptosis resolved at 2 months but with residual left eye exotropia.

CASE 3
Viral infection
A 20-year-old male student presented to the ED for evaluation of acute-onset diplopia that was present upon awakening from sleep 4 days earlier. There was no ptosis or other neurologic symptoms. He had no history of trauma or viral illness. Examination revealed limited adduction, depression, levo-elevation, levo-depression, and dextro-depression in the right eye (FIGURE 4). Both pupils were reactive. There was no sign of aberrant third nerve regeneration. The optic nerve and other CN functions were intact. A systemic neurologic examination was unremarkable, and the fundus was normal, with no optic disc swelling. All blood work was negative for diabetes, hypercoagulability, and hyperlipidemia.

CT angiography (CTA) and MR angiography (MRA) did not reveal any vascular abnormalities such as intracranial aneurysms, arteriovenous malformations, or berry aneurysm. We treated the patient for right eye partial TNP secondary to presumed prior viral infection that led to an immune-mediated palsy of the third nerve. He was given a short course of low-dose oral prednisolone (30 mg/d for 5 days). He achieved full recovery of his ocular motility after 2 weeks.
Continue to: CASE 4
CASE 4
Trauma
A 33-year-old woman was brought to the ED after she was knocked off her motorbike by a car. A passerby found her unconscious and still wearing her helmet. En route to the hospital, the patient regained consciousness but had retrograde amnesia.
She was referred to us for evaluation of complete ptosis of her left eye. She was fully conscious during the examination. Her left eye vision was 6/9. Complete ptosis with exotropia was noted. Pupillary examination revealed a sluggish dilated left eye pupil of 7 mm with no reverse relative afferent pupillary defect. Extraocular movement was restricted at elevation, depression, and adduction with diplopia (FIGURE 5). All other CN functions were preserved.

CT of the brain and orbit revealed acute right frontotemporal subarachnoid hemorrhage (FIGURE 6). There was no radiologic evidence of orbital wall fractures or extraocular muscle entrapment. She remained stable during the first 24 hours of monitoring and was given a diagnosis of

Repeat CT of the brain 5 days later revealed complete resolution of the subarachnoid hemorrhage. The patient's clinical condition improved 2 weeks later and included resolution of ptosis and recovery of ocular motility.
Key takeaways from the cases
Case 1: Herpes zoster ophthalmicus
Clinical diagnosis of HZO is straightforward, with painful vesicular lesions occurring along the trigeminal nerve (V1) dermatome, as was seen in this case. The oculomotor nerve is the CN most commonly involved; the trochlear nerve is the least-often affected.6 In a report from the Mayo Clinic, 3 of 86 patients with HZO had oculomotor nerve palsies (3.4%).7 A separate review from an eye hospital study stated that 9.8% (n = 133) of 1356 patients with HZO had extraocular muscle palsy, with TNP in 4 of the patients.8
Ocular complications such as blepharitis, keratoconjunctivits, or iritis occur in 20% to 70% of HZO cases.9 Ophthalmoplegia, which most often involves the oculomotor nerve, is seen in 7% to 31% of HZO cases (mostly in the elderly) and usually occurs within 1 to 3 weeks of the onset of rash.6 Our patient immediately underwent contrast CT of the brain to rule out meningitis and nerve compression.
Treatment with a systemic antiviral agent is crucial. Acyclovir, valaciclovir, and famciclovir are available treatment options, used for treating the skin lesions, reducing the viral load, and reducing the risk for ocular involvement or its progression. Our patient started a 2-week course of oral acyclovir 800 mg 5 times per day. Ophthalmoplegia is usually self-limiting and has a good prognosis. Time to resolution varies from 2 to 18 months. Diplopia, if present, resolves within 1 year.6 Our patient achieved full recovery of his extraocular movement after completing 4 weeks of antiviral treatment.
Continue to: Case 2
Case 2: Posterior communicating artery aneurysm
Given the patient’s high BP, ruling out a hypertensive emergency with CT was the first priority. TNP caused by microvascular ischemia is not uncommon in the elderly. However, her pupil involvement and persistent headache called for an MRI to better evaluate the soft tissues and to rule out possible vascular pathologies. Left posterior communicating artery aneurysm was discovered with MRI, and urgent cerebral angiography and coiling was performed successfully.
Incidence. One report of 1400 patients with TNP confirmed that aneurysm was the cause in 10% of cases, with posterior communicating artery aneurysm accounting for the greatest number, 119 (25.7%).10 Of these cases of posterior communicating artery aneurysm, pupillary involvement was detected in 108 (90.8%). The oculomotor nerve lies adjacent to the posterior communicating artery as it passes through the subarachnoid space of the basal cisterns, where it is susceptible to compression.3
A high index of suspicion for posterior communicating artery aneurysm is crucial for early detection and lifesaving treatment. The patient in this case did well after the coiling. Her ptosis resolved at 2 months, although she had residual left eye exotropia.
Case 3: Viral infection
We chose CTA of the brain instead of contrast CT to rule out the possibility of intracranial aneurysm. CTA has been shown to be an adequate first-line study to detect aneurysms, particularly those greater than 4 mm in diameter.2,11 One study demonstrated an 81.8% sensitivity for aneurysms smaller than 3 mm when performed on a 320-slice CT.12
Additional imaging selection. We also selected MRA to rule out berry aneurysm, which is often asymptomatic. We decided against MRI because of its higher cost and longer acquisition time. It is usually reserved for patients with a negative initial work-up with CT or cerebral angiography if suspicion of a possible aneurysm remains.11 The MRA finding in this case was negative, and we made a presumptive diagnosis of TNP secondary to viral infection.
Isolated TNP following viral infection is a clinical diagnosis of exclusion. In 1 reported case, a 39-year-old man developed a superior division palsy after a common cold without fever, underwent no serologic study, and recovered spontaneously 6 weeks later.13 A 5-year-old boy who experienced a superior division palsy immediately after a common cold with fever was found on serologic examination to have an increased titre of influenza A virus. His palsy resolved in 4 months.14
The exact mechanism of viral-induced palsy is unknown. The possibility of postinfectious cranial neuropathy has been postulated, as most reported cases following a flu-like illness resolved within a few months.15 Although the pathogenesis remains speculative, an autoimmune process might have been involved.16 Our patient recovered fully in 1 month following a short course of oral prednisolone 30 mg/d for 5 days.
Case 4: Trauma
Trauma accounts for approximately 12% of all TNP cases.17 Traumatic TNPs are usually sustained in severe, high-speed, closed-head injuries, and are often associated with other CN injuries and neurologic deficits. The damage may be caused indirectly by compression, hemorrhage, or ischemia, or directly at certain vulnerable points including the nerve’s exit from the brainstem and the point at which it crosses the petroclinoid ligament.17 In our case, despite the patient having complete TNP, there was no sign of localized orbital trauma on the CT other than the presence of subarachnoid hemorrhage at the right frontotemporal region.
In a similar reported case, the patient had a right traumatic isolated TNP and was found to have left frontal subarachnoid hemorrhage with no sign of orbital trauma.18 However, the mechanisms of isolated TNP caused by traumatic brain injury are not clear. Possible causes include rootlet avulsion, distal fascicular damage, stretching of the nerve (including the parasellar segment), and decreased blood supply.18
It has been suggested that TNP is more frequently observed in cases of frontal region injury. As orbitofrontal regions are predominantly affected by cortical contusions, the risk for ocular involvement increases.19
Keep these fundamentals in mind
The diagnosis and management of isolated TNP are guided by the patient’s age, by the degree to which each of the oculomotor nerve’s 2 major functions—pupillomotor and oculomotor—are affected, and by the circumstances preceding the onset of TNP.2 Cases 1 and 3 in our series presented with partial TNP, while Cases 2 and 4 exhibited complete TNP. Pupillary involvement was detected only in Case 2. Nevertheless, radiologic imaging was ordered for all 4 cases after the diagnosis of TNP was made, to exclude the most worrying neurologic emergencies. The choice of imaging modality depends on not only the availability of the services but also the clinical signs and symptoms and presumptive clinical diagnosis. A tailored and thoughtful approach with consideration of the anatomy and varied pathologies help clinicians to skillfully discern emergencies from nonurgent cases.
CORRESPONDENCE
Lott Pooi Wah, MSOphth, FRCOphth, Department of Ophthalmology, Faculty of Medicine, Universiti Malaya, 50603 Kuala Lumpur, Malaysia; lottpw@yahoo.com Orcid no: 0000-0001-8746-1528
1. Radia M, Stahl M, Arunakirinathan M, et al. Examination of a third nerve palsy. Brit J Hosp Med. 2017;78:188-192. doi: 10.12968/hmed.2017.78.12.C188
2. Bruce BB, Biousse V, Newman NJ. Third nerve palsies. Semin Neurol. 2007;27:257-268. doi: 10.1055/s-2007-979681
3. Motoyama Y, Nonaka J, Hironaka Y, et al. Pupil-sparing oculomotor nerve palsy caused by upward compression of a large posterior communicating artery aneurysm. Case report. Neurol Med Chir (Tokyo). 2012;52:202-205. doi: 10.2176/nmc.52.202
4. Fang C, Leavitt JA, Hodge DO, et al. Incidence and etiologies of acquired third nerve palsy using a population-based method. JAMA Ophthalmol. 2017;135:23-28. doi: 10.1001/jamaophthal mol.2016.4456
5. Wyatt K. Three common ophthalmic emergencies. JAAPA. 2014;27:32-37. doi: 10.1097/01.JAA.0000447004.96714.34
6. Daswani M, Bhosale N, Shah VM. Rare case of herpes zoster ophthalmicus with orbital myositis, oculomotor nerve palsy and anterior uveitis. Indian J Dermatol Venereol Leprol. 2017;83:365-367. doi: 10.4103/0378-6323.199582
7. Womack LW, Liesegang TJ. Complications of herpes zoster ophthalmicus. Arch Ophthalmol. 1983;101:42-45. doi: 10.1001/archopht.1983.01040010044004
8. Marsh RJ, Dulley B, Kelly V. External ocular motor palsies in ophthalmic zoster: a review. Br J Ophthalmol. 1977;61:667-682. doi: 10.1136/bjo.61.11.677
9. Lim JJ, Ong YM, Zalina MCW, et al. Herpes zoster ophthalmicus with orbital apex syndrome – difference in outcomes and literature review. Ocul Immunol Inflamm. 2017;26:187-193. doi: 10.1080/09273948.2017.1327604
10. Keane JR. Third nerve palsy: analysis of 1400 personally-examined patients. Can J Neurol Sci. 2010;37:662-670. doi: 10.1017/s0317167100010866
11. Yoon NK, McNally S, Taussky P, et al. Imaging of cerebral aneurysms: a clinical perspective. Neurovasc Imaging. 2016;2:6. doi: 10.1186/s40809-016-0016-3
12. Wang H, Li W, He H, et al. 320-detector row CT angiography for detection and evaluation of intracranial aneurysms: comparison with conventional digital subtraction angiography. Clin Radiol. 2013;68:e15-20. doi: 10.1016/j.crad.2012.09.001
13. Derakhshan I. Superior branch palsy with spontaneous recovery. Ann Neurol. 1978;4:478-479. doi: 10.1002/ana.410040519
14. Engelhardt A, Credzich C, Kompf D. Isolated superior branch palsy of the oculomotor nerve in influenza A. Neuroophthalmol. 1989;9:233-235. doi: 10.3109/01658108908997359
15. Knox DL, Clark DB, Schuster FF. Benign VI nerve palsies in children. Pediatrics. 1967;40:560-564.
16. Saeki N, Yotsukura J, Adachi E, et al. Isolated superior division oculomotor palsy in a child with spontaneous recovery. J Clin Neurosci. 2000;7:62-64. doi: 10.1054/jocn.1998.0152
17. Nagendran ST, Lee V, Perry M. Traumatic orbital third nerve palsy. Brit J Oral Maxillofac Surg. 2019;57:578-581. doi: 10.1016/j.bjoms.2019.01.029
18. Kim T, Nam K, Kwon BS. Isolated oculomotor nerve palsy in mild traumatic brain injury: a literature review. Am J Phys Med Rehabil. 2020;99:430-435. doi: 10.1097/PHM.0000000000001316
19. Sharma B, Gupta R, Anand R, et al. Ocular manifestations of head injury and incidence of post-traumatic ocular motor nerve involvement in cases of head injury: a clinical review. Int Ophthalmol. 2014;34:893-900. doi: 10.1007/s10792-014-9898-8
Of all the cranial nerve (CN) palsies that affect the eye, the third (oculomotor) nerve palsy (TNP) requires the most urgent evaluation.1 Third nerve dysfunction may signal an underlying neurologic emergency, such as ruptured cerebral aneurysm or giant cell arteritis. Early recognition and prompt treatment choices are key to reversing clinical and visual defects. The classic presentation of isolated TNP is a “down and out eye” deviation and ptosis with or without pupillary involvement.1
Recognize varying clinical presentations. TNPs, isolated or not, may be partial or complete, congenital or acquired, pupil involving or pupil sparing. In many cases, patients may have additional constitutional, ocular, or neurologic symptoms or signs, such as ataxia or hemiplegia.2 Recognition of these clinical findings, which at times can be subtle, is crucial. Appropriate clinical diagnosis and management rely on distinguishing isolated TNP from TNP that involves other CNs.2
Further clues to underlying pathology. Disruption of the third nerve can occur anywhere along its course from the oculomotor nucleus in the brain to its terminus at the extraocular muscles in the orbit.2 TNP’s effect on the pupil can often aid in diagnosis.3 Pupil-sparing TNP is usually due to microvascular ischemia, as may occur with diabetes or hypertension. Pupil involvement, though, may be the first sign of a compressive lesion.
Influence of age. Among individuals older than 60 years, the annual incidence of isolated TNP has been shown to be 12.5 per 100,000, compared with 1.7 per 100,000 in those younger than 60 years.4 In those older than 50 years, microvascular ischemia tends to be the dominant cause.4 Other possible causes include aneurysm, trauma, and neoplasm, particularly pituitary adenoma and metastatic tumor. In childhood and young adulthood, the most common cause of TNP is trauma.5
Use of vascular imaging is influenced by an individual’s age and clinical risk for an aneurysm. Isolated partial TNP or TNP with pupil involvement suggest compression of the third nerve and the need for immediate imaging. Given the dire implications of intracranial aneurysm, most physicians will focus their initial evaluation on vascular imaging, if available.2 If clinical findings instead suggest underlying microvascular ischemia, a delay of imaging may be possible.
In the text that follows, we present 4 patient cases describing the clinical investigative process and treatment determinations based on an individual’s history, clinical presentation, and neurologic findings.
CASE 1
Herpes zoster ophthalmicus
An 84-year-old man with no known medical illness presented to the emergency department (ED) with vesicular skin lesions that had appeared 4 days earlier over his scalp, right forehead, and periorbital region. The vesicles followed the distribution of the ophthalmic division of the trigeminal nerve (FIGURE 1). The patient was given a diagnosis of shingles. The only notable ocular features were the swollen right upper eyelid, injected conjunctiva, and reduced corneal sensation with otherwise normal right eye vision at 6/6. For right eye herpes zoster ophthalmicus (HZO), he was prescribed oral acyclovir 800 mg 5 times per day for 2 weeks.
Continue to: Two days later...
Two days later, he returned after experiencing a sudden onset of binocular diplopia and ptosis of the right eye. Partial ptosis was noted, with restricted adduction and elevation. Pupils were reactive and equal bilaterally. Hutchinson sign, which would indicate an impaired nasociliary nerve and increased risk for corneal and ocular sequelae,6 was absent. Relative afferent pupillary defect also was absent. All other CN functions were intact, with no systemic neurologic deficit. Contrast CT of the brain and orbit showed no radiologic evidence of meningitis, space-occupying lesion, or cerebral aneurysm.
Given the unremarkable imaging findings and lack of symptoms of meningism (eg, headache, vomiting, neck stiffness, or fever), we diagnosed right eye pupil-sparing partial TNP secondary to HZO. The patient continued taking oral acyclovir, which was tapered over 6 weeks. After 4 weeks of antiviral treatment, he recovered full extraocular movement and the ptosis subsided.
CASE 2
Posterior communicating artery aneurysm
A 71-year-old woman with hypercholesterolemia, hypertension, and ischemic heart disease presented to the ED with a 4-day history of headache, vomiting, and neck pain and a 2-day history of a drooping left eyelid. When asked if she had double vision, she said “No.” She had no other neurologic symptoms. Her blood pressure (BP) was 199/88 mm Hg. An initial plain CT of the brain ruled out ischemia, intracranial hemorrhage, and space-occupying lesion.
Once her BP was stabilized, she was referred to us for detailed eye assessment. Her best corrected visual acuity was 6/12 bilaterally. In contrast to her right eye pupil, which was 4 mm in diameter and reactive, her left eye pupil was 7 mm and poorly reactive to light. Optic nerve functions were preserved. There was complete ptosis of the left eye, with exotropia and total limitation of elevation, depression, and abduction (FIGURE 2). There was no proptosis; intraocular pressure was normal. Fundus examination of the left eye was unremarkable. All other CN and neurologic examinations were normal. We diagnosed left eye pupil-involving TNP.
Further assessment of the brain with magnetic resonance imaging (MRI) revealed a left posterior communicating artery aneurysm. We performed cerebral angiography (FIGURE 3) with coiling. Postoperatively, her ptosis resolved at 2 months but with residual left eye exotropia.
CASE 3
Viral infection
A 20-year-old male student presented to the ED for evaluation of acute-onset diplopia that was present upon awakening from sleep 4 days earlier. There was no ptosis or other neurologic symptoms. He had no history of trauma or viral illness. Examination revealed limited adduction, depression, levo-elevation, levo-depression, and dextro-depression in the right eye (FIGURE 4). Both pupils were reactive. There was no sign of aberrant third nerve regeneration. The optic nerve and other CN functions were intact. A systemic neurologic examination was unremarkable, and the fundus was normal, with no optic disc swelling. All blood work was negative for diabetes, hypercoagulability, and hyperlipidemia.
CT angiography (CTA) and MR angiography (MRA) did not reveal any vascular abnormalities such as intracranial aneurysms, arteriovenous malformations, or berry aneurysm. We treated the patient for right eye partial TNP secondary to presumed prior viral infection that led to an immune-mediated palsy of the third nerve. He was given a short course of low-dose oral prednisolone (30 mg/d for 5 days). He achieved full recovery of his ocular motility after 2 weeks.
Continue to: CASE 4
CASE 4
Trauma
A 33-year-old woman was brought to the ED after she was knocked off her motorbike by a car. A passerby found her unconscious and still wearing her helmet. En route to the hospital, the patient regained consciousness but had retrograde amnesia.
She was referred to us for evaluation of complete ptosis of her left eye. She was fully conscious during the examination. Her left eye vision was 6/9. Complete ptosis with exotropia was noted. Pupillary examination revealed a sluggish dilated left eye pupil of 7 mm with no reverse relative afferent pupillary defect. Extraocular movement was restricted at elevation, depression, and adduction with diplopia (FIGURE 5). All other CN functions were preserved.
CT of the brain and orbit revealed acute right frontotemporal subarachnoid hemorrhage (FIGURE 6). There was no radiologic evidence of orbital wall fractures or extraocular muscle entrapment. She remained stable during the first 24 hours of monitoring and was given a diagnosis of
Repeat CT of the brain 5 days later revealed complete resolution of the subarachnoid hemorrhage. The patient's clinical condition improved 2 weeks later and included resolution of ptosis and recovery of ocular motility.
Key takeaways from the cases
Case 1: Herpes zoster ophthalmicus
Clinical diagnosis of HZO is straightforward, with painful vesicular lesions occurring along the trigeminal nerve (V1) dermatome, as was seen in this case. The oculomotor nerve is the CN most commonly involved; the trochlear nerve is the least-often affected.6 In a report from the Mayo Clinic, 3 of 86 patients with HZO had oculomotor nerve palsies (3.4%).7 A separate review from an eye hospital study stated that 9.8% (n = 133) of 1356 patients with HZO had extraocular muscle palsy, with TNP in 4 of the patients.8
Ocular complications such as blepharitis, keratoconjunctivits, or iritis occur in 20% to 70% of HZO cases.9 Ophthalmoplegia, which most often involves the oculomotor nerve, is seen in 7% to 31% of HZO cases (mostly in the elderly) and usually occurs within 1 to 3 weeks of the onset of rash.6 Our patient immediately underwent contrast CT of the brain to rule out meningitis and nerve compression.
Treatment with a systemic antiviral agent is crucial. Acyclovir, valaciclovir, and famciclovir are available treatment options, used for treating the skin lesions, reducing the viral load, and reducing the risk for ocular involvement or its progression. Our patient started a 2-week course of oral acyclovir 800 mg 5 times per day. Ophthalmoplegia is usually self-limiting and has a good prognosis. Time to resolution varies from 2 to 18 months. Diplopia, if present, resolves within 1 year.6 Our patient achieved full recovery of his extraocular movement after completing 4 weeks of antiviral treatment.
Continue to: Case 2
Case 2: Posterior communicating artery aneurysm
Given the patient’s high BP, ruling out a hypertensive emergency with CT was the first priority. TNP caused by microvascular ischemia is not uncommon in the elderly. However, her pupil involvement and persistent headache called for an MRI to better evaluate the soft tissues and to rule out possible vascular pathologies. Left posterior communicating artery aneurysm was discovered with MRI, and urgent cerebral angiography and coiling was performed successfully.
Incidence. One report of 1400 patients with TNP confirmed that aneurysm was the cause in 10% of cases, with posterior communicating artery aneurysm accounting for the greatest number, 119 (25.7%).10 Of these cases of posterior communicating artery aneurysm, pupillary involvement was detected in 108 (90.8%). The oculomotor nerve lies adjacent to the posterior communicating artery as it passes through the subarachnoid space of the basal cisterns, where it is susceptible to compression.3
A high index of suspicion for posterior communicating artery aneurysm is crucial for early detection and lifesaving treatment. The patient in this case did well after the coiling. Her ptosis resolved at 2 months, although she had residual left eye exotropia.
Case 3: Viral infection
We chose CTA of the brain instead of contrast CT to rule out the possibility of intracranial aneurysm. CTA has been shown to be an adequate first-line study to detect aneurysms, particularly those greater than 4 mm in diameter.2,11 One study demonstrated an 81.8% sensitivity for aneurysms smaller than 3 mm when performed on a 320-slice CT.12
Additional imaging selection. We also selected MRA to rule out berry aneurysm, which is often asymptomatic. We decided against MRI because of its higher cost and longer acquisition time. It is usually reserved for patients with a negative initial work-up with CT or cerebral angiography if suspicion of a possible aneurysm remains.11 The MRA finding in this case was negative, and we made a presumptive diagnosis of TNP secondary to viral infection.
Isolated TNP following viral infection is a clinical diagnosis of exclusion. In 1 reported case, a 39-year-old man developed a superior division palsy after a common cold without fever, underwent no serologic study, and recovered spontaneously 6 weeks later.13 A 5-year-old boy who experienced a superior division palsy immediately after a common cold with fever was found on serologic examination to have an increased titre of influenza A virus. His palsy resolved in 4 months.14
The exact mechanism of viral-induced palsy is unknown. The possibility of postinfectious cranial neuropathy has been postulated, as most reported cases following a flu-like illness resolved within a few months.15 Although the pathogenesis remains speculative, an autoimmune process might have been involved.16 Our patient recovered fully in 1 month following a short course of oral prednisolone 30 mg/d for 5 days.
Case 4: Trauma
Trauma accounts for approximately 12% of all TNP cases.17 Traumatic TNPs are usually sustained in severe, high-speed, closed-head injuries, and are often associated with other CN injuries and neurologic deficits. The damage may be caused indirectly by compression, hemorrhage, or ischemia, or directly at certain vulnerable points including the nerve’s exit from the brainstem and the point at which it crosses the petroclinoid ligament.17 In our case, despite the patient having complete TNP, there was no sign of localized orbital trauma on the CT other than the presence of subarachnoid hemorrhage at the right frontotemporal region.
In a similar reported case, the patient had a right traumatic isolated TNP and was found to have left frontal subarachnoid hemorrhage with no sign of orbital trauma.18 However, the mechanisms of isolated TNP caused by traumatic brain injury are not clear. Possible causes include rootlet avulsion, distal fascicular damage, stretching of the nerve (including the parasellar segment), and decreased blood supply.18
It has been suggested that TNP is more frequently observed in cases of frontal region injury. As orbitofrontal regions are predominantly affected by cortical contusions, the risk for ocular involvement increases.19
Keep these fundamentals in mind
The diagnosis and management of isolated TNP are guided by the patient’s age, by the degree to which each of the oculomotor nerve’s 2 major functions—pupillomotor and oculomotor—are affected, and by the circumstances preceding the onset of TNP.2 Cases 1 and 3 in our series presented with partial TNP, while Cases 2 and 4 exhibited complete TNP. Pupillary involvement was detected only in Case 2. Nevertheless, radiologic imaging was ordered for all 4 cases after the diagnosis of TNP was made, to exclude the most worrying neurologic emergencies. The choice of imaging modality depends on not only the availability of the services but also the clinical signs and symptoms and presumptive clinical diagnosis. A tailored and thoughtful approach with consideration of the anatomy and varied pathologies help clinicians to skillfully discern emergencies from nonurgent cases.
CORRESPONDENCE
Lott Pooi Wah, MSOphth, FRCOphth, Department of Ophthalmology, Faculty of Medicine, Universiti Malaya, 50603 Kuala Lumpur, Malaysia; lottpw@yahoo.com Orcid no: 0000-0001-8746-1528
Of all the cranial nerve (CN) palsies that affect the eye, the third (oculomotor) nerve palsy (TNP) requires the most urgent evaluation.1 Third nerve dysfunction may signal an underlying neurologic emergency, such as ruptured cerebral aneurysm or giant cell arteritis. Early recognition and prompt treatment choices are key to reversing clinical and visual defects. The classic presentation of isolated TNP is a “down and out eye” deviation and ptosis with or without pupillary involvement.1
Recognize varying clinical presentations. TNPs, isolated or not, may be partial or complete, congenital or acquired, pupil involving or pupil sparing. In many cases, patients may have additional constitutional, ocular, or neurologic symptoms or signs, such as ataxia or hemiplegia.2 Recognition of these clinical findings, which at times can be subtle, is crucial. Appropriate clinical diagnosis and management rely on distinguishing isolated TNP from TNP that involves other CNs.2
Further clues to underlying pathology. Disruption of the third nerve can occur anywhere along its course from the oculomotor nucleus in the brain to its terminus at the extraocular muscles in the orbit.2 TNP’s effect on the pupil can often aid in diagnosis.3 Pupil-sparing TNP is usually due to microvascular ischemia, as may occur with diabetes or hypertension. Pupil involvement, though, may be the first sign of a compressive lesion.
Influence of age. Among individuals older than 60 years, the annual incidence of isolated TNP has been shown to be 12.5 per 100,000, compared with 1.7 per 100,000 in those younger than 60 years.4 In those older than 50 years, microvascular ischemia tends to be the dominant cause.4 Other possible causes include aneurysm, trauma, and neoplasm, particularly pituitary adenoma and metastatic tumor. In childhood and young adulthood, the most common cause of TNP is trauma.5
Use of vascular imaging is influenced by an individual’s age and clinical risk for an aneurysm. Isolated partial TNP or TNP with pupil involvement suggest compression of the third nerve and the need for immediate imaging. Given the dire implications of intracranial aneurysm, most physicians will focus their initial evaluation on vascular imaging, if available.2 If clinical findings instead suggest underlying microvascular ischemia, a delay of imaging may be possible.
In the text that follows, we present 4 patient cases describing the clinical investigative process and treatment determinations based on an individual’s history, clinical presentation, and neurologic findings.
CASE 1
Herpes zoster ophthalmicus
An 84-year-old man with no known medical illness presented to the emergency department (ED) with vesicular skin lesions that had appeared 4 days earlier over his scalp, right forehead, and periorbital region. The vesicles followed the distribution of the ophthalmic division of the trigeminal nerve (FIGURE 1). The patient was given a diagnosis of shingles. The only notable ocular features were the swollen right upper eyelid, injected conjunctiva, and reduced corneal sensation with otherwise normal right eye vision at 6/6. For right eye herpes zoster ophthalmicus (HZO), he was prescribed oral acyclovir 800 mg 5 times per day for 2 weeks.
Continue to: Two days later...
Two days later, he returned after experiencing a sudden onset of binocular diplopia and ptosis of the right eye. Partial ptosis was noted, with restricted adduction and elevation. Pupils were reactive and equal bilaterally. Hutchinson sign, which would indicate an impaired nasociliary nerve and increased risk for corneal and ocular sequelae,6 was absent. Relative afferent pupillary defect also was absent. All other CN functions were intact, with no systemic neurologic deficit. Contrast CT of the brain and orbit showed no radiologic evidence of meningitis, space-occupying lesion, or cerebral aneurysm.
Given the unremarkable imaging findings and lack of symptoms of meningism (eg, headache, vomiting, neck stiffness, or fever), we diagnosed right eye pupil-sparing partial TNP secondary to HZO. The patient continued taking oral acyclovir, which was tapered over 6 weeks. After 4 weeks of antiviral treatment, he recovered full extraocular movement and the ptosis subsided.
CASE 2
Posterior communicating artery aneurysm
A 71-year-old woman with hypercholesterolemia, hypertension, and ischemic heart disease presented to the ED with a 4-day history of headache, vomiting, and neck pain and a 2-day history of a drooping left eyelid. When asked if she had double vision, she said “No.” She had no other neurologic symptoms. Her blood pressure (BP) was 199/88 mm Hg. An initial plain CT of the brain ruled out ischemia, intracranial hemorrhage, and space-occupying lesion.
Once her BP was stabilized, she was referred to us for detailed eye assessment. Her best corrected visual acuity was 6/12 bilaterally. In contrast to her right eye pupil, which was 4 mm in diameter and reactive, her left eye pupil was 7 mm and poorly reactive to light. Optic nerve functions were preserved. There was complete ptosis of the left eye, with exotropia and total limitation of elevation, depression, and abduction (FIGURE 2). There was no proptosis; intraocular pressure was normal. Fundus examination of the left eye was unremarkable. All other CN and neurologic examinations were normal. We diagnosed left eye pupil-involving TNP.
Further assessment of the brain with magnetic resonance imaging (MRI) revealed a left posterior communicating artery aneurysm. We performed cerebral angiography (FIGURE 3) with coiling. Postoperatively, her ptosis resolved at 2 months but with residual left eye exotropia.
CASE 3
Viral infection
A 20-year-old male student presented to the ED for evaluation of acute-onset diplopia that was present upon awakening from sleep 4 days earlier. There was no ptosis or other neurologic symptoms. He had no history of trauma or viral illness. Examination revealed limited adduction, depression, levo-elevation, levo-depression, and dextro-depression in the right eye (FIGURE 4). Both pupils were reactive. There was no sign of aberrant third nerve regeneration. The optic nerve and other CN functions were intact. A systemic neurologic examination was unremarkable, and the fundus was normal, with no optic disc swelling. All blood work was negative for diabetes, hypercoagulability, and hyperlipidemia.
CT angiography (CTA) and MR angiography (MRA) did not reveal any vascular abnormalities such as intracranial aneurysms, arteriovenous malformations, or berry aneurysm. We treated the patient for right eye partial TNP secondary to presumed prior viral infection that led to an immune-mediated palsy of the third nerve. He was given a short course of low-dose oral prednisolone (30 mg/d for 5 days). He achieved full recovery of his ocular motility after 2 weeks.
Continue to: CASE 4
CASE 4
Trauma
A 33-year-old woman was brought to the ED after she was knocked off her motorbike by a car. A passerby found her unconscious and still wearing her helmet. En route to the hospital, the patient regained consciousness but had retrograde amnesia.
She was referred to us for evaluation of complete ptosis of her left eye. She was fully conscious during the examination. Her left eye vision was 6/9. Complete ptosis with exotropia was noted. Pupillary examination revealed a sluggish dilated left eye pupil of 7 mm with no reverse relative afferent pupillary defect. Extraocular movement was restricted at elevation, depression, and adduction with diplopia (FIGURE 5). All other CN functions were preserved.
CT of the brain and orbit revealed acute right frontotemporal subarachnoid hemorrhage (FIGURE 6). There was no radiologic evidence of orbital wall fractures or extraocular muscle entrapment. She remained stable during the first 24 hours of monitoring and was given a diagnosis of
Repeat CT of the brain 5 days later revealed complete resolution of the subarachnoid hemorrhage. The patient's clinical condition improved 2 weeks later and included resolution of ptosis and recovery of ocular motility.
Key takeaways from the cases
Case 1: Herpes zoster ophthalmicus
Clinical diagnosis of HZO is straightforward, with painful vesicular lesions occurring along the trigeminal nerve (V1) dermatome, as was seen in this case. The oculomotor nerve is the CN most commonly involved; the trochlear nerve is the least-often affected.6 In a report from the Mayo Clinic, 3 of 86 patients with HZO had oculomotor nerve palsies (3.4%).7 A separate review from an eye hospital study stated that 9.8% (n = 133) of 1356 patients with HZO had extraocular muscle palsy, with TNP in 4 of the patients.8
Ocular complications such as blepharitis, keratoconjunctivits, or iritis occur in 20% to 70% of HZO cases.9 Ophthalmoplegia, which most often involves the oculomotor nerve, is seen in 7% to 31% of HZO cases (mostly in the elderly) and usually occurs within 1 to 3 weeks of the onset of rash.6 Our patient immediately underwent contrast CT of the brain to rule out meningitis and nerve compression.
Treatment with a systemic antiviral agent is crucial. Acyclovir, valaciclovir, and famciclovir are available treatment options, used for treating the skin lesions, reducing the viral load, and reducing the risk for ocular involvement or its progression. Our patient started a 2-week course of oral acyclovir 800 mg 5 times per day. Ophthalmoplegia is usually self-limiting and has a good prognosis. Time to resolution varies from 2 to 18 months. Diplopia, if present, resolves within 1 year.6 Our patient achieved full recovery of his extraocular movement after completing 4 weeks of antiviral treatment.
Continue to: Case 2
Case 2: Posterior communicating artery aneurysm
Given the patient’s high BP, ruling out a hypertensive emergency with CT was the first priority. TNP caused by microvascular ischemia is not uncommon in the elderly. However, her pupil involvement and persistent headache called for an MRI to better evaluate the soft tissues and to rule out possible vascular pathologies. Left posterior communicating artery aneurysm was discovered with MRI, and urgent cerebral angiography and coiling was performed successfully.
Incidence. One report of 1400 patients with TNP confirmed that aneurysm was the cause in 10% of cases, with posterior communicating artery aneurysm accounting for the greatest number, 119 (25.7%).10 Of these cases of posterior communicating artery aneurysm, pupillary involvement was detected in 108 (90.8%). The oculomotor nerve lies adjacent to the posterior communicating artery as it passes through the subarachnoid space of the basal cisterns, where it is susceptible to compression.3
A high index of suspicion for posterior communicating artery aneurysm is crucial for early detection and lifesaving treatment. The patient in this case did well after the coiling. Her ptosis resolved at 2 months, although she had residual left eye exotropia.
Case 3: Viral infection
We chose CTA of the brain instead of contrast CT to rule out the possibility of intracranial aneurysm. CTA has been shown to be an adequate first-line study to detect aneurysms, particularly those greater than 4 mm in diameter.2,11 One study demonstrated an 81.8% sensitivity for aneurysms smaller than 3 mm when performed on a 320-slice CT.12
Additional imaging selection. We also selected MRA to rule out berry aneurysm, which is often asymptomatic. We decided against MRI because of its higher cost and longer acquisition time. It is usually reserved for patients with a negative initial work-up with CT or cerebral angiography if suspicion of a possible aneurysm remains.11 The MRA finding in this case was negative, and we made a presumptive diagnosis of TNP secondary to viral infection.
Isolated TNP following viral infection is a clinical diagnosis of exclusion. In 1 reported case, a 39-year-old man developed a superior division palsy after a common cold without fever, underwent no serologic study, and recovered spontaneously 6 weeks later.13 A 5-year-old boy who experienced a superior division palsy immediately after a common cold with fever was found on serologic examination to have an increased titre of influenza A virus. His palsy resolved in 4 months.14
The exact mechanism of viral-induced palsy is unknown. The possibility of postinfectious cranial neuropathy has been postulated, as most reported cases following a flu-like illness resolved within a few months.15 Although the pathogenesis remains speculative, an autoimmune process might have been involved.16 Our patient recovered fully in 1 month following a short course of oral prednisolone 30 mg/d for 5 days.
Case 4: Trauma
Trauma accounts for approximately 12% of all TNP cases.17 Traumatic TNPs are usually sustained in severe, high-speed, closed-head injuries, and are often associated with other CN injuries and neurologic deficits. The damage may be caused indirectly by compression, hemorrhage, or ischemia, or directly at certain vulnerable points including the nerve’s exit from the brainstem and the point at which it crosses the petroclinoid ligament.17 In our case, despite the patient having complete TNP, there was no sign of localized orbital trauma on the CT other than the presence of subarachnoid hemorrhage at the right frontotemporal region.
In a similar reported case, the patient had a right traumatic isolated TNP and was found to have left frontal subarachnoid hemorrhage with no sign of orbital trauma.18 However, the mechanisms of isolated TNP caused by traumatic brain injury are not clear. Possible causes include rootlet avulsion, distal fascicular damage, stretching of the nerve (including the parasellar segment), and decreased blood supply.18
It has been suggested that TNP is more frequently observed in cases of frontal region injury. As orbitofrontal regions are predominantly affected by cortical contusions, the risk for ocular involvement increases.19
Keep these fundamentals in mind
The diagnosis and management of isolated TNP are guided by the patient’s age, by the degree to which each of the oculomotor nerve’s 2 major functions—pupillomotor and oculomotor—are affected, and by the circumstances preceding the onset of TNP.2 Cases 1 and 3 in our series presented with partial TNP, while Cases 2 and 4 exhibited complete TNP. Pupillary involvement was detected only in Case 2. Nevertheless, radiologic imaging was ordered for all 4 cases after the diagnosis of TNP was made, to exclude the most worrying neurologic emergencies. The choice of imaging modality depends on not only the availability of the services but also the clinical signs and symptoms and presumptive clinical diagnosis. A tailored and thoughtful approach with consideration of the anatomy and varied pathologies help clinicians to skillfully discern emergencies from nonurgent cases.
CORRESPONDENCE
Lott Pooi Wah, MSOphth, FRCOphth, Department of Ophthalmology, Faculty of Medicine, Universiti Malaya, 50603 Kuala Lumpur, Malaysia; lottpw@yahoo.com Orcid no: 0000-0001-8746-1528
1. Radia M, Stahl M, Arunakirinathan M, et al. Examination of a third nerve palsy. Brit J Hosp Med. 2017;78:188-192. doi: 10.12968/hmed.2017.78.12.C188
2. Bruce BB, Biousse V, Newman NJ. Third nerve palsies. Semin Neurol. 2007;27:257-268. doi: 10.1055/s-2007-979681
3. Motoyama Y, Nonaka J, Hironaka Y, et al. Pupil-sparing oculomotor nerve palsy caused by upward compression of a large posterior communicating artery aneurysm. Case report. Neurol Med Chir (Tokyo). 2012;52:202-205. doi: 10.2176/nmc.52.202
4. Fang C, Leavitt JA, Hodge DO, et al. Incidence and etiologies of acquired third nerve palsy using a population-based method. JAMA Ophthalmol. 2017;135:23-28. doi: 10.1001/jamaophthal mol.2016.4456
5. Wyatt K. Three common ophthalmic emergencies. JAAPA. 2014;27:32-37. doi: 10.1097/01.JAA.0000447004.96714.34
6. Daswani M, Bhosale N, Shah VM. Rare case of herpes zoster ophthalmicus with orbital myositis, oculomotor nerve palsy and anterior uveitis. Indian J Dermatol Venereol Leprol. 2017;83:365-367. doi: 10.4103/0378-6323.199582
7. Womack LW, Liesegang TJ. Complications of herpes zoster ophthalmicus. Arch Ophthalmol. 1983;101:42-45. doi: 10.1001/archopht.1983.01040010044004
8. Marsh RJ, Dulley B, Kelly V. External ocular motor palsies in ophthalmic zoster: a review. Br J Ophthalmol. 1977;61:667-682. doi: 10.1136/bjo.61.11.677
9. Lim JJ, Ong YM, Zalina MCW, et al. Herpes zoster ophthalmicus with orbital apex syndrome – difference in outcomes and literature review. Ocul Immunol Inflamm. 2017;26:187-193. doi: 10.1080/09273948.2017.1327604
10. Keane JR. Third nerve palsy: analysis of 1400 personally-examined patients. Can J Neurol Sci. 2010;37:662-670. doi: 10.1017/s0317167100010866
11. Yoon NK, McNally S, Taussky P, et al. Imaging of cerebral aneurysms: a clinical perspective. Neurovasc Imaging. 2016;2:6. doi: 10.1186/s40809-016-0016-3
12. Wang H, Li W, He H, et al. 320-detector row CT angiography for detection and evaluation of intracranial aneurysms: comparison with conventional digital subtraction angiography. Clin Radiol. 2013;68:e15-20. doi: 10.1016/j.crad.2012.09.001
13. Derakhshan I. Superior branch palsy with spontaneous recovery. Ann Neurol. 1978;4:478-479. doi: 10.1002/ana.410040519
14. Engelhardt A, Credzich C, Kompf D. Isolated superior branch palsy of the oculomotor nerve in influenza A. Neuroophthalmol. 1989;9:233-235. doi: 10.3109/01658108908997359
15. Knox DL, Clark DB, Schuster FF. Benign VI nerve palsies in children. Pediatrics. 1967;40:560-564.
16. Saeki N, Yotsukura J, Adachi E, et al. Isolated superior division oculomotor palsy in a child with spontaneous recovery. J Clin Neurosci. 2000;7:62-64. doi: 10.1054/jocn.1998.0152
17. Nagendran ST, Lee V, Perry M. Traumatic orbital third nerve palsy. Brit J Oral Maxillofac Surg. 2019;57:578-581. doi: 10.1016/j.bjoms.2019.01.029
18. Kim T, Nam K, Kwon BS. Isolated oculomotor nerve palsy in mild traumatic brain injury: a literature review. Am J Phys Med Rehabil. 2020;99:430-435. doi: 10.1097/PHM.0000000000001316
19. Sharma B, Gupta R, Anand R, et al. Ocular manifestations of head injury and incidence of post-traumatic ocular motor nerve involvement in cases of head injury: a clinical review. Int Ophthalmol. 2014;34:893-900. doi: 10.1007/s10792-014-9898-8
1. Radia M, Stahl M, Arunakirinathan M, et al. Examination of a third nerve palsy. Brit J Hosp Med. 2017;78:188-192. doi: 10.12968/hmed.2017.78.12.C188
2. Bruce BB, Biousse V, Newman NJ. Third nerve palsies. Semin Neurol. 2007;27:257-268. doi: 10.1055/s-2007-979681
3. Motoyama Y, Nonaka J, Hironaka Y, et al. Pupil-sparing oculomotor nerve palsy caused by upward compression of a large posterior communicating artery aneurysm. Case report. Neurol Med Chir (Tokyo). 2012;52:202-205. doi: 10.2176/nmc.52.202
4. Fang C, Leavitt JA, Hodge DO, et al. Incidence and etiologies of acquired third nerve palsy using a population-based method. JAMA Ophthalmol. 2017;135:23-28. doi: 10.1001/jamaophthal mol.2016.4456
5. Wyatt K. Three common ophthalmic emergencies. JAAPA. 2014;27:32-37. doi: 10.1097/01.JAA.0000447004.96714.34
6. Daswani M, Bhosale N, Shah VM. Rare case of herpes zoster ophthalmicus with orbital myositis, oculomotor nerve palsy and anterior uveitis. Indian J Dermatol Venereol Leprol. 2017;83:365-367. doi: 10.4103/0378-6323.199582
7. Womack LW, Liesegang TJ. Complications of herpes zoster ophthalmicus. Arch Ophthalmol. 1983;101:42-45. doi: 10.1001/archopht.1983.01040010044004
8. Marsh RJ, Dulley B, Kelly V. External ocular motor palsies in ophthalmic zoster: a review. Br J Ophthalmol. 1977;61:667-682. doi: 10.1136/bjo.61.11.677
9. Lim JJ, Ong YM, Zalina MCW, et al. Herpes zoster ophthalmicus with orbital apex syndrome – difference in outcomes and literature review. Ocul Immunol Inflamm. 2017;26:187-193. doi: 10.1080/09273948.2017.1327604
10. Keane JR. Third nerve palsy: analysis of 1400 personally-examined patients. Can J Neurol Sci. 2010;37:662-670. doi: 10.1017/s0317167100010866
11. Yoon NK, McNally S, Taussky P, et al. Imaging of cerebral aneurysms: a clinical perspective. Neurovasc Imaging. 2016;2:6. doi: 10.1186/s40809-016-0016-3
12. Wang H, Li W, He H, et al. 320-detector row CT angiography for detection and evaluation of intracranial aneurysms: comparison with conventional digital subtraction angiography. Clin Radiol. 2013;68:e15-20. doi: 10.1016/j.crad.2012.09.001
13. Derakhshan I. Superior branch palsy with spontaneous recovery. Ann Neurol. 1978;4:478-479. doi: 10.1002/ana.410040519
14. Engelhardt A, Credzich C, Kompf D. Isolated superior branch palsy of the oculomotor nerve in influenza A. Neuroophthalmol. 1989;9:233-235. doi: 10.3109/01658108908997359
15. Knox DL, Clark DB, Schuster FF. Benign VI nerve palsies in children. Pediatrics. 1967;40:560-564.
16. Saeki N, Yotsukura J, Adachi E, et al. Isolated superior division oculomotor palsy in a child with spontaneous recovery. J Clin Neurosci. 2000;7:62-64. doi: 10.1054/jocn.1998.0152
17. Nagendran ST, Lee V, Perry M. Traumatic orbital third nerve palsy. Brit J Oral Maxillofac Surg. 2019;57:578-581. doi: 10.1016/j.bjoms.2019.01.029
18. Kim T, Nam K, Kwon BS. Isolated oculomotor nerve palsy in mild traumatic brain injury: a literature review. Am J Phys Med Rehabil. 2020;99:430-435. doi: 10.1097/PHM.0000000000001316
19. Sharma B, Gupta R, Anand R, et al. Ocular manifestations of head injury and incidence of post-traumatic ocular motor nerve involvement in cases of head injury: a clinical review. Int Ophthalmol. 2014;34:893-900. doi: 10.1007/s10792-014-9898-8
PRACTICE RECOMMENDATIONS
› Consider microvascular ischemia if third nerve palsy is pupil sparing. C
› Consider computerized tomography (CT) angiography as an alternative to plain CT for first-line study of suspected aneurysm. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series

We have seen the future of healthy muffins, and its name is Roselle
Get ‘em while they’re hot … for your health
Today on the Eating Channel, it’s a very special episode of “Much Ado About Muffin.”
The muffin. For some of us, it’s a good way to pretend we’re not having dessert for breakfast. A bran muffin can be loaded with calcium and fiber, and our beloved blueberry is full of yummy antioxidants and vitamins. Definitely not dessert.
Well, the muffin denial can stop there because there’s a new flavor on the scene, and research suggests it may actually be healthy. (Disclaimer: Muffin may not be considered healthy in Norway.) This new muffin has a name, Roselle, that comes from the calyx extract used in it, which is found in the Hibiscus sabdariffa plant of the same name.
Now, when it comes to new foods, especially ones that are supposed to be healthy, the No. 1 criteria is the same: It has to taste good. Researchers at the Norwegian University of Science and Technology and Amity University in India agreed, but they also set out to make it nutritionally valuable and give it a long shelf life without the addition of preservatives.
Sounds like a tall order, but they figured it out.
Not only is it tasty, but the properties of it could rival your morning multivitamin. Hibiscus extract has huge amounts of antioxidants, like phenolics, which are believed to help prevent cell membrane damage. Foods like vegetables, flax seed, and whole grains also have these antioxidants, but why not just have a Roselle muffin instead? You also get a dose of ascorbic acid without the glass of OJ in the morning.
The ascorbic acid, however, is not there just to help you. It also helps to check the researcher’s third box, shelf life. These naturally rosy-colored pastries will stay mold-free for 6 days without refrigeration at room temperature and without added preservatives.
Our guess, though, is they won’t be on the kitchen counter long enough to find out.
A sobering proposition
If Hollywood is to be believed, there’s no amount of drunkenness that can’t be cured with a cup of coffee or a stern slap in the face. Unfortunately, here in the real world the only thing that can make you less drunk is time. Maybe next time you’ll stop after that seventh Manhattan.
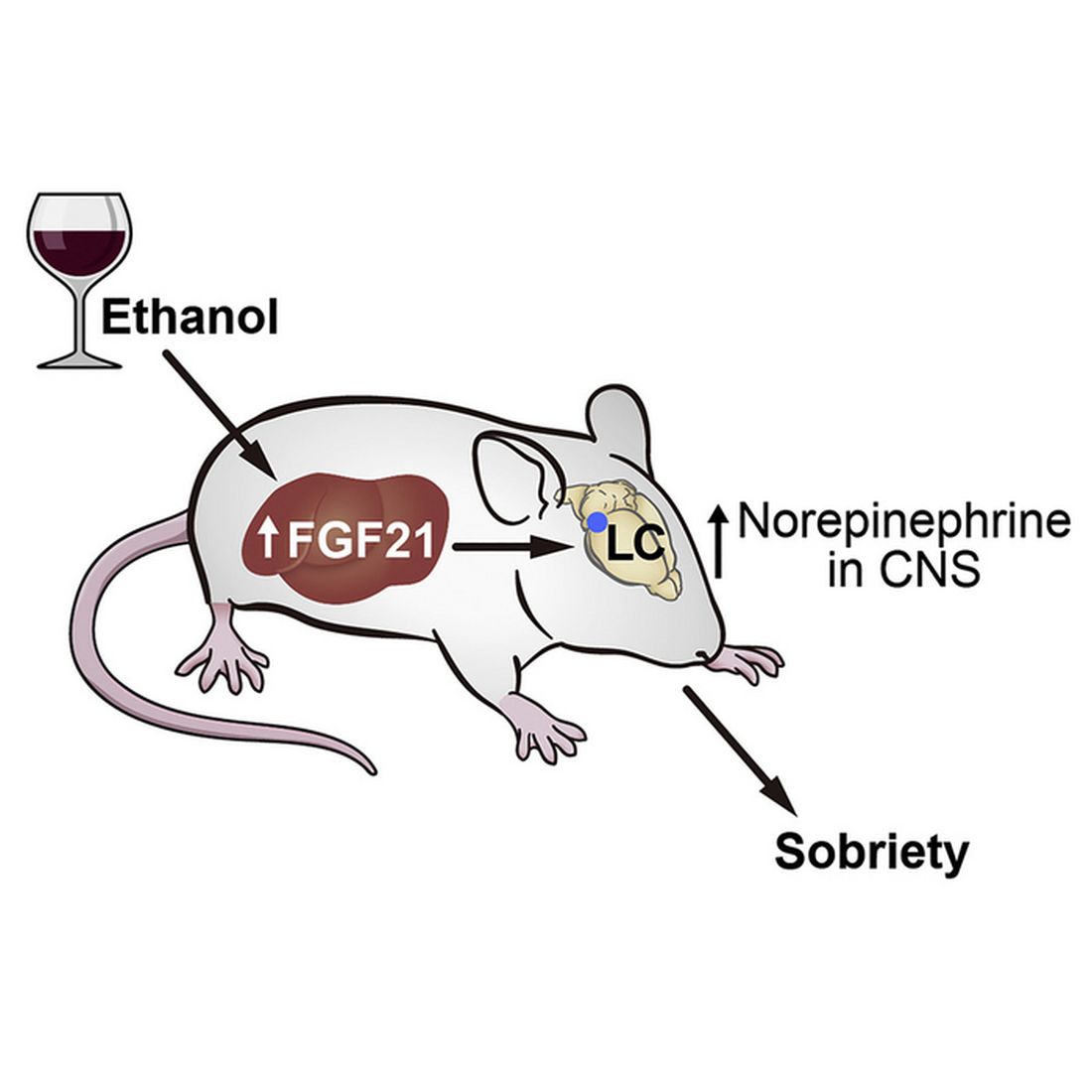
But what if we could beat time? What if there’s an actual sobriety drug out there?
Say hello to fibroblast growth factor 21. Although the liver already does good work filtering out what is essentially poison, it then goes the extra mile and produces fibroblast growth factor 21 (or, as her friends call her, FGF21), a hormone that suppresses the desire to drink, makes you desire water, and protects the liver all at the same time.
Now, FGF21 in its current role is great, but if you’ve ever seen or been a drunk person before, you’ve experienced the lack of interest in listening to reason, especially when it comes from within our own bodies. Who are you to tell us what to do, body? You’re not the boss of us! So a group of scientists decided to push the limits of FGF21. Could it do more than it already does?
First off, they genetically altered a group of mice so that they didn’t produce FGF21 on their own. Then they got them drunk. We’re going to assume they built a scale model of the bar from Cheers and had the mice filter in through the front door as they served their subjects beer out of tiny little glasses.
Once the mice were nice and liquored up, some were given a treatment of FGF21 while others were given a placebo. Lo and behold, the mice given FGF21 recovered about 50% faster than those that received the control treatment. Not exactly instant, but 50% is nothing to sniff at.
Before you bring your FGF21 supplement to the bar, though, this research only applies to mice. We don’t know if it works in people. And make sure you stick to booze. If your choice of intoxication is a bit more exotic, FGF21 isn’t going to do anything for you. Yes, the scientists tried. Yes, those mice are living a very interesting life. And yes, we are jealous of drugged-up lab mice.
Supersize your imagination, shrink your snacks
Have you ever heard of the meal-recall effect? Did you know that, in England, a biscuit is really a cookie? Did you also know that the magazine Bon Appétit is not the same as the peer-reviewed journal Appetite? We do … now.

The meal-recall effect is the subsequent reduction in snacking that comes from remembering a recent meal. It was used to great effect in a recent study conducted at the University of Cambridge, which is in England, where they feed their experimental humans cookies but, for some reason, call them biscuits.
For the first part of the study, the participants were invited to dine at Che Laboratory, where they “were given a microwave ready meal of rice and sauce and a cup of water,” according to a statement from the university. As our Uncle Ernie would say, “Gourmet all the way.”
The test subjects were instructed not to eat anything for 3 hours and “then invited back to the lab to perform imagination tasks.” Those who did come back were randomly divided into five different groups, each with a different task:
- Imagine moving their recent lunch at the lab around a plate.
- Recall eating their recent lunch in detail.
- Imagine that the lunch was twice as big and filling as it really was.
- Look at a photograph of spaghetti hoops in tomato sauce and write a description of it before imagining moving the food around a plate.
- Look at a photo of paper clips and rubber bands and imagine moving them around.
Now, at last, we get to the biscuits/cookies, which were the subject of a taste test that “was simply a rouse for covertly assessing snacking,” the investigators explained. As part of that test, participants were told they could eat as many biscuits as they wanted.
When the tables were cleared and the leftovers examined, the group that imagined spaghetti hoops had eaten the most biscuits (75.9 g), followed by the group that imagined paper clips (75.5 g), the moving-their-lunch-around-the-plate group (72.0 g), and the group that relived eating their lunch (70.0 g).
In a victory for the meal-recall effect, the people who imagined their meal being twice as big ate the fewest biscuits (51.1 g). “Your mind can be more powerful than your stomach in dictating how much you eat,” lead author Joanna Szypula, PhD, said in the university statement.
Oh! One more thing. The study appeared in Appetite, which is a peer-reviewed journal, not in Bon Appétit, which is not a peer-reviewed journal. Thanks to the fine folks at both publications for pointing that out to us.
Get ‘em while they’re hot … for your health
Today on the Eating Channel, it’s a very special episode of “Much Ado About Muffin.”
The muffin. For some of us, it’s a good way to pretend we’re not having dessert for breakfast. A bran muffin can be loaded with calcium and fiber, and our beloved blueberry is full of yummy antioxidants and vitamins. Definitely not dessert.
Well, the muffin denial can stop there because there’s a new flavor on the scene, and research suggests it may actually be healthy. (Disclaimer: Muffin may not be considered healthy in Norway.) This new muffin has a name, Roselle, that comes from the calyx extract used in it, which is found in the Hibiscus sabdariffa plant of the same name.
Now, when it comes to new foods, especially ones that are supposed to be healthy, the No. 1 criteria is the same: It has to taste good. Researchers at the Norwegian University of Science and Technology and Amity University in India agreed, but they also set out to make it nutritionally valuable and give it a long shelf life without the addition of preservatives.
Sounds like a tall order, but they figured it out.
Not only is it tasty, but the properties of it could rival your morning multivitamin. Hibiscus extract has huge amounts of antioxidants, like phenolics, which are believed to help prevent cell membrane damage. Foods like vegetables, flax seed, and whole grains also have these antioxidants, but why not just have a Roselle muffin instead? You also get a dose of ascorbic acid without the glass of OJ in the morning.
The ascorbic acid, however, is not there just to help you. It also helps to check the researcher’s third box, shelf life. These naturally rosy-colored pastries will stay mold-free for 6 days without refrigeration at room temperature and without added preservatives.
Our guess, though, is they won’t be on the kitchen counter long enough to find out.
A sobering proposition
If Hollywood is to be believed, there’s no amount of drunkenness that can’t be cured with a cup of coffee or a stern slap in the face. Unfortunately, here in the real world the only thing that can make you less drunk is time. Maybe next time you’ll stop after that seventh Manhattan.
But what if we could beat time? What if there’s an actual sobriety drug out there?
Say hello to fibroblast growth factor 21. Although the liver already does good work filtering out what is essentially poison, it then goes the extra mile and produces fibroblast growth factor 21 (or, as her friends call her, FGF21), a hormone that suppresses the desire to drink, makes you desire water, and protects the liver all at the same time.
Now, FGF21 in its current role is great, but if you’ve ever seen or been a drunk person before, you’ve experienced the lack of interest in listening to reason, especially when it comes from within our own bodies. Who are you to tell us what to do, body? You’re not the boss of us! So a group of scientists decided to push the limits of FGF21. Could it do more than it already does?
First off, they genetically altered a group of mice so that they didn’t produce FGF21 on their own. Then they got them drunk. We’re going to assume they built a scale model of the bar from Cheers and had the mice filter in through the front door as they served their subjects beer out of tiny little glasses.
Once the mice were nice and liquored up, some were given a treatment of FGF21 while others were given a placebo. Lo and behold, the mice given FGF21 recovered about 50% faster than those that received the control treatment. Not exactly instant, but 50% is nothing to sniff at.
Before you bring your FGF21 supplement to the bar, though, this research only applies to mice. We don’t know if it works in people. And make sure you stick to booze. If your choice of intoxication is a bit more exotic, FGF21 isn’t going to do anything for you. Yes, the scientists tried. Yes, those mice are living a very interesting life. And yes, we are jealous of drugged-up lab mice.
Supersize your imagination, shrink your snacks
Have you ever heard of the meal-recall effect? Did you know that, in England, a biscuit is really a cookie? Did you also know that the magazine Bon Appétit is not the same as the peer-reviewed journal Appetite? We do … now.
The meal-recall effect is the subsequent reduction in snacking that comes from remembering a recent meal. It was used to great effect in a recent study conducted at the University of Cambridge, which is in England, where they feed their experimental humans cookies but, for some reason, call them biscuits.
For the first part of the study, the participants were invited to dine at Che Laboratory, where they “were given a microwave ready meal of rice and sauce and a cup of water,” according to a statement from the university. As our Uncle Ernie would say, “Gourmet all the way.”
The test subjects were instructed not to eat anything for 3 hours and “then invited back to the lab to perform imagination tasks.” Those who did come back were randomly divided into five different groups, each with a different task:
- Imagine moving their recent lunch at the lab around a plate.
- Recall eating their recent lunch in detail.
- Imagine that the lunch was twice as big and filling as it really was.
- Look at a photograph of spaghetti hoops in tomato sauce and write a description of it before imagining moving the food around a plate.
- Look at a photo of paper clips and rubber bands and imagine moving them around.
Now, at last, we get to the biscuits/cookies, which were the subject of a taste test that “was simply a rouse for covertly assessing snacking,” the investigators explained. As part of that test, participants were told they could eat as many biscuits as they wanted.
When the tables were cleared and the leftovers examined, the group that imagined spaghetti hoops had eaten the most biscuits (75.9 g), followed by the group that imagined paper clips (75.5 g), the moving-their-lunch-around-the-plate group (72.0 g), and the group that relived eating their lunch (70.0 g).
In a victory for the meal-recall effect, the people who imagined their meal being twice as big ate the fewest biscuits (51.1 g). “Your mind can be more powerful than your stomach in dictating how much you eat,” lead author Joanna Szypula, PhD, said in the university statement.
Oh! One more thing. The study appeared in Appetite, which is a peer-reviewed journal, not in Bon Appétit, which is not a peer-reviewed journal. Thanks to the fine folks at both publications for pointing that out to us.
Get ‘em while they’re hot … for your health
Today on the Eating Channel, it’s a very special episode of “Much Ado About Muffin.”
The muffin. For some of us, it’s a good way to pretend we’re not having dessert for breakfast. A bran muffin can be loaded with calcium and fiber, and our beloved blueberry is full of yummy antioxidants and vitamins. Definitely not dessert.
Well, the muffin denial can stop there because there’s a new flavor on the scene, and research suggests it may actually be healthy. (Disclaimer: Muffin may not be considered healthy in Norway.) This new muffin has a name, Roselle, that comes from the calyx extract used in it, which is found in the Hibiscus sabdariffa plant of the same name.
Now, when it comes to new foods, especially ones that are supposed to be healthy, the No. 1 criteria is the same: It has to taste good. Researchers at the Norwegian University of Science and Technology and Amity University in India agreed, but they also set out to make it nutritionally valuable and give it a long shelf life without the addition of preservatives.
Sounds like a tall order, but they figured it out.
Not only is it tasty, but the properties of it could rival your morning multivitamin. Hibiscus extract has huge amounts of antioxidants, like phenolics, which are believed to help prevent cell membrane damage. Foods like vegetables, flax seed, and whole grains also have these antioxidants, but why not just have a Roselle muffin instead? You also get a dose of ascorbic acid without the glass of OJ in the morning.
The ascorbic acid, however, is not there just to help you. It also helps to check the researcher’s third box, shelf life. These naturally rosy-colored pastries will stay mold-free for 6 days without refrigeration at room temperature and without added preservatives.
Our guess, though, is they won’t be on the kitchen counter long enough to find out.
A sobering proposition
If Hollywood is to be believed, there’s no amount of drunkenness that can’t be cured with a cup of coffee or a stern slap in the face. Unfortunately, here in the real world the only thing that can make you less drunk is time. Maybe next time you’ll stop after that seventh Manhattan.
But what if we could beat time? What if there’s an actual sobriety drug out there?
Say hello to fibroblast growth factor 21. Although the liver already does good work filtering out what is essentially poison, it then goes the extra mile and produces fibroblast growth factor 21 (or, as her friends call her, FGF21), a hormone that suppresses the desire to drink, makes you desire water, and protects the liver all at the same time.
Now, FGF21 in its current role is great, but if you’ve ever seen or been a drunk person before, you’ve experienced the lack of interest in listening to reason, especially when it comes from within our own bodies. Who are you to tell us what to do, body? You’re not the boss of us! So a group of scientists decided to push the limits of FGF21. Could it do more than it already does?
First off, they genetically altered a group of mice so that they didn’t produce FGF21 on their own. Then they got them drunk. We’re going to assume they built a scale model of the bar from Cheers and had the mice filter in through the front door as they served their subjects beer out of tiny little glasses.
Once the mice were nice and liquored up, some were given a treatment of FGF21 while others were given a placebo. Lo and behold, the mice given FGF21 recovered about 50% faster than those that received the control treatment. Not exactly instant, but 50% is nothing to sniff at.
Before you bring your FGF21 supplement to the bar, though, this research only applies to mice. We don’t know if it works in people. And make sure you stick to booze. If your choice of intoxication is a bit more exotic, FGF21 isn’t going to do anything for you. Yes, the scientists tried. Yes, those mice are living a very interesting life. And yes, we are jealous of drugged-up lab mice.
Supersize your imagination, shrink your snacks
Have you ever heard of the meal-recall effect? Did you know that, in England, a biscuit is really a cookie? Did you also know that the magazine Bon Appétit is not the same as the peer-reviewed journal Appetite? We do … now.
The meal-recall effect is the subsequent reduction in snacking that comes from remembering a recent meal. It was used to great effect in a recent study conducted at the University of Cambridge, which is in England, where they feed their experimental humans cookies but, for some reason, call them biscuits.
For the first part of the study, the participants were invited to dine at Che Laboratory, where they “were given a microwave ready meal of rice and sauce and a cup of water,” according to a statement from the university. As our Uncle Ernie would say, “Gourmet all the way.”
The test subjects were instructed not to eat anything for 3 hours and “then invited back to the lab to perform imagination tasks.” Those who did come back were randomly divided into five different groups, each with a different task:
- Imagine moving their recent lunch at the lab around a plate.
- Recall eating their recent lunch in detail.
- Imagine that the lunch was twice as big and filling as it really was.
- Look at a photograph of spaghetti hoops in tomato sauce and write a description of it before imagining moving the food around a plate.
- Look at a photo of paper clips and rubber bands and imagine moving them around.
Now, at last, we get to the biscuits/cookies, which were the subject of a taste test that “was simply a rouse for covertly assessing snacking,” the investigators explained. As part of that test, participants were told they could eat as many biscuits as they wanted.
When the tables were cleared and the leftovers examined, the group that imagined spaghetti hoops had eaten the most biscuits (75.9 g), followed by the group that imagined paper clips (75.5 g), the moving-their-lunch-around-the-plate group (72.0 g), and the group that relived eating their lunch (70.0 g).
In a victory for the meal-recall effect, the people who imagined their meal being twice as big ate the fewest biscuits (51.1 g). “Your mind can be more powerful than your stomach in dictating how much you eat,” lead author Joanna Szypula, PhD, said in the university statement.
Oh! One more thing. The study appeared in Appetite, which is a peer-reviewed journal, not in Bon Appétit, which is not a peer-reviewed journal. Thanks to the fine folks at both publications for pointing that out to us.
Inclusive reminder: LGBTQ community may donate stem cells
In fact, gay men have been able to donate stem cells in the United States since 2015. That’s when National Marrow Donor Program’s Be the Match registry lifted restrictions on men who have sex with men (MSM).
Physicians say advocacy is still necessary, because LGBTQ people may assume they can’t donate or be wary of clinicians. “The LGBTQIA+ population in general has experienced a lot of issues with the medical-industrial complex in terms of discrimination and inappropriate care,” said UT Southwestern Medical Center pathologist Brian Adkins, MD, who manages the blood bank at Children’s Health in Dallas, in an interview. “There’s a weariness there that may produce some hesitancy to interact with the donation process.”
An estimated 6.8 million people give blood in the United States each year, and an estimated 9 million people are registered as potential stem cell donors. A total of 22,013 hematopoietic cell transplantation procedures were performed in 2020, according to the U.S. Health Resources and Services Administration.
Expanding the number of LGBTQ donors, especially those born as biological males, could pay major dividends. As Dr. Adkins noted, the ideal stem cell donor is young – Be the Match says doctors generally prefer donors aged 18-35 – and male. According to a 2021 Gallup Poll, 21% of those born from 1997 to 2003 (Generation Z) say they’re LGBTQ, as do 11% of those born from 1981 to 1996 (Millennials).
In North America, the most extensive outreach to the LGBTQ community about stem cell donation has been launched in Canada. There, an organization called Stem Cell Club focuses on encouraging college students and other young people to register as potential stem cell donors.
Stem Cell Club has several campaigns aimed at ethnic minority groups, and its Saving Lives With Pride project focuses on MSM. The project’s web page includes testimonials from a woman whose life was saved by an unrelated gay male donor and from a gay male nurse who recovered from blood cancer thanks to a stem cell donation. The site also includes videos about stem cell donation featuring LGBTQ young people and Canadian hematologists.
“Our specialized collection center will treat donors with the highest levels of respect and courtesy, indeed as heroes of their unselfish gift that can truly save a life,” says Ottawa Hospital transplant hematologist David Allan, MD, in one of the videos.
Stem Cell Club was founded by transplant hematologist Warren Fingrut, MD, a research fellow at Memorial Sloan Kettering Cancer Center. In an interview, he said the organization’s LGBTQ project has promoted stem cell donation at several annual gay pride events and will continue the outreach this coming summer. In 2018 and 2019, advocates recruited 354 potential stem-cell donors (40% male, 42 non-White) at five pride events, Dr. Fingrut and colleagues reported last year in the journal Bone Marrow Transplantation.
For a new study, researchers interviewed 37 gay and bisexual men from five Canadian provinces about stem cell donation. Dr. Fingrut and colleagues reported the findings in February in an abstract at the Transplantation & Cellular Therapy Meetings.
Most participants didn’t know they “are eligible to donate stem cells, with many confusing stem cell versus blood donor eligibility criteria,” the researchers reported. According to Dr. Fingrut, some of the men “felt they were treated as second-class citizens, and that translated into frustration and decreased motivation to donate. There were concerns that they would be treated as though they shouldn’t be there.”
Canada has allowed gay men to donate stem cells for at least 10 years, Dr. Fingrut said. In 2022, Canadian officials said blood banks would no longer require MSM donors to have been abstinent from sex for 3 months, the BBC reported. However, donors will be asked about high-risk sexual behaviors.
The United States, where HIV spread through the blood supply during the early years of the AIDS pandemic and killed thousands of hemophiliacs, has much been slower to change its policies. For decades, starting in the 1980s, both blood banks and stem cell donation programs chose to lower the risk by turning away MSM donors.
Policies only began to change in recent years. Be the Match’s registry led the way by welcoming MSM in 2015. Stem cell donations go through more extensive testing than blood donations, Dr. Adkins said, so it’s more likely that HIV will be screened out. Also, he said, officials probably realized “it was necessary to widen the donor pool in order to best serve the patients” because it’s so hard to find matched stem-cell donors.
Be the Match has also stepped up its outreach to the LGBTQ community. “During Pride Month in 2022, Be The Match sponsored booths at events in 12 major markets from coast to coast,” said Jamie Margolis, senior vice president of Donor Services. “These efforts enabled us to increase awareness among more than 500,000 festival attendees and added more than 2,000 new members to the Be The Match Registry. We also produced a social media awareness campaign featuring one of our own employees, who is a cofounder of the Pride Employee Resource Group at Be The Match and a recent blood stem cell donor.”
In 2020 as blood banks became desperate for donations during the early days of the COVID-19 pandemic, the FDA changed its policy and required MSM to be abstinent for 3 months instead of 1 year before giving blood. (Prior to December 2014, any man who’d had sex with a man, even once, was indefinitely banned from giving blood.)
The 3-month policy instituted in 2020 drew fire from critics such as the American Medical Association, which noted the regulation treated men differently if they had unprotected sex with a single man versus with multiple women.
Now, the FDA is proposing that it once again change the policy about blood donations: It is recommending that there be no special polices regarding MSM. “All prospective donors who report having a new sexual partner or more than one sexual partner and had anal sex in the past 3 months would be deferred from donation.”
Under the proposal, anyone who’s ever had HIV will not be able to donate. (They can’t donate stem cells either.) And the FDA proposes restrictions on those who take pre-exposure prophylaxis or postexposure prophylaxis for HIV.
Margolis, of Be the Match, noted that some members of the LGBTQ community may not be able to donate to Be The Match BioTherapies, which works with cell and gene therapy developers worldwide to provide cellular starting material. “These therapies may have different requirements than those for blood stem-cell transplants. Men who have had sex with men in the past 5 years or women who have had sex with a man who has had sex with a man in the past 5 years may not be able to donate to Be The Match BioTherapies. While we understand this could be upsetting or frustrating for someone who desires to be a part of these therapies, we are committed to following medical guidelines and regulations, while also advocating for our donors and the LBGTQIA+ community as a whole.”
MSM aren’t the only target of outreach by proponents of stem cell donation. In 2019, UT Southwestern’s Dr. Adkins and colleagues wrote a commentary in Bone Marrow Transplantation that called for bone marrow donation centers to do more to be welcoming to transgender donors. “The largest age group identifying as transgender is 18-24 years of life, which overlaps considerably with the population of hematopoietic stem cell donors, which tend to be younger individuals,” the researchers wrote.
The transgender community was “simply overlooked,” Dr. Adkins said. Since then, as he pointed out, things have changed. Now, Be the Match’s website notes that “members of the LGBTQIA+ community CAN join the registry and donate.” The organization says that “for medical reasons, everyone is asked to provide their sex assigned at birth when they register. Should you be called as a match, pronouns and gender identity are respected throughout the process.”
In addition, the site says people on prescription hormone therapy are not excluded from joining the registry. Patients who have undergone surgery within the last 12 months, including sex-reassignment procedures, “will be asked about the current status of their recovery and whether they are still seeing a physician for follow-up in regards to the surgery.”
What’s next? Dr. Fingrut said he expects the lifting of strict rules about MSM and blood donation will boost stem cell donation in the community.
There seems to be plenty of room for more outreach. Cole Williams, founder of Pride & Plasma, which advocates for allowing gay men to give blood, suggested in an interview that advocates who want to increase stem cell donation in the LGBTQ community reach out to its community centers, health organizations, providers, and clinics.
So far, though, “I haven’t seen a big call for registration of any individuals unless they have a personal relation to bone marrow donation,” he said.
Dr. Fingrut and Dr. Adkins report no disclosures.
In fact, gay men have been able to donate stem cells in the United States since 2015. That’s when National Marrow Donor Program’s Be the Match registry lifted restrictions on men who have sex with men (MSM).
Physicians say advocacy is still necessary, because LGBTQ people may assume they can’t donate or be wary of clinicians. “The LGBTQIA+ population in general has experienced a lot of issues with the medical-industrial complex in terms of discrimination and inappropriate care,” said UT Southwestern Medical Center pathologist Brian Adkins, MD, who manages the blood bank at Children’s Health in Dallas, in an interview. “There’s a weariness there that may produce some hesitancy to interact with the donation process.”
An estimated 6.8 million people give blood in the United States each year, and an estimated 9 million people are registered as potential stem cell donors. A total of 22,013 hematopoietic cell transplantation procedures were performed in 2020, according to the U.S. Health Resources and Services Administration.
Expanding the number of LGBTQ donors, especially those born as biological males, could pay major dividends. As Dr. Adkins noted, the ideal stem cell donor is young – Be the Match says doctors generally prefer donors aged 18-35 – and male. According to a 2021 Gallup Poll, 21% of those born from 1997 to 2003 (Generation Z) say they’re LGBTQ, as do 11% of those born from 1981 to 1996 (Millennials).
In North America, the most extensive outreach to the LGBTQ community about stem cell donation has been launched in Canada. There, an organization called Stem Cell Club focuses on encouraging college students and other young people to register as potential stem cell donors.
Stem Cell Club has several campaigns aimed at ethnic minority groups, and its Saving Lives With Pride project focuses on MSM. The project’s web page includes testimonials from a woman whose life was saved by an unrelated gay male donor and from a gay male nurse who recovered from blood cancer thanks to a stem cell donation. The site also includes videos about stem cell donation featuring LGBTQ young people and Canadian hematologists.
“Our specialized collection center will treat donors with the highest levels of respect and courtesy, indeed as heroes of their unselfish gift that can truly save a life,” says Ottawa Hospital transplant hematologist David Allan, MD, in one of the videos.
Stem Cell Club was founded by transplant hematologist Warren Fingrut, MD, a research fellow at Memorial Sloan Kettering Cancer Center. In an interview, he said the organization’s LGBTQ project has promoted stem cell donation at several annual gay pride events and will continue the outreach this coming summer. In 2018 and 2019, advocates recruited 354 potential stem-cell donors (40% male, 42 non-White) at five pride events, Dr. Fingrut and colleagues reported last year in the journal Bone Marrow Transplantation.
For a new study, researchers interviewed 37 gay and bisexual men from five Canadian provinces about stem cell donation. Dr. Fingrut and colleagues reported the findings in February in an abstract at the Transplantation & Cellular Therapy Meetings.
Most participants didn’t know they “are eligible to donate stem cells, with many confusing stem cell versus blood donor eligibility criteria,” the researchers reported. According to Dr. Fingrut, some of the men “felt they were treated as second-class citizens, and that translated into frustration and decreased motivation to donate. There were concerns that they would be treated as though they shouldn’t be there.”
Canada has allowed gay men to donate stem cells for at least 10 years, Dr. Fingrut said. In 2022, Canadian officials said blood banks would no longer require MSM donors to have been abstinent from sex for 3 months, the BBC reported. However, donors will be asked about high-risk sexual behaviors.
The United States, where HIV spread through the blood supply during the early years of the AIDS pandemic and killed thousands of hemophiliacs, has much been slower to change its policies. For decades, starting in the 1980s, both blood banks and stem cell donation programs chose to lower the risk by turning away MSM donors.
Policies only began to change in recent years. Be the Match’s registry led the way by welcoming MSM in 2015. Stem cell donations go through more extensive testing than blood donations, Dr. Adkins said, so it’s more likely that HIV will be screened out. Also, he said, officials probably realized “it was necessary to widen the donor pool in order to best serve the patients” because it’s so hard to find matched stem-cell donors.
Be the Match has also stepped up its outreach to the LGBTQ community. “During Pride Month in 2022, Be The Match sponsored booths at events in 12 major markets from coast to coast,” said Jamie Margolis, senior vice president of Donor Services. “These efforts enabled us to increase awareness among more than 500,000 festival attendees and added more than 2,000 new members to the Be The Match Registry. We also produced a social media awareness campaign featuring one of our own employees, who is a cofounder of the Pride Employee Resource Group at Be The Match and a recent blood stem cell donor.”
In 2020 as blood banks became desperate for donations during the early days of the COVID-19 pandemic, the FDA changed its policy and required MSM to be abstinent for 3 months instead of 1 year before giving blood. (Prior to December 2014, any man who’d had sex with a man, even once, was indefinitely banned from giving blood.)
The 3-month policy instituted in 2020 drew fire from critics such as the American Medical Association, which noted the regulation treated men differently if they had unprotected sex with a single man versus with multiple women.
Now, the FDA is proposing that it once again change the policy about blood donations: It is recommending that there be no special polices regarding MSM. “All prospective donors who report having a new sexual partner or more than one sexual partner and had anal sex in the past 3 months would be deferred from donation.”
Under the proposal, anyone who’s ever had HIV will not be able to donate. (They can’t donate stem cells either.) And the FDA proposes restrictions on those who take pre-exposure prophylaxis or postexposure prophylaxis for HIV.
Margolis, of Be the Match, noted that some members of the LGBTQ community may not be able to donate to Be The Match BioTherapies, which works with cell and gene therapy developers worldwide to provide cellular starting material. “These therapies may have different requirements than those for blood stem-cell transplants. Men who have had sex with men in the past 5 years or women who have had sex with a man who has had sex with a man in the past 5 years may not be able to donate to Be The Match BioTherapies. While we understand this could be upsetting or frustrating for someone who desires to be a part of these therapies, we are committed to following medical guidelines and regulations, while also advocating for our donors and the LBGTQIA+ community as a whole.”
MSM aren’t the only target of outreach by proponents of stem cell donation. In 2019, UT Southwestern’s Dr. Adkins and colleagues wrote a commentary in Bone Marrow Transplantation that called for bone marrow donation centers to do more to be welcoming to transgender donors. “The largest age group identifying as transgender is 18-24 years of life, which overlaps considerably with the population of hematopoietic stem cell donors, which tend to be younger individuals,” the researchers wrote.
The transgender community was “simply overlooked,” Dr. Adkins said. Since then, as he pointed out, things have changed. Now, Be the Match’s website notes that “members of the LGBTQIA+ community CAN join the registry and donate.” The organization says that “for medical reasons, everyone is asked to provide their sex assigned at birth when they register. Should you be called as a match, pronouns and gender identity are respected throughout the process.”
In addition, the site says people on prescription hormone therapy are not excluded from joining the registry. Patients who have undergone surgery within the last 12 months, including sex-reassignment procedures, “will be asked about the current status of their recovery and whether they are still seeing a physician for follow-up in regards to the surgery.”
What’s next? Dr. Fingrut said he expects the lifting of strict rules about MSM and blood donation will boost stem cell donation in the community.
There seems to be plenty of room for more outreach. Cole Williams, founder of Pride & Plasma, which advocates for allowing gay men to give blood, suggested in an interview that advocates who want to increase stem cell donation in the LGBTQ community reach out to its community centers, health organizations, providers, and clinics.
So far, though, “I haven’t seen a big call for registration of any individuals unless they have a personal relation to bone marrow donation,” he said.
Dr. Fingrut and Dr. Adkins report no disclosures.
In fact, gay men have been able to donate stem cells in the United States since 2015. That’s when National Marrow Donor Program’s Be the Match registry lifted restrictions on men who have sex with men (MSM).
Physicians say advocacy is still necessary, because LGBTQ people may assume they can’t donate or be wary of clinicians. “The LGBTQIA+ population in general has experienced a lot of issues with the medical-industrial complex in terms of discrimination and inappropriate care,” said UT Southwestern Medical Center pathologist Brian Adkins, MD, who manages the blood bank at Children’s Health in Dallas, in an interview. “There’s a weariness there that may produce some hesitancy to interact with the donation process.”
An estimated 6.8 million people give blood in the United States each year, and an estimated 9 million people are registered as potential stem cell donors. A total of 22,013 hematopoietic cell transplantation procedures were performed in 2020, according to the U.S. Health Resources and Services Administration.
Expanding the number of LGBTQ donors, especially those born as biological males, could pay major dividends. As Dr. Adkins noted, the ideal stem cell donor is young – Be the Match says doctors generally prefer donors aged 18-35 – and male. According to a 2021 Gallup Poll, 21% of those born from 1997 to 2003 (Generation Z) say they’re LGBTQ, as do 11% of those born from 1981 to 1996 (Millennials).
In North America, the most extensive outreach to the LGBTQ community about stem cell donation has been launched in Canada. There, an organization called Stem Cell Club focuses on encouraging college students and other young people to register as potential stem cell donors.
Stem Cell Club has several campaigns aimed at ethnic minority groups, and its Saving Lives With Pride project focuses on MSM. The project’s web page includes testimonials from a woman whose life was saved by an unrelated gay male donor and from a gay male nurse who recovered from blood cancer thanks to a stem cell donation. The site also includes videos about stem cell donation featuring LGBTQ young people and Canadian hematologists.
“Our specialized collection center will treat donors with the highest levels of respect and courtesy, indeed as heroes of their unselfish gift that can truly save a life,” says Ottawa Hospital transplant hematologist David Allan, MD, in one of the videos.
Stem Cell Club was founded by transplant hematologist Warren Fingrut, MD, a research fellow at Memorial Sloan Kettering Cancer Center. In an interview, he said the organization’s LGBTQ project has promoted stem cell donation at several annual gay pride events and will continue the outreach this coming summer. In 2018 and 2019, advocates recruited 354 potential stem-cell donors (40% male, 42 non-White) at five pride events, Dr. Fingrut and colleagues reported last year in the journal Bone Marrow Transplantation.
For a new study, researchers interviewed 37 gay and bisexual men from five Canadian provinces about stem cell donation. Dr. Fingrut and colleagues reported the findings in February in an abstract at the Transplantation & Cellular Therapy Meetings.
Most participants didn’t know they “are eligible to donate stem cells, with many confusing stem cell versus blood donor eligibility criteria,” the researchers reported. According to Dr. Fingrut, some of the men “felt they were treated as second-class citizens, and that translated into frustration and decreased motivation to donate. There were concerns that they would be treated as though they shouldn’t be there.”
Canada has allowed gay men to donate stem cells for at least 10 years, Dr. Fingrut said. In 2022, Canadian officials said blood banks would no longer require MSM donors to have been abstinent from sex for 3 months, the BBC reported. However, donors will be asked about high-risk sexual behaviors.
The United States, where HIV spread through the blood supply during the early years of the AIDS pandemic and killed thousands of hemophiliacs, has much been slower to change its policies. For decades, starting in the 1980s, both blood banks and stem cell donation programs chose to lower the risk by turning away MSM donors.
Policies only began to change in recent years. Be the Match’s registry led the way by welcoming MSM in 2015. Stem cell donations go through more extensive testing than blood donations, Dr. Adkins said, so it’s more likely that HIV will be screened out. Also, he said, officials probably realized “it was necessary to widen the donor pool in order to best serve the patients” because it’s so hard to find matched stem-cell donors.
Be the Match has also stepped up its outreach to the LGBTQ community. “During Pride Month in 2022, Be The Match sponsored booths at events in 12 major markets from coast to coast,” said Jamie Margolis, senior vice president of Donor Services. “These efforts enabled us to increase awareness among more than 500,000 festival attendees and added more than 2,000 new members to the Be The Match Registry. We also produced a social media awareness campaign featuring one of our own employees, who is a cofounder of the Pride Employee Resource Group at Be The Match and a recent blood stem cell donor.”
In 2020 as blood banks became desperate for donations during the early days of the COVID-19 pandemic, the FDA changed its policy and required MSM to be abstinent for 3 months instead of 1 year before giving blood. (Prior to December 2014, any man who’d had sex with a man, even once, was indefinitely banned from giving blood.)
The 3-month policy instituted in 2020 drew fire from critics such as the American Medical Association, which noted the regulation treated men differently if they had unprotected sex with a single man versus with multiple women.
Now, the FDA is proposing that it once again change the policy about blood donations: It is recommending that there be no special polices regarding MSM. “All prospective donors who report having a new sexual partner or more than one sexual partner and had anal sex in the past 3 months would be deferred from donation.”
Under the proposal, anyone who’s ever had HIV will not be able to donate. (They can’t donate stem cells either.) And the FDA proposes restrictions on those who take pre-exposure prophylaxis or postexposure prophylaxis for HIV.
Margolis, of Be the Match, noted that some members of the LGBTQ community may not be able to donate to Be The Match BioTherapies, which works with cell and gene therapy developers worldwide to provide cellular starting material. “These therapies may have different requirements than those for blood stem-cell transplants. Men who have had sex with men in the past 5 years or women who have had sex with a man who has had sex with a man in the past 5 years may not be able to donate to Be The Match BioTherapies. While we understand this could be upsetting or frustrating for someone who desires to be a part of these therapies, we are committed to following medical guidelines and regulations, while also advocating for our donors and the LBGTQIA+ community as a whole.”
MSM aren’t the only target of outreach by proponents of stem cell donation. In 2019, UT Southwestern’s Dr. Adkins and colleagues wrote a commentary in Bone Marrow Transplantation that called for bone marrow donation centers to do more to be welcoming to transgender donors. “The largest age group identifying as transgender is 18-24 years of life, which overlaps considerably with the population of hematopoietic stem cell donors, which tend to be younger individuals,” the researchers wrote.
The transgender community was “simply overlooked,” Dr. Adkins said. Since then, as he pointed out, things have changed. Now, Be the Match’s website notes that “members of the LGBTQIA+ community CAN join the registry and donate.” The organization says that “for medical reasons, everyone is asked to provide their sex assigned at birth when they register. Should you be called as a match, pronouns and gender identity are respected throughout the process.”
In addition, the site says people on prescription hormone therapy are not excluded from joining the registry. Patients who have undergone surgery within the last 12 months, including sex-reassignment procedures, “will be asked about the current status of their recovery and whether they are still seeing a physician for follow-up in regards to the surgery.”
What’s next? Dr. Fingrut said he expects the lifting of strict rules about MSM and blood donation will boost stem cell donation in the community.
There seems to be plenty of room for more outreach. Cole Williams, founder of Pride & Plasma, which advocates for allowing gay men to give blood, suggested in an interview that advocates who want to increase stem cell donation in the LGBTQ community reach out to its community centers, health organizations, providers, and clinics.
So far, though, “I haven’t seen a big call for registration of any individuals unless they have a personal relation to bone marrow donation,” he said.
Dr. Fingrut and Dr. Adkins report no disclosures.
Pulmonary function may predict frailty
Pulmonary function was significantly associated with frailty in community-dwelling older adults over a 5-year period, as indicated by data from more than 1,000 individuals.
The pulmonary function test has been proposed as a predictive tool for clinical outcomes in geriatrics, including hospitalization, mortality, and frailty, but , write Walter Sepulveda-Loyola, MD, of Universidad de Las Americas, Santiago, Chile, and colleagues.
In an observational study published in Heart and Lung, the researchers reviewed data from adults older than 64 years who were participants in the Toledo Study for Healthy Aging.
The study population included 1,188 older adults (mean age, 74 years; 54% women). The prevalence of frailty at baseline ranged from 7% to 26%.
Frailty was defined using the frailty phenotype (FP) and the Frailty Trait Scale 5 (FTS5). Pulmonary function was determined on the basis of forced expiratory volume in the first second (FEV1) and forced vital capacity (FVC), using spirometry.
Overall, at the 5-year follow-up, FEV1 and FVC were inversely associated with prevalence and incidence of frailty in nonadjusted and adjusted models using FP and FTS5.
In adjusted models, FEV1 and FVC, as well as FEV1 and FVC percent predicted value, were significantly associated with the prevalence of frailty, with odds ratios ranging from 0.53 to 0.99. FEV1 and FVC were significantly associated with increased incidence of frailty, with odds ratios ranging from 0.49 to 0.50 (P < .05 for both).
Pulmonary function also was associated with prevalent and incident frailty, hospitalization, and mortality in regression models, including the whole sample and after respiratory diseases were excluded.
Pulmonary function measures below the cutoff points for FEV1 and FVC were significantly associated with frailty, as well as with hospitalization and mortality. The cutoff points for FEV1 were 1.805 L for men and 1.165 L for women; cutoff points for FVC were 2.385 L for men and 1.585 L for women.
“Pulmonary function should be evaluated not only in frail patients, with the aim of detecting patients with poor prognoses regardless of their comorbidity, but also in individuals who are not frail but have an increased risk of developing frailty, as well as other adverse events,” the researchers write.
The study findings were limited by lack of data on pulmonary function variables outside of spirometry and by the need for data from populations with different characteristics to assess whether the same cutoff points are predictive of frailty, the researchers note.
The results were strengthened by the large sample size and additional analysis that excluded other respiratory diseases. Future research should consider adding pulmonary function assessment to the frailty model, the authors write.
Given the relationship between pulmonary function and physical capacity, the current study supports more frequent evaluation of pulmonary function in clinical practice for older adults, including those with no pulmonary disease, they conclude.
The study was supported by the Spanish Ministry of Economy, Industry, and Competitiveness, financed by the European Regional Development Funds, and the Centro de Investigacion Biomedica en Red en Fragilidad y Envejecimiento Saludable and the Fundacion Francisco Soria Melguizo. Lead author Dr. Sepulveda-Loyola was supported by the Brazilian National Council for Scientific and Technological Development.
A version of this article first appeared on Medscape.com.
Pulmonary function was significantly associated with frailty in community-dwelling older adults over a 5-year period, as indicated by data from more than 1,000 individuals.
The pulmonary function test has been proposed as a predictive tool for clinical outcomes in geriatrics, including hospitalization, mortality, and frailty, but , write Walter Sepulveda-Loyola, MD, of Universidad de Las Americas, Santiago, Chile, and colleagues.
In an observational study published in Heart and Lung, the researchers reviewed data from adults older than 64 years who were participants in the Toledo Study for Healthy Aging.
The study population included 1,188 older adults (mean age, 74 years; 54% women). The prevalence of frailty at baseline ranged from 7% to 26%.
Frailty was defined using the frailty phenotype (FP) and the Frailty Trait Scale 5 (FTS5). Pulmonary function was determined on the basis of forced expiratory volume in the first second (FEV1) and forced vital capacity (FVC), using spirometry.
Overall, at the 5-year follow-up, FEV1 and FVC were inversely associated with prevalence and incidence of frailty in nonadjusted and adjusted models using FP and FTS5.
In adjusted models, FEV1 and FVC, as well as FEV1 and FVC percent predicted value, were significantly associated with the prevalence of frailty, with odds ratios ranging from 0.53 to 0.99. FEV1 and FVC were significantly associated with increased incidence of frailty, with odds ratios ranging from 0.49 to 0.50 (P < .05 for both).
Pulmonary function also was associated with prevalent and incident frailty, hospitalization, and mortality in regression models, including the whole sample and after respiratory diseases were excluded.
Pulmonary function measures below the cutoff points for FEV1 and FVC were significantly associated with frailty, as well as with hospitalization and mortality. The cutoff points for FEV1 were 1.805 L for men and 1.165 L for women; cutoff points for FVC were 2.385 L for men and 1.585 L for women.
“Pulmonary function should be evaluated not only in frail patients, with the aim of detecting patients with poor prognoses regardless of their comorbidity, but also in individuals who are not frail but have an increased risk of developing frailty, as well as other adverse events,” the researchers write.
The study findings were limited by lack of data on pulmonary function variables outside of spirometry and by the need for data from populations with different characteristics to assess whether the same cutoff points are predictive of frailty, the researchers note.
The results were strengthened by the large sample size and additional analysis that excluded other respiratory diseases. Future research should consider adding pulmonary function assessment to the frailty model, the authors write.
Given the relationship between pulmonary function and physical capacity, the current study supports more frequent evaluation of pulmonary function in clinical practice for older adults, including those with no pulmonary disease, they conclude.
The study was supported by the Spanish Ministry of Economy, Industry, and Competitiveness, financed by the European Regional Development Funds, and the Centro de Investigacion Biomedica en Red en Fragilidad y Envejecimiento Saludable and the Fundacion Francisco Soria Melguizo. Lead author Dr. Sepulveda-Loyola was supported by the Brazilian National Council for Scientific and Technological Development.
A version of this article first appeared on Medscape.com.
Pulmonary function was significantly associated with frailty in community-dwelling older adults over a 5-year period, as indicated by data from more than 1,000 individuals.
The pulmonary function test has been proposed as a predictive tool for clinical outcomes in geriatrics, including hospitalization, mortality, and frailty, but , write Walter Sepulveda-Loyola, MD, of Universidad de Las Americas, Santiago, Chile, and colleagues.
In an observational study published in Heart and Lung, the researchers reviewed data from adults older than 64 years who were participants in the Toledo Study for Healthy Aging.
The study population included 1,188 older adults (mean age, 74 years; 54% women). The prevalence of frailty at baseline ranged from 7% to 26%.
Frailty was defined using the frailty phenotype (FP) and the Frailty Trait Scale 5 (FTS5). Pulmonary function was determined on the basis of forced expiratory volume in the first second (FEV1) and forced vital capacity (FVC), using spirometry.
Overall, at the 5-year follow-up, FEV1 and FVC were inversely associated with prevalence and incidence of frailty in nonadjusted and adjusted models using FP and FTS5.
In adjusted models, FEV1 and FVC, as well as FEV1 and FVC percent predicted value, were significantly associated with the prevalence of frailty, with odds ratios ranging from 0.53 to 0.99. FEV1 and FVC were significantly associated with increased incidence of frailty, with odds ratios ranging from 0.49 to 0.50 (P < .05 for both).
Pulmonary function also was associated with prevalent and incident frailty, hospitalization, and mortality in regression models, including the whole sample and after respiratory diseases were excluded.
Pulmonary function measures below the cutoff points for FEV1 and FVC were significantly associated with frailty, as well as with hospitalization and mortality. The cutoff points for FEV1 were 1.805 L for men and 1.165 L for women; cutoff points for FVC were 2.385 L for men and 1.585 L for women.
“Pulmonary function should be evaluated not only in frail patients, with the aim of detecting patients with poor prognoses regardless of their comorbidity, but also in individuals who are not frail but have an increased risk of developing frailty, as well as other adverse events,” the researchers write.
The study findings were limited by lack of data on pulmonary function variables outside of spirometry and by the need for data from populations with different characteristics to assess whether the same cutoff points are predictive of frailty, the researchers note.
The results were strengthened by the large sample size and additional analysis that excluded other respiratory diseases. Future research should consider adding pulmonary function assessment to the frailty model, the authors write.
Given the relationship between pulmonary function and physical capacity, the current study supports more frequent evaluation of pulmonary function in clinical practice for older adults, including those with no pulmonary disease, they conclude.
The study was supported by the Spanish Ministry of Economy, Industry, and Competitiveness, financed by the European Regional Development Funds, and the Centro de Investigacion Biomedica en Red en Fragilidad y Envejecimiento Saludable and the Fundacion Francisco Soria Melguizo. Lead author Dr. Sepulveda-Loyola was supported by the Brazilian National Council for Scientific and Technological Development.
A version of this article first appeared on Medscape.com.
Do artificial sweeteners alter postmeal glucose, hunger hormones?
Drinking a sugar-sweetened beverage (SSB), however, had a different effect on postprandial levels of glucose and the hormones insulin, glucagonlike peptide–1 (GLP-1), gastric inhibitory polypeptide (GIP), peptide YY (PYY), ghrelin, leptin, and glucagon.
These findings are from a new meta-analysis by Roselyn Zhang and colleagues, supported by the nonprofit organization Institute for the Advancement of Food and Nutrition Sciences. The study was published recently in Nutrients.
“Nonnutritive sweeteners have no acute metabolic or endocrine effects and they are similar to water in that respect, and they show a different response from caloric sweeteners,” study author Tauseef Khan, MBBS, PhD, summarized in an interview following a press briefing from the IAFNS.
“Our study supports that nonnutritive sweeteners are a healthier alternative to sugar-sweetened beverages or caloric beverages,” said Dr. Khan, an epidemiologist in the department of nutritional sciences, University of Toronto.
Most participants in the 36 trials included in the meta-analysis were healthy, he noted. However, for certain types of NNS beverages, “we had enough studies for type 2 diabetes to also assess that separately, and the results were the same: Nonnutritive sweeteners were no different from water; however, they were different from caloric sweeteners.”
Of note, none of the studies included erythritol – a sugar alcohol (polyol) increasingly used as an artificial sweetener in keto and other types of foods – which was associated with a risk for adverse cardiac events in a paper in Nature Medicine.
Are these NNS drinks largely inert?
“This [meta-analysis] implies that sweeteners are largely inert,” in terms of acute postprandial glucose and hormone response, but the review did not include newer reports that differ, Duane Mellor, PhD, RD, RNutr, who was not involved with the research, noted in an email.
“This is possibly,” he said, because the study “only reviewed the literature up until January 2022 and therefore it missed the World Health Organization review ‘Health Effects of the Use of Non-Sugar Sweeteners’ published in April [2022], and a study published in August 2022 in the journal Cell suggesting that some nonnutritive sweeteners may have a minor effect on gut microbiome and glucose response.
“Although there is a place of nonnutritive sweeteners as a way to reduce sugar intake, they are a small part of dietary pattern and lifestyle which can help reduce risk of disease,” said Dr. Mellor, a registered dietitian and senior teaching fellow at Aston University, Birmingham, England.
“So, although we are clear we need to reduce our intake of sugar-sweetened beverages, switching to non-nutritive sweetened beverages (such as diet sodas) is not necessarily the healthiest option, as unlike water, it seems that some nonnutritive sweeteners may influence glucose responses and levels of related hormones in more recent studies.”
NNS beverages ‘are similar to water’
Dr. Khan pointed out that the meta-analysis addressed two major concerns about NNS beverages.
First, the “sweet uncoupling hypothesis” proposes that low-calorie sweeteners affect sweet taste by separating sweet taste from calories. “The body is confused, and then there is hormonal change. Our study shows that actually that’s not true, and [NNS beverages] are similar to water.”
Second, when no-calorie or low-calorie sweeteners are taken with calories (coupling), a concern is that “then you eat more somehow, or your response is different. However, the results [in this meta-analysis] also show that that is not the case for glucose response, insulin response, and other hormonal markers.”
“The strength is not that low-calorie sweeteners have some benefit per se,” he elaborated. “The advantage is that they replace caloric beverages.
“We are not saying that anybody who is not taking low-calorie sweeteners should start taking [them],” he continued. “What we are saying is somebody who is taking sugar-sweetened beverages and has a problem of taking excess calories, if you replace those calories with low-calorie sweetener, replacement of calories itself may be beneficial, and also they should not be concerned of any [acute] issues with a moderate amount of low-calorie sweeteners.”
Postprandial effect of NNS beverages, SSBs, water
Eight NNS are currently approved by the Food and Drug Administration: aspartame, acesulfame potassium (ace-K), luo han guo (monkfruit) extract, neotame, saccharin, stevia, sucralose, and advantame, the researchers noted.
Ms. Zhang and colleagues searched the literature up until Jan. 15, 2022, for studies of NNS beverages and acute postprandial glycemic and endocrine responses.
Trials were excluded if they involved sugar alcohols (eg, erythritol) or rare sugars (eg, allulose), or if they were shorter than 2 hours, lacked a comparator arm, or did not provide suitable endpoint data.
They identified 36 randomized and nonrandomized clinical trials of 472 predominantly healthy participants: 21 trials (15 reports, n = 266) with NNS consumed alone (uncoupled), 3 trials (3 reports, n = 27) with NNS consumed in a solution containing a carbohydrate (coupled), and 12 trials (7 reports, n = 179) with NNS consumed up to 15 minutes before oral glucose carbohydrate load (delayed coupling).
The four types of beverages were single NNS (ace-K, aspartame, cyclamate, saccharin, stevia, and sucralose), NNS blends (ace-K + aspartame; ace-K + sucralose; ace-K + aspartame + cyclamate; and ace-K + aspartame + sucralose), SSBs (glucose, sucrose, and fructose), and water (control).
In the uncoupled interventions, NNS beverages (single or blends) had no effect on postprandial glucose, insulin, GLP-1, GIP, PYY, ghrelin, and glucagon, with responses similar to water.
In the uncoupled interventions, SSBs sweetened with caloric sugars (glucose and sucrose) increased postprandial glucose, insulin, GLP-1, and GIP responses, with no differences in postprandial ghrelin and glucagon responses.
In the coupled and delayed coupling interventions, NNS beverages had no postprandial glucose and endocrine effects, with responses similar to water.
The studies generally had low to moderate confidence.
The study was supported by an unrestricted grant from IAFNS. Dr. Khan has received research support from the Canadian Institutes of Health Research, the International Life Sciences Institute, and the National Honey Board. He has received honorariums for lectures from the International Food Information Council and the IAFNS. Dr. Mellor has no disclosures.
A version of this article first appeared on Medscape.com.
Drinking a sugar-sweetened beverage (SSB), however, had a different effect on postprandial levels of glucose and the hormones insulin, glucagonlike peptide–1 (GLP-1), gastric inhibitory polypeptide (GIP), peptide YY (PYY), ghrelin, leptin, and glucagon.
These findings are from a new meta-analysis by Roselyn Zhang and colleagues, supported by the nonprofit organization Institute for the Advancement of Food and Nutrition Sciences. The study was published recently in Nutrients.
“Nonnutritive sweeteners have no acute metabolic or endocrine effects and they are similar to water in that respect, and they show a different response from caloric sweeteners,” study author Tauseef Khan, MBBS, PhD, summarized in an interview following a press briefing from the IAFNS.
“Our study supports that nonnutritive sweeteners are a healthier alternative to sugar-sweetened beverages or caloric beverages,” said Dr. Khan, an epidemiologist in the department of nutritional sciences, University of Toronto.
Most participants in the 36 trials included in the meta-analysis were healthy, he noted. However, for certain types of NNS beverages, “we had enough studies for type 2 diabetes to also assess that separately, and the results were the same: Nonnutritive sweeteners were no different from water; however, they were different from caloric sweeteners.”
Of note, none of the studies included erythritol – a sugar alcohol (polyol) increasingly used as an artificial sweetener in keto and other types of foods – which was associated with a risk for adverse cardiac events in a paper in Nature Medicine.
Are these NNS drinks largely inert?
“This [meta-analysis] implies that sweeteners are largely inert,” in terms of acute postprandial glucose and hormone response, but the review did not include newer reports that differ, Duane Mellor, PhD, RD, RNutr, who was not involved with the research, noted in an email.
“This is possibly,” he said, because the study “only reviewed the literature up until January 2022 and therefore it missed the World Health Organization review ‘Health Effects of the Use of Non-Sugar Sweeteners’ published in April [2022], and a study published in August 2022 in the journal Cell suggesting that some nonnutritive sweeteners may have a minor effect on gut microbiome and glucose response.
“Although there is a place of nonnutritive sweeteners as a way to reduce sugar intake, they are a small part of dietary pattern and lifestyle which can help reduce risk of disease,” said Dr. Mellor, a registered dietitian and senior teaching fellow at Aston University, Birmingham, England.
“So, although we are clear we need to reduce our intake of sugar-sweetened beverages, switching to non-nutritive sweetened beverages (such as diet sodas) is not necessarily the healthiest option, as unlike water, it seems that some nonnutritive sweeteners may influence glucose responses and levels of related hormones in more recent studies.”
NNS beverages ‘are similar to water’
Dr. Khan pointed out that the meta-analysis addressed two major concerns about NNS beverages.
First, the “sweet uncoupling hypothesis” proposes that low-calorie sweeteners affect sweet taste by separating sweet taste from calories. “The body is confused, and then there is hormonal change. Our study shows that actually that’s not true, and [NNS beverages] are similar to water.”
Second, when no-calorie or low-calorie sweeteners are taken with calories (coupling), a concern is that “then you eat more somehow, or your response is different. However, the results [in this meta-analysis] also show that that is not the case for glucose response, insulin response, and other hormonal markers.”
“The strength is not that low-calorie sweeteners have some benefit per se,” he elaborated. “The advantage is that they replace caloric beverages.
“We are not saying that anybody who is not taking low-calorie sweeteners should start taking [them],” he continued. “What we are saying is somebody who is taking sugar-sweetened beverages and has a problem of taking excess calories, if you replace those calories with low-calorie sweetener, replacement of calories itself may be beneficial, and also they should not be concerned of any [acute] issues with a moderate amount of low-calorie sweeteners.”
Postprandial effect of NNS beverages, SSBs, water
Eight NNS are currently approved by the Food and Drug Administration: aspartame, acesulfame potassium (ace-K), luo han guo (monkfruit) extract, neotame, saccharin, stevia, sucralose, and advantame, the researchers noted.
Ms. Zhang and colleagues searched the literature up until Jan. 15, 2022, for studies of NNS beverages and acute postprandial glycemic and endocrine responses.
Trials were excluded if they involved sugar alcohols (eg, erythritol) or rare sugars (eg, allulose), or if they were shorter than 2 hours, lacked a comparator arm, or did not provide suitable endpoint data.
They identified 36 randomized and nonrandomized clinical trials of 472 predominantly healthy participants: 21 trials (15 reports, n = 266) with NNS consumed alone (uncoupled), 3 trials (3 reports, n = 27) with NNS consumed in a solution containing a carbohydrate (coupled), and 12 trials (7 reports, n = 179) with NNS consumed up to 15 minutes before oral glucose carbohydrate load (delayed coupling).
The four types of beverages were single NNS (ace-K, aspartame, cyclamate, saccharin, stevia, and sucralose), NNS blends (ace-K + aspartame; ace-K + sucralose; ace-K + aspartame + cyclamate; and ace-K + aspartame + sucralose), SSBs (glucose, sucrose, and fructose), and water (control).
In the uncoupled interventions, NNS beverages (single or blends) had no effect on postprandial glucose, insulin, GLP-1, GIP, PYY, ghrelin, and glucagon, with responses similar to water.
In the uncoupled interventions, SSBs sweetened with caloric sugars (glucose and sucrose) increased postprandial glucose, insulin, GLP-1, and GIP responses, with no differences in postprandial ghrelin and glucagon responses.
In the coupled and delayed coupling interventions, NNS beverages had no postprandial glucose and endocrine effects, with responses similar to water.
The studies generally had low to moderate confidence.
The study was supported by an unrestricted grant from IAFNS. Dr. Khan has received research support from the Canadian Institutes of Health Research, the International Life Sciences Institute, and the National Honey Board. He has received honorariums for lectures from the International Food Information Council and the IAFNS. Dr. Mellor has no disclosures.
A version of this article first appeared on Medscape.com.
Drinking a sugar-sweetened beverage (SSB), however, had a different effect on postprandial levels of glucose and the hormones insulin, glucagonlike peptide–1 (GLP-1), gastric inhibitory polypeptide (GIP), peptide YY (PYY), ghrelin, leptin, and glucagon.
These findings are from a new meta-analysis by Roselyn Zhang and colleagues, supported by the nonprofit organization Institute for the Advancement of Food and Nutrition Sciences. The study was published recently in Nutrients.
“Nonnutritive sweeteners have no acute metabolic or endocrine effects and they are similar to water in that respect, and they show a different response from caloric sweeteners,” study author Tauseef Khan, MBBS, PhD, summarized in an interview following a press briefing from the IAFNS.
“Our study supports that nonnutritive sweeteners are a healthier alternative to sugar-sweetened beverages or caloric beverages,” said Dr. Khan, an epidemiologist in the department of nutritional sciences, University of Toronto.
Most participants in the 36 trials included in the meta-analysis were healthy, he noted. However, for certain types of NNS beverages, “we had enough studies for type 2 diabetes to also assess that separately, and the results were the same: Nonnutritive sweeteners were no different from water; however, they were different from caloric sweeteners.”
Of note, none of the studies included erythritol – a sugar alcohol (polyol) increasingly used as an artificial sweetener in keto and other types of foods – which was associated with a risk for adverse cardiac events in a paper in Nature Medicine.
Are these NNS drinks largely inert?
“This [meta-analysis] implies that sweeteners are largely inert,” in terms of acute postprandial glucose and hormone response, but the review did not include newer reports that differ, Duane Mellor, PhD, RD, RNutr, who was not involved with the research, noted in an email.
“This is possibly,” he said, because the study “only reviewed the literature up until January 2022 and therefore it missed the World Health Organization review ‘Health Effects of the Use of Non-Sugar Sweeteners’ published in April [2022], and a study published in August 2022 in the journal Cell suggesting that some nonnutritive sweeteners may have a minor effect on gut microbiome and glucose response.
“Although there is a place of nonnutritive sweeteners as a way to reduce sugar intake, they are a small part of dietary pattern and lifestyle which can help reduce risk of disease,” said Dr. Mellor, a registered dietitian and senior teaching fellow at Aston University, Birmingham, England.
“So, although we are clear we need to reduce our intake of sugar-sweetened beverages, switching to non-nutritive sweetened beverages (such as diet sodas) is not necessarily the healthiest option, as unlike water, it seems that some nonnutritive sweeteners may influence glucose responses and levels of related hormones in more recent studies.”
NNS beverages ‘are similar to water’
Dr. Khan pointed out that the meta-analysis addressed two major concerns about NNS beverages.
First, the “sweet uncoupling hypothesis” proposes that low-calorie sweeteners affect sweet taste by separating sweet taste from calories. “The body is confused, and then there is hormonal change. Our study shows that actually that’s not true, and [NNS beverages] are similar to water.”
Second, when no-calorie or low-calorie sweeteners are taken with calories (coupling), a concern is that “then you eat more somehow, or your response is different. However, the results [in this meta-analysis] also show that that is not the case for glucose response, insulin response, and other hormonal markers.”
“The strength is not that low-calorie sweeteners have some benefit per se,” he elaborated. “The advantage is that they replace caloric beverages.
“We are not saying that anybody who is not taking low-calorie sweeteners should start taking [them],” he continued. “What we are saying is somebody who is taking sugar-sweetened beverages and has a problem of taking excess calories, if you replace those calories with low-calorie sweetener, replacement of calories itself may be beneficial, and also they should not be concerned of any [acute] issues with a moderate amount of low-calorie sweeteners.”
Postprandial effect of NNS beverages, SSBs, water
Eight NNS are currently approved by the Food and Drug Administration: aspartame, acesulfame potassium (ace-K), luo han guo (monkfruit) extract, neotame, saccharin, stevia, sucralose, and advantame, the researchers noted.
Ms. Zhang and colleagues searched the literature up until Jan. 15, 2022, for studies of NNS beverages and acute postprandial glycemic and endocrine responses.
Trials were excluded if they involved sugar alcohols (eg, erythritol) or rare sugars (eg, allulose), or if they were shorter than 2 hours, lacked a comparator arm, or did not provide suitable endpoint data.
They identified 36 randomized and nonrandomized clinical trials of 472 predominantly healthy participants: 21 trials (15 reports, n = 266) with NNS consumed alone (uncoupled), 3 trials (3 reports, n = 27) with NNS consumed in a solution containing a carbohydrate (coupled), and 12 trials (7 reports, n = 179) with NNS consumed up to 15 minutes before oral glucose carbohydrate load (delayed coupling).
The four types of beverages were single NNS (ace-K, aspartame, cyclamate, saccharin, stevia, and sucralose), NNS blends (ace-K + aspartame; ace-K + sucralose; ace-K + aspartame + cyclamate; and ace-K + aspartame + sucralose), SSBs (glucose, sucrose, and fructose), and water (control).
In the uncoupled interventions, NNS beverages (single or blends) had no effect on postprandial glucose, insulin, GLP-1, GIP, PYY, ghrelin, and glucagon, with responses similar to water.
In the uncoupled interventions, SSBs sweetened with caloric sugars (glucose and sucrose) increased postprandial glucose, insulin, GLP-1, and GIP responses, with no differences in postprandial ghrelin and glucagon responses.
In the coupled and delayed coupling interventions, NNS beverages had no postprandial glucose and endocrine effects, with responses similar to water.
The studies generally had low to moderate confidence.
The study was supported by an unrestricted grant from IAFNS. Dr. Khan has received research support from the Canadian Institutes of Health Research, the International Life Sciences Institute, and the National Honey Board. He has received honorariums for lectures from the International Food Information Council and the IAFNS. Dr. Mellor has no disclosures.
A version of this article first appeared on Medscape.com.
FROM NUTRIENTS